obstet gynecol. 2011 apr;117(4)777 87
TRANSCRIPT

Original Research
Effective Treatment of Heavy MenstrualBleeding With Estradiol Valerate and DienogestA Randomized Controlled Trial
Jeffrey T. Jensen, MD, MPH, Susanne Parke, MD, PhD, Uwe Mellinger, PhD, Andrea Machlitt, MD,and Ian S. Fraser, MD
OBJECTIVE: To estimate the efficacy of a fixed estrogenstep-down and progestin step-up 28-day estradiol (E2)valerate and dienogest oral contraceptive regimen inwomen with heavy menstrual bleeding, prolonged men-strual bleeding, or heavy and prolonged menstrual bleed-ing without organic pathology.
METHODS: This double-blind, placebo-controlled studyrandomized women aged 18 years or older with prolonged,frequent, or heavy menstrual bleeding, objectively con-firmed during a 90-day run-in phase, to treatment with E2valerate and dienogest or placebo (2:1) for 196 days. Data
from the last 90 days of treatment and the run-in phasewere compared. The primary variable was the “completeresponse” rate (complete resolution of qualifying abnormalmenstrual symptoms, including a 50% or greater reductionin pretreatment menstrual blood loss volume in womenwith heavy menstrual bleeding). Secondary variables includedobjective changes in menstrual blood loss volume (alkalinehematin methodology) and iron metabolism parameters.Overall, 180 women were needed to provide 90% power.
RESULTS: There were no marked differences in the char-acteristics of E2 valerate and dienogest (n�120) andplacebo (n�70) recipients. The proportion of “completeresponders” in the evaluable group was significantlyhigher in E2 valerate and dienogest (35/80; 43.8%) com-pared with placebo (2/48, 4.2%, P<.001) recipients. Themean [standard deviation] reduction in menstrual bloodloss with E2 valerate and dienogest from the run-in phaseto the efficacy phase was substantial (�353 mL [309 mL];mean �64.2%; median �70.6%) and significantly greaterthan that in placebo recipients (�130 mL [338 mL]; mean�7.8%; median �18.7%; P<.001). Significant improve-ments in hemoglobin, hematocrit, and ferritin were seenwith E2 valerate and dienogest, but not with placebo.
CONCLUSION: Oral E2 valerate and dienogest washighly effective compared with placebo in the treatmentof women with heavy menstrual bleeding, prolongedmenstrual bleeding, or heavy and prolonged menstrualbleeding without organic pathology.
CLINICAL TRIAL REGISTRATION: ClinicalTrials.gov,www.clinicaltrials.gov, NCT00293059.(Obstet Gynecol 2011;117:777–87)DOI: 10.1097/AOG.0b013e3182118ac3
LEVEL OF EVIDENCE: I
Abnormal uterine bleeding describes a range ofmenstrual bleeding symptoms, the most common
of which is heavy bleeding. The estimated worldwideprevalence of subjective, self-defined abnormal uter-ine bleeding varies greatly from 4% to 52%.1 Women
See related editorial on page 773.
From the Department of Obstetrics and Gynecology, Oregon Health & ScienceUniversity, Portland, Oregon; the Departments of Clinical Development, Clin-ical Statistics, and Global Medical Affairs Women’s Healthcare, Bayer Health-Care Pharmaceuticals, Berlin, Germany; and the Department of ReproductiveMedicine, University of Sydney, Sydney, New South Wales, Australia.
Supported by Bayer HealthCare Pharmaceuticals.
The authors thank Lyndal Staples and Phil Jones (inScience Communications,a Wolters Kluwer business, Chester, United Kingdom) for medical writingsupport during manuscript preparation. Funding for editorial assistance wasprovided by Bayer HealthCare Pharmaceuticals.
Presented as an abstract and oral presentation at the 65th Annual Meeting of theAmerican Society for Reproductive Medicine, October 17–21, 2009, Atlanta, Georgia.
Corresponding author: Jeffrey T. Jensen, Department of Obstetrics & Gynecology,Oregon Health & Science University, 3181 SW Sam Jackson Park Road,Portland 97239, OR; e-mail: [email protected].
Financial DisclosureDr. Jensen is a consultant and speaker for Bayer HealthCare Pharmaceuticals Inc.,Wyeth Pharmaceuticals, and Schering Plough and has received research funding fromBayer HealthCare Pharmaceuticals Inc, Wyeth Pharmaceuticals, Warner Chilcott,the Population Council, and the National Institutes of Health (NIH); Dr. Parke, Dr.Mellinger, and Dr. Machlitt are employees of Bayer HealthCare Pharmaceuticals.Dr. Machlitt owns stock in Bayer HealthCare Pharmaceuticals. Dr. Fraser is aconsultant and speaker for Bayer HealthCare Pharmaceuticals, Schering Plough, andDaiichi Sankyo Pharmaceuticals and has received research support from the NIH, theAustralian National Health and Medical Research Council, the Population Council,Bayer HealthCare Pharmaceuticals, and Schering Plough.
© 2011 by The American College of Obstetricians and Gynecologists. Publishedby Lippincott Williams & Wilkins.ISSN: 0029-7844/11
VOL. 117, NO. 4, APRIL 2011 OBSTETRICS & GYNECOLOGY 777

with abnormal bleeding have a reduced quality of lifecompared with the general female population.1,2
No common agreement has been reached on theclassification of abnormal uterine bleeding symptoms;however, symptom-oriented descriptive terminologysuch as heavy menstrual bleeding is generally pre-ferred to poorly defined historical terms such asmenorrhagia.3
It is generally agreed that a normal bleedingepisode comprises a menstrual blood loss volume inthe range of 30–40 mL,4,5 with an upper limit of 80mL.6 The prevalence of objectively measured heavymenstrual bleeding (ie, a blood loss volume of 80 mLor more per cycle as determined using the alkalinehematin method to quantify hemoglobin extractedfrom used sanitary items)6 has been reported to be9–14% in a review of epidemiologic studies.1 In themajority of women, the duration of menstruation is3–8 days.7
Limited studies indicate that oral contraceptivepills (OCPs) can reduce menstrual blood loss inwomen with heavy menstrual bleeding.8,9 The prop-erties of an OCP combining estradiol (E2) valerate(which circulates as E2) and dienogest (a progestinwith high endometrial potency) in an estrogen step-down and progestin step-up regimen was hypothe-sized to be beneficial in this setting. A phase IIIclinical study showed that the cycle control andbleeding pattern achieved with E2 valerate and dieno-gest was comparable to that of a monophasic OCPcontaining ethinyl E2 20 micrograms and levonorg-estrel 100 micrograms.10 Moreover, E2 valerate anddienogest was associated with shorter (median dura-tion 4 compared with 5 days), lighter (rated signifi-cantly more often as only spotting or of light intensity)menstrual bleeding, or more often absent (P�.001).10
As such, we undertook this phase III study in NorthAmerica to determine the efficacy and explore safetyof E2 valerate and dienogest in women with con-firmed heavy menstrual bleeding, prolonged men-strual bleeding, or heavy and prolonged menstrualbleeding without organic cause.
