
Yves BENHAMOU
Management of Patients with HIV/HBV Co-infection
Yves Benhamou
Hepatology Department
Groupe Hospitalier Pitié Salpétrière
Paris, France

Influence of HIV on HBVHIV in HBsAg positive patients (compared to HBV mono-
infected):
– Increases the risk of chronicity after HBV contamination
– Reduces the seroconversion rate to anti-HBe
– Increases reactivation rate
– Increases HBV replication
– Accelerates fibrosis progression
– Increases the risk of liver decompensation, HCC and liver deathBodsworth, JID 1989 ; Hadler, JID 1991 ; Krogsgaard, Hepatology 1987 ; Bodsworth, JID 1989 ; Gilson, AIDS 1997. Piroth, J Hepatol 2002
Vogel Cancer Res 1991; Corallini Cncer Res 1993 ; Altavilla Am J Pathol 2000 ; Bodsworth, JID 1989 ; Mills, Gastroenterol 1990 ; Goldin, J Clin Pathol 1990 ;Gilson, AIDS 1997 ; Thio, Lancet 2002. RR 8.3 (4.8-14.3) ; Di Martino, Gastroenterol 2002 ; Colin : Hepatol 1999 ; Di Martino, Gastroenterol ;
Perillo, Ann Int Med 1986 ; McDonald, J Hepatol 1987 ; Colin, Hepatology 1999 ; Gilson, AIDS 1997
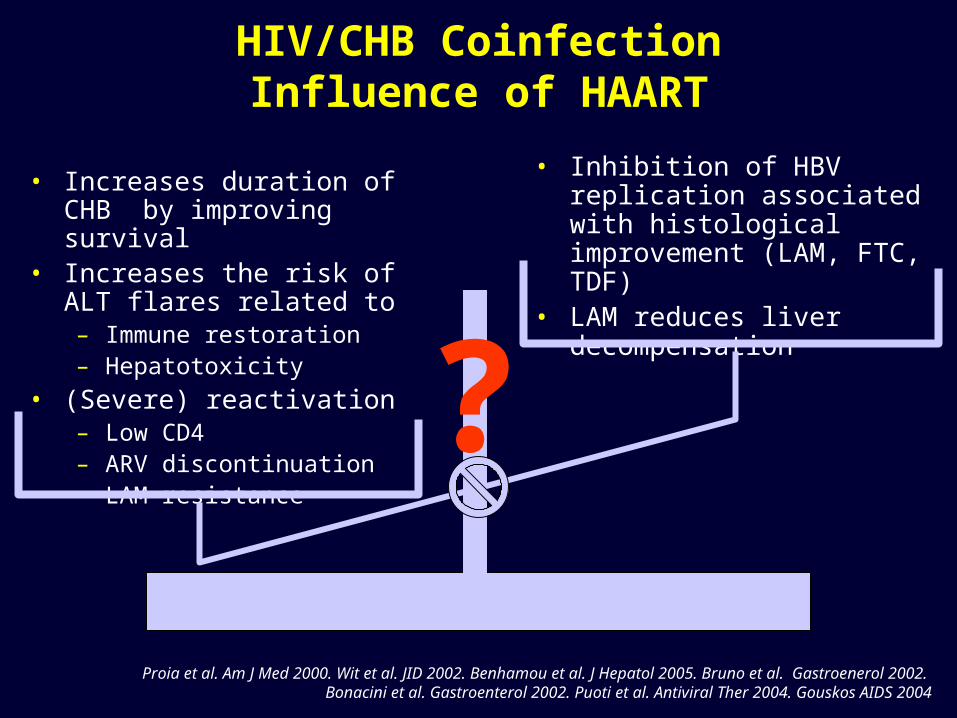
HIV/CHB CoinfectionInfluence of HAART
• Increases duration of CHB by improving survival
• Increases the risk of ALT flares related to – Immune restoration– Hepatotoxicity
• (Severe) reactivation– Low CD4– ARV discontinuation– LAM resistance
• Inhibition of HBV replication associated with histological improvement (LAM, FTC, TDF)
• LAM reduces liver decompensation
?
Proia et al. Am J Med 2000. Wit et al. JID 2002. Benhamou et al. J Hepatol 2005. Bruno et al. Gastroenerol 2002. Bonacini et al. Gastroenterol 2002. Puoti et al. Antiviral Ther 2004. Gouskos AIDS 2004

HIV negativeN=504
HIV positiveN=164
P
Median ALTALT< 2xULN (%)
50 (45-56)26.7
57 (47-74)29.1
NS
HBeAg + (%) 49.9 78.8% <.0001
LAM-R HBV (%) 17.1 34.8% <.0001
HBVDNA> 6 log (%) 37.8 62.1% <.0001
Liver biopsy*
Fibrosis (median)- Cirrhosis (%)
Inflammation (median)- A2/3 (%)
N=469
1 (1-2)16
130.1
N=54
2 (2-2)29.6%
134.7
<.0001
<.0001
Assessed by the METAVIR scoring system.
