
10/2/17
1
COMMON RESPIRATORY INFECTIONS – ARE THERE UPDATES?
Kelly E Wood, MD Clinical Associate Professor University of Iowa Stead Family Children’s Hospital Stead Family Department of Pediatrics
I have a financial relationship with McGraw Hill Professional for a pediatric board review textbook I co-edited.
Objectives
¨ Review common pediatric respiratory infections including ¤ Pathophysiology ¤ Management ¤ Complications
¨ Provide evidence based recommendations when available
Date of download: 6/24/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
From: Head Exploring Essential Radiology, 2014
What is shown on this x-ray?

10/2/17
2
Croup Laryngotracheitis
¨ Inflammation of the larynx and subglottic
¨ Viral or Spasmodic
¨ Clinical diagnosis ¤ Consider X ray if atypical presentation
Treatment
¨ Cool mist ineffective
¨ Steroids ¤ Dexamethasone preferred ¤ Low (0.15 mg/kg) or high dose (0.6 mg/kg) ¤ PO as good as IM
¨ Racemic epinephrine nebulization n Can use levo epinephrine n Rapid, short term
Croup
¨ RED FLAGS ¤ Hypoxia ¤ Hypercapnia ¤ Somnolence ¤ Softening of cough / stridor ¤ Drooling ¤ Tripod ¤ Unimmunized ¤ < 6 months or > 5 yr old ¤ Recurrent, protracted episode
Date of download: 6/24/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
From: IV. Nontrauma Emergencies CURRENT Diagnosis & Treatment Emergency Medicine, 7e, 2011
What is shown on this x-ray?

10/2/17
3
Clinical Presentation
Drooling and wants to be upright!
Balfour-Lynn I et al. Acute Infections that Produce Upper Airway Obstruction. Kendig and Chernick’s Disorders of the Respiratory Tract in Children. 2012:424-436.
Epiglottis
¨ Bacterial infection – Haemophilus influenzae type b (Hib)
¨ Unimmunized / asplenia
¨ Life Threatening
¨ Treatment ¤ Secure airway first ¤ Antibiotics
Epiglottis
Rogers D et al. Epiglottitis due to nontypeable Haemophilus influenzae in a vaccinated child. International Journal of Pediatric Otorhinolaryngology. 2010;74(2):218-220. Congenital Disorders of the Larynx. http://clinicalgate.com/congenital-disorders-of-the-larynx. Accessed August 16, 2016.
From Benjamin B. The pediatric airway, slide #2, Slide Lecture Series. American Academy of Otolaryngology–Head and Neck Surgery, 1992.
Date of download: 6/24/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
From: Part 2. Specialty Areas The Atlas of Emergency Medicine, 3e, 2010
What is shown on this x-ray?

10/2/17
4
Retropharyngeal abscess
¨ Polymicrobial including MRSA ¨ Retropharyngeal nodes
¤ Drain nasopharynx, adenoids, paranasal sinuses, middle ear
¨ Progresses from cellulitis -> phlegmon -> abscess ¨ Space extends from base of skull to mediastinum
Limited neck movement especially extension!
Date of download: 6/24/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved.
Contrasted CT of a left retropharyngeal abscess (arrow).
Legend:
From: Section 19. Eyes, Ears, Nose, Throat, and Oral Surgery Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e, 2011
Management
¨ Admission ¤ Access to Otolaryngologists
¨ Imaging
¨ Antibiotics ¤ Include MRSA and anaerobic coverage
¨ Surgery ¤ Airway impingement ¤ Mature abscess > 2-3 cm ¤ Failed 24-48 IV antibiotics
¨ Dexamethasone Source: Influenza, Parainfluenza, Respiratory Syncytial Virus, Adenovirus, and Other Respiratory Viruses, Sherris Medical Microbiology, 6e Citation: Ryan KJ, Ray C. Sherris Medical Microbiology, 6e; 2014 Available at: http://accessmedicine.mhmedical.com/ViewLarge.aspx?
figid=56989069 Accessed: August 16, 2017Copyright © 2017 McGraw-Hill Education. All rights reserved

10/2/17
5
Figure 1
Viral Bronchiolitis Bronchiolitis
¨ #1 cause of hospital admission
¨ Risk factors for severe disease: < 8 weeks old, prematurity, chronic health condition
¨ Sloughing of epithelial cells, edema and mucous
¨ Treatment – supportive ¤ No hypotonic fluids ¤ Early enteral feeding ¤ No hypertonic saline nebs ¤ Avoid continuous pulse oximetry if on room air
Right lower lobe pneumonia
Bennett NJ. Imaging in Pediatric Pneumonia. Medscape. http://emedicine.medscape.com/article/1926980-overview. Accessed August 16, 2016.
What is shown on this X-ray?
Pneumonia
¨ Viral ¨ Bacterial – lobar
¤ Streptococcus pneumoniae ¤ Haemophilus influenzae
¨ Atypical ¤ Mycoplasma pneumoniae ¤ Chlamydia pneumoniae
¨ Aspiration
Ask about immunizations!

