white matter abnormalities in pediatric obsessive-compulsive disorder
TRANSCRIPT

Psychiatry Research: Neuroimaging 213 (2013) 154–160
Contents lists available at SciVerse ScienceDirect
Psychiatry Research: Neuroimaging
0925-49http://d
n CorrE-m
journal homepage: www.elsevier.com/locate/psychresns
White matter abnormalities in pediatric obsessive-compulsive disorder
Timothy Silk a,n, Jian Chen a, Marc Seal a,c, Alasdair Vance b
a Developmental Imaging, Murdoch Childrens Research Institute, Royal Children's Hospital, Melbourne 3052, Australiab Academic Child Psychiatry Unit, Department of Paediatrics, University of Melbourne, Royal Children's Hospital, Melbourne, Australiac Department of Paediatrics, University of Melbourne, Melbourne, Australia
a r t i c l e i n f o
Article history:Received 16 May 2012Received in revised form4 December 2012Accepted 25 April 2013
Keywords:Diffusion tensor imaging (DTI)OCDAxial diffusivity
27/$ - see front matter & 2013 Elsevier Irelanx.doi.org/10.1016/j.pscychresns.2013.04.003
esponding author. Tel.: +61 3 9936 6708.ail address: [email protected] (T. Silk).
a b s t r a c t
Diffusion tensor imaging (DTI) has been useful in allowing us to examine the nature and extent ofneuronal disruption associated with obsessive-compulsive disorder (OCD). However, little is knownabout the underlying brain structure in OCD. Diffusion-weighted magnetic resonance imaging wasperformed in 16 children with OCD and 22 typically developing children. Tract-based spatial statistics(TBSS) was used to compare the microstructure of white-matter tracts of OCD children with those oftypically developing children. Correlation/regression analyses were also performed on each diffusionmeasure in order to detect any correlation of white-matter microstructure with scales of symptomseverity. Analysis revealed significantly greater axial diffusivity in both the genu and the splenium of thecorpus callosum in the control compared to the OCD group; these regions consecutively connect bilateralmedial frontal regions and bilateral parietal regions. Secondly, correlation and voxel-based regressionanalysis revealed that lower axial diffusion correlated with greater severity of symptoms within the OCDgroup, as measured by the Child Behaviour Checklist-Obsessive Compulsive Scale (CBCL-OCS). Thefindings demonstrated a correlation of axial diffusivity with severity of symptoms in children with OCD.DTI may provide novel ways to help reveal the relationships between clinical symptoms and alteredbrain regions.
& 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Obsessive-compulsive disorder (OCD) is one of the mostdisabling anxiety disorders, involving a recurrent pattern ofintrusive thoughts, dysphoric feelings and maladaptivecompulsive behaviors that interfere with young people'sacademic, social and home life. Key neurobiological models ofOCD have implicated substructures and connections of a fronto–striatal–thalamic–cortical network, the most widely acceptedinvolving the orbitofrontal cortex (OFC), anterior cingulate,thalamus and and striatum (Modell et al., 1989; Saxena et al.,1998; Graybiel and Rauch, 2000). In general, the model of fronto–striatal–thalamic–cortical involvement in OCD has been wellsupported by both structural and functional neuroimaging. Thereare several informative reviews on neuroimaging in adult OCD(e.g. Saxena and Rauch, 2000; Kwon et al., 2009), but few over-views in pediatric OCD (MacMaster et al., 2008; Huyser et al.,2009; MacMaster, 2010). Although morphometric studies of OCDhave been somewhat inconsistent, the most consistent findings inOCD are gray matter volumetric abnormalities involving theorbitofrontal cortex and the basal ganglia.
d Ltd. All rights reserved.
While conventional structural magnetic resonance imaging(MRI) can provide valuable information about brain regionalmacrostructure and volume, diffusion tensor imaging (DTI) allowsfurther examination of microstructure of cortical gray and whitematter. This technique estimates the direction and extent ofdiffusion of water within the brain and is particularly sensitiveto the organization of white matter tracts. Diffusion properties aretypically quantified by measures derived from three principaldirections of diffusion; primary (λ1), secondary (λ2), and tertiary(λ3) eigenvalues. The primary eigenvalue (also known as axialdiffusivity; λ∥) denotes water diffusivity parallel to nerve axons.The secondary and tertiary eigenvalues correspond to diffusionorthogonal to λ1 and can generate a measure of radial diffusivity(λ⊥). Mean diffusivity (MD) is a composite of the three eigenvaluesand represents apparent mobility of water, which is simply themagnitude of diffusion in each measured voxel; and fractionalanisotropy (FA) is an index of the ‘directionality’ of diffusion ineach voxel. Therefore, because the direction and extent of waterdiffusion is dependent on the underlying structure of tissue,differences in cellular structure can be inferred from thesemeasures. Diffusion parameters can be biomarkers of changes inthese axonal properties with particular measures differentiallysensitive to different white-matter development and pathology.For example, radial diffusivity appears to be modulated by dys- orde-myelination (cell membrane and cytoskeleton) in white matter,

T. Silk et al. / Psychiatry Research: Neuroimaging 213 (2013) 154–160 155
whereas the axial diffusivity may be more specific to axonaldegeneration (volume and organization) (Harsan et al., 2006).
DTI studies of OCD are few; of the 14 studies to date, only twostudies have been conducted in adolescents and/or children, andfindings have been variable. All studies have reported FA as themain measure of diffusion. A few studies have also includedadditional measures of diffusivity including MD (or apparentdiffusion coefficient) (Saito et al., 2008; Nakamae et al., 2011;Lochner et al., 2012), axial diffusivity (or principal diffusiondirection) (Garibotto et al., 2010; Bora et al., 2011; Jayarajanet al., 2012) and radial diffusivity (Bora et al., 2011; Jayarajanet al., 2012). FA changes in adult OCD have been reported in anumber of brain regions, including the anterior cingulate (Szeszkoet al., 2005; Ha et al., 2009) and the cingulum bundle (Cannistraroet al., 2007; Garibotto et al., 2010; Chiu et al., 2011; Nakamae et al.,2011; Zarei et al., 2011), corpus callosum (CC) (Yoo et al., 2007;Saito et al., 2008; Garibotto et al., 2010; Bora et al., 2011; Nakamaeet al., 2011; Zarei et al., 2011), internal capsule (Cannistraro et al.,2007; Yoo et al., 2007; Nakamae et al., 2011), parietal regions(Szeszko et al., 2005; Menzies et al., 2008), medial frontal regions(Menzies et al., 2008; Zarei et al., 2011), the inferior fronto-occipital fasciculus (Garibotto et al., 2010; Zarei et al., 2011) andthe anterior thalamic radiation (Chiu et al., 2011), bilateral cen-trum semiovale and sub-insular region (Nakamae et al., 2008), anda region superolateral to the right caudate (Yoo et al., 2007).
