
Glaucoma/OHT in the Community
Suspect Investigation &
Stable Management
eCare Ipswich
20-03-2019
Christian Dutton
Education & Compliance Lead OptometristBSc(Hons.) MScClinOpt FCOptom Prof.Cert.Glauc
Mr. Simon Hardman-Lea
Lead Consultant OphthalmologistMA (Oxon.) FRCS FRCOphth
Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
• Second leading cause of blindness worldwide (10% of UK blindness)
• 50% is still undetected
• 2010 - 60.5 million people (OAG and ACG) – 500,000 in England• Blind: 4.5 million OAG, 4 million ACG
• 2020 - 79.6 million• Blind: 6 million OAG, 5 million ACG
• 75% OAG
• 60% are women (make up 55% of OAG and 70% of ACG)
• 50% are Asian (85% of ACG)
Statistics

HES:
• 30% of all outpatient follow-ups (over 1 million appts)
• 15% of all new assessments
Statistics

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s

Definitions
OHT
• IOP ≥ 22mmHg
• Open angle
• Normal fields
• Normal discs
• ~10% of individuals with IOPs between 22-30mmHg develop POAG over 5 yrs
COAG suspect
• Open angle
• Suspicious fields
• Suspicious discs
• POAG suspect if IOP ≥ 22mmHg
• NTG suspect if IOP <22mmHg
Definitions

Glaucoma
• Group of diseases
• Acquired progressive optic neuropathy
• Progressive loss of visual function if• Undetected
• Untreated
• Undertreated
Definitions

Definitions
CLASSIFICATION
• Appearance of the aqueous drainage pathway at the TM• Open-angle glaucoma
• Normal clinical appearance
• Aqueous outflow may be restricted
• Angle closure glaucoma• Access to the TM is physically obstructed
• Mechanisms that push the iris forward from behind
• Mechanisms that pull it forward

PRIMARY ANGLE CLOSURE• Primary angle closure suspect (PACS)
• Contact between peripheral iris and posterior TM possible • IOP, discs and visual fields are normal
• Primary Angle Closure (PAC)• Obstruction of the TM by the peripheral iris has occurred• Raised IOP (appositional PAC) and/or peripheral anterior synechiae (synaechial PAC)• Disc and fields are normal
• Primary Angle Closure Glaucoma (PACG)• PAC with damage to the optic nerve and visual field change.• Damage caused by:
• Episodes of severe IOP elevation (so IOP might be normal or raised on presentation)• Long-term elevated IOP
Definitions
Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
Specific to the eye
• Raised IOP• 15.5mmHg (SD 2.5mmHg) 10-21
• Refractive error• > –8D ocular connective tissue disorder
• Hypermetropic small ‘crowded’ ACs
• Thin CCT
Risk factors

Systemic
• Age• Increased TM resistance to outflow
• Family history• First-degree relatives = 10x risk
• Vascular disease• Poor optic nerve head blood flow (NTG)
• Migraine, Raynaud’s, Diabetes
• Obstructive sleep apnoea (?diurnal IOP variation)
Risk factors

Racial
• POAG• Afro- Caribbean and West African
• PAC/PACG• Far-East Asian and Inuit
Risk factors
Secondary
• Steroid
• PDS
• PXF
• Uveitis
• Iris neovascularisation from retinal ischaemia (e.g. CRVO)
Risk factors

Structure vs function
• Structure (physical measurable pathology e.g. cell loss)
• Function (field and VA)
• Combining structural & functional tests improves diagnostic accuracy
• Can get structural or functional defects first• Rarely both at the same time
Clinical Investigations

Optic disc• Vertical disc diameter
• 1.5mm small, 2.1mm large• Helps in C:D interpretation• 66D 1:1 (1/mag x graticule)
• C:D ratio• ≥0.7, 0.2 difference, progression
• Rim contour • Diffuse narrowing / localized notching / both• Loss from inner edge of rim, especially ST/IT
Clinical Investigations
Optic disc
• Haemorrhage(s)• 2-5x more common in NTG than POAG
• Associated with rapid progression, notches and B PPA
• Usually in RNFL (IT/ST)
• Frequency increases then decreases
• Often self-resolve within 2/12
Clinical Investigations
Optic disc• Vascular changes (due to structural NRR loss)
• Baring of circumlinear vessels• Bayonetting (advanced disease)• ‘Fly-over’ vessels - lose contact with the previously underlying NRR• Nasalisation of central vessels
• PPA• Beta Zone (next to disc margin)
• RPE atrophy since choriocapillaris closed (absolute scotoma)
• Risk factor for progression• Extent proportional to disc and field damage• Precedes disc haemorrhage in 80% of cases
Clinical Investigations
Progression - optic disc
• Structural qualitative changes (photos, clinical notes)• Vessel changes
• Notching
• Haemorrhages
• Enlarging PPA
• Quantitative changes• C:D progression
• OCT progression analysis (disc map volumetric data)
Clinical Investigations

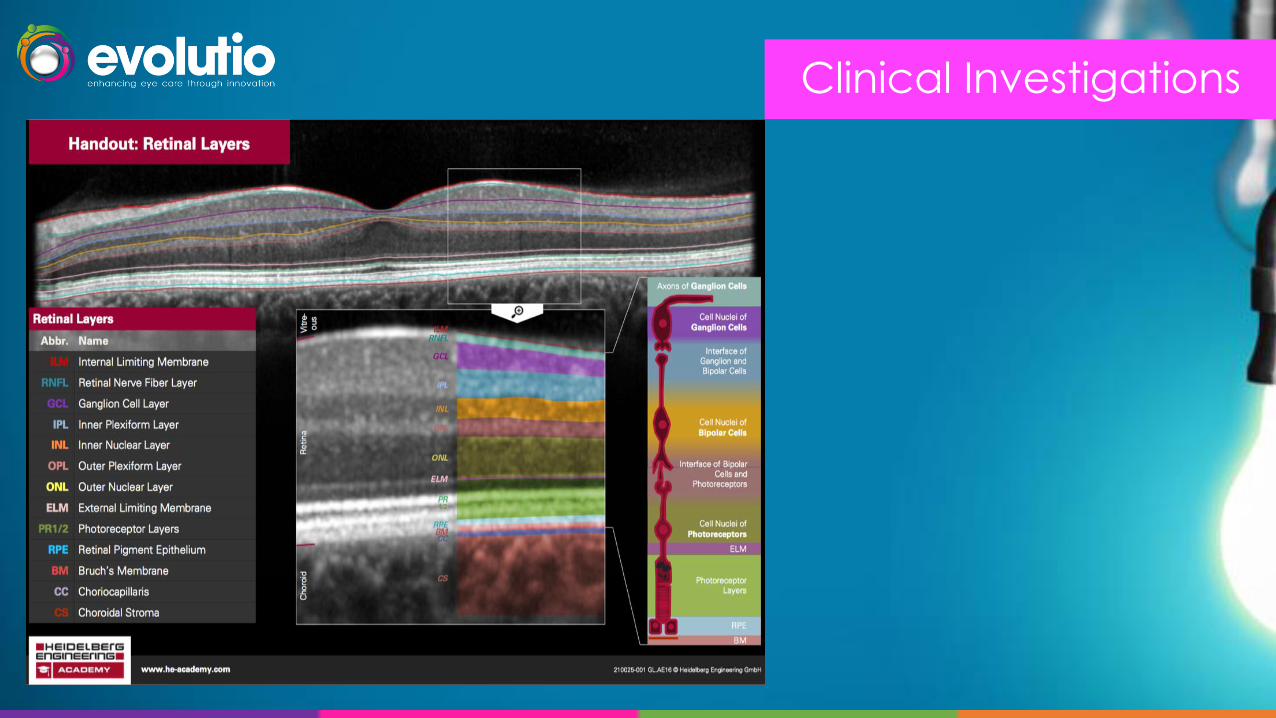
RNFL (axons of retinal ganglion cells)• Identify pre-perimetric damage
• Qualitative (red free photo)• Initially small slit/groove bundle defects• Coalesce to form large wedge defects• Later =diffuse loss
• Quantitative• OCT disc map (circumpapillary RNFL thickness)• OCT GCC map (segmentation algorithm)
• Over 50% of all RGC’s are in macula
Clinical Investigations
Clinical Investigations

