south australian health and medical research institute
TRANSCRIPT
South Australian Health and Medical Research Institute (SAHMRI) Submission to the South Australian Productivity Commission Health and Medical Research Inquiry
8 May 2020
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 2
TABLE OF CONTENTS
ACRONYMS & DEFINITIONS ...........................................................................................................................................5
EXECUTIVE SUMMARY ...................................................................................................................................................7
SUMMARY OF RECOMMENDATIONS ........................................................................................................................... 10
Investment ................................................................................................................................................................. 10 Strategy & Leadership ................................................................................................................................................ 10 Commercialisation & Collaboration ........................................................................................................................... 10 Funding and Infrastructure ........................................................................................................................................ 11 Local Health Networks (LHNs) .................................................................................................................................... 11 Universities ................................................................................................................................................................. 11 Data Access ................................................................................................................................................................ 12
BACKGROUND ............................................................................................................................................................. 13
WHY WAS SAHMRI ESTABLISHED? ........................................................................................................................................ 13 SAHMRI’S COLLABORATIVE MODEL ....................................................................................................................................... 14
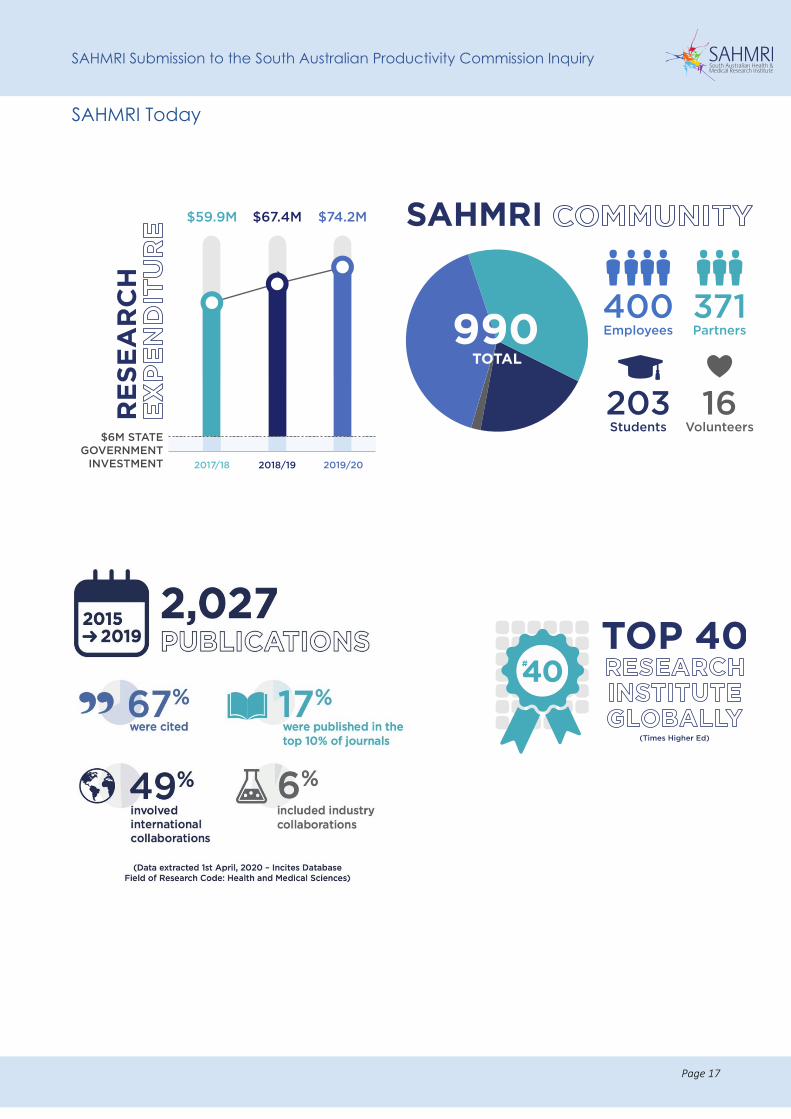
A Collaborative Governance Structure ....................................................................................................................... 16 SAHMRI TODAY................................................................................................................................................................. 17
SAHMRI’S VISION FOR THE FUTURE OF HEALTH AND MEDICAL RESEARCH IN SOUTH AUSTRALIA ............................... 18
STRENGTHENED INTERACTION BETWEEN SAHMRI AND THE SA HEALTH SYSTEM.............................................................................. 19 IMPORTANCE OF CONTINUED STATE GOVERNMENT SUPPORT FOR SAHMRI ................................................................................... 20
SAHMRI’S RESPONSE TO THE SAPC INQUIRY ............................................................................................................... 22
PERFORMANCE OF HMR AND DEVELOPMENT IN SOUTH AUSTRALIA .......................................................................... 22
AN INDEPENDENT REVIEW OF SAHMRI’S IMPACT ..................................................................................................................... 22 PERFORMANCE OF SAHMRI ................................................................................................................................................. 23
SAHMRI’s share of national grant funding and publication output ........................................................................... 23 SAHMRI’s publication output – comparison with our peers ....................................................................................... 25 Improving health outcomes through innovative translational research .............................................................. 28 Economic benefits and cost savings to the health system ......................................................................................... 29 Staff development at SAHMRI .................................................................................................................................... 29 NHMRC Fellowships as an employment strategy at SAHMRI .................................................................................... 30
THE POLICY ENVIRONMENT AND ITS IMPACT ON HMR IN SOUTH AUSTRALIA ................................................................................... 31 Research Priority Setting ............................................................................................................................................ 31 Research Ethics and Governance Processes ............................................................................................................... 31
KEY FACTORS INFLUENCING LEVEL OF PUBLIC AND PRIVATE SECTOR HEALTH AND MEDICAL RESEARCH OUTPUT ...... 33
SAHMRI’S COMMUNITY ...................................................................................................................................................... 33 Our leaders recognised by the Australian Academy of Health and Medical Sciences ................................................ 34 SAHMRI Faculty Appointments .................................................................................................................................. 34 Clinician Researchers .................................................................................................................................................. 36 Students at SAHMRI ................................................................................................................................................... 36 Aboriginal health research workforce at SAHMRI ...................................................................................................... 37 Gender diversity at SAHMRI ....................................................................................................................................... 37
CAPACITY TO RECRUIT TALENTED STAFF .................................................................................................................................... 38 Recruiting talented clinician researchers to South Australia ..................................................................................... 39
ACCESS TO DATA: REGULATION AND EFFICIENCY ...................................................................................................................... 41 Registries at SAHMRI .................................................................................................................................................. 42
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 3
SA/NT DataLink .......................................................................................................................................................... 42 Artificial Intelligence and Machine Learning .............................................................................................................. 42
CONNECTIVITY OF THE ADELAIDE BIOMED CITY AND THE PLANNED FLINDERS PRECINCT ............................................................... 44 RESEARCH INFRASTRUCTURE AT SAHMRI ................................................................................................................................ 44
COLLABORATIVE MODELS TO DRIVE HMR AND DEVELOPMENT .................................................................................. 46
SAHMRI COLLABORATIVE RESEARCH PROJECTS ......................................................................................................................... 46 Industry and International Collaborations ................................................................................................................. 48
COLLABORATION – HEALTH OUTCOMES DRIVEN ......................................................................................................................... 49 Collaborative approaches to co-location of researchers ............................................................................................ 49 Collaboration with the Universities ............................................................................................................................ 50 Collaboration with Non-Government agencies: an example of cross-sector collaboration ....................................... 50
OPPORTUNITIES FOR INCREASED COMMERCIALISATION OF HEALTH AND MEDICAL RESEARCH ................................. 52
SAHMRI HAS ADOPTED A UNIQUE APPROACH TO COMMERCIALISATION ........................................................................................ 52 SAHMRI Ventures ....................................................................................................................................................... 53 Medical Research Commercialisation Fund (MRCF) ................................................................................................... 53 Barriers to commercialisation .................................................................................................................................... 53 Intellectual property (IP) policy .................................................................................................................................. 54
PRODUCTIVITY MEASURES AND IMPACT OF RESEARCH ACTIVITY ............................................................................... 55
NHMRC FUNDING TO SOUTH AUSTRALIA ............................................................................................................................... 55 SAHMRI FUNDING SUCCESS ................................................................................................................................................. 57
NHMRC success at SAHMRI ........................................................................................................................................ 57 Limitations of NHMRC funding metrics ...................................................................................................................... 58 The Medical Research Future Fund (MRFF): a new mechanism to support medical research ................................... 59 Australian Research Council Funding ......................................................................................................................... 60 National Collaborative Research Infrastructure Strategy (NCRIS) ............................................................................. 61 State Government Funding to SAHMRI ...................................................................................................................... 61
THE COST OF TURNING MEDICAL RESEARCH INTO IMPACT ............................................................................................................. 63 THE STATE OF PLAY ACROSS AUSTRALIA: A COMPARATIVE OVERVIEW ............................................................................................. 64
CHARACTERISTICS OF SOUTH AUSTRALIA AND ITS POPULATION AND AREAS OF COMPETITIVE ADVANTAGE ............. 66
AREAS OF COMPETITIVE ADVANTAGE AT SAHMRI ..................................................................................................................... 66 COMPETITIVE ADVANTAGE – CLINICAL RESEARCH ...................................................................................................................... 67 OPPORTUNITY FOR CLINICAL TRIALS IN SOUTH AUSTRALIA ........................................................................................................... 69 COMPETITIVE ADVANTAGE – COLLABORATION AND PRECINCTS ..................................................................................................... 70
APPENDICES ................................................................................................................................................................ 73
APPENDIX I: SHINE YOUNG OBJECTIVES APPENDIX II: SAHMRI STRUCTURE AND THEMES APPENDIX III: RESEARCH ADVISORY COMMITTEE APPENDIX IV: FINAL REPORT, DANDOLO PARTNERS (APRIL 2020) APPENDIX V: RESEARCH IMPACT STORIES APPENDIX VI: LEADERSHIP STATEMENTS APPENDIX VII: SAHMRI INFRASTRUCTURE APPENDIX VIII: UNIVERSITY RENT SUBSIDIES APPENDIX IX: CARDIOLOGY CLINICAL TRIALS, EXAMPLES
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 4
List of Figures and Tables
FIGURE 1: SAHMRI’S STRUCTURE AND THEMES ............................................................................................................................ 15 FIGURE 2: SCHEMATIC DIAGRAM OF SAHMRI’S POSITION IN THE SOUTH AUSTRALIAN HEALTH AND MEDICAL RESEARCH LANDSCAPE ............. 18 FIGURE 3: INCREASING TREND IN SAHMRI REVENUE STREAMS, 2017-2019...................................................................................... 24 FIGURE 4: SAHMRI SHARE OF NHMRC FUNDING AWARDED STEADILY INCREASES, 2016 – 2019 ................................................... 24 FIGURE 5: SAHMRI RECEIVES THE MAJORITY OF NHMRC ABORIGINAL AND TORRES STRAIT ISLANDER HEALTH FUNDING COMPARED TO THE
REST OF SOUTH AUSTRALIA (2013-2019) ........................................................................................................................... 25 FIGURE 6: SOUTH AUSTRALIAN PUBLICATION OUTPUT, 2005-2019 .............................................................................................. 25 FIGURE 7: IMPROVED CITATION IMPACT WHEN PUBLISHING WITH SAHMRI (2012-2019) AS MEASURED BY A) CATEGORY NORMALISED
CITATION IMPACT AND B) PERCENTAGE OF DOCUMENTS IN TOP 10% ........................................................................................ 26 FIGURE 8: SAHMRI PUBLICATION OUTPUTS (2012-2019) COMPARE FAVOURABLY TO OTHER COMPARATIVE, INDEPENDENT MRIS AS
MEASURED BY A) CATEGORY NORMALISED CITATION IMPACT AND B) PERCENTAGE OF DOCUMENTS IN TOP 10% ................................ 27 FIGURE 9: INCREASING PROPORTION OF NHMRC FELLOWSHIP FUNDING AWARDED TO SAHMRI, 2016-2018. ...................................... 30 FIGURE 10: BREAKDOWN OF FACULTY APPOINTMENTS ................................................................................................................... 35 FIGURE 11: ABORIGINAL AND TORRES STRAIT ISLANDER WORKFORCE ACROSS ALL SAHMRI THEMES (AS AT APRIL 2020) .......................... 37 FIGURE 12: A STRONG FEMALE WORKFORCE ACROSS CAREER LEVELS AT SAHRMI (2010 – 2019) ......................................................... 37 FIGURE 13: SAHMRI’S WORKFORCE (AS AT MARCH 2020) BALANCE OF YOUNGER RESEARCHERS TO ALLOW SCIENTIFIC SUCCESSION ............ 38 FIGURE 14: SAHMRI COLLABORATIONS WITHIN THE PAST FIVE YEARS ............................................................................................... 47 FIGURE 15: SAHMRI IS A LEADER AMONG INDEPENDENT HMRIS IN TERMS OF A) INDUSTRY AND B) INTERNATIONAL COLLABORATIONS, 2012-
2019 ........................................................................................................................................................................... 48 FIGURE 16: NHMRC FUNDING TO SOUTH AUSTRALIA OVER THE 2012 – 2019 PERIOD ....................................................................... 56 FIGURE 17: ANNUAL NHMRC EXPENDITURE TO SOUTH AUSTRALIA RELATIVE TO POPULATION AND SDP ................................................. 56 FIGURE 18: INCREASING PERCENTAGE OF SOUTH AUSTRALIAN NHMRC FUNDING AWARDED TO SAHMRI, 2016 – 2019 ....................... 57 FIGURE 19: SAHMRI RECEIVES THE MAJORITY OF NHMRC ABORIGINAL AND TORRES STRAIT ISLANDER HEALTH FUNDING COMPARED TO THE
REST OF SOUTH AUSTRALIA (2013-2019) ........................................................................................................................... 58 FIGURE 20: SA GOVERNMENT CONTRIBUTION TO SAHMRI 2010-2018. ......................................................................................... 63
TABLE 1: AAHMS STATE MEMBERS – SAHMRI REPRESENTATION .................................................................................................. 34 TABLE 2: FACULTY APPOINTMENTS BY INSTITUTION AND LEVEL......................................................................................................... 35 TABLE 3: MRFF FUNDING SUCCESS IN SOUTH AUSTRALIA ............................................................................................................... 59 TABLE 4: EXAMPLES OF DIVERSITY OF FUNDING SOURCES.: ............................................................................................................... 62 TABLE 5: INCOME FOR INDIRECT COSTS AT ONLY INDEPENDENT HMRIS ............................................................................................. 64
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 5
ACRONYMS & DEFINITIONS
AAHMS Australian Academy of Health and Medical Sciences
AAMRI Association of Australian Medical Research Institutes
AAS Australian Academy of Science
ABMC Adelaide BioMed City
AHMS University of Adelaide, Health and Medical Sciences
AHRTC Advanced Health and Research Translation Centre
AIML Australian Institute for Machine Learning
ALL Acute Lymphoblastic Leukaemia
ANZDATA Australia New Zealand Dialysis and Transplant Registry
AOA Australian Orthopaedic Association
ARC Australian Research Council
ARWU Academic Ranking of World Universities
BCP Beat Cancer Project
CALHN Central Adelaide Local Health Network
CEIH Commission on Excellence and Innovation in Health
CML Chronic Myeloid Leukaemia
CRIC Clinical Research and Imaging Centre
DBS Dried Blood Spot
EMBL European Molecular Biology Laboratory
ERA Excellence in Research Australia
HARC Health Analytics Research Collaborative
HERDC Higher Education Research Data Collection
HREC Human Research Ethics Committee
HMR Health and Medical Research
HMRI Health and Medical Research Institute
HTSA Health Translation SA
IP Intellectual Property
LHN Local Health Network
MHH Microbiome and Host Health
MITRU Molecular Imaging Therapy Research Unit
MRCF Medical Research Commercialisation Fund
MRFF Medical Research Future Fund
NCRIS National Collaborative Research Infrastructure Strategy
NHMRC National Health and Medical Research Council
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 6
PIRL Preclinical Imaging Research Laboratories
RAC Research Advisory Committee
RAH Royal Adelaide Hospital
ROSA Registry of Senior Australians
REC Research Executive Committee
SACCR South Australian Clinical Cancer Registry (SACCR) – Central Coordination Unit
SAHMRI South Australian Health & Medical Research Institute
SALHN Southern Adelaide Local Health Network
SAPC South Australian Productivity Commission
SDP State Domestic Product
WCH Women’s and Children’s Hospital
WCHN Women’s and Children’s Health Network
Definitions
Clinical researcher: Clinical researchers find new and better ways to detect, diagnose, treat, and prevent disease. Clinician researcher: A medical health care professional who works with patients and carries out research projects. Clinician researchers are defined as those researchers with a concurrent clinical role/duties and appointment in the clinical setting. Allied health clinician researcher: A non-medical health care professional (e.g. dieticians,) who work with patients and carries out research projects. LHN: Includes all State Government hospitals and health services
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 7
EXECUTIVE SUMMARY Constituted in 2009, SAHMRI opened its state-of-the-art flagship research facility on North Terrace in December 2013. In SAHMRI’s short history, we have contributed enormously to increasing South Australia’s health and medical research capacity.
SAHMRI is the only independent Health and Medical Research Institute in South Australia. Building on the collaborative networks and infrastructure platforms we have already established, SAHMRI is at the centre of health and medical research and translational activities in the State, and is perfectly placed to be the interface between the health system and medical research for the state. SAHMRI will continue to make its mark by accelerating the delivery of high-impact translational research needed for effective and efficient health care delivery in the State, and should lead a strategic forum to set a comprehensive health and medical research direction for the State.
SAHMRI’s model is fundamentally about collaboration. It is in our DNA and is evidenced by, amongst other things:
• Significant national and international research collaborations on important issues to the state.
• Co-location of researchers from multiple disciplines and institutions.
• Governance which is inclusive of University and State Government members, and
• Collaborative arrangements for grant administration across Universities and for publication affiliations.
SAHMRI’s impact has already been significant. We have established a coordinated approach and clear focal point to increase South Australia’s health and medical research capacity, which is consistent with the objectives set out by the Shine Young Review in 2008 (See Appendix I: Shine Young Objectives).
At SAHMRI, research excellence is a key strategic objective. We have:
• Evolved into a highly renowned, internationally recognised independent health and medical research institute, recently placed in the top 40 institutes in the World by the Times Higher Education World Rankings (2018).
• Contributed significantly to the State’s research income evidenced by bringing in approximately $30 million annually in research grant funding (not including commercial research funding).
• Received more than 55% of the MRFF funding awarded to South Australian researchers to date (April 2020).
• Published a total of 62 papers in the highest impact journals (NEJM, JAMA, Lancet, Nature, Science, Cell) in the three years from 2016 to 2018 (inclusive), the majority (about 60%) of which were clinical research papers.
• Recruited exceptional external leaders who brought in significant research funds to the State (for example Prof Stephen Nicholls (now Director Monash Heart Health) and Prof Alex Brown, who collectively brought in more than $100 million in collaborative research funding).
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 8
Other noteworthy achievements include:
• SAHMRI researchers are overrepresented amongst the members of the prestigious Australian Academy of Health and Medical Sciences (AAHMS). Of the 41 South Australians who have been recognised as Fellows of the AAHMS, eighteen (44%) are affiliated with SAHMRI, either as direct employees or as SAHMRI Faculty appointments.
• SAHMRI has led the establishment of the SAHMRI 2 project, which will include Australia’s first Proton Therapy Unit. To date, the project has secured $70 million in Federal funds and $370 million private investment and will generate 1000 jobs and an estimated $1 billion in economic activity to the State.
• SAHMRI has built research infrastructure that is accessible to local and national researchers, enhancing State research capacity, including:
• A genomics suite with state-of-the-art sequencing equipment valued at $2 million.
• SAHMRI proteomics, metabolomics and MS-Imaging core facility, with over $4 million of equipment with funding from the Australian Cancer Research Foundation and Ian Potter Foundation.
• A sophisticated flow-cytometry facility, funded by Australian Cancer Research Foundation and the Zero Childhood Cancer initiative together with a philanthropic contribution from the Detmold Group with equipment valued at over $5 million.
• The only full-service biospecimen repository in SA, valued at $600,000.
• Secured funding through Bioplatforms Australia and research partners representing a $7 million investment.
• A SPF and germ-free animal house services, valued at about $10 million, and
• Clinical Research Imaging Centre (CRIC) – a partnership with Jones and Partners with imaging equipment valued at approximately $16 million.
• Since taking over the facility at Gilles Plains, SAHMRI has transformed the Preclinical Imaging Research Laboratories (PIRL) as a nationally-accredited imaging service for researchers state-wide for accessing large animal imaging facilities and other essential preclinical services.
• Through the establishment of Molecular Imaging Therapeutic Research Unit (MITRU, including $15 million cyclotron facility), SAHMRI supplies a growing market for radio-isotopes locally and interstate for cancer diagnostics and research.
• Created a ‘home’ for some of Australia’s national medical registries, which includes:
• The Australian Orthopaedic Association (AOA, Joint Replacement Registry);
• The Australia and New Zealand Dialysis and Transplant registry (ANZDATA);
• The newly established but highly successful Registry of Senior Australians (ROSA, founded by SAHMRI and funded by the Premier’s Research and Infrastructure Fund) that has also received more than $6 million research funding since being established in 2018.
• Consolidated and coordinated clinical trial capacity and a Clinical Trials Platform that supports global clinical trials delivery in South Australia and has generated more than $89 million in clinical research funding since 2010.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 9
• Facilitated data access for our researchers to critical SA Health datasets required for clinical trials through the implementation of the OACIS Access Deed.
• Built the Aboriginal Health Equity Theme, establishing the largest team of Aboriginal or Torres Strait Islander researchers in Australia. Across SAHMRI, 8% of all staff identify as Aboriginal or Torres Strait Islander.
- Over the past seven years, SAHMRI as a lead or partner, has received 90% of all NHMRC funding to South Australia for Aboriginal and Torres Strait Islander Health research (2013-2019).
• Established the Health Policy Centre which has been instrumental in providing evidence-based advice to the SA Chief Medical Officer overseeing the COVID-19 pandemic.
• Created an Artificial Intelligence (AI) platform that has enabled strong collaborations with University of Adelaide’s Lot Fourteen1, which will allow future joint funding opportunities.
• Led and facilitated the establishment of Health Translation SA, an NHMRC-accredited Advanced Health Research and Translation Centre, with the secretariat functions currently administered and housed at SAHMRI.
• Supported the establishment of Adelaide BioMed City, a partnership between RAH, the three main South Australian based Universities and SAHMRI, with the secretariat currently administered and housed at SAHMRI.
• Increased commercialisation and entrepreneurship of ideas and innovation into business, with 32% of our total revenue being derived from commercial income.
• Publication of first Framework for Consumer and Community Engagement in Research in Australia and creation of the first state-wide consumer registry, to advance quality consumer engagement in research across the State.
Our response and series of recommendations to the South Australian Productivity Commission (SAPC) Inquiry into Health and Medical Research in South Australia highlights the important position of SAHMRI within the State’s health and medical research ecosystem. It provides clear direction for the SAPC’s consideration of the South Australian health and medical research landscape, aligned to their terms of reference.
We are delighted to provide you with our submission and welcome the opportunity to discuss at any time.
Professor Steve Wesselingh
Executive Director
1 https://www.adelaide.edu.au/aiml/news/tag/lot-fourteen
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 10
SUMMARY OF RECOMMENDATIONS SAHMRI’s position at the centre of health and medical research in South Australia should be consolidated and enhanced through:
Investment
R1: The State Government operating grant to SAHMRI should be increased to a base amount of $10 million per annum (commencing in 2021). The annual operating grant should be:
• Increased annually in accordance with CPI; and
• As a further incentive for SAHMRI to contribute to the State's total economic activity (Gross StateProduct), increased in line with our contribution.
Strategy & Leadership
R2: SAHMRI, in collaboration with the Universities, LHNs and Health Translation SA, should convene a strategic forum and take a leadership role in the preparation of the following state-wide strategies:
• Comprehensive health and medical research strategy – based on strengths of the State as well ascommunity need, with the objective being to promote collaboration, increase competitiveness andidentify and recommend optimum resourcing and implementation plans.
• Impact Framework to measure the success of health and medical research across the State overthe next 10 years.
• Recruitment and retention strategy for high performing researchers – actively targeting clinicianresearchers, as well as identifying, attracting and developing the next generation of researchleaders; identifying and recommending recruitment packages that are competitive with otherjurisdictions.
• MRFF grant success strategy – targeted at supporting researchers through the provision ofmatched funding/Government support; building the capacity of clinician researchers with an aim toincrease the number of successful funding outcomes; increased political lobbying to attract non-competitive funding.
• Coordinated provision of research support and preclinical services on a State-wide basis – to avoidduplication and maximise scarce resources, including a long-term strategy for the services currentlyprovided at PIRL Gilles Plains.
R3: SAHMRI, in collaboration with the State Government, should take a leadership role in development of a Clinical research strategy – building on the work already being undertaken by the Department of Health and Wellbeing under the leadership of the Chief Scientist.
R4: The State Government should take a leadership role in implementing the recommendations of the Birch report.
Commercialisation & Collaboration
R5: Financial support to kick start the establishment of a new Venture Capital fund, aimed specifically at addressing the early “valleys of death” in research commercialisation.
R6: Disruptive model of IP identification and commercialisation adopted by SAHMRI in partnership with Bright Arena over the past two years should be supported and endorsed.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 11
R7: To enhance IP commercialisation capabilities, the staff and activities of AusHealth2 (formerly MedVet) should be merged into SAHMRI.
R8: AusHealth could fulfil a coordination role regarding IP management once merged into SAHMRI.
R9: Acknowledging that collaborative links between SAHMRI and the South Australian based Universities are already strong and multi-facetted, research linkages between SAHMRI and each of the LHN’s should be actively pursued. With the support and encouragement of the State Government, this would position SAHMRI to assist the Government in the provision of research-led health care.
Funding and Infrastructure
R10: Additional investment in health and medical research at a State Government level is critical to enhance the national competitiveness of South Australian researchers. The following funding schemes are suggested:
• Co-investment in Stage 2 MRFF Frontiers applications; matched funding for other MRFFapplications, when appropriate.
• Fellowships aimed at supporting and attracting our brightest minds, undertaking research in areasof specific interest and significance to the State.
• Consideration should be given as to whether the funds currently being administered by the HealthServices Charitable Gifts Board could be leveraged as a catalyst to scale up health and medicalresearch in the State.
Local Health Networks (LHNs)
R11: The LHNs, with the endorsement and support of the State Government, should embed health and medical research within their operations, with the aim of seamlessly integrating research into their core business in a manner that is complementary to clinical care, including by:
• Creating research-related KPIs for Chief Executive Officers. Research should be viewed as a valuablepart of core business.
• Encouraging greater profile of the Research Director and Research Office at each LHN, withinteraction of these functions with equivalent staff across the sector.
• Re-imagine incentives for research success within the LHN’s, including access to promotionalopportunities and infrastructure funds that are linked to research grants, as well as rewards forresearch that is successful commercially.
Universities
R12: The merger of University of SA and University of Adelaide should be actively considered, given the synergies between the two institutions, the potential economies of scale and the significant state-wide advantages that could ensue.
2 https://www.aushealth.com.au/
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 12
Data Access
R13: The SAHMRI/CALHN Research Affiliate Status arrangement (to allow researchers access to data for ethically approved projects) should be adopted by other LHNs.
R14: Infrastructure is required to support the capture of clinical trials in South Australia, through a centralised database.
R15: The Government should seek to support initiatives such as the HTSA Health Analytics Research Collaboration (HARC) in order to build analytical expertise across the sector.
R16: The “AI in Health” platform should be expanded dramatically across the State, with a significant node in ABMC.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 13
BACKGROUND
Why was SAHMRI established? In 2008, the SA Government, led by Minister for Health the Honourable John Hill, commissioned Professor John Shine and Mr Alan Young to undertake a review of health and medical research in South Australia. The aim of the review was to determine ways of increasing South Australia’s competitiveness in health and medical research.
At the time of the review, South Australia had one very small independent research institute – the Children’s Health Research Institute3, which was located within the Women’s and Children’s Hospital. Appreciating this, and that the Universities had established several internal institutes/research centres, Shine and Young acknowledged that in order for the State to increase competitiveness and have a focal point for health and medical research, the establishment of an independent health and medical research institute (HMRI) was critical. Size and scope of this independent HMRI were key considerations – critical mass and a state-wide focus were crucial for success.
Following a comprehensive analysis of the sector, the Shine Young Review made three key recommendations aimed at supporting the strategic directions for health and medical research in South Australia:
• Establish an independent health and medical research institute.
• House the health and medical research institute in a new ‘flagship’ research facility, and
• Build and maintain a health and medical research fund.
Following receipt of the recommendations from the Shine Young Review, the State Government realised that this was a once in a lifetime opportunity to develop a health and medical research precinct that would attract a large cohort of researchers across the research spectrum and combine best practice in health care delivery, education and research. They committed to establishing the South Australian Health and Medical Research Institute (SAHMRI), with the vision that SAHMRI would:
• Be a centre of excellence for health and medical research in South Australia.
• Support new and leading areas of research in human medicine and health.
• Attract national and international researchers.
• Build partnerships between researchers and research bodies to promote research excellence.
• Foster the application of research knowledge to benefit health and wellbeing of people within and outside of South Australia.
• Offer significant economic advantages to the State, by attracting significant funding from national and international sources.
3 Subsequently absorbed into SAHMRI in partnership with WCH and University of Adelaide.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 14
• Support South Australian and Australian Federal research objectives.
• Create synergies between researchers and care providers, through the co-location with the new Royal Adelaide Hospital and collaboration with other State hospitals, and
• Be housed within a ‘flagship’ research facility adjacent to the new Royal Adelaide Hospital.4
SAHMRI was established based on the above objectives as an independent, state-wide health and medical research institute as a company limited by guarantee. Our model demonstrates the initial collaborative intent under which SAHMRI was established and achieved through the membership of the Company and beyond into research themes and collaborative ventures.
SAHMRI’s Collaborative model The SAHMRI model is very different to other independent health and medical research institutes across Australia – a collaborative venture with all three Universities and the State Government as partners. Given this, a flexible model was created whereby SAHMRI employees and partner staff from the Universities and CSIRO work alongside each other in our world-class facility. This provides benefits to both SAHMRI and our partners in relation to collaborative opportunities, access to infrastructure and animal house services, co-supervision of students and subsidised rent (at around the third of the cost of rent when benchmarked against office space in the Adelaide CBD). Furthermore, this co-location brings multidisciplinary teams together across ‘bench to bedside’ translational research and facilitates innovative approaches to research practices.
EXAMPLE OF MULTIDISCIPLINARY RESEARCH ACROSS ‘BENCH TO BEDSIDE’
As a discovery scientist, Dr Tim Sargeant provides the ‘bench side’ scientific expertise to multidisciplinary translational research programs that are currently exploring the role of lysosomal biology and autophagy in atherosclerosis. He works synergistically with Dr Peter Psaltis (vascular cardiologist, RAH and Co-Director, SAHMRI Vascular Research Centre) to better understand the potential cardiovascular benefits of colchicine (an anti-inflammatory therapy) and the mechanistic basis of its anti-atherosclerotic and plaque-stabilising properties with conjoint awards, publications and supervisory roles. These vital multidisciplinary collaborations provide novel insights into the use of repurposed therapies for cardiovascular disease.
Our structure includes researchers working right across the discovery continuum, from basic science right through to population health. This depth of research focus provides us with the agility to quickly respond to emerging priorities that arise in a crisis scenario, much like the environment we’re working in today with COVID-19. With about 15 COVID-related projects, we have responded quickly and brought together multidisciplinary teams to support governments in their response to the pandemic.
In 2019, we created a new theme structure to build on our early success (Figure 1). We wanted to better reflect our vision for the future of health and medical research and the health care system, to
4 SA Health Media Release - 2008
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 15
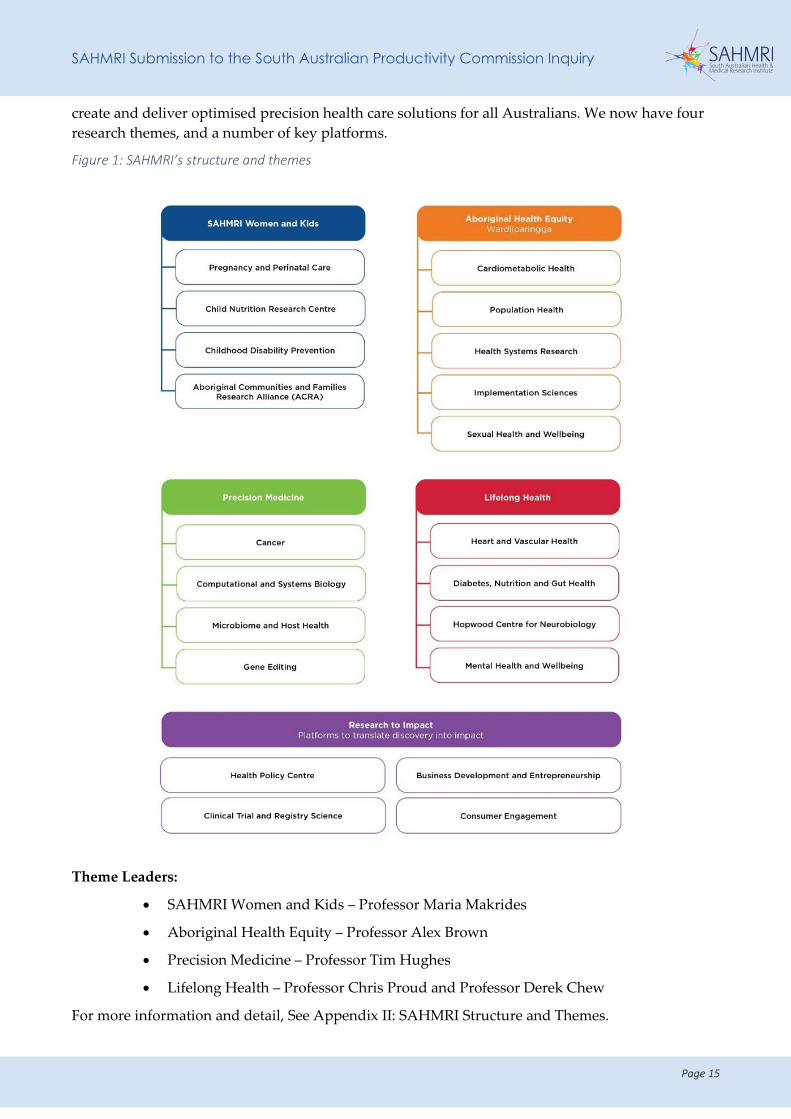
create and deliver optimised precision health care solutions for all Australians. We now have four research themes, and a number of key platforms.
Figure 1: SAHMRI’s structure and themes
Theme Leaders:
• SAHMRI Women and Kids – Professor Maria Makrides
• Aboriginal Health Equity – Professor Alex Brown
• Precision Medicine – Professor Tim Hughes
• Lifelong Health – Professor Chris Proud and Professor Derek Chew
For more information and detail, See Appendix II: SAHMRI Structure and Themes.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 16
A Collaborative Governance Structure
SAHMRI exists as an independent state-wide health and medical research institute as a company limited by guarantee.
We are bound by a Constitution, which outlines the Members of the company, namely:
• The Minister for Health and Wellbeing
• The Minister for Innovation and Skills
• The Treasurer
• The University of Adelaide
• The University of South Australia
• Flinders University.
Each of the Members has representation on the SAHMRI Board.
SAHMRI is accredited as an Administering Institution with the National Health and Medical Research Council (NHMRC).
SAHMRI has a Research Executive Committee (REC, made up of Theme, Program and Platform Leaders plus key leaders from partner organisations) which meets on a bi-monthly basis to discuss issues associated with research strategy and priorities across the Institute.
On a biennial basis, SAHMRI’s research strategy and performance are assessed by our Research Advisory Committee (RAC) – current membership is provided below:
• Professor John Shine, President Australian Academy of Science (Chair)
• Professor Ian Frazer FAA, Founding CEO and Director of Research, Translational Research Institute
• Professor Doug Hilton FAA, Director, Walter and Eliza Hall Institute
• Professor John Mattick, AO FAA
• Professor Vicki Anderson, Director, Critical Care and Neurosciences Research at the Murdoch Children’s Research Institute
• Professor Peter Libby, Chair of Cardiology, Harvard Medical School
• Professor Justin McArthur, Chair and Head of Neurology Johns Hopkins
• Professor Papaarangi Reid, University of Auckland
• Professor Steve Wesselingh, Executive Director, SAHMRI (ex-officio).
Research Advisory Committee Reports, 2016 and 2019 are provided for information (See Appendix III: Research Advisory Committee).
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 17
SAHMRI Today
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 18
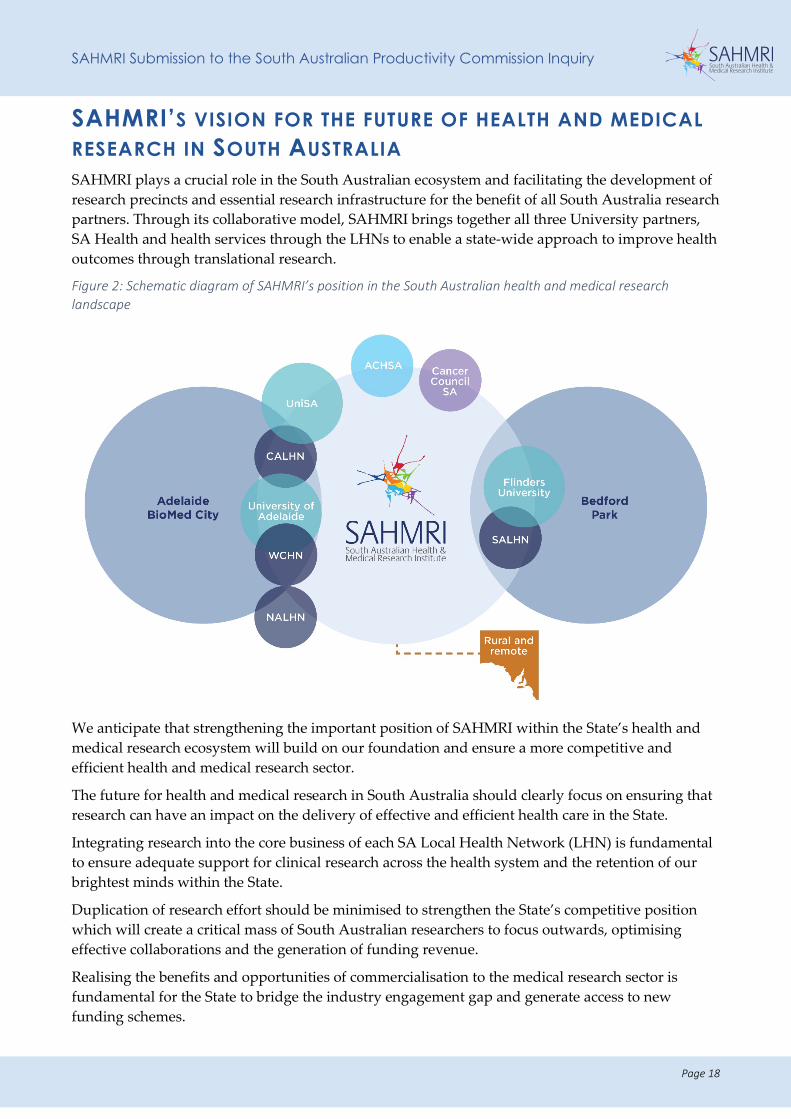
SAHMRI’S VISION FOR THE FUTURE OF HEALTH AND MEDICAL RESEARCH IN SOUTH AUSTRALIA SAHMRI plays a crucial role in the South Australian ecosystem and facilitating the development of research precincts and essential research infrastructure for the benefit of all South Australia research partners. Through its collaborative model, SAHMRI brings together all three University partners, SA Health and health services through the LHNs to enable a state-wide approach to improve health outcomes through translational research.
Figure 2: Schematic diagram of SAHMRI’s position in the South Australian health and medical research landscape
We anticipate that strengthening the important position of SAHMRI within the State’s health and medical research ecosystem will build on our foundation and ensure a more competitive and efficient health and medical research sector.
The future for health and medical research in South Australia should clearly focus on ensuring that research can have an impact on the delivery of effective and efficient health care in the State.
Integrating research into the core business of each SA Local Health Network (LHN) is fundamental to ensure adequate support for clinical research across the health system and the retention of our brightest minds within the State.
Duplication of research effort should be minimised to strengthen the State’s competitive position which will create a critical mass of South Australian researchers to focus outwards, optimising effective collaborations and the generation of funding revenue.
Realising the benefits and opportunities of commercialisation to the medical research sector is fundamental for the State to bridge the industry engagement gap and generate access to new funding schemes.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 19
The support of the State Government in defining South Australia as a knowledge state and major scientific destination is essential to attract researchers and their work to the world-class infrastructure now available within the precincts. Innovative incentives to support our research sector are an alternative approach and imperative for South Australia to continue to succeed beyond its expectations and advance its reputation.
SAHMRI has the capacity and capability to support a new approach. We are committed to a state-wide translational interaction with the health system and have established the networks and infrastructure needed to enhance the clinical-research interface.
Our existing collaborative working relationships with the South Australian Universities is vital – through joint appointments, faculty memberships, student supervision and joint research activities. The continuation of these relationships is an important part of our future moving forward.
Strengthened interaction between SAHMRI and the SA health system We believe that, beyond the collaborative activities that we have with the Universities and those we expect to continue into the future, SAHMRI should be viewed as the centre of ongoing sustainability and excellence in health and medical research in South Australia, playing a critical role in delivering research-led healthcare in areas of importance for the State Government, and relevance to national priorities.
• We are committed to improving the health of all South Australians through the conduct and translation of health and medical research at a level of international excellence.
• We can play a critical role in ensuring that health and equity are improved in a collaborative and strategic way with SA Health, including the LHNs and the Commission on Excellence and Innovation in Health (CEIH).
SAHMRI’s existing relationships with SA Health and the LHNs should continue to be strengthened through the formalisation of agreements at both the level of SA Health and each of the LHNs. It is also important that SAHMRI maintains its strong relationship with Health Translation SA.
This arrangement would (from a strategic/governance perspective):
• Allow SA Health (and therefore the State Government) to work directly with SAHMRI to have key research questions identified and answered in a timely fashion (e.g. COVID-19), in the absence of the often-cumbersome bureaucracy within University systems.
• Embed SAHMRI in the health ecosystem, recognising it as the key research partner.
• Strengthen the role of Health Translation SA in research activities, and coordination activities to enable health service research and health care innovation through close collaborations with SAHMRI.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 20
It would also:
• Improve the pipeline from bioscience research through to direct translation into healthcare.
• Increase the number of high-performing clinician researchers within the health system, with SAHMRI creating a pathway and invigorating ‘research home’ that links and enhances their clinical and research work.
• Build the capacity of the next generation of research leaders for the State and the nation.
• Align research with NHMRC and Medical Research Future Fund (MRFF) priorities, as well as those identified at a State level.
• Further build clinical trials capacity across the sector and increase the number of trials driven by and conducted within the public health system.
• Build registry and analytic capabilities for the betterment of the health of South Australians, and
• Facilitate consumer engagement, particularly through consumer/clinician partnerships.
Importance of continued State Government support for SAHMRI Continuing to support SAHMRI as the State’s only independent health and medical research institute should be a priority for the State Government.
The significant return on investment, and the significant contribution we have made directly to the State’s economy demonstrates the importance and value of investment in health and medical research through SAHMRI.
As an Institution, we play a complementary role to the research undertaken within the university and clinical settings. As a sector, with appropriate Government support, this collaborative venture will continue to grow, which will also enable the further enhancement of research partners outputs as observed to date.
Our commitment and approach to state-wide coordinated efforts, as opposed to cross-institutional competition within the State, is critical to positioning South Australia as a rival to other state and international research competitors, and the financial, commercial and ‘knowledge capital’ benefits that this would realise for the State both now and in the future.
Re-imagining South Australia as a knowledge economy, and as a magnet for innovation, talent and biotechnology research and development is an essential next step, and will require investment into the health and medical research sector more broadly, and SAHMRI specifically.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 21
RECOMMENDATIONS
We offer the following recommendations in relation to the future of health and medical research in South Australia:
R1: The State Government operating grant to SAHMRI should be increased to a base amount of $10 million per annum (commencing in 2021). The annual operating grant should be:
• Increased annually in accordance with CPI; and
• As a further incentive for SAHMRI to contribute to the State's total economic activity (Gross StateProduct), increased in line with our contribution.
R9: Acknowledging that collaborative links between SAHMRI and the South Australian based Universities are already strong and multi-facetted, research linkages between SAHMRI and each of the LHN’s should be actively pursued. With the support and encouragement of the State Government, this would position SAHMRI to assist the Government in the provision of research-led health care.
R11: The LHNs, with the endorsement and support of the State Government, should embed health and medical research within their operations, with the aim of seamlessly integrating research into their core business in a manner that is complementary to clinical care, including by:
• Creating research-related KPIs for Chief Executive Officers. Research should be viewed as a valuablepart of core business.
• Encouraging greater profile of the Research Director and Research Office at each LHN, withinteraction of these functions with equivalent staff across the sector.
• Re-imagine incentives for research success within the LHN’s, including access to promotionalopportunities and infrastructure funds that are linked to research grants, as well as rewards forresearch that is successful commercially.
R12: The merger of University of SA and University of Adelaide should be actively considered, given the synergies between the two institutions, the potential economies of scale and the significant state-wide advantages that could ensue.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 22
SAHMRI’S RESPONSE TO THE SAPC INQUIRY SAHMRI is pleased to make this response to the SAPC Inquiry and have the opportunity to share our vision for the future of health and medical research in South Australia. In making this response, we address the specific SAPC Terms of Reference and respond to the questions outlined in the Issues Paper (13 March 2020).
PERFORMANCE OF HMR AND DEVELOPMENT IN SOUTH AUSTRALIA Terms of Reference. Assess the performance of health and medical R&D in South Australia, including a comparative analysis of South Australia's share of national grant funding benchmarked against other jurisdictions, with particular reference to how health and medical R&D in South Australia:
• Fosters innovation and improvements in health care service delivery that lead to improved health outcomes for the community and provide cost savings to the health system
• Encourages staff development that promotes high professional standards and supports recruitment and retention.
An independent review of SAHMRI’s impact While SAHMRI regularly reviews our own performance, and our Research Advisory Committee reviews our strategic directions and outputs on a biennial basis, we determined that it was timely to commission an independent review of SAHMRI’s performance.
SAHMRI commissioned dandolopartners (a management consulting firm specialising in public policy) to undertake this review, focussing on our value as a health and medical research institute.
Dandolo reviewed SAHMRI in terms of impact across a variety of fields, including knowledge, social, health, economic, leadership. A copy of the report is included (See Appendix IV: Final Report, dandolopartners, April 2020).
DANDOLO’S FINAL REPORT HIGHLIGHTS THE FOLLOWING IN RELATION TO SAHMRI:
SAHMRI balances its role as a vehicle to improve health outcomes for South Australia and its role as a world-class MRI.
• SAHMRI contributes substantially to the State’s grant income and publications. It also contributes significantly to the research output of South Australian universities.
• 27% of South Australia’s research output in HMR is associated with SAHMRI, despite accounting for only approximately 10% of the HMR workforce in South Australia.
• More importantly, SAHMRI is having a significant impact on the State’s healthcare system – and contributing changes in clinical practice to the world. This is a result of its focus at the right end of the translational medicine continuum, closest to real-world patient impact and its broad remit across diseases and ages.
• Within a relatively short period of six years in operation, SAHMRI activity has saved 1000s of lives and millions of dollars. As part of this, SAHMRI is improving health equity in South Australia.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 23
SAHMRI brings together researchers across the State to harness their collective research strength and reduce unnecessary competition.
• SAHMRI collaborates extensively and has led establishment of many new state-wide initiatives – particularly clinical research and health translation space. Not least of these is Health Translation South Australia.
• SAHMRI is enhancing the health and medical research rankings of South Australian Universities.
• Dandolo estimates that SAHMRI contributes directly to 20% of University of Adelaide ranking points in the Academic Ranking of World Universities (ARWU) assessment for Medicine and Life Sciences, principally via top publications and highly cited researchers.
• University of Adelaide jumped from below 150th to above 100th in its Medical and Life Sciences ARWU rankings around 2015, based on SAHMRI’s contribution of approximately 20% of ranking points. Dandolo’s believes that University of Adelaide’s jump in Medical and Life Sciences rankings is largely influenced by SAHMRI, which reached maturation about that time.
• SAHMRI is securing diverse income streams, especially compared to other MRIs. It is less reliant on traditional grant incomes, instead performing exceptionally well at attracting commercial income streams.
• SAHMRI ranks second in Australia in terms of commercial income for MRIs, which accounts for 32% of total income. This is highly indicative of its credibility and its focus on real-world research.
SAHMRI attracts diverse talent and novel research infrastructure (including clinical registries and datasets) to South Australia.
• SAHMRI has a more diverse workforce and community than most other health and medical research organisations in Australia, conferring a competitive advantage in the research it undertakes and its attractiveness to new talent.
• As two indicative measures of diversity, SAHMRI attracts and retains far more female health and medical researcher workers and staff from Indigenous backgrounds than the national average.
Performance of SAHMRI
SAHMRI’s share of national grant funding and publication output
SAHMRI receives revenue from multiple sources for health and medical research and development, including grant funding, government support, commercial and philanthropic income. Over the last three years, grant and commercial income has increased by about 20% as demonstrated in Figure 3.

SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 24
Figure 3: Increasing trend in SAHMRI revenue streams, 2017-2019
Since 2016, SAHMRI has steadily increased its share of funding at a State level, with 42% of South Australian NHMRC funding being awarded to researchers associated with SAHMRI in 2019 (Figure 4).
Figure 4: SAHMRI share of NHMRC Funding awarded steadily increases, 2016 – 2019
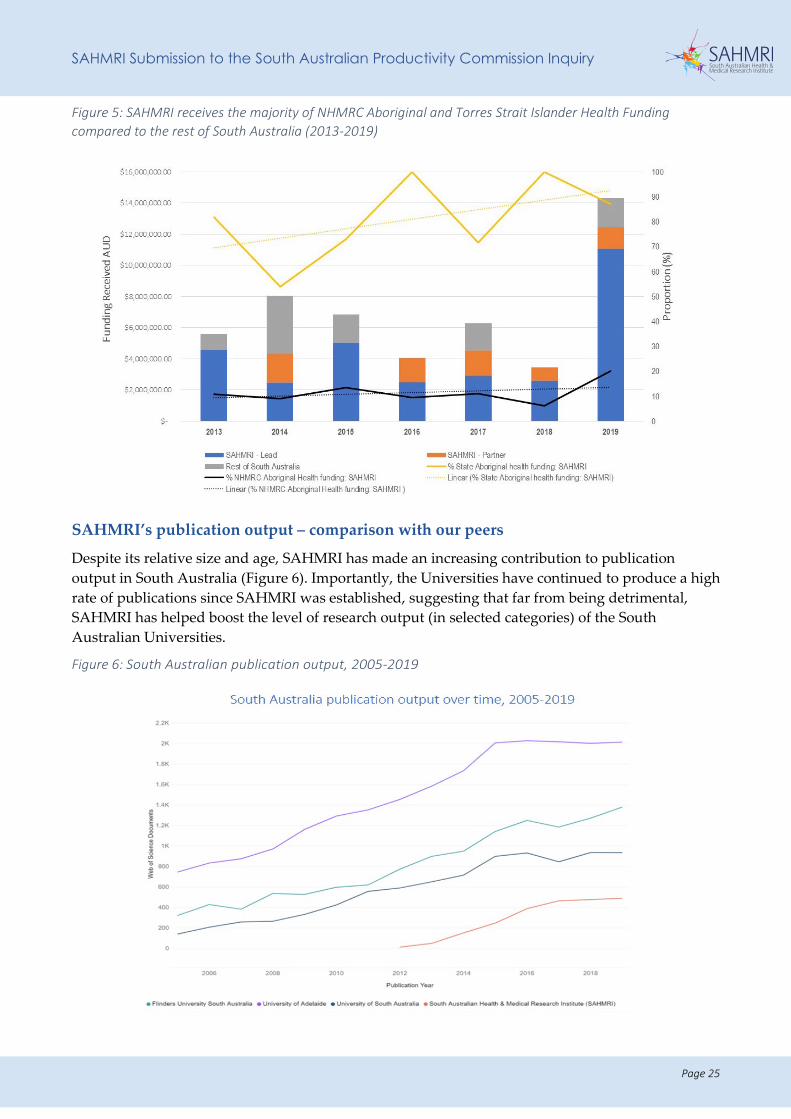
SAHMRI, through its Aboriginal Health Equity Theme, has been highly successful in NHMRC funding for Aboriginal and Torres Strait Islander Health research: over the past seven years, SAHMRI as a lead or partner, has received 90% of all NHMRC funding to South Australia for Aboriginal and Torres Strait Islander Health research (2013-2019) (Figure 5).
$0
$10,000,000
$20,000,000
$30,000,000
$40,000,000
$50,000,000
$60,000,000
$70,000,000
$80,000,000
FY17 FY18 FY19
Research Grants State Government Contribution Commerical Income Other Income
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
$-
$10,000,000.00
$20,000,000.00
$30,000,000.00
$40,000,000.00
$50,000,000.00
$60,000,000.00
$70,000,000.00
$80,000,000.00
$90,000,000.00
2016 2017 2018 2019
TOTAL SA: SAHMRI: %
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 25
Figure 5: SAHMRI receives the majority of NHMRC Aboriginal and Torres Strait Islander Health Funding compared to the rest of South Australia (2013-2019)
SAHMRI’s publication output – comparison with our peers
Despite its relative size and age, SAHMRI has made an increasing contribution to publication output in South Australia (Figure 6). Importantly, the Universities have continued to produce a high rate of publications since SAHMRI was established, suggesting that far from being detrimental, SAHMRI has helped boost the level of research output (in selected categories) of the South Australian Universities.
Figure 6: South Australian publication output, 2005-2019
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 26
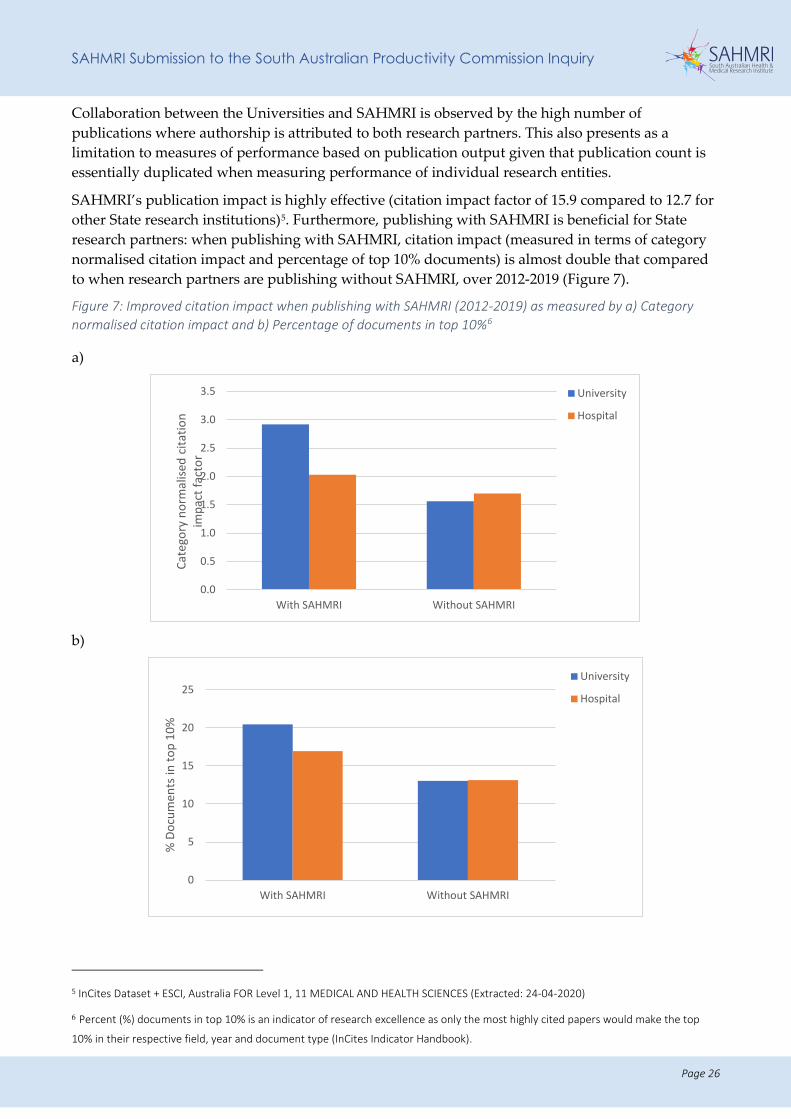
Collaboration between the Universities and SAHMRI is observed by the high number of publications where authorship is attributed to both research partners. This also presents as a limitation to measures of performance based on publication output given that publication count is essentially duplicated when measuring performance of individual research entities.
SAHMRI’s publication impact is highly effective (citation impact factor of 15.9 compared to 12.7 for other State research institutions)5. Furthermore, publishing with SAHMRI is beneficial for State research partners: when publishing with SAHMRI, citation impact (measured in terms of category normalised citation impact and percentage of top 10% documents) is almost double that compared to when research partners are publishing without SAHMRI, over 2012-2019 (Figure 7).
Figure 7: Improved citation impact when publishing with SAHMRI (2012-2019) as measured by a) Category normalised citation impact and b) Percentage of documents in top 10%6
a)
b)
5 InCites Dataset + ESCI, Australia FOR Level 1, 11 MEDICAL AND HEALTH SCIENCES (Extracted: 24-04-2020)
6 Percent (%) documents in top 10% is an indicator of research excellence as only the most highly cited papers would make the top
10% in their respective field, year and document type (InCites Indicator Handbook).
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
With SAHMRI Without SAHMRI
Cate
gory
nor
mal
ised
cita
tion
impa
ct fa
ctor
University
Hospital
0
5
10
15
20
25
With SAHMRI Without SAHMRI
% D
ocum
ents
in to
p 10
%
University
Hospital
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 27
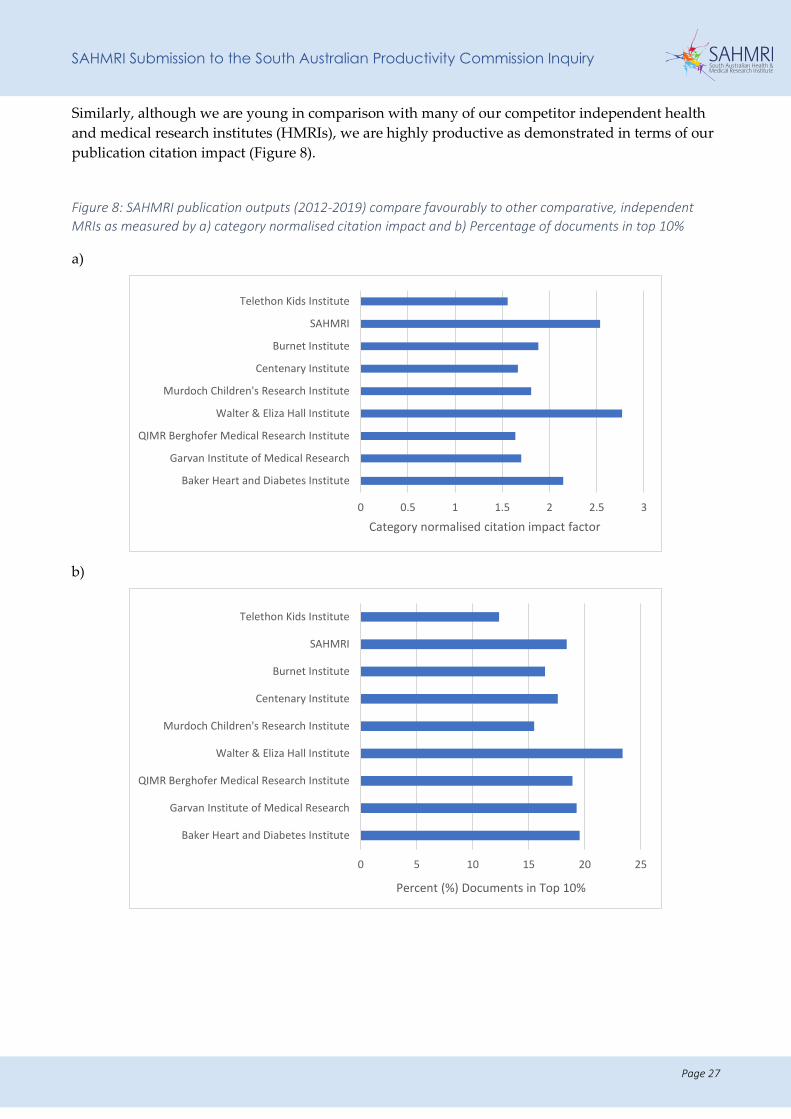
Similarly, although we are young in comparison with many of our competitor independent health and medical research institutes (HMRIs), we are highly productive as demonstrated in terms of our publication citation impact (Figure 8).
Figure 8: SAHMRI publication outputs (2012-2019) compare favourably to other comparative, independent MRIs as measured by a) category normalised citation impact and b) Percentage of documents in top 10%
a)
b)
0 0.5 1 1.5 2 2.5 3
Baker Heart and Diabetes Institute
Garvan Institute of Medical Research
QIMR Berghofer Medical Research Institute
Walter & Eliza Hall Institute
Murdoch Children's Research Institute
Centenary Institute
Burnet Institute
SAHMRI
Telethon Kids Institute
Category normalised citation impact factor
0 5 10 15 20 25
Baker Heart and Diabetes Institute
Garvan Institute of Medical Research
QIMR Berghofer Medical Research Institute
Walter & Eliza Hall Institute
Murdoch Children's Research Institute
Centenary Institute
Burnet Institute
SAHMRI
Telethon Kids Institute
Percent (%) Documents in Top 10%
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 28
Improving health outcomes through innovative translational research
SAHMRI was originally established as an HMRI focused on the translation of research findings directly into healthcare for improved community health outcomes. We continue to have a very strong focus on this translational approach today, as evidenced by examples of our research demonstrating impact on health outcomes (See Appendix V: Research Impact Stories).
EXAMPLES OF TRANSLATIONAL IMPACT
Aboriginal Health Equity: Across the State, and increasingly the nation, the Aboriginal Health Equity Theme, led by Professor Alex Brown is recognised for its expertise across a wide range of public and population health research and translation capabilities. This includes:
• Leadership of novel, nationally relevant, landmark studies of chronic disease epidemiology and biology, sociocultural determinants of health, inequity and adolescent health, changing modes of health care delivery to Aboriginal communities.
• Development of state-wide plans (Heart and Stroke, Diabetes, Cancer, Prisoner Health), provision of support to government departments in epidemiological monitoring and community engagement, supported the establishment of key interagency relationships and driven mixed method health system research to guide action.
• Building the next generation of Aboriginal and Torres Strait Islander researchers through a consolidated commitment to capacity building across the sector.
• Professor James Ward worked alongside State and Federal Government to influence policy and practice, whilst delivering meaningful and culturally appropriate solutions to reduce the transmission of blood borne viruses and sexually transmitted infections. Professor Ward is now in a key leadership position at the University of Queensland.
SAHMRI Women and Kids: Professor Maria Makrides has led clinical trials which were influential in causing The Australasian Society for Clinical Allergy and Immunology, as well as other like international societies, to change their feeding guidance for infants to have diets that are more inclusive of allergenic foods, such as cooked egg and peanut paste, from the time a child is ready to start eating solid foods. Her group provided key information to integrate guidance about the early inclusion of these allergenic foods with nutritional guidance (relating to iron rich foods and duration of breastfeeding), which was used by the Australasian Society for Clinical Immunology and Allergy and the Centre for Food and Allergy Research (NHMRC Centre of Research Excellence) to harmonise wording for infant feeding guidance.
A Cochrane Review (published by Associate Professor Philippa Middleton): ‘Omega-3 fatty acid addition during pregnancy’ is already having an impact on the national pregnancy guidelines. This new evidence of substantial reductions in preterm birth with omega-3 supplementations has led to a recommended policy change for women with a singleton pregnancy to take a daily supplement of omega-3 long chain polyunsaturated fatty acids from around the 12th week of pregnancy. This recommendation is currently being integrated into the update of the NHMRC national pregnancy guidelines.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 29
Economic benefits and cost savings to the health system
SAHMRI has indirectly generated revenue for the State through such innovations as:
• SAHMRI 2: $370 million private investment, $70 million federal government investment and projected 1000 jobs and $1 billion revenue generation for the State.
• Generation of approximately $90 million from clinical research coordinated through SAHMRI.
• Research and commercial income 10x the State Government contribution (for every dollar we receive from the State Government we have generated $10).
As a relatively young organisation, SAHMRI researchers have already achieved significant translational outcomes across a range of disease states and health service settings, including cardiovascular health, cancer and precision medicine, emergency medicine and aged care. Examples are included for more detail.
TRANSLATION OF RESEARCH EVIDENCE INTO HEALTH AND ECONOMIC BENEFITS
As examples, the projects below have been quantified in terms of true cost savings to the health system7:
Chronic Myeloid Leukaemia (CML) nationally
• cost savings from pioneering treatment cessation in patients achieving deep molecular response of approximately $250 million nationally over 10 years
• removal of need for 3 monthly bone marrow tests for 5000 CML patients nationally – saving at least $600,000 annually
• avoidance of bone marrow transplants nationally – saving $18 million annually
Improving care for newborns in SA
• Predicted or estimated future savings of $43,000 annually with reduced preterm births resulting in cerebral palsy
• Lifetime cost saving of $5.57 million per cerebral palsy case
• Projected estimated cost-savings of $200,000 per year from reducing newborn length of stay and $242,000 per year from reduced maternal length of stay through better targeting of antibiotics
Staff development at SAHMRI
SAHMRI leads various initiatives to instil a culture of high professional standards amongst all our staff and students. These are evident with receipt of the SAGE Athena Swan bronze award8 and includes a range of internal initiatives such as the SAHMRI mentoring and gender equity programs.
7 Kathy Mott and Associates, 2020
8 An Athena SWAN Bronze Institution Award recognises an institution’s commitment to advancing the careers of women, trans and
gender diverse individuals in STEMM disciplines in Higher Education and Research. Achieving a Bronze Institution Award requires an
institution to demonstrate a solid foundation for improving gender equity in STEMM.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 30
SAHMRI maintains high levels of research integrity aligned to the NHMRC Australian Code of Responsible Research Conduct (2018), overseen through our Research Executive Committee (REC) and the Governance Committee of the SAHMRI Board.
Students, and early- and mid-career researchers are supported and mentored through two self-managed committees that report to REC and the SAHMRI Board.
Furthermore, SAHMRI has a nation-leading initiative to recruit and retain young Aboriginal staff and mentor them as future leaders through the SAHMRI Indigenous Collective. SAHMRI creates opportunities for Aboriginal and Torres Strait Islander people in health and medical research by building a culturally responsive workforce, and includes ways of working which unite the physical, spiritual and emotional wellbeing of all people.
NHMRC Fellowships as an employment strategy at SAHMRI
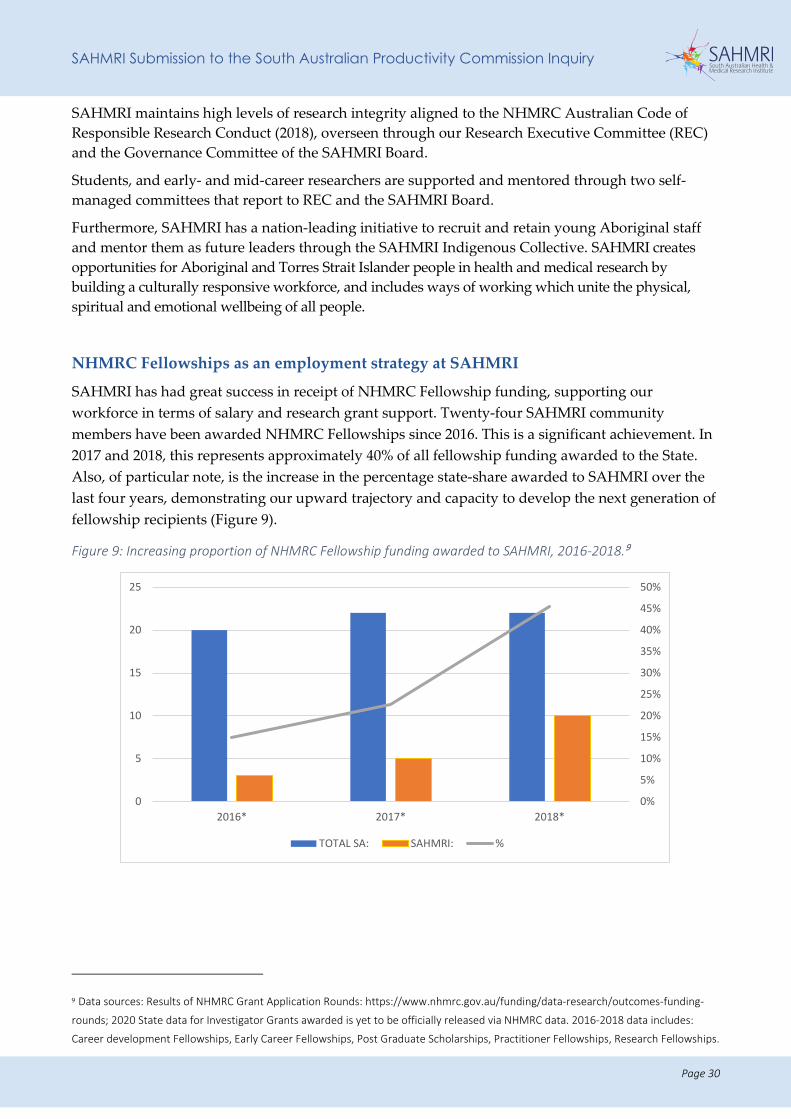
SAHMRI has had great success in receipt of NHMRC Fellowship funding, supporting our workforce in terms of salary and research grant support. Twenty-four SAHMRI community members have been awarded NHMRC Fellowships since 2016. This is a significant achievement. In 2017 and 2018, this represents approximately 40% of all fellowship funding awarded to the State. Also, of particular note, is the increase in the percentage state-share awarded to SAHMRI over the last four years, demonstrating our upward trajectory and capacity to develop the next generation of fellowship recipients (Figure 9).
Figure 9: Increasing proportion of NHMRC Fellowship funding awarded to SAHMRI, 2016-2018.9
9 Data sources: Results of NHMRC Grant Application Rounds: https://www.nhmrc.gov.au/funding/data-research/outcomes-funding-
rounds; 2020 State data for Investigator Grants awarded is yet to be officially released via NHMRC data. 2016-2018 data includes:
Career development Fellowships, Early Career Fellowships, Post Graduate Scholarships, Practitioner Fellowships, Research Fellowships.
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
0
5
10
15
20
25
2016* 2017* 2018*
TOTAL SA: SAHMRI: %
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 31
The policy environment and its impact on HMR in South Australia
Information request 3.1: policy environment
• What is the potential for further simplifying or streamlining current HREC approval processes?
Research Priority Setting
SAHMRI researchers operate within and are generally very good at navigating the national and state policy requirements.
At the highest level, our researchers are required to adhere to the Australian Code of Responsible Research Conduct (2018). SAHMRI has a series of internal policies requiring compliance with the Code, and these are consistent with similar policies issued by the Universities.
The identification of health and medical priorities is undertaken at the level of the Federal and State Governments, and while these offer some guidance in relation to priority research areas, there is not one single source of research priority-setting. The NHMRC has a series of targeted research calls, designed to address particular pressing health needs, and each of the smaller funding agencies call for research applications according to their own research priorities e.g. Heart Foundation, Cancer Council.
Given this, there is an opportunity for the State in identifying our strengths at a state level and ensuring that we apply these strengths to our competitive advantage. This will require collaboration and alignment amongst South Australian research institutions in order to have a shared vision for the State. A research strategy, adopted universally by all research institutions, would be one way of achieving this (See Recommendations).
Research Ethics and Governance Processes
While we understand that reforms to the research ethics and governance processes, including Site Specific Assessments, are the focus of the Birch Review10, it is important to recognise them as part of this Inquiry.
Delays in research ethics and governance processes are significant impediments to the timely commencement of research in South Australia. Mutual acceptance models of Human Research Ethics Committee (HREC) review have certainly improved the current system, but there is a long way to go in relation to streamlining governance approvals. Without resolution of these issues, the State will miss the opportunity to thrive.
SAHMRI is actively engaged on the Clinical Governance Committee, chaired by Professor Caroline McMillen, tasked with reviewing clinical research governance in the State (Professor Maria Makrides represents SAHMRI on this Committee).
10 Birch (2018). Review of Research Governance in the Department for Health and Wellbeing (SA) and related LHNs.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 32
RECOMMENDATIONS
We offer the following recommendations in relation to the policy environment:
R3: SAHMRI, in collaboration with the State Government, should take a leadership role in development of a Clinical research strategy – building on the work already being undertaken by the Department of Health and Wellbeing under the leadership of the Chief Scientist.
R4: The State Government should take a leadership role in implementing the recommendations of the Birch report.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 33
KEY FACTORS INFLUENCING LEVEL OF PUBLIC AND PRIVATE SECTOR HEALTH AND MEDICAL RESEARCH OUTPUT Terms of Reference. Identify and assess the key factors influencing the level of public sector (including universities) and private sector health and medical research output and activity in South Australia including:
• Talent and the capacity to attract new talent
• Industry structure and composition
• Funding, including Australian government funding
• Access to data: regulation affecting access to data; and efficiency of collection and acquisition
• Connectivity of the Biomedical Precinct and the planned Flinders precinct
• Potential for greater connectivity between the Local Health Network medical workforce and university recruitment
• Integration of research partners with SA Health.
SAHMRI’s Community
Information request 5.1: workforce
• What strategies are being used by institutions to attract talented researchers and postgraduates and how successful have they been?
SAHMRI has led the State in the recruitment of research leaders. As a newly established HMRI, SAHMRI was a ‘green-fields’ site with the opportunity to create a set of research themes that would allow the conduct of internationally competitive research led by experts in their selected fields.
Leadership at SAHMRI – original recruitment
• Executive Director: Professor Steve Wesselingh
• Theme Leaders: Professor Steve Nicholls, Professor Charles Mullighan, Professor Julio Licinio, Professor Alex Brown, Professor Chris Proud, Professor Maria Makrides
The SAHMRI Community has steadily grown under the leadership of notable experts in their respective fields over the last 6 years since we moved into our North Terrace facility. SAHMRI now has approximately 400 employees, spread across our various sites:
• North Terrace = 325
• Women’s and Children’s Hospital = 40
• Preclinical Research Imaging Laboratory (PIRL) – Gilles Plains = 21
• Flinders Medical Centre = 9
• Country SA = 2
• Interstate = 4
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 34
SAHMRI provides significant funding to all recruits over and above competitive funding, and on occasion, draws on additional funding support from the University (where it is a joint-appointment). Information regarding these recruitment packages is available upon request (confidentially).
Our Community extends beyond only our employees. It is made up of SAHMRI employees, students and partner staff from the Universities and CSIRO (n=371, as of February 2020). This model provides mutual benefit to both SAHMRI and partner staff who have increased opportunities for collaboration on areas of shared research interest.
Our leaders recognised by the Australian Academy of Health and Medical Sciences
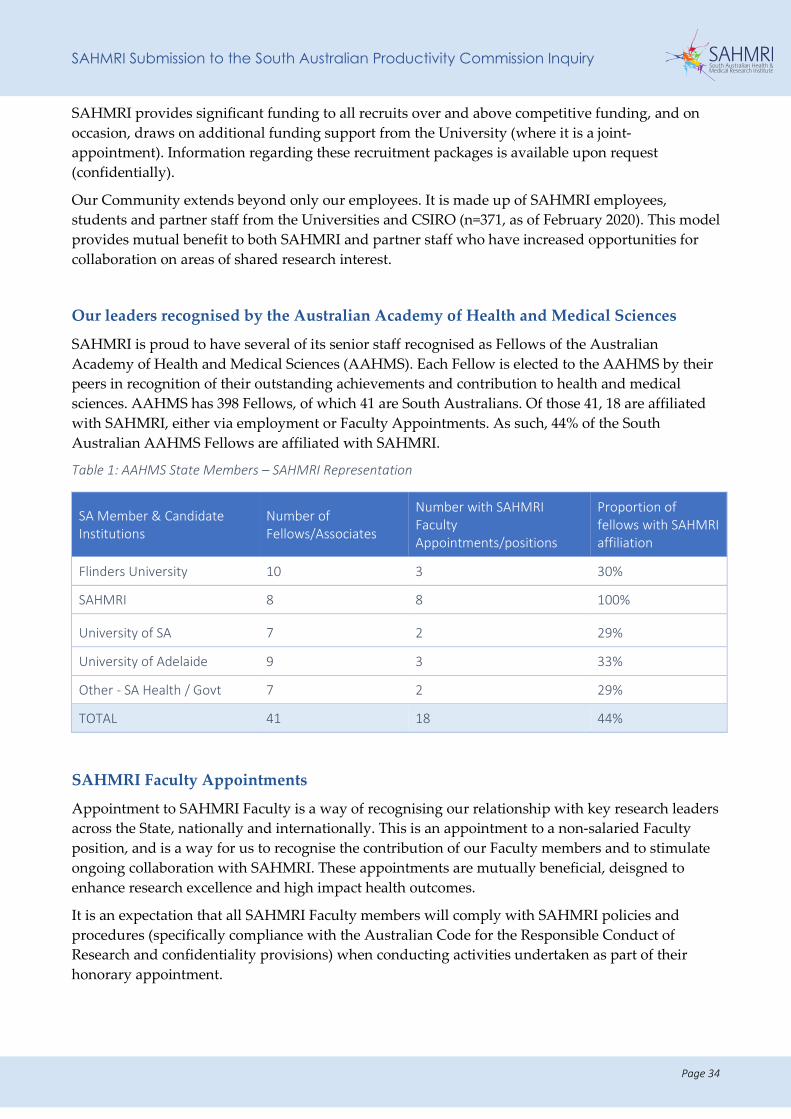
SAHMRI is proud to have several of its senior staff recognised as Fellows of the Australian Academy of Health and Medical Sciences (AAHMS). Each Fellow is elected to the AAHMS by their peers in recognition of their outstanding achievements and contribution to health and medical sciences. AAHMS has 398 Fellows, of which 41 are South Australians. Of those 41, 18 are affiliated with SAHMRI, either via employment or Faculty Appointments. As such, 44% of the South Australian AAHMS Fellows are affiliated with SAHMRI.
Table 1: AAHMS State Members – SAHMRI Representation
SA Member & Candidate Institutions
Number of Fellows/Associates
Number with SAHMRI Faculty Appointments/positions
Proportion of fellows with SAHMRI affiliation
Flinders University 10 3 30%
SAHMRI 8 8 100%
University of SA 7 2 29%
University of Adelaide 9 3 33%
Other - SA Health / Govt 7 2 29%
TOTAL 41 18 44%
SAHMRI Faculty Appointments
Appointment to SAHMRI Faculty is a way of recognising our relationship with key research leaders across the State, nationally and internationally. This is an appointment to a non-salaried Faculty position, and is a way for us to recognise the contribution of our Faculty members and to stimulate ongoing collaboration with SAHMRI. These appointments are mutually beneficial, deisgned to enhance research excellence and high impact health outcomes.
It is an expectation that all SAHMRI Faculty members will comply with SAHMRI policies and procedures (specifically compliance with the Australian Code for the Responsible Conduct of Research and confidentiality provisions) when conducting activities undertaken as part of their honorary appointment.
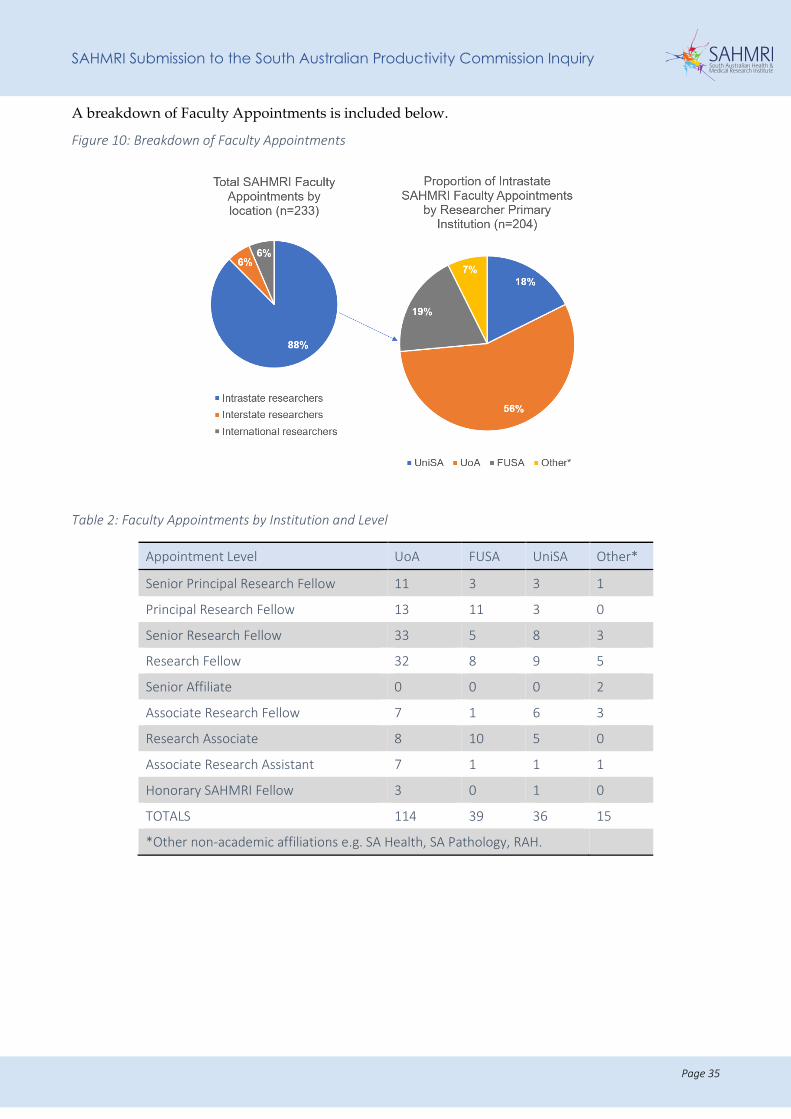
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 35
A breakdown of Faculty Appointments is included below.
Figure 10: Breakdown of Faculty Appointments
Table 2: Faculty Appointments by Institution and Level
Appointment Level UoA FUSA UniSA Other*
Senior Principal Research Fellow 11 3 3 1
Principal Research Fellow 13 11 3 0
Senior Research Fellow 33 5 8 3
Research Fellow 32 8 9 5
Senior Affiliate 0 0 0 2
Associate Research Fellow 7 1 6 3
Research Associate 8 10 5 0
Associate Research Assistant 7 1 1 1
Honorary SAHMRI Fellow 3 0 1 0
TOTALS 114 39 36 15
*Other non-academic affiliations e.g. SA Health, SA Pathology, RAH.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 36
Clinician Researchers
Information request 5.1: workforce
• Are there barriers to clinicians participating in research? How can any barriers be addressed?
Over time, and through disinvestment in research within the health system, the number of clinician researchers in the State has steadily decreased.
SAHMRI has recognised the importance of clinician researchers, and have a number working within our Themes. These researchers have direct contact with the health care system and offer us the ability to directly translate research findings into evidence-based improvements to health service delivery.
SAHMRI has both medical and allied health clinicians (dieticians) working within our Themes.
• Professor Maria Makrides (dietitian) is the Theme Leader of the SAHMRI Women and Kids Theme, a member of the AAHMS and Australian Academy of Science (AAS). Her role demonstrates the importance of allied health researchers in the clinical setting.
• Professor Tim Hughes (haematologist, RAH) is the Theme Leader of our Precision Medicine Theme.
• Professor Steve Wesselingh (infectious disease specialist) is the Executive Director, SAHMRI and a key clinician researcher, working specifically at Flinders Medical Centre.
• Dr Peter Psaltis (cardiologist, RAH) plays a critical role as the Co-Director of our Vascular Research Centre.
Other clinician researchers working at SAHMRI include Professor Stephen McDonald, Dr David Yeung, Dr Devendra Hiwase and Dr Dan Thomas, all clinicians with links to the Royal Adelaide Hospital; Dr Amy Keir (neonatologist), Dr Monica Skubisz (obstetrician), Dr Carmel Collins (nurse), and Dr Merryn Netting (paediatric dietitian), all work within the Women’s and Children’s Hospital.
To enable clinician researchers to have the greatest translational impact, they must be granted quarantined research time and research support as key components to success.
South Australia needs a recruitment and retention strategy for clinician researchers to ensure that as a State we attract and maintain the foremost clinical research expertise as a key capability in translational research.
Students at SAHMRI
SAHMRI currently has approximately 200 students working within our facilities, supervised by SAHMRI and partner staff. Our student population includes those undertaking Honours, Masters and PhD degrees.
Our students are a critical part of the SAHMRI community and we are very proud of the work that they are undertaking. While each of these students is academically registered at one of the three Universities, SAHMRI plays a critical role in supporting them in the conduct of their research through direct supervision, teaching and provision of infrastructure.
SAHMRI has established a Student Committee, run by the students themselves. Critically, the co-chairs of the Committee attend and are a key part of the SAHMRI Research Executive Committee.
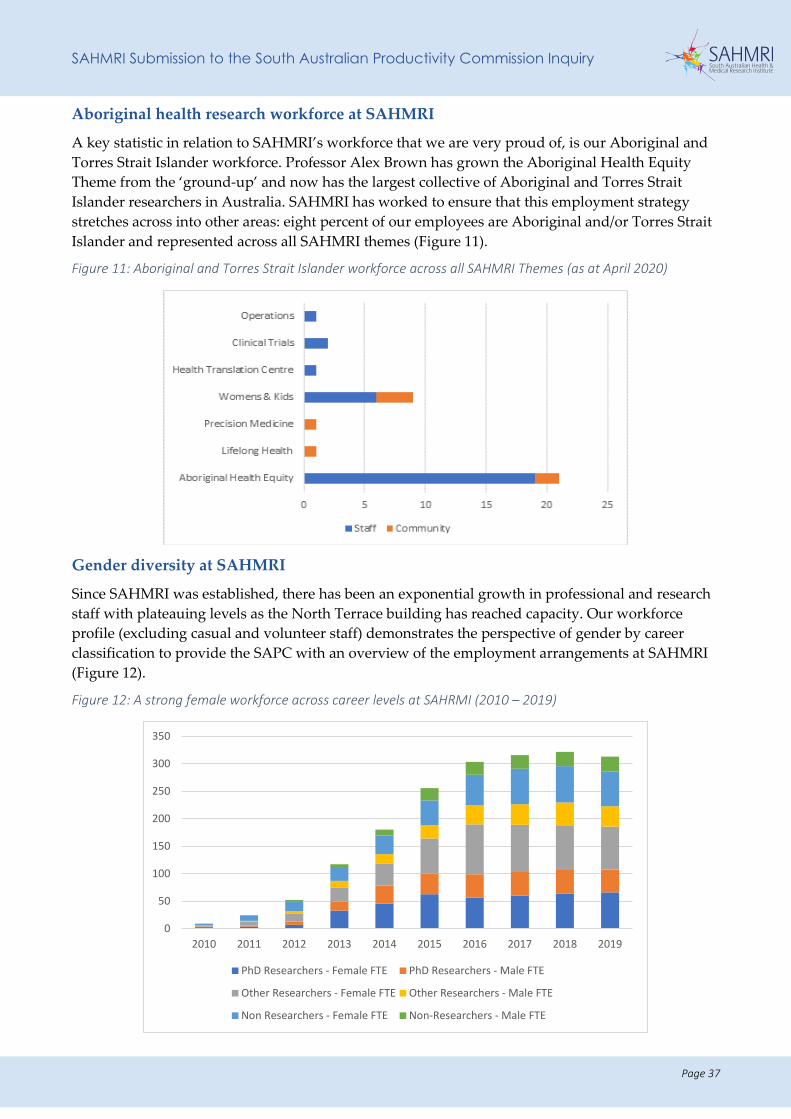
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 37
Aboriginal health research workforce at SAHMRI
A key statistic in relation to SAHMRI’s workforce that we are very proud of, is our Aboriginal and Torres Strait Islander workforce. Professor Alex Brown has grown the Aboriginal Health Equity Theme from the ‘ground-up’ and now has the largest collective of Aboriginal and Torres Strait Islander researchers in Australia. SAHMRI has worked to ensure that this employment strategy stretches across into other areas: eight percent of our employees are Aboriginal and/or Torres Strait Islander and represented across all SAHMRI themes (Figure 11).
Figure 11: Aboriginal and Torres Strait Islander workforce across all SAHMRI Themes (as at April 2020)
Gender diversity at SAHMRI
Since SAHMRI was established, there has been an exponential growth in professional and research staff with plateauing levels as the North Terrace building has reached capacity. Our workforce profile (excluding casual and volunteer staff) demonstrates the perspective of gender by career classification to provide the SAPC with an overview of the employment arrangements at SAHMRI (Figure 12).
Figure 12: A strong female workforce across career levels at SAHRMI (2010 – 2019)
0
50
100
150
200
250
300
350
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019
PhD Researchers - Female FTE PhD Researchers - Male FTE
Other Researchers - Female FTE Other Researchers - Male FTE
Non Researchers - Female FTE Non-Researchers - Male FTE
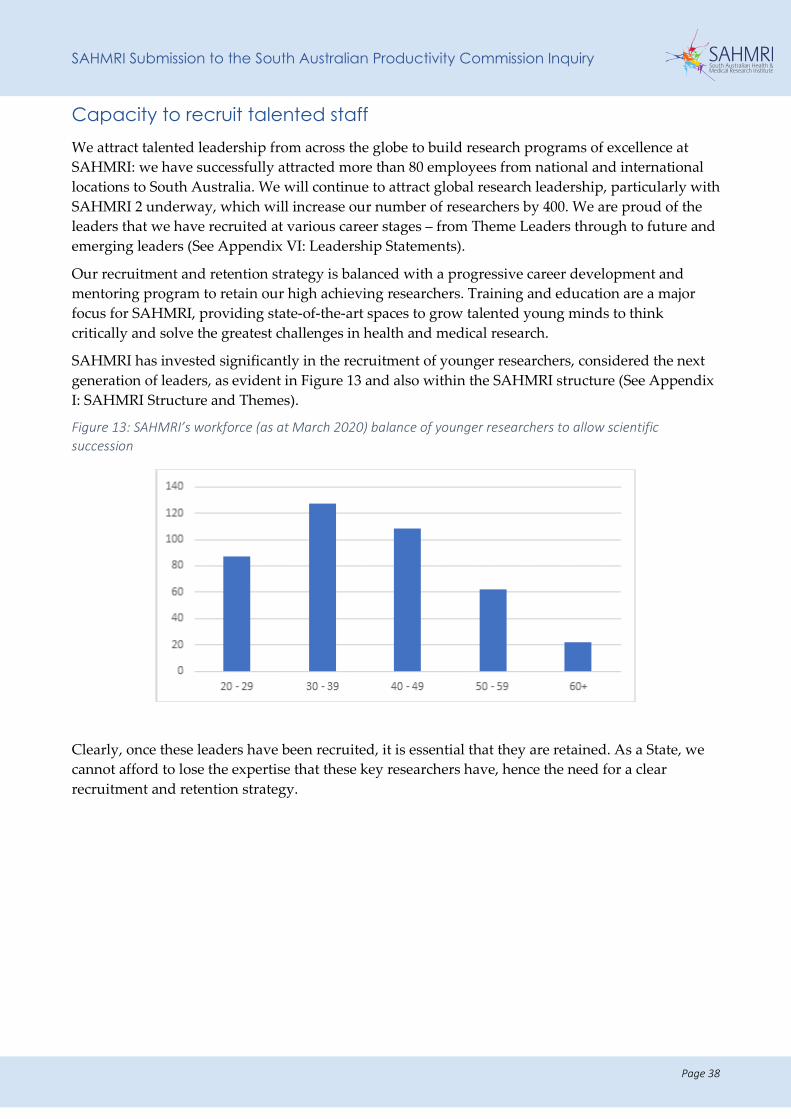
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 38
Capacity to recruit talented staff We attract talented leadership from across the globe to build research programs of excellence at SAHMRI: we have successfully attracted more than 80 employees from national and international locations to South Australia. We will continue to attract global research leadership, particularly with SAHMRI 2 underway, which will increase our number of researchers by 400. We are proud of the leaders that we have recruited at various career stages – from Theme Leaders through to future and emerging leaders (See Appendix VI: Leadership Statements).
Our recruitment and retention strategy is balanced with a progressive career development and mentoring program to retain our high achieving researchers. Training and education are a major focus for SAHMRI, providing state-of-the-art spaces to grow talented young minds to think critically and solve the greatest challenges in health and medical research.
SAHMRI has invested significantly in the recruitment of younger researchers, considered the next generation of leaders, as evident in Figure 13 and also within the SAHMRI structure (See Appendix I: SAHMRI Structure and Themes).
Figure 13: SAHMRI’s workforce (as at March 2020) balance of younger researchers to allow scientific succession
Clearly, once these leaders have been recruited, it is essential that they are retained. As a State, we cannot afford to lose the expertise that these key researchers have, hence the need for a clear recruitment and retention strategy.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 39
Recruiting talented clinician researchers to South Australia
Information request 5.1: workforce
• What connections are there between SA Health and university workforces and how do these affect recruitment and retention of HMR researchers?
Many key researchers have been attracted to South Australia because of the interaction and co-location of clinical/health service delivery, research laboratories and academic institutions. However, we must do more to increase the pool of world-class researchers and be more competitive and effective through the following:
1. Shared appointment model
For South Australia to compete with the eastern states in relation to attraction of the best health and medical research talent, the State must consider a state-wide and competitive recruitment and retention strategy.
Many high performing researchers will come to South Australia because they are offered an opportunity to work across various institutions within the sector – occupying clinical duties within the health system, an academic role at one of the Universities and a research role at SAHMRI. The ability to work across institutions is appealing to many and should be considered in the context of a state-wide recruitment and retention strategy.
We can point to examples that have applied this shared appointment model such as the recruitment of Dr Dan Thomas and Dr Dan Worthley (Precision Medicine), both recognised for excellence in their respective fields and attracted back to South Australia (from overseas) on joint appointment arrangements between the University of Adelaide and SAHMRI.
2. Optimised recruitment packages
Until recently, hospitals have been less inclined to invest in research active clinicians and scientists. As a State, we must be willing to commit to funding these researchers to ensure active translation of evidence into improved outcomes in health care.
The shared appointment model could be supported through the provision of funds from the State Government to allow a health system component of the cross-institutional employment. This model has been adopted in Queensland where clinician researchers (medical and allied health) are supported financially.
3. Future young leaders
Interstate researchers tend not to move to South Australia (young people tend to want to be in the big dynamic cities) and international people generally do not have Adelaide on their radar. More could be done to promote Adelaide as a major scientific destination, especially with the creation of Adelaide BioMed City (e.g. as the State Government does for tourism).
Instead of attracting a ‘lone-star’, we must bring in a capability, which may be their whole team or aligning them to an established team.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 40
RECOMMENDATIONS
We offer the following recommendations in relation to workforce strategy and talent recruitment in SA:
R2: SAHMRI, in collaboration with the Universities, LHNs and Health Translation SA, should convene a strategic forum and take a leadership role in the preparation of the following state-wide strategies:
• Recruitment and retention strategy for high performing researchers – actively targeting clinician researchers, as well as identifying and attracting and developing the next generation of research leaders; identifying and recommending recruitment packages that are competitive with other jurisdictions.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 41
Access to data: regulation and efficiency
Information request 5.2: access to data
• Is the current regulatory environment at the national level conducive to data generation and sharing?
• What types of data are important to share in HMR?
• What barriers are there to sharing data for HMR?
• What data related bottlenecks constrain HMR and what can be done to remove them?
Our clinician researchers, translational scientists and trialists rely on patient data to complete their work. Our Aboriginal Health researchers rely on de-identified data to allow large cohort studies. Data is essential to our routine research work.
While appreciating the responsibilities of data custodians, data access is one of the largest issues facing researchers in South Australia, and barrier to translational research for the benefit of the State’s health system and community. Given the issues associated with data access, South Australian researchers are at a significant disadvantage to their interstate counterparts where data is more readily made available for research purposes.
It is difficult to negotiate access to SA Health data, even when ethics and privacy issues are appropriately accounted for. A risk-adverse approach to data access, not adequately balanced against potential benefits and opportunities lost, prevents South Australian researchers from accessing the specific health and demographic data required to undertake research with any level of efficiency. This substantially increases the cost of conducting research and is a real barrier to feasibility and grant success. It is a significant impediment to South Australia’s increased competitiveness. It also hampers translational research for the health system.
SAHMRI has worked tirelessly over the last eight years in collaboration with SA Health to ensure that our clinical researchers have efficient access to the patient data that they require to undertake timely clinical and health systems research. Primarily this relates to OACIS access – SA Health’s patient management system. Gains in this area will have direct benefits in improved quality and reduced costs for SA Health while at the same time improving grant success.
SAHMRI has established an OACIS Access Deed with SA Health which enables a small number of approved SAHMRI staff to receive access to OACIS data for clinical trials. SAHMRI led the development of this arrangement, and the University of Adelaide now directly benefits from the arrangement that SAHMRI brokered.
More recently, we commenced work with Central Adelaide LHN (CALHN) to grant our staff ‘Research Affiliate Status’ within the LHN. This will allow the approved researcher to access the same datasets available to those with LHN employment status. This is a significant benefit to our researchers who work collaboratively with the RAH. We are hoping to demonstrate the success of the Research Affiliate Agreement CALHN and seek expansion of this with the other LHNs.
While the Access Deed and the Research Affiliate Status arrangements are significant improvements to data access for our researchers, significant reform is required in this area to ensure efficient and timely access.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 42
Registries at SAHMRI
SAHMRI houses a number of key national registries that offer a competitive advantage to South Australia:
• Registry of Senior Australians (ROSA);
• Australian Orthopaedic Association (AOA, Joint Replacement Registry);
• Australia and New Zealand Dialysis and Transplant registry (ANZDATA);
• Transcatheter Aortic Valve Implantation (TAVI) Registry;
• South Australian Clinical Cancer Registry (SACCR) Central Coordination Unit
• Australian Corneal Graft Registry.
The co-location of these registries in the SAHMRI building offers opportunities in relation to consolidation of infrastructure, as well as shared knowledge and generation of new expertise. Importantly, the SAHMRI IT department has created significant IP in the development of clinical trial platforms for these registries, which can be accessed nationwide.
SA/NT DataLink
SA/NT DataLink is co-located in the SAHMRI North Terrace Facility. They have secure facilities on Level 8 of our building to allow them to access/link data under incredibly regulated conditions.
SA/NT DataLink is a critical piece of data infrastructure in the State and must be supported. Its capacity to undertake analysis on big data is critical for researchers in the State. In addition, the return on investment in data linkage is significant – we are able to link data to answer significant questions of specific interest to the Government.
Artificial Intelligence and Machine Learning
SAHMRI has recently established an Artificial Intelligence and Machine Learning Platform, in collaboration with the Australian Institute for Machine Learning (AIML, University of Adelaide) to achieve world-class AI-in-Health research capability in South Australia, and the health impact this transformative technology enables. The AI Platform will bring together the AI and health research community to build a long-term research base, realise the potential of AI’s capacity to improve health outcomes and efficiency, and generate novel AI methods that will have significant and sustainable health impact. The focus on novel and transformative methods over applied AI is essential if we are to capitalise on the opportunity and achieve the desired long-term impact.
Discussions are currently underway with SA Health in relation to the advancement of AI within the health system – through the establishment of a “AI in Health” platform.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 43
RECOMMENDATIONS
We offer the following recommendations in relation to data access:
R13: The SAHMRI/CALHN Research Affiliate Status arrangement (to allow researchers access to data for ethically approved projects) should be adopted by other LHNs.
R14: Infrastructure is required to support the capture of clinical trials in South Australia, through a centralised database.
R15: The Government should seek to support initiatives such as the HTSA Health Analytics Research Collaboration (HARC) in order to build analytical expertise across the sector.
R16: The “AI in Health” platform should be expanded dramatically across the State, with a significant node in ABMC.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 44
Connectivity of the Adelaide BioMed City and the planned Flinders precinct
Information request 5.3: infrastructure
• What role do precincts, neighbourhoods and physical proximity play in promoting collaboration?
SAHMRI is actively engaged in the work of Adelaide BioMed City (ABMC). SAHMRI has been key in driving the process towards a formalised partnership and the recruitment of the general manager, Yvette Van Eenennaam (October 2018; located within SAHMRI).
With a current investment of almost $4 billion in medical, research and education infrastructure, the precinct accommodates more than 15,000 South Australians.
AMBC play a critical role in terms of collaboration, as will the Flinders precinct upon its formal establishment. Given our role as a state-wide institute, our research activity already spans the breadth of the Adelaide metropolitan region and SAHMRI is actively collaborating in many of the initiatives of AMBC and the planned Flinders precinct.
SAHMRI has staff already co-located within the planned Flinders precinct: Professor Geraint Rogers and his team (Microbiome and Host Health) have offices and laboratories on site at Flinders University; various clinical trials led by Professor Maria Makrides occupy space and recruit participants from Flinders Medical Centre; a number of our staff have joint appointments with Flinders University (Professor David Lynn, Professor Stuart Brierley and Dr Cedric Bardy).
Research infrastructure at SAHMRI
Information request 5.3: infrastructure
• How well is existing SA public and private HMR infrastructure being utilised?
• Could existing HMR infrastructure be better utilised or shared more effectively to deliver improvements in HMR performance?
• Can the competing demands on infrastructure of delivering health care and conducting research be better managed?
A key component of the SAHMRI North Terrace Facility is the infrastructure that we have been able to provide to the State. We house a comprehensive suite of equipment, services and expertise to deliver sophisticated analysis and research support to researchers, partners and health services, both locally and nationally.
We bring the list of infrastructure provided in Appendix VII to the attention of the SAPC because without SAHMRI much of this would not have been made available to the State. For example, MITRU exists because there was commitment to build a cyclotron in the basement of SAHMRI; we were responsible for saving PIRL from closure when SA Pathology decided to de-invest in the facility; SAHMRI negotiated the agreement with Jones and Partners and invested heavily (approximately $6 million) in the establishment of CRIC.
SAHMRI plays a critical role in enabling access to this infrastructure to the whole research community in South Australia, particularly across ABMC: core facility collaborations exist within the Biomedical precinct.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 45
These shared arrangements, which include significantly subsidised rates for partner staff (usually in excess of 50% subsidy), are critical to the ongoing success of health and medical research and to the avoidance of duplication of equipment, infrastructure and effort across South Australia.
We are aware that ABMC has a committee dedicated to managing the utilisation of infrastructure across the precinct, and that discussions are occurring at this level to determine more effective and efficient ways of managing this.
The new SA Genomics Centre has already been discussed but in general all the core facilities collaborate to some extent.
EXAMPLE OF CORE FACILITY COLLABORATIONS THAT EXIST WITHIN THE PRECINCT
An agreement is currently in place between the University of Adelaide, Health and Medical Sciences (AHMS) and SAHMRI that sees both organisations Flow Cytometry facilities jointly provide service to the Biomedical precinct. An agreement is also being finalised for Proteomics services to be provided in the same manner in a three-way collaboration with SAHMRI and two faculties of the University of Adelaide (AHMS & Sciences). In addition, under separate employment agreements, the Confocal Microscopy facilities at both SAHMRI and Centre of Cancer Biology are managed by the same Core Manager.
These agreements and arrangements draw upon the shared service culture and cohesive nature in which SAHMRI runs its core facilities.
The benefits are:
• Increased capacity, flexibility and improved stability of the staffing profile and services.
• Reduced duplication of technology, allowing for diversification of the assets to service the diverse technological requirements for researchers in both institutions.
• Improved outcomes for both quality and quantity of work performed.
• New opportunities to promote and initiate collaboration opportunities.
• Enhanced joint facilities benefit current and future grant and contract research bids.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 46
COLLABORATIVE MODELS TO DRIVE HMR AND DEVELOPMENT Terms of Reference. Identify and assess existing collaboration on health and medical research between research organisations (public and private) and linkages between organisations and industry. Identify innovative collaboration models to drive R&D.
Information request 5.4: collaboration
• How important is collaboration to securing research funding and to the achievement of HMR outcomes – both between researchers and between research institutions and industry, nationally or globally?
• What steps could be taken to enhance collaboration amongst research institutions, including universities, and between research institutions and industry?
Information request 5.11: competitive advantage – collaboration and precincts
• The size and culture of South Australia and Adelaide is said to make collaboration easier. Does this apply in HMR?
• How competitive is South Australia in attracting leading researchers and talented postgraduates to HMR?
SAHMRI collaborative research projects SAHMRI is very proud of the collaborative approach that we have adopted in relation to the conduct of health and medical research. The premise of our model centres on collaboration (See Background).
Our collaborations extend across University partners, industry, national and international partnerships and a range of other partners (such as government and non-government agencies) to ensure research success in South Australia.
EXAMPLES OF SOME OF OUR KEY NATIONAL COLLABORATIVE PROJECTS
Creation of blood spot, patent, partnership with University of Adelaide and Trajan
The SAHMRI Women and Kids Theme are world leaders in the development of dried blood spot (DBS) technology for the assessment of nutrient status in humans. The DBS system (for measuring the unstable long chain fatty acids in blood) has been patented by the University of Adelaide and licenced to Xerion Pty Ltd. This technology has driven a partnership with Trajan Scientific and Medical, a Melbourne-based company, that has resulted in the formation of Trajan Nutrition a joint venture with the University of Adelaide and SAHMRI. Through Trajan Scientific and Medical, Trajan Nutrition has agencies in Malaysia, the UK and the USA. The tools developed by Trajan Nutrition are being used in the large-scale clinical trials administered by SAHMRI Women and Kids and provide a distinct advantage in the area of perinatal nutrition where the volume of blood can be critical, such as in the case of early preterm infants.
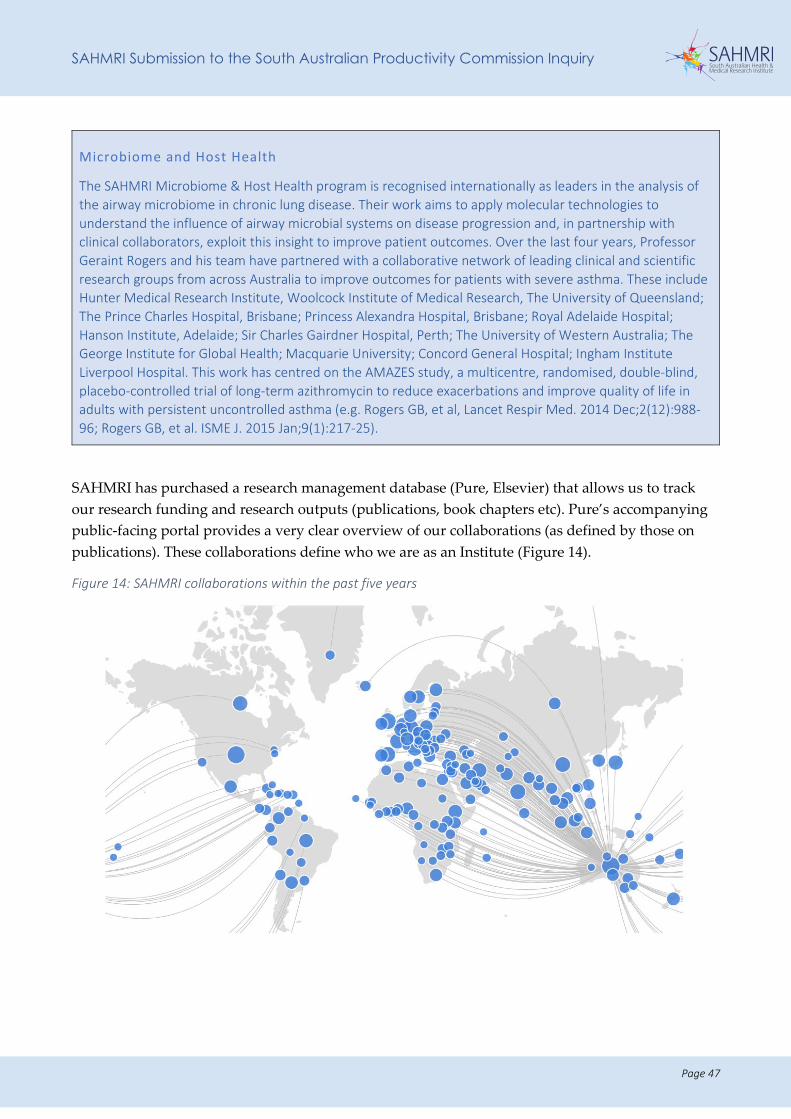
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 47
Microbiome and Host Health
The SAHMRI Microbiome & Host Health program is recognised internationally as leaders in the analysis of the airway microbiome in chronic lung disease. Their work aims to apply molecular technologies to understand the influence of airway microbial systems on disease progression and, in partnership with clinical collaborators, exploit this insight to improve patient outcomes. Over the last four years, Professor Geraint Rogers and his team have partnered with a collaborative network of leading clinical and scientific research groups from across Australia to improve outcomes for patients with severe asthma. These include Hunter Medical Research Institute, Woolcock Institute of Medical Research, The University of Queensland; The Prince Charles Hospital, Brisbane; Princess Alexandra Hospital, Brisbane; Royal Adelaide Hospital; Hanson Institute, Adelaide; Sir Charles Gairdner Hospital, Perth; The University of Western Australia; The George Institute for Global Health; Macquarie University; Concord General Hospital; Ingham Institute Liverpool Hospital. This work has centred on the AMAZES study, a multicentre, randomised, double-blind, placebo-controlled trial of long-term azithromycin to reduce exacerbations and improve quality of life in adults with persistent uncontrolled asthma (e.g. Rogers GB, et al, Lancet Respir Med. 2014 Dec;2(12):988-96; Rogers GB, et al. ISME J. 2015 Jan;9(1):217-25).
SAHMRI has purchased a research management database (Pure, Elsevier) that allows us to track our research funding and research outputs (publications, book chapters etc). Pure’s accompanying public-facing portal provides a very clear overview of our collaborations (as defined by those on publications). These collaborations define who we are as an Institute (Figure 14).
Figure 14: SAHMRI collaborations within the past five years
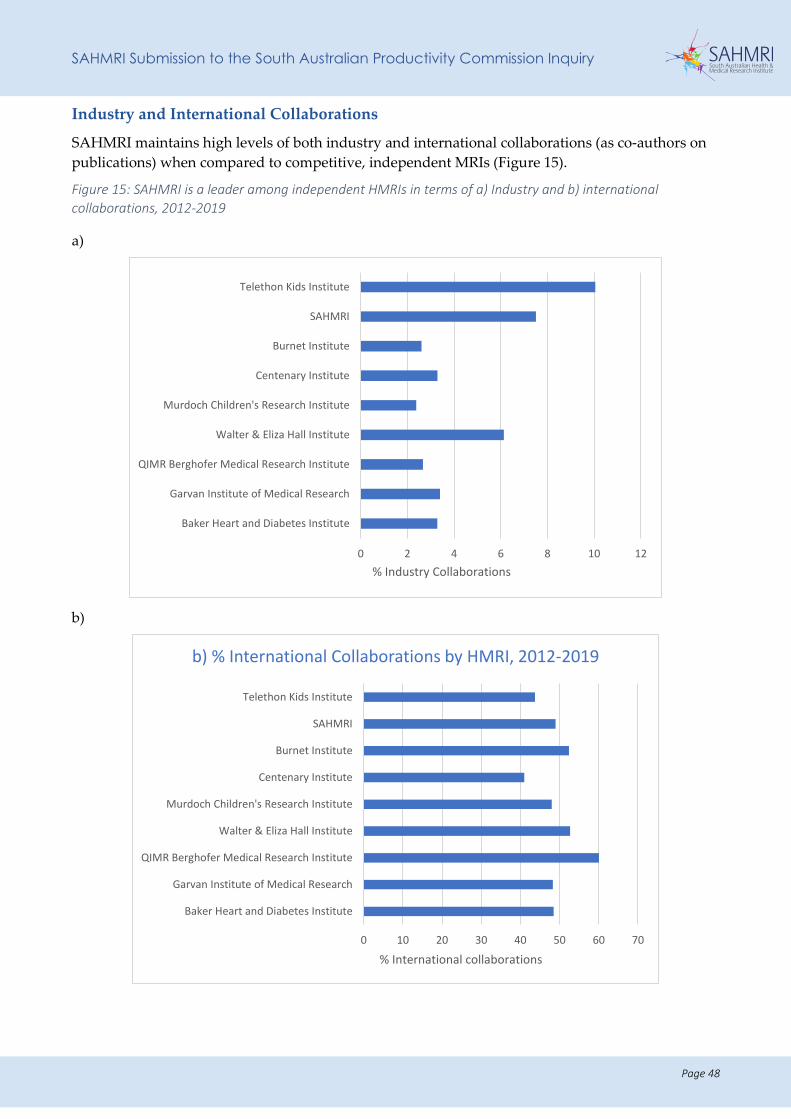
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 48
Industry and International Collaborations
SAHMRI maintains high levels of both industry and international collaborations (as co-authors on publications) when compared to competitive, independent MRIs (Figure 15).
Figure 15: SAHMRI is a leader among independent HMRIs in terms of a) Industry and b) international collaborations, 2012-2019
a)
b)
0 2 4 6 8 10 12
Baker Heart and Diabetes Institute
Garvan Institute of Medical Research
QIMR Berghofer Medical Research Institute
Walter & Eliza Hall Institute
Murdoch Children's Research Institute
Centenary Institute
Burnet Institute
SAHMRI
Telethon Kids Institute
% Industry Collaborations
0 10 20 30 40 50 60 70
Baker Heart and Diabetes Institute
Garvan Institute of Medical Research
QIMR Berghofer Medical Research Institute
Walter & Eliza Hall Institute
Murdoch Children's Research Institute
Centenary Institute
Burnet Institute
SAHMRI
Telethon Kids Institute
% International collaborations
b) % International Collaborations by HMRI, 2012-2019
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 49
Collaboration – health outcomes driven The unique collaborative model allows SAHMRI and other research partners to maximise their research outputs and ensure outcomes are driven by the health needs of the South Australian population. Our collaborative approach facilitates outputs that are health outcome driven through:
• Co-location that brings multidisciplinary teams together across ‘bench to bedside’ translational research and facilitates innovative approaches to research practices.
• SAHMRI’s important role in the South Australian ecosystem and facilitating the development of research precincts and essential research infrastructure for the benefit of all South Australia research partners.
• SAHMRI’s strong commitment and established track record in consumer engagement, with the involvement of consumers in many areas of research along different elements of the research pathway: our research partners are similarly adopting SAHMRI’s Consumer and Community Engagement Framework11.
Collaborative approaches to co-location of researchers
The SAHMRI building on North Terrace was designed to house SAHMRI staff as well as researchers from our key partners. This is still a reality today, with a number of key researchers from the three Universities and CSIRO occupying space within the building. This co-location is mutually beneficial for all parties.
Agreements have been implemented with each of our partner organisations, to specify the rent that they pay for occupying space within the SAHMRI building. The agreement also specifies the rates that they pay for accessing infrastructure within the building. Both the rent and the infrastructure costs are at a significantly subsidised rate (about one-third of market CBD office rate for sophisticated research facilities/space). Appendix VIII (University Rent Subsidies) provides an overview of the arrangement that is in place with the partner organisations regarding occupation of the SAHMRI facility. SAHMRI is of the view that this arrangement is extremely beneficial to partner organisations, considering the benefits associated with occupation of a world-class facility, access to infrastructure and the collaborative opportunities available to the research staff.
The co-location of the SAHMRI building with the RAH is significantly advantageous from the perspective of clinical research. The RAH was designed without key lab space – SAHMRI offers this to clinician researchers, along with key diagnostic infrastructure and space. This arrangement is working well, with additional researchers seeking space within SAHMRI to conduct their research.
Access to laboratory space within SAHMRI by hospital staff is funded by SAHMRI, the Universities and grants, not directly via hospital funds.
11 https://www.sahmri.org/research-theme/resource-13/
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 50
Collaboration with the Universities
SAHMRI has a very proud association of working collaboratively with the three Universities, as evidenced throughout our submission. We share a commitment to undertaking excellent nationally and internationally competitive health and medical research, and to building the capacity of the next generation of researchers state-wide.
Our collaboration extends to joint projects, co-location of University staff within the SAHMRI building and our associated sites, the joint appointment of key international recruits and the administration of a large proportion of SAHMRI staff grants directly via a University partner. We also hold a critical leadership role within the shared vision of Adelaide BioMed City (ABMC).
As previously outlined, the three Universities are represented on the SAHMRI Board and are represented within the structure of each of our Themes (with some University staff occupying leadership roles within the Thematic structure).
A number of SAHMRI staff are jointly employed by one of the Universities, occupying important teaching and research roles.
We have arrangements in place with each of the Universities in relation to the administration of our Category 1 Australian Competitive Grants, specifically MRFF and NHMRC awards. This relationship is managed directly at the level of the Research Offices, and to date has worked very well. SAHMRI has made the recent decision to administer all of its NHMRC grants via the Universities. This arrangement means that the University is able to count SAHMRI grant success towards its Excellence in Research for Australia (ERA) and other rankings and is counted in Higher Education Research Data Collection (HERDC) data.
All SAHMRI staff with a university affiliation are required to attribute both SAHMRI and the University in the authorship by-line, for all peer-reviewed publications. This ensures that both organisations receive mutual recognition for the publication. In addition, many University researchers who occupy space within the SAHMRI building also include SAHMRI within publication by-lines. This recognises the benefit of co-location and sharing of infrastructure.
Collaboration with Non-Government agencies: an example of cross-sector collaboration
Since 2011, SAHMRI has provided the administrative management of Cancer Council SA’s Beat Cancer Project. The Beat Cancer Project is a South Australian state-wide initiative intended to support and advance cancer research within the State. It is funded by Cancer Council SA, the SA Government (through SA Health) and the Australian Government Medical Research Future Fund (MRFF).
The objectives of the Beat Cancer Project are to increase funding for cancer research, increase the capacity for researchers to attract more national and international research grants, and build a stronger cancer research workforce and broader research infrastructure in South Australia.
SAHMRI provides the executive support function for the Beat Cancer Project, which includes facilitation of all leadership meetings, management of funding rounds, coordination of peer review, and the awarding and administration of funding.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 51
RECOMMENDATIONS
We offer the following recommendations in relation to collaboration:
R2: SAHMRI, in collaboration with the Universities, LHNs and Health Translation SA, should convene a strategic forum and take a leadership role in the preparation of the following state-wide strategies:
• Comprehensive health and medical research strategy – based on strengths of the state as well as community need, with the objective being to promote collaboration, increase competitiveness and identify and recommend optimum resourcing and implementation plans.
• Impact Framework to measure the success of health and medical research across the State over the next 10 years.
• MRFF grant success strategy – targeted at supporting researchers through the provision of matched funding/Government support; building the capacity of clinician researchers with an aim to increase the number of successful funding outcomes; increased political lobbying to attract non-competitive funding.
• Coordinated provision of research support and preclinical services on a State-wide basis – to avoid duplication and maximise scarce resources, including a long-term strategy for the services currently provided at PIRL Gilles Plains.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 52
OPPORTUNITIES FOR INCREASED COMMERCIALISATION OF HEALTH AND MEDICAL RESEARCH Terms of Reference. Identify and assess opportunities for increased commercialisation of health and medical research in South Australia
Information request 5.6: translation of research
• What opportunities are there to increase commercialisation of HMR in SA?
• What barriers, if any, are there to commercialisation of HMR?
• What steps can be taken to remove or reduce these barriers?
SAHMRI has adopted a unique approach to commercialisation Since 2017, SAHMRI has partnered with Bright Arena to support commercialisation activities within the Institute.
Our approach to commercialisation is quite different to the traditional approaches adopted by Universities and Government Departments. This new approach to commercialisation focuses on impact, both at the level of the individual researcher, and the Institute as a whole.
Our goal is to build a culture of entrepreneurship at SAHMRI, enabling researchers and staff to pursue their ideas and develop their science and ideas through a commercial lens from day one. This new approach involves:
• Building a pipeline of opportunities to actively engage all members of the institute to identify and prioritise promising technology and talent for support.
• Building commercial capability and capacity in SAHMRI researchers and staff through accelerator programs. These programs teach crucial commercial and entrepreneurial skills that researchers apply to current and future research opportunities.
• Providing hands on support for researchers that have identified a commercial opportunity from their research.
• Expanding research portfolios working with industry and develop ideas into commercial and economic impact.
• Connecting researchers with the right skills and expertise at the right time to scale their impact, and
• Supporting researchers in negotiations with industry, company establishment and growth.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 53
Over the last two years, SAHMRI in collaboration with Bright Arena, has been able to demonstrate success utilising this approach, namely:
• 76 project teams engaged in commercial/entrepreneurial programs
• 128 researchers trained in industry skills
• 7 new companies created
• 3 new products in development
• 3 new research groups recruited with commercial interests:
- Dr Fiona Kerr : NeuroTech Institute
- Dr Dan Worthley: private company
- Dr Petranel Ferrao: Personalised Theragnostics
SAHMRI Ventures
In addition to delivering the core program, Bright Arena is in the process of raising an Early Stage Venture fund for SAHMRI. Over the past two years, this work has supported researchers through early validation and has found innovative ways to create new businesses, products and build entrepreneurial capability. The goal is to have an Early Stage Venture fund established by mid-2020. These funds will increase the pipeline of commercial opportunities emerging from SAHMRI. It also acts as a support and enabler to build the biomedical and biotechnology ecosystem as a key pillar in South Australia.
Medical Research Commercialisation Fund (MRCF)
At a national level, the Medical Research Commercialisation Fund (MRCF) provides dedicated, investment funding to support the commercialisation of early-stage medical research discoveries that originate from its member institutes. The collaborative nature of the MRCF seeks to foster best practice in the commercialisation of medical innovations.12
SAHMRI is a financial member of MRCF, which allows access for researchers across the State.
Brandon Capital Partners, which manages MRCF, has a staff member – Dr Melissa McBurnie – working in the SAHMRI building. Having Dr McBurnie in our building assists in raising the profile of SAHMRI researchers and also ensures that we are capitalising on the opportunities that the MRCF has to offer our researchers.
Barriers to commercialisation
Early stage commercialisation is impacted upon by lack of funding for preclinical and early clinical work, as well as data collection. This must be addressed in order to ensure future success of commercial and economic impact. We must ensure that researchers receive funding to support these activities that are often considered too early for support from venture capital companies, but too late for academic funding from bodies such as the NHMRC and ARC.
12 www.mcrf.com.au

SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 54
Intellectual property (IP) policy
South Australia has several diverse approaches to the management of intellectual property. Each hospital and research organisation manage their own intellectual property (IP) and provide advice to their own staff. South Australia should consider avoiding duplication of effort and coordinating some of this centrally through the creation of a centralised IP network.
RECOMMENDATIONS
We offer the following recommendations in relation to commercialisation of research:
R5: Financial support to kick start the establishment of a new Venture Capital fund, aimed specifically at addressing the early “valleys of death” in research commercialisation.
R6: Disruptive model of IP identification and commercialisation adopted by SAHMRI in partnership with Bright Arena over the past 2 years should be supported and endorsed.
R7: To enhance IP commercialisation capabilities, the staff and activities of AusHealth13 (formerly MedVet) should be merged into SAHMRI.
R8: AusHealth could fulfil a coordination role regarding IP management once merged into SAHMRI.
13 https://www.aushealth.com.au/
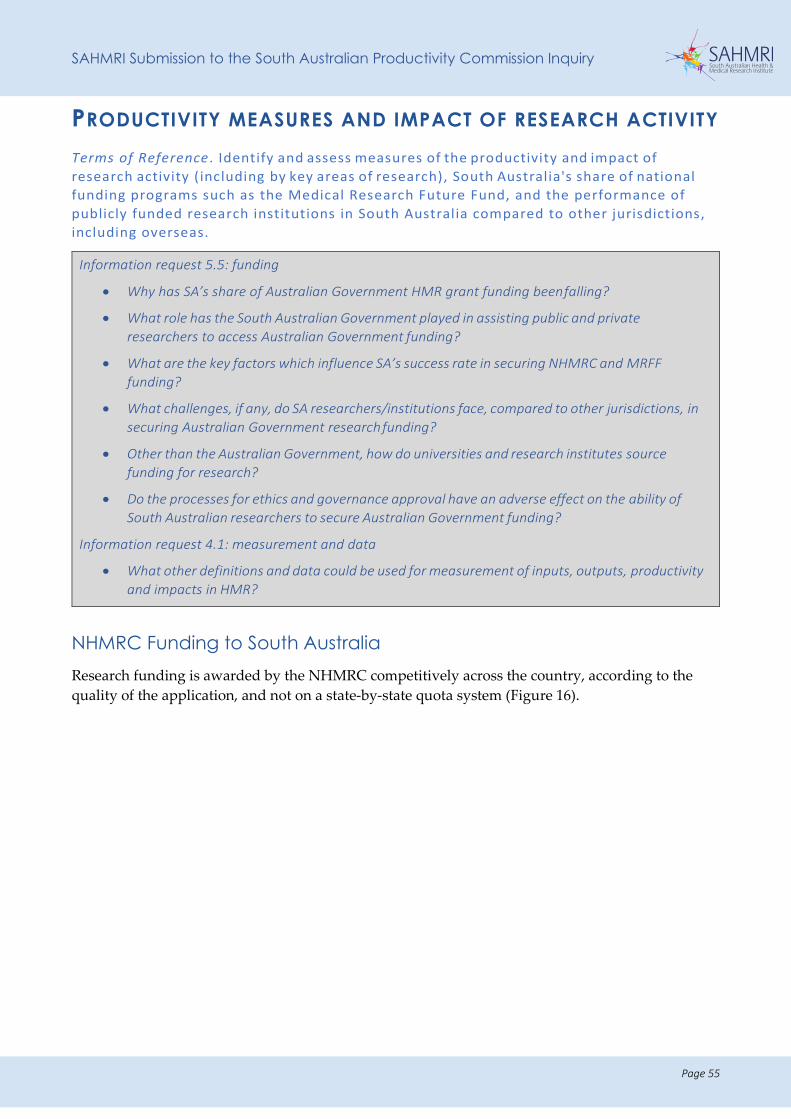
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 55
PRODUCTIVITY MEASURES AND IMPACT OF RESEARCH ACTIVITY Terms of Reference . Identify and assess measures of the productivity and impact of research activity (including by key areas of research), South Australia's share of national funding programs such as the Medical Research Future Fund, and the performance of publicly funded research institutions in South Australia compared to other jurisdictions, including overseas.
Information request 5.5: funding
• Why has SA’s share of Australian Government HMR grant funding been falling?
• What role has the South Australian Government played in assisting public and private researchers to access Australian Government funding?
• What are the key factors which influence SA’s success rate in securing NHMRC and MRFF funding?
• What challenges, if any, do SA researchers/institutions face, compared to other jurisdictions, in securing Australian Government research funding?
• Other than the Australian Government, how do universities and research institutes source funding for research?
• Do the processes for ethics and governance approval have an adverse effect on the ability of South Australian researchers to secure Australian Government funding?
Information request 4.1: measurement and data
• What other definitions and data could be used for measurement of inputs, outputs, productivity and impacts in HMR?
NHMRC Funding to South Australia Research funding is awarded by the NHMRC competitively across the country, according to the quality of the application, and not on a state-by-state quota system (Figure 16).
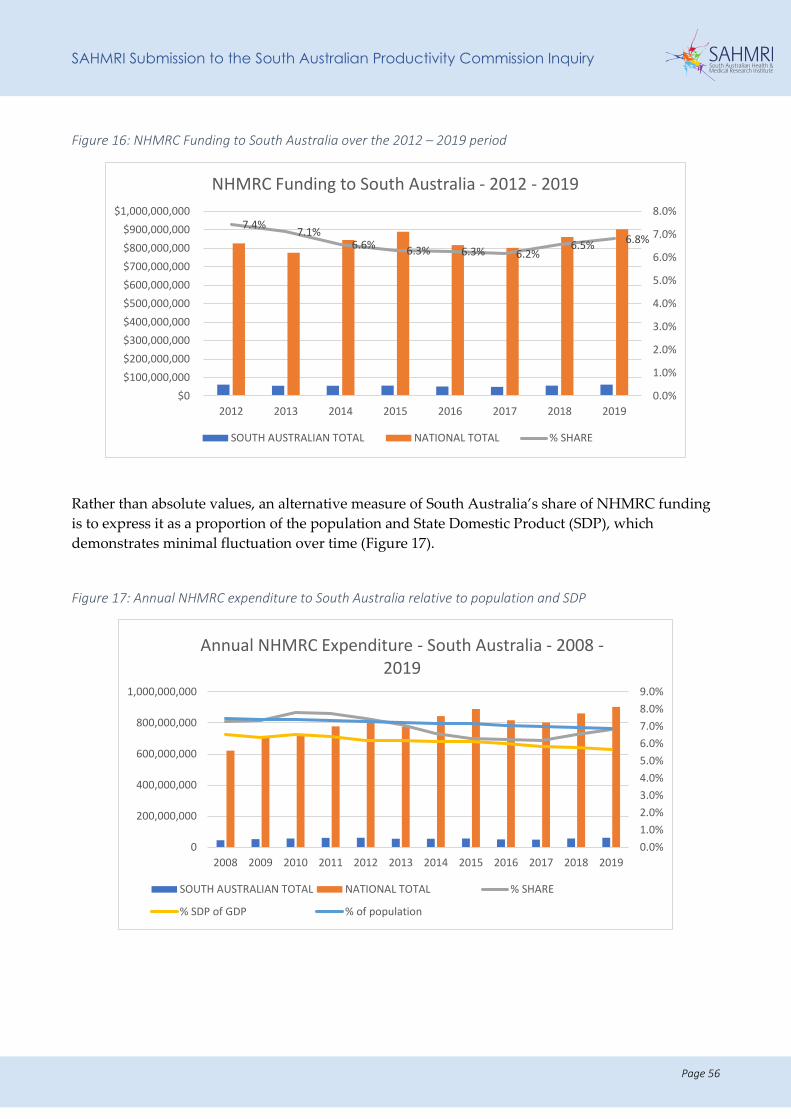
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 56
Figure 16: NHMRC Funding to South Australia over the 2012 – 2019 period
Rather than absolute values, an alternative measure of South Australia’s share of NHMRC funding is to express it as a proportion of the population and State Domestic Product (SDP), which demonstrates minimal fluctuation over time (Figure 17).
Figure 17: Annual NHMRC expenditure to South Australia relative to population and SDP
7.4% 7.1%6.6% 6.3% 6.3% 6.2%
6.5% 6.8%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
$0$100,000,000$200,000,000$300,000,000$400,000,000$500,000,000$600,000,000$700,000,000$800,000,000$900,000,000
$1,000,000,000
2012 2013 2014 2015 2016 2017 2018 2019
NHMRC Funding to South Australia - 2012 - 2019
SOUTH AUSTRALIAN TOTAL NATIONAL TOTAL % SHARE
0.0%1.0%2.0%3.0%4.0%5.0%6.0%7.0%8.0%9.0%
0
200,000,000
400,000,000
600,000,000
800,000,000
1,000,000,000
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019
Annual NHMRC Expenditure - South Australia - 2008 -2019
SOUTH AUSTRALIAN TOTAL NATIONAL TOTAL % SHARE
% SDP of GDP % of population
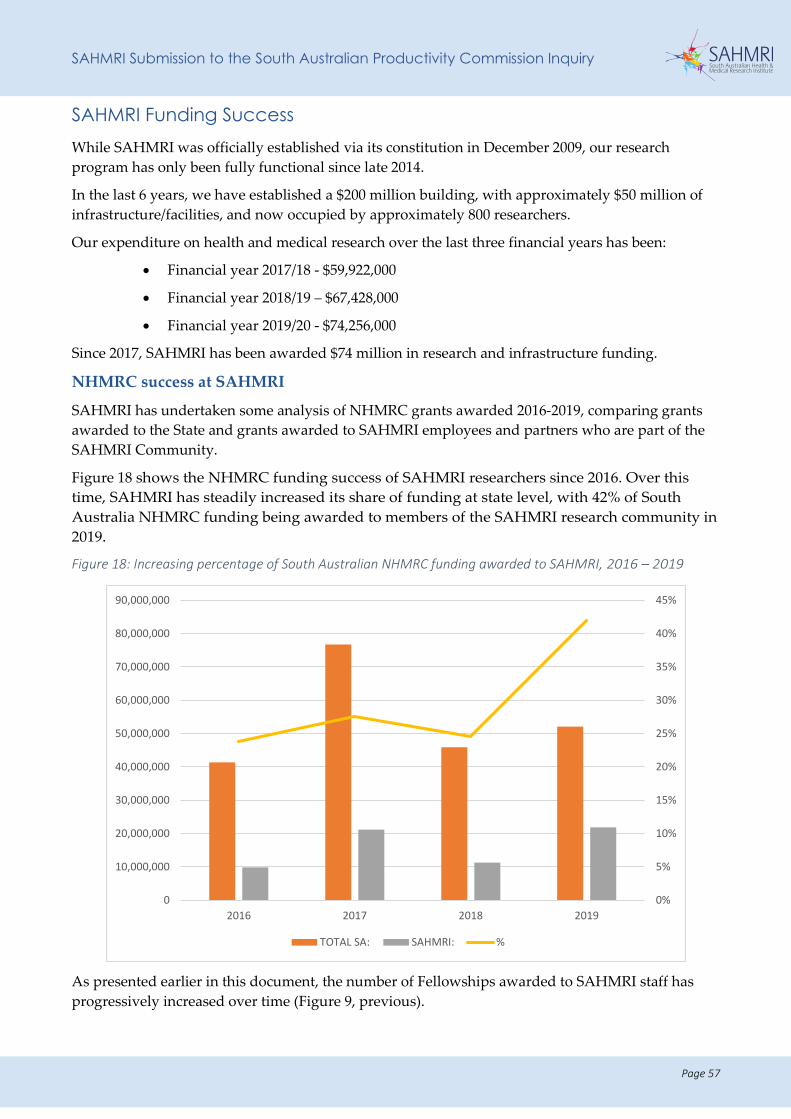
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 57
SAHMRI Funding Success While SAHMRI was officially established via its constitution in December 2009, our research program has only been fully functional since late 2014.
In the last 6 years, we have established a $200 million building, with approximately $50 million of infrastructure/facilities, and now occupied by approximately 800 researchers.
Our expenditure on health and medical research over the last three financial years has been:
• Financial year 2017/18 - $59,922,000
• Financial year 2018/19 – $67,428,000
• Financial year 2019/20 - $74,256,000
Since 2017, SAHMRI has been awarded $74 million in research and infrastructure funding.
NHMRC success at SAHMRI
SAHMRI has undertaken some analysis of NHMRC grants awarded 2016-2019, comparing grants awarded to the State and grants awarded to SAHMRI employees and partners who are part of the SAHMRI Community.
Figure 18 shows the NHMRC funding success of SAHMRI researchers since 2016. Over this time, SAHMRI has steadily increased its share of funding at state level, with 42% of South Australia NHMRC funding being awarded to members of the SAHMRI research community in 2019.
Figure 18: Increasing percentage of South Australian NHMRC funding awarded to SAHMRI, 2016 – 2019
As presented earlier in this document, the number of Fellowships awarded to SAHMRI staff has progressively increased over time (Figure 9, previous).
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
0
10,000,000
20,000,000
30,000,000
40,000,000
50,000,000
60,000,000
70,000,000
80,000,000
90,000,000
2016 2017 2018 2019
TOTAL SA: SAHMRI: %
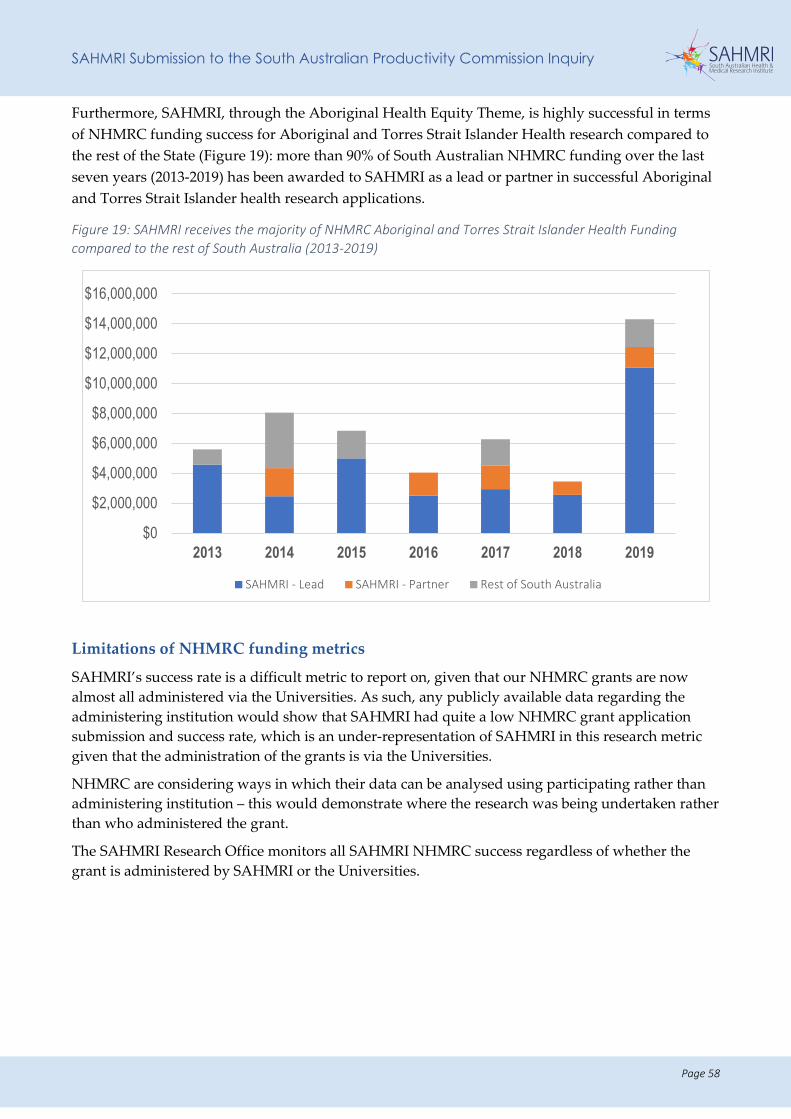
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 58
Furthermore, SAHMRI, through the Aboriginal Health Equity Theme, is highly successful in terms of NHMRC funding success for Aboriginal and Torres Strait Islander Health research compared to the rest of the State (Figure 19): more than 90% of South Australian NHMRC funding over the last seven years (2013-2019) has been awarded to SAHMRI as a lead or partner in successful Aboriginal and Torres Strait Islander health research applications.
Figure 19: SAHMRI receives the majority of NHMRC Aboriginal and Torres Strait Islander Health Funding compared to the rest of South Australia (2013-2019)
Limitations of NHMRC funding metrics
SAHMRI’s success rate is a difficult metric to report on, given that our NHMRC grants are now almost all administered via the Universities. As such, any publicly available data regarding the administering institution would show that SAHMRI had quite a low NHMRC grant application submission and success rate, which is an under-representation of SAHMRI in this research metric given that the administration of the grants is via the Universities.
NHMRC are considering ways in which their data can be analysed using participating rather than administering institution – this would demonstrate where the research was being undertaken rather than who administered the grant.
The SAHMRI Research Office monitors all SAHMRI NHMRC success regardless of whether the grant is administered by SAHMRI or the Universities.
$0
$2,000,000
$4,000,000
$6,000,000
$8,000,000
$10,000,000
$12,000,000
$14,000,000
$16,000,000
2013 2014 2015 2016 2017 2018 2019
SAHMRI - Lead SAHMRI - Partner Rest of South Australia
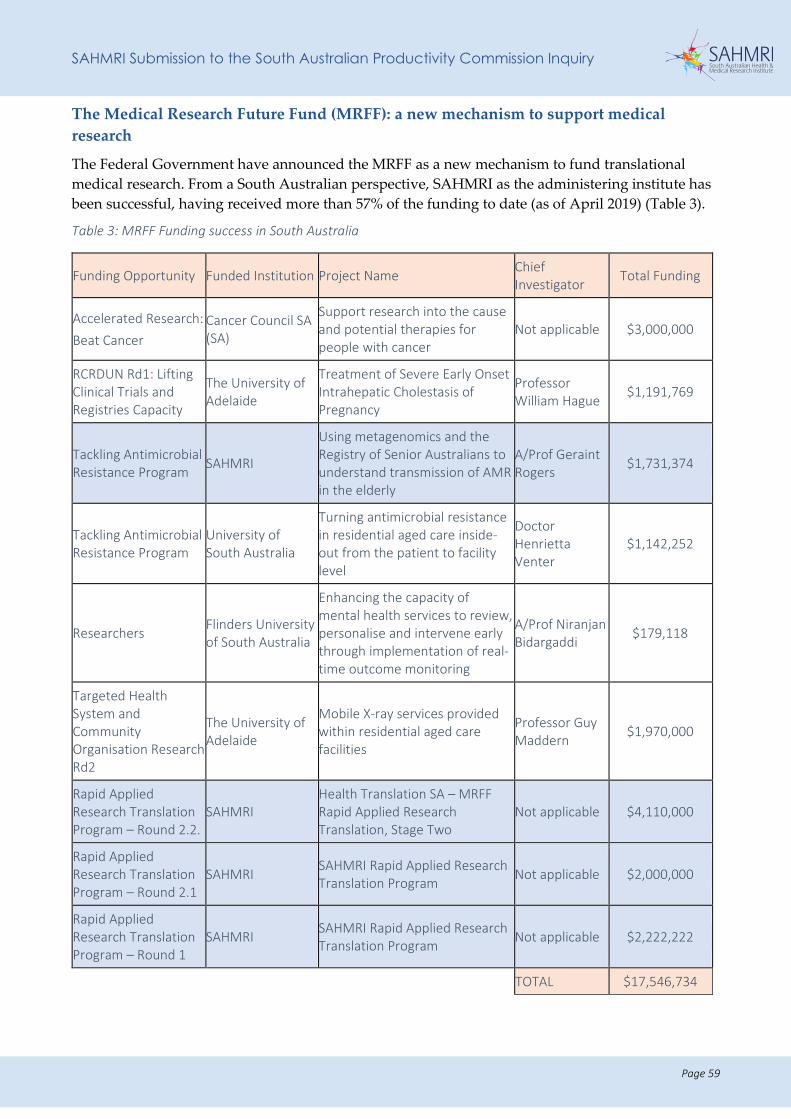
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 59
The Medical Research Future Fund (MRFF): a new mechanism to support medical research
The Federal Government have announced the MRFF as a new mechanism to fund translational medical research. From a South Australian perspective, SAHMRI as the administering institute has been successful, having received more than 57% of the funding to date (as of April 2019) (Table 3).
Table 3: MRFF Funding success in South Australia
Funding Opportunity Funded Institution Project Name Chief Investigator Total Funding
Accelerated Research: Beat Cancer
Cancer Council SA (SA)
Support research into the cause and potential therapies for people with cancer
Not applicable $3,000,000
RCRDUN Rd1: Lifting Clinical Trials and Registries Capacity
The University of Adelaide
Treatment of Severe Early Onset Intrahepatic Cholestasis of Pregnancy
Professor William Hague $1,191,769
Tackling Antimicrobial Resistance Program SAHMRI
Using metagenomics and the Registry of Senior Australians to understand transmission of AMR in the elderly
A/Prof Geraint Rogers $1,731,374
Tackling Antimicrobial Resistance Program
University of South Australia
Turning antimicrobial resistance in residential aged care inside-out from the patient to facility level
Doctor Henrietta Venter
$1,142,252
Researchers Flinders University of South Australia
Enhancing the capacity of mental health services to review, personalise and intervene early through implementation of real-time outcome monitoring
A/Prof Niranjan Bidargaddi $179,118
Targeted Health System and Community Organisation Research Rd2
The University of Adelaide
Mobile X-ray services provided within residential aged care facilities
Professor Guy Maddern $1,970,000
Rapid Applied Research Translation Program – Round 2.2.
SAHMRI Health Translation SA – MRFF Rapid Applied Research Translation, Stage Two
Not applicable $4,110,000
Rapid Applied Research Translation Program – Round 2.1
SAHMRI SAHMRI Rapid Applied Research Translation Program Not applicable $2,000,000
Rapid Applied Research Translation Program – Round 1
SAHMRI SAHMRI Rapid Applied Research Translation Program Not applicable $2,222,222
TOTAL $17,546,734
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 60
While the attraction of $17 million into the State from the MRFF is a significant achievement, consideration must be given to ways of improving our success rate as a State. MRFF funding to SAHMRI also includes the support of Health Translation SA which is currently administered by SAHMRI.
Significant lobbying occurs in relation to the MRFF – directly to the Minister and Chairs of the Missions. This has been a very successful strategy for the eastern states, but has not been adopted as dramatically in South Australia: South Australia has only received an estimated 1% of MRFF non-competitive funding (i.e. targeted and emerging priorities) suggesting an opportunity for greater political lobbying/advocacy for key health issues reflective of the South Australian population.
The MRFF currently has 2018-2020 priorities which guide their research funding schemes. Every two years, the Australian Medical Research Advisory Board (AMRAB) consults the public regarding MRFF priorities. SAHMRI leadership, and researchers across our Themes, will actively participate in the consultation process to set the next round of MRFF priorities – expected in late 2020.
The NHMRC and MRFF have quite different strategic objectives and fund projects based on different criteria. The MRFF aims to transform health and medical research and innovation to improve lives, build the economy and contribute to health system sustainability.14 Successful projects must demonstrate the ability to meet all three of these criteria.
Essential to this therefore are clinical researchers – an area already identified as a growth area for the State. With a state-wide recruitment and retention strategy in this area, South Australia would have the capacity to increase receipt of MRFF funding. Given SAHMRI’s interest in health service improvement, and focus on translation, this is a key area in which we could play a significant role.
In addition, the MRFF has a number of competitive rounds across a number of missions, all with varying research areas and research approaches (e.g. clinical trials, infrastructure). SAHMRI is perfectly positioned to benefit from the MRFF as more competitive schemes roll-out.
SAHMRI has appointed a member of the Research Office 0.5FTE to work with researchers on developing applications for submission to the MRFF. This staff member is dedicated to also ensuring that SAHMRI has a comprehensive understanding of the funding available, upcoming funding schemes and awareness of the funding rules.
Health Translation SA, in collaboration with the three Universities and the State Government, facilitate a MRFF working group designed to work collaboratively to improve South Australia’s success at securing MRFF grants. It is an important forum for the exchange of information, discussion of collaborative opportunities across institutions, and information-sharing to develop a state-wide MRFF strategy. SAHMRI is an active member of this group and strongly encourages the State Government to ensure that this group continues.
Australian Research Council Funding
As an HMRI, we are ineligible to apply for funding from the Australian Research Council (ARC). Our researchers are often named as co-investigators on ARC grant applications but SAHMRI cannot be named as the lead institution of the submission. Where SAHMRI researchers have an affiliation with a University, they may choose to submit the ARC grant utilising their affiliate appointment (with the University named as the lead (administering) institution).
14 https://www.health.gov.au/initiatives-and-programs/medical-research-future-fund
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 61
National Collaborative Research Infrastructure Strategy (NCRIS)
SAHMRI has received NCRIS funding to support our work both at PIRL and in our North Terrace Facility in relation to the SA Genome Editing Facility. SAHMRI hosts the South Australian arm of both the National Imaging Facility and the Australian Phenomics Network, which has contributed millions of dollars in funding since initiated by SAHMRI and offers substantial research infrastructure benefit to the State.
State Government Funding to SAHMRI
At the time of the acceptance of the Shine Young Review recommendations, the State Government made a conscious decision to divest in health and medical research given the establishment of SAHMRI. This resulted in a number of research groups transitioning from SA Pathology to SAHMRI:
• The Large Animal Research Imaging Facility – now located at PIRL
• Prof John Hopwood and his laboratory – the Lysosomal Diseases Research Unit (now part of the Hopwood Centre for Neurobiology
• Prof Deb White and her laboratory – now within the Precision Medicine Theme.
Had SAHMRI not seen the value offered by each of these groups, and transitioned them to the SAHMRI structure, these groups would have experienced further funding cuts and been unable to continue their essential research.
EXAMPLE OF SAHMRI’S UNIQUE PRECLINICAL AND DIAGNOSTIC FACILITIES FOR RESEARCHERS NATIONALLY
Prof Deb White is the Director of the Cancer Program at SAHMRI, the Acute Lymphoblastic Leukaemia (ALL) Project Lead for the Australian Genomics Program and the SA Scientific Lead for Zero Childhood Cancer.
Acute Lymphoblastic Leukaemia (ALL) is the most common childhood cancer and remains the leading cause of non-traumatic death in children. For adolescents and young adults with ALL the therapeutic outcomes are poor. Most older adults will die of their disease. ALL is characterised by recurrent gene fusions and concomitant structural abnormalities. In the absence of genomic testing, current clinical prognostic approaches do not identify the significant number of patients with high risk disease. This means that they are only identified when they fail therapy at which time the possibility of good clinical outcomes is significantly reduced and escalated therapeutic strategies increase toxicity. Next generation sequencing (NGS) has enabled the identification of genomic lesions, not otherwise identifiable, which are hallmarks of high-risk disease in patients otherwise classified as standard or good risk. Furthermore, for some of these lesions rational therapies are available, for others identification provides an opportunity for drug development, or the use of immune based therapies. As the National Referral Centre for genomic screening, ethically consented, ALL paediatric and adult samples, newly diagnosed and/or relapsed patients across Australia are referred to Prof White’s laboratory for genomic analysis (NGS). Results are curated in collaboration with Prof White’s bioinformatic and scientific team and presented back to the requesting clinician through research reports and national MTBs (Molecular Tumour Boards) chaired by Prof White. This federated approach, enables genomic and clinical data to be used to significantly improve patient care with a precision medicine approach for risk stratification and therapeutic triage.
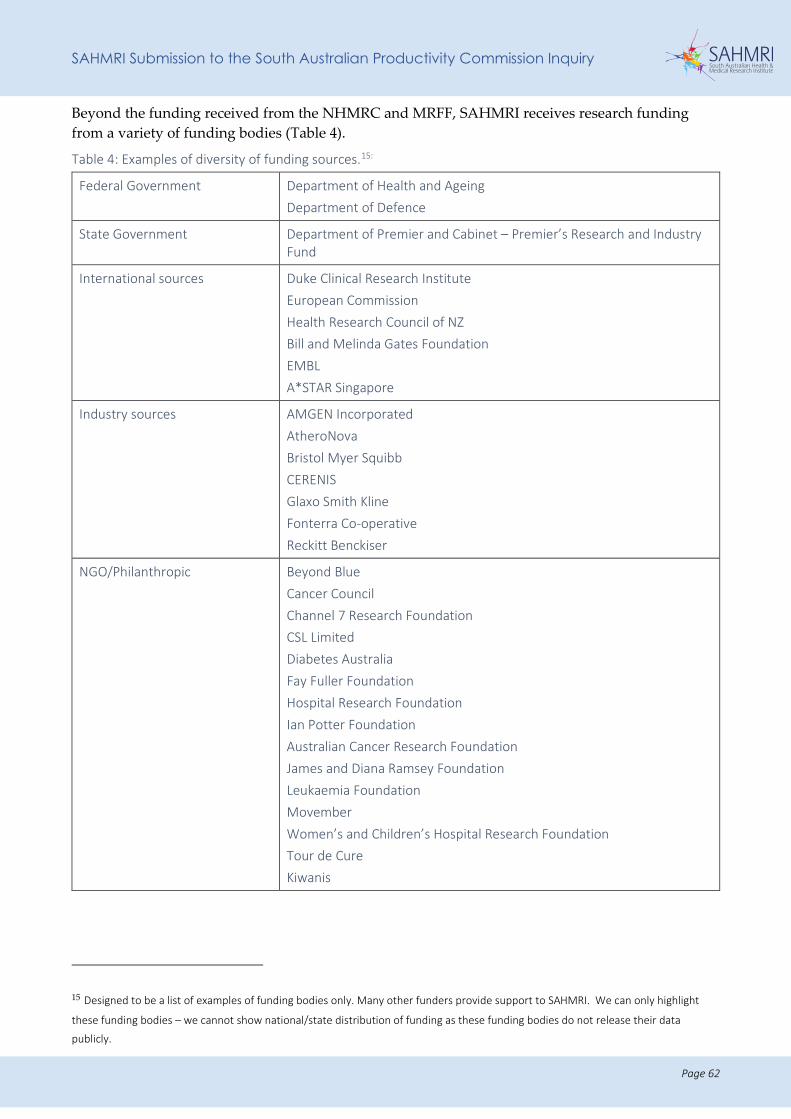
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 62
Beyond the funding received from the NHMRC and MRFF, SAHMRI receives research funding from a variety of funding bodies (Table 4).
Table 4: Examples of diversity of funding sources.15:
Federal Government Department of Health and Ageing Department of Defence
State Government Department of Premier and Cabinet – Premier’s Research and Industry Fund
International sources Duke Clinical Research Institute European Commission Health Research Council of NZ Bill and Melinda Gates Foundation EMBL A*STAR Singapore
Industry sources AMGEN Incorporated AtheroNova Bristol Myer Squibb CERENIS Glaxo Smith Kline Fonterra Co-operative Reckitt Benckiser
NGO/Philanthropic Beyond Blue Cancer Council Channel 7 Research Foundation CSL Limited Diabetes Australia Fay Fuller Foundation Hospital Research Foundation Ian Potter Foundation Australian Cancer Research Foundation James and Diana Ramsey Foundation Leukaemia Foundation Movember Women’s and Children’s Hospital Research Foundation Tour de Cure Kiwanis
15 Designed to be a list of examples of funding bodies only. Many other funders provide support to SAHMRI. We can only highlight
these funding bodies – we cannot show national/state distribution of funding as these funding bodies do not release their data
publicly.
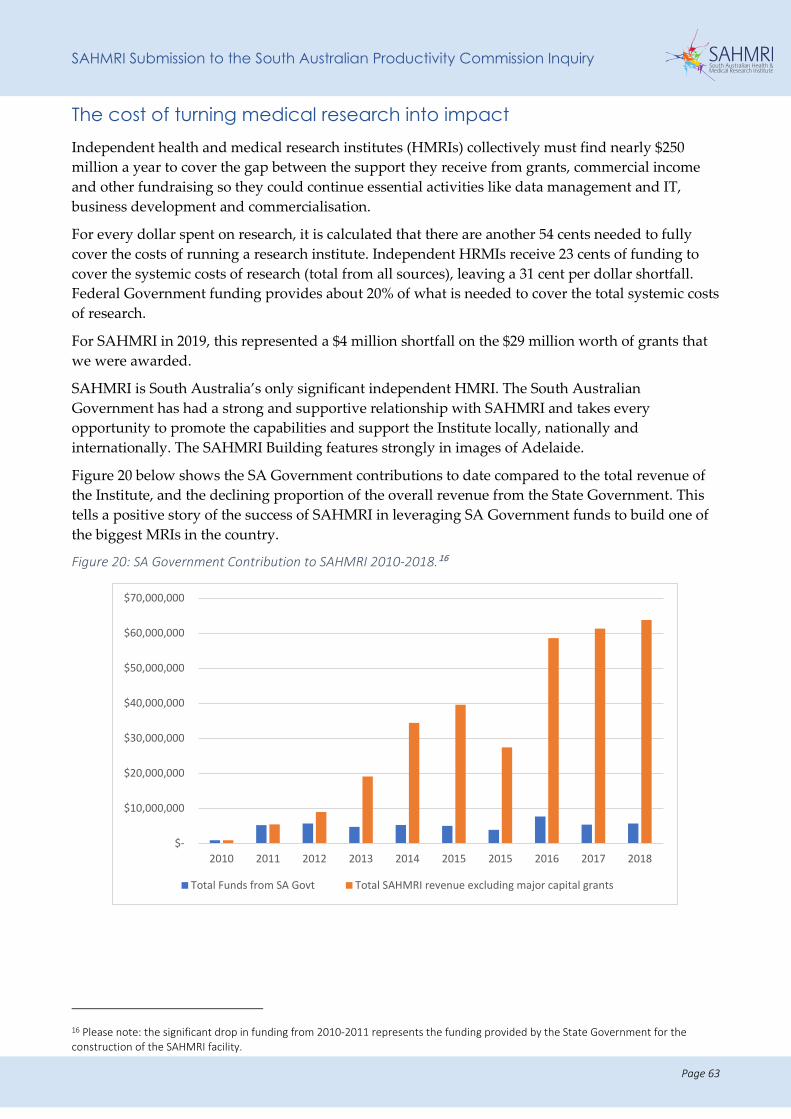
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 63
The cost of turning medical research into impact Independent health and medical research institutes (HMRIs) collectively must find nearly $250 million a year to cover the gap between the support they receive from grants, commercial income and other fundraising so they could continue essential activities like data management and IT, business development and commercialisation.
For every dollar spent on research, it is calculated that there are another 54 cents needed to fully cover the costs of running a research institute. Independent HRMIs receive 23 cents of funding to cover the systemic costs of research (total from all sources), leaving a 31 cent per dollar shortfall. Federal Government funding provides about 20% of what is needed to cover the total systemic costs of research.
For SAHMRI in 2019, this represented a $4 million shortfall on the $29 million worth of grants that we were awarded.
SAHMRI is South Australia’s only significant independent HMRI. The South Australian Government has had a strong and supportive relationship with SAHMRI and takes every opportunity to promote the capabilities and support the Institute locally, nationally and internationally. The SAHMRI Building features strongly in images of Adelaide.
Figure 20 below shows the SA Government contributions to date compared to the total revenue of the Institute, and the declining proportion of the overall revenue from the State Government. This tells a positive story of the success of SAHMRI in leveraging SA Government funds to build one of the biggest MRIs in the country.
Figure 20: SA Government Contribution to SAHMRI 2010-2018.16
16 Please note: the significant drop in funding from 2010-2011 represents the funding provided by the State Government for the construction of the SAHMRI facility.
$-
$10,000,000
$20,000,000
$30,000,000
$40,000,000
$50,000,000
$60,000,000
$70,000,000
2010 2011 2012 2013 2014 2015 2015 2016 2017 2018
Total Funds from SA Govt Total SAHMRI revenue excluding major capital grants
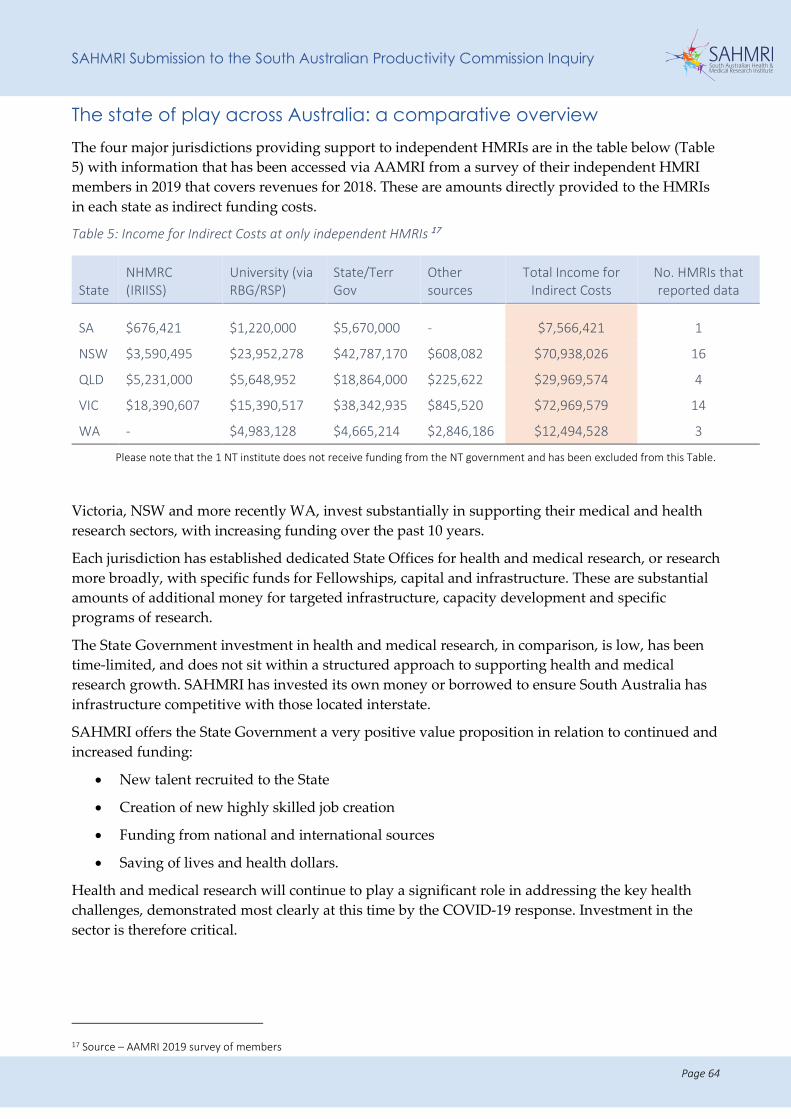
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 64
The state of play across Australia: a comparative overview The four major jurisdictions providing support to independent HMRIs are in the table below (Table 5) with information that has been accessed via AAMRI from a survey of their independent HMRI members in 2019 that covers revenues for 2018. These are amounts directly provided to the HMRIs in each state as indirect funding costs.
Table 5: Income for Indirect Costs at only independent HMRIs 17
State NHMRC (IRIISS)
University (via RBG/RSP)
State/Terr Gov
Other sources
Total Income for Indirect Costs
No. HMRIs that reported data
SA $676,421 $1,220,000 $5,670,000 - $7,566,421 1
NSW $3,590,495 $23,952,278 $42,787,170 $608,082 $70,938,026 16
QLD $5,231,000 $5,648,952 $18,864,000 $225,622 $29,969,574 4
VIC $18,390,607 $15,390,517 $38,342,935 $845,520 $72,969,579 14
WA - $4,983,128 $4,665,214 $2,846,186 $12,494,528 3
Please note that the 1 NT institute does not receive funding from the NT government and has been excluded from this Table.
Victoria, NSW and more recently WA, invest substantially in supporting their medical and health research sectors, with increasing funding over the past 10 years.
Each jurisdiction has established dedicated State Offices for health and medical research, or research more broadly, with specific funds for Fellowships, capital and infrastructure. These are substantial amounts of additional money for targeted infrastructure, capacity development and specific programs of research.
The State Government investment in health and medical research, in comparison, is low, has been time-limited, and does not sit within a structured approach to supporting health and medical research growth. SAHMRI has invested its own money or borrowed to ensure South Australia has infrastructure competitive with those located interstate.
SAHMRI offers the State Government a very positive value proposition in relation to continued and increased funding:
• New talent recruited to the State
• Creation of new highly skilled job creation
• Funding from national and international sources
• Saving of lives and health dollars.
Health and medical research will continue to play a significant role in addressing the key health challenges, demonstrated most clearly at this time by the COVID-19 response. Investment in the sector is therefore critical.
17 Source – AAMRI 2019 survey of members
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 65
As an independent HMRI, SAHMRI has the ability to work across all areas of research, free of the bias and bureaucracy evident in the university system. SAHMRI has strength in helping to play a role in ensuring that South Australia is responsive to modern day challenges.
However, we can only truly be effective at delivering improvements to health service delivery and the health outcomes of the community if the Institute works off a viable base. A long-term commitment of funding will allow SAHMRI to be agile and responsive to the needs of the State and the health service needs of the South Australian population.
RECOMMENDATIONS
We offer the following recommendations in relation to funding:
R1: The State Government operating grant to SAHMRI should be increased to a base amount of $10 million per annum (commencing in 2021). The annual operating grant should be:
• Increased annually in accordance with CPI; and
• As a further incentive for SAHMRI to contribute to the State's total economic activity (Gross StateProduct), increased in line with that contribution.
R10: Additional investment in health and medical research at a State Government level is critical to enhance the national competitiveness of South Australian researchers. The following funding schemes are suggested:
• Co-investment in Stage 2 MRFF Frontiers applications; matched funding for other MRFF applications, when appropriate.
• Fellowships aimed at supporting and attracting our brightest minds, undertaking research in areas of specific interest and significance to the State.
• Consideration should be given as to whether the funds currently being administered by the Health Services Charitable Gifts Board could be leveraged as a catalyst to scale up health and medical research in the State.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 66
CHARACTERISTICS OF SOUTH AUSTRALIA AND ITS POPULATION AND AREAS OF COMPETITIVE ADVANTAGE Terms of Reference. Identify and assess the characteristics of South Australia and its population that may give rise to areas of competitive advantage compared to other jurisdictions in health and medical R&D, and identify methods of maximising these opportunities.
Information request 5.9: competitive advantage – areas and phases of research
• Does South Australia have areas of research excellence of national or global renown? What are they?
• What are South Australia’s competitive strengths and weaknesses in various fields and phases in HMR?
South Australia has a collective of researchers who are incredibly talented, with extraordinary expertise. We must celebrate this, while at the same time, consider ways in which we can continue to foster this expertise including the next generation of researchers.
At SAHMRI, our Themes were selected based on the most important health issues we were facing as a State, but also their intersection with each other, and the research collaborations they would create. In doing so, we attracted world class leaders in their fields to lead an array of research programs.
We must continue to keep the South Australian population at the front of our minds when we conduct health and medical research – we are ultimately doing what we do to improve their health and the services that they receive.
Areas of competitive advantage at SAHMRI We would like to highlight some of our exciting research activities, that also represent competitive strengths both nationally and internationally.
Aboriginal Health Equity: Led by Professor Alex Brown, the Aboriginal Health Equity Theme conducts research that is of direct relevance to the health and wellbeing of Aboriginal people in South Australia and across the country with a focus on reducing inequity in health and wellbeing among Australia’s First Peoples, and the next generation of Indigenous research leaders. This group is the largest cohort of Aboriginal researchers in Australia.
Women and Kids Research: SAHMRI’s research, led by Professor Maria Makrides, in the area of nutrition in pregnancy and early life, leads the way in Australia. It has led to the development of guidelines, has been published in leading journals (JAMA and NEJM) and continues to define new programs leading to reductions in pre-term birth and improvements in childhood development.
Leukaemia: Our Chronic Myeloid Leukaemia (CML) and Acute Lympoblastic Leukaemia (ALL) research groups are exemplar of the precision medicine model. In CML, our researchers have led the charge at moving CML from a fatal illness to a chronic disease, with individualised treatments using biomarkers and analytics. This is now moving into ALL.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 67
Health Data: Through the use of health data, along with Monash University, we play a leadership role in the use of data and registries in improving the delivery of health care. This is emphasised by the registry capacity at SAHMRI and the use of data in rolling out powerful clinical trials.
Neurobiology: There is a long tradition in the development of treatments for neurological disorders, from genetically inherited disorders to Dementia and Parkinson’s. This research is continuing within SAHMRI today. More recently, SAHMRI has developed leadership in this area, specifically in relation to gut health, immune responses and anti-microbial resistance.
Competitive advantage – Clinical Research We note the SAPCs focus on clinical trials, but we would like to expand this to consider the clinical research occurring across the State.
SAHMRI’s impact is greatest, and most immediate, in the area of clinical research. SAHMRI has had a strong and consistent focus on clinical research, and particularly clinical trials since inception.
SAHMRI’s success in clinical research is already exemplified in various ways, including:
• Papers in high impact journals. High impact papers strongly influence thinking and behaviour amongst clinicians and policymakers, and in some cases the public, when media covers the research outputs. In the 3-year period 2016 to 2018, SAHMRI researchers published a total of 62 papers in the highest impact journals (NEJM, JAMA, Lancet, Nature, Science, Cell). The majority (about 60%) were clinical research papers.
• Influencing clinical practice, clinical guidelines and policy. SAHMRI researchers have generated new evidence that has influenced clinical practice, or health policies locally, nationally and internationally.
EXAMPLES OF OUR CLINICAL RESEARCH IMPACT
SAHMRI Women and Kids
- changed national and international infant feeding guidance for introduction of solid foods (STAR and STEP trials) and policy guidance in the USA regarding iodine fortification of the food supply.
- instigated a global change in the composition of the protein content of human milk fortifier marketed by Nestle (PiPIN trial).
- brought about changes to the Aboriginal Birthing Program to enhance the support to women.
Aboriginal Health Equity
- developed new, evidence-based community embedded plans for SA in diabetes, cancer, cardiac and prisoner health.
- developed culturally-informed solutions for serious sexual health problems in Aboriginal communities.
- improved access to health care and better management of diabetes, and detection and management of chronic conditions across the State through the assessment of over a thousand Aboriginal people (Aboriginal Diabetes Study).
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 68
Precision Medicine
- influenced policies for access to colonoscopy.
- influenced the management of Chronic Myeloid Leukaemia globally through work to promote kinase inhibitor therapy for curative intent.
- has led the establishment of Genomic Testing for all newly diagnosed and relapsed Acute Lymphoblastic Leukaemia (ALL) cases. To date approximately 600 cases have had complete transcriptomic sequencing (mRNA Seq) performed. In the last year this has translated to therapeutic change for ~30 patients and a change in risk stratification for a further ~50 patients.
Lifelong Health
- has driven changes to bariatric surgery.
- improved surgical treatments for patients with hypothalamic obesity.
- developed better treatments to manage bladder pain and co-morbidities of Irritable Bowel Syndrome (IBS).
Registry of Senior Australians (ROSA)
- The ROSA database was used to develop benchmark reports on the quality of aged care providers. The reports have been disseminated to the Department of Health and Aged Care Quality and Safety Commission.
- The ROSA research team has been involved in the Royal Commission into Aged Care Quality and safety investigation through providing expert testimony and serving in Steering Committees.
The opportunities for growth are strong. Continued growth will be contingent on high quality infrastructure being developed and maintained over time. The MRFF opportunities for clinical research are significant. Those institutions that prepare themselves well by developing robust, comprehensive clinical trial platforms will be able to compete nationally for those funds and continue to attract the industry sponsored and collaborative trials internationally.
Our vision for SAHMRI is to strengthen our clinical research platform to effectively support the completion of internationally recognised, impactful clinical research across diverse disciplines:
• Create new partnerships and expand existing partnerships to build capability.
• Grow the next generation of clinical research leaders collaboratively.
• Maintain diversity of revenue sources – competitive grants and industry funding.
• Update our infrastructure to ensure efficiency and quality are high.
• Ensure clinical research is highly relevant to clinical needs.
• Support and encourage sustained publication in high impact journals.
Key to success will be the partnership with Health Translation SA and Adelaide Biomedical City, which are both driving integration and collaboration in systems and information sharing.
Clinical research has generated approximately $10 million a year in grant or commercial revenue for SAHMRI on average since 2014. This in turn has generated over $2 million in infrastructure revenue via block funding or in budgeted infrastructure lines within budgets for commercial clients.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 69
Opportunity for clinical trials in South Australia
Information request 5.10: competitive advantage – clinical trials
• What type of clinical trials are being undertaken in South Australia?
• Does South Australia have any competitive advantages in conducting clinical trials?
South Australia has a number of substantial benefits as a location for conducting clinical trials:
• SAHMRI’s clinical research platform
• Several key registries from which clinical trials can be run
• Co-location with the RAH, the State's flagship hospital
• One centralised health system, with ease of patient access.
Early revenue from clinical trials at SAHMRI was driven largely by our Heart Health Theme, but over the last few years there has been a significant diversification and breadth of clinical research and researchers.
Three Theme leaders – Professors Maria Makrides, Tim Hughes and Alex Brown – have substantial track records of clinical research funded by grants and industry. The appointment of Professor Derek Chew and attraction of other clinical researchers to SAHMRI continues to grow our profile for clinical research.
We attach for the SAPCs information, an overview of key cardiology clinical trials being undertaken at SAHMRI as an example of clinical trial activity (See Appendix IX: Cardiology Clinical Trials, Examples).
SAHMRI is currently planning to invest in the following to support clinical trials within our institution, which will significantly enhance the conduct of clinical trials and can act as a resource for other trialists within the State:
• Participant management system
• Data integration and intelligence system
• Clinical trial management system.
Also of note, SAHMRI has two chief investigators involved in the Centre for Research Excellence in Clinical Trial Statistics (Prof Maria Makrides and Dr Lisa Yelland). Dr Yelland leads the South Australian node of this project. This has resulted in our ability to appoint a new 0.6 FTE appointment at the beginning of July 2020, significantly increasing our clinical trial statistics capability.
Barriers to conducting clinical trials include:
• Lack of infrastructure to support clinical trials
• Lack of streamlined ethics and governance processes
• Limited access to patient data for clinical trials
• High cost of large quantities of drugs for clinical trials
• Lack of recruitment of clinical researchers
• Low level commitment to the conduct of health and medical research in LHNs, recognising the potential for clinical trials as a standard of patient care
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 70
At both the state and national level, improvements must be made in relation to the capture of data in relation to clinical trials, to ensure knowledge of the research occurring and identification of collaborative opportunities.
Competitive advantage – collaboration and precincts
Information request 5.11: competitive advantage – collaboration and precincts
• Do Adelaide’s innovation precincts provide it with a competitive edge in HMR and translation?
Health Translation SA (HTSA): is the State’s NHMRC-accredited Advanced Health Research and Translation Centre (AHRTC).
SAHMRI coordinated the submission to have an AHRTC in South Australia. Given our state-wide focus, we were able to effectively engage all partners and work collaboratively with them to develop a submission representative of all strengths in the State.
SAHMRI provides space for the secretariat function of HTSA, and Professor Steve Wesselingh was the inaugural Director and Chair of the Board. He has, in the last year, handed this over to the CEO (Wendy Keech) and new Board Chair, Dr Leanna Read (previous SA Chief Scientist).
Without the coordinating role and leadership shown by SAHMRI, HTSA would not exist today.
SAHMRI enjoys our collaborative relationship with HTSA, however it must be recognised that HTSA occupies quite a unique position within the State. While HTSA provides a key piece in the collaboration puzzle in South Australia, it cannot and does not employee researchers which differentiates it from SAHMRI.
Connectivity of Adelaide BioMed City (AMBC) and the Planned Flinders precinct: SAHMRI is a key partner within Adelaide BioMed City. We share the vision of ABMC Partners, who are aiming to utilise our collective strengths for the benefit of South Australia. We have a significant opportunity to continue to grow the capacity within the precinct, through shared infrastructure, co-supervision of students and shared research interests. Professor Steve Wesselingh was the inaugural Chair of ABMC, but has recently handed this role over to Professor Caroline McMillen (current Chief Scientist).
The growth of the Flinders precinct is of specific interest to SAHMRI, given the co-location of SAHMRI staff at Flinders University. In addition, a number of our researchers have joint appointments with the University, and clinical staff occupy positions within the Southern Adelaide LHN (SALHN).
Proton Therapy, SAHMRI 2
SAHMRI 2 is an innovative ‘next step’ that will bring together leading researchers from around the globe with ground-breaking technology to shape the future of health care practice. In particular, the proton therapy unit (housed within the Australian Bragg Centre for Proton Therapy and Research) – a significant advancement in radiation for cancer – will be available in this ultra-modern building for use in clinical trials and other research, in collaboration with other high-performance global research organisations. To be located within the Adelaide BioMed City and adjacent to the SAHMRI building, SAHMRI 2 provides an opportunity for South Australia to cement its reputation as a leader in international health and medical research.
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 71
SAHMRI leadership led to $70 million of Federal funding to be secured to purchase the proton therapy equipment, as well as an additional $370 million which has been secured from private investment to build the bunker and additional research space above the ground.
The Proton Therapy Unit provides highly focused precision treatment
• Minimal entry and exit dose
• Delivers a very high radiation dose to the tumour
• Delivers nearly all the dose directly to the tumour
• Can treat tumours that lie within millimetres of vital tissue
• Reduces risk of treatment induced second cancer
• Wide range of non-patient research opportunities in areas such as radiobiology, bioengineering.
RECENT EXAMPLE OF OUR COMPETITIVE STRENGTHS BOTH NATIONALLY AND INTERNATIONALLY.
Over the last month, SAHMRI has demonstrated its ability to respond in an agile and timely manner to health challenges, specifically COVID-19.
The recent challenges raised by the COVID-19 virus are a salient reminder of the critical importance of an internationally recognised, dynamic and capable research institute closely aligned with government healthcare priorities – a unique resource for provision of immediate expert advice relevant to the State’s and community interests.
Through this challenging time, now more than ever, SAHMRI is committed to being flexible, adaptable and to pivot rapidly to shift focus to where it is needed most.
The following are newly established research projects which are being undertaken by SAHMRI researchers to counteract COVID-19's impact on our community:
- BRACE Trial aims to protect frontline health care workers – Professor Steve Wesselingh and Professor David Lynn
o SAHMRI is partnering with SA Health and the Murdoch Children’s Institute (MCRI) to become a remote site for the MCRI’s BRACE Trial.
o The trial will investigate whether an established tuberculosis vaccine called Bacille Calmette-Guerin (BCG) can provide an immune system boost to lessen the prevalence or severity of COVID-19 symptoms.
o Initially this arm of the trial will involve 500 South Australian health care workers who are involved with patient care. It's hoped the project will be expanded and, if successful, provide benefits to the broader community.
o The Bill and Melinda Gates Foundation has recently committed $10 million to this project, which already has funding of $700,000 from Sarah and Lachlan Murdoch, $400,000 from the Royal Children’s Hospital Foundation (RCHF), $1.5million from The Minderoo Foundation and $200,000 from the South Australian Government.
- Wellbeing and Resilience - Free online training: Joseph Van Agteren
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 72
- Health Policy Centre – Rapid evidence synthesis to answer priority questions from the State’s COVID-19 Task Force: Professor Caroline Miller (Commission on Excellence and Innovation in Health collaboration)
- Viral pneumonia hospitalisations and aged care: Associate Professor Maria Inacio, SAHMRI Registry of Senior Australians (ROSA)
- FFX enhanced public health response and study: Tracking COVID-19 symptoms and cases within households to understand transmission of COVID-19; First few hundred cases of infection: Professor Caroline Miller (SA Health and Doherty Institute collaboration; World Health Organization sponsored study).
- Seroprevalence study – measuring the presence of antibodies to SARS-COV-2 in blood samples, to gauge community exposure to COVID-19 and potential for immunity: Professor Caroline Miller (SA Pathology and Kirby Institute Collaboration).
- Global survey of patients with chronic myeloid leukaemia (CML) who have had COVID-19 infections: Professor Tim Hughes
- Using ultraviolet sanitiser for parents/staff to protect premature babies in the neonatal nurseries (Women’s and Children’s Hospital joint initiative): Dr Amy Kier
- RNA sequencing to profile immune gene expression response in blood of patients: Professor David Lynn
- Surveying behaviours to slow the spread with follow-up instructional video: Dr Johan Verjans
- Outreach program participants – checking in on Aboriginal and Torres Strait Islander communities offering pathways to social and health support services: Dr Natasha Howard
- Clinical Trials: Antiviral COVID-19 clinical trial and Targeted Humanised Antibody COVID-19 Therapy Clinical Trial (Royal Adelaide Hospital collaboration) Dr Paul Wabnitz
- Smartphone app to track virus spread and send proactive alerts: (Flinders University collaboration) Associate Professor Niranjan Bidargaddi
- Cell signalling group - connections to SARS-CoV-2 biology: Dr Kirk Jensen
- Developing low cost easy-to-use ventilators to help poorer nations – partnership with Uni SA and lung imaging company, 4DX
SAHMRI Submission to the South Australian Productivity Commission Inquiry
Page 73
APPENDICES


Appendix I: Shine Young Objectives
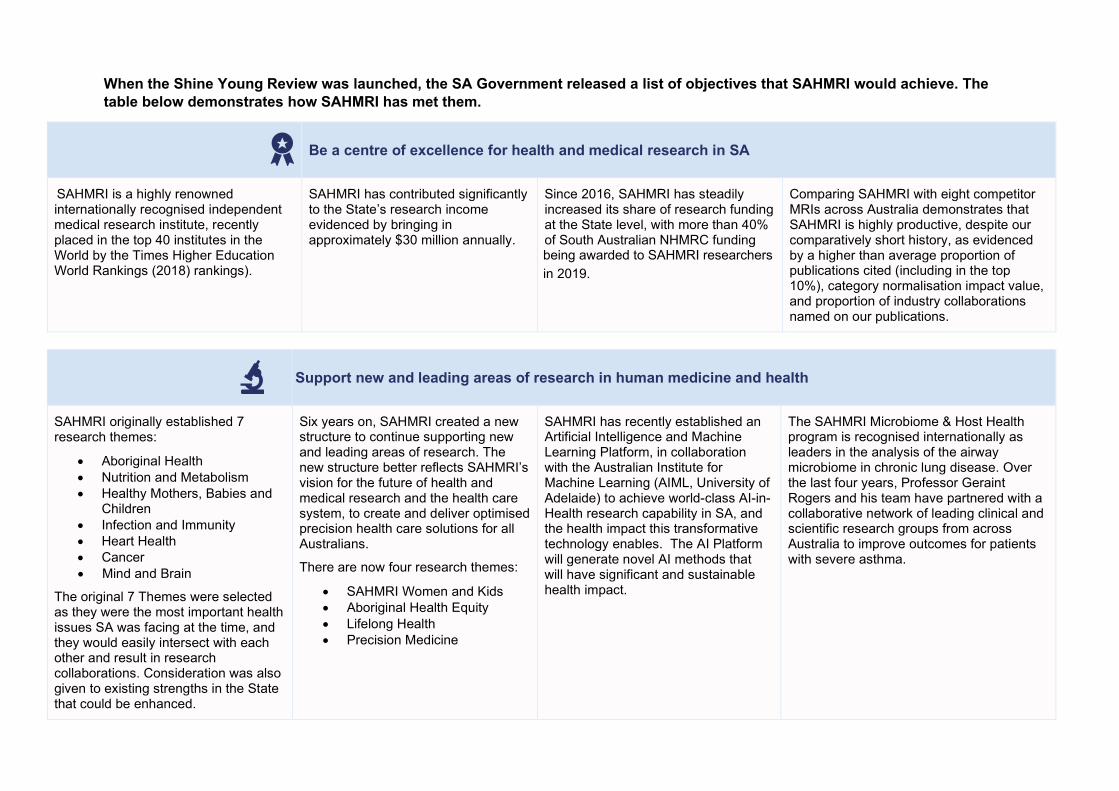
When the Shine Young Review was launched, the SA Government released a list of objectives that SAHMRI would achieve. The table below demonstrates how SAHMRI has met them.
Be a centre of excellence for health and medical research in SA
SAHMRI is a highly renowned internationally recognised independent medical research institute, recently placed in the top 40 institutes in the World by the Times Higher Education World Rankings (2018) rankings).
SAHMRI has contributed significantly to the State’s research income evidenced by bringing in approximately $30 million annually.
Since 2016, SAHMRI has steadily increased its share of research funding at the State level, with more than 40% of South Australian NHMRC funding
in 2019.
Comparing SAHMRI with eight competitor MRIs across Australia demonstrates that SAHMRI is highly productive, despite our comparatively short history, as evidenced by a higher than average proportion of publications cited (including in the top 10%), category normalisation impact value, and proportion of industry collaborations named on our publications.
Support new and leading areas of research in human medicine and health
SAHMRI originally established 7 research themes:
• Aboriginal Health• Nutrition and Metabolism• Healthy Mothers, Babies and
Children • Infection and Immunity• Heart Health• Cancer• Mind and Brain
The original 7 Themes were selected as they were the most important health issues SA was facing at the time, and they would easily intersect with each other and result in research collaborations. Consideration was also given to existing strengths in the State that could be enhanced.
Six years on, SAHMRI created a new structure to continue supporting new and leading areas of research. The new structure better reflects SAHMRI’s vision for the future of health and medical research and the health care system, to create and deliver optimised precision health care solutions for all Australians.
There are now four research themes:
• SAHMRI Women and Kids• Aboriginal Health Equity• Lifelong Health• Precision Medicine
SAHMRI has recently established an Artificial Intelligence and Machine Learning Platform, in collaboration with the Australian Institute for Machine Learning (AIML, University of Adelaide) to achieve world-class AI-in-Health research capability in SA, and the health impact this transformative technology enables. The AI Platform will generate novel AI methods that will have significant and sustainable health impact.
The SAHMRI Microbiome & Host Health program is recognised internationally as leaders in the analysis of the airway microbiome in chronic lung disease. Over the last four years, Professor Geraint Rogers and his team have partnered with a collaborative network of leading clinical and scientific research groups from across Australia to improve outcomes for patients with severe asthma.
being awarded to SAHMRI researchers
Attract national and international researchers
SAHMRI attracted world class leaders in their fields to lead SAHMRI: Prof Steve Wesselingh (Executive Director), a highly regarded infectious diseases physician, recruited from Monash University and is now the Chair of the National Health and Medical Research Council’s (NHMRC) Research Committee, Australia’s foremost medical research funding body.
SAHMRI recruited exceptional external Theme Leaders who brought in significant research funds to the State (for example Prof Stephen Nicholls and Prof Alex Brown, who collectively brought in more than $100 million in research funding).
The recruitment of clinician leaders is important for the success of health and medical research in South Australia. SAHMRI has recently recruited Associate Professor Dan Thomas. Moving back to Australia after six years of a unique training and mentoring experience while working as a haematology research fellow at Stanford School of Medicine (USA), A/Prof Thomas brings a novel skill set to the SAHMRI Precision Medicine Theme. A/Prof Thomas is a clinical haematologist and pathologist with more than 45 peer-reviewed publications (more than three quarters in high impact journals), 14 awards and more than $5 million in competitive grant funding, including a prestigious five-year CSL Centenary Fellowship grant to help build his translational cancer research team.
Approximately 20% of SAHMRI staff (professional and researchers) have been attracted from overseas and interstate to work at SAHMRI, such as Prof James Ward (Head, Sexual Health and Wellbeing); Dr Cedric Bardy (Head, Laboratory for Human Neurophysiology and Genetics); Associate Prof Maria Inacio (Director, Registry of Senior Australians); Prof Geraint Rogers (Director, Microbiome and Host Health); Prof David Lynn (Director, Computational and Systems Biology).
Build partnerships between researchers and research bodies to promote research excellence
Partnerships have been established with our founding members: The University of Adelaide; University of South Australia; Flinders University; and SA Health as evidenced through executed partnership agreements as well as collaborations on research projects and publications.
Partnerships have been established with CSIRO (collaborations on research projects and publications), EMBL Australia (the South Australian node of EMBL Australia is hosted at SAHMRI).
SAHMRI partners with Cancer Council SA to administer the Beat Cancer Project and since 2012 has distributed approximately $30 million in funding to cancer researchers in South Australia.
Partnerships have been established with Health Translation SA and Adelaide BioMed City which support and promote research excellence across the State.
Foster the application of research knowledge to benefit health and wellbeing of people within and outside of SA
Aboriginal Health Equity led by Professor Alex Brown has developed state-wide plans (Heart and Stroke, Diabetes, Cancer, Prisoner Health) and has also provided support to Government departments in epidemiological monitoring and community engagement.
A Cochrane Review (published by Associate Professor Philippa Middleton): ‘Omega-3 fatty acid addition during pregnancy’ is already having an impact on the national pregnancy guidelines. This new evidence of substantial reductions in preterm birth with omega-3 supplementations has led to a recommended policy change for women with a singleton pregnancy. This recommendation is currently being integrated into the update of the NHMRC national pregnancy guidelines.
The Registry of Senior Australians (ROSA) monitors the health, service utilisation, medication use, mortality, and other outcomes of people receiving aged care services in South Australia. ROSA produces evidence to guide decision-making for quality, coordinated, efficient, innovative and age-friendly services and practices. ROSA is contributing to the Royal Commission in Aged Care Quality and Safety.
The BRACE Trial, run by the Murdoch Children’s Research Institute’s (MCRI) and coordinated by SAHMRI is designed to test whether the Bacillus Calmette-Guerin (BCG) vaccine, which boosts ‘frontline’ immunity, can protect healthcare workers who contract COVID-19 from developing severe symptoms. The original enrolment target was 4000 healthcare workers. Already more than 2500 have been enrolled in Australia. A $10 million grant from the Bill & Melinda Gates Foundation will allow the trial to more than double its reach to 10,000 healthcare workers across Australia, Spain and The Netherlands.
Offer significant economic advantages to the State, by attracting significant funding from national and international sources
SAHMRI has contributed significantly to the State’s research income evidenced by bringing in approximately $30 million annually.
Consolidated and coordinated clinical trial capacity and a Clinical Trials Platform that support global clinical trials delivery in South Australia and has generated more than $89 million in clinical research funding since 20.
Increased commercialisation and entrepreneurship of ideas and innovation into business, with 32% of our total revenue being derived from commercial income.
SAHMRI has led the establishment of SAHMRI 2 and the Proton Therapy Unit that generated $70 million Federal and $370 million private investment and will generate 1000 jobs and an estimated $1 billion in economic revenue to the State.
Support South Australian and Australian Government research objectives
Aboriginal Health Equity led by Professor Alex Brown has developed state-wide plans (Heart and Stroke, Diabetes, Cancer, Prisoner Health) and has also provided support to government departments in epidemiological monitoring and community engagement.
Other research groups in SAHMRI have entered into tenders/contracts with the State and Federal Government in relation to smoking rates and Aboriginal sexual health plans.
ROSA's work enables governments to make evidence-based decisions promoting quality, efficient, innovative
The Health Policy Centre at SAHMRI has been working with the SA Government to synthesise evidence and respond to queries around COVID-19.
SAHMRI facilitated data access to critical SA Health datasets for the researchers who required it for clinical trials. This was achieved with the execution of the OACIS Access Deed. SAHMRI led the development of this arrangement, and the University of Adelaide now directly benefits from the arrangement that SAHMRI brokered.
Gains in this area will have direct benefits in improved quality and reduced costs for SA Health while at the same time improving grant success.
aged care services and practices.
ROSA contributes to the Royal Commission in Aged Care Quality and Safety.
Create synergies between researchers and care providers, through the co-location with the new Royal Adelaide hospital, and collaboration with other State hospitals
Clinician researchers are an incredibly important part of the research team at SAHMRI. These researchers have direct contact with the health care system and offer us the ability to directly translate research findings into evidence-based service delivery.
SAHMRI has both medical and non-medical clinicians (dieticians, nutritionists) working within our Themes.
The researchers who form the Women and Kids theme at SAHMRI are located on the 7th floor of the Adelaide Women's and Children’s Hospital (this space was formerly the Children’s Health Research Institute). SAHMRI has renovated the floor and leases the space for the SAHMRI researchers to be located there so that they can continue to build relationships and create collaborations with the Women's and Children’s Hospital.
SAHMRI has collaborated with multiple universities and hospitals across Australia (e.g. Royal Women’s Children Hospital in Melbourne, Murdoch Children Research Institute) as part of the NHMRC Centre of Research Excellence (CRE) in Targeted Nutrition to Improve Maternal and Child Outcomes. SAHMRI provided oversight and coordinated the CRE’s projects and developed new tools for accurate assessment of nutritional status in large scale trials.
This CRE has resulted in more than 60 peer-reviewed publications, 3 new NHMRC investigator grants and the creation of a new company.
SAHMRI fully supports the establishment of Adelaide BioMed City, a partnership between RAH, the South Australian Universities and SAHMRI.
Be housed within a ‘flagship’ research facility adjacent to the new Royal Adelaide Hospital
In 2009, SA Heath received funding from the Commonwealth Government to build a $200 million Health and Medical ‘Flagship’ Research Facility next door to the new Royal Adelaide Hospital in Adelaide's west end.
In 2013, SAHMRI opened its doors and now houses approximately 750 researchers. In the past 7 years, approximately $50 million of infrastructure/facilities, has been acquired, helping to make SAHMRI a world-class research facility.
The SAHMRI building on North Terrace houses SAHMRI staff and also has partner staff from the three Universities and CSIRO occupying space within the building. This co-location provides benefits to both SAHMRI and our partners in relation to collaborative opportunities, access to infrastructure and animal house services, co-supervision of students and subsidised rent (at around the third of the cost of rent when benchmarked against office space in the Adelaide CBD). Furthermore, this co-location brings multidisciplinary teams together across ‘bench to bedside’ translational research and facilitates innovative approaches to research practices.
SAHMRI is incredibly proud to be a leader of SAHMRI 2, which will establish a world-class proton therapy facility that will impact so many aspects, from teaching and clinical studies, through to patient care and treatment.
SAHMRI 2 will comprise world-class facilities and sit alongside the Royal Adelaide Hospital, SAHMRI, the University of Adelaide Health and Medical Sciences Building, and the University of South Australia’s Health Innovation Building.
This unique infrastructure represents South Australia’s highest priority project for health, research and education, providing a focal point for research of international calibre into the most serious chronic illnesses. Unprecedented numbers of health care professionals will be trained here to address current and future capacity constraints and surging health care demands.

