systems for tracking minimally invasive surgical instruments
TRANSCRIPT
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [TU University of Technology Delft]On: 15 September 2008Access details: Access Details: [subscription number 732450797]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Minimally Invasive Therapy and Allied TechnologiesPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713683124
Systems for tracking minimally invasive surgical instrumentsM. K. Chmarra a; C. A. Grimbergen ab; J. Dankelman a
a Department of BioMechanical Engineering, Delft University of Technology, Delft, The Netherlands b
Department of Medical Physics, University of Amsterdam, The Netherlands
First Published on: 17 October 2007
To cite this Article Chmarra, M. K., Grimbergen, C. A. and Dankelman, J.(2007)'Systems for tracking minimally invasive surgicalinstruments',Minimally Invasive Therapy and Allied Technologies,16:6,328 — 340
To link to this Article: DOI: 10.1080/13645700701702135
URL: http://dx.doi.org/10.1080/13645700701702135
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
REVIEW ARTICLE
Systems for tracking minimally invasive surgical instruments
M. K. CHMARRA1, C. A. GRIMBERGEN1,2 & J. DANKELMAN1
1Department of BioMechanical Engineering, Delft University of Technology, Delft, The Netherlands, and 2Department of
Medical Physics, University of Amsterdam, The Netherlands
AbstractMinimally invasive surgery (e.g. laparoscopy) requires special surgical skills, which should be objectively assessed. Severalstudies have shown that motion analysis is a valuable assessment tool of basic surgical skills in laparoscopy. However, to usemotion analysis as the assessment tool, it is necessary to track and record the motions of laparoscopic instruments. Thisarticle describes the state of the art in research on tracking systems for laparoscopy. It gives an overview on existing systems,on how these systems work, their advantages, and their shortcomings. Although various approaches have been used, none ofthe tracking systems to date comes out as clearly superior. A great number of systems can be used in training environmentonly, most systems do not allow the use of real laparoscopic instruments, and only a small number of systems provide forcefeedback.
Key words: Minimally invasive surgery, tracking system, motion analysis, objective assessment, skills
Introduction
Minimally invasive surgery (e.g. laparoscopy) is a
technique that requires special surgical skills (1).
Traditionally, resident surgeons start their surgical
education observing experienced surgeons in the
operating room (OR). Afterwards, they are allowed
to contribute to the operation (e.g. they perform a
number of basic techniques). Finally, they become
primary surgeons; however, this generally occurs
without an objective assessment of their skills.
Since the skill and the level of experience of the
surgeons are not exactly known, the current
method of training is potentially unsafe for the
patient (2).
Since the emphasis on medical safety and the
complexity of laparoscopic techniques and equip-
ment continuously increases, it is essential to
develop new, safe training and assessment methods
for laparoscopic skills. Training methods, such as
box trainers and virtual reality (VR) trainers, have
already been developed to learn basic laparoscopic
skills outside the operating room (3–6). However,
the objective assessment of residents’ skills still
remains a challenge (7).To date, there is no one
widely used automatic assessment method of the
basic minimally invasive surgical skills. Commonly,
assessment relies heavily on the expert surgeons and,
therefore, is not always objective (8–10). An
objective assessment of skills is a very important
factor in developing an effective curriculum, since it
motivates residents to actively engage with training
of his/her skills and provides valuable feedback as to
whether that engagement translates into gaining
experience.
In the literature, it has been demonstrated that
basic psychomotor laparoscopic skills can be
assessed by analysing motions of the instrument
(7,10). Several measures have been proposed (e.g.
the length of the curve described by the tip of the
instrument, the total distance travelled by the
instrument along its axis, economy of the move-
ment, changes in instrument velocity over time)
(4,7,11–13). In order to use motion analysis as the
assessment tool, a system is needed to track and
record these motions. In VR trainers such tracking
systems are inherently present. Tracking systems
that can track real laparoscopic instruments during
surgery or in the box trainer are still in their
infancy.
Correspondence: M. K. Chmarra, Department of BioMechanical Engineering, Faculty of Mechanical, Maritime and Materials Engineering (3mE), Delft
University of Technology, Mekelweg 2, 2628 CD Delft, The Netherlands. Fax: 31-15-278 4717. E-mail: [email protected]
Minimally Invasive Therapy. 2007; 16:6; 328–340
ISSN 1364-5706 print/ISSN 1365-2931 online # 2007 Taylor & Francis
DOI: 10.1080/13645700701702135
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

In general, one may consider the tracking system
as an independent component of a training system,
not directly related to the choice of exercises and
scoring measures. The sole task of the tracking
system is to measure the position (x, y, and z
coordinates) and the orientation (yaw, pitch, and
roll) of the laparoscopic instrument with respect to a
fixed reference frame.
Presently, there is a number of (commercially)
available devices for tracking movements of laparo-
scopic instruments. These devices are specific for
different environments: Box trainers, virtual reality
trainers, and operating rooms. Our study of the
literature showed that no overview of the systems
used for tracking motions of the laparoscopic
instruments has been published. Since there is a
number of such systems already available, and since
new systems are being developed, it is difficult for a
potential customer to find appropriate information
and to choose a proper tracking system. To produce
a complete and structured overview of tracking
systems, a large number of journals and proceedings
available via PubMed, Scholar Google, and patents
have been studied. In this article, special care was
taken to ensure that presented information is correct
and up-to-date; for each approach it was attempted
to answer the following questions:
N How does it work?
N Where can it be used?
N What are its chief advantages?
N What are its shortcomings?
For this reason, nine features were used to evaluate
the systems: the kind of system (active or passive),
the mechanics, the number of degrees of freedom,
possibility of using real laparoscopic instruments,
environment (box trainer, VR trainer, and/or oper-
ating room), haptic feedback, portability, reported
accuracy, and commercial availability.
Tracking systems
Aspects of general tracking systems
Tracking systems are intended as an interface
between humans and computers. In terms of hard-
ware, three components required in such systems
can be distinguished: A source that generates a
signal, a sensor that receives the signal, and a data
acquisition system, which processes the signal and
communicates with the computer (14). Depending
on the technology, either the source or the sensor is
attached to the object, while the other serves as a
reference point and is located at a fixed point in the
environment. Many of the currently used tracking
systems are active; the sensor, which measures the
actual movement, is attached to the target to be
tracked. Passive tracking systems localise (from a
distance) markers/transmitters that have been placed
on instruments (or objects) to be tracked in the field.
Current tracking devices are based on mechanical,
optical, acoustic, or electromagnetic technologies.
Mechanical tracking devices, typically taking the
form of small volume mechanical arms, use a direct
mechanical connection between a reference point
and a target (angles formed by each joint) to
measure the position and orientation of the object
in the environment. Optical position trackers work
one of two ways:
N One or several cameras are connected to the
object, and a set of light emitting diodes (LEDs)
is placed at the fixed reference points, or
N the cameras are mounted at fixed points, while a
set of LEDs is placed on the object.
