science horizon - odisha bigyan academy
TRANSCRIPT


Science HorizonEditorial BoardProf. Niranjan BarikProf. Ramesh Chandra ParidaDr. Choudhury Satyabrata NandaDr. Rajballav MohantyDr. Nilambar BiswalGuest Editorial BoardDr. Sidhartha GiriDr. Manoranjan PattnaikDr. A M Khan
President, Odisha Bigyan AcademyProf. Bibhuti Bhusan MishraEditorEr. Mayadhar SwainGuest EditorDr. Sanghamitra PatiManaging EditorDr. Puspasree PuhanSecretary, Odisha Bigyan AcademyLanguage ExpertProf. Sachidananda Tripathy
Issue 4Volume 7 April, 2022
Cover Design : Kalakar Sahoo
CONTENTSSubject Author PageEditorial : Tuberculosis in India Sanghamitra Pati 147
1. Epidemiology of Tuberculosis: An Update Sidhartha Giri 148Sanghamitra PatiA.M. Khan
2. Mycobacterium Tuberculosis: The Bacteria Ratnaprava Mohapatra 151Causing Tuberculosis Ipsita Jena
Paresh Nath Mohanty3. Immunological Concepts in Tuberculosis Sonalika Rath 156
Ira Praharaj4. Symptoms of Tuberculosis Manoranjan Pattanaik 161
S. Pothal5. Laboratory Diagnosis of Tuberculosis Sujeet Kumar 164
Sarita KarHimadri Bhusan BalSunil Swick RoutDasarathi DasSidhartha Giri &NRL Laboratory Team
6. Treatment of Tuberculosis Thitta Mohanty 173Geetanjali Panda

146 Science Horizon:Volume 7: Issue 4
APRIL, 2022
CONTENTSSubject Author Page
7. Drug-Resistant Tuberculosis Baijayantimala Mishra 1768. HIV and TB Prasanta Raghab Mohapatra 1829. Tuberculosis Prevention: Vaccines & Behavioural Abhinav Sinha 190
Aspects Srikanta Kanungo10. Tuberculosis in Diabetic Population Tahziba Hussain 19511. COVID-19 and Tuberculosis: Tackling The Sampat Dash 201
Dual Problem in Future12. Stigma Related to Tuberculosis (TB) in India Krushna Chandra Sahoo 204
Pranab Mahapatra13. NTM: The Hidden Menace Jyotirmayee Turuk 207
Sunil Swick RoutSudarshan Biswal
14. Tuberculosis and Environment Jaya Krushna Panigrahi 21215. Role of ICMR-Regional Medical Research Centre Sidhartha Giri 219
(RMRC), Bhubaneswar in Tuberculosis Control Jyotimayee Turukand Prevention Dasarathi Das
Sanghamitra Pati

147Science Horizon:Volume 7: Issue 4
APRIL, 2022
TUBERCULOSIS IN INDIA
EditorialEditorial
Tuberculosis (TB) is caused bybacteria, Mycobacterium tuberculosis, andcommonly affects the lungs of humans,although it can affect other organs also. Thedisease is curable and can be prevented.Approximately, one fourth of the world’shumanpopulation is infected with TBbacteria. However, most people infected byTB bacteria are not ill, or do not have thedisease, and hence cannot transmit theinfection. Although all the age groups are atrisk of developing active TB disease, itmostly affects adults in their productive agegroup. About 95% of active TB cases anddeaths occur in developing countries. In2020, approximately 10 million people fell illwith TB worldwide, including 5.6 millionmen, 3.3 million women, and 1.1 millionchildren. According to the India TB report2020, the incidence of TB in India in 2019was 26.9 lakhs. TB is the leading cause ofsevere illness and death among peopleliving with HIV. India ranks second in theworld and accounts for 9% of the global
burden of HIV associated with TBinfection.
In this regard, a special issue on TBhas been prepared by ICMR-RMRCBhubaneswar, along with other institutes ofOdisha, to spread the scientific knowledgeabout TB among the general population ofOdisha. It is specially tailored for the youngand enthusiastic school and college students.Apart from covering the scientific aspects,the issue also focusses on the impact of TBon the mental health of the population, andother issues including the effect on theenvironment. This is extremely necessary toincrease the scientific awareness regardingTB infection and disease among the youngergeneration so as to infuse the spirit ofscientific excellence and requisite skills andknowledge to address such public healthevent in the future.
I hope the readers of this special issuewill find the contents highly valuable.
Sanghamitra Pati
Guest Editor
148 Science Horizon:Volume 7: Issue 4
APRIL, 2022
1
EPIDEMIOLOGY OFTUBERCULOSIS: AN UPDATE
1Sidhartha Giri2Sanghamitra Pati
3A.M. KhanTuberculosis (TB) is caused by bacteria,Mycobacterium tuberculosis, and primarilyaffects the lungs of humans, although it canaffect other organs also. The disease is curableand can be prevented. Tuberculosis infectionis transmitted/spread from person to personthrough the air. The infection spreads when aperson with lung TB (pulmonary TB) coughs,sneezes, or spits, and releases substantialnumber of bacteria into the air. A healthyperson gets infected with TB when he/sheinhales the bacteria.
Approximately, one fourth of the world’shuman population is infected with TB bacteria.However, most people infected by TB bacteriaare not ill, or do not have the disease, and hencecannot transmit the infection. For those peopleinfected with the TB bacteria, the life time riskof developing TB disease is 5-10%. The peoplewho fall ill with TB are primarily those who aremalnourished and have weak immune systemsuffering from diabetes, or infected with humanimmunodeficiency virus (HIV), or those whouse tobacco and alcohol regularly.
When a person develops activetuberculosis disease, he/she developssymptoms such as fever, cough, weight loss,night sweat, chest pain, loss of appetite, etc.,
which can persist for months. As the initialsymptoms may be mild, there is a delay inseeking health care, and hence the symptomaticperson continues to transmit the infection toother healthy people in the communityespecially household contacts. A person withactive TB disease can transmit the infection to5-15 healthy persons who are in close contactduring a period of 1 year. In the absence ofearly detection and appropriate treatment,approximately 45% of HIV-negative peoplewith TB, and almost all people with HIV andTB, will lose their life.Who are at Maximum Risk of TB Disease?
Although all the age groups are at risk ofdeveloping active TB disease, it mostly affectsadults in their productive age group. About95% of active TB cases and deaths occur indeveloping countries. People who are infectedwith TB and HIV are 18 times more likely todevelop active TB disease, compared to peoplewho do not have HIV infection. The risk ofactive TB disease is 3 times higher in peoplewho are malnourished, as poor nutrition affectsthe normal functioning of the immune system.In 2020, there were 1.9 million new cases ofTB worldwide in those who had undernutrition.

