Quality improvement in the neonatal unit – how can nurses contribute?
Denise EvansLead Nurse Y&H Neonatal ODNMarch 16th 2015
Denise Evans March 2015 2
What do we want
QUALITY IMPROVEMENT
an essential or distinctive characteristic, property, or attribute : peculiar and essential character : An inherent or distinguishing characteristic; a property: the non-inferiority or superiority of something.
Improvement is the process of a thing moving from one state to a state considered to be better, usually through some action intended to bring about that better state.
Denise Evans March 2015 3
Industry & NHSASQ is a global leader in quality and
consists of a community of passionate people who use their tools, ideas and expertise to make our world better.
[quality is] the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.
Denise Evans March 2015 4
VisionThere is evidence of poor patient
experiences and outcomesEconomic downturn response - not
indiscriminate cuts1. Improving efficiency2. Driving up quality 3. Reducing levels of harm 4. initiatives such as quality accounts and
the Commissioning for Quality and Innovation (CQUIN) payment framework.
Denise Evans March 2015 5
The Dimensions
Safe – avoiding harmEffective - evidence of benefitPatient-centred - partnershipTimely – avoid harmful delaysEfficient – avoid waste Equitable – does not vary in
quality
Denise Evans March 2015 6
Nurse Led ChangeParalysis –Fixed head position.Visiting – Visitors corridorAccess – NO ENTRYPain reliefSeparation – bonding -
developmental care
Denise Evans March 2015 7
MinutiaSometimes used to describe
trivia but the smallest details are what we share today.
‘How do we know what constitutes good care?’
Denise Evans March 2015 8
10 key challenges
1. Convincing people that there is a problem 2. Convincing people that the solution chosen is the
right one 3. Getting data collection and monitoring systems right 4. Excess ambitions and ‘projectness’ 5. The organisational context, culture and capacities 6. Tribalism and lack of staff engagement 7. Leadership 8. Balancing carrots and sticks – harnessing
commitment through incentives and potential sanctions
9. Securing sustainability 10. Considering the side effects of change.
Denise Evans March 2015 9
Bespoke Neonatal Safety Thermometer
Harm Free Care “Its not just counting its caring”
Neonatal Unit & Postnatal Care 1. Is there a measurable outcome of harm?
(can we define what the harm is?) 2. Does it happen enough on one day each
month to be picked up in point prevalence testing?
3. Is the information accessible and quick and easy to collect?
4. Does this affect the patient in all settings?
Denise Evans March 2015 10
MeasuresDeteriorationExtravasationPainSkin Integrity
Measurement and gathering data are vital elements ofany attempt to improve performance or quality, and arealso needed to assess its impact.
Denise Evans March 2015 11
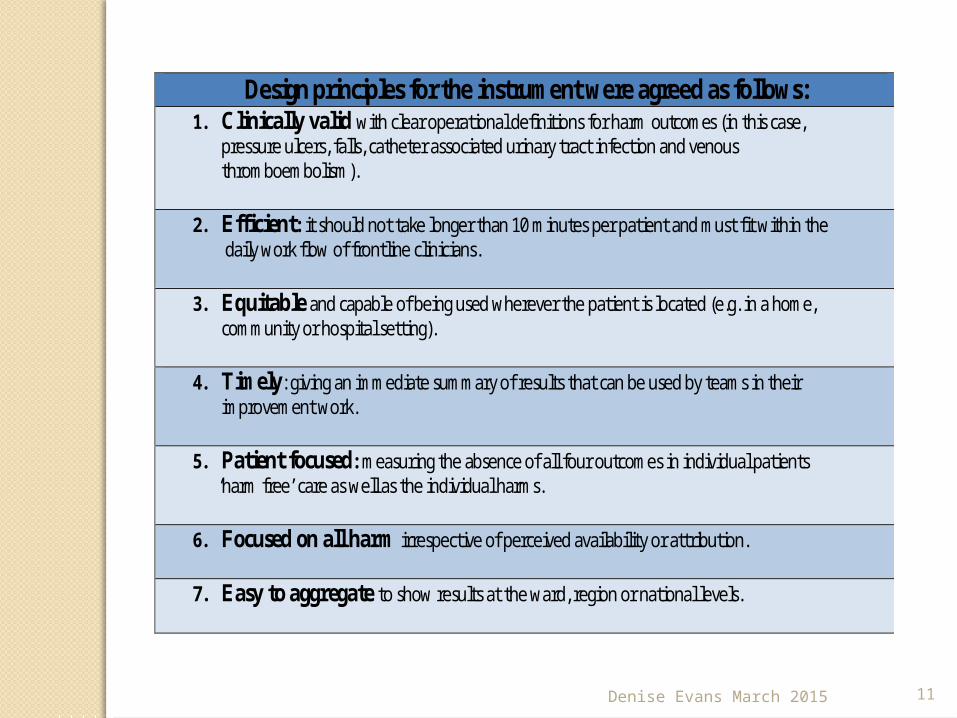
Design principles for the instrument were agreed as follows: 1. Clinically valid with clear operational definitions for harm outcomes (in this case,
pressure ulcers, falls, catheter associated urinary tract infection and venous thromboembolism).
