self-directed e-learning at a tertiary hospital in malawi – a qualitative evaluation and lessons...
TRANSCRIPT

Self-directed e-learning at a tertiary hospital in Malawi –A qualitative Evaluation and Lessons learnt
AbstractBackground: Malawi faces a severe lack of health workers. Despiteinitiatives to address this problem, a critical shortage of health care
Sandra Barteit1
Philip Hoepffner2staff remains. This lack challenges the education and training of juniorSören Huwendiek3
medical staff, especially medical interns in their final and crucial trainingyear before they independently work as medical doctors. Angela Karamagi4Project description: We have introduced an e-learning platform in themedical department of the Kamuzu Central Hospital (KCH) in Malawi.
Charles Munthali5
Antje Theurer4With the support of computer-assisted instruction, we aimed to improveFlorian Neuhann1the quality of medical training and education, as well as access to cur-
rent medical materials, in particular for interns.Method: From March to April 2012, we conducted a qualitative evalu-ation to assess relevance and appropriateness of the e-learning plat- 1 Heidelberg University,
Institute of Public Health,Heidelberg, Germanyform. Data was collected via face-to-face interviews, a guided group
discussion and a checklist based observation log. Evaluation data was2 University Hospital ofWürzburg, Clinic and
recorded and coded using content analysis, interviewees were chosenvia purposive sampling.
Polyclinic for Psychiatry andResults: E-learning proved to be technically feasible in this setting. Usersconsidered the e-learning platform to be relevant and appropriate.
Psychotherapy, Würzburg,Germany
Concerns were raised about sustainability, accessibility and technical3 University of Bern, Instituteof Medical Education,
infrastructure, as well as limited involvement and responsibilities ofMalawian partners. Interest in e-learning was high, yet, awareness of
Department of Assessmentand knowledge about the e-learning platform among potential users and Evaluation, Bern,Switzerlandwas low. Evaluation results indicated that further adaptions to local
needs are necessary to increase usage and accessibility.4 ESTHER Germany, MalawiGerman Networking for
Conclusions: Interview results and our project experiences showed that,in the given setting, e-learning requires commitment from local stake-
Capacity Building inholders, adequate technical infrastructure, identification and assignationof responsibilities, as well as specific adaption to local needs.
Treatment, Training andResearch at Kamuzu CentralHospital (MAGNET), GermanyKeywords: computer-assisted instruction, multimedia, Medical
Education, capacity, ICT, understaffed, teaching hospital, virtual patients,Sub-saharan Africa
5 Kamuzu Central Hospital,Medical Department,Lilongwe, Malawi
IntroductionMalawi faces an immense shortage of health personnelpaired with poor access to health information. In 2013,Malawi had a ratio of 0.2 physicians and 3.4 nurses andmidwives per 10.000 population [http://www.who.int/countries/mwi/en/], compared to the WHO recommend-ation of 23 doctors, nurses and midwives [http://www.who.int/hrh/workforce_mdgs/en/]. Initiatives toaddress this issue included a short 3-year diploma forclinical officers to alleviate the lack of medical doctors[1], extending medical education within Malawi by open-ing the College of Medicine in 1991 [2], [http://www.medcol.mw/?page_id=1194] and an emergency
training plan for health care workers in 2005 [http://www.who.int/countryfocus/cooperation_strategy/ccs_mwi_en.pdf]. Facing the dire lack of senior clinical doctorsfor supervision and teaching during internship, we intro-duced an e-learning platform [http://www.esther-magnet.org] in the medical department of the KamuzuCentral Hospital (KCH). The intention was to compensatefor the lack of medical teaching staff, to increase accessand to improve quality of medical education in the depart-ment with the support of information and communicationstechnology (ICT) and by providing access to up-to-datemedical information [3]. E-learning programs were suc-cessfully used to train healthcare workers in low- andmiddle-income-countries, like e-learning for evidence-
1/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
article – project reportThis is the original (English) version.
The translated (German) version starts at p. 8.OPEN ACCESSmedicine

basedmedicine [4] and for nursing education inMalaysia[5]. We targetedmedical interns during the critical phasefrom trainee to an independent medical professional.The introduction of e-learning was embedded in a widerapproach to improve quality of care and in service trainingat the medical department, supported by a hospitalpartnership [http://www.esther.eu].In the following, we present the concept and implement-ation of e-learning, as well as its evaluation and corres-ponding results one year after its introduction.
Project DescriptionKCH is a tertiary 800-bed-hospital administered by theMinistry of Health [6]. It serves as a teaching hospital andas a referral hospital for central Malawi with a catchmentpopulation of around 6 million [7], [http://www.who.int/patientsafety/implementation/apps/first_wave/malawi_middlesbrough/en/index.html]. Themedical departmenthas a bed capacity of around 90 and runs daily outpa-tient’s clinics, an admitting ward and is further respons-ible for the tuberculosis ward off campus.In Malawi, the College of Medicine (CoM) provides fullmedical training since 1991 [2], [http://www.medcol.mw/?page_id=415]. Currently, there are about forty newmedical doctors graduating per year [8], whereby first-year intake numbers are gradually increased [2]. Gradu-ates intern at a hospital, rotating through departmentsof Medicine, Surgery, Paediatrics and Obstetrics-Gynae-cology. After the internship, the majority works in theMalawian public sector [2].Another essential medical cadre are clinical officers (CO)[1]. They provide medical care, give anesthesia, do sur-gical procedures and perform around 80% of all Malawiancaesarian sections [9]. After 3 years, CO studentsgraduate with a diploma in clinical medicine, followed bya one year hospital internship [1].The lack of senior medical doctors impairs the learningopportunities for interns, especially during their vital in-ternship-year. During the project period there were twodepartmental senior doctors responsible for intern train-ing, in addition to their tasks in patient care and adminis-tration. Improving the education during the internship ispivotal in order to sustain good quality of treatment andcare.
Implementation and content
The e-learning platform was initially setup by the Germanproject partners with medical materials created withinthe project.
Technical setup
With a preference for open source software, the e-learningplatform was setup in Moodle [http://docs.moodle.org/26/en/About_Moodle], which is also used at the partner-ing University. The on-site computer equipment consists
out of 2 workstations and 2 laptops. To save cost andtime, we rented an already setup Linux virtual server,located in Germany. We contracted the Malawi basedInternet service provider Globe Internet Ltd. For the LocalArea Network (LAN), Globe Internet Ltd. installed aWiMAXantenna. The maximum data transfer rate was 256kbps,full duplex. Currently, the department uses a prepaid 3Gmobile network with a data transfer rate of up to 21Mbps.
Content
The needs of medical interns guided the content creationfor and the design of the e-learning platform, particularlyconsidering local relevance and country-specific pathology[2, 6, 7]. Educational needs were specified according tothe requirements in the interns’ logbook of the depart-ment that has been developed with senior medical staffand project partners. Content is geared to support rotatinginterns to meet the defined requirements at the end oftheir rotation with regards to practical knowledge for pa-tient management and demonstration of skills - e.g.lumbar puncture.The platform is organized into four sections: medicallessons and materials, mortality audits, presentationsand workshops, and virtual patients (see Figure 1). Virtualpatients (VP) are a focal element of the e-learning plat-form and defined as “an interactive computer simulationof real-life clinical scenarios for the purpose of healthcareand medical training, education or assessment” [10],[11] (see Table 1 and 2 ). Other projects and studiesprove the relevance of VPs for healthcare education andtheir successful application in developing countries [12].Also, the platform features the medical online librariesHINARI [http://www.who.int/hinari/en/] and UpToDate[http://www.uptodate.com]. Access to the platform isrestricted to clinical personnel and interns.
Didactics
Interns learn self-directed: they work through medicaltexts, watch recorded presentations and step-by-stepwork through VP, which offer also direct feedback to eachdecisionmade, multiple-choice questions and referencesto further relevant materials on third-party websites.Knowledge acquisition during these self-directed learningphases is supported by multimedia activities that coverinformation, communication and exercise activities torapidly qualify learners with instructional knowledge [13],[14].
EvaluationWe qualitatively evaluated the project in May 2012, oneyear after its introduction, focusing on the researchquestion what factors influence the use of the e-learningplatform.
2/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Self-directed e-learning at a tertiary hospital in ...