Progression - RNFL (axons of retinal ganglion cells)
• Qualitative changes (red free photo)• Enlarging defects compared with previous photos
• Quantitative changes• OCT disc and macular map
• Progression analysis or subjective assessment
Clinical Investigations
Visual Fields
• Diagnosis and monitor progression
• Main functional measurement
• Standard automated perimetry (central thresholding)• Gold standard
• Not optimal for early detection but good for monitoring
• Time consuming/tiresome so use intelligent algorithms
Clinical Investigations

Visual Fields• Reliability
• Variability is normal in glaucoma• Patient performance• Fixation losses• Fatigue• Learning effects• Changes in pupil size• Improper refractive correction• True physiological variability• Artefacts (ptosis, spectacle/lens rim)
Clinical Investigations

Clinical Investigations
Reliability indices
• Fixation losses• Poor blindspot plotting• Field loss close to fixation
• False positives• Trigger happy• Under 20%
• False negatives• Inattentive• Common in glaucoma
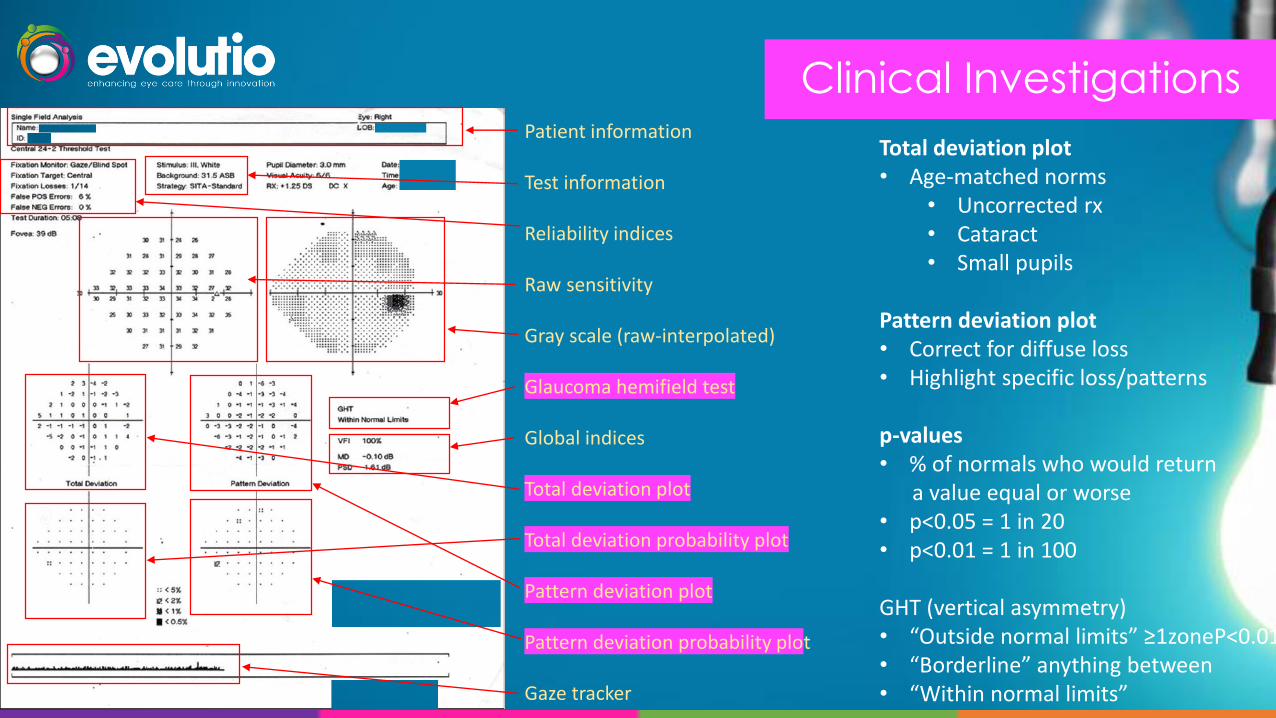
Patient information
Test information
Reliability indices
Raw sensitivity
Gray scale (raw-interpolated)
Glaucoma hemifield test
Global indices
Total deviation plot
Total deviation probability plot
Pattern deviation plot
Pattern deviation probability plot
Gaze tracker
Clinical InvestigationsPatient information
Test information
Reliability indices
Raw sensitivity
Gray scale (raw-interpolated)
Glaucoma hemifield test
Global indices
Total deviation plot
Total deviation probability plot
Pattern deviation plot
Pattern deviation probability plot
Gaze tracker
Total deviation plot• Age-matched norms
• Uncorrected rx• Cataract• Small pupils
Pattern deviation plot• Correct for diffuse loss• Highlight specific loss/patterns
p-values• % of normals who would return
a value equal or worse• p<0.05 = 1 in 20• p<0.01 = 1 in 100
GHT (vertical asymmetry)• “Outside normal limits” ≥1zoneP<0.01• “Borderline” anything between• “Within normal limits”

Clinical InvestigationsPatient information
Test information
Reliability indices
Raw sensitivity
Gray scale (raw-interpolated)
Glaucoma hemifield test
Global indices
Total deviation plot
Total deviation probability plot
Pattern deviation plot
Pattern deviation probability plot
Gaze tracker
Global indicesMathematical evaluations of the visual field
Mean deviation (MD) index (-)• Reflects diffuse change• Weighted average of all the points
in the total deviation plot
Pattern SD (PSD) index (+)• Reflects variability across field• Higher = focal loss
(p) of the result being normal
Hodapp classificationEarly COAG MD > -6 dB.Moderate COAG -6 dB to -12 dB

Visual fields (RNFL bundle defects)
• Paracentral• Deep, close to fixation, especially in NTG
• Follow RNFL distribution and abruptly stop at horizontal midline
• Arcuate• Coalition of a group of smaller defects, more extensive than paracentral,
respect horiz midline
• Nasal step• Due to sensitivity difference above and below horizontal midline
• Normal patients may have shallow small steps (over 5 degrees is significant)
• Depth (deep = more likely to be real)
• Clustering (more than 2 abnormal points likely to be significant)
Clinical Investigations

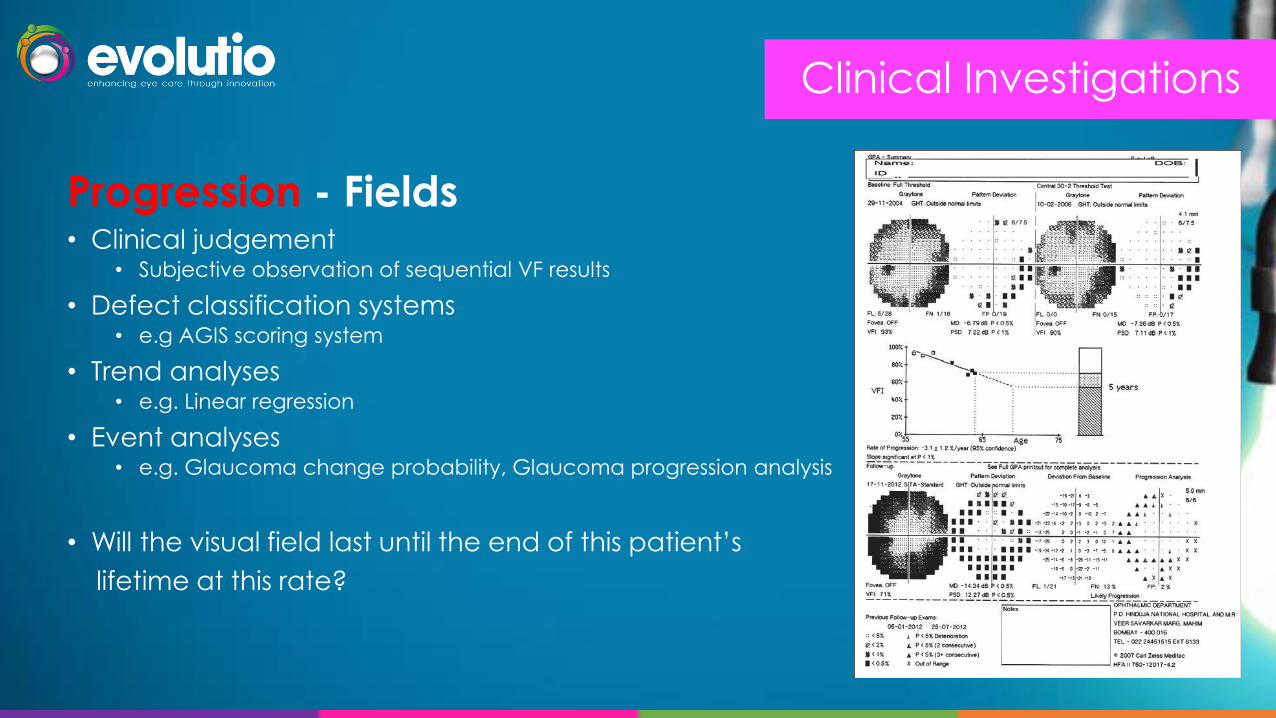
Progression - Fields• Clinical judgement
• Subjective observation of sequential VF results
• Defect classification systems• e.g AGIS scoring system
• Trend analyses• e.g. Linear regression
• Event analyses• e.g. Glaucoma change probability, Glaucoma progression analysis
Clinical Investigations
Progression - Fields• Clinical judgement
• Subjective observation of sequential VF results
• Defect classification systems• e.g AGIS scoring system
• Trend analyses• e.g. Linear regression
• Event analyses• e.g. Glaucoma change probability, Glaucoma progression analysis
• Will the visual field last until the end of this patient’s
lifetime at this rate?
Clinical Investigations
IOP
• Errors• Lids, misaligned, meniscus width, prolonged contact
• Short term changes• Diurnal range (3-6 normal, glaucoma 13) • Increase if accommodating, blinking, squeezing, raised
intrathoracic pressure (strain, hold breath, tight collar)
• Other factors• Corneal thickness (thin = underestimate)• Curvature (flat = underestimate)• Elasticity (stiff = overestimate)• Hydration
Clinical Investigations