Two studies also used fiber tracking to examine a priori regionsof interest (ROIs) in OCD adults (Garibotto et al., 2010; Chiu et al.,2011). Garibotto et al. (2010) examined the inferior fronto-occipitalfasciculus and found decreased fiber tract coherency and direc-tionality in the connections of the orbitofrontal and occipitalcortex in OCD. Chiu et al. (2011) found lower generalized FA inthe right anterior thalamic radiation and the left anterior segmentof the cingulum bundle in adults with OCD compared to healthycontrol participants.
The most consistent finding from DTI studies in OCD is thatof diffusion differences in the CC. The CC is the largest white-matter commissure and allows interhemispheric communication.While varying in their approaches and the regions of the CCselected, most studies found lower FA in OCD (Saito et al., 2008;Garibotto et al., 2010; Bora et al., 2011; Nakamae et al., 2011) withsome exceptions (Yoo et al., 2007; Zarei et al., 2011). Involvementof the CC is also supported by morphometric studies (Rosenberget al., 1997; Farchione et al., 2002; Chen et al., in preparation).
While previous studies have often used VBM methods forwhole-brain analysis, this approach has several limitations whenapplied to DTI data (Smith et al., 2006). Methodologically, limita-tions relate to difficulties in accurate inter-subject image registra-tion, which is crucial for DTI data in which large image intensityboundaries exist between white-matter tracts (relatively high FAvalues) and cortical gray matter or subcortical nuclei (relativelylow FA values). White-matter structure is inherently highly vari-able between individuals, and therefore registration for whitematter between individuals at a voxel basis is critical. Tract-basedspatial statistics (TBSS) is an analytic method developed specifi-cally for DTI data that restricts analysis to just the center of majorwhite-matter tracts, rather than indiscriminately across thewhole-brain volume (Smith et al., 2006). TBSS minimizes inter-subject registration problems and problems of multiple compar-isons by first determining a mean FA ‘skeleton’, representing onlythe center of major white-matter fiber tracts, then mapping eachparticipant's DTI data directly onto that skeleton. TBSS methodsare therefore highly sensitive to changes in microstructure withinthe major white-matter fiber pathways of the brain. Two recentstudies have used TBSS to analyze DTI results in examining OCDadults (Bora et al., 2011; Nakamae et al., 2011), and two inadolescents/children (Zarei et al., 2011; Jayarajan et al., 2012).
Both adult studies found significantly lower FA in the body of theCC. Nakamae et al. (2011), additionally found a trend toward lowerFA across a larger proportion of the CC, the right cingulum, and theleft anterior limb of the internal capsule. In adolescents, Zarei et al.(2011) reported higher FA in the splenium and genu of the CC, aswell as a number of other tracts including the major and minorforceps and the cingulum. In children, Jayarajan et al. (2012) foundno difference between patients and controls for FA. However, therewas widespread difference reported in both axial and radialdiffusivity in regions including the CC, superior and inferior long-itudinal fascicule, cingulum, anterior thalamic radiation and cere-bellar peduncle.
Significantly, several findings suggest that anomalies in whitematter may vary according to symptom severity. Seven of the DTIstudies have explored whether there is a correlation betweenFA and clinical assessments, most commonly the Yale–BrownObsessive-Compulsive Scale (Y-BOCS) (Szeszko et al., 2005; Saitoet al., 2008; Garibotto et al., 2010; Chiu et al., 2011; Nakamae et al.,2011; Zarei et al., 2011; Lochner et al., 2012), the obsession orcompulsion subscores from the Y-BOCS (Ha et al., 2009; Chiu et al.,2011) or the children's Y-BOCS (Jayarajan et al., 2012), but also aDepression Scale (Saito et al., 2008), and a battery of testsexamining visuospatial ability, working memory, and decisionmaking (Garibotto et al., 2010). Negative correlations (higherscores on the Y-BOCS correlated with lower FA) have beenreported in the CC, fronto-occipital fasciculus, superior longitudi-nal fasciculus (SLF), optic radiation and parietal regions (Szeszkoet al., 2005; Saito et al., 2008; Garibotto et al., 2010), positivecorrelations in the anterior cingulum bundle and the anteriorcingulate (Ha et al., 2009; Chiu et al., 2011), the CC and major andminor forceps (Zarei et al., 2011) and also no significant correlationwith respects to FA (Nakamae et al., 2011; Lochner et al., 2012). Nocorrelation was found with scores on a depression scale (Saitoet al., 2008), but Garibotto et al. (2010) found a negative correla-tion of FA with performance in a spatial attention and a decisionmaking task in the fronto-occipital fasciculus, the superiorlongitudinal fasciculus, and the whole CC. Given theseinconsistent findings to date, the current study examined ifdifferent diffusion parameters in white matter vary with respectto two measures of OCD symptom severity (Children's Yale–BrownObsessive Compulsive Scale (Children's Y-BOCS) and ChildBehavior Checklist-Obsessive Compulsive Scale (CBCL-OCS)) andtwo depression/anxiety measures (Children's Depression Inven-tory (CDI) and Child Behavior Checklist-Anxiety and Depressionscale (CBCL-AD)).
In the present study, we examined the microstructure of whitematter in children and adolescents with OCD compared withhealthy age-, handedness- and IQ-matched control participants.Utilizing TBSS (Smith et al., 2006), we examined four diffusivitymeasures (FA, MD, axial and radial diffusivity) within major white-matter pathways throughout the whole brain. Additionally, corre-lation/regression analyses were performed on each diffusionmeasure over the white matter of the whole brain in order todetect any correlation of white-matter microstructure with scoreson standard cognitive tests and scales of symptom severity.
2. Methods
2.1. Participants
Sixteen children fulfilling DSM-IV criteria for OCD (6 males, 10 females), aged8–18 years (mean 12.7772.83 years), were identified at the Royal Children'sHospital, Melbourne, Australia. OCD is defined categorically, using a semi-structured clinical interview with the participant's parent(s) and the young personsthemselves, and the Anxiety Disorders Interview Schedule for Children(A-DISC); (Silverman and Albano, 1996), in addition to dimensionally using the

T. Silk et al. / Psychiatry Research: Neuroimaging 213 (2013) 154–160156
clinician rating of OCD (CY-BOCS). Participants had a full scale IQ above 70,according to an age-appropriate Wechsler test (2004: mean performance IQ:100.3715.8; mean verbal IQ: 95.6717.2); and there were no known neurologicalor endocrine conditions, mood disorders, autistic disorders, psychotic disorders,attention deficit hyperactivity disorder, combined type, reading/spelling/arithmeticlearning disorders, developmental coordination disorder or alcohol/substanceabuse/dependence disorders. Three of the patients had comorbid generalizedanxiety disorder. All participants were medication-naïve except for two patients;one had been on fluoxetine (20 mg) for 6 months, and one had been on sertraline(50 mg) and ritalin (10 mg) for 12 months. These two participants were withdrawnfrom medication for 24 h before scanning.
