dr alexander miras mrc clinical research fellow imperial...
TRANSCRIPT

Bariatric surgery–from morbid obesity to obese morbidity
Dr Alexander Miras
MRC Clinical Research Fellow
Imperial Weight Centre - Charing Cross Hospital
Metabolic Imaging Group - Hammersmith Hospital
What’s happening in the UK?
• No money!
• Some authorities have stopped bariatric surgery
• Others follow the NICE guidelines (BMI>35 or
40)
• Others operate only on patients with BMI>50

London underground newspaper
North West London
• We operate on patients with BMI>35 and:
• Sleep apnoea/hypopnoea
• Uncontrolled hypertension/stable CVD
• Type 2 Diabetes Mellitus
• Infertility
Case 1
• 43 year old lady
• BMI 45
• No cardiovascular/respiratory disease
• No evidence of Type 2 Diabetes
• 2 children, peri menopausal
• University lecturer
• Plays tennis twice a week
• On Thyroxine 100mcg od

Case 2
• 43 year old lady
• BMI 45
• No cardiovascular/respiratory disease
• Impaired fasting glycaemia
• Fasting glucose 6.8 mmol/l (122.4 mg/dl)
• Fasting Insulin 20 mu/l
• 2 children, regular periods
• University lecturer
• Plays tennis twice a week
• On Thyroxine 100mcg od
Case 3
• 43 year old lady
• BMI 45
• No cardiovascular/respiratory disease
• No evidence of Type 2 Diabetes
• 2 children, regular periods
• University lecturer-just quit
• Mobilises with crutches, severe knee OA
• Needs 3rd party assistance for daily life
• “My quality of life is very poor”
• On Thyroxine 100mcg od and painkillers
Case 4
• 43 year old lady
• BMI 45
• Home oxygen-cor pulmonale
• Exercise tolerance 10 meters
• Type 2 Diabetes with microvascular complications
• 2 children, regular periods
• Unemployed
• House bound
• Polypharmacy
Case 5
• 55 year old gentleman
• BMI 60
• Sleep apnoea on CPAP
• 2 cardiac stents, BP 149/96
• Type 2 Diabetes for 5 years
• HbA1c 10.6% (92.3 mmol/mol)
• Total cholesterol/HDL ratio 9.2
• University lecturer
• Walks twice a week
• On 4 agents for T2DM, Antiplatelets, statin, 4
antihypertensives, Thyroxine 100mcg od

