tobacco advertising, environmental smoking bans, and smoking in chinese urban areas
TRANSCRIPT

G
D
Tu
Ta
b
c
a
ARR2AA
KTWHSTC
1
tftattgtpPibro
agR
0d
ARTICLE IN PRESS Model
AD-4337; No. of Pages 7
Drug and Alcohol Dependence xxx (2012) xxx– xxx
Contents lists available at SciVerse ScienceDirect
Drug and Alcohol Dependence
jo u rn al hom epage: www.elsev ier .com/ locate /drugalcdep
obacco advertising, environmental smoking bans, and smoking in Chineserban areas
ingzhong Yanga,∗, Ian R.H. Rockettb, Mu Li c, Xiaochao Xua, Yaming Gua
Center for Tobacco Control Research, Zhejiang University School of Medicine, Hangzhou 310058, ChinaInjury Control Research Center and Department of Community Medicine, West Virginia University, Morgantown, WV, USASydney School of Public Health, University of Sydney, Australia
r t i c l e i n f o
rticle history:eceived 25 June 2011eceived in revised form0 December 2011ccepted 21 December 2011vailable online xxx
eywords:
a b s t r a c t
Objectives: To evaluate whether cigarette smoking in Chinese urban areas was respectively associatedwith exposure to tobacco advertising and smoking bans in households, workplaces, and public places.Methods: Participants were 4735 urban residents aged 15 years and older, who were identified throughmulti-stage quota-sampling conducted in six Chinese cities. Data were collected on individual sociode-mographics and smoking status, and regional tobacco control measures. The sample was characterizedin terms of smoking prevalence, and multilevel logistic models were employed to analyze the associationbetween smoking and tobacco advertising and environmental smoking restrictions, respectively.
obacco control public placeorkplace
ouseholdmoking restrictionobacco advertisinghina
Results: Smoking prevalence was 30%. Multilevel logistic regression analysis showed that smoking waspositively associated with exposure to tobacco advertising, and negatively associated with workplaceand household smoking bans.Conclusions: The association of smoking with both tobacco advertising and environmental smoking bansfurther justifies implementation of comprehensive smoking interventions and tobacco control programsin China.
. Introduction
Exposure to tobacco smoke causes serious disease and prema-ure death. Globally, the tobacco-smoking epidemic is responsibleor approximately 5.4 million deaths each year, including morehan 600,000 non-smokers (World Health Organization, 2008). Thennual death toll is projected to exceed 8 million by 2030. Morehan 80% of these deaths will occur in less developed nations, andhe epidemic will strike hardest in those countries with rapidlyrowing economies (World Health Organization, 2008). China leadshe world in tobacco consumption and approximately one millionersons Chinese die each year from tobacco-related causes (Theeople’s Republic of China Ministry of Health, 2007). This death tolls projected to reach two million annually by 2025 and three milliony 2050. A projected 100 million Chinese will die from smoking-elated causes over the next 50 years if the current high prevalencef smoking persists (Doll et al., 2004; Peto et al., 1996).
Exposure to tobacco smoke in public places is common in China,
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
nd occurs in most restaurants and 70% of schools and hospitals,overnment buildings, and train stations (Stillman et al., 2007).estrictions on smoking in public places were associated with a
∗ Corresponding author.E-mail address: [email protected] (T. Yang).
376-8716/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.drugalcdep.2011.12.021
© 2011 Elsevier Ireland Ltd. All rights reserved.
higher probability of delaying smoking uptake and lowering smok-ing prevalence (US Department of Health and Human Services,2006; Wakefield et al., 2000). Smoke-free laws may reduce smok-ing prevalence substantially (New York State Department of Health,2011). In a report in 2000, the US Surgeon-General stated thatsmoke-free policies are the most effective way to reduce exposureto tobacco smoke (Wakefield et al., 2000). Many studies have shownthat smoke-free workplace policies substantially reduce workerexposure to tobacco smoke (Fichtenberg and Glantz, 2002; Skeeret al., 2005), and encourage smokers to quit or reduce their smok-ing (Eriksen and Cerak, 2008; Moher et al., 2005). Studies have alsodemonstrated that restricting smoking in the home is effective inreducing exposure to passive tobacco smoke, and such restrictioncould help reduce experimental smoking among children and ado-lescents, and more generally encourage smoking cessation (Keglerand Malcoe, 2002; Li et al., 2009). We found that almost all of thestudies on the association between smoking restrictions and smok-ing came from the more economically developed countries, such asthe United States, various European countries, Australia, Canada,and Japan (US Department of Health and Human Services, 2006;Wakefield et al., 2000; Fichtenberg and Glantz, 2002; Skeer et al.,
ronmental smoking bans, and smoking in Chinese urban areas. Drug
2005; Moher et al., 2005; Mackay et al., 2010). There have been nostudies reporting on this relationship in China. This emerges as avery important gap to close in order to develop appropriate tobaccocontrol strategies.

ING Model
D
2 ol Dep
OTbp2tmsto2pCstaamP2tAilahmoF
ataOpf(2
StJsotaccpap2B
Cet
2
2
sda
ARTICLEAD-4337; No. of Pages 7
T. Yang et al. / Drug and Alcoh
To counter the global spread of tobacco use, the World Healthrganization (WHO) established the Framework Convention onobacco Control (FCTC) in 1999. This framework was fully endorsedy member states on May 21, 2003. The Chinese National Peo-le’s Congress ratified the FCTC on August 27, 2005 (Yang et al.,005). The FCTC provides clear guidance through Article 8 (Protec-ion from Exposure to Tobacco Smoke). Article 8 outlines specific
easures and approaches for reducing population-wide tobaccomoke exposure. More than 739 million people worldwide are pro-ected by comprehensive, national smoke-free laws, an increasef more than 385 million since 2008 (World Health Organization,011). Implementation of FCTC recommended activities has beenrogressing slowly in China. Nevertheless, by ratifying the FCTC,hina has agreed that all workplaces and public places should bemoke-free by 2011. Moreover, efforts have recently been madeo expand the number of smoke-free places. China does not have
comprehensive smoke-free law. However, several national lawsnd policies regulate smoking in public places. The central govern-ent is revising the Regulations on the Sanitary Administration of
ublic Places to strengthen controls on secondhand smoke (Li et al.,010). In recent years, Ministry of Health and Ministry of Educa-ion regulations have required smoke-free schools and hospitals.t present, nearly half of the Chinese midsize and large cities have
mplemented smoke-free policies or regulations pertaining to pub-ic places. In many cases, however, extant policies or regulationsre weak due to limited enforcement (Li et al., 2010). On the otherand, Chinese organizations are now creating smoke-free environ-ents, and nationwide campaigns are being waged to ban smoking
n university campuses and in hospitals (Yang et al., 2009b; Lin andraser, 2011).
