
1
Help patients with immunotherapy designed to reduce risk of GVHD in stem cell transplantations
Unlock full potential of haploidentical hematopoietic stem cell transplantations (HSCT), with allo-depleted T-cell product ATIR
Company presentation, February 25, 2018
Amsterdam, The NetherlandsEuronext (KDS)
Disclaimer
These slides and the accompanying oral presentation contain forward-looking statements and information. Forward-looking statements are subject to known and unknown risks, uncertainties, and other factors that may cause our or our industry’s actual results, levels or activity, performance or achievements to be materially different from those anticipated by such statements. The use of words such as “may”, “might”, “will”, “should”, “could”, “expect”, “plan”, “anticipate”, “believe”, “estimate”, “project”, “intend”, “future”, “potential” or “continue”, and other similar expressions are intended to identify forward looking statements. For example, all statements we make regarding (i) the initiation, timing, cost, progress and results of our preclinical and clinical studies and our research and developmentprograms, (ii) our ability to advance product candidates into, and successfully complete, clinical studies, (iii) the timing or likelihood of regulatory filings and approvals, (iv) our ability to develop, manufacture and commercialize our product candidates and to improve the manufacturing process, (v) the rate and degree of market acceptance of our product candidates, (vi) the size and growth potential of the markets for our product candidates and our ability to serve those markets, and (vii) our expectations regarding our ability to obtain and maintain intellectual property protection for our product candidates, are forward looking. All forward-looking statements are based on current estimates, assumptions and expectations by our management that, although we believe to be reasonable, are inherently uncertain. All forward-looking statements are subject to risks and uncertainties that may cause actual results to differ materially from those that we expected. Any forward-looking statement speaks only as of the date on which it was made. We undertake no obligation to publicly update or revise any forward-looking statement, whether as a result of new information, future events or otherwise, except as required by law. This presentation is not, and nothing in it should be construed as, an offer, invitation or recommendation in respect of our securities, or an offer, invitation or recommendation to sell, or a solicitation of an offer to buy, any of our securities in any jurisdiction. Neither this presentation nor anything in it shall form the basis of any contract or commitment. This presentation is not intended to be relied upon as advice to investors or potential investors and does not take into account the investment objectives, financial situation or needs of any investor.
2

Novel cell therapies establishing themselves
3
Selected companies Product Status Company valuation
Kymriah(list price $475,000)
FDA approved
Yescarta(list price $373,000)
FDA approved $11.9bn 8/2017 acquisition by Gilead
liso-celPotential FDA filing 2H 2018
$9.0bn 1/2018 offer by Celgene
darvadstrocelEMA positive CHMP opinion
$596M12/2017 acquisition by Takeda
tabelecleucel Phase 3 $1.7bn* market capitalization 1/2018 $128m capital raise
* As of market close February 13, 2018

The very first cell therapy: allogeneic HSCT
Allogeneic Hematopoietic Stem Cell Transplantation (HSCT):
• Curative intent: replace disease blood/immune system with healthy one from donor
• Risk of Graft versus Host disease (GVHD): Donor immune system attacks the patient
• Mostly blood cancers (85%) and adults (82%)
4
Adoption of HSCT
limited by high risk
Blood cancers: Only 20-30% long term GVHD-Free and
Relapse-Free Survival (GRFS)
Inherited blood disorders or autoimmune disease:
Risk of replacing chronic disease with (chronic) GVHD
AML, 39%(early AML 21%,advanced AML 12%,transformed AML 6%)
CML, 2%
MDS/MPN, 12%MPN, 35%
ALL, 16%
Others, 1%AID, 0.1%
IDM, 0.8%PID, 3%
Thal/sickle, 3%
CLL, 2%
HD, 3%
NHL, 4%
PCD, 7.1%
Solid tumors, 0.2%BMF, 5%
Source: Solh 2017; McCurdy 2017; Broder 2017; Passweg 2017; CIBMTR 2016 summary slides; Besse 2015
MPN, 3%
Disease indications for allogeneic HSCT in Europe in 2015

Kiadis: aim to enable HSCT with reduced risk of GVHD
5
FUNDAMENTALLY
SAFER HSCT
CLOSE TO
MARKET
STRONG PATIENT
BENEFIT
PLATFORM FOR
GROWTH
• ATIR allo-depleted T-Cell product, given after HSCT, designed to
reduce risk of GVHD, can unlock full HSCT potential
• Improvement in GVHD-Free and Relapse-Free Survival (GRFS) vs.