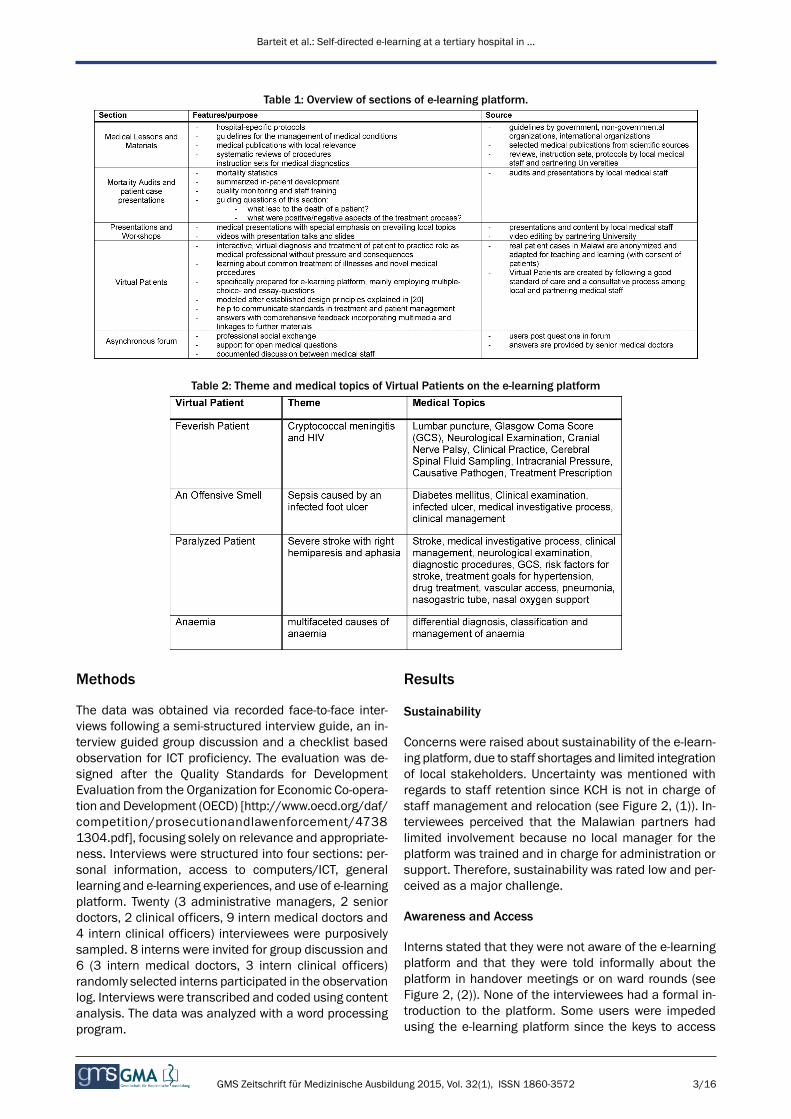
Table 1: Overview of sections of e-learning platform.
Table 2: Theme and medical topics of Virtual Patients on the e-learning platform
Methods
The data was obtained via recorded face-to-face inter-views following a semi-structured interview guide, an in-terview guided group discussion and a checklist basedobservation for ICT proficiency. The evaluation was de-signed after the Quality Standards for DevelopmentEvaluation from the Organization for Economic Co-opera-tion and Development (OECD) [http://www.oecd.org/daf/competition/prosecutionandlawenforcement/47381304.pdf], focusing solely on relevance and appropriate-ness. Interviews were structured into four sections: per-sonal information, access to computers/ICT, generallearning and e-learning experiences, and use of e-learningplatform. Twenty (3 administrative managers, 2 seniordoctors, 2 clinical officers, 9 intern medical doctors and4 intern clinical officers) interviewees were purposivelysampled. 8 interns were invited for group discussion and6 (3 intern medical doctors, 3 intern clinical officers)randomly selected interns participated in the observationlog. Interviews were transcribed and coded using contentanalysis. The data was analyzed with a word processingprogram.
Results
Sustainability
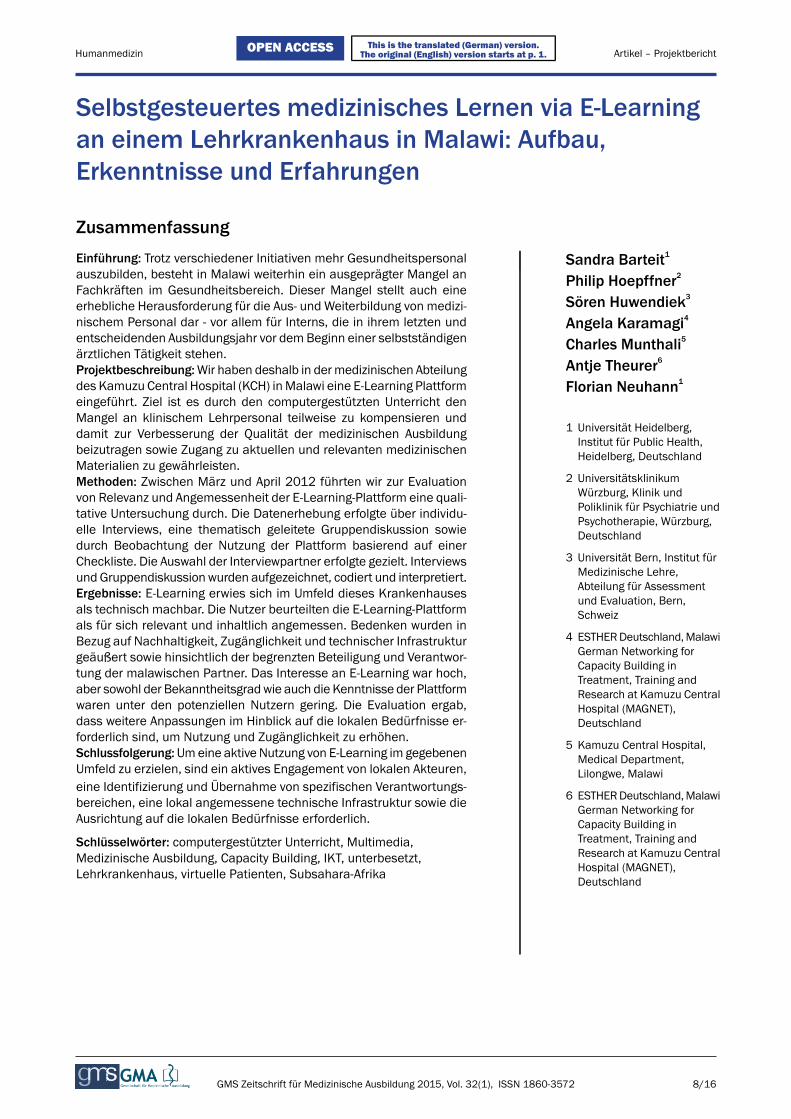
Concerns were raised about sustainability of the e-learn-ing platform, due to staff shortages and limited integrationof local stakeholders. Uncertainty was mentioned withregards to staff retention since KCH is not in charge ofstaff management and relocation (see Figure 2, (1)). In-terviewees perceived that the Malawian partners hadlimited involvement because no local manager for theplatform was trained and in charge for administration orsupport. Therefore, sustainability was rated low and per-ceived as a major challenge.
Awareness and Access
Interns stated that they were not aware of the e-learningplatform and that they were told informally about theplatform in handover meetings or on ward rounds (seeFigure 2, (2)). None of the interviewees had a formal in-troduction to the platform. Some users were impededusing the e-learning platform since the keys to access
3/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Self-directed e-learning at a tertiary hospital in ...
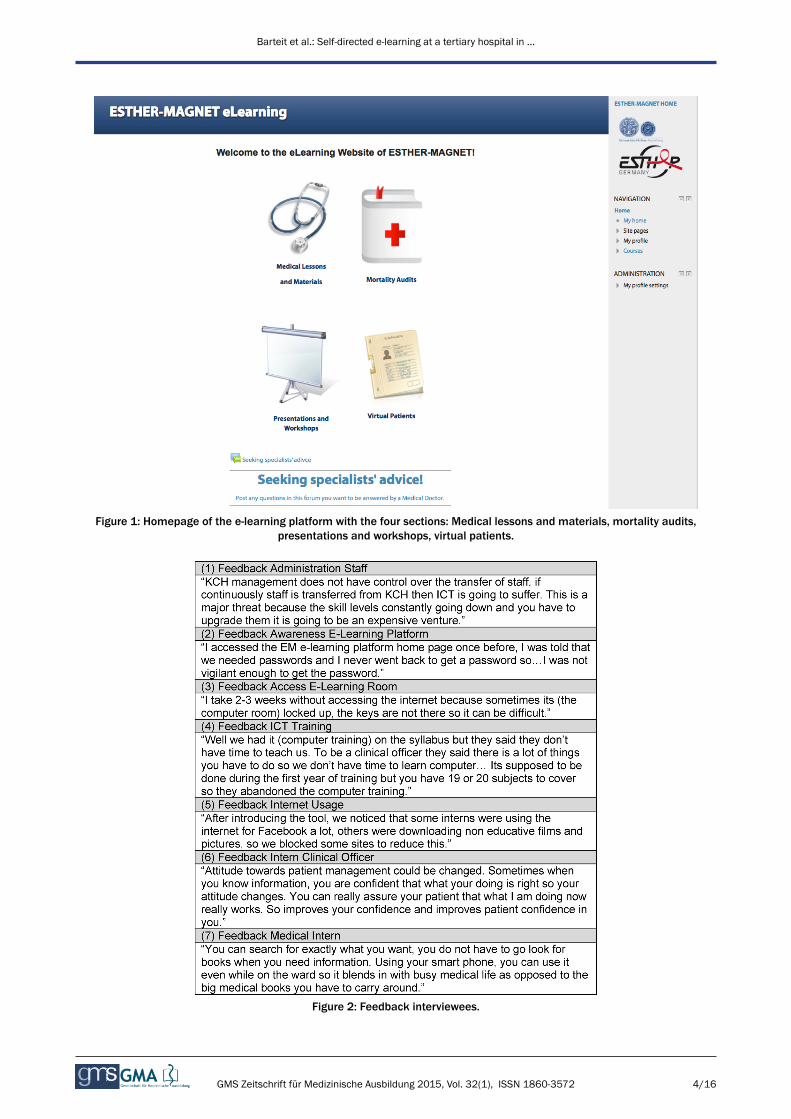
Figure 1: Homepage of the e-learning platform with the four sections: Medical lessons and materials, mortality audits,presentations and workshops, virtual patients.
