do#we#need#neuromuscular#blockers#...
TRANSCRIPT

Dr. J. P. Mulier, MD PhD
Geneeskundige dagen Antwerpen
September 16 th 2010
Antwerpen, Italy
Do we need Neuromuscular blockers (NMB) in morbid obese pa8ents
undergoing laparoscopy?
1 16 sept 2010 Geneesk dagen Antwerpen

Introduction Obesity is a growing general health problem
2 16 sept 2010 Geneesk dagen Antwerpen

Bariatric surgery is more effec7ve in reducing weight
3 16 sept 2010 Geneesk dagen Antwerpen

Bariatric surgery reduces morbidity ORIGINAL ARTICLE
Surgery Decreases Long-term Mortality, Morbidity, andHealth Care Use in Morbidly Obese Patients
Nicolas V. Christou, MD, PhD, John S. Sampalis, PhD, Moishe Liberman, MD, Didier Look, MD,Stephane Auger, BSc, Alexander P.H. McLean, MD, and Lloyd D. MacLean MD, PhD
Objective: This study tested the hypothesis that weight-reduction(bariatric) surgery reduces long-term mortality in morbidly obesepatients.Background: Obesity is a significant cause of morbidity andmortality. The impact of surgically induced, long-term weight losson this mortality is unknown.Methods: We used an observational 2-cohort study. The treatmentcohort (n ! 1035) included patients having undergone bariatricsurgery at the McGill University Health Centre between 1986 and2002. The control group (n ! 5746) included age- and gender-matched severely obese patients who had not undergone weight-reduction surgery identified from the Quebec provincial health insur-ance database. Subjects with medical conditions (other then morbidobesity) at cohort-inception into the study were excluded. The cohortswere followed for a maximum of 5 years from inception.Results: The cohorts were well matched for age, gender, andduration of follow-up. Bariatric surgery resulted in significant re-duction in mean percent excess weight loss (67.1%, P " 0.001).Bariatric surgery patients had significant risk reductions for devel-oping cardiovascular, cancer, endocrine, infectious, psychiatric, andmental disorders compared with controls, with the exception ofhematologic (no difference) and digestive diseases (increased ratesin the bariatric cohort). The mortality rate in the bariatric surgerycohort was 0.68% compared with 6.17% in controls (relative risk0.11, 95% confidence interval 0.04–0.27), which translates to areduction in the relative risk of death by 89%.Conclusions: This study shows that weight-loss surgery signifi-cantly decreases overall mortality as well as the development of newhealth-related conditions in morbidly obese patients.
(Ann Surg 2004;240: 416–424)
In recent years, morbid obesity has emerged as a seriouspublic health threat. After smoking, it is the second leading
cause of preventable, premature death in the United States. Itis estimated that there are 400,000 deaths attributable toobesity in the United States each year.1 The World HealthOrganization has recognized an epidemic of obesity through-out most of the developed and developing world.2 Canadianadult obesity trends have grown during a 13-year period from5.6% in 1985 to 14.8% in 1998.
Obesity is associated with multiple complications andrelated comorbidities that lead to both physical and psycho-logic problems.3–6 Bariatric surgery has been shown to be aneffective method for producing weight loss in obese patientsin both the short and long term7–11 and to be more effectivethan dieting in producing sustained weight loss.12 To date,there has not been a population-based study demonstrating asignificant impact of surgically induced permanent weightloss on mortality and the prevention of comorbidity in severeobesity. The current study addresses these issues by compar-ing the outcomes in 2 cohorts of morbidly obese patients.
METHODS
Study DesignThis was an observational 2-cohort study that compared
the morbidity and mortality of a cohort of morbidly obesepatients treated with bariatric surgery at the McGill Univer-sity Health Centre (MUHC) to that of matched morbidlyobese controls who had not been treated surgically. Theinception time of the bariatric cohort was the time of admis-sion for surgery. The inception time for the control group wasthe date of surgery of their matched bariatric patients. Amaximum of 6 controls were identified for each bariatricsubject. The 2 cohorts were followed for a maximum of 5years. The MUHC Research Institute ethics board approvedthe study.
