the contribution of european case registers to research on
TRANSCRIPT

26
The Contribution ofEuropean Case Registersto Research onSchizophrenia
by Heinz HBfner and Wolframan der Helden
Abstract
Psychiatric case registers havebecome important instruments forepidemiological research and for theevaluation of care provided forpersons suffering from schizophrenia.Under the condition of a sufficientprovision of care, case registerspermit relatively reliable estimates of"treated" incidence and prevalence,and enable the investigation ofassociations between morbidity risks,disease courses, and variables such asecological, social, and occupationalfactors. The linkage with twin,adoption, and birth registers providesnew opportunities for the investi-gation of the impact of genetic versusenvironmental factors on the proba-bility of becoming ill with schizo-phrenia. On the basis of long-termutilization figures, case registersenable a valid measure forcontrolling utilization, effectiveness,quality, and costs of care. Becausecase registers take demographic andregional factors into account, theyenable better planning of mentalhealth services—a task that growsmore important with the shift fromhospital-based to community-basedtreatment, especially for the chronicpatients.
Cumulative Psychiatric CaseRegisters: Composition andOrganization
Cumulative psychiatric case registersare health information systems of ageographically delimited region.They register all contacts of theirpopulation with psychiatric servicesover long periods of time. Caseregisters were preceded by hospitalstatistics, which in general are basedon aggregate data and therefore areof minor value to research.They werealso preceded by disease registers towhich hospitals and physicians
reported all cases of a certaindiagnosis. Disease registers weremostly used to collect large enoughnumbers of cases with rare diseasesto enable clinical and genetic studiesto be carried out. Only relativelyrecently have more and more diseaseregisters, such as cancer registers,been run as population-related caseregisters, so that findings can begeneralized, and changes inmorbidity and environmental impactcan be assessed. Cumulativepsychiatric case registers collect andcompile their data in relation to casesand exclude multiple counting.Contrary to disease registers, theycover the entire spectrum ofdiagnoses given to inhabitants of thecatchment area when they contact apsychiatric service.
The functions of psychiatric caseregisters are determined by the extentto which they can be used.According to Wing, Wing, andHailey (1970), there are four possibleuses, namely correlation andcomparison with other population-related registers and statistics, follow-up of utilization cohorts and oflong-term utilization trends in anentire health care region, and finallydrawing of defined, representativepatient samples.
Case Identification. The procedure ofcase identification leading to regis-tration in a case register is based ona diagnosis given by a psychiatristwho contributes to the provision ofmental health care. Therefore, caseregisters could only be started inthose areas where all psychiatristshad learned to diagnose according tocommon, sufficiently precise defini-tions—for example, in Norway after
Reprint requests should be sent to Prof.Dr. H. Hafner, Zentrahnstitut furSeelische Gesundheit, J5, D-6800Mannheim, Federal Republic of Germany.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL 12, NO. 1, 1986 27
the adoption of Kraepelin's scheme ofdiagnoses in 1926 (0degard 1971b)or after the introduction of the ICDin various European countries about1960 (Kendell 1975). The use of caseregisters for epidemiological researchdepends on the reliability ofdiagnoses and on the proportion ofcases recorded in the register inrelation to the total number ofindividuals of a population whosuffer from the same disease.
The possibilities of epidemiologicaland service-related evaluationimprove when, in addition to themain diagnosis, secondary diagnosesare also registered (e.g., threeadditional diagnoses are recorded inthe Danish register (Dupont 1979)) orwhen diagnoses are based on a multi-axial classification.
In diseases that have a long course,the reliability of attribution to adiagnostic category is increased in acase register, because successivediagnoses by several services, as wellas observation of the course, can beused to validate the first diagnosticjudgment. Because the reliability ofthe diagnosis of schizophrenia hasbeen satisfactory since the 7th and8th revisions of the ICD (Klug 1983),the course of schizophrenia proves tobe long term in about 70 percent offirst onsets, and nearly all schizo-phrenics contact a psychiatric servicein their lifetimes (0degard 1971b;Nielsen and Nielsen 1977), caseregisters are important instruments ofresearch on schizophrenia. Forpsychiatric disturbances which havelow diagnostic reliability, or ofwhich only a minor proportionreceive care from psychiatricservices—for instance, neuroses—theuse of psychiatric case registers israther limited. Because of theincreasing period over which diseasecourses can be observed and thegrowing amount of information to beevaluated, the scientific value of a
case register increases with the lengthof its existence (Baldwin 1970;Helgason 1979).
Size of Catchment Area andPopulation. Registers are either runon a national level, as is done inNorway and Denmark (0degard1952, 1971a, 1971b; Kiselev 1972;Dupont, Videbech, and Weeke 1974;Weeke, Kastrup, and Dupont 1979),or on a regional or local basis.National registers cover largepopulation figures (about 5 million inDenmark, about 250 million in theU.S.S.R.). Thus, they compriserelatively large case figures of aspecific diagnosis. National registersallow epidemiologists to investigatethe relation of morbidity risk andcourse of schizophrenia to factorsshowing an uneven regional distri-bution, such as occupational statusor ecological variables.
Regional or local registers usuallycomprise the catchment area of acommunity mental health service.Therefore, the population at riskincluded in these registers iscomparatively small: Lomest, Italy—88,000 (Torre, Marinoni, and Allegri1982); Salford, U.K.-130,000-140,000 (Wing and Fryers 1976);Iceland—about 110,000 (Helgason1977); Mannheim, F.R.G.—about 300,000 (Hafner and Klug1982). The non-European caseregisters are organized on a regionallevel, but most of them cover alarger population; e.g., Maryland,U.S.A.—about 3.5 million; MonroeCounty, U.S.A.—about 700,000;Victoria, Australia—about 3.5million.
Since their catchment areas areeasy to survey, most of the regionalcase registers cover all contacts withpsychiatric services. They are able tofurnish additional information aboutservices and context variables ofutilization or course of illness. Also,
on the basis of regional registers, it isconvenient to carry out followupstudies in neighboring medical orsocial facilities. Regional caseregisters can contribute to researchon schizophrenia, especially in theevaluation of mental health caresystems and services, and in theinvestigation of epidemiologicalsamples—for instance, prospectivecohorts which allow the analysis ofchanges over long periods of time.
Information systems based onindividual data—similar to caseregisters—originated in centralizednational health care systems (e.g., inFinland). These information systemshave the advantage of compilingutilization data from all branches ofthe health care system. Even thoughthis approach reduces the reliabilityof relevant psychiatric data, generalhealth registers can be used formaking important epidemiologicalevaluations.
Services and Facilities Affiliated witha Register. When interpreting epide-miological data from case registers,one should take into considerationhow extensive the network ofservices providing data is. TheNorwegian register recordsadmissions to all psychiatrichospitals and departments run inNorway (0degard 1971a, 1971b).The Danish register additionallyincludes data on all admissions topsychotherapeutic sanatoriums andpsychiatric day and night clinics. Ingeneral, regional registers alsoreceive information about contactswith psychiatric outpatient services;this information is nearly complete incentralized health care systems (e.g.,the United Kingdom and theU.S.S.R.). In countries where alarger proportion of outpatient careis provided by psychiatrists inprivate practice (Federal Republic ofGermany, Netherlands, Italy), outpa-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

28 SCHIZOPHRENIA BULLETIN
tient utilization is often registeredincompletely.
If a register also covers neigh-boring fields of the social or healthcare system, it improves the possi-bilities of evaluating interdisciplinarycare provided to some patientgroups. Thus, the CamberwellRegister also includes data onhomeless persons who contact apsychiatric service or are providedsocial care in homes of the catchmentarea (Wing and Hailey 1972; Wingand Fryers 1976). While the majorityof the registers compile only data onmentally ill adults, a few areaffiliated with mental health servicesfor children and adolescents and withfacilities for the mentally retarded(e.g., the Camberwell Register ofPsychiatric Illness and Mental Retar-dation and the Register of EssexHospital Region in the UnitedKingdom). The Mannheim Registercomprises a subregister recording allparasuicidal acts seen in generalhospitals of the region. The inclusionof these acts, which can be identifiedrather reliably, makes possible epide-miological studies on the risk ofsuicide and attempted suicide.Furthermore, the Mannheim Registercomprises all psychiatric homes,sheltered apartments, and shelteredworkshops. Case identification ismade by a consultant psychiatrist.The inclusion of these facilitiesallows studies to be carried out ofthe utilization of alternative andcomplementary services by schizo-phrenic patients, and changes in themental health care system to beevaluated (Hafner and an der Heiden1982, 1983).
Diagnostic Groups Recorded. TheNorwegian Case Register recordsonly psychoses (ICD no. 295-299),whereas the majority of case registerscover all psychiatric diagnoses andcontacts with mental health services.
Number of Items Registered. Thenumber of registered items variesbetween 12 in the U.S.S.R. (Kiselev1972) and a maximum of 126 inAberdeen, Scotland (Baldwin 1971).Mean values are between 20 and 40items (Camberwell, 20; Denmark, 26;Iceland, 29; Mannheim, 42). Therestriction to a smaller number ofitems is generally dictated by theneed to keep the proportion ofmissing information as small aspossible. Although detailed social,health, and treatment data are ofvalue to epidemiological research, aregister that provides a minimum ofinformation about each patient in acommunity is more important thanone that provides more detailedinformation only from specific facil-ities, as pointed out by Murphy(1975).
Different levels of information—e.g., between inpatient and outpa-tient facilities—are bridged by blocksystems of data registration(Jakubaschk et al. 19.78).
One exception is the Icelandic CaseRegister. Since 1960, it has registeredonly first contacts of all persons whoutilize a psychiatric service, a generalhospital, or a nursing home andreceive a psychiatric diagnosis. Thisregister is therefore exclusively usedfor epidemiological research (Mazer1966; Helgason 1975, 1979) (seetable 1).
Access to and Crossing With PublicStatistics. In principle, diseaseregisters need aggregate data frompopulation statistics in order to getpopulation-related, age-correctedrates and to be able to compute onthe basis of parallelized controlgroups. Additionally, the localauthorities (registrar's offices, publichealth offices, residents' registrationoffices) transmit case-related infor-mation about social and demographicindicators, deaths and causes of
death, to most of the registers. Thismakes it possible to undertakeinvestigations on mortality (e.g., themortality of suicide) and to eliminatethe deceased. But it also improvesthe completeness and quality of theregistered items.
The crossing of psychiatric caseregisters with population registers,such as twin and adoption registers,is of great importance to epide-miology, especially for hypothesistesting. The best prerequisites forcrossing registers are to be found inthe Northern countries, which haverelatively stable populations,excellent population registers, andpsychiatric registers containing largecase numbers without essentialregional distortions.
Epidemiological Data
Indicators of True Morbidity. Underthe conditions of a sufficientprovision of care for the populationand high utilization rates for theinvestigated disease group, as applyin schizophrenia, first contactscompiled by a case register can beregarded as indicators of truemorbidity. Investigating the relationsamong morbidity risks, diseasecourses, and environmental variablesis only appropriate if a diagnosticgroup is sufficiently large and repre-sentative. The analysis of suchrelations or trends over longerperiods of time on the basis of caseregister cohorts is more valid thancross-sectional comparisons or longi-tudinal studies among hospitalpopulations. Besides, long-termcollection of data on representativepatient groups—starting with firstadmissions—is an excellentinstrument for observing the manifes-tation of diseases over a long periodand for assessing changes that mayoccur due to therapeutic measures
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 29
Table 1. Some psychiatric case registers in
Registers
Norway/Oslo
Denmark/Aarhus
Iceland/Reykjavic1
U.S.S.R./Moscow
U.K./Nottingham
U.K./Salford
U.K./Aberdeen
U.K./Camberwell
F.R.G./Mannheim
Netherlands/Groningen
Ireland/ThreeCounty PsychiatricCase Register
Italy/Lomest
West DublinCounty Register
Year ofstarting
1936
1937
1968
1968
1958
1959
1962
1964
1973
1973
1973
1975
1973
Informationgoing back to
1916
1905
1908
1968
1958
1959
1962
1964
1973
1973
1973
1975
Europe
Catchmentarea
National
National
Regional
National
Regional/local
Regional/local
Regional/local
Regional/local
Regional/local
Regional/local
Regional
Regional/local
Regional
Populationat risk
(approximate)
8 million
5 million
40,000
250 million
390,000
135,000
200,000
155,000
300,000
43,000
150,000
81,000
230,500
Registered population(case definition andaffiliated services)
Psychoses; psychiatricinpatlent services
All mental disorders; psychi-atric Inpatient services &partial hospitalization
All mental disorders; psychi-atric inpatients & outpa-tients; general hospitals
All mental disorders; mentalhospitals & mental healthdispensaries
All mental disorders; mentalhealth services
All mental disorders; mentalhealth services
All mental disorders; mentalhealth services
All mental disorders; mentalretardation; mental healthservices; homeless people
All mental disorders; mentalhealth services & psychi-atric components of socialservices
All mental disorders; mentalhealth services
All mental disorders; mentalhealth services
All mental disorders; mentalhealth services
Inpatient & outpatientservices; public & private
Note. — Further psychiatric case registers are run in the Netherlands on a national level and in Maastricht, In Geneva (Switzerland), Cardiff,Oxford, Southampton, Worcester (U.K.), Verona (Italy), and Basque Country (Spain).1 Not cumulative; first ever contacts only.
and health care provisions. Theinvestigation of groups at high riskand the comparison with the rest ofthe population with regard tomorbidity patterns, environmentalconditions, and long-term changesmay provide information aboutdistribution processes of morbidity
risks, connections with possible stressfactors, and special needs for care.
Exact comparisons of "admin-istrative" annual incidence rates forschizophrenia from several caseregisters cannot be made because ofdifferences in definitions (e.g.,diagnosis, first contact with a certain
facility or with the register) and indenominators (e.g., total populationor population aged 15 and over). Theinfluence of differing denominators(total population versus populationaged 15 and over) is shown by acomparison of incidence rates fromthe Mannheim Case Register calcu-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

30 SCHIZOPHRENIA BULLETIN
Table 2. Annual incidence rates for schizophrenia inMannheim—1974-80
Year
1974197519761977197819791980
First onsets0)159176210195193174190
Rate of first
Total populationper 1,000
.48
.56
.67
.63
.63
.57
.62
.59
onsets related to
Population aged> 15 per 1,000
.58
.67
.81
.75
.75
.67
.72
.71
Source: Psychiatric Case Register, Mannheim.
lated according to both methods forthe period 1974-1980 (see table 2).
