nonintubated thoracoscopic anatomical segmentectomy for lung tumors
TRANSCRIPT

THORACIC
GENERAL
Nonintubated Thoracoscopic AnatomicalSegmentectomy for Lung TumorsMing-Hui Hung, MD, MS, Hsao-Hsun Hsu, MD, PhD, Ke-Cheng Chen, MD,Kuang-Cheng Chan, MD, Ya-Jung Cheng, MD, PhD, and Jin-Shing Chen, MD, PhDDepartment of Anesthesiology, Division of Thoracic Surgery, Experimental Surgery, Department of Surgery, National TaiwanUniversity Hospital and National Taiwan University College of Medicine, Graduate Institute of Clinical Medicine, National TaiwanUniversity College of Medicine, Taipei, Taiwan
Background. Intubated general anesthesia with one-lung ventilation is considered mandatory for anatomicalpulmonary resections. Nonintubated thoracoscopic seg-mentectomy for management of lung tumors, which istechnically challenging, has not been reportedpreviously.The goal of this study was to evaluate the feasibility andsafety of thoracoscopic anatomical segmentectomywithout endotracheal intubation.
Methods. From August 2009 to December 2012, 21 pa-tients with lung tumors were treated using thoracoscopicanatomical segmentectomy without endotracheal intuba-tion using a combination of thoracic epidural anesthesia,intrathoracic vagal blockade, and target-controlledsedation.
Results. There were 16 patients with primary or met-astatic lung cancers and 5 patients with nonmalignanttumors. Left upper lobe apical trisegmentectomy wasmost commonly performed (n [ 6), followed by superior
Accepted for publication May 21, 2013.
Address correspondence to Dr Cheng, Department of Anesthesiology,National Taiwan University Hospital and National Taiwan UniversityCollege of Medicine, 7, Chung-Shan South Road, Taipei 10002, Taiwan; e-mail: [email protected]; [email protected].
� 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
segmentectomy of the right lower lobe (n [ 4) and leftlower lobe (n [ 4). One patient required conversion tointubated single-lung ventilation because of vigorousmediastinal and diaphragmatic movement. No patientrequired conversion to a thoracotomy or lobectomy.Operative complications developed in 1 patient who hadan air leak for more than 3 days postoperatively. Themean duration of postoperative chest tube drainage andmean hospital stay were 2.5 days and 6.0 days, respec-tively. Anesthetic induction and the operation required amean 26.5 minutes and 148.0 minutes, respectively.Conclusions. Nonintubated thoracoscopic segmentec-
tomy is technically feasible and safe. It can be analternative to intubated single-lung ventilation for man-agement of lung tumors in selected patients.
(Ann Thorac Surg 2013;96:1209–16)� 2013 by The Society of Thoracic Surgeons
ntroduction of the double-lumen endotracheal tube
Iand endobronchial blocker for one-lung ventilationwas a major milestone in thoracic surgical procedures [1].For decades, intubated one-lung ventilation was consid-ered mandatory. However, complications after generalanesthesia and endotracheal intubation are not negligible[2–5]. To reduce the adverse effects of general anesthesiawith intubation, a nonintubated technique has been re-ported in a variety of thoracic procedures with encour-aging results [6–18].Although the standard resection for lung cancers orcentrally located lung tumors is a lobectomy, anatomicalsegmentectomy is being increasingly reevaluated, notonly in patients with compromised pulmonary functionwho cannot tolerate a lobectomy but also in patients withsmall peripheral lung cancers 2.0 cm or smaller [19–21].The video-assisted thoracoscopic surgery (VATS)approach is also superior to conventional thoracotomy
in reducing postoperative pain, shortening the hospitalstay, and facilitating a fast recovery [22, 23]. A combina-tion of thoracoscopic segmentectomy and nonintubatedanesthesia could be a less invasive operation for themanagement of selected patients with small lung cancersor centrally located lung tumors. In this study, we reportour initial experience with this nonintubated thoraco-scopic approach for anatomical segmentectomy in pa-tients presenting with lung tumors.
Patients and Methods
This study was reviewed and approved by the ResearchEthics Committee of National Taiwan University Hospital(approval No: 201301079RINC).
Study Design and PatientsA prospectively maintained database of all patients under-going nonintubated thoracoscopic surgery was used toidentify patients who underwent anatomical segmentec-tomy for lung tumors between August 2009 and December2012. In our hospital, the thoracic surgical team, comprisingsurgeons and anesthesiologists, selected the patients fornonintubated thoracoscopic segmentectomy after a
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.05.065
1210 HUNG ET AL Ann Thorac SurgNONINTUBATED SEGMENTECTOMY 2013;96:1209–16
GENERALTHORACIC
review of their medical records and discussion with thepatients. Patients considered appropriate for non-intubated thoracoscopic segmentectomy included thosewith clinical stage I lung cancer with tumors smallerthan 2 cm, those with centrally located benign lung tu-mors, and those with marginal cardiopulmonary functionwho were not suitable for a lobectomy (elderly patientswith a New York Heart Association functional classifi-cation of II or higher, patients with a history ofcongestive heart failure, or those with a preoperativeforced expiratory volume in 1 second <70% predicted).Patients with an American Society of Anesthesiologistsstatus of 4 or greater, a bleeding disorder, sleep apnea,evidence of pleural adhesions, and unfavorable airwayfeatures or spinal anatomical characteristics were excludedfrom nonintubated operative procedures. Consent wasobtained after explaining the type of anesthesia and thesurgical procedure to the patients.
