submicrometer precision biometry of the anterior segment of the human eye
TRANSCRIPT

Submicrometer Precision Biometry of the AnteriorSegment of the Human Eye
Wolfgang Drexler * Angela Baumgartner,* Oliver Findl,\ Christoph K. Hitzenberger,*Harold Sattmann,* and Adolf F. Fercher*
Purpose. To demonstrate the feasibility of measuring the anterior structures of the humaneye by partial coherence interferometry and to determine its precision for eyes under normaland cycloplegic conditions.
Methods. The dual-beam version of partial coherence interferometry, a recendy developednoninvasive optical ranging technique, enables high resolution measurements of several intra-ocular distances with unprecedented precision. A modified, more sensitive scanning versionof this technique was used to assess the central and peripheral corneal thickness, the anteriorchamber depth, and the lens thickness of 20 healthy, emmetropic to moderately myopic eyes.Furthermore the anterior structures of three eyes were measured under cycloplegia (1%cyclopentolate) to investigate the influence on the precision of this technique after suppres-sion of residual accommodations.
Results. The mean geometric precision (standard deviation) of the measurement of the centralcorneal thickness was 0.29 fxm (range, 0.22 //m to 0.38 /um) and 0.43 /um (range, 0.27 /v,m to0.56 /urn) for the peripheral corneal thickness at a distance 2 mm from its apex. The precisionfor measuring the anterior chamber depth and the lens thickness for fixation at infinity was8.7 fj,m (range, 3.9 ^m to 16.8 fj.m) and 8.9 yum (range, 2.9 fim to 14.4 /urn) for noncycloplegiceyes and 1.9 fj,m (range, 1.7 /urn to 2 m) and 1.4 fini (range, 0.7 fim to 1.8 /um) for cycloplegiceyes, respectively.
Conclusions. The dual-beam partial coherence interferometry enables fast, noninvasive, submi-crometer precision biometry of the anterior segment of the eye. The precision of determiningthe anterior chamber depth and the lens thickness is more than one order of magnitudebetter than that of the currently used ultrasound and optical techniques, and it can beimproved by a factor of 5 by using cycloplegia. Invest Ophthalmol Vis Sci. 1997; 38:1304-1313.
1 he precise biometry of several intraocular distancesis fundamental to many applications in modern oph-thalmology. Exact measurement of corneal thicknessis needed in many physiological and clinical studiesand is helpful in diagnosis of several corneal disorders,including corneal degenerations, endothelial dysfunc-
From the * Inslitut far MedizinisrJie Physik, Universitat Wien, and the•fUniversit/itsklinik fur Augenheilkunde, Allgemeines Kmnkenhaus Wien, Wien,Austria.Presented in part at the annual meeting of the Association for Research in Visionand Ophthalmology, April 1996, Fort l^auderdale, Florida.Supported by the Austrian Fonds zur Forderung der wissenschafllichm Forschung(grant P 97S1-MHO).Submitted for publication October 15, 1996; revised February 3, 1997; acceptedFebruary 4, 1997.Proprietary interest category: P.lieprint requests: Wolfgang Drexler, Inslitut fur Medizinische Physik, WahringerSlrasse 13, A-1090 Vienna, Austria.
tion, and different types of stromal dystrophy.1'2 A par-ticularly important domain, which demands accurateassessment of the central and peripheral corneal thick-ness, is corneal refractive surgery.3 Radial keratotomyis a common procedure, where radial incisions areperformed in the corneal stroma down to Descemet'smembrane. These incisions are made using a bladewith a length of 10 fxm less than the thinnest part ofthe cornea. Therefore, a corneal thickness measure-ment with a precision better than 10 /im is needed.4
In photorefractive keratectomy the cornea is ablatedby laser photo ablation.5 For correcting 10 D of myo-pia, only 90 fj,m of the stroma must be removed.6 Inthe examination of new types of contact lenses, theswelling of the cornea resulting from edema causedby hypoxia needs exact measurement.78 The applica-
1304Investigative Ophthalmology & Visual SciiCopyright © Association for Research in '
::e,June 1997, Vol. 38, No. 7ion and Ophthalmology

Submicrometer Precision Biometry of the Anterior Eye Segment 1305
tions of these measurements also might be useful fordetermining which type of contact lens is toleratedbest by a patient.
Currently, measurements of corneal thickness areperformed mainly with the classic optical slit-lamp pa-chometers of the Haag-Streit type or with ultrasoundpachometers, whose principles and sources of errorare discussed in detail in the literature.9"" With ultra-sound pachometers, the central corneal thickness canbe determined with a precision of 5 /im, peripheralmeasurements can be performed with a precision of10 fim. Optical pachometers measure the central cor-neal thickness with a precision of approximately 13fj,m. Because of interobserver and interinstrumentvariabilities, large deviations are encountered in usingthese techniques.12 With a new high-frequency ultra-sound technique incorporating digital signal pro-cessing, topographic measurements of the cornea andthe epithelium can be performed with a precision(standard deviation) of 4.8 //m and 2 fj,m, employingA-scan and I-scan, respectively.13'14
Besides the corneal power, an accurate measure-ment of the axial eye length and the anterior chamberdepth—for the assumption of the postoperative pseu-dophakic chamber depth—are indispensable for thecalculation of the appropriate power of the intraocu-lar lenses in cataract surgery.15>lb Accurate biometry ofocular components that influence refractive error—human crystalline lens, for instance—can yield infor-mation about the genesis and development of myopia,emmetropization of children, or about normal eyegrowth.17"19
Biometry of the anterior chamber depth and thelens thickness are currently mainly performed withinstruments based on the ultrasound technique. How-ever, this method is limited in its longitudinal resolu-tion. The precision of the ultrasound technique forthe determination of the anterior chamber depth isreported to be 290 pun, and that for measurementof lens thickness 200 /j.m.20 Another drawback of theultrasound technique is the mechanical contact be-tween the eye and the instrument as well as differentapplanation depths of the cornea by the ultrasoundprobe. Using the ultrasound technique, there is a con-sequent need of anesthesia and risk of infection.
