the roles of persistence and perseveration in psychopathology
TRANSCRIPT
www.elsevier.com/locate/bt
Available online at www.sciencedirect.com
Behavior Therapy 40 (2009) 260–271
The Roles of Persistence and Perseveration in Psychopathology
Lucy SerpellUniversity College London and Central and North West London NHS Foundation Trust
Glenn WallerInstitute of Psychiatry, King's College London, and Central and North West London
NHS Foundation Trust
Pasco FearonUniversity of Reading
Caroline MeyerUniversity of Loughborough
Two constructs were hypothesized to be of importance inpsychological disorders: persistence (the ability to keepgoing to reach a goal, even when the task is difficult ordrawn out) and perseveration (the tendency to continue abehavior, even when it ceases to be effective or rewarding).These are contrasted with perfectionism (having highstandards for oneself or others). A measure was developedto address these constructs (the Persistence, Perseverationand Perfectionism Questionnaire; PPPQ). The PPPQ wasadministered to 325 nonclinical participants, alongside ameasure of psychological disturbance. Factor analysisresulted in a 22-item version of the measure, consisting ofsubscales with good psychometric properties correspondingto the 3 theoretical constructs. Persistence was associatedwith lower levels of psychopathology, whereas persevera-
Research reported in this paper was submitted for the Doctoratein Clinical Psychology at University College London by the firstauthor. The authors would like to thank Janet Feigenbaum,Howard Steele, Ann Schlotmann and Nick Harrison for help withrecruitment.
Address correspondence to Lucy Serpell, Research Department ofClinical, Educational&HealthPsychology,UniversityCollegeLondon,1-19 Torrington Place, LondonWC1E 7HB; e-mail: [email protected]/08/0260–0271$1.00/0© 2008 Association for Behavioral and Cognitive Therapies. Published byElsevier Ltd. All rights reserved.
tion was associated with higher levels of psychopathology.Perfectionism was weakly associated with psychopathology.Further work is needed to develop these constructs withclinical groups, but the findings support the hypothesis thatpersistence is an adaptive construct whereas perseveration ismaladaptive.
The Roles of Persistence and Perseverationin PsychopathologyPersonality and cognitive styles have commonlybeen found to be associated with different domainsof psychopathology (Arnkoff & Glass, 1982;Ingram & Kendall, 1992; Macleod & Mathews,1991; Marcus, Gurley, Marchi, & Bauer, 2007;Zohar, LaBuda, & Moschel-Ravid, 1995). Onesuch domain is the pattern of compulsivity thatunderpins many psychological disorders. Thatpattern underlies the behaviors that are found indisorders such as obsessive-compulsive disorder,compulsive exercise, eating disorders, and neurolo-gical disorders (Ames, Cummings, Wirshing, Quinn,& Mahler, 1994; Davis, Kapstein, Kaplan,Olmsted, & Woodside, 1998; Matsunaga, Kiriike,Iwasaki, Yamagami, & Kaye, 1999; Serpell, Hirani,Willoughby, Neiderman, & Lask, 2006; Serpell,

261p er s i s t ence and pers everat ion
Livingstone, Neiderman, & Lask, 2002). It has beensuggested that the core pathology behind suchbehaviors is perfectionism (Bulik et al., 2003;Enns, Cox, & Clara, 2002; Frost & Steketee,1997; Shafran, Cooper, & Fairburn, 2002; Shafran& Mansell, 2001). However, perfectionism canalso be an adaptive characteristic (Bieling, Israeli,& Antony, 2004; Chang, Watkins, & Banks,2004; Vitousek, 2003). Instead of simply treatingcompulsivity as a manifestation of perfectionism, itmay be useful to consider the functions of thecompulsive behaviors. One such function is theability to keep going with a behavior or activity toreach a goal, even when the task is difficult or takesa long time—persistence. A contrasting function isthe tendency to continue a particular learnedresponse or behavior, even when it ceases to berewarding—perseveration. Different definitions andmeasures of perfectionism appear to contain differ-ent degrees of each of these constructs, potentiallyexplaining why different measures of perfectionismfail to correlate well and why perfectionism ispresented as either adaptive or maladaptive indifferent models (Chang et al., 2004; Davis, 1997;Enns et al., 2002; Shafran et al., 2002; Terry-Short,Owens, Slade, & Dewey, 1995).As defined here, persistence overlaps with the
concept of sustained attention, as described byBarkley (1997). In keeping with learned indus-triousness theory (Eisenberger, Kuhlman, & Cot-terell, 1992), task persistence is linked with ahistory of reward for high levels of effort. It canbe seen as an adaptive trait, which is associatedwith targeted, goal-related behaviors. For example,there is evidence that high persistence is a positivetrait, associated with success in a smoking-cessationtrial (Brandon, Herzog, Juliano, Irvin, & Lazev,2003). Another way of conceptualizing persistenceis in terms of Perceptual Control Theory (PCT;Carver & Scheier, 1982; Mansell, 2005; Powers,1973). This theory suggests that behavior ismanaged using a hierarchical goal structure,wherein lower-order goals are directed in theservice of higher-order goals. Successfully mana-ging the pursuit of goals requires flexible awarenessthroughout the hierarchy. It is suggested that thiskind of flexible awareness is demonstrated withinpersistent responding, whereas perseverationinvolves either the pursuit of lower-order goals atthe expense of keeping higher-order goals in mind,or (even more problematically) the pursuit of abehavior which was originally intended to meet agoal, but without continuing to consider whetherthe goal has been met or is still relevant.Perseveration is broadly a maladaptive trait.
Although it can be seen in neurological damage
(Ames et al., 1994), perseveration is also acharacteristic of functional disorders. It is mostclearly seen in the safety-seeking behaviors thatcharacterize the anxiety disorders (e.g., Salkovskis,1996; Salkovskis, Clark, Hackmann, Wells, &Gelder, 1999) and in superstitious behaviors.Safety-seeking behaviors are behaviors that areused to prevent threat from being realized, but thathave the side effect of preventing disconfirmation ofunrealistic fears (Salkovskis, 1996). However,perseveration cannot be as easily applied to under-standing the repetitive behaviors seen in obsessive-compulsive disorder, as that disorder is motivatedby an attempt (albeit misguided) to achieve thehigher-order goal of avoiding future negativeconsequences.To summarize, persistence is the ability to
continue with an activity in order to reach ahigher-order goal, even when the task is arduousor lasts for a long time (Lufi & Cohen, 1987). It ismore likely to be voluntary (i.e., under some degreeof conscious control). In contrast, perseveration isthe tendency to continue with a particular behavioror activity beyond the point at which the behaviorceases to be appropriate or rewarding. This is arelatively automatic process, which is not underconscious control. The behaviors characteristic ofpersistence and perseveration may be superficiallysimilar, but the cognitive components differ mark-edly. For example, someone who brushes their teethfor 5 minutes might be persistent (deciding to do sofor a long time because it is seen to be necessary,even if arduous or boring) or might be perseverant(i.e., continuing because once the activity hasstarted, it has a tendency to be continued ratherthan stopped).Given this model, we hypothesize that persis-
tence and perseveration will form distinct factors.Those factors will have different levels ofadaptiveness, and hence, different patterns ofassociation with psychopathology. Persistence islikely to be a protective factor, whereas perse-veration is likely to be a vulnerability factor forpsychological distress. As no measure exists thatcontrasts these two constructs directly, the currentresearch attempted to develop a self-report mea-sure of persistence and perseveration andvalidate it against a measure of psychopathologicalcharacteristics in a nonclinical group of youngadults.
