stroke among women, ethnic groups, young adults, and children
TRANSCRIPT

Handbook of Clinical Neurology, Vol. 92 (3rd series)Stroke, Part IM. Fisher, Editor# 2009 Elsevier B.V. All rights reserved
Chapter 17
Stroke among women, ethnic groups,
young adults, and children
JONATHAN W. STURM1, MARK T. MACKAY2, AND AMANDA G. THRIFT3*
1Department of Neurology, Gosford Hospital, Central Coast Area Health, Gosford, Australia2Department of Neurology, Royal Children’s Hospital, Parkville, Australia
3Baker Heart Research Institute, Melbourne, Australia
There are a number of different groups of people among
whom the incidence and etiology of stroke differ. Inci-
dence is somewhat lower among women than men, and
is considerably lower among young adults and children.
There are some ethnic groups amongwhom the incidence
and the composition of the subtypes of stroke vary con-
siderably. Stroke in children is more commonly asso-
ciated with other disorders, such as non-atherosclerotic
arteriopathies and cardiac disorders.Among young adults
similar disorders are also associated with stroke; how-
ever, other factors such as recreational drug use and
migraine play a role, as well as the development of
atherosclerosis. In this chapter we will discuss the most
important differences among these groups.
17.1. Stroke in women
The incidence of stroke has consistently been shown to
be lower in women than in men (Sudlow and Warlow,
1997). In the majority of incidence studies, however,
the number of strokes occurring among women is
greater (Bamford et al., 1988; Ricci et al., 1991;
D’Alessandro et al., 1992; J�rgensen et al., 1992; Bonitaet al., 1993; Czlonkowska et al., 1994; Feigin et al.,
1995; Brown et al., 1996; Thrift et al., 2000). This
apparent disparity is due to the fact that stroke incidence
increases with age and there are more elderly women
than elderly men in the population.
There are many physiological differences between
women and men that predispose them to diseases in
different ways. For stroke these differences are largely
*Correspondence to: Dr Amanda G. Thrift, Head, Population Hea
Road, Melbourne, Victoria 8008, Australia. E-mail: Amanda.Th
1100.
attributed to childbearing, pregnancy, contraception,
and maintenance of hormone levels during and after
menopause. In addition, there is some evidence that
other risk and protective factors for women are not the
same as for men, and that some factors may require
higher exposures in one group than the other. For exam-
ple, in a cohort study in the USA, serum albumin con-
centrations of more than 4.4 g/dl have been shown to
be associated with reduced stroke risk among men aged
65–74 years but the same association has not been
observed among women (Gillum et al., 1994). Many
of these findings have either not been replicated by
others, are inconsistent, or the studies have low power,
and so these factors will not be discussed further.
17.1.1. Pregnancy
Women are at increased risk of stroke during pregnancy,
with approximately 11 ischemic strokes and nine intra-
cerebral hemorrhages being reported to occur with
every 100 000 deliveries in the 15–45-year age group
(Kittner et al., 1996). The incidence was lower in a study
conducted in France, being 4.3 per 100 000 deliveries for
non-hemorrhagic stroke and 4.6 per 100 000 deliveries
for intraparenchymal hemorrhage (Sharshar et al., 1995).
The reason for this lower incidence may partly be the
inclusion of a longer postpartum period in the former
study, with the majority of strokes occurring during this
period.
During pregnancy and the 6-week postpartum per-
iod combined Kittner and colleagues (1996) found that
lth Research, Baker Heart Research Institute, 75 Commercial
[email protected]; Tel: (613) 8532-1111; Fax: (613) 8532-

Current OCP use
Estrogen dose
Progesterone typeFirst generation
Second generation
Third generation
0.5 1.0
Relative Risk (95% CI)
10.0
High (>50µg)
Medium (50µg)
Low (<50µg)
Fig. 17.1. Summary of relative risk (and 95% confidence
intervals (CI)) of the oral contraceptive pill for ischemic
stroke. (Adapted from Gillum et al., 2000.)
RM
the relative risk (RR) for cerebral infarction was 1.6
(95% confidence interval (CI) 1.0–2.7), and for intra-
cerebral hemorrhage was 5.6 (95% CI 3.0–10.5). The
greatest risk of stroke occurred during the early post-
partum period, being 5.4 (95% CI 2.9–10.0) for
ischemic stroke and 18.2 (95% CI 8.7–38.1) for intra-
cerebral hemorrhage. In another investigation of the
role of pregnancy in ischemic stroke risk, no such
association was found (Nightingale and Farmer, 2004).
However, in this latter study there were only two preg-
nancies among the women with ischemic stroke and the
confidence intervals were wide (1.23, 95% CI 0.34–
4.41), encompassing the point estimate of the previous
investigation. Therefore it appears that there is an
increased risk of stroke among women during pregnancy
and in the early postpartum period.
In a recent case-control study conducted in the
USA, Brown and colleagues (2006) investigated the
association between a history of pre-eclampsia and
ischemic stroke risk. They found that women with a
history of pre-eclampsia more often had a non-
pregnancy-related ischemic stroke than women with-
out a history of this condition (odds ratio (OR) 1.63,
95% CI 1.02–2.62). Therefore, although the greatest
risk of stroke appears to be in the early postpartum
period, it may be that people with this condition con-
tinue to be at elevated risk of ischemic stroke beyond
the postpartum period.
There are a number of potential mechanisms for an
increased predisposition to stroke during pregnancy
and the early postpartum period, including athero-
sclerosis, cardioembolism, arterial dissection during
labor, hematological disorders, paradoxical embolism
from the venous system of the pelvis or legs, and fat,
air, or amniotic fluid embolism (Sharshar et al.,
1995; Jeng et al., 2004). In addition Sharshar and col-
leagues (1995) reported that eclampsia was associated
with 47% of pregnancy-related non-hemorrhagic
strokes and 44% of intraparenchymal hemorrhages in
the northern region of France. Thus, the association
between pregnancy and stroke is biologically plausible.
17.1.2. Oral contraceptive pill
There have been numerous investigations of the asso-
ciation between the oral contraceptive pill and stroke
since this possibility was first raised in 1962 (Lorentz,
1962). Evidence for an association has been conflict-
ing. In studies conducted in the 1960s and 1970s the
relative risk of stroke associated with the oral contra-
ceptive pill was reported to be between 3.14 and 8.80
(Sartwell et al., 1969; Vessey and Doll, 1969; Colla-
borative Group for the Study of Stroke in Young
338 J.W. STU
Women, 1973, 1975). Over the next few decades this
association diminished somewhat, with relative risk
estimates tending towards lower values of between 2
and 4 (Petitti et al., 1996; WHO Collaborative Study
of Cardiovascular Disease and Steroid Hormone Con-
traception, 1996a, b; Schwartz et al., 1997, 1998; Hei-
nemann et al., 1998; Lidegaard, 1999; Poulter et al.,
1999; Lidegaard and Kreiner, 2002).
The decline in the risk of stroke associated with the
oral contraceptive pill over the past few decades has
largely been attributed to its changing composition.
This is demonstrated by the results of a recent meta-
analysis (Gillum et al., 2000), where a dose–response
relationship between estrogen levels and ischemic
stroke risk was observed (Fig. 17.1). The relative risk
for ischemic stroke increased from 2.08 (95% CI
1.55–2.80) among those taking low dose estrogen oral
contraceptive pills (<50 mg) to 2.78 (95% CI 2.00–
3.85) among those taking medium doses (50 mg) and4.53 (95% CI 2.17–9.50) for those taking high
(�50 mg) doses (Gillum et al., 2000). Most modern
oral contraceptive pills contain 30–35 mg of estrogen
and so it is possible that the risk of stroke with the oral
contraceptive pill will decline further. Evidence for
this has been provided by the results of a recent Danish
case-control study that included 626 women with
ischemic stroke or transient ischemic attack (TIA)
(Lidegaard and Kreiner, 2002). In this study the rela-
tive risk of ischemic stroke or transient ischemic attack
was 1.6 (95% CI 1.3–2.0) among those taking oral
contraceptive pills with an estrogen dose of 30–
40 mg, which is somewhat lower than that reported
among those taking doses less than 50 mg in the recent
meta-analysis (Gillum et al., 2000).
Investigation of the effect of the progesterone
type of oral contraceptive pill on the risk of ischemic
stroke provides some conflicting results. In the large
ET AL.

OU
meta-analysis conducted by Gillum and colleagues
(2000) there was a non-significant decrease in risk of
ischemic stroke with third-generation preparations. A
similar decline with the newer preparations was
reported by Lidegaard and Kreiner (2002), where a
lower relative risk was found among those taking
third-generation preparations (OR 1.4; 95% CI 1.0–
1.9) than first-generation preparations (OR 4.5; 95%
CI 2.6–7.7). In contrast to this, Kemmeren and collea-
gues (2002) found no difference in the adjusted odds
ratio for ischemic stroke between the different prepara-
tions of progesterone. The reason for this disparity is
unclear, although it is possible that prescribing practices
may account for some of the observed differences. If the
newer preparations are seen as being safer and are pre-
scribed to higher-risk women in some areas, this might
potentially bias the results.
There have been few investigations of the risk of
either intracerebral hemorrhage or subarachnoid
hemorrhage among users of the oral contraceptive pill
(Hannaford et al., 1994; Thrift et al., 1996; Jick et al.,
1999). As shown in Table 17.1, these studies provide
evidence that the oral contraceptive pill does not infer
a greater risk of either intracerebral hemorrhage (Han-
naford et al., 1994; Thrift et al., 1996; Jick et al., 1999)
or subarachnoid hemorrhage (Hannaford et al., 1994).
Similar results have been reported from investigations
among a combined group of hemorrhagic strokes
(Collaborative Group for the Study of Stroke in Young
Women, 1975; Hirvonen and Idanpaan-Heikkila, 1990;
Petitti et al., 1996). This provides evidence that the oral
contraceptive pill does not appear to predispose to
either of the major hemorrhagic stroke subtypes.
Some investigators have reported that the risk of
stroke among oral contraceptive pill users is greater
among those who are hypertensive (Collaborative
Group for the Study of Stroke in Young Women,
1975), who smoke (Collaborative Group for the Study
of Stroke in Young Women, 1975; WHO Collaborative
Study of Cardiovascular Disease and Steroid Hormone
Contraception, 1996b; Heinemann et al., 1998), or who
suffer migraines (Collaborative Group for the Study
of Stroke in Young Women, 1975; Schwartz et al.,
1998; Bousser, 2004; Etminan et al., 2005). In contrast,
in their meta-analysis Gillum and colleagues (2000)
reported that oral contraceptive pill use appeared to
impart similar risks of ischemic stroke among smokers
and non-smokers, those with and without hypertension,
and those with and without migraine (Gillum et al.,
2000). Although this is reassuring, it is possible that
these additional risk factors are imbalanced between
groups because of prescribing practices. Such imbal-
ances may relate to the level of blood pressure or to
STROKE AMONG WOMEN, ETHNIC GR
the amount that women smoke. Therefore it might be
more prudent to avoid prescribing oral contraceptive
pills to women with these additional risk factors.