Anesthetic Setting, Induction, and MaintenanceAnesthetic management of nonintubated thoracoscopicoperations has been described in previous studies [14, 17,18, 24, 25]. All patients were premedicated with intrave-nous fentanyl (50 to 100 mg/mL). Standard monitoringof the electrocardiogram, noninvasive blood pressuremonitoring, and pulse oximetry was applied for estab-lishing thoracic epidural anesthesia. With full sterilepreparation, an epidural catheter was inserted into theT5–6 thoracic interspace to achieve and maintain a sen-sory block between the T2 and T9 dermatomes using 2%lidocaine. After confirmation of working epidural anes-thesia, patients were sedated with intravenous propofol1% using a target-controlled infusion method. The levelof sedation aimed to achieve a bispectral index valuebetween 40 and 60, and incremental intravenous in-jections of fentanyl 25 mg were given to maintain a res-piratory rate between 12 and 20 breaths/min. Meanwhile,continuous monitoring of the arterial blood pressure,urine output, and end-tidal carbon dioxide by insertion ofa detector into 1 nostril was done. The patients wereplaced in the lateral decubitus position.
During the procedure, patients spontaneously breathedoxygen through a ventilation mask to keep the oxygensaturation at more than 90%. A chest wall incision wascreated for a thoracoscopy, which caused an iatrogenicpneumothorax. The operated lung collapsed gradually.To prevent patients coughing during thoracoscopicmanipulation, intrathoracic vagal blockade was producedby infiltration of 0.25% bupivacaine (3 mL) adjacent to thevagal nerve at the level of the lower trachea for right-sided procedures and at the level of the aortopulmonarywindow for left-sided procedures under direct thoraco-scopic vision. This vagal blockade effectively inhibited thecough reflex for 3 hours or longer [17].
During wound closure and chest tube insertion, theoperated lung was manually expanded through positive-pressure mask ventilation to check for air leakage, afterwhich the propofol infusion was stopped. At the end of theoperation, patients were fully awake and asked to breathedeeply and cough to further reexpand the collapsed lung.
Surgical Technique for Anatomical Segmentectomy ofLung TumorsAll patients underwent a complete anatomical segmen-tectomy. Meanwhile, mediastinal lymph node dissectionwas also performed in patients with confirmation of pri-mary lung cancer. Thoracoscopic segmentectomy wasperformed using a 3-port method, as described byMcKenna [26]. In brief, the patient was placed in the fulllateral decubitus position, with slight flexion of the tableat the level of the midchest. The thoracoscope was placedin the seventh or eighth intercostal space in the mid-axillary line. A working port was placed in the sixth orseventh intercostal space in an auscultatory triangle, andan anterior 3- to 5-cm utility incision was placed anteri-orly in the fifth intercostal space.After collapse of the lung, interlobar fissures, pulmo-
nary vessels, bronchi, and the pulmonary parenchyma tothe affected segment were divided and sectioned withendoscopic stapling devices. The resected lung segmentwas removed in an organ retrieval bag through the utilityincision. For patients with primary lung cancer, stagingmediastinal lymph node dissection was performed, andthe rough pleural surface of the lung was sutured using4–0 Prolene (Ethicon, Somerville, NJ). After the operation,a 28F chest tube was placed through the lowest incision.Rib spreading, rib cutting, and retractor use were avoidedin all patients.
Anesthetic ConversionThe attending surgeon and anesthesiologist decidedwhether to convert from nonintubated anesthesia tointubated one-lung ventilation in cases of ineffectiveepidural anesthesia, profound respiratory movement,massive pleural adhesions, persistent hypoxemia (oxygensaturation on pulse oximetry <80%), unstable hemody-namic status, or intraoperative bleeding requiring a tho-racotomy [14, 17, 18, 25]. For conversion, the surgicalwounds were sealed with transparent waterproof dress-ings (Tegaderm Film, 3M Health Care, Neuss, Germany)after insertion of a chest tube to reexpand the lung. Thetrachea was then intubated under bronchoscopic guid-ance, followed by insertion of a bronchial blocker for one-lung ventilation without a change in the patient’sposition.
Postoperative Analgesics and CarePostoperative analgesia was administrated with acontinuous epidural infusion of bupivacaine 0.1% andfentanyl (1.25 mg/mL) for 3 days. Additional analgesicsincluded oral nonsteroidal analgesics and acetaminophenonce patients resumed oral intake 2 to 4 hours afteroperation. On postoperative days 1 and 2, patients wereasked to evaluate the intensity of postoperative pain us-ing a visual analog scale (VAS) in which 0 represented nopain and 10 represented intractable pain. Chest radiog-raphy was performed immediately postoperatively or thenext morning. The chest tube was removed if no air leakwas present and drainage was less than 200 mL in a 24-hour period. An air leak was defined as prolonged

1211Ann Thorac Surg HUNG ET AL2013;96:1209–16 NONINTUBATED SEGMENTECTOMY
GENERALTHORACIC
when it lasted longer than 3 days [14]. All postoperativecomplications were recorded.
