
Fibrillazione atriale e terapia anticoagulante
Clinica Geriatrica
Centro di Eccellenza Europeo e di Riferimento Regionale per
l’Aterosclerosi, l’Ipertensione Arteriosa e le Dislipidemie
Università “G. d’Annunzio” Chieti
Francesco Cipollone
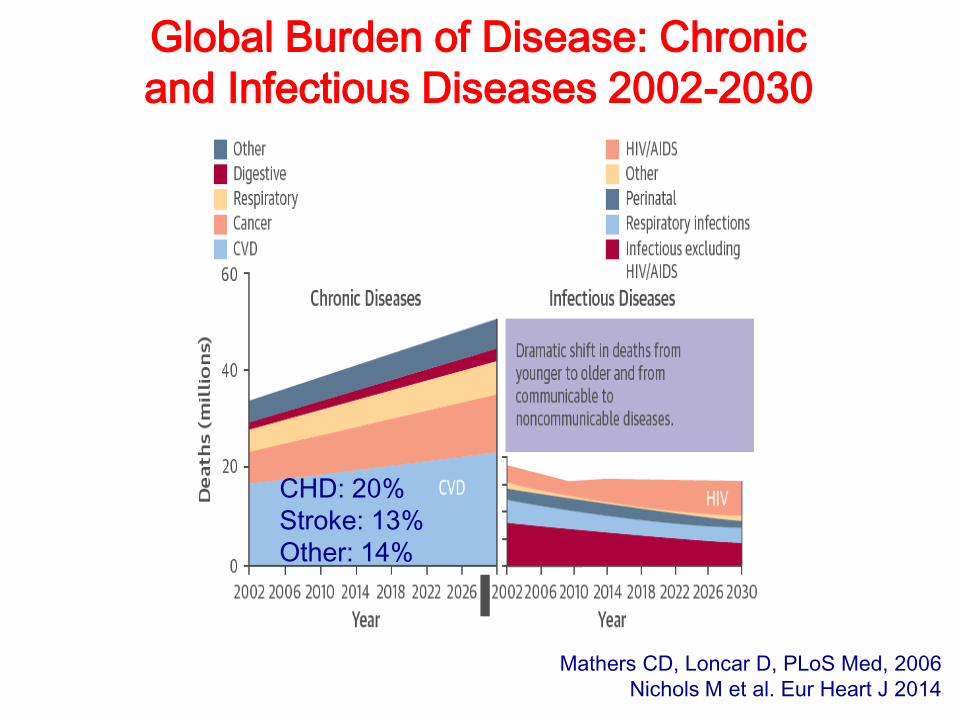
Global Burden of Disease: Chronic
and Infectious Diseases 2002-2030
Mathers CD, Loncar D, PLoS Med, 2006
Nichols M et al. Eur Heart J 2014
CHD: 20%
Stroke: 13%
Other: 14%
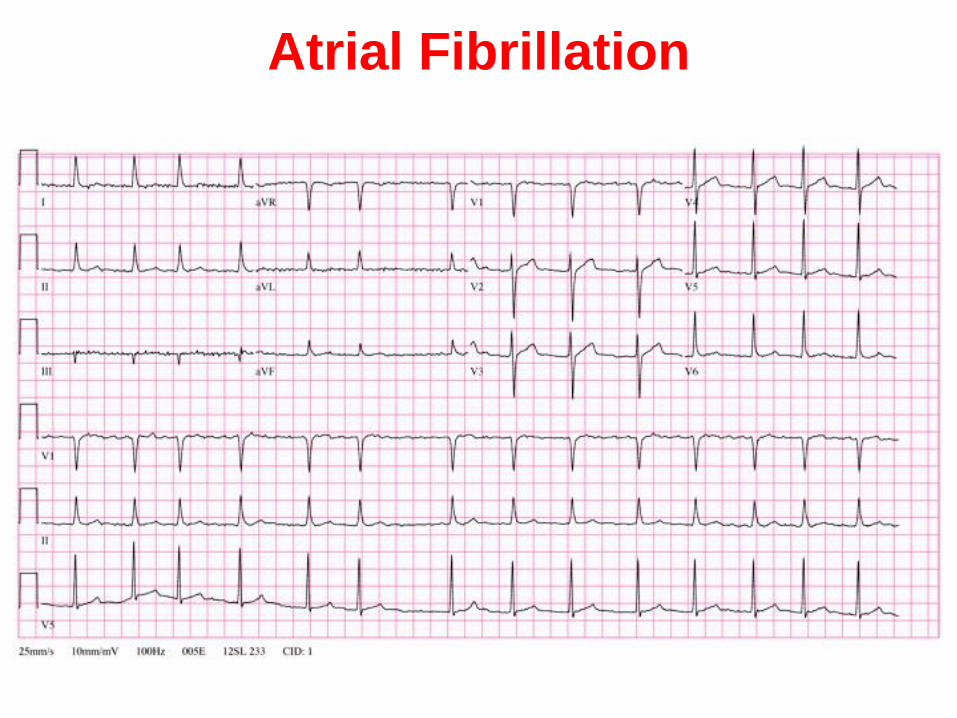
Atrial Fibrillation
Rising prevalence in Europe
• AF is the most common sustained arrhythmia
in the general population1 currently affecting
approximately 1.5-2% of the population
worldwide2
• With an aging population in Europe, the
prevalence of atrial fibrillation is expected to
double (to 3.3%) on the continent
representing an increase from 8.8 to 17.9
million adults aged over 55 years between
2010 and 20602.
• ITALY:
• Prevalence: 600.000-1.200.000
• Incidence: + 120.000/year
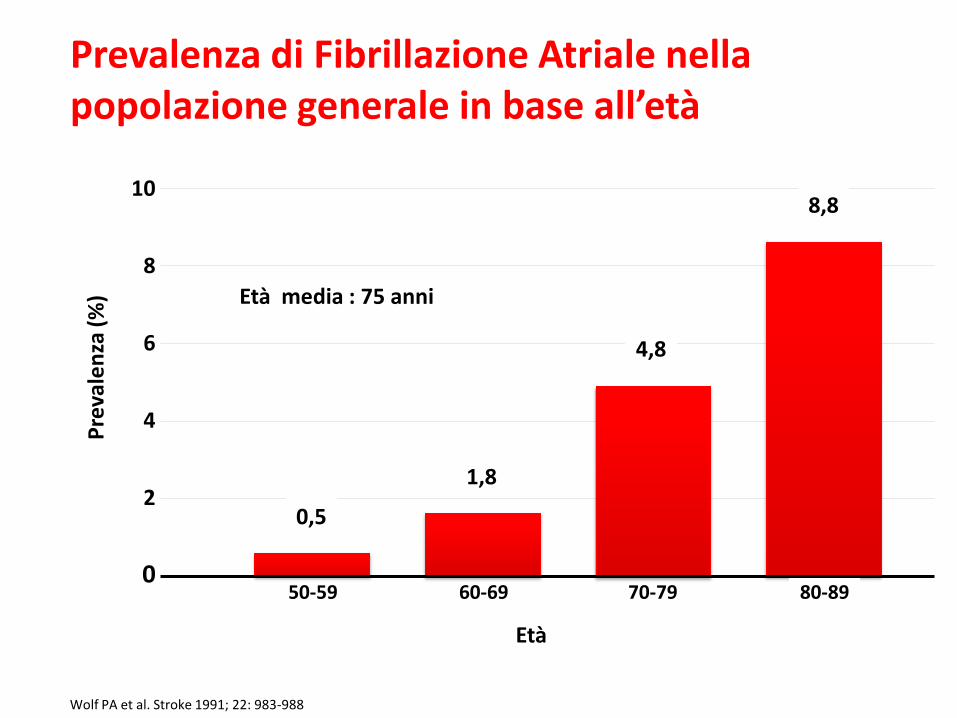
Wolf PA et al. Stroke 1991; 22: 983-988
10
8
6
4
2
0 60-69
Pre
vale
nza
(%
)
50-59 70-79
8,8
0,5
Età
1,8
4,8
Età media : 75 anni
Prevalenza di Fibrillazione Atriale nella popolazione generale in base all’età
80-89

The SPAF Investigators. AIM 1992; 116: 1 – 5
Incidenza annuale di stroke:
Pz con FA: 4.5% Pz in ritmo sinusale:0.2%-1.4%
Fibrillazione Atriale: stroke
tromboembolico
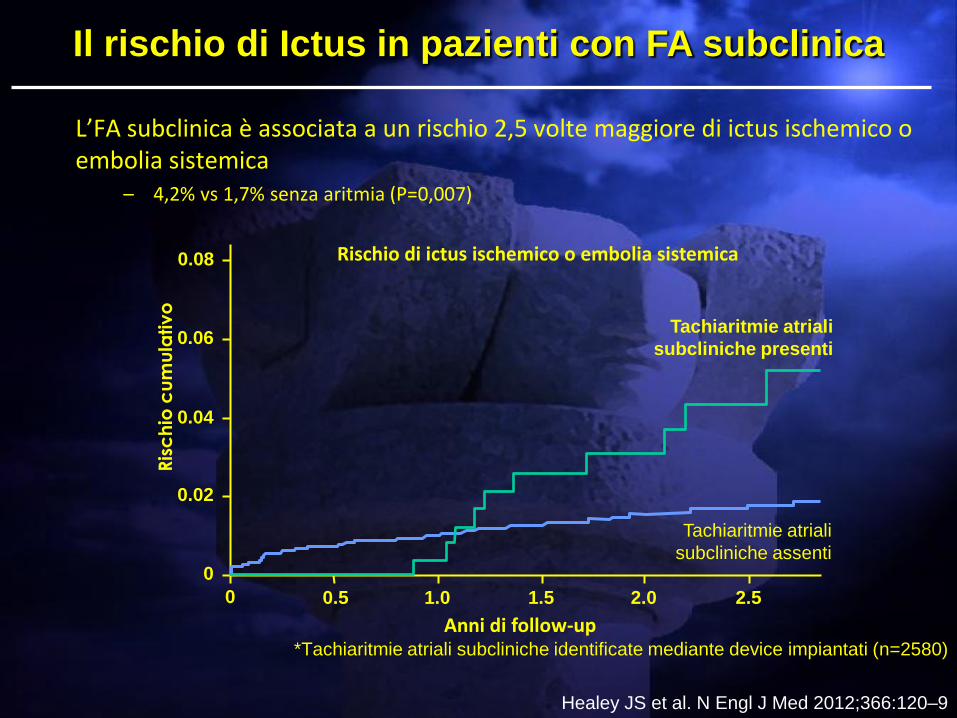
L’FA subclinica è associata a un rischio 2,5 volte maggiore di ictus ischemico o embolia sistemica
– 4,2% vs 1,7% senza aritmia (P=0,007)
*Tachiaritmie atriali subcliniche identificate mediante device impiantati (n=2580)
Healey JS et al. N Engl J Med 2012;366:120–9
Rischio di ictus ischemico o embolia sistemica
Anni di follow-up
0.06
0.08
0 0.5 1.0
Ris
ch
io c
um
ula
tiv
o
0.04
0.02
0
1.5 2.0 2.5
Tachiaritmie atriali
subcliniche assenti
Tachiaritmie atriali
subcliniche presenti
Il rischio di Ictus in pazienti con FA subclinica

Strategie Terapeutiche
After an incident in 1951, where a US
Army inductee unsuccessfully attempted
suicide with multiple doses of warfarin in
rodenticide and recovered fully after
presenting to a hospital, and being treated
with vitamin K (by then known as a
specific antidote),studies began in the use
of warfarin as a therapeutic anticoagulant.
It was found to be generally superior to
dicoumarol, and in 1954 was approved for
medical use in humans. A famous early recipient of warfarin was
US president Dwight Eisenhower, who
was prescribed the drug after having a
heart attack in 1955.
Warfarin and anticoagulation
LA DIFFICILE GESTIONE DEL FARMACO
+ ? ?