The anterior chamber depth was measured witha noninvasive optical technique for the first time inthe early 1960s.21 In the past several years a newoptical ranging technique, based on interferometryand employing partially coherent light has been de-veloped, having the potential to measure intraoculardistances and structures of the eye with unprece-dented precision and resolution. Corneal thicknessand anterior chamber depth were measured in vitroand in vivo using a conventional interferometricsetup, which, however, is sensitive to longitudinal
object motions.22 24 The dual-beam version of theinterferometric technique is completely insensitiveto longitudinal eye motions. After first obtaining pre-cise measurements of axial eye length in healthyeyes25'26 and in those with cataract27 and measure-ments of the fundus of the eye,26'28 this techniquealso was used to assess the central29'30 and peripheralcorneal thickness, corneal thickness profiles,31 ante-rior chamber depth, and lens thickness.32 Based onthis technique, a new fully computer-controlledscanning partial coherence interferometer (SPCI)was developed that is capable of measuring intraocu-lar distances at arbitrary angles to the vision axis.3S'84
The first topographic measurements of the humaneye fundus, using this technique, revealed the capa-bility of this instrument to quantitatively obtain thecontour and the thickness profile of retinal layers,with a precision (standard deviation) of 2 to 3 /j,m.35
Two-dimensional tomographic false color images ofthe fundus in the human eye with high axial resolu-tion showing the microstructure of the retina alsowere synthesized.S3~35
The purpose of this article is to demonstrate thefeasibility of this new instrument for measuring centraland peripheral corneal thickness, anterior chamberdepth, and lens thickness, and to evaluate the precisionof these measurements. The arrangement of instrumentand eye were optimized for measuring the anterior eyesegments by means of ray-tracing calculations,32 based onGullstrand's schematic eye.36 Furthermore, the influenceof residual accommodations on the measuring precisionof anterior chamber depth and lens thickness were investi-gated by means of a cycloplegic agent.
METHODS
Scanning Partial Coherence Interferometer
The principle of measuring intraocular distances bypartial coherence interferometry and the insensi-tiveness to longitudinal eye motions of the dual-beamversion of this technique have been described in previ-
ous reports.' The improved version of this in-strument, SPCI, that is also based on the dual-beamtechnique has been reported and described re-cently.33'34 Therefore, only a short summary of thisnew instrument is presented here, stressing the mainimprovements in the light source, sensitivity, preci-sion, resolution, and measurement time.
Figure 1 shows a schematic of the SPCI, that con-sists of five parts: the light sources, the interferometerunit (an external Michelson interferometer), thetransversal scanning unit, the detection and observa-tion unit, and the control unit with electronics. Informer versions of this instrument, multimode semi-conductor lasers (resolution approximately 120 /jm in

1306 Investigative Ophthalmology & Visual Science, June 1997, Vol. 38, No. 7
PersonalComputer
i
DiaitalBand Pass
Filter
1Amplifier
1 Photo-1Idetectorp
Control Unit
FIGURE 1. Schematic of the scanning partial coherence interferometer. Measurements at aspecific angle between the vision axis and the measurement beam, or along a completelinear or circular scan, are performed by a fully computer-controlled scanning unit.
air), and superluminescent diodes (resolution approx-imately 20 /Ltm in air) were used. The first version ofthe SPCI used a superluminescent diode yielding aresolution of 15 fj,m in air.33'34 All these light sourcesproduce sidelobes caused by the mode structure ofthe emission spectrum of the diode.37 These sidelobesappear in an optical A-scan as additional signal peaks,which are artifacts. They occur at multiples of theoptical length of the laser crystal (usually 1.1 to 1.3mm) from the central peak and can cause problemsespecially in measuring the anterior structures of theeye. If the position of one of these sidelobes coincideswith the signal from an intraocular distance, the lattermight be covered and, hence, missed.31'32 The recentversion of the SPCI uses an infrared superluminescentdiode (C86142E; Optoelectronics, Montreal, Quebec,Canada) with a central wavelength of 855 nm, a maxi-mum output power of 5 mW, a spectral bandwidth ofapproximately 25 nm (full width at half maximum[FWHM]) and a coherence length of approximately12 fim (FWHM) in air. This provides a resolution of~9 /im within the eye media (that is, 12 £tm dividedby the group-refractive index of the respective eye me-dium). This superluminescent diode has a very lowspectral modulation, thereby eliminating the prob-lems with subsidiary maxima. The light emitted by this
superluminescent diode is collimated to an approxi-mately parallel beam with a near infrared precisionmicroscope objective (numeric aperture, 0.6; magni-fication, X40; NACHET Vision; Newport, Irvine, CA).At the position of the cornea, this beam has an ellipticprofile of approximately 0.8 mm X 0.5 mm (1/e2 =decay of the maximum power). Because of power losscaused by the collimating objective and optical ele-ments (beam splitters, lenses, and mirrors) of the SPCI(Fig. 1), the eye is illuminated with approximately 220jiiW when a decreased output power of 3 mW is used.