Data Collection and AnalysesThe clinical data, operative findings, operative andanesthetic results, treatment outcomes, side effects andcomplications, and pathologic characteristics of the lungtumors were collected from the medical records. Thearterial blood gas analyses were performed before skinincision (preoperative), after segmentectomy (intra-operative), and after wound closure (postoperative). TheVAS data were collected from the nursing records.
Results
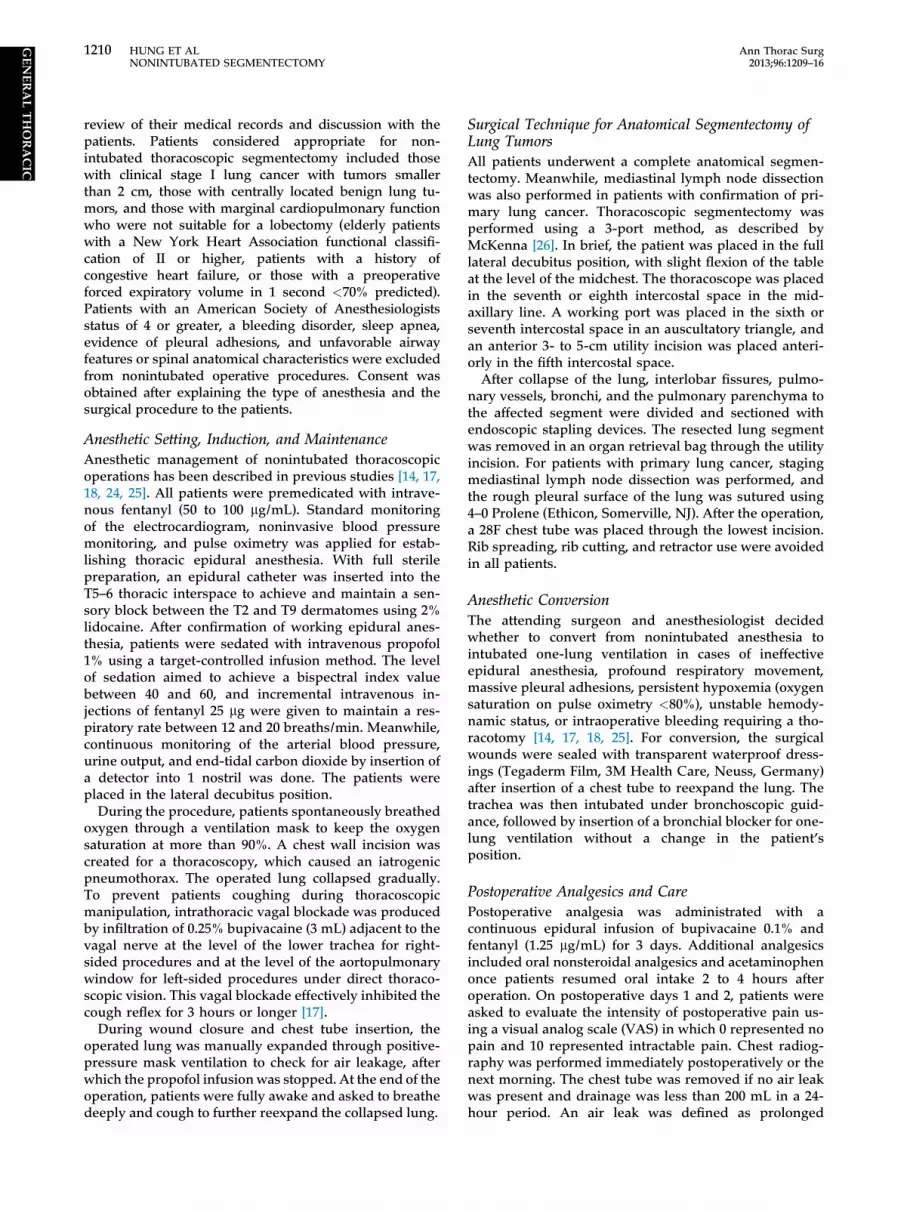
The algorithm for patient selection is shown in Figure 1.From August 2009 through December 2012, nonintubatedVATS was performed in 309 patients with lung tumors.Among them, 21 patients underwent segmentectomywithout endotracheal intubation for management of theirlung tumors, and their data are reported in Table 1. Themedian patient age was 61.0 years, and 16 patients (76.2%)were women. The median body mass index of the pa-tients was 22.2 kg/m2. The median tumor size was 1.5 cm.The pulmonary function of the patients was generallygood, with a mean forced vital capacity of 105.4% pre-dicted and forced expiratory volume in 1 second of105.5% predicted. At the time of the procedure, theAmerican Society of Anesthesiologists physical status was1 in 2 patients, 2 in 11 patients, and 3 in 8 patients. Thelung tumors were malignant in 16 patients (76.2%) andincluded primary non–small-cell lung cancer (NSCLC) in13 patients, mucosa-associated lymphoid tissue lym-phoma in 1 patient, and metastatic lung cancer in 2
patients. The remaining 5 patients (23.8%) had benigndiseases, including atypical adenomatous hyperplasia,aspergilloma, hamartoma, organizing pneumonia, andsclerosing hemangioma. Four of 13 patients with primarylung cancer underwent compromised segmentectomybecause of advanced age or marginal cardiopulmonaryfunction (median, 77 years; range, 70–83 years), althoughtheir tumors were larger than 2.5 cm (range, 2.5–3.5 cm).The remaining 9 patients received intentional segmen-tectomy because their tumors were small and peripheral(median, 0.78 cm; range, 0.5–2.2 cm).