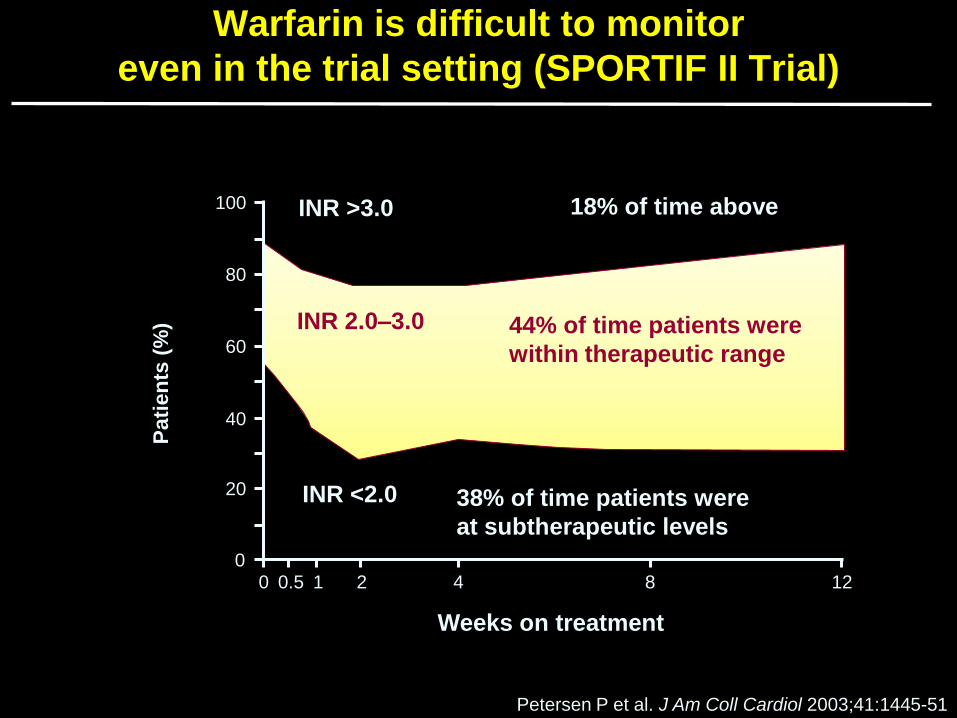
Warfarin is difficult to monitor
even in the trial setting (SPORTIF II Trial)
Petersen P et al. J Am Coll Cardiol 2003;41:1445-51
44% of time patients were
within therapeutic range
38% of time patients were
at subtherapeutic levels
18% of time above
Pati
en
ts (
%) INR 2.0–3.0
100
80
60
40
20
0 0 0.5 1 2 4 8 12
Weeks on treatment
INR >3.0
INR <2.0
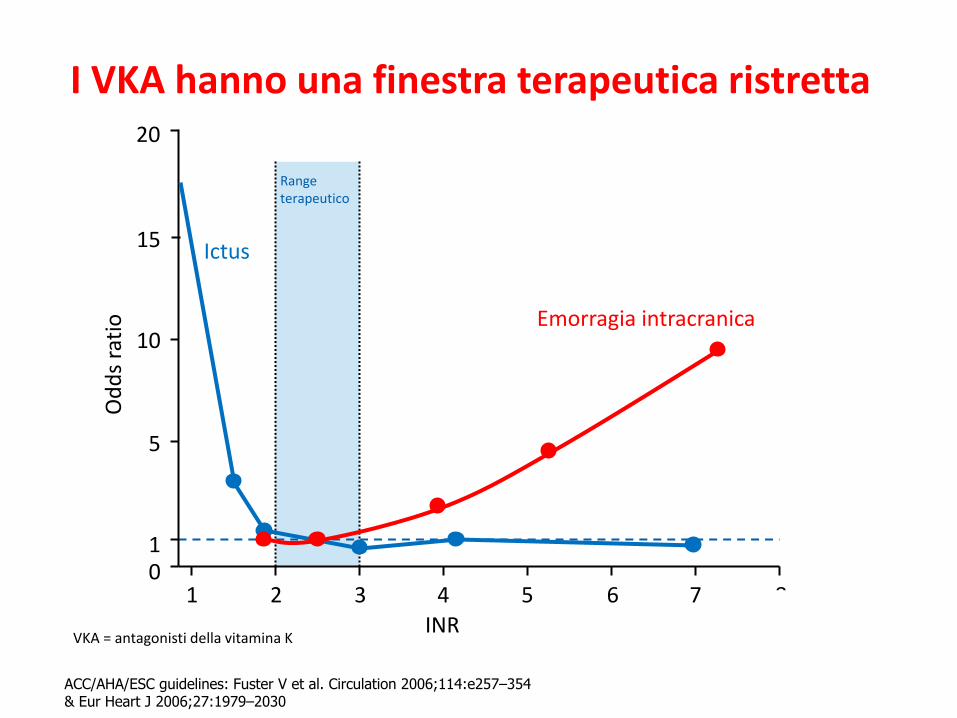
I VKA hanno una finestra terapeutica ristretta
19 ACC/AHA/ESC guidelines: Fuster V et al. Circulation 2006;114:e257–354 & Eur Heart J 2006;27:1979–2030
1
INR
Od
ds
rati
o
2
15
8
10
5
0 1
3 4 5 6 7
Ictus
Emorragia intracranica
Range terapeutico
20
VKA = antagonisti della vitamina K
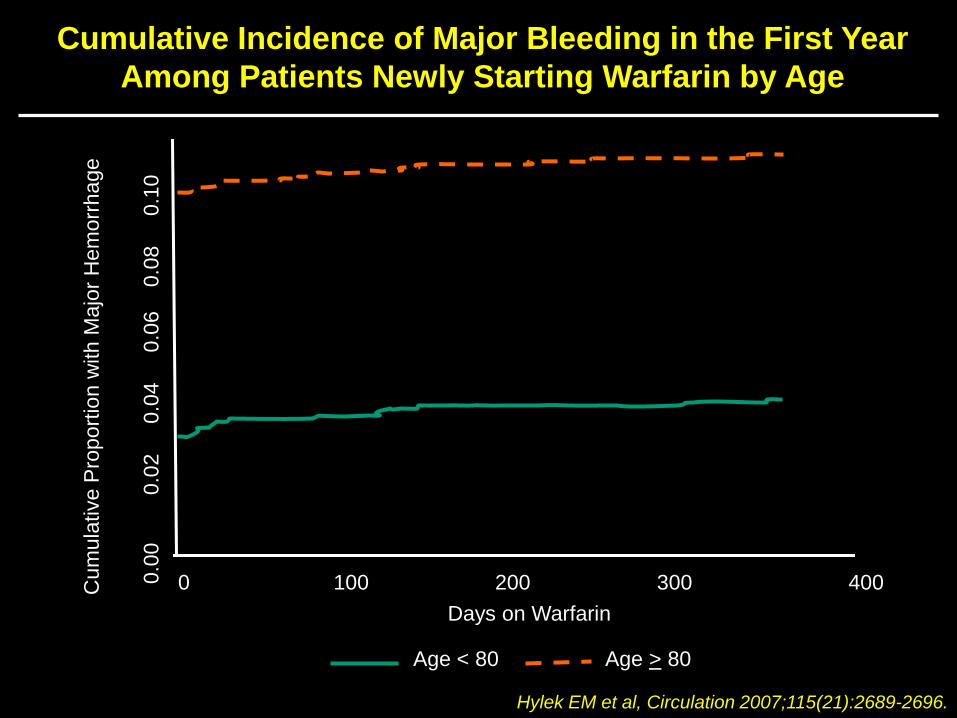
Cumulative Incidence of Major Bleeding in the First Year
Among Patients Newly Starting Warfarin by Age
Hylek EM et al, Circulation 2007;115(21):2689-2696.
0 100 200 300 400
Days on Warfarin
Age < 80 Age > 80
Cum
ula
tive P
roport
ion w
ith M
ajo
r H
em
orr
hage
0.0
0
0.0
2
0
.04
0
.06
0.0
8
0
.10
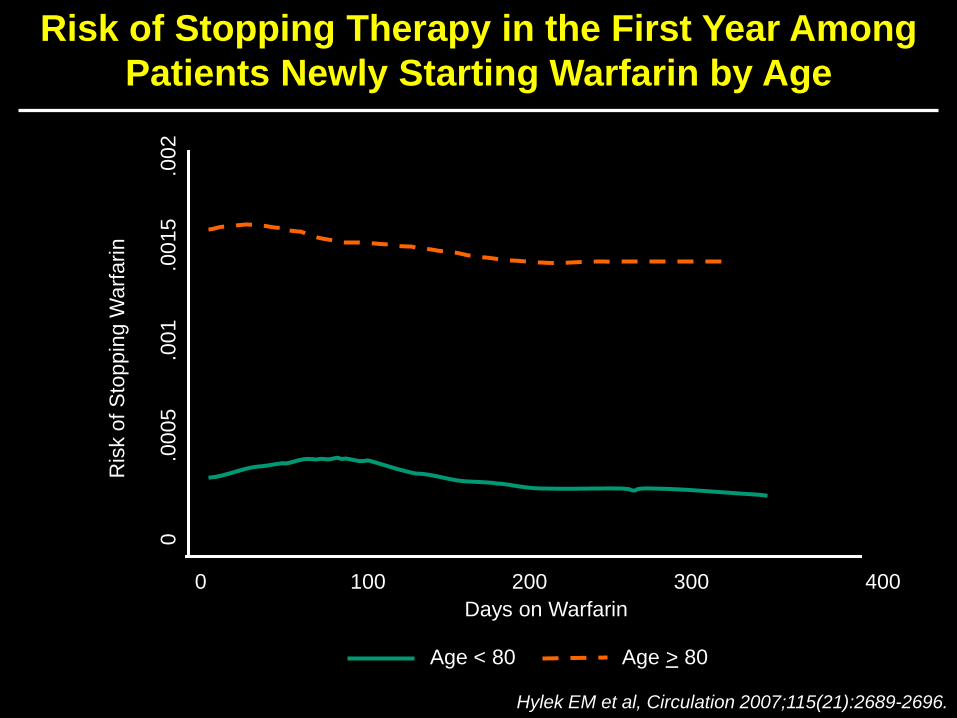
Risk of Stopping Therapy in the First Year Among
Patients Newly Starting Warfarin by Age
Hylek EM et al, Circulation 2007;115(21):2689-2696.
0 100 200 300 400
Days on Warfarin
Age < 80 Age > 80
Ris
k o
f S
top
pin
g W
arf
arin
0
.00
05
.00
1
.0
01
5
.0
02
consequences…

Warfarin è utilizzato solo in metà dei pazienti con FA
Age (yrs)
Uso d
el w
arf
arin n
ei pazie
nti
ele
ggib
ili (
%)
Utilizzo globale= 55%
100
<55
80
60
40
20
0 55–64 65–74 75–84 85
44%
58% 61%
57%
35%
Go A et al. Ann Intern Med 1999;131:927
Il warfarin è sotto-utilizzato soprattutto nei pazienti anziani che sono quelli a più alto rischio di ictus

Lo scarso impiego della TAO nei
pazienti con FA a rischio elevato è
stato riscontrato nella maggior parte
dei 54 studi (1998-2008)
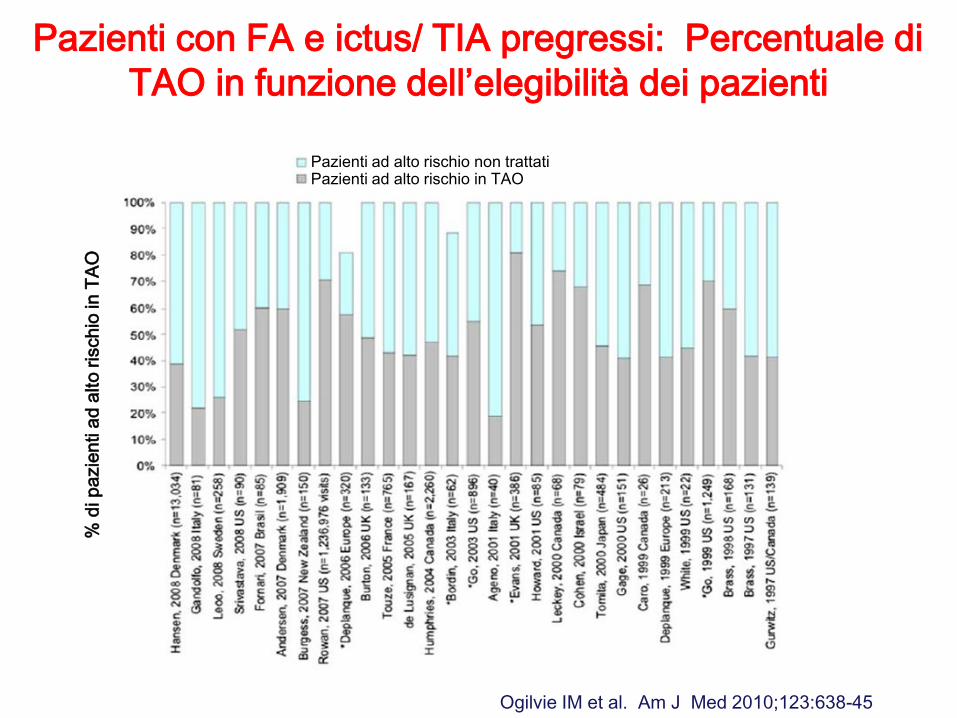
Ogilvie IM et al. Am J Med 2010;123:638-45
% d
i p
azie
nti a
d a
lto
ris
ch
io in
TA
O
Pazienti ad alto rischio non trattati Pazienti ad alto rischio in TAO
Pazienti con FA e ictus/ TIA pregressi: Percentuale di
TAO in funzione dell’elegibilità dei pazienti

Profilo dell’anticoagulante ideale
Furie & Furie. N Engl J Med 2008;359:938–949
Turpie. Eur Heart J 2007;29:155–165
Ampia
finestra
terapeutica
Somministrazione
orale e dosaggio
fisso
Rapidi onset e
offset d’azione
Dose-risposta
Prevedibile
Assenza di
monitoraggio
esami di
laboratorio
Ridotto rischio
di
sanguinamento
Interazioni
minime con
altri farmaci e
cibo
Reversibile
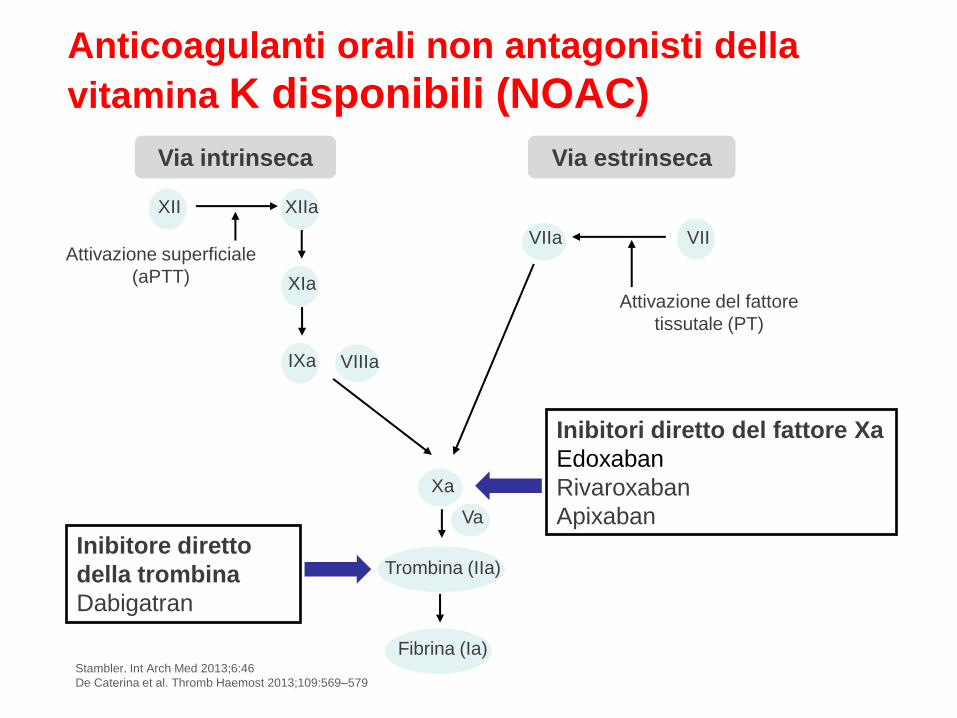
Stambler. Int Arch Med 2013;6:46