Twenty-two healthy control participants (16 males, 6 females) were matched inage (8–18 years; mean 11.2472.13 years) and IQ (mean performance IQ:104.7710.3; mean verbal IQ: 102.7714.8) to the OCD group. All participants wereright-handed. After complete description of the study to the subjects, writtenconsent was obtained. All procedures were approved by the Human ResearchEthics Committee of the Royal Children's Hospital, Melbourne, Australia.
2.2. Clinical assessment
Children's Yale–Brown Obsessive Compulsive Scale (CY-BOCS): The CY-BOCS is asemi-structured interview assessing the severity of both obsessions and compul-sions separately, as well as giving an overall score (Scahill et al., 1997). ChildBehavior Checklist (CBCL): The CBCL is an extensively used rating scale question-naire for parents to detail the frequency and intensity of behavioral and emotionalproblems exhibited by their child (Achenbach and Edelbrock, 1983). It contains 118items covering problems that have occurred over the preceding 6 months. Anumber of subscores are derived for the CBCL including the Anxiety and Depression(CBCL-AD) scale, which is used in the current study. A CBCL Obsessive-CompulsiveScale (CBCL-OCS) was developed (Nelson et al., 2001) using eight items (creating arange between 0 and 16) with the aim of predicting OCD. It has been shown to beboth reliable and valid (Geller et al., 2006; Hudziak et al., 2006; Storch et al., 2006).Although there have been various adaptations of the CBCL-OCS tested, with feweritems including versions with six items (Storch et al., 2006), three items (Gelleret al., 2006), and even just two items (Ivarsson and Larsson, 2008), we used theoriginal eight-item scale (Nelson et al., 2001) for the purposes of our research. TheCBCL-OCS was the main scale of interest. The CBCL-AD was included for validationas the 13-item scale contains four of the eight items in the CBCL-OCS scale.Children's Depression Inventory (CDI): The CDI is a 27-item self-report measure ofdepressive symptoms in children and adolescents (Kovacs, 1985).
2.3. Data acquisition and analysis
Neuroimaging data were acquired on the 3T Siemens TIM Trio scanner(Siemens, Erlangen, Germany) at the Murdoch Children's Research Institute, RoyalChildren's Hospital, Melbourne. Participants lay supine with their head supportedin a 12-channel head coil. Diffusion weighted echo-planar images (EPI) wereacquired along 60 diffusion gradient directions for acquisition of 36 slices throughthe whole brain (TR¼5200 ms, TE¼88 ms, flip angle¼901, b value¼1000 s/mm2,FOV¼220 mm2, 128�128 matrix, 1.72 mm in-plane resolution, slice thickness¼3 mm, b0 images¼10).
Analyses of diffusion-weighted images were done using FMRIB's SoftwareLibrary (FSL; Oxford, UK): FMRIB's Diffusion Toolbox (FDT). Initially, Eddy CurrentCorrection was run to correct for gradient-coil distortions and small head motions,using affine registration to a b0 reference volume. A diffusion tensor model wasfitted to each voxel, generating FA, MD, and diffusivity along the principal λ1, λ2, λ3directions. Finally, we used TBSS (Smith et al., 2006) to carry out voxel-wisestatistical analyses for relevant diffusivity measures (FA, MD and axial and radialdiffusivity) along major white matter tracts. The TBSS method minimizes thepotential misalignment problems of other voxel-based whole-brain analysismethods by determining a white-matter “skeleton” restricted only to the centerof major white-matter tracts, and mapping diffusion values from each individualdirectly onto this standard skeleton for group comparison. Images from allindividuals were aligned to each other using non-linear registration (IRTK localmatrix deformation) in order to determine the most representative individual (i.e.the closest to the mean of the group) to be defined as the target image. This targetimage was then aligned, using affine registration to the Montreal NeurologicalInstitute (MNI) brain template. A white-matter skeleton was then generatedrepresenting a single line running down the centers of all the common white-matter fibers. Group statistical analysis was then conducted only on voxels withinthe white-matter skeleton mask, therefore restricting the voxel-wise analysis onlyto voxels with high confidence of lying within equivalent major white-matterpathways in each individual. Differences in FA, MD and axial and radial diffusivitybetween OCD and control groups were assessed using voxel-wise independenttwo-sample t-tests by Randomize, the nonparametric analysis tool in FSL. TheThreshold-Free Cluster Enhancement (TFCE (Smith and Nichols, 2009)) option wasemployed at po0.05 to obtain cluster inferences.
To further characterize pathways of the white-matter tracts in which differ-ences in axial diffusivity were found, the probabilistic tractography method
implemented within FSL software (Oxford, UK) was used to track likely pathsextending from the clusters identified as abnormal by the TBSS analysis. Two ROImasks were generated, one for the cluster in the genu of the CC and one for thecluster in the splenium of the CC. These ROI masks were then back-projected to theoriginal FA images for each individual. Probabilistic fiber-tracking, as implementedwithin FSL, was then conducted using each of these ROI masks as “seed” regions,with a step length of 0.5 mm, a maximum of 2000 steps, and a curvature thresholdof 0.2. Probabilistic tracks for each individual are then normalized back to standardspace and averaged across the group. Using this method, we obtained probabilisticconnectivity maps representing the most likely paths extending from the clustersin which abnormalities in axial diffusivity had been found. Finally, correlation ofclinical measures to diffusion measures were conducted using TBSS General LinearModel (GLM) regression. Each demeaned clinical measure was entered as anexplanatory variable in the design matrix and tested for positive or negativecorrelation. Voxel-wise independent t-tests were conducted using Randomize, andthe TFCE approach was used to obtain cluster inferences.
3. Results
3.1. Between-group TBSS analysis of regional white matter
TBSS analysis identified several clusters of significantly greateraxial diffusivity in the control group compared to OCD aftercorrection for multiple comparisons. Regions of significant differ-ences included fibers in both the genu and the splenium(see Fig. 1a). Mean axial diffusivity measures in the ROIs of theclusters identified from the TBSS analysis were: OCD: 1.5170.02(�10−3 mm2/s); Controls: 1.4470.04 (�10−3 mm2/s). No signifi-cant between-group differences were identified in FA, MD, orradial diffusivity after correction for multiple comparisions.
