sense of coherence – a mediator between disability and handicap
TRANSCRIPT
Regular Article
Psychother Psychosom 1999;68:102–110
Sense of Coherence – A Mediatorbetween Disability and Handicap?
Ulrich Schnyderb Stefan Büchia Hanspeter Mörgelib Tom Senskyc
Richard Klaghofera
aDivision of Psychosocial Medicine, bPsychiatric Outpatient Department, University Hospital, Zurich, Switzerland;cDivision of Neurosciences and Psychological Medicine, Imperial College School of Medicine, West Middlesex
Hospital, Isleworth, Middlesex, UK
Dr. Ulrich Schnyder, MDPsychiatric Outpatient Department, University HospitalRämistrasse 100CH–8091 Zurich (Switzerland)Tel. +41 1 255 52 80, Fax +41 1 255 43 83, E-Mail [email protected]
ABCFax + 41 61 306 12 34E-Mail [email protected]
© 1999 S. Karger AG, Basel0033–3190/99/0682–0102$17.50/0
Accessible online at:http://BioMedNet.com/karger
Key WordsDisability W Impairment W Handicap W Accidents W
Rheumatoid arthritis W Salutogenesis W Sense of
coherence
AbstractBackground: The aim of this study was first to analyze
the associations between disability and handicap and
Antonovsky’s concept of sense of coherence (SOC); sec-
ondly, to find out how the SOC concept could be inte-
grated in the WHO model of impairments, disabilities,
and handicaps (ICIDH). Methods: Data from two studies
were used: one on patients with rheumatoid arthritis,
one on severely injured accident victims. Objective mea-
sures of the illness or the injury were conceptualized as
indicator variables for disability, whereas variables relat-
ed to the patients’ subjective judgement were concep-
tualized as indicator variables for handicap. Correlations
were calculated between both sets of variables and the
SOC scale total score. Results: SOC showed no signifi-
cant correlation with ‘disability variables’ (rheumatoid
arthritis: HAQ, SF36 physical functioning; accidental inju-
ries: ISS, GCS). However, significant correlations were
found between SOC and all ‘handicap variables’ (rheu-
matoid arthritis: HAD, SF36 social functioning; accidental
injuries: CAPS-2, IES, SCL-90-R depression subscale).
Conclusions: SOC is related to the psychosocial effects of
health problems. It may be understood as a mediator
between disability and handicap. Prospective studies are
needed to clarify whether the SOC scale can be used as
an outcome predictor with regard to psychosocial adap-
tation, in acute as well as in chronic health problems.
Introduction
Disability is a serious public health and social issue allover the world. For instance, in the United States, about35 million persons experience activity limitations owingto chronic health problems or impairments, incurringhigh health care costs [1]. In view of the manifest impor-tance of this problem, it would be valuable to have modelspredictive of handicap easily applicable to large popula-tions. If it were possible to provide a simple measure pre-dicting the amount of handicap a patient with a given dis-ability will have to face, it would be easier to identify per-sons at risk and to offer those patients specifically tailoredprevention or rehabilitation programs, according to theirindividual needs.

Sense of Coherence Psychother Psychosom 1999;68:102–110 103
Several attempts have been made in order to under-stand and conceptualize the process of disease or im-paired health in a general way. According to the Interna-tional Classification of Impairments, Disabilities, andHandicaps (ICIDH), a trial supplement to the WHO clas-sification of diseases, four concepts should be distin-guished: disease, impairment, disability, and handicap.ICIDH recognizes that ‘whether a person performs asocially expected activity depends not simply on the char-acteristics of the person but also on the larger context ofsocial and physical environments’ [1]. Within this frame-work, disease (or injury) is seen as pure ‘pathology’.Impairment refers to losses of mental, anatomical, orphysiological structure or function directly attributable toinjury or disease (‘structural loss’). Impairment can resultin disability, which refers to limitations in physical ormental function, in carrying out socially defined tasks androles that individuals generally are expected to be able todo (‘functional limitation’). Finally, handicap is definedas limitation in an individual’s roles which may or maynot occur as a consequence of disability (‘role limitation’)[1]. In rheumatoid arthritis (RA) for example, the diseaseprocess consists of a joint inflammation, while impair-ment corresponds to degenerative processes in the joints;difficulties in walking or gripping are signs of disability,and loss of work capacity as a housewife or a cook refer tothe handicap dimension.
How these components of ill health may be operation-ally defined remains complex, as are the relationshipsbetween the components. In the studies described in thispaper, it is assumed that objective measures of illnessdefine disability, while psychological and other subjectivefactors as well as disability contribute to handicap.
Factors which may mediate between disability andhandicap are of substantial clinical and research interest.One putative factor with such a role is sense of coherence(SOC), which arose from the concept of salutogenesis,developed by the medical sociologist Aaron Antonovsky[2] from studies with menopausal women, some of whomhad survived the holocaust. Antonovsky argued that therewere no such states as ‘health’ or ‘illness’ in a strict sense,but rather an ‘ease-disease continuum’ on which we allmove back and forth during our life cycle. Being well doesnot merely imply the absence of pathology; the key featureof salutogenesis is that good health can be directly sus-tained by positive factors. Antonovsky [3] defined coher-ence as ‘a global orientation that expresses the extent towhich one has a pervasive, though dynamic feeling of con-fidence that (1) the stimuli deriving from one’s internaland external environments in the course of living are
structured, predictable, and explicable; (2) the resourcesare available to one to meet the demands posed by thesestimuli; and (3) these demands are challenges, worthy ofinvestment and engagement’.
The SOC scale was developed by Antonovsky to mea-sure salutogenesis. The SOC scale is a self-rating question-naire which measures the extent to which an individual islikely to construe a stressor as comprehensible and worthovercoming, and the individual’s appraisal that he or shewill manage to overcome such stressors [3]. SOC is essen-tially a measure of an individual’s resilience in the face ofstress, and capacity to cope with it. However, while con-ventional coping measures assess preferences for particu-lar coping strategies, SOC measures the individual’s ca-pacity to respond to stressors by the appropriate applica-tion of a variety of coping and other strategies [4]. Indi-viduals with high SOC scores are those likely to perceivestressors as predictable and explicable, have confidence intheir capacity to overcome stressors, and judge it worth-while to rise to the challenges they face. Low SOC mea-sures the relative absence of these beliefs. The concept hassimilarities with other theories of stress resistance such aslocus of control [5], self-efficacy [6], hardiness [7], disposi-tional optimism [8], and psychological well-being [9].However, SOC is a broader concept than each of these,including individual as well as societal dimensions ofmeaningfulness, thus making the concept applicablethroughout different cultures.
