video-assisted thoracoscopic clipping of patent ductus arteriosus: close to the gold standard and...
TRANSCRIPT

Cop
Original article
Video-assisted thoracoscopic clipping of patent ductusarteriosus: close to the gold standard and minimally invasivecompetitor of percutaneous techniquesEmmanuel Villa, Thierry Folliguet, Diego Magnano, Frederic Vanden Eynden,Emmanuel Le Bret and Francois Laborde
Objective To review our 12-year experience in video-
assisted thoracoscopic surgery (VATS) for patent ductus
arteriosus.
Methods VATS was performed in 743 patients. Three
groups were compared: 24 low-birth-weight infants
(LBWIs), 676 children between 2.5–25 kg and 43 boys
> 25 kg. A diameter of > 8 mm was the main
contraindication. For 85 consecutive patients, hospital stay
underwent cost analysis.
Results Median age was 1.6 years (range 5 days–33 years)
and median weight 9.0 kg (range 1.2–65 kg). Mortality was
nil. Median operative time was 20 min and hospital stay
2 days. Residual patency at discharge was 0% in LBWIs, 0.7%
in children, and 4.7% in boys (P U NS) and 0, 0.3, and 4.7% at
follow-up (P U 0.001). Persistent recurrent laryngeal nerve
dysfunction was recorded in 4.2% of LBWIs, 0.3% of children
yright © Italian Federation of Cardiology. Unauth
1558-2027 � 2006 Italian Federation of Cardiology
and 0% of boys (P U 0.012). Total mean cost was
s 5954 W 2110.
Conclusions The success rate of VATS clipping compares
favorably with the thoracotomic approach but without chest
wall trauma and it may have a very favorable cost-effective
therapeutic balance compared to transcatheter techniques.
J Cardiovasc Med 7:210–215 Q 2006 Italian Federation of
Cardiology.
Journal of Cardiovascular Medicine 2006, 7:210–215
Keywords: low-birth-weight infants, minimally invasive surgical procedures,patent ductus arteriosus, pediatrics, video-assisted thoracic surgery
Cardiac Pathology Department, Institut Mutualiste Montsouris, Paris, France
Correspondence and requests for reprints to Dr Emmanuel Villa, Cardiochirurgia,Fondazione Poliambulanza, Via Bissolati 57, 25124 Brescia, Italye-mail: [email protected]
Received 28 January 2005 Revised 26 July 2005Accepted 1 August 2005
IntroductionMinimally invasive surgery has been one of the most
important surgical advances in recent years along with a
great development of techniques and materials for per-
cutaneous procedures aiming at treating heart diseases.
Nevertheless, division of a patent ductus arteriosus
(PDA) by means of posterolateral thoracotomy is still
considered the gold standard [1]. Actually, in the unre-
ported experience of congenital surgical teams and in
published series [2], the interruption of PDA via open
thoracotomy is a safe and reproducible surgical procedure
that provides very reliable results.
In recent years, closure by percutaneous techniques has
been increasingly adopted thanks to it being less inva-
sive, although burdened by some limitations related to
body weight and ductal morphology [1,3]. From the
surgical standpoint, advances also in equipment and
instruments have been attained and a net reduction in
morbidity has been obtained by means of minimally
invasive techniques. In the early 1990s, video-assisted
thoracoscopic surgery (VATS) began to be employed in
the pediatric field [4,5]. Although not yet widely
accepted, VATS for PDA closure is supposed to offer
the same results and safety standards as the traditional
approach having a reduced invasiveness like the
percutaneous approach.
This study aims at supporting this hypothesis reporting
our results and cost analysis on PDA closure with VATS
in order to compare them with data from conventional
treatment and those from catheter-based approaches.
MethodsPatientsReferring areas were the Paris regions, some hospitals
from northern France and from overseas domains. Pre-
sence of a clinically or instrumentally significant shunt
indicated closure of the arterial duct in low-birth-weight
neonates, whereas in older children persistent patency
was the indication. Pediatricians and pediatric cardiolo-
gists of referring hospitals chose the type of approach
(medical, surgical or percutaneous) for each patient. All
children referred to our institution for surgical strategy
were evaluated for VATS. The following criteria were
considered contraindications to VATS clipping: a duct
diameter of > 8 mm, previous thoracotomy, presence
of calcifications, active infection, or aneurysm. From
September 1991 to February 2004, a total of 794 patients
were referred to our institution for isolated arterial
orized reproduction of this article is prohibited.

