usaid okoa maisha dhibiti malaria (omdm) activity - pdf
TRANSCRIPT
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity QUARTERLY PERFORMANCE REPORT: YEAR 2, QUARTER 1
Submitted: January 31, 2020 This report was made possible by the generous support of the American people through the United States Agency for International Development (USAID) and the U.S. President’s Malaria Initiative (PMI). It was prepared by RTI International for the USAID | Okoa Maisha Dhibiti Malaria Activity.

USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity
QUARTERLY PERFORMANCE REPORT October 1–December 31, 2019
Cooperative Agreement Number: 72062118CA-00002 Contractual Period: August 7, 2018–August 6, 2023
Prepared for:
USAID | Tanzania U.S. Agency for International Development Office of Acquisition and Assistance
Prepared by
RTI International 3040 Cornwallis Road P.O. Box 12194 Research Triangle Park, NC 22709-2194
RTI International is one of the world’s leading research institutes, dedicated to improving the human condition by turning knowledge into practice. Our staff of more than 3,700 provides research and technical services to governments and businesses in more than 75 countries in the areas of health and pharmaceuticals, education and training, surveys and statistics, advanced technology, international development, economic and social policy, energy and the environment, and laboratory testing and chemical analysis.
RTI International is a registered trademark and a trade name of Research Triangle Institute.
The contents of this report are the responsibility of RTI International and do not necessarily reflect the views of USAID/PMI or the United States Government.
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report iii
Table of Contents 1. PROGRAM OVERVIEW ...........................................................................................................................1
1.1 Program Description ..........................................................................................................................1
1.2 Y2, Q1 Achievements ........................................................................................................................2
2. ACTIVITY IMPLEMENTATION PROGRESS ...........................................................................................7
2.2 Result 1: Malaria Surveillance Is Improved ........................................................................................7
Mainland Tanzania ....................................................................................................................................7
2.2.1 Activity 1A.1: Provide technical support to the SME community ..........................................7
2.2.2 Activity 1A.2: Support HMIS/DHIS2, eIDSR, and malaria surveillance implementation ....................................................................................................................8
2.2.3 Activity 1A.3: Strengthen MoHCDGEC and NMCP outbreak response capacity ............... 22
Zanzibar 24
2.2.4 Activity 1B.1: Support ZAMEP to update and implement the malaria surveillance strategy .............................................................................................................................. 24
2.2.5 Activity 1B.2: Develop interoperability between key HIS .................................................... 28
2.2.6 Activity 1B.3: Enhance and strengthen MCN ICT architecture and sustainability ............... 29
2.2.7 Activity 1B.4: Support MCN implementation ...................................................................... 31
2.2.8 Activity 1B.5: Refine operational thresholds and triggers as MCN data are analyzed ............................................................................................................................ 33
2.2.9 Activity 1B.6: Develop strategy and implementation plan to minimize malaria importation ......................................................................................................................... 34
2.3 Result 2: Entomological monitoring is improved ............................................................................... 35
2.3.1 Activity 2.1: Compile and review entomological monitoring data ........................................ 36
2.3.2 Activity 2.2: Conduct entomological monitoring planning and implementation ................... 37
2.3.3 Activity 2.4: Provide equipment and supplies for entomological monitoring ....................... 42
2.3.4 Activity 2.5: Entomological investigation and response in hot spot areas/active foci (Zanzibar only) ............................................................................................................ 42
2.3.5 Activity 2.6: Capacity building of new entomological field team in new emerging hot spots (Zanzibar only) ................................................................................................... 42
2.3.6 Activity 2.7: Strengthen national malaria vector control strategies, policies, and guidelines .......................................................................................................................... 42
2.4 Result 3: Drug efficacy monitoring is improved ................................................................................ 43
2.4.1 Activity 3.2: Plan, monitor, and implement TES ................................................................. 43
2.4.2 Activity 3.3: Provide equipment and supplies for TES ........................................................ 44
2.4.3 Activity 3.5: Strengthen national malaria case management strategies, policies, and guidelines ................................................................................................................... 45
2.5 Result 4: GOT’s evidence-based decision making is improved ........................................................ 45
2.5.1 Activity 4.1: Strengthen Tanzania’s capacity for state-of-the-art (SOTA) analysis and interpretation of surveillance, entomological, and drug efficacy data .......................... 45
2.5.2 Activity 4.2: Conduct SOTA analysis and interpretation of surveillance, entomological, and drug efficacy data ............................................................................... 46
2.5.3 Activity 4.3: Disseminate OMDM results through various channels ................................... 46
2.5.4 Activity 4.4: Implement Learning Agenda .......................................................................... 48
3. IMPLEMENTATION CHALLENGES ...................................................................................................... 49
4. GENDER CONSIDERATIONS ............................................................................................................... 50
5. ENVIRONMENTAL COMPLIANCE ........................................................................................................ 50
6. MEL PLAN: PROGRESS ON OMDM PERFORMANCE INDICATORS ................................................ 50
iv USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
7. MANAGEMENT ...................................................................................................................................... 50
7.1 Collaboration with OMDM partners and stakeholders ...................................................................... 50
7.2 List of all documents submitted to the Development Experience Clearinghouse ............................. 51
7.3 Certification that all participant training information has been entered in the TraiNet database .......................................................................................................................................... 51
8. UPCOMING EVENTS ............................................................................................................................. 51
ANNEX 1. PERFORMANCE INDICATOR SUMMARY TABLE .................................................................... 52
ANNEX 2. OMDM SUCCESS STORY ........................................................................................................... 59
List of Figures Figure 1. OMDM Results Framework ........................................................................................................1
Figure 2. Number of malaria cases 2017–2019 ...................................................................................... 17
Figure 3. Number of malaria cases by region 2017–2019 ....................................................................... 18
Figure 4. Malaria positivity by region 2017–2019 .................................................................................... 18
Figure 5. mRDT QC Results ................................................................................................................... 25
Figure 6. Screenshot from the MCN system highlighting the threshold features to trace an abnormal increase in malaria cases in December 2019 .................................................................. 30
Figure 7. Distribution of malaria cases investigated and classified October–December 2019 ............... 34
Figure 8. Efficacy residue of Actellic 300 CS in Zanzibar ........................................................................ 41
List of Tables
Table 1. Summary of progress during OMDM’s Y2, Q1 ............................................................................2
Table 2. DHIS2 Malaria Version 2 Dashboard issues raised with UDSM ............................................... 10
Table 3. Data review findings .................................................................................................................. 18
Table 4. Recommendations/follow-up from data review workshop ......................................................... 19
Table 5. Malaria data by lab register and OPD register .......................................................................... 23
Table 6. SWOT analysis of District Council Management Office visit ..................................................... 23
Table 7. Results of proficiency test per facility ........................................................................................ 25
Table 8. List of issues discussed during CMSO feedback meetings ....................................................... 32
Table 9. Q1 ACD activities ...................................................................................................................... 34
Table 10. Malaria vector collected per collection method, October–December 2019 .............................. 38
Table 11. Number of Anopheles collected by collection method and location ......................................... 39
Table 12. Treatment outcomes on day 28 ............................................................................................... 44
Table 13. OMDM implementation challenges ......................................................................................... 49
Table 14. OMDM Q1 collaboration with partners and stakeholders ........................................................ 50
Table 15. Upcoming events .................................................................................................................... 51
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report v
Abbreviations and Acronyms
ABER annual blood examination rate
ACD active case detection
ACPR adequate clinical and parasitological response
ALMA African Leadership Malaria Alliance
ALu artemether lumefantrine
ANC antenatal care
AOR Agreement Officer’s Representative
API application programming interface
App mobile application
ASTMH American Society of Tropical Medicine and Hygiene
CBR CDC light traps with collection bottle rotators
CBS case-based surveillance
CD continuous distribution
CDC U.S. Center for Disease Control and Prevention
CHMT Council Health Management Team
CHW community health worker
CLA Collaborating, Learning, and Adapting
CMC Community Mosquito Collectors
CMO Chief Medical Officer
CMS Central Medical Store
CMSO Council Malaria Surveillance Officer
CRT Council Response Teams
CUHAS Catholic University and Allied Sciences
DHIS2 District Health Information System 2
dLAB Tanzania Data Lab
DMO District Malaria Officer
EDS electronic data system
eIDSR electronic Integrated Disease Surveillance and Response
EHO environmental health officer
ETF early treatment failure
FAA fixed amount award
FELTP Field Epidemiology and Laboratory Training Program
FY fiscal year
vi USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
GFATM Global Fund to Fight AIDS, Tuberculosis and Malaria
GOT Government of Tanzania
HBC home-based care
HC health center
HFR health facility register
HIS health information system
HLC human landing catch
HMIS health management information system
ICT information and communication technology
ICT4D Information and Communications Technologies for Development
IDSR Integrated Disease Surveillance Response
IDWE infectious disease weekly ending
IHI Ifakara Health Institute
IPD inpatient department
IPTp3 intermittent preventive treatment in pregnancy 3
IRS indoor residual spraying
JPPM Joint Partner Program Monitoring
KCMC Kilimanjaro Christian Medical Centre
LOA letter of authorization
LLIN long-lasting insecticidal net
LCF late clinical failure
LPF late parasitological failure
LTC CDC-light trap collection
MDA mass drug administration
M&E monitoring and evaluation
MCN malaria case notification
MEEDS Malaria Epidemic Early Detecting System
MEL monitoring, evaluation, and learning
MERLA monitoring, evaluation, research, learning, and adapting
MLC man-landing catches
MoEST Ministry of Education, Science and Technology
MOHZ Ministry of Health (Zanzibar)
MoHCDGEC Ministry of Health, Community Development, Gender, Elderly and Children
mRDT malaria rapid diagnostic test
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report vii
MSD medical store department
MSDQI malaria services and data quality improvement
MTR malaria mid-term review
MUHAS Muhimbili University of Health and Allied Sciences
MVS malaria vector surveillance
MVES malaria vector entomological surveillance
NIMR National Institute for Medical Research
NMCP National Malaria Control Program
OAA Office of Assistance and Acquisition
OMDM Okoa Maisha Dhibiti Malaria Activity (Save Lives, End Malaria)
OPD outpatient department
OR operational research
PBO piperonyl butoxide
PCR polymerase chain reaction
PHLB Private Health Laboratories Board
PMI U.S. President’s Malaria Initiative
PO-RALG President’s Office—Regional Administration and Local Government
PSC pyrethrum spray catch
PTC pit trap catch Q1/2/3/4 quarter 1/2/3/4
QA quality assurance
QC quality control
RCH reproductive and child health
RDT rapid diagnostic test
RHMT Regional Health Management Team
RMFP Regional Malaria Focal Person
RMO Regional Medical Officer
SBCC social behavior change communication
s.l. sensu lato
SME surveillance, monitoring and evaluation
SMPS School Malaria Parasitemia Survey
SMSP Supplemental Malaria Strategic Plan 2018–2020
SOTA state of the art
s.s. sensu stricto
viii USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
SUA Sokoine University of Agriculture
Swiss TPH Swiss Tropical and Public Health Institute
TA technical assistance
TAPAMA Tanzania Parliamentarians Against Malaria
TBD to be determined
TES therapeutic efficacy studies
TMDA Tanzania Medicine & Medical Devices Authority
ToR terms of reference
TWG technical working group
UDSM University of Dar es Salaam
USAID U.S. Agency for International Development
USSD Unstructured Supplementary Service Data
VEO village executive officer
WEO ward executive officer
WHO World Health Organization
Y1/2/3/4 Year 1/2/3/4
ZAMEP Zanzibar Malaria Elimination Program
ZBC Zanzibar Broadcasting Corporation
ZMEAC Zanzibar Malaria Elimination Advisory Committee
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 1
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity
1. Program Overview
Program Name: Okoa Maisha Dhibiti Malaria (OMDM) Activity
Activity Start and End Dates: August 7, 2018 to August 6, 2023
Prime Implementing Partner: RTI International
Cooperative Agreement Number:
72062118CA00002
Geographic Coverage: Mainland Tanzania and Zanzibar
Reporting Period: Year 2, Quarter 1: October 1–December 31, 2019
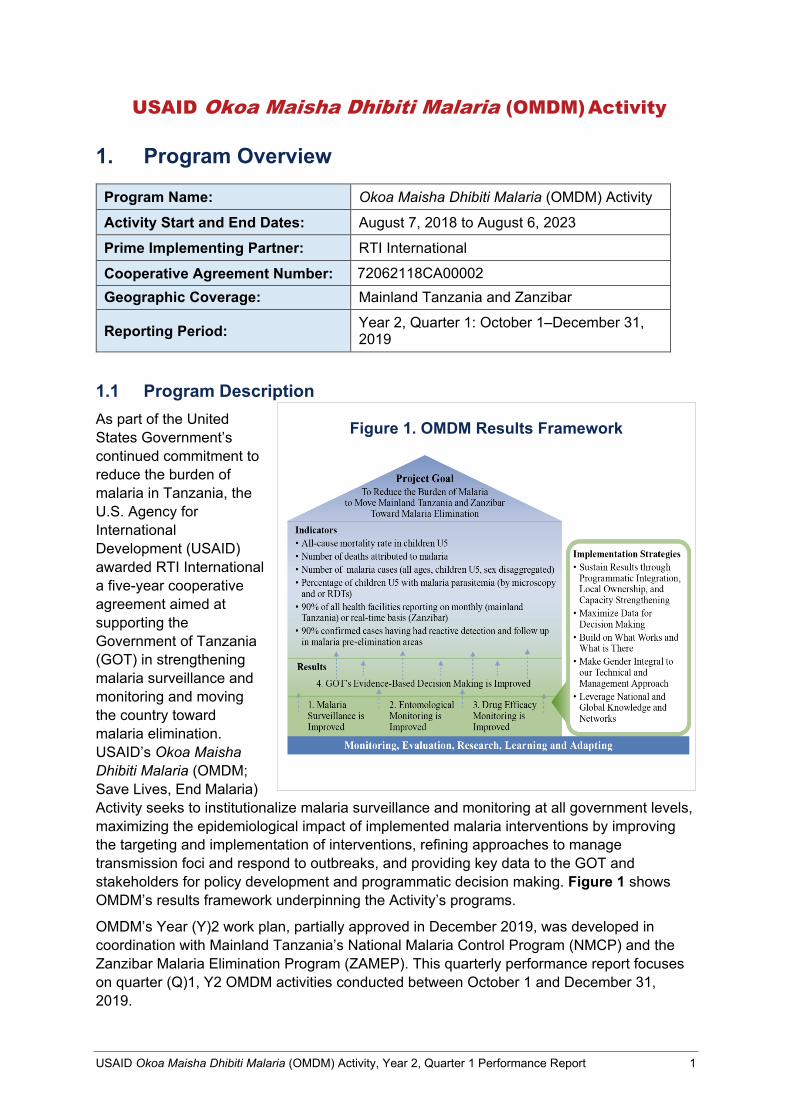
1.1 Program Description As part of the United States Government’s continued commitment to reduce the burden of malaria in Tanzania, the U.S. Agency for International Development (USAID) awarded RTI International a five-year cooperative agreement aimed at supporting the Government of Tanzania (GOT) in strengthening malaria surveillance and monitoring and moving the country toward malaria elimination. USAID’s Okoa Maisha Dhibiti Malaria (OMDM; Save Lives, End Malaria) Activity seeks to institutionalize malaria surveillance and monitoring at all government levels, maximizing the epidemiological impact of implemented malaria interventions by improving the targeting and implementation of interventions, refining approaches to manage transmission foci and respond to outbreaks, and providing key data to the GOT and stakeholders for policy development and programmatic decision making. Figure 1 shows OMDM’s results framework underpinning the Activity’s programs.
OMDM’s Year (Y)2 work plan, partially approved in December 2019, was developed in coordination with Mainland Tanzania’s National Malaria Control Program (NMCP) and the Zanzibar Malaria Elimination Program (ZAMEP). This quarterly performance report focuses on quarter (Q)1, Y2 OMDM activities conducted between October 1 and December 31, 2019.
Figure 1. OMDM Results Framework
2 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
1.2 Y2, Q1 Achievements Table 1 summarizes OMDM’s progress toward achieving results during Q1. Please see Section 2 and Annex 1 for additional detailed information regarding progress under each activity.
Table 1. Summary of progress during OMDM’s Y2, Q1
OMDM Result Areas Y2, Q1 Achievements Result 1: Malaria surveillance is improved MAINLAND TANZANIA
Activity 1A.1: Provide technical support to Surveillance, Monitoring, and Evaluation Unit (SME) community
• OMDM reviewed and provided inputs into the terms of reference (TOR) of the Surveillance, Monitoring, and Evaluation Unit’s (SME) Technical Working Group (TWG). Technical assistance (TA) was provided to the NMCP to ensure the TWG becomes operational.
Activity 1A.2: Support Health Information Management System (HMIS)/District Health Information System 2 (DHIS2), electronic Integrated Disease Surveillance and Response (eIDSR), and malaria surveillance implementation
• From October 22–29, 2019, The Ministry of Health, Community Development, Gender, Elderly, and Children (MoHCDGEC) convened various stakeholders in Arusha to review and adopt the 3rd edition of the eIDSR Guidelines.
• On November 5, 2019, OMDM’s Information and Communication Technology (ICT) Specialist met with representatives from the University of Dar es Salaam (UDSM), NMCP, and Swiss Tropical and Public Health (Swiss TPH) to discuss the latest system upgrades to the DHIS2 led by UDSM. This meeting the Activity to help the NMCP and Swiss TPH to monitor progress on the system upgrades and enhancements, and plan for follow-up discussions with UDSM to ensure timely completion of the upgrades.
• From November 11–16, 2019, OMDM facilitated a meeting in Morogoro between the NMCP and MoHCDGEC to discuss in depth the status of the malaria composite database. Nineteen participants from OMDM, NMCP, MoHCDGEC (ICT, HMIS & Epidemiology Units), Swiss TPH, USAID Boresha Afya, and Ifakara Health Institute (IHI) were part of the discussions.
• OMDM conducted its first data review workshop with the NMCP on December 11, 2019 in Dodoma. Nine participants comprised of staff from the SME, Vector Control and Case Management Units and three OMDM staff were part of the data review meeting.
• From November 19–22, 2019, OMDM staff visited our new office at the NMCP’s University of Dodoma compound. Having OMDM staff onsite increases opportunities for hands-on coaching, mentoring, and support to the NMCP’s SME Unit. OMDM’s space is on the 2nd floor of the NMCP’s office.
• From November 26–29, 2019, OMDM participated in a workshop organized by the African Leadership Malaria Alliance (ALMA) and the NMCP in Morogoro. The workshop, Operationalizing Tanzania’s malaria scorecard management tool, was designed to orient Regional Malaria Focal Persons (RMFP) on the tool.
Activity 1A.3: Strengthen MoHCDGEC and NMCP outbreak response capacity
• OMDM completed preliminary analysis of eIDSR data in Q4 of Y1 and initiated development of a draft publication. This publication will be completed over the course of Y2 in collaboration with U.S. President’s Malaria Initiative (PMI) and NMCP.
• OMDM participated in the NMCP’s 5-day Case Based Surveillance (CBS) Workshop in Moshi from October 6–12 2019.
ZANZIBAR
Activity 1B.1: Support ZAMEP to update and implement malaria surveillance strategy
• Under ZAMEP’s fixed amount award (FAA) with OMDM, the Case Management and Diagnosis Unit undertook 5,176 blood microscopy examinations for malaria diagnosis as part of quality assurance (QA)/quality control (QC) monitoring. 30 slides tested positive, with sensitivity at 93.3% and specificity at 100%.
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 11
OMDM Result Areas Y2, Q1 Achievements • Proficiency testing of malaria examinations conducted by individual
laboratory technicians was done during ZAMEP’s supervision visits in Q1. 6 of the 24 technicians assessed scored above 85% in malaria parasite speciation and quantification. However, overall performance did not reach the World Health Organization’s (WHO) recommendations.
• Supervision visits were conducted by ZAMEP at 91 public health facilities to assess the usage, availability, and quality of diagnostic services. Of the 99,754 patients across Zanzibar’s 93 health facilities, 16.2% (n=16,118) were screened for malaria antigens using SD-Bio line malaria rapid diagnostic test (mRDT) kits. Of these, 276 (1.7%) revealed malaria antigens with differentiate of Plasmodium falciparum (64.13%; n=177), Pan (1.8%; n=5) and P. falciparum plus Plan (34.05%; n=94).
• ZAMEP conducted a 3-day training for 30 health care providers from public and private health facilities on current malaria management recommendations from the WHO. The training was designed was to update the health care providers’ knowledge, skills and practices on understanding a patient’s prior history and current management of malaria cases.
• Monitoring and supervision of continuous net distribution activities was conducted in 52 health facilities (30 Pemba, 22 Unguja) that distribute long lasting insecticide nets (LLIN) and in 65 shehia (30 Pemba, 35 Unguja). The objective of this activity was to assess the progress of net distribution activities and provide technical support to ensure that distribution is implemented as planned.
• A total of eight live television programs and ten live radio programs were aired in Q1. The programs were designed to increase community understanding of key malaria elimination interventions.
• ZAMEP’s Social Behavior Communication Change (SBCC) Unit printed and distributed a total of 845 calendars embedded with malaria elimination messages. The embedded messages emphasize utilization of key malaria elimination interventions including continuous net use, participation in indoor residual spraying (IRS) activities, larviciding, early health-seeking behavior, and cleanness of living environment to eliminate malaria breeding sites and other malaria risk factors.
• ZAMEP conducted 16 community meetings in malaria hotspot areas. The meetings were designed to sensitize community members living in those areas on the importance of adhering to malaria elimination interventions. Meetings were conducted in the following shehia in Unguja: Mnazi Mmoja, Kiponda, Malini, Shangani, Mkunazini, Kikwajuni Bondeni, Kikwajuni Juu, Kisiwandui, Kisima Majongoo, Mtowa Pwani (Fungu Refu), Bumbwini and Kiongwe. The same meetings were conducted in Tumbe Mashariki and Piki shehia in Pemba.
Activity 1B.2: Develop interoperability between key health information systems (HIS)
• In Q1 of Y2, OMDM continued work on the following integration activities: 1. Finalized malaria indicators to be integrated across malaria
surveillance systems; 2. Added selected indicators into a DHIS2 test server; 3. Harmonized organizational units between the malaria case
notification (MCN) system and DHIS2; 4. Developed scripts for synchronizing aggregated data between the
MCN and DHIS2; and, 5. Defined required dashboards and began developing them within
DHIS2.
Activity 1B.3: Enhance and strengthen malaria case notification (MCN) information and ICT architecture and sustainability
• In Q1, OMDM developed a capacity building plan detailing relevant training and mentoring required over the course of Y2 to capacitate ZAMEP staff to manage malaria surveillance systems. Essentially, we are proposing to follow the approach used by DHIS2 which distinguishes between end users, integrators and developers. End users refer to people that use the system and includes both data collection-oriented users like Council Malaria Surveillance Officers (CMSO) as well as data consuming users like the SME unit at ZAMEP. Integrators are those responsible for configuring and updating the system so that it continues to meet the ZAMEP’s needs. Developers are focused on a full understanding of the system architecture and software and are responsible for managing the server and database
4 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
OMDM Result Areas Y2, Q1 Achievements and making necessary changes to the software in order to facilitate new
features or fix bugs. • Based on existing threshold values utilized by ZAMEP, OMDM introduced a
feature in the MCN system that automatically detects abnormal increases in malaria cases.
• In addition to the epidemic thresholds feature that was activated in the MCN, OMDM has continued to improve on the automated weekly report, based on useful feedback from PMI and other partners who receive the weekly reports from ZAMEP.
Activity 1B.4: Support MCN implementation
• Throughout Q1, OMDM made small updates to questions and skip logics in the Coconut App, specifically related to the travel history component of the tool, based on feedback from CMSOs using this software on their tablets during household visits.
• ZAMEP’s SME Unit continues to emphasize the importance of reporting data on time. In Q1, 82.5% of facilities submitted their reports on time (Monday). Unguja’s reporting rate was 85% for the period; in Pemba, the reporting rate was 80%.
• In Q1, supervision activities were conducted to 18 CMSOs (10, Unguja; 8, Pemba) to monitor data management performance, identify and correct any implementation challenges reported by CMSOs from health facilities to the household level. Additionally, ZAMEP conducted feedback meetings for CMSOs in both Pemba and Unguja.
Activity 1B.5: Refine operational thresholds and triggers as MCN data are analyzed
• During this quarter, 15 active case detection (ACD) events have been organized and conducted throughout Unguja and Pemba triggered by an abnormal increase of malaria cases following the continued rains. Eight ACD events were conducted in Unguja involving 3,194 mRDTs performed; 62 (1.9%) were positive for malaria infection. ZAMEP supported Council Response Teams (CRT) in Pemba to implement seven ACD events; 6,376 mRDTs were performed and 6 (0.09%) were positive for malaria infection.
Activity 1B.6: Develop strategy and implementation plan to minimize malaria importation
• In Q1, ZAMEP with support from OMDM continued monitoring the question sets in the Coconut app to detect any problems that may impact case classification outcomes. Of the 1,836 malaria cases investigated and classified, 1,092 (58%) were classified as imported, 768 as indigenous, 5 as introduced and 1 as induced.
Result 2: Entomological monitoring is improved
Activity 2.1: Compile and review entomological monitoring data
• In Q1, a draft report of compiled entomological surveillance data was submitted to ZAMEP for review. On November 15–16 2019, OMDM met with ZAMEP’s Entomology Unit to discuss the draft report and to support the team to write their annual entomological surveillance report. The final report of compiled entomological surveillance data will be disseminated in Q2.
• On November 28–29 2019, OMDM met with the NMCP’s Vector Control Unit to discuss and agree on the implementation plan for entomological monitoring activities in Y2. Issues discussed include the following: ⇒ How we can work together to continue activities initiated in Y1, such as
modalities to accelerate the inclusion of entomological indicators into a composite database. OMDM was requested to continue supporting the NMCP to create the malaria entomological database to be uploaded in DHIS2.
⇒ How we can work together to develop a mechanism to upload entomological monitoring data into a DHIS2 composite database.
⇒ The need to strengthen QA/QC of the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) supported malaria vector entomological surveillance (MVES) in 62 districts.
⇒ The need for a meeting to triangulate and analyze data and write a comprehensive report resulting from ongoing MVES activities.
⇒ The timeline of the vector control TWG meeting to discuss progress made in entomological surveillance.
• OMDM worked with the National Institute for Medical Research (NIMR) Mwanza and PMI and the US Centers for Disease Control and Prevention
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 5
OMDM Result Areas Y2, Q1 Achievements (CDC) to review the sentinel sites for entomological monitoring for 2019–
2020. This review focused on entomological monitoring in the 4 regions— Mwanza, Kagera, Geita, and Kigoma—where piperonyl butoxide (PBO) LLINs have been distributed. Entomological monitoring is required in these regions to align with NIMR Mwanza’s planned activities. All 4 regions where PBO nets are used have at least one non-IRS control district for entomological monitoring except for Mwanza; as such, one additional district (Magu) was added in Mwanza.
• In Q1, OMDM initiated development of a protocol to analyze the impact of IRS in Tanzania’s Lake Zone and Zanzibar.
Activity 2.2: Conduct entomological monitoring planning and implementation
• OMDM issued FAAs to NIMR Mwanza, NIMR Amani, and ZAMEP to support entomological monitoring in mainland Tanzania and Zanzibar in Y2.