17.1.3. Hormone replacement therapy
A recently carefully conducted meta-analysis of nine
observational studies provided evidence for an increa-
sed risk of stroke among ever users of hormone replace-
ment therapy (RR 1.12; 95% CI 1.01–1.23) (Nelson
et al., 2002). The authors calculated that for every
10 000 postmenopausal women treated with hormone
replacement therapy per year there would be one extra
stroke among those aged 55–64 years, three extra strokes
among those aged 65–74 years, and six extra strokes
among those aged 75–84 years. Further analysis by stroke
subtype revealed that the increased risk of stroke was
largely attributable to an increased risk of ischemic stroke
(RR 1.20; 95% CI 1.01–1.40) (Nelson et al., 2002). In
contrast, there was no elevated risk of either subara-
chnoid haemorrhage (RR 0.80; 95% CI 0.57–1.04) or
intracerebral hemorrhage (RR 0.81; 95% CI 0.25–1.29).
Despite the fact that ischemic stroke was increased
among those taking hormone replacement therapy, the
authors of this meta-analysis suggested caution when
assessing the results (Nelson et al., 2002). This is
because women who take hormone replacement therapy
differ in ways that are known to decrease the risk of
cardiovascular disease. These women tend to be more
affluent, are leaner, have higher educational attainment,
exercise more often, and drink alcohol more regularly.
There have been three recent randomized trials of
hormone replacement therapy and stroke; two of these
were for secondary prevention of stroke (Simon et al.,
2001; Viscoli et al., 2001) while one was a primary
prevention study (Wassertheil-Smoller et al., 2003;
Anderson et al., 2004). In the secondary prevention
studies there was no evidence of a benefit or a detri-
mental effect of hormone replacement therapy on the
risk of stroke among either those with pre-existing cor-
onary heart disease (Simon et al., 2001) or those with a
prior ischemic stroke or transient ischemic attack
(Viscoli et al., 2001). There were two arms of the
Women’s Health Initiative, one involving the use of
estrogen plus progestin among postmenopausal
women aged 50–79 years (Wassertheil-Smoller et al.,
2003) and one on postmenopausal use of estrogen
among women aged 50–79 years with a prior hyster-
ectomy (Anderson et al., 2004). In the former of these
arms, a 31% increase in strokes was reported among
those taking estrogen plus progestin when compared
to placebo (Wassertheil-Smoller et al., 2003). This
was equivalent to about eight extra strokes for every
PS, YOUNG ADULTS, AND CHILDREN 339

Table 17.1
Summary of relative risk or odds ratio (and 95% confidence intervals (CI)) of the oral contraceptive pill for intracerebral hemorrhage
and subarachnoid hemorrhage
Location
Study
population Cases Controls
Oral contraceptive
pill status
Risk/odds ratio
(95% CI) Adjustments
Intracerebral hemorrhage
United Kingdom (Hannaford et al.,
1994)
GP database 22 66 Never user 1.0 Smoking and socioeconomic
status
Ever user 1.3 (0.5–3.8)
Current user 1.1 (0.2–7.1)
Former user 1.4 (0.5–4.2)
United Kingdom (Jick et al., 1999) GP database 29 116 Second generation
users
1.0 Nil
Use of desogestrel 1.2 (0.2–6.8)
Use of gestodene 1.4 (0.2–8.2)
Melbourne, Australia (Thrift et al.,
1996)
Cases-control
study
331 331 Ever used oral
contraceptive pills
0.89 (0.38–2.09) Hypertension, cholesterol,
previous cardiovascular
disease, exercise, body mass
index, smoking, and alcohol
consumption.
Subarachnoid hemorrhage
United Kingdom (Hannaford et al.,
1994)
GP database 73 219 Never user 1.0 Smoking and socioeconomic
status.Ever user 1.3 (0.7–2.5)
Current user 1.5 (0.6–3.7)
Former user 1.3 (0.7–2.5)
95% CI, 95% confidence interval.

OU
10 000 women-years of treatment. Moreover, when the
hazard ratios were adjusted for multiple comparisons
the confidence intervals crossed unity and so the asso-
ciation was no longer statistically significant (Nelson
et al., 2002; Patel et al., 2002). Similar results were
found for the use of estrogen therapy among postme-
nopausal women with a prior hysterectomy (Anderson
et al., 2004).
Although there is inconclusive evidence regarding
excessive stroke risk among postmenopausal women
taking hormone replacement therapy, there is now a
large body of evidence from meta-analysis and rando-
mized controlled trials that hormone replacement ther-
apy does not provide protection against ischemic
stroke (Simon et al., 2001; Viscoli et al., 2001; Nelson
et al., 2002; Wassertheil-Smoller et al., 2003; Ander-
son et al., 2004). Therefore there is no longer support
for the use of these agents in either the primary or
secondary prevention of ischemic stroke.
17.1.4. Summary
Women have a number of risk factors for stroke that are
unique. Many of these involve their reproductive capa-
city, although other factors may also be involved. An
increased risk of both ischemic stroke and intracerebral
hemorrhage has been observed during pregnancy, with
the highest risk occurring early in the postpartum per-
iod. There has been conflicting evidence for a role of
the oral contraceptive pill on ischemic stroke risk, which
appears to be mainly attributable to changing doses and
preparations over the decades. However, despite the fact
that there has been an amelioration of the risk of stroke
associated with use of the oral contraceptive pill with
the introduction of newer lower-dose preparations, a
significant risk persists. Similar conflicting evidence
was apparent for the use of hormone replacement ther-
apy in preventing stroke. However, with the publication
of a recent meta-analysis of observational studies as
well as the completion of several randomized controlled
trials, the evidence no longer supports a role for these
preparations in protecting against stroke and so these
drugs should not be prescribed for this purpose.
17.2. Ethnicity
17.2.1. Incidence and type of stroke
There have been a number of reports of differences in
subtypes of stroke between people of different ethnic
backgrounds. Early work conducted in Japan (Tanaka
et al., 1982; Ueda et al., 1988) demonstrated that hemor-
rhagic stroke comprised a larger proportion of strokes
(approximately 30%) than those occurring in European,
STROKE AMONG WOMEN, ETHNIC GR
Australian, or American populations (15–20%) (Bam-
ford et al., 1990; Giroud et al., 1991; Ricci et al., 1991;
D’Alessandro et al., 1992; Tuomilehto et al., 1992;
Wolf et al., 1992; Anderson et al., 1993; Brown et al.,
1996). Intracerebral hemorrhages are also more com-
mon in China, with this subtype of stroke comprising
between 17% and 39% of strokes in different regions
(Zhang et al., 2003). In addition, there is some evidence
from hospital-based registries that hemorrhagic stroke
may account for between 26% and 46% of strokes in
South America (Saposnik et al., 2003). These are likely
to be overestimates, however, as hemorrhages usually
comprise the more severe strokes and are therefore more
likely to result in hospitalization.
In studies conducted in the USA and the UK the inci-
dence of stroke among blacks has been shown to be
approximately twice that of whites (Kittner et al., 1990;
Giles et al., 1995; Sacco et al., 1998; Stewart et al.,
1999; Kissela et al., 2004). Furthermore, the incidence
was greater among blacks for each of ischemic stroke,
intracerebral hemorrhage, and subarachnoid hemorrhage
(Stewart et al., 1999; Kissela et al., 2004). Similarly high
incidence rates were also observed among Hispanics
living in northern Manhattan (Sacco et al., 1998).
17.2.2. Risk factors
Differences in the incidence of stroke among different
ethnic groups have not been explained by differences
in social class, age, or sex (Stewart et al., 1999). How-
ever, there have been observed differences in other
risk factors. The prevalence of hypertension and dia-
betes was found to be greater among blacks than
whites in a multicenter study conducted in Europe,
while the prevalence of atrial fibrillation and smoking
was greater in whites (Hajat et al., 2004). In addition
to hypertension and diabetes, the prevalence of obesity
and inadequate physical activity was also greater
among blacks in a study conducted in the USA
(McGruder et al., 2004). In contrast, Hispanics had a
greater prevalence of diabetes than whites but a similar
prevalence of other risk factors (McGruder et al.,
2004). These differences in risk factors can be used
to guide community-based prevention strategies in dif-
ferent ethnic groups. Tailoring strategies toward those
risk factors that are particularly high in distinct ethnic
groups will ensure that prevention strategies are opti-
mized.
17.3. Stroke in young adults
A relatively small proportion of strokes occurs in
adults aged between 15 and 45 years. However, stroke
in young adults requires special consideration as the
PS, YOUNG ADULTS, AND CHILDREN 341
RM
relative frequencies of underlying pathophysiological
mechanisms differ from those of the general stroke
population and because of the potential long-term
impact on independence and performance of familial,
occupational, and societal roles.
17.3.1. Incidence
In Western countries between 2% (Marini et al., 2001)
and 8% (Jacobs et al., 2002) of first-ever strokes occur
in people aged between 15 and 45 years, and in specia-
lized stroke centers the proportion may be as high as
12% (Bogousslavsky and Pierre, 1992). In developing
countries, 20–30% of strokes may occur in young
adults (Radhakrishan et al., 1986; Al Radjeh and
Awada, 2002). Annual incidence rates for first-ever
strokes at the age of less than 45 years are between
10 and 23 per 100 000 (Marini et al., 2001; Jacobs
et al., 2002). Even within the category of ‘young
stroke’, incidence increases with age, with only 30%
occurring in those aged less than 35 years (Marini
et al., 2001). Men have generally been found to have
greater incidence rates than women at all ages (Marini
et al., 2001; Jacobs et al., 2002); however, in those
aged less than 30 years a greater incidence has been
reported in women than men (Naess et al., 2002).
Similar to the general stroke population, incidence var-
ies among ethnic groups in people aged less than 45
years, with greater rates of stroke (Jacobs et al.,
2002) in blacks and Hispanics and greater rates of
transient ischemic attack (Kleindorfer et al., 2005) in
blacks than whites in the USA.