C
VATS clipping of patent ductus arteriosus Villa et al. 211
duct surgical treatment. VATS clipping was performed
in 743 of these cases and the series was retrospectively
analyzed. Of the remaining patients, 28 participated in a
study previously made at our institution for a robotically
assisted procedure [6], and the final 23 underwent a
standard thoracotomy due to contraindications to VATS.
Preoperative procedureStandard laboratory analysis and chest radiography were
performed primarily on an outpatient basis. Transtho-
racic echocardiography was systematically repeated on
the admission day for confirmation of the indication to
VATS. Angiography and cardiac catheterization were not
routinely performed if accurate anatomical and functional
definition was obtained by ultrasound. The degree of
pulmonary hypertension not allowing PDA closure by
VATS referred to the standard limits commonly accepted
[1]. The hospital governance committee evaluated the
procedures and informed approval from patients or
parents was obtained.
Surgical procedureTechnique and materials used have been reported in
previous studies and remained unchanged for the study
period with a few exceptions [4,7]. The principal steps
included two thoracotomy incisions for the introduction
of 5 mm trocars (L-shaped electrocautery and camera),
one smaller incision for direct nerve hook insertion (two
hooks for lung retraction, one for pleural reflection),
positioning of two 9 mm titanium clips through the
central incision after trocar removal, and pleural drainage
by one small-diameter wound drain catheter placed
through the same incision.
AnesthesiaAnesthesia was settled for a short-course operation. Pres-
sure monitoring, perfusion lines, and ventilation strategy
were employed as previously described [4,7]. Modifi-
cations in the pharmacological protocol were made in
recent years and new drugs introduced. The current
scheme is the following: propofol, sufentanil, atracurium
besylate for induction and sevoflurane and sufentanil
for maintenance.
Postoperative eventsEchocardiography was performed immediately after
VATS, either in the operating room, in the recovery
room, or in the intensive care unit depending on the
patient’s age and clinical status. If a persistent patency
was present, the patient was returned to the operating
room. In case of complete flow suppression, chest radi-
ography and extubation were then performed. Another
echocardiographic study was always conducted prior
to discharge.
All unfavorable events were recorded paying attention to
the following occurrences: residual shunt, VATS redo
opyright © Italian Federation of Cardiology. Unau
clipping, thoracotomy for bleeding or residual patency,
transfusion for bleeding, clinically detected transient
laryngeal nerve dysfunction (hoarseness, stridor, voice
changes), persistent laryngeal nerve dysfunction (ORL
confirmed), phrenic nerve injury, pneumothorax (if
requiring placement of a new drain), chylothorax, wound
infection, aneurysm formation, pulmonary artery steno-
sis, inadvertent clipping of another vessel, endarteritis/
endocarditis, or hemolysis. A complicated course was
defined if any of the cited morbid events occurred at
any moment after the operation. Intensive care unit and
surgical pediatric ward stay at our department were
considered postoperative stay. Continuation in neonatal
nursery due to the premature condition (lung immaturity,
weight deficit, etc.) was not considered as requiring
further stay due to surgical morbidity.
Referring pediatric cardiologists provided follow-up visits
on postoperative days 7 to 10 and after 6 months.
CostThe cost of hospitalization at our department (general
logistic, medical logistic, direct charges, meals, laundry,
sterilization) and the cost of the facility were determined
by a computer-based monitoring system of the function-
ing of our hospital. Consequently a daily mean charge was
obtained retrospectively. Technical consumption was
instead prospectively recorded using the scoring system
of the French National Health Organization. Data about
medical and administrative actions were collected and
linked. Every caring act was scored considering consump-
tion of medical, nursing, and technical resources (further
information available at www.le-pmsi.org).
