onse health activity malawi - pdf server
TRANSCRIPT

This report is made possible by the support of the American People through the US Agency for International Development (USAID). The
contents of this report are the sole responsibility of Organized Network of Services for Everyone’s (ONSE) Health Activity and do not
necessarily reflect the views of USAID or the United States Government.
ONSE HEALTH ACTIVITY MALAWI
QUARTERLY ACTIVITY REPORT
PY6 Quarter 2: January 1, 2022 to March 31, 2022 Submission Date: April 29, 2022
Contract Number: AID-612-C-17-00001
COR Name: Reuben Ligowe
Submitted by: Ann Phoya, Chief of Party
Management Sciences for Health (MSH)
Mercantile Office Building
Area 13/138
P Bag 398
Lilongwe, Malawi
PHOTO CREDIT: ERIK SCHOUTEN
PHOTO CREDIT: REJOICE PHIRI
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 2
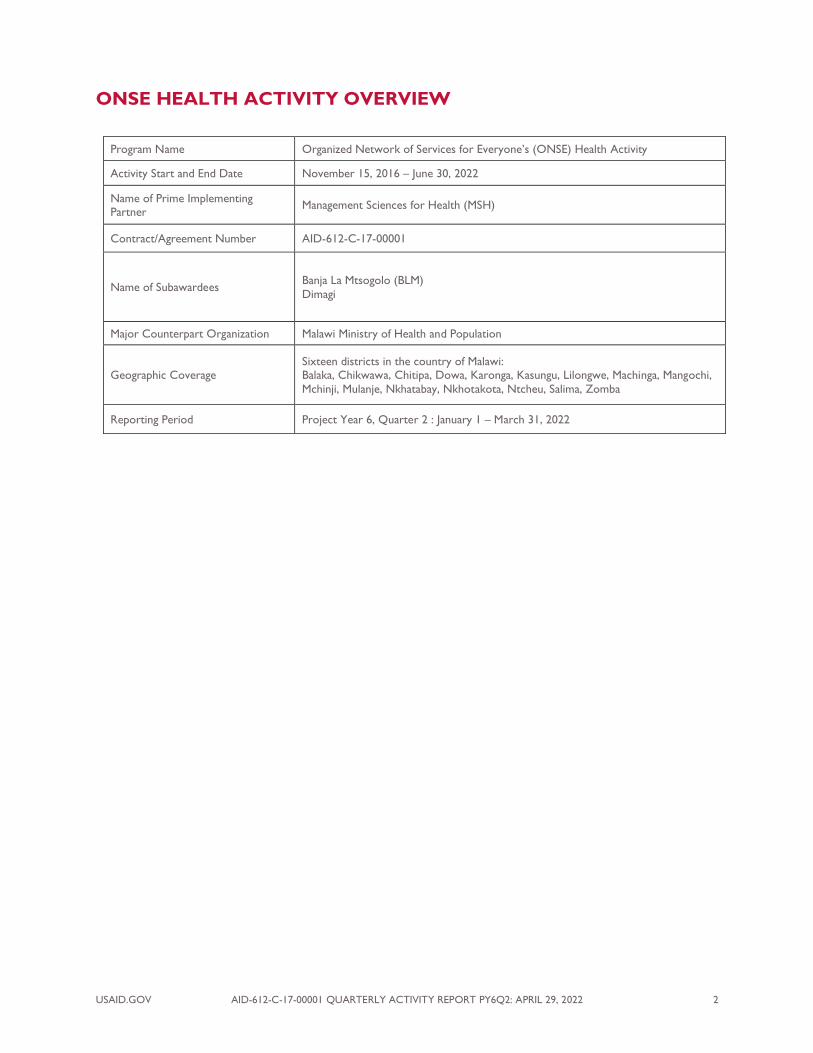
ONSE HEALTH ACTIVITY OVERVIEW
Program Name Organized Network of Services for Everyone’s (ONSE) Health Activity
Activity Start and End Date November 15, 2016 – June 30, 2022
Name of Prime Implementing Partner
Management Sciences for Health (MSH)
Contract/Agreement Number AID-612-C-17-00001
Name of Subawardees Banja La Mtsogolo (BLM)
Dimagi
Major Counterpart Organization Malawi Ministry of Health and Population
Geographic Coverage Sixteen districts in the country of Malawi: Balaka, Chikwawa, Chitipa, Dowa, Karonga, Kasungu, Lilongwe, Machinga, Mangochi,
Mchinji, Mulanje, Nkhatabay, Nkhotakota, Ntcheu, Salima, Zomba
Reporting Period Project Year 6, Quarter 2 : January 1 – March 31, 2022

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 3
CONTENTS
ONSE HEALTH ACTIVITY OVERVIEW 2
ACRONYMS AND ABBREVIATIONS 4
EXECUTIVE SUMMARY 7
PROGRAM OVERVIEW 10
STRATEGIC PRINCIPLES 11
COVID-19 RESPONSE 15
CROSS CUTTING AREAS 23
CLINICAL SERVICES 25
PERFORMANCE OF HEALTH SYSTEMS STRENGTHENED 64
DEMAND CREATION AND COMMUNITY ENGAGEMENT 69
PROJECT MANAGEMENT 74
IMPLEMENTATION CHALLENGES AND LESSONS LEARNED 84
ANNEX A. ACTIVITY M&E PLAN 85
ANNEX B. RCCE 94
ANNEX C. PARTNER COLLABORATION AND COORDINATION 96
ANNEX D. PY6 Q2 SUCCESS STORIES 97

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 4
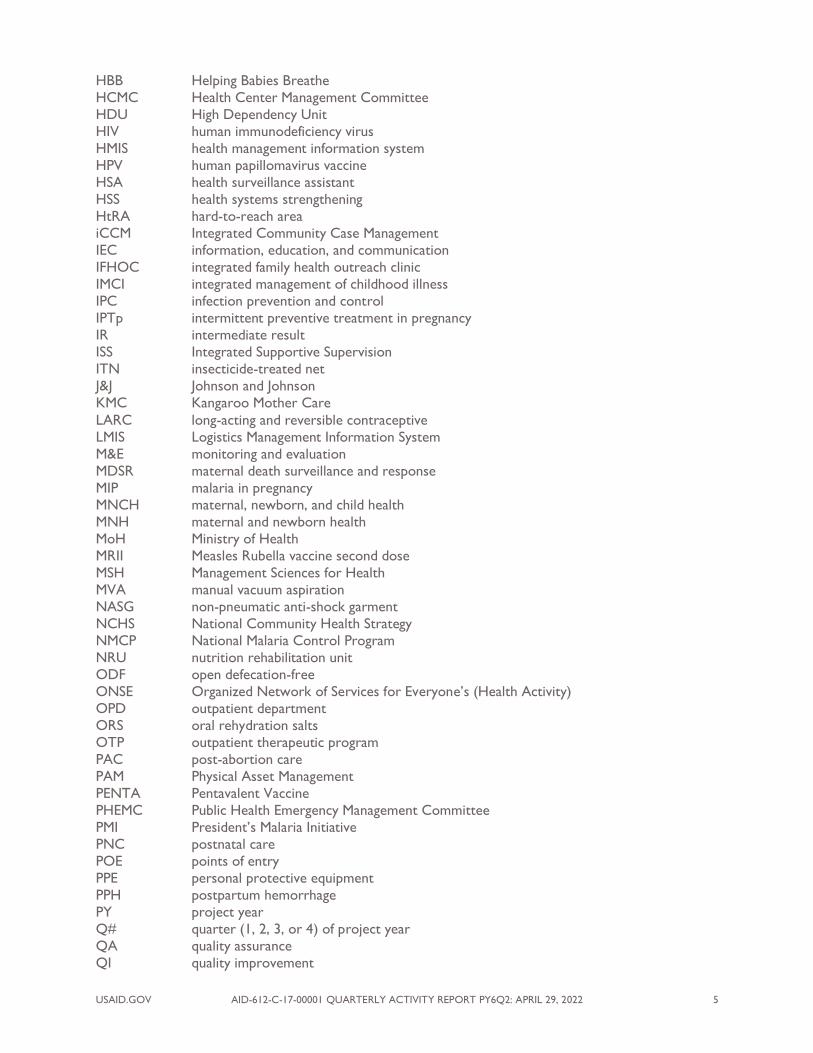
ACRONYMS AND ABBREVIATIONS
5S sort, set in order, shine, standardize, and sustain
ADC Area Development Committee
ANC antenatal care
ART anti-retroviral therapy
AZD AstraZeneca
BEmONC basic emergency obstetric and newborn care
BFHI baby-friendly hospital initiative
BLM Banja La Mtsogolo
BTL bilateral tubal ligation
CAC Community Action Cycle
CBMNC community-based maternal and neonatal care
CC Champion Community
CDCS Country Development Cooperation Strategy
CEmONC comprehensive emergency obstetric and newborn care
CHAI Clinton Health Access Initiative
CHAG Community Health Action Group
CHAM Christian Health Association Malawi
CHSU Community Health Services Unit
CMAM community-based management of acute malnutrition
CMED Central Monitoring and Evaluation Division
CMT Community Mobilization Team
COIN Care of the Infant and Newborn
COR USAID Contract Officer’s Representative
CPD continuous professional development
CSC community score card
CYP couple years protection
DHIS2 District Health Information System 2
DHMT District Health Management Team
DHO district health office
DHPO district health promotion officer
DHSS Director of Health and Social Services
DIP district implementation plan
DMO District Medical Office
DMPA Depo-Provera
DMPA-IM Depo-Provera Intramuscular
DMPA-SC Depo-Provera Subcutaneous (Sayana Press)
DPT1 Diphtheria Tetanus Pertussis vaccine - first dose
DPT3 Diphtheria Tetanus Pertussis vaccine - third dose
DQA data quality assurance
DRRT District Rapid Response Team
DTC Drug and Therapeutics Committee
EC emergency contraception
EMMP Environmental Monitoring and Mitigation Plan
EPI Expanded Program on Immunization
ETAT emergency triage assessment and treatment
FGD focus group discussion
FHP family health package (district)
FP family planning
FP/RH family planning/reproductive health
GIZ Deutsche Gesellschaft für Internationale Zusammenarbeit
GOM Government of Malawi
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 5
HBB Helping Babies Breathe
HCMC Health Center Management Committee
HDU High Dependency Unit
HIV human immunodeficiency virus
HMIS health management information system
HPV human papillomavirus vaccine
HSA health surveillance assistant
HSS health systems strengthening
HtRA hard-to-reach area
iCCM Integrated Community Case Management
IEC information, education, and communication
IFHOC integrated family health outreach clinic
IMCI integrated management of childhood illness
IPC infection prevention and control
IPTp intermittent preventive treatment in pregnancy
IR intermediate result
ISS Integrated Supportive Supervision
ITN insecticide-treated net
J&J Johnson and Johnson
KMC Kangaroo Mother Care
LARC long-acting and reversible contraceptive
LMIS Logistics Management Information System
M&E monitoring and evaluation
MDSR maternal death surveillance and response
MIP malaria in pregnancy
MNCH maternal, newborn, and child health
MNH maternal and newborn health
MoH Ministry of Health
MRII Measles Rubella vaccine second dose
MSH Management Sciences for Health
MVA manual vacuum aspiration
NASG non-pneumatic anti-shock garment
NCHS National Community Health Strategy
NMCP National Malaria Control Program
NRU nutrition rehabilitation unit
ODF open defecation-free
ONSE Organized Network of Services for Everyone’s (Health Activity)
OPD outpatient department
ORS oral rehydration salts
OTP outpatient therapeutic program
PAC post-abortion care
PAM Physical Asset Management
PENTA Pentavalent Vaccine
PHEMC Public Health Emergency Management Committee
PMI President’s Malaria Initiative
PNC postnatal care
POE points of entry
PPE personal protective equipment
PPH postpartum hemorrhage
PY project year
Q# quarter (1, 2, 3, or 4) of project year
QA quality assurance
QI quality improvement

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 6
QIST quality improvement support team
QoC quality of care
QMD Quality Management Directorate
RCCE risk communication and community engagement
RHD Reproductive Health Directorate
RUTF ready-to-use therapeutic food
SAM severe acute malnutrition
SBC social and behavior change
SBCC SBC communication
SP Sulfadoxine-pyrimethamine
SRH sexual and reproductive health
TA traditional authority
TWG technical working group
UNICEF United Nations Children’s Fund
USAID US Agency for International Development
USG US Government
WASH water, sanitation, and hygiene
WHO World Health Organization
WIT ward improvement team
WPC water point committee
VAT value-added tax
VHC Village Health Committee
YFHS youth-friendly health services

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 7
EXECUTIVE SUMMARY
The overall purpose of the US Agency for International Development’s (USAID) Organized Network of
Services for Everyone’s (ONSE) Health Activity is to support Malawi in reducing maternal, newborn, and
child morbidity and mortality. In pursuit of this goal, ONSE works closely with the Ministry of Health
(MoH) and key stakeholders at the national and district levels to deliver on four intermediate results
(IRs): (1) Improving access to priority health services, (2) improving quality of priority health services,
(3) strengthening performance of health systems, and (4) increasing demand for priority health services.
Through the ONSE Health Activity, Management Sciences for Health (MSH) and its partners provide
technical assistance to improve the capacity of the health system and of key health system and
community actors to expand the availability, quality, and utilization of essential health services. ONSE
focuses on sustainable health system interventions, aligning and coordinating with partners in the
Malawian government and civil society to support better planning; more effective and transparent
leadership, management, and governance; and improved evidence-based citizen and community
advocacy.
ONSE’s activities are based on four core principles that promote self-reliance:
1. Data-driven, district-specific targeting to jointly identify needs for high-impact interventions
with districts, facilities, and communities - targeting our assistance where it is most needed and
will have the greatest impact.
2. Systemic capacity building coupled with smart capacity building approaches, to improve
performance and quality, including improved competencies of the individuals and teams who
work within and with the system. Approaches such as mentorship, coaching, and simulations
strengthen processes and competencies on the job.
3. Mutual accountability between the system and the communities that it serves to ensure that
health system transformations are responsive to priority health issues and wholly owned by
citizens, health workers, and health leaders.
4. Dignity for the clients who access services, for the providers working within the health system,
and for all health system actors. Leveraging systems and community engagement interventions
to strengthen the availability and quality of person-centered services, including ensuring that
clients who access services do so with dignity, and that providers feel they are treated with
dignity within the system.
January-March 2022 (Project Year [PY] 6, Quarter [Q] 2) marks the last quarter of the last year of
implementation of the ONSE project. ONSE’s efforts in P6Q2 continued to demonstrate that the
Activity is doing essential work, meeting its objectives, achieving sustainable results, using resources
effectively, and reaffirming the commitment of the US Government (USG) and the American people to
Malawi. The final year for ONSE is a critical period for communicating Activity strategies and successes,
as well as relating its legacy and impact to key target audiences in both Malawi and the US. The Activity
is placing a focus on the sustainability of its contributions to the health sector, as well as on advancing
Malawi on its journey to self-reliance.
Despite the COVID-19 pandemic’s continued threat to the Malawian health system, ONSE continues to
support essential activities while providing operational support in local preparedness and response
activities. By April 9, 2022, a cumulative total of 85,702 confirmed COVID-19 cases with 2,628
cumulative total number of deaths (with a case fatality rate of 3.07%) were reported since the pandemic
was declared in April 2020. During the quarter, ONSE assisted the government’s efforts in increasing
uptake of the COVID-19 vaccines by supporting vaccination supervision; new vaccines orientation; and
dissemination of COVID-19 messages in communities through mobile van awareness campaigns,
integrated family health outreach clinic (IFHOC) services, and community sensitization and engagement
meetings and radio programs. As a result of these efforts, 411,549 people were vaccinated in ONSE-
supported districts. Additionally, ONSE continues to support the MoH in intensified screening of

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 8
travelers at all points of entry (POE) to prevent importation of COVID-19 cases, including requiring a
negative PCR test from travelers no older than 72 hours upon arrival. ONSE, with its strong district
footprint, continued providing crucial operational and technical support to strengthen various aspects of
the response, while complementing response efforts through several elements of its routine
programming. ONSE works closely with USAID, the Government of Malawi (GOM), and other
implementing partners so that the country responds effectively and efficiently to the pandemic. A
COVID-19 section has been included in this report to highlight key areas of ONSE support, specifically
under the following critical pillars of immunization readiness and implementation; risk communication
and community engagement (RCCE); surveillance, case finding, rapid response teams, case investigation,
and contact tracing; infection prevention and control (IPC); case management; and coordination and
operations.
This quarterly report presents ONSE’s PY6Q2 achievements against ONSE’s PY6 annual targets. By the
end of PY6Q2, 42% (14) of the 33 indicators that are monitored quarterly were achieved, with another
18% (6) almost achieved and 40% (13) not achieved. The details of the categorization are included as a
footnote in figure 1, and the same scale has been applied in each summary table at the start of section in
the report.
FIGURE 1. INDICATOR ACHIEVEMENT DASHBOARD
CLINICAL SERVICES
MATERNAL AND NEWBORN HEALTH (MNH): Between January and March 2022, ONSE
continued to strengthen the capacity of health workers at community and facility levels to deliver high-
impact interventions including antenatal care (ANC), basic emergency obstetric and newborn care
(BEmONC), and community-based maternal and neonatal care (CBMNC):
◼ In PY6Q2, 13,050 pregnant women-initiated ANC in the first trimester, compared to 12,389
pregnant women in PY5Q2, contributing to a 107% achievement of the PY6 target at the end of
the second quarter.
◼ The number of women giving birth who received uterotonics in the third stage of labor (or
immediately after birth) through USG-supported programs (EPMM indicator) reached a
cumulative achievement of 119,461 for a 96% achievement of the annual target.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 9
CHILD HEALTH AND EXPANDED PROGRAM ON IMMUNIZATION (EPI): In PY6Q2,
ONSE continued to support the MoH to deliver high-impact neonatal and child health interventions in
the 11 family health package (FHP) districts. Of the six indicators ONSE tracks related to child health,
three are on track, two are almost on track, and one is not on track as of PY6Q2.
◼ By the end of the second quarter, the number of children 12-23 months who received measles-
rubella second dose through USG-assisted programs reached a cumulative 67,896 for a 99%
achievement against the annual target.
◼ The Diphtheria Tetanus Pertussis vaccine-first dose (DPT1) to third dose (DPT3) drop-out-rate
reached 5.1%, contributing to a 100% achievement of the annual target.
FAMILY PLANNING (FP): During PY6Q2, ONSE continued to support FP activities at both the
facility and community level, with an emphasis on building capacity for the provision of long-acting and
reversible contraceptive (LARC) and permanent methods. PY6Q2 highlights included the following:
◼ At the end of PY6Q2, couple years protection (CYP) for the 11 FP districts reached a
cumulative 341,843, 85% of the annual target. Currently PY6Q2 accounts for only January and
February 2022 data (remaining data for the quarter will be reflected in PY6 annual report) so
the cumulative total of CYPs cannot be compared between PY5Q2 and PY6Q2, however CYP
from LARCs increased from 45% to 50%.
YOUTH: ONSE tailors services and activities to meet the needs of young people and women and to
support the engagement of women and youth in planning and monitoring health services intended for
their benefit. During PY6Q2:
◼ In PY6Q2, 292,065 youth (10-24 years) utilized youth-friendly health services (YFHS) in the
ONSE supported facilities, marking a cumulative 571,469 or 571% achievement against the
annual target.
MALARIA: ONSE’s progress in malaria is tracked against three key indicators—tracking diagnostics,
case management, and intermittent preventive treatment in pregnancy (IPTp)—in line with National
Malaria Control Program (NMCP) and President’s Malaria Initiative (PMI) priorities. In PY6Q2:
◼ 54% of pregnant women received three or more doses of IPTp during ANC, maintaining at
106% achievement against the annual target.
NUTRITION: ONSE supports both community- and facility-level interventions, including outreach
clinics, community-based management of acute malnutrition (CMAM), and nutrition counseling for
pregnant women and new babies as part of ANC and postnatal care (PNC). Other highlights during
PY6Q2 included:
◼ In this quarter, a total of 93,643 children under five (0-59 months) were reached by USG-
supported nutrition programs, contributing to a 106% achievement of the annual target.
◼ A total of 79,598 pregnant women were reached with nutrition interventions through USG-
supported programs, marking a cumulative 158,979 or 145% achievement against the annual
target.
WATER, SANITATION, AND HYGIENE (WASH): In PY6Q2, ONSE continued to make efforts
to integrate WASH activities with priority health areas and district- and community-based systems
strengthening activities. Highlights from PY6Q2 included:
◼ In PY6Q2, 17 institutional settings gained access to basic drinking water services as a result of
USG assistance, contributing to a 94% achievement of the annual target.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 10
HEALTH SYSTEMS STRENGTHENING
GOVERNANCE AND PLANNING: The MoH continues to devolve its authority and resources to
the district councils to make health services more efficient and cost effective. Through integrated
interventions that strengthen health governance at district level, ONSE has enhanced the capacity of
District Health Offices (DHOs) to plan and allocate resources for health. Highlights included:
◼ By the end of PY6Q2, ONSE supported 3 additional district implementation plan (DIP) reviews
in ONSE-supported districts, contributing to a 118% achievement of the annual target.
LEADERSHIP AND MANAGEMENT:
◼ ONSE supported DHMT Integrated Supportive Supervision (ISS) of 403 (260M, 143F) health
workers from 78 health facilities in 9 districts, where 114 action points were developed as per
the ISS Dashboard. At the end of the quarter, ONSE’s achievement on the ISS indicator is 86%
against the annual target.
HEALTH MANAGEMENT INFORMATION SYSTEMS (HMIS): ONSE targeted HMIS at the
district level, and District Health Information System 2 (DHIS2) data reporting steadily improved. In
PY6Q2, 238 health facilities submitted DHIS2 data in line with national standards each quarter,
representing 80% of the annual target.
COMMUNITY MOBILIZATION AND ENGAGEMENT
ONSE engages and mobilizes communities to disseminate critical health information and messages,
increase demand for and utilization of high-quality services, and strengthen and elevate the voices of
citizens and communities to ensure that health services are accountable to their users. Highlights during
PY6Q2 included:
◼ As of PY6Q2, ONSE has supported 58% of communities using community score card (CSC)
methodology, a 104% achievement of the annual target at the end of the second quarter.
PROGRAM OVERVIEW
The ONSE Health Activity is funded by USAID. ONSE is supporting Malawi’s efforts to improve
effective coverage of essential health care services in the priority areas of maternal, newborn, and child
health (MNCH); malaria; FP/reproductive health (FP/RH); nutrition; and WASH across 16 districts in
Malawi.
CONCEPTUAL FRAMEWORK
The overall purpose of the ONSE Health Activity is to improve maternal, newborn, and child survival
and well-being in Malawi. ONSE’s activities are directed toward four main objectives, or IRs:
◼ Increasing access to priority health services (IR1)
◼ Improving the quality of priority health services (IR2)
◼ Strengthening the performance of health systems (IR3)
◼ Increasing the demand for priority health services (IR4)
ONSE’s approach builds on previous advances in the health sector, and focuses on district-based service
provision and systems strengthening. Recognizing that one size does not fit all, ONSE co-designs and
targets its approaches with the MoH, health facilities, community groups, and youth based on locally
available evidence. As illustrated in Figure 2 below, ONSE implements activities in three key areas:
clinical services, HSS, and community mobilization and engagement. Clinical services encompasses IR1
and IR2 as ONSE aims to increase access to quality health services. HSS draws largely from IR3 activities
geared toward strong leaders and managers, transparent governance practices, data-driven decision-
making, and improved access to commodities. Community mobilization and engagement is cross cutting
across all IRs, but specifically encompasses IR4 activities empowering communities and generating