The FCTC requires that each party to the Convention “undertake comprehensive ban, and restrict tobacco advertising, promo-ion, and sponsorship on radio, television, print media, and also,s appropriate, other media such as the Internet” (World Healthrganization, 2003). Several studies have documented that com-lete bans on tobacco advertising and promotion can protect youthrom initiating smoking and adults from continuing to smokeBiener and Siegel, 2006; Blecher, 2008; Chapman, 1996; Li et al.,009; Martínez-Donate et al., 2005; Nelson, 2003).
China has been tightening up bans on tobacco advertising. Thetanding Committee of the National People’s Congress approvedhe Law of the People’s Republic of China on Tobacco Monopoly inune 1991. According to this Law “advertising for tobacco productshall be banned on radio and television stations, or in newspapersr periodicals”. However, there is no comprehensive legislationhat specifically bans tobacco advertising and promotion. Tobaccodvertising remains widespread (Li et al., 2009). Noteworthy, theomprehensive legislation that has banned tobacco advertisingovers all forms of tobacco advertising and sponsorship. The com-rehensive legislation for smoke-free air covers 100% of indoorreas in all workplaces and public places. Such legislation hasroven effective in many countries (World Health Organization,008; Fong et al., 2006; Edwards et al., 2008; Mackay et al., 2010;raverman and Aarø, 2004; Saffer and Chaloupka, 2000).
This study will explore the association between smoking inhinese urban areas and exposure to tobacco advertising andnvironmental restrictions on smoking. Results will inform futureobacco control policies and interventions in China.
. Methods
.1. Study design
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
This study used a cross-sectional multistage sampling design. In Stage 1,ix Chinese cities were selected based on geographic location and economicevelopment status. The six study cities and their respective population sizend economic focus were Hangzhou (6.7 million, light industry and tourism),
PRESSendence xxx (2012) xxx– xxx
Nanjing (6.2 million, education and light industry), Guangzhou (7.7 million, lightindustry and commerce), Taiyuan (3.5 million, manufacturing), Yinchuan (1.6million, agriculture and light industry), and Harbin (9.9 million, manufacturing).They are capital cities and located in the southeast, southeast and partial west,south, north, northwest, and northeast China, respectively. In terms of relativeeconomic development, Harbin, Yinchuan and Taiyuan are underdeveloped,Nanjing has moderate development, and Hangzhou and Guangzhou possessadvanced economies (Department of Comprehensive Statistics of National Bureauof Statistics, 2008). In all cities except Taiyuan, the local government had issuedsmoke-free policies in public places at the time of the survey. More recently, thelocal People’s Congress issued smoke-free regulations in Hangzhou, Guangzhou,Harbin, and Yinchuan. These regulations commonly cover kindergartens andnurseries, cinemas, libraries, exhibition halls, mass transit systems, schools, andhospitals. Stage 2 comprised the selection of residential districts within each city.Two residential districts with a high density of family households were randomlyselected from the sampling frame in each study city. In Stage 3, four ‘Jiedao’ (asub-district neighborhood administration) were randomly selected within eachresidential district and then sixteen building blocks were randomly selected fromeach ‘Jiedao’. In Stage 4, a family household registration (“hukou”) list was usedto randomly sample households within the selected building blocks. Individualsaged 15 years and older, who had lived in their home for at least one year, wereidentified within each household. Finally, one respondent was randomly selectedfrom each family, with eligibility being determined by the birth date closest to thecontact date (Yang et al., 2011). Data were collected between March and May 2008.
2.2. Methodology
A face-to-face interview was scheduled once an individual was identified andagreed to participate. All interviews were conducted by the interviewers using a briefquestionnaire. Interviewers were fourth-year medical students from a local medi-cal college who received a one-day training on the study protocol and interviewingprocedures. The survey was administered privately to participants in their homeor in a designated quiet place, such as a backyard or community park. Appoint-ments were scheduled by phone through a community organization. Interviewswere conducted on Saturdays, Sundays, or during the evening or other times whenparticipants were available. Appointments were rescheduled whenever necessary.Upon receiving survey instructions explained by assistants, participants were askedto fill out a survey questionnaire of approximately 30 min duration. Each partici-pant was given an opportunity to answer or clarify questions regarding the surveyor survey items, and adequate time for survey completion.
A common interview protocol was used across the six study cities to assurehomogeneity of interview and data collection. The study was approved by the EthicsCommittee at the Medical Center, Zhejiang University, and informed written consentwas obtained from all respondents prior to commencement of the study. Possess-ing acceptable psychometric properties, the data collection procedures have beenextensively employed in smoking research in China (Yang et al., 2011).
A total of 5333 individuals were identified, with 5012 available for contact and4981 consenting to interview. There were 4735 complete questionnaires returned,for a response rate of 89%. No reasons were given for non-participation.
2.3. Measures
2.3.1. Dependent variable. Smoking status: information regarding smoking status,frequency and quantity of smoking, and smoking history was assessed through self-report. For our smoking measure, we employed the standard method recommendedby the World Health Organization (World Health Organization, 1998), and consis-tent with the Global Adult Tobacco Survey (GATS). We defined a current smokeras someone who smoked cigarettes at time of interview, a daily smoker as some-one who smoked every day, and an occasional smoker as someone who smoked onsome days (World Health Organization, 1998; Yang et al., 2010, 2011). The depen-dent variable in this study was current smoking, and was coded dichotomously as1 = current smoking and 0 = no smoking.
