therapy of auricular keloids: review of different treatment modalities and proposal for a...
TRANSCRIPT

Eur Arch Otorhinolaryngol (2007) 264:1497–1508
DOI 10.1007/s00405-007-0383-0MISCELLANEOUS
Therapy of auricular keloids: review of diVerent treatment modalities and proposal for a therapeutic algorithm
K. Froelich · R. Staudenmaier · N. Kleinsasser · R. Hagen
Received: 5 February 2007 / Accepted: 14 June 2007 / Published online: 13 July 2007© Springer-Verlag 2007
Abstract Keloids are abnormal wound reactions of con-nective tissue. Auricular keloids can develop as a result of,e.g., otoplasty, ear piercing, or skin trauma. A wide varietyof therapeutic options exists, including surgery as primarytreatment. Furthermore, there are medical, physical, radio-therapeutic and experimental options. The present paperfocuses on the diVerent techniques including the therapeu-tic outcome and quality rating for each chosen pathway. Inaddition to the experience of the university hospitals, athorough review of the literature was performed in order toupdate and compare today’s therapeutic options. Surgicaltechniques are customized to the lesion’s speciWc localiza-tion and extent. They may include revision of otoplasty.With medical treatment, established modalities such as ste-roid injection have to be distinguished from experimentalmethods like interferon, 5-FU, verapamil, imiquimod, ormitomycin C. Radiation is generally accepted to be eVec-tive, especially applied accompanying surgery, but needs tobe restricted due to possible side eVects. Physical therapy,e.g., pressure in a variety of application modalities, hasgained a profound position in the therapy of auricularkeloids. The success rates of the diVerent treatment modali-ties vary markedly, and the number of patients per study isconsiderably low. Resuming the results, a periodic follow-up and good patients’ compliance are mandatory to earlyrealize and treat auricular keloids. However, studies are
needed to evaluate accepted and experimental therapiesincluding larger number of patients.
Keywords Auricular keloids · Keloid therapy · Surgery of auricular keloids
Introduction
Keloids are abnormal wound reactions, which develop fromconnective tissue as a result of skin trauma such as inXam-mation, burns, piercing or surgery in predisposed individu-als. This Wbrous growth occurs spontaneously within 1 yearafter local injury, extends beyond the boundaries of theoriginal wound and rarely regresses. Keloids have a thickand glassy appearance. These characteristics distinguishkeloids from hypertrophic scars, which are conWned to theoriginal wound and show spontaneous regression.
Morphology and histopathology
Both keloids and hypertrophic scars are characterized byuncontrolled synthesis and excessive depositing of collagenand glycoprotein. However, there are histopathologicaldiVerences between these two entities of abnormal scarring.This makes an accurate distinction mandatory when plan-ning surgical excision or necessary aftercare treatment. Inkeloids, whorls and nodules of thicker, larger and wavy col-lagen Wbers with a mucinous base substance are present. Incontrast to normal scars, the collagen bundles are notsorted. In hypertrophic scars, little or no keloidal collagenis found [2, 20, 39]. Whether increased synthesis ordecreased resorption of collagen due to reduced generationof collagenase or direct enzyme inhibition is responsibleremains uncertain. The combination of both mechanisms
K. Froelich (&) · N. Kleinsasser · R. HagenDepartment of Otolaryngology, Head and Neck Surgery, University of Wuerzburg, Josef-Schneider-Strasse 11, 97080 Würzburg, Germanye-mail: [email protected]
R. StaudenmaierDepartment of Otolaryngology, Head and Neck Surgery, Technical University Munich, Munich, Germany
123

1498 Eur Arch Otorhinolaryngol (2007) 264:1497–1508
can be considered a reason for these typical histopathologi-cal changes in keloids as well [31]. Several studies focus onthe mechanistic processes of keloid formation. On onehand, it is suggested that keloid keratinocytes inXuenceunderlying Wbroblasts, thereby playing an important role inkeloidogenesis. They may promote more proliferation andless apoptosis in the Wbroblasts through paracrine eVects,e.g., increased expression of TGF-�, Bcl-2 (proto-oncogene)and increased signal-regulated kinase-phosphorylation[2, 26, 41, 60, 61]. Transforming growth factor (TGF)-� issupposed to be a component of these epithelial–mesenchy-mal interactions from both TGF-� production and activa-tion by the keloid keratinocytes as well as elevated TGF-�expression, utilization and signaling in Wbroblasts [2, 60].However, it is not yet fully understood which concretemechanism is responsible for keloidogenesis.
Epidemiology and etiology
Keloids are common in Black, Hispanic and Asian popula-tions with an incidence of 4.5 up to 16% [1, 22, 31, 39].Other suggested predisposing factors are hormone imbal-ances as well as pregnancy. Familial occurrence also indi-cates congenital factors [2, 10, 31].
A history of ear piercing is found in most cases of ear-lobe keloids, but infection due to a nickel allergy can alsobe responsible [49]. Furthermore, in cases of patient predis-position, earlobe keloids are frequently found bilaterally[10, 40]. Aköz et al. [1] examined 12 patients with keloidsof the auricle, 9 of which had keloids of the earlobe. Allwomen in this group showed bilateral keloids of the ear-lobes [1]. Besides the earlobe, other parts of the auricle canbe aVected as well. Keloids on the back side of the auricleare also often described after otoplasty in cases wherepatients are predisposed [10]. The period from trauma, orrather ear piercing, until the appearance of keloid formationcan vary from a few months to several years [36, 40].
Symptoms
Patients with auricular keloids complain about various symp-toms. Apart from the unsatisfactory cosmetic appearance andfunctional constrictions in cases of large keloids, patientsreport pain, pruritus, numbness and redness in the area of thelesion [40, 58]. The cosmetic impairment is dependent onboth the localization as well as the extent of the keloids.
Therapy
Keloids are still a therapeutic challenge and the optimaltreatment remains undeWned with a wide variety of tech-niques characterizing the management of keloids. TheeYcacy of treatment as represented by a low recurrence rate
and satisfactory aesthetic result varies markedly. Recur-rences range from 50 to 100% in case of excision alone tolower recurrence rates by combining diVerent therapeuticmethods [9, 34, 43]. Besides surgical treatment, many othernonsurgical therapeutic procedures such as steroid injection,radiation therapy, silicone-gel sheeting and pressure or int-ralesional application of diVerent drugs are implemented oradapted based on the particular localization.
The present paper focuses on the wide spectrum of auric-ular keloids and their diVerent therapeutic managementtechniques including the therapeutic outcome and qualityrating for each chosen pathway. It summarizes surgical andmedical therapies of established and experimental charac-ter, physical modalities and radiation as possible measures.
