the contribution of therapist beliefs to psychological distress in therapists: an investigation of...
TRANSCRIPT

Behavioural and Cognitive Psychotherapy, 2003, 31, 417–428Printed in the United Kingdom DOI: 10.1017/S135246580300403X
THE CONTRIBUTION OF THERAPIST BELIEFS TOPSYCHOLOGICAL DISTRESS IN THERAPISTS: AN
INVESTIGATION OF VICARIOUS TRAUMATIZATION,BURNOUT AND SYMPTOMS OF AVOIDANCE AND
INTRUSION
Sara McLean and Tracey D. Wade
Flinders University, Adelaide, Australia
Jason S. Encel
CAMHS, South Australia, Australia
Abstract. The present study surveyed a sample of 116 Australian therapists who identifiedthemselves as working primarily with traumatized clients. Outcome variables were measuresof vicarious traumatization (VT), burnout and trauma symptomatology (intrusion andavoidance). A measure of beliefs about the therapeutic process was constructed for thepresent study and examined along with other predictor variables, namely years of experienceas a therapist, percentage of time spent in clinical work with clients, predominant clientgroup, and recent and direct exposure to trauma in the therapist. Therapist beliefs werefound to predict vulnerability to VT and burnout, supporting a cognitive model of therapistdistress. Implications of the findings for maintaining therapist health are discussed.
Keywords: Vicarious traumatization, therapist beliefs, burnout, therapist distress.
Introduction
Over the last decade there has been increased interest in the psychological impact on mentalhealth professionals of undertaking therapy with traumatized clients. A number of adverseoutcomes can arise for the therapist, and Vicarious Traumatization (VT) has been used todescribe one such outcome. VT is defined as the disruptive and painful psychological symp-toms that result from exposure to clients’ traumatic memories although the therapist has notexperienced the trauma directly (McCann & Pearlman, 1990). These symptoms, analogousto post-trauma symptoms, can include sleep disturbance, intrusive images, and disruption tocore schema about safety in the world, trust, intimacy and control. In common with otherconceptualizations of trauma, cumulative exposure to a client’s trauma material is seen to
Reprint requests to Tracey Wade, School of Psychology, Flinders University, GPO Box 2100, Adelaide 5001, SA,Australia. E-mail: [email protected]
2003 British Association for Behavioural and Cognitive Psychotherapies
S. McLean et al.418
be a necessary but not sufficient condition for the development of VT. VT is seen to bequalitatively different from burnout, which is defined as the emotional exhaustion thatemerges gradually after long-term work with difficult clients.Although intuitively appealing, clarity around the parameters of VT is still somewhat
lacking (Figley, 1995) and support for the construct validity of VT has been variable thusfar. In support of VT as a construct separate from burnout, Schauben and Frazier (1995), intheir work with counsellors of survivors of sexual violence, found that a higher percentageof clinical work involving trauma was related to higher self-reports of VT symptomatology,but not to burnout. Similarly, Chrestman (1995) found an increasing proportion of clinicalwork involving trauma was related to symptoms of dissociation, anxiety, sleep disturbance,intrusion and avoidance. However, this relationship has not been replicated consistently(Fleming, 1999; Pearlman & MacIan, 1995) and some studies find a significant overlapbetween measures of VT and burnout, suggesting that there might not be a clear distinctionbetween these two constructs (Adams, Matto, & Harrington, 2001). Clearly, such support iskey to the argument that VT is a separate construct from other forms of therapist distress.While it is highly likely, in common with a range of other psychological disorders, that
the onset of VT is multi-determined, further research is required to identify specific variablesthat may contribute to VT. Four such factors are of interest to the current research. First, aconsistent finding in the literature has been that therapist experience mediates vulnerabilityto psychological distress, such that less experienced therapists are more vulnerable to dis-tress, including VT (Chrestman, 1995; Pearlman & MacIan, 1995; Ackerley, Burnell,Holder, & Kurdeck, 1988). Second, while research finds a childhood history of abuse intrauma therapists as being predictive of VT (Pearlman & MacIan, 1995), though this findinghas not been supported consistently (Fleming, 1999; Follette, Polunsky, & Milbeck, 1994;Schauben & Frazier, 1995), the more fundamental question has been overlooked. In nostudy have respondents been asked whether they have experienced direct and recent traumain their personal lives in order to conclude that any traumatic symptomatology in the therap-ist has indeed arisen vicariously, rather than as a result of their recent life history. Third,given that the notion of empathic engagement is central to VT, it seems reasonable toassume that therapists who are involved in more frequent contact with their clients may bemore vulnerable to VT than those having less client contact. Finally, while working withchildren is anecdotally reported to be more distressing than working with adults (Beaton &Murphy, 1995; Dyregrov & Mitchell, 1992), this notion has not been explicitly examinedwith respect to VT.In addition to these variables, and of relevance to the cognitive model of secondary