In spite of these differences, theincidence rates of various caseregisters range rather precisely abouttwo mean values: the rates fromBritish registers are about a mean of15-20/100,000/year; those from theU.S.A., Ireland, and the F.R.G.amount to 50-60/100,000/year (seetable 3). With respect to confidenceintervals, this is a minor difference,but it is impossible to concludewhether it reflects a true difference inmorbidity. It might stem, forexample, from a wide or narrowdefinition of schizophrenia, theproportion of age groups at risk(especially the proportion of personsaged 20-40 years) in the totalpopulation, and the density ofmental health services affiliated to acase register.
The point or period prevalence,i.e., the rate of manifestly ill personsin a population who are in contactwith mental health services, has agreater probability of being completeand consistent. However, these ratesare influenced by regional differencesin morbidity (e.g., higher prevalenceof chronically ill in large cities or inpopulations with a higher life expec-
tancy in general). Furthermore, withlong-lasting diseases in particular,they are also influenced by the caresystem, and by high proportions oflong-term hospital patients (e.g., inIreland) (Hafner and Klug 1982;Hafner and an der Heiden 1983) (seetable 4).
Long-term Epidemiology. TheScandinavian case registers collectlarge numbers of first admissionsover long periods, and thus mayserve as a basis for investigatingcorrelations and differential processesof distribution for relevant socialvariables. While first admission ratesremained stable over several decadesin Iceland (Helgason 1975), inDenmark (Dupont and Weeke 1977;Weeke and Stromgren 1978), and inNorway (0degard 1971b) (the sameis true for the admission rates ofpersons aged up to 35 (Weeke andStromgren 1978) and of persons upto 30 years (Ugelstad 1978)), pointprevalence rates and length ofhospital stays of schizophrenicpatients varied greatly. In Norway,the sharpest decline took place in theperiod 1936-59 (0degard 1964). InDenmark, the number of schizo-phrenic patients in mental hospitals
dramatically decreased by about 30percent between 1957 and 1962(Dupont and Weeke 1977; Weekeand Stromgren 1978). By 1971, therehad been only a slight furtherreduction, which has remainedconstant since then. Preceded by asteady increase, in England andWales, the number of hospitalizedschizophrenics continuously declinedby over 50 percent in the period1956-73. These trends reflectsystematic efforts to curtail thelength of hospital stays of thechronically mentally ill and toaccommodate them in comple-mentary facilities.
Following 0degard's model,Astrup (1982) studied first admissionsfor schizophrenia recorded in theNorwegian Register from 1926 to1978. He calculated the lifetime riskof ten 5-year cohorts and one 3-yearcohort in a period of investigationcovering 53 years. He took the lifeexpectancy of the same age classes ofthe total population as a basis(timetable method). The lifetime riskfor schizophrenia declined in malesfrom 194/100,000 in 1926-30 to42/100,000 in 1977-78; in females itdecreased from 179/100,000 in1926-30 to 35/100,000 in 1977-78.To the same extent, the "lifetime riskfor the diagnostic group of reactivepsychoses and paranoid syndromes"increased from 43/100,000 to167/100,000 in males and from52/100,000 to 220/100,000 infemales. In the more comprehensivediagnostic category of "functionalpsychoses," the lifetime risk correctedfor age and age group remainedstable over a period of 53 years.According to Astrup (1982), thedecrease in first admission rates forschizophrenia can be explained bythe increasing tendency of Norwegianpsychiatrists to diagnose schizo-phrenic disorders that are precipi-tated by life events, and show severe
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 31
Table 3. Incidence rates for schizophrenia from psychiatric caseregisters
Place
NorwayNorwayIcelandCamberwell, U.K.Salford, U.K.DenmarkVictoria, AustraliaNetherlandsSouth-Verona, ItalyMaryland, U.S.A.Mannheim, F.R.G.
Mannheim, F.R.G.Rochester, U.S.A.Oberbayern, F.R.G.
Author
Astrup (1982)Astrup (1982)Helgason (1977)Hailey et al. (1974)Fryers et al. (1974)Dupont and Weeke (1977)Krupinski (1984) •Giel et al. (1980)Tansella et al. (1985)Warthen et al. (1967)Hafnerand Reimann
(1970)HafnerBabigian (1975)Dilling and Weyerer
(1975)
Year
1926-301977/781966/67
19711971
1972/731978
1978/7919831963
1965 7
1974-80 '1970
1974/75 7
Rate/1,000
.23'
.24'
.27
.13
.11.12 2/.O6 '
.16
.11 4
.08 '••
.50
.54
.59
.69
.48
Note —Includes data from case registers in Europe, United States (survey based oncomparable sources of data collection), and Australia. Incidence rate = first contacts with apsychiatric case register per year and per 1,000 total population' "Lifetime expectancy rate," hospitalized cases only, schizophrenia, and "reactivepsychoses."1 Rate separately for men (hospitalized cases of schizophrenia without "reactivepsychoses").' Rate separately for women (hospitalized cases of schizophrenia without "reactivepsychoses")- Including ICD 297.0-297.9; 298.3-298.9.' Rate for first-ever contacts.' Rate for schizophrenia and other functional psychoses.' Survey based on comparable sources of data collection1 Data from the Cumulative Psychiatric Case ReQlster of the Central Institute of MentalHealth, Mannheim, F R.G.' Personal communication.
Table 4. Prevalence rates for schizophrenia from psychiatriccase registers
Place
Baltimore, U.S.A.Camberwell, U.K.Rochester, U.S.A.IrelandMannheim, F.R.G.
Author
Wing et al. (1967)Wing et al. (1967)Babigian (1975)Walsh et al. (1980)Hafner3
Year
1963196519701973
1974-80
Rate/1,000
5.1 '3.4'4.7 2
8 . 3 '2.3 2
1 Census day prevalence.* Period prevalence.1 Data from the Cumulative Psychiatric Case Register of the Central Institute of MentalHealth, Mannheim, F.R.G.
affective symptoms or comprehen-sible delusional ideas, as a "reactivepsychosis" or a "paranoid syndrome"(0degard 1967; Astrup 1982). Thisassumption was confirmed by cohortstudies of Achte (1961), Noreik et al.(1967), and Welner and Stromgren(1958) (see, also, Kringlen 1980).
Although the provision of comple-mentary services and outpatient carereceived much greater emphasis inrecent years, the long-term studycarried out in Iceland among a muchsmaller register population (Helgason1975, 1977) showed stable rates offirst contacts with mental healthservices for schizophrenia when threeperiods were compared: 1926-27,1946-47, and 1966-67. In theregisters of Camberwell and Salford,Wing and Fryers (1976) found stablerates of first contacts for schizo-phrenia in the period 1964-74. Thefact that the admission rate forschizophrenic patients aged under 30years had remained stable in theDanish Case Register from 1957 to1976 (Ugelstad 1978) also supported0degard's assumption: The aston-ishing stability of first admissionrates over half a century indicatesthat in the countries investigated thetrue incidence of schizophreniaremained essentially unchanged. Thefindings also tallied with Goldhamerand Marshall's (1953) studies inMassachusetts. Due to non-age-corrected data from the Norwegianregister, Astrup had assumed in 1956that the frequency of schizophreniawould particularly increase in theperiod of rapid industrialization as aconsequence of the capitalist society.However, Astrup corrected hisresults and their interpretation in his1982 publication. As Astrup (1982)stated, his data are consistent withthe hypothesis that functionalpsychoses are biological reactiontypes that are relatively independentof the social environment.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

32 SCHIZOPHRENIA BULLETIN
Ecological Factors. In the industrialCity of Mannheim, which thencounted 300,000 inhabitants, Hafnerand Reimann (1970) once againfound a concentric distributionpattern of first admission for schizo-phrenia, similar to the one found inChicago by Faris and Dunham(1939). The analysis of deviatingaccumulation—e.g., in subcenters onthe outskirts of the city—indicatedthat mobility steered by sociopoli-tical measures (such as housingprojects) influences the distributionof morbidity. 0degard (1972) couldnot furnish proof of a concentricdistribution pattern of first admis-sions in Norwegian towns, althoughthe first admission rates in the Cityof Oslo, like those from Copenhagen(Dupont and Weeke 1977), werehigher than the national average.Levy and Rowitz (1970, 1973), intheir replication of the study by Farisand Dunham (1939), were able todemonstrate in Chicago a zonaldistribution pattern of the origin ofpatients readmitted for schizo-phrenia, but not of first admissions.0degard took this finding to be aconfirmation of his assumption:Within the complex structure ofmodern cities, the migrationprocesses of individuals at risk forschizophrenia cannot be described byunidimensional ecological models.Although the greatest concentrationof domiciles of persons alreadysuffering from schizophrenia is incheap dwelling areas as a conse-quence of downward mobility,0degard's findings based on caseregister data were confirmed by Hare(1956) in Bristol and Stein (1957) inLondon. They showed that firstonsets have a stronger connectionwith social isolation than withpoverty.
Civil Status. At the time of firstadmission, schizophrenics are signifi-
cantly more often unmarried than thepopulation of the same age (0degard1946; Dupont and Weeke 1977). Acomparison of two time periods(1931-45 and 1956-65) showed thatin Norway the proportion ofunmarried males among first admis-sions for schizophrenia rose from 4.3to 7.7 and that of unmarried femalesfrom 3.7 to 4.5 times the amount ofthe same age group in the generalpopulation. 0degard attributed thesedifferences to prepsychotic charactertraits. Social disability preceding thepsychosis affects men more stronglythan women, since in Europeanculture men have to play a moreactive role in matchmaking. It is truethat the rate of unmarried personsamong schizophrenics rose in aperiod in which the frequency ofmarriage declined and the averageage at marriage increased (1931-65).But the disproportionately higherincrease in unmarried schizophrenicmales reflects their disproportionatelylarger difficulties in active match-making due to prepsychoticdisturbances in the ability to estab-lish interpersonal relationships(0degard 1971a). Widowed personshave a considerably higher firstadmission rate compared to marriedones, but a lower rate thanunmarried persons. 0degard (1971a)attributes this to the missingprotective factor of matrimony,which at least in cases of less severeillness, diminishes the probability ofhospital admission.
Social Class. The uneven distributionof schizophrenia over social classesor socioeconomic strata, beingmaximal in the lower class, is aconsistent finding over nations andcontinents, with rare exceptions.Because schizophrenia frequentlyentails social disability, the unevendistribution of prevalence rates over
social classes is much more obviousthan the inequality of first admissionor true incidence rates (Adelstein etal. 1968; Goldberg and Morrison1963). However, the construct of"socioeconomic class" is tooimprecise to be used to assessdetailed hypotheses proposed toaccount for the distribution processesof individuals at risk for schizo-phrenia (0degard 1975).
Employment. Various factorsunevenly distributed over time mayhave contributed to the long-termtrend toward shorter hospital staysand extramural care of schizophrenicpatients in industrial countries(Brown 1960; Hafner and Klug1982). At first, the decrease in hospi-talized schizophrenic patients resultedexclusively from the decline of long-term hospitalized patients (Wing andFryers 1976; Fryers 1979; Hafner andKlug 1982; Hafner and an der Heiden1983). As was earlier stated byBrenner (1967) in his study coveringa 60-year period of hospitalization inNew York (1900-60), 0degard (1971)and Astrup (1982) pointed to thecorrelation of time between changesin the length of hospital stays ofschizophrenic patients and theemployment situation. The reversedtrend observed by Fryers in Salfordsince 1973 and by Weeke andStromgren on the basis of the DanishCase Register since 1971—a newincrease in the accumulation rate forlong-term hospitalized schizophrenicpatients—is clearly connected withdeclining economic activity andincreased unemployment in bothcountries. In the Federal Republic ofGermany, where unemploymentincreased more recently, theproportion of long-term hospitalizedpatients decreased until 1980. Inprinciple, the entry of psychosociallydisabled persons into the free labor
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 33
market must be understood as athreshold phenomenon: Wheneverunemployment rates and demands onthe applicants for a position are high,the number of schizophrenics who,due to their psychosocial disability,cannot find employment on the freelabor market grows disproportion-ately in relation to the totalpopulation.
Therapeutic Measures. <3degardattached only partial importance tothe introduction of psychotropicdrugs, since in Norway the greatestchanges had already occurred in the1936-50 period following the intro-duction of electroshock therapy. Insome European countries, theprovision of complementary servicesand their influence on the length ofhospital stays of schizophrenicpatients came to the forefrontbetween 1960 and 1980 (Wing andFryers 1976; Weeke and Stromgren1978; Fryers 1979; Hafner and an derHeiden 1982, 1983), but thisinfluence was counterbalanced by theunfavorable effects of the highunemployment rate (Wing and Fryers1976; Weeke and Stromgren 1978;Weeke, Kastrup, and Dupont J979;Dupont 1979). An increasedprovision of complementary services,especially of sheltered homes, apart-ments, and workshops, can keep theproportion of schizophrenic long-staypatients low even in times ofeconomic recession and make itpossible for the majority (about 75percent) of schizophrenic patientsneeding care for over 1 year to livein the community (Hafner and an derHeiden 1983).
Occupation and Social Mobility.From an analysis of the age-correcteddistribution of first admissions forschizophrenia over various occupa-tional groups in the period 1926-65,0degard (1971a, 1971k) deduced that
the largest proportion was to befound in occupational groups withlittle practical and theoretical trainingand low social prestige. He foundhigh rates in sailors and farmlaborers, and considerably lowerrates in first mates of the merchantmarine and farmers, although theirsituation in life and work iscomparable. Since the morbidity riskof Norwegian seamen was abouttwice as high as that of industrialworkers belonging to the same socialclass, 0degard concluded that theeconomic status had no direct effecton the morbidity risk.