149Science Horizon:Volume 7: Issue 4
APRIL, 2022
Chronic alcohol use and tobacco smokingalso increases the risk of developing activeTB disease by 3.3 and 1.6 times respectively.In 2020, 0.74 million and 0.73 million newTB cases were attributed to chronic alcoholuse and tobacco smoking respectively.
Impact of TB WorldwideTuberculosis occurs in countries across
the globe. In 2020, approximately 10 millionpeople fell ill with TB worldwide, including5.6 million men, 3.3 million women, and 1.1million children. In 2020, TB was the 13th
leading cause of death worldwide, and thesecond highest infectious disease killer aftercoronavirus disease 2019 (COVID-19).Approximately 1.5 million people died due toTB in 2020, including 2,14,000 people withHIV (along with TB).
In 2020, 43% of all new TB cases werereported from the World Health Organization(WHO) South-East Asian region, followedby 25% from the African region, and 18%from the Western Pacific region. In 2020, 30high burden countries contributed 86% of allthe new TB cases worldwide. The top eighthigh burden countries accounted for two thirdof all the new TB cases, which included India,China, Indonesia, the Philippines, Pakistan,Nigeria, Bangladesh, and South Africa.
TB is a curable disease, and active TBdisease which is susceptible to drugs can becured with a 6 months therapy using 4 anti-tubercular drugs (rifampicin, isoniazid,pyrazinamide, ethambutol). Between 2000 and2020, approximately 66 million people havebeen successfully treated through proper TBdiagnosis and appropriate therapy.
Anti-tubercular drugs have been used formany years, and M. tuberculosis bacteriastrains that are resistant to one or more ofthese drugs have been documented. Resistanceof M. tuberculosis bacteria to anti-tuberculardrugs develops due to inappropriate use ofdrugs, such as incorrect prescription bydoctors/ heath care workers, patients notcompleting the course of therapy, and poorquality medicines. Multidrug-resistanttuberculosis (MDR-TB) is caused by M.tuberculosis bacteria which are resistant torifampicin and isoniazid, the two mosteffective anti-tubercular drugs. However,MDR-TB can be treated using other anti-tubercular drugs, although the duration oftreatment can prolong upto 2 years. In 2020,only 1 in 3 people with MDR-TB accessedtreatment, and hence, MDR-TB has become apublic health threat with far reachingconsequences. In 2018, the success rate ofMDR-TB treatment was 59% worldwide.
Globally, the incidence of tuberculosishas been decreasing by approximately 2%every year, and the cumulative reduction inTB between 2015 and 2020 was 11%. TBhas resulted in severe economic costs aswell. Worldwide, approximately one in everytwo households affected with TB face costswhich is higher than 20% of their totalhousehold income. In 2022, about 13 billionUS dollars is required for TB diagnosis,treatment, and prevention, worldwide.Unfortunately, the funding in low- andmiddle- income countries (LMICs), that havealmost 98% of the total TB cases, is farbelow the required target.
150 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Tuberculosis in IndiaIndia has the highest number of TB cases
in the world. According to the India TB report2020, the incidence of TB in India in 2019was 26.9 lakhs.TB is the leading cause ofsevere illness and death among people livingwith HIV. India ranks second in the world andaccounts for 9% of the global burden of HIVassociated with TB infection. With the rise insocio-economic status of people in India, theincidence of diabetes mellitus (DM) hasincreased dramatically. Evidence frommodelling studies indicate that approximately20% of all tuberculosis cases in India alsosuffer from diabetes. Diabetes increase therisk of TB by 3 times. Diabetes can lead toworsening of the clinical condition in TBcases, and presence of TB disease can lead tobad control of blood sugar levels in peoplewith diabetes. In 2019, 64% of the notified TBpatients had their blood sugar screened. Amongall the TB patients screened for blood sugar,7% had diabetes-TB, and 52% among thesewere linked to diabetic therapy.
India is the second largest consumer oftobacco worldwide, and is the third largestproducer of tobacco after China and Brazil.Under the National Tuberculosis EliminationProgram (NTEP), 57% of notified TB patientshad their tobacco usage status known, and14% among them were known tobacco users.Among the TB cases who were tobacco users,24% were linked to tobacco cessation centres,in addition to brief counselling being providedto all TB patients. Undernutrition is also astrong risk factor for developing TB disease.Undernutrition contributes to about 55% of
the annual incidence of TB in India. TheGovernment of India (GoI) has committed600 crores INR for nutritional support of Rs.500 per month to every TB patient throughdirect benefit transfer into the bank accountof the beneficiary. Till December 2019,approximately 38 lakh beneficiaries have beenpaid under the scheme.
TB is also a disease of concern duringchildhood and in pregnancy. Women ofreproductive age group (15-49 years)contribute to a significant burden of TB inIndia and worldwide. In 2011, India hadapproximately 44,500 pregnant women withTB, and contributed to 20.6% of the globalburden of TB in pregnancy. Pediatric TB isone of the 10 major causes of death worldwidein children below 15 years of age. In India,approximately 3,42,000 new cases of pediatricTB are reported every year, and accounts for13% of overall TB in the country.
The United Nations SustainableDevelopment Goals (SDGs) targets to end thetuberculosis epidemic by 2030. In India, theTB National Strategic Plan (NSP) 2020-2025,is a plan formulated by the Government ofIndia (GoI) which aims to eliminate TB inIndia by 2025, five years ahead of the SDGgoals for 2030. The vison of NSP is to have aTB-free India, with zero deaths, disease, andpoverty due to tuberculosis by 2025. The NSPemphasizes on prompt diagnosis of all TBcases using highly sensitive diagnostic testsavailable in the public and private sector. The
......To be Continued at Page No.-172

151Science Horizon:Volume 7: Issue 4
APRIL, 2022
PhysiologyMycobacterium tuberculosis is an
intracellular organism, obligate, highly aerobicand require high level of oxygen. M.tuberculosis is straight and slightly curved
rod measuring about 1 to 4 µ long and 0.2 to0.8 µ wide. It may be arranged in groupsor single, pairs, beaded form or inclusters.
PathophysiologyHumans are the only known
reservoirs ofM.tuberculosis. Amisconception is that M.tuberculosis can be spread by shakinghands, making contact with toilet seats,sharing food or drink, or sharingtoothbrushes. Kissing could be a
IntroductionMycobacterium tuberculosis is a species
of pathogenic bacteria in the familymycobacteriaceae and the causative agent oftuberculosis, discovered in 1882 by RobertKoch. M. tuberculosis has an unusual waxycoating on its cell surface primarily due to thepresence of mycolic acid. This bacterium isalso known as “Kochbacillus”.
Tuberculosis (TB) is caused byM.tuberculosis. The bacteria usually attackthe lungs known as pulmonary tuberculosis.The bacteria also affect other parts of thebody such as spine, kidney, brain (except hairand nail) known as extra pulmonarytuberculosis.
Figure-1
Figure-2
2
MYCOBACTERIUMTUBERCULOSIS: THE BACTERIA
CAUSING TUBERCULOSIS
1Ratnaprava Mohapatra2Ipsita Jena
3Paresh Nath Mohanty

152 Science Horizon:Volume 7: Issue 4
APRIL, 2022
possible route of transmission if the person isexcreting many mycobacteria through thesputum. However, the major spread isthrough air droplets originating from a personwho has the disease either through coughing,sneezing, speaking, singing, or laughing.
When in the lungs, M.tuberculosisis phagocytosed by alveolar macrophages(pneumocyte Type I & II), but they are unableto kill and digest the bacterium. Its cell wallprevents the fusion of the phagosome withthe lysosome, which contains a host ofantibacterial factors. Specifically, M.tuberculosis blocks the bridging molecule,early endosomal autoantigen however, thisblockade does not prevent fusion of vesiclesfilled with nutrients. Consequently, the bacteria
multiply unchecked within the macrophage.
MicroscopyOther bacteria are commonly identified
with a microscope by staining them with Gramstain. However, the mycolic acid in the cellwall of M. tuberculosis does not absorb thestain. Instead, acid-fast stains such as Ziehl–Neelsen stain, or fluorescent stains suchas auramine are used. Cells are curved rod-shaped and are often seen wrapped together,due to the presence of fatty acids in the cellwall that stick together. This appearance isreferred to as cording, like strands of cordthat make up a rope. M. tuberculosis ischaracterized in tissue by caseating granulomascontaining Langhans giant cells, which have a“horseshoe” pattern of nuclei.
Figure-3

