Download - Managememt of Carcinoma Nasopharynx

Management of carcinoma nasopharynx
By- Dr. Isha JaiswalModerator- Dr. Madhup Rastogi
Date: 17th February 2015
Nasopharyngeal carcinoma (particularly non keratinizing type) is different from other H&N cancers in terms of: Geographic & ethnic distribution association with Epstein–Barr virus (EBV) aggressive natural behaviour high predilection for distant metastases
Challenges in management: Detection is difficult: silent deep seated location treatment is difficult: anatomical proximity to critical structures role of surgery is limited to biopsy and salvage
Fortunately, this cancer is highly radiosensitive and chemosensitive; excellent tumor control can be achieved with RT ±CT However, the therapeutic margin is narrow, and the most conformal and precise radiotherapy is
demanded
“Treatment of NPC is one of the greatest challenges for oncologists and it is also one of the most gratifying”

Topics to be discussed:
• Pre-treatment evaluation• Staging• Management overview
• Evidence based treatment• NCCN guidelines
Radiotherapy Chemotherapy Surgery
Pre-treatment evaluation
History & physical examination Endoscopic examination & biopsy Radiological tests Metastatic workup Laboratory studies: CBC LFT,KFT Epstein –bar virus specific serologic tests
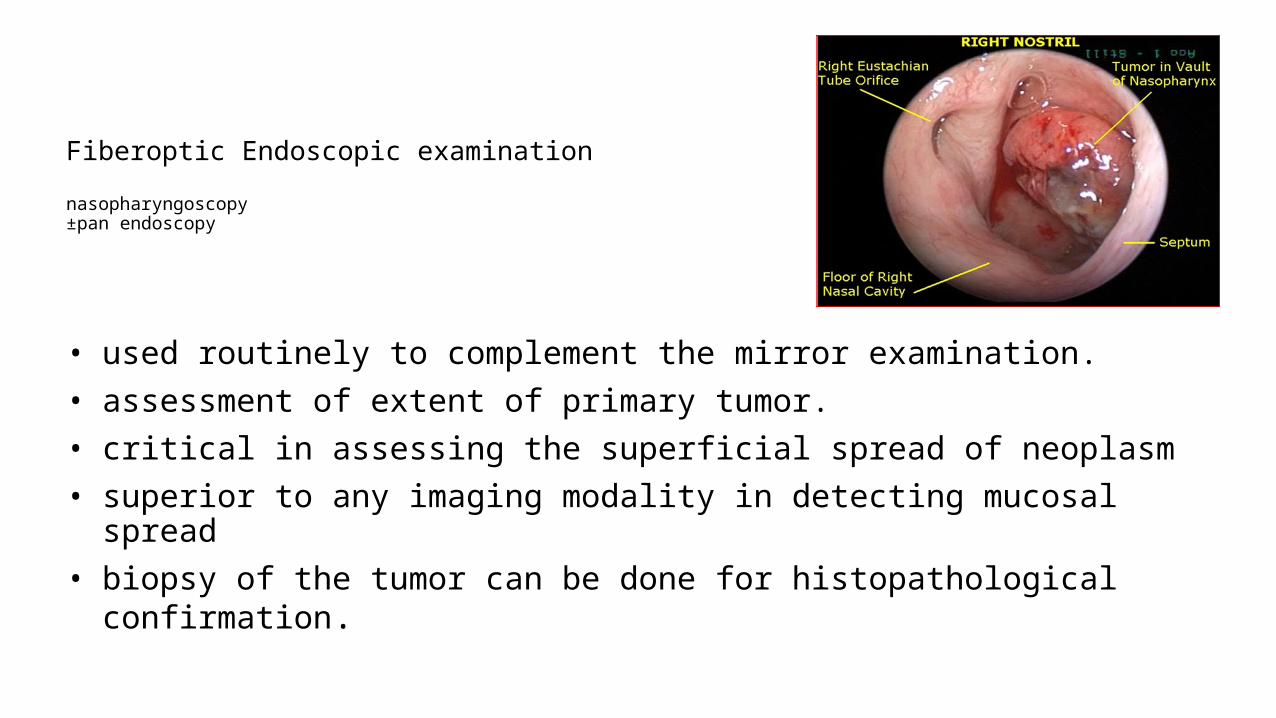
Fiberoptic Endoscopic examination
nasopharyngoscopy±pan endoscopy
• used routinely to complement the mirror examination. • assessment of extent of primary tumor.• critical in assessing the superficial spread of neoplasm• superior to any imaging modality in detecting mucosal spread• biopsy of the tumor can be done for histopathological confirmation.
Nasopharyngeal biopsy Tumor visible on clinical examination: biopsy performed with local anaesthesia in an outpatient setting. Tumor not visible or patient cannot cooperate: biopsy by direct visualization under general anaesthesia. For suspicious cases of a nasopharyngeal primary tumor with lack of visible tumor:
random biopsies of the pharyngeal recess (fossa of Rosenmüller).
FNAC of a suspicious neck mass :may be performed prior to biopsy of the nasopharynx when primary tumor is not clinically detectable

Radiological studiesCECT head & neckContrast enhanced MRI of head and neck

Contrast enhanced MRI head and neck
Includes imaging of nasopharynx ,paranasal sinus, nasal cavity , base of skull & neck
When utilizing MRI, thin slices (3 mm) should be used
preferred imaging technique for staging.
The AJCC T-classification requires details for tumor invasion into the soft tissue (e.g., parapharyngeal space) and bony structures so MRI necessary for proper staging

A:Axial T1-weighted magnetic resonance image (MRI) with 5-mm slices. B: Axial T1 MRI with 3-mm slices; skull-base invasion (arrow) upstaged this tumor from T1 to T3.

MRI is considered superior to CT for assessing primary tumour invasion into surrounding soft tissue bony structures pharyngobasilar fascia invasion infiltration of prevertebral muscles invasion into sinus of Morgagni skull base invasion cavernous sinus extension perineural disease (Liao et al., 2008; Sakata, 1999)Liao XB, Mao YP, Liu LZ, et al: How does magnetic resonance imaging influence staging according to AJCC staging system for nasopharyngeal carcinoma compared with computed tomography IJROBP 72:1368-1377, 2008
MRI is also more reliable for differentiating between the primary tumor and retropharyngeal adenopathy(Chang, 2005; Chong, 1996; Chung, 2004; King, 2000)

A: Axial T1-weighted MRI demonstrating involvement of maxillary branch of trigeminal nerve by nasopharyngeal carcinoma (V2) (arrow).
B: Coronal contrast-enhanced MRI showing involvement of the trigeminal cave (also known as Meckel’s cave) by nasopharyngeal carcinoma (arrow)

A: Axial T1-weighted magnetic resonance image (MRI) showing tumor infiltration of the right parapharyngeal space (left arrow). Note the resultant serous otitis media (right arrow).A: Axial contrast-enhanced magnetic resonance image (MRI) demonstrating involvement of the cavernous sinus by nasopharyngeal carcinoma
Contrast enhanced CT scan head and neck
Acceptable alternative imaging Relatively inexpensive Rapid image acquisition
Som P.M 1 defined lymph node metastases radiologically by following criteria
Size: greatest nodal diameter is 1.5cm for jugulodigastric and submandibular nodes 0.8 cm for retropharyngeal nodes &1 cm for all other cervical nodes.
More accurate size criterion is shortest axial diameter exceeds 1 1 mm in the jugulodigastric, 5mm in retropharyngeal & 10 mm in all other cervical nodes
Shape: metastatic nodes are spherical (hyperplastic node is bean shaped) Extracapsular spread central necrosis Localized nodal groupings in node-draining area (three or more contiguous & confluent L.N
each of which has maximal diameter of 8-15 mm or minimal axial diameter of 8-1 0 mm)
Detection of occult lymph node metastasis
1Som PM. Detection of metastasis in cervical lymph nodes: CT and MR criteria and differential diagnosis. AJR Am J Roentgenol 1992;158(5):961–969.

METASTATIC WORKUP
• Routine: Chest X ray• Additional: if clinically indicated or N3 diseaseCT Thorax: CT Abdomen: Bone Scan :PET-CT
In detection of unknown /small primary tumorIn evaluating clinically occult nodal involvementCan be used in place of conventional staging by CT, bone, scans and
ultrasound for detection of distant metastasisIn follow up to differentiate between treatment sequelae & tumor
recurrence/residual
Role Of 18FDG PET-CT
EBV specific Serological tests:
• association of EBV with NPC (non keratinizing type) provides basis for serological test may enhance early detection of the primary disease/ relapses, supplement TNM staging & improve
prognostication• for diagnosis: anti -VCA & anti EA Ab are both sensitive however IgA anti-VCA has better specificity1 &
may serve as screening test in high-risk patients.• for prognosis: prognostic effects of pre & post treatment Ab titre have been controversial due to inconsistent
results in various studies2
titers remained persistently high even in patients who achieved remission. there was no reliable cut-off value for differentiating between recurrence and remission.
Ig A antiviral capsule antigen ( Ig A anti –VCA) Ig G anti early antigen (IgG anti EA A)
1Neel HB 3rd. Nasopharyngeal carcinoma: diagnosis, staging, and management. Oncology (Williston Park), 1992;6(2):87–95;2 Neel HB 3rd, Taylor WF. Epstein-Barr virus-related antibody. Changes in titers after therapy for nasopharyngealCa. Arch Otolaryngol Head Neck Surg 1990;116(11):1287–1290.

• PCR based technique makes it possible to detect EBV DNA levels• Plasma EBV DNA is superior to serum anti-EBV Ab in prognostication
• Diagnosis: has high sensitivity (96%) & specificity (93%) for detecting NPC• Levels correlated significantly with tumor load, TNM staging, recurrence rate, and survival.
• Prognosis: study by Leung et al* on 376 NPC pts. showed pretherapy DNA load was an independent prognostic factor for OS
• Risk grouping: identify poor-risk among early-stage pts. & can complement TNM staging and guide treatment decision.
• *Leung SF, Zee B, Ma BB, et al: Plasma Epstein-Barr viral deoxyribonucleic acid quantitation complements tumor-node-metastasis staging prognostication in nasopharyngeal carcinoma. J Clin Oncol 24:5414- 5418, 2006
Plasma Epstein Virus DNA Levels
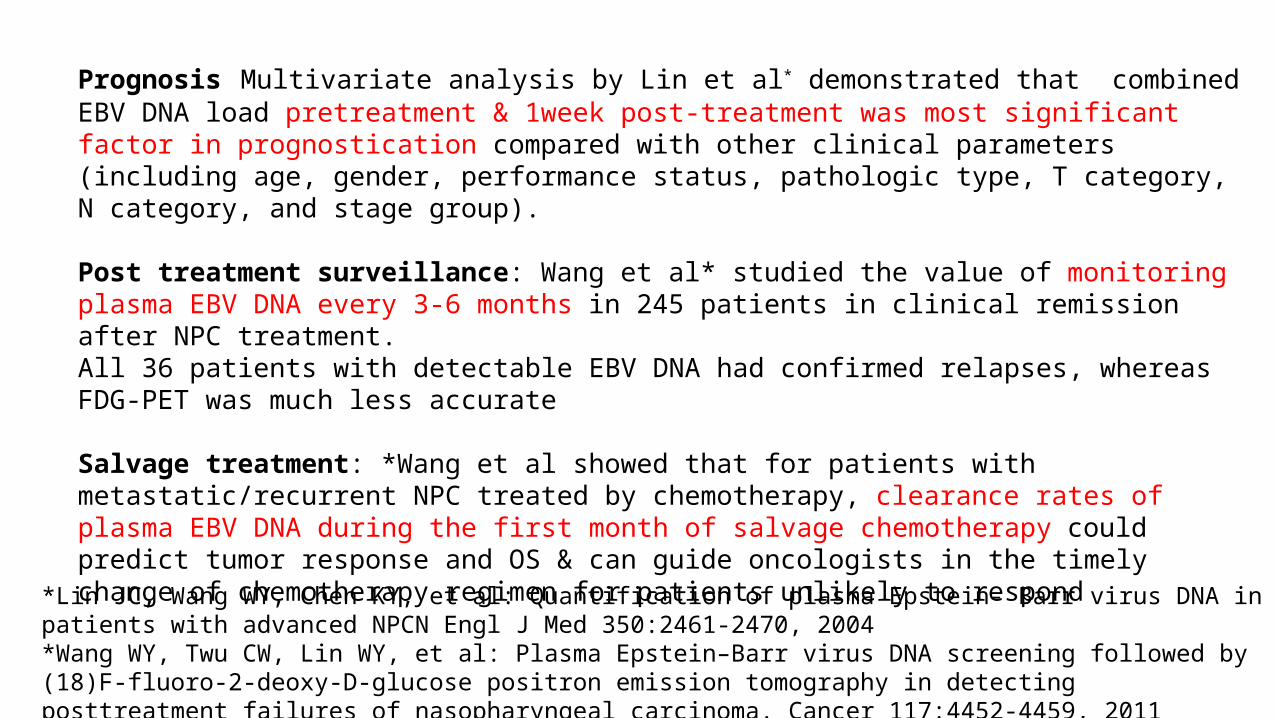
Prognosis Multivariate analysis by Lin et al* demonstrated that combined EBV DNA load pretreatment & 1week post-treatment was most significant factor in prognostication compared with other clinical parameters (including age, gender, performance status, pathologic type, T category, N category, and stage group).
Post treatment surveillance: Wang et al* studied the value of monitoring plasma EBV DNA every 3-6 months in 245 patients in clinical remission after NPC treatment. All 36 patients with detectable EBV DNA had confirmed relapses, whereas FDG-PET was much less accurate
Salvage treatment: *Wang et al showed that for patients with metastatic/recurrent NPC treated by chemotherapy, clearance rates of plasma EBV DNA during the first month of salvage chemotherapy could predict tumor response and OS & can guide oncologists in the timely change of chemotherapy regimen for patients unlikely to respond
*Lin JC, Wang WY, Chen KY, et al: Quantification of plasma Epstein- Barr virus DNA in patients with advanced NPCN Engl J Med 350:2461-2470, 2004*Wang WY, Twu CW, Lin WY, et al: Plasma Epstein–Barr virus DNA screening followed by (18)F-fluoro-2-deoxy-D-glucose positron emission tomography in detecting posttreatment failures of nasopharyngeal carcinoma. Cancer 117:4452-4459, 2011

