seroprevalence of antibodies to pertussis and diphtheria among healthy adults in china
TRANSCRIPT

Title: 1
Seroprevalence of antibodies to pertussis and diphtheria among asymptomatic adults in 2
China 3
4
5
6
Authors: 7
Qi Zhang, Ph.D.,1 email: [email protected] 8
Fulian Han, M.D.,2 email: [email protected] 9
Qing Nie,Ph.D.,2 email: [email protected] 10
Hongyu Ren,1 email: [email protected] 11
Baoqiang Zhang,M.D.,2 email: [email protected] 12
Qiyong Liu, M.D.,1 email: [email protected] 13
Zhujun Shao, Ph.D.,*1 email: [email protected] 14
15
Institutes: 16
1 Institute for Communicable Disease Control and Prevention, State Key Laboratory of 17
Infectious Diseases, Chinese Center for Disease Control and Prevention, Beijing 102206, 18
P.R.China 19
2 Weifang Municipal Center for Disease Control and Prevention, Weifang, Shandong 20
261041, P.R.china 21
22
23
*Corresponding author: 24
Zhujun Shao, Professor and Director of Department of Respiratory Infectious Disease, 25
Institute for Communicable Disease Control and Prevention, Chinese Center for Disease 26
Control and Prevention, P.O.Box5, Changping,Beijing 102206, P.R.China 27
Tel: 86-010-58900752: Fax: 86-010-58900700; Email: [email protected] 28
29
30
31
32
Abstract 1
Background. Diphtheria and pertussis are vaccine-preventable respiratory diseases. 2
Because of the absent coverage of Tetanus- diphtheria- pertussis vaccine in adults, there 3
is a general shift in the age distribution of pertussis to adults who are considered as 4
source of infection for younger infants, and potential increased risk of re-emergence of 5
diphtheria in China. This study aims to determine the seroprevalence of pertussis and 6
diphtheria among 18-50 years old adults in the province of Shandong, China. 7
Methods. A total of 210 sera samples of subjects were tested by commercial enzyme 8
immunoassay for IgG of pertussis and diphtheria, respectively. 9
Results. The results of anti-pertussis IgG showed a mean level of 74.35 U/mL, and 10
76.7% of the studied subjects were seropositive to Bordetella pertussis. No subjects had 11
diphtheria antibody level of ≤0.0 1IU/mL. Diphtheria antibody level of ≥0.1 IU/mL was 12
found in 161 subjects (76.6%), while 49 (23.3%) had antitoxin levels of 0.01-0.099 IU/mL. 13
Conclusions. High seroprevalence of pertussis in 18-50 years age adults is possibly 14
due to natural infection with B.pertussis. Although the overall a high proportion of 15
population had a protective level of immunity against diphtheria, the antibody level of 16
diphtheria gradually decreased with increasing age. Vaccines combined with pertussis, 17
diphtheria and tetanus toxoids should be booster injection in adults. 18
19
20
Background 1
Diphtheria and pertussis are vaccine-preventable respiratory diseases. A combined 2
Tetanus- diphtheria-whole cell pertussis vaccine (DTwP) was introduced in 1980s in China. 3
Since 2007, a combined Tetanus- diphtheria- acelluar pertussis vaccine (DTaP) has been 4
used in place of DTwP. In several provinces of China including Shandong and Beijing, 5
combined vaccine is administered in the 3th, 4th and 5th months of life, in combination with 6
three booster doses one administered in month 18-24 and the other two doses 7
tetanus-diphtheria combined vaccine in the years 7 and 12. 8
9
Vaccination against diphtheria has resulted in less than 10 cases reported to this disease 10
from 2003 to present in China mainland. In recent years, several imported cases of 11