Surgical therapy
Conventional surgery
In general, to avoid keloids or recurrences, nonessentialcosmetic surgery should not be performed on predisposedpatients like Blacks or Asian people [29, 34]. Incisionsshould be made along the skin tension lines without cross-ing them and wounds should be closed without any tension[49]. Furthermore, intradermal, subcuticular closure is to bepreferred [2]. Surgical excision neglecting any aftertreat-ment is not suYcient when keloids have appeared, andleads to recurrence rates between 45 and 100% [9, 19, 34,43, 46, 47]. Therefore, adjuvant treatment with, e.g., steroidinjection or silicone sheeting is mandatory.
Keloids develop on the earlobe usually after ear piercingand on the posterior side of the auricle following otoplasty,and the surgical treatment depends on the lesion’s speciWclocalization and extent. The surgeon should always attemptto remove the keloid completely and to achieve wound clo-sure with normal tension. When the keloids are small, sim-ple excision followed by undermining the skin and primarywound closure is recommended. In cases of larger lesions,sometimes extensive skin deWcits result. To resurface thesedefects the use of full thickness skin grafts may be reason-able. However, it is essential to consider that, in the predis-posed patient, additional traumatization of the skin byharvesting a skin graft should be avoided. If done, coveringthe defect with local Xaps, such as transposition Xaps fromthe retroauricular sulcus, is to be favoured over skin graftsfrom other localizations (Fig. 1a, b). However, otherauthors [49] reported on satisfactory results without localrecurrence in the treatment of earlobe keloids with surgicalexcision and grafting with a split thickness skin graft. Also,no keloid developed at the site of graft harvesting.
Large defects after major excisions are a very challeng-ing problem (Fig. 2). Many are resistent to treatment and,
123

Eur Arch Otorhinolaryngol (2007) 264:1497–1508 1499
despite careful resection and wound closure with local Xapsand normal tension, these keloids often recur [43]. Radia-tion therapy following the operation should be consideredin such cases. Although a satisfactory aesthetic result is aprimary objective of surgical treatment, often the simulta-neous relief of symptoms and maintenance of the anatomyof the auricle cannot be achieved.
Keloids following an otoplasty can be found either in thearea of the helix or the posterior side of the pinna. Com-monly, the cartilage beneath the skin is under tension andthus permanently applies pressure on the skin. Therefore, inaddition to excision of the keloid, revision of the otoplastyis mandatory (Fig. 3).
A wide variety of surgical techniques have beendescribed in the literature. Options range from primaryresurfacing, wound healing by second intention to the useof full thickness skin grafts or local Xaps [32, 36]. Particu-larly concerning the surgical treatment of the earlobe, manydiVerent methods exist. Kim et al. [36] liberated and pre-served the skin of the keloid by “Wlleting” the skin fromthe keloid mass and removed the keloid tissue completely.The remaining skin was used to reconstruct the earlobe.
The authors described recurrence in four of their nine cases,which were treated with triamcinolone injections [36]. Zic-cardi [62] reports on a defect resurfacing technique with theuse of a full thickness skin graft harvested from the keloidskin after removing the auricular keloid. However, whenusing these or other techniques the surgeon should keepclearly in mind that the earlobe tends to shrink in the post-operative course. Hatoko et al. [32] tried to solve this prob-lem with a subcutaneous island pedicle Xap from theposterior side of the auricle. They used this technique espe-cially for grafting skin defects on the posterior side aftersurgical excision of earlobe keloids and obtained satisfatoryresults with respect to aesthetics and recurrence rates.
In general, surgical removal followed by plastic recon-struction is the primary therapeutic management techniquefor large keloids. Many diVerent procedures and drugs areavailable for aftertreatment and should be taken into con-sideration.
Cryosurgery
Cryosurgery may be used either as monotherapy orcombined with other modalities [23].
Fig. 1 a Keloid of the helix in a female patient. b After surgical exci-sion of the keloid lesion, the resulting defect was grafted by a transpo-sition Xap harvested from the retroauricular sulcus
Fig. 2 Large keloid of the auricle with destruction of the pinna in ablack male patient. In such cases it is diYcult to preserve the anatomyof the auricle and large skin defects result which need closure usinglocal Xaps
123

1500 Eur Arch Otorhinolaryngol (2007) 264:1497–1508
Mode of action
Freezing keloid lesions with liquid nitrogen, which is themost frequently used agent, causes cell and microvasculardamage followed by selective tissue necrosis [22, 23, 34].The result is tissue Xattening.
Application
Thaw cycles of 20–30 s each should be performed every2–3 weeks from 2 to 12 times, depending on the scar size[23, 34].
Side eVects
Generally, local pain during and immediately after thetreatment occurs. In addition, lesional hypopigmentationand atrophy are the major side eVects that have beenreported [22, 23, 34, 48]. Rarely, cartilage damage canoccur in the treatment of auricle keloid or nasal lesions[23].
Evaluation
Results with a therapeutic success rate from 61 to 100% arereported, whereas duration of the lesions and scar volumeseems to have an inXuence on the therapeutic outcome.Reports show that younger keloids seem to respond betterto cryosurgery [22, 23, 48]. Rusciani et al. [48] treated 135patients and achieved a volume reduction of the initial massof more than 80 in 79.5% of the treated lesions. Cryosur-gery is a successful alternative therapeutic management forkeloids, but many patients do not return for follow-up treat-ments because of local pain and slow healing [34]. Studysizes vary from 7 to 135 patients [23, 48].
Medical therapy
Steroid injection
Intralesional injection of triamcinolone acetonide, one ofthe long-term standards of keloid therapy, is the Wrst-linemonotherapy in cases of small keloids and adjuvant treat-ment after surgical excision to diminish local recurrencerates.
Mode of action
Injection of corticosteroids leads to inhibition of collagensynthesis and a decrease in collagenase activity by inhibit-ing �2-makroglobulin, which in turn, inhibits collagenase[1, 2, 14, 34]. Further proliferation of Wbroblasts is proba-bly reduced by steroid-induced suppression of endogenousvascular endothelial growth factor (VEGF) [59].
Application
Usually a 10% triamcinolone acetonide crystal suspensionis used in combination with lidocain. Injecting lidocaingreatly reduces the pain of intralesional injection, which issigniWcant [34, 43]. For injection into the keloid a needle ora dermojet-injector is applied. Generally, a series of severalinjections of triamcinolone acetonide (10–40 mg/ml) every2–3 weeks is performed to obtain a satisfactory result. Top-ical steroid creams have shown varying success rates [43].
Fig. 3 a, b Keloids on the posterior side of the auricle followingotoplasty
123

Eur Arch Otorhinolaryngol (2007) 264:1497–1508 1501
Side eVects
Intralesional corticosteroid injections are associated withdiVerent side eVects: injections can be quite painful and canlead to skin atrophy, depigmentation and teleangiectasias in63% of all patients [43]. The steroid should be injecteddirectly into the lesion to reduce damage to the surroundingnormal skin and should be put into the papillary dermiswhere collagenase is produced. Subcutaneous tissue must beconserved to avoid underlying fat atrophy [34]. Skin lesionsas a result of steroid injection can remain for months or evenyears. Particularly in the treatment of patients with dark skin,hypo- or depigmentation and the importance of maintainingthe perilesional, healthy skin should be considered [22].