Historical Classifications - Sharma AM , Int J Obes 2009

“Morbid Obesity” – Scott and Law 1970

Recent Classifications
• Before 1985: Metropolitan Life Insurance
Company height-weight tables
• 1985: NIH Consensus Conference
recommended the use of BMI
• 1997: WHO adopts BMI
• Waist Circumference and Waist-to-Hip ratio also
recommended
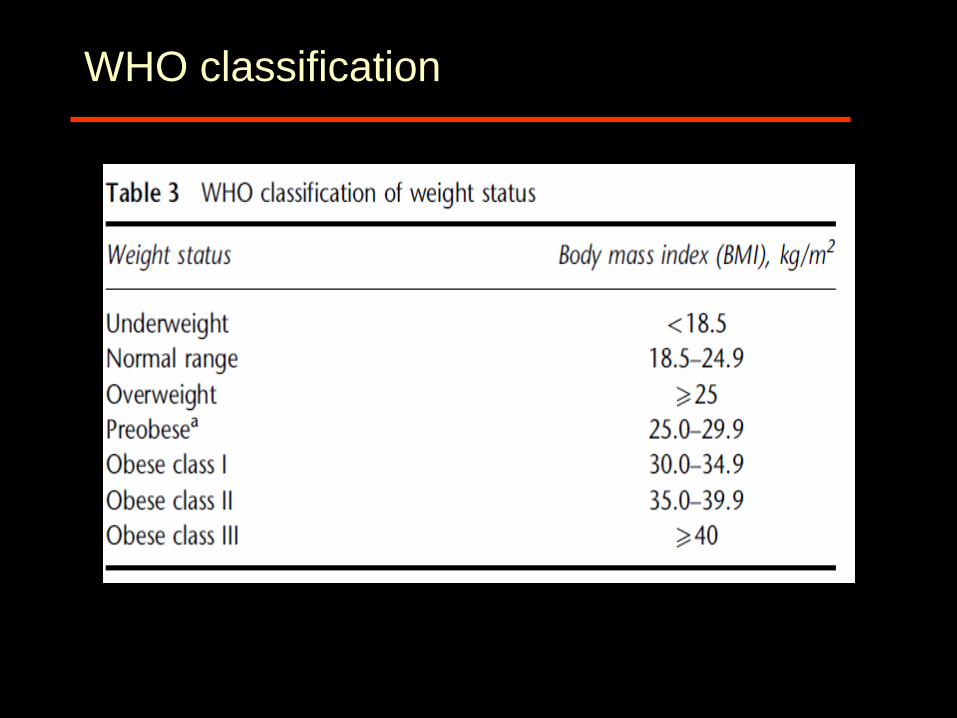
WHO classification
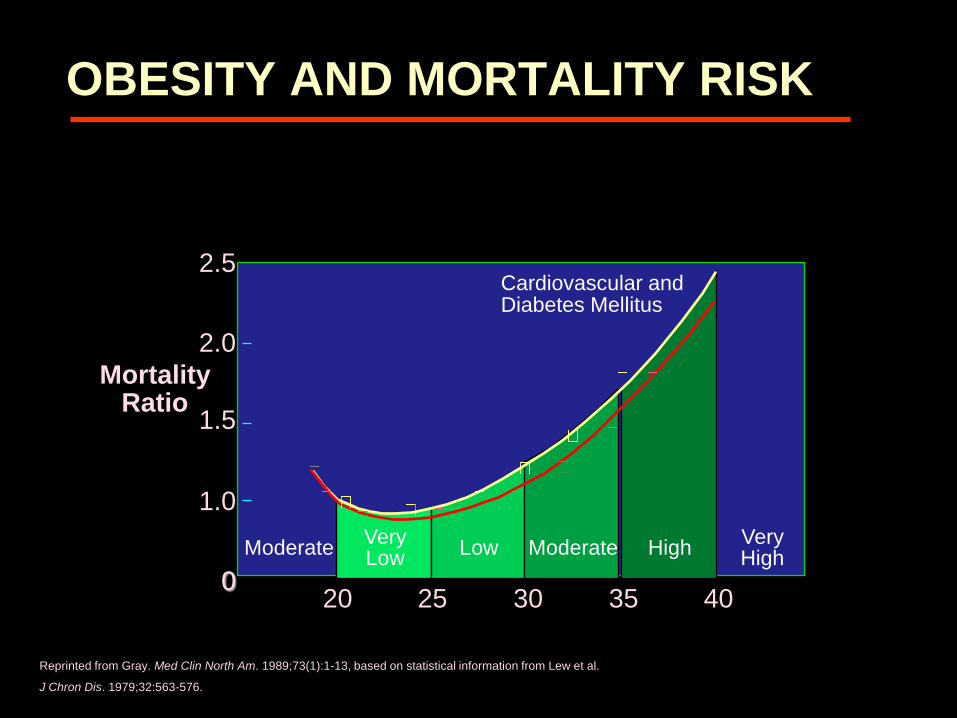
2.5
2.0
1.5
1.0
0 20 25 30 35 40
BMI
Mortality Ratio
Cardiovascular and Diabetes Mellitus
Moderate Very Low
Low Moderate High Very High
Reprinted from Gray. Med Clin North Am. 1989;73(1):1-13, based on statistical information from Lew et al.
J Chron Dis. 1979;32:563-576.
OBESITY AND MORTALITY RISK
Limitations
• Lack of sensitivity and specificity
• No incorporation of comorbidities
• No measure of functionality, QoL, risk
• Poor correlation with overall health

Weight Management vs Obese Morbidity
Clinic Treatment
kg Weight
management Stop
coming
Multi-
modal
Strategy
Morbid Obesity Obese Morbidity
9 domain
assessment
P1
P2
P3
Weight sensitive?
Weight resistant?
Non-weight related?
Therapy specific?