Corynebacterium diphtheriae infection were reported in United States, France and 12
neighbor countries [1, 2]. The absent coverage of diphtheria vaccination in adolescents 13
and adults threaten the healthy safety of population, especially potential increased risk of 14
re-emergence of diphtheria in China, and surggest that an evaluation of the antibody level 15
of diphtheria in adults is necessary. 16
17
Vaccination-based prevention of pertussis is widely practiced to infants and young 18
Children in China, and has resulted in a dramatic decrease in the morbidity and mortality 19
caused by this disease. Over the past two decades, pertussis continues to be a global 20
concern with increased incidence in many countries including Argentina, Australia, 21
Canada, Italy, Japan, the Netherlands, Switzerland and the US [3]. In recent years, there 22
is a general shift in the age distribution of pertussis, with adolescents and adults an 1
underdetermined but significant source of infection for neonates and younger infants [4-8]. 2
The Strategic Advisory Group of Experts (SAGE) in World Health Organization (WHO) 3
recommended that the target of reducing mortality caused by vaccine-preventable 4
disease by two thirds by 2015 compared with 2000 levels, as well as the Millennium 5
Development Goals that aim to reduce child mortality. The importance of pertussis 6
control’s contribution towards the goal of reduced mortality should be recognized [9]. In 7
China, reported incidence of pertussis fluctuated a rate of 1 per 100,000 after introduction 8
of vaccination of pertussis [10, 11]. But it is obvious that due to atypical symptom of adults 9
patients and lack of evidence of laboratory diagnosis, the real incidence of pertussis is 10
underestimated [12]. These groups maybe act as a source of infection for younger infants. 11
12
In this study, in order to assess the need for pertussis and diphtheria booster vaccination 13
in adults, our goal was to determine the seroprevalence of Pertussis and diphtheria 14
among 18-50 years old adults population in the province of Shandong, China. 15
16
Methods 17
Sample collection. Healthy adults aged 18-50 years adults attending health checkup 18
clinic in Shandong province for starting public service work from May to June 2010 were 19
enrolled in a cross-sectional sero-epidemiological study. All individuals were 20
asymptomatic while entering the study. Individual with any respiratory diseases or 21
conditions affecting immunocompetence was excluded from the study. A total of 210 22
subjects were classified into three age groups: 18-24 years, 25-34 years, 35-50 years. 1
Basic epidemiological data like age, gender and address was recorded. 2
3
Laboratory processes. 3-5mL of venous blood was drawn. Serum was extracted from 4
blood samples soon after arrival to local lab and stored at -20℃ refrigerator until 5
transported to China CDC laboratory using cold chain. IgG antibodies against Bordetella 6
pertussis and corynebacterium diphtheriae antigens were measured quantitatively by 7
CE-marked sandwich ELISAs (IBL International, Hamburg, Germany) respectively 8
according to the instructions for use. Results of pertussis are interpreted as positive, 9
negative and equivocal. Subjects bearing more than 24 U/mL of IgG to B. pertussis 10
antigens were considered as seropositive, below 16 U/mL as seronegative, between 16 11