traumatization, is the role of therapist beliefs on the development and severity of VT. Todate, no systematic attempt has been made to examine these beliefs with respect to VT.Beliefs about therapy that can result in therapist distress identified previously in the literatureinclude the need to work at peak efficiency, over all situations, and with all clients (Deutsch,1984); attitudes of rigidity, inflexibility and dogmatism with respect to the application oftherapeutic models and process (Hellman, Morrison, & Abramowitz, 1987; Norcross, 1981);and perfectionist expectations and ideals regarding performance and treatment outcome(Pearlman & Saaktvitne, 1995). In addition, the need to appear knowledgeable, having alow tolerance for ambiguity, and the need for emotional and therapeutic control (Deutsch,1984; Hellman, Morrison, & Abramowitz, 1986; Rodolfa, Kraft, & Reilly, 1988) have alsobeen implicated in therapist distress, as has an intolerance for client emotionality (Deutsch,

Contribution of therapist beliefs to distress 419
1984; Farber, 1983) and need for approval (Forney, Wallace-Schutzman, & Wiggers, 1982).The primary aim of this study is therefore to examine the association of both therapist
beliefs and the four variables previously outlined with VT, burnout, and trauma symptomato-logy. It is predicted that therapists’ endorsement of unhelpful beliefs will contribute signi-ficantly to both VT and burnout and, further, being less experienced, working with children,having experienced direct trauma recently, and having more contact time with traumatizedclients (in duration and frequency) will increase therapist distress. A secondary aim is toassess support for VT as a construct separate from burnout, where it is expected that meas-ures of VT and burnout will not be completely independent constructs but, rather, be some-what over-lapping.
Method
Participants
One hundred and sixteen professionals who identified themselves as working withtraumatized clients volunteered to take part in the study, including 85 females (73%) and31 males (27%). This gender distribution is similar to that obtained by others (Pearlman &MacIan, 1995). Of these participants, 31% were psychologists, 53.4% were social workersand the remaining 15.6% were mental health professionals from other disciplines (nursing,psychiatry, occupational therapy). The majority of these professionals worked in a govern-ment setting (87%), with the remainder working for either non-government agencies (10%)and private practice or other settings (3%). Most professionals classified their work as indi-vidual therapy (48%), followed by a combination of family and individual therapy (12%)or some other combination of therapies (10%). Altogether, 30% of the professionals sur-veyed worked primarily in a brief intervention model (assessment, preventative/educationalwork or phone contacts). The age ranges of the participants were reasonably evenly distrib-uted, with most participants falling in the two largest age brackets – 45–55 (33%), followedby 35–45 (20%). There were equal numbers of participants in the lower age ranges 25–30(18%) and 30–35 (18%), and fewer in the 20–25 (3%) or 55–65 (8%) year range.
Procedure
The questionnaire and materials used in this study were approved by the Flinders UniversitySocial and Behavioural Research Ethics Committee. Participants were advised of the volun-tary nature of the study and were assured that neither individuals nor organizations wouldbe identified. One hundred and ninety-one questionnaires were sent, and 116 completedpackages were returned, yielding a response rate of 61%. This represents a higher responserate than that obtained by previous studies; previous comparable studies with mental healthprofessionals have yielded response rates ranging from 37% (Pearlman & MacIan, 1995),52% (Follette et al., 1994), 53% (Fleming, 1999) to 58% (Pope & Feldman-Summers, 1992).
Independent measures
Situational variables. Participants were asked to identify the percentage of time spent inclinical work with clients, whether their primary clients were predominantly children or
S. McLean et al.420
adults. Other background information was obtained about work setting, age, and profession.Additionally, participants were asked to indicate whether or not they had personal directexperience of traumatic events within the past 6 months i.e., ‘‘Have you yourself beendirectly involved in a traumatic incident in your personal or work life in the past sixmonths?’’