MATERIALS AND METHODSThis was a phase III, randomized, double-blind,placebo-controlled study that was conducted to inves-tigate the efficacy and safety of E2 valerate anddienogest for the treatment of confirmed heavy men-strual bleeding, prolonged menstrual bleeding, or heavyand prolonged menstrual bleeding (ClinicalTrials.govidentifier: NCT00293059). The study was conductedat 47 centers in the United States and Canada be-tween December 2005 and May 2008 in accordance
with the ethical principles of the Declaration of Hel-sinki and the guidelines of the International Confer-ence on Harmonization on Good Clinical Practice.The study protocol was approved by each study site’sInstitutional Review Board before the start of thestudy. All participants provided written informedconsent before entering the study.
The study comprised a screening phase thatlasted up to 28 days, a 90-day run-in interval, a196-day treatment interval, and a 30-day follow-upphase. After the screening phase, participants enteredthe 90-day run-in interval during which the symptomsof heavy bleeding (at least two bleeding episodes witha measured menstrual blood loss volume of 80 mL ormore), prolonged bleeding (at least two bleedingepisodes each lasting 8 days or more), or frequentbleeding (more than five bleeding episodes with aminimum of 20 bleeding days overall) or a combina-tion of any of the three were objectively confirmed bythe use of electronic diaries and quantification ofmenstrual blood loss by hemoglobin extraction fromcollected sanitary protection.
The study recruited women aged at least 18 yearswho had heavy menstrual bleeding, prolonged men-strual bleeding, frequent menstrual bleeding, or anycombination thereof and who fulfilled the additionalcriteria for inclusion. To satisfy these criteria, individ-uals had to be willing to use a barrier method ofcontraception and to use (and collect) all sanitaryprotection items (pads and tampons) provided tothem for use during the study. Participants alsoneeded to have a normal endometrial biopsy or, atmost, mild simple endometrial hyperplasia during the6 months before study entry. Women older than 40years had to have follicle-stimulating hormone levelof less than 40 milli-international units/mL. Womenwere excluded if, at screening before study entry, theyhad an abnormal transvaginal ultrasonogram (definedas the presence of uterine pathology, eg, fibroids orpolyps whose size or localization would be associatedwith heavy menstrual bleeding) or clinically signifi-cant abnormal values for any laboratory examination,or if they had undergone in the 2 months before thestudy endometrial ablation or dilatation and curet-tage. Women were also excluded if they had organicpathology (including von Willebrand disease, chronicendometritis, adenomyosis, endometriosis, endome-trial polyps, significant leiomyomas, or uterine malig-nancy). Exclusion criteria also included the use ofagents intended for the treatment of symptoms of ab-normal uterine bleeding (eg, tranexamic acid, nonsteroi-dal antiinflammatory drugs, and sex steroids); a bodymass index (calculated as weight (kg)/[height (m)]2) of
778 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding OBSTETRICS & GYNECOLOGY

more than 32; smoking more than 10 cigarettes per day(in women older than 35 years); and criteria consistentwith contraindications for the use of combined OCPs.For ethical reasons in this placebo-controlled trial, use ofiron supplementation was allowed if the attending phy-sician considered it necessary.
After the run-in, participants with at least onequalifying symptom were randomized (2:1) to E2 valer-ate and dienogest (NATAZIA, QLAIRA) or matchingplacebo for 196 days (seven cycles) according to apermuted-block, computer-generated (RANDO SASMacro, Version 9.1 for Windows) schedule generatedby the study sponsor using blocks of six. Eligibleindividuals were given study drug according to therandomization code. The randomization number wasfound on the label of the blister card. Randomizationachieved balanced treatment allocation in each block.
The E2 valerate and dienogest regimen com-prised E2 valerate 3 mg on days 1–2 (1 mg of E2valerate is equivalent to 0.76 mg of E2), E2 valerate 2mg and dienogest 2 mg on days 3–7, E2 valerate 2 mgand dienogest 3 mg on days 8–24, E2 valerate 1 mgon days 25–26, and placebo on days 27–28. E2valerate and dienogest was packaged in blister cards,each containing 28 tablets. Participants and investiga-tors were blinded to treatment. For this reason, theplacebo and E2 valerate and dienogest blister cardswere identical in appearance. All participants com-pleted an electronic diary on a daily basis throughoutthe study (including during the run-in interval) todocument drug intake (during the treatment interval),the number of items of sanitary protection used, andtheir perception of menstrual bleeding. Participantsrated their daily bleeding intensity as none, spotting,or bleeding (light, normal, or heavy). Spotting wasdefined as bleeding that was lighter than the partici-pant’s normal experience during menstruation, withno need for sanitary protection other than pantyliners. In addition, participants were carefully in-structed on how to collect all used sanitary protection(pads and tampons) and blood “clots” so that men-strual blood loss volume could be objectively assessedusing a modification of the alkaline hematin methodto quantify hemoglobin in menstrual fluid after TritonX detergent extraction.11 Care was taken to counselparticipants about ways of maximizing the collectionof their total menstrual loss. All sanitary protectionitems were processed and analyzed at a central labo-ratory (Specialty Labs, Valencia, CA).
The primary outcome was the proportion ofparticipants with a complete response to treatment (ie,a return to complete menstrual normality). Data fromthe last 90 days of treatment (efficacy period) and 90
days of run-in phase were compared. The efficacyinterval had to start on the first day of a treatmentcycle. For participants who completed up to day 6 oftreatment cycle 7, the efficacy phase started on thefirst day of treatment cycle 4. For participants whoprematurely discontinued or who had incompletedata, the 90-day efficacy phase was shifted backward.A “complete response” was rigorously defined as acomposite of the absence of all qualifying conditions:no bleeding episodes that lasted more than 7 days; nomore than four bleeding episodes overall; no bleedingepisodes that involved a blood loss volume of 80 mLor more; no more than one bleeding episode increasefrom baseline; no more than 24 days of bleedingoverall; and no increase from baseline in an individ-ual participant’s total number of bleeding days. Forindividuals with prolonged bleeding, the decrease inthe maximum duration of a bleeding episode betweenthe run-in and efficacy phases had to be at least 2days. Similarly, for participants with heavy bleeding,the blood loss volume for each episode had to be lessthan 80 mL and had to represent a decrease of at least50% from the average of the qualifying bleedingepisodes (ie, those episodes with a blood loss volumeof at least 80 mL during the run-in phase). Theprimary efficacy outcome was a responder analysisconducted in the intention-to-treat population (ie, allrandomized participants). Participants were categorizedas complete responders (no abnormal bleeding symp-toms and achievement of all relevant criteria during the90-day efficacy interval); partial or nonresponders(missed at least one of the relevant criteria for a com-plete response during the efficacy phase [for participantsenrolled with heavy bleeding this included the achieve-ment of a reduction in menstrual blood loss volume of50% or more]); or as participants with missing data(received no study medication, did not complete theminimum 90 days of treatment [early drop-outs], or hadtoo many missing bleeding data to define a valid 90-dayefficacy phase [ie, more than 1 day in sequence withmissing bleeding information or more than 9 noncon-secutive days in a 90-day interval with missing bleedinginformation]). The primary efficacy outcome was alsoassessed in those participants with an evaluable response(ie, excluding individuals with missing data). The pri-mary efficacy variable was analyzed by the difference inthe proportions of responders in the two groups and thecorresponding unconditional two-sided 95% confidenceinterval (CI).12 This unconditional CI was calculated byinverting two separate one-sided tests of half the nomi-nal significance level each.