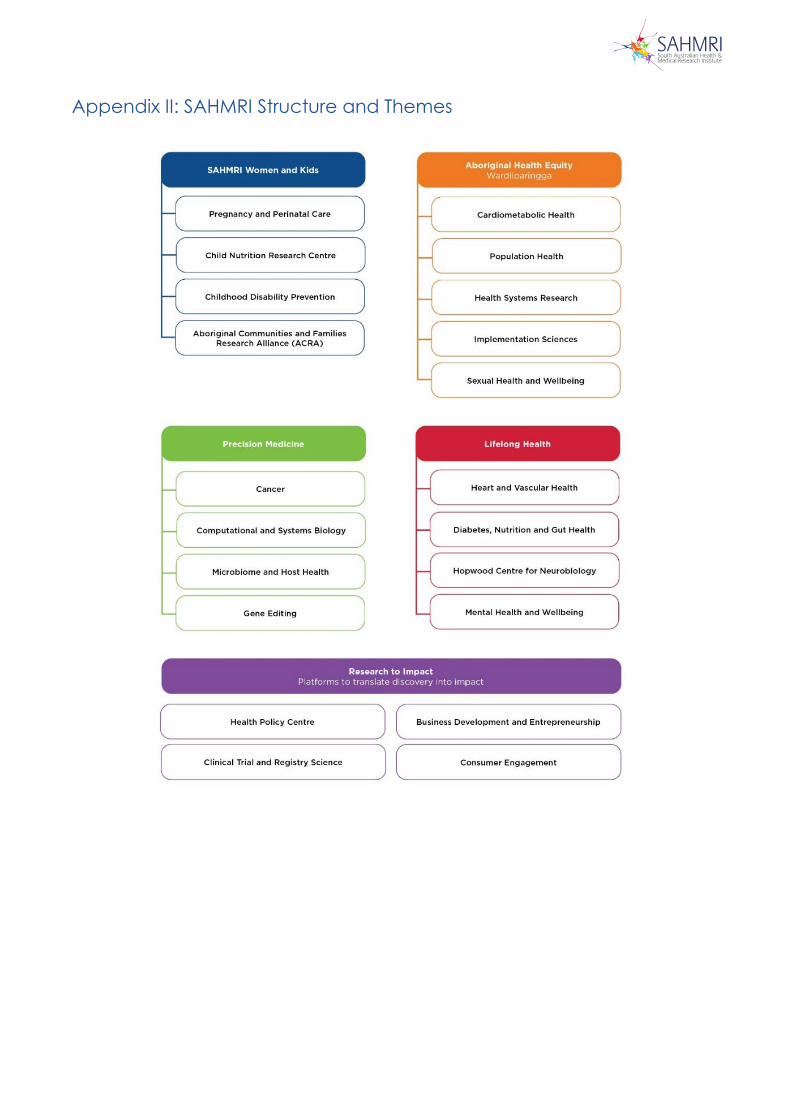
Appendix II: SAHMRI Structure and Themes
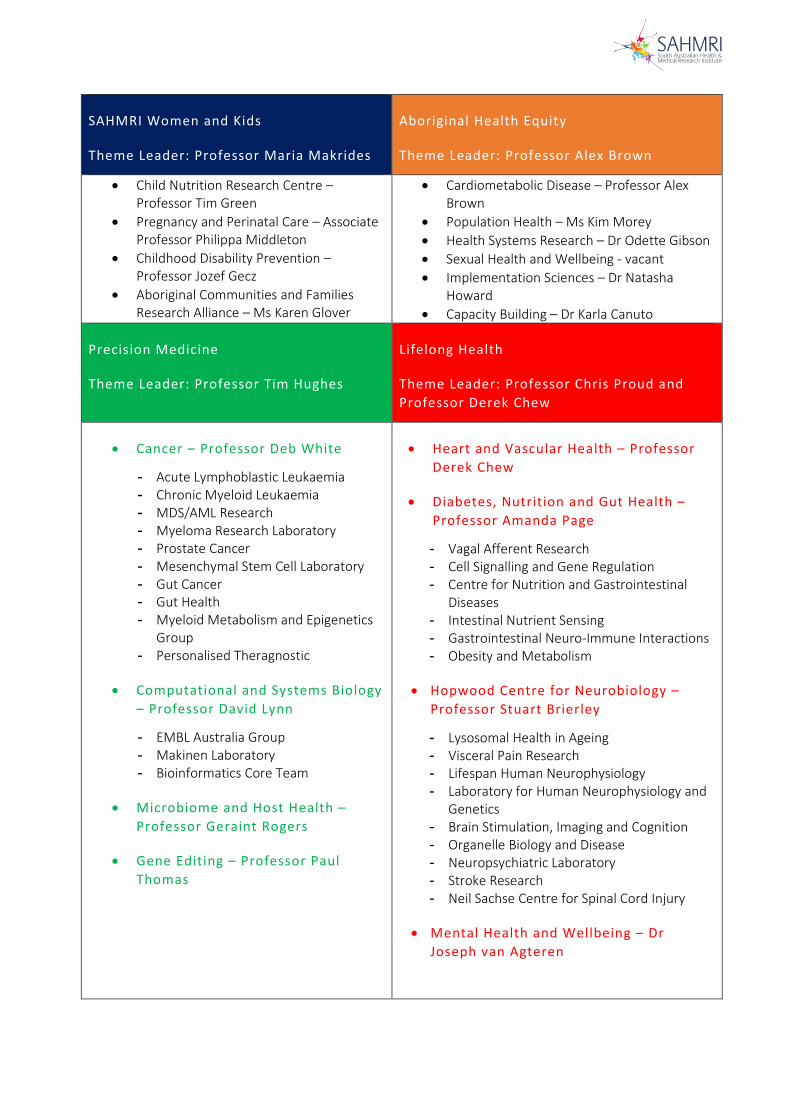
SAHMRI Women and Kids
Theme Leader: Professor Maria Makrides
Aboriginal Health Equity
Theme Leader: Professor Alex Brown
• Child Nutrition Research Centre –Professor Tim Green
• Pregnancy and Perinatal Care – AssociateProfessor Philippa Middleton
• Childhood Disability Prevention –Professor Jozef Gecz
• Aboriginal Communities and FamiliesResearch Alliance – Ms Karen Glover
• Cardiometabolic Disease – Professor AlexBrown
• Population Health – Ms Kim Morey• Health Systems Research – Dr Odette Gibson• Sexual Health and Wellbeing - vacant• Implementation Sciences – Dr Natasha
Howard• Capacity Building – Dr Karla Canuto
Precision Medicine
Theme Leader: Professor Tim Hughes
Lifelong Health
Theme Leader: Professor Chris Proud and Professor Derek Chew
• Cancer – Professor Deb White
- Acute Lymphoblastic Leukaemia- Chronic Myeloid Leukaemia- MDS/AML Research- Myeloma Research Laboratory- Prostate Cancer- Mesenchymal Stem Cell Laboratory- Gut Cancer- Gut Health- Myeloid Metabolism and Epigenetics
Group- Personalised Theragnostic
• Computational and Systems Biology– Professor David Lynn
- EMBL Australia Group- Makinen Laboratory- Bioinformatics Core Team
• Microbiome and Host Health –Professor Geraint Rogers
• Gene Editing – Professor PaulThomas
• Heart and Vascular Health – ProfessorDerek Chew
• Diabetes, Nutrition and Gut Health –Professor Amanda Page
- Vagal Afferent Research- Cell Signalling and Gene Regulation- Centre for Nutrition and Gastrointestinal
Diseases- Intestinal Nutrient Sensing- Gastrointestinal Neuro-Immune Interactions- Obesity and Metabolism
• Hopwood Centre for Neurobiology –Professor Stuart Brierley
- Lysosomal Health in Ageing- Visceral Pain Research- Lifespan Human Neurophysiology- Laboratory for Human Neurophysiology and
Genetics- Brain Stimulation, Imaging and Cognition- Organelle Biology and Disease- Neuropsychiatric Laboratory- Stroke Research- Neil Sachse Centre for Spinal Cord Injury
• Mental Health and Wellbeing – DrJoseph van Agteren

SAHMRI PLATFORMS
Health Policy Centre – Professor Caroline Miller
Key areas of research are health behaviours and health policy:
• Tobacco control• Obesity prevention• Alcohol• Collaborations in bowel cancer screening, cancer registries and PROMs (patient-reported
outcome measures) for cancer.
Clinical Trial and Registry Science – Ms Liddy Griffith and Associate Professor Maria Inacio
• Provides a central resource for conducting clinical trials and other clinical research includingproject and data management
• Supports clinical trial activity embedded within SAHMRI based registries
Registries housed at SAHMRI
• Registry of Senior Australians (ROSA)• Australian Orthopaedic Association National Joint Replacement Registry• Australia and New Zealand Dialysis and Transplant Registry• Transcatheter Aortic Value Implementation (TAVI) Registry
(ROSA, AOA and ANZDATA are 3 of the largest registries in Australia)
Business Development and Entrepreneurship – Mr Dougal Edwards
The Platform – led by Bright Arena – works with researchers affiliated with SAHMRI to commercialise and translate SAHMRI promising research into high impact treatments and therapies.


Appendix III: Research Advisory Committee Letter to SAPC from RAC Chair, Prof John Shine
Research Advisory Committee Report, 2016 and 2019

President Professor John Shine AC PresAA
9:2_14 "04111k‘.
1 April 2020
Dr Matthew Butlin
Chair and Chief Executive
South Australian Productivity Commission
Australian Academy of
Science
Dear Dr Butlin
RE: Inquiry into Health and Medical Research in South Australia
I have read with interest the issues paper released regarding the Productivity Commission's Inquiry into
Health and Medical Research in South Australia.
I am writing to you both as the co-author of the Shine Young Review (Review of Health and Medical
Research in South Australia — May 2008) as well as in my current role as the Chair of the SAHMRI
Research Advisory Committee.
In 2008 when Alan Young and I undertook the Shine Young Review, we were excited by the opportunity
to contribute to the transformation of the health and medical research sector in South Australia. It was
clear then, as it is in South Australia now, that the State has a significant number of high calibre
researchers, undertaking impressive and internationally competitive health and medical research.
Following our assessment of many key factors impacting on health and medical research in the State,
including diminishing grant funding, critical mass, infrastructure gaps and the attraction and retention of
staff, we concluded and ultimately recommended to the then Health Minister, Hon John Hill, that South
Australia establish an independent health and medical research institute.
Both Alan and I were very proud and pleased that the Government immediately acted upon our
recommendation and established SAHMRI in the following year. I think that the speed in which the
Government acted emphasised how great the need was for South Australia to have a flagship health and
medical research institute.
I am pleased to continue to be involved in the work of SAHMRI in my role as the Chair of the Research
Advisory Committee, comprising a group of national and international experts aligned to SAHMRI's
research themes. I have been in this role formally since 2011 and am grateful that I have had the
opportunity to continue to witness the vision that Alan and I had for the State coming to fruition.
To me, it is clear that over the last five years (the point at which SAHMRI's Theme Leaders were all
appointed and the themes were actively undertaking research) SAHMRI has developed a clear unity of
purpose. The Institute has made rapid progress in establishing a strategic direction for health and medical
research and has embedded itself in the health and medical research sector not only at the State level,
but nationally and internationally as well.
Ian Potter House, GPO Box 783
T +61 (0)2 6201 9400 E [email protected]
9 Gordon Street, Acton ACT 2601 Canberra ACT 2601 Australia
F +61 (0)2 6201 9494 www.science.org.au

As Chair of the Research Advisory Committee, it is clear that the scientific quality and research output of
the Institute has continued to improve, soundly positioning the Institute in a very competitive position. The
unanimous view of the Committee is that SAHMRI has a clear upward trajectory both in quality and quantity
of research and has matured to become one of Australia's leading Health and Medical Research Institutes.
In particular it has very clear leadership status in Aboriginal health and in the areas of translation, health
services and policy. There is a clear and shared passion for working within the Institute, and in working
towards the SAHMRI vision of improving the health of the community through research. The recent
challenges raised by the COV1D-19 virus are a salient reminder of the critical importance of an
internationally excellent research institute closely aligned with government healthcare priorities — a unique
resource for provision of immediate expert advice relevant to the State.
SAHMRI is performing well in what is a very competitive funding landscape and has an impressive record
in publications in high impact journals. While these are important metrics, the Research Advisory
Committee has also been very pleased with the efforts made by SAHMRI researchers in relation to the
translation of their findings into direct health care benefits, through policy interventions or via direct health
delivery changes. This is where SAHMRI has a unique advantage and this must be harnessed and not
overlooked or undervalued.
Of critical importance is the collaborative nature of SAHMRI and the engagement with the three
Universities and the SA Health system in undertaking critical health and medical research. The co-location
of SAHMRI with the Royal Adelaide Hospital, and its important role within Adelaide BioMed City, highlights
the importance of this collaboration, and the statewide leadership presence that SAHMRI has in a number
of areas.
I would impress upon the Government the importance of continuing to support SAHMRI as the State's only
independent health and medical research institute. SAHMRI and its researchers play a complementary role
to the research undertaken within the university and clinical settings, and as a sector, with Government
support, this collaborative venture can continue to grow.
I wish you well with the Review and look forward to hearing the outcomes in due course.
Yours sincerely,
Professor John Shine AC PresAA
President, Australian Academy of Science
Chair, SAHMRI Research Advisory Committee
Ian Potter House, GPO Box 783
9 Gordon Street, Acton ACT 2601 Canberra ACT 2601 Australia
T +61 (0)2 6201 9400 E [email protected]
F -i-61 (0)2 6201 9494 www.science.orgau
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
1
RESEARCH ADVISORY COMMITTEE REPORT - 2016 The SAHMRI Research Advisory Committee met at SAHMRI on Thursday 11th and Friday 12th August, 2016.
The Committee comprised:
Professor John Shine (Garvan Institute, Sydney (Chair)) Professor Vicki Anderson (Royal Children’s Hospital, Melbourne) Professor Ian Frazer (Translational Research Institute, Brisbane) Professor Doug Hilton (Walter and Eliza Hall Institute, Melbourne) Professor Peter Libby (Harvard Medical School, USA) Professor John Mattick (Garvan Institute, Sydney) Professor Justin McArthur (John Hopkins Medicine, USA) Professor Melanie Wakefield (Cancer Council, Victoria) Professor Steve Wesselingh, SAHMRI Ms Sarah Lawson (Secretariat)
Apologies were received from Professor Nadia Rosenthal.
EXECUTIVE SUMMARY The RAC expressed their appreciation to the Executive Director and his staff for the efficient and professional organisation of the Review and the comprehensive quality of the pre–review materials.
The RAC was unanimously very impressed with the rapid progress made in establishing the strategic direction of SAHMRI research, the cohesiveness of the institute’s research programs and specifically the development of each of the SAHMRI Themes. It was noted that implementation of most of the recommendations of the 2014 Review had been progressed well, including the effective transition of the Lysosomal Disease Research Unit into the Nutrition and Metabolism Theme, restructuring of core facilities and the establishment of a gender equity and diversity committee. On the other hand, RAC members were disappointed that Flinders University has declined the opportunity to contribute financially to SAHMRI 2, and encouraged SAHMRI to continue to explore further opportunities to involve Flinders more in the development of the precinct.
It is clear that SAHMRI has developed a unity of purpose which was applauded by members. Of specific note is the Aboriginal Health research effort at SAHMRI and how this permeates all Themes. It creates a common ground and a shared endeavour - a unique feature of SAHMRI and something that the Institute should be significantly proud of. The recruitment of Alex Brown has allowed SAHMRI to position itself as the Australian leader in Aboriginal and Torres Strait Islander research.
General Recommendations:
• Collaboration with the Universities needs to be a key part of all senior researchersroles – while all Themes currently have clear links with at least one of theUniversities, continuing pro-active collaborations with all three universities shouldremain a priority.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
2
• The SAHMRI Executive Director has three Deputies (Steve Nicholls, Alex Brown and Julio Licinio) – the RAC supports the review of the effectiveness of these initial arrangements now that SAHMRI is well established.
• Should SAHMRI decide to expand its research focus, the clear gap is in the area of musculoskeletal research. Consideration could be given to ways in which this could be integrated into current SAHMRI themes.
• The need for bioinformatics support was identified by every Theme as an area of
need – SAHMRI should establish a bioinformatics core, with a specialist in this area sitting within each theme to support researchers. This will build capacity which will benefit the themes in the future.
• The need for Health Economics support was identified by many of the Themes –
SAHMRI should work with the three universities to see how researchers can be better supported in this area.
• SAHMRI should facilitate cross-theme meetings of post-doctoral researchers to facilitate discussion about issues such as experimental design, allow them to practice presentations etc. Following an initial meeting, rotating responsibility for this could be taken up by a post-doc researcher.
• SAHMRI should consider establishing a Faculty Senate, to allow regular
discussions between key researchers regarding research-related issues at SAHMRI.
• The appointment of the Development Manager should occur as soon as possible
given the importance of this position in relation to fundraising and philanthropic support to the Institute.
• SAHMRI could also consider dedicating a resource to assist in the preparation of
grants to Trusts and Foundations, recognising the different nature of these funding applications.
• In terms of impact metrics, SAHMRI could consider “alt-metrics” to review social
media and other impact factors. This would complement the research metrics that can be generated from PURE.
• Steve Nicholls should be formally appointed as Co-Chair of the Gender Equity
Committee.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
3
THEME REPORTS – Cancer The RAC was very impressed with the workings of the Cancer Theme as an excellent example of the close integration of clinicians and basic researchers. Although the six groups are each run relatively independently (financially, research direction etc), all are very interactive, both within the Theme and across SA. It was clear that the Theme boasts a very engaged leadership with Tim Hughes and Deb White co-leading a very synergistic group. There is an exciting opportunity unfolding for SAHMRI to be the centre of cancer biobanking in SA and a major force nationally. The excellent clinical trial networks are adding value to the research and the group is well poised to add corresponding research value to the trials. This is well evidenced by the high quality publication record in haematology/cancer as well as biomedical journals. While embracing the opportunities presented by genomics, bioinformatics expertise will become a limiting factor unless bioinformaticians are actively embedded into the Theme. Recommendations:
• Further work is required to interact more effectively with the SAHMRI Population
Health Research Group, who have a specific focus on cancer-related issues e.g. tobacco control, obesity prevention.
• A specific plan should be developed to resource and integrate bioinformatics into the Theme as part of a SAHMRI–wide bioinformatics initiative.
• The interaction of SAHMRI with the Centre for Cancer Biology in SA
Pathology/UNI SA should be formalised with a view to further collaborative research.
THEME REPORTS – Heart Health The Heart Health Theme has progressed very well over the past two years and demonstrates a strong sense of teamwork, with excellent leadership evident, both of the overall theme and from the section heads. The RAC was pleased to see the successful development of a cellular biology program, as foreshadowed in the 2014 Review. It was also evident that there is a genuine concern for the development of trainees and younger colleagues. The presentations by more junior speakers were polished and professional, suggesting a level of performance indicative of careful coaching and good mentorship. The very substantive collaboration with the Aboriginal Health Theme represents an enormous strength and opportunity for the Group as well as for SAHMRI as a whole. Although this is currently the most extensive collaborative program, there is also smaller and emerging collaborations with Mind and Brain and Healthy Mothers and Babies – both of which should be actively encouraged.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
4
It was also noted that the Theme has bought together much of the cardiology activity in the State with a lot of effort placed into engaging with all SA researchers. This leading collaborative approach is also evidenced by the involvement of Theme researchers in two NHMRC Program grant applications – a significant achievement. As with several other SAHMRI groups, the Heart Theme identified the aspiration to both develop more genomics and bioinformatics and the cardiovascular biobank. Both areas are supported by the RAC as the clinical expertise is available in the Theme to properly interrogate the data collected. Recommendations: • Develop a strategic plan for future genetic testing via the CV Biobank (ie genetic
consent from trial and biobank participants)
• A specific plan should be developed to resource and integrate bioinformatics into the Theme as part of a SAHMRI–wide bioinformatics initiative.
• Build on the opportunities presented by the molecular imaging pod, the cyclotron and co-location with the RAH, specifically to translate molecular imaging from mouse models to patients.
• The theme is very well placed to move into cardio-oncology, collaborating with the Cancer Theme. This is a new and important research area well aligned with SAHMRI’s vision.
THEME REPORTS - Mind and Brain The Mind and Brain Theme has a broad and ambitious portfolio of ongoing and future projects ranging from depression, pharmacogenomics, the impact of anti-depressants on obesity, to wellness/resilience and spinal cord injury. Unfortunately, an integrated program of research was not evident in the theme presentations. The 2014 Review suggested building up the Wellness Centre and recruiting another senior staff member to help build the Theme beyond the initial single research group. The RAC was impressed with the Wellness/Resilience project which was presented extremely well. It has developed key links with industry which will facilitate translation of knowledge and has great potential for research, provided that appropriate leadership is available from an academician. A well-qualified, but junior, faculty member, Cedric Bardy has been recruited from the USA. He has expertise in developing induced pluripotent stem cells in Parkinson disease and will develop this capability in depression. However, he will need high level mentoring to support him to develop. The spinal cord injury (SCI) project appears to be relatively nascent in its evolution, and the logistics of the patient population to be studied is unclear. The reviewers felt that studying acute SCI would have insurmountable challenges, and considerations might be given to studying sub-acute phases of SCI. The ‘future directions’ of the project, specifically the potential impact on clinical management are also unclear. Further discussion with the potential donor for this work may be necessary to design a feasible, mutually agreed research program.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
5
Several themes, including Aboriginal Health and Nutrition, identified potential areas of collaboration that could be developed more aggressively in concert with MBT. While a number of cross theme collaborations were apparent, the opportunity for MBT to ‘value add’ to other themes is enormous, and should be embraced more. Other groups commented on the challenge of working with the Mind and Brain theme, which would be a lost opportunity for both SAHMRI and the Theme.
Recommendations • While the RAC recognises the important work being undertaken by the Theme,
Mind and Brain is the least developed of all of the SAHMRI Themes and has made the least progress since the last RAC visit. It is therefore recommended that a review is undertaken of the Theme to address the breadth of the work currently being undertaken and to identify a niche area for SAHMRI to make a significant contribution to this important area. This may result in a change of direction for the Theme, and consequently consideration may need to be given to the leadership structure, including the position of Theme Leader.
• As part of this review, consideration must be given to ways in which the Theme can be more collaborative across the Institute, and with other like research groups from across Australia.
• The Wellbeing and Resilience Centre offers significant strength to SAHMRI and is
an area that should be supported further. For example, a Fellow in Behavioural Health could be appointed.
• While considered to be potentially a worthwhile scientific endeavour, the spinal cord injury research program needs to be re-visited and better framed from a research perspective. This may require the appointment of an academic lead.
• The Theme needs to maximize the opportunities presented by the new
imaging pod
THEME REPORTS – Infection and Immunity
The RAC was impressed with the enthusiasm and clear plans articulated by the Theme and the three group leaders. There is clear evidence of the three areas working well together and proactively trying to link their goals. James Ward was specifically identified as a key future leader and as an individual who can have real impact in his research field.
Each program is relatively new, exciting and of considerable practical/translational merit. Each lead researcher’s program is quite diverse, and it’s likely that increasing focus will develop and be required in future. Bioinformatics is also an area that will require further staffing support. The agreement for a carriage study to be undertaken as part of an agreement with GSK for vaccination of all year 11 and 12 students against meningococcal B is an outstanding example of facilitating effective interaction with industry and public health.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
6
Recommendations: • Consideration could be given (at some point in the near future) to identifying the
key areas of focus for the theme, given the current breadth of research activity. • The Aboriginal and Torres Strait Islander research should be a key focus for the
theme moving forward.
• The Theme could consider appointing an individual with experience in basic immunology to build Tcell capacity.
• The SA Advanced Health Research and Translation Centre could link with the
Aboriginal Health groups that form part of James’ research to strengthen the focus of the Centre on Aboriginal Health research.
• In relation to germ-free mice, consideration could be given to out-sourcing this to another institution such as WEHI.
• A specific plan should be developed to further resource and integrate
bioinformatics into the Theme as part of a SAHMRI–wide bioinformatics initiative.
THEME REPORTS – Aboriginal Health The Director should be congratulated on the appointment of Alex Brown. Alex and the team he has built have not only grown to be the best Aboriginal Health Research group in the country, they have been important catalysts in creating the unique "SAHMRI culture". However, the primary leadership of Alex also brings succession and delegation into sharp focus, highlighting the importance of identifying a deputy with the key skills required. At least two other potential faculty members need to be found, together with explicit leadership development programs for all staff in the Theme. Odette Gibson should also be considered for appointment as a faculty member. Some successful collaborations have been consolidated since the last review and very productive links have been developed with other themes, especially Infection and Immunity, Healthy Mothers, Babies and Children and Heart Themes. These should be sustained while, without spreading resources more thinly, there are some obvious synergies that could be created with the Cancer theme and especially with the Mind and Brain theme (given Alex's background). It may be necessary in the latter case to find a resource to place in the Mind and Brain Theme to initiate a viable collaboration. Recommendations: • A Deputy Director should be appointed for the Theme.
• A second tier of leadership staff should be appointed within the Theme to both
support Alex Brown as Theme Leader and allow these post-doctoral researchers to advance their careers.
• The Theme should implement a mentoring plan for postdoctoral staff.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
7
• The Cancer Theme could be engaged to assist with educating Aboriginal communities on genomics. This would provide important content knowledge in this area and make more optimal use of the current genomics opportunities.
• Consider interaction with Poche Centers and with AAHMS to introduce indigenous
medical students to SAMRHI's research program.
THEME REPORTS – Nutrition and Metabolism The RAC noted that the Theme has a broad and wide-ranging portfolio of longstanding (lysosomal disorders) and relatively new projects (cell signalling based upon Chis Proud’s research). The LDRU has successfully integrated into the Theme and is broadening its research from a decades-long and very productive focus on MPS-IIIa to now include the study of lysosomal disorders in late-onset neurodegenerative disorders including Alzeimer’s. The recruitment of Dr. Tim Sargeant from Cambridge will consolidate this expanded work. Chris Proud presented an excellent overview of the theme and acknowledged that there was a tremendous diversity of research within the theme. This included a number of projects, in addition to the Alzheimer’s work, that involve neurobiological elements: visceral pain, sweet taste sensation within the gut, satiety, and optical coherence tomography studies of the retina. Given the large number of neuroscience-related projects, one would hope to see a very strong collaboration with the Mind and Brain Theme. This has not yet occurred for various reasons. For these projects to reach their maximal potential there clearly needs to be a much stronger convergence of research interests. The work of CSIRO theme members is principally focused on the testing of healthy foodstuffs and weight control. While scientifically and fiscally productive, the research directions of this group are not clear and the unit appears somewhat disconnected from the rest of the theme. The future directions of the LDRU should be clarified, especially since tremendous progress has already been made in the development of therapeutics for MPS-IIIa. The LDRU is encouraged to ask what unanswered questions remain, and where is the field moving. The lysosomal work planned for Alzheimer’s is obviously addressing a disease epidemic of almost unprecedented proportions for the country. Research into Alzheimer’s and related dementias is a very competitive field and the investigators should be encouraged to establish ties with other investigators both nationally and internationally. In addition, the anticipated arrival into Mind and Brain of Dr. Cedric Bardy will infuse experience with neurodegenerative disorders that could provide for additional synergies between the two themes. Recommendations: • The theme should consider linkages with the SAHMRI Population Health
Research Group, particularly in relation to sugar sweetened beverages work.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
8
• The Theme should continue the work associated with the reorientation of the LDRU towards neurodegeneration, including the rebranding of the Unit based on this.
• The Theme is encouraged to give consideration to the areas in which the Theme can have a more global focus.
THEME REPORTS – Healthy Mothers, Babies and Children Progress in this theme has been impressive with a great team atmosphere and significant strengths in clinical trials. There is also strong national relevance evidenced by their impact on guideline development and uptake of research evidence into policy/practice change. They also enjoy an international reputation for their high quality research. This clear translational framework within the theme is driven by the very effective leadership style of Maria Makrides. The Baby Bundles project was particularly impressive, as was the blood spot technology. It was clear that one of the major challenges is capacity building in strengthening the Aboriginal health care workforce and teaching Aboriginals and non-Aboriginals to work together effectively in this space. The organization of the site visit was excellent and evidence of strong and effective leadership and logistic skills. More importantly, the tight coordination of the interests in the Theme and the collegiality of the team were evident at the site visit. The program for perinatal care in the Aboriginal community was inspiring. The passion and commitment of the research team was evident and admirable. It is an outstanding example of real-world implementation of a program that appears to be making a significant impact in “Closing the Gap”. Recommendations: • The Theme could consider linking with the Burnet Institute and their research
program re healthy mothers in Papua New Guinea.
• Engage with a health economist to support the work of the theme (this could be a resource made available to other themes across SAHMRI).
• The non-doctoral staff who are critical to the Baby Bundles project may need
additional support as their lack of advanced degrees limits access to traditional means of support for their essential work and mission. Among other options, perhaps Nursing Fellowship awards could be considered.
RESEARCH GROUP REPORT – Population Health The RAC acknowledged that this is a small group which nevertheless has performed well and was highly focused on a number of key projects with strong engagement with government. These positive relationships are key to the success of their work.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
9
The limited resources available have tended to result in mostly reactive linkages where external collaborators have approached the Group seeking help with clinical epidemiology advice and technical assistance. It will be important to train Group researchers to continue the existing work by linking them with organisations that David Roder has been working with long-term, as well as ensuring that they are offered training in epidemiology and health economics.
Recommendations: o The research group should consider developing stronger linkages with the
SAHMRI themes, particularly Cancer, Heart Health and Nutrition and Metabolism (in relation to sugar sweetened beverages work).
RESEARCH GROUP REPORT - Research services (Bioresources, Molecular Imaging, MITRU) The RAC was impressed with the enthusiasm and quality of the research services. The Bioresources staff are focused on animal breeding and on training researchers. It would be useful for them to be involved more directly in some of the research procedures where appropriate and to visit other facilities to gain experience. Molecular Imaging is clearly a developing service which is not yet fully utilized. They are correctly planning for the future and focused on promoting the opportunities the service offers to researchers who currently do not use it. MITRU is best-in-class, TGA approved and competent in both the production of clinically proven radiotracers as well as development of novel products. The Program could benefit from a leader with experience in radiology and from interactions with user groups from the core facilities where those don't currently exist. Recommendations: • User groups should be established for each of the core facilities.
RESEARCH GROUP REPORT – Clinical Platform Steve Nicholls and Liddy Griffith spoke to the RAC about the Clinical Platform and the extensive Registry capacity at SAHMRI. It was acknowledged that the registries offer significant opportunities for clinical trials and facilitate innovation in clinical research. Recommendations: • Continue to support the ongoing development of the Clinical Platform in the
support of clinical trial activity by SAHMRI researchers.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
10
RESEARCH ADVISORY COMMITTEE REPORT 2019 SAHMRI RESEARCH ADVISORY COMMITTEE MEETING The SAHMRI Research Advisory Committee met at SAHMRI on Thursday 4th and Friday 5th April 2019. The Committee comprised: Professor John Shine (Garvan Institute, Sydney (Chair)) Professor Vicki Anderson (Royal Children’s Hospital, Melbourne) Professor Ian Frazer (Translational Research Institute, Brisbane) Professor Doug Hilton (Walter and Eliza Hall Institute, Melbourne) Professor John Mattick (Oxford University, UK) Professor Papaarangi Reid (University of Auckland, NZ) Professor Justin McArthur (Johns Hopkins Medicine, USA) Professor Steve Wesselingh, SAHMRI Ms Sarah Lawson (Secretariat) Apologies were received from Professor Nadia Rosenthal, Professor Peter Libby and Professor Melanie Wakefield. EXECUTIVE SUMMARY The RAC expressed their appreciation to the Executive Director and his staff for the efficient and professional organisation of the Review and the comprehensive quality of the pre–review materials. RAC members agreed that the scientific quality and research output of the Institute had continued to improve and progress over the last two years. The institute had followed a clear upward trajectory both in quality and quantity and had matured to become one of Australia’s leading Health and Medical Research Institutes (HMRIs). In particular it had very clear leadership status in Aboriginal health and the translational, health services and policy area. There is a clear and shared passion for working within the Institute, and in working towards the SAHMRI vision of improving the health of the community through research. Steve is to be congratulated on his leadership of SAHMRI and particularly in ensuring the growth and integration of the Institute. The RAC were strongly encouraged by the presentations delivered by the Themes, specifically at the Theme visits where the enthusiasm and passion of the researchers was evident. Members agreed that it was great to see some of the same faces since the last meeting, but equally it was encouraging to see new faces to complement existing staff and research ambitions. In relation to the recent restructure of the organisation, members strongly agreed that the refinement of four themes and key platform areas gives SAHMRI greater clarity of vision and a clear research agenda for the next five years. The challenge for the Institute will be to ensure that there is a clear narrative regarding the role of each Theme and the ways in which collaborations across Themes are continued and encouraged. Members agreed that the re-organisation of the Institute from seven themes to four has excellent potential to concentrate scientific focus.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
11
The comments and recommendations provided below are predicated on the obvious excellence and enthusiasm for research, and the skills in research leadership that are evident across the Institute. SAHMRI OVERVIEW Restructure of SAHMRI Themes The Committee was introduced to the new SAHMRI organisational structure:
• Four Themes (with 17 programs): o Precision Medicine o Lifelong Health o Aboriginal Health Equity o SAHMRI Women and Kids
• SAHMRI Impact Platforms, including o Health Policy Centre o Clinical Trial and Registry Science
• Research Support Services; and • The strong partnership with Health Translation SA.
Of particular note is that 8 programs are led by women and 5 are led by Indigenous researchers. Two Deputy Directors have been appointed within the new structure – Prof Alex Brown and Prof Maria Makrides. The RAC agreed that Steve Wesselingh could draw on Alex and Maria more strategically in their capacity as Deputy Directors by having them shadow or deputise for him at strategic meetings, and in the long-term strategic visioning of the Institute. The RAC agreed that the restructure represents a much more coherent organisational approach. Members noted and acknowledged that the revised structure provides improved visibility of leaders beyond the Theme Leaders. While essentially the restructure does not change the research that is happening at SAHMRI, it does represent a number of structural and functional changes that have brought key and ‘like’ groups together. There are clear intersections that still exist across Themes, but the RAC agreed that the restructure provides the Institute with the opportunity to enhance both intra-theme and cross-theme collaborations. In order to support the restructure and alignment of groups within Themes, leaders are encouraged to have weekly theme meetings - PhD student and postdoc talks, technology talks, current trends, talks from visiting scientists, etc. – to ensure strength in Theme culture and a shared research vision. Within the context of the restructure, consideration could be given to the way in which work within the social sciences and bioethics could be strengthened within SAHMRI. With the commitment of additional resources in these areas, this could sit within the Health Policy Centre. Engagement with the national funding bodies and alignment with the priorities of these funding bodies is essential for SAHMRI. The Institute is strongly encouraged to ensure that it is engaged (via researcher representation) on relevant Committees e.g. establishment of the MRFF Missions. Proactive approaches should be made to these funders to be engaged in this way. Every Theme should try to embed at least one
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
12
person in the relevant steering groups that are attempting to plan the various MRFF missions, in the way that Alex has done for Indigenous medicine. SAHMRI Values and Strategic Plan There was key support from the RAC for the inclusion of equity as a SAHMRI value. Given the restructure to include the Aboriginal Health Equity theme, and the general principle of equity across all research streams, RAC members agreed that this would be an advantageous inclusion. The current SAHMRI strategic plan has been written for a 3-year period (up until 2020). Members thought that this should be extended to a 5-year plan, with an annual operational plan. This will provide a longer term to achieve what is planned, as well as demonstrating aspirational targets. The Committee discussed discretionary funds allocated by the Executive Director and whether there was a common philosophy regarding expenditure. There could be incentives introduced based on the SAHMRI values of excellence and impact. The Reconciliation Action Plan was recognised as being a real asset of the Institute. The Plan should be accompanied by a formal Indigenous Research Workforce Strategy that is fully funded to allow implementation. Researcher support Members were interested in the appointment and re-appointment of research staff at SAHMRI, with the primary objective of ensuring that SAHMRI has the best quality researchers within each Theme. A mid-point review in staff contracts is recommended to assess KPIs and action points for improvement. Other ‘best practices’ in career development should be explored: peer writing groups, presentation skills, mentoring the mentors, formal 360 evaluations for theme leaders, use of social media such as SLACK for research work groups to avoid email overload, and leadership development courses. Theme and Platform leaders must ensure that they are actively supporting their staff in understanding career opportunities relevant to them. It is essential that SAHMRI does not lose talent because of uncertainty. Leaders must ensure that they are actively mentoring and supporting their staff in this way. This may require support from HR to achieve this with, e.g. mentoring programs. Trials and Big Data SAHMRI has a clear strength in conducting large clinical research projects and cohort studies. Members discussed the possibility of leveraging all trials/patient engagement by seeking consent for access to all clinical records – to underpin and empower investigation of large datasets. SAHMRI Brand Recognition With the recent restructure, it will be important to ensure that the new research structure of the Institute is communicated effectively – both from a research perspective but importantly from a community perspective (recognition and fundraising). Scientific Seminar Series Members recommended that the weekly seminar should broaden from science and medicine to include social perspectives e.g. Garvan’s Leaders in Science and Society series.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
13
SAHMRI 2 SAHMRI 2 was of specific interest to the Committee, given that the current SAHMRI building is almost at capacity. SAHMRI has three floors in the SAHMRI 2 building – one floor will be dedicated to clinical research space, with two floors dedicated to computational activities (dry space). Members agreed that this was complementary to the research activity already occurring within the SAHMRI building. Given experience interstate, SAHMRI was encouraged to discuss developer responsibility and cost for infrastructure and building maintenance. The inclusion of the proton therapy unit in SAHMRI 2 provides the State with the opportunity to consider a centre of excellence in cancer research – through the work being undertaken in the Precision Medicine Theme, the CCB at Uni SA, work at Adelaide University, RAH and the proton therapy unit. Future RAC Meetings It would be useful for the RAC to meet with the SAHMRI Board when it next visits SAHMRI. GENERAL RECOMMENDATIONS
• Consider extending the Strategic Plan to a rolling five-year plan (2020-2025), accompanied by an annual operational plan.
• Utilise Deputy-Directors Alex Brown and Maria Makrides in the long-term strategic planning of the Institute and to represent SAHMRI in state and national forums.
• In order to support the restructure and alignment of groups within Themes, leaders are encouraged to have weekly theme meetings - PhD student and postdoc talks, technology talks, current trends, talks from visiting scientists, etc. – to ensure strength in Theme culture and a shared research vision.
• Ensure that SAHMRI is represented at the table of national funding bodies when planning their funding priorities and strategies e.g. MRFF Missions. This should be through proactive engagement with the funders to ensure inclusion in committees. Every Theme should try to embed at least one person in the steering groups that are attempting to plan the various MRFF missions, in the way that Alex has done for Indigenous medicine.
• Include equity as an over-arching value of the Institute.
• Consider the ways in which the social sciences and bioethics can be strengthened within the SAHMRI research program.
• Consider the appointment and re-appointment processes for research staff across SAHMRI to aid retention but also ensure ongoing strengthening of the research faculty.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
14
• Other ‘best practices’ in career development should be explored: peer writing groups, presentation skills, mentoring the mentors, formal 360 evaluations for theme leaders, use of social media e.g. SLACK for research work groups to avoid email overload, and leadership development courses.
• Ensure that SAHMRI Theme Leaders and Program Leaders are mentoring their staff effectively to ensure development and retention of talent.
• Support Theme Leaders, Program Leaders and junior staff to attend leadership programs.
• Ensure that the restructure is communicated effectively via the website – both from a research perspective but also for community engagement purposes. This must capture the totality of the work across the Institute.
• Consideration could be given running a brand recognition survey for SAHMRI within the SA community.
• The Institute should consider the possibility of leveraging all trials/patient engagement by seeking consent for access to all clinical records to underpin and empower the investigation of large datasets.
• Consider the introduction of financial incentives for researchers – via ED
discretionary funds – to acknowledge success and demonstration with SAHMRI values.
• Executive must ensure that sufficient support is provided to the ongoing implementation and management of the SAHMRI Reconciliation Action Plan.
o This should include implementation of a formal Indigenous Research Workforce Strategy that is sponsored by Executive to ensure that people have funding to seek workforce/training support.
o Ongoing engagement and training should be offered and provided to non-Indigenous staff and researchers at SAHMRI.
• Consider trying to capture lateral information from all studies, e.g., requesting participants in cohort and clinical studies to allow (de-identified) access to their broader medical records, smart sensor data etc., to allow the development of a rich data ecology amenable to AI interrogation.
• As teams continue to engage in big data and cohort studies, consideration should be given to the associated ethics and data governance issues.
• The Health Policy Centre, Clinical Trials and Registry Science, and Health Translation SA place SAHMRI in a very unique position and therefore these teams should be fostered and supported in their growth and ongoing capacity development.
• The weekly seminar should broaden from science and medicine to including a social perspective e.g. Garvan’s Leaders in Science and Society series.
• In relation to SAHMRI 2, and given the experience interstate, SAHMRI is
encouraged to discuss developer responsibility for infrastructure and building maintenance.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
15
• The inclusion of the proton therapy unit in SAHMRI 2 provides the State with
the opportunity to consider a centre of excellence in cancer research – through the work being undertaken in the Precision Medicine Theme, the CCB at Uni SA, work at Adelaide University and the proton therapy unit.
• Continue to ensure that support is provided to early-career researchers to ensure that business and commercialisation advice is provided early in individuals careers.
THEME REPORTS – Precision Medicine The Committee acknowledged that the Precision Medicine Theme has only been operational as a collective for a few months. The comments provided should be considered in this context. The Theme has a number of very talented and world-leading researchers who should be recognized and congratulated for their outstanding science and research outputs. There is a strong and shared sense of the importance of precision medicine in the research and health delivery landscape, which sets the Theme on a positive path. By bringing together the cancer researchers, those working in computational biology and systems, the microbiome and gene editing, the diversity of the research undertaken within the Theme has increased significantly. The leadership of the Theme is strong, and therefore the potential of what can be achieved as a collective is high. The challenge for the Theme moving forward is to ensure that there is a clear, exciting and shared vision and narrative, and that all members (as well as the Institute as a whole) take advantage of the expertise and capacity within the Theme as well as the collaborations that are possible across Themes (the work of Ville Makkinen with the Hopwood Centre is an excellent example of this). The vision must reach beyond cancer, which dominates the Theme. Weekly meetings with the entire theme will assist in bringing the Theme together and for Tim to demonstrate the leadership and culture that he wants for the Theme. The Theme Leader is encouraged to be ambitious in developing the vision for the Theme and opportunistic in relation to what the new theme can offer. Having a shared and exciting vision will then result in the potential to provide leadership and partnership with the universities to transform healthcare. Microbiome studies is a clear strength at SAHMRI and are likely to be increasingly relevant in many areas of medicine into the future. Members agreed that this area of research should be given greater focus at SHAMRI, possibly with the recruitment of additional investigators, and by intentionally adding microbiome studies within each of the themes. In relation to the clinical research being undertaken by the Theme, discussion should occur with Alex Brown and the Aboriginal Health Equity Theme to ensure representation of the Aboriginal community in these studies.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
16
There is the opportunity for the Theme to engage with the Proton Therapy Unit once established within SAHMRI 2. Given the focus on improvements to patient care, it will be important that the Theme has very strong collaborations with the health system. Recommendations:
• This is an exciting research leadership opportunity for SAHMRI. The theme should be encouraged to develop a shared and exciting vision for the Precision Medicine Theme that is accompanied by a clear statement of what the Theme is aiming to achieve. This vision must be inclusive of all of the groups within the Theme, and not focus only on cancer. The Committee encourages the Theme Leader to be ambitious in the development of this vision, highlighting what the Theme can achieve as a collective in the area of precision medicine.
• Tim Hughes’ role as Theme Leader and Lab Group Leader should be considered in the context of ensuring sufficient time available to act as Theme Leader of a diverse group of research interests, while also ensuring that the CML group’s success is maintained.
• Ensure that the various components of the theme are connected to the clinical
environment in the SA health system.
• Weekly Theme meetings are encouraged. These will allow a cohesive team culture, opportunities for sharing research findings (especially for postdocs and PhD students) and allow the leadership team to communicate their desired objectives.
• Consideration should be given to the way in which the teams are represented – labs vs cores vs groups.
• Recruitment priorities for the next 3-5 years need to be identified, specifically
in the areas of cancer, the ‘omics’ technologies, computational analyses and microbiome research.
• Consideration should be given to the way in which cross-theme collaborations can be strengthened and included (as a Venn diagram approach) – for example, how can Precision Medicine draw on the expertise offered by Josef Gecz in the SAHMRI Women and Kids Theme. There are clearly other teams working in precision medicine and this expertise should be exploited.
• Consideration should be given to the way in which other bioinformatics, biostatistics and computational biology functions from across the Institute can be integrated with the key teams within the Precision Medicine theme.
• Additional investigators should be recruited to the microbiome team given the increase in interest in this nationally. This would then allow intentional inclusion of microbiome studies within each of the themes across SAHMRI.
• In relation to the clinical research being undertaken by the Theme, discussion
should occur with Alex Brown and the Aboriginal Health Equity Theme to ensure representation of the Aboriginal community in these studies.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
17
• Consider the way in which health economics could be built in to the work of the Theme, through collaboration with expertise available at Flinders University.
• Recognise and build on the opportunities that medical and artificial intelligence will offer the Theme.
• Consider ways in which the Theme can engage with the Proton Therapy Unit once established within SAHMRI 2.
THEME REPORTS – Lifelong Health The Committee acknowledged that the Lifelong Health Theme has only been operational as a collective for a few months. The comments provided should be considered in this context. The Committee was impressed with the leadership provided by both Chris Proud and Derek Chew, particularly given Derek’s recent appointment as Theme Leader. The Theme overall has a visionary approach to building the team as a collective with a very positive culture. The creation of the Lifelong Health Theme made sense to the RAC from the perspective of collaborations and areas of shared interest in chronic disease. There are clear collaborations within the Theme and across Themes within the Institute, and these can clearly continue to be nurtured. There is however a clear opportunity to build on the relationship with Aboriginal Health Equity and SAHMRI Women and Kids in relation to the early prevention areas that contribute to lifelong health. The Leadership team is encouraged to think about when/how all of the teams are brought together for networking, idea generation and planning. The Theme has a clear interest in big data. It would be useful for SAHMRI to consider investing in this area to set the institute up as a world leader in the use of big data to avoid disease risk. The Vascular program is outstanding but quite large and with quite a ‘flat’ structure. The Theme Leaders are encouraged to consider ways in which this could be broken down into smaller teams, led by new young high potential group leaders, mentored by theme/program leaders. It would also be worth considering incorporating cerebrovascular disease, both micro- and macrovascular into the ongoing (and exciting) studies of atherogenesis. There are clearly great strengths here with Dr Simon Koblar, and merging some of the lines of research would be useful. The work on dementia within the Hopwood Centre was recognized as a positive area of research, working on issues not explored elsewhere in Australia. Given this, and to ensure the continued success, RAC members recommended the bolstering of research staff in this area. The work on visceral pain is to be commended. To enhance this area of work, consideration could be given to including input from pain psychologists.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
18
Greater consideration needs to be given to the way in which the Mental Health and Wellbeing team can be expanded to have greater impact across a broader range of research areas and to specifically ensure that it is focused on the mental health aspects of chronic disease which are the focus of the Theme. For example, ways in which the wellbeing and resilience approach can be inserted into a cardiac clinical trial to see if there is an effect. This could include a psycho-social approach. The Neil Sasche Centre was recognized as being quite small, but delivering on an important area of research. The Centre has very limited collaborations with other areas of the Institute and this should be explored further. There needs to be clear messaging re the distinction between the community engagement role of the Centre, and the research team of the Centre. It was also acknowledged that within the research component of the Centre, limited funding success has been achieved. This may require mentoring so that better research applications are prepared. Consideration should also be given to the clinical studies being undertaken and whether these will lead to new understandings of spinal cord injuries. Recommendations:
• The Theme Leaders are encouraged to think about when/how all of the teams within the Theme are brought together for networking, idea generation and planning.
• Build on the collaborative opportunities with Aboriginal Health Equity and SAHMRI Women and Kids to address early prevention areas, by reaching out to Alex Brown and Maria Makrides and their teams to explore collaborative research.
• The Theme has a clear interest in big data. It would be useful for SAHMRI to consider investing in this area to set the institute up as a world leader in the use of big data to avoid disease risk.
• Consider ways in which a genetics perspective could be incorporated into the research being undertaken within the Theme.
• In relation to the Vascular Research program, consider ways in which the team could be parsed into smaller teams/groups led by new young high potential group leaders, mentored by theme/program leaders.
• Consider the incorporation of cerebrovascular disease, both micro- and macrovascular into the ongoing (and exciting) studies of atherogenesis. There are clearly great strengths here with Dr Simon Koblar, and merging some of the lines of research would be useful.
• Consider increasing the number of staff working on dementia within the Hopwood Centre, in recognition of the fact that this focus on dementia is important and different to investigations at other HMRIs.
• The work on visceral pain is to be commended. To enhance this area of work, consideration could be given to including input from pain psychologists.
• Greater consideration needs to be given to the way in which the Mental Health and Wellbeing team can be expanded to have greater impact across a broader range of research areas and to specifically ensure that it is focused on the
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
19
mental health aspects of chronic disease focus of the Theme. This may be achieved through focus on psycho-social components of chronic disease.
• There needs to be clear messaging re the distinction between the community engagement role of the Neil Sasche Centre, and the research team of the Centre.
• It was also acknowledged that within the research component of the Neil Sasche Centre, limited funding success has been achieved. This may require mentoring so that better research applications are prepared.
• The Neil Sasche Centre has very limited collaborations with other areas of the Institute and this should be explored further.
THEME REPORTS – Aboriginal Health Equity The Committee was extremely impressed and motivated by the enthusiasm within the Aboriginal Health Equity Theme, and the determination of staff who are committed to the vision of improving the health of Aboriginal and Torres Strait Islander people. The visit to the Theme demonstrated this passion through discussions with younger researchers. The foundations of the theme have been built strongly over the last five years, and as a group, they are now well placed to deliver health impact. The restructure of the Theme has allowed the next tier of researchers to be elevated to leadership positions, which has also provided Alex as Theme Leader with greater support and time to commit to his own research activities. It was however acknowledged that James Ward may need to appoint a deputy to allow him greater time to focus on the number of successful projects being completed in the area of sexual health and wellbeing. The number of Indigenous researchers working within the Theme is admirable. As suggested by James Ward, the goal is to recruit an Indigenous Post-Doc within his team. In terms of funding, MRFF opportunities should be explored, including the Frontiers of Science program. The Theme undertakes important clinical research but could benefit from being integrated to a higher level with other clinically focussed project groups within the Institute and the infrastructure that supports them that could contribute to the agenda of understanding the basis of health disadvantage in the aboriginal communities. In order to increase the capacity of staff within the Theme, it was suggested that training could be provided by other staff across SAHMRI, or via visits to other HMRIs. This could ensure that individuals are effectively trained by rotating them through some of the other groups where a short and intensive exposure to research outside the Aboriginal context may help both the researcher and the other group. Cross-theme collaborations is an area that could be considered further, both from a research as well as an educational perspective.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
20
Recommendations:
• Recruit a deputy lead for James Ward’s Sexual Health and Wellbeing program, and support James to appoint an Indigenous post-doctoral researcher.
• Cross-theme collaborations is an area that could be considered further, both from a research as well as an educational perspective. This could also include joint-appointments across Themes to enhance capacity and increase depth of research expertise.
• Develop ways of integrating with other clinically focussed project groups within the Institute and the infrastructure that supports them that could contribute to the agenda of understanding the basis of health disadvantage in the Aboriginal communities.
• Consider the ways in which MRFF funding opportunities can be applied for e.g. Frontier Health and Medical Research Program, to attract significant funding to implement programs of research to support true population level improvements.
• Engage with the other Themes to provide training for Indigenous researchers in methodologies that would specifically enhance and grow the current research agenda of the theme. This could also be achieved by staff visiting key staff at other HMRIs.
• The Theme must persist in its efforts to interact positively with the teams at the Royal Adelaide Hospital in order to improve patient care. This could also be supported by Health Translation SA.
• Consider ways in which the Theme can interact positively with Health Translation SA to impact upon Aboriginal participation in clinical trials (given this is recognized as a statewide and potentially national issue).
THEME REPORTS – SAHMRI Women and Kids The Committee applauded the enthusiasm and impressive energy of the Theme Leader and her staff. They are all clearly very proud to work for SAHMRI and are committed to making a difference for the health of pre-term babies and their families. The positive interaction between researchers and strong support for other team members across Platforms within the Theme was evident, highlighting the multi-disciplinary nature of the Theme. The program of work of the Theme is excellent and the continued emphasis on translation across all programs of the Theme was recognized as being a key success indicator of the Theme e.g. guideline development and uptake of research evidence into policy/practice change. Since the last meeting of the RAC, the growth of the Aboriginal workforce within the Theme has improved significantly and should be commended. The connections with the Aboriginal Health Equity Theme are evident and should continue.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
21
The co-location of the team with the Women’s and Children’s Hospital offers clear opportunities for direct interaction with clinicians and the ability to therefore impact directly upon uptake of evidence directly into patient care. The employment of clinicians within the team also strengthens the capacity of already excellent researchers. The new facilities in which the Theme is now located are excellent and appear fit for purpose for the work that they Theme engages in. While this co-location with the hospital is beneficial, it is important for the Theme to ensure that it engages and integrates with the work being undertaken within the SAHMRI building on North Terrace. The Committee noted that the Theme has a number of strong cross-Theme collaborations but these could be increased with more exposure within the SAHMRI North Terrace facility. The Theme has significant skills that could be shared with other Themes for mutual benefit. There appears to be the opportunity to expand consent to build multi-lateral datasets for interrogation, irrespective of the reason for recruiting the participant in the first place. Recommendations:
• Ensure that cross-Theme collaborations are continued and strengthened through greater exposure of the SAHMRI Women and Kids Theme within the SAHMRI building, to ensure sharing of skills for mutual benefit.
• The Theme is encouraged to continually develop and strengthen the relationship of the Theme with the WCH executive and key clinicians, in the context of the benefit that the Theme can offer in the translation of evidence into improved patient care.
• Consider ways in which imaging (utilizing the imaging modalities available within the Clinical Research Imaging Centre at SAHMRI) can be built into the studies currently being undertaken within the Theme or any future planned projects.
• While the Committee agreed that there is significant strength in the work
undertaken by Josef Gecz, the interaction of this research with other teams within the Theme and across the Institute should be highlighted and potentially strengthened to make the best use of the genetics expertise.
• Consideration could be given to genotyping all those who are involved in the
number of successful cohort studies undertaken by the Theme. This would provide a significant data capacity currently not possible.
• The Theme is encouraged to take part in/seek funding from the relevant MRFF missions (million minds, indigenous health, traumatic brain injury).
• There appears to be the opportunity to expand consent to build multi-lateral datasets for interrogation, irrespective of the reason for recruiting the participant in the first place.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
22
RESEARCH GROUP REPORT – Health Policy Centre The Committee noted that the Health Policy Centre, Clinical Trials and Registry Science, and Health Translation SA place SAHMRI in a very unique position. These teams offer the Institute a focus not present at many other HMRIs, and a strategic advantage. Therefore, these teams should be fostered and supported in their growth and ongoing capacity development. Caroline Miller and Jacquie Bowden presented to the Committee. The RAC acknowledged the significant growth in this team since the last visit, particularly their success in attracting category one funding. The expertise offered by members of the Centre is a true asset to the Institute and should be drawn upon by other Themes in collaborative projects, for example, in the mental health and wellbeing area. The Centre is also encouraged to proactively approach other teams within SAHMRI to collaborate and offer expertise. With increased capacity, the team could set SAHMRI up as the place to come for health policy advice. It was noted that the team is often engaged to produce reports for Government, which comes with significant advantages, but potential delays in publications. The team has been asked recently to provide advice in a new area of illicit drugs. Recommendations:
• The Health Policy Centre should consider opportunities for collaboration with
SAHMRI Women and Kids Theme in relation to the research projects that have a focus on prevention and behavioural change e.g. fish oil study. There are clear areas of shared expertise across the two groups that would benefit both teams.
• Stronger collaborations should also be fostered with the Mental Health and Wellbeing team.
• The Health Policy Centre should proactively interact with the Themes and Programs to determine ways in which their expertise can be used in collaborative projects.
• Given SA Government interest in the area of illicit drugs, and recent requests
made of the team, consideration could be given to building capacity in this particular area.
• One area of future focus could be climate action.
RESEARCH GROUP REPORT - Research Support Services Sophia Degner and Tim Kuchel presented to the Committee.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
23
Significant structural changes have been made to the way in which Research Support Services are managed at SAHMRI, with all core facilities now reporting centrally rather than through a Theme. Members recognized the efficiencies that this will deliver. Members were supportive of the core facilities that SAHMRI has and the support provided to staff to access this equipment. A key infrastructure improvement will be the replacement of the animal management database. SAHMRI is encouraged to discuss the option that WEHI has adopted. RAC members agreed that Adelaide BioMed City provided opportunities regarding equipment sharing and management. The cost-recovery policy of SAHMRI was discussed, with members suggesting that this is reviewed in the context of the position of other HMRIs. In relation to PIRL at Gilles Plains, members recognised the world-class facility and the high-quality research infrastructure provided to the State. It was acknowledged however that very few SAHMRI researchers make use of PIRL. The opportunities offered by the impressive imaging equipment at PIRL should be exploited. Recommendations:
• Ensure that the operations at PIRL break-even.
• The opportunities offered by the impressive imaging equipment at PIRL should be
exploited.
• In relation to the introduction of a new animal management database at SAHMRI, discussions should occur with WEHI regarding the system that they have implemented.
• NATA accreditation should be sought for both the genomics and flow cytometry
core facilities.
• Consider the difference between a core facility manager as a researcher and as an equipment manager, and how SAHMRI can ensure that the staff are included on publications when appropriate.
• Give consideration to implementing a full cost recovery model at SAHMRI, with
developmental exceptions, offset by vouchers to groups. This improves transparency, equity, more considered/efficient usage and better ability to manage costs.
RESEARCH GROUP REPORT – Clinical Trial and Registry Science The Committee noted that the Health Policy Centre, Clinical Trials and Registry Science, and Health Translation SA place SAHMRI in a very unique position. These teams offer the Institute a focus not present at many other HMRIs, and a strategic advantage. Therefore, these teams should be fostered and supported in their growth and ongoing capacity development.
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
24
Liddy Griffith and Maria Inacio presented to the Committee. In relation to the clinical trial platform, the presentation clearly outlined the key opportunities afforded to trials utilising the platform, and also the success of the platform more broadly in the management of clinical trials (primarily in the areas of heart health and healthy mothers and children). It would be good to see trials conducted by staff in other Themes utilising the support of the platform. The RAC explored the way in which the clinical trial platform provided advice on the quality of the design of the clinical trial. It was acknowledged that this was any area that could be improved on with further resources. The importance of conducting clinical trials within the registries was highlighted and acknowledged as an area that should continue to be advanced. The registries at SAHMRI were acknowledged as some of the best in Australia and the Committee supported the continuing leadership in this area. Recommendations:
• Consideration should be given to ways in which other Themes can be encouraged to utilise the skills of the platform in the management of trials.
• In order to see the continued success of the platform, SAHMRI should invest in increased IT platforms and data capacity.
• Increase the capacity of the clinical trial platform by employing senior research epidemiologists who could work with researchers to ensure quality clinical trial design.
RESEARCH GROUP REPORT – Health Translation SA The Committee noted that the Health Policy Centre, Clinical Trials and Registry Science, and Health Translation SA place SAHMRI in a very unique position. These teams offer the Institute a focus not present at many other HMRIs, and a strategic advantage. Therefore, these teams should be fostered and supported in their growth and ongoing capacity development. Wendy Keech presented to the Committee. The RAC congratulated Health Translation SA on its success to date, noting that it was recognized across Australia as the leading Advanced Health Research and Translation Centre. The truly statewide nature of the Centre, and the engagement of the primary health sector, are admired. The strength lies in the success of Health Translation SA in bringing together the disparate groups to plan meaningful research with practical outcomes. The way in which Health Translation SA can play a role in attracting funding to the State was highlighted by RAC members. While it was noted that the Board of Health Translation SA is made up of representatives from partners, members wondered if in fact it would be good to have
RESEARCH ADVISORY COMMITTEE Reports – 2016 and 2019
25
primary care expertise (separate from the PHN representation) on the Board e.g. a GP. Recommendations:
• Consideration should be given to ways in which Health Translation SA can assist
in attracting funding from category one sources to the State, and SAHMRI.
• Consider expanding the Board to include primary care expertise e.g. GPs, given the focus of this within the Centre priorities.
RESEARCH GROUP REPORT – Business Development and Commercialisation While the Research Advisory Committee did not have sufficient time to hear from the Business Development and Commercialisation team at this meeting, they were encouraged to see that SAHMRI had chosen to include this as one of its key platforms. Recommendations
• The Entrepreneurial Research Commercialisation group was acknowledged for
their work with young researchers and encouraged to continue to support early-career researchers with business and commercialisation advice provided early in their careers. (This recommendation has been included under the general SAHMRI recommendations)

Appendix IV: Final report, dandolopartners (April 2020)
DANDOLO LETTER OF COMPLETION - SAHMRI REVIEW | 1
Professor Steven Wesselingh Executive Director South Australian Health and Medical Research Institute (SAHMRI) By email
5 May 2020
COVER LETTER FOR SAHMRI REVIEW To Whom It May Concern:
dandolopartners (dandolo) is pleased to present this final report “The South Australian Health and Medical Research Institute (SAHMRI) – delivering real world benefits from medical research in South Australia: An independent review of SAHMRI’s value to South Australia.”
About dandolo
dandolo is a public policy consulting firm with extensive experience across the innovation, health and medical research (HMR) and education sectors in particular. We have worked with dozens of medical research organisations in recent years, undertaking reviews, analysis and strategic planning for Australia’s best health and medical research institutions – particularly across the Eastern Seaboard.
One of dandolo’s most significant reviews in the HMR space was for Victoria’s medical research institutes where we undertook a detailed analysis of their contribution to Victoria’s economy and international standings. This work demonstrated the unique value that MRI’s play alongside universities, including the benefits they provide through improving global rankings which ultimately attract students and staff, supervising Honours and PhD students and boosting publications and grant income.
Based on our experience with the HMR sector, and our close links with and understanding of government policy and decision making, dandolopartners (dandolo) was engaged by SAHMRI to undertake an independent review of the institute’s performance and value to South Australia and beyond.
About our review of SAHMRI
Our review demonstrated that SAHMRI occupies a unique and important role in the South Australian HMR sector – and indeed in the Australian MRI landscape. More importantly, it is clear from the evidence that SAHMRI is playing a direct role to save lives and healthcare costs for the State in line with its mandate from the government. For example:
• 27% of SA’s research output in HMR is associated with SAHMRI, despite accounting for only ~10% of the HMR workforce in South Australia.
• Within a relatively short period of six years in operation, SAHMRI activity has saved 1000s of lives and millions of dollars. As part of this, SAHMRI is improving health equity in SA.
SAHMRI’s actions are bringing together researchers from across the State to harness their collective research strengths, reduce unnecessary competition and boost international rankings for SA’s universities. For example:
• We estimate SAHMRI contributes directly to 20% of University of Adelaide ranking points in the ARWU assessment for Medicine and Life Sciences – principally via top publications and highly cited researchers.
DANDOLO LETTER OF COMPLETION - SAHMRI REVIEW | 2
• SAHMRI ranks second in Australia in terms of commercial income for MRIs, which accounts for 32% of total income. This is highly indicative of its credibility and its focus on real-world research.
Finally, SAHMRI attracts diverse talent and novel research infrastructure (including clinical registries and datasets) to South Australia. For example:
• SAHMRI has a more diverse workforce and community than most other HMR organisations in Australia, conferring a competitive advantage in the research it undertakes and its attractiveness to new talent. As two indicative measures of diversity, SAHMRI attracts and retains far more female HMR workers and staff from Indigenous backgrounds than that national average.
In conclusion we believe SAHMRI is contributing significantly to South Australia’s health and innovation sectors. We propose a range of measures to build on these strengths and to continue to deliver knowledge, health and economic benefits for Australia.
Please don’t hesitate to contact us should you wish to discuss any aspects of our prior work or our review of SAHMRI.
Kind regards
Joseph Connell
Director
dandolopartners