literature for PTCy/Baltimore protocol
• EMA potential approval 4Q18 (CHMP); Potential initial EU launch 2H19; FDA RMAT ‘breakthrough’ designation; Phase 3 enrolling
• Potential >27,900 target patients per year; Sustainable;
Attractive economics vs. CAR-T
• Ability to leverage cell therapy infrastructure: manufacturing,
supply chain, medical, commercial
ATTRACTIVE BUSINESS
OPPORTUNITY

HSCT challenge: give potent donor T-cells, yet avoid GVHD
Protect against viruses and tumor cells
Attack patient tissue
Donor stem cells (CD34+)
Source: Walker 2004
The ‘holy grail’ of HSCT: Give donor T-cells that protect
Remove donor T-cells that attackAvoid immunosuppressants
6
Donor T-cells (CD3+)
Immunosuppressants(reduce GVHD, but
hamper engraftment and protection)
Stem cells engraft in patient bone marrow: create blood and immune system
But, stem cells alone not enough: T-cells take 6-12 months to re-emerge from stem cells; survival without T-cells 10-20%

Graft Versus Host Disease (GVHD): a terrible disease
Types Acute: can be life threatening (grade III/IV) Chronic: can be severely debilitating
Organs Skin, mouth, eyes, liver, GI tract, lungs
Manifestations Scleroderma, rash, ulceration, erythema, cirrhosis, immunodeficiency
EffectsSkin disease, infections, muscle constriction, bone loss, pulmonary disease, thyroid disfunction, ophthalmology, solid tumors, sleep deprivation, depression
Treatment Immunosuppression (steroids, MMF, MTX)
Subpopulation of mature T-cells from donor attack antigenically foreign antigens on patient tissues, due to
genetic differences between patient and donor (MHC Class II proteins)
Source: Jones 2016; Koreth 2013 7MMF: mycophenolate mofetilMTX: methotrexate
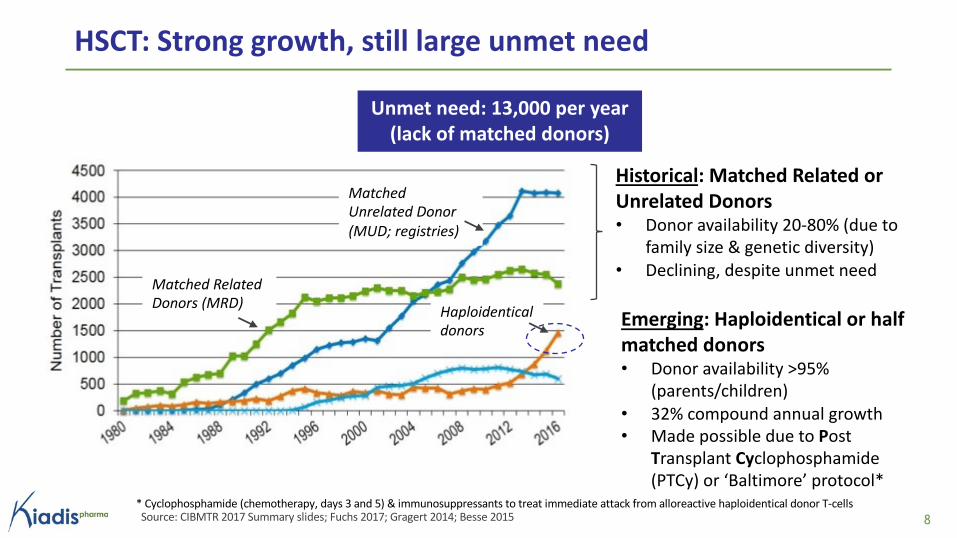
HSCT: Strong growth, still large unmet need
8Source: CIBMTR 2017 Summary slides; Fuchs 2017; Gragert 2014; Besse 2015
Historical: Matched Related or Unrelated Donors• Donor availability 20-80% (due to
family size & genetic diversity)• Declining, despite unmet need
Emerging: Haploidentical or half matched donors• Donor availability >95%
(parents/children)• 32% compound annual growth• Made possible due to Post
Transplant Cyclophosphamide (PTCy) or ‘Baltimore’ protocol*
Haploidentical donors
Matched Unrelated Donor (MUD; registries)
Matched Related Donors (MRD)
Unmet need: 13,000 per year (lack of matched donors)
* Cyclophosphamide (chemotherapy, days 3 and 5) & immunosuppressants to treat immediate attack from alloreactive haploidentical donor T-cells

Haplo PTCy/Baltimore vs MUD: improved GVHD, worse relapse
9
* Not a ‘true’ average: Mix of indications (AML, NHL, HL), follow up (1.5, 2 and 3 yr) and patient populations; analysis based on ratio within each of the publications in the review paper shows similar resultsSource: Fuchs E 2017
38%
53%
38%
51%
26% 27%
45%49%
'Average'MatchedUnrelated Donor
'Average'Haploidentical(PTCy)*
Acute GVHD II-IV
Chronic GVHD
Relapse Survival
Post Transplant Cyclophosphamide (PTCy or Baltimore protocol): Trigger immediate ‘GVHD attack’ by activation of half-matched donor T-cells in the patient, treated with chemotherapy on days 3&5 and immunosuppressants
• Lower GVHD for PTCy than MUD (ie effective depletion of alloreactive T-cells)
• Higher relapse for PTCy than MUD (ie also depleting protective T-Cells)
MUD: Matched Unrelated Donor

Haplo HSCT 30 days after Haplo HSCT
GVHD Treatment/Prophylaxis Approach
KiadisT-cell depleted (‘safe’ stem cells)
ATIR: subset of T-cells, depleted of alloreactive T-cells (‘safe’ T cells)
No prophylactic immunosuppressant
PreventGVHD
PTCy or Baltimore protocol
T-cell replete (stem cells plus all T-cells)
Chemo (cyclophosphamide) & immunosuppressants to treat immediate attack from alloreactive donor T-cells
TreatGVHD
Kiadis: potential improvement versus PTCy/Baltimore
Kiadis: reduce risk of GVHD: give T-cells that protect; not T-cells that attack
10Table provided for illustrative purposes, not for direct comparison
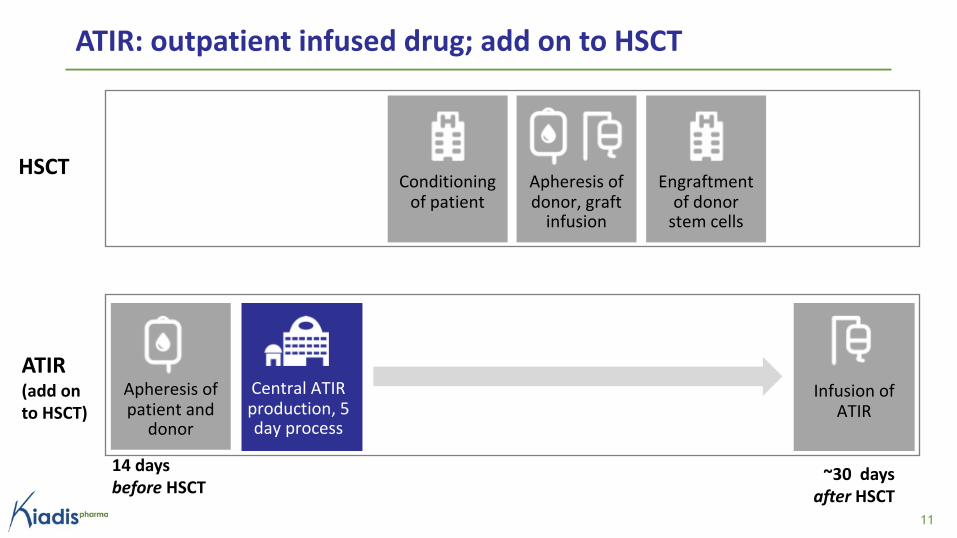
