task sharing in rural haiti: qualitative assessment of a brief, structured training with and without...
TRANSCRIPT
Copyrig
Task sharing in rural Haiti: qualitativeassessment of a brief, structuredtraining with and without
McLean et al.
apprenticeship supervision for
community health workerser, Ashley K. Hagaman,rosme & Brandon A. Kohrt
Key Implications forPractice� Qualitative research is crucial for
determining best practice for tasksharing training and supervising.
� Apprenticeship with supervision isneededtoassuree¡ectiveandethicalservice delivery.
� Motivation levels of non specialists isamarker of eventual clinical compe-tency.
� Incorporate mental health and psy-chosocial needs of non specialists
Kristen E. McLean, Bonnie N. KaisBradley H.Wagenaar,Tatiana P. The
Despite growing support for supervision after task
sharing trainings in humanitarian settings, there
is limited research on the experience of trainees in
apprenticeship and other supervision approaches.
Studying apprenticeships from trainees’perspectives
is crucial to re¢ne supervision and enhance moti-
vation for service implementation. The authors
implemented a multi-stage, transcultural adap-
tation for a pilot, task sharing training in Haiti
entailing three phases:1) literature review and qual-
itative research to adapt a mental health and psycho-
social support training; 2) implementation and
qualitative process evaluation of a brief, structured
group training; and 3) implementation and qualita-
tive evaluation of an apprenticeship training,
including a two year follow-up of trainees. Struc-
tured group training revealed limited knowledge
acquisition, low motivation, time and resource con-
straints on mastery and limited incorporation of
skills into practice. Adding an apprenticeship com-
ponent was associated with subjective clinical com-
petency, increased of con¢dence regarding utilising
skills and career advancement. Qualitative ¢ndings
support the added value of apprenticeship according
to trainees.
Keywords: apprenticeship, Haiti, tasksharing, task shifting, training
Introduction
ht © War Trauma Foundation. Unautho
BackgroundGlobally there is a projected shortage of1.2 million mental health professionals, with
this gap being greatest in low and middleincome countries (LMICs) (Kakuma et al.,2011; World Health Organization (WHO),2000). This shortage has led to increasinge¡orts of task sharing of mental healthcare(Patel et al., 2007;WHO,2006).Task sharing,also known as task shifting, refers to theinvolvement of non specialist service provi-ders delivering health care that traditionallyresided within the domain of expert healthworkers (WHO, 2008). Within the contextof global mental health, ‘non specialist’ refers
into task sharing initiatives.
rized reproduction of this article is prohibited.
to a person who lacks prior professional, orother specialised, training in mental healthcare delivery. Non specialists, in both low
135

Copyrig
a
, I
and high resource settings, may include:community health volunteers, peer helpers,social workers, midwives, auxiliary healthsta¡, teachers, primary care workers andthose without a professional service role.Task sharing includes: building humancapacity among healthcare workers, enhan-cing the capacity to provide needed careand strengthening health systems so thatscale-up of services is sustainable (WHO,2008). This approach has been recom-mended as a pragmatic, cost e¡ective wayto assure higher coverage of care in LMICsthatbear a large portionof the global burdenof mental disorders (Somasundram, 2006;WHO, 2010).Randomised controlled trials of interven-tions implemented by non specialists forpersons with mental, neurological and sub-stance abuse disorders suggest improvementfor some mental health outcomes in LMICs(van Ginneken et al., 2013). Ventevogel andcolleagues (2012) argue that individuals,with little to no experience in mental health-care, can be trained to deliver serviceswithin systems of care that include regularsupervision and refresher trainings. A num-ber of resources exist regarding guidelinesand appropriate content for mental health-care interventions in LMICs. The WHOlaunched the mental health Gap Action Pro-
gramme (mhGAP) in order to address sys-tematic mental health needs in LMICs,including an intervention guide for generalhealthcare workers (WHO, 2010). In LMICsettings, such as Haiti, community basedhealthcare personnel may be ideal for tasksharing initiatives as they are more likely tounderstand (lay) explanatory models andto be able to utilise local idioms of distress(Keys, Kaiser, Kohrt, Khoury, & Brewster,2012). However, important questions remainregarding the best approach to train nonspecialist healthcare workers to providemental health services. Additionally, best
Task sharing in rural Haiti: qualitative assessment of
apprenticeship supervision for community health workers
ht © War Trauma Foundation. Unautho
practice for mental health training are stillunder evaluated, as compared for example,to guidance provided for task sharing
136
in HIV/AIDS care (Murray et al., 2011;Perez-Sales, Fernandez-Liria, Baingana, &Ventevogel, 2011;WHO, 2008).Murray and colleagues (2011) argue thatexisting guidelines are overly broad andlimit replication e¡orts. Lack of adequateevidence results in brief, one time trainingapproaches and a limited participatoryframework. Studies from both high incomecountries (HICs) and LMICs have shownthat such one o¡ approaches, with little posttraining supervision, may result in changesin knowledge, but rarely in changes in prac-tice (Beidas & Kendall, 2010; Budosan, 2011;Herschell, Kolko, Baumann, & Davis, 2010).For more e¡ective and sustainable interven-tions, mental health training needs to becoupled with continued supervision andassistance from a mental healthcareprofessional (Baingana & Mangen, 2011;Saxena, Thornicroft, Knapp, & Whiteford,2007; van derVeer & Francis, 2011). In theirevidence based review of supervision litera-ture, Milne et al. (2008) stress that the useof multiple trainingmodalities (e.g. instruct-ing, feedback, modelling, observing) arekey to e¡ective supervision. Apprenticeshipapproaches, where training is reinforcedthrough intensive supervision, coachingand feedback, may thus lead to increased¢delity and e¡ectiveness of psychosocialinterventions in LMICs, and thereforewarrant further consideration (Murrayet al., 2011).Currently, there is limited qualitativeresearch describing the process of imple-mentation ofmental health andpsychosocialsupport (MHPSS)1 trainings and supervi-sion in LMICs within larger systems of care(Flisher et al., 2007;WHO & Wonca, 2008).Therefore, this article attempts to addressthis gap, by describing a qualitative evalu-ation of a pilot project and by documentingsuccesses and challenges that arose in theprocess. As Baingana and Mangen note
brief, structured training with and without
ntervention 2015, Volume 13, Number 2, Page 135 - 155
rized reproduction of this article is prohibited.
(2011), there is often a tension in the imple-mentation literature between rigorous quan-titative methodologies and more qualitative

Copyrig
and participatory methods. This article istherefore designedas a descriptionof a processand is meant to raise critical questions fordiscussion and re£ection regarding tasksharing initiatives in LMICs.
Mental health and psychosocialsupport in rural HaitiMental health and psychosocial support(MHPSS) resources in Haiti are insu⁄cientdue to lack of infrastructure, particularly inrural areas (WHO, 2003). Approximatelyhalf of rural Haitians lack access to primarycare and mental health services are extrem-ely limited (Caribbean Country Manage-ment Unit, 2006). A Pan American HealthOrganization (PAHO)/WHO (2003) reportestimated only ten psychiatrists and ninepsychiatric nurses working in the publicsector, most of whom were located in Port-
ht © War Trauma Foundation. Unautho
au-Prince. Recent reports suggest slightlyhigher numbers (around 20 psychiatrists)but still attest to a dearth of mental health
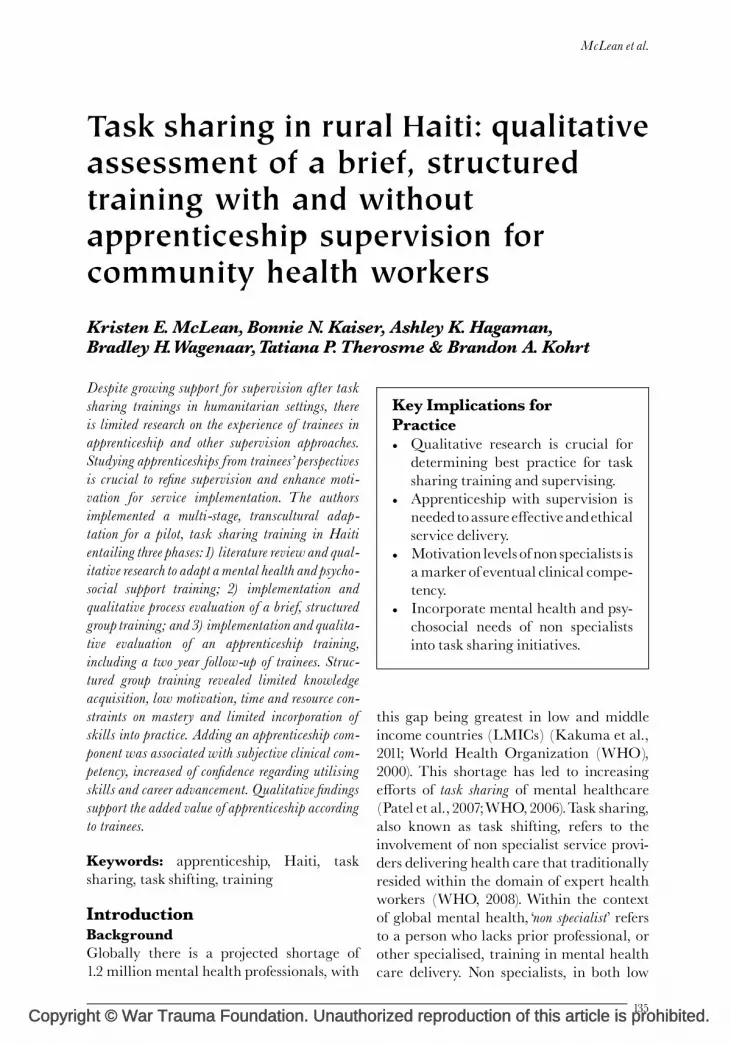
• Identify conte August 2010• Qualitative da notes)• Manual revisi
Content development
• Pilot training• Qualitative da semi-structur• Design of alte
Group psychosocialtraining pilot
• Pilot training• Qualitative da during trainin structured int• Qualitative da during couns
Apprenticeship pilot
Figure 1: Structure of training development:
training pilot and apprenticeship pilot.
providers in the country (WHO, 2011). Alocal a⁄liate of Partners in Health (ZanmiLasante) has recently begun to scale-upcommunity based mental health servicesin the Central Plateau and Artibonitedepartments (Raviola, Eustache, Oswald.& Belkin, (2012)).When su¡ering frommental, emotional andphysical problems, Haitians often seek carefrom herbalists (dokte' fey),Vodoupriests (hou-gan or mambo) and religious leaders (Bijoux,2010; Hagaman et al., 2013; Khoury, Kaiser,Keys, Brewster, & Kohrt, 2012; Miller,2000; Wagenaar, Kohrt, Hagaman,McLean, & Kaiser, 2013). Only 29% ofrespondents in the Central Plateau said theywould ¢rst seek care from hospitals or clinicswhen su¡ering from psychological distress,as the clinic was perceived to provide strictlybiomedical care (Wagenaar et al., 2013).
McLean et al.
rized reproduction of this article is prohibited.
Respondents also reported seekinghelp fromfamily. These preliminary ¢ndings suggestthat community health workers and local
nt (literature search; ethnographic data from June to)ta collection (key informant interviews x18; field
on
ta collection (participant observation during training;ed interviews x2; focus group discussions x2)rnative approach
ta collection: immediate (participant observationg, counseling sessions and debriefing; semi-erviews x3)ta collection: long-term (participant observationeling sessions; semi-structured interviews x2)
content development, group psychosocial
137