Identification of Study CohortsA total of 1118 patients underwent bariatric surgery for
the treatment of morbid obesity at the MUHC betweenJanuary 7, 1986, and June 8, 2002. The unique health insur-
From the Section of Bariatric Surgery, Division of General Surgery, Depart-ment of Surgery, McGill University, Montreal, Quebec, Canada.
Reprints: Nicolas V. Christou, MD, PhD, Room s9.30, 687 Pine Ave. W., Montreal,Quebec, Canada H3A1A1. E-mail: [email protected].
Copyright © 2004 by Lippincott Williams & WilkinsISSN: 0003-4932/04/24003-0416DOI: 10.1097/01.sla.0000137343.63376.19
Annals of Surgery • Volume 240, Number 3, September 2004416
morbidity indicators, ie, excluding those with a history of theoutcomes, and matching the controls with respect to theduration of disease and age are key elements of the study’sdesign. These elements make the current study an excellentsimulation of a prospective cohort study and a valid repre-sentation of a “real-life” situation.
The results of the current study show that for up to 16years after bariatric surgery, patients experience significantand sustained weight loss. This result is expected and com-patible with those reported in other studies. The resultsshowing reduced mortality, reduction in the development of
new comorbid conditions, and reduced health care use aftersurgery in combination with the demonstrated effectivenessin weight loss are unique findings of the current study.
The effects of morbid obesity on the risk for hyperten-sion, coronary artery disease, and vascular disorders23,24;diabetes25,26; cancer27; and respiratory conditions28,29 havebeen well documented. In the current study, patients havingundergone bariatric surgery had significantly reduced risk ofdeveloping cancer, cardiovascular disease, endocrinologicaldisorders, infectious diseases, musculoskeletal disorders, andrespiratory conditions.
The increased risk for gastrointestinal disorders in thesurgery cohort was expected, and one that we feel serves asan internal consistency check of the analysis. After surgery,some patients experience stenosis of the vertical bandedoutlet, stenosis of the gastrojejunostomy, stomal ulcers, gas-tro-gastric fistula, small bowel obstructions, incisional her-nias, dumping syndrome, and diarrhea.30 Thus, one expects tosee increased physician visits and hospitalizations for treat-ment of these conditions.
Morbid obesity increases the risk for mortality.31,32 Thecurrent study demonstrates that in patients being treated withbariatric surgery, the risk of 5-year mortality is reduced by89%. This is a significant observation because it not onlysuggests the role of morbidity as a risk factor for earlymortality but also provides evidence that surgical treatment ofobesity produces a significant reduction in mortality. We feelthat the improved weight loss due to the efficacy of the RYgastric bypass and the conversion of the failed verticalbanded gastroplasty patients to RY gastric bypass, which
TABLE 4. Five-Year Morbidity and Mortality
Condition/disease
Cohort
Relative Risk Reduction
P Value
BariatricSurgery Controls
n % n % Estimate 95% CI
Blood and blood-forming organs 4 0.39 41 0.72 0.54 0.19 1.50 0.230Cancer 21 2.03 487 8.49 0.24 0.17 0.39 0.001Cardiovascular and circulatory 49 4.73 1530 26.69 0.18 0.12 0.22 0.001Digestive 377 36.43 1414 24.66 1.48 1.42 1.78 0.001Endocrinological 98 9.47 1566 27.25 0.35 0.32 0.38 0.001Genitourinary 77 7.44 551 9.61 0.77 0.63 0.97 0.027Infectious diseases 90 8.70 2140 37.33 0.23 0.17 0.25 0.001Musculoskeletal 50 4.83 682 11.90 0.41 0.32 0.55 0.001Nervous system 25 2.42 228 3.98 0.61 0.44 0.93 0.010Psychiatric and mental 45 4.35 470 8.20 0.53 0.41 0.73 0.001Respiratory 28 2.71 651 11.36 0.24 0.17 0.36 0.001Skin 38 3.67 305 5.32 0.69 0.48 0.96 0.027Mortality 7 0.68 354 6.17 0.11 0.04 0.27 0.001
FIGURE 2. Survival by group (Kaplan Meier survival analysis).
Christou et al Annals of Surgery • Volume 240, Number 3, September 2004
© 2004 Lippincott Williams & Wilkins420
ORIGINAL ARTICLE
Surgery Decreases Long-term Mortality, Morbidity, andHealth Care Use in Morbidly Obese Patients
Nicolas V. Christou, MD, PhD, John S. Sampalis, PhD, Moishe Liberman, MD, Didier Look, MD,Stephane Auger, BSc, Alexander P.H. McLean, MD, and Lloyd D. MacLean MD, PhD
