thinner prefrontal cortex in veterans with posttraumatic stress disorder
TRANSCRIPT

www.elsevier.com/locate/ynimg
NeuroImage 41 (2008) 675–681Thinner prefrontal cortex in veterans withposttraumatic stress disorder
Elbert Geuze,a,b,⁎ Herman G.M. Westenberg,b Armin Heinecke,c
Carien S. de Kloet,a Rainer Goebel,c,d and Eric Vermettena,b
aResearch Centre, Military Mental Healthcare, Ministry of Defence, Utrecht, The NetherlandsbDepartment of Psychiatry, Rudolf Magnus Institute of Neuroscience, Utrecht University Medical Centre, Utrecht, The NetherlandscBrain Innovation, Maastricht, The NetherlandsdDepartment of Cognitive Neuroscience, Faculty of Psychology, Maastricht University, Maastricht, The Netherlands
Received 19 October 2007; revised 27 February 2008; accepted 6 March 2008Available online 20 March 2008
Structural neuroimaging studies in posttraumatic stress disorder(PTSD) have focused primarily on structural alterations in the medialtemporal lobe, and only a few have examined grey matter reductions inthe cortex. Recent advances in computational analysis provide newopportunities to use semi-automatic techniques to determine corticalthickness, but these techniques have not yet been applied in PTSD.Twenty-five male veterans with PTSD and twenty-five male veteranswithout PTSD matched for age, year and region of deployment wererecruited. All the subjects were scanned using MRI. Subjects' brainswere aligned using cortex-based alignment in a region of interest basedapproach. Individual cortical thickness maps were calculated from theMR images. Regions of interest examined included the bilateral superiorfrontal gyri, bilateral middle frontal gyri, bilateral inferior frontal gyri,bilateral superior temporal gyri, and bilateral middle temporal gyri. Ina large number of patients and controls, IQ scores and memory scoreswere also obtained. Individual cortical thickness maps were calculatedfrom the MR images. Veterans with PTSD revealed reduced corticalthickness in the bilateral superior and middle frontal gyri, the leftinferior frontal gyrus, and the left superior temporal gyrus. Veteranswith PTSD performed significantly worse on memory measurescompared to control veterans. Cortical thickness correlated withmemory measures in the veterans without PTSD, but not in the veteranswith PTSD. Cortical thinning in these regions may thus correspond tofunctional abnormalities observed in patients with PTSD.© 2008 Elsevier Inc. All rights reserved.
Keywords: PTSD; Cortical thickness; MRI; Frontal cortex; Veterans
⁎ Corresponding author. Research Centre, Military Mental Healthcare andDivision of Neuroscience, Utrecht University Medical Centre, PO Box90.000, 3509 AA Utrecht, The Netherlands. Fax: +31 30 250 2282.
E-mail address: [email protected] (E. Geuze).Available online on ScienceDirect (www.sciencedirect.com).
1053-8119/$ - see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1016/j.neuroimage.2008.03.007
Introduction
Neuroimaging studies in posttraumatic stress disorder (PTSD)have identified a number of functional and structural alterations thatare associated with this disorder. Structural neuroimaging studies inPTSD have focused primarily on manual based hippocampalvolumetry. These studies have shown that patients with PTSD areassociated with bilateral smaller hippocampal volume (Geuze et al.,2005; Kitayama et al., 2005). A recent meta-analysis, confirmed thepresence of significantly smaller hippocampal volumes and leftamygdala volumes in patients with PTSD compared to controls withand without trauma exposure (Karl et al., 2006).
However, while considerable attention has been placed onvolume changes in subcortical structures, very little attention hasbeen directed to grey matter reductions in the cortex. Manual tracingof the anterior cingulate cortex has shown that this area is alsosmaller in patients with PTSD compared to controls (Woodwardet al., 2006; Rauch et al., 2003). Several voxel-based morphometrystudies, a whole-brain analysis technique, have been applied inPTSD. These studies have shown reduced grey matter density in theanterior cingulate gyrus, hippocampus, and insula (Chen et al., 2006;Corbo et al., 2005; Yamasue et al., 2003; Kasai et al., 2007). A recentmeta-analysis of these studies confirmed that patients with PTSDrevealed significantly smaller anterior cingulate cortex volumecompared to trauma-exposed controls (Karl et al., 2006). In pediatricpatients with PTSD, significantly smaller prefrontal lobe volumeand corpus callosum volume have been found (De Bellis et al., 1999,2002b). The findings of smaller corpus callosum volume have notbeen replicated in a sample of adult patients with PTSD (Kitayamaet al., 2007). Functional neuroimaging studies have also identified anumber of brain areas with altered activity in patients with PTSD,including the prefrontal cortex, temporal cortex, insula, amygdala,and hippocampus (Francati et al., 2007; Nemeroff et al., 2006; Hull,2002).

676 E. Geuze et al. / NeuroImage 41 (2008) 675–681
Cortical thickness and volumetric analysis receive increasinginterest in the imaging community because it allows relation ofcognitive abilities, effects of aging, and effects of diseases to (subtle)structural changes in the brain. Practical constraints, however, re-lated to intensive measurement technique and the use of postmortemsamples, make it difficult to compare differences in cytoarchitectureacross the cortex. Whole brain volumetric techniques are alsocompromised by large inter-individual differences in neuroanatomymaking it difficult to match the same macroscopic regions betweensubjects. Recent advances in computational analysis, provide newopportunities to use imaging data to derive more knowledge oncortical thickness. In this study, we have applied the new corticalthickness analysis tools in Brainvoyager QX to compare veteranswith PTSD to veterans without PTSD. In order to maximize thespatial correspondence mapping between cortical macrostructures,we also made use of the new technique of cortex-based alignment,which aligns reconstructed cortices using curvature informationreflecting the gyral/sulcal folding pattern. It has been shown that acortical matching approach substantially improves statisticalanalysis across subjects by reducing anatomical variability (Fischlet al., 1999a,b; Dale et al., 1999).