Copyrig
a
, I
religious leaders would be an appropriatechoice in this setting to train in basic mentalhealthcare. Traditional and primary careproviders have reported feeling inadequatelyprepared to supply mental healthcare(Khoury et al., 2012) and often adhered toa protocol of sending severe cases to Haiti’stwo distant psychiatric hospitals when thefamily could a¡ord it (Hagaman et al., 2013).Following the 2010 earthquake, e¡orts toscale up mental health resources have calledattention to chronic mental health needsthroughout the country (Budosan & Bruno,2011; de Ville de Goyet, Sarmiento, &Grunewald, 2011; Raviola, Eustache,Oswald, & Belkin, 2013; Rose, Hughes,Ali, & Jones, 2011). Budosan and Bruno(2011) found that establishing a referral
Task sharing in rural Haiti: qualitative assessment of
apprenticeship supervision for community health workers
ht © War Trauma Foundation. Unautho
systembetween the community and health-care sector in Haiti was feasible by imple-menting a series of short (three-to-¢ve
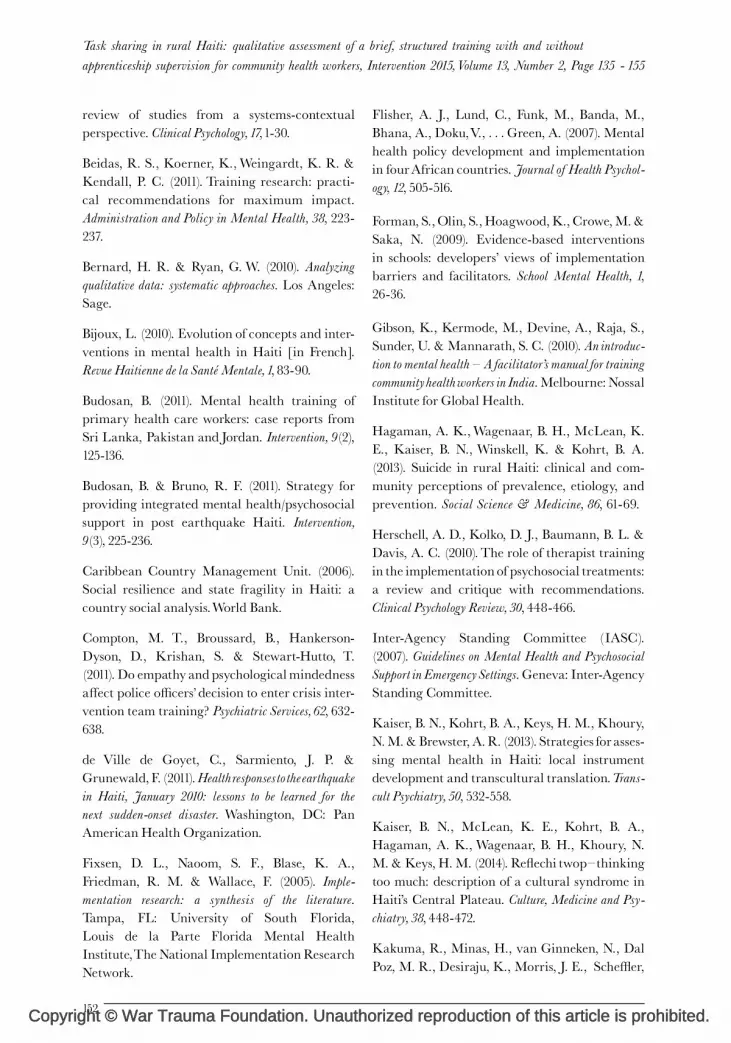
Key findings• Local terminology for mental distress• Recognizing signs and symptoms• Community identified coping mechanisms and sources of support• Identification of CHWs as training population• Need for basic psychotherapy skills with emphasis on referral
Key findings• Increased knowledge regarding mental illness and psychosocial support skills• Iterative critique of training was lacking• Active learning and role play most useful• Mixed results regarding confidence to implement new skills learned• Minimal behaviour change observed
Key findings
• Improvement in knowledge of concepts and demonstrated ability to implement skills• Ability to distinguish mild from severe cases of distress and when to refer for further care• Apprentices expressed desire to train other psychosocial workers• Continued utilisation of skills at two year follow-up
(a) Content development
(b) Group training pilot
(c) Apprenticeship pilot
Figure2: Relationshipbetweenkey¢ndingswith
of training development. CHW, community hea
138
day) mental health trainings. While thisapproach improved case ¢nding, com-munity level workers reported low motiv-ation and low levels of perceived e⁄cacyin care delivery; both of which are hall-marks of task sharing endeavours thathave not succeeded (Kane, Gerretsen,Scherpbier, Dal Poz, & Dieleman, 2010).These challenges and outcomes highlightthe need for ongoing professional supportfor non specialists participating in tasksharing endeavours (Figure 2).
Objectives of current studyThe study objective was to implementand evaluate a culturally relevant tasksharing training, meant to provide MHPSSservices for mild to moderate mental dis-
brief, structured training with and without
ntervention 2015, Volume 13, Number 2, Page 135 - 155
rized reproduction of this article is prohibited.
tress in order to overcome the region’s short-age of mental health care professionals.Included in the study was a description of
Application/modifications• Ongoing training and supervision is key for skill consolidation and confidence building• Self-selection of trainees and consideration of structural barriers to taking on new roles• Predictable and consistent remuneration• Consideration of trainee’s mental health and psychosocial needs• More rigorous evaluation methods
Application/modifications• More experiential learning to reinforce skills, including observation followed by supervised counseling sessions• Provision of printed materials• Recruitment of highly motivated individuals• Consideration of career development and other incentives
Application/modifications
• Cultural adaptation of didactic style segments• Incorporation of role play and small group learning activities• Development of locally contextualised case vignettes• Establishment of referral system
adaptationsandmodi¢cationsforeachstage
lth workers.