MethodEthical approval for the study was obtained fromthe local Research Ethics Committee, working tostandards compatible with those of the American

262 s erpe ll e t al .
Psychological Association and the British Psycho-logical Society.
participants
To ensure a sufficient sample for factor analysis(Mundfrom, Shaw, & Ke, 2005), a sample of 325participants completed the measures. This sampleconsisted of undergraduate and postgraduatestudents (51.1%) and adults in full- or part-timeemployment (48.9%). Student participants wererecruited by attending lectures and asking for theirparticipation. Questionnaire packs were handedout, and students were asked to return them usinginternal university mail. A cover sheet was includedon which participants could provide contact detailsto be entered into a drawing to win a £25 booktoken. Nonstudents were recruited via email—friends and acquaintances of the first author wereemailed to request their participation with ques-tionnaires sent as an attachment. They were alsoasked to pass on the questionnaire pack to theirown friends and acquaintances. Questionnairepacks could be returned by email or post. Allemailed responses were printed out for data entryand to maintain anonymity. The respondents’meanage was 22.4 years (SD=6.64), and 254 (78.2%)were female.
measures
Development of the self-report measure of persis-tence and perseveration. An initial pool of itemswas generated by the researchers to reflect theconstructs of persistence and perseveration. Inorder to determine whether these constructs weresufficiently well defined that they could be distin-guished from perfectionism, items were generatedthat reflected that construct. The perfectionismitems aimed to be heterogeneous, covering differentaspects of perfectionism (including high personalstandards, concern over mistakes and the impor-tance of organization and order1). Eleven itemswere generated for each construct.The 33 resulting items were given to 27
independent raters, who were educated to at leastthe graduate level and were naïve to the hypothesesof the study. These individuals were given theconstruct definitions (as outlined in the Introduc-tion and above) and were asked to rate each of the33 items according to how well it matched each ofthe three constructs, using a Likert-type scale
1 It should be noted that one item that was generated for thismeasure (qOne of my goals is to be perfect in everything I doq) is thesame as an item on the Hewitt-Flett Multidimensional Perfection-ism Scale (Hewitt & Flett, 1991). This items was generated withoutreference to that previous scale.
(1=does not fit the definition at all; 7= fits thedefinition very well). Items were retained if themean rating on one of the constructs was greaterthan 5 and if this mean was at least one standarddeviation above the mean ratings on both of theother two constructs. Five items failed to meet thesecriteria, indicating that they were not as distinctiveas necessary. Thus, 28 items were retained (11reflecting persistence, 8 reflecting perseveration,and 9 reflecting perfectionism), which were rela-tively distinct and pure descriptors of the construct.Those 28 items are given in Table 2. Each was ratedby the sample of 325 participants, using a 5-pointLikert-type scale (0=not at all true of me; 5= totallytrue of me).Brief Symptom Inventory (BSI; Derogatis, 1993;
Derogatis & Melisaratos, 1983). In addition tothose 28 items, the participants completed the BSI.The BSI is a short version of the SymptomChecklist-90 (SCL-90; Derogatis, Lipman, Rickels,Uhlenhuth, & Covi, 1974; Derogatis, Rickels, &Rock, 1976), a well-validated measure of a range ofpsychiatric symptoms. The BSI consists of 53 items,which make up nine subscales (Somatization,Obsessive-Compulsive, Interpersonal Sensitivity,Depression, Anxiety, Hostility, Phobic Anxiety,Paranoid Ideation, Psychoticism). It is also possibleto calculate a Global Severity Index, which is ameasure of overall symptom severity on allsubscales. The BSI has good psychometric proper-ties (Derogatis, 1993; Derogatis et al., 1976).
procedure
Student participants returned the two measures bymail. Nonstudent participants returned the ques-tionnaires by email. The response rate was 34%.For test-retest purposes, a subset of participantswere asked to complete the measure of persistence,perseveration and perfectionism again (between 7and 14 days after they had originally completed it).Fifty-two participants (a mixture of students andnonstudents) were contacted for this purpose, and42 (80.8%) completed and returned the measure.
data analysis
All analyses were conducted using SPSS (v. 11.0).Factor analysis was used to establish the factorstructure of the new measure. Exploratory factoranalysis was used (rather than principal componentsanalysis), as the goal was to explore the multivariatefactor structure of the measure, rather than to reducethe number of items (Floyd & Widaman, 1995). Avarimax rotation was used for the final solution, asthis yielded a more meaningful outcome than theunrotated solution. A non-orthogonal solution(direct oblimin) failed to converge. Cronbach's

263p er s i s t ence and pers everat ion
alpha was calculated to determine the internalconsistency of subscales, and test-retest reliabilitywas determined using Pearson's correlations andpaired-sample t-tests. Finally, multiple linear regres-sion was used to establish the relationship betweenthe resultant scales and psychopathology (i.e., BSIsubscale scores).
Resultssample characteristics
Table 1 shows the participants’ means on the BSIscales, comparing them with published norms(Derogatis & Melisaratos, 1983). Their scoreswere in the nonclinical range, as one would expectfor this group. In keeping with the sample's meanage, their mean BSI scores generally fell between thenorms for adolescents and adults.