In this study our goal was to employ this relatively new techniqueto examine cortical thickness in patients with PTSD. We hypoth-esized that patients with PTSD would reveal reduced cortical thick-ness in frontal and temporal brain areas. Due to technical limitationsof the cortical thickness algorithm, which performed less accuratelyin the inferior temporal lobe, and medial prefrontal cortex, we onlyexamined cortical thickness in the bilateral superior, middle, andinferior frontal gyri, as well as the bilateral superior and middletemporal gyri.
Materials and methods
Subjects
The sample consisted of twenty-five male Dutch veterans withPTSD, and twenty-five agematched control veterans without PTSD.All patients were recruited from the Department of MilitaryPsychiatry at the Central Military Hospital in Utrecht. Controlsubjects were recruited via direct mail to veterans who wereregistered at the Veterans Institute in Doorn, The Netherlands. Allparticipants had served in UN peacekeeping missions in Lebanon,Cambodia, or Bosnia. Control veterans were matched to the patientgroup with respect to age, year of deployment, and country ofdeployment. None of the veterans included was physically injured atthe time of deployment. At study entry, twenty of the twenty-fivepatients were drug naive. The other five subjects had not taken anypsychotropic medications or abused substances for at least 6months.Subjects with a history of neurological illness, psychiatric illnessother than mood and anxiety disorders, were excluded. This studywas approved by the Institutional Review Board of the UniversityMedical Centre of Utrecht, The Netherlands. Written informedconsent was obtained from all subjects who participated in the studyafter a complete written and verbal description of the study. Thestudy was performed between August 2002 and September 2005.
Clinical assessments
All subjects were assessed using the Structured Clinical Inter-view for DSM-IV (First et al., 1997) and the Clinician AdministeredPTSD Scale (CAPS) (Blake et al., 1995). Diagnosis of PTSD was
confirmed by the CAPS and through consensus by three clinicians(EG, EV, andCdK). Only subjects with a CAPS score greater than 50were included in the patient group. Subjects with a CAPS scoregreater than 20 were excluded from the trauma control group.Hamilton Depression Scale (HAM-D), and the Hamilton AnxietyScale (HAM-A) scores were also obtained for all subjects.
Neuropsychological testing
Total IQ of the subjects was estimated based upon a prorated scoreincluding the followingWechsler Adult Intelligence Scale (WAIS-III)subtests: Similarities,Vocabulary, BlockDesign, andPictureArrange-ment, to provide a measure of intelligence. The Dutch version of theRey Auditory Verbal Learning Task (AVLT; (Rey, 1964; Brand andJolles, 1985) was collected in subjects to provide a measure ofmemory. The AVLT consists of five presentations of a 15-word list,followed by a delayed free recall and recognition testing after a periodof 30 min. Variables of interest for the AVLT included the sum ofcorrectly recalled words from the list for trials 1–5, and the number ofcorrectly recalled words after a delay of 30 min.
MRI
Magnetic resonance imaging (MRI) of all subjects was performedat the Department of Radiology of the University Medical Centre ofUtrecht. MRIs were acquired using a 1.5 Tscanner (Philips Gyroscan;Philips Medical Systems, Best, The Netherlands). T1-weighted, 3D,fast field echo scanswith 160 to 180 1.2mmcontiguous coronal slices(echo time, 4.6ms; repetition time, 30ms; flip angle 30°; field of view256 mm; and in-plane voxel sizes 1×1 mm2) of the whole head wereused for cortical thickness analysis.
Preprocessing and advanced segmentation analysis
All image data preparation and preprocessing, cortical thicknessanalysis, and cortex-based alignment, were carried out usingBrainvoyager QX 1.7 (Brain Innovation, Maastricht, The Nether-lands). The anatomical data (DICOM format) of each subject wasloaded and converted into Brainvoyager's internal data format. Thedatawas resampled into 1mm resolution, and transformed intoACPCand Talairach standard space. The spatial transformations werecombined and applied backward in one step to avoid quality loss dueto successive data sampling (Goebel et al., 2006). Prior to corticalthickness analysis, several preparatory advanced segmentation stepswere performed. However, since the advanced segmentation tools inBrainvoyager work in a 0.5×0.5×0.5 mm resolution space, theresulting data set (in Talairach space) had to be resampled once moreto 0.5 mm iso-voxels using sinc interpolation. Then the brain wassegmented from surrounding head tissue using an automatic “brainpeeling” tool (Goebel et al., 2006). Subcortical structures and thecerebellum were removed using a mask. Tissue contrast andhomogeneity were enhanced using a sigma filter (which smoothesintensity values around each voxel while taking care that only voxelsincluded in this process contain intensity values close to the intensityof a considered voxel). Next the white matter–grey matter border wassegmented automatically using an adaptive region growing stepwhich uses two sources of information to separate white from greymatter voxels (locally computed histograms and gradient informa-tion). Then the grey matter–cerebrospinal fluid (CSF) border wassegmented using a dilation process which begins at the white matter–grey matter boundary and labels grey matter voxels by moving

Fig. 1. Regions of interest. This figure shows the selected regions of interestfor the left hemisphere (regions of interest for the right hemisphere were thesame). These included the superior frontal gyrus, middle frontal gyrus,inferior frontal gyrus, superior temporal gyrus, and middle temporal gyrus.
677E. Geuze et al. / NeuroImage 41 (2008) 675–681
towards the CSF boundary. This process is controlled by computedgradient fields and histogram analysis of grey matter–CSF thresholdvalues. Both the white matter–grey matter and grey matter–CSFborders were ‘polished’ by calculating a magnitude map based on thecomputed gradient maps of the binary segmentation results.