HBsAg+ vs HBsAg+/HIVGHPS cohort
Benhamou et al CROI 2005
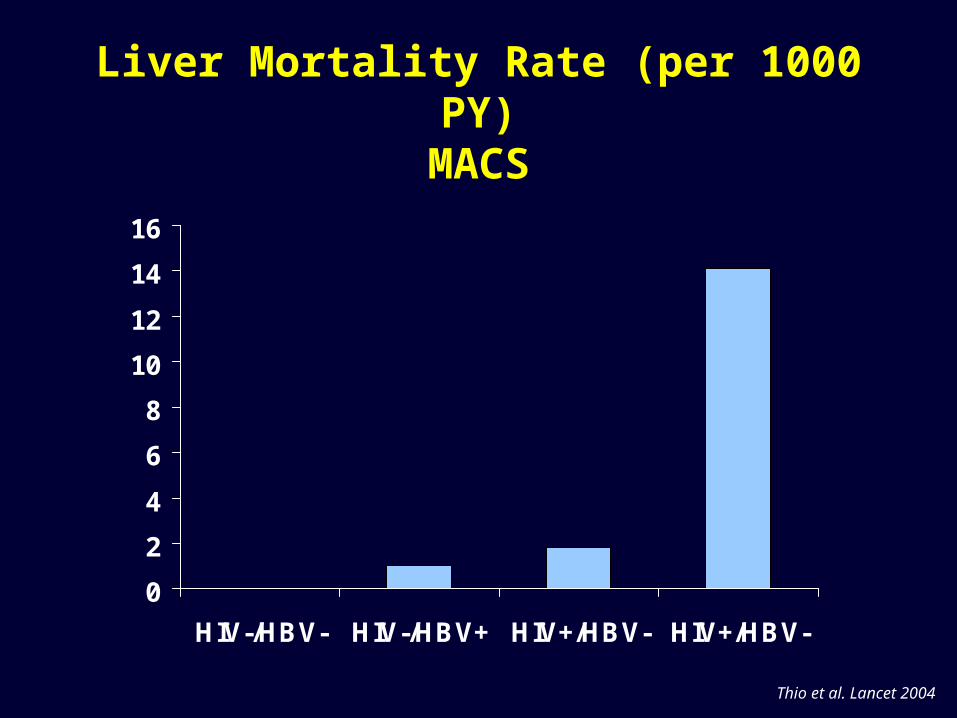
Liver Mortality Rate (per 1000 PY)MACS
0
2
4
6
8
10
12
14
16
HIV-/HBV- HIV-/HBV+ HIV+/HBV- HIV+/HBV-
Thio et al. Lancet 2004
0
0.25
0.50
0.75
1
0 75 150 225 300
Follow up (months)
Pro
po
rtio
n o
f p
atie
nts
fre
e
Of
live
r d
eco
mp
ensa
tio
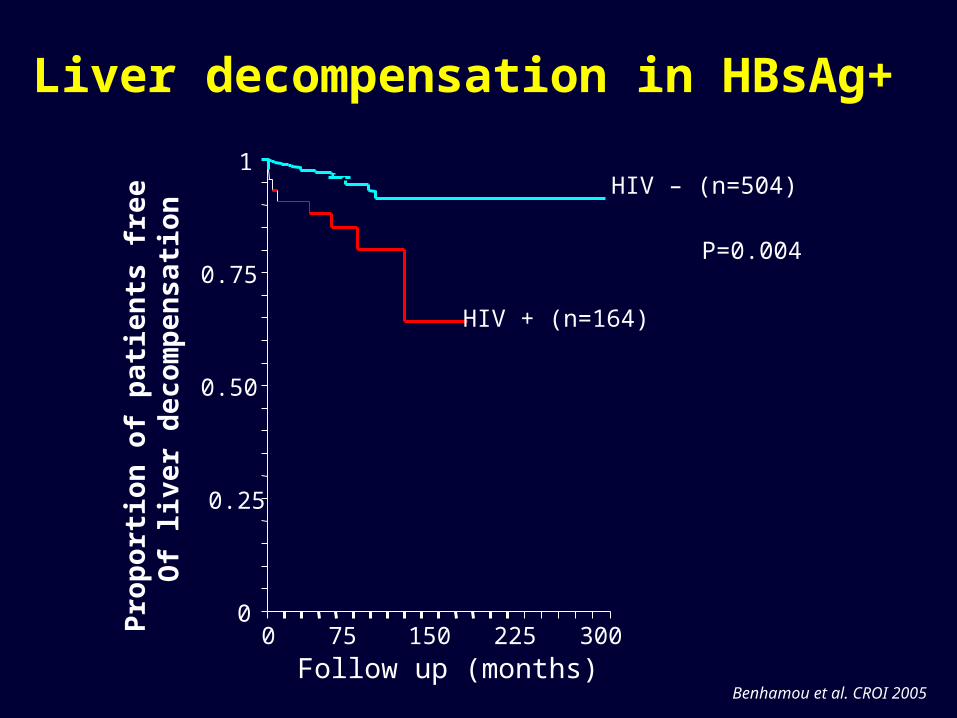
nHIV – (n=504)
HIV + (n=164)
P=0.004
Liver decompensation in HBsAg+
Benhamou et al. CROI 2005

Anti-HBV therapy
• Objective: Decrease liver inflammation and fibrosis progression
• Criteria for anti-HBV initiation:– HBV DNA
• AgHBe+ > 20 000 UI/ml HBeAg+/- > 2000 UI/mL• AgHBe- > 2000 UI/ml
Alberti A et al. J Hepatol. 2005
– Histology• METAVIR A≥2 or F≥2
Thresholds based on HBV mono-infected knowledgeMay be used in HIV/HBV co-infected patients
Alberti A et al. J Hepatol. 2005
HIV/HBV: Treatment
Licensed for Treatment of CHB
• Lamivudine
• Adefovir dipivoxil
• Entecavir
• IFN/Pegylated IFN
Licensed for Treatment of HIV Only with Demonstrated Anti-HBV Activity
• Tenofovir DF
• Emtricitabine
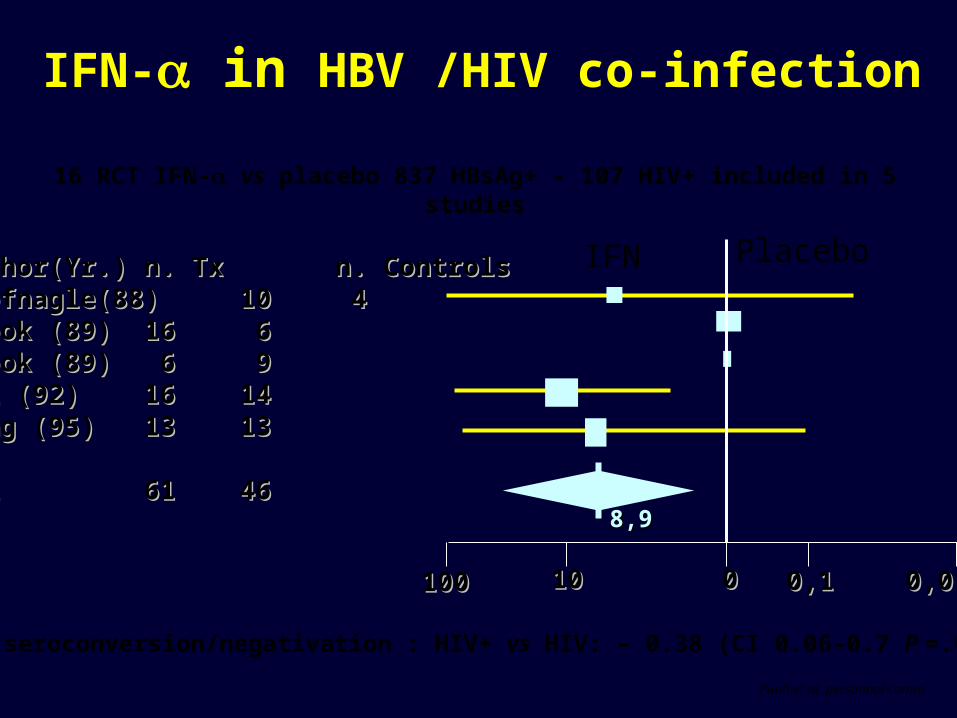
Author(Yr.)Author(Yr.) n. Tx n. Tx n. Controlsn. ControlsHoofnagle(88)Hoofnagle(88) 1010 4 4Brook (89)Brook (89) 1616 6 6Brook (89)Brook (89) 6 6 9 9Pol (92)Pol (92) 1616 1414Wong (95)Wong (95) 1313 1313
All All 6161 4646
100100 1010 00 0,10,1 0,010,01
8,98,9
16 RCT IFN- vs placebo 837 HBsAg+ - 107 HIV+ included in 5 studies
HBe seroconversion/negativation : HIV+ vs HIV: – 0.38 (CI 0.06-0.7 P =.02)
IFN- in HBV /HIV co-infection
IFN Placebo
Puoti et al. personnal comm.