Acoustic tracking devices employ high frequency
(20 kHz or greater) ultrasonic sound waves in the
form of time-to-flight transducers/sensors or phase-
referent systems. The latter class of systems relies on
comparing the phase of a reference signal to that of a
sensed emitted signal. In a time-to-flight system, the
duration of the travel of an emitted signal is
correlated with the distance travelled in the air at a
given temperature. Electromagnetic tracking is
based on the movement of a number of small sensor
units, each housing three small (orthogonally posi-
tioned) wire coils, within a low frequency electro-
magnetic field generated by a second three-coil
source or transmitter.
Aspects of tracking systems for minimally invasive
surgery
Minimally invasive surgery requires unique psycho-
motor skills that are different from those needed to
perform open surgery. The surgeon’s hand move-
ments are transmitted through the incision point via
a trocar (instrument shaft) to the tip of the
instrument. This limits the range of motions from
six to four degrees of freedom (DOFs): translation of
the instrument along its axis (z coordinate – 1st
DOF), rotation of the instrument around its axis
(roll – 2nd DOF), left–right and forward-backward
rotations of the instrument around the incision point
(yaw – 3rd DOF, and pitch – 4th DOF, respectively).
Information about instrument motions in all four
DOFs provides valuable information, which can be
used during the assessment of basic laparoscopic
skills. Therefore, tracking systems should track
motions in all four DOFs.
Tracking minimally invasive instruments 329
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

A great number of active systems contain a
mechanical part that mimics the incision (pivoting
point). Many of these systems use a gimbal
mechanism, which allows the control and measure-
ment of the object’s rotations in three-dimensional
Euclidean space. Usually, the gimbal consists of a set
of two or three rings, mounted on axes at right angles
(15). These rings provide a stable reference to the
position and attitude in all three dimensions. Since it
is necessary to define a reference point (position,
space) in the environment in order to measure the
movements of the object, it seems reasonable to use
the pivoting point as a reference point in active
systems.
A wide variety of different instruments is available
for use in minimally invasive surgery. Instruments
are made by various companies and have different
purposes, consequently, the length, the diameter,
the handgrip, and the tip of real laparoscopic
instruments can differ largely. The variation in
instruments has an influence on the design of a
tracking system, which should ideally be suitable for
any laparoscopic instrument.
Motions of the laparoscopic instruments can be
tracked and recorded in three environments: In the
operating room (during an operation), in a box
trainer, or a virtual reality trainer (during training).
The operating room is the most realistic environ-
ment, where a surgeon uses real laparoscopic
instruments, which provide natural instrument-
tissue interaction with realistic force feedback. The
box trainer also presents a realistic environment
where force feedback is obtained due to the use of
real laparoscopic instruments. The virtual reality
trainer presents a less realistic (virtual) environment
for the training of laparoscopic skills, where simu-
lated laparoscopic instruments are often used. Force
feedback in VR trainers (if present) is far from that
provided by real laparoscopic instruments. The use
of simulated laparoscopic instruments in a VR
trainer, however, results in simplified tracking in a
VR trainer. Designing a system that can track real
laparoscopic instruments in the OR seems to be the
most difficult, since factors such as patient safety and
ergonomics in the OR play a critical role. In box
trainers, tracking systems have to track real laparo-
scopic instruments. Ideally, a tracking system should
be designed in such a way that it is possible to use it
in all three environments. Besides, the system should
be small in order to be portable and easy to place at a
desired position.
Surgeons execute laparoscopy using hand-held
instruments that provide little haptic information
(16–18). It is still unknown how important haptic
feedback is during a laparoscopic task and, therefore,
it is very difficult to say whether force feedback is
needed during training of basic laparoscopic skills.
Precision, a degree to which measurements show
the same or similar results, is a very important
characteristic of each tracking system. The precision
with which instrument movements can be measured
depends on the resolution and accuracy of the
system (15). The resolution is defined by the
smallest change detected by the sensor, and is fixed
for a given system. The accuracy of the system is
defined by the range within which a measured
position is correct.
A number of tracking systems is provided only in
combination with VR trainers, while other systems
can be acquired separately. In the paragraphs that
follow, we present both tracking systems that are
currently commercially available and prototypes, i.e.
systems that are still being developed. The practical
use of these tracking systems will also be described.
Passive tracking systems
In the ProMIS simulator (Haptica Inc., Boston,
USA, www.haptica.com), the measurement of the
instrument movements is taken using a passive
tracking system (Figure 1) (19). Three separate
cameras capture the video images of the internal
movement of the laparoscopic instrument from three
different angles (20). This design allows for mea-
Figure 1. In the ProMIS surgical simulator from Haptica
(courtesy of Haptica Inc.), the MIS instrument movements are
tracked using a passive system. Laparoscopic instruments are
covered with two stripes of yellow tape (a marker). Internal
movements of the instruments are captured with three separate
cameras.
330 M. K. Chmarra et al.
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

surement of the motions in the x, y, and z directions.
Standard laparoscopic instruments are covered with
two strips of yellow tape – markers for the camera
tracking system. The tracking system is situated in a
large mannequin, thus not easily portable. The
system is commercially available as a combination
of a real and a virtual environment. It cannot be used
during operation (in the OR), however. The ProMIS
simulator provides force feedback.
Sokollik et al. used a 3-D ultrasound measure-
ment system to record the motion along the
trajectories of the instruments (Zebris Medial
GmbH, Isny, Germany, www.zebris.de) (21). The
system (Figure 2) determines the spatial coordinates
(x, y, and z together with rotation) of miniature
ultrasound transmitters placed on the instruments
by means of the relative position of these transmit-
ters to a fixed system of three microphones. The
system is portable and commercially available.
Natural haptic feedback is obtained due to the use
of real laparoscopic instruments. Since ultrasound
transmitters can be sterilised, the 3-D ultrasound
measurement system can be used in the operating
room as well as in a box trainer and VR trainers.
An ultrasound wireless positioning system is being
developed at Delft University of Technology (Delft
University of Technology, Delft, the Netherlands,
wwwetis.et.tudelft.nl). This system is intended to be
used in the operating room to detect the exact 3-D
location and orientation of the instrument in the
patient (22). An array of ultrasound receivers detects
the positions of the two markers/transmitters placed
on each of the instruments, outside the patient’s
body (Figure 3). This allows readings with an
accuracy of 40 mm at a distance of about 1 m
between transmitter and receiver. The resolution of
the system is about 5 mm (23). This prototype
measures movements in one DOF. The size of the
system is rather large and, therefore, the system is
not easily portable. Natural haptic feedback is
obtained due to the use of real laparoscopic
instruments.
Active tracking systems
Laparoscopic Surgical Workstation, Virtual
Laparoscopic Interface, and Laparoscopic Impulse
Engine are the best known hardware interfaces
designed for laparoscopic virtual simulations offered
by Immersion Inc. (Immersion Inc. Gaithersburg,
USA, http://www.immersion.com). The Laparos-
copic Surgical Workstation and the Virtual
Laparoscopic Interface offer two fully instrumented
tools (Figure 4). The movements of the instrument
in four DOFs are measured and recorded using four
electromechanical transducers mounted in the gim-
bal mechanism (24–28). The Laparoscopic Surgical
Workstation provides force feedback. The sensor
resolution is 8 mm for translation, 0.03˚ for roll
(rotation), and 0.01˚ for pitch and yaw. The
Laparoscopic Surgical Workstation is rather big
(300 mm6340 mm) and, therefore, not easily
portable.
