vegf administration in chronic myocardial ischemia in pigs
TRANSCRIPT

Cardiovascular Research 40 (1998) 272–281
VEGF administration in chronic myocardial ischemia in pigsa ,b a ,b c a ,d fJohn J. Lopez , Roger J. Laham , Alon Stamler , Justin D. Pearlman , Stuart Bunting ,
e b c a ,b ,*Aaron Kaplan , Joseph P. Carrozza , Frank W. Sellke , Michael SimonsaAngiogenesis Research Center, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA
bCardiovascular Division, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USAcDepartment of Surgery, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA
dDepartment of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USAeLocal Med, Palo Alto, CA, USA
fGenentech, Inc., South San Francisco, CA, USA
Received 1 December 1997; accepted 6 April 1998
Abstract
Objective: Previous investigations have shown the effectiveness of sustained intra- or extravascular administration of vascularendothelial growth factor (VEGF) in chronic myocardial ischemia in improvement of left ventricular function. The present investigationswere undertaken in order to evaluate efficacy of a single bolus or local intracoronary delivery. Methods: Yorkshire pigs underwentplacement of a left circumflex artery ameroid occluder. Three weeks later the animals were randomized to treatment with VEGF (20 mg)
TMaccomplished by local intracoronary delivery system (InfusaSleeve , n510), intracoronary bolus infusion (n57) or by epicardialimplantation of an osmotic delivery system (n57). An additional group of animals received intracoronary administration of saline andserved as a control (n59). Three weeks after initiation of therapy, the animals were evaluated with regard to myocardial perfusion andglobal as well as regional ventricular function. Results: All three VEGF treatment groups but not the control animals demonstrated asignificant increase in the left-to-left (but not right-to-left) collateral index, myocardial blood flow (pre-therapy LCX vs. LAD (average of
21 21 21 21* *all groups): 0.7660.35 vs. 0.9660.38 ml*min g , p50.03; post-therapy: LCX vs. LAD: 1.1660.39 vs. 1.1560.28 ml*min g ,p5NS) and coronary vasodilatory reserve 3 weeks after growth factor administration. The observed increase in VEGF-induced perfusioncorrelated with improvement in regional ventricular function in all VEGF-treated groups (pre-therapy vs. post-therapy: i.c. VEGF 2065.1vs. 3364.8; local VEGF 1662.8 vs. 33.6; pump VEGF 1763.8 vs. 3464.9 p,0.05 for all) but not control animals (2163.3 vs. 2765.8,p5NS). Conclusion: Single intracoronary delivery (intravascular bolus or local delivery) of VEGF is effective in stimulatingphysiologically significant angiogenesis in porcine model of chronic myocardial ischemia. 1998 Elsevier Science B.V. All rightsreserved.
Keywords: Angiogenesis; VEGF; Myocardial ischemia; Growth factors; Magnetic Resonance Imaging
1. Introduction attempt to induce growth and development of new collater-al vessels [1,2]. Recently, a number of studies have
Therapeutic approaches to management of chronic evaluated the therapeutic potential of administering variousmyocardial ischemia traditionally include manipulations angiogenic growth factors in chronic myocardial ischemiadesigned to reduce myocardial oxygen demand or to [3–7]. Several of these studies have demonstrated im-increase blood supply to compromised territories by pro- proved collateral blood flow and myocardial function inviding new (coronary artery bypass grafting) or restoring the setting of chronic ischemia after vascular endothelialold (coronary angioplasty) pathways for blood flow. A growth factor (VEGF) administration [5,7] although apotential alternative to these approaches may include an recent study suggested a lack of therapeutic efficacy of
VEGF in these settings [8]. However, all of these studies*Corresponding author. Tel.: 11 (617) 667 5364; Fax: 11 (617) 972
5201; e-mail: [email protected] Time for primary review 43 days
0008-6363/98/$ – see front matter 1998 Elsevier Science B.V. All rights reserved.PI I : S0008-6363( 98 )00136-9
by guest on Septem
ber 4, 2016D
ownloaded from
J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281 273
typically employed a prolonged form of VEGF delivery, formed through an 8F JR4 guiding catheter (Cordis Corp,relying either on continuous intracoronary or extracoronary Miami, FL) via a right femoral cutdown, in multiple LAOinfusions or repeat intra-arterial administration. These and RAO projections using ionic contrast, was employedmethods of cytokine delivery, however, raise a number of to document LCX occlusion at the site of ameroid place-practical issues for application to human trials. Clearly, a ment as well as to assess the extent of collateral circulationone time, single intracoronary administration of the growth (collateral index) in this territory. A set of colored micro-factor would have significant advantages over repeat spheres was injected into the left atrium to determinedosing and/or continuous infusions given the significant myocardial blood flow prior to initiation of VEGF therapy.vasoactive properties of VEGF [9–11]. In addition, magnetic resonance imaging was carried out to
In evaluating different forms of intracoronary delivery, a obtain quantitative measures of global and regional leftdistinction needs to be made between local delivery and ventricular function (ejection fraction, radial wall motion,intracoronary bolus administration. The former approach regional wall thickening) as well as to assess regionalcreates a local extravascular depot of the growth factor, myocardial perfusion using previously validated myocar-while the latter relies on the ability of capillary beds dial contrast density mapping [14].and/or cardiac tissues in the ischemic territory to retain the Following this baseline evaluation, animals were as-growth factor. To date there is no convincing evidence signed to one of four treatment groups: (1) VEGF pumpsuggesting a beneficial effect with either local or in- delivery; (2) local intracoronary catheter-based VEGFtracoronary bolus administration of VEGF. delivery; (3) local intracoronary bolus VEGF injection; and
With these considerations in mind we set out to de- (4) local intracoronary catheter-based saline delivery (con-termine the ability of VEGF to improve myocardial blood trol). All animals were pretreated with aspirin, bretyliumflow and function in the setting of established coronary (50 mg i.v.) and intravenous heparin (3000 U) prior to aischemia, to evaluate two forms of intracoronary VEGF coronary intervention. Animals randomized to localdelivery, and to compare them to a previously studied catheter-based VEGF underwent two directional in-method of sustained-release periadventitial administration. tracoronary deliveries of 10 mg of recombinant human
VEGF (rhVEGF, Genentech, South San Francisco, CA)165
in a volume of 2 ml saline each using a 10 mmTM2. Methods InfusaSleeve catheter (Local Med, Palo Alto, CA)
loaded over a 3.0 mm320 mm angioplasty balloon,All animal experiments in this study were conducted in delivered over a 0.014 inch angioplasty guidewire. VEGF