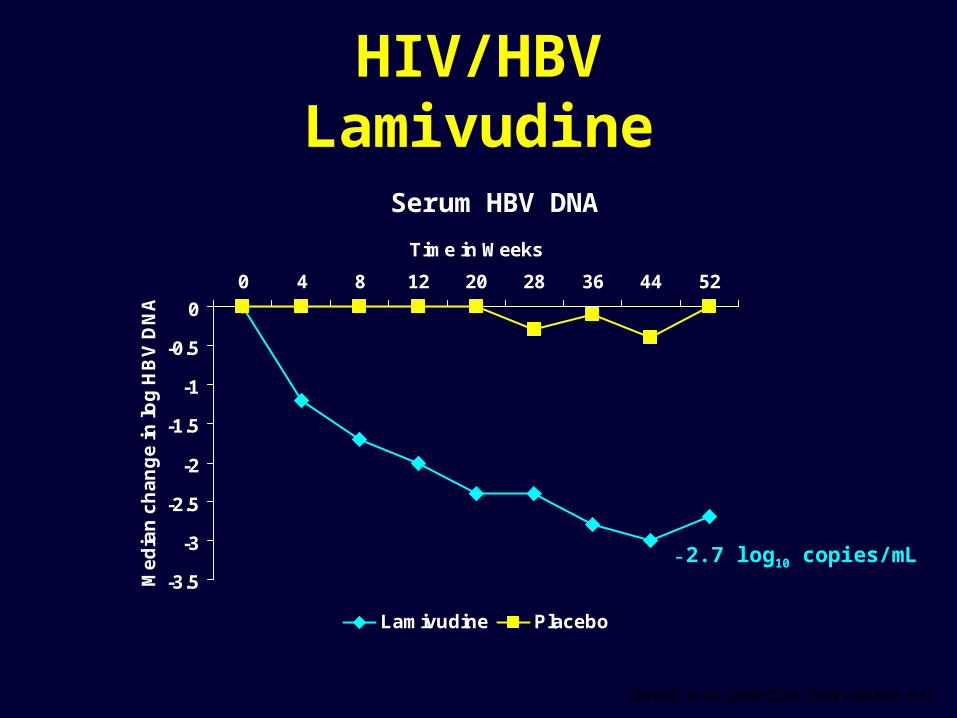
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0 4 8 12 20 28 36 44 52
Time in Weeks
Me
dia
n c
ha
ng
e in
log
HB
V D
NA
Lamivudine Placebo
Serum HBV DNA
Dore GJ, et al. J Infect Dis. 1999;180:607-613.
HIV/HBVLamivudine
-2.7 log10 copies/mL

0
50
100
150
200
250
300
Baseline 2 4 6 8 10 12
AL
T (
UI/L
)
HBV DNA >5x105 copies/mL at baseline
HBV DNA <5x105 copies/mL at baseline
P<0.05
Lamivudine therapy duration (months)
Changes in ALT (UI/mL) during lamivudine therapy
Y Benhamou et al. Ann Intern Med. 1996;125:705-712.
HIV/HBVLamivudine

Lo
g1
0 H
BV
DN
A
24 22 20 20 1733 33 33 33 3310 10 10 7 7
FTC HBV+HIVFTC HBV
d4T HBV+HIV
FTC is not licensed for the treatment of HBV.Raffi F. IAS Conference, July 13-16, 2003, Abstract # 215.