Figure 2: Feedback interviewees.
4/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Self-directed e-learning at a tertiary hospital in ...

the computer room stayed with one person, who was notalways around (see Figure 2, (3)).
ICT proficiency
The level of ICT-proficiency varied between internmedicaldoctors and intern clinical officers. While intern medicaldoctors are trained in ICT usage during their studies, in-tern clinical officers reported to receive either no or littleICT training (see Figure 2, (4)). One intern clinical officerneeded support with basic computer tasks, another internmedical doctors, as well as 2 intern clinical officersshowed proficiency for all checkpoints on the observationchecklist. Interviewees stated that if they felt the contentwas of interest to them, they feel encouraged to use ICTs.Several intern clinical officers expressed a need fortraining in the usage of the e-learning platform and gen-eral ICT usage.
ICT infrastructure
Although 1 out of 4 intern clinical officers and 5 out of12 intern medical doctors had access to a private laptop,interns perceived the numbers of computers as insuffi-cient to cover the departmental ICT need, as there arepeak-times for computer usage in the medical depart-ment. Usage is high during lunchtime and after theworkday. Non-professional Internet usage was remarkedas a negative side effect (see Figure 2, (5)).
Relevance
Interviewees confirmed the relevance of content andappropriateness of the e-learning platform to their setting.The medical staff identified the e-learning platform asbeneficial to compensate for the lack of senior medicalstaff and for limitations in access to current and relevantmedical information.
Potential effects
Respondents viewed the e-learning platform as positiveand beneficial. It was affirmed that the e-learning platformimproves their clinical skill set, especially in regard topatient management (see Figure 2, (6)). Furthermore,the e-learning platform was perceived as a central re-source of reliable and up-to-datemedical information thatreduces effort and time for research (see Figure 2, (7)).
DiscussionWe described the development, technical set up, imple-mentation and user experiences of the e-learning platformas part of a broader approach to improve quality oftraining and care at the medical department of the KCH.Various e-learning approaches in developing countrieshave shown the appropriateness, relevance and the greatinterest of users [5], [8], [15] to use such a medium formedical training. At KCH, interviewees confirmed these
aspects, highlighting the impact on their medical skill set.However, to yield the potential benefits, several issuesappear noteworthy: awareness and acceptance, technicalchallenges and adequacy of IT infrastructure, as well ascontent design, managerial competence and the need ofat least one local e-learning coordinator.Our evaluation showed that just to provide an e-learningplatform is not sufficient. Hence before helping to com-pensate the lack of clinical teachers, it needs efforts toset up and to maintain it. Medical teachers and involvedlocal staff need commitment to the project [5] to promoteawareness, which was perceived low. In our setting,awareness was further impeded by the forced move andtemporary shutdown of the computer lab due to recon-struction work of the department for a few months andlocal financial mismanagement of project funds that cutoff Internet access for a longer time period.Also needed are ICT expertise, infrastructure and supportsystems, continuous IT support, the commitment andstrategies to cooperate, as well as a suitable didacticapproach [16]. ICT proficiency to use the platform provedjust sufficient, however structured introductions seemadvisable for optimal use, as shown in similar e-learningsettings [3], [15]. The target group confirmed the positivepotential and local preparedness of the technology.Currently, the number of computers is not sufficient,which has been shown to lower usage [17]. Another infra-structural challenge is the poor broadband network con-nection with low download speeds diminishing the overalle-learning experience [8].Further, results showed the need for support and dedica-tion of the department, the identification and integrationof stakeholders [3] as well as faculty and intern engage-ment [5].The critical remarks on lack of involvement and ownershipof local capacity have been taken up and we have identi-fied an e-learning coordinator who handles administrativeplatform tasks,manages content, and offers ICT capacitybuilding and supports interns. As the project started, aperson with the respective skills and sufficient time forthis task was not available.In order to improve awareness, we see potentials instructured introductory sessions for new interns of thedepartment and active promotion of the e-learning plat-form within the department. Also, the e-learning platformis integrated in the interns’ curriculum. This needs to bean ongoing activity because of the relatively fast turnaround of interns who are in the medical ward for 10weeks.Rewards have proven to encourage usage and involve-ment [15]. In the next phase, we take up this approachwith a prize competition for interns, so they engage increating new VP from patient cases or other relevantmaterial for the e-learning platform [15].In order to cut access times and stabilize the networkconnection, we will test and integrate the following: ageneral caching system [3] andDNS caching [16], a delay-tolerant network [17], a transfer protocol like BitTorrent[3], off-peak hour downloading for large files and data
5/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Self-directed e-learning at a tertiary hospital in ...

compression [18]. The range of wireless LAN was exten-ded since interviewees reported to own a laptop.After the first comprehensive training sessions, we willevaluate didactics and contents of the platform.Education is amajor driving force of a country’s economy[19] and essential to alleviateMalawi’s poverty [20]. ICTsare part of the millennium development goals [http://www.un.org/millenniumgoals] due to their substantialimpact on a country’s development [15] and are integ-rated more and more into the political agenda, such asthe Malawian eHealth agenda [17]. As technological ac-cess and competition increases, cost for its usage de-crease. It makes e-learning a tool of growing importanceto sustain and extend access to education, especially incountries that lack skilled health personnel. Studiesshowed that e-learning has a positive effect in traininghealthcare workers in similar settings [5], as well as influ-encing the quality of the training and quantity of trainedmedical personnel [21].
ConclusionsWe have introduced an e-learning platform at a tertiaryhospital in Malawi that centralizes access to relevant andup-to-date medical materials and information that mayotherwise be unavailable. It provides a source to refer tostandard in treatment guidelines, reduces time for re-searching and aids the training of medical skills and pa-tient management.After a qualitative evaluation, we found that for an e-learning platform to work, it requires an appropriate ICTinfrastructure with corresponding support, integration ofstakeholders and the commitment of the department andinvolved faculty. Users value the opportunity of an e-learning platform to partially compensate for the lack ofclinical teachers, as well as to improve the quality oftraining for interns and access to medical up-to-date in-formation in the medical department of the KCH.
LimitationsWe appreciate the limitations of our evaluation as weexplored only the perceptions of the personnel of onehospital over a limited time span and relatively early afterthe introduction which limits the potential experience ofusers. This early evaluation however was done to guidethe future development and direction of the platformdevelopment. Furthermore, we think the lessons learntcan be helpful for others initiating similar projects.
Authors’ contributionsAll authors were involved in the conception and designof the study and have all approved the final version ofthe manuscript to be published. All authors have beenresponsible for redrafting and revising the intellectual
content of this article. The corresponding author wrotethe first draft, the first and last author contributed equallyto the paper.
Ethical ConsiderationsPrior to the study, the study protocol was submitted toand approved by the Ethics Committee of the MedicalFaculty in Heidelberg (Germany) and the National HealthScienceResearch Committee ofMalawi. Themanagementof the KCH approved and permitted the study. Informedconsent was given from all respondents prior to interviewsand group discussions. Permission to record was alsorequested. All information shared was kept confidential.The information would not be used to identify them asthe respondent.
AcknowledgementsThe hospital partnership project received funding throughtheGerman technical cooperation (GIZ), PROFILE (GermanESTHER secretariat), within the ESTHER (Ensemble pourune Solidarité Thérapeutique Hospitalière En Réseau)initiative in cooperation with the partnership projectMAGNET (Malawi German Networking for CapacityBuilding in Treatment, Training and Research at KamuzuCentral Hospital).
Competing interestsThe authors declare that they have no competing in-terests. The authors alone are responsible for the contentand the writing of the paper.
References1. Muula A. Case for Clinical Officers and Medical Assistants in
Malawi. Croat Med J. 2009;50(1):77-78. DOI:10.3325/cmj.2009.50.77
2. Zijlstra E, Broadhead R. The College of Medicine in the Republicof Malawi: towards sustainable staff development. Hum ResourHealth. 2007;5:10. DOI: 10.1186/1478-4491-5-10
3. Crow J, Broussard R, Dong L, Finn J, Wiley B, Geisler G. Asynthesis of research on ICT adoption and use by medicalprofessionals in Sub-Saharan Africa. Proceedings of the 2ndACMSIGHIT International Health Informatics Symposium;Miami,Florida, USA. 2110384: ACM; 2012. p. 161-70.
4. Kulier R, Gülmezoglu A, Zamora J, Plana MN, Carroli G, CecattiJG, Germar MJ, Pisake L, Mittal S, Pattison R, Wolomby-MolondoJJ, Bergh AM, May VV, Souza JP, Koppenhoefer S, Khan KS.Effectiveness of a clinically integrated e-learning course inevidence-based medicine for reproductive health training: Arandomized trial. JAMA. 2012;308(21):2218-2225. DOI:10.1001/jama.2012.33640
6/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Self-directed e-learning at a tertiary hospital in ...
