Download - PDC_2008_Headwall Boom Study

Medical Gas Booms vs. Traditional Headwalls
James A.Thomas, M.D., Associate Professor, UT Southwestern Medical CenterDebayjoti Pati, PhD, AIIA, Director of Research, HKS Architects
Jennie Evans, RN, BS, Director of Clinical Operations, HKS Architects
2008 International Conference and Exhibition on Planning, Design and Construction™

• What is optimal for patient care?• What are the differences between caregivers’ needs g
and wants?• Is there a safety component in the choice of medical
gas delivery systems?
2008 International Conference and Exhibition on Planning, Design and Construction™

Learning Objectives• Identify what clinicians prefer between medical gas
booms and headwalls.A hi h f id h d idi• Assess which factors to consider when deciding between the medical gas options.
• Discuss the family considerations as it relates to the• Discuss the family considerations as it relates to the provision of the medical gas booms vs headwalls while in the ICU.
2008 International Conference and Exhibition on Planning, Design and Construction™

Acknowledgments• Study participants, Children’s Medical Center of Dallas
• Getinge USA Inc for partial funding support• Getinge USA, Inc. for partial funding support
2008 International Conference and Exhibition on Planning, Design and Construction™

Agenda• Why the question• Study methodology• Assessment framework• Definitions• Caregivers preferences• Family considerations
h i i b• When to invest in booms• Future directions
2008 International Conference and Exhibition on Planning, Design and Construction™

Why the Question• Current drivers of
decision-making• Problem definition
– Arbitrary decision-ki– Early technology
adoption– Peer competition
making– Absence of empirical
data to support or Peer competition– Perceived efficiency– Perceived safety
data to suppo t orefute contentions
y
2008 International Conference and Exhibition on Planning, Design and Construction™

Study Methodology• Objectives
– Assess the relative impacts of headwalls
• Simulation scenarios– Admission
I t b tiimpacts of headwalls and ceiling booms
• Study Design
– Intubation– Surgery– Code
– Simulation runs of real life situations
– ECMO
2008 International Conference and Exhibition on Planning, Design and Construction™

Methodology Cont.• Hospital:
– Children’s Medical Center of DallasCenter of Dallas
– 66-bed ICU has both headwalls and ceiling bbooms
• Setting1 ICU room with ceiling– 1 ICU room with ceiling boom
– Headwall mock-up
2008 International Conference and Exhibition on Planning, Design and Construction™

Methodology Cont.• Participants:
– 2 physicians2 titi– 2 nurse practitioners
– 2 respiratory therapists– 4 ICU nurses
• Patient:– 1 pediatric manikin
• Data:– Video recording; Notes
2008 International Conference and Exhibition on Planning, Design and Construction™

Assessment Framework• Physical Elements
– Intravenous tubingEl t i l d
• Performance Dimensions
Fl ibilit– Electrical cord– Medical gas tubing– Equipment
– Flexibility– Ergonomics– Teamworkq p
2008 International Conference and Exhibition on Planning, Design and Construction™

Flexibility• Definition
– Conceptual definitioni h
• Measure– Bed positioning
• Distance the bed could be moved • Responsive to change;
adaptable
– Operational definition
from the wall• Maximum turn angle achievable
in relation to original position
– Equipment• The ability to offer
optimum layout of bed, caregivers and equipment for various levels of
Equipment• # of equipment pieces affecting
circulation in a particular scenario
– Caregiverfor various levels of acuity and procedures
Caregiver• # of caregivers accommodated in
a scenario, without affecting circulation + patient access by caregivers and mobile equipment
2008 International Conference and Exhibition on Planning, Design and Construction™
g q p

Ergonomics• Definition
– ConceptualM i i d ti it b
• Measure– In a particular scenario, count measure
of the number of times the following are obser ed in iolation of the criteria• Maximize productivity by
reducing operator fatigue and discomfort
– Operational
are observed in violation of the criteria outlined in the operational definition: bending, stretching, reaching
• The ability of caregiver to move about the space and attend to all tasks void of reaching greater than 70” AFF, reaching lower than 24” AFF reaching greaterthan 24 AFF, reaching greater than 30” from center of gravity and twisting of the spine.
2008 International Conference and Exhibition on Planning, Design and Construction™
Teamwork• Definition
– Conceptual definition:• Cooperation between those
• Measure– In a particular scenario, count
measure of the number of time th f ll i h h tp
who are working together on a task
– Operational definition:
the following happens when at least 2 clinicians are working together:
• Losing timeI i t f t l t f• Ability to work together, by
virtue of the layout vis-à-vis patient bed, in an orderly, comfortable and safe
• Inappropriate space for at least one of the clinicians
• Inappropriate adjacency for at least one pair of the clinicians
• Unsafe body mechanics for at least f th li i imanner, void of any time
delays in accessing crucial services within the patient room.
one of the clinicians
2008 International Conference and Exhibition on Planning, Design and Construction™

Clinician’s Preference
2008 International Conference and Exhibition on Planning, Design and Construction™

