treatment of status epilepticus in a large community hospital
TRANSCRIPT

Epilepsy & Behavior 23 (2012) 235–240
Contents lists available at SciVerse ScienceDirect
Epilepsy & Behavior
j ourna l homepage: www.e lsev ie r .com/ locate /yebeh
Treatment of status epilepticus in a large community hospital
Christoph Kellinghaus ⁎, Florian StögbauerDept. of Neurology, Klinikum Osnabrück, Osnabrück, Germany
⁎ Corresponding author at: Dept. of Neurology, Kliniku1, 49076 Osnabrück, Germany. Fax: +49 541 405 6599.
E-mail address: [email protected]
1525-5050/$ – see front matter © 2012 Elsevier Inc. Alldoi:10.1016/j.yebeh.2011.12.020
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 8 October 2011Revised 6 December 2011Accepted 12 December 2011Available online 16 February 2012Keywords:IntravenousAnticonvulsantOutcomeEfficacyStatus epilepticus
Background: Status epilepticus (SE) is a neurological emergency usually requiring immediate medical treat-ment. Due to the lack of adequate studies, treatment guidelines and their application vary between countriesand institutions. We intended to analyze current treatment of SE in a German community hospital.Methods: We retrospectively identified patients from a large community hospital in northern Germany whohad been diagnosed with SE between August 2008 and December 2010. Their charts were reviewed regardingsociodemographic variables, treatment and outcome.Results:We studied the first SE episode in 172 patients with amedian age of 69 years (range 18–90 years). Theetiology was acute symptomatic in 30 patients, progressive symptomatic in 22 patients and remote symptom-atic in 120 patients. Presentation was generalized convulsive in 60 patients, non-convulsive in 72 patients andsimple motor/aura in 40 patients. Median latency from onset to treatment start was 0.75 h (range 0.2–336 h).Initial treatment had a success rate (SR) of 40%. Second line treatment had a success rate of 54%. In patients
whose seizures were refractory to the first two drugs, success rates were between 31% and 55%, with only aminority of the patients receiving established drugs such as phenytoin or barbiturates.Multivariate analysis revealed non-convulsive semiology as the only factor significantly associated withrefractoriness. SE could be terminated in 95% of the patients and in-hospital mortality was 10%. Benzodiaze-pines and phenytoin had the most severe side effects.Conclusions: Status epilepticus can be terminated successfully and with low in-hospital mortality in the vastmajority of the patients treated in a large community hospital. The success rate of each treatment step isbetween 30% and 55% regardless of the substances used.© 2012 Elsevier Inc. All rights reserved.
1. Introduction
Status epilepticus (SE), i.e. a prolonged and sustained epilepticseizure, is a potentially life-threatening neurological emergency.According to population-based studies, its incidence is estimated as10–20/100,000/year in western industrialized countries [1–3].
In spite of the incidence and emergency character of SE, there are onlyvery few randomized, blinded, and controlled trials regarding SE therapy[4–6]. These studies suggest that lorazepam, diazepam, phenobarbital andphenytoin are more or less equally efficient in initial treatment of SEwhen phenytoin is combined with benzodiazepines. Valproate may beequally effective as phenytoin, but has not been compared to phenytoinand benzodiazepines in combination [7]. Based on these few studies, cur-rent SE treatment guidelines propose intravenous (i.v.) administration oflorazepam or diazepam followed by i.v. administration of phenytoin asfirst treatment steps [8,9]. Since most of the randomized studies wereperformed more than 15 years ago when modern non-sedating i.v.anticonvulants like valproate, levetiracetam, fosphenytoin and lacosa-mide were not available, their role in initial treatment of SE is
mOsnabrück, Am Finkenhügel
e (C. Kellinghaus).
rights reserved.
undetermined. Data regarding treatment of refractory status epilepticusalmost exclusively consist of uncontrolled prospective or retrospectivecase series, and thus treatment recommendations vary greatly betweenauthors and countries. As a consequence, surveys among epileptologistsand critical care neurologists in the U.S. as well as in Europe have dem-onstrated that there is no consensus over treatment strategies oncebenzodiazepines and phenytoin have failed [10,11]. Particularly uncer-tain is the value of the new agents that as yet have mainly been used inrefractory SE. Most authors retrospectively analyzed single cases orsmall series with a large range of success rates and without comparisonto standard treatment or other new drugs [12–15].
It is very likely that treatment approaches differ significantlybetween hospitals or departments of a region. The best way to reachconsensus about the optimal treatment of SE would be a large pro-spective, randomized and controlled multicenter study that includesbenzodiazepines and phenytoin as well as valproate, levetiracetamand lacosamide. However, there are many legal, ethical and financialobstacles that have yet precluded such an approach. Prospective casedocumentations or registries are second best, but have been limitedto a single agent [16], to university hospitals [17,18], were performedbefore modern non-sedating i.v. anticonvulsants were available [19],or were performed in countries with predominantly infectious etiolo-gies [20]. However, most cases of SE are treated in non-academic,

236 C. Kellinghaus, F. Stögbauer / Epilepsy & Behavior 23 (2012) 235–240
community-based hospitals that care for distinctly different patientcohorts and rely on different resources and hospital policies than thetertiary-level academic hospitals where most scientific publicationsare generated.