U/mL and 24 U/mL as equivocal. In the case of diphtheria, the classification into specific 12
titer ranges for the evaluation of immunization protection is based on practical and 13
theoretical considerations. Diphtheria antibody levels of ≤0.01 IU/mL was defined as no 14
immune protection or seronegativity and susceptibility. A value of >0.01 IU/mL is given for 15
a secure individual protection. For safety reasons a tenfold higher value (0.1 IU/mL) than 16
the internationally specified minimum titer for a prophylaxis was recommended. 17
18
Statistical analysis. Data analysis was performed using SPSS 13.0 software (SPSS Inc, 19
Chicago, USA). For statistical analysis, subjects were categorized into three groups 20
according to their age: 18-24, 25-34, 35-50 years. The total prevalence of seropositive 21
results and mean level of pertussis and diphtheria IgG of subjects were descriptively 22
calculated. The serological change trends of each pertussis and diphtheria IgG results by 1
age were demonstrated by scatter figure. Mean IgG levels between the age subgroups 2
were examined by one-way ANOVA. Significance level was set at P<0.05. 3
4
Ethical considerations. This study was approved by the Institutional Review Board (IRB) 5
of Chinese Center for Disease Control and Prevention. Informed consent was received 6
from all subjects before the blood samples were collected. 7
8
Results 9
A total of 210 sera samples of subjects (64 for the 18-24 years age group, 68 for the 25-34 10
years age group and 78 for the 35-50 years age group) were tested in this study. 11
12
Humoral immunity to pertussis The results of anti-pertussis IgG showed a mean level 13
of 74.35 U/mL (95% Confidence Interval CI: 57.54-91.16), and 76.7% of the studied 14
subjects were seropositive to B.pertussis, while 9.5% and 13.8% fell into negative and 15
equivocal category respectively. Of all the 210 sera samples, seropositivity for each group 16
of subjects was 71.9% (n=46), 76.5% (n=52) and 80.8% (n=63) for group 18-24 years, 17
25-34 years and 35-50 years age respectively (table 1). The mean IgG levels was 67.69 18
U/mL in subjects aged 18-24 years (95% CI, 38.05-97.32), 62.55 U/mL (95%CI, 19
41.24-83.86) for those aged 25-34 years and 90.1 U/mL (95%CI, 56.09-124.11) for 35-50 20
years age group (figure1 left). There were no significant difference in the mean IgG levels 21
among the age groups (P=0.389). Local regression (loess) analysis was used to estimate 22
serological trends because the data did not conform to a single overall linear regression 1
model. The graph also showed that levels of B.pertussis for subjects 18-50 years did not 2
change vigorously (figure2 left). 3
4
Humoral immunity to Diphtheria Of all sera samples, no subjects had an diphtheria 5
antibody level of ≤0.01 IU/mL (no immune protection). An diphtheria antibody level of ≥0.1 6
IU/mL (full protection) was found in 161 subjects (76.6%), while 49 (23.3%) had antibidy 7
levels of 0.01-0.099 IU/mL (basic protection). In each age group of subjects, percentage of 8
full protection was highest at 87.5% in 18-24 years age group, while lowest at 74.4% in 9
35-50 years age group (table1). The mean level of diphtheria antibody was 0.61 IU/mL 10
(95% CI, 0.511-0.71) in all subjects aged 18-50 years, while 0.94 IU/mL (95% CI, 11
0.74-1.15) for those aged 18-24 years, 0.79 IU/mL (95% CI, 0.48-0.86) for 25-34 years 12
age subjects and 0.28 IU/ML (95% CI, 0.21-0.36) for 35-50 years age group (figure1 right). 13