Copyrig
implementing two MHPSS task sharingtraining approaches: (1) a structured grouptraining pilot of community health workers(CHWs) and (2) a structured group trainingplus an apprenticeship based supervision pi-lot. Both approaches were intended to trainCHWs to identify cases of mental distress,provide basic MHPSS services and to referindividuals required it to specialist services.The training and supervision approacheswere evaluated in a process researchapproach2 using qualitative methods (Saun-ders, Evans, & Joshi, 2005).
MethodsSetting and contextThe present project is part of mixedmethodsresearch examining perceptions, experi-ences, care seeking and supports availablefor persons with mental illness in Haiti’sCentral Plateau (Hagaman et al., 2013;Kaiser, Kohrt, Keys, Khoury, & Brewster,2013; Kaiser et al., 2014; Keys et al., 2012;Khoury et al., 2012; Wagenaar, Hagaman,Kaiser, McLean, & Kohrt, 2012; Wagenaaret al., 2013).The study team formed apartnership along-side a local nongovernmental organisation(NGO) interested in providing feasibleforms of mental health support. Situatedin a remote and rural region of the CentralPlateau, the study location contained onebasic health centre serving zones within atwo hour walk. The clinic’s care focusedmainly on mild to moderate health con-ditions, ranging from infectious diseases tomaternal andchild health.More severe caseswere referred to one of three larger hospitalswithin a two hour drive. One physician,one nurse, twoauxiliary nurses, one lab tech-nician and one social worker served patients.Outreach in the form of mobile clinicsoccurred once every three months withineach surrounding subregion. Only thephysician and social worker had received
ht © War Trauma Foundation. Unautho
any formal mental health training, whichconsisted of a standard psychiatric curricu-lum delivered in medical school and a post
baccalaureate training programme, respect-ively.The training activities described belowwere implemented during May^June 2011,in partnership with a local NGO. Projectactivities were based in the communalsection, roughly equivalent to a county,of Lahoye. Apprenticeship trainees werefollowed-up in 2013.The authors conducted a multi-stage, trans-cultural training adaptation for a pilot men-tal health task sharing intervention. Theprocess involved three phases: 1) review ofthe literature and qualitative data collectionto adapt a MHPSS training; 2) implementa-tion and qualitative process evaluation ofa structured group pilot training; and3) implementation and evaluation ofan apprentice style pilot training (seeFigure 1). Prior to implementing the study,the researchers had only planned for Phase1andPhase 2.However, basedontheprocessresearch approach, the need for a modi¢edtraining approach and supervision wasidenti¢ed. Therefore, Phase 3 was added toaddress trainees’ and researchers’ concernsabout the limitations identi¢ed in Phase 2.Trilingual (Creole, French, English)Haitianresearch assistants were recruited from thecommunity to conduct onsite translationfor interviews and focus group discussions,translate training materials and facilitategroup trainings. One week of training famil-iarised research assistants with project aimsand methods, techniques for providingliteral translation and issues relating toethics and con¢dentiality. Because manyrural Haitians are illiterate, all participantsprovided verbal consent in Creole or French.The project was approved by the Institu-tional Review Board of Emory Universityand the Haitian Ministry of Health.Throughout the process, the study teamusedthe terms tris (sadness), ke' pakontan (unhappyheart) and stre' s (stress) to refer to mild tomoderate emotional distress because these
McLean et al.
rized reproduction of this article is prohibited.
local terms were more salient than psychia-tric diagnostic terminology (Kaiser et al.,2014; Keys et al., 2012). After a more speci¢c
139

Copyrig
a
, I
idiom of distress that captured psychologicaldistress was identi¢ed, maladi kalkilasyon
(thinking/calculating sickness) (Kaiseret al., 2014), this term was added.
Phase 1: Curriculum developmentFollowing development of provisionalmodules, in country qualitative data collec-tion was conducted to adapt the modulesusing elements of a participant orientedapproach (van der Veer & Francis, 2011).Eighteen key informant interviews wereconductedwith religious leaders, traditionalhealers, clinicians, teachers, municipal¢gures and other community leaders.Theseinterviews relied on an open ended, semistructured format to allow for £exibility ofquestioning and responses.Topics addressedin the interviews included: local signsof mental distress, care seeking, problemsolving and coping mechanisms. Partici-pants were asked whether they would ¢ndan MHPSS training useful, and if so, whattopics would be most valuable. Interviewswere conducted in French or Creole, facili-tatedby carefully trained trilingual researchassistants, and lasted between 30 minutesandone hour each. Responseswere recordedin detailed, handwritten notes by membersof the research team in English, and thenentered into a laptop computer on the sameday for later thematic analysis (Bernard &Ryan, 2010). The research team met daily todiscussmodi¢cation of questions in the inter-viewguide, review each other’s notes, discussemerging ¢ndings and identify importantthemes to be coded for analysis.
Phase 2: Structured training pilotQualitative post training data collectionwasconducted to explore perceptions regardingtraining and to identify areas for improve-ment.This included participant observationand semi structured follow-up interviewswith two of the trainees.Two teammembers
Task sharing in rural Haiti: qualitative assessment of
apprenticeship supervision for community health workers
ht © War Trauma Foundation. Unautho
observed the training and took detailednotes regarding participant engagement intraining activities, interactions between
140
participants and trainers, and amongparticipants, and topics covered.
Phase 3: Structured training plussupervised apprenticeshipInformedbydata collectedduring phase twoof the intervention, the study team adaptedtraining materials to ¢t an apprenticeshipstyle approach. The apprenticeship wasintended to address problems identi¢ed inthe ¢rst training, in particular the lowcon¢dence among trainees to implementand integrate skills learned into daily prac-tice. The new approach was to begin with astructured training similar to that providedto the entire group of CHWs. Prior to thePhase 3 training and apprenticeship, twofocus group discussions (FGD) were con-ducted, one among local teachers and com-munity leaders (n¼ 7), and another amongyouth leaders (n¼ 5), to inform this phaseof adaptation. The purpose of further datacollection was to gather insight into usefultraining modalities from individuals in thecommunity with experience in teachingand conducting trainings. FGD were facili-tated by the team’s social worker, with a sec-ond team member present to take detailed,almost verbatim notes. These data werecollected, recorded, and analysed similarlyto the prior semi structured interviews.Identi¢ed themes related to perceiveduseful-ness of various training methodologies, pre-ferred learning styles, logistics of hostingtrainings, mechanisms of evaluation andgeneral recommendations.Qualitative data were collected throughouteach apprenticeship, and included semistructured interviews with apprentices andparticipant observation during training,counselling sessions, and debrie¢ng. Longterm, follow-up data were collected twoyears later.The follow-up interviews focusedon recent cases, including strategies for pro-viding support and outcomes, and long term
brief, structured training with and without
ntervention 2015, Volume 13, Number 2, Page 135 - 155
rized reproduction of this article is prohibited.
re£ection on the training, including mostand least useful components. In addition,the initial apprentice was shadowed,

Copyrig
including observation of home visits withtwo current cases under his care. Detailedobservation notes were taken regarding con-tent of the conversation and visual cues(e.g. eye contact, facial expressions). Withparticipants’ permission, interactions withthe apprenticewere audio recorded. All datawere analysed to determine knowledgegained, satisfaction, con¢dence, intentionto apply skills learned in daily practice andappropriateness of counselling provided.
ResultsPhase 1: Content developmentProcess description: Based on the team’sprior qualitative research in Haiti’s CentralPlateau during June^August 2010 (Kaiseret al., 2013; Kaiser et al., 2014; Keys et al.,2012; Khoury et al., 2012) and an exten-sive literature search, provisional trainingmodules were developed by the study team,which included a Haitian clinical psycho-logist and an US based cultural psychiatristwith experience in multiple LMICs.Modules drew upon mental health trainingmanuals developed by mhGAPandTiyatienHealth3 for CHWs in India and Liberia(Gibsonet al.,2010;WHO,2010).Case studiestaken from stories gathered during previousethnographic data collection (Hagamanet al., 2013; Kaiser et al., 2014; Keys et al.,2012; Khoury et al., 2012) were used to placeconcepts and skills learned into a local con-text, as well as to encourage discussionregarding identifying signs and symptomsof distress, suggesting coping mechanismsand deciding when to refer someone to seekprofessional care.A body mapping exercise was developed forthe ¢rst module, to aid participants in con-ceptualising a psychosocial model of mentalhealth (IASC, 2007; Psychosocial WorkingGroup, 2003). Body mapping is a researchand training technique based on participa-
ht © War Trauma Foundation. Unautho
tory research methods for cross-culturalpopulations and bene¢ciaries with limitededucation. Participants draw a ¢gure and
then indicate the location in or on the bodywhere di¡erent aspects of distress are experi-enced. This approach is bene¢cial in cross-cultural settings to counter bias introducedby biomedical, psychiatric categories andsymptoms. Local idioms of distress associ-ated with psychosomatic complaints can beidenti¢ed through body mapping exercises.This method had been utilised in the team’sprior work to understand how emotionalexperiences and cognitive processes arelocalised within various parts of the bodyin terms of idioms of distress (Keys et al.,2012) and was selected as a teachingmodality that would have local relevance.
Key ¢ndingsTerminology for training: ‘weak limbs’
(fe' b nan manm), ‘strange face’ (¢gi dwo' l), ‘loss
of good sense’ (pe' di bon sans), and ‘lack of motiv-
ation’ (mank motivasyon). ‘Thinking/calculating
sickness’ (maladi kalkilasyon) and ‘thinking
too much’ (re£echi two' p) are idioms markedby intense rumination, social isolationand prolonged sadness (Kaiser et al.,2014). These terms were all incorporatedin the modules.Selecting appropriate types of train-ees: MHPSS provided by healthcareworkers and other community supports wasreported to be low by community members.Participants reported that CHWs did nottalk to them about their feelings andsuggested that it would be helpful to trainthem to listen better. The sacristan at thelocal Catholic Church noted that currently,‘the local leaders do not have enough knowledge
to support or talk to these individuals’. Such ¢nd-ings encouraged the team to include CHWsin the training, with a focus on basic com-munication skills such as supportive listen-ing.Content of training: In addition to a focuson listening skills, Phase1respondents calledfor training in coping mechanisms, includ-
McLean et al.
rized reproduction of this article is prohibited.
ing relaxation exercises. Suggested copingmechanisms included: reading the Bible, lis-tening to music, sewing, going on a picnic
141