The South Australian Health and Medical Research Institute (SAHMRI) – delivering real world benefits from medical research in South AustraliaAn independent review of SAHMRI’s value to South Australia
May 2020
1
SAHMRI’s operating environment is changing
The purpose of this document
The South Australian Health and Medical Research Institute (SAHMRI) has an opportunity to demonstrate its value during a period of national and State focus on health and medical research and outcomes.
The most important driver for SAHMRI is a current and wide-ranging South Australia Productivity Commission (SAPC) inquiry into health and medical research and development commissioned by the South Australian (SA) Government. SAPC recently released an issues paper that is likely to:• Be highly influential on State Government economic policy• Impact SAHMRI’s current funding arrangements with the SA
Government.
In addition to the SAPC issues paper, SAHMRI also has opportunities to demonstrate its value in the context of:• A renewed government focus on the importance of research in
developing competitive advantages and growing the economy. • The COVID-19 pandemic, which has thrown the country’s reliance on
our health and medical research capabilities into sharp relief. SAHMRI is contributing to crisis response and treatment research in many ways.
Given this context there is a need for a compelling, robust and pithy outline of the value SAHMRI delivers for SA, Australia and the world.
Section Page
1. SAHMRI’s value proposition 2
2. SAHMRI’s impact 5
3. Conclusions 22
This document is designed to support SAHMRI’s submission to the SA Productivity Commission and to position SAHMRI to make the most of the opportunities in the changing operating environment.
5. Appendices: Methodologies 31
4. Future Opportunities for SAHMRI 24
SAHMRI engaged dandolo to review and present SAHMRI’s value proposition. This document summarises our findings based on:• Analysis of evidence relating to SAHMRI’s performance• The expert opinion of dandolopartners based on its extensive experience reviewing
Australian medical research institutes (MRIs) – especially in Victoria and NSW.
The remainder of this document follows this structure:
SAHMRI’s value proposition
2
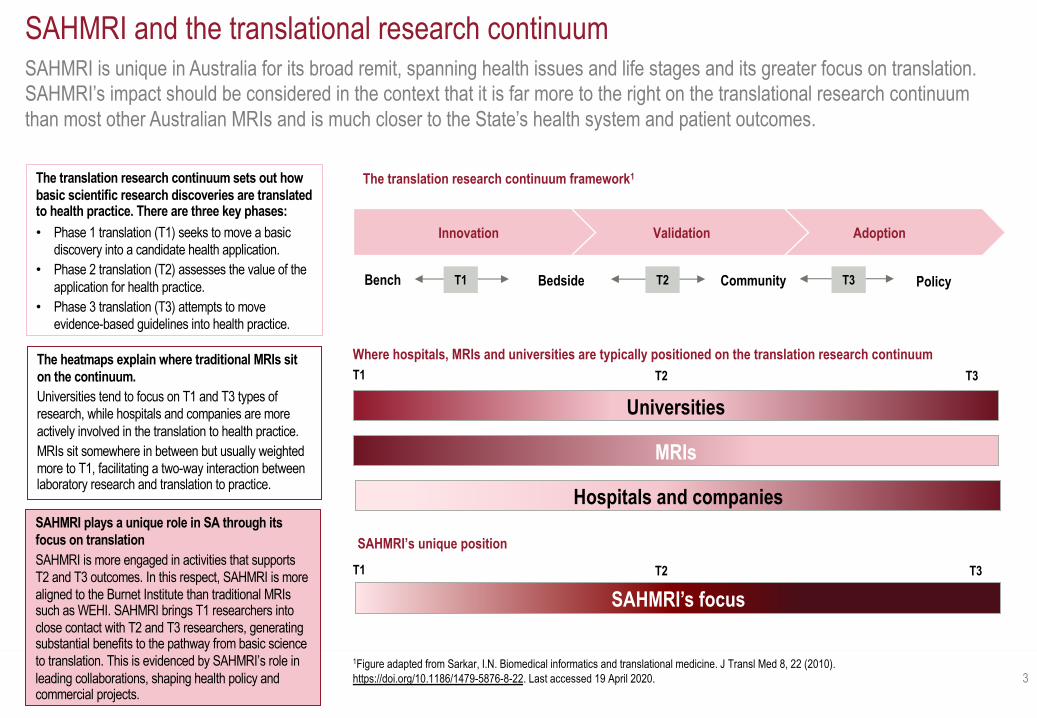
SAHMRI is unique in Australia for its broad remit, spanning health issues and life stages and its greater focus on translation. SAHMRI’s impact should be considered in the context that it is far more to the right on the translational research continuum than most other Australian MRIs and is much closer to the State’s health system and patient outcomes.
3
SAHMRI and the translational research continuum
1Figure adapted from Sarkar, I.N. Biomedical informatics and translational medicine. J Transl Med 8, 22 (2010). https://doi.org/10.1186/1479-5876-8-22. Last accessed 19 April 2020.
AdoptionValidationInnovation
Bench Bedside Community PolicyT1 T2 T3
The translation research continuum framework1
Where hospitals, MRIs and universities are typically positioned on the translation research continuum
The translation research continuum sets out how basic scientific research discoveries are translated to health practice. There are three key phases:• Phase 1 translation (T1) seeks to move a basic
discovery into a candidate health application.• Phase 2 translation (T2) assesses the value of the
application for health practice.• Phase 3 translation (T3) attempts to move
evidence-based guidelines into health practice.
The heatmaps explain where traditional MRIs sit on the continuum. Universities tend to focus on T1 and T3 types of research, while hospitals and companies are more actively involved in the translation to health practice. MRIs sit somewhere in between but usually weighted more to T1, facilitating a two-way interaction between laboratory research and translation to practice.
SAHMRI plays a unique role in SA through its focus on translation SAHMRI is more engaged in activities that supports T2 and T3 outcomes. In this respect, SAHMRI is more aligned to the Burnet Institute than traditional MRIs such as WEHI. SAHMRI brings T1 researchers into close contact with T2 and T3 researchers, generating substantial benefits to the pathway from basic science to translation. This is evidenced by SAHMRI’s role in leading collaborations, shaping health policy and commercial projects.
SAHMRI’s focus
SAHMRI’s unique positionT1 T2 T3
Hospitals and companies
T1 T2 T3
Universities
MRIs
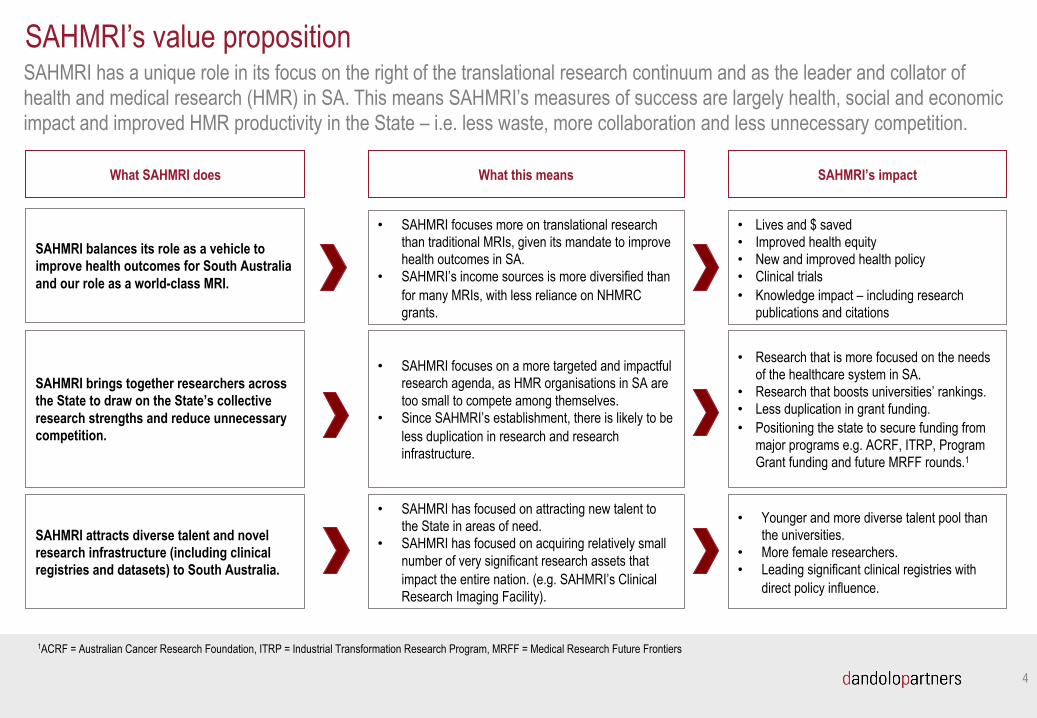
SAHMRI has a unique role in its focus on the right of the translational research continuum and as the leader and collator of health and medical research (HMR) in SA. This means SAHMRI’s measures of success are largely health, social and economic impact and improved HMR productivity in the State – i.e. less waste, more collaboration and less unnecessary competition.
4
SAHMRI’s value proposition
What SAHMRI does What this means SAHMRI’s impact
SAHMRI balances its role as a vehicle to improve health outcomes for South Australia and our role as a world-class MRI.
SAHMRI brings together researchers across the State to draw on the State’s collective research strengths and reduce unnecessary competition.
SAHMRI attracts diverse talent and novel research infrastructure (including clinical registries and datasets) to South Australia.
• SAHMRI focuses more on translational research than traditional MRIs, given its mandate to improve health outcomes in SA.
• SAHMRI’s income sources is more diversified than for many MRIs, with less reliance on NHMRC grants.
• SAHMRI focuses on a more targeted and impactful research agenda, as HMR organisations in SA are too small to compete among themselves.
• Since SAHMRI’s establishment, there is likely to be less duplication in research and research infrastructure.
• SAHMRI has focused on attracting new talent to the State in areas of need.
• SAHMRI has focused on acquiring relatively small number of very significant research assets that impact the entire nation. (e.g. SAHMRI’s Clinical Research Imaging Facility).
• Lives and $ saved• Improved health equity • New and improved health policy• Clinical trials• Knowledge impact – including research
publications and citations
• Research that is more focused on the needs of the healthcare system in SA.
• Research that boosts universities’ rankings. • Less duplication in grant funding.• Positioning the state to secure funding from
major programs e.g. ACRF, ITRP, Program Grant funding and future MRFF rounds.1
• Younger and more diverse talent pool than the universities.
• More female researchers. • Leading significant clinical registries with
direct policy influence.
1ACRF = Australian Cancer Research Foundation, ITRP = Industrial Transformation Research Program, MRFF = Medical Research Future Frontiers

SAHMRI’s impact
5
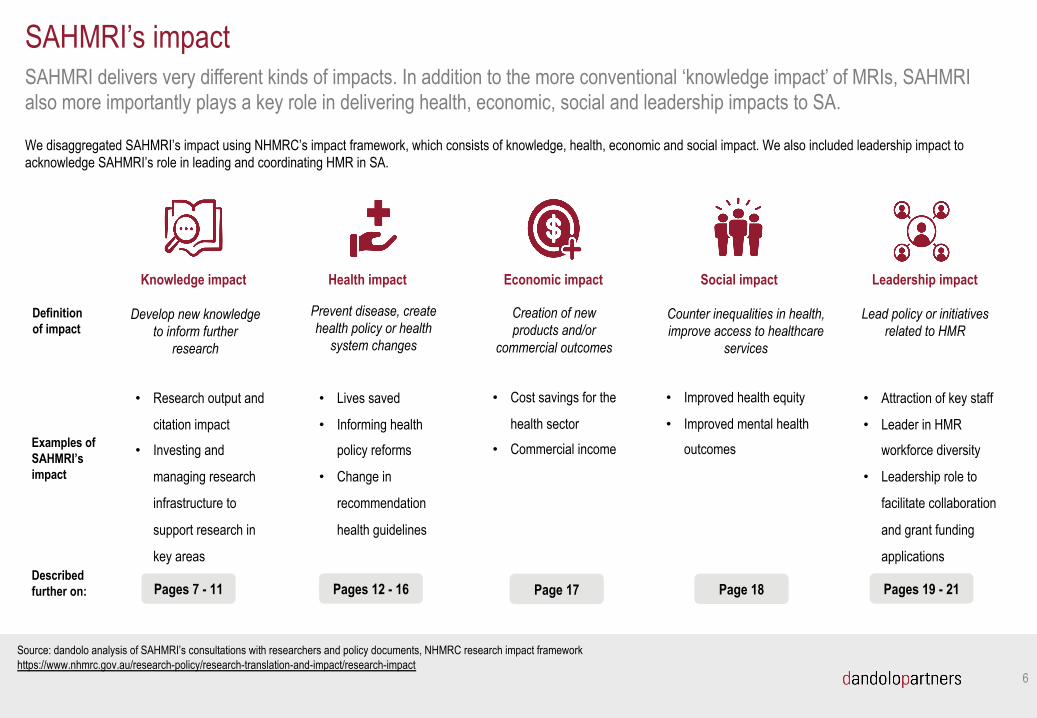
Knowledge impact
SAHMRI delivers very different kinds of impacts. In addition to the more conventional ‘knowledge impact’ of MRIs, SAHMRI also more importantly plays a key role in delivering health, economic, social and leadership impacts to SA.
6
SAHMRI’s impact
Pages 7 - 11Described further on:
Health impact Economic impact Social impact Leadership impact
Examples of SAHMRI’s impact
• Research output and
citation impact
• Investing and
managing research
infrastructure to
support research in
key areas
• Lives saved
• Informing health
policy reforms
• Change in
recommendation
health guidelines
• Cost savings for the
health sector• Commercial income
• Improved health equity
• Improved mental health outcomes
• Attraction of key staff
• Leader in HMR
workforce diversity
• Leadership role to
facilitate collaboration
and grant funding
applications
Pages 12 - 16 Page 17 Page 18 Pages 19 - 21
Definition of impact
Prevent disease, create health policy or health
system changes
Creation of new products and/or
commercial outcomes
Counter inequalities in health, improve access to healthcare
services
Lead policy or initiatives related to HMR
Develop new knowledge to inform further
research
Source: dandolo analysis of SAHMRI’s consultations with researchers and policy documents, NHMRC research impact framework https://www.nhmrc.gov.au/research-policy/research-translation-and-impact/research-impact
We disaggregated SAHMRI’s impact using NHMRC’s impact framework, which consists of knowledge, health, economic and social impact. We also included leadership impact to acknowledge SAHMRI’s role in leading and coordinating HMR in SA.
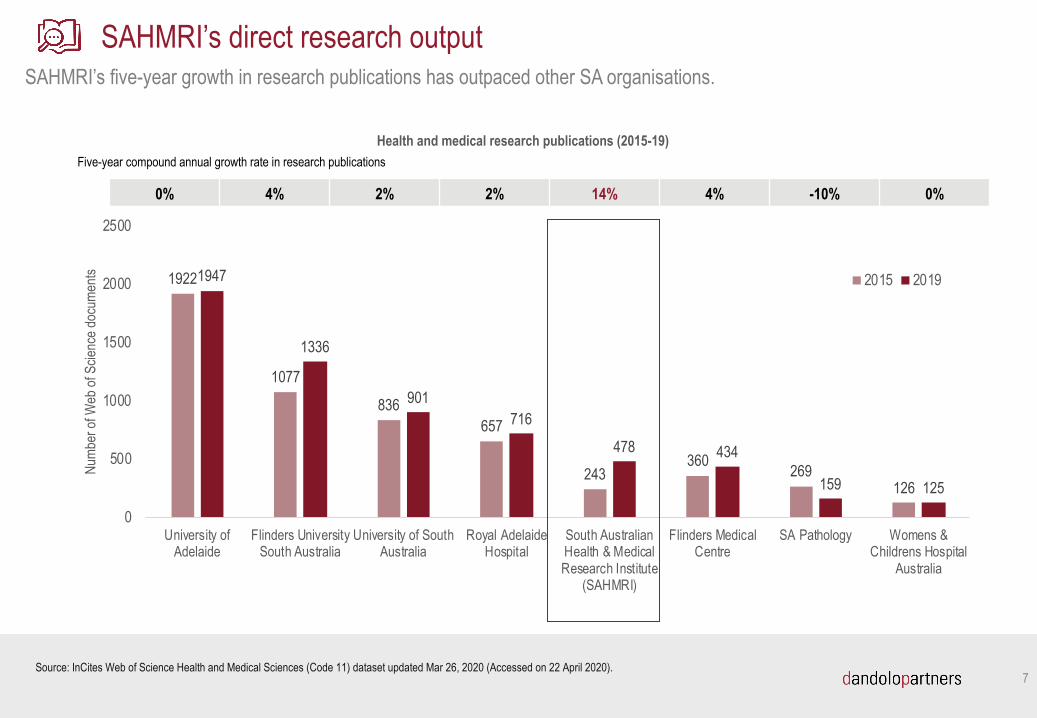
1922
1077
836657
243360 269
126
1947
1336
901716
478 434
159 125
0
500
1000
1500
2000
2500
University ofAdelaide
Flinders UniversitySouth Australia
University of SouthAustralia
Royal AdelaideHospital
South AustralianHealth & MedicalResearch Institute
(SAHMRI)
Flinders MedicalCentre
SA Pathology Womens &Childrens Hospital
Australia
Numb
er of
Web
of S
cienc
e doc
umen
ts
Health and medical research publications (2015-19)
2015 2019
SAHMRI’s five-year growth in research publications has outpaced other SA organisations.
7
SAHMRI’s direct research output
Source: InCites Web of Science Health and Medical Sciences (Code 11) dataset updated Mar 26, 2020 (Accessed on 22 April 2020).
0% 4% 2% 2% 14% 4% -10% 0%
Five-year compound annual growth rate in research publications
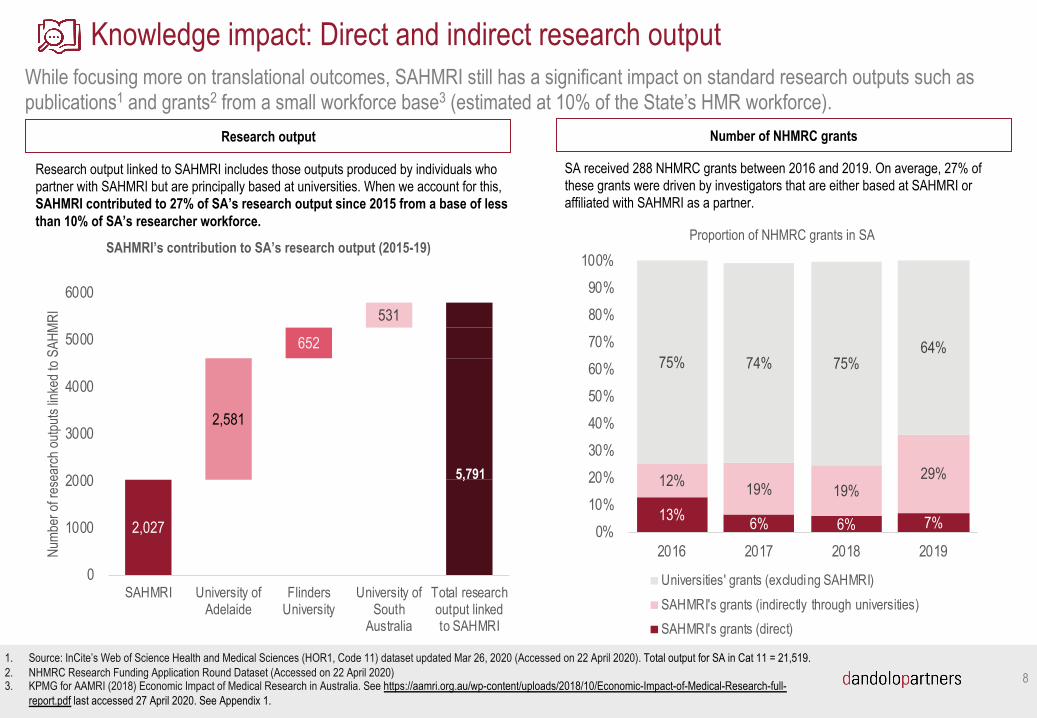
While focusing more on translational outcomes, SAHMRI still has a significant impact on standard research outputs such as publications1 and grants2 from a small workforce base3 (estimated at 10% of the State’s HMR workforce).
8
Knowledge impact: Direct and indirect research output
2,027
2,581
652531
0
1000
2000
3000
4000
5000
6000
SAHMRI University ofAdelaide
FlindersUniversity
University ofSouth
Australia
Total researchoutput linkedto SAHMRI
Numb
er of
rese
arch
outpu
ts lin
ked t
o SAH
MRI
SAHMRI’s contribution to SA’s research output (2015-19)
5,791
1. Source: InCite’s Web of Science Health and Medical Sciences (HOR1, Code 11) dataset updated Mar 26, 2020 (Accessed on 22 April 2020). Total output for SA in Cat 11 = 21,519.2. NHMRC Research Funding Application Round Dataset (Accessed on 22 April 2020)3. KPMG for AAMRI (2018) Economic Impact of Medical Research in Australia. See https://aamri.org.au/wp-content/uploads/2018/10/Economic-Impact-of-Medical-Research-full-
report.pdf last accessed 27 April 2020. See Appendix 1.
Research output linked to SAHMRI includes those outputs produced by individuals who partner with SAHMRI but are principally based at universities. When we account for this, SAHMRI contributed to 27% of SA’s research output since 2015 from a base of less than 10% of SA’s researcher workforce.
SA received 288 NHMRC grants between 2016 and 2019. On average, 27% of these grants were driven by investigators that are either based at SAHMRI or affiliated with SAHMRI as a partner.
Research output Number of NHMRC grants
13% 6% 6% 7%
12% 19% 19%29%
75% 74% 75%64%
0%10%20%30%40%50%60%70%80%90%
100%
2016 2017 2018 2019
Proportion of NHMRC grants in SA
Universities' grants (excluding SAHMRI)SAHMRI's grants (indirectly through universities)SAHMRI's grants (direct)
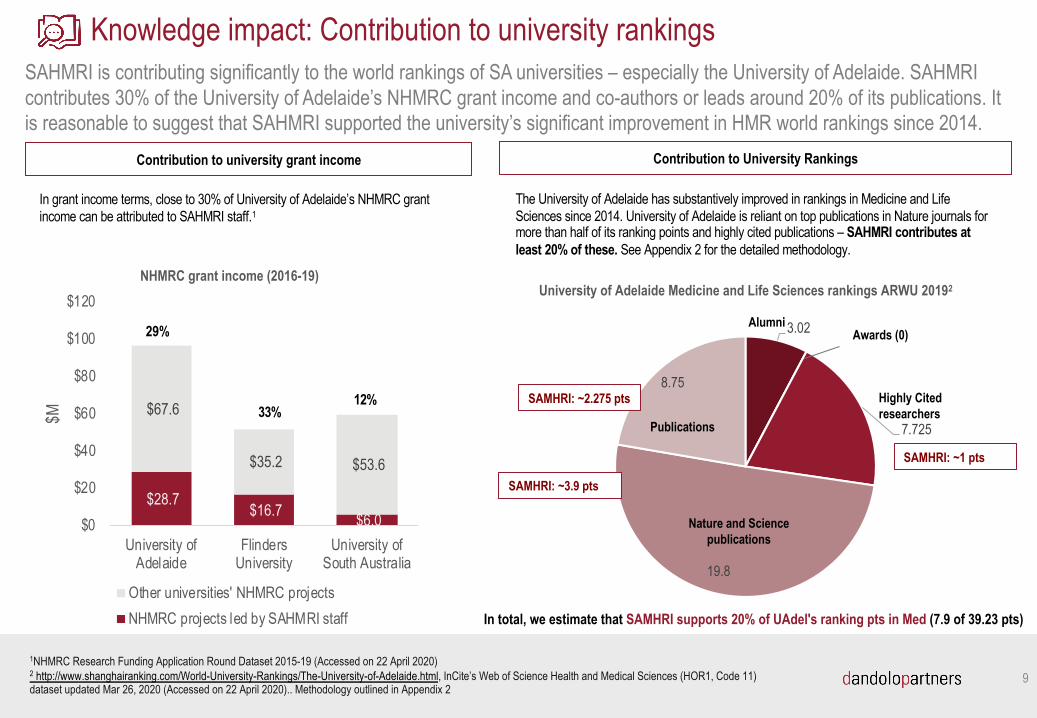
SAHMRI is contributing significantly to the world rankings of SA universities – especially the University of Adelaide. SAHMRI contributes 30% of the University of Adelaide’s NHMRC grant income and co-authors or leads around 20% of its publications. It is reasonable to suggest that SAHMRI supported the university’s significant improvement in HMR world rankings since 2014.
9
Knowledge impact: Contribution to university rankings
1NHMRC Research Funding Application Round Dataset 2015-19 (Accessed on 22 April 2020)2 http://www.shanghairanking.com/World-University-Rankings/The-University-of-Adelaide.html, InCite’s Web of Science Health and Medical Sciences (HOR1, Code 11) dataset updated Mar 26, 2020 (Accessed on 22 April 2020).. Methodology outlined in Appendix 2
Contribution to university grant income Contribution to University Rankings
In grant income terms, close to 30% of University of Adelaide’s NHMRC grant income can be attributed to SAHMRI staff.1
3.02
7.725
19.8
8.75
University of Adelaide Medicine and Life Sciences rankings ARWU 20192
SAMHRI: ~3.9 pts
Publications
AlumniAwards (0)
Highly Cited researchers
Nature and Science publications
SAMHRI: ~1 pts
SAMHRI: ~2.275 pts
The University of Adelaide has substantively improved in rankings in Medicine and Life Sciences since 2014. University of Adelaide is reliant on top publications in Nature journals for more than half of its ranking points and highly cited publications – SAHMRI contributes at least 20% of these. See Appendix 2 for the detailed methodology.
In total, we estimate that SAMHRI supports 20% of UAdel's ranking pts in Med (7.9 of 39.23 pts)
$28.7 $16.7 $6.0
$67.6
$35.2 $53.6
$0
$20
$40
$60
$80
$100
$120
University ofAdelaide
FlindersUniversity
University ofSouth Australia
$M
NHMRC grant income (2016-19)
Other universities' NHMRC projectsNHMRC projects led by SAHMRI staff
29%
33%12%
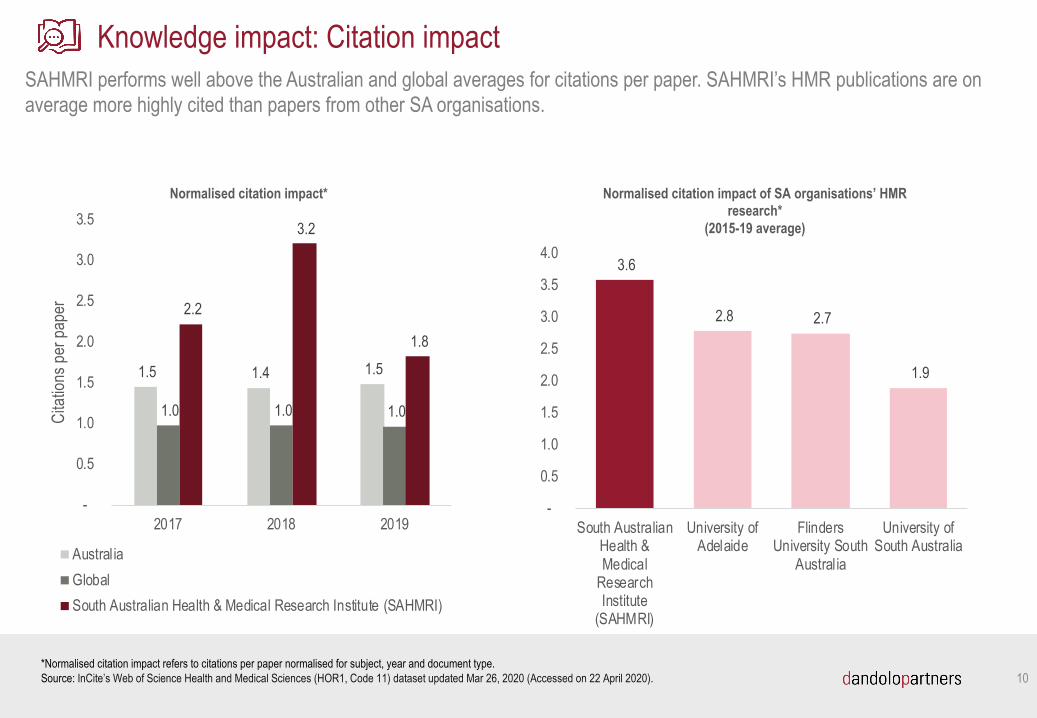
SAHMRI performs well above the Australian and global averages for citations per paper. SAHMRI’s HMR publications are on average more highly cited than papers from other SA organisations.
10
Knowledge impact: Citation impact
*Normalised citation impact refers to citations per paper normalised for subject, year and document type. Source: InCite’s Web of Science Health and Medical Sciences (HOR1, Code 11) dataset updated Mar 26, 2020 (Accessed on 22 April 2020).
1.5 1.4 1.5
1.0 1.0 1.0
2.2
3.2
1.8
-
0.5
1.0
1.5
2.0
2.5
3.0
3.5
2017 2018 2019
Cita
tions
per
pap
er
Normalised citation impact*
AustraliaGlobalSouth Australian Health & Medical Research Institute (SAHMRI)
3.6
2.8 2.7
1.9
-
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
South AustralianHealth &Medical
ResearchInstitute
(SAHMRI)
University ofAdelaide
FlindersUniversity South
Australia
University ofSouth Australia
Normalised citation impact of SA organisations’ HMR research*
(2015-19 average)
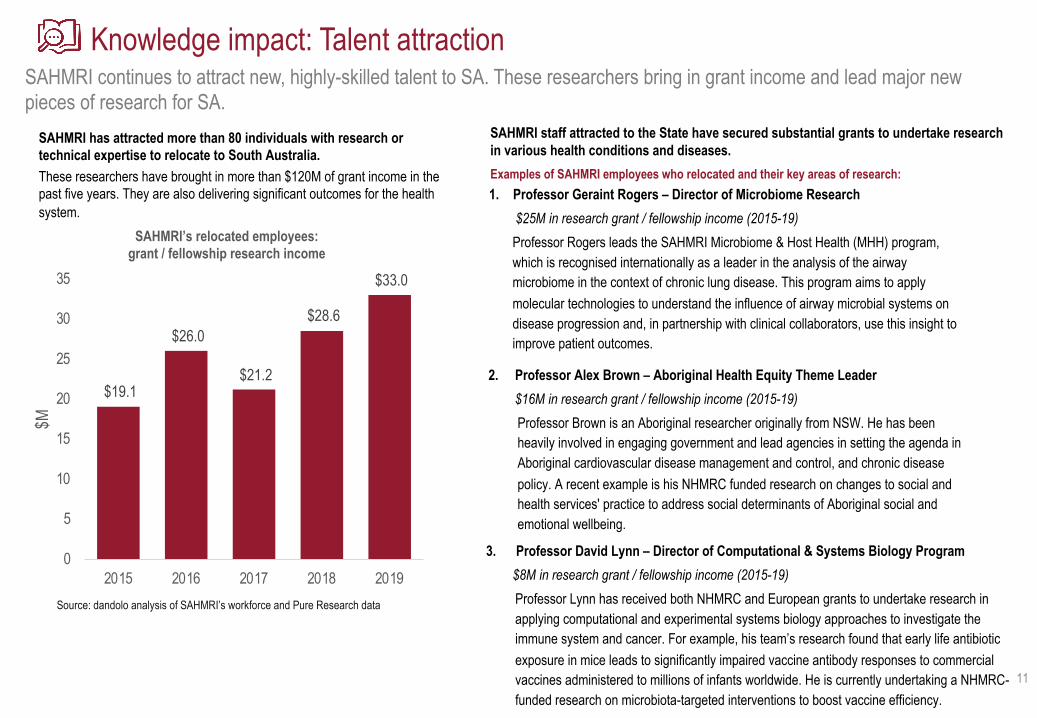
SAHMRI continues to attract new, highly-skilled talent to SA. These researchers bring in grant income and lead major new pieces of research for SA.
11
Knowledge impact: Talent attraction
SAHMRI has attracted more than 80 individuals with research or technical expertise to relocate to South Australia. These researchers have brought in more than $120M of grant income in the past five years. They are also delivering significant outcomes for the health system.
$19.1
$26.0
$21.2
$28.6
$33.0
0
5
10
15
20
25
30
35
2015 2016 2017 2018 2019
$M
SAHMRI’s relocated employees: grant / fellowship research income
1. Professor Geraint Rogers – Director of Microbiome Research$25M in research grant / fellowship income (2015-19)
Professor Rogers leads the SAHMRI Microbiome & Host Health (MHH) program, which is recognised internationally as a leader in the analysis of the airway microbiome in the context of chronic lung disease. This program aims to apply molecular technologies to understand the influence of airway microbial systems on disease progression and, in partnership with clinical collaborators, use this insight to improve patient outcomes.
Source: dandolo analysis of SAHMRI’s workforce and Pure Research data
3. Professor David Lynn – Director of Computational & Systems Biology Program$8M in research grant / fellowship income (2015-19)
Professor Lynn has received both NHMRC and European grants to undertake research in applying computational and experimental systems biology approaches to investigate the immune system and cancer. For example, his team’s research found that early life antibiotic exposure in mice leads to significantly impaired vaccine antibody responses to commercial vaccines administered to millions of infants worldwide. He is currently undertaking a NHMRC-funded research on microbiota-targeted interventions to boost vaccine efficiency.
SAHMRI staff attracted to the State have secured substantial grants to undertake research in various health conditions and diseases.
2. Professor Alex Brown – Aboriginal Health Equity Theme Leader$16M in research grant / fellowship income (2015-19)
Professor Brown is an Aboriginal researcher originally from NSW. He has been heavily involved in engaging government and lead agencies in setting the agenda in Aboriginal cardiovascular disease management and control, and chronic disease policy. A recent example is his NHMRC funded research on changes to social and health services' practice to address social determinants of Aboriginal social and emotional wellbeing.
Examples of SAHMRI employees who relocated and their key areas of research:
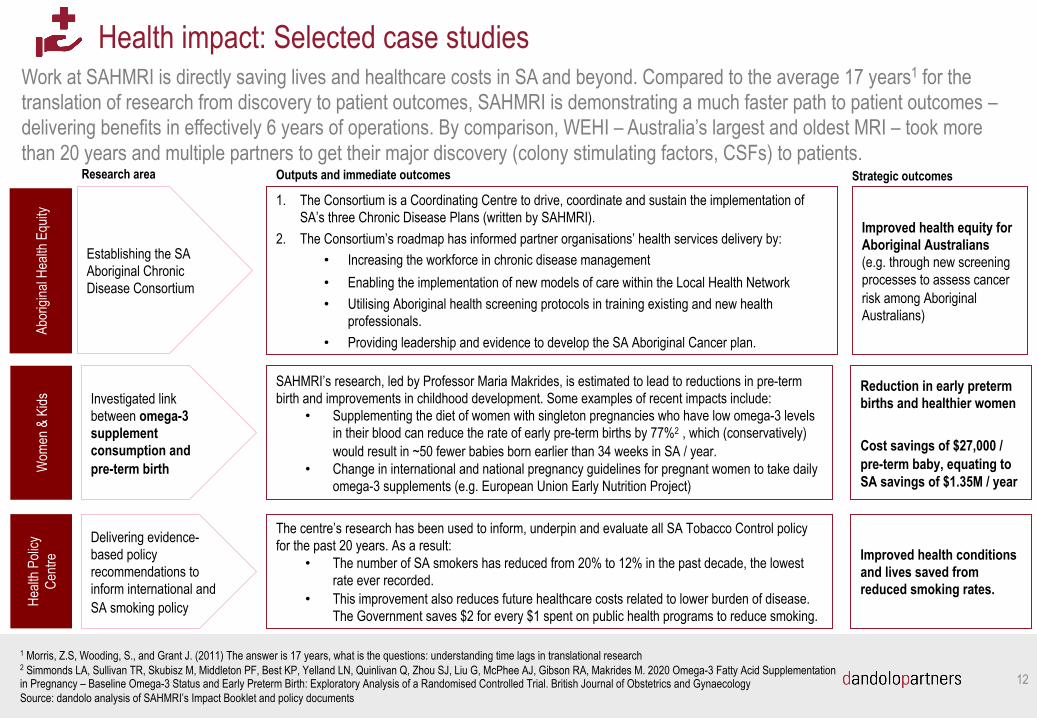
Work at SAHMRI is directly saving lives and healthcare costs in SA and beyond. Compared to the average 17 years1 for the translation of research from discovery to patient outcomes, SAHMRI is demonstrating a much faster path to patient outcomes –delivering benefits in effectively 6 years of operations. By comparison, WEHI – Australia’s largest and oldest MRI – took more than 20 years and multiple partners to get their major discovery (colony stimulating factors, CSFs) to patients.
Health impact: Selected case studies
1 Morris, Z.S, Wooding, S., and Grant J. (2011) The answer is 17 years, what is the questions: understanding time lags in translational research2 Simmonds LA, Sullivan TR, Skubisz M, Middleton PF, Best KP, Yelland LN, Quinlivan Q, Zhou SJ, Liu G, McPhee AJ, Gibson RA, Makrides M. 2020 Omega-3 Fatty Acid Supplementation in Pregnancy – Baseline Omega-3 Status and Early Preterm Birth: Exploratory Analysis of a Randomised Controlled Trial. British Journal of Obstetrics and GynaecologySource: dandolo analysis of SAHMRI’s Impact Booklet and policy documents
Abor
igina
l Hea
lth E
quity
Establishing the SA Aboriginal Chronic Disease Consortium
1. The Consortium is a Coordinating Centre to drive, coordinate and sustain the implementation of SA’s three Chronic Disease Plans (written by SAHMRI).
2. The Consortium’s roadmap has informed partner organisations’ health services delivery by:• Increasing the workforce in chronic disease management• Enabling the implementation of new models of care within the Local Health Network• Utilising Aboriginal health screening protocols in training existing and new health
professionals.• Providing leadership and evidence to develop the SA Aboriginal Cancer plan.
Outputs and immediate outcomesResearch area Strategic outcomes
Improved health equity for Aboriginal Australians (e.g. through new screening processes to assess cancer risk among Aboriginal Australians)
Wom
en &
Kids Investigated link
between omega-3 supplement consumption and pre-term birth
SAHMRI’s research, led by Professor Maria Makrides, is estimated to lead to reductions in pre-term birth and improvements in childhood development. Some examples of recent impacts include:
• Supplementing the diet of women with singleton pregnancies who have low omega-3 levels in their blood can reduce the rate of early pre-term births by 77%2 , which (conservatively) would result in ~50 fewer babies born earlier than 34 weeks in SA / year.
• Change in international and national pregnancy guidelines for pregnant women to take daily omega-3 supplements (e.g. European Union Early Nutrition Project)
Reduction in early preterm births and healthier women
Cost savings of $27,000 / pre-term baby, equating to SA savings of $1.35M / year
Healt
h Poli
cy
Centr
e
Delivering evidence-based policy recommendations to inform international and SA smoking policy
The centre’s research has been used to inform, underpin and evaluate all SA Tobacco Control policy for the past 20 years. As a result:
• The number of SA smokers has reduced from 20% to 12% in the past decade, the lowest rate ever recorded.
• This improvement also reduces future healthcare costs related to lower burden of disease. The Government saves $2 for every $1 spent on public health programs to reduce smoking.
Improved health conditions and lives saved from reduced smoking rates.
12
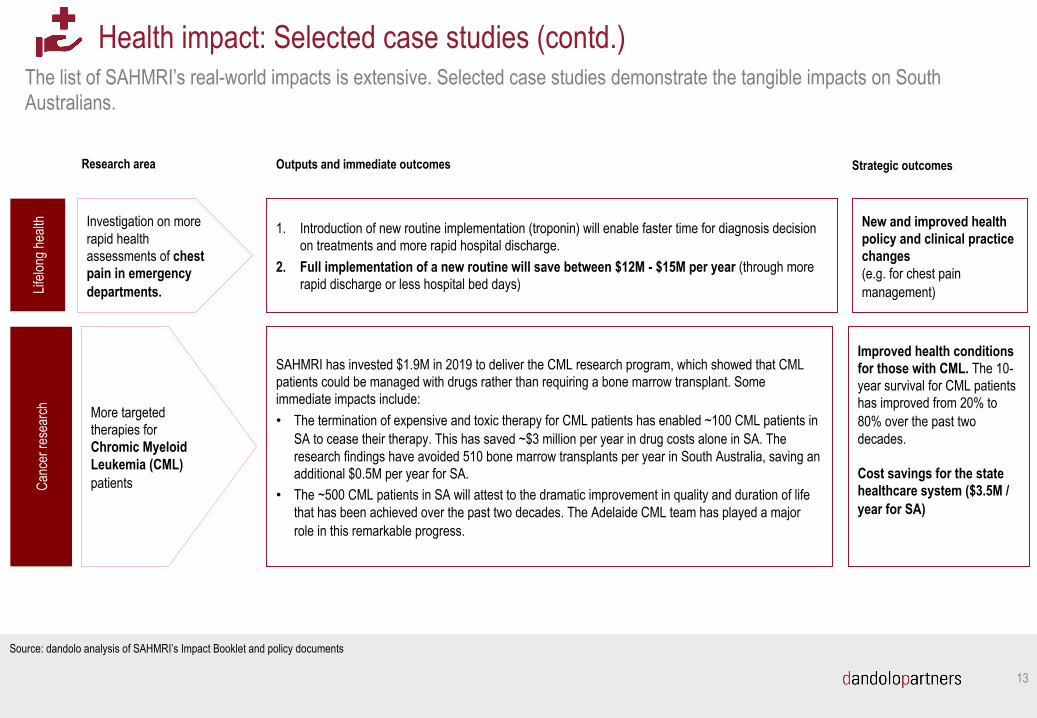
The list of SAHMRI’s real-world impacts is extensive. Selected case studies demonstrate the tangible impacts on South Australians.
Health impact: Selected case studies (contd.)
Source: dandolo analysis of SAHMRI’s Impact Booklet and policy documents
Lifelo
ng he
alth Investigation on more
rapid health assessments of chest pain in emergency departments.
1. Introduction of new routine implementation (troponin) will enable faster time for diagnosis decision on treatments and more rapid hospital discharge.
2. Full implementation of a new routine will save between $12M - $15M per year (through more rapid discharge or less hospital bed days)
Outputs and immediate outcomesResearch area Strategic outcomes
New and improved health policy and clinical practice changes (e.g. for chest pain management)
Canc
er re
sear
ch More targeted therapies for Chromic Myeloid Leukemia (CML) patients
SAHMRI has invested $1.9M in 2019 to deliver the CML research program, which showed that CML patients could be managed with drugs rather than requiring a bone marrow transplant. Some immediate impacts include:• The termination of expensive and toxic therapy for CML patients has enabled ~100 CML patients in
SA to cease their therapy. This has saved ~$3 million per year in drug costs alone in SA. The research findings have avoided 510 bone marrow transplants per year in South Australia, saving an additional $0.5M per year for SA.
• The ~500 CML patients in SA will attest to the dramatic improvement in quality and duration of life that has been achieved over the past two decades. The Adelaide CML team has played a major role in this remarkable progress.
Improved health conditions for those with CML. The 10-year survival for CML patients has improved from 20% to 80% over the past two decades.
Cost savings for the state healthcare system ($3.5M / year for SA)
13
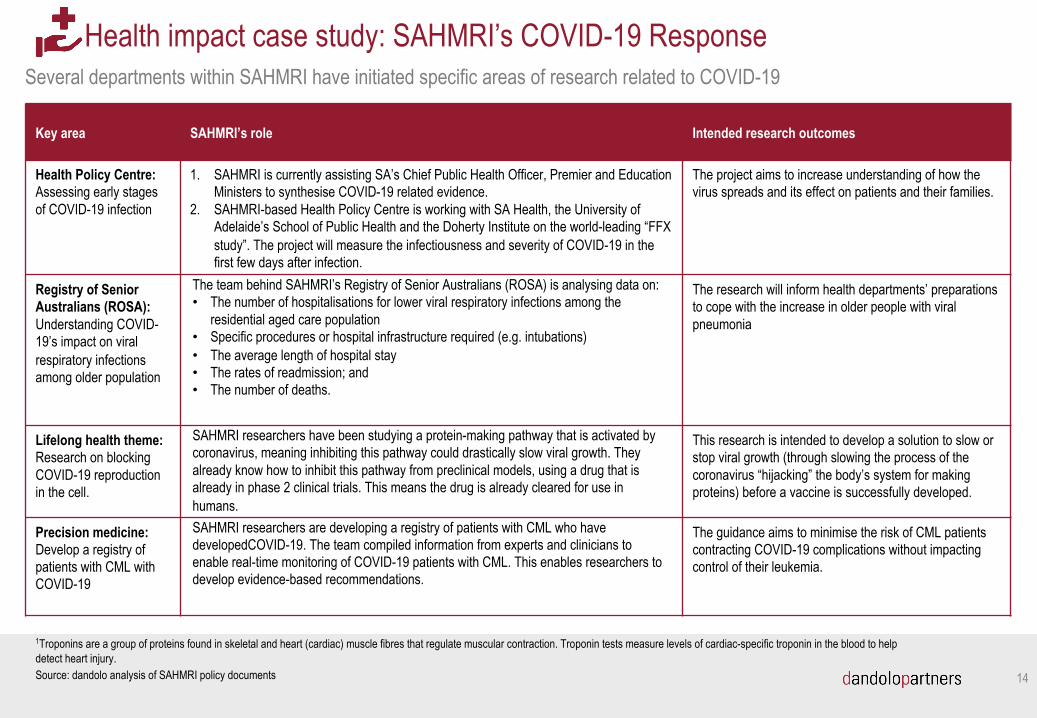
Health impact case study: SAHMRI’s COVID-19 ResponseSeveral departments within SAHMRI have initiated specific areas of research related to COVID-19
1Troponins are a group of proteins found in skeletal and heart (cardiac) muscle fibres that regulate muscular contraction. Troponin tests measure levels of cardiac-specific troponin in the blood to help detect heart injury.
Key area SAHMRI’s role Intended research outcomes
Health Policy Centre: Assessing early stages of COVID-19 infection
1. SAHMRI is currently assisting SA’s Chief Public Health Officer, Premier and Education Ministers to synthesise COVID-19 related evidence.
2. SAHMRI-based Health Policy Centre is working with SA Health, the University of Adelaide’s School of Public Health and the Doherty Institute on the world-leading “FFX study”. The project will measure the infectiousness and severity of COVID-19 in the first few days after infection.
The project aims to increase understanding of how the virus spreads and its effect on patients and their families.
Registry of Senior Australians (ROSA): Understanding COVID-19’s impact on viral respiratory infections among older population
The team behind SAHMRI’s Registry of Senior Australians (ROSA) is analysing data on:• The number of hospitalisations for lower viral respiratory infections among the
residential aged care population • Specific procedures or hospital infrastructure required (e.g. intubations)• The average length of hospital stay• The rates of readmission; and • The number of deaths.
The research will inform health departments’ preparations to cope with the increase in older people with viral pneumonia
Lifelong health theme: Research on blocking COVID-19 reproduction in the cell.
SAHMRI researchers have been studying a protein-making pathway that is activated by coronavirus, meaning inhibiting this pathway could drastically slow viral growth. They already know how to inhibit this pathway from preclinical models, using a drug that is already in phase 2 clinical trials. This means the drug is already cleared for use in humans.
This research is intended to develop a solution to slow or stop viral growth (through slowing the process of the coronavirus “hijacking” the body’s system for making proteins) before a vaccine is successfully developed.
Precision medicine: Develop a registry of patients with CML with COVID-19
SAHMRI researchers are developing a registry of patients with CML who have developedCOVID-19. The team compiled information from experts and clinicians to enable real-time monitoring of COVID-19 patients with CML. This enables researchers to develop evidence-based recommendations.
The guidance aims to minimise the risk of CML patients contracting COVID-19 complications without impacting control of their leukemia.
Source: dandolo analysis of SAHMRI policy documents 14
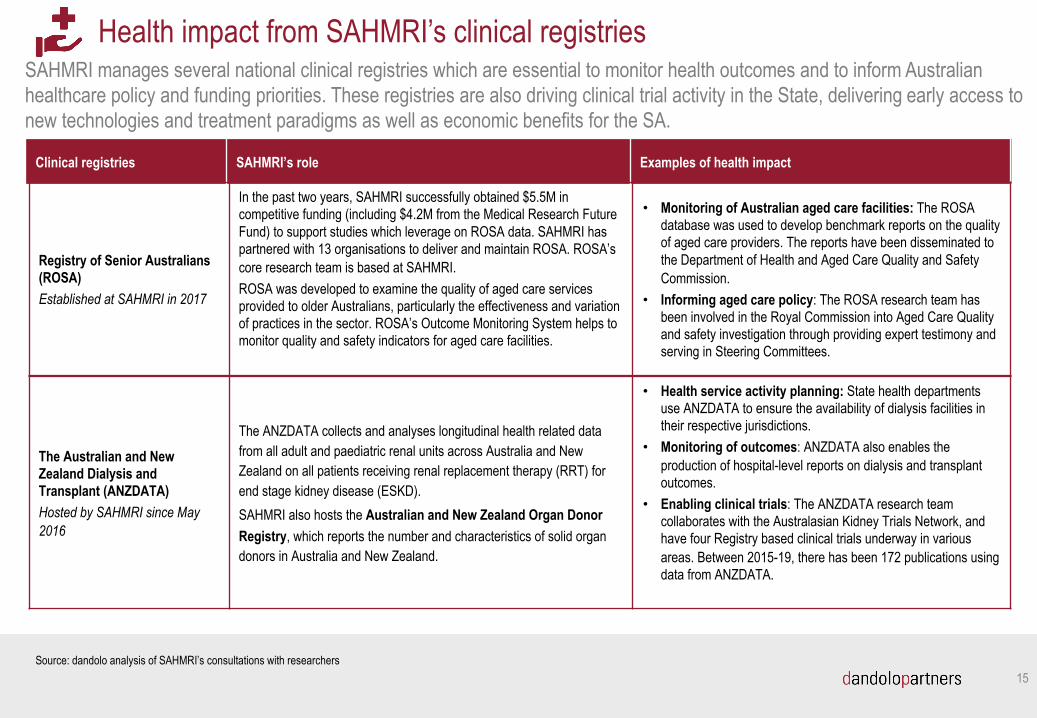
SAHMRI manages several national clinical registries which are essential to monitor health outcomes and to inform Australian healthcare policy and funding priorities. These registries are also driving clinical trial activity in the State, delivering early access to new technologies and treatment paradigms as well as economic benefits for the SA.
15
Health impact from SAHMRI’s clinical registries
Clinical registries SAHMRI’s role Examples of health impact
Registry of Senior Australians(ROSA)Established at SAHMRI in 2017
In the past two years, SAHMRI successfully obtained $5.5M in competitive funding (including $4.2M from the Medical Research Future Fund) to support studies which leverage on ROSA data. SAHMRI has partnered with 13 organisations to deliver and maintain ROSA. ROSA’s core research team is based at SAHMRI. ROSA was developed to examine the quality of aged care services provided to older Australians, particularly the effectiveness and variation of practices in the sector. ROSA’s Outcome Monitoring System helps to monitor quality and safety indicators for aged care facilities.
• Monitoring of Australian aged care facilities: The ROSA database was used to develop benchmark reports on the quality of aged care providers. The reports have been disseminated to the Department of Health and Aged Care Quality and Safety Commission.
• Informing aged care policy: The ROSA research team has been involved in the Royal Commission into Aged Care Quality and safety investigation through providing expert testimony and serving in Steering Committees.
Source: dandolo analysis of SAHMRI’s consultations with researchers
The Australian and New Zealand Dialysis and Transplant (ANZDATA)Hosted by SAHMRI since May 2016
The ANZDATA collects and analyses longitudinal health related data from all adult and paediatric renal units across Australia and New Zealand on all patients receiving renal replacement therapy (RRT) for end stage kidney disease (ESKD).SAHMRI also hosts the Australian and New Zealand Organ Donor Registry, which reports the number and characteristics of solid organ donors in Australia and New Zealand.
• Health service activity planning: State health departments use ANZDATA to ensure the availability of dialysis facilities in their respective jurisdictions.
• Monitoring of outcomes: ANZDATA also enables the production of hospital-level reports on dialysis and transplant outcomes.
• Enabling clinical trials: The ANZDATA research team collaborates with the Australasian Kidney Trials Network, and have four Registry based clinical trials underway in various areas. Between 2015-19, there has been 172 publications using data from ANZDATA.
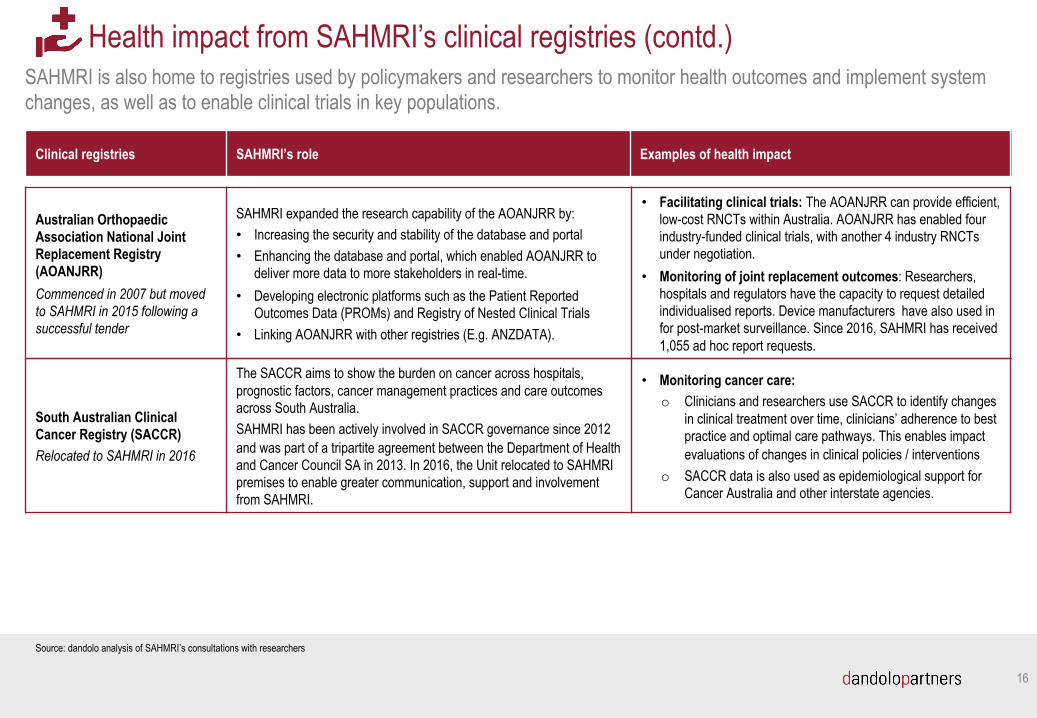
SAHMRI is also home to registries used by policymakers and researchers to monitor health outcomes and implement system changes, as well as to enable clinical trials in key populations.
16
Health impact from SAHMRI’s clinical registries (contd.)
Clinical registries SAHMRI’s role Examples of health impact
South Australian Clinical Cancer Registry (SACCR)Relocated to SAHMRI in 2016
The SACCR aims to show the burden on cancer across hospitals, prognostic factors, cancer management practices and care outcomes across South Australia. SAHMRI has been actively involved in SACCR governance since 2012 and was part of a tripartite agreement between the Department of Health and Cancer Council SA in 2013. In 2016, the Unit relocated to SAHMRI premises to enable greater communication, support and involvement from SAHMRI.
• Monitoring cancer care: o Clinicians and researchers use SACCR to identify changes
in clinical treatment over time, clinicians’ adherence to best practice and optimal care pathways. This enables impact evaluations of changes in clinical policies / interventions
o SACCR data is also used as epidemiological support for Cancer Australia and other interstate agencies.
Source: dandolo analysis of SAHMRI’s consultations with researchers
Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR)Commenced in 2007 but moved to SAHMRI in 2015 following a successful tender
SAHMRI expanded the research capability of the AOANJRR by:• Increasing the security and stability of the database and portal• Enhancing the database and portal, which enabled AOANJRR to
deliver more data to more stakeholders in real-time. • Developing electronic platforms such as the Patient Reported
Outcomes Data (PROMs) and Registry of Nested Clinical Trials• Linking AOANJRR with other registries (E.g. ANZDATA).
• Facilitating clinical trials: The AOANJRR can provide efficient, low-cost RNCTs within Australia. AOANJRR has enabled four industry-funded clinical trials, with another 4 industry RNCTs under negotiation.
• Monitoring of joint replacement outcomes: Researchers, hospitals and regulators have the capacity to request detailed individualised reports. Device manufacturers have also used in for post-market surveillance. Since 2016, SAHMRI has received 1,055 ad hoc report requests.
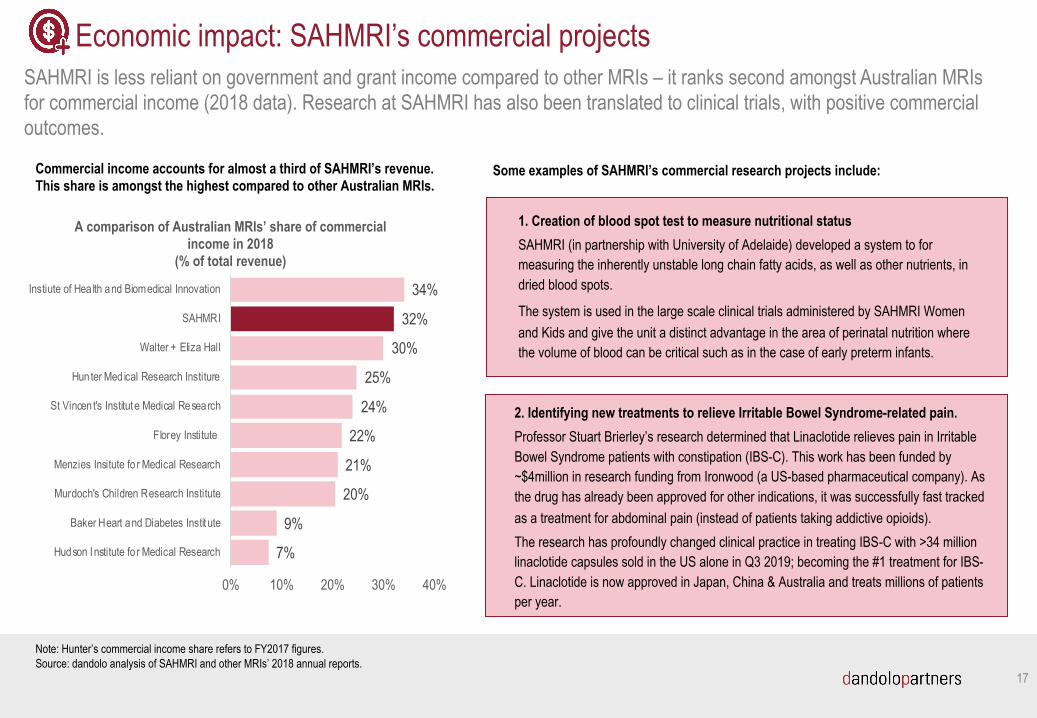
SAHMRI is less reliant on government and grant income compared to other MRIs – it ranks second amongst Australian MRIs for commercial income (2018 data). Research at SAHMRI has also been translated to clinical trials, with positive commercial outcomes.
17
Economic impact: SAHMRI’s commercial projects
Commercial income accounts for almost a third of SAHMRI’s revenue. This share is amongst the highest compared to other Australian MRIs.
7%
9%
20%
21%
22%
24%
25%
30%
32%
34%
0% 10% 20% 30% 40%
Hudson Institute fo r Medical Research
Baker Heart and Diabetes Instit ute
Murdoch's Children Research Institute
Menzies Insitute fo r Medical Research
Florey Institute
St Vincent's Institute Medical Research
Hunter Med ical Research Institure
Walter + Eliza Hall
SAHMRI
Instiute of Hea lth and Biomedical Innovation
A comparison of Australian MRIs’ share of commercial income in 2018
(% of total revenue)
Note: Hunter’s commercial income share refers to FY2017 figures. Source: dandolo analysis of SAHMRI and other MRIs’ 2018 annual reports.
Some examples of SAHMRI’s commercial research projects include:
1. Creation of blood spot test to measure nutritional statusSAHMRI (in partnership with University of Adelaide) developed a system to for measuring the inherently unstable long chain fatty acids, as well as other nutrients, in dried blood spots.
The system is used in the large scale clinical trials administered by SAHMRI Women and Kids and give the unit a distinct advantage in the area of perinatal nutrition where the volume of blood can be critical such as in the case of early preterm infants.
2. Identifying new treatments to relieve Irritable Bowel Syndrome-related pain.Professor Stuart Brierley’s research determined that Linaclotide relieves pain in Irritable Bowel Syndrome patients with constipation (IBS-C). This work has been funded by ~$4million in research funding from Ironwood (a US-based pharmaceutical company). As the drug has already been approved for other indications, it was successfully fast tracked as a treatment for abdominal pain (instead of patients taking addictive opioids). The research has profoundly changed clinical practice in treating IBS-C with >34 million linaclotide capsules sold in the US alone in Q3 2019; becoming the #1 treatment for IBS-C. Linaclotide is now approved in Japan, China & Australia and treats millions of patients per year.
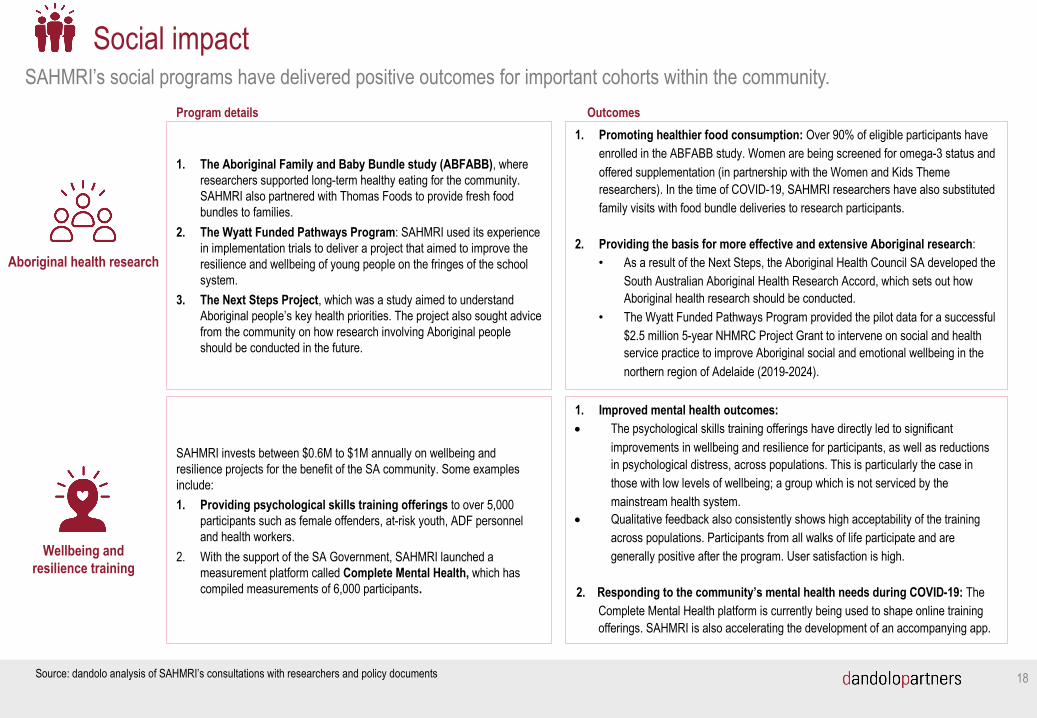
SAHMRI’s social programs have delivered positive outcomes for important cohorts within the community.
18
Social impact
Aboriginal health research
1. The Aboriginal Family and Baby Bundle study (ABFABB), where researchers supported long-term healthy eating for the community. SAHMRI also partnered with Thomas Foods to provide fresh food bundles to families.
2. The Wyatt Funded Pathways Program: SAHMRI used its experience in implementation trials to deliver a project that aimed to improve the resilience and wellbeing of young people on the fringes of the school system.
3. The Next Steps Project, which was a study aimed to understand Aboriginal people’s key health priorities. The project also sought advice from the community on how research involving Aboriginal people should be conducted in the future.
Program details1. Promoting healthier food consumption: Over 90% of eligible participants have
enrolled in the ABFABB study. Women are being screened for omega-3 status and offered supplementation (in partnership with the Women and Kids Theme researchers). In the time of COVID-19, SAHMRI researchers have also substituted family visits with food bundle deliveries to research participants.
2. Providing the basis for more effective and extensive Aboriginal research: • As a result of the Next Steps, the Aboriginal Health Council SA developed the
South Australian Aboriginal Health Research Accord, which sets out how Aboriginal health research should be conducted.
• The Wyatt Funded Pathways Program provided the pilot data for a successful $2.5 million 5-year NHMRC Project Grant to intervene on social and health service practice to improve Aboriginal social and emotional wellbeing in the northern region of Adelaide (2019-2024).
Outcomes
Wellbeing and resilience training
SAHMRI invests between $0.6M to $1M annually on wellbeing and resilience projects for the benefit of the SA community. Some examples include: 1. Providing psychological skills training offerings to over 5,000
participants such as female offenders, at-risk youth, ADF personnel and health workers.
2. With the support of the SA Government, SAHMRI launched a measurement platform called Complete Mental Health, which has compiled measurements of 6,000 participants.
1. Improved mental health outcomes: • The psychological skills training offerings have directly led to significant
improvements in wellbeing and resilience for participants, as well as reductions in psychological distress, across populations. This is particularly the case in those with low levels of wellbeing; a group which is not serviced by the mainstream health system.
• Qualitative feedback also consistently shows high acceptability of the training across populations. Participants from all walks of life participate and are generally positive after the program. User satisfaction is high.
2. Responding to the community’s mental health needs during COVID-19: The Complete Mental Health platform is currently being used to shape online training offerings. SAHMRI is also accelerating the development of an accompanying app.
Source: dandolo analysis of SAHMRI’s consultations with researchers and policy documents
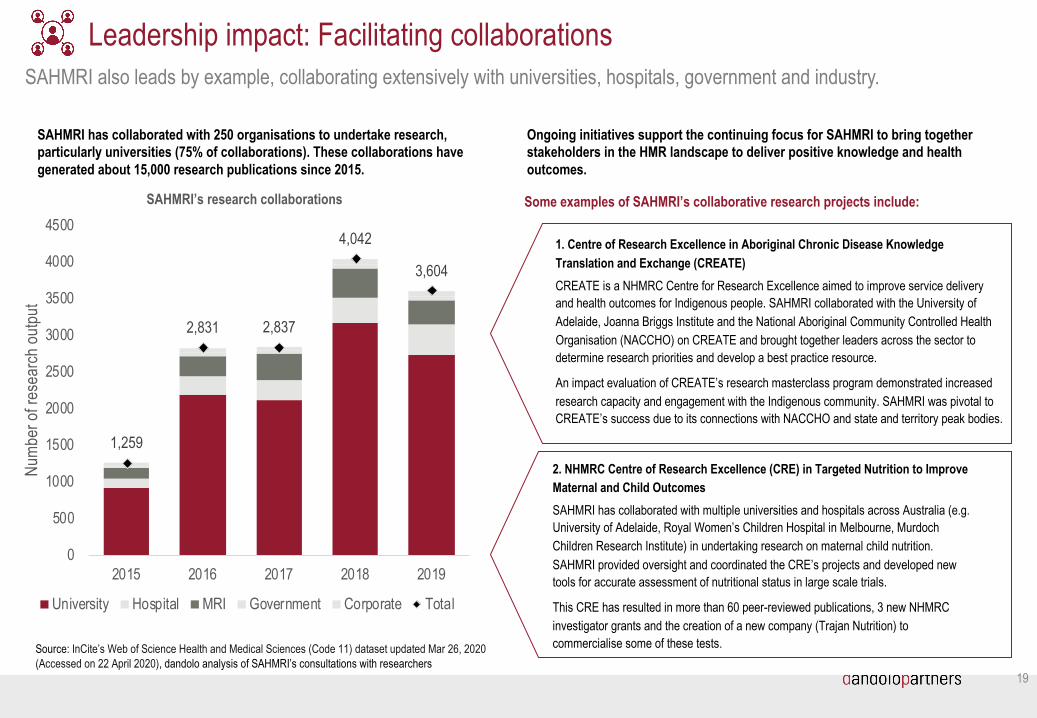
SAHMRI also leads by example, collaborating extensively with universities, hospitals, government and industry.
19
Leadership impact: Facilitating collaborations
SAHMRI has collaborated with 250 organisations to undertake research, particularly universities (75% of collaborations). These collaborations have generated about 15,000 research publications since 2015.
1,259
2,831 2,837
4,042
3,604
0
500
1000
1500
2000
2500
3000
3500
4000
4500
2015 2016 2017 2018 2019
Num
ber o
f res
earc
h ou
tput
SAHMRI’s research collaborations
University Hospital MRI Government Corporate Total
Ongoing initiatives support the continuing focus for SAHMRI to bring together stakeholders in the HMR landscape to deliver positive knowledge and health outcomes.
Some examples of SAHMRI’s collaborative research projects include:
1. Centre of Research Excellence in Aboriginal Chronic Disease Knowledge Translation and Exchange (CREATE)CREATE is a NHMRC Centre for Research Excellence aimed to improve service delivery and health outcomes for Indigenous people. SAHMRI collaborated with the University of Adelaide, Joanna Briggs Institute and the National Aboriginal Community Controlled Health Organisation (NACCHO) on CREATE and brought together leaders across the sector to determine research priorities and develop a best practice resource.
An impact evaluation of CREATE’s research masterclass program demonstrated increased research capacity and engagement with the Indigenous community. SAHMRI was pivotal to CREATE’s success due to its connections with NACCHO and state and territory peak bodies.
2. NHMRC Centre of Research Excellence (CRE) in Targeted Nutrition to Improve Maternal and Child Outcomes SAHMRI has collaborated with multiple universities and hospitals across Australia (e.g. University of Adelaide, Royal Women’s Children Hospital in Melbourne, Murdoch Children Research Institute) in undertaking research on maternal child nutrition. SAHMRI provided oversight and coordinated the CRE’s projects and developed new tools for accurate assessment of nutritional status in large scale trials.
This CRE has resulted in more than 60 peer-reviewed publications, 3 new NHMRC investigator grants and the creation of a new company (Trajan Nutrition) to commercialise some of these tests. Source: InCite’s Web of Science Health and Medical Sciences (Code 11) dataset updated Mar 26, 2020
(Accessed on 22 April 2020), dandolo analysis of SAHMRI’s consultations with researchers
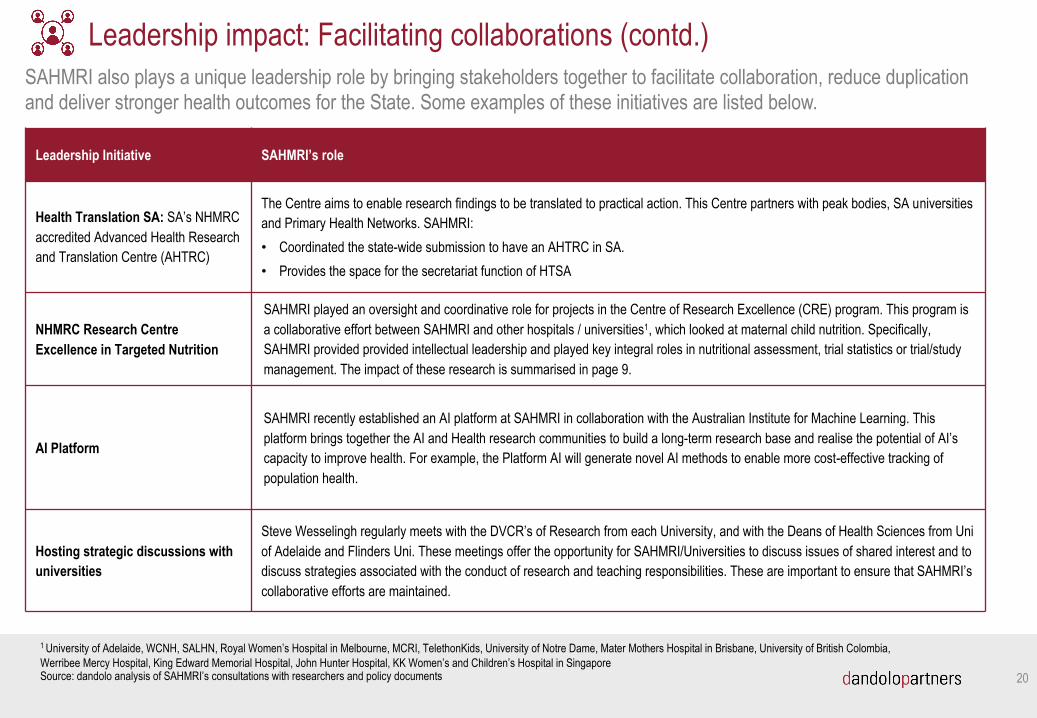
SAHMRI also plays a unique leadership role by bringing stakeholders together to facilitate collaboration, reduce duplication and deliver stronger health outcomes for the State. Some examples of these initiatives are listed below.
20
Leadership impact: Facilitating collaborations (contd.)
Leadership Initiative SAHMRI’s role
Health Translation SA: SA’s NHMRC accredited Advanced Health Research and Translation Centre (AHTRC)
The Centre aims to enable research findings to be translated to practical action. This Centre partners with peak bodies, SA universities and Primary Health Networks. SAHMRI:• Coordinated the state-wide submission to have an AHTRC in SA. • Provides the space for the secretariat function of HTSA
NHMRC Research Centre Excellence in Targeted Nutrition
SAHMRI played an oversight and coordinative role for projects in the Centre of Research Excellence (CRE) program. This program is a collaborative effort between SAHMRI and other hospitals / universities1, which looked at maternal child nutrition. Specifically, SAHMRI provided provided intellectual leadership and played key integral roles in nutritional assessment, trial statistics or trial/study management. The impact of these research is summarised in page 9.
AI Platform
SAHMRI recently established an AI platform at SAHMRI in collaboration with the Australian Institute for Machine Learning. This platform brings together the AI and Health research communities to build a long-term research base and realise the potential of AI’s capacity to improve health. For example, the Platform AI will generate novel AI methods to enable more cost-effective tracking of population health.
Hosting strategic discussions with universities
Steve Wesselingh regularly meets with the DVCR’s of Research from each University, and with the Deans of Health Sciences from Uni of Adelaide and Flinders Uni. These meetings offer the opportunity for SAHMRI/Universities to discuss issues of shared interest and to discuss strategies associated with the conduct of research and teaching responsibilities. These are important to ensure that SAHMRI’s collaborative efforts are maintained.
1 University of Adelaide, WCNH, SALHN, Royal Women’s Hospital in Melbourne, MCRI, TelethonKids, University of Notre Dame, Mater Mothers Hospital in Brisbane, University of British Colombia, Werribee Mercy Hospital, King Edward Memorial Hospital, John Hunter Hospital, KK Women’s and Children’s Hospital in SingaporeSource: dandolo analysis of SAHMRI’s consultations with researchers and policy documents