To obtain short measurement times, a special het-erodyne detection technique, called laser Doppler in-terferometry, is used.26'34 The Doppler shift of the lightfrequency caused by moving the measurement mirrorof the interferometer unit moved with constant speedis used to judge the coincidence of the path differencewithin the eye with that of the external interferometer.In case of path length coincidence, the intensity ofthe corresponding interference pattern, consisting ofcircular, Newton-like interference fringes, is modu-lated by the Doppler frequency and detected by anavalanche-diode photodetector. To record a well mod-ulated interference signal, the width of the photode-tector entrance pupil has to be smaller than the widthof the interference fringes. For this purpose, the pho-

Submicrometer Precision Biometry of the Anterior Eye Segment 1307
-1.5 -1.0 -0.5 0.0 +0.5 +1.0 +1.5Interferometer arm length difference (mm)
FIGURE 2. Measurement of the central corneal thickness. The interference fringe contrast isplotted versus the difference in interferometer arm-lengths. Signal peak ACS is caused bythe anterior corneal surface. The peak labeled PCSl denotes the position of the posteriorcorneal surface. The distance between ACS and PCSl equals the optical thickness of thecentral cornea. Because of the symmetry of the coherence function, the signal is symmetricat ~0. Hence, a second peak PCS2 is obtained at the opposite side of PCSl and at the samedistance from the ACS peak. The distance between PCSl and PCS2 equals twice the opticalcorneal thickness. ACS = anterior corneal surface; PCSl, PCS2 = posterior corneal surface.
todiode is equipped with a multimode fiber pigtailwith 50-^m core diameter (Fig. 1). After amplificationand filtering by a bandpass filter, the envelope of themeasured signal is recorded and displayed as a func-tion of the stepper motor position in a personal com-puter (Figs. 2, 3). The positions of the recorded signalpeaks that are used to determine the intraocular dis-tances are determined by a cursor readout on thepersonal computer. The resolution of the cursor read-out is 0.5 //m and is independent of the scan length.Compared with former versions of the instrument, themeasurement time has been reduced by a factor of 3,which is especially important for the measurement ofthe whole anterior segment, in that a distance largerthan 10 mm has to be scanned for a single longitudinalA-scan. A single measurement of the corneal thicknesstakes ~0.25 seconds and of the whole anterior eyesegment, less than 2 seconds. By improving the qualityof the bandpass filter that separates the Doppler fre-quency signal from noise, the dynamic range of theinstrument is enhanced.
The half-wave (\/2) and quarter-wave plates ( \ /4) are retardation plates, or phase shifters, that areused in combination with a polarizing beam splitterto optimize the power of laser light illuminating the
eye and the amount of reflected light from the eyethat is detected by the detector fiber (Fig. 1).
Furthermore, the SPCI offers the possibility of ob-taining measurements not only parallel to the visionaxis but at arbitrary horizontal and vertical angles toit. This is achieved by a stepper motor-controlledscanning mirror that is imaged onto the nodal pointof the human eye by special scanning optics. The max-imum scanning range in horizontal and vertical direc-tions, (that is, the maximum angle between die visionaxis and the measurement direction) is approximately±25°, permitting measurements of the cornea in anapproximate 6-mm diameter region. The resolutionin both directions is 20 angular seconds. A specificangle between the vision axis and the measurementbeam or a complete linear or circular scan—a seriesof equidistant measurement points—can be selectedby special software on the personal computer. Hencethe corneal thickness at different peripheral positionsor complete corneal thickness profiles, anterior cham-ber depth, and lens thickness along specific angles tothe vision axis can easily be obtained. In contrast withthe former version of the SPCI, a separate fixationlight, focused to infinity, is offered directly to the ex-amined eye (and not to the fellow eye, as in the previ-
1308 Investigative Ophthalmology & Visual Science, June 1997, Vol. 38, No. 7
Interferometer arm length difference (mm)
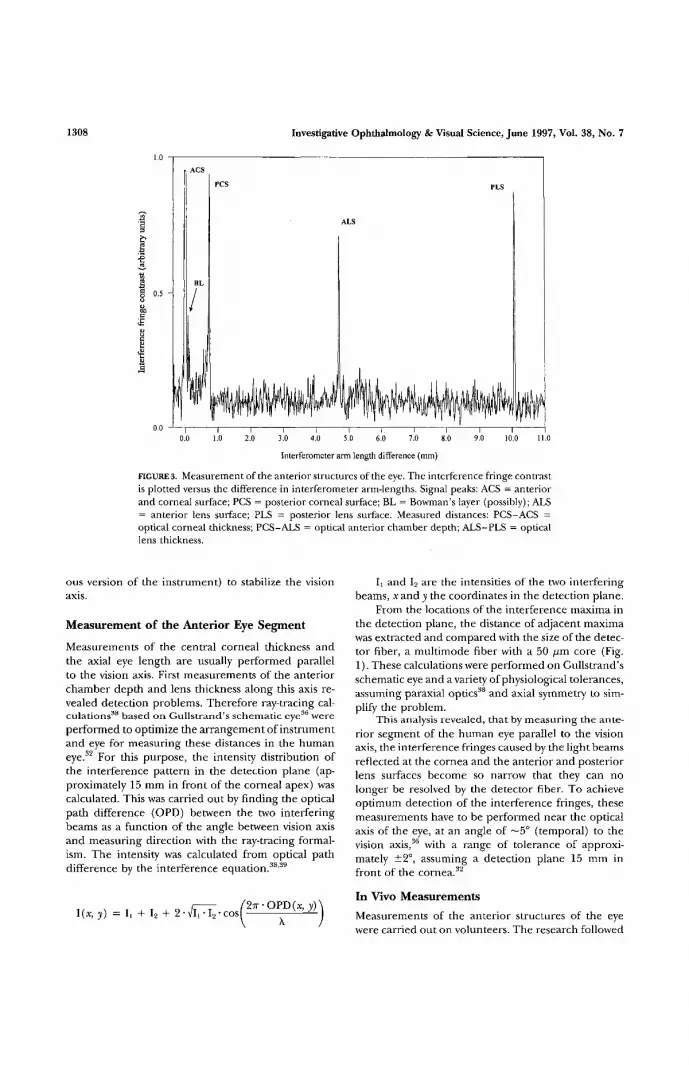
FIGURE 3. Measurement of the anterior structures of the eye. The interference fringe contrastis plotted versus the difference in interferometer arm-lengths. Signal peaks: ACS = anteriorand corneal surface; PCS = posterior corneal surface; BL = Bowman's layer (possibly); ALS= anterior lens surface; PLS = posterior lens surface. Measured distances: PCS-ACS =optical corneal thickness; PCS-ALS = optical anterior chamber depth; ALS-PLS = opticallens thickness.