In population-based studies a higher proportion of
intracerebral hemorrhage and subarachnoid hemor-
rhage has been found in young adults compared to
342 J.W. STU
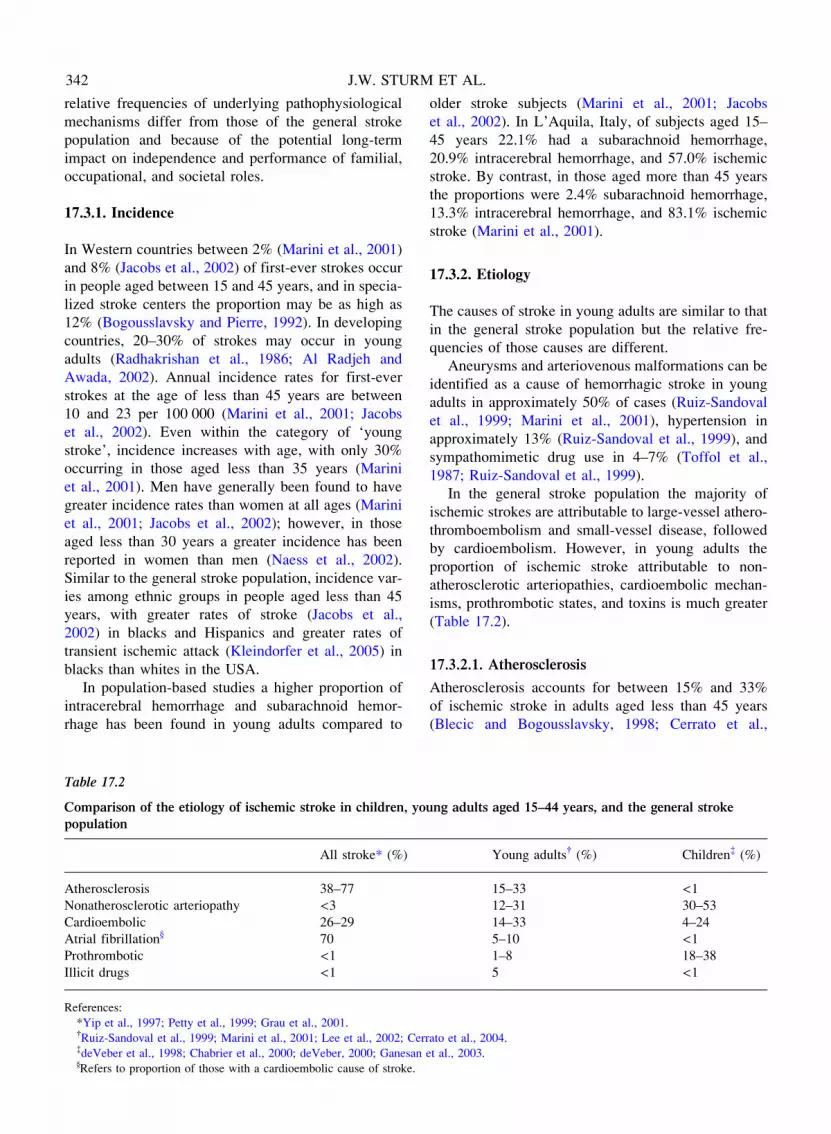
Table 17.2
Comparison of the etiology of ischemic stroke in children, yo
population
All stroke* (%)
Atherosclerosis 38–77
Nonatherosclerotic arteriopathy <3Cardioembolic 26–29
Atrial fibrillation} 70
Prothrombotic <1Illicit drugs <1
References:
*Yip et al., 1997; Petty et al., 1999; Grau et al., 2001.{Ruiz-Sandoval et al., 1999; Marini et al., 2001; Lee et al., 2002; Cer{deVeber et al., 1998; Chabrier et al., 2000; deVeber, 2000; Ganesan}Refers to proportion of those with a cardioembolic cause of stroke.
older stroke subjects (Marini et al., 2001; Jacobs
et al., 2002). In L’Aquila, Italy, of subjects aged 15–
45 years 22.1% had a subarachnoid hemorrhage,
20.9% intracerebral hemorrhage, and 57.0% ischemic
stroke. By contrast, in those aged more than 45 years
the proportions were 2.4% subarachnoid hemorrhage,
13.3% intracerebral hemorrhage, and 83.1% ischemic
stroke (Marini et al., 2001).
17.3.2. Etiology
The causes of stroke in young adults are similar to that
in the general stroke population but the relative fre-
quencies of those causes are different.
Aneurysms and arteriovenous malformations can be
identified as a cause of hemorrhagic stroke in young
adults in approximately 50% of cases (Ruiz-Sandoval
et al., 1999; Marini et al., 2001), hypertension in
approximately 13% (Ruiz-Sandoval et al., 1999), and
sympathomimetic drug use in 4–7% (Toffol et al.,
1987; Ruiz-Sandoval et al., 1999).
In the general stroke population the majority of
ischemic strokes are attributable to large-vessel athero-
thromboembolism and small-vessel disease, followed
by cardioembolism. However, in young adults the
proportion of ischemic stroke attributable to non-
atherosclerotic arteriopathies, cardioembolic mechan-
isms, prothrombotic states, and toxins is much greater
(Table 17.2).
17.3.2.1. Atherosclerosis
Atherosclerosis accounts for between 15% and 33%
of ischemic stroke in adults aged less than 45 years
(Blecic and Bogousslavsky, 1998; Cerrato et al.,
ET AL.
ung adults aged 15–44 years, and the general stroke
Young adults{ (%) Children{ (%)
15–33 <112–31 30–53
14–33 4–24
5–10 <11–8 18–38
5 <1
rato et al., 2004.
et al., 2003.
OU
2004; Varona et al., 2007), and in only 5% in those less
than 30 years (Bogousslavsky and Regli, 1987). Large-
vessel disease is more common in Western populations
(Adams et al., 1995), while small-vessel disease is
greater among blacks in the USA (Qureshi et al.,
1995) and among Taiwanese (Lee et al., 2002). By con-
trast, atherosclerosis accounts for between 38% and
77% of ischemic stroke in the general population
(large-artery and small-vessel disease combined; Yip
et al., 1997). Risk factors for atherosclerosis in young
adults are the same as in the general population:
hypertension, diabetes, smoking, and hyperlipidemia
(Cerrato et al., 2004).
17.3.2.2. Non-atherosclerotic arteriopathies
This heterogeneous group of disorders accounts for
12–31% of ischemic strokes in young adults (Blecic
and Bogousslavsky, 1998; Varona et al., 2007). This is
considerably greater than the proportion attributable to
these conditions in the general stroke population
(<3%; Petty et al., 1999; Grau et al., 2001). Carotid
and vertebral arterial dissection causes approximately
10% of strokes among those less than 40 years of age
and 20% among those less than 30 years of age (Guillon
et al., 1998). Dissection is usually spontaneous but can
be secondary to trauma, fibromuscular dysplasia, or
connective tissue disorders. A less common arteriopathy
is fibromuscular dysplasia, which occurs predominantly
in white women and usually involves the distal extracra-
nial vertebral and carotid arteries. Abnormalities in the
smooth muscle layer result in widening and narrowing
of the arterial lumen, leading to the characteristic ‘string
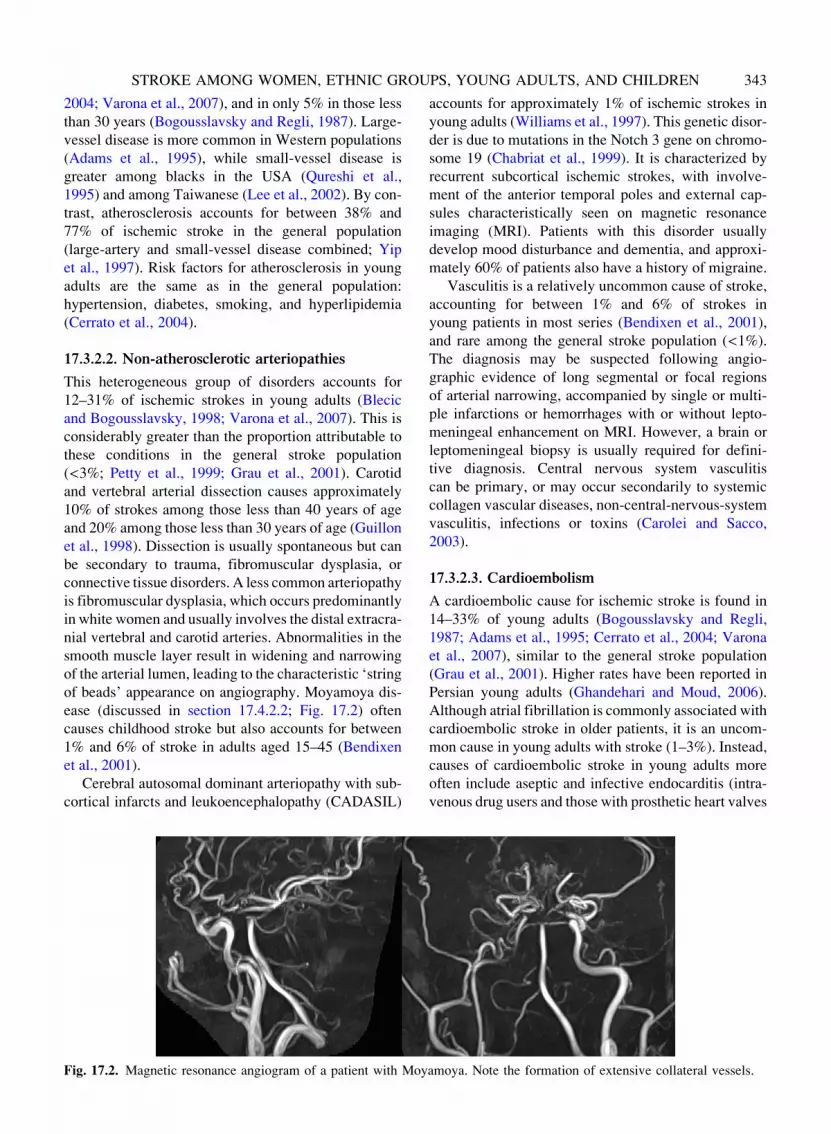
of beads’ appearance on angiography. Moyamoya dis-
ease (discussed in section 17.4.2.2; Fig. 17.2) often
causes childhood stroke but also accounts for between
1% and 6% of stroke in adults aged 15–45 (Bendixen
et al., 2001).
Cerebral autosomal dominant arteriopathy with sub-
cortical infarcts and leukoencephalopathy (CADASIL)
STROKE AMONG WOMEN, ETHNIC GR
Fig. 17.2. Magnetic resonance angiogram of a patient with Moy
accounts for approximately 1% of ischemic strokes in
young adults (Williams et al., 1997). This genetic disor-
der is due to mutations in the Notch 3 gene on chromo-
some 19 (Chabriat et al., 1999). It is characterized by
recurrent subcortical ischemic strokes, with involve-
ment of the anterior temporal poles and external cap-
sules characteristically seen on magnetic resonance
imaging (MRI). Patients with this disorder usually
develop mood disturbance and dementia, and approxi-
mately 60% of patients also have a history of migraine.
Vasculitis is a relatively uncommon cause of stroke,
accounting for between 1% and 6% of strokes in
young patients in most series (Bendixen et al., 2001),
and rare among the general stroke population (<1%).
The diagnosis may be suspected following angio-
graphic evidence of long segmental or focal regions
of arterial narrowing, accompanied by single or multi-
ple infarctions or hemorrhages with or without lepto-
meningeal enhancement on MRI. However, a brain or
leptomeningeal biopsy is usually required for defini-
tive diagnosis. Central nervous system vasculitis
can be primary, or may occur secondarily to systemic
collagen vascular diseases, non-central-nervous-system
vasculitis, infections or toxins (Carolei and Sacco,
2003).
17.3.2.3. Cardioembolism
A cardioembolic cause for ischemic stroke is found in
14–33% of young adults (Bogousslavsky and Regli,
1987; Adams et al., 1995; Cerrato et al., 2004; Varona
et al., 2007), similar to the general stroke population
(Grau et al., 2001). Higher rates have been reported in
Persian young adults (Ghandehari and Moud, 2006).
Although atrial fibrillation is commonly associated with
cardioembolic stroke in older patients, it is an uncom-
mon cause in young adults with stroke (1–3%). Instead,
causes of cardioembolic stroke in young adults more
often include aseptic and infective endocarditis (intra-
venous drug users and those with prosthetic heart valves
PS, YOUNG ADULTS, AND CHILDREN 343
amoya. Note the formation of extensive collateral vessels.

RM
are at high risk), left ventricular thrombus associated
with dilated cardiomyopathy or acute myocardial
infarction, and rarely atrial myxoma (Bendixen et al.,
2001; Cerrato et al., 2004). Another potential cause of
cardioembolic stroke is patent foramen ovale, which
appears to be a risk factor for ischemic stroke only in
those aged less than 55 years, not in older people (Over-
ell et al., 2000). Although patent foramen ovale is found
in approximately one-quarter of the normal population,
it is found at higher frequencies in people with crypto-
genic stroke. Whether a patent foramen ovale suspected
of causing a stroke should be closed is uncertain, as
there are no randomized clinical trials comparing medi-
cal therapy to surgical closure. In contrast to patent fora-
men ovale, evidence from recent studies suggests that
uncomplicated mitral valve prolapse is not a risk factor
for stroke (Orencia et al., 1995).