Cortical thickness analysis
Cortical thickness maps for each subject were calculated. Sincecortical thickness varies substantially across space, a simple orthog-onal measurement technique – going in a fixed, orthogonal directionfrom one side of grey matter to the other side –may lead to erroneousthickness estimates. To avoid these problems, the cortical thicknessmeasurements in Brainvoyager QX are based on the Laplace method(Jones et al., 2000). Laplace's equation is a partial differentialequation, which is used inmany fields of science, notably the fields ofelectromagnetism, astronomy and fluid dynamics. In three dimen-sions, the problem is to find twice-differentiable real-valued functionsΦ (phi) of real variables x, y, and z such that
j2U ¼ ∂2U∂x2
þ ∂2U∂y2
þ ∂2U∂z2
¼ 0
Solutions of this partial differential equation have to fulfill theconstraint that the sum of the (unmixed) second partial derivatives iszero. This is fulfilled if the gradient slopes do not change along eachdimension. For cortical thicknessmeasures, Brainvoyager defines twodifferent “potential” (intensity) values, one at the white–grey matter(WM–GM) boundary and one at the grey matter–CSF (GM–CSF)boundary. A solution of Laplace's equation then results in a smoothtransition of voltages (intensities) from one boundary to the other(▿2Φ=0). Such a solution can be found simply by keeping the valuesat the boundaries fixed and by smoothing the “voltage” values inbetween (grey matter voxels). From the obtained smooth field, agradient value (▿Φ) can be calculated at each voxel. Integrating alongthese gradient values allows calculation of “field lines” or “stream-lines”. To calculate a cortical thickness value, the program starts at anyboundary voxel, checks the gradient and performs a small step alongthe gradient direction. Then the gradient is re-evaluated at the newpoint and the next step along the gradient direction is performed. Thisprocedure is repeated until the other boundary is reached. The sum ofthe performed small step sizes provides the cortical thickness value.By going in both gradient directions (“up” and “down”), thicknessvalues for any voxel between the boundary-voxels may be calculatedby simply adding up two partial streamlines.
Cortical alignment
To improve the spatial correspondence mapping between subjects'brains beyond Talairach space matching, reconstructed cortices werealigned using curvature information reflecting the gyral/sulcal foldingpattern. While functional areas do not precisely follow corticallandmarks, it has been shown that a cortical matching approachsubstantially improves statistical analysis across subjects by reducinganatomical variability (Fischl et al., 1999b). First, the reconstructedfolded cortical representations of each subject and hemisphere weremorphed into a spherical representation, which provides a parameter-izable surface well-suited for across-subject non-rigid alignment. Eachvertex on the sphere (spherical coordinate system) corresponds to avertex of the folded cortex (Cartesian coordinate system) and viceversa. The curvature information computed in the folded representa-
tion was preserved as a curvature map on the spherical representation.The curvature information (folding pattern) was smoothed along thesurface to provide spatially extended gradient information drivingintercortex alignment minimizing the mean squared differencesbetween the curvature of a source and a target sphere. The alignmentproceeded iteratively following a coarse-to-fine matching strategy,which starts with highly smoothed curvature maps and progresses toonly slightly smoothed representations. Starting with a coarsealignment as provided by Talairach space, this method ensures thatthe smoothed curvature of the two cortices possesses enough overlapfor a locally operating gradient-descent procedure to converge withoutuser intervention (Goebel et al., 2006; Formisano et al., 2004).
Although tests have shown that alignment results are very similarwhen using different target spheres, the selection of a specific targetbrain might lead to suboptimal results in brain regions where theselected brain has an idiosyncratic folding pattern, therefore allbrains were aligned using a moving target approach. In the movingtarget group averaging approach, the selection of a target sphere isnot required. In this approach, the goal function is specified as amoving target computed repeatedly during the alignment process asthe average curvature across all hemispheres at a given alignmentstage. The procedure starts with the coarsest curvature maps. Thenthe next finer curvature maps are used and averaged with the ob-tained alignment result of the previous level.