Objective: This study tested the hypothesis that weight-reduction(bariatric) surgery reduces long-term mortality in morbidly obesepatients.Background: Obesity is a significant cause of morbidity andmortality. The impact of surgically induced, long-term weight losson this mortality is unknown.Methods: We used an observational 2-cohort study. The treatmentcohort (n ! 1035) included patients having undergone bariatricsurgery at the McGill University Health Centre between 1986 and2002. The control group (n ! 5746) included age- and gender-matched severely obese patients who had not undergone weight-reduction surgery identified from the Quebec provincial health insur-ance database. Subjects with medical conditions (other then morbidobesity) at cohort-inception into the study were excluded. The cohortswere followed for a maximum of 5 years from inception.Results: The cohorts were well matched for age, gender, andduration of follow-up. Bariatric surgery resulted in significant re-duction in mean percent excess weight loss (67.1%, P " 0.001).Bariatric surgery patients had significant risk reductions for devel-oping cardiovascular, cancer, endocrine, infectious, psychiatric, andmental disorders compared with controls, with the exception ofhematologic (no difference) and digestive diseases (increased ratesin the bariatric cohort). The mortality rate in the bariatric surgerycohort was 0.68% compared with 6.17% in controls (relative risk0.11, 95% confidence interval 0.04–0.27), which translates to areduction in the relative risk of death by 89%.Conclusions: This study shows that weight-loss surgery signifi-cantly decreases overall mortality as well as the development of newhealth-related conditions in morbidly obese patients.
(Ann Surg 2004;240: 416–424)
In recent years, morbid obesity has emerged as a seriouspublic health threat. After smoking, it is the second leading
cause of preventable, premature death in the United States. Itis estimated that there are 400,000 deaths attributable toobesity in the United States each year.1 The World HealthOrganization has recognized an epidemic of obesity through-out most of the developed and developing world.2 Canadianadult obesity trends have grown during a 13-year period from5.6% in 1985 to 14.8% in 1998.
Obesity is associated with multiple complications andrelated comorbidities that lead to both physical and psycho-logic problems.3–6 Bariatric surgery has been shown to be aneffective method for producing weight loss in obese patientsin both the short and long term7–11 and to be more effectivethan dieting in producing sustained weight loss.12 To date,there has not been a population-based study demonstrating asignificant impact of surgically induced permanent weightloss on mortality and the prevention of comorbidity in severeobesity. The current study addresses these issues by compar-ing the outcomes in 2 cohorts of morbidly obese patients.
METHODS
Study DesignThis was an observational 2-cohort study that compared
the morbidity and mortality of a cohort of morbidly obesepatients treated with bariatric surgery at the McGill Univer-sity Health Centre (MUHC) to that of matched morbidlyobese controls who had not been treated surgically. Theinception time of the bariatric cohort was the time of admis-sion for surgery. The inception time for the control group wasthe date of surgery of their matched bariatric patients. Amaximum of 6 controls were identified for each bariatricsubject. The 2 cohorts were followed for a maximum of 5years. The MUHC Research Institute ethics board approvedthe study.
Identification of Study CohortsA total of 1118 patients underwent bariatric surgery for
the treatment of morbid obesity at the MUHC betweenJanuary 7, 1986, and June 8, 2002. The unique health insur-
From the Section of Bariatric Surgery, Division of General Surgery, Depart-ment of Surgery, McGill University, Montreal, Quebec, Canada.
Reprints: Nicolas V. Christou, MD, PhD, Room s9.30, 687 Pine Ave. W., Montreal,Quebec, Canada H3A1A1. E-mail: [email protected].
Copyright © 2004 by Lippincott Williams & WilkinsISSN: 0003-4932/04/24003-0416DOI: 10.1097/01.sla.0000137343.63376.19
Annals of Surgery • Volume 240, Number 3, September 2004416
4 16 sept 2010 Geneesk dagen Antwerpen