Statistical analysisMeans were expressed � 1 SD; range was added if con-
sidered helpful to data interpretation. Patients were
divided into groups by body weight according to the
cut-off reported in the literature [8,9]. Pearson x2 test
or Fisher’s exact test when appropriate was used to
evaluate differences in the incidence of complications.
Statistical difference between data was achieved defining
the P significance according to the degrees of freedom.
Data were analyzed using a SPSS for Windows 11.5 (SPSS
Inc., Chicago, Illinois, USA).
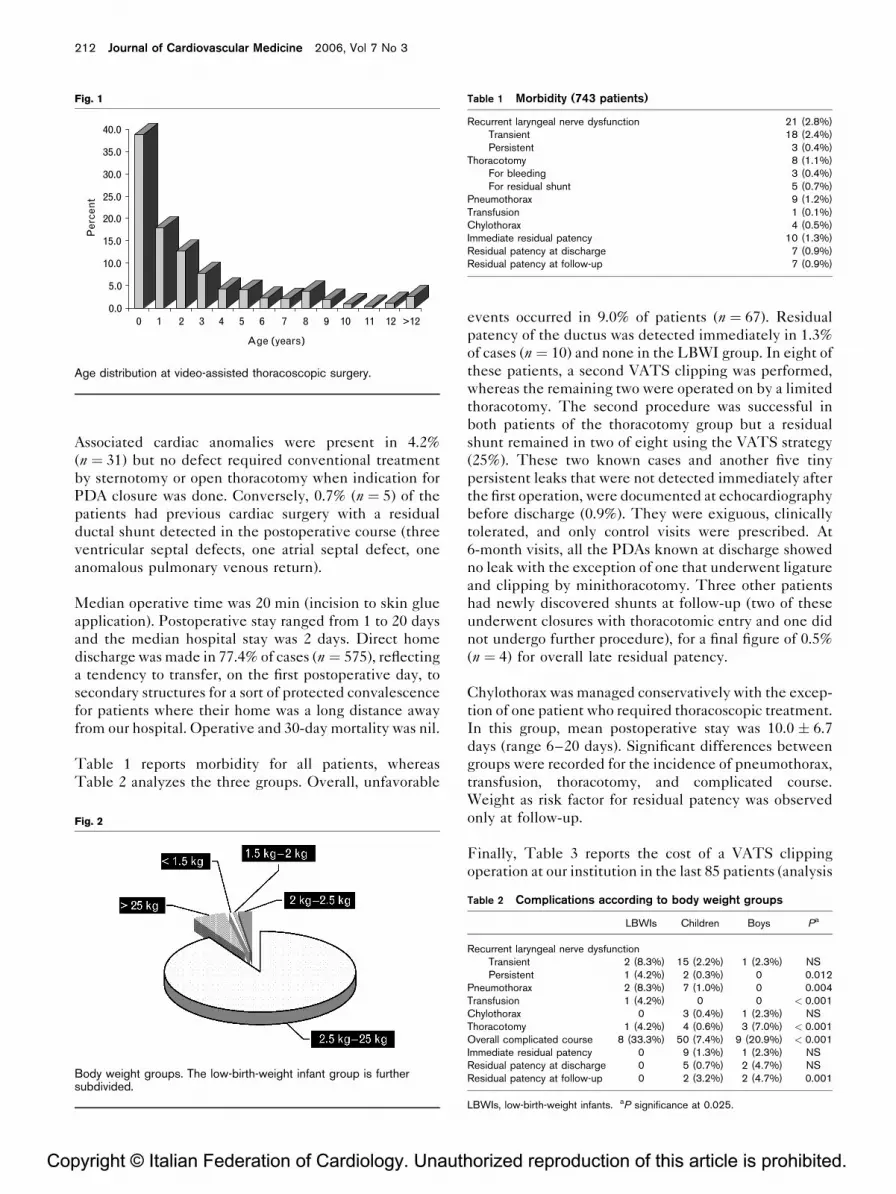
ResultsMean age at surgery was 2.9 � 3.7 years ranging from
5 days to 33 years (Fig. 1). The male/female ratio was
0.6. The overall mean weight was 10.7 � 8.0 kg (range
1.2–65 kg). The subdivision into three groups was
made according to body weight and the composition of
the study population was the following: low-birth-
weight infants (LBWIs) 3%, children (between 2.5–
25 kg) 91%, boys (> 25 kg) 6% (Fig. 2). Mean weight
of LBWIs was 2.1 � 0.4 kg and the male/female ratio
was 0.8.
thorized reproduction of this article is prohibited.