Long-term changes in the charac-teristic features of occupationalgroups gave further opportunities tocompare two competing hypotheses.The "selection" hypothesis attributesthe low socioeconomic status ofschizophrenics to their preexistingdisorder or to their predisposition todevelop disorder. By contrast, thesociogenetic or "breeder" hypothesislinks the development of schizo-phrenia to preexisting social precipi-tants or stressors. In Norway, theoccupational groups with unusuallyhigh first admission rates for schizo-phrenia (seamen and farm workers),which continued to increase in theperiod of observation, showed asharp decline in employment.0degard demonstrated this processby the example of female domesticservants, an occupation thatnowadays has almost died out inNorway: The exceptionally high firstadmission rates for schizophrenia inthis occupational group contrastedwith significantly lower rates forsingle housewives withoutoccupation, a group which differedvery little from the domestics withrespect to their life and worksituation. From this, 0degardconcluded that occupations which aredying out and offer little chance ofsuccess are the domain of individuals
who, because of their socialdisability, avoid changing to morepromising occupations. They arejoined by newly disabled individualsfrom other occupational groups, forwhom the lower threshold of qualifi-cation makes it possible to findemployment. These data do notsupport the sociogenetic hypothesisthat schizophrenia is caused orprecipitated by social strain.However, the selection hypothesis issupported by the substance anddimension of the described processesof distribution over social situations.Thus, 0degard's findings in caseregister studies point in the samedirection as the findings of Goldbergand Morrison (1963) on intragenera-tional mobility of individualssuffering from schizophrenia. Eaton(1980) recently used a stochasticmodel to demonstrate that socialintergenerational and intragenera-tional mobility in male schizo-phrenics, compared to normal males,fully explains the quantitative differ-ences in social class distribution.
Selective Effects of PremorbidBehavioral Patterns. Since theprocesses leading to uneven distri-bution in marriage, in the choice ofan occupation, and in migration werein effect before first admission, theymust have been determined bypremorbid traits of those who laterwould develop schizophrenia. Noreikand 0degard (1966) retrospectivelyexamined the school files of a sampleof schizophrenic patients andcompared them with a matchedcontrol group. They found that thosepupils who later developed schizo-phrenia, on the average, hadobtained lower grades and had hadfewer social relations than their class-mates. These findings, which havesince been verified by prospectivestudies of individuals at high risk forschizophrenia (Garmezy 1981),
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

34 SCHIZOPHRENIA BULLETIN
support 0degard's (1972) andAstrup's (1982) assumption that thesocial processes which lead to anuneven distribution of the morbidityrisk are initiated by the preexistingpersonality traits of individuals wholater develop schizophrenia.
Schizothymic personality traits,lack of social contact, rigidity, andlack of self-assertiveness can also befound more frequently in the lowerclasses (Odegard 1975). From thisapparent evidence of social selection,Odegard (1975) deduced that schizo-phrenia is deeply rooted in thepatient's past and that its causesshould be sought, not at the time ofonset, but in the premorbid period,©degard considers it possible that theearliest manifested disturbances arenot character traits, but initialsymptoms of a psychosis that istaking a very slow course. At thisearly stage, the personality changecan barely be recognized as patho-logical. 0degard's conclusion hasimplications for theories about theproductive (positive) symptoms thatcharacterize schizophrenia. The factthat the productive symptoms are notpowerful predictors of long-termoutcome (Strauss and Carpenter1977; Tsuang, Woolson, and Fleming1979; Schubart et al. 1982) could beexplained as follows: The realprocess of schizophrenia, which isaccompanied by the development ofsocial disability and is of greatestprognostic value, in general precedesand is largely independent of,episodes of productive symptoms,which may be precipitated byadditional factors.
Geographic Mobility (Migration).The first comprehensive empiricalstudy of the relation betweenmorbidity rates for schizophrenia andmigration was published by 0degardin 1932. It was based on data fromthe Norwegian Case Register and on
hospital admission data fromMinnesota. The studies demonstratedelevated first admission rates inNorwegians who had emigrated tothe United States in comparison tothe native population in the UnitedStates and in Norway. Even inNorwegians who had reemigratedfrom the United States, the firstadmission rates for schizophreniawere elevated (0degard 1973).Malzberg (1969) demonstrated thatthe differences diminished whenanalyses controlled for the variablesof age and sex. The tendency,however, remained.
Jointly with members of his staff,0degard then carried out severalsystematic studies on the influence ofmigration processes on the morbidityrate for schizophrenia. Within thecountry, Dalgard (1971), Astrup andOdegard (1960), and 0degard (1975)found significantly lower firstadmission rates for schizophrenia inmigrants from rural to urban areasand from large cities to suburbs.However, the frequency of firstadmission was increased in migrantsfrom urban to rural areas. Inconnection with his findings onprocesses of labor migration,0degard favored an explanationsuggested by the selective hypothesis:Premorbid personality traits,especially the lack of social relation-ships and occupational success, makeit easier to decide to leave home andoccupation. This explains the factthat in migration streams connectedwith social ascent there are relativelyfew, whereas in migration streams ofindividuals with little social successthere are relatively many, individualswith a disposition to schizophrenia.
The morbidity rate for schizo-phrenia in Hungarian emigrants toNorway, who had left their homecountry mainly for political reasons,was investigated by Eitinger andGriinfeld (1966) on the basis of the
Norwegian register. In the periodfrom 1956 to 1963, hospitaladmission rates for schizophreniawere slightly elevated in emigrantscompared with the Norwegianpopulation and showed a trend toassimilate after a longer stay inNorway.
On the basis of hospital statisticsfor England and Wales, Cochrane(1977, 1979) found significantlyhigher first admission rates forschizophrenia in Irish women (butnot men) and in immigrants from theWest Indies and Pakistan.Bebbington et al. (1981) comparedthe morbidity rates of West Indianimmigrants with those of Irishimmigrants and of the nativepopulation. Their study used datafrom the Camberwell Register andfrom an additional population studycovering the catchment area of theregister. The purpose of the studywas to test the following three alter-native hypotheses: (1) The morbidityhypothesis—the morbidity of schizo-phrenia is dependent on racial ornational differences. (2) The selectionhypothesis—previous abnormalitiesreflecting a predisposition to schizo-phrenia influence the decision toemigrate. (3) The stress hypothesis—stress due to emigration and confron-tation with a foreign culture increasesmorbidity.
A comparison between immigrantsand the population born in Englandcorrected for age showed signifi-cantly higher true incidence rates forschizophrenia in immigrants from theWest Indies, in females moremarkedly than in males. Admissionrates and rates for treated prevalencewere also elevated in this group. Inimmigrants born in Ireland,Bebbington et al. (1981) could onlypartially verify Cochrane's findings,which had not been corrected forage: Incidence rates for schizophreniawere clearly lower in Irish men and
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL 12, NO. 1, 1986 35
dearly, although not considerably,higher in Irish women than in thelocal population. Bebbington et al.points out that the three hypothesesare not exclusive, but they attributethe greatest importance to theselection hypothesis.
The case register study on psychi-atric morbidity of foreign workers inMannheim done by Hafner (1980)underlines the extraordinary impor-tance of the selection hypothesis. Inthe period of investigation—1974-78—about 13 percent of theMannheim population wereforeigners. The age composition offoreign workers showed anoverrepresentation of younger agegroups and thus differed markedlyfrom the German population.Consequently, the rates of psychi-atric morbidity among foreignworkers were correspondingly lower.When corrected for age, the rates oftreated schizophrenic episodes (acomparison of first admission rateswas not appropriate because of thelow number) were still significantlylower than those of the Germanpopulation. The lowest rates werefound among Turks and slightlyreduced rates were found amongItalians, whereas Yugoslavs and thegroup of other foreigners in whichrefugees prevailed did not differsignificantly from the nativepopulation. The distribution of therates for alcohol-related diseases andorganic brain syndromes wasanalogous; however, the rates foraffective psychoses and for neuroticand psychosomatic disorders showedno marked differences between theforeign groups and the Germanpopulation. Hafner (1980) assumedthat both the decision to go abroadto work and the chances of passing amedical screening before emigrationare influenced by an early onset ofchronic disease courses and bypremorbid abnormalities of person-
ality. Medical examination by theGerman labor administration is mostsevere for Turkish workers. Highermorbidity rates among women ofmigratory workers may be explainedby the fact that they contribute lessto the decision to emigrate and areexamined less thoroughly. In contrastto the earlier mentioned emigrantgroups, in Germany foreign workersrepresent an example of positiveselection (reduced disposition toschizophrenia and other long-termmental disorders). As a consequence,in comparably poorer regions inwhich large proportions of thehealthy population emigrate, theremaining individuals tend to bethose who are old and at risk forchronic mental disorders. This mayresult not only in an unhealthypopulation structure, but also in arelative increase in the morbidityrates for schizophrenia, as was foundin Istria, a region in Yugoslavia thatwas affected by several waves ofemigration (Lemkau et al. 1980), andin Ireland (Scheper-Hughes 1979).
Morbidity Risk for SchizophreniaAfter Extreme Stress. In severalstudies, Eitinger (1959, 1960, 1967)used data from the Norwegian CaseRegister to investigate the morbidityrate for schizophrenia in individualswho had spent several years inGerman displaced persons (DP) andconcentration camps by means ofdata from the Norwegian CaseRegister. In a first study, he found 14persons suffering from schizophreniaamong a total of 19,000 personsreturned from German concentrationand DP camps. Thus, in this group,the rate for the lifetime risk ismarkedly higher than in Norwegians.However, the group could not becompared for age, social class, orother factors.
In a later study, Eitinger andStrtfm (1973) compared a total of
4,447 Norwegians who had returnedfrom German concentration campswith a control group matched forage, sex, and socioeconomic status.The investigators aimed at a moreprecise determination of mortalityand morbidity following severestress. A representative sample of 480males and 18 females out of thisgroup were interviewed. The preva-lence rate for schizophrenia amongsurvivors of concentration campswas identical with that found in thecontrol group of the Norwegianpopulation. In each of the twointerview samples, three cases ofschizophrenia had occurred since thewar. In contradiction to his formerassumption and to the assumption ofother authors (e.g., Baeyer andBinder 1982), which were not basedon epidemiological results, Eitingerthus could not find any indicationthat the risk of schizophreniaincreases after the severe stress of astay in a concentration camp. Thesefindings, as well as the unchangedincidence rates for schizophrenia inbelligerent countries, are of impor-tance for the hypothesis that any sortof mental stress precipitatespsychoses.
Risk for Subgroups of Schizophrenia.As long as clinical diagnosis is notbased on standardized diagnosticinstruments and as long as detailedfindings are not recorded, caseregister data do not allow inferencesto be drawn about changes in theincidence of certain symptoms,syndromes, or subgroups of schizo-phrenia. Only syndromes that arereliably identified, such as febrilecatatonia, are an exception. On thebasis of hospital statistics andcatamnestic samples, Pauleikoff(1969), Huber (1969) and M. Bleuler(1972) had assumed that thesyndrome of febrile catatonia hadceased to occur since 1960 as a result
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

36 SCHIZOPHRENIA BULLETIN
of improved therapy. By means ofcase register data and data on theutilization of a unit for intensivepsychiatric care in Mannheim,Hafner and Kasper (1982) showedthat in the period 1974-81, acute life-threatening catatonia occurred withan almost unchanged frequency ofepisodes per year, about 1/300,000total population.
The fact that this syndromedisappeared from the psychiatrichospitals in the F.R.G. may beexplained by changes in the systemof medical care: After the opening ofintensive care units at hospitals ordepartments for internal medicine,neurology, and anesthesiology fromabout 1960 on, the treatment of life-threatening syndromes was shiftedfrom the psychiatric hospitals, mostof which are insufficiently equipped,to these units.
Special Population Groups at Riskfor Schizophrenia. Noreik andOdegard (1966) compared theadmission rates of a cohort consistingof about 13,000 Norwegians who inthe period 1916 to 1925 had finishedsecondary education, with those ofGypsies and homeless persons andthose of neglected and criminaladolescents in Norway. While theacademic cohort showed a slightlylower prevalence rate for schizo-phrenia in both sexes compared tothe total population corrected forage, the rate of schizophrenia wassignificantly higher than expectedamong individuals without fixedabode and dissocial adolescents,©degard's cohort studies allowstatements on the morbidity risk ofthe investigated population group,whereas the increased prevalencerates for schizophrenics amonghomeless persons found inCamberwell (Wing et al. 1972) pointto an augmented risk of social deteri-oration and social disintegration in
persons suffering from schizophrenia.The followup investigation of repre-sentative samples, drawn from theCamberwell Case Register, in thecommunity (Wing and Olsen 1979)confirmed this tendency: Many ofthem lived in poor circumstances,were out of work, and not able toaccomplish their tasks at home.Nevertheless, few members of thissocially neglected group wanted toaccept offers made by mental healthor welfare services. Apparently incontradiction to this, Wing andBrown (1970) had found that mostschizophrenic patients who had beenliving in mental hospitals for manyyears preferred to stay there. Chronicschizophrenic patients seem to bemore afraid of a change in theirpresent circumstances than of the lowquality of life often characterizingconditions in the hospital or in thecommunity.
Genetic Studies.1 After Luxenburger(1936) had used twin registers to getundistorted concordance rates forschizophrenia, Tienari first examineda larger series in 1963: 903 out of1,053 pairs of male twins from theFinnish Twin Register. Among 15monozygotic pairs with a clearlyschizophrenic index twin, he foundno cotwin who met strict criteria forschizophrenia. When a widerdefinition was applied, three cotwinscould be identified as cases: one asreactive psychosis and two asborderline schizophrenia. LaterTienari (1975) crossed the originaltwin population with the register ofall psychiatric hospitals and psychi-
1 E. Kringlen (1980) described most ofthe results of the epidemiological studiescarried out among twins and adoptedpersons in his report on the contributionof the Scandinavian countries to researchon schizophrenia. We therefore confineourselves to a short survey.
atric outpatient departments inFinland. The result was essentiallyunchanged. Only the cotwin firstdiagnosed with a reactive psychosislater received a diagnosis ofschizophrenia.