TNM STAGING- AJCC 7th edition (2010)* T STAGE
T1: Tumor confined to nasopharynx or extends to oropharynx* & or nasal cavity* without parapharyngeal extension
T2: Tumor with parapharyngeal extension* ( *posterolateral infiltration beyond the pharyngobasilar fascia)
T3: Tumors involving bony structures of skull base & or paranasal sinuses
T4 Tumors with intracranial extension & or involvement of cranial nerves, hypopharynx, orbit or with extension to the infratemporal fossa* or masticator space* (*masticator space and infratemporal fossa: extension beyond the ant. surface of lateral pterygoid muscle, or lateral extension beyond the posterolateral wall of maxillary antrum & pterygomaxillary fissure.)
*Edge SB, Byrd DR, Compton CC, et al. AJCC cancer staging handbook, 7th ed. New York: Springer, 2010.*
(*Nasal cavity : ant. extension beyond the post. margin of choana*Oropharynx: inferior extension beyond the level of free border of soft palate. The junction at C1/C2 is recommended as a more consistent radiologic landmark)
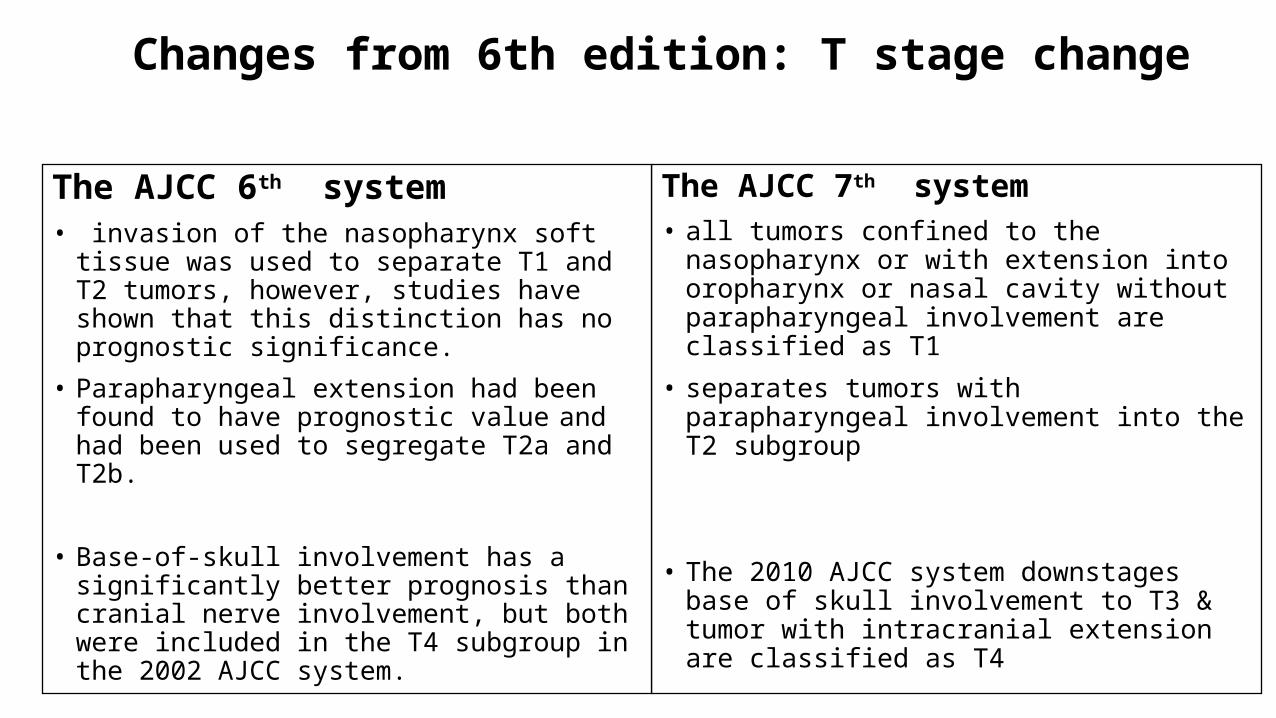
Changes from 6th edition: T stage change
The AJCC 7th system• all tumors confined to the nasopharynx or with
extension into oropharynx or nasal cavity without parapharyngeal involvement are classified as T1
• separates tumors with parapharyngeal involvement into the T2 subgroup
• The 2010 AJCC system downstages base of skull involvement to T3 & tumor with intracranial extension are classified as T4
The AJCC 6th system• invasion of the nasopharynx soft tissue was used to
separate T1 and T2 tumors, however, studies have shown that this distinction has no prognostic significance.
• Parapharyngeal extension had been found to have prognostic value and had been used to segregate T2a and T2b.
• Base-of-skull involvement has a significantly better prognosis than cranial nerve involvement, but both were included in the T4 subgroup in the 2002 AJCC system.
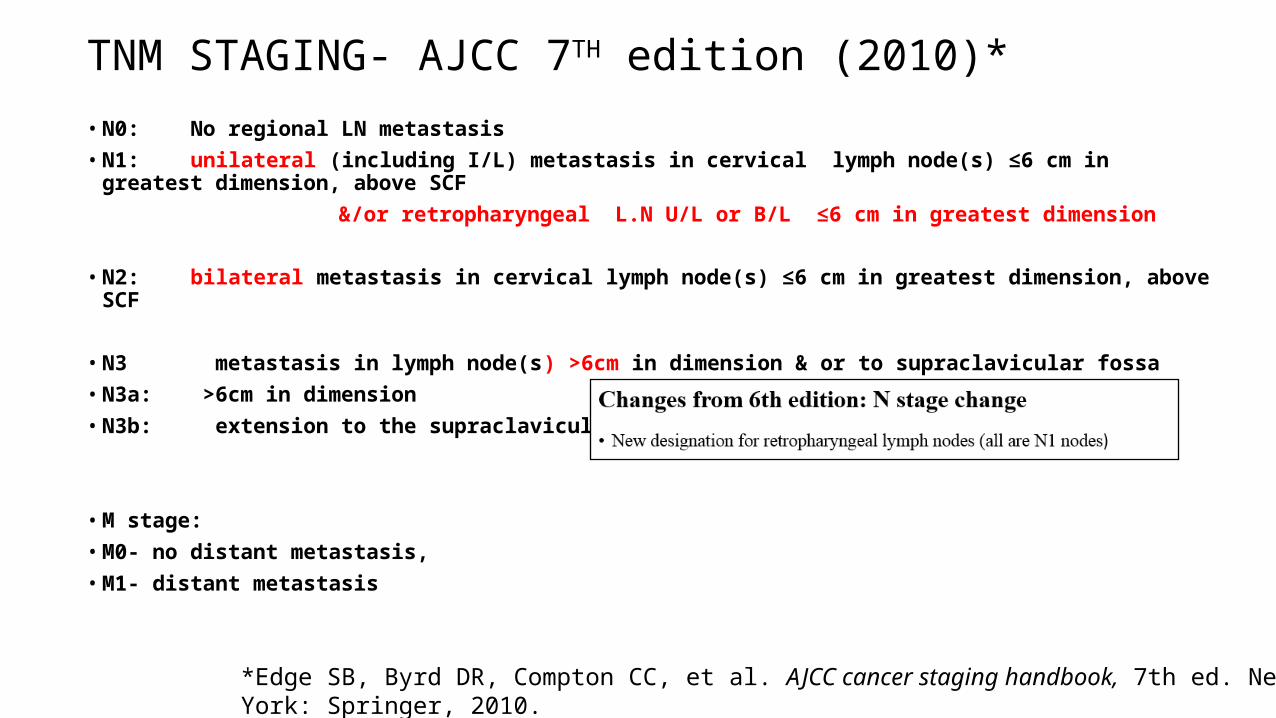
TNM STAGING- AJCC 7TH edition (2010)*• N0: No regional LN metastasis• N1: unilateral (including I/L) metastasis in cervical lymph node(s) ≤6 cm in greatest dimension, above SCF &/or retropharyngeal L.N U/L or B/L ≤6 cm in greatest dimension
• N2: bilateral metastasis in cervical lymph node(s) ≤6 cm in greatest dimension, above SCF
• N3 metastasis in lymph node(s) >6cm in dimension & or to supraclavicular fossa• N3a: >6cm in dimension• N3b: extension to the supraclavicular fossa
• M stage: • M0- no distant metastasis, • M1- distant metastasis
*Edge SB, Byrd DR, Compton CC, et al. AJCC cancer staging handbook, 7th ed. New York: Springer, 2010.
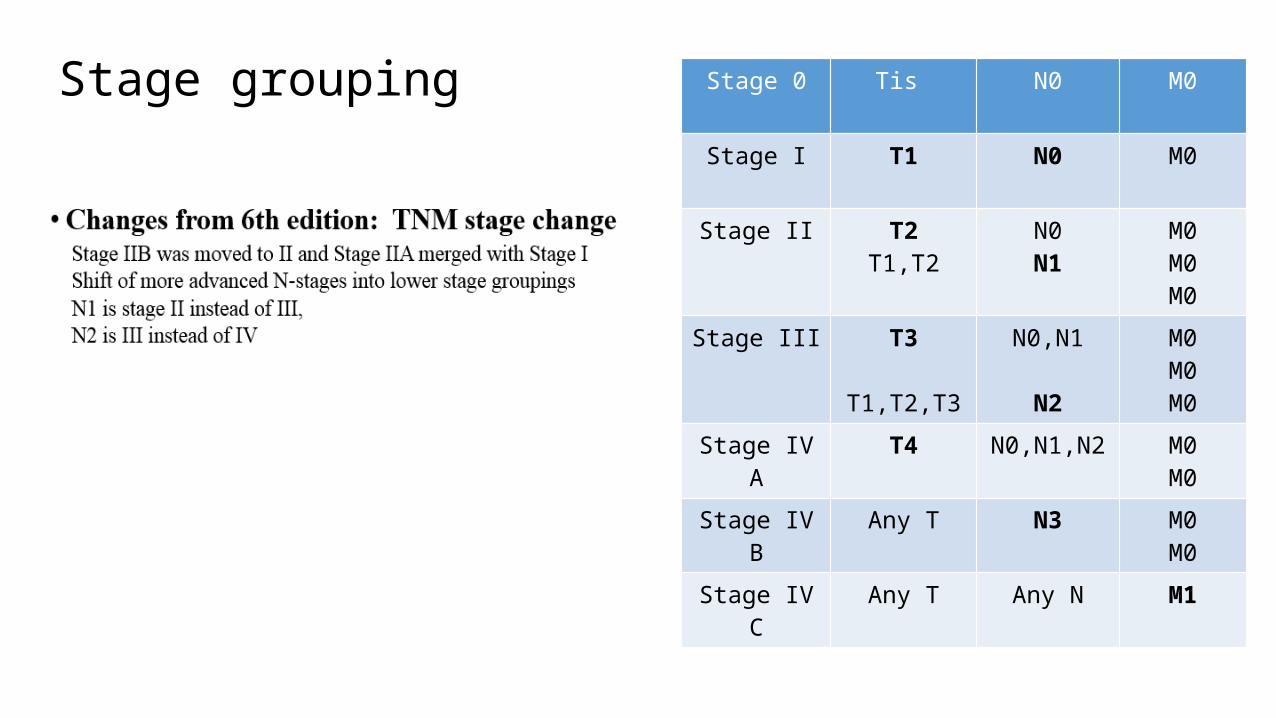
Stage grouping Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage II T2T1,T2
N0N1
M0M0M0
Stage III T3
T1,T2,T3
N0,N1
N2
M0M0M0
Stage IV A T4 N0,N1,N2 M0M0
Stage IV B Any T N3 M0M0
Stage IV C Any T Any N M1