The anatomical locations of the VATS segmentectomiesare reported in Table 2. Left upper lobe apicaltrisegmentectomy was most commonly performed (Fig 2),followed by superior segmentectomy of the right lowerlobe and left lower lobe.The operative and anesthetic results are reported in
Table 3. The mean duration of anesthesia induction was26.5 minutes, and the mean operative duration was148.0 minutes. The mean intraoperative ratio of arterialoxygen tension to inspired oxygen fraction (PaO2/FiO2)during one-lung breathing was significantly lower(223 � 60) when compared with preoperative or post-operative PaO2/FiO2 ratio (p < 0.001). During the opera-tion, the mean lowest oxygen saturation was 95.5%(range, 88% to 100%), and the mean highest partialpressure of arterial carbon dioxide during one-lungventilation was 51.8 mm Hg (range, 34.1–68.4 mm Hg).Conversion to intubated one-lung ventilation wasrequired in a 69-year-old woman with a body mass indexof 30.0 kg/m2 because of vigorous mediastinal anddiaphragmatic movement during the operation. Theconversion was accomplished within 20 minutes withoutany sequelae. No patients required conversion to a
Fig 1. Flow chart of 21 patients screenedduring the study period.
Table 1. Clinical Characteristics of Patients
Variablea Frequency (N ¼ 21)
Age, y 61 (32–83) 61.0 � 15.2Male, sex 5 (23.8%)Height, cm 162.3 (152.7–176) 162.0 � 6.8Weight, kg 58.5 (48–81.2) 59.6 � 8.4Body mass index, kg/m2 22.2 (16.8–30.0) 22.8 � 3.6Smokers 4 (19.0%)Tumor size, cm 1.5 (0.5–4.5) 1.72 � 1.1Pulmonary function test, % of
predictionForced vital capacity 104.5 (75.0–133.8) 105.4 � 18.1Forced expiratory volume
in 1 sec103.5 (65.7–149.2) 105.5 � 20.2
ComorbidityExtrapulmonary malignancy 6 (28.6%)Hypertension 6 (28.6%)Diabetes mellitus 4 (19.0%)Chronic hepatitis 4 (19.0%)Heart disease 2 (9.5%)Chronic obstructive
pulmonary disease1 (4.8%)
American Society ofAnesthesiologists class
1 2 (9.5%)2 11 (52.4%)3 8 (38.1%)
DiagnosisNon–small-cell lung cancer 13 (61.9%)MALToma 1 (4.8%)Metastatic lung cancer 2 (9.5%)Benign lung tumor 5 (23.8%)
a Continuous data are shown as median (range) and mean � standarddeviation, and categorical data are shown as number (%).
MALToma ¼ mucosa-associated lymphoid tissue lymphoma.
Table 2. Type of Segmental Resection by Anatomical Location
Location No. (%) (N ¼ 21)
Right upper lobeAnterior segmentectomy 3 (14.3%)Apicoposterior segmentectomy 1 (4.8%)
Right lower lobeSuperior segmentectomy 4 (19.0%)
Left upper lobeLingulectomy 3 (14.3%)Apical trisegmentectomy 6 (28.6%)
Left lower lobeSuperior segmentectomy 4 (19.0%)
1212 HUNG ET AL Ann Thorac SurgNONINTUBATED SEGMENTECTOMY 2013;96:1209–16
GENERALTHORACIC
thoracotomy or lobectomy and no blood transfusion wasrequired in any patient.
Complications after anesthesia occurred in 1 patientwho had a sore throat, headache, and vomiting requiringmedication. The mean postoperative VAS pain score was1.8 on the first postoperative day and 1.9 on the secondpostoperative day. The mean duration of postoperativechest tube drainage was 2.5 days, and the postoperativehospital stay was 6 days. One patient had air leaks lastingmore than 3 days after operation. No deaths or majorcomplications occurred (Table 4).