CCT
• Normal distribution 540 ±30 μm (mean +/- SD)
• Thin CCT (less than 555μm) risk factor for:• Development of POAG
• Progression of POAG
• Visual field progression
• CCT can influence accuracy of IOP measurement• No verified algorithm to apply
• Ehler: 1mmHg correction for every 15 μm
Clinical Investigations

Anterior Eye
• Cornea• Epi oedema, posterior embryotoxin, KP
• A/C• Trauma, uveitic, pigmentary, lens related• Cells, flare, pigment, protein, lens particles
• Iris• Atrophy (diffuse, sector), deposits, pupil margin, TI, neovasc
• Lens• PXF, glaucomflecken (anterior subcaps), phacodonesis (zonular
weakness in PXF – wobbly iris), phacomorphic, phacolytic
Clinical Investigations

Anterior Chamber Depth
• Limbal Depth• Van Herick
• 600, narrow, bright beam, nasal & temporal• AC:cornea - record as % and equivalent VH• <25% occludable
• A-S OCT• Qualitative image, quantitative analysis possible
• Gonioscopy• Raised IOP requiring treatment (open angle vs angle closure)• Patients at risk of acute angle closure (VH <25%)
Clinical Investigations

Anterior Chamber Depth
• Central Depth• Smith technique
• Illumination at 600, beam horizontal and short
• Cornea in focus temporally
• Move nasally until the beam just touches nasal pupil margin
• Increase beam height until images touch
• Multiply result by 1.4 (gives central A/C depth in mm)
• <1.8 shallow, >2.5 deep
Clinical Investigations

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
• 4 Principles
• IOP is the only modifiable risk factor
• Reduction in IOP reduces the rate of damage
• Damage occurs at the presenting IOP
• Treatment should reduce IOP to a ‘target pressure’
Treatment Philosophy
• Estimated upper limit
• To slow progression to maintain vision-related quality of life
• For the expected lifetime of the patient• MD <-14dB visual impairment• MD <-22dB statutory blindness
• 20-35% (5-7 mmHg)
• Set by consultant• Rate of progression, risk factors (e.g. CCT)• TargetIOP.com
Target Pressure

OHT/Suspected POAG (IOP 24 or more)
• Are they at risk of future visual impairment?
• Consider: IOP, CCT, FH, life expectancy
• Old CG85 - categories which might be at risk
• Not at risk• No treatment
• Regular EE
Treatment
OHT/Suspected POAG (IOP 24 or more)
• At risk of visual impairment in lifetime• Generic PGA (e.g. latanoprost od nocte R&L)
• If non-tol:• Another generic PGA / Beta Blocker / Non-generic PGA/other class of drug
• If preservative allergy• Consider preservative free (e.g. monoprost) if significant OSD and
• High risk of COAG conversion
• If ineffective• Different therapeutic class or combination
Treatment

COAG
• Generic PGA (e.g. latanoprost od nocte R&L)• If non-tol
• Try different therapeutic class
• If preservative allergy• Consider preservative free if significant OSD
• If ineffective:• Discuss adherence
• Check eye drop instillation technique
• Try different therapeutic class or combo
• Surgery if 2 classes don’t work
Treatment

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s

• Start with 1 drug
• Show how to put in
• If IOP not at target • Change if IOP reduced 2 or less
• Add second drug if IOP reduced more than 2
• Generally treat both eyes (give px choice)• Less confusing
• Cosmetic balance with PGA
• Avoid • Beta Blocker if asthma, heart disease, poor
circulation
• PGA in pregnancy
Treatment Algorithm & Considerations
• Prostaglandin analogues (latanoprost)• Prostamide (bimatoprost)
• Beta blockers (timolol)
• Sympathomimetics (brimonidine)
• Carbonic Anhydrase Inhibitors (brinzolamide)
• Miotics (pilocarpine)
• Combination products (above plus timolol)
Glaucoma Medications
Prostaglandin analogues
• Action: increase (uveoscleral) aqueous outflow
• Examples:• Gutt Latanoprost 50microgram/ml OD nocte (Branded = Xalatan)• Monopost (PF)• Travoprost (Travatan), Tafluprost (Saflutan)
• Avoid:• Aphake, pseudophake, A/C implant• Severe asthma• Herpetic diease• Induces labour
Glaucoma Medications

Prostamide
• Action: increase (uveoscleral) aqueous outflow
• Examples:• Gutt Bimatoprost 100microgram/ml (0.01%) OD (Lumigan)• Gutt Bimatoprost 300microgram/ml (0.03%) (PF) (Lumigan)
• Avoid: • Aphake, pseudophake, A/C implant• Severe asthma• Renal disease
Glaucoma Medications
Glaucoma Medications
Beta-blockers
• Action: Reduce aqueous production
• Examples:
• Gutt Timolol 0.25% / 0.5% bd (or LA mane) – available unit dose
(PF)
• Timolol 1mg/g gel mane (Tiopex)
• Levobunolol (Betagan), Betaxolol (Betoptic)
• Avoid:
• Heart probs (reduce HR)
• Asthma/COPD (bronchoconstriction)
• Worsen vasc disease
• ACE inhib, anti arythmias (amiodarone), calcium channel blocker
(verapamil), parasympathomimetic (pilo), sympathomimetic
(adrenaline) – very rare in clinical practice

Sympathomimetics
• Action: Reduce aqueous production and increase outflow
• Examples:• Gutt Brimonidine 0.2% bd (Alphagan)• Apraclonidine (Iopidine)
• Avoid: • Heart/vascular disease (smooth muscle/vaso constriction,
heart works harder and incr. BP)• MAOI’s (phenelzine, isocarboxazid)• Tricyclic antidepressants (amitryptilline, doxepin)• Alpha stimulation also: Eyelid retraction, mydriasis, increase
outflow
Glaucoma Medications

Carbonic anhydrase inhibitors
• Action: reduce aqueous production
• Examples:
• Gutt Brinzolamide 10mg/ml bd (Azopt)
• Dorzolamide 2% bd/tds (Trusopt)
• PO 250mg Acetazolamide take two tablets up to max QDS
• Avoid:
• Sulphonamide allergy e.g. trimethoprim (since it is a sulphonamide derivative)
• Electrolyte imbalance/renal disease
• Pregnancy
Glaucoma Medications