Secondary efficacy variables included changes inmenstrual blood loss volume; the number of sanitary
VOL. 117, NO. 4, APRIL 2011 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding 779

protection items used; changes in the number ofbleeding days and episodes; the proportion of partic-ipants cured of individual symptoms; and changes iniron metabolism parameters. Other secondary endpoints included the proportion of participants with animprovement in menstrual bleeding symptoms as-sessed by investigators using a global assessment scaleand by individuals using a patient’s overall assessmentscale. Both assessment scales were administered ondays 84 and 196 (when investigators and participantswere still blinded to treatment). Each seven-categoryscale ranged from very much improved to very muchworse compared with symptoms at study admission.Secondary efficacy outcomes were analyzed using theintention-to-treat population, irrespective of re-sponder status. If a 90-day efficacy interval could notbe defined for a given woman (ie, if she had missingdata), she was excluded from any analyses that com-pared data from the 90-day run-in interval with the90-day efficacy interval. Such participants, however,were included in any analyses that referred to per-cycle data. Continuous secondary efficacy variableswere analyzed using an analysis of variance or ananalysis of covariance model. Noncontinuous second-ary efficacy variables were analyzed by differences ofproportions and the corresponding CIs.
Safety assessments included measurement of vitalsigns and physical and gynecologic examinations.Data relating to adverse events were gathered byallowing participants to spontaneously volunteer in-formation rather than by direct questioning. Adverseevents were coded using MedDRA 10.0; as such, cate-gories were mandated by standard adverse event report-ing requirements. Safety outcomes were assessed in allrandomized participants who took at least one dose ofstudy medication (the safety analysis population).
It was estimated that the success rate (based onthe complete response rate) for the E2 valerate anddienogest and placebo groups would be 50% and20%, respectively, and that the overall dropout ratewould be 30%. Using these assumptions, it was calcu-lated that 120 participants would be required for theE2 valerate and dienogest group and 60 for theplacebo group (180 in total) to provide 90% power totest the null hypothesis (ie, that the two treatmentgroups would have an equal rate of success) at a 5%significance level. All variables were analyzed de-scriptively. Numbers, means, standard deviations,minima, quartiles, medians, and maxima were calcu-lated for metric data. Frequency tables were gener-ated for categorical data. Statistical analyses wereperformed using SAS for Windows.
Randomized to estradiolvalerate and dienogest
(intention-to-treat population) n=120
Excluded: n=887Consent withdrawn: 138Inclusion/exclusion criteria
not met: 604Patient lost to follow-up: 88Other: 57
Randomized to placebo(intention-to-treat population)
n=70
ScreenedN=1,077
Randomized (2:1 ratio)n=190
Medication administered(safety population)
n=119
Medication administered(safety population)
n=66
Did not complete studymedication: n=35
Discontinued study medication: 31
Unknown: 4
Did not complete studymedication: n=15
Discontinued study medication: 13
Unknown: 2
Completed study coursen=85
Completed study coursen=51
Completed study medicationn=84
Completed study medicationn=51
Fig. 1. Flow of participants throughthe study.Jensen. Estradiol Valerate and Dienogestfor Menstrual Bleeding. Obstet Gynecol2011.
780 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding OBSTETRICS & GYNECOLOGY

Bleeding intensity data from the diaries that weremissed on nonconsecutive days were replaced usingthe highest intensity value for bleeding obtained onthe bordering days. No more than 9 nonconsecutivedays were replaced per 90-day interval. Consecutivedays with missing bleeding intensity data were notreplaced.
RESULTSThe flow of participants through the study is shown inFigure 1. A total of 1,077 women were screened; ofthese, 190 were randomized to treatment and com-prised the intention-to-treat population: 120 wererandomized to E2 valerate and dienogest and 70 toplacebo. The most common reason for not beingrandomized to treatment was failure to meet the strictinclusion or exclusion criteria (n�604).
The demographic and baseline characteristics ofparticipants are shown in Table 1. Participants in thetwo treatment groups were generally well matched interms of age and body mass index. The most commonmenstrual bleeding symptom at baseline was heavybleeding (75.8–85.7%), followed by prolonged bleed-ing (17.1–21.7%). The proportion of frequent bleedersin both treatment groups was very low. Only oneenrolled participant (a 46-year-old woman, gravida 5para 4, enrolled for heavy menstrual bleeding andwas randomly assigned to placebo) had an endome-trial ablation (7 years before entering the study) in hersurgical history. An overview of the responder status(and the reasons for a partial or nonresponse) in eachtreatment group is shown in Table 2. The proportionof complete responders (ie, participants who met all ofthe strict response criteria and who had a return tomenstrual normality) was significantly higher in theE2 valerate and dienogest group than in the placebo
Table 1. Demographic and BaselineCharacteristics of Participants Assignedto Estradiol Valerate and Dienogest orPlacebo (Intention-to-Treat Population)
E2 Valerate andDienogest(n�120)
Placebo(n�70)
Age (y) 36.9�7.5 37.0�6.7Ethnicity
White 71 (59.2) 46 (65.7)Black 38 (31.7) 14 (20.0)Hispanic 8 (6.7) 6 (8.6)
Weight (kg) 71.3�11.1 69.5�11.8Body mass index (kg/m2) 26.3�3.6 25.8�3.6Bleeding symptoms*
Prolonged bleeding 26 (21.7) 12 (17.1)Frequent bleeding 4 (3.3) 2 (2.9)Heavy bleeding 91 (75.8) 60 (85.7)
E2, estradiol.Data are mean�standard deviation or n (%).* Some participants presented with multiple symptoms.
Table 2. Responder Status in Women Who Received Estradiol Valerate and Dienogest or Placebo(Intention-to-Treat Population)
E2 Valerate andDienogest(n�120)
Placebo(n�70)
Complete responder 35 (29.2) 2 (2.9)Partial or non-responder 45 (37.5) 46 (65.7)Missing data 40 (33.3) 22 (31.4)
Patients classified as partial or nonresponders failed to meet the following criteria*No bleeding episodes lasting more than 7 d 25 (20.8) 18 (25.7)No more than four bleeding episodes overall 7 (5.8) 0 (0.0)No bleeding episodes with a menstrual blood loss volume of 80 mL or more 30 (25.0) 42 (60.0)No more than one bleeding episode increase from baseline 7 (5.8) 2 (2.6)No more than 24 bleeding days overall 12 (10.0) 8 (11.4)No increase from baseline in the total number of bleeding days 22 (18.3) 18 (25.7)If enrolled with prolonged bleeding n�26 n�12
(Decrease of at least 2 d from the run-in phase to the efficacyphase in the maximum duration of bleeding)
6 (23.1) 5 (41.7)
If enrolled with heavy bleeding n�91 n�60(Menstrual blood loss associated with each episode less than
80 mL and decreased by at least 50% from the average ofthe qualifying bleeding episodes during the run-in phase)
30 (33.0) 39 (65.0)
E2, estradiol.Data are n (%).* Women could have been classified as nonresponders for multiple reasons.