Morbidity and weight loss sensitivity or resistance
Metabolic
Ventilatory
Reproductive
CV risk
Perceived health status
ADL / QoL
Eating behaviour
Anxiety / depression
Body Image dysphoria
Economic cost
-5 -10 -15 -20 -25 -30
% weight
loss to
improve
morbidity
Aylwin 2005

Benefits of a good classification system
• Stratification of patients
• Treatment decision making
• Application of guidelines
• Audit/Research

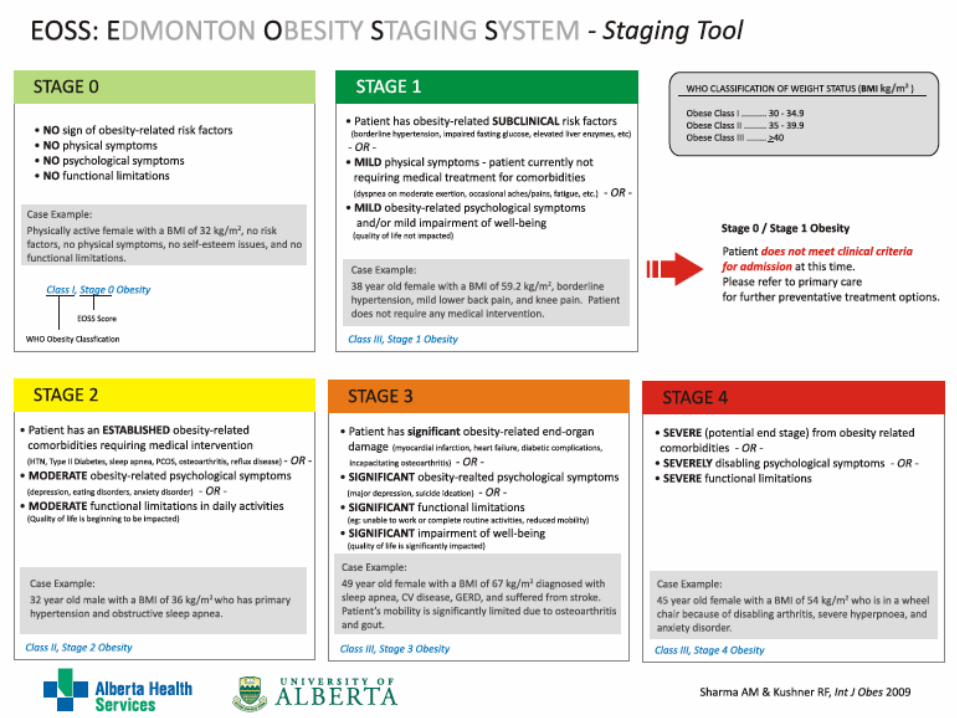
Edmonton Obesity Staging System (EOSS)
Stage 0
Sharma AM & Kushner RF, Int J Obes 2009
Stage 1
Stage 2
Stage 3
Stage 4
co-morbidity
moderate
moderate
Obesity