Probabilistic tractography was then used to illustrate the path-ways of the white-matter tracts by representing the most likelypaths extending from the clusters in which abnormalities in axialdiffusivity had been found. Fig. 1b shows that the fibers runningthrough the genu of the CC connecting bilateral medial frontalregions, and the fibers running through the splenium of the CCconnecting bilateral parietal regions as well as extending down tosuperior temporal regions.
Previous DTI studies have found differential developmental tra-jectories between males and females during childhood and adoles-cence (Schmithorst et al., 2008). Given the OCD and control groupswere not matched for gender, examination of potential genderdifferences in diffusivity revealed no significant differences on anyof the diffusion measures between males and females in the meandiffusion values in either the whole white-matter skeleton or in ROIsof the clusters identified from the TBSS analysis (difference in axialdiffusivity between OCD and control participants).
3.2. Whole brain correlation analysis in OCD
Pearson correlation analyses were performed on the mean ofeach diffusion measure over the whole-brain white-matter skele-ton in order to detect any correlation of white-matter microstruc-ture with scores on the clinical assessments within the OCD group.Scores on the CBCL-OCS, showed a significant negative correlationwith axial diffusivity (r¼−0.45, p¼0.041) (see Fig. 2c). Scores onthe CBCL-AD also showed a significant negative correlation(r¼−0.51, p¼0.021). There were no significant correlations forscores on the CY-BOCS or the CDI.
3.3. Voxel-based regression analysis in OCD
To locate specific regions that correlated scores on the clinicalassessment in the OCD group with white-matter microstructure,linear regressions were used to examine correlations betweenclinical assessment scores and diffusion measures. The threshold ofpo0.05 was considered significant. Regression analysis of axialdiffusivity shows significant negative correlation with scores on the
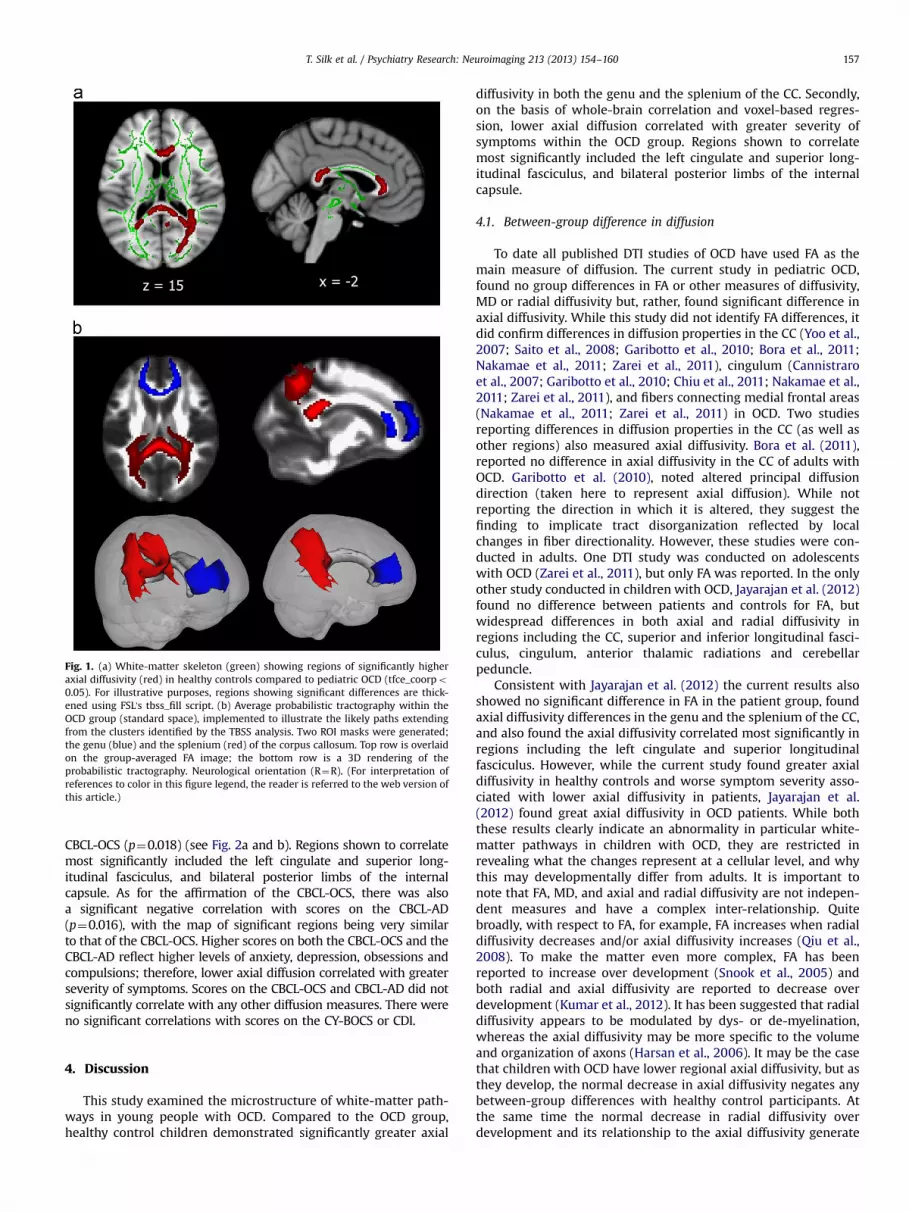
Fig. 1. (a) White-matter skeleton (green) showing regions of significantly higheraxial diffusivity (red) in healthy controls compared to pediatric OCD (tfce_coorpo0.05). For illustrative purposes, regions showing significant differences are thick-ened using FSL's tbss_fill script. (b) Average probabilistic tractography within theOCD group (standard space), implemented to illustrate the likely paths extendingfrom the clusters identified by the TBSS analysis. Two ROI masks were generated;the genu (blue) and the splenium (red) of the corpus callosum. Top row is overlaidon the group-averaged FA image; the bottom row is a 3D rendering of theprobabilistic tractography. Neurological orientation (R¼R). (For interpretation ofreferences to color in this figure legend, the reader is referred to the web version ofthis article.)