Comment
This is the first report showing that VATS anatomicalsegmentectomy is feasible and can be safely performedwithout endotracheal intubation in highly selected patientswith lung tumors. Because enhanced com-puted tomography screening protocols have identifiedincreasing numbers of small lung tumors in patientswith high surgical risk [20], there is increasing interestin minimally invasive surgical approaches, including
thoracoscopic incisions, parenchyma-sparing resection,and less invasive anesthesia for management of lungtumors.Lobectomy, either by thoracotomy or thoracoscopy, is
currently considered the standard operation for early-stage NSCLC [22, 27, 28]. The role of thoracoscopic seg-mentectomy for NSCLC is still limited and controversial[20, 21]. Traditionally, it is used as a parenchyma-sparingprocedure in high-risk patients with significantly reducedpulmonary function or a compromised medical condition.However, it is being increasingly reevaluated for themanagement of small NSCLC (tumor < 2.0 cm), and hasshown oncologic results comparable with the well-established lobectomy [19]. In addition, thoracoscopicsegmentectomy may also be the choice of operation forpatients with metastatic disease or undiagnosed pulmo-nary nodules that are not amenable to wedge resectionbecause of their proximity to large bronchovascularstructures. In our cohort, compromised VATS segmen-tectomy was performed in 4 patients with NSCLCbecause of advanced age or marginal cardiopulmonaryfunction, although their tumors were larger than 2.5 cm(range, 2.5–3.5 cm). The remaining 17 patients receivedintentional VATS segmentectomy because of smallNSCLC (<2.0 cm) or centrally located benign or malig-nant lesions.In this study, 76% of the patients were women, with a
median body height of 158 cm. We believe that non-intubated thoracoscopic surgical procedures are mostapplicable in small-bodied female patients. These pa-tients are prone to have a small tracheal caliber and aresusceptible to intubation-related complications such ashoarseness, subglottic stenosis, and airway injuries,especially when double-lumen endotracheal tubes areused [29].Although patient satisfaction with nonintubated thor-
acoscopic segmentectomy was not assessed, the operativeand anesthetic results were satisfactory in this study. Ourprevious study showed that patients who underwentnonintubated lobectomy had lower rates of sore throatand earlier resumption of oral intake compared with theirintubated counterparts [17]. Because muscle relaxantswere not used, the patients resumed water and foodintake between 2 and 4 hours postoperatively. Only

Table 3. Operative and Anesthetic Results
Variablea Frequency (N ¼ 21)
Anesthetic inductionduration, min
20 (10–50) 26.5 � 12.4
Surgical duration, min 156 (78–209) 148.0 � 43.2Global operating room
duration, min210 (140–290) 209.3 � 41.3
Perioperative PaO2/FiO2 ratioPreoperative (n ¼ 13) 406 (229–512) 408 � 78Intraoperative (n ¼ 21)b 237 (131–349) 223 � 60Postoperative (n ¼ 9) 379 (305–434) 380 � 34
Perioperative PaCO2, mm HgPreoperative (n ¼ 13) 40.9 (29.5–44.9) 39.0 � 4.6Intraoperative (n ¼ 21)c 52.4 (34.1–68.4) 51.8 � 9.0Postoperative (n ¼ 9) 40.5 (34.5–43.4) 39.7 � 2.8
Lowest SpO2 during operation, % 97 (88–100) 95.5 � 4.2Peak EtCO2 during
operation, mm Hg42 (35–53) 42.0 � 6.2
Lymph nodes dissected, no.d 5 (0–18) 6.5 � 5.9Conversion to intubation 1 (4.8%)Conversion to lobectomy 0Conversion to thoracotomy 0
a Continuous data are shown as median (range) and mean � standarddeviation, and categorical data are shown as number (%). b In-traoperative PaO2/FiO2 ratio was significantly lower when compared withpreoperative or postoperative PaO2/FiO2 ratio (p < 0.001). c Intraoper-ative PaCO2 was significantly higher when compared with preoperative orpostoperative PaCO2 (p < 0.001). d Performed in 13 patients with non–small-cell lung cancer.
EtCO2 ¼ end tidal carbon dioxide; PaCO2 ¼ partial pressure of arterialcarbon dioxide; PaO2/FiO2 ratio ¼ ratio of arterial oxygen tension toinspired oxygen fraction; SpO2 ¼ oxyhemoglobin saturation by pulseoximetry.
Fig 2. Operative views of a patientundergoing nonintubated thoracoscopic api-cal trisegmentectomy of the left upper lobe.(A) The patient was anesthetized withouttracheal intubation. The sedation level wasmonitored by bispectral index (arrow). (B)After hilar dissection, an apicoposteriorsegmental artery was identified (red vasculartape) and divided.(C) The upper division of left superior pul-monary vein was identified (blue vasculartape) and divided. (D) The upper division ofleft upper bronchus was identified (yellowvascular tape) and divided. (LA ¼ lingualartery; LV ¼ lingual vein.)