Since surgical excision in combination with steroid treat-ment can lead to disturbed wound healing and wounddehiscence, sutures should be left in place longer than usualwhen postoperative steroid injection is intended [1, 22, 34].Systemic eVects such as Cushing’s syndrome generally donot occur with triamcinolone treatment, but rare cases havebeen described [2].
Evaluation
Descriptions of therapeutic results of this major keloid ther-apy diVer widely in the literature. No consistent statementsexist with respect to recurrence rates even for the most fre-quent management technique of combining surgery withadjuvant triamcinolone acetonide injection [1]. Thedescribed recurrence rates range from 3 to 60% [4, 19, 36].Chowdri et al. [13] gave an account of a response rate with-out relapse of 91.9% in the treatment of keloids and 95% intreating hypertrophic scars. They injected triamcinoloneintraoperatively and repeated the injections at 1-week inter-vals for 2–5 weeks followed by monthly injections for afurther 6 months [13]. Shons et al. [53] treated 31 earlobekeloids with triamchinolone postoperatively for 2 monthsand found only one recurrence after a mean follow-upperiod of 35 months. Overall, published data seem to con-Wrm that the combination of surgical excision with postop-erative injection of triamcinolone acetonide and steroidmonotherapy in cases of small keloids represents an eVec-tive procedure for the treatment of auricular keloids.
Verapamil
The intralesional verapamil hydrochloride injection has alsoshown a beneWcial eVect in the treatment of keloids in the past.
Mode of action
Calcium antagonists are thought to decrease collagen syn-thesis in the extracellular matrix and increase collagenase
synthesis, thus reducing Wbrous tissue production, althoughthe precise mechanism is still unknown [15, 16, 37]. Leeand Ping [38], however, ascertained that calcium antago-nists, like verapamil can disrupt the cellular calcium metab-olism which appears to regulate the extracellular matrixproduction. There are various studies, which focus on theeVectiveness of verapamil in the treatment and preventionof keloids. Primary cultures of central keloid Wbroblaststreated with verapamil showed a decrease in interleukin 6(IL-6) and vascular endothelial growth factor (VEGF)release. Moreover, reduced cell proliferation and increasedapoptosis could also be determined [27].
Application
Like other therapeutic options, verapamil injections may beperformed alone or in combination with surgical excisionor other therapies. Depending on the size of the keloid, 0.5–2 ml verapamil are injected per application at a concentra-tion of 2.5 mg/ml. Commonly, the calcium antagonistverapamil is used as a relapse prophylaxis and is injectedon the seventh postoperative day followed by three to fourfurther applications at intervals of 1 week [16, 37].
Evaluation
In general, satisfactory results could be obtained by severalinvestigators by combining surgical excision with verapamilinjection and other procedures like silicone sheeting or pres-sure earrings [15, 16, 37]. In cases of earlobe keloids, Law-rence [37] achieved a response rate without relapse of 55% inall patients combining surgical excision, postoperative verap-amil injection and application of pressure earrings. Thus,verapamil injection also appears to be an encouraging thera-peutic option in the treatment and prevention of keloids.
5-Flourouracil
Although it is well known as a chemotherapeutic agent, 5-Flourouracil (5-FU) is an experimental therapy for keloids thathas shown some potential due to its antiproliferative eVect.
Mode of action
5-FU is a pyrimidine analogon with antimetabolite activitywhich inhibits the proliferation of Wbroblasts. It also has aninhibitory eVect on human Wbroblasts and myoWbroblastdiVerentiation in Dupuytren Wbroblasts in vitro [33].
Application
The application of 5-Flourouracil is carried out at a concen-tration of 50 mg/ml with a cumulative dose from 50 to
123

1502 Eur Arch Otorhinolaryngol (2007) 264:1497–1508
150 mg per application. Frequently, this drug is used incombination with corticosteroids, where better results canbe obtained when 0.1 ml of triamcinolone acetonide(10 mg/ml) is added to 0.9 ml of 5-FU (50 mg/ml) [34].Others [3] used 1.6 ml of 5-FU at the same concentrationand 0.4 ml of betamethasone with success.
The injection series starts with three injections a week.Depending on therapeutic response, frequency of applica-tions diminishes over the course of treatment [24]. On aver-age, a total of 16 injections repeated at 1-week intervalwere performed by Gupta and Kalra [30]. In the treatmentof small keloids they could achieve a signiWcant Xatteningof the lesions of more than 50% in about half the patientswith injections of 5-FU as an independent therapeuticagent. A better therapeutic response was found in patientswith keloids existing for over 5 years [30].
Side eVects
Systemic side eVects like blood count modulation were notobserved using this therapeutic modality, although injectionpain, purpura at the injection site, temporary hyperpigmen-tation and, rarely, also temporary ulcerations can appear[30, 44].
Evaluation
Overall, this therapeutic method is a safe and eVectiveoption for the treatment of small isolated keloids of shortduration, and the results are comparable with those of othersingle-use treatment modalities [24, 30, 31, 34, 44]. How-ever, speciWc investigations which focus on the treatment ofthe auricle with 5-FU are lacking thus far.
Interferon
A further experimental modality is the use of interferons.These are cytokines which have considerable side eVectsand a controversial eYcacy in keloid treatment.
Mode of action
Interferon-� and interferon-� cause a reduction in keloidWbroblasts, reduce collagen type I and III synthesis and alsoinhibit glycosaminoglycan production. Furthermore, theymarkedly increase collagenase production and inhibitsecretion of collagenase inhibitors [9, 17, 22, 31, 34].
Application
Injection of 1 million units/cm (1 MU/cm) along the con-Wnes of resection can markedly reduce chances of recur-rence [9, 22].
Side eVects
Side eVects such as Xu-like symptoms with fever, headacheand myalgias are possible; they can be relieved by prophy-lactic administration of 500 mg paracetamol [9, 22, 31].
Evaluation
Berman and Flores [4] examined the recurrence rate afterpostoperative interferon therapy in comparison with theresults after postoperative triamcinolone injection. Amaz-ingly, they reported a recurrence rate of 58.4% after surgi-cal excision combined with triamcinolone injection and arecurrence rate of 18.7% after surgical excision and inter-feron-�2b treatment. Surgical excision alone led to 50%relapse in their examination. Granstein et al. [28] observedearly signiWcant Xattening of the keloids for about 30%, butlong-term recurrences with sole injection of interferon-�. Incontrast, other studies failed to demonstrate any beneWtfrom intralesional injection of interferon-�2b [17].