153Science Horizon:Volume 7: Issue 4
APRIL, 2022
CultureM. tuberculosis can be grown in the
laboratory. Compared to other commonlystudied bacteria, M. tuberculosis has aremarkably slow growth rate, doubling roughlyonce per day. Commonly used media includeliquids such as Middlebrook 7H9 or 7H12,egg-based solid media such as Lowenstein-Jensen, and solid agar-based suchas Middlebrook 7H11 or 7H10. Visiblecolonies require several weeks to grow onagar plates. It is distinguished from othermycobacteria by its productionof catalase and niacin.
Signs & SymptomsSymptoms of M. tuberculosis include
coughing that lasts for more than threeweeks, hemoptysis (blood in cough), chestpain when breathing or coughing, weight loss,fatigue, fever, night sweats, chills, and loss ofappetite. M. tuberculosis also has the potentialof spreading to other parts of the body.
Antibiotic Resistance (ABR)Resistance to antibiotics in M.
tuberculosis typically occurs due to eitherthe accumulation of mutations in the genestargeted by the antibiotic or a change in
titration of the drug. M. tuberculosis isconsidered to be multidrug-resistant (MDRTB) if it has developed drug resistance toboth rifampicin and isoniazid, which are themost important antibiotics used in treatment.Additionally, extensively drug-resistant M.tuberculosis (XDR TB) is characterized byresistance to both isoniazid and rifampin,plus any fluoroquinolone and at least one ofthree injectable second-line drugs (i.e.,amikacin, kanamycin, or capreomycin).
GenomeThe genome of the H37Rv strain was
published in 1998. Its size is 4 million basepairs, with 3,959 genes; 40% of these geneshave had their function characterized, withpossible function postulated for another 44%.
EvolutionThe M. tuberculosis complex evolved in
Africa and most probably in the Horn ofAfrica. In addition to M. tuberculosis, the M.tuberculosis complex (MTBC) has a numberof members infecting various animal species,these include M. africanum, M. bovis(Dassie’s bacillus), M. caprae , M.microti, M. mungi, M. orygis, and M.pinnipedii.
Figure-4 Figure-5 Figure-6

154 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Tests for TB InfectionThe screening of groups with a high risk
for developing tuberculosis (TB) is a priorityin order to control this disease. Since there isno gold standard for the diagnosis of latent TBinfection (LTBI), both the tuberculin skin test
(TST) and the interferon-gamma release assays(IGRA) have been used for this purpose.
Identification of the M. Tuberculosiscomplex by the Molecular Line probe Assay
Polymerase chain reaction (PCR) wasinvented by Karry Mullis in 1983. It is a techniquethat takes a small amount of a specific DNAsequence and amplifies it for further testing. It isalso called “Molecular Photocopier”.
Hybridization – Detection StepsReverse Hybridization – Unlabeled probespecific for Mtuberculosis complex or othermycobacterial species are bound to the strips.Biotin labeled target DNA binds to thecomplementary probe on strip.
Probe target complex is detected-Streptavidin conjugated reagent detects biotinlabeled target probe complex.
TST IGRAGood for serial testing Not as good for
serial testingInexpensive More expensiveUniversally accessible Skill, equipment and
timeframe needed limitaccessibility
Low specificity in certain High specificity in allpopulations (BCG-60%) populationsTwo visits One visitVariability in test interpret- Low variability in testation by reader *** interpretation byreader
TST Vs. IGRA
Figure-7

155Science Horizon:Volume 7: Issue 4
APRIL, 2022
CBNAAT – Cartridge-Based NucleicAcid Amplification Test
CBNAAT system detects DNA sequencesfor M. Tuberculosis and rifampicin resistanceby polymerase chain reaction (PCR). It purifiesand concentrates M. tuberculosis bacilli, fromsputum samples, isolates genomic materialsfrom captured bacteria by sonication andsubsequently amplifies the genomic DNA byPCR. The process identifies clinically relevant,rifampicin resistance inducing mutations inthe RNA polymerase beta (rpobeta) gene inthe M. Tuberculosisgenome in the real timeformat using fluorescent probes calledmolecular beacons. Results are obtained fromunprocessed sputum samples in 90 minutes.
Liquid Culture MGIT 960The MGIT (Mycobacteria Growth
Indicator Tube) consists of liquid brothmedium that is known to yield better recoveryand faster growth of mycobacteria. The MGITcontains 7.0 ml of modified Middlebrook7H9 broth base. This medium is terminallysterilized by autoclaving. An enrichment, MGITOADC (Oleic acid, Albumin, Dextrose andCatalase) or MGIT 960 Growth Supplement,is added to make the medium complete. Thisgrowth supplement is essential for growth ofmany mycobacteria, especially those belongingto M. tuberculosis complex. Addition of theMGIT PANTA is necessary to suppresscontamination.
In addition to Middlebrook 7H9 liquidmedia, the MGIT tube contains an oxygen-quenched fluorochrome, tris 4, 7-diphenyl-1,10-phenonthroline ruthenium chloride
pentahydrate, embedded in silicone at thebottom of the tube. During bacterial growthwithin the tube, the free oxygen is utilized andis replaced with carbon dioxide. With depletionof free oxygen, the fluorochrome is no longerinhibited, resulting in fluorescence within theMGIT tube when visualized under UV light.The intensity of fluorescence is directlyproportional to the extent of oxygen depletion.
MGIT tubes may be incubated at 37ºCand read manually under a UV light or enteredinto a MGIT 960 instrument where they areincubated and monitored for increasingfluorescence every 60 minutes. Growth ofbacteria as well as mycobacteria increases thefluorescence. In case of M. tuberculosis, atthe time of positivity, there are approximately105 – 106 colony- forming units (CFU) perml of medium. The instrument declares a tubenegative if it remains negative for six weeks(42 days). The detection of growth can also bevisually observed by the presence of a non-homogeneous light turbidity or small granular/flaky appearance in the medium. Growth ofsome non tuberculous mycobacteria or NTM(most commonly rapid growers) results inlight turbidity, while contaminating bacteriagenerally produce heavy turbidity.
Drug susceptibility testing can beperformed based on the same principle. TwoMGIT tubes are inoculated with the test culture.A known concentration of a test drug is addedto one of the MGIT tubes, and growth iscompared with the MGIT tube without thedrug (growth control). If the test drug is active
......To be Continued at Page No.-160

156 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Fig.1:Simple representation of the spectrum of tuberculosis disease and association with cell-mediated immunity, especially the role of CD4+ T lymphocytes and IFN
investigation. Proper understanding of theimmunological aspects of tuberculosis is vitalin the endeavour to develop effective vaccinesagainst the pathogen and disease.
The BCG vaccine, a live attenuatedbacterial vaccine has been around for more
Primary TuberculosisPrimary tuberculosis is characterized by
granulomas in the lungs. TB granulomas arecomprised of lymphocytic infiltration,consisting of both T and B lymphocytes, inaddition to macrophages which surround them
3
IMMUNOLOGICAL CONCEPTS INTUBERCULOSIS
1Sonalika Rath2Ira Praharaj
Although Mycobacterium tuberculosis(M.tuberculosis) is one of the oldest bacterialpathogens known to man and grown in culture,the understanding of immunity to this pathogenis still evolving with newer methods of
than 100 years now and has been usedworldwide but has not been effective inreducing the burden of TB disease.
Spectrum of TB disease