VOL. 117, NO. 4, APRIL 2011 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding 781
group; this was the case when results were analyzed inthe intention-to-treat population and in the popula-tion of participants with evaluable data.
Using the most conservative approach, that is,categorizing all randomized participants (intention-to-treat population) with missing data as nonresponders,35 of 120 individuals (29.2%) in the E2 valerate anddienogest group and 2 of 70 participants (2.9%) in theplacebo group had a complete response to treatment(P�.001). In an analysis of evaluable participantsaccording to the complete response criteria (ie, ex-cluding those individuals with missing data), thecomplete response rate was 43.8% (35/80) in womenwho received E2 valerate and dienogest comparedwith only 4.2% (2/48) in women who received pla-cebo (P�.001).
The majority of participants (ie, 91/120 [75.8%]treated with E2 valerate and dienogest and 60/70[85.7%] with placebo) were recruited for heavy bleed-ing. If resolution of heavy bleeding (defined as lessthan 80 mL menstrual blood loss volume for eachepisode) was considered the only response criterionrequired, 51 of 91 (56.0%) participants treated with E2valerate and dienogest and 16 of 60 (26.7%) withplacebo would be defined as cured of heavy bleedingat the end of study.
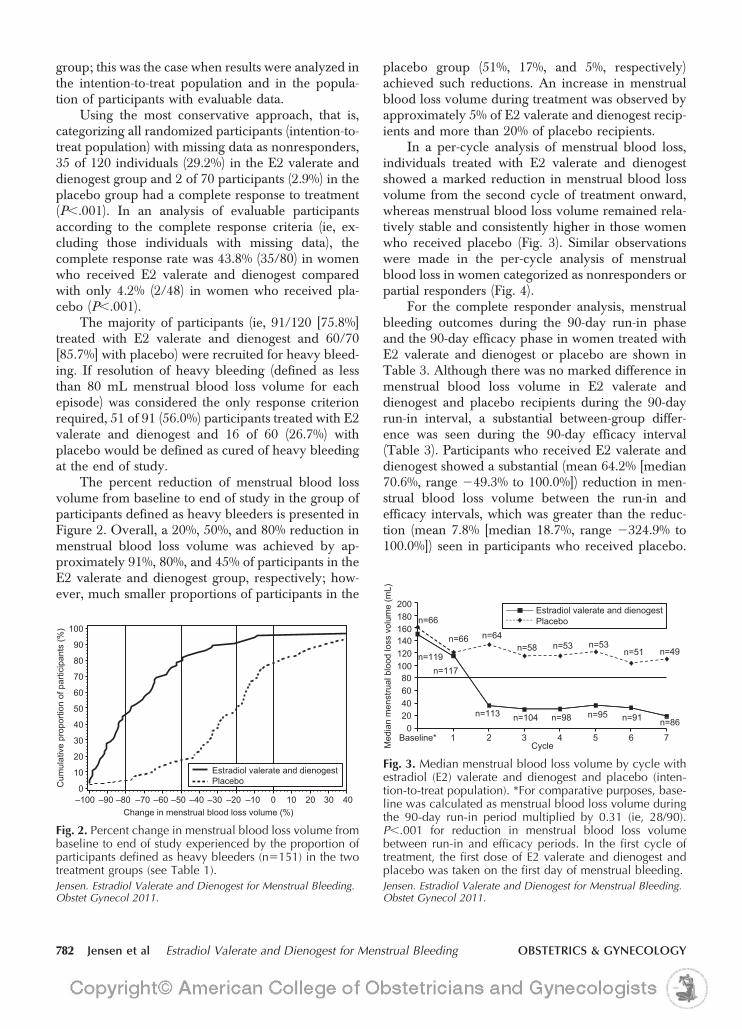
The percent reduction of menstrual blood lossvolume from baseline to end of study in the group ofparticipants defined as heavy bleeders is presented inFigure 2. Overall, a 20%, 50%, and 80% reduction inmenstrual blood loss volume was achieved by ap-proximately 91%, 80%, and 45% of participants in theE2 valerate and dienogest group, respectively; how-ever, much smaller proportions of participants in the
placebo group (51%, 17%, and 5%, respectively)achieved such reductions. An increase in menstrualblood loss volume during treatment was observed byapproximately 5% of E2 valerate and dienogest recip-ients and more than 20% of placebo recipients.
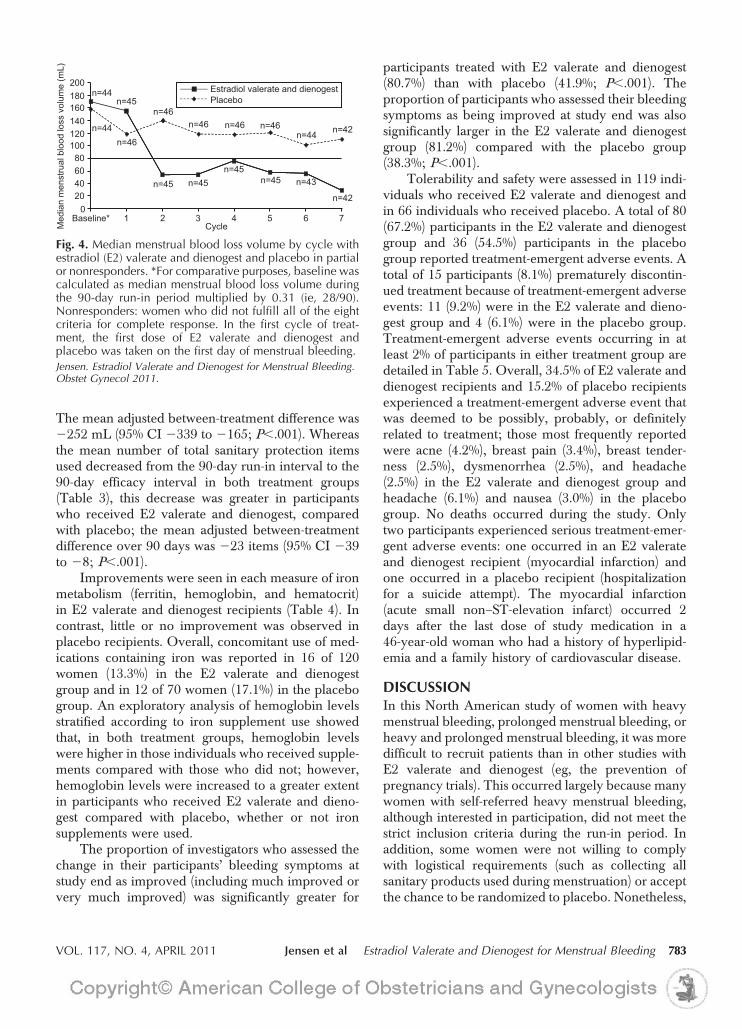
In a per-cycle analysis of menstrual blood loss,individuals treated with E2 valerate and dienogestshowed a marked reduction in menstrual blood lossvolume from the second cycle of treatment onward,whereas menstrual blood loss volume remained rela-tively stable and consistently higher in those womenwho received placebo (Fig. 3). Similar observationswere made in the per-cycle analysis of menstrualblood loss in women categorized as nonresponders orpartial responders (Fig. 4).
