Transposition of great arteriesEpidemiological Data
Relatively common malformation(5 - 7% of all congenital heartdisease)
The incidence is 20-30 per 100,000 live births
Provision for women (60-70%)

Atrio-ventricularconcordance
Ventricles-greatarteriesDiscordance
Transposition of great arteriesAnatomy
TGA with intact ventricular septum
TGA with VSD
TGA with VSD and pulmonary stenosis
TGA with systemic outflow obstruction) (Subaortic stenosis, CoAo,)
Transposition of great arteriesAnatomical shapes
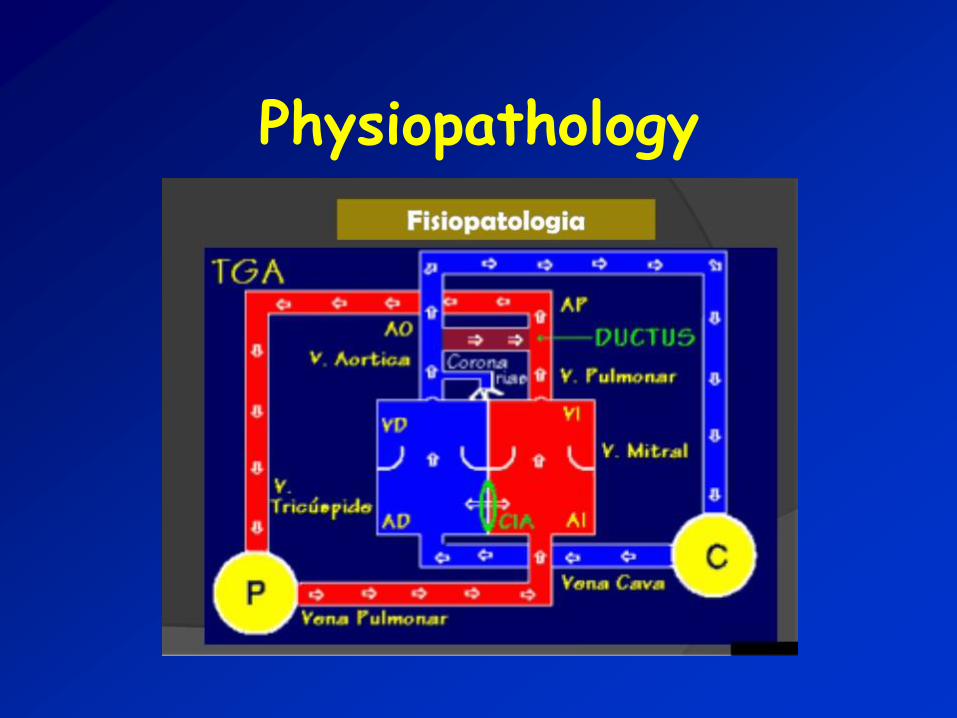
Physiopathology

TRANPOSITION OF GREAT ARTERIES
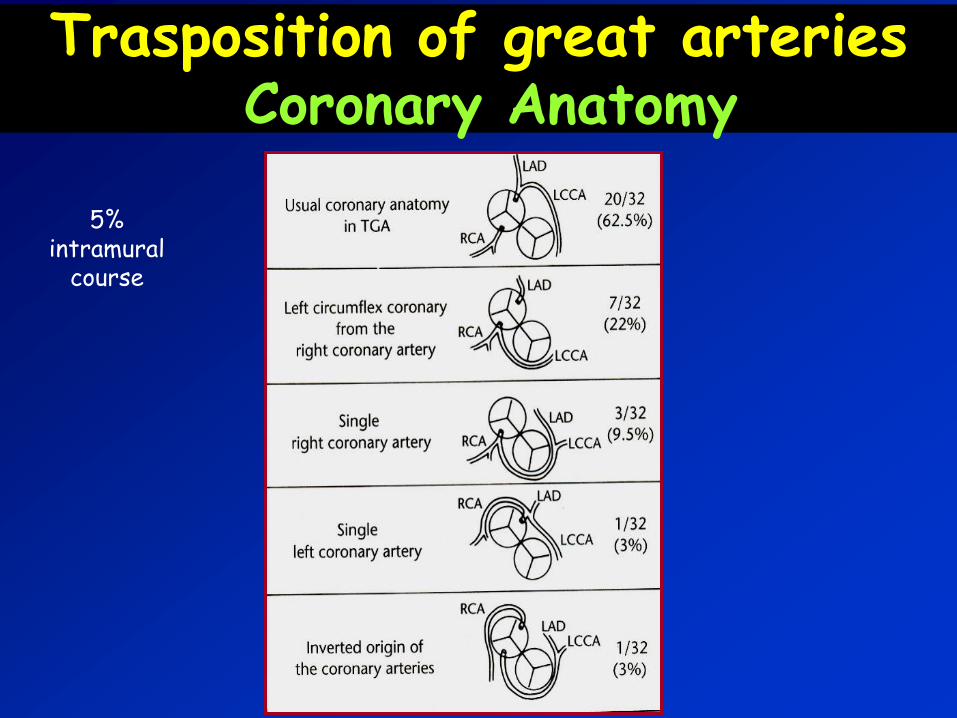
Trasposition of great arteriesCoronary Anatomy
5% intramural
course
Transposition of great arteriesClinical pictures
Transposition of great arteriesClinical pictures
TGA with intact septum: severe cyanosis and tendency metabolic acidosis with compensatory tachypnea, in the presence of inadequate blood mixing(DIA/foramen ovale restrictive. Small PDA )
Transposition of great arteriesClinical pictures
TGA with intact septum
Neonatal clinical emergency
Prenatal diagnosis reduces mortality and
neonatal morbidity
( Bonnet D et al: Circulation 1999)

Transposition of great arteriesClinical pictures
TGA + DIV: cyanosis and signs of heart failure (tachypnea, intercostal retractions, tachycardia, hepatomegaly, excessive sweating) appear gradually in the first days of life in relation to the reduction in pulmonary vascular resistance.