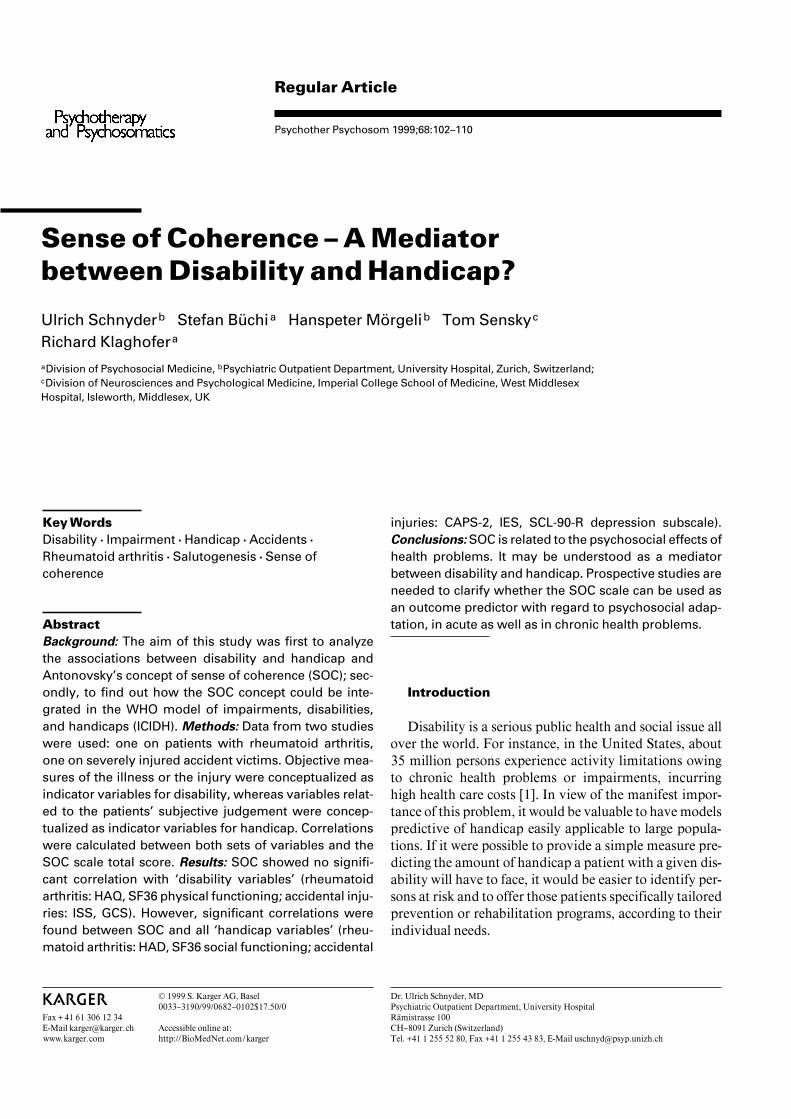
The SOC scale has been used in a large number of stud-ies in mental health [10, 11], psychosomatic medicine[12–14], public health [15, 16], and stress research [17,18]. Although it is known that SOC can predict short-termor long-term outcome of psychiatric and somatic healthproblems [19–21], it is unclear how SOC exerts itsinfluence on the course of an illness. Therefore, the aim ofthis study was first to analyze the associations betweendisability and handicap and SOC; and secondly, to findout how Antonovsky’s concept could be integrated in theWHO model of impairments, disabilities, and handicaps(ICIDH). For this purpose, data from two studies recentlycarried out by our research group were analyzed for possi-ble correlations between SOC and a number of indicatorvariables of disability and handicap. Our hypothesis wasthat SOC acts as a mediator between disability and handi-cap, exerting its impact mainly on variables related to thepatient’s subjective valuation of a perceived disability(fig. 1).
104 Psychother Psychosom 1999;68:102–110 Schnyder/Büchi/Mörgeli/Sensky/Klaghofer
Fig. 1. The SOC within the WHO model, the ICIDH.
Method
Measurement of SOCThe SOC questionnaire [3] consists of 29 items. Answers have to
be given using a 7-point Likert scale on which the extreme answers (1and 7) are formulated for each question. For instance, patients areasked ‘Until now your life has had: No clear goals or purpose at all(answer 1) ... Very clear goals and purpose (answer 7)’; ‘Do you havethe feeling that you’re being treated unfairly? Very often (answer 1) ...Very seldom or never (answer 7)’. Test properties such as test-retestreliability and internal consistency of the SOC scale are excellent [4,22]. In previous studies, factor analyses have failed to reproduce thethree subscales (comprehensibility, manageability, meaningfulness).It has therefore been recommended that only the total SOC score beused in research [4, 13, 14, 23] and the present study followed thisconvention.
Study AA study on the psychosocial outcome of patients with RA was
chosen as an example of a chronic and disabling disease [24]. Thissample allowed us to study the SOC in patients who had been suffer-ing from their disease for a long period of time, and had reached arelatively stable steady state, with a degree of disability and handi-cap.
Measures in Study A. Functional limitation (disability) was mea-sured using the Health Assessment Questionnaire (HAQ) [25], one ofthe most widely used measures of limitation in activities of daily liv-ing in RA [26]. The HAQ is a self-report questionnaire measuringdifficulties in eight domains, including dressing, arising, eating, walk-ing, hygiene, reaching, and gripping. A total score is derived from themean of its subscales. The Hospital Anxiety and Depression Scale(HAD) [27] was used to assess psychological parameters. This is areliable measure of depression in people with physical illness [28].For the purpose of this study, the HAD depression subscale was usedas an indicator variable for handicap. The Short Form Health SurveyQuestionnaire (SF36) [29, 30] is a well-known and often used genericinstrument to assess health-related quality of life. It consists of eight
scales (physical functioning, role limitations due to physical andemotional problems, pain, general health perceptions, vitality, socialfunctioning, and emotional well-being). For the analyses presented inthis paper, the SF36 physical functioning scale served as an indicatorvariable for disability, while the SF36 social functioning scale wasused as an indicator variable for handicap (see below).
Procedure in Study A. The sample was drawn from patientsattending a rheumatology outpatient clinic. Inclusion criteria for thestudy were (a) age at least 25 years and (b) signs and symptoms meet-ing the 1987 criteria of the American College of Rheumatology [31].Patients with significant comorbidity or a past psychiatric historywere excluded. Of 110 consecutive patients eligible for the study, 89(81%) agreed to participate. Nonparticipants did not differ from thestudy sample in gender, age, employment status or duration of ill-ness. Sociodemographic and clinical characteristics of the RA studysample are presented in table 1.