Miotics
• Action: increase aqueous outflow
• Examples:
• Gutt Pilocarpine 1%, 2% max qds
• Avoid:
• Heart problems (reduce HR)
• Asthma/COPD (bronchoconstriction)
• Peptic ulcer (increase secretions)
• Anterior uveitis, secondary glaucoma
Glaucoma Medications

• Latanoprost 50micrograms & timolol 5mg/ml Xalacom
• Travoprost 40 micrograms & timolol 5mg/ml eye drops DuoTrav
• Bimatoprost 0.03% & timolol 0.5% eye drops Ganfort(also Ganfort PF available)
• Brimonidine 0.2% & timolol 0.5% eye drops Combigan
• Brinzolamide 10mg & timolol 5mg/ml eye drops Azarga
• Dorzolamide 2% & timolol 0.5% eye drops Cosopt
• Brinzolamide 10mg/ml & Brimonidine 2mg/ml eye drops Simbrinza
Glaucoma Medications

Miotics
Pilocarpine
Generic
Pilocarpine 1/2/4% qds
Unit dose (2% only)
S/E
Reduce HR, bronchoconstriction,
increase secretions, headaches
Avo
id
Heart probs, Asthma/COPD,
peptic ulcer, anterior uveitis,
secondary glaucoma
Rx
Gutt Pilocarpine 1%, 2% max qds
Reduce HR, Bronchoconstrict
Heart probs, asthma/COPD, worsen vascular
disease. ACE inhib, anti arythmias
(amiodarone), calcium channel blocker
(verapamil), parasympathomimetic (pilo),
sympathomimetic (adrenaline) – very rare
Travoprost 0.4mg/ml / Timolol 5mg/ml - mane - branded only
Latanoprost 0.05mg/ml / Timolol 5mg/ml - mane - branded,
generic
Taptiqom®
Cosopt®
/ Tidomat® / Eylamdo
®
Simbrinza®
Aphake, A/C implant, severe asthma,
herpetic disease, induces labour.
Prostamide (Bimatoprost): aphake,
pseudophake, A/C implant, severe
asthma, renal disease
Gutt Latanoprost 50microgram/ml (also
PF) od
Gutt Travoprost 40microgram/ml od
Gutt Tafluprost 15microgram/ml (PF) od
Gutt Bimatoprost 100microgram/ml
Sulphonamide allergy e.g.
trimethoprim (since it is a
sulphonamide derivative)
Watch for skin rash, electrolyte
imbalance/renal disease,
pregnancy
Gutt Brinzolamide 10mg/ml bd
Gutt Dorzolamide 2% bd/tds
PO 250mg Acetazolamide take
two tablets up to max QDS
Duotrav®
Xalacom®
Ganfort® Bimatoprost 0.3mg/ml / Timolol 5mg/ml - mane - branded only
Tafluprost
Saflutan® 15mg/ml nocte
Available in unpreserved form only
Gutt Timolol 0.25% / 0.5% bd (also 0.1% LA pres
free od)
Gutt Levobunolol 0.5% od / bd
Gutt Brimonidine 0.2% bd
Heart/vascular disease. MAOI’s
(phenelzine, isocarboxazid),
tricyclic antidepressants
(amitryptilline, doxepin)
Smooth muscle/vaso constriction
(heart works harder and
increases BP). Alpha stimulation
also: Eyelid retraction, mydriasis,
increase outflow
First c
ho
ice
Last c
ho
ice
Prostaglandin Analogues Carbonic Anhydrase
Inhibitors
Bimatoprost Betaxolol
Betoptic®
0.5% bd
Betoptic-S®
0.25% bd Generic
Unit dose (0.25% only)
Lumigan® 0.01% nocte
Preserved = 0.01% or 0.03%
Unpreserved = 0.03% only
Generics (0.03% only)
PF unit dose = Lumigan UD®
PF multidose = Eyreida®
Generic
Travatan® does NOT contain BAK Generic
Travoprost DOES contain BAK
Unit dose
Pres-free multi-dose
(Eydelto® )
Generic
Unit dose
Generic
NB cost of unit dose:
1% available only in unit dose
0.5% available only in multi dose
Generics Generic PF multidose = Eysano®
Generic 0.25 & 0.5%
Unit dose
(Generics include ‘Brymont’) Generic
Travoprost
Travatan® 0.004% nocte
Dorzolamide
Trusopt® 2% bd/tds
Levobunolol
Betagan®
0.5% bd
Apraclonidine
Iopidine® 0.5/1% tds
Latanoprost
Xalatan® 0.005% nocte
Pres-free option = Monopost
Brinzolamide
Azopt® 1% bd/tds
Timolol (gel and guttae)
Timoptol®
0.25/0.50% bd
Tiopex® 1mg/g gel mane
Timoptol-LA® 0.25/0.5% mane
Brimonidine
Alphagan® 0.2% bd
Beta-Blockers Adrenergics
Dorzolamide 20mg/ml / Timolol 5mg/ml - bd - branded multi/ unit dose, generic
Brimonidine 2mg/ml / Timolol 5mg/ml - bd - branded only
Brinzolamide 10mg/ml / Timolol 5mg/ml - bd - branded only
Brinzolamide 10mg/ml / Brimonidine 2mg/ml - bd/tds - branded onlyTafluprost 0.015mg/ml / Timolol 5mg/ml - mane - branded only
Combigan®
Azarga®

• The disease• Symptomless but irreversible loss
• What the treatment does
• How to instil drops
• Side-effects (& what to do)
• How to get repeat rx
• Sources of info/support
• Importance of regular review
Patient Information

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
• Usually in 4-8 weeks
• Verify medication
• Check compliance and understanding
• Assess possible side-effects (‘tolerance’)
• Check logistics for repeat prescriptions
• Check effectiveness of treatment
• Answer any unresolved queries
Tolerating well, self-reported compliance good, has repeat rx from GP.See in x/12 (high presenting IOP/suspicious disc) with fields
Review
• Treated OHT/suspected COAG• Discharge if OHT not requiring treatment or COAG suspect no longer suspect
• No conversion to COAG:
• 18-24/12 (12-18/24 for COAG suspect)
• Conversion to COAG uncertain:
• 1-4/12 (and review treatment plan) if IOP not controlled
• Else 6-12/12
• Conversion: see COAG section
• COAG• No progression:
• 1-4/12 (and review treatment plan) if IOP not controlled
• Else 6-12/12 if high risk or 12-18/24 if low risk
• Progression/uncertain:
• 1-2/12 (and review treatment plan) if IOP not controlled
• Else 2-6/12
Recall

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
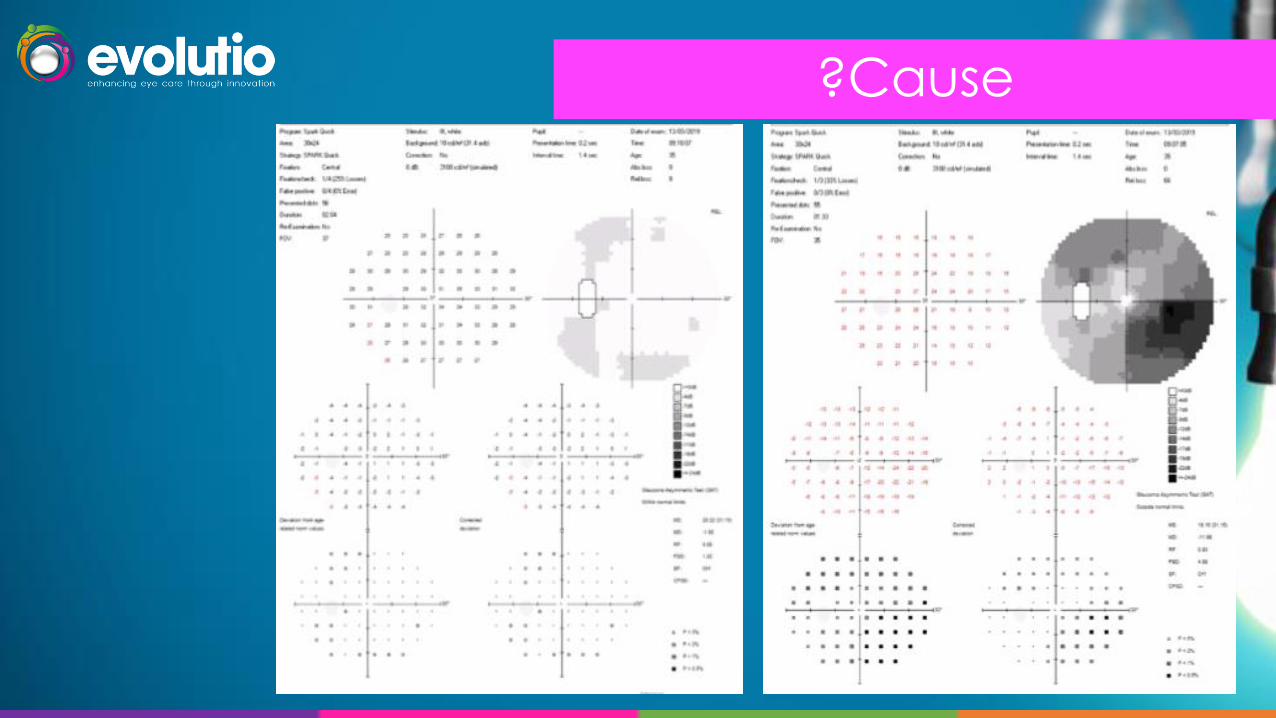
?Cause