Bariatric surgery reduces mortality
5 16 sept 2010 Geneesk dagen Antwerpen

Bariatric surgery reduces health costs
AFer 2 years cost for society of lap surgery is lower than no surgery
6 16 sept 2010 Geneesk dagen Antwerpen

Stop nega8ve aKtude!
• Self inflicted -‐> no cure ?
• 1. Preven8ve measures in children remains very important.
• 2. Bariatric surgery is more than weight reduc8on. – Prevents cardiovascular diseases – Prevents cancer – Treats diabetes – Treats hypertension
• 3. Bariatric surgery -‐> Metabolic surgery! 7 16 sept 2010 Geneesk dagen Antwerpen

Laparoscopy in morbid obesity.
• 1/3 of pa8ents requiring laparoscopy are obese.
• Bariatric surgery is now preferen8al laparoscopic.
• Why is morbid obese laparoscopy difficult for the
– Anesthesiologist ? – Surgeon ?
8 16 sept 2010 Geneesk dagen Antwerpen

16 sept 2010 Geneesk dagen Antwerpen 9
Surgical comments
• S8ll a lot of complaints – Pa8ent presses en s8ll the anesthe8st tell that the pa8ent is relaxed. (TOF 0) !
– Some anesthe8sts can give be^er relaxa8on than others. Why?
– I have no surgical workspace and the anesthe8st is not willing to do anything!
– Other surgeon can work at lower pressures while I am not able to do this?
– Pa8ent is breathing at end opera8on although recovery s8ll takes a long 8me!

Anesthesiologische vragen
• Ik kan pa8ent onvoldoende beademen wegens hoge luchtwegdrukken.
• Chirurg wil intra abdominale druk niet doen dalen.
• Et CO2 loopt te hoog op. TV, freq reeds maximaal.
• Sommige chirurgen klagen nooit, hebben geen spierrelaxa8e nodig, werken veel sneller,…
• Locoregionale niet mogelijk
10 16 sept 2010 Geneesk dagen Antwerpen

On the abdominal pressure volume rela8on
0 2 4 6 8
10 12 14 16 18
0 1 2 3
intr
a ab
dom
inal
pre
ssur
e m
mHg
!
intra abdominal volume Liter!
J Mulier, B Dillemans, M Crombach, C Missant, A Sels (2009) On the abdominal pressure volume rela7onship. The Internet Journal of Anesthesiology. 2009; 21: 1.
PV0 = 5
E = 4 mmHg/l
Higher insuffla8on pressures needed
Insufficient intra abdominal volume
11 16 sept 2010 Geneesk dagen Antwerpen

Abdominal E and PV0
• Measure the abdominal pressure volume rela8on in the op8mal posi8on. – Inflate the abdomen to reach a volume of 3 L. Keep this
pressure constant. – Measure three points (vol-‐pressure) and calculate E and
PV0.
• Calculate the pressure to reach 3 L • Set the inflator to this pressure.
Simplified: Set at the pressure when a volume of 3 L is reached.
12 16 sept 2010 Geneesk dagen Antwerpen

16 sept 2010 Geneesk dagen Antwerpen Mulier JP 2008
13

16 sept 2010 Geneesk dagen Antwerpen 14
BMI effect on abdominal P/V rela8on
• J Mulier ISPUB 2009 – Pressure volume rela8on is linear
– PV0 and E define each pa8ent
• J Mulier IFSO 2007

16 sept 2010 Geneesk dagen Antwerpen
Waist to Hip ra8o (WHR)
• Man normal WHR: 0,9 • Woman normal WHR: 0,7
• Android fat distribu8on – WHR > 0,8
• Gynoid fat distribu8on – WHR < 0,8
15

16 sept 2010 Geneesk dagen Antwerpen 16
Android versus Gynoid fat distribu8on has a different Elastance

16 sept 2010 Geneesk dagen Antwerpen 17
Two types of android obesity
Intra visceral adiposity Extra visceral adiposity Subcutaneus fat is scant and Subcutaneus fat is thick and intra abdominal fat is thick and intra abdominal fat is scant.