The most important study is theone carried out by Kringlen (1964).For the period 1901-30, he drew atotal of 25,588 twin pairs out of theNorwegian national birth statisticsand matched them with the CentralRegister of Psychoses. Theconcordance rate of monozygotictwins was 25 percent when narrow,and 38 percent when broad, defini-tions of schizophrenia were applied.The corresponding rates for dizygotictwins were 4 percent and 10 percent,respectively. Kringlen also found that38 percent of monozygotic cotwinshaving schizophrenic partners weregiven the diagnosis of neurosis or"borderline" disease and that about30 percent were clinically healthy.Similar to Slater (1953) and Tienari(1963), Kringlen showed that themore dependent, submissive twin isat greater risk to develop schizo-phrenia in the course of his life thanthe dominant one.
Fischer, Harvald, and Hauge(1969) and Fischer (1973) crossed allsame-sexed twin pairs listed in theDanish Twin Register as being bornin the period 1870-1920 with theNational Psychiatric Register inAarhus. Among the 21 monozygoticand 41 dizygotic twins of the samesex who had a schizophrenic partner,they found concordance rates ofschizophrenia of 24 percent inmonozygotic and 10 percent indizygotic twins. Furthermore, Fischerexamined the children of healthymonozygotic cotwins. The morbidityrate of these children almost equalsthe rate of monozygotic partners ofschizophrenic twins. The number isstill too small, however, for thesefindings to be generalized. The
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL 12, NO. 1, 1986 37
difference between the consistentlylower concordance rates from studiesusing case register data and themostly much higher and morestrongly varying risk figures fromnonrepresentative twin populations ismainly due to different samplingmethods. The introduction of registerstrategies greatly contributed toprogress in psychiatric genetics(Rosenthal 1962; Kringlen 1967;Shields 1975).
The Danish adoption studies weredesigned to test the alternativehypotheses of a genetic transmissionof schizophrenia versus afamily/environmental transmission ofschizophrenia. They were based oncrossing an adoption register with theDanish Case Register. A sample of5,483 children from the Province ofCopenhagen who had been legallyadopted by nonrelatives in the period1924-47 formed the basis of atwo-part investigation: (1) acomparison between adopted-awaychildren of schizophrenic patientsand adopted children of nonschizo-phrenic parents (Rosenthal et al.1968) and (2) a comparison betweenthe biological and adoptive relativesof schizophrenic adoptees and thoseof nonschizophrenic controladoptees. For case identification inthe parents, the register data weresupplemented by reports on theparents taken from the adoption files(Kety et al. 1968).
The adopted-away children ofschizophrenic and control parentsunderwent a blind interview and alarge battery of tests. Three out of 76index cases were given a diagnosis ofschizophrenia by at least one rater,whereas none of the control caseshad developed schizophrenia. As thefindings were not significant becauseof the small sample size, the investi-gators extended the case definition tothe so-called "schizophrenia spectrumdisorder," a rather imprecise
diagnostic group. They then found 24(31.6 percent) positive cases among76 index cases and 12 (17.9 percent)among 67 control cases, a differencethat was significant on the 0.5percent level. The same casedefinition and the same method ofdata collection were applied in thesecond phase of the study, whichtook as its point of departureadopted persons who developedschizophrenia. In this phase, thebiological parents were comparedwith the adoptive parents.
Meanwhile repeated secondaryanalyses were made on the basis ofthese data (Haier, Rosenthal, andWender 1978; Kendler, Gruenberg,and Strauss 1981a, 1981b, 1981c;Iidz, Blatt, and Cook 1981). Thefindings, partially processedaccording to the criteria of DMS-III(Kendler, Gruenberg, and Strauss1981a, 1981b, 1981c), generallyaffirmed that neither the number ofbiological relatives who received areliable diagnosis of schizophrenianor the number of index cases amongthe adoptees were sufficiently largefor definite conclusions to be drawn.There remains a clear trend toward agreater probability of developingschizophrenia in genetic as comparedto adoptive parent and child relation-ships. This trend needs to beconfirmed on the basis of larger casenumbers and of precise criteria ofcase definition and identification. Asa next step, the adoption registerscould be crossed with a psychiatriccase register on a national level.
Quite a few of the Scandinavianregister studies were carried out inpopulations at risk. Mednick andSchulsinger (1971) undertook aprospective longitudinal study amongchildren of schizophrenic mothers inDenmark. Out of 173 children, whowere re-examined at an average ageof 28, eight (4.6 percent) comparedto one (1.1 percent) out of 91
controls had developed schizo-phrenia. Tienari et al. (1979)identified all females who had beengiven the diagnosis of schizophreniaand had been recorded in the FinnishCase Register between 1960 and1970. By crossing these data with thebirth register, he formed a sample ofthose 120 children who had beenseparated from their genetic mothersby adoption. Kringlen (1978) investi-gated a sample of 48 married couplesin which both partners had afunctional psychosis recorded in theNorwegian Register and had beenhospitalized. The average age of theparents was 38 years. Five out of 25children (20 percent) developedschizophrenia; seven (28 percent)developed a reactive psychosis. Whencorrected for age, the lifetime expec-tancy rate of schizophrenia wasrelatively low, at 29 percent.Kringlen emphasized that 28 percentof the children of two schizophrenicparents had remained clinicallynormal.
Evaluative and ServicesResearch
Assessment of Needs, Planning, andEvaluation of Services. Case registerscover only treated morbidity. Aprecise assessment of changes inmorbidity, especially in themorbidity of those mental disordersin which only a minority receivemental health services, requiresadditional field studies or datacollection in primary health services,particularly in general practice(Odegard 1972; Fryers 1979). A largeamount of work is required in suchstudies. L. Wing et al. (1968) pointedout that about 100,000 personswould have to be examined per yearin order to find 15 new (first onset)cases of schizophrenia. Therefore,field studies are carried out only inrare cases in needs assessment and, if
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

38 SCHIZOPHRENIA BULLETIN
so, with a precise formulation of theresearch questions to be addressed.
Although they cannot contributemuch tc fhe direct assessment ofunserved needs of a population,registers are of great importance inevaluating the adequacy of servicesand care systems. They allow us toascertain which group of patientsutilized which elements of availableservices at what time and to whatextent. They enable us to identifypatients who do not utilize offers ofcare recommended to them, andfacilitate the assessment of specificneeds of patient groups, e.g., foralternative offers of care, which arestill uncovered (Fryers 1979). T"hispresupposes the use of existingknowledge of specific needs of certainpatient groups, which—in case theyare not covered—lead tomisplacement or lack of care.
Demand and Utilization. The utili-zation of mental health servicescannot be equated with a region'sactual needs. Data on utilization alsodo not permit direct conclusions onthe effectiveness of services to bedrawn. To determine the uncoveredproportion of need (see Matthew1971; Alderson 1976; Hafner 1979;Jakubaschk et al. 1978; Klug, an derHeiden, and Scheel 1980), it wouldbe necessary to do field studies asdescribed above. The field studieswould include persons who rejectpsychiatric care although it is clearlyindicated or turn to other medicaldisciplines (see Weyerer et al. 1982).With only a few exceptions, psychi-atric case registers are restricted toutilization data from psychiatricservices. The amount of missinginformation resulting from thisrestriction lessens the generalizabilityof findings, but this problem appliesmuch less to the group of schizo-phrenic patients than to those withmilder conditions. When data are
also collected from alternative andcomplementary services, as is doneby the Mannheim Case Register(Hafner and Klug 1980, 1981, 1982),changes of care provided to chronicschizophrenic patients—following therecommendations laid down underthe concept of "comprehensivecommunity mental health care"(World Health Organization 1973)—can be described continuously.
A crude comparison of census dataon treated prevalence collected byeight case registers for all diagnosticgroups shows considerable differ-ences at the first glance (see table 5).The data partially reflect differentstages of the development ofoutpatient and complementaryservices in the respective regions.Besides, they reveal differences in theproportion of long-term hospitalizedpatients and the completeness of datacollection by the institutionscontributing to mental health care(see, also, Walsh et al. 1980).
Planning. In the past, changes in thefield of mental health care were oftenmade without taking into consider-ation the scientific knowledge aboutfactors that influence the extent ofdisease and impairment in a
population and also the provision ofoptimal care (Wing and Hailey 1972).For this reason—often to an unusualdegree and unacceptable to thepersons affected—political ideologiesfound expression in laws or measuresalleged to improve mental healthcare.
The prediction of future need onthe basis of utilization trends, anddemographic and social develop-ments, is important for planningservices. Its reliability increases whenthe factors influencing a large part ofthe variation are analyzed and thetrends are observed over a longerperiod of time (0degard 1972).
There are numerous examples ofvaluable contributions by caseregisters to the planning of psychi-atric services. Thus, in 1976, theneed for psychiatric hospital beds inthe Danish provinces was assessed onthe basis of the Danish Case Registerfollowing a request of thegovernment. The findings were usedto prepare the transfer of responsi-bility for psychiatric hospitals fromthe state government to theprovincial governments (Stromgren etal. 1979). In the United Kingdom,case register studies have long beenused to interpret the misleading
Table 5. Point prevalence rates of some European caseregisters '
Register
Camberwell, U.K.Salford, U.K.Mannheim, F.R.G.Randers, DenmarkThree County, IrelandGroningen,
NetherlandsLomest, ItalyAberdeen, U.K.
Rate
769538681822'
1770834
268682
Pointprevalence
Dec. 12, 1974Dec. 31, 1974May 15, 1974March 1, 1977March 31, 1973Dec. 31, 1975
Dec. 31, 1975Dec. 31, 1966
Source
Wing & Fryers (1976)Wing & Fryers (1976)Hafner & Klug 1981Kastrup & Bille (1980)Walsh et al. (1980)Giel & ten Horn (1981)
Marinoni et al. (1983)Baldwin (1971)
• Inpatient and outpatient care; rates per 100,000 total population.' Census data added.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL 12, NO. 1, 1986 39
aggregate data of hospital statisticsand of the National Health Service,and also to correct prognoses of needfor hospital beds and alternativefacilities (Department of Health andSocial Security 1975).
Evaluation of Utilization. In the lastdecades, a transition from hospital-centered to community mental healthcare, including outpatient andcomplementary services, took placein many European countries (WorldHealth Organization 1973;Department of Health and SocialSecurity 1975; Report of the ExpertCommission on Psychiatry, F.R.G.,1975). This process of marked changein the system of care, which wasaccompanied by a considerableincrease in treatment prevalence, hasbeen evaluated in various countrieson the basis of case register data(Wing and Bransby 1970; Wing andFryers 1976; Hafner and Klug 1980,1981, 1982; Giel and ten Horn 1982).
It appears that the different levelsof psychiatric care have contributedto the increase in treatment preva-lence to a varying extent. The ratefor contacts with complementary andoutpatient services rose drastically,whereas the population-related rateof occupied beds declined in theregions analyzed or, in case of lowerinitial values, remained stable (Wingand Fryers 1976; Hafner and Klug1982; Hafner and an der Heiden1983).
In Mannheim, for example, thetotal number of treated episodes peryear of schizophrenic patientsincreased from 485 to 756 in theperiod 1974-79; in the same period,the number of occupied bedsdecreased from 243 to 209 (Hafnerand Klug 1981). There are tworeasons for this trend: (1) theincreased provision of outpatient andcomplementary services, accom-panied by changes in the help-seeking
behavior of schizophrenic patients(an der Heiden and Klug 1980;Hafner and an der Heiden 1982);(2) the drastic shortening of stays ininpatient services, as reported fromother case registers (Gam 1980; Wingand Bransby 1970; Fryers 1974). Thereduction of long-term hospital stays(over 1 year) is followed by a rise inshort- and medium-term stays so thatin spite of unchanged or decreasingrates of occupied beds, an equalnumber of schizophrenic patients hasto be cared for at more frequentintervals during the same period oftime.
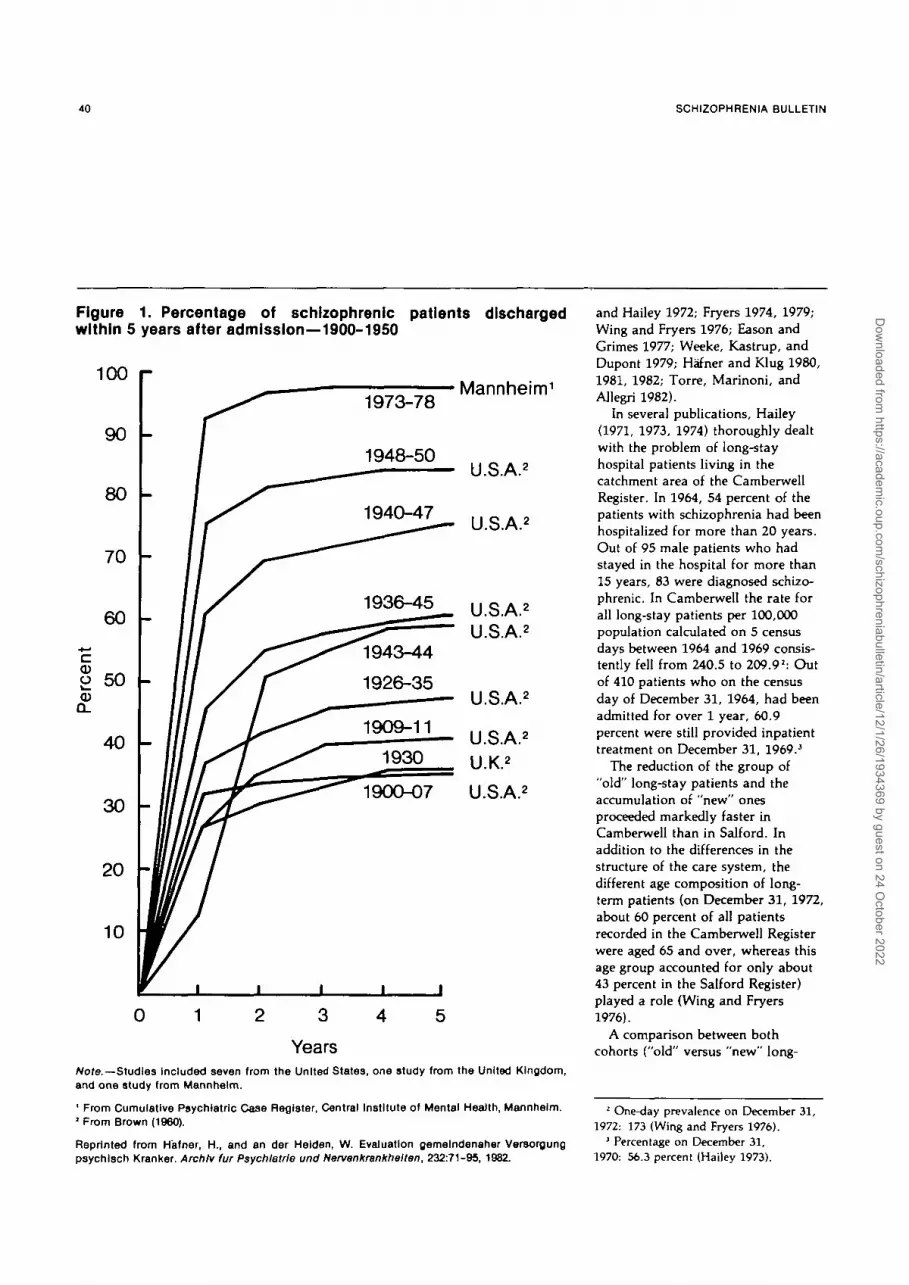
This historical trend in the care ofschizophrenic patients is clarifiedwhen the respective rates for theyears 1974-79 from the MannheimCase Register (Hafner and an derHeiden 1982) are added to a reviewof eight studies on discharge rates forschizophrenic patients 1-5 years aftertheir first admission carried outbetween 1900 and 1950 (Brown1960). The proportion of schizo-phrenics who, after first admission,stay in the hospital for more than 1year has consistently declined sincethe turn of the century, from about70 percent to about 5 percent in 1980(see figure 1).