ATIR: outpatient infused drug; add on to HSCT
Apheresis of patient and
donor
Infusion of ATIR
Central ATIR production, 5 day process
14 days before HSCT
~30 days after HSCT
11
Conditioning of patient
Apheresis of donor, graft
infusion
Engraftment of donor
stem cells
ATIR (add on to HSCT)
HSCT

ATIR production: subset of T-cells that protect, but not attack
Step 1 (Day 1–4)
Patient cells inactivated by radiation
Healthy donor
Patient
Immune cells are collected and mixed
Step 3 (Day 5)Step 2 (Day 5)donor
patient
```
ATIR: remaining potent non-
alloreactive donor T-cells, infused on
day 28-32 after HSCT
Add TH9402*, which accumulates only in
activated T-cells (MDR pump is switched off in
activated T-cells)
*TH9402 – proprietary selective rhodamine derivative, modified to become cytotoxic under green light
Mix patient cells & haplo donor T-cells: alloreactive donor
T-cells become activated (Mixed
Lymphocyte Reaction)
Expose to green light: TH9402* induces
apoptosis: activated and thus alloreactive
T-cells are killed
Protect: Retain protective T-cells to fight relapse and infections
& Not attack: Reduce risk of GVHD by depleting alloreactive T-cells ex vivo
12

ATIR production: fast & simple, own facility secured
13
ü 5 day process
ü No genetic engineering (No viral vector production/transfection)
ü Clean rooms with LAF cabinets (No BL2; No bioreactors)
ü 42 hour hold time for ingoing material, final product frozen down
ü Own commercial manufacturing facility secured (lease)
Lower COGS per batch and capex compared to e.g. CAR-T

ATIR: Past and current clinical trials in blood cancers
14
Phase 1 Phase 2 Phase 3
CR-GVH-001• Dose finding • 19 patients; Complete
CR-AIR-006• Historic observational cohort
(control)• 35 patients; Complete
CR-AIR-009• Randomized/controlled• 195 patients; Enrolling
CR-AIR-007• Open label single arm efficacy • 23 patients; Complete
CR-AIR-008• 9 patients only 1st dose; 6
patients also 2nd dose • 15 patients; Enrolment complete
ATIR as add on to haploidential CD34+ HSCTAML/ALL/MDS

Phase 2 (007): potent T-cell product, yet low GVHD (1 yr)
• no acute grade III/IV
• 3 acute grade II (13%)• 1 chronic (4%)
007: Haplo CD34+ plus single dose ATIR
• Open label single arm 2013-18
• 23 AML/ALL patients receiving ATIR (MITT)
• 4 sites Canada/EU
• Dose 2 million cells/kg*
006: Haplo CD34+
• Historical observational cohort 2006-13
• 35 patients, similar indications/sites
• Protocol based on EMA scientific advice
Low GVHD due to ATIR
2 million cells/kg of potent T-cells:
increasing survival 3x, yet
low GVHD**
No need for prophylactic immunosuppression
15* Non allodepleted donor lymphocyte infusion can cause severe GVHD at 10,000 cells/kg
Improved Overall Survival due to ATIR
CD34+ stem cells
with ATIR
CD34+ stem cells
without ATIR
3x
61%
20%

0% 0%
4%5%
8%**
24%
Acute
GVHD III/IV
Chronic
GVHD
Severe
Chronic
GVHD
Phase 2 (007): relapse & GVHD vs literature for PTCy (1 yr)
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials* PTCy: Relapse: of which 11% relapsed and 18% relapsed and died
** Solomon 2012; Ciurea 2012; Esquirol 2016
*** Ciurea 2015; Piemontese 2017, Solomon 2012, Ciurea 2012; Devillier 2016; Di Stasi 2014; Esquirol 2016; Sugita 2015
**** Ciurea 2015; McCurdy 2017, Devillier 2016, Sugita 2015 (normalization based on Armand 2014); DRI CR-AIR-AIR-007: 53% high/47% intermediate
Overall SurvivalATIR Phase 2, 007
(MITT, n=23)
PTCy/Baltimore
Literature, at least 50%
AML/ALL*** (n=571)
Relapse and NRM*
9%
30%29%
22%
Relapse Non Relapse
Mortality
PTCy: results from
EBMT/CIBMTR databases,
Johns Hopkins (Baltimore)
and Northside (Atlanta)
61% 60%57%
Overall Survival
PTCy/Baltimore
Literature, adjusted for
DRI**** (n=561)
GVHD
16
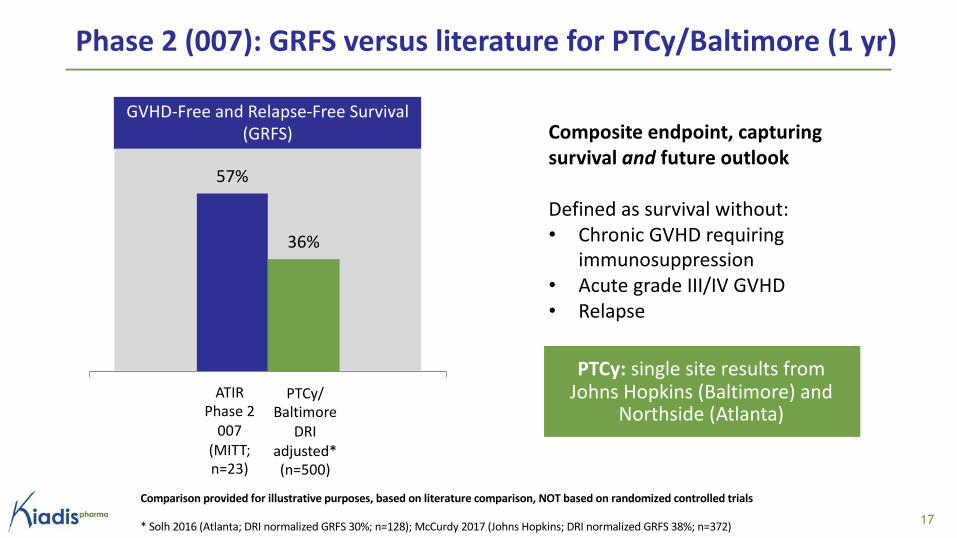
Phase 2 (007): GRFS versus literature for PTCy/Baltimore (1 yr)
GVHD-Free and Relapse-Free Survival (GRFS) Composite endpoint, capturing
survival and future outlook
Defined as survival without:• Chronic GVHD requiring
immunosuppression• Acute grade III/IV GVHD• Relapse