Figure 2. The Zebris ultrasound system adapted for laparoscopic
surgery application (courtesy of C. Sokollik). In this passive
tracking system, ultrasound transmitters are placed on the
laparoscopic instruments. Spatial coordinates are determined by
means of relative positions of the transmitters to a fixed system of
three microphones.
Figure 3. An ultrasound wireless positioning system that is being
developed at Delft University of Technology (courtesy of F.
Tatar). In this passive tracking system, an array of ultrasound
receivers detects the positions of the two markers/transmitters
placed on each of the instruments.
Tracking minimally invasive instruments 331
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

The Virtual Laparoscopic Interface does not
provide force feedback. The sensor resolution is
22 mm for translation, 0.26˚ for roll (rotation), and
0.064˚ for pitch and yaw. The Virtual Laparoscopic
Interface is easily portable. Both the Laparoscopic
Surgical Workstation and the Virtual Laparoscopic
Interface are commercially available. The
Laparoscopic Impulse Engine is a tool-based force
feedback device that uses servo-motor actuators
(Figure 5). Laparoscopic Impulse Engine allows
movements in four DOFs. A variety of surgical tools
(or tool handles) can be fitted in the device. The
Immersion devices cannot be used in the operating
room.
The CELTS (Computer Enhanced Laparoscopic
Training System) is a prototype simulator (Figure 6)
developed at the Center for Integration of Medicine
and Innovative Technology (CIMIT, Boston, USA,
www.cimit.org). CELTS is a modified Virtual
Laparoscopic Interface from Immersion Inc.; tool
handles and main shafts from the Virtual
Laparoscopic Interface were replaced with a system
that allows for the use of real laparoscopic instru-
ments to detect the trajectories of these instruments
in a simulator (7,29,30). Pitch, yaw, roll, and
translation are measured with the original Virtual
Laparoscopic Interface sensors. CELTS can be used
in a box trainer as well as in a virtual reality
environment. It is not possible to use this system in
the OR during operations. The system is easily
transportable, just like the Virtual Laparoscopic
Interface. The possibility of using real laparoscopic
instruments in the CELTS results in a natural haptic
feedback.
The ADEPT (Advanced Dundee Endoscopic
Psychomotor Tester) was developed at the
University of Dundee (University of Dundee,
Dundee Tayside, Scotland). The ADEPT consists
of a gimbal mechanism that accepts real endoscopic
instruments (Figure 7) (31,32). This active system
tracks and records positions of the instrument in 3-D
space, and detects rotational movements. The
measurements are taken using potentiometers
mounted in the gimbal mechanism; this allows
readings to within a millimetre. The accuracy of
the x, y, and z coordinates (at a distance of 300 mm
from the pivoting point) is within 0.5 mm. The
smallest angle recognised by the ADEPT is approxi-
mately 0.005 .̊ Real laparoscopic instruments can be
used in the ADEPT; nevertheless, it is not possible
to use this system to record instrument movements
during an operation in the OR. The commercially
used ADEPT provides natural haptic feedback.
The Simendo (Figure 8) is a virtual reality
simulator for minimally invasive surgery
(DelltaTech, Delft, the Netherlands, www.dellta-
tech.nl) (33). DelltaTech manufactures the
Simendo, which comprises both the instrument
interface and the virtual reality training software.
The tracking system in the instrument interface
consists of a gimbal mechanism. Translation and
rotation of the simulated laparoscopic instruments
are measured by an optical sensor, while pitch and
yaw are measured by optical encoders. This combi-
nation allows measuring the movements of the
Figure 4. The Laparoscopic Surgical Workstation (left) and
Virtual Laparoscopic Interface (right) from Immersion (www.im-
mersion.com). These active tracking systems measure movements
of laparoscopic instruments using four electromechanical trans-
ducers mounted in the gimbal mechanism.
Figure 5. The Laparoscopic Impulse Engine from Immersion
(www.immersion.com). This active tracking system is a tool-
based force feedback device that uses servo-motor actuators.
332 M. K. Chmarra et al.
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

instrument in four DOFs. As the Simendo was
especially developed for application in virtual reality
simulation, it does not accept real laparoscopic
instruments and does not provide force feedback.
The instrument interface of the Simendo is small
and light and, therefore, easy to transport. The
Simendo is commercially available.
The BlueDRAGON tracking system was devel-
oped at the University of Washington (University of
Washington, Seattle, USA, http://brl.ee.washington.
edu). This system consists of two four-bar passive
mechanisms that are connected to the instruments
(Figure 9) (34,35). The measurements of the
instrument positions, orientations, and translation
are taken with multi turn potentiometers integrated
into four joints of the mechanism. The system is
rather large, and thus not easily portable. The
Figure 6. The CELTS interface device from Center for Integration of Medicine and Innovative Technology (courtesy of N. Stylopoulos).
This tracking system is a modified Virtual Laparoscopic Interface from Immersion Inc. The main shafts and tool handles are replaced with a
system that allows the use of real laparoscopic instruments.
Figure 7. The ADEPT system from the University of Dundee
(courtesy of M. Schijven). This active tracking system measures
the position of the laparoscopic instrument using potentiometers
mounted in the gimbal mechanism.
Figure 8. The Simendo from DelltaTech (courtesy of
DelltaTech). In this active tracking system, translation and
rotation of laparoscopic instrument are measured with an optical
sensor, while pitch and yaw are measured with encoders.
Figure 9. The BlueDRAGON from the University of Washington
(courtesy of J. Rosen). This active tracking system consists of two
four-bar passive mechanisms that are connected to the instru-
ment. Multi turn potentiometers are integrated into four joints of
the mechanism in order to measure movements of laparoscopic
instrument.
Tracking minimally invasive instruments 333
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

BlueDRAGON allows the use of real laparoscopic
instruments and can be used in the OR during
operation.
The Patriot is a dual sensor tracking system
produced by Polhemus (Polhemus, Colchester,
USA, www.polhemus.com/). The Patriot consists
of an electromagnetic transmitter and receiver. The
transmitter serves as the system’s reference frame for
receiver measurements; the receiver detects mag-
netic fields emitted by the transmitter (Figure 10)
(36). In laparoscopic training setups (e.g.
SimSurgery), the receiver is placed on the laparo-
scopic instrument. The Patriot has a resolution of
0.038 mm for the x, y, and z positions, and 0.1˚ for
the receiver orientation. Static accuracy of the
system is 2.54 mm, and 0.75 .̊ Since the Patriot
can be used to track real laparoscopic instruments, it
is possible to use the Patriot in training setups (VR
and box trainers). The Patriot system is not certified
for medical or bio-medical use; therefore, it should
not be used in the OR.
Xitact ITP (Instrument Tracking Port) and Xitact
IHP (Instrument Haptic Port) are virtual reality
simulation platforms produced by Xitact S.A.