For the complete responder analysis, menstrualbleeding outcomes during the 90-day run-in phaseand the 90-day efficacy phase in women treated withE2 valerate and dienogest or placebo are shown inTable 3. Although there was no marked difference inmenstrual blood loss volume in E2 valerate anddienogest and placebo recipients during the 90-dayrun-in interval, a substantial between-group differ-ence was seen during the 90-day efficacy interval(Table 3). Participants who received E2 valerate anddienogest showed a substantial (mean 64.2% [median70.6%, range �49.3% to 100.0%]) reduction in men-strual blood loss volume between the run-in andefficacy intervals, which was greater than the reduc-tion (mean 7.8% [median 18.7%, range �324.9% to100.0%]) seen in participants who received placebo.
Estradiol valerate and dienogestPlaceboC
umul
ativ
e pr
opor
tion
of p
artic
ipan
ts (%
) 100
90
80
70
60
50
40
30
20
10
0
Change in menstrual blood loss volume (%)–100 –90 –80 –70 –60 –50 –40 –30 –20 –10 0 10 20 30 40
Fig. 2. Percent change in menstrual blood loss volume frombaseline to end of study experienced by the proportion ofparticipants defined as heavy bleeders (n�151) in the twotreatment groups (see Table 1).Jensen. Estradiol Valerate and Dienogest for Menstrual Bleeding.Obstet Gynecol 2011.
200
140160180 n=66
n=64
100120
n=66n=58 n=53 n=53
n=51 n=49n=119n=117
20406080
n=113 n=980
n=91 n=86
Estradiol valerate and dienogestPlacebo
CycleBaseline* 1 32
Med
ian
men
stru
al b
lood
loss
vol
ume
(mL)
4 5 6 7
n=104 n=95
Fig. 3. Median menstrual blood loss volume by cycle withestradiol (E2) valerate and dienogest and placebo (inten-tion-to-treat population). *For comparative purposes, base-line was calculated as menstrual blood loss volume duringthe 90-day run-in period multiplied by 0.31 (ie, 28/90).P�.001 for reduction in menstrual blood loss volumebetween run-in and efficacy periods. In the first cycle oftreatment, the first dose of E2 valerate and dienogest andplacebo was taken on the first day of menstrual bleeding.Jensen. Estradiol Valerate and Dienogest for Menstrual Bleeding.Obstet Gynecol 2011.
782 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding OBSTETRICS & GYNECOLOGY
The mean adjusted between-treatment difference was�252 mL (95% CI �339 to �165; P�.001). Whereasthe mean number of total sanitary protection itemsused decreased from the 90-day run-in interval to the90-day efficacy interval in both treatment groups(Table 3), this decrease was greater in participantswho received E2 valerate and dienogest, comparedwith placebo; the mean adjusted between-treatmentdifference over 90 days was �23 items (95% CI �39to �8; P�.001).
Improvements were seen in each measure of ironmetabolism (ferritin, hemoglobin, and hematocrit)in E2 valerate and dienogest recipients (Table 4). Incontrast, little or no improvement was observed inplacebo recipients. Overall, concomitant use of med-ications containing iron was reported in 16 of 120women (13.3%) in the E2 valerate and dienogestgroup and in 12 of 70 women (17.1%) in the placebogroup. An exploratory analysis of hemoglobin levelsstratified according to iron supplement use showedthat, in both treatment groups, hemoglobin levelswere higher in those individuals who received supple-ments compared with those who did not; however,hemoglobin levels were increased to a greater extentin participants who received E2 valerate and dieno-gest compared with placebo, whether or not ironsupplements were used.
The proportion of investigators who assessed thechange in their participants’ bleeding symptoms atstudy end as improved (including much improved orvery much improved) was significantly greater for
participants treated with E2 valerate and dienogest(80.7%) than with placebo (41.9%; P�.001). Theproportion of participants who assessed their bleedingsymptoms as being improved at study end was alsosignificantly larger in the E2 valerate and dienogestgroup (81.2%) compared with the placebo group(38.3%; P�.001).
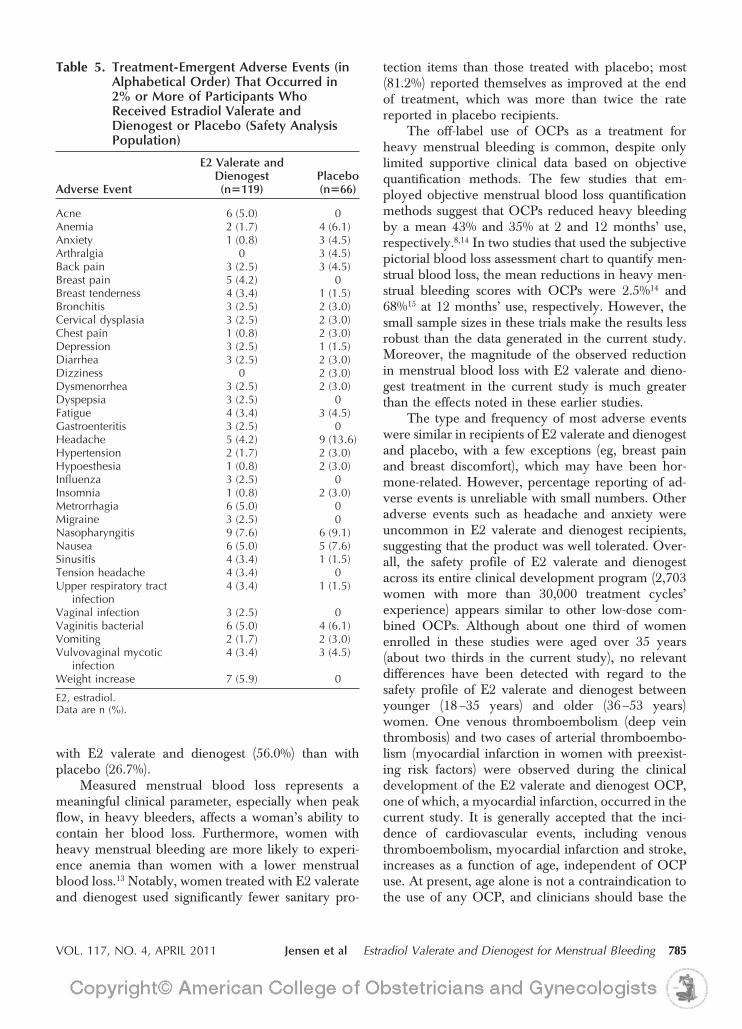
Tolerability and safety were assessed in 119 indi-viduals who received E2 valerate and dienogest andin 66 individuals who received placebo. A total of 80(67.2%) participants in the E2 valerate and dienogestgroup and 36 (54.5%) participants in the placebogroup reported treatment-emergent adverse events. Atotal of 15 participants (8.1%) prematurely discontin-ued treatment because of treatment-emergent adverseevents: 11 (9.2%) were in the E2 valerate and dieno-gest group and 4 (6.1%) were in the placebo group.Treatment-emergent adverse events occurring in atleast 2% of participants in either treatment group aredetailed in Table 5. Overall, 34.5% of E2 valerate anddienogest recipients and 15.2% of placebo recipientsexperienced a treatment-emergent adverse event thatwas deemed to be possibly, probably, or definitelyrelated to treatment; those most frequently reportedwere acne (4.2%), breast pain (3.4%), breast tender-ness (2.5%), dysmenorrhea (2.5%), and headache(2.5%) in the E2 valerate and dienogest group andheadache (6.1%) and nausea (3.0%) in the placebogroup. No deaths occurred during the study. Onlytwo participants experienced serious treatment-emer-gent adverse events: one occurred in an E2 valerateand dienogest recipient (myocardial infarction) andone occurred in a placebo recipient (hospitalizationfor a suicide attempt). The myocardial infarction(acute small non–ST-elevation infarct) occurred 2days after the last dose of study medication in a46-year-old woman who had a history of hyperlipid-emia and a family history of cardiovascular disease.