2.3.2. Individual-level independent variables. Sociodemographics: data were col-lected on age, gender, ethnicity, marital status, educational level, occupation, andsmoking status and tobacco control measures.
Exposure to tobacco advertising: respondents were asked whether they hadseen any tobacco advertisements in the last six months (never/seldom/sometimes/often/almost always) with the responses recoded as 1 = never/seldom and2 = sometimes/often/almost always.
Smoking restrictions in public places: respondents were asked two questions.First, had they witnessed smoking in restaurants, hospitals, shops, buses, and otherpublic places in their city in the last six months (yes/no)? Secondly, if answering inthe affirmative, they were asked whether they had observed any smoking restric-
ronmental smoking bans, and smoking in Chinese urban areas. Drug
tions with smoke free organizations (for example, smoke free campus or hospitals)signage or notification in outside or no-smoking signage or any publicity materi-als for a smoke-free policy displayed within these venues, with optional responsescovering no restrictions/restrictions/no attention. Responses were recoded dichoto-mously as 1 = no smoking restrictions 2 = smoking ban.

ING Model
D
ol Dep
ri1ots
rprt
2raa
2swtvm2tm2ac
cvtiIlvaabwlfipdsiu
Whp
3
3if(Satr94s
argpw
ARTICLEAD-4337; No. of Pages 7
T. Yang et al. / Drug and Alcoh
Smoking restrictions in workplaces: respondents were asked what smokingestrictions were implemented in their present workplace, with options cover-ng none/in some places/in all places. Responses were recoded dichotomously as
= no smoking restrictions or partial restrictions and 2 = smoking ban. For retiredr unemployed respondents, ‘workplace’ referred to the place where they went foremporary work, leisure, or community activities. For students, workplace covereduch places as classrooms and libraries.
Smoking restrictions in households: respondents were asked what smokingestrictions were currently in their household, with options covering none/in somelaces/in all places. Responses were recoded dichotomously as 1 = no smokingestrictions or partial restrictions and 2 = smoking ban. Household smoking restric-ions were internally imposed only.
.3.3. Regional-level independent variable. The contextual independent variable,egion, was categorized as south or north. Of our six study cities, Hangzhou, Nanjing,nd Guangzhou are located in southern China, and Taiyuan, Yinchuan, and Harbinre located in the north.
.3.4. Data analysis. Data analysis was conducted in several stages using SAS ver-ion 6.12 and MLwiN Version 2.02 (Rashash et al., 2001). Smoking prevalenceas calculated for the sample, and Chi-square tests were performed to analyze
he univariate association between individual-level and regional-level independentariables and smoking. Multilevel logistic regression models were used in assessingultivariate associations (Fone and Dunstan, 2006; Goldstein, 1995; Rashash et al.,
001). A nested hierarchical multilevel modeling technique has substantial advan-ages over a single-level regression procedure, when there is both a defined outcome
easure and clear differentiation of ‘individual’ and ‘place’ (Fone and Dunstan,006). Individuals were nested by region (N = 4735). By modeling random variationt both individual and regional levels, effects of ecological and atomistic fallaciesould be avoided.
Model building started with the ‘null’ model, a two-level model of random inter-epts. This null model was confined to a constant, which accounted for smokingariation across the six study cities, and was used for subsequent comparisons. Herehe variation in smoking was modeled by random intercept terms for cities and anndividual random error term. The final model was an expansion of the base model.n the final model, we could assess compositional fixed effects and residual cityevel random variances. Here the compositional fixed effects are individual-levelariables, namely, personal sociodemographics and respective exposure to tobaccodvertising and environmental smoking restrictions, and a single contextual vari-ble, region. The individual-level variables were entered as fixed main effects on theasis of significant univariate associations with current smoking. The fixed effectsere expressed by odds ratios which indicated the likelihood of smoking preva-
ence for each level of a variable compared to the referent. A preferred methodor exploratory analyses, forward-stepwise regression, enabled us to assess thesendependent variables individually. In the final model we incorporated those inde-endent variables that manifested a statistically significant association with theependent variable. Our final model also sought to explain variation in currentmoking status across cities. Model fitting was assessed by the likelihood of a changen the −2 log. Significance of the random effect variance estimates was assessedsing the Wald joint X2 test statistic (Goldstein, 1995).
Analyses were weighted by city population size, as were the reported statistics.e did not consider district, sub-district, blocks of apartment buildings, or house-
olds in our weighting, since differences in general characteristics and smokingrevalence were minimal within a given city (Yang et al., 2011).