Consequently, although preliminary Wndings appearedencouraging, further studies yielded equivocal results. Becauseof diVerent systemic side eVects and questionable beneWt ofinterferon, its use in keloid therapy has to be reconsidered.
Imiquimod therapy
Another therapeutic alternative which has become the focusof recent research is imiquimod cream.
Mode of action
Imiquimod 5% cream is a novel immune modulator that,topically applied, enhances the local production of cyto-kines like interleukin-6 and interferon-� at the site of appli-cation [55].
Application
Berman and Kaufman [5] treated 12 patients with imiqui-mod 5% cream after surgical excision of the keloids. Theystarted immediately after surgery and continued the topicalapplication for 8 weeks. After 24 weeks the patients wereevaluated and none of them showed recurrence of thekeloid lesion.
Side eVects
More than 50% of the patients in the study developedhyperpigmentation during therapy. Two cases of irritationsecondary to the application cleared with discontinuation ofthe medication. However, therapy could be resumed after-wards without any diYculties. In case of large surgical sites
123

Eur Arch Otorhinolaryngol (2007) 264:1497–1508 1503
and wounds closed with tension or grafts, imiquimod ther-apy should not be started immediately after the operation,because early treatment can cause wound dehiscence [5,34]. Moderate to severe local skin reactions secondary toimiquimod treatment were observed by other authors [41].
Evaluation
Imiquimod’s eYcacy in the prevention of recurrences wasalso examined speciWcally for the treatment of earlobekeloids after surgical excision [41, 55]. Martin-García et al.[41] showed imiquimod 5% cream to be successful in pre-venting keloid recurrence in 75% of the treated earlobes ata 24-week follow-up.
In conclusion, it can be suggested that imiquimod 5%cream is an eVective therapeutic alternative for preventionof keloid recurrence after surgical excision of earlobekeloids, but larger studies comparing imiquimod with sur-gical monotherapy and other adjuvant therapies with long-term follow-up are mandatory [41, 55].
Mitomycin C
Mitomycin C has been reported as a successful therapyoption for laryngeal or tracheal stenosis. Several studiesdeal with its use in keloid therapy.
Mode of action
Mitomycin C is a chemotherapeutic agent produced byStreptomyces caespitosus that inhibits Wbroblast prolifera-tion [12, 50, 56, 57]. It interferes with the ability of Wbro-blasts to produce a scar without causing changes inepithelialization [50]. Besides these eVects, Simman et al.[54] found an increase in Wbroblasts treated with mitomycinC in vitro after 3 weeks.
Application
Chen et al. [12] conclude from their investigations that aclinically ideal concentration of mitomycin C could slowWbroblast proliferation and not cause cell death to enable awound healing response. These criteria are satisWed in vitroby the exposure of 0.4 mg/ml mitomycin C for 4 min. Both,inhibition of Wbroblasts’ proliferation and increase ofgrowth factor synthesis enabling wound healing response,are assured [12]. A further group also used a concentrationof 0.4 mg/ml for 5 min in vivo [50].
Side eVects
Hyperpigmentation and skin atrophy are observed sideeVects [51].
Evaluation
Whereas mitomycin C has been reported to be successfulin upper airway stenosis [12], regarding the eVectiveness inkeloid treatment, diVerent therapeutic results are found inthe literature [35, 56, 57]. A newer study showed encourag-ing results with injections of bleomycin in keloids whichare unresponsive to intralesional steroid therapy [34, 51].
Physical modalities
Pressure
Pressure therapy has been standard therapy for hypertro-phic burn scars and is most frequently used as a postopera-tive adjunct for earlobe keloids, e.g., in the form ofearrings.
Mode of action
Pressure seems to decrease scar hydration, which results inmast cell stabilization and a decrease in neovascularizationand extracellular matrix production [34]. Another possiblemechanism is local hypoxia at the site of application, whichleads to degeneration of Wbroblasts and collagen [8, 34].Moreover, pressure seems to increase collagenase activity[34].
Application
Frequently, this therapeutic option is combined with otherslike steroid injection or silicon sheeting and is used for pre-vention of recurrence after surgical excision [8, 37].Depending on localization of the lesion, a wide variety ofdiVerent forms and materials are applied, such as speciallydesigned earrings for earlobe keloids [1, 31]. After surgeryand postoperative pressure therapy at diVerent sites, 18%recurrence of keloids could be found in comparison to 67%after surgical monotherapy [45]. Similarly good resultscould be achieved in a small patient collective involvingtreatment of earlobe keloids with postoperative pressuretherapy using special earrings [8]. In addition, these ear-rings can be coated with silicone [1].
Evaluation
Therapeutic results, however, depend on patient compli-ance, since to achieve satisfactory results it is mandatory towear these earrings consistently 12–24 h a day for a longerperiod of time [1, 2, 31, 34, 37]. Nonetheless, particularlyfor earlobe keloids, it is an eVective and feasible manage-ment technique with only minimal side eVects.
123

1504 Eur Arch Otorhinolaryngol (2007) 264:1497–1508
Tab
le1
Sum
mar
y of
trea
tmen
t str
ateg
ies
and
ther
apeu
tic
resu
lts
Pat
ient
s/ke
loid
sT
reat
men
t reg
ime
Res
ults
Ster
oid
inje
ctio
n
Akö
z et
al. [
1]n
=9/
n=
12Su
rger
y w
ith in
tral
esio
nal t
riam
cino
lone
and
pre
ssur
e si
lico
ne s
heet
ing
11%
rec
urre
nces
Ber
man
and
Flo
res
[4]
n=
65Su
rger
y an
d in
tral
esio
nal t
riam
cino
lone
58.4
% r
ecur
renc
es
Cho
wdr
i eta
l. [1
3]n
=58
Surg
ery
and
intr
ales
iona
l tri
amci
nolo
ne8.
1% r
ecur
renc
es
Scl
afan
i eta
l. [5
2]n
=12
/n=
12Su
rger
y an
d in
tral
esio
nal t
riam
cino
lone
33%
rec
urre
nces
Sho
ns e
tal.
[53]
n=
20/n
=31
Surg
ery
and
intr
ales
iona
l tri
amci
nolo
ne3.
2% r
ecur
renc
es
Dav
ison
eta
l. [1
7]n
=26
kel
oids
Surg
ery
and
intr
ales
iona
l tri
amci
nolo
ne15
% r
ecur
renc
es
Ver
apam
il
Cop
cu e
tal.
[15]
n=
21/n
=21
Surg
ery
and
intr
ales
iona
l ver
apam
il9.