Region of interest analysis
In order to increase statistical power a region of interest (ROI)approach was applied. After the target (group) brain was aligned tothe atlas brain provided by Brainvoyager QX, several ROIs wereselected for analysis (see Fig. 1). Conform our hypothesis the ROIselected included the bilateral superior frontal gyri, bilateral middlefrontal gyri, bilateral inferior frontal gyri, bilateral superiortemporal gyri, and bilateral middle temporal gyri. Due to technicallimitations of the cortical thickness algorithm, which performedless accurately in the inferior temporal lobe and medial prefrontalcortex, the inferior temporal gyri and anterior cingulate gyri werenot selected. Cortical thickness maps for each of the ROIs in thetwo groups were averaged and displayed on the target (group)cortex (see Fig. 2). Individual cortical thickness values from these
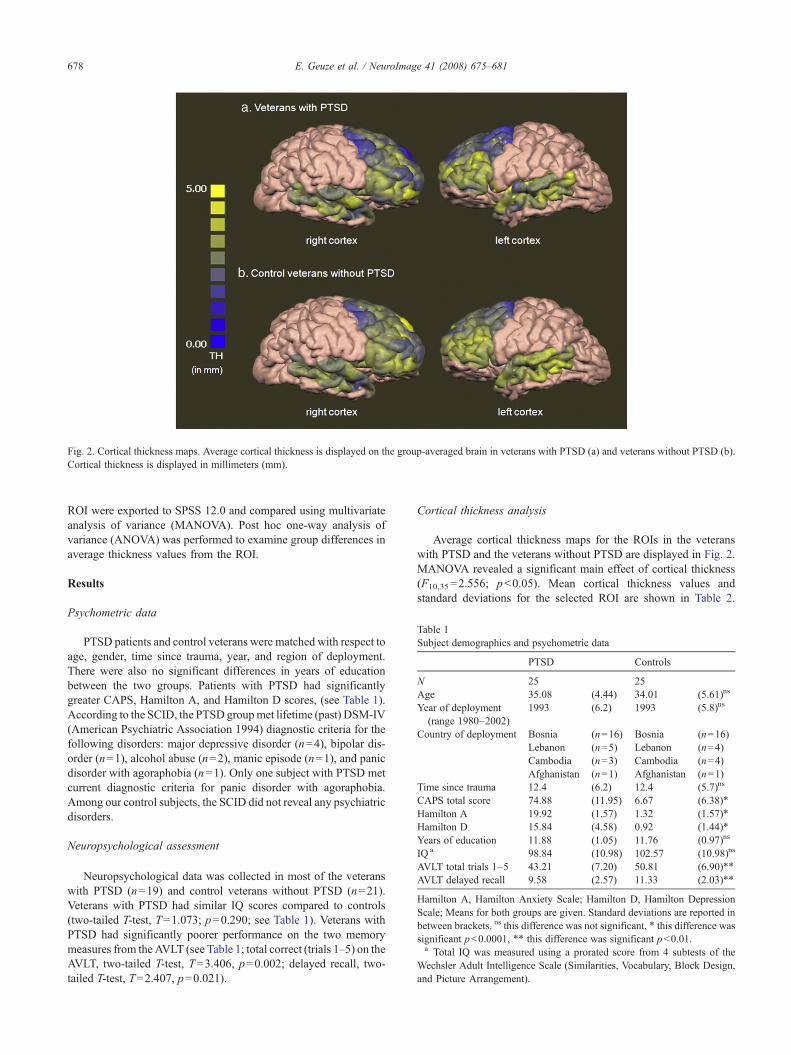
Fig. 2. Cortical thickness maps. Average cortical thickness is displayed on the group-averaged brain in veterans with PTSD (a) and veterans without PTSD (b).Cortical thickness is displayed in millimeters (mm).
Table 1Subject demographics and psychometric data
PTSD Controls
N 25 25Age 35.08 (4.44) 34.01 (5.61)ns
Year of deployment(range 1980–2002)
1993 (6.2) 1993 (5.8)ns
Country of deployment Bosnia (n=16) Bosnia (n=16)Lebanon (n=5) Lebanon (n=4)Cambodia (n=3) Cambodia (n=4)Afghanistan (n=1) Afghanistan (n=1)
Time since trauma 12.4 (6.2) 12.4 (5.7)ns
CAPS total score 74.88 (11.95) 6.67 (6.38)⁎
Hamilton A 19.92 (1.57) 1.32 (1.57)⁎
Hamilton D 15.84 (4.58) 0.92 (1.44)⁎
Years of education 11.88 (1.05) 11.76 (0.97)ns
IQ a 98.84 (10.98) 102.57 (10.98)ns
AVLT total trials 1–5 43.21 (7.20) 50.81 (6.90)⁎⁎
AVLT delayed recall 9.58 (2.57) 11.33 (2.03)⁎⁎
Hamilton A, Hamilton Anxiety Scale; Hamilton D, Hamilton DepressionScale; Means for both groups are given. Standard deviations are reported inbetween brackets. ns this difference was not significant, ⁎ this difference wassignificant pb0.0001, ⁎⁎ this difference was significant pb0.01.a Total IQ was measured using a prorated score from 4 subtests of the
Wechsler Adult Intelligence Scale (Similarities, Vocabulary, Block Design,and Picture Arrangement).
678 E. Geuze et al. / NeuroImage 41 (2008) 675–681
ROI were exported to SPSS 12.0 and compared using multivariateanalysis of variance (MANOVA). Post hoc one-way analysis ofvariance (ANOVA) was performed to examine group differences inaverage thickness values from the ROI.
Results
Psychometric data
PTSD patients and control veterans were matched with respect toage, gender, time since trauma, year, and region of deployment.There were also no significant differences in years of educationbetween the two groups. Patients with PTSD had significantlygreater CAPS, Hamilton A, and Hamilton D scores, (see Table 1).According to the SCID, the PTSD groupmet lifetime (past) DSM-IV(American Psychiatric Association 1994) diagnostic criteria for thefollowing disorders: major depressive disorder (n=4), bipolar dis-order (n=1), alcohol abuse (n=2), manic episode (n=1), and panicdisorder with agoraphobia (n=1). Only one subject with PTSD metcurrent diagnostic criteria for panic disorder with agoraphobia.Among our control subjects, the SCID did not reveal any psychiatricdisorders.
Neuropsychological assessment
Neuropsychological data was collected in most of the veteranswith PTSD (n=19) and control veterans without PTSD (n=21).Veterans with PTSD had similar IQ scores compared to controls(two-tailed T-test, T=1.073; p=0.290; see Table 1). Veterans withPTSD had significantly poorer performance on the two memorymeasures from theAVLT (see Table 1; total correct (trials 1–5) on theAVLT, two-tailed T-test, T=3.406, p=0.002; delayed recall, two-tailed T-test, T=2.407, p=0.021).
Cortical thickness analysis
Average cortical thickness maps for the ROIs in the veteranswith PTSD and the veterans without PTSD are displayed in Fig. 2.MANOVA revealed a significant main effect of cortical thickness(F10,35=2.556; pb0.05). Mean cortical thickness values andstandard deviations for the selected ROI are shown in Table 2.