What Booms Change• Booms reduce the area of restricted access• Booms reduce the area of restricted access
to the patient (Concept #1)Headwall Boom
Boom or headwall
Patient access area
Bed
2008 International Conference and Exhibition on Planning, Design and Construction™
Area of restricted access

Wh t B ChWhat Booms Change• Booms mobilize area of access restriction
(Concept #2)Restricted Head/Neck
AUnrestricted Head/Neck
AAccess Access
Boom or headwall
Patient access area
Bed
2008 International Conference and Exhibition on Planning, Design and Construction™
Area of restricted access

Physician
Flexibility Ergonomics Teamwork CommentsIV TubingEl t i l Boom (+) in Boom (+) in Boom (+) in Majority of powerElectricalCords
Boom (+) in situations needing access to head of bedHeadwall (-)
Boom (+) in situations needing access to head of bedHeadwall (-)
Boom (+) in situations needing access to head of bedHeadwall (-)
Majority of poweroutlets are on the boom
Medical Boom (+) in situations needing
Boom (+) in situations needing
Boom (+) in situations needing
Could be addressed with gases on one
Gasessituations needing access to head of bedHeadwall (-)
situations needing access to head of bedHeadwall (-)
situations needing access to head of bedHeadwall (-)
with gases on one side of bed in headwalls
Equipment
2008 International Conference and Exhibition on Planning, Design and Construction™

Nurse Practitioner
Flexibility Ergonomics Teamwork CommentsbiIV Tubing
ElectricalCords
Boom (+) in situations needing access to head of bedHeadwall (-)
Boom (+) in situations needing access to head of bedHeadwall (-)
Boom (+) in situations needing access to head of bedHeadwall (-)
Majority of poweroutlets are on the boom
Headwall ( ) Headwall ( ) Headwall ( )
Medical Gases
Boom (+) in situations needing access to head of bedHeadwall (-)
Boom (+) in situations needing access to head of bedHeadwall (-)
Boom (+) in situations needing access to head of bedHeadwall (-)
Could be addressed with gases on one side of bed in headwalls
Equipment
2008 International Conference and Exhibition on Planning, Design and Construction™
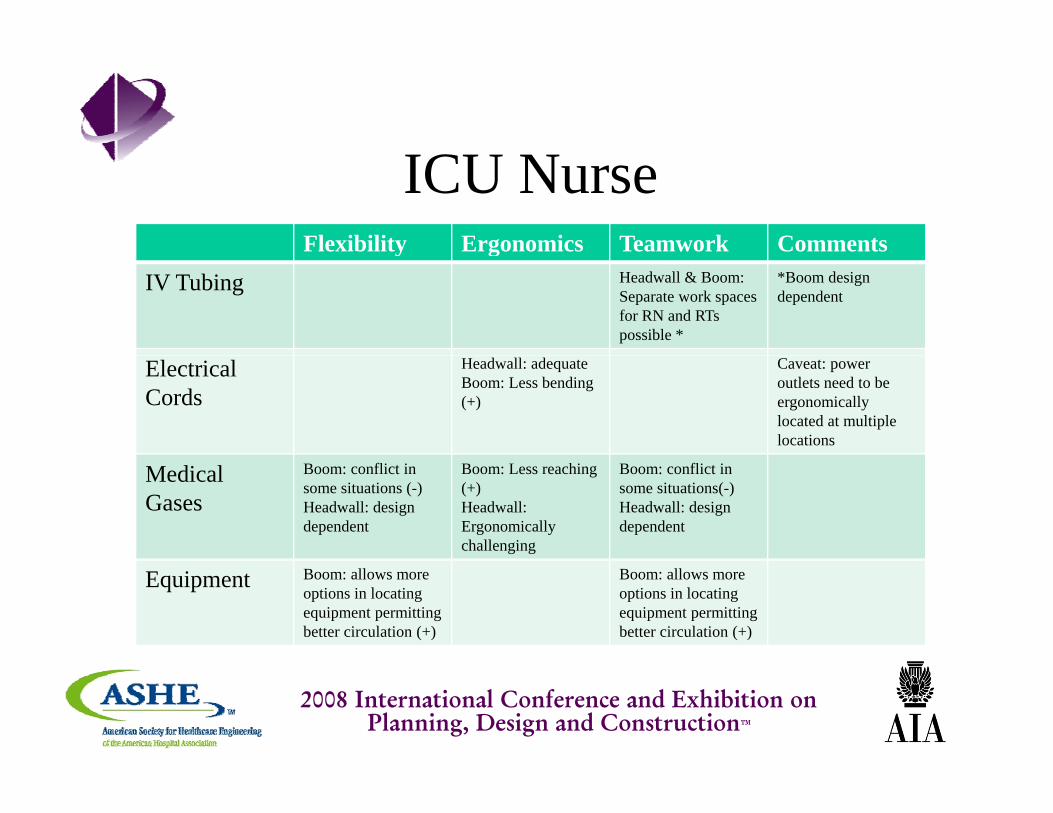
ICU NurseFlexibility Ergonomics Teamwork Commentsy g
IV Tubing Headwall & Boom: Separate work spaces for RN and RTs possible *
*Boom design dependent
ElectricalCords
Headwall: adequateBoom: Less bending (+)
Caveat: power outlets need to be ergonomically located at multiple locations
Medical Gases
Boom: conflict in some situations (-)Headwall: design dependent
Boom: Less reaching (+)Headwall: Ergonomically challenging
Boom: conflict in some situations(-)Headwall: design dependent
Equipment Boom: allows more options in locating equipment permittingbetter circulation (+)
Boom: allows more options in locating equipment permittingbetter circulation (+)
2008 International Conference and Exhibition on Planning, Design and Construction™