5% r
ecur
renc
es (
smal
ler)
9.5%
hyp
ertr
ophi
c sc
ars
D’A
ndre
a et
al. [
16]
n=
22/n
=22
Surg
ery
with
sili
cone
she
etin
g an
d in
tral
esio
nal v
erap
amil
36%
rec
urre
nces
of
smal
ler
kelo
ids
9% r
ecur
renc
es o
f w
orse
kel
oids
Law
renc
e [3
7]n
=35
/n=
45Su
rger
y w
ith in
tral
esio
nal v
erap
amil
and
pre
ssur
e th
erap
y45
% r
ecur
renc
es
5-Fl
ouro
urac
il
Fitz
patr
ick
[24]
n>
1,00
0 ke
loid
s an
d H
SIn
tral
esio
nal i
njec
tion
/com
bina
tion
wit
h pu
lse
dye
lase
r or
Ken
alog
No
recu
rren
ce r
ates
/eV
ectiv
e tr
eatm
ent
Gup
ta a
nd K
alra
[30
]n
=24
/n=
24In
tral
esio
nal i
njec
tion
50>
50%
Xat
teni
ng33
>75
% X
atte
ning
Nan
da a
nd R
eddy
[44
]n
=28
/n=
28In
tral
esio
nal i
njec
tion
>50
% im
prov
emen
t0%
rec
urre
nce
afte
r 24
wee
ks f
ollo
w-u
p
Api
kian
and
Goo
dman
[3]
n=
2/n
=2
Intr
ales
iona
l inj
ecti
on w
ith
beta
met
haso
ne10
0% im
prov
emen
t
Inte
rfer
on
Ber
man
and
Flo
res
[4]
n=
16Su
rger
y an
d in
terf
eron
-�2b
18.7
% r
ecur
renc
es
Dav
ison
eta
l. [1
7]n
=13
kel
oids
Surg
ery
and
inte
rfer
on-�
2b (
at s
urge
ry a
nd o
ne w
eek
late
r)54
% r
ecur
renc
es
Gra
nste
in e
tal.
[28]
n=
6/n
=6
Intr
ales
iona
l inj
ecti
on o
f in
terf
eron
�R
educ
tion
in s
ize
(30.
4% h
eigh
t red
uctio
n)
Imiq
uim
od 5
%
Ber
man
and
Kau
fman
[5]
n=
12/n
=13
Surg
ery
with
topi
cal i
miq
uim
od0%
rec
urre
nces
Mar
tin-
Gar
cía
etal
. [41
]n
=6/
n=
8Su
rger
y w
ith to
pica
l im
iqui
mod
25%
rec
urre
nces
Sta
show
er [
55]
n=
4/n
=8
Surg
ery
with
topi
cal i
miq
uim
od0%
rec
urre
nces
Mit
omyc
in C
Kim
eta
l. [3
6]n
=10
/n=
10Su
rger
y w
ith to
pica
l mito
myc
in-C
10%
rec
urre
nces
San
ders
eta
l. [5
0]n
=15
Surg
ery
with
topi
cal m
itom
ycin
-C27
% r
ecur
renc
es
Pres
sure
ther
apy
Law
renc
e [3
7]n
=35
/n=
45Su
rger
y w
ith in
tral
esio
nal v
erap
amil
and
pre
ssur
e th
erap
y45
% r
ecur
renc
es
Akö
z et
al. [
1]n
=9/
n=
12Su
rger
y w
ith in
tral
esio
nal t
riam
cino
lone
and
pre
ssur
e si
lico
ne s
heet
ing
11%
rec
urre
nces
Bre
nt [
8]n
=5/
n=
10Su
rger
y an
d pr
essu
re e
arri
ng0%
rec
urre
nce
123
Eur Arch Otorhinolaryngol (2007) 264:1497–1508 1505
Silicone gel sheeting
Silicone gel is eVective in the treatment of keloids, but islimited by patient compliance.
Mode of action
Treatment with silicone gel is a new and painless therapeu-tic option whose mode of action on keloids and hypertro-phic scars is yet unknown. It is supposed that heightenedhydration of the skin following the occlusion is responsiblefor cellular remodelling in the lesions [1, 25, 58]. Penetra-tion of silicone from the silicone sheet into the tissue with adirect eVect on Wbroblasts or collagen metabolism could notbe ascertained [58].
Application
Silicone sheeting is used as monotherapy and in combina-tion with triamcinolon-acetonide injections or pressuretherapy after surgery. Also in cases of fresh scars, siliconesheeting can lead to satisfactory results. Over the course oftreatment elasticity increases, scars become softer anddiminish and even symptoms like pruritus and pain disap-pear. Moreover, in predisposed persons, including children,it acts as an eVective, painless prophylaxis after surgery ortraumata [21, 25, 34, 58]. Flattening of the lesions could beachieved in 85% with sole silicone gel application partiallycombined with steroid injection [25]. The silicone sheetshould be worn consistently for several hours a day (12–24 h) for several months (2–12 months) [22, 25, 34]. There-fore, the use of silicone gel, especially as sheets, is also lim-ited by the patient’s daily compliance. Most sheets have adurability of about 2–3 weeks and should be cleansed anddried carefully every day to prevent bacterial irritations orimpetiginization [25, 34, 58].
Side eVects
Side eVects at the site of application include occasional skinmaceration, erosion, rash and pruritus. All of these symp-toms disappear upon removal of the gel [2].
Evaluation
A recently invented sheet made of polyurethane seems to actlike silicone gel sheets and softens keloids by daily applica-tion over several weeks. Others observed that silicone andnonsilicone dressings are equally eVective in keloid treat-ment. [18]. This raises the question of whether silicone istruly an important component of the sheets [16]. Therapeu-tic success of the sheet could also be enhanced by pressure[1, 34, 58]. With respect to the auricle, sheet application canT
able
1co
ntin
ued
HS
hype
rtro
phic
sca
r
Pat
ient
s/ke
loid
sT
reat
men
t reg
ime
Res
ults
Rad
iatio
n th
erap
y
Cha
udhr
y et
al. [
11]
n=
44Su
rger
y w
ith im
med
iate
pos
tope
rati
ve r
adia
tion
ther
apy
(1,8
00cG
y in
thre
e fr
acti
ons)
2.8%
rec
urre
nces
Scla
fani
eta
l. [5
2]n
=16
/n=
16Su
rger
y pl
us r
adat
ion
ther
apy
(700
or
1,00
0cG
y/on
e fr
acti
on)
12.5
% r
ecur
renc
es
Rag
oow
ansi
eta
l. [4
7]n
=80
/n=
80Su
rger
y w
ith im
med
iate
pos
tope
rati
ve
radi
atio
n th
erap
y (1
0G
y, s
ingl
e fr
actio
n)9%
rec
urre
nces
aft
er 1
year
16%
rec
urre
nces
aft
er 5
year
s
Rag
oow
ansi
eta
l. [4
6]n
=35
/n=
35Su
rger
y w
ith im
med
iate
pos
tope
rati
ve
radi
atio
n th
erap
y (1
0G
y, s
ingl
e fr
actio
n)8.