24
Pathological classification: WHO 2005• WHO classes
• based on light microscopy findings
• 3 histological types • type I – Keratinizing SCC • type IIa – Nonkeratinizing Differentiated Carcinoma• type IIb – Nonkeratinizing Undifferentiated Carcinoma• Type III-basaloid squamous cell carcinoma

25
• Differences between type I and types II & III
Viral associations• Type I - HPV• Types IIa IIb – EBV
5-year overall survival (OS) rate 60-80% in WHO type II NPC - high degree of radiosensitivity 20-40% in WHO type I NPC - low degree of radiosensitivity
Basaloid squamous cell carcinoma is quite rare, with a frequency of <0.2%
Tumor relatedTNM staging: most important prognostic factor. • advanced T-category: associated with worse local control and overall survival; • advanced N-category: increased risk of distant metastasis and worse survival. • M1 stage: poor prognosisHistopathology: nonkeratinizing and undifferentiated carcinomas more radiosensitive and
offer better prognosis than keratinizing SCC Plasma EBV DNA & anti EBV antibodies
PROGNOSTIC FACTORS*
*Lin JC 2009:prognostic factors in NPC

Patient related
Ethnicity: no prognostic difference between ethnic Asian and non-Asian patients with nonkeratinizing carcinoma
Age: better prognosis younger patients Gender : not significant Performance status, weight loss & anaemia before treatment :not significant in pts. treated definitively
Diagnosis & treatment related
Treatment delay > 8 weeks after diagnosis or extending break during RT adversely effect outcome Treatment strategy & techniques: use of Chemo RT & IMRT improves tt. outcome compared to
conventional therapy Tumor regression during RT: not significant
*Lin JC 2009:prognostic factors in NPC
• Radiotherapy:
• Chemotherapy :
• Surgery:
Concurrent Neoadjuvant Adjuvant
Treatment Options
Definitive treatment: EBRT: Conventional, 3DCRT, IMRT Dose escalation with altered fractionation, brachytherapy
Limited role
Role of radiation therapy: treatment of choice
• Historically, RT alone was used, and resulted in• 5-year OS 35-50%
• Early-stage (I-II) outcomes were good, with 5-year DFS 75-95% and OS 70-80%• For advanced-stage (III-IV) 5-year DFS was ~50%, and OS only 10-40%
• Early stage disease (Stage I-II) :continues to be managed with RT alone• Advanced stage disease (Stage III-IV) & some bulky stage II is managed with
chemotherapy and radiotherapy
Role of surgery
• Due to deep location of nasopharynx, and anatomic proximity to critical structures, radical surgery is typically not used
• Limited to biopsy for histological confirmationNeck dissections for persistently enlarged lymph nodesNasopharyngectomy in persistent or recurrent disease
RADIATION THERAPY: definitive treatment
Total Dose Time & Fractionation Radiation Technique Dose Escalation Addition Of Chemotherapy
Impact Of DoseHigh dose is needed for NPC tumor despite its radiosensitivity
The general recommendation is : 70 Gy to the gross tumor @1.8-2 Gy /# 50-60 Gy to potential risk sites @ 1.8-2 Gy /#
1,2Retrospective studies shown that T1-2 tumors had good local control rate of 90-100% for >70 Gy, compared to 80% for 66 to 70 Gy.However, local control for patients with T3-4 tumours remained <55%, even with total dose >70 Gy. Higher doses did not significantly improve outcomes in T3-4 tumors. These observations suggest that, besides consideration of the prescribed dose, the problem of
sufficient coverage has to be overcome for advanced tumors.
1 Perez CA, et al. Carcinoma nasopharynx: factors affecting prognosis. IJROBP 1992;23(2):271–2802 Mesic JB,. Megavoltage irradiation of epithelial tumors of the nasopharynx. IJROBP 1981;7(4):447–453.
Impact of time & fractionation• 1Prolongation of treatment significantly jeopardizes local control
• Benefit of accelerated fractionation is uncertain (no benefit in local control, increased toxicities)
• Retrospective study by Lee et al.2 in 1,008 patients with T1 tumours irradiated by four different fractionation schedules demonstrated that total dose was the most important radiation factor (p = .01).
• Dose per fraction did not affect local control; however, it was a significant risk factor for temporal lobe necrosis.
• Therefore, a fractional dose of >2-2.12 Gy should be avoided
1. Kwong DL, Sham JS, Chua DT, et al: The effect of interruptions and prolonged treatment time in radiotherapy for nasopharyngeal carcinoma.IJROBP 39:703-710, 1997
2. Lee AW, Kwong DL, Leung SF, et al: Factors affecting risk of symptomatic temporal lobe necrosis: Significance of fractional dose and treatment timeIJROBP53:75-85, 2002

TRIALS FOR ALTERED FRACTIONATION1Teo et al randomized 159 pts. Of NPC into 2 arms(38% of cases were T3-4)
Arm A 2.5 Gy/#QD for 8# f/b 1.6 Gy b.id 32#Arm B: 2.5Gy/# QD for 24 #.
Results: prematurely terminated by significant increase in neurological complications
5-year local FFR did not improve (89% vs 85%), but there were excessive neurological toxicities (49% vs 23%).
1Teo et al: Final report of a randomized trial on altered-fractionated radiotherapy in nasopharyngeal carcinoma. IJROBP 48:1311-1322, 2000
Trial Comparing Conventional Radiotherapy To Split Course Bifractionated Radiation Therapy In Patients With Nasopharyngeal Carcinoma
• 2Daoud et al randomized 154 patients of NPC into 2 arms• (45% T3-4 tumors)• Arm A: 1.6 Gy/# b.id to 70.4Gy/6 weeks with split course• Arm B: 2 Gy/# QD to 70 Gy/7 weeks
• Results: 5-yearlocoregional FFR did not improve significantly (81% vs78%), though major excessive toxicities were observed.
• 2Daoud J, et al: Results of a prospective randomised trial comparing conventional radiotherapy to split course bifractionated radiation therapy in patients with nasopharyngeal carcinoma. Radiother Oncol 85:17-23, 2007

NPC-9902 Trial:IJROBP 2006
Aim: to assess the therapeutic benefit of AF and/or concurrent-adjuvant chemoradiotherapy (CRT). • randomized 189 patients with locally advanced NPC (T3-T4, N0-1, M0) to four arms:(i) conventional fractionation (CF) alone, (ii) AF (six fractions/week) alone,(iii) CF with concurrent chemotherapy,(iv) AF with concurrent chemotherapy.Preliminary Results*: median follow-up of 2.9 years • AF did not demonstrate significant improvement in event-free survival (EFS) when compared to CF (AF vs. CF: HR 0.68, p = .22). • A significant increase in acute and late toxicity in the AF arm
*Further results discussed with chemotherapy trials
Lee, et al. Preliminary results of a randomized study on therapeutic gain by concurrent chemotherapy and/or accelerated fractionation for locally advanced NPC. IJROBP 2006;66(1):142–15

RADIOTHERAPY TECHNIQUE
• 2D: conventional• 3D:conformal• IMRT

Nasopharyngeal carcinoma presents most typically as a concave tumor, allowing for computerized three-dimensional (3D) treatment plans to be an important technical advance for improved radiation delivery.When compared to conventional 2D plans, 3D planning demonstrated better tumor dose coverage while decreasing normal tissue dose in several studies.1,2,3,4
2D Vs 3DCRT
1Chau RM, Teo PM, Choi PH, et al. Three-dimensional dosimetric evaluation of a conventional radiotherapy technique for treatment of nasopharyngeal carcinoma. Radiother Oncol 2001;58(2):143–1532Kutcher GJ, Fuks Z, Brenner H, et al. Three-dimensional photon treatment planning for carcinoma of the nasopharynx. IJROBP1991;21(1):169–182.3Leibel SA, Kutcher GJ, Harrison LB, et al. Improved dose distributions for 3D conformal boost treatments in carcinoma of the nasopharynx. Int J Radiat Oncol Biol Phys 1991;20(4):823–834Jen et al. Parotid gland-sparing 3-dimensional conformal radiotherapy results in less severe dry mouth in nasopharyngeal cancer patients: a dosimetric and clinical comparison with conventional radiotherapy. Radiother Oncol 2005;75(2):204–209.
IMRT IMRT has supplanted conventional radiotherapy in the treatment of NPC & is preferred
for NPC if resources permit
The intensity of the radiation beams can be modulated to deliver a high dose to the tumor with a superior target volume coverage while significantly limiting the dose to surrounding normal structures.
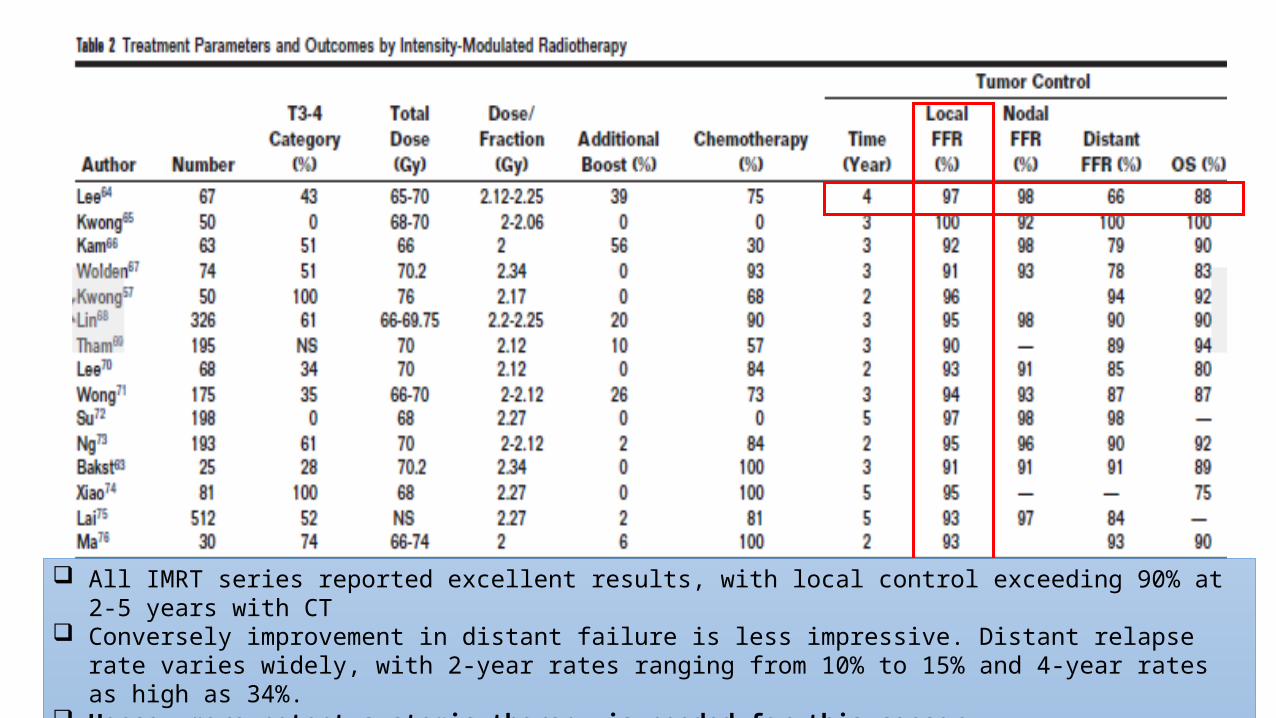
All IMRT series reported excellent results, with local control exceeding 90% at 2-5 years with CT Conversely improvement in distant failure is less impressive. Distant relapse rate varies widely, with 2-year rates
ranging from 10% to 15% and 4-year rates as high as 34%. Hence, more potent systemic therapy is needed for this cancer.