• ZAMEP. Entomological monitoring in Zanzibar was conducted in 10 sites in both Unguja and Pemba. The entomological indicator monitored in Q1 was density; other parameters are awaiting completion of laboratory work.
• ZAMEP. Under their FAA with OMDM, ZAMEP continued IRS quality assurance activities in six shehias across Unguja and Pemba. Fifteen houses were selected for WHO cone bioassays in each shehia reflecting various wall surfaces including mud, cement, oil paint, water paint and stone block. Three houses representing each wall surface type were tested in each Shehia. Results indicate that Actellic 300 CS insecticide aged 210 days showed high mortality among malaria vectors in Pemba (mortality rate of >90%) as compared to Unguja (mortality rate of 64-72%) on all wall surfaces. At 240 days, Actellic 300 CS maintained the minimum effectiveness in Pemba and Unguja.
• NIMR Mwanza. In Q1, NIMR Mwanza conducted cone and fumigant bioassays in Muleba and Biharamuro following IRS operations using clothianidin. Similar bioassays were conducted in Kibondo, Kakonko and Kasulu districts which were sprayed with pirimiphos methyl (Actellic® 300CG) during IRS operations. The observed mortality for the wall cone bioassays on all surfaces was 100% days 2–6 post clothianidin exposure. A strong fumigant effect of clothianidin was also observed, with 100% mortality shown 1-2 days after insecticide exposure. Pirimiphos methyl (Actellic® 300CG) also showed a strong fumigant effect with 100% mortality shown one day after insecticide exposure. Two months post-IRS insecticide efficacy continued to retain up to 100% in all surfaces on all sites except in Kibondo district where mud, painted and whitewash surfaced were less than 50% mortality after 24 hours.
• Both NIMR Mwanza and ZAMEP continued maintaining their Anopheles gambiae s.s. colonies (Kisumu strain) in Q1. Production of adult mosquitoes continued to meet the required demands for IRS quality assessments and residual efficacy testing.
Activity 2.4: Provide equipment and supplies for entomological monitoring
• Worked with NIMR Mwanza, NIMR Amani and ZAMEP to identify entomological monitoring equipment, supplies and reagents needed for Y2 activities. Procurement of the identified equipment, supplies and reagents is underway.
Activity 2.5: Entomological investigation and response in hot spot areas/active foci (Zanzibar only)
• ZAMEP conducted foci investigations in three foci in Unguja and Pemba following an abnormal increase of local cases. The investigation aimed to assess the risk factors associated with disease transmission and develop recommendations to keep the situation under control. The risk factors investigated included demographic information, vector control interventions—particularly IRS and LLINs—at the household level, malaria vector characterization and presence of mosquito breeding sites. General findings showed the presence of outdoor biting of malaria vectors with the presence of mosquito breeding sites close to households. Larviciding was highly recommended as a way of reducing malaria transmission. SBCC intensification was also recommended to increase LLIN usage in foci areas.
Activity 2.6: Capacity building of new entomological field
No activities were conducted during the October–December 2019 reporting period.
6 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
OMDM Result Areas Y2, Q1 Achievements team in new emerging hot spot (Zanzibar only)
Activity 2.7: Strengthen national malaria vector control strategies, policies, and guidelines
• In Q1, OMDM discussed plans and potential dates for the vector control TWG meeting in Q2 with the NMCP.
• On November 14–16, 2019, OMDM supported ZAMEP to develop the larval source management operational guideline; the guideline was then reviewed by ZAMEP staff in a second meeting on 13th December. The final tool will be presented to ZAMEP management in Q2.
• On December 19, 2019, OMDM participated in a stakeholders meeting to kickstart the malaria midterm review (MTR) of ZAMEP’s malaria strategic plan; the MTR is planned for Q2.
Result 3: Drug efficacy monitoring is improved
Activity 3.2: Plan, monitor, and implement therapeutic efficacy studies (TES)
• OMDM initiated the process to issue an FAA with the Catholic University of Health and Allied Sciences (CUHAS) for TES implementation in 2020.
• OMDM supported the FY19 TES implementing partner, Muhimbili University of Health and Allied Sciences (MUHAS), in data analysis, interpretation and dissemination following 2019 TES.
• MUHAS analyzed other outcomes, including early treatment failure (ETF), late clinical failure (LCF), late parasitological failure (LPF) according to the 2009 WHO guidelines.
• The summary on adverse events, risk of recurrent infections per study sites and proportions of patients with parasitemia on days 1 to 3 and day 28 were also provided. These findings were presented at the TES TWG meeting held on November 5, 2019 at MUHAS.
Activity 3.3: Provide equipment and supplies for TES
• Supported the procurement of reagents and supplies to support NIMR Tanga’s molecular analysis activities of samples collected between 2018 and 2020.
Activity 3.5: Strengthen national malaria case management strategies, policies, and guidelines
• OMDM supported the TES TWG meeting on November 5, 2019, including participants from NMCP, MUHAS, NIMR and CUHAS; representatives from Kilimanjaro Christian Medical Centre (KCMC) and CDC/PMI were absent with apology. The meeting was updated on the progress of TES Implementation for 2019, supervision using the harmonized checklist, and planned training and molecular analysis 2017-2019 at NIMR and Sokoine University of Agriculture (SUA). Meeting minutes have been shared with all stakeholders.
Result 4: GOT’s evidence-based decision making is improved Activity 4.1: Strengthen Tanzania’s capacity for state- of-the-art (SOTA) analysis and interpretation of surveillance, entomological, and drug efficacy data
• In Q1, OMDM staff provided continuous mentorship and coaching around DHIS2, including its use and analysis, and in data review. Additionally,
OMDM’s Data Scientist was in Dodoma at the NMCP to support the SME Unit in their day to day activities from the December 8– 13, 2019.
Activity 4.2: Conduct SOTA analysis and interpretation of surveillance, entomological, and drug efficacy data
• Working with NMCP and ZAMEP, OMDM supported the analysis and interpretation of epidemiological and entomological data, specifically data showcasing malaria trends, case classification and seasonal variation in Zanzibar, and routine entomological data from both Zanzibar and mainland. Regular data review meetings with the NMCP has provided OMDM the opportunity to showcase useful information on malaria trends; these meetings are ongoing in Y2.
Activity 4.3: Disseminate OMDM results through various channels
• On November 20, 2019, OMDM participated in a meeting of representatives from national malaria programs in Washington, DC including representatives from five countries—Burkina Faso, Guinea, Senegal, Thailand, Tanzania, and Zanzibar. The primary meeting objective was to make connections to facilitate the sharing of best practices and lessons learned, discuss mutual priorities and challenges, and to highlight RTI’s network of programs working in malaria in other countries.
• OMDM worked with the NMCP to develop and disseminate the 8th edition of the Malaria Bulletin. Using routine data generated from DHIS2, the issue highlighted the malaria burden in Mainland Tanzania and provided an
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 7
OMDM Result Areas Y2, Q1 Achievements update on malaria indicators including the diagnosis of uncomplicated and
severe malaria; performance of intermittent preventive therapy of malaria in pregnant women (IPTp); and LLIN distribution at health facilities.
• On November 21–22, 2019, OMDM presented three posters (2 from OMDM staff; one from NIMR Mwanza Staff) at the American Society Tropical Medicine and Health (ASTMH) 68th Annual Meeting at National Harbor in Maryland, USA.
• On December 4–6, 2019, OMDM supported six participants (two from the NMCP; two from OMDM; one from HMIS-Zanzibar and one from ZAMEP) to attend the Data Tamasha workshop. Data Tamasha is a unique, local platform that facilitated discussions around the theme of ‘how data can make a difference in our community’.
• OMDM began working on the first draft of the eIDSR analysis report and is reviewing other drafts of manuscripts for possible publication.
Activity 4.5: Implement Learning Agenda
OMDM, in coordination with RTI’s home office based MERLA team, drafted and submitted the Activity’s Learning Agenda in Q3 Y1. Based on feedback from PMI, the Activity resubmitted the revised Learning Agenda and the proposed Operational Research (OR) separately. The OR document has been expanded and tied OMDM’s support of the recommendations presented in the Zanzibar Malaria Elimination Advisory Committee (ZMEAC) report published in FY2019.
2. Activity Implementation Progress 2.2 Result 1: Malaria Surveillance Is Improved MAINLAND TANZANIA OMDM continued building on Activity achievements in mainland Tanzania in Q1 of Y2. Facilitated through OMDM’s direct partnership with the NMCP, our team provided TA to a activities including developing the ToR to revitalize the SME TWG; reviewing the 3rd edition of eIDSR guidelines; and discuss development of the malaria composite database. OMDM led the first data review workshop with the NMCP and staff from the MoHCDGEC’s Vector Control and Case Management Units in December of 2019. Also in Q1, OMDM established within the at NMCP’s University of Dodoma office, facilitating on-site coaching and mentoring to NMCP and SME Unit staff. Additional details follow:
2.2.1 Activity 1A.1: Provide technical support to the SME community Serve as members of and participate in relevant HMIS/DHIS2 coordinating bodies Progress in Y2, Q1
In Q1, NMCP held discussions with OMDM to assist with the relaunch of the malaria-specific SME TWG. This SME TWG is comprised of partners from GFATM, USAID vector control implementing partners, PMI, and the WHO that advise on various strategies to implement appropriate SME activities, including systems strengthening and use of data generated in the decision-making process. Although the NMCP leads coordination, the SME TWG is defunct, having not held regular meetings since 2017. In Q1, OMDM collaborated with the SME Unit to obtain a copy of the existing ToR so that the Activity could review and provide inputs to update this document, and work with the NMCP to ensure that the TWG becomes operational.
Planned for Q2
OMDM will share the revised draft ToR with the NMCP and work with the SME Unit to finalize the document. After executing the updated ToR and ensuring key partners and
8 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
experts are well represented in this group, OMDM will support the NMCP to formally relaunch the SME TWG.
Support the NMCP in future review and updates of health sector strategic, policy, and technical documents Progress in Y2, Q1
OMDM participated in an NMCP-led workshop to finalize the review of the National Malaria Diagnosis and Treatment Guidelines 2014-2019 from October 23–25, 2019 in Morogoro. Workshop participants provided inputs to a draft developed in August 2019 draft aligned with strategies outlined in the Supplementary Malaria Strategic Plan 2018–2020 (SMSP) and new global developments in malaria diagnosis and treatment. The workshop was attended by representatives from the WHO, NMCP, Swiss TPH, NIMR Tanga, MUHAS, Tanzania Medicine and Medical Devices Authority (TMDA), Pharmacy Council, Private Health Laboratories Board (PHLB), USAID implementing partners, Clinton Health Access Initiative (CHAI) and Morogoro’s Regional Medical Officer (RMO). Inputs will be compiled by a consultant hired by the NMCP hired and the final draft will be presented to stakeholders early 2020.
2.2.2 Activity 1A.2: Support HMIS/DHIS2, eIDSR, and malaria surveillance implementation
Continuously engage with MoHCDGEC, NMCP, and other stakeholders to ensure that HMIS/DHIS2 and eIDSR are functional and that data flow is adhered to in terms of timely collection and transfer of data, data completeness, and quality Progress in Y2, Q1
Meeting to review eIDSR Guidelines
The MoHCDGEC conducted a workshop on October 22– 29, 2019, in Arusha, convening various stakeholders to review and draft the third edition of the eIDSR guidelines. The meeting’s primary objective was to gather feedback about the second edition, the current eIDSR guidelines in use, and then draft the third edition based on these discussions. The second edition covers twenty-three diseases; the third edition will be expanded and will cover thirty-four diseases, including re-emerging infectious diseases and viral hemorrhagic fever (e.g., dengue, Ebola, etc.) Some of the key points highlighted in the workshop included constitution of the eIDSR Expert Working Group, overview of the second edition of the guidelines, and the NMCP’s implementation plans using the eIDSR and revised guidelines.
• eIDSR Expert Working Group. presented the ToR for the eIDSR Expert Working Group and recommended that the group should constitute 12–16 experts in disease, epidemiology, and health systems. He proposed that the Expert Working Group meeting quarterly, with an annual meeting that convenes a wider range of stakeholders.
• Overview of the second edition of eIDSR guidelines. The second edition of the eIDSR Guidelines for African countries was presented by
Epidemiology Unit. The primary aim of the Guideline is to integrate and report on notifiable diseases using the country’s standard surveillance system.
Opening session of the eIDSR guideline review meeting. Photo: RTI International
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 9
• NMCP’s implementation plans using the eIDSR and revised guidelines. The NMCP presented on the malaria component of the eIDSR and their plans to implement case-based malaria surveillance in the areas of very low malaria prevalence.
DHIS2 system upgrades
On November 5, 2019, , OMDM’s ICT Specialist,. met with officials from the University of Dar es Salaam (UDSM), NMCP, and Swiss TPH to receive updates from UDSM on the following DHIS2 system upgrades:
• DHIS2 malaria composite database
• Malaria Services and Data Quality Improvement (MSDQI) mobile application
• DHIS2 Malaria Version 2 Dashboard
• District Profiles/Bulletin in Dashboard
During the meeting, also supported the NMCP and Swiss TPH to monitor progress on the enhancements and conduct regular follow-up with UDSM to ensure timely completion of the upgrades.
Progress through Q1 includes the following:
• The development of malaria composite database is complete. However, two outstanding steps need to be completed before the database can be activated and officially launched:
▪ A subdomain must be assigned to the database. NMCP is waiting for the ICT Unit from MoHCDGEC to provide the subdomain.
▪ Some data elements and indicators need to be refined. NMCP has already shared the required datasets and indicators with UDSM.
• MSDQI mobile application has been finalized. The tool underwent field testing in Q4 of FY19 in Morogoro. However, the migration of previous data used in the old electronic data system (EDS) format to the current MSDQI app is underway, though not yet completed by UDSM.
• DHIS2 Malaria Version 2 Dashboard. OMDM reviewed the malaria dashboard and recommended additional changes (e.g., further refinement of charts and features).
• District Profiles/Bulletin in Dashboard. This is pending, awaiting execution of a ToR between the NMCP and UDSM; the ToR is being developed by the NMCP and Swiss TPH.
10 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
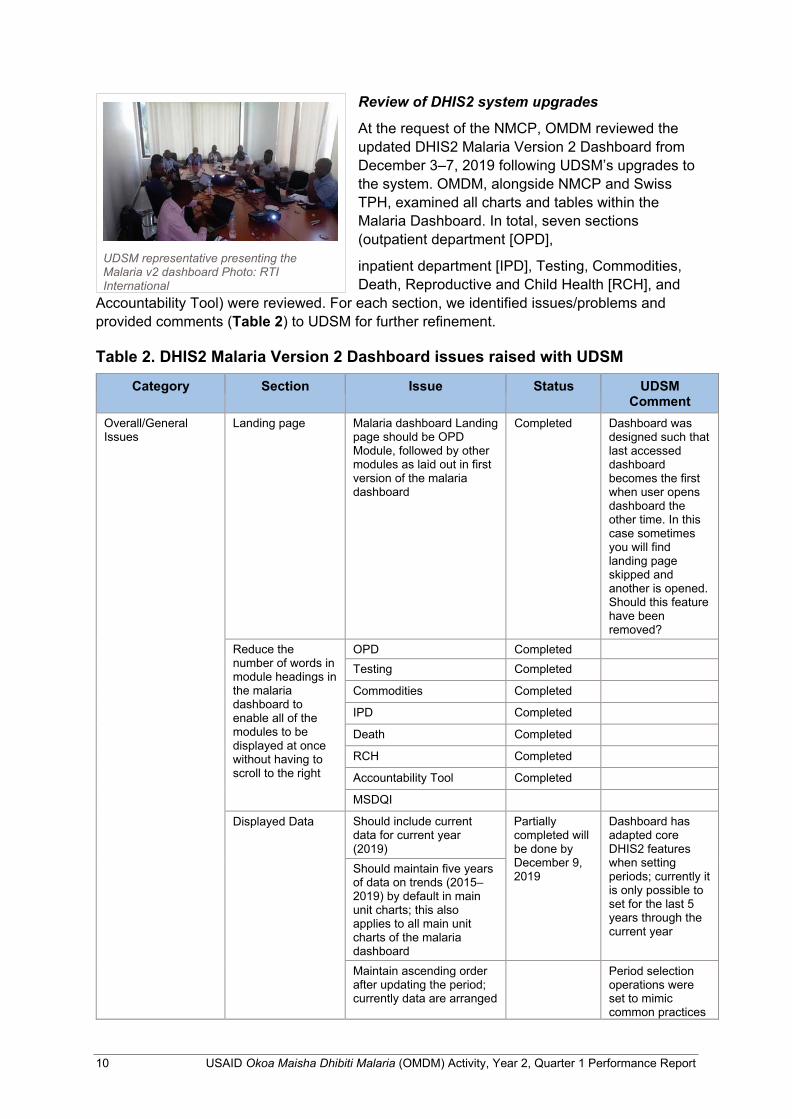
Review of DHIS2 system upgrades
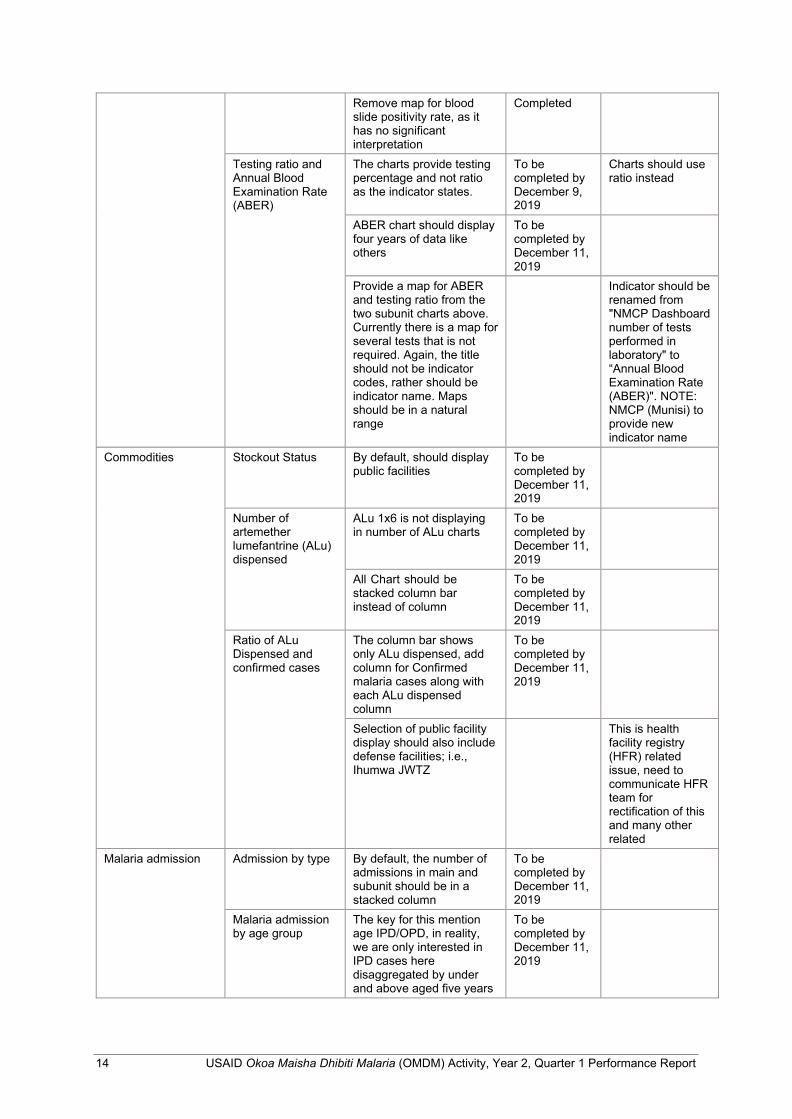
At the request of the NMCP, OMDM reviewed the updated DHIS2 Malaria Version 2 Dashboard from December 3–7, 2019 following UDSM’s upgrades to the system. OMDM, alongside NMCP and Swiss TPH, examined all charts and tables within the Malaria Dashboard. In total, seven sections (outpatient department [OPD],
inpatient department [IPD], Testing, Commodities, Death, Reproductive and Child Health [RCH], and
Accountability Tool) were reviewed. For each section, we identified issues/problems and provided comments (Table 2) to UDSM for further refinement.
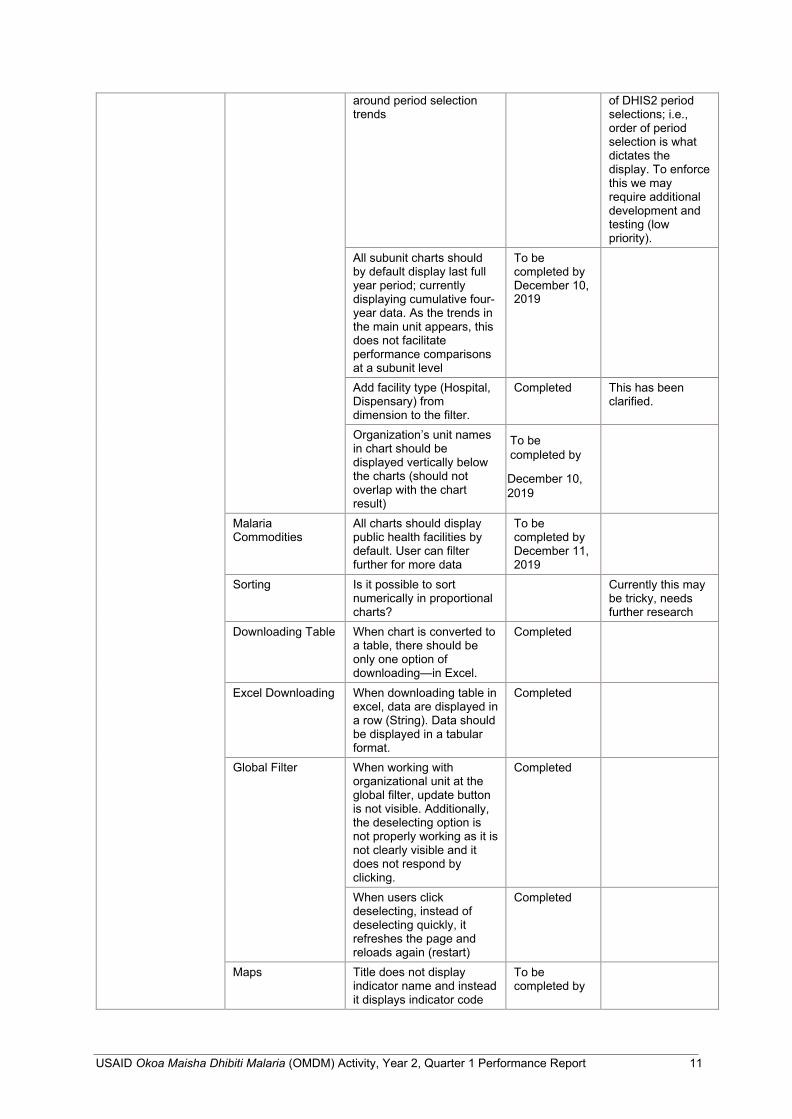
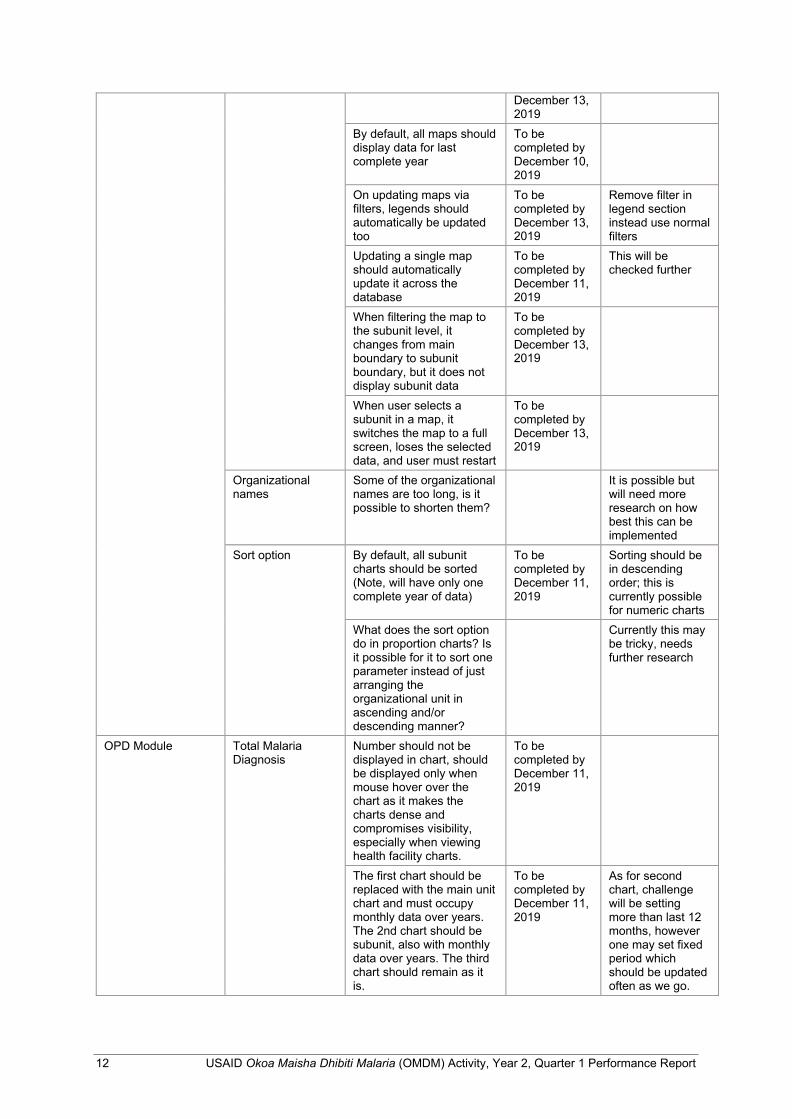
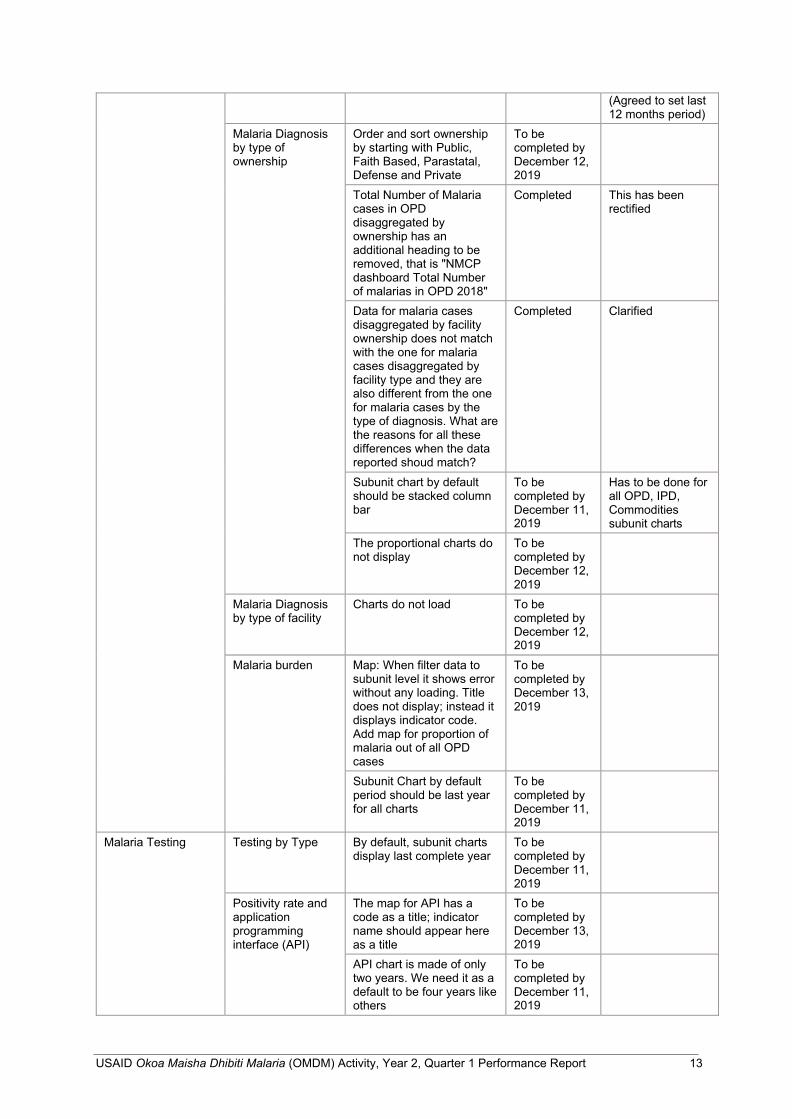
Table 2. DHIS2 Malaria Version 2 Dashboard issues raised with UDSM
Category Section Issue Status UDSM Comment
Overall/General Issues
Landing page Malaria dashboard Landing page should be OPD Module, followed by other modules as laid out in first version of the malaria dashboard
Completed Dashboard was designed such that last accessed dashboard becomes the first when user opens dashboard the other time. In this case sometimes you will find landing page skipped and another is opened. Should this feature have been removed?