Copyrig
a
, I
and playing soccer. These were then, there-fore, incorporated into the trainingmodules.The training also emphasised the need toidentify coping mechanisms on an individ-ual case basis, so that recommendations(including faith based activities) came frompatients themselves and did not risk furtherstigmatisation or alienation. Con¢dentialitywas additionally highlighted as an import-ant training topic. Participants had reportedthat they do not often talk about theirproblems with neighbours and friendsbecause they fear people will not practisecon¢dentiality (kenbe yon bagay sekre' , lit. holdsomething secret): ‘The other women are not
reliable and they gossip too much. If you ask another
for help, they may be tempted to speak badly about
you to other women in the community’ (Femalefarmer).Of all the participants that were inter-viewed prior to the training, only one, adeacon, mentioned that he ever referredindividuals to a nearby psychologist. Toraise awareness of the need for referrals, amodule on this topic was included. Becausethere were no speciality services availablethrough the partner NGO, the study teamworked with a di¡erent organisation,Zanmi Lasante,4 to establish a referral sys-tem for individuals exhibiting the need forimmediate care. The team was giventailored referral sheets, to share with trai-nees, to document the name, location,relevant history and mental health symp-toms of any referred individual. Any carereceived was at no cost to the patient andall travel related expenses were reimbursedby Zanmi Lasante.
Phase 2: Group MHPSS training pilotProcess descriptionThe partner NGO hosted a pilot training.Trainees included fourteen CHWs currentlyworkingwith theNGO, both ajan sante (com-munity health workers) and promoters
Task sharing in rural Haiti: qualitative assessment of
apprenticeship supervision for community health workers
ht © War Trauma Foundation. Unautho
(community members who provide healtheducation through song). They wereassigned to participate by the local NGO
142
and were initially selected for the trainingbecause they expressed a desire to partici-pate. At the time of the training, CHWswerelargely providing services for HIV/AIDSand cholera prevention.The six modules were delivered by Haitiantrainers in Creole during a three day train-ing period (see Box 1). An average of fourhours per day was spent on training.At participants’ request, skills covered in thetraining were framed within a seven stepprocedure for providing MHPSS withinthe local context (see Box 2).
Key ¢ndingsKnowledge: After the training, partici-pants reported having acquired knowledgeon identifying signs and symptoms of mentaldistress, describing what it means to be asupportive listener, practising con¢dentia-lity and identifying coping methods. Fewrespondentswere able to identify under whatcircumstances it is necessary to break con¢-dentiality (e.g., danger to self or others).Instead, most respondents felt it was import-ant always to maintain con¢dentiality, inorder to gain trust.Satisfaction: Participants reported overallsatisfaction with the training. One femaleCHW reported; ‘everything about the training
went well. If I thought it wasn’t good or useful,
I wouldn’t have left my house and trekked through
the mud all the way to [the training centre]’.However, when asked what they had likedor disliked about the training, participantswere hesitant to provide any criticismand would respond that they liked every-thing. This may be due to the fact thatparticipants perceived trainers as experts;‘I don’t think I can tell you what to improve
because you know more than I do’ (FemaleCHW).Usefulness and preferred trainingmethod: A body map exercise was utilisedto help participants visually illustrate the
brief, structured training with and without
ntervention 2015, Volume 13, Number 2, Page 135 - 155
rized reproduction of this article is prohibited.
di¡erent domains of ‘self ’ (e.g. head, soul)and to describe the psychological andemotional issues faced by community

Copyright © War Trauma Foundation. Unauthorized reproduction of this article is prohibited.
Box 1: Content of psychosocial training for community health workersDay1Developing a psychosocial model for mental health
1 Participants arewelcomedand introduced tomembers of the study team.Anover-view of the programme purpose and objectives is provided.
2 A case study is presented to the group about awoman in the community who hasexperienced mental distress. Participants are asked to identify signs and symptoms ofherdistress andhowtheymighthelp if shecametothem for support.Designedto exploreparticipants’understanding and knowledge of mental health.To go beyond concepts offou (psychosis),mental illnesses arede¢nedmorebroadlyasunhealthy thoughts, feelingsand behaviours,
3 Brainstorming activity helps participants to understand factors that contribute tomental distress and how members of the community experience su¡ering. Di¡erentdomains a¡ected by distress (e.g. head, heart, body, etc.) are listed on a £ip chart. Usedto facilitate understanding of a psychosocial model of mental heath.Recognising signs and symptoms of distress
4 Brainstormingactivityusedto identify local signsand symptomsofmentaldistress.Responses are recorded on a £ip chart. Participants are asked to identify the e¡ects ofmental illness on individuals and their families, including in regard to farmwork, com-merce, cooking and caring for the home and participation in community activities.Included also is a conversation on stigma and its impact on peoples’wellbeing.
5 Bodymapping exercise used to illustrate concepts learned in previousbrainstorm-ing activity. Signs and symptoms of distress as experienced in various domains of ‘self ’aredrawnonhandout.Participantsbreakupintogroupsof threetocompletetheactivity.Results are then shared with the group as awhole.
6 Participants split up into groups andare asked to identify three things they learnedfrom the session, two things they were still unclear about and one thing they felt theycould teach to another. Designed to summarise the session and identify areas needingfurther discussion.
Day 2Demonstrating active and supportive listening
1 Participants re£ect onDay1of the training.Major themes andmessages are ident-i¢ed and concepts clari¢ed as needed.
2 Participants are introduced to the concept of supportive listening. In small groups,major steps to implementing supportive listening are identi¢ed and recorded on a £ipchart. Groups then come together to compare ¢ndings.
3 Roleplay isusedtodemonstrate theapplicationof principlesof supportive listeningand to identify social and psychological bene¢ts of applying supportive listening withina therapeutic environment. Participants are then split into groups of three to practiseconcepts learned.Practising confidentiality when people come to you for help
4 Atrained local socialworker speakstoparticipantsontheconceptofcon¢dentialityandunderwhatcircumstances con¢dentialitymaybebroken. Participants are informed
McLean et al.
143

Copyrig
that if apersonmentionswanting to in£ict harmtohimself or another person, theymustinform amental health professional.
5 Case studies are used to explore ways that breach of con¢dentiality can negativelya¡ect people su¡ering frommental healthproblems.Designedto emphasise the import-ance of patient/client privilege.
6 Participants split up into groups andare asked to identify three things they learnedfrom the session, two things they were still unclear about, and one thing they felt theycould teach to another. Designed to summarise the session and identify areas needingfurther discussion.
Day 3Managing and coping with mental distress
1 Participants re£ect onDay 2 of the training.Major themes andmessages are ident-i¢ed and concepts clari¢ed as needed.
2 Asagroup,participantsbrainstormdi¡erenttypesofcopingresources inthe familyand/or community. Coping mechanisms are divided according to mental, social, spiri-tual and physical strategies.
3 Roleplay isusedto illustratehowonemightaidcommunitymembers in identifyingtheir owncoping strategies, so that theyare relevantonacase-by-casebasis. Participantsare then split up into small groups to practise problem solving and scenarios where theyhelp the individual to elicit certain help seeking behaviours and coping mechanisms.Depending on referral strategies and resource networking
4 Participants ¢rst discuss commonpathways to care seeking in the community andfactors that contribute to healthcare seeking, e.g. cost, trust, stigma, etc. Bene¢ts andpotentialdangersof referring individualstovarious sectorsofcarewithinthecommunityare discussed.
5 When to refer someone to a health professional is then discussed.Where to refersomeone, depending on the circumstances, is then covered.
6 A case study involving someone who is severely mentally distressed is used as anexample to illustrate when and how to refer someone to a professional.
7 A summary of the training is provided andparticipants are thanked for their time
Task sharing in rural Haiti: qualitative assessment of a brief, structured training with and without
apprenticeship supervision for community health workers, Intervention 2015, Volume 13, Number 2, Page 135 - 155
members within each of these domains(Karki, Kohrt, & Jordans, 2009; Keyset al., 2012). This exercise, role play, groupdiscussions and case studies were all con-sidered useful. Eliciting peer feedbackduring role play was challenging becauseparticipants perceived constructive criticismas losing face in front of the group. Duringrole play, trainers repeatedly rephrased
and participation.
ht © War Trauma Foundation. Unautho
questions to avoid appearing to ask partici-pants to criticise one of their co workers bysuggesting ways to improve their response.
144
The use of a participatory method was also,initially, challenging because CHWs wereuncomfortable providing their opinions inwhat was perceived as a formal teaching set-ting. In several unrelated trainings con-ducted by the host NGO, the teamobserved limited participation of traineesin proceedings.The training teammitigatedthis challenge, in part, by explaining their
rized reproduction of this article is prohibited.
role to be more that of a facilitator and byemphasising that the participants were the‘experts’ in this cultural context.