AS
VS
AP
VD
AO
Transposition of great arteriesClinical pictures
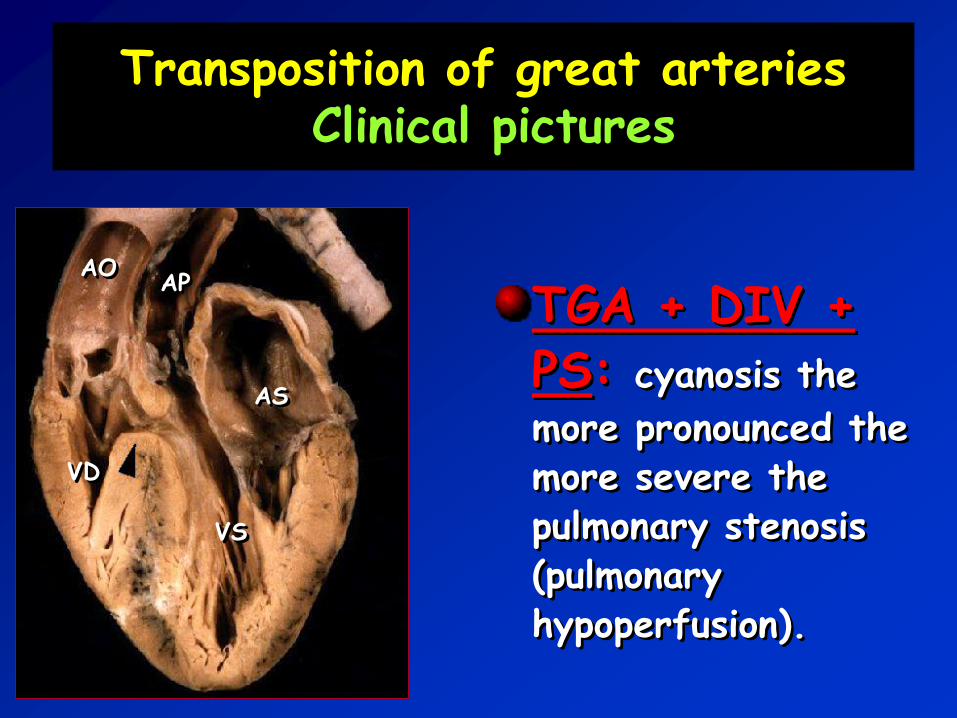
TGA + DIV + PS: cyanosis the
more pronounced the more severe the pulmonary stenosis (pulmonary hypoperfusion).