1213Ann Thorac Surg HUNG ET AL2013;96:1209–16 NONINTUBATED SEGMENTECTOMY
GENERALTHORACIC
1 patient experienced minor side effects of vomiting, sorethroat, and headache. The postoperative VAS pain scoreswere low, probably because of routine use of patient-controlled epidural analgesics. The mean postoperativehospital stay was relatively long in our patients (6 days)because of our National Health Insurance policy.Copayment is not required for patients with malignantdiseases in Taiwan.Conversion to intubated general anesthesia was
necessary in only 1 patient with a body mass index of 30.0kg/m2 because of a vigorous diaphragmatic breathingpattern and significant mediastinal movement that madebronchovascular dissection difficult and dangerous. Theanesthesiologist and the surgeon both agreed on trachealintubation and the patient was intubated and extubatedsmoothly. The conversion rate to intubation was 4.8% inpatients undergoing segmentectomy, which was similarto our nonintubated VATS lobectomy cases [17, 18]. Ourexperience suggests that patients with a body mass indexof 30.0 kg/m2 or more frequently experience vigorousdiaphragmatic and mediastinal movement, and non-intubated thoracoscopic segmentectomy or lobectomy isnot suitable for them.Although none of our patients in this study required
emergency conversion to intubation or a thoracotomybecause of uncontrolled bleeding, it happened in ourearly experience and it is important to be aware of thepossibility [17]. We suggest that proper patient selec-tion, accumulated experience from performing minornonintubated thoracoscopic procedures, and conver-sion to intubated general anesthesia without hesitationare mandatory to decrease the risk of emergency

Table 4. Treatment Outcome
Variablea Frequency (N ¼ 21)
Anesthetic side effectsVomiting requiring medication 1 (4.8%)Sore throat 1 (4.8%)Headache 1 (4.8%)
Operative complicationsAir leak > 3 d 1 (4.8%)
Postoperative visual analog scaleDay 1 1.8 (0–6)Day 2 1.9 (0–6)
Postoperative chest drainage, d 2 (1–6) 2.5 � 1.1Postoperative hospital stay, d 5 (3–14) 6 � 2.8Perioperative deaths (30 d) 0
a Continuous data are shown as median (range) and mean � standarddeviation, and categorical data are shown as number (%)
1214 HUNG ET AL Ann Thorac SurgNONINTUBATED SEGMENTECTOMY 2013;96:1209–16
GENERALTHORACIC
conversion, especially at the beginning of the learningcurve.
There are concerns about using the nonintubatedtechnique for VATS segmentectomy. One major anes-thetic concern is how respiratory function is maintainedin a spontaneously breathing patient with an openpneumothorax (ie, in severe hypoxemia and hypercap-nia), especially when the surgical duration is usually aslong as a VATS lobectomy. To our surprise, our patientstolerated the procedure well, and supplemental oxygenby facemask was enough to maintain satisfactoryoxygenation. Although carbon dioxide rebreathing mightoccur, these patients had only mild hypercapnia, whichwas not clinically relevant and resolved soon after ter-minating sedation. Atelectasis of the dependent lungduring mechanical ventilation has been demonstrated tobe a major contributing factor in ventilation-perfusionmismatch during one-lung ventilation and predisposespatients to severe hypoxemia [30]. Therefore, an alveolarrecruitment strategy with application of positive end-expiratory pressure during one-lung ventilation wasshown to be substantially effective in decreasing both aright-to-left shunt fraction and dead space ventilationfrom the dependent lung to improve oxygenation [30, 31].We believe that preservation of diaphragm function ispivotal in a single-lung spontaneous breathing scenario,and the lower rate of atelectasis in the dependent lungcompared with that in the intubated technique mayexplain the satisfactory oxygenation results in ourpatients.
The other major concern is whether it is feasible andsafe to perform a surgical procedure on a nondependentlung, especially when intense pulmonary manipulationduring segmentectomy might trigger coughing in spon-taneously breathing patients. With intrathoracic vagalblockade to abolish the cough reflex, we previouslydemonstrated that this procedure was effective duringnonintubated lobectomy [17, 18] and was also effectiveduring nonintubated segmentectomy. Empirically,retraction of the ipsilateral upper lobe is necessary toexpose the intrathoracic vagal nerve. Before lung
retraction and injection of local anesthetics, the level ofsedation is transiently deepened to prevent triggering acough reflex. After vagal blockade with bupivacaine, thelevel of sedation was returned to moderate and invasivepulmonary dissection was permitted for more than 3hours. Transient recurrent laryngeal nerve palsy is occa-sionally noted after vagal blockade, but it resolves spon-taneously after operation. Dissection of the subcarinallymph nodes occasionally contacts or irritates thecontralateral main bronchus, which might induce tran-sient coughing.To our satisfaction, nonintubated patients reported less
postoperative nausea and vomiting, early recovery of oralintake and clear consciousness, and better postoperativeanalgesia in comparison with intubated patients. Inaddition, intubation-related complications are essentiallyavoided [14, 17, 18]. Most of our patients were satisfiedwith their own choices of what they wanted duringoperation.We acknowledge that this study was limited by its
retrospective design and a small number of patients.Meanwhile, the lack of a control group who receivedintubated general anesthesia makes differentiation ofspecific benefits of the nonintubated technique for VATSsegmentectomy difficult. However, the low conversionrate from nonintubated to intubated general anesthesiaand the low complication rate indicate that nonintubatedVATS segmentectomy can be safely performed inselected patients. Further investigation is encouraged toclarify the applicability and benefits of nonintubatedVATS segmentectomy for specific patient groups.In summary, our experience showed that a VATS seg-
mentectomy without tracheal intubation is technicallyfeasible and clinically safe for management of lung tu-mors. In selected patients with NSCLC, it can be anattractive alternative both in compromised patients andfor intentional purposes. The true benefits of non-intubated VATS segmentectomy should be further veri-fied in larger prospective studies.
References
1. Ovassapian A. Conduct of anesthesia. In: Shields TW,LoCicero J, Ponn RB, eds. General Thoracic Surgery. Phila-delphia: Lippincott Williams & Wilkins; 2000:327–44.