Copyrig
Box 2: Seven step approach to providing psychosocial support1 Askquestions to determine the emotional state of the client.Participants identi¢ed
questions such as: how are things going in your life right now?
2 Look for signs and symptoms of distress.Local signs and symptoms that partici-pants identi¢ed included: loss of weight, facial expressions like frowning or looking down, andnot liking yourself.
3 Identify the source of the problem by asking for client’s history.One way that aparticipant addressed this in a role play activity was by asking: what is causing you to feelsadness or stress?
4 Help the client to identify positive aspects of his or her life.Participants mightencourage client to: list activities they enjoy doing in their free time or things in their life that theyare thankful for. Suggestions provided by community health workers during role playincluded: listening to the radio, playing soccer, going to Church, and talking with friends.
5 Identify or help client to identify coping resources.The participant might ask, forexample: what do you like to do for fun? Activities identi¢ed by community membersincluded: listening to the radio and playing dominoes.
6 Decide whether it is necessary to refer client to a professional.Things that partici-pantswere encouraged to consider in their decisionmaking processwere:whether the per-son mentioned in£icting harm to another or to oneself (including threats of suicide).
7 End the conversation on a positive note.In one role play scenario, a participantended a conversation by pointing out that his colleague had successfully suggested several copingmechanisms to try.
McLean et al.
Con¢dence: Results were mixed regardinghaving the con¢dence to implement andintegrate skills learned into daily practice.Prior to the training, CHWs expressed dis-comfort providing emotional support tocommunity members; ‘I can help someone whohasexperiencedmild issuesorwhohasmoderate dis-
tress (tonbe yon ti kras) [lit. ‘fallen some’], but
not someone who has severe distress (tonbe anpil)’
[lit.‘fallen a lot’] (Male CHW). Immediatelyfollowing the training, several participantsindicated that they would feel more able tosucceed in helping someone who came tothem with mental distress. Such responsesillustrate increased con¢dence in providingassistance as a result of the training. How-ever, several follow-up, semi structuredinterviews revealed that trainees’ con-¢dence to apply their new skills wasactually low. These interviews also helpedto identify elements of the training thatparticipants thought could be improved to
ht © War Trauma Foundation. Unautho
provide increased con¢dence. Respondentsexpressed concern that the trainings werenot long enough to su⁄ciently teach skillsneeded to help those experiencing distress.OneCHWstated that hewouldprefer longertrainings, spread over time, to reinforceideas as he was concerned about forgettinginformation learned in the training. Partici-pants also expressed the desire for infor-mation to be presented in written form sothat they could take the information homewith them and concepts could be practisedas needed over time. Other respondentsreported that some aspects of the trainingremained unclear.
‘It was still somewhat unclear how to tellwhen
a person is experiencing stress (stre' s) or
anxiety (ankyete) without that person saying
it. In this culture, we know of stress, but we
don’t really know what it does or how to tell if
someone is stressed.This training was a good
rized reproduction of this article is prohibited.145

Copyrig
a
, I
start, but I would like to have more infor-
mation and strategies to help someone with
stress’ (Male CHW).
A longer training period would haveallowed for su⁄cient time to address signsand symptoms of local manifestations of dis-tress and to practise engaging individualswith such symptoms.Behaviour change and implementa-tion: Observation and interviews followingthe training revealed that the interventionresulted in minimal changes in behaviour:no trainees provided accounts of implement-ing skills covered in the training in the twoweeks following it. From limited qualitativedata collected immediately following thetraining, the CHWs seemed to be anxiousthat the training would expose them notonly to new skills, but also to an entirelynew role in the community ^ that of mentalhealthcare provider. Upon completion of thetraining, traineeswere providedwith a certi-¢cate of participation. However, partici-pants expressed frustration that they werebeing asked to take on new and time inten-sive responsibilities without any monetarybene¢t. During a post training interview, aCHW provided an unsolicited detailed dis-cussion of her own ¢nancial hardships andsources of distress related to family problems,which she viewed as a barrier to providing
Task sharing in rural Haiti: qualitative assessment of
apprenticeship supervision for community health workers
MHPSS services to others.
Phase 3: Apprenticeship pilotProcess descriptionRevisions of the structured training com-ponent included: di¡erentiation of severemental distress from mild distress, referralresources to link individuals to immediatecare and clarifying circumstances in whichto break con¢dentiality. Trainees wereprovided printed materials detailing train-ing topics (e.g., signs and symptoms ofdistress, practising active listening, con-
ht © War Trauma Foundation. Unautho
veying con¢dentiality and building trust,identifying coping mechanisms and under-standing health seeking behaviours). Such
146
information was listed, along with referralstrategies, so that they could easily draw onthese resources in the future, and link clientsto appropriate caregivers.Discussion, role play and case study vign-ettes were used to build up a basic level ofknowledge and skill, as well as to assessunderstanding of the problems, causes andpotential MHPSS within the local setting.Additionally, apprentices were exposed tothe seven stepapproach to providing supportwithin the context of a home visit (see Box2). Following each role play, trainers andapprentices discussedhoweachmember per-formed, how they could improve and keyissues raised. Within this small motivatedgroup, feedback became the cornerstone ofsuccess of this exercise.After the structured training, the appren-ticeship approach included oneweekof dailyobservation by a licensed counsellor con-ducting sessions with community members(approximately 1^2 session per day), fol-lowedbyanother weekof supervised sessionswhere the trainee could practise new skillslearned. Brie¢ng and debrie¢ng aroundthese sessions were to facilitate learningand active problem solving. Furthermore,because experience showed that individualswere reticent to take on new, time intensiveroles within the community without addedmonetary bene¢t, it was decided that onlyhighly motivated individuals with adequatetime availability would be recruited toparticipate in the second training pilot.Three traineeswere selected for the structuredtraining plus apprenticeship pilot. Based on ¢nd-ings from Phase 2, we did not restrict partici-pants only to health workers. Instead, anyindividuals who expressly demonstratedinterest in MHPSS were included. Thismeant including one CHWparticipant fromthe group MHPSS training (Phase 2) whohad expressed a desire for further skill build-ing in the post training assessment. The
brief, structured training with and without
ntervention 2015, Volume 13, Number 2, Page 135 - 155
rized reproduction of this article is prohibited.
two additional apprentices were a sacristanfrom the local Catholic Church and a wellrespected woman from the community.

Copyrig
Despite not being CHWs, these individualswere selected because they were highlymotivated, expressing interest in receivingtraining and members of the local com-munity identi¢ed them as currently pro-viding advice and help to others. Neitherhad received any former mental healthrelated training. Apprentices selected thefrequency and timing of training sessions inorder to ¢t within their schedules anddaily tasks.Following the classroom portion of therevised training, apprentices observed alicensed counsellor conducting counsellingsessions with community members. Theseindividuals were identi¢ed by our concur-rent epidemiological survey (Wagenaaret al., 2012) as having depressive symptomol-ogy. These case visits included referral tolocal mental health professionals if thecounsellor deemed it necessary. Individualswith severe mental distress, thoughts ofsuicide, or other needs requiring a psycholo-gist or mental health physicianwere referredto Zanmi Lasante’s mental healthcare pro-gramme, with two facilities within a 30^45minute drive from the community. Case vis-its progressed from the apprentice shadow-ing the licensed social worker on housevisits, followed by debrie¢ng and discussion,to the apprentice conducting home visitswhile being shadowed by the licensed socialworker, again followedbydebrie¢nganddis-cussion. The apprentices observed approxi-mately ¢ve one-hour counselling sessionsover the course of one week before conduct-ing their own supervised sessions. Follow-up debrie¢ngs included a discussion of whatthe apprentice did well and ways they couldimprove, as well as moments that wereparticularly challenging and how to addresssuch situations in the future.
Key ¢ndingsActivities at follow-up: Two years after
ht © War Trauma Foundation. Unautho
starting the apprenticeship process, all threetrained apprentices were engaged in activi-ties related to training, including providing
mental health support and referring seriouscases to professionals. Apprentices reportedhelpingbetween15 and 35 individuals in thattime period, typically for relationship prob-lems and ‘problems of life, Haitian problems’.They engaged in multiple visits with eachindividual, usually over a period of 1^3months. Apprentices reported that theirvisits focused on helping to identify thesource of problems, encouraging continuedactivity and goal setting, enabling indivi-duals to focus on positive things in life andsources of support. There were no accountsof CHWswhounderwentonly the ¢rst groupMHPSS training providing organised men-tal health support or referring individualswith serious mental disorders.Service provision observation: Obser-vation of apprentices in the ¢eld and feed-back following MHPSS sessions showedthat apprenticeship training was successfulin promoting understanding of conceptsrelated to providing mental health support.Participants seemed to understand the pur-pose of the sessions and how to integratethe concepts learned in the training intopractice. One apprentice displayed hisunderstanding of the counselling techniqueas follows: ‘at the beginning we tried to make nicewith this person, make her feel comfortable being
honest. In the middle, we underlined the problem.
At the end, we tried to ¢nish with a positive note’(Male CHW). In conversation with theCHW, the client admitted to experiencingthoughts of suicide.The apprentice was suc-cessfully able to identify the source of distressand help the client identify positive aspectswithin her life, including coping resources.The apprentice referred her for professionalcare. During follow-up observations, theapprentice demonstrated active listeningskills, a focus on encouraging individualsto identify coping resources and sources ofhope and knowledge of when to referindividuals.These examples illustrate under-
McLean et al.
rized reproduction of this article is prohibited.
standing of skills learned in the apprentice-ship training, including how to maintaincohesion and £ow within a MHPSS session,
147