There was significant difference when the mean levels of 35-50 years group compared to 14
those of 25-34 years group and 18-24 years group respectively (P=0.00 and 0.002). The 15
graph of loess analysis also demonstrated that there were two peaks concentration of 16
antibody between 18 and 30 years age subjects, and whose mean concentration of 17
antibody were significantly greater than 31-50 years age subjects’(figure2 right). 18
19
Discussion 20
In this study, we documented a 76.7% seroprevalence of pertussis antibodies in the adults 21
population in China between the ages of 18 and 50 years, which was independent of age 22
(within this age range). This result fell into the range of seroprevalence rates of 30-97% in 1
adults reported from China and various other countries [10, 13-18]. China took formally 2
part in WHO Expanded Programme on Immunization (EPI) which included pertussis, 3
diphtheria and tetanus combined vaccine in 1981, subjects of present study can be 4
grouped into a vaccine-eligible age group in which subjects were vaccinated during 5
childhood and a vaccine-ineligible age group in which subjects didn’t accept vaccine 6
according to the ages. The vaccine-eligible age groups and the vaccine-ineligible age 7
group were under 30 years old and over 31 years old, respectively. Pertussis booster 8
vaccine for adolescences and adults were still not introduced in China yet. Because 9
vaccine antibodies begin to wane 4 years after the last dose, thus immunity to pertussis 10
vaccine diminishes to 0%-20% over a 10-year interval [13, 19], it can be concluded that 11
high pertussis seroprevalence in 18-50 years age adults is due to natural infection with 12
B.pertussis. Results of loess analysis also demonstrated that mean levels of pertussis of 13
vaccine-eligible age group (18-30 years age) did not differ significantly from 14
vaccine-ineligible age group (31-50 years age). 15
16
The current study showed a considerable number of adults used to be infected by B. 17
pertussis, also verified this pathogen still circulated in the societies, especially in the adult 18
population. But the clinical manifestation of the adult pertussis was atypical or difficult to 19
diagnose because of using antibiotics at home and late appearing at out-patient of 20
hospital, which resulted in these population as potential source of infection of the disease 21
in the younger infants (< 6 months of age). Main numbers of subjects in this study were 22

from rural area of China and were going to work on Food and beverage industry and 1
public services, their customers who lost protective antibody of pertussis or uncompleted 2
the basic immunity would have to undertake the harmful consequence of transmission of 3
disease. Therefore, it may be time to discuss the need for the administration of pertussis 4
booster vaccine to adults, especially, public servers. 5
6
In present study, none of our subjects had a diphtheria antitoxin level of ≤0.01IU/mL (no 7
immune protection). But in some other countries, the proportion of individuals susceptible 8
to diphtheria with antibody concentration of <0.01IU/mL varied from 5.3% to 37.6% 9
[20-26]. Compared with the threshold (75%) indicated by Dadswell [27] as sufficient to 10
prevent an outbreak of diphtheria, the percentages of 76.6% full protected subjects and 11
23.3% basic protected subjects were significantly above the safety limits. Similar results 12