T. Silk et al. / Psychiatry Research: Neuroimaging 213 (2013) 154–160 157
CBCL-OCS (p¼0.018) (see Fig. 2a and b). Regions shown to correlatemost significantly included the left cingulate and superior long-itudinal fasciculus, and bilateral posterior limbs of the internalcapsule. As for the affirmation of the CBCL-OCS, there was alsoa significant negative correlation with scores on the CBCL-AD(p¼0.016), with the map of significant regions being very similarto that of the CBCL-OCS. Higher scores on both the CBCL-OCS and theCBCL-AD reflect higher levels of anxiety, depression, obsessions andcompulsions; therefore, lower axial diffusion correlated with greaterseverity of symptoms. Scores on the CBCL-OCS and CBCL-AD did notsignificantly correlate with any other diffusion measures. There wereno significant correlations with scores on the CY-BOCS or CDI.
4. Discussion
This study examined the microstructure of white-matter path-ways in young people with OCD. Compared to the OCD group,healthy control children demonstrated significantly greater axial
diffusivity in both the genu and the splenium of the CC. Secondly,on the basis of whole-brain correlation and voxel-based regres-sion, lower axial diffusion correlated with greater severity ofsymptoms within the OCD group. Regions shown to correlatemost significantly included the left cingulate and superior long-itudinal fasciculus, and bilateral posterior limbs of the internalcapsule.
4.1. Between-group difference in diffusion
To date all published DTI studies of OCD have used FA as themain measure of diffusion. The current study in pediatric OCD,found no group differences in FA or other measures of diffusivity,MD or radial diffusivity but, rather, found significant difference inaxial diffusivity. While this study did not identify FA differences, itdid confirm differences in diffusion properties in the CC (Yoo et al.,2007; Saito et al., 2008; Garibotto et al., 2010; Bora et al., 2011;Nakamae et al., 2011; Zarei et al., 2011), cingulum (Cannistraroet al., 2007; Garibotto et al., 2010; Chiu et al., 2011; Nakamae et al.,2011; Zarei et al., 2011), and fibers connecting medial frontal areas(Nakamae et al., 2011; Zarei et al., 2011) in OCD. Two studiesreporting differences in diffusion properties in the CC (as well asother regions) also measured axial diffusivity. Bora et al. (2011),reported no difference in axial diffusivity in the CC of adults withOCD. Garibotto et al. (2010), noted altered principal diffusiondirection (taken here to represent axial diffusion). While notreporting the direction in which it is altered, they suggest thefinding to implicate tract disorganization reflected by localchanges in fiber directionality. However, these studies were con-ducted in adults. One DTI study was conducted on adolescentswith OCD (Zarei et al., 2011), but only FA was reported. In the onlyother study conducted in children with OCD, Jayarajan et al. (2012)found no difference between patients and controls for FA, butwidespread differences in both axial and radial diffusivity inregions including the CC, superior and inferior longitudinal fasci-culus, cingulum, anterior thalamic radiations and cerebellarpeduncle.
Consistent with Jayarajan et al. (2012) the current results alsoshowed no significant difference in FA in the patient group, foundaxial diffusivity differences in the genu and the splenium of the CC,and also found the axial diffusivity correlated most significantly inregions including the left cingulate and superior longitudinalfasciculus. However, while the current study found greater axialdiffusivity in healthy controls and worse symptom severity asso-ciated with lower axial diffusivity in patients, Jayarajan et al.(2012) found great axial diffusivity in OCD patients. While boththese results clearly indicate an abnormality in particular white-matter pathways in children with OCD, they are restricted inrevealing what the changes represent at a cellular level, and whythis may developmentally differ from adults. It is important tonote that FA, MD, and axial and radial diffusivity are not indepen-dent measures and have a complex inter-relationship. Quitebroadly, with respect to FA, for example, FA increases when radialdiffusivity decreases and/or axial diffusivity increases (Qiu et al.,2008). To make the matter even more complex, FA has beenreported to increase over development (Snook et al., 2005) andboth radial and axial diffusivity are reported to decrease overdevelopment (Kumar et al., 2012). It has been suggested that radialdiffusivity appears to be modulated by dys- or de-myelination,whereas the axial diffusivity may be more specific to the volumeand organization of axons (Harsan et al., 2006). It may be the casethat children with OCD have lower regional axial diffusivity, but asthey develop, the normal decrease in axial diffusivity negates anybetween-group differences with healthy control participants. Atthe same time the normal decrease in radial diffusivity overdevelopment and its relationship to the axial diffusivity generate
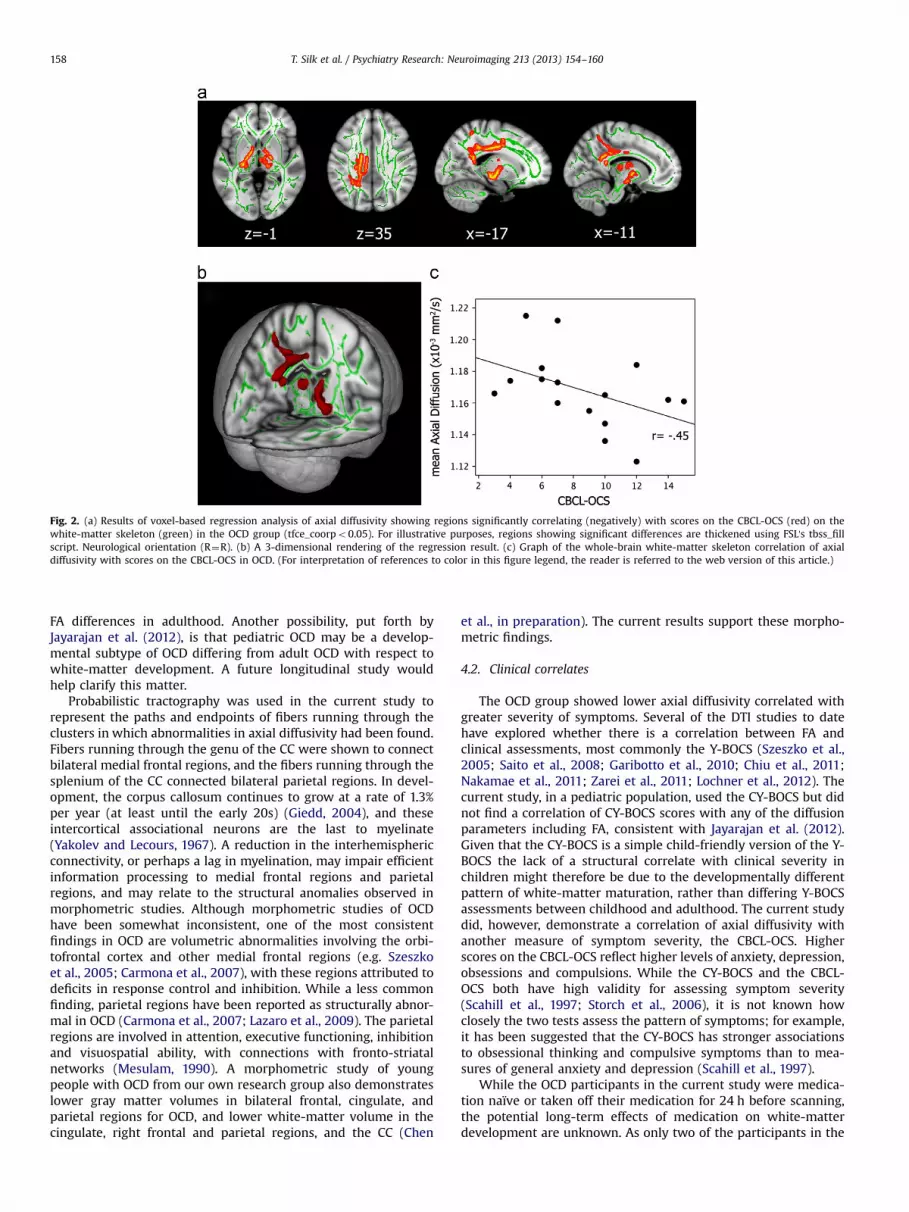
Fig. 2. (a) Results of voxel-based regression analysis of axial diffusivity showing regions significantly correlating (negatively) with scores on the CBCL-OCS (red) on thewhite-matter skeleton (green) in the OCD group (tfce_coorpo0.05). For illustrative purposes, regions showing significant differences are thickened using FSL's tbss_fillscript. Neurological orientation (R¼R). (b) A 3-dimensional rendering of the regression result. (c) Graph of the whole-brain white-matter skeleton correlation of axialdiffusivity with scores on the CBCL-OCS in OCD. (For interpretation of references to color in this figure legend, the reader is referred to the web version of this article.)