8% r
ecur
renc
es a
fter
1ye
ar20
.6%
rec
urre
nces
aft
er 5
year
s
Sur
gery
alo
ne
Scla
fani
eta
l. [5
2]n
=3/
n=
3M
onot
hera
py33
% r
ecur
renc
es
Ber
man
and
Flo
res
[4]
n=
43M
onot
hera
py51
.1%
rec
urre
nces
Cry
osur
gery
Fikr
le a
nd P
izin
ger
[23]
n=
7/n
=11
Mon
othe
rapy
0% r
ecur
renc
es10
0% r
educ
tion
of s
car
volu
me
Rus
cian
i eta
l. [4
8]n
=13
5/n
=16
6M
onot
hera
py0%
rec
urre
nces
6% u
nsat
isfa
ctor
y vo
lum
e re
duct
ion
123

1506 Eur Arch Otorhinolaryngol (2007) 264:1497–1508
often be diYcult, so frequently special pressure earringswith silicone backing are used as important therapeuticadjuncts for the prevention of recurrence after surgical ther-apy of earlobe keloids [1]. More recently, a silicone gel hasbecome available which makes application on other, morediYcult localizations of the auricle possible. Furthermore,silicone gel sheeting is especially useful in children as wellas those who cannot tolerate other therapeutic procedures.
Radiation therapy
A further important pillar in keloid therapy, mainly as adju-vant treatment to prevent recurrence, is radiation therapy.
Mode of action
It has been hypothesized that Wbroblasts, connective tissuestem cells and acute imXammatory cells are destroyed. Inthis way, a balance between collagen formation and degra-dation can be created [2, 11, 19].
Application
Radiation therapy is most promising as a preventative pro-cedure when it is applied immediately, ideally on the day ofactual surgery or at the latest within 48 h after surgicalexcision. Descriptions of single doses, cumulative dosesand intervals between applications diVer in the literature.These range from 3 to 10 Gy either single or multiple (3–4)fractions [19, 34, 58]. The combination of surgical excisionwith adjuvant radiotherapy can obtain satisfactory cosmeticresults without recurrence in up to 97% [6, 11, 19, 31, 40,47]. Radiation monotherapy, however, is less eVective [34].
Ragoowansi et al. [46] treated 35 patients with earlobekeloids which showed no regression after conservativetreatment. A complete surgical excision was followed by asingle fraction with 10 Gy within 24 h after the operation.This management led to a therapeutic success rate of 79.4%of all cases without recurrence in 5 years [46]. Similarlyencouraging results regarding earlobe keloid treatment withsurgical excision and adjuvant radiotherapy have beenreported by others as well [11, 19, 52].
Side eVects
Important after-eVects are hyperpigmentation, pruritus anderythema [2, 19, 52]. Furthermore, uncertainty exists as tothe carcinogenic eVects of radiation therapy. Keloid is abenign lesion and most patients are young, so radiationtherapy is recommended critically [19] and contraindicatedin pediatric and pregnant patients [2].
One case of medullary carcinoma of the thyroid in an 11-year-old child which appeared 8 years after surgery andpostoperative radiation therapy of a chin keloid and onecase of bilateral breast carcinoma 30 years after treatmentof chest wall keloids are described in the literature [7, 11,31]. Recently, Mizuno et al. [42] reported a squamous cellcarcinoma of the auricle 30 years after keloid excision andpostoperative radium needle therapy, however. Furtherreports regarding an increased incidence of malignanttumors are lacking [31].
Evaluation
Clearly, radiotherapy as an adjuvant therapeutic option inkeloid treatment has produced encouraging results withrespect to reduced recurrence rates. The small risk of devel-oping a radiation-induced malignant tumor must always beconsidered when treating young patients with low-doseadjuvant radiotherapy. Furthermore, the eVectiveness ofsurgery with postoperative radiotherapy is comparable topostoperative corticosteroid injection [52].
Conclusion
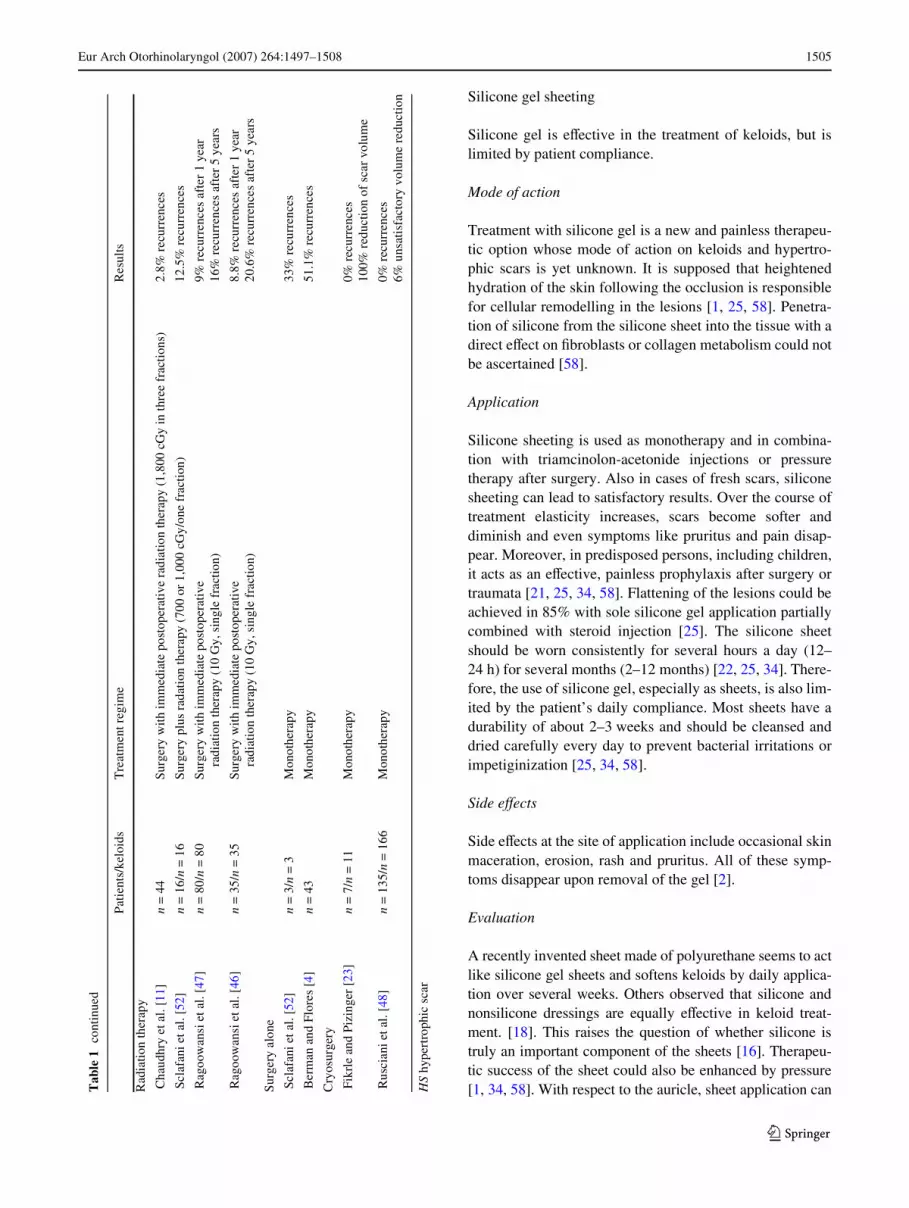
Auricular keloids can develop as a result of otoplasty, earpiercing or skin trauma. Initial and small keloids can beeVectively treated with steroid injection or silicone sheet-ing. In the case of more extensive lesions, surgical interven-tion is the primary therapeutic management option. Table 1summarizes the treatment strategies and therapeutic resultsof the cited studies. Figure 4 shows an algorithm that mayhelp to Wnd the customized treatment for the individualpatient.