(Xitact S.A. Morges, Switzerland, www.xitact.com).
Both systems (Figure 11) measure movements of the
instruments in four DOFs. Both Xitact systems
consist of the PantoScope (Hybrid Parallel Serial
drive), and the LinRot (Linear and Rotational
drive). The longitudinal and angular positions of
the instruments are measured using optical sensors
placed in the LinRot (37). The yaw and pitch are
measured using two optical encoders situated in the
PantoScope. The sensor resolution is 0.057 mm for
translation, 0.58˚ for roll, and 0.03˚ for both pitch
and yaw. The footprint and the weight of the Xitact
ITP are smaller than those of the Xitact IHP. Both
systems are easy to transport. Contrary to the Xitect
ITP, the Xitect IHP provides force feedback.
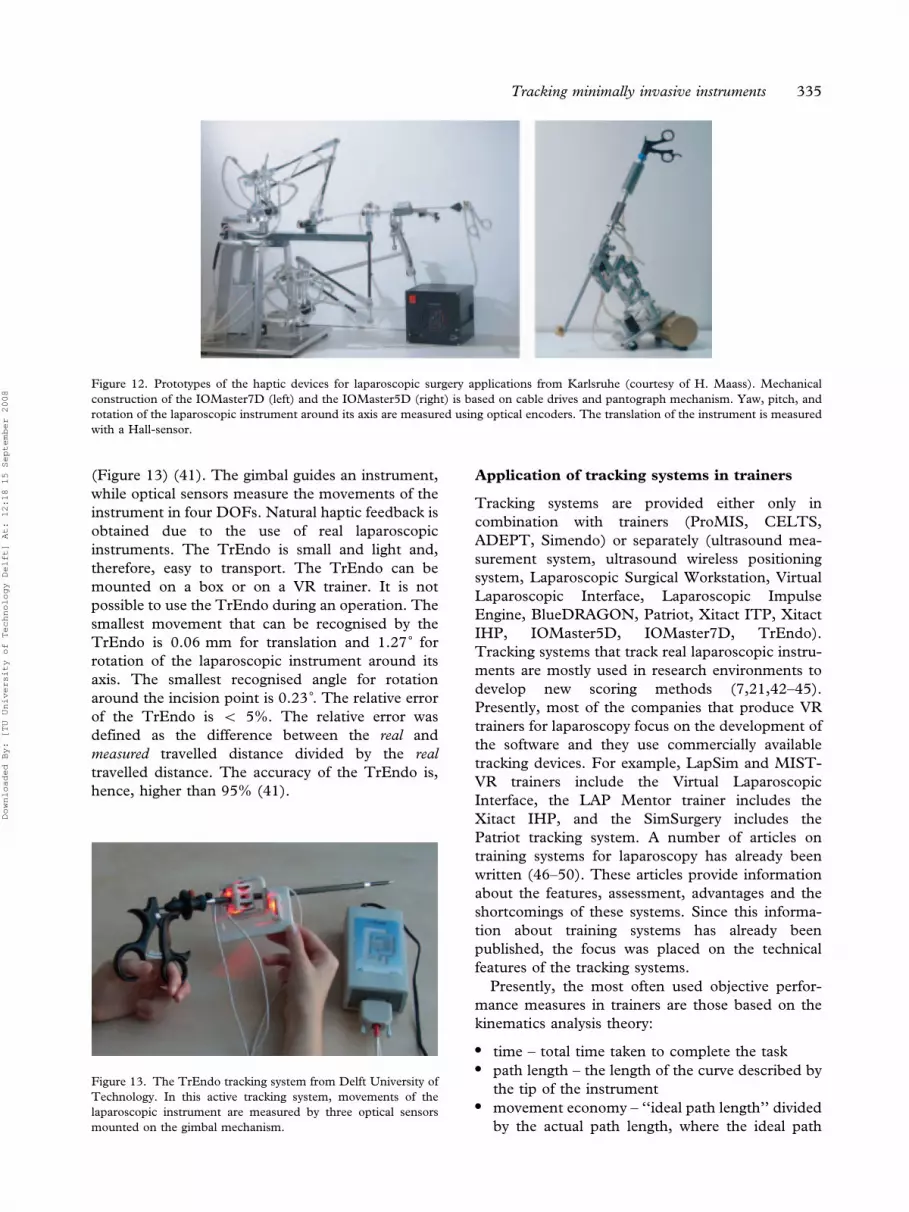
The IOMaster5D and the IOMaster7D are pro-
totype hardware interfaces designed at the Research
Centre Karlsruhe (Karlsruhe, Germany, www-
kismet.iai.fzk.de). The mechanical construction of
these systems is based on cable drives and a
pantograph mechanism (Figure 12) (38–40). This
combination allows movements in four DOFs in the
IOMaster5D and six DOFs in the IOMaster7D.
Additionally, the IOMaster7D captures the move-
ments of the trocar. The yaw, pitch, and angular
position of the simulated laparoscopic instrument
are measured by optical encoders; the translation is
measured with a Hall-sensor. The IOMaster5D and
the IOMaster7D have been designed for laparo-
scopic virtual simulation and are not able to track
real laparoscopic instruments. Both systems provide
force feedback (38–40). The IOMaster7D has a
large working space (600 mm (W)6600 mm
(H)6300 mm (D)) and, therefore, is not easily
portable.