With this study we document and analyze the current treatmentof SE in a large community hospital in Germany. Although formallyit is a retrospective study, data quality is high because we could relyon SE-specific patient treatment documentation that has been usedin our department since 2007. With this study we try to narrow thegap between the urgently needed but unavailable data from largerandomized controlled trials and the currently available small caseseries that mainly serve as ‘proof of principle’ for one of the new i.v.anticonvulsants.
2. Methods
We retrospectively identified all patients treated for SE in ourhospital between July 2008 and December 2010. For identificationwe searched the hospital database using the search terms ‘statusepilepticus’, ‘prolonged epileptic seizure’ as well as the ICD-10 codesG41.xx that cover status epilepticus. In addition, the EEG databasewas searched using the same search terms. If a patient was admittedmore than once for treatment of SE during the study period, only thedata of the first admission were analyzed further. Patients with post-anoxic status epilepticus were excluded.
The hospital charts were reviewed for sociodemographic data,etiology, semiology, onset of SE, and discharge. Time, dose and effectof anticonvulsant treatment were taken from a standardized SEdocumentation form that was introduced in our institution for qualitycontrol purposes in 2007. Once the diagnosis of SE has beenmade, theform is introduced into the individual patient chart and documentstime, efficacy and tolerability of each treatment step, starting withpreclinical treatment. Original imaging data were reviewed by atleast one of the authors, and all EEG data were reviewed by an expe-rienced electroencephalographer (C.K.). All patients underwent neu-rological examination and cranial imaging (CT or MRI) at admission.EEG was performed for at least 20 min using the electrodes of the in-ternational 10/20 systemwith additional anterior temporal electrodes(FT9/FT10) in all patients to document cessation of SE and get infor-mation about seizure onset at latest at the first working day followingadmission. Ictal EEG could be performed in 91/172 patients. Comor-bidity and clinical outcome were assessed with the modified RankinScale (mRS) [21,22] that allows an overview of the patient's disabil-ities using basic information about neurological symptoms and thepatient's need for support in everyday life. AmRS score of 0 is assignedwhen the patient is free of symptoms, a score of 1 when the patienthas no significant disabilities despite some symptoms, a score of 2when there is a slight disability, a score of 3 when the patient requiressome help but is able to walk unassisted, a score of 4 when the patientis unable to attend to own bodily needswithout assistance, a score of 5when the patient requires constant nursing care and attention, and ascore of 6 when the patient is dead. The mRS score was determinedusing all available information about the patient's state before onsetof SE and at the time of discharge from hospital. In addition, wecounted the ICD-10 diagnoses that were assigned to the case by med-ical documentation specialists for reimbursement purposes. Epilepsydiagnoses (ICD 10G 40.xx and G41.xx) were subtracted from thetotal count. SE was defined as a) seizures lasting >10 min, or b) recur-rent seizures without regaining recovery of awareness. In EEG, SE wasdefined according to the criteria stated by Young et al. [23]. SE semiol-ogy was categorized pragmatically into generalized convulsive, loss ofconsciousness without major motor symptoms, aphasic/dyscognitive,simple motor and other simple partial (e.g. aura). Loss of consciousnessand aphasic/dyscognitive was lumped into the category ‘non-convul-sive’ for some analyses. If SE started with a generalized convulsive sei-zure followed by EEG-confirmed non-convulsive SE, it was
nevertheless considered as ‘generalized convulsive’ because this typeof SE, also described as ‘subtle SE’, most likely has similar pathophysio-logical and treatment implications. Time of cessation of SE was definedby the timewhen the seizure symptoms ceased, or – if in doubt – by thetime of the first EEG showing cessation of the electroencephalographicsigns of SE.
An anticonvulsant drug was considered as successful when nofurther anticonvulsant was introduced until cessation of SE. Differentsubstances of the benzodiazepine class such as lorazepam, diazepam,midazolam and clonazepam were lumped into the group ‘benzodiaze-pine’. Equivalent doses were calculated according to established phar-macologic tables [24,25]: 10 mg diazepam=1mg lorazepam=0.5 mgclonazepam=7.5 mg midazolam.
Two subgroups were formed retrospectively according to theresponse to the first two substances used for treatment. If SE ceasedafter the first or second anticonvulsant, SE was considered ‘non-refractory’. If SE did not cease after the second anticonvulsant, SE wasconsidered ‘refractory’. Different benzodiazepines were considered asone anticonvulsant.