DOSE ESCALATION• ALTERED FRACTIONATION• BRACHYTHERAPY

BRACHYTHERAPY• Intracavitary/ interstitial implants have been used in NPC
• Indications:as a boost treatment following EBRT in the treatment of recurrent disease.

ADJUVANT BRACHYTHERAPY BOOST FOR PRIMARY TREATMENT OF NASOPHARYNGEAL CARCINOMA
Table :summarizes reports on the use of brachytherapy as a boost for dose escalation. Most studies demonstrated that local control of up to 90% to 95% could be achieved for T1-2 tumors without excessive late damages
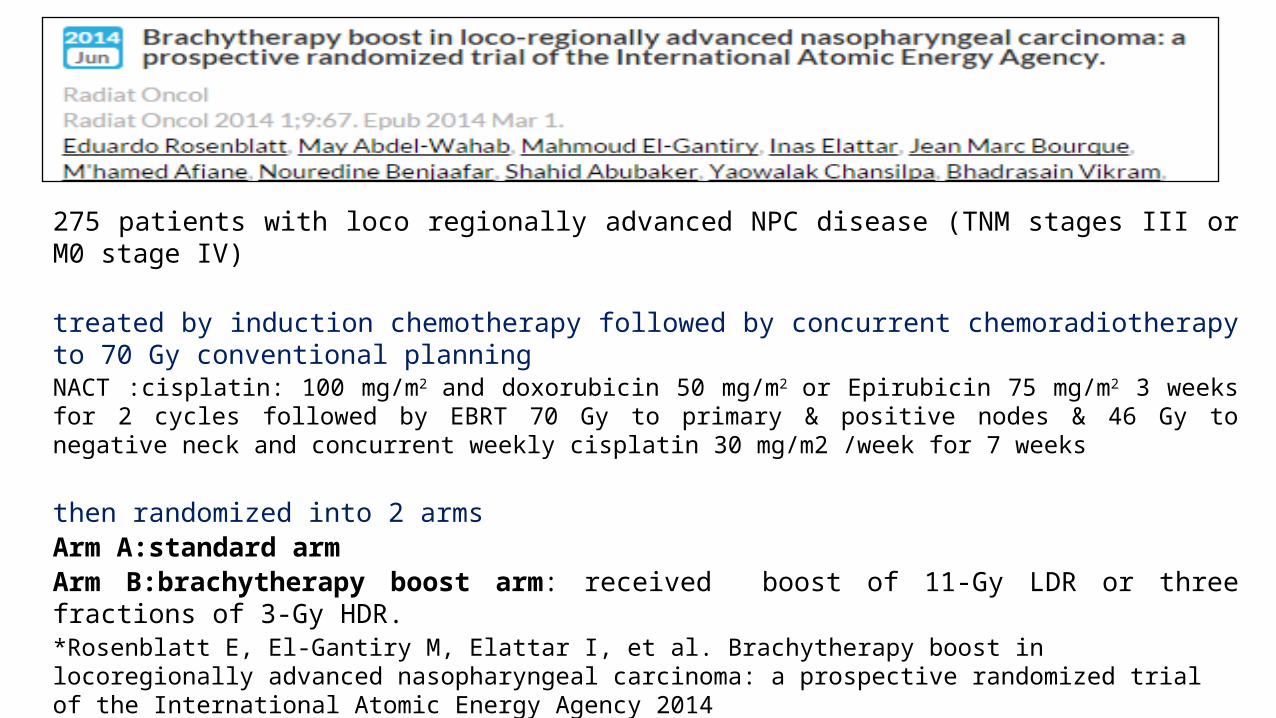
275 patients with loco regionally advanced NPC disease (TNM stages III or M0 stage IV)
treated by induction chemotherapy followed by concurrent chemoradiotherapy to 70 Gy conventional planningNACT :cisplatin: 100 mg/m2 and doxorubicin 50 mg/m2 or Epirubicin 75 mg/m2 3 weeks for 2 cycles followed by EBRT 70 Gy to primary & positive nodes & 46 Gy to negative neck and concurrent weekly cisplatin 30 mg/m2 /week for 7 weeks
then randomized into 2 armsArm A:standard armArm B:brachytherapy boost arm: received boost of 11-Gy LDR or three fractions of 3-Gy HDR.
*Rosenblatt E, El-Gantiry M, Elattar I, et al. Brachytherapy boost in locoregionally advanced nasopharyngeal carcinoma: a prospective randomized trial of the International Atomic Energy Agency 2014

RESULTS:With a median follow-up of 29 months no additional benefit of brachytherapy boost compared with chemoradiotherapy alone distant-metastasis–free survival (52.6% vs. 59.8%, p = .496) 3-year OS (63.3% vs. 62.9%, p = .742) . locoregional-FFR (54.4% vs. 60.5%, p = .647)
Rotterdam nasopharyngeal applicator
ConclusionsThe addition of a brachytherapy boost to external beam radiotherapy and chemotherapy did not improve outcome in loco-regionally advanced nasopharyngeal carcinoma
Limitations of brachytherapy:
dose delivered is adequate only for superficial nonbulky tumors. not suitable for treatment of tumors with intracranial extension because of the rapid reduction of dose with distanceoptimal positioning of the applicators depends both on clinician’s skill and patient’s anatomic features
Present status of brachytherapy
Since the advent of IMRT as primary radiotherapy for nasopharyngeal carcinoma and with its excellent local control, the use of brachytherapy as a boost treatment following definitive EBRT has declined
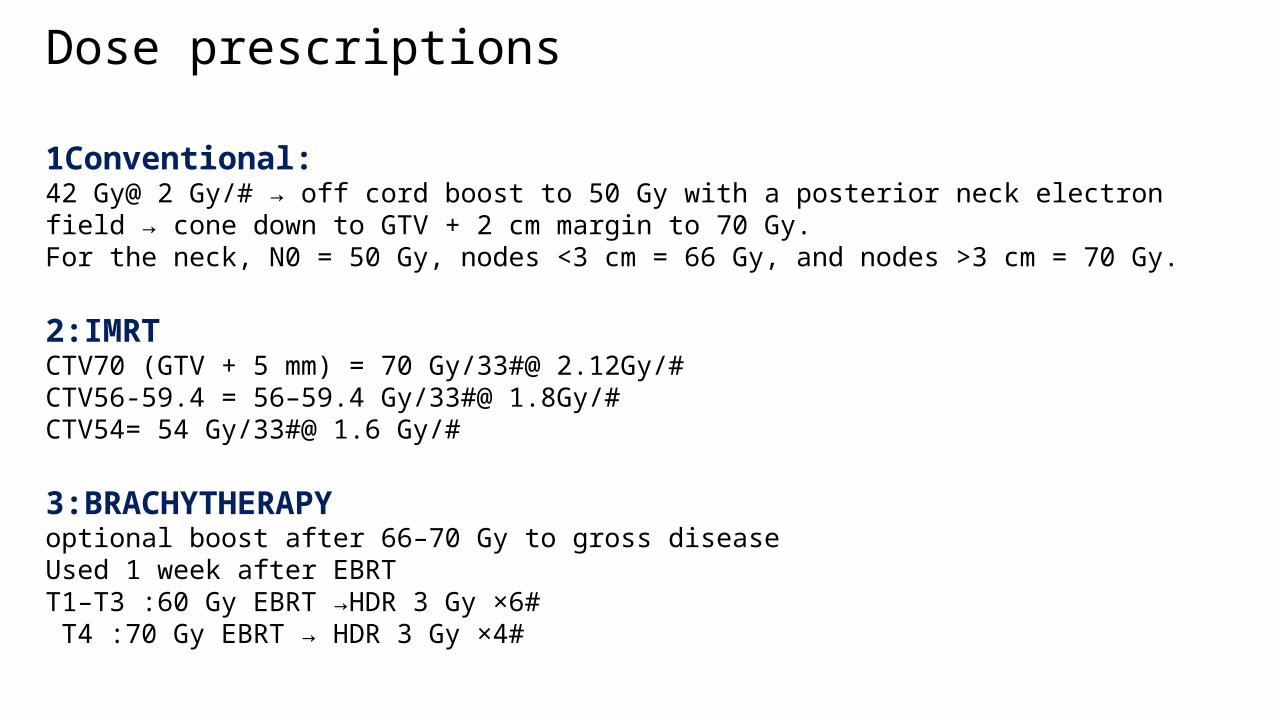
Dose prescriptions
1Conventional: 42 Gy@ 2 Gy/# → off cord boost to 50 Gy with a posterior neck electron field → cone down to GTV + 2 cm margin to 70 Gy.For the neck, N0 = 50 Gy, nodes <3 cm = 66 Gy, and nodes >3 cm = 70 Gy.
2:IMRT CTV70 (GTV + 5 mm) = 70 Gy/33#@ 2.12Gy/#CTV56-59.4 = 56–59.4 Gy/33#@ 1.8Gy/# CTV54= 54 Gy/33#@ 1.6 Gy/#
3:BRACHYTHERAPYoptional boost after 66–70 Gy to gross disease Used 1 week after EBRT T1–T3 :60 Gy EBRT →HDR 3 Gy ×6# T4 :70 Gy EBRT → HDR 3 Gy ×4#
CHEMOTHERAPY• Concurrent Chemo radiotherapy• Neoadjuvant/induction Chemotherapy• Adjuvant Chemotherapy
RT RT-ACCRT-AC
CRT
IC-RT
IC-CRT
NPC is well known for its chemo-responsiveness.
However review of available clinical trials on efficacy of chemotherapy in NPC shows inconsistent conclusions
Up to 2004 there were 11 RCTs comparing combined chemoradiotherapy (CRT) treatment versus RT alone
five trials on induction chemotherapy combined with RT (I-CRT) :only 1 showed significant benefit
three trials on adjuvant chemotherapy combined with RT(A-CRT) :none achieved significant benefit
Three trials on concurrent chemotherapy showed relatively more consistent conclusions.
First trial to achieve significant survival benefit was the IGS (Intergroup-0099 Study), which used concurrent and adjuvant chemotherapy combined with RT (CA-CRT)When compared with RT alone, the magnitude of gain in EFS & OS was so impressive that this regimen became the standard treatment for patients with loco regional advanced NPC