17.3.2.4. Prothrombotic states
Antiphospholipid antibodies (e.g., lupus anticoagulant,
anticardiolipin antibody) have been associated with
arterial thromboembolism and ischemic stroke (Asher-
son et al., 1989; Galli et al., 2003), accounting for a
small proportion (<1–8%) of stroke in young adults
(Bendixen et al., 2001; Cerrato et al., 2004). People with
sickle cell disease are also at high risk of ischemic
stroke, with 7–10% of people with this disease having
strokes before the age of 20 years (Adams, 1995). Those
with other hemoglobinopathies are at lesser risk of
stroke (Ohene-Frempong et al., 1998). Inherited throm-
bophilias, such as deficiencies in protein C, protein S,
antithrombin III, and factor V and II mutations, are risk
factors for venous thromboembolism but appear not to
be for stroke (Hankey et al., 2001).
17.3.2.5. Migraine
Migraine is a risk factor for ischemic stroke in young
adults aged less than 45 years with a relative risk of
2.36 (95%CI 1.92–2.90) (Etminan et al., 2005). The risk
of ischemic stroke associated with migraine is poten-
tiated among women, tripled among women who
smoke, and quadrupled among those taking the oral con-
traceptive pill. The triad of migraine, smoking, and oral
contraceptive pill use may increase the risk of ischemic
stroke 30-fold (Bousser, 2004; Etminan et al., 2005).
17.3.2.6. Drugs
Sympathomimetic agents in over-the-counter cold
remedies and herbal medications have been associated
with hemorrhagic stroke (Kernan et al., 2000). Illicit
drugs are a rare cause of stroke in older adults but may
cause up to 5% of stroke in people aged 15–44 years
(Sloan et al., 1998). Cocaine, amphetamines, heroin,
344 J.W. STU
and phencyclidine have been implicated. Potential
mechanisms of stroke include acute hypertension, vaso-
constriction, cerebral vasculitis, and cardiomyopathy.
Sympathomimetic drugs may also promote rupture of
aneurysms or arteriovenous malformations (Bendixen
et al., 2001).
17.3.3. Prognosis
17.3.3.1. Mortality
In most studies case fatality at 30 days post-stroke in
young adults (aged <45 years) is 10–23% (Jacobs
et al., 2002), similar to that in the general stroke popu-
lation (Thrift et al., 2000; Jacobs et al., 2002). Greater
30-day case fatality has been reported in South African
blacks (34%; Rosman, 1986), US blacks (33%; Jacobs
et al., 2002), and in hemorrhagic subtypes (intracerebral
hemorrhage 36%, subarachnoid hemorrhage 12%,
ischemic stroke 6%; Thrift et al., 2000; Jacobs et al.,
2002). Young stroke survivors remain at greatly
increased risk of death over the subsequent 10 years
compared to those of the same age and sex in the general
population, although estimates are imprecise because of
the small number of deaths occurring (OR 77.8; 95% CI
20.2–135.4; Hardie et al., 2003). Among those aged 15–
45 years with ischemic stroke, average annual mortality
rates are approximately 5% in the first year and 1% per
year thereafter (Marini et al., 1999; Leys et al., 2002;
Varona et al., 2004).
17.3.3.2. Stroke recurrence, myocardial infarction,
and seizures
The average annual rate of stroke recurrence for young
adults with ischemic stroke (1.4–3.6% in the first year
and 0.5–1.7% thereafter; Marini et al., 1999; Leys
et al., 2002; Varona et al., 2004) is lower than among
older people with stroke (12.5% at 1 year, average
of 3% per year thereafter; Hankey et al., 1998). Aver-
age annual rates of myocardial infarction are between
0.2% (Leys et al., 2002) and 1.7% (Marini et al.,
1999). An annual rate of vascular death, recurrent
stroke, or non-fatal myocardial infarction was reported
to be 2.6% over 6 years (Kappelle et al., 1994).
Post-stroke seizures occur in 6.6–10% of survivors
(Leys et al., 2002; Naess et al., 2002; Varona et al.,
2004).
17.3.3.3. Functional outcome
Of surviving young adults, more than 90% return to
independent living after stroke (Leys et al., 2002; Var-
ona et al., 2004), a much greater proportion than in the
general stroke population. However, only 42–58% were
employed at 6–12 years post-stroke (Kappelle et al.,
ET AL.

OU
1994; Naess et al., 2002; Varona et al., 2004),
one-quarter to one-half have depressive symptoms
(Kappelle et al., 1994; Varona et al., 2004), and the
majority report reduced quality of life (Kappelle et al.,
1994).
17.3.4. Summary
In summary, people aged less than 45 years with
stroke require special consideration. The frequencies
of underlying etiology differ from the older stroke
population and a greater breadth of investigation is
generally required (e.g., transesophageal echocardio-
graphy, angiography, antiphospholipid antibodies).
Young adults with stroke have fewer comorbidities
than older patients and have a better prognosis for
long-term survival and return to independence. None-
theless, the burden of stroke on young adults, their
families, and society is considerable, with approxi-
mately half never returning to employment and the
majority living with reduced quality of life.
17.4. Childhood stroke
Although considered a rare disorder by adult stan-
dards, childhood stroke (stroke in those aged <15years) is more common than brain tumors and is
among the top 10 causes of death in childhood, with
the highest mortality in the first 12 months of life
(Murphy, 2000). In comparison to adult stroke there
is limited understanding of the etiology, treatment,
and predictors of outcome of childhood stroke. Sys-
tematic coordinated care and research are only now
being initiated for these children.
17.4.1. Incidence
17.4.1.1. Arterial ischemic stroke
The incidence of stroke has increased over time, partly
because of better diagnosis due to increased awareness
and improved neuroimaging techniques (Lynch et al.,
2002). The best epidemiological data on childhood
stroke comes from the Canadian Pediatric Ischemic
Stroke Registry (CPISR; deVeber, 2000), showing an
incidence of arterial ischemic stroke of 2.7/100 000
population per year with a male to female ratio of
1.5:1. The stroke recurrence rate is as high as 20–40%
and recurrence is more likely with vasculopathies such
as sickle cell and Moyamoya disease. The age distribu-
tion of children with arterial ischemic stroke is skewed,
with approximately 25% occurring in infants less than 1
year of age (deVeber, 2000). Neonatal arterial ischemic
stroke (in infants<28 days of age) has an estimated inci-
dence of 1:4000 live births per year (Estan and Hope,
STROKE AMONG WOMEN, ETHNIC GR
1997) but a lower recurrence rate, estimated at 3–5%.
It is under-recognized, with seizures the most common
mode of presentation. Hemiparesis is rarely noted,
occurring in less than 25% of newborns with stroke
(deVeber, 2000).
17.4.1.2. Sinovenous thrombosis
In the CPISR sinovenous thrombosis was less common
than arterial ischemic stroke, with an incidence of
0.67/100 000 per year. The age distributionwas skewed,
with infants less than 1 year of age comprising 54% of
cases and neonates 43% of cases. Thrombosis more
often involved the superficial venous system and was
associated with venous infarction in 41% of cases. In
76% of cases signs and symptoms were non-specific,
including headache, altered consciousness, and papille-
dema. Seizures were reported in 58% of children (deVe-
ber et al., 2001). Neonatal sinovenous thrombosis has an
estimated incidence of 41/100 000 population per year
(deVeber, 1999) with seizures and lethargy the most fre-
quent presentation. Clot propagation can occur without
clinical signs of deterioration. Infarction has been
reported in 50% and intraventricular hemorrhage in
33% of cases (Wu et al., 2003).
17.4.1.3. Hemorrhagic stroke
Hemorrhagic stroke has an estimated incidence of 1.5–
2.9/100 000 population per year (Broderick et al.,
1993; Lynch et al., 2002). In a series of 63 children
the most common presenting symptoms were head-
ache or vomiting due to raised intracranial pressure
(59% of cases), followed by seizures (37%) and hemi-
paresis (16%) (Al-Jarallah et al., 2000). Arteriovenous
malformations and fistulae are the most commonly
identified cause of hemorrhagic stroke and are asso-
ciated with a 2–4% risk of re-bleeding per year (Fults
and Kelly, 1984). Other causes of hemorrhagic stroke
include hematological disorders, coagulopathies,
trauma, brain tumors, cavernomas, and, rarely, aneur-
ysms (Lynch et al., 2002).
17.4.2. Risk factors for arterial ischemic strokeand sinovenous thrombosis
Risk factors for childhood arterial ischemic stroke are
age-dependent and include arteriopathies, cardiac disor-
ders, congenital or acquired thrombophilia, local or sys-
temic infections, and rare genetic/metabolic disorders
(Table 17.3). The majority of childhood stroke occurs
in those with pre-existing medical conditions (Chabrier
et al., 2000; Kirkham et al., 2000), the type and fre-
quency of which differ between countries. In 22–26%
of children with arterial ischemic stroke no identifiable
PS, YOUNG ADULTS, AND CHILDREN 345
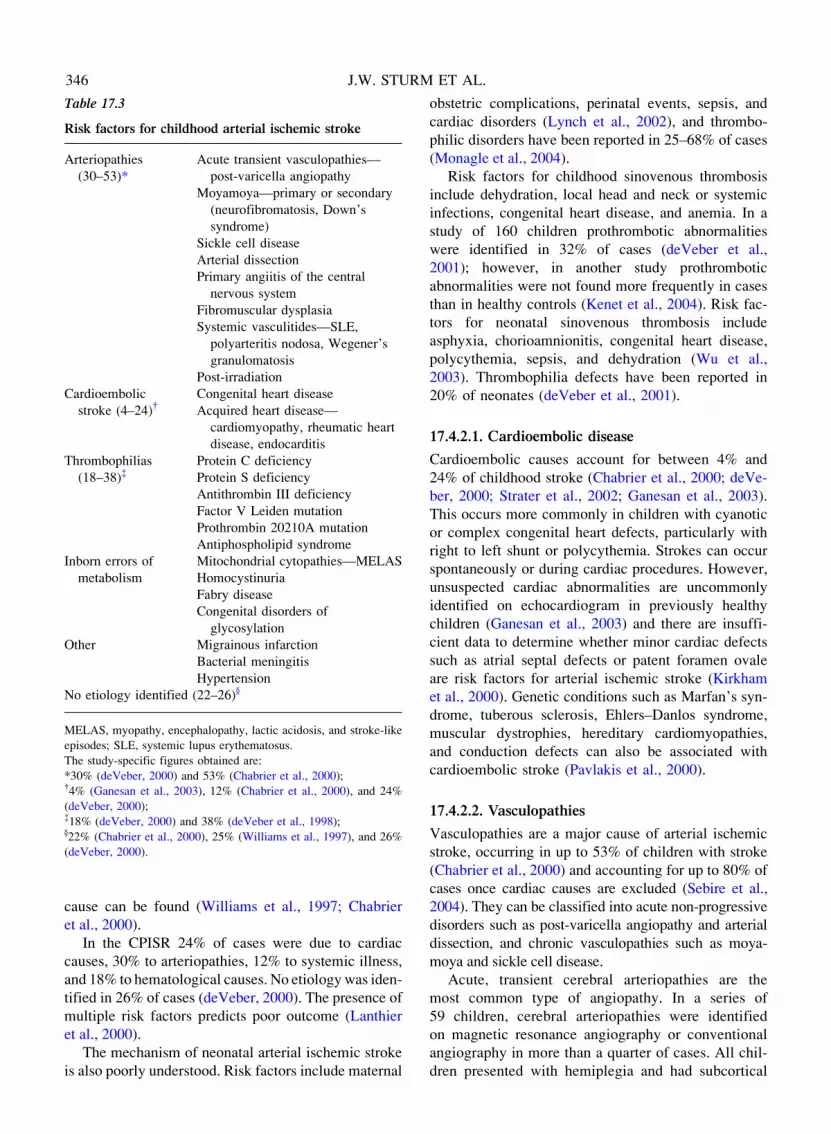
Table 17.3
Risk factors for childhood arterial ischemic stroke
Arteriopathies
(30–53)*
Acute transient vasculopathies—
post-varicella angiopathy
Moyamoya—primary or secondary
(neurofibromatosis, Down’s
syndrome)
Sickle cell disease
Arterial dissection
Primary angiitis of the central
nervous system
Fibromuscular dysplasia
Systemic vasculitides—SLE,
polyarteritis nodosa, Wegener’s
granulomatosis
Post-irradiation
Cardioembolic
stroke (4–24){Congenital heart disease
Acquired heart disease—
cardiomyopathy, rheumatic heart
disease, endocarditis
Thrombophilias
(18–38){Protein C deficiency
Protein S deficiency
Antithrombin III deficiency
Factor V Leiden mutation
Prothrombin 20210A mutation
Antiphospholipid syndrome
Inborn errors of
metabolism
Mitochondrial cytopathies—MELAS
Homocystinuria
Fabry disease
Congenital disorders of
glycosylation
Other Migrainous infarction
Bacterial meningitis
Hypertension
No etiology identified (22–26)}
MELAS, myopathy, encephalopathy, lactic acidosis, and stroke-like
episodes; SLE, systemic lupus erythematosus.