FTC HBV+HIV
d4T HBV+HIV
FTC in Chronic HBV (FTCB-102)
HIV/HBVFTC
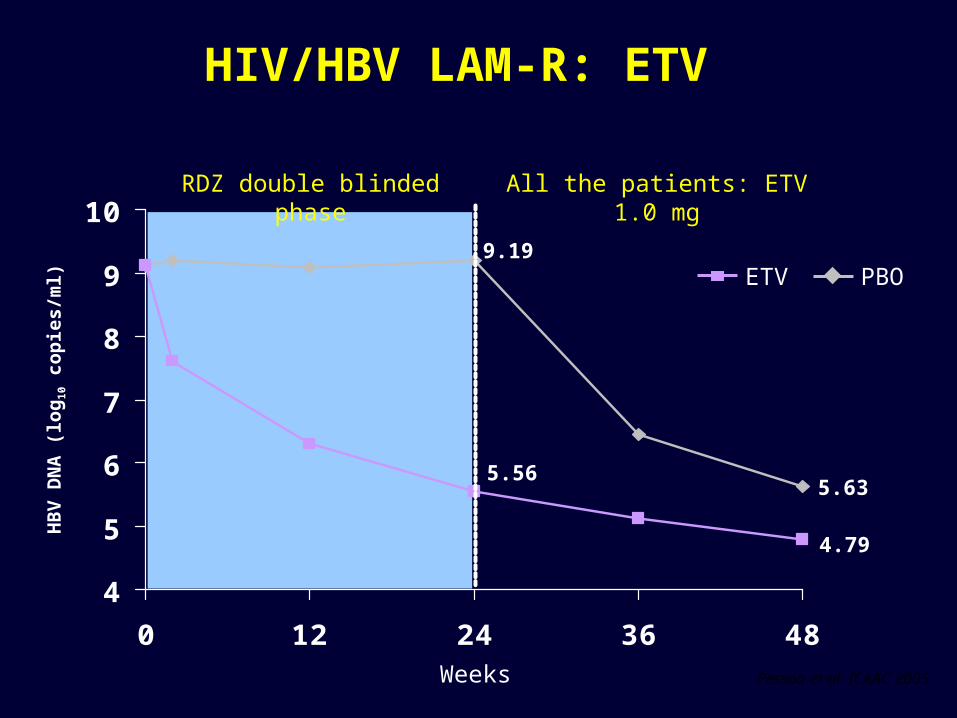
4
5
6
7
8
9
10
0 12 24 36 48
ETV PBO
5.56
HB
V D
NA
(lo
g1
0 c
op
ies/
ml)
9.19
4.79
5.63
Weeks
RDZ double blinded phase All the patients: ETV 1.0 mg
HIV/HBV LAM-R: ETV
Pessoa et al. ICAAC 2005

Number of patients (%)
ETV
W24
ETV
W48
PBO
W24
PBO ETV
W48
ALT 5 (10) 2 (4) 0 (0) 2 (12)
AST 5 (10) 0 0 (0) 2(12)
Pessoa et al. ICAAC 2005
HIV/HBV LAM-R: ETV
ALT/AST flares (>3 x ULN) during ETV therapy
HB
V D
NA
(lo
g10 c
op
ies/
ml)
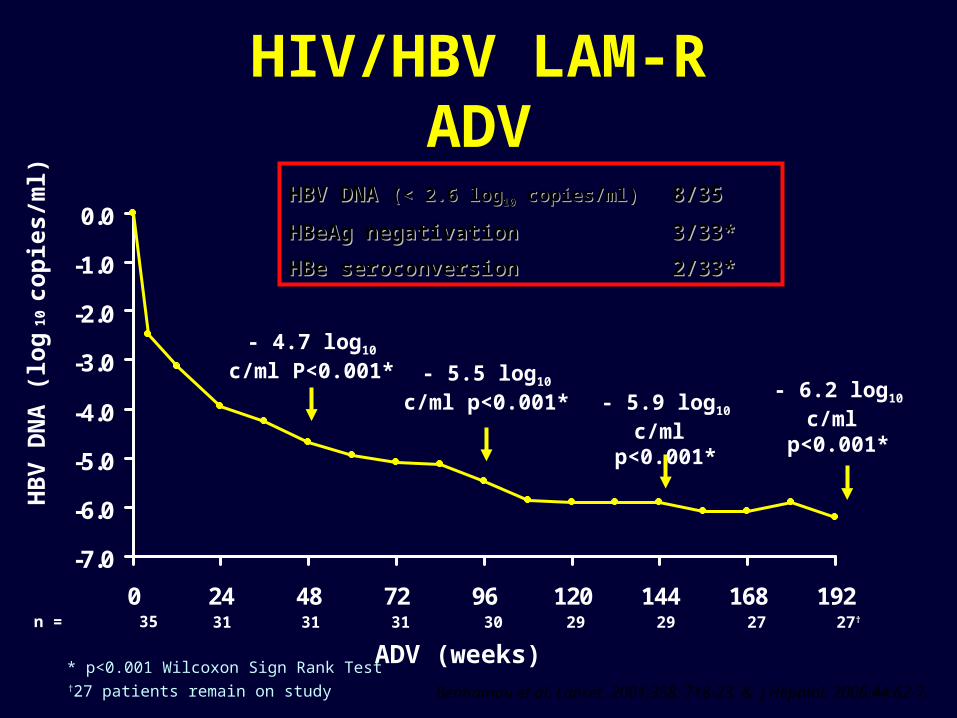
- 6.2 log10 c/ml p<0.001*
-7.0
-6.0
-5.0
-4.0
-3.0
-2.0
-1.0
0.0
0 24 48 72 96 120 144 168 192
ADV (weeks)
- 5.9 log10 c/ml p<0.001*
- 4.7 log10 c/ml P<0.001* - 5.5 log10 c/ml
p<0.001*
31 29 31 30 31 29 27†27n = 35
†27 patients remain on study
* p<0.001 Wilcoxon Sign Rank Test
Benhamou et al. Lancet. 2001;358: 718-23. & J Hepatol. 2006;44:62-7.