Cop
212 Journal of Cardiovascular Medicine 2006, Vol 7 No 3
Fig. 1
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Per
cen
t
>121211 10 9 8 7 6 5 4 3 2 10
Age (years)
Age distribution at video-assisted thoracoscopic surgery.
Table 1 Morbidity (743 patients)
Recurrent laryngeal nerve dysfunction 21 (2.8%)Transient 18 (2.4%)Persistent 3 (0.4%)
Thoracotomy 8 (1.1%)For bleeding 3 (0.4%)For residual shunt 5 (0.7%)
Pneumothorax 9 (1.2%)Transfusion 1 (0.1%)Chylothorax 4 (0.5%)Immediate residual patency 10 (1.3%)Residual patency at discharge 7 (0.9%)Residual patency at follow-up 7 (0.9%)
Associated cardiac anomalies were present in 4.2%
(n ¼ 31) but no defect required conventional treatment
by sternotomy or open thoracotomy when indication for
PDA closure was done. Conversely, 0.7% (n ¼ 5) of the
patients had previous cardiac surgery with a residual
ductal shunt detected in the postoperative course (three
ventricular septal defects, one atrial septal defect, one
anomalous pulmonary venous return).
Median operative time was 20 min (incision to skin glue
application). Postoperative stay ranged from 1 to 20 days
and the median hospital stay was 2 days. Direct home
discharge was made in 77.4% of cases (n ¼ 575), reflecting
a tendency to transfer, on the first postoperative day, to
secondary structures for a sort of protected convalescence
for patients where their home was a long distance away
from our hospital. Operative and 30-day mortality was nil.
Table 1 reports morbidity for all patients, whereas
Table 2 analyzes the three groups. Overall, unfavorable
yright © Italian Federation of Cardiology. Unauth
Fig. 2
Body weight groups. The low-birth-weight infant group is furthersubdivided.
events occurred in 9.0% of patients (n ¼ 67). Residual
patency of the ductus was detected immediately in 1.3%
of cases (n ¼ 10) and none in the LBWI group. In eight of
these patients, a second VATS clipping was performed,
whereas the remaining two were operated on by a limited
thoracotomy. The second procedure was successful in
both patients of the thoracotomy group but a residual
shunt remained in two of eight using the VATS strategy
(25%). These two known cases and another five tiny
persistent leaks that were not detected immediately after
the first operation, were documented at echocardiography
before discharge (0.9%). They were exiguous, clinically
tolerated, and only control visits were prescribed. At
6-month visits, all the PDAs known at discharge showed
no leak with the exception of one that underwent ligature
and clipping by minithoracotomy. Three other patients
had newly discovered shunts at follow-up (two of these
underwent closures with thoracotomic entry and one did
not undergo further procedure), for a final figure of 0.5%
(n ¼ 4) for overall late residual patency.
Chylothorax was managed conservatively with the excep-
tion of one patient who required thoracoscopic treatment.
In this group, mean postoperative stay was 10.0 � 6.7
days (range 6–20 days). Significant differences between
groups were recorded for the incidence of pneumothorax,
transfusion, thoracotomy, and complicated course.
Weight as risk factor for residual patency was observed
only at follow-up.
Finally, Table 3 reports the cost of a VATS clipping
operation at our institution in the last 85 patients (analysis
orized reproduction of this article is prohibited.