Simultaneously with the reductionof the average length of stay, thecase/episode ratio has increased. In1974, one hospitalized schizophrenicpatient in Mannheim accounted for1.16 inpatient treatment episodes peryear, but this value increased to 1.28by 1979 (Hafner and an der Heiden1982), including long-term patients.
Long-term Patients. In the past,schizophrenics constituted by far thelargest proportion of long-termhospitalized patients. On December31, 1972, for example, 60.3 percentof all long-term hospital patients inCamberwell had been given adiagnosis of schizophrenia; in Salford
they amounted to 66.8 percent in thesame period (Wing and Fryers 1976).A 1-day census carried out inMannheim on May 30, 1973, ascer-tained a proportion of 53 percent(Hafner and Klug 1982).
When the composition ofinpatients over several census days isexamined on the basis of case registerdata, the following trend can bediscerned: In all diagnostic groups,the proportion of long-term patientsin the total number of occupied bedsis continuously diminishing;however, the rate of decrease greatlydiffers in the various areas of care(Wing and Bransby 1970; Wing andFryers 1976; Hafner and Klug 1980,1981, 1982; Giel and ten Horn 1982).An example from England and Walesreported by Wing and Fryers (1976)may illustrate this: In the period1964-74, the rate of schizophrenicpatients fell from 72.9 percent to 59.9percent in Camberwell, whereas inSalford it remained stable between1967 and 1973 at a high mean of 82percent.
Comparison of "Old" and "New"Long-stay Cohorts. To show thechanges in the need for long-termhospital admission in the context of acommunity mental health service, thetotal cohort of long-term patients canbe divided into the following twosubcohorts: (1) Patients who on agiven census day had beenhospitalized for over 1 year; to alarge part, these are the inheritanceof a past hospital policy. (2) Patientswho from this census day on becomenew long-stay patients under theconditions afforded by moderntreatment.
In all case register areas, a corre-sponding accumulation of "new"long-stay patients can be observed,and does not seem to have yetreached its peak (Wing and Bransby1970; Hailey 1971, 1973, 1974; Wing
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022
40 SCHIZOPHRENIA BULLETIN
Figure 1. Percentage of schizophrenic patients dischargedwithin 5 years after admission—1900-1950
Mannheim1
U.S.A.2
U.S.A.2
U.S.A.2
U.S.A.2
U.S.A.2
U.S.A.2
U.K.2
U.S.A.2
0 1 3 4
YearsNora—Studies included seven from the United States, one study from the United Kingdom,and one study from Mannheim.
' From Cumulative Psychiatric Case Register, Central Institute of Mental Health, Mannheim.1 From Brown (1960).
Reprinted from Hafner, H., and an der Helden, W. Evaluation gemelndenaher Versorgungpsychlsch Kranker. Archlv fur Psychlatrle und Nervenkrankhelten, 232:71-95, 1982.
and Hailey 1972; Fryers 1974, 1979;Wing and Fryers 1976; Eason andGrimes 1977; Weeke, Kastrup, andDupont 1979; Hafner and Klug 1980,1981, 1982; Torre, Marinoni, andAllegri 1982).
In several publications, Hailey(1971, 1973, 1974) thoroughly dealtwith the problem of long-stayhospital patients living in thecatchment area of the CamberwellRegister. In 1964, 54 percent of thepatients with schizophrenia had beenhospitalized for more than 20 years.Out of 95 male patients who hadstayed in the hospital for more than15 years, 83 were diagnosed schizo-phrenic. In Camberwell the rate forall long-stay patients per 100,000population calculated on 5 censusdays between 1964 and 1969 consis-tently fell from 240.5 to 209.9J: Outof 410 patients who on the censusday of December 31, 1964, had beenadmitted for over 1 year, 60.9percent were still provided inpatienttreatment on December 31, 1969.3
The reduction of the group of"old" long-stay patients and theaccumulation of "new" onesproceeded markedly faster inCamberwell than in Salford. Inaddition to the differences in thestructure of the care system, thedifferent age composition of long-term patients (on December 31, 1972,about 60 percent of all patientsrecorded in the Camberwell Registerwere aged 65 and over, whereas thisage group accounted for only about43 percent in the Salford Register)played a role (Wing and Fryers1976).
A comparison between bothcohorts ("old" versus "new" long-
! One-day prevalence on December 31,
1972: 173 (Wing and Fryers 1976).
' Percentage on December 31,
1970: 56.3 percent (Hailey 1973).
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 41
term patients) made in Mannheim(census day: May 30, 1973; Hafnerand Klug 1982) showed that, under acommunity mental health service,fewer schizophrenics needed long-term hospitalization than before;their rate decreased from 53 percentof the old to 35 percent of the newlong-stay patients (Hafner and 'Klug1982). Moreover, schizophrenicsbecame long-stay patients at aconsiderably later time—mostly onlyafter several preceding hospital stays.Parallels to the findings fromMannheim are to be found in theUnited Kingdom (Fryers 1979).
Beds Needed for Long-stay Patients.Before case register data wereavailable, estimations of future needsfor hospital beds were based on-extrapolations from the change inbed occupancy over a defined period(e.g., Tooth and Brooke 1961) or ona retrospective analysis of theprobability of discharge in relation todifferent lengths of stay in psychi-atric hospitals (e.g., Baldwin andHall 1967). Only the case-relatedinclusion of accumulating new long-stay patients in case registers allowedplanners to make a differentiatedanalysis of changes in bed needs andresidential placements resulting fromchanges in the mental health caresystem (Eason and Grimes 1977;Weeke, Kastrup, and Dupont 1979;Fryers 1974, 1979; Hafner and Klug1982). Thus, case register data alsopermit a better interpretation of thetrends observed in hospital statistics.
Complementary Services for Schizo-phrenics in the Community. Manychronically ill patients, who formerlywould have been consigned to long-term residence in a psychiatrichospital, can now live in thecommunity due to the extensivenetwork of complementary servicesavailable. Studies carried out in the
United Kingdom (Mann and Sproule1972; Mann and Cree 1976; Magnus1967) showed that, according toclinical judgment, even a largepercentage of the new long-termhospitalized patients did not requiretreatment in a psychiatric hospital.
Wing (1982) investigated thespecific needs of patients from theCamberwell Register who on June 30,1979, had had contact with ahalfway or complementary facilityfor at least 1 year. The studycomprised institutions providing 24-hour care (hospital departments,homes) and also day clinics, daycenters, and sheltered workshops.Patients with one episode oftreatment of less than 1 year andpatients who had been hospitalizedfor more than 1 year at the censusday were excluded. Out of the 181patients aged over 18—correspondingto a rate of 139 per 100,000population—who met the criteria,almost half had received a diagnosisof schizophrenia. Regarding thedistribution of sociodemographicvariables, the composition wassimilar to that found in long-termhospital patients. In three quarters ofthe patients, the first contact with apsychiatric institution was more than10 years in the past; only four ofthem had never been hospitalizedbefore. Although the findings of thisinvestigation primarily reflect thespecific aspects of the mental healthservice in Camberwell, some generalstatements can be formulated. Thus,Wing (1982) emphasizes the need toexamine each patient regularly inorder to adjust the patient'splacement to his needs and toimprove his abilities in anenvironment that optimallyencourages his independence.
The provision of support andadvice to relatives as part of comple-mentary health care for schizophrenicpatients is of special importance.
Over 40 percent of the sample drawnfrom the Camberwell Register hadrelatives who more or less regularlylooked after them. The relatives oftenhad to meet the same requirements asthe staff of homes and nursing homeswithout being provided comparableinstitutional support.
A study based on data from theMannheim Case Register (Hafner andan der Heiden 1983) showed to whatextent the focus of care for chronicschizophrenic patients can be trans-ferred from the psychiatric hospitalto alternative services. In the periodbetween the two census days,December 15, 1974, and December15, 1979, the proportion of patientswho remained in the hospital formore than 1 year among the totalnumber of schizophrenic patientstreated in psychiatric hospitals andhomes (about 200-220) decreasedfrom 85 percent (=> 164) to 68percent (= 148). In the same period,admissions of "new" long-staypatients from Mannheim, a city ofabout 310,000 inhabitants, to psychi-atric homes increased from 7 in 1974to 30 in 1979. Thus, in 1979, aboutthree quarters of the annual admis-sions of all new long-stay patientswith schizophrenia were made topsychiatric homes, whereas onlyabout one quarter went to psychiatrichospitals. This distribution hasremained stable to date.
Further Research on the Basis of CaseRegister Data. The necessity ofcontinuous psychiatric treatment andof comprehensive care for chronicschizophrenic patients, including thefields of housing, occupation, leisuretime, and social contacts, led to theimplementation of a network ofservices. The evaluation of thesecomplex patterns of care, their effec-tiveness, and the functions of everysingle service therefore gained signif-icance (see Wing and Bransby 1970;
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

42 SCHIZOPHRENIA BULLETIN
ten Horn 1980; Giel and ten Horn1982; an der Heiden and Klug 1980).
Research on utilization of thenetwork of community mental healthservices. Ten Horn (1980) demon-strated the multiple utilizations ofoutpatient facilities by 1,594 patientswith different diagnoses who hadbeen recorded in the Groningen CaseRegister (Netherlands) in 1974-75.The complex pattern of use ofvarious services was even morestriking in a cohort of 148 schizo-phrenic patients from Mannheimwho had been admitted to inpatientservices between October 1, 1977,and September 30, 1978 (Hafner andan der Heiden 1982, 1983). Afterhospital discharge, 116 (78.4 percent)patients contacted three to sevenfacilities of extramural care eithersimultaneously or successively. Inmost of the patients, it was a suitablecombination of visits to a physician,home care, and attendance at asheltered workshop and/or patients'club. These results demonstrate theinterrelatedness of components ofcomprehensive community mentalhealth care, a factor that should beconsidered in planning, coordinating,and analyzing the costs of such anextensive service. The effectiveness ofintensive extramural care wasdemonstrated by the fact that theintensity of utilization considerablyreduced the probability of rehospital-ization.
Leff and Vaughn (1972) exploreddisease variables and socialindicators that differentiated patientswho used extramural care facilitiesfrom those who did not. Acomparison between two samples ofschizophrenic or manic-depressivepatients drawn from the CamberwellRegister (50 patients "in contact" and40 patients "out of contact") revealedthe following: Patients "in contact"had more frequently been treated in ahospital and to a larger extent
received medication. This mayindicate that the extent of care isflexibly adapted to the severity of thedisease. Patients with more severedisabilities are provided morefrequent and more intensive care. Aninvestigation by Hafner and an derHeiden (1982) also showed a signif-icant relation between the number ofpreceding hospital admissions andthe intensity of use of outpatient andcomplementary services. In the studyby Leff and Vaughn (1972), patients"in contact" had more frequent andalso a larger number of symptoms,as reported by their relatives, andboth family and occupational tieswere less stable. Furthermore, thestudy indicated that among thepatients who had no outpatientcontacts, those receiving medicationshowed a better social adjustment(see Leff and Wing 1971).
Experimental research on the basisof case register data. Methodologicalproblems in the retrospective analysisand interpretation of changes and offactors influencing them often reducethe generalizability of epidemio-logical research findings. This alsoapplies to intervention studies carriedout in a nonrepresentative utilizationpopulation, such as patients of aspecific hospital. It is an inherentdeficiency of many clinical andtreatment studies. The combinationof epidemiological and experimentaldesigns is an excellent way of solvingthis problem.
Wing et al. (1972) made an inter-esting attempt to combine anepidemiological with a quasi-experimental approach. Out of agroup of 380 schizophrenic patientsrecorded in the Camberwell Registerin 1968, 75 were found who had beenliving at home for at least 1 yearwithout occupation. Twenty-eight ofthese patients were divided into twoequal groups. In order to evaluatethe effectiveness of preparatory
training for occupational rehabili-tation, the experimental group wasassigned to a day clinic program. Allof the patients had severe secondaryhandicaps. Even though a followupexamination after 2 years indicatedno differences between the groupswith respect to occupational reinte-gration (four patients from eachgroup were employed) or socialadjustment, the study neverthelesshad some intriguing results: Obser-vations during the phase of socialactivation indicated, for example,that intensive methods of socialtreatment, as well as pressure by thefamily, may lead to deterioration oracute relapses (Vaughn and Leff1976). In addition, five patients fromthe original group were found tohave committed suicide. So thesuicide rate was 11 times as high(132/100,000) as that of theCamberwell population (12/100,000).From this study, it was concludedthat the appropriate accommodationfor the majority of chronic schizo-phrenics would be an environment inwhich permanent handicaps areaccepted and excessive activation isavoided.