Study BBy contrast, as an example representing health problems with
acute onset and good prognosis, we chose a study on patients whohad sustained severe injuries following a life-threatening accident,requiring treatment in an intensive care unit [32]. These patientswere suddenly and unexpectedly confronted with severe injuries,impairments, and disabilities, and with a considerable uncertaintyabout physical and psychosocial sequelae. In other words, thesepatients had to cope with current handicaps as well as with the threatof possible long-term handicaps in the future.
Measures in Study B. The Injury Severity Score (ISS) [33, 34] per-mits an evaluation of the gravity of injuries by a surgeon specializedin accidents: every area of the body concerned is given a score (1 =minimum; 6 = fatal injury). The scores of the three most badly dam-aged areas of the body are squared and then added up, producing amaximum score of 75. Patients with a score of 10 or more are gener-ally considered severely injured. The Glasgow Coma Scale (GCS)[35] is an outside rating for the clinical appraisal of the gravity of acoma following injury to the skull and brain. Patients with severeskull and brain trauma generally have a score of under 9. ISS andGCS were conceptualized as indicator variables for disability (seebelow). Posttraumatic psychological symptoms were assessed usingthe Impact of Event Scale (IES) [36], a 15-item self-rating question-naire comprising two subscales (intrusion and avoidance) that isamong the most frequently used research instruments in traumaticstress research. The questionnaire has high reliability and validity asa screening instrument for posttraumatic stress disorder (PTSD) [37,38]. To assess the specific symptoms of posttraumatic stress disorder,the Clinician-Administered PTSD Scale (CAPS-2) [39–41] was ad-ministered. This instrument allows quantification of the frequencyplus intensity of each of the 17 PTSD symptoms according to theDSM-III-R. The CAPS-2 has excellent psychometric properties [39,41]. Finally, the Symptom Checklist (SCL-90-R) [42, 43] was used toassess a broad spectrum of psychological complaints. In the evalua-tion, nine symptom factors can be distinguished: somatization,obsessive-compulsive, interpersonal sensitivity, depression, anxiety,aggression, hostility, phobic anxiety, paranoid ideation and psychoti-cism. IES, CAPS-2, and SCL-90-R depression subscale served asindicator variables for handicap (see below).
Procedure in Study B. Inclusion criteria for this study were 18–70years of age, an ISS of 10 or more, a GCS score of 9 or more (thusexcluding all patients with severe head injuries), and the capacity tocooperate in an extensive interview within 1 month after the acci-
Sociodemographic variables
Sense of Coherence Psychother Psychosom 1999;68:102–110 105
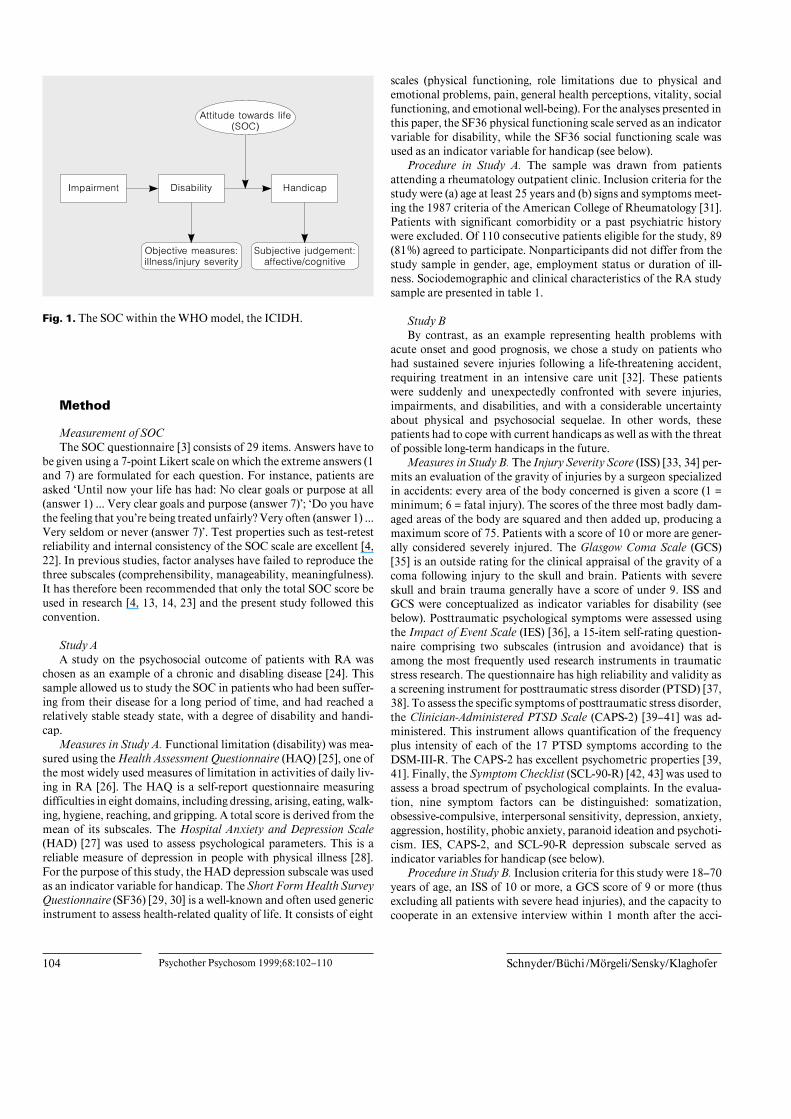
Table 1. Sample characteristics ofpatients with RA (n = 89) and of severelyinjured accident victims (n = 112)
RA Accidental injuries
Age, yearsBSD 61.3B13.8 37.9B13.4Sex
Male 24 (27.0%) 83 (74.1%)Female 65 (73.0%) 29 (25.9%)
Marital statusSingle 11 (12.4%) 50 (44.6%)Married 50 (56.2%) 48 (42.9%)Divorced, separated 16 (18.0%) 14 (12.5%)Widowed 12 (13.5%) 0 (0.0%)
Living arrangementsAlone 26 (29.5) 24 (21.4%)With others (family, partner, friends) 62 (70.5) 88 (78.6%)Missing 1 0
Employment statusPaid work (full- or part-time) 21 (23.6%) 96 (85.7%)Homemaker 28 (31.5%) 2 (1.8%)Retired 37 (41.6%) 3 (2.7%)Unemployed, student 3 (3.4%) 11 (9.8%)
Clinical variablesSOC total score (range 29–203) 144.1B27.9 155.3B20.7Years since diagnosis 12.6B9.7HAQ (range 0–3) 1.1B0.7HAD depression score (range 0–21) 6.0B3.2SF36 physical functioning 29.0B26.9SF36 social functioning 48.9B27.0
Number of days between accident and interview (t1) 13.5B6.6ISS (range 0–75) 21.8B10.0GCS (range 0–15) 14.5B1.4CAPS-2 total score (range 0–136) 20.8B14.4IES total score (range 0–75) 14.5B14.6SCL-90-R depression subscale score (range 0–4) 0.58B0.53
Figures are numbers (%) of patients and mean values (B SD).
