
Court Outcomes Data Project
Thursday, February 26, 2015
@HSJCC
Michael Dunn, Provincial HSJCC Co-ChairSarah Gauthier, Canadian Mental Health Association - Sudbury/ ManitoulinHélène Philbin-Wilkinson, North Bay Regional Health Centre

HSJCC Webinar
Thank you to CMHA Ontario and the Evidence Exchange Network (EENet) for providing support to host this webinar!
• To ask a question, please type your question in the chat box.
• Power-point presentation will be emailed to you following the webinar.
• Please complete the brief feedback survey following the webinar.
2@HSJCC

Overview of Presentation
1. About the HSJCC
2. Northeast Regional Outcomes Project
3. Live Tour of Online Portal
4. Questions & Comments
3@HSJCC

Presenters
• Michael Dunn, Director of Research, Evaluation & Quality Improvement, Canadian Mental Health Association - Simcoe County Branch, Co-Chair of the Provincial HSJCC
• Sarah Gauthier, Justice Program Coordinator at CMHA - Sudbury/ Manitoulin Branch, Chair of the Sudbury /Manitoulin District HSJCC and Co-chair of the Northeast Regional HSJCC
• Hélène Philbin-Wilkinson, Director of Dual Diagnosis and Mental Health & the Law Services at North Bay Regional Health Centre, Northeast Regional HSJCC Member
4@HSJCC

HSJCC Network
• Established based on the Provincial Strategy to Coordinate Human Services and Criminal Justice Systems in Ontario (1997)
• Responding to a recognized need in the province to coordinate resources and services, and plan more effectively for people who are in conflict with the law
• Priority consideration is for people with a serious mental illness, developmental disability, acquired brain injury, drug and alcohol addiction, and/or fetal alcohol syndrome
5@HSJCC

HSJCC Network
HSJCC Network is comprised of• 43 Local HSJCCs
• 14 Regional HSJCCs
• Provincial HSJCC
• Each HSJCC is a voluntary collaboration between health and social service organizations, community mental health and addictions organizations and partners from the justice sector including crown attorneys, judges, police services and correctional service providers
• Funded by the Ministry of Health and Long-Term Care
6@HSJCC

Provincial HSJCC
Provincial HSJCC consists of
• Regional HSJCC Chairs representing their Regions
• Ex-officio members from important stakeholder groups such as Correctional Service of Canada, Ontario Provincial Police and Ontario Association of Chiefs of Police, Legal Aid Ontario, and Community Networks of Specialized Care
• Ex-officio representatives from 5 Provincial Ministries:– Attorney General– Children and Youth Services – Community and Social Services– Community Safety and Correctional Services– Health and Long-Term Care
7@HSJCC
Upcoming Webinars
1. March 26, 2015, 12 pm to 1 pm – Pre-Charge Diversion
2. April (date and time to be determined), 2015 – Hamilton Rapid Response Team
Stay tuned for further details on these webinars!
8@HSJCC

Contact Information
For more information about the Provincial HSJCC, or to join the mailing list visit: www.hsjcc.on.ca
For more information about CMHA Ontario, visit: www.ontario.cmha.ca
For more information about EENet, visit: www.eenet.ca
9@HSJCC

Northeast Regional Outcomes Project
Sarah Gauthier BAHélène Philbin-Wilkinson BScN, Reg. N., MN

Agenda• Background
• Development Process
• Measures
• Regional & District Trends
• Implications
• Lessons Learned
• Live Tour of Online Portal

Northeast Region• Spans 400 000 square kilometers• Represents over 40% of Ontario’s land mass• With 4.2& of population• Compared to rest of the province we have higher rates of:
o Alcohol abuse, smokingo Chronic conditionso Unscheduled emergency department visits for mental health and substance abuseo Hospitalizations related to mental illness and self-injury (ages 15years and older)
• 25 hospitals (4 x Schedule 1, 1 x Regional Health Centre)• 48 community mental health and addictions services• 1 CCAC
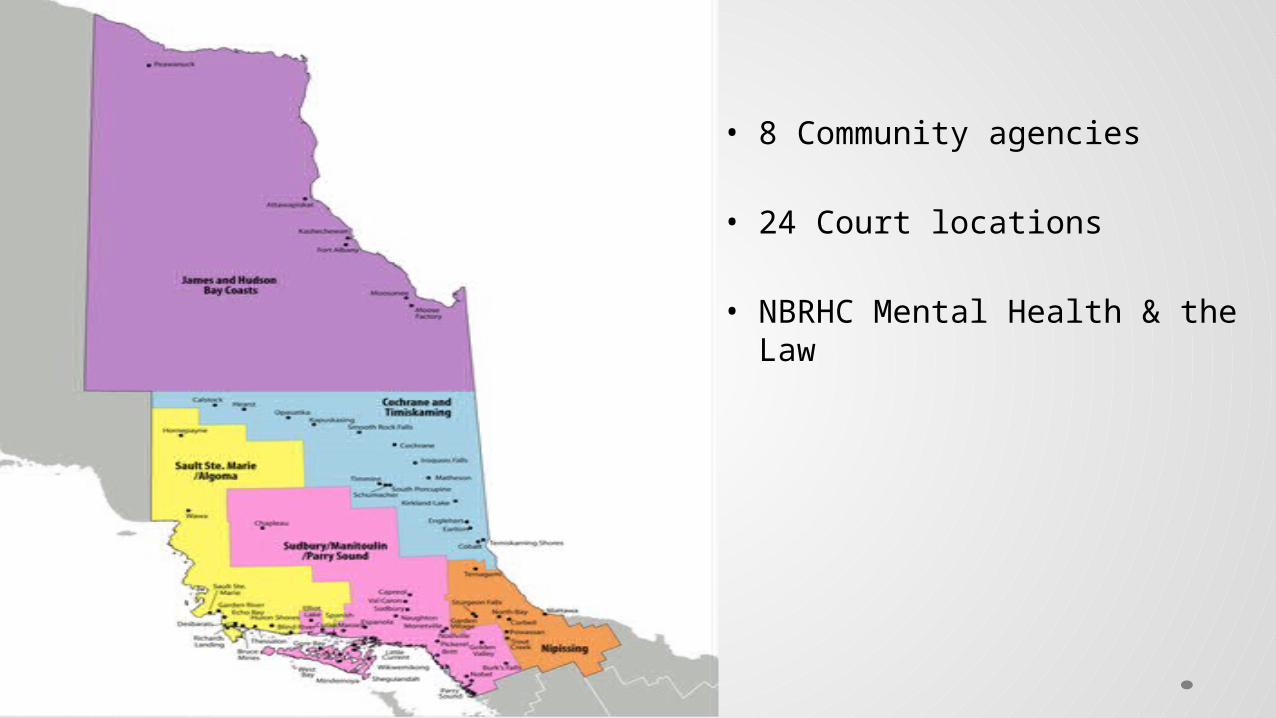
• 8 Community agencies
• 24 Court locations
• NBRHC Mental Health & the Law