only by the International Nasopharynx Cancer Study Group VUMCA1trial using cisplatin, epirubicin, and bleomycin showed significant improvement in disease-free survival (40% vs 30% at 5years; p < 0.01), but no benefit in OS was shown even with longer follow-up.
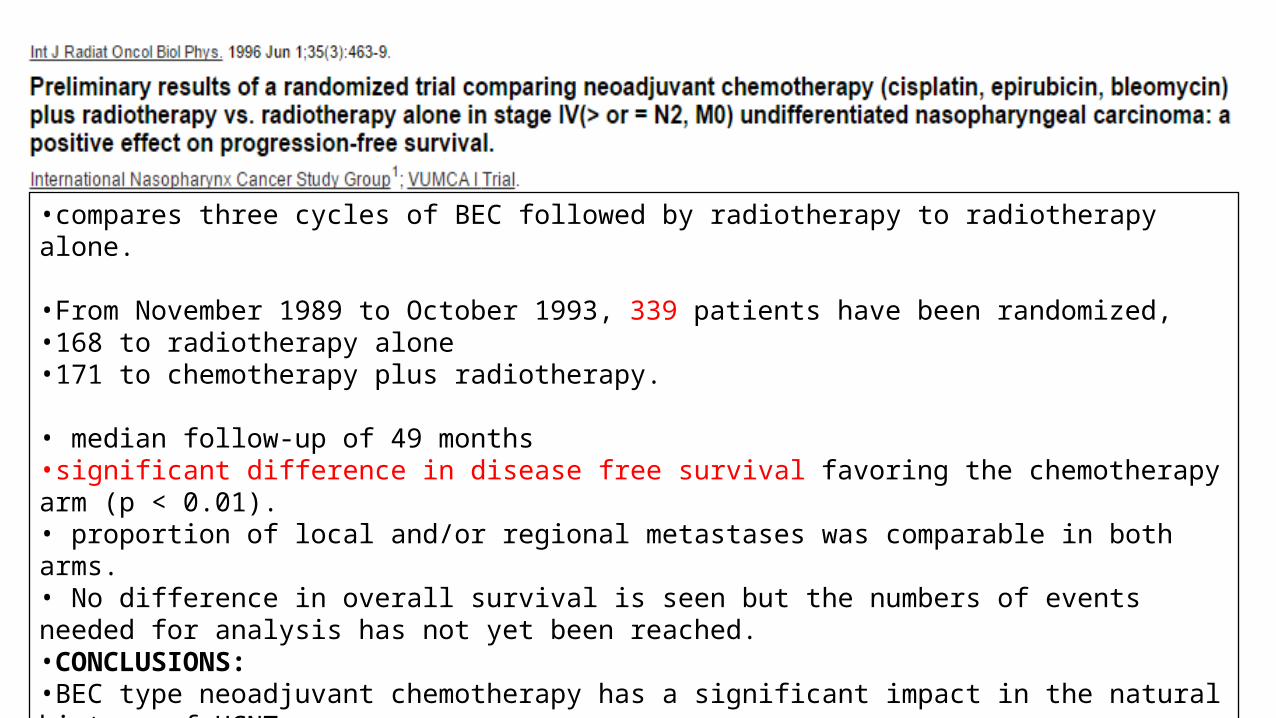
•compares three cycles of BEC followed by radiotherapy to radiotherapy alone.
•From November 1989 to October 1993, 339 patients have been randomized, •168 to radiotherapy alone •171 to chemotherapy plus radiotherapy.
• median follow-up of 49 months•significant difference in disease free survival favoring the chemotherapy arm (p < 0.01). • proportion of local and/or regional metastases was comparable in both arms.• No difference in overall survival is seen but the numbers of events needed for analysis has not yet been reached.•CONCLUSIONS:•BEC type neoadjuvant chemotherapy has a significant impact in the natural history of UCNT. •Further follow-up is needed to establish an eventual overall survival difference.
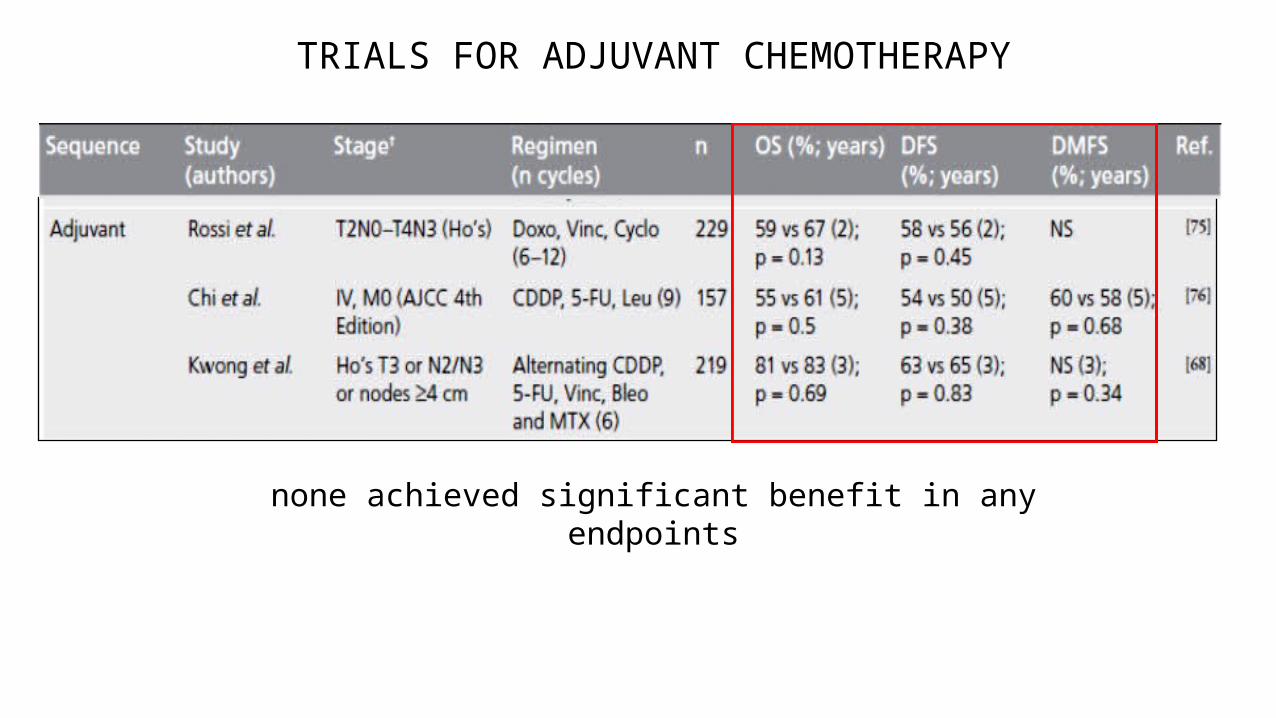
TRIALS FOR ADJUVANT CHEMOTHERAPY
none achieved significant benefit in any endpoints
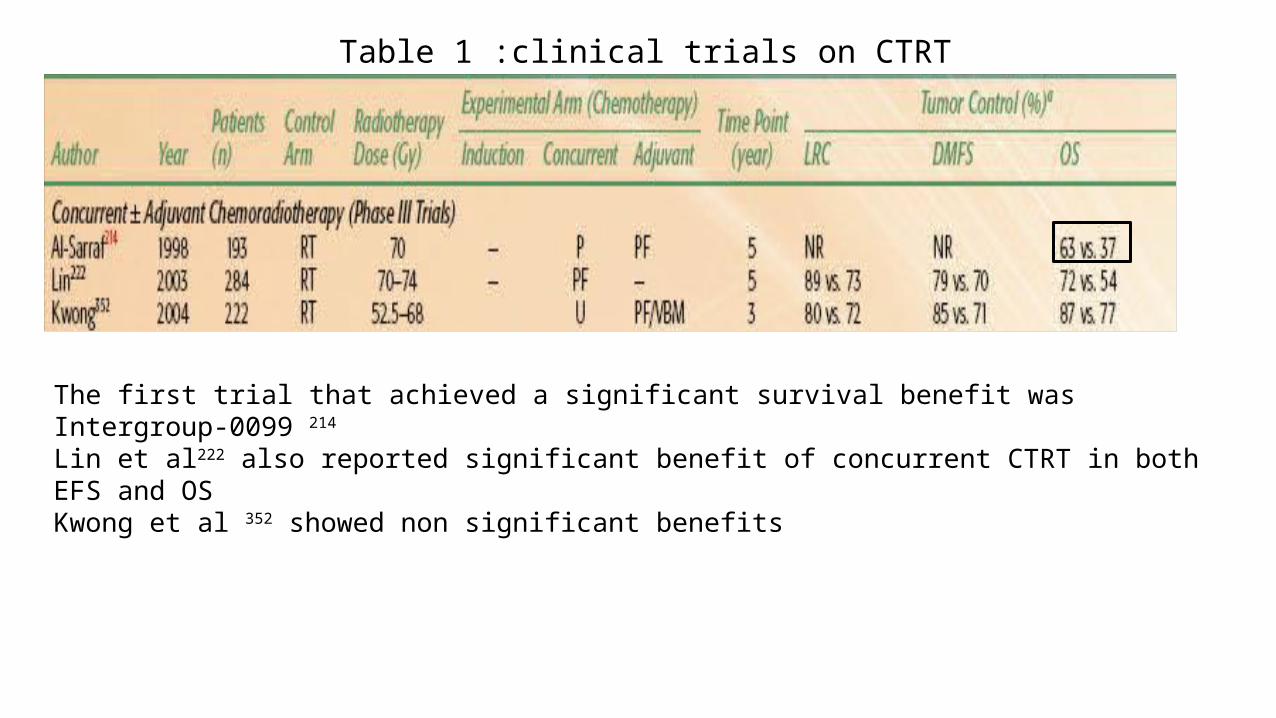
The first trial that achieved a significant survival benefit was Intergroup-0099 214 Lin et al222 also reported significant benefit of concurrent CTRT in both EFS and OSKwong et al 352 showed non significant benefits
Table 1 :clinical trials on CTRT

Chemoradiotherapy Versus Radiotherapy in Patients With Advanced Nasopharyngeal Cancer: Phase III Randomized Intergroup Study 0099Muhyi Al-Sarraf, et al
Journal of Clinical Oncology, Vol 16, No 4 (April), 1998: pp 1310-1317
• Pts. were stratified by tumor stage, nodal stage, performance status & histology
• Radiotherapy 1.8- to 2.0-Gy/d fractions for 35 to 39 fractions for a total dose of 70 Gy.
• investigational arm received chemotherapy with cisplatin 100 mg/m 2 on days 1, 22, and 43 during radiotherapy;
• adjuvant chemotherapy with cisplatin 80 mg/m 2 on day 1 and fluorouracil 1,000 mg/m 2/d on days 1 to 4 was administered every 4 weeks for three courses.
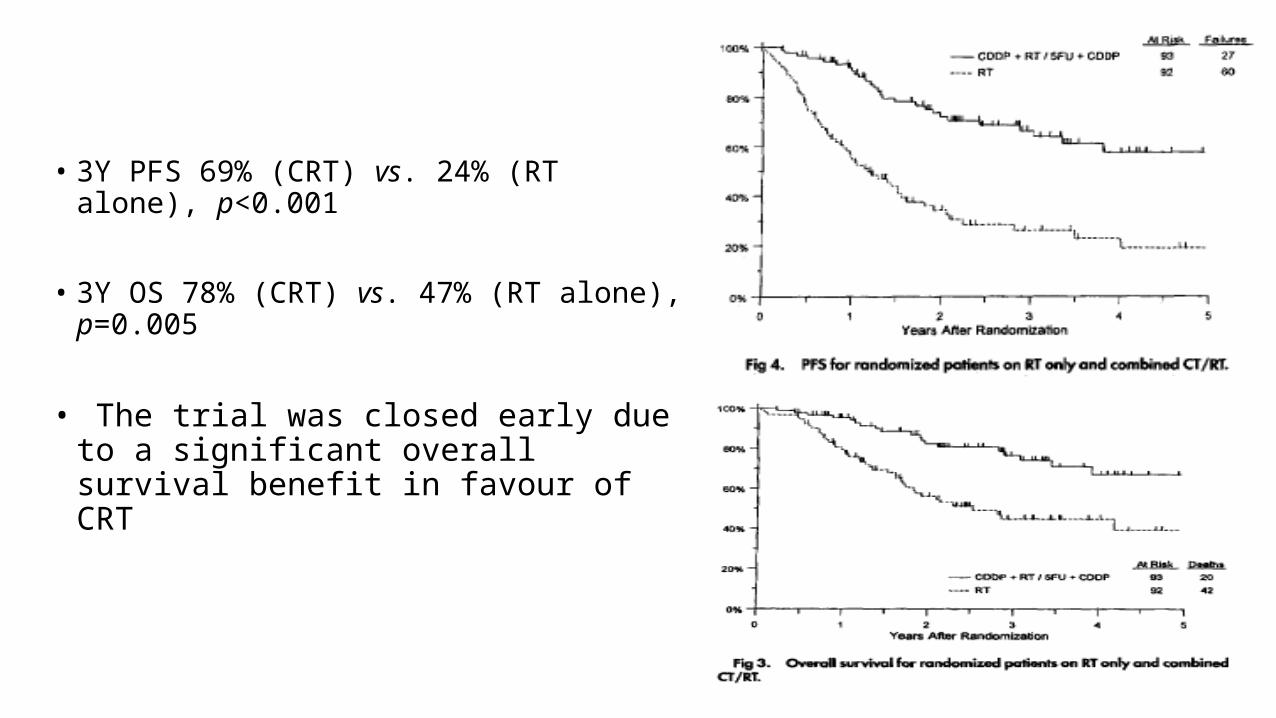
• 3Y PFS 69% (CRT) vs. 24% (RT alone), p<0.001
• 3Y OS 78% (CRT) vs. 47% (RT alone), p=0.005
• The trial was closed early due to a significant overall survival benefit in favour of CRT