T. Silk et al. / Psychiatry Research: Neuroimaging 213 (2013) 154–160158
FA differences in adulthood. Another possibility, put forth byJayarajan et al. (2012), is that pediatric OCD may be a develop-mental subtype of OCD differing from adult OCD with respect towhite-matter development. A future longitudinal study wouldhelp clarify this matter.
Probabilistic tractography was used in the current study torepresent the paths and endpoints of fibers running through theclusters in which abnormalities in axial diffusivity had been found.Fibers running through the genu of the CC were shown to connectbilateral medial frontal regions, and the fibers running through thesplenium of the CC connected bilateral parietal regions. In devel-opment, the corpus callosum continues to grow at a rate of 1.3%per year (at least until the early 20s) (Giedd, 2004), and theseintercortical associational neurons are the last to myelinate(Yakolev and Lecours, 1967). A reduction in the interhemisphericconnectivity, or perhaps a lag in myelination, may impair efficientinformation processing to medial frontal regions and parietalregions, and may relate to the structural anomalies observed inmorphometric studies. Although morphometric studies of OCDhave been somewhat inconsistent, one of the most consistentfindings in OCD are volumetric abnormalities involving the orbi-tofrontal cortex and other medial frontal regions (e.g. Szeszkoet al., 2005; Carmona et al., 2007), with these regions attributed todeficits in response control and inhibition. While a less commonfinding, parietal regions have been reported as structurally abnor-mal in OCD (Carmona et al., 2007; Lazaro et al., 2009). The parietalregions are involved in attention, executive functioning, inhibitionand visuospatial ability, with connections with fronto-striatalnetworks (Mesulam, 1990). A morphometric study of youngpeople with OCD from our own research group also demonstrateslower gray matter volumes in bilateral frontal, cingulate, andparietal regions for OCD, and lower white-matter volume in thecingulate, right frontal and parietal regions, and the CC (Chen
et al., in preparation). The current results support these morpho-metric findings.
4.2. Clinical correlates
The OCD group showed lower axial diffusivity correlated withgreater severity of symptoms. Several of the DTI studies to datehave explored whether there is a correlation between FA andclinical assessments, most commonly the Y-BOCS (Szeszko et al.,2005; Saito et al., 2008; Garibotto et al., 2010; Chiu et al., 2011;Nakamae et al., 2011; Zarei et al., 2011; Lochner et al., 2012). Thecurrent study, in a pediatric population, used the CY-BOCS but didnot find a correlation of CY-BOCS scores with any of the diffusionparameters including FA, consistent with Jayarajan et al. (2012).Given that the CY-BOCS is a simple child-friendly version of the Y-BOCS the lack of a structural correlate with clinical severity inchildren might therefore be due to the developmentally differentpattern of white-matter maturation, rather than differing Y-BOCSassessments between childhood and adulthood. The current studydid, however, demonstrate a correlation of axial diffusivity withanother measure of symptom severity, the CBCL-OCS. Higherscores on the CBCL-OCS reflect higher levels of anxiety, depression,obsessions and compulsions. While the CY-BOCS and the CBCL-OCS both have high validity for assessing symptom severity(Scahill et al., 1997; Storch et al., 2006), it is not known howclosely the two tests assess the pattern of symptoms; for example,it has been suggested that the CY-BOCS has stronger associationsto obsessional thinking and compulsive symptoms than to mea-sures of general anxiety and depression (Scahill et al., 1997).
While the OCD participants in the current study were medica-tion naïve or taken off their medication for 24 h before scanning,the potential long-term effects of medication on white-matterdevelopment are unknown. As only two of the participants in the

T. Silk et al. / Psychiatry Research: Neuroimaging 213 (2013) 154–160 159
current study had a history of medication, and both for a relativelyshort period (one of 6 and one of 12 months), any potentiallong-term effects would not be expected to have had a significantimpact on these results, but this issue will be important for futureresearch to investigate.
4.3. Conclusions
The current study has provided further insight into the orga-nization and the structure of white-matter pathways in OCD inchildren. While the etiology and the cognitive and behavioralimplications of the identified structural abnormalities are unclear,it is apparent that the axial diffusivity anomalies in children withOCD correspond to symptom severity as measured by the CBCL-OCS. DTI can potentially be important in allowing us to examinethe nature and extent of neuronal disruption associated with OCDthat conventional MRI cannot identify, and in the future, providingnew avenues to help reveal the relationships between the clinicalsymptoms and the affected brain regions. In the future, diffusionmeasures may potentially serve as an important biomarker forOCD.
Acknowledgments
This work was supported by the Eric Ormond Baker Trust, theNational Health and Medical Research Council, by the VictorianGovernment's Operational Infrastructure Support Program and bythe Royal Children's Hospital staff and patients. TS was supportedby a NHMRC Career Development Award.