Statistical analysis was performed using OPENSTAT (http://statpages.org, Version June 2010). Ranked variables were describedusing mean and standard deviation, and median/quartiles whennormal distribution could not be assumed. For univariate analysis ofcategorical data, chi-square test and Fisher's exact test (2×2 tables)were used. Interval-scaled or ordinal-scaled data were analyzedwith the Mann–Whitney U test (comparison of two groups), or theKruskal–Wallis test (comparison of three or more groups). In a sec-ond step, backward multiple logistic regression was performed(p=0.05 for inclusion, p=0.10 for exclusion) to determine thecontribution of individual treatment-independent factors to therefractoriness (i.e. no cessation after the second anticonvulsant).
3. Results
During the 29 months that were analyzed, 204 episodes of SEwere documented in 172 patients. One hundred forty-nine patientshad one episode, 17 patients had two episodes, three patients hadthree episodes, and three patients had four episodes of SE. Only thefirst episode during this time period was analyzed.
Most patients were elderly patients above 65 years of age, and halfof them were women (see Table 1). In the majority of patients, theunderlying etiology was remote symptomatic. Thirty patients (17%)had an acute, non-progressive CNS lesion (e.g. stroke, trauma), and22 patients (13%) a progressive CNS lesion (tumor, metastasis). Semi-ology was generalized convulsive in a third of the patients, whileonly 3 patients were treated for an aura status. More than half ofthe patients were treated with anticonvulsant drugs (AED) beforeSE onset. Most patients suffered from moderate or major impairmentaccording to the mRS score. Only a third had a mRS score of 2 or lowerbefore SE, and less than a quarter of the patients were discharged withless than 5 diagnoses.
Treatment started after a median of 45 min (range 10 min to336 h), with approximately half of the patients having received thefirst medication between 10 and 30 min after SE onset. The firstdrug was almost always a benzodiazepine (lorazepam, diazepam,clonazepam or midazolam, or a successive combination) (see Table 2).SE ceased after administration of the first drug in 69 patients (40%)after a median of 0.13 h. In the remaining 103 patients, a second drugwas administered after a median latency of 0.4 h. Most patients (78)received levetiracetam, a minority was treated with other intravenousAEDs such as valproate, phenytoin or lacosamide. Six patients weredirectly treated with anesthetic agents. The second substance wassuccessful in terminating the SE in 56 patients (54%). Seizures in theother 47 patients were considered refractory. In one patient with glio-blastoma multiforme, treatment and life support were withdrawnaccording to the patients previously-stated wishes after failure of the

Table 1Sociodemographic characteristic.
Variable All patients (N=172)
Age (years) Mean/standard deviation 64.56/+/−17.98Median/range 69 (18–90)
Gender Female 82 (48%)Etiology Acute symptomatic 30 (17%)
Remote symptomatic first man 44 (26%)Remote symptomatic old 76 (44%)Remote sympt all 120 (70%)Progressive symptomatic 22 (13%)
Semiology Generalized convulsive 60 (35%)LOC only 45 (26%)Simple Motor 37 (22%)Aphasic/dyscognitive 27 (16%)Other simple partial 3 (1%)
Ictal EEG No ictal EEG performed 81 (47%)Generalized 15 (9%)Lateralized 46 (27%)Regional 29 (17%)
AED before SE Yes 74 (43%)No. of diagnoses Median/range 9 (0–33)
0–4 37 (22%)5–9 53 (30%)10–14 41 (24%)15–19 20 (12%)20 or more 21 (12%)
mRS before SE Median 30 30 (17%)1+2 33 (19%)3 48 (28%)4 33 (19%)5 28 (16%)
AED = anticonvulsant drug; SE = status epilepticus; mRS = modified Rankin Scale;LOC = loss of consciousness.first man = first manifestation of seizures/epilepsy; old = established epilepsy.
Table 2Course of treatment.
Latency SE onset- treatmentonset (n=172)
Median/range (hours) 0.75 (0.2–336)
10–30 min 90 (52%)31–60 min 18 (10%)61–120 min 17(10%)121 min to 6 h 25 (15%)>6 h to 24 h 13 (8%)>24 h 9 (15%)
Latency treatment onset-SEend (hours) (n=163)
Median/range 1.5 (0.1–814.25)
No. of patients Successrate*
AED 1 Benzo 168 39%other 4All 172 40%
Latency AED1–AED2 (h) Median/range 0.4/0.15–91.3AED 2 LEV 78 49%
other 24 52%All 102 54%
Latency AED 2–AED 3(h) Median/range 0.5/0.1–61AED3 PHT 15 40%
LCM 21 33%other 10 30%All 46 35%
Latency AED 3–AED 4 (h) Median/range 17/0.25–208AED 4 PHT 10 50%
LCM 9VPA 6other 5All 30 37%
Latency AED 4–AED 5 (h) Median/range 27.5/2–319AED 5 PHT 3
VPA 3CBZ/OXC 5Other 4All 16 31%
Latency AED 5–AED 6 (h) Median/range 37/0.5–470AED 6 All 11 55%Latency AED 6–AED 7 (h) Median/range 121/43–168AED 7 All 3 33%Latency AED 7–AED 8 (h) Median/range 317.5/216–419AED 8 All 2 0AED 9 All 1 0AED 10 All 1 0
SE = status epilepticus; AED = anticonvulsant drug; benzo = benzodiazepine;LEV = levetiracetam; PHT = phenytoin; LCM = lacosamide; VPA = valproate;CBZ = carbamazepine; OXC = oxcarbazepine.