Edmonton score
Sharma et al, IJO 2009
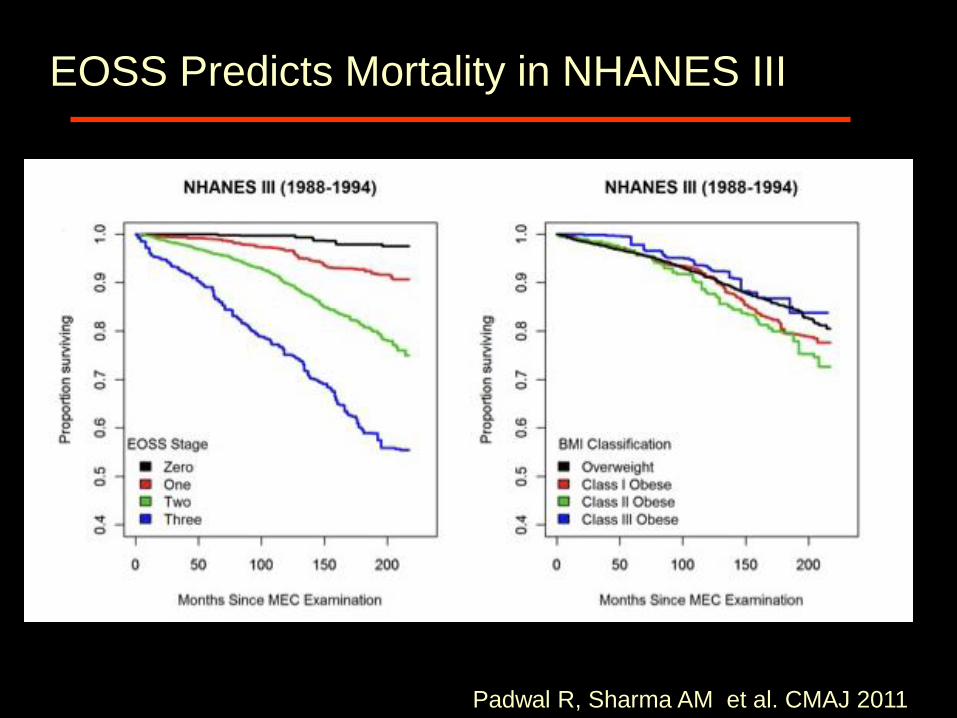
EOSS Predicts Mortality in NHANES III
Padwal R, Sharma AM et al. CMAJ 2011

EOSS Predicts Mortality at Every Level of BMI
Padwal R, Sharma AM et al. CMAJ 2011
Overweight
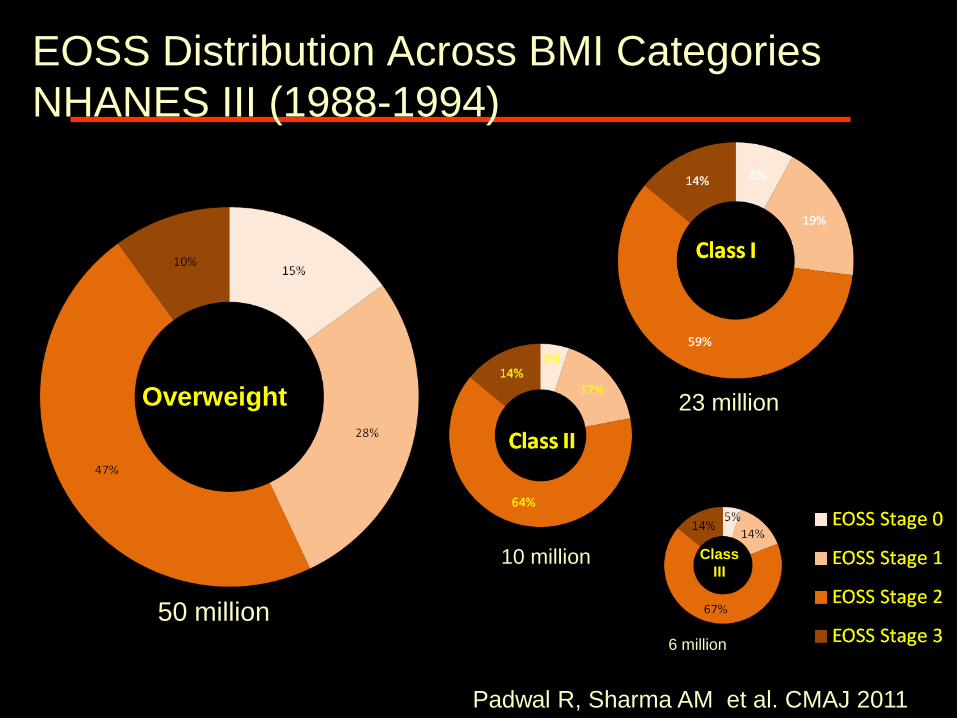
EOSS Distribution Across BMI Categories
NHANES III (1988-1994)
Overweight
Class
III
Padwal R, Sharma AM et al. CMAJ 2011
50 million
23 million
10 million
6 million