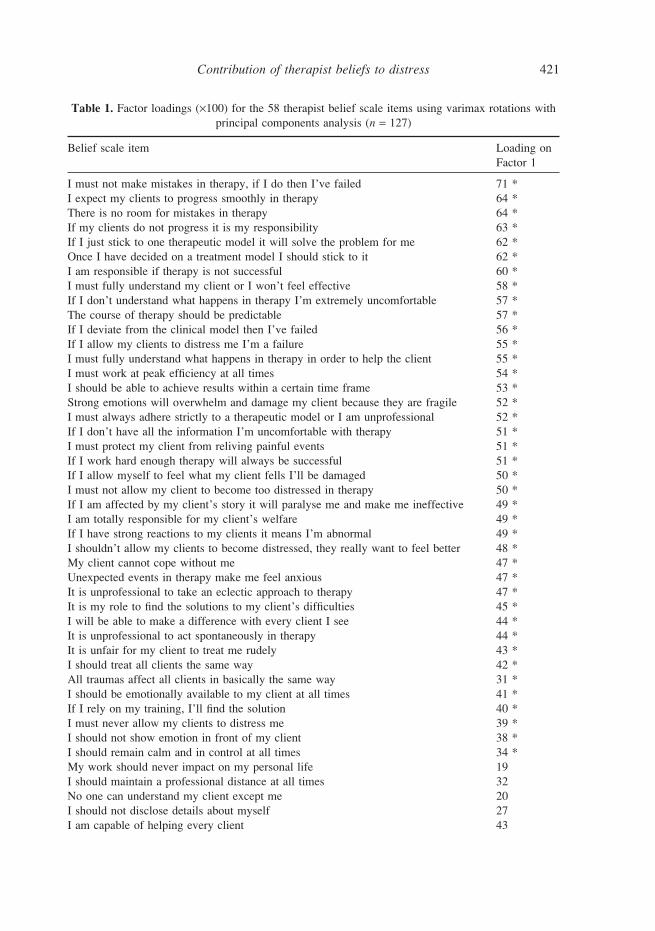
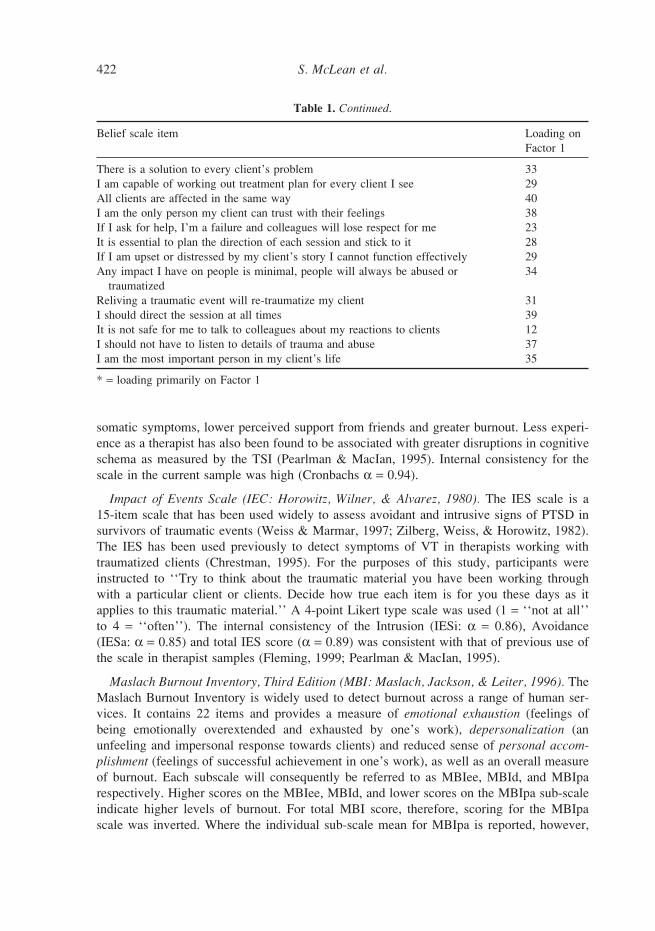
Therapist beliefs. A therapist belief scale was constructed for this study using a four-stepprocedure. First, the literature on therapist stress and related concepts was reviewed and anextensive list of potential negatively valanced thoughts was generated. Second, a group of20 psychologists from a variety of workplace backgrounds participated in a structured dis-cussion about trauma work. They were asked: a) to generate unhelpful or irrational thoughtsthat they felt influenced a therapist’s ability to work effectively with traumatized clients;and b) to rate their endorsement of items on the list of irrational and exaggerated thoughtsgenerated from the review of relevant literature. Third, the resultant items were refined bydrawing on general principles of cognitive distortions relevant to the development of emo-tional distress, such as perfectionism, over-control, all or nothing (absolutist) thinking, andcatastrophizing. In this way, a final list of 58 items was generated, each using a 6-pointLikert scale (1 = ‘‘disagree strongly’’ to 6 = ‘‘agree strongly’’). Respondents were told that‘‘This questionnaire is about automatic thoughts that people can have about their work.There are no right or wrong answers. Please indicate your agreement with each statementby placing a number from 1–6 next to each statement.’’ Fourth, an exploratory factor ana-lysis using varimax rotation was used to investigate the data generated from this question-naire by 127 therapists (including 116 therapists who are the focus of the current study). Acriterion of 0.32 for the correlation between the item and the factor was set (Tabachnick &Fidell, 1996). Results supported the existence of one primary factor, with 69% of items (40out of 58) clustered around one factor (see Table 1). Further, 9 of the 18 items not loadingprimarily on this primary factor correlated at 0.32 or above with the factor. While the resultsare unlikely to be stable given that this analysis is underpowered, they do provide prelimin-ary support for the validity of using a total score as an indicator of unhelpful therapistbeliefs.For the 116 therapists that worked primarily with traumatized clients, and who are the
focus of the remaining analyses, the mean total belief scale score was 129.4 (SD = 24.4).The sample was normally distributed (Kolmogorow-Smirnov statistic = .11, p > .01). Theinternal consistency for the scale was 0.92.
