documentation. outline overview value of excellent documentation define, discuss, review soap...
TRANSCRIPT

DOCUMENTATION

OUTLINE
Overview value of excellent documentation
Define, discuss, review SOAP notes
Review how it should look in MEMSRR
Questions and discussion

WHY?
Patient Legacy
Continuity of Care
Legal Document
Billing

MEMSMEMS patient/run record will be legible and thoroughly
completed for each call or for each patient when more than one
patient is involved in a call. This document is our legacy of patient
care and holds information valuable to hospital providers.
Services are encouraged to leave a completed copy of the
patient/run report at the hospital before they leave. In rare
circumstances, when it is not possible to complete this record
before leaving the hospital, the services may provide the hospital
with a Maine EMS approved, one page, patient care summary.
THIS DOCUMENT DOES NOT REPLACE THE COMPLETED RUN
REPORT. Services must complete this report and make the report
available to the hospital as soon as possible.
BILLING
Be clear • Emergency vs. Transfer• Transport? • All procedures, treatments, interventions and
medications need to be listed • Spelling, Grammar, Abbreviations

SOAP
S ~ Subjective ~ What happened?
O~ Objective ~ What did you find?
A ~ Assessment ~What do you think?
P ~ Plan ~ What did you do?

THE CALL
Called to XYZ Office for a woman
who fainted

SUBJECTIVE
Tell the StoryInclude:
• Age• Chief Complaint• MOI/NOI• What, when, where, how?• SAMPLE…..OPQRST• Pertinent meds and medical history

Ambulance 7 responded for a 40 year old female who had a
syncopal episode from a standing position. Patient reports she
was at work and began to feel nauseous. Walked into break room
and passed out on floor. Coworkers report pt. slumped forward
onto recliner then slid onto carpeted floor. No obvious head or
neck involvement and no significant traumatic mechanism. No
seizure type activity noted. Pt. reports waking on the floor cold
and shivering. Pt. moved to couch with assistance. Pt. denies
head, neck, chest or back pain, sob, headache, vomiting, blurred
vision, numbness, or tingling in extremities. Pt. does report mild
dizziness and ongoing weakness. Coworkers called 911 for
assistance.

OBJECTIVE
Get Technical… do the Investigation
Include:• LOC• Head to toe report with emphasis on
appropriate detailed assessment• Vitals including skin• + ( positive findings) and – (pertinent
negatives)• Some overlap
Upon initial contact, patient lying on couch in break room, alert and
oriented to name, place, time and event. Skin warm and dry with
normal color and tone. Mild muscle tremors (shivers) in arms and
legs. Pt. does report feeling cold. Head normocephalic without
abnormality on visualization or palpation. Neck midline and intact
without pain on palpation or movement. Thoracic, lumbar and sacral
spine intact without pain on palpation or spontaneous movement.
Chest intact with equal expansion, unremarkable on visualization and
palpation. Lung sounds clear and equal bilaterally with normal tidal
volume. Breathing pattern normal. No odor on breath noted.
Abdomen soft, non- tender, atraumatic and unremarkable on
visualization and palpation to all quadrants, without masses or
rigidity noted.

Pelvis and hips stable and intact without pain or crepitus on
palpation anterior or lateral. Incontinent to urine. Legs and
knees intact and atraumatic. Arms are intact and atraumatic.
No language barrier existed between patient and providers.
Neurological Exam: Pt.’s pupils equal, round and reactive to
light. Pt. does not present with observable short or long term
memory loss or confusion. Major motor neuros intact. Gross
sensory assessment intact with normal sensation throughout.
Assessment revealed no abnormal neurological findings. CiSS
negative. All observable neurological assessments remained
unchanged during and after transport to hospital.

ASSESSMENT
What do you think is going on with
the patient
• Unsure? List what you think as possibilities

PLAN
Details of interventions and how the patient
respondedInclude :
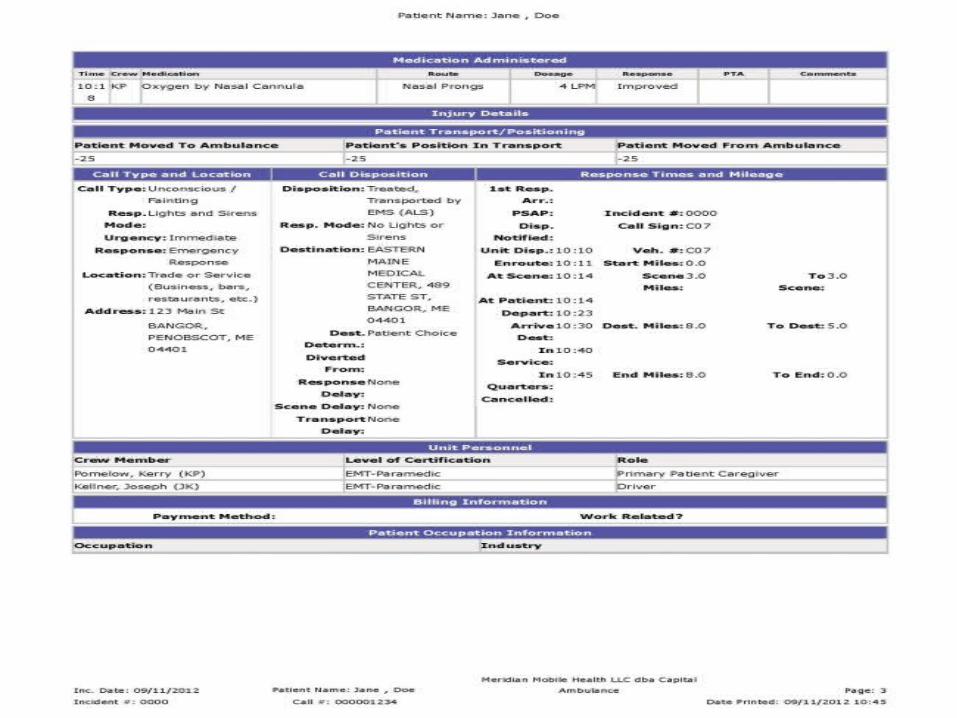
• Treatments (splints, nebs, CPAP, etc…)• Medications (02, Normal Saline, D50, etc…)• Interventions ( Monitor, IV/INT, Bg….)

Pt. transported non-emergent to XYZ emergency
room. Pt. transported without change in status or
level of consciousness. Patients treatment plan
included full secondary assessment, detailed
neurological examination, vital signs, cardiac
monitoring, 12 lead, pulse oximetry, Bg, IV left
hand tko and supplemental oxygen. Following
hand off report to staff, patient left in hospital bed
with rails up and staff in attendance.



THANKS!
Remember if you didn’t write it, it didn’t happen
Documentation is patient care!
Be thorough and take pride in what you write
Use SOAP as a guideline
Make the most of the available drop down boxes in
MEMSRR!