2. Murphy GS, Szokol JW, Avram MJ, et al. Postoperative re-sidual neuromuscular blockade is associated with impairedclinical recovery. Anesth Analg; 2013 Jan 21. [Epub ahead ofprint] http://dx.doi.org/10.1213/ANE.0b013e3182742e75.
3. Murphy GS, Szokol JW, Marymont JH, Greenberg SB,AvramMJ, Vender JS. Residual neuromuscular blockade andcritical respiratory events in the postanesthesia care unit.Anesth Analg 2008;107:130–7.
4. Gothard J. Lung injury after thoracic surgery and one-lungventilation. Curr Opin Anaesthesiol 2006;19:5–10.
5. Fitzmaurice BG, Brodsky JB. Airway rupture from double-lumen tubes. J Cardiothorac Vasc Anesth 1999;13:322–9.
6. Campos JH, Hallam EA, Van Natta T, Kernstine KH. Devicesfor lung isolation used by anesthesiologists with limitedthoracic experience: comparison of double-lumen endotra-cheal tube, univent torque control blocker, and Arndt wire-guided endobronchial blocker. Anesthesiology 2006;104:261–6.

1215Ann Thorac Surg HUNG ET AL2013;96:1209–16 NONINTUBATED SEGMENTECTOMY
GENERALTHORACIC
7. Ishikawa S, Lohser J. One-lung ventilation and arterialoxygenation. Curr Opin Anaesthesiol 2011;24:24–31.
8. Guarracino F, Gemignani R, Pratesi G, Melfi F,Ambrosino N. Awake palliative thoracic surgery in a high-risk patient: one-lung, non-invasive ventilation combinedwith epidural blockade. Anaesthesia 2008;63:761–3.
9. Mukaida T, Andou A, Date H, Aoe M, Shimizu N. Thor-acoscopic operation for secondary pneumothorax underlocal and epidural anesthesia in high-risk patients. AnnThorac Surg 1998;65:924–6.
10. Sugimoto S, Date H, Sugimoto R, et al. Thoracoscopicoperation with local and epidural anesthesia in the treatmentof pneumothorax after lung transplantation. J Thorac Car-diovasc Surg 2005;130:1219–20.
11. Pompeo E, Tacconi F, Mineo D, Mineo TC. The role of awakevideo-assisted thoracoscopic surgery in spontaneous pneu-mothorax. J Thorac Cardiovasc Surg 2007;133:786–90.
12. Tacconi F, Pompeo E, Fabbi E, Mineo TC. Awake video-assisted pleural decortication for empyema thoracis. Eur JCardiothorac Surg 2010;37:594–601.
13. Pompeo E, Mineo D, Rogliani P, Sabato AF, Mineo TC.Feasibility and results of awake thoracoscopic resection ofsolitary pulmonary nodules. Ann Thorac Surg 2004;78:1761–8.
14. Tseng YD, Cheng YJ, Hung MH, Chen KC, Chen JS. Non-intubated needlescopic video-assisted thoracic surgery formanagement of peripheral lung nodules. Ann Thorac Surg2012;93:1049–54.
15. Pompeo E, Mineo TC. Awake pulmonary metastasectomy.J Thorac Cardiovasc Surg 2007;133:960–6.
16. Mineo TC, Pompeo E, Mineo D, Tacconi F, Marino M,Sabato AF. Awake nonresectional lung volume reductionsurgery. Ann Surg 2006;243:131–6.
17. Chen JS, Cheng YJ, Hung MH, Tseng YD, Chen KC, Lee YC.Nonintubated thoracoscopic lobectomy for lung cancer. AnnSurg 2011;254:1038–43.
18. Wu CY, Chen JS, Lin YS, et al. Feasibility and safety ofnonintubated thoracoscopic lobectomy for geriatric lungcancer patients. Ann Thorac Surg 2013;95:405–11.
19. Okada M, Nishio W, Sakamoto T, et al. Effect of tumor sizeon prognosis in patients with non-small cell lung cancer: therole of segmentectomy as a type of lesser resection. J ThoracCardiovasc Surg 2005;129:87–93.
� 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
20. Yang CF, D’Amico TA. Thoracoscopic segmentectomy forlung cancer. Ann Thorac Surg 2012;94:668–81.
21. Swanson SJ. Video-assisted thoracic surgery segmentectomy:the future of surgery for lung cancer? Ann Thorac Surg2010;89:S2096–7.
22. Whitson BA, Groth SS, Duval SJ, Swanson SJ, Maddaus MA.Surgery for early-stage non-small cell lung cancer: a sys-tematic review of the video-assisted thoracoscopic surgeryversus thoracotomy approaches to lobectomy. Ann ThoracSurg 2008;86:2008–16.
23. Atkins BZ, Harpole DH Jr, Mangum JH, Toloza EM,D’Amico TA, Burfeind WR Jr. Pulmonary segmentectomy bythoracotomy or thoracoscopy: reduced hospital length of staywith a minimally-invasive approach. Ann Thorac Surg2007;84:1107–12.
24. Tsai TM, Chen JS. Nonintubated thoracoscopic surgery forpulmonary lesions in both lungs. J Thorac Cardiovasc Surg2012;144:e95–7.