5. Frehywot S, Vovides Y, Talib Z, Mikhail N, Ross H, Wohltjen H,Bedada S, Korhumel K, Koumare AK, Scott J. E-learning inmedical education in resource constrained low- and middle-income countries. Hum Resour Health. 2013;11(1):4. DOI:10.1186/1478-4491-11-4
6. Huwendiek S, Reichert F, Bosse H, de Leng B, van der VleutenC, Haag M, et al. Design principles for virtual patients: a focusgroup study among students. Med Educ. 2009;43:580-588. DOI:10.1111/j.1365-2923.2009.03369.x
7. Agyeman-Duah J, Theurer A, Munthali C, Alide N, Neuhann F.Understanding the barriers to setting up a healthcare qualityimprovement process in resource-limited settings: a situationalanalysis at the Medical Department of Kamuzu Central Hospitalin Lilongwe, Malawi. BMC Health Serv Res. 2014;14(1):1. DOI:10.1186/1472-6963-14-1
8. Mains EA, Blackmur J, Dewhurst D, Ward R, Garden O, WigmoreS. Study on the feasibility of provision of distance learningprogrammes in surgery toMalawi. Surgeon. 2011;9(6):322-325.DOI: 10.1016/j.surge.2010.11.032
9. Mullan F, Frehywot S. Non-physician clinicians in 47 sub-SaharanAfrican countries. Lancet. 2007;370(9605):2158-2163. DOI:10.1016/S0140-6736(07)60785-5
10. Ellaway R, Candler C, Greene P, Smothers V. An ArchitecturalModel for MedBiquitous Virtual Patients. Baltimore, MD:MedBiquitous; 2006.
11. Huwendiek S, De leng BA, Zary N, Fischer MR, Ruiz JG, EllawayR. Towards a typology of virtual patients. Med Teach.2009;31(8):743-748. DOI: 10.1080/01421590903124708
12. Dewhurst D, Borgstein E, GrantM, BeggM. Online virtual patients- A driver for change in medical and healthcare professionaleducation in developing countries?Med Teach. 2009;31(8):721-724. DOI: 10.1080/01421590903124732
13. Czaputa C. Didaktische Reflexionen zumUnterrichtseinsatz. Ref.4.7. Dillingen: eLearning Kompetenzzentrum Akademie fürLehrerfortbildung und Personalführung; 2009.
14. Kerres M. Mediendidaktik?: Konzeption und Entwicklungmediengestützter Lernangebote. München: Oldenbourg; 2013.DOI: 10.1524/9783486736038
15. Bhuasiri W, Xaymoungkhoun O, Zo H, Rho JJ, Ciganek AP. Criticalsuccess factors for e-learning in developing countries: Acomparative analysis between ICT experts and faculty. CompEduc. 2012;58(2):843-55. DOI:10.1016/j.compedu.2011.10.010
16. Chen J, Subramanian L. Interactive web caching for slow orintermittent networks. Proceedings of the 4th Annual Symposiumon Computing for Development. Cape Town, South Africa: ACM;2013. S.1-10.
17. Isaacman S, Martonosi M. Potential for collaborative cachingand prefetching in largely-disconnected villages. Proceedings ofthe 2008 ACM workshop on Wireless networks and systems fordeveloping regions. San Francisco, California, USA: ACM; 2008.S.23-30.
18. Johnson DL, Belding EM, Almeroth K, Stam Gv. Internet usageand performance analysis of a rural wireless network in Macha,Zambia. Proceedings of the 4th ACM Workshop on NetworkedSystems for Developing Regions. San Francisco, California: ACM;2010. S.1-6.
19. Bank W. World Development Report 1998-1999: Knowledge forDevelopment. Washington/DC: World Bank; 1998.
20. Ajakaiye O, Kimenyi MS. Higher Education and EconomicDevelopment in Africa: Introduction and Overview. J Afr Econom.2011;20(Supplement 3):iii3-iii13. DOI: 10.1093/jae/ejr027
21. Chen C, Buch E, Wassermann T, Frehywot S, Mullan F, OmaswaF, Greysen SR, Kolars JC, Dovlo D, El Gali Abu Bakr DE,Haileamlak A, Koumare AK, Olapade-Olaopa EO. A survey of Sub-Saharan African medical schools. Hum Resour Health.2012;10(1):4. DOI: 10.1186/1478-4491-10-4
22. Kanwischer D, Quennet F. Distance Education and SpatialCitizenship in Africa–Challenges and Prospects. Rev Int GeographEduc Online. 2012;2(1). Zugänglich unter/available from: http://www.rigeo.org/vol2no1/2.6.RIGEO-VOL.2.NO.1-6.pdf
23. Dev P, Hoffer E, Barnett GO. Computers in Medical Education.In: Shortliffe E, Cimino J (Hrsg). Biomedical Informatics. HealthInformatics. New York: Springer; 2006. S.737-762. DOI:10.1007/0-387-36278-9_21
24. Mars M. Building the capacity to build capacity in e-health in sub-Saharan Africa: the KwaZulu-Natal experience. Telemed J EHealth. 2012;18(1):32-37. DOI: 10.1089/tmj.2011.0146
Corresponding author:Sandra Barteit, M.A.Heidelberg University, Institute of Public Health,Bergheimer Straße 20, D-69115 Heidelberg, Germany,Phone: +49 (0)6221/[email protected]
Please cite asBarteit S, Hoepffner P, Huwendiek S, Karamagi A, Munthali C, Theurer A,Neuhann F. Self-directed e-learning at a tertiary hospital in Malawi –A qualitative Evaluation and Lessons learnt. GMS Z Med Ausbild.2015;32(1):Doc7.DOI: 10.3205/zma000949, URN: urn:nbn:de:0183-zma0009497
This article is freely available fromhttp://www.egms.de/en/journals/zma/2015-32/zma000949.shtml
Received: 2014-04-30Revised: 2014-09-22Accepted: 2014-12-01Published: 2015-02-11
Copyright©2015 Barteit et al. This is an Open Access article distributed underthe terms of the Creative Commons Attribution 4.0 License. See licenseinformation at http://creativecommons.org/licenses/by/4.0/.
7/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Self-directed e-learning at a tertiary hospital in ...
Selbstgesteuertes medizinisches Lernen via E-Learningan einem Lehrkrankenhaus in Malawi: Aufbau,Erkenntnisse und Erfahrungen
ZusammenfassungEinführung: Trotz verschiedener Initiativen mehr Gesundheitspersonalauszubilden, besteht in Malawi weiterhin ein ausgeprägter Mangel an
Sandra Barteit1
Philip Hoepffner2Fachkräften im Gesundheitsbereich. Dieser Mangel stellt auch eineSören Huwendiek3
erhebliche Herausforderung für die Aus- und Weiterbildung von medizi-Angela Karamagi4nischem Personal dar - vor allem für Interns, die in ihrem letzten und
entscheidenden Ausbildungsjahr vor demBeginn einer selbstständigenärztlichen Tätigkeit stehen.
Charles Munthali5
Antje Theurer6Projektbeschreibung:Wir haben deshalb in dermedizinischen Abteilungdes Kamuzu Central Hospital (KCH) inMalawi eine E-Learning Plattform Florian Neuhann1
eingeführt. Ziel ist es durch den computergestützten Unterricht denMangel an klinischem Lehrpersonal teilweise zu kompensieren und
1 Universität Heidelberg,Institut für Public Health,Heidelberg, Deutschland
damit zur Verbesserung der Qualität der medizinischen Ausbildungbeizutragen sowie Zugang zu aktuellen und relevanten medizinischenMaterialien zu gewährleisten.
2 UniversitätsklinikumWürzburg, Klinik und
Methoden: Zwischen März und April 2012 führten wir zur Evaluationvon Relevanz und Angemessenheit der E-Learning-Plattform eine quali-
Poliklinik für Psychiatrie undtative Untersuchung durch. Die Datenerhebung erfolgte über individu- Psychotherapie, Würzburg,Deutschlandelle Interviews, eine thematisch geleitete Gruppendiskussion sowie
durch Beobachtung der Nutzung der Plattform basierend auf einer3 Universität Bern, Institut fürMedizinische Lehre,
Checkliste. Die Auswahl der Interviewpartner erfolgte gezielt. InterviewsundGruppendiskussion wurden aufgezeichnet, codiert und interpretiert.
Abteilung für AssessmentErgebnisse: E-Learning erwies sich im Umfeld dieses Krankenhausesals technisch machbar. Die Nutzer beurteilten die E-Learning-Plattform
und Evaluation, Bern,Schweiz
als für sich relevant und inhaltlich angemessen. Bedenken wurden in4 ESTHERDeutschland,MalawiGerman Networking for
Bezug auf Nachhaltigkeit, Zugänglichkeit und technischer Infrastrukturgeäußert sowie hinsichtlich der begrenzten Beteiligung und Verantwor-
Capacity Building intung der malawischen Partner. Das Interesse an E-Learning war hoch, Treatment, Training andaber sowohl der Bekanntheitsgradwie auch die Kenntnisse der Plattform Research at Kamuzu Centralwaren unter den potenziellen Nutzern gering. Die Evaluation ergab, Hospital (MAGNET),
Deutschlanddass weitere Anpassungen im Hinblick auf die lokalen Bedürfnisse er-forderlich sind, um Nutzung und Zugänglichkeit zu erhöhen. 5 Kamuzu Central Hospital,
Medical Department,Lilongwe, Malawi
Schlussfolgerung:Umeine aktive Nutzung von E-Learning im gegebenenUmfeld zu erzielen, sind ein aktives Engagement von lokalen Akteuren,eine Identifizierung und Übernahme von spezifischen Verantwortungs-
6 ESTHERDeutschland,MalawiGerman Networking forbereichen, eine lokal angemessene technische Infrastruktur sowie die
Ausrichtung auf die lokalen Bedürfnisse erforderlich. Capacity Building inSchlüsselwörter: computergestützter Unterricht, Multimedia,Medizinische Ausbildung, Capacity Building, IKT, unterbesetzt,Lehrkrankenhaus, virtuelle Patienten, Subsahara-Afrika
Treatment, Training andResearch at Kamuzu CentralHospital (MAGNET),Deutschland
8/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Artikel – ProjektberichtThis is the translated (German) version.