Dependent measures
The Traumatic Stress Institute (TSI) Scale (Pearlman, 1996). The scale measures one ofthe postulated outcomes of VT, disruptions in cognitive schema relating to the need forsafety, trust, control, esteem and intimacy. The version of the scale used in this study (TSIRevision M) contains 77 items. Participants rated their endorsement of each statement on a6-point scale (1 = ‘‘disagree strongly’’ to 6 = ‘‘agree strongly’’). Given the lack of psycho-metric information available about sub-scale structure, and in keeping with previous use ofthe scale (Fleming, 1999), only a total score was used in the analyses. A report on thevalidity of the TSI in masters’ level clinical social workers (Adams et al., 2001) suggeststhat greater disruptions in cognitive schema are associated with younger age, more reported
Contribution of therapist beliefs to distress 421
Table 1. Factor loadings (×100) for the 58 therapist belief scale items using varimax rotations withprincipal components analysis (n = 127)
Belief scale item Loading onFactor 1
I must not make mistakes in therapy, if I do then I’ve failed 71 *I expect my clients to progress smoothly in therapy 64 *There is no room for mistakes in therapy 64 *If my clients do not progress it is my responsibility 63 *If I just stick to one therapeutic model it will solve the problem for me 62 *Once I have decided on a treatment model I should stick to it 62 *I am responsible if therapy is not successful 60 *I must fully understand my client or I won’t feel effective 58 *If I don’t understand what happens in therapy I’m extremely uncomfortable 57 *The course of therapy should be predictable 57 *If I deviate from the clinical model then I’ve failed 56 *If I allow my clients to distress me I’m a failure 55 *I must fully understand what happens in therapy in order to help the client 55 *I must work at peak efficiency at all times 54 *I should be able to achieve results within a certain time frame 53 *Strong emotions will overwhelm and damage my client because they are fragile 52 *I must always adhere strictly to a therapeutic model or I am unprofessional 52 *If I don’t have all the information I’m uncomfortable with therapy 51 *I must protect my client from reliving painful events 51 *If I work hard enough therapy will always be successful 51 *If I allow myself to feel what my client fells I’ll be damaged 50 *I must not allow my client to become too distressed in therapy 50 *If I am affected by my client’s story it will paralyse me and make me ineffective 49 *I am totally responsible for my client’s welfare 49 *If I have strong reactions to my clients it means I’m abnormal 49 *I shouldn’t allow my clients to become distressed, they really want to feel better 48 *My client cannot cope without me 47 *Unexpected events in therapy make me feel anxious 47 *It is unprofessional to take an eclectic approach to therapy 47 *It is my role to find the solutions to my client’s difficulties 45 *I will be able to make a difference with every client I see 44 *It is unprofessional to act spontaneously in therapy 44 *It is unfair for my client to treat me rudely 43 *I should treat all clients the same way 42 *All traumas affect all clients in basically the same way 31 *I should be emotionally available to my client at all times 41 *If I rely on my training, I’ll find the solution 40 *I must never allow my clients to distress me 39 *I should not show emotion in front of my client 38 *I should remain calm and in control at all times 34 *My work should never impact on my personal life 19I should maintain a professional distance at all times 32No one can understand my client except me 20I should not disclose details about myself 27I am capable of helping every client 43
S. McLean et al.422
Table 1. Continued.
Belief scale item Loading onFactor 1
There is a solution to every client’s problem 33I am capable of working out treatment plan for every client I see 29All clients are affected in the same way 40I am the only person my client can trust with their feelings 38If I ask for help, I’m a failure and colleagues will lose respect for me 23It is essential to plan the direction of each session and stick to it 28If I am upset or distressed by my client’s story I cannot function effectively 29Any impact I have on people is minimal, people will always be abused or 34traumatized
Reliving a traumatic event will re-traumatize my client 31I should direct the session at all times 39It is not safe for me to talk to colleagues about my reactions to clients 12I should not have to listen to details of trauma and abuse 37I am the most important person in my client’s life 35
* = loading primarily on Factor 1
somatic symptoms, lower perceived support from friends and greater burnout. Less experi-ence as a therapist has also been found to be associated with greater disruptions in cognitiveschema as measured by the TSI (Pearlman & MacIan, 1995). Internal consistency for thescale in the current sample was high (Cronbachs α = 0.94).
Impact of Events Scale (IEC: Horowitz, Wilner, & Alvarez, 1980). The IES scale is a15-item scale that has been used widely to assess avoidant and intrusive signs of PTSD insurvivors of traumatic events (Weiss & Marmar, 1997; Zilberg, Weiss, & Horowitz, 1982).The IES has been used previously to detect symptoms of VT in therapists working withtraumatized clients (Chrestman, 1995). For the purposes of this study, participants wereinstructed to ‘‘Try to think about the traumatic material you have been working throughwith a particular client or clients. Decide how true each item is for you these days as itapplies to this traumatic material.’’ A 4-point Likert type scale was used (1 = ‘‘not at all’’to 4 = ‘‘often’’). The internal consistency of the Intrusion (IESi: α = 0.86), Avoidance(IESa: α = 0.85) and total IES score (α = 0.89) was consistent with that of previous use ofthe scale in therapist samples (Fleming, 1999; Pearlman & MacIan, 1995).