factor analysis
Factors were included if they had eigenvaluesgreater than 1 and if examination of the scree plotindicated that it was appropriate to do so. A three-factor solution was the most appropriate, inkeeping with the study's hypothesis (distinct factorsof persistence, perseveration and perfectionism).Therefore, the analysis was repeated, this timeforcing a three-factor solution (with a varimaxrotation) and imposing a cut-off of a factor loadingof .40 for each item to be included. If an item loadedon more than one factor at .40 or greater, it wasincluded in the factor on which its loading washighest, unless the two loadings were close toidentical. The loadings of the 28 items on each of
Table 1Levels of psychopathology (mean scores and SDs) on Brief Sympt
Measure Current study(N=325)
DemographicsAge (years) 22.4 (6.64)Gender 21.8% male
BSI subscaleGlobal 0.63 (0.51)Somatization 0.45 (0.55)Obsessive-compulsive 1.01 (0.69)Interpersonal sensitivity 0.91 (0.85)Depression 0.68 (0.74)Anxiety 0.66 (0.64)Hostility 0.62 (0.61)Phobic anxiety 0.30 (0.56)Paranoid ideation 0.62 (0.69)Psychoticism 0.49 (0.64)
Notes. BSI=Brief Symptom Inventory. Nonpatient norms from Derogatis
the three factors are shown in Table 2. All itemloadings were positive, indicating that there wereno items that needed to be reverse-scored. Factor 1corresponded to the hypothesised construct ofPersistence, Factor 2 corresponded to the constructof Perseveration, and Factor 3 corresponded toPerfectionism. Therefore, those labels are usedhereafter for the scales.Six items were removed from the measure at this
point (see Table 2). Two items had loadings belowthe cut-off on all three scales and were removedfrom consideration. A further three items loadedonto two scales at roughly similar levels and weretherefore not clear descriptors of a distinct con-struct. One item was deleted because it wasoriginally developed to be a perseveration item,but it loaded more strongly on the perfectionismfactor. After removal of these six items, Cronbach'salphas for the three subscales were calculated, andare shown in Table 2. The internal consistency ofeach scale was acceptable, although the Cronbach'salpha for Factor 2 (Perseveration) was slightlybelow the level of 0.7 suggested by Nunnally(1978). Removing the item with the lowest item-total correlation did not improve the internalconsistency of this subscale.Intercorrelations between subscales were gener-
ally statistically significant, but low to moderate insize (persistence-perseveration: r=.22, pb .01; per-sistence-perfectionism: r=.47, pb .01; persevera-tion-perfectionism: r=.39, pb .01), suggesting thatthe subscales are reasonably independent and thatthey measure sufficiently distinct constructs. It isnoteworthy that the persistence-perseveration
om Inventory scales and comparison with nonpatient norms
Adult nonpatientnorms (N=974)
Adolescent nonpatientnorms (N=2402)
46.0 (14.7) 15.8 (1.10)50.7% male 66.5% male
0.30 (0.31) 0.83 (0.59)0.29 (0.40) 0.63 (0.64)0.43 (0.48) 0.94 (0.75)0.32 (0.48) 0.99 (0.84)0.28 (0.46) 0.82 (0.79)0.35 (0.45) 0.78 (0.68)0.35 (0.42) 1.02 (0.86)0.17 (0.36) 0.54 (0.64)0.34 (0.45) 1.13 (0.82)0.15 (0.30) 0.73 (0.73)
& Melisaratos (1983).
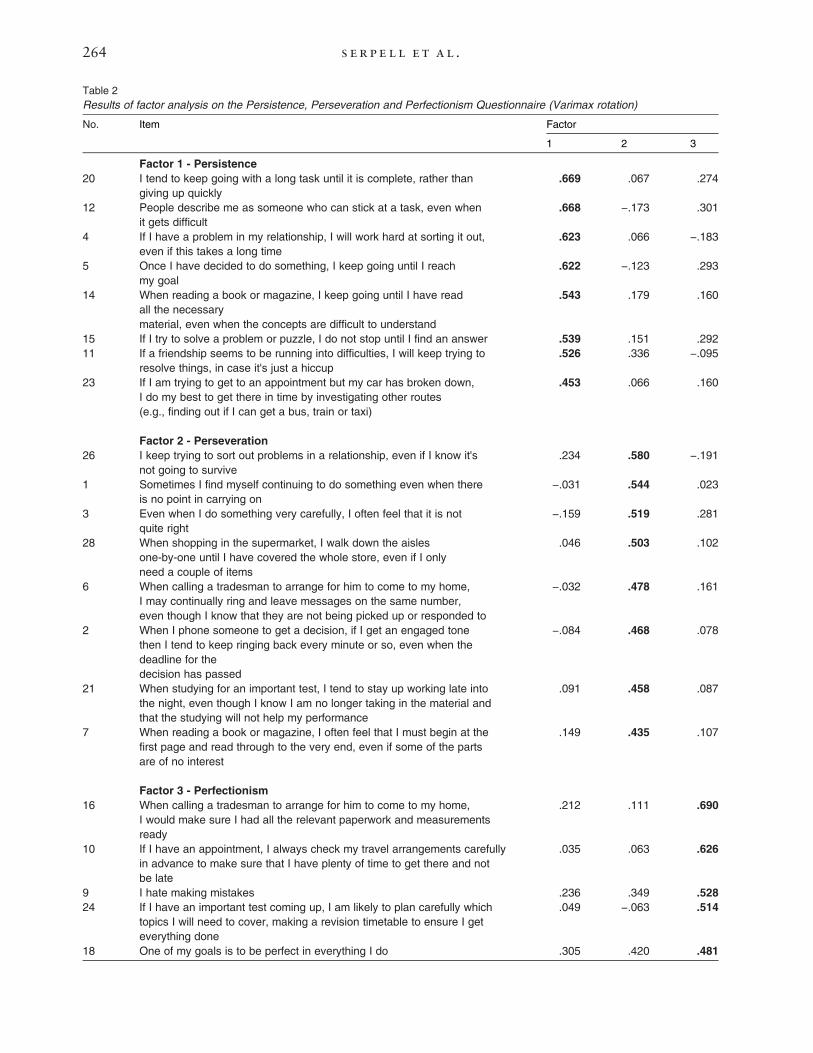
Table 2Results of factor analysis on the Persistence, Perseveration and Perfectionism Questionnaire (Varimax rotation)
FactorNo. Item
1 2 3
Factor 1 - Persistence
20 I tend to keep going with a long task until it is complete, rather thangiving up quickly
.669 .067 .274
12 People describe me as someone who can stick at a task, even whenit gets difficult
.668 −.173 .301
4 If I have a problem in my relationship, I will work hard at sorting it out,even if this takes a long time
.623 .066 −.183
5 Once I have decided to do something, I keep going until I reachmy goal
.622 −.123 .293
14 When reading a book or magazine, I keep going until I have readall the necessarymaterial, even when the concepts are difficult to understand
.543 .179 .160
15 If I try to solve a problem or puzzle, I do not stop until I find an answer .539 .151 .29211 If a friendship seems to be running into difficulties, I will keep trying to
resolve things, in case it's just a hiccup.526 .336 −.095
23 If I am trying to get to an appointment but my car has broken down,I do my best to get there in time by investigating other routes(e.g., finding out if I can get a bus, train or taxi)
.453 .066 .160
Factor 2 - Perseveration
26 I keep trying to sort out problems in a relationship, even if I know it'snot going to survive
.234 .580 −.191
1 Sometimes I find myself continuing to do something even when thereis no point in carrying on
−.031 .544 .023
3 Even when I do something very carefully, I often feel that it is notquite right
−.159 .519 .281
28 When shopping in the supermarket, I walk down the aislesone-by-one until I have covered the whole store, even if I onlyneed a couple of items
.046 .503 .102
6 When calling a tradesman to arrange for him to come to my home,I may continually ring and leave messages on the same number,even though I know that they are not being picked up or responded to
−.032 .478 .161
2 When I phone someone to get a decision, if I get an engaged tonethen I tend to keep ringing back every minute or so, even when thedeadline for thedecision has passed
−.084 .468 .078
21 When studying for an important test, I tend to stay up working late intothe night, even though I know I am no longer taking in the material andthat the studying will not help my performance
.091 .458 .087
7 When reading a book or magazine, I often feel that I must begin at thefirst page and read through to the very end, even if some of the partsare of no interest
.149 .435 .107
Factor 3 - Perfectionism
16 When calling a tradesman to arrange for him to come to my home,I would make sure I had all the relevant paperwork and measurementsready
.212 .111 .690
10 If I have an appointment, I always check my travel arrangements carefullyin advance to make sure that I have plenty of time to get there and notbe late
.035 .063 .626
9 I hate making mistakes .236 .349 .528
24 If I have an important test coming up, I am likely to plan carefully whichtopics I will need to cover, making a revision timetable to ensure I geteverything done
.049 −.063 .514
18 One of my goals is to be perfect in everything I do .305 .420 .481
264 s erpe ll e t al .