Table 2Cortical thickness in veterans with and without PTSD
ROI PTSD Controls ANOVA p
n M a SD n M a SD
Left hemisphereSuperior frontal
gyrus25 2.19 0.52 25 2.64 0.41 F(1,48)=11.54 0.001
Middle frontalgyrus
25 2.12 0.50 25 2.52 0.42 F(1,48)=9.36 0.004
Inferior frontalgyrus
25 2.57 0.52 25 2.89 0.31 F(1,48)=6.86 0.012
Superior temporalgyrus
25 2.74 0.45 25 2.97 0.25 F(1,48)=4.87 0.032
Middle temporalgyrus
25 3.21 0.58 25 3.26 0.25 F(1,48)=0.20 0.659
Right hemisphereSuperior frontal
gyrus24 2.34 0.56 23 2.72 0.50 F(1,45)=6.00 0.018
Middle frontalgyrus
24 2.35 0.52 23 2.68 0.47 F(1,45)=5.30 0.026
Inferior frontalgyrus
24 2.71 0.47 23 2.91 0.35 F(1,45)=2.58 0.115
Superior temporalgyrus
23 2.80 0.38 23 2.87 0.27 F(1,44)=0.446 0.507
Middle temporalgyrus
24 3.03 0.51 23 3.00 0.28 F(1,45)=0.050 0.825
Multivariate analysis (MANOVA) was used to compare the two groups onthese measures; post hoc one-way ANOVA results are presented in the table.a In mm.
679E. Geuze et al. / NeuroImage 41 (2008) 675–681
Post hoc ANOVAs revealed significantly lower cortical thicknessvalues in the bilateral superior and middle frontal gyri, left inferiorfrontal gyrus, and the left superior temporal gyrus in veterans withPTSD compared to control veterans (see Table 2). There was nosignificant interaction between diagnosis, cortical thickness, anddelayed recall.
Correlations
Since age, years of education, IQ, and time since trauma did notdiffer significantly between the groups; we looked within the wholegroup of veterans combined whether cortical thickness correlatedwith these measures. Cortical thickness did not correlate with age,years of education, and time since trauma. The left inferior frontalgyrus was correlated with total IQ (Pearson's r=0.327, p=0.040).Within each of the groups, we also checked for correlations ofcortical thickness with total CAPS score, total number of wordsrecalled after trials 1–5, and delayed recall. Within the veteranswithout PTSD, the inferior frontal gyrus correlated with the totalnumber of words recalled after trials 1–5 (r=−0.571, p=0.007) anddelayed recall (r=−0.503, p=0.020). There were no other sig-nificant correlations within either the veterans without PTSD or theveterans with PTSD.
Discussion
This is the first study in the field of PTSD that provides data onthe cortical thickness of veterans with PTSD compared to healthycontrol veterans. Cortical thickness is a relatively new semi-automatic technique that has recently also been implemented in the
neuroimaging program Brainvoyager QX 1.7. In this ROI basedanalysis, patients revealed reduced cortical thickness in the bilateralprefrontal cortex and the left superior temporal gyrus compared tocontrols.
In PTSD several different areas of the prefrontal cortex includingthe dorsolateral prefrontal cortex, the ventrolateral prefrontal cortex,the medial prefrontal cortex, the anterior cingulate cortex, and theorbital frontal cortex have revealed altered function compared tocontrols (Bremner et al., 2004a,b, 2000, 1999, 1997; Britton et al.,2005; Shin et al., 2005; Lindauer et al., 2004). Several other studieshave also shown that veterans with PTSD show altered function ofthe prefrontal cortex in pain processing (Geuze et al., 2007b) andduring memory processing (Clark et al., 2003; Weber et al., 2005;Karl et al., 2006; Geuze et al., 2007a). PTSD has long been thoughtto be associated with a “hypofrontality”, or reduced bloodflow andneural activation in frontal areas (Nemeroff et al., 2006). Reducedcortical thickness in frontal areas could possibly contribute toreduced working memory performance in patients with PTSD.Cortical thinning in patients with PTSD was less pronounced in theright inferior frontal gyrus, and not significantly different comparedto controls. In a large sample, this effect might also have beensignificant. In a recent workingmemory imaging study, patients withPTSD revealed reduced activation in left dorsolateral prefrontalcortex DLPFC), and increased activation in the right DLPFC (Clarket al., 2003).
Several neurocircuitry models of anxiety and PTSD haveproposed a role for the (medial) prefrontal cortex in the extinctionof fear conditioning (Rauch et al., 2006; Bremner et al., 2005). It hasbeen postulated that PTSD is characterized by a failure of extinction offear conditioning. Interventions such as EMDR, cognitive behaviour-al therapy, and exposure therapy may be effective at restoring theextinction of fear conditioning in a therapeutic setting.
Deficits in the temporal lobe (particularly the medial temporallobe) are frequently witnessed in patients with PTSD (Nemeroffet al., 2006; Francati et al., 2007; Geuze et al., 2005; Karl et al.,2006). PTSD subjects show less activation in the superior temporalgyrus in response to traumatic scripts (Lindauer et al., 2004). In astudy of associative memory processing, however, veterans withPTSD revealed increased left superior temporal gyrus activationduring encoding (Geuze et al., 2007a). Patients with PTSD hadsimilar cortical thickness in the right temporal gyri compared tocontrols. The right superior temporal gyrus has been linked todissociation symptoms in patients with PTSD (Hopper et al., 2007;Lanius et al., 2002). Children with PTSD show significantly greaterright superior temporal gyrus grey matter volume (De Bellis et al.,2002a).