Copyrig
Task sharing in rural Haiti: qualitative assessment of a brief, structured training with and without
apprenticeship supervision for community health workers, Intervention 2015, Volume 13, Number 2, Page 135 - 155
as well as when and where to refer cases ofsevere distress.Satisfaction: Apprentices reported over-all satisfaction with training goals andmethods. They expressed a desire to trainmore individuals using the apprenticeshipmodel. After completing the training, themale sacristan explained the importanceof providing nearby regions with localcounsellors.
‘I live here, I can help people nearby. If in
another zone, however, that person cannot
get to me. There needs to be someone there.
You need to train and give a respected com-
munity leader this knowledge in every zone
so everyone can have access to this support.
If you train me, we can take one week in
Lahoye and go train them too.We can help
you train others.’
Apprentices reported that it was helpful toobserve a trained professional conduct acounselling session in the ¢eld. In debrie¢ngfollowing a case visit, one participant said,‘it has been helpful to see this. The more that you
spoke with this person, the more comfortable they
felt sharing with you’ (Male CHW). Afterobserving the counsellor discuss copingmechanisms, the sacristan stated, ‘I really
appreciate the positive method you used to let the
lady know that there are a lot of things that she can
do [. . .] When you say that you are supposed to
empoweraperson tosolve theirownproblems, Ididn’t
understand it before, but I now understand.’ Atthe two year follow-up, apprentices notedthat the training skills that they used mostoften were identifying signs and symptomsof distress and helping people to identifycoping resources, such as community sup-ports and engaging in activities.Con¢dence: Not giving direct advice wasa challenge for each apprentice to over-come, as witnessed both in role play andobservation of the MHPSS sessions. A sig-ni¢cant portion of initial training wasspent practising how to handle situationswhere individuals were slow to suggest
ht © War Trauma Foundation. Unautho148
solutions on their own. Several role plays,involving feedback from both trainers andpeers as well as question and answerperiods, helped the apprentices gain con¢-dence and question posing skills. Oneapprentice, when asked by a supervisorwhat he thought he did well following asolo session, replied (with a smile), ‘I intro-duced myself and began the session well. I did best
when the woman mentioned that it would be sum-
mer vacation soon, and she could save money then
to go towards starting a business. She came up with
her own solution.’ At a two year follow-upobservation, there was a decrease in directadvice, with the apprentice solely askingquestions and encouraging individuals toidentify their own solutions.When asked at follow-up for examples ofcases that they would not have felt able tohelp prior to training, one apprentice namedfamily problems, feelings of abandonmentand hopelessness, and suicidal ideation.Another apprentice explained that hehelpedto intervene in a community disagreementand used his new skills to facilitate a resol-ution between neighbours. Additionally, allapprentices appear to have gained com-munity recognition for their roles, reportingexamples of individuals seeking them outfor support. In other cases, they approachedcommunity members known to be su¡eringfrom mental distress or identi¢ed casesthrough typical encounters (in the case ofthe CHW).
DiscussionWith the aim of contributing to identifyingbest practices for task sharing in humanitar-ian and LMICs settings, we described thedevelopment and implementation of twomodels for a task sharing mental healthtraining in rural Haiti. After a groupbased, three day training, participantsdemonstrated increased knowledge; how-ever, motivation and intention to apply con-cepts were lacking. Several participantsexpressed concern that they would forgetconcepts learned or did not fully understand
rized reproduction of this article is prohibited.

Copyrig
how to implement skills taught. Addition-ally, no behavioural changes were observedor recounted following the initial pilot train-ing. Incontrast, anapprenticeship approach,which built upon a didactic-style train-ing and included supportive supervision,demonstrated more positive outcomes.Given the various ¢nancial, logistical, andemotional barriers faced by these appren-tices, we consider it particularly noteworthythat all three continued identifying, counsel-ling, and referring community members atleast two years after the training, and oneformer apprentice became an o⁄cial volun-teer for a large Haitian healthcare NGOas a psychosocial worker in a volunteercapacity. Factors that potentially explainthese di¡erences include training structure,recruitment of trainees and motivation toparticipate in the training in order to gainskills for future use.
Training structureGroup training may have limited bene¢t inpractice because of the modality, while stillimportant for knowledge gain. Teachingnovel concepts within a classroom setting,especially concepts related to providing apublic service, may be less e¡ective for pro-moting skill building than coaching individ-uals through hands on practice within thecommunity (Beidas, Koerner, Weingardt,& Kendall, 2011).While role play and otheractivities remain helpful teaching tools, theydo not elicit the same level of practice andfeedback compared to observed ¢eld activi-ties. Moreover, post training supervision isone of the strongest predictors of behaviourchange (Fixsen, Naoom, Blase, Friedman,& Wallace, 2005). Trainees in LMICs preferexposure to real life experience when apply-ing skills learned during trainings (Flisheret al., 2007).The second pilot intervention providedpractice based learning within an appren-
ht © War Trauma Foundation. Unautho
ticeship model built on a structured founda-tional training. Our initial ¢ndings suggestthat increased e¡orts to integrate elements
of the apprenticeship approach, includingactive, participatory learning, ongoingsupervision and on-site feedback are war-ranted. This is consistent with recommen-dations that trainings should be active andpractical, incorporatingbehavioural rehear-sal (Herschell et al., 2010; Murray et al.,2011). The supervision in the apprenticeshiptraining model that enabled bidirectionalcollaboration and assurance of back-up sup-port may be responsible for observed beha-viour change following the intervention.Bidirectional teaching that treats traineesas engaged, rather than passive, partici-pants, as well as supervision, is consideredcritical (Beidas et al., 2011). Such bidirec-tional collaboration is also an important pre-dictor of e¡ective interventions (Forman,Olin, Hoagwood, Crowe, & Saka, 2009),with assurance of a back-up system of sup-port shown to be a key ingredient in somesuccessful task sharing interventions (Kaneet al., 2010). Future research should explorethe impact of di¡erent durations of supervi-sion processes in promoting capacity andmotivation to provide MHPSS services.
Identifying appropriate traineesOne of the reasons that this apprentice-ship model may have been successful wasbecause only motivated, community iden-ti¢ed volunteers were trained. They werealready working to provide emotionalsupport within the community and hadexpressed interest in learning additionalskills. It is often assumed that training ofindividuals who self-select into interventionprogrammes is good practice, despite evalu-ations showing no signi¢cant di¡erences inempathy and psychological mindedness ofvolunteer versus non volunteer trainees(Compton, Broussard, Hankerson-Dyson,Krishan, & Stewart-Hutto, 2011). Researchrelated to the e¡ectiveness of programmesthat recruit on a volunteer basis is further
McLean et al.
rized reproduction of this article is prohibited.
warranted. Motivation, anticipation ofbeing valued by the community and assur-ance of back-up support are important
149

Copyrig
a
, I
factors, as task sharing personnel mayalreadybe overburdenedwithmultiple com-munity health demands (Kane et al., 2010;Maes, Kohrt, & Closser, 2010). In this case,task sharing runs the risk of becoming ‘taskdumping.’Our team may have mistakenly concludedthat CHWs would be the most appropriategroup for this training because of theirhealth related experience, mobility andregular access to individuals in their homes.However, this failed to account for structuralbarriers that may have prevented them frome¡ectively incorporating new MHPSS skillsinto their daily activities. Such barriersinclude monetary compensation and avail-able timeand resources. Again,CHWs livingin low resource settings, especially postdisaster settings, are often over burdenedwith numerous tasks (Maes, Shi¡eraw,Hadley, & Tesfaye, 2011).Following the group training, CHWsrequested additional pay for implementingnew skills learned. Although the CHWs inthis training did receive a salary for theiremployment, we were asking them totake on additional responsibilities withoutadditional compensation. It is worth consid-ering whether this was a fair expectation.CHWs and other mid level healthcare pro-viders are often overburdened with day-to-day responsibilities of caregiving, coupledwith their own economic stress (Maeset al., 2010; Maes et al., 2011). On a globalscale, there is general reluctance by donorsto direct funds toward creating healthcarejobs in low income countries, despite criticalshortages in sta⁄ng (Ooms, van Damme,& Temmerman, 2007). As a result, cheap orvolunteer labour has become the norm inmany LMICs. Although the apprenticeswere not paid, our ¢ndings suggest thatappropriate compensation should accom-pany the expectation that CHWs take onnew skills and responsibilities.
Task sharing in rural Haiti: qualitative assessment of
apprenticeship supervision for community health workers
ht © War Trauma Foundation. Unautho
In addition to increased wages, an addedincentive, such as a recognised certi¢cationfor the training, is important. Several
150
participants conveyed the desire for concrete‘proof ’ that they had received new skills.Although this was a pilot training, task shar-ing initiatives may be more e¡ective if careproviders can be formally recognised bynational or community wide educationorganisations (WHO, 2008). Certi¢cationhas also been shown to improve overalle¡ectiveness of health related trainings(Necochea,2006;WHO,2003). Furthermore,Farmer and colleagues argue that CHWsshould be incorporated into the publicsector, which would have the dual bene¢tof ensuring government recognition andstrengthening public health systems(Mukherjee&Eustache,2007; Public Broad-casting System (PBS), 2009).Additionally, it is also important to considerwhether recruits for task sharing trainingswithin global mental health care are havingtheir own emotional and mental healthneeds addressed. During post training inter-views, participants cited familyand ¢nancialproblems and related personal emotionaldistress as barriers to engaging in MHPSSservices for others. Petersen, Ssebunnya,Bhana, and Baillie (2011) emphasise theimportance of support and supervision forhealth care workers exhibiting stress as partof care delivery within task sharing initiat-ives.
Strengths and limitationsThis was a pilot intervention with a smallsample size nested within the particularsocial and cultural milieu of one Haitiancommunity. The evaluation of the trainingre£ected in this analysis is purely qualitativeand therefore lacks standardised measuresof knowledge acquisition. Ideally, theoptimal measure of e¡ectiveness would havebeen an evaluation of patient outcomesthrough both qualitative and quantitativeapproaches. The supervisor trainer for bothstudies was an American social worker who
brief, structured training with and without
ntervention 2015, Volume 13, Number 2, Page 135 - 155
rized reproduction of this article is prohibited.
did not speak the local language. Though aHaitianpsychologist was originally intendedto ful¢l this role, she unexpectedly withdrew