SAHMRI prides itself for having a diverse workforce, with a high representation of female and Indigenous researchers relative toaverages.
21
Leadership impact: SAHMRI’s contribution to SA’s workforce diversity
SAHMRI has a diverse community of students and researchers
The share of female researchers in SAHMRI is higher relative to other research organisation
400(40%) 371
(37%)
201(21%)
16 (2%)
Employees Partners Students Volunteers
SAHMRI has the largest Indigenous researcher workforce in Australia
• SAHMRI’s community consists of partners, employees and students.
• SAHMRI partners are typically employed by SA hospitals or universities. Eight partners hold a position within the formal SAHMRI organisational structure.
• Six SAHMRI employees have joint appointments with SA universities, which facilitates a high number of research collaborations.
7%
3%
1%
SAHMRI
• Females make up two-thirds of the SAHMRI researcher workforce. This is significantly higher than the average share in both health and medical research as well as the broader researcher workforce in Australia.
• Female leaders are also leading ground-breaking research, such as Professor Maria Makrides in nutrition for women, Professor Deborah White’s CML research and Professor Caroline Miller who is Director of the Health Policy Centre at SAHMRI.
65%
52%44%
SAHMRI Medical and health sciences
workforce
Australia researcher workforce
*Sector average reflects the average share of employees in the professional, scientific and technical services who are of ATSI descent in 2016. Source: dandolo analysis of SAHMRI demographic data, ABS ATSI Census and Labour Market Statistics (2016), ARC speech on increasing female participation in research (2018) https://www.arc.gov.au/news-publications/media/media-releases/increasing-female-participation-research
SAHMRI community by employee type Share of female researchers Share of staff identifying as Indigenous
• The share of people who identify as Indigenous (Indigenous) in SAHMRI (7%) is significantly higher than sector and national averages. The Aboriginal Health Equity Theme has the largest cohort of Indigenous researchers.
• This has enabled research on common health issues affecting the Indigenous community and the design of more targeted health preventative measures (see page 9 for additional information).
Sector average*
National average

Conclusions
22
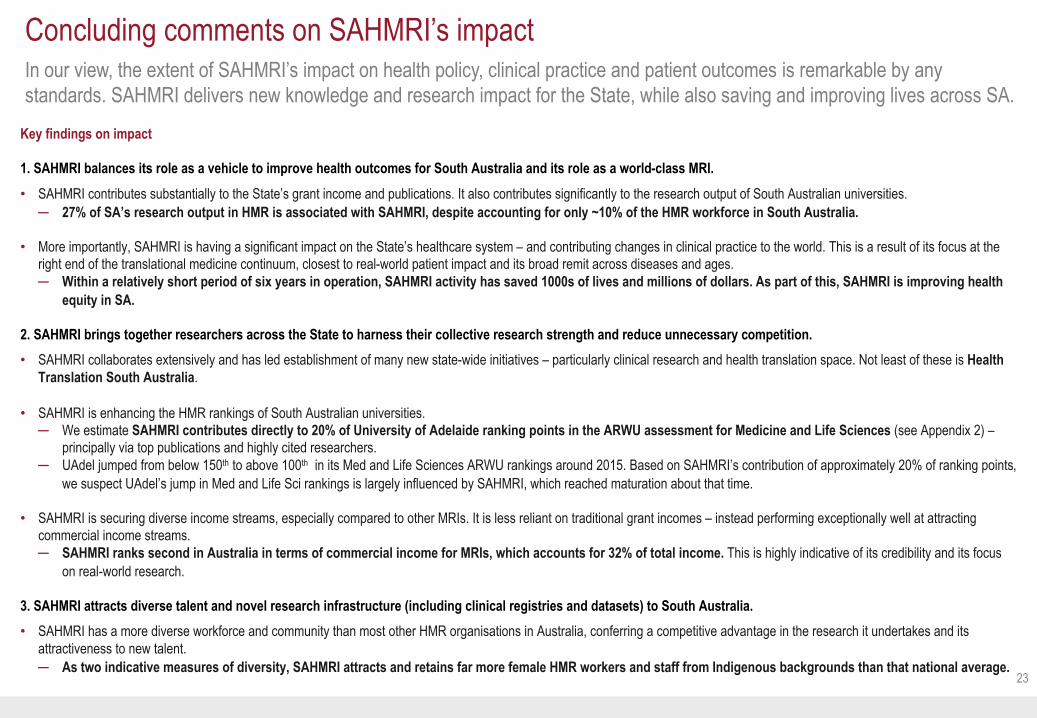
In our view, the extent of SAHMRI’s impact on health policy, clinical practice and patient outcomes is remarkable by any standards. SAHMRI delivers new knowledge and research impact for the State, while also saving and improving lives across SA.
23
Key findings on impact
1. SAHMRI balances its role as a vehicle to improve health outcomes for South Australia and its role as a world-class MRI. • SAHMRI contributes substantially to the State’s grant income and publications. It also contributes significantly to the research output of South Australian universities.
─ 27% of SA’s research output in HMR is associated with SAHMRI, despite accounting for only ~10% of the HMR workforce in South Australia.
• More importantly, SAHMRI is having a significant impact on the State’s healthcare system – and contributing changes in clinical practice to the world. This is a result of its focus at the right end of the translational medicine continuum, closest to real-world patient impact and its broad remit across diseases and ages. ─ Within a relatively short period of six years in operation, SAHMRI activity has saved 1000s of lives and millions of dollars. As part of this, SAHMRI is improving health
equity in SA.
2. SAHMRI brings together researchers across the State to harness their collective research strength and reduce unnecessary competition.• SAHMRI collaborates extensively and has led establishment of many new state-wide initiatives – particularly clinical research and health translation space. Not least of these is Health
Translation South Australia.
• SAHMRI is enhancing the HMR rankings of South Australian universities. ─ We estimate SAHMRI contributes directly to 20% of University of Adelaide ranking points in the ARWU assessment for Medicine and Life Sciences (see Appendix 2) –
principally via top publications and highly cited researchers. ─ UAdel jumped from below 150th to above 100th in its Med and Life Sciences ARWU rankings around 2015. Based on SAHMRI’s contribution of approximately 20% of ranking points,
we suspect UAdel’s jump in Med and Life Sci rankings is largely influenced by SAHMRI, which reached maturation about that time.
• SAHMRI is securing diverse income streams, especially compared to other MRIs. It is less reliant on traditional grant incomes – instead performing exceptionally well at attracting commercial income streams. ─ SAHMRI ranks second in Australia in terms of commercial income for MRIs, which accounts for 32% of total income. This is highly indicative of its credibility and its focus
on real-world research.
3. SAHMRI attracts diverse talent and novel research infrastructure (including clinical registries and datasets) to South Australia. • SAHMRI has a more diverse workforce and community than most other HMR organisations in Australia, conferring a competitive advantage in the research it undertakes and its
attractiveness to new talent. ─ As two indicative measures of diversity, SAHMRI attracts and retains far more female HMR workers and staff from Indigenous backgrounds than that national average.
Concluding comments on SAHMRI’s impact

Future opportunities for SAHMRI
24
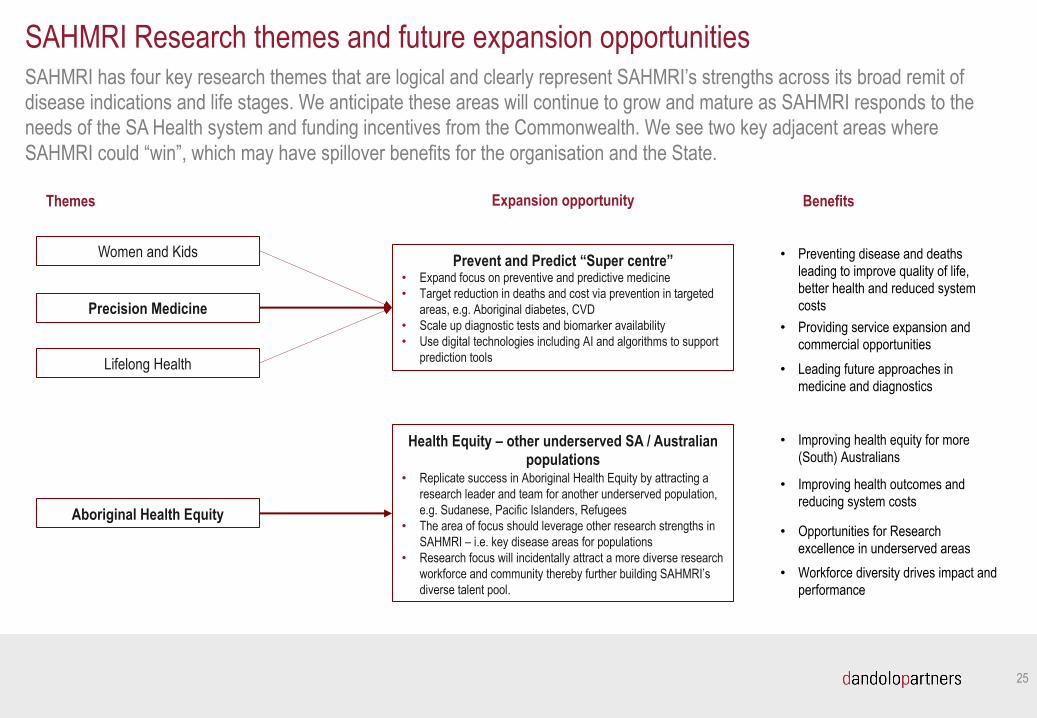
SAHMRI has four key research themes that are logical and clearly represent SAHMRI’s strengths across its broad remit of disease indications and life stages. We anticipate these areas will continue to grow and mature as SAHMRI responds to the needs of the SA Health system and funding incentives from the Commonwealth. We see two key adjacent areas where SAHMRI could “win”, which may have spillover benefits for the organisation and the State.
25
Women and Kids
SAHMRI Research themes and future expansion opportunities
Themes
Aboriginal Health Equity
Precision Medicine
Lifelong Health
Health Equity – other underserved SA / Australian populations
• Replicate success in Aboriginal Health Equity by attracting a research leader and team for another underserved population, e.g. Sudanese, Pacific Islanders, Refugees
• The area of focus should leverage other research strengths in SAHMRI – i.e. key disease areas for populations
• Research focus will incidentally attract a more diverse research workforce and community thereby further building SAHMRI’s diverse talent pool.
Expansion opportunity Benefits
Prevent and Predict “Super centre”• Expand focus on preventive and predictive medicine • Target reduction in deaths and cost via prevention in targeted
areas, e.g. Aboriginal diabetes, CVD• Scale up diagnostic tests and biomarker availability• Use digital technologies including AI and algorithms to support
prediction tools
• Workforce diversity drives impact and performance
• Improving health equity for more (South) Australians
• Improving health outcomes and reducing system costs
• Opportunities for Research excellence in underserved areas
• Preventing disease and deaths leading to improve quality of life, better health and reduced system costs
• Providing service expansion and commercial opportunities
• Leading future approaches in medicine and diagnostics
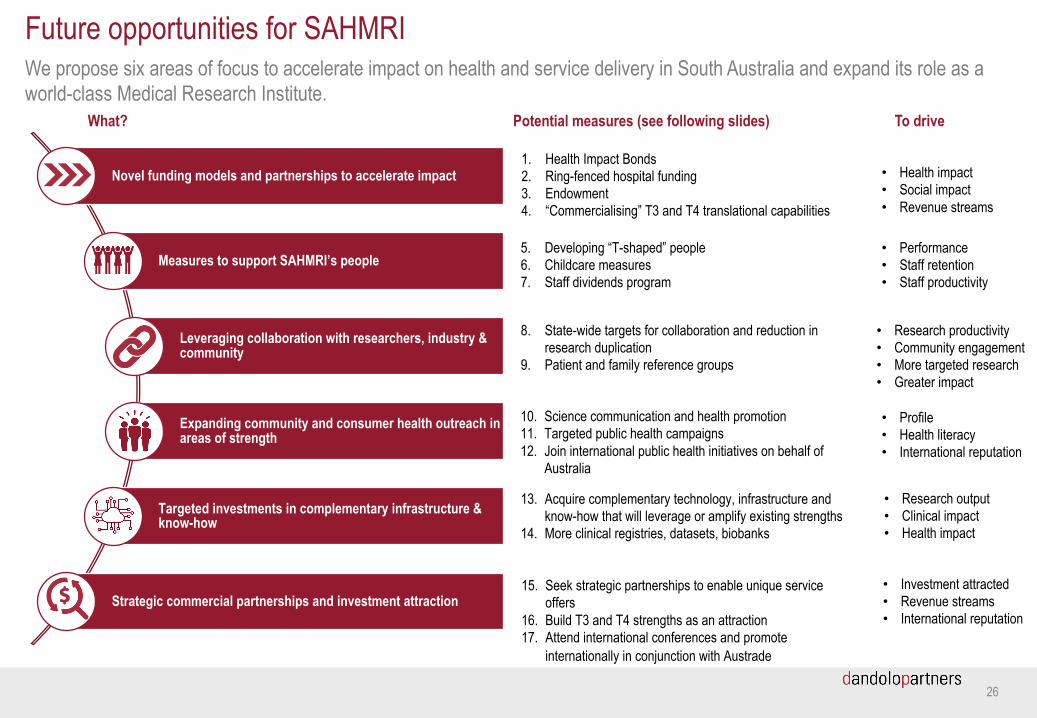
Novel funding models and partnerships to accelerate impact
Measures to support SAHMRI’s people
Leveraging collaboration with researchers, industry & community
Expanding community and consumer health outreach in areas of strength
Targeted investments in complementary infrastructure & know-how
Strategic commercial partnerships and investment attraction
We propose six areas of focus to accelerate impact on health and service delivery in South Australia and expand its role as aworld-class Medical Research Institute.
26
Future opportunities for SAHMRI
What? Potential measures (see following slides) To drive
1. Health Impact Bonds2. Ring-fenced hospital funding3. Endowment4. “Commercialising” T3 and T4 translational capabilities
8. State-wide targets for collaboration and reduction in research duplication
9. Patient and family reference groups
5. Developing “T-shaped” people6. Childcare measures7. Staff dividends program
• Performance• Staff retention• Staff productivity
13. Acquire complementary technology, infrastructure and know-how that will leverage or amplify existing strengths
14. More clinical registries, datasets, biobanks
10. Science communication and health promotion 11. Targeted public health campaigns 12. Join international public health initiatives on behalf of
Australia
15. Seek strategic partnerships to enable unique service offers
16. Build T3 and T4 strengths as an attraction17. Attend international conferences and promote
internationally in conjunction with Austrade
• Health impact• Social impact• Revenue streams
• Research productivity• Community engagement• More targeted research• Greater impact
• Profile• Health literacy• International reputation
• Research output• Clinical impact• Health impact
• Investment attracted• Revenue streams• International reputation
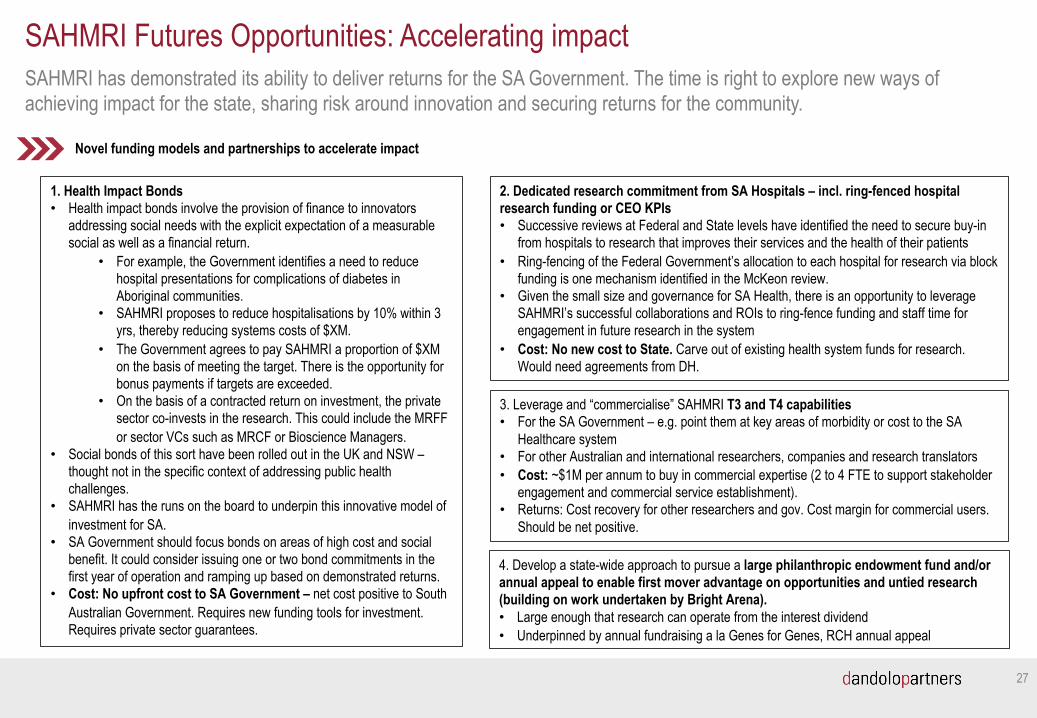
SAHMRI has demonstrated its ability to deliver returns for the SA Government. The time is right to explore new ways of achieving impact for the state, sharing risk around innovation and securing returns for the community.
27
SAHMRI Futures Opportunities: Accelerating impact
4. Develop a state-wide approach to pursue a large philanthropic endowment fund and/or annual appeal to enable first mover advantage on opportunities and untied research (building on work undertaken by Bright Arena). • Large enough that research can operate from the interest dividend • Underpinned by annual fundraising a la Genes for Genes, RCH annual appeal
Novel funding models and partnerships to accelerate impact
1. Health Impact Bonds • Health impact bonds involve the provision of finance to innovators
addressing social needs with the explicit expectation of a measurable social as well as a financial return.
• For example, the Government identifies a need to reduce hospital presentations for complications of diabetes in Aboriginal communities.
• SAHMRI proposes to reduce hospitalisations by 10% within 3 yrs, thereby reducing systems costs of $XM.
• The Government agrees to pay SAHMRI a proportion of $XM on the basis of meeting the target. There is the opportunity for bonus payments if targets are exceeded.
• On the basis of a contracted return on investment, the private sector co-invests in the research. This could include the MRFF or sector VCs such as MRCF or Bioscience Managers.
• Social bonds of this sort have been rolled out in the UK and NSW –thought not in the specific context of addressing public health challenges.
• SAHMRI has the runs on the board to underpin this innovative model of investment for SA.
• SA Government should focus bonds on areas of high cost and social benefit. It could consider issuing one or two bond commitments in the first year of operation and ramping up based on demonstrated returns.
• Cost: No upfront cost to SA Government – net cost positive to South Australian Government. Requires new funding tools for investment. Requires private sector guarantees.
2. Dedicated research commitment from SA Hospitals – incl. ring-fenced hospital research funding or CEO KPIs• Successive reviews at Federal and State levels have identified the need to secure buy-in
from hospitals to research that improves their services and the health of their patients• Ring-fencing of the Federal Government’s allocation to each hospital for research via block
funding is one mechanism identified in the McKeon review. • Given the small size and governance for SA Health, there is an opportunity to leverage
SAHMRI’s successful collaborations and ROIs to ring-fence funding and staff time for engagement in future research in the system
• Cost: No new cost to State. Carve out of existing health system funds for research. Would need agreements from DH.
3. Leverage and “commercialise” SAHMRI T3 and T4 capabilities• For the SA Government – e.g. point them at key areas of morbidity or cost to the SA
Healthcare system• For other Australian and international researchers, companies and research translators• Cost: ~$1M per annum to buy in commercial expertise (2 to 4 FTE to support stakeholder
engagement and commercial service establishment). • Returns: Cost recovery for other researchers and gov. Cost margin for commercial users.
Should be net positive.
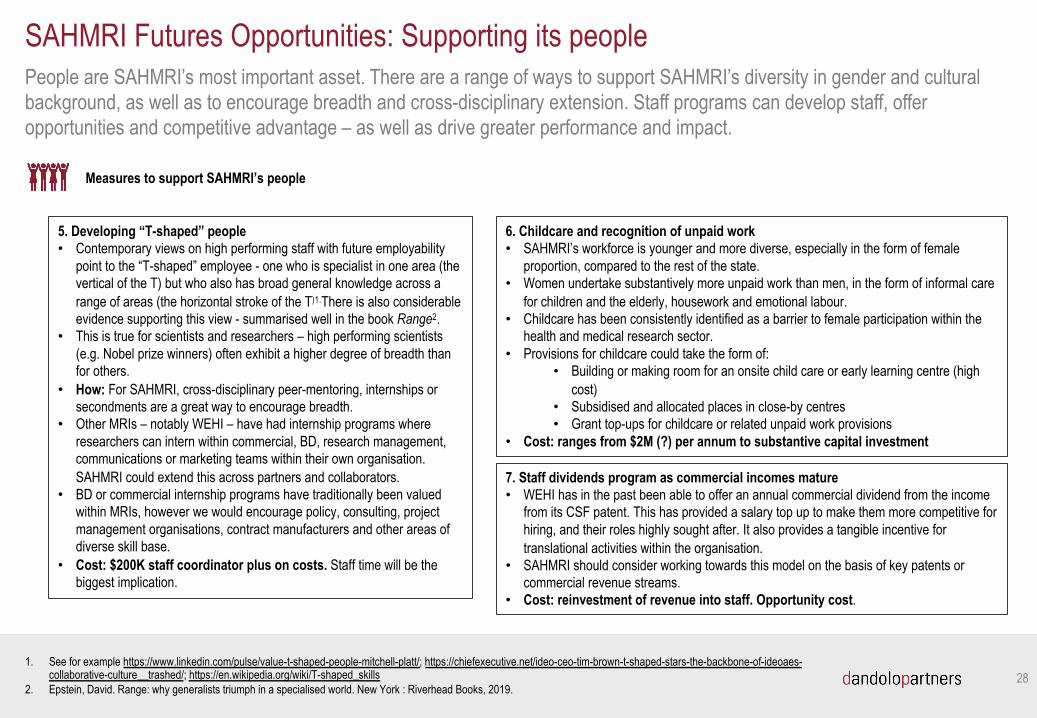
People are SAHMRI’s most important asset. There are a range of ways to support SAHMRI’s diversity in gender and cultural background, as well as to encourage breadth and cross-disciplinary extension. Staff programs can develop staff, offer opportunities and competitive advantage – as well as drive greater performance and impact.
28
7. Staff dividends program as commercial incomes mature• WEHI has in the past been able to offer an annual commercial dividend from the income
from its CSF patent. This has provided a salary top up to make them more competitive for hiring, and their roles highly sought after. It also provides a tangible incentive for translational activities within the organisation.
• SAHMRI should consider working towards this model on the basis of key patents or commercial revenue streams.
• Cost: reinvestment of revenue into staff. Opportunity cost.
Measures to support SAHMRI’s people
SAHMRI Futures Opportunities: Supporting its people
5. Developing “T-shaped” people• Contemporary views on high performing staff with future employability
point to the “T-shaped” employee - one who is specialist in one area (the vertical of the T) but who also has broad general knowledge across a range of areas (the horizontal stroke of the T)1.There is also considerable evidence supporting this view - summarised well in the book Range2.
• This is true for scientists and researchers – high performing scientists (e.g. Nobel prize winners) often exhibit a higher degree of breadth than for others.
• How: For SAHMRI, cross-disciplinary peer-mentoring, internships or secondments are a great way to encourage breadth.
• Other MRIs – notably WEHI – have had internship programs where researchers can intern within commercial, BD, research management, communications or marketing teams within their own organisation. SAHMRI could extend this across partners and collaborators.
• BD or commercial internship programs have traditionally been valued within MRIs, however we would encourage policy, consulting, project management organisations, contract manufacturers and other areas of diverse skill base.
• Cost: $200K staff coordinator plus on costs. Staff time will be the biggest implication.
1. See for example https://www.linkedin.com/pulse/value-t-shaped-people-mitchell-platt/; https://chiefexecutive.net/ideo-ceo-tim-brown-t-shaped-stars-the-backbone-of-ideoaes-collaborative-culture__trashed/; https://en.wikipedia.org/wiki/T-shaped_skills
2. Epstein, David. Range: why generalists triumph in a specialised world. New York : Riverhead Books, 2019.
6. Childcare and recognition of unpaid work • SAHMRI’s workforce is younger and more diverse, especially in the form of female
proportion, compared to the rest of the state. • Women undertake substantively more unpaid work than men, in the form of informal care
for children and the elderly, housework and emotional labour. • Childcare has been consistently identified as a barrier to female participation within the
health and medical research sector. • Provisions for childcare could take the form of:
• Building or making room for an onsite child care or early learning centre (high cost)
• Subsidised and allocated places in close-by centres• Grant top-ups for childcare or related unpaid work provisions
• Cost: ranges from $2M (?) per annum to substantive capital investment
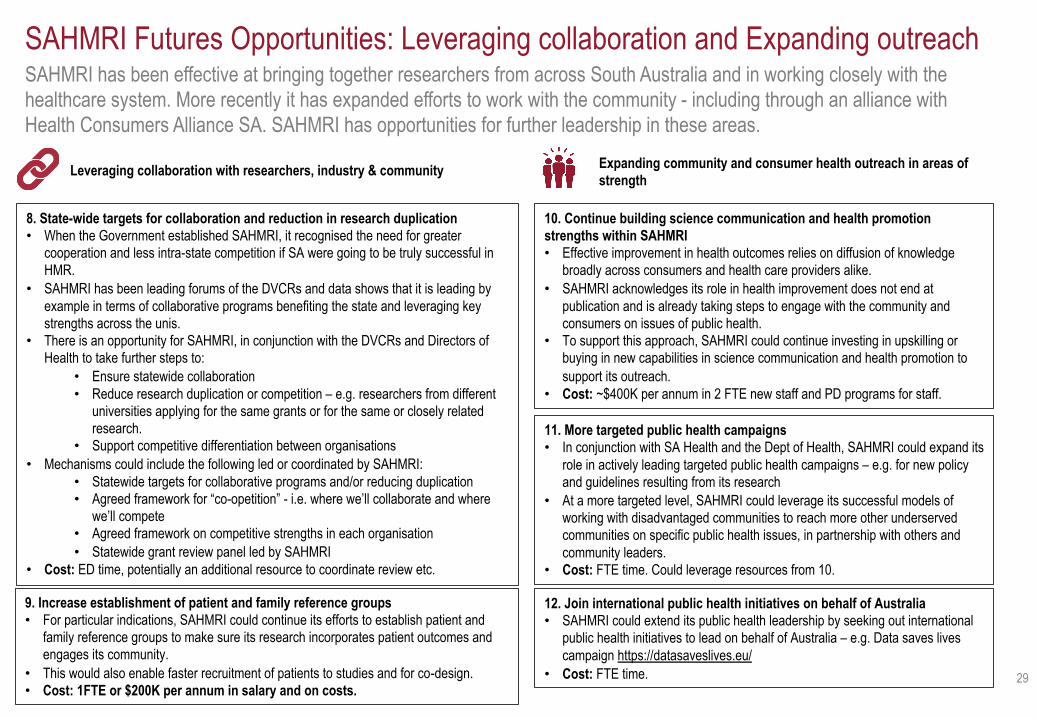
SAHMRI has been effective at bringing together researchers from across South Australia and in working closely with the healthcare system. More recently it has expanded efforts to work with the community - including through an alliance with Health Consumers Alliance SA. SAHMRI has opportunities for further leadership in these areas.
29
Leveraging collaboration with researchers, industry & community Expanding community and consumer health outreach in areas of strength
SAHMRI Futures Opportunities: Leveraging collaboration and Expanding outreach
8. State-wide targets for collaboration and reduction in research duplication• When the Government established SAHMRI, it recognised the need for greater
cooperation and less intra-state competition if SA were going to be truly successful in HMR.
• SAHMRI has been leading forums of the DVCRs and data shows that it is leading by example in terms of collaborative programs benefiting the state and leveraging key strengths across the unis.
• There is an opportunity for SAHMRI, in conjunction with the DVCRs and Directors of Health to take further steps to:
• Ensure statewide collaboration • Reduce research duplication or competition – e.g. researchers from different
universities applying for the same grants or for the same or closely related research.
• Support competitive differentiation between organisations• Mechanisms could include the following led or coordinated by SAHMRI:
• Statewide targets for collaborative programs and/or reducing duplication• Agreed framework for “co-opetition” - i.e. where we’ll collaborate and where
we’ll compete• Agreed framework on competitive strengths in each organisation• Statewide grant review panel led by SAHMRI
• Cost: ED time, potentially an additional resource to coordinate review etc.
10. Continue building science communication and health promotion strengths within SAHMRI• Effective improvement in health outcomes relies on diffusion of knowledge
broadly across consumers and health care providers alike. • SAHMRI acknowledges its role in health improvement does not end at
publication and is already taking steps to engage with the community and consumers on issues of public health.
• To support this approach, SAHMRI could continue investing in upskilling or buying in new capabilities in science communication and health promotion to support its outreach.
• Cost: ~$400K per annum in 2 FTE new staff and PD programs for staff.
9. Increase establishment of patient and family reference groups• For particular indications, SAHMRI could continue its efforts to establish patient and
family reference groups to make sure its research incorporates patient outcomes and engages its community.
• This would also enable faster recruitment of patients to studies and for co-design. • Cost: 1FTE or $200K per annum in salary and on costs.
11. More targeted public health campaigns • In conjunction with SA Health and the Dept of Health, SAHMRI could expand its
role in actively leading targeted public health campaigns – e.g. for new policy and guidelines resulting from its research
• At a more targeted level, SAHMRI could leverage its successful models of working with disadvantaged communities to reach more other underserved communities on specific public health issues, in partnership with others and community leaders.
• Cost: FTE time. Could leverage resources from 10.
12. Join international public health initiatives on behalf of Australia• SAHMRI could extend its public health leadership by seeking out international
public health initiatives to lead on behalf of Australia – e.g. Data saves lives campaign https://datasaveslives.eu/
• Cost: FTE time.
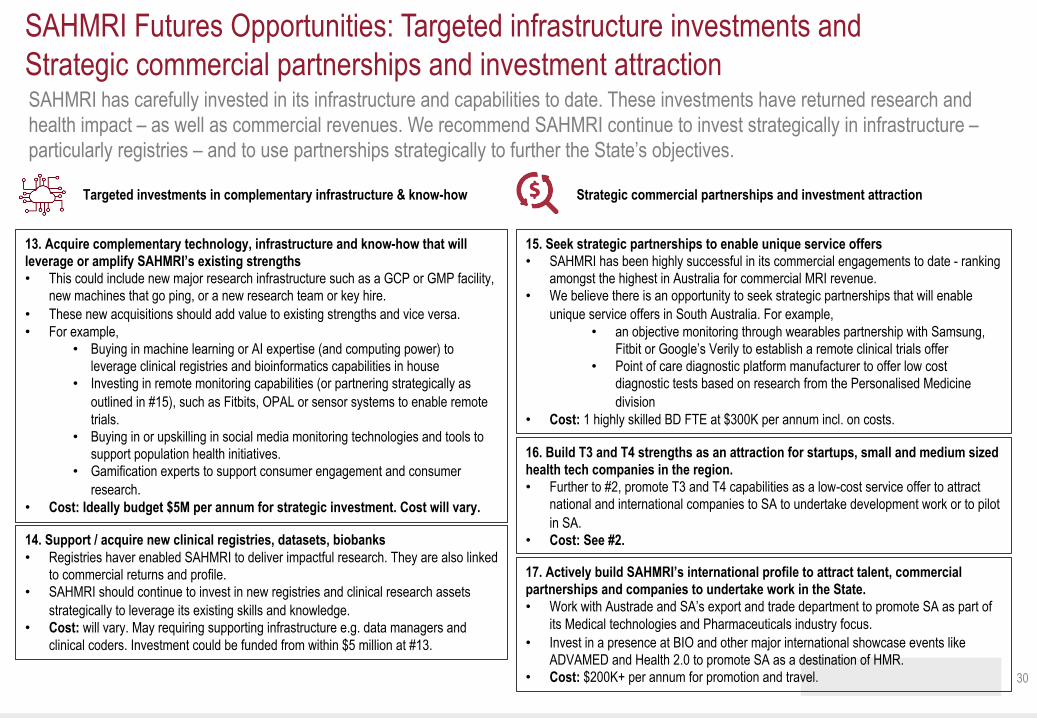
SAHMRI has carefully invested in its infrastructure and capabilities to date. These investments have returned research and health impact – as well as commercial revenues. We recommend SAHMRI continue to invest strategically in infrastructure –particularly registries – and to use partnerships strategically to further the State’s objectives.
30
Targeted investments in complementary infrastructure & know-how Strategic commercial partnerships and investment attraction
SAHMRI Futures Opportunities: Targeted infrastructure investments and Strategic commercial partnerships and investment attraction
13. Acquire complementary technology, infrastructure and know-how that will leverage or amplify SAHMRI’s existing strengths• This could include new major research infrastructure such as a GCP or GMP facility,
new machines that go ping, or a new research team or key hire. • These new acquisitions should add value to existing strengths and vice versa. • For example,
• Buying in machine learning or AI expertise (and computing power) to leverage clinical registries and bioinformatics capabilities in house
• Investing in remote monitoring capabilities (or partnering strategically as outlined in #15), such as Fitbits, OPAL or sensor systems to enable remote trials.
• Buying in or upskilling in social media monitoring technologies and tools to support population health initiatives.
• Gamification experts to support consumer engagement and consumer research.
• Cost: Ideally budget $5M per annum for strategic investment. Cost will vary.
15. Seek strategic partnerships to enable unique service offers• SAHMRI has been highly successful in its commercial engagements to date - ranking
amongst the highest in Australia for commercial MRI revenue. • We believe there is an opportunity to seek strategic partnerships that will enable
unique service offers in South Australia. For example, • an objective monitoring through wearables partnership with Samsung,
Fitbit or Google’s Verily to establish a remote clinical trials offer• Point of care diagnostic platform manufacturer to offer low cost
diagnostic tests based on research from the Personalised Medicine division
• Cost: 1 highly skilled BD FTE at $300K per annum incl. on costs.
14. Support / acquire new clinical registries, datasets, biobanks • Registries haver enabled SAHMRI to deliver impactful research. They are also linked
to commercial returns and profile. • SAHMRI should continue to invest in new registries and clinical research assets
strategically to leverage its existing skills and knowledge. • Cost: will vary. May requiring supporting infrastructure e.g. data managers and
clinical coders. Investment could be funded from within $5 million at #13.
16. Build T3 and T4 strengths as an attraction for startups, small and medium sized health tech companies in the region. • Further to #2, promote T3 and T4 capabilities as a low-cost service offer to attract
national and international companies to SA to undertake development work or to pilot in SA.
• Cost: See #2.
17. Actively build SAHMRI’s international profile to attract talent, commercial partnerships and companies to undertake work in the State. • Work with Austrade and SA’s export and trade department to promote SA as part of
its Medical technologies and Pharmaceuticals industry focus. • Invest in a presence at BIO and other major international showcase events like
ADVAMED and Health 2.0 to promote SA as a destination of HMR. • Cost: $200K+ per annum for promotion and travel.

Appendices
31
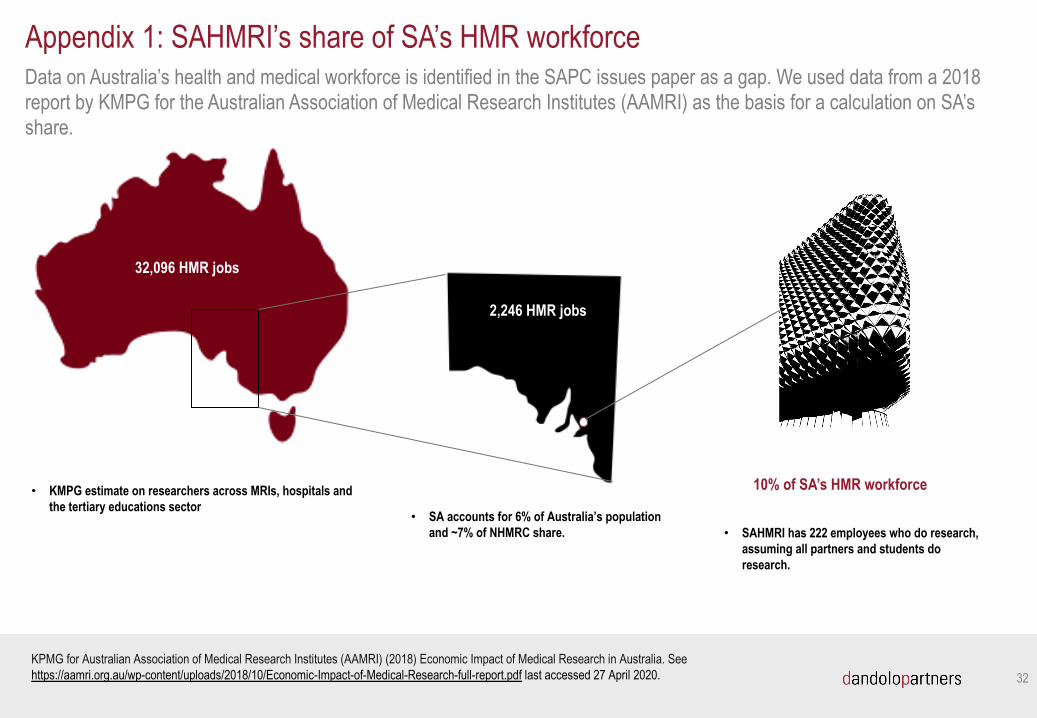
Data on Australia’s health and medical workforce is identified in the SAPC issues paper as a gap. We used data from a 2018 report by KMPG for the Australian Association of Medical Research Institutes (AAMRI) as the basis for a calculation on SA’s share.
32
Appendix 1: SAHMRI’s share of SA’s HMR workforce
KPMG for Australian Association of Medical Research Institutes (AAMRI) (2018) Economic Impact of Medical Research in Australia. See https://aamri.org.au/wp-content/uploads/2018/10/Economic-Impact-of-Medical-Research-full-report.pdf last accessed 27 April 2020.
32,096 HMR jobs
• KMPG estimate on researchers across MRIs, hospitals and the tertiary educations sector
2,246 HMR jobs
• SA accounts for 6% of Australia’s population and ~7% of NHMRC share. • SAHMRI has 222 employees who do research,
assuming all partners and students do research.
10% of SA’s HMR workforce
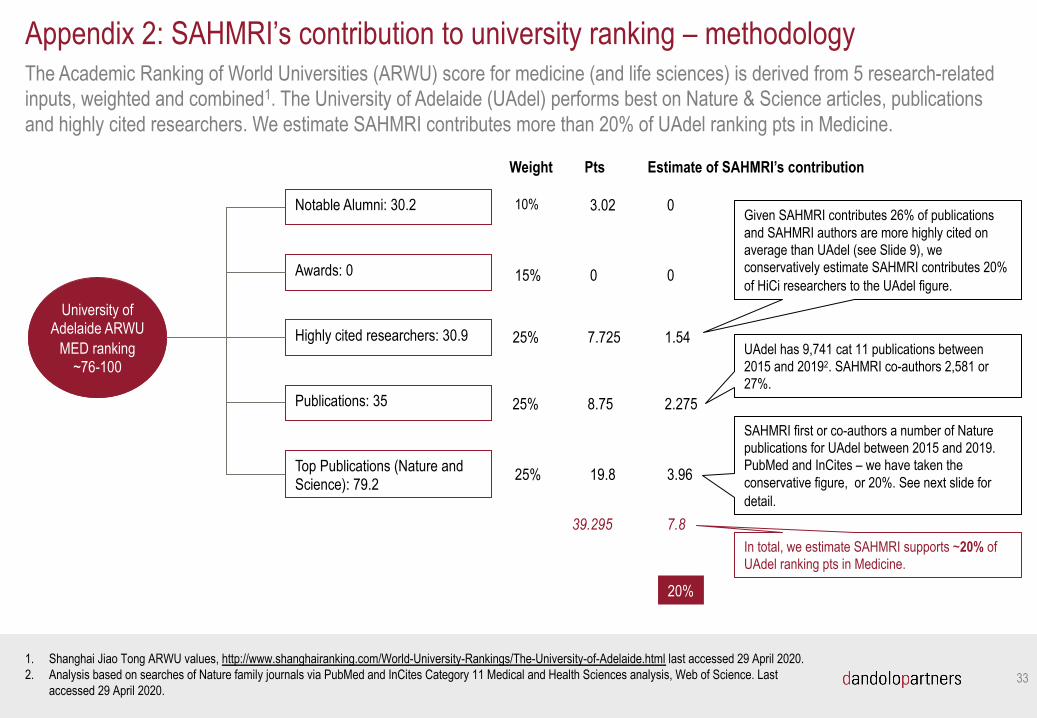
The Academic Ranking of World Universities (ARWU) score for medicine (and life sciences) is derived from 5 research-related inputs, weighted and combined1. The University of Adelaide (UAdel) performs best on Nature & Science articles, publications and highly cited researchers. We estimate SAHMRI contributes more than 20% of UAdel ranking pts in Medicine.
33
Appendix 2: SAHMRI’s contribution to university ranking – methodology
University of Adelaide ARWU
MED ranking ~76-100
Notable Alumni: 30.2
Awards: 0
Highly cited researchers: 30.9
Publications: 35
Top Publications (Nature and Science): 79.2
Weight
10%
15%
25%
25%
25%
Estimate of SAHMRI’s contribution
0
0
1.54
2.275
3.96
Pts
3.02
0
7.725
8.75
19.8
Given SAHMRI contributes 26% of publications and SAHMRI authors are more highly cited on average than UAdel (see Slide 9), we conservatively estimate SAHMRI contributes 20% of HiCi researchers to the UAdel figure.
UAdel has 9,741 cat 11 publications between 2015 and 20192. SAHMRI co-authors 2,581 or 27%.
1. Shanghai Jiao Tong ARWU values, http://www.shanghairanking.com/World-University-Rankings/The-University-of-Adelaide.html last accessed 29 April 2020.2. Analysis based on searches of Nature family journals via PubMed and InCites Category 11 Medical and Health Sciences analysis, Web of Science. Last
accessed 29 April 2020.
SAHMRI first or co-authors a number of Nature publications for UAdel between 2015 and 2019. PubMed and InCites – we have taken the conservative figure, or 20%. See next slide for detail.
7.839.295In total, we estimate SAHMRI supports ~20% of UAdel ranking pts in Medicine.
20%
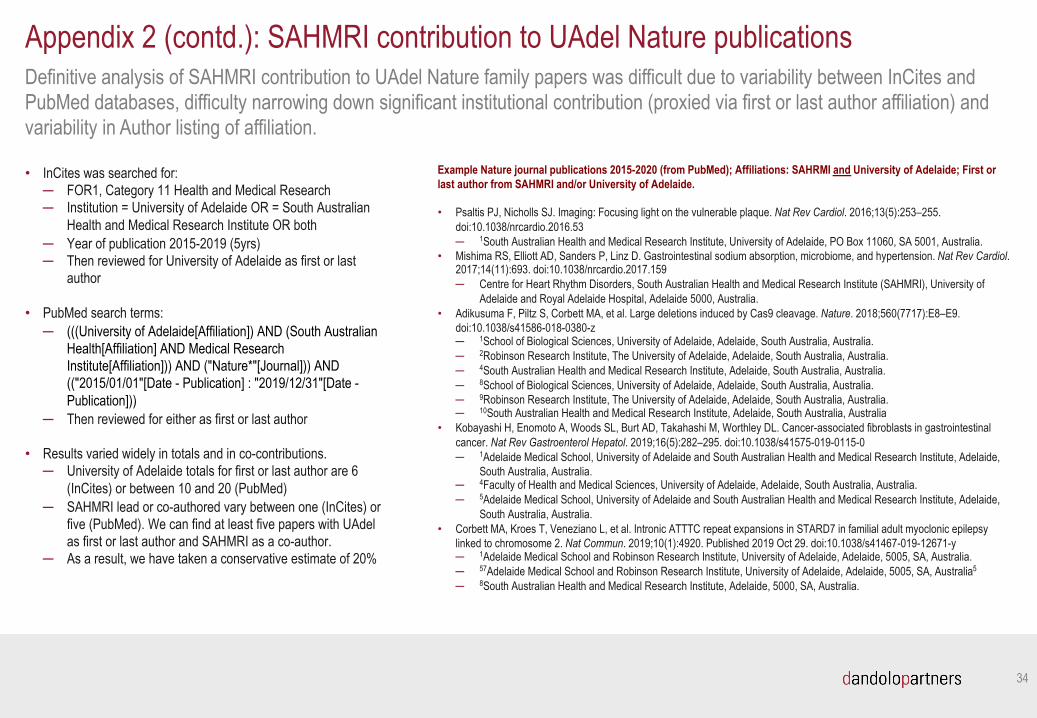
Definitive analysis of SAHMRI contribution to UAdel Nature family papers was difficult due to variability between InCites andPubMed databases, difficulty narrowing down significant institutional contribution (proxied via first or last author affiliation) and variability in Author listing of affiliation.
34
• InCites was searched for:─ FOR1, Category 11 Health and Medical Research─ Institution = University of Adelaide OR = South Australian
Health and Medical Research Institute OR both─ Year of publication 2015-2019 (5yrs)─ Then reviewed for University of Adelaide as first or last
author
• PubMed search terms:─ (((University of Adelaide[Affiliation]) AND (South Australian
Health[Affiliation] AND Medical Research Institute[Affiliation])) AND ("Nature*"[Journal])) AND (("2015/01/01"[Date - Publication] : "2019/12/31"[Date -Publication]))
─ Then reviewed for either as first or last author
• Results varied widely in totals and in co-contributions.─ University of Adelaide totals for first or last author are 6
(InCites) or between 10 and 20 (PubMed)─ SAHMRI lead or co-authored vary between one (InCites) or
five (PubMed). We can find at least five papers with UAdel as first or last author and SAHMRI as a co-author.
─ As a result, we have taken a conservative estimate of 20%
Appendix 2 (contd.): SAHMRI contribution to UAdel Nature publications
Example Nature journal publications 2015-2020 (from PubMed); Affiliations: SAHRMI and University of Adelaide; First or last author from SAHMRI and/or University of Adelaide.
• Psaltis PJ, Nicholls SJ. Imaging: Focusing light on the vulnerable plaque. Nat Rev Cardiol. 2016;13(5):253–255.doi:10.1038/nrcardio.2016.53─ 1South Australian Health and Medical Research Institute, University of Adelaide, PO Box 11060, SA 5001, Australia.
• Mishima RS, Elliott AD, Sanders P, Linz D. Gastrointestinal sodium absorption, microbiome, and hypertension. Nat Rev Cardiol. 2017;14(11):693. doi:10.1038/nrcardio.2017.159─ Centre for Heart Rhythm Disorders, South Australian Health and Medical Research Institute (SAHMRI), University of
Adelaide and Royal Adelaide Hospital, Adelaide 5000, Australia.• Adikusuma F, Piltz S, Corbett MA, et al. Large deletions induced by Cas9 cleavage. Nature. 2018;560(7717):E8–E9.
doi:10.1038/s41586-018-0380-z─ 1School of Biological Sciences, University of Adelaide, Adelaide, South Australia, Australia.─ 2Robinson Research Institute, The University of Adelaide, Adelaide, South Australia, Australia.─ 4South Australian Health and Medical Research Institute, Adelaide, South Australia, Australia.─ 8School of Biological Sciences, University of Adelaide, Adelaide, South Australia, Australia. ─ 9Robinson Research Institute, The University of Adelaide, Adelaide, South Australia, Australia.─ 10South Australian Health and Medical Research Institute, Adelaide, South Australia, Australia
• Kobayashi H, Enomoto A, Woods SL, Burt AD, Takahashi M, Worthley DL. Cancer-associated fibroblasts in gastrointestinalcancer. Nat Rev Gastroenterol Hepatol. 2019;16(5):282–295. doi:10.1038/s41575-019-0115-0─ 1Adelaide Medical School, University of Adelaide and South Australian Health and Medical Research Institute, Adelaide,
South Australia, Australia.─ 4Faculty of Health and Medical Sciences, University of Adelaide, Adelaide, South Australia, Australia.─ 5Adelaide Medical School, University of Adelaide and South Australian Health and Medical Research Institute, Adelaide,
South Australia, Australia. • Corbett MA, Kroes T, Veneziano L, et al. Intronic ATTTC repeat expansions in STARD7 in familial adult myoclonic epilepsy
linked to chromosome 2. Nat Commun. 2019;10(1):4920. Published 2019 Oct 29. doi:10.1038/s41467-019-12671-y─ 1Adelaide Medical School and Robinson Research Institute, University of Adelaide, Adelaide, 5005, SA, Australia.─ 57Adelaide Medical School and Robinson Research Institute, University of Adelaide, Adelaide, 5005, SA, Australia5
─ 8South Australian Health and Medical Research Institute, Adelaide, 5000, SA, Australia.