Deficits in frontal and temporal lobe in PTSD have beenhypothesized to underlie the cognitive deficits often present in thispopulation (Isaac et al., 2006; Clark et al., 2003; Weber et al., 2005;Yehuda et al., 2005, 1995). In this study, veterans with PTSDdisplayed both reduced cortical thickness in frontal and temporal lobe,as well as poor performance on memorymeasures. It might have beenexpected that cortical thickness would be correlated with age.However, several of the correlations failed to reach significance.Partly this may be attributed to a sample size problem, but moreimportantly, it should be noted that the age range was very narrow(30–40 years). Total IQ correlated with the left inferior frontal gyrus.Previous studies have shown that prefrontal cortical thickness andgreymatter density are correlated to IQ in healthy controls (Narr et al.,2006; Frangou et al., 2004). Within the veterans with PTSD groupcortical thickness did not correlate with memory measures, or symp-

680 E. Geuze et al. / NeuroImage 41 (2008) 675–681
tom severity. Surprisingly, within the control veteran group, subjectswith a thinner left inferior frontal gyrus actually performed better onthe memory task. This counterintuitive finding is hard to explain. Theinferior frontal gyrus is known to play a role in verbal learning andmemory (Hagino et al., 2002). However caution should be taken ininterpreting this finding, as verbal learning and memory depend on amuch larger network than the left inferior frontal gyrus alone, and thecorrelation was found in a small sample.
Cortical thickness is a reflection of the size, density, and arrange-ment of neurons, glial cell and nerve fibers, thus cortical thinning inthese areas likely reflects changes in the grey–white matter boundaryrelated to a loss of dendrites and dendritic spines or changes inmyelination within specific brain systems (Narr et al., 2005; Harrison,1999). Alternatively, cortical thinning may also indicate changes inthe cortical mantle related to the size and density of neurons (Shawet al., 2006).
In earlier structural MRI studies in PTSD, which focused onhippocampal volume loss, it had been postulated that increasedglucocorticoid release during periods of stress may result inapoptosis, and thus loss of neural tissue (see Yehuda (2001) andBremner (2001) for a review). However, due to the absence oflongitudinal MRI studies, it is still unclear whether smallerhippocampal volumes are present prior to trauma (i.e. a vulnerabilityfactor), or acquired as a direct consequence of PTSD. In a study withmonozygotic twins discordant for trauma exposure, Gilbertson et al.(2002) provided evidence that smaller hippocampal volume mayconstitute a risk factor for the development of stress-relatedpsychopathology. On the other hand, a new analysis of the sametwin sample using voxel-based morphometry was unable to confirmthese findings, and instead supported the hypothesis that diminishedACC volume was acquired as a result of combat exposure, PTSDitself, or both (Kasai et al., 2007). A recent meta-analysis showedthat trauma-exposed persons without PTSD also have significantlysmaller bilateral hippocampal volumes compared to non-exposedcontrols (Karl et al., 2006). One could propose that the corticalthinning we observe in patients with PTSD might be explained byincreased glucocorticoid exposure during stress, however, only aprospective MRI study will be able to provide a definitive answer tothis question.
In this ROI based analysis, we defined several gyri a priori,however, this type of analysis precludes us frommaking conclusionsabout other gyri in the brain. We preferred the ROI analysis to awhole-brain method of analysis, because at this time, a propercorrection for multiple comparisons had not been implemented yet,in addition the cortical thickness algorithm performed weakly insome areas in which we were also interested, such as the medialprefrontal cortex. Future research should also attempt to relatecortical thickness values to known functions or psychopathologyassociated with these gyri. It would be of interest to examine corticalthickness in medial prefrontal and parietal areas (such as the anteriorcingulate cortex, posterior cingulate cortex, and the precuneus) aswell. This would provide valuable information, not only for PTSDand the psychiatric field, but perhaps more importantly for the wholefield of neuroscience.
Acknowledgments
This work was financially supported by the Dutch Ministry ofDefence. The authors would also like to thank the RadiologyDepartment of Utrecht University Medical Centre for acquisition ofMRI scans, and Arthur Rademaker, MSc for clinical assessments.
References
Blake, D.D., Weathers, F.W., Nagy, L.M., Kaloupek, D.G., Gusman, F.D.,Charney, D.S., et al., 1995. The development of a Clinician-AdministeredPTSD Scale. J. Trauma Stress 8, 75–90.
Brand, N., Jolles, J., 1985. Learning and retrieval rate of words presentedauditorily and visually. J. Gen. Psych. 112, 201–210.
Bremner, J.D., 2001. Hypotheses and controversies related to effects ofstress on the hippocampus: an argument for stress-induced damage to thehippocampus in patients with posttraumatic stress disorder. Hippocam-pus 11, 75–81 (discussion 82–4).
Bremner, J.D., Innis, R.B., Ng, C.K., Staib, L.H., Salomon, R.M., Bronen,R.A., et al., 1997. Positron emission tomography measurement of cerebralmetabolic correlates of yohimbine administration in combat-relatedposttraumatic stress disorder. Arch. Gen. Psychiatry 54, 246–254.
Bremner, J.D., Innis, R.B., Southwick, S.M., Staib, L., Zoghbi, S., Charney,D.S., 2000. Decreased benzodiazepine receptor binding in prefrontalcortex in combat-related posttraumatic stress disorder. Am. J. Psychiatry157, 1120–1126.
Bremner, J.D., Staib, L.H., Kaloupek, D., Southwick, S.M., Soufer, R.,Charney, D.S., 1999. Neural correlates of exposure to traumatic picturesand sound in Vietnam combat veterans with and without posttraumaticstress disorder: a positron emission tomography study. Biol. Psychiatry45, 806–816.
Bremner, J.D., Vermetten, E., Schmahl, C., Vaccarino, V., Vythilingam, M.,Afzal, N., et al., 2005. Positron emission tomographic imaging of neuralcorrelates of a fear acquisition and extinction paradigm in women withchildhood sexual-abuse-related post-traumatic stress disorder. Psychol.Med. 35, 791–806.
Bremner, J.D., Vermetten, E., Vythilingam, M., Afzal, N., Schmahl, C.,Elzinga, B., et al., 2004a. Neural correlates of the classic color andemotional stroop in women with abuse-related posttraumatic stressdisorder. Biol. Psychiatry 55, 612–620.