accordance with the National Institutes of Health guide- delivery was accomplished by first inflating the angioplastylines for the care and use of laboratory animals and the balloon to 30 psi, and then delivering the cytokine throughstudy protocol was approved by the Beth Israel Deaconess the local delivery catheter at 80 psi over 30 s. In all casesMedical Center Animal Care and Use Committee. an attempt was made to deliver VEGF into the LCX artery
proximal to the ameroid occluder, as well as into the left2.1. Ameroid constrictor model and study design anterior descending (LAD) artery at the level of LCX
ameroid occluder placement. In those animals in which aYorkshire pigs (25–30 kg.) were instrumented with a proximal LCX injection could not be carried out, the
size-matched ameroid constrictor (Research Instruments, second dose of VEGF was delivered into the LAD at theCorvalis, OR) on the proximal circumflex coronary artery same site as the original delivery. Animals randomized tounder general anesthesia as described previously [4,5]. In the control group received two intracoronary deliveries ofaddition, implantation of an osmotic polymer pump (Alza saline in a similar manner. Intracoronary bolus infusion ofCorporation) containing heparinized saline (50 U heparin / VEGF was accomplished by a manual injection of 20 mg2 ml saline) was carried out in animals randomized to of VEGF through an Ultrafuse-X dual lumen catheterpump VEGF delivery with tip of the pump catheter (SciMed, Minneapolis, MN) into the proximal LAD arterypositioned over the adventitial surface of the LCX artery carried out over 10 minutes. Animals randomized to pump1–2 cm distal to the ameroid occluder. In all animals, a set VEGF therapy were taken to the operating room and,of colored microspheres was injected into the left atrium following repeat thoracotomy, the osmotic pump primedduring transient LCX occlusion to enable subsequent with heparinized saline was replaced with a pump con-determination of the of LCX territory at risk (see below). taining 25 mg VEGF and 50 U heparin in 2 ml ofPostoperatively all animals were treated with antibiotics phosphate-buffered saline. With 80% of the materialfor 48 h and narcotic analgesics were used as needed. delivered over 3 weeks by the pump, the final estimated
Three weeks later, a period of time sufficient for delivered dose in each animal was 20 mg.ameroid closure and development of myocardial ischemia Three weeks after initiation of therapy, animals werein this model [12,13], the animals underwent a set of brought back for a final evaluation. This consisted ofbaseline studies carried out under general anesthesia with repeat coronary angiography (collateral index assessment),hemodynamic monitoring. Coronary angiography, per- microsphere coronary blood flow studies at rest and after
by guest on Septem
ber 4, 2016D
ownloaded from

274 J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281
administration of a maximal vasodilatory dose of in- Coronary resistance prior to and during adenosinetracoronary adenosine, and MRI studies to assess myocar- infusion was calculated as mean arterial pressure (mm Hg)
21 21dial function and perfusion. At the end of these studies, divided by coronary blood flow (ml min g ). For dataanimals were sacrificed by direct intracardiac administra- presentation, myocardial blood flow is given as a weightedtion of KCl. Myocardial samples were collected for average of flows in subendocardial, mid-myocardial, anddetermination of coronary flow in ischemic and normally subepicardial regions.perfused myocardium as previously described [4,5].
2.4. Magnetic Resonance (MR) imaging2.2. Coronary angiographic evaluation
MR imaging was performed in the body coil of a 1.5Evaluation of angiographic collateral density was per-Tesla whole-body Siemens Vision system. Baselineformed by two experienced angiographers, blinded toanatomic images were obtained by a turboFLASH tech-treatment assignment. The ‘collateral index’ was assessednique [19] to identify coordinates for apical four-chamber,for left to left (LAD to LCX or LCX to LCX) and right totwo-chamber, and short-axis views and to locate any areasleft (RCA to LCX) collaterals using a standard 4 pointof myocardial infarctions. Functional imaging was per-scale (05no visible collateral vessels, 15faint filling offormed during breath-hold and the time series of imagesside branches of the main epicardial vessel, without fillingwere then analyzed to define the size and severity of thethe main vessel, 25partial filling of the main epicardialcontrast arrival deficit. MR image analysis was performedvessel, 35complete filling of the main vessel) [15,16].on a dedicated Sun Microsystems workstation using auto-Differences in score assignment between the observersmated object recognition software to define myocardialwere resolved by joint film review.borders, to correct misregistrations, and to explore atinteractive speed the time intensity curves. From the
2.3. Myocardial blood flow endocardial border image, the floating centroid center ofmass was determined with the aid of computer software
To determine the extent of the LCX territory at risk, a and radials were extended to the epicardial border [20].set of colored microspheres (1560.1 mm diameter, Triton For assessment of myocardial perfusion and infarctionTechnology Inc., San Diego, CA) was injected prior to the size, the presence of myocardial blood flow was de-ameroid constrictor placement [5] with the LCX artery termined by measuring the intensity of the gadodiamide-held transiently occluded. At the time of analysis, sections enhanced signal in the different parts of the LV wall andof the myocardium containing ,10% of microspheres generating a space-time map of myocardial perfusion asfrom this set were considered to belong to the LCX previously described [14]. Areas of myocardium demon-territory at risk. strating no increase in contrast intensity (defined as ,25%
For determination of regional myocardial blood flow 3 increase in baseline value) were considered to have noand 6 weeks after ameroid placement, an angiographic significant perfusion and were taken to represent areas ofcatheter was advanced into the left atrium retrograde infarction. The extent of such territories as well asthrough the mitral valve and a set of colored microspheres territories demonstrating delayed contrast arrival was6(10 ) was forcefully injected after verification of catheter calculated as previously described [14] as a percent of totalplacement. Reference blood samples were withdrawn using LV volume. In addition, the presence of myocardiala syringe pump at a constant rate of 4 ml /min through the necrosis was confirmed by visual macroscopic and his-femoral artery. In addition to resting blood flow determi- tological analysis of myocardial tissues.nation at the time of final study, an additional set ofmicrospheres was injected after maximal coronary vasodi-lation was achieved by adenosine infusion (1.25 mg/kg/ 2.5. Statisticsmin) into the central circulation [17].