The study-specific figures obtained are:
*30% (deVeber, 2000) and 53% (Chabrier et al., 2000);{4% (Ganesan et al., 2003), 12% (Chabrier et al., 2000), and 24%
(deVeber, 2000);{18% (deVeber, 2000) and 38% (deVeber et al., 1998);}22% (Chabrier et al., 2000), 25% (Williams et al., 1997), and 26%
(deVeber, 2000).
346 J.W. STURM
cause can be found (Williams et al., 1997; Chabrier
et al., 2000).
In the CPISR 24% of cases were due to cardiac
causes, 30% to arteriopathies, 12% to systemic illness,
and 18% to hematological causes. No etiologywas iden-
tified in 26% of cases (deVeber, 2000). The presence of
multiple risk factors predicts poor outcome (Lanthier
et al., 2000).
The mechanism of neonatal arterial ischemic stroke
is also poorly understood. Risk factors include maternal
obstetric complications, perinatal events, sepsis, and
cardiac disorders (Lynch et al., 2002), and thrombo-
philic disorders have been reported in 25–68% of cases
(Monagle et al., 2004).
Risk factors for childhood sinovenous thrombosis
include dehydration, local head and neck or systemic
infections, congenital heart disease, and anemia. In a
study of 160 children prothrombotic abnormalities
were identified in 32% of cases (deVeber et al.,
2001); however, in another study prothrombotic
abnormalities were not found more frequently in cases
than in healthy controls (Kenet et al., 2004). Risk fac-
tors for neonatal sinovenous thrombosis include
asphyxia, chorioamnionitis, congenital heart disease,
polycythemia, sepsis, and dehydration (Wu et al.,
2003). Thrombophilia defects have been reported in
20% of neonates (deVeber et al., 2001).
17.4.2.1. Cardioembolic disease
Cardioembolic causes account for between 4% and
24% of childhood stroke (Chabrier et al., 2000; deVe-
ber, 2000; Strater et al., 2002; Ganesan et al., 2003).
This occurs more commonly in children with cyanotic
or complex congenital heart defects, particularly with
right to left shunt or polycythemia. Strokes can occur
spontaneously or during cardiac procedures. However,
unsuspected cardiac abnormalities are uncommonly
identified on echocardiogram in previously healthy
children (Ganesan et al., 2003) and there are insuffi-
cient data to determine whether minor cardiac defects
such as atrial septal defects or patent foramen ovale
are risk factors for arterial ischemic stroke (Kirkham
et al., 2000). Genetic conditions such as Marfan’s syn-
drome, tuberous sclerosis, Ehlers–Danlos syndrome,
muscular dystrophies, hereditary cardiomyopathies,
and conduction defects can also be associated with
cardioembolic stroke (Pavlakis et al., 2000).
17.4.2.2. Vasculopathies
Vasculopathies are a major cause of arterial ischemic
stroke, occurring in up to 53% of children with stroke
(Chabrier et al., 2000) and accounting for up to 80% of
cases once cardiac causes are excluded (Sebire et al.,
2004). They can be classified into acute non-progressive
disorders such as post-varicella angiopathy and arterial
dissection, and chronic vasculopathies such as moya-
moya and sickle cell disease.
Acute, transient cerebral arteriopathies are the
most common type of angiopathy. In a series of
59 children, cerebral arteriopathies were identified
on magnetic resonance angiography or conventional
angiography in more than a quarter of cases. All chil-
dren presented with hemiplegia and had subcortical
ET AL.

OU
stroke identified on neuroimaging (Chabrier et al.,
1998). Post-varicella angiopathy is the best described
form of this condition. A greater proportion of chil-
dren with a history of varicella in the previous 12
months had stroke when compared to control in a
French study (Sebire et al., 1999) and a causal rela-
tionship was subsequently confirmed in a prospective
Canadian cohort study (Askalan et al., 2001). Post-
varicella angiopathy typically causes focal or segmen-
tal stenosis of the distal internal carotid or proximal
segment of the middle cerebral artery resulting in
basal ganglia infarction (Askalan et al., 2001). Chil-
dren can have recurrent strokes up to 8 months fol-
lowing presentation but the arteriopathy takes a
monophasic course with subsequent regression of ste-
nosis within 2 years (Sebire et al., 1999; Lanthier
et al., 2005).
Moyamoya accounts for 7–20% of infarcts in chil-
dren and is most commonly seen in the Japanese popu-
lation (Chabrier et al., 2000). Angiography shows
progressive bilateral distal internal carotid artery ste-
nosis and occlusion with the development of a network
of collateral vessels forming the characteristic ‘puff of
smoke’ (Fig. 17.2). In children, Moyamoya is usually
associated with progressive motor and cognitive dete-
rioration, seizures, transient ischemic attacks, and
arterial ischemic stroke, in contrast to adults, where
hemorrhagic stroke is more common (Suzuki and
Kodama, 1983). Neurofibromatosis type 1, Down’s
syndrome, and tuberous sclerosis have also been asso-
ciated with Moyamoya disease.
Sickle cell disease is associated with distal internal
carotid or proximal middle cerebral artery stenosis.
Patients with sickle cell disease have a 10% untreated
risk per year of stroke (Adams et al., 1998) and at least
10% of homozygotes will have a stroke by 20 years of
age (Ohene-Frempong et al., 1998). Recurrent transi-
ent ischemic attacks and transcranial Doppler veloci-
ties above 200 cm/s are predictive of stroke (Adams
et al., 1997). These strokes can be prevented by regu-
lar transfusion to reduce sickle hemoglobin below
30% (Adams et al., 1998).
Arterial dissection accounts for 9–20% of cases of
arterial ischemic stroke. It more often involves the
intracranial and anterior circulations (Fullerton et al.,
2001).
Primary angiitis of the central nervous system has
been rarely described in children. This progressive
disorder has a high mortality rate. Children with
large- to medium-sized artery involvement and evi-
dence of granulomatous angiitis on biopsy have a
poorer outcome than those with small-vessel involve-
ment and a lymphocytic inflammatory infiltrate (Lan-
thier et al., 2001). Other rare causes of vasculopathy
STROKE AMONG WOMEN, ETHNIC GR
include postcranial irradiation arteriopathy and fibro-
muscular dysplasia.
17.4.2.3. Thrombophilias
The thrombophilias are congenital or acquired states that
increase the risk of thromboembolic disease. The most
common congenital thrombophilic defect in the general
population is caused by a mutation in clotting factor V
that makes it resistant to the inhibition of activated pro-
tein C (activated protein C resistance, factor V Leiden
mutation; Bertina et al., 1994). A mutation in the precur-
sor of thrombin (prothrombin gene mutation) is another
well established congenital thrombophilic defect (Poort
et al., 1996). The most common acquired thrombophilic
defect is development of antiphospholipid antibodies
(Ehrenforth et al., 1999; Greaves, 1999). They occur tran-
siently following tissue injury, infection, and drug expo-
sure or develop as part of a broader autoimmune
disease. Antiphospholipid antibodies are associated with
an increased risk of arterial and venous thromboembo-
lism as well as an increased risk of stroke in adults.
Recently, an increase in the frequency of thrombo-
philia in children with stroke has been reported (Angel-
ini et al., 1994; Ganesan et al., 1996; Becker et al., 1998;
Bonduel et al., 1999; Heller et al., 1999; Nowak-Gottl
et al., 1999a, b; Strater et al., 1999). Prothrombotic
abnormalities have been identified in 38% of children
with acute stroke (deVeber et al., 1998) and may indi-
cate increased risk of recurrence (Chabrier et al.,
1998). Others, however, have found no relationship
between prothrombotic abnormalities and stroke (Gane-
san et al., 1998; Zenz et al., 1998; McColl et al., 1999).
Many of these studies hadmethodological flaws, includ-
ing highly selected, non-prospective populations and a
lack of systematic thrombophilic work up on all
patients. Acquired protein S deficiency is known to
occur after varicella infection and may explain the
increased incidence of childhood stroke following
chicken pox infection (Humphries, 1995). Elevated
anticardiolipin antibodies do not seem to be associated
with childhood stroke (Lanthier et al., 2004). Impor-
tantly, no investigators have documented a relationship
between thrombophilia and severity, recurrence, or
neurological outcome of arterial ischemic stroke.
17.4.2.4. Other causes
Raremetabolic causes of arterial ischemic stroke include:
homocystinuria; mitochondrial disorders such as mito-
chondrial myopathy, encephalopathy, lactic acidosis,
and stroke-like episodes (MELAS); Fabry’s disease, an
X linked lysosomal disorder; congenital disorders of gly-
cosylation; urea cycle defects; and amino and organic
acidemias (Pavlakis et al., 2000).
PS, YOUNG ADULTS, AND CHILDREN 347
RM
17.4.3. Outcome following stroke
The outcome of childhood arterial ischemic stroke is
worse than for sinovenous thrombosis. The reported
mortality for arterial ischemic stroke ranges from 7%
to 28% (Lynch et al., 2002), with death being caused
either by the stroke or by the underlying disease. The
reported frequency of long-term neurological deficits
following childhood arterial ischemic stroke ranges
from 50% to 85%, with post-stroke epilepsy occurring
in 15–20% of survivors. Stroke recurs in approximately
19–40% of children with arterial ischemic stroke (deVe-
ber, 2000; Ganesan et al., 2000). Factors associated with
greater risk of recurrent stroke include recurrent tran-
sient ischemic attacks, Moyamoya disease, vasculitis,
5–10 methylenetetrahydrofolate reductase homozygos-
ity, elevated homocysteine, anticardiolipin antibodies,
systemic disease, and embolic stroke (Chabrier et al.,
2000; Lynch et al., 2002). In children with middle cere-
bral artery strokes there is correlation between an infarct
volume of more than 10% (Ganesan et al., 1999),
younger age at time of stroke (Ganesan et al., 2000),
and poor outcome.