De Caterina et al. Thromb Haemost 2013;109:569–579
Anticoagulanti orali non antagonisti della
vitamina K disponibili (NOAC)
Attivazione superficiale
(aPTT)
Attivazione del fattore
tissutale (PT)
Via intrinseca Via estrinseca
Inibitori diretto del fattore Xa
Edoxaban
Rivaroxaban
Apixaban
Inibitore diretto
della trombina
Dabigatran
XII XIIa
XIa
VIIa VII
VIIIa IXa
Xa
Trombina (IIa)
Fibrina (Ia)
Va
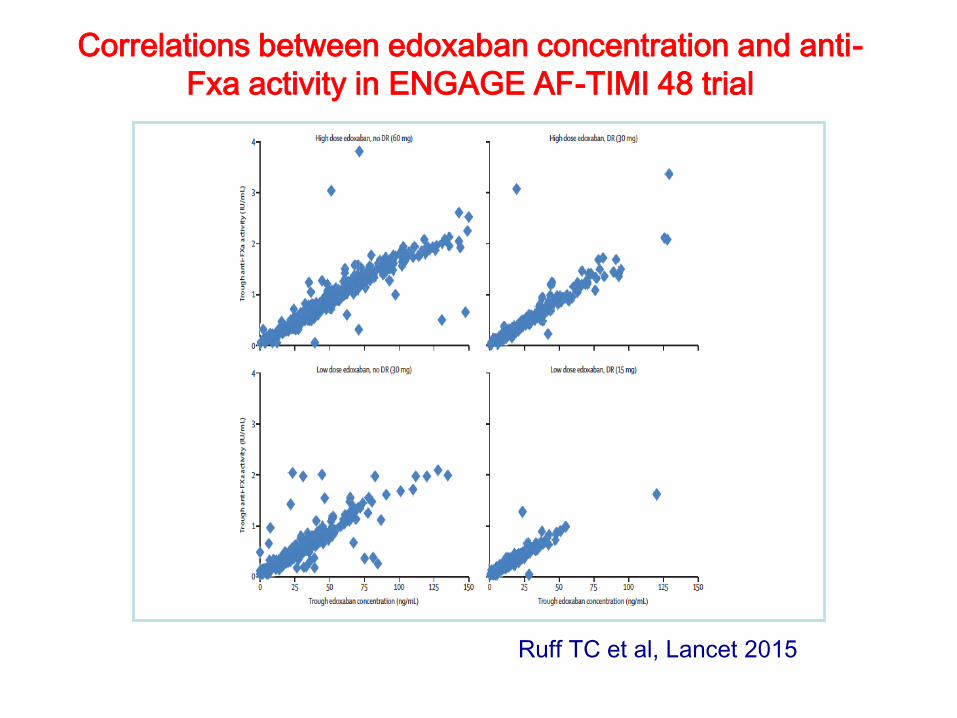
Correlations between edoxaban concentration and anti-
Fxa activity in ENGAGE AF-TIMI 48 trial
Ruff TC et al, Lancet 2015
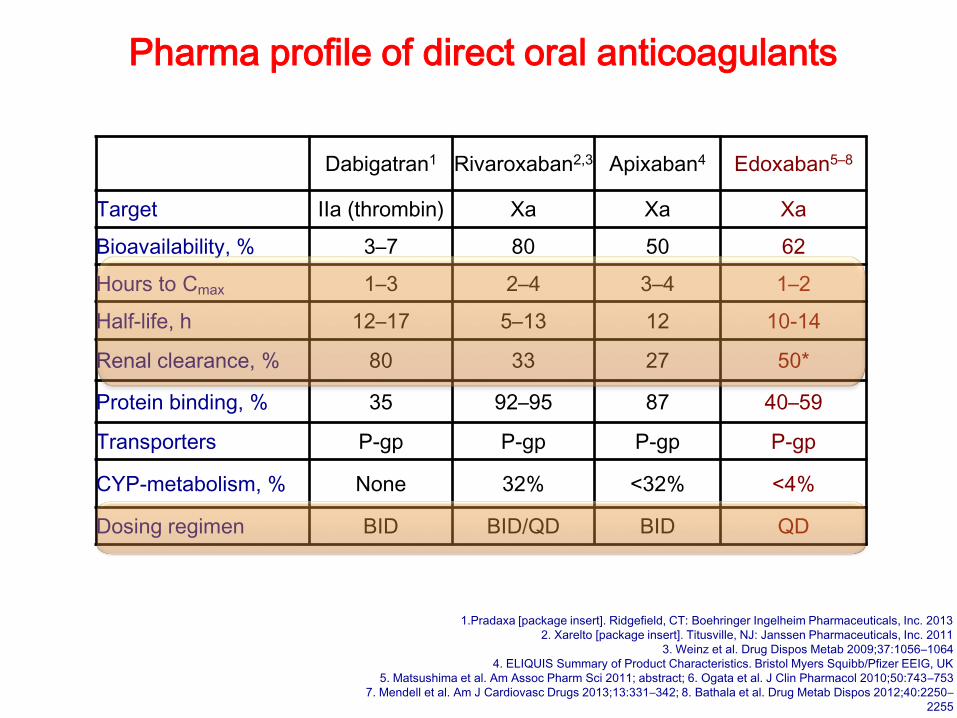
Pharma profile of direct oral anticoagulants
1.Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc. 2013
2. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc. 2011
3. Weinz et al. Drug Dispos Metab 2009;37:1056–1064
4. ELIQUIS Summary of Product Characteristics. Bristol Myers Squibb/Pfizer EEIG, UK
5. Matsushima et al. Am Assoc Pharm Sci 2011; abstract; 6. Ogata et al. J Clin Pharmacol 2010;50:743–753
7. Mendell et al. Am J Cardiovasc Drugs 2013;13:331–342; 8. Bathala et al. Drug Metab Dispos 2012;40:2250–
2255
Dabigatran1 Rivaroxaban2,3 Apixaban4 Edoxaban5–8
Target IIa (thrombin) Xa Xa Xa
Bioavailability, % 3–7 80 50 62
Hours to Cmax 1–3 2–4 3–4 1–2
Half-life, h 12–17 5–13 12 10-14
Renal clearance, % 80 33 27 50*
Protein binding, % 35 92–95 87 40–59
Transporters P-gp P-gp P-gp P-gp
CYP-metabolism, % None 32% <32% <4%
Dosing regimen BID BID/QD BID QD
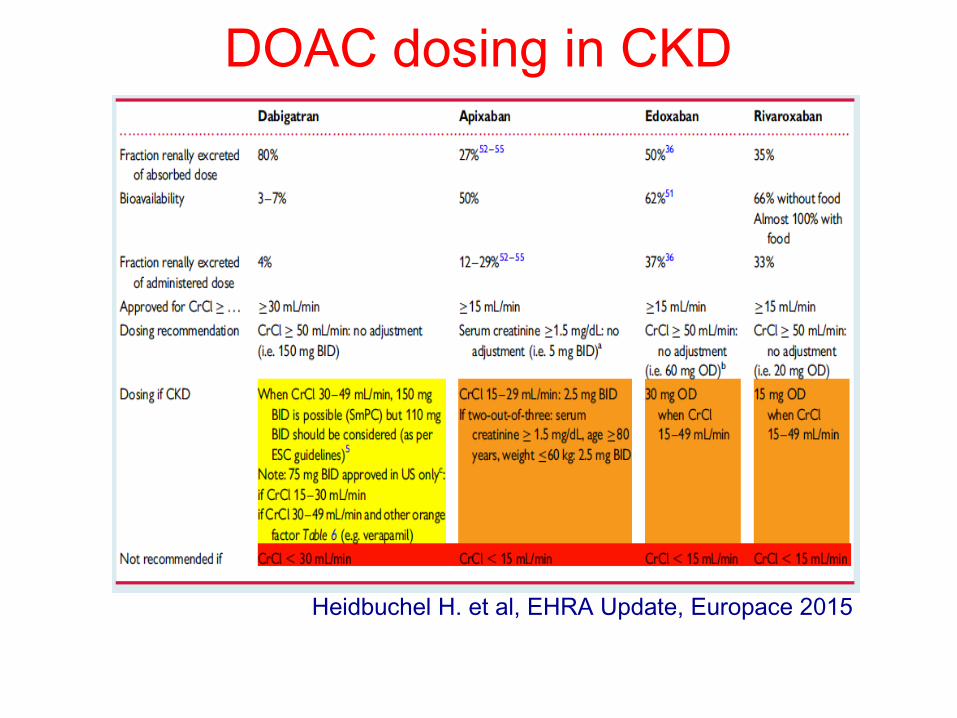
DOAC dosing in CKD
Heidbuchel H. et al, EHRA Update, Europace 2015
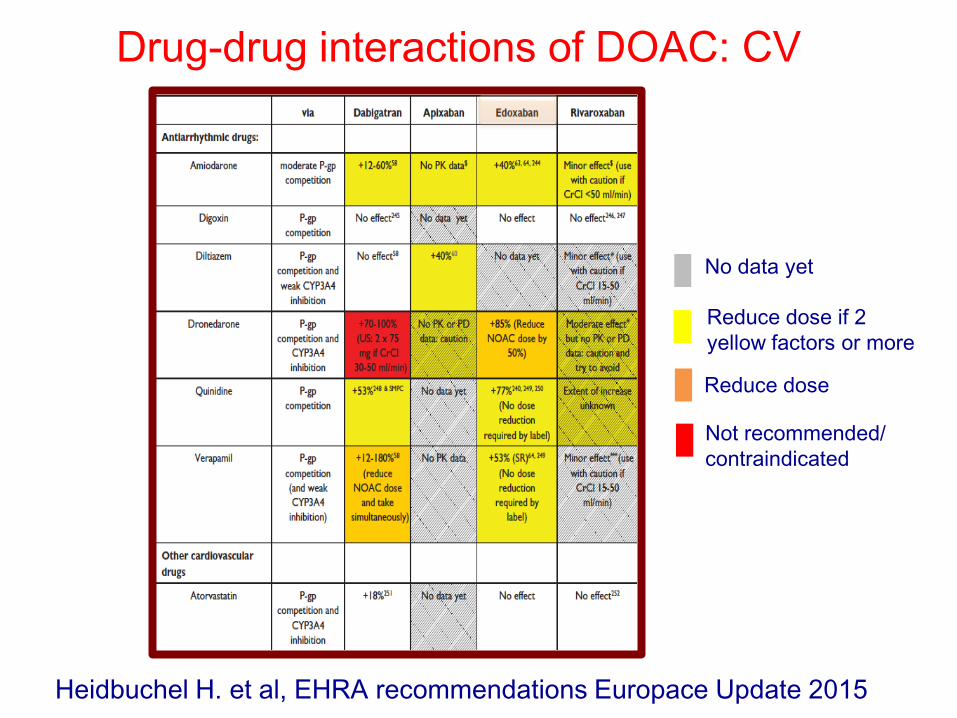
Drug-drug interactions of DOAC: CV
Not recommended/
contraindicated
Reduce dose
No data yet
Reduce dose if 2
yellow factors or more
Heidbuchel H. et al, EHRA recommendations Europace Update 2015
Efficacia e sicurezza
I quattro studi clinici randomizzati sui NAO nella prevenzione dell’ictus nella fibrillazione atriale
1. Connolly SJ et al. N Engl J Med. 2009;361(12):1139-1151; 2. Granger CB et al. N Engl J Med. 2011;365(11):981-992; 3. Patel MR et al. N Engl J Med. 2011;365(10):883-891; 4. Giugliano RP et al. N Engl J Med. 2013;369(22):2093-2104
1 2
3 4
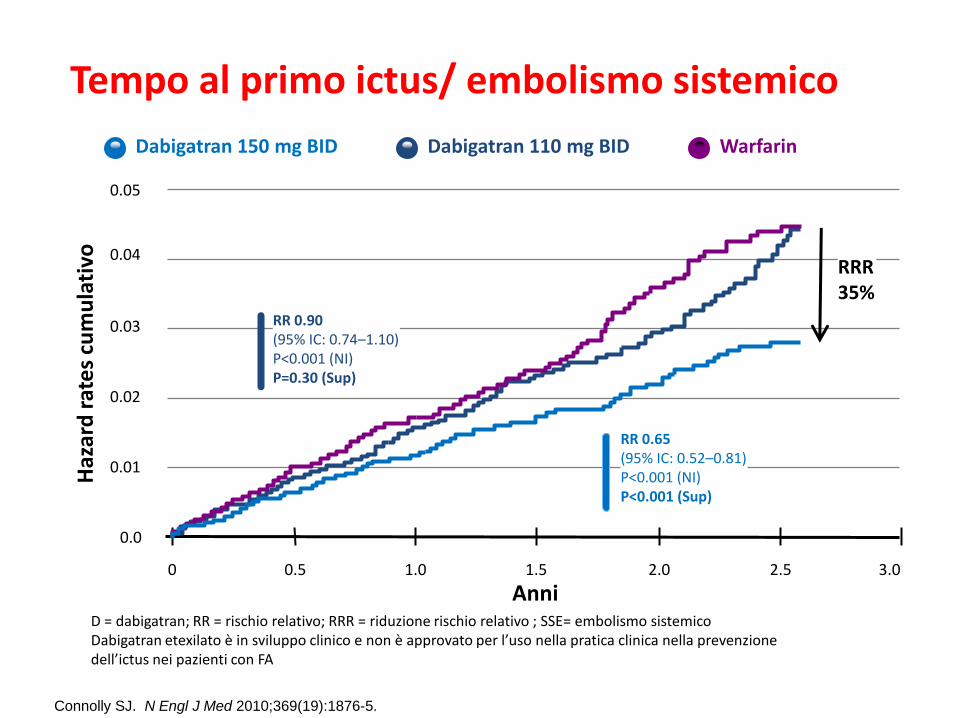
Tempo al primo ictus/ embolismo sistemico
Warfarin
Anni
RRR 35%
Haz
ard
rat
es
cum
ula
tivo
0
0.01
0.02
0.03
0.05
0.04
0.0
0.5 1.0 1.5 2.0 2.5
RR 0.90 (95% IC: 0.74–1.10) P<0.001 (NI) P=0.30 (Sup)
RR 0.65 (95% IC: 0.52–0.81) P<0.001 (NI) P<0.001 (Sup)
Dabigatran 150 mg BID Dabigatran 110 mg BID
3.0
Connolly SJ. N Engl J Med 2010;369(19):1876-5.