dent. Patients were excluded who had been suffering from any seri-ous illness (particularly from any psychiatric disorder) prior to theaccident, as were those with injuries due to a suicide attempt or to aphysical attack. The sample thus consisted of severely injured acci-dent victims who have not sustained a major head injury and whohad no major somatic or psychological health problems prior to thetraumatic event. During a recruitment period of 18 months, 135patients were eligible for the study. One hundred and twenty-one(89.6%) gave their informed consent. Sociodemographic and clinicalcharacteristics of this sample are presented in table 1. With regard tothe scales analyzed in this paper, complete sets of data were availablein 112 patients. The mean number of days between accident andinterview were 13.5 (standard deviation, SD 6.6).
Assessment of Disability and HandicapIn keeping with the definition of disability according to the
ICIDH [1], objective measures of illness (RA study: HAQ, SF36
physical functioning) or injury severity (accident study: ISS, GCS)were judged to be indicators of disability for this study. On the otherhand, we assumed that limitations in social roles (i.e. handicap) arereflected well in measures of the patients’ subjective judgementregarding their health problem. Therefore, we chose the HADdepression subscale and SF36 social functioning in the RA study, andthe IES, CAPS-2, and SCL-90-R depression subscale in the accidentstudy as indicator variables for handicap.
Statistical AnalysesData were analyzed using the Statistical Package for Social
Sciences SPSS [44]. Pearson’s correlation coefficients were calcu-lated to assess correlations between SOC and all other variables. Tocontrol for correlations between disability and handicap variables,partial correlation coefficients were also calculated.
HAQ
106 Psychother Psychosom 1999;68:102–110 Schnyder/Büchi/Mörgeli/Sensky/Klaghofer
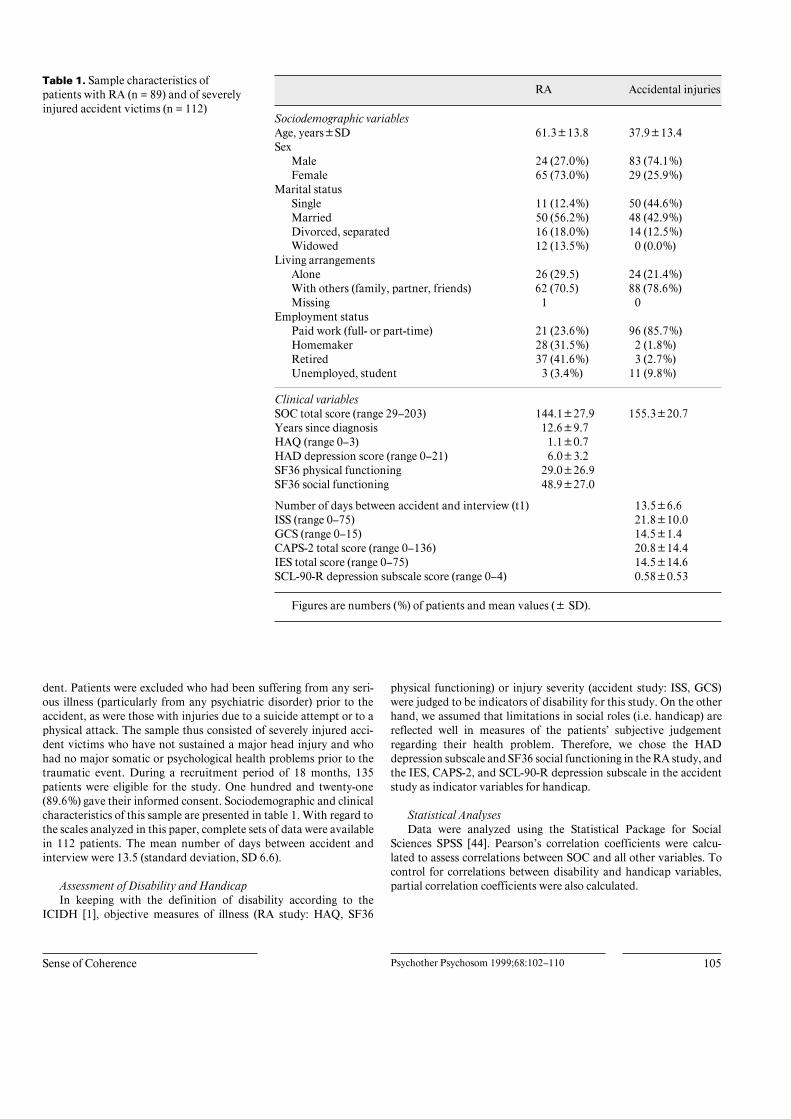
Table 2. Correlation matrix for SOCand indicator variables for disability andhandicap in RA (n = 89)
SOC HAQ SF36physicalfunctioning
HADdepression
–0.19p = 0.090
SF36 physical functioning 0.20p = 0.068
–0.79p = 0.000
HAD depression –0.55p = 0.000
0.45p = 0.000
–0.47p = 0.000
SF36 social functioning 0.37p = 0.001
–0.61p = 0.000
0.62p = 0.000
–0.63p = 0.000
Partial correlation coefficients for ‘disability variables’, controlling for HAD depression andSF36 social functioningHAQ 0.08
p = 0.470SF36 physical functioning –0.08
p = 0.468
Partial correlation coefficients for ‘handicap variables’, controlling for HAQ and SF36physical functioningHAD depression –0.53
p = 0.000SF36 social functioning 0.33
p = 0.003
Pearson’s correlation coefficients.
Results
Study A (RA)The mean SOC total score was 144.1 (SD 27.9). No
significant correlations with SOC were found for age.Mean SOC scores did not differ significantly betweenmales and females (t = –0.37, d.f. = 81, p = 0.71). Thecorrelation matrix for SOC, disability, and handicap vari-ables is presented in table 2. HAQ and SF36 physicalfunctioning, the two variables measuring bodily damageand thus serving as indicator variables for disability in ourmodel, did not correlate significantly with SOC. Signifi-cant correlations were found between SOC and all thechosen handicap variables, i.e. a negative correlation withthe HAD subscale for depression and a positive correla-tion with the SF36 social functioning. The results re-mained unchanged after calculating partial correlations,controlling for the mutual influence of the disability andhandicap variables, respectively, on their correlationswith SOC.