A 10% mortality has been reported in neonatal arter-
ial ischemic stroke, and two-thirds have neurological
deficits (deVeber et al., 1995). Motor sequelae includ-
ing hemiplegia, dystonia, and spasticity occur less fre-
quently in neonates than in older children but are more
likely if there is concomitant involvement of the basal
ganglia, internal capsule, and cortex (Mercuri et al.,
1999). Recurrence risk is lower than in older children,
occurring in fewer than 5%.
The outcome of childhood sinovenous thrombosis,
although better than for arterial ischemic stroke, is
still guarded. In the CPISR there was 8% mortality,
with death being directly attributable to sinovenous
thrombosis in one-quarter of children. Some 38%
had neurological deficits, including motor impair-
ment, cranial nerve palsies, or delayed intellectual
development, and 15% had seizures. The presence
of venous infarct predicted a worse outcome (deVe-
ber et al., 2001). In a multicenter European study of
42 children there was 12% mortality and 62% had
neurological sequelae. Older age, absence of venous
infarction, anticoagulant therapy, and lateral and/or
venous sinus involvement were independent predic-
tors of good outcome (Sebire et al., 2005). By con-
trast 74% of neonates have no neurological sequelae
(deVeber et al., 2000).
There is scarce literature on the functional impact
of childhood stroke. In a study of 17 children with
unilateral middle cerebral artery territory stroke, 47%
had mild to moderate activity limitations affecting
motor function, self-care, and education. There were
348 J.W. STU
correlations between impairment of bodily functions
and activity limitation, and between the extent of brain
injury on neuroimaging and physical health (Gordon
et al., 2002).
Cognitive outcome following stroke has been exam-
ined in a few studies. In a Canadian series of 163 neo-
nates and children with arterial ischemic stroke and
sinovenous thrombosis, speech and cognitive deficits
were rare (deVeber et al., 2000); however, in a UK series
of 90 children, 59% had educational difficulties and
42% had speech and language deficits (Ganesan et al.,
2000). Higher cortical function impairments are also
common in children with congenital hemiplegia due to
presumed perinatal strokes, with 54% having speech,
behavior, or learning problems and 23% having seizures
(Golomb et al., 2001).
First-year costs of stroke for adult patients have been
estimated to be US$14 361 (Dewey et al., 2001). The
types and magnitude of health care costs generated by
childhood stroke have not been assessed but are likely
to be much greater than in adults because children sur-
viving stroke will have more years living with disabil-
ity. The psychological and social impact of childhood
stroke has not been estimated and warrants further
study.
ET AL.
17.4.4. Summary
Although considered rare, stroke is more common
than brain tumors in children. One-quarter of arterial
ischemic stroke and more than half of sinovenous
thrombosis cases occur in children less than 1 year of
age. Arteriopathies are the most commonly identified
risk factor for arterial ischemic stroke, followed by car-
diac and thromboembolic disorders. Neurological
sequelae are common in arterial ischemic stroke and
sinovenous thrombosis.
Prospective registries are necessary to increase
understanding of childhood stroke and to establish accu-
rate recurrence risks. Outcome studies using validated
measures are needed to determine the long-term impact
of stroke on children and their families, and to plan
interventional studies to improve the outcome of chil-
dren with stroke. Because of the relatively small number
of strokes that occur in children, multicenter collabora-
tion will be required to ensure that adequate cases are
accrued. Such a collaboration, termed the International
Pediatric Stroke Study, has been formed through a
consortium of pediatric neurologists and hematologists
who are currently enrolling patients in an international
childhood stroke registry. A multicenter randomized
controlled trial of aspirin versus Coumadin in the sec-
ondary prevention of childhood stroke is also planned
OUPS, YOUNG ADULTS, AND CHILDREN 349
to assess whether childhood stroke can be prevented
(International Pediatric Stroke Study: https://www.sick-
kids.on.ca/cstrokestudy).
References
Adams HPJ, Kapelle LJ, Biller J, et al. (1995). Ischaemic
stroke in young adults: experience in 329 patients enrolled
in the Iowa Registry of stroke in young adults. Arch Neu-
rol 52: 491–495.
Adams RJ (1995). Sickle cell disease and stroke. J Child
Neurol 10: 75–76.
Adams RJ, McKie VC, Carl EM, et al. (1997). Long-term
stroke risk in children with sickle cell disease screened
with transcranial Doppler. Ann Neurol 42: 699–704.
Adams RJ, McKie VC, Hsu L, et al. (1998). Prevention of a
first stroke by transfusions in children with sickle cell ane-
mia and abnormal results on transcranial Doppler ultraso-
nography. N Engl J Med 339: 5–11.
Al-Jarallah A, Al-Rifai MT, Riela AR, et al. (2000). Nontrau-
matic brain hemorrhage in children: etiology and presenta-
tion. J Child Neurol 15: 284–289.
Al Radjeh S, Awada A (2002). Stroke in Saudi Arabia. Cere-
brovasc Dis 13: 3–8.
Anderson CS, Jamrozik KD, Burvill PW, et al. (1993). Deter-
mining the incidence of different subtypes of stroke:
results from the Perth Community Stroke Study, 1989–
1990. Med J Aust 158: 85–89.
Anderson GL, Limacher M, Assaf AR, et al. (2004). Effects
of conjugated equine estrogen in postmenopausal women
with hysterectomy: the Women’s Health Initiative rando-
mized controlled trial. JAMA 291: 1701–1712.
Angelini L, Ravelli A, Caporali R, et al. (1994). Antipho-
spholipid antibodies in children with idiopathic cerebral
ischaemia. Lancet 344: 1232.
Asherson RA, Khamashta MA, Ordi-Ros J, et al. (1989). The
‘primary’ antiphospholipid syndrome: major clinical and
serological features. Medicine 68: 366–374.
Askalan R, Laughlin S, Mayank S, et al. (2001). Chickenpox
and stroke in childhood: a study of frequency and causa-
tion. Stroke 32: 1257–1262.
Bamford J, Sandercock P, Dennis M, et al. (1988). A pro-
spective study of acute cerebrovascular disease in the
community: the Oxfordshire Community Stroke Project
1981–86. I. Methodology, demography and incident cases
of first-ever stroke. J Neurol Neurosurg Psychiatry 51:
1373–1380.
Bamford J, Sandercock P, Dennis M, et al. (1990). A pro-
spective study of acute cerebrovascular disease in the
community: the Oxfordshire Community Stroke Project
1981–86. 2. Incidence, case fatality rates and overall out-
come at one year of cerebral infarction, primary intracere-
bral and subarachnoid haemorrhage. J Neurol Neurosurg
Psychiatry 53: 16–22.
Becker S, Heller C, Gropp F, et al. (1998). Thrombophilic
disorders in children with cerebral infarction. Lancet
352: 1756–1757.
Bendixen BH, Posner J, Lango R (2001). Stroke in young
adults and children. Curr Neurol Neurosci Rep 1: 54–66.
STROKE AMONG WOMEN, ETHNIC GR
Bertina RM, Koeleman BP, Koster T, et al. (1994). Mutation
in blood coagulation factor V associated with resistance to
activated protein C. Nature 369: 64–67.
Blecic S, Bogousslavsky J (1998). Stroke in young adults.
In: HJM Barnett, JP Mohr, BM Stein, et al. (Eds.), Stroke:
Pathophysiology, Diagnosis, and Management, 3rd edn.
Churchill Livingstone, Philadelphia, PA.
Bogousslavsky J, Pierre P (1992). Ischemic stroke in patients
under age 45. Neurol Clin 10: 113–124.
Bogousslavsky J, Regli F (1987). Ischemic stroke in adults
younger than 30 years of age. Arch Neurol 44: 479.
Bonduel M, Sciuccati G, Hepner M, et al. (1999). Prethrom-
botic disorders in children with arterial ischemic stroke
and sinovenous thrombosis. Arch Neurol 56: 967–971.
Bonita R, Broad JB, Beaglehole R (1993). Changes in stroke
incidence and case-fatality in Auckland, New Zealand,
1981–91. Lancet 342: 1470–1473.
Bousser MG (2004). Estrogens, migraine and stroke. Stroke
35: 2652–2656.
Broderick J, Talbot GT, Prenger E, et al. (1993). Stroke in chil-
dren within a major metropolitan area: the surprising impor-
tance of intracerebral hemorrhage. J Child Neurol 8:
250–255.
Brown DW, Dueker N, Jamieson DJ, et al. (2006). Pree-
clampsia and the risk of ischemic stroke among young
women: results from the Stroke Prevention in Young
Women Study. Stroke 37: 1055–1059.
Brown RD, Whisnant JP, Sicks JD, et al. (1996). Stroke inci-
dence, prevalence, and survival. Secular trends in Roche-
ster, Minnesota, through 1989. Stroke 27: 373–380.
Carolei A, Sacco S (2003). Central nervous system vasculitis.
Neurol Sci S8–S10.
Cerrato P, Grasso M, Imperiale D, et al. (2004). Stroke in
young patients: etiopathogenesis and risk factors in differ-
ent age classes. Cerebrovasc Dis 18: 154–159.
Chabriat H, Tournier-Lasserve E, Bousser MG (1999). Vascu-
lopathies. In: MJ Alberts (Ed.), Genetics of Cerebrovascu-
lar Disease. Futura, New York, pp. 195–208.
Chabrier S, Rodesch G, Lasjaunias P, et al. (1998). Transient
cerebral arteriopathy: a disorder recognized by serial angio-
grams in children with stroke. J Child Neurol 13: 27–32.
Chabrier S, Husson B, Lasjaunias P, et al. (2000). Stroke in
childhood: outcome and recurrence risk by mechanism in
59 patients. J Child Neurol 15: 290–294.
Collaborative Group for the Study of Stroke in YoungWomen
(1973). Oral contraception and increased risk of cerebral
ischemia or thrombosis. N Engl J Med 288: 871–878.
Collaborative Group for the Study of Stroke in Young
Women (1975). Oral contraceptives and stroke in young
women: associated risk factors. JAMA 231: 718–722.
Czlonkowska A, Ryglewicz D, Weissbein T, et al. (1994). A
prospective community-based study of stroke in Warsaw,
Poland. Stroke 25: 547–551.
D’Alessandro G, Di Giovanni M, Roveyaz L, et al. (1992).
Incidence and prognosis of stroke in the Valle d’Aosta,
Italy. Stroke 23: 1712–1715.
deVeber G (1999). Cerebrovascular diseases in children. In:
KF Swainman, S Ashwal (Eds.), Pediatric Neurology: Prin-
ciples and Practice. Mosby, St Louis, MO, pp. 1099–1124.
350 J.W. STURM ET AL.
deVeber G (2000). The Canadian Pediatric Ischemic Stroke
Study Group. Canadian pediatric ischaemic stroke study
registry: analysis of children with arterial ischaemic
stroke. Ann Neurol 48: 514.
deVeber G, Adams M, Andrew M (1995). The Canadian
Pediatric Ischaemic Stroke Study Group. Neonatal cere-
bral thromboembolism: clinical and radiographic features.