also have been reported in Beijing (91.59%) and Jiangsu province (81.99%) [28, 29]. The 13
variation results between China and some countries can be explained by different 14
vaccination programs and booster schedules, awareness among population, and by 15
different study designs and methods. Schneerson’s study pointed out that the ELISA test 16
have led to an over-estimation of the subjects really protected, since the antibodies 17
revealed might not always be efficient [30]. 18
19
Distinguished from pertussis vaccination program in Shandong province, diphtheria and 20
tetanus combined booster vaccine was injected to individuals at 7 years old and 21
adolescences who attended secondary school and university in first year. According to 22
WHO’s summary, following the primary immunization series, the average duration of 1
protection is about 10 years, booster dose of diphtheria toxid beyond infancy and early 2
school age are required to maintain protective immunity [31]. These could explain that the 3
peak concentrations of vaccine eligible group (18-30 years old) in the graph of loess 4
analysis were due to correspond to a boost in the concentration of antibody after routine 5
immunization and the very high vaccine coverage in Shandong province. Both of results of 6
ANOVA and loess analysis demonstrated that there was an overall trend of decreasing 7
immunity with increasing age. Although the vaccine ineligible group (31-50 years old) who 8
was not immunized against diphtheria also had a high titer of protective diphtheria 9
antibody, this was considered to be the effect of inapparent or apparent natural diphtheria 10
infection during the period of absent diphtheria vaccine. Similar seroepidemiologic 11
findings have also been observed in several other countries [32-34]. 12
13
Our data from China were in accordance with other reports that B.pertussis was a problem 14
amongst adolescents and adults, and the antibody level of diphtheria gradually decreased 15
with increasing age, although the overall a high proportion of population had a protective 16
level of immunity against diphtheria. According to the Ministry of Health of China, the 17
immunization coverage rates and number districts achieved with 3 doses of DTP 18
vaccination in childhood were over 90% and 99%, respectively from years of 2000 to 19
present. Despite universal immunization of children with DTP vaccine, adults were at high 20
risk of acquiring pertussis, at a time when vaccine-induced immunity has waned. Acellular 21
pertussis vaccines confer safe and effective protection against pertussis in adolescents 22

and adults [35]. In March 2006, the American Academy of Paediatrics published their 1
recommendation that adolescents 11 to 18 years of age should receive a single dose of 2
acellular pertussis vaccines combined with diphtheria and tetanus toxoids (DTaP) instead 3
of tetanus and diphtheria toxoids vaccine for booster immunization. Our data would 4
suggest that this strategy should be considered for China. Regards to diphtheria immunity, 5
adults, especially over 30 years old people, may not be adequately protected. We strongly 6
encourage booster injections subsequently every 10 years throughout life for diphtheria. 7
8
The limitation of our study is that we applied commercial ELISA kit rather than in-house 9
anti-PT of B.pertussis and antitoxin of C.diphtheria ELISA recommended by WHO, which 10