• July’12 - Optom referral – C:D asymmetry and ?field defect
• IOP 20/18
• C:D 0.5/0.4
• Fields ?mildly enlarged blind spot
• Sept ‘12 - Community glaucoma service
• IOP 28/26
• C:D 0.5/0.4
• Fields normal R&L
• CCT 573/584
• A/C Deep
Impression – OHT, no treatment indicated, review 6/12
Case 1 – OHT (stable, untreated)
Female, Caucasian, Age 68
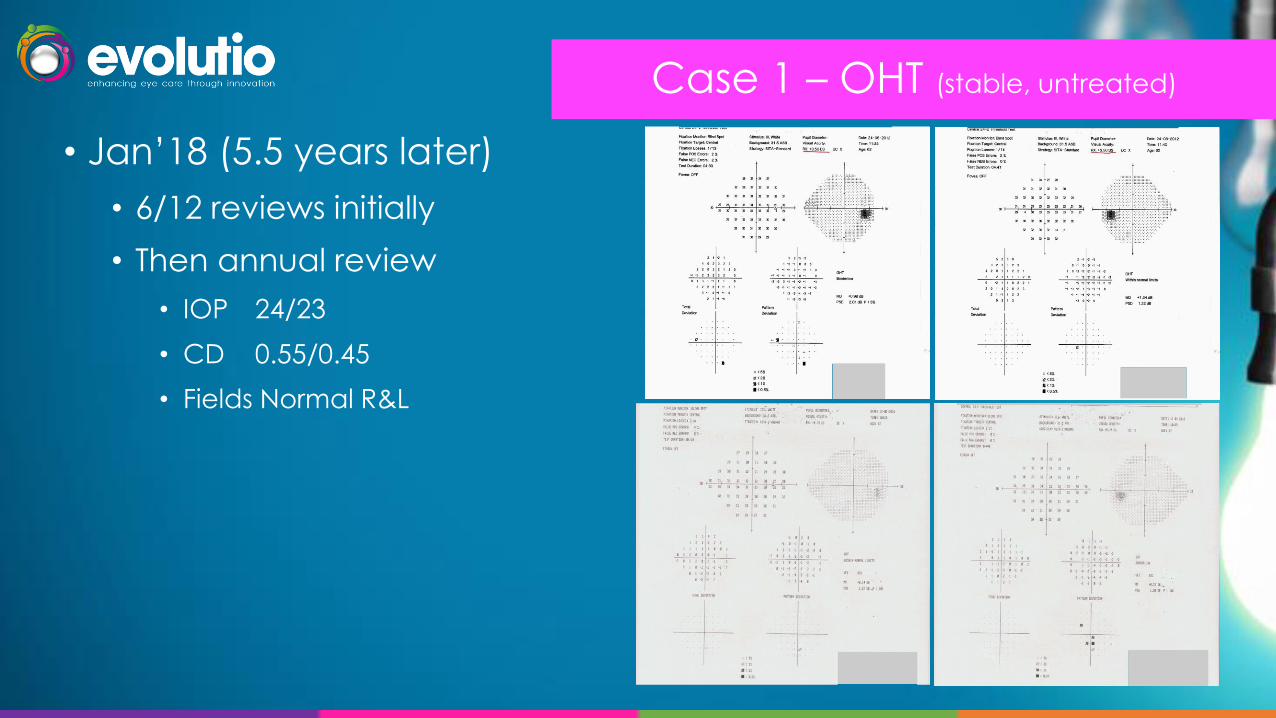
• Jan’18 (5.5 years later)
• 6/12 reviews initially
• Then annual review
• IOP 24/23
• CD 0.55/0.45
• Fields Normal R&L
Case 1 – OHT (stable, untreated)

Case 1 – OHT (stable, untreated)
Name:
ID:
DOB:
Age:
410630
68
Exam date:
Gender:
Eye: Both
21/11/18
Female
Comments:
Version: 8.0.2 SOCT Copernicus REVO Device SN: 1550974/11 OPTOPOL Technology Sp. z o.o.Print date: 21/11/18
LR21/11/18 10:04:42
3D 6x6 mm
21/11/18 10:04:14
3D 6x6 mm
DISC | BOTH EYES
NFL signification
%
NFL signification
%
NFL thickness
µm
NFL thickness
µm
Ring diameter 2.40 mm. Ring thickness 0.40 mm. Ring diameter 2.40 mm. Ring thickness 0.40 mm.
Name:
ID:
DOB:
Age:
410630
68
Exam date:
Gender:
Eye: Both
21/11/18
Female
Comments:
Version: 8.0.2 SOCT Copernicus REVO Device SN: 1550974/11 OPTOPOL Technology Sp. z o.o.Print date: 21/11/18
LR21/11/18 10:04:57
3D 7x7 mm
21/11/18 10:03:54
3D 7x7 mm
RETINA | BOTH EYES | GANGLION
NFL+GCL+IPL thickness
µm
NFL+GCL+IPL thickness
µm
NFL+GCL+IPL signification
%
NFL+GCL+IPL signification
%
NFL+GCL+IPL deviation
%
NFL+GCL+IPL deviation
%
S - I Hemisphere asymmetry
µm
I - S
S - I Hemisphere asymmetry
µm
I - S
R - L Asymmetry
µm
L - R Asymmetry
µm
% %
• Oct ’18 eCare transfer
• IOP 26/25
• C:D 0.6/0.5
• Fields Normal R&L
• Impression:
• Stable OHT
• Plan:
• No treatment indicated
• Review 12/12