AS
VS
AP
VD
AO
Transposition of great arteriesClinical pictures
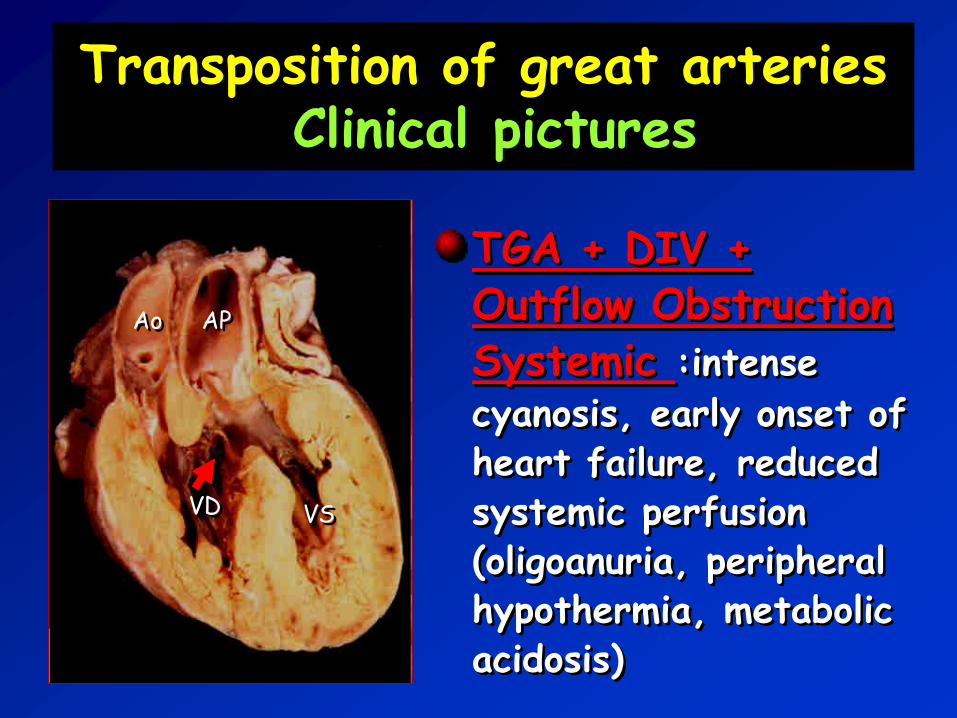
TGA + DIV + Outflow ObstructionSystemic :intense
cyanosis, early onset ofheart failure, reducedsystemic perfusion(oligoanuria, peripheralhypothermia, metabolicacidosis)
Ao AP
VD VS

TRANSPOSITION OF GREAT ARTERIES
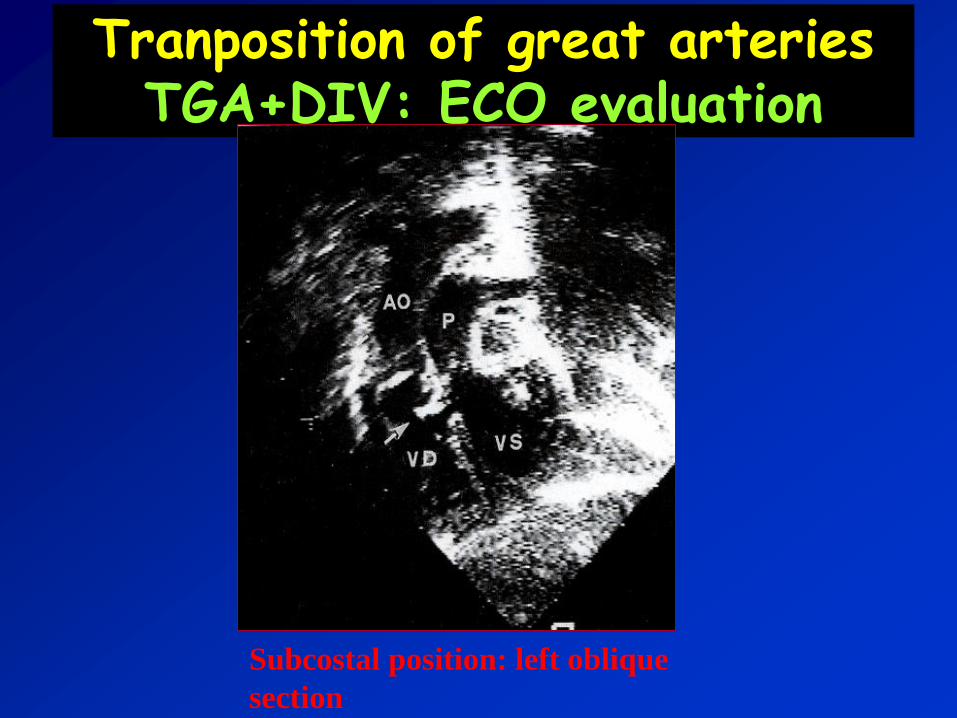
Tranposition of great arteriesTGA+DIV: ECO evaluation
Subcostal position: left oblique
section

EchocardiogramTranposition of great arteries
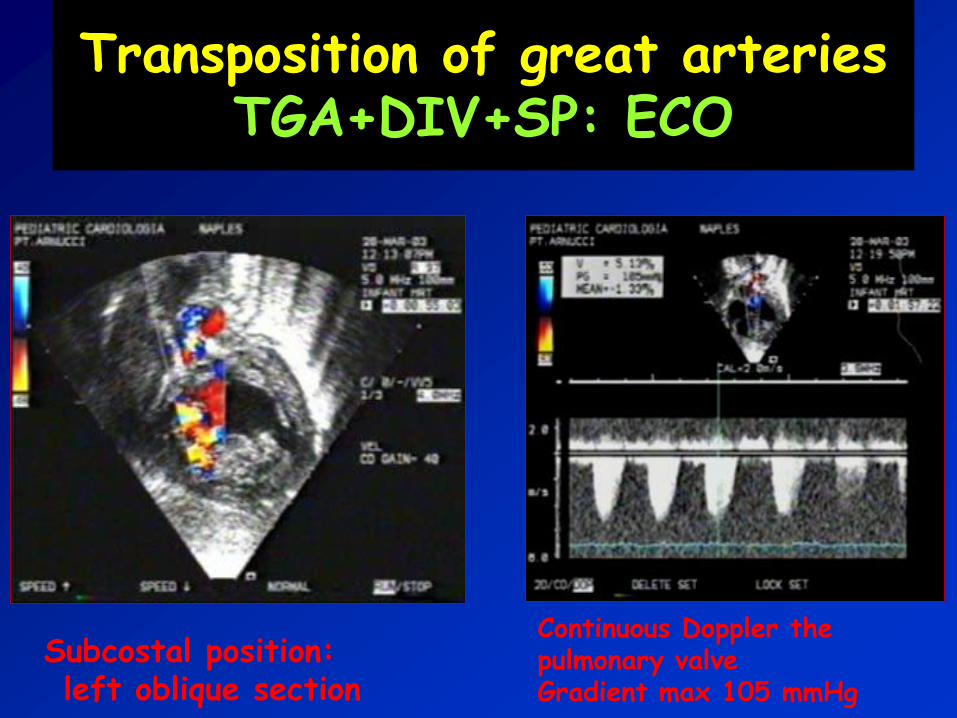
Transposition of great arteriesTGA+DIV+SP: ECO
Subcostal position:left oblique section
Continuous Doppler the pulmonary valveGradient max 105 mmHg