HBV DNA HBV DNA (< 2.6 log(< 2.6 log1010 copies/ml) copies/ml) 8/358/35
HBeAg negativationHBeAg negativation 3/33*3/33*
HBe seroconversion HBe seroconversion 2/33*2/33*
HIV/HBV LAM-RADV
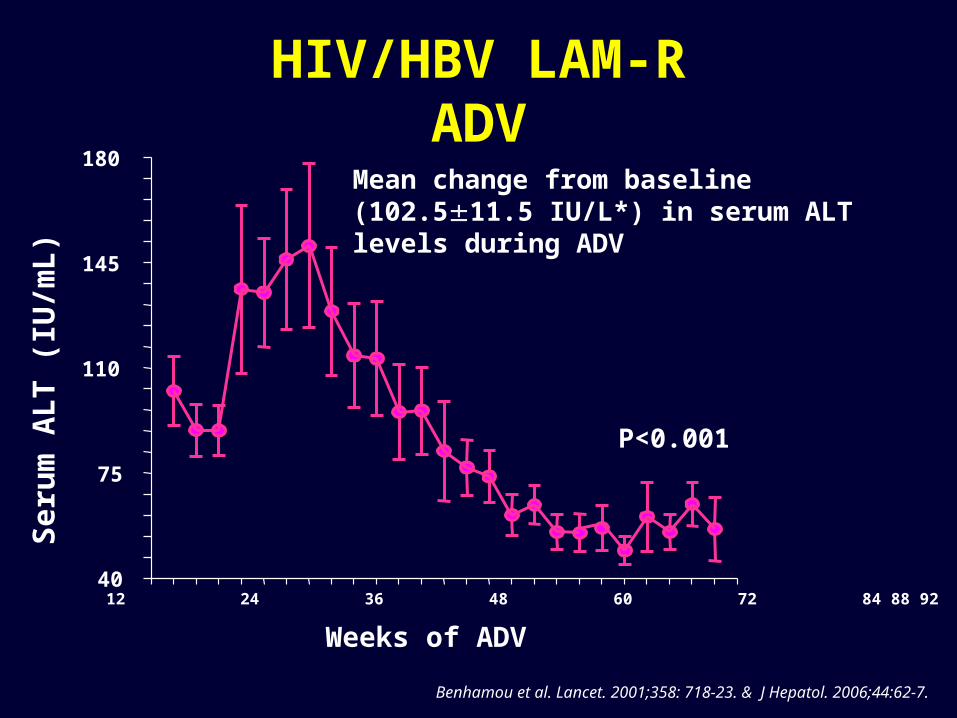
Mean change from baseline (102.511.5 IU/L*) in serum ALT levels during ADV
40
75
110
145
180
Weeks of ADV
Se
rum
AL
T (
IU/m
L)
Bas. 12 24 36 48 60 72 84 88 92
P<0.001
Benhamou et al. Lancet. 2001;358: 718-23. & J Hepatol. 2006;44:62-7.
HIV/HBV LAM-RADV
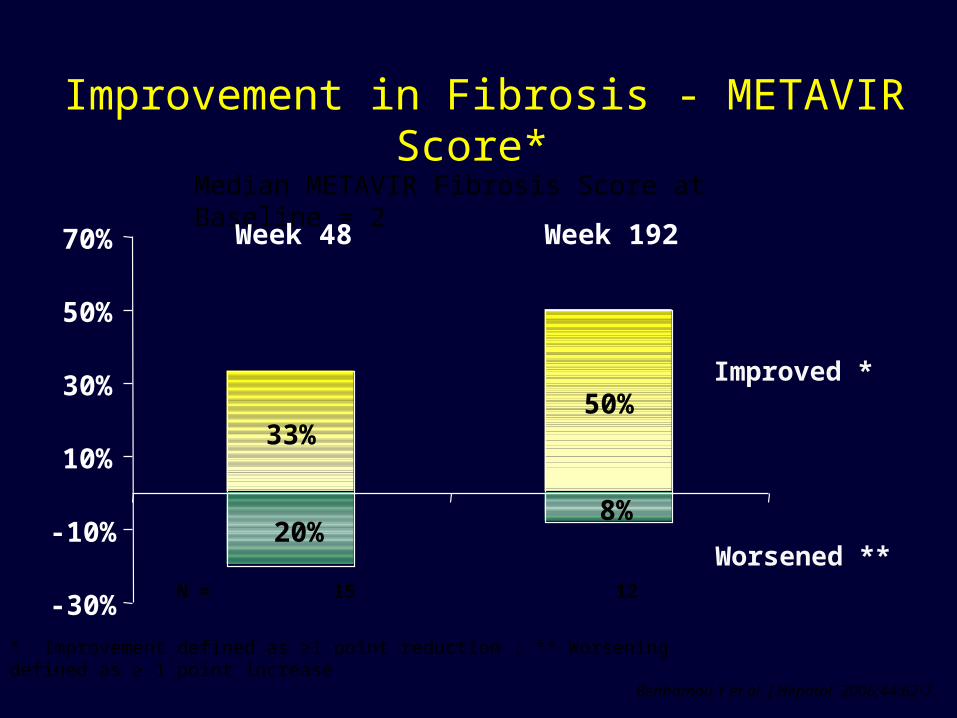
Improvement in Fibrosis - METAVIR Score*
* Improvement defined as ≥1 point reduction ; ** Worsening defined as ≥ 1 point increase
Median METAVIR Fibrosis Score at Baseline = 2
Improved *
Worsened **
N = 15 12
33%50%
20% 8%
-30%
-10%
10%
30%
50%
70% Week 48 Week 192
Benhamou Y et al. J Hepatol. 2006;44:62-7.
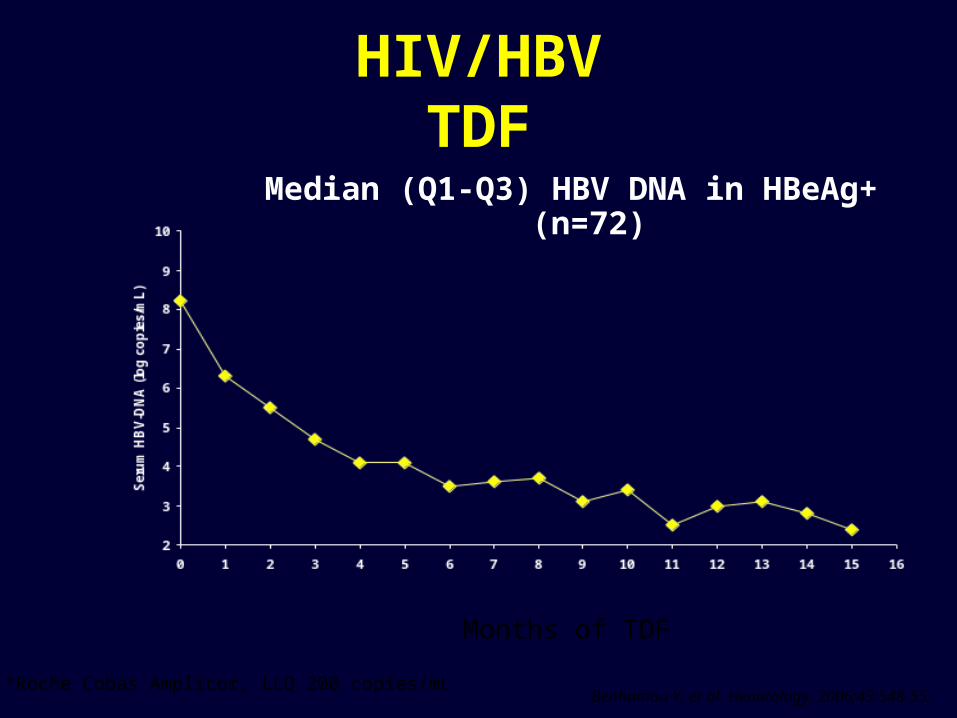
Median (Q1-Q3) HBV DNA in HBeAg+ (n=72)
Benhamou Y, et al. Hepatology. 2006;43:548-55.