Bremner, J.D., Vythilingam,M., Vermetten, E., Vaccarino, V., Charney, D.S.,2004b. Deficits in hippocampal and anterior cingulate functioning duringverbal declarative memory encoding in midlife major depression. Am. J.Psychiatry 161, 637–645.
Britton, J.C., Phan, K.L., Taylor, S.F., Fig, L.M., Liberzon, I., 2005.Corticolimbic blood flow in posttraumatic stress disorder during script-driven imagery. Biol. Psychiatry 57, 832–840.
Chen, S., Xia, W., Li, L., Liu, J., He, Z., Zhang, Z., et al., 2006. Graymatter density reduction in the insula in fire survivors with posttraumaticstress disorder: a voxel-based morphometric study. Psychiatry Res. 146,65–72.
Clark, C.R., McFarlane, A.C., Morris, P., Weber, D.L., Sonkkilla, C., Shaw,M., et al., 2003. Cerebral function in posttraumatic stress disorder duringverbal working memory updating: a positron emission tomographystudy. Biol. Psychiatry 53, 474–481.
Corbo, V., Clement, M.H., Armony, J.L., Pruessner, J.C., Brunet, A., 2005.Size versus shape differences: contrasting voxel-based and volumetricanalyses of the anterior cingulate cortex in individuals with acuteposttraumatic stress disorder. Biol. Psychiatry 58, 119–124.
Dale, A.M., Fischl, B., Sereno, M.I., 1999. Cortical surface-based analysis.I. Segmentation and surface reconstruction. NeuroImage 9, 179–194.
De Bellis, M.D., Keshavan, M.S., Clark, D.B., Casey, B.J., Giedd, J.N.,Boring, A.M., et al., 1999. A.E. Bennett Research Award. Develop-mental traumatology. Part II: Brain development. Biol. Psychiatry 45,1271–1284.
De Bellis, M.D., Keshavan, M.S., Frustaci, K., Shifflett, H., Iyengar, S.,Beers, S.R., et al., 2002a. Superior temporal gyrus volumes in maltreatedchildren and adolescents with PTSD. Biol. Psychiatry 51, 544–552.
De Bellis, M.D., Keshavan, M.S., Shifflett, H., Iyengar, S., Beers, S.R.,Hall, J., et al., 2002b. Brain structures in pediatric maltreatment-relatedposttraumatic stress disorder: a sociodemographically matched study.Biol. Psychiatry 52, 1066–1078.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1997. StructuredClinical Interview for DSM-IVAxis I Disorders.

681E. Geuze et al. / NeuroImage 41 (2008) 675–681
Fischl, B., Sereno,M.I., Dale, A.M., 1999a. Cortical surface-based analysis. II:Inflation, flattening, and a surface-based coordinate system. NeuroImage 9,195–207.
Fischl, B., Sereno, M.I., Tootell, R.B., Dale, A.M., 1999b. High-resolutionintersubject averaging and a coordinate system for the cortical surface.Hum. Brain Mapp. 8, 272–284.
Formisano, E., Esposito, F., Di Salle, F., Goebel, R., 2004. Cortex-basedindependent component analysis of fMRI time series. Magn. Reson.Imaging 22, 1493–1504.
Francati, V., Vermetten, E., Bremner, J.D., 2007. Functional neuroimagingstudies in posttraumatic stress disorder: review of current methods andfindings. Depress Anxiety 24, 202–218.
Frangou, S., Chitins, X., Williams, S.C., 2004. Mapping IQ and gray matterdensity in healthy young people. NeuroImage 23, 800–805.
Geuze, E., Vermetten, E., Bremner, J.D., 2005. MR-based in vivohippocampal volumetrics: 2. Findings in neuropsychiatric disorders.Mol. Psychiatry 10, 160–184.
Geuze, E., Vermetten, E., Ruf, M., de Kloet, C.S., Westenberg, H.G., 2007a.Neural correlates of associative learning and memory in veteranswith posttraumatic stress disorder. J. Psychiatr. Res. doi:10.1016/j.jpsychres.2007.06.007.
Geuze, E., Westenberg, H.G., Jochims, A., de Kloet, C.S., Bohus, M.,Vermetten, E., et al., 2007b. Altered pain processing in veterans withposttraumatic stress disorder. Arch. Gen. Psychiatry 64, 76–85.
Gilbertson, M.W., Shenton, M.E., Ciszewski, A., Kasai, K., Lasko, N.B., Orr,S.P., et al., 2002. Smaller hippocampal volume predicts pathologicvulnerability to psychological trauma. Nat. Neurosci. 5, 1242–1247.
Goebel, R., Esposito, F., Formisano, E., 2006. Analysis of functional imageanalysis contest (FIAC) data with brainvoyager QX: From single-subjectto cortically aligned group general linear model analysis and self-organizing group independent component analysis. Hum. Brain Mapp.27, 392–401.
Hagino,H., Suzuki,M.,Mori, K., Nohara, S., Yamashita, I., Takahashi, T., et al.,2002. Proton magnetic resonance spectroscopy of the inferior frontal gyrusand thalamus and its relationship to verbal learning task performance inpatientswith schizophrenia: a preliminary report. PsychiatryClin. Neurosci.56, 499–507.
Harrison, P.J., 1999. The neuropathology of schizophrenia. A critical reviewof the data and their interpretation. Brain 122 (Pt 4), 593–624.
Hopper, J.W., Frewen, P.A., van der Kolk, B.A., Lanius, R.A., 2007. Neuralcorrelates of reexperiencing, avoidance, and dissociation in PTSD:symptom dimensions and emotion dysregulation in responses to script-driven trauma imagery. J. Trauma. Stress 20, 713–725.