Following sacrifice, with the heart excised and the left All data are expressed as mean6SD. A p value of lessventricle dissected free of other structures, a trans-axial than or equal to 0.05 was considered significant. Com-slice approximately 1 cm thick was cut at the mid- parison of angiographic collateral density via the ‘collater-ventricular level. From this slice, eight radial samples were al index’ was assessed among all groups by the Kruskall–obtained and processed as previously described [4,5]. Wallis test for non-parametric, ordinal data. Changes in
21 21Regional myocardial flow (expressed in ml min g ) was angiographic collateral scores before and after treatmentcalculated as [18]: over the course of the study within a group were assessed
by the Wilcoxon rank-sum test for paired ordinal non-Blood flow(tissue sampleX)parametric data. One way analysis of variance and Bonfer-
215Withdrawal rate(ml min ) /weight(tissue sampleX)(g) roni-corrected t-tests were used for multiple group com-
3 OD(tissue sampleX) /OD(reference blood sample) parisons.
by guest on Septem
ber 4, 2016D
ownloaded from
J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281 275
3. Results therapy, (6 weeks after ameroid placement), there was nosignificant differences among the groups with regard to
Forty animals underwent placement of ameroid constric- LAD territory perfusion. Analysis of flow in the LCXtors. Two animals died in the immediate post-op period territory showed that all three VEGF-treated groups dem-and another two died prior to 3 week base-line evaluation onstrated a significant increase in the resting blood flowpoint. In all cases the cause of death appeared to be acute compared to pre-treatment flow (paired t-test) whilemyocardial infarction due to premature LCX occlusion. control animals showed no significant change in LCXThree animals died during surgery for VEGF pump place- perfusion (Fig. 2). Analysis of variance showed no differ-ment due to surgical complications of repeat thoracotomy. ence between the three VEGF treatment groups with regardThe remaining thirty-three animals (local VEGF, n510, to LCX perfusion. Combining all VEGF groups togetherintracoronary bolus VEGF, n57, pump VEGF, n57, showed that VEGF treatment resulted in LCX perfusioncontrol, n59) completed the entire study. MR data were that was equal to that seen in the LAD territory (LCX vs.
21 21not available in two control animals due to data acquisition *LAD: 1.1660.39 vs. 1.1560.28 ml*min g , p5NS).problems. At the same time LCX flow in VEGF-treated animals was
significantly higher than in controls (VEGF vs. control:21 21*1.1660.39 vs. 0.8560.21 ml*min g , p50.04).3.1. Coronary angiography
To further assess the impact of VEGF treatment oncoronary perfusion, coronary vasodilation was induced byAll coronary angiograms were analyzed with blinding toadministration of adenosine into the central circulation inthe treatment group and the timing (first or second) of thethe amount previously demonstrated to induce maximalangiogram. Disagreement in assignment of collateral indexcoronary vasodilation [17] and maximal increase in cor-score was adjudicated by joint film review in 12.5% of allonary blood flow in this model [21]. Calculations ofangiograms.coronary resistance demonstrated an expected significantAnalysis of changes in the extent of coronary collaterals
(collateral index) and the origin (LAD or LCX→LCX or reductions in resistance in the LAD territory in all fourRCA→LCX) of collateral vessels was carried out for each groups (Fig. 3A). At the same time, LCX resistanceof four groups by comparing angiograms performed before following adenosine infusion significantly decreased in theand after therapy. There was a significant increase in three VEGF-treated groups but not in control animalscollateral index for left-to-left (LAD→LCX or (compared to pre-adenosine values; paired t-test, see Fig.LCX→LCX) collaterals for all three VEGF-treated but not 3B), suggesting the presence of impaired vasodilatorycontrol group (Fig. 1A, Wilcoxon signed rank test). reserve in the LCX bed in control animals that wasHowever, there was no change in the number of reversed by VEGF administration. The reductions inRCA→LCX collaterals in any of the groups as assessed by coronary resistance (and the increase in coronary bloodthe collateral index (Fig. 1B). Thus, administration of flow) in these settings is somewhat lower than the 3.5–4VEGF into the left coronary system resulted in a direction- fold change usually seen in dogs due to a rapid drop inal increase in collateral circulation regionally restricted to systemic blood pressure that limits coronary perfusionthe left but not right coronary system suggesting a local during colored microspheres injections. However, directeffect of VEGF administration. measurements of coronary blood flow during adenosine
infusion in this model demonstrate on the average a 3.5fold increase in coronary blood flow [21].3.2. Myocardial blood flow
In addition to coronary blood flow analysis, MR-basedperfusion assessment of the myocardium was carried out atTo confirm the angiographic evidence of improved3 and 6 week time points. The size of the zone of delayedperfusion following VEGF therapy, regional myocardialcontract arrival was similar in all groups 3 weeks afterblood flow in the LCX and LAD territories was analyzedameroid occluder implantation (control: 1565.5, localimmediately before and after initiation of VEGF therapy.VEGF: 2266.4, i.c. VEGF: 18613, pump VEGF:In addition, coronary resistance in both the LCX and LAD1668.3% LV volume, F51.77, p5NS by ANOVA).beds was assessed during adenosine-induced maximalHowever, at the time of final study all VEGF groupsvasodilation at the time of final study.
Three weeks after implantation of ameroid occluders demonstrated a marked reduction in the size of delayedresting myocardial blood flow in the LCX territory was arrival zone while the control group showed no significantsimilarly reduced in all four groups and was significantly change (Fig. 4). Comparison of the size of the zone at thelower than flow in the LAD territory in all animals (LCX time of final study between the four groups demonstrated
21 21*vs. LAD: 0.7660.35 vs. 0.9660.38 ml*min g , p5 marked differences (F55.17, p50.006) with significant0.03). At the same time, there were no differences between reductions ( p,0.05 by Bonferroni t-tests) in animalsthe groups with regard to both LCX (Fig. 2) and LAD treated with local intracoronary and pump administration(data not shown) flows. Three weeks following initiation of of VEGF.