Thromb Haemostasis 77: 725.
deVeber G, Monagle P, Chan A, et al. (1998). Prothrombotic
disorders in infants and children with cerebral thromboem-
bolism. Arch Neurol 55: 1539–1543.
deVeber GA,MacGregor D, Curtis R, et al. (2000). Neurologic
outcome in survivors of childhood arterial ischemic stroke
and sinovenous thrombosis. J Child Neurol 15: 316–324.
deVeber G, AndrewM, Adams C, et al. (2001). Cerebral sino-
venous thrombosis in children. N Engl JMed 345: 417–423.
Dewey HM, Thrift AG, Mihalopoulos C, et al. (2001). Cost
of stroke in Australia from a societal perspective: results
from the North East Melbourne Stroke Incidence Study
(NEMESIS). Stroke 32: 2409–2416.
Ehrenforth S, Junker R, Koch HG, et al. (1999). Multicentre
evaluation of combined prothrombotic defects associated
with thrombophilia in childhood. Childhood Thrombophi-
lia Study Group. Eur J Pediatr 158: S97–S104.
Estan J, Hope P (1997). Unilateral neonatal cerebral infarc-
tion in full term infants. Arch Dis Child Fetal and Neona-
tal Ed 76: F88–F93.
Etminan M, Takkouche B, Isorna FC, et al. (2005). Risk of
ischaemic stroke in people with migraine: systematic
review and meta-analysis of observational studies. Br
Med J 330: 63.
Feigin VL, Wiebers DO, Nikitin YP, et al. (1995). Stroke
epidemiology in Novosibirsk, Russia: a population-based
study. Mayo Clin Proc 70: 847–852.
Fullerton HJ, Johnston SC, Smith WS (2001). Arterial dis-
section and stroke in children. Neurology 57: 1155–1160.
Fults D, Kelly DL Jr (1984). Natural history of arteriovenous
malformations of the brain: a clinical study. Neurosurgery
15: 658–662.
Galli M, Luciano D, Bertolini G, et al. (2003). Lupus anti-
coagulants are stronger risk factors for thrombosis than
anticardiolipin antibodies in the antiphospholipid syn-
drome: a systematic review of the literature. Blood 101:
1827–1832.
Ganesan V, Kelsey H, Cookson J, et al. (1996). Activated
protein C resistance in childhood stroke. Lancet 347: 260.
Ganesan V, McShane MA, Liesner R, et al. (1998). Inherited
prothrombotic states and ischaemic stroke in childhood.
J Neurol Neurosurg Psychiatry 65: 508–511.
Ganesan V, Ng V, Chong WK, et al. (1999). Lesion volume,
lesion location, and outcome after middle cerebral artery
territory stroke. Arch Dis Child 81: 295–300.
Ganesan V, Hogan A, Shack N, et al. (2000). Outcome after
ischaemic stroke in childhood. Dev Med Child Neurol 42:
455–461.
Ganesan V, Prengler M, McShane MA, et al. (2003). Investi-
gation of risk factors in children with arterial ischemic
stroke. Ann Neurol 53: 167–173.
Ghandehari K, Moud ZI (2006). Incidence and etiology of
ischemic stroke in Persian young adults. Acta Neurol
Scand 113: 121–124.
Giles WH, Kittner SJ, Hebel RJ, et al. (1995). Determinants
of black–white differences in the risk of cerebral infarc-
tion. Arch Intern Med 155: 1319–1324.
Gillum LA, Mamidipudi SK, Johnston SC (2000). Ischemic
stroke risk with oral contraceptives: a meta-analysis. JAMA
284: 72–78.
Gillum RF, Ingram DD, Makuc DM (1994). Relation
between serum albumin concentration and stroke inci-
dence and death: the NHANES I Epidemiologic Follow-
up Study. Am J Epidemiol 140: 876–888.
Giroud M, Milan C, Beuriat P, et al. (1991). Incidence and
survival rates during a two-year period of intracerebral
and subarachnoid haemorrhages, cortical infarcts, lacunes
and transient ischaemic attacks. The stroke registry of
Dijon: 1985–1989. Int J Epidemiol 20: 892–899.
Golomb MR, MacGregor DL, Domi T, et al. (2001). Pre-
sumed pre- or perinatal arterial ischemic stroke: risk fac-
tors and outcomes. Ann Neurol 50: 163–168.
Gordon AL, Ganesan V, Towell A, et al. (2002). Functional
outcome following stroke in children. J Child Neurol 17:
429–434.
Grau AJ, Weimar C, Buggle F, et al. (2001). Risk factors,
outcome, and treatment in subtypes of ischemic stroke.
The German Stroke Data Bank. Stroke 32: 2559–2566.
Greaves M (1999). Antiphospholipid antibodies and throm-
bosis. Lancet 354: 1031.
Guillon B, Levy C, Bousser MG (1998). Internal carotid
artery dissection: an update. J Neurol Sci 153: 146–158.
Hajat C, Tilling K, Stewart JA, et al. (2004). Ethnic differ-
ences in risk factors for ischemic stroke: a European
case-control study. Stroke 35: 1562–1567.
Hankey GJ, Jamrozik KD, Broadhurst RJ, et al. (1998).
Long-term risk of first recurrent stroke in the Perth Com-
munity Stroke Study. Stroke 29: 2491–2500.
Hankey GJ, Eikelboom JW, van Bockxmeer FM, et al.
(2001). Inherited thrombophilia in ischemic stroke and
its pathogenic subtypes. Stroke 32: 1793–1799.
Hannaford PC, Croft PR, Kay CR (1994). Oral contraception
and stroke. Evidence from the Royal College of General
Practitioners’ Oral Contraception Study. Stroke 25:
935–942.
Hardie K, Hankey GJ, Jamrozik K, et al. (2003). Ten-year
survival after first-ever stroke in the Perth Community
Stroke Study. Stroke 34: 1842–1846.
Heinemann LA, Lewis MA, Spitzer WO, et al. (1998).
Thromboembolic stroke in young women. A European
case-control study on oral contraceptives. Transnational
Research Group on Oral Contraceptives and the Health
of Young Women. Contraception 57: 29–37.
Heller C, Becker S, Scharrer I, et al. (1999). Prothrombotic
risk factors in childhood stroke and venous thrombosis.
Eur J Pediatr 158: S117–S121.
Hirvonen E, Idanpaan-Heikkila J (1990). Cardiovascular
death among women under 40 years of age using low-
estrogen oral contraceptives and intrauterine devices in
STROKE AMONG WOMEN, ETHNIC GROUPS, YOUNG ADULTS, AND CHILDREN 351
Finland from 1975 to 1984. Am J Obstet Gynecol 163:
281–284.
Humphries JE (1995). Thrombophilia and complex acquired
deficiencies of antithrombin, protein C, and protein S.
Semin Hematol 32: 8–16.
Jacobs BS, Boden-Albala B, Lin I-F, et al. (2002). Stroke in
the young in the Northern Manhattan Stroke Study. Stroke
33: 2789–2796.
Jeng JS, Tang SC, Yip PK (2004). Incidence and etiologies
of stroke during pregnancy and puerperium as evidenced
in Taiwanese women. Cerebrovasc Dis 18: 290–295.
Jick SS, Myers MW, Jick H (1999). Risk of idiopathic cere-
bral haemorrhage in women on oral contraceptives with
differing progestagen components. Lancet 354: 302–303.
J�rgensen HS, Plesner A-M, Hubbe P, et al. (1992). Marked
increase of stroke incidence in men between 1972 and
1990 in Frederiksberg, Denmark. Stroke 23: 1701–1704.
Kappelle LJ, Adams HPJ, Heffner ML, et al. (1994). Prog-
nosis of young adults with ischemic stroke: a long-term
follow-up study assessing recurrent vascular events and
functional outcome in the Iowa registry of stroke in young
adults. Stroke 25: 1360–1365.
Kemmeren JM, Tanis BC, van den Bosch MA, et al.
(2002). Risk of Arterial Thrombosis in Relation to Oral
Contraceptives (RATIO) study: oral contraceptives and
the risk of ischemic stroke. Stroke 33: 1202–1208.
Kenet G, Waldman D, Lubetsky A, et al. (2004). Paediatric
cerebral sinus vein thrombosis. A multi-center, case-
controlled study. Thromb Haemostasis 92: 713–718.
Kernan WN, Viscoli CM, Brass LM, et al. (2000). Phenylpro-
panolamine and the risk of haemorrhagic stroke. N Engl J
Med 343: 1826–1832.
Kirkham FJ, Prengler M, Hewes DK, et al. (2000). Risk fac-
tors for arterial ischemic stroke in children. J Child Neurol
15: 299–307.
Kissela B, Schneider A, Kleindorfer D, et al. (2004). Stroke
in a biracial population: the excess burden of stroke
among blacks. Stroke 35: 426–431.
Kittner SJ, White LR, Losonczy KG, et al. (1990). Black–
white differences in stroke incidence in a national sample:
the contribution of hypertension and diabetes mellitus.
JAMA 264: 1267–1270.
Kittner SJ, Stern BJ, Feeser BR, et al. (1996). Pregnancy and
the risk of stroke. N Engl J Med 335: 768–774.
Kleindorfer D, Panagos P, Pancioli A, et al. (2005). Incidence
and short-term prognosis of transient ischemic attack in a
population-based study. Stroke 36: 720–723.
Lanthier S, Carmant L, David M, et al. (2000). Stroke in
children: the coexistence of multiple risk factors predicts
poor outcome. Neurology 54: 371–378.
Lanthier S, Lortie A, Michaud J, et al. (2001). Isolated angii-
tis of the CNS in children. Neurology 56: 837–842.
Lanthier S, Kirkham FJ, Mitchell LG, et al. (2004). Increased
anticardiolipin antibody IgG titers do not predict recurrent
stroke or TIA in children. Neurology 62: 194–200.
Lanthier S, Armstrong D, Domi T, et al. (2005). Post-vari-
cella arteriopathy of childhood: natural history of vascular
stenosis. Neurology 64: 660–663.
Lee T-H, Hsu W-C, Chen C-J, et al. (2002). Etiologic study of
young ischemic stroke in Taiwan. Stroke 33: 1950–1955.
Leys D, Bandu L, Henon H, et al. (2002). Clinical outcome
in 287 consecutive young adults (15 to 45 years) with
ischemic stroke. Neurology 59: 26–33.
Lidegaard O (1999). Smoking and use of oral contraceptives:
impact on thrombotic diseases. Am J Obstet Gynecol 180:
S357–S363.
Lidegaard O, Kreiner S (2002). Contraceptives and cerebral
thrombosis: a five-year national case-control study. Con-
traception 65: 197–205.
Lorentz IT (1962). Parietal lesion and Enavid. Br Med J 2:
1191.
Lynch JK, Hirtz DG, DeVeber G, et al. (2002). Report of the
National Institute of Neurological Disorders and Stroke
workshop on perinatal and childhood stroke. Pediatrics
109: 116–123.
McColl MD, Chalmers EA, Thomas A, et al. (1999). Factor V
Leiden, prothrombin 20210G!A and the MTHFR C677T
mutations in childhood stroke. Thromb Haemost 81:
690–694.
McGruder HF, Malarcher AM, Antoine TL, et al. (2004).
Racial and ethnic disparities in cardiovascular risk factors
among stroke survivors: United States 1999 to 2001.
Stroke 35: 1557–1561.