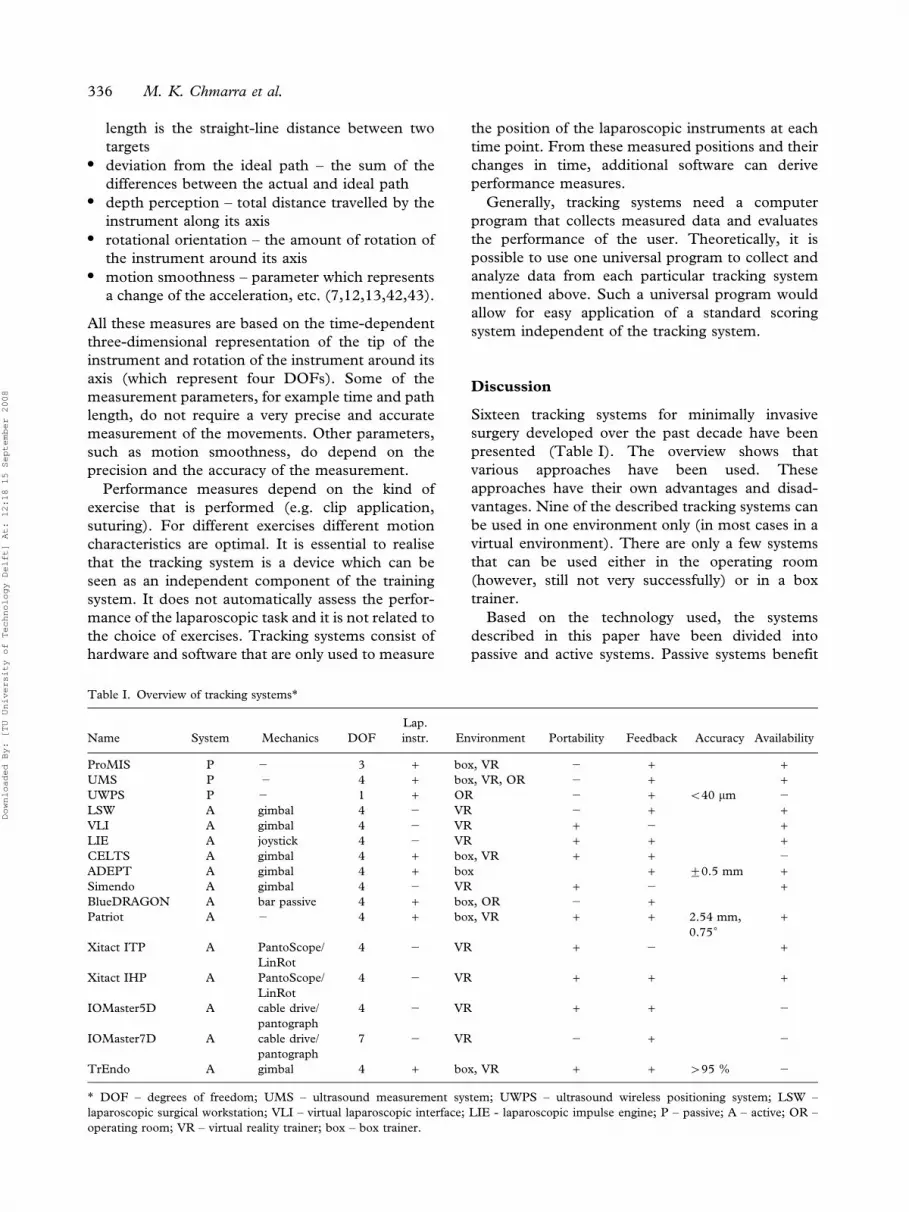
The TrEndo (Delft University of Technology,
Delft, the Netherlands, www.3me.tudelft.nl) is a
prototype tracking system, which consists of a two-
axis gimbal mechanism with three optical sensors
Figure 10. The Patriot, a dual sensor tracking system produced
by Polhemus (www.polhemus.com). Patriot is an active tracking
system, which uses electromagnetic transmitter and receiver to
measure the movements of laparoscopic instrument.
Figure 11. The Xitact ITP (left) and Xitact IHP (right) from
Xitact S.A. (www.xitact.com). In both Xitact interfaces, transla-
tion and angular position of the instrument are measured with
optical sensors placed in the LinRot (Linear and Rotational drive),
while the yaw and pitch are measured using optical encoders
placed in the PantoScope (Hybrid Parallel Serial drive).
334 M. K. Chmarra et al.
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008
(Figure 13) (41). The gimbal guides an instrument,
while optical sensors measure the movements of the
instrument in four DOFs. Natural haptic feedback is
obtained due to the use of real laparoscopic
instruments. The TrEndo is small and light and,
therefore, easy to transport. The TrEndo can be
mounted on a box or on a VR trainer. It is not
possible to use the TrEndo during an operation. The
smallest movement that can be recognised by the
TrEndo is 0.06 mm for translation and 1.27˚ for
rotation of the laparoscopic instrument around its
axis. The smallest recognised angle for rotation
around the incision point is 0.23 .̊ The relative error
of the TrEndo is v 5%. The relative error was
defined as the difference between the real and
measured travelled distance divided by the real
travelled distance. The accuracy of the TrEndo is,
hence, higher than 95% (41).
Application of tracking systems in trainers
Tracking systems are provided either only in
combination with trainers (ProMIS, CELTS,
ADEPT, Simendo) or separately (ultrasound mea-
surement system, ultrasound wireless positioning
system, Laparoscopic Surgical Workstation, Virtual
Laparoscopic Interface, Laparoscopic Impulse
Engine, BlueDRAGON, Patriot, Xitact ITP, Xitact
IHP, IOMaster5D, IOMaster7D, TrEndo).
Tracking systems that track real laparoscopic instru-
ments are mostly used in research environments to
develop new scoring methods (7,21,42–45).
Presently, most of the companies that produce VR
trainers for laparoscopy focus on the development of
the software and they use commercially available
tracking devices. For example, LapSim and MIST-
VR trainers include the Virtual Laparoscopic
Interface, the LAP Mentor trainer includes the
Xitact IHP, and the SimSurgery includes the
Patriot tracking system. A number of articles on
training systems for laparoscopy has already been
written (46–50). These articles provide information
about the features, assessment, advantages and the
shortcomings of these systems. Since this informa-
tion about training systems has already been
published, the focus was placed on the technical
features of the tracking systems.
Presently, the most often used objective perfor-
mance measures in trainers are those based on the
kinematics analysis theory:
N time – total time taken to complete the task
N path length – the length of the curve described by
the tip of the instrument
N movement economy – ‘‘ideal path length’’ divided
by the actual path length, where the ideal path
Figure 12. Prototypes of the haptic devices for laparoscopic surgery applications from Karlsruhe (courtesy of H. Maass). Mechanical
construction of the IOMaster7D (left) and the IOMaster5D (right) is based on cable drives and pantograph mechanism. Yaw, pitch, and
rotation of the laparoscopic instrument around its axis are measured using optical encoders. The translation of the instrument is measured
with a Hall-sensor.
Figure 13. The TrEndo tracking system from Delft University of
Technology. In this active tracking system, movements of the
laparoscopic instrument are measured by three optical sensors
mounted on the gimbal mechanism.
Tracking minimally invasive instruments 335
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008
length is the straight-line distance between two
targets
N deviation from the ideal path – the sum of the
differences between the actual and ideal path
N depth perception – total distance travelled by the
instrument along its axis
N rotational orientation – the amount of rotation of
the instrument around its axis
N motion smoothness – parameter which represents
a change of the acceleration, etc. (7,12,13,42,43).
All these measures are based on the time-dependent
three-dimensional representation of the tip of the
instrument and rotation of the instrument around its
axis (which represent four DOFs). Some of the
measurement parameters, for example time and path
length, do not require a very precise and accurate
measurement of the movements. Other parameters,
such as motion smoothness, do depend on the
precision and the accuracy of the measurement.
Performance measures depend on the kind of
exercise that is performed (e.g. clip application,
suturing). For different exercises different motion
characteristics are optimal. It is essential to realise
that the tracking system is a device which can be
seen as an independent component of the training
system. It does not automatically assess the perfor-
mance of the laparoscopic task and it is not related to
the choice of exercises. Tracking systems consist of
hardware and software that are only used to measure
the position of the laparoscopic instruments at each
time point. From these measured positions and their
changes in time, additional software can derive
performance measures.
Generally, tracking systems need a computer
program that collects measured data and evaluates
the performance of the user. Theoretically, it is
possible to use one universal program to collect and
analyze data from each particular tracking system
mentioned above. Such a universal program would
allow for easy application of a standard scoring
system independent of the tracking system.