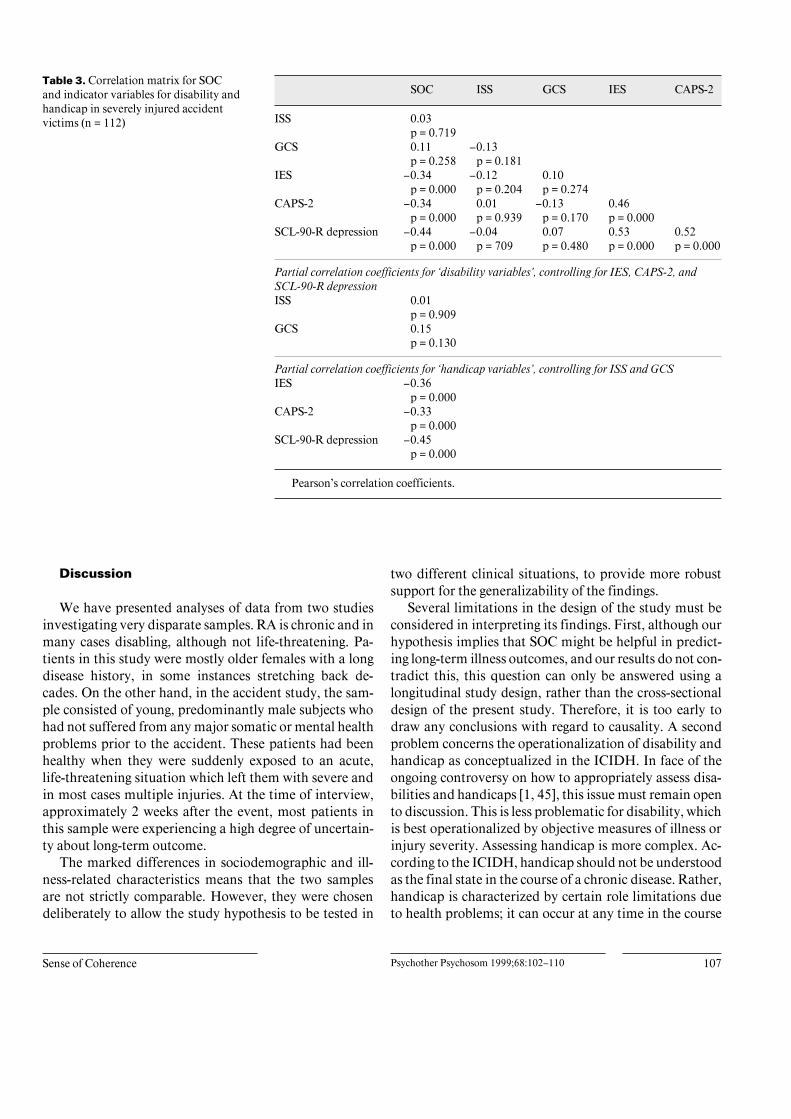
Study B (Accident Victims)The mean SOC total score in this sample was 155.3
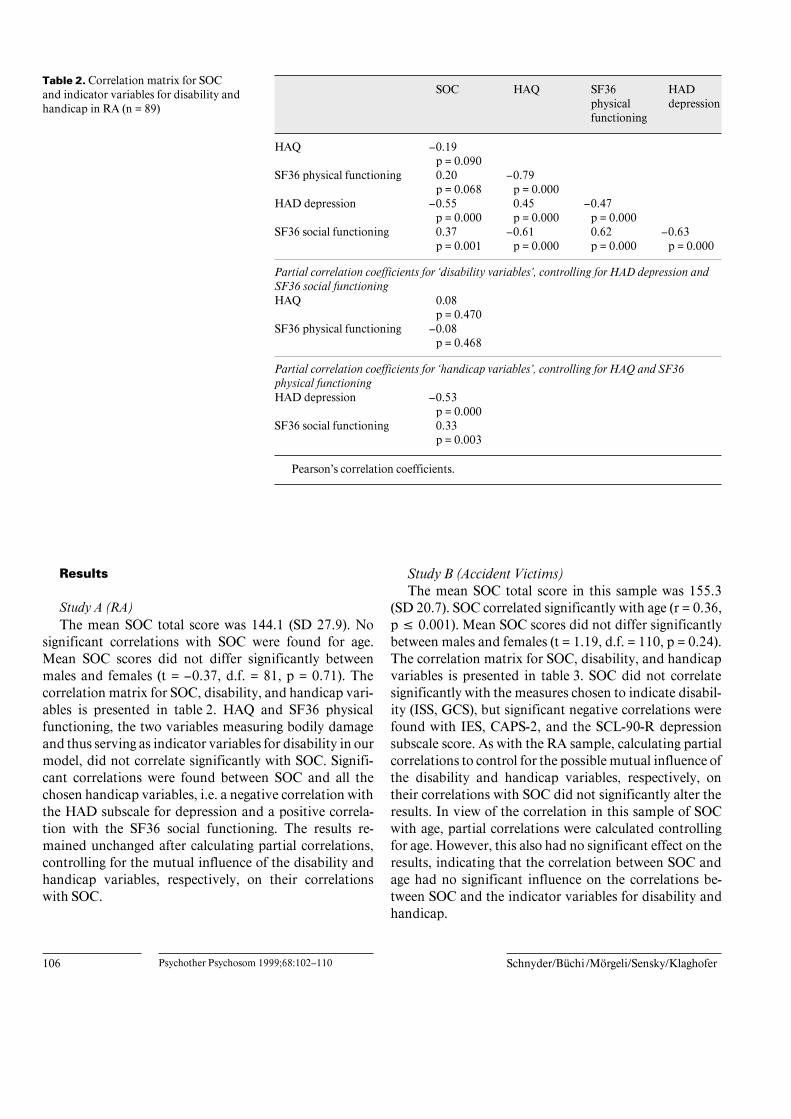
(SD 20.7). SOC correlated significantly with age (r = 0.36,p ^ 0.001). Mean SOC scores did not differ significantlybetween males and females (t = 1.19, d.f. = 110, p = 0.24).The correlation matrix for SOC, disability, and handicapvariables is presented in table 3. SOC did not correlatesignificantly with the measures chosen to indicate disabil-ity (ISS, GCS), but significant negative correlations werefound with IES, CAPS-2, and the SCL-90-R depressionsubscale score. As with the RA sample, calculating partialcorrelations to control for the possible mutual influence ofthe disability and handicap variables, respectively, ontheir correlations with SOC did not significantly alter theresults. In view of the correlation in this sample of SOCwith age, partial correlations were calculated controllingfor age. However, this also had no significant effect on theresults, indicating that the correlation between SOC andage had no significant influence on the correlations be-tween SOC and the indicator variables for disability andhandicap.