Maslach Burnout Inventory, Third Edition (MBI: Maslach, Jackson, & Leiter, 1996). TheMaslach Burnout Inventory is widely used to detect burnout across a range of human ser-vices. It contains 22 items and provides a measure of emotional exhaustion (feelings ofbeing emotionally overextended and exhausted by one’s work), depersonalization (anunfeeling and impersonal response towards clients) and reduced sense of personal accom-plishment (feelings of successful achievement in one’s work), as well as an overall measureof burnout. Each subscale will consequently be referred to as MBIee, MBId, and MBIparespectively. Higher scores on the MBIee, MBId, and lower scores on the MBIpa sub-scaleindicate higher levels of burnout. For total MBI score, therefore, scoring for the MBIpascale was inverted. Where the individual sub-scale mean for MBIpa is reported, however,
Contribution of therapist beliefs to distress 423
it is based on original scoring. Participants were required to record the frequency with whichthey experience feelings related to each sub-scale on a 6-point scale (0 = ‘‘never’’ to 6 =‘‘everyday’’). The internal consistency (Cronbach alphas) for the scale in this study was0.75 for MBIpa and 0.82 for MBId. Internal consistency for both the MBI total score andMBIee subscale was 0.89, similar to those reported elsewhere (Maslach et al., 1996;Schauben & Frazier, 1995).
Results
Preliminary investigation of the data
Scores for depersonalization and years working were significantly positively skewed andunderwent square root transformation. In both cases this improved normality. Data werescreened for univariate and multivariate outliers (Tabachnick & Fidell, 1996), and werefound to be satisfactory.
Descriptive statistics
Therapists had been working with traumatized clients for an average of 11 years (M = 11.01,SD = 8.9) and spent an average of 39% of their work time in direct clinical activities withclients: 47% of therapists identified that they worked primarily with child clients, 35%worked predominantly with adult clients, and 18% divided their clinical workload evenlybetween adult and child clients. Approximately one-third of the therapists had been directlytraumatized in their work or personal life in the past 6 months (34% yes, 63% no, 3%missing). Of those therapists working with adults, children, or both adults and children,28%, 34% and 50% respectively had experienced direct trauma in the past 6 months.Overall, the mean scores and standard deviations found for the sample of therapists
working with traumatized clients are representative of those found in previous studies. Meanscores for MBIee and MHId, of 18.7 (16.5) and 5.3 (4.9) respectively, parallel those reportedfor a sample of 730 American mental health workers, while the mean MBIpa score in thissample of 10.6 (5.9) is slightly higher than those found previously (Maslach et al., 1996).The mean IES total score in this sample, 28 (7.9), is slightly less than the cut-off score of35 found to have optimal diagnostic specificity (Joseph, 2000), but higher than the meanscore of 16.7 reported in a nonclinical sample with a prior history of traumatization(Briere & Elliot, 1998). The mean score for the TSI scale in this sample, 157.6 (32.2), wassomewhat lower than that obtained for an earlier 79-item version of the scale (Pearlman &MacIan, 1995), but consistent with that obtained earlier using the identical 77-item revisionused in this study (Fleming, 1999).Gender differences were examined for each of the dependent variables. Males and females
did not differ on mean scores for TSI total, MBI total, MBId, MBIee, MBI pa, IESi or IESa.A significant difference was found between the mean IES total scores for males and femalesin the sample, such that the 29 males scored significantly lower than the 82 females whocompleted this scale, with respective means of 25.4 and 28.9 (t = 2.06, p < .05). Hence infurther analysis of the IES total score, gender was added as a covariate.Pearson correlations were conducted on the dependent variables to identify any relation-
ship between the variables used. All correlations were in the moderate to high range. For
S. McLean et al.424
Table 2. Pearson correlations between independent measures
Measures MBIe MBId MBIp IESi IESa MBI IESe a total total
Traumatic stress .584 .513 .449 .461 .383 .675 .474Institute scale – totalImpact of events scale .521 .442 .230 .872 .899 .531 —(IES) – totalMalach burnout .880 .799 .635 .522 .423 — —Inventory (MBI) – total
Note: all results significant at the p < .01 level (one-tailed).
total scores, the highest correlation was found between TSI total score and MBI total score(see Table 2).