Fig. 4 Proposal for a therapeu-tic algorithm
?
Primary keloid
Large keloid (disturbing cosmetics)
Small keloid (no disturbing
cosmetics)
Intralesionalsteroid
injection,
Siliconesheeting,
Pressuretherapy
+
Radiotherapy
Experimentalmethods:
Verapamil
Mitomycin C
Interferon
Imiquimod etc. Surgery
Surgery
Auricularkeloid
Recurrentkeloid
123

Eur Arch Otorhinolaryngol (2007) 264:1497–1508 1507
For prevention of local recurrence, various modalitiessuch as silicone sheeting, pressure therapy, radiation ther-apy and several medical therapeutic options exist. Sinceeach of these diVer with respect to therapeutic success andside eVects, it is imperative that therapy is adjusted on anindividual basis. Consistent aftercare and good patient com-pliance is also mandatory to ensure the expeditious treat-ment of potential recurrence.
References
1. Aköz T, Gideroglu K, Akan M (2002) Combination of diVerenttechniques for the treatment of earlobe keloids. Aesthetic PlastSurg 26:184–188
2. Al-Attar A, Mess S, Thomassen JM, KauVman CL, Davison SP(2006) Keloid pathogenesis and treatment. Plast Reconstr Surg117:286–300
3. Apikian M, Goodman G (2004) Intralesional 5-Xuorouracil in thetreatment of keloid scars. Australas J Dermatol 45:140–143
4. Berman B, Flores F (1997) Recurrence rates of excised keloidstreated with postoperative triamcinolone acetonide injections orinterferon alfa-2b injections. J Am Acad Dermatol 37:755–757
5. Berman B, Kaufman J (2002) Pilot study of the eVect of postoper-ative imiquimod 5% cream on the recurrence rate of excised ke-loids. J Am Acad Dermatol 47:S209–S211
6. Borok TL, Bray M, Sinclair I, Plafker J, Labirth L, Rollins C(1988) Role of ionizing irradiation for 393 keloids. Int J RadiatOncol Biol Phys 15:865–870
7. Botwood N, Lewanski C, Lowdell C (1999) The risks of treatingkeloids with radiotherapy. Br J Radiol 72:1222–1224
8. Brent B (1978) The role of pressure therapy in management of ear-lobe keloids. Ann Plast Surg 1:579–581
9. Brown LA, Pierce HE (1986) Keloids: scar revision. J DermatolSurg Oncol 12:51–56
10. Buchwald C, Nielsen LH, Rosborg J (1992) Keloids of the exter-nal ear. ORL J Otorhinolaryngol Relat Spec 54:108–112
11. Chaudhry MR, Akhtar S, Duvalsaint F, Garner L, Lucente FE(1994) Ear lobe keloids, surgical excision followed by radiationtherapy: a 10-year experience. Ear Nose Throat J 73:779–781
12. Chen T, Kunnavatana SS, Koch RJ (2006) EVects of mitomycin-Con normal dermal Wbroblasts. Laryngoscope 116:514–517
13. Chowdri NA, Masarat M, Mattoo A, Darzi MA (1999) Keloidsand hypertrophic scars: results with intraoperative and serial post-operative corticosteroid injection therapy. Aust N Z J Surg69:655–659
14. Cohen IK, Diegelmann RF, Johnson ML (1977) EVect of corticos-teroids on collagen synthesis. Surgery 82:15–20
15. Copcu E, Sivrioglu N, Oztan Y (2004) Combination of surgeryand intralesional verapamil injection in the treatment of the keloid.J Burn Care Rehabil 25:1–7
16. D’Andrea F, Brongo S, Ferraro G, Baroni A (2002) Prevention andtreatment of keloids with intralesional verapamil. Dermatology204:60–62
17. Davison SP, Mess S, KauVman LC, Al-Attar A (2006) IneVectivetreatment of keloids with interferon alpha-2b. Plast Reconstr Surg117:247–252
18. de Oliveira GV, Nunes TA, Magna LA, Cintra ML, Kitten GT,Zarpellon S, Raposo Do Amaral CM (2001) Silicone versus non-silicone gel dressings: a controlled trial. Dermatol Surg 27:721–726
19. Dinh Q, Veness M, Richards S (2004) Role of adjuvant radiother-apy in recurrent earlobe keloids. Australas J Dermatol 45:162–166
20. Ehrlich HP, Desmouliere A, Diegelmann RF, Cohen IK, ComptonCC, Garner WL, Kapanci Y, Gabbiani G (1994) Morphologicaland immunochemical diVerences between keloid and hypertrophicscar. Am J Pathol 145:105–113
21. Eishi K, Bae SJ, Ogawa F, Hamasaki Y, Shimizu K, Katayama I(2003) Silicone gel sheets relieve pain and pruritus with clinicalimprovement of keloid: possible target of mast cells. J DermatologTreat 14:248–252
22. Englisch RS, Shenefelt PD (1999) Keloids and hypertrophic scars.Dermatol Surg 25:631–638
23. Fikrle T, Pizinger K (2005) Cryosurgery in the treatment of ear-lobe keloids: report of seven cases. Dermatol Surg 31:1728–1731
24. Fitzpatrick RE (1999) Treatment of inXamed hypertrophic scarsusing intralesional 5-FU. Dermatol Surg 25:224–232
25. Fulton JE (1995) Silicone gel sheeting for the prevention and man-agement of evolving hypertrophic and keloid scars. Dermatol Surg21:947–951
26. Funayama E, Chodon T, Oyama A, Sugihara T (2003) Keratino-cytes promote proliferation and inhibit apoptosis of the underlyingWbroblasts: an important role in the pathogenesis of keloid. J InvestDermatol 121:1326–1331
27. Giugliano G, Pasquali D, Notaro A, Brongo S, Nicoletti G, D’An-drea F, Bellastella A, Sinisi AA (2003) Verapamil inhibits inter-leukin-6 and vascular endothelial growth factor production inprimary cultures of keloid Wbroblasts. Br J Plast Surg 56:804–809
28. Granstein RD, Rook A, Flotte TJ, Haas A (1990) A controlled trialof intralesional recombinant interferon-� in the treatment of keloi-dal scarring. Arch Dermatol 126:1295–1301
29. Grimes PE, Hunt SG (1993) Considerations for cosmetic surgeryin the black population. Clin Plast Surg 20:27–34