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials
* Solh 2016 (Atlanta; DRI normalized GRFS 30%; n=128); McCurdy 2017 (Johns Hopkins; DRI normalized GRFS 38%; n=372)
57%
36%
GRFSATIR Phase 2
007 (MITT; n=23)
PTCy/ Baltimore
DRI adjusted* (n=500)
PTCy: single site results from Johns Hopkins (Baltimore) and
Northside (Atlanta)
17

Future options for patients: ATIR after CD34+ or after PTCy
18
Stem cells (CD34+; Phase 2)
PTCy/ Baltimore
(literature*)
+ ATIR20%
+ATIR ?57%
61%
future study
Overall Survival (OS) GVHD
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials
* Ciurea 2015; McCurdy 2017, Devillier 2016, Sugita 2015 (normalization based on Armand 2014); DRI CR-AIR-AIR-007: 53% high/47% intermediate

Filed in EU & received ‘breakthrough’ in US, based on Phase 2
* Various hemato-oncology products EMA (conditionally) approved based on Phase 2, e.g., Zalmoxis (MolMed, 36 patients, versus matched historical control), Blincyto, Venclexta, Bosulif
EMA (EU)
Marketing Authorization Application filed, potential (conditional) approval Q4 2018
• ATMP certificate for quality and non-clinical data in 2015
• Pediatric Investigation Plan agreed
• Phase 2 and historical control accepted for filing and review*
• Day 120 questions received, adequate response end Q1 2018
FDA (US)
Regenerative Medicine Advanced Therapy designation received (same benefits as Breakthrough)
• Increased access to FDA (not limited to customary timepoints)
• Possibility for priority/rolling review of BLA
• Development support (program/endpoints)
19

Objectives: demonstrate superior clinical benefit and collect pharmacoeconomical data (cost, days in hospital, incidence of severe infections and quality of life)
Phase 3 (009): ATIR vs. PTCy/Baltimore protocol
R
RandomizedControlled(1:1)
HSCT plus ATIR: CD34+ HSCT + single dose ATIR101
PTCy/Baltimore protocol: post-HSCT cyclophosphamide & immunosuppressant
Primary endpoint: GVHD-Free and Relapse-Free Survival (GRFS**)
Secondary endpoints: OS, Progression Free Survival, Relapse Related Mortality, Transplant Related Mortality
Event driven:Primary analysis at 93 GRFS events, Interim analysis at half GRFS events
195 patients* with acute leukemia or MDS40-50 sites in US, Canada and EU
Aligned with FDA and regulators in EU; Enrolling patients
* 80% powered to detect 20% GRSF difference; 15% difference will be statistically significant; allowed under protocol to increase sample size; 245 pts would give 80% power to detect 18% difference** Survival without chronic GVHD requiring immunosuppression, acute grade III/IV GVHD or relapse 20

ATIR potential: target >27,900 annual patients US/EU
* EU Not Known; ** EU 2000, US 900Provided for illustrative purposesSource: CIBMTR summary slides 2017, Passweg 2017, Besse 2015;
21
TBD
12,000
13,000 (US*)
2,900
Haploidentical transplants 2016**
Unmet need(lack of matched
donors)
Matched Unrelated Donor
Blood disorders, auto-immune
disease
Potential haploidentical
transplants
Growth haploidentical HSCT: Historic 32% compound annual growth with PTCy; potential for acceleration upon increased benefits of ATIR
>27,900

1 in 3
1 in 12
1 in 4Overallchronic GVHD
SeverechronicGVHD
Relapse
Reduce risk of (severe) GVHD and relapse
22
Death• 50% five year mortality for
severe chronic GVHD
Quality of life• QALY loss: 27% for severe
GVHD (up to 68%) and 20% for
moderate GVHD *
• Quality of life with severe
GVHD worse than vision
impairment, MS, loss of
arm/leg, diabetes
• Impact on patients, donors,
families, physicians
Loss of income• 75% of patients lose 3 years of
earnings
• 25% of patients permanently
lose earnings
Risk with PTCy Risk with ATIR
1 in 28
1 in 9
0

ATIR market survey 100 US/EU KOLs (2013)
Note: Needs to be updatedSource: ATIR Assessment, September 2013 by Defined Health, based on Phase 1 data: 100 transplant physicians/KOLs (50/50 US/EU; eg Harvard, Johns Hopkins, MD Anderson, Stanford, Dresden, Saint Antoine)
In what percent of your haplo’swould you use ATIR given strong
Phase 3 data and formal approval?