Reduce the number of words in module headings in the malaria dashboard to enable all of the modules to be displayed at once without having to scroll to the right
OPD Completed
Testing Completed
Commodities Completed
IPD Completed
Death Completed
RCH Completed
Accountability Tool Completed
MSDQI
Displayed Data Should include current data for current year (2019)
Partially completed will be done by December 9, 2019
Dashboard has adapted core DHIS2 features when setting periods; currently it is only possible to set for the last 5 years through the current year
Should maintain five years of data on trends (2015– 2019) by default in main unit charts; this also applies to all main unit charts of the malaria dashboard Maintain ascending order after updating the period; currently data are arranged
Period selection operations were set to mimic common practices
UDSM representative presenting the Malaria v2 dashboard Photo: RTI International
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 11
around period selection trends
of DHIS2 period selections; i.e., order of period selection is what dictates the display. To enforce this we may require additional development and testing (low priority).
All subunit charts should by default display last full year period; currently displaying cumulative four- year data. As the trends in the main unit appears, this does not facilitate performance comparisons at a subunit level
To be completed by December 10, 2019
Add facility type (Hospital, Dispensary) from dimension to the filter.
Completed This has been clarified.
Organization’s unit names in chart should be displayed vertically below the charts (should not overlap with the chart result)
To be completed by
December 10, 2019
Malaria Commodities
All charts should display public health facilities by default. User can filter further for more data
To be completed by December 11, 2019
Sorting Is it possible to sort numerically in proportional charts?
Currently this may be tricky, needs further research
Downloading Table When chart is converted to a table, there should be only one option of downloading—in Excel.
Completed
Excel Downloading When downloading table in excel, data are displayed in a row (String). Data should be displayed in a tabular format.
Completed
Global Filter When working with organizational unit at the global filter, update button is not visible. Additionally, the deselecting option is not properly working as it is not clearly visible and it does not respond by clicking.
Completed
When users click deselecting, instead of deselecting quickly, it refreshes the page and reloads again (restart)
Completed
Maps Title does not display indicator name and instead it displays indicator code
To be completed by
12 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
December 13, 2019
By default, all maps should display data for last complete year
To be completed by December 10, 2019
On updating maps via filters, legends should automatically be updated too
To be completed by December 13, 2019
Remove filter in legend section instead use normal filters
Updating a single map should automatically update it across the database
To be completed by December 11, 2019
This will be checked further
When filtering the map to the subunit level, it changes from main boundary to subunit boundary, but it does not display subunit data
To be completed by December 13, 2019
When user selects a subunit in a map, it switches the map to a full screen, loses the selected data, and user must restart
To be completed by December 13, 2019
Organizational names
Some of the organizational names are too long, is it possible to shorten them?
It is possible but will need more research on how best this can be implemented
Sort option By default, all subunit charts should be sorted (Note, will have only one complete year of data)
To be completed by December 11, 2019
Sorting should be in descending order; this is currently possible for numeric charts
What does the sort option do in proportion charts? Is it possible for it to sort one parameter instead of just arranging the organizational unit in ascending and/or descending manner?
Currently this may be tricky, needs further research
OPD Module Total Malaria Diagnosis
Number should not be displayed in chart, should be displayed only when mouse hover over the chart as it makes the charts dense and compromises visibility, especially when viewing health facility charts.
To be completed by December 11, 2019
The first chart should be replaced with the main unit chart and must occupy monthly data over years. The 2nd chart should be subunit, also with monthly data over years. The third chart should remain as it is.
To be completed by December 11, 2019
As for second chart, challenge will be setting more than last 12 months, however one may set fixed period which should be updated often as we go.
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 13
(Agreed to set last 12 months period)
Malaria Diagnosis by type of ownership
Order and sort ownership by starting with Public, Faith Based, Parastatal, Defense and Private
To be completed by December 12, 2019
Total Number of Malaria cases in OPD disaggregated by ownership has an additional heading to be removed, that is "NMCP dashboard Total Number of malarias in OPD 2018"
Completed This has been rectified
Data for malaria cases disaggregated by facility ownership does not match with the one for malaria cases disaggregated by facility type and they are also different from the one for malaria cases by the type of diagnosis. What are the reasons for all these differences when the data reported shoud match?
Completed Clarified
Subunit chart by default should be stacked column bar
To be completed by December 11, 2019
Has to be done for all OPD, IPD, Commodities subunit charts
The proportional charts do not display
To be completed by December 12, 2019
Malaria Diagnosis by type of facility
Charts do not load To be completed by December 12, 2019
Malaria burden Map: When filter data to subunit level it shows error without any loading. Title does not display; instead it displays indicator code. Add map for proportion of malaria out of all OPD cases
To be completed by December 13, 2019
Subunit Chart by default period should be last year for all charts
To be completed by December 11, 2019
Malaria Testing Testing by Type By default, subunit charts display last complete year
To be completed by December 11, 2019
Positivity rate and application programming interface (API)
The map for API has a code as a title; indicator name should appear here as a title
To be completed by December 13, 2019
API chart is made of only two years. We need it as a default to be four years like others
To be completed by December 11, 2019
14 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Remove map for blood slide positivity rate, as it has no significant interpretation
Completed
Testing ratio and Annual Blood Examination Rate (ABER)
The charts provide testing percentage and not ratio as the indicator states.
To be completed by December 9, 2019
Charts should use ratio instead
ABER chart should display four years of data like others
To be completed by December 11, 2019
Provide a map for ABER and testing ratio from the two subunit charts above. Currently there is a map for several tests that is not required. Again, the title should not be indicator codes, rather should be indicator name. Maps should be in a natural range
Indicator should be renamed from "NMCP Dashboard number of tests performed in laboratory" to “Annual Blood Examination Rate (ABER)". NOTE: NMCP (Munisi) to provide new indicator name
Commodities Stockout Status By default, should display public facilities
To be completed by December 11, 2019
Number of artemether lumefantrine (ALu) dispensed
ALu 1x6 is not displaying in number of ALu charts
To be completed by December 11, 2019
All Chart should be stacked column bar instead of column
To be completed by December 11, 2019
Ratio of ALu Dispensed and confirmed cases
The column bar shows only ALu dispensed, add column for Confirmed malaria cases along with each ALu dispensed column
To be completed by December 11, 2019
Selection of public facility display should also include defense facilities; i.e., Ihumwa JWTZ
This is health facility registry (HFR) related issue, need to communicate HFR team for rectification of this and many other related
Malaria admission Admission by type By default, the number of admissions in main and subunit should be in a stacked column
To be completed by December 11, 2019
Malaria admission by age group
The key for this mention age IPD/OPD, in reality, we are only interested in IPD cases here disaggregated by under and above aged five years
To be completed by December 11, 2019
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 15
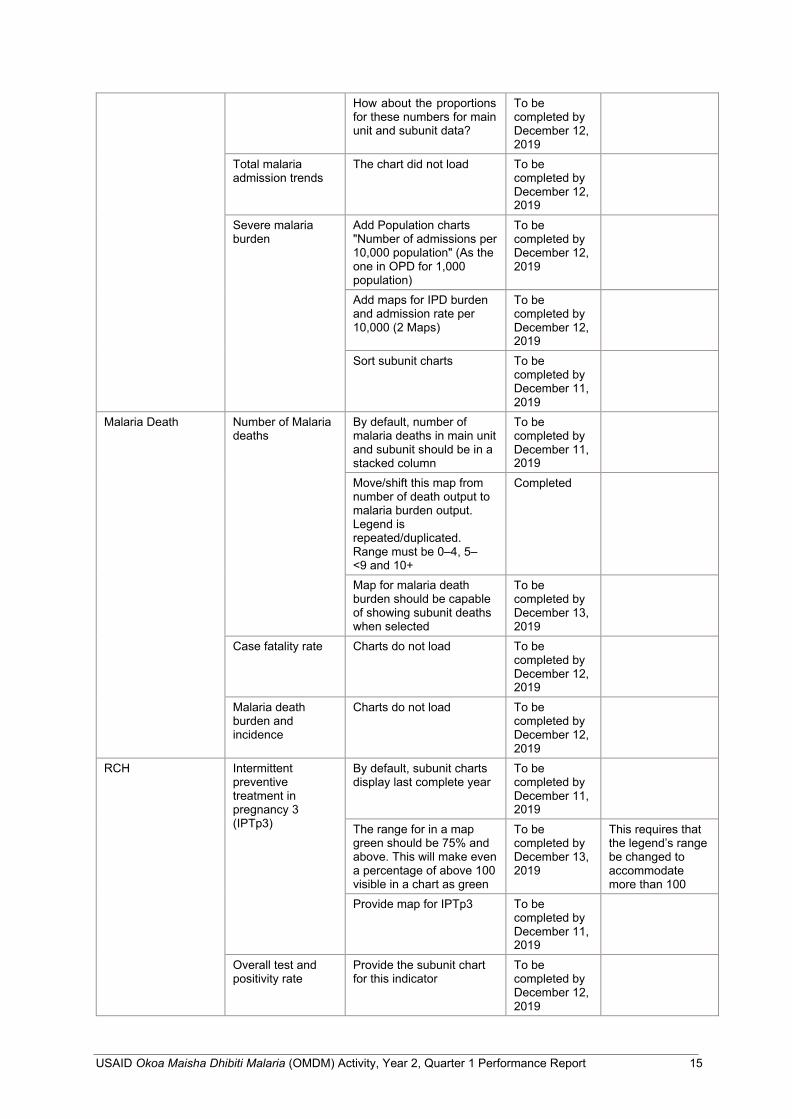
How about the proportions for these numbers for main unit and subunit data?
To be completed by December 12, 2019
Total malaria admission trends
The chart did not load To be completed by December 12, 2019
Severe malaria burden
Add Population charts "Number of admissions per 10,000 population" (As the one in OPD for 1,000 population)
To be completed by December 12, 2019
Add maps for IPD burden and admission rate per 10,000 (2 Maps)
To be completed by December 12, 2019
Sort subunit charts To be completed by December 11, 2019
Malaria Death Number of Malaria deaths
By default, number of malaria deaths in main unit and subunit should be in a stacked column
To be completed by December 11, 2019
Move/shift this map from number of death output to malaria burden output. Legend is repeated/duplicated. Range must be 0–4, 5– <9 and 10+
Completed
Map for malaria death burden should be capable of showing subunit deaths when selected
To be completed by December 13, 2019
Case fatality rate Charts do not load To be completed by December 12, 2019
Malaria death burden and incidence
Charts do not load To be completed by December 12, 2019
RCH Intermittent preventive treatment in pregnancy 3 (IPTp3)
By default, subunit charts display last complete year
To be completed by December 11, 2019
The range for in a map green should be 75% and above. This will make even a percentage of above 100 visible in a chart as green
To be completed by December 13, 2019
This requires that the legend’s range be changed to accommodate more than 100
Provide map for IPTp3 To be completed by December 11, 2019
Overall test and positivity rate
Provide the subunit chart for this indicator
To be completed by December 12, 2019
16 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
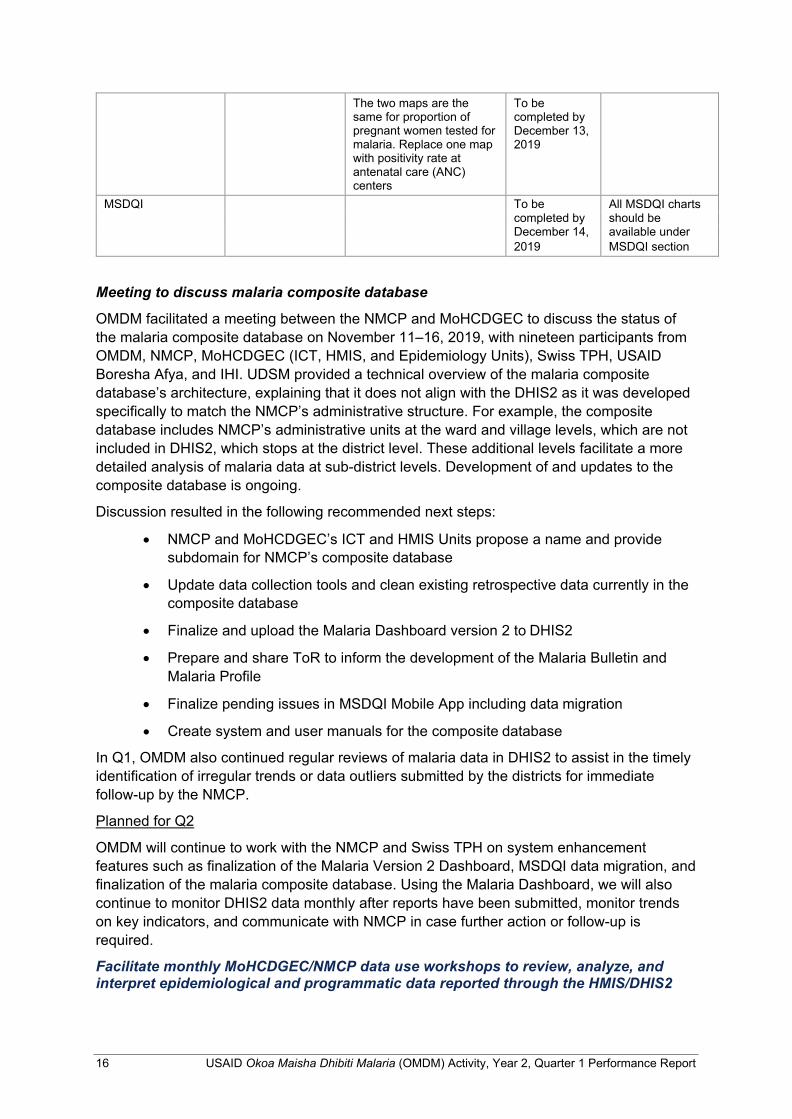
The two maps are the same for proportion of pregnant women tested for malaria. Replace one map with positivity rate at antenatal care (ANC) centers
To be completed by December 13, 2019
MSDQI To be All MSDQI charts completed by should be December 14, available under 2019 MSDQI section
Meeting to discuss malaria composite database
OMDM facilitated a meeting between the NMCP and MoHCDGEC to discuss the status of the malaria composite database on November 11–16, 2019, with nineteen participants from OMDM, NMCP, MoHCDGEC (ICT, HMIS, and Epidemiology Units), Swiss TPH, USAID Boresha Afya, and IHI. UDSM provided a technical overview of the malaria composite database’s architecture, explaining that it does not align with the DHIS2 as it was developed specifically to match the NMCP’s administrative structure. For example, the composite database includes NMCP’s administrative units at the ward and village levels, which are not included in DHIS2, which stops at the district level. These additional levels facilitate a more detailed analysis of malaria data at sub-district levels. Development of and updates to the composite database is ongoing.
Discussion resulted in the following recommended next steps:
• NMCP and MoHCDGEC’s ICT and HMIS Units propose a name and provide subdomain for NMCP’s composite database
• Update data collection tools and clean existing retrospective data currently in the composite database
• Finalize and upload the Malaria Dashboard version 2 to DHIS2
• Prepare and share ToR to inform the development of the Malaria Bulletin and Malaria Profile
• Finalize pending issues in MSDQI Mobile App including data migration
• Create system and user manuals for the composite database
In Q1, OMDM also continued regular reviews of malaria data in DHIS2 to assist in the timely identification of irregular trends or data outliers submitted by the districts for immediate follow-up by the NMCP.
Planned for Q2
OMDM will continue to work with the NMCP and Swiss TPH on system enhancement features such as finalization of the Malaria Version 2 Dashboard, MSDQI data migration, and finalization of the malaria composite database. Using the Malaria Dashboard, we will also continue to monitor DHIS2 data monthly after reports have been submitted, monitor trends on key indicators, and communicate with NMCP in case further action or follow-up is required.
Facilitate monthly MoHCDGEC/NMCP data use workshops to review, analyze, and interpret epidemiological and programmatic data reported through the HMIS/DHIS2
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 17
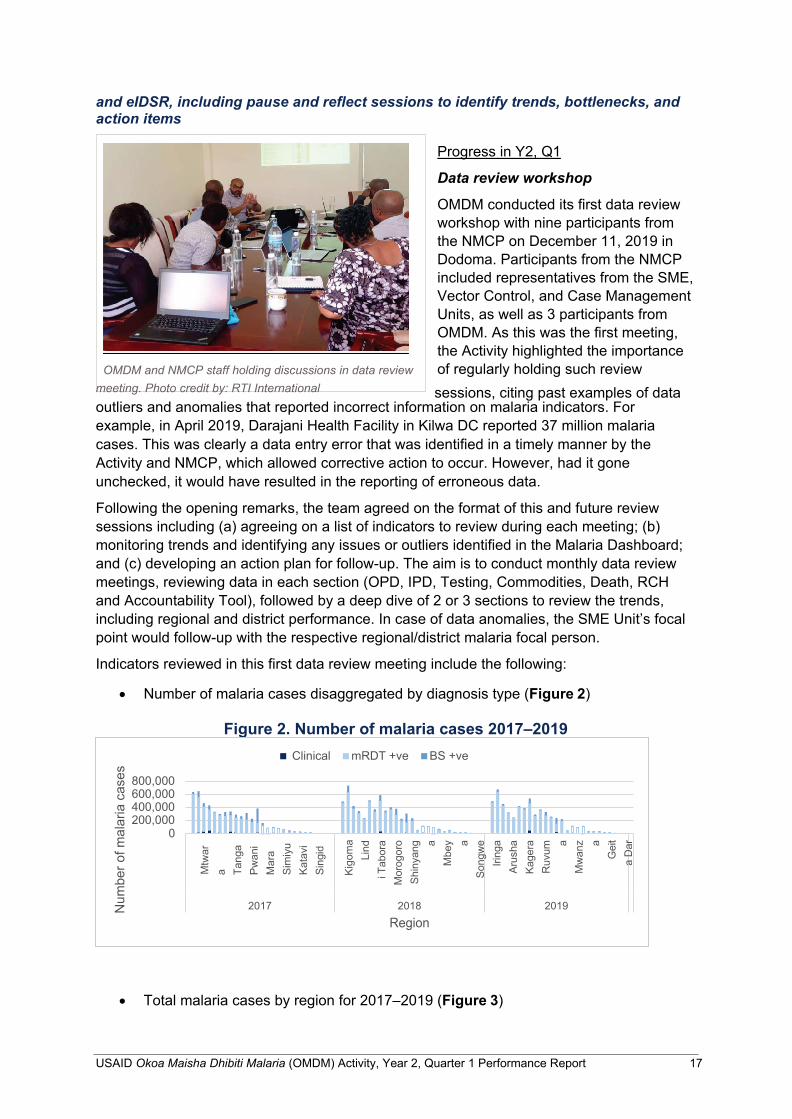
OMDM and NMCP staff holding discussions in data review meeting. Photo credit by: RTI International
and eIDSR, including pause and reflect sessions to identify trends, bottlenecks, and action items
Progress in Y2, Q1
Data review workshop
OMDM conducted its first data review workshop with nine participants from the NMCP on December 11, 2019 in Dodoma. Participants from the NMCP included representatives from the SME, Vector Control, and Case Management Units, as well as 3 participants from OMDM. As this was the first meeting, the Activity highlighted the importance of regularly holding such review sessions, citing past examples of data
outliers and anomalies that reported incorrect information on malaria indicators. For example, in April 2019, Darajani Health Facility in Kilwa DC reported 37 million malaria cases. This was clearly a data entry error that was identified in a timely manner by the Activity and NMCP, which allowed corrective action to occur. However, had it gone unchecked, it would have resulted in the reporting of erroneous data.
Following the opening remarks, the team agreed on the format of this and future review sessions including (a) agreeing on a list of indicators to review during each meeting; (b) monitoring trends and identifying any issues or outliers identified in the Malaria Dashboard; and (c) developing an action plan for follow-up. The aim is to conduct monthly data review meetings, reviewing data in each section (OPD, IPD, Testing, Commodities, Death, RCH and Accountability Tool), followed by a deep dive of 2 or 3 sections to review the trends, including regional and district performance. In case of data anomalies, the SME Unit’s focal point would follow-up with the respective regional/district malaria focal person.
Indicators reviewed in this first data review meeting include the following:
• Number of malaria cases disaggregated by diagnosis type (Figure 2)
Figure 2. Number of malaria cases 2017–2019
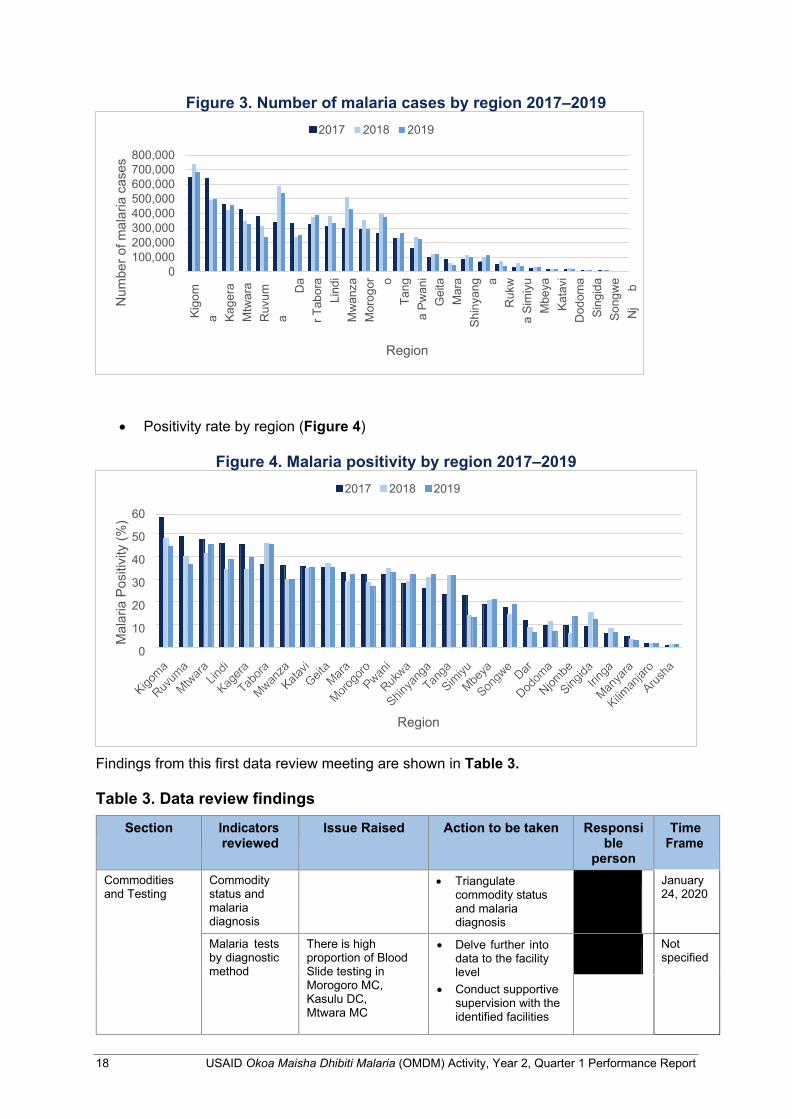
• Total malaria cases by region for 2017–2019 (Figure 3)
2019 2018 Region
2017
800,000 600,000 400,000 200,000
0
Clinical mRDT +ve BS +ve
Num
ber o
f mal
aria
cas
es
Mtw
ara Ta
nga
Pwan
i M
ara
Sim
iyu
Kata
vi
Sing
id
Ki
gom
a Li
ndi T
abor
a M
orog
oro
Shin
yang a
Mbe
y a So
ngw
e Iri
nga
Arus
ha
Kage
ra
Ruv
uma
Mw
anz a
Gei
ta
Dar
18 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
2017 2018 2019
800,000 700,000 600,000 500,000 400,000 300,000 200,000 100,000
0
Region
2017 2018 2019
60
50
40
30
20
10
0
Region
Figure 3. Number of malaria cases by region 2017–2019
• Positivity rate by region (Figure 4)
Figure 4. Malaria positivity by region 2017–2019
Findings from this first data review meeting are shown in Table 3.