ISS
Sense of Coherence Psychother Psychosom 1999;68:102–110 107
Table 3. Correlation matrix for SOCand indicator variables for disability andhandicap in severely injured accidentvictims (n = 112)
SOC ISS GCS IES CAPS-2
0.03p = 0.719
GCS 0.11p = 0.258
–0.13p = 0.181
IES –0.34p = 0.000
–0.12p = 0.204
0.10p = 0.274
CAPS-2 –0.34p = 0.000
0.01p = 0.939
–0.13p = 0.170
0.46p = 0.000
SCL-90-R depression –0.44p = 0.000
–0.04p = 709
0.07p = 0.480
0.53p = 0.000
0.52p = 0.000
Partial correlation coefficients for ‘disability variables’, controlling for IES, CAPS-2, andSCL-90-R depressionISS 0.01
p = 0.909GCS 0.15
p = 0.130
Partial correlation coefficients for ‘handicap variables’, controlling for ISS and GCSIES –0.36
p = 0.000CAPS-2 –0.33
p = 0.000SCL-90-R depression –0.45
p = 0.000
Pearson’s correlation coefficients.
Discussion
We have presented analyses of data from two studiesinvestigating very disparate samples. RA is chronic and inmany cases disabling, although not life-threatening. Pa-tients in this study were mostly older females with a longdisease history, in some instances stretching back de-cades. On the other hand, in the accident study, the sam-ple consisted of young, predominantly male subjects whohad not suffered from any major somatic or mental healthproblems prior to the accident. These patients had beenhealthy when they were suddenly exposed to an acute,life-threatening situation which left them with severe andin most cases multiple injuries. At the time of interview,approximately 2 weeks after the event, most patients inthis sample were experiencing a high degree of uncertain-ty about long-term outcome.
The marked differences in sociodemographic and ill-ness-related characteristics means that the two samplesare not strictly comparable. However, they were chosendeliberately to allow the study hypothesis to be tested in
two different clinical situations, to provide more robustsupport for the generalizability of the findings.
Several limitations in the design of the study must beconsidered in interpreting its findings. First, although ourhypothesis implies that SOC might be helpful in predict-ing long-term illness outcomes, and our results do not con-tradict this, this question can only be answered using alongitudinal study design, rather than the cross-sectionaldesign of the present study. Therefore, it is too early todraw any conclusions with regard to causality. A secondproblem concerns the operationalization of disability andhandicap as conceptualized in the ICIDH. In face of theongoing controversy on how to appropriately assess disa-bilities and handicaps [1, 45], this issue must remain opento discussion. This is less problematic for disability, whichis best operationalized by objective measures of illness orinjury severity. Assessing handicap is more complex. Ac-cording to the ICIDH, handicap should not be understoodas the final state in the course of a chronic disease. Rather,handicap is characterized by certain role limitations dueto health problems; it can occur at any time in the course

108 Psychother Psychosom 1999;68:102–110 Schnyder/Büchi/Mörgeli/Sensky/Klaghofer
of an illness or a rehabilitation process and is thus alwayssubject to change [45, 46]. A further complication isthat mental disorders such as depression are themselvesclassified in the ICIDH as impairments. However, themeasures of depression used in our study (HAD and SCL-90-R depression subscales, respectively) refer to depres-sive symptoms or ‘depressivity’ rather than to the clinicalsyndrome of depression. Because depressive symptoms,impaired social functioning or the presence of specificposttraumatic stress symptoms almost always lead to rolelimitations, we consider that it is justified to use these asindicator variables for handicap. A further limitation ofany study using SOC is that it is uncertain that SOC accu-rately reflects salutogenesis, because there is no ‘gold stan-dard’ measure available to assess this aspect of the validi-ty of SOC. In view of the observed correlations betweenSOC and our indicator variables of handicap, it could beargued that SOC is merely a proxy measure of depression(see below).
The mean SOC total score in our patients with RA issimilar to that found in other similar patient samples [13].The mean SOC score in the sample of severely injuredaccident victims is relatively high, even higher than ingeneral population samples [47–49]. This finding can beinterpreted in two ways. First, it may represent thepatients’ readiness to face the challenges and demandsrelated to their current situation as an accident victim,and the salience of coping in their lives at the time. Sec-ond, the high SOC scores may also be understood as areflection of a transient state characterized by feelings ofoptimism and strength in persons who have recentlyescaped a life-threatening situation.
In spite of the marked disparity between the two sam-ples, they yielded similar answers to the main hypothesisof the study. No significant correlations were foundbetween SOC and any objective measures of illness orinjury severity, conceptualized as indicator variables fordisability. On the other hand, SOC correlated significant-ly with all variables related to subjective judgement, con-ceptualized as indicator variables for handicap. Relatingthis finding to the WHO model of impairments, disabili-ties, and handicaps (ICIDH) [1], these results lend sup-port to the idea that SOC might exert its effect indepen-dently of a given disability (disease or injury) somewhereon the pathway between disability and handicap (fig. 1). Ifthese findings could be confirmed in prospective studies(which is not unlikely, given the relative stability of theSOC construct), handicap could be seen as the result of aninteraction between disability and salutogenic resources.Given a defined level of disability, a patient with a high
SOC would then be expected to move more toward thehealth end on the ‘ease-disease continuum’ [3] and there-fore suffer less handicap than a patient with low SOC.
Studies in different fields of medicine have alreadyreported similar relations between SOC, impairment, andhandicap. In patients with oral and pharyngeal cancer,more severe disturbances after surgery were found inpatients with lower SOC but no significant correlationsbetween extensiveness of surgery and disturbances werefound [50]. Similarly, in women with a range of chronicphysical disabilities, long-term psychosocial adaptationwas predicted only by socioeconomic status and SOC butnot by disability status variables [51]. In a study on trafficaccident victims, SOC correlated significantly with post-traumatic symptoms but not with injury severity [52].Also, in an experimental study exposing the participantsto a controlled stressful situation, subjects with low SOCreported significantly more stress, anxiety and anger, andwere also less approach-oriented in their coping behaviorthan high SOC subjects [17].