D = dabigatran; RR = rischio relativo; RRR = riduzione rischio relativo ; SSE= embolismo sistemico Dabigatran etexilato è in sviluppo clinico e non è approvato per l’uso nella pratica clinica nella prevenzione dell’ictus nei pazienti con FA
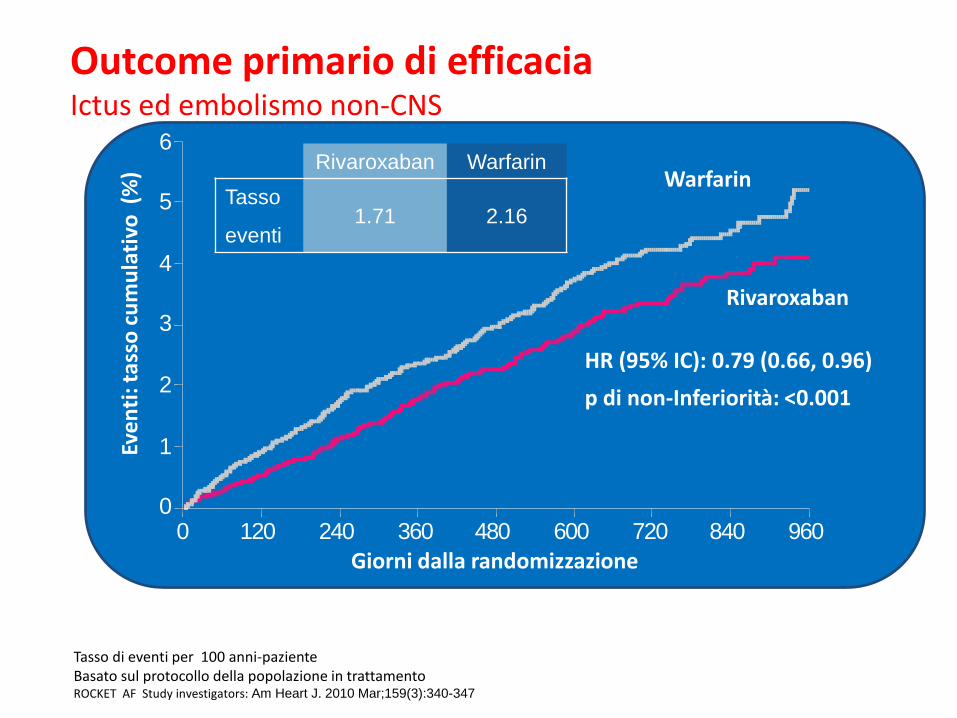
Outcome primario di efficacia Ictus ed embolismo non-CNS
Tasso di eventi per 100 anni-paziente Basato sul protocollo della popolazione in trattamento ROCKET AF Study investigators: Am Heart J. 2010 Mar;159(3):340-347
0
1
2
3
4
5
6
0 120 240 360 480 600 720 840 960
Warfarin
HR (95% IC): 0.79 (0.66, 0.96)
p di non-Inferiorità: <0.001
Giorni dalla randomizzazione
Eve
nti
: tas
so c
um
ula
tivo
(%
)
Rivaroxaban
Rivaroxaban Warfarin
Tasso
eventi 1.71 2.16
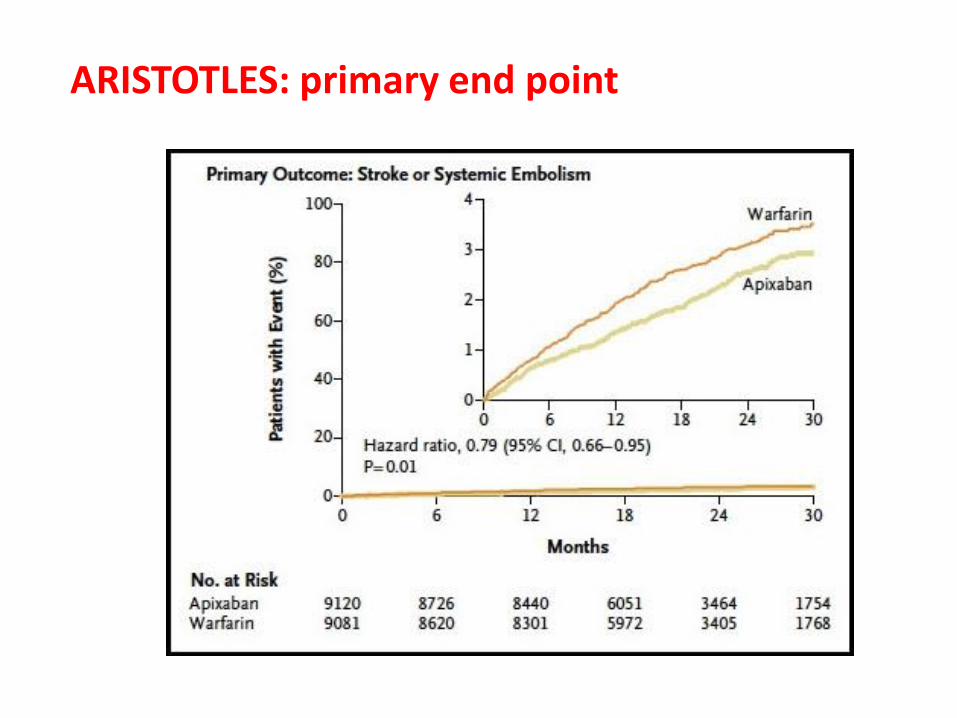
ARISTOTLES: primary end point
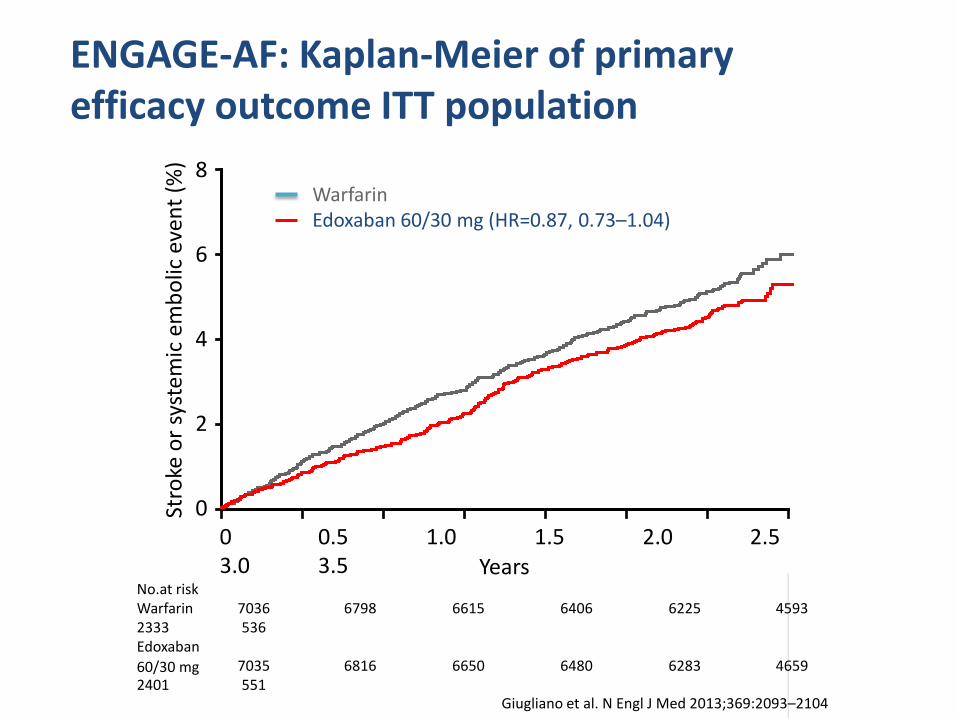
ENGAGE-AF: Kaplan-Meier of primary efficacy outcome ITT population
Warfarin Edoxaban 60/30 mg (HR=0.87, 0.73–1.04)
8
6
4
2
0 Stro
ke o
r sy
stem
ic e
mb
olic
eve
nt
(%)
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
No.at risk Warfarin 7036 6798 6615 6406 6225 4593 2333 536 Edoxaban 7035 6816 6650 6480 6283 4659 2401 551
Years
Median TTR=68.4%
Giugliano et al. N Engl J Med 2013;369:2093–2104
60/30 mg
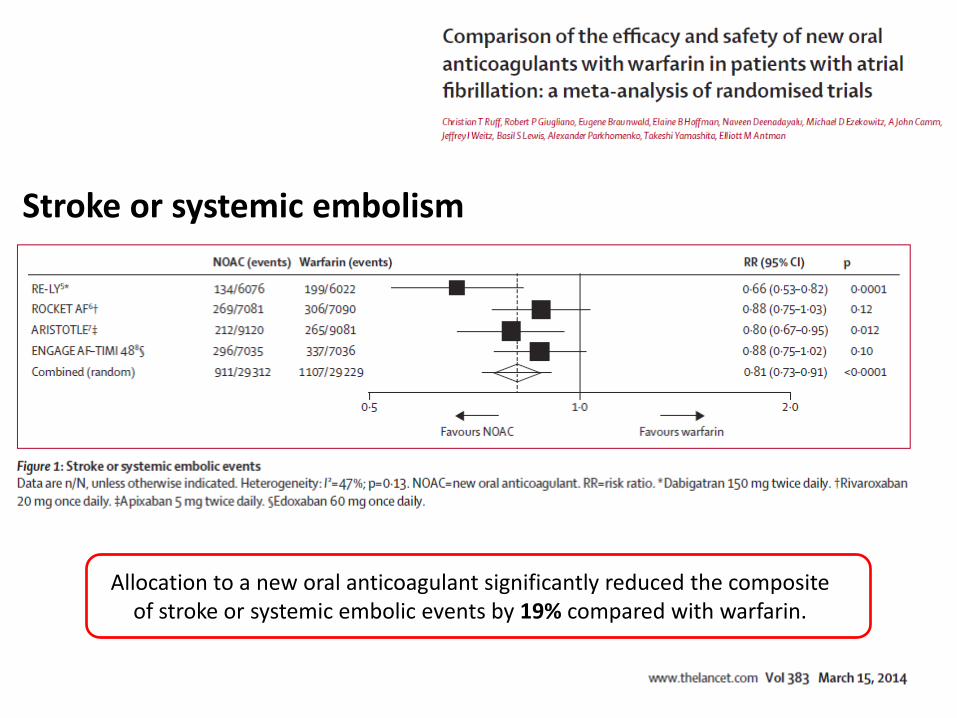
Allocation to a new oral anticoagulant significantly reduced the composite of stroke or systemic embolic events by 19% compared with warfarin.
Stroke or systemic embolism
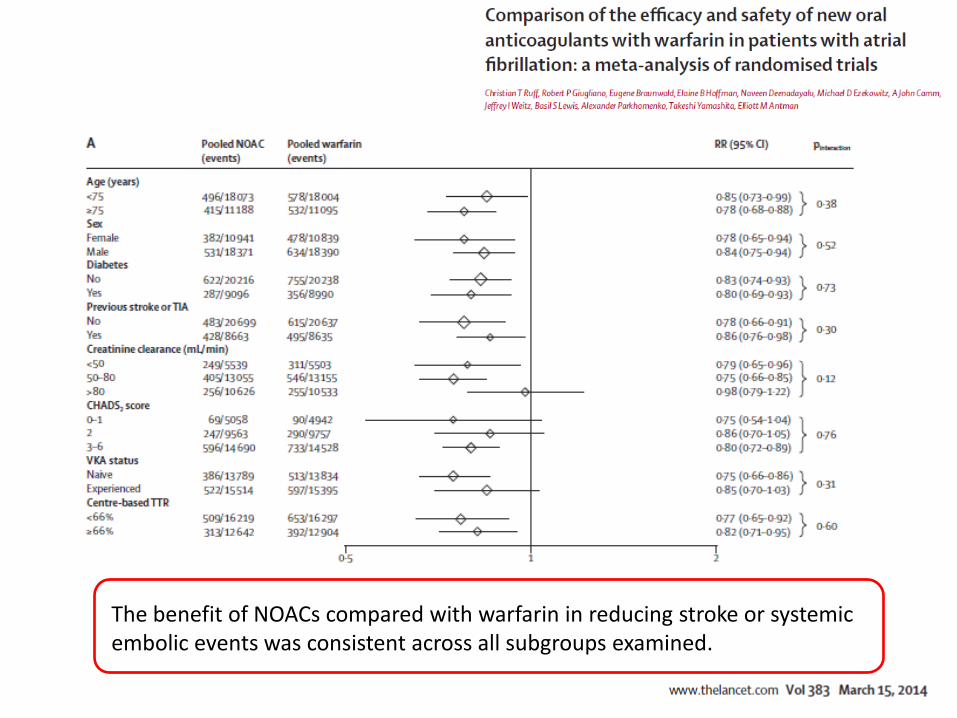
The benefit of NOACs compared with warfarin in reducing stroke or systemic embolic events was consistent across all subgroups examined.