Table 3Outcome.
Variable Patients
SE terminated Yes 163 (95%)mRS at discharge 0 22 (13%)
1+2 33 (19%)3 43 (25%)4 31 (18%)5 25 (15%)6 18 (10%)
mRS difference −6 3 (2%)−5 1 (0.5%)−4 1 (0.5%)−3 4 (2%)−2 8 (5%)−1 15 (9%)0 140 (82%)
SE = status epilepticus; mRS = modified Rankin Scale.
237C. Kellinghaus, F. Stögbauer / Epilepsy & Behavior 23 (2012) 235–240
secondAED. All other patients received a third AED – inmost cases laco-samide or phenytoin – after a median latency of 0.5 h. The third AEDwas successful in 16 (35%) of the patients. The fourth effort of treatmentin the 30 remaining non-responders also consistedmainly of phenytoinand lacosamide, with some patients already receiving an enteral AEDsuch as carbamazepine or oxcarbazepine. In the fourth to seventh stepof treatment, success rates were between 30 and 50% using a varietyof intravenous and enteral AEDs. All further efforts in the few patientsremaining in SE were unsuccessful. Anesthesia for treatment of refrac-tory SEwas performedwith propofol in 9 patients andwith thiopenthalin 1 patient. Only 4 of these patients had a nonconvulsive SE, all otherpatients were admitted for generalized convulsive SE.
SE was terminated successfully in 163 patients (95%). In 140patients (82%), mRS at discharge was the same as before SE onset(see Table 3). Eighteen patients died, the majority of them aftercessation of SE.
Patients with refractory SE did not differ from those successfullytreated with the first or second AED regarding age, gender, or broadetiological categories as used here (see Table 4). The number of diag-noses was significantly higher in the patients with drug-resistant sei-zures, whereas mRS before SE onset only numerically differed.Significantly more patients with nonconvulsive SE (i.e. loss of con-sciousness or aphasia or cognitive dysfunction) had drug-resistantseizures, and latency until treatment start tended to be longer inthese patients without reaching statistical significance. As expected,patients with drug-resistant seizures had more adverse events andworse global outcome as expressed as higher mRS scores. However,median benzodiazepine and levetiracetam bolus doses did not differ.
Multiple logistic regression was performed using refractoriness asdependent variable. Independent variables were age, gender, etiology(remote symptomatic yes/no as dummy variable), semiology (noncon-vulsive semiology yes/no as dummy variable), latency from SE onset totreatment, mRS before admission, benzodiazepine dose. Backward
multiple logistic regression showed nonconvulsive semiology as theonly independently contributing variable (Beta 0.167, standard error0.068, t=2.212, p=0.028).