Table 2 Complications according to body weight groups
LBWIs Children Boys Pa
Recurrent laryngeal nerve dysfunctionTransient 2 (8.3%) 15 (2.2%) 1 (2.3%) NSPersistent 1 (4.2%) 2 (0.3%) 0 0.012
Pneumothorax 2 (8.3%) 7 (1.0%) 0 0.004Transfusion 1 (4.2%) 0 0 < 0.001Chylothorax 0 3 (0.4%) 1 (2.3%) NSThoracotomy 1 (4.2%) 4 (0.6%) 3 (7.0%) < 0.001Overall complicated course 8 (33.3%) 50 (7.4%) 9 (20.9%) < 0.001Immediate residual patency 0 9 (1.3%) 1 (2.3%) NSResidual patency at discharge 0 5 (0.7%) 2 (4.7%) NSResidual patency at follow-up 0 2 (3.2%) 2 (4.7%) 0.001
LBWIs, low-birth-weight infants. aP significance at 0.025.

C
VATS clipping of patent ductus arteriosus Villa et al. 213
Table 3 Cost analysis of hospital stay (85 patients)a
Department stay 3517 � 1848Facility 214 � 112Technical consumption
Operating theater 975 � 239Anesthesia 994 � 234Imaging 100 � 51
Total cost 5800 � 211095% confidence interval 5351 � 6248
Costs are expressed in Euro. aanalysis refers to all consecutive patients treated inthe last 18 months. 2002 was the reference currency year.
Table 4 Overall cost analysis according to body weight groups
LBWIs Children Boys Pa
Total mean cost 6976 � 917 5957 � 2180 5579 � 1350 NS
Costs are expressed in Euro. LBWIs, low-birth-weight infants. aP significance at0.025.
was limited to the last 18 months owing to administrative
reasons and not to case selection) while Table 4 shows the
subdivision according to body weight.
DiscussionIn infancy closure of an isolated PDA removes the
hemodynamic burden of the left-to-right shunt. In older
children and boys suppression of the shunt is advised to
prevent infective endarteritis, pulmonary hypertension,
heart failure, aneurysm formation and pulmonary/
systemic thromboembolism [1,3]. PDA in premature
newborns presents some particularities [10] and surgery
is generally indicated in case of failure or contraindica-
tions to the pharmacological options [1].
After more than half a century of practice worldwide,
standard surgical approach has reached a high level of
safety and efficacy and it has been indicated as the gold
standard of treatment [2]. PDA may be simply ligated or
clipped; otherwise it may be sectioned and sutured. The
thoracotomy approach is still largely adopted owing to
the possibility of such an intervention at any age and to
the versatility offered to correct varied anatomical occur-
rences. However, it has resulted in some concerns about
long-term sequelae (rib deformity, scoliosis, shoulder
dysfunction) [11] besides postoperative pain, respiratory
dysfunction, and duration of hospital stay [12]. Today,
cosmetics and length of incision are questionably more
and more important, but is a fact that muscle cutting and
rib spreading are invasive parts of the standard surgical
approach.
At the beginning of the 1990s, we developed the pro-
cedure of VATS clipping to reduce the morbidity of open
thoracotomy. The series studied in this manuscript is the
largest reported to date. Instruments are introduced
through two trocars and only a supplemental incision
of a few millimeters is required to expose, dissect, and
opyright © Italian Federation of Cardiology. Unau
clip the PDA. Damage to the chest wall is reduced thanks
to the limited number of thoracotomies. Temperature
management, particularly relevant to younger patients, is
more facilitated with VATS than with thoracotomy, in the
absence of a wide thoracic cage opening and very short
operative time. The use of skin glue appeared be very
beneficial and no wound infections were recorded.
From our experience, VATS demonstrated a comparable
level of efficacy and a low level of morbidity to standard
techniques. Recurrent laryngeal nerve injury was noted
as a complication in 2.8% of our patients, whereas the
incidence with standard PDA ligation is reported to be
4.2% by Fan et al. [13]. Symptoms attributable to vocal
cord paralysis regressed in most of our cases and only
0.4% had long-lasting dysfunction, the cause being prob-
ably the trauma induced by traction or by electrocautery.
The incidence of long-lasting laryngeal nerve dysfunc-
tion in LBWIs was significantly higher (4.2%, P ¼ 0.012).
Zbar et al. [14] report a series of PDAs treated using open
thoracotomy and indicate an incidence of recurrent
laryngeal nerve injury of 22.7% in extremely low-weight
babies. This confirms the importance of the issue in
premature neonates and why the decreased incidence
achieved with VATS by improved vision from the video
camera is significant.