Copyrig
from ¢eld participation prior to training. Forthe structured group training, severalparticipants declined to be interviewedfollowing completion of the training due toissues related to lack of time and resources,and reporteddisinterest. Our present projectalso does not formally compare the twoapproaches. More rigorous methods areneeded to fully evaluate the apprenticeshipapproach and other training models. Inparticular, anonymous feedback approacheswould have been a useful complement toin-depth interviews.Another limitation is that at the time of thestudy, the CHW training modules formhGAP were not available, and thistraining relied upon modi¢ed versions ofmhGAP-IG. Finally, whereas this approachinvolved task sharing of mental health ser-vices to CHW, a collaborative care modelin which health workers at multiple levelswere trained would have been preferableand would have increased the likelihoodof appropriate division of responsibilities.Overburdening community health workerswithout adequate access to higher levels ofexpertise is a disincentive to appropriateprovision of care. Another limitation is thatthis study only employed selected elementsof participant oriented approaches as out-lined by van der Veer and Francis (2011).Implementing the process with exclusiveallegiance to participant oriented method-ology may have produced di¡erent qualita-tive outcomes.On the other hand, this project had severalstrengths. The training was developedalongside community members andresearch assistants within a participatoryformat. Qualitative methodologies allowedthe team to explore perceptions and beha-viour in greater depth and to uncovercontext speci¢c challenges to providingMHPSS services. In the case of smallsamples, qualitative evaluation is preferable
ht © War Trauma Foundation. Unautho
to quantitative measures, as the former canprovide detailed information of knowledgegained and how to improve training content
and structure. Our study incorporated longterm follow-up data attesting to the utilityof the apprenticeship model.This is import-ant, given that few studies have documentedsustained changes in practice beyond sixmonths following training (Flisher et al.,2007).
ConclusionsQualitative process assessment of two train-ing models that were iteratively designedand implemented supports use of a cultur-ally adapted apprenticeship model withsupportive supervision. More studies thatevaluatemethods to recruit, train and super-vise mid level mental health workers inlow resource settings are needed, especiallythose that utilise rigorous randomisationmethods and long term follow-up. Withoutrigorous evaluation of trainings, it is di⁄cultto determine if interventions succeed or failbecause of the intervention content orbecause of the approaches used to trainpractitioners.Going forward, it will also be important toensure that community based trainingactivities are embedded within approachesto build multi layered systems of care (Patel& Thornicroft, 2009). CHW and othernon specialists involved in mental healthcare provision serve as an important linkbetween community members and healthcare providers, especially whenprofessionalsare in short supply. For post con£ict, postdisaster and poverty stricken populationsthere is a crucial need to identify trainingstrategies for CHW with the greatest likeli-hood of improving individual and com-munity wellbeing.
ReferencesBaingana, F.&Mangen, P.O. (2011). Scaling up ofmental health and trauma support among wara¡ectedcommunities innorthernUganda: lessonslearned. Intervention, 9(3), 291-303.
McLean et al.
rized reproduction of this article is prohibited.
Beidas, R. S. & Kendall, P. C. (2010). Trainingtherapists in evidence-based practice: a critical
151
Copyrig
Task sharing in rural Haiti: qualitative assessment of a brief, structured training with and without
apprenticeship supervision for community health workers, Intervention 2015, Volume 13, Number 2, Page 135 - 155
review of studies from a systems-contextualperspective. Clinical Psychology, 17,1-30.
Beidas, R. S., Koerner, K.,Weingardt, K. R. &Kendall, P. C. (2011). Training research: practi-cal recommendations for maximum impact.Administration and Policy in Mental Health, 38, 223-237.
Bernard, H. R. & Ryan, G. W. (2010). Analyzingqualitative data: systematic approaches. Los Angeles:Sage.
Bijoux, L. (2010). Evolution of concepts and inter-ventions in mental health in Haiti [in French].Revue Haitienne de la Sante¤ Mentale, 1, 83-90.
Budosan, B. (2011). Mental health training ofprimary health care workers: case reports fromSri Lanka, Pakistan andJordan. Intervention, 9(2),125-136.
Budosan, B. & Bruno, R. F. (2011). Strategy forproviding integrated mental health/psychosocialsupport in post earthquake Haiti. Intervention,
9(3), 225-236.
Caribbean Country Management Unit. (2006).Social resilience and state fragility in Haiti: acountry social analysis.World Bank.
Compton, M. T., Broussard, B., Hankerson-Dyson, D., Krishan, S. & Stewart-Hutto, T.(2011). Do empathyandpsychologicalmindednessa¡ect police o⁄cers’decision to enter crisis inter-vention team training? Psychiatric Services, 62, 632-638.
de Ville de Goyet, C., Sarmiento, J. P. &Grunewald,F. (2011).Healthresponsestotheearthquakein Haiti, January 2010: lessons to be learned for the
next sudden-onset disaster. Washington, DC: PanAmerican Health Organization.
Fixsen, D. L., Naoom, S. F., Blase, K. A.,Friedman, R. M. & Wallace, F. (2005). Imple-
mentation research: a synthesis of the literature.Tampa, FL: University of South Florida,Louis de la Parte Florida Mental HealthInstitute,TheNational ImplementationResearchNetwork.
ht © War Trauma Foundation. Unautho152
Flisher, A. J., Lund, C., Funk, M., Banda, M.,Bhana, A., Doku,V., . . . Green, A. (2007). Mentalhealth policy development and implementationin fourAfrican countries. Journal of Health Psychol-ogy, 12, 505-516.
Forman, S.,Olin, S.,Hoagwood,K.,Crowe,M.&Saka, N. (2009). Evidence-based interventionsin schools: developers’ views of implementationbarriers and facilitators. School Mental Health, 1,26-36.
Gibson, K., Kermode, M., Devine, A., Raja, S.,Sunder, U. &Mannarath, S. C. (2010).An introduc-tion to mental health ^ Afacilitator’s manual for training
communityhealthworkers in India.Melbourne:NossalInstitute for Global Health.
Hagaman, A. K.,Wagenaar, B. H., McLean, K.E., Kaiser, B. N., Winskell, K. & Kohrt, B. A.(2013). Suicide in rural Haiti: clinical and com-munity perceptions of prevalence, etiology, andprevention. Social Science & Medicine, 86, 61-69.
Herschell, A. D., Kolko, D. J., Baumann, B. L. &Davis, A. C. (2010).The role of therapist trainingin the implementation of psychosocial treatments:a review and critique with recommendations.Clinical Psychology Review, 30, 448-466.
Inter-Agency Standing Committee (IASC).(2007). Guidelines on Mental Health and Psychosocial
Support inEmergency Settings. Geneva: Inter-AgencyStanding Committee.
Kaiser, B. N., Kohrt, B. A., Keys, H.M., Khoury,N.M.&Brewster,A.R. (2013). Strategies forasses-sing mental health in Haiti: local instrumentdevelopment and transcultural translation.Trans-cult Psychiatry, 50, 532-558.
Kaiser, B. N., McLean, K. E., Kohrt, B. A.,Hagaman, A. K., Wagenaar, B. H., Khoury, N.M.&Keys, H.M. (2014). Re£echi twop^thinkingtoo much: description of a cultural syndrome inHaiti’s Central Plateau. Culture, Medicine and Psy-
chiatry, 38, 448-472.
Kakuma, R., Minas, H., van Ginneken, N., DalPoz, M. R., Desiraju, K., Morris, J. E., Sche¥er,
rized reproduction of this article is prohibited.
Copyrig
R. M. (2011). Human resources for mental healthcare: current situation and strategies for action.Lancet, 378,1654-1663.
Kane, S. S., Gerretsen, B., Scherpbier, R., DalPoz, M. & Dieleman, M. (2010). A realistsynthesis of randomised control trials involvinguse of community health workers for deliveringchild health interventions in low and middleincome countries. BMC Health Services Research,
10, 286.
Karki, R.,Kohrt, B. A.& Jordans,M. J. D. (2009).Child Led Indicators: pilot testing a childparticipation tool for psychosocial support pro-grammes for former child soldiers in Nepal. Inter-vention, 7, 92-109.
Keys, H.M., Kaiser, B. N., Kohrt, B. A., Khoury,N.M. & Brewster, A. R. (2012). Idioms of distress,ethnopsychology, and the clinical encounter inHaiti’s Central Plateau. Social Science & Medicine,
75, 555-564.
Khoury, N. M., Kaiser, B. N., Keys, H. M.,Brewster,A.R.&Kohrt, B.A. (2012). Explanatorymodels and mental health treatment: isVodou anobstacle to psychiatric treatment in rural Haiti?Culture,Medicine and Psychiatry, 36, 514-534.
Maes,K.C.,Kohrt, B.A.&Closser, S. (2010).Cul-ture, status and context in community healthworker pay: pitfalls and opportunities for policyresearch. A commentary on Glenton et al. (2010).Social Science & Medicine, 71, 1375-1378 discussion1379-1380.
Maes,K.C., Shi¡eraw,S.,Hadley,C.&Tesfaye,F.(2011). Volunteer home-based HIV/AIDS careand food crisis in Addis Ababa, Ethiopia: sustain-ability in the face of chronic food insecurity.HealthPolicy Plan, 26, 43-52.
Miller, N. L. (2000). Haitian ethnomedical sys-tems and biomedical practitioners: directions forclinicians. JTranscult Nurs, 11, 204-211.
ht © War Trauma Foundation. Unautho
Milne,D.,Aylott,H., Fitzpatrick,H.&Ellis,M.V.(2008). How Does Clinical Supervision Work?Using a ‘‘Best Evidence Synthesis’’ Approach to
Construct a Basic Model of Supervision. The
Clinical Supervisor, 27,170-190.
Mukherjee, J. S. & Eustache, F. E. (2007). Com-munity health workers as a cornerstone for inte-grating HIVand primary healthcare. AIDS Care,19(Suppl1), S73-S82.
Murray, L. K., Dorsey, S., Bolton, P., Jordans, M.J.,Rahman,A., Bass, J.&Verdeli,H. (2011). Build-ing capacity in mental health interventions inlow resource countries: an apprenticeship modelfor training local providers. InternationalJournal ofMental Health Systems, 5, 30.
Necochea, E. (2006). Building stronger humanresources for health through licensure, certi¢ca-tion and accreditation. Chapel Hill: The Capcity
Project .
Ooms, G., van Damme, W. & Temmerman, M.(2007). Medicines without doctors: why theGlobal Fund must fund salaries of healthworkers to expand AIDS treatment. PLoSMed, 4,e128.
Pan American Health Organization. (2003).Haiti: pro¢le of the health services system.Washington, DC.
Patel,V., Araya, R., Chatterjee, S., Chisholm, D.,Cohen, A., De Silva, M., . . . van Ommeren, M.(2007). Treatment and prevention of mental dis-orders in low-income and middle-incomecountries. Lancet, 370, 991-1005.
Patel,V.&Thornicroft,G. (2009).Packagesof carefor mental, neurological, and substance use dis-orders in low- andmiddle-income countries. PLoSMed, 6, e1000160.
Public Broadcasting System (PBS) (2009). Africa:house calls and health care. http://www.pbs.org/now/shows/537/index.html
Perez-Sales, P., Fernandez-Liria, A., Baingana, F.&Ventevogel, P. (2011). Integratingmental health
McLean et al.
rized reproduction of this article is prohibited.
into existing systems of care duringandafter com-plex humanitarian emergencies: rethinking theexperience. Intervention, 9, 345-357.
153