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 11
demand for high-quality health services. The relationships and alignment of approaches and activities
across these areas is essential to build sustainable systemic capacity for improved health.
FIGURE 2. ONSE CONCEPTUAL FRAMEWORK
CONSORTIUM PARTNERS
ONSE is implemented by a consortium of partners with complementary areas of expertise. ONSE has
established a solid collaborative framework and will continue to draw on the partners’ complementary
technical expertise, experience, and resources to support project implementation. ONSE staff are
housed in ONSE offices under a unified project team and management structure to ensure day-to-day
continuous, integrated, and systematic planning and implementation of project activities with a strong
project focus and identity. MSH brings decades of experience in HSS and a novel approach for systemic
capacity building, including smart capacity building of system’s actors, to improve maternal and child
survival and well-being. Banja La Mtsogolo (BLM) increases access to and quality of FP/RH services
through its community outreach and facility-based service-delivery platforms. The mobile youth
outreach clinics are contributing to provision of essential FP/RH services at the community level during
COVID-19. Dimagi CommCare is the digital platform that houses the ISS toolkit, which supports district
facility supervision. With an online dashboard, ISS empowers decision makers and other stakeholders
with data for real-time facility performance monitoring to enable them to provide targeted support to
facilities and programs and steer performance improvement.
STRATEGIC PRINCIPLES
SMART CAPACITY BUILDING
To enable stronger overall systemic capacity—and thus improve the performance capacity of individuals
working in and with that system—ONSE needs to intervene at multiple levels of Malawi’s health system.
ONSE therefore employs a systemic capacity-building approach modeled on the framework proposed by
Potter and Brough that includes interventions targeting various components of systemic capacity. These
elements are illustrated in Figure 3.
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 12
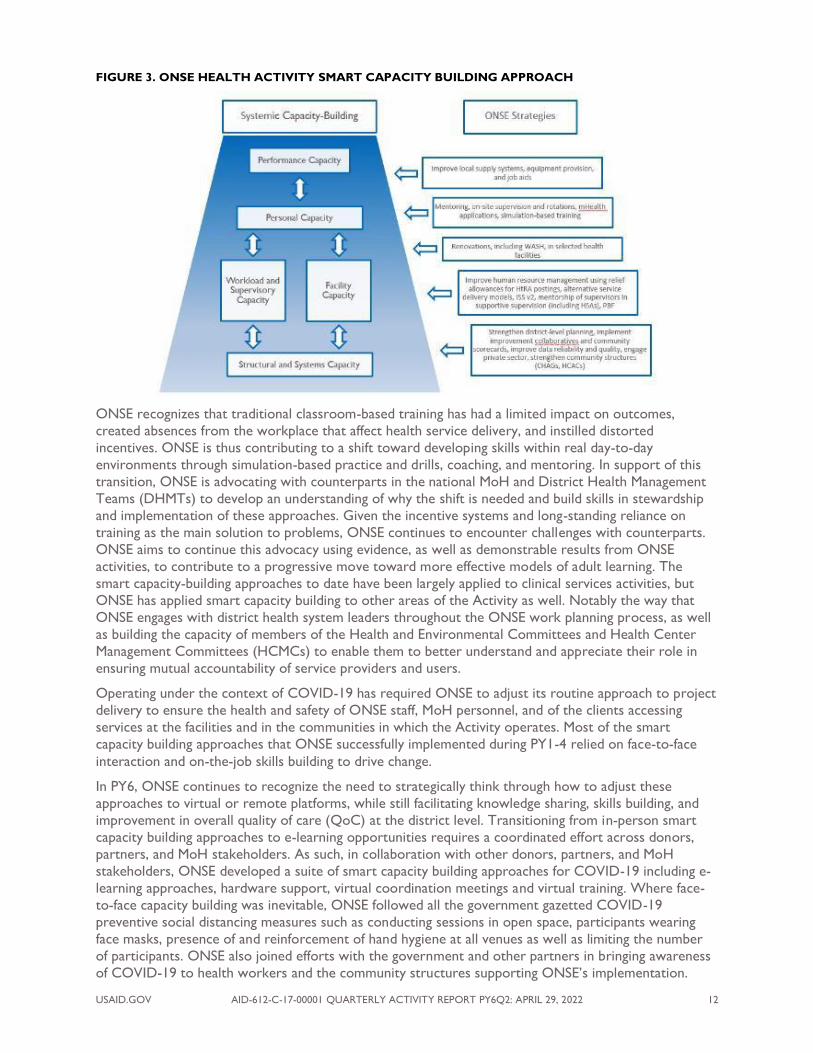
FIGURE 3. ONSE HEALTH ACTIVITY SMART CAPACITY BUILDING APPROACH
ONSE recognizes that traditional classroom-based training has had a limited impact on outcomes,
created absences from the workplace that affect health service delivery, and instilled distorted
incentives. ONSE is thus contributing to a shift toward developing skills within real day-to-day
environments through simulation-based practice and drills, coaching, and mentoring. In support of this
transition, ONSE is advocating with counterparts in the national MoH and District Health Management
Teams (DHMTs) to develop an understanding of why the shift is needed and build skills in stewardship
and implementation of these approaches. Given the incentive systems and long-standing reliance on
training as the main solution to problems, ONSE continues to encounter challenges with counterparts.
ONSE aims to continue this advocacy using evidence, as well as demonstrable results from ONSE
activities, to contribute to a progressive move toward more effective models of adult learning. The
smart capacity-building approaches to date have been largely applied to clinical services activities, but
ONSE has applied smart capacity building to other areas of the Activity as well. Notably the way that
ONSE engages with district health system leaders throughout the ONSE work planning process, as well
as building the capacity of members of the Health and Environmental Committees and Health Center
Management Committees (HCMCs) to enable them to better understand and appreciate their role in
ensuring mutual accountability of service providers and users.
Operating under the context of COVID-19 has required ONSE to adjust its routine approach to project
delivery to ensure the health and safety of ONSE staff, MoH personnel, and of the clients accessing
services at the facilities and in the communities in which the Activity operates. Most of the smart
capacity building approaches that ONSE successfully implemented during PY1-4 relied on face-to-face
interaction and on-the-job skills building to drive change.
In PY6, ONSE continues to recognize the need to strategically think through how to adjust these
approaches to virtual or remote platforms, while still facilitating knowledge sharing, skills building, and
improvement in overall quality of care (QoC) at the district level. Transitioning from in-person smart
capacity building approaches to e-learning opportunities requires a coordinated effort across donors,
partners, and MoH stakeholders. As such, in collaboration with other donors, partners, and MoH
stakeholders, ONSE developed a suite of smart capacity building approaches for COVID-19 including e-
learning approaches, hardware support, virtual coordination meetings and virtual training. Where face-
to-face capacity building was inevitable, ONSE followed all the government gazetted COVID-19
preventive social distancing measures such as conducting sessions in open space, participants wearing
face masks, presence of and reinforcement of hand hygiene at all venues as well as limiting the number
of participants. ONSE also joined efforts with the government and other partners in bringing awareness
of COVID-19 to health workers and the community structures supporting ONSE’s implementation.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 13
COVID-19 is now the first agenda in all capacity building activities. In the Cost Extension period, ONSE
planned to pilot remote supervision by engaging facility in-charges and senior health surveillance
assistants (HSAs) in a bid to minimize movement of district level staff traveling to health centers for
supervision thereby reducing the spread of the virus between facilities.
COMMUNITY MOBILIZATION
The community is an essential platform for much of ONSE’s work, including community health service
delivery and community engagement and mobilization. As a key partner of the MoH for implementation
of the National Community Health Strategy (NCHS), at the national and district level, ONSE
collaborates with the MoH Preventive Health Section and key implementing partners to eliminate
harmful practices and promote increased health-seeking and healthy behaviors in all districts. ONSE
continues to expand and strengthen community-based structures to ensure meaningful engagement of
communities in service delivery and planning and monitoring of government and facility commitments,
including the provision of quality health care services. All of ONSE’s community work rests on the
following principles:
◼ Promoting self-reliance and resilience in hard-to-reach areas (HtRAs)
◼ Integrating participatory communications across all demand generation and community
mobilization activities
◼ Strengthening social accountability through community participation in monitoring health
services and systems activities
◼ Coordinating and collaborating with the Community Health Services Unit (CHSU) and other
partners to implement the NCHS
ONSE focuses on intensifying community participation in health issues affecting communities by
improving the functionality of community structures such as Community Health Action Groups
(CHAGs), providing necessary support to Champion Community (CC) groups, and ensuring that both
districts and communities are responding to community health needs through capacity-building
investments. Key community mobilization and engagement activities supported by ONSE to promote
the sustainability of and access to quality health services include:
◼ Building the capacity of districts to develop district-specific social and behavior change (SBC)
plans to be used as a resource mobilization tool to inform DIP activities. ONSE is well-
positioned to link district health promotion officers (DHPOs) and community health workers to
engage them fully in the DIP process, as well as ensure participation of community structures
and civil society organizations at key moments in the planning and review process.
◼ Establishment and revitalization of CHAGs, to enhance communities’ roles in supporting the
implementation of community-led approaches with the involvement of Village Health
Committees (VHCs) and care groups.
◼ Fostering opportunities for collaboration and sharing among CHAGs and other community
groups (care groups, VHCs, and CCs) as well as governance structures with a role in
community health (VHCs, Community Mobilization Teams [CMTs], HCMCs, and DHMTs).
ONSE supports coordination of these structures in collaboration with government partners to
advocate for continuity beyond the project’s lifespan to ensure sustainability of the
interventions.
◼ The COVID-19 pandemic provided a substantial impetus towards engaging the assistance of
community structures including CHAGs, Area Development Committees (ADCs), village
development committees, Chiefs, Religious Leaders and different structures such as police
forums and market committees to implement pandemic response measures.
◼ CSC sessions between health facilities and catchment communities as a mechanism for reviewing
and planning interventions targeted to the improvement of health priorities in the community.
HCMCs, CHAGs, CCs, VHCs, and other volunteers are part of the sessions, as are service
providers in both facilities and communities. Women and youth are also included in these
discussions.
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 14
More information on ONSE’s community mobilization and engagement work can be found in the
corresponding section beginning on page 72.
DISTRICT AND NATIONAL GOVERNMENT COORDINATION
The GoM, and especially the DHMTs, remain the key counterparts for ONSE and the project has been
able to maintain strong and collaborative relationships with many, if not most, of our key counterparts in
the MoH. The Reproductive Health Directorate (RHD), NMCP, and Physical Asset Management (PAM)
are three examples where very strong coordination and collaboration has contributed to the
achievement of many of our program targets and indicators to date. The Activity remains focused on the
people of Malawi, and the support provided to all levels of the MoH to improve health services and the
systems that support those services. ONSE has also maintained strong collaboration with other
implementing partners including those supported by USAID. Of particular mention is Clinton Health
Access Initiative (CHAI) which is supporting the planning of leadership structures in all the 26 districts.
ONSE is closely working with CHAI in all 16 districts we support.
Each district has also identified a counterpart for ONSE within the DHMT, who is the focal person for
identifying priorities, resolving issues, and ensuring a smooth and productive relationship between the
Activity and the district. ONSE has a similar counterparts within the MoH at national level, including at
the Directorates of Planning and Policy Development; Health Technical Support Services; Central
Monitoring and Evaluation Division (CMED); integrated management of childhood illness (IMCI) unit,
which includes the emergency triage assessment and treatment (ETAT) unit; Environmental Health
Services Section; EPI; Environmental Health Department; Health Education Unit; Human Resources
Management Section; NMCP; Pharmaceutical Services; Preventive Health Services, particularly the
CHSU; Quality Management Directorate (QMD); and the RHD. The Ministry of Agriculture, Irrigation,
and Water Development and the Ministry of Youth and Gender are also important government
counterparts.
During the COVID-19 pandemic, ONSE has continued to participate actively in all national- and district-
level committees established by the government. At the national level, ONSE is a member of the
National Health Cluster which includes representation from different ministries, departments, and
agencies, and several sub-clusters including the RCCE, Case Management Sub-Cluster, IPC, Equipment
and Supplies, sexual and reproductive health (SRH) rights partners technical working group (TWG),
oxygen TWG and RCCE partners on COVID-19. At the district level, ONSE’s involvement includes,
among others, participating in district-based Public Health Emergency Management Committee
(PHEMC) and District Rapid Response Team (DRRT) meetings. Our team provides technical support,
shares COVID-19 updates, learns what others are doing in order to complement efforts, and provides
financial support through the provision of lunch allowances and transport refunds for participants. In
quarter 2 of PY6, ONSE continued to participate and support targeted meetings including COVID-19
related activities that are aimed at strengthening national and district coordination.
PARTNER COLLABORATION AND COORDINATION
ONSE routinely seeks support and collaboration with other partners and stakeholders, particularly
USAID implementing partners such as Global Health Supply Chain - Procurement and Supply
Management towards achievement of the USAID Country Development Cooperation Strategy (CDCS)
and coordination, colocation, and collaboration approach. The Activity also works closely with other
donors, for example Foreign, Commonwealth and Development Office, CHAI, and Deutsche
Gesellschaft für Internationale Zusammenarbeit (GIZ), for specific areas of work, and multilateral
partners including United Nations Children’s Fund (UNICEF), and United Nations Population Fund. The
below table provides illustrative examples of our collaboration activities. ONSE will seek to engage
partners more effectively and document that engagement as part of a strategy to strengthen external
visibility. See Annex C Table C1 for a list of key partners and collaboration activities.
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 15
COVID-19 RESPONSE
OVERVIEW
In support of the GoM’s National COVID-19 Preparedness and Response Plan, in PY6Q2, ONSE
continued to provide critical operational support to district-level teams engaged in local preparedness
and response activities, while complementing response efforts through several elements of its routine
programming (per the modes of support described in Table 1). The program’s activities, implemented
across the 16 ONSE-supported districts covering more than 60% of the population, helped to
strengthen Malawi’s health system to meet the challenge of COVID-19 and maintain essential health
services. ONSE leveraged its extensive district footprint to support pandemic control measures initiated
by DHMTs during the initial and the sustained period of response. ONSE’s district-level support was
built off a rapid assessment and subsequent district planning conducted during May to June 2020, which
was aligned to the national response plan. ONSE’s response anticipated evolving and newly emerging
approaches such as the introduction of HSAs to support community-based surveillance and revised case
management approaches adapted to the local situation. Activities supported critical pillars under the
World Health Organization’s (WHO’s) operational guidelines for country preparedness and response,
including country-level coordination, planning, and monitoring; RCCE; surveillance, rapid response
teams, and case investigation; POE; IPC; case management and the newly introduced pillar of COVID-19
vaccine roll out.
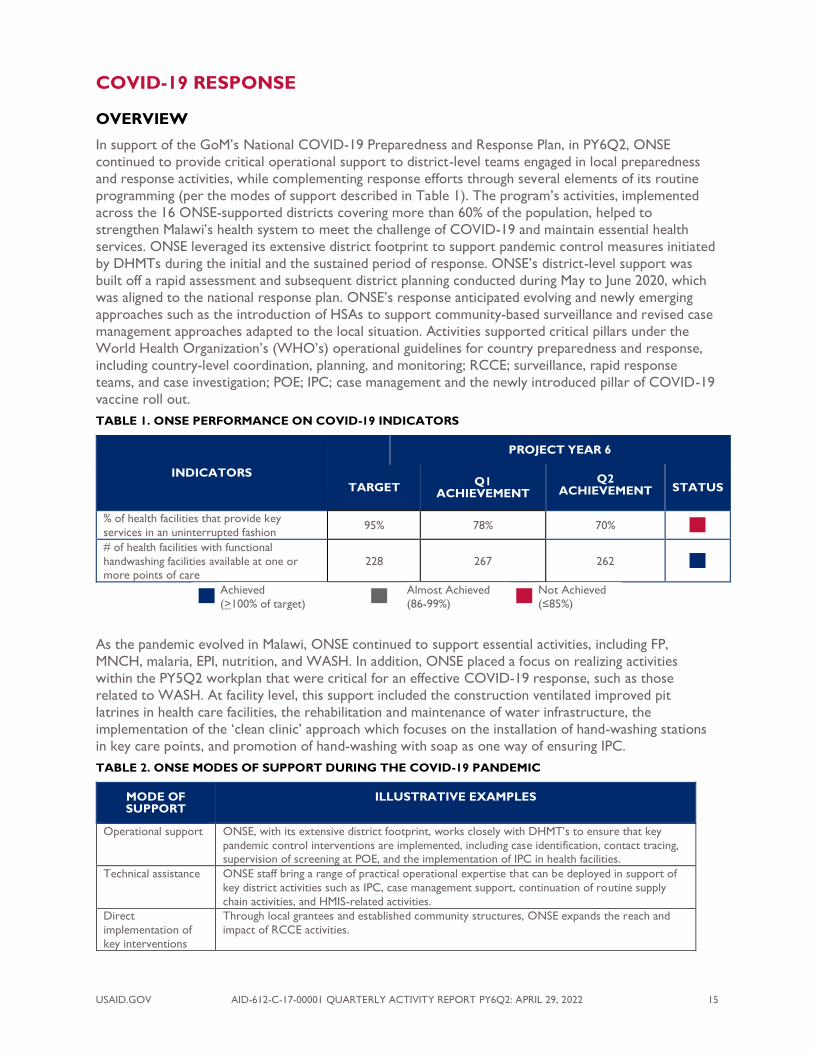
TABLE 1. ONSE PERFORMANCE ON COVID-19 INDICATORS
INDICATORS
PROJECT YEAR 6
TARGET Q1
ACHIEVEMENT
Q2 ACHIEVEMENT STATUS
% of health facilities that provide key
services in an uninterrupted fashion 95% 78% 70%
# of health facilities with functional
handwashing facilities available at one or more points of care
228 267 262
Achieved
(>100% of target)
Almost Achieved
(86-99%) Not Achieved
(≤85%)
As the pandemic evolved in Malawi, ONSE continued to support essential activities, including FP,
MNCH, malaria, EPI, nutrition, and WASH. In addition, ONSE placed a focus on realizing activities
within the PY5Q2 workplan that were critical for an effective COVID-19 response, such as those
related to WASH. At facility level, this support included the construction ventilated improved pit
latrines in health care facilities, the rehabilitation and maintenance of water infrastructure, the
implementation of the ‘clean clinic’ approach which focuses on the installation of hand-washing stations
in key care points, and promotion of hand-washing with soap as one way of ensuring IPC.
TABLE 2. ONSE MODES OF SUPPORT DURING THE COVID-19 PANDEMIC
MODE OF SUPPORT
ILLUSTRATIVE EXAMPLES
Operational support ONSE, with its extensive district footprint, works closely with DHMT’s to ensure that key
pandemic control interventions are implemented, including case identification, contact tracing, supervision of screening at POE, and the implementation of IPC in health facilities.
Technical assistance ONSE staff bring a range of practical operational expertise that can be deployed in support of
key district activities such as IPC, case management support, continuation of routine supply
chain activities, and HMIS-related activities.
Direct
implementation of
key interventions
Through local grantees and established community structures, ONSE expands the reach and
impact of RCCE activities.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 16
Support for coordination of
activities
In collaboration with the MoH, ONSE convenes stakeholders actively engaged in key focus areas for effective district response, including RCCE, surveillance, case identification, and
contact tracing. Such activities involve the participation of several stakeholders such as the Red
Cross, GIZ, care groups, and other community structures.
Support for the continuation of
essential services
ONSE provides support for the continuation of outreach clinics and an appropriate suite of FP activities. ONSE develops and disseminates guidelines to ensure continuity of essential services
amidst COVID-19. Through subgrantees, ONSE helps integrate messages of continued
availability of essential services.
However, ONSE’s interventions were affected by the pandemic in several ways. For example, some
resources (MoH staff) were redirected towards the pandemic control leaving little bandwidth for
program related activities. The government imposed restrictions in Malawi, affected operations as
supervisory visits and other activities requiring direct physical contact were curtailed. Support of
services provided through IFHOCs were affected as some clinicians and nurses were deployed in
COVID-19 treatment centers and vaccination services delivery. Additionally, some clients were
reluctant to frequent the clinics as they were afraid of getting infected. Further, coordination with other
key stakeholders was a challenge as meetings were virtually conducted.
IMMUNIZATION READINESS AND IMPLEMENTATION
During the reporting period, ONSE supported MoH efforts to increase COVID-19 vaccination uptake
while also reducing vaccine wastage. By March 31, 2022, Malawi had vaccinated nationally a total of
1,142,421 people with the first dose (AstraZeneca [AZD] and Pfizer), and 892,414 were fully vaccinated.
Supporting the government’s efforts to increase COVID-19 vaccination uptake, ONSE conducted
various activities in supported districts including social mobilization meetings for local leaders; door-to-
door campaigns; and vaccinations in non-traditional places like shopping malls, markets, and in hard-to-
reach areas like on islands of Lake Chirwa in Zomba district. These activities contributed to an increase
in the number of people vaccinated in the ONSE supported districts. In the ONSE supported districts, a
total number of 411,549 people were vaccinated with COVID-19 vaccines. ONSE contribution was
179,574 which is 44% of the total vaccinated during the quarter.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 17
FIGURE 4. PROPORTION OF PEOPLE VACCINATED WITH COVID-19 VACCINES IN ONSE SUPPORTED DISTRICTS - PY6Q2
COVID-19 SUPERVISION
In Karonga, ONSE supported COVID-19 vaccination supervision at Lwezga and Sangilo health centers,
benefitting 5 (2M, 3F) staff. Some of the observations included the following: issues such as booster
vaccination administration had not started, Pfizer and AZD vaccines were not available, and inconsistent
refrigerator temperature monitoring. Some of the actions undertaken included advice to the health
facilities to start administering booster doses, the health facility to order vaccines Pfizer and AZD and
that refrigerator temperature should be consistently monitored. All the actions were assigned to the
SHSA of the facility and were conducted by March 2022.
ORIENTATION OF VACCINATORS ON NEW VACCINES
In Chikwawa, Karonga, Machinga, Mchinji, and Nkhatabay, ONSE supported orientation of 435 (217M,
218F) vaccinators (HSAs, clinicians and nurses) on administration of new COVID-19 vaccines such as
Pfizer, Johnson and Johnson, Moderna, and Sinapharm vaccines.
FLOOD DISASTER RESPONSE
In February, Malawi was hit by floods due to Cyclone Ana, and among the affected districts were Balaka,
Chikwawa, Machinga, Mulanje, and Zomba. Chikwawa and Mulanje were the hardest hit districts, with
102,224 households affected. ONSE provided a quick response to the floods by providing hypochlorite
chlorine for water chlorination, hand soap for hand hygiene, and cloth face masks for COVID-19
prevention and control for use by the displaced people in camps. Additionally, ONSE supported
IFHOCs, a rapid needs assessment on the flood situation, and had meetings with DHMTs in the affected
areas. A total of 131 camps were established in Chikwawa and Mulanje districts.
0
10
20
30
40
50
60
70
80
90
Perc
enta
ge
District

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 18
ONSE DISTRIBUTING RELIEF ITEMS AT MULANJE DHO (L) AT CHIKWAWA DHO. PICTURE COURTESY OF REJOICE PHIRI, COMMUNICATIONS MANAGER
THE CAMP RESIDENTS AT MAKHUWILA SCHOOL IN CHIKWAWA. PICTURE COURTESY OF REJOICE PHIRI, COMMUNICATIONS MANAGER
RISK COMMUNICATION AND COMMUNITY ENGAGEMENT (RCCE)
SBC communication (SBCC) involves the use of communication to change behaviors including service
utilization, it also promotes social change by positively influencing knowledge, attitudes and social norms.
In the reporting quarter, ONSE supported the dissemination of COVID-19 messages in the communities
through IFHOC services, mobile vans, radio messaging on community radio, and community engagement
meetings. The aim of these activities was to increase uptake of the COVID-19 vaccination at community
level, to orient community structures on their role in COVID-19 vaccination awareness and
sensitization meetings, and to dispel myths and misconceptions concerning the COVID-19 vaccines.
Outcome expectation was that the number of community members accessing and getting vaccinated
increases and the community members follow all COVID-19 preventive measures. Key messages
disseminated during the exercise included signs and symptoms of COVID-19, importance of
handwashing with soap to prevent COVID-19, how to use face masks to prevent COVID-19, COVID-19
vaccination sites in the district, eligibility for receiving the COVID-19 vaccination, social distancing, and
importance of reporting close contacts.
In the reporting period, ONSE focused and supported COVID-19 sensitization messages through mobile
van awareness campaigns, IFHOC services, community sensitization and engagement meetings and radio
program as follows:
◼ Support for 12 mobile vans community awareness and sensitization messages in 8 districts
(Balaka, Chikwawa, Chitipa, Karonga, Machinga, Mchinji, Mulanje, and Zomba), reaching 324,992
(160,873M, 163,619F) in 40 markets, 17 villages, and around 24 health facilities. A total of 1,767
(751M, 1,016F) persons got vaccinated through the mobile van activity.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 19
◼ Supported 100 FHOC services in 6 districts (Balaka, Chitipa, Karonga, Machinga, Mulanje and
Nkhotakota) where 17,873 (6,694M, 11,179F) people were reached with COVID-19 messages
during IFHOC activities. This also included provision of routine IFHOC services and COVID-19
vaccine.
◼ Supported 5 community sensitization meetings for influential, faith-based, and local leaders
drawn from 13 traditional authorities (TAs) in 3 districts (Karonga, Mulanje, Salima). The aim of
increasing vaccine awareness among community members in order to increase vaccine uptake. A
total of 633 (387M, 246F) leaders participated in these meetings.
◼ Supported 3 community sensitization awareness meetings for local leaders and communities
around marketplaces in 3 districts (Chikwawa, Mulanje, and Nkhotakota) reaching 13,128
(5,652M, 7,476F) COVID-19 messages and 108 (68M, 50F) received the COVID vaccine.
◼ Supported Tuntufye Radio Station in Karonga with two sessions of COVID-19 radio
programming. The radio station is accessible to the whole Northern region of Malawi which
caters to I.6 million people. The Tuntufye Radio program also included a phone-in radio
program conducted by three male MoH health workers from Karonga District Hospital who
updated listeners about COVID-19, including total number of confirmed cases at national and
district levels, total number of recoveries, total number of deaths due to COVID-19, COVID-19
preventive measures, and information on the COVID-19 vaccines.
The overall COVID-19 messages of all of the above activities were to inform the community on where
and how to access to COVID-19 vaccine in respective catchment areas, the importance of COVID-19
vaccine, eligibility criteria for COVID vaccine, preventive measures on COVID-19, why is it important to
avoid unnecessary travel during the COVID-19 pandemic, and dispelling myths and misconceptions of
COVID-19 vaccines as well as providing an update of COVID statistics for districts.
COVID-19 VACCINATION AT CHINGALE HC. PICTURE COURTESY OF ELLINA MAKWAWA, ASSISTANT PRO ZOMBA

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 20
MOBILE VAN MOBILIZATION AT MULOMBA HC CATCHMENT AREA. PICTURE COURTESY OF ALBERT PHIRI
SURVEILLANCE, CASE FINDING, RAPID RESPONSE TEAMS, CASE
INVESTIGATION, AND CONTACT TRACING
As of April 9, 2022, a cumulative total of 85,702 confirmed COVID-19 cases with 2,628 cumulative total
number of deaths (with a case fatality rate of 3.07%) were reported since the pandemic was declared in
April 2020. This is much higher as compared to a cumulative total number of 79,987 cases with 2,413
cumulative total number of deaths as reported on January 9, 2022.
POINT OF ENTRY (POE) SCREENING
TABLE 3. SUMMARY OF REQUIREMENTS FOR TRAVELERS ENTERING MALAWI
1. All arriving travelers of all nationalities, including Malawians, will be expected to show a valid, electronically
verifiable COVID-19 full vaccination certificate at point of entry. 2. Arriving travelers that are not able to show an electronically verifiable certificate at point of entry shall be
expected to access COVID-19 vaccine that will be available for free at the point of entry before being processed
to enter/re-enter the country, as a preventive measure.
3. Travelers that are not able to produce a valid electronically verifiable COVID-19 certificate and refuse to access COVID-19 vaccine offered at point of entry will be required to undergo institutional quarantine for symptoms
monitoring for 10 days at their cost.
4. Those without a valid negative PCR-based COVID-19 test certificate will be subjected to a Rapid Antigen Test on
site at the point of entry before proceeding through immigration services, without exception, and at their cost. 5. Those that test positive on the Rapid Antigen Test will have a PCR test processed, also at their cost, and they will
be conveyed to the District Health System where they are proceeding, where they will be managed according to
standard national protocols.
During the reporting period, ONSE supported POE screening in Lilongwe, Mchinji, Chitipa, Karonga,
Nkhatabay, and Mulanje. A total number of 24,549 (14,450M, 10,071F) travelers were screened and a
total number of 925 (702M, 223F) travelers were tested for COVID-19, and five (5M, 0F) tested
positive.
In Karonga, ONSE supported DHMTs to conduct joint border meetings at Songwe and Muloza Border.
A total of 50 (35M, 15F) people attended the meeting at both sites. Issues discussed are that the
Tanzania border side is not recognizing Malawi COVID-19 negative certificates due to lack of equipment
(pan bios platform) and that some certificates issued from Tanzania were not valid certificates. At

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 21
Muloza they discussed poor sanitation at the border. At Songwe, members agreed to approach their
counterparts in Kasumulu on the issue of the certificates and in Muloza members agreed towards
improvement of sanitation at the border post.
Also in Karonga, ONSE supported DHMT supervision at Songwe port health office to assess the
performance of the port in terms of POE service provision. A total number of 10 (6M, 4F) port health
staff were supervised. The following were findings:
TABLE 4. SUMMARY OF POE SUPERVISION - KARONGA
STRENGTHS ISSUE ACTION POINT
◼ Services were being offered at the clinic
◼ COVID-19 tests were
being done
◼ There was a small room being used for COVID-19 testing
◼ There were no lights and curtains in
the testing room
◼ Port Health Officers trained in COVID-19 testing had not yet started
their work despite the training
◼ Inadequate COVID-19 supplies
(personal protective equipment [PPE]) from the Wellness Center
◼ Need to construct a new COVID-19 testing laboratory at Songwe port health office
◼ Lights and curtains to be fixed by end of the
month
◼ District Medical Office (DMO) and Director of Health and Social Services (DHSS) were
actioned to facilitate the operationalization of
COVID-19 testing using the Port Health
Officers ◼ Port Health Officers should order PPE
INFECTION PREVENTION AND CONTROL (IPC)
In PY6Q2, ONSE supported the implementation of various IPC/WASH interventions in the context of
COVID-19. Supported activities included IPC/WASH supervision and mentorship, IPC committee
meetings, and IPC orientations and training. Due to many districts being heavily engaged in COVID-19
vaccinations, other activities were given less attention and some IPC activities were combined with
COVID-19 prevention components, such as general facility cleaning and IPC assessments.
ONSE supported IPC/WASH supervision in 8 districts (Chitipa, Karonga, Balaka, Mangochi, Chikwawa,
Kasungu, Salima and Nkhata Bay). The first three districts were visited twice. A total of 99 health
facilities were supervised and 342 (172M, 170F) were supervised. Eleven of the facilities were village
health clinics. The supervision aimed at checking and supporting health workers comply with the
IPC/WASH standards with emphasis to COVID-19 prevention and control. At the village clinics, it was
noted that safe water was available in all sites that were visited except Ngoya, where the borehole was
broken down in January 2021. All HSAs washed hands with soap or sanitizer, used facemasks, and were
maintaining social distances. All HSAs used safety boxes when handling sharp objects. There was rational
use of PPE. Pit latrines and refuse pits were available and in use. However, the following challenges were
noted in some clinics including inadequate supply of soap or sanitizer, low community participation in
IPC like digging new refuse pits that were almost full, and disposal sites (refuse pits) were not fenced and
were accessible to children and domestic animals.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 22
TABLE 5. SUMMARY FINDINGS OF IPC SUPERVISION, PY6Q2
STRENGTHS GAPS ACTION POINTS
◼ Most facilities observe COVID-19 preventive measures
◼ Availability of running water in all facilities
visited
◼ Availability of hand washing facilities in all health facilities visited
◼ At health posts, HSAs do comply with
COVID-19 prevention through hand
hygiene ◼ All HSAs use safety boxes when handling
sharps
◼ Pit latrines and refuse pits are available
and in use ◼ A number of health workers are trained
in IPC/WASH.
◼ Surroundings were generally clear except
a few with bushy surroundings
◼ Inadequate PPE and cleaning materials
◼ Knowledge gap in IPC/WASH
guidelines
◼ Some facilities did not have incinerators, placenta pit, and
ash pit
◼ Chlorine has been scarce for
some time especially in health posts
◼ Poor waste segregation due to
lack of waste segregation
buckets
◼ In-charges to ensure availability of adequate PPE and cleaning materials
◼ Need to train facility staff in
IPC/WASH guidelines
◼ DHMT to facilitate construction of incinerator, placenta pit and ash pit
◼ HSAs to be provided with chlorine
from DHO
◼ IPC focal person to lobby for buckets
In Karonga, ONSE supported the district to conduct a follow up on IPC/WASH action points at 10
health facilities. The activity was conducted by 5 (4M, 1F) quality improvement (QI)/IPC supervisors who
engaged a total of 30 (20M, 10F) participants comprising clinical, nursing staff, HSAs, and hospital
attendants. It was noted that most of the previously agreed action points had been carried out. It was
noted that all facilities had functional hand washing facilities and that most facilities were observing
COVID-19 measures.
ONSE supported the orientation of 372 (163M, 209F) health workers from 48 health facilities in 5
districts (Chikwawa, Balaka, Zomba, Mangochi, and Nkhata Bay). The orientation covered the following
topics: introduction to IPC/WASH, instrument processing, linen, management, environmental cleaning,
waste management, basic microbiology, hand hygiene, standard precautions, rational use of PPE, and
health facility associated infections. It is expected that with the orientation, there will be better
compliance to IPC/WASH in COVID-19 prevention and control.
In Nkhatabay, ONSE supported one IPC committee, which was attended by 15 (5M, 10F) members. The
following are major action points from the meeting:
◼ IPC focal person to lobby for an increase in funding for IPC/WASH resources from DHMT and
partners
◼ IPC focal person to lobby for establishment of waste storage area at the incinerator from
DHMT and partners
◼ IPC team to intensify health talk programs which include COVID-19 topics in the ward and at
outpatient department (OPD)
◼ IPC team to introduce motivational activities to increase positive attitudes among health
workers in implementing IPC standards
◼ IPC team replanning how to implement IPC/WASH activities supported by ONSE
COORDINATION AND OPERATIONS
During the reporting period, ONSE supported various district coordination meetings. Six DRRT
meetings were supported, two meetings in Chitipa with 15 (11M, 4F) attendees and one meeting each in
Machinga with 25 (15M, 10F) attendees, Zomba with 14 (7M, 7F) attendees, Mangochi with 25 (17M, 8F)
attendees and Chikwawa with 21 (9M, 12F) attendees. The aim of the meetings was to share COVID-19
updates including reports on contact tracing, sample collection and testing operations, as well as
COVID-19 supplies updates. A few challenges and points came out of the Chitipa discussions. One
challenge with COVID-19 case management was the lack of normal saline. Guardians were being asked
to buy from private pharmacies. It was also agreed to audit all COVID-19 deaths for proper
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 23
classification. Additionally, it was learned that every health facility in the Chitipa district has the capacity
to test COVID-19 following training of non-laboratory personnel. Flood updates were also shared in
these meetings. For efficient disaster management post Cyclone Ana in Zomba, there is a need to
decentralize disaster response teams for better management, for health facilities close to the affected
areas and camps to lead.
A total of three PHEMC meetings were supported, one meeting in Chitipa with 30 attendees (26M, 4F)
and two meetings in Karonga with 20 attendees (14M, 6F). The meetings were conducted to share
COVID-19 updates, successes, challenges, and proposed solutions in combating the pandemic. In
Karonga, there were difficulties in introducing the Pfizer vaccine due to inadequate resources to
sensitize teachers and parents. Cholera and flood preparedness updates were also shared. The Karonga
district had not registered any cases related to cholera. The district has inadequate stocks of chlorine
and has reached out to stakeholders for chlorine support, to ensure the district is prepared in case of an
outbreak. Members were also updated on the flood response and evacuation plan project to be
implemented by the Red Cross in collaboration with the district council. The Council installed early
warning gadgets in rivers that are prone to flooding to warn community members.
CROSS CUTTING AREAS
OVERVIEW
ONSE’s approach to improving maternal, newborn, and child survival and well-being requires special
emphasis on several cross-cutting areas that span clinical services, HSS, and demand for priority services.
Cross-cutting areas are incorporated into the planning and implementation of the Activity whenever
applicable and are central to the achievement of equitable, sustainable health outcomes. These areas
include youth and gender, and private-sector engagement.
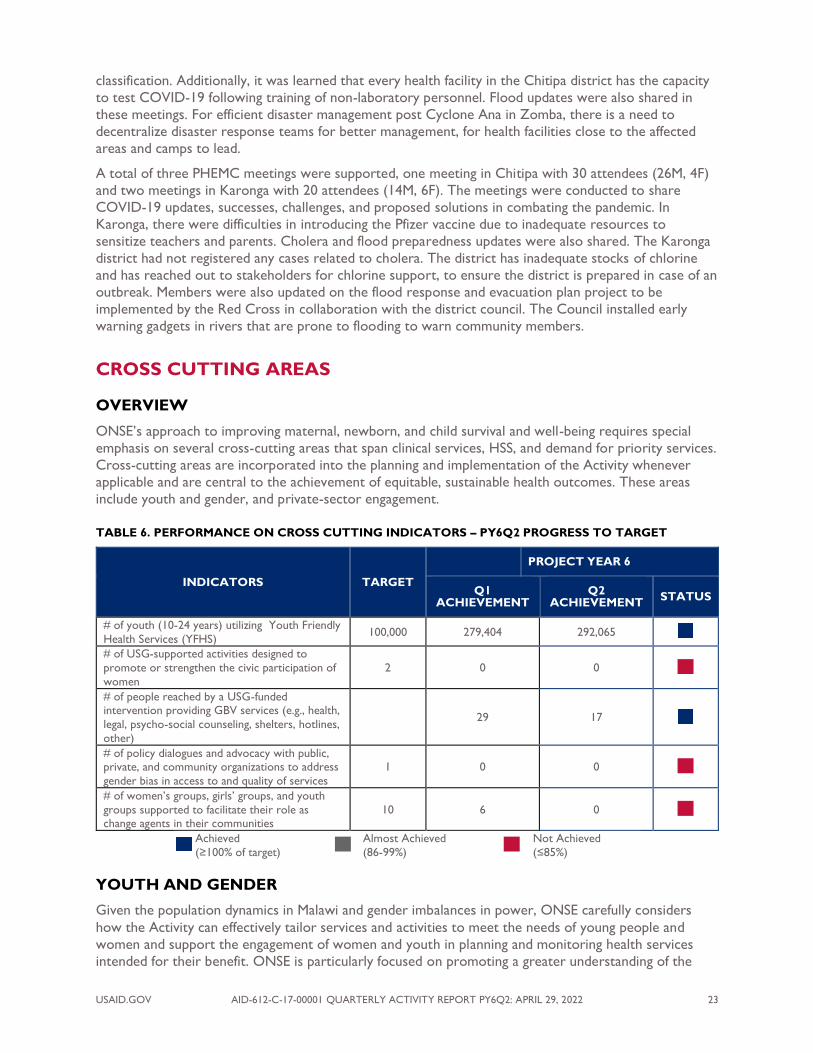
TABLE 6. PERFORMANCE ON CROSS CUTTING INDICATORS – PY6Q2 PROGRESS TO TARGET
INDICATORS TARGET
PROJECT YEAR 6
Q1 ACHIEVEMENT
Q2 ACHIEVEMENT
STATUS
# of youth (10-24 years) utilizing Youth Friendly
Health Services (YFHS) 100,000 279,404 292,065
# of USG-supported activities designed to
promote or strengthen the civic participation of
women
2 0 0
# of people reached by a USG-funded intervention providing GBV services (e.g., health,
legal, psycho-social counseling, shelters, hotlines,
other)
5 29 17
# of policy dialogues and advocacy with public, private, and community organizations to address
gender bias in access to and quality of services
1 0 0
# of women’s groups, girls’ groups, and youth
groups supported to facilitate their role as change agents in their communities
10 6 0
Achieved
(≥100% of target) Almost Achieved
(86-99%) Not Achieved
(≤85%)
YOUTH AND GENDER
Given the population dynamics in Malawi and gender imbalances in power, ONSE carefully considers
how the Activity can effectively tailor services and activities to meet the needs of young people and
women and support the engagement of women and youth in planning and monitoring health services
intended for their benefit. ONSE is particularly focused on promoting a greater understanding of the

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 24
unique needs of young people to grow into healthy, productive, and responsible adults and providing
opportunities to participate in decisions regarding their health, including SRH services.
During the quarter, ONSE supported YFHS supportive supervision targeting 24 health facilities in
Kasungu and Chitipa aimed at assessing provision of quality YFHS in the targeted facilities. A total of 60
(42M, 18F) providers were supervised. The supervisors used a national YFHS monitoring tool to
conduct the exercise. Details of key issues are highlighted in the table below.
TABLE 7. SUMMARY OF YFHS – KASUNGU, CHITIPA
STRENGTHS CHALLENGES ACTION POINTS
Kasungu ◼ Supervisions were done in
all targeted facilities.
◼ All facilities visited are
offering services to youths.
◼ Logistics such as fuel were being provided on time
every day
◼ Good collaboration from
facility teams ◼ YFHS are offered in all the
supervised facilities
◼ Unavailability of YFHS recreation materials.
◼ Few trained YFHS providers in most
facilities.
◼ Late reporting experienced in some facilities.
◼ Some providers have been reluctant in
providing YFHS.
◼ Some facilities trained providers have been transferred and there is no
provider to offer the services.
◼ Need to lobby funds from partners to procure YFHS recreation materials for
the facilities.
◼ Need to train more YFHS providers,
focusing much on facilities whose providers were transferred or have
retired.
◼ Those facilities, which were reporting
late, have been advised and are expected to change and start timely reporting.
◼ Revamp facilities, which are not active in
offering YFHS.
◼ Engaging the reluctant providers to resume their duties as before.
Chitipa ◼ Facilities are offering YFHS
◼ Supervisees were ready for the supervision
◼ No trained providers in YFHS in most
facilities ◼ No information, education, and
communication (IEC) materials targeting
young people
◼ No youth SRH policy on YFHS in all facilities
◼ No utilization of data collected
◼ No sign post for YFHS at Wenya
◼ No youth corner room at Kameme ◼ No recreation materials at Kameme
◼ Lobby for a training for new YFHS
providers ◼ Collect some IEC materials from DHO
on the next probable trip
◼ Follow up and collect youth policies from
HMIS ◼ Follow up supervision to the YFHS sites
◼ Lobby for support from other partners
In Zomba, ONSE supported data review meetings targeting the city and Thondwe cluster, drawing
participation from 51 (23M, 28F) health care workers and facilitated by three (1M, 2F) coordinators (2
nurse midwives, one clinical officer). YFHS focal persons and data clerks from targeted clusters
participated in the meeting. The aim of the activity was to review facility and district data on YFHS
reporting rates and completeness, including reviewing of YFHS data sources and reporting tools.
Strengths observed included an increase in clients accessing FP methods between July and December
2021 (compared to the same period in 2020) and an improvement in timeliness and completeness of the
YFHS reports. Weaknesses observed included high rates of teenage pregnancies, inadequate numbers of
staff trained in YFHS due to turnover, and poor data management of some facilities (e.g., City Clinic and
Lambulira Health Center). Actions identified included arranging mentorship and orientation to facilities
with no trained providers; conducting quarterly data reviews; providing support to outreach clinics
targeting youth clubs; revamping facilities currently not offering YFHS; and starting awareness meetings
in schools, youth clubs, and faith-based gathering centers. All identified actions are expected to be
achieved by end of May 2022.
In Karonga, ONSE supported YFHS data management mentoring at five facilities, where a total of 10
(6M, 4F) health care workers were engaged. The YFHS coordinator and HMIS Officer conducted the
mentorship session to follow-up on the previous action points, distribute YFHS reporting forms, and
mentor facility data clerks on YFHS report writing. Strengths observed included that most facilities
visited had written and submitted their reports for the last quarter; for those missing in the last visit,