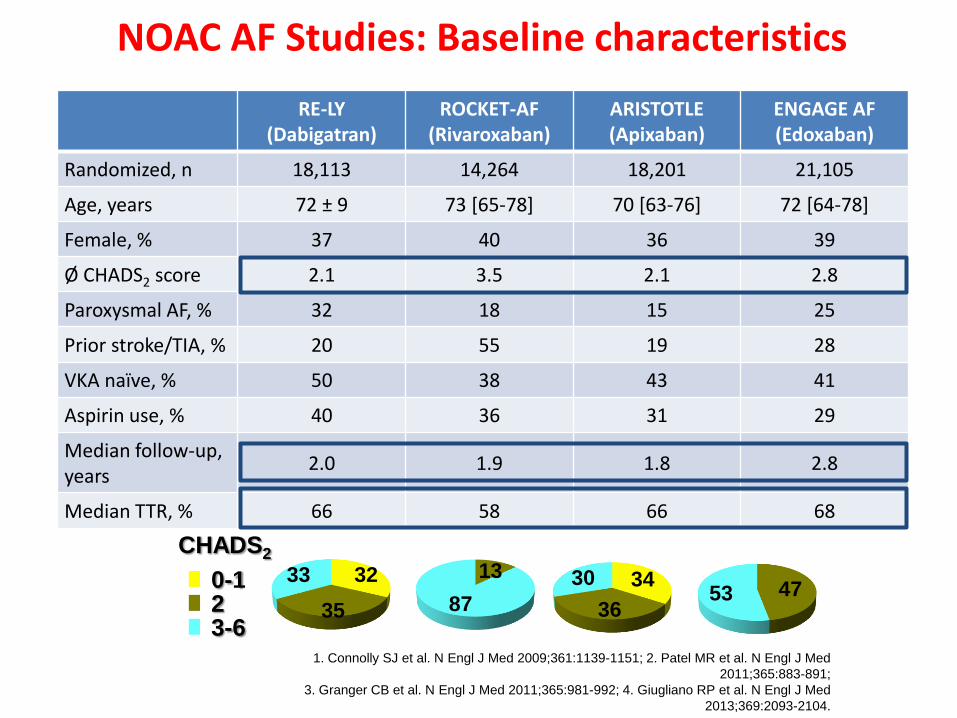
NOAC AF Studies: Baseline characteristics
RE-LY (Dabigatran)
ROCKET-AF (Rivaroxaban)
ARISTOTLE (Apixaban)
ENGAGE AF (Edoxaban)
Randomized, n 18,113 14,264 18,201 21,105
Age, years 72 ± 9 73 [65-78] 70 [63-76] 72 [64-78]
Female, % 37 40 36 39
Ø CHADS2 score 2.1 3.5 2.1 2.8
Paroxysmal AF, % 32 18 15 25
Prior stroke/TIA, % 20 55 19 28
VKA naïve, % 50 38 43 41
Aspirin use, % 40 36 31 29
Median follow-up, years
2.0 1.9 1.8 2.8
Median TTR, % 66 58 66 68
32
35
33 13
87 47 53
34
36
30
CHADS2
2 3-6
0-1
1. Connolly SJ et al. N Engl J Med 2009;361:1139-1151; 2. Patel MR et al. N Engl J Med
2011;365:883-891;
3. Granger CB et al. N Engl J Med 2011;365:981-992; 4. Giugliano RP et al. N Engl J Med
2013;369:2093-2104.
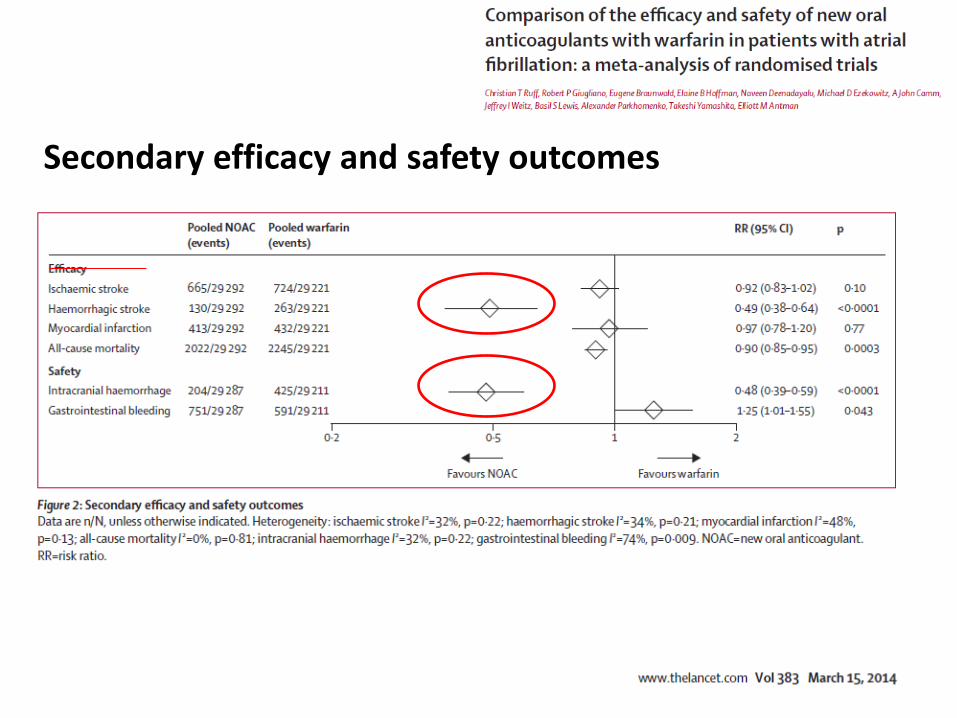
Secondary efficacy and safety outcomes
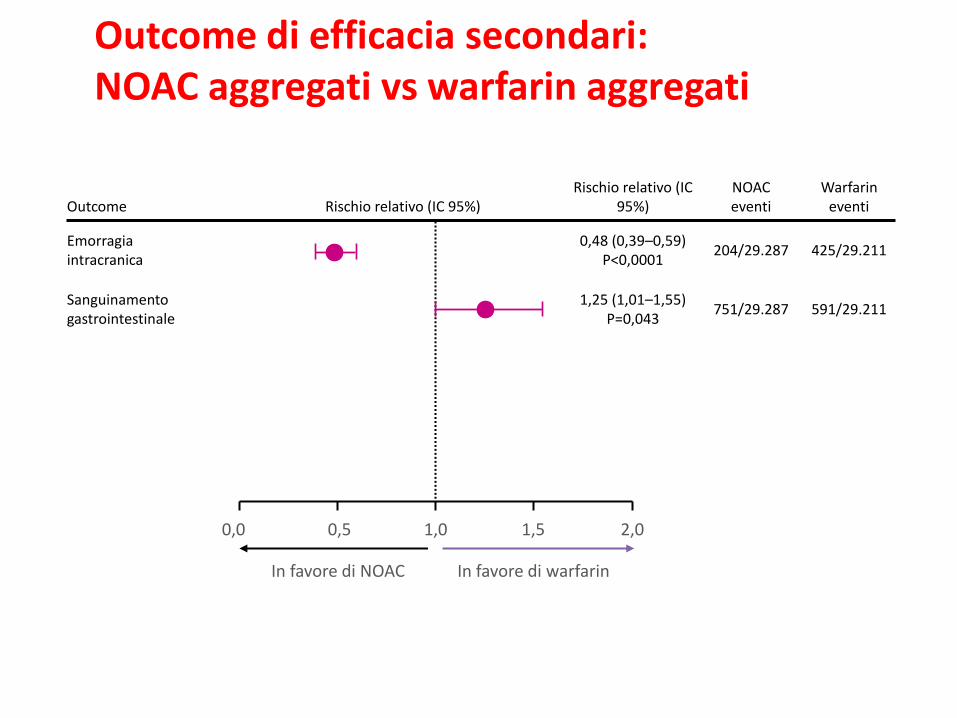
Rischio relativo (IC 95%) NOAC eventi
Warfarin eventi Outcome
Rischio relativo (IC 95%)
Emorragia intracranica
0,48 (0,39–0,59) P<0,0001
204/29.287 425/29.211
Sanguinamento gastrointestinale
1,25 (1,01–1,55) P=0,043
751/29.287 591/29.211
Outcome di efficacia secondari: NOAC aggregati vs warfarin aggregati
0,0 1,0 2,0 1,5 0,5
In favore di NOAC In favore di warfarin
Meta-analysis of data from RE-LY®, ROCKET AF, ARISTOTLE, ENGAGE AF-TIMI 48
Ruff et al. Lancet 2013
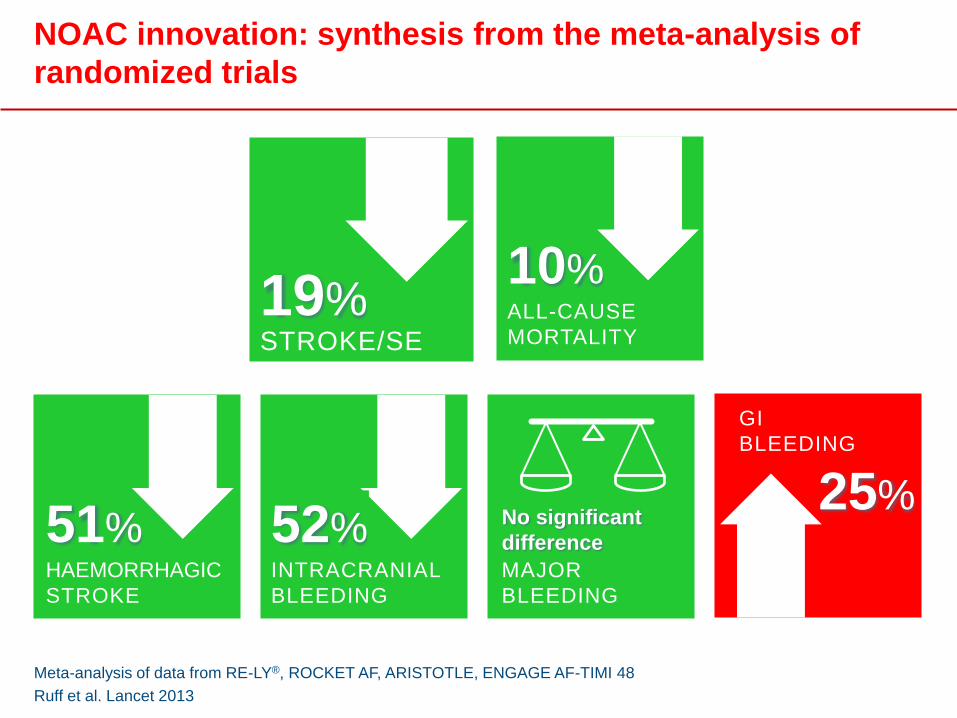
NOAC innovation: synthesis from the meta-analysis of
randomized trials
ALL-CAUSE
MORTALITY
10%
STROKE/SE
19%
INTRACRANIAL
BLEEDING
52% MAJOR
BLEEDING
No significant
difference
GI
BLEEDING
25%
HAEMORRHAGIC
STROKE
51%
Cosa dicono le linee guida?