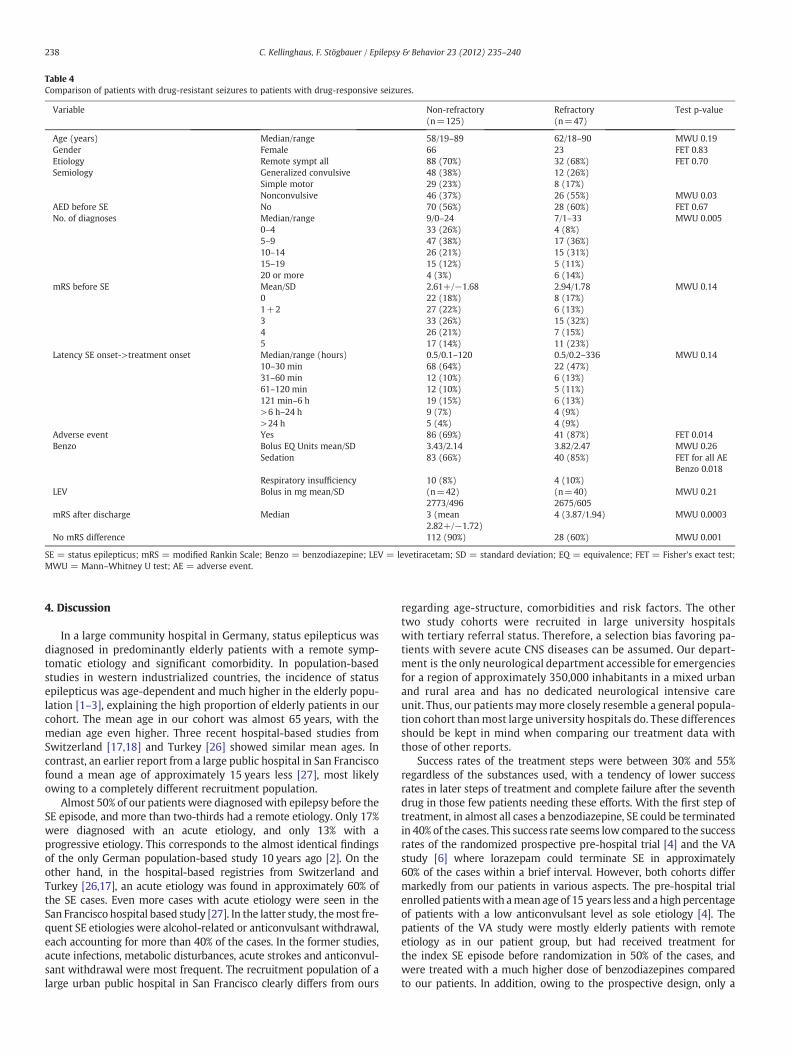
Table 4Comparison of patients with drug-resistant seizures to patients with drug-responsive seizures.
Variable Non-refractory(n=125)
Refractory(n=47)
Test p-value
Age (years) Median/range 58/19–89 62/18–90 MWU 0.19Gender Female 66 23 FET 0.83Etiology Remote sympt all 88 (70%) 32 (68%) FET 0.70Semiology Generalized convulsive 48 (38%) 12 (26%)
Simple motor 29 (23%) 8 (17%)Nonconvulsive 46 (37%) 26 (55%) MWU 0.03
AED before SE No 70 (56%) 28 (60%) FET 0.67No. of diagnoses Median/range 9/0–24 7/1–33 MWU 0.005
0–4 33 (26%) 4 (8%)5–9 47 (38%) 17 (36%)10–14 26 (21%) 15 (31%)15–19 15 (12%) 5 (11%)20 or more 4 (3%) 6 (14%)
mRS before SE Mean/SD 2.61+/−1.68 2.94/1.78 MWU 0.140 22 (18%) 8 (17%)1+2 27 (22%) 6 (13%)3 33 (26%) 15 (32%)4 26 (21%) 7 (15%)5 17 (14%) 11 (23%)
Latency SE onset->treatment onset Median/range (hours) 0.5/0.1–120 0.5/0.2–336 MWU 0.1410–30 min 68 (64%) 22 (47%)31–60 min 12 (10%) 6 (13%)61–120 min 12 (10%) 5 (11%)121 min–6 h 19 (15%) 6 (13%)>6 h–24 h 9 (7%) 4 (9%)>24 h 5 (4%) 4 (9%)
Adverse event Yes 86 (69%) 41 (87%) FET 0.014Benzo Bolus EQ Units mean/SD 3.43/2.14 3.82/2.47 MWU 0.26
Sedation 83 (66%) 40 (85%) FET for all AEBenzo 0.018
Respiratory insufficiency 10 (8%) 4 (10%)LEV Bolus in mg mean/SD (n=42)
2773/496(n=40)2675/605
MWU 0.21
mRS after discharge Median 3 (mean2.82+/−1.72)
4 (3.87/1.94) MWU 0.0003
No mRS difference 112 (90%) 28 (60%) MWU 0.001
SE = status epilepticus; mRS = modified Rankin Scale; Benzo = benzodiazepine; LEV = levetiracetam; SD = standard deviation; EQ = equivalence; FET = Fisher's exact test;MWU = Mann–Whitney U test; AE = adverse event.
238 C. Kellinghaus, F. Stögbauer / Epilepsy & Behavior 23 (2012) 235–240
4. Discussion
In a large community hospital in Germany, status epilepticus wasdiagnosed in predominantly elderly patients with a remote symp-tomatic etiology and significant comorbidity. In population-basedstudies in western industrialized countries, the incidence of statusepilepticus was age-dependent and much higher in the elderly popu-lation [1–3], explaining the high proportion of elderly patients in ourcohort. The mean age in our cohort was almost 65 years, with themedian age even higher. Three recent hospital-based studies fromSwitzerland [17,18] and Turkey [26] showed similar mean ages. Incontrast, an earlier report from a large public hospital in San Franciscofound a mean age of approximately 15 years less [27], most likelyowing to a completely different recruitment population.