Prediction of therapist trauma
A series of ANOVAs was conducted with exposure to direct trauma, predominantly clientgroup, percentage time spent in clinical work with traumatized clients, years experience astherapist, and total belief scale score and all two-way interactions as independent variables.This approach is comparable to a series of regressions but is more appropriate when analysisinvolves non-continuous independent variables. Selection of the model that best predicted thedependent variable under examination was based on the most parsimonious fit between theleast number of predictor variables and proportion of variance accounted for by the model. Asinitial solutions (i.e. full models) accounted for between 20–30% of the variance, significantmodels (p < .05) accounting for approximately 30% of the total variance were considered.The therapist belief scale total score was solely predictive of the TSI total score and the
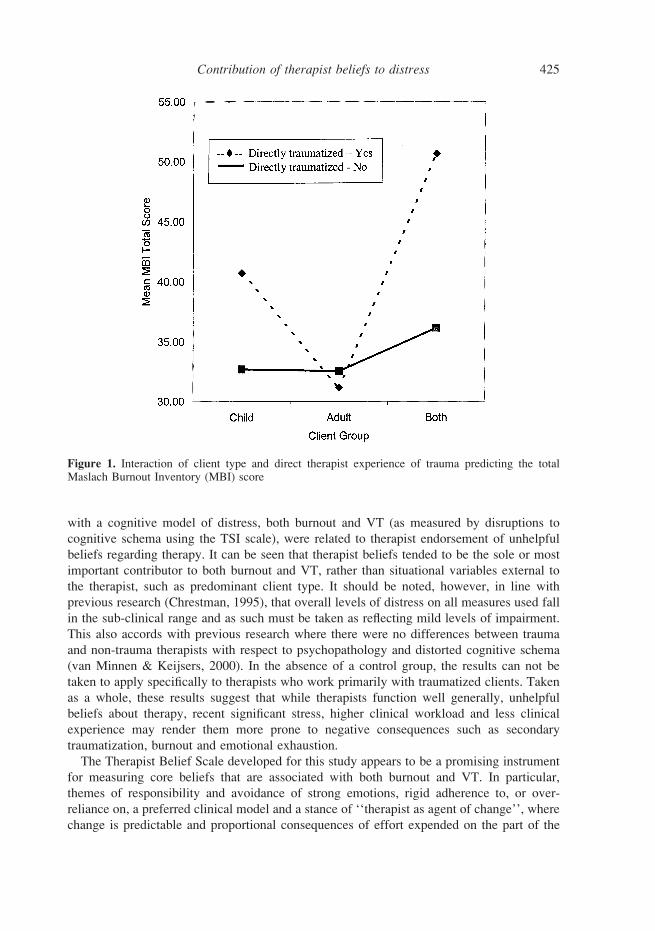
MBId, with a R2 of .36 and .27 respectively. The therapist belief score also predicted theMBI total score and the MBIee score, along with an interaction between direct trauma andpredominant client type, with respective R2 of .29 and .31. These interactions both showedthat therapists who had been recently and directly traumatized and who are working withchildren predominantly experienced higher levels of burnout (MBI total score) than thoseworking with traumatized children who had not experienced recent direct trauma. Amongsttherapists working with traumatized adults, however, therapists with recent direct experienceof trauma were no more vulnerable to burnout than those who had not been traumatized.Interestingly, the highest level of burnout was reported by those therapists who had experi-enced recent and direct trauma and split their workload between both traumatized adultsand children. This interaction is illustrated for the total MBI score in Figure 1.Avoidance symptoms (IESa) were predicted by percentage of time spent in clinical work
with clients, such that increasing clinical workload was related to increase in reported avoid-ance symptomatology (R2 = .32). Overall IES total score was predicted by years experience(p < .01), such that less experienced therapists reported higher IES scores (R2 = .27).