Transposition of great arteriesTGA+DIV+Subpulmonary stenosis :
ECO
Without treatment it has a mortality
rate of:
- 30% in the first week of life ,
- 50% within first month,
- 70% in the first six months
- 90% by the year.
Transposition of great arteriesNatural History

Transposition of great arteriesManagement in the neonatal period and TGA SI / DIV
➢Ensure adeguate mixing intercircolatory
➢Correction acidosis( if present)
➢Early surgicalcorrection
✓ PGE1 ev
✓ Septostomy atrial (Rashkind)
✓ Bicarbonate ev
Anatomicalcorrection
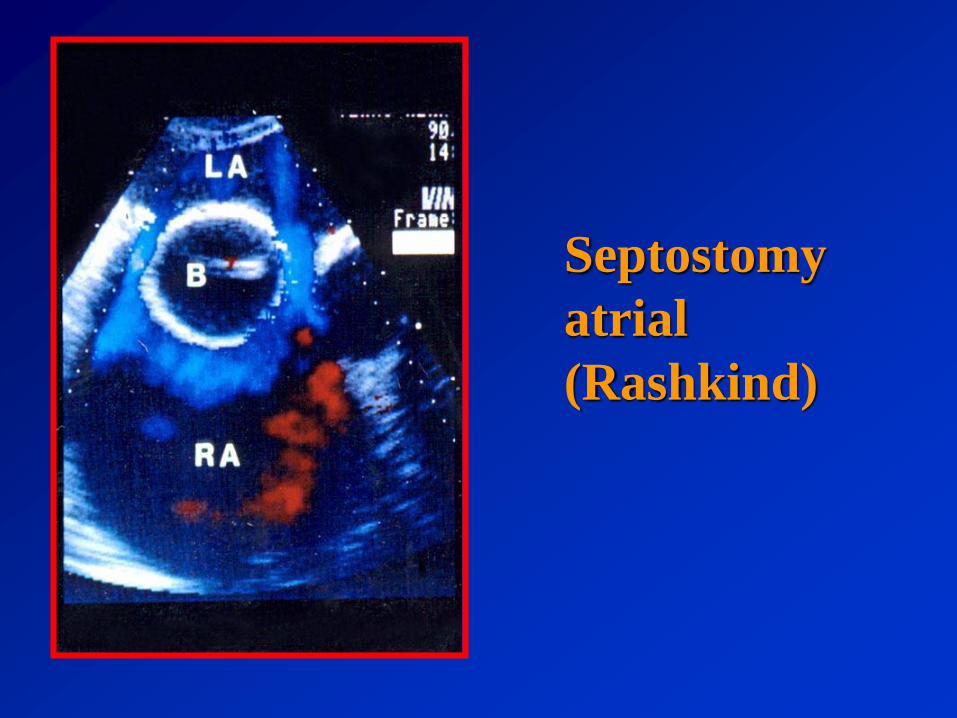
Septostomy
atrial
(Rashkind)

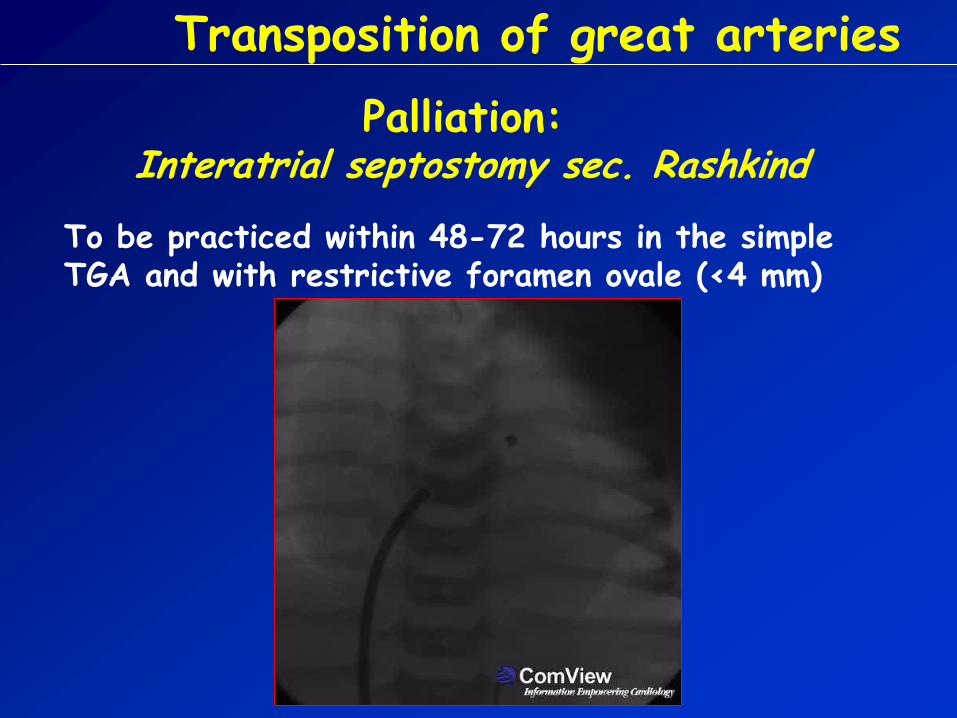
Transposition of great arteries