Table 3. Data review findings
Section Indicators reviewed
Issue Raised Action to be taken Responsi ble
person
Time Frame
Commodities and Testing
Commodity status and malaria diagnosis
• Triangulate commodity status and malaria diagnosis
January 24, 2020
Malaria tests by diagnostic method
There is high proportion of Blood Slide testing in Morogoro MC, Kasulu DC, Mtwara MC
• Delve further into data to the facility level
• Conduct supportive supervision with the identified facilities
Not specified
Mal
aria
Pos
itivi
ty (%
) N
umbe
r of m
alar
ia c
ases
Kigo
ma Ka
gera
M
twar
a R
uvum
a D
ar T
abor
a Li
ndi
Mw
anza
M
orog
or o Ta
nga
Pwan
i G
eita
M
ara
Shin
yang a
Ruk
wa
Sim
iyu
Mbe
ya
Kata
vi
Dod
oma
Sing
ida
Song
we
Nj
b
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 19
Section Indicators reviewed
Issue Raised Action to be taken Responsi ble
person
Time Frame
OPD Total malaria cases by region for 2017, 2018, 2019
Variance in case diagnosis is prominent for some regions; e.g., Mtwara and Tabora, both showing increase in malaria over the last 3 years
• NMCP will share this chart with its respective units as part of informing them on the malaria trends
Dec 2020
Testing Positivity rate by region and districts
Nzega DC: The trend for positivity rate decreased over time. 88% in 2017, 69% in 2018, and 65% in 2019
• Continue monitoring trends over time
All Not specified
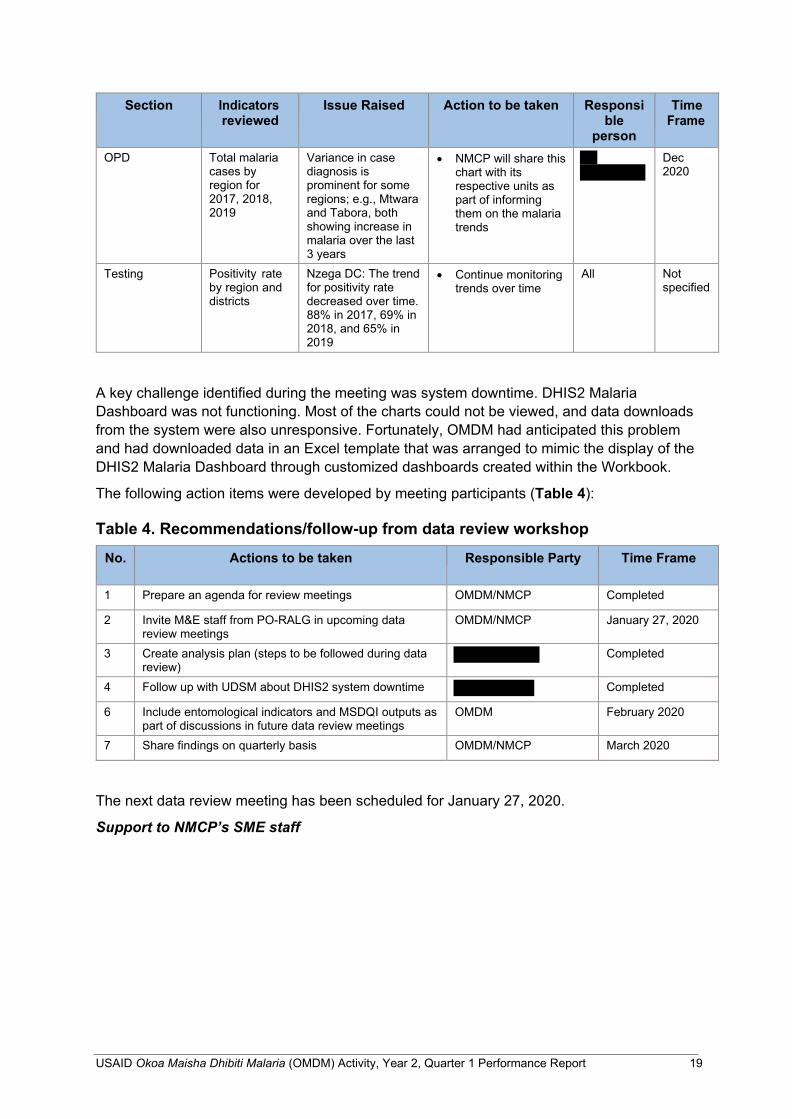
A key challenge identified during the meeting was system downtime. DHIS2 Malaria Dashboard was not functioning. Most of the charts could not be viewed, and data downloads from the system were also unresponsive. Fortunately, OMDM had anticipated this problem and had downloaded data in an Excel template that was arranged to mimic the display of the DHIS2 Malaria Dashboard through customized dashboards created within the Workbook.
The following action items were developed by meeting participants (Table 4):
Table 4. Recommendations/follow-up from data review workshop
No.
Actions to be taken Responsible Party Time Frame
1 Prepare an agenda for review meetings OMDM/NMCP Completed
2 Invite M&E staff from PO-RALG in upcoming data review meetings
OMDM/NMCP January 27, 2020
3 Create analysis plan (steps to be followed during data review)
Completed
4 Follow up with UDSM about DHIS2 system downtime
Completed
6 Include entomological indicators and MSDQI outputs as part of discussions in future data review meetings
OMDM February 2020
7 Share findings on quarterly basis OMDM/NMCP March 2020
The next data review meeting has been scheduled for January 27, 2020.
Support to NMCP’s SME staff
20 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
On November 19–22, 2019, OMDM’s Data Scientist,
visited the new OMDM office identified by the NMCP to co- locate OMDM Staff in their University of Dodoma compound. The thinking behind this co- location is that OMDM staff will be able to provide hands-on coaching, support, and mentoring to the NMCP’s SME Unit in
their day-to-day activities. The office is on the 2nd floor of the NMCP office, equipped with two wall tables and two metal cabinets. It was noted that the door lock was faulty and needs replacement, also there is need to have a router to ensure internet connectivity.
During the November visit, OMDM worked on the NMCP’s data request [detailed summary of total malaria positive (OPD+IPD) against total tested for malaria (any method)] required for malaria commodities quantification. The required data elements were downloaded from DHIS2 and a pivot table was created to summarize the required data elements, with data disaggregated by year, month, region, and council. The next support visit is scheduled for January 27–28, 2020.
Operationalize Tanzania’s malaria scorecard management tool
On November 26–29, 2019, OMDM participated in a workshop Operationalizing Tanzania’s malaria scorecard management tool, organized by ALMA and the NMCP in Morogoro. The workshop focused on orienting RMFPs on the malaria scorecard management tool. Other participants included representatives from PO-RALG and Tanzania Parliamentarians Against Malaria (TAPAMA). Workshop objectives included the following:
• Gain an understanding of how other countries are using scorecards
• Gain an understanding of Tanzania’s scorecard indicators and thresholds
• Learn how to access and use the online scorecard web platform management tool
• Integrate the scorecard into existing accountability mechanisms at all levels
• Analyze the first Q3 (July–September 2019) scorecard and recommendations
• Learn how to use the “work plan manager” to manage regional operational plans
• Agree on roles and responsibilities and next steps
OMDM office space at University of Dodoma. Photo credit by: RTI International
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 21
Workshop outcomes
• ALMA will support the implementation of the malaria scorecard in four high malaria burden regions (Kigoma, Kagera, Mtwara, and Geita) with their respective councils,
beginning in February 2020.
• ALMA will conduct a training to Members of Parliament in February 2020.
• ALMA will conduct high-level sensitization meetings for the MoHCDGEC and PO- RALG.
• NMCP will train RHMT members and partners about how to use the malaria scorecard and add their accounts to the web platform by end January 2020.
• Regional Malaria Focal Persons (RMFP) provided immediate feedback on the malaria scorecard to stakeholders by December 7, 2019.
• RMFPs should orient councils about the malaria scorecard.
Maximize the use of the malaria interactive dashboard within DHIS2 and promote its use at all levels Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
OMDM will participate in Zonal review meetings that include a data review component.
Support the NMCP and other stakeholders in the implementation of the MSDQI framework by facilitating the interpretation and utilization of the outcomes of the routine supportive supervision activities Progress in Y2, Q1
Although the MSDQI App is complete, it continues to be refined with feedback from the Regional and Council Health Management Teams. Data from the health facilities are currently being housed in the MSDQI Dashboard within DHIS2.
Planned for Q2
As indicated in Table 4, we plan to discuss MSDQI outputs in future data review meetings. It will give the Activity and NMCP the opportunity to review progress and results on key outputs related to malaria services and data quality improvement plans.
ALMA facilitator orienting participants on malaria scorecard in Morogoro. Photo: RTI International
22 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
2.2.3 Activity 1A.3: Strengthen MoHCDGEC and NMCP outbreak response capacity
Support the MoHCDGEC/NMCP to define thresholds and triggers indicating malaria outbreak, including implementing them as predictors and automated notifications in eIDSR and DHIS2 and continuously monitoring and analyzing malaria data in the national DHIS2 system Progress in Y2, Q1
OMDM completed the first part of the analysis of eIDSR data in July–September reporting period of fiscal year 2019. A first draft of the publication is already under development. Revisions will continue during Y2 in collaboration with PMI and NMCP. The second part of the analysis involves customized thresholds and triggers; the Activity will first discussed the analysis and potential publication with our internal MERLA team to determine how best to advance before engaging with the wider team, including the NMCP and Tulane University.
Case Based Surveillance (CBS) workshop and field visit
Also during the reporting period, OMDM was invited by the NMCP to participate in a five-day CBS workshop held in Moshi MC from October 6–12, 2019. The objectives of the workshop follow:
• Introduction of the strategic context of CBS within the SMSP
• Understand the epidemiology of malaria in low transmission areas in Tanzania
• Share outputs from Arusha baseline data gathered by the NMCP prior to the workshop
• Introduce principles of malaria surveillance in very low malaria transmission settings targeting elimination
• Identify operational priorities for introduction of CBS in very low malaria transmission settings
• Develop CBS protocol based on NMCP’s available first draft
In addition to the standard workshop format, the team also undertook a field visit. Using customized checklists, four groups were assigned to collect information from the community, health facility with more than one case per month, health facility with less than one case per month, and a visit to the District Council Management Office. OMDM staff were part of the group that visited Lyamungo Health Center (HC) and the District Council Management Office. A summary of both visits follows.
Field visit report
Lyamungo HC
The Facility serves an average of 10,179 patients from the catchments area (Moshi DC and MC) and from neighboring villages (Lyamungo Kati, Kilanya, and Sinde). Lyamungo HS consists of eleven medical professionals, two support staff, and five community health workers (CHW). Each village is assigned one CHW, responsible for raising awareness of community health services available; the two other CHWs assigned to Lyamungo HC specifically conduct home-based care (HBC).
Microscopy services are available at Lyamungo HC, though they are not currently being used due to the lack of reagents; malaria tests are being conducted via mRDTs. The eleven
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 23
medical staff are able to test for malaria using mRDTs, with three having received formal training and the rest on-the-job training.
The field visit team checked the facility’s registers and observed that all—OPD register, monthly summary, tally sheet—were available to be checked and were found to be well managed and completed. Malaria data is collected using two sources (Table 5)—lab and OPD registers.
Table 5. Malaria data by lab register and OPD register
terms of reported malaria cases.
Upon observation, it was noted that there was a data inconsistency between the lab and OPD registers in the month of October 2019 in
All positive malaria cases were identified as imported, with the majority of cases verbally identified as originating through Lyamungo Secondary School.
Lyamungo HC believes they are able to implement CBS due to the availability of trained staff, presence of malaria commodities (mRDT, ALu), and cooperation with local GOT representatives. HCWs believe CBS will limit transmission of malaria infection from infected persons to other community members.
OMDM Staff ( ) explains the purpose of the visit to Facility in charge at Lyamungo HC. Photo: RTI International
District Council Management Office Visit
As part of the field visit, the team visited the Moshi District Council, introducing themselves and the purpose of the field visit. A strengths, weaknesses, opportunities and threats (SWOT) analysis was conducted; results follow in (Table 6).
Table 6. SWOT analysis of District Council Management Office visit
Strength Threats/Weakness
• RRT in place and active following the June 2019 Anthrax outbreak
• Data use is observed • RRT composition known • Good linkage between HFs with community through
CHWs • Political engagement to address outbreaks • Over 91% of the health facilities conduct malaria testing
for ANC
• District Medical Officer’s (DMO), Medical Stores Department (MSD) account for receipt in kind has no funds
• Shortage of health staff, especially Environmental Health Officer (EHO) and laboratory technicians
• No government HFs at lower Moshi where most of the malaria cases are reported
• Transport and logistics issues
Lab Register OPD Register July-Sept 2019 8 8 October 2019 1 2
24 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Opportunities Willingness
• 5 private health laboratories were provided with OPD registers to document testing
• Use of administrative structure (e.g., ward executive officer (WEO), village executive officer (VEO) and community health workers) in responding to outbreaks
• Team revealed willingness of the district to conduct CBS but asking for capacity building in terms of resources and logistics
Planned for Q2
The Activity will continue working on the draft publication for part one of the eIDSR analysis. We will also continue providing technical assistance to the NMCP in the development of the CBS protocol.
ZANZIBAR OMDM’s support to ZAMEP continued in Q1, including financial support through the Activity’s FAA with ZAMEP for activities managed by the Case Management Diagnosis and Treatment and SBCC Units and through TA to the HMIS and ICT Units related to the management of malaria surveillance systems. Through TA from RTI’s ICT staff based in Nairobi, Kenya, initial capacity building plans have been developed to facilitate the transfer of ownership of the MCN to ZAMEP over the life of OMDM. Additional questions and skip logics have been added to the MCN, and introduced a feature that automatically detects and abnormal increase in malaria cases at the health facility, district, and shehia levels. Additionial updates follow:
2.2.4 Activity 1B.1: Support ZAMEP to update and implement the malaria surveillance strategy
Coordinate malaria surveillance and response system strengthening efforts through the Malaria Surveillance TWG Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
OMDM will work with ZAMEP to schedule a Malaria Surveillance TWG in Q2.
Strengthen public and private sector facility malaria diagnosis and treatment capacity Progress in Y2, Q1
Case Management—Diagnosis
In the October–December 2019 reporting period, 5,176 patients were tested for malaria via microscopy examination at 96 health facilities using microscopy QA/QC. Among them, 2,863 (55.3%) were female and 2,313 (44.6%) male. Of the total tested, 30 slides tested positive. Slide cross-checking was done to assess the overall sensitivity and specificity of the health facilities’ technicians. On average, the sensitivity was 93.3% and specificity was 100%. The lowest sensitivity was recorded at Magharibi and Mjini district with 92.8% and 93.3%, respectively.
In this reporting period, in addition to P. falciparum malaria species, P. malariae and P. ovale were also detected.
Supervision Activities
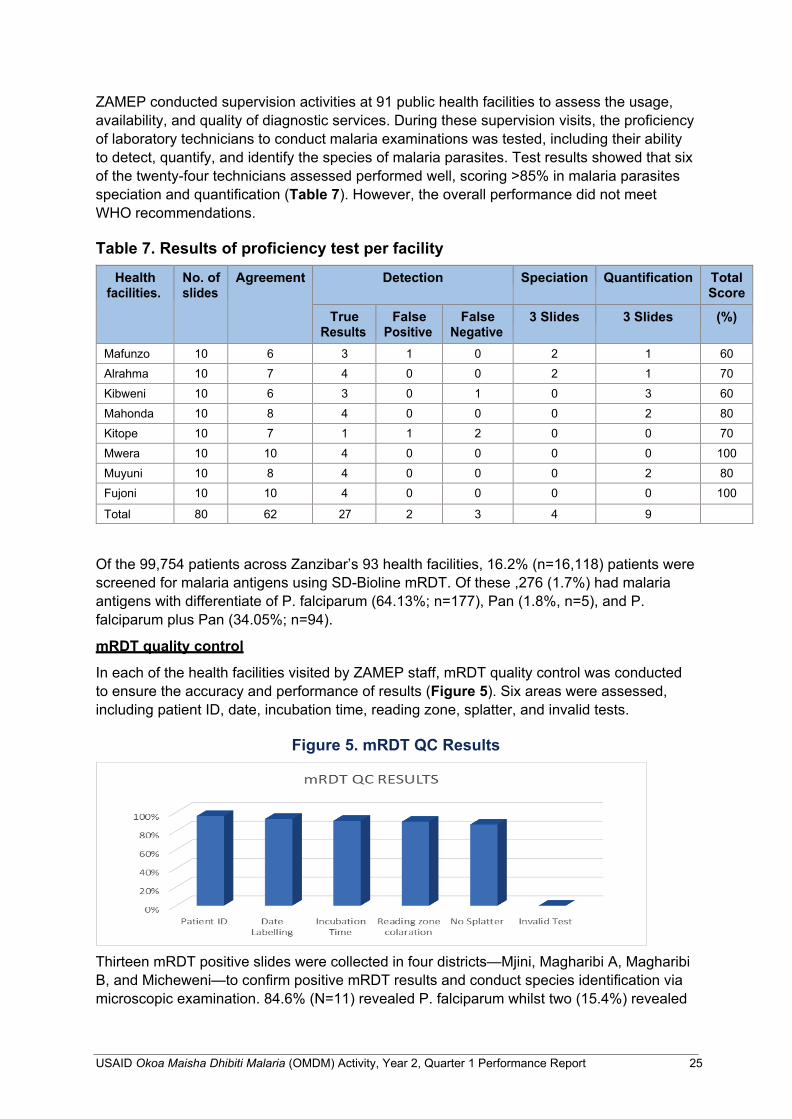
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 25
ZAMEP conducted supervision activities at 91 public health facilities to assess the usage, availability, and quality of diagnostic services. During these supervision visits, the proficiency of laboratory technicians to conduct malaria examinations was tested, including their ability to detect, quantify, and identify the species of malaria parasites. Test results showed that six of the twenty-four technicians assessed performed well, scoring >85% in malaria parasites speciation and quantification (Table 7). However, the overall performance did not meet WHO recommendations.
Table 7. Results of proficiency test per facility
Health facilities.
No. of slides
Agreement Detection Speciation Quantification Total Score
True Results
False Positive
False Negative
3 Slides 3 Slides (%)
Mafunzo 10 6 3 1 0 2 1 60 Alrahma 10 7 4 0 0 2 1 70 Kibweni 10 6 3 0 1 0 3 60 Mahonda 10 8 4 0 0 0 2 80 Kitope 10 7 1 1 2 0 0 70 Mwera 10 10 4 0 0 0 0 100 Muyuni 10 8 4 0 0 0 2 80 Fujoni 10 10 4 0 0 0 0 100
Total 80 62 27 2 3 4 9
Of the 99,754 patients across Zanzibar’s 93 health facilities, 16.2% (n=16,118) patients were screened for malaria antigens using SD-Bioline mRDT. Of these ,276 (1.7%) had malaria antigens with differentiate of P. falciparum (64.13%; n=177), Pan (1.8%, n=5), and P. falciparum plus Pan (34.05%; n=94).
mRDT quality control
In each of the health facilities visited by ZAMEP staff, mRDT quality control was conducted to ensure the accuracy and performance of results (Figure 5). Six areas were assessed, including patient ID, date, incubation time, reading zone, splatter, and invalid tests.
Figure 5. mRDT QC Results
Thirteen mRDT positive slides were collected in four districts—Mjini, Magharibi A, Magharibi B, and Micheweni—to confirm positive mRDT results and conduct species identification via microscopic examination. 84.6% (N=11) revealed P. falciparum whilst two (15.4%) revealed
26 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
P. malariae. Two (15.4%) slides revealed trophozoite of P. ovale, 7.7% mixed infection of P. falciparum and malaria and gametocyte of P. falciparum, malaria and ovale (Pfg, Pm and PO), no auto-fixation was reported in this period. All slides agreed with the first and second reader with speciation and were quantified by blood per microliters of parasites.
Procurement of diagnostic supplies
Procurement activities are underway to augment ZAMEP’s diagnostic activities via support from OMDM. The Activity is working with ZAMEP to ensure sufficient quantities of malaria microscopy commodities and consumables to eliminate stock-outs at health facilities.
Case Management—Treatment
HCW Training on 2018 Malaria Treatment Guidelines
The WHO conducted a three-day training to 30 health care providers from public and private health facilities across Zanzibar. The objective of the training was to update the knowledge, skills and practices of the HCWs to record patient history and appropriately respond to and manage current malaria cases.
Specifically, the training covered complicated and uncomplicated malaria case management and diagnosis; managing various manifestations of malaria across health facilities; ensuring the correct dosage of artesunate for intravenous/intramuscular injections and managing malaria cases for special groups (e.g, patients with HIV and pregnant women).
Quarterly feedback meetings
In this reporting period, ZAMEP conducted one-day quarterly feedback meetings with district-level teams—DMOs and District Logistics Officers (DLO)—to determine antimalarial stock status at HF levels. It was observed that all of the HFs had sufficient stock of at least 2–4 categories of antimalarial (e.g., infant, toddler, child, adult doses). ZAMEP recommended redistribution of malaria commodities to avoid under-stock at any HF.
Strengthen health facility and community-level SBCC capacity Progress in Y2, Q1
Continuous net distribution (CD)
Monitoring and supervision of continuous net distribution activities was conducted in 52 health facilities (30 Pemba; 22 Unguja) that provide distribute LLINs and 65 shehia (30 Pemba; 35 Unguja). The objective of this activity was to assess the progress of distribution activities and to provide technical support to ensure the high-quality of service delivery throughout the net distribution network. ZAMEP observed that most of the health facilities visited had a 6-month supply of nets due to a previous LLIN distribution to all 179 health facilities in September 2019 conducted by ZAMEP and the Central Medical Store (CMS). Similarly, all of the 35 Shehia visited had adequate stocks of coupons in support of net distribution activities.
The biggest challenge identified was the failure of assistant Shehas to provide coupons in a timely manner to eligible community members. In addition, ZAMEP identified that some community members delayed collecting nets from their nearest health facilities. With the technical support from USAID Tulonge Afya, ZAMEP is preparing to launch an intensive SBCC campaign to address these issues among others. The SBCC campaign will begin on January 6, 2020 across Zanzibar.
CD planning, coordination, and feedback meetings with shehias and district authorities
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 27
In this reporting period, ZAMEP conducted a series of planning, coordination, and feedback meetings with shehias and district authorities on CD progress. These meetings targeted district authorities given their key stakeholder role in net distribution, given that all community-based distribution is managed by sheha and their assistants.
Two meetings were conducted—one each on Unguja and Pemba—with attendance from 59 participants representing district-level stakeholders. Among the issues discussed was the shortage of coupons amongst some shehia and the delayed distribution of coupons to targeted community members from the Central and North B districts for Unguja and Micheweni for Pemba.
Rapid assessment for LLIN utilization
With support from USAID’s Tulonge Afya project, ZAMEP conducted a rapid assessment for LLIN utilization to establish a baseline against which future net distribution activities can be measured. Information was collected via focus group discussions with shehas, assistant shehas, caretakers, pregnant women, and heads of households. Findings will be used to improve net distribution.
LLIN consignment through support from GFATM
A total of 331,000 LLINs were received from GFATM for support to Zanzibar’s net distribution intervention. This funding ensures the availability of nets at health facilities and seamless operation of distribution channels all over the Islands. A portion of the nets are stored at the Central Medical Store warehouse; a second portion is stored at the Ministry of Health Zanzibar’s (MoHZ) IRS warehouse in Mombasa.
Mass media campaigns
Eight live television programs aired on Zanzibar Broadcasting Corporation (ZBC) television and ten live radio programs were prepared and broadcasted on ZBC radio and Micheweni FM radio in Pemba. The programs aimed to increase the communities’ understanding of key malaria elimination activities. The major topics covered included CD of LLINs, malaria prevention for travelers, malaria case management, and community-based malaria case follow-up.
Print/distribute educational malaria materials
ZAMEP’s SBCC Unit printed and distributed 845 calendars with embedded malaria elimination messages emphasizing key malaria elimination interventions, including continuous net use, participating in IRS, larviciding, early health-seeking behavior, and cleanness of living environment to eliminate malaria breeding sites and other malaria risk factors. The calendars were distributed to local government and private institutions.
ZAMEP is coordinating printing of car stickers with malaria elimination messages. A vendor has been identified and ZAMEP sent the file with the final messages that will be printed and applied to its fleet of 80 cars to further disseminate malaria elimination messages to the general public.
Conduct malaria sensitization meetings with community members living in malaria foci areas
During the reporting period, sixteen community meetings were conducted in malaria hotspot areas. to sensitize community members about the importance of adopting malaria elimination strategies. Meetings were conducted in the following shehia in Unguja—Mnazi Mmoja, Kiponda, Malini, Shangani, Mkunazini, Kikwajuni Bondeni, Kikwajuni Juu,
28 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Kisiwandui, Kisima Majongoo, Mtowa Pwani (Fungu refu), Bumbwini and Kiongwe; in Pemba, meetings were conducted Tumbe Mashariki and Piki shehia.
Regional and district IRS advocacy meetings
Through support from the USAID VectorLink project, ZAMEP conducted two meetings—one in Unguja and one in Pemba—to update regional and district authorities on the upcoming IRS campaign scheduled for February 2020 in 63 Shehia across Unguja and Pemba.
2.2.5 Activity 1B.2: Develop interoperability between key HIS Complete ongoing electronic interoperability efforts between MCN and DHIS2 to enable ZAMEP to compare, analyze, and visualize data from multiple sources in DHIS2, including the ability to automatically generate necessary program and data elements in DHIS2 Progress in Y2, Q1
The MoHZ uses DHIS2 to report on routine health indicators collected across health facilities in Zanzibar. The MCN system, also known as Coconut Surveillance, is another platform used by ZAMEP to capture and track individual cases, as well as to track performance of CMSOs in reaching positively identified indexed and secondary malaria cases across Pemba and Unguja.
ZAMEP also utilizes another system called the Malaria Early Epidemic Detection System (MEEDS). Established in 2008, MEEDS uses mobile phones to transmit weekly summaries of aggregated malaria cases (among other parameters) from the health facilities to ZAMEP. Both MEEDS and MCN are independently run by ZAMEP. However, the focus now is to integrate parallel systems, including MEEDS and MCN, into the ministry-owned DHIS2 platform to sustain and optimize MoHZ-owned resources and systems.
In Q1, OMDM continued to work on specific activities to integrate DHIS2 and Coconut including syncing selected indicators across both systems. The following activities were conducted:
1. Finalized malaria indicators that will be integrated including the following:
− Malaria cases disaggregated by detection (Active/Passive) − Malaria cases by age (<5 and ≥5 years) − Malaria cases by gender − Malaria cases by classification − Malaria cases disaggregated by location
2. Created the aforementioned selected indicators in DHIS2 (on a DHIS2 test server that is not live. It will only be activated after testing of integration activities is complete).
3. Harmonized organizational units between MCN and DHIS2.This was the most challenging phase because in DHIS2, the only shehias listed are those that are attached to an existing health facility. However, in the MCN, all shehias are listed since CMSOs can visit any household across the two islands and would be required to record this information. Although we have harmonized most of the shehias between DHIS2 and MCN, we are still streamlining this process.
4. Developed scripts for synchronizing aggregated data between MCN and DHIS2. The scripts are programmed to enable data to be pulled from MCN into DHIS2 for the selected indicators. The scripts were also tested to ensure that it was functioning correctly in terms of allowing the right data to be pulled from Coconut into DHIS2
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 29
5. Define required dashboards. We began working on building dashboards that could emulate a malaria dashboard like on the Mainland, to show the data in a meaningful way to the users. This is still in process.
Also, there is a wider plan by the MOHZ to roll out an Integrated Diseases Weekly Ending (IDWE) report in 2020. This reports notifiable diseases on a weekly basis through DHIS2. It also includes malaria indicators. Once in place, it will replace MEEDS, the current weekly reporting platform. However, OMDM will continue to use MEEDS until we are ready to launch the Integrated Diseases Weekly Ending report.
Planned for Q2
OMDM will continue working on integration activities. We will begin reviewing the data in DHIS2 and compare it against Coconut. Our plan is to finalize the dashboards in DHIS2 and share them with ZAMEP and the HMIS Unit of the MOHZ to capture their opinions and feedback on ways of improving their functionality.
Link Zanzibar’s Integrated Logistic System (ZILS) to DHIS2 to improve ZAMEP’s ability to monitor and manage the supply of antimalarial drugs, RDTs and insecticide- treated nets (ITNs) to health care facilities and districts Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
OMDM will initially schedule a meeting with representatives from the ZILS to explore indicators that could be included within DHIS2. We need to determine what could be useful for ZAMEP to track and how often (monthly, quarterly). Once the groundwork is in place, we can plan to work with the HMIS and ICT Units to determine how data for the selected indicators can be pulled from ZILS into DHIS2.