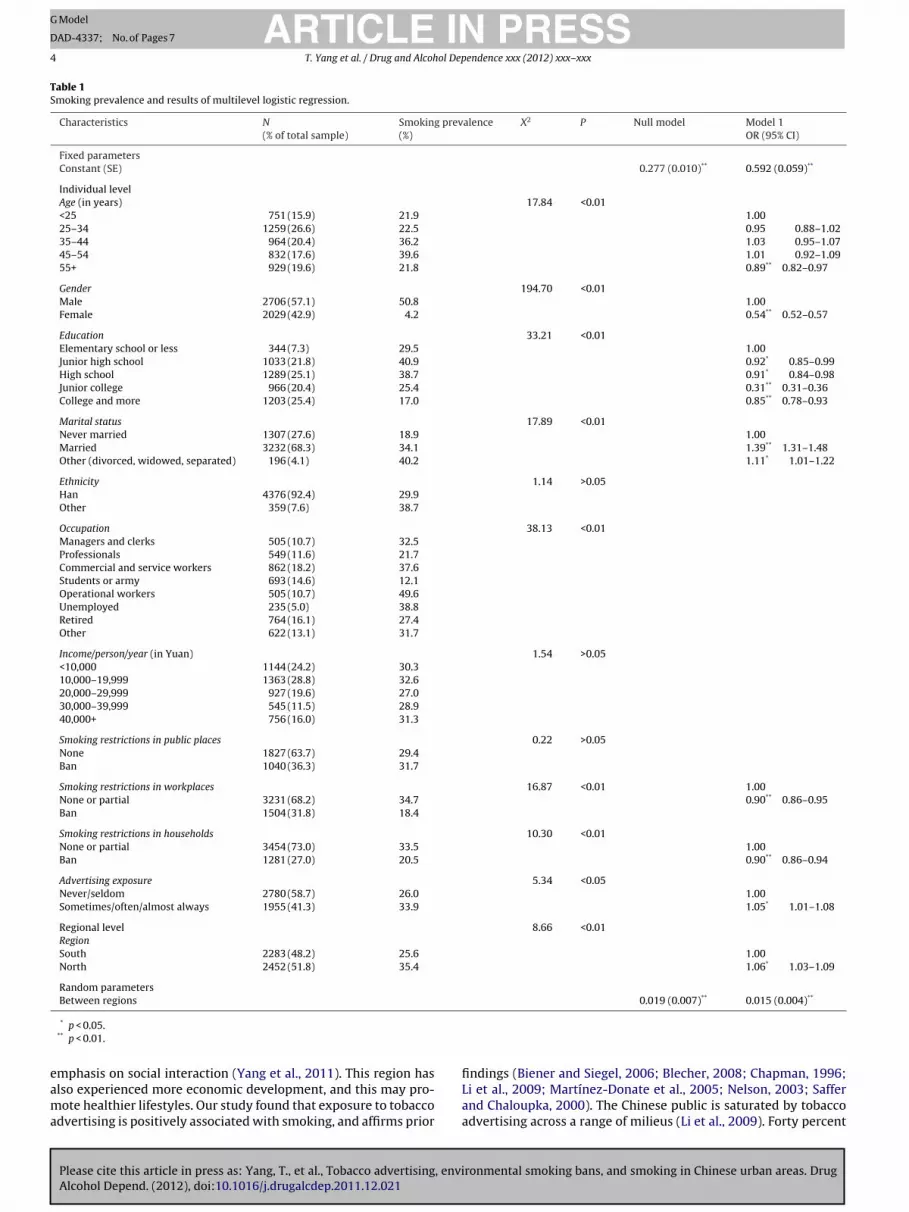
. Results
Among the 4735 respondents, current smoking prevalence was0%, daily smoking prevalence was 23%, and occasional smok-
ng prevalence was 7%. Sample characteristics resembled thoserom national surveys, except for a higher male-to-female ratioDepartment of Comprehensive Statistics of National Bureau oftatistics, 2008). Current smoking prevalence was associated withge, gender, education, marital status, occupation, smoking restric-ions in households, workplaces, and advertising exposure, andegional location (Table 1). Of the 4735 respondents in this study,1.4% (4329) witnessed smoking in public places. Of this subset of329, 66.2% (2867) were sensitive to the existence of a restrictivemoking policy.
We now present the estimates generated by the multilevelnalysis (Table 1). The null model estimation showed that the
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
andom effect between cities was 0.019 (P = 0.01), which sug-ested inter-city variation in smoking prevalence. The table showsarameter estimates for compositional variables as fixed effects,hich are adjusted for all variables included in the model. Several
PRESSendence xxx (2012) xxx– xxx 3
individual-level sociodemographic variables were associatedwith smoking. Females were less likely than males to smoke.The married, divorced, or separated were more likely to smokethan the never-married. People aged 55 years and older wereless likely than their younger referent to smoke. People with ahigher education manifested a lower prevalence of smoking thanthe lesser educated. Those living in the north were more likely tosmoke than those in the south. Current smoking was negativelyassociated with both workplace and household restrictions, butpositively associated with exposure to tobacco advertising.
Exposure to tobacco advertising by watching television,billboards, visiting tobacconist shops was 54%, 28% and 25%, respec-tively. Thirty-seven percent of the smokers, who were exposedto tobacco advertising, reported that this exposure influencedtheir smoking expenditures. Twenty-seven percent of participantsreported complete smoking restrictions in their household; withthe likely impact that 48% of the smokers cut back a little onsmoking cigarettes, 21% somewhat more, and 16% much more.Restriction on smoking (31.7%) in households of married peoplewas significantly higher than in the other households (17.8%) thatwere distinguished by marital status (i.e., married versus nevermarried, divorced, widowed, and separated) (X2: 6.56, P < 0.01).Smokers reported that workplace restrictions made 44.5% of themdecrease smoking cigarettes somewhat, 21.4% decrease more, and19.4% decrease much more. However, only 31.8% of workplacescaptured in our study implemented smoking bans. The prevalenceof banning smoking in the workplace ranged from 23.8% to 40.7%across age groups (X2: 12.58, P < 0.01), was 33.8% in the case offemales and 24.6% in the case of males (X2: 88.22, P < 0.05), andranged from 22.1% to 40.3% across occupational groups.
4. Discussion
This study is the first in China to investigate the associationbetween tobacco control measures implemented in major urbanareas and smoking status. We focus our discussion on the informa-tion generated by the multilevel analyses. The ‘null’ model has theonly constant term, a city-level random effect. This term accountsfor variation in smoking prevalence across the six study cities.The ‘null’ model shows the proportion of variation explained byattributes of living in different cities. Addition of fixed-effect vari-ables to the null model for estimating the final model only slightlyreduced the higher-level random variances. This finding furtherindicated the influence of regional heterogeneity. While we iden-tified a subset of individual-level variables that were statisticallysignificantly associated with current smoking, the random effectnonetheless retained its significance. This finding likely reflects theinfluence of both regional cultural and socioeconomic heterogene-ity upon smoking. In the final model, several variables were statis-tically significantly associated with current smoking. Our findingson the impact of sociodemographics on smoking prevalence con-firmed those from prior studies (Fichtenberg and Glantz, 2002;Biener and Siegel, 2006; Yang et al., 2009a,b). Smoking was over-whelmingly a male phenomenon. This observation is consistentwith smoking norms in China (Yang, 2010). Similar gender-basedprevalence gaps are reported for other less developed nations (Jhaet al., 2002), and were observed in Western countries prior to thetobacco industry targeting females (Graham, 1996). Collectively,these findings raise an important need and opportunity to pre-vent diffusion of smoking among females. Smoking prevalence washigher in northern than southern China. Culturally, the north has
ronmental smoking bans, and smoking in Chinese urban areas. Drug
been influenced by a nomadic culture that encourages social inter-action outside the family. In the north, cigarettes acquire an impor-tant role in social etiquette, which facilitates adoption and contin-uation of smoking. In the south, an agricultural heritage places less
ARTICLE IN PRESSG Model
DAD-4337; No. of Pages 7
4 T. Yang et al. / Drug and Alcohol Dependence xxx (2012) xxx– xxx
Table 1Smoking prevalence and results of multilevel logistic regression.