Palliation:Interatrial septostomy sec. Rashkind
To be practiced within 48-72 hours in the simple TGA and with restrictive foramen ovale (<4 mm)
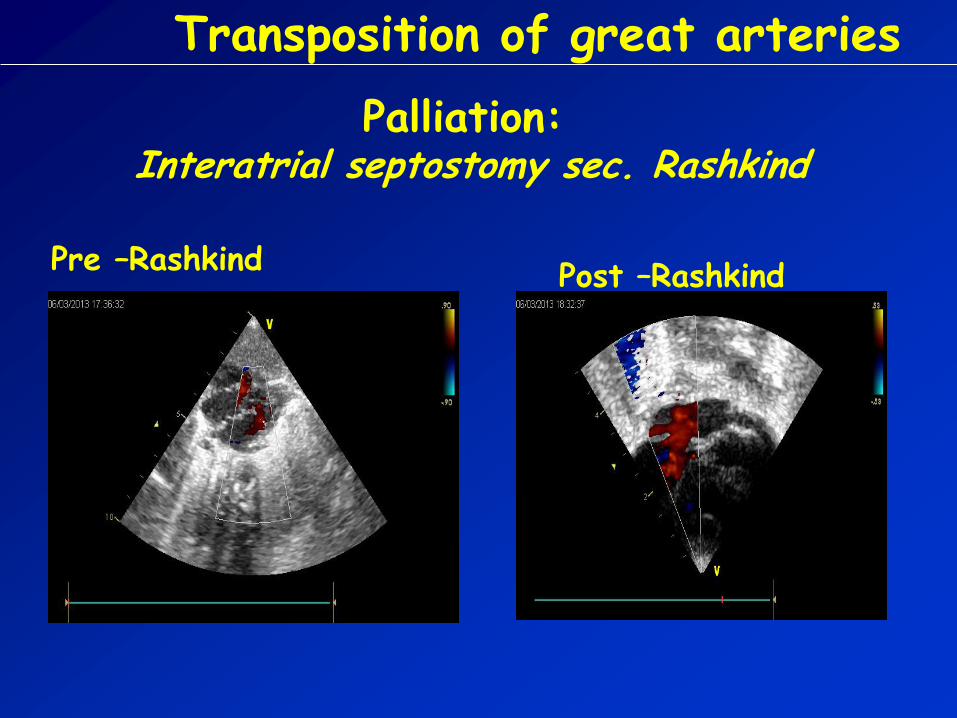
Transposition of great arteries
Palliation:Interatrial septostomy sec. Rashkind
Post –RashkindPre –Rashkind
Transposition of great arteriesSurgical approach
TGA with intact septum or DIV:* Physiological correction (Mustard/Senning)* Anatomical correction (arterlai switch )
TGA + DIV + SP:* shunt systemic-pulmonary (palliation)* Rastelli operation* REV
Ao AP
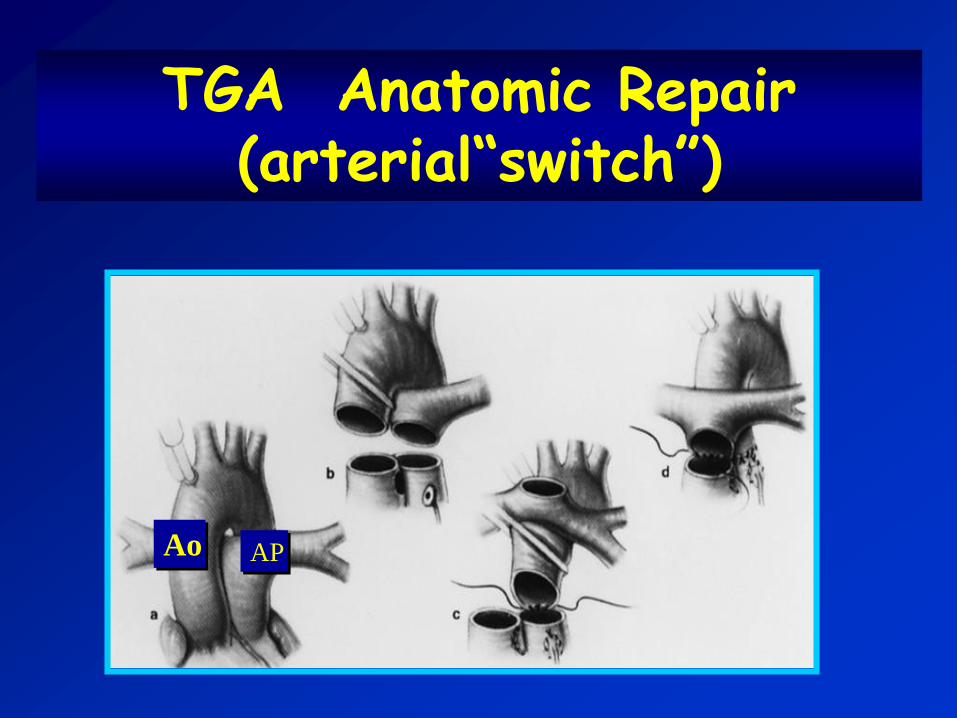
TGA Anatomic Repair (arterial“switch”)

TRANSPOSITION GREAT ARTERIES
Risult surgical anatomical correction
Early mortality : 2-15%