Research with impact.
IMPACT: NOW IMPACT: SOON IMPACT: FUTURE
y Better treatmentsfor Chronic MyeloidLeukaemia
y Improved diagnosisof heart attacks inemergency departments
y Reducing impacts ofchronic conditions inAboriginal people
y High quality and safeaged care
y Better treatments forchronic abdominal andpelvic pain
y Reducing smoking rates
y Improving outcomes forleukaemia
y Reducing preterm births
y Improving care ofnewborns in SouthAustralia
y Reducing risk ofCerebral Palsy
y Reducing unnecessaryuse of antibiotics
y Reducing the risk ofdeveloping dementia
y Preventing obesity
Appendix V: Research Impact Stories
IMPACT: NOW
BETTER TREATMENTS FOR CHRONIC MYELOID LEUKAEMIA
Better treatments for Chronic Myeloid Leukaemia
COLLABORATION WITHIN SA
• The University of Adelaide
• SA Pathology and Centre for Cancer Biology (UniSA)
• SA Health
NATIONAL & INTERNATIONAL
• Victorian Comprehensive Cancer Centre and Royal Melbourne Hospital (Melbourne)
• The Australian Leukaemia and Lymphoma Group (25 centres nationally)
• St Jude Children’s Research Hospital (Memphis, USA)
• Comprehensive Cancer Centre (Freiburg, Germany)
• International CML Foundation (20 CML Centres of Excellence globally)
SAHMRI is a global leader in the treatment of Chronic Myeloid Leukaemia - one of the most remarkable cancer success stories this century.
BACKGROUND
Chronic Myeloid Leukaemia (CML) is a blood cancer. The treatment of CML has been one of the most remarkable cancer success stories this century. Ten-year survival for CML patients has improved from 20 per cent in the 1990s to more than 80 per cent today. This has been achieved through the clinical application of tyrosine kinase inhibitor (TKIs) therapy.
SAHMRI is making a differenceProfessor Tim Hughes, Professor Deborah White and their SAHMRI Precision Medicine Theme team have pioneered the concept that TKI therapy for CML can and should be used as a curative rather than just maintenance therapy.
SAHMRI’s CML team showed that patients who achieve excellent molecular responses can in many cases stop their therapy altogether and remain in treatment-free remission (TFR). Their recommendations for TFR are now included in international CML guidelines. Currently around 25% of patients can achieve TFR.
This work was enabled by previous breakthroughs tracking the dynamics of molecular response to treatment, which is done using the polymerase chain reaction (PCR) assay that the Adelaide team developed and standardised. This ‘precision medicine’ approach to therapy selection has led to improved outcomes for even the most severe cases of CML and has been adopted globally.
BETTER TREATMENTS FOR CHRONIC MYELOID LEUKAEMIA
1. Hughes TP, Mauro MJ, Cortes JE, Minami H, Rea D, DeAngelo DJ, Breccia M, Goh YT, Talpaz M, Hochhaus A, leCoutre P, Ottmann O, Heinrich MC. Steehmann JL, Deininger MW, Janssen JJ, Mahon FX, Minami Y, Yeung DT, Ross DM, Tallman MS, Park JH, Druker BJ, Hynds D, Duan Y, Meille C, Hourcade-Potelleret F, Vanasse G, Lang F, Kim DW. 2019. Asciminib in Chronic Myeloid Leukemia after ABL Kinase Inhibitor Failure. New England Journal of Medicine. 381(24) 2315-2326
2. Branford S, Kim DDH, Apperley JF, Eid Ca, Mustjoki S, Ong ST, Nteliopoulos G, Ernst T, Chuah C, Gam-barcort-Passerini C, Mauro MJ, Druker BJ, Kim DW, Mahon FX, Cortes J, Radich JP, Hochhaus A, Hughes TP. 2019. Laying the foundation for genomically-based risk assessment in chronic myeloid leukemia. Leukemia 33(8) 1835-1850 CIT 5
3. Branford S, Wang P, Yeung DT, Thomson D, Purins A, Wadham C, Shahrin NH, Marum JE, Nataren N, Parker WT, Georghegan J, Feng J, Shanmuganathan N, Mueller MC, Dietz C, Stangl D, Donaldson Z, Altamura H, Georgievski J, Braley J, Brown A, Hahn C, Walker I, Kim SH, Choi SY, Park SH, Kim DW, White DL, Yong A,
• Professor Hughes is the Cancer Council “Beat Cancer” Professor at the University of Adelaide • Australasian Leukaemia and Lymphoma Group (ALLG)International CML Foundation • US Leukemia and Lymphoma Society • National Health and Medical Research Council (NHMRC) - Professor Hughes is an NHMRC Principal Research Fellow • Royal Adelaide Hospital (RAH), Professor Hughes is a consultant haematologist at RAH
Ross DM, Scott HS, Schreiber AW, Hughes TP. 2018. Integrative genomic analysis reveals cancer-associ-ated mutations at diagnosis of CML in patients with high-risk disease. Blood 132(9) 948-961 CIT 22
4. Hughes TP, Ross DM. 2016. Moving treatment-free remission into mainstream clinical practice in CML. BLOOD 128 (1) 17-23 CIT 190
5. Yeung D, Osborn MP, White DL, Branford S, Braley J, Herschtal, Kornhauser M, Issa S, Hiwase DK, Hertzberg M, Schwarer A, Filshie R, Arthur C, Kwan YL, Trotman J, Forsyth CJ, Taper J, Ross DM, Beresford J, Tam C, Mills AK, Grigg AP, Hughes TP. 2015. TIDEL-II: first-line use of imatinib in CML with early switch to nilotinib for failure to achieve time-de-pendent molecular targets. BLOOD; 125: 915 - 923 CIT 83
6. Yeung D, Osborn MP, White DL, Branford S, Braley J, Herschtal, Kornhauser M, Issa S, Hiwase DK, Hertzberg M, Schwarer A, Filshie R, Arthur C, Kwan YL, Trotman J, Forsyth CJ, Taper J, Ross DM, Beresford J, Tam C, Mills AK, Grigg AP, Hughes TP. 2015.TIDEL-II: first-line use of imatinib in CML with early switch to nilotinib for
failure to achieve time-dependent molecular targets. BLOOD; 125: 915 - 923 CIT 83
7. Hughes TP, Saglio G, Kantarjian HM, Guilhot F, Niederwieser D, Rosti G, Nakaseko C, De Souza CA, Kalaycio ME, Meier S, Fan X, Menssen HD, Larson RA, Hochhaus A. 2014. Early molecular response predicts outcomes in patients with chronic myeloid leukemia in chronic phase treated with frontline nilotinib or imatinib. Blood. 27;123(9):1353-60 CIT 204
8. Ross DM, Branford S, Seymour JF, Schwarer AP, Ar-thur C, Yeung DT, Dang P, Goyne JM, Slader C, Filshie RJ, Mills AK, Melo JV, White DL, Grigg AP, Hughes TP. 2013. Safety and efficacy of imatinib cessation for CML patients with stable undetectable minimal resid-ual disease: results from the TWISTER study. Blood. 25;122(4): 515-522 CIT 534
9. Hughes, T., Lipton, J., et al. (2014). Deep molecular responses achieved in patients with CML-CP who are switched to nilotinib after long-term imatinib. Blood, 124(5), 729-736.
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS
Professor Hughes’ leadership has ensured South Australia is nationally and internationally recognised as world-class with its CML research and clinical care, guiding global projects such as the Phase I Asciminib Trial. Asciminib is a novel TKI which is generally much better tolerated by patients and is also effective for some patients who have developed resistance to every other TKI.
SAHMRI-based studies and expertise have helped save the Pharmaceutical Benefits Scheme around $9 million annually by transitioning patients to TFR. The team’s molecular monitoring innovations have saved at least $600,000 annually through replacing bone marrow aspirations and cytogenetic testing. The work means around 120 bone marrow transplants can be avoided each year, saving the system around $18 million and more importantly saving 35 an average of 35 lives lost each year to BMT complications.
Around 25% of people with CML can now experience treatment-free remission (TFR) saving them significant financial costs of treatment and significant physical and emotional costs from side-effects and reduced quality of life.
Molecular monitoring allows better targeted therapies and confidence in prognosis.
In the past decade, this work has saved around 450 South Australian lives and has saved the SA health system about $250 million. The impacts continue to be enjoyed around the world.
IMPACT: NOW
IMPROVED DIAGNOSIS OF HEART ATTACKS IN EMERGENCY DEPARTMENTS
Improved diagnosis of heart attacks in emergency departments
COLLABORATION WITHIN SA
• Flinders University
• SA Health
• The University of Adelaide
NATIONAL & INTERNATIONAL
• University of Western Australia (Perth)
• Royal Brisbane and Women’s Hospital (Brisbane)
• Queensland University of Technology (Brisbane)
• University of Queensland (Queensland)
• Swinburne University (Melbourne)
• University of Technology (Sydney)
• University of New South Wales (Sydney)
Rapid, accurate diagnosis of patients presenting to emergency departments with chest pain delivers significant savings from reduced ED crowding and fewer hospital admissions.
BACKGROUND
High-sensitivity troponin assays promise earlier discrimination of myocardial infarction and the ability to intervene rapidly to protect the heart from damage.
Troponins are a group of proteins found in skeletal and cardiac muscle fibres that regulate muscular contraction. Troponin tests measure levels of cardiac-specific troponin in the blood to help detect heart injury.
SAHMRI is making a differenceProfessor Derek Chew led the evaluation of the benefits and harms of a more rapid protocol for assessment of possible heart attack in patients who present to emergency departments with chest pain.
Professor Chew’s South Australian in-practice evaluation in four EDs involved a follow-up troponin test for acute coronary syndrome (ACS) after just one hour, rather than the traditional protocol of three hours. The more rapid testing resulted in earlier average discharge from the ED and less average hospital admissions while maintaining patient health outcomes1.
IMPROVED DIAGNOSIS OF HEART ATTACKS IN EMERGENCY DEPARTMENTS
1. Chew, D et al. 2019, ‘A Randomized Trial of
a 1-Hour Troponin T Protocol in Suspected
Acute Coronary Syndromes’, Circulation, vol.
140, no. 19, 1543–1556, https://doi.org/10.1161/
CIRCULATIONAHA.119.042891
2. Chew, Derek P. et al. 2016, ‘National Heart
Foundation of Australia & Cardiac Society of
Australia and New Zealand: Australian Clinical
Guidelines for the Manage- ment of Acute
Funded by the National Health and Medical Research Council of Australia and unrestricted grant from Roche Diagnostics International.
Coronary Syndromes 2016’, Heart, Lung and
Circulation, vol. 25, no. 9, 895-951, http://dx.
doi. org/10.1016/j.hlc.2016.06.789
3. Mauro, M, Nelson, A, Stokes, M 2017. ‘Tro-
ponin test- ing in the primary care setting’,
FOCUS Chest Pain, vol. 46, no. 11, 823-826,
accessed 5 March 2020, <https:// www.racgp.
org.au/download/Documents/AFP/2017/ No-
vember/AFP-2017-11-Focus-Troponin.pdf>
4. Deloitte Access Economics Pty Ltd 2011,
‘ACS in perspective - The importance of
secondary prevention’, commissioned by
AstraZeneca Australia
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS
About 30,000 presentations to the state’s EDs each year are for chest pain and suspected acute coronary syndrome. This represents around 12% of all presentations. Chest pain assessment uses the equivalent of about 17,500 bed days each year but the vast majority of these patients are found to have no ACS or other cardiac-related cause for their admission.
Professor Chew’s study demonstrates the feasibility of embedding randomised research within routine time-critical clinical care, leading to an evidence-base that is directly relevant and immediately implementable within the local health system. It provides an exemplar for evidence translation and the self-learning health system. The findings of this trial are being implemented across the system leading to shorter length of stays. If fully implemented across the state’s health system its estimated this protocol would save up to 7000 bed days a year and between $12-15M per year.
Faster diagnosis for patients presenting with chest pain.
Reduced time for patients in ED and less hospital admissions.
Saving the health system around 7000 bed days and more than $12 million annually.
IMPACT: NOW
REDUCING IMPACTS OF CHRONIC CONDITIONS IN ABORIGINAL PEOPLE
Reducing impacts of chronic conditions in Aboriginal people
COLLABORATION WITHIN SA
• Health Translation SA
• Rural Doctors Workforce Agency
• SA Health
• SA Ambulance Service
NATIONAL & INTERNATIONAL
• Aboriginal Community Controlled Health Organisations sector
• Royal Flying Doctor Service
• Rural Country Support Services
SAHMRI’s Wardliparingga Aboriginal Health Equity Theme is partnering with Indigenous communities to reduce inequitable burdens of chronic diseases including diabetes, cancer and heart disease.
BACKGROUND
Collectively, diabetes, cancer and heart disease account for 80% of the life expectancy difference between Aboriginal and Non-Aboriginal people.
In South Australia 20% of Aboriginal and Torres Strait Islander people have diabetes. The state’s Indigenous population is three times as likely to experience peripheral arterial disease, 10 times as likely to be hospitalised with foot complications and 38 times more likely to have lower limbs amputated.
Data gathered between 1990 and 2010 show Aboriginal South Australians diagnosed with cancer are on average 10 years younger than the wider community and are often diagnosed with cancer at a more advanced stage. Records over a 30-year period show Aboriginal and non-Aboriginal five-year survivals for all cancer sites combined show a disparity of between 40.0% and 56.8%.
Cardiovascular disease (CVD) is the major cause of premature death experienced by Aboriginal and Torres Strait Islander Australians, on average striking around 10 to 20 years younger than other Australians. The emotional, societal and economic implications of premature CVD are devastating, and in many ways preventable.
SAHMRI is making a differenceThese conditions are critical targets for research and health system and policy reform. Professor Alex Brown and his Wardliparingga (Aboriginal Health Equity) team focus on these leading causes of inequity. These conditions are the major causes contributing to poor quality of life and reduced life expectancy experienced by Aboriginal people. The South Australian Aboriginal Chronic Disease Consortium has been established to drive, coordinate, support and partner with health sector organisations in implementing South Australian evidence in these chronic conditions.
REDUCING IMPACTS OF CHRONIC CONDITIONS IN ABORIGINAL PEOPLE
1. Australian Bureau of Statistics (ABS) 2014.
Australian Health Survey: National Aboriginal
and Torres Strait Islander Health Measures
Survey 2012–13. Canberra: ABS.
2. Government of South Australia, 2016, South
Australian Aboriginal Cancer Plan, 2016-2020,
SA Health, Adelaide, South Australia
3. Keech, W; Mckivett, A; Morey, K; Stewart, H;
Clinch, D; Saltmarsh, A; Brown, A; 2017, South
Australian Chronic Disease Consortium Road
Map 2017-2021, SAHMRI, Adelaide.
REFERENCES
BENEFITS
The South Australian Aboriginal Chronic Disease Consortium is a flagship program of work and is aligned with SAHMRI’s Wardliparingga Theme - the largest group of Aboriginal and Torres Strait Islander researchers in Australia.
The Consortium’s work is underpinned by partnerships with the Aboriginal community. It has a community reference group of Aboriginal and Torres Strait Islander people who live with chronic disease or care for someone who does.
The Consortium’s extensive networks reduce duplication while driving implementation of the existing evidence. By increasing health literacy, the Consortium improved prevention of chronic disease and promotes earlier identification which leads to better management and reduced complications experienced by Aboriginal people.
SAHMRI’s Aboriginal Health Equity Theme (Wardliparingga) is the largest dedicated Indigenous health research unit In Australia.
Engaging Indigenous communities with every step of the research pathway is the most effective and efficient way to truly address inequity.
Better health literacy improves prevention and early identification of chronic disease, leading to better management and fewer complications.
The Consortium is a comprehensive network of health organisations with responsibility to contribute to disease prevention, management, service delivery and policy. The network includes health researchers, policy makers, systems planners, clinicians, service providers and community to oversee and drive evidence-based responses to meeting the challenges in improving Aboriginal health outcomes. State-wide plans for cancer control, diabetes and heart disease management were developed by Wardliparingga in partnership with Aboriginal communities and health system partners and endorsed by the State Government in 2017/2018.
Significant progress has been made to influence the way services are being delivered to Aboriginal and Torres Strait Islander people.
IMPACT: NOW
HIGH QUALITY AND SAFE AGED CARE
High quality and safe aged careCOLLABORATION WITHIN SA
• University of South Australia
• The University of Adelaide
• Flinders University
• Health Translation SA
• Helping Hand
• Silver Chain
• ECH
• Council On The Ageing SA
• Health Consumers Alliance of SA
• SA NT DataLink
• Adelaide & Country SA PHN
• SA Health
NATIONAL & INTERNATIONAL
• Royal Australasian College of Surgeons - Australian Safety and Efficacy Register of New Interventional Procedures - Surgical
• Australian Dementia Network
• Monash University (Melbourne)
• Dalhouise University (Halifax, Canada)
ROSA’s work enables governments and the private sector to make evidence-based decisions promoting quality, efficient, innovative aged-care services and practices.
BACKGROUND
More than 1.2 million people received aged care services during the 2017-18 financial year1, with most (77%) receiving support in their home or other community-based settings. More than 3,000 aged care providers in Australia deliver care through nearly 9,000 services, at a total cost to governments of $18.4 billion.2 In SA people aged 65 years and over make up 18.3% of the 2016 population. By 2031, 19% of Australia’s population is expected to be aged over 65.
SAHMRI is making a differenceThe SAHMRI-based Registry of Senior Australians (ROSA) is a powerful data platform that uses big data and sophisticated computational research to, for the first time in Australia, examine the intersection between the aged care and health care sectors at the population level.
Professor Steve Wesselingh, Associate Professor Maria Inacio and their ROSA team produces evidence to guide decision-making for quality, efficient, innovative and age-friendly services and practices.
ROSA has informed the national understanding of the prevalence and trends in major diseases, evaluating of the quality use of medicines and variations in practices and models of care nationally.
The Registry has developed an Outcome Monitoring System which is a pragmatic, efficient, low burden tool to support evidence-based quality improvement efforts through transparency and best practice in aged care.

HIGH QUALITY AND SAFE AGED CARE
1.https://quickstats.censusdata.abs.gov.au/
census_services/getproduct/census/2016/
quickstat/4?opendocument
2. https://www.aihw.gov.au/reports/austra-
lias-welfare/aged-care/
3. Moldovan M, Khadka J, Visvanathan R,
Wesselingh S, Inacio M. 2020. Using elastic
ROSA is supported by the South Australian Government through the Department for Innovation and Skills (2017-2021), Silver Chain, and ECH Inc.
Additional support for ROSA has been obtained from the Medical Research Future Fund, The Hospital Research Foundation, the National Health and
Medical Research Council, Health Translation SA, and SAHMRI.
nets to estimate frailty burden from routinely
collected national aged care data. J Am Med
Inform Assoc, 27:3:419–428.
4. Harrison SL, Sluggett JK, Lang C, White-
head C, Crotty M, Corlis M, Wesselingh SL,
Inacio MC. 2020. The dispensing of psycho-
tropic medicines to older people before and
after they enter residential aged care. Medical
Journal of Australia. https://doi.org/10.5694/
mja2.50501
5. Inacio, M, Khadka, J, Lang, C, Harrison, S,
Crotty, M, Whitehead, C & Wesselingh, S 2019,
‘Young people in aged care: trends in the use
of aged care services by younger Australians,
2008–2016’, Disability and rehabilitation.
https://doi.org/10.1080/09638288.2019.1652
703
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS
ROSA positions South Australia as a national leader in aged care planning, conducting ground-breaking research that answers vital questions for governments, NGOs and the aged care industry. This evidence has short, medium and long-term benefits, saving money through reduced inefficiencies and targeted use of resources and improving lives through more appropriate care and services.
Providing evidence to the Royal Commission into Aged Care Quality and Safety across a broad range of issues relating to care and service delivery.
Developing tools including an Outcome Monitoring System and Frailty Index to inform decision making and improve care.
Targeting research in areas that can produce short-term benefits including assessing psychotropic medication and antibiotic use in residential aged care, impacts of respite care on long-term outcomes and national trends in rates of dementia.
ROSA has also developed a Frailty Index with clinical relevance at the time of assessment by an Aged Care Assessment Team (ACAT), enabling appropriate interventions to reverse the frailty or to prioritise those with high frailty scores.3
IMPACT: NOW
IMPROVED DIAGNOSIS OF HEART ATTACKS IN EMERGENCY DEPARTMENTS
Better treatments for chronic abdominal and pelvic painCOLLABORATION WITHIN SA
• Flinders University
• University SA
• The University of Adelaide
NATIONAL & INTERNATIONAL
• University of Queensland
• Monash Institute of Pharmaceutical Sciences (Melbourne)
• Illawarra Health and Medical Research Institute, University of Wollongong
• University of Melbourne
• Florey Institute (Melbourne)
• Melbourne Royal Women’s Hospital
• University of Sydney
• Harvard University (Boston, USA)
• Johns Hopkins University (Baltimore, USA)
• Columbia University (New York, USA)
• University of California (Los Angeles, USA)
• University of California (San Francisco, USA)
• University of Sheffield (UK)
• University of Cambridge (UK)
• Universite de Toulouse (France)
• University of Vienna (Austria)
• Takeda Pharmaceuticals (Tokyo, Japan)
• Ironwood Pharmaceuticals (Boston, USA)
• Arena Pharmaceuticals (San Diego, USA)
SAHMRI’s successful research into the underlying causes of irritable bowel syndrome, inflammatory bowel disease, bladder pain syndrome and endometriosis is providing safer pain relief options and better quality of life for sufferers.
BACKGROUND
Irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), bladder pain syndrome (BPS) and endometriosis share common symptoms of chronic abdominal and pelvic (visceral) pain. These conditions are of such concern that the Australian Government Minister for Health has released national action plans for chronic pain, IBD and Endometriosis.
Nearly 85,000 Australians, most aged from 5 to 49 years, are living with IBD, which is the collective term used for Crohn’s disease and ulcerative colitis. Australia has one of the highest rates of prevalence and incidence of IBD in the world with the rate increasing each year. Presently, there is no cure. 1 The estimated health and economic cost of IBD to Australia is more $3 billion annually.2
Endometriosis is a common disease in which tissue that is similar to the lining of the womb grows in other parts of the body. More than 830,000 Australian women suffer from endometriosis at some point in their life with the disease often starting during the teenage years. An Australian government report estimated the cost of endometriosis to be $9.7 billion annually. Two-thirds of that cost is attributed to a loss in productivity with the remaining $2.5 billion being direct healthcare costs.3
SAHMRI is making a differenceProfessor Stuart Brierley, Director of the Visceral Pain Research Group and the Hopwood Centre for Neurobiology in SAHMRI’s Lifelong Health Theme, is recognised as a world leader in the field of visceral pain. Professor Brierley’s research investigates the causes of IBS, IBD, BPS and endometriosis with a focus on finding new treatments for these debilitating conditions.
IMPROVED DIAGNOSIS OF HEART ATTACKS IN EMERGENCY DEPARTMENTS
1. https://www.crohnsandcolitis.com.au
2. https://www.crohnsandcolitis.com.au/site/wp-content/uploads/PwC-Report-2013-Exec-utive-Summary.pdf
3. https://www.endometriosisaustralia.org
4. Grundy, L., Harrington, AM., Castro, J., Gar-cia-Cara- ballo, S., Deiteren, A., Maddern, J.,
• Flinders University • Funding by National Health and Medicial Research Council (NHMRC) of Australia, Australian Research Council (ARC), National
Institutes of Health (NIH), USA.
Rychkov, G. Y., Ge, P., Peters, S., Feil, R., Miller, P., Ghetti, A., Hannig, G., Kurtz, CB., Silos-San-tiago, I., Brierley, SM. 2018. Chronic linaclotide treatment reduces colitis-induced neuro- plasticity and reverses persistent bladder dysfunction. JCI insight, 3(19), e121841. https://doi.org/10.1172/jci. insight.121841
5. Castro J et al. 2013 Linaclotide Inhibits Colonic Nociceptors and Relieves Abdominal
Pain via Guanylate Cyclase-C and Extracellu-lar Cyclic Guanosine 3’, 5’ Mo- nophosphate Journal of Gastroenterology 145:6:1334- 46.e11 https://doi.org/10.1053/j.gastro.2013.08.017 6. https://investor.ironwoodpharma.com/press-releas- es/press-release-de-tails/2019/Ironwood-Pharmaceuticals-Re-ports-Third-Quarter-2019-Results-Raises-Full- Year-2019-Guidance/default.aspx
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS
Research by Professor Brierley’s team has profoundly changed clinical practice. But the demand for further breakthroughs in visceral pain management are clear. Approximately 25% of South Australians would potentially benefit from better pain control associated with their internal organs if the novel treatments being researched by Professor Brierley’s team reach clinical trial and translation stages.
The potential for significant improvements in quality of life are clear, as are the reductions on costs to the public health system and increase in productivity.
Better diagnosis leading to more effective pain management.
New drug candidates for specific targeting of chronic visceral.
Improved quality of life and productivity through more effective treatments.
Professor Brierley’s research has provided a significant paradigm shift by targeting the underlying causes of these conditions to provide clinically relevant pain relief and improve patient quality of life.4, 5 His work with Ironwood Pharmaceuticals determined how Linaclotide relieves pain in IBS patients with constipation (IBS-C). Linaclotide targets nerves within the gut, inhibiting signals being sent to the brain, relieving pain without systematic side-effects.
Linaclotide has become the number one treatment in the US.6 Linaclotide is now approved in Japan, China and Australia where it helps millions of patients each year. The ‘mechanism of action data’ derived by Professor Brierley’s group appears in the prescription box globally.6
IMPACT: NOW
REDUCING SMOKING RATES
Reducing smoking rates
COLLABORATION WITHIN SA
• SA Government
• The University of Adelaide
• Flinders University
NATIONAL & INTERNATIONAL
• Australian Government Department of Health
• Cancer Council Victoria
• National University of Singapore
• Health Promotion Board, Singapore
The SAHMRI Health Policy Centre’s research has directly influenced state and national tobacco control policy to reduce smoking - saving lives and significantly relieving the burden on health systems.
BACKGROUND
Annual health care expenditure attributable to smoking in Australia is around $6.8 billion.1 That equates to around $500 million from the South Australian health budget.
Tracheal, bronchus and lung cancer are the most significant tobacco-attributable deaths in Australia (6500 annually), followed by chronic obstructive pulmonary disease and ischaemic heart disease.1
While enormous progress has been made, tobacco is still the leading risk factor for disease in Australia, contributing 9.3% of the total burden of disease in 2015. This includes 41% of the burden of respiratory disease, 22% of cancer and 11% of cardiovascular disease.2
SAHMRI is making a differenceThe SAHMRI Health Policy Centre (HPC) makes a substantial contribution to evidence-based policy and practice in tobacco control locally, nationally and internationally. Research by the Centre, led by Professor Caroline Miller, contributed to Australia’s successful defence of plain packaging laws against legal challenges at the World Trade Organisation. Professor Miller has spent several years as the lead international adviser to the Singapore Government as it prepared to legislate for tobacco plain packaging. Professor Miller was commissioned to lead the development of evidence-based standards for Australia’s Quitline services and her work has also been instrumental in the advancement of the National Tobacco Campaign and graphic health warnings on tobacco packaging.
We are now seeing the lowest rates of smoking ever recorded in South Australia and this can be attributed to a strong tobacco control program, underpinned by evidence generated and synthesized by the SAHMRI HPC.

REDUCING SMOKING RATES
1. Whetton S, Tait RJ, Scollo M, Banks E, Chapman J, et al. Identifying the social costs of tobacco use to Australia in 2015/16. Perth, Western Australia: The National Drug Research Institute at Curtin University, 2019. Available from: http://ndri.curtin.edu.au/NDRI/media/documents/publica-tions/T273.pdf
2. Australian Institute of Health and Welfare. Australian burden of disease study: Impact and causes of illness and death in Australia 2015. Australian Burden of Disease, Canberra: AIHW, 2019. Available from: https:// www.aihw.gov.au/reports/burden-of-disease/burden- disease-study-illness-death-2015/contents/summary.
3. Martin, K., Dono, J., Stewart, H., Sparrow, A., Miller, C., Roder, D., & Bowden, J. Evaluation of an intervention to train health professionals working with Aboriginal and Torres Strait Islander people to provide smoking cessation advice. Australian and New Zealand Journal of Public Health, 2019; 43(2):156-162. https://www.ncbi.nlm.nih.gov/pubmed/30786129
4. Frazer K, Callinan JE, McHugh J, van Baarsel S, Clarke A, et al. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database of Systematic
• SA Government • Singapore Government • National Health and Medical Research Council • Beat Cancer Project
Reviews, 2016; 2:CD005992. Available from: https://www.ncbi.nlm.nih.gov/pubmed/26842828
5. Dono, J., et al., Taking the pressure off the spring: the case of rebounding smoking rates when antitobacco campaigns ceased. Tobacco Control, 2019. 28(2):233-6. Available from: https://tobaccocontrol.bmj.com/con-tent/28/2/233
6. Extrapolated from: Australian Burden of Disease Study: Impact and causes of illness and death in Australia, 2015. Appendix D: Additional tables and figures. Australian In-stitute of Health and Welfare, 2019. Available from: https://www.aihw.gov.au/reports/burden-of-disease/burden-dis-ease-study-illness- death-2015
7. Martin K, Bowden J & Miller C. Key Smoking Statistics for SA – 2018. Adelaide, Australia. South Australian Health and Medical Research Institute (SAHMRI), March 2019. Available from: https://www.sahmri.org/sahmri-impact-theme/re-source-19/
8. Kahende JW, Loomis BR, Adhikari B, and Mar- shall L. A review of economic evaluations of tobacco control programs. International Journal of Environmental Research and Public Health, 2009; 6(1):51- 68. Available from: https://www.ncbi.nlm.nih.gov/pubmed/19440269
9. Applied Economics. Returns on investment in public health: An epidemiological and economic analysis Depart-ment of Health and Ageing, 2003. Available from: http://www.appliedeconomics.com.au/pubs/reports/health/index.htm#TopOfPage.
10. VicHealth Centre for Tobacco Control, Tobacco control: A bluechip investment in public health. 2003, The Cancer Council of Victoria: Melbourne. Available from: https://www.tobaccoinaustralia.org.au/downloads/chapters/TCMaster-April2003.pdf
11. Atusingwize E, Lewis S, and Langley T. Economic evalua-tions of tobacco control mass media campaigns: A system-atic review. Tobacco Control, 2015; 24(4):320-7. Available from: https://www.ncbi.nlm.nih.gov/pubmed/2498573012. Hurley SF and Matthews JP. Cost-effectiveness of the Australian national tobacco campaign. Tobacco Control, 2008; 17(6):379-84. Available from: https://www.ncbi.nlm.nih.gov/pubmed/18719075
13. McCaffrey N and Carter R. Economic evaluation of the Victorian quitline service. Melbourne: Deakin University and Cancer Council Victoria, 2018. Available from: https://www.quit.org.au/documents/245/Economic_evaluation_of_the_Victorian_Quitline_service.pdf.
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS
The HPC has been integral in the implementation of smoke-free legislation which has been clearly shown to lead to rapid savings for the health care system from reduced smoking-related illness.4 The decline in smoking rates reduces the preventable burdens of heart disease and cancer saving thousands of lives.
A 2019 HPC publication demonstrated increases in smoking rates when a mass media campaign was abruptly ceased.5 The SA Minister consequently reinstated $1m of annual funding for the campaign which reversed the trend. An Access Economics study estimated that the Australian Government saved $2 for every $1 spent on public health programs to reduce smoking. Tobacco control programs are vital to maintain the downward pressure on smoking rates to reduce health care expenditure in SA.
The SAHMRI Health Policy Centre’s work has supported a broad spectrum of tobacco control policies and legislation that have contributed to declining smoking rates.
The HPC’s expertise are utilized locally, nationally and internationally.
The HPC continues to focus on smoking rates among high prevalence groups including people living in disadvantaged areas and those with mental illness.
The centre, in partnership with SAHMRI’s Aboriginal Health Equity Theme continues to assist evaluation of programs aimed at reducing the impact of tobacco in Aboriginal and Torres Strait Islander communities. Recently, SAHMRI led the evaluation and subsequent publication of the national health worker trained ‘Quitskills’ program.3 This evaluation was reported to Commonwealth Government and formed the basis for continued funding of the program.
IMPACT: NOW
IMPROVING OUTCOMES FOR LEUKAEMIA
Improving outcomes for leukaemiaCOLLABORATION WITHIN SA
• SA Pathology
• The University of Adelaide
• Royal Adelaide Hospital
• University of SA
• Queen Elizabeth Hospital
• The Women’s and Children’s Hospital
NATIONAL & INTERNATIONAL
• Hospitals and Medical Research Centres & Institutes in WA, NSW, VIC, QLD, ACT
• Australasian Leukaemia and Lymphoma Group (Melbourne)
• Australian and New Zealand Children’s Haematology/Oncology Group (Melbourne)
• Australian Genomics (Melbourne)
• Zero Childhood Cancer (Sydney)
• St Jude Children’s Research Hospital (Memphis, USA)
• Harvard University (Boston, USA)
• National Cancer Institute (Brasilia, Brazil)
• University of Technology (Sydney)
• University of New South Wales (Sydney)
SAHMRI’s acute lymphoblastic leukaemia laboratory is the National Referral Centre for genomic screening of ALL cases across all age groups.
Acute lymphoblastic leukaemia (ALL) is the most common childhood cancer and the leading cause of non-traumatic death in young people. The recent wealth of genomic information has seen the identification of new lesions known to confer a high risk of treatment failure. Of clinical importance is that these genomic changes cannot be identified using current diagnostic approaches, meaning patients carrying these lesions are only identified as high-risk when they relapse or fail to respond to treatment.
Professor Deborah White was one of the first researchers to describe resistance to targeted therapies in ALL in 2016. She detailed the high prevalence of relapse in a form of ALL related to the Philadelphia chromosome, despite the application of risk-adapted personalised therapy.1,2,3 Until recently, it was almost impossible to target treatments to a person’s unique genetic makeup. Historically, cancer medicine has been a one-size-fits-all approach.
Professor White’s laboratory is the National Referral Centre for genomic screening of ALL cases across all age groups. The team has identified a significant number of alterations and novel gene fusions for investigation. Their research aims to understand additional factors that impact both disease initiation and therapeutic response, in particular the effects of the genome, immune system and gut microbiota. This critical work, in addition to providing therapeutic impact, has enabled the genomic landscape mapping of ALL in this country, which from an ethnicity perspective has been critically important. This work will become integral to ongoing guidelines in the near future.
This year, it’s estimated more than 800 new cases of cancer will be diagnosed in people aged 0-14.5 The number of deaths from blood cancers and the quality of life of people living with blood cancer, can be substantially improved by applying what is already known today. Adoption of novel therapies in use globally could potentially reduce the number of expected deaths by up to one third in total.6
Precision medicine is now at the forefront of innovative cancer treatment, targeting specific changes in a patient’s tumour DNA to treat the disease, while also taking into account the genetic variations between people who have been influenced by environmental and lifestyle factors.6

IMPROVING OUTCOMES FOR LEUKAEMIA
1. Forgione, M. O., McClure, B. J., Eadie, L. N., Yeung, D. T., & White, D. L. (2019). KMT2A rearranged acute lymphoblastic leukaemia: unravelling the genomic complexity and heterogeneity of this high-risk disease. Cancer letters.
2. Eadie, L., Dang, P., Saunders, V., Yeung, D., Osborn, M., Grigg, A., White, D. (2017). The clinical significance of ABCB1 overexpression in predicting outcome of CML patients undergoing first-line imatinib treatment. Leukemia, 31(1), 75-82.
3. Heatley, S., Sadras, T., Kok, C., Nievergall, E., Quek, K., Dang, P., White, D. (2017). High prevalence of relapse in children with Philadelphia-like acute lym-phoblastic leukemia despite risk-adapted treatment. Haematologica, 102(12), e490-e493.
4. Zaliova M, Moorman AV, Cazzaniga G, Stanulla, M,
• National Health and Medical Research Council (NHMRC) • The University of Adelaide • Beat Cancer – Cancer Council SA • Leukaemia Foundation • Tour de Cure • Cancer Australia • The Kids’ Cancer Project • Channel 7 Research Foundation • AMP’s Tomorrow Fund • J & D Ramsay Foundation • Kiwanis • Australian Federal Government
Harvey RC, Roberts KG, Heatley SL, Loh ML, Kono-pleva M, Chen I, Zimmermannova O, Schwab C, Smith O, Mozziconacci MJ, Chabannon C, Kim M, Falken-burg JHF, Norton A, Marshall K, Haas OA, Starkova J, Stuchly J, Hunger SP, White DL, Mullighan CG, Willman CL, Stary J, Trka J, Zuna J. (2016) Characterization of leukemias with ETV6-ABL1 fusion. Haematologica. 2016 Sep;101(9):1082-93.
5. https://www.aihw.gov.au/getmedia/8c9f- cf52-0055-41a0-96d9-f81b0feb98cf/aihw-can-123. pdf.aspx?inline=true
6. https://www.leukaemia.org.au/wp-content/up- loads/2019/09/State-of-the-Nation-Blood-Cancer-in- Australia_Leukaemia-Foundation.pdf
7. Trahair TN, Lock RB, Sutton R, Sia KCS, Evans K, Richmond J, Law T, Venn NC, Irving JA, Moore S,
Eva Nievergall E, Dang P, Heatley SL, White DL and Revesz T. Xenograft-directed personalized therapy for a patient with post-transplant relapse of ALL. Bone Marrow Transplantation 51, 1279-1282 September 2016
8. Richmond J, Robbins A, Evans K, Beck D, Raushan T. Kurmasheva RT, Billups CA, Carol H, Heatley S, Sut-ton R, Marshall GM, White DL, Pimanda J, Houghton PJ, Smith MA, Lock RB. Acute Sensitivity of Ph-like Acute Lymphoblastic Leukemia to the SMAC-Mimetic Birinapant. Cancer Res 2016 76 (15) 4579-1591
9. Dolai S, Sia KCS, Robbins AK, Zhong L, Heatley SL, Vincent TL, Hochgräfe F, Sutton R, Kurmasheva RT, Revesz T, White DL, Houghton PJ, Smith MA, Teachey DT, Daly RJ, Raftery MJ, Lock RB. Quantitative phos-photyrosine profiling of patient-derived xenografts identifies therapeutic targets in pediatric leukemia. Cancer Research 2016 76 (9), 2766-2777
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS FOR SA
The population of people diagnosed with leukaemia is small in SA, however the burden they carry physically and economically is significant. Any improvements in treatment targeting will extend lives and reduce burdens on families and individuals. SA has a national profile in ALL diagnosis, genotyping and treatments.
THE NEXT FRONTIER
Older cancer treatments, such as intensive chemotherapy regimens, have often come with significant side-effects, including secondary cancers and heart problems. Adult survivors of childhood ALL experience significant co-morbidities and an increased rate of secondary cancers. While we can successfully treat ALL, the life-long effects are significant. We need to better understand the disease so that therapies can be targeted for more effective treatment and reduced long-term effects.
1. Accurate disease risk stratification
a. The accurate identification of High Risk versus standard Risk ALL disease for therapeutic risk stratification and better use of health resources.
i. Which patients need expensive immune therapies up front?
ii. Which patients have standard risk ALL and will likely do well on a de-escalated chemotherapeutic regimen with less short and long-term side effects?
iii. Which patients would benefit from re-purposed drugs (ie TKIs)?
2. Analysing the gut microbiota and immune system from diagnosis through to post therapy
a. Can we modify the gut microbiota to reduce toxicity, and increase therapeutic effectiveness?
b. Can we reduce long term co-morbidities?
• 600 leukaemia cases with complete transcriptomic sequencing (mRNA Seq)
• Therapeutic change for around 30 patients per year with that capacity increasing
• Change in risk stratification for around 50 patients per year
• Targeted use of expensive treatments
• Reduced comorbidities leading to reduced health resource use
The cost for the initial phase of Leukaemia treatment is $36,176 (2013 dollars), the continuing phase is $15,070 and the terminal phase is $63,462.4
ALL Treatments
Cost per course of treatment (before government subsidy)
Blinatumomab $122,900
Inotuzumab ozogamicin $122,900
CAR T therapy $500,000
IMPACT: SOON
REDUCING PRETERM BIRTHS
Reducing preterm births
COLLABORATION WITHIN SA
• The University of Adelaide
• Women’s and Children’s Health Network
• Southern Adelaide Local Health Network
• Northern Adelaide Local Health Network
NATIONAL & INTERNATIONAL
• Mater Mothers Hospital (Brisbane)
• Joondalup Health Campus, University of Notre Dame (Perth)
• Werribee Mercy Hospital (Melbourne)
• Trajan Scientific and Medical (Melbourne)
• Cochrane Pregnancy and Childbirth Group (London, UK)
• Statens Serum Institut (Copenhagen, Denmark)
• Australian Preterm Birth Prevention Alliance
SAHMRI Women and Kids is leading international investigations into omega-3 fish oil as a safe, easily accessible intervention against preterm birth.
BACKGROUND
Preterm birth complications are the leading cause of death of children under five years old in Australia.
Preterm babies have an average hospital stay more than twice that of babies delivered at term. Around 80% of preterm babies are admitted to a neonatal intensive care unit compared with 12% of babies delivered at term. Mortality rates were highest among babies born at 20 - 27 weeks gestation (694 per 1,000 births) and lowest among babies born at term (2 per 1,000 births).1
Early preterm children (born before 34 weeks) are at greater risk of developmental delays and potentially face a range of issues including visual and hearing impairments, respiratory problems and poor health outcomes.
Parents of children born early preterm are more likely to report moderate to severe anxiety, have symptoms of depression, experience poorer family functioning and have higher levels of parenting stress compared with parents of children born at term.2
SAHMRI is making a differenceProfessor Maria Makrides and her team at SAHMRI Women and Kids conducted one of the largest studies of omega-3 fish oil supplementation and preterm birth. Known as the ORIP trial, the study showed that women with single pregnancies and low omega-3 status are at higher risk of preterm birth so are most likely to benefit from omega-3 supplements. The study also showed that women with multiple pregnancies might not benefit from supplementation and women who already have higher omega-3 status could be harmed by additional supplementation. This indicated that a targeted rather than a universal approach to supplementation was needed.3,4
REDUCING PRETERM BIRTHS
1. Lain, S, Nassar, N, Bowen, J, Roberts, C. Risk factors and costs of hospital admissions in first year of life: a population based study. Journal of Pediatrics 2013;163:1014-1019. 2. Australian Institute of Health and Welfare. 2019 Australia’s mothers and babies 2017—in brief. Perinatal statistics series no. 35. Cat. no. PER 100. Canberra: AIHW.
3. Simmonds LA, Sullivan TR, Skubisz M, Middleton
• Health Translation SA • The project was supported by the Australian Government’s Medical Research Future Fund as part of the Rapid Applied
Research Translation program. Support is acknowledged from the NHMRC (Project Grant and Centre of Research Excellence) and the Thyne Reid
Foundation.
PF, Best KP, Yelland LN, Quinlivan J, Zhou SJ, Liu G, McPhee AJ, Gibson RA, Makrides M. 2020 Omega-3 Fatty Acid Supplementation in Pregnancy – Baseline Omega-3 Status and Early Preterm Birth: Exploratory Analysis of a Randomised Controlled Trial. British Journal of Obstetrics and Gynaecology [ahead of print] PMID: 32034969 DOI: 10.1111/1471-0528.16168
4. Holditch-Davis D, Bartlett TR, Blickman AL, Miles MS. Posttraumatic stress symptoms in mothers of premature infants. Journal Obstet Gynecol Neonatal Nurs 3003;32:151-71
5. Treyvaud, K et al. Very Preterm Birth Influences Parental Mental Health and Family Outcomes Seven Years after Birth. Journal of Pediatrics 2014;164:515-21
6. Makrides M, Best K, Yelland L, McPhee A, Zhou SJ, Quinlivan J, et al. A randomized trial of prenatal n-3 fatty acid supplementation and preterm delivery. New England Journal of Medicine. 2019;381:1035-45
REFERENCES
ACKNOWLEDGEMENTS
BENEFITS
There are about 1500 preterm births in SA each year with around 370 of these occurring before 34 weeks of gestation. Providing fish oil supplements to women with single pregnancies who have low omega-3 levels can reduce the rate of early preterm births by 77%.4 This would mean about 50 South Australian babies each year are saved from being born before 34 weeks. It’s estimated each early preterm baby costs the hospital system $27,000 in its first year of life alone, which equates to an annual saving to the state of $1.35 million.
If 50 fewer babies are born before 34 weeks, then at least 50 parents per year will also be prevented from unnecessary stress, depression and anxiety.5,2 Up to 50 babies per year will be less likely to rely on health and disability services throughout their lives.
Reducing preterm birth means healthier babies, parents and families.
Reducing preterm birth means less short, medium and long term associated costs on the health system.
Commercialisation of the Adelaide-developed dried blood spot testing can reduce service costs to the system and generate income through business development and royalties.
SAHMRI is partnering with Trajan Nutrition to commercialise a simple omega-3 screening test to identify who would most benefit from supplementation. Based at SAHMRI, Trajan Nutrition is a joint venture between Trajan Scientific and Medical in Melbourne, SAHMRI and the University of Adelaide. The novel dried blood spot technology at the core of the testing was developed in Adelaide. The goal is to embed the testing into existing health services and workflows so that it is routinely available.
IMPACT: SOON
IMPROVING CARE OF NEWBORNS IN SOUTH AUSTRALIA
Improving care of newborns in South Australia
• Reducing risk of Cerebral Palsy
• Reducing unnecessary use of antibiotics
COLLABORATION WITHIN SA
• Women’s and Children’s Health Network
• Southern Area Local Health Network
• SA Ambulance Service
• Robinson Research Institute and Adelaide Medical School, The University of Adelaide
SAHMRI Women and Kids is helping give South Australian babies the best start to life.
Almost 17,000 babies are born each year in South Australia. Most are born healthy and at term but approximately 1500 of these are born before 37 weeks of gestation (preterm) and about 370 babies are born before 34 weeks (early preterm). Preterm babies often need varying degrees of specialist neonatal care and can have ongoing medical issues. Preterm birth complications are the leading cause of death for children under five years of age in Australia. Dr Amy Keir of SAHMRI’s Women and Kids is working with her clinical and research colleagues to translate the best available research evidence into practice to ensure babies get the best start in life. Dr Keir is leading a continuous quality improvement program to close the ‘evidence-to-practice’ gap in perinatal care.
BENEFITS FOR SA
Every 15 hours, an Australian child is born with cerebral palsy. Giving magnesium sulphate to women in threatened early labour (before 30 weeks of gestation) reduces the risk of cerebral palsy and protects gross motor function in these infants born preterm.1 Until recently, just over half of eligible women were treated with magnesium sulphate at the Women’s and Children’s Hospital in Adelaide. Dr Keir and her team have succeeded in raising this rate to more than 90%. Identifying and addressing the barriers to the use of this neuroprotective medication has resulted in increased uptake, and this will reduce the risk of cerebral palsy in these children.
Early onset sepsis is a rare but significant cause of health issues and death in newborn babies. The current South Australian guidelines lead clinicians to prescribe antibiotics to a number of babies who may not benefit, which might have unintended consequences. As many as 90% of newborns prescribed antibiotics did not need the medication, as they did not end up having an infection.
Antibiotic overuse is costly and contributes to antibiotic-resistant infections in hospitals. Antibiotic treatment results in a longer length of admission for mother and baby and could impact negatively on breastfeeding rates if the baby needs to be separated from its mother. Dr Keir and her team have implemented the use of an existing early onset sepsis risk calculator within the Women’s and Children’s Hospital. Preliminary data indicates this approach is already reducing the numbers of blood tests in babies as well as decreasing the incidence of antibiotic intervention.

IMPROVING CARE OF NEWBORNS IN SOUTH AUSTRALIA
1. Peebles DM, Kenyon AP. 2011. Magnesium Sulphate to Prevent Cerebral Palsy following Preterm Birth. Royal College of Obstetricians and Gynaecologists London UK
2. Gong, C.L., Dasgupta-Tsinikas, S., Zangwill, K.M. et al. 2019. Early onset sepsis calculator-based manage-ment of newborns exposed to maternal intrapartum fever: a cost benefit analysis. J Perinatol 39, 571–580. https:// doi.org/10.1038/s41372-019-0316-y
• SAHMRI Women and Kids • Dr Keir is in receipt of National Health and Medical Research Council (NHMRC) Fellowships (APP1161379). The views expressed in this article are solely the responsibility of the authors and do not reflect the views of the NHMRC • Health Services Charitable Gifts Board (BP Storen Estate)
3. Based on costs of hospital stay SA 2019 - does not include savings in pathology testing, other medica-tions and other related costs
4. Australia, Sydney NSW https://cpaustralia.com.au/ media/20379/access_economics_report.pdf
5. Kaiser Permanente https://neonatalsepsiscalculator. kaiserpermanente.org/
6. Access Economics. 2008. The Economic Cost of Cerebral Palsy in Australia in 2007. Cerebral Palsy
7. Pettinger KJ, Mayers K, McKechnie L, Phillips B. 2020. Sensitivity of the Kaiser Permanente early-onset sepsis calculator: A systematic review and meta-analy- sis EClinical Medicine (Lancet) 19:100227 DOI https:// doi.org/10.1016/j.eclinm.2019.11.020
REFERENCES
ACKNOWLEDGEMENTS
CLOSING THE EVIDENCE GAP
Efforts to improve uptake of evidence-based care are unlikely to be successful if they are one dimensional or focus only on individual health professionals. Through harnessing the enthusiasm and drive of healthcare professionals on the frontline of perinatal care, Dr Keir and colleagues are improving outcomes for babies and their families. This quality improvement platform is a collaborative solution. It works alongside healthcare professionals, administrators and families of former preterm infants to drive effective, sustainable practice changes at a state-wide level across South Australia.
THE NEXT FRONTIER
Dr Keir and her colleagues are working on a state-wide approach to scale up the continuous quality improvement program to close the evidence-to-practice gaps and improve the effectiveness of care in public hospitals. The same efforts could be applied in other major public obstetric and neonatal units, and potentially to private hospitals, to improve the use of magnesium sulphate for fetal neuroprotection and to reduce the use of antibiotics in newborn babies. This could deliver significant cost savings from reduced antibiotic use and reduced length of stay while helping in the fight against antibiotic resistance.
Total savings of $43,000 per year from reduced incidents of cerebral palsy due to preterm birth.2
Lifetime savings of $5.57 million per case of cerebral palsy.2
50% reduction in use of antibiotics in newborns.
Better targeted use of antibiotics saves $202,285 per year from reduced length of newborn hospital stays and $242,857 per year from reduced length of maternal hospital stays.3
CEREBRAL PALSY
Cerebral Palsy Australia estimates 600-700 infants are born with cerebral palsy in Australia each year. Total health expenditure for the disorder in 2007 was estimated at $40.5 million.
EARLY-ONSET SEPSIS RISK CALCULATOR
A calculator-based approach resulted in a net monetary benefit of $3998 per infant with a 60% likelihood of net benefit in probabilistic sensitivity analysis. This published model predicted a 67% decrease in antibiotic use in the calculator arm. Compared to existing guidelines, a calculator-based approach for newborns exposed to maternal intrapartum fever yields a robust net monetary benefit, largely by preventing unnecessary antibiotic treatment.5
NEONATAL ANTIOBIOTICS
Neonatal antibiotic administration has been reported to be associated with childhood asthma, allergy and autoimmune disease, pain and parental anxiety and separation. It also incurs significant workload and financial costs on the health system.4
IMPACT: FUTURE
REDUCING THE RISK OF DEVELOPING DEMENTIA
Reducing the risk of developing dementiaCOLLABORATION WITHIN SA
• European Molecular Biology Laboratory (at SAHMRI)
• University of South Australia and the Centre for Cancer Biology
• CSIRO
• The University of Adelaide
NATIONAL & INTERNATIONAL
• University of Queensland
Collaborative genetic research within SAHMRI is explaining a cell system that drives Alzheimer’s disease, promising mid-life interventions that could delay or prevent the disease’s onset and severity.
BACKGROUND
In 2017, there were 34,916 South Australians living with dementia. Without a medical breakthrough, the number of people with dementia is expected to more than double by 2056. In 2017, dementia was the leading cause of death of women, and the third leading cause of death of men. Overall, dementia accounts for 13,729 Australian deaths each year.1
Dementia is the single greatest cause of disability in Australians aged 65 years or older and is the third leading cause of disability burden overall. In 2018, dementia is estimated to cost Australia more than $15 billion. By 2025, the total cost of dementia is predicted to increase to about $19 billion and by 2056 to about $37 billion. People with dementia account for 52% of all residents in residential aged care facilities.1
SAHMRI is making a differenceDr Tim Sargeant and his team in the Hopwood Centre for Neurobiology within SAHMRI’s Lifelong Health Theme are working to reduce the risk of developing dementia in late-life by developing mid-life interventions. His team researches the lysosomal system which is the recycling centre of our cells – removing damaged cell machinery to slow aging and promote healthy brain function.
Using genetic information from more than 60,000 people, Dr Sargeant and his colleagues demonstrated that the lysosomal system drives Alzheimer’s disease.2 Further, they found the lysosomal system could be influenced by nutrition, meaning interventions in mid-life could slow or potentially even halt the onset of dementia.
REDUCING THE RISK OF DEVELOPING DEMENTIA
1. Dementia Statistics. 2020. Dementia Aus-
tralia, accessed 13 March 2020, https://www.
dementia.org.au/statistics>
2. Gao S, Casey AE, Sargeant TJ, Mäkinen V-P.
2018. Genetic variation within endolysosomal
system is associated with late-onset Alzhei-
mer’s disease, Brain, 141:9:2711-20, https://doi.
org/10.1093/brain/awy197
3. NATSEM. 2017. Economic Cost of Dementia
in Australia 2016-2056, Dementia Australia,
Sydney. https://www.dementia.org.au/files/
NATIONAL/documents/The-economic-cost-
of-dementia-in-Australia-2016-to-2056.pdf
4. Whyte LS, Hassiotis S, Hattersley KJ,
Hemsley KM, Hopwood JJ, Lau AA, Sargeant
TJ. Lysosomal Dysregulation in the Murine
AppNL-G-F/NL-G-F Model of Alzheimer’s
Disease. Neuroscience. 2020 Mar 1;429:143-
155. doi:10.1016/j.neuroscience.2019.12.042.
Epub2020 Jan 7.
5. Hassiotis S, Manavis J, Blumbergs PC,
Hattersley KJ, Carosi JM, Kamei M, Sargeant
TJ. Lysosomal LAMP1immunoreactivity exists
in both diffuse and neuritic amyloid plaques
in the human hippocampus. Eur J Neurosci.
2018 May;47(9):1043-1053. doi: 10.1111/ejn.13913.
Epub 2018 Apr 2.
REFERENCES
BENEFITS
Without intervention, the direct and indirect costs of dementia in SA are around $800 million annually and rising. The annual financial impost on Australia’s health system is almost $40,000 per dementia patient and rising by almost 3% each year. This represents a total annual cost of about $15 billion.
The impact of funding research to reduce hospitalisation costs for people with dementia is also estimated to reduce dementia incidence by 10%.1 A 5% reduction in the annual incidence of dementia in people aged 65 years and over leads to a 23.7% reduction in the number of people with dementia by 2056, generating direct cost savings of $76.6 billion and indirect cost savings of $43.8 billion over the next 40 years.3
SAHMRI has investigated how cells’ recycling centres – the lysosomal system – impact the development of dementia.
With this knowledge, the team is developing nutrition as a mid-life intervention to slow or stop the onset of dementia.
A novel blood test for anti-ageing lysosomal activity has been developed for human use to identify people at risk of dementia and monitor interventions such as nutrition.
The team is now developing a blood test to measure lysosomal activity to help determine risk of dementia and assess efficacy of interventions.
IMPACT: FUTURE
PREVENTING OBESITY
Preventing obesity
COLLABORATION WITHIN SA
• SA Government
• The University of Adelaide
• Flinders University
• University of SA
NATIONAL & INTERNATIONAL
• LaTrobe University (Melbourne)
• Monash University (Melbourne)
• University of Sydney
• University of Wollongong
• Griffith University (Gold Coast)
• The George Institute for Global Health (Sydney)
• Obesity Policy Coalition
• Cancer Council VIC & NSW
• Singapore Government
The SAHMRI Health Policy Centre researches and advises a broad spectrum of obesity-related topics to help policy-makers reduce the burden of disease and save health systems significant related costs.
BACKGROUND
Overweight and obesity contributed to 8.4% of the burden of disease in Australia in 2015. Estimates for South Australia show that about half of the population was overweight or obese, with that figure jumping to almost three-quarters for people in country SA.1
Obesity increases the risk of serious health problems including type 2 diabetes, high blood pressure, respiratory issues, sleep disorders and liver disease as well as psychological problems such as anxiety and depression.
SAHMRI is making a differenceThe SAHMRI Health Policy Centre (HPC) actively contributes to policy discussions on obesity prevention and conducts projects aimed at reducing over-consumption of highly processed food and beverages, with a focused program of work in sugar-sweetened beverages.
Professor Caroline Miller and her team lead projects aimed at reducing sugar-sweetened beverage consumption and collaborate on projects in food labelling, food advertising, social marketing and cultural drivers of consumption. The team has contributed original research which was cited to underpin changes, since adopted, to the way beverages are labelled under the ANZ Health Star Rating system.1 HPC continues to generate policy-ready evidence to assist policy makers in determining most effective labelling for consumers, with the format for added sugar labelling under active consideration.

PREVENTING OBESITY
1. https://www.aihw.gov.au/getmedia/762dea8d- 07fb-47c7-8f40-83a3933f66c7/aihwmhc-hpf-27-Over- weight-Obesity-December-2016.pdf.aspx?inline=true
2. Lal A, Mantilla-Herrera AM, Veerman L, Backholer K, Sacks G, Moodie M, et al. (2017) Modelled health bene- fits of a sugar-sweetened beverage tax across different socioeconomic groups in Australia: A cost-effective- ness and equity analysis. PLoS Med 14(6): e1002326. https://doi.org/10.1371/journal.pmed.1002326
3. Australian Bureau of Statistics. 2015. Australian Health Survey: Nutrition First Results - Foods and Nu- trients, 2011-12. Consumption of sweetened beverages. ABS, Canberra.
4. Sohn W, Burt BA, Sowers MR. 2006. Carbonated soft drinks and dental caries in the primary dentition. J Dent Res 85(3):262-66. doi:10.1177/154405910608500311.
5. Malik VS, Pan A, Willett WC, et al. 2013. Sugar-sweet- ened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am J Clin Nutr 98(4):1084-102. doi:10.3945/ajcn.113.058362.
6. Te Morenga L, Mallard S, Mann J. 2012. Dietary sugars and body weight: Systematic review and me- ta-analy-ses of randomised controlled trials and cohort studies. BMJ 346:e7492. doi: 10.1136/bmj.e7492. doi:10.1136/bmj.e7492. Te Morenga LA, Howatson AJ, Jones RM, et al.
7. Te Morenga LA, Howatson AJ, Jones RM, Mann J. 2014. Dietary sugars and cardiometabolic risk: Sys- tematic review and meta-analyses of randomized con- trolled trials of the effects on blood pressure and lipids. Am J Clin Nutr 100:65-79. 10.3945/ajcn.113.081521
8. Van Rompay MI, McKeown NM, Goodman E, et al. 2015. Sugar-sweetened beverage intake is positively associated with baseline triglyceride concentra- tions, and changes in intake are inversely associated with changes in hdl cholesterol over 12 months in a multi-ethnic sample of children. J Nutr 145:2389-95. doi:10.3945/jn.115.2126625
9. Vartanian LR, Schwartz MB, Brownell KD. 2007. Ef- fects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am J Public Health 97(4):667-75
10. AIHW. 2015 Australian Burden of Disease study, AIHW.
11. Miller C, Wakefield M, Braunack-Mayer A, Roder D, O’Dea K, Ettridge K, et al. 2019. Who drinks sugar sweetened beverages and juice? An Australian popula- tion study of behaviour, awareness and attitudes. BMC Obes. 6(1).
12.http://www.oecd.org/australia/Heavy-bur- den-of-obesity-Media-country-note-AUSTRALIA.pdf
13. https://www.aihw.gov.au/getmedia/45f6ecc6- 0caf-4af4-9ffc-a44c885b33d2/aihw-phe-216.pdf. aspx?inline=true 14. https://www.who.int/elena/titles/ssbs_childhood_ obesity/en/
15. PwC Australia 2015. Weighing the cost of obesity: a case for action. Australia: PwC Australia Sydney.
16. https://www.oecd.org/health/health-systems/ Heavy-burden-of-obesity-Policy-Brief-2019.pdf
REFERENCES
BENEFITS
The SAHMRI Health Policy Centre produces evidence for the South Australian and other governments to formulate and justify policy in the highly challenging context of sugar intake regulation.
Reducing obesity, with sugar intake a major contributor, has significant benefits for the individual and community health as well as public expenditure. Obesity-related diseases are estimated to reduce average life expectancy in Australia by 2.7 years and cost the health system $87.7 billion in the decade between 2015 and 2025. Obesity costs the SA government $270.30 extra in health costs for every person every year.2
Modelling indicates a 20% sugar-sweetener beverage tax would lead to significant health gains and reduced health care costs or $1,733 million over the lifetime of the population.
The HPC is making significant evidence-based contributions to ongoing reform of the Health Star Rating system and food labelling regulations.
Reducing obesity will reduce risks of heart disease, type II diabetes, cancer and other conditions, and will improve productivity and labour market outcomes.
HPC research shows there is strong public support for government action in reducing the consumption of sugar-sweetened beverages and this support is building. This can facilitate Australian policy makers to move forward with confidence knowing they have public support to follow international leaders in implementing levies on sugary drinks, as well as stronger labelling and restrictions on marketing to children.