ous version of the instrument) to stabilize the visionaxis.
Measurement of the Anterior Eye Segment
Measurements of the central corneal thickness andthe axial eye length are usually performed parallelto the vision axis. First measurements of the anteriorchamber depth and lens thickness along this axis re-vealed detection problems. Therefore ray-tracing cal-culations38 based on Gullstrand's schematic eye36 wereperformed to optimize the arrangement of instrumentand eye for measuring these distances in the humaneye.32 For this purpose, the intensity distribution ofthe interference pattern in the detection plane (ap-proximately 15 mm in front of the corneal apex) wascalculated. This was carried out by finding the opticalpath difference (OPD) between the two interferingbeams as a function of the angle between vision axisand measuring direction with the ray-tracing formal-ism. The intensity was calculated from optical pathdifference by the interference equation.38'39
I, and I2 are the intensities of the two interferingbeams, xandji the coordinates in the detection plane.
From the locations of the interference maxima inthe detection plane, the distance of adjacent maximawas extracted and compared with the size of die detec-tor fiber, a multimode fiber with a 50 fim core (Fig.1). These calculations were performed on Gullstrand'sschematic eye and a variety of physiological tolerances,assuming paraxial optics38 and axial symmetry to sim-plify the problem.
This analysis revealed, that by measuring the ante-rior segment of the human eye parallel to the visionaxis, the interference fringes caused by the light beamsreflected at the cornea and the anterior and posteriorlens surfaces become so narrow that they can nolonger be resolved by the detector fiber. To achieveoptimum detection of the interference fringes, thesemeasurements have to be performed near the opticalaxis of the eye, at an angle of ~5° (temporal) to thevision axis,36 with a range of tolerance of approxi-mately ±2°, assuming a detection plane 15 mm infront of the cornea.32
In Vivo Measurements
Measurements of the anterior structures of the eyewere carried out on volunteers. The research followed

Submicrometer Precision Biometry of the Anterior Eye Segment 1309
the tenets of the Declaration of Helsinki. Informedconsent was obtained after the nature and all possibleconsequences of the study had been explained.
Corneal thickness measurements were performedon 20 eyes of 10 healthy subjects (3 women and 7men). The average age of the patients was 30 years(mean ± standard deviation, 29.9 ± 5.6 years; range,22 to 39 years). Six eyes were emmetropic (±0.5 Dspherical equivalent [SE)), 10 were myopic, up to —6D (SE), and 4 were hyperopic, up to +2 D SE. Therefractive error was measured in noncycloplegic statewith an autorefractometer (Topcon [Paramus, NJ] KR3500 Auto Kerato-Refraktometer). Ten measurementswere performed in each eye and mean value and stan-dard deviation were calculated for each eye separately.Contact lens users (2 subjects) did not wear the lensesfor a minimum of 12 hours before the measurements.For measurements of the central corneal thickness,the subject had to fixate the measurement beam. Thiswas possible, because the broad emission spectrum ofthe superluminescent diode contains also faintly visi-ble wavelengths. For the peripheral measurements,the subject had to fixate a green light-emitting diodethat was aligned coaxially to the measurement beambefore the beam-tilting for peripheral measurements.Measurements at 15° nasal and 15° temporal were per-formed, corresponding to a location ±2 mm off theapex of the cornea (assuming a corneal radius of 7.7mm).31 A minimum of eight measurements were usedto determine the mean value and the standard devia-tion of the corneal thickness at each of the three loca-tions.
Measurements of the anterior chamber depth andlens thickness were performed on 20 healthy, eyes of10 healthy volunteers (4 women and 6 men). Thesubjects of this study group were partly different fromthose of the corneal-thickness study. Six eyes were em-metropic (±0.5 D SE), 14 were myopic, up to -5.5 DSE. The average age of the subjects was 36 years (mean± SD, 35.7 ± 15.6 years; range, 25 to 69 years). Themeasurements were performed parallel to the opticalaxis at an angle of 5° (±2°) to the vision axis. In somecases, only one peak from either the anterior or theposterior lens surface was detected at 5°. In these casesseveral measurements, ranging from 3° temporal to 7°temporal in steps of 1°, and from 2° inferior to 2°superior at 5° temporal in steps of 1°, were performedto find a measurement direction where the signalpeaks of both lens surfaces could be detected simulta-neously. Eight or more measurements containingboth of these peaks were then used to determine themean value and the standard deviation of the anteriorchamber depth and lens thickness in each of the 20eyes.