% survival:84 % in 1 month82 % in 1 year82 % in 3 years82 % in 5 years
Kirklin et al Circulation 1992
TRANSPOSITION OF GREAT ARTERIES
Functional status / quality of life post anatomical correction
All subjects in NYHA I class(fully active/no limitation)
Exercise testing : 94% normalexercise capacity
Good quality of life
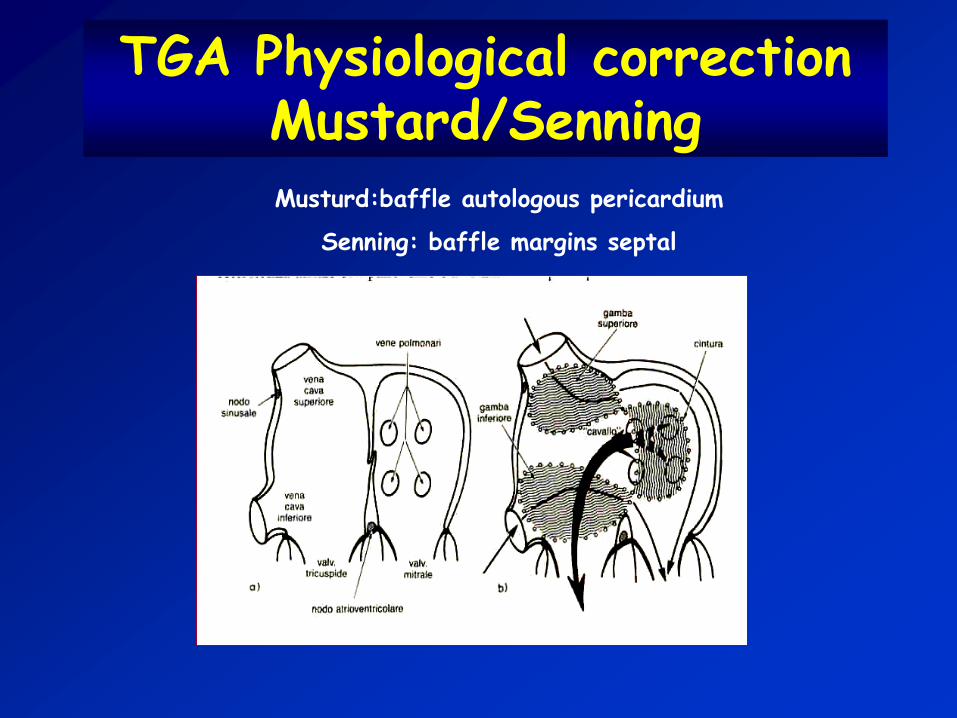
TGA Physiological correction Mustard/SenningMusturd:baffle autologous pericardium
Senning: baffle margins septal
TGA Physiological correction (Mustard) Issues in the post-operative follow-up
Right ventricular disfunction
Tricuspid regurgitation
Dynamic LVOT stenosis (subpulmonary)
Obstruction pulmonary venous return