maybe overestimate the antibody titer of subjects. The other hand, further surveillance 11
with large sample size including adolescences should be conducted to monitor the 12
pertussis and diphtheria immunity in China. Further evaluation might be necessary to 13
establish the most appropriate booster vaccine program in China. 14
15
Conclusions 16
High seroprevalence of pertussis in 18-50 years age adults is possibly due to natural 17
infection with B.pertussis. Although the overall a high proportion of population had a 18
protective level of immunity against diphtheria, the antibody level of diphtheria gradually 19
decreased with increasing age. Vaccines combined with pertussis, diphtheria and tetanus 20
toxoids should be booster injection in adults. 21
22
Competing interests 1
The authors declare that they have no competing interests. 2
3
Authors’ contributions 1
Q Zhang, FL Han, QY Liu and ZJ Shao planned the study design and drafted and edited 2
the manuscript. Q Zhang carried out the immunoassays. BQ Zhang and Q Nie were in 3
charge of data collection and blood samples collection. Q Zhang performed the statistical 4
analysis. 5
All authors read and approved the final manuscript. 6
7
8
Acknowledgments and Funding 1
We acknowledge the technicians from the Institute for Communicable Disease Control 2
and Prevention and Weifang Municipal Center for Disease Control and Prevention, who 3
assisting with data collection and blood samples collection. 4
This work was supported by China the Ministry of Health and the Ministry of Science and 5
Technology [2008ZX10004-008]. 6
7
8
9

References 1
1. Lartigue MF MX, Le Flèche A, Grimont PA, Benet JJ, Durrbach A, Fabre M, Nordmann 2
P: Corynebacterium ulcerans in an immunocompromised patient with diphtheria 3
and her dog. J Clin Microbiol 2005, 43(2):999-1001 4
2. Tiwari TS GA, Yu DT, Ehresmann KR, Jones TF, Hill HE, Cassiday PK, Pawloski LC, 5
Moran JS, Popovic T, Wharton M.: Investigations of 2 cases of diphtheria-like 6
illness due to toxigenic Corynebacterium ulcerans. Clin Infect Dis 2008, 7
46(3):395-401 8
3. Tan T, Trindade E, Skowronski D: Epidemiology of pertussis. Pediatr Infect Dis J 9
2005, 24(5 Suppl):S10-18 10
4. Cherry JD, Grimprel E, Guiso N, Heininger U, Mertsola J: Defining pertussis 11
epidemiology: clinical, microbiologic and serologic perspectives. Pediatr Infect 12
Dis J 2005, 24(5 Suppl):S25-34 13
5. Forsyth K, Tan T, von Konig CH, Caro JJ, Plotkin S: Potential strategies to reduce 14
the burden of pertussis. Pediatr Infect Dis J 2005, 24(5 Suppl):S69-74 15
6. Greenberg DP: Pertussis in adolescents: increasing incidence brings attention 16
to the need for booster immunization of adolescents. Pediatr Infect Dis J 2005, 17
24(8):721-728 18
7. Edwards K, Freeman DM: Adolescent and adult pertussis: disease burden and 19
prevention. Curr Opin Pediatr 2006, 18(1):77-80 20
8. Forsyth KD, Wirsing von Konig CH, Tan T, Caro J, Plotkin S: Prevention of pertussis: 21
recommendations derived from the second Global Pertussis Initiative 22
roundtable meeting. Vaccine 2007, 25(14):2634-2642 1
9. WHO: Meeting of the Strategic Advisory Group of Experts on immunization, 2
October 2009-conclusions and recommendations. WklyEpidemiolRec 2009, 3
84:517-532 4
10. Jian. F, Yue-fang. W, Bao-xiang. X: Analysis on Pertussis Epidemiology in 5
Zhejiang Province in 1954-2004. Chinese Journal of Vaccines and Immunization 6
2005, 11(4):279-281 7