Respiratory TherapistFlexibility Ergonomics Teamwork Commentsy g
IV Tubing Headwall & Boom: Separate work spaces for RN and RTs possible *
*Boom design dependent
ElectricalCords
Headwall: adequateBoom: Less bending (+)
Caveat: power outlets need to be ergonomically located at multiple locations
Medical Gases
Boom: conflict in situations needing suction (-)Headwall: design dependent
Boom: Less reaching (+)Headwall: Ergonomically challenging
Boom: conflict in situations needing suction (-)Headwall: design dependent
Equipment Boom: allows more options in locating equipment permittingbetter circulation (+)
Boom: allows more options in locating equipment permittingbetter circulation (+)
2008 International Conference and Exhibition on Planning, Design and Construction™

Med Gas Tubing andMed Gas Tubing and Electrical Cords Management
2008 International Conference and Exhibition on Planning, Design and Construction™

TeamworkTeamwork
2008 International Conference and Exhibition on Planning, Design and Construction™

Flexibility: BedFlexibility: Bed placement; Equipment
2008 International Conference and Exhibition on Planning, Design and Construction™

Ergonomics
2008 International Conference and Exhibition on Planning, Design and Construction™

Clinician’s Comments• Physicians:
– prefer the boom
• Nurse Practitioners:P f h d ll d t i t d di t bilit– Prefer headwall due to consistency and predictability of equipment location across all patient rooms
– Perceive the benefit of boom over headwall as ‘low impact’ in high acuity scenarios
ICU N• ICU Nurses:– Prefer booms, because it is movable and all the gases
come off from one central place. Reduces figuring out which gas is plugged in where and less tripping over cables and connectionsover cables and connections.
• Respiratory Therapists:– Prefer booms owing to ergonomic advantages and
flexibility in equipment location
2008 International Conference and Exhibition on Planning, Design and Construction™

Family Considerations• Patient visibility
– In life threatening situations it is secondary to clinicians’
• Access to patient– In life threatening situations it
is secondary to clinicians’ needs.
– In lesser acuity situations no difference in visibility
Ci l i i / f
needs.– In lesser acuity situations no
difference in visibilityWh th hild i t bili d• Circulation in/out of room
– Patient population and acuity affects family circulation in and out of the room
– When the child is stabilized a pathway could be made in either scenario for parents to access their childrenand out of the room
– Not significantly affected by headwall vs boom
2008 International Conference and Exhibition on Planning, Design and Construction™

Parent CirculationSightline to PatientSightline to PatientAccess to Patient
2008 International Conference and Exhibition on Planning, Design and Construction™

When to invest in Booms• Anticipated level of acuity
– Frequency of ECMO, High Frequency Ventilator, Nitric
• Anticipated head access frequency– Frequency of 1) Intubation, 2)
Oxide ventilator, and Intracranial Pressure Monitoring
A ti i t d i l
q y ) )Cervical spine precautions and care, and 3) EEG monitoring
i i d b d• Anticipated surgical procedures
– Planned surgical procedures in the patient room
• Anticipated budget– budget limited, but encounter
some or all of the critical scenarios listed in this slidein the patient room scenarios listed in this slide
2008 International Conference and Exhibition on Planning, Design and Construction™

Some considerations
• Progressing reduction in invasiveness -means more surgery in patient rooms.
• How important is caregivers’ perception of flexibility?y
2008 International Conference and Exhibition on Planning, Design and Construction™

Shortcomings• Small sample
– One simulation of each scenario, with– Same subjects
• Day-to-day care delivery not includedy y y• Generalizability:
– Decision matrix could be generalized– Decision matrix could be generalized– Adult bed used to expand inferences to adult
ICUs2008 International Conference and Exhibition on
Planning, Design and Construction™
ICUs

Further Studies
• Multiple sites and larger sample to enhance generalizability
• Inclusion of medical gas columns• Examine headwalls with sufficient number• Examine headwalls with sufficient number
of duplicate medical gases
2008 International Conference and Exhibition on Planning, Design and Construction™

Further Studies
• Association between ceiling booms and adverse events (patient safety)
• Day-to-day care; bed repositioning; impact of view
2008 International Conference and Exhibition on Planning, Design and Construction™

Questions
2008 International Conference and Exhibition on Planning, Design and Construction™