Obstruction systemic venous return
Residual interatrial shunt
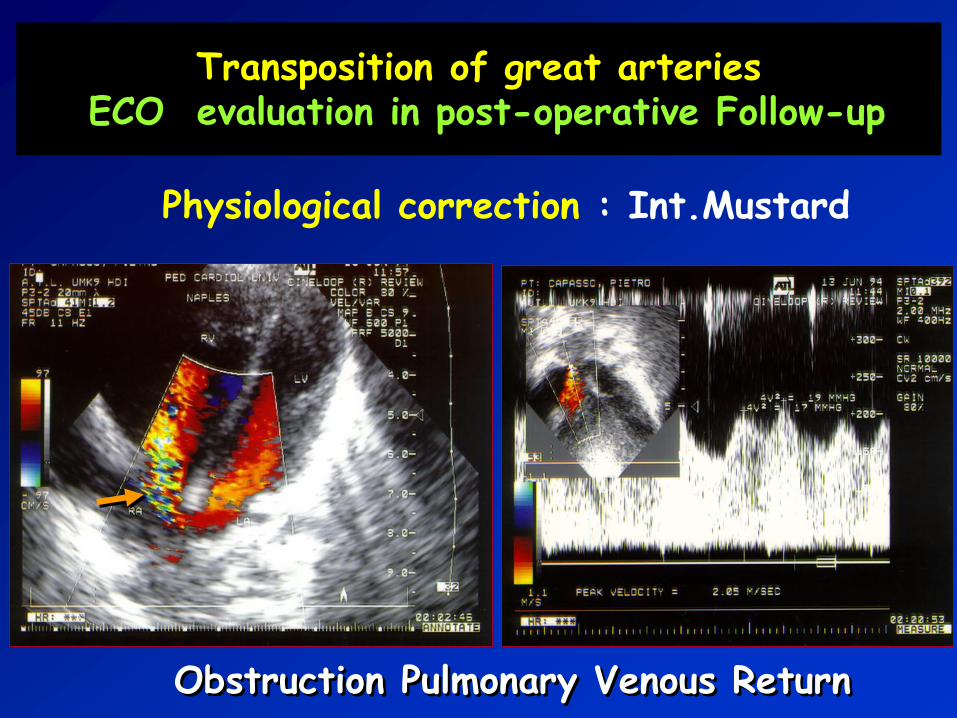
Transposition of great arteriesECO evaluation in post-operative Follow-up
Physiological correction : Int.Mustard
Obstruction Pulmonary Venous Return
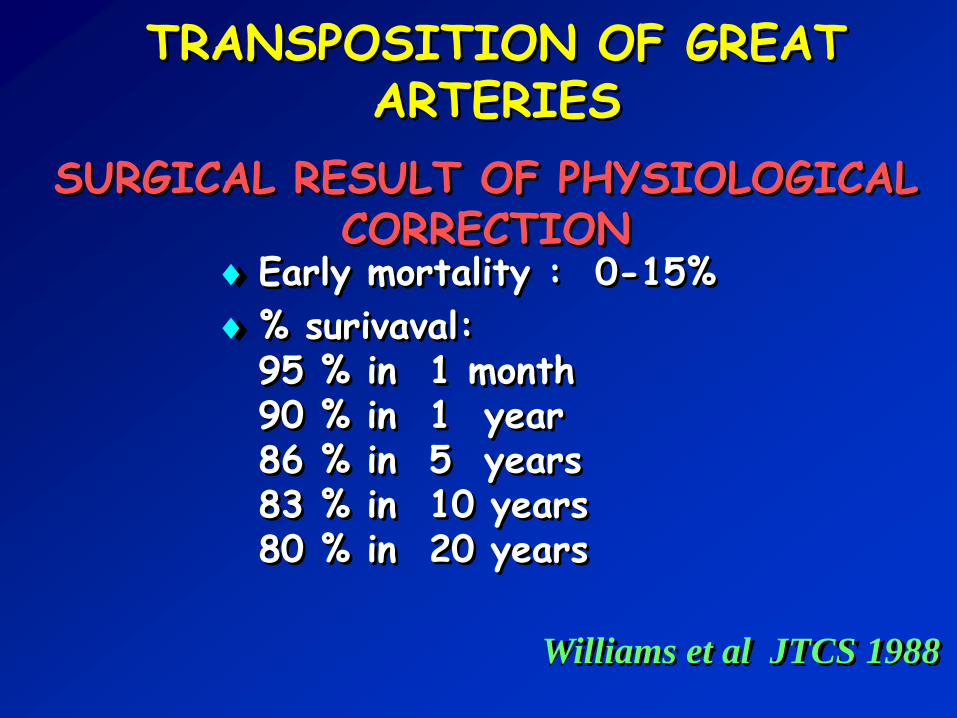
TRANSPOSITION OF GREAT ARTERIES
SURGICAL RESULT OF PHYSIOLOGICAL CORRECTION
Early mortality : 0-15%
% surivaval:95 % in 1 month90 % in 1 year86 % in 5 years83 % in 10 years80 % in 20 years
Williams et al JTCS 1988

TRANPOSITION OF GREAT ARTERIES
Subjects in I-II NYHA class
Exercise testing: exercisecapacity reduced by 50%
Residues / Physiological sequelae after correction