Methodology
Stability of Diagnoses. Thecumulative case-related registrationof successive contacts drew attentionto the diagnoses attributed to apatient who had been repeatedlyrecorded in the register. Quite a fewpublications deal with the search forexplanations of changes in thediagnoses recorded. In addition tothe possibility of a patient'sdeveloping two independent psychi-atric disorders, or expressingdifferent states characteristic of thesame basic disorder over the courseof time, the influence of external,disease-related variables was
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL 12, NO. 1, 1986 43
examined. In one of the first studiesbased on case register data, Babigianet al. (1965) investigated the stabilityof diagnoses in 1,215 patients in theMonroe County Psychiatric CaseRegister who had contacted a psychi-atric institution at least twice during1961-62. When patients wereassigned to four diagnostic categories(schizophrenia, affective psychoses,organic brain syndromes, and miscel-laneous), the concordance of first andsecond diagnoses varied between 69percent and 88 percent. The patient'ssetting and social class had nodiscernible influence, but the insti-tution giving a first diagnosis seemedto play an important role, especiallywith respect to a change indiagnosis: In three quarters of allcases, the diagnosis "worsened," inthe direction of a psychosis, if thefirst contact was with a physician inpractice.
In the study of Babigian et al. theperiod between each contact did notinfluence diagnostic consistency, butJakubaschk and Hurry (1977), usingdata from the Camberwell Register,found that concordance diminished inparallel with the length of theinterval between two diagnoses.Concordance was assessed withrespect to the 13 diagnostic categoriesof the register (not identical with theICD classification) in a randomsample of 144 patients entered in1970 who had had at least one subse-quent contact. In 50.5 percent of thecases, the diagnoses given at the firstand last contact were identical; therewas no significant connectionbetween diagnostic changes andchanges of the attending physiciansor the institution.
A central register containing alldata on admissions to and dischargesfrom psychiatric hospitals in Englandand Wales was used by Cooper(1967) to investigate the reliabilityand quality of the recorded
diagnoses. In a sample of 293patients who were registered as firstadmissions in the second half of 1955and had three readmissions in thefollowing 2 years, the diagnoses wereidentical (four-figure ICD classifi-cation) in only 20 percent of cases.Unlike Jakubaschk and Hurry (1977),Cooper found an importantconnection between change ofphysician and change of diagnosis:A change of physician increased theprobability of being given a differentdiagnosis. Cooper concluded thatmost diagnostic changes are notbased on changes in the clinicalpicture, but on inadequate diagnosticcriteria and classificatory systems.
In a study using the MannheimPsychiatric Case Register, Klug(1983) included data for 2,028persons who had had 2-12 contactswith psychiatric facilities betweenMay 31, 1973, and July 31, 1976. Forthe 17 diagnostic categories investi-gated (ICD, 8th revision), diagnosticconcordance between the first twodates of utilization was about 67percent when both primary andsecondary diagnoses were taken intoaccount. The average time differencebetween the two diagnoses was 244days. The comparatively high levelof diagnostic agreement found byKlug (1983) may reflect improve-ments in the classificatory systemand effects of training among thediagnosing psychiatrists. Amongindividual diagnostic groups, lifelongdisturbances (chronic and recurrentdiseases such as mental retardationand schizophrenia) showed thehighest levels of stability.
In Klug's study, the intervalbetween two treated episodes had anunexpected influence: If time differ-ences were small, concordance rateswere much lower than with largerdifferences of time. This result mayreflect a tendency to stabilize adiagnosis when the amount of infor-
mation, particularly on indicators ofcourse, is growing. A further aspectpoints into the same direction: Incase of a change of institution, thestability of diagnoses grew contin-uously, from 55 percent to 63percent, between the first and thethird change.
Although their findings on theeffects of a change of physician andinstitution or on diagnostic habitsdiffer, all investigators concludedthat the type of psychiatric disorderis an important factor. Theconcordance rate for schizophreniawas about 70 percent throughout(see, also, Kaelbling and Volpe 1963)and was relatively insensitive toinfluences of time and institution.The effects of external factors, partic-ularly of multimorbidity, on thestability of diagnoses may be dimin-ished by giving primary andsecondary diagnoses and byattaching different weights to them(Dupont 1980). The reduction andstandardization of diagnosticcategories (Babigian et al. 1965;Cooper 1967; Jakubaschk and Hurry1977; Klug 1983) may also lead to anincrease in stability, albeit at theprice of a loss of information. Theintroduction of a multi-axial classifi-cation makes it possible to classifyimportant variables on differentlevels of stability. Diagnosticreliability can be improved ifstandardized diagnoses are made byspecially trained staff of the caseregister (Cooper 1967; see, also,Walsh et al. 1980).
Data Processing and Evaluation. Theamount and quality (in the sense ofmeasurement theory) of informationdelivered to a case register requireincreasingly differentiated methods ofdata processing and analysis. Bydeveloping a special documentationsystem, an der Heiden and Klug
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022
44 SCHIZOPHRENIA BULLETIN
(1980) illustrated the use of intra-mural and extramural institutions byschizophrenic patients in Mannheimover an 18-month period on the basisof 14-day intervals. The system madeit possible to calculate the probabilityof transition between various stagesof care over the course of time. Witha time series analysis (Markovchain), they showed that after about6 months, roughly 63 percent of acohort utilized aftercare services, 17percent got inpatient care, and 20percent were not provided any care.These proportions remained stable atevery further cross-section within the18-month period (Hafner and an derHeiden 1982). This method couldalso be useful in cost-effectivenessanalyses.
Summary
Because schizophrenia often takes along-term course and is linked withsocially conspicuous disturbances,the probability that a schizophrenicwill contact a mental health serviceat least once in his lifetime approxi-mates 100 percent if a sufficientlydeveloped network of care isprovided. Case registers therefore areimportant instruments of research onschizophrenia. In particular, theirvalue to epidemiological and servicesresearch increases with the length ofperiod they cover.
The first cumulative psychiatriccase register was established in Osloin 1936. The data of this nationalregister of psychoses go back to1916. Most local and regionalregisters in European countries werestarted in the 1960's in connectionwith the introduction of the ICDclassification. These registers coversmaller populations, but record allcontacts with psychiatric inpatientservices, and a portion of contactswith complementary and outpatient
facilities, irrespective of the diagnosisgiven.
The validity of cross-sectionalcomparisons of rates for first admis-sions and treated prevalence islimited because of the varyingregistration-density, differing defini-tions, and—reflecting the age-dependent morbidity risk—differentdenominators. The development offirst admission rates, which can beobserved over a period of 53 years inthe Norwegian register and over 30years in the Icelandic and Danishregisters, proved to be an indicatorof the long-term trend inmorbidity: In schizophrenia, themorbidity risk, controlled for age,seems not to have changed in thesecountries for about half a century.The correlations between therates for first admissions anddemographic, ecological, and socialfactors—primarily investigated by©degard et al. on the basis of theNorwegian Case Register—stronglysuggest the validity of selectionhypotheses.
In investigations of the frequencyof schizophrenia among migratingpopulation groups, the results wereinconsistent: In Norwegianimmigrants to the United States andin Southeast Asian immigrants toGreat Britain, the frequency ofschizophrenia was higher, whereasthe age-corrected rates for foreignworkers in the F.R.G. were lower.These findings can be interpreted onthe basis of different selectiveprocesses: Those selective factorsleading to an unequal distribution atthe onset of the disease seem toreflect certain traits of the premorbidpersonality of preschizophrenicpatterns of social behavior. Long-term epidemiology and the analysisof geographic migration and socialmobility could not verify thehypothesis that environmentalfactors—such as social systems.
social context variables, or severestress—might heighten the risk ofbecoming schizophrenic. Some of thefindings tend to refute theassumption that the risk of illness iscausally dependent on environmental
• factors.By crossing data from twin and
case registers, genetic research onschizophrenia for the first timeobtained valid empirical data onhereditary factors in schizophrenia.The hypothesis of a genetic trans-mission of the predisposition todevelop schizophrenia wasconfirmed, although some portion ofthe risk appeared to depend onenvironmental factors. Adoptionstudies based on Danish populationregisters have made an importantcontribution to the assessment ofgenetic versus familial/environmentalfactors in the transmission of schizo-phrenia. However, the results of theadoption studies need to beconfirmed in larger samples.
Long-term trends in utilization ofmental health services can bediscerned in analyses of case registerdata, which permit relatively reliabledeterminations of future needs.Because they take demographic andregional factors into account, caseregisters contribute to a better inter-pretation of aggregate data fromhospital statistics and to more validplanning of mental health services.The evaluation of mental health caresystems and services on the basis ofcase registers has enhanced signif-icance because of recent fundamentalchanges in mental health care.Schizophrenics are the main targetgroup of the reform in the mentalhealth care system, and they alsoprovide the largest group of patientsfor whom care has been transferredfrom hospital to complementaryservices. In this context, caseregisters are an indispensableinstrument for assessing utilization.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 45
effectiveness, quality, and costs ofinterrelated components of anincreasingly complex system of care.. In addition, case registers havebeen used as a basis for combiningepidemiological and quasi-experimental methods of research onschizophrenia. This approach hascontributed findings (e.g., on thespecific vulnerability of chronicschizophrenics) that can begeneralized. The possibilities of usingcase register data to follow thecourse of a disease and itsdependence on intervening variables,to study the stability of syndromesand diagnoses, and to develop newmethodologies have not yet beenfully exhausted.
References
Achte, K.A. Der Verlauf der Schizo-phrenien und der schizophrenifonnenPsychosen. Eine vergleichende Unter-suchung der Veranderungen in denKrankheitsbildern, der Prognosenund des Verhal misses zwischen denKranken und dem Arzt in den Jahren1933-1935 und 1953-1955. ActaPsychiatrica Scandinavica, Suppl.155, 1961.
Adelstein, A.M.; Downham, D.Y.;Stein, Z.; and Susser, M.W. Theepidemiology of mental illness in anEnglish city: Inceptions recognizedby Salford psychiatric services.Social Psychiatry, 3:47-59, 1968.Alderson, M.R. Indicators of need,demand, and use. In: Acheson,R.M.; Hall, D.J.; and Aird, L, eds.Seminars in CommunityMedicine: Health Information,Planning, and Monitoring. Vol. 2.London: Oxford University Press,1976. pp. 29-40.Astrup, C. Nervose Erkrankungenund soziale Verhaltnisse. Berlin:Volk und Gesundheit, 1956.
Astrup, C. "The Increase of MentalDisorders." Unpublished manuscriptfrom the National Case Register ofMental Disorder, Gaustad Hospital,Oslo, Norway, 1982.
Astrup, C , and Odeg&rd, 0 .Internal migration and mental diseasein 'Norway. Psychiatric Quarterly,Suppl. 34:116-130, 1980.
Babigian, H.M.; Gardner, E.A.;Miles, H.C.; and Romano, J.Diagnostic consistency and change ina follow-up study of 1215 patients.American Journal of Psychiatry,121:895-901, 1965.
Babigian, H.M. Schizophrenia:Epidemiology. In: Freedman, A.M.;Kaplan, H.I.; and Sadock, B.J., eds.Comprehensive Textbook ofPsychiatry. Vol. II. Baltimore:Williams and WUkins, 1975. pp.860-866.Baeyer, W. von, and Binder, W.Endomorphe Psychosen beiVerfolgten. Berlin-Heidelberg-NewYork: Springer, 1982.
Baldwin, J.A. The register as amental health service informationsystem. In: Wing, J.K., and Bransby,E.R., eds. Psychiatric Case Registers.DHSS, Statistical Report Series No 8.London: Her Majesty's StationeryOffice, 1970. pp. 9-13.Baldwin, J.A. The Mental Hospital inthe Psychiatric Service: A Case-Register Study. London-New York-Toronto: Oxford University Press,1971.
Baldwin, J.A., and Hall, I.J.Estimation of the outcome of astanding mental hospital population.British Journal of Preventive andSocial Medicine, 21:56-65, 1967.
Bebbington, P.B.; Hurry, J.;Tennant, C ; and Wing, J.K. Theepidemiology of mental disorders inthe Camberwell community. Psycho-logical Medicine, 11:561-579, 1981.
Bleuler, M. Die schizophrenenGeistesstorungen: im Lichtelangjahriger Kranken- und Familien-geschichten. Stuttgart: Thieme, 1972.Brenner, M.H. Economic change andmental hospitalization: New YorkState, 1910-1960. Social Psychiatry,2:180-188, 1967.Brown, G.W. Length of hospital stayand schizophrenia: A review ofstatistical studies. Acta Psychiatricaet Neurologica Scandinavica,35:414-430, 1960.
Cochrane, R. Mental illness inimmigrants to England andWales: An analysis of mentalhospital admissions. SocialPsychiatry, 12:25-35, 1977.
Cochrane, R. Psychological andbehavioural disturbance in WestIndians, Indians and Pakistanis inBritain: A comparison of ratesamong children and adults. BritishJournal of Psychiatry, 134:201-210,1979.
Cooper, J.E. Diagnostic change in alongitudinal study of psychiatricpatients. British Journal ofPsychiatry, 113:129-142, 1967.
Dalgard, O.S. Migration andFunctional Psychoses in Oslo.Oslo: Universitetsforlaget, 1971.
Department of Health and SocialSecurity. Better Services for theMentally III. London: Her Majesty'sStationery Office, Oct., 1975.
Dilling, H., and Weyerer, S. ZurBehandlungsinzidenz und -pravalenzin drei Kreisen Oberbayerns.In: Bericht uber die Lage derPsychiatrie in der BundesrepublikDeutschland—Zur Psychiatrischenund psychotherapeutisch/psychoso-matischen Versorgung derBevdlkerung. Drs. 7/4201.Bonn: Deutscher Bundestag, 1975.
Dupont, A. Psychiatric case registers.In: Hafner, H., ed. Estimating Needs
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022
46 SCHIZOPHRENIA BULLETIN
for Mental Health Care. Berlin-Heidelberg-New York: Springer,1979. pp. 43-51.
Dupont, A. "Entry in a Case Registeras a Definition of a 'Case.' " Paperpresented at the WPA Symposium"What is a Case." London, May14-16, 1980.
Dupont, A.; Videbech, T.; andWeeke, A. A cumulative nationalpsychiatric register: Its structure andapplication. Acta PsychiatricaScandinavica, 50:161-175, 1974.