157Science Horizon:Volume 7: Issue 4
APRIL, 2022
as well as fibroblast cells. The major roleplayed by the granuloma is in containing theM.tuberculosis infection which in manyendemic areas occurs early on in life.
Latent TuberculosisAfter infection with M.tuberculosis, in
a number of instances, the bacteria are notcompletely eradicated from the body inspiteof immune responses, both cell mediatedand humoral. A latent state of existence inthe body is seen in a considerable proportionof individuals infected with tuberculosis.This has been estimated to be as much asone-third of the global population. Of them,only 5-15% of individuals with latenttuberculosis ever progress to active diseaseduring their lifetime.Mycobacterium tuberculosis as aparadigm of an intracellular pathogen
The capacity to survive and multiplyinside cells and especially macrophages isconsidered one of the important virulencefactors for M.tuberculosis.The bacteria persistin phagosomes that prevent fusion withlysosomes.M.tuberculosis targetsmacrophages, especially the alveolarmacrophages in primary infection, whichalthough engulf the bacteria do not kill themand may in fact lead to their persistence andmultiplication intracellularly.M.tuberculosis,once internalized by macrophages preventsphagolysosomal fusion and infact persists inthe phagosomes.
The pathogen has a highly evolvedmechanism for evading the host immuneresponse against it and multiplying even in thepresence of substantial host immune response.
The intracellular location protects theorganism from antibody mediated immuneresponse and cell mediated immune responsewith different effector T-cell populations needto be in force for clearing the organism. Cellmediated immunity plays an especiallyimportant role in tuberculosis.
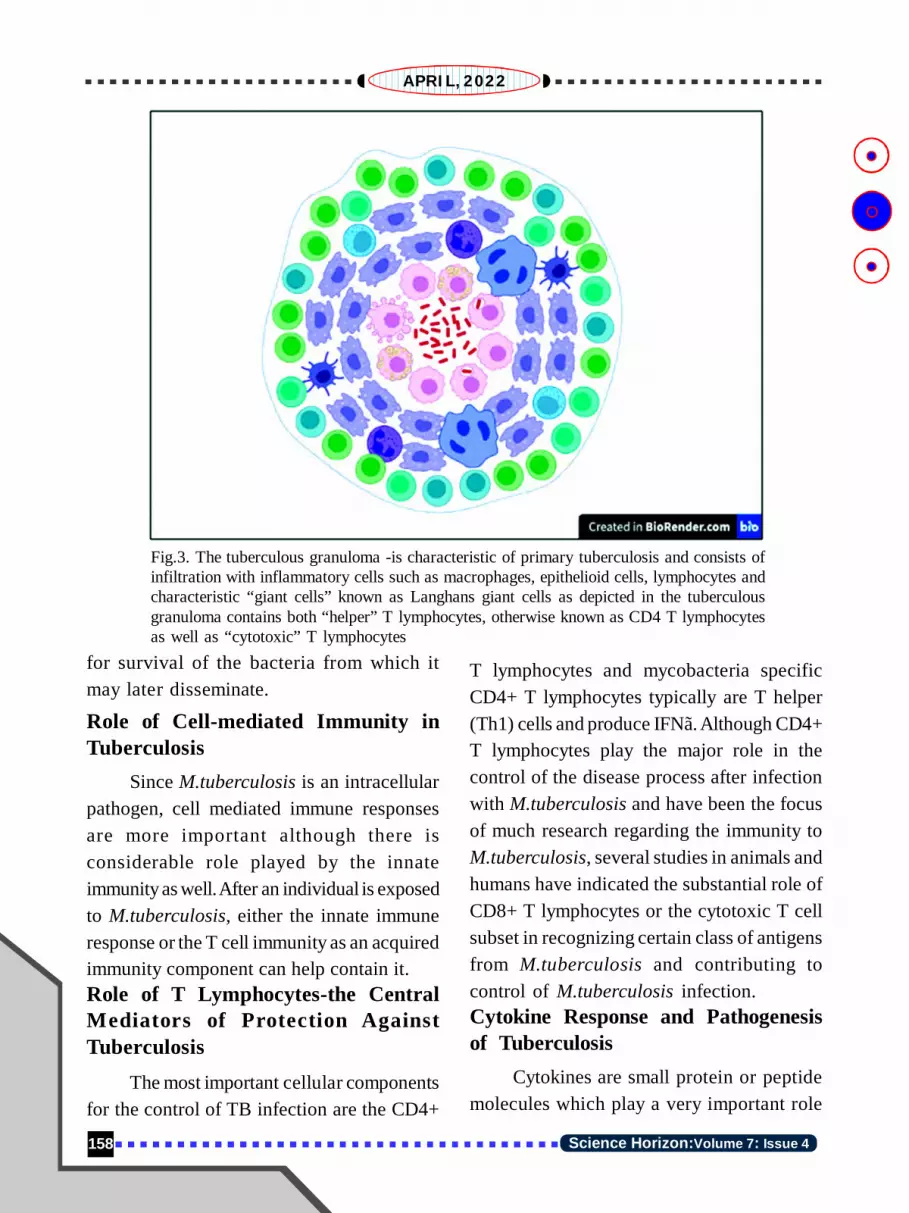
The characteristic pathological hallmarkof tuberculosis infection is the tuberculargranuloma. It is an aggregate of differentinflammatory and immune cell types such asmacrophages, other mononuclear cells,lymphocytes and characteristic giant cellscalled as “Langhans Giant Cells”. Althoughlong considered essential for control oftuberculosis infection, recent conceptsabout tubercular granulomas have seen ashift in the perception of their role as niches
Fig. 2: Depicting the persisting ofM.tuberculosis bacteria intact inmacrophages (phagosomes) without phago-lysosomal fusion
158 Science Horizon:Volume 7: Issue 4
APRIL, 2022
for survival of the bacteria from which itmay later disseminate.
Role of Cell-mediated Immunity inTuberculosis
Since M.tuberculosis is an intracellularpathogen, cell mediated immune responsesare more important although there isconsiderable role played by the innateimmunity as well. After an individual is exposedto M.tuberculosis, either the innate immuneresponse or the T cell immunity as an acquiredimmunity component can help contain it.Role of T Lymphocytes-the CentralMediators of Protection AgainstTuberculosis
The most important cellular componentsfor the control of TB infection are the CD4+
T lymphocytes and mycobacteria specificCD4+ T lymphocytes typically are T helper(Th1) cells and produce IFNã. Although CD4+T lymphocytes play the major role in thecontrol of the disease process after infectionwith M.tuberculosis and have been the focusof much research regarding the immunity toM.tuberculosis, several studies in animals andhumans have indicated the substantial role ofCD8+ T lymphocytes or the cytotoxic T cellsubset in recognizing certain class of antigensfrom M.tuberculosis and contributing tocontrol of M.tuberculosis infection.Cytokine Response and Pathogenesisof Tuberculosis
Cytokines are small protein or peptidemolecules which play a very important role
Fig.3. The tuberculous granuloma -is characteristic of primary tuberculosis and consists ofinfiltration with inflammatory cells such as macrophages, epithelioid cells, lymphocytes andcharacteristic “giant cells” known as Langhans giant cells as depicted in the tuberculousgranuloma contains both “helper” T lymphocytes, otherwise known as CD4 T lymphocytesas well as “cytotoxic” T lymphocytes