References
Achenbach, T.M., Edelbrock, C.S., 1983. Manual for the Child Behaviour Checklistand Behaviour Profile. University of Vermont, Burlington.
Bora, E., Harrison, B.J., Fornito, A., Cocchi, L., Pujol, J., Fontenelle, L.F., Velakoulis, D.,Pantelis, C., Yucel, M., 2011. White matter microstructure in patients withobsessive-compulsive disorder. Journal of Psychiatry & Neuroscience 36, 42–46.
Cannistraro, P.A., Makris, N., Howard, J.D., Wedig, M.M., Hodge, S.M., Wilhelm, S.,Kennedy, D.N., Rauch, S.L., 2007. A diffusion tensor imaging study of whitematter in obsessive-compulsive disorder. Depression & Anxiety 24, 440–446.
Carmona, S., Bassas, N., Rovira, M., Gispert, J.D., Soliva, J.C., Prado, M., Tomas, J.,Bulbena, A., Vilarroya, O., 2007. Pediatric OCD structural brain deficits inconflict monitoring circuits: a voxel-based morphometry study. NeuroscienceLetters 421, 218–223.
Chen, J., Silk, T.J., Seal, M., Dally, K., Vance, A. Widespread decreased grey and whitematter in paediatric Obsessive-Compulsive Disorder (OCD): a voxel-basedmorphometric MRI study. Psychiatry Research: Neuroimaging, in preparation.
Chiu, C.H., Lo, Y.C., Tang, H.S., Liu, I.C., Chiang, W.Y., Yeh, F.C., Jaw, F.S., Tseng, W.Y.,2011. White matter abnormalities of fronto-striato-thalamic circuitry inobsessive-compulsive disorder: a study using diffusion spectrum imagingtractography. Psychiatry Research: Neuroimaging 192, 176–182.
Farchione, T.R., Lorch, E., Rosenberg, D.R., 2002. Hypoplasia of the corpus callosumand obsessive-compulsive symptoms. Journal of Child Neurology 17, 535–537.
Garibotto, V., Scifo, P., Gorini, A., Alonso, C.R., Brambati, S., Bellodi, L., Perani, D.,Alonso, C.R., 2010. Disorganization of anatomical connectivity in obsessivecompulsive disorder: a multi-parameter diffusion tensor imaging study in asubpopulation of patients. Neurobiology of Disease 37, 468–476.
Geller, D.A., Doyle, R., Shaw, D., Mullin, B., Coffey, B., Petty, C., Vivas, F., Biederman,J., 2006. A quick and reliable screening measure for OCD in youth: reliabilityand validity of the obsessive compulsive scale of the Child Behavior Checklist.Comprehensive Psychiatry 47, 234–240.
Giedd, J.N., 2004. Structural magnetic resonance imaging of the adolescent brain.Annals of the New York Academy of Sciences 1021, 77–85.
Graybiel, A.M., Rauch, S.L., 2000. Toward a neurobiology of obsessive-compulsivedisorder. Neuron 28, 343–347.
Ha, T.H., Kang, D.H., Park, J.S., Jang, J.H., Jung, W.H., Choi, J.S., Park, J.Y., Jung, M.H.,Choi, C.H., Lee, J.M., Ha, K., Kwon, J.S., 2009. White matter alterations in malepatients with obsessive-compulsive disorder. Neuroreport 20, 735–739.
Harsan, L.A., Poulet, P., Guignard, B., Steibel, J., Parizel, N., de Sousa, P.L., Boehm, N.,Grucker, D., Ghandour, M.S., 2006. Brain dysmyelination and recovery assess-ment by noninvasive in vivo diffusion tensor magnetic resonance imaging.Journal of Neuroscience Research 83, 392–402.
Hudziak, J.J., Althoff, R.R., Stanger, C., van Beijsterveldt, C.E., Nelson, E.C., Hanna, G.L.,Boomsma, D.I., Todd, R.D., 2006. The Obsessive Compulsive Scale of the ChildBehavior Checklist predicts obsessive-compulsive disorder: a receiver operating
characteristic curve analysis. Journal of Child Psychology & Psychiatry & AlliedDisciplines 47, 160–166.
Huyser, C., Veltman, D.J., de Haan, E., Boer, F., 2009. Paediatric obsessive-compulsive disorder, a neurodevelopmental disorder? Evidence from neuroi-maging. Neuroscience & Biobehavioral Reviews 33, 818–830.
Ivarsson, T., Larsson, B., 2008. The Obsessive-Compulsive Symptom (OCS) scale ofthe Child Behavior Checklist: a comparison between Swedish children withObsessive-Compulsive Disorder from a specialized unit, regular outpatients anda school sample. Journal of Anxiety Disorders 22, 1172–1179.
Jayarajan, R.N., Venkatasubramanian, G., Viswanath, B., Reddy, J., Srinath, S.,Vasudev, M.K., Chandrashekar, C.R., 2012. White matter abnormalities inchildren and adolescents with obsessive-compulsive disorder: a diffusiontensor imaging study. Depression and Anxiety 29 (9), 780–788.
Kovacs, M., 1985. The Children's Depression, Inventory (CDI). PsychopharmacologyBulletin 21, 995–998.
Kumar, R., Nguyen, H.D., Macey, P.M., Woo, M.A., Harper, R.M., 2012. Regional brainaxial and radial diffusivity changes during development. Journal of Neu-roscience Research 90, 346–355.
Kwon, J.S., Jang, J.H., Choi, J.S., Kang, D.H., 2009. Neuroimaging in obsessive-compulsive disorder. Expert Review of Neurotherapeutics 9, 255–269.
Lazaro, L., Bargallo, N., Castro-Fornieles, J., Falcon, C., Andres, S., Calvo, R., Junque, C.,2009. Brain changes in children and adolescents with obsessive-compulsivedisorder before and after treatment: a voxel-based morphometric MRI study.Psychiatry Research: Neuroimaging 172, 140–146.
Lochner, C., Fouche, J.-P., Plessis, S.d., Spottiswoode, B., Seedat, S., Fineberg, N.,Chamberlain, S., Stein, D.J., 2012. Evidence for fractional anisotropy and meandiffusivity white matter abnormalities in the internal capsule and cingulum inpatients with obsessive-compulsive disorder. Journal of Psychiatry & Neu-roscience 37, 193–199.
MacMaster, F.P., 2010. Translational neuroimaging research in pediatric obsessive-compulsive disorder. Dialogues in Clinical Neuroscience 12, 165–174.