Residual accommodations, which occur duringfixation at infinity, might influence the measuring pre-
cision of anterior chamber depth and lens thickness.To assess this influence, measurements under cyclo-plegia also were performed. Because cyclopentolate isknown to produce psychogenic side effects, mainlyin children through its effect on the central nervoussystem,40'41 the anterior structures of only 3 of the 20eyes were measured in a cycloplegic state. One dropof 1 % cyclopentolate was instilled, followed by anotherdrop, 5 minutes later. After 25 minutes, biometry ofthese three eyes was performed at the same angle tothe vision axis, as was done in the noncycloplegic mea-surements.
Because all the distances obtained by partial co-herence interferometry are optical distances, theyhave to be divided by the group-refractive index42 ofthe respective eye medium for the used wavelength of855 nm to obtain the geometric distances.26 Thegroup-refractive indexes—the quotients of vacuumlight speed c and the group velocity of the light in themedia—of the eye media for \ = 855 nm are notavailable in the literature, but only the usual phase-refractive indexes—the quotients of c and the speedof the phase velocity in the media at A. = 550 nm —are available.36 Because the eye consists mainly of wa-ter and because of a lack of dispersion data on theeye media, the dispersion of water and the knownphase-refractive indexes at 550 nm43 were used to cal-culate the group-refractive index values of the investi-gated eye media for A. = 855 nm. Even for the corneaand the lens, this approximation was used, althoughthe water content is smaller. In this study values of1.3851 and 1.3454 were used for the group-refractiveindex of the cornea and the aqueous humor, respec-tively. Because the human crystalline lens has a sig-nificant refractive index gradient, a mean value of1.4065 was used for the group-refractive index. Henceits geometric thickness is less well known than that ofthe other more homogeneous ocular components(the cornea also has inhomogeneities, but the stroma,which makes up approximately 90% of its thickness,is relatively homogeneous). It should be mentionedthat ultrasound measurements suffer from the samedifficulty because they depend on the exact knowl-edge of the sound speed in the eye media.
During measurement the eye was illuminated witha center wavelength of approximately 855 nm withpower of ~220 yuW or an intensity of 572 ^iW/cm2
(averaged for a 7-mm aperture according to lasersafety regulations). To meet laser safety regulations,the retinal irradiance has to be regarded. The maxi-mum illumination time of the eye for a certain powerand wavelength is determined by calculating the inten-sity averaged for a 7-mm aperture , even if a beamsmaller in diameter is used. For in vivo measurementswith the SPCI, a maximum illumination time of ap-proximately 28 minutes is allowed for 220 .W at X.

1310 Investigative Ophthalmology & Visual Science, June 1997, Vol. 38, No. 7
= 855 nm.44 A single measurement of the cornealthickness and of the whole anterior segment takes0.5 seconds and 2 seconds, respectively. The wholemeasuring time for 8 to 10 consecutive longitudinalscans is not more than 20 seconds. This is well withinthe safety limits.
RESULTS
Corneal Thickness Measurements
In a typical measurement of the central corneal thick-ness, the signal intensity (ordinate), which is propor-tional to the interference fringe contrast, is plottedas a function of the interferometer arm length differ-ence (abscissa; Fig. 2). In this case, the measurementmirror (Fig. 1) was scanned from —1.5 mm to +1.5mm, which takes approximately 0.5 seconds. In con-trast to earlier measurements with other lightsources, described previously, only peaks caused byintraocular interfaces are observed—in this casethree peaks. At the difference in interferometer arm-lengths of 0 a strong signal is observed. The peaklabeled ACS indicates equal path lengths of the twointerferometer arms and denotes the position of theanterior corneal surface. This peak is distorted be-cause of nonlinearities of the amplifier, making anexact location of the signal's maximum difficult. Be-cause the intensities of the PCS peaks are less thanthat of the ACS peak, they are not distorted. There-fore their positions can be determined with higherprecision. To measure the corneal thickness, the po-sition of PCS1 and PCS2 are determined by a manualcursor readout on the personal computer. Their dis-tance equals twice the optical corneal thickness,which is 763.5 ^m in this case. The resolution of thiscursor readout on the personal computer is 0.5 /xm.For determination of the corneal thickness with theSPCI, the distance between PCS1 and PCS2 is dividedby 2 (Fig. 2). Hence, a precision less than the resolu-tion of this cursor readout is achieved. The meancentral optical thickness of the cornea (Fig. 2) is763.4 ± 0.34 p,m. The corresponding geometricthickness is 551.1 ± 0.26 fxm, which is the opticalthickness divided by the group-refractive index of thecornea at the wavelength of 855 nm. All other mea-surements of the central and peripheral cornea wereobtained in the same way. The mean value of centralcorneal thickness ± standard deviation, averaged forall 20 eyes is 538.4 ± 25.3 fim (range, 482.2 fim to 562fim). The corresponding values of mean peripheralcorneal thickness, at a 2-mm distance from its apexare 539.5 ± 22.1 /xm temporally (range, 500.4 /L«n to554.3 fim) and 557.7 ± 43.4 ^m nasally (range, 507.6fim to 582.9 /um). The mean precision (standard devi-ation) for central corneal thickness measurements,
which is the mean value of the standard deviationsobtained in the individual corneal thickness mea-surements is 0.29 fim (range, 0.22 fim to 0.38 fxm)and for peripheral measurements 0.43 im (range,0.27 jum to 0.56 //m). In this case the precision isequivalent to the repeatability.