5 year update• A 5-year update confirmed progression-free survival (58% vs. 29%) and overall
survival (67% vs. 37%) in favour of CRT
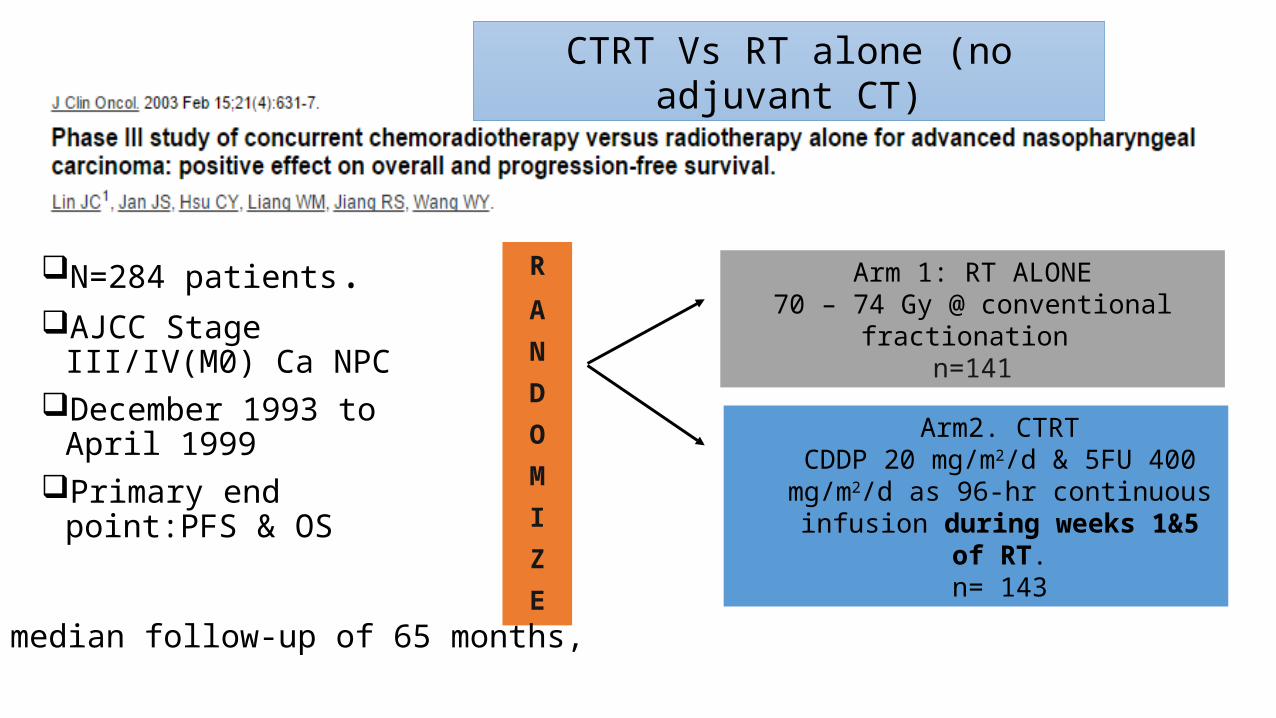
N=284 patients.AJCC Stage III/IV(M0) Ca
NPCDecember 1993 to April
1999Primary end point:PFS & OS
R
ANDOMIZE
Arm2. CTRTCDDP 20 mg/m2/d & 5FU 400
mg/m2/d as 96-hr continuous infusion during weeks 1&5 of RT.
n= 143
median follow-up of 65 months,
CTRT Vs RT alone (no adjuvant CT)
Arm 1: RT ALONE70 – 74 Gy @ conventional fractionation
n=141
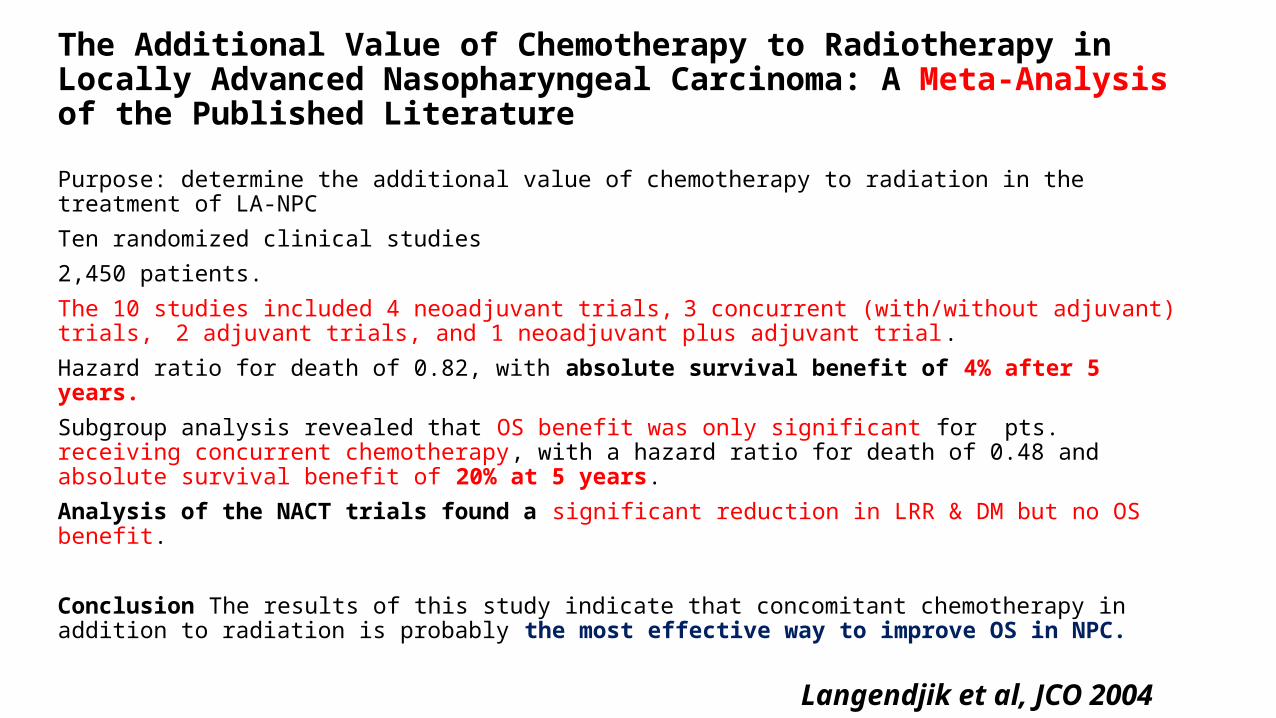
The Additional Value of Chemotherapy to Radiotherapy in Locally Advanced Nasopharyngeal Carcinoma: A Meta-Analysis of the Published Literature
Purpose: determine the additional value of chemotherapy to radiation in the treatment of LA-NPC Ten randomized clinical studies 2,450 patients. The 10 studies included 4 neoadjuvant trials, 3 concurrent (with/without adjuvant) trials, 2 adjuvant trials, and 1 neoadjuvant plus adjuvant trial. Hazard ratio for death of 0.82, with absolute survival benefit of 4% after 5 years.Subgroup analysis revealed that OS benefit was only significant for pts. receiving concurrent chemotherapy, with a hazard ratio for death of 0.48 and absolute survival benefit of 20% at 5 years.Analysis of the NACT trials found a significant reduction in LRR & DM but no OS benefit.
Conclusion The results of this study indicate that concomitant chemotherapy in addition to radiation is probably the most effective way to improve OS in NPC.
Langendjik et al, JCO 2004
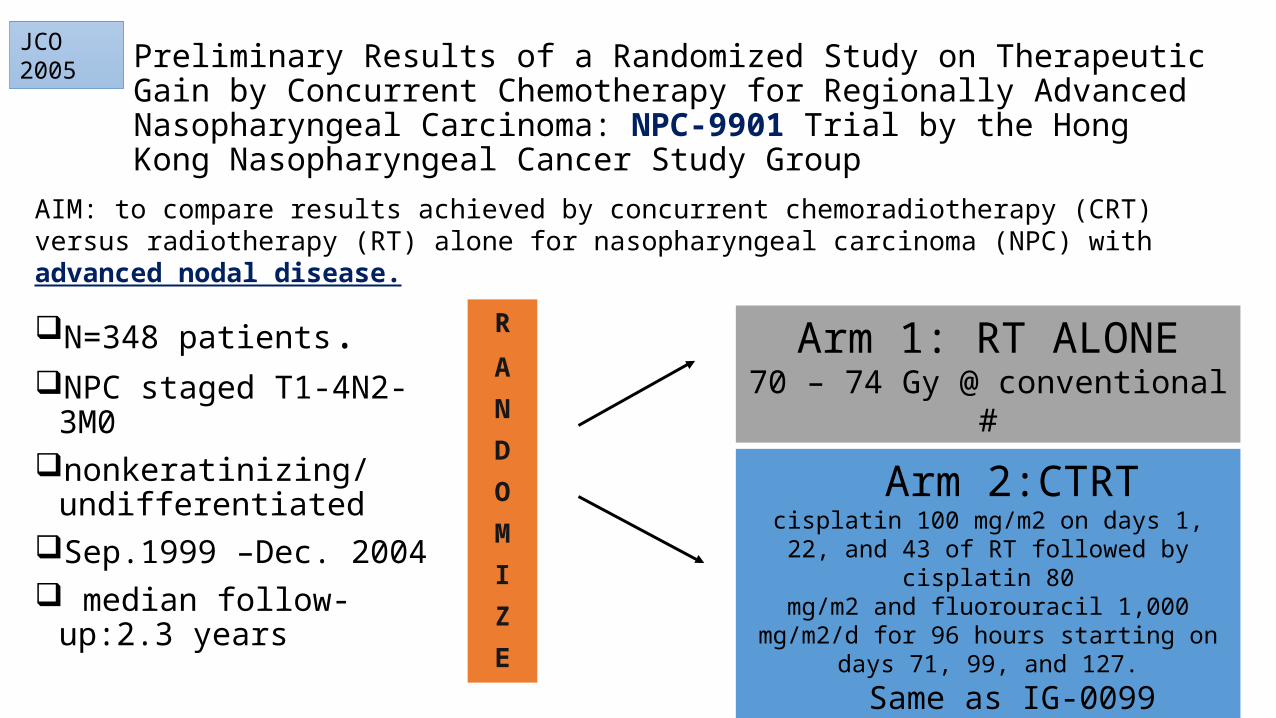
N=348 patients.NPC staged T1-4N2-3M0nonkeratinizing/
undifferentiated Sep.1999 –Dec. 2004 median follow-up:2.3 years
Preliminary Results of a Randomized Study on Therapeutic Gain by Concurrent Chemotherapy for Regionally Advanced Nasopharyngeal Carcinoma: NPC-9901 Trial by the Hong Kong Nasopharyngeal Cancer Study Group
R
ANDOMIZE
Arm 2:CTRTcisplatin 100 mg/m2 on days 1, 22, and 43 of RT
followed by cisplatin 80mg/m2 and fluorouracil 1,000 mg/m2/d for 96
hours starting on days 71, 99, and 127.Same as IG-0099
Arm 1: RT ALONE70 – 74 Gy @ conventional #
JCO 2005
AIM: to compare results achieved by concurrent chemoradiotherapy (CRT) versus radiotherapy (RT) alone for nasopharyngeal carcinoma (NPC) with advanced nodal disease.
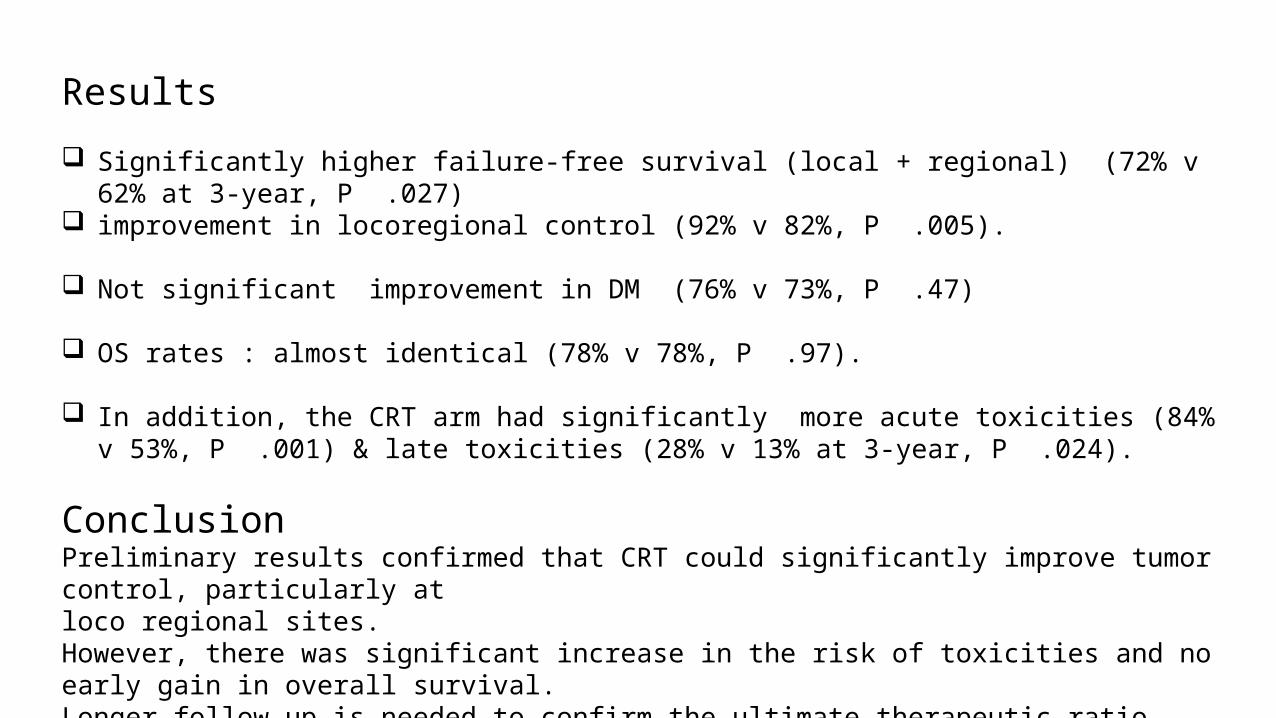
Results
Significantly higher failure-free survival (local + regional) (72% v 62% at 3-year, P .027) improvement in locoregional control (92% v 82%, P .005).
Not significant improvement in DM (76% v 73%, P .47)
OS rates : almost identical (78% v 78%, P .97).
In addition, the CRT arm had significantly more acute toxicities (84% v 53%, P .001) & late toxicities (28% v 13% at 3-year, P .024).
ConclusionPreliminary results confirmed that CRT could significantly improve tumor control, particularly atloco regional sites.However, there was significant increase in the risk of toxicities and no early gain in overall survival. Longer follow-up is needed to confirm the ultimate therapeutic ratio.