• Oct ’17 - High street optometry - ?glaucoma
• IOP 22/23 (NCT)
• Discs 0.3/0.45
• Fields Full R&L
• Nov ‘17 – Community glaucoma service
• IOP 21/21 (GAT)
• Discs 0.4 tilted/0.5 tilted
• Fields Normal R&L
• CCT 558/550
• A/C Deep
Glaucoma suspect, no treatment indicated
Case 2 – OHT (stable, untreated)
Male, Caucasian, 33
Case 2 – OHT (stable, untreated)
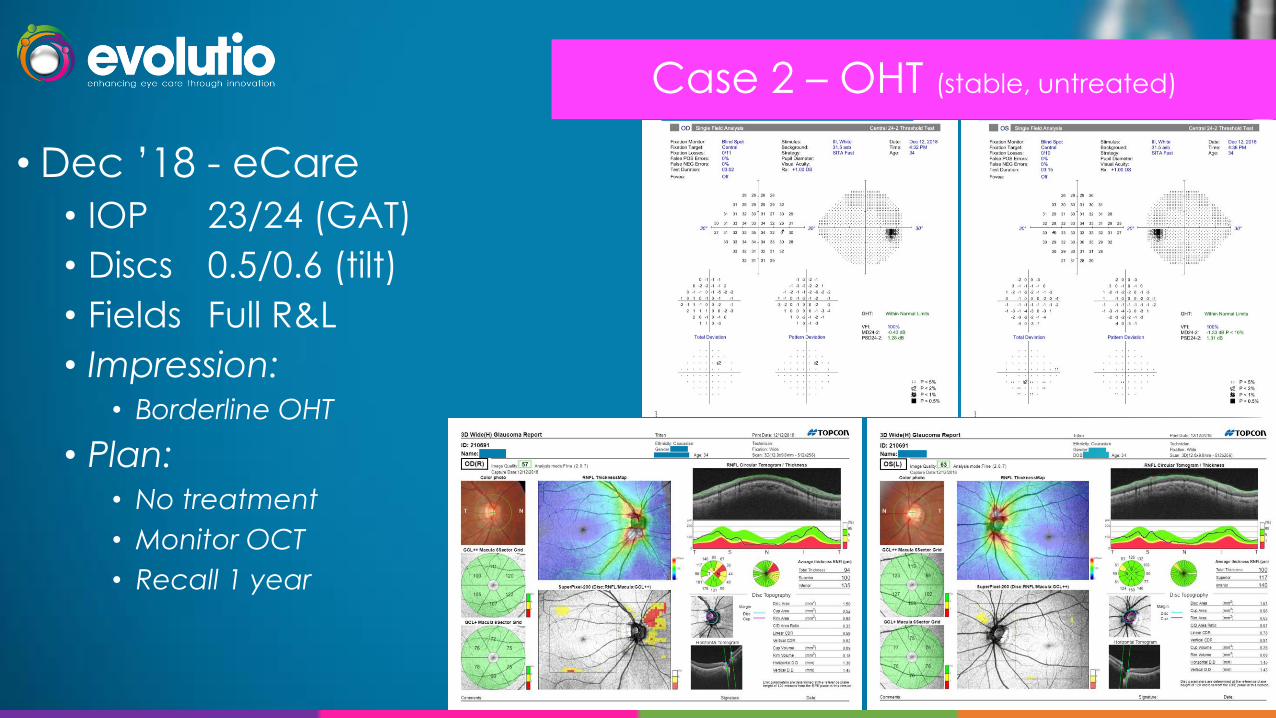
• Dec ’18 - eCare
• IOP 23/24 (GAT)
• Discs 0.5/0.6 (tilt)
• Fields Full R&L
• Impression:• Borderline OHT
• Plan:• No treatment
• Monitor OCT
• Recall 1 year
• Jan’17 – Community ophthalmology service (Optom referral for raised IOP)
• IOP 22/29
• C:D 0.1/0.1
• Fields Full R&L
• CCT 570/570
• A/C Deep, no PDS/PXF
Impression - LE OHT, commence latanoprost OD LE only, review 6/52 (initially)
• Nov ‘17 - Community glaucoma service
• IOP 20/20
• C:D 0.1/0.1
• Fields Full R&L
Impression – LE treated OHT, continue LE latanoprost, review 12/12
Case 3 – OHT (stable, treated)
Male, Caucasian, Age 64

• Nov’18 – eCare transfer
• IOP 27/20
• C:D 0.1/0.1
• Fields Full R&L
• A/C VH3/VH4
• Impression:
• LE treated OHT
• RE OHT
• Plan:
• Continue latanoprost LE nocte
• Commence latanoprost RE nocte
• Target IOP 20 R&L
• Review 3/12
Case 3 – OHT (UNstable, treated)

• Jan ’16 – Optom referral for suspicious discs and fields
• IOP 23/24
• C:D 0.6/0.5
• Fields Early loss R&L
• Apr ‘16 - Community glaucoma service
• IOP 24/24
• C:D 0.65/0.5
• Fields RE early paracentral loss, LE full
• CCT 599/595
• A/C Wide open angles
Impression – RE glaucoma suspect, LE OHT
Plan – No treatment indicated; Review 6/12
Case 4 – Glaucoma suspect (stable, untreated)
Female, Afrocarribean, Age 62
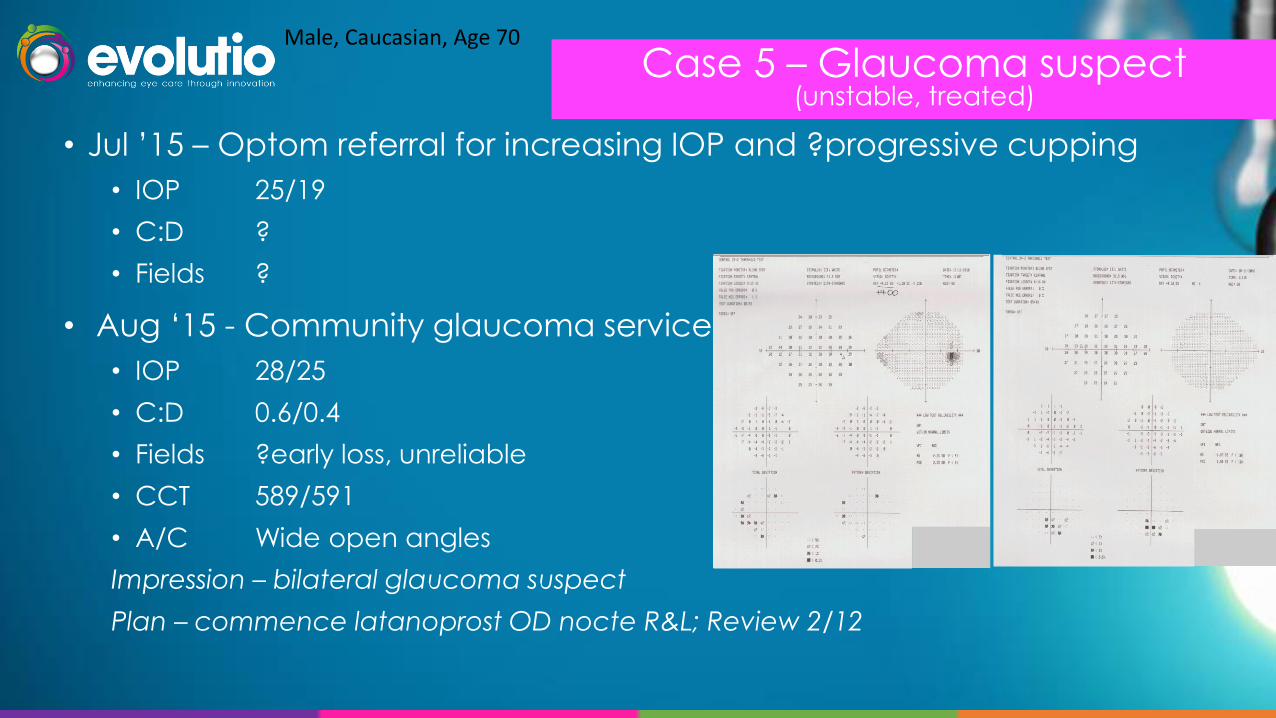
• Jul ’15 – Optom referral for increasing IOP and ?progressive cupping
• IOP 25/19
• C:D ?
• Fields ?
• Aug ‘15 - Community glaucoma service
• IOP 28/25
• C:D 0.6/0.4
• Fields ?early loss, unreliable
• CCT 589/591
• A/C Wide open angles
Impression – bilateral glaucoma suspect
Plan – commence latanoprost OD nocte R&L; Review 2/12
Case 5 – Glaucoma suspect (unstable, treated)
Male, Caucasian, Age 70

• Nov ‘18 – Transfer to eCare
• IOP 28/16
• C:D 0.7/0.4
• Fields RE ?mild loss, LE unreliable but ?early loss
• Impression
• RE glaucoma suspect, inadequate control (but compliant)
• LE glaucoma suspect, well controlled
• Plan
• RE continue latanoprost o.d. nocte, add brinzolamide b.d.
• LE continue latanoprost o.d. nocte
• Target IOP R19 L 17
• Review 2/12 (IOP)
Case 5 – Glaucoma suspect (unstable, treated)

• Oct ’16 – optometrist referral for suspicious discs & field defect
• IOP 22/21
• C:D 0.7/0.7
• Fields Arcuate defect L>R (repeatable)
• Nov ‘16 – community glaucoma clinic
• IOP 21/21
• C:D 0.8/0.8
• Fields Bilateral superior and inferior arcuate loss R>L
• Plan:
• Commence latanoprost o.d. nocte R&L
• Review 2/12
Case 6 – Glaucoma(stable, treated)
Male, Caucasian, Age 67