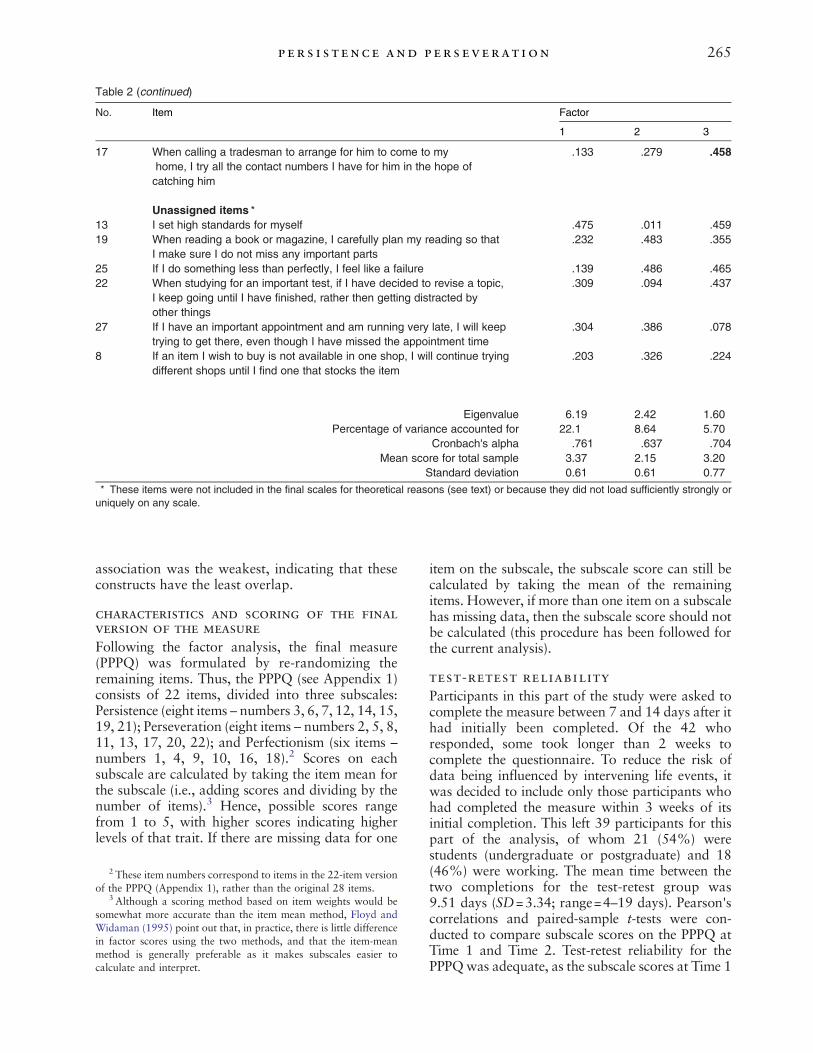
Table 2 (continued)
FactorNo. Item
1 2 3
17 When calling a tradesman to arrange for him to come to myhome, I try all the contact numbers I have for him in the hope ofcatching him
.133 .279 .458
Unassigned items ⁎13 I set high standards for myself .475 .011 .45919 When reading a book or magazine, I carefully plan my reading so that
I make sure I do not miss any important parts.232 .483 .355
25 If I do something less than perfectly, I feel like a failure .139 .486 .46522 When studying for an important test, if I have decided to revise a topic,
I keep going until I have finished, rather then getting distracted byother things
.309 .094 .437
27 If I have an important appointment and am running very late, I will keeptrying to get there, even though I have missed the appointment time
.304 .386 .078
8 If an item I wish to buy is not available in one shop, I will continue tryingdifferent shops until I find one that stocks the item
.203 .326 .224
Eigenvalue 6.19 2.42 1.60Percentage of variance accounted for 22.1 8.64 5.70
Cronbach's alpha .761 .637 .704Mean score for total sample 3.37 2.15 3.20
Standard deviation 0.61 0.61 0.77
⁎ These items were not included in the final scales for theoretical reasons (see text) or because they did not load sufficiently strongly oruniquely on any scale.
265p er s i s t ence and pers everat ion
association was the weakest, indicating that theseconstructs have the least overlap.
characteristics and scoring of the finalversion of the measure
Following the factor analysis, the final measure(PPPQ) was formulated by re-randomizing theremaining items. Thus, the PPPQ (see Appendix 1)consists of 22 items, divided into three subscales:Persistence (eight items – numbers 3, 6, 7, 12, 14, 15,19, 21); Perseveration (eight items – numbers 2, 5, 8,11, 13, 17, 20, 22); and Perfectionism (six items –numbers 1, 4, 9, 10, 16, 18).2 Scores on eachsubscale are calculated by taking the item mean forthe subscale (i.e., adding scores and dividing by thenumber of items).3 Hence, possible scores rangefrom 1 to 5, with higher scores indicating higherlevels of that trait. If there are missing data for one
2 These item numbers correspond to items in the 22-item versionof the PPPQ (Appendix 1), rather than the original 28 items.