OBJECTIVE:To study the effect of adding CT to RT on OS & EFS for patients with NPC8 trials, 1753 pts median follow-up was 6 yearsHR for death=0.82 (95% CI 0.71-0.95p = 0.006)) corresponding to 6% absolute survival benefit at 5 years
from the addition of chemotherapy (from 56% to 62%). HR for tumor failure or death was 0.76 (95% confidence interval, 0.67-0.86; p < 0.0001), corresponding to
an absolute EFS benefit of 10% at 5 years from the addition of chemotherapy (from 42% to 52%). A significant interaction was observed between the timing of chemotherapy and overall survival (p =
0.005), explaining the heterogeneity observed in the treatment effect (p = 0.03), with the highest benefit resulting from concomitant chemotherapy.
Greatest benefit from concurrent chemo Baujat, IJROBP, 2006
H=0.60 (concurrent) HRR=0.97 (adjuvant) HR=0.99 (induction)
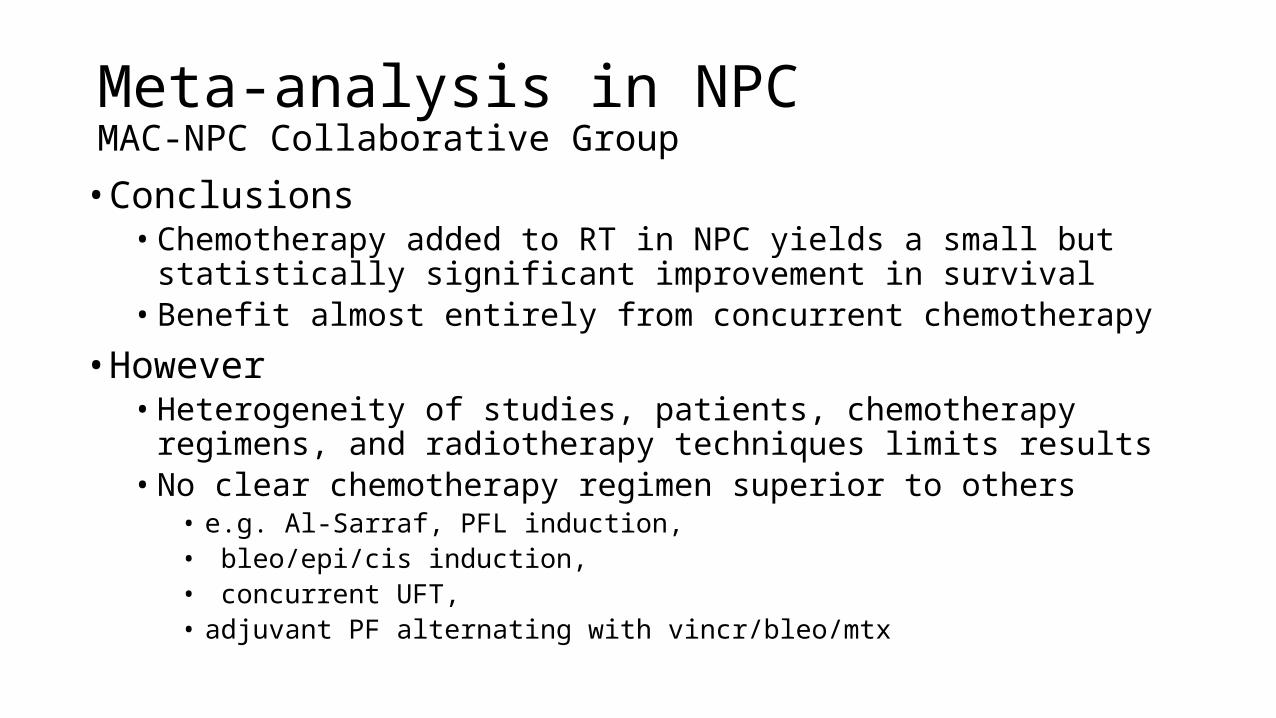
Meta-analysis in NPCMAC-NPC Collaborative Group
• Conclusions• Chemotherapy added to RT in NPC yields a small but statistically significant
improvement in survival• Benefit almost entirely from concurrent chemotherapy
• However• Heterogeneity of studies, patients, chemotherapy regimens, and radiotherapy
techniques limits results• No clear chemotherapy regimen superior to others
• e.g. Al-Sarraf, PFL induction,• bleo/epi/cis induction,• concurrent UFT, • adjuvant PF alternating with vincr/bleo/mtx

N=189 patients. NPC (T3-T4, N0-1, M0)Sep. 1999 and April 2004 median follow-up:2.9 yearstrial terminated early
because of slow accrual
R
ANDOMIZE
(i) conventional fractionation (CF) alone > or =66 Gy at 2 Gy/#,5#/week
IJROBP 2006
AIM: To compare the benefit achieved by concurrent chemoradiotherapy (CRT) and/or accelerated fractionation (AF) vs. radiotherapy (RT) alone with conventional fractionation (CF) for patients with T3-4N0-1M0 NPC.
(ii) Accelerated fractionation (AF) alone > or =66 Gy at 2 Gy/# 6 #/week
(iii) CF with concurrent chemotherapy Intergroup 0099 regimen
( (iv) AF with concurrent chemotherapy Intergroup 0099 regimen .