Dupont, A., and Weeke, A. Antaletaf psykiatriske indlaggelser iDanmark. Ugeskrift for Lager,139:1241-1242, 1977.
Eason, R.J., and Grimes, J.A.Inpatient care of the mentally ill: Astatistical study of future provision.Health Trends, 8:13-18, 1977.Eaton, W.W. A formal theory ofselection for schizophrenia. AmericanJournal of Sociology, 86:149-158,1980.
Eitinger, L. Incidence of mentaldisease among refugees in Norway.Journal of Mental Science,105:326-338, 1959.Eitinger, L. The symptomatology ofmental disease among refugees inNorway. Journal of Mental Science,106:947-966, 1960.
Eitinger, L. Schizophrenia amongconcentration camp survivors. Inter-national Journal of Psychiatry,3:403-406, 1967.
Eitinger, L., and Grunfeld, B.Psychoses among refugees inNorway. Acta PsychiatricaScandinavica, 42:315-328, 1966.
Eitinger, L., and Str^m, A. Mortalityand Morbidity After Excessive Stress.New York: Humanities Press, 1973.
Faris, R.E.L., and Dunham, H.W.Mental Disorders in UrbanAreas: An Ecological Study ofSchizophrenia and Other Psychoses.
Chicago: University of ChicagoPress, 1939.
Fischer, M. Genetic and environ-mental factors in schizophrenia. ActaPsychiatrica Scandinavica, Suppl.238, 1973.
Fischer, M.; Harvald, B.; and Hauge,M. A Danish twin study of schizo-phrenia. British Journal ofPsychiatry, 115:981-990, 1969.Fryers, T. Psychiatric in-patients in1982—how many beds7 Psycho-logical Medicine, 4:196-211, 1974.
Fryers, T. Estimation of need on thebasis of case register studies: Britishcase register data. In: Hafner, H.,ed. Estimating Needs for MentalHealth Care. Berlin-Heidelberg-NewYork: Springer, 1979. pp. 52-63.
Fryers, T.; Newton, P.; Sousa, R.;and Wooff, K. Psychiatric Services inCamberwell and Salford: StatisticsFrom the Camberwell and SalfordRegister: 1964-1973. London: MRCSocial Psychiatric Unit, 1974.
Gam, J. A 5-year retrospectiveinvestigation of all first admittedschizophrenics to Danish psychiatricinstitutions in the fiscal year fromApril 1st, 1970, to April 1st, 1971.In: Stromgren, E.; Dupont, A.; andAchton-Nielsen, ]., eds. Epidemio-logical Research as a Basis for theOrganization of ExtramuralPsychiatry. Copenhagen: Munks-gaard, 1980. pp. 332-336.
Garmezy, N. The current status ofresearch with children at risk forschizophrenia and other forms ofpsychopathology. In: Regier, D.A.,and Allen, G.A., eds. Risk FactorResearch in the Major MentalDisorders. (Publication No. ADM81-1068) Washington, DC: Superin-tendent of Documents, U.S.Government Printing Office, 1981.pp. 23-39.Giel, R.; Sauer, H.C.; Slooff, C.J.;and Wiersma, D. Epidemiological
observations on schizophrenia anddisability in the Netherlands.Tijdschrift voor Psychiatrie,11-12:710-722, 1980.
Giel, R., and ten Horn, G.H.M.M."Mental Health in Pilot StudyAreas: The Dutch Experience—Introduction to the Participation ofthe Department of SocialPsychiatry." Unpublishedmanuscript, The Netherlands,August, 1981.
Giel, R., and ten Horn, G.H.M.M.Patterns of mental health care in aDutch register area. SocialPsychiatry, 17:117-123, 1982.
Goldberg, E.M., and Morrison, S.L.Schizophrenia and social class.British Journal of Psychiatry,109:785-802, 1963.Goldhamer, H., and Marshall, A.Psychosis and Civilization. Glencoe,IL: Free Press, 1953.
Hafner, H., ed. Estimating Needs forMental Health Care. Berlin-Heidelberg-New York: Springer,1979.
Hafner, H. Psychiatrische Morbiditatvon Gastarbeitern in Mannheim.Epidemiologische Analyse einerInanspruchnahmepopulation. Nerve-narzt, 51:672-683, 1980.
Hafner, H., and an der Heiden, W.Evaluation gemeindenaherVersorgung psychisch Kranker.Ergebnisse von 4 Jahren wissenschaft-licher Begleitung der Aufbauphasedes Mannheimer Modells. Archiv furPsychiatrie und Nervenkrankheiten,232:71-95, 1982.
Hafner, H., and an der Heiden, W.The impact of a changing system ofcare on patterns of utilization byschizophrenics. Social Psychiatry,18:153-160, 1983.
Hafner, H., and Kasper, S. Akutelebensbedrohliche Katatonie.Epidemiologie und klinische Befunde.Nervenarzt, 53:385-394, 1982.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 47
Hafner, H., and Klug, ]. First evalu-ation of the Mannheim communitymental health service. In: Stromgren,E., ed. "Epidemiological Research asBasis for the Organization of Extra-mural Psychiatry." Ada PsychiatricaScandinavica, 62 (Suppl. 285):68-78,1980.
Hafner, H., and Klug, J. Wissen-schaftliche Begleitung derEntwicklung einer gemeindenahenpsychiatrischen Versorgung in Mann-heim. In: Haase, H.J., ed.Burgernahe Psychiatrie imWirkungsbereich des psychiatrischenKrankenhauses. Erlangen: PerimedFachbuch-Verlagsgesellschaf t, 1981.pp. 23-58.
Hafner, H., and Klug, ]. The impactof an expanding community mentalhealth service on patterns of bedusage: Evaluation of a four-yearperiod of implementation. Psycho-logical Medicine, 12:177-190, 1982.
Hafner, H., and Reimann, H. Spatialdistribution of mental disorders inMannheim 1965. In: Hare, E.H., andWing, J.K., eds. Psychiatric Epidemi-ology. London-New York-Toronto: Oxford University Press,1970. pp. 341-354.
Haier, R.J.; Rosenthal, D.; andWender, P.H. MMPI assessment ofpsychopathology in the adopted-away offspring of schizophrenics.Archives of General Psychiatry,35:171-175, 1978.
Hailey, A.M. Long-stay psychiatricinpatients: A study based on theCamberwell register. PsychologicalMedicine, 1:128-142, 1971.
Hailey, A.M. The chronic mentalhospital population: A six-yearfollow-up study. British Journal ofPreventive and Social Medicine,27:255-260, 1973.
Hailey, A.M. The new chronicpsychiatric population. British
]ournal of Preventive and SocialMedicine, 28:180-186, 1974.Hailey, A.M.; Hurry, L.J.; Powell,M.; Shannon, B.; Wing, J.K.; andWing, L. Psychiatric Services inCamberwell and Salford: StatisticsFrom the Camberwell and SalfordRegister: 1964-1973. London: MRCSocial Psychiatric Unit, 1974.
Hare, E.H. Family setting and theurban distribution of schizophrenia.journal of Mental Science,102:753-760, 1956.
an der Heiden, W., and Klug, J. Anintegrated record system for theobservation of the demand formedical and social aftercare as basisfor organizing extramural services.Ada Psychiatrica Scandinavica, 62(Suppl. 285):54-59, 1980.
Helgason, L. Psychiatric services andmental illness in Iceland. AdaPsychiatrica Scandinavica, Suppl.268, 1977.
Helgason, T. Studies on prevalenceand incidence of mental disorders inIceland with a health questionnaireand a psychiatric case register.In: Astrup, C, ed. Troms'o Seminarin Medicine. Tromsb: University ofTromso, 1975. pp. 172-183.Helgason, T. Estimation of need onthe basis of case register studies:Discussion. In: Hafner, H., ed.Estimating Needs for Mental HealthCare. Berlin-Heidelberg-NewYork: Springer, 1979. pp. 64-68.ten Horn, G.H.M.M. Registerstudy: A small cohort of multiple-service-users from a geographicallycircumscribed area. Ada PsychiatricaScandinavica, Suppl. 285:305-314,1980.
Huber, G. Psychiatrische Syndromebei endogenen Intoxikationen undlebensbedrohlichen Katatonien.Verhandlungen der deutschenCessellschaft fur innere Medizin. Vol.75. Miinchen: Bergmann, 1969.
Jakubaschk, J., and Hurry, ]. DieDiagnosen im Camberwell-Register,einem kumulativen psychiatrischenFallregister. Schweizer Archiv furNeurologie, Neurochirurgie undPsychiatrie, 120:243-255, 1970.
Jakubaschk, ].; Klug, J.; Weyerer, S.;and Dilling, H. Behandlungsbedurft-igkeit—Uberlegungen zur psychi-atrischen Versorgung. PsychiatrischePraxis, 5:203-211, 1978.Kaelbling, R., and Volpe, P.A.Constancy of psychiatric diagnosis inre-admissions. ComprehensivePsychiatry, 4:29-38, 1963.
Kastrup, M., and Bille, M. A censusstudy with special regard to long-staypsychiatric patients. In: Stromgren,E.; Dupont, A.; and Achton-Nielsen,]., eds. Epidemiological Research asBasis for Organization of ExtramuralPsychiatry. Copenhagen: Munks-gaard, 1980. pp. 270-278.
Kastrup, M.; Nakane, A.; Dupont,A.; and Bille, M. Psychiatrictreatment in a delimited population—With particular reference tooutpatients. Ada PsychiatricaScandinavica, 53:35-50, 1976.
Kendell, R.E. The Role of Diagnosisin Psychiatry. Oxford-London-Edinburgh-Melbourne: BlackwellScientific Publications, 1975.
Kendler, K.S.; Gruenberg, A.M.; andStrauss, J.S. An independent analysisof the Copenhagen sample of theDanish adoption study of schizo-phrenia. I. The relationship betweenanxiety disorder and schizophrenia.Archives of General Psychiatry,38:973-977, 1981a.
Kendler, K.S.; Gruenberg, A.M.; andStrauss, J.S. An independent analysisof the Copenhagen sample of theDanish adoption study of schizo-phrenia. II. The relationship betweenschizotypal personality disorder andschizophrenia. Archives of GeneralPsychiatry, 38:982-984, 1981b.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

48 SCHIZOPHRENIA BULLETIN
Kendler, K.S.; Gruenberg, A.M.; andStrauss, J.S. An independent analysisof the Copenhagen sample of theDanish adoption study of schizo-phrenia. III. The relationship betweenparanoid psychosis (delusionaldisorder) and the schizophreniaspectrum disorders. Archives ofGeneral Psychiatry, 38:985-987,1981c.Kety, S.S.; Rosenthal, D.; Wender,P.H.; and Schulsinger, F. The typesand prevalence of mental illness inthe biological and adoptive familiesof adopted schizophrenics.In: Rosenthal, D., and Kety, S.S.,eds. The Transmission of Schizo-phrenia. Oxford: Pergamon Press,Ltd., 1968. pp. 345-362.
Kiselev, A.S. Centralized system forcollection and analysis of data onpatients in the U.S.S.R. AmericanJournal of Psychiatry, 128:1019-1022, 1972.
Klug, J. Psychiatrische Diagnosen.Einflussfaktoren auf die Stabilitat imzeitlichen Verlauf. Weinheim: Beltz,1983.Klug, }.; an der Heiden, W.; andScheel, R. Psychiatrische Versorgungim Wandel—Determinanten derBedarfsplanung. In: Biefang, S., ed.Evaluationsforschung in der Psychi-atrie: Fragestellungen und Methoden.Stuttgart: Enke, 1980. pp. 250-285.
Kringlen, E. Schizophrenia in malemonozygotic twins. Ada Psychi-atrica Scandinavica, Suppl. 178,1964.
Kringlen, E. Twins—Still our bestmethod. Schizophrenia Bulletin,2:429-433, 1967.
Kringlen, E. Adult offspring of twopsychotic parents, with specialreference to schizophrenia.In: Wynne, L.C.; Cromwell, R.L.;and Matthysse, S., eds. The Natureof Schizophrenia: New Approachesto Research and Treatment. New
York: John Wiley & Sons, Inc.,1978. pp. 9-24.
Kringlen, E. Schizophrenia in theNordic countries. SchizophreniaBulletin, 6:566-578, 1980.Leff, J., and Vaughn, C. Psychiatricpatients in contact and out of contactwith services: A clinical and socialassessment. In: Wing, J.K., andHailey, A.M., eds. Evaluating aCommunity Psychiatric Service.London: Oxford University Press,1972. pp. 259-274.
Leff, J., and Wing, J. Trial of mainte-nance therapy in schizophrenia.British Medical Journal, 3:599-608,1971.
Lemkau, P.V.; Kulcar, Z.; Kesic, B.;and Kovacic, L. Selected aspects ofthe epidemiology of psychoses inCroatia, Yugoslavia. IV. Represent-ative sample and results of thesurvey. American Journal ofEpidemiology, 112:661-674, 1980.
Levy, L., and Rowitz, L. The spatialdistribution of mental disorders inChicago. Social Psychiatry, 5:1-11,1970.
Levy, L., and Rowitz, L. TheEcology of Mental Disorders inChicago. New York: BehavioralPublications, 1973.
Iidz, T.; Blatt, S.; and Cook, B.Critique of the Danish-Americanstudies of the adopted-away offspringof schizophrenic parents. AmericanJournal of Psychiatry, 138:1063-1068, 1981.
Luxenburger, H. Untersuchungen anschizophrenen Zwillingen und ihrenGeschwistern zur Prufung derRealitat von Manifestationsschwank-ungen. Zentralblatt fur die gesamteNeurologie und Psychiatrie,154:351-394, 1936.
Magnus, R.V. The new chronics.British Journal of Psychiatry,113:555-556, 1967.
Malzberg, B. Important statisticaldata about mental illness. In: Arieti,S., ed. American Handbook ofPsychiatry. Vol. I. New York: BasicBooks, Inc., 1969. pp. 161-174.
Mann, S.A., and Cree, W. "New"long-stay psychiatric patients: Anational sample survey of fifteenmental hospitals in England andWales 1972/73. PsychologicalMedicine, 6:603-616, 1976.