It’s got to show an advantage over PTCysomewhere. I’m not saying necessarily
superiority of survival but even if there’s a
superiority in terms of infection rate, it’s got to show that it’s better in
some respect
EU
US
23
““55%
58%

ATIR potential reimbursement: drug, separate from HSCT
24
ATIR (Medicare: Part B, J-code)
• Outpatient infused drug (~30 days after HSCT, 1-2 weeks after end of hospitalization); no hospitalization for infusion*
• Cost of drug billed to payer (‘buy & bill’, mark up for physician); Apheresis reimbursed via procedure code or bundled into ATIR
• Examples: Checkpoint inhibitors
HSCT(Medicare: MS-DRG-14)
• Covers HSCT procedure, including hospitalizations and follow ups• Additional CD34 selection already routinely reimbursed within DRG • Cost savings to hospital due to reduced use of cyclophosphamide and
AEs (e.g., Hemorrhagic cystitis)
• CAR-T SAEs require hospitalization and thus inpatient/DRG• Source: interviews
Likely differentiated from CAR-T*

ATIR protection: patents, orphan drug, know how
Patents (owned/ licensed)
• Methods for reducing GVHD including composition (P015; October 2021)• More rhodamine derivatives (P019; January 2024)• Improved photodynamic process (P040; February 2036 – if granted)
Orphan drug designation
• US (7 years from launch): for prevention of GVHD or TRM• EU (10 years from launch): for treatment in HSCT regardless of disease,
for treatment of AML, for prevention of GVHD
Proprietary know how
• Manufacturing critical process parameters• Release assays based on critical quality attributes• Cell handling, storage, formulation and shipment• Patient specific supply chain and communication
Biosimilar unfeasible: head to head comparative trial not possible for patient specific cell therapy product
25

Kiadis management: track record commercial/medical/ops
26
Arthur Lahr (April 2017) Chief Executive OfficerChief Strategy Officer Crucell (8 years; head BD, M&A, M&S US/EU); Supervisory Board Sanquin (Dutch blood bank); McKinsey; Unilever
Robbert van HeekerenChief Financial OfficerHead Global Finance & Control Organon
Jan Feijen (April 2017)Chief Operations OfficerEVP Operations J&J Vaccines and VP Manufacturing and Ops J&J Vaccines & Advanced Therapies; VP Crucell Asia; Managing Director Operations Avebe; Gist-Brocades
Andrew Sandler (Oct 2017)Chief Medical OfficerSVP Medical Affairs Medivation; CMO Dendreon and Spectrum Pharma; Bayer; Berlex; Seattle Genetics; Board certified medical oncologist
Karl Hård (Sept 2017)Head IR & communicationsHead investor relations AstraZeneca; 10 years investor relations; 10 years pharma R&D; Assistant Professor chemistry
Margot HoppeGeneral Counsel20+ years in corporate legal,including Gist-Brocades, DSM

Kiadis: company at a glance
• Management track record operations, development and commercial (Crucell, Medivation, J&J, AstraZeneca, Organon, DSM, McKinsey)
• Strong supervisory board (Cipla CEO/Novartis ExCom; Actelion COO, Prosensa/Jerini CFO; Prof Dana Farber)
• Euronext Amsterdam/Brussels, listed in 2015
• Major shareholders (>5%): LSP, Draper Esprit, Alta
• Analysts: Jefferies, Canaccord, Oppenheimer, Chardan, KBC, Kempen, LifeSci
• Market cap: ~$248M / €202M
• 17.5 million shares outstanding
• Raised €40M in equity & debt since June 2017; €77M in/since IPO
27
ORGANIZATION
SHAREHOLDERS
FINANCIALS (February 21, 2018)

Kiadis key (potential) milestones
28
2017
EMA submission of ATIR for marketing authorization approval ✔
First patient enrolled for ATIR Phase 3 ✔
Updates enrollment, regulatory, new clinical sites ✔
FDA Regenerative Medicine Advanced Therapy designation ✔ (extra)
Secured own commercial manufacturing facility (lease) ✔ (extra)
New management and supervisory board members ✔ (extra)
2018
Completion of enrolment of second Phase 2 (CR-AIR-008) ✔
Submission of answers to EMA Day 120 questions (End Q1)
Potential (conditional) EMA approval in EU (CHMP opinion, Q4)
Updates Phase 2 data and Phase 3 enrollment
2019Potential initial commercial launch ATIR in first of EU5 countries (H2)
Initiate trial with ATIR as adjunctive to PTCy
Potential interim read out Phase 3

Kiadis: aim to enable HSCT with reduced risk of GVHD
29
FUNDAMENTALLY
SAFER HSCT
CLOSE TO
MARKET
STRONG PATIENT
BENEFIT
PLATFORM FOR
GROWTH
• ATIR allo-depleted T-Cell product, given after HSCT, designed to
reduce risk of GVHD, can unlock full HSCT potential
• Improvement in GVHD-Free and Relapse-Free Survival (GRFS) vs.