16 sept 2010 Geneesk dagen Antwerpen
Large intra visceral fat volume, or liver steatosis makes the rela8on non linear !
• If the abdominal fascia is already circular instead of ellip8c – No deforma8on possible
– No radius decrease with increasing volume
18

16 sept 2010 Geneesk dagen Antwerpen 19
Pig: High dose desfl sevo • Zelfde spier relaxa8e effect sevo en desfl
• data JPMulier 2009

16 sept 2010 Geneesk dagen Antwerpen
20
E en PV0 determined by ?
factors PV0 PVO sig E E sig
Age Neg 0.828 Pos 0.003*
Length Neg 0.356 Neg 0.245
Body weigth Pos 0.012* Pos 0.294
Bmi neg 0.054 Neg 0.272
Sex Neg 0.596 Neg 0.536
Gravidity Neg 0.305 Neg 0.049*
Prev abd operation Neg 0.191 Neg 0.009*
Muscle relaxation Neg 0.001* Neg 0.376
* Sig p<0.05
• Mulier Dillemans ESA 2007

16 sept 2010 Geneesk dagen Antwerpen 21
NMB effect on E -‐ PV0
• E or Compliance unchanged by NMB – E determined by fascia, size and shape
• PV0 drops by NMB – = extra volume at same pressure

16 sept 2010 Geneesk dagen Antwerpen 22
Is deep relaxa8on needed and possible?
• Time between end pneumoperitoneum and end opera8on is very short: – in 5 min from TOF 0/4 -‐¼ 8ll 90% – is not possible with neos8gmine.
• Sugammadex – TOF 0/4 8ll end pneumoperitoneum – Very deep NMB PTC < 5 is possible 8ll the end

16 sept 2010 Geneesk dagen Antwerpen
23
Effect of deep muscle relaxa8on on IAP with constant IAV
• Gradual pressure drop un8l flat line • Max effect at TOF = 0/4 • No need to drop un8l PTC = 0

16 sept 2010 Geneesk dagen Antwerpen
24
Effect of deep muscle relaxa8on on abdominal PV loop
• TOF > 90%
• TOF = 0/4
• TOF 0/4 and PTC < 5

Only leg flexion affects E in mmHg/L
E: 3,6 > E: 2,6 vol increase: 1100ml
J P Mulier, B Dillemans Impact of trunk posi8oning and leg flexion on the abdominal elastance during bariatric surgery. :Eur J Anesth 2008; 25, S44:234
Only table inclination affects PV0 in mmHg
PV0: 4,8 > 4,1 > 3,8 vol increase: 200ml 900 ml
25 16 sept 2010 Geneesk dagen Antwerpen

16 sept 2010 Geneesk dagen Antwerpen 26
How to change E : hip flexion
• Mulier JP, Dillemans B Obes Surg 2009

Worst Best
airway pres in cmH20:
27,6 > 27,3 > 25,4 > 25 > 24,4
Effect of posi8on on airway pressure cmH2O
P decreases with an8 trendelenburg and leg flexion
J P Mulier, B Dillemans Impact of leg flexion and reverse trendelenburg on airway pressure during laparoscopic bariatric surgery. Obes Surg 2008; 18:444 27 16 sept 2010 Geneesk dagen Antwerpen

Volume instead of pressure controlled abdominal insufflation in morbid obese patients.
J P Mulier, B Dillemans Volume instead of pressure controlled abdominal insuffla8on in morbid obese pa8ents. Obes Surg 2007; 17:1000 28 16 sept 2010 Geneesk dagen Antwerpen

16 sept 2010 Geneesk dagen Antwerpen 29
Why giving insufficient NMB? • Rest relaxa8on is very anxious • To prevent bad respira8on post op, low satura8on, high et CO2
• Relaxa8on sufficient ended to allow neos8gmine to work – TOF minimum one count
• Be^er no neos8gmine as – Bradycardia -‐ total AV block risico – Bronchospasm (asthma8c pa8ents?) – Vomi8ng and nausea post op
No reason now with Sugammadex (brideon)