11. Yan. Y, Lin-qi. D, Zhen-yuan. S: Analysis on Epidemiology in 1963-2002 and 8
Control Strategy on Pertussis in Henan Province. Chinese Journal of Vaccines 9
and Immunization 2005, 11(5):402-404 10
12. Cheng-yan. M, Wen-hong. Z: Current Status and Perspective of Worldwide 11
Disease Burden of Pertussis. Chinese Journal of Vaccines and Immunization 2006, 12
12(4):318-321 13
13. Cattaneo LA, Reed GW, Haase DH, Wills MJ, Edwards KM: The seroepidemiology 14
of Bordetella pertussis infections: a study of persons ages 1-65 years. J Infect 15
Dis 1996, 173(5):1256-1259 16
14. Arav-Boger. R, Ashkenazi. S, Gdalevich. M, Cohen. D, Danon. YL: Seroprevalence 17
of pertussis antibodies among adolescents in Israel. Isr Med Assoc J 2000, 18
2(2):174-177 19
15. Okada K, Ueda K, Morokuma K, Kino Y, Tokugawa K, Nishima S: Seroepidemiologic 20
study on pertussis, diphtheria, and tetanus in the Fukuoka area of southern 21
Japan: seroprevalence among persons 0-80 years old and vaccination program. 22

Jpn J Infect Dis 2004, 57(2):67-71 1
16. Wilder-Smith A, Ng S, Earnest A: Seroepidemiology of pertussis in the adult 2
population of Singapore. Ann Acad Med Singapore 2006, 35(11):780-782 3
17. Hashemi. SH, Ranjbar. M, Hajilooi. M, Seif-Rabiei. M-A, Bolandi. M, Moghimi. J: 4
Seroprevalence of Immunoglobulin G antibodies against pertussis toxin among 5
asymptomatic medical students in the west of Iran: a cross sectional study. 6
BMC Infect Dis 2009, 9(9):1-4 7
18. Syed. MA, Said. F, Bukhari SHA: Seroepidemiology of Bordetella pertussis 8
infections in the twin cities of Pakistan. North American Journal of Medical 9
Sciences 2009, 1(7):353-355 10
19. Campins-Marti M, Cheng HK, Forsyth K, Guiso N, Halperin S, Huang LM, Mertsola J, 11
Oselka G, Ward J, Wirsing von Konig CH et al: Recommendations are needed for 12
adolescent and adult pertussis immunisation: rationale and strategies for 13
consideration. Vaccine 2001, 20(5-6):641-646 14
20. Maple PA, Efstratiou A, George RC, Andrews NJ, Sesardic D: Diphtheria immunity 15
in UK blood donors. Lancet 1995, 345(8955):963-965 16
21. Ballereau F, Schrive I, Fisch A, Speich M, Laurichesse H, Tournade S, Rey M: A 17
multicentre serosurvey on diphtheria immunity in a French population of 1004 18
subjects. Eur J Epidemiol 1998, 14(5):499-503 19
22. de Melker HE, Berbers GA, Nagelkerke NJ, Conyn-van Spaendonck MA: Diphtheria 20
antitoxin levels in the Netherlands: a population-based study. Emerg Infect Dis 21
1999, 5(5):694-700 22
23. Marlovits S, Stocker R, Efstratiou A, Broughton K, Kaider A, Vecsei V, Wiedermann G, 1
Kollaritsch H: Seroprevalence of diphtheria immunity among injured adults in 2
Austria. Vaccine 2000, 19(9-10):1061-1067 3
24. von Hunolstein C, Rota MC, Alfarone G, Ricci ML, Salmaso S: Diphtheria antibody 4
levels in the Italian Population. Eur J Clin Microbiol Infect Dis 2000, 19(6):433-437 5
25. Redwan EM, El-Awady MK: Status of diphtheria immunity in the Egyptian 6
population. Ann Trop Med Parasitol 2005, 99(1):93-99 7
26. Valinsky L, Simhoni S, Bassal R, Agmon V, Yishai R, Green MS, Cohen D: 8
Prevalence and correlates of diphtheria toxoid antibodies in children and adults 9
in Israel. Clin Microbiol Infect 2006, 12(10):968-973 10
27. Kjeldsen K, Simonsen O, Heron I: Immunity against diphtheria 25-30 years after 11
primary vaccination in childhood. Lancet 1985, 1(8434):900-902 12
28. Wen-sheng. W, Ai-hua. L, Yin-hua. G: Surveillance and Analysis of Diphtheria 13