25. Chen KC, Cheng YJ, Hung MH, Tseng YD, Chen JS. Non-intubated thoracoscopic lung resection: a 3-year experiencewith 285 cases in a single institution. J Thorac Dis 2012;4:347–51.
26. McKenna RJ Jr. Lobectomy by video-assisted thoracic sur-gery with mediastinal node sampling for lung cancer.J Thorac Cardiovasc Surg 1994;107:879–81.
27. Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomyversus limited resection for T1N0 non-small cell lung cancer.Lung cancer study group. Ann Thorac Surg 1995;60:615–22.
28. Demmy TL, Curtis JJ. Minimally invasive lobectomy directedtoward frail and high-risk patients: a case-control study. AnnThorac Surg 1999;68:194–200.
29. Kim J, Lim T, Bahk JH. Tracheal laceration during intubationof a double-lumen tube and intraoperative fiberoptic bron-choscopic evaluation through an LMA in the lateral position:a case report. Korean J Anesthesiol 2011;60:285–9.
30. Tusman G, Bohm SH, Melkun F, et al. Alveolar recruitmentstrategy increases arterial oxygenation during one-lungventilation. Ann Thorac Surg 2002;73:1204–9.
31. Tusman G, Bohm SH, Sipmann FS, Maisch S. Lung recruit-ment improves the efficiency of ventilation and gas exchangeduring one-lung ventilation anesthesia. Anesth Analg2004;98:1604–9.
INVITED COMMENTARY
In this issue of The Annals, Hung and coworkers [1]explore the feasibility of nonintubated thoracoscopicsegmentectomy in 21 selected patients, 16 of whom had amalignant lesion. The eligibility criteria included pe-ripheral stage I non-small cell lung cancer, central ma-lignant lesions in marginal surgical candidates,and central benign lesions. The most frequent typeof resection was left upper lobe apical trisegmentectomy,followed by superior segmentectomy of the lower lobes.
The current study corroborates and extends the find-ings of other groups on regional anesthesia strategiesused to perform several lung surgical procedures,including wedge resection, lobectomy, lung volumereduction, and bullectomy. It also adds to previous find-ings coming from the same group on the feasibility ofnonintubated lobectomy.
The anesthesia protocol proposed by Hung and co-workers differs somewhat from that reported by others inrecent years and may have benefited from some historicalwork by pioneer surgeons such as Buckingham [2], whofirst reported in 1950 on major lung resections performed
through sole thoracic epidural anesthesia, and Visch-nevski [3], who reported on a multistep local anesthesiaprotocol including vagal blockade.In their modern protocol, Hung and coworkers not only
adopted selective vagal blockade to temporarily abolishthe cough reflex and thus avoid unexpected and as yetdangerous lung movements during surgical maneu-vering, but also used a bispectral index monitoring tokeep the level of sedation at an optimal level while as-suring the maintenance of spontaneous ventilation.By this particular strategy, the authors achieved satis-
factory results, inasmuch as optimal oxygenation wasmaintained for more than 2 hours during the operation, 1obese patient only required conversion to general anes-thesia because of excessive diaphragmatic movements,and operative morbidity was limited to one case of pro-longed air leaks.Nonetheless, it is conceivable that this article will
reinvigorate criticism from those who may consider itsomewhat hazardous to perform major lung proceduresentailing fine vascular dissection in mildly sedated,
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.06.021

1216 HUNG ET AL Ann Thorac SurgNONINTUBATED SEGMENTECTOMY 2013;96:1209–16
GENERALTHORACIC
spontaneously ventilating patients, provided that deepsedation with amnesia of the surgical event and animmobile collapsed lung during the operation areoffered, as a counterpart, by general anesthesia withsingle-lung ventilation.
As properly acknowledged by the authors, the mainlimitations of the current study include the small series,the retrospective design, and the lack of a control groupfor comparison of the results.
This implies that further detailed investigation by largecontrolled studies is needed. Among the several issues tobe analyzed, the impact of the different anesthesia pro-tocols on perioperative physiology and stress hormoneresponse seems crucial because it could affect not onlyearly outcomes and promptness of recovery but, asrecently hypothesized, even cancer metastatization andoverall survival.
In summary, Hung and coworkers must be congratu-lated for providing us with a provocative study that willcertainly contribute to animate the debate and promote
further investigation in an attempt to develop safer, moreeffective, and globally less invasive surgical strategies foran optimal treatment of lung cancer.
Eugenio Pompeo, MD, FETCS
Department of Thoracic SurgeryPoliclinico Tor Vergata UniversityV.le Oxford, 81Rome, Italy 00133e-mail: [email protected]
References
1. Hung M-H, Hsu H-H, Chen K-C, Chan K-C, Cheng Y-J,Chen J-S. Nonintubated thoracoscopic anatomical segmen-tectomy for lung tumors. Ann Thorac Surg 2013;96:1209–16.
2. Buckingham WW, Beatty AJ, Brasher CA, Ottosen P. Thetechnique of administering epidural anesthesia in thoracicsurgery. Dis Chest 1950;17:561–8.
3. Vischnevski AA. Local anesthesia in thoracic surgery: lungs,heart, and esophagus. Minerva Anestesiol 1954;20:432–5.