16 sept 2010 Geneesk dagen Antwerpen 30
Are surgeons right to be difficult?
• Even with max NMB, abdomen can be under tension with insufficient space.
• Other techniques are needed Abd infla8on volume at 15mmHg

16 sept 2010 Geneesk dagen Antwerpen 31
Laparoscopy without muscle relaxants ?
• Laparoscopy is possible without NMB if – Abdominal compliance > 0,5 L/mmHg – IAV > 4 L at 15 mmHg at start laparoscopy
• Gravidity > 3 • Previous mul8ple laparoscopies/laparotomies • > 10 kg weight reduc8on • No man with android fat distribu8on
– AFer several hours abdominal compliance rises and
– Sufficient deep sleep • As pa8ent should not breath against ven8lator.
– Pressure support ven8la8on • Easier to prevent breathing against ven8lator
16 sept 2010 Geneesk dagen Antwerpen
32
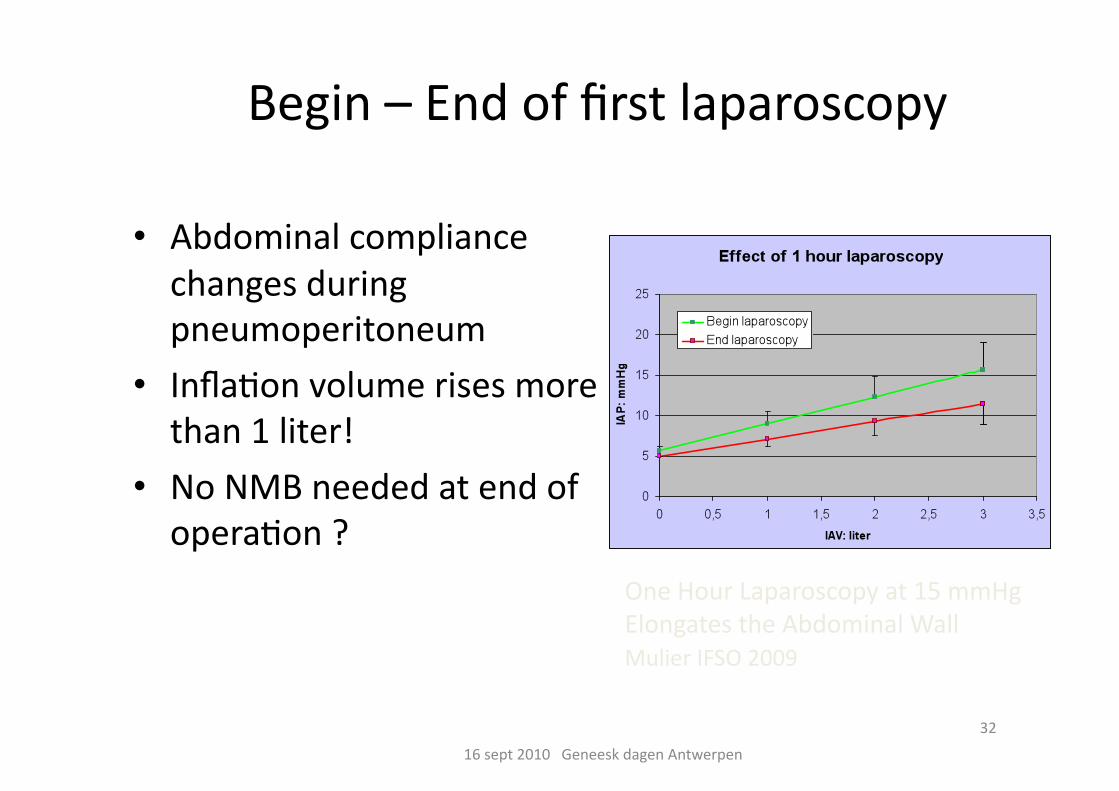
Begin – End of first laparoscopy
• Abdominal compliance changes during pneumoperitoneum
• Infla8on volume rises more than 1 liter!
• No NMB needed at end of opera8on ?
One Hour Laparoscopy at 15 mmHg Elongates the Abdominal Wall Mulier IFSO 2009