Measurements of the Anterior Structures of theEyeFigure 3 shows a measurement of the anterior struc-tures of a human eye during fixation at infinity. Again,(Fig. 2) the interference fringe contrast is plotted ver-sus the difference in interferometer arm-lengths. Inthis case the measurement mirror is scanned over adistance from —0.5 mm to +11 mm, which takes lessthan 2 seconds. This measurement was performed at6° temporal to the vision axis (at the cornea). In con-trast to previous measurements of the anterior struc-tures,32 no sidelobes are observed and therefore—comparable to ultrasound A-scan—only signal peakscaused by intraocular interfaces are detected. Fourstrong peaks can be distinguished. The peaks labeledACS and PCS originate from the anterior and poste-rior corneal surface (Fig. 2). The distance betweenthe centers of these peaks equals the optical cornealthickness. In this case the optical corneal thickness is735.1 ± 0.7 //m, the geometric thickness is 530.7 ± 0.5fim. Mean value ± standard deviation of the geometriccorneal thickness of the 20 investigated eyes was 532.4± 37.5 //m, ranging from 437.3 /im to 575.4 /im. Themean precision (standard deviation) was 1.1 ± 0.4(im, ranging from 0.5 yum to 1.8 //.m. Another, smallerand very narrow peak (BL) can also be observed (Fig.3) at an optical distance of 83.4 fim from the centralpeak (ACS), which is at a geometric distance of ap-proximately 60.2 j^ra (by using the group-refractiveindex of the cornea for X. 855 nm). The exact originof this peak is not quite clear yet, but it may be causedby the interface of corneal epithelium with Bowman'slayer, enabling the measurement of the thickness ofthe corneal epithelium.
The peaks labeled ALS and PLS are caused bylight beams reflected at the anterior and posteriorlens surface. The distance between PCS and ALS, andALS and PLS, respectively equal the optical anteriorchamber depth (ACD) and the optical lens thickness(LT). In this case the optical ACD = 3.967 mm ± 2.5//m (mean value of 10 measurements and standarddeviation) and the optical LT = 5.373 mm ± 1 fim.After dividing them by the group-refractive index ofthe respective medium, described earlier, the ACD =2.949 mm ± 1.9 //m and the LT = 3.82 mm ± 0.7fim. All other measurements of the anterior structureswere performed in the same way. The mean geometricACD and LT ± standard deviation of the 20 measuredeyes were: ACD = 3.26 ± 0.38 mm (range, 2.63 mm

Submicrometer Precision Biometry of the Anterior Eye Segment 1311
to 3.82 mm) and LT = 3.89 ± 0.39 mm (range, 3.22mm to 4.92 mm). The mean precision (standard devia-tion) of ACD and LT measurements, which is themean value of the standard deviations obtained in theindividual ACD and LT measurements, were 8.7 yumfor the ACD (range, 3.9 ^m to 16.8 /im) and 8.9 fimfor the LT (range, 2.9 yum to 14.4 /um). The precisionof the ACD and LT measurement of Figure 3 is betterthan the mean standard deviation mentioned above,because the scan in this figure is taken from a measure-ment of a cycloplegic eye.
To investigate the influence of residual accommo-dations during fixation at infinity on the measuringprecision, 3 of the 20 eyes were also measured undercycloplegia. These measurements showed that the pre-cision of the measurement of the ACD and the LTcan be improved by a factor of 5 by using cycloplegia.The mean standard deviation for the measurement ofthe ACD and the LT were reduced to 1.9 /im (range,1.7 /zm to 2 ^m) and 1.4 /um (range, 0.7 fim to 1.8^m), respectively. Furthermore, a mean increase ofthe ACD of 112 pm (range, 83 ^m to 164 //m), anda mean decrease of the LT of 107 fxm (range, 58 fimto 191 //m) were detected when measuring the sameeye in a cycloplegic state.
DISCUSSION
We have shown that the improved version of the SPCIis able to perform central and peripheral cornealthickness measurements with submicrometer preci-sion. The decrease of the precision in the peripheralregion—2 mm from the apex of the cornea—iscaused by the parabolic shape of the corneal thicknessprofile.31
With former versions of this technique a precisionfor measuring the central corneal thickness of 7 /urnand 1.5 fj,m (standard deviation), had been ob-tained.29'30 Corneal thickness profiles could be as-sessed with a precision of 1.6 to 3.7 /zm.31 Further-more, it was demonstrated that this technique has nointerobserver variability.31 With the new version of theSPCI, the precision could be improved further to ap-proximately 0.3 /jm for central corneal thickness. Thisis an improvement by a factor of 15 to 40 comparedwith the precision of the usually used ultrasound oroptical pachometers9"12 and a factor 5 to 10 bettercompared with precision in high-frequency ultra-sound techniques that incorporate digital signal pro-cessing.1314 Because the signals reflected at the ante-rior and posterior lens surface are less intense thanthose reflected at the anterior and posterior cornealsurface, these last two signal peaks are often distortedif the amplifier gain is set to optimum detection ofthe lens surface peaks. Therefore the measurementof the corneal thickness as the distance between the
centers of these two peaks is less precise comparedwith the amplifier gain optimized for measurement ofjust the corneal thickness.