Discussion
Sixteen tracking systems for minimally invasive
surgery developed over the past decade have been
presented (Table I). The overview shows that
various approaches have been used. These
approaches have their own advantages and disad-
vantages. Nine of the described tracking systems can
be used in one environment only (in most cases in a
virtual environment). There are only a few systems
that can be used either in the operating room
(however, still not very successfully) or in a box
trainer.
Based on the technology used, the systems
described in this paper have been divided into
passive and active systems. Passive systems benefit
Table I. Overview of tracking systems*
Name System Mechanics DOF
Lap.
instr. Environment Portability Feedback Accuracy Availability
ProMIS P 2 3 + box, VR 2 + +UMS P 2 4 + box, VR, OR 2 + +UWPS P 2 1 + OR 2 + v40 mm 2
LSW A gimbal 4 2 VR 2 + +VLI A gimbal 4 2 VR + 2 +LIE A joystick 4 2 VR + + +CELTS A gimbal 4 + box, VR + + 2
ADEPT A gimbal 4 + box + ¡0.5 mm +Simendo A gimbal 4 2 VR + 2 +BlueDRAGON A bar passive 4 + box, OR 2 +Patriot A 2 4 + box, VR + + 2.54 mm,
0.75˚+
Xitact ITP A PantoScope/
LinRot
4 2 VR + 2 +
Xitact IHP A PantoScope/
LinRot
4 2 VR + + +
IOMaster5D A cable drive/
pantograph
4 2 VR + + 2
IOMaster7D A cable drive/
pantograph
7 2 VR 2 + 2
TrEndo A gimbal 4 + box, VR + + w95 % 2
* DOF – degrees of freedom; UMS – ultrasound measurement system; UWPS – ultrasound wireless positioning system; LSW –
laparoscopic surgical workstation; VLI – virtual laparoscopic interface; LIE - laparoscopic impulse engine; P – passive; A – active; OR –
operating room; VR – virtual reality trainer; box – box trainer.
336 M. K. Chmarra et al.
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008
from not requiring any type of cables wiring attached
to the instrument. For that reason, this approach is
to be favoured from the user’s perspective. However,
there is a number of factors that limit the passive
systems (for tracking hand-held objects). The most
significant is the need for line-of-sight. Objects held
in hand are, by definition, partially hidden behind a
person’s hand, and totally hidden behind a person’s
body from certain perspectives. A solution to this
problem can be to add extra trackers (localisers).
However, this will introduce additional cost and
computational complexity. Therefore, many of the
currently used tracking systems for minimally
invasive surgical instruments are active. Most of
the active systems use gimbal mechanisms to guide
and measure the movements of the instrument in
four degrees of freedom. Such a mechanism benefits
from its simplicity; a gimbal is an easy and
inexpensive-to-produce mechanism. On the other
hand, it would be very complex to use gimbal
mechanisms to guide the motions of the laparoscopic
instrument during real surgery.
In laparoscopy, the surgeon’s hand movements
are transmitted through the incision point to the tip
of the instrument. This results in a reduced number
of degrees of freedom from six to four. Since
information of these four DOFs provides valuable
information that can be used to assess basic
laparoscopic skills, the focus of this article was only
on these DOFs. Nevertheless, laparoscopic instru-
ments also provide a fifth DOF: The opening and
closing of the instrument handles. Therefore, a
number of tracking systems (mainly for VR trainers)
tracks and records also this fifth DOF.
Precision and accuracy are important character-
istics of each tracking device. Ideally, a measurement
device (or system) is both precise and accurate. In
laparoscopy, small movements in the incision point
can result in large movements of the tip of the
instrument. Therefore, sensors that record the
instrument’s movements at the incision point should
be able to recognise small movements. The literature
survey showed that there is no study which defines
how precise and accurate the measurements of the
laparoscopic instrument motions should be.
Therefore, it is difficult to say whether the precision
and accuracy of the present tracking systems are high
enough to be used to track motions of instruments.
Some systems have to be calibrated before use in
order to make measurements more reliable and
accurate. Often, such calibration is done by posi-
tioning the laparoscopic instrument in a predefined
start position. Since all measurements start at the
same position, it is easy to compare the results of the
measurements.
Presently, a single method of establishing and
presenting the accuracy of tracking systems for
laparoscopy is lacking. Usually, the precision and
accuracy are established by the manufacturer by
repeatedly measuring some traceable reference
standard. In this manner, the accuracy can be
calculated in different ways, depending on what is
important for the manufacturer or designer.
Additionally, a number of manufacturers do not
provide any information about the accuracy of their
systems. This can be confusing for customers.
In laparoscopy, the assessment of the basic
laparoscopic skills is preferably done based on the
movements of the instrument tip; therefore, this
study focuses only on systems that track the tip of
laparoscopic instruments. Nevertheless, there is a
number of tracking systems that can track various
hand-held objects (e.g. PHANTOM (51)). Some of
these systems can be easily adapted and used for
tracking motions of laparoscopic instruments.
Additionally, systems have been developed for
tracking various parts of the human body (e.g. arms,
legs, head). These systems can also be modified and
used for tracking surgical movements. Examples of
such systems are: The Imperial College Surgical
Assessment Device (ICSAD) (52,53), which tracks
the movements of the hands, and the ultrasound
measurement system, which was adapted to track
the movements of the laparoscopic instrument (21).
There are also robotic systems, such as da Vinci
(54,55), RobIn Heart (56,57), and a spherical
mechanism (58) which contain tracking systems.
These systems can be used to assess the motions
when performing minimally invasive surgery with a
robot (59,60).
Motion analysis is purely used for objective
assessment of basic technical skills. However, even
a simple task in laparoscopy requires the use of
several different skills at the same time (e.g.
anatomical knowledge, protocol knowledge, instru-
ment use, eye-hand coordination) (2). Furthermore,
a competent surgeon must possess not only basic
technical skills, but also cognitive and clinical skills,
which require other assessment methods, e.g. multi-
ple choice questionnaires, assessment of patient
management problems, observation and assessment
by a skilled trainer, and video analysis (61–64).
Motion analysis alone fails to demonstrate the actual
surgical competence of the individual.
This study does not focus on the costs of the
presented tracking systems. However, the accep-
tance of a system strongly depends on its cost.
Currently, there is a great variation between costs of
the systems; the cheapest system costs around 1.000
Euro, while the most expensive systems cost more
Tracking minimally invasive instruments 337
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

than 50.000 Euro. Nevertheless, it is still very
difficult to compare the costs of the tracking systems,
since a number of these systems is at a prototype
stage, and the systems available on the market are
often sold with additional products (e.g. software, a
VR trainer). In order to make training and assess-
ment of the basic laparoscopic skills feasible in every
surgical education, it seems to be necessary to
reduce the costs of both training and assessment.
The introduction of new competitive tracking
systems and new technologies that can be used
in these systems will hopefully lead to decreased
costs.