159Science Horizon:Volume 7: Issue 4
APRIL, 2022
in cell to cell signaling and in the immuneresponse to different pathogens by enablingcommunication between different cell types.In case of tuberculosis, protection andcontrol of TB disease is conferred by aspecific kind of immune response known asthe Th1 response which leads to aproinflammatory response important forkilling of intracellular pathogens likeMycobacterium tuberculosis. IFN-ã is also thecytokine type majorly responsible for the cross-talk between T-lymphocyte subsets and theeffector cells, i.e. macrophages. The majorcytokines responsible for a Th1 type of responseare IFNã and IL-12. The IFNã response is alsothe basis of some common diagnostic tests forTB infection and exposure such as the InterferonGamma Release Assay (IGRA).
The other important cytokine in thepathogenesis and control of TB is TNF-á whichis important in granuloma formation and hencecontrolling the disease. It is also the cytokineresponsible for destruction of lung tissue dueto host response against M.tuberculosis.
Tuberculosis and HIVHuman Immunodeficiency Virus (HIV)
disease is one of the major risk factors foractive tuberculosis diseases as well as TBreactivation. The Human immunodeficiencyvirus specifically affects particular subsets ofthe cell-mediated immunity in the human body,i.e. the CD4 T lymphocytes, otherwise knownas the “helper” T cells.
HIV disease not only increases thepropensity for developing active TB diseasebut also changes the clinical presentation.HIV positive individuals and patients with
active disease have a higher likelihood ofdeveloping extrapulmonary TB or TB whichaffects organs other than the respiratorysystem. Therefore, screening for TB infectionand disease is very important in HIV positiveindividuals.Immunity to TB, Current TB Vaccineand Translation to Newer TB Vaccines
The oldest vaccine against tuberculosis,Bacillus Calmette Guerin (BCG) developedover 13 years between 1908 and 1921 is aweakened or attenuated strain ofMycobacterium bovis, closely related toMycobacterium tuberculosis. BCG vaccinehas been used in many countries but has notbeen effective in preventing many forms oftuberculosis including the severemanifestations of tuberculosis. The efficacyof the BCG vaccine can range from 0 to 80%with some protection for childhoodmanifestations of tuberculosis such astuberculous meningitis. The vaccine efficacyfor BCG appears to be closely related to thegeographical location and is lowest in areas ofthe world where the TB burden is high and thepopulation is exposed frequently and early toM.tuberculosis as well as multiple species ofenvironmental non-tuberculous mycobacteria.Owing to the many limitations of the BCGvaccine and its limited efficacy in preventingmost forms of TB in adults in many parts ofthe world, there is considerable emphasis onnovel TB vaccines and vaccine strategies aimedat both preventive TB vaccines which shouldbe administered early on in life in infancybefore exposure to M. tuberculosis orenvironmental mycobacteria, as well as
160 Science Horizon:Volume 7: Issue 4
APRIL, 2022
therapeutic vaccines which are aimed at beingused along with the anti-TB chemotherapeuticagents/drugs and to prevent recurrent disease.The major types of preventive TB vaccinesinclude whole-cell vaccines, subunit vaccinesand inactivated vaccines. Although a number ofTB vaccine candidates, numbering more than20 have progressed through clinical studies andclinical trials in the last 2 decades, for a numberof them the disappointing results have onlyrevealed the lack of complete understanding ofthe immune response to tuberculosis and itscomplexity in different host conditions.
Among the different new-age vaccinesin various stages of development are vaccinecandidates using whole-cell, viral vectorvaccines and vaccines using recombinantproteins.One of the major hurdles faced inpre-clinical phases for TB vaccinedevelopment is the absence of appropriateanimal models in which these vaccines canbe tested before being tested in humans.Lack of clinical/immunological correlatesof protection makes the process ofevaluating efficacy of newer tuberculosisvaccines difficult.
Going forward, the evolving concepts inimmune response to tuberculosis as well asbetter animal models and relevant correlatesof protection against TB disease need to beincorporated in the quest to develop effectivevaccines against this organism.
References1. Berger, A. “Th1 and Th2 responses: what are
they?.” BMJ (Clinical research ed.) vol.321,7258 (2000): 424. doi:10.1136/bmj.321.7258.424.
2. O’Garra, A. and Britton, W.J. (2008).Cytokines in Tuberculosis. In Handbook ofTuberculosis (eds S.H.E. Kaufmann, E. Rubin,W.J. Britton and P. Helden). https://doi.org/10.1002/9783527611614.ch25.
3. Flynn JL.Immunology of tuberculosis andimplications in vaccine development.Tuberculosis (2004) 84, 93–101
4. Ehlers, Stefan, and Ulrich E Schaible. “Thegranuloma in tuberculosis: dynamics of a host-pathogen collusion.” Frontiers inimmunology vol. 3 411. 7 Jan. 2013,doi:10.3389/fimmu.2012.00411.
5. Cobelens, Frank et al.Accelerating researchand development of new vaccines againsttuberculosis: a global roadmap. The LancetInfectious Diseases, 28 Feb 2022.
ICMR- Regional MedicalResearch Centre,
Bhubaneswar
against the isolated mycobacteria, it willinhibit the growth and thus there will besuppression of fluorescence, while thegrowth control will grow uninhibited andwill have increasing fluorescence. Growthis monitored by the BACTEC 960instrument which automatically interpretsresults as susceptible or resistant.
TrueNaTDetection of rifampicin resistance in
M. tuberculosisusingTruenat MTB/MTBPlus aids in the diagnosis of MDR-TB. Thistest detects the presence of major mutations(SNPs) in the MTB genome that are knownto cause resistance to rifampicin.
Intermediate Reference Laboratory (IRL), ATD&TC,
SCB Medical College, Cuttack
.....Continuing from Page No.-155

161Science Horizon:Volume 7: Issue 4
APRIL, 2022
4
SYMPTOMS OF TUBERCULOSIS
1Manoranjan Pattanaik2S. PothalIntroduction
Tuberculosis (TB) is caused by a bacteriacalled Mycobacterium tuberculosis. Medicalscience has advanced a lot in the 21st centurybut clinical history still holds the pride ofplace and symptomatology remains the key toapproach for the diagnosis of tuberculosis.Application of the knowledge regarding thesymptoms & signs by the common man cansave tremendous resources in respect offinances, equipment and personnel requirementfor case finding campaign particularly in ahuge population like India. Based on patient’sclinical symptoms and other investigations,doctor can understand the nature, severity andextent of TB.
However, clinical approach has itslimitation. At times clinical evidence may beabsent or insufficient or at times evenmisleading. Doctor used to apply his/herclinical skill with help of different investigationsfor the diagnosis & proper management of TB.Demonstration of TB bacteria in patient sampleswill confirm the definite diagnosis.
Clinical HistoryFamily history of TB, particularly infant
& children,are important but may not always
be present. Other possible source ofinfection from close contact other than familymember should be kept in mind which helpsthe doctor to treat TB in a precise way. TBpatients should provide details of previousillness (like diabetics, peptic ulcer, HIV,chronic kidney diseases, cancer, emotionalstress etc.), drug history (steroid, otherimmunosuppressive drug, cancer treatment)to treating physicians as, exposure to diseases/drugs could be a potential source for decreasedimmunity in patients leading to developmentof TB disease. Even past history of any anti TBdrugs with duration of treatment should beexplained by the patient or by previousdocument which helps the physician forprescribing proper anti TB medication. Apatient’s past & present occupation (e.g. coalmines), working environment, nature of workmay predispose his/her susceptibility to TB.Patient’s general pattern of life comprisinghis/her habits, recreation and behavior mayinfluence his/her health. Malnutrition,excessive drinking, smoking, indifferent familylife, inadequate rest also undermine health anddecreases the immunity of patients, whichlead to development of TB. Doctors usually

162 Science Horizon:Volume 7: Issue 4
APRIL, 2022
ask the patient to tell his/her history in his/herown words, as many important links in thechain of evidence may thus be discoveredwhich may otherwise be missed.
SymptomatologySymptoms of Pulmonary TB (TB inside
lung) do not provide a clear-cut diagnosis; asthey are common to many non-tuberculosisconditions affecting the lungs. Symptoms maybe absent, not only during the early phase ofdevelopment of disease but at times even inadvanced stage of the disease. Appearance ofsymptoms, early or late, depends not onlyupon the extent and situation of the lesionbut also primarily upon the human body’sresponse to the disease. High immunity ofpatient may inhibit the activity of TB bacteriaand prevent any tissue reaction or, as usuallyhappens, the disease may progress slowly.Moreover, symptoms may persist even afterthe lesion is healed.
The following symptoms are common inTB; cough, fever, weakness, weight loss, chestpain, loss of appetite, haemoptysis(coughingup blood) etc. Of the above symptoms, themost common symptoms are cough for morethan two weeks. Even some other respiratorydisease can be cause of cough, still TB shouldbe suspected as two diseases may also bepresent simultaneously. Blood in sputum mayoccur due to other diseases, but TB is morecommon than other diseases. Blood in sputummay be due to healed TB too. TB can affectany organ of body except nail & hair, but inabout 80% of TB cases, the lungs areaffected. So, chest symptoms are commonlyencountered in TB patients. TB which affects
lung is called as Pulmonary TB, whereas TBoutside the lung is called as extra-pulmonaryTB. Symptoms of extra-pulmonary TB dependon the site of affected organ. Out of extra-pulmonary TB, TB in lymph node (usuallyneck swelling), pleural effusion(accumulation of water outside the lung butinside the chest) are common.
Lassitude (physical or mental tiredness,lack of energy) is one of the earliest symptoms.In the beginning, it is experienced only towardsthe end of the day and disappears after a shortrest. Gradually, the patient begins to feeltired earlier and more easily. Even the night’srest may not relieve him/her. Digestivedisturbances are sometimes prominent. Theyare characteristically vague and of the nature ofdyspepsia, such as fullness after meals,flatulence. Loss of weight, slow but progressive,is frequent. Every case of Pulmonary TBexhibits some degree of fever. In early phases,the fever is slight and of short duration, usuallyoccurring in the late afternoon or evening.
SignsThough Pulmonary TB is more common,
still extra-pulmonary TB is frequentlyassociated with it. So, a thorough generalphysical examination is required covering allthe systems (respiratory, cardiac, digestive,neurological, etc). It helps the physician notonly in the identification of other sites of TB,but also in the detection of other non-tuberculardiseases (Chronic Kidney Diseases, DiabeticsMellitus, etc) which may require modificationof patient management.Through generalexamination, physician can identify; anemia(low hemoglobin), cyanosis (bluish