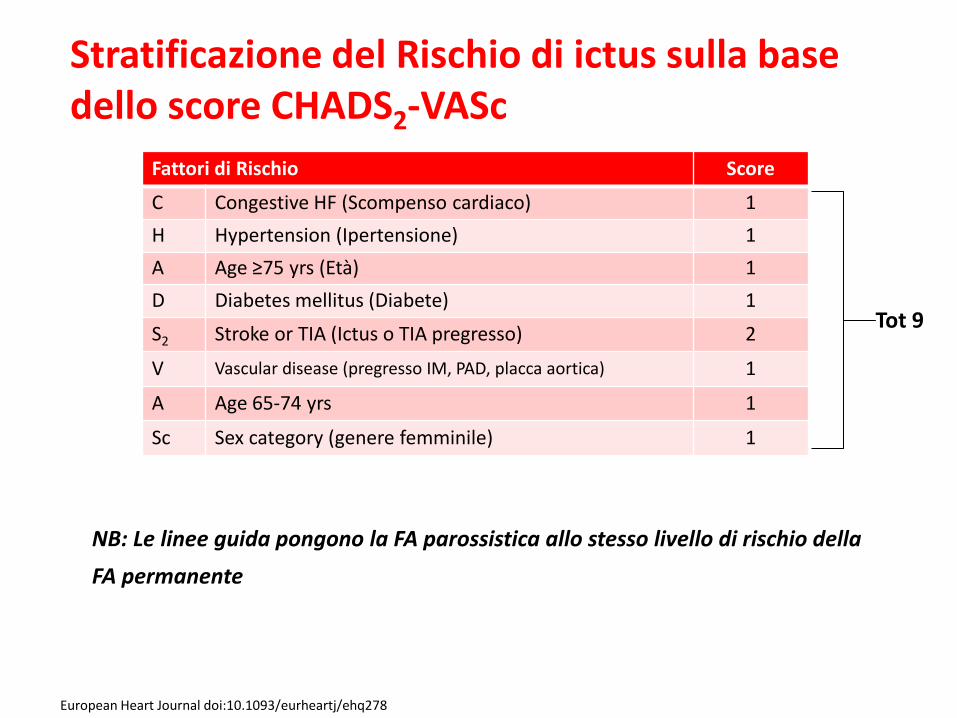
Stratificazione del Rischio di ictus sulla base dello score CHADS2-VASc
Fattori di Rischio Score
C Congestive HF (Scompenso cardiaco) 1
H Hypertension (Ipertensione) 1
A Age ≥75 yrs (Età) 1
D Diabetes mellitus (Diabete) 1
S2 Stroke or TIA (Ictus o TIA pregresso) 2
V Vascular disease (pregresso IM, PAD, placca aortica) 1
A Age 65-74 yrs 1
Sc Sex category (genere femminile) 1
European Heart Journal doi:10.1093/eurheartj/ehq278
NB: Le linee guida pongono la FA parossistica allo stesso livello di rischio della
FA permanente
Tot 9
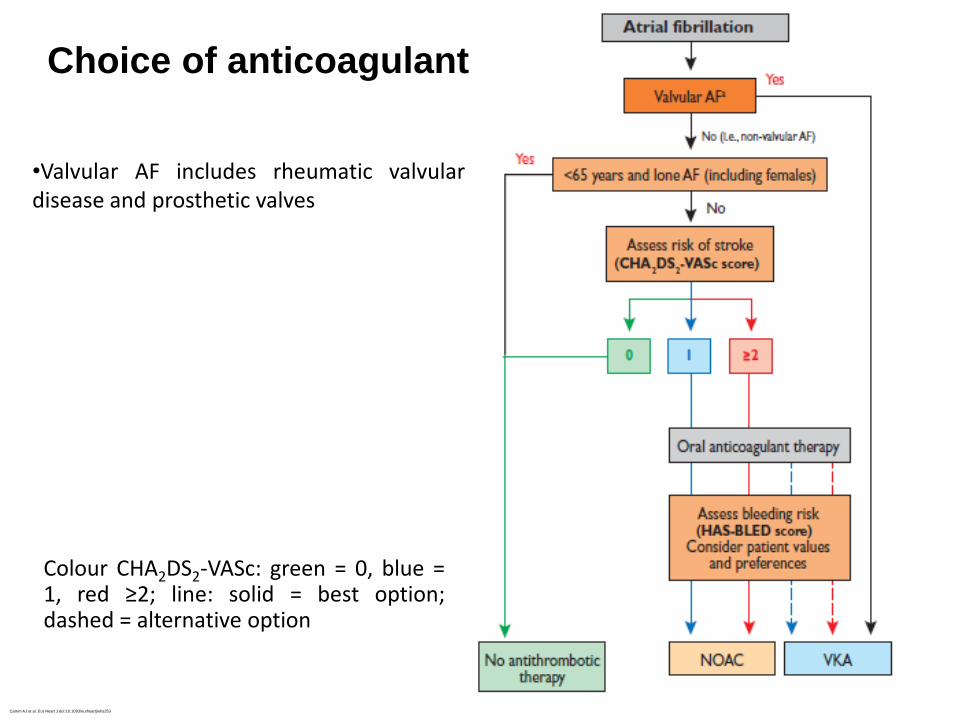
Choice of anticoagulant
Camm AJ et al. Eur Heart J doi:10.1093/eurheartj/ehs253
•Valvular AF includes rheumatic valvular disease and prosthetic valves
Colour CHA2DS2-VASc: green = 0, blue = 1, red ≥2; line: solid = best option; dashed = alternative option
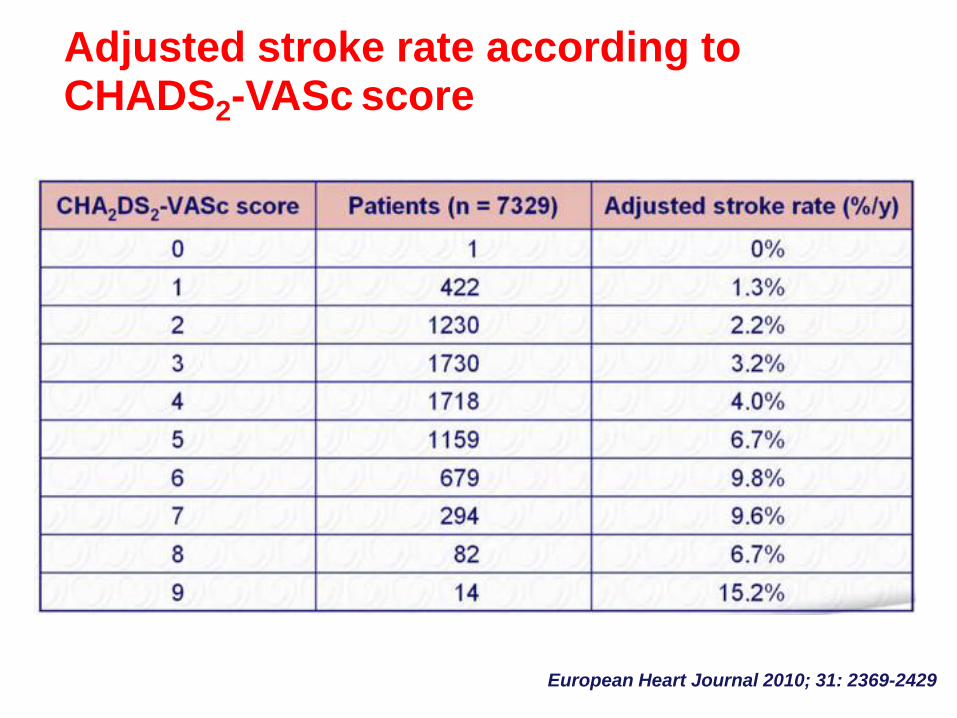
Adjusted stroke rate according to CHADS2-VASc score
European Heart Journal 2010; 31: 2369-2429
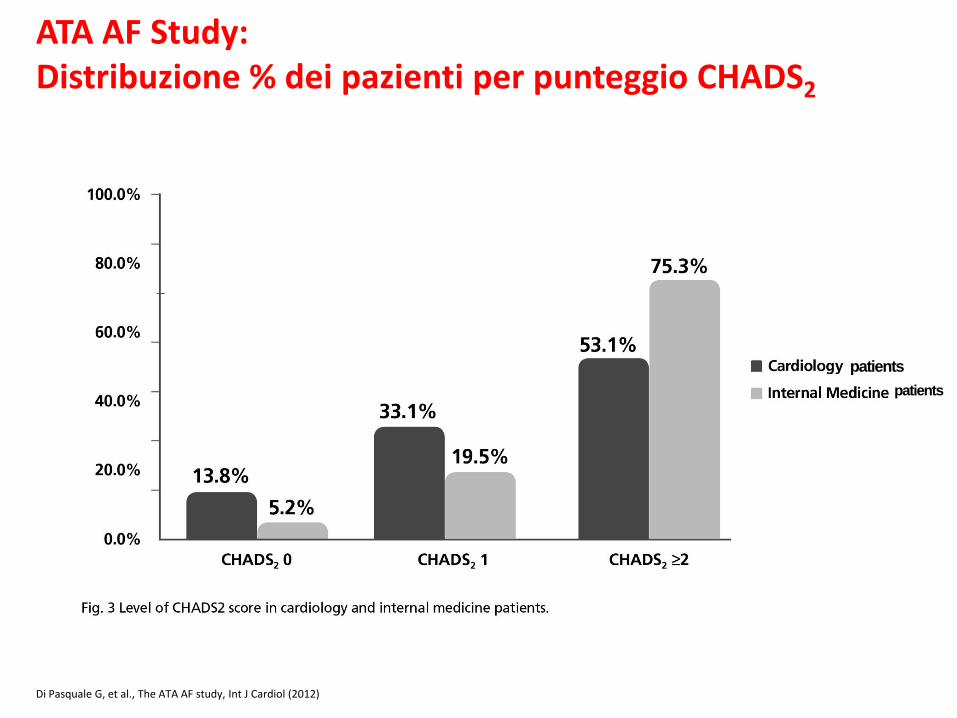
Di Pasquale G, et al., The ATA AF study, Int J Cardiol (2012)
patients
patients
ATA AF Study: Distribuzione % dei pazienti per punteggio CHADS2
… ed invece il mondo reale
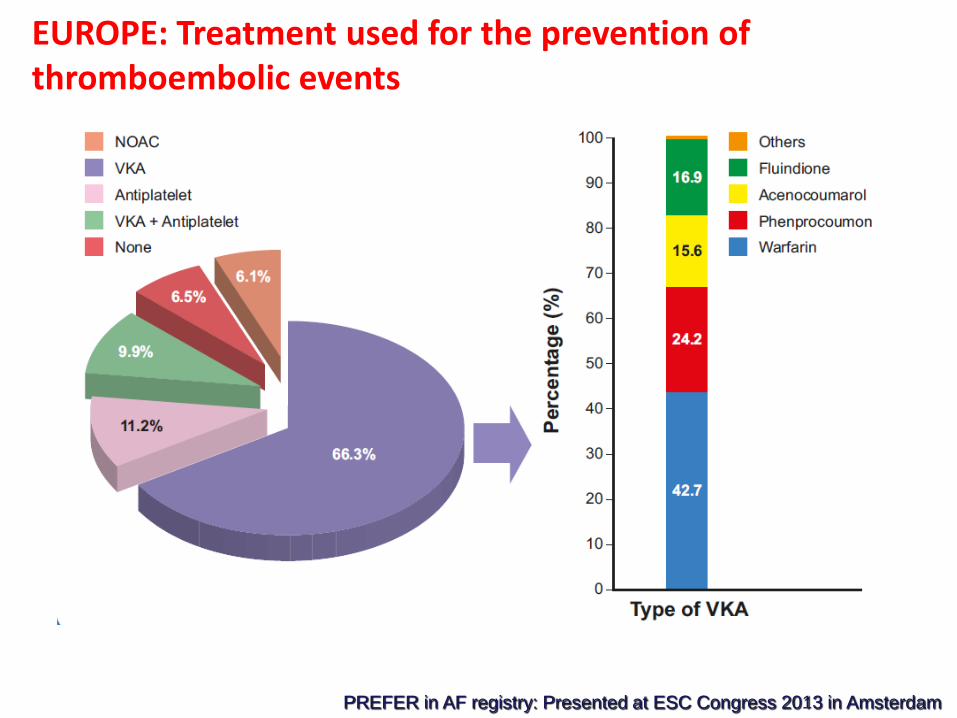
EUROPE: Treatment used for the prevention of thromboembolic events
PREFER in AF registry: Presented at ESC Congress 2013 in Amsterdam
I dati Italia 2015
•37% dei pazienti con FA in terapia con
ASA.
•17% dei pazienti senza alcuna terapia
anticoagulante o antiaggregante.
I (falsi) luoghi comuni
•Evidenze non ancora sufficienti.
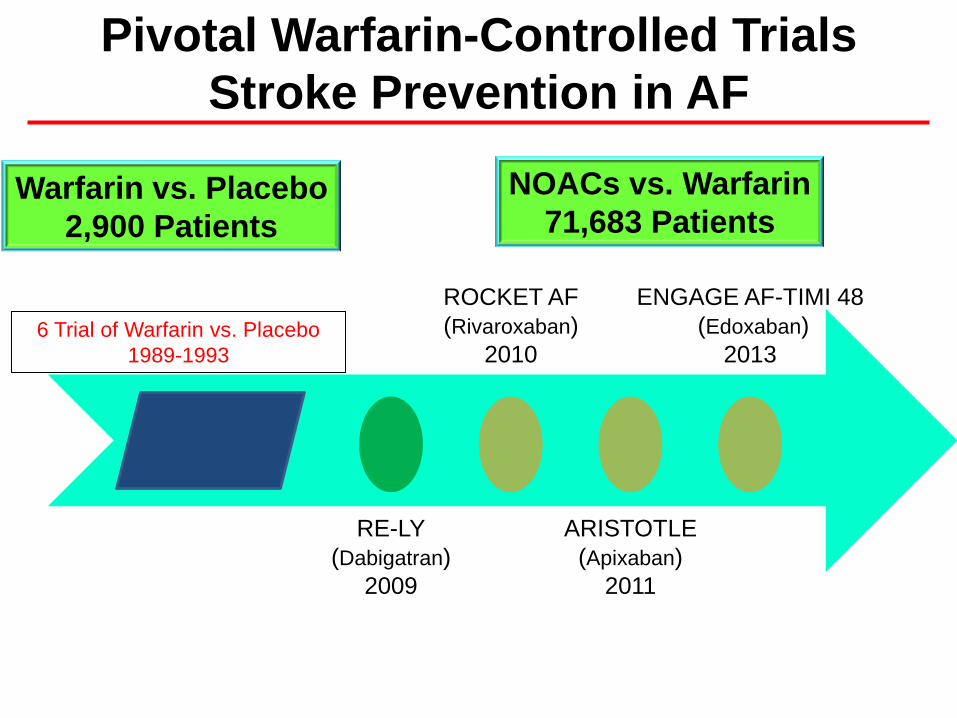
Pivotal Warfarin-Controlled Trials
Stroke Prevention in AF
6 Trial of Warfarin vs. Placebo
1989-1993
RE-LY
(Dabigatran)
2009
ROCKET AF
(Rivaroxaban)
2010
ARISTOTLE
(Apixaban)
2011
ENGAGE AF-TIMI 48
(Edoxaban)
2013
Warfarin vs. Placebo
2,900 Patients
NOACs vs. Warfarin
71,683 Patients
I (falsi) luoghi comuni
•Dati derivati solo da trials e non dal
mondo reale.