Almost 50% of our patients were diagnosedwith epilepsy before theSE episode, and more than two-thirds had a remote etiology. Only 17%were diagnosed with an acute etiology, and only 13% with aprogressive etiology. This corresponds to the almost identical findingsof the only German population-based study 10 years ago [2]. On theother hand, in the hospital-based registries from Switzerland andTurkey [26,17], an acute etiology was found in approximately 60% ofthe SE cases. Even more cases with acute etiology were seen in theSan Francisco hospital based study [27]. In the latter study, themost fre-quent SE etiologies were alcohol-related or anticonvulsant withdrawal,each accounting for more than 40% of the cases. In the former studies,acute infections, metabolic disturbances, acute strokes and anticonvul-sant withdrawal were most frequent. The recruitment population of alarge urban public hospital in San Francisco clearly differs from ours
regarding age-structure, comorbidities and risk factors. The othertwo study cohorts were recruited in large university hospitalswith tertiary referral status. Therefore, a selection bias favoring pa-tients with severe acute CNS diseases can be assumed. Our depart-ment is the only neurological department accessible for emergenciesfor a region of approximately 350,000 inhabitants in a mixed urbanand rural area and has no dedicated neurological intensive careunit. Thus, our patients maymore closely resemble a general popula-tion cohort thanmost large university hospitals do. These differencesshould be kept in mind when comparing our treatment data withthose of other reports.
Success rates of the treatment steps were between 30% and 55%regardless of the substances used, with a tendency of lower successrates in later steps of treatment and complete failure after the seventhdrug in those few patients needing these efforts. With the first step oftreatment, in almost all cases a benzodiazepine, SE could be terminatedin 40% of the cases. This success rate seems low compared to the successrates of the randomized prospective pre-hospital trial [4] and the VAstudy [6] where lorazepam could terminate SE in approximately60% of the cases within a brief interval. However, both cohorts differmarkedly from our patients in various aspects. The pre-hospital trialenrolled patientswith amean age of 15 years less and a high percentageof patients with a low anticonvulsant level as sole etiology [4]. Thepatients of the VA study were mostly elderly patients with remoteetiology as in our patient group, but had received treatment forthe index SE episode before randomization in 50% of the cases, andwere treated with a much higher dose of benzodiazepines comparedto our patients. In addition, owing to the prospective design, only a

239C. Kellinghaus, F. Stögbauer / Epilepsy & Behavior 23 (2012) 235–240
fraction of the screened patients finally was enrolled into both studies,suggesting a relevant sampling bias.
Levetiracetam was used as second treatment step in the majorityof the patients with ongoing SE after benzodiazepine treatment. Itwas able to stop the SE in almost half of the cases. This is well withinthe range of previous retrospective series focussing on levetiracetamthat found success rates between 26% [28] and 89% [14]. In a recentlarge prospective observational series, levetiracetam was successfulas a second step of treatment in 52% [17]. A retrospective studycomparing levetiracetam with phenytoin and valproate suggested alower success rate for levetiracetam, but the mean bolus dose wasonly 1600 mg and thus much lower than in our study [17]. In arandomized prospective study comparing lorazepam with levetirace-tam as first-line treatment in status epilepticus, both drugs showed asuccess rate of more than 70% [29]. However, the protocol used a veryaggressive treatment approach resulting in a significantly higheradverse event rate. In addition, the patient cohort was recruited inIndia where etiologies are different from European or U.S. cohorts.As of yet, there has been no randomized trial comparinglevetiracetam with other anticonvulsants for treatment of SE afterfailure of benzodiazepines.
Although it is supposed to be common knowledge that the successrate of anticonvulsant therapy in SE decreases strongly with thenumber of previously failed anticonvulsants, our data do not supportthis view. Success rates were between 31% and 50% after the failure ofthe second drug. This may be due to the small group sizes in latterstages of treatment that do not allow us to find a consistent trendin our data. Indeed, our data suggest the existence of truly ‘super-refractory’ status epilepticus. Although the retrospective designprecludes proper comparison of the efficacy of the substances used,our success rates and refractoriness rates are similar to other studiesusing different proportions of established and new drugs.
General outcome in our cohort was good. The overall in-hospitalmortality was less than 10%, compared to 18% both in the Swissstudy [18] and the Turkish study [26]. Our in-hospital mortality closelyresembles the case fatality rate of 9.3% found in the Germanpopulation-based study [2]. Five percent of our patients remained inSE at the time of their death or discharge.
Seizures in only 27% of our patients were refractory according toour definition (failure of both first-line and second-line therapy).This is in line with the prospective study from Switzerland thatfound a slightly lower rate of 22% [18] and in contrast to the Turkishregistry with a higher rate of 38% [26]. Both studies used comparablecriteria for defining refractoriness. When using the definition ‘intuba-tion and admission to ICU’, as other studies did [30,31], our rate of re-fractory SE episodes would be about 10% compared to 30% and 45% inthose studies. This is most likely due to the inclusion of hypoxic/anox-ic patients into the SE group as well as to the selection of the patientsmainly from the ICU.