DISCUSSIONIn this North American study of women with heavymenstrual bleeding, prolonged menstrual bleeding, orheavy and prolonged menstrual bleeding, it was moredifficult to recruit patients than in other studies withE2 valerate and dienogest (eg, the prevention ofpregnancy trials). This occurred largely because manywomen with self-referred heavy menstrual bleeding,although interested in participation, did not meet thestrict inclusion criteria during the run-in period. Inaddition, some women were not willing to complywith logistical requirements (such as collecting allsanitary products used during menstruation) or acceptthe chance to be randomized to placebo. Nonetheless,
200
140160180 n=44
n=45n=46
80100120
n=46
n=46 n=46 n=46n=44 n=42n=44
204060
n=45 n=45n=45
n=45 n=43
n=420
CycleBaseline* 1 32
Med
ian
men
stru
al b
lood
loss
vol
ume
(mL)
4 5 6 7
Estradiol valerate and dienogestPlacebo
Fig. 4. Median menstrual blood loss volume by cycle withestradiol (E2) valerate and dienogest and placebo in partialor nonresponders. *For comparative purposes, baseline wascalculated as median menstrual blood loss volume duringthe 90-day run-in period multiplied by 0.31 (ie, 28/90).Nonresponders: women who did not fulfill all of the eightcriteria for complete response. In the first cycle of treat-ment, the first dose of E2 valerate and dienogest andplacebo was taken on the first day of menstrual bleeding.Jensen. Estradiol Valerate and Dienogest for Menstrual Bleeding.Obstet Gynecol 2011.
VOL. 117, NO. 4, APRIL 2011 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding 783

a sufficient number of women participated to demon-strate that E2 valerate and dienogest is an effectiveand well-tolerated treatment for heavy menstrualbleeding, prolonged menstrual bleeding, or heavyand prolonged menstrual bleeding. Participants usingE2 valerate and dienogest were significantly morelikely to achieve a complete response, a novel pri-mary efficacy variable based on stringent criteriadeveloped in consultation with the U.S. Food andDrug Administration. Classification as a completeresponder required that participants fulfill a compos-ite of up to eight individual criteria during a 90-dayefficacy interval. Participants had to show an absenceof previous symptoms plus a defined improvement in
condition. To the authors’ knowledge, no other stud-ies have used such strict criteria. Excluding individu-als with missing data, the complete response rate withE2 valerate and dienogest was 43.8%. Moreover, asubstantial reduction in menstrual blood loss percycle was observed in E2 valerate and dienogest–treated participants categorized as partial or nonre-sponders and in participants with missing diary data.
E2 valerate and dienogest recipients showed arapid, large, and sustained decrease in menstrualblood loss volume. Furthermore, the proportion ofparticipants who experienced resolution of heavybleeding, that is, no bleeding episodes with a men-strual blood loss of 80 mL or more, was much higher
Table 3. Characteristics of Menstrual Bleeding During the 90-Day Run-In Phase and the 90-Day EfficacyPhase in Women Treated With Estradiol Valerate and Dienogest or Placebo
E2 Valerate and Dienogest Placebo
P forBetween-
GroupDifference
90-d Run-In Phase
90-dEfficacyPhase
ChangeFrom 90-dRun-In to
90-d EfficacyPhase
90-d Run-In Phase
90-dEfficacyPhase
ChangeFrom 90-
Day Run-Into 90-Day
Efficacy Phase
Menstrual bloodloss (mL)
(n�119)518�382
(n�80)196�267
(n�79)�353�309
(n�66)618�432
(n�48)444�306
(n�46)�130�338
�.001
Bleeding andspotting (d)
(n�120)25.1�10.5
(n�80)23.5�13.1
(n�80)�1.1�14.0
(n�70)24.7�9.7
(n�48)22.9�10.2
(n�48)�2.3�6.7
Not available
Bleeding only (d) (n�120)18.6�7.5
(n�80)15.3�9.6
(n�80)�2.8�10.8
(n�70)17.9�6.5
(n�48)16.0�6.1
(n�48)�2.2�4.6
.024
Spotting only (d) (n�120)6.5�6.0
(n�80)8.2�8.4
(n�80)�1.7�8.2
(n�70)6.8�6.2
(n�48)6.9�6.7
(n�48)�0.2�4.9
Not available
Bleeding episodes (n�119)3.5�0.8
(n�80)3.0�1.2
(n�79)�0.5�1.5
(n�66)3.5�0.8
(n�48)3.2�0.7
(n�46)�0.30�0.9
.080
Sanitary protection(no. of items)
(n�119)90�42
(n�80)51�49
(n�79)�44�41
(n�66)96�45
(n�48)69�29
(n�46)�21�43
�.001
E2, estradiol.Data are mean�standard deviation unless otherwise specified.Only those participants with evaluable data (ie, no missing data) were included in this analysis.
Table 4. Levels of Hemoglobin, Hematocrit, and Ferritin at Baseline and Adjusted Mean Change FromBaseline in Participants Who Received Estradiol Valerate and Dienogest or Placebo
E2 Valerate and Dienogest Placebo
BaselineAdjusted Mean Change
From Baseline BaselineAdjusted Mean Change
From Baseline
Hemoglobin (g/dL) (n�120)12.2�1.3
(n�108)�0.6*
(n�70)12.0�1.4
(n�59)�0.1
Hematocrit (%) (n�120)37.3�3.6
(n�108)�1.4†
(n�70)37.0�3.8
(n�59)�0.05
Ferritin (ng/mL) (n�120)23.2�35.1
(n�112)�2.9‡
(n�68)21.2�18.6
(n�59)�0.4
E2, estradiol.Baseline data are mean�standard deviation.* P�.004 compared with change from baseline with placebo.† P�.001 compared with change from baseline with placebo.‡ P�.011 compared with change from baseline with placebo.
784 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding OBSTETRICS & GYNECOLOGY
with E2 valerate and dienogest (56.0%) than withplacebo (26.7%).
Measured menstrual blood loss represents ameaningful clinical parameter, especially when peakflow, in heavy bleeders, affects a woman’s ability tocontain her blood loss. Furthermore, women withheavy menstrual bleeding are more likely to experi-ence anemia than women with a lower menstrualblood loss.13 Notably, women treated with E2 valerateand dienogest used significantly fewer sanitary pro-
tection items than those treated with placebo; most(81.2%) reported themselves as improved at the endof treatment, which was more than twice the ratereported in placebo recipients.