3 Although a scoring method based on item weights would besomewhat more accurate than the item mean method, Floyd andWidaman (1995) point out that, in practice, there is little differencein factor scores using the two methods, and that the item-meanmethod is generally preferable as it makes subscales easier tocalculate and interpret.
item on the subscale, the subscale score can still becalculated by taking the mean of the remainingitems. However, if more than one item on a subscalehas missing data, then the subscale score should notbe calculated (this procedure has been followed forthe current analysis).
test-retest reliability
Participants in this part of the study were asked tocomplete the measure between 7 and 14 days after ithad initially been completed. Of the 42 whoresponded, some took longer than 2 weeks tocomplete the questionnaire. To reduce the risk ofdata being influenced by intervening life events, itwas decided to include only those participants whohad completed the measure within 3 weeks of itsinitial completion. This left 39 participants for thispart of the analysis, of whom 21 (54%) werestudents (undergraduate or postgraduate) and 18(46%) were working. The mean time between thetwo completions for the test-retest group was9.51 days (SD=3.34; range=4–19 days). Pearson'scorrelations and paired-sample t-tests were con-ducted to compare subscale scores on the PPPQ atTime 1 and Time 2. Test-retest reliability for thePPPQwas adequate, as the subscale scores at Time 1

266 s erpe ll e t al .
and Time 2 were strongly and significantly corre-lated for persistence (r=.89, pb .001), perseveration(r=.79, pb .001) and perfectionism (r=.73, pb .001)and there was no significant difference in scores overtime (tb1.80; ns, in all cases).
relationship between pppq subscales anddemographic variables
Pearson's correlations were calculated between thePPPQ subscales and age. The alpha level was set to.01 to reduce the likelihood of a Type I errorresulting from multiple correlations. A significantnegative correlation was found between age andperseveration (r= -.29, pb .001), but no othercorrelations were significant. Nor were there anydifferences in PPPQ scores between the studentsand the nonstudents (MANCOVA, correcting forage differences between the groups). Finally, t-testsshowed no significant differences in PPPQ subscalescores across genders. To summarize, the onlyrelationship between demographic factors andPPPQ scores was a negative relationship betweenperseveration and age, indicating that perseverationis stronger at the younger end of this age range.
clinical validation: associations of pppqscores with psychopathology
Pearson's correlations were used to examine theindividual relationships between PPPQ and BSIsubscales (see Table 3). To reduce the risk of Type Ierrors, the acceptable alpha level was set at .01.Perseveration was associated with the greatestrange of BSI psychopathology scales, and perfec-tionism with slightly fewer. Persistence was notassociated with any elements of psychopathology.Given that the PPPQ scales were all associated
with each other, it was important to determine the
Table 3Correlations (Pearson's r) between subscales of the Brief Symptom IQuestionnaire
PPPQ scaleBSI scale
Persistence
Somatization .022Obsessive-compulsive −.014Interpersonal sensitivity −.027Depression −.125Anxiety .014Hostility −.053Phobic anxiety .054Paranoia .011Psychoticism −.049
Notes. BSI=Brief Symptom Inventory. PPPQ=Persistence, Perseverat⁎ Correlation is significant at the 0.05 level (2-tailed)
⁎⁎ Correlation is significant at the 0.01 level (2-tailed)
pattern of association when those intercorrelationswere accounted for. Therefore, multiple regressionanalysis was used to test the relationship betweenPPPQ subscales and psychopathology (i.e., BSIscales). Age was included as a potential predictor,given its association with perseveration (above).Table 4 shows the relationships between theindependent variables (PPPQ scales and age) andeach BSI scale. Only the statistically significantindependent variables are shown.Perseveration was consistently the best predictor
of psychopathology, as measured by the BSI (evenwhen the impact of age was taken into account). Itwas significantly positively associated with all BSIsubscales. Although perfectionism was positivelyassociated with some aspects of psychopathology(Global BSI, Obsessive-Compulsive, InterpersonalSensitivity, Depression, Phobic Anxiety, ParanoidIdeation), it was a less powerful factor thanperseveration. In contrast, persistence was negativelyassociatedwithmost types of psychopathology (highpersistence was associated with lower psychopathol-ogy scores on all but three BSI subscales).
DiscussionThis paper reports the development of a self-reportmeasure of persistence and perseveration, designedto distinguish those constructs that are adaptive/healthy and maladaptive/unhealthy in a nonclinicalgroup. The factor analysis demonstrated threefactors that were both psychometrically and clini-cally valid, corresponding to the hypothesizeddistinct constructs of persistence, perseverationand perfectionism. The three constructs wererelated to psychopathology in different ways,consistent with the hypothesis that perseveration
nventory and the Persistence, Perseveration and Perfectionism
Perseveration Perfectionism
.331 ⁎⁎ .136
.468 ⁎⁎ .192 ⁎
.395 ⁎⁎ .206 ⁎⁎
.330 ⁎⁎ .106
.385 ⁎⁎ .159 ⁎
.275 ⁎⁎ .084
.381 ⁎⁎ .236 ⁎⁎
.398 ⁎⁎ .197 ⁎⁎
.352 ⁎⁎ .124
ion and Perfectionism Questionnaire.
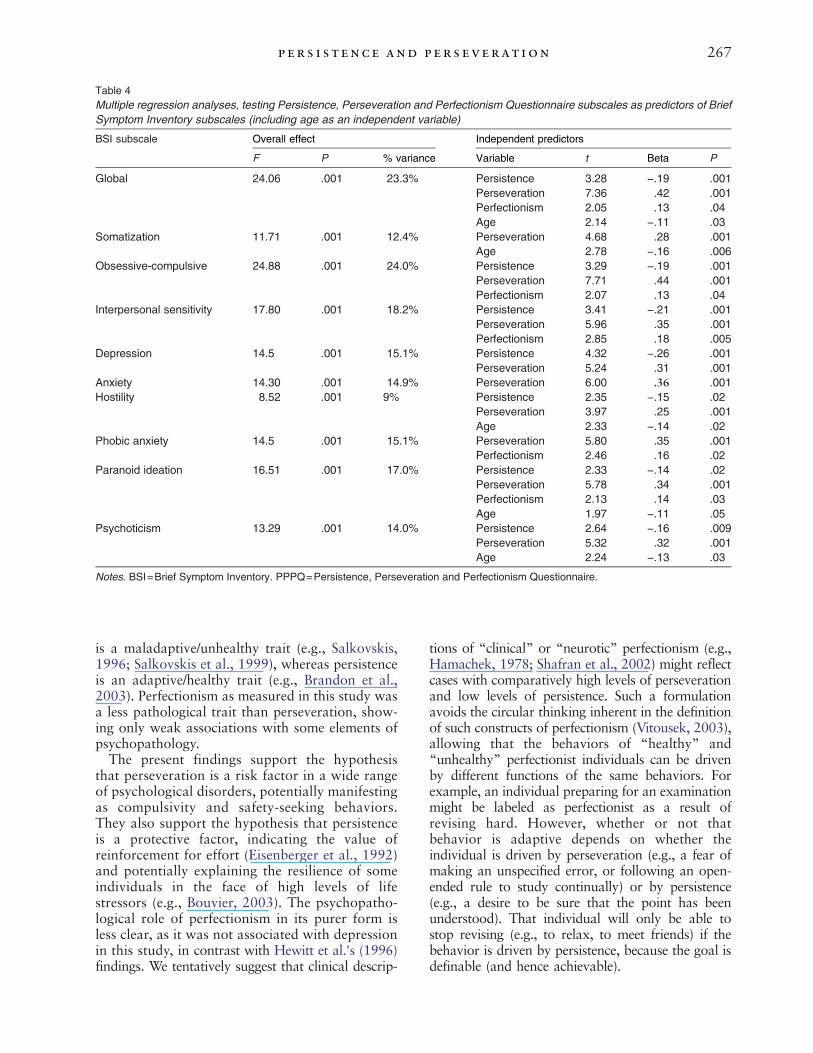
Table 4Multiple regression analyses, testing Persistence, Perseveration and Perfectionism Questionnaire subscales as predictors of BriefSymptom Inventory subscales (including age as an independent variable)
Overall effect Independent predictorsBSI subscale
F P % variance Variable t Beta P
Global 24.06 .001 23.3% Persistence 3.28 −.19 .001Perseveration 7.36 .42 .001Perfectionism 2.05 .13 .04Age 2.14 −.11 .03
Somatization 11.71 .001 12.4% Perseveration 4.68 .28 .001Age 2.78 −.16 .006
Obsessive-compulsive 24.88 .001 24.0% Persistence 3.29 −.19 .001Perseveration 7.71 .44 .001Perfectionism 2.07 .13 .04
Interpersonal sensitivity 17.80 .001 18.2% Persistence 3.41 −.21 .001Perseveration 5.96 .35 .001Perfectionism 2.85 .18 .005
Depression 14.5 .001 15.1% Persistence 4.32 −.26 .001Perseveration 5.24 .31 .001
Anxiety 14.30 .001 14.9% Perseveration 6.00 .36 .001Hostility 8.52 .001 9% Persistence 2.35 −.15 .02
Perseveration 3.97 .25 .001Age 2.33 −.14 .02
Phobic anxiety 14.5 .001 15.1% Perseveration 5.80 .35 .001Perfectionism 2.46 .16 .02
Paranoid ideation 16.51 .001 17.0% Persistence 2.33 −.14 .02Perseveration 5.78 .34 .001Perfectionism 2.13 .14 .03Age 1.97 −.11 .05
Psychoticism 13.29 .001 14.0% Persistence 2.64 −.16 .009Perseveration 5.32 .32 .001Age 2.24 −.13 .03
Notes. BSI=Brief Symptom Inventory. PPPQ=Persistence, Perseveration and Perfectionism Questionnaire.
267p er s i s t ence and pers everat ion
is a maladaptive/unhealthy trait (e.g., Salkovskis,1996; Salkovskis et al., 1999), whereas persistenceis an adaptive/healthy trait (e.g., Brandon et al.,2003). Perfectionism as measured in this study wasa less pathological trait than perseveration, show-ing only weak associations with some elements ofpsychopathology.The present findings support the hypothesis