RESULTS:
When compared with the CF arm, both the AF arm and the CF+C arm were insignificant (p > or = 0.38).
significant improvement in failure-free survival (FFS) was achieved by the AF+Chemotherapy arm (94% vs. 70% at 3 years, p = 0.008)
Multivariate analyses showed that CRT was a significant factor: hazard ratio (HR) = 0.52 (0.28-0.97), AF per se was insignificant: HR = 0.68 (0.37-1.25);Interaction of CRT by AF was strongly significant (p = 0.006).
TOXICITY: Both CRT arms had significant increase in acute toxicities (p < 0.005), AF+C arm also incurred increase in late toxicities (34% vs. 14% at 3 years, p = 0.05).
CONCLUSIONS:Preliminary results suggest that concurrent chemoradiotherapy with accelerated fractionation could significantly improve tumor control when compared with conventional RT alonefurther confirmation of therapeutic ratio is warranted
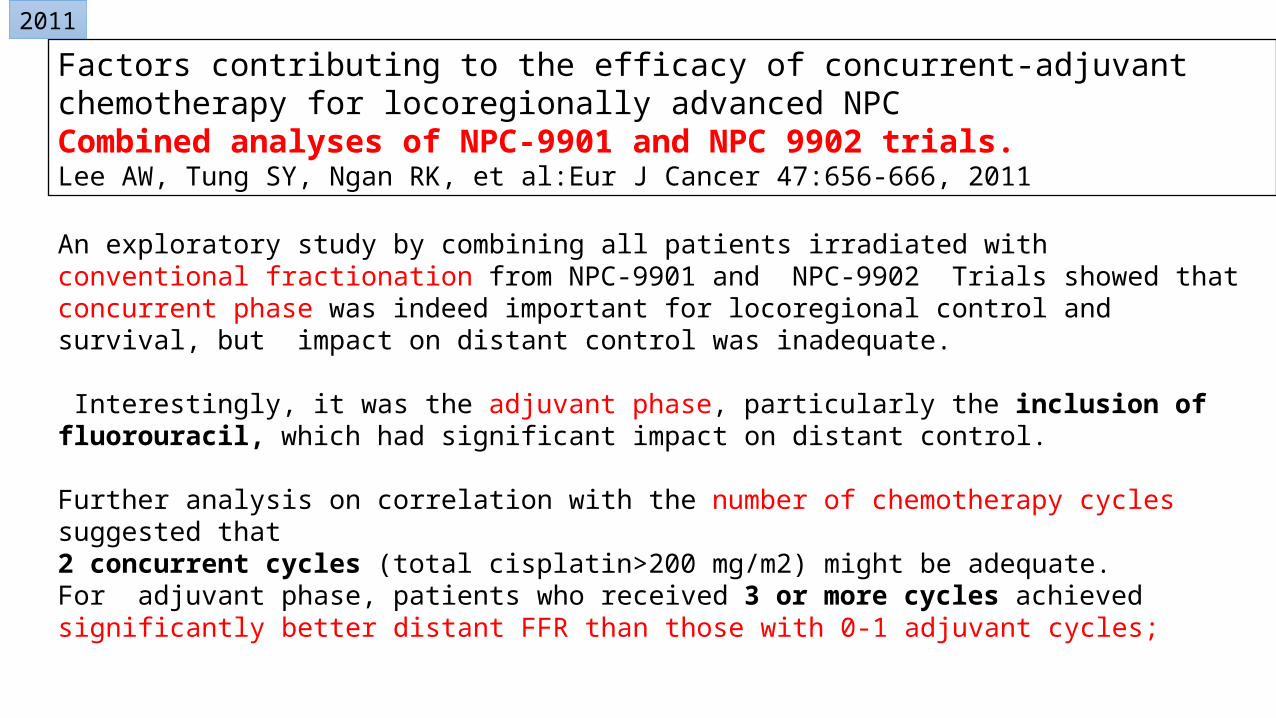
An exploratory study by combining all patients irradiated with conventional fractionation from NPC-9901 and NPC-9902 Trials showed thatconcurrent phase was indeed important for locoregional control and survival, but impact on distant control was inadequate.
Interestingly, it was the adjuvant phase, particularly the inclusion of fluorouracil, which had significant impact on distant control.
Further analysis on correlation with the number of chemotherapy cycles suggested that 2 concurrent cycles (total cisplatin>200 mg/m2) might be adequate.For adjuvant phase, patients who received 3 or more cycles achieved significantly better distant FFR than those with 0-1 adjuvant cycles;
Factors contributing to the efficacy of concurrent-adjuvant chemotherapy for locoregionally advanced NPCCombined analyses of NPC-9901 and NPC 9902 trials. Lee AW, Tung SY, Ngan RK, et al:Eur J Cancer 47:656-666, 2011
2011
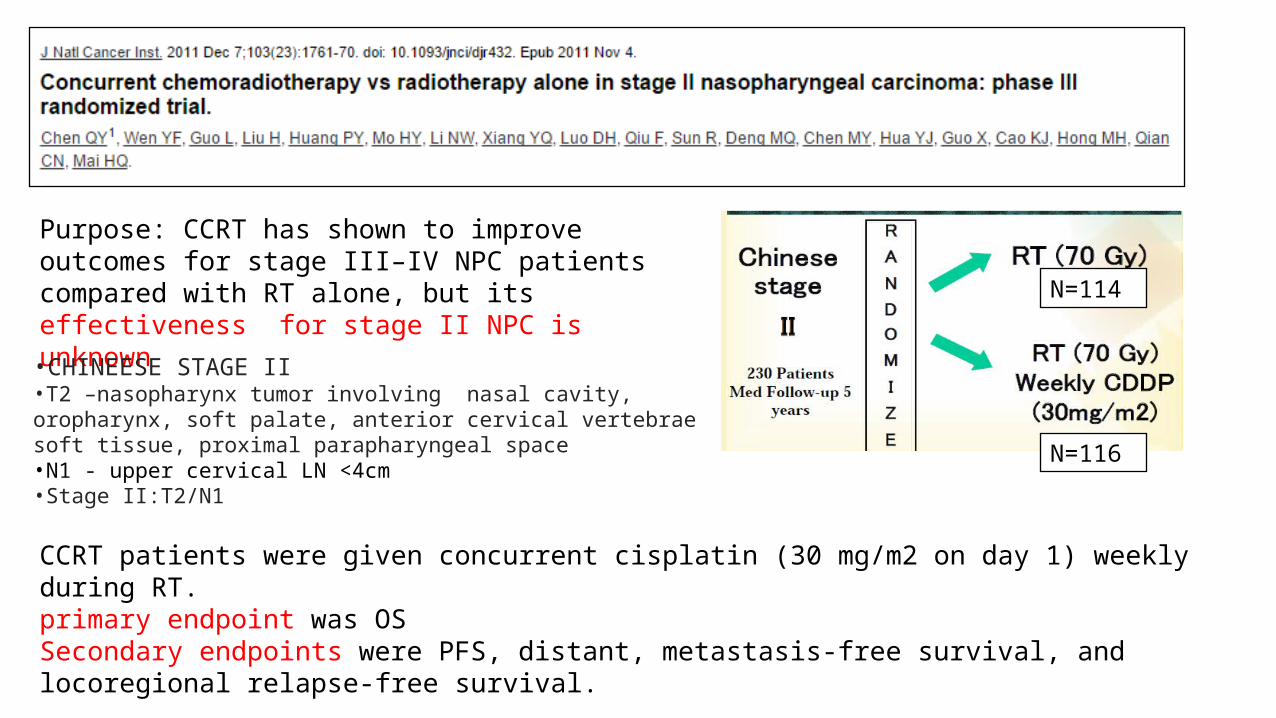
Purpose: CCRT has shown to improve outcomes for stage III–IV NPC patients compared with RT alone, but its effectiveness for stage II NPC is unknown
CCRT patients were given concurrent cisplatin (30 mg/m2 on day 1) weekly during RT.primary endpoint was OSSecondary endpoints were PFS, distant, metastasis-free survival, and locoregional relapse-free survival.
N=114
N=116
•CHINEESE STAGE II•T2 –nasopharynx tumor involving nasal cavity, oropharynx, soft palate, anterior cervical vertebrae soft tissue, proximal parapharyngeal space•N1 - upper cervical LN <4cm•Stage II:T2/N1
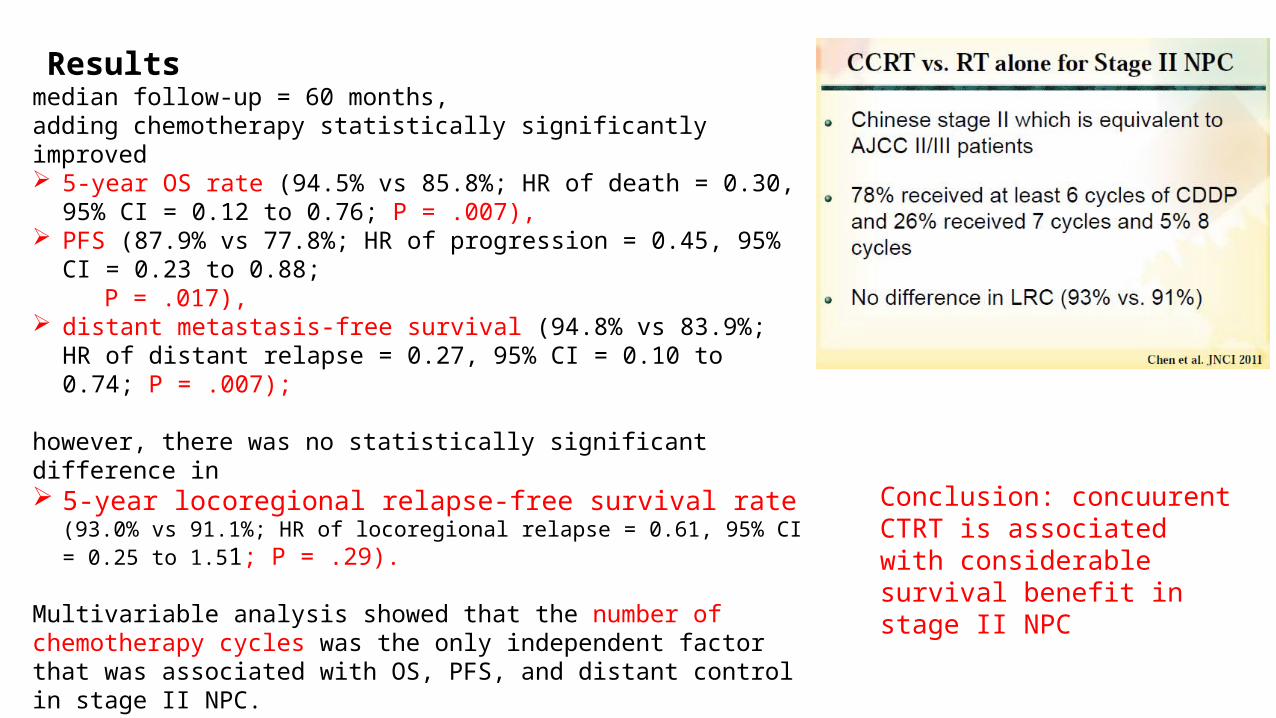
Results median follow-up = 60 months, adding chemotherapy statistically significantly improved 5-year OS rate (94.5% vs 85.8%; HR of death = 0.30, 95% CI = 0.12 to 0.76;
P = .007), PFS (87.9% vs 77.8%; HR of progression = 0.45, 95% CI = 0.23 to 0.88; P = .017), distant metastasis-free survival (94.8% vs 83.9%; HR of distant relapse =
0.27, 95% CI = 0.10 to 0.74; P = .007);
however, there was no statistically significant difference in 5-year locoregional relapse-free survival rate (93.0% vs 91.1%; HR of
locoregional relapse = 0.61, 95% CI = 0.25 to 1.51; P = .29).
Multivariable analysis showed that the number of chemotherapy cycles was the only independent factor that was associated with OS, PFS, and distant control in stage II NPC.
The CCRT arm experienced statistically significantly more acute toxic effects (P = .001), although the rate of late toxic effects did not increase statistically significantly.
Conclusion: concuurent CTRT is associated with considerable survival benefit in stage II NPC

One strategy to further improve the efficacy of chemotherapy is to use an induction-concurrent sequence.
Advantages of Induction chemotherapy better tolerated than adjuvant chemotherapy;early use of a potent combination of cytotoxic drugs at full dose may eradicate micrometastases. can shrink primary tumor to give a wider margin for irradiation, can save adjacent critical neural structures during RT
INDUCTION CHEMOTHERAPY

MRI showing shrinkage of primary tumor by induction chemotherapy before proceeding to concurrent chemoradiotherapy. (From Lee AW, Lau KY, Hung WM, et al. Potential improvement of tumor control probability by induction chemotherapy for advanced nasopharyngeal carcinoma. Radiother Oncol. 2008;87(2):204–210, with permission from Elsevier.)
Lee et al showed that 3 cycles of IC(cisplatin+5FU) could significantly reduce the primary GTV by an average of 61%, leading to significant increase in the minimum tumor dose & consequent improvement in the estimated tumor control probability (P= 0.002).

Currently, there are 3 ongoing randomized trials to evaluate this strategy.
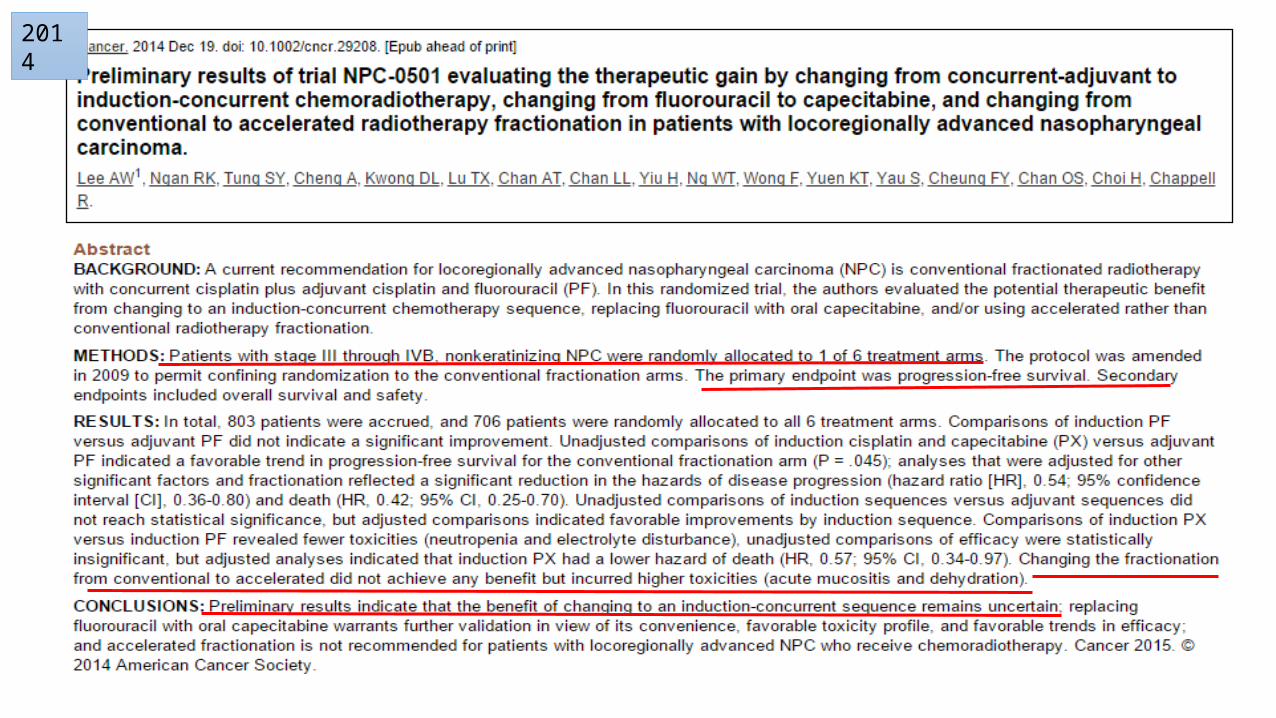
The NPC-0501 Trial aims to compare the benefit of changing the chemotherapy sequence from concurrent- adjuvant chemotherapy (the Intergroup-0099 regimen)to induction-concurrent and RT fractionation from conventional to accelerated.
The GORTEC-NPC2006 Trial aims to compare concurrent CRT at conventional fractionation versus CRT plus induction chemotherapy (docetaxel,cisplatin, and fluorouracil).
A third randomized trial from Singapore also tests the benefits of induction chemotherapy in the setting of concurrent chemoradiation.
The results from these trials will provide valuable data for future direction
2014

THANKYOU