163Science Horizon:Volume 7: Issue 4
APRIL, 2022
discoloration of finger/lip/tongue), clubbingof fingers(swelling of dorsal surface of distalend of finger), edema (swelling of body/feet)etc. Physical examination of the chest, likeany other diagnostic measure, has its value aswell as limitation. None of the observedphysical signs is pathognomonic oftuberculosis. Many clinical findings like;pleural rub, pericardial friction, bronchospasm,localized wheeze help physician in precisediagnosis which may be missed by otherinvestigations. Clinical examination also helpsphysician for further exploration duringtreatment, which may not be possible by otherinvestigations particularly in low resourcesettings; for example, identification of idealsite for aspiration of fluid from pleural spacein pleural effusion(fluid outside lung but withinchest). Physical examination usually enhancesthe doctors’ ability to interpret the varied anddifferent investigation reports. Pulmonarytuberculosis mostly occurs in apical andposterior segments of upper lobes and apical
segments of lowerlobes of the lungs.Thus early physicalsigns are usually foundposterior over thoseregions.
Skeletal deformities,poor expansion ofchest, asymmetricalabnormalities in chestwall, retraction orprominence of any partof chest can be
appreciated by physician by only observingthe patient without touching him/her.Displacement of trachea (wind pipe), apexbeat of heart suggest the nature of underlyingpathology. Pattern of swelling of lymph node(consistency, size, conglomeration) at timeshelps physician for further effective mode ofinvestigation for firm diagnosis oftuberculosis. Type of appreciation of voicesound by hand by physician over chest wall ofpatients gives many information of underlyinglung pathology. Changes in percussion noteover chest wall gives many physiological orpathological information of lung condition.Finally, stethoscope helps physician foridentification of underlying lung physiologyor pathology by listening to the type of breathsound, adventitious sound, voice sound,whispered sound over chest wall.
1Department of Pulmonary Medicine
SCB Medical College, Cuttack2Department of Pulmonary Medicine,
VIMSAR, Burla

164 Science Horizon:Volume 7: Issue 4
APRIL, 2022
5LABORATORY DIAGNOSIS OF
TUBERCULOSIS
1Sujeet Kumar, 2Sarita Kar,3Himadri Bhusan Bal, 4Sunil Swick Rout,
5Dasarathi Das, 6Sidhartha Giri, & NRLLaboratory Team*
Tuberculosis (TB), is a highly infectiousdisease caused by Mycobacteriumtuberculosis (M.tb) and primarily affects thelungs.According to the World HealthOrganization (WHO), 1.5 million people diedfrom the disease in 2020. TB is usually curableand preventable under the right conditions andwith appropriate therapy. A variety of TB strainsexist, and some of these have become resistantto available anti-tubercular drugs.
TB is transmitted from person to personby respiratory droplets.Almost one in fourpeople in the world are infected with TBbacteria. People with well-functioning immunesystems may not experience TB symptoms,even if they are infected with the bacteria, andthis is known as latent or inactive TBinfection. Latent tuberculosis infection (LTBI)itself progresses to active disease inapproximately 5% to 10% of infected persons.The rate of progression is much greater inimmune compromised individuals such as HIV,advancing age, diabetes or other immunecompromising illnesses.
Strategies to combat tuberculosis aim,first, to identify and treat persons who haveactive disease. Tools for the diagnosis of activedisease include clinical suspicion, response
to treatment, chest radiographs, staining andmicroscopy for detection of for acid-fastbacilli (AFB), culture for mycobacteria, and,more recently, nucleic acid amplification(NAA) assays.
An ideal test for tuberculosis wouldprovide rapid results (available within 1 day),would have high sensitivity and specificity,low cost, and robustness (ability to providereproducible results in a variety of settings),would be highly automated or easily performedwithout the need for excessive samplepreparation or technical expertise, and wouldbe able to provide drug-susceptibility data.Ideally, such a test would also be able todistinguish between LTBI and active disease.
Did you know?Researchers have traced Tuberculosis or TBback to the days of the ancient Egyptiancivilization, more than 5,000 years ago.However, the first written documentsdescribing TB were found in India and inChina. In 1720, for the first time, theinfectious origin of TB was conjectured bythe English physician Benjamin Marten, in

165Science Horizon:Volume 7: Issue 4
APRIL, 2022
his publication “A new theory ofConsumption”. Both terms consumption andphthisis were used in the 17th and18th centuries, until in the mid-19th centurywhen Johann Lukas Schönlein coined theterm “tuberculosis” in the 1834.Currently Available Diagnostics Canbe Classified as Those That• Directly detect the actively growing
bacilli or the nuclei acids of bacilli.• Indirectly detect the immune response
against the bacilli.Direct Methods of M. TuberculosisDetection
Direct detection of TB infectionincludes microscopy, culture, antigendetection and nucleic acid detection methods,whereas indirect methods of detection includedetection of immune response by tuberculinskin testing (TST) and interferon gammarelease assays (IGRAs).
MicroscopySputum smear microscopy forms the
backbone for diagnosis of TB. The most regularpractice is acid fast staining using carbolfuschin, Ziehl–Neelsen (ZN) method andfluorochrome dyeauramine/rhodamineFluorescence microscopy (FM). In ZNstaining, the bacilli appear pink in a bluebackground while in auramine staining, thebacilli appear as bright yellow luminous rods,against a dark background. Microscopy isrelatively fast, inexpensive and specific forTB in high incidence areas. Sputummicroscopy has varied sensitivity and can detectthe bacilli in sputum when the load of bacilli is5000-10000 bacilli/ml. Routine microscopycannot differentiate between live and dead bacilliand hence it is not suitable to monitor TBtreatment response. It can neither be used topredict drug resistance nor the presence of nontuberculous mycobacteria (NTM).
Figure 1: Microscopy: A) Microscope; B) ZN stain; C) FM Microscopy