EOSS Case 1
24 year-old physically active female,
BMI of 32 Kg/m2
no demonstrable risk factors, no functional
limitations, or mental health issues
Class I, Stage 0 Obesity
- Focus on prevention of further weight gain
- Health benefits of more aggressive obesity
treatment likely marginal
Sharma AM & Kushner RF, Int J Obes 2009

EOSS Case 2
32 year-old male
BMI of 36 Kg/m2
hypertension, sleep apnea, depression
Class 2, Stage 2 Obesity
- Clear benefits of obesity treatment
Sharma AM & Kushner RF, Int J Obes 2009
EOSS Case 3
63 year-old male
BMI of 54 Kg/m2
disabling osteoarthritis (wheel chair)
severe hypoventilation, fibromyalgia, generalized
anxiety disorder
Class 3, Stage 4 Obesity
- Aggressive obesity treatment unless deemed
palliative
Sharma AM & Kushner RF, Int J Obes 2009
Good points
• Incorporates comorbidities, function, QoL,
psychology
• Does not use BMI
• Management suggestions (?)
Bad points
• Relies on constantly changing definitions
• Are the conditions obesity related or not?
• Subjective parameters
• Difficult to confidently allocate patients
• Difficult to capture success of treatment
Aims
• To study the utility of King’s Criteria in assessing obese patients
A. Patient health stage scores
144 obese patients assessed before bariatric surgery
(BMI48±7)
and again 1 year after surgery (BMI 37±7)
B. Observer consistency
11 clinicians scored the same 12 patients in the 9 health
domains
(based on written information)

Obesity Staging Score: Aylwin et al Front Horm Res 2008
Aasheim E et al, Clinical Obesity 2011