The original (English) version starts at p. 1.OPEN ACCESSHumanmedizin

EinleitungInMalawi besteht ein immenserMangel an Gesundheits-personal mit gleichzeitigem schlechten Zugang zu aktuel-len medizinischen Wissensquellen. Das Verhältnis vonÄrzten, Krankenpflegepersonal und Hebammen betrug2013 0,2 bzw. 3,4 pro 10.000 Einwohner [http://www.who.int/countries/mwi/en/], und steht in starkemKontrast zu WHO Empfehlungen, die ein Verhältnis von23 Ärzten, Krankenschwestern undHebammen vorsehen[http://www.who.int/hrh/workforce_mdgs/en/]. Initiativengegen diesen Mangel umfassen u.a. eine 3-jährige Aus-bildung zumClinical Officer [1], die Ausweitung dermedi-zinischen Ausbildungskapazität durch das College ofMedicine, das seit 1991 ein volles Medizinstudium inMalawi gewährleistet [2] [http://www.medcol.mw/?page_id=1194] sowie ein Notfall-Ausbildungs-Programm fürGesundheitsfachkräfte, das 2005 eingeführt wurde[http://www.who.int/countryfocus/cooperation_strategy/ccs_mwi_en.pd].Aufgrund des kritischen Mangels an erfahrenen Ärztenfür Lehre und klinische Supervision u.a. während des In-ternships (äquivalent zumPraktischen Jahr des deutschenMedizinstudiums), haben wir eine E-Learning Plattform[http://www.esther-magnet.org] für die medizinische Ab-teilung des Kamuzu Central Hospital (KCH) in Lilongwe,Malawi, aufgebaut. Der Aufbau der E-Learning Plattformzielt darauf ab, durch den Einsatz von Informations- undKommunikationstechnologien (IKT) den Mangel an klini-schem Lehrpersonal zumindest teilweise zu kompensie-ren, den Zugang zu medizinischen Informationsquellenzu erleichtern und die Qualität der medizinischen Ausbil-dung und Versorgung in der Abteilung zu verbessern [3].E-Learning Programme wurden bereits erfolgreich imGesundheitsbereich in Ländernmit niedrigem undmittle-remEinkommeneingesetzt, wie beispielsweise E-Learningfür evidenzbasierte Medizin [4] und für die Pflegeausbil-dung in Malaysia [5]. Primäre Zielgruppe sind die Internsund deren gezielte Unterstützung während der kritischenPhase von der praktischen Ausbildung zur unabhängigenärztlichen Tätigkeit.Die Einführung von E-Learning ist Teil eines umfassende-ren Ansatzes die Qualität der Ausbildung und Versorgungin dermedizinischen Abteilung des KCH imRahmen einerKrankenhaus-Partnerschaft [http://www.esther.eu] zuverbessern. Im Folgenden beschreiben wir Konzept,Umsetzung sowie die Ergebnisse der Evaluation, die einJahr nach Einführung der E-Learning Plattform durchge-führt wurde.
ProjektbeschreibungDas KCH ist ein tertiäres 800-Betten-Krankenhaus, dasdem malawischen Gesundheitsministerium untersteht[6]. Es dient als Lehr- und Referenzkrankenhaus fürZentral-Malawi und umfasst ein Einzugsgebiet von rund6 Millionen Einwohnern [7], [http://www.who.int/patientsafety/implementation/apps/first_wave/malawi_
middlesbrough/en/index.html]. Die medizinische Abtei-lung verfügt über etwa 90 Betten und bietet täglich am-bulante Schwerpunktdienste an, wie z.B. Diabetes- oderTumor-Sprechstunden. Die Abteilung hat eine zentraleAufnahmestation, in der täglich etwa 40 Patienten betreutwerden. Zudem ist die Abteilung zuständig für die Tuber-kulose-Station, die außerhalb des Krankenhausgeländesliegt.Seit 1991 bietet das College of Medicine (CoM) ein voll-ständiges Medizinstudium in Malawi an [2], [http://www.medcol.mw/?page_id=415]. Derzeit schließen etwa40 Medizinstudenten jährlich ihr Studium ab [8], wobeihöhere Abschlusszahlen angestrebt werden und die Zahlder Neueinschreibungen schrittweise erhöht werden [2].Nach Abschluss des Studiums erfolgt ein einjähriges In-ternship in einem Krankenhaus, während welchem In-terns die Abteilungen Geburtshilfe, Pädiatrie, Chirurgieund Allgemeine Medizin durchlaufen. Danach arbeitendie Mehrzahl der Absolventen als Arzt in einem staatli-chen Krankenhaus [2].Ebenso wichtig für diemedizinische Versorgung inMalawisind die Clinical Officers (CO) [1]. Nach einer 3-jährigenpraxisorientierten Ausbildung erhalten CO Studenten einDiplom in klinischer Medizin, auf das ein einjährigesKrankenhaus-Praktikum folgt [1]. Nach erfolgreichemAbschluss des Krankenhaus-Praktikums, werden COssehr vielfältig in der allgemeinen medizinischen Versor-gung eingesetzt. Sie führen anästhetische und chirurgi-sche Eingriffe durch, beispielsweise nehmen sie rund80% aller Kaiserschnitte in Malawi vor [9].Allerdings beeinträchtigt der Mangel an Lehr-Ärzten dieAusbildung der Interns während dieser prägenden undwichtigen Phase der Internship. Im Durchschnitt sind zweileitende Ärzte für die Ausbildung der Interns in der Abtei-lung verantwortlich, neben ihren Aufgaben in der Patien-tenversorgung und Verwaltung. Dabei ist eine Verbesse-rung der praktischen Ausbildung entscheidend, um einequalitative angemessene medizinische Behandlung undBetreuung in Malawi sicherzustellen.
Umsetzung und Inhalt
Inhaltlich und technisch wurde die E-Learning Plattforminitial von den deutschen Projektpartnern aufgebaut.
Technische Einrichtung
Die E-Learning Plattform nutzt die Open-Source-SoftwareMoodle [http://docs.moodle.org/26/en/About_Moodle],die auch an der Partner-Universität verwendet wird. DieComputerausrüstung vor Ort besteht aus 2 feststehendenRechnern und 2 Laptops. Um anfangs Kosten und Zeitzu sparen, wurde ein Linux Virtual-Server in Deutschlandangemietet. Das Netzwerk in dermedizinischen Abteilungwurde von demMalawi-basierten Internet-Anbieter GlobeInternet Ltd bereitgestellt, der dafür eineWiMAX-Antenneinstalliert hatte. Die maximale Datenübertragungsratelag bei 256 KBit/s, Vollduplex. Derzeit nutzt die Abteilung
9/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...

ein kostengünstigeresmobiles 3G-Netz (Prepaid)mit einerDatenübertragungsrate von bis zu 21 Mbps.
Inhalt
Inhalte und die Gestaltung der E-Learning Plattformrichteten sich in erster Linie nach den Bedürfnissen derInterns, insbesondere wurden lokale Relevanz und lan-desspezifische Pathologie berücksichtigt [2], [7], [8]. DerAusbildungsbedarf wurde von den verantwortlichen Ärztenin Malawi entsprechend relevanter Richtlinien festgelegtund in Absprache mit den deutschen Projektpartnern ineinem Anforderungsbegleitheft der medizinischen Abtei-lung für die Interns spezifiziert. Der Inhalt ist darauf aus-gerichtet, die Interns während ihrer Internship in dermedizinischen Abteilung zu unterstützen, vor allem hin-sichtlich der geforderten Ausbildungsziele der Abteilung.Dabei liegt der Fokus auf praktischen Kenntnissen, wiebeispielsweise Patientenmanagement undDemonstrationvon medizinischen Prozeduren, z.B. Lumbalpunktion.Die Plattform ist in vier Abschnitte unterteilt: medizinischeLektionen undMaterialien, Sterblichkeitsberichte, Präsen-tationen undWorkshops, sowie virtuelle Patienten (sieheAbbildung 1). Virtuelle Patienten (VP) sind ein Schwer-punkt der E-Learning Plattform und definiert als „eineinteraktive Computer-Simulation aus realen klinischenSzenarien für das Gesundheitswesen, für die medizini-sche Praxis, Ausbildung oder Überprüfung“ [10], [11](siehe Tabelle 1 und 2 ). Andere Projekte und Studienzeigen die Relevanz der VP für das Gesundheitswesenhinsichtlich Bildung und ihrer erfolgreichen Anwendungin Entwicklungsländern [12]. Die Plattform bietet zusätz-lich Zugang zu den medizinischen Online-BibliothekenHINARI [http://www.who.int/hinari/en/] und UpToDate[http://www.uptodate.com]. Neben den Interns habennur registrierte Mitarbeiter der Abteilung Zugang zurPlattform.