166 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Did you know?The famous scientist Robert Koch was ableto isolate the tubercle bacillus. He usedmethylene blue staining recommended byPaul Ehrlich and identified, isolated andcultivated the bacillus in animal serum.Finally, he succeeded in reproducing thedisease by inoculating the bacillus intolaboratory animals. This result waspresented by Robert Koch on 24thMarch 1882to the Society of Physiology in Berlin,marking a milestone in the history of fightagainst TB and this date is nowcommemorated annually as the World TBDay. Koch was awarded the Nobel prize inMedicine in 1905 for his contribution to theelucidation of the infectious etiology of TBand for his scientific results.In his early studies on the bacteria, Kochnoted that this organism was much moredifficult to stain than other bacteria that hehad previously discovered, including Bacillusanthracis. We now know that M.tuberculosis resists staining because ofits exceptionally resilient cell wall structurecontaining mycolic acids, long chainhydrocarbons akin to paraffin wax. Thisobservation led to development of a specialstaining method by Franz Ziehl, which waslater modified by Friedrich Neelsen. Thismethod also known as the Ziehl-Neelsen (ZN)stain, and the method uses heat to allowstain to penetrate the waxy surface ofmycobacteria. Use of a strong acid as adecolorizer removes the stain from allorganisms without such a waxy coat andgives the method its common name “acid-
fast staining.” The Ziehl-Neelsen methodwas further improved on by Joseph Kinyoun,who omitted the heating step, thereforelimiting the infectious risk inherent withaerosolization of M. tuberculosis. Later, bythe 1930s, E. Lowenstein and K. Jensen(their first names appear to have been lostto history) developed selective mediacontaining malachite green, now known asLöwenstein-Jensen (LJ) medium, which isstill commonly used for culture ofmycobacteria.
Culture
Culture remains the gold standard fordiagnosis of TB, and it helps in diagnosis ofdrug resistance and monitoring the TBtreatment response. However, M.tb growsextremely slowly in comparison to otherbacteria as the doubling time of M.tb is about18 hours. So, TB diagnosis and its DST byculture method is time consuming. Culturesare generally performed using solid and liquidculture medium. Traditional egg based(Lowenstein Jensen) and agar based(Middlebrook 7H10/11) media are widelyused. The conventional egg based mediumtakes from 4 to 8 weeks for visible growth ofbacteria. The growth rate of the bacteria ismore rapid in liquid medium. The mostcommon liquid culture method adopted by thelaboratories, is using Middlebrook 7H9 broth- the mycobacterial growth indicator tube(MGIT), a non-radiometric detection methodwhich measures the consumption of oxygenby fluorescence. As bacteria grow in theculture, the oxygen is utilized causing it to befluorescent when placed under UV light. The

167Science Horizon:Volume 7: Issue 4
APRIL, 2022
limit of detection by culture is 100 bacilli/ml,thus increasing the sensitivity compared tosputum microscopy.
The major limitations of culture methodsare requirement of bio-safety facilities thatare expensive to build and maintain andspecially trained laboratory technicians toperform the procedure. Hence, TB culturesare performed only at National ReferenceLaboratories (NRLs) or in hospitallaboratories having TBcontainment facility inlarge cities.M o l e c u l a rDetection: NucleicAcid AmplificationTests (NAAT)
Advent ofPolymerase ChainReaction (PCR) hasrevolutionized the areaof molecular biology.The polymerase chain
reaction (PCR) is used to make millions ofcopies of a target piece of DNA. It is anindispensable tool in modern molecularbiology and has transformed scientificresearch and diagnostic medicine.PCR and itsvariations have a wide range of specializedapplications and are used by scientists in allfields of biology. Gene amplification canachieve the goal of reducing the generationtime of microorganisms to minutes. Most
Figure 2: Culture of M. tuberculosis in LJ (solid) and MGIT (liquid) medium
Figure 3: Biosafety level 3 (BSL 3) laboratory for culture of TB bacilli

168 Science Horizon:Volume 7: Issue 4
APRIL, 2022
molecular methods detect the nucleic acid(DNA) of both live and dead bacilli. Becausethe DNA based molecular methods also candetect the DNA of a dead bacilli, they are notsuitable to monitor the TB treatment response.The major advantage of the NAAT assays isthese tests are recommended for thepaucibacillary samples like extrapulmonaryand pediatric samples.Xpert MTB/RIF and Xpert MTB/RIFUltra (CBNAAT)
Xpert MTB/RIF (Cepheid, United States)often referred to as Cartridge Based NucleicAcid Amplification Test (CBNAAT), is a rapid
molecular test, for the detection of the M.tuberculosis complex and rifampicin (RIF)resistance screening in presumptive cases.The Xpert MTB/RIF assay uses semi-quantitative nested real-time PCR to amplify a
fragment containing the 81 bp hotspot regionof the rpoB gene (codons 507–533) that isthen hybridized to five molecular beaconprobes. The whole experiment is performed ina self-contained cartridge, like a minilaboratory, to minimize carryover-contamination between samples. Compared tothe standard culture based DST, it significantlydecreases the detection time of RIF resistancefrom 4 to 8 weeks (culture and DST) to only2 hours. Recently, the next-generation XpertMTB/RIF Ultra system (Cepheid) that has alarger amplification chamber to increase theamount of sputum and two additional targets
(IS1081 and IS6110) to identify MTB hasbeen launched. It has higher MTB detectionsensitivity (16 bacilli/ml compared with 131bacilli/ml for the current Xpert MTB/RIFcartridge) and facilitates MTB screening in
Figure 4: A) CBNAAT system; B) Sample report