HIV/HBVTDF
Months of TDF
*Roche Cobas Amplicor, LLQ 200 copies/mL

HIV/HBV: TDFRetrospective Analysis
TDF added to 3TC HBV LAM-R vs TDF+ 3TC first line
Mauss S. et al. EASL 2006
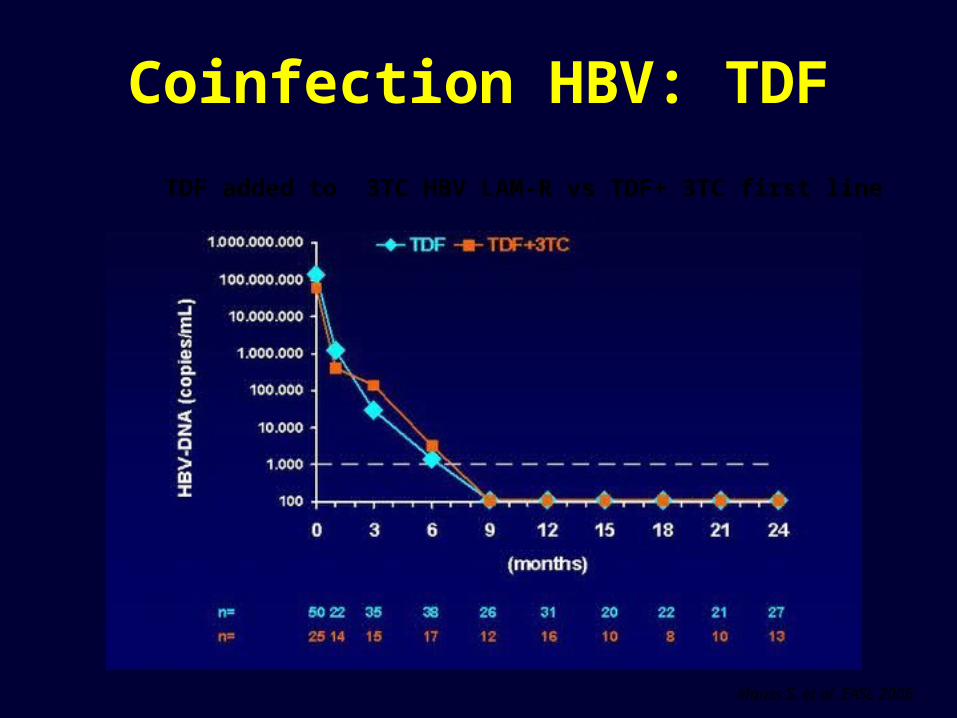
Coinfection HBV: TDF
TDF added to 3TC HBV LAM-R vs TDF+ 3TC first line
Mauss S. et al. EASL 2006
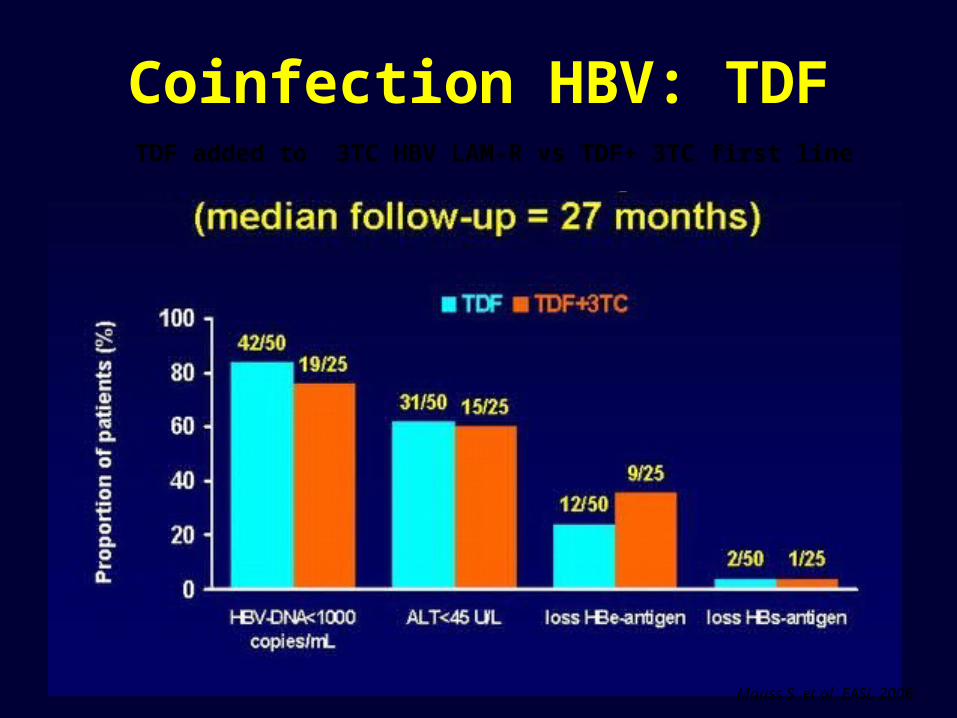
Coinfection HBV: TDFTDF added to 3TC HBV LAM-R vs TDF+ 3TC first line
Mauss S. et al. EASL 2006

Peters M et al. CROI 2005.