Didaktik
Das didaktische Konzept beruht auf selbstgesteuertemLernen: die Interns lesen problem- bzw. fallorientiertemedizinische Texte, sehen sich aufgezeichnete Präsenta-tionen an und arbeiten sich Schritt-für-Schritt durch virtu-elle Patienten anhand von Multiple-Choice-Fragen, dieeine direkte Rückmeldung zu jeder Entscheidung gebensowie zusätzlich auf thematisch relevantes Material ver-weisen. Der Wissenserwerb während dieser Selbstlern-phasen wird durch Multimedia-Aktivitäten unterstützt,die informative und kommunikative Elemente sowie Akti-vität im Rahmen von Aufgaben abdecken, um so einezügiges Qualifizieren der Interns mit Handlungswissenzu erreichen [13], [14].
EvaluationWir evaluierten das Projekt qualitativ im Mai 2012, einJahr nach seiner Einführung. Der Fokus der Fragestellung
lag dabei auf den Faktoren, welche die Nutzung der E-Learning Plattform beeinflussen.
Methoden
Die Daten wurden anhand aufgezeichneter Interviewsgewonnen, die nach einem semi-strukturierten Leitfadengeführt wurden, anhand einer Gruppendiskussion undeiner Checkliste, auf derenGrundlage durch BeobachtungIKT-Kenntnisse eingeschätzt wurden. Die Bewertungwurde nach den Qualitätsstandards der Organisation fürwirtschaftliche Zusammenarbeit und Entwicklung (OECD)[http://www.oecd.org/daf/competition/prosecutionandlawenforcement/47381304.pdf] vorgenommen undkonzentriert sich ausschließlich auf Relevanz und Ange-messenheit.Die Interviews wurden in vier Abschnitte gegliedert: per-sönliche Informationen, Zugang zu Computern/IKT, allge-meine Lern- und E-Learning Erfahrungen, sowie Nutzungder E-Learning Plattform. Zwanzig Personen (3 leitendeMitarbeiter der Administration, 2 leitende Ärzte, 2 ClinicalOfficers, 9 Medical Interns und 4 Clinical Officer Interns)wurden gezielt für Interviews ausgewählt. 8 Interns wur-den zur Gruppendiskussion eingeladen und 6 (3MedicalInterns, 3 Clinical Officer Interns) zufällig ausgewählteInterns haben an der Beobachtung teilgenommen. Inter-views wurden transkribiert und anhand einer Inhaltsana-lyse codiert. Die Daten selbst wurden mit einem Textver-arbeitungs-Programm analysiert.
Ergebnisse
Nachhaltigkeit
Die Interviewpartner äußerten Bedenken in Bezug aufdie Nachhaltigkeit der E-Learning Plattform, vor allemmitBlick auf den Personalmangel und der bis dahin begrenz-ten Integration der lokalen Akteure. Eine Schwierigkeitwurde darin gesehen, eine kontinuierlicheMitarbeit einersolchen lokalen Person zu gewährleisten, da das KCHnicht selbst verantwortlich für die Personalverwaltung seiund unerwartete Versetzungen an einen anderen Arbeits-platz erfolgen können (siehe Abbildung 2, (1)). Die Betei-ligung der malawischen Partner sei eingeschränkt, insbe-sondere weil in der Entwicklungs- und Aufbauphase keineAusbildung eines lokalen Mitarbeiters für Administrationund Support erfolgte und es dadurch keine lokalen Zu-ständigkeiten für Administration oder Support der Platt-form gab.Nachhaltigkeit wurde deshalb als niedrig bewertet undals große Herausforderung gesehen.
Bewusstsein und Zugang
Die befragten Interns erklärten, dass sie keine strukturier-te Einführung zur E-Learning Plattform erhalten und teilsnur informell von der Zugangsmöglichkeit zur E-Plattformbei der Morgenbesprechung oder während der Visite ge-hört hätten (siehe Abbidlung 2 , (2)). Zudem sei der Zu-
10/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...
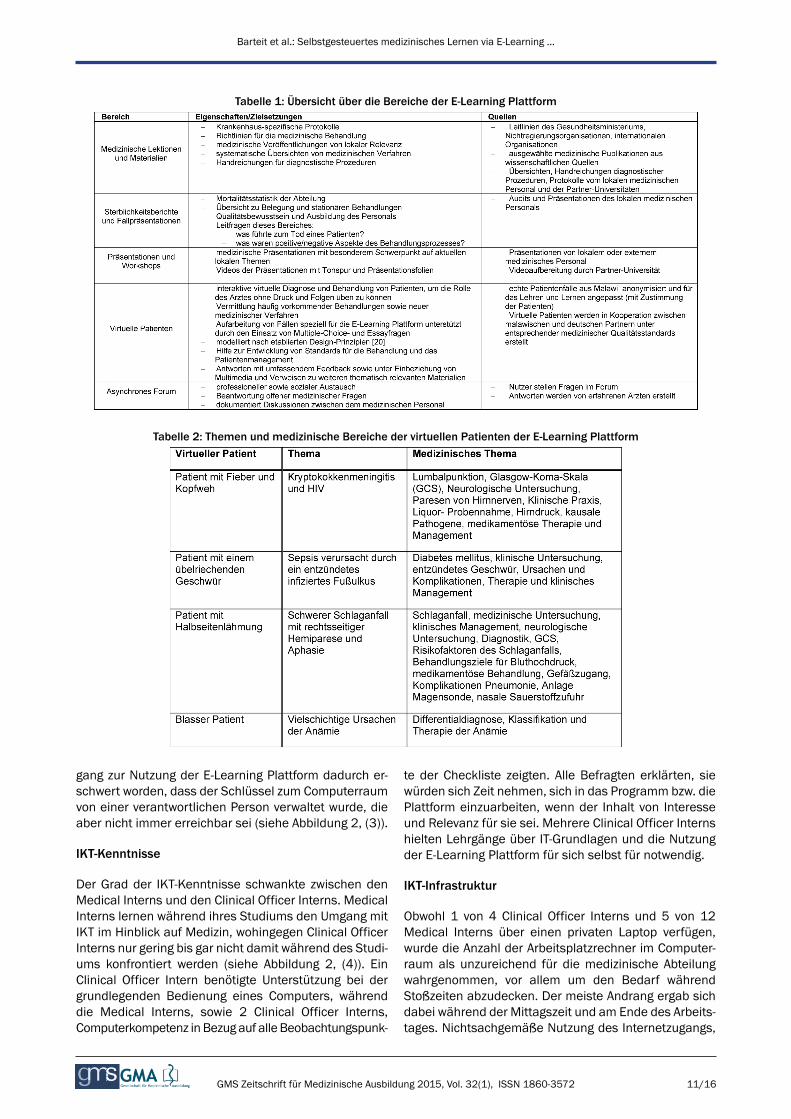
Tabelle 1: Übersicht über die Bereiche der E-Learning Plattform
Tabelle 2: Themen und medizinische Bereiche der virtuellen Patienten der E-Learning Plattform
gang zur Nutzung der E-Learning Plattform dadurch er-schwert worden, dass der Schlüssel zum Computerraumvon einer verantwortlichen Person verwaltet wurde, dieaber nicht immer erreichbar sei (siehe Abbildung 2, (3)).
IKT-Kenntnisse
Der Grad der IKT-Kenntnisse schwankte zwischen denMedical Interns und den Clinical Officer Interns. MedicalInterns lernen während ihres Studiums den Umgang mitIKT im Hinblick auf Medizin, wohingegen Clinical OfficerInterns nur gering bis gar nicht damit während des Studi-ums konfrontiert werden (siehe Abbildung 2, (4)). EinClinical Officer Intern benötigte Unterstützung bei dergrundlegenden Bedienung eines Computers, währenddie Medical Interns, sowie 2 Clinical Officer Interns,Computerkompetenz in Bezug auf alle Beobachtungspunk-
te der Checkliste zeigten. Alle Befragten erklärten, siewürden sich Zeit nehmen, sich in das Programm bzw. diePlattform einzuarbeiten, wenn der Inhalt von Interesseund Relevanz für sie sei. Mehrere Clinical Officer Internshielten Lehrgänge über IT-Grundlagen und die Nutzungder E-Learning Plattform für sich selbst für notwendig.
IKT-Infrastruktur
Obwohl 1 von 4 Clinical Officer Interns und 5 von 12Medical Interns über einen privaten Laptop verfügen,wurde die Anzahl der Arbeitsplatzrechner im Computer-raum als unzureichend für die medizinische Abteilungwahrgenommen, vor allem um den Bedarf währendStoßzeiten abzudecken. Der meiste Andrang ergab sichdabei während der Mittagszeit und am Ende des Arbeits-tages. Nichtsachgemäße Nutzung des Internetzugangs,
11/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...

Abbildung 1: Homepage der E-Learning Plattform mit den vier Bereichen: medizinische Lektionen und Materialien,Sterblichkeitsberichte, Präsentationen und Workshops, virtuelle Patienten.
wie das Aufrufen unangemessenerer Webseiten, wurdeals ein negativer Nebeneffekt angemerkt (siehe Abbildung2, (5)).
Relevanz
Die Befragten bestätigten die Relevanz der Inhalte unddie Zweckmäßigkeit der E-Learning-Plattform für den ge-gebenen Rahmen der Abteilung. Das befragte medizini-sche Personal beurteilte die E-Learning Plattform alsdienlich, um denMangel anmedizinischem Lehrpersonalzu kompensieren und den Zugang zu aktuellen und rele-vanten medizinischen Informationen zu ermöglichen.