literature for PTCy/Baltimore protocol
• EMA potential approval 4Q18 (CHMP); Potential initial EU launch 2H19; FDA RMAT ‘breakthrough’ designation; Phase 3 enrolling
• Potential >27,900 target patients per year; Sustainable;
Attractive economics vs. CAR-T
• Ability to leverage cell therapy infrastructure: manufacturing,
supply chain, medical, commercial
ATTRACTIVE BUSINESS
OPPORTUNITY

30
‘Practice two things in your dealings with disease: either help or do not harm the patient’
Epidemics, Book I, of the Hippocratic school
‘I will prevent disease whenever I can but I will always look for a path to a cure for all diseases’
Hippocratic oath, Louis Lasagna, Academic Dean of the School of Medicine at Tufts University (1964)

Attachments
31

Additional information
• Competition
• Pricing
• ATIR product characteristics
• Clinical trial information
• Disease Risk Index adjustment for literature comparisons
32

Haplo HSCTHaplo donor T-cell Product (after HSCT)
GVHD Treatment/Prophylaxis (in patient)
Approach to GVHD
ATIR (Kiadis) T-cell depleted
‘Safe’ subset of T-cells, depleted of alloreactive T-cells
No prophylactic immunosuppressant Prevent
Zalmoxis (MolMed)BPX-501 (Bellicum)
T-cell depleted
All T-cells, but engineered with ‘suicide gene’
Eliminate activated T-cells by infusing suicide agent, if GVHD occurs
Treat
PTCy or Baltimore protocol
T-cell replete (All T-cells)
Post Transplant Cyclo-phosphamide & immunosuppressants
Treat
Comparison Kiadis with MolMed/Bellicum
33Table provided for illustrative purposes, not for direct comparison

Patients
Effect of
product* Survival** Relapse NRM
Status
EMA
ATIR
(Kiadis)
Adult
Potential CHMP
Q4 2018
Zalmoxis
(MolMed)Adult
Approval Q4 2016
BPX-501
(Bellicum)Pediatric
Submission 2019
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials
* ATIR 007 MITT data (N=23). Matched historical control for Zalmoxis includes T-cell replete and T-cell deplete, thus effect of product cannot be determined** Leukemia Free Survival for BPX-501 (BPX-501 Overall Survival is 89%, Overall Survival not reported for controls); *** Adults PTCy, pediatric MUD; except for ATIR not DRI adjusted/matchedLow GVHD for all three; 5% Grade III/IV for BPX-501 (resolved after rimiducid) Source: CHMP Assessment report (Zalmoxis); Merli EHA 2017 (BPX-501); Locatelli 2017 (BPX-501)
3.0x
1.1x
29
29
19
21
20
15
42
9
22
5
60
3
20
30
46
22
Competitive overview – available data January 2018 (1 year)
Product (Matched) Historical Control MUD or PTCy***
34
77
57
57
77
34
20
83
51
61

Zalmoxis (MolMed) – EMA filing data and EU pricing
Survival Relapse and NRM
9%
30%
42%
20%
29%
22%
Relapse Non RelapseMortality
61%
51%
60%
Overall Survival
4%7% 6%
5%
24%
AcuteGVHD III/IV
ChronicGVHD
GVHD
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials * CHMP Assessment report (aGVHD III/IV: Kempen 2017 report); CD34+ HSCT; 74% AML; 10% ALL; 16%MDS/NHL/HD; patients receiving Zalmoxis** Ciurea 2015 (CIBMTR); Piemontese 2017 (EBMT), Solomon 2012 (Atlanta), Ciurea 2012; Devillier 2016; Di Stasi 2014; Esquirol 2016; Sugita 2015*** Prices as at 16 January 2018 and 13 December 2017, respectively
ATIR Phase II (007, MITT, n=23)
Zalmoxis (MolMed)Phase II data in EMA filing, n=36*
Zalmoxis pricing/dose*** (1-4 doses per patient):
Germany: €163,900Italy: €149,000
0%
35
PTCy/BaltimoreLiterature, at least 50% AML/ALL** (n=571)

BPX-501 (Bellicum): AML/ALL pediatric (Zhou 2014)
36
Population• Pediatric, aged 3-17, 10 pts• CD34+ HSCT
1 Year data• Survival 80%• Relapse 30%• Non Relapse Mortality 0%
Observations• Low GVHD, at high doses of T
cells (incl. alloreactive T-cells)• 3 out of 4 patients treated with
rimiducid to treat GVHD subsequently died from relapse (day 158, 164, 591)
Infused T cells/kg
aGVHD cGVHD Administration of AP1903
Current status (day after SCT*
1x106 Grade I/II
None Yes Alive, CR (D+1440)
1x106 Grade I None Yes Relapse of ALL (D+552), death D+591
3X106 None None None Alive, CR (D+1388)
3X106 Grade I None Yes Relapse of ALL (D+57), death D+158
1X107 Grade I None Yes Relapse of ALL (D+158), death D+164
1X106 None None None Alive, CR (D+1016)
1X107 None None None Alive, CR (D+954)
1X107 None None None Alive, CR (D+835)
1X107
1X106None None None Relapse (D+312), alive, CR (D+475)
second allo-HSCT)
1X107
5X106None None None Death from respiratory failure secondary
to refractory AIHA (D+615)

CAR-T therapies
• First products approved by FDA (B-cell lymphomas), EU approval expected in 2018̶ Kymriah (Novartis): list price $475,000 (outcome based)̶ Yescarta (Kite/Gilead): list price $373,000
• In most cases used as a bridge to a HSCT• Most successes from targeting CD19
(i.e., ALL, CLL, B-cell lymphomas; esp. refractory ALL)• Also pursued by Juno, Cellectis, Amgen, Pfizer, Celgene, Merck KgaA• Reported issues