2.2.6 Activity 1B.3: Enhance and strengthen MCN ICT architecture and sustainability
Improve MCN documentation for technical support and SOPs, transfer routine MCN technology support responsibilities to ZAMEP through mentoring, develop local MCN software development and support capacity, and transfer Tier 1 MCN software development and support responsibility to an identity identified by ZAMEP Progress in Y2, Q1
ZAMEP is committed to sustaining the Coconut Surveillance MCN system in the long term; the Program is committed to building the capacity of existing staff in Zanzibar to manage all aspects of the Coconut system and how it is used by ZAMEP. In Q1, OMDM developed a capacity building plan that detailed relevant training and mentoring required in Y2. Essentially, we propose to follow the approach used by DHIS2 that distinguishes between end users, integrators, and developers. End users are people that use the system and includes both data collection-oriented users like CMSOs and data-consuming users like the SME Unit at ZAMEP. Integrators are those who are responsible for configuring and updating the system. Activities include managing users and updating or changing the questions that are being captured in the field. Developers need a full understanding of the system architecture and software and are responsible for managing the server and database and making software changes to add new features or fix bugs.
For end users and integrators, a capacity building and training of trainers-focused approach is proposed. This will also include documents with screenshots as resources. Developers will
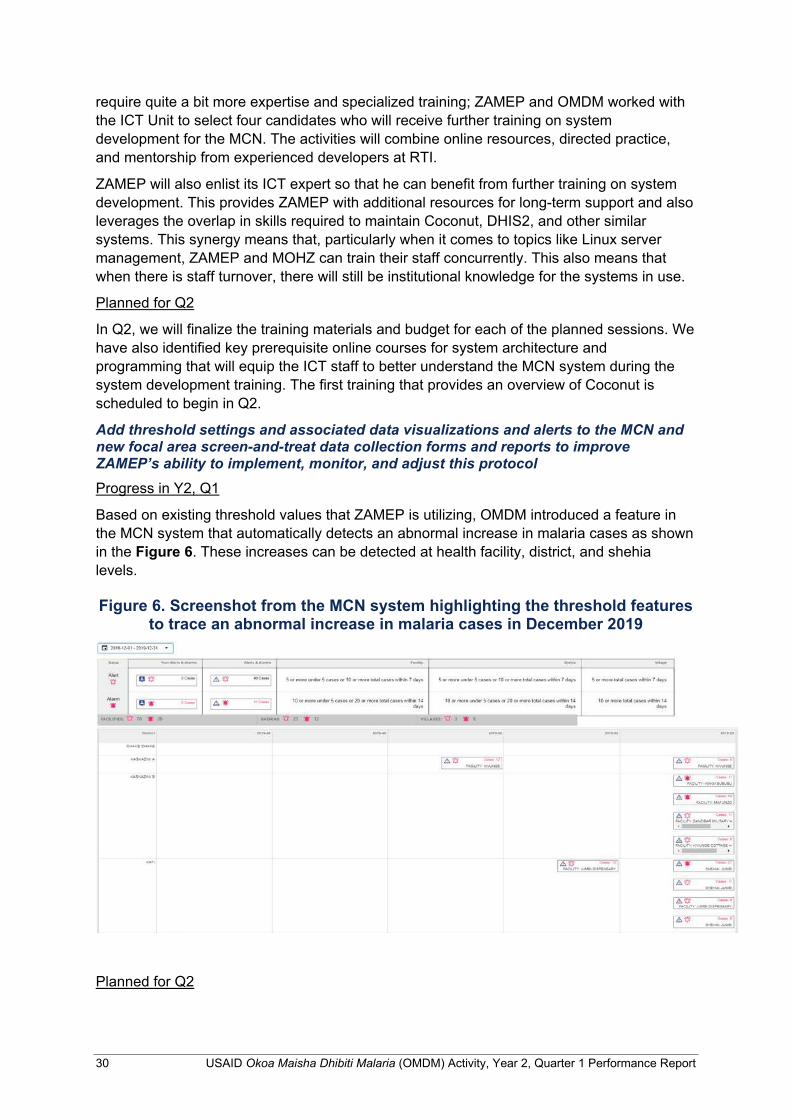
30 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
require quite a bit more expertise and specialized training; ZAMEP and OMDM worked with the ICT Unit to select four candidates who will receive further training on system development for the MCN. The activities will combine online resources, directed practice, and mentorship from experienced developers at RTI.
ZAMEP will also enlist its ICT expert so that he can benefit from further training on system development. This provides ZAMEP with additional resources for long-term support and also leverages the overlap in skills required to maintain Coconut, DHIS2, and other similar systems. This synergy means that, particularly when it comes to topics like Linux server management, ZAMEP and MOHZ can train their staff concurrently. This also means that when there is staff turnover, there will still be institutional knowledge for the systems in use.
Planned for Q2
In Q2, we will finalize the training materials and budget for each of the planned sessions. We have also identified key prerequisite online courses for system architecture and programming that will equip the ICT staff to better understand the MCN system during the system development training. The first training that provides an overview of Coconut is scheduled to begin in Q2.
Add threshold settings and associated data visualizations and alerts to the MCN and new focal area screen-and-treat data collection forms and reports to improve ZAMEP’s ability to implement, monitor, and adjust this protocol Progress in Y2, Q1
Based on existing threshold values that ZAMEP is utilizing, OMDM introduced a feature in the MCN system that automatically detects an abnormal increase in malaria cases as shown in the Figure 6. These increases can be detected at health facility, district, and shehia levels.
Figure 6. Screenshot from the MCN system highlighting the threshold features
to trace an abnormal increase in malaria cases in December 2019
Planned for Q2
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 31
As shown above, the recent uptick in cases was detected by the MCN system. We are not currently sending out emails when these are detected. However, OMDM will work with ZAMEP to get feedback on the threshold settings, and in future, decide who should receive notifications when an alert or alarm is detected. This is configurable and can be done in the administrative section of the Coconut website.
Continue to adapt and enhance MCN reports and data visualizations to meet emerging ZAMEP needs Progress in Y2, Q1
In addition to the epidemic thresholds feature that was activated in the MCN, OMDM has continued to improve the automated weekly report, based on useful feedback from PMI and other partners who receive the reports from ZAMEP on weekly basis.
Planned for Q2
The Activity has started working on another feature that aims to reflect malaria foci at the shehia level. OMDM aims to add foci classification that can be seen on a map, and show active, residual active, and cleared areas of transmission for a specified time period. We are currently in the development stage and once complete, will conduct usability and beta testing before being deployed for use by ZAMEP’s SME team.
2.2.7 Activity 1B.4: Support MCN implementation Provide software technology and equipment support to CMSO Progress in Y2, Q1
In Q1, OMDM made small updates to the travel history questions and skip logics in the Coconut app, based on feedback from CMSOs who regularly use this software on their tablets during household visits.
Some CMSOs were experiencing problems with their Coconut App such as the application not loading, or data unable to be saved. The main reason for this problem was due to lack of memory available on the tablets. We resolved this by requesting ZAMEP’s SME teams instruct CMSOs to clear photos/movies and other personal files from the tablets to free up space and allow the application to function optimally.
Planned for Q2
We will continue to provide support for the MCN system and software maintenance and ensure that it continues to function well.
Continuously engage with ZAMEP and CMSOs to ensure that MCN is functional and data flow is adhered to in terms of timely collection and transfer of data, data completeness, and quality, and that reactive case follow-up occurs within stipulated time windows Progress in Y2, Q1
Improve MEEDS reporting timeliness
ZAMEP’s SME Unit continues to emphasize the importance of reporting data on time. The SME Unit uses two approaches to increase reporting timeliness. First, it follows up with facilities by calling them when they observe a delay in submitting reports or when incorrect data are sent. Second, visits are scheduled with facilities where the problem continues to persist over a long period.

32 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Between October–December 2019, 82.5% of the facilities submitted their reports on time (Monday). The reporting rate for Unguja was 85%; in Pemba it was 80%. The major challenge observed was receiving notifications of delivered messages once health care providers submit their reports. Some health facilities delayed submitting their current reports waiting to get a notification while their reports were already received in the system. The problem was reported to Selcom for further follow up and rectification.
Health facility results
95% of identified malaria cases were well registered in all three data systems—MCN, MEEDS and HMIS—with only one patient not documented in the MCN. ZAMEP followed up with all ten cases identified at the household level. Nine cases were notified within the 48 hour timeframe; only one case missed the 48 hour target.
Household results
Between October–December 2019, 6,631 additional household members were tested during the CMSOs’ visits at the household level; 143 additional malaria cases were confirmed. The highest number of household members revealed in Mjini (1,365) and the lowest (97) additional household members tested reported in Kusini, Unguja..
Quarterly supporting supervision visits with CMSOs
Supervision is one monitoring mechanism that provides an opportunity to track and improve the performance of health workers to meet their main objective to collect and report quality data at the national level.
In Q1, supervision activities were conducted by 18 CMSOs (10 in Unguja; 8 in Pemba) through support from ZAMEP under their FAA with OMDM. The primary objective of this supervision was to monitor data management performance and identify and correct any implementation challenges identified amongst CMSOs from the health facility to the household level.
16 malaria cases—two cases per CMSO—were identified during the supervision activities conducted in Q1. All visited cases were reported from 10 health facilities—six in Unguja (Bwejuu, Kizimkazi Dimbani, Donge Mchangani, Nungwi, Kizimbani and Kiembe Samaki) and four in Pemba (Tumbe, Abdalla Mzee, Chonga and Jadida).
Feedback meetings with CMSOs in Unguja and Pemba
ZAMEP’s SME Unit routinely conducts CMSOs feedback meetings in Unguja and Pemba in order to review data reported by CMSOs during their case investigation activities and to share any operational challenges during implementation. In Q1, six meetings were conducted as planned. The main issues raised during the meeting included failure to auto- switch between the forms within the Coconut app and increased malaria cases in almost all districts across Unguja and Pemba. Table 8 summarizes some of the issues discussed during the meeting.
Table 8. List of issues discussed during CMSO feedback meetings
SN Issue Status Way forward 1 Duplication of cases Facilities report more than one
case in single day. This is due to missed delivery reports from the system.
This a long existing problem and it is not 100% resolved. This issue was reported to RTI/SELCOM.
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 33
SN Issue Status Way forward 2 Delayed addition of some
additional menu options related to Household data during case follow-up.
This issue has been reported by CMSOs from both Unguja and Pemba. During their household visits, when CMSOs pressed the Household button it takes too long to run.
This issue was already reported to the programmer and he advised CMSOs to uninstall/remove unnecessary programs on their tablets to speed up the processing operation of their tablets.
3 Increasing malaria cases This was one of the major issues discussed. Participants agreed that CMSOs continue with their case follow-up despite the case fluctuations in most areas. It was well elaborated that more focus should be given in areas that report many cases like Kikwajuni Shehia in Unguja.
This was agreed and action has been taken to respond with increases of malaria cases in Kikwajuni.
Facilitate data use workshops to review, analyze, and interpret epidemiological and programmatic data reported through DHIS2 and MCN Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
OMDM will schedule and conduct a data review meeting with ZAMEP in Q2.
2.2.8 Activity 1B.5: Refine operational thresholds and triggers as MCN data are analyzed
Use MERLA approach to continuously support ZAMEP to assess sensitivity and specificity of thresholds and triggers, that change and adapt, as appropriate, to further increase interventions’ programmatic effectiveness Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities to be initiated in Q3.
Collaborate with ZAMEP, PMI, and stakeholders to update, as necessary, guidance and intervention strategies to prevent and respond to the emergency of case clusters at village or Shehia level Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities to take place as necessary following routine data reviews.
Conduct ACD and foci investigation Progress in Y2, Q1
In Q1, 15 ACD events were organized and conducted across Unguja and Pemba, triggered by an abnormal increase of malaria cases following the continued rains. Eight ACD events were conducted in Unguja involving 3,194 mRDT tests resulting in where 62 (1.9%) had positive results. ZAMEP supported Council Response Teams (CRTs) to implement seven
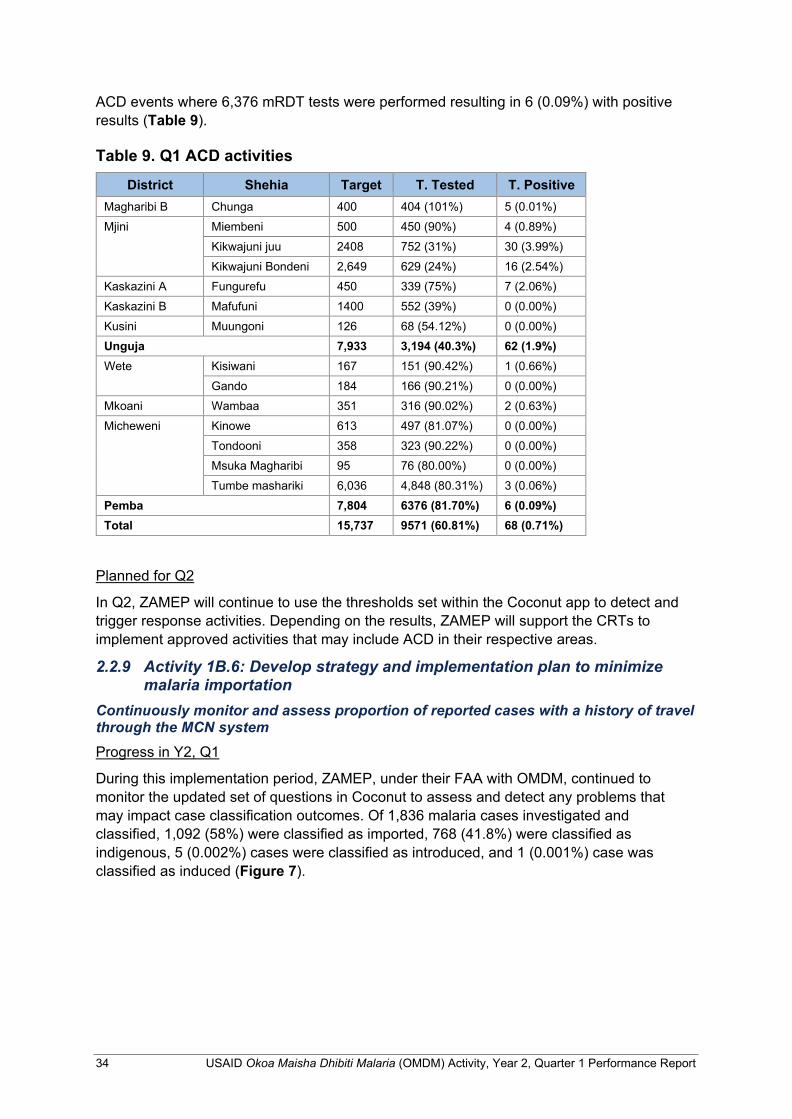
34 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
ACD events where 6,376 mRDT tests were performed resulting in 6 (0.09%) with positive results (Table 9).
Table 9. Q1 ACD activities
District Shehia Target T. Tested T. Positive Magharibi B Chunga 400 404 (101%) 5 (0.01%) Mjini Miembeni 500 450 (90%) 4 (0.89%)
Kikwajuni juu 2408 752 (31%) 30 (3.99%) Kikwajuni Bondeni 2,649 629 (24%) 16 (2.54%)
Kaskazini A Fungurefu 450 339 (75%) 7 (2.06%) Kaskazini B Mafufuni 1400 552 (39%) 0 (0.00%) Kusini Muungoni 126 68 (54.12%) 0 (0.00%) Unguja 7,933 3,194 (40.3%) 62 (1.9%) Wete Kisiwani 167 151 (90.42%) 1 (0.66%)
Gando 184 166 (90.21%) 0 (0.00%) Mkoani Wambaa 351 316 (90.02%) 2 (0.63%) Micheweni Kinowe 613 497 (81.07%) 0 (0.00%)
Tondooni 358 323 (90.22%) 0 (0.00%) Msuka Magharibi 95 76 (80.00%) 0 (0.00%) Tumbe mashariki 6,036 4,848 (80.31%) 3 (0.06%)
Pemba 7,804 6376 (81.70%) 6 (0.09%) Total 15,737 9571 (60.81%) 68 (0.71%)
Planned for Q2
In Q2, ZAMEP will continue to use the thresholds set within the Coconut app to detect and trigger response activities. Depending on the results, ZAMEP will support the CRTs to implement approved activities that may include ACD in their respective areas.
2.2.9 Activity 1B.6: Develop strategy and implementation plan to minimize malaria importation
Continuously monitor and assess proportion of reported cases with a history of travel through the MCN system Progress in Y2, Q1
During this implementation period, ZAMEP, under their FAA with OMDM, continued to monitor the updated set of questions in Coconut to assess and detect any problems that may impact case classification outcomes. Of 1,836 malaria cases investigated and classified, 1,092 (58%) were classified as imported, 768 (41.8%) were classified as indigenous, 5 (0.002%) cases were classified as introduced, and 1 (0.001%) case was classified as induced (Figure 7).
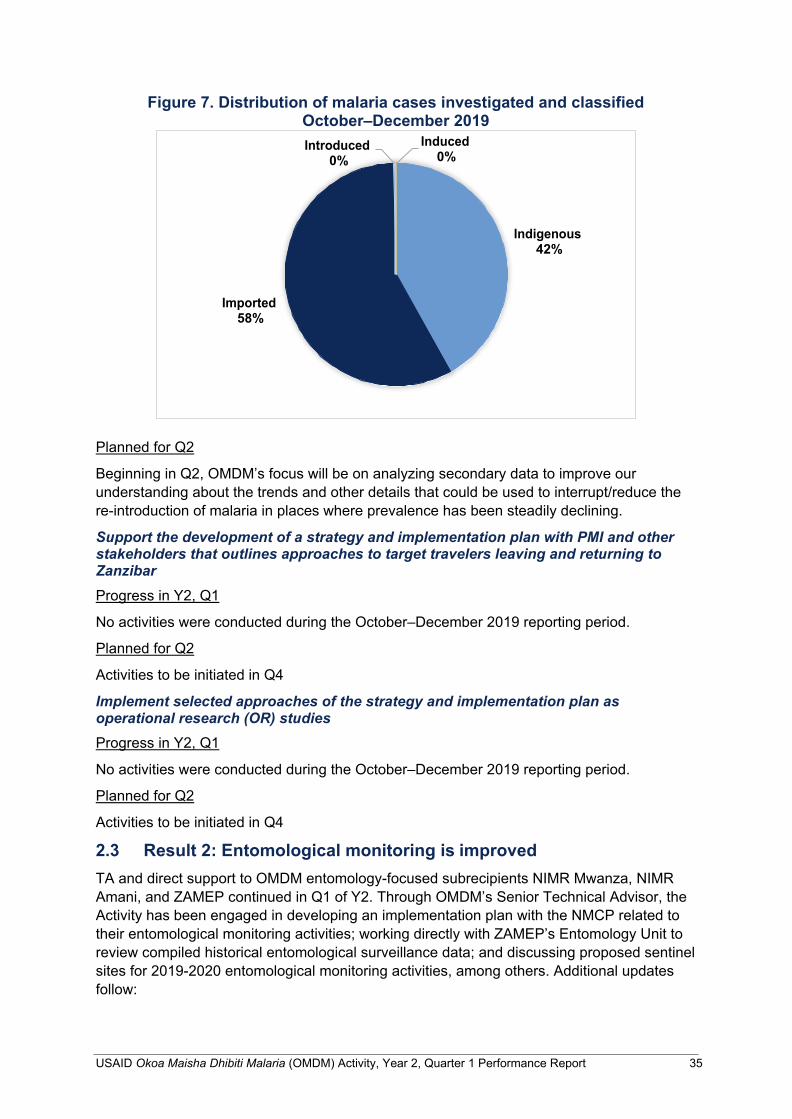
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 35
Figure 7. Distribution of malaria cases investigated and classified October–December 2019
Planned for Q2
Beginning in Q2, OMDM’s focus will be on analyzing secondary data to improve our understanding about the trends and other details that could be used to interrupt/reduce the re-introduction of malaria in places where prevalence has been steadily declining.
Support the development of a strategy and implementation plan with PMI and other stakeholders that outlines approaches to target travelers leaving and returning to Zanzibar Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities to be initiated in Q4
Implement selected approaches of the strategy and implementation plan as operational research (OR) studies Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities to be initiated in Q4
2.3 Result 2: Entomological monitoring is improved TA and direct support to OMDM entomology-focused subrecipients NIMR Mwanza, NIMR Amani, and ZAMEP continued in Q1 of Y2. Through OMDM’s Senior Technical Advisor, the Activity has been engaged in developing an implementation plan with the NMCP related to their entomological monitoring activities; working directly with ZAMEP’s Entomology Unit to review compiled historical entomological surveillance data; and discussing proposed sentinel sites for 2019-2020 entomological monitoring activities, among others. Additional updates follow:
Imported 58%
Indigenous 42%
Induced 0%
Introduced 0%
36 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
2.3.1 Activity 2.1: Compile and review entomological monitoring data Carry out a desk-based review of all entomological monitoring efforts in the past decade in Tanzania Progress in Y2, Q1
The desk-based review of entomological monitoring efforts in mainland Tanzania and Zanzibar initiated in Y1 continued in Q1 of Y2. OMDM submitted the draft report of the compiled entomological surveillance data to ZAMEP for review and met with their Entomology Unit on November 15–16, 2019 to briefly discuss the report and support them to write their annual entomological surveillance report. The final report of the compiled entomological surveillance data will be produced in Q2.
On November 28–29, 2019, OMDM met with the NMCP’s Vector Control Unit to discuss and agree on the implementation plan of entomological monitoring activities in Y2. We discussed the following issues:
• Working together to continue activities initiated in Y1 (such as modalities to accelerate the inclusion of entomological indicators into composite database). OMDM requested to continue supporting the NMCP to create the malaria entomological database to be uploaded in DHIS2
• Collaborating to develop a mechanism to upload entomological monitoring data in the DHIS2 composite database
• Strengthening the QA/QC of the GFATM-supported MVES in 62 districts
• Scheduling a meeting to triangulate and analyze data and write a comprehensive report resulting from ongoing MVES
• Developing a timeline of planned vector control TWG meetings to discuss entomological surveillance progress
Planned for Q2
In Q2, OMDM will:
• Work with ZAMEP to finalize the compiled entomological surveillance data report;
• Facilitate vector control TWG meetings to discuss entomological surveillance progress. Among other things, this meeting will focus on discussing modalities to accelerate the inclusion of entomological indicators into a composite database and a mechanism to upload entomology data into DHIS2; and,
• Support the NMCP to finalize the development of indicators in a composite database and facilitate data entry from relevant institutions.
Review entomological monitoring sites and their current operational and analytical capacity to successfully conduct entomological monitoring Progress in Y2, Q1
OMDM worked with NIMR Mwanza and PMI/CDC to review the sentinel sites for entomological monitoring for 2019–2020.We did this review to incorporate the data from entomological monitoring in regions where PBO LLINs have been distributed—Mwanza, Kagera, Geita, and Kigoma. Entomological monitoring is needed in these regions and must be synced with NIMR Mwanza’s Y2 workplan. All four regions where PBO nets are used
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 37
have at least one non-IRS control district for entomological monitoring except the Mwanza region; as a result, the Magu district has been proposed as an additional site to ensure coverage of the Mwanza region.
Planned for Q2
In Q2, OMDM will continue engaging with the NMCP, ZAMEP and key stakeholders to discuss the need to review and/or expand entomological monitoring sites aligned with the current malaria situation. We will additionally support orientation of ZAMEP’s entomologists to use the MCN, including training on data collection forms.
Conduct an IRS impact evaluation study Progress in Y2, Q1
In this reporting period, OMDM began developing a protocol to analyze the impact of IRS in Tanzania’s Lake Zone and Zanzibar.
Planned for Q2
In Q2, OMDM will:
• Finalize the protocol to analyze the impact of IRS in the Lake Zone and Zanzibar and present to NMCP/ZAMEP for approval;
• Using the new protocol, we will Initiate the analysis of the impact of IRS in Tanzania’s Lake Zone and Zanzibar;
• Lead data collection activities and analysis; and,
• Work with NMCP/ZAMEP to convene vector control TWGs to present initial findings and gather feedback.
Provide TA to NMCP for entomological monitoring and data analysis Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
In Q2, OMDM will liaise with the NMCP and provide them TA to plan, coordinate, and implement GFATM’s MVES, data triangulation, analysis and report writing.
2.3.2 Activity 2.2: Conduct entomological monitoring planning and implementation
Entomological surveillance, including Anopheles mosquito vector distribution, density, seasonality, biting behavior, human blood index, sporozoite rate, and entomological inoculation rate (EIR) Progress in Y2, Q1
OMDM issued fixed amount awards (FAAs) to NIMR Mwanza and ZAMEP to support entomological monitoring in Mainland Tanzania and Zanzibar. Summary data for Y2 Q1 is reported below.
ZAMEP. In Q1, ZAMEP completed entomological monitoring at sites in both Unguja and Pemba to assess the impact of IRS and LLINs, focusing on the entomological parameters that facilitate malaria transmission including vector density, infection rate, biting and resting behavior, and species composition. Pit trap catch (PTC), human landing catch (HLC), light trap collection (LTC), pyrethrum spray catch (PSC) and Prokopack were the methods used
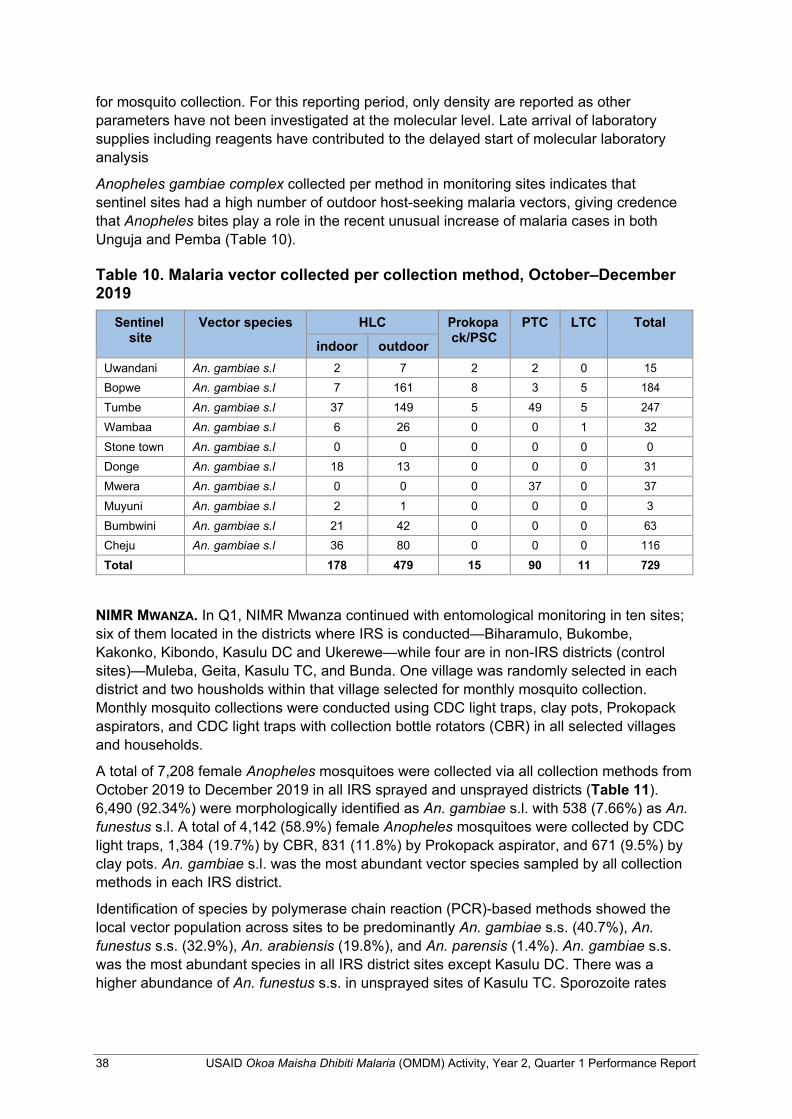
38 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
for mosquito collection. For this reporting period, only density are reported as other parameters have not been investigated at the molecular level. Late arrival of laboratory supplies including reagents have contributed to the delayed start of molecular laboratory analysis
Anopheles gambiae complex collected per method in monitoring sites indicates that sentinel sites had a high number of outdoor host-seeking malaria vectors, giving credence that Anopheles bites play a role in the recent unusual increase of malaria cases in both Unguja and Pemba (Table 10).