that perseveration is a risk factor in a wide rangeof psychological disorders, potentially manifestingas compulsivity and safety-seeking behaviors.They also support the hypothesis that persistenceis a protective factor, indicating the value ofreinforcement for effort (Eisenberger et al., 1992)and potentially explaining the resilience of someindividuals in the face of high levels of lifestressors (e.g., Bouvier, 2003). The psychopatho-logical role of perfectionism in its purer form isless clear, as it was not associated with depressionin this study, in contrast with Hewitt et al.'s (1996)findings. We tentatively suggest that clinical descrip-
tions of “clinical” or “neurotic” perfectionism (e.g.,Hamachek, 1978; Shafran et al., 2002) might reflectcases with comparatively high levels of perseverationand low levels of persistence. Such a formulationavoids the circular thinking inherent in the definitionof such constructs of perfectionism (Vitousek, 2003),allowing that the behaviors of “healthy” and“unhealthy” perfectionist individuals can be drivenby different functions of the same behaviors. Forexample, an individual preparing for an examinationmight be labeled as perfectionist as a result ofrevising hard. However, whether or not thatbehavior is adaptive depends on whether theindividual is driven by perseveration (e.g., a fear ofmaking an unspecified error, or following an open-ended rule to study continually) or by persistence(e.g., a desire to be sure that the point has beenunderstood). That individual will only be able tostop revising (e.g., to relax, to meet friends) if thebehavior is driven by persistence, because the goal isdefinable (and hence achievable).

268 s erpe ll e t al .
An alternative possibility is that persistenceand perseveration are simply alternative ways oflabeling the constructs of adaptive andmaladaptiveperfectionism. This is an empirical question, whichcould be addressed through examining the associa-tion of these PPPQ scales and appropriate measuresof adaptive and maladaptive perfectionism. Suchresearch should also consider whether the hypothe-sized corresponding constructs (adaptive perfec-tionism and persistence; maladaptive perfectionismand perseveration) predict the same or distinctelements in the variance in measures of psycho-pathology.It should be acknowledged that the cross-
sectional nature of the current study is a limitation.Without prospective methodology, it is not possibleto show that perseveration and persistence areactually responsible for exacerbating or reducing/protecting against psychological symptoms. Anadditional limitation is that the discriminantvalidity of the PPPQ has not been established.Future studies should examine the relationshipbetween the new measure and preexisting measuresof related constructs (such as attentional control,perfectionism, self-efficacy, and experiential avoid-ance). Such findings will elucidate whether thePPPQ is tapping elements of preexisting scales ormeasuring new concepts. It is possible that theattempt to make the perfectionism scale hetero-geneous may have meant that some items (such asthose concerned with organization and order) didnot tap core aspects of perfectionism. It may bethat the perfectionism scale should be revised inline with recent research relating to the corecomponents of the perfectionism construct (e.g.Dunkley et al., 2006a, 2006b). Finally, the lowresponse rate in the current study might haveresulted in those who responded being unrepre-sentative of the normal population in some way.This possibility should also be explored in futureresearch.It will be important for future research to
examine the psychometric properties of the PPPQin a range of clinical samples, in order to determinethe clinical validity of the PPPQ. In particular, it willbe critical for future research to examine the PPPQ'sclinical validity with patient groups who demon-strate compulsive features and the use of safety-seeking behaviors. It will also be necessary todetermine whether the perseveration scale's con-struct validity is enhanced in clinical groups. Suchstudies might also examine the impact of these twocore constructs on therapy outcome. For example,high levels of persistence might predict a lowerlikelihood of dropping out of treatment and agreater engagement in the process (e.g., completion
of homework tasks), whereas high perseverationmay result in poorer outcomes from therapies thatrequire flexible thinking and taking alternativeperspectives on problems (e.g., cognitive-behavioraltherapy). The validity of the PPPQ needs to bedetermined with a wider age range, and prospectivestudies are needed to determine the development,maintenance and casual links of these traits. It isalso necessary to determine whether the use ofemail contacts for recruitment could have influ-enced the results, although Naglieri et al. (2004)conclude that there are advantages as well asdisadvantages to using this method of administra-tion (compared to pencil-and-paper methods), asuse of electronic methods might encourage accu-racy of scoring, honesty in participants, and accessto more diverse populations.The work of Harvey and colleagues (2004) and
others has suggested that certain dysfunctionalprocesses may be common to a range of psycholo-gical disorders. This approach stands in contrast tothe recent proliferation of specific cognitive beha-vioral models developed for different conditionsand suggests that such conditions have manycommonalities as well as differences (e.g., Norton,2006). The correlations between the perseverationand persistence subscales and a large number of thesubscales of the BSI suggest that these may beadditional “core processes” (one more adaptive,one more maladaptive), which could lend supportto a transdiagnostic approach.In clinical terms, the findings of a protective role
of persistence suggests that there is a potential rolefor “effort training,” in which individuals aretrained to increase persistence by manipulatingthe schedule on which rewards are given forparticular behaviour (Eisenberger et al., 1992).Adaptations of these techniques might be a usefuladdition to current therapy techniques (e.g., activityscheduling). Patients’ levels of task persistencemight also indicate their suitability for treatmentssuch as cognitive-behavioral therapy, in whichpersistence is more likely to be an asset, assistingthe patient to continue in the face of challenges. Themore pathological facet of perseveration mightindicate the need for therapies that enable indivi-duals to refocus their attention on higher ordergoals, shifting perspective and examining a range ofpossible solutions or approaches to problems.Many of these aspects could be addressed withina cognitive behavioral approach. However, theremight also a role for Cognitive RemediationTherapy, an approach used to improve cognitiveflexibility and “seeing the wood for the trees”(Davies & Tchanturia, 2005; Tchanturia, Davies,& Campbell, 2007).