•Physiologicalcorrection•AnatomicalCorrection•Rastelli - REV
vd
vs
AoAP
Ao AP

Rastelli - REV in TGA+VSD+PS
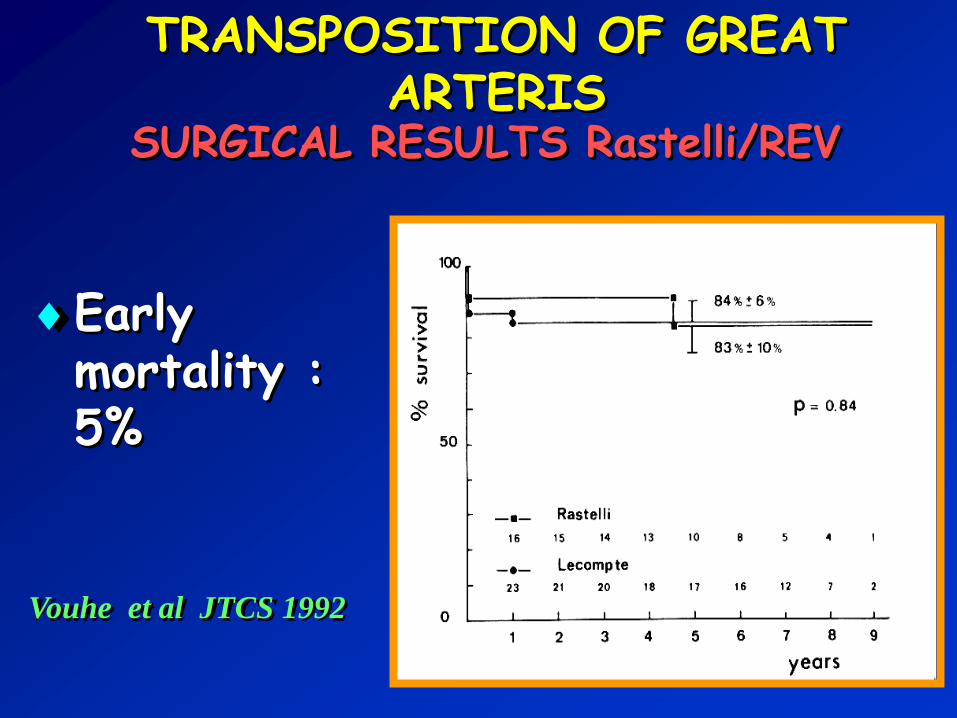
TRANSPOSITION OF GREAT ARTERIS
SURGICAL RESULTS Rastelli/REV
Earlymortality : 5%
Vouhe et al JTCS 1992

TRANSPOSITION OF GREAT ARTERIES
Functional status /Quality of life di post Rastelli/REV
98% in I-II NYHA class
Good quality of life




![Developing Country of Pakistan Great Arteries in a ... · congenitally corrected transposition of the great arteries (CCTGA) [1]. CCTGA is a defect whereby the right atrium is connected](https://cdn.vdocuments.mx/doc/165x107/5cace22d88c99376788cec5d/developing-country-of-pakistan-great-arteries-in-a-congenitally-corrected.jpg)