MacMaster, F.P., O'Neill, J., Rosenberg, D.R., 2008. Brain imaging in pediatricobsessive-compulsive disorder. Journal of the American Academy of Child &Adolescent Psychiatry 47, 1262–1272.
Menzies, L., Williams, G.B., Chamberlain, S.R., Ooi, C., Fineberg, N., Suckling, J.,Sahakian, B.J., Robbins, T.W., Bullmore, E.T., 2008. White matter abnormalitiesin patients with obsessive-compulsive disorder and their first-degree relatives.American Journal of Psychiatry 165, 1308–1315.
Mesulam, M.M., 1990. Large-scale neurocognitive networks and distributed proces-sing for attention, language, and memory. Annals of Neurology 28, 597–613.
Modell, J.G., Mountz, J.M., Curtis, G.C., Greden, J.F., 1989. Neurophysiologic dysfunc-tion in basal ganglia/limbic striatal and thalamocortical circuits as a pathoge-netic mechanism of obsessive-compulsive disorder. Journal of Neuropsychiatry& Clinical Neurosciences 1, 27–36.
Nakamae, T., Narumoto, J., Sakai, Y., Nishida, S., Yamada, K., Nishimura, T., Fukui, K.,2011. Diffusion tensor imaging and tract-based spatial statistics in obsessive-compulsive disorder. Journal of Psychiatric Research 45, 687–690.
Nakamae, T., Narumoto, J., Shibata, K., Matsumoto, R., Kitabayashi, Y., Yoshida, T.,Yamada, K., Nishimura, T., Fukui, K., 2008. Alteration of fractional anisotropyand apparent diffusion coefficient in obsessive-compulsive disorder: a diffusiontensor imaging study. Progress in Neuro-Psychopharmacology & BiologicalPsychiatry 32, 1221–1226.
Nelson, E.C., Hanna, G.L., Hudziak, J.J., Botteron, K.N., Heath, A.C., Todd, R.D., 2001.Obsessive-compulsive scale of the child behavior checklist: specificity, sensi-tivity, and predictive power. Pediatrics 108, E14.
Qiu, D., Tan, L.H., Zhou, K., Khong, P.L., 2008. Diffusion tensor imaging of normalwhite matter maturation from late childhood to young adulthood: voxel-wiseevaluation of mean diffusivity, fractional anisotropy, radial and axial diffusivities,and correlation with reading development. Neuroimage 41, 223–232.
Rosenberg, D.R., Keshavan, M.S., Dick, E.L., Bagwell, W.W., MacMaster, F.P., Birma-her, B., 1997. Corpus callosal morphology in treatment-naive pediatric obses-sive compulsive disorder. Progress in Neuro-Psychopharmacology & BiologicalPsychiatry 21, 1269–1283.
Saito, Y., Nobuhara, K., Okugawa, G., Takase, K., Sugimoto, T., Horiuchi, M., Ueno, C.,Maehara, M., Omura, N., Kurokawa, H., Ikeda, K., Tanigawa, N., Sawada, S.,Kinoshita, T., 2008. Corpus callosum in patients with obsessive-compulsivedisorder: diffusion-tensor imaging study. Radiology 246, 536–542.
Saxena, S., Brody, A.L., Schwartz, J.M., Baxter, L.R., 1998. Neuroimaging and frontal-subcortical circuitry in obsessive-compulsive disorder. British Journal of Psy-chiatry Supplementum 35, 26–37.
Saxena, S., Rauch, S.L., 2000. Functional neuroimaging and the neuroanatomy ofobsessive-compulsive disorder. Psychiatric Clinics of North America 23,563–586.
Scahill, L., Riddle, M.A., McSwiggin-Hardin, M., Ort, S.I., King, R.A., Goodman, W.K.,Cicchetti, D., Leckman, J.F., 1997. Children's Yale-Brown Obsessive CompulsiveScale: reliability and validity. Journal of the American Academy of Child &Adolescent Psychiatry 36, 844–852.
Schmithorst, V.J., Holland, S.K., Dardzinski, B.J., 2008. Developmental differences inwhite matter architecture between boys and girls. Human Brain Mapping 29,696–710.
Silverman, W.K., Albano, A.M., 1996. Anxiety Disorders Interview Schedule forDSM-IV. Graywind, Texas.
Smith, S.M., Jenkinson, M., Johansen-Berg, H., Rueckert, D., Nichols, T.E., Mackay, C.E., Watkins, K.E., Ciccarelli, O., Cader, M.Z., Matthews, P.M., Behrens, T.E., 2006.Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data.Neuroimage 31, 1487–1505.
T. Silk et al. / Psychiatry Research: Neuroimaging 213 (2013) 154–160160
Smith, S.M., Nichols, T.E., 2009. Threshold-free cluster enhancement: addressingproblems of smoothing, threshold dependence and localisation in clusterinference. Neuroimage 44, 83–98.
Snook, L., Paulson, L.A., Roy, D., Phillips, L., Beaulieu, C., 2005. Diffusion tensorimaging of neurodevelopment in children and young adults. Neuroimage 26,1164–1173.
Storch, E.A., Murphy, T.K., Bagner, D.M., Johns, N.B., Baumeister, A.L., Goodman, W.K., Geffken, G.R., 2006. Reliability and validity of the Child Behavior ChecklistObsessive-Compulsive Scale. Journal of Anxiety Disorders 20, 473–485.
Szeszko, P.R., Ardekani, B.A., Ashtari, M., Malhotra, A.K., Robinson, D.G., Bilder, R.M.,Lim, K.O., 2005. White matter abnormalities in obsessive-compulsive disorder:a diffusion tensor imaging study. Archives of General Psychiatry 62, 782–790.
Yakolev, P.I., Lecours, A.R., 1967. The myelogenic cycles of regional maturation ofthe brain. In: Minkowski, A. (Ed.), Regional Development of the Brain in EarlyLife. Blackwell, Oxford, pp. 3–70.
Yoo, S.Y., Jang, J.H., Shin, Y.W., Kim, D.J., Park, H.J., Moon, W.J., Chung, E.C., Lee, J.M.,Kim, I.Y., Kim, S.I., Kwon, J.S., 2007. White matter abnormalities in drug-naivepatients with obsessive-compulsive disorder: a diffusion tensor study beforeand after citalopram treatment. Acta Psychiatrica Scandinavica 116, 211–219.
Zarei, M., Mataix-Cols, D., Heyman, I., Hough, M., Doherty, J., Burge, L., Winmill, L.,Nijhawan, S., Matthews, P.M., James, A., 2011. Changes in gray matter volumeand white matter microstructure in adolescents with obsessive-compulsivedisorder. Biological Psychiatry 70, 1083–1090.