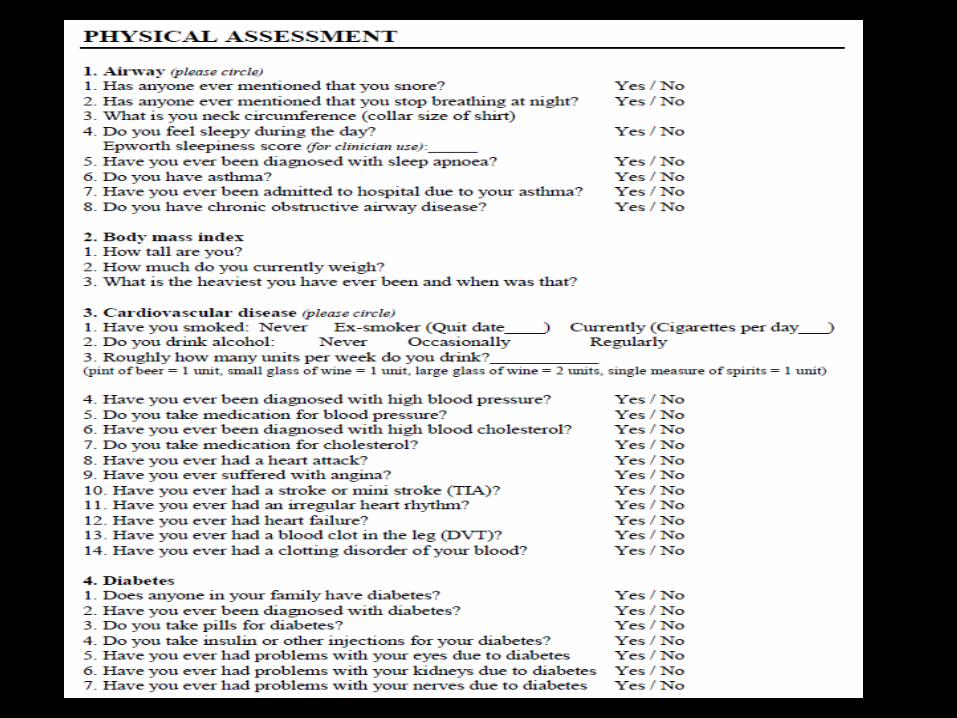
Methods
Basis for assigning King’s Criteria scores:
Medical history
Clinical examination
Test results
“New Patient Questionnaire”
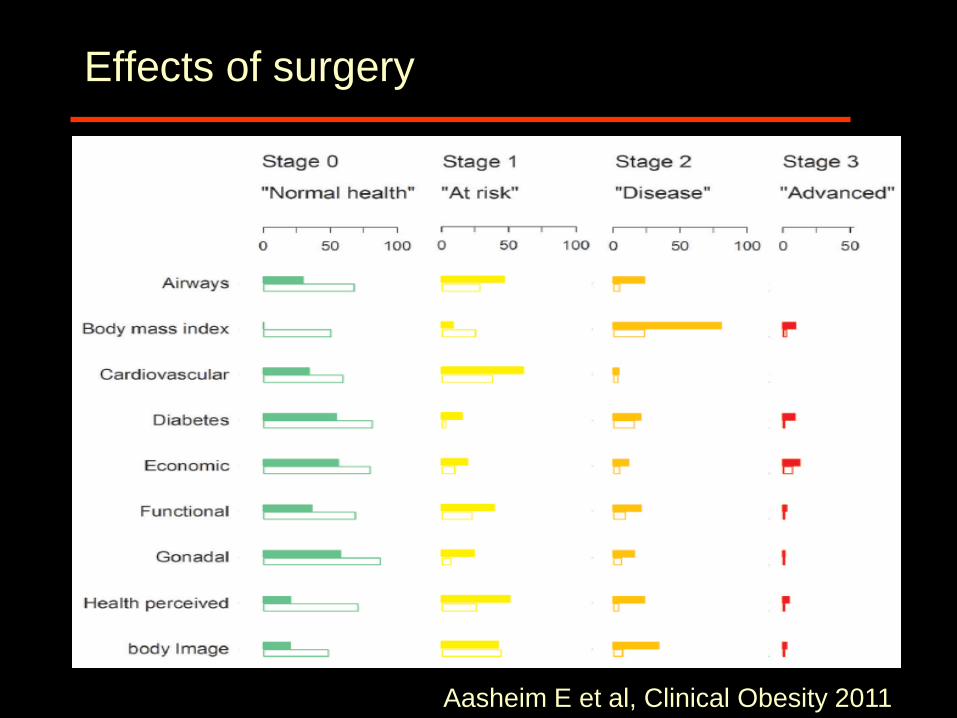
Effects of surgery
Aasheim E et al, Clinical Obesity 2011
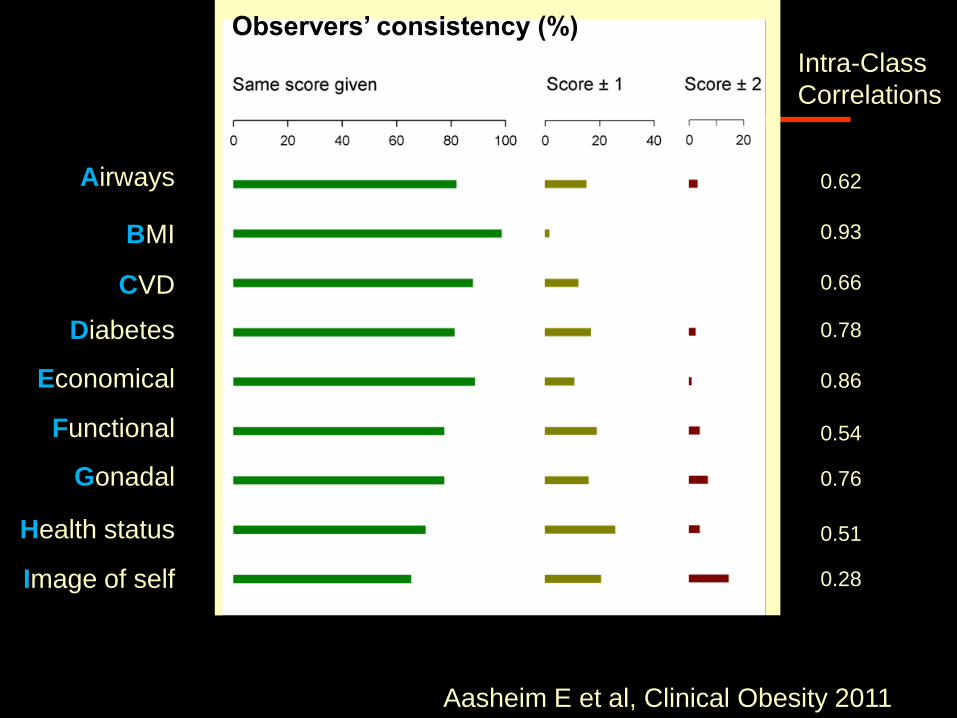
Intra-Class
Correlations
0.62
0.93
0.66
0.78
0.86
0.54
0.76
0.51
0.28
Observers’ consistency (%)
Airways
BMI
CVD
Diabetes
Economical
Functional
Gonadal
Health status
Image of self
Aasheim E et al, Clinical Obesity 2011
Results: summary
King’s Criteria
• Captured obesity-related disease and tracked health
improvements after weight loss.
• Reasonable consistency in scoring among clinicians
Clinically useful
• Identifies which patients may gain most from treatment
• Provides baseline for later comparison
• Adds structure to MDT communication
• Shifts focus from losing weight to improving health
Limitations of King’s Criteria
• Relies on constantly changing definitions, but can be
adapted
• Are the conditions obesity related or not?
• Subjective parameters
• Potential improvements
• Refine staging definitions and weigh them
• Add more domains:
Junction of the gastro-esophagus
Kidneys
Liver