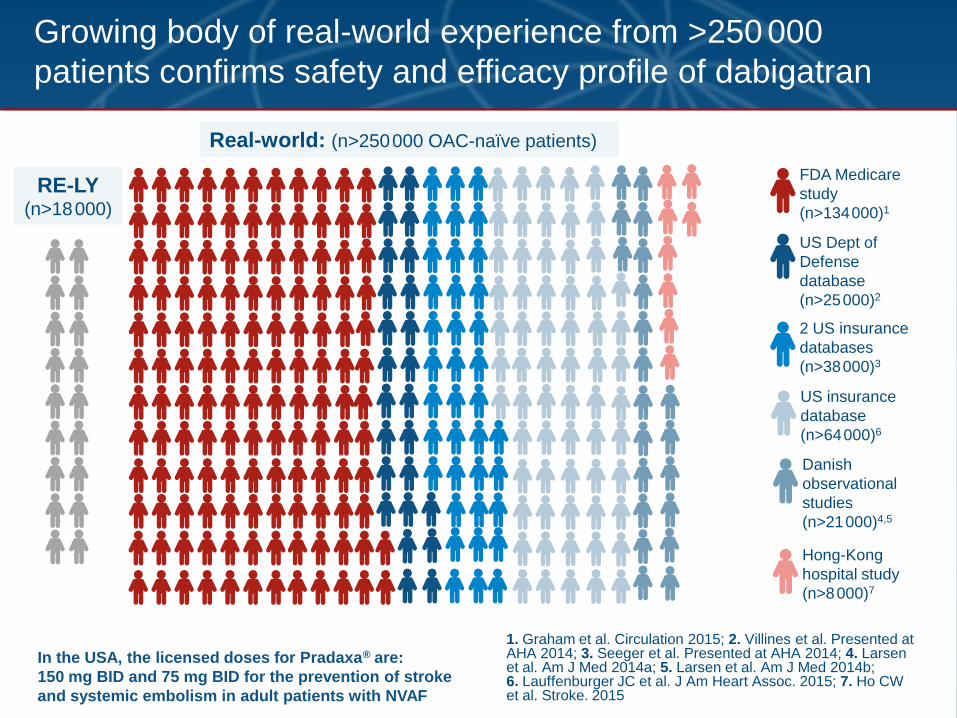
Growing body of real-world experience from >250 000
patients confirms safety and efficacy profile of dabigatran
RE-LY (n>18 000)
Real-world: (n>250 000 OAC-naïve patients)
FDA Medicare
study
(n>134 000)1
2 US insurance
databases
(n>38 000)3
US Dept of
Defense
database
(n>25 000)2
US insurance
database
(n>64 000)6
Hong-Kong
hospital study
(n>8 000)7
Danish
observational
studies
(n>21 000)4,5
In the USA, the licensed doses for Pradaxa® are:
150 mg BID and 75 mg BID for the prevention of stroke
and systemic embolism in adult patients with NVAF
1. Graham et al. Circulation 2015; 2. Villines et al. Presented at AHA 2014; 3. Seeger et al. Presented at AHA 2014; 4. Larsen et al. Am J Med 2014a; 5. Larsen et al. Am J Med 2014b; 6. Lauffenburger JC et al. J Am Heart Assoc. 2015; 7. Ho CW et al. Stroke. 2015
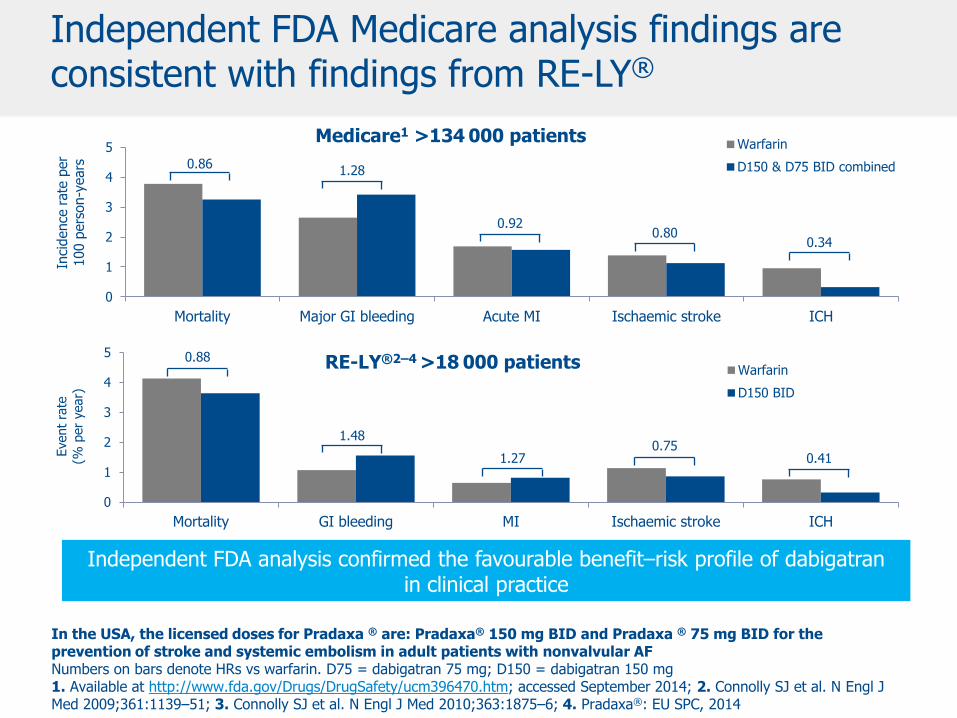
0
1
2
3
4
5
Mortality Major GI bleeding Acute MI Ischaemic stroke ICH
Inci
dence
rate
per
100 p
ers
on-y
ears
Warfarin
D150 & D75 BID combined
0
1
2
3
4
5
Mortality GI bleeding MI Ischaemic stroke ICH
Event
rate
(% p
er
year)
Warfarin
D150 BID
RE-LY®2–4 >18 000 patients
Medicare1 >134 000 patients
0.86 1.28
0.92 0.80
0.34
0.88
1.48
1.27 0.75
0.41
Independent FDA Medicare analysis findings are consistent with findings from RE-LY®
In the USA, the licensed doses for Pradaxa ® are: Pradaxa® 150 mg BID and Pradaxa ® 75 mg BID for the prevention of stroke and systemic embolism in adult patients with nonvalvular AF Numbers on bars denote HRs vs warfarin. D75 = dabigatran 75 mg; D150 = dabigatran 150 mg 1. Available at http://www.fda.gov/Drugs/DrugSafety/ucm396470.htm; accessed September 2014; 2. Connolly SJ et al. N Engl J Med 2009;361:1139–51; 3. Connolly SJ et al. N Engl J Med 2010;363:1875–6; 4. Pradaxa®: EU SPC, 2014
Independent FDA analysis confirmed the favourable benefit–risk profile of dabigatran in clinical practice
I (falsi) luoghi comuni
•I NOACs non hanno antidoto, il
warfarin si.
•L’unico anticoagulante che ha un vero
antidoto (solfato di protamina) è l’eparina
sodica.
•La vitamina K NON è un antidoto per il
warfarin.
•I NOACs hanno una emivita di 12-14 ore
circa, il warfarin di 120 ore.
•Sono ora disponibli antidoti per i NOACs.
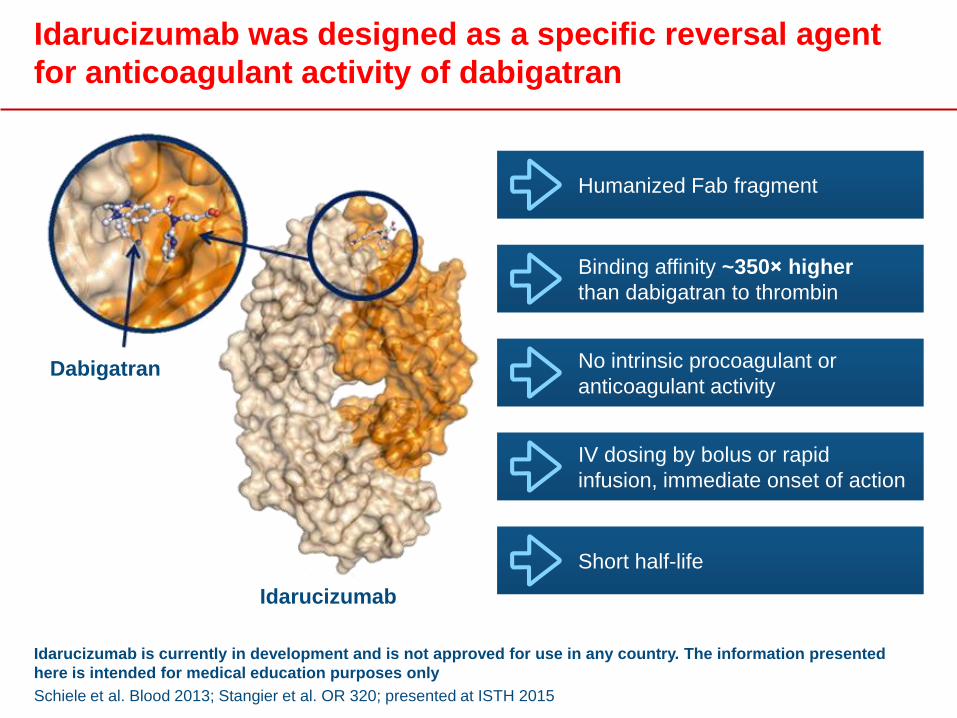
Idarucizumab is currently in development and is not approved for use in any country. The information presented
here is intended for medical education purposes only
Schiele et al. Blood 2013; Stangier et al. OR 320; presented at ISTH 2015
Idarucizumab was designed as a specific reversal agent
for anticoagulant activity of dabigatran
Dabigatran
Idarucizumab
Humanized Fab fragment
IV dosing by bolus or rapid
infusion, immediate onset of action
Binding affinity ~350× higher
than dabigatran to thrombin
No intrinsic procoagulant or
anticoagulant activity
Short half-life
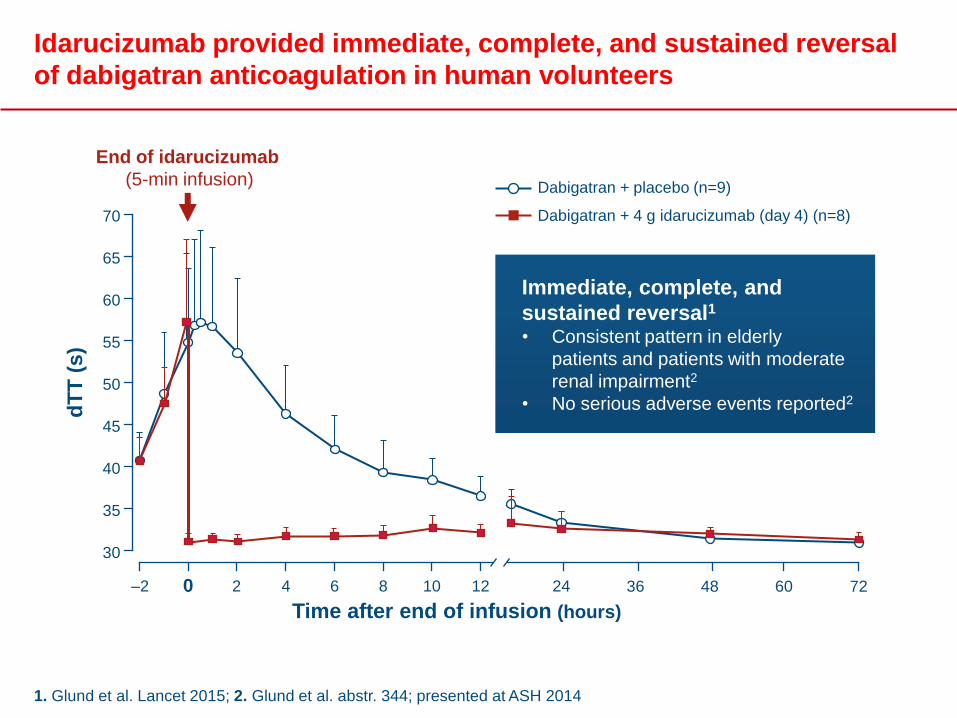
1. Glund et al. Lancet 2015; 2. Glund et al. abstr. 344; presented at ASH 2014
Idarucizumab provided immediate, complete, and sustained reversal
of dabigatran anticoagulation in human volunteers
Dabigatran + placebo (n=9)
–2
Time after end of infusion (hours)
dT
T (
s)
70
65
60
55
50
45
40
35
30
0 2 4 6 8 10 12 24 36 48 72 60
End of idarucizumab
(5-min infusion)
Dabigatran + 4 g idarucizumab (day 4) (n=8)
Immediate, complete, and
sustained reversal1
• Consistent pattern in elderly
patients and patients with moderate
renal impairment2
• No serious adverse events reported2
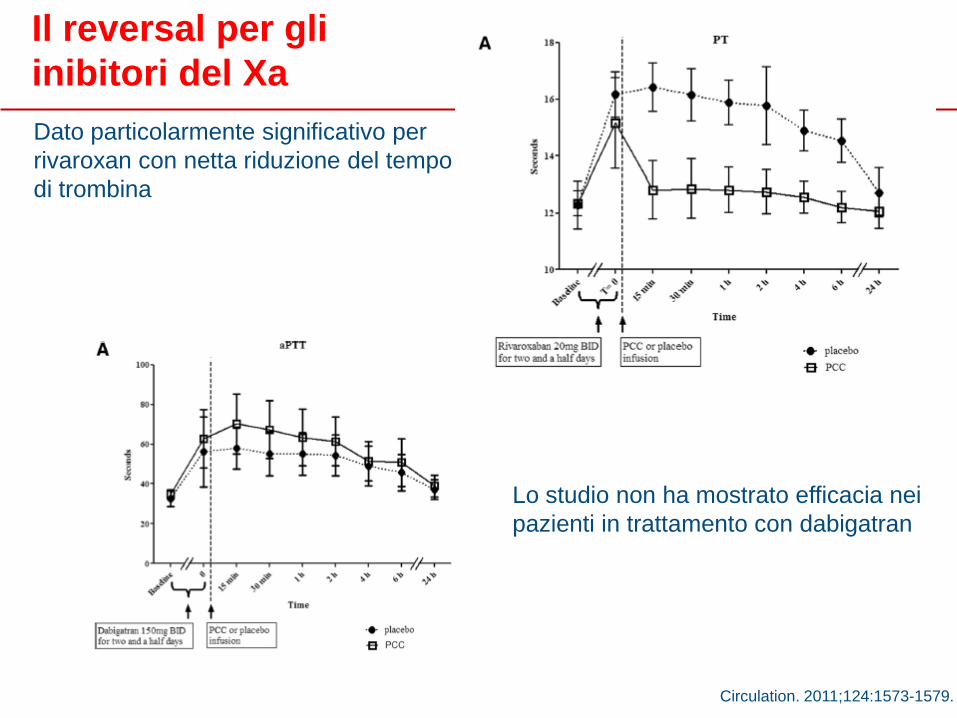
Dato particolarmente significativo per
rivaroxan con netta riduzione del tempo
di trombina
Lo studio non ha mostrato efficacia nei
pazienti in trattamento con dabigatran
Circulation. 2011;124:1573-1579.