Marini C, Totaro R, Carolei A for the National Research
Council Study Group on stroke in the young (1999).
Long-term prognosis of cerebral ischemia in young adults.
Stroke 30: 2320–2325.
Marini C, Totaro R, De Santis F, et al. (2001). Stroke in
young adults in the community-based L’Aquila registry.
Incidence and prognosis. Stroke 32: 52–56.
Mercuri E, Rutherford M, Cowan F, et al. (1999). Early
prognostic indicators of outcome in infants with neo-
natal cerebral infarction: a clinical, electroencephalogram,
and magnetic resonance imaging study. Pediatrics 103:
39–46.
Monagle P, Chan A, Massicotte P, et al. (2004). Antithrom-
botic therapy in children: the Seventh ACCP Conference
on Antithrombotic and Thrombolytic Therapy. Chest
126: 645S–687S.
Murphy SL (2000). Deaths: final data for 1998. Natl Vital
Stat Rep 48: 1–105.
Naess H, Nyland HI, Thomassen L, et al. (2002). Incidence
and short-term outcome of cerebral infarction in young
adults in Western Norway. Stroke 33: 2105–2108.
Nelson HD, Humphrey LL, Nygren P, et al. (2002). Postme-
nopausal hormone replacement therapy: scientific review.
JAMA 288: 872–881.
Nightingale AL, Farmer RD (2004). Ischemic stroke in young
women: a nested case-control study using the UK General
Practice Research Database. Stroke 35: 1574–1578.
Nowak-Gottl U, Junker R, Hartmeier M, et al. (1999a).
Increased lipoprotein(a) is an important risk factor for
venous thromboembolism in childhood. Circulation 100:
743–748.
Nowak-Gottl U, Strater R, Heinecke A, et al. (1999b). Lipo-
protein (a) and genetic polymorphisms of clotting factor

352 J.W. STURM ET AL.
V, prothrombin, and methylenetetrahydrofolate reductase
are risk factors of spontaneous ischemic stroke in child-
hood. Blood 94: 3678–3682.
Oehne-Frempong K, Weiner SJ, Sleeper LA, et al. (1998).
Cerebrovascular accidents in sickle cell disease: rates
and risk factors. Blood 91: 288–294.
Orencia A, Petty GW, Khandherica BK, et al. (1995). Risk
of stroke with mitral valve prolapse in a population-based
cohort study. Stroke 26: 7–13.
Overell JR, Bone I, Less KR (2000). Interatrial septal
abnormalities and stroke. A meta-analysis of case-control
studies. Neurology 55: 1172–1179.
Patel A, Norton R, MacMahon S (2002). The HRT furore:
getting the message right. Med J Aust 177: 345–346.
Pavlakis SG, Kingsley PB, Bialer MG (2000). Stroke in chil-
dren: genetic and metabolic issues. J Child Neurol 15:
308–315.
Petitti DB, Sidney S, Bernstein A, et al. (1996). Stroke in
users of low-dose oral contraceptives. N Engl J Med
335: 8–15.
Petty GW, Brown RD, Whisnant JP, et al. (1999). Ischemic
stroke subtypes. A population-based study of incidence
and risk factors. Stroke 30: 2513–2516.
Poort SR, Rosendaal FR, Reitsma PH, et al. (1996). A com-
mon genetic variation in the 30-untranslated region of the
prothrombin gene is associated with elevated plasma pro-
thrombin levels and an increase in venous thrombosis.
Blood 88: 3698–3703.
Poulter NR, Chang CL, Farley TM, et al. (1999). Effect on
stroke of different progestagens in low oestrogen dose oral
contraceptives. WHO Collaborative Study of Cardiovascu-
lar Disease and Steroid Hormone Contraception. Lancet
354: 301–302.
Qureshi AI, Safdar K, Patel M, et al. (1995). Stroke in young
black patients. Risk factors, subtypes, and prognosis.
Stroke 26: 1995–1998.
Radhakrishan K, Ashok PP, Sridharan R, et al. (1986). Stroke
in the young: incidence and pattern in Benghazi, Libya.
Acta Neurol Scand 73: 434–438.
Ricci S, Celani MG, La Rosa F, et al. (1991). SEPIVAC: a
community-based study of stroke incidence in Umbria,
Italy. J Neurol Neurosurg Psychiatry 54: 695–698.
Rosman KD (1986). The epidemiology of stroke in an urban
black population. Stroke 17: 667–669.
Ruiz-Sandoval JL, Cantu C, Barinagarrementeria F (1999).
Intracerebral hemorrhage in young people: analysis of risk
factors, location, causes and prognosis. Stroke 30: 537–541.
Sacco RL, Boden-Albala B, Gan R, et al. (1998). Stroke inci-
dence among white, black and Hispanic residents of an
urban community. The Northern Manhattan Stroke Study.
Am J Epidemiol 147: 259–268.
Saposnik G, Del Brutto OH for the IberoAmerican Society
of Cerebrovascular Diseases (2003). Stroke in South
America: a systematic review of incidence, prevalence,
and stroke subtypes. Stroke 34: 2103–2107.
Sartwell PE, Masi AT, Arthes FG, et al. (1969). Thromboem-
bolism and oral contraceptives: an epidemiological case-
control study. Am J Epidemiol 90: 365–380.
Schwartz SM, Siscovick DS, Longstreth WT Jr, et al.
(1997). Use of low-dose oral contraceptives and stroke in
young women. Ann Intern Med 127: 596–603.
Schwartz SM, Petitti DB, Siscovick DS, et al. (1998). Stroke
and use of low-dose oral contraceptives in young women:
a pooled analysis of two US studies. Stroke 29: 2277–2284.
Sebire G, Meyer L, Chabrier S (1999). Varicella as a risk
factor for cerebral infarction in childhood: a case-control
study. Ann Neurol 45: 679–680.
Sebire G, Fullerton H, Riou E, et al. (2004). Toward the defi-
nition of cerebral arteriopathies of childhood. Curr Opin
Pediatr 16: 617–622.
Sebire G, Tabarki B, Saunders DE, et al. (2005). Cerebral
venous sinus thrombosis in children: risk factors, presenta-
tion, diagnosis and outcome. Brain 128: 477–489.
Sharshar T, Lamy C, Mas JL (1995). Incidence and causes of
stroke associated with pregnancy and puerperium. Stroke
26: 930–936.
Simon JA, Hsia J, Cauley JA, et al. (2001). Postmenopausal
hormone therapy and risk of stroke: the Heart and Estro-
gen-progestin Replacement Study (HERS). Circulation
103: 638–642.
Sloan MA, Kittner SJ, Feeser BR, et al. (1998). Illicit drug-
associated ischemic stroke in the Baltimore–Washington
young stroke study. Neurology 50: 1688–1693.
Stewart JA, Dundas R, Howard RS, et al. (1999). Ethnic dif-
ferences in incidence of stroke: prospective study with
stroke register. BMJ 318: 967–971.
Strater R, Vielhaber H, Kassenbohmer R, et al. (1999).
Genetic risk factors of thrombophilia in ischaemic child-
hood stroke of cardiac origin. A prospective ESPED sur-
vey. Eur J Pediatr 158: S122–S125.
Strater R, Becker S, von Eckardstein A, et al. (2002). Pro-
spective assessment of risk factors for recurrent stroke
during childhood—a 5-year follow-up study. Lancet 360:
1540–1545.
Sudlow CLM, Warlow CP (1997). Comparable studies of the
incidence of stroke and its pathological types. Results
from an international collaboration. Stroke 28: 491–499.
Suzuki J, Kodama N (1983). Moyamoya disease—a review.
Stroke 14: 104–109.
Tanaka H, Ueda Y, Hayashi M, et al. (1982). Risk factors for
cerebral hemorrhage and cerebral infarction in a Japanese
rural community. Stroke 13: 62–73.
Thrift AG, McNeil JJ, Forbes A, et al. (1996). Risk factors
for cerebral haemorrhage in the era of well-controlled
hypertension. Stroke 27: 2020–2025.
Thrift AG, Dewey HM, Macdonell RAL, et al. (2000). Stroke
incidence on the east coast of Australia: the North East
Melbourne Stroke Incidence Study (NEMESIS). Stroke
31: 2087–2092.
Toffol GJ, Biller J, Adams HPJ (1987). Nontraumatic intra-
cerebral haemorrhage in young adults. Arch Neurol 44:
483.
Tuomilehto J, Sarti C, Narva EV, et al. (1992). The FINMO-
NICA Stroke Register. Community-based stroke registra-
tion and analysis of stroke incidence in Finland, 1983–
1985. Am J Epidemiol 135: 1259–1270.

STROKE AMONG WOMEN, ETHNIC GROUPS, YOUNG ADULTS, AND CHILDREN 353
Ueda K, Hasuo Y, Kiyohara Y, et al. (1988). Intracerebral
hemorrhage in a Japanese community, Hisayama: inci-
dence, changing pattern during long-term follow-up, and
related factors. Stroke 19: 48–52.
Varona JF, Bermejo F, Guerra JM, et al. (2004). Long-term
prognosis of ischemic stroke in young adults: study of
272 cases. J Neurol 251: 1507–1514.
Varona JF, Guerra JM, Bermejo F, et al. (2007). Causes of
ischemic stroke in young adults, and evolution of the etio-
logical diagnosis over the long term. Eur Neurol 57:
212–218.
Vessey P, Doll R (1969). Investigation of relation between
use of oral contraceptives and thromboembolic disease.
A further report. Br Med J 2: 651–657.
Viscoli CM, Brass LM, Kernan WN, et al. (2001). A clinical
trial of estrogen-replacement therapy after ischemic
stroke. N Engl J Med 345: 1243–1249.
Wassertheil-Smoller S, Hendrix SL, Limacher M, et al.
(2003). Effect of estrogen plus progestin on stroke in post-
menopausal women: the Women’s Health Initiative: a ran-
domized trial. JAMA 289: 2673–2684.
WHO Collaborative Study of Cardiovascular Disease and
Steroid Hormone Contraception (1996a). Haemorrhagic
stroke, overall stroke risk, and combined oral contracep-
tives: results of an international, multicentre, case-control
study. Lancet 348: 505–510.
WHO Collaborative Study of Cardiovascular Disease and Ster-
oid Hormone Contraception (1996b). Ischaemic stroke and
combined oral contraceptives: results of an international,
multicentre, case-control study. Lancet 348: 498–505.
Williams LS, Garg BP, Cohen M, et al. (1997). Subtypes of
ischemic stroke in children and young adults. Neurology
49: 1541–1545.
Wolf PA, D’Agostino RB, O’Neal A, et al. (1992). Secular
trends in stroke incidence and mortality. The Framingham
Study. Stroke 23: 1551–1555.
Wu YW, Miller SP, Chin K, et al. (2003). Multiple risk factors
in neonatal sinovenous thrombosis. Neurology 59: 438–440.
Yip P-K, Jeng J-S, Lee T-K, et al. (1997). Subtypes of
ischemic stroke. A hospital-based registry in Taiwan
(SCAN-IV). Stroke 28: 2507–2512.
Zenz W, Bodo Z, Plotho J, et al. (1998). Factor V Leiden and
prothrombin gene G 20210 A variant in children with
ischemic stroke. Thromb Haemostasis 80: 763–766.
Zhang LF, Yang J, Hong Z, et al. (2003). Proportion of dif-
ferent subtypes of stroke in China. Stroke 34: 2091–2096.