-7
-6
-5
-4
-3
-2
-1
0
0 12 24 36 48
ADVTDF
HB
V D
NA
(lo
g 10
c/m
L)*
ADV 25 24 23 20 18 17
TDF 27 26 23 18 17 18
HIV/HBVADV vs TDF
*Roche Cobas Amplicor, LLQ 200 copies/mL

PEG 2a + ADV in HIV/HBV LAM-R
0123456789
Baseline 12 24 48 72
Weeks
Seru
m H
BV D
NA (l
og
copi
es/m
L)
PEGASYS + ADV
0
20
40
60
80
100
Weeks
Seru
m A
LT (I
U/L)
PEGASYS + ADV
HBV DNA ALT
Benhamou Y et al. ADPEG Study Preliminary report

HBV resistance
Lai C et al. N Engl J Med 1998. Leung N et al. J Hepatol 1999. Chang T et al. Antiv Ther 2000. Benhamou Y et al. Hepatology 1999. Benhamou Y et al. Lancet 2001 and AADSL 2003. Data on file. NV-02B-003. Idenix.
HIV/HBV HIV/HBV HBV HBV
0
00
0
0
0
0
50
90
0
4%
024%
18
4%
9
19%24
38
49
67%
0
10
20
30
40
50
60
70
80
90
1
3
LMVFTC LdT ADV
LMV+LdT
ETVLMV
LMV+ADV
LMV+TDF
ETV +
LAM
Years
Patien
ts (%)
Patien
ts (%)
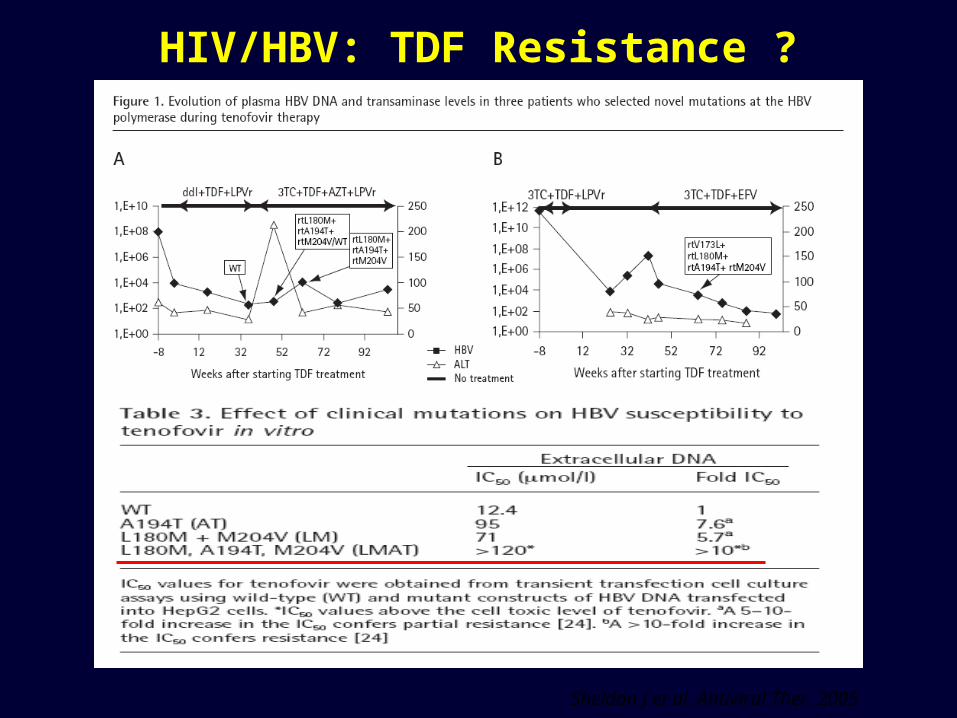
HIV/HBV: TDF Resistance ?
Sheldon J et al. Antiviral Ther. 2005
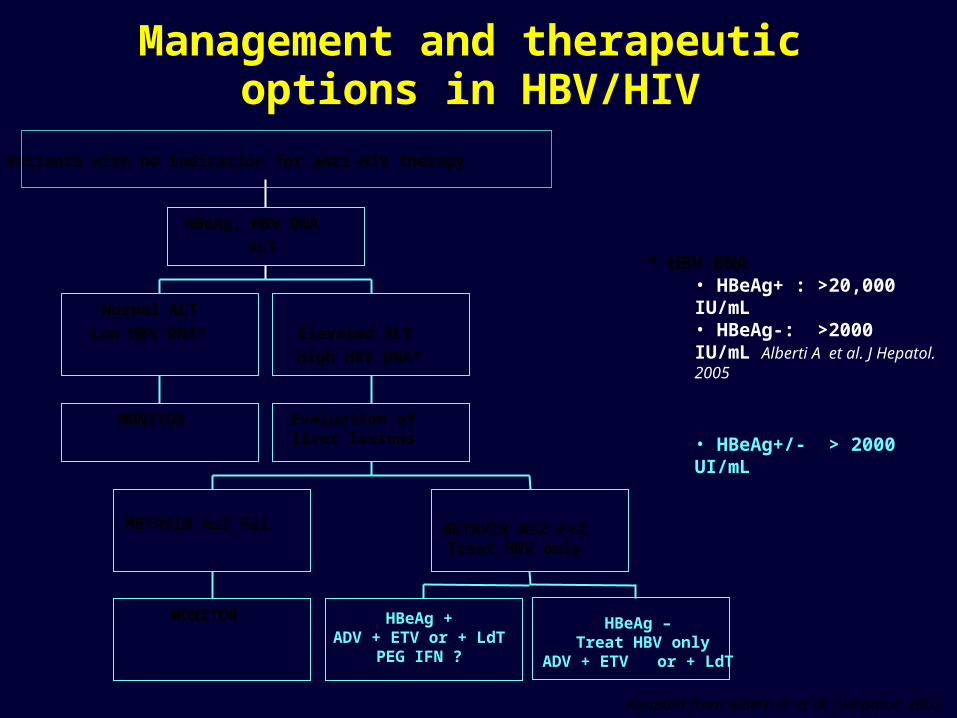
Management and therapeutic options in HBV/HIV
MONITOR
Normal ALT
Low HBV DNA*
MONITOR
METAVIR A≤1 F≤1 METAVIR A≥2 F≥2Treat HBV only
Evaluation of liver lesions
Elevated ALT
High HBV DNA*
HBeAg, HBV DNA
ALT
Patients with no indication for anti-HIV therapy
HBeAg – Treat HBV only
ADV + ETV or + LdT
HBeAg +ADV + ETV or + LdT
PEG IFN ?