by guest on Septem
ber 4, 2016D
ownloaded from

276 J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281
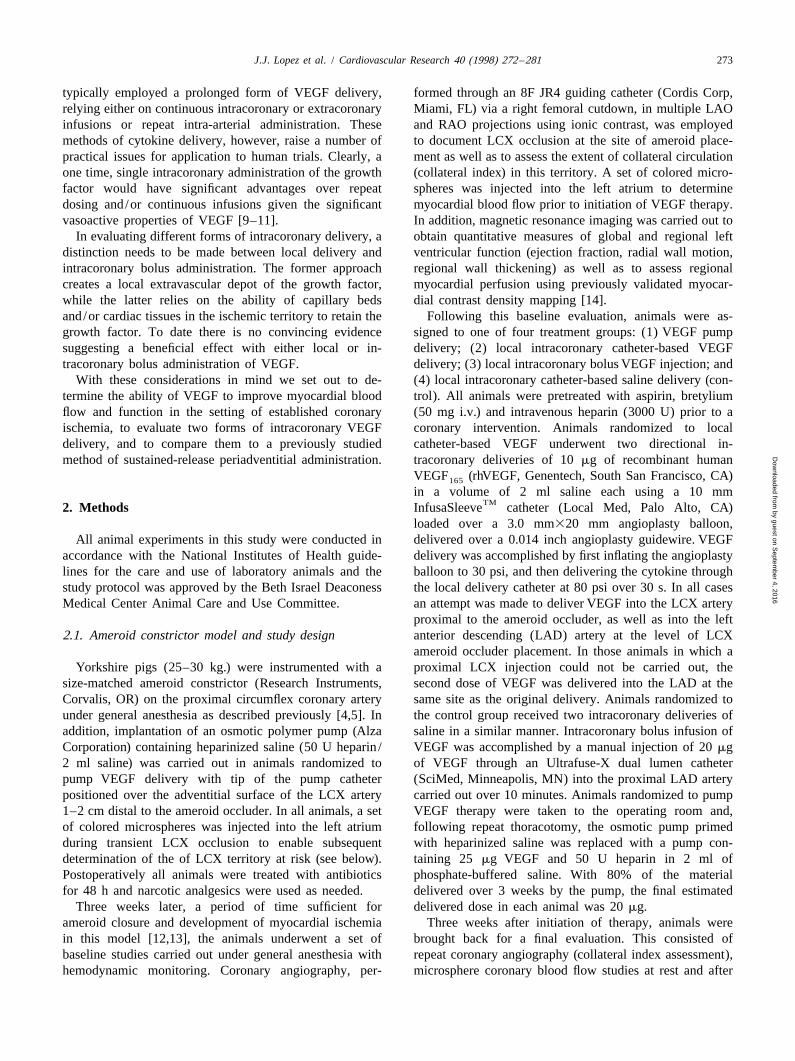
Fig. 1. Collateral index. Changes in the collateral index scores between initial (3 week pre-treatment) and follow-up (6 weeks post-treatment) angiogramsfor collaterals originating from the left anterior descending or left circumflex coronary arteries (Fig. 1A), or the right coronary artery (Fig. 1B) in pigssubjected to local delivery of VEGF (top left), intracoronary VEGF infusion (bottom left), control local delivery (top right), and VEGF pump implantation(bottom right). P-values are for Wilcoxon rank sum test for paired non-ordinal data.
by guest on Septem
ber 4, 2016D
ownloaded from
J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281 277
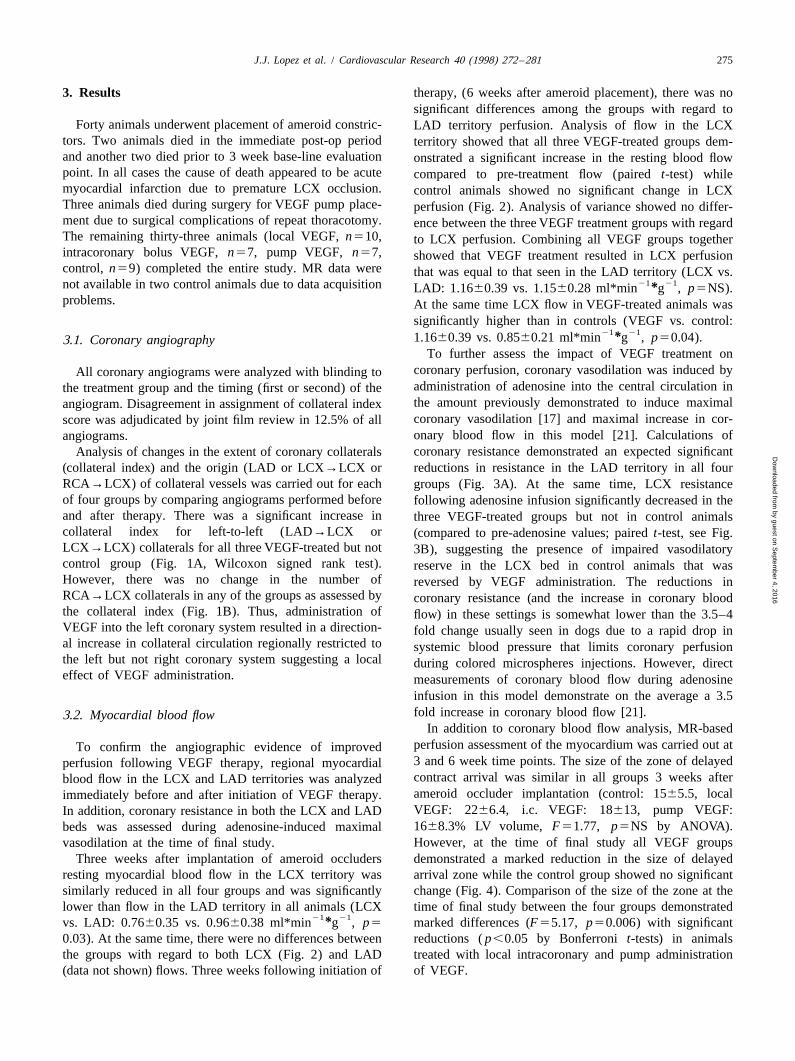
Fig. 2. Effect of VEGF administration on coronary blood flow. ChangesFig. 3. Effect of VEGF Administration on coronary flow reserve.in the pre-treatment (black bars) and post-treatment (gray bars) micro- -1 -1*21 21 Coronary resistance (mm Hg/ml*min g ) was determined prior to*sphere-determined rest coronary blood flow (ml*min g ) for the left(dark bars) and following administration of maximally vasodilating dosecircumflex (Fig. 2A) and left anterior descending (Fig. 2B). Noteof adenosine. A significant decline in the LAD territory resistance is seenincreased rest coronary blood flow in all 3 VEGF treatment groupsall 4 groups (Fig. 3A) while only VEGF-treated groups showed a(Local, local VEGF delivery; i.c., intracoronary VEGF bolus delivery;significant decline in coronary resistance in the LCX territory (Fig. 3B).pump, pump VEGF delivery) in the LCX but not the LAD territory.(Local, local VEGF delivery; i.c., intracoronary VEGF bolus delivery;* p,0.05, post-treatment vs. pre-treatment (paired t-test).pump, pump VEGF delivery). * p,0.05 vs. control (ANOVA, Bonferronit-test); 3p,0.05 post-adenosine vs. pre-adenosine (paired t-test).