Table 10. Malaria vector collected per collection method, October–December 2019
Sentinel site
Vector species HLC Prokopa ck/PSC
PTC LTC Total
indoor outdoor Uwandani An. gambiae s.l 2 7 2 2 0 15 Bopwe An. gambiae s.l 7 161 8 3 5 184 Tumbe An. gambiae s.l 37 149 5 49 5 247 Wambaa An. gambiae s.l 6 26 0 0 1 32 Stone town An. gambiae s.l 0 0 0 0 0 0 Donge An. gambiae s.l 18 13 0 0 0 31 Mwera An. gambiae s.l 0 0 0 37 0 37 Muyuni An. gambiae s.l 2 1 0 0 0 3 Bumbwini An. gambiae s.l 21 42 0 0 0 63 Cheju An. gambiae s.l 36 80 0 0 0 116 Total 178 479 15 90 11 729
NIMR MWANZA. In Q1, NIMR Mwanza continued with entomological monitoring in ten sites; six of them located in the districts where IRS is conducted—Biharamulo, Bukombe, Kakonko, Kibondo, Kasulu DC and Ukerewe—while four are in non-IRS districts (control sites)—Muleba, Geita, Kasulu TC, and Bunda. One village was randomly selected in each district and two housholds within that village selected for monthly mosquito collection. Monthly mosquito collections were conducted using CDC light traps, clay pots, Prokopack aspirators, and CDC light traps with collection bottle rotators (CBR) in all selected villages and households.
A total of 7,208 female Anopheles mosquitoes were collected via all collection methods from October 2019 to December 2019 in all IRS sprayed and unsprayed districts (Table 11). 6,490 (92.34%) were morphologically identified as An. gambiae s.l. with 538 (7.66%) as An. funestus s.l. A total of 4,142 (58.9%) female Anopheles mosquitoes were collected by CDC light traps, 1,384 (19.7%) by CBR, 831 (11.8%) by Prokopack aspirator, and 671 (9.5%) by clay pots. An. gambiae s.l. was the most abundant vector species sampled by all collection methods in each IRS district.
Identification of species by polymerase chain reaction (PCR)-based methods showed the local vector population across sites to be predominantly An. gambiae s.s. (40.7%), An. funestus s.s. (32.9%), An. arabiensis (19.8%), and An. parensis (1.4%). An. gambiae s.s. was the most abundant species in all IRS district sites except Kasulu DC. There was a higher abundance of An. funestus s.s. in unsprayed sites of Kasulu TC. Sporozoite rates
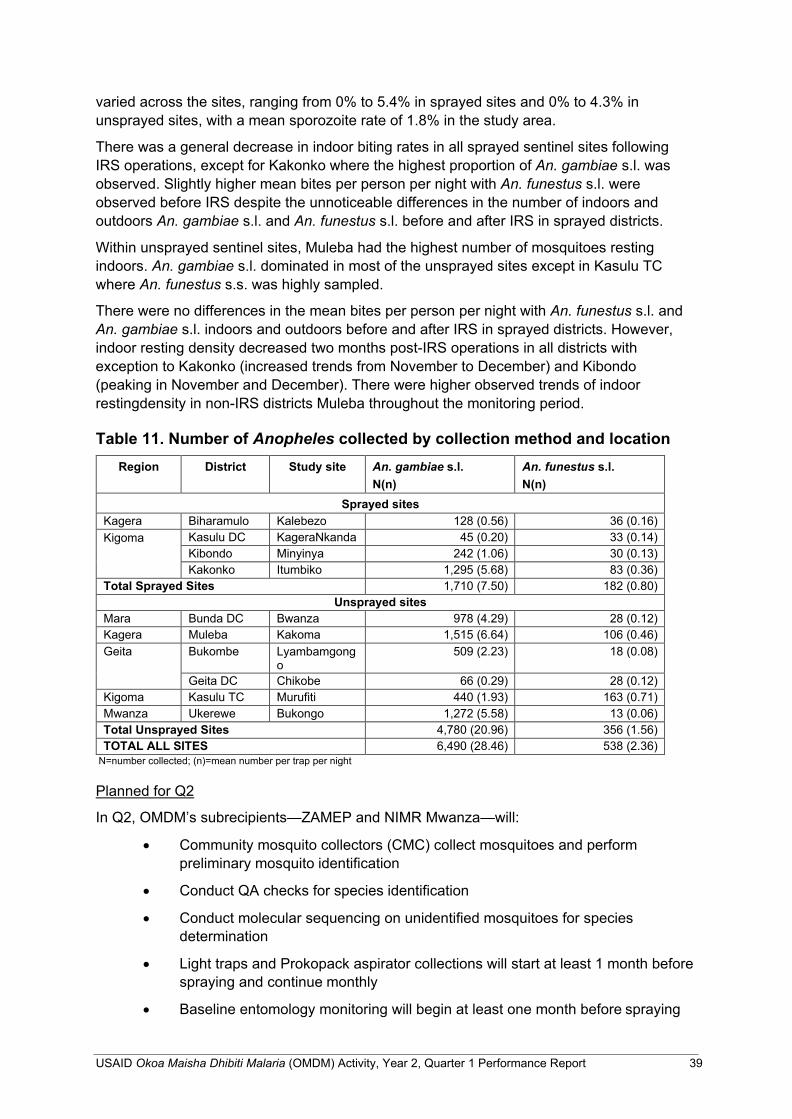
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 39
varied across the sites, ranging from 0% to 5.4% in sprayed sites and 0% to 4.3% in unsprayed sites, with a mean sporozoite rate of 1.8% in the study area.
There was a general decrease in indoor biting rates in all sprayed sentinel sites following IRS operations, except for Kakonko where the highest proportion of An. gambiae s.l. was observed. Slightly higher mean bites per person per night with An. funestus s.l. were observed before IRS despite the unnoticeable differences in the number of indoors and outdoors An. gambiae s.l. and An. funestus s.l. before and after IRS in sprayed districts.
Within unsprayed sentinel sites, Muleba had the highest number of mosquitoes resting indoors. An. gambiae s.l. dominated in most of the unsprayed sites except in Kasulu TC where An. funestus s.s. was highly sampled.
There were no differences in the mean bites per person per night with An. funestus s.l. and An. gambiae s.l. indoors and outdoors before and after IRS in sprayed districts. However, indoor resting density decreased two months post-IRS operations in all districts with exception to Kakonko (increased trends from November to December) and Kibondo (peaking in November and December). There were higher observed trends of indoor restingdensity in non-IRS districts Muleba throughout the monitoring period.
Table 11. Number of Anopheles collected by collection method and location
Region District Study site An. gambiae s.l. N(n)
An. funestus s.l. N(n)
Sprayed sites Kagera Biharamulo Kalebezo 128 (0.56) 36 (0.16) Kigoma Kasulu DC KageraNkanda 45 (0.20) 33 (0.14)
Kibondo Minyinya 242 (1.06) 30 (0.13) Kakonko Itumbiko 1,295 (5.68) 83 (0.36)
Total Sprayed Sites 1,710 (7.50) 182 (0.80) Unsprayed sites
Mara Bunda DC Bwanza 978 (4.29) 28 (0.12) Kagera Muleba Kakoma 1,515 (6.64) 106 (0.46) Geita Bukombe Lyambamgong
o 509 (2.23) 18 (0.08)
Geita DC Chikobe 66 (0.29) 28 (0.12) Kigoma Kasulu TC Murufiti 440 (1.93) 163 (0.71) Mwanza Ukerewe Bukongo 1,272 (5.58) 13 (0.06) Total Unsprayed Sites 4,780 (20.96) 356 (1.56) TOTAL ALL SITES 6,490 (28.46) 538 (2.36)
N=number collected; (n)=mean number per trap per night
Planned for Q2
In Q2, OMDM’s subrecipients—ZAMEP and NIMR Mwanza—will:
• Community mosquito collectors (CMC) collect mosquitoes and perform preliminary mosquito identification
• Conduct QA checks for species identification
• Conduct molecular sequencing on unidentified mosquitoes for species determination
• Light traps and Prokopack aspirator collections will start at least 1 month before spraying and continue monthly
• Baseline entomology monitoring will begin at least one month before spraying

40 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
• Indoor biting rates determined by CDC light traps—collect mosquitoes for 14 nights during two consecutive weeks each month. NIMR Mwanza to survey two different houses per night.
• Outdoor biting rates monitored using CDC light traps with bottle rotators— sampling on nights near new moon
• Vector feeding time and location monitored indoors and outdoors using CDC light traps with bottle rotators—mosquitoes collected 10 days of lunar month
• Outdoor and indoor resting densities measured using Prokopack aspiration in five houses each day
• 100 Anopheles will be analyzed to determine the proportion of mosquito blood meals from humans versus other animals.
QA and insecticide residual efficacy monitoring following IRS Progress in Y2, Q1
NIMR MWANZA. Under their FAA with OMDM, NIMR Mwanza conducted wall cone and fumigant bioassays in Muleba and Biharamuro following the IRS campaign using clothianidin. Similar bioassays were conducted in Kibondo, Kakonko, and Kasulu districts that were sprayed with pirimiphos methyl (Actellic® 300CS) during IRS operations. The observed mortality for the wall cone bioassays was 100% on all surfaces 2–6 days following exposure to clothianidin. A strong fumigant effect of clothianidin was also observed, with 100% mortality shown 1–2 days after insecticide exposure. Pirimiphos methyl (Actellic® 300CG), also showed a strong fumigant effect with 100% mortality shown one day after insecticide exposure. Two months post-IRS insecticide efficacy was retained up to 100% in all surfaces on all sites except in Kibondo district where mud, painted and whitewash surfaced were less than 50% mortality after 24 hours.
ZAMEP. Under their FAA with OMDM, ZAMEP continued with IRS QA activities in six shehias across Unguja and Pemba. Specifically, ZAMEP selected 15 houses to conduct WHO cone bioassays reflecting various wall surfaces, including mud, cement, oil paint, lime wash, water paint, and stone block. Three houses representing each wall surface type were tested in each shehia. Results indicate that Actellic 300 CS insecticide aged 210 days showed high mortality among malaria vectors in Pemba (mortality rate of >90%) as compared with Unguja (mortality rate of 64%–72%) on all wall surfaces. At 240 days, Actellic 300 CS still maintained the minimum effectiveness in Pemba and Unguja (Figure 8).
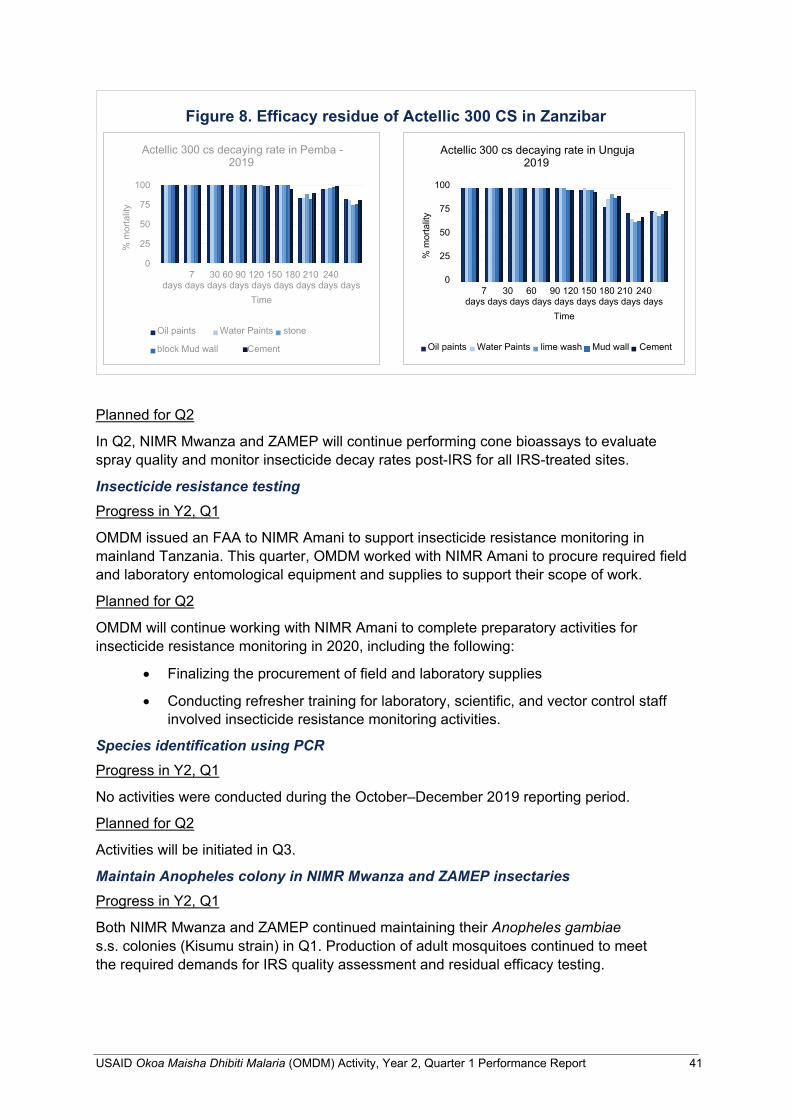
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 41
Figure 8. Efficacy residue of Actellic 300 CS in Zanzibar
Actellic 300 cs decaying rate in Unguja 2019
100
75
50
25
0 7 30 60 90 120 150 180 210 240
days days days days days days days days days Time
Oil paints Water Paints lime wash Mud wall Cement
Actellic 300 cs decaying rate in Pemba - 2019
100
75
50
25
0 7 30 60 90 120 150 180 210 240
days days days days days days days days days Time
Oil paints Water Paints stone
block Mud wall Cement
Planned for Q2
In Q2, NIMR Mwanza and ZAMEP will continue performing cone bioassays to evaluate spray quality and monitor insecticide decay rates post-IRS for all IRS-treated sites.
Insecticide resistance testing Progress in Y2, Q1
OMDM issued an FAA to NIMR Amani to support insecticide resistance monitoring in mainland Tanzania. This quarter, OMDM worked with NIMR Amani to procure required field and laboratory entomological equipment and supplies to support their scope of work.
Planned for Q2
OMDM will continue working with NIMR Amani to complete preparatory activities for insecticide resistance monitoring in 2020, including the following:
• Finalizing the procurement of field and laboratory supplies
• Conducting refresher training for laboratory, scientific, and vector control staff involved insecticide resistance monitoring activities.
Species identification using PCR Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities will be initiated in Q3.
Maintain Anopheles colony in NIMR Mwanza and ZAMEP insectaries Progress in Y2, Q1
Both NIMR Mwanza and ZAMEP continued maintaining their Anopheles gambiae s.s. colonies (Kisumu strain) in Q1. Production of adult mosquitoes continued to meet the required demands for IRS quality assessment and residual efficacy testing.
% m
orta
lity
% m
orta
lity
42 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Planned activities for Q2 Anopheles gambiae s.s. colonies (susceptible Kisumu strain) colonies will be maintained in insectaries in Q2 by NIMR Mwanza and ZAMEP.
2.3.3 Activity 2.4: Provide equipment and supplies for entomological monitoring
Progress in Y2, Q1
OMDM staff worked with NIMR Mwanza, NIMR Amani, and ZAMEP to identify entomological monitoring equipment, supplies, and reagents needed for Y2 activities. Procurement is underway.
Planned for Q2
OMDM will continue to work with NIMR Mwanza, NIMR Amani and ZAMEP to finalize the procurement of the identified equipment, supplies and reagents, with the goal of having all supplies in country early in Q2.
2.3.4 Activity 2.5: Entomological investigation and response in hot spot areas/active foci (Zanzibar only)
Progress in Y2, Q1
Under their FAA with OMDM, ZAMEP conducted foci investigations in three foci in Unguja and Pemba following an abnormal increase of local cases. The investigations aimed to assess the risk factors associated with disease transmission and provide recommendations to effectively manage disease transmission. The risk factors investigated were demographic information, vector control application particularly IRS and LLINs at the household level, malaria vector characterization and the presence of mosquito breeding sites.
General findings showed the presence of outdoor biting of malaria vectors with the presence of mosquito breeding sites close to the households. The team recommended the use of vector control that will reduce residual malaria transmission. Additionally, they recommended intensifying SBCC messaging to increase LLIN usage in the foci areas.
Planned for Q2
Under their subaward with OMDM, ZAMEP will continue foci investigation and address identified challenges in Q2.
2.3.5 Activity 2.6: Capacity building of new entomological field team in new emerging hot spots (Zanzibar only)
Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities to be initiated in Q3
2.3.6 Activity 2.7: Strengthen national malaria vector control strategies, policies, and guidelines
Engage with the respective subcommittees and TWGs Progress in Y2, Q1
In Q1, OMDM and the NMCP agreed to hold the vector control TWG meeting in Q2. Also see section 2.3.1 above.
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 43
Planned for Q2
In Q2, OMDM will support the vector control TWG meeting of the NMCP and will initiate the development of ToR for the vector control TWG for ZAMEP.
Review and update relevant policy and technical guidelines Progress in Y2, Q1
On November 14–16, 2019, OMDM supported ZAMEP to develop the larval source management opererational tool. As a follow-up, OMDM met with ZAMEP on December 13, 2019, to validate the tool. The final larviciding tool will be presented to ZAMEP management in Q2.
On December 19, 2019, OMDM participated in a stakeholders’ meeting to launch the midterm review of ZAMEP’s malaria strategic plan. The actual midterm review will be conducted in Q2.
Planned for Q2
In Q2, OMDM will:
• Work with ZAMEP to finalize the larval source management operational tool; and
• Participate in the midterm review of ZAMEP’s malaria strategic plan.
Provide financial and logistic support to disseminate updated guidance documents Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities will be initiated in Q2
2.4 Result 3: Drug efficacy monitoring is improved In Q1 of Y2, OMDM continued support to the TES 2019 implementing partner—MUHAS— while also preparing the FAA to the TES 2020 implementing partner, CUHAS. Additionally, OMDM supported the initiation of molecular analysis activities completed by NIMR Tanga, including procurement of necessary equipment and supplies through support from RTI’s home office. Additional details follow:
2.4.1 Activity 3.2: Plan, monitor, and implement TES Mainland Tanzania: Plan, monitor, and implement TES Progress in Y2, Q1
In Q1, OMDM initiated the process to put an FAA in place with CUHAS to support their management of TES implementation activities in 2020.
Additionally, OMDM supported MUHAS to conduct data analysis, interpretation, and dissemination of data from TES 2019. MUHAS analyzed TES outcomes, including early treatment failure, late clinical failure, and late parasitological failure according to the 2009 WHO guidelines. The summary on adverse events, risk of recurrent infections per study site, and proportions of patients with parasitemia on day 28 (Table 12) were also provided. These findings were presented at the TES TWG meeting held on November 5, 2019, at MUHAS.
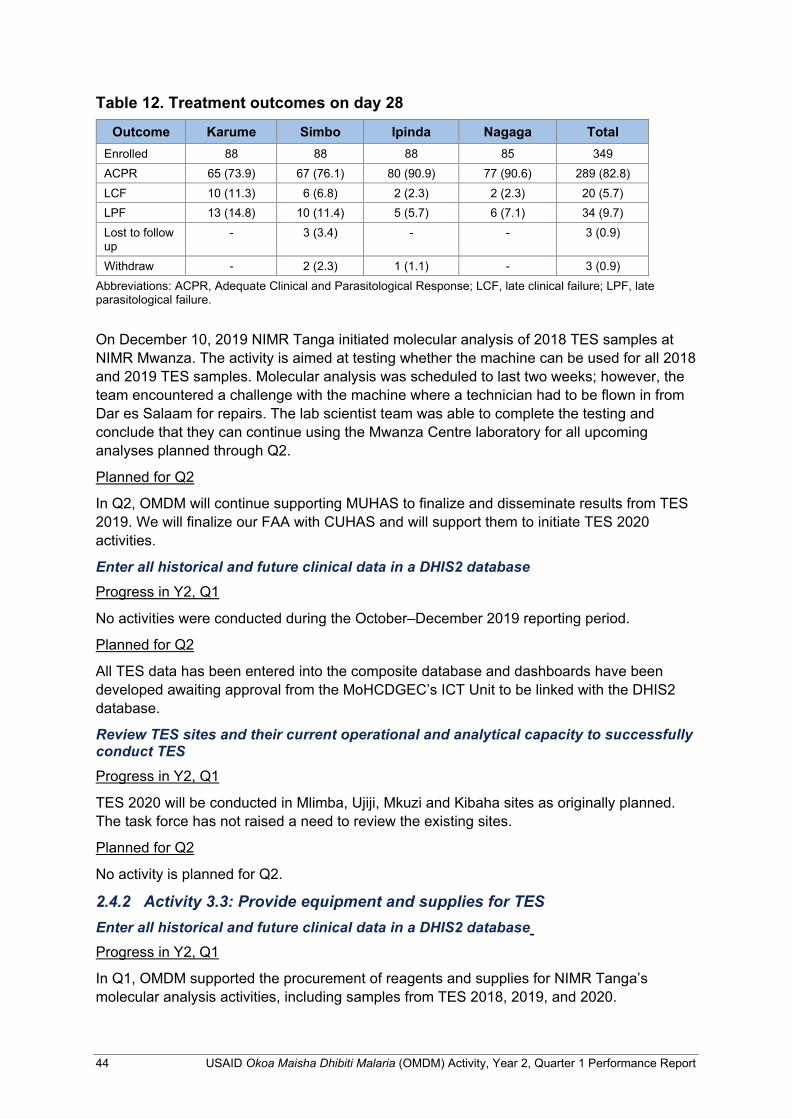
44 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Table 12. Treatment outcomes on day 28
Outcome Karume Simbo Ipinda Nagaga Total Enrolled 88 88 88 85 349 ACPR 65 (73.9) 67 (76.1) 80 (90.9) 77 (90.6) 289 (82.8) LCF 10 (11.3) 6 (6.8) 2 (2.3) 2 (2.3) 20 (5.7) LPF 13 (14.8) 10 (11.4) 5 (5.7) 6 (7.1) 34 (9.7) Lost to follow up
- 3 (3.4) - - 3 (0.9)
Withdraw - 2 (2.3) 1 (1.1) - 3 (0.9) Abbreviations: ACPR, Adequate Clinical and Parasitological Response; LCF, late clinical failure; LPF, late parasitological failure.
On December 10, 2019 NIMR Tanga initiated molecular analysis of 2018 TES samples at NIMR Mwanza. The activity is aimed at testing whether the machine can be used for all 2018 and 2019 TES samples. Molecular analysis was scheduled to last two weeks; however, the team encountered a challenge with the machine where a technician had to be flown in from Dar es Salaam for repairs. The lab scientist team was able to complete the testing and conclude that they can continue using the Mwanza Centre laboratory for all upcoming analyses planned through Q2.
Planned for Q2
In Q2, OMDM will continue supporting MUHAS to finalize and disseminate results from TES 2019. We will finalize our FAA with CUHAS and will support them to initiate TES 2020 activities.
Enter all historical and future clinical data in a DHIS2 database Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
All TES data has been entered into the composite database and dashboards have been developed awaiting approval from the MoHCDGEC’s ICT Unit to be linked with the DHIS2 database.
Review TES sites and their current operational and analytical capacity to successfully conduct TES Progress in Y2, Q1
TES 2020 will be conducted in Mlimba, Ujiji, Mkuzi and Kibaha sites as originally planned. The task force has not raised a need to review the existing sites.
Planned for Q2
No activity is planned for Q2.
2.4.2 Activity 3.3: Provide equipment and supplies for TES Enter all historical and future clinical data in a DHIS2 database Progress in Y2, Q1
In Q1, OMDM supported the procurement of reagents and supplies for NIMR Tanga’s molecular analysis activities, including samples from TES 2018, 2019, and 2020.
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 45
Planned for Q2
In Q2, OMDM will finalize procurement activities to ensure all materials and supplies are delivered to NIMR Tanga to facilitate their molecular analysis activities. Additionally, OMDM will work with CUHAS to ensure that subagreements to local partners are executed in a timely fashion to allow TES 2020 activities to proceed.
2.4.3 Activity 3.5: Strengthen national malaria case management strategies, policies, and guidelines
Engage with the respective subcommittees and TWGs Progress in Y2, Q1
OMDM supported the TES TWG meeting held on November 5, 2019, bringing together representatives from OMDM, the NMCP, MUHAS, NIMR Tanga, and CUHAS. Members from Kilimanjaro Christian Medical Centre (KCMC) and CDC/PMI were absent with apology. Participants discussed the TES progress report of Implementation for 2019, Report of project supervision using the harmonized checklist, and Planned training and molecular analysis 2017-2019 at NIMR Tanga and Sokoine University of Agriculture (SUA). The minutes have been shared with all stakeholders.
Planned for Q2
In Q2, OMDM will continue supporting MUHAS to finalize data analysis, interpretation and dissemination of TES 2019 results. Additionally, we will continue supporting NIMR Tanga to finalize molecular analysis of samples from 2017 and 2018 TES. We will also support the implementation of TES 2020 through an FAA issued to CUHAS.
2.5 Result 4: GOT’s evidence-based decision making is improved OMDM continued direct technical assistance via hands-on coaching and mentoring of NMCP and ZAMEP staff through Q1 of Y2. Co-location of OMDM staff in the NMCP’s office at the University of Dodoma and within ZAMEP’s offices in Zanzibar facilitates hands-on coaching and mentoring, the ability to quickly address and troubleshoot challenges as they arise, and continue capacitating each team for ensure sustainability of program achievements into perpetuity. Additional details follow:
2.5.1 Activity 4.1: Strengthen Tanzania’s capacity for state-of-the-art (SOTA) analysis and interpretation of surveillance, entomological, and drug efficacy data
Provide and/or support attendance of short courses Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
The Activity has identified potential short courses for interested applicants from the NMCP and ZAMEP. Courses such as the online DHIS2 Academy, MEASURE Evaluation’s M&E of Malaria Programs, etc. have been earmarked for the selected applicants. A participant list will be shared in advance with USAID and PMI for review and approval.
Support for FELTP trainees Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
46 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Planned for Q2
OMDM will continue supporting FELTP trainees in the 3-month frontline worker training program. In Y2, three FELTP trainees will be selected in collaboration with the NMCP, PO- RALG, ZAMEP, USAID, and the Tanzania FELTP team. In Q2, we will liaise with the FELTP Coordinator to obtain the dates for upcoming trainings and ensure that the selected candidates are registered.
Hold scientific stature/data analysis workshops Progress in Y2, Q1
No activities were conducted during the October–December 2019 reporting period.
Planned for Q2
Activities will be initiated in Q3.