In our group, refractoriness was associated with non-convulsivesemiology, more adverse events and worse outcome despite similarlyhigh doses of first- and second-line drugs. In univariate analysis, theTurkish study also found an association between non-convulsive SEand refractoriness that failed to remain significant in multivariateanalysis [26]. Loss of consciousness as well as nonconvulsive SE incoma are relevant scoring points in the Status Epilepticus SeverityScore (STESS) [32], which is strongly associated with mortality aswell as refractoriness in SE [18,32,33,6]. The majority of our patientsclassified as having non-convulsive SE had significantly impairedconsciousness. Most likely, loss of consciousness in associationwith SE signals either a more severe underlying brain disorder ormore significant extracerebral comorbidity, or both. No significantimpact of time from SE onset to treatment onset was found. Thisis in agreement with the literature [26,34,32,35,36], althoughsome authors found development of refractoriness over time inSE [37,6].
Our study has several limitations. First, the retrospective designmay result in selection bias and poor data quality. However, caseascertainment was made thoroughly and by using all available data.Therefore, only a small number of patients with SE will have beenmissed. In addition, standardized documentation of treatment and ef-fect that has been established in our hospital was extremely helpful inextracting all important treatment data retrospectively. Thus, our se-ries is close to a prospective design. A second limitation when compar-ing treatment steps is the lack of randomization, resulting in selectionbias that is inherent in all non-randomized studies. Finally, our cohortrepresents the patients and the resources and policies of one single cen-ter. Although our cohort is quite similar to a German population-basedcohort in several aspects, our results and experiences cannot be trans-ferred on a one-to-one basis to other institutions, let alone other coun-tries. However, our data represent a coherent and detailed exploratorydataset that could be used to design and develop prospective or evenrandomized studies that are urgently needed.
Conflict of interest statement
Dr. Kellinghaus received honoraria and travel support from UCB,Eisai, Pfizer, Desitin, Novartis and Sanofi-Aventis. He has served onadvisory boards for UCB (2010 to present).
Dr. Stögbauer received honoraria and travel support fromBayer, Biogen TAD, Novartis, Biogen, Merck Serono, Pfizer, TEVAand Sanofi-Aventis.
References
[1] Hesdorffer DC, Logroscino G, Cascino G, Annegers JF, Hauser WA. Incidence of sta-tus epilepticus in Rochester, Minnesota, 1965-1984. Neurology 1998;50:735–41.
[2] Knake S, Rosenow F, Vescovi M, et al. Incidence of status epilepticus in adults inGermany: a prospective, population-based study. Epilepsia 2001;42:714–8.
[3] Vignatelli L, Tonon C, D'Alessandro R. Incidence and short-term prognosis ofstatus epilepticus in adults in Bologna, Italy. Epilepsia 2003;44:964–8.
[4] Alldredge BK, Gelb AM, Isaacs SM, et al. A comparison of lorazepam, diazepam,and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med2001;345:631–7.
[5] Leppik IE, Derivan AT, Homan RW, Walker J, Ramsay RE, Patrick B. Double-blindstudy of lorazepam and diazepam in status epilepticus. JAMA 1983;249:1452–4.
[6] Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatmentsfor generalized convulsive status epilepticus. Veterans Affairs Status EpilepticusCooperative Study Group. N Engl J Med 1998;339:792–8.
[7] Misra UK, Kalita J, Patel R. Sodium valproate vs phenytoin in status epilepticus:a pilot study. Neurology 2006;67:340–2.
[8] Meierkord H, Boon P, Engelsen B, et al. EFNS guideline on the management ofstatus epilepticus in adults. Eur J Neurol 2009;17:348–55.
[9] Minicucci F, Muscas G, Perucca E, Capovilla G, Vigevano F, Tinuper P. Treatmentof status epilepticus in adults: guidelines of the Italian League against Epilepsy.Epilepsia 2006;47(Suppl 5):9–15.
[10] Claassen J, Hirsch LJ, Mayer SA. Treatment of status epilepticus: a survey of neu-rologists. J Neurol Sci 2003;211:37–41.
[11] Holtkamp M, Masuhr F, Harms L, Einhaupl KM, Meierkord H, Buchheim K. Themanagement of refractory generalised convulsive and complex partial statusepilepticus in three European countries: a survey among epileptologists andcritical care neurologists. J Neurol Neurosurg Psychiatry 2003;74:1095–9.
[12] Berning S, Boesebeck F, Van Baalen A, Kellinghaus C. Intravenous levetiracetam astreatment for status epilepticus. J Neurol 2009;256:1634–42.
[13] Kellinghaus C, Berning S, Immisch I, et al. Intravenous lacosamide for treatmentof status epilepticus. Acta Neurol Scand 2011;123:137–41.