Discussion
The findings of this study provide support for the view that the beliefs that therapists holdabout their work and their clients can impact on their psychological adjustment. Consistent
Contribution of therapist beliefs to distress 425
Figure 1. Interaction of client type and direct therapist experience of trauma predicting the totalMaslach Burnout Inventory (MBI) score
with a cognitive model of distress, both burnout and VT (as measured by disruptions tocognitive schema using the TSI scale), were related to therapist endorsement of unhelpfulbeliefs regarding therapy. It can be seen that therapist beliefs tended to be the sole or mostimportant contributor to both burnout and VT, rather than situational variables external tothe therapist, such as predominant client type. It should be noted, however, in line withprevious research (Chrestman, 1995), that overall levels of distress on all measures used fallin the sub-clinical range and as such must be taken as reflecting mild levels of impairment.This also accords with previous research where there were no differences between traumaand non-trauma therapists with respect to psychopathology and distorted cognitive schema(van Minnen & Keijsers, 2000). In the absence of a control group, the results can not betaken to apply specifically to therapists who work primarily with traumatized clients. Takenas a whole, these results suggest that while therapists function well generally, unhelpfulbeliefs about therapy, recent significant stress, higher clinical workload and less clinicalexperience may render them more prone to negative consequences such as secondarytraumatization, burnout and emotional exhaustion.The Therapist Belief Scale developed for this study appears to be a promising instrument
for measuring core beliefs that are associated with both burnout and VT. In particular,themes of responsibility and avoidance of strong emotions, rigid adherence to, or over-reliance on, a preferred clinical model and a stance of ‘‘therapist as agent of change’’, wherechange is predictable and proportional consequences of effort expended on the part of the

S. McLean et al.426
therapist, are associated with poor outcome. Such themes are consistent with beliefs sug-gested previously that place therapists at risk of work-related psychological distress (Figley,1995; Deutsch, 1984; Forney et al., 1982; Pearlman & Saakvitne, 1995; Pope & Tabachnick,1994).A secondary aim of this study was to explore support for VT as a construct separate from
burnout. As predicted, results suggest that the two are neither identical nor completelyindependent constructs, but are somewhat over-lapping. First, the correlation between bur-nout and the TSI was moderate, where the two measures shared approximately 45% of thevariance, consistent with previous findings (Adams et al., 2001). Second, the predictiveprofile was similar but slightly different for burnout and VT (TSI scale). While the TherapistBelief Scale was a powerful predictor of both VT and burnout, demographic variables alsoappear to contribute to vulnerability to burnout. Further work is required to better understandthe meaningful differences between VT and burnout.Given the general implications of these findings, it appears that the active identification
and disputation of unhelpful beliefs in therapist training and supervision, with a view todeveloping more adaptive, helpful alternative beliefs, may be important in maintaining ther-apist mental health. Further, the concept of a ‘‘self-care plan’’ (Saakvitne & Pearlman,1996; Skovholt, 2001) has gained acceptance in the literature, underlining the need to takepractical steps to minimize deleterious secondary impacts on therapists. An examination oftherapist beliefs could form a central component of such a plan. Newer therapists appearedto be more susceptible to the symptoms of intrusion and avoidance, and therefore expertsupervision and self-care plans in this population are critical. This study also highlightsthe importance of providing support for additional therapist self-care (Skovholt, 2001) andorganizational or supervisory support at times of personal stress or crisis for the therapist.This raises the question of making temporary adjustments to caseloads in terms of type orquantity, at times of recent direct therapist exposure to traumatic stress, especially if thetherapist is working with children or dividing their clinical workload between both childrenand adults.The results of this study should be interpreted in the context of four limitations. First,
longitudinal examination of the nature of therapist distress is required in order to draw anycausal implications about the contribution of beliefs to the mental health of therapists.Second, self-selection biases may have influenced our results. Therapists more able to copewith trauma work may remain in the field longer and feel better able to answer questionsabout mental health. Alternatively, those therapists who felt that they were suffering distressmay have elected to become involved in such a study. Third, while the Therapist BeliefScale shows good internal consistency and possible predictive ability, further developmentof the scale is required. An important next step is to carry out a factor analysis of the scalein a larger and more varied population of therapists. Finally, the measurement of prior directand recent traumatic stress in the lives of therapists needs to be expanded in future studiesto allow for measurement of the nature, intensity and manner of resolution of prior traumaso that it can be adequately controlled in future investigations.
Acknowledgements
This research was partly funded through the Flinders University Research Budget. We thankall those participants who gave their time to be involved in this study.
Contribution of therapist beliefs to distress 427
References
ACKERLEY, G. D., BURNELL, J., HOLDER, D. C., & KURDEK, L. A. (1988). Burnout among licensedpsychologists. Professional Psychology: Research and Practice, 19, 624–631.
ADAMS, K. B., MATTO, H. C., & HARRINGTON, D. (2001). The Traumatic Stress Institute Belief Scaleas a measure of vicarious trauma in a national sample of clinical social workers. Families in Society,82, 363–371.
BEATON, R. D., & MURPHY, S. A. (1995). Working with people in crisis: Research implications. InC. R. Figley (Ed.), Compassion fatigue: Coping with secondary traumatic stress disorder in thosewho treat the traumatised (pp. 51–81). New York: Brunner/Mazel.
BRIERE, J., & ELLIOT, D. M. (1998). Clinical utility of the impact of event scale: Psychometrics in thegeneral population. Assessment, 5, 171–180.
CHRESTMAN, K. R. (1995). Secondary exposure to trauma and self-reported distress amongst therapists.In B. H. Stamm (Ed.), Secondary traumatic stress: Self care issues for clinicians, researchers andeducators (pp. 29–36). Maryland: Sidran Press.
DEUTSCH, C. J. (1984). Self reported sources of stress among psychotherapists. Professional Psycho-logy: Research and Practice, 15, 833–845.
DYREGROV, A., & MITCHELL, J. T. (1992). Work with traumatised children: Psychological effects andcoping strategies. Journal of Traumatic Stress, 5, 5–17.
FARBER, B. A. (1983). Psychotherapists receptions of stressful patient behaviour. Professional Psycho-logy: Research and Practice, 14, 697–705.