Mögliche Auswirkungen
Die E-Learning Plattform wurde von den Befragten alspositiv und nützlich wahrgenommen. Es wurde bestätigt,dass sich durch die Inhalte der Plattform klinische Fertig-keiten, insbesondere in Bezug auf das Patienten-Mana-gement (siehe Abbidlung 2 , (6)), verbessern können. DieE-Learning Plattform wird als zentrale Ressource wahrge-nommen, die zuverlässige und aktuelle medizinische In-formationen bereitstellt und damit Aufwand und Zeit imAlltag für Informationssuche (siehe Abbildung 2, (7)) re-duziert.
DiskussionIn der vorliegenden Arbeit beschreiben wir die Entwick-lung, die technischen Aspekte, die Einführung und dieErfahrungen der Benutzer der E-Learning Plattform - dieTeil eines umfassenderen Ansatzes zur Verbesserung derAusbildungs- und Behandlungsqualität dermedizinischenAbteilung des KCH ist.Verschiedene Ansätze zu E-Learning in ressourcenarmenLändern zeigen dessen Zweckmäßigkeit und Relevanz inder medizinischen Ausbildung sowie das Interesse derNutzer [5], [8], [15]. Diese Einschätzung bestätigten auchdie im KCH Befragten und unterstrichen zudem die Aus-wirkung auf ihremedizinische Fertigkeiten. Um allerdingseine aktive Nutzung des E-Learnings zu erzielen, sindmehrere Aspekte zu berücksichtigen: der Bekanntheits-grad der E-Learning Plattform und deren Akzeptanz, dieBewältigung technischer Herausforderungen und dieAngemessenheit der IT-Infrastruktur gegenüber der loka-len Gegebenheiten, eine ansprechende Gestaltung undein angemessener didaktischer Ansatz der Plattform,sowie personelle Ressourcen für lokale Administrationund Support (E-Learning Koordinator).Unsere Evaluation ergab, dass es nicht ausreicht eine E-Learning Plattform mit Inhalten zur Verfügung zu stellen.Für einen zielführenden Einsatzmuss in die Aufbauphaseinvestiert werden und die Frage der Pflege und Wartunggeklärt werden. Ärztliches Personal und beteiligte Mitar-
12/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...

Abbildung 2: Antworten und Rückmeldung der Befragten.
beiter vor Ort müssen Engagement für das Projekt zeigen[5], um Bekanntheit und Nutzungsgrad der Plattformdauerhaft zu fördern, welche bisher niedrig waren. Aller-dings traten während der Projektlaufzeit unvorhergesehe-ne Behinderungen auf, wie der Umzug der Bettenstationauf eine andere Etage des Krankenhauses. Dadurch warder Computerraum fürmehrereMonate nicht zugänglich.Außerdem führte die nicht ordnungsgemäße Abrechnungvon Projektmitteln für einen längeren Zeitraum zur Sper-rung des Netzwerkzugangs durch den Dienstleistungsan-bieter.Deutlich zeigte sich in unserem Projekt, dass für eine er-folgreiche Umsetzung IT-Kompetenzen, räumliche undtechnische Infrastruktur, eine kontinuierliche IT Support-Struktur, lokales Engagement, verbindliche Kooperations-vereinbarungen sowie ein geeigneter didaktischer Ansatzerforderlich sind [16].Kenntnisse, um die Plattform sinnvoll nutzen zu können,erwiesen sich als gerade ausreichend. Daher erscheinenstrukturierte Einführungen als zweckmäßig für eine ver-besserte Nutzung, wie E-Learning Ansätze in ähnlichenKontexten [3], [15] zeigen. Die Evaluation der Zielgruppebestätigte ein vorhandenes Potential und die Angemes-senheit der eingesetzten Technik.Derzeit ist die zur Verfügung stehende Anzahl der Compu-terarbeitsplätze nicht ausreichend, was sich nachweislich
negativ auf die Nutzung [17] auswirkt. Eine andere infra-strukturelle Herausforderung ist die limitierende Breitban-danbindung mit geringer Datentransferrate, die den Ge-samteindruck des E-Learnings beeinträchtigt [8].Darüber hinaus zeigten die Ergebnisse der Evaluation,wie wichtig es ist, die Abteilung, lokale Akteure [3], Dozen-ten und auch Interns [5] aktiv in das Projekt einzubinden,um so die lokale Unterstützung und das Engagementdafür innerhalb der Abteilung zu steigern.Die Kritik hinsichtlich der mangelnden Beteiligung undEigenverantwortung der lokalen Projektbeteiligten sindaufgenommenworden: wir haben einen E-Learning-Koor-dinator identifiziert, der verwaltungsspezifische Aufgabender Plattform übernimmt, Inhalte verwaltet und Internsunterstützt, auch in Bezug auf ihre IKT-Fertigkeiten. ZuProjektbeginn stand eine Person mit entsprechendenKompetenzen und zeitlicher Kapazität für diese Aufgabenicht zur Verfügung.Um das Wissen um die Plattform zu verbessern, sindstrukturierte Einführungsveranstaltungen für neue Internsder Abteilung zweckdienlich sowie eine aktive Förderungdes E-Learnings innerhalb der Abteilung nötig. Diesmusskontinuierlich geschehen, da im Schnitt alle 10 Wochenneue Interns in die Abteilung rotieren. Die Nutzung desE-Learnings soll integraler Bestandteil der Rotation derInterns in der medizinische Abteilung werden. Gezielte
13/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...

Anreize haben sich als nützlich erwiesen die Beteiligungam E-Learning [15] zu fördern. In der nächsten Phasemöchten wir diesen Ansatz in Form eines Wettbewerbsfür Interns einführen, der das Erstellen von Lehrmateria-lien, wie beispielsweise einer Falldarstellung für einenneuen virtuellen Patienten oder das Erstellen von anderenrelevanten Materialien für die E-Learning-Plattform [15],auszeichnet.Um die geringe Datentransferrate zu kompensieren,werden wir folgende Ansätze testen und gegebenenfallsimplementieren: ein allgemeines Caching-System [3] undDNS-Caching [16], ein Verzögerung-tolerantes Netzwerk[17], ein Übertragungsprotokoll wie BitTorrent [3], sowieOff-Peak-Downloads bei großen Dateien und Datenkom-primierung [18]. Der Sendebereich des Wireless-LANwurde erweitert, da einige Befragte einen Laptop besitzen,um damit den Zugang zur Plattform nutzen können. Nachden ersten strukturierten Einführungen zur Nutzungwerden wir Didaktik und Inhalte der Plattform erneutevaluieren.Bildung ist eine wichtige treibende Kraft für dieWirtschafteines Landes [19] und Bestandteil von Strategien zurArmutsbekämpfung [20]. IKTs sind Teil der Millennium-Entwicklungsziele [http://www.un.org/millenniumgoals],da sie einen erheblichen Einfluss auf die Entwicklung ei-nes Landes [15] haben und daher bereits in die politischeAgenda integriert werden, wie die malawische eHealthAgenda zeigt [17]. Nicht nur der Zugang zu Technologieerhöht sich, sondern auch der Wettbewerb in diesemBereich, was die Kosten für deren Nutzung in Afrika weitersinken lässt. In der Folge kann die Bedeutung von E-Learning wachsen, als ein Werkzeug, das Zugang zu Bil-dung ermöglicht und erweitern kann. Insbesondere inLändern, in denen es z.B. anmedizinischemFachpersonalmangelt. Studien mit ähnlichen Rahmenbedingungenhaben gezeigt, dass E-Learning die Ausbildung von Ge-sundheitspersonal unterstützt [5] und die Qualität derAusbildung und die Anzahl des ausgebildeten medizini-schen Personals positiv beeinflusst [21].
SchlussfolgerungWir haben eine E-Learning Plattform in einem tertiärenKrankenhaus in Malawi eingeführt, die den Zugang zurelevanten und aktuellen medizinischen Informationenermöglicht, die ansonsten nicht zur Verfügung stünden.Die E-Learning Plattform wird als Referenzquelle für Be-handlungsleitlinien genutzt, sie reduziert Zeit und Auf-wand bei der Suche nach Informationen und unterstütztdie Ausbildung in Bezug auf medizinische Fähigkeitenund Patientenmanagement.Die qualitative Evaluation der E-Learning Plattform unter-streicht die Bedeutung eine angemessene IT-Infrastrukturmit entsprechender Unterstützung bereitzustellen, aktivAkteure zu integrieren und kontinuierliches Engagementder Institution bzw. der Abteilung und der beteiligten Do-zenten zu fördern.
Positiv schätzen die Nutzer die Möglichkeiten der E-Learning Plattform den Mangel an klinischen Lehrernteilweise zu kompensieren und damit eine qualitätsgesi-cherte Ausbildung von Interns zu unterstützen und denZugang zu aktuellen und relevanten Informationen in dermedizinischen Abteilung des KCH zu verbessern.
EinschränkungenDas Konzept unserer Evaluation weist Einschränkungenauf. Die Untersuchung bezog sich auf das Personal einesKrankenhauses und auf einen begrenzten Zeitraum, be-reits früh nach der Einführung der E-Learning Plattform.Dadurch waren die Anzahl der Nutzer und deren Erfah-rung begrenzt. Diese frühe Evaluierung wurde jedochdurchgeführt, um Informationen für dieWeiterentwicklungder Plattform-Entwicklung zu gewinnen, die auch für dieEinführung ähnlicher Projekte hilfreich sein können.