Conversion to thoracotomy for bleeding was necessary in
very few cases (three patients). Overall, thoracotomy was
required in 1.1% of patients: in addition to the three
previously mentioned, it was performed in five for diffi-
cult closure of the ductus (two immediate and three
residual shunts). Other authors report a number of
unplanned thoracotomies ranging from 1 to 7% in mixed
patient populations [15,16]. In our study, heavier patients
were found to be at risk of conversion. Therefore, a careful
echocardiographic evaluation of the size and anatomy of
the ductus is essential to adequately select patients for
VATS in order to minimize the incidence of conversion
and to manage larger PDA directly by thoracotomy.
Different issues are involved when caring for premature
and/or small babies. We did not have formal inferior
weight limit for VATS, but our patient recruitment was
influenced by the absence of a neonatal intensive care
unit in our hospital. Therefore, our VATS experience in
LBWIs is still limited, even though smaller instruments
and other strategies are under consideration [17,18].
Echo-Doppler studies have detected flow in clinically
silent ducts that have been only ligated [19]. Con-
sequently, because we were not dividing the ductus,
we always performed a double echographic check during
the hospital stay. Our protocol has allowed detecting
1.3% of incomplete closures. Each of these patients
underwent additional surgery and the second procedure
was unsuccessful in one-quarter of patients re-operated
thorized reproduction of this article is prohibited.

Cop
214 Journal of Cardiovascular Medicine 2006, Vol 7 No 3
using VATS. Therefore, it seems wise to remedy with
open surgery in the event that the first VATS operation
fails. This would allow shortcomings in clip size, ana-
tomic anomalies and difficult visualization to be more
easily overcome. Heavier patients require greater care
because of thicker duct walls. Indeed, residual patency at
follow-up (total incidence 0.5%) was significantly associ-
ated with body weight > 25 kg, as was the overall inci-
dence of thoracotomy.
Interventional PDA closure is now available in many
cardiac centers and it seems to have a high level of
reproducibility. Only recently, however, after use of coils
and accumulation of sufficient experience, results have
been comparable to surgery. Intermediate (1-year)
residual shunt was present in 5% of patients enrolled
in the European Registry [20]. Immediate residual
patency, however, was 41% and it is unknown in how
much time complete occlusion occurs. Consequently
concerns about effective complete closure, repeat exam-
inations, duration of follow-up, and necessity of long-
term antibiotic prophylaxis exist [21]. Superseding the
Rashkind double umbrella PDA occluder, the Amplatzer
occluder is an alternative to coils in large ducts. All of
these devices, however, maintain disadvantages and
potential intraprocedural risks such as embolization of
the occluder and peripheral vascular injury. Intravascular
foreign corps may protrude creating iatrogenic pulmonary
or isthmic stenosis or may be responsible for thromboem-
bolic events, hemolysis, infection, aneurysm, or recana-
lization [1,3,21–23]. Cases of vocal cord paralysis have
also recently been attributed to closure by coils [24].
The VATS technique is safely applicable to cohorts of
patients younger and lighter than those generally treated
in cardiological series [20,25]. We successfully performed
clip closure in a wide range of body size and age with a
simple set of instruments. Further, in our study a high
degree of efficacy was demonstrated for duct diameters
up to 8 mm. Multiple coils, conversely, are usually
required for duct diameters ranging from 3 to 8 mm,
increasing the risk of complications.
Sedation and local anesthesia generally allow very short
hospital stays in interventional practice. We deem home
discharge the morning of the second day advisable to
assure a safe early postoperative course and we consider
this practice as having an acceptable cost. Although we
did not systematically survey pain or cosmetic evaluation
of scars after VATS, patients (when possible) and parents
have often reported satisfaction with the smooth and
rapid course of recovery.
No extensive cost-effectiveness comparisons of VATS
clipping versus open surgery or versus currently adopted
transcatheter techniques are available in the literature.