269p er s i s t ence and pers everat ion
Appendix 1. Persistence, Perseveration and Perfectionism Questionnaire (PPPQ) Instructions:
This questionnaire contains a number of statements about how people might behave or think. Please read each itemcarefully and place a tick in the column that most applies to you.
Not at alltrue of me
A littletrue of me
Somewhattrue of me
Very trueof me
Totallytrue of me
1. I hate making mistakes.
2. I keep trying to sort out problems in a relationship,even if I know it's not going to survive.3. If a friendship seems to be running into difficulties,I will keep trying to resolve things, in case it's justa hiccup.
4. If I have an appointment, I always check my travelarrangements carefully in advance to make sure thatI have plenty of time to get there and not be late.
5. When reading a book or magazine, I often feel thatI must begin at the first page and read through to thevery end, even if some of the parts are of no interest.
6. When reading a book or magazine, I keep goinguntil I have read all the necessary material, evenwhen the concepts are difficult to understand.
7. I tend to keep going with a long task until it iscomplete, rather than giving up quickly.
8. When I phone someone to get a decision, if I get anengaged tone then I tend to keep ringing back everyminute or so, even when the deadline for thedecision has passed.
9. If I have an important test coming up, I am likely toplan carefully which topics I will need to cover,making a revision timetable to ensure I get everythingdone.
10. One of my goals is to be perfect in everything I do.
11. When studying for an important test, I tend to stayup working late into the night, even though I knowI am no longer taking in the material and that thestudying will not help my performance.12. People describe me as someone who can stick ata task, even when it gets difficult.
13. When calling a tradesman to arrange for him tocome to my home, I may continually ring and leavemessages on the same number, even though I knowthat they are not being picked up or responded to.
14. If I try to solve a problem or puzzle, I do not stopuntil I find an answer.
15. Once I have decided to do something, I keep goinguntil I reach my goal.
16. When calling a tradesman to arrange for him tocome to my home, I try all the contact numbersI have for him in the hope of catching him.
17. Even when I do something very carefully, I oftenfeel that it is not quite right.
18. When calling a tradesman to arrange for him tocome to my home, I would make sure I had all therelevant paperwork and measurements ready.
19. If I have a problem in my relationship, I will workhard at sorting it out, even if this takes a long time.
270 s erpe ll e t al .
(continued)Appendix I (continued)
Not at alltrue of me
A littletrue of me
Somewhattrue of me
Very trueof me
Totallytrue of me
20. When shopping in the supermarket, I walk downthe aisles one-by-one until I have covered the wholestore, even if I only need a couple of items.
21. If I am trying to get to an appointment but my carhas broken down, I do my best to get there in time byinvestigating other routes (e.g., finding out if I can geta bus, train or taxi).
22. Sometimes I find myself continuing to do somethingeven when there is no point in carrying on.
References
Ames, D., Cummings, J., Wirshing, W., Quinn, B., & Mahler,M. (1994). Review of reported cases: Repetitive andcompulsive behavior in frontal lobe degenerations. Journalof Neuropsychiatry and Clinical Neuroscience, 6, 100–113.
Arnkoff, D. B., & Glass, C. R. (1982). Clinical cognitiveconstructs: Examination, evaluation and elaboration. In P. C.Kendall (Ed.),Advances in cognitive-behavioral research andtherapy, Vol. 1. (pp. 1–34)New York: Academic Press.
Barkley, R. (1997). Behavioral inhibition, sustained attention,and executive functions: Constructing a unifying theory ofADHD. Psychological Bulletin, 121, 65–94.
Bieling, P., Israeli, A., & Antony, M. (2004). Is perfectionismgood, bad or both? Examining models of the perfec-tionism construct. Personality and Individual Differences,36, 1373–1385.
Bouvier, P. (2003). Child sexual abuse: Vicious circles of fate orpaths to resilience? Lancet, 361, 446–447.
Brandon, T., Herzog, T., Juliano, L., Irvin, J., & Lazev, A.(2003). Pre-treatment task persistence predicts smokingcessation outcome. Journal of Abnormal Psychology, 112,448–456.
Bulik, C., Tozzi, F., Anderson, C., Mazzeo, S., Aggen, S., &Sullivan, P. (2003). The relation between eating disorders andcomponents of perfectionism.American Journal of Psychiatry,160, 366–368.
Carver, C. S., & Scheier, M. F. (1982). Control theory: Auseful conceptual framework for personality-social, clin-ical, and health psychology. Psychological Bulletin, 92,111–135.
Chang, E., Watkins, A., & Banks, K. (2004). How adaptive andmaladaptive perfectionism relate to positive and negativepsychological functioning: Testing a stress-mediationmodel inBlack and White female college students. Journal of Counsel-ling Psychology, 51, 93–102.
Davies, H., & Tchanturia, K. (2005). Cognitive remediationtherapy as an intervention for acute anorexia nervosa: A casereport. European Eating Disorders Review, 13, 311–316.
Davis, C. (1997). Normal and neurotic perfectionism in eatingdisorders: An interactive model. International Journal ofEating Disorders, 22, 421–426.
Davis, C., Kapstein, S., Kaplan, A., Olmsted, M., & Woodside,D. B. (1998). Obsessionality in anorexia nervosa: Themoderating influence of exercise. Psychosomatic Medicine,60, 192–197.