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 25
facilities in-charge were able to delegate the task of report writing, and providers are able to follow up
information and write YFHS reports. One challenge observed was that facilities were writing and
submitting the reports on time but the HMIS office was not entering the reports in time. As a way
forward, the HMIS officer was tasked to facilitate timely entry of YFHS reports and the YFHS
Coordinator was tasked to help in entering reports in DHIS2.
CLINICAL SERVICES
OVERVIEW
ONSE is designed to strengthen the continuum of care for priority health services in each of the
supported districts from communities to district hospitals. Over the life of the activity, ONSE is
supporting infrastructure improvements, filling gaps in essential equipment, and strengthening capacity of
health workers for the continuous provision of quality health services and improving referral systems.
As ONSE seeks to improve the availability of and access to priority health care services, the Activity is
testing and scaling (as appropriate) approaches to reduce barriers to service access, including
community-based delivery of IPTp and the self-administered Sayana Press injectable (Depo-Provera
Subcutaneous [DMPA-SC]) contraceptives.
ONSE’s approaches to enhancing the availability, accessibility, and quality of priority health services are
intertwined. The Activity supports district and facility leadership and local partners to strengthen quality
assurance (QA) systems and implement QI interventions in line with the MoH’s vision for quality
management in Malawi. Working with the MoH QMD, the Activity supports district and facility
leadership and local partners to strengthen QA systems and implement QI interventions. In addition,
ONSE is strengthening the quality of services by improving the technical and interpersonal capacities of
health care workers through competency-based “smart” approaches, such as supportive supervision,
mentoring, and working with individuals, facility and departmental teams as well as clusters of staff from
across service sites. Simulations, drills and clinical practice sessions are embedded within these
approaches. Smart capacity building approaches adopted and implemented by ONSE ensure the
development and mastery of high-quality practice and ability to identify other barriers to acceptable
levels of performance without taking health providers for prolonged periods away from their duty
stations to allow continuity of care within the constrained health care workforce.
Of the 25 clinical services indicators that ONSE monitors quarterly, 11 (44%) have achieved or
surpassed the annual target, 4 (16%) are on track for achievement, and 10 (40%) are not on track.
COVID-19 second surge affected clinical service delivery as many health providers got sick, some
preventive measures meant a pause of some capacity building interventions like cluster mentorship,
some MoH Program Coordinators who are key in implementing ONSE’s supported activities were
supporting service delivery at the emergency treatment units.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 26
TABLE 8. PERFORMANCE ON SELECT CLINICAL SERVICES INDICATORS, PY6Q2 PROGRESS TO TARGET
INDICATORS PROJECT YEAR 6
TARGET Q1
ACHIEVEMENT Q2
ACHIEVEMENT STATUS
# pregnant women initiating ANC visits in
the first trimester 25,000 13,794 13,050
# of newborns not breathing at birth
resuscitated in USG-supported programs 3,500 3,024 2,942
# cases of child diarrhea treated in USG-
assisted programs 125,000 67,422 73,345
# children received DPT3 (Pentavalent
Vaccine [PENTA] III) by 12 months of age in USG-assisted programs
137,100 72,801 69,920
Couple Years Protection 400,000 184,126 157,717
% of pregnant women who received three or
more doses of IPTp during ANC 52% 56% 54%
# of children under five (0-59 months)
reached by USG-supported nutrition programs
175,000 91,558 93,643
# institutional settings gaining access to a
basic drinking water service as a result of
USG assistance
18 0 17
Achieved
(≥100% of target) Almost Achieved
(86-99%) Not Achieved
(≤85%)
RENOVATION OF HEALTH FACILITIES AND EQUIPMENT PROVISION
In PY6Q2, ONSE completed a number of infrastructure improvement works including water systems
improvement, construction of waste disposal facilities and supply and installation of medical waste
mechanical incinerators in ONSE supported districts.
◼ WATER SYSTEM IMPROVEMENTS. ONSE has completed implementation of water
systems improvement of 17 sites in Balaka (Dziwe, Utale 2); Dowa (Dowa DH); Mpata, Ngana,
Chilumba, Nyungwe in Karonga District; Mpepa, Lodjwa in Kasungu; Mngoni and Chitedze in
Lilongwe District; Nkhotakota (Kawongozi and Dwambadzi); and Mulanje (Mulomba, Chonde,
Chambe and Kambenje). In Karonga, the sites have been officially handed over and are in use.
The remaining sites will be handed over in PY6Q3. The works involved drilling/rehabilitation of
boreholes, installation of submersible water pumps, construction of water towers and septic
tanks, and installation of water tanks. A site called Tchesamu in Nkhatabay District has been
dropped as it was inaccessible due to bad road conditions caused by heavy rain in the area.
◼ SUPPLY AND INSTALLATION OF MECHANICAL INCINERATORS IN 5
HOSPITALS. ONSE has completed installation of 5 mechanical incinerators for Bwaila
Hospital, Machinga, Dowa, Chikwawa and Chitipa District Hospitals. The supplier has also
trained the operators and electricians on the operations and maintenance of the mechanical
incinerators.
◼ WASTE DISPOSAL FACILITIES (INCINERATORS, ASH AND PLACENTA PITS).
ONSE has completed construction of waste disposal facilities by PAM in the following districts:
◼ Chikwawa – incinerators at Kakoma and Ndakwera, ash pit at Chikwawa District Hospital
◼ Dowa – incinerator and ash pit at Chankhungu and placenta pit at Chinkhwili
◼ Lilongwe – ash pit at Bwaila Hospital.
◼ Mulanje – placenta pit at Mulanje District Hospital and incinerator, ash and placenta pits at
Milonde and Chonde
◼ Machinga – ash pit at Machinga District Hospital and incinerator and ash pit at Nainunje

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 27
◼ Zomba – incinerator at Likangala Health Center
◼ MINOR WORKS IN HEALTH FACILITIES. ONSE has commenced minor renovation
works which involve plumbing, carpentry, electrical, building, painting, etc. The sites are LOT 1 -
Kapenda HC in Chitipa, Kaporo Rural Hospital in Karonga; LOT 2 – Chisepo and Bowe in
Dowa, Mdunga in Kasungu, Chileka and Khongoni in Lilongwe, Mwansambo in Nkhotakota,
Chinguluwe in Salima; and LOT 3 – Chikweo and Nainunje in Machinga, Nandumbo and
Kalembo in Balaka, Mbiza in Mulanje, Chingale and Bimbi in Zomba. All materials have been
procured and delivered to the sites and the renovation works have started. The renovation
works will be completed by the end of April 2022.
QUALITY OF CARE
A sustainable strategy for achieving continuous delivery of quality health services is to apply QI principles
to all priority health interventions including components of HSS and demand creation. Consequently,
ONSE supports the MoH QMD to strengthen and harmonize quality management systems and build
capacity in QA and improvement activities, as well as supporting Malawi’s participation in the Global
Network for MNCH QoC, spearheaded by WHO. Malawi has now finalized a harmonized QI training
manual to be used by all stakeholders and implementing partners supporting the MoH with QI efforts.
Malawi’s harmonized QI strategy reflects a systems approach with an emphasis on the use of quality
improvement support team (QIST) to champion improvement approaches at all levels of the health
system. ONSE continued to support the MoH QMD to strengthen and build capacity in QA and
improvement activities.
NATIONAL LEVEL SUPPORT
ONSE supported the establishment of district based QI mentors in all the 11 family health ONSE
districts. For effective implementation of QI projects, it requires frequent on-site coaching and
mentoring which was not happening because of inadequate QI mentors at the national level and
restriction of travel due to COVID-19. It is expected that with district-based mentors, there will be
adequate coaching of ward improvement teams (WITs) resulting in having successful QI projects. As the
mentors are based at district level, mentorship is expected to continue beyond ONSE presence. Two
QI providers from each district and all ONSE clinical coordinators were trained as QI mentors. A total
of 22 (11M, 11F) health care providers and 9 (4M, 5F) ONSE clinical coordinators were trained as QI
mentors. The training was facilitated by 3 (1M, 2F) national trainers identified by QMD.
ONSE funded 26 (11M, 15F) delegates from 8 facilities (Mulanje, Machinga, Dowa and Nkhotakota
district hospitals; Zomba Central Hospital, Matawale, Nasawa and Likangala in Zomba) and managers
from QMD head office for a collaborative learning meeting from March 23 to 25, 2022. This was the
first national collaborative meeting and facilities displayed their successful QI projects. It felt great to
have the ONSE supported facilities (Matawale and Nasawa) being recognized as the best so far. Dowa
and Nkhotakota presentations also show remarkable progress. Mulanje and Machinga did not make their
presentations, as their participation was solely to learn from others. Examples of QI projects presented
include:
◼ DOWA DISTRICT HOSPITAL: Worked on increasing the percentage of documentation in
the sick neonate registers from 40% to 70% by using a guide on hand overs. The hospital
developed and oriented staff on the guide, achieving 80% (surpassing their target of 70%).
◼ NKHOTAKOTA DISTRICT HOSPITAL: Worked on reducing incidence of birth asphyxia
from 7% to 5% from September 1, 2021 to November 30, 2021 by conducting spot checks
during handovers. This resulted in improved monitoring of women in labor, which consequently
reduced incidence of babies born asphyxiated as evidenced by a shift on the run chart depicted
in Figure 5.
◼ ZOMBA CENTRAL HOSPITAL: Their project aimed to reduce the percentage of
hypothermia of newborns on admission from 71% to 50% from April 1, 2021 to October 30,

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 28
2021 by checking temperature in the labor ward on newborns and treat hypothermia if noted,
before referring them to nursery.
◼ NASAWA HEALTH CENTER (ZOMBA): Worked on increasing the percentage of
newborns receiving comprehensive rapid initial and subsequent postpartum assessment from
12% to 80% from July 1, 2021 to September 30, 2021. The facility managed to achieve above
87% by use of a number of change ideas. In addition to this project, the facility also worked on a
number of QI projects such as development of referral protocols, handover policy, consent and
companion of choice forms, oxygen concentrator monitoring tool, daily complication tally
charts, postnatal assessment tool that includes mental health assessment and tracing vaccine
defaulters.
◼ MATAWALE HEALTH CENTER (ZOMBA): The facility worked on a project to reduce
the percentage of health center manageable maternal referrals from 64% to 30% from October
20, 2021 to December 31, 2021. The facility surpassed their target as wrong referrals were
reduced to below 15%. Refer to the examples of the run chart in Figure 6 below for the change
ideas used as illustrated by annotation in the run chart.
FIGURE 5. NKHOTAKOTA DISTRICT HOSPITAL BIRTH ASPHYXIA RUN CHART

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 29
FIGURE 6. MATAWALE HEALTH CENTER MATERNAL COMPLICATIONS REFERRAL RUN CHART
DISTRICT LEVEL SUPPORT
In Karonga, ONSE supported a collaborative learning session at the district hospital on February 2,
2022, drawing participation from 20 (10M, 10F) members of the QIST and 8 WITs from different
departments to share their QI updates and experiences. Four departments reported formation of WITs
that are working on some QI projects. The other four had not yet formed WITs. Knowledge gaps by
most WITs were noted. Even the active WITs had challenges in documenting QI projects in a journal.
There is a need for mentorship of the WITs on proper documentation of the QI projects.
QISTS/WITS MEETINGS
ONSE supported 47 QIST/WIT (14 QIST and 33 WIT) meetings in 8 districts (Zomba, Mangochi, Dowa,
Nkhotakota, Salima, Mulanje, Chitipa and Lilongwe), drawing participation from 548 (294M, 254F)
members. Major topics discussed during QIST meetings included updates from WITs on QI projects,
identifying performance challenges that require, and following up on QI action plans. During WIT
meetings, major topics included progress on QI projects, initiating new projects, and performing
interventions such as general cleaning for their departments and doing sort, set in order, shine,
standardize, and sustain (5S). For example, in Nkhotakota during the WIT meeting they conducted
general cleaning and in Machinga, implemented 5S, as illustrated in the photo respectively.
BEFORE 5S (LEFT) AND AFTER 5S (RGIHT). PICTURE COURTESY OF NIXON CHIDZERE, CLINICAL COORDINATOR FOR MACHINGA
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 30
PICTURE COURTESY OF LILIAN CHIMBAYO, ENVIRONMENTAL HEALTH OFFICER IN NKHOTAKOTA
BENCHMARKING QI IMPLEMENTATION
ONSE supported Machinga and Mulanje district hospitals to benchmark proper implementation of QI
projects as conducted at Matawale and Nasawa health centers in Zomba to provide a learning
opportunity for district QI teams to properly implement QI projects. A total of 6 (1M, 5F) WIT and
QIST members from Machinga, and 5 (3M, 2F) WIT and QIST members from Mulanje benefited from
the activity and three (3F) providers from Machinga and Mulanje district hospitals facilitated the
benchmarking. Providers coached the QIST and WIT members on proper documentation of QI
projects, commitment of facility staff, general cleanliness of facilities, comprehensive handovers, and the
importance of DHMT support for the QIST to work effectively. The districts also appreciated the fact
that it is possible to implement QI projects with little available resources. It is hoped that the
benchmarking will help the visiting facilities improve on their QI projects implementation.
QI COACHING/MENTORSHIP
In the quarter, ONSE supported follow-up coaching/mentorship by four (1M, 3F) QMD QI mentors.
There were two teams, each comprising two mentors. Apart from routine QI coaching, the team
reviewed the previous action plans and assisted the team to develop new action plans. The mentorship
also aimed at assessing the functionality of QISTs and WITs. The activity reached 60 (24M, 34F) QI
providers from 7 district hospitals (Bwaila maternity, Dowa, Kasungu, Nkhotakota, Salima, Karonga and
Chitipa), who were mentored on QI processes including documentation of QI projects for reporting.
TABLE 9. QI COACHING AND MENTORSHIP HIGHLIGHTS PY6Q2
STRENGTHS CHALLENGES ACTIONS TAKEN
◼ Team work
◼ Availability of QI projects ◼ Newly trained QI mentors started
their work in some districts
◼ National mentors provided technical
support as necessary
◼ Lack of 5S materials and
supplies ◼ No clear QI plans in some
districts
◼ QIST/WITs meetings not being
done routinely ◼ Documentation of QI projects
still a challenge
◼ DHMTs asked to support
procurement of basic 5S materials ◼ Discussed the need for having clear
schedule to adhere to
◼ National mentors provided technical
support as necessary

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 31
IPC/WASH
In Karonga and Machinga, ONSE supported 13 health centers to conduct routine IPC/ WASH. A total of
106 (57M, 49F) health care workers were reached. Major challenges include knowledge gaps among
staff, especially on waste management and erratic water supply due to low pressure. Other challenges
include lack of incinerators and placenta pits in some facilities. Mentorship on waste management was
done during the supervision. The DHMT will support the maintenance of the water tanks, incinerators
and placenta pits.
In Mangochi, ONSE supported the DHMT to conduct internal assessment on IPC/WASH in 9 of their
health facilities. A total of 68 (23M, 45F) participated in the assessment. The score range was from 21%
to 61%, an average of 51% and median of 52%.
ONSE also supported Balaka DHO to conduct cleaning exercises in 13 health facilities, reaching 315
(175M, 140F). It is expected that the activity will improve the standards of IPC in the facilities thereby
improving the quality of services provided by the facility.
INTEGRATED FAMILY HEALTH OUTREACH CLINICS IFHOCs are an important strategy by which the MoH and ONSE aim to provide integrated health
services to clients, especially in HtRAs. IFHOC services include FP, ANC, PNC, immunization (EPI),
OPD consultations for children under-five, human immunodeficiency virus (HIV) testing services, and
growth monitoring and promotion.
TABLE 10. NUMBER OF PLANNED AND SUPPORTED IFHOCS IN ONSE DISTRICTS IN PY6Q2
DISTRICT # OF
IFHOCS PLANNED
# OF IFHOCS
SUPPORTED TOTAL # OF
BENEFICIARIES
Balaka 39 17 3623
Chitipa 36 37 7371
Dowa 36 17 3542
Karonga 45 71 12947
Kasungu 105 28 3735
Lilongwe 87 54 16364
Machinga 48 33 10397
Mulanje 33 17 1947
Nkhotakota 39 33 10766
Ntcheu 0 2 732
Salima 33 42 8740
Zomba 60 83 9687
Total 561 434 91,741
By the end of PY6Q2, ONSE had supported 91,741 people to access essential services through 434
IFHOCs. ONSE will continue to provide both operational and technical support to IFHOCs, ensuring
that services reach those people living in HtRAs. IFHOCs also present a unique opportunity to leverage
clients for demand generation, health talks, and other counseling and community mobilization services.
Highlights from IFHOC services include:
◼ 6,612 pregnant women attended an ANC visit at an IFHOC, of these women, 2,262 (34%)
received HIV counseling and testing during ANC. 340 women initiated ANC in their first
trimester
◼ 2,087 pregnant women received their third dose of IPTp during ANC visits conducted during an
IFHOC
◼ 10,644 people received FP services, including 2,292 new users
◼ 3,432 children were fully immunized

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 32
◼ 16,682 children had caregivers who received nutrition counseling through USG-supported
nutrition programs and 3,044 pregnant or lactating women were reached with nutrition
interventions through USG-supported programs
◼ 5,713 (2,738 under-five, 2,975 over-five) people that had confirmed malaria received antimalarial
medication at IFHOCs
MATERNAL HEALTH
In PY6Q2, ONSE continued to work with the MoH and other partners to improve access to quality,
high-impact, cost-effective MNH interventions at both the community and facility levels. ONSE
strengthened activities through smart capacity building (mentorship and supervision) of both community
and facility-based health workers. In the period under review, ONSE continued to support maternal
death surveillance and response (MDSR) and follow-up of action points.
In PY6Q2, 13,050 pregnant women-initiated ANC in the first trimester, compared to 12,462 pregnant
women in PY5Q2. For emergency obstetric and newborn care sites, in PY6Q2, 20% of facilities were
fully functional (n = 15) and another 20% were partially functional compared to 17% that were functional
in the same period last year. A total of 2,942 newborns not breathing at birth were resuscitated
compared to 3,024 during the PY6Q1. Further to this, 60,442 women received uterotonics during the
third stage of labor compared to 59,019 in PY6Q1.
TABLE 11. PERFORMANCE ON MATERNAL HEALTH INDICATORS, PY6Q2 PROGRESS TO TARGET
INDICATORS
PROJECT YEAR 6
TARGET Q1 ACHIEVEMENT
Q2 ACHIEVEMENT
STATUS
# pregnant women initiating ANC visits in the
first trimester 25,000 13,794 13,050
% of USG-supported facilities providing
BEmONC in the past three months 65% 21% 20%
# of women giving birth receiving uterotonics
in the third stage of labor (or immediately after birth) through USG-supported programs
125,000 59,019 60,442
# of newborns not breathing at birth
resuscitated in USG-supported programs 3,500 3,024 2,942
# of newborns receiving PNC within two days of childbirth in USG-supported programs
102,834 28,361 23,397
# newborn infants receiving antibiotic
treatment for infection through USG-
supported programs
5,000 2,060 2,031
% of USG-supported communities establishing
an emergency transport system (ETS) for
pregnant women within the reporting period*
70% 17% 71%
Achieved (≥100% of target)
Almost Achieved (86-99%)
Not Achieved (≤85%)
ANTENATAL CARE
In PY6Q2, 13,050 pregnant women-initiated ANC in the first trimester compared to 12,462 who
initiated ANC in the first trimester during the same period in PY5. ONSE worked with the MoH
through the RHD and the district level MoH as well as community-based staff to implement activities
that increase uptake and quality of ANC services. These activities included capacity building of health
workers, and provision of services in hard-to-reach areas through IFHOCs. In Dowa, ONSE supported
orientation of health workers to the revised national ANC guidelines in line with the 2016 WHO
recommendation on ANC that changed from four FANC visits now to eight contacts. A total of 96
(32M, 64F) providers from the 24 health facilities in the district were reached. With this activity, Dowa

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 33
facilities have at least one person at a minimum who knows the guidelines and will be able to provide
peer coaching to other providers who were not reached due to scheduling. It is expected that the
facilities will be adhering to the guidelines that promote provision of quality and comprehensive ANC.
All districts implemented ANC activities through IFHOCs and at static MCH clinics.
INTRAPARTUM AND ESSENTIAL NEWBORN CARE
In PY6Q2, 20% of facilities were fully functional (n = 15) and another 20% (n = 24) were partially
functional compared to 17% that were functional in the same period last year. Below in Table 12 is a
summary of the proportion of facilities offering each signal function, disaggregated by BEmONC and
comprehensive emergency obstetric and newborn care (CEmONC) facilities for Q2.
TABLE 12. PROPORTION OF BEMONC AND CEMONC FACILITIES PROVIDING EACH SIGNAL FUNCTION
% BEMONC FACILITIES OFFERING SERVICE IN THE LAST 3 MONTHS
% CEMONC FACILITIES OFFERING SERVICE IN THE LAST 3 MONTHS
Oxytocin 100% 100% Asphyxia 89% 89% Antibiotics 89% 89% Vacuum Extraction 58% 100% Anticonvulsive 54% 72% MRP 54% 56% Post-abortion care (PAC) 54% 94% Blood Transfusions - 94% C sections - 100%
Health providers continue to appreciate ONSE for providing facilities with KIWI vacuum extractors that
gives them comfort and confidence in conducting vacuum extractions, especially at CEmONC facilities
where there has been a 100% achievement. The improvement is slightly lower at BEmONC due to lack
of transport on site in case of a failed procedure.
Figure 7 below summarizes signal function data for all BemONC and CEmONC facilities aggregated
together.
FIGURE 7. PROPORTION OF FULLY, PARTIALLY, AND NON-FUNCTIONAL BEMONC FACILITIES
The achievement could be attributed to the following activities that ONSE supported in the FHP
districts. ONSE health activity supported BEmONC mentorship at 24 health facilities in Dowa, Kasungu,
Lilongwe, Salima, Nkhotakota, Machinga and Karonga districts. A total of 136 (49M, 87F) health

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 34
providers were mentored on various parameters of BEmONC including documentation of signal
functions. A breakdown per district is as follows: Lilongwe 22 (1M, 21F) providers; Kasungu 15 (6M, 9F)
from six facilities; Salima 5 (2M, 3F) from two facilities; and Karonga 55 (25M, 30F) providers.
HELPING BABIES BREATHE (HBB) PRACTICAL SESSIONS AT NYUNGWE & DISTRICT HOSPITAL. PICTURE COURTESY OF DUNCAN NYIRONG & JOSEPH KASILILIKA
In Machinga, ONSE supported PAC orientations in six (Nyambi, Chikweo, Ngokwe, Mangamba,
Nainunje, and Ntaja) health facilities. The aim of the activity was to improve the quality of post abortal
services provided, conducted by 4 (0M, 4F) district mentors orienting a total of 31 (16M, 15F) health
care workers. Each facility has one manual vacuum aspiration (MVA) set so the Safe Motherhood
Coordinator and PAC focal person are to receive additional PAC equipment and job aids from RHD and
other partners by June 2022.
SUPERVISOR DEMONSTRATING HOW TO DO MVA DURING PAC ONSITE ORIENTATION AT NAINUNJE HEALTH CENTER PIC BY NIXON CHIDZERE
ONSE supported BEmONC supervision in all six BEmONC and CEmONC facilities in Mulanje. The aim
of the supervision was to assess how the facilities had performed in terms of functionality for BEmONC
and CEmONC and to provide support on documentation in registers. A total of 6 (4M, 2F) providers
were supervised. Findings showed that both CEmONC facilities in Mulanje are fully functional achieving
all the nine signal functions, while two BEmONC sites (Chonde and Kambenje) achieved full functionality
of the seven signal functions, and Namulenga achieved six signal functions, and M’biza achieved five.
Namulenga was coached on vacuum extraction as this was the only signal function that was not
performed.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 35
At Machinga District Hospital, ONSE supported non-pneumatic anti-shock garment (NASG) care
practices and IPC on-site orientations for a total of 20 (7M, 13F) hospital support staff. The aim of the
activity was to orient supporting staff on infection prevention and how to take care of NASG. This
orientation improved the cleaners’ skills in caring for the NASG equipment after donning it off the
patient as it is usually soaked with blood and other birth secretions; previously, days would pass without
it being cleaned. On IPC, the orientation is anticipated to improve environmental cleanliness of the
facility. On practical experiences of the participants, it was discovered that the postnatal and female
ward sluices were not in good working condition, and the matter was raised with the maintenance
supervisor.
In Kasungu, ONSE supported BEmONC refresher orientations to 15 (8M, 7F) participants. The activity
was organized with the essence of addressing the skills gaps that were identified through BEmONC
camping, integrated MNH supportive supervision, and cluster review meetings conducted in the facilities.
The training proved a success as the majority of the participants admitted to have been deployed into
facilities without adequate knowledge on BEmONC and acknowledged that the training has increased
their knowledge and confidence in BEmONC required skills.
ONSE supported a team of four female service providers from Nkhotakota High Dependency Unit
(HDU) department to benchmark best practices at Kamuzu Central Hospital. The activity aimed to
provide health workers with skills and knowledge on the care and management of critically ill patients
and overall management of the HDU. Key skills learned include:
◼ Team spirit and collaboration among health workers
◼ Always getting ready to respond to emergencies
◼ Observation of 5S in the HDU
◼ The providers are being supported to establish and institutionalize the lessons learnt
POSTPARTUM CARE
A total of 23,397 newborns received PNC within 48 hours after delivery compared to 32,798 reached
within the same period in PY5. There has been an improvement in documentation in most facilities.
However, during this period, there was a national crisis of lack of postnatal registers in health facilities.
Due to the processes followed for printing registers, ONSE only managed to print and distribute 500
registers in April 2022, thus outside the reporting period. The MoH were unable to print because they
lacked resources, and the lack of registers contributed to data losses. ONSE in its transition has
recommended retrospective data entry using few elements on the partograph to fill this data gap.
During the reporting period, ONSE supported Lilongwe DHO to conduct PNC mentorship in four
facilities of Mabang’ombe 2, Chiunjiza, Khongoni, and Matapila. The mentorship was undertaken by a
team of midwives from Bwaila (1M, 3F) with the goal of equipping midwives and other clinical staff with
skills and knowledge on the management of babies and mothers in the 48 hours postnatal period. A total
of 15 (5M, 10F) health workers were mentored in the four visited facilities. The facilities were provided
with MNH resources such as partographs, HBB guidelines, PNC reporting booklets, and handwashing
guidelines. In all the facilities, the mentors managed to find postnatal women for the case
demonstrations. The health workers managed to appreciate their gaps especially in the documentation
and pledged to improve.
In the reporting period, ONSE supported PNC and HBB register orientations in Chitipa. In total, 58
health workers (33M, 25F) were oriented from 10 health facilities. The objectives of the activity were to
refresh health care workers on use and documentation in postnatal and HBB registers and to discuss the
importance of proper documentation of registers in MNH. The orientation addressed timing, number of
postnatal checks, and content of PNC for all mothers and babies during the six weeks after birth, which
will help in capturing some complications that could have been missed due to incomplete assessment.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 36
INTEGRATED MNH SUPERVISION
In Dowa, Nkhotakota, Kasungu, Karonga and Lilongwe districts, ONSE supported integrated MNH
supervision and coaching for 146 (79M, 67F) providers from 43 health facilities. The activity aimed at
supporting the facilities in the provision of quality MNH services. Strengths and gaps were identified and
recommendations to address the gaps were provided. Table 13 summarizes some of the findings and
recommendations.
TABLE 13. SUMMARY OF SUPPORTIVE SUPERVISION IN INTEGRATED MNH CONDUCTED WITH ONSE SUPPORT
STRENGTHS CHALLENGES RECOMMENDATIONS
Kasungu (12 facilities), 23 supervised (10M, 13F)
◼ Availability of most drugs (e.g., ferrous
sulfate, folic acid, TTV, and insecticide-
treated nets [ITNs]) ◼ All staff were trained in BEmONC
◼ Use of partographs when monitoring
women in labor
◼ Availability of parenteral antibiotics; benzylpenicillin and gentamicin
◼ Availability of anticonvulsants
◼ Stockouts of syphilis test kits
◼ No piped water at Wimbe due
to stolen pump
◼ Facility in-charges was advised to
make emergency requests from the
DHO ◼ HCMC is working with local leaders
to ensure security of hospital
property and are lobbying with the
DHO for a new pump
Dowa (6 facilities), 16 supervised (6M, 10F)
◼ Essential drugs were available ◼ ITNs are being provided according to
protocol
◼ Poor documentation in the registers especially for signal
functions like parenteral
antibiotics
◼ Poor utilization of partographs
◼ Coaching on partograph use was done
◼ Coaching was done on the day of
the visit and included the importance
of partograph use
Chitpa (6 facilities), 22 supervised (8M, 14F)
◼ Availability of most essential drugs in
ANC
◼ All staff were trained in BEmONC ◼ Use of partographs when monitoring
women in labor
◼ Availability of parental antibiotics and anticonvulsants
◼ HB check not being done at
ANC due to unavailability of
haemacule ◼ No misoprostol and
chlorhexidine for IP
◼ Facility in-charge to lobby for
haemacule from mother facility
◼ The facility to source misoprostol and chlorhexidine from mother
facility
Nkhotakota (11 facilities), 24 supervised (10M, 14F)
◼ Clean environment at both facilities
◼ No BBAs reported at Mtosa for a period of six months
◼ Monitoring of postnatal mothers done
according to protocol at both facilities
◼ Lack of a stepping stool for
pregnant women at Mtosa ◼ HB not checked due to lack of
cuvettes
◼ Emergency tray not updated at
Mtosa
◼ Lobby for a stepping stool
◼ Place an order for cuvettes ◼ Emergency tray was updated on day
of visit and encouraged providers to
maintain
Zomba (11 facilities), 58 supervised (23M, 35F)
◼ Emergency tray available and updated at Likangala Health Center in Zomba
◼ Kangaroo Mother Care (KMC) corner
available and all information pasted on
the wall in 50% of the supervised health facilities in Zomba
◼ Excellent 5S at Likangala Health Center
◼ Antenatal matrix not followed at 40% of the supervised health
facilities in Zomba
◼ IP practices for MNH not fully
adhered to in some facilities
◼ Coaching was done and additional matrixes were provided
◼ Provided were coached on
adherence to IP protocols and given
examples of facilities like Likangala that are doing well in the district
Mulanje (5 facilities), 10 supervised (4M, 6F)
◼ Postnatal report well written at
Namphimba in Mulanje
◼ Improved documentation in KMC and
postnatal register at Naphimba ◼ Vital signs monitoring equipment
available in the facilities
◼ No protocols and missing KMC
register at Thuchira Maternity
◼ Early discharge of postnatal
mothers at Thuchira and Chambe health centers
◼ Maternity in-charge to source these
from their stores and order if still
not available
◼ Discussed with providers to adhere to the national discharge protocol
In Zomba, ONSE supported MNCH awareness meetings with the local leaders at Domasi rural hospital
to raise awareness among the communities on MNCH. A total of 24 (17M, 7F) chiefs and 18 (8M, 10F)

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 37
health care workers attended the meeting. The objectives of this activity were to ensure local leaders
are able to deliver MNCH messages to their community members and to inform communities about
their roles on MNCH especially safe motherhood issues. The DHO support team advised the chiefs to
conduct village meetings to share MNCH information with community members. It is expected that
continued engagement of the local leaders in safe motherhood issues would improve uptake of MNH
services in the district.
In Machinga, ONSE supported an obstetric ultrasound scanning orientation at the district hospital to
equip nurses and clinicians on diagnosing obstetric cases using ultrasound scanning. A total of 31 (19M,
12F) clinicians and nurses were orientated by 3 (3M) district facilitators. It is expected that delays in
initiating appropriate care will be minimized with the timely diagnosis using the USS machines in labor.
DISTRICT RADIOGRAPHIC TECHNICIAN DEMONSTRATING TO A CLINICAL OFFICER ON HOW AN ULTRASOUND SCANNING MACHINE WORKS PICTURE COURTESY OF
NIXON CHIDZERE
In Kasungu and Salima, ONSE supported six cluster-based MNH review meetings idrawing participation
from a total of 245 (76M, 169F) health providers from 18 facilities. The main objective of the review was
to identify issues and challenges affecting the MNH program and update DHMT for support. There was
a good relationship between the community and the facilities through community existing structures
such as HCMCs. Male involvement was evident in all the facilities. Most essential drugs like parenteral
antibiotics were available. Some challenges included increased workload affecting QoC, monitoring, and
documentation of care rendered. Late reporting was noted, as some women were coming to deliver
while in the second stage of labor in almost all the facilities. A lot of ANC and PNC data was incorrectly
reported because of the misunderstanding of the cohorts in Kasungu. Late referrals were also noted due
to transport challenges. The DNOs and DHSS are to lobby for the recruitment of more skilled birth
attendants as most facilities are understaffed and intensify quarterly supportive supervision and
mentorship in all districts. Participants were encouraged to intensely use community structures to
ensure early reporting to the facilities.
MATERNAL DEATH SURVEILLANCE AND RESPONSE (MDSR)
In the period under review, ONSE supported MDSR for 11 maternal deaths in Nkhotakota, Balaka,
Machinga, Zomba, Lilongwe, and Zomba districts with the aim of collecting adequate information on
maternal deaths and coming up with actionable points for preventing future deaths. The causes of the