Characteristics N(% of total sample)
Smoking prevalence(%)
X2 P Null model Model 1OR (95% CI)
Fixed parametersConstant (SE) 0.277 (0.010)** 0.592 (0.059)**
Individual levelAge (in years) 17.84 <0.01<25 751 (15.9) 21.9 1.0025–34 1259 (26.6) 22.5 0.95 0.88–1.0235–44 964 (20.4) 36.2 1.03 0.95–1.0745–54 832 (17.6) 39.6 1.01 0.92–1.0955+ 929 (19.6) 21.8 0.89** 0.82–0.97
Gender 194.70 <0.01Male 2706 (57.1) 50.8 1.00Female 2029 (42.9) 4.2 0.54** 0.52–0.57
Education 33.21 <0.01Elementary school or less 344 (7.3) 29.5 1.00Junior high school 1033 (21.8) 40.9 0.92* 0.85–0.99High school 1289 (25.1) 38.7 0.91* 0.84–0.98Junior college 966 (20.4) 25.4 0.31** 0.31–0.36College and more 1203 (25.4) 17.0 0.85** 0.78–0.93
Marital status 17.89 <0.01Never married 1307 (27.6) 18.9 1.00Married 3232 (68.3) 34.1 1.39** 1.31–1.48Other (divorced, widowed, separated) 196 (4.1) 40.2 1.11* 1.01–1.22
Ethnicity 1.14 >0.05Han 4376 (92.4) 29.9Other 359 (7.6) 38.7
Occupation 38.13 <0.01Managers and clerks 505 (10.7) 32.5Professionals 549 (11.6) 21.7Commercial and service workers 862 (18.2) 37.6Students or army 693 (14.6) 12.1Operational workers 505 (10.7) 49.6Unemployed 235 (5.0) 38.8Retired 764 (16.1) 27.4Other 622 (13.1) 31.7
Income/person/year (in Yuan) 1.54 >0.05<10,000 1144 (24.2) 30.310,000–19,999 1363 (28.8) 32.620,000–29,999 927 (19.6) 27.030,000–39,999 545 (11.5) 28.940,000+ 756 (16.0) 31.3
Smoking restrictions in public places 0.22 >0.05None 1827 (63.7) 29.4Ban 1040 (36.3) 31.7
Smoking restrictions in workplaces 16.87 <0.01 1.00None or partial 3231 (68.2) 34.7 0.90** 0.86–0.95Ban 1504 (31.8) 18.4
Smoking restrictions in households 10.30 <0.01None or partial 3454 (73.0) 33.5 1.00Ban 1281 (27.0) 20.5 0.90** 0.86–0.94
Advertising exposure 5.34 <0.05Never/seldom 2780 (58.7) 26.0 1.00Sometimes/often/almost always 1955 (41.3) 33.9 1.05* 1.01–1.08
Regional level 8.66 <0.01RegionSouth 2283 (48.2) 25.6 1.00North 2452 (51.8) 35.4 1.06* 1.03–1.09
Random parametersBetween regions 0.019 (0.007)** 0.015 (0.004)**
eama
* p < 0.05.** p < 0.01.
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
mphasis on social interaction (Yang et al., 2011). This region haslso experienced more economic development, and this may pro-ote healthier lifestyles. Our study found that exposure to tobacco
dvertising is positively associated with smoking, and affirms prior
ronmental smoking bans, and smoking in Chinese urban areas. Drug
findings (Biener and Siegel, 2006; Blecher, 2008; Chapman, 1996;Li et al., 2009; Martínez-Donate et al., 2005; Nelson, 2003; Safferand Chaloupka, 2000). The Chinese public is saturated by tobaccoadvertising across a range of milieus (Li et al., 2009). Forty percent

ING Model
D
ol Dep
obtobatsos‘LaCam(grmHvfbf
ianrirdtwotsiYiaictaWotstmomsppivlfcaic
ARTICLEAD-4337; No. of Pages 7
T. Yang et al. / Drug and Alcoh
f respondents in our study reported ‘sometimes’ or ‘very often’eing exposed to tobacco advertising. Highest exposures occurredhrough watching television, observing billboards, and proximityf tobacconist shops. These results are similar to those reportedy Li and associates (Li et al., 2009). Banning tobacco advertisingnd promotion is an important component in a comprehensiveobacco control program to curb the tobacco epidemic. Manytudies suggest that comprehensive tobacco advertising bans notnly reduce tobacco consumption, but send a clear message tomokers and non-smokers alike that smoking contravenes socialnorms’ (Biener and Siegel, 2006; Blecher, 2008; Chapman, 1996;i et al., 2009; Martínez-Donate et al., 2005; Nelson, 2003; Saffernd Chaloupka, 2000). The FCTC requires that each party to theonvention “undertake a comprehensive ban, and restrict tobaccodvertising, promotion, and sponsorship on radio, television, printedia, and also, as appropriate, other media such as the Internet”
World Health Organization, 2003). Since the 1990s, the Chineseovernment has endeavored to implement laws and regulationsestricting tobacco advertising and banning tobacco advertise-ents on radio and television, and in newspapers and periodicals.owever, indirect tobacco advertising is common on Chinese tele-ision, and smoking scenes in television programs are increasinglyrequent. We urge the government to legislate a comprehensivean on tobacco advertising, promotion, and sponsorship in all theirorms.