The possibility of recording the movements of
standard laparoscopic instruments with tracking
systems is an important issue; residents must learn
how to use various laparoscopic instruments for
different purposes. They should also get a sense of
what they actually can feel when performing laparo-
scopic tasks. Standard laparoscopic instruments
provide exactly the same haptic feedback as during
surgery. Some of the current tracking systems for
virtual reality also offer force feedback. However,
feedback in these systems is still distant from the
feedback provided by the real laparoscopic instru-
ment during an operation. In order to understand
the way the sensory cues can be delivered or
simulated, the development and use of haptic
feedback in laparoscopy should be further investi-
gated. Since a high level of fidelity of sensory cues
can be very expensive and may not always be
advantageous, it is very important to investigate
when, how, and how accurate sensory cues should be
used during training of basic laparoscopic skills.
Conclusions
Tracking both the position and orientation of
minimally invasive surgical instruments is an impor-
tant challenge when creating a scoring system based
on motion analysis for the performance of trainees.
Although various approaches to this challenge have
been studied, none has come out as clearly superior;
each system has some advantages and some dis-
advantages. There is no tracking system that could
easily be used in all three environments: The
operating room, the pelvi trainer, and the virtual
reality trainer. A great number of systems do not
allow use of real laparoscopic instruments, and only
a small number of systems provide force feedback.
Additionally, the cost of the systems currently
present on the market is rather high. There is still
much work to be done in order to develop simple
and affordable tracking systems for the various
training environments.
References
1. Arregui ME, Fitzgibbons RJ, Kathouda N, McKernan JB,
et al. Principles of laparoscopic surgery: basic and advanced
techniques. Springer-Verlag: New York Inc.; 1995.
2. Dankelman J, Chmarra MK, Verdaasdonk EGG,
Stassen LPS, et al. Fundamental aspects of learning
minimally invasive surgical skills. Minim Invasiv Ther.
2005;14:247–56.
3. Aggarwal R, Moorthy K, Darzi A. Laparoscopic skills training
and assessment. Br J Surg. 2004;91:1549–58.
4. Gallagher AG, Lederman AB, McGlade K, Satava RM, et al.
Discriminative validity of the minimally invasive surgical
trainer in virtual reality (MIST-VR) using criteria levels based
on expert performance. Surg Endosc. 2004;18:660–5.
5. McClusky DAM, van Sickle K, Gallagher AG. Relationship
between motion analysis, time, accuracy, and errors during
performance of a laparoscopic suturing task on an augmented
reality simulator. 12th International Congress of the European
Association for Endoscopic Surgery, Barcelona, June 2004:
O207.
6. Munz Y, Kumar BD, Moorthy K, Bann S, et al. Laparoscopic
virtual reality and box trainers: is one superior to the other?
Surg Endosc. 2004;18:485–94.
7. Cotin S, Stylopoulos N, Ottensmeyer M, Neumann P, et al.
Metrics for Laparoscopic Skills Trainers: The Weakest Link!
LNCS. 2002;2488:35–43.
8. Darzi A, Smith S, Taffinder N. Assessing operative skill.
Needs to become more objective. BMJ. 1999;318:887–8.
9. Martin JA, Regehr G, Reznick R, MacRae H, et al. Objective
structured assessment of technical skills (OSATS) for surgical
residents. Brit J Surg. 1997;84:273–8.
10. Moorthy K, Munz Y, Sarker SK, Darzi A. Objective
assessment of technical skills in surgery. BMJ. 2003;327:
1032–7.
11. Van Sickle KR, McKlusky DA, Gallagher AG, Smith CD.
Construct validation of the ProMIS simulator using a novel
laparoscopic suturing task. Surg Endosc. 2005;19:1227–31.
12. Acosta E, Temkin B. Haptic laparoscopic skills trainer with
practical user evaluation metrics. Stud Health Techn Inform.
MMVR. 2005;111:8–11.
13. Cavallo F, Megali G, Sinigaglia S, Tonet O, et al. A
biomechanical analysis of surgeon’s gesture in a laparoscopic
virtual scenario. Stud Health Techn Inform. MMVR. 2006;
119:79–84.
14. Baratoff G, Blanksteen S. Tracking Devices. The
Encyclopedia of Virtual Environments, Human Interface
Technology Laboratory, University of Washington. http://
www.hitl.washington.edu/scivw/EVE/, 1993.
15. ‘‘Wikipedia, The Free Encyclopedia,’’ http://www.wikipedia.
org/.
16. Heijnsdijk EAM, Pasdeloup A, van der Pijl AJ, Dankelman J,
et al. The influence of force feedback and visual feedback in
grasping tissue laparoscopically. Surg Endosc. 2004;18:
980–5.
17. Bholat OS, Haluck RS, Kutz RH, Gorman PJ, et al. Defining
the role of haptic feedback in minimally invasive surgery. Stud
Health Technol Inform. 1999;62:62–6.
18. Bholat OS, Haluck RS, Murray WB, Gorman PJ, et al.
Tactile feedback is present during minimally invasive surgery.
J Am Coll Surg. 1999;189:349–55.
19. Lacey G. A Surgical Training Simulator. Patent Number
IE20030351.
20. van Sickle KR, McClusky DA, Gallagher AG, Smith CD.
Construct validation of the ProMIS simulator using a novel
laparoscopic suturing task. Surg Endosc. 2005;19:1227–31.
338 M. K. Chmarra et al.
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

21. Sokollik C, Gross J, Buess G. New model for skills assessment
and training progress in minimally invasive surgery. Surg
Endosc. 2004;18:495–500.
22. Tatar F, Mollinger JR, Den Dulk RC, van Duyl WA, et al.
Ultrasonic sensor for measuring position and orientation of
laparoscopic instruments in minimally invasive surgery. 2nd
Annual International IEEE-EMBS Special Topic Conference
on Microtechnologies in Medicine & Biology, Madison,
Wisconsin USA, 2002.
23. Tatar F, Bastemeijer J, Mollinger JR, Bossche A. Two-
frequency method for measuring the position of surgical tools
with mm precision. Eurosensors XIX Conference, Barcelona,
Spain, 2005.
24. Rosenberg LB. Computer interface or control input device for
laparoscopic surgical instrument and other elongated
mechanical objects. Patent Number 5,623,582.
25. Jacobus CJ, Griffin JL. Method and system for simulating
medical procedures including virtual reality and control
method system for use therein. Patent Number 5,769,640.
26. Jacobus CJ, Riggs AJ, Taylor MJ. Force feedback system.
Patent Number 5,629,594.
27. Martin KM, Levin MD, Rosenberg LB. Mechanical interface
having multiple grounded actuators. Patent Number
5,828,197.
28. Rosenberg LB. Physically realistic computer simulation on
medical procedures. Patent Number 6,654,000.
29. Stylopoulos N, Cotin S, Dawson S, Ottensmeyer M, et al.
CELTS: a clinically-based computer enhanced laparoscopic
training system. Stud Health Technol Inform. 2003;94:
336–42.
30. Stylopoulos N, Cotin S, Maithel SK, Ottensmeyer M, et al.
Computer-enhanced laparoscopic training system (CELTS):
bridging the gap. Surg Endosc. 2004;18:782–9.