AutorenbeiträgeAlle Autoren waren an der Konzeption und dem Entwurfder Evaluation beteiligt und haben alle der Veröffentli-chung der endgültigen Fassung des Manuskripts zuge-stimmt. Alle Autoren waren an der Revision des Inhaltsdieses Artikels beteiligt. Der korrespondierende Autorschrieb dasManuskript, der erste und letzte Autor trugengleichermaßen zu dem Artikel bei.
Ethische AspekteDas Protokoll für die Evaluation wurde durch die Ethik-kommission der Medizinischen Fakultät Heidelberg(Deutschland) und das National Health Science ResearchCommittee (Malawi) genehmigt.Das Management des KCH hat der Durchführung derEvaluation zugestimmt. Alle Befragten gaben ihre Einwil-ligung zur Durchführung der Interviews, Gruppendiskus-sionen und Audio-Aufnahmen. Alle persönlich gegebenenInformationen werden vertraulich behandelt und die indi-viduelle Identifizierung von Befragten wird verhindert.
DanksagungDas Krankenhaus-Partnerschafts-Projekt erhielt Mitteldurch die DeutscheGesellschaft für Internationale Zusam-menarbeit (GIZ), PROFILE (deutsches ESTHER Sekretari-at), innerhalb der ESTHER (Ensemble pour une SolidaritéThérapeutique Hospitalière En Réseau) Initiative in Zu-sammenarbeit mit dem Partnerschaftsprojekt MAGNET(Malawi German Networking for Capacity Building inTreatment, Training and Research at Kamuzu CentralHospital).
14/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...
InteressenkonfliktDie Autoren erklären, dass sie keine Interessenkonflikteim Zusammenhangmit diesemArtikel haben. Die Autorenallein zeichnen sich für den Inhalt und das Verfassen desArtikels verantwortlich.
Literatur1. Muula A. Case for Clinical Officers and Medical Assistants in
Malawi. Croat Med J. 2009;50(1):77-78. DOI:10.3325/cmj.2009.50.77
2. Zijlstra E, Broadhead R. The College of Medicine in the Republicof Malawi: towards sustainable staff development. Hum ResourHealth. 2007;5:10. DOI: 10.1186/1478-4491-5-10
3. Crow J, Broussard R, Dong L, Finn J, Wiley B, Geisler G. Asynthesis of research on ICT adoption and use by medicalprofessionals in Sub-Saharan Africa. Proceedings of the 2ndACMSIGHIT International Health Informatics Symposium;Miami,Florida, USA. 2110384: ACM; 2012. p. 161-70.
4. Kulier R, Gülmezoglu A, Zamora J, Plana MN, Carroli G, CecattiJG, Germar MJ, Pisake L, Mittal S, Pattison R, Wolomby-MolondoJJ, Bergh AM, May VV, Souza JP, Koppenhoefer S, Khan KS.Effectiveness of a clinically integrated e-learning course inevidence-based medicine for reproductive health training: Arandomized trial. JAMA. 2012;308(21):2218-2225. DOI:10.1001/jama.2012.33640
5. Frehywot S, Vovides Y, Talib Z, Mikhail N, Ross H, Wohltjen H,Bedada S, Korhumel K, Koumare AK, Scott J. E-learning inmedical education in resource constrained low- and middle-income countries. Hum Resour Health. 2013;11(1):4. DOI:10.1186/1478-4491-11-4
6. Huwendiek S, Reichert F, Bosse H, de Leng B, van der VleutenC, Haag M, et al. Design principles for virtual patients: a focusgroup study among students. Med Educ. 2009;43:580-588. DOI:10.1111/j.1365-2923.2009.03369.x
7. Agyeman-Duah J, Theurer A, Munthali C, Alide N, Neuhann F.Understanding the barriers to setting up a healthcare qualityimprovement process in resource-limited settings: a situationalanalysis at the Medical Department of Kamuzu Central Hospitalin Lilongwe, Malawi. BMC Health Serv Res. 2014;14(1):1. DOI:10.1186/1472-6963-14-1
8. Mains EA, Blackmur J, Dewhurst D, Ward R, Garden O, WigmoreS. Study on the feasibility of provision of distance learningprogrammes in surgery toMalawi. Surgeon. 2011;9(6):322-325.DOI: 10.1016/j.surge.2010.11.032
9. Mullan F, Frehywot S. Non-physician clinicians in 47 sub-SaharanAfrican countries. Lancet. 2007;370(9605):2158-2163. DOI:10.1016/S0140-6736(07)60785-5
10. Ellaway R, Candler C, Greene P, Smothers V. An ArchitecturalModel for MedBiquitous Virtual Patients. Baltimore, MD:MedBiquitous; 2006.
11. Huwendiek S, De leng BA, Zary N, Fischer MR, Ruiz JG, EllawayR. Towards a typology of virtual patients. Med Teach.2009;31(8):743-748. DOI: 10.1080/01421590903124708
12. Dewhurst D, Borgstein E, GrantM, BeggM. Online virtual patients- A driver for change in medical and healthcare professionaleducation in developing countries?Med Teach. 2009;31(8):721-724. DOI: 10.1080/01421590903124732
13. Czaputa C. Didaktische Reflexionen zumUnterrichtseinsatz. Ref.4.7. Dillingen: eLearning Kompetenzzentrum Akademie fürLehrerfortbildung und Personalführung; 2009.
14. Kerres M. Mediendidaktik?: Konzeption und Entwicklungmediengestützter Lernangebote. München: Oldenbourg; 2013.DOI: 10.1524/9783486736038
15. Bhuasiri W, Xaymoungkhoun O, Zo H, Rho JJ, Ciganek AP. Criticalsuccess factors for e-learning in developing countries: Acomparative analysis between ICT experts and faculty. CompEduc. 2012;58(2):843-55. DOI:10.1016/j.compedu.2011.10.010
16. Chen J, Subramanian L. Interactive web caching for slow orintermittent networks. Proceedings of the 4th Annual Symposiumon Computing for Development. Cape Town, South Africa: ACM;2013. S.1-10.
17. Isaacman S, Martonosi M. Potential for collaborative cachingand prefetching in largely-disconnected villages. Proceedings ofthe 2008 ACM workshop on Wireless networks and systems fordeveloping regions. San Francisco, California, USA: ACM; 2008.S.23-30.
18. Johnson DL, Belding EM, Almeroth K, Stam Gv. Internet usageand performance analysis of a rural wireless network in Macha,Zambia. Proceedings of the 4th ACM Workshop on NetworkedSystems for Developing Regions. San Francisco, California: ACM;2010. S.1-6.
19. Bank W. World Development Report 1998-1999: Knowledge forDevelopment. Washington/DC: World Bank; 1998.
20. Ajakaiye O, Kimenyi MS. Higher Education and EconomicDevelopment in Africa: Introduction and Overview. J Afr Econom.2011;20(Supplement 3):iii3-iii13. DOI: 10.1093/jae/ejr027
21. Chen C, Buch E, Wassermann T, Frehywot S, Mullan F, OmaswaF, Greysen SR, Kolars JC, Dovlo D, El Gali Abu Bakr DE,Haileamlak A, Koumare AK, Olapade-Olaopa EO. A survey of Sub-Saharan African medical schools. Hum Resour Health.2012;10(1):4. DOI: 10.1186/1478-4491-10-4
22. Kanwischer D, Quennet F. Distance Education and SpatialCitizenship in Africa–Challenges and Prospects. Rev Int GeographEduc Online. 2012;2(1). Zugänglich unter/available from: http://www.rigeo.org/vol2no1/2.6.RIGEO-VOL.2.NO.1-6.pdf
23. Dev P, Hoffer E, Barnett GO. Computers in Medical Education.In: Shortliffe E, Cimino J (Hrsg). Biomedical Informatics. HealthInformatics. New York: Springer; 2006. S.737-762. DOI:10.1007/0-387-36278-9_21
24. Mars M. Building the capacity to build capacity in e-health in sub-Saharan Africa: the KwaZulu-Natal experience. Telemed J EHealth. 2012;18(1):32-37. DOI: 10.1089/tmj.2011.0146
Korrespondenzadresse:Sandra Barteit, M.A.Universität Heidelberg, Institut für Public Health,Bergheimer Straße20, D-69115Heidelberg, Deutschland,Tel.: +49 (0)6221/[email protected]
Bitte zitieren alsBarteit S, Hoepffner P, Huwendiek S, Karamagi A, Munthali C, Theurer A,Neuhann F. Self-directed e-learning at a tertiary hospital in Malawi –A qualitative Evaluation and Lessons learnt. GMS Z Med Ausbild.2015;32(1):Doc7.DOI: 10.3205/zma000949, URN: urn:nbn:de:0183-zma0009497
Artikel online frei zugänglich unterhttp://www.egms.de/en/journals/zma/2015-32/zma000949.shtml
15/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...

Eingereicht: 30.04.2014Überarbeitet: 22.09.2014Angenommen: 01.12.2014Veröffentlicht: 11.02.2015
Copyright©2015 Barteit et al. Dieser Artikel ist ein Open-Access-Artikel und stehtunter den Lizenzbedingungen der Creative Commons Attribution 4.0License (Namensnennung). Lizenz-Angaben siehehttp://creativecommons.org/licenses/by/4.0/.
16/16GMS Zeitschrift für Medizinische Ausbildung 2015, Vol. 32(1), ISSN 1860-3572
Barteit et al.: Selbstgesteuertes medizinisches Lernen via E-Learning ...