The association between tobacco advertising and current smok-ng attained slight significance in this study. We comparedlternative coding for the advertising exposure variable (i.e.,ever/seldom/sometimes vs. often/almost always). However, theesults were similar. Smoking prevalence was 26.5% and 35.7%n the never/seldom/sometimes and often/almost always groups,espectively; OR: 1.07 (95% CI: 1.03–1.10) a statistically significantifference. We found that many smokers reported that exposure toobacco advertising influenced their smoking expenditures. Note-orthy, there was no sociodemographic variation in the prevalence
f exposure to tobacco advertising. Any family member can poten-ially develop health problems from exposure to passive tobaccomoke, with children being especially vulnerable. The Chinese arencreasingly being exposed to passive smoking (Li et al., 2009;ang et al., 2005). The number of smoke-free homes has reportedly
ncreased in some more developed countries in recent years (Keglernd Malcoe, 2002; Li et al., 2009). Our study revealed that smok-ng restrictions in their household can induce smokers to curb theirigarette consumption. Our findings highlight an imperative to con-inue educational campaigns aimed at raising public awarenessbout the harmful consequences of exposure to tobacco smoke.e recommend that all media educate the public about the perils
f both smoking and exposure to second-hand smoke. At the sameime, it is important to advocate for a change in attitudes towardsmoking restrictions in households. The prevalence of reportedotal smoking bans in households was higher among females than
ales, and for the married than the never married, divorced, wid-wed, and separated. Gender differences in smoking prevalenceay relate to variation across households in the impact of marital
tatus; a possibility which warrants in-depth research. The higherrevalence of smoking restrictions in the households of marriedeople may be cultural. Perhaps most salient in Chinese culture
s the value of family to individuals and society. Chinese familyalues emphasize the collective quality in the nature of individualife and behavior. A strong sense of obligation and responsibility toamily is a cherished virtue. In this context, smoking may be per-eived as a threat to familial health and financial solvency. Family
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
nd peer influences have been associated with smoking behaviorn China (Unger et al., 2002; Yang et al., 2011). Our findings areonfirmatory. Ninety-two percent of smokers had received advice
PRESSendence xxx (2012) xxx– xxx 5
to quit smoking, with the source of three-quarters of this advicebeing family members.
Exposure to tobacco smoke in the workplace is correlated withincreased risk for heart disease and lung cancer among adultnon-smokers (Fichtenberg and Glantz, 2002; Skeer et al., 2005).Studies have shown that implementing workplace smoking restric-tions substantially reduces the likelihood of self-reported exposureto passive tobacco smoke among employees, and also the dura-tion of that exposure (Fichtenberg and Glantz, 2002; Skeer et al.,2005). Furthermore, smoke-free workplaces not only protect non-smokers from deleterious effects, but encourage smokers to reduceor quit cigarette smoking (Eriksen and Cerak, 2008; Stillman et al.,2007). In our study, smokers reported that workplace restrictionsassociated with smoking decreasing. However, only one-third ofworkplaces captured in our study implemented smoking bans. Thisprevalence is lower than reported elsewhere (Farrelly et al., 1999;Fichtenberg and Glantz, 2002; World Health Organization, 2007);a reporting gap that argues for expanding smoke-free policies inChinese workplaces.
Based on self-reports, our study determined that the preva-lence of smoking bans in the workplace varies across age, gender,and occupation. More research is necessary to inform these datagaps. In addition, interactions between workplace restrictions andsociodemographics did not enter our final model.
Many studies have shown that restrictions on smoking in publicplaces were associated both with a higher probability of delayingsmoking uptake, and lowering smoking prevalence (US Departmentof Health and Human Services, 2006; Wakefield et al., 2000).However, we found no association between smoking and smok-ing restrictions in public places. An explanation may be that wecould only examine extant policies and not their actual imple-mentation. Thus, we could not assess true smoking restrictionstatus. Moreover, implementation of smoke-free policies in publicplaces is poor, even within Chinese hospitals and schools (Li et al.,2010). While Guangzhou, Hangzhou, Harbin, and Yinchuan haverecently issued smoke-free legislation that covers public places,far short of the ideal of 100% of public venues and workplaces aresmoke-free. In addition, there is a lack of strong penalties for vio-lating this legislation. In May 2011, the Chinese Health Ministrylaunched a national ban on lighting up tobacco products in hotels,restaurants, and other “indoor public spaces”. Again enforcementis problematic. Exposure to tobacco smoke in public places is com-mon, including in most restaurants and 70% of schools, hospitals,government buildings, and train stations (Stillman et al., 2007). Ina recent Chinese study, approximately 82% (95% CI: 81.1–82.5%)of respondents supported a ban on smoking in public places (Yanget al., 2005). We endorse the need for government, and more specif-ically, legislative departments, to assume responsibility for tobaccocontrol, and for the Chinese Government to implement a com-prehensive national smoke-free law. Efforts to restrict smoking inpublic places should focus on achieving bans across China, whilesimultaneously raising public awareness of the perils of second-hand smoke.
Reinforced by Chinese social and cultural norms that favorsmoking, public ignorance of the health risks from secondhandsmoke or passive smoking has contributed to this harmful expo-sure (Abdullah et al., 2011). Smoking is socioculturally acceptable.People routinely smoke during their social interactions and on thejob. They offer cigarettes to each other as a compliment; thus try-ing to prohibit others from smoking would induce “loss of face”. Inaddition to restricting smoking in public places, the Chinese Gov-ernment is utilizing the mass media to intensify public education on
ronmental smoking bans, and smoking in Chinese urban areas. Drug
the hazards of secondhand smoking. The aim is to create positiveattitudes towards tobacco control, while campaigning to changesocietal attitudes and norms about smoking.