• Nov ‘18 - eCare
• IOP 21/21
• C:D 0.8/0.8
• Fields Bilateral superior and inferior arcuate loss R>L (unchanged)
• CCT 528/521
• A/C Wide open angles
Case 6 – Glaucoma(stable, treated)

Impression:
Bilateral stable glaucoma R>L
Plan:
Continue latanoprost OD nocte R&L
Review 12/12
Case 6 – Glaucoma(stable, treated)

• Aug ‘18 – optom referral for raised IOP with narrow angles
• IOP 25/24
• Discs 0.35/0.35
• Fields ‘Abnormal’ & unreliable
• A/C VH2
• Oct ‘18 - eCare
• IOP 27/26
• Discs 0.2/0.2
• Fields ‘Abnormal’ & unreliable
• A/C VH1 R&L N&T
Case 7 – Narrow AnglesFemale, Chinese, Age 48

• Impression
• Shallow A/C with raised IOP and field defect ?PAC
• Plan
• Refer to HES for angle assessment & ?prophylactic treatment
Case 7 – Narrow Angles
Gonioscopy if increased risk of acute angle closure and patients we treat
• At risk of acute angle closure (V/H<2)• Onward refer if gonioscopy not available
• Onward refer if raised IOP with angle closure
• Raised IOP requiring treatment• Classify as ‘open angle’ or ‘angle closure’
• ?corporate clinic at first review after starting treatment
Case 7 – Narrow Angles

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
Glaucoma protocol

Glaucoma protocol (quick reference)
NB – this quick reference guide is not a substitute for the clinical protocol

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s
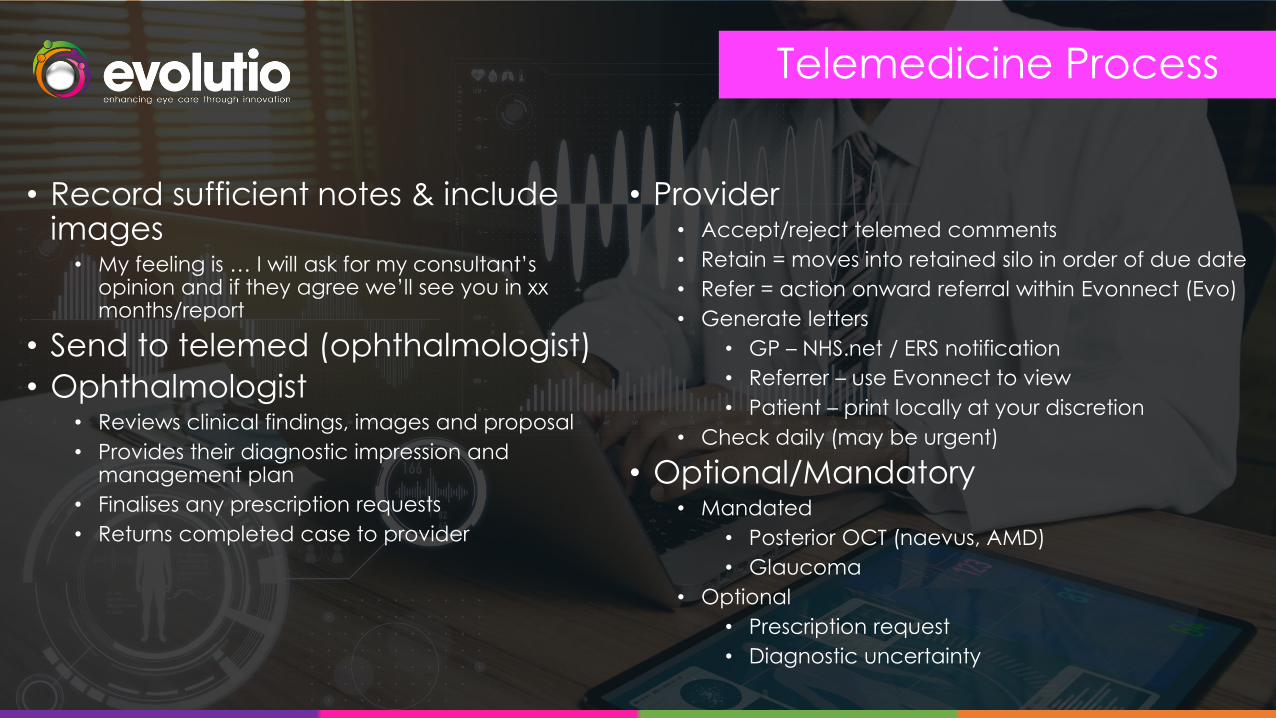
Telemedicine Process
• Record sufficient notes & include images
• My feeling is … I will ask for my consultant’s opinion and if they agree we’ll see you in xx months/report
• Send to telemed (ophthalmologist)
• Ophthalmologist• Reviews clinical findings, images and proposal
• Provides their diagnostic impression and management plan
• Finalises any prescription requests
• Returns completed case to provider
• Provider• Accept/reject telemed comments
• Retain = moves into retained silo in order of due date
• Refer = action onward referral within Evonnect (Evo)
• Generate letters
• GP – NHS.net / ERS notification
• Referrer – use Evonnect to view
• Patient – print locally at your discretion
• Check daily (may be urgent)
• Optional/Mandatory• Mandated
• Posterior OCT (naevus, AMD)
• Glaucoma
• Optional
• Prescription request
• Diagnostic uncertainty

““The consultant’s opinion was sought for confirmation and responded with the
following comments the next day:
Agreed, likely POAG.
Request sent to GP for
gutt. Latanoprost
0.005% nocte. Target
IOP is 18 R&L. Suggest
review in 3/12.”
The process of monitoring for change and proposing target pressures and treatments is robust and ultimately the consultant decides on the management plan. Telemedicine is a great opportunity to
bridge the gap between optometry and ophthalmology and develop your skills within practice.

Telemedicine

• If a patient requires a prescription• Complete ‘suggested medication’ box
• Send to telemedicine
• ‘Accept’ when ‘from telemed’• If consultant agrees/prescribes
• “Do you want to view printing options?”
• “Prescription request to mailroom”
• Dedicated request to GP (GMC no.)
• In addition to main report
Prescription Requests

Tips from the Consultants
Escalation of
treatment algorithm
IOP exceeds target
VF or ONH progression
despite 'adequate' IOP
control
Stable, IOP
within target
Continue
Monitoring
Monitoring
Lowering of
target IOP
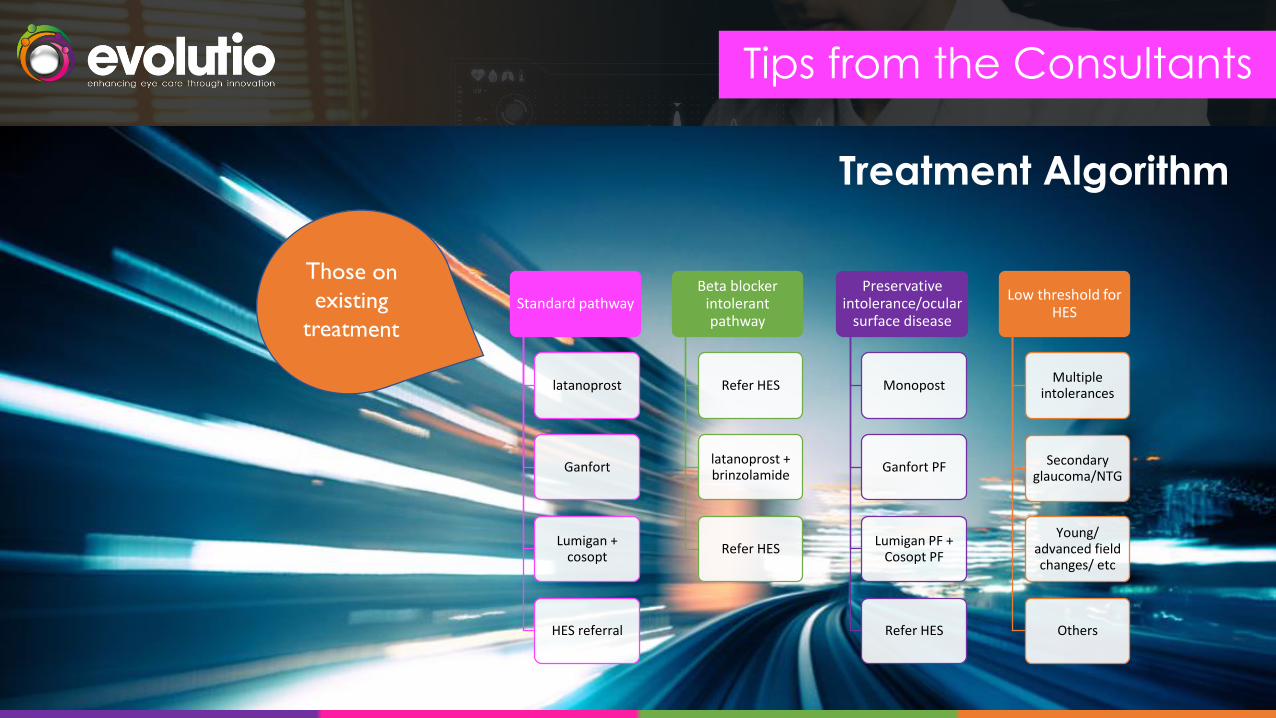
Tips from the Consultants
Treatment Algorithm
Standard pathway
latanoprost
Ganfort
Lumigan + cosopt
HES referral
Beta blocker intolerant pathway
Refer HES
latanoprost + brinzolamide
Refer HES
Preservative intolerance/ocular
surface disease
Monopost
Ganfort PF
Lumigan PF + Cosopt PF
Refer HES
Low threshold for HES
Multiple intolerances
Secondary glaucoma/NTG
Young/ advanced field changes/ etc
Others