Il reversal per gli
inibitori del Xa
Conclusioni

Profilo dell’anticoagulante ideale:
i NAO quali punti soddisfano?
Furie & Furie. N Engl J Med 2008;359:938–949
Turpie. Eur Heart J 2007;29:155–165
Ampia
finestra
terapeutica
Somministrazione
orale e dosaggio
fisso
Rapidi onset e
offset d’azione
Dose-risposta
Prevedibile
Assenza di
monitoraggio
esami di
laboratorio
Ridotto rischio
di
sanguinamento
Interazioni
minime con
altri farmaci e
cibo
Reversibile
Grazie
“Quando penso ad una malattia, non è per trovarvi rimedio, ma, invece, per prevenirla” L. Pasteur
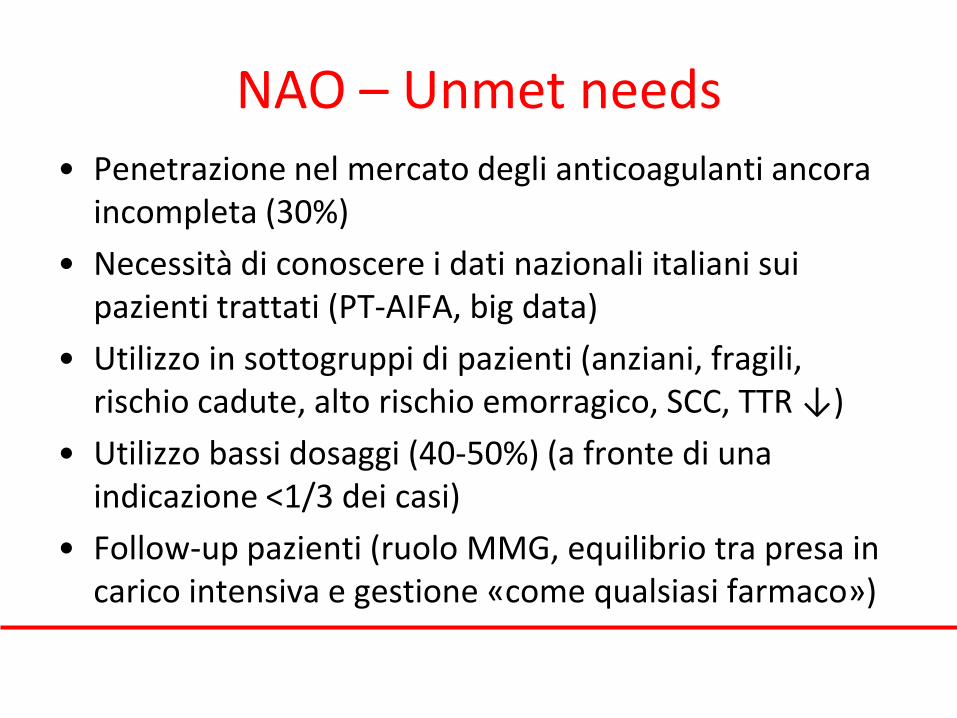
NAO – Unmet needs • Penetrazione nel mercato degli anticoagulanti ancora
incompleta (30%)
• Necessità di conoscere i dati nazionali italiani sui pazienti trattati (PT-AIFA, big data)
• Utilizzo in sottogruppi di pazienti (anziani, fragili, rischio cadute, alto rischio emorragico, SCC, TTR ↓)
• Utilizzo bassi dosaggi (40-50%) (a fronte di una indicazione <1/3 dei casi)
• Follow-up pazienti (ruolo MMG, equilibrio tra presa in carico intensiva e gestione «come qualsiasi farmaco»)
L’unico rischio da evitare
Trasformare la facilità d’impiego dei NOACs (pregio) in una banalizzazione d’impiego (difetto).
ESC AF GUIDELINES 2010

Dabigatran Rivaroxaban Apixaban
Condizioni di ingresso Paziente con
Fibrillazione Atriale
Non Valvolare (FANV)
Età >18 anni
Paziente con
Fibrillazione Atriale
Non Valvolare (FANV)
Età >18 anni
Paziente con
Fibrillazione Atriale
Non Valvolare (FANV)
Età ≥18 anni
Ai fini dell'eleggibilità bisogna rientrare in una delle seguenti
condizioni (1, 2 o 3)
Gruppo 1 CHA2DS2-VASc ≥1
e HAS-BLED >3
CHA2DS2-VASc >3
e HAS-BLED >3
CHA2DS2-VASc ≥1
e HAS-BLED >3
Gruppo 2 TTR negli ultimi 6
mesi ≤70
TTR negli ultimi 6
mesi ≤60
TTR negli ultimi 6
mesi ≤70
Gruppo 3 Il trattamento
anticoagulante non è
attuabile per difficoltà
oggettive ad eseguire i
controlli di INR.
Il trattamento
anticoagulante non è
attuabile per difficoltà
oggettive ad eseguire i
controlli di INR.
Il trattamento
anticoagulante non è
attuabile per difficoltà
oggettive ad eseguire i
controlli di INR.
Piani terapeutici AIFA a confronto: 2 luglio 2014
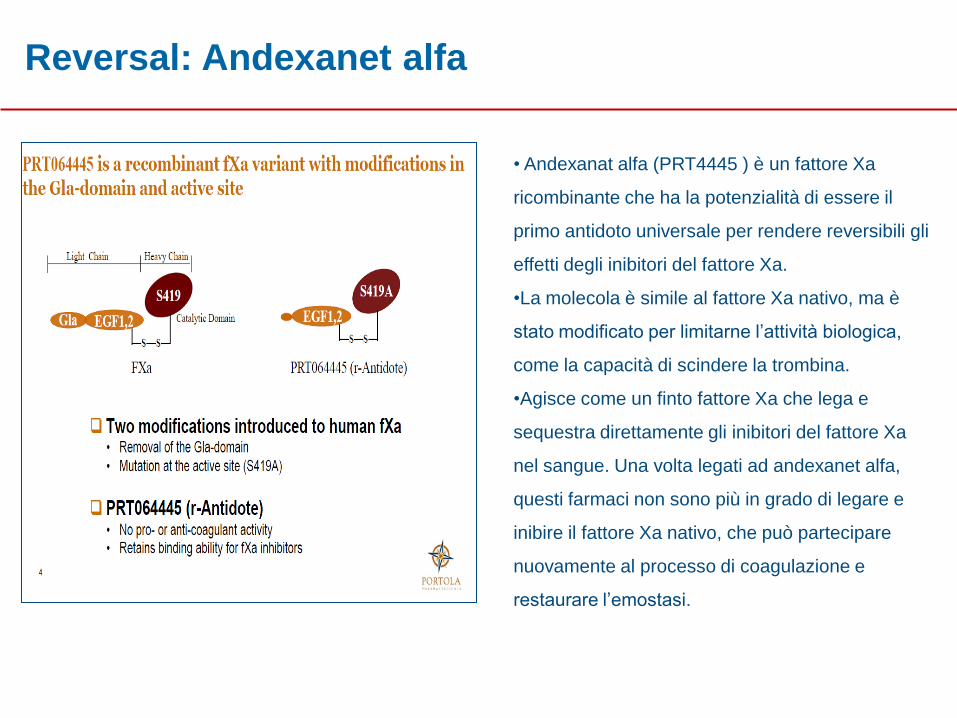
• Andexanat alfa (PRT4445 ) è un fattore Xa
ricombinante che ha la potenzialità di essere il
primo antidoto universale per rendere reversibili gli
effetti degli inibitori del fattore Xa.
•La molecola è simile al fattore Xa nativo, ma è
stato modificato per limitarne l’attività biologica,
come la capacità di scindere la trombina.
•Agisce come un finto fattore Xa che lega e
sequestra direttamente gli inibitori del fattore Xa
nel sangue. Una volta legati ad andexanet alfa,
questi farmaci non sono più in grado di legare e
inibire il fattore Xa nativo, che può partecipare
nuovamente al processo di coagulazione e
restaurare l’emostasi.
Reversal: Andexanet alfa
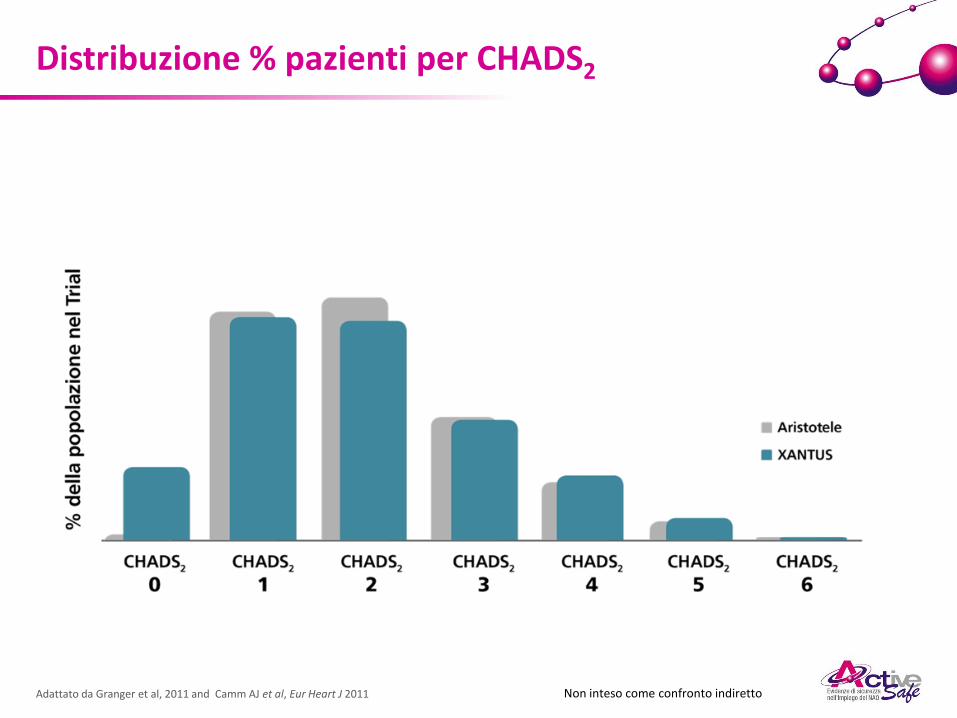
Adattato da Granger et al, 2011 and Camm AJ et al, Eur Heart J 2011
Distribuzione % pazienti per CHADS2
Non inteso come confronto indiretto
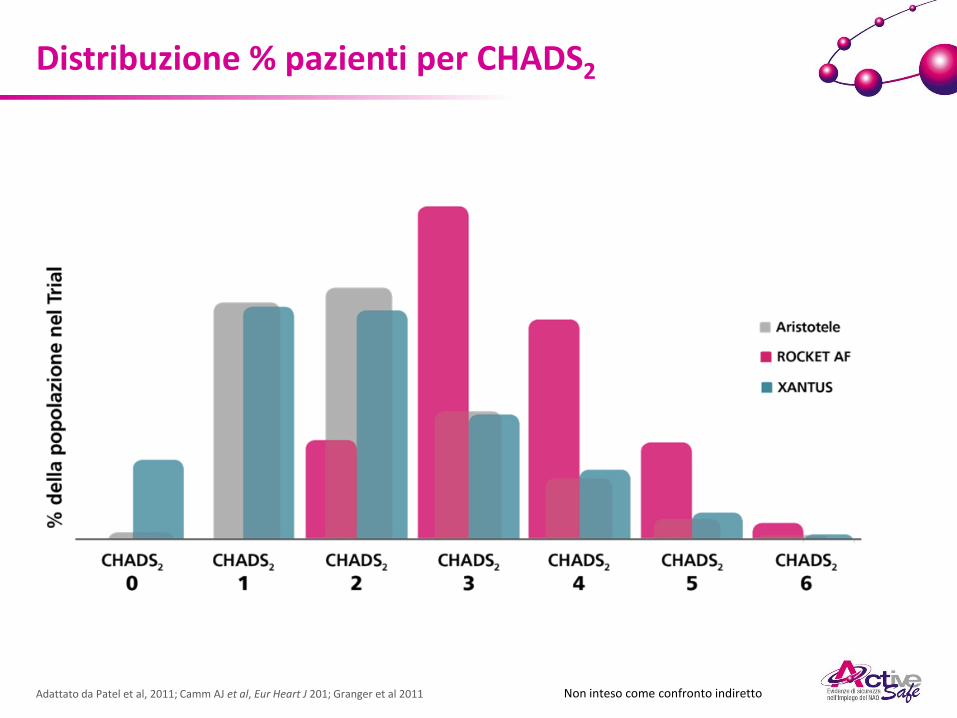
Adattato da Patel et al, 2011; Camm AJ et al, Eur Heart J 201; Granger et al 2011
Distribuzione % pazienti per CHADS2
Non inteso come confronto indiretto
… ed invece il mondo reale
(eminence-based medicine)