Mann, S.A., and Sproule, J. Reasonsfor six months stay. In: Wing, J.K.,and Hailey, A.M., eds. Evaluating aCommunity Psychiatric Service.London: Oxford University Press,1972. pp. 233-248.Marinoni, A.; Torre, E.; Allegri, G.;and Comelli, M. Lomest psychiatriccase register: The statistical contextrequired for planning. Ada Psychi-atrica Scandinavica, 67:109-117,1983.
Matthew, G.K. Measuring need andevaluating services. In: McLachlan,G., ed. Portfolio for Health:Problems and Progress in MedicalCare. 6th series. London-New York-Toronto: Oxford University Press,1971. pp. 27-46.Mazer, M. A psychiatric andparapsychiatric register for an islandcommunity. Archives of GeneralPsychiatry, 14:366-371, 1966.
Mednick, S., and Schulsinger, F.Breakdown in individuals at high riskfor schizophrenia: Possible predis-positional perinatal factors. MentalHygiene, 54:50-63, 1971.Murphy, H.B.M. Evaluation ofcommunity psychiatric programmes.In: Psychiatrie der Gegenwart. Bd.3: Soziale und angewandte Psychi-atrie. 2. Aufl. Berlin-Heidelberg-NewYork: Springer, 1975. pp. 361-427.
Nielsen, J., and Nielsen, J.A. Acensus study of mental illness inSams0. Psychological Medicine,7:491-503, 1977.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 49
Noreik, K.; Astrup, C ; Dalgard,O.S.; and Holmboe, R.A. Aprolonged follow-up of acute schizo-phrenic and schizophreniformpsychoses. Ada Psychiatrica Scandi-navica, 43:432-443, 1967.Noreik, K., and 0degard, 0 .Psychosis in Norwegians with abackground of higher education.British Journal of Psychiatry,112:43-55, 1966.
0degard, 0 . Immigration andinsanity: A study of mental diseaseamong the Norwegian-bornpopulation in Minnesota. AdaPsychiatrica et Neurologica Scandi-navica, Suppl. 4:1-206, 1932.0degard, 0 . Marriage and mentaldisease. Journal of Mental Science,92:35-49, 1946.0degard, 0 . The incidence of mentaldiseases as measured by censusinvestigations versus admissionstatistics. Psychiatric Quarterly,26:212-218, 1952.0degard, 0 . Pattern of dischargefrom Norwegian psychiatric hospitalsbefore and after the introduction ofpsychotropic drugs. AmericanJournal of Psychiatry, 120:772-778,1964.
0degard, 0 . Reactive psychoses.Acta Psychiatrica Scandinavica,Suppl. 203, 1967.
0degard, 0 . Epidemiologie derPsychosen. Nervenarzt, 42:569-575,1971a.0degard, 0 . Hospitalized psychosesin Norway: Time trends 1926-1965.Social Psychiatry, 6:53-58, 1971k.
0degard, 0 . Epidemiology of thepsychoses. In: Kisker, K.P.; Meyer,J.E.; Muller, C.; and Stromgren, E.,eds. Psychiatrie der Gegenwart.Berlin-Heidelberg-New York: Sprin-ger, 1972. pp. 213-258.
0degard, 0 . Norwegian emigration,re-emigration and internal migration.In: Zwingmann, C , and Pfister-
Ammende, M., eds. Uprooting andAfter. . . . Berlin-Heidelberg-NewYork: Springer, 1973. pp. 161-177.
0degard, 0 . Social and ecologicalfactors in the etiology, outcome,treatment and prevention of mentaldisorders. In: Kisker, K.P.; Meyer,J.E.; Muller, C ; and Strbmgren, E.,eds. Psychiatrie der Gegenwart. Vol.II, 2nd ed. Berlin-Heidelberg-NewYork: Springer, 1975. pp. 151-198.
Pauleikoff, B. Die Katatonie(1868-1968). Fortschritte der Neuro-logie, Psychiatrie und Ihrer Grenzge-biete, 37:461-496, 1969.Report of the Expert Commission onPsychiatry, F.R.G. [Bericht uber dieLage der Psychiatrie in der Bundes-republik Deutschland—Zur psychi-atrischen und psychothera-peutisch/psychosomatischen Versor-gung der Bevblkerung.] Drs. 7/4200,7/4201. Bonn: Deutscher Bundestag,1975.
Rosenthal, D. Problems of samplingand diagnosis in the major twinstudies of schizophrenic twins.Journal of Psychiatric Research,2:116-134, 1962.
Rosenthal, D.; Wender, P.H.; Kety,S.S.; Schulsinger, F.; Welner, ].; and0stergard, L. Schizophrenics'offspring reared in adoptive homes.In: Rosenthal, D., and Kety, S.S.,eds. The Transmission of Schizo-phrenia. Oxford: Pergamon PressLtd., 1968. pp. 377-391.
Scheper-Hughes, N. Saints, Scholars,and Schizophrenics: Mental Illness inRural Ireland. Berkeley: Universityof California Press, 1979.
Schubart, C ; Krumm, B.; Biehl, H.;and Schwarz, R. 'The Measurementof Disability in a SchizophrenicPatient Group—Definition,Assessment and Outcomes Over TwoYears." Presented at the 1982Symposium of the Section ofEpidemiology and Community
Psychiatry of the World PsychiatricAssociation on the ChronicallyMentally 111, Baltimore, May 10-13,1982.
Shields, J. Some recent developmentsin psychiatric genetics. Archiv furPsychiatrie und Nervenkrankheiten,220:347-360, 1975.
Slater, E. Psychotic and NeuroticIllness in Twins. Medical ResearchCouncil, Special Reports Series, No.278. London: Her Majesty'sStationery Office, 1953.
Stein, L. "Social class" gradient inschizophrenia. British Journal ofPreventive and Social Medicine,11:181-195, 1957.
Strauss, J.S., and Carpenter, W.T.,Jr. Prediction of outcome in schizo-phrenia. Archives of GeneralPsychiatry, 34:159-163, 1977.
Tansella, M.; Faccincani, C ;Mignolli, G.; Balestrieri, M.; andZimmermann-Tansella, C. II registropsichiatrico di Verona-Sud. Epide-miologia per la valutazione dei nuoviservizi territoriali. In: Tansella, M.,ed. L'Approcio Epidemiologico inPsychiatria. Torino: Boringhieri,1985. pp. 225-259.Tienari, P. Psychiatric illnesses inidentical twins. Acta PsychiatricaScandinavica, Suppl. 171, 1963.
Tienari, P. Schizophrenia in Finnishmale twins. In: Lader, M.H., ed.Studies of Schizophrenia. (BritishJournal of Psychiatry, Special Publi-cation No. 10) Ashford, Kent,England: Headley Brothers Ltd.,1975. pp. 29-35.
Tienari, P.; Lahti, I.; Naarala, M.;Sorri, A.; and Vaisanen, E. Schizo-phrenics' offspring reared in adoptivehomes: A family-dynamic study.In: Obiols, J.; Ballus, C ; GonzalezMonclus, E.; and Pujol, J., eds.Biological Psychiatry Today.Amsterdam: Elsevier/North-HollandBiomedical Press, 1979. pp. 27-32.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

50 SCHIZOPHRENIA BULLETIN
Tooth, G.C., and Brooke, E.M.Trends in the mental hospitalpopulation. Lancet, 1:710-713, 1961.
Torre, E.; Marinoni, A.; andAllegri, G. Lomest psychiatric caseregister: Old and new long-staypatients. Social Psychiatry,17:125-131, 1982.Tsuang, M.T., and Dempsey, G.M.Long-term outcome of majorpsychoses: II. Schizoaffectivedisorder compared with schizo-phrenia, affective disorders, and asurgical control group. Archives ofGeneral Psychiatry, 36:1302-1304,1979.Tsuang, M.T.; Woolson, R.F.; andFleming, J.A. Long-term outcome ofmajor psychoses: I. Schizophreniaand affective disorders comparedwith psychiatrically symptom-freesurgical conditions. Archives ofGeneral Psychiatry, 36:1295-1301,1979.
Ugelstad, E. PsykiatriskeLangtidspasienter i PsykiatriskeSykehus—Nye Behandlingsforstfk.Oslo: Universitetsforlaget, 1978.
Vaughn, C.E., and Leff, J. Theinfluence of family and social factorson the course of psychiatricillness: A comparison of schizo-phrenic and depressed neuroticpatients. British Journal ofPsychiatry, 129:125-137, 1976.
Walsh, D.; O'Hare, A.; Blake, B.;Holpenny, J.V.; and O'Brian, P.F.The treated prevalence of mentalillness in the Republic of Ireland—The three county case register study.Psychological Medicine, 10:465-470,1980.
Warthen, F.J.; Klee, G.C., Bahn,A.K.; and Gorwitz, K. DiagnosedSchizophrenia in Maryland.Psychiatric Research Report 22.Washington, DC: AmericanPsychiatric Association, 1967.
Weeke, A.; Kastrup, M.; andDupont, A. Long-stay patients inDanish psychiatric hospitals. Psycho-logical Medicine, 9:551-556, 1979.
Weeke, A., and Stromgren, E. Fifteenyears later: A comparison of patientsin Danish psychiatric institutions in1957, 1962, 1967, and 1972. ActaPsychiatrica Scandinavica,57:129-144, 1978.
Welner, J., and Stromgren, E.Clinical and genetic studies on benignschizophreniform psychoses based ona follow-up. Acta PsychiatricaScandinavica, 57:129-144, 1958.
Weyerer, S.; Dilling, H.; Kohl, R.;and Martens, H. Social class andmental disorders. Social Psychiatry,17:133-141, 1982.
Wing, J.K., ed. Long-termcommunity care: Experience in aLondon borough. PsychologicalMedicine, Suppl. 2, 1982.Wing, J.K., and Bransby, E.R.Psychiatric Case Register.(Department of Health and SocialSecurity, Statistical Report Series,No. 8) London: Her Majesty'sStationery Office, 1970.
Wing, J.K., and Brown, G.W.Institutionalism and Schizo-phrenia: A Comparative Study ofThree Mental Hospitals 1960-1968.Cambridge: University Press, 1970.
Wing, J.K., and Fryers, T., eds.Psychiatric Services in Camberwelland Salford: Statistics From theCamberwell and Salford PsychiatricRegisters, 1964-1974. MedicalResearch Council Social PsychiatryUnit, London, and Department ofCommunity Medicine, University ofManchester, 1976.
Wing, J.K., and Hailey, A.M.Evaluating a Community PsychiatricService. London: Oxford UniversityPress, 1972.
Wing, J.K., and Olsen, R., eds.Community Care for the MentallyDisabled. Oxford: Oxford UniversityPress, 1979.
Wing, J.K.; Wing, L.; and Hailey, A.The use of case registers inevaluating and planning psychiatricservices. In: Wing, J.K., andBransby, R., eds. Psychiatric CaseRegisters. (Department of Health andSocial Security, Statistical ReportSeries No. 8) London: Her Majesty'sStationery Office, 1970. pp. 3-8.
Wing, L.; Bramley, C ; Hailey, A.;and Wing, J.K. Camberwellcumulative psychiatric caseregister: Part I. Aims and methods.Social Psychiatry, 3:116-123, 1968.
Wing, L.; Wing, J.K.; Hailey, A.;Bahn, A.K.; Smith, H.E.; andBaldwin, J.A. The use of psychiatricservices in three urban areas: Aninternational case register study.Social Psychiatry, 2:158-167, 1967.Wing, L.; Wing, J.K.; Stevens, B.;and Griffiths, D. An epidemiologicaland experimental evaluation ofindustrial rehabilitation of chronicpsychotic patients in the community.In: Wing, J.K., and Hailey, A.M.,eds. Evaluating a Community Psychi-atric Service: The CamberwellRegister. London: Oxford UniversityPress, 1972. pp. 283-308.
World Health Organization, RegionalOffice for Europe. The Developmentof Comprehensive Mental HealthServices in the Community. Reporton a conference, Peebles, Scotland,May 24-30, 1972. Copenhagen:EURO 5414 I, 1973.
The Authors
Heinz Hafner, Dr. med.. Dr. phil., isProfessor of Psychiatry, Universityof Heidelberg, and Head of the
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022

VOL. 12, NO. 1, 1986 51
Central Institute of Mental Health,Mannheim, Federal Republic ofGermany. Wolfram an der Heiden,
Dipl. psych., is also affiliated withthe Central Institute of Mental
Health, Mannheim, Federal Republicof Germany.
Audio Tapes onSchizophreniaAvailable
Guilford Publications announcesSchizophrenia: Interview Strategiesfor Detecting CharacteristicSymptoms, a training model byBMA Audio Cassettes. Developed atthe UCLA Neuropsychiatric Instituteby Dr. Ian Falloon and Dr. DavidLukoff, the package includes twocassette tapes and a useful manualwith instructive information designedfor researchers, psychiatric residents,and psychology interns.
The program focuses onperceptual, thought, and communi-cation dysfunctions specific to schizo-phrenia. Drs. Falloon and Lukoff usean experiential, interactive approachto demonstrate how to elicit andevaluate distinctive qualities of apatient's experience and to relate thisinformation to today's complexdiagnostic standards. The programaddresses the assessment of thoughtinterference, hallucinations,delusions, and speech and behavioraldisturbances. Clear definitions ofsymptoms, dramatized interviews,and critical commentary encouragelisteners to develop their ability to
detect characteristic indicators ofschizophrenia, as they compare theirown conclusions with those of theauthors.
BMA also offers The InitialInterview: Evaluation Strategies forDSM-III Diagnosis, by RobertSpitzer, M.D., and Janet Williams,D.S.W., A.C.S.W. This set of tapespresents interviewing strategies whichcan be applied across the full rangeof DSM-III, while focusing on fourrepresentative symptom types(anxiety, depression, crisisadjustment, and psychosis). Theprogram demonstrates the StructuredClinical Interviews for DSM-Hl(SCID) method which Drs. Spitzerand Williams pioneered to gathermore reliable information fromconfused or relatively inarticulatepatients and to establish proceduralguidelines for interviewing.
For more information or to order,write to BMA Audio Cassettes, 200Park Avenue South, New York, NY10003 or call toll-free 800-221-3966(in New York State and Canada, call212-674-1900).
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/1/26/1934369 by guest on 24 O
ctober 2022