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 38
maternal deaths were PPH (3), eclampsia (1), anemia (1), ruptured uterus (1), and high spinal anesthesia
(1). Contributing factors were from all levels including patient, health worker, and administrative factors.
There was a delay in initiating or providing the right treatment as well as in reaching facilities. For
example, a 16-year-old woman reported timely in labor but providers delayed identifying cephalo-pelvid
disproportion (CPD) and ended up having prolonged labor. Vacuum extraction was attempted, but
failed, and the woman was then referred to the next level where a cesarean section was done. Days
later, she developed bowel obstruction and a laparotomy was done where a uterus rupture was
discovered. Another woman reported walking to the facility for an elective cesarean section due to
having two previous cesarean section scars. She developed cardiac arrest at the theater table and passed
away. Mentorship has been organized to address these gaps which will be led by the district medical
officers. A 17-year-old woman delivered through a cesarean section and got discharged. The woman
started bleeding profusely at home and reported back to the hospital in a bad state. Uterine evacuation
through D&C was done to no avail and proceeded to do subtotal hysterectomy where retained
membranes were discovered. After receiving four units of blood and other medications, the young
woman could still not make it and died of PPH. There were delays in identifying underlying causes of
complications, delays in reporting to the facility, and there were no ambulances with fixed oxygen
cylinders for patients on transfer. Action points were drawn and assigned to individuals.
KANGAROO MOTHER CARE (KMC)
ONSE supported KMC supportive supervision at two facilities in Machinga to improve care provided to
children born underweight. A total of 7 (3M, 4F) health workers were supervised and mentored by 2
(1M, 1F) District KMC supervisors. There was a knowledge gap on how to write KMC reports in both
facilities, inadequate documentation in KMC register, no KMC protocols and guidelines in both the
facilities, and no feeding cups and buckets at Nyambi. Mentorship was done on the gaps identified. The
KMC Coordinator and facility in-charge are to source KMC equipment and supplies from RHD. They
were advised to document all KMC babies in the KMC register.
ONSE supported orientation of Family Led Care in care of preterm babies in Balaka at Phalula Health
Center to equip the participants with knowledge and skills for managing preterm and low birth weight
babies. A total of 10 (3M, 7F) were oriented by 3 (1M, 2F) facilitators. The areas for the mentorship
included admission criteria for KMC, how to put a baby in KMC position, how to use counseling for
Family Led Care/KMC, monitoring chart, feeding chart, and discharge criteria, as well as criteria for re-
admission. Participants acquired the planned skills, a follow-up in March was done to see how they are
internalizing the skills imparted to them during this training.
During the reporting period, ONSE supported on-site coaching on HBB and KMC in Dowa and
Kasungu. The aim of the activity was to establish the gaps in HBB and KMC and coaching the health
workers in those specific gaps. A total of 19 (6M, 11F) health workers from 10 facilities were mentored.
Most midwives do not document in the HBB register at Kasungu District Hospital. Midwives were
reminded of the importance of documentation for any program including HBB. HBB resuscitation area
was not set at Mnyanja Health Center because there were no tables to improvise for the resuscitation
area. They were advised to use the bedside and always have equipment ready. KMC babies are not fed
as per guidelines in Dowa. Both districts are using non-standardized KMC monitoring. The districts
were advised to always make sure that the standard monitoring forms are available.
COMMUNITY-BASED MATERNAL AND NEONATAL CARE (CBMNC)
During the reporting period, ONSE supported CBMNC supervision, coaching, and mentoring in Zomba,
Salima, and Kasungu. The aim of the activity was to observe and assess performance of HSAs when
conducting the CBMNC services. A total of 122 (75M, 47F) HSAs from 12 facilities were mentored. The
identified issues included lack of equipment such as thermometers, scales, and bags for the majority of
HSAs. Some CBMNC providers had no reporting and referral forms in Salima and there was a lack of
knowledge on how to use the new CBMNC registers and reporting tools. Some HSAs were not able to
carry out the CBMNC counseling using counseling and baby cards. Recommendations included working

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 39
with RHD to identify funds for refresher trainings as the HSAs were trained more than two years ago
and the package has been revised. In addition, continuing with supportive supervision and onsite
coaching was recommended. The providers were provided with the necessary forms.
In Nkhotakota, ONSE supported CBMNC review meetings at four clusters of DHO, Nkhunga, Kapiri,
Kasitu, and Alinafe health facilities. It was attended by a total of 125 (89M, 36F) participants from all the
21 health facilities of the district. Health centers presented their experiences in the CBMNC program
on what was working and not working well.
TABLE 14. SUMMARY OF CBMNC REVIEW MEETING FINDINGS
STRENGTHS CHALLENGES AND SOLUTIONS
◼ Successfully barred three influential traditional birth attendants surrounding Nkhotakota DHO and Chididi
Health Centers from conducting deliveries
◼ Increased number of women delivering at health facilities
especially at Mpamantha Health Center ◼ Consistent reporting by almost all health centers and data
is updated in DHIS2
◼ Supportive supervision was done to almost all active HSAs
◼ Deployment of Community Midwifery Assistants to three communities that often delivered at TBAs
◼ Few HSAs underwent the revised CBMNC guidelines course, sourcing funds for capacity building of the
remaining HSAs
◼ Some women do not disclose to the HSAs whenever
they are pregnant, and HSAs were advised to conduct awareness on the importance of disclosing pregnancies
so that they are well supported.
◼ Lack of counseling cards and other teaching aids during
home visits. RHD is working with partners to print counseling cards
CHILD HEALTH AND EPI
Of the six indicators that ONSE tracks related to child health, three achieved the annual target, two
almost achieved the annual target, and one did not achieve the annual target as of the end of PY6Q2.
The number of cases of child diarrhea treated in USG-supported facilities reached a cumulative 140,767
for 113% achievement against the annual target at the end of the second quarter. This can be attributed
to a substantial availability of oral rehydration salts (ORS) and Zinc tablets for treatment of diarrhea,
however the medicines for diarrhea are inconsistent and still in short supply. The number of children
under-five suspected with pneumonia receiving antibiotics reached a cumulative number of 269,102
represent an achievement of 83% of the annual target at the end of the second quarter. This
achievement is a lower achievement for this indicator. The lower achievement can be attributed to
continuous intermittent and stock out supply of dispersible amoxicillin especially at village clinic level.
This has also led to increased referrals of children suspected with pneumonia who could not be treated
at village clinic level but referred to next level of care.
TABLE 15. PERFORMANCE ON CHILD HEALTH INDICATORS, PY6Q2 PROGRESS TO TARGET
INDICATORS
PROJECT YEAR 6
TARGET Q1
ACHIEVEMENT Q1
ACHIEVEMENT STATUS
# cases of child diarrhea treated in USG-assisted
programs 125,000 67,422 73,345
# children <5 suspected with pneumonia received antibiotics by trained facility or community health
workers in USG-assisted programs
325,000 117,798 151,304
% of health service delivery points offer community-
based child health services* 90% 81% 78%
# children received DPT3 (Pentavalent Vaccine
[PENTA] III) by 12 months of age in USG-assisted
programs
137,100 72,801 69,920
# children 12-23 months received measles-rubella second dose (MRII) through USG-assisted programs
68,550 39,589 28,307
Diphtheria Tetanus Pertussis vaccine - first dose
(DPT1) to DPT3 dropout rate* 5% -1.1% 6.2%
Achieved (≥100% of target)
Almost Achieved (86-99%)
Not Achieved (≤85%)
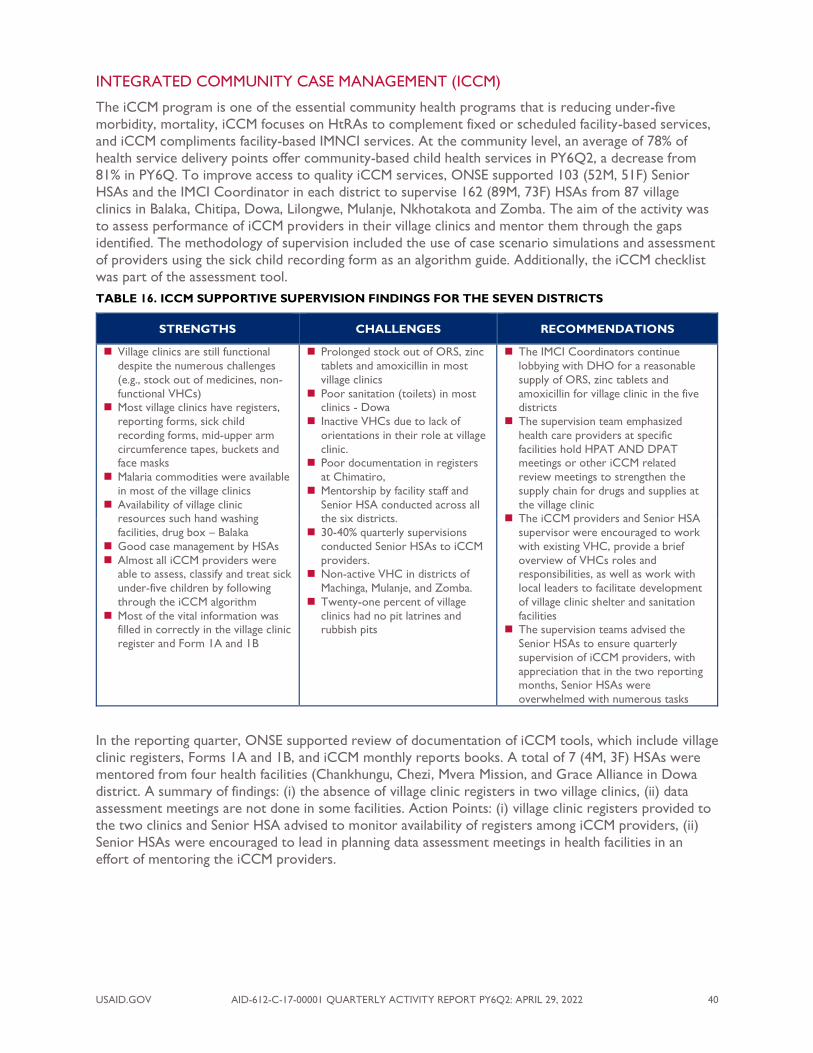
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 40
INTEGRATED COMMUNITY CASE MANAGEMENT (ICCM)
The iCCM program is one of the essential community health programs that is reducing under-five
morbidity, mortality, iCCM focuses on HtRAs to complement fixed or scheduled facility-based services,
and iCCM compliments facility-based IMNCI services. At the community level, an average of 78% of
health service delivery points offer community-based child health services in PY6Q2, a decrease from
81% in PY6Q. To improve access to quality iCCM services, ONSE supported 103 (52M, 51F) Senior
HSAs and the IMCI Coordinator in each district to supervise 162 (89M, 73F) HSAs from 87 village
clinics in Balaka, Chitipa, Dowa, Lilongwe, Mulanje, Nkhotakota and Zomba. The aim of the activity was
to assess performance of iCCM providers in their village clinics and mentor them through the gaps
identified. The methodology of supervision included the use of case scenario simulations and assessment
of providers using the sick child recording form as an algorithm guide. Additionally, the iCCM checklist
was part of the assessment tool.
TABLE 16. ICCM SUPPORTIVE SUPERVISION FINDINGS FOR THE SEVEN DISTRICTS
STRENGTHS CHALLENGES RECOMMENDATIONS
◼ Village clinics are still functional
despite the numerous challenges
(e.g., stock out of medicines, non-
functional VHCs) ◼ Most village clinics have registers,
reporting forms, sick child
recording forms, mid-upper arm
circumference tapes, buckets and face masks
◼ Malaria commodities were available
in most of the village clinics
◼ Availability of village clinic resources such hand washing
facilities, drug box – Balaka
◼ Good case management by HSAs
◼ Almost all iCCM providers were able to assess, classify and treat sick
under-five children by following
through the iCCM algorithm
◼ Most of the vital information was filled in correctly in the village clinic
register and Form 1A and 1B
◼ Prolonged stock out of ORS, zinc
tablets and amoxicillin in most
village clinics
◼ Poor sanitation (toilets) in most clinics - Dowa
◼ Inactive VHCs due to lack of
orientations in their role at village
clinic. ◼ Poor documentation in registers
at Chimatiro,
◼ Mentorship by facility staff and
Senior HSA conducted across all the six districts.
◼ 30-40% quarterly supervisions
conducted Senior HSAs to iCCM
providers. ◼ Non-active VHC in districts of
Machinga, Mulanje, and Zomba.
◼ Twenty-one percent of village
clinics had no pit latrines and rubbish pits
◼ The IMCI Coordinators continue
lobbying with DHO for a reasonable
supply of ORS, zinc tablets and
amoxicillin for village clinic in the five districts
◼ The supervision team emphasized
health care providers at specific
facilities hold HPAT AND DPAT meetings or other iCCM related
review meetings to strengthen the
supply chain for drugs and supplies at
the village clinic ◼ The iCCM providers and Senior HSA
supervisor were encouraged to work
with existing VHC, provide a brief
overview of VHCs roles and responsibilities, as well as work with
local leaders to facilitate development
of village clinic shelter and sanitation
facilities ◼ The supervision teams advised the
Senior HSAs to ensure quarterly
supervision of iCCM providers, with
appreciation that in the two reporting months, Senior HSAs were
overwhelmed with numerous tasks
In the reporting quarter, ONSE supported review of documentation of iCCM tools, which include village
clinic registers, Forms 1A and 1B, and iCCM monthly reports books. A total of 7 (4M, 3F) HSAs were
mentored from four health facilities (Chankhungu, Chezi, Mvera Mission, and Grace Alliance in Dowa
district. A summary of findings: (i) the absence of village clinic registers in two village clinics, (ii) data
assessment meetings are not done in some facilities. Action Points: (i) village clinic registers provided to
the two clinics and Senior HSA advised to monitor availability of registers among iCCM providers, (ii)
Senior HSAs were encouraged to lead in planning data assessment meetings in health facilities in an
effort of mentoring the iCCM providers.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 41
ICCM MENTORSHIP SESSION AT MVERA MISSION FACILITY
CARE OF INFANTS AND NEWBORNS (COIN)
COIN is an advanced skill concept that was designed to enable clinical staff and nurses to provide
important, best-practice and evidence care for every newborn and young infant less than two months
old who is sick and admitted to the special care neonatal unit. In Mulanje, ONSE supported 6 (3M, 3F)
national trainers to conduct COIN training for 15 (5M, 10F) health care providers. Of these fifteen
participants, five were clinical officers and ten nurse/midwives. The participants were drawn from
maternity, neonatal care units, postnatal, and pediatric wards. The aim of the training was to impart
knowledge on how to manage sick newborn babies and young infants using modern technologies and to
impart basic maintenance skills for troubleshooting equipment used in neonatal care units. This was a
five-day training, divided into several daily sections to help participants achieve objectives. Delivery of
content was through lectures, videos, drills, and scenarios methods. It is anticipated that after the COIN
training, the participants will be able to provide standardized care for sick newborn and young infants
and avert death. Topics covered during the training included:
◼ Care and use of essential equipment (suction machine, baby resuscitator, radiant warmers,
oxygen concentrators and splitters, pulse oximeters, glucometers, phototherapy)
◼ Triage drills
◼ Newborn and infant resuscitation
◼ Management of breathing difficulties and birth asphyxia
◼ Management of low birth weight babies (KMC)
◼ Prevention and management of hypoglycemia
◼ Prevention and management of hypothermia
◼ Management of shock and sepsis
◼ Fluid management
◼ Review of neonatal tools
◼ How to stabilize and refer a sick newborn or young infant
In Balaka, ONSE supported COIN mentorship for five facilities (Comfort Mission Hospital, Kwitanda,
Nandumbo, Utale 1, and Ulongwe) for 20 (10M, 10F) providers. The aim of the supervision was to
assess health care providers’ knowledge on the management of neonates and young infants with
breathing problems and to address the identified gaps. Key findings observed were that in most facilities
oxygen concentrators and suction machines were not cleaned sufficiently for use by the next patient.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 42
The mentorship team will continue to mentor health workers on the use and care of equipment used in
emergencies.
TABLE 17. FINDINGS AND RECOMMENDATIONS OF THE BALAKA COIN SUPPORTIVE SUPERVISION
STRENGTHS CHALLENGES RECOMMENDATIONS
◼ The facilities had the most basic equipment for
resuscitation
◼ The health care providers
were knowledgeable on resuscitation skills and
administration of oxygen
therapy
◼ Infection prevention practices were followed
according to standards
◼ Suction machines at Nandumbo HC and Comfort
MH were not working
◼ Health care providers at
Comfort MH demonstrated little knowledge on
administration of vitamin K.
◼ Comfort Mission Hospital
neonatal care unit does not have a CPAP machine.
◼ Health care providers at
Utale did not administer the
recommended amount of oxygen to neonates and
young infants
◼ Poor documentation in sick
newborn registers and in patient case notes
◼ Balaka Maintenance Officer was contacted and informed of the status of all machines, which
required his attention
◼ The supervising team conducted a mentorship
session of benefits of vitamin K, when to administer, and how it is administered.
◼ Comfort Mission Hospital were referred to NEST
360 for the request of a CPAP machine, However,
Comfort MH was informed to buy the gadget from NEST 360 as the CPAP machine for donation had
been exhausted
◼ The health care providers were mentored through
criteria for administering oxygen therapy, placing a neonate/young infant on oxygen and monitoring
neonate on oxygen therapy
◼ The supervising team conducted a coaching session
on documentation of sick newborn register and the related neonatal care standardized tools
NEONATAL DEATH AUDIT
ONSE supported 5 neonatal death audits in Chitipa (1), Karonga (2), Kasungu (1), and Mulanje (1). The
aim of the audits were to assess the QoC provided to neonates and to find strategies and develop
action points that would lead to improvement in the QoC provided at unit level. The audit process was
conducted by 92 (45M, 47F) health care providers. Chitipa, Karonga and Kasungu audited neonatal death
cases for the district hospitals, while Mulanje audited neonatal cases for both the district and mission
hospitals combined. A total of 51 neonatal death cases were audited in this period. The major causes of
death were: birth asphyxia (47%), hypoxemia (22%), prematurity (14%), respiratory distress syndrome
(10%), neonatal sepsis (4%), meconium aspiration (2%), and dehydration (12%). Of importance to note is
that hypoxemia and respiratory distress syndrome are direct signs and symptoms linked to neonates
born with prematurity; however, the audit teams in districts attributed the two conditions as primary
cause of death rather than prematurity itself. The major leading cause of neonatal death continues to be
birth asphyxia, which is linked to management of women during labor and delivery.
TABLE 18. FINDINGS OF THE NEONATAL DEATH AUDITS IN THE FOUR-DISTRICTS
CHALLENGES IDENTIFIED PROPOSED SOLUTION AND RECOMMENDATIONS
◼ Inadequate assessment of sick neonate at time of admission – insufficient notes
◼ The DMO to take up responsibility of allocating a second clinician for the neonatal unit who will review neonates as a routine process
◼ The DMO’s Chitipa and Kasungu DHs to ensure the neonatal care unit
Rota for clinicians is available and followed as per allocation
◼ Sensitizing all nurse’s working in neonatal care units to call for a clinician for every admission and very sick neonate
◼ Inadequate review of neonates with severe
illness by clinicians
◼ Critically ill neonate not reviewed during weekends
◼ DMO responsibility, to allocate clinicians responsible for neonatal units
who could review babies on a daily basis
◼ The DMO’s Chitipa and Karonga DH’s to ensure the neonatal care unit Rota for clinicians is available and followed as per allocation
◼ Inadequate maternal and labor and delivery
notes/records
◼ Incomplete history taking and documentation.
◼ The Neonatal Care Unit In-charge to emphasize on attaching mother’s
partograph on every admission to the neonatal care unit
◼ Emphasize on complete filling of nursery admission form
◼ Inadequate oxygen supply to the ward
during electricity black outs – Karonga DH
◼ The Hospital Administrator - Karonga DH tasked to liaises with
DHMT on strategy to source for backup power for electricity
◼ Insufficient checks of oxygen saturation and blood glucose
◼ The Unit In-charges will ensure the availability of resources (e.g., pulse oximeter and glucometer) and conduct case note spot checks to

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 43
ensure that neonates are tested on the two parameters and results are documented
◼ Delayed change of treatment by clinician despite observing abnormal readings on
several occasions
◼ Inadequate routine monitoring of neonates
admitted in neonatal care units ◼ Inadequate monitoring of vital signs as per
required standard
◼ The neonatal care unit In-charge as well as Head of Clinicians in neonatal unit assigned to routinely monitor patient care and set
reminders to nursing and clinical staff on importance of initial
assessment, daily routine patient monitoring, clinician and nurses be in
position to timely alert providers with advanced skills to assist when the patient is not making good progress
◼ Prescribed feeds not given at the
appropriate times
◼ The Safe Motherhood Coordinators for the three districts to facilitate
mentorship sessions on nutrition and feeding for neonates and reoriented health care providers to the feeding landscape for neonates
EMERGENCY TRIAGE, ASSESSMENT, AND TREATMENT (ETAT)
ETAT complements IMCI and iCCM services as a point for emergency care of the under-five conditions;
it is an essential process of saving lives of very sick under-five children by identifying children with
immediately life-threatening conditions. ONSE targeted 65 BEmONC sites across the 11 FHP districts
to ensure the facilities are able to provide the 7/9 signal functions. ETAT as a child health program also
targeted the 65 BEmONC facilities to ensure there were functional ETAT corners, at end PY6Q2 there
were 43 (67%) functional ETAT corners in the designated BEmONC facilities. The major focus on ETAT
was to strengthen functionality of existing ETAT stabilization corners rather than establishing new ones.
ONSE supported ETAT supportive supervision for 29 (15M, 14F) providers from nine health facilities of
Balaka (4) and Dowa (5). The health care providers were supervised by 6 (2M, 4F) supervisors from
Balaka and Dowa District Hospitals. The general findings across all the facilities:
TABLE 19. ETAT SUPERVISION FINDINGS FOR BALAKA AND DOWA HEALTH FACILITIES.
STRENGTHS CHALLENGES RECOMMENDATIONS
◼ Health care providers
follow the IMCI/ETAT concept guidelines to
care
◼ Treatment guidelines -
IMCI and ETAT flow charts available and
pasted on walls
◼ IMCI Chart booklets
were used as reference text for Dowa facilities
◼ Emergency trays were
available
◼ Some emergency drugs were available
◼ No tool to facilitate triaging
(e.g. lack of color code rulers or ETAT stamps for Dowa
facilities)
◼ Stock out of essential
medicines (e.g., amoxicillin for most facilities in both districts)
◼ The treatment rooms for
Comfort Mission Hospital and
Nandumbo and Utale 1 health centers were dirty
◼ Lack of treatment guidelines
for artesunate and 10%
glucose at Comfort Hospital ◼ Emergency trays were not
updated at all the facilitie
◼ Some health workers were
not trained in ETAT
◼ The ETAT Coordinator to request partners and
DHMT of the possibility of developing ETAT stamps of ETAT color code rulers
◼ The ETAT Coordinator liaised with DMO Dowa on
how to source for essential medicines that are out of
stock ◼ The In-charges for Comfort Mission Hospital,
Nandumbo and Utale 1 health centers were advised
to ensure that the treatment rooms are cleaned on a
daily basis and whenever there is need ◼ The ETAT Coordinator to source for artesunate and
10% glucose guidelines
◼ The emergency trays were updated on the day of the
supervision and they were mentored on the process of replenishing the emergency trays
◼ The In-charges for the facilities should make sure that
the emergency trays are updated regularly
◼ The ETAT Coordinator and DMO to lobby for funds from partners in the district to support this initiative
In Karonga, ONSE supported the ETAT coordinator (1M) to conduct ETAT orientation for 20 (12M,
8F) health workers from two facilities (Mpata and Kayelekera). The objective of the mentorship was to
impart knowledge and skills in ETAT from gaps identified during the previous supportive supervision.
The orientation session had a practical session on triaging, and participants practiced the triage process
on the available patients at the facilities. Topics included in the orientation were identification of danger
signs in sick under-five children, importance of using colored rulers or an ETAT stamp, treatment of
emergency signs (airway, breath, circulation, coma, convulsion, and severe dehydration) and a list of
basic equipment required for an ETAT stabilization room/corner. Mpata and Kayelekera health facilities
are partially functional on ETAT as some essential basic equipment like oxygen concentrators and

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 44
nebulisers are not available. The basic equipment for stabilization corners will be sourced from DHO
and other health partners in the district. It is anticipated that each facility will be collecting triaging data
which will be analyzed at the end of every month.
In Lilongwe and Kasungu, ONSE supported ETAT Program Coordinators (3M, 1F) to conduct
mentorship and supervision of 54 (21M, 33F) health care providers from 12 facilities (7 Lilongwe, 5
Kasungu). The activity aimed at equipping health center staff with knowledge and lifesaving skills in the
management of childhood emergencies and illnesses. The mentorship focus for Kasungu team was cross
checking on the triage system, availability of treatment guidelines, availability of emergency medicines,
and functional equipment. The Lilongwe ETAT mentorship focused on knowledge, skills and
organizational gaps in ETAT as well impart knowledge and skills in the organization preparedness and
delivery of ETAT services. The Lilongwe mentorship was delivered through a one-on-one model of
mentorship using a checklist while Kasungu conducted a group mentorship model using the ETAT
supervision tool. Achievements observed and action points from mentorship provided at Kasungu
District Hospital are included in the table below.
TABLE 20. ACHIEVEMENTS OBSERVED AND ACTION POINT FOR KASUNGU DISTRICT HOSPITAL, ETAT MENTORSHIP
ACHIEVEMENTS OBSERVED ACTION POINTS FOR KASUNGU DH
◼ The mentorship team managed to reorganize the
emergency units in the 12 facilities ◼ The team debriefed staff on the list of medicines required
in the emergency and ensured availability of essential
accessories (e.g., cannulas, intravenous fluids and the
intravenous giving sets). ◼ Discussed the importance of teamwork in ETAT between
clinical and support staff so that all eligible cases are
triaged and treated with urgency
◼ Kasungu observation showed that nurses, clinicians, and supporting staff like hospital attendance and hospital
guards were able to triage sick children with emergency
signs like airway, breathing problems, and also convulsions
as well as manage the illnesses with urgency
◼ Kasungu DMO to allocate an additional Medical
Assistant at Simlemba Health center ◼ ONSE supported the printing of treatment guidelines for
management of under-five children
◼ The ETAT Coordinator lobbied with Kasungu DMO to
source emergency equipment like oxygen concentrator, nebulizer, glucometer, and suctioning machine for the
health facilities
In Karonga, ONSE supported the ETAT Coordinator (1M) to facilitate an ETAT Review Meeting at
Chilumba Rural Hospital, drawing participation from 10 (4M, 6F) providers. The overall aim of the
activity was to improve functionality of ETAT corners in the facilities as well as create a platform
through which health facilities shared best practices and experiences in the implementation of ETAT.
The activity involved auditing case files for children admitted at the facility from November 2021 to
January 2022. The health care providers were also oriented briefly to the assessment, treatment and
management of a child’s airway and breathing, circulation (shock), level of consciousness, coma,
convulsions, and severe dehydration problems. It was observed that there was an increase in providers
correctly prescribing and administering medicines for malaria cases, with an improvement from 30% in
June 2021 to 53% in February 2022. All admission files were contained in the critical care pathway sheet
to facilitate patient care monitoring and providers are using the standardized pediatric admission sheet,
whereas previously they were using outdated health passport books. The health facility was supported
with treatment and admission sheets and was recommended to institute routine pediatric reviews as
part of QoC checks.
PEDIATRIC DEATH AUDIT
In Kasungu, ONSE supported three pediatric death audit sessions where 13 cases were reviewed by 24
(13M, 11F) health care providers. The cases audited were for children 8 to 45 months old. The major
cause of death was malaria (7) compounded by sepsis and anemia. Other conditions included
hypoglycemia (2), severe anemia (1), severe pneumonia (1), severe dehydration and gastroenteritis (1),
and sepsis (1).
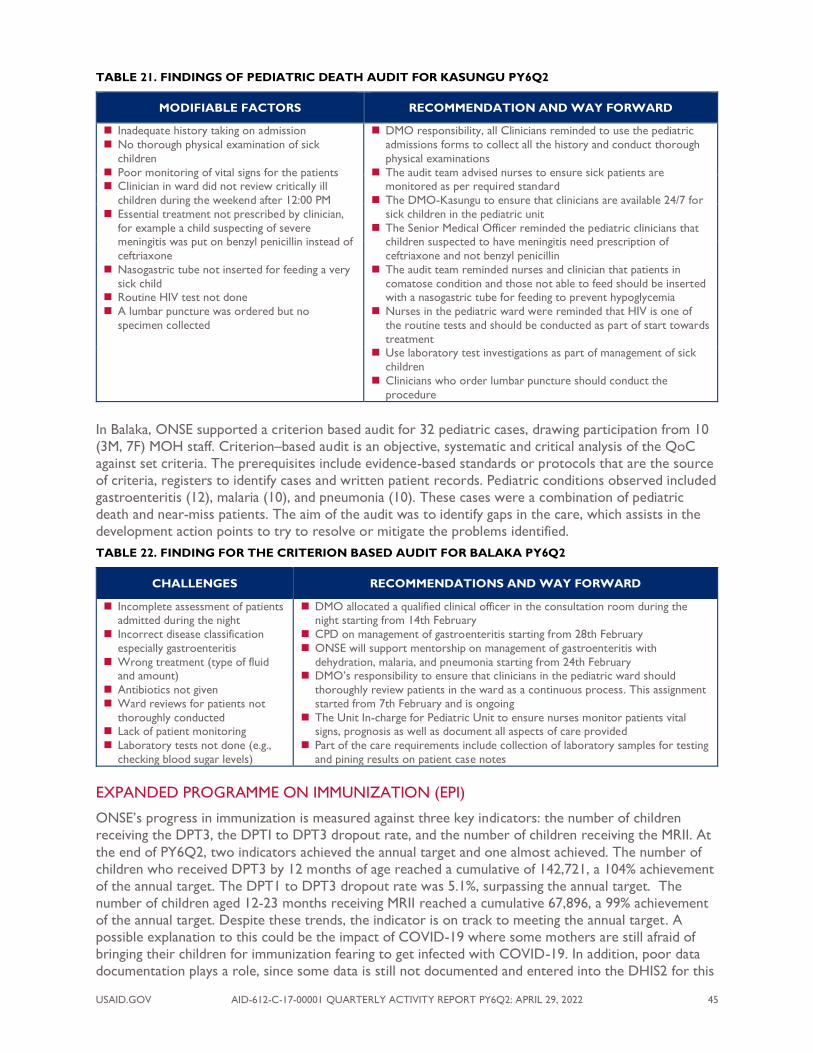
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 45
TABLE 21. FINDINGS OF PEDIATRIC DEATH AUDIT FOR KASUNGU PY6Q2
MODIFIABLE FACTORS RECOMMENDATION AND WAY FORWARD
◼ Inadequate history taking on admission
◼ No thorough physical examination of sick
children
◼ Poor monitoring of vital signs for the patients ◼ Clinician in ward did not review critically ill
children during the weekend after 12:00 PM
◼ Essential treatment not prescribed by clinician,
for example a child suspecting of severe meningitis was put on benzyl penicillin instead of
ceftriaxone
◼ Nasogastric tube not inserted for feeding a very
sick child ◼ Routine HIV test not done
◼ A lumbar puncture was ordered but no
specimen collected
◼ DMO responsibility, all Clinicians reminded to use the pediatric
admissions forms to collect all the history and conduct thorough
physical examinations
◼ The audit team advised nurses to ensure sick patients are monitored as per required standard
◼ The DMO-Kasungu to ensure that clinicians are available 24/7 for
sick children in the pediatric unit
◼ The Senior Medical Officer reminded the pediatric clinicians that children suspected to have meningitis need prescription of
ceftriaxone and not benzyl penicillin
◼ The audit team reminded nurses and clinician that patients in
comatose condition and those not able to feed should be inserted with a nasogastric tube for feeding to prevent hypoglycemia
◼ Nurses in the pediatric ward were reminded that HIV is one of
the routine tests and should be conducted as part of start towards
treatment ◼ Use laboratory test investigations as part of management of sick
children
◼ Clinicians who order lumbar puncture should conduct the
procedure
In Balaka, ONSE supported a criterion based audit for 32 pediatric cases, drawing participation from 10
(3M, 7F) MOH staff. Criterion–based audit is an objective, systematic and critical analysis of the QoC
against set criteria. The prerequisites include evidence-based standards or protocols that are the source
of criteria, registers to identify cases and written patient records. Pediatric conditions observed included
gastroenteritis (12), malaria (10), and pneumonia (10). These cases were a combination of pediatric
death and near-miss patients. The aim of the audit was to identify gaps in the care, which assists in the
development action points to try to resolve or mitigate the problems identified.
TABLE 22. FINDING FOR THE CRITERION BASED AUDIT FOR BALAKA PY6Q2
CHALLENGES RECOMMENDATIONS AND WAY FORWARD
◼ Incomplete assessment of patients admitted during the night
◼ Incorrect disease classification
especially gastroenteritis
◼ Wrong treatment (type of fluid and amount)
◼ Antibiotics not given
◼ Ward reviews for patients not
thoroughly conducted ◼ Lack of patient monitoring
◼ Laboratory tests not done (e.g.,
checking blood sugar levels)
◼ DMO allocated a qualified clinical officer in the consultation room during the night starting from 14th February
◼ CPD on management of gastroenteritis starting from 28th February
◼ ONSE will support mentorship on management of gastroenteritis with
dehydration, malaria, and pneumonia starting from 24th February ◼ DMO’s responsibility to ensure that clinicians in the pediatric ward should
thoroughly review patients in the ward as a continuous process. This assignment
started from 7th February and is ongoing
◼ The Unit In-charge for Pediatric Unit to ensure nurses monitor patients vital signs, prognosis as well as document all aspects of care provided
◼ Part of the care requirements include collection of laboratory samples for testing
and pining results on patient case notes
EXPANDED PROGRAMME ON IMMUNIZATION (EPI)
ONSE’s progress in immunization is measured against three key indicators: the number of children
receiving the DPT3, the DPTI to DPT3 dropout rate, and the number of children receiving the MRII. At
the end of PY6Q2, two indicators achieved the annual target and one almost achieved. The number of
children who received DPT3 by 12 months of age reached a cumulative of 142,721, a 104% achievement
of the annual target. The DPT1 to DPT3 dropout rate was 5.1%, surpassing the annual target. The
number of children aged 12-23 months receiving MRII reached a cumulative 67,896, a 99% achievement
of the annual target. Despite these trends, the indicator is on track to meeting the annual target. A
possible explanation to this could be the impact of COVID-19 where some mothers are still afraid of
bringing their children for immunization fearing to get infected with COVID-19. In addition, poor data
documentation plays a role, since some data is still not documented and entered into the DHIS2 for this