Impact of laparoscopy depends on
16 sept 2010 Geneesk dagen Antwerpen
33
0
0.5
1
1.5
2
2.5
3
• J P Mulier, I Casier, K Verbeke, B Vanacker 2010 ESA
Vol increase at end lap

16 sept 2010 Geneesk dagen Antwerpen 34
But if pa8ent breaths against ven8lator: Valsalva effect
• Valsalva is an ac8ve muscle contrac8on different from breathing – It increases the abdominal pressure to block inspira8on
• Preventable by support ven8la8on

Peri opera8ve pain medica8on depends on Gravidity or previous laparoscopy
• ASA 2010 JPMulier
0
10
20
30
40
50
60
BMI Piritramide Sufentanyl
G:0 lap:0
G>0 lap>0
35 16 sept 2010 Geneesk dagen Antwerpen
Piritramide mg Sufentanyl ug Total peri opera8ve dose
Perfusalgan 2 gr/4 hours

16 sept 2010 Geneesk dagen Antwerpen 36
Con8nuous NMB needed ?
• Yes – Larger surgical work-‐volume at lower pressures – Workspace some8mes remains insufficient making surgeons angry : try to do everything.
– Prevent breathing against ven8lator – At low pressures less structural damage and less post op pain?
• No – Abdominal compliance some8mes large enough – Work at higher intra abdominal pressure?
– 2 MAC inhala8on has same effect? – Effect of posi8on and of 8me?

16 sept 2010 Geneesk dagen Antwerpen 37
If Yes -‐> decurarisa8on needed
• Only Bridion is able to do allow full muscle relaxa8on 8ll the end.
• Use con8nuous infusion of Rocuronium (Esmeron) adapted to TOF measurements. – Induc8on dose of 0,6 -‐ 1,2 mg/kg IBW – Con8nuous infusion of 50 mg/h -‐> …

Sugammadex Dose adapta8on? • Sorgenfrei 2006 78 sec • Vanacker 94 sec • P Van Lancker T Bogaert J P Mulier • BMI 44,5 2mg/kg sugammadex at T1 – T2 • All pa8ent were full decurarised above 90% in max 6 minutes
16 sept 2010 Geneesk dagen Antwerpen 38
0
50
100
150
200
250
300
350
IBW IBW + 20% IBW + 40%
7me to T4>0.9
8me to T4>0.9

16 sept 2010 Geneesk dagen Antwerpen 39
Measure Depth of Blockade
• Intense block: 16 mg/kg • Deep block: 4 mg/kg • Moderate block: 2 mg/kg • Superficial block: 1 mg/kg + Neos8gmine? • No block: 0 mg/kg
PTC 0 PTC ≥1
Intense block Deep block Moderate block
TOF count 0 TOF count 0 TOF count 1-3
Level of block
Response to TOF
Response to PTC
PTC, posttetanic count; TOF, train-of-four. Fuchs-Buder T et al. Acta Anaesthesiol Scand. 2007;51:789-808.
Posttetanic count
Twitch response
Twitch percentage
Superficial block TOF count 4
T1/T4 %

16 sept 2010 Geneesk dagen Antwerpen 40
Immediate effects in morbid obese pa8ents of Bridion
• Deep breaths possible – Less lung collaps
• Aurosal effect – Like Amfetamine awakening – Sudden muscle fiber s8mula8on gives aurosal
• Pa8ent transfers him/her self in bed – 50 % of cases instead of only10%
• Spontaneous movements easier – Deep venous trombosis preven8on
• No non invasive assist since introduc8on of sugammadex

Old method: rolling mat
16 sept 2010 Geneesk dagen Antwerpen 41

Self in bed aFer Bridion?
16 sept 2010 Geneesk dagen Antwerpen 42

JPM 9 9 2010 Anesthesie voor bariatrische heelk 43
Second ESPCOP Scien8fic mee8ng
Mul8disciplinarity
Pordenone, Italy 18 sept 2010