Mentor and coach MoHCDGEC/NMCP and MOHZ/ZAMEP staff Progress in Y2, Q1
In Q1, OMDM staff provided continuous mentorship and coaching in areas of DHIS2, including its use and analysis, as well as in data review. Additionally, OMDM’s Data Scientist, traveled to Dodoma at the NMCP to work onsite and alongside the SME Unit to support their day-to-day activities.
Planned for Q2
In Q2, OMDM staff will continue coaching and mentoring activities with the NMCP and ZAMEP under their respective funding mechanisms, through one-on-one engagement of team members, as well as through TA provided through various TWGs.
2.5.2 Activity 4.2: Conduct SOTA analysis and interpretation of surveillance, entomological, and drug efficacy data
Progress in Y2, Q1
Working with the NMCP and ZAMEP, OMDM continues to identify various areas for further analysis and interpretation of epidemiological and entomological data. Our staff provide ongoing support including sharing data showcasing malaria trends, case classification, and seasonal variations in Zanzibar, as well as providing support in the analysis of routine entomological data for both mainland Tanzania and Zanzibar. Additionally, the monthly data review meetings with the NMCP will continue to provide OMDM the opportunity to highlight useful information on malaria trends over the course of Y2.
Planned for Q2
In partnership with the NMCP and ZAMEP, we will continue to provide support to analyze routine malaria data, including entomological information.
2.5.3 Activity 4.3: Disseminate OMDM results through various channels Provide regular updates on SOTA analyses Progress in Y2, Q1
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 47
On November 20, 2019, OMDM met with RTI home office staff in Washington, DC, and leaders for national malaria programs from five countries (Burkina Faso, Guinea, Senegal, Thailand, Tanzania, and Zanzibar). The main objective of the meeting was to share program priorities and challenges, and to engage with malaria programs implemented by RTI in other countries . The national leaders shared insights about their daily routines, experiences and challenges in the fight against malaria. Program Managers from the NMCP and ZAMEP were
appreciative of RTI for coordinating this event and raising the visibility of various malaria control programs engaged in the fight against malaria.
Planned for Q2
In Q2, OMDM will begin work with the NMCP on the upcoming edition of the Malaria Bulletin.
Support drafting and disseminating programmatic updates Progress in Y2, Q1
OMDM worked with NMCP on the eighth edition of the Malaria Bulletin. Using routine data generated from DHIS2, the issue highlighted the malaria burden in mainland Tanzania, as well as provided an update on some malaria indicators including diagnosis of uncomplicated and severe malaria; performance of IPTp for women; and LLIN distribution at health facilities.
Planned for Q2
In Q2, OMDM will continue supporting the NMCP and ZAMEP to develop and disseminate programmatic updates. Additionally, OMDM will finalize the Activity’s draft Communications Plan to guide future communications activities, including publications, press releases, brochures, etc.
Develop policy and advocacy briefs No activities planned for Y2.
Attend national, regional, and international conferences and workshops Progress in Y2, Q1
On November 21–22, 2019, OMDM presented two posters at ASTMH’s 68th Annual Meeting at the National Harbor in Maryland, as follows:
• Malaria surveillance in Tanzania electronic Integrated Disease Surveillance and Response (eIDSR) system completeness and timelines, presented by
OMDM’s ICT Specialist
• Malaria Surveillance in Zanzibar: Patterns of Case Notification and Investigation in Line with WHO’s “1-3-7 Days” Approach, presented by OMDM’s
Director
On December 4–6, 2019, OMDM supported six participants (2 staff from NMCP; 2 staff from OMDM; 1 staff from MOHZ’s HMIS Unit, and 1 staff from ZAMEP) to attend the Data Tamasha workshop. Data Tamasha is a unique local platform that facilitates the sharing of ‘how data can make a difference in our community’. It brings together data enthusiasts,
Leaders of National Malaria programs. Photo credit by: RTI International
48 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
leaders, and practitioners across industries, the public sector, and academia. Every two years, this event is organized and hosted by the Tanzania Data Lab (dLab), a nongovernmental organization that envisions frequent and effective data use to inform policy and decision making at all levels by strengthening data ecosystems and data usage in Tanzania and Africa.
The 2019 Data Tamasha theme was “The Power of Data for Inclusive Sustainable Development.” The workshop included dialogues, panel discussions, presentations, demonstrations, interactive sessions, exhibitions, and public outreach activities.
Planned for Q2
No activities will be conducted during Q2.
Manuscript submitted for peer review
Progress in Y2, Q1
OMDM began working on the first draft of the eIDSR analysis that we conducted in Y1. This is still in progress. In addition, we are brainstorming and drafting other manuscripts.
Planned for Q2
We will develop a plan of action for each of the proposed manuscripts that identifies the topic, lead person, and estimated timeline for their finalization. Additionally, we will establish a SharePoint site to facilitate collaboration on the manuscript drafts .
Success stories Progress in Y2, Q1
OMDM has drafted a success story for submission with this quarterly report. Please see Annex 2 to read the success story around ZAMEP’s three-day scientific stature workshop in September 2019.
Planned for Q2
OMDM will continue identifying topics to be developed into success stories.
2.5.4 Activity 4.4: Implement Learning Agenda Progress in Y2, Q1
OMDM, in coordination with RTI’s home office based MERLA team, drafted and submitted the Activity’s Learning Agenda in Q3 Y1. Based on feedback from PMI, the Activity resubmitted the revised Learning Agenda and the proposed OR separately. The OR document has been expanded and tied to how OMDM can support some of the recommendations listed in the most recent ZMEAC report. A summary is provided below.
Quantifying the flow of travel to the Mainland OMDM hosted a meeting to highlight key challenges, including the substantial threat of imported malaria cases. Our proposed OR will identify entry points with high malaria importation risk that can be used as a guide to plan interventions. Furthermore, our research will provide critical information for Recommendation SME.11—to incorporate a multi-sectoral approach to ensure strong surveillance, including using community identification of people entering from outside Zanzibar in addition to or instead of the formal air and sea ports—and SME.12—analyze case classification data to understand the extent of imported and introduced case burden and include analysis of port of entry for imported cases.
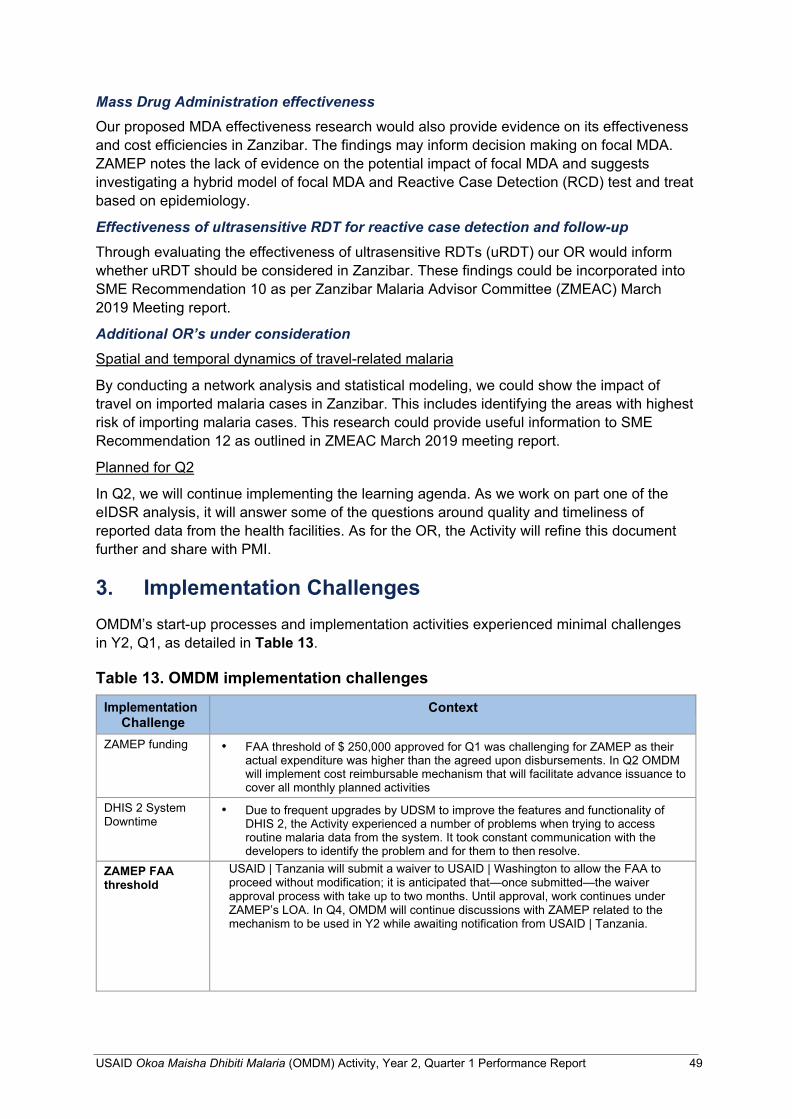
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 49
Mass Drug Administration effectiveness Our proposed MDA effectiveness research would also provide evidence on its effectiveness and cost efficiencies in Zanzibar. The findings may inform decision making on focal MDA. ZAMEP notes the lack of evidence on the potential impact of focal MDA and suggests investigating a hybrid model of focal MDA and Reactive Case Detection (RCD) test and treat based on epidemiology.
Effectiveness of ultrasensitive RDT for reactive case detection and follow-up Through evaluating the effectiveness of ultrasensitive RDTs (uRDT) our OR would inform whether uRDT should be considered in Zanzibar. These findings could be incorporated into SME Recommendation 10 as per Zanzibar Malaria Advisor Committee (ZMEAC) March 2019 Meeting report.
Additional OR’s under consideration Spatial and temporal dynamics of travel-related malaria
By conducting a network analysis and statistical modeling, we could show the impact of travel on imported malaria cases in Zanzibar. This includes identifying the areas with highest risk of importing malaria cases. This research could provide useful information to SME Recommendation 12 as outlined in ZMEAC March 2019 meeting report.
Planned for Q2
In Q2, we will continue implementing the learning agenda. As we work on part one of the eIDSR analysis, it will answer some of the questions around quality and timeliness of reported data from the health facilities. As for the OR, the Activity will refine this document further and share with PMI.
3. Implementation Challenges OMDM’s start-up processes and implementation activities experienced minimal challenges in Y2, Q1, as detailed in Table 13.
Table 13. OMDM implementation challenges
Implementation Challenge
Context
ZAMEP funding • FAA threshold of $ 250,000 approved for Q1 was challenging for ZAMEP as their actual expenditure was higher than the agreed upon disbursements. In Q2 OMDM will implement cost reimbursable mechanism that will facilitate advance issuance to cover all monthly planned activities
DHIS 2 System Downtime
• Due to frequent upgrades by UDSM to improve the features and functionality of DHIS 2, the Activity experienced a number of problems when trying to access routine malaria data from the system. It took constant communication with the developers to identify the problem and for them to then resolve.
ZAMEP FAA threshold
USAID | Tanzania will submit a waiver to USAID | Washington to allow the FAA to proceed without modification; it is anticipated that—once submitted—the waiver approval process with take up to two months. Until approval, work continues under ZAMEP’s LOA. In Q4, OMDM will continue discussions with ZAMEP related to the mechanism to be used in Y2 while awaiting notification from USAID | Tanzania.
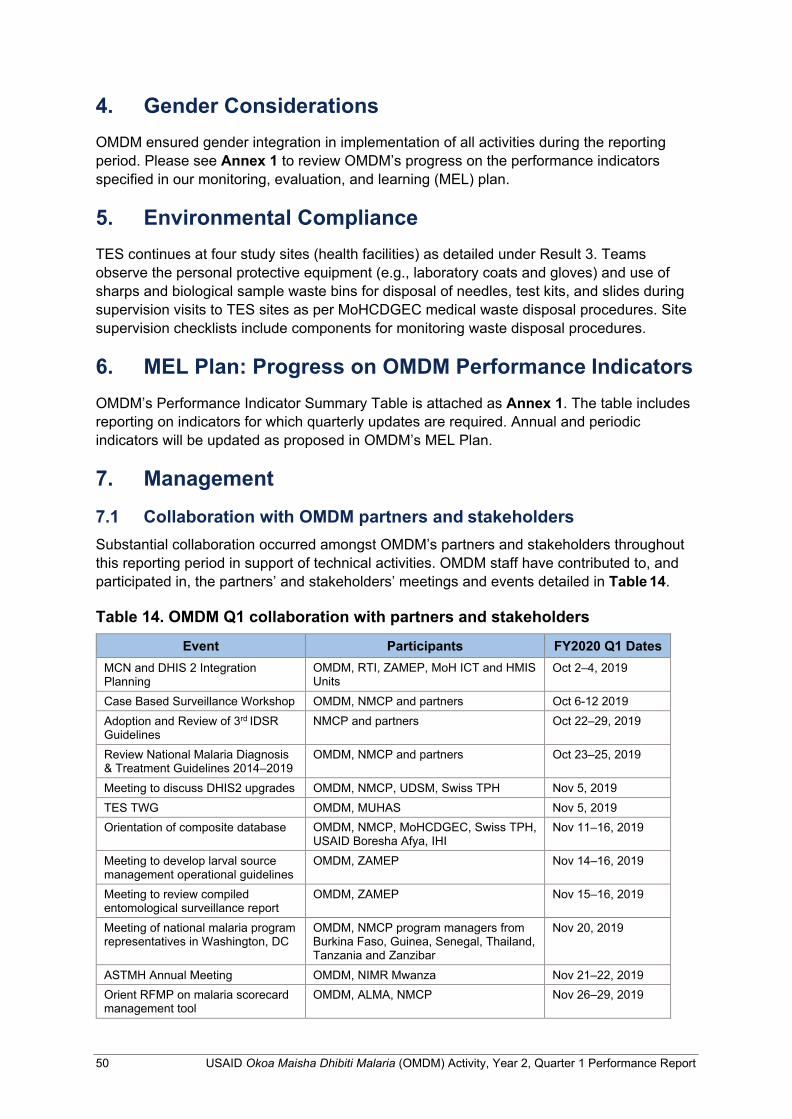
50 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
4. Gender Considerations OMDM ensured gender integration in implementation of all activities during the reporting period. Please see Annex 1 to review OMDM’s progress on the performance indicators specified in our monitoring, evaluation, and learning (MEL) plan.
5. Environmental Compliance TES continues at four study sites (health facilities) as detailed under Result 3. Teams observe the personal protective equipment (e.g., laboratory coats and gloves) and use of sharps and biological sample waste bins for disposal of needles, test kits, and slides during supervision visits to TES sites as per MoHCDGEC medical waste disposal procedures. Site supervision checklists include components for monitoring waste disposal procedures.
6. MEL Plan: Progress on OMDM Performance Indicators OMDM’s Performance Indicator Summary Table is attached as Annex 1. The table includes reporting on indicators for which quarterly updates are required. Annual and periodic indicators will be updated as proposed in OMDM’s MEL Plan.
7. Management 7.1 Collaboration with OMDM partners and stakeholders Substantial collaboration occurred amongst OMDM’s partners and stakeholders throughout this reporting period in support of technical activities. OMDM staff have contributed to, and participated in, the partners’ and stakeholders’ meetings and events detailed in Table 14.
Table 14. OMDM Q1 collaboration with partners and stakeholders
Event Participants FY2020 Q1 Dates MCN and DHIS 2 Integration Planning
OMDM, RTI, ZAMEP, MoH ICT and HMIS Units
Oct 2–4, 2019
Case Based Surveillance Workshop OMDM, NMCP and partners Oct 6-12 2019 Adoption and Review of 3rd IDSR Guidelines
NMCP and partners Oct 22–29, 2019
Review National Malaria Diagnosis & Treatment Guidelines 2014–2019
OMDM, NMCP and partners Oct 23–25, 2019
Meeting to discuss DHIS2 upgrades OMDM, NMCP, UDSM, Swiss TPH Nov 5, 2019 TES TWG OMDM, MUHAS Nov 5, 2019 Orientation of composite database OMDM, NMCP, MoHCDGEC, Swiss TPH,
USAID Boresha Afya, IHI Nov 11–16, 2019
Meeting to develop larval source management operational guidelines
OMDM, ZAMEP Nov 14–16, 2019
Meeting to review compiled entomological surveillance report
OMDM, ZAMEP Nov 15–16, 2019
Meeting of national malaria program representatives in Washington, DC
OMDM, NMCP program managers from Burkina Faso, Guinea, Senegal, Thailand, Tanzania and Zanzibar
Nov 20, 2019
ASTMH Annual Meeting OMDM, NIMR Mwanza Nov 21–22, 2019 Orient RFMP on malaria scorecard management tool
OMDM, ALMA, NMCP Nov 26–29, 2019

USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 51
Event Participants FY2020 Q1 Dates Meeting to finalize implementation plan for Y2 entomological monitoring activities
OMDM, NMCP Nov 28–29, 2019
Review of Malaria Dashboard Version 2
OMDM, NMCP, Swiss TPH Dec 3–7, 2019
Data Tamasha Workshop OMDM, NMCP, MOHZ’s HMIS Unit, ZAMEP
Dec 4–6, 2019
Hands-on coaching/mentoring site visit to SME Unit
OMDM, NMCP, SME Unit Dec 8–13, 2019
Pemba and Unguja site vistis OMDM, PMI, Boresha Afya, ZAMEP Dec 10–13, 2019 Data Review Meeting OMDM, NMCP Dec 11, 2019 Meeting to review/finalize larval source management operational guidelines
OMDM, ZAMEP Dec 13, 2019
Stakeholder meeting to kickstart malaria midterm review of ZAMEP’s malaria strategic plan
OMDM, ZAMEP Dec 19, 2019
Site visit to NMCP office and co- located OMDM office space
OMDM, NMCP Dec 19–22, 2019
7.2 List of all documents submitted to the Development Experience Clearinghouse Work continued in Q1 to ensure that performance reports to date meet 508 compliance requirements in terms of redaction and readability to allow posting to the DEC. All Y1 reports through Q3 have been posted; OMDM’s Annual Report is being made 508 compliant and will be posted to the DEC in Q2.
7.3 Certification that all participant training information has been entered in the TraiNet database No participant trainings were conducted in Y2, Q1. OMDM will ensure timely updates to the TraiNet database as trainings occur throughout the life of the Activity.
8. Upcoming Events Table 15 highlights planned events involving OMDM and key implementing partners in Y1, Q2.
Table 15. Upcoming events
Event Lead FY2020, Q4 Dates
Case Based Surveillance Phase 2 Workshop NMCP Jan 6–16, 2020 Data Management for the School Malaria Parasitemia Survey (SMPS) 2019
NMCP Jan 8–13, 2020
Zonal Meeting Dar es Salaam NMCP Jan 16–17, 2020 Zonal Meeting Mwanza NMCP Jan 27–28, 2020 Data Review Meeting OMDM (ZAMEP) Jan 29, 2020 Data Review Meeting OMDM(NMCP) Jan 31, 2020 Joint Partner Planning Meeting OMDM 12th February 2020 MCN users training – session 1 OMDM (ZAMEP) TBD March 2020
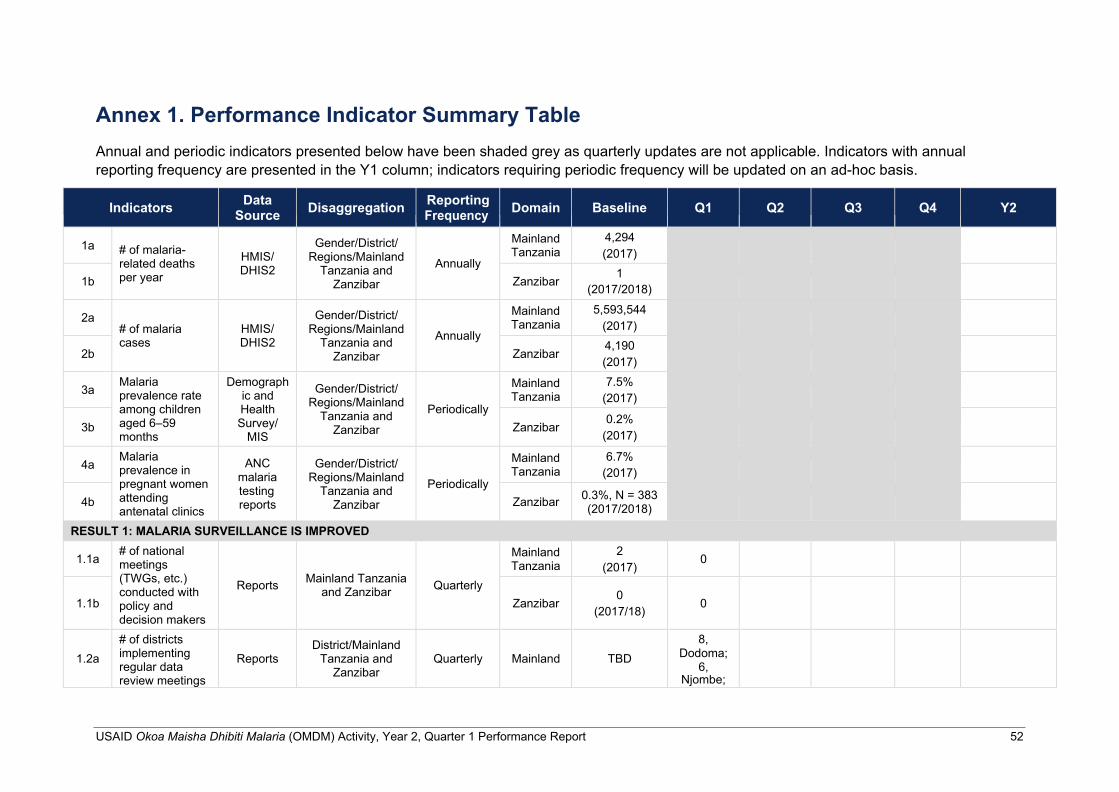
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 52
Annex 1. Performance Indicator Summary Table Annual and periodic indicators presented below have been shaded grey as quarterly updates are not applicable. Indicators with annual reporting frequency are presented in the Y1 column; indicators requiring periodic frequency will be updated on an ad-hoc basis.