* HBV DNA • HBeAg+ : >20,000 IU/mL• HBeAg-: >2000 IU/mL Alberti A et al. J Hepatol. 2005
• HBeAg+/- > 2000 UI/mL
Adapted from Alberti A et al. J Hepatol. 2005
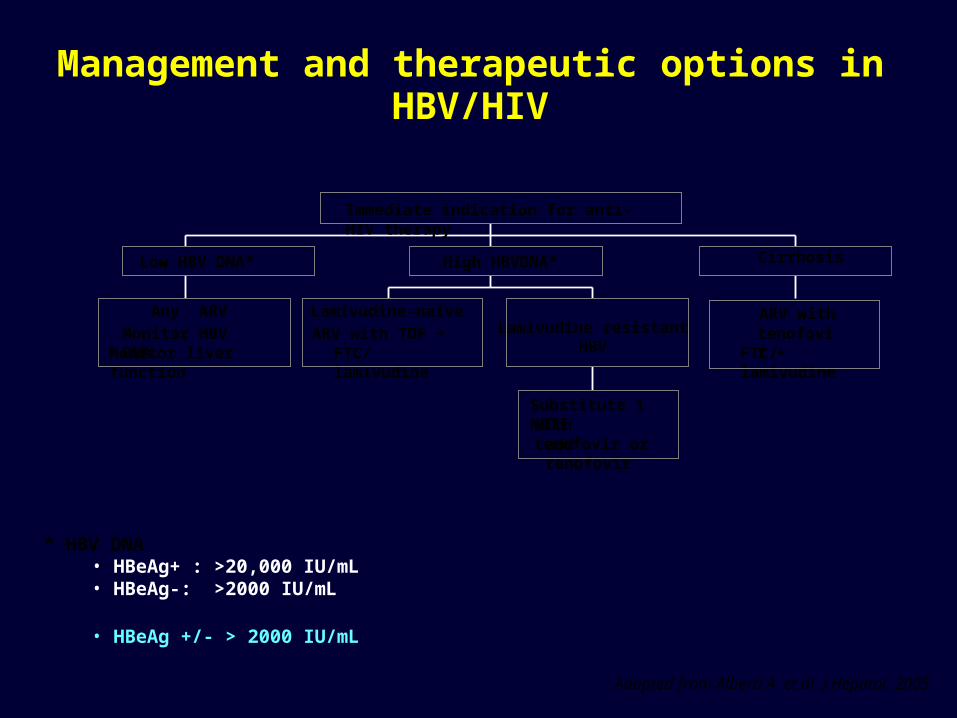
Management and therapeutic options in HBV/HIV
* HBV DNA • HBeAg+ : >20,000 IU/mL• HBeAg-: >2000 IU/mL
• HBeAg +/- > 2000 IU/mL
Adapted from Alberti A et al. J Hepatol. 2005
Monitor HBV DNAMonitor liver function
Low HBV DNA*
Lamivudine-naive
ARV with TDF +FTC/lamivudine
Substitute 1 NRTIwith tenofovir or
add tenofovir
Lamivudine resistantHBV
High HBVDNA*
ARV withtenofovir +
FTC/lamivudine
Cirrhosis
Immediate indication for anti-HIV therapy
Any ARV
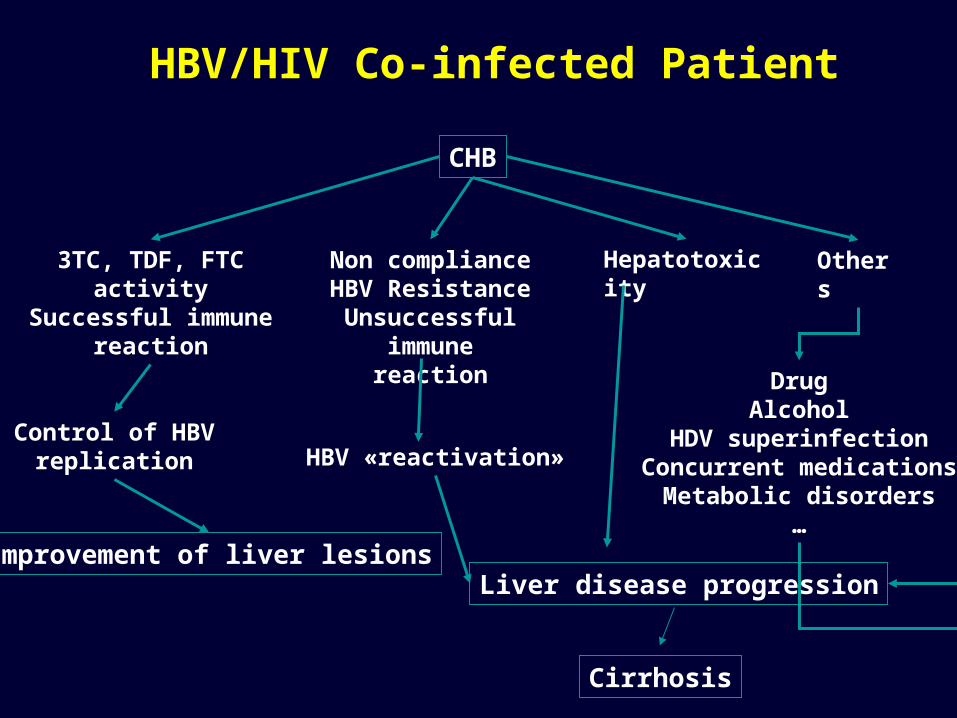
HBV/HIV Co-infected Patient
CHB
Non complianceHBV Resistance
Unsuccessful immunereaction
HBV «reactivation»
Hepatotoxicity Others
DrugAlcohol
HDV superinfectionConcurrent medications
Metabolic disorders…
Liver disease progression
3TC, TDF, FTC activity
Successful immunereaction
Control of HBVreplication
Improvement of liver lesions
Cirrhosis