SOS NEJM 2007
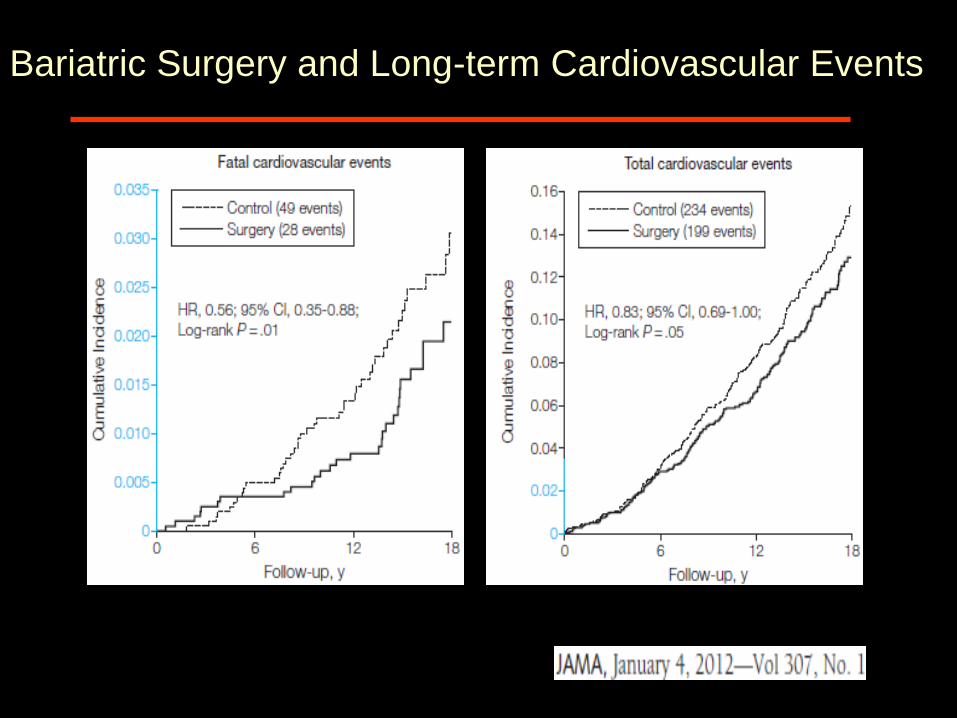
Bariatric Surgery and Long-term Cardiovascular Events