With the new light source, partial coherence inter-ferometry scans similar to that shown Figure 3 containonly signal peaks caused directly by intraocular inter-faces. Any side lobes that could be mistaken for realinterfaces are suppressed. Therefore these scans, so-called optical A-scans, can be directly compared withultrasound A-scans. However, the signal peaks of anoptical A-scan are very narrow (only approximately9 //m) compared with those of ultrasound A-scans.Therefore resolution and precision are much better.The resolution is on the order of the peak width.The precision of anterior chamber depth and lensthickness measurements for noncycloplegic eyes wasshown to be also approximately 9 /um. This is morethan one order of magnitude better than the measur-ing precision of the ultrasound technique—290 fimfor ACD and 200 fj,m for LT of cycloplegic adult eyes,20
and 240 fim for ACD and 150 /xm for LT of cycloplegicchildren eyes,45 respectively. Furthermore, ACD mea-surements performed by the ultrasound technique areless reliable because of different applanation depthsof the cornea by the ultrasound probe. These applana-tion depths are estimated to be as high as 140 //m.46
The high precision of the SPCI enabled the dem-onstration of the effect of cycloplegia on the measure-ments of ACD and LT. The measuring precision ofcycloplegic eyes was improved by a factor of 5, to 1 to2 fim. This is an improvement by a factor of approxi-mately 100 compared with the precision of the ultra-sound A-scan technique. It seems that residual accom-modations during fixation at infinity cause a de-creased precision of ACD and LT measurements innoncycloplegic eyes. This is contrary to the commonview47 that no accommodative fluctuations occur in arelaxed eye focusing on its far point. Furthermore, amean increase of the ACD of 112 (xm and a meanflattening of the lens of 107 /um was detected whenmeasuring the same eye in a cycloplegic state.
The advantages of this improved version of theSPCI are high precision, high resolution (approxi-mately 8 to 10 jum), short measurement time (espe-cially for ACD and LT measurements), no mistakableartifact signal peaks, and the ability to perform mea-surements not only parallel to the vision axis, but alsoat arbitrary angles to it. Finally, vergence eye move-ments during measurement are prevented, becausethe fixation light is offered directly to the examinedeye to stabilize the vision axis.
This examination technique offers a high degreeof comfort for the patient. No mydriatic agents forpupil dilatation are needed, it is a noncontact methodwith no need for anesthesia, and it ensures decreasedrisk of corneal infection.
1312 Investigative Ophthalmology & Visual Science, June 1997, Vol. 38, No. 7
Key Words
anterior eye segment, biometry, cycloplegia, interferometry,partial coherence interferometry
Acknowledgments
The authors thank Leopold Schachinger from the Instituteof Medical Physics, University of Vienna, Austria, for techni-cal assistance.
References
1. Olsen T, Nielsen CB, Ehlers E. On the optical mea-surements of corneal thickness: II: The measuringconditions and sources of error. Ada Ophthalmol.1980;58:975-984.
2. Ehlers N, Bramsen T. Central thickness in cornealdisorders. Ada Ophthalmol. 1978; 56:412-416.
3. Hoffmann F: Refractive corneal surgery. In: Blodi FC,Mackensen G, Neubauer H, eds. Surgical OphthalmologyI. Berlin, Gottingen, Heidelberg: Springer-Verlag;1986:523-546.
4. Waring GO III, Lynn MJ, McDonnell PJ. Results of theProspective Evaluation of Radial Keratotomy (PERK)Study 10 years after surgery for myopia. Arch Ophthal-mol. 1994; 112:1298-1308.
5. Muller-Stolzenburg N. Refractive corneal surgery withlasers. In: Blodi FC, Mackensen G, Neubauer H, eds.Surgical Ophthalmology I. Berlin, Gottingen, Heidel-berg: Springer Verlag; 1991:540-546.
6. Talley A, Hardten D, Sher N, et al. Results one yearafter using the 193 nm excimer laser for photorefrac-tive keratectomy in mild to moderate myopia. Am JOphthalmol. 1994; 118:304-311.
7. Holden BA, Mertz GW, McNallyJJ. Corneal swellingresponse to contact lenses worn under extended wearconditions. Invest Ophthalmol Vis Sci. 1983; 24:218-226.
8. Armitage BS, Schoessler JP. Overnight corneal swell-ing response in adapted and unadapted extendedwear patients. Am J Optom Physiol Opt. 1988;65:155-161.
9. Ehlers N, Hansen FK. On the optical measurement ofcorneal thickness. Ada Ophthalmol. 1971;49:65-81.
10. Mishima S, Hedbys BO. Measurement of cornealthickness with the Haag—Streit pachometer. ArchOphthalmol. 1986;80:710-713.
11. Olsen T, Ehlers N. The thickness of the human corneaas determined by a specular method. Ada Ophthalmol.1984; 62:859-871.
12. Reader AL and Salz JJ. Differences among ultrasonicpachymeters in measuring corneal thickness. J RefractSurg. 1987;3:7-11.
13. Reinstein DZ, Silverman RH, Rondeau MJ, ColemanDJ. Epithelial and corneal thickness measurements byhigh-frequency ultrasound digital signal processing.Ophthalmology. 1994; 101:140-146.
14. Reinstein DZ, Silverman RH, Trokel SL, Coleman DJ.Corneal pachymetric topography. Ophthalmology.1994; 101:432-438.
15. Boerringter RMM, Thijssen JM, Verbeck AM. Intraoc-ular lens power calculations: The optimal approach.Ophthalmology. 1985; 191:89-94.
16. Olsen T. Sources of error in intraocular lens powercalculation. / Cataract Refract Surg. 1992; 18:125-129.
17. Larsen JS. The sagittal growth of the eye: I: Ultrasoundmeasurement of the depth of the anterior chamberfrom birth to puberty. Ada Ophthalmol. 1971; 49:239-262.
18. Larsen JS. The sagittal growth of die eye: II: Ultrasonicmeasurement of the axial diameter of the lens andthe anterior segment from birth to puberty. Ada Oph-thalmol. 1971;49:427-440.