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 46
reporting period. We also expect the DPT1 to DPT3 dropout rate to change with full data from the
quarter, as some sites have missing data for DPT1. This indicator is expected to improve through
sensitizing mothers to bring their children for vaccination. Additionally, DHMTs need to intensify
supervision to ensure COVID-19 measures are being applied and that the data for all children vaccinated
is well documented and entered into the DHIS2.
VACCINE COLLECTION AND DISTRIBUTION
In PY6Q2, ONSE supported the collection and distribution of EPI supplies from the central vaccine
stores to an average number of 310 health facilities per month in the 11 FHP districts. Some of the EPI
supplies that were transported included: vaccines and gas cylinders for gas refrigerators, safety boxes,
vaccine carriers, freeze tags, syringes (5ml, 2ml, 0.5ml, and 0.05ml), cotton wool, and EPI posters. The
distribution was based on monthly consumption and current stock status per commodity. This
contributed to the availability of vaccines and other supplies at the health facility and assisted in
improving immunization coverage. During the distribution, some spot-checks on EPI were conducted in
Kasungu and the major issues were presented in the table below.
TABLE 23. SUMMARY OF EPI SPOT CHECKS - DOWA AND KASUNGU
STRENGTHS CHALLENGES ACTIONS/RECOMMENDATIONS
Dowa
◼ Availability of all antigens at
central region vaccine stores
(CRVS) ◼ Gas cylinders were collected
◼ Collected two refrigerators
from RVS and replaced at
Chizolowondo and Grace Alliance
◼ Lack of EPI reporting tools such as
reporting booklets, immunization
monitoring charts and child health passports at the regional vaccine stores
◼ Impassable roads due to heavy rains in
some areas
◼ Vandalizing of EPI equipment (refrigerator) at Kainja Health Post
◼ Lobby with the EPI unit and partners
for provision of EPI reporting tools
◼ DHO assigned to allocate a security guard at Kainja health post to
prevent issues of vandalism
Kasungu
◼ No stock-outs of vaccines in all
the facilities.
◼ During distribution, 23 cold chain equipment were installed
with remote temperature
monitoring device
◼ Timely provision of fuel for distribution by ONSE
◼ Inconsistent temperature monitoring in
some health facilities
◼ Stock books for vaccines (including COVID-19 vaccines) and injection
materials not updated in some facilities
◼ Lack of EPI performance monitoring
charts ◼ Non-functional cold chain equipment at
Simlemba, Dwangwa, Kamboni, Livwezi,
and Santhe
◼ Health facilities were reminded to
consistently monitor refrigerator
temperatures ◼ Facilities were reminded to update
all stock books for vaccines and
injection materials
◼ To lobby EPI and partners for EPI monitoring charts
◼ DHO and partners to support cold
chain technician to conduct
prevention maintenance in the district for cold chain equipment
IMMUNIZATIONS AT IFHOC CLINICS
During the reporting period, the EPI immunization activities continued to be supported through the
IFHOCs. According to the IFHOC records, immunization coverage for the reporting period is lower as
compared to the duration in PY5Q2. This is contributed to COVID-19 as many people are afraid to visit
clinics for fear of contacting COVID-19.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 47
TABLE 24. IMMUNIZATIONS PROVIDED AT IFHOCS - PY5Q2 AND PY6Q2 COMPARISON
IMMUNIZATION PY5Q2 PY6Q2
M F Total M F Total
PENTA I 2,440 2,599 5,039 1,7570 1,674 3,454
PENTA III 2,303 2,972 5,275 1,742 1,651 3,393 MR I 2,291 2,299 4,590 1,592 1,529 3,121 MR II 1,855 1,966 3,821 1,356 1,243 2,599 Total 8,889 9,836 18,725 6,107 6,460 12,567
SUPPORT FOR THE INSTALLATION OF REMOTE TEMPERATURE MONITORING DEVICE
In Mulanje, ONSE supported the installation of remote temperature monitoring devices for the EPI
fridge at Chonde Health Center. The aim of the activity was to assist the district in monitoring cold
chain maintenance in health centers through installation of special devices which will help the district in
early rectification of problems in cold chain. ONSE supported the activity with lunch allowances and fuel
for a vehicle.
A COLD CHAIN TECHNICIAN INSTALLING A MONITORING DEVICE AT CHONDE HEALTH CENTRE. PICTURE COURTESY OF ZIMA NINDI
EPI SUPPORTIVE SUPERVISION AND MENTORSHIP
During the reporting period, EPI supportive supervision was conducted in Machinga, Mulanje, Salima and
Lilongwe districts. The aim of the activity was to provide support and guidance to HSAs in the EPI
program and to provide onsite mentorship on EPI. The activity benefited a total number of 40 health
facilities and 112 (76M, 36F) health workers in all the four districts supervised. The supervision findings
are summarized below:

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 48
TABLE 25. SUMMARY OF EPI SUPPORTIVE SUPERVISION FINDINGS
STRENGTHS ISSUES ACTIONS
◼ Availability of vaccines
and supplies
◼ Availability of an EPI
updated schedule for clinics
◼ No active surveillance being done at Mpala
◼ Vaccine monitoring charts not updated to stock out
of chart
◼ Vaccines are not provided every day in some facilities (Dzenje)
◼ HSAs not taking action despite having no electricity
for a week at Makokola health post
◼ No immunization posters at Kamwendo health post ◼ Some facilities visited did not have updated
microplans for 2022
◼ Lack of well-established mechanisms for defaulter
tracing for the children who are not immunized or under-immunized. Replan for every canceled clinic
◼ To improve on active disease
surveillance
◼ District to provide vaccine
monitoring charts to health facilities
◼ HSA at Makokola advised to
write a report on vaccine status
to District Hospital ◼ Health Facilities were advised to
update their microplans for
2022.
◼ Health facilities were advised to have a well-established means of
defaulter tracing
In Machinga, ONSE supported EPI review meetings for 5 health facilities (Mpiri, Nsanama, Namandanje,
Chikweo, and Namanja) and benefited a total number of 115 (76M, 39F) health workers. Some of the
issues discussed at the meeting included: vaccination data analysis using health facility-based tools,
mentorship on calculation of annual vaccination coverage, dropout rates, unimmunized children, and
general issues affecting vaccine delivery in the district.
SHOWING EPI REVIEW MEETING AT CHIKWEO. PICYURE COURSEY OF MAONONGA (HSAS)
In Dowa, ONSE supported a mentorship on immunization in practice for 55 (38M, 17F) staff from 15 EPI
reporting facilities in the district. The selection of the facilities was based on gaps identified in the said
health facilities regarding data capturing and reporting.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 49
TABLE 26. SUMMARY OF EPI MENTORSHIP
STRENGTHS ISSUES ACTIONS
◼ Availability of data monitoring tools, clinic
schedules demographic data
and meeting minutes
◼ Adherence to COVID-19 preventive measures
◼ Lack of EPI monitoring tools such as immunization monitoring charts, and
health passports.
◼ Vitamin A and albendazole was not
available in some health facilities ◼ Health facilities had no means of
reliable transportation such as a
motorcycle
◼ Poor data recording in some health centers
◼ EPI to lobby the national vaccine store to supply the district the following items:
reporting booklets, immunization
monitoring charts, child health profiles,
Vitamin A, and albendazole ◼ DHSS through DEHO to relocate some
motor cycles within the district to ease
transportation problems
◼ On-the-job training in data capturing was conducted
POLIO SUPPLEMENTARY IMMUNIZATION ACTIVITY (SIA)
During the reporting period, ONSE supported the national and district Training of Trainers (ToT) in
Lilongwe and Mponela for 29 (22M, 7F) health workers. The national level meeting was attended by high
level trainers from Government, NGOs, and international partners such as WHO (AFRO, Geneva,
Brazzaville), UNICEF, CDC, and GPEI.
In Dowa, Machinga, and Nkhotakota ONSE supported polio SIA supervision of 15 (12M, 3F) to assess
how the SIA implementation was going on in the districts. Some of the challenges noted included the
vaccinators were not passing to the child care takers messages about the need for the child to be
brought back for vaccination after a month and hand washing to prevent polio. Additionally, marking of
the households after vaccination was not consistently done. This would pose a great challenge with
follow up. Additionally, it was noted that integration of polio and COVID-19 vaccination was not
happening as earlier anticipated. The integration did not take place due to a number of factors of which
one of them is the COVID-19 vaccine hesitancy. Some of the actions taken were that the vaccinators
and their supervisors were advised to consistently follow the guidelines by ensuring that all procedures
required are followed such as marking of the households.
POLIO VACCINATION IN NKHOTAKOTA AND MCHINJI: PICTURE COURTESY OF BLESSINGS MAJAWA
FAMILY PLANNING
In PY6Q2, ONSE focused its efforts on consolidation of gains from the activity implementation of PY5
and PY6Q1 more especially those that would be sustained by the MoH as the project concludes. These
activities include IFHOCs, follow up on public sector strengthening mentors, strengthening quality of FP
data at both the community and facility level through data cleaning, and supervisions and mentorship.
Aside from this routine outreach clinic for youth, adults at health centers and underserved communities,
and harmonization of the outreach clinic reference guide for RHD were supported in the targeted

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 50
districts. Furthermore, ONSE supported orientation of community FP providers on the emergency
contraception (EC) strategy that allows HSAs and CBDAs to provide ECs at the community level in the
districts that had not yet finalized these activities. In order to be adherent to US abortion and FP
requirements, ONSE conducted FP compliance monitoring visits to facilities providing FP services.
TABLE 27. PERFORMANCE ON FAMILY PLANNING INDICATORS PY6Q2 PROGRESS TO TARGET
INDICATORS
PROJECT YEAR 6
TARGET Q1
ACHIEVEMENT Q2
ACHIEVEMENT STATUS
Couple Years Protection 400,000 184,126 157,717 % of health service delivery points offering
community-based FP services* 92% 52% 66%
# of USG-assisted community health workers
providing FP services during the year 1,421 1,399 1,099
Achieved
(≥100% of target) Almost Achieved
(86-99%) Not Achieved
(≤85%)
COUPLE YEARS PROTECTION (CYP)
At the end of PY6Q2, CYP for the 11 FP districts reached a cumulative 341,843 representing 85% of the
annual target. Between PY5Q2 and PY6Q2, CYP from LARCs increased from 45% to 50%. A drop was
seen in permanent methods from 8% to 6% within the same period in the 11 FP districts respectively
and there has been a downward trend in permanent methods since the onset of the COVID-19
pandemic. A similar trend was noted in both nine youth and four facility outreach teams done by ONSE-
BLM, a decline of 11% for client visits and 27% for CYP. LARCs, at 47%, continue to contribute largely
to the CYP in the FHP districts. The slight increase in the proportion of CYP from LARCs this quarter
could be attributed to a number of factors which include: a short implementation period due to the
holiday break, seasonal drop because of the growing season coupled with effects of COVID-19
pandemic where most hospitals suspended permanent FP services, and unavailability of staff to provide
LARC due to competing priorities in the management of the COVID-19 pandemic. However, in all the
ONSE districts, continued support was provided to the MoH for continuous services within the
established MNH-FP COVID-19 service provision guidelines.
FIGURE 8. NATIONAL HMIS CYP BY QUARTER

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 51
COMMUNITY-LEVEL FAMILY PLANNING
IFHOCS
ONSE provides essential support to MoH and DHOs to ensure the operation of IFHOCs across all 11
districts. ONSE supports specific outreach targeting HtRAs around the hospital catchment area and in
Christian Health Association Malawi (CHAM) facilities where FP methods, especially LARCs, are not
widely available. Outreach clinics are intended to bring a variety of services closer to the community
hence addressing the barriers to access services that ONSE champions in the districts. ONSE also
provides technical support to ensure that the teams provide comprehensive services and capture data
using proper data collection tools. Cancellation of some IFHOCs and Cyclones Ana and Gombe have
affected the uptake of FP services due to unavailability of MoH vehicles and competing flood response as
a result of the cyclones. During PY6Q2, a total of 434 IFHOCs were conducted in HtRAs in the 11
ONSE districts, where 10,644 clients (2,292 new and 8,352 revisit clients) accessed a full method mix,
generating 5,110 CYP. These outreach clinics targeted underserved communities and CHAM catholic
facilities where FP services are not provided. In some districts, the IFHOCs also integrate cervical
cancer screening services. COVID-19 preventive measures such as hand washing and social distancing
were observed in most sites.
TABLE 28. IFHOC FP SERVICES – JAN TO MARCH 2022
METHOD NEW VISIT REVISIT TOTAL
CLIENTS CYP
Male Condoms 950 1270 2220 19
Female Condoms 85 378 463 3.9
Oral Contraceptives 153 531 684 45.6
Depo-Provera Intramuscular (DMPA-IM) 823 5404 6227 1557
Implanon 145 349 494 1580.8
Jadelle 77 269 346 1315
Levoplant 46 142 188 470
Intrauterine Contraceptive Device 9 9 18 82.8
Bilateral Tubal Ligation (BTL) 4 0 4 37.2 TOTAL 2292 8352 10644 5110.3
TABLE 29. SUMMARY OF CERVICAL CANCER SCREENING CLIENTS REACHED
CERVICAL CANCER SCREENING NUMBER OF CLIENTS
Clients tested using VIA 165
Clients tested using human papillomavirus vaccine (HPV)/DNA 6
Clients tested HPV/DNA negative 1
Clients tested HPV/DNA positive 1
Clients with other Gynae problems 16
Clients referred for further management 5

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 52
FIGURE 9. CYP CONTRIBUTION BY AGE DURING IFHOCS IN 11 DISTRICTS
Twenty percent (2,112) of the total 10,644 IFHOC FP clients were youth aged 10-19 years, with the
vast majority (8,460) reporting their age to be 20 years and above. At the IFHOCs, 884 CYPs were
generated for youth aged 10-19 years of which 68% were from LARCs. Across all FP clients, 65% (3,035)
of the CYP contribution was from LARC methods (compared to 79% in PY5Q2). Across all FP clients,
34% of IFHOC clients CYP was from a short-term method (compared to 19% in PY5Q2). This could be
attributed to some IFHOCs being supported by MoH, shortages of DMPA-IM and SC, and male
condoms seen nationally.
In Karonga, ONSE supported EC orientation of 66 (39M, 27F) providers (nurses, midwives, and HSAs)
from three health clusters. The activity was aimed at equipping the participants with knowledge and
skills on how to safely provide emergency contraceptives at the community level. Key topics covered
included the definition of ECs, types and formulation of EC pills available in Malawi, explaining how ECs
work, characteristics of ECs, medical eligibility of ECs, myths and misconceptions associated with ECs,
instructions given to clients using ECs, and key counseling messages and ECs strategy in Malawi.
In Zomba, ONSE supported Depo-Provera (DMPA) supportive supervision and coaching of 12 (8M, 4F)
DMPA providers from three facilities (Domasi, Bimbi, and Zilindo). The activity was aimed at assessing
current clinical practice, stock status level of FP commodities, availability of registers and if filled
correctly, and check status of the monthly reports. Strengths noted included provision of FP services at
outreach clinics and good documentation and record keeping by 70% of supervised providers.
Challenges included a lack of FP IEC materials and 40% of providers not trained on DMPA-SC. Action
points identified included conducting on-site mentorship on proper FP register documentation, FP
Coordinator to lobby for refresher and initial DMPA-SC trainings, and for the FP Coordinator to liaise
with health promotion officers on IEC materials to be distributed to outreach clinics.
In Zomba, ONSE conducted CBDA supportive supervision and coaching of 58 (25M, 33F) providers
from three facilities (Likangala, Magomero, and Mayaka). The activity was aimed at assessing current
clinical practice, stock status level of FP, commodities, availability of registers and if filled correctly, and
also checking availability and status of monthly reports. Strengths observed that all CBDAs are reporting
using tally sheets, good record keeping and documentation by 75% of supervised CBDAs, and CBDAs
able to understand the new pill formulation of 21 per pack instead of the previous 28 per pack.
Challenges included outdated knowledge as the majority of the CBDAs were trained in 2012, mobility
problems due to lack of push bicycles, lack of enablers and identifiers (i.e., backpacks for carrying
documents, t-shirts, caps), and a lack of drug boxes for storage of contraceptives and other items.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 53
Action items include the FP Coordinator to lobby with other partners for CBDA refresher training,
drug boxes, and push bicycles, and to conduct supervision for remaining CBDAs.
DISTRICT YOUTH OUTREACH TEAMS
Access to underserved Malawians, particularly youth, has been addressed primarily through the rollout
of nine mobile youth outreach teams to cover the 11 FHP districts. ONSE teams worked with District
FP Coordinators and FP partners on site selection to ensure that there was no duplication of efforts or
competition for sites. Teams coordinate with youth clubs, HSAs, and MoH staff running under-five
clinics to mobilize clients. All clients are welcome, with the clinic seeing mainly older women in the
mornings, and then focusing on youth in the afternoons.
In the first two quarters of PY6, the mobile youth outreach teams saw 43,851 client visits which
generated 53,298 CYPs. A total of 64% of clients served by the youth teams in PY6 were under the age
of 25 years, of which 30% were below 20 years old. When compared with PY5, this data reveals an
increase of both 8% in the youth and adolescent reach by the Youth-Focused Outreach teams. Teams
provided 718,281 pieces of condoms, 14,447 doses of DMPA (6,683 of which were DMPA-IM and 7,764
were DMPA-SC [7,412 provider injected and 352 self-injected]), and 6,072 pill cycles over 2,268 client
visits. Short term methods (STMs) made up approximately 73% of the method mix provided under
Youth teams in PY6. The other methods provided were LARCs and permanent methods – 27% of the
method mix - of which 10,677 were implants, 316 were intra-uterine contraceptive devices IUCDs and
630 were BTLs.
FP CAMPAIGNS
In Zomba, ONSE supported FP mobile outreach clinics during market days. The activity was conducted
at Sunuzi, Mayaka, and Jali market places. The activity aimed at increasing access to FP services in the
hard to reach areas of the district that are predominantly catholic catchment areas. A total of 11 (5M;
6F) FP providers were involved during the campaign and reached 523 clients generating 447 CYPs. 80%
of clients accessed LARC while only 20% sought for short acting and reversible contraceptives. More
clients turned up for the services, especially at Mayaka market, there was teamwork among providers
and more clients previously on DMPA-IM were counseled on DMPA–SC self-injection. Availability of
public addressing systems in all days of the activity assisted to mobilize more clients. However, there
was an inadequate supply of lignocaine.
In Machinga, ONSE supported distribution of FP IEC material and job aids in Machinga HC. The activity
was aimed at ensuring provision of quality FP services and dissemination of FP messages. The activity
was conducted in collaboration with FP retrospective data collection exercise. Distribution was done to
Nayuchi, Ngokwe, Chikweo, Ntaja, Nyambi, and Mkwepere health facilities. The materials include kulera
posters and flip charts, PPFP protocols, management of hormonal side effects, implant insertion, and
removal protocol.
In Chitipa, ONSE supported integrated FP and COVID-19 vaccine campaigns in selected communities
under Kapoka, Ifumbo, Kapenda, Kameme, Nthalire, Wenya, Misuku, and Msumbe health facilities. The
activity was aimed at providing an opportunity for communities in hard to reach areas to access LARCs
and COVID-19 vaccines. A total of 89 clients accessed FP methods generating 111 CYPs while 82 (45M,
37F) people accessed J&J COVID-19 vaccine as per the details below.
TABLE 30. SUMMARY OF INTEGRATED FP CAMPAIGN FINDINGS
STRENGTHS CHALLENGES ACTION POINTS
◼ Clients accessed a variety of FP
services
◼ Misconception and myths on FP
methods and COVID-19 vaccine were cleared
◼ Sensitization was not adequate hence
low uptake in some areas
◼ Some hard-to-reach areas were not
involved in the campaign, as they needed DSAs
◼ Conduct sensitization a week prior
to service delivery
◼ Conduct regular campaigns
◼ Intensify IEC on myths and misconceptions of FP and COVID-
19 vaccines

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 54
FACILITY-LEVEL FAMILY PLANNING
FACILITY FOCUSED OUTREACH TEAMS
The two Facility-Focused Outreach Teams covered three districts (Karonga, Chitipa and Balaka) and
primarily support clients at health facilities with all methods, but the highest uptake is usually LARCs and
BTLs. In PY6Q1-2 the Facility-Focused teams saw 8,022 client visits generating 19,139 CYPs. Two
voluntary vasectomy procedures were conducted by the Karonga team, 556 voluntary BTLs were
provided, along with 112 IUCDs and 3,541 implants. In addition, 2,714 DMPA injections, of which 1,969
were DMPA-IM and 745 were DMPA-SC (455 provider injected and 290 self-injected) and 56,351
condoms were provided to 891 clients. Overall, 7% of the clients received voluntary permanent
methods, 46% accessed LARC methods and 47% opted for STMs.
PUBLIC SECTOR STRENGTHENING (PSS)
In the first two quarters of PY6, the PSS providers of the 29 facilities across 10 districts provided
voluntary FP services to 83,920 clients generating a total of 55,687 CYPs. PSS providers offered 351
voluntary TLs, 229 IUCDs and 10,186 implants. 69,316 doses of DMPA were provided, including 29,195
DMPA-IM and 40,121 DMPA-SC (23,396 provider injection and 16,725 self-injection) and 15,682 pill
cycles were provided to 5,585 client visits. During PY6, ONSE focused on the close-out of the project,
ensuring the interventions made during previous months would leave long term improvements for FP
service provision in Malawi. Therefore, ONSE concentrated on training and mentorship to the PSS
facilities, to ensure the public facilities are able to continue the work commenced under the project, as
detailed in the sections below.
Throughout PY6, ONSE-BLM has also prioritized a sustainable approach under the interventions
implemented. Thus, BLM teams have focused on additional training for providers from the 29 PSS sites
supported by ONSE. In December, BLM conducted a Training of Trainers (ToT) on LARC and PM
mentorship for 41 public personnel. This classroom training focused on transferring the necessary skills
for the district staff (District FP Coordinators, YFHS Coordinator, BTL Clinical Officers, Midwifery
Officers and DNOs) to conduct LARC and BTL mentorship and supportive supervision to the providers
trained under the project – this will allow the districts to continue supporting the sites once the project
phases out. Following the training, the Clinical Quality team conducted supervision visits and mentorship
to all the mentors trained to ensure any competency gap was addressed. Furthermore, in February,
ONSE-BLM M&E team conducted a data training for 145 staff covering the PSS facilities. The training
provided orientation on the FP registers, roles, responsibilities and guidance on how disaggregate data
prior to entering it into DHIS2. This was aimed at improving the data reported to the national data tool.
In PY6, shortages of commodities and supplies remained a challenge, varying across the months and
districts. PSS facilities experienced stockout of lignocaine in the last months of 2021 affecting the ability
of PSS sites to offer implants or tubal ligation methods. Over the first months of 2022, the facilities have
seen an improvement on the stock of this supply. With regards to the commodities, the erratic supply
has affected the ability of some teams to offer certain methods. To minimize these challenges, ONSE-
BLM supported the MoH in February on their annual quantification exercise of FP commodities to
ensure the availability of FP commodities at national and district level.
In February, BLM-ONSE piloted the integration of both Outreach and PSS channels during mentorship.
PSS providers joined Outreach teams for a full week to receive mentorship on FP methods during
outreach clinic days. Overall, 28 PSS providers were mentored by the Outreach teams during service
provision. Furthermore, ONSE-BLM PSS coordinator and clinical quality teams also conducted
competency assessment visits to ensure high standards during PSS service provision and assess the
District Mentors’ work. In November 2021, BLM Operations team also conducted a joint assessment
visit to 9 PSS facilities with MSH and RHD. The aim of the visit was not only meant to conduct an
assessment but also involve the RHD and advocate for their support to aid in addressing the challenges
observed over the course of the project, such as shortages of supplies/commodities and availability of
service providers.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 55
FACILITY-BASED SERVICE PROVISION
In its effort to improve the quality of FP data, ONSE supported the RHD to conduct a data cleaning
exercise in the districts of Lilongwe, Dowa, Nkhotakota, Karonga, Zomba, Machinga and Mulanje. This
was necessitated due to the drop in PY5 CYPs which revealed gaps or missing FP reports in the DHIS2
aside from low uptake of FP services due to increase in COVID-19 cases. To effectively carry out this
activity, a data quality assurance (DQA) tool was developed and an orientation done to HMIS officers
and FP coordinators for the targeted districts. Key issues and questions on the tool were clarified and
later the team set out to conduct the activities in the samples 42 facilities. A total of 96 (45M, 49F)
providers and data clerks were reached during the exercise.
Some of the issues revealed by this exercise included that most facilities had the data tools for FP but
there was underreporting in most districts and that some facilities especially in CHAM and private for
profit facilities were using outdated registers. The FP coordinators were tasked to intensify
comprehensive supervision and mentorship on FP register documentation in all facilities including
CHAM and private facilities. They were also asked to link up with CMED and RHD for registers which
are to be distributed to facilities that were using outdated registers. Missing reports affected DQA
exercise in Nkhotakota at Kasitu and at Lilongwe City council and Chinsapo Clinic. There were missing
reports in some facilities like in Nkhotakota at Kasitu, at Lilongwe City council, and Chinsapo Clinic in
Lilongwe district and this affected the DQA exercise. There were data discrepancies between DHIS2,
the registers, and the hard copies of the reports. The FP and HMIS officers follow up on filling of reports
and registers, eliminating chances of errors and making it a custom for all reports.
In Kasungu, ONSE supported redistribution of FP commodities from facilities that had over stocks to
understocked facilities. The activity was aimed at ensuring continued provision of FP services.
Observations included that all facilities visited have trained pharmacy personnel except Kakwale, well
updated stock cards and monthly physical counts are being done, good stocks of malaria commodities in
most facilities, and good storage areas in most facilities except for Kakwale. Challenges included
insufficient MNH and FP supplies and medications in most facilities, stock outs of oxytocin, misoprostol,
and magnesium sulphate at the Kasungu DHO, storage space challenges at Kakwale, and heavy rains
affecting accessibility to other facilities. Action points were for FP and pharmacy to source commodities
from central medical stores, DHO/donors to assist to improve storage space at Kakwale, and
MoH/DHO to provide Kakwale Health Center with trained pharmacy personnel.
TABLE 31. SUMMARY OF FP COMMODITIES REDISTRIBUTED
COMMODITY FROM TO
240 Implanon Mnyanja Health Center
Kasungu DHO 200 Jadelle Kapyanga Health Center 100 Levoplant Mdunga Health Center
200 DMPA-SC (each) Kasungu DHO
Mziza Health Center
Mpepa Health Center
Kakwale Health Center
Kapelula Health Center
ONSE supported Lilongwe DHO to conduct BTL mentorship in the health facilities of Mitundu, Bwaila,
and Kabudula. The main aim of the mentorship was to reach women in hard to reach areas with BTL
services for the three facilities. The specific objectives for the BTL mentorship were to support skill
development of BTL outreach teams for Mitundu, Bwaila, and Kabudula and reach out to women of
reproductive age who seek BTLs in hard to reach areas. A team of nurses, clinicians, and hospital
attendants who were trained and groomed to mentor other providers does the BTL mentorships. The
team conducted mobilization and sensitization of clients for the available BTL services. All clients who
opted for BTLs were booked on the designated days, and the mentored teams conducted BTLs on these

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 56
scheduled days. A total of 16 health care workers participated in the BTL mentorship (10M, 6F). During
the mentorship, a total of 22 BTLs were done (10 BTLs were done at Mitundu, 7 at Bwaila, and 5 at
Kabudula) generating 205 CYPs.
In Nkhotakota, ONSE in Nkhotakota supported FP supportive supervision at St. Anne’s Hospital and
Chididi Health Center. The visit was aimed at supporting the facility in the provision of quality FP
services. The exercise was conducted by 2 (0M, 2F) supervisors who engaged 4 (1M, 3F) health facility
staff. The supervisors used the MoH FP checklist to assess the quality of health education given to
clients, availability and stock levels of FP commodities, and to identify any other factors that may hinder
provision of FP services. Below are key highlights from the supervision.
TABLE 32. SUMMARY OF FP SUPERVISION FINDINGS
STRENGTHS CHALLENGES ACTION POINTS
◼ FP services provided on a daily basis at both health facilities
◼ Availability of a wide range of
FP methods at both health
facilities ◼ Comprehensive group and
individual counseling is done
according to standards
◼ A conducive environment for both client and provider (i.e.,
both audio and visual privacy)
◼ Both health facilities
consistently submit monthly reports and update in DHIS2
timely
◼ Use of outdated register at St. Anne’s Hospital
◼ Lack of page summaries in the FP
register at St Anne’s
◼ Low uptake of LARC methods at both health facilities
◼ FP coordinator to provide St Anne’s Hospital with new version of the FP
register
◼ Facility in-charge and hospital attendant
to mop the floors and remove cobwebs and follow a cleaning schedule
of at least twice a day at Chididi
◼ Conduct facility based mentorship
session on provision of LARC at both facilities
◼ Liaised with health workers including
HSAs to continue giving information to
communities on the availability of a wide range of contraceptives at the
facility
FP COMPLIANCE MONITORING
During the quarter, ONSE supported FP compliance monitoring in Lilongwe, Zomba, Machinga, Balaka,
Dowa, Kasungu, and Salima districts. The activity aimed at assessing facility adherence to US abortion
and FP requirements during provision of FP services, identifying any compliance violation issues, and
instituting mitigation measures to identified compliance issues. A total of 104 facilities were reached, and
147 providers and 219 clients were interviewed. All facilities were compliant to FP compliance
requirements and those with vulnerabilities, had the issues addressed and planned to be sorted out in
due course as indicated in the recommendations. Below is a summary of the exercise.
TABLE 33. SUMMARY OF FP COMPLIANCE MONITORING FINDINGS
DISTRICT NUMBER OF
FACILITIES PROVIDERS MONITORED BY
GENDER CLIENTS
INTERVIEWED
Dowa 21 39 (11M, 28F) 62
Lilongwe 36 33 (12M, 21F) 67
Kasungu 16 17 (3M, 14F) 25
Salima 12 26 (9M, 17F) 21
Zomba 7 6 (3M, 3F) 15
Machinga 10 23 29
Balaka 2 3 (2M, 1F) 0 Total 104 147 219
HARMONIZATION OF OUTREACH CLINIC GUIDELINES
During the reporting period, ONSE supported the RHD to kick start the harmonization of the outreach
clinic guidelines and later validation of the guidelines. The activity aimed at identifying existing outreach
guidelines and supervision checklists, review the existing outreach guidelines and supervision checklists

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 57
and develop a zero draft of comprehensive outreach guidelines, and supervision checklists. All MoH
departments whose programs are included in the checklist contribute to the process. A total of 32
(17M, 15F) people participated in the activity including ONSE technical team, RHD, Planning department,
HIV unit, QMD, EPI, Environmental health department, PSI, BLM and FPAM. The team reviewed existing
guidelines and checklists from PSI, BLM, and searched for other guidelines from neighboring countries.
Participants worked in groups that reviewed and where necessary adapted the checklists and guidelines.
Each day, groups made presentations on progress made as per the given task. By the end of the 2
sessions the first draft was developed. Next steps include editing of the guide including the supervision
checklists, RHD to lobby with other organizations to fund the remaining processes. It is expected that
by the end of June, a final guideline and supervision checklist will be finalized.
MALARIA
ONSE supports PMI in its global effort to decrease malaria morbidity and malaria-related deaths. In PY5,
ONSE’s efforts on malaria support were significantly reduced to focus only on issues related to malaria
in pregnancy (MIP) and collaboration with other partners. ONSE’s approach in PY6 continues to include
targeted supportive supervision, mentoring, cluster based data reviews, and on-the-job coaching to scale
up quality prevention, treatment, and diagnosis services.
TABLE 34. PERFORMANCE ON MALARIA INDICATORS, PY6Q2 PROGRESS TO TARGET
INDICATORS TARGET
PROJECT YEAR 6
Q1 ACHIEVEMENT Q1 ACHIEVEMENT STATUS
% of pregnant women who received three
or more doses of IPTp during ANC 52% 56% 54%
Achieved
(≥100% of target) Almost Achieved
(86-99%) Not Achieved
(≤85%)
ONSE supported MIP supervision of 78 (30M, 48F) health workers from 21 health facilities from 5
Districts (Machinga, Balaka, Dowa, Nkhotakota, and Zomba). The main aim was to check the
implementation of MIP and provide mentorship on the identified gaps. Key observations include
Sulfadoxine-pyrimethamine (SP) being given under DOT and verified, register documentation for SP1-3
is adequate, long-lasting insecticidal nets are in stock, IPTp is provided at ANC, and essential equipment
and supplies are available at all supervised health facilities (BP machines, stethoscopes, tape measures,
and fetal scopes). Gaps and action points are detailed in the table below.
TABLE 35. SUMMARY OF MIP SUPERVISION GAPS AND ACTION POINTS
GAPS ACTIONS POINTS
Some do not bring personal cups Encourage women to bring a personal bottle for water for DOT Data reviews and use not being done Facilities to conduct monthly data review session to facilitate use of data
for decision making (e.g., ordering for supplies) Lack of IEC materials on MIP in some facilities Coordinators to check with MNCP for availability of MIP IEC materials Lack of health education roster ANC in-charges advised to develop roster for health education at ANC Health workers not oriented on the revised MIP
guidelines Malaria Coordinator to liaise with partners for the orientation of health
workers to new MIP guidelines ANC register not filled according to matrix at 75%
of the supervised health facilities Mentorship on how to fill ANC register according to the matrix was
done
In the reporting quarter, ONSE supported training of MIP trainers organized by the NMCP. The aim was
to create a pool of trainers at district level who will cascade the same to other health facilities in their
districts. Participants were drawn from 10 of the 11 ONSE supported Family Health districts. Kasungu
was not included in the list because the district was supported by Impact Malaria on Malaria issues. A
total of 9 officers from each district were oriented on the revised guidelines. The orientation was
facilitated by 5 (2M, 3F) trainers from NMCP, RHD, and QMD. Two officers from Impact Malaria and