Prieto et al. [25] stated that coil occlusion is as effective as
yright © Italian Federation of Cardiology. Unauth
and less costly than conventional surgery. Their con-
clusions are principally based on the cost of postsurgical
stay while considering the presence of persistent leaks
clinically negligible. Regarding these issues, we estimate
that the thoracoscopic approach may favorably influence
the cost-effective therapeutic balance thanks to a shorter
inpatient hospital stay (compared with conventional
surgery) and less residual shunts (compared with transca-
theter procedure).
Our retrospective and single-center study has some
limitations. Transcatheter techniques are not a thera-
peutic option available at our hospital; direct comparison
with VATS was therefore not possible and data of
patients not referred to our institution were not available
for outcome analysis. As previously mentioned, the
cohort of LBWIs was small and results in this group
are not completely conclusive. Other limitations are
related to cost comparisons between different systems
and institutions because they are always something hazar-
dous. Nonetheless, this study records a long experience
of continuous practice ranging from neonates to adults. It
wishes to provide data for evaluation of VATS in con-
genital practice and for indirect comparison with percu-
taneous techniques. Interest in VATS is growing
worldwide [16,18,26–28].
In conclusion, VATS clipping for PDA is a safe procedure
close to the efficacy of the gold standard thoracotomic
closure. This technique has been pioneered in the field of
less invasive congenital cardiac surgery and can be a valid
competitor of transcatheter procedures. With correct pre-
operative evaluation, VATS clipping may be performed in
all ductus diameters < 9 mm, but experience in LBWIs is
limited. The technique requires minimal operating time
and avoids morbidity related to chest wall trauma, percu-
taneous vascular access and intravascular foreign bodies.
References1 Benson LN, Cowan KN. The arterial duct: its persistence and its patency.
In: Anderson RH, Baker EJ, Macartney FJ, Rigby ML, Shinebourne EA,Tynan M, editors. Paediatric cardiology, 2nd ed. London: ChurchillLivingstone; 2002, pp. 1405–1459.
2 Mavroudis C, Backer CL, Gevitz M. Forty-six years of patent ductusarteriosus division at Children’s Memorial Hospital of Chicago. Standardsfor comparison. Ann Surg 1994; 220:402–409.
3 Therrien J, Connelly MS, Webb GD. Patent ductus arteriosus. Curr TreatOptions Cardiovasc Med 1999; 1:341–346.
4 Laborde F, Noirhomme P, Karam J, Batisse A, Bourel P, Saint Maurice O. Anew video-assisted thoracoscopic surgical technique for interruption ofpatent ductus arteriosus in infants and children. J Thorac Cardiovasc Surg1993; 105:278–280.
5 Burke RP, Wernovsky G, van der Velde M, Hansen D, Castaneda AR.Video-assisted thoracoscopic surgery for congenital heart disease.J Thorac Cardiovasc Surg 1995; 109:499–508.
6 Le Bret E, Papadatos S, Folliguet T, Carbognani D, Petrie J, Aggoun Y, et al.Interruption of patent ductus arteriosus in children: robotically assistedversus videothoracoscopic surgery. J Thorac Cardiovasc Surg 2002;123:973–976.
7 Laborde F, Folliguet TA, Etienne PY, Carbognani D, Batisse A, Petrie J.Video-thoracoscopic surgical interruption of patent ductus arteriosus.Routine experience in 332 pediatric cases. Eur J Cardiothorac Surg 1997;11:1052–1055.
orized reproduction of this article is prohibited.

C
VATS clipping of patent ductus arteriosus Villa et al. 215
8 Backer CL, Mavroudis C. Congenital Heart Surgery Nomenclature andDatabase Project: patent ductus arteriosus, coarctation of the aorta,interrupted aortic arch. Ann Thorac Surg 2000; 69(Suppl):S298–S307.
9 Burke RP, Jacobs JP, Cheng W, Trento A, Fontana GP. Video-assistedthoracoscopic surgery for patent ductus arteriosus in low birth weightneonates and infants. Pediatrics 1999; 104(Pt 1):227–230.
10 Cassady G, Crouse DT, Kirklin JW, Strange MJ, Joiner CH, Godoy G, et al.A randomized, controlled trial of very early prophylactic ligation of theductus arteriosus in babies who weighed 1000 g or less at birth. N Engl JMed 1989; 320:1511–1516.