The off-label use of OCPs as a treatment forheavy menstrual bleeding is common, despite onlylimited supportive clinical data based on objectivequantification methods. The few studies that em-ployed objective menstrual blood loss quantificationmethods suggest that OCPs reduced heavy bleedingby a mean 43% and 35% at 2 and 12 months’ use,respectively.8,14 In two studies that used the subjectivepictorial blood loss assessment chart to quantify men-strual blood loss, the mean reductions in heavy men-strual bleeding scores with OCPs were 2.5%14 and68%15 at 12 months’ use, respectively. However, thesmall sample sizes in these trials make the results lessrobust than the data generated in the current study.Moreover, the magnitude of the observed reductionin menstrual blood loss with E2 valerate and dieno-gest treatment in the current study is much greaterthan the effects noted in these earlier studies.
The type and frequency of most adverse eventswere similar in recipients of E2 valerate and dienogestand placebo, with a few exceptions (eg, breast painand breast discomfort), which may have been hor-mone-related. However, percentage reporting of ad-verse events is unreliable with small numbers. Otheradverse events such as headache and anxiety wereuncommon in E2 valerate and dienogest recipients,suggesting that the product was well tolerated. Over-all, the safety profile of E2 valerate and dienogestacross its entire clinical development program (2,703women with more than 30,000 treatment cycles’experience) appears similar to other low-dose com-bined OCPs. Although about one third of womenenrolled in these studies were aged over 35 years(about two thirds in the current study), no relevantdifferences have been detected with regard to thesafety profile of E2 valerate and dienogest betweenyounger (18–35 years) and older (36–53 years)women. One venous thromboembolism (deep veinthrombosis) and two cases of arterial thromboembo-lism (myocardial infarction in women with preexist-ing risk factors) were observed during the clinicaldevelopment of the E2 valerate and dienogest OCP,one of which, a myocardial infarction, occurred in thecurrent study. It is generally accepted that the inci-dence of cardiovascular events, including venousthromboembolism, myocardial infarction and stroke,increases as a function of age, independent of OCPuse. At present, age alone is not a contraindication tothe use of any OCP, and clinicians should base the
Table 5. Treatment-Emergent Adverse Events (inAlphabetical Order) That Occurred in2% or More of Participants WhoReceived Estradiol Valerate andDienogest or Placebo (Safety AnalysisPopulation)
Adverse Event
E2 Valerate andDienogest(n�119)
Placebo(n�66)
Acne 6 (5.0) 0Anemia 2 (1.7) 4 (6.1)Anxiety 1 (0.8) 3 (4.5)Arthralgia 0 3 (4.5)Back pain 3 (2.5) 3 (4.5)Breast pain 5 (4.2) 0Breast tenderness 4 (3.4) 1 (1.5)Bronchitis 3 (2.5) 2 (3.0)Cervical dysplasia 3 (2.5) 2 (3.0)Chest pain 1 (0.8) 2 (3.0)Depression 3 (2.5) 1 (1.5)Diarrhea 3 (2.5) 2 (3.0)Dizziness 0 2 (3.0)Dysmenorrhea 3 (2.5) 2 (3.0)Dyspepsia 3 (2.5) 0Fatigue 4 (3.4) 3 (4.5)Gastroenteritis 3 (2.5) 0Headache 5 (4.2) 9 (13.6)Hypertension 2 (1.7) 2 (3.0)Hypoesthesia 1 (0.8) 2 (3.0)Influenza 3 (2.5) 0Insomnia 1 (0.8) 2 (3.0)Metrorrhagia 6 (5.0) 0Migraine 3 (2.5) 0Nasopharyngitis 9 (7.6) 6 (9.1)Nausea 6 (5.0) 5 (7.6)Sinusitis 4 (3.4) 1 (1.5)Tension headache 4 (3.4) 0Upper respiratory tract
infection4 (3.4) 1 (1.5)
Vaginal infection 3 (2.5) 0Vaginitis bacterial 6 (5.0) 4 (6.1)Vomiting 2 (1.7) 2 (3.0)Vulvovaginal mycotic
infection4 (3.4) 3 (4.5)
Weight increase 7 (5.9) 0
E2, estradiol.Data are n (%).
VOL. 117, NO. 4, APRIL 2011 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding 785

decision to prescribe on established criteria that eval-uate potential medical contraindications.16 The risksof rare but serious adverse events with the E2 valerateand dienogest pill are currently being assessed in alarge active surveillance postmarketing study, Inter-national Active Surveillance Study–Safety of Contra-ceptives: Role of Estrogens (INAS-SCORE).
E2 valerate and dienogest may represent anattractive alternative to current medical treatments forheavy menstrual bleeding. The levonorgestrel-releas-ing intrauterine system is an effective, well-toleratedmedical therapy in women with heavy menstrualbleeding, but is not suitable for or accepted by allwomen.17 Although cyclical progestins administeredduring the luteal phase are much less effective thanother treatments,18 extended regimens of high-dosecyclical oral medroxyprogesterone acetate and nore-thisterone have been shown to reduce menstrualblood loss volume.19,20 That said, these doses are notapproved and may be associated with reduced toler-ability. Oral tranexamic acid (recently approved inthe United States for the treatment of heavy menstrualbleeding) is associated with a reduction in menstrualblood loss volume,21 but it is not a contraceptive andcannot regulate the menstrual cycle. In addition, in atrial (that used the alkaline hematin method to quan-tify blood loss), a 40% reduction from baseline inmean menstrual blood loss was observed withtranexamic acid 3,900 mg/d,22 suggesting that E2valerate and dienogest may be more effective inrestoring normal menstrual blood loss. Nonsteroidalantiinflammatory drugs approved for the treatment ofheavy menstrual bleeding (eg, mefenamic acid) mayalleviate accompanying dysmenorrhea; however,their ability to reduce heavy menstrual bleeding islimited.8,23
This study has a number of limitations that haveto be considered when making generalizations rela-tive to clinical practice. Women recruited to ourstudy, with its stringent recruitment criteria, may notbe truly representative of those seeking treatment inroutine clinical practice. In addition, it is possible thatthe laborious process of collecting used sanitary itemsmay have resulted in some women not collecting allitems used, particularly overtime, and therefore, re-sult in otherwise greater reductions in measuredblood loss than would otherwise be expected as aresult of fewer sanitary items collected. However, thewillingness to continue to comply with collection ofsanitary items would more likely be an issue if thepatient perceived that her medication was not work-ing. Therefore participants in the placebo group mayhave had less incentive to persist with study protocols,
exaggerating the reduction in measured menstrualblood loss. Nonetheless, the reduction in menstrualblood loss observed in E2 valerate and dienogestgroup was accompanied by significant improvementin iron metabolism parameters, but this was not thecase in the placebo group.
The unique dosing regimen (estrogen step-downand progestogen step-up) and the hormonal compo-nents of this novel OCP may account for its ability toreduce heavy menstrual bleeding. The regimen en-sures estrogen dominance in the first part of the cycleand progestogen dominance in the mid-to-late part ofthe cycle.10 Furthermore, the treatment regimen in-corporates 22 days of continuous treatment withdienogest, a progestin with a pronounced endometrialactivity,24–26 followed by 6 progestogen-free days thatprovide almost continuous E2 exposure,27 which isthought to support endometrial stability.