10/2/17
6
Treatment
¨ Blood cultures not routinely recommended ¨ Chest x ray not routinely recommended ¨ Consider influenza testing and treat
¨ Antibiotics ¤ High dose amoxicillin first line ¤ Augmentin if conjunctivitis, recent antibiotics, unimmunized ¤ Macrolide if atypical
¨ Close follow up
Treatment – inpatient
¨ Blood culture and chest x ray (AP and lateral)
¨ Consider influenza testing and treat
¨ Antibiotics ¤ Ampicillin – simple lobar, immunized ¤ Ceftriaxone – complicated, unimmunized, high PCN
resistance ¤ Azithromycin – atypical pathogens
No allergies PCN allergy
Outpatient
< 5 years Amoxicillin Alt: Augmentin 2nd or 3rd generation
cephalosporin (cefpodoxime, cefuroxime, cefprozil) Alt: Levofloxacin, Azithromycin
≧5 years Amoxicillin Alt: Augmentin +/- Azithromycin
Inpatient (all ages)
Immunized Ampicillin or PCN Alt: Ceftriaxone*
Ceftriaxone* Alt: Levofloxacin, Vancomycin
Unimmunized, high PCN resistance
Ceftriaxone* Alt: Levofloxacin
Ceftriaxone* Alt: Levofloxacin
Life threatening, empyema Ceftriaxone* +/- MRSA coverage
Ceftriaxone* Alt: Levofloxacin +/- MRSA coverage
Adapted from 2011 IDSA guidelines: CAP in infants and children
What is shown on this x ray?
Pandian TK and Hamner C, Surgical management for complications of pediatric lung injury. Seminars in Pediatric Surgery. 2015;24(1):50-58.
Empyema
10/2/17
7
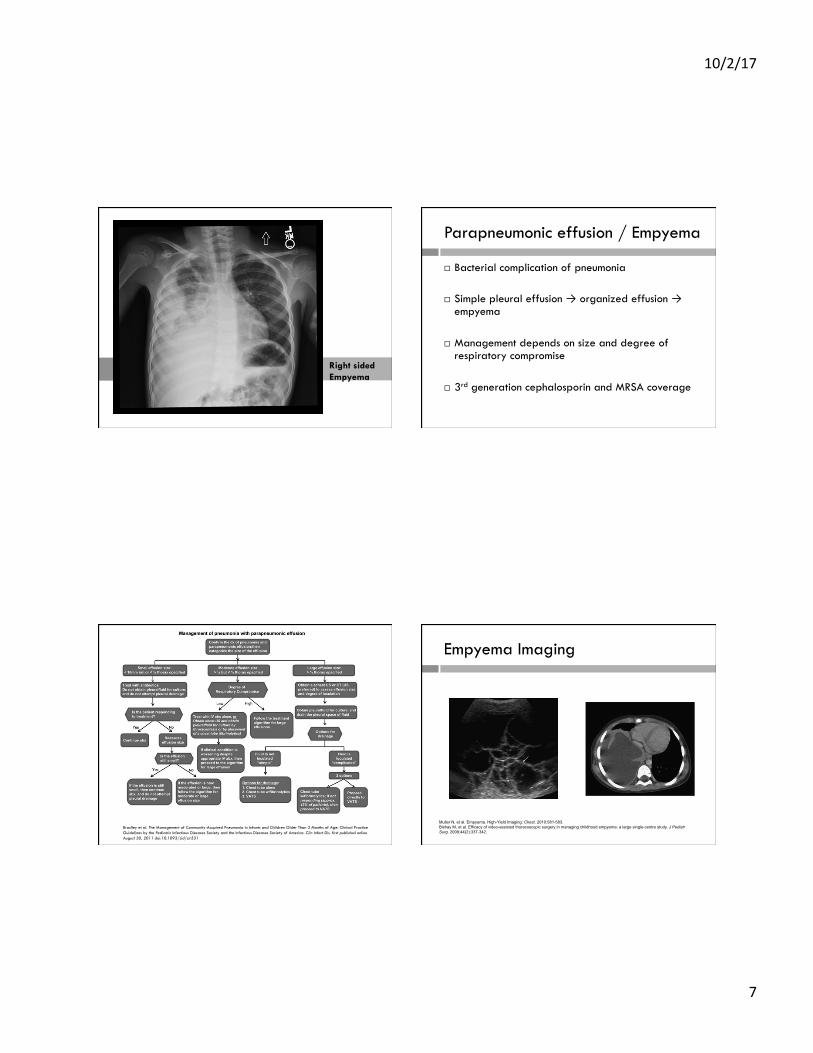
Right sided Empyema
Parapneumonic effusion / Empyema
¨ Bacterial complication of pneumonia ¨ Simple pleural effusion → organized effusion →
empyema
¨ Management depends on size and degree of respiratory compromise
¨ 3rd generation cephalosporin and MRSA coverage
Bradley et al. The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. first published online August 30, 2011 doi:10.1093/cid/cir531
Empyema Imaging
Muller N, et al. Empyema. High-Yield Imaging: Chest. 2010:581-583. Bishay M, et al. Efficacy of video-assisted thoracoscopic surgery in managing childhood empyema: a large single-centre study. J Pediatr Surg. 2009;44(2):337-342.

10/2/17
8
References
¨ Bjornson CJ, Johnson DW. Croup in children. CMAJ. 2013;185:1317-1323. ¨ Bradly JS, Byington CL, Shah SS, et al. The management of community-
acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clinical Infectious Diseases. 2011. http://cid.oxfordjournals.org/content/early/2011/08/30/cid.cir531.full. Accessed November 11, 2016.
¨ Escobar ML and Needleman J. Stridor. Pediatrics in Review. 2015;36:135-137.
¨ Marinati LC and Boner AL. Clinical diagnosis of wheezing in early childhood. Allergy. 1995;50:701-710.
¨ Richards AM. Pediatric Respiratory Emergencies. Emerg Med Clin N Am. 2016; 34:77–96.
¨ Virbalas J and Smith L. Upper Airway Obstruction. Pediatrics in Review. 2016;36;62-73.