In accordance with other reported findings [13, 14, 18],our results indicate that SOC and depression are related.In fact, some authors claimed that SOC may be mainly areflection of psychiatric (mainly affective) morbidity [13,14]. Low SOC superficially resembles some of the cogni-tive features of depression. However, several lines of evi-dence indicate that SOC and depression are fundamental-ly different measures. First, some findings of the currentstudy are inconsistent with SOC being simply a measureof depression. For instance, in our RA study sample thereis a significant correlation between the SF36 physicalfunctioning and HAD depression (r = 0.47, p ^ 0.001),but a nonsignificant correlation between SF36 physicalfunctioning and SOC (r = 0.20, n.s.). The two correlationsare significantly different from each other (p ^ 0.05).This finding could not be replicated in the accident studythough, where we found no significant correlations ofinjury severity with either SCL-90-R depression or SOC.Secondly, even allowing for some overlap between lowSOC and the cognitive aspects of depression, there is noreason why high SOC should equate with absence ofdepressive symptoms alone. It has been demonstrated inan earlier paper of our study group that depression canalso occur in RA patients with high SOC, and, conversely,not 100% but only 56% of RA patients with low SOCdevelop depression [24]. Thirdly, while depression is astate which changes over time, evidence that SOC be-haves more like a trait measure comes from data on theconsistency of SOC scores over time [4, 53] and their cor-relation with other trait measures [49, 54]. Nevertheless,

Sense of Coherence Psychother Psychosom 1999;68:102–110 109
SOC must not necessarily be seen as a stable personalitytrait. Rather, it can best be understood as an individual’s‘world view’ that remains largely stable but also has adegree of plasticity, being subject to modification byexceptional experiences.
In the RA sample, age did not correlate significantlywith SOC, whereas in the accidentally injured patients, asignificant positive correlation was found. Partial correla-tion showed that psychological symptoms have no effecton this correlation. The accident victims were almost 25years younger than the patients with RA, although thestandard deviation was the same in both samples. Anto-novsky claimed that the SOC develops in childhood andadolescence and remains stable during adulthood [3].From a perspective of life span development [55, 56], itcould be argued that 10 years make a greater difference ina person’s twenties than in his or her sixties. In the sampleof accident victims, some of the patients may not yet havereached their full psychological maturity and thus theirSOC is still subject to further development. In a study on asample of 461 patients attending a psychosomatic outpa-
tient clinic, showing a similar age distribution, age alsocorrelated significantly with SOC [12].
In conclusion, disability is a sine qua non for the devel-opment of a handicap. However, variance of handicapappears not to be exclusively determined by the varianceof disability. Handicap seems to be associated with lowSOC scores. Our findings suggest that SOC might beunderstood as a mediator between disability and handi-cap, influencing the psychosocial effects of a given healthproblem. However, further evaluation in prospectivestudies is necessary before robust conclusions can bedrawn on the relevance of SOC to the development of dis-ease-related handicap.
Acknowledgements
This study was supported by the Swiss National Science Founda-tion (U. Schnyder: project No. 32-43640.95; S. Büchi: fellowship).We wish to thank Prof. C. Buddeberg, Zurich, and Prof. E. Heim,Oberhofen, for their critical remarks and helpful suggestions withregard to an earlier version of this paper.
References
1 Pope AM, Tarlow AR (eds): Disability inAmerica: Toward a National Agenda for Pre-vention. Washington, National AcademyPress, 1991.
2 Antonovsky A: Health, Stress and Coping. SanFrancisco, Jossey-Bass, 1979.
3 Antonovsky A: Unraveling the Mystery ofHealth: How People Manage Stress and StayWell. San Francisco, Jossey-Bass, 1987.
4 Antonovsky A: The structure and properties ofthe sense of coherence scale. Soc Sci Med 1993;36:725–733.
5 Rotter JB: Generalized expectancies for inter-nal versus external control of reinforcement.Psychol Monogr 1966;80.
6 Bandura A: Self-efficacy: Toward a unifyingtheory of behavioral change. Psychol Rev 1977;84:191–215.
7 Kobasa SC: Stressful life events, personalityand health: An inquiry into hardiness. J PersSoc Psychol 1979;37:1–11.
8 Scheier MF, Carver CS: Optimism, coping, andhealth: Assessment and implications of gener-alized outcome expectancies. Health Psychol1985;3:219–247.
9 Ryff CD, Singer B: Psychological well-being:Meaning, measurement, and implications forpsychotherapy research. Psychother Psycho-som 1996;65:14–23.
10 Kushner MG, Riggs DS, Foa EB, Miller SM:Perceived controllability and the developmentof posttraumatic stress disorder (PTSD) incrime victims. Behav Res Ther 1993;31:105–110.
11 Eriksson NG, Lundin T: Early traumatic stressreactions among Swedish survivors of the m/sEstonia disaster. Br J Psychiatry 1996;169:713–716.
12 Sack M, Künsebeck H-W, Lamprecht F: Senseof coherence and psychosomatic outcome: Anempirical investigation on salutogenesis. Psy-chother Psychosom Med Psychol 1996;47:149–155.
13 Hawley DJ, Wolfe F, Cathey MA: The sense ofcoherence questionnaire in patients with rheu-matoid arthritis. J Rheumatol 1992;19:1912–1918.
14 Callahan LF, Pincus T: The sense of coherencescale in patients with rheumatoid arthritis. Ar-thritis Care Res 1995;8:28–35.
15 Udris I, Kraft U, Mussmann C: Personal andorganisational resources of salutogenesis; inDauwalder J-P (ed): Psychology and Promo-tion of Health. Seattle, Hogrefe & Huber, 1994,pp 3–7.
16 Lundberg O, Nyström Peck M: Sense of coher-ence, social structure and health: Evidencefrom a population survey in Sweden. Eur JPublic Health 1994;4:252–257.
17 McSherry WC, Holm JE: Sense of coherence:Its effects on psychological and physiologicalprocesses prior to, during, and after a stressfulsituation. J Clin Psychol 1994;50:476–487.
18 Flannery RB, Perry JC, Penk WE, FlanneryGJ: Validating Antonovsky’s Sense of Coher-ence scale. J Clin Psychol 1994;50:575–577.
19 Flannery RB, Flannery GJ: Sense of coherence,life stress, and psychological distress: A pro-spective methodological inquiry. J Clin Psy-chol 1990;46:415–420.
20 Chamberlain K, Petrie K, Azariah R: The roleof optimism and sense of coherence in predict-ing recovery following surgery. Psychol Health1992;7:301–310.