3.3. Left ventricular functionextent of myocardial necrosis among any groups at either 3
To assess the functional significance of VEGF-mediated weeks (control: 1.363.1, local VEGF: 1.663.5, i.c. VEGF:improvement in myocardial blood flow, we employed MR 3.067.3, pump VEGF: 3.064.8% LV volume, ANOVA,imaging to assess global and regional myocardial function p5NS) or 6 weeks (control: 1.162.8, local VEGF:in all study animals. The porcine ameroid occlusion model 1.763.5, i.c. VEGF 4.767.8, pump VEGF: 3.464.4% LVis associated with the development of small areas of left volume, ANOVA, p5NS).ventricular myocardial necrosis in most animals [13]. To Left ventricular ejection fraction determined at rest threeexclude the possibility that differences in infarct size could weeks following occluder implantation was similar in allaffect comparisons of ventricular function between differ- treatment groups and was within normal limits for thisent groups, the extent of myocardial necrosis in each group model of intubated closed-chest pigs (control, 4662.6;was assessed by MR imaging at the time of treatment local, 4861.2%; intracoronary, 4962.7%; pump,initiation (3 weeks post-ameroid implantation) and at the 4962.1%; ANOVA, p5NS). Analysis of wall thickeningtime of final study (6 weeks), with myocardial infarction in the anterior wall (LAD territory) likewise demonstrateddefined as areas of myocardium showing no increase in no difference among the groups (data not shown). At thecontrast signal intensity on perfusion imaging. Using this same time, there was evidence of impaired regional wallparameter, there was no significant differences in the motion (% wall thickening) in the LCX territory in all
by guest on Septem
ber 4, 2016D
ownloaded from
278 J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281
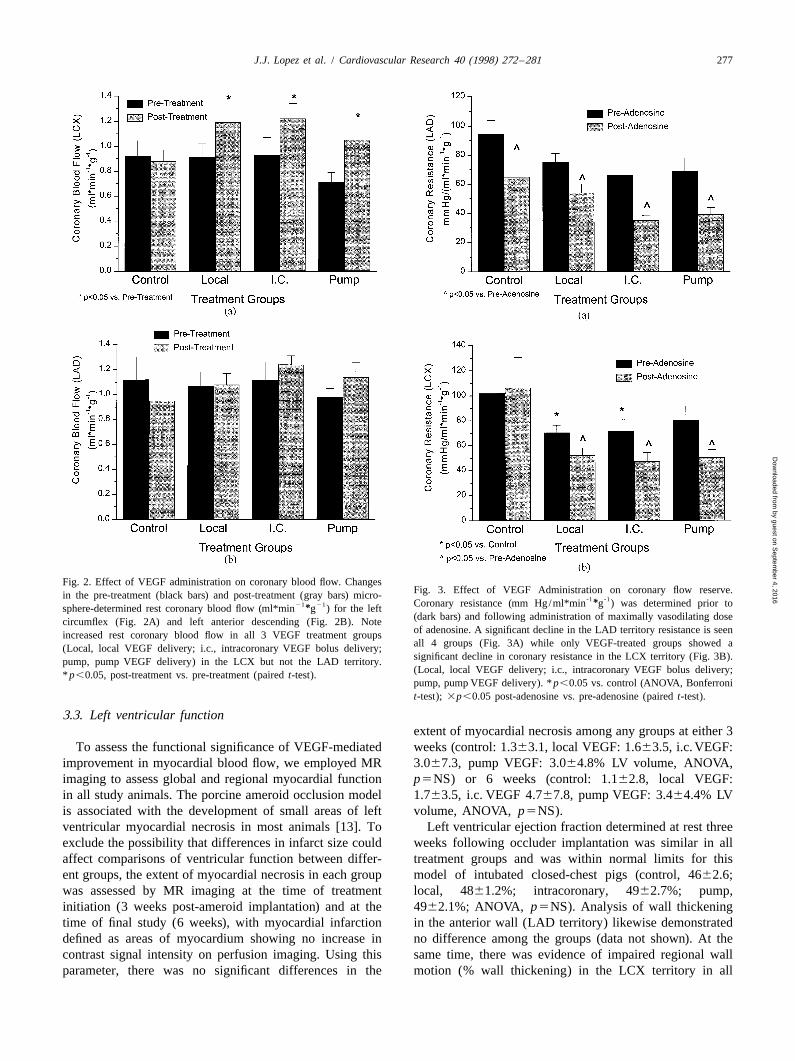
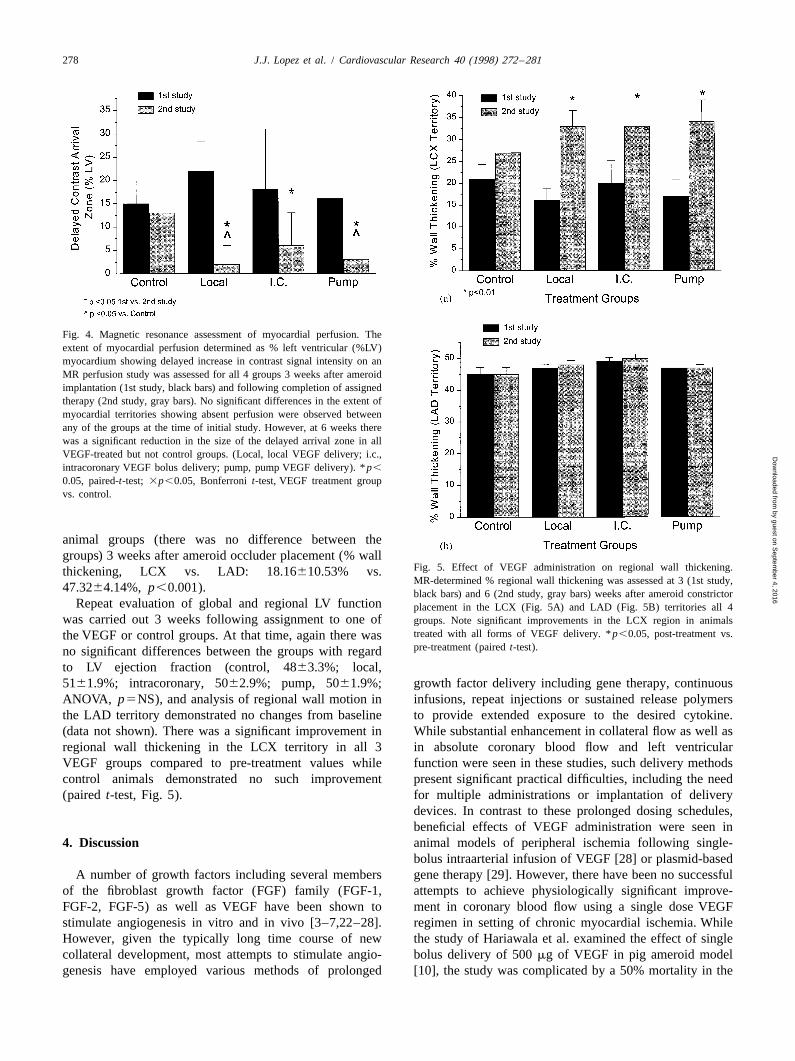
Fig. 4. Magnetic resonance assessment of myocardial perfusion. Theextent of myocardial perfusion determined as % left ventricular (%LV)myocardium showing delayed increase in contrast signal intensity on anMR perfusion study was assessed for all 4 groups 3 weeks after ameroidimplantation (1st study, black bars) and following completion of assignedtherapy (2nd study, gray bars). No significant differences in the extent ofmyocardial territories showing absent perfusion were observed betweenany of the groups at the time of initial study. However, at 6 weeks therewas a significant reduction in the size of the delayed arrival zone in allVEGF-treated but not control groups. (Local, local VEGF delivery; i.c.,intracoronary VEGF bolus delivery; pump, pump VEGF delivery). * p,
0.05, paired-t-test; 3p,0.05, Bonferroni t-test, VEGF treatment groupvs. control.
animal groups (there was no difference between thegroups) 3 weeks after ameroid occluder placement (% wall
Fig. 5. Effect of VEGF administration on regional wall thickening.thickening, LCX vs. LAD: 18.16610.53% vs.MR-determined % regional wall thickening was assessed at 3 (1st study,
47.3264.14%, p,0.001). black bars) and 6 (2nd study, gray bars) weeks after ameroid constrictorRepeat evaluation of global and regional LV function placement in the LCX (Fig. 5A) and LAD (Fig. 5B) territories all 4
was carried out 3 weeks following assignment to one of groups. Note significant improvements in the LCX region in animalstreated with all forms of VEGF delivery. * p,0.05, post-treatment vs.the VEGF or control groups. At that time, again there waspre-treatment (paired t-test).no significant differences between the groups with regard
to LV ejection fraction (control, 4863.3%; local,5161.9%; intracoronary, 5062.9%; pump, 5061.9%; growth factor delivery including gene therapy, continuousANOVA, p5NS), and analysis of regional wall motion in infusions, repeat injections or sustained release polymersthe LAD territory demonstrated no changes from baseline to provide extended exposure to the desired cytokine.(data not shown). There was a significant improvement in While substantial enhancement in collateral flow as well asregional wall thickening in the LCX territory in all 3 in absolute coronary blood flow and left ventricularVEGF groups compared to pre-treatment values while function were seen in these studies, such delivery methodscontrol animals demonstrated no such improvement present significant practical difficulties, including the need(paired t-test, Fig. 5). for multiple administrations or implantation of delivery
devices. In contrast to these prolonged dosing schedules,beneficial effects of VEGF administration were seen in
4. Discussion animal models of peripheral ischemia following single-bolus intraarterial infusion of VEGF [28] or plasmid-based