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 58
STA for ONSE co-facilitated the activity. The training covered the following main areas: malaria
transmission & prevention, treatment of uncomplicated and severe malaria, health education, monitoring
and evaluation (M&E), filling in MIP registers, calculation of SP uptake indicators and ITINs, and a
discussion on major challenges. ONSE also supported the orientation of 166 (67M, 99F) providers from
61 health facilities from Chitipa, Dowa and Mulanje districts. These orientations were conducted by the
district based trainers.
MALARIA IN PREGNANCY (MIP) SUPERVISION
In the reporting period, ONSE also supported MIP supervision in Nkhotakota and Salima districts. A
total of 15 health facilities; one in Nkhotakota and 14 in Salima were supervised. 49 (30M, 19F)
providers were supervised. The supervision aimed at building the capacity of health center staff in
providing comprehensive care to ANC women in preventing and managing malaria in accordance with
the national guidelines.
ONSE participated in one National Malaria Control Partnership Meeting which was attended by several
partners. The following are some of the presentations made during the meeting: PMI presented the PMI
STRATEGIC FRAMEWORK 2021-2026 with the following objectives: reduce deaths by 33% from 2015
level, and reduce illness by 40% from 2015 level. World Vision presented their work on Integrated
Vector Management Indoor Residual Spray (IRS). USAID Global Health Supply Chain talked about their
work on commodity forecasting and supply planning (FASP), procurement, receiving and warehousing,
distribution, and Logistics Management Information System (LMIS) support. Impact Malaria provided
support to the government through the MoH National Malaria Program (NMP), National Parasitology
Reference Laboratory (NPRL), and three districts of Kasungu, Mchinji, and Nkhatabay. Save the Children
provided school-based health services and enables learners to access testing and treatment for malaria
and other minor ailments during learning hours at school. ONSE shared a presentation on malaria
support since 2017 to date, highlighting the fact that now ONSE’s support is confined to MIP which was
concluded with a call for continued support from other partners and DHMTs as the ONSE project is
phasing out activities at the end of March.
NUTRITION
ONSE’s progress in nutrition is tracked against four key indicators at the health facility level: number of
health facilities that maintain international SPHERE standards for the treatment of severe acute
malnutrition (SAM), the number of children under five (0-59 months) reached by USG-supported
nutrition programs, the number of children under two (0-23 months) reached by USG-supported
nutrition programs, and the number of pregnant women reached with nutrition interventions through
USG-supported program. In the quarter, the number of facilities that maintain international SPHERE
standards for the treatment of SAM was 276; and a total of 2,260 under two (0-23 months); 93,643
children under five (0-59 months) and 79,598 pregnant women were reached with nutrition programs
respectively.
Children are reached with nutrition interventions through a number of ways, but the information is not
always accurately captured. For example, children reached through the baby-friendly hospital initiative
(BFHI) have just started being captured in DHIS2 but most districts are not yet familiar and therefore
not yet capturing the data. Women are assisted in ANC where iron supplementation and nutrition
counseling take place but documentation is not completed. ONSE continues to strengthen mentorship
and supportive supervision at the health facility level, where immediate supervisors regularly support
service providers in order to address these challenges.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 59
TABLE 36. PERFORMANCE ON NUTRITION INDICATORS - PY6Q2 PROGRESS TO TARGET
INDICATORS TARGET
PROJECT YEAR 6
Q1 ACHIEVEMENT
Q2 ACHIEVEMENT STATUS
# of children under five (0-59 months) reached by
USG-supported nutrition programs 175,000 91,558 93,643
# of children under two (0-23 months) reached
with community-level nutrition interventions
through USG-supported programs
56,000 3,071 2,260
# pregnant women reached with nutrition interventions through USG-supported programs
110,000 79,381 79,598
# of health facilities that maintain international
standards for treatment of SAM* 230 259 276
Achieved (≥100% of target)
Almost Achieved (86-99%)
Not Achieved (≤85%)
NUTRITION SERVICE PROVISION
In PY6Q2, ONSE reached 93,643 children under-five with nutrition services respectively, marking a
106% achievement of the PY6 target. At the national level, ONSE supported MoH to review IEC
materials on nutrition including two review workshops and pretesting of the draft package of the
materials. The draft packages included 5 radio jingles/slots, 6 posters, 1 leaflet, 1 flip chart. Pretesting of
the materials was done in all the 3 regions of the country and valuable feedback was received. The
audience for the pretesting included the targeted users such as caregivers of under-fives and local
leaders. MoH will still need support to refine the materials to accommodate feedback from pre testing
sessions and printing & distribution of the materials.
COMMUNITY MANAGEMENT OF ACUTE MALNUTRITION (CMAM)
ONSE supported CMAM supervision in Chitipa, Dowa, Kasungu, Machinga, and Nkhotakota, where 19
(7M, 12F) supervisors reached 83 (44M, 39F) service providers in 27 health facilities. The aim of the
activity was to assess service providers’ adherence to the recommended CMAM guidelines. Key issues
observed are summarized below:
TABLE 37. CMAM SUPPORTIVE SUPERVISION
STRENGTHS CHALLENGES ACTIONS TAKEN
Chitipa ◼ Very sick children are prioritized
through triage before clinic starts except
at Chisansu Health Center
◼ At Msumbe, SFP clients linked to other
structures such as care groups for continuity of management
◼ Triage not being done at Chisansu Health Centre
◼ Reports not filed at Chisansu,
Kapenda, Msumbe(CHAM), Mahowe
and Ifumbo
◼ Immediate mentorship was done on triaging at Chisansu HC
◼ Facilities to create/have special
arch files for CMAM programs
Dowa ◼ Reports submitted on time
◼ Admissions done correctly
◼ Shortages of ready-to-use therapeutic
food (RUTF) in most facilities due to delays from Central Medical Stores
◼ Shortages of reporting booklets
◼ Liaise with central medical stores
to provide RUTF timely ◼ Provide reporting booklets to
the facilities
Kasungu ◼ During previous supervision Wimbe
health facility was keeping all the
monitoring cards of those in program
and discharges in the same folder but
now they are keeping them separately
◼ Routine medications like amoxicillin not administered to clients as it is
mostly out of stock
◼ The Pharmacy assistant to order routine drugs each month end
Machinga ◼ Health talk roster available and pasted
on walls at Chikweo and Namanja health
centers
◼ Unavailability of CMAM guidelines,
stock cards and ration cards at
Chikweo, Namanja and Nsanama
◼ District Nutrition coordinator to
mobilize and distribute the out of
stock stationery
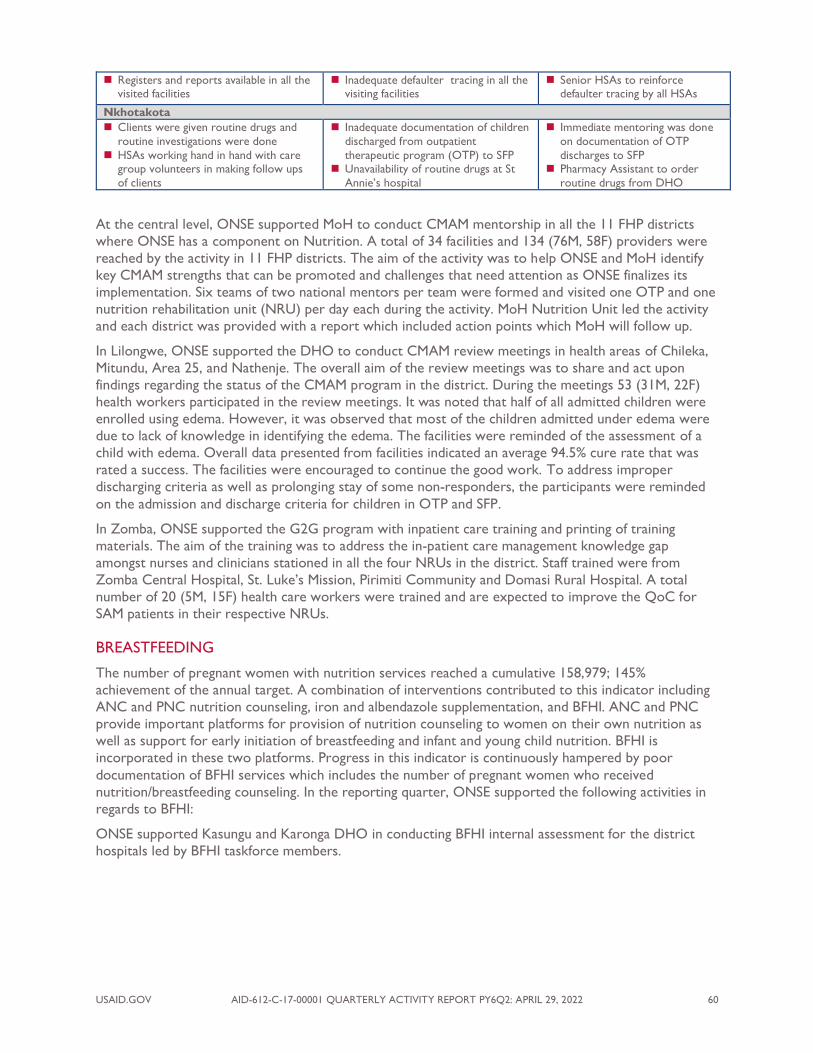
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 60
◼ Registers and reports available in all the visited facilities
◼ Inadequate defaulter tracing in all the visiting facilities
◼ Senior HSAs to reinforce defaulter tracing by all HSAs
Nkhotakota ◼ Clients were given routine drugs and
routine investigations were done
◼ HSAs working hand in hand with care group volunteers in making follow ups
of clients
◼ Inadequate documentation of children
discharged from outpatient
therapeutic program (OTP) to SFP ◼ Unavailability of routine drugs at St
Annie’s hospital
◼ Immediate mentoring was done
on documentation of OTP
discharges to SFP ◼ Pharmacy Assistant to order
routine drugs from DHO
At the central level, ONSE supported MoH to conduct CMAM mentorship in all the 11 FHP districts
where ONSE has a component on Nutrition. A total of 34 facilities and 134 (76M, 58F) providers were
reached by the activity in 11 FHP districts. The aim of the activity was to help ONSE and MoH identify
key CMAM strengths that can be promoted and challenges that need attention as ONSE finalizes its
implementation. Six teams of two national mentors per team were formed and visited one OTP and one
nutrition rehabilitation unit (NRU) per day each during the activity. MoH Nutrition Unit led the activity
and each district was provided with a report which included action points which MoH will follow up.
In Lilongwe, ONSE supported the DHO to conduct CMAM review meetings in health areas of Chileka,
Mitundu, Area 25, and Nathenje. The overall aim of the review meetings was to share and act upon
findings regarding the status of the CMAM program in the district. During the meetings 53 (31M, 22F)
health workers participated in the review meetings. It was noted that half of all admitted children were
enrolled using edema. However, it was observed that most of the children admitted under edema were
due to lack of knowledge in identifying the edema. The facilities were reminded of the assessment of a
child with edema. Overall data presented from facilities indicated an average 94.5% cure rate that was
rated a success. The facilities were encouraged to continue the good work. To address improper
discharging criteria as well as prolonging stay of some non-responders, the participants were reminded
on the admission and discharge criteria for children in OTP and SFP.
In Zomba, ONSE supported the G2G program with inpatient care training and printing of training
materials. The aim of the training was to address the in-patient care management knowledge gap
amongst nurses and clinicians stationed in all the four NRUs in the district. Staff trained were from
Zomba Central Hospital, St. Luke’s Mission, Pirimiti Community and Domasi Rural Hospital. A total
number of 20 (5M, 15F) health care workers were trained and are expected to improve the QoC for
SAM patients in their respective NRUs.
BREASTFEEDING
The number of pregnant women with nutrition services reached a cumulative 158,979; 145%
achievement of the annual target. A combination of interventions contributed to this indicator including
ANC and PNC nutrition counseling, iron and albendazole supplementation, and BFHI. ANC and PNC
provide important platforms for provision of nutrition counseling to women on their own nutrition as
well as support for early initiation of breastfeeding and infant and young child nutrition. BFHI is
incorporated in these two platforms. Progress in this indicator is continuously hampered by poor
documentation of BFHI services which includes the number of pregnant women who received
nutrition/breastfeeding counseling. In the reporting quarter, ONSE supported the following activities in
regards to BFHI:
ONSE supported Kasungu and Karonga DHO in conducting BFHI internal assessment for the district
hospitals led by BFHI taskforce members.
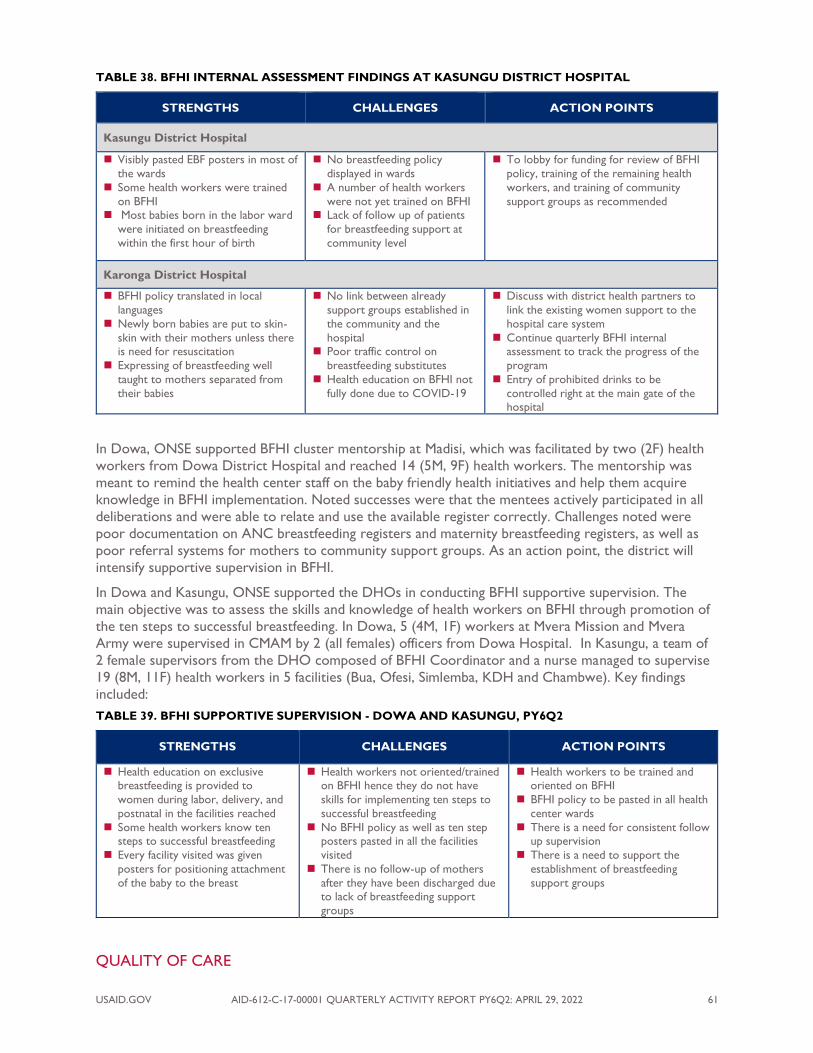
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 61
TABLE 38. BFHI INTERNAL ASSESSMENT FINDINGS AT KASUNGU DISTRICT HOSPITAL
STRENGTHS CHALLENGES ACTION POINTS
Kasungu District Hospital
◼ Visibly pasted EBF posters in most of
the wards
◼ Some health workers were trained
on BFHI ◼ Most babies born in the labor ward
were initiated on breastfeeding
within the first hour of birth
◼ No breastfeeding policy
displayed in wards
◼ A number of health workers
were not yet trained on BFHI ◼ Lack of follow up of patients
for breastfeeding support at
community level
◼ To lobby for funding for review of BFHI
policy, training of the remaining health
workers, and training of community
support groups as recommended
Karonga District Hospital
◼ BFHI policy translated in local
languages
◼ Newly born babies are put to skin-
skin with their mothers unless there is need for resuscitation
◼ Expressing of breastfeeding well
taught to mothers separated from
their babies
◼ No link between already
support groups established in
the community and the
hospital ◼ Poor traffic control on
breastfeeding substitutes
◼ Health education on BFHI not
fully done due to COVID-19
◼ Discuss with district health partners to
link the existing women support to the
hospital care system
◼ Continue quarterly BFHI internal assessment to track the progress of the
program
◼ Entry of prohibited drinks to be
controlled right at the main gate of the hospital
In Dowa, ONSE supported BFHI cluster mentorship at Madisi, which was facilitated by two (2F) health
workers from Dowa District Hospital and reached 14 (5M, 9F) health workers. The mentorship was
meant to remind the health center staff on the baby friendly health initiatives and help them acquire
knowledge in BFHI implementation. Noted successes were that the mentees actively participated in all
deliberations and were able to relate and use the available register correctly. Challenges noted were
poor documentation on ANC breastfeeding registers and maternity breastfeeding registers, as well as
poor referral systems for mothers to community support groups. As an action point, the district will
intensify supportive supervision in BFHI.
In Dowa and Kasungu, ONSE supported the DHOs in conducting BFHI supportive supervision. The
main objective was to assess the skills and knowledge of health workers on BFHI through promotion of
the ten steps to successful breastfeeding. In Dowa, 5 (4M, 1F) workers at Mvera Mission and Mvera
Army were supervised in CMAM by 2 (all females) officers from Dowa Hospital. In Kasungu, a team of
2 female supervisors from the DHO composed of BFHI Coordinator and a nurse managed to supervise
19 (8M, 11F) health workers in 5 facilities (Bua, Ofesi, Simlemba, KDH and Chambwe). Key findings
included:
TABLE 39. BFHI SUPPORTIVE SUPERVISION - DOWA AND KASUNGU, PY6Q2
STRENGTHS CHALLENGES ACTION POINTS
◼ Health education on exclusive breastfeeding is provided to
women during labor, delivery, and
postnatal in the facilities reached
◼ Some health workers know ten steps to successful breastfeeding
◼ Every facility visited was given
posters for positioning attachment
of the baby to the breast
◼ Health workers not oriented/trained on BFHI hence they do not have
skills for implementing ten steps to
successful breastfeeding
◼ No BFHI policy as well as ten step posters pasted in all the facilities
visited
◼ There is no follow-up of mothers
after they have been discharged due to lack of breastfeeding support
groups
◼ Health workers to be trained and oriented on BFHI
◼ BFHI policy to be pasted in all health
center wards
◼ There is a need for consistent follow up supervision
◼ There is a need to support the
establishment of breastfeeding
support groups
QUALITY OF CARE

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 62
Of the facilities targeted by ONSE in PY6Q2, 276 continue to maintain SPHERE standards of care, a
core set of humanitarian standards in key life-saving sectors: water supply, sanitation, and hygiene
promotion; food security and nutrition; shelter, settlement, and non-food items; and health action. This
can, in part, be attributed to Malawi’s adoption of the SPHERE standards for NRUs and facilities
providing CMAM services, and the requirements are nearly routine.
In the reporting period, ONSE supported Chitipa, Kasungu, Machinga, Mulanje, Salima and Zomba
districts to conduct NRU death audits. The audits were conducted by a total of 100 (41M, 59F) NRU QI
team members and 12 deaths were audited. The audit findings are summarized below:
TABLE 40. SUMMARY FINDINGS OF NRU DEATH AUDITS
KEY CONTRIBUTING FACTORS RECOMMENDATIONS
Salima District Hospital
◼ Inadequate clinical assessment and management ◼ Inadequate monitoring of vital signs
◼ Regular checks by Ward in charge to ensure all protocols are adhered to
Kasungu District Hospital
◼ Poor clinical participation
◼ Poor documentation on treatment charts
◼ Administration of blood and intravenous fluids without following CMAM guidelines
◼ Enforce clinical participation for all NRU patients
◼ Proper documentation and adherence to protocols in
managing NRU patients
Chitipa District Hospital
◼ Poor management of dehydration in NRU patients
◼ Lab results not attached to case files
◼ Unavailability of Resomal for management of diarrhea in malnourished children and weighing scales
◼ To conduct ward meetings/CPDs on the management of
dehydration in SAM
◼ Follow up results from lab and attach all results to case files
◼ Nutritionist to order ReSoMal and weighing scales
Domasi Hospital, Machinga District Hospital, Mulanje District Hospital, Mulanje Mission Hospital
◼ Incorrect diagnosis and treatment of dehydration
(ReSoMal was out of stock) in Mulanje
◼ Late transitioning of feeds to RUTF ◼ Catch up feeds were not given according to protocol
◼ Guardians of one patient refused NGT and oxygen
therapy in Machinga
◼ NRU ward in-charges to advise the ward team to work on
the recorded vital signs
◼ Clinical in-charge to facilitate onsite orientation on initial management chart of NRU
◼ Machinga NRU Ward in-charge to facilitate proper
counseling of guardians on the benefit of other
management (i.e., NGT and oxygen)
ONSE supported NRU QI meetings at Mulanje Mission and Mulanje DH drawing participation from 20
(7M, 13F) facility staff. The aim of the meeting was to assess how the facilities were performing in the
management of SAM by reviewing their records. Areas reviewed were anthropometric measurements
on admission for NRU files, adherence to monitoring of SAM patients, 10 steps Management of SAM
patients and assessment of SAM entry points (OPD and NRU). Strengths observed were that
management of SAM cases was done according to 10 steps and anthropometric measurements were
being done correctly and staff are able to admit children according to correct admission criteria.
Challenges included that weight for height calculations were not done daily for all patients, target weight
was not recorded on all patients’ charts, and iron supplementation was being missed for some patients.
As a way forward, regular supportive supervision will be conducted by the DHO to ensure adherence
to recommended guidelines.
WATER, SANITATION, AND HYGIENE (WASH)
In PY6Q2, ONSE continued to provide WASH support to its supported districts. The emphasis shifted
towards building resilience to ensure the activities implemented by ONSE are sustainable after project
closeout. Of the two indicators tracked quarterly for WASH, zero indicators are on track to meet the
annual target and one almost already achieved the LOA target. Based on the PY3 achievements for

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 63
increasing access to drinking water services in the community, achieving life of award targets, the focus
is now on improving facility-level WASH.
TABLE 41. PERFORMANCE ON WASH INDICATORS, PY6Q2 PROGRESS TO TARGET
INDICATORS TARGET
PROJECT YEAR 6
Q1 ACHIEVEMENT
Q1 ACHIEVEMENT
STATUS
# institutional settings gaining access to a basic
drinking water service as a result of USG assistance 18 0 17
# of health facilities that have implemented their facility level WASH action plan
22 0 0
Achieved
(≥100% of target) Almost Achieved
(86-99%) Not Achieved
(≤85%)
WATER
ONSE continues to prioritize WASH in health facilities through the facilitation of the Clean Clinic
Approach to ensure health facilities are always kept clean and have well-functioning toilets with drop
hole covers, handwashing facilities and soap, and toilets are segregated according to gender. ONSE
focuses on assessment of WASH conditions in health care facilities to identify issues or gaps, and
developing action plans highlighting what should be done, and facilitating the implementation of the
action plan to address the issues. ONSE also works to support the district environmental health
sections to monitor communities already declared open defecation-free (ODF), but certification was not
done due to COVID-19 constraints. In order to consolidate the gains made in the past fiscal year, ONSE
continues to support follow up visits to areas that were already declared ODF.
FACILITY WATER SUPPLY
In the reporting quarter, ONSE supported the water supply improvement systems in 18 health facilities
in 8 districts of Karonga (4), Nkhata Bay (1), Lilongwe (2), Kasungu (2), Dowa (1), Nkhota Kota (2),
Balaka (2), and Mulanje (4). The intervention aimed at increasing access to priority health services
through improving the availability of health services, reducing structural barriers to access health
services and increasing the quality of priority health services by allowing health workers to wash their
hands with soap before and after attending to each patient. The intervention involved drilling of new
boreholes/rehabilitation of existing boreholes, construction of water tank tower with cement blocks,
and installation of the submersible pump and water storage tank.
COMMUNITY WATER SUPPLY
ONSE supported the water quality testing of all the 316 boreholes in the WASH supported districts of
Chitipa, Karonga, Kasungu, Dowa, Nkhotakota, Salima, Lilongwe, Balaka, Machinga Zomba and Mulanje.
The aim of the exercise was to ensure the compliance to the provision of safe drinking water to
communities at all times. This is also in line with the Sustainable Development Goal number 6.1. The
water quality is monitored against the Malawi Standards (MS 733:2005) which are also in reference to
the WHO Standards and the US Environmental Protection Agency (USEPA) Standards. The Water
Quality Testing is focusing on the eight (8) parameters such as: health-related parameters (arsenic, fecal
coliform, fluoride, nitrate [as NO3]) and operational-related parameters (electrical conductivity, total
dissolved solids [TDS], pH, and turbidity). The Malawi Central Water Laboratory, ONSE pre-qualified
laboratory, has been subcontracted to conduct the water quality testing.
ONSE supported 10 water point committees (WPCs) supervision in Machinga and Karonga Districts. In
the Machinga District, 5 WPCs (Simba, Mejala, Tiole, Mwitiya, and Mkumba) were visited from March 11
to 15, 2022, while in Karonga, another 5 WPCs (Ipinda [Ngana], Shalison [Kaporo], Muzang’unya [CRH],
MliraSambo, and Chilawira [Lwezga]) were supervised from February 23 to 27, 2022. The aim of the
activity was to appreciate how WPCs were managing their boreholes. Some of the findings were: good
sanitation surrounding the facilities; written work plan on maintenance; funds availability in their

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 64
accounts for borehole maintenance; committee members are trained; good collaboration with other
community structures; and the WPCs were able to dismantle, clean, reassemble the borehole and
replace worn out parts on their own (including women).
SANITATION
SANITATION MONITORING
In Machinga, ONSE supported a sanitation marketing review meeting at Nyambi, Mangamba and
Ntholowa drawing participation from 54 (39M, 15F) people. During the exercise, it was observed that
four new latrines were constructed and sand screened. It was also encouraging to find out that the
trained masons were very active and that chiefs were participating in the activity and motivating their
communities. This is good for the project sustainability.
DISASTER RESPONSE
In the reporting period, ONSE continued its leadership stewardship in the time of disasters. In the
reporting period, ONSE supported Zomba District Council with 20 liters of fuel for transportation of
10 temporary pit latrines to be mounted in different camps to improve sanitation during Cyclone Ann.
CHOLERA PREPAREDNESS
In Machinga, ONSE supported a cholera preparedness and briefing meeting to update the DRRT on the
new case of Cholera which was recorded in the district and strategies to prevent further spread of the
infection. A total of 12 (8M, 4F) participated in the activity. The following activities were performed to
contain the spread of the epidemic: inspection of food premises, pot to pot chlorination in all villages
prone to cholera, and sensitization of the local leaders.
PERFORMANCE OF HEALTH SYSTEMS STRENGTHENED
OVERVIEW
ONSE’s HSS interventions are interrelated, interdependent, and foundational to improving service
provision and serve to reinforce access to and quality of health services and accountability to the
community. ONSE’s support to HSS focuses on three key results: (1) improved strategic management
and supervision of human resources for health; (2) improved district-level governance, management, and
policy implementation; and (3) institutionalized use of a health information system to inform
management of district-level health services. Although supply chain is situated in the clinical services area
of the results framework, ONSE will discuss supply chain interventions in this section, as the
improvement of availability of supplies and commodities is an important health systems component and
ONSE continued this support in PY6Q2. By the end of PY6Q2, out of the four HSS indicators that
ONSE tracks quarterly, one was achieved and three were not on track for achievement.
TABLE 42. PERFORMANCE ON HEALTH SYSTEMS STRENGTHENING INDICATORS, PY6Q2 PROGRESS TO TARGET
INDICATORS TARGET
PROJECT YEAR 6
Q1 ACHIEVEMENT
Q2 ACHIEVEMENT
STATUS
# of DIPs reviews conducted to monitor DIP
activities or budgets with stakeholder 11 10 6
% of health facilities with functional HCMCs 96% 41% 46% % of health facilities supervised based on
performance standards in the ISS Tool that complete
follow-up actions
89% 76% 73%
# of health facilities submitting DHIS2 data in line with national standards
308 253 238
Achieved
(≥100% of target) Almost Achieved
(86-99%) Not Achieved
(≤85%)

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 65
GOVERNANCE AND PLANNING
DISTRICT PLANNING
ONSE participated in the January and March 2022 monthly DIP Task Team meetings; there was no
monthly meeting in February 2022 because of other competing priorities for the MoH Department of
Planning and Policy Development who chairs the meeting. The key updates and discussion areas during
these meetings were: update on District Planning, support to District TWGs & Stakeholder Engagement
Checklist, aligning council budgets prepared outside of DIP tool to the districts, linkage of DIP Action
Trackers to the JAR (Power BI dashboard), platform for district planning documents, planning module in
the HFMT curriculum, and brief on HSSP III development.
ONSE also supported DIP Review meetings in Chitipa, Karonga, Salima, Lilongwe, Machinga and Mulanje.
In Chitipa, ONSE supported the DIP/HMIS semi-annual review meeting for Chitipa District Health
Sector at Fwasa Lodge drawing participation from 72 (55M, 17F) people (DHMT members, health
facilities representatives, program coordinators, heads of units/sections, and ONSE staff). The aim of the
DIP DIP/HMIS semi-annual meeting was to review implementation of activities and the corresponding
health indicators for respective programs for July to December 2021 through presentations by various
program coordinators and selected health facilities. In the presentations some indicator that were
presented as improved are as follows:
◼ 86.9% of postnatal women were receiving care with 48 hours which is almost the same as the
national target of 87%
◼ The contraceptive prevalence rate is at 62% which is higher than the national target of 60%
The meeting also reviewed implementation of the previous meeting action plan and developed a new
action plan. In Karonga, ONSE supported a DIP/HMIS semi-annual review meeting at Mikoma Lodge on
March 17 and 18, 2022. The activity was attended by 70 people, 54 males and 16 females. In Salima,
ONSE supported a DIP review meeting at Eclipse Lodge on March 30 and 31, 2022. The activity was
attended by 47 (29M, 18F) including health center in-charges, program coordinators, DHMT members.
In Machinga DIP review meeting which was conducted on March 24 and 25, 2022. The meeting reviewed
data and activity implementation for the June to December 2021 period. There were 49 (43M, 22F)
participants, made up of DHMT, Program Coordinators and Facility Charges. The health facility in-
charges also made presentations, and the key highlights from the presentations were: (a) there was
improvement in all facilities on monthly reports submission, and (b) there was an increased number of
new ANC visits in the first trimester at Mkwepere Health Centre. In Lilongwe DIP review meeting was
supported from February 23 to 25, 2022, and the DIP review led to development of 2022/2023 District
Implementation Plans. The review was attended by program coordinators, DHMT and few partners in
the district. The objectives were to review the planned activities for each and every department of the
sector in order to understand how far planned activities are being implemented, and discuss critical
issues affecting the sector. In Mulanje, the DIP Review meeting was held from March 24 to 26, 2022. The
objective was to review activities from July 2021 to February 2022. During the meeting, presentations
were made at cluster level and 6 health clusters presented. ONSE and other partners had one
consolidated report. A total of 60 (40M, 20F) participants including TA Mabuka and 6 Councilors
attended the meeting.
In Mangochi, ONSE provided technical support to the Mangochi District Health Sector on DIP
development, drawing participation from 55 (34M, 21F) program coordinators, departmental heads and
health stakeholders participated in the DIP development. Activities to be implemented from April 2022
to March 2023 were listed and budgeted in specific programs. Health implementing partners were asked
to come up with plans and budgets of activities that they intend to implement within the stated period
to be incorporated in the DIP. Finally, all the departmental plans and budgets were merged into one
document.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 66
GOVERNANCE
ONSE supported Chitipa, Balaka, Dowa, Karonga, Nkhotakota, Lilongwe, Salima and Zomba DHOs to
conduct HCMC supervision and mentorship in 80 facilities, supervising a total of 631 members (388M,
243F). In general, 46% of the HCMCs were found to be functional. The objectives of the HCMC
supervisions were to follow up on how HCMCs are executing their roles, appreciate projects that are
implemented in the facilities by HCMCs with support from different stakeholders, identify challenges
hindering the quality of services and appreciate the strengths of health workers and HCMC members,
and check if monthly meetings are being conducted evidenced by availability of minutes.
TABLE 43. SELECT OUTCOMES OF HCMC SUPERVISION PY6Q2 (CHITIPA, DOWA, KARONGA, LILONGWE, NKHOTAKOTA)
DISTRICT HCMC STRENGTHS
Chitipa Kapenda,
Kameme and
Ifumbo
◼ All HCMCs are holding monthly meetings and minutes were available
◼ All the HCMCs have quarterly work plans
Dowa Chinsepo ◼ Chisepo HCMC is in a project of rehabilitating the security guard house following his transfer from Chankhungu Health Centre. Looking at the resource mobilization, the
HCMC chair asked the DHO to help so that the house can be finished with urgency
since the officer is being accommodated at the guardian shelter. The DHO pledged to
assist with 2 bags of cement for plastering the sitting room
Karonga Iponga ◼ Iponga HCMC took leadership in constructing a fence around the facility's rubbish pit
Lilongwe Kang’oma ◼ Kang’oma HCMC has conducted a general cleaning activity at the Facility and also they
have dug a rubbish pit
Ukwe and Ngoni
◼ Ukwe and Ngoni HCMCs have built staff houses through lobbying funds and their own initiatives
Nkhotakota Mtosa and
Mwansambo
◼ They raised funds through monthly contributions for the smooth running of their
committees
◼ The committees initiated facility clean-up campaign which done every fortnight ◼ Drug Monitoring Subcommittees active in their roles and responsibilities
LEADERSHIP AND MANAGEMENT
INTEGRATED SUPPORTIVE SUPERVISION (ISS)
During PY6Q2 ONSE held several coordination meetings with QMD Director, DH Coordinator and
QMD National ISS Coordinator. These meetings were held to ensure the implementation of the agreed
work plans and ensure ISS institutionalization in MoH. ONSE through Dimagi also performed checklist
revisions and other technical tasks in preparation for local hosting. In checklist revisions, the following
tasks were done:
◼ Explored how the indicator report for HIV is built and developed the plan for implementation in
the technical document and reordered the indicators based on the order in the checklist
◼ Changed the setup of lookup table for FP methods
◼ Monitored superset dashboard to see if data needs cleaning and cleaned data
◼ Updated technical documents with "How to create indicators"
◼ HIV and TB checklist updates - added new questions and indicators
Dimagi in PY6Q2 also focused on building local ownership and knowledge of the CommCare platform
and the ISS application active in Malawi. This was done through STTA which focused specifically on
training the MoH TAs on how to conduct application building and maintenance of the ISS application. A
total of 16 MoH participants were trained. The CommCare App Building, and ISS App Training were
very successful. During the training we managed to cover all topics that were planned for the three days
and the trainees showed to have strong technical aptitude and a strong interest in the application
development and management aspects. Following the training DHD team is performing the ongoing
maintenance tasks are recurring activities.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 67
In the reporting quarter, ONSE also supported DHMT ISS in Balaka, Chitipa, Dowa, Karonga, Lilongwe,
Machinga, Mulanje, Nkhotakota, and Salima districts reaching 78 facilities and supervising 403 (260M,
143F) health workers. During the supervision, 114 action points were developed and 79 were
implemented. 86% of health facilities successfully supervised for the quarter.
SUPPLY CHAIN
Beginning in PY5Q1, district support towards supply chain activities has tremendously shifted to mostly
collaboration with sister projects like the USAID-funded GHSC project implemented by Chemonics, the
district pharmacy personnel and other partners. This collaboration is critical especially in ensuring that
facilities supported by ONSE have adequate supplies for increasing access to quality essential services. At
the district level, ONSE continues to collaborate with pharmacy personnel in redistributing drugs and
supplies to ensure some facilities are not overstocked while other facilities within the district are
stocked out. This is done as a gap filling measure which is integrated within other ONSE activities such
as supportive supervision. ONSE also continues to integrate the collection of LMIS reports within the
routine data collection supported every month. Activities directly supported with ONSE resources this
quarter are stipulated below.
DRUG AND MEDICAL SUPPLY REDISTRIBUTION
In PY6Q2, ONSE supported redistribution of the tracer commodities in Dowa and Kasungu with the
aim of ensuring equal access to essential health services through uninterrupted availability of essential
health commodities in public health facilities. A total of 4 facilities in Dowa and 15 in Kasungu benefitted
from this exercise. The table below provides a summary of the commodities that were redistributed and
the number of facilities that got involved.
TABLE 44. QUANTITY OF HEALTH COMMODITY REDISTRIBUTED PER FACILITY
HEALTH COMMODITY QUANTITY
REDISTRIBUTED
FROM HOW MANY
FACILITIES
TO HOW MANY
FACILITIES
Lumefantrine/Artemether 120mg/20mg 26,800 10 1
LA 3X6 27000 8 2
Depo Provera IM 300 1 3
Jadelle 100 1 3
Microgynon 90 1 2
Oxytocin 1700 1 5
Misoprostol 600 1 5
Magnesium Sulphate 600 1 13
SUPPORT TO DRUG AND THERAPEUTICS COMMITTEES (DTCS)
In Kasungu, ONSE supported the monthly DTC meeting drawing participation from 12 (8M, 4F)
Pharmacy Technicians, Clinical Officers, Registered Nurse Midwives among others. Reviewing and
resolving last DTC meeting minutes. The objectives of the meeting were to brief members on annual
budget statements and the status of drug resource management, update on the availability of additional
funds to cover for the drug budget from the MoH, and to order medicines and other medical products
using an order template from the LMIS form. Participants discussed several key issues and action points
raised from the previous meeting, including the issue of distribution of benzyl benzoate paint to
outreach clinics to manage scabies outbreak in the district. However, members suggested that it would
be ideal if the clinics are given the opportunity to order their own drugs rather than wait for outreach
clinics because the facilities will be able to manage their cases in time.
During the deliberations it was also noted that all albendazole was contraindicated for use in pregnant
and breastfeeding mothers, posing concern from maternal and neonatal health care providers. This
prompted members to request the pharmacy to make all necessary communication with central medical
stores to have the appropriate albendazole that is suitable for pregnant and breastfeeding mothers.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 68
HEALTH MANAGEMENT INFORMATION SYSTEMS
DHIS2 SUPPORT
DATA COLLECTION
ONSE supported data collection from the health centers to report to the district level for data entry
into DHIS2; the support included provision of fuel and allowances to statistical clerks from the HMIS
office who went to facilities to mentor and to coach data clerks at a facility level. A total number of 223
(149M, 74F) HMIS personnel conducted data collection in 277 facilities in the quarter. In Zomba, data
collection is integrated with G2G routine data collection. Some notable issues during the exercise were
incomplete documentation in registers such as OPR. During the exercise, mentorship on documentation
in antenatal and outpatient registers was done. Availability of registers, improved documentation
especially in OPR where page summaries are written, as well as updated graphs in some facilities were
some of the observations during the exercise.
RETROSPECTIVE DATA COLLECTION
To improve on reporting, ONSE supported retrospective data collection in the quarter for missing
reports in DHIS2 in Karonga and Chitipa. The activity targeted all missing reports in DHIS2 from Oct
2020 to September 2021. The aim was to generate reports and enter in DHIS2. The reports that had
high numbers missing in DHIS2 were: YFHS, HBB, Ante-natal care, Maternity, HMIS15, and FP. By the
end of the exercise, all reports collected were entered in DHIS2. A total number of 26 facilities were
visited by 7 (4M, 3F) people comprising of midwives and data clerks
HMIS SUPERVISION AND DATA MENTORSHIP
ONSE supported HMIS supervision in Dowa, Balaka, Salima, and Nkhotakota. The exercise focused on
reviewing registers and reporting tools as well as data mentorship in MNH tools, another objective was
to strengthen data quality in the health facilities as well as data plotting on run charts to enhance data
use and visibility. The team reached 16 facilities including a new facility in Dowa, and 45 (16M, 29F)
health facility staff were supervised. Issues identified during supervision were incomplete documentation
in registers, lack of capacity to plot graphs. The team was mentored on how to plot graphs and the
importance of complete documentation in registers was also emphasized.
STRENGTHENING DATA QUALITY
DATA VERIFICATION
In the reporting period, ONSE supported data verification exercise in 7 districts to verify reported data
in DHIS2 with primary data sources at service delivery points. The objective of the exercise was to
verify reported data in DHIS2 with primary data sources at service delivery points. The activity also
served as a preparatory visit to sampled facilities for USAID data verification and the focus was on
ONSE fixed fee indicators. A total number of 45 (33M, 12F) district staff including HMIS personnel and
nurses verified data from 31 facilities. A summary of the data verification exercise can be found in the
table below.
TABLE 45. SUMMARY OF DATA VERIFICATION EXERCISE - PY6Q2
OBSERVATIONS AND CHALLENGES WAY FORWARD
◼ Variations in reported and verified data
◼ Few or no graphs pasted in facilities
◼ Good systematic filing in some facilities
◼ The verified data was corrected both in the hard copy
reports and also in the system
◼ Mentorship on plotting of graphs was done ◼ Continue proper filing