Hull, A.M., 2002. Neuroimaging findings in post-traumatic stress disorder.Systematic review. Br. J. Psychiatry 181, 102–110.
Isaac, C.L., Cushway, D., Jones, G.V., 2006. Is posttraumatic stress disorderassociated with specific deficits in episodic memory? Clin. Psychol. Rev.
Jones, S.E., Buchbinder, B.R., Aharon, I., 2000. Three-dimensional mappingof cortical thickness using Laplace's equation. Hum. Brain Mapp. 11,12–32.
Karl, A., Schaefer, M., Malta, L.S., Dorfel, D., Rohleder, N., Werner, A.,2006. A meta-analysis of structural brain abnormalities in PTSD.Neurosci. Biobehav. Rev. 30, 1004–1031.
Kasai, K., Yamasue, H., Gilbertson, M.W., Shenton, M.E., Rauch, S.L.,Pitman, R.K., 2007. Evidence for acquired pregenual anterior cingulategray matter loss from a twin study of combat-related posttraumatic stressdisorder. Biol. Psychiatry.
Kitayama, N., Brummer, M., Hertz, L., Quinn, S., Kim, Y., Bremner, J.D.,2007. Morphologic alterations in the corpus callosum in abuse-related
posttraumatic stress disorder: a preliminary study. J. Nerv. Ment. Dis.195, 1027–1029.
Kitayama, N., Vaccarino, V., Kutner, M., Weiss, P., Bremner, J.D., 2005. Mag-netic resonance imaging (MRI) measurement of hippocampal volume inposttraumatic stress disorder: a meta-analysis. J. Affect. Disord. 88, 79–86.
Lanius, R.A., Williamson, P.C., Boksman, K., Densmore, M., Gupta, M.,Neufeld, R.W., et al., 2002. Brain activation during script-drivenimagery induced dissociative responses in PTSD: a functional magneticresonance imaging investigation. Biol. Psychiatry 52, 305–311.
Lindauer, R.J., Booij, J., Habraken, J.B., Uylings, H.B., Olff, M., Carlier, I.V.,et al., 2004. Cerebral blood flow changes during script-driven imagery inpolice officers with posttraumatic stress disorder. Biol. Psychiatry 56,853–861.
Narr, K.L., Toga, A.W., Szeszko, P., Thompson, P.M., Woods, R.P.,Robinson, D., et al., 2005. Cortical thinning in cingulate and occipitalcortices in first episode schizophrenia. Biol. Psychiatry 58, 32–40.
Narr, K.L., Woods, R.P., Thompson, P.M., Szeszko, P., Robinson, D.,Dimtcheva, T., et al., 2006. Relationships between IQ and regional corticalgray matter thickness in healthy adults. Cereb. Cortex.
Nemeroff, C.B., Bremner, J.D., Foa, E.B., Mayberg, H.S., North, C.S.,Stein, M.B., 2006. Posttraumatic stress disorder: a state-of-the-sciencereview. J. Psychiatr. Res. 40, 1–21.
Rauch, S.L., Shin, L.M., Phelps, E.A., 2006. Neurocircuitry models ofposttraumatic stress disorder and extinction: human neuroimagingresearch — past, present, and future. Biol. Psychiatry 60, 376–382.
Rauch, S.L., Shin, L.M., Segal, E., Pitman, R.K., Carson, M.A., McMullin,K., et al., 2003. Selectively reduced regional cortical volumes in post-traumatic stress disorder. NeuroReport 14, 913–916.
Rey, A., 1964. L'examen clinique en psychologie. Presses Universitaires deFrance, Paris.
Shaw, P., Lerch, J., Greenstein, D., Sharp, W., Clasen, L., Evans, A., et al.,2006. Longitudinal mapping of cortical thickness and clinical outcomein children and adolescents with attention-deficit/hyperactivity disorder.Arch. Gen. Psychiatry 63, 540–549.
Shin, L.M., Wright, C.I., Cannistraro, P.A., Wedig, M.M., McMullin, K.,Martis, B., et al., 2005. A functional magnetic resonance imaging studyof amygdala and medial prefrontal cortex responses to overtly presentedfearful faces in posttraumatic stress disorder. Arch. Gen. Psychiatry 62,273–281.
Weber, D.L., Clark, C.R., McFarlane, A.C., Moores, K.A., Morris, P., Egan,G.F., 2005. Abnormal frontal and parietal activity during workingmemory updating in post-traumatic stress disorder. Psychiatry Res. 140,27–44.
Woodward, S.H., Kaloupek, D.G., Streeter, C.C., Martinez, C., Schaer, M.,Eliez, S., 2006. Decreased anterior cingulate volume in combat-relatedPTSD. Biol. Psychiatry 59, 582–587.
Yamasue, H., Kasai, K., Iwanami, A., Ohtani, T., Yamada, H., Abe, O., et al.,2003. Voxel-based analysis of MRI reveals anterior cingulate gray-matter volume reduction in posttraumatic stress disorder due toterrorism. Proc. Natl. Acad. Sci. U. S. A. 100, 9039–9043.
Yehuda, R., 2001. Are glucocortoids responsible for putative hippocampaldamage in PTSD? How and when to decide. Hippocampus 11, 85–89(discussion 82–4).
Yehuda, R., Golier, J.A., Tischler, L., Stavitsky, K., Harvey, P.D., 2005.Learning and memory in aging combat veterans with PTSD. J. Clin.Exp. Neuropsychol. 27, 504–515.
Yehuda, R., Keefe, R.S., Harvey, P.D., Levengood, R.A., Gerber, D.K.,Geni, J., et al., 1995. Learning and memory in combat veterans withposttraumatic stress disorder. Am. J. Psychiatry 152, 137–139.