19. Sorsby A, Lear)' GA. A longitudinal study of refraction andits components during growth. Medical Research Council,Special Report Series No. 301. London: Her Majesty'sStationary Office, 1961.
20. Zadnik K, Mutti DO, Adams AJ. The repeatability ofmeasurements of the ocular components. Invest Oph-thalmol Vis Sci. 1992; 33:2325-2333.
21. Bleeker GM. Evaluation of three methods of re-cording the anterior chamber depth of the eye. ArchOphthalmol. 1961; 65:369-376.
22. Huang D, WangJ, Lin CP, Puliafito CA, FujimotoJG.Micron-resolution ranging of cornea anterior cham-ber by optical Reflectometry. Lasers Surg Med.1991; 11:419-425.
23. Huang D, Swanson EA, Lin CP, et al. Optical coher-ence tomography. Science. 1991; 254:1178-1181.
24. IzaltJA, Hee MR, Swanson EA, et al. Micrometer-scaleresolution imaging of the anterior eye in vivo withoptical coherence tomography. Arch Ophthalmol.1994; 112:1584-1589.
25. Fercher AF, Roth E. Ophthalmic laser interferometry.ProcSPIE. 1986;658:48-51.
26. Hitzenberger CK. Optical measurement of the axialeye length by laser Doppler interferometry. Invest Oph-thalmol Vis Sci. 1991; 32:616-624.
27. Hitzenberger CK, Drexler W, Dolezal C, et al. Mea-surement of the axial length of cataract eyes by laserDoppler interferometry. Invest Ophthalmol Vis Sci.1993;34:1886-1893.
28. Fercher AF, Hitzenberger CK, Drexler W, Kamp G,Sattmann H. In vivo optical coherence tomography.Am J Ophthalmol. 1993; 116:113-114.
29. Hitzenberger CK, Drexler W, Fercher AF. Measure-ment of corneal thickness by laser Doppler interfer-ometry. Invest Ophthalmol Vis Sci. 1992; 33:98-103.
30. Hitzenberger CK. Measurement of corneal thicknessby low-coherence interferometry. Appl Opt. 1992;31:6637-6642.
31. Hitzenberger CK, Baumgartner A, Drexler W, FercherAF. Interferometric measurement of corneal thick-ness with micrometer precision. Am J Ophthalmol.1994; 118:468-476.
32. Baumgartner A, Hitzenberger CK, Drexler W, Satt-mann H, Fercher AF. Measurement of the anteriorstructures of the human eye by partial-coherence in-terferometry. Progress in Biomedical Optics, Lille1994 in Lasers in Ophthalmology II. Brancato R, FercherAF, Melamed AS, Rol PO, Katzir A. Proc SPIE.1995;2330:146-151.
33. Drexler W, Hitzenberger CK, Sattmann H andFercher AF. In vivo optical coherence tomography
Submicrometer Precision Biometry of the Anterior Eye Segment 1313
and topography of the fundus of the human eye. Prog-ress in Biomedical Optics, Lille 1994 in Lasers in Oph-thalmology II. Brancato R, Fercher AF, Melamed AS,Rol PO, Katzir A, Proc SPIE. 1995; 2330:134-145.
34. Drexler W, Hitzenberger CK, Sattmann H, FercherAF. Measurement of the thickness of fundus layers bypartial coherence tomography. OptEng. 1995; 34:701-710.
35. Drexler W, Hitzenberger CK, Baumgartner A, et al.(Sub)micrometer precision biometry of the humaneye by optical coherence tomography and topogra-phy. ARVO Abstracts. Invest Ophthalmol Vis Sci.1996;37:S956.
36. Obstfeld H. Optics in Vision. London: Butterworth;1982:30-42.
37. NingY, Grattan KTV, MeggittBT, Palmer AW. Charac-teristics of laser diodes for interferometric use. ApplOpt. 1989; 28:3657-3661.
38. Klein MV, Furtrak TE. Optics. J Wiley: New York,1986:129-164, 264-270.
39. Born M, Wolf E. Interference and diffraction withpartially coherent light. In: Principle of Optics. Oxford:Pergamon Press; 1980:491-555.
40. Awan KJ. Adverse systemic reactions of topical cyclo-
pentolate hydrochlorid. Ann Ophthalmol. 1976;8:695-698.
41. Binkhorst RD, Weinstein GW, Baretz RM, ClahaneAC. Psychotic reaction induced by cyclopentolate(cyclogyl). Am J Ophthalmol. 1963;55:1243-1245.
42. Pancharatnam S. Partial polarisation, partial coher-ence and their spectral description for polychromaticlight—part II, Proc Ind Acad Sci. 1963;57:231-243.
43. Landolt-Bornstein. Zahlenwerte und Funktionen aus Phy-sik, Chemie, Astronomie, Geophysik, Technih. Vol. 2, 6thed. Optische Konstanten; Berlin, Gottingen, Heidel-berg: Springer Verlag; 1962:565-566.
44. American National Standards Institut. Safe Use of La-sers. ANSI Z 136.1, New York: American National Stan-dards Institute, 1986.
45. Mutti DO, Zadnik K, Egashira S, Kish L, Twelker JD,Adams AJ. The effect of cycloplegia on measurementsof the ocula components. Invest Ophthalmol Vis Sci.1994; 35:515-527.
46. Olsen T, Nielsen PJ. Immersion versus contact tech-nique in the measurement of axial length by ultra-sound. Ada Ophthalmol Copenh. 1989;67:101-102.
47. Moses RA. Accommodation. In: Moses RA, Hart WM,eds. Adler's Physiology of the Eye. Clinical Application. 8thed. St. Louis: CV Mosby; 1987:291-310.