Indicators Data Source Disaggregation Reporting
Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
1a
# of malaria- related deaths per year
HMIS/ DHIS2
Gender/District/ Regions/Mainland
Tanzania and Zanzibar
Annually
Mainland Tanzania
4,294 (2017)
1b Zanzibar 1 (2017/2018)
2a # of malaria cases
HMIS/ DHIS2
Gender/District/ Regions/Mainland
Tanzania and Zanzibar
Annually
Mainland Tanzania
5,593,544 (2017)
2b Zanzibar 4,190 (2017)
3a Malaria prevalence rate among children aged 6‒59 months
Demograph ic and Health Survey/
MIS
Gender/District/ Regions/Mainland
Tanzania and Zanzibar
Periodically
Mainland Tanzania
7.5% (2017)
3b
Zanzibar
0.2% (2017)
4a Malaria prevalence in pregnant women attending antenatal clinics
ANC malaria testing reports
Gender/District/ Regions/Mainland
Tanzania and Zanzibar
Periodically
Mainland Tanzania
6.7% (2017)
4b
Zanzibar 0.3%, N = 383
(2017/2018)
RESULT 1: MALARIA SURVEILLANCE IS IMPROVED
1.1a # of national meetings (TWGs, etc.) conducted with policy and decision makers
Reports
Mainland Tanzania and Zanzibar
Quarterly
Mainland Tanzania
2 (2017)
0
1.1b
Zanzibar
0 (2017/18)
0
1.2a
# of districts implementing regular data review meetings
Reports
District/Mainland Tanzania and
Zanzibar
Quarterly
Mainland
TBD
8, Dodoma;
6, Njombe;
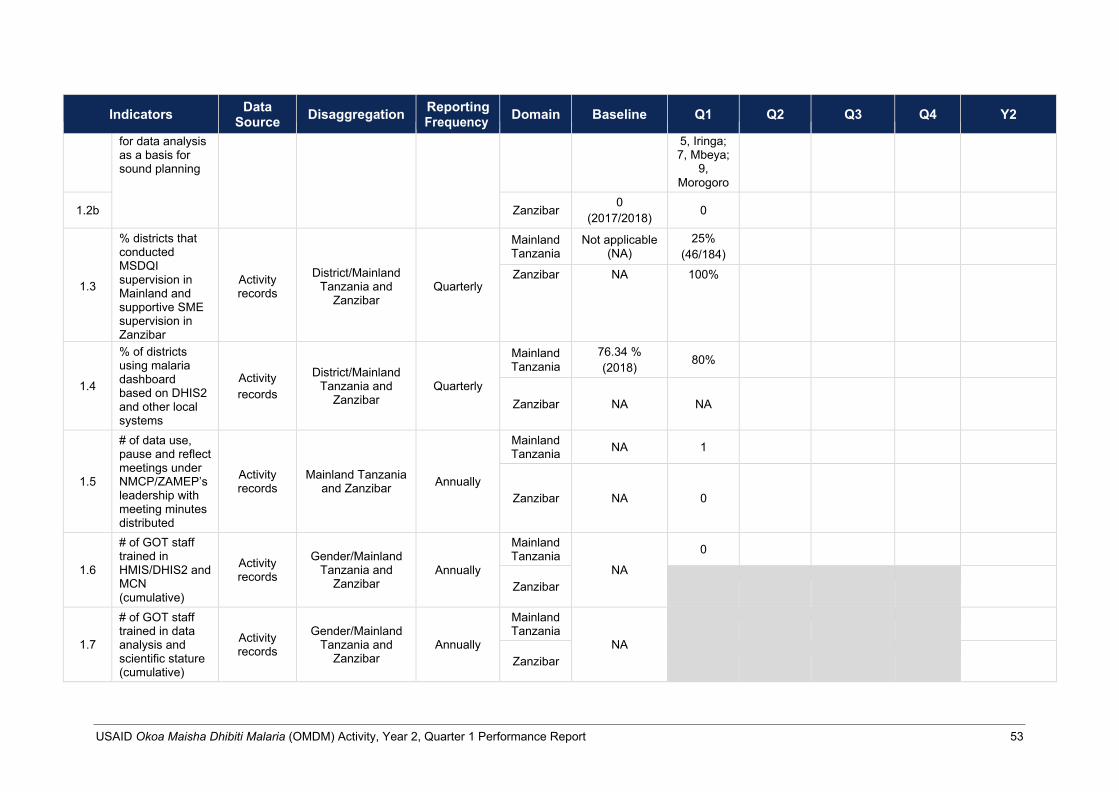
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 53
Indicators Data
Source Disaggregation Reporting Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
for data analysis as a basis for sound planning
5, Iringa; 7, Mbeya;
9, Morogoro
1.2b Zanzibar 0 (2017/2018) 0
1.3
% districts that conducted MSDQI supervision in Mainland and supportive SME supervision in Zanzibar
Activity records
District/Mainland Tanzania and
Zanzibar
Quarterly
Mainland Tanzania
Not applicable (NA)
25% (46/184)
Zanzibar NA 100%
1.4
% of districts using malaria dashboard based on DHIS2 and other local systems
Activity records
District/Mainland
Tanzania and Zanzibar
Quarterly
Mainland Tanzania
76.34 % (2018) 80%
Zanzibar
NA
NA
1.5
# of data use, pause and reflect meetings under NMCP/ZAMEP’s leadership with meeting minutes distributed
Activity records
Mainland Tanzania and Zanzibar
Annually
Mainland Tanzania NA 1
Zanzibar
NA
0
1.6
# of GOT staff trained in HMIS/DHIS2 and MCN (cumulative)
Activity records
Gender/Mainland
Tanzania and Zanzibar
Annually
Mainland Tanzania
NA
0
Zanzibar
1.7
# of GOT staff trained in data analysis and scientific stature (cumulative)
Activity records
Gender/Mainland
Tanzania and Zanzibar
Annually
Mainland Tanzania
NA
Zanzibar
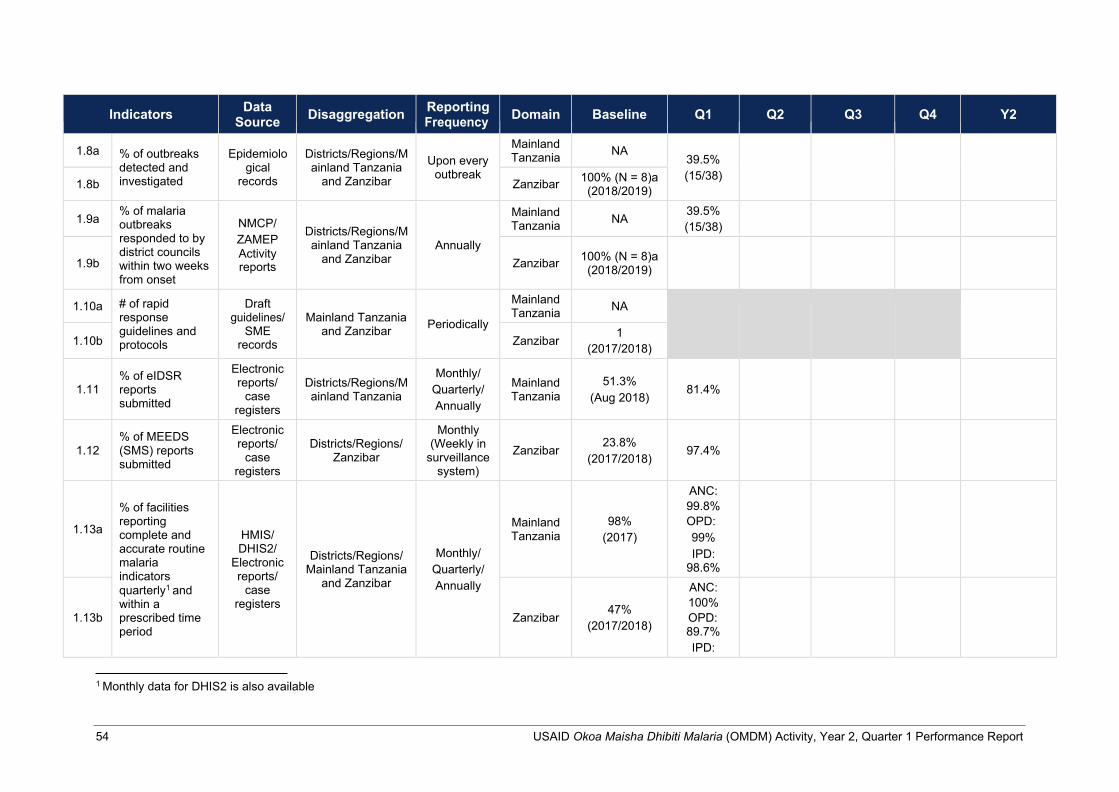
54 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Indicators Data
Source Disaggregation Reporting Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
1.8a
% of outbreaks detected and investigated
Epidemiolo
gical records
Districts/Regions/M ainland Tanzania
and Zanzibar
Upon every
outbreak
Mainland Tanzania NA
39.5% (15/38)
1.8b Zanzibar 100% (N = 8)a (2018/2019)
1.9a % of malaria outbreaks responded to by district councils within two weeks from onset
NMCP/ ZAMEP Activity reports
Districts/Regions/M ainland Tanzania
and Zanzibar
Annually
Mainland Tanzania NA 39.5%
(15/38)
1.9b
Zanzibar
100% (N = 8)a (2018/2019)
1.10a # of rapid response guidelines and protocols
Draft guidelines/
SME records
Mainland Tanzania
and Zanzibar
Periodically
Mainland Tanzania NA
1.10b Zanzibar 1 (2017/2018)
1.11 % of eIDSR reports submitted
Electronic reports/
case registers
Districts/Regions/M ainland Tanzania
Monthly/ Quarterly/ Annually
Mainland Tanzania
51.3%
(Aug 2018)
81.4%
1.12
% of MEEDS (SMS) reports submitted
Electronic reports/
case registers
Districts/Regions/
Zanzibar
Monthly (Weekly in
surveillance system)
Zanzibar
23.8%
(2017/2018)
97.4%
1.13a
% of facilities reporting complete and accurate routine malaria indicators quarterly1 and within a prescribed time period
HMIS/ DHIS2/
Electronic reports/
case registers
Districts/Regions/ Mainland Tanzania
and Zanzibar
Monthly/ Quarterly/ Annually
Mainland Tanzania
98% (2017)
ANC: 99.8% OPD: 99% IPD:
98.6%
1.13b
Zanzibar
47% (2017/2018)
ANC: 100% OPD: 89.7% IPD:
1 Monthly data for DHIS2 is also available
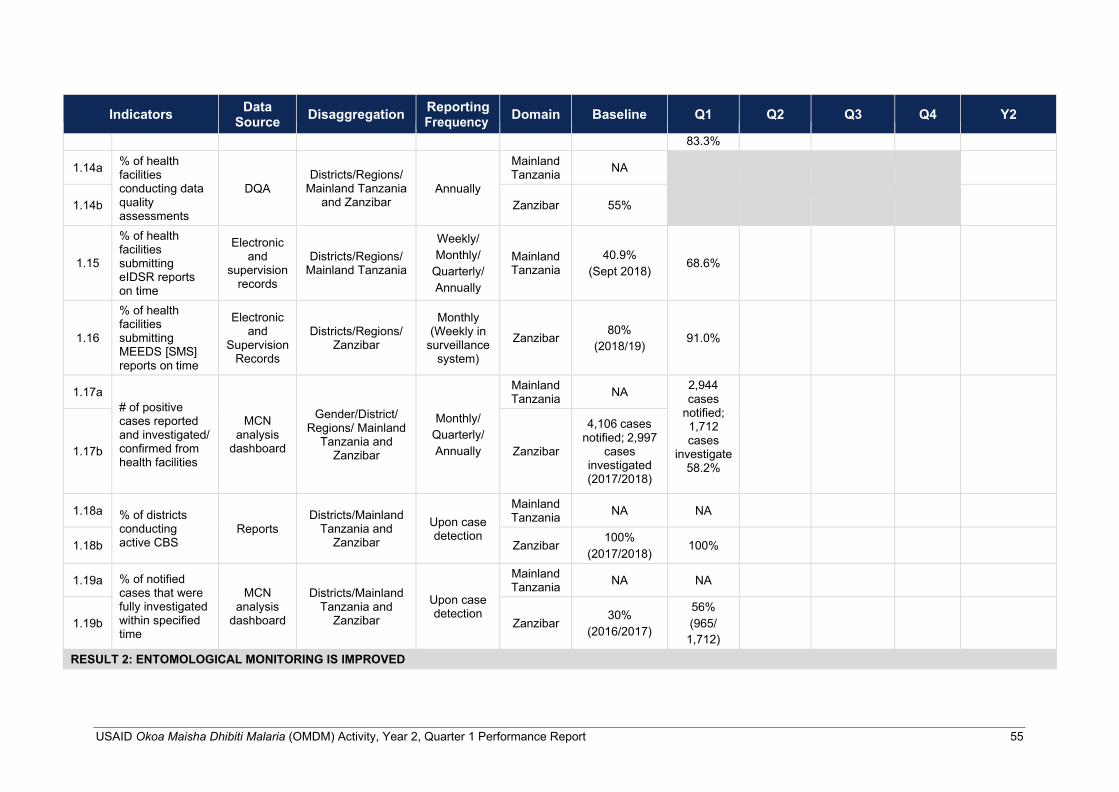
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 55
Indicators Data
Source Disaggregation Reporting Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
83.3%
1.14a % of health facilities conducting data quality assessments
DQA
Districts/Regions/
Mainland Tanzania and Zanzibar
Annually
Mainland Tanzania NA
1.14b
Zanzibar
55%
1.15
% of health facilities submitting eIDSR reports on time
Electronic and
supervision records
Districts/Regions/
Mainland Tanzania
Weekly/ Monthly/
Quarterly/ Annually
Mainland Tanzania
40.9%
(Sept 2018)
68.6%
1.16
% of health facilities submitting MEEDS [SMS] reports on time
Electronic and
Supervision Records
Districts/Regions/ Zanzibar
Monthly (Weekly in
surveillance system)
Zanzibar
80%
(2018/19)
91.0%
1.17a
# of positive cases reported and investigated/ confirmed from health facilities
MCN analysis
dashboard
Gender/District/ Regions/ Mainland
Tanzania and Zanzibar
Monthly/ Quarterly/ Annually
Mainland Tanzania NA 2,944
cases notified; 1,712 cases
investigate 58.2%
1.17b
Zanzibar
4,106 cases notified; 2,997
cases investigated (2017/2018)
1.18a
% of districts conducting active CBS
Reports
Districts/Mainland
Tanzania and Zanzibar
Upon case detection
Mainland Tanzania NA NA
1.18b Zanzibar 100%
(2017/2018) 100%
1.19a % of notified cases that were fully investigated within specified time
MCN
analysis dashboard
Districts/Mainland
Tanzania and Zanzibar
Upon case detection
Mainland Tanzania NA NA
1.19b
Zanzibar
30% (2016/2017)
56% (965/
1,712)
RESULT 2: ENTOMOLOGICAL MONITORING IS IMPROVED
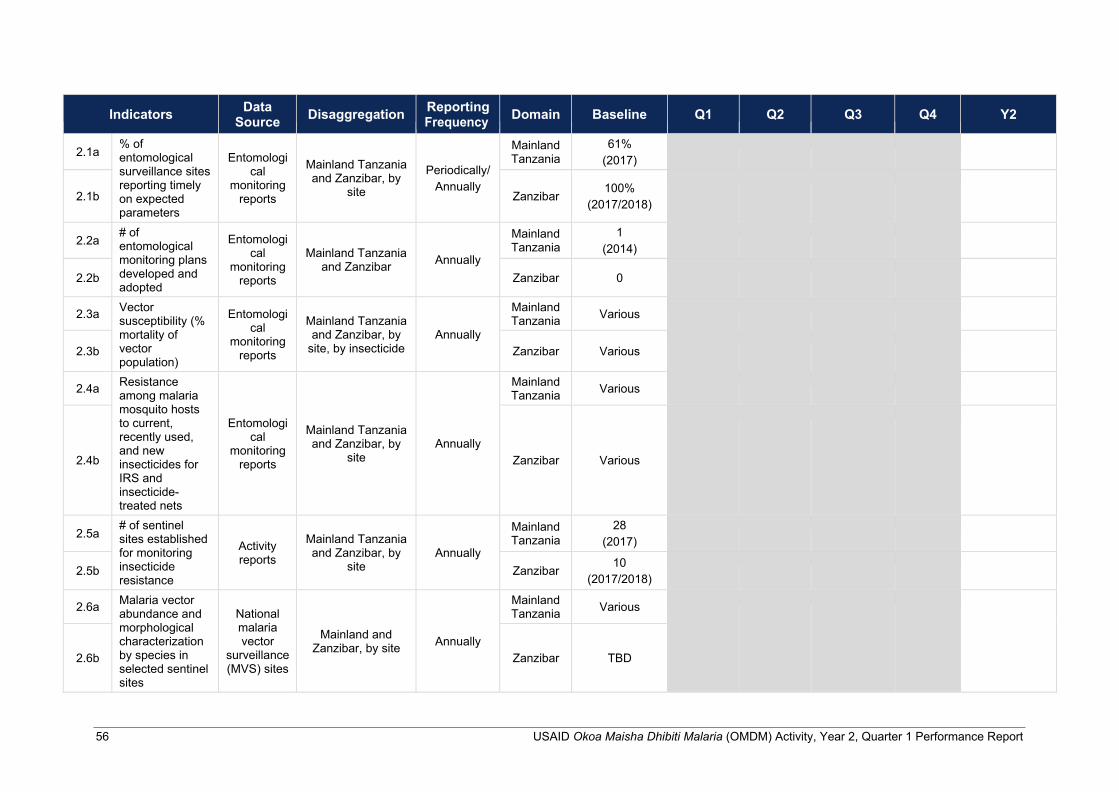
56 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Indicators Data
Source Disaggregation Reporting Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
2.1a % of entomological surveillance sites reporting timely on expected parameters
Entomologi
cal monitoring
reports
Mainland Tanzania and Zanzibar, by
site
Periodically/ Annually
Mainland Tanzania
61% (2017)
2.1b
Zanzibar
100% (2017/2018)
2.2a # of entomological monitoring plans developed and adopted
Entomologi cal
monitoring reports
Mainland Tanzania
and Zanzibar
Annually
Mainland Tanzania
1 (2014)
2.2b
Zanzibar
0
2.3a Vector susceptibility (% mortality of vector population)
Entomologi cal
monitoring reports
Mainland Tanzania and Zanzibar, by
site, by insecticide
Annually
Mainland Tanzania Various
2.3b
Zanzibar
Various
2.4a Resistance among malaria mosquito hosts to current, recently used, and new insecticides for IRS and insecticide- treated nets
Entomologi cal
monitoring reports
Mainland Tanzania and Zanzibar, by
site
Annually
Mainland Tanzania Various
2.4b
Zanzibar
Various
2.5a # of sentinel sites established for monitoring insecticide resistance
Activity reports
Mainland Tanzania and Zanzibar, by
site
Annually
Mainland Tanzania
28 (2017)
2.5b
Zanzibar 10
(2017/2018)
2.6a Malaria vector abundance and morphological characterization by species in selected sentinel sites
National malaria vector
surveillance (MVS) sites
Mainland and Zanzibar, by site
Annually
Mainland Tanzania Various
2.6b
Zanzibar
TBD
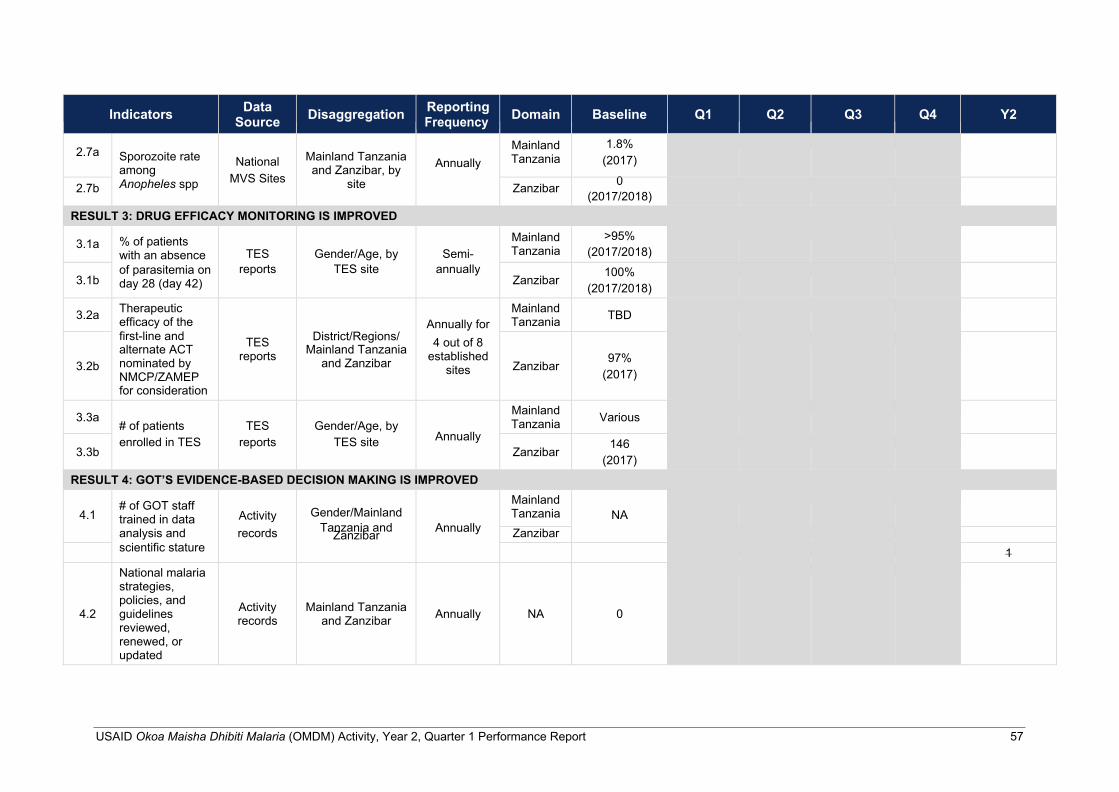
USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 57
Indicators Data
Source Disaggregation Reporting Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
2.7a
Sporozoite rate among
National
Mainland Tanzania and Zanzibar, by
Annually
Mainland Tanzania
1.8% (2017)
2.7b Anopheles spp MVS Sites site Zanzibar 0 (2017/2018)
RESULT 3: DRUG EFFICACY MONITORING IS IMPROVED
3.1a % of patients with an absence
TES
Gender/Age, by
Semi-
Mainland Tanzania
>95% (2017/2018)
3.1b of parasitemia on day 28 (day 42)
reports TES site annually Zanzibar 100%
(2017/2018)
3.2a Therapeutic efficacy of the
Annually for
Mainland Tanzania TBD
3.2b
first-line and alternate ACT nominated by NMCP/ZAMEP for consideration
TES reports
District/Regions/ Mainland Tanzania
and Zanzibar
4 out of 8 established
sites
Zanzibar
97%
(2017)
3.3a # of patients
TES
Gender/Age, by
Mainland Tanzania Various
3.3b enrolled in TES reports TES site Annually
Zanzibar 146 (2017)
RESULT 4: GOT’S EVIDENCE-BASED DECISION MAKING IS IMPROVED
4.1
# of GOT staff trained in data
Activity
Gender/Mainland
Mainland Tanzania
NA
analysis and records Tanzania and Zanzibar Annually Zanzibar scientific stature 1
4.2
National malaria strategies, policies, and guidelines reviewed, renewed, or updated
Activity records
Mainland Tanzania and Zanzibar
Annually
NA
0
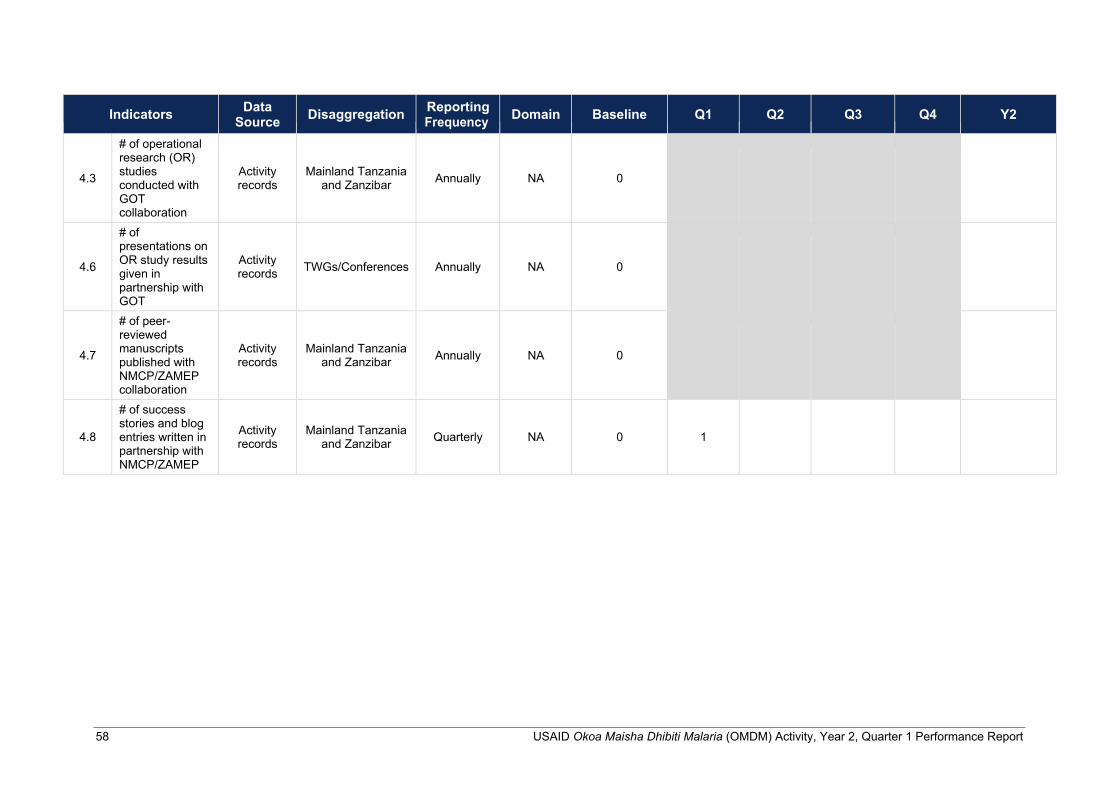
58 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Indicators Data
Source Disaggregation Reporting Frequency Domain Baseline Q1 Q2 Q3 Q4 Y2
4.3
# of operational research (OR) studies conducted with GOT collaboration
Activity records
Mainland Tanzania and Zanzibar
Annually
NA
0
4.6
# of presentations on OR study results given in partnership with GOT
Activity records
TWGs/Conferences
Annually
NA
0
4.7
# of peer- reviewed manuscripts published with NMCP/ZAMEP collaboration
Activity records
Mainland Tanzania and Zanzibar
Annually
NA
0
4.8
# of success stories and blog entries written in partnership with NMCP/ZAMEP
Activity records
Mainland Tanzania
and Zanzibar
Quarterly
NA
0
1

USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report 59
Annex 2. OMDM Success Story
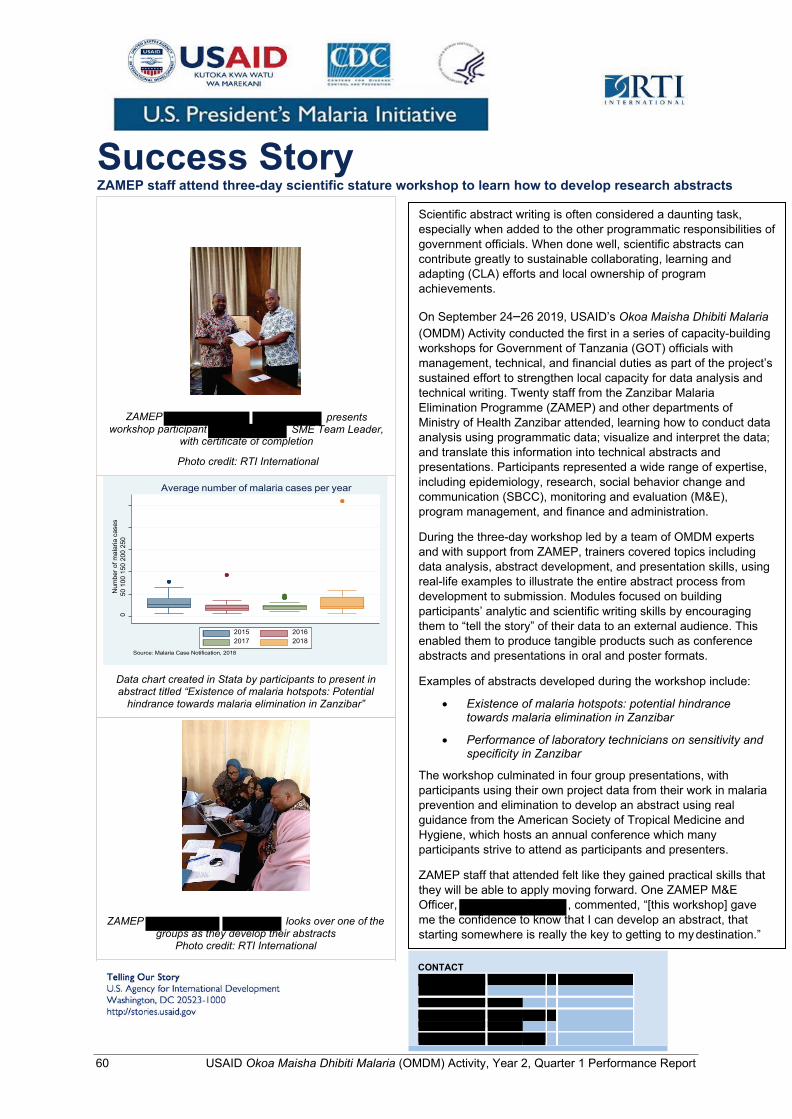
60 USAID Okoa Maisha Dhibiti Malaria (OMDM) Activity, Year 2, Quarter 1 Performance Report
Success Story ZAMEP staff attend three-day scientific stature workshop to learn how to develop research abstracts
Scientific abstract writing is often considered a daunting task, especially when added to the other programmatic responsibilities of government officials. When done well, scientific abstracts can contribute greatly to sustainable collaborating, learning and adapting (CLA) efforts and local ownership of program achievements.
On September 24–26 2019, USAID’s Okoa Maisha Dhibiti Malaria (OMDM) Activity conducted the first in a series of capacity-building workshops for Government of Tanzania (GOT) officials with management, technical, and financial duties as part of the project’s sustained effort to strengthen local capacity for data analysis and technical writing. Twenty staff from the Zanzibar Malaria Elimination Programme (ZAMEP) and other departments of Ministry of Health Zanzibar attended, learning how to conduct data analysis using programmatic data; visualize and interpret the data; and translate this information into technical abstracts and presentations. Participants represented a wide range of expertise, including epidemiology, research, social behavior change and communication (SBCC), monitoring and evaluation (M&E), program management, and finance and administration.
During the three-day workshop led by a team of OMDM experts and with support from ZAMEP, trainers covered topics including data analysis, abstract development, and presentation skills, using real-life examples to illustrate the entire abstract process from development to submission. Modules focused on building participants’ analytic and scientific writing skills by encouraging them to “tell the story” of their data to an external audience. This enabled them to produce tangible products such as conference abstracts and presentations in oral and poster formats.
Examples of abstracts developed during the workshop include:
• Existence of malaria hotspots: potential hindrance towards malaria elimination in Zanzibar
• Performance of laboratory technicians on sensitivity and specificity in Zanzibar
The workshop culminated in four group presentations, with participants using their own project data from their work in malaria prevention and elimination to develop an abstract using real guidance from the American Society of Tropical Medicine and Hygiene, which hosts an annual conference which many participants strive to attend as participants and presenters.
ZAMEP staff that attended felt like they gained practical skills that they will be able to apply moving forward. One ZAMEP M&E Officer, , commented, “[this workshop] gave me the confidence to know that I can develop an abstract, that starting somewhere is really the key to getting to my destination.”
CONTACT
ZAMEP looks over one of the groups as they develop their abstracts
Photo credit: RTI International
Data chart created in Stata by participants to present in abstract titled “Existence of malaria hotspots: Potential
hindrance towards malaria elimination in Zanzibar”
with certificate of completion
Photo credit: RTI International
presents SME Team Leader,
ZAMEP workshop participant
2016 2018
2015 2017
Source: Malaria Case Notification, 2018
Average number of malaria cases per year
Num
ber o
f mal
aria
cas
es
50 1
00 1
50 2
00 2
50
0