Partnerships with Purpose• Service agreements since 2000
o Outlining roles and responsibilitieso Timely accesso Optimizing resource utilizationo Track service trends
• Inconsistent definitions and unclear rational for data collection• Inconsistent methods of reporting• Unclear understanding of the system demands in each area • Inability to validate trends and inform funding• How do we hold ourselves accountable?• Common goal of improving access and connections to service


Background• How do we know we are making a difference?
• How do we measure program & system performance?
• Surveyed other programs across the province
• No provincial standard measures or common definitions
• Traditional data collection aka “ caseload statistics”
• Support from Northeast Regional HSJCC & North Bay Regional Health Centre

Timeline• CMHA- Sudbury/ Manitoulin went live 2012 with three process
measures
• Demonstrated data after 6 months to HSJCC and partners
• Partners agreed to the development of a Regional portal building on
the three measures
• Agreement to engage consultant and financial commitment
• Northeast Regional Portal went live April 1, 2013
• Phase 2 was funded by the NE LHIN to enhance current measures
and further develop system outcomes measures

Development Process
Improvement

Collaborative process guided by Brian Tramontini

Measures• Phase 1
o Diversion Success Rate: How successfully are people diverted from the criminal justice system and into the mental health system?
o Alternate Disposition (diversion) Success Rate:Are we successful in advocating for improved dispositions?
o Admission Aversion Rate:How many clients inappropriate admissions to forensic units are avoided?

Measures• Phase 2
o Diversion Recidivism: How many people, while on a mental health diversion, were known to reoffend within the diversion period?
o Fitness Recommendation Consistency Rate: Was the agency fitness recommendation consistent with the physician assessment recommendation?
o Release from Custody Rate: How many clients are released on a recognizance back to the community based on the involvement of the mental health court worker?

Data Collection• No unique identifiers
• Each agency utilizes their own client data base reference #
• Agency & Court
• Demographics: age category, sex, aboriginal, primary and
secondary diagnosis, needs

Data Collection• Use of OCAN categories / language
• Data integrity – permissions, mandatory fields
• Integrated into current practices
Outcomes
Dx
gender
age

2013 2014 2015 2013 2014 2015Alternate Diversion
0
5
10
15
20
25
30
35
40
45
50Diversion Counts CMHA Sudbury-Manitoulin
CMHA Sault Ste. Marie
CMHA Nipissing
CMHA Cochrane -Temiskaming - Kirkland Lake
Muskoka-Parry Sound Community Mental Health Service
CMHA Cochrane-Temiskaming Timmins Of-fice
Hearst Kapuskasing Smooth Rock Falls Counselling Services
Sudbury Community Service Centre
Weeneebayko Area Health Authority
Adult (18-64) Youth (12-17) Senior (65+)Diversion
0
50
100
150
200
250
300Diversion Counts by Age and Diagnosis
Dissociative Disorders
_None
Acquired Brain Injury
Disorder of Childhood/ adolescence
Personality Disorders
Substance Related Dis-orders
Unknown
Developmental Disability
Schizophrenia and other psychotic Disorders
Anxiety disorder
Mood Disorder

District and Regional Trends• Youth recidivism rates are higher in Sudbury & Nipissing
• Intervention increases success rate of release on bail for Dual Diagnosis population
• Courts consistently follow recommendation of Justice Programs when ordering Fitness to Stand Trial assessments
• Demographics: more males being diverted than females in most districts, gap is narrowed with youth


Implications• Combines qualitative and quantitative data
• Common language and measures to achieve our common goal
• Allows for flexibility in processes within the districts
• Outcome based accountability framework that informs service delivery
• Relevant evidence to identify system pressures
• Starting to understand cost savings at a program and system level
• Supports a culture of quality improvement in line with the Excellent Care for
All Act
• Despite barriers of geography and distance it fosters collaboration and a
supportive partnership
• Assists in determining allocations of funds and resources

Lessons learned• Commitment at all levels
• Different levels of readiness
• Need a champion and evidence that it works
• Competing priorities and needs
• Common language early on to motivate engagement
• Essential to have expertise in outcome performance and data
management
• Requires training and on-going support and involvement of all partners
• Utilizing partnership agreement

Future Directions• Continued data collection & analysis
• Quality Improvement Planning
• Re-establishing the baseline and targets
• Setting the standard for an evaluative framework

Online Portal Tour
Thank you / Questions?