A number of growth factors including several members gene therapy [29]. However, there have been no successfulof the fibroblast growth factor (FGF) family (FGF-1, attempts to achieve physiologically significant improve-FGF-2, FGF-5) as well as VEGF have been shown to ment in coronary blood flow using a single dose VEGFstimulate angiogenesis in vitro and in vivo [3–7,22–28]. regimen in setting of chronic myocardial ischemia. WhileHowever, given the typically long time course of new the study of Hariawala et al. examined the effect of singlecollateral development, most attempts to stimulate angio- bolus delivery of 500 mg of VEGF in pig ameroid modelgenesis have employed various methods of prolonged [10], the study was complicated by a 50% mortality in the
by guest on Septem
ber 4, 2016D
ownloaded from
J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281 279
treatment group (four of eight animals) secondary to coronary flow in the chronically ischemic myocardium atrefractory VEGF-induced hypotension thereby rendering rest were seen following bFGF administration in the samethe results less than conclusive. model [26]. Additional evidence of VEGF-enhanced perfu-
With these considerations in mind, the present study was sion comes from examination of coronary resistancedesigned to assess the effectiveness of two forms of following adenosine infusion. As expected, there was aintracoronary delivery: single bolus intracoronary infusion substantial decline in resistance in the LAD territory in alland local catheter-based intracoronary delivery using a animals. At the same time, there was no significantlocal delivery catheter, and to compare them to a previous- reduction in LCX resistance in control animals suggestingly studied local adventitial delivery system using an decreased vasodilatory reserve in this territory. In contrast,implantable osmotic polymer pump, with regard to stimu- VEGF therapy was associated with restoration of adeno-lation of physiologically meaningful angiogenesis in a sine-induced vasodilation in the LCX territory thus demon-porcine model of chronic myocardial ischemia. strating improvement in vasodilatory reserve. MR analysis
To study these different means of VEGF delivery, we of tissue perfusion demonstrated marked reduction in theinitiated therapy three weeks after placement of ameroid size of the zone of delayed contrast arrival in VEGF-constrictors. This study design allowed us to document the treated but not control animals.ameroid occlusion prior to initiation of therapy and to In accord with microsphere-and MR-based determina-obtain serial data with regard to changes in coronary flow tions of improved tissue perfusion, angiographic analysisand left ventricular function in all study animals. Further- of collateral density demonstrated a significant increase inmore, this study protocol avoided potential complications the number of visible collateral vessels in all three VEGFassociated with initiation of therapy prior to the occluder groups but not in control animals. Interestingly, while thereplacement, given the theoretical potential of heparin-bind- was an increase in the number of left-to-left collaterals,ing growth factors such as VEGF to influence the rate of there was no increase in the number of right-to-leftconstrictor closure and thereby affect the final outcome. collaterals. It is not clear whether this spatial inhomo-
We found that ameroid constrictors were occluded in all geneity of collateral development is the result of growthstudy animals 3 weeks after placement. Comparison of left factor administration into the left coronary system, theventricular infarct sizes as well as global and regional left relative proximity of LAD and LCX but not LCX andventricular function parameters showed no differences RCA coronary branches in porcine hearts or some otheramong the four groups prior to initiation of treatment. unknown effect.Furthermore, the size of myocardial infarcts in all 4 groups In addition to improvement in angiographic collateral(1.2 to 5%) were within the range reported for this model index, and myocardial blood flow, VEGF therapy was[13]. Likewise, there were no significant differences in associated with significant recovery of regional left ven-absolute coronary flow values or the extent of MR-de- tricular wall motion in the LCX territory thus documentingtermined perfusion in either LCX or LAD territories functional benefit of cytokine-augmented angiogenesis inbetween the groups. We conclude, therefore, that all 4 this single dose treatment regimen.groups were closely matched with regard to coronary flow, This demonstration of VEGF efficacy in improvingleft ventricular function and infarction size prior to initia- coronary flow and function in myocardial ischemia furthertion of VEGF delivery. supports our prior observation demonstrating the beneficial