Bariatric Surgery and Long-term Cardiovascular Events
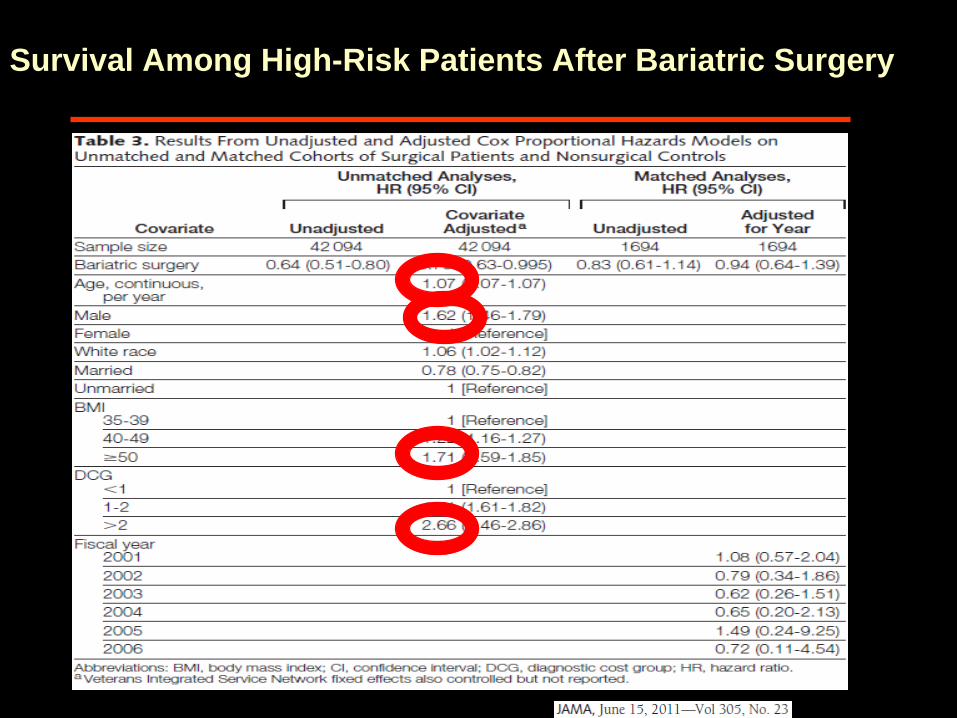
Survival Among High-Risk Patients After Bariatric Surgery

RCT – At last

Bariatric surgery won’t:
• make you thin
• make you happy

Bariatric surgery will:
• make you healthier
• make you more functional

Acknowledgements
• Imperial Weight Centre • Dr Carel le Roux • Mr Torsten Olbers • Dr Florian Seyfried • Dr Ling Ling Chua • Miss Sabrina Jackson
• Institute of Clinical Sciences
• Prof Jimmy Bell • Dr Tony Goldstone • Dr Samantha Scholtz • Dr Christina Prechtl • Dr Sarah Ali • Miss Giuliana Durighel
• King’s College London • Dr Simon Aylwin
Case 6
• 43 year old lady
• BMI 45
• No cardiovascular/respiratory disease
• No evidence of Type 2 Diabetes
• 2 children, regular periods, divorced
• University lecturer-just quit
• Severe depression, house bound, regular
psychiatric follow up
• On Thyroxine 100mcg od and antidepressants
Case 7
• 70 year old lady
• BMI 45
• No cardiovascular/respiratory disease
• No evidence of Type 2 Diabetes
• 2 children, peri menopausal
• Retired University lecturer
• Plays tennis twice a week
• On Thyroxine 100mcg od

Case 8
• 43 year old Asian lady
• BMI 33.9
• 2 cardiac stents, BP 149/96
• Type 2 Diabetes for 5 years
• HbA1c 10.6% (92.3 mmol/mol)
• Total cholesterol/HDL ratio 9.2
• 2 children, regular periods
• University lecturer
• Plays tennis twice a week
• On 4 agents for T2DM, Antiplatelets, statin, 4
antihypertensives, Thyroxine 100mcg od