‒ Persistence: Even in ALL with remissions of 90%, many patients relapse (most in ALL)‒ Antigen-negative relapse: CAR-T no longer able to target because cells no longer display the desired antigen, so far
only with CD19‒ Safety: severe cytokine release syndrome and neurotoxicity correlated with efficacy‒ Manufacturing (viral vectors): complexity, time, capacity, yields, batch failures, costs
Source: Evaluate Pharma report 2016; Novartis and Gilead/Kite press releases 37

Healthcare costs of Allogeneic HSCTs*
38
* Includes Inpatient/Outpatient/pharmacy costs** Includes different physician charges, graft procurement costs
Total HSCT costs Period / Source
$401,000 (MA)$301,000 (RIC)
100 days; Broder 2017
$549,000 (MA)$432,000 (RIC)
1 year; Broder 2017
$893,000 180 days; Milliman 2017**
Excludes lifelong costs of chronic GVHD
MA: myeloablative conditioningRIC: reduced intensity conditioning

Costs of HSCT complications
HSCT complications Costs to healthcare system (US)
Cancer death $165,000
Relapse $69,000*
Hemorrhagic cystitis $242,000*/**
Acute GVHD $527,000*
Chronic GVHD moderate/mild $124,000 ($14,400 per year***)
Chronic GVHD severe $322,000 ($37,400 per year***)
39
* Cost based on Broder total cost and cost multiplier Khera
** Side effect of cyclophosphamide
*** 10 years, discounted
Sources: Mariotto 2011; Yu 2017; Broder 2017; Khera 2014; literature PTCy analysis

Examples EU conditionally approved ATMPs/leukemia drugs
40
Approved indication Trial Design Trial size List Price
Treatment of patients with ADA-SCID who cannot be treated by a bone-marrow transplant because they do not have a suitable, matched, related donor
Open-label, prospective, sequential study in children with SCID due to ADA deficiency who lacked a healthy HLA-identical sibling
12 patients GBP 594,000 (UK)
Treatment of moderate to severe limbalstem-cell deficiency caused by burns, including chemical burns, to the eyes
Two retrospective, multicentre, case series based, non-randomised, and uncontrolled observational studies
135 patients over 9 years
GBP 80,000 (UK)
Adjunctive treatment to CD34+ haploidentical stem cell transplantation
Open label, single arm phase II study 36 patients €163,900 per dose (DE); €149,000 per dose (Italy)
Treatment of adults with Philadelphia chromosome negative relapsed or refractory B-precursor acute lymphoblastic leukaemia (ALL)
Open-label, multicentre, single-arm Phase 2 study
€87,000 (UK, DE; per course)
Second or third-line treatment in chronic lymphocytic leukaemia (CLL) in the presence of 17p deletion or TP53 mutation in adult patients
Open-label, single-arm Phase 1 and 2 studies
€99,000 (DE)

ATIR101: alloreactive T-cells depleted, potency retained
Functional release assay based on Quality Target Product Profile
& Critical Quality Attributes
41Source: Bonig ISCT 2017
*
Control: no donorreactivity
Safety: depleted
allo-reactivity
Potency:other reactivity
retained
12
6
1.6
1.4
1.2
1.0Autologous Recipient 3rd Party CD3/28
Prol
ifera
tion
Inde
x (PI
) DonorATIR101

ATIR101: T-cells reactive against infections & tumor retained
Donor
ATIR Control
Myb628multimer
CD8 T-cells
Collaboration with Prof. Angela Krackhardt, Medizinische Klinik III, Klinikum Rechts der Isar, TU Munich, Munich, Germany 42Source: Bonig ISCT 2017

ATIR101: T-cells reactive against EBV retained – examples
Examples of two patients in clinical study with ATIR:
EBV reactivation triggered response of (viral specific) T-cells in several patients• Increase in CD3+ T-cells detected in
peripheral blood• EBV copy numbers reduced after
increase in CD3+ T-cells, indicating effective immunological T-cell response
43

Phase 1 (CR-GVH-001): Overall Survival (5 year)
Patients: 19 with advanced hematological malignancies (14 not in remission at transplant)
ATIR101 doses: 10k cells/kg to 5 mln cells/kg; 31 days after HSCT
Results:
• 67% Overall Survival at middle dose level after 5 years
• No acute grade III/IV GVHD related to ATIR101 at any dose
Overall Survival (OS)
Dose L1-L3
Dose L4-L6
Dose L7
0%
20%
40%
60%
80%
100%
0 6 12 18 24 30 36 42 48 54 60
Time after HSCT (months)
3 patients; 2,6-5M cells/kg)
7 patients, 10-130k cells/kg
9 patients, 320k-2M cells/kg
Note: un-manipulated haplo-identical Donor Lymphocyte Infusion escalated above 10k T cells/kg induce GVHDSource: Lewalle 2003 44

Phase 2 (CR-AIR-007): trial characteristics & endpoints
45
Design: Open-label, single arm, multi-center study
Patient population:• AML or ALL in first remission with high-risk features or in second or higher remission• No suitable matched donor• Haploidentical family
Locations: CA, BE , DE, UK (8 sites in total, patients from 4 sites)
Primary endpoint: Transplant Related Mortality (TRM) at 6 months
Secondary endpoints:
• Acute and chronic GVHD• Immune reconstitution• Infections• TRM, relapse, Overall Survival (OS)
Patient follow-up (per 27 September 2016):
Median 485 days (range 110 – 744)
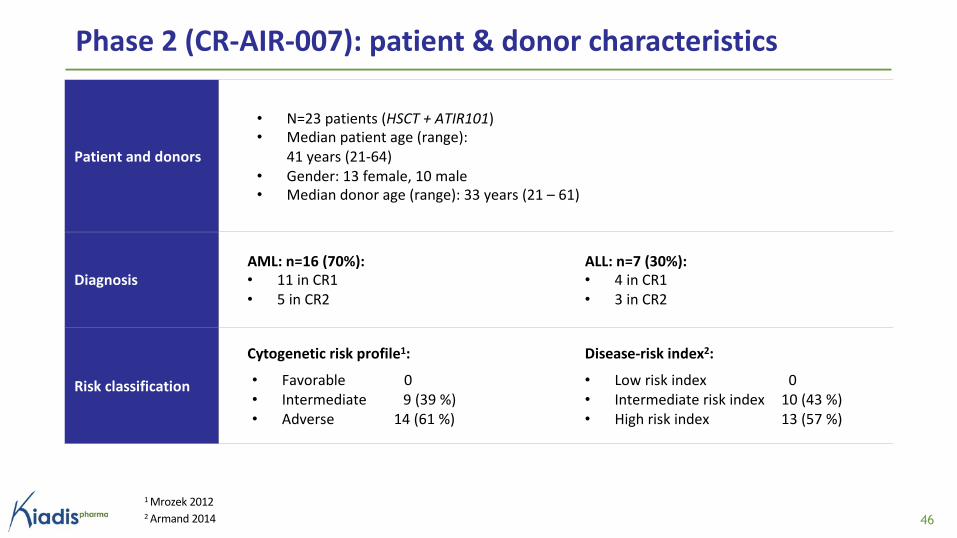
Phase 2 (CR-AIR-007): patient & donor characteristics
1 Mrozek 20122 Armand 2014 46
Patient and donors
• N=23 patients (HSCT + ATIR101)• Median patient age (range):
41 years (21-64)
• Gender: 13 female, 10 male• Median donor age (range): 33 years (21 – 61)
DiagnosisAML: n=16 (70%):• 11 in CR1
• 5 in CR2
ALL: n=7 (30%):• 4 in CR1
• 3 in CR2
Risk classification
Cytogenetic risk profile1:
• Favorable 0
• Intermediate 9 (39 %)
• Adverse 14 (61 %)
Disease-risk index2:
• Low risk index 0
• Intermediate risk index 10 (43 %)
• High risk index 13 (57 %)

Phase 2 (CR-AIR-007): causes of deathPeriod post HSCT Classification No. of pts Classification of cause of death
< 6 months
Relapse 1
TRM – Infections 2 Adenovirus and JC virus infections
TRM – Other 1 Pulmonary embolism
6-12 months
Relapse 1
TRM – Infections 3 Respiratory/pulmonary infections/distress
TRM – Other 1 Multi-organ failure
12-24 months
Relapse 2
TRM-Infections 3* Pneumonia/sepsis/septic shock
Total 14 (61%)
* All 3 patients immunosuppressed, subsequently contracted infections, leading to death: 2 patients who received un-manipulated DLI’s and subsequently developed severe acute GVHD; 1 patient with chronic GVHD 47

Objective Extend the length of protection (further improve TRM); investigate flexibility for physicians
Design HSCT followed with ATIR101 at day 30, and additional dose of ATIR101 at day 72
Patients AML, ALL and MDS
StatusEnrolment completed: 15 patients treated with ATIR101: 9 with one dose (of which 5 with > 1 year follow up) and 6 with two doses (all with > 1 year follow up)Study ongoing, not all data yet monitored and thus subject to change
Interim results
Two doses (for 6 patients): grade III/IV acute GVHD in two patients within 30 days of 2nd doseSingle dose (for 5 patients that have > 1 year follow up): • No grade III/IV GVHD• 80% Overall Survival; 20% 1 year Relapse, 0% 1 year Non Relapse MortalitySingle dose (for 4 patients that have < 1 year follow up): 1 suspected grade III acute GVHD
Interim conclusion
Confirming safety/efficacy findings of 007 in the 5 patients with a single dose that have >1 year follow up; Not confirmed with two doses or with remainder of single dose patients.Phase 3 009 based on 007, not based on 008
Phase 2 (CR-AIR-008): second dose (January 2018)
48

Phase 2 (007 & 007/008) vs. PTCy literature (1 yr)ATIRPhase 2 007/008 (MITT; pts receiving ATIR; n=28*)
PTCyLiterature, adjusted for 007 DRI for OS (n=561)** & for GRFS (n=500)**
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials: * 23 AML/ALL patients from 007 (study completed) plus 5 AML/ALL patients from 008 that have completed 1 year follow up with single dose (008 data not all monitored and thus subject to change); for 28 AML/ALL 007/008 patients: Relapse rate 11% and NRM 25%, chronic GVHD 4%** Ciurea 2015 (CIBMTR); McCurdy 2017 (Baltimore), Devillier 2016, Sugita 2015 (57% high DRI; normalization based on Armand 2014) *** Solh 2016 (Atlanta; DRI normalized GRFS 30%; n=128); McCurdy 2017 (Johns Hopkins; DRI normalized GRFS 38%; n=372) 49
Survival GRFS
61%57%
54%
36% 37%
ATIRPhase 2 007 (ITT; pts receiving HSCT; n=26)
ATIRPhase 2 007 (MITT; pts receiving ATIR; n=23)
64%61%
58% 57% 59%
OS
PTCyLiterature, adjusted for 007/008 DRI for OS (n=561)* & for GRFS (n=500)**

Disease• Anemia due to defects in haemoglobin and red blood cells• Transfusion dependency and iron overload, leading to high mortality
HSCT• Potential cure of blood forming system, yet high risk• ATIR201 to increase safety
Trial design• ATIR201 as adjunctive to αβ T-cell depleted HSCT• 10 pediatric patients with β-thalassemia major
Status• No patient dosed yet• Postponed
ATIR201 Phase 1/2: β-thalassemia
50

DRI adjustment (Armand 2014)
DRI adjusted 1-year survival (OS)
comparison ATIR vs all HSCT
Comparison provided for illustrative purposes, based on literature comparison, NOT based on randomized controlled trials
Armand 2014: 9849 HSCT patients
(CIBMTR 2008-2010):
• MRD, non-MRD, MUD, mismatched
• PB, BM, cord
• Leukemia, lymphoma, MM, etc
• Myeloablative, RIC
61%55%
GRFSATIR101
Phase 2
007
(n=25)
Average HSCT
in Armand 2014;
DRI adjusted
0 6 12 18 24
Months from transplantation
0
20
40
60
80
100
Ove
rall S
urv
iva
l (%
)
Very High Risk
High Risk
Intermediate Risk
Low Risk
P<0.0001
51
Conclusion: Disease Risk Index (DRI) is strongest prognostic factor for Overall Survival

52
…so that many more patients with otherwise incurable diseases will have a reasonable chance of long survival and cure
Dr. E. Donnall Thomasestablished bone marrow transplantation as a treatment for leukemiaNobel Lecture | 1990