Implantation of ameroid occluders resulted in decreased effect of VEGF pump delivery in a similar model [5], asresting blood flow in the LCX compared to the LAD well as studies of Banai et al. in a dog ameroid constrictorterritory in all animals that was accompanied by reduced model [7] and single bolus VEGF administration inleft ventricular wall thickening and radial wall motion. The peripheral circulation model of chronic ischemia [28].subsequent recovery of these parameters suggests the However, these findings contrast with a recent study thatpresence of hibernating myocardium in this model. The found no beneficial effects of repetitive left atrial bolusespresence of chronically reduced blood flow in the LCX of VEGF in a canine model of myocardial ischemia [8].territory in control animals correlates with previously Potential explanations for this difference in outcomeobserved increases in expression of VEGF [5] as well as include handling of the growth factor, presence of adequateVEGF and bFGF receptors [30], all known to be sensitive amounts of heparin to prevent VEGF binding to tubing,to ischemia /hypoxia induction of expression [2], in the timing of growth factor delivery, as well as fundamentalLCX but not in normal (LAD) myocardium seen as long as physiological differences between the extensively col-8 weeks after ameroid implantation. lateralized dog and substantially less collateralized pig
VEGF administration by either local, intracoronary or ischemia models. The latter point is perhaps particularlyextravascular delivery was associated with a significant relevant given that previous studies using the same porcineimprovement in the coronary flow in the circumflex ameroid model have shown gradual improvements interritory at 3 weeks following initiation of therapy com- control animals progressing to almost complete restorationpared to flow values prior to treatment, while control of resting myocardial blood flow and function due toanimals showed no such improvement. Similar changes in spontaneous collateral development [31]. The time course
by guest on Septem
ber 4, 2016D
ownloaded from

280 J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281
[2] Ware JA, Simons M. Angiogenesis in ischemic heart disease. Natureof these changes however, is considerably longer thanMed 1997;3:158–164.could be monitored in the present study, suggesting that
[3] Yanagisawa-Miwa A, Uchida Y, Nakamura F, et al. Salvage ofVEGF therapy accelerates and perhaps augments endogen-infarcted myocardium by angiogenic action of basic fibroblast
ous angiogenesis. growth factor. Science 1992;257(5075):1401–1403.We did not observe any significant differences between [4] Harada K, Grossman W, Friedman M, et al. Basic fibroblast growth
factor improves myocardial function in chronically ischemic porcinethe three forms of VEGF delivery employed in this study.TM hearts. J Clin Invest 1994;94(2):623–630.InfusaSleeve , a local delivery catheter used in this
[5] Harada K, Friedman M, Lopez JJ, et al. Vascular endothelial growthstudy, achieves significant deposition of material into thefactor administration in chronic myocardial ischemia. Am J Physiolarterial wall with moderate (6 atm) pressure inflation [32].1996;270(5 Pt 2):H1791–H802.
Higher pressure inflations (30 atm) as used in this study, [6] Unger EF, Banai S, Shou M, et al. Basic fibroblast growth factorresults in periadventitial and intramyocardial deposition of enhances myocardial collateral flow in a canine model. Am J
Physiol 1994;266(4 Pt 2):H1588–H1595.the material; however the efficiency of this delivery system[7] Banai S, Jaklitsch MT, Shou M, et al. Angiogenic-induced enhance-still remains rather low (,2% of the total load, M. Simons
ment of collateral blood flow to ischemic myocardium by vascularand A. Kaplan, unpublished observations). The use of aendothelial growth factor in dogs. Circulation 1994;89(5):2183–local delivery device is potentially associated with a risk of2189.
local arterial complications (thrombosis, dissection, suba- [8] Lazarous DF, Shou M, Scheinowitz M, et al. Comparative effects ofcute closure) and a long-term risk of restenosis secondary basic fibroblast growth factor and vascular endothelial growth factor
on coronary collateral development and the arterial response toto injury-induced neointimal proliferation, although noneinjury. Circulation 1996;94:1074–1082.of these complications were observed in the current study.
[9] Ku DD, Zaleski JK, Liu S, Brock TA. Vascular endothelial growthThe potential benefit of local administration is the abilityfactor induces EDRF-dependent relaxation in coronary arteries. Amto achieve a desirable effect with a smaller dose of VEGFJ Physiol 1993;265(2 Pt 2):H586–H592.
thus minimizing hemodynamic effects associated with [10] Hariawala MD, Horowitz JJ, Esakof D, et al. VEGF improvesintracoronary bolus delivery [21]. myocardial blood flow but produces EDRF-mediated hypotension in
porcine hearts. J Surg Res 1996;63(1):77–82.It is important to consider several limitations of the[11] Yang R, Thomas G, Bunting S, et al. Effects of vascular endothelialstudy. First, the statistical analysis of inter-group com-
growth factor on hemodynamic and cardiac performance. J Cardiov-parison is based on post-hoc combination of control andasc Pharmacol 1996;27:838–844.heparin groups. Second, three VEGF pump animals that
[12] Longhurst J, Ordway G, Buja L. Evaluation of coronary native anddied during pump replacement may have had especially coronary collateral pressure gradients in the conscious dog. Am Jdeficient collateral supply thus contributing to a selection Cardiovasc Pathol 1987;1:79–90.