Antibody in Healthy Population During 1996 - 2000 in Beijing. Zhongguo Ji Hua 14
Mian Yi 2002, 8(5):264-265 15
29. Huang LM, Xu EP, Yang LX: [Observation of immunity level of 16
pertussis-diphtheria-tetanus in healthy people in Hangzhou City during 17
1995-2006]. Zhongguo Ji Hua Mian Yi 2009, 15(1):68-71 18
30. Schneerson R, Robbins JB, Taranger J, Lagergard T, Trollfors B: A toxoid vaccine 19
for pertussis as well as diphtheria? Lessons to be relearned. Lancet 1996, 20
348(9037):1289-1292 21
31. WHO: Diphtheria vaccine-WHO position paper. Wkly epidemiol Rec 2006, 22
81(3):21-32 1
32. Rappuoli R, Perugini M, Falsen E: Molecular epidemiology of the 1984-1986 2
outbreak of diphtheria in Sweden. N Engl J Med 1988, 318(1):12-14 3
33. WHO: WHO Expanded programme on Immunization. Diphtheria and measles 4
control, China. Wkly Epidemiol Rec 1988, 63:225-227 5
34. Galazka AM, Robertson SE: Diphtheria: changing patterns in the developing 6
world and the industrialized world. Eur J Epidemiol 1995, 11(1):107-117 7
35. Edwards KM: Is pertussis a frequent cause of cough in adolescents and adults? 8
Should routine pertussis immunization be recommended? Clin Infect Dis 2001, 9
32(12):1698-1699 10
11
12
Figures legends 1
Figure 1. Mean levels ±95% confidence interval of anti-pertussis IgG and anti-diphtheria 2
IgG by age group. Left for pertussis, right for diphtheria. 3
Figure 2. Serologic response (as determined by ELISA) to pertussis and diphtheria by age 4
(18-50 years of age). Each symbol represent one subject. Solid line present mean level of 5
IgG using local regression analysis; left: IgG of pertussis; right: IgG of diphtheria. 6
7
8
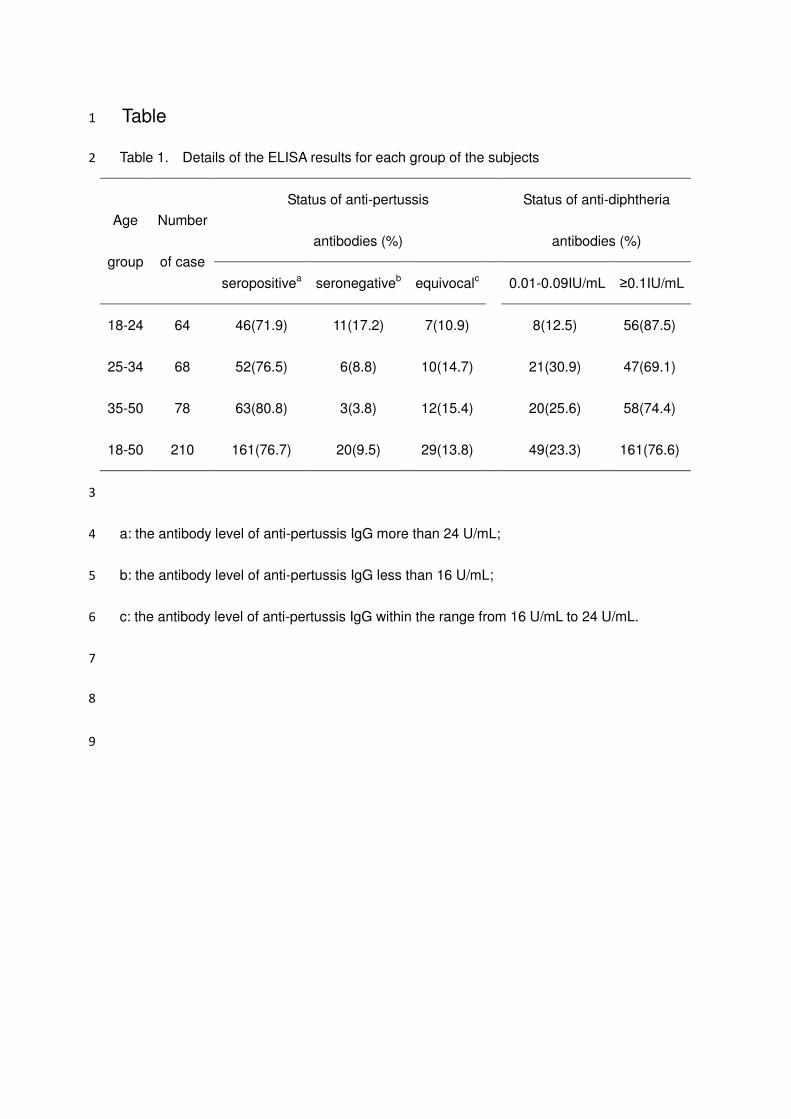
Table 1
Table 1. Details of the ELISA results for each group of the subjects 2
Status of anti-pertussis
antibodies (%)
Status of anti-diphtheria
antibodies (%)
Age
group
Number
of case
seropositivea seronegativeb equivocalc 0.01-0.09IU/mL ≥0.1IU/mL
18-24 64 46(71.9) 11(17.2) 7(10.9) 8(12.5) 56(87.5)
25-34 68 52(76.5) 6(8.8) 10(14.7) 21(30.9) 47(69.1)
35-50 78 63(80.8) 3(3.8) 12(15.4) 20(25.6) 58(74.4)
18-50 210 161(76.7) 20(9.5) 29(13.8) 49(23.3) 161(76.6)
3
a: the antibody level of anti-pertussis IgG more than 24 U/mL; 4
b: the antibody level of anti-pertussis IgG less than 16 U/mL; 5
c: the antibody level of anti-pertussis IgG within the range from 16 U/mL to 24 U/mL. 6
7
8
9
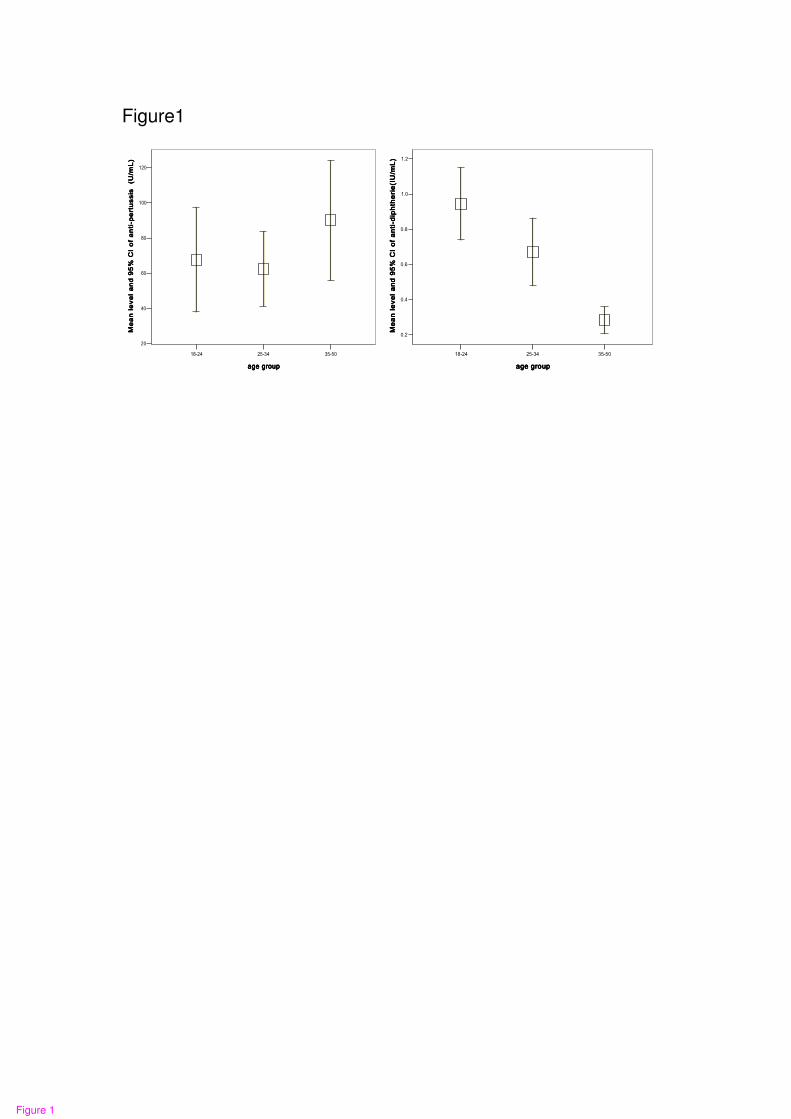
Figure1
57/7247/563:/46
cig"itqwrcig"itqwrcig"itqwrcig"itqwr
342
322
:2
82
62
42
Ogcp"ng
xgn"cpf";7'"EK"qh"cpvk/rgtvwuu
ku""*W
1oN+
Ogcp"ng
xgn"cpf";7'"EK"qh"cpvk/rgtvwuu
ku""*W
1oN+
Ogcp"ng
xgn"cpf";7'"EK"qh"cpvk/rgtvwuu
ku""*W
1oN+
Ogcp"ng
xgn"cpf";7'"EK"qh"cpvk/rgtvwuu
ku""*W
1oN+
57/7247/563:/46
cig"itqwrcig"itqwrcig"itqwrcig"itqwr
304
302
20:
208
206
204
Ogc
p"ngxg
n"cpf
";7'
"EK"qh"cpvk/fkrj
vjgtkg*KW1o
N+Ogc
p"ngxg
n"cpf
";7'
"EK"qh"cpvk/fkrj
vjgtkg*KW1o
N+Ogc
p"ngxg
n"cpf
";7'
"EK"qh"cpvk/fkrj
vjgtkg*KW1o
N+Ogc
p"ngxg
n"cpf
";7'
"EK"qh"cpvk/fkrj
vjgtkg*KW1o
N+
�
Figure 1

Figure2 ��
73726;6:69686766656463625;5:59585756555453524;4:49484746454443423;3:
cigcigcigcig
32220222
:220222
8220222
6220222
4220222
20222
KiI"qh"D0rgtvwuu
kuKiI"qh"D0rgtvwuu
kuKiI"qh"D0rgtvwuu
kuKiI"qh"D0rgtvwuu
ku
73726;6:69686766656463625;5:59585756555453524;4:49484746454443423;3:
cigcigcigcig
60222
50222
40222
30222
20222
KiI"qh"fkrjvjg
tkc
KiI"qh"fkrjvjg
tkc
KiI"qh"fkrjvjg
tkc
KiI"qh"fkrjvjg
tkc
��
���
Figure 2