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 69
DEMAND CREATION AND COMMUNITY ENGAGEMENT
OVERVIEW
Through community mobilization and engagement activities, ONSE supports communities to identify
their own problems and mobilize their resources or identify other local resources to achieve solutions.
ONSE helps communities access tools and platforms to hold health care workers and local governments
accountable to provide high-quality services and participate in planning and other local government
processes. ONSE continues to support district health teams to engage with communities to ensure
active participation of communities in health promotion activities as well as capacitating them to demand
quality health services. Activities supported included SBCC and strengthening capacity of CHAGs to
apply the Community Action Cycle (CAC) in their health promotion activities.
Of the two community mobilization and engagement indicators that ONSE monitors annually, one is
achieved, and one is not on track for achievement of the annual target.
TABLE 46. PERFORMANCE ON COMMUNITY MOBILIZATION & ENGAGEMENT INDICATORS – PY6Q2
INDICATORS TARGET
PROJECT YEAR 6
Q1 ACHIEVEMENT
Q2 ACHIEVEMENT
STATUS
% of communities using CSC
methodology 57% 61% 58%
# of civil society organizations receiving
USG assistance engaged in advocacy
interventions
5 1 0
Achieved (≥100% of target)
Almost Achieved (86-99%)
Not Achieved (≤85%)
COMMUNITY ACTION CYCLE
Strong community structures and community-level engagement are critical in ensuring successful
community health programmes. The key issues of priority focus were on supportive supervision for
CHAGs and CCs includes to a) increase community-level engagement, participation, and ownership of
community health services, and b) to develop a strong community-level structures and sufficient clarity
on their roles and responsibilities during the participation in the community health programs.
COMMUNITY HEALTH ACTION GROUP (CHAG) SUPERVISIONS
In the reporting quarter, ONSE in the districts of Balaka, Chitipa, Dowa, Karonga, Kasungu and
Machinga supported the supervision of 52 CHAG’s and reached 891 (411M, 480F) members. The
supportive supervision was conducted by DHPOs in collaboration with CMT members and HSA’s for
the respective catchment areas. The aim of the supportive supervision was to review the progress of
activities made since the last supervision visit, assess the challenges and actions developed to address the
issues, review COVID-19 related issues and activities, and take an opportunity to collect CHAG reports
from the members.
KEY FINDINGS FOR CHAG SUPPORTIVE SUPERVISION
Strengths
The supportive supervision meetings acted as refresher sessions for old and new CHAG members, the
supervision was an opportunity of orienting the new CHAG members on the essential interventions for
community mobilization and engagement. During the CHAG supervisions in Kasungu, CHAG members
came in large numbers for the meeting and showed a willingness to continue working for the
community. Additionally, the CHAG members were able to recall community mobilization and
engagement concepts they were trained on some few years’ back. In Machinga, there were active
HCMC members and there was good coordination between CHAG members and HCMC. The cordial

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 70
relationship between HCMC and CHAGs was evidenced by the ability of the two groups to ensure
availability of emergency transport at community level for Machinga CHAGs. The positive side was that
almost all CHAGs supervised were active and conducting meetings. CHAGs in Dowa and Machinga
were able to work with VHCs and other community health volunteers and a reasonable number of
activities were implemented in this quarter.
Challenges
There was a lack of supportive supervision in all the six districts, this has led to a lack of CHAG active
work plans in three-quarters of the districts supervised. The lack of consistent supportive supervision
led to inconsistent or no submission of reports by CHAGs across the districts. In Dowa, some CHAG
members left thereby creating a gap in activity implementation. This prompted co-opting new CHAG
members into the groups. However, the new CHAG members are unable to generate a report for
implemented activities. There is a need therefore to orient the new CHAG members for them to play
their roles meaningfully. Districts that require this orientation include Balaka (Maera, Chiyaka,
Nyang’ona, Maserema, and Ligwangw’a). Additionally, a reasonable number of CHAG members in
Machinga have not been working since the outbreak of COVID-19 due to various misconceptions and
lack of motivation. These will also require refresher trainings.
Action Points
The CMT supervision team emphasized the need for CHAGs to remain vibrant and follow through the
action points on a monthly basis. Across all the six districts, CHAGs without action points were
reminded of the importance of developing one within the shortest period of one month. CHAGs were
encouraged to hold monthly meetings. The HSAs were encouraged to work with CMT and the CHAGs
and find community-based solutions to challenges identified. Additionally, CHAG members were
encouraged to follow up with ADC to facilitate progress of identified issues that require attention. In
Dowa, the CMT supervisors supplied CHAGs with enough blank reporting forms for the coming
quarter.
TABLE 47. ACHIEVEMENTS/HIGHLIGHTS FROM CHAG’S AND CC’S IN THE SIX DISTRICTS
THEMATIC AREA ACHIEVEMENTS/ HIGHLIGHTS
WASH and Hygiene ◼ In Chitipa, Sayini and Ridwell village had broken boreholes since 2017. The CC reported
this issue to the district Water Development Officer; through CHAG initiative, the
boreholes have been maintained ◼ Nkhangwa CHAG in Chitipa has ensured that the 440 households are able to access clean
water through the introduction of new boreholes in some areas as well as ensuring that
every house has a toilet and a hand washing facility to be used soon after using the toilet
◼ Nkhangwa CHAG is active and the group was able to display a work plan with health challenges affecting the community. However, the CHAG was encouraged to develop and
work through sustainable action points
Health Issues ◼ Kafora CC in Chitipa is plastering a community built iCCM provider, staff house and
kitchen to be completed by May 2022 ◼ CHAG in Chitipa was able to conduct household visits to assess the usage of ITNs - this
was a follow-up action point from previous meeting Action Points. Six of the 95
households did not sleep under ITLN
◼ The CHAG in Chitipa held a meeting where they discussed issues to do with malnutrition. In collaboration with Tuwalere II (Local NGO), the CHAG encouraged households to
come up with vegetable gardens
Income Generating
Activities ◼ In Chitipa, the CC and CHAG have failed to grow maize and beans because of late coming
of rains ◼ Chitipa CHAG – Each member is encouraged to have a garden of groundnuts and later
shall contribute 2 bags of 50 kilograms each for CHAG IGA

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 71
CHAG SUPPORT SUPERVISION AT MANKHOKWE- DOWA. PICTURE COURTESY BY ROGERS KUMWENDA
COMMUNITY SCORE CARDS
CSC is a process, or voice card, that enables communities to voice their assessment of apriority public
services. It also enables community members, health providers, and government officials to work
together to identify and overcome health coverage quality and equity obstacles. The purpose of CSC
sessions was to a) create awareness of health issues to the community, b) enhance collaboration and
coordination in issues of promoting health between the community and the health facilities, and c)
strengthen facility and community linkage system in promotion of health care services delivery. In the
reporting quarter, ONSE therefore supported CSC activities in Chitipa, Karonga, Lilongwe, Dowa,
Kasungu, Mulanje, Zomba and Nkhota-kota. Sixty one (61) of 106 Group Village Headmen participated
in the Community Scorecard process in the eight districts representing 58% for this reporting period.
The CSC sessions were conducted in 3-day sessions per district.
TABLE 48. SHOWING DISTRICTS, FACILITIES AND PEOPLE REACHED WITH COMMUNITY SCORECARD ACTIVITY.
DISTRICT FACILITY
NAME FOCUS
GROUPS
PARTICIPATING
GROUP VILLAGE
HEAD (GVH)
TOTAL
GVHS TOTAL
PARTICIPANT MALE FEMALE
Chitipa Ifumbo HC 4 5 8 117 75 42
Karonga Atupele
Community Hospital
2 2 6 59 34 25
Nkhota-
kota Nkhota-kota
DHO 5 6 10 52 34 18
Lilongwe Khongoni HC 6 38 68 64 37 27
Dowa 2 2
Kasugu 3 3
Mulanje 4 4
Zomba 1 5
Total 17 61 106 292 180 112
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 72
BRIEF OUTLINE OF CSC ACTIVITIES IN THE THREE-DAY SESSIONS
DAY 1: GENERATION OF ISSUES
Day 1 involved the use of checklists with standard thematic areas at community level; the facilitating
teams probed what is working well and what is not working. The emphasis was on generation of issues
that contribute to poor indicators. For each district, the participants divided themselves into focus
group discussions (FGDs) and the common group formulations were: male, female, youth, health care
workers and community leaders.
DAY 2: CONSOLIDATION AND SCORING
Day 2 saw a generation of issues from the different FGDs, as per CSC guidance. The issues generated in
the various groups at each specific district were consolidated into one graphic table on flip charts.
DAY 3: INTERFACE MEETING
On Day 3, which was the Interface meeting for all the four-districts, the community members met
members of the District Council, DHMTs, ADCs, Management of the Health Facilities, Chiefs and
HCMC. The common arrangement was that the issues generated on Day 1 were displayed on flip charts
and pasted on a wall or tree and this was common across all districts that participated in the CSC
session. All participants discussed pertinent issues and action points were drawn. The generation of
issues was based on the following thematic areas across all four districts:
◼ Attendance of ANC, Maternity & PNC services
◼ Community involvement on MNCH issues
◼ Availability of ambulance in referring pregnant mothers to the district hospital
◼ Attitude of health worker
◼ Attitude of community members
◼ Availability of adequate & quality maternity services
◼ Availability of FP services
◼ Availability of YFHS
◼ Availability of Health Centre Management Committee
◼ WASH

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 73
TABLE 49. COMMON INDICATORS, ISSUES, AND ACTION POINTS ACROSS THE FOUR DISTRICTS
INDICATORS ISSUES ACTION POINTS
Availability of
ambulances for
referring women to the
district hospital
(Lilongwe and Chitipa)
◼ Ambulance arrives late – after 4
hours of being called
◼ Bad status of the road
◼ Poor mobile phone network
◼ Transport Officers to timely send the
ambulance to health centers to pick patients up
and transport them to the next level of care
◼ A hardcover notebook to be provided for recording time at which an ambulance was
called for help; the hardcover notebook will
also record the recipient of a message at a
referral facility ◼ Lilongwe District Council will consider
reallocation of vehicles across the high volume
facilities
Community involvement on MNH
issues
(Karonga)
◼ The community has provided bricks and sand for the construction of a
guardian shelter at Atupele
Community Hospital
◼ Lack of transport from community to the hospital. Provision of emergency
transport for pregnant women
◼ Chiefs Council at District Council level will map the furthest areas that require
transportation
◼ The ADC to table the issue of community
transport to chiefs in the next ADC Meeting for Karonga
◼ The District Council will ensure that
construction materials and supplies are
available by end-March and construction to start early April 2022
Low ANC, Maternity &
PNC services
attendance
(Lilongwe)
◼ Most older pregnant women delay in
starting ANC within the first
trimester ◼ Belief in traditional medicine and
delivering under the supervision of
traditional birth attendants
◼ Long distances to health facilities delay women in starting ANC
◼ HSAs to conduct door-to-door follow-ups on
pregnant women and newborn babies within
their catchment area ◼ HCMC to strengthen the existing bylaws on
ANC attendance, maternity, and PNC services
◼ The DHSS Karonga and Atupele CH In-charge
will mobilize resources to support community outreach clinics
◼ The responsible officers on the issue are Head
of Community Health (Atupele) assisted by
HCMC & Chiefs and the follow up to action to implementation of the activity will be provided
by the DHSS Lilongwe
Low Staffing Levels (Nkhota -kota)
◼ There are few staff at labor ward
(maternity unit) and only one clinician who does not reside at the facility but
conducts periodic routine visits at
Chisoti Health Center
◼ Local Government in Nkhota-kota assured the
community that it will recruit additional staff ◼ The DHO - Nkhotakota has recruited three
nurse/midwives, but on temporary basis to
work at the Chisoti Health center Maternity
unit
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 74
PROJECT MANAGEMENT
OPERATIONAL HIGHLIGHTS
In line with its approved PY6 Workplan, the Activity has ended implementation of major activities on
March 31, 2022 except for few activities that were carried forward to April 2022. The activities that
were carried forward to April 2022 include PY5 fee verification, project endline survey, HMIS data
collection for the last month of the reporting quarter (i.e., March 2022); minor infrastructure
improvement/renovation works in 16 selected health facilities; BLM outreach activities, and activity
closeout/transition meetings with ONSE district focal persons, DHMTs, and program managers. All of
those remaining activities will be completed by the end of April 2022.
ONSE will conduct administrative closeout during the remaining period of April-June 2022. As per the
closeout plan submitted to USAID on March 1, 2022, the closeout activities include: transition of
technical activities to the DHMTs and other health actors, dissemination event (conference), final
programmatic and financial reporting, demobilization of key personnel, disposition of non-expendable
properties, final payments to vendors, submission of monthly invoices, demobilization of zonal and
district teams and offices, and project office closure.
PROCUREMENT
During the reporting quarter, the Activity had completed the following major procurements:
◼ Supply, installation, and commissioning of five medical waste mechanical incinerators at Bwaila,
Dowa, Machinga, Chikwawa, and Chitipa District Hospitals. The handing over of the Mechanical
Incinerators to the respective district hospitals will be done in April 2022.
◼ Server for local hosting of digital health application systems by MOH Digital Health Unit. The
installation, migration of the application systems, training of the MOH technical team on local
hosting and commissioning of the server has also been completed within the reporting quarter.
◼ Procured 57 pieces of sterilizing units with spare parts to be distributed to selected ONSE
legacy facilities. Distribution of the sterilizing units will be done in the month of April 2022.
◼ Completed drilling and rehabilitation of boreholes in 17 health facilities under the Central (7),
North (4), and South (6) regions. The drilling and rehabilitation works were done at
Chankhungu, Mpepa, Lodjwa, Maluwa, Mngoni, Dwambadzi, and Kawongozi in the Central
Region; Mpata, Ngana, Nyungwe, and Chilumba in the North; and Dziwe, Utale, Mulomba,
Chonde, Nkomaula and Kambenje in the South Region. The drilling and rehabilitation activities
were done by three subcontractors named Drill Max, GIMM Water Experts & Drilling, and
WaterTech Drilling Contractors. ONSE canceled the planned borehole drilling work at
Tchesamu Health Facility in Nkhatabay district as it was not possible to access the facility due to
bad road conditions caused by rain. Handing over of the boreholes to the facilities in the North
Region was completed in the reporting quarter while that of the facilities in the Central and
South Region will be done in April 2022.
◼ Supply and delivery of construction materials for minor improvement/renovation works in 16
health facilities. The materials were delivered to all the 16 sites and the improvement/renovation
activities have started in the reporting quarter. The improvement/renovations works include
plumbing, electrical fittings, painting, carpentry, and tiling works and will be completed by the
end of April 2022. The renovations will be made to Chikweo and Nainuje Health Centers in
Machinga District; Chinguluwe Health Center in Salima District; Kalembo and Nandumbo Health
Centers in Balaka District; Kapenda Health Center in Chitipa District; Kapora Rural Hospital in
Karonga District; Mbidza Health Center in Mulanje District; Bowe and Chisepo Health Centers
in Dowa District; Chileka and Khongoni Health Centers in Lilongwe District; Chingale and Bimbi
Health Centers in Zomba District; Mdunga Health Center in Kasungu District; and Mwansambo
Health Center in Nkhotakota District. ONSE has supplied the materials and is providing
technical support while the renovation works are done by the maintenance team under the
PAM Unit of the respective DHO.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 75
SUB-CONTRACTORS MANAGEMENT
Due to completion of activities under the subcontract, ONSE has terminated Dimagi’s subcontract on
March 31, 2022. ONSE will also terminate BLM’s subcontract when the activities are completed on May
31, 2022.
VALUE-ADDED TAX (VAT) REIMBURSEMENT
During the reporting quarter, ONSE continued offsetting the outstanding VAT balance against monthly
payroll taxes and withholding taxes deducted from vendors on procurement transactions. A total VAT
amount of Malawi Kwacha 95 million ($115K) has been offset in the reporting quarter. However, we still
have an outstanding balance of Malawi Kwacha 41 million ($57K) under BLM, which is yet to be
refunded by MRA. Unlike MSH, BLM did not get authorization to offset VAT against PAYE and
Withholding taxes deducted from vendors on procurement transactions.
STAFFING
As the Activity is coming to an end on June 30, 2022, ONSE has planned to demobilize the TCN (i.e.,
DCOP-F&A) by the end of June 2022. Termination of contracts for the national staff will be done
through a phased approach with the first batch ending their contract on April 15, 2022, the second
batch and the largest number on May 31, 2022, and the last batch on June 30, 2022.
DELIVERABLES
In PY6Q2, the ONSE Health Activity submitted all required deliverables to USAID’s Contract Officer’s
Representative (COR) on time as per the terms of the contract.
TABLE 50. ONSE DELIVERABLES SUBMITTED IN PY6Q2
DELIVERABLES SUBMITTED COR APPROVAL STATUS
COMMENTS
PY6Q1 Quarterly Financial
and Progress Report
January 28, 2022 N/A COR did not acknowledge
receipt
PY6Q1 Quarterly Activity
Report
January 28, 2022 N/A COR did not acknowledge
receipt
Draft Closeout Plan February 14, 2022 N/A COR did not acknowledge
receipt
January Monthly COVID
Report
February 15, 2022 N/A COR did not acknowledge
receipt
Draft Disposition Plan
(COR)
February 28, 2022 N/A COR acknowledged receipt
on 2/28. Revised version submitted on April 1, 2022.
Disposition approval request
to be submitted to USAID
CO in April 2022
February Monthly Update February 28, 2022 N/A COR did not acknowledge
receipt
February Monthly COVID
Report
February 28, 2022 N/A COR did not acknowledge
receipt
March Monthly Update March 30, 2022 N/A COR did not acknowledge
receipt
March Monthly COVID Report
March 30, 2022 N/A COR did not acknowledge receipt
PY6Q1 Quarterly Financial
and Progress Report
January 28, 2022 N/A COR did not acknowledge
receipt
COMMUNICATIONS
Within the past quarter, ONSE published and shared the following success stories and communication
products in a range of formats, including media appearances, social media links, written stories. These

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 76
strategically illustrated ONSE’s accomplishments and impact on, FP, maternal and child health, COVID
19 prevention and response and awareness campaigns. Key pieces were shared with USAID for
potential redistribution and message leveraging and with targeted audiences and the larger global health
community through the MSH website, emails, and other platforms.
TABLE 51. ONSE COMMUNICATIONS PRODUCTS, PY6Q2
TYPE TITLE DESCRIPTION DATE REPORT
Written success
story
Availability of
supervision data helps in
decision
making at
health facility level
ONSE works to support data for decision making through
DHMT supervision at Machinga DHO.
March
2022
PY6Q2
Report
Written success
story
YFHS
enhances lives
of youth in Nkhotakota
ONSE works to support YFHS at Mpamantha Health
Center, bringing the total adolescent girl pregnancies from
40% to 20% in 6 months after the initiation of community youth group program.
February
2022
PY6Q2
Report
Media
Appearance
Awareness
programs on
COVID vaccinations
ONSE supported radio program on Tuntufye Radio on 10,
11, and 14th January 2022. The aim of the activity was to
provide correct information on COVID-19 pandemic including vaccination. The radio program targets the
whole Northern Region of Malawi, which has an estimated
audience of about one million six hundred people
January
2022
PY6Q2
Report
Media appearance
Flood Response
ONSE donated assorted sanitary items to Mulanje District Hospital to respond to health concerns in congested
evacuation camps during the recent floods in Southern
Malawi.
The items donated include buckets of chlorine, face masks
and tablets of lifebuoy soap for hand washing.
https://www.facebook.com/120942427951729/posts/5008
483229197600/
February 2022
Zodiak News
Media
Appearances
ONSE joined the rest of the world in commemorating
International Women’s Day with a social media post on
USAID’s Facebook, page highlighting a mother’s role in
caring for preterm infants in a KMC with support from ONSE
https://www.facebook.com/109280417135017/posts/8739
05240672527/
March
2022
International
Women's
day USAID
social media
ENVIRONMENTAL MONITORING AND MITIGATION PLAN (EMMP)
SUMMARY
In PY6Q2, ONSE completed construction of waste disposal facilities (comprising incinerators, placenta,
and ash pits) in Nkhotakota, Lilongwe (Bwaila), Zomba, Mulanje, Machinga, Dowa, and Chikwawa
districts. ONSE also completed water system improvement works in 17 selected health centers which
included drilling/rehabilitation of boreholes, installation of submersible pumps, construction of water
towers, installation of water tanks; and reticulating water into the facilities. ONSE has also completed
installation of General/Medical Waste Mechanical Incinerators in 5 health facilities namely Bwaila,
Chitipa, Chikwawa, Dowa, and Machinga District Hospitals.
This EMMP fully aligns with required mitigation measures and systematically ensure compliance with the
GOM requirements as well as with the 2013-2018 Initial Environmental Examination (IEE), which
addresses all activities anticipated under the USAID/Malawi Health Office, specifically ONSE Health
Activity Portfolio and applies to all health activities implemented under Malawi’s 2013-2018 CDCS.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 77
Take note that this IEE has been superseded with the Malawi Integrated Health and HIV Prevention
Portfolio IEE 2018-2023, except those ongoing activities operating under an approved EMMP conforming
to the requirements of the 2013 – 2018 IEE which may continue operating under that EMMP.
CONSTRUCTION EMMP SUMMARY
PRE-DEPLOYMENT
TABLE 52. PRE-DEPLOYMENT SUMMARY
MITIGATION MEASURE SITE NAME YES/NO
Contracts in place ◼ Construction of waste disposal facilities in Nkhotakota, Lilongwe, Zomba, Mulanje,
Machinga, Zomba, and Chikwawa
◼ Water system improvement works in Karonga,
Nkhatabay, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
Yes. Memorandum of understanding with
DHMTs for construction of IPAs.
Contracts with 3 subcontractors for
drilling/rehabilitation of boreholes
Communities have been
notified through media,
meetings, and/or public announcements
◼ Construction of waste disposal facilities in
Nkhotakota, Lilongwe, Zomba, Mulanje,
Machinga, Zomba, and Chikwawa ◼ Water system improvements works in Karonga,
Nkhatabay, Nkhotakota, Dowa, Balaka,
Lilongwe, and Mulanje
Yes, through meetings and site
assessment visits
Permits obtained ◼ Construction of waste disposal facilities in Nkhotakota, Lilongwe, Zomba, Mulanje,
Machinga, Zomba and Chikwawa
◼ Water system improvement works in Karonga,
Nkhatabay, Nkhotakota, Dowa, Balaka, Lilongwe, and Mulanje
Yes, from MoH Planning Department, PAM in districts
Workers PPE compliant ◼ Construction of waste disposal facilities in
Nkhotakota, Lilongwe, Zomba, Mulanje,
Machinga, Zomba, and Chikwawa ◼ Water system improvements works in Karonga,
Nkhatabay, Nkhotakota, Dowa, Balaka,
Lilongwe, and Mulanje
Yes ONSE issued personal protective
clothing and equipment to the
workers. The subcontractors also provided PPE to their site workers
Signage available informing workers of
rules and regulations
◼ Construction of waste disposal facilities in Nkhotakota, Lilongwe, Zomba, Mulanje,
Machinga, Zomba, and Chikwawa
◼ Water system improvement works in Karonga,
Nkhatabay, Nkhotakota, Dowa, Balaka, Lilongwe, and Mulanje
Yes the sites have sign posts
HIV/AIDS prevention
measures in place at work
sites
◼ Construction of waste disposal facilities in
Nkhotakota, Lilongwe, Zomba, Mulanje,
Machinga, Zomba, and Chikwawa ◼ Water system improvement works in Karonga,
Nkhatabay, Nkhotakota, Dowa, Balaka,
Lilongwe, and Mulanje
Yes, through awareness creation
during kickoff meetings
Relevant photos from sites in this stage:

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 78
PPE COMPLIANT BY GIMM WATER EXPERT AT CHAMBE HEALTH CENTRE. PICTURE COURTESY OF KONDWANI MSISKA
SAFETY POSTERS, BARRICADING THE WORKS AND PROTECTION OF PUMP IN PLACE AT CHONDE HC IN MULANJE. PICTURE COURTESY OF KONDWANI MSISKA

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 79
SITE PREPARATION
TABLE 53. SITE PREPARATION SUMMARY
MITIGATION MEASURE SITE NAME YES/NO
Site chosen to create least impact ◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa ◼ Water System Improvement works in Karonga,
Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and Machinga Hospitals
Yes, some existing
sites for Mechanical Incinerators
Slope less than 5%
◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa
◼ Water System Improvemens works in Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, gently rolling
land requiring minimal
levelling
Site of Borehole at a minimum of
30 meters from sanitation
facilities
◼ Water System Improvement works in Karonga,
Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
Yes
Design infrastructure to ensure the least impact and raised above
flood plain
◼ Construction of waste disposal facilities in Nkhotakota, Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa
◼ Water System Improvement works in Karonga, Nkhatabay,
Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, the slab was raised to avoid run off
water flooding into
the water point
surrounding
Minimize disturbance to native
flora and fauna ◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa ◼ Water System Improvement works in
Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and Machinga Hospitals
Yes, by minimal
clearance of vegetation in the
construction area.
Soil erosion measures in place ◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa
◼ Water System Improvement works in Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, by planting grass
and construction of
retaining wall
Relevant photos from sites in this stage:

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 80
MINIMUM DISTURBANCE OF FLORA AND FAUNA AND SLAB ABOVE GROUND AT MACHINGA DH. PICTURE COURTESY OF KONDWANI MSISKA
PAVEMENT AND RETAINING WALL FOR DISABILITY FRIENDLY AND CONTROL OF SOIL EROSION AT MACHINGA DH. PHOTO COIURTESY OF KONDWANI MSISKA

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 81
DRILLING, CONSTRUCTION AND INSTALLATION
TABLE 54. SUMMARY OF BOREHOLE DRILLING, CONSTRUCTION AND INSTALLATION OF IPA
MITIGATION MEASURE SITE NAME YES/NO
Construction and installation activities during day hours
◼ Construction of waste disposal facilities in Nkhotakota, Lilongwe, Zomba, Mulanje, Machinga, Dowa and
Chikwawa
◼ Water System Improvement works in Karonga,
Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje ◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes
Using Environmentally friendly Building Materials
◼ Construction of waste disposal facilities in Nkhotakota, Lilongwe, Zomba, Mulanje, Machinga, Dowa and
Chikwawa
◼ Water System Improvements works in Karonga,
Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje ◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, Sand Cement Blocks and Firebricks
were used for
Construction for both
Water Improvement works like Water
towers, Fences,
Substructure, and
Incinerators
Avoid timber from
unsustainable source
◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and
Chikwawa
◼ Water System Improvement works in Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, timber was bought
from recognized
suppliers
Avoid lead paint ◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and
Chikwawa
◼ Water System Improvement works in Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, paint was bought
from recognized
suppliers, and the paint
had no lead.
Whenever feasible the
contractor will reuse and
recycle appropriate and viable
materials (except asbestos)
◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and
Chikwawa
◼ Water System Improvement works in Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, when backfilling the
foundation, some debris
were used for backfilling
Noise levels kept to a minimum ◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and
Chikwawa
◼ Water System Improvement works in Karonga, Nkhotakota, Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical
Incinerators at Bwaila, Chikwawa, Chitipa, Dowa and
Machinga Hospitals
Yes, live sites and noise
levels were kept to a
minimum
Relevant photos from sites in this stage:

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 82
USING ENVIRONMENTAL-FRIENDLY MATERIAL LIKE BLOCKS AND FIREBRICKS FOR IPAS AT NAINUNJE IN MACHINGA. PICTURE COURTESY OF KONDWANI
COMPLETION
TABLE 55. COMPLETION SUMMARY
MITIGATION MEASURE SITE NAME YES/NO
Landscaping program to restore site
to original form
◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa ◼ Water System Improvement works in Karonga, Nkhotakota,
Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical Incinerators
at Bwaila, Chikwawa, Chitipa, Dowa and Machinga Hospitals
Yes
Completed sites minimize
stormwater and surface runoff
◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa
◼ Water System Improvement works in Karonga, Nkhotakota,
Dowa, Balaka, Lilongwe and Mulanje ◼ Installation of General/Medical Waste Mechanical Incinerators
at Bwaila, Chikwawa, Chitipa, Dowa and Machinga Hospitals
Yes
Disposal of waste and materials
done in accordance with GOM and USAID standards
◼ Construction of waste disposal facilities in Nkhotakota,
Lilongwe, Zomba, Mulanje, Machinga, Dowa and Chikwawa ◼ Water System Improvement works in Karonga, Nkhotakota,
Dowa, Balaka, Lilongwe and Mulanje
◼ Installation of General/Medical Waste Mechanical Incinerators
at Bwaila, Chikwawa, Chitipa, Dowa and Machinga Hospitals
Yes
Relevant photos from sites in this stage:

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 83
MINIMIZING STORM WATER AND SURFACE RUNOFF ON COMPLETED SITE AT CHIKWAWA INCINERATOR SITE. PICTURE COURTESY OF KONDWANI
ONGOING EMMP SUMMARY
In building capacity of health workers through mentoring, and supportive supervision, ONSE staff have
continued to ensure the following:
◼ Proper handling, use, and disposal of hazardous and medical waste. ONSE promotes waste
segregation and proper disposal of such waste. Ongoing support is provided where gaps are
identified such as promotion of hand washing before wearing and removing gloves as well as face
masks.
◼ Facilities have sharp boxes and IPC equipment available and in use. Boxes for sharp disposals
were always available in-service delivery points in the quarter in question.
◼ Facilities with improper management of waste identified and corrective action taken to address
weaknesses. ONSE has supported construction of disposal facilities to facilitate good waste
management as explained above.
◼ Commodities and equipment are managed according to USG and GOM standards and
regulations.
SBCC activities:
◼ Events minimally used high-frequency broadcasting equipment during road shows
◼ Refuse bins available and ONSE encouraged correct usage
◼ Site selection for minimal disruption during COVID-19 awareness campaigns and messaging
mostly integrated with routine activities. For instance, correct disposal of disposable face masks
was integrated during health education and client counseling

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 84
IMPLEMENTATION CHALLENGES AND LESSONS LEARNED
CHALLENGES
◼ Due to the heavy storms that rocked the country within the quarter, health facilities are
experiencing power outages. For instance, lack of power to the vaccine fridge compromises
vaccine storage at Chipoka due to a faulty transformer affecting Santhe, Anchor farm, and
Mkhota. As a result, vaccines are stored at another facility called Khoma. Other facilities have
had their vaccines swept away due to the floods in the country early in the year.
◼ Some village clinics in Nkhotakota do not have a shelter hence services are provided at a
volunteer’s house and in some instances in an open area. This is even more of a challenge during
the rainy season like now.
◼ In some areas like the Chisoti clinic in Nkhotakota, there are few staff members at the labor
ward and only one clinician who only comes during routine visits. This has contributed to a
rising number of home deliveries in the area and fewer women starting ANC during the first
trimester.
◼ There have been orientations aimed at sensitizing the local leaders on COVID-19 vaccines and
introducing Pfizer to the local leaders to take lead in sensitizing the community and alert them
on the importance of vaccinating 12-17 age groups as they also do transmit the
disease. However, some people are still resistant to get the COVID-19 vaccine and have
discouraged the children since the targeted population requires consent to get the vaccine.
LESSONS LEARNED
◼ Due to the heavy storms that rocked the country within the quarter, health facilities are
experiencing power outages. For instance, lack of power to the vaccine fridge compromises
vaccine storage at Chipoka due to a faulty transformer affecting Santhe, Anchor farm, and
Mkhota. As a result, vaccines are stored at another facility called Khoma. Other facilities have
had their vaccines swept away due to the floods in the country early in the year.
◼ Some village clinics in Nkhotakota do not have a shelter hence services are provided at a
volunteer’s house and in some instances in an open area. This is even more of a challenge during
the rainy season like now.
◼ In some areas like the Chisoti clinic in Nkhotakota, there are few staff members at the labor
ward and only one clinician who only comes during routine visits. This has contributed to a
rising number of home deliveries in the area and fewer women starting ANC during the first
trimester.
◼ There have been orientations aimed at sensitizing the local leaders on COVID-19 vaccines and
introducing Pfizer to the local leaders to take lead in sensitizing the community and alert them
on the importance of vaccinating 12-17 age groups as they also do transmit the disease.
However, some people are still resistant to get the COVID-19 vaccine and have discouraged the
children since the targeted population requires consent to get the vaccine.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 85
ANNEX A. ACTIVITY M&E PLAN
Disaggregation
Project Year 6
Comments for Q2 Target
Quarter 1
Achievement
Quarter 2
Achievement
Achieved
to Date Balance
%
Achievement
IR 1: Access to priority health services increased
1-1. Couple Years Protection N/A 400,000 184,126 157,717 341,843 58,157 85%
SIR 1.1: Availability of priority health services in targeted districts improved
1.1-1. Percent of USG-supported
facilities that provided BEmONC in the
past three months
65% 21% 20% 21% 44% 32%
1.1-2. Number of newborns not
breathing at birth who were
resuscitated in USG-supported
programs
3,500 3,024 2,942 5,966 -2,466 170%
1.1-3. Percent of non-public health
facilities (including CHAM, NGO, and
private-for profit institutions)
supported by USG to provide priority health services
70% N/A N/A N/A N/A N/A
1.1-4. Number of people gaining access
to basic drinking water services as a
result of USG assistance
N/A N/A N/A N/A N/A N/A
1.1-5. Number of people gaining access
to a basic sanitation service in WASH
targeted districts as a result of USG
assistance
N/A N/A N/A N/A N/A N/A
1.1-6. Number of institutional settings
gaining access to a basic drinking water
services as a result of USG assistance
18 0 17 17 1 94%
Due to the rainy season, it was
impossible to do one facility in
Nkhatabay (Tchesamu) as such
17 facilities were done of the 18 facilities.
1.1-7. Number of basic sanitation
facilities provided in institutional
settings as a result of USG assistance
N/A N/A N/A N/A N/A N/A
1.1.8 -Number of cases of child
diarrhoea treated in USG-assisted
programs
Boys 125,000
35,059 38,139 73,198 -15,767 113%
Girls 32,363 35,206 67,569
67,422 73,345 140,767

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 86
1.1.9-Number of women giving birth who received uterotonics in the third
stage of labor (or immediately after
birth) through USG-supported
programs (EPMM indicator)
125,000 59,019 60,442 119,461 5,539 96%
1.1.10. Number of calls received
through CCPF N/A N/A N/A N/A N/A N/A
1.1.11 Number of facilities with
improved infrastructure as a results of USG assistance
N/A N/A N/A N/A N/A N/A
1.1-12. Percent of newborns that
received at least one dose of
chlorhexidine to the cord on the first day of birth (ENAP indicator)
N/A N/A N/A N/A N/A N/A
1.1-13. Number of newborn infants
receiving antibiotic treatment for
infection through USG supported programs
5,000 2,060 2,031 4,091 909 82%
1.1-14. Number of children who
received DPT3 (PENTA III) by 12
months of age in USG-assisted programs
137,100 72,801 69,920 142,721 -5,621 104%
1.1-15. Number of children 12-23
months who received measles-rubella
second dose through USG-assisted programs
68,550 39,589 28,307 67,896 654 99%
1.1-16. DPT1 to DPT3 drop-out-rate
(percent) 5% -1.1% 6.2% 5.1% -0.1% 100%
1.1-17. Number of children under five years of age suspected with pneumonia
receiving antibiotics by trained facility
or community health workers in USG-
assisted programs
325,000 117,798 151,304 269,102 55,898 83%
1.1-18. Estimated potential beneficiary
population for maternal and child
survival program
750,000 N/A N/A N/A N/A N/A Will be included in annual report
SIR 1.2: Barriers to accessing priority health services reduced
1.2. Percent of health facilities offering
priority health services
Child Health 92% N/A N/A N/A N/A N/A Will be included in annual report
Family Planning 95% N/A N/A N/A N/A N/A Will be included in annual report
Maternal and
Newborn health 80% N/A N/A N/A N/A N/A Will be included in annual report
Malaria N/A N/A N/A N/A N/A N/A Will be included in annual report
KMC 85% N/A N/A N/A N/A N/A Will be included in annual report

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 87
1.2-1. Number of youth (10-24 years) utilizing youth-friendly health services in
facilities supported with USG funds
100,000 279,404 292,065 571,469 -471,469 571%
1.2-2. Number of vulnerable people
benefitting from USG-supported social services
N/A N/A N/A N/A N/A N/A
1.2-3. Number of children under five
(0-59 months) reached by USG-
supported nutrition programs
175,000 91,558 93,643 185,201 -10,201 106%
1.2-4. Number of children under two
(0-23 months) reached with
community-level nutrition interventions
through USG-supported programs
56,000 3,071 2,260 5,331 50,669 10%
1.2-5. Number of pregnant women
reached with nutrition interventions
through USG-supported programs
110,000 79,381 79,598 158,979 -48,979 145%
1.2-6. Percent of health service delivery
points offering community-based child
health services
Child Health 90% 81% 78% 80% 11% 88%
Family Planning 92% 52% 66% 59% 33% 64%
This performance is a result of a
variety of factors including,
persistent shortage of DMPA
both IM and SC, reduction in number IFHOCs in some districts
for the PY6 work-plan to allow
DHOs to absorb some sites as a
sustainability drive. Lastly the response to cyclone Ana and
polio affected MoH as the same
staff that provide FP at
community level were also required to support the response
1.2-7. Percent of USG-supported
communities establishing an emergency
transport system for pregnant women within the reporting period
70% 17% 71% 71% -1% 101%
12 of 17 (Balaka, Machinga,
Chitipa and Karonga) BEmONC
sites have established emergency transport systems. This
represents 71%.
1.2-8. Number of USG-assisted
community health workers (CHWs) providing Family Planning services
during the year
Men
1,421
539 307 846
-1077 176% Women 113 51 164
Total 1399 1099 2498

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 88
1.2-9. Number of people receiving improved service quality from an
existing basic drinking or safely
managed water services as a result of
USG assistance
N/A N/A N/A N/A N/A N/A
1.2-10. Percent of communities (group
villages) using Community Scorecard
(CSC) methodology
57% 61% 58% 60% -3% 104%
In this reporting period, 8
(Lilongwe, Chitipa, Karonga,
Dowa, Kasungu, Mulanje, Zomba
and Nkhotakota) districts conducted the Community
Scorecard. A total of 61
communities participated in the
process of 106 communities representing 58%. Overall, for
PY6, the indicators has surpassed
the target of 57%.
SIR 1.3: Availability of priority health commodities and supplies in targeted districts improved
1.3-1. Percent of facilities overstocked
with a package of malaria, FP, oral
rehydration solution, and zinc tracer
commodities
Malaria N/A N/A N/A N/A N/A N/A
Family Planning N/A N/A N/A N/A N/A N/A
MNCH N/A N/A N/A N/A N/A N/A
ORS N/A N/A N/A N/A N/A N/A
Zinc N/A N/A N/A N/A N/A N/A
1.3-2. Average stock out rate of
contraceptive commodities at Family
Planning (FP) service points
N/A N/A N/A N/A N/A N/A
1.3-3. Number of health facilities that
have equipment considered basic to
quality client services available in the
general outpatient service area
158 N/A N/A N/A N/A N/A
IR 2: Quality of priority health services improved
2.1. Number of newborns who received
postnatal care within two days of
childbirth in USG supported programs
102,834 28,361 23,397 51,758 51,076 50%
2-2. Percent of suspected malaria cases
tested by either microscopy or rapid
diagnostic test
N/A N/A N/A N/A N/A N/A
2.3. Percent of pregnant women who received three or more doses of IPTp
during ANC
52% 56% 54% 55% -3% 106%
2.4. Percent of clients satisfied with
quality of services. 45% N/A N/A N/A N/A N/A

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 89
2.5 Overall service utilization rate among USAID-supported facilities
implementing quality improvement (QI)
0.50 N/A N/A N/A N/A N/A
2.6 a Average of the service gaps
between a) ANC1 and ANC4 b) DPT1 and DPT3 in USAID-supported districts
Total 0.81 N/A N/A N/A N/A N/A
ANC N/A N/A N/A N/A N/A N/A
DPT N/A N/A N/A N/A N/A N/A
2.7 Proportion of facilities (static) that
provide key services in an
uninterrupted fashion – deliveries conducted, ANC services provided, FP
services provided, child health services
provided (EPI, IMCI)
95% 78% 70% 74% 17% 78%
Total number of facilities providing services in an uninterrupted fashion
320 251 225 226 69 78%
2.8 Number of health facilities with
functional handwashing facilities
available at one or more points of care
228 267 262 265 -39 116%
SIR 2.1: Competencies of health service providers in targeted districts improved
2.1.1 Number of individuals receiving
nutrition-related professional training
through USG-supported programs (CMAM, Care groups, BFHI)
Men 0 N/A
N/A N/A
Women
Men 0 N/A
N/A N/A
Women
2.1.2 Number of individuals receiving
malaria-related training (ACT, Case
management, Lab diagnostics, IPTp)
Men 0 N/A
N/A N/A
Women
Men 0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women 2.1.3. Number of individuals receiving
family planning-related training (CBDA,
LARC, PPFP, BTL)
Men 0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women
USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 90
Men 0 N/A
N/A N/A
Women 2.1-4. Percent of key staff (ONSE, partners and sub-grantees) complete
annual Global Health and PLHA
eLearning course on U.S. abortion and
FP compliance within first half of each fiscal year (Oct –Mar)
100% N/A N/A N/A
2.1.4 Number of individuals receiving
WASH-related training (Water
Resource management)
Men
0 N/A
N/A N/A
Women
2.1.5 Number of individuals receiving
maternal and neonatal health-related
training
Men 0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women
2.1.6 Number of individuals receiving
child health-related training
Men 0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women Men
0 N/A
N/A N/A
Women SIR 2.2: Quality assurance systems in targeted districts improved

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 91
2.2-1. Number of health facilities that maintain international SPHERE
standards for the treatment of severe
acute malnutrition
230 259 276 267.5 -37.5 116%
2.2-2. Percent of confirmed malaria cases receiving first line antimalarial
medication
N/A N/A N/A N/A N/A N/A
SIR 3: Performance of Health Systems Strengthened
SIR 3.1: Strategic management and supervision of human resources for health improved
3.1-1. Percent of health facilities
supervised based on performance
standards in Integrated Supportive
Supervision Tool that complete follow-up actions
89% 76% 73% 75% 15% 84%
SIR 3.2: District-level governance, management, and policy implementation improved
3.2-1. Number of DIP reviews
conducted to monitor DIP activities or
budgets with stakeholder
11 10 6 16 -5 145%
During the reporting period, 6
(Salima, Chitipa, Lilongwe, Machinga, Mulanje and Karonga)
districts were supported to
conduct DIP annual reviews. This
brings total DIP reviews to 16 for PY6.
3.2-2. Percent of health facilities with
functional Health Center Management
Committees
96% 41% 46% 44% 53% 45%
3.2-3. Number of health facilities that
have implemented their facility level
WASH action plan
10 0% 0% 0% 10 0%
Limited activities in Q2. Only
activities are the WASH
renovations.
3.2-4. Number of districts with an operational area mechanics network as
a result of USG assistance
N/A N/A N/A N/A N/A N/A
3.2-5. Number of districts regularly
monitoring water point functionality as a result of USG assistance
N/A N/A N/A N/A N/A N/A
SIR 3.3: Use of a health information system to inform management of district-level health services institutionalized
3.3-1. Number of health facilities
submitting data in line with national standards
DHIS 2 308 253 238 246 63 80%
Open LMIS 388 N/A N/A N/A N/A N/A
IR 4: Demand for quality priority health services increased
4.1. Percent of population reporting
unmet need for Family Planning, Maternal, Newborn and Child Health.
FP 13% N/A N/A N/A N/A N/A Will be reported in EOP report
EmONC N/A N/A N/A N/A N/A N/A Will be reported in EOP report
3

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 92
4.1-1. Number of pregnant women who
initiate ANC visits in the first trimester
Women < 19 Yrs
25,000
3,466 3,278 6,744
-1,844 107%
Women > 19
Yrs 10,365 9,805 20,170
Total 13,794 13,050 26,844
4.1-2. Number of facilities with low-
literacy SBC materials and/or messages
for facility-based patient education and
community mobilization
National N/A N/A N/A N/A N/A N/A
4.1-3 Number of communities verified
as ODF National N/A N/A N/A N/A N/A N/A
4.1-4. Percentage of targeted
communities reporting access to improved sanitation products or
services as a result of USG assistance
N/A N/A N/A N/A N/A N/A
SIR 4.2: Participatory process for community empowerment to safeguard health improved
4.2-1. Percent of communities with functional Community Health Action
Groups
N/A N/A N/A N/A N/A N/A
4.2-2. Number of USG-supported
activities designed to promote or strengthen the civic participation of
women
2 0 0 0 2 0%
4.2-3. Number of civil society
organizations receiving USG assistance engaged in advocacy interventions
5 1 0 1 4 20%
4.2-4. Number of Champion
Communities established N/A N/A N/A N/A N/A N/A
4.2-5. Number of sanitation enterprises (e.g. Local masons) that have improved
capacity in sanitation supply service
delivery as a result of USG assistance
N/A N/A N/A N/A N/A N/A
Integration
IN-1. Number of integration
interventions completed N/A 6 3 1 4 2 67%
Worked with World Relief on
conducting the COVID-19
vaccination in Blantyre, and
Mangochi
Cross Cutting
CC-1. Number of people reached by a
USG-funded intervention providing
gender-based violence services (e.g., health, legal, psycho-social counseling,
shelters, hotlines, other)
N/A 5 29 17 46 -41 920%
2 female cases in Balaka and 15
(3M, 12F) cases in Nkhotakota were reached.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 93
CC-2. Number of policy dialogues and advocacy with public, private, and
community organizations to address
gender bias in access to and quality of
services
N/A 1 0 0 0 1 0%
CC-3. Number of women’s groups,
girls’ groups, and youth groups
supported to facilitate their role as
change agents in their communities
N/A 10 6 0 6 4 60%
CC-4. At least one FP compliance
questionnaire completed for each
project supported facility per year
during supervisory visits
N/A 196 34 0 34 162 17%

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 94
ANNEX B. RCCE
TABLE B1. COMMUNITIES REACHED WITH MOBILE VAN WITH COVID MESSAGES
DISTRICT AREAS WITH REACHED WITH MOBILE VAN
Balaka Mkweta, Mpale, Kasiyo, Kuntiyani, Kapalamula, Tsoka, Khoswe, Mbaza, Chisinkha Chikwawa Lundu at Tizola and Biasi, Maseya at Kalima, Mulilima at Kajawo, Makhwira at Tsapa and Chapananga at
Kakoma. Makhwira at Nkhate and Lundu at Chambuluka. (7 T/A’s). Chitipa Bugulira – Wenya, Kapilinkhonde – Nthalire, Lufita, Misuku, Kapoka, Ifumbo, Mwamukumbwa and Kameme Karonga Ighembe trading, Pusi trading, Lutengano area, Mbughuyo area up to Songwe, Ndemange, Mwabulambo ,
Mapwa, Kansewe, Mwesha, Kasikizi, Chesa, Ndembwera, Mlare Market, Kasimba, Kayerekera , Wiliro,
Folotia, Chinsewe Malungo Machinga Nayuchi, Ninja, Namanja and Mpiri Mbanira, Ntaja, Kawinga, Mlomba, Nainunje, Mkwepere, Ntholowa,
Nsanama, Nyambi, and Mposa Health Facilities Mulanje
(Villages) Musisi, Nkumbi, Chinakanaka, Chitambi, Robeni, Sinoya, Mlatha, Mphika, Mwamadi, Kandulu, Nakutho,
Bwanali, Maonga, Muhiyo, Nankuyu, Richard, Chimbanga, Nkatasi CBO, Nankonya, Mphwesha, Mawindo,
Khwalala, Mchoma, Tonthola, Sanjama, Juma, Nguwo, Muhunguzi, Makina, Misomali, Khoviwa, Mpheni,
Drawesi, Mwanamvula, Namijingo, and Sitolo Mulanje
(Facilities) Mulanje DHO, Mulanje Mission Hospital, Lujeri HC , Milonde HC, Mimosa HC, Bondo HC, ChondeHC,
Thuchira HC, Namphungo HC, MulozaHC , Namasalima HC, Chinyama HC and Mbiza HC. Zomba Mayaka HC, Chanda HC, H Parker HC, Machinjiri HC, Namikango HC, Namadidi HC and Sadzi HC,
Machinjiri HC, Likangala HC, Namadidi HC and Makwapa HC
TABLE B2. COMMUNITY AWARENESS AND SENSITIZATION MESSAGES THROUGH IFHOCS
DISTRICTS TYPE OF
ACTIVITY MALE FEMALE TOTAL PEOPLE
REACHED NUMBER OF IFHOC
VISITED
Chitipa IFHOC 1,736 3370 5,506 30
Balaka IFHOC 441 646 1087 6
Karonga IFHOC 3,506 3,534 7,040 43
Machinga IFHOC 427 818 1,245 4
Nkhota-kota IFHOC 584 2411 2,995 17
Total
6,694 11,179 17,873 100
TABLE B3. COMMUNITY STRUCTURE ENGAGEMENT MEETINGS – SENSITIZATION ON COVID-19
DISTRICTS TYPE OF
ACTIVITY COMMUNITY
STRUCTURE MALE FEMALE TOTAL
PEOPLE
REACHED
NUMBER OF
TAS
Karonga Community
Sensitization meeting
Volunteers 29 21 50 2
Kasungu Community
Sensitization
meeting Influential Leaders 34 16 50 2
Mulanje Community
Sensitization
meeting Faith Based Leaders 101 103 204
TA Mthiramanja,
Tombondia and
Juma 3
Mchinji Community
Sensitization
meeting Local Leaders 130 59 189 3
Salima Community Sensitization
meeting Local Leaders 93 47 140 3
Total 387 246 633 13

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 95
TABLE B4. COMMUNITY STRUCTURE SENSITIZATION MEETING ON COVID-19
DISTRICTS TYPE OF
ACTIVITY AREAS
REACHED TOTAL PEOPLE
REACHED PEOPLE
VACCINATED FACILITIES T/A
Male Female Total Male Female Total
Chikwawa Community
Sensitization and COVID- vaccination
TA
Makhwira at
Nkhate and TA Lundu at
Chambuluka
4,976 6,544 11,520 36 27 53 5
Mangochi
Community
Sensitization and
Local leader meeting
Namcholi,
Nangalamu, Chiponde,
Malembo,
Nkope,
Monkeybay and
Nankhwali
health
centres.
72 32 108 7
Nkhota-kota
Community
Sensitization and
COVID-
vaccination- Market
Mkaika and
Chibothera Markets
600 900 1500 32 23 55
Total 5,652 7,476 13,128 68 50 108 7 5

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 96
ANNEX C. PARTNER COLLABORATION AND COORDINATION
TABLE C1. PARTNER COLLABORATION AND COORDINATION TABLE C1. PARTNER COLLABORATION AND COORDINATION
PARTNER COLLABORATION ACTIVITIES
GHSC-PSM
(Chemonics/USAID)
ONSE strives to work collaboratively with GHSC-PSM with the aim of strengthening supply chain
management at the district level in critical areas such as OpenLMIS where ONSE supports aspects
such as data collection and data capturing. The collaboration is in particular very important in
ensuring the availability of FP methods in ONSE district.
Rice University The strong collaboration between USAID, Rice University and ONSE is enabling the establishment
of a ‘nursery movement’ through district hospitals and other large hospitals in Malawi. This will
ultimately support the development of high quality service delivery for neonates in Malawi.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 97
ANNEX D. PY6 Q2 SUCCESS STORIES
In Q2, the following success stories were produced:
1. AVAILABILITY OF SUPERVISION DATA HELPS IN DECISION MAKING AT
HEALTH FACILITY LEVEL
ONSE Health Activity supports the Machinga District Health Office to improve availability of supervision
data as they implement digital ISS and dashboard. By combining the ISS tool and the data in the DHIS 2,
ISS is linked with data.
2. WATER AND WASTE MANAGEMENT RENOVATIONS IMPROVE LIVES IN
HEALTH FACILITIES
ONSE supported the Government of Malawi on an assessment of 424 health facilities in 16 districts to
identify service delivery gaps and the gaps’ root causes. The work contributes to improved access to
safe water to the facilities and surrounding communities, clean and safe sanitation facilities, more health
hygiene facilities at points of care and latrines, and appropriate waste disposal systems.
3. YOUTH FRIENDLY HEALTH SERVICES ENHANCES LIVES OF YOUTH IN
NKHOTAKOTA
Mpamantha, a community in Nkhotakota district, struggled with youth-related issues like early
pregnancies and marriages, gender-based violence, and anti-retroviral therapy defaulting. In partnership
with ONSE, youth friendly health services introduced a youth program for the community to create a
safe space where youth could meet frequently and discuss issues affecting their lives. Since the
introduction, the community has seen lower teenage pregnancies, reported sexual abuses cases, and
ART treatment defaults among the youth.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 98
ONSE SUCCESS STORY
AVAILABILITY OF SUPERVISION DATA HELPS IN DECISION
MAKING AT HEALTH FACILITY LEVEL
MSOLORA HIGHLIGHTING THE IMPORTANCE OF THE DASHBOARD TO ONSE’S MISOMALI
Machinga District for quite a long time was faring badly in regards to data usage. One would assume
that with the availability of a specific department on Health Management Information System (HMIS),
things would run smoothly, but that was not the case. In 2019, their reporting rate was less than 60
percent and as DHMT they sat and devised mechanisms on how this area could be improved into
DHIS2.
“One of the strategies we looked at was on how we could marry the supervision to the reporting of
programs into DHIS 2. We met with ONSE Machinga staff to discuss how this could be possible and
thankfully they took us through the dashboard and we learnt that it was possible to use it to see which
areas would need improvement. This led us to combine the ISS tool and the data in the DHIS 2 that
when the team is going out for DHMT integrated supportive supervision (ISS) it should be combined
with the data and it has been very helpful strategy” said Madalitso Msolora, Machinga Hospital
administrator
Availability of supervision data via the dashboard has improved their ability to monitor facilities or
programs and be able to tailor target their support as DHMT to particular areas of need. For instance,
through this, they have been able to uncover deficiencies in facility and use data captured to affect some
decisions at the District Health Office (DHO). Machinga is one of the districts that is benefitting from
digital ISS and dashboard with financial support from ONSE. However, the district encountered
challenges to implement supportive supervision which were thankfully addressed.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 99
“There were times when we had problems with our reporting into national platform but through
DHMT supervision, we noted that we needed additional staff and thankfully government responded
rapidly. It provided us with data clerks that are able to assist the team in picking data and reporting
through a WhatsApp group that I created so that we would be able to get data quickly, so I would give
credit to the DHMT ISS tool that helped us to uncover the deficiencies at facility level and respond
immediately by deploying data clerks” further commented Msolora
Some of the notable changes at Machinga DHO include damages to structure that can be covered when
the team goes out for supervision. Furthermore, staff discipline has improved in that it can now be
addresses without having to wait for reports from incharges to call the staff for disciplinary hearing,
these issues are dealt with right there and then when the team goes out for supervision. All that has
been possible with readily available data.
“The benefits for using this tool are too numerous and surpass the negatives. If the Ministry could take
up this function through the department of quality of management, we would not see differences once
ONSE phases out. The Ministry has to understand what ONSE is doing and be able to train and employ
people to take up the role without problems. This will help us manage transition without glitches along
the way” concluded Msolora
The district manages 23 fully operational facilities. However, there are people that have registered small
clinics that rarely operate even 5 days in a week bringing the total number to 43. When DHMT makes a
trip to supervise them, one finds them closed. A decision is being made to ensure that any facility that is
being supervised should be one that is fully functional.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 100
ONSE SUCCESS STORY
WATER AND WASTE MANAGEMENT RENOVATIONS IMPROVE
LIVES IN HEALTH FACILITIES
1DR PHOYA HANDING OVER AN INCINERATOR TO MULANJE DHMT MEMBERS
The Government of Malawi increasingly recognizes the important role that water, sanitation, and
hygiene (WASH) plays in infection prevention, saving lives, and improving QoC. As such, implementing
partners and donors, including ONSE Health Activity, were asked to invest more in this critical
component for health and wellbeing.
In May 2017, ONSE conducted an assessment of 424 public and private-for-profit health facilities in the
16 supported districts, identifying crucial service delivery gaps, as well as the root causes of those gaps
Some of the challenges identified included blocked plumbing systems, lack of functional taps, latrines and
showers, unrepaired water tanks and water pumps and lack of proper waste management systems like
ash and placenta pits. ONSE has since then been working to ensure healthcare facilities have a safe and
accessible water supply; clean and safe sanitation facilities; hand hygiene facilities at points of care and at
latrines; and appropriate waste disposal systems.
As the project is coming to an end, management has for the past few weeks been going around the
districts to appreciate what has been done and to officially hand over the construction works of water
supply improvements and waste disposal in these health facilities.
“Our work as ONSE is to support the 16 districts to achieve its health goals of which one of it is
improving access to safe water at the facility and surrounding communities. With the coming of COVID

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 101
19, we have come to appreciate
more the need to have readily
available water at facility level and
with financial support from USAID,
we are happy to finally handover all
these developments to various
districts. We however hope that
District Health Office alongside the
Physical Asset Management team
will ensure that maintenance is
being done regularly and that
communities will also take
ownership of these projects to
protect it from vandalism”
Commented Dr Ann Phoya, COP
for ONSE
Dziwe and Utale 2 Health facilities
are beneficiaries of these
construction works and in a
meeting with District Health
Management Team (DHMT)
members, they indicated that it has
been a problem to retain health
workers over a long period of time
as most would complain and ask
for a transfer due to this problem.
“Dziwe and Utale 2 Health facility
in Balaka district are among some
of our many facilities that have had
poor water supply for many years
which has affected the operations
of the facility particularly at the
maternity wing and staff houses.
We have had many health personnel resigning due to the water challenges problems, so when we first
heard that ONSE is coming to rectify these problems, we were very excited and thankful. The
beneficiary of these projects is not only for the facility but even surrounding communities and for this
we are grateful” Thomas Bizeki Representative of DHMT, Balaka
ONSE has drilled new boreholes, erected water towers, built septic tanks, did some plumbing works
and installed submersible pumps in various facilities. Currently, ONSE has handed over 17 boreholes in
8 districts and 12 incinerators in selected districts across the country.
2. A WATER TANK AND TOWER BUILT AT UTALE 2 HEALTH FACILITY BY ONSE

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 102
ONSE SUCCESS STORY
YFHS ENHANCES LIVES OF YOUTH IN NKHOTAKOTA
3. SOME OF THE YOUTH UTILIZING RECREATIONAL MATERIALS FROM ONSE
15-year-old Patricia Mukiwa got pregnant in 2019 while she was in grade 8. By then she had no idea
what it meant to be pregnant, and it took her mother to notice that her daughter was expecting.
Unfortunately, her parents chased her away out of anger. She went to tell her boyfriend of the same
age,but his parents refused to take them in, and they decided to rent a small house where they lived
together for two years.
“Life was so hard, we didn’t know what we were doing. Every day we would go out to look for piece
work, sometimes we would find it and other times not. We slept hungry more times than I could count
and unfortunately I was expecting my baby by then. Our families didn’t want to have anything to do
with us because they said since we wanted to be adults, we have to fend for ourselves.” Commented
Patricia
But in 2021, she was approached by members of Mpamantha youth group, who heard from the
community’s Mother group, a structure that looks out for the welfare of young girls, during their
monthly meeting. She was encouraged to join the group and learn more about YFHS. That is how her
life changed. With the help of the youth group, she asked her parents if she could come back home and
resume school, and thankfully her parents let her come back home.
Mpamantha is a community in Nkhotakota district under TA Malengachanzi, which has struggled with
many youth-related issues for many years. Some of these issues include early pregnancies and
marriages, Gender Based Violence; and anti-retroviral therapy (ART) defaulting which has had
detrimental consequences on the youth including the development of viral resistance, treatment failure,
and increased risof disease progression.

USAID.GOV AID-612-C-17-00001 QUARTERLY ACTIVITY REPORT PY6Q2: APRIL 29, 2022 103
“When we did an assessment with the officer in charge of Mpamantha, Mr Tambulasi, and ONSE as our
partner in July 2021, some of the issues we discovered included that we had 104 ART defaulters and, of
that, 30 were young people. That is when we knew that we needed to do something about it,”
commented Maliseni Pikausi, Youth Friendly Coordinator at Mpamantha Health Center.
The team decided to involve all community structures like the traditional leaders, community policing,
parents, and other structures because after an assessment, it was discovered that a lot of the problems
were related to culture and misinformation. For instance, there were a lot of myths about ARVs where
some said they caused mental problems and some family planning (FP) methods caused infertility issues
in women.
The youth-friendly and other structures decided to work with other youth networks in surrounding
communities to set up a youth group that would meet up every Friday at Mpamantha Health Center to
ensure there was a safe space where youth could meet frequently to discuss issues affecting their lives,
which demonstrated success.
“We started with less than 10 youth members. Knowing the importance of making sure our youth
remain active, we asked ONSE to provide them with recreational materials. So they bought them a lot
of board games and football and netballs to ensure that they have something to do when we meet. So,
Fridays have become youth days here where apart from playing sports, we invite different specialists in
various topics including FP, Gender Based Violence and these are discussed in depth with the youth. So
now we have over 70 youth coming together every Friday," commented Tambulasi, Officer in Charge of
Mpamantha.
Over a period of approximately 6 months that the program has been operational, no sexual abuse cases
were reported in Mpamantha Health Center, when prior to this, every month they cases reported. In
regards to teenage pregnancies, before the introduction of this program, at least 40% of antenatal cases
were adolescent girls, but now they have reduced to less than 20%. Furthermore, the number of young
people who default on ART treatment has decreased from 30 to less than 18.
“ONSE has been very instrumental in all these improvements. Apart from all the recreational materials
they provided for the youth, they have also financially supported supervision and mentorship programs
for our youth coordinators as well as supported FP and YFHS,” said Maliseni Pikausi, Youth Friendly
Coordinator at Mpamantha Health Center.
Through this YFHS program at Mpamantha Health Center, a lot of youth have found meaning to life.
“I led a very pathetic life that had no direction. All I did was hang around with bad company and make
bad decisions. That is why I will be eternally grateful for Mpamantha Health Center management for
introducing this program. Now our youth group has a pond where we have over 4,000 fish that will be
sold soon. The money from this will be used to reinvest in other income generating activities to
generate more income to help pay school fees and provide needs to other youth,” commented Dyson
Nkhoma, a member of the youth club.
Apart from fish farming, some of the young people have had the opportunity to go for youth vocational
training where some of them are now tailors, carpenters, plumbers, and welders. Some of the money
from fish farming is planned to send more young people for more training to ensure that everyone is
financially stable.
Due to how the district has improved its performance in all of its 21 health facilities, Nkhotakota was
recently awarded a Best Performing District Shield in YFHS making it a force to reckon with.