[13] Roth D, Maruoka Y, Rogers J, White F, Longhurst J, Bloor C.bias. Finally, degree of coronary vasodilation in responseDevelopment of coronary collateral circulation in left circumflexto adenosine seen in this study was somewhat less thanAmeroid-occluded swine myocardium. Am J Physiol 1987;253(5 Pttypically observed in similar settings. To some extent this2):H1279–1288.
difference may be attributable to general anesthesia and a [14] Pearlman JD, Hibberd MG, Chuang ML, et al. Magnetic resonancesomewhat low mean blood pressure in our study. mapping demonstrates benefits of VEGF-induced myocardial angio-
In summary, we observed significant improvements in genesis. Nat Med 1995;1(10):1085–1089.[15] Rentrop KP, Cohen M, Blanke H, Phillips RA. Changes in collateralmyocardial blood flow and regional myocardial function
channel filling immediately after controlled coronary artery occlu-following initiation of VEGF therapy in the setting of fullysion by an angioplasty balloon in human subjects. J Am Coll Cardiolestablished chronic myocardial ischemia in a porcine1985;5(3):587–592.
model. Thus single bolus intracoronary or local VEGF [16] Fujita M, Sasayama S, Asanoi H, Nakajima H, Sakai O, Ohno A.administration may prove to be useful therapeutic strate- Improvement of treadmill capacity and collateral circulation as agies for treatment of myocardial ischemia. result of exercise with heparin pretreatment in patients with effort
angina. Circulation 1988;77(5):1022–1029.[17] Carroll SM, White FC, Roth DM, Bloor CM. Heparin accelerates
coronary collateral development in a porcine model of coronaryAcknowledgements artery occlusion. Circulation 1993;88:198–207.
[18] Kowallik P, Schulz R, Guth BD, et al. Measurement of regionalSupported in part by NIH grants HL-46716 (FWS), myocardial blood flow with multiple colored microspheres. Circula-
tion 1991;83(3):974–982.HL-53793 (MS) and a grant from Genentech, Inc. Dr.[19] VanRugge FP, Botreel JJ, Van der Walls EE, et al. Cardiac first passLopez and Dr. Simons were also supported by the Clinical
myocardial perfusion in normal subjects assessed by sub-secondInvestigator Training Program, Beth Israel Hospital-Har- Gd-DPTA enhanced MR imaging. J Comp Assisted Tomogrvard /MIT Health Science and Technology, in collabora- 1991;15:959–965.tion with Pfizer, Inc. [20] Pearlman J, Hogan R, Wiske P, Franklin T, Weyman A. Ech-
ocardiographic definition of the left ventricle centroid; analysis ofmethods for centroid calculation from a single tomogram. J Am CollCardiol 1990;16(4):986–992.
References [21] Lopez J, Laham RJ, Carrozza JC, et al. Hemodynamic effects ofintracoronary VEGF delivery: evidence of tachyphylaxis and NO
[1] Folkman J, Shing Y. Angiogenesis. J Biol Chem 1992;267:10931– dependence of response. Am J Physiol 1997;273:H1317–H1323.10934. [22] Bauters C, Asahara T, Zheng LP, et al. Physiological assessment of
by guest on Septem
ber 4, 2016D
ownloaded from

J.J. Lopez et al. / Cardiovascular Research 40 (1998) 272 –281 281
augmented vascularity induced by VEGF in ischemic rabbit hind- artery augmentation in a rabbit model of chronic limb ischemia.limb. Am J Physiol 1994;267:H1263–H1271. Circulation 1994;90:II228–II234.
[23] Bauters, C., Asahara, T., Zheng, L.P. et al. Site-specific therapeutic [28] Takeshita S, Zheng LP, Brogi E, et al. Therapeutic angiogenesis. Aangiogenesis after systemic administration of vascular endothelial single intraarterial bolus of vascular endothelial growth factorgrowth factor. J Vasc Surg. 1995; 21(2): 314-24; discussion 324-5. augments revascularization in a rabbit ischemic hind limb model. J
[24] Banai S, Jaklitsch MT, Casscells W, et al. Effects of acidic fibroblast Clin Invest 1994;93(2):662–670.growth factor on normal and ischemic myocardium. Circ Res [29] Isner J, Walsh K, Symes J, et al. Arterial gene therapy for1991;69(1):76–85. therapeutic angiogenesis in patients with peripheral artery disease.
[25] Baffour R, Berman J, Garb JL, Rhee SW, Kaufman J, Friedmann P. Circulation 1995;91:2687–2692.Enhanced angiogenesis and growth of collaterals by in vivo ad- [30] Sellke FW, Wang SY, Stamler A, et al. Enhanced microvascularministration of recombinant basic fibroblast growth factor in a rabbit relaxations to VEGF and bFGF in chronically ischemic porcinemodel of acute lower limb ischemia: dose-response effect of basic myocardium. Am J Physiol 1996;271:H713–H720.fibroblast growth factor. J Vasc Surg 1992;16(2):181–191. [31] White F, Carroll S, Magnet A, Bloorm C. Coronary collateral
[26] Lopez JJ, Edelman ER, Stamler A, et al. Basic fibroblast growth development in swine after coronary artery occlusion. Circ Resfactor in a porcine model of chronic myocardial ischemia: a 1992;71(6):1490–1500.comparison of angiographic, echocardiographic and coronary flow [32] Gottsauner-Wolf M, Jang Y, Penn MS, et al. Quantitative evaluationparameters. J Pharmacol Exp Ther 1997;282:385–390. of local drug delivery using the InfusaSleeve catheter. Cathet
[27] Takeshita S, Pu LQ, Stein LA, et al. Intramuscular administration of Cardiovasc Diagn 1997;42(1):102–108.vascular endothelial growth factor induces dose-dependent collateral
by guest on Septem
ber 4, 2016D
ownloaded from