ING Model
D
6 ol Dep
atss
ssnawsirposav
5
iecpemia
R
0(
C
sdtmfi
C
A
f(LlAo
R
A
ARTICLEAD-4337; No. of Pages 7
T. Yang et al. / Drug and Alcoh
In summary, variation of smoking prevalence in urban areasppears contingent on the degree to which respective tobacco con-rol programs can suppress or curb tobacco advertising, and thetrength of environmental smoking restrictions. Our results furtherupport the argument for large-scale tobacco control.
This study has several major limitations. First, our cross-ectional research design precluded causal inference. Secondly, thetudy was confined to the individual level. More research will beecessary to examine the association between smoking prevalencend smoking restrictions at the contextual level; that is, in homes,orkplaces, and public places. Reflecting a third study limitation,
moking prevalence will need to be evaluated in relation to chang-ng exposures to tobacco advertising and environmental smokingestrictions. Fourthly, in measuring smoking restrictions in publiclaces, our study was confined to inferring just extant policy thoughbservation of smoke-free organizations or no-smoking signs. Con-equently, we could not assess compliance with restrictive policies,nd therefore measure true smoking restriction status in publicenues. Further study is necessary.
. Conclusion
The association of current smoking with both tobacco advertis-ng and environmental smoking bans, which emerged from thisxploratory research, holds very important public health impli-ations for China. Our findings should be most informative forolicymakers, and encourage them to develop and implementffective tobacco control policies and interventions. Given the enor-ity of the Chinese smoking-related healthcare burden, reductions
n smoking will inevitably increase both population life expectancynd healthy life expectancy.
ole of funding source
This study was partly funded by WHO (WP/2002/IC/TFI/2.2/001/3.02.AW.03), and the National Social Science Foundation of China01BSH030).
ontributors
TY conceived the study design, conceptualized the ideas, andupervised the data management and analyses. XX and YG con-ucted the data collection. ML drafted the manuscript. IR providedechnical support for the data analysis, and in revising the
anuscript. All authors reviewed previous drafts and approved thenal version.
onflict of interest
No conflict declared.
cknowledgements
We thank local teams from the “Building advocacy capacityor tobacco control among the public health workforce in Chinasupported by The International Union Against Tuberculosis andung Disease)” project for organizing the data collection. We wouldike to thank Yan Lin and Trish Fraser from the International Uniongainst Tuberculosis and Lung Disease for her advice and editingf this article.
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
eferences
bdullah, A.S., Hua, F., Xia, X., Hurlburt, S., Ng, P., MacLeod, W., Siegel, M., Griffiths, S.,Zhang, Z., 2011. Second-hand smoke exposure and household smoking bans in
PRESSendence xxx (2012) xxx– xxx
Chinese families: a qualitative study. Health Social Care Community, publishedonline: 27 October 2011, doi:10.1111/j.1365-2524.2011.01035.x.
Biener, L., Siegel, M., 2006. The role of tobacco advertising and promotion in smokinginitiation. Smok. Tob. Control Monogr. 14, 201–212.
Blecher, E., 2008. The impact of tobacco advertising bans on consumption in devel-oping countries. J. Health Econ. 27, 930–942.
Braverman, M.T., Aarø, L.F., 2004. Adolescent smoking and exposure to tobacco mar-keting under a tobacco advertising ban: findings from 2 Norwegian nationalsamples. Am. J. Public Health 94, 1230–1238.
Chapman, S., 1996. The ethics of tobacco advertising and advertising bans. Br. Med.Bull. 52, 121–131.
Department of Comprehensive Statistics of National Bureau of Statistics, 2008. ChinaStatistics China Yearbook for Regional Economy 2008. China Statistics Press,Beijing.
Doll, R., Peto, R., Boreham, J., Sutherland, I., 2004. Mortality in relation to smoking:50 years’ observations on male British doctors. BMJ 328, 1519–1527.
Edwards, R., Thomson, G., Wilson, N., Waa, A., Bullen, C., O’Dea, D., Gifford, H., Glover,M., Laugesen, M., Woodward, A., 2008. After the smoke has cleared: evaluationof the impact of a new national smoke-free law in New Zealand. Tob. Control17, e2.
Eriksen, M.P., Cerak, R.L., 2008. The diffusion and impact of clean indoor air laws.Annu. Rev. Public Health 29, 171–185.
Farrelly, M.C., Evans, W.N., Sfekas, A.E.S., 1999. The impact of workplace smokingbans: results from a national survey. Tob. Control 8, 272–277.
Fichtenberg, C.M., Glantz, S.A., 2002. Effect of smoke-free workplaces on smokingbehavior: systematic review. BMJ 325, 188.
Fong, G.T., Hyland, A., Borland, R., Hammond, D., Hastings, G., McNeill, A., Ander-son, S., Cummings, K.M., Allwright, S., Mulcahy, M., Howell, F., Clancy, L.,Thompson, M.E., Connolly, G., Driezen, P., 2006. Reductions in tobacco smokepollution and increases in support for smoke-free public places following theimplementation of comprehensive smoke-free workplace legislation in theRepublic of Ireland: findings from the ITC Ireland/UK Survey. Tob. Control 15,iii51–iii58.
Fone, D.L., Dunstan, F., 2006. Mental health, places and people: a multilevelanalysis of economic inactivity and social deprivation. Health Place 12,332–344.
Goldstein, H., 1995. Multilevel Statistical Models, 2nd ed. Edward Arnold, London.Graham, H., 1996. Smoking prevalence among women in the European Community
1950–1990. Soc. Sci. Med. 43, 243–254.Jha, P., Ranson, M.K., Nguyen, S.N., Yach, D., 2002. Estimates of global and regional
smoking prevalence in 1995, by age and sex. Am. J. Public Health 92, 1002–1006.Kegler, M.C., Malcoe, L.H., 2002. Smoking restrictions in the home and car among
rural native American and white families with young children. Prev. Med. 35,334–342.
Li, L., Yong, H.H., Borland, R., Fong, G.T., Thompson, M.E., Jiang, Y., Yang, Y., Siri-rassamee, B., Hastings, G., Harris, F., 2009. Reported awareness of tobaccoadvertising and promotion in China compared to Thailand, Australia and theUSA. Tob. Control 18, 222–227.