In conclusion, E2 valerate and dienogest is aneffective and well-tolerated treatment in women withheavy menstrual bleeding, prolonged menstrualbleeding, or heavy and prolonged menstrual bleedingwithout organic pathology. E2 valerate and dienogestprovides an important new oral, daily, self-adminis-tered noninvasive and fertility-sparing treatment op-tion that is reversible and provides reliable contracep-tive efficacy.28
REFERENCES1. Fraser IS, Langham S, Uhl-Hochgraeber K. Health-related
quality of life and economic burden of abnormal uterinebleeding. Exp Rev Obstet Gynecol 2009;4:179–89.
2. Liu Z, Doan QV, Blumenthal P, Dubois RW. A systematicreview evaluating health-related quality of life, work impair-ment, and health-care costs and utilization in abnormal uterinebleeding. Value Health 2007;10:183–94.
3. Fraser IS, Critchley HO, Munro MG, Broder M; WritingGroup for This Menstrual Agreement Process. A processdesigned to lead to international agreement on terminologiesand definitions used to describe abnormalities of menstrualbleeding. Fertil Steril 2007;87:466–76.
4. Fraser IS, Weisberg E, Minehan E, Johansson ED. A detailedanalysis of menstrual blood loss in women using Norplant andNestorone progestogen-only contraceptive implants or vaginalrings. Contraception 2000;61:241–51.
5. Hale GE, Manconi F, Luscombe G, Fraser IS. Quantitativemeasurements of menstrual blood loss in ovulatory and anovu-latory cycles in middle- and late-reproductive age and themenopausal transition. Obstet Gynecol 2010;115(2 pt1):249–56.
6. Hallberg L, Hogdahl AM, Nilsson L, Rybo G. Menstrual bloodloss–a population study. Variation at different ages andattempts to define normality. Acta Obstet Gynecol Scand1966;45:320–51.
7. National Institute for Health and Clinical Excellence. Clin-ical guideline: heavy menstrual bleeding. January 2007.Available from: http://www.nice.org.uk/nicemedia/pdf/CG44FullGuideline.pdf. Accessed February 15, 2011.
786 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding OBSTETRICS & GYNECOLOGY

8. Fraser IS, McCarron G. Randomized trial of 2 hormonal and2 prostaglandin-inhibiting agents in women with a complaintof menorrhagia. Aust N Z J Obstet Gynaecol 1991;31:66–70.
9. Nilsson L, Rybo G. Treatment of menorrhagia. Am J ObstetGynecol 1971;110:713–20.
10. Ahrendt HJ, Makalova D, Parke S, Mellinger U, Mansour D.Bleeding pattern and cycle control with an estradiol-based oralcontraceptive: a seven-cycle, randomized comparative trial ofestradiol valerate/dienogest and ethinyl estradiol/levonorg-estrel. Contraception 2009;80:436–44.
11. Shaw ST Jr, Aaronson DE, Moyer DL. Quantitation of men-strual blood loss–further evaluation of the alkaline hematinmethod. Contraception 1972;5:497–513.
12. Chan IS, Zhang Z. Test-based exact confidence intervals forthe difference of two binomial proportions. Biometrics 1999;55:1201–9.
13. Hallberg L, Hogdahl AM, Nilsson L, Rybo G. Menstrual bloodloss and iron deficiency. Acta Med Scand 1966;180:639–50.
14. Shabaan MM, Zakherah MS, El-Nashar SA, Sayed GA.Levonorgestrel-releasing intrauterine system compared to lowdose combined oral contraceptive pills for idiopathic menor-rhagia: a randomized clinical trial. Contraception 2011;83:48–54.
15. Endrikat J, Shapiro H, Lukkari-Lax E, Kunz M, Schmidt W,Fortier M. A Canadian, multicentre study comparing theefficacy of a levonorgestrel-releasing intrauterine system to anoral contraceptive in women with idiopathic menorrhagia.J Obstet Gynaecol Can 2009;31:340–7.
16. Peterson HB, Curtis KM, Jamieson D, Lehnherr J, March-banks P. U S. Medical Eligibility Criteria for ContraceptiveUse, 2010: adapted from the World Health OrganizationMedical Eligibility Criteria for Contraceptive Use, 4th edition.MMWR Recomm Rep 2010;59(RR-4): 1–86.
17. Lethaby AE, Cooke I, Rees M. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding.The Cochrane Database of Systematic Reviews 2005, Issue 4.Art. No.: CD002126. DOI: 10.1002/14651858.CD002126.pub2.
18. Lethaby A, Irvine G, Cameron I. Cyclical progestogens forheavy menstrual bleeding. The Cochrane Database of System-
atic Reviews 2008, Issue 1. Art. No.: CD001016. DOI:10.1002/14651858.CD001016.pub2.
19. Fraser IS. Treatment of ovulatory and anovulatory dysfunc-tional uterine bleeding with oral progestogens. Aust N Z JObstet Gynaecol 1990;30:353–6.
20. Irvine GA, Campbell-Brown MB, Lumsden MA, Heikkila A,Walker JJ, Cameron IT. Randomised comparative trial of thelevonorgestrel intrauterine system and norethisterone for treat-ment of idiopathic menorrhagia. Br J Obstet Gynaecol 1998;105:592–8.
21. Wellington K, Wagstaff AJ. Tranexamic acid: a review of itsuse in the management of menorrhagia. Drugs 2003;63:1417–33.
22. Lukes AS, Moore KA, Muse KN, Gersten JK, Hecht BR,Edlund M, et al. Tranexamic acid treatment for heavy men-strual bleeding: a randomized controlled trial. Obstet Gynecol.2010;116:865–75.
23. Reid PC, Virtanen-Kari S. Randomised comparative trial ofthe levonorgestrel intrauterine system and mefenamic acid forthe treatment of idiopathic menorrhagia: a multiple analysisusing total menstrual fluid loss, menstrual blood loss andpictorial blood loss assessment charts. BJOG 2005;112:1121–5.
24. Oettel M, Breitbarth H, Elger W, Graser T, Hubler D,Kaufmann G, et al. The pharmacological profile of dienogest.Eur J Contracept Reprod Health Care 1999;4(suppl 1):2–13.
25. Oettel M, Graser T, Hoffmann H, Moore C, Zimmermann H,Zimmermann T. The preclinical and clinical profile of dieno-gest: a short overview. Drugs Today 1999;35(suppl C):3–12.
26. Sasagawa S, Shimizu Y, Kami H, Takeuchi T, Mita S, Imada K,et al. Dienogest is a selective progesterone receptor agonist intransactivation analysis with potent oral endometrial activitydue to its efficient pharmacokinetic profile. Steroids 2008;73:222–31.
27. Zeun S, Lu M, Uddin A, Zeiler B, Morrison D, Blode H.Pharmacokinetics of an oral contraceptive containing oestra-diol valerate and dienogest. Eur J Contracept Reprod HealthCare 2009;14:221–32.
28. Palacios S, Wildt L, Parke S, Machlitt A, Romer T, Bitzer J.Efficacy and safety of a novel oral contraceptive based onoestradiol (oestradiol valerate/dienogest): a Phase III trial. EurJ Obstet Gynecol Reprod Biol 2010;149:57–62.
VOL. 117, NO. 4, APRIL 2011 Jensen et al Estradiol Valerate and Dienogest for Menstrual Bleeding 787