31. Hanna GB, Drew T, Clinch P, Hunter B, et al. A
microprocessor-controlled psychomotor tester for minimal
access surgery. Surg Endosc. 1996;10:965–9.
32. Hanna GB, Drew T, Clinch P, Hunter B, et al. Computer-
controlled endoscopic performance assessment system. Surg
Endosc. 1998;12:997–1000.
33. Demirtas D, Post JJ, Dankelman J. Joystick. Patent Number
WO2005088419.
34. Rosen J, Brown JD, Chang L, Barreca M, et al. The
BlueDRAGON – a system for measuring the kinematics
and the dynamics of minimally invasive surgical tools in-vivo.
Proc. IEEE Intl. Conf. on Robotics and Automation ICRA,
Washington, DC, 2002.
35. Rosen J, Brown JD, Barreca M, Chang L, et al. The Blue
DRAGON - A system for Monitoring the Kinematics and
Dynamics of Endoscopic Tools in Minimally Invasive Surgery
for Objective Laparoscopic Skill Assessment. Stud Health
Techn Inform. MMVR. 2002;85:412–8.
36. Polhemus, ‘‘Patriot brochure,’’ www.polhemus.com/
PATRIOT/PATRIOT_brochure.pdf.
37. Vecerina I, Zoethout J, Betrisay S. Device for determining the
longitudinal and angular position of a rotationally symme-
trical apparatus. Patent Number 20050075558.
38. Maass H, Chantier BBA, Cakmak HK, Kuhnapfel UG. How
to Add Force Feedback to a Surgery Simulator. LNCS.
2003;2673:165–74.
39. Kuhnapfel U, Cakmak HK, Chantier B, Maass H, et al.
HapticIO: Haptic Interface-Systems for Virtual-Reality
Training in Minimally-Invasive Surgery. Proceedings
Internationale Statustagung ‘‘Virtuelle und Erweiterte
Realitat, 2004.
40. Maass H, Cakmak HK, Kuhnapfel UG, Trantakis C, et al.
Providing More Possibilities for Haptic Devices in Surgery
Simulation. CARS, International Congress Series. 2005;
1281:725–9.
41. Chmarra MK, Bakker NH, Grimbergen CA, Dankelman J.
TrEndo, a device for tracking minimally invasive surgical
instruments in training set-ups. Sensor Actuat A-Phys.
2006;126:328–34.
42. Strom P, Kjellin A, Hedman L, Johnson E, et al. Training in
tasks with different visual-spatial components does not
improve virtual arthroscopy performance. Surg Endosc.
2004;18:115–20.
43. Smith CD, Farrell TM, McNatt SS, Metrveli RE. Assessing
laparoscopic manipulative skills. Am J Surg. 2001;181:
547–50.
44. Rosen J, Brown JD, Chang L, Sinanan M, et al. Generalized
Approach for Modeling Minimally Invasive Surgery as a
Stochastic Process Using a Discrete Markov Model.
IEEE Transactions on Biomedical Engineering. 2006;53:
399–413.
45. Chmarra MK, Jansen FW, Wentink M, Grimbergen CA, et al.
Performance during distinct phases in laparoscopic surgery.
10th World Congress of Endoscopic Surgery, 2006:112.
46. Schijven M, Jakimowicz J. Virtual reality surgical laparoscopic
simulators. How to choose. Surg Endosc. 2003;17:1943–50.
47. Halvorsen FH, Elle OJ, Fosse E. Simulators in surgery.
Minim Invasiv Ther. 2005;14:214–223.
48. Cosman PH, Cregan PC, Martin CJ, Cartmill JA. Virtual
reality simulators: Current status in acquisition and assess-
ment of surgical skills. ANZ J Surg. 2002;72:30–4.
49. Sutherland LM, Middleton PF, Anthony A, Hamdorf J, et al.
Surgical simulation. A systematical review. Ann Surg. 2006;
243:291–300.
50. Dunkin B, Adrales GL, Apelgren K, Mellinger JD. Surgical
simulation: a current review. Surg Endosc. 2007;21:357–66.
51. Massie TH, Salisbury JK. The PHANTOM Haptic Interface:
A Device for Probing Virtual Objects. Proceedings of the
ASME winter annual meeting, symposium on haptic inter-
faces for virtual environments and teleoperator systems,
Chicago, IL, 1994.
52. Datta V, Mackay S, Mandalia M, Darzi A. The use of
electromagnetic motion tracking analysis to objectively
measure open surgical skill in the laboratory-based model. J
Am Coll Surg. 2001;193:479–85.
53. Moorthy K, Munz Y, Dossis A, Bello F, et al. Motion analysis
in the training and assessment of minimally invasive surgery.
Min Invas Ther & Allied Technol. 2003;12:137–42.
54. Binder J, Kramer W. Point of technique. Robotically-assisted
laparoscopic radical prostatectomy. BJU International. 2001;
87:408–10.
55. Lanfranco AR, Castellanos AE, Desai JP, Meyers WC.
Robotic surgery. A current perspective. Ann Surg. 2004;239:
14–21.
56. Nawrat Z, Malota Z, Kostka P, Religa Z. The polish project
of telemanipulator for cardiac minimal invasive surgery with
preplanning and advisory system - assumptions and actual
state of art of RobIn Heart. 8th IEEE International
Conference on Methods and Models in Automation and
Robotics, Szczecin, Poland, 2002.
57. Podsedkowski L, Mianowski K, Wroblewski P, Nawrat Z.
Kinematic aspects of selected manipulators for cardiac
surgery. 8th IEEE International Conference on Methods
and Models in Automation and Robotics, Szczecin, Poland,
2002.
58. Rosen J, Lum M, Trimble D, Hannaford B, et al. Spherical
mechanism analysis of a surgical robot for minimally invasive
surgery – analytical and experimental approaches. MMVR.
2005;13:422–8.
Tracking minimally invasive instruments 339
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008

59. Prasad SM, Prasad SM, Maniar HS, Chu C, et al. Surgical
Robotics: Impact of Motion Scaling on Task Performance.
Am J Surg. 2004;199:863–8.
60. Lin HC, Shafran I, Murphy TE, Okamura AM, et al.
Automatic Detection and Segmentation of Robot-Assisted
Surgical Motions. MICCAI, LNCS. 2005;3749:802–10.
61. Satava RM, Cuschieri A, Hamdorf J. Metrics for objective
assessment. Preliminary summary of the Surgical Skills
Workshop. Surg Endosc. 2003;17:220–6.
62. Satava RM, Gallagher AG, Pellegrini CA. Surgical compe-
tence and surgical proficiency: definitions, taxonomy, and
metrics. J Am Coll Surg. 2003;196:933–7.
63. Yule S, Flin R, Paterson-Brown S, Maran N. Non-technical
skills for surgeons in the operating room: A review of the
literature. Surgery. 2006;139:140–9.
64. Healey AN, Undre S, Vincent CA. Developing observational
measures of performance in surgical teams. Qual Saf Health
Care. 2004;13:33–40.
340 M. K. Chmarra et al.
Downloaded By: [TU University of Technology Delft] At: 12:18 15 September 2008