[14] Knake S, Gruener J, Hattemer K, et al. Intravenous levetiracetam in the treatmentof benzodiazepine refractory status epilepticus. J Neurol Neurosurg Psychiatry2008;79:588–9.
[15] Möddel G, Bunten S, Dobis C, et al. Intravenous levetiracetam: a new treatmentalternative for refractory status epilepticus. J Neurol Neurosurg Psychiatry 2009;80:689–92.
[16] Stephani U, Esser W, Evers S, et al. Intravenous levetiracetam in clinical practice —
90 patients reported to an independent registry. Epilepsia 2009;50 48-P212.[17] Alvarez V, Januel JM, Burnand B, Rossetti AO. Second-line status epilepticus treat-
ment: comparison of phenytoin, valproate, and levetiracetam. Epilepsia 2011;52:1292–6.
[18] Novy J, Logroscino G, Rossetti AO. Refractory status epilepticus: a prospectiveobservational study. Epilepsia 2010;51:251–6.
[19] Martin PJ, Millac PA. Status epilepticus: management and outcome of 107 episodes.Seizure 1994;3:107–13.
[20] Kalita J, Nair PP, Misra UK. A clinical, radiological and outcome study of statusepilepticus from India. J Neurol 2010;257:224–9.

240 C. Kellinghaus, F. Stögbauer / Epilepsy & Behavior 23 (2012) 235–240
[21] Rankin L. Cerebral vascular accidents in patients over the age of 60. II. Prognosis.Scott Med J 1957;2:200–15.
[22] van Swieten JC, Koudstaal PJ, VisserMC, SchoutenHJ, van Gijn J. Interobserver agree-ment for the assessment of handicap in stroke patients. Stroke 1988;19:604–7.
[23] Young GB, Jordan KG, Doig GS. An assessment of nonconvulsive seizures in theintensive care unit using continuous EEGmonitoring: an investigation of variablesassociated with mortality. Neurology 1996;47:83–9.
[24] Ashton CH. Benzodiazepines —How they work and how to withdraw (The Ashtonmanual). URL http://www.benzo.org.uk/manual/ accessed 20-April-2011.
[25] Sostmann HJ, Sostmann H, Crevoisier C, Bircher J. Dose equivalence of midazolamand triazolam. A psychometric study based on flicker sensitivity, reaction timeand digit symbol substitution test. Eur J Clin Pharmacol 1989;36:181–7.
[26] Agan K, Afsar N, Midi I, Us O, Aktan S, Aykut-Bingol C. Predictors of refractorinessin a Turkish status epilepticus data bank. Epilepsy Behav 2009;14:651–4.
[27] Lowenstein DH, Alldredge BK. Status epilepticus at an urban public hospital in the1980s. Neurology 1993;43:483–8.
[28] Rossetti AO, Bromfield EB. Levetiracetam in the treatment of status epilepticus inadults: a study of 13 episodes. Eur Neurol 2005;54:34–8.
[29] Misra UK, Kalita J,Maurya PK. Levetiracetam versus lorazepam in status epilepticus: arandomized, open labeled pilot study. J Neurol 2011 Sep 6. doi:10.1007/s00415-011-6227-2 [Electronic publication ahead of print].
[30] Holtkamp M, Othman J, Buchheim K, Meierkord H. Predictors and prognosis ofrefractory status epilepticus treated in a neurological intensive care unit. J NeurolNeurosurg Psychiatry 2005;76:534–9.
[31] Rossetti AO, Logroscino G, Bromfield EB. Refractory status epilepticus: effect oftreatment aggressiveness on prognosis. Arch Neurol 2005;62:1698–702.
[32] Rossetti AO, Logroscino G, Bromfield EB. A clinical score for prognosis of statusepilepticus in adults. Neurology 2006;66:1736–8.
[33] Rossetti AO, Logroscino G, Milligan TA, Michaelides C, Ruffieux C, Bromfield EB.Status Epilepticus Severity Score (STESS): a tool to orient early treatment strategy.J Neurol 2008;255:1561–6.
[34] Logroscino G, Hesdorffer DC, Cascino G, Annegers JF, Hauser WA. Short-termmortality after a first episode of status epilepticus. Epilepsia 1997;38:1344–9.
[35] Rossetti AO, Hurwitz S, Logroscino G, Bromfield EB. Prognosis of status epilepticus:role of aetiology, age, and consciousness impairment at presentation. J NeurolNeurosurg Psychiatry 2006;77:611–5.
[36] Towne AR, Pellock JM, Ko D, DeLorenzo RJ. Determinants of mortality in statusepilepticus. Epilepsia 1994;35:27–34.
[37] DeLorenzo RJ, Waterhouse EJ, Towne AR, et al. Persistent nonconvulsive statusepilepticus after the control of convulsive status epilepticus. Epilepsia 1998;39:833–40.