21 Petrie K, Brook R: Sense of coherence, self-esteem, depression and hopelessness as corre-lates of reattempting suicide. Br J Clin Psychol1992;31:293–300.
22 Frenz AW: Measuring Antonovsky’s sense ofcoherence construct: A psychometric study.Diss Abstr Int 1990;51:6141.
23 Frenz AW, Carrey MP, Jorgensen RS: Psycho-metric evaluation of Antonovsky’s sense of co-herence scale. Psychol Assess 1993;5:145–153.
24 Büchi S, Sensky T, Allard S, Stoll T, SchnyderU, Klaghofer R, Buddeberg C: Sense of coher-ence: A protective factor for depression inrheumatoid arthritis. J Rheumatol 1998;25:869–875.
25 Fries JF, Spitz PW, Kraines RG, Holman HR:Measurements of patients outcome in arthritis.Arthritis Rheum 1980;23:137–145.
26 Radanov BP, Schwarz HA, Frost SA, Augusti-ny KF: Relationship between self-rated func-tional status and psychosocial stress in patientssuffering from rheumatoid arthritis. Psycho-ther Psychosom 1997;66:252–257.
27 Zigmond AS, Snaith RP: The Hospital Anxietyand Depression Scale. Acta Psychiatr Scand1983;67:361–370.
110 Psychother Psychosom 1999;68:102–110 Schnyder/Büchi/Mörgeli/Sensky/Klaghofer
28 Aylard PR, Gooding JH, McKenna PJ, SnaithRP: A validation study of three anxiety anddepression self-assessment scales. J PsychosomRes 1987;31:261–268.
29 Ware JE, Sherbourne CD: A 36-item ShortForm Health Survey (SF36): Conceptualframework and item selection. Med Care 1992;30:473–483.
30 Jenkinson C, Coulter A, Wright L: Short Form(SF 36) Health Survey questionnaire: Norma-tive data for adults of working age. BMJ 1993;306:1437–1440.
31 Arnett FC, Edworthy SM, Bloch DA: TheAmerican Rheumatism Association 1987 re-vised criteria for the classification of rheuma-toid arthritis. Arthritis Rheum 1988;31:315–324.
32 Schnyder U: Psychotraumatological aspects ofaccidents. Arch Neuropsychiatry 1997;34:88–96.
33 Baker SP, O’Neill B, Haddon W: The injuryseverity score: A method for describing pa-tients with multiple injuries and evaluatingemergency care. J Trauma 1974;14:187–196.
34 Baker SP, O’Neill B: The injury severity score:An update. J Trauma 1976;16:882–885.
35 Teasdale G, Jennett B: Assessment of comaand impaired consciousness: A practical scale.Lancet 1974;ii:81.
36 Horowitz MJ, Wilner N, Alvarez W: Impact ofEvent Scale: A measure of subjective stress.Psychosom Med 1979;41:209–218.
37 McFall ME, Smith DE, Roszell DK, TarverDJ, Malas KL: Convergent validity of mea-sures of PSD in Vietnam combat veterans. AmJ Psychiatry 1990;147:645–648.
38 Ferring D, Filipp S-H: Teststatistische Über-prüfung der Impact of Event-Skala: Befunde zuReliabilität und Stabilität. Diagnostica 1994;40:344–362.
39 Weathers FW, Litz BT: Psychometric proper-ties of the Clinician-Administered PTSD Scale,CAPS-1. PTSD Res Q 1994;5:2–6.
40 Blake DD, Weathers FW, Nagy L, KaloupekDG, Klauminzer G, Charney DS, Keane TM:A clinician rating scale for assessing currentand lifetime PTSD: The CAPS-1. Behav Thera-pist 1990;18:187–188.
41 Blake DD, Weathers FW, Nagy L, KaloupekDG, Gusmann FD, Charney DS, Keane TM:The development of a Clinician-AdministeredPTSD Scale. J Trauma Stress 1995;8:75–90.
42 Derogatis LR: SCL-90 R: Administration,Scoring and Procedure Manual-II for the Re-vised Version. Towson, Clinical PsychometricResearch, 1986.
43 Franke G: Eine weitere Überprüfung derSymptom-Check-Liste (SCL-90 R) als For-schungsinstrument. Diagnostica 1992;38:160–167.
44 SPSS-7.5: SPSS 7.5 syntax reference guide.Chicago, SPSS, 1997.
45 Matthesius RG, Jochheim KA, Barolin GS,Heinz C (eds): ICIDH – International Classifi-cation of Impairments, Disabilities, and Han-dicaps. Berlin, Ullstein/Mosby, 1995.
46 WHO: International Classification of Impair-ments, Disabilities and Handicaps: A Manualof Classification Relating to the Consequencesof Disease. Geneva, World Health Organiza-tion, 1980.
47 Cederblad M, Dahlin L, Hagnell O, HanssonK: Coping with life-span crises in a group atrisk for mental and behavioral disorders: Fromthe Lundby study. Acta Psychiatr Scand 1995;91:322–330.
48 Kalimo R, Vouri J: Work factors and health:The predictive role of pre-employment experi-ences. J Occup Psychol 1991;64:97–115.
49 Langius A, Bjorwell H: Coping ability andfunctional status in a Swedish population sam-ple. Scand J Caring Sci 1993;7:3–10.
50 Langius A, Lind MG: Well-being and coping inoral and pharyngeal cancer patients. Eur J Can-cer 1995;31B:242–249.
51 Dangoor N, Florian V: Women with chronicphysical disabilities: Correlates of their long-term psychosocial adaptation. Int J RehabilRes 1994;17:159–168.
52 Frommberger U, Stieglitz RD, Nyberg E,Straub S, Berger M: Der Einfluss des «Kohä-renzgefühls» auf die Entwicklung posttrauma-tischer Belastungsstörungen nach Verkehrsun-fällen; in Schüffel W, Brucks U, Johnen R,Köllner V, Lamprecht F, Schnyder U (eds):Handbuch der Salutogenese: Konzept undPraxis. Wiesbaden, Ullstein Medical, 1998.
53 Carmel S, Bernstein J: Trait-anxiety and senseof coherence: A longitudinal study. PsycholRev 1989;65:221–222.
54 Hart KE, Hittner JB, Paras KC: Sense of coher-ence, trait anxiety, and the perceived availabili-ty of social support. J Res Pers 1991;25:137–145.
55 Baltes PB, Reese HW, Lipsitt LP: Life-spandevelopmental psychology: Personality and so-cialisation. Annu Rev Psychol 1980;31:65–110.
56 Featherman D, Lerner RM: Life-Span Devel-opment. New York, Academic Press, 1986.