Derogatis, L. (1993). The Brief Symptom Inventory: Adminis-tration, scoring and procedures manual, 3rd ed. Minneapolis:National Computer Systems Inc.
Derogatis, L., Lipman, R., Rickels, K., Uhlenhuth, E.,&Covi, L.(1974). The Hopkins Symptom Checklist (HSCL): A
measure of primary symptom dimensions. In P. Pichot(Ed.), Psychological measurements in psychopharmacology(pp. 79–110). Basel, Switzerland: Karger.
Derogatis, L., & Melisaratos, N. (1983). The Brief SymptomInventory: An introductory report. Psychological Medicine,13, 595–605.
Derogatis, L., Rickels, K., & Rock, A. (1976). The SCL-90 andtheMMPI: A step in the validation of a new self-report scale.British Journal of Psychiatry, 128, 280–289.
Dunkley, D., Blankstein, K., Zuroff, D., Lecce, S., & Hui, D.(2006). Self-critical and personal standards factors ofperfectionism located within the five-factor model of person-ality. Personality and Individual Differences, 40, 409–420.
Dunkley, D., Blankstein, K., Masheb, R., & Grilo, C. (2006).Personal standards and evaluative concerns dimensions of“clinical” perfectionism: A reply to Shafran et al. (2002, 2003)and Hewitt et al. (2003). Behaviour Research and Therapy,44, 63–84.
Eisenberger, R., Kuhlman, D., & Cotterell, N. (1992). Effects ofsocial values, effort training and goal structure on taskpersistence. Journal of Research in Personality, 26, 258–272.
Enns, M., Cox, B., & Clara, I. (2002). Adaptive and maladaptiveperfectionism: Developmental origins and association withdepression proneness. Personality and Individual Differences,33, 921–935.
Floyd, F., & Widaman, K. (1995). Factor analysis in the devel-opment and refinement of clinical assessment instruments.Psychological Assessment, 7, 286–299.
Frost, R., & Steketee, G. (1997). Perfectionism in obsessive-compulsive disorder patients.Behavior Research and Therapy,35, 291–296.
Hamachek, D. (1978). Psychodynamics of normal and neuroticperfectionism. Psychology, 15, 27–33.
Harvey, A. G., Watkins, E., Mansell, W., & Shafran, S. (2004).Cognitive behavioural processes across psychologicaldisorders: A transdiagnostic approach to research andtreatment. Oxford: Oxford University Press.
Hewitt, P., Flett, G., & Ediger, E. (1996). Perfectionism anddepression: Longitudinal assessment of a specific vulner-ability hypothesis. Journal of Abnormal Psychology, 105,276–280.
Ingram, R. E.,&Kendall, P. C. (1992). The evolution of cognitionin clinical theory and research: Cognitive vulnerability topsychopathology. Cognitive Therapy and Research, 16,375–377.
Lufi, D., & Cohen, A. (1987). A scale for measuring persistencein children. Journal of Personality Assessment, 51, 178–185.
Macleod, C., & Mathews, A. (1991). Biased cognitive opera-tions in anxiety: Accessibility of information or assignmentof processing priorities. Behaviour Research and Therapy,29, 599–610.
271p er s i s t ence and pers everat ion
Mansell, W. (2005). Control theory and psychopathology: Anintegrative approach.Psychology andPsychotherapy:Theory,Research and Practice, 78, 141–178.
Marcus, D. K., Gurley, J. R., Marchi, M. M., & Bauer, C.(2007). Cognitive and perceptual variables in hypochon-driasis and health anxiety: A systematic review. ClinicalPsychology Review, 27, 127–139.
Matsunaga, H., Kiriike, N., Iwasaki, Y., Yamagami, S., & Kaye,W. (1999). Clinical characteristics in patients with anorexianervosa and obsessive-compulsive disorder. PsychologicalMedicine, 29, 407–414.
Mundfrom, D. J., Shaw, D. G., & Ke, T. L. (2005). Minimumsample size recommendations for conducting factor analyses.International Journal of Testing, 5, 159–168.
Naglieri, J. A., Drasgow, F., Schmit, M., Handler, L., Prifitera,A., Margolis, A., & Velasquez, R. (2004). Psychologicaltesting on the internet: New problems, old issues. AmericanPsychologist, 59, 150–162.
Norton, P. (2006). Toward a clinically-oriented model of anxietydisorders. Cognitive Behaviour Therapy, 35, 88–105.
Nunnally, J. (1978). Psychometric theory, 2nd ed. New York:McGraw-Hill.
Powers, W. T. (1973). Behaviour: The control of perception.Chicago: Aldine.
Salkovskis, P. (1996). The cognitive approach to anxiety:Threat beliefs, safety-seeking behavior and the special caseof health anxiety and obsessions. In P. Salkovskis (Ed.),Frontiers of cognitive therapy New York: Guilford Press.
Salkovskis, P., Clark, D., Hackmann, A., Wells, A., & Gelder,M. (1999). An experimental investigation of the role ofsafety-seeking behaviors in the maintenance of panic disorderwith agoraphobia. Behaviour Research and Therapy, 37,559–574.
Serpell, L., Hirani, V., Willoughby, K., Neiderman, M., & Lask,B. (2006). Personality or pathology?: Obsessive-compulsivesymptoms in children and adolescents with anorexianervosa. European Eating Disorders Review, 14, 404–413.
Serpell, L., Livingstone, A., Neiderman, M., & Lask, B. (2002).Anorexia nervosa: Obsessive compulsive disorder, obsessivecompulsive personality or neither.Clinical PsychologyReview,647–669.
Shafran, R., Cooper, Z., & Fairburn, C. (2002). Clinicalperfectionism: A cognitive behavioral analysis. BehaviourResearch and Therapy, 40, 773–791.
Shafran, R., & Mansell, W. (2001). Perfectionism andpsychopathology: A review of research and treatment.Clinical Psychology Review, 21, 879–906.
Tchanturia, K., Davies, H., & Campbell, I. (2007). Cognitiveremediation therapy for patients with anorexia nervosa:Preliminary findings. Annals of General Psychiatry, 6, 14.
Terry-Short, L. A., Owens, R. G., Slade, P. D., & Dewey, M. E.(1995). Positive and negative perfectionism. Personality andIndividual Differences, 18, 663–668.
Vitousek, K. (2003, May). Perfectionism and anorexia nervosa;Vulnerability, value or job requirements. London: Paperpresented at the Sixth London International Conference onEating Disorders, Imperial College.
Zohar, A., LaBuda, M., & Moschel-Ravid, O. (1995).Obsessive-compulsive behaviors and cognitive functioning:A study of compulsivity, frame shifting and Type A activitypatterns in a normal population. Neuropsychiatry, Neurop-sychology and Behavioral Neurology, 8, 163–167.
RECEIVED: January 25, 2008ACCEPTED: July 23, 2008Available online 5 November 2008