30. Gupta S, Kalra A (2002) EYacy and safety of intralesional 5-Xourouracil in the treatment of keloids. Dermatology 204:130–132
31. Hackert I, AschoV R, Sebastian G (2003) Keloide und ihre Thera-pie. Hautarzt 54:1003–1015
32. Hatoko M, Kuwahara M, Shiba A, Tada H, Okazaki T, MuramatsuT, Shirai T (1998) Earlobe reconstruction using a subcutaneous is-land pedicle Xap after resection of “earlobe keloid”. DermatolSurg 24:257–261
33. Jemec B, Linge C, Grobbelaar AO, Smith PJ, Sanders R, McGrou-ther DA (2000) The eVect of 5-Xuorouracil on Dupuytren Wbro-blast proliferation and diVerentiation. Chir Main 19:15–22
34. Kelly AP (2004) Medical and surgical therapies for keloids.Dermatol Ther 17:212–218
35. Kim JY, Stewart CE (2004) Application of Mitomycin-C for headand neck keloids. Otolaryngol Head Neck Surg 131(2):P73
36. Kim DY, Kim ES, Eo SR, Kim KS, Lee SY, Cho BH (2004) A sur-gical approach for earlobe keloid: keloid Wllet Xap. Plast ReconstrSurg 113:1668–1674
37. Lawrence WT (1996) Treatment of earlobe keloids with surgeryplus adjuvant intralesional verapamil and pressure earrings. AnnPlast Surg 37:167–169
38. Lee RC, Ping JA (1990) Calcium antagonists retard extracellularmatrix production in connective tissue equivalent. J Surg Res49:463–466
39. Lee J, Yang CC, Chao SC, Wong TW (2004) HistopathologicaldiVerential diagnosis of keloid and hypertrophic scar. Am JDermatopathol 26:379–384
40. Mall JW, Pollmann C, Müller JM, Buttemeyer R (2002) Keloidbil-dung des Ohrläppchens nach Ohrlochstechen. Chirurg 73:514–516
41. Martin-García RF, Busquets AC (2005) Postsurgical use of imiq-uimod 5% cream in the prevention of earlobe keloid recurrences:results of an open-label, pilot study. Dermatol Surg 31:1394–1398
42. Mizuno H, Cagri Uysal A, Koike S, Hyakusoku H (2006) Squa-mous cell carcinoma of the auricle arising from keloid after radiumneedle therapy. J Craniofac Surg 17:360–362
123

1508 Eur Arch Otorhinolaryngol (2007) 264:1497–1508
43. Mustoe TA, Cooter RD, Gold MH, Hobbs FD, Ramelet AA,Shakespeare PG, Stella M, Teot L, Wood FM, Ziegler UE (2002)International clinical recommendations on scar management. PlastReconstr Surg 110:560–571
44. Nanda S, Reddy BS (2004) Intralesional 5-Xuorouracil as a treat-ment modality of keloids. Dermatol Surg 30:54–57
45. Nason KH (1942) Keloids and their treatment. N Engl J Med226:883–886
46. Ragoowansi R, Cornes PG, Glees JP, Powell BW, Moss AL(2001) Ear-lobe keloids: treatment by a protocol of surgical exci-sion and immediate postoperative adjuvant radiotherapy. Br J PlastSurg 54:504–508
47. Ragoowansi R, Cornes PG, Moss AL, Glees JP (2003) Treatmentof keloids by surgical excision and immediate postoperative sin-gle-fraction radiotherapy. Plast Reconstr Surg 111:1853–1859
48. Rusciani L, Paradisi A, Alfano C, Chiummariello S, Rusciani A(2006) Cryotherapy in the treatment of keloids. J Drugs Dermatol5:591–595
49. Saha SS, Kumar V, Khazanchi RK, Aggarwal A, Garg S (2004)Primary skin grafting in ear lobule keloid. Plast Reconstr Surg114:1204–1207
50. Sanders KW, Gage-White L, Stucker FJ (2005) Topical mitomy-cin C in the prevention of keloid scar recurrence. Arch Facial PlastSurg 7:172–175
51. Saray Y, Gulec AT (2005) Treatment of keloids and hypertrophicscars with dermojet injections of bleomycin: a preliminary study.Int J Dermatol 44:777–784
52. Sclafani AP, Gordon L, Chadha M, Romo T III (1996) Preventionof earlobe keloid recurrence with postoperative corticosteroidinjections versus radiation therapy: a randomized, prospectivestudy and review of the literature. Dermatol Surg 22:569–574
53. Shons AR, Press BH (1983) The treatment of earlobe keloids bysurgical excision and postoperative triamcinolone injection. AnnPlast Surg 10:480–482
54. Simman R, Alani H, Williams F (2003) EVect of mitomycin C onkeloid Wbroblasts: an in vitro study. Ann Plast Surg 50:71–76
55. Stashower ME (2006) Successful treatment of earlobe keloidswith imiquimod after tangential shave excision. Dermatol Surg32:380–386
56. Stewart CE IV, Kim JY (2006) Application of mitomycin-C forhead and neck keloids. Otolaryngol Head Neck Surg 135:946–950
57. Talmi YP, Orenstein A, Wolf M, Kronenberg J (2005) Use ofmitomycin C for treatment of keloid: a preliminary report. Otolar-yngol Head Neck Surg 132:598–601
58. Worret WI, Vogt HJ (2004) Narbentherapie in der Dermatologie.Dtsch Arztebl 101:2819–2824
59. Wu WS, Wang FS, Yang KD, Huang CC, Kuo YR (2006)Dexamethasone induction of keloid regression through eVectivesuppression of VEGF expression and keloid Wbroblast prolifera-tion. J Invest Dermatol 126:1264–1271
60. Xia W, Phan TT, Lim IJ, Longaker MT, Yang GP (2004) Complexepithelial–mesenchymal interactions modulate transforminggrowth factor-beta expression in keloid-derived cells. Wound Re-pair Regen 12:546–556
61. Xia W, Phan TT, Lim IJ, Longaker MT, Yang GP (2006) DiVer-ential transcriptional responses of keloid and normal keratinocytesto serum stimulation. J Surg Res 135:156–163
62. Ziccardi VB, Lamphier J (2000) Use of keloid skin as an autograftfor earlobe reconstruction after excision. Oral Surg Oral Med OralPathol Oral Radiol Endod 89:674
123