Li, Q., Hyland, A., O’Connor, R., Zhao, G., Du, L., Li, X., Fong, G., 2010. Support forsmoke free policies among smokers and non-smokers in six cities in China. Tob.Control 19 (Suppl. 2), i40–i466.
Lin, Y., Fraser, T., 2011. A review of smoke-free health care in mainland China. Int. J.Tuberc. Lung Dis. 15, 453–458.
Martínez-Donate, A.P., Hovell, M.F., Hofstetter, C.R., González-Pérez, G.J., Adams,M.A., Sánchez, J.D.J., Guzmán-Cerda, G., 2005. Smoking, exposure to secondhandsmoke, and smoking restrictions in Tijuana, Mexico. Rev. Panam. Salud Publica18, 412–417.
Mackay, D.F., Irfan, M.O., Haw, S., Pell, J.P., 2010. Meta-analysis of the effect ofcomprehensive smoke-free legislation on acute coronary events. Heart 96,1525–1530.
Moher, M., Hey, K., Lancaster, T., 2005. Workplace interventions for smoking cessa-tion. Evidence-Based Med. Cochrane Database Syst. Rev. CD003440.
Nelson, J.P., 2003. Cigarette demand, structural change, and advertising bans: inter-national evidence, 1970–1995. Controv. Econ. Anal. Policy 2, 10–15.
New York State Department of Health, 2011. Youth Prevention and Adult Smokingin New York, http://www.nyhealth.gov/prevention/tobacco control/docs/2011-03-11 ny state brief report prevention.pdf (accessed 23.08.11).
Peto, R., Chen, Z., Boreham, J., 1996. Tobacco – the growing epidemic in China. Nat.Med. 5, 15–17.
Rashash, J., Steele, F., Browne, W.J., Goldstein, H., 2001. A User’s Guide to MLinNVersion 2.10. Centre for Multilevel Modeling, Institute of Education, London.
Saffer, H., Chaloupka, F., 2000. The effect of tobacco advertising bans on tobaccoconsumption. J. Health Econ. 19, 1117–1137.
Skeer, M., Cheng, D.M., Rigotti, N.A., Siegel, M., 2005. Secondhand smoke exposurein the workplace. Am. J. Prev. Med. 28, 331–337.
Stillman, F., Navas-Acien, A., Ma, J., Ma, S., Avila-Tang, E., Breysse, P., Yang, G., Samet,J., 2007. Second-hand tobacco smoke in public places in urban and rural China.Tob. Control 16, 229–234.
The People’s Republic of China Ministry of Health, 2007. The 2007 China TobaccoControl Report, Beijing.
Unger, J.B., Yan, L., Shakib, S., Rohrbach, L.A., Chen, X., Qian, G., Chou, C.P., Jianguo, S.,
ronmental smoking bans, and smoking in Chinese urban areas. Drug
Azen, S., Zheng, H., Johnson, C.A., 2002. Peer influences and access to cigarettes ascorrelates of adolescent smoking: a cross-cultural comparison of Wuhan, China,and California. Prev. Med. 34, 476–484.
US Department of Health and Human Services, 2006. Reducing Tobacco Use: AReport of the Surgeon General. U.S. Department of Health and Human Services,

ING Model
D
ol Dep
W
W
W
W
W
ARTICLEAD-4337; No. of Pages 7
T. Yang et al. / Drug and Alcoh
Centers for Disease Control and Prevention, National Center for Chronic DiseasePrevention and Health Promotion, Office on Smoking and Health, Atlanta, GA.
akefield, M.A., Chaloupka, F.J., Kaufman, N.J., Orleans, C.T., Barker, D.C., Ruel, E.E.,2000. Effect of restrictions on smoking at home, at school, and in public placeson teenage smoking: cross sectional study. BMJ 321, 333–337.
orld Health Organization, 2003. WHO Framework Convention on Tobacco Control.World Health Organization, Geneva, Switzerland.
orld Health Organization, 2007. Only 100% smoke-free environments adequatelyprotected from dangers of second-hand., http://www.who.int/mediacentre/news/releases/2007/pr26/en/index.html.
Please cite this article in press as: Yang, T., et al., Tobacco advertising, enviAlcohol Depend. (2012), doi:10.1016/j.drugalcdep.2011.12.021
orld Health Organization, 2008. WHO Report on the Global Tobacco Epidemic2008: The MPOWER Package. World Health Organization, Geneva.
orld Health Organization, 1998. Guidelines for Controlling and Mon-itoring the Tobacco Epidemic. World Health Organization, Geneva,pp. 61–99.
PRESSendence xxx (2012) xxx– xxx 7
Yang, G.H., Ma, J.M., Liu, N., Zhou, L.N., 2005. Smoking and passive smoking in Chi-nese, 2002. Chin. J. Epidemiol. 26, 77–83.
Yang, T., 2010. Tobacco Control Theory and Implementation. People’s Health House,Beijing, pp. 77–105.
Yang, T., Wu, J., Rockett, I.R.H., Abdullah, A.S., Beard, J., Ye, J., 2009a. Smoking patternsamong Chinese rural–urban migrant workers. Public Health 123, 743–749.
Yang, T., Yang, X., Lv, Q., Zhao, Q., Ke, X., 2009b. China’s first historic efforts to developa tobacco control advocacy workforce via schools of public health. Tob. Control18, 422–424.
Yang, T., Shiffman, S., Rockett, I.R.H., Cui, X., Cao, R., 2011. Nicotine dependence
ronmental smoking bans, and smoking in Chinese urban areas. Drug
among Chinese city dwellers: a population-based cross-sectional study. NicotineTob. Res., doi:10.1093/ntr/ntr040.
Yang, T., Rockett, I.R., Wu, Y., Chen, W.W., Lu, Z., 2010. Agreement among multiplemeasures of self-reported smoking status in Chinese urban residents. PublicHealth 124, 437–443.