FIGLEY, C. R. (1995). Compassion fatigue: Toward a new understanding of the costs of caring. InB. H. Stamm (Ed.), Secondary traumatic stress: Self care issues for clinicians, researchers andeducators (pp. 3–28). Maryland: Sidran Press.
FLEMING, A. L. (1999). Factors predicting the development of vicarious traumatisation in the helpingprofessions: The role of perceived helplessness. Unpublished manuscript, Flinders University ofSouth Australia, Adelaide, Australia.
FOLLETTE, V. M., POLUNSKY, M. M., & MILBECK, K. (1994). Mental health and law enforcementprofessionals: Trauma history, psychological symptoms and impact of providing services to childsexual abuse survivors. Professional Psychology: Research and Practice, 25, 3, 275–282.
FORNEY, D., WALLACE-SCHUTZMAN, F., & WIGGERS, T. T. (1982). Burnout among career developmentprofessionals: Preliminary findings and implications. Personnel and Guidance Journal, 60, 435–439.
HELLMAN, I. D., MORRISON, T. L., & ABRAMOWITZ, S. I. (1986). The stresses of psychotheraeuticwork: A replication and extension. Journal of Clinical Psychology, 42, 197–205.
HELLMAN, I. D., MORRISON, T. L., & ABRAMOWITZ, S. I. (1987). Therapist flexibility/rigidity and workstress. Professional Psychology: Research and Practice, 18, 21–27.
HOROWITZ, M. J., WILNER, N., & ALVAREZ, W. (1980). Signs and symptoms of post-traumatic stressdisorder. Archives of General Psychiatry, 37, 85–92.
JOSEPH, S. (2000). Psychometric evaluation of Horowitz’s impact of event scale: A review. Journalof Traumatic Stress, 13, 101–113.
MASLACH, C., JACKSON, S. E., & LEITER, M. P. (1996). Maslach Burnout Inventory-Manual (3rd ed.).Palo Alto, CA: Consulting Psychologist Press.
MCCANN, I. L., & PEARLMAN, L. A. (1990). Vicarious traumatization: A framework for understandingthe psychological effects of working with victims. Journal of Traumatic Stress, 3, 131–149.
NORCROSS, J. C. (1981). All in the family? On therapeutic commonalitites. American Psychologist,36, 1544–1545.
PEARLMAN, L. A. (1996). Review of the TSI Belief Scale. In B. H. Stamm (Ed.), Measurement ofstress, trauma and adaptation (pp. 414–416). Lutherville: Sidran.
PEARLMAN, L. A., & MACIAN, P. S. (1995). Vicarious traumatization: An empirical study of the effects

S. McLean et al.428
of trauma work on trauma therapists. Professional Psychology: Research and Practice, 26, 558–565.
PEARLMAN, L. A., & SAAKVITNE, K. W. (1995). Trauma and the therapist: Countertransference andvicarious traumatization in psychotherapy with incest survivors. New York: Norton.
POPE, K. S., & FELDMAN-SUMMERS, S. (1992). National survey of psychologist’s sexual and physicalabuse history and their evaluation of training and competence in these areas. Professional Psycho-logy: Research and Practice, 19, 43–49.
POPE, K. S., & TABACHNICK, B. G. (1994). Therapists as patients: A national survey of psychologists’experiences, problems, and beliefs. Professional Psychology, Research and Practice, 25, 247–258.
RODOLFA, E. R., KRAFT, W. A., & REILLEY, R. R. (1988). Stressors of professional and trainees atAPA-approved counseling and VA Medical Center internship sites. Professional Psychology:Research and Practice, 19, 43–49.
SAAKVITNE, K. W., & PEARLMAN, L. A. (1996). Transforming the pain: A workbook on vicarioustraumatization. New York: Norton.
SCHAUBEN, L. J., & FRAZIER, P. A. (1995). Vicarious trauma: The effects on female counselors ofworking with sexual violence survivors. Psychology of Women Quarterly, 19, 49–54.
SKOVHOLT, T. M. (2001). The resilient-practitioner: Burnout prevention and self-care strategies forcounselors, therapists, teachers, and health professionals. Boston: Allyn and Bacon.
TABACHNICK, B. G., & FIDELL, L. S. (1996). Using multivariate statistics (3rd Ed.). New York: HarperCollins.
VAN MINNEN, A., & KEIJSERS, G. P. J. (2000). A controlled study into the (cognitive) effects ofexposure treatment on trauma therapists. Journal of Behavior Therapy and Experimental Psychiatry,31, 189–200.
WEISS, D. S., & MARMAR, C. R. (1997). The impact of event scale. In J. Wilson (Ed.), Assessingpsychological trauma and PTSD (pp. 399–411). New York: Guilford.
ZILBERG, N., WEISS, D., & HOROWITZ, M. (1982). Impact of event scale: A cross validation study andsome empirical evidence supporting a conceptual model of stress response syndromes. Journal ofConsulting and Clinical Psychology, 30, 401–414.