Copyrig
Task sharing in rural Haiti: qualitative assessment of a brief, structured training with and without
apprenticeship supervision for community health workers, Intervention 2015, Volume 13, Number 2, Page 135 - 155
Petersen, I., Ssebunnya, J., Bhana,A.&Baillie,K.(2011). Lessons from case studies of integratingmental health into primary health care in SouthAfrica and Uganda. InternationalJournal of Mental
Health Systems, 5, 8.
Psychosocial Working Group. (2003). PsychosocialIntervention in Complex Emergencies: A Framework for
Practice. Edinburgh: Queen Margaret UniversityCollege.
Raviola,G.,Eustache,E.,Oswald,C.&Belkin,G.S. (2012). Mental health response in Haiti in theaftermath of the 2010 earthquake: A case studyfor building long-term solutions. Harvard Review
of Psychiatry, 20, 68-77.
Raviola, G., Severe, J.,Therosme,T., Oswald, C.,Belkin, G. & Eustache, E. (2013). The 2010 Haitiearthquake response. Psychiatric Clinics of North
America, 36, 431-450.
Rose,N.,Hughes,P.,Ali, S.&Jones,L. (2011). Inte-grating mental health into primary health caresettings after an emergency: lessons from Haiti.Intervention, 9, 211-224.
Saunders, R. P., Evans, M. H. & Joshi, P. (2005).Developing a Process-Evaluation Plan for Asses-singHealthPromotionProgramImplementation:A How-To Guide. Health Promotion Practice, 6(2),134-147.
Saxena, S., Thornicroft, G., Knapp, M. &Whiteford,H. (2007).Resources formentalhealth:scarcity, inequity, and ine⁄ciency. Lancet, 370,878-889.
Somasundram, D. (2006). Disaster mental healthin Sri Lanka. InJ. Diaz, R. Murthy, & Lakshmi-narayana (Eds.), Advances in disaster mental health
and psychological support. Delhi:VHAIPress.
van derVeer, G. & Francis, F.T. (2011). Field basedtraining for mental health workers, communityworkers, psychosocial workers and counselors: aparticipant-oriented approach. Intervention, 9,145-153.
vanGinneken,N.,Tharyan, P., Lewin, S., Rao,G.N., Meera, S. M., Pian, J., . . . Patel, V. (2013).
ht © War Trauma Foundation. Unautho154
Non-specialist health worker interventions forthe care of mental, neurological and substance-abuse disorders in low- and middle-incomecountries. Cochrane Database Syst Rev11, CD009149.
Ventevogel, P., van de Put, W., Faiz, H., vanMierlo, B., Siddiqi, M. & Komproe, I. H. (2012).Improving access to mental health care andpsychosocial support within a fragile context:a case study from Afghanistan. PLoS Med, 9,e1001225.
Wagenaar, B. H., Hagaman, A. K., Kaiser, B. N.,McLean, K. E. &Kohrt, B. A. (2012). Depression,suicidal ideation, and associated factors: a cross-sectional study in rural Haiti. BMCPsychiatry, 12,149.
Wagenaar, B. H., Kohrt, B. A., Hagaman, A. K.,McLean, K. E. & Kaiser, B. N. (2013). Determi-nants of care seeking for mental health problemsin rural Haiti: culture, cost, or competency. Psy-chiatric Services, 64(4), 366-372.
WHO (2000). International Consortium of Psy-chiatric Epidemiology. Cross-national compari-sons of mental disorders. Bulletin of the World
Health Organization, 78, 413-426.
WHO (2003). Quality and accreditation in health careservices: a global review. Geneva: World HealthOrganization.
WHO (2006). Disease control priorities related to
mental, neurological, developmental and substance abuse
disorders. Geneva:World Health Organization.
WHO (2008).Task shifting: rational redistribution oftasks among health workforce teams. Geneva: WorldHealth Organization.
WHO (2010). mhGAP intervention guide for mental,
neurological and substance use disorders in non-speci¢ed
health settings. Geneva: World Health Organiz-ation.
WHO (2011). Le syste' me sante¤ mentale en Ha|« ti:rapport d’e¤ valuation du syste' me de Sante¤ mentaleen Ha|« ti a l’aide de l’instrument d’evaluationconcu par L’Organization Mondiale de la Sante¤
rized reproduction of this article is prohibited.

Copyrig
Mentale (OMS).Ministe' rede laSante¤ Publiqueetde la Population,;1; Organisation Mondiale de laSante¤ , Organisation Paname¤ ricaine de la Sante¤ .
WHO&Wonca (2008). Integratingmental health intoprimary care: a global perspective. Geneva: WorldHealth Organization.
1 We employ the Inter-Agency Standing Committee
Guidelines to operationalise mental health andpsychosocial support (MHPSS) to ‘describe any typeof local or outside support that aims to protect or promote
psychosocialwell-beingand/or prevent or treatmental dis-
order,’ (IASC, 2007, p. 1). The term psychosocial isde¢ned according to The Psychosocial WorkingGroup as ‘well-being of an individual... with respect tothree coredomains: human capacity, social ecologyand cul-
ture and values.These domains map in turn the human,
ht © War Trauma Foundation. Unautho
to the challenges of prevailing events and conditions,’
(The Psychosocial Working Group, Centre for
KristenMcLean,MPH, is a doctoral student in the
Bonnie Kaiser,MA, is a doctoral student in the Depa
Ashley Hagaman, MPH, is a doctoral student in the
Evolution and Social Change, at Arizona State Univ
BradleyWagenaar, MPH, is a doctoral student in t
Health, at the University ofWashington.
TatianaTherosme,BA, isapsychologicalpractitioner
social SupportTeam at Zanmi Lasante/Partners in H
Brandon Kohrt,MD, PhD is a psychiatrist and anth
Global Health, and Cultural Anthropology at the Du
Psychiatry and Behavioral Sciences at Duke Univers
email: [email protected]
International Health Studies Queen MargaretUniversity College, 2003, p. 2).2 Process evaluation research refers to methodsand theories employed to monitor and docu-ment the implementation of interventionprogrammes. It is used to elucidate how inter-vention elements and pathways contribute tointervention outcomes (Saunders, Evans, &Joshi, 2005). Qualitative methods are commonlyused to document intervention processes thatare not amenable to categorical or other formsof quantitative reporting.3 Unpublished training manual provided byTiyatien Health and used with permission.Tiyatien Health has been renamed as Last MileHealth (‘‘http://www.lastmilehealth.org/’’ www.lastmilehealth.org).4 Zanmi Lasante is a nongovernmental health-
McLean et al.
care provider in Haiti and a sister organisation of
social and cultural capital available to people respondingrized reproduction of this article is prohibited.
Partners in Health (www.pih.org/country/haiti/about).
Department of Anthropology atYale University.
rtment of Anthropology at Emory University.
Department of Global Health, School of Human
ersity.
he Department of Epidemiology, School of Public
. She isamemberof theMentalHealth andPsycho-
ealth in Haiti’s Central Plateau.
ropologist. He is Assistant Professor of Psychiatry,
ke Global Health Institute and the Department of
ity School ofMedicine.
155