Appendix VI: Leadership Statements
Leadership at SAHMRI
Leadership at SAHMRI is integral to its success. SAHMRI’s approach is to recruit national and international experts in their respective fields combined with nurturing the leaders of the future through active mentoring, fostering diversity, and empowerment. The leadership team of Professors Wesselingh, Makrides and Brown reflect national and international leaders in research excellence and translational science, maternal-infant nutrition and Aboriginal health. With more than 750 publications between them, the SAHMRI research leadership team exemplifies the collective impact of SAHMRI research on an international scale.
The broader leadership team of theme leaders, past and present, further exemplifies the calibre of the leadership group to contribute to world class research programs pursing excellence in medical science with a focus on translating the highest quality research into practical health improvements for the broader community. SAHMRI leadership also reflects extraordinary capability in developing the next generation of research leaders to tackle the biggest health challenges in society, today and in the future.
International business leader steers SAHMRI success
Raymond Spencer is a South Australian businessman who returned to Australia in 2009, following more than three decades of living and working in the USA, India and Europe. Highly experienced in directing international projects, Raymond Spencer has worked in eighteen countries and has advised corporations and not-for-profit groups on organisational, cultural, and leadership initiatives.
Raymond Spencer brings high calibre leadership experience in international business, management planning, technology, finance, organisational culture and mergers and acquisitions to his role as Chair of the SAHMRI Board. He holds numerous positions of chair on several boards, including the Global Centre for Modern Ageing and the South Australian Venture Capital Fund. He is a Founding Partner of RSVP Ventures and holds the position of Chair or Director in several of its portfolio companies. Raymond currently holds the position of Chair, Central Adelaide Local Health Network (CALHN) Governing Board.
SAHMRI Executive Director chairs Australia’s most prestigious Research Committee
Professor Steve Wesselingh (MBBS, PhD, FRACP, FAHMS) is a recognised leader amongst his peers, both nationally and internationally. He is the current Executive Director of the South Australian Health and Medical Research Institute (SAHMRI), recruited from Monash University (Victoria) in 2012 where he held the position of Dean, Faculty of Medicine, Nursing and Health Sciences (2007-2011). This is the largest Faculty at Monash, and the one that offers the most comprehensive suite of professional health training in Victoria, Australia, consistently ranking in the top 50 universities worldwide for clinical, pre-clinical and health sciences. Prof Wesselingh is a highly regarded infectious diseases physician with an international reputation in HIV-associated neurological disease, describing an important role for the innate immune system. He has considerable expertise in translational research, particularly infectious diseases and health services policy, with more than 250 publications and over 10,000 citations. He continually pushes the translational agenda and was instrumental in the establishment of Health Translation SA, one of the first four NHMRC-accredited Advanced Health Research and Translation Centres in Australia and the only state and system-wide partnership across all Universities, Local Health Networks and Primary Health Networks.
At a national level, Prof Wesselingh’s promotion of research excellence and innovation are recognised in his appointment by the Federal Minister of Health as Chair of the National Health and Medical Research Council’s (NHMRC) Research Committee, Australia’s foremost medical research funding body and former chair of the Australian Health Research Alliance (AHRA), an alliance of NHMRC-accredited research translation centres across Australia.
SAHMRI Deputy Director elected to prominent Academy of Science
Professor Maria Makrides (BNutrDiet, BSc, PhD, FAA, FAHMS) has received several prominent national and international awards and honours in recognition of her outstanding contributions to nutrition research. She is a Deputy Director at SAHMRI and recruited from the Women's & Children's Health Research Institute where she continues to hold a joint appointment. Prof Makrides is an international leader in maternal-infant nutrition, with a focus on optimising the cognition, growth and immune development of children. She is especially recognised for her rigorous nutritional intervention studies during the first 1000 days of life—between conception and a child’s second birthday. In 2019, she was one of eight women elected by her peers as a Fellow of the Australian Academy of Science, one of the highest categories of research award for Australian scientists. Prof Makrides has over 270 peer reviewed publications, 70% of which are cited more often than the average paper published across similar journals over the same period. Her work has made significant and direct contributions to changes in the composition of infant formulae, and on setting specific nutrient recommendations for pregnancy and lactation worldwide: outcomes from large-scale randomised controlled trials she has conducted to investigate the health effects of iodine nutrition for pregnancy resulted in the USA FDA making the monumental recommendation of not fortifying foods, or supplementing diets for pregnant women with iodine in the USA.
Internationally recognised, Prof Makrides is regularly invited to provide expert opinion and evidence to policy reviews and changing international food laws: in early 2020 as the only invited speaker from outside North America, she provided new evidence on nutrition during pregnancy and lactation to update the National Academies of Sciences, Engineering, and Medicine Nutrition During Pregnancy and Lactation policy documents, which are also influential globally.
SAHMRI Deputy Director recognised as a world leader in Indigenous health
Professor Alex Brown (MBBS, MPH, PhD, FCSANZ, FRACP (Hon)) is one of the leading Aboriginal clinician-researchers in Australia and recognised internationally for his research programs on chronic disease in vulnerable communities. He is a Deputy Director at SAHMRI and recruited from the Baker IDI Heart and Diabetes Institute’s Centre for Indigenous Vascular and Diabetes Research in Alice Springs (NT). Prof Brown leads the Wardliparingga Aboriginal Health Equity Theme at SAHMRI which is the nation’s leading research unit focused on reducing inequity in health and wellbeing among Australia’s First peoples, with a concomitant focus on developing the next generation of Indigenous research leaders. Soon after receiving his PhD, Alex was awarded the prestigious Viertel Senior Medical Research Fellowship and has since published more than 200 peer-reviewed publications. He has mentored more than 25 Aboriginal staff and students at Wardliparingga and established a state-wide Aboriginal Health Research Network of more than 30 Aboriginal researchers at different stages of their career.
Prof Brown is also well regarded for his significant input to national policy in Aboriginal health throughout his career. His advisory and advocacy contributions are highly sought, holding numerous positions on national committees including Ministerial Advisory Councils, the National Health and Medical Research Committee (NHMRC), the National Aboriginal Community
Controlled Health Organisation (NACCHO) and the Australian Institute of Health and Welfare (AIHW). More recently, Prof Brown’s contribution to setting the agenda in Aboriginal cardiovascular disease management and chronic disease policy more broadly were recognised with his appointment as co-chair of the 10 year, $160 million MRFF Indigenous Health Research Fund, the first national research fund led by Indigenous people and conducted with close engagement with Indigenous communities.
SAHMRI Theme leader at the forefront of global improvements in cancer survival
Professor Tim Hughes (MBBS, PhD, FRACP, FRCPA) is a clinician-scientist and haematologist, internationally recognised for his pioneering work in improving diagnosis and therapy for blood cancers (specifically chronic myeloid leukaemia, CML). He was recruited to SAHMRI in 2015 as the Precision Medicine Theme Leader and holds a joint appointment as Consultant Haematologist in the Division of Haematology, SA Pathology. Prof Hughes is an international expert in the biology and treatment of leukaemia. He led the establishment of the molecular response criteria that are used world-wide to measure response in CML and overseen many of the key global and national trials. His group has successfully developed predictive bioassays and molecular targets that influence the way CML patients are managed world-wide. He has published more than 250 papers that have been cited over 40,000 times. In 2017, he was awarded the prestigious GSK Award for Research Excellence in recognition of his outstanding achievement in medical research that has had a global impact on patients’ lives.
Prof Hughes has extensive experience in clinical trials research and precision medicine as recognised in his appointments as the Cancer Council Chair in Cancer Research, Chair of the International Chronic Myeloid Leukemia Foundation, and Fellow of the Australian Academy of Health and Medical Sciences (AAHMS). More recently, he was appointed to the National Blood Cancer Taskforce, convened by the Leukaemia Foundation with the support of the Federal Government, to develop Australia’s first National Strategic Action Plan for Blood Cancer.
SAHMRI leukaemia expert extends leadership to the broader research community
Professor Deborah White (PhD FFSc RCPA) is a highly awarded academic that provides strategic leadership to the broader research community through her numerous committee roles. Recruited to SAHMRI in 2013, Prof White is the Director of the Cancer Program at SAHMRI, and Deputy Precision Medicine Theme Leader with holds an affiliate appointment in the Discipline of Medicine and Discipline of Paediatrics at The University of Adelaide. Prof White is internationally recognised for her leadership of large multidisciplinary research teams that focus on Chronic Myeloid (CML) and Acute Lymphoblastic Leukaemia (ALL) and integrate cutting-edge technologies that aim to transform the treatment and outcomes for patients diagnosed with CML and ALL. Her research is recognised world-wide with memberships of the American, European and Australian Societies of Haematology, the Australian and New Zealand Children’s Haematology/Oncology Group (ANZCHOG) and the International (USA) Children’s Oncology Group (COG) and a member of the Editorial Board for Cancer Letters. Prof White has presented more than 170 papers at national and international scientific meetings and authored more than 100 scientific publications as well as being an inventor on several international patents. Her numerous awards include the Australian Society for Medical Research (ASMR) Leading Light award (2014), the University of Adelaide James McWha medal (2016) and in 2019 she was awarded a prestigious NHMRC Research Excellence Award.
Prof White generously offers her knowledge and experience to the wider research community through her roles as the National Flagship Lead for the ALL Stream of Australian Genomics, and SA scientific lead for Zero Children’s Cancer. She is an active member of the National Health & Medical Research Council (NHMRC) being a member of the NHMRC Academy, the Translational Research Program Advisory Committee, and the Women in Health Science (WiHS) Committee and plays an active role in Pharmaceutical Advisory Boards.
Infectious disease expert helps protect the most vulnerable from infection outbreaks
Professor Geraint Rogers (BSc Hons, PhD) was recruited from the Mater Medical Research Institute (Qld) by Prof Wesselingh to lead the Microbiome and Host Health Programme at SAHMRI with a joint appointment at Flinders University. Prof Rogers is a NHMRC Senior Research Fellow and a Matthew Flinders Research Fellow with more than 110 publications, of which he is first or senior author on more than 60 percent. He is an internationally recognised molecular microbiologist and microbial ecologist, specialising in respiratory disease and antimicrobial resistance (AMR), and is frequently invited to make addresses at international meetings. Since moving to SAHMRI, Prof Rogers has secured more than $20 million in competitive research funding. His growing research team has expanded the range of analytical strategies available for human microbiome research and now provides an integrated platform for collaborations across state, national and international research groups. His team is at the forefront of research into the application of precision medicine to infectious diseases and the translation of basic research into clinical improvements in a range of settings including aged care, hospital, regional and resource-limited settings: the pathogen genomics programme in his team demonstrated that respiratory infections in intensive care units (ICUs) were caused by a common source, namely mouthwash contaminated during manufacture.
Prof Rogers is nationally well-regarded as a leader in infectious diseases and regularly contributes to the investigation of national infection outbreaks, including in ICU patients diagnosed with COVID-19. Internationally, Prof Rogers (in collaboration with Hunter Medical Research Institute) was recognised as identifying the importance of precision medicine in the management of patients diagnosed with severe asthma (Lancet Respiratory Medicine 2016). Outcomes from these studies provided a significant advance in understanding the composition of the airway microbiome in severe asthma, that led to the application of a novel antibiotic therapy (Lancet 2017). These findings informed the development of international clinical guidelines (Global Initiative for Asthma, 2019) and are essential to guide future clinical management of patients with severe asthma.
National leader in tobacco control leads SAHMRI Health Policy Centre
Professor Caroline Miller (BA (Hons), BEc, MPH, PhD) is nationally and internationally recognised in tobacco control. She was recruited from Cancer Council SA in 2012 to lead the SAHMRI Health Policy Centre, a public health research group that applies the science and experience from tobacco control to dietary risk (obesity prevention) and alcohol consumption. Prof Miller has worked for 20 years at the interface of research and policy in population health, being actively involved in the translation of research into policy through direct engagement with policy makers and non-government advocates. Her research has directly contributed to evidence-based policy change, most notably tobacco but also food and alcohol policy, both locally and at a national level. Prof Miller has previously chaired Cancer Council Australia and the National Heart Foundation’s joint Tobacco Issues Committee and was the past Deputy Chair of Cancer Council Australia’s Nutrition, Physical Activity (and Alcohol) Committee. Prof Miller is a highly awarded research fellow with a Beacon Fellowship, NHMRC Career Development Fellowship, Heart Foundation Future Leader Fellow and
Beat Cancer Project Principal Research Fellow with more than 80 publications and secured more than $13 million from both government and non-government sources since being at SAHMRI.
Under Prof Miller’s leadership, the Centre delivers evidence to inform state and national public health policy and population-based public health and health promotion interventions to reduce the preventable burden of non-communicable disease. More recently, Prof Miller’s capacity to effectively translate research in health policy is evident with her involvement with the SA Commission on Excellence and Innovation in Health to rapidly deliver and present the best available evidence to the South Australian COVID-19 Taskforce to inform its response.
Esteemed molecular biologist facilitates international relations
Professor Christopher Proud (BSc, PhD) has recently announced his retirement from his position as Director of the Hopwood Centre for Neurobiology, and co-Director of the Lifelong Health Theme at SAHMRI. Recruited to SAHMRI in 2014 following a move from UK, Prof Proud has had a distinguished scientific career, holding senior university positions in UK and Canada and >25 years’ of highly productive track record. He holds visiting professorships in China and the UK and is also a Professor in Biological Sciences at the University of Adelaide. Prof Proud has an international reputation in the molecular mechanisms by which nutrients and hormones regulate mammalian cell function, especially protein metabolism, and their roles in health and disease. His research includes studies on the roles of controlling protein synthesis in cancer cell metabolism, neurological disease, and cardiovascular disorders and the molecular mechanisms involved in insulin resistance and type 2 diabetes. He is widely published with more than 350 publications and member of three Editorial Boards. In the last five years, he has presented more than 50 papers in more than 10 countries and since 2011, has organised five international conferences.
Despite his retirement from his leadership role at SAHMRI, Prof Proud continues his supervisory role of the next generation of researchers. Throughout his academic career, Professor Proud has actively supervised and mentored a large cohort of future researchers with more than 80 HDR students and postdoctoral research fellows, including some of the future SAHMRI leaders such as Professor Stuart Brierley and Dr Tim Sargent. His vast array of academic collaborations in the UK, Europe, Norway, Israel, Canada, the USA, Australia, Japan and China, industry collaborations including GSK, AstraZeneca, and Janssen; and interactions with commercial or academic drug discovery programmes in China, Australia and Singapore, also paves the way for his research team and students to embark on future national and international collaborations in translational science.
SAHMRI Theme leader at forefront of data sharing principles to accelerate cardiac research
Professor Derek Chew (MBBS, MPH, FRACP, FACC) is a clinical and interventional cardiologist and eminent clinical trialist and outcomes researcher in cardiovascular medicine. A highly awarded clinician-researcher, Prof Chew was recruited to SAHMRI in 2019 to co-lead the Lifelong Health Theme, holding joint appointments as the Roy and Marjory Edwards Heart Foundation Senior Principal Research Fellow in Cardiovascular Outcomes Research at Flinders University, the Regional Head of Cardiology for the Adelaide Health Service (Southern Region), Head of the Flinders Clinical Trial Centre, and Chair of the State-wide Cardiology Clinical Network. He has an honorary appointment at the George Institute for Global Health and maintains strong international links with the Duke Clinical Research Institute and Cleveland Clinic C5 (US). His clinical and research career is centred on the translation of current and future therapies and technologies in cardiology to improve patient outcomes in a clinically effective manner, enabled through his extensive network of academic, clinical and health policy collaborators. Prof Chew’s reputation is
recognised nationally with his roles as chair of the Cardiovascular Disease Expert Advisory Group, the primary cardiovascular disease monitoring body of the Australian Institute of Health and Welfare (AIHW); and he provides expert advice to the Australian Commission for Quality and Safety in Health Care (ACQSHC). He has served as the national co-ordinator on several international multi-centre clinical trials and also chairs the Quality Standards Committee of the Cardiac Society of Australia and New Zealand, and the Clinical Committee of the Heart Foundation. He has authored over 280 manuscripts and book chapters.
Prof Chew has numerous leadership roles that enable the translation of evidence into real improvements in care and outcomes for the Australian community, and influence practice internationally. Through collaborations with the Adelaide Institute for Machine Learning (AIML), the Digital Health Centre for Research Excellence (University of Sydney) the Cardiac Outcomes Centre for Research Excellence (Monash University), the AIHW and ACQHSC combined with his roles as chair of the National Acute Coronary Syndromes Data Definitions and the Acute Coronary Syndrome Electronic Decision Support working groups, Prof Chew has driven the national standard for health data definitions in Australia and the development of data sharing principles for the electronic data collection methods to facilitate national collaboration and accelerate cardiovascular outcomes research.
EMBL group leader applies advanced computational systems to preclinical research
Professor David Lynn (BA, MSc, PhD) is an European Molecular Biology Laboratory (EMBL) Australia Group Leader and Director of the Computational and Systems Biology Program at SAHMRI. He also holds a full academic faculty position as Professor at the Flinders University School of Medicine. Prof Lynn has an international track record, having worked in Canada and Ireland before moving to Australia in 2014. He has been an invited speaker at conferences across six continents and has also served on the organising committees for both national and international conferences. Prof Lynn’s multidisciplinary team at SAHMRI is equally divided between computational and experimental systems researchers to investigate the immune system. Using these advanced preclinical models enables his research to be translated into clinical trials more quickly. Prof Lynn also lead the systems biology aspects of the recently established ACRF funded ($2.5 million) Centre for Integrated Cancer Systems Biology at SAHMRI, and is one of the lead PIs on PRIMES, a €12 million EU-funded international colorectal cancer project. He has more than 70 publications with many in the leading systems and experimental biology journals, with more than 5300 citations.
Since 2014, Prof Lynn was awarded the highly prestigious position of an EMBL Australia Group Leader, with only 15 awarded in Australia. EMBL is Europe’s flagship life sciences institution: EMBL Australia’s flagship program is its network of research groups embedded in existing research institutes and universities across the country, of which SAHMRI is one under Prof Lynn’s leadership. The EMBL award supports ambitious research projects and provides access to infrastructure and training and offers up to nine years of secure funding to outstanding early and mid-career Australian scientists.
Tall Poppy now leading world-renowned SAHMRI Hopwood Centre
Professor Stuart Brierley (BSc (Hons), PhD) is an international authority on visceral pain and the mechanisms underlying the debilitating conditions such as irritable bowel syndrome (IBS), bladder pain syndrome (BPS) and endometriosis. He leads the Visceral Pain Research Group, a unit within the College of Medicine and Public Health at Flinders University co-located within the SAHMRI
Hopwood Centre for Neurobiology, which he now leads following Prof Proud’s recent retirement. Prof Brierley is a foremost research fellow being highly awarded with a NHMRC Research Excellence Award (2016) and a Matthew Flinders Fellow in Gastrointestinal Neuroscience (2016). His outstanding career is recognised amongst his peers as a South Australian Tall Poppy recipient (2011), a NHMRC R.D Wright Biomedical Fellow (2017), President-Elect of the Australasian Neurogastroenterology and Motility Association (ANGMA), and co-chair of the Federation of Neurogastroenterology and Motility (FNM) 2020 meeting.
Prof Brierly maintains significant collaborations with academic and industry partners, with a distinguished track record in coordinating multi-faceted research programs that result in highly cited publications in top tier journals, such as Nature and Cell. His recent collaborations with industry partners identified the mechanism of pain relief of a new drug, linaclotide, in treating patients with Irritable Bowel Syndrome with Constipation (IBS-C). Linaclotide, a guanylate cyclase-C (GC-C) agonist is effective in relieving abdominal pain associated with IBS-C and is already available and registered for use by IBS-C patients in the USA and Europe.
Past leaders that shaped the SAHMRI vision
Bringing research royalty returns to South Australia
Emeritus Professor John Hopwood (AM FAA), an international leader in the field of lysosomal biology, established the former Lysosomal Diseases Research Unit (LDRU) (now known as the Hopwood Centre for Neurobiology) at SAHMRI, a large multidisciplinary group researching lysosomal storage disorders (rare inherited metabolic diseases) nationally and internationally. Under Professor Hopwood's stewardship, the LDRU became world-renowned for its research capabilities in this area and the translation of research findings into state-of-the-art diagnostic services and therapeutics. The LDRU has remained at the international forefront of research into the diagnosis, treatment and biology of lysosomal diseases. Professor Hopwood has mentored 23 PhD students and 35 Post-Doctoral scientists; has over 400 peer-reviewed scientific publications, over 30 international patents and more than $35 million in competitive research funding. Professor Hopwood continues his association with SAHMRI as a member of the Board.
The LDRU has generated several world firsts, particularly the isolation of the genes involved in some of these disorders and the development of first-ever FDA- approved treatments for two disorders, which in 2005 and 2006 were marketed world-wide. These outcomes have led to improved quality of life for patients and multi-million dollar royalty returns to South Australia. This represents one of the largest public sector commercialisation outcomes in South Australia and possibly Australia.
Visionary veterinarian leaves a legacy in preclinical research
Dr Tim Kuchel AM (1951-2019), a highly regarded academic veterinarian with more than 30 years’ experience, foresaw the need for large animal work and its translation into important clinical diagnostics and treatment regimens to establish a world class imaging and research facility at SAHMRI. As Director of the Preclinical Imaging and Research Laboratories (PIRL), Dr Kuchel advanced national and international collaborations with researchers, clinicians and pharmaceutical companies to facilitate all stages of preclinical research from proof-of-concept and efficacy to clinical translation and meeting regulatory requirements for safety/toxicity. The integral role that the Large Animal Research Imaging Facility within PIRL has with the Australian research community is recognised with it becoming a node within the National Imaging Facility (NIF) network, that also enabled significant investment from the National Collaborative Research Infrastructure Strategy (NCRIS).
Dr Kuchel creatively opened the PIRL facility to workshops providing surgeons the opportunity to trial new procedures and test new equipment: surgical training has now become a core activity at PIRL with more than 40 workshops conducted. He was a highly valued member on several institutional animal ethics and welfare committees and in 2015 he was recognised in the Queen’s Birthday Honours list for significant services to veterinary science, advocated for the humane treatment and welfare of animals in medical research.
Agent of change in cardiovascular prevention
Professor Stephen Nicholls (MBBS, PhD, FRACP, FACC, FESC, FAHA, FCSANZ, FAHMS) made significant contributions to cardiovascular prevention and leadership roles over the six years at SAHMRI (2012-2018). Returning to Adelaide from the prestigious Cleveland Clinic (US), Prof Nicholls was appointed as Deputy Director and Hearth Health Theme Leader at SAHMRI, with conjoint roles as Professor of Cardiology at The University of Adelaide and consultant cardiologist with the Central Adelaide Local Health Network. A clinician-researcher, his work spans the translational spectrum from ‘bench to bedside’, with a focus on understanding the factors that promote plaque formation, novel vascular imaging and leadership of large-scale clinical trials of new therapies designed to reduce the risk of heart disease. He has extensive academic and industry collaborations, having raised more than $100 million in research funding with over 400 peer-reviewed publications cited more than 20,000 times. He was appointed as an inaugural Fellow of the Australian Academy of Health and Medical Sciences, a member of numerous national and global industry advisory boards and assumed various leadership positions including past-president of the Australian Atherosclerosis Society and Treasurer of the Cardiac Society of Australia and New Zealand.
Prof Nicholls is globally regarded as one of the leading lights in the field of cardiovascular prevention, making seminal contributions in dyslipidemia, plaque imaging and cardiovascular clinical trials. His work has directly influenced patient care and is rapidly integrated into treatment guidelines for cardiovascular prevention and widely cited in the field and the popular media. Prof Nicholls has supervised and mentored 50 young scientists with trainees progressing to roles in academia, clinical practice and industry. Following his leadership success at SAHMRI, in 2018 he was appointed to the position of Director of MonashHeart, Monash Health, the largest public health service in Melbourne, Victoria.
Future Leaders
ROSA Director wins award for using big data to help the Aged Care sector
Associate Professor Maria Inacio (MS, PhD) was recruited to SAHMRI in 2017 by Prof Wesselingh to lead the newly established Registry of Senior Australians (ROSA), the unique SA-based Clinical Quality Registry developed to support the monitoring and evaluation of the quality of ageing and aged care services provided to older Australians. A mid-career researcher originally from USA, A/Prof Inacio has an international reputation in registry science and utilisation of existing data and informatics to enhance clinical systems being the former lead epidemiologist at the world-renowned Kaiser Permanente Implant Registries (USA). Moving to Australia, A/Prof Inacio established new relationships with national leaders in registry and health services research including becoming a Specialist Advisor for the Australian Government Therapeutic Goods Administration Advisory Committees on medical device surveillance. Under A/Prof Inacio’s leadership within three years at SAHMRI, the ROSA team has grown to 11 staff, secured more than $5.5 million collaborative funding and received numerous awards including being recognised as the best application of business intelligence to leverage value from Big Data at the Information Technology in Aged Care (ITAC) 2020 Conference.
A/Prof Inacio is recognised nationally as an emerging leader and works closely with the Royal Commission into Aged Care Quality and Safety: ROSA is recognized as being the only registry of its kind in Australia to monitor the health, service utilization, medication use, mortality and other outcomes of Australians receiving aged care services with outcomes regularly being incorporated into Commission recommendations (e.g. chemical-induced restraint in aged care facilities).
Longstanding contributor to evidence-based health care for early childbirth
Associate Professor Philippa Middleton (BScHons, GradDipLibSt, MPH, PhD) was recruited to SAHMRI by Prof Makrides and now co-leads the Pregnancy and Perinatal Care Pillar of SAHMRI Women and Kids, being internationally recognised for her work in evidence-based maternal and child health care. Since completing her PhD in 2015 (University of Adelaide), she has secured over $12 million from competitive funding sources, including two NHMRC Centres of Research Excellence. A/Prof Middleton holds leadership roles in the NHMRC Stillbirth Centre of Research Excellence and Cochrane Pregnancy and Childbirth with an extensive network of national and international collaborators addressing stillbirth and preterm birth prevention. She is a founding member of the Australian Preterm Birth Prevention Alliance that aims to implement prevention strategies for preterm births, recently leading the design of the smoking cessation component of a national stillbirth education program for midwives and obstetricians (the Stillbirth Safer Baby Bundle) for Aboriginal families.
Appointed to the NHMRC Synthesis and Translation of Research Evidence, A/Prof Middleton is integrally involved in the formulation of international research reporting standards and standards for NHMRC guidelines. As a member of the NHMRC Pregnancy Care Guidelines Expert Advisory Committee, she has facilitated the development of six NHMRC-endorsed clinical guidelines. With more than 200 peer-reviewed publications, her research has contributed to over 100 policy documents, including WHO guidelines and evidence maps, The National Institute for Health and Care Excellence (NICE, UK), UK Parliament, American College of Obstetrics and Gynaecology, and the Society of Obstetrics and Gynaecology Canada. Her research has widespread and immediate benefit for the community: she led the landmark Cochrane systematic review that highlighted that

an increased intake of omega-3 long-chain fatty acids during pregnancy reduced the risk of premature birth and having a direct impact on national and international maternity policy.
Returning clinical haematologist at the forefront of a new era in cancer therapy
Associate Professor Dan Thomas (BMedSc (Hons), MBBS, PhD) was recruited back to Adelaide by Professor Tim Hughes to provide exciting and emerging expertise in molecularly targeted therapy in myeloid leukaemia. Moving back to Australia after six years of a unique training and mentoring experience while working as a haematology research fellow at Stanford School of Medicine (US), A/Prof Thomas brings a novel skill set to the SAHMRI Precision Medicine Theme. A/Prof Thomas is a clinical haematologist and pathologist with more than 45 peer-reviewed publications (more than three quarters in high impact journals), 14 awards and more than $5 million in competitive grant funding, including a prestigious five-year CSL Centenary Fellowship grant to help build his translational cancer research team.
A/Prof Thomas is an emerging leader with ambition to foster the successful careers and research impact of junior team members. With his novel skill set established while overseas, together with his extensive trial experience and global collaborations, he is in a strong position to make innovative advances in the discovery and development of new drugs for the treatment of blood cancers using a variety of cutting-edge technologies.
High achieving cardiologist spanning bench to bedside research
A/Prof Peter Psaltis (MBBS, PhD, FRACP, FCSANZ), a highly awarded academic cardiologist and vascular biologist, was recruited to SAHMRI from Monash University (Victoria). A/Prof Psaltis is the deputy leader of the Heart and Vascular Program and co-director of the Vascular Research Centre. Ranking outright first in each of six years of medical school and recipient of 25 academic awards and prizes, he brings a unique skill set to his vascular research program with internationally recognised expertise in non-invasive and invasive imaging techniques. His team of more than 15 students and staff are similarly high achieving with six awards for research excellence in the past three years. An early-to mid-career researcher, A/Prof Psaltis has more than 120 peer-reviewed publications, half of which as first or senior author. He is recognised nationally and internationally as an emerging leader in his field with regular speaking invitations to professional meetings.
A/Prof Psaltis contributed to the significant paradigm shift in the demonstration that stem cells are present in the wall of adult blood vessels (previously considered to only comprise differentiated cell types) with follow up studies exploring the contribution of these unique cells in normal vascular health and disease in both mice models and human tissue. A/Prof Psaltis’ unique expertise that spans all three disciplines of basic, translational and clinical research, enables him to directly apply findings from preclinical studies to clinical trial settings, as demonstrated with funding received to study cell therapy in cancer patients receiving anthracycline therapy who are at increased risk of developing cardiomyopathy.
Emerging Leaders
Young Dutch cardiologist leading the way in the application of AI in medical research
Associate Professor Johan Verjans (MD, PhD), a physician-researcher originally from the Netherlands, was recruited by Professor Stephen Nicholls to join the SAHMRI Heart Health Theme. Moving to Adelaide in 2018, A/Prof Verjans was also appointed as Deputy Director, Medical Machine Learning at the Australian Institute for Machine Learning (AIML), Australia’s first institute dedicated to research in machine learning. His role with AIML includes enhancing collaborations to connect the world-class machine learning capabilities of the AIML to the medical and research communities across the Biomedical Precinct in Adelaide: using complex data to develop solutions to help healthcare professionals and improve patient outcomes. A/Prof Verjans has contributed to the development of guidelines for the rapid uptake of AI in medical research and health care including being invited to the American College of Cardiologists Working group for the Consensus statement on use of AI, co-authored PRIME guidelines for Standardised use of Machine Learning in Cardiac Imaging, edited a Special Issue on Machine Learning (Netherlands Heart Journal) and co-authored the Cardiology chapter for Springer Nature’s first book on Artificial Intelligence in Medical Imaging.
He has received several young investigator awards and recently was awarded the Ahrens Researcher Award by the Australian Heart Foundation. Holding combined clinical and research appointments, A/Prof Verjans’ research program focuses on imaging biomarkers from large datasets using supervised and unsupervised machine learning strategies. Since moving to Australia, he has facilitated numerous collaborations across Australia to integrate machine learning capabilities into medical research, including as associate investigator with the ARC Centre of Excellence for Nanoscale BioPhotonics, and to image analysis in cardiovascular problems and neurological diseases, such as transient ischaemic attack, stroke and vascular dementia research being undertaken at SAHMRI.
SAHMRI neurobiologist’s trailblazing 'brain in a dish' to revolutionise brain research
Dr Cedric Bardy (PhD) was recruited back to Australia in 2016 from the Salk Institute (California, US) by Professor Julio Licinio to lead the Laboratory for Neurophysiology and Genetics (Lifelong Health Theme) at SAHMRI. Dr Bardy is a mid-career researcher and holds a conjoint appointment at Flinders University. Since returning to Australia, he’s published more than 20 peer-reviewed publications in high-impact journals. He is a neurobiologist with unique and in-depth expertise in human neural stem cell models, electrophysiology and single cell genetics to better understand the effect of neurological disorders on brain cells. His laboratory of ten staff and students is at the forefront of human cellular neuroscience research and translational applications that advance the understanding of human neuronal physiology in health and disease.
Dr Bardy develops and applies innovative stem cell biotechnologies to discover new treatments for brain disorders. His expertise in the stem cell field is highly sought after with scientific consultations for biotech companies and numerous collaborations across Australia and overseas. He developed a new culture medium, BrainPhys, that supports the fundamental electrophysiological functions of human neurons in vitro. BrainPhys represents a technical paradigm shift, which identified and remedied serious limitations in media that was being used by the research community for decades without improvement. BrainPhys is now commercialised and distributed internationally to the scientific community, used in more than 1000 laboratories world-wide.
SAHMRI cell biologist unlocks clues for translational research
Dr Timothy Sargeant (PhD) was recruited to SAHMRI from University of Cambridge (UK) by Prof John Hopwood, Director of the then Lysosomal Diseases Research Unit to lead the Lysosomal Health in Ageing program. Under the mentorship of Prof Hopwood, Dr Sargeant has established his own research program to investigate lysosome-mediated cell death and neurodegeneration and the role of the lysosome in age-related disease. With a unique skill set in the creation and analysis of complex cell and animal models of lysosomal dysfunction, Dr Sargeant has developed novel testing regimens to measure the biological recycling machinery in human tissue (autophagic flux) that has direct application in clinical trials. Such testing provides novel insights into cell-death and the role in age-related disease across a range of human tissue (including brain and heart).
As a discovery scientist, Dr Sargeant provides the ‘benchside’ scientific expertise to multidisciplinary translational research programs that are currently exploring the role of lysosomal biology and autophagy in atherosclerosis. He works synergistically with clinician-researchers to better understand the potential cardiovascular benefits of colchicine (an anti-inflammatory therapy) and the mechanistic basis of its anti-atherosclerotic and plaque-stabilising properties with conjoint awards, publications and supervisory roles. These vital multidisciplinary collaborations provide novel insights into the use of repurposed therapies for cardiovascular disease.
Next generation of Indigenous research leaders
The Wardliparingga Aboriginal Health Equity Theme of SAHMRI is regarded as the nation’s leading Aboriginal Health research unit, not only with respect to the high-quality research outputs, but also one that actively facilitates and mentors the next generation of Indigenous research leaders. With half of the Theme’s more than 50 academic, professional and clinical staff from Aboriginal and/or Torres Strait Islander backgrounds, the Theme is recognised as being at the forefront of strengthening the capacity of Aboriginal and Torres Strait Islanders engaged in or leading research in Australia.
Extraordinary research trajectory of Rising Star Indigenous researcher
Professor James Ward (PhD) is a Pitjantjatjara and Narungga man, and a national leader in Aboriginal and Torres Strait Islander research. He has recently been appointed as the Director of the Poche Centre for Indigenous Health and Professor within the School of Public Health at the University of Queensland following his recruitment to SAHMRI by Prof Wesselingh (Executive Director) in 2014 as the Head of the Infection Diseases Research Program, Aboriginal Health. Prior to joining SAHMRI, Prof Ward had a long history of working in Aboriginal communities, beginning as a men’s health educator for 29 remote communities in central Australia and held various roles in Aboriginal public health policy for both government and non-government organisations. In 2007, Prof Ward made a key career change into research being appointed as the Inaugural Program Head of the Aboriginal Program at the Kirby Institute, University of New South Wales, and then Deputy Director of the Baker Institutes’ Aboriginal Health Program (Alice Springs) in 2012. In 2016, Prof Ward completed his PhD focused on epidemiology of sexually transmissible infections in Aboriginal communities and in 2017 he was recognised by the NHMRC with the Rising Star Research Excellence Award for the top-ranked application by an Indigenous researcher in the Early Career Fellowship scheme.
In his relatively short research-dedicated career, Prof Ward has established himself as one of Australia’s leading researchers in the area of Aboriginal Health and translational research. He has been awarded funding totalling $23 million; including $7.14 million as CIA on NHMRC funded
grants and has authored 100 publications and led national research projects in sexually transmissible infections and blood borne viruses, including issues surrounding injecting drug use. His work over the last five years has influenced policy and practice through contributions to national guidelines, and regularly advice to the Federal Government. He has been instrumental in initiating and advocating for action to address an ongoing syphilis outbreak that affects predominantly young people living in remote communities which has resulted in $8.8 million government funding being allocated to address the outbreak and the establishment of the Commonwealth Government Syphilis Taskforce. His numerous collaborations fostered over many years with the Aboriginal Community Controlled Health Sector, Government and the non-Government sector, enabled active engagement of the broader SAHMRI community with Aboriginal and Torres Strait Islander communities and ensures research relevance and research translation opportunities continue to be maximised despite his recent departure.
Recognized as the ‘beating heart’ of SAHMRI Aboriginal Health Equity
Kim Morey (MPH) is recognised as the ‘beating heart’ of the Wardliparingga Aboriginal Health Equity Theme at SAHMRI with extensive policy experience working within the Aboriginal Health and Housing portfolios in the South Australian Public Sector. Kim Morey is of Anmatyerre/Eastern Arrente descent and has an excellent knowledge of the health and wellbeing issues facing Aboriginal peoples both from a South Australian perspective and at a National level. As manager for Knowledge Transition and Exchange, she brings the policy perspective to research being undertaken in the Theme drawing on her sound understanding and experience in Senior Government positions of how research and evidence links within the policy frameworks across Aboriginal health. Kim Morey has been a delegate of the National Congress of Australia’s First People and continues to volunteer on local Aboriginal Community based Boards of Management. In 2019, she was awarded the highly sought SAHMRI Executive Director’s award that recognises leadership and integrity among the SAHMRI community.
Kim Morey currently leads the South Australian (SA) Aboriginal Chronic Disease Consortium (SA ACDC) to operationalise the implementation of the three SA health care plans across Diabetes, Heart and Stroke and Cancer themes. Through her leadership, she supports the collaborative, jurisdictional partnership formed to govern the Consortium, and ensures that Aboriginal Health research is contributing to making a difference at policy and practice level in South Australia.
Young Torres Strait Islander woman transforming SA Aboriginal Health Plans
Dr Odette Pearson (GradCert (ResMethods), GradCert (HealthEc), BAppHSci (IPHC), PhD) is a Kuku Yalanji/Torres Strait Islander woman and a mid-career researcher who is transforming South Australian Aboriginal Health Plans. A Senior Research Fellow, Dr Pearson leads the Health Equity Population Health Platform within the Wardliparingga Aboriginal Health Equity Theme at SAHMRI. Her research draws on a unique and comprehensive skillset relevant to existing and emerging complexities of Aboriginal and Torres Strait Islander health and well-being. Specifically, Dr Pearson seeks to understand how institutional policies and practices drive health and social inequities experienced by Indigenous populations. Her novel approach is the use of community-level quantitative data to show and explore the reasons for variations in disadvantage both within the Aboriginal community and between the Aboriginal and non-Aboriginal community.
In her role with Wardliparingga Aboriginal Health Equity Theme, Dr Pearson coordinated the development of the South Australian Aboriginal Diabetes Strategy, which is regarded as the most inclusive and integrated Diabetes strategy for Aboriginal communities in Australia. Her
epidemiological research expertise combined with strong community and cross sector engagement is further recognised with her appointment as the senior researcher on the Australian Commission on Safety and Quality in Healthcare implementation guide for the first ever Aboriginal and Torres Strait Islander actions (National Safety and Quality Health Service Standards user guide for Aboriginal and Torres Strait Islander Health, 2017). She is regularly invited to advise on consultation processes with the Aboriginal and Torres Strait Islander community nationally and has contributed to clinical guideline working groups for the clinical care of Aboriginal and Torres Strait Islander people with chronic disease.
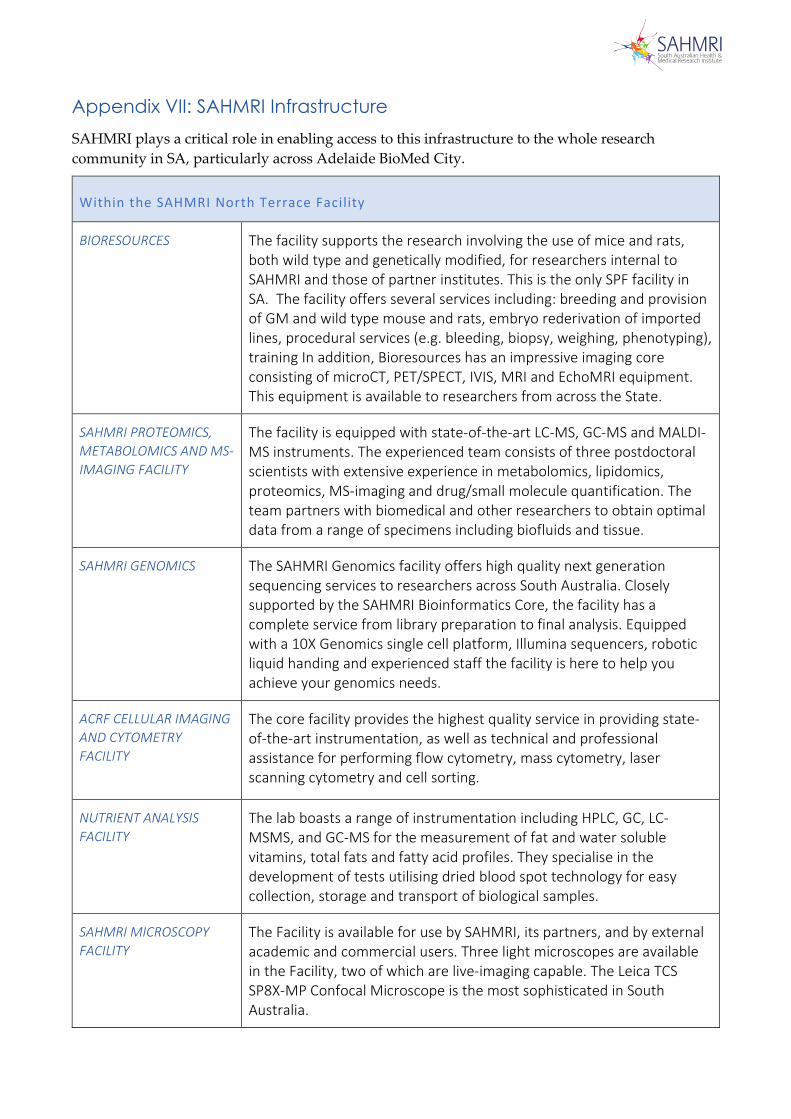
Appendix VII: SAHMRI Infrastructure SAHMRI plays a critical role in enabling access to this infrastructure to the whole research community in SA, particularly across Adelaide BioMed City.
Within the SAHMRI North Terrace Facility
BIORESOURCES The facility supports the research involving the use of mice and rats, both wild type and genetically modified, for researchers internal to SAHMRI and those of partner institutes. This is the only SPF facility in SA. The facility offers several services including: breeding and provision of GM and wild type mouse and rats, embryo rederivation of imported lines, procedural services (e.g. bleeding, biopsy, weighing, phenotyping), training In addition, Bioresources has an impressive imaging core consisting of microCT, PET/SPECT, IVIS, MRI and EchoMRI equipment. This equipment is available to researchers from across the State.
SAHMRI PROTEOMICS, METABOLOMICS AND MS-IMAGING FACILITY
The facility is equipped with state-of-the-art LC-MS, GC-MS and MALDI-MS instruments. The experienced team consists of three postdoctoral scientists with extensive experience in metabolomics, lipidomics, proteomics, MS-imaging and drug/small molecule quantification. The team partners with biomedical and other researchers to obtain optimal data from a range of specimens including biofluids and tissue.
SAHMRI GENOMICS The SAHMRI Genomics facility offers high quality next generation sequencing services to researchers across South Australia. Closely supported by the SAHMRI Bioinformatics Core, the facility has a complete service from library preparation to final analysis. Equipped with a 10X Genomics single cell platform, Illumina sequencers, robotic liquid handing and experienced staff the facility is here to help you achieve your genomics needs.
ACRF CELLULAR IMAGING AND CYTOMETRY FACILITY
The core facility provides the highest quality service in providing state-of-the-art instrumentation, as well as technical and professional assistance for performing flow cytometry, mass cytometry, laser scanning cytometry and cell sorting.
NUTRIENT ANALYSIS FACILITY
The lab boasts a range of instrumentation including HPLC, GC, LC-MSMS, and GC-MS for the measurement of fat and water soluble vitamins, total fats and fatty acid profiles. They specialise in the development of tests utilising dried blood spot technology for easy collection, storage and transport of biological samples.
SAHMRI MICROSCOPY FACILITY
The Facility is available for use by SAHMRI, its partners, and by external academic and commercial users. Three light microscopes are available in the Facility, two of which are live-imaging capable. The Leica TCS SP8X-MP Confocal Microscope is the most sophisticated in South Australia.
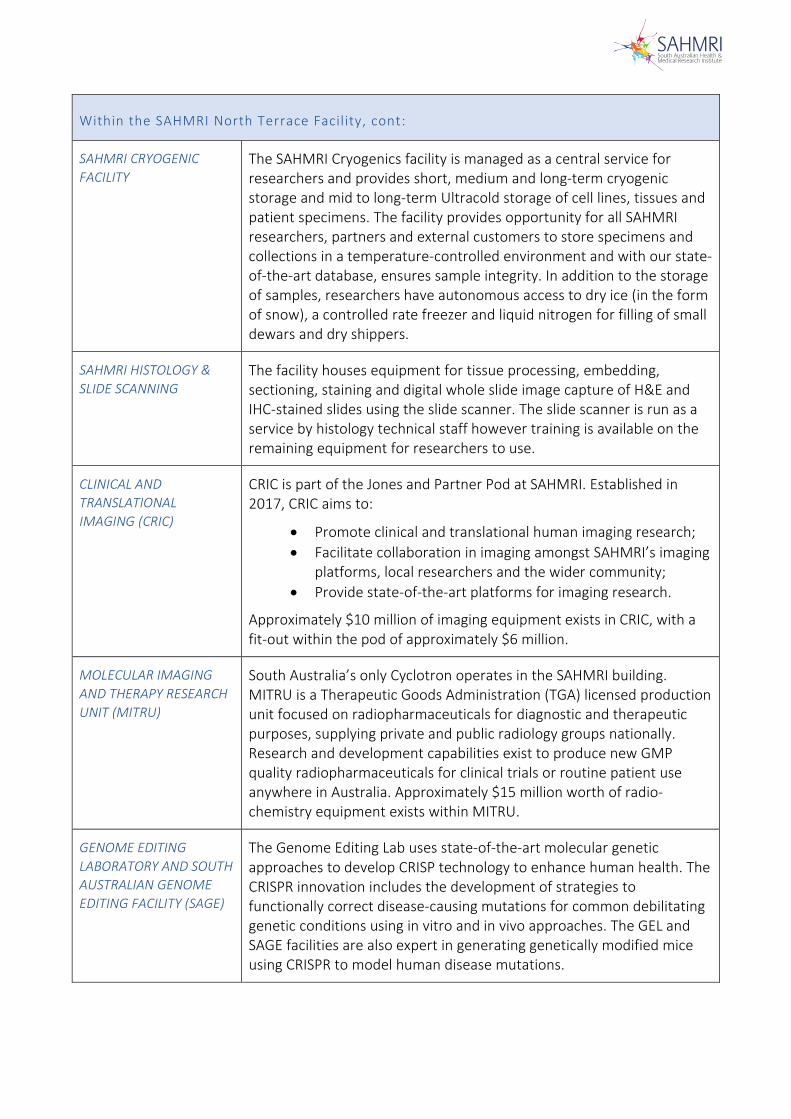
Within the SAHMRI North Terrace Facility, cont:
SAHMRI CRYOGENIC FACILITY
The SAHMRI Cryogenics facility is managed as a central service for researchers and provides short, medium and long-term cryogenic storage and mid to long-term Ultracold storage of cell lines, tissues and patient specimens. The facility provides opportunity for all SAHMRI researchers, partners and external customers to store specimens and collections in a temperature-controlled environment and with our state-of-the-art database, ensures sample integrity. In addition to the storage of samples, researchers have autonomous access to dry ice (in the form of snow), a controlled rate freezer and liquid nitrogen for filling of small dewars and dry shippers.
SAHMRI HISTOLOGY & SLIDE SCANNING
The facility houses equipment for tissue processing, embedding, sectioning, staining and digital whole slide image capture of H&E and IHC-stained slides using the slide scanner. The slide scanner is run as a service by histology technical staff however training is available on the remaining equipment for researchers to use.
CLINICAL AND TRANSLATIONAL IMAGING (CRIC)
CRIC is part of the Jones and Partner Pod at SAHMRI. Established in 2017, CRIC aims to:
• Promote clinical and translational human imaging research;• Facilitate collaboration in imaging amongst SAHMRI’s imaging
platforms, local researchers and the wider community;• Provide state-of-the-art platforms for imaging research.
Approximately $10 million of imaging equipment exists in CRIC, with a fit-out within the pod of approximately $6 million.
MOLECULAR IMAGING AND THERAPY RESEARCH UNIT (MITRU)
South Australia’s only Cyclotron operates in the SAHMRI building. MITRU is a Therapeutic Goods Administration (TGA) licensed production unit focused on radiopharmaceuticals for diagnostic and therapeutic purposes, supplying private and public radiology groups nationally. Research and development capabilities exist to produce new GMP quality radiopharmaceuticals for clinical trials or routine patient use anywhere in Australia. Approximately $15 million worth of radio-chemistry equipment exists within MITRU.
GENOME EDITING LABORATORY AND SOUTH AUSTRALIAN GENOME EDITING FACILITY (SAGE)
The Genome Editing Lab uses state-of-the-art molecular genetic approaches to develop CRISP technology to enhance human health. The CRISPR innovation includes the development of strategies to functionally correct disease-causing mutations for common debilitating genetic conditions using in vitro and in vivo approaches. The GEL and SAGE facilities are also expert in generating genetically modified mice using CRISPR to model human disease mutations.
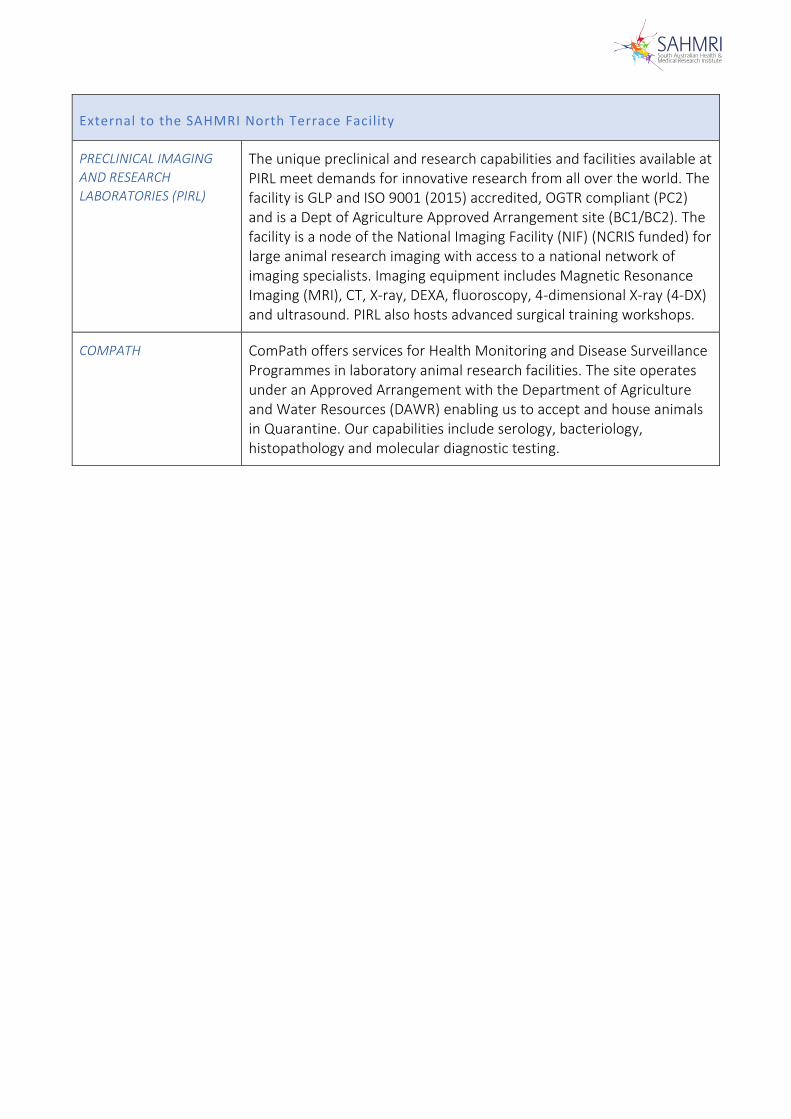
External to the SAHMRI North Terrace Facility
PRECLINICAL IMAGING AND RESEARCH LABORATORIES (PIRL)
The unique preclinical and research capabilities and facilities available at PIRL meet demands for innovative research from all over the world. The facility is GLP and ISO 9001 (2015) accredited, OGTR compliant (PC2) and is a Dept of Agriculture Approved Arrangement site (BC1/BC2). The facility is a node of the National Imaging Facility (NIF) (NCRIS funded) for large animal research imaging with access to a national network of imaging specialists. Imaging equipment includes Magnetic Resonance Imaging (MRI), CT, X-ray, DEXA, fluoroscopy, 4-dimensional X-ray (4-DX) and ultrasound. PIRL also hosts advanced surgical training workshops.
COMPATH
ComPath offers services for Health Monitoring and Disease Surveillance Programmes in laboratory animal research facilities. The site operates under an Approved Arrangement with the Department of Agriculture and Water Resources (DAWR) enabling us to accept and house animals in Quarantine. Our capabilities include serology, bacteriology, histopathology and molecular diagnostic testing.
Appendix VIII: University Rent Subsidies
Summary of:
1.) Cost per sqm over the 10-year period based on fit out contributions from the Partners, as well as cost per sqm per year
2.) Outgoings from each Partner
3.) Infrastructure funding received from University of Adelaide, for researcher groups who occupy seats, but these seats are not included in the Licence Agreement
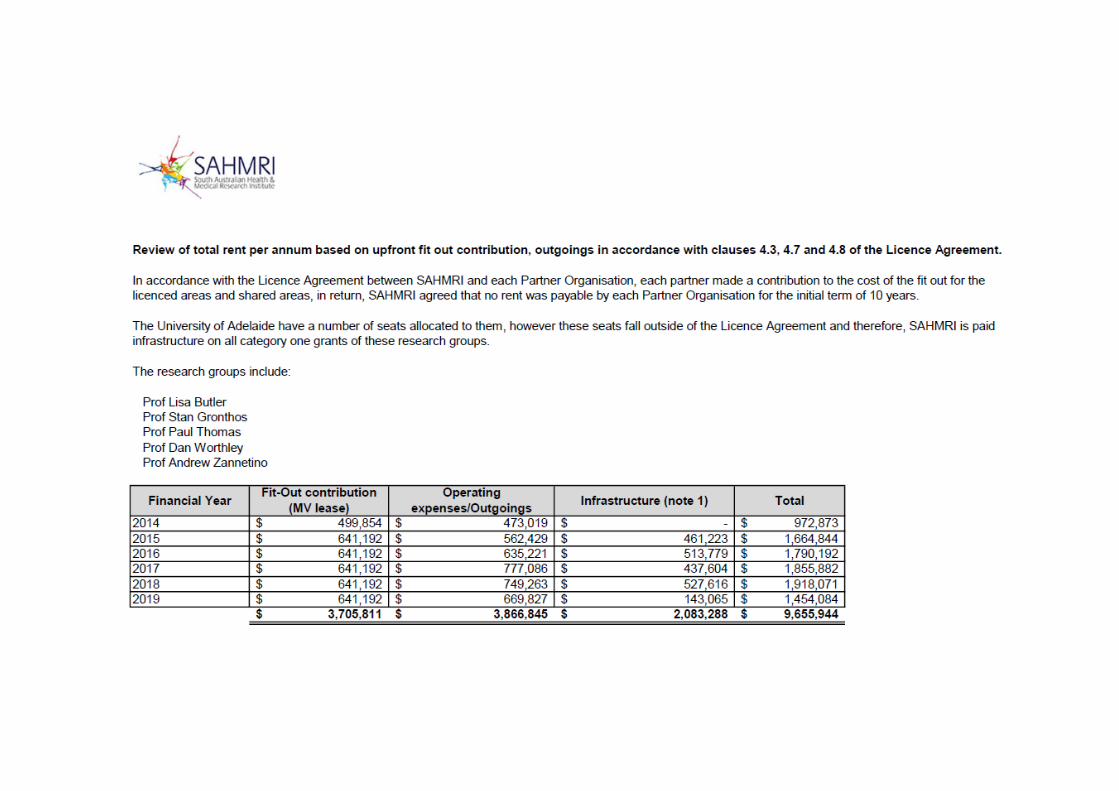
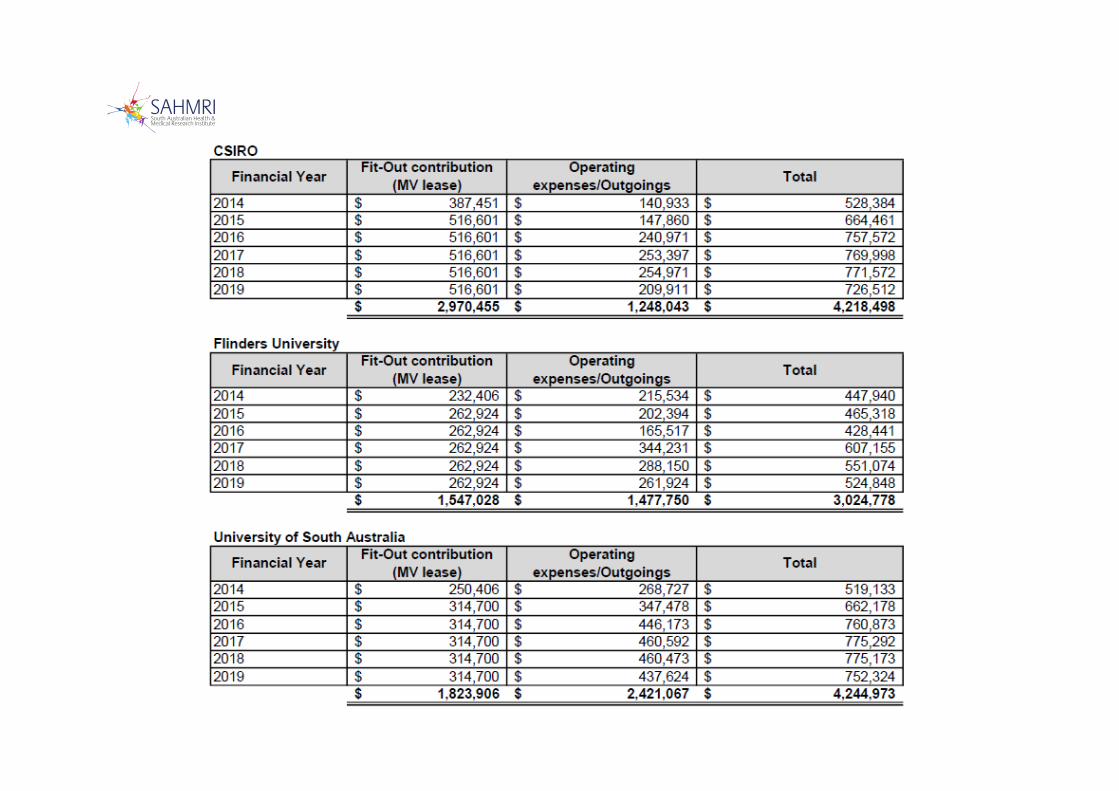
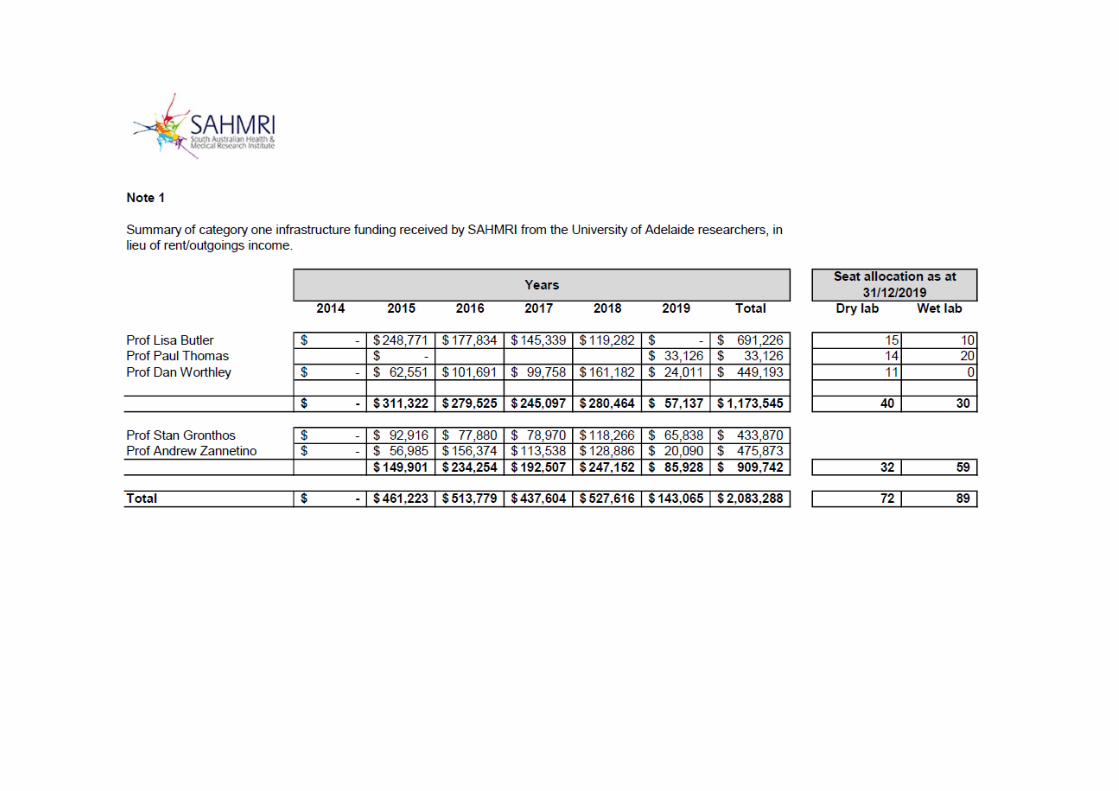
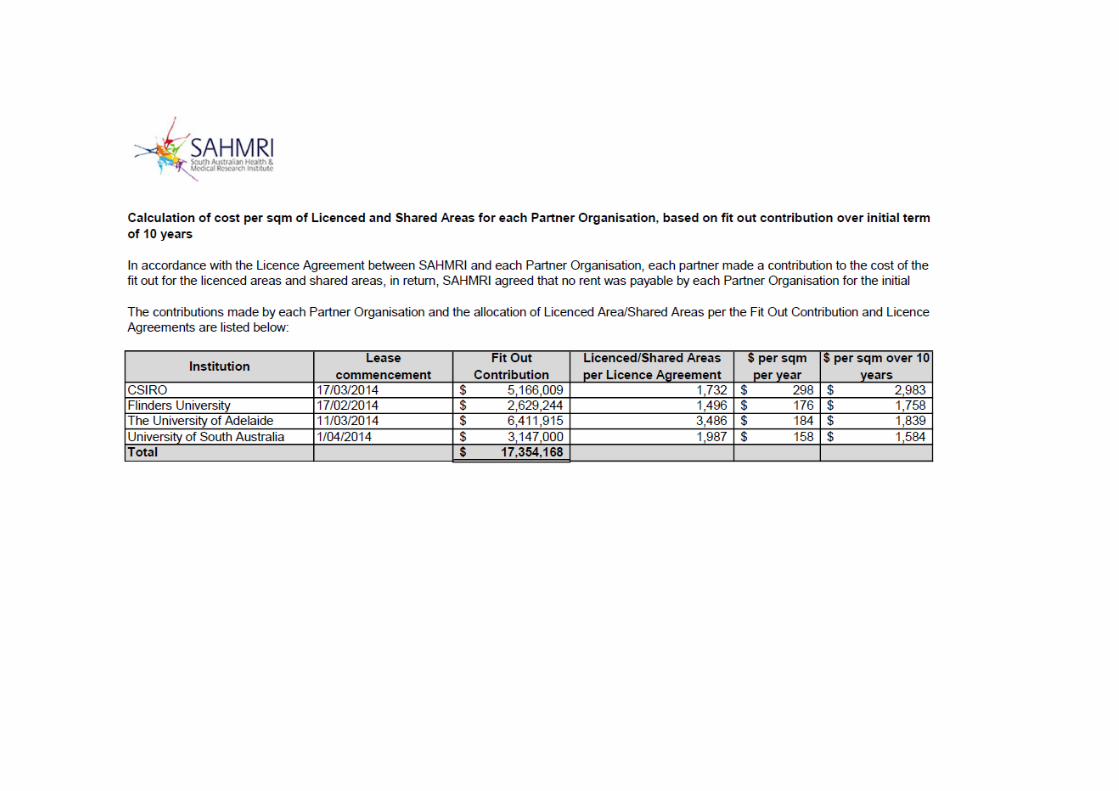

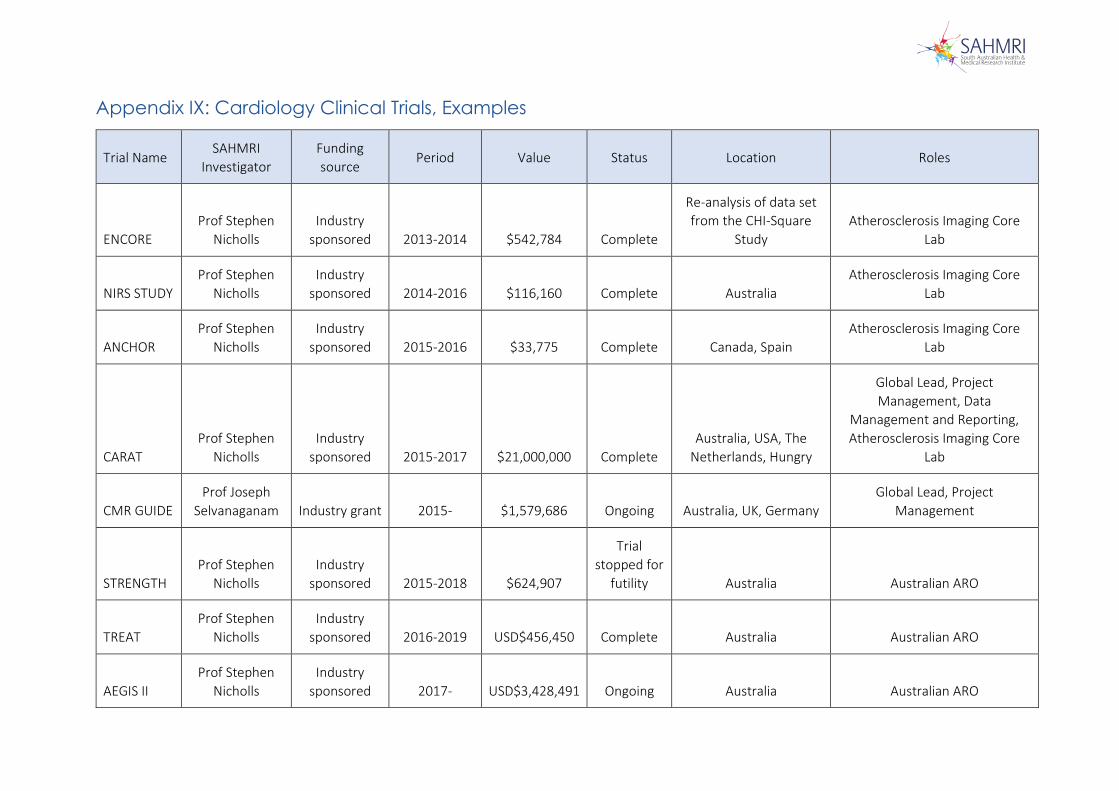
Appendix IX: Cardiology Clinical Trials, Examples
Trial Name SAHMRI
Investigator Funding source
Period Value Status Location Roles
ENCORE Prof Stephen
Nicholls Industry
sponsored 2013-2014 $542,784 Complete
Re-analysis of data set from the CHI-Square
Study Atherosclerosis Imaging Core
Lab
NIRS STUDY Prof Stephen
Nicholls Industry
sponsored 2014-2016 $116,160 Complete Australia Atherosclerosis Imaging Core
Lab
ANCHOR Prof Stephen
Nicholls Industry
sponsored 2015-2016 $33,775 Complete Canada, Spain Atherosclerosis Imaging Core
Lab
CARAT Prof Stephen
Nicholls Industry
sponsored 2015-2017 $21,000,000 Complete Australia, USA, The
Netherlands, Hungry
Global Lead, Project Management, Data
Management and Reporting, Atherosclerosis Imaging Core
Lab
CMR GUIDE Prof Joseph
Selvanaganam Industry grant 2015- $1,579,686 Ongoing Australia, UK, Germany Global Lead, Project
Management
STRENGTH Prof Stephen
Nicholls Industry
sponsored 2015-2018 $624,907
Trial stopped for
futility Australia Australian ARO
TREAT Prof Stephen
Nicholls Industry
sponsored 2016-2019 USD$456,450 Complete Australia Australian ARO
AEGIS II Prof Stephen
Nicholls Industry
sponsored 2017- USD$3,428,491 Ongoing Australia Australian ARO
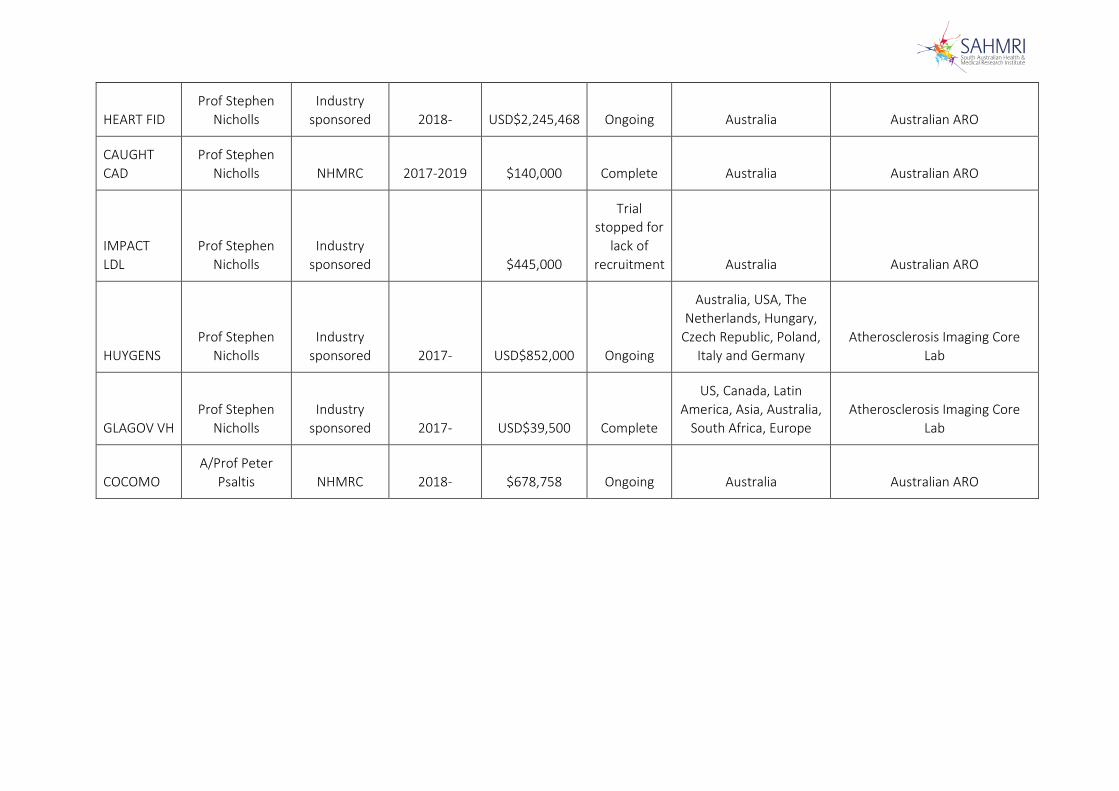
HEART FID Prof Stephen
Nicholls Industry
sponsored 2018- USD$2,245,468 Ongoing Australia Australian ARO
CAUGHT CAD
Prof Stephen Nicholls NHMRC 2017-2019 $140,000 Complete Australia Australian ARO
IMPACT LDL
Prof Stephen Nicholls
Industry sponsored
$445,000
Trial stopped for
lack of recruitment Australia Australian ARO
HUYGENS Prof Stephen
Nicholls Industry
sponsored 2017- USD$852,000 Ongoing
Australia, USA, The Netherlands, Hungary,
Czech Republic, Poland, Italy and Germany
Atherosclerosis Imaging Core Lab
GLAGOV VH Prof Stephen
Nicholls Industry
sponsored 2017- USD$39,500 Complete
US, Canada, Latin America, Asia, Australia,
South Africa, Europe Atherosclerosis Imaging Core
Lab
COCOMO A/Prof Peter
Psaltis NHMRC 2018- $678,758 Ongoing Australia Australian ARO