2. Efficient: it should not take longer than 10 minutes per patient and must fit within the daily work flow of frontline clinicians.
3. Equitable and capable of being used wherever the patient is located (e.g. in a home, community or hospital setting).
4. Timely: giving an immediate summary of results that can be used by teams in their improvement work.
5. Patient focused: measuring the absence of all four outcomes in individual patients ‘harm free’ care as well as the individual harms.
6. Focused on all harm irrespective of perceived availability or attribution.
7. Easy to aggregate to show results at the ward, region or national levels.
Denise Evans March 2015 12
Meaningful Actions
Involving the clinical team early on when setting aspirations and goals
Ensuring senior clinical involvement and peer influence
Obtaining credible endorsement – for example, from the royal colleges
Involving clinical networks across organisational boundaries
Providing evidence that the change has been successful elsewhere
Embedding an understanding of quality improvement into training and education of healthcare professionals.
Denise Evans March 2015 13
Planning, Doing, Studying, Acting
‘What are we trying to accomplish?’––‘How will we know that a change is
an improvement?’ ––‘What changes can we make that
will result in improvement?’
Each cycle starts with hunches, theories and ideas and helps them evolve into knowledge that can inform action and, ultimately, produce positive outcomes.
Denise Evans March 2015 14
Focus on Quality
Focus on quality, not targets – if effective care is delivered and the focus is on quality, safety and outcomes, the targets are delivered as a consequence of that process, not the other way around.
Denise Evans March 2015 15
Hurdles need to find ways of freeing up
staff time to take part in training programmes
‘We want everybody to feel that they have the opportunity to solve problems and improve the things that they see every day,’
The team across the pathway all need to work together with one goal. Improved outcomes not looking to blame “Not me”
Denise Evans March 2015 16
What clinical care do neonates need?
Safe delivery &stabilisation +/-resuscitation at birth &
minimal handling!!!!
Competent staff to undertake procedures safely & deliver optimal care in hospital & on transport
Effective assessment of medical & nursing needs
Denise Evans March 2015 17
Morecambe Bay ReportAll showed evidence of the same
problems of poor clinical competence, insufficient recognition of risk, inappropriate pursuit of normal childbirth and failures of team-working, as seen previously. Initial investigation was again deficient and failed to identify manifest problems.
Denise Evans March 2015 18
Morecambe Bay We found clear evidence of distortion of
the truth in responses to investigation, including particularly the supposed universal lack of knowledge of the significance of hypothermia in a newborn baby
staffed and equipped to provide a restricted range of neonatal care, but not to deal with more pre-term babies who needed more intensive forms of care.
Denise Evans March 2015 19
Paperless
Jeremy Hunt, Secretary of State for Health, has set a clear expectation of a Paperless NHS by 2018, stating that technology will be the saviour of the NHS. Only with world class information systems will the NHS deliver world class care.
Denise Evans March 2015 20
If you have never measured it how do you know it has improved?
Thank you
Denise Evans March 2015 21
References
Quality improvement made simple Second edition, August 2013.
© 2013 Health Foundation ISBN 978-1-906461-47-8© 2015 The Health Foundation
Building the foundations for improvement is published by the Health Foundation, 90 Long Acre, London WC2E 9RA
The Report of the Morecambe Bay Investigation March 2015