11 Seghaye MC, Grabitz R, Alzen G, Trommer F, Hornchen H, Messmer BJ,von Bernuth G. Thoracic sequelae after surgical closure of the patentductus arteriosus in premature infants. Acta Paediatr 1997; 86:213–216.
12 Landreneau RJ, Hazelrigg SR, Mack MJ, Dowling RD, Burke D, Gavlick J,et al. Postoperative pain-related morbidity: video-assisted thoracic surgeryversus thoracotomy. Ann Thorac Surg 1993; 56:1285–1289.
13 Fan LL, Campbell DN, Clarke DR, Washington RL, Fix EJ, White CW.Paralyzed left vocal cord associated with ligation of patent ductusarteriosus. J Thorac Cardiovasc Surg 1989; 98:611–613.
14 Zbar RIS, Chen AH, Behrendt DM, Bell EF, Smith RJ. Incidence of vocalfold paralysis in infants undergoing ligation of patent ductus arteriosus. AnnThorac Surg 1996; 61:814–816.
15 Hines MH, Bensky AS, Hammond JW Jr, Pennington DG. Video-assistedthoracoscopic ligation of patent ductus arteriosus: safe and outpatient. AnnThorac Surg 1998; 66:853–859.
16 Nezafati MH, Mahmoodi E, Hashemian SH, Hamedanchi A. Video-assistedthoracoscopic surgical (VATS) closure of patent ductus arteriosus: reportof three-hundred cases. Heart Surg Forum 2002; 5:57–59.
17 Villa E, Mazzera E, Galetta D, Di Donato RM. Patent ductus arteriosus inneonates and new approaches. Ann Thorac Surg 2005; 79:1827–1828.
18 Hines MH, Raines KH, Payne RM, Covitz W, Cnota JF, Smith TE, et al.Video-assisted ductal ligation in premature infants. Ann Thorac Surg 2003;76:1417–1420.
19 Sorensen KE, Kristensen B, Hansen OK. Frequency of occurrence ofresidual ductal flow after surgical ligation by color-flow mapping. Am JCardiol 1991; 67:653–654.
20 Magee AG, Huggon IC, Seed PT, Qureshi SA, Tynan M, on behalf of theAssociation for European Cardiology. Transcatheter coil: occlusion of thearterial duct. Results of the European Registry. Eur Heart J 2001;22:1817–1821.
21 Sullivan ID. Patent arterial duct: when should it be closed? Arch Dis Child1998; 78:285–287.
22 Soares AM, Aiello VD, Andrade JL, Kajita LJ, Soares J Jr, Morhy SS, et al.Doppler flow evaluation can anticipate abnormal left lung perfusion aftertranscatheter closure of patent ductus arteriosus. Eur J Cardiol 2004;25:1927–1933.
23 Lozier JS, Cowley CG. Reactivity of the ductus arteriosus: implications fortranscatheter therapy. Catheter Cardiovasc Interv 2004; 61:268–270.
24 Liang CD, Ko SF, Huang SC, Niu CK. Vocal cord paralysis aftertranscatheter coil embolization of patent ductus arteriosus. Am Heart J2003; 146:367–371.
25 Prieto LP, DeCamillo DM, Konrad DJ, Scalet-Longworth L, Latson LA.Comparison of cost and clinical outcome between transcatheter coilocclusion and surgical closure of isolated patent ductus arteriosus.Pediatrics 1998; 101:1020–1024.
26 Kim BY, Choi HH, Park JB, Yu BS, Oh BS. Video assisted thoracoscopicligation of patent ductus arteriosus. Technique of sliding loop ligation.J Cardiovasc Surg (Torino) 2000; 41:69–72.
27 Vida VL, Rubino M, Bottio T, Padalino MA, Milanesi O, Pittarello D, StellinG. Thoracoscopic closure of the patent arterial duct. Cardiol Young 2004;14:164–167.
28 Georgeson KE, Robertson DJ. Minimally invasive surgery in the neonate:review of current evidence. Semin Perinatol 2004; 28:212–220.
opyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.