Tips from the Consultants
Monitoring
Group 1. 4monthly for
at least 12 months
Glaucomatous visual field changesPOAG, NTGs
Group 2. 6 monthly for at
least 12 months
Glaucomatous disc changes, normal fieldsGl. suspects
Group 3. Annual Review
OHTSuspected anomalous discs, glaucoma unlikelyStable group 1 and 2 patients
Tips from the Consultants
A compact, targeted history
A complete set of relevant observations
Ideally with a conclusion
In a perfect world, we should be able to go straight to your conclusion first, then scan back to make sure the
details are correct
Eg 63 year old lady, no risks for glaucoma, IOP 25 corrected, normal disc, OCT, field = glaucoma suspect.
And a suggestion about follow up
Plus any relevant patient related issues
Eg prefers not to be treated at present/ worried about possible cancer
What do we like to see on your records?

Tips from the Consultants
History taking and reportingHow old is the patient
How long for /when did it start
Ever had it before
One eye or both
Anything makes it better / worse
For vision – when it’s at its worst, what would you be able to see
if you were looking at me.
Any previous ophthalmic history**. (They won’t tell you)
If there are previous notes, check through them for
eg highest IOP before treatment
PLEASE DO NOT MANIPULATE THE HISTORY TO MATCH WHAT YOU THINK IS HAPPENING.

Tips from the Consultants
Avoid abbreviations
Need to be understood by GP and other stakeholders
Helpful to start with age, sex and highest IOP first
Comment on the reliability of fields/OCT
Disc photos are essential, especially for tilted/anomalous discs
If the fields/OCT show progression review early e.g. 2/12
When prescribing, unless contraindicated consider:
1. Latanoprost
2. Ganfort (i.e. Bimatoprost with timolol)
3. Lumigan (bimatoprost) & cosopt (i.e. dorzolamide & timolol) … or refer!
Tips from the Consultants
Their letter is taken straight from your notes
They don’t know our abbreviations
So CRVO / LO / RD / ERM doesn’t mean anything to them
Beware your own pet abbreviations – I keep reading ones I have no idea about!
Remember to spell out RIGHT and LEFT
Quite apart from confusion over LVA, it’s frowned on medico-legally
Remember those poor GPs

Tips from the Consultants
However, you’ll need to remember to take that statement out when the record comes back from telemed.
If you are really concerned about a telemed decision, best to
email either
We’ll never get troubled if you say – “I really don’t know what is
going on here – what do you think?”
Remember

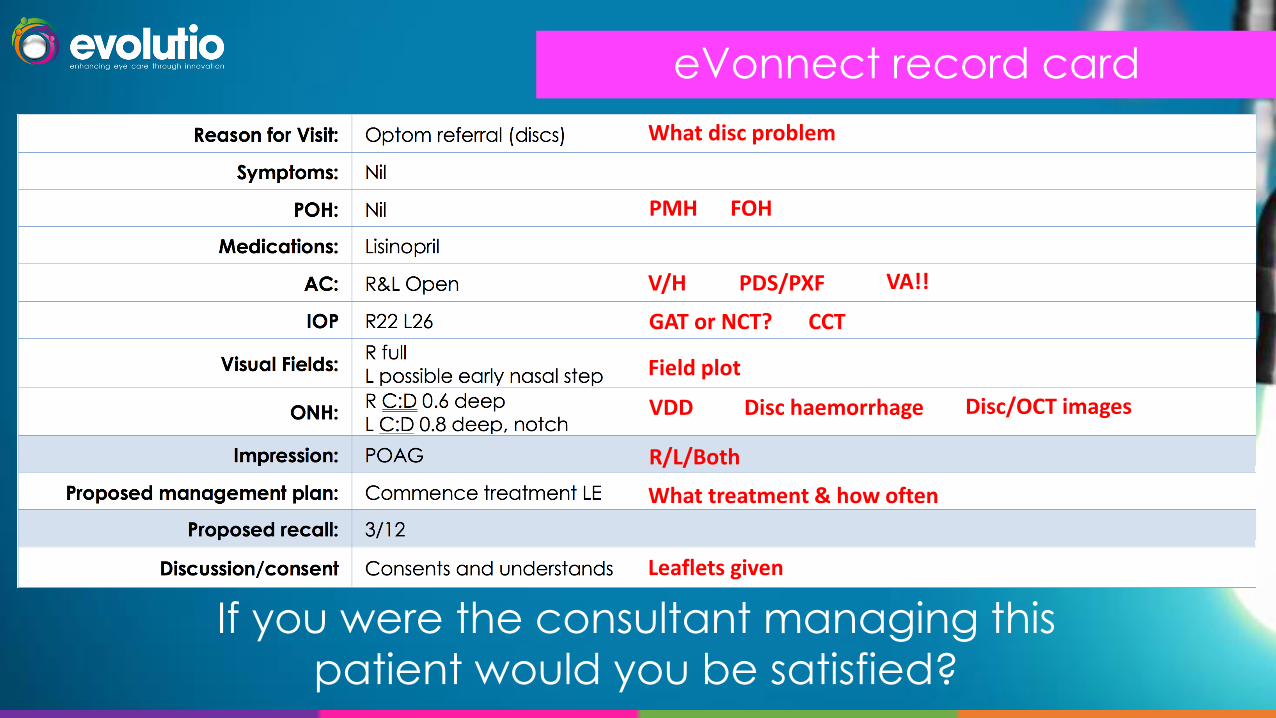
eVonnect record card
If you were the consultant managing this
patient would you be satisfied?
eVonnect record card
If you were the consultant managing this
patient would you be satisfied?
What disc problem
PMH FOH
VA!!
GAT or NCT? CCT
V/H
Field plot
Disc/OCT images
PDS/PXF
VDD Disc haemorrhage
R/L/Both
What treatment & how often
Leaflets given

Overview
Assessing Risk in Glaucoma
• Statistics
• Definitions
• Clinical Investigations• Discs / RNFL / Fields• IOP / CCT• A/C
• Treatment Philosophy• Target Pressure
• Treatment• Treatment Algorithm• Glaucoma Medications• Patient Information
• Review• Progression• Recall
Glaucoma Cases & Telemedicine
• Clinical case studies
• Clinical protocols
• Telemedicine
• Tips from the telemedicine consultants
• Validation & MCQ’s

• 12 MCQ’s
• Completed online• Eloomi training platform or Survey Monkey – link will be sent
• Minimum of 9/12 must be correctly answered to pass
Validation & MCQ’s

Thank you