169Science Horizon:Volume 7: Issue 4
APRIL, 2022
specimens with low numbers of bacilli, suchas sputum samples from children and frompatients co-infected by HIV, and in difficult-to-diagnose cases, such as smear-negativepulmonary and extra-pulmonary TB.
TruenatTruenat (Molbio Diagnostics/Bigtec
Labs, Goa/Bengaluru, India), is a new chip-based, micro real-time -PCR test that detectstubercle bacilli in sputum samples inapproximately one hour. Upon receiving apositive test result, an “add-on” chip can beused to detect RIF-resistance status, addinganother one hour of test time. The test isprepared and run on the battery-poweredTruelab system, which includes the samplepreparation device (i.e., machine for DNAextraction and purification from the sputumsample) and the PCR analyzer device, available
in 1-, 2-, or 4-module configurations with thelatter most capable of testing four samplessimultaneously. Due to the portability of thistesting platform, Truenat may be valuable inperipheral healthcare settings, such as
designated microscopy centers (DMCs) andprimary healthcare facilities in India. It has adetection limit of 100 CFU/ml.
DNA Line Probe Assays Line probe assays (LPAs) are basically DNA–DNA hybridization assays that allow thesimultaneous detection of different mutationsby using multiple probes. After DNA extractionand target amplification, amplicons arehybridized to specific oligonucleotide probesthat are complementary to the target sequencesand are immobilized on the surface of a strip.After several post-hybridization washes toremove non-specific binding, the amplicon-
Figure 5: TrueNAT system: a) PCR microchip; b) Trueprep for DNA extraction; c) PCR analyzer; d)Sample report
170 Science Horizon:Volume 7: Issue 4
APRIL, 2022
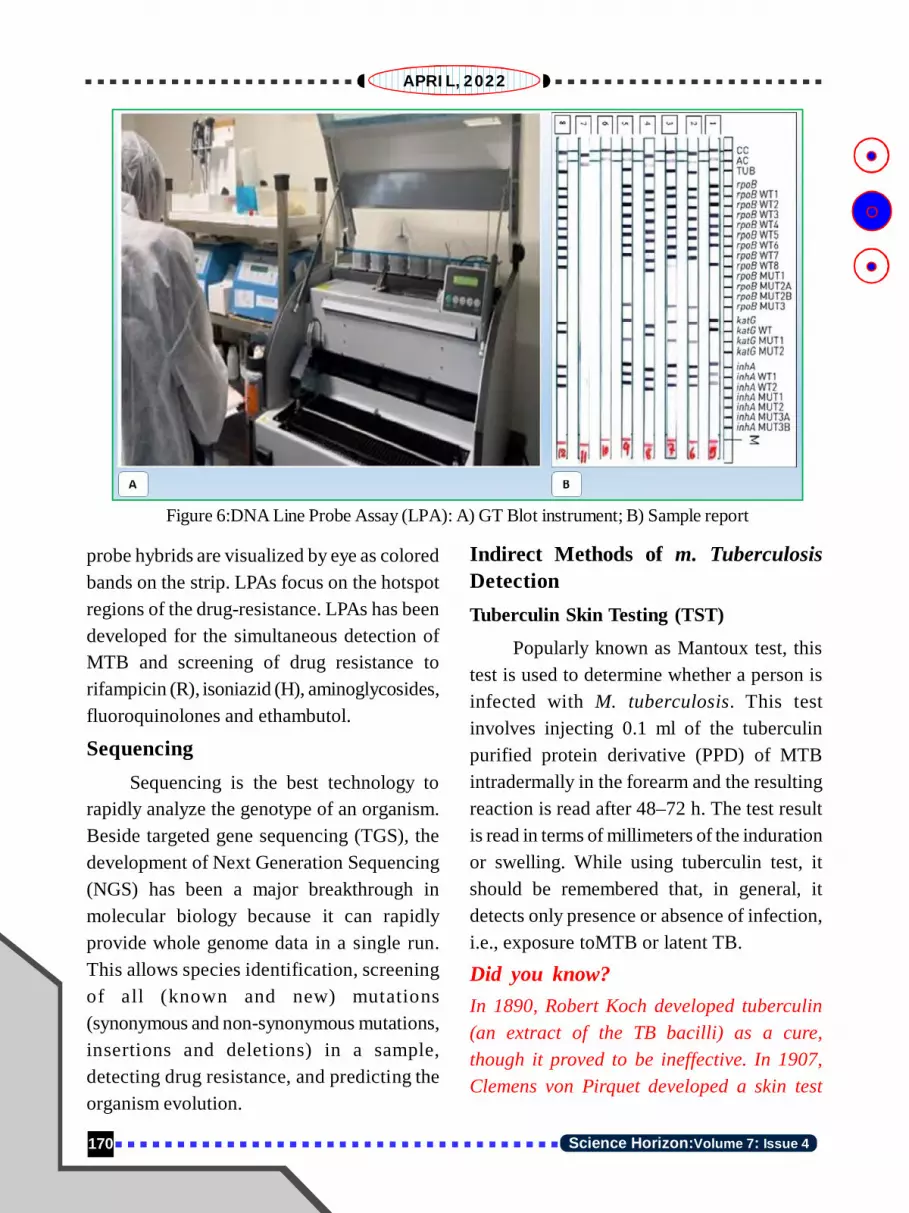
probe hybrids are visualized by eye as coloredbands on the strip. LPAs focus on the hotspotregions of the drug-resistance. LPAs has beendeveloped for the simultaneous detection ofMTB and screening of drug resistance torifampicin (R), isoniazid (H), aminoglycosides,fluoroquinolones and ethambutol.
SequencingSequencing is the best technology to
rapidly analyze the genotype of an organism.Beside targeted gene sequencing (TGS), thedevelopment of Next Generation Sequencing(NGS) has been a major breakthrough inmolecular biology because it can rapidlyprovide whole genome data in a single run.This allows species identification, screeningof all (known and new) mutations(synonymous and non-synonymous mutations,insertions and deletions) in a sample,detecting drug resistance, and predicting theorganism evolution.
Figure 6:DNA Line Probe Assay (LPA): A) GT Blot instrument; B) Sample report
Indirect Methods of m. TuberculosisDetectionTuberculin Skin Testing (TST)
Popularly known as Mantoux test, thistest is used to determine whether a person isinfected with M. tuberculosis. This testinvolves injecting 0.1 ml of the tuberculinpurified protein derivative (PPD) of MTBintradermally in the forearm and the resultingreaction is read after 48–72 h. The test resultis read in terms of millimeters of the indurationor swelling. While using tuberculin test, itshould be remembered that, in general, itdetects only presence or absence of infection,i.e., exposure toMTB or latent TB.
Did you know?In 1890, Robert Koch developed tuberculin(an extract of the TB bacilli) as a cure,though it proved to be ineffective. In 1907,Clemens von Pirquet developed a skin test

171Science Horizon:Volume 7: Issue 4
APRIL, 2022
that put a small amount of tuberculin underthe skin and measured the body’s reaction.Pirquet also invented the term “latent TBinfection” in 1909. In 1908, Charles Mantouxupdated the skin test method by using aneedle and syringe to inject the tuberculin.In the 1930s, American Florence SeibertPhD developed a process to create a purifiedprotein derivative of tuberculin (PPD) forthe TB skin test. Prior to this, the tuberculinused in skin tests was not consistent orstandardized. Seibert did not patent thetechnology, but the United States governmentadopted it in 1940.
The TB skin test is still used today and hasremained virtually unchanged for almosteighty years. A more recent advancement inTB testing has been the interferon-gammarelease assays (IGRAs).Interferon Gamma Release Assay(IGRA)
Interferon-Gamma Release Assays(IGRAs) are whole blood tests which can helpin the diagnosis of M. tuberculosis infection.However, the test cannot differentiate betweenactive tubercular disease and latenttuberculosis infection (LTBI). IGRAs measurethe reactivity of a person’s immune system to
Figure 7: Flow chart for laboratory diagnosis of TB
172 Science Horizon:Volume 7: Issue 4
APRIL, 2022
M. tuberculosis. The white blood cells (WBCs)of most people infected with M. tuberculosis,will release interferon-gamma (IFN-g) whenmixed with antigens (substances which caninduce an immune response) derived from theM. tuberculosis bacteria. For the test, freshblood sample collected from a person is mixedwith antigens and controls. The test requires asingle patient visit, and the results can beavailable within 24 hours. Another advantageof IGRA test is that prior BCG vaccinationdoes not cause a false positive test result.
Did you know?
Diagnosis of TB by any microbiological toolsand treatment for TB are available FREE ofcost at all health facilities under NationalTuberculosis Elimination Program (NTEP),India to both public and private sectorpatients by Government of India (GOI).Treatment adherence to regular and completetreatment is important for successful
treatment outcome and relapsefree cure fromTB. The TB patients are traced and treatedunder NTEP and are monitored by dedicatedNTEP treatment supervisors. In May 2012,Government of India issued a gazettenotification which makes it mandatory forprivate practitioners to notify any case ofTB that they diagnose or treat. Themechanisms provided for notification includeboth paper and case-based web based onlinereporting system called NIKSHAY. Under thescheme NIKSHAY Poshan Yojana all notifiedTB patients are provided incentive of Rs 500per month during anti-TB treatment forNutritional support in cash or in-kind supportthrough Direct benefit transfer (DBT).
1-2, 4-6ICMR- Regional Medical Research Centre,
Bhubaneswar- 7510233FIND-India, New Delhi
*Laboratory Team: Prakash Kumar Nayak, Satya NarayanSingh, Kumari Shweta, Sudarsan Biswal, Baikuntha BihariSahoo, Tapaswini Hota, Chinmayee Mohanty, Sadruddin
Khan, Subrat Kumar Barik, Sarthak Mahapatra
.....Continuing from Page No.-150network of laboratories for TB diagnosisunder the NTEP includes 6 NationalReference Laboratories (NRLs), 31Intermediate Reference Laboratories(IRLs), 50 certified laboratories for liquidculture and drug susceptibility testing(DST) services, 64 certified laboratoriesfor line probe assay (LPA) services, alongwith 20356 designated microscopy centres.
References1. Tuberculosis. World Health Organization
(WHO). www.who.int2. National Strategic Plan for Tuberculosis
Elimination 2017-2025.www.tbcindia.gov.in
3. India TB report 2020. www.tbcindia.gov.in
1&2ICMR- Regional Medical Research Centre,Bhubaneswar
3ICMR Headquarters, New Delhi

173Science Horizon:Volume 7: Issue 4
APRIL, 2022
6TREATMENT OF TUBERCULOSIS
1Thitta Mohanty2Geetanjali Panda
The basis of treating tuberculosis lies onkilling the Mycobacteria and preventingdevelopment of drug resistance by the organismfor which appropriate combination of atleastthree effective drugs in correct dosage forstipulated duration and directly observed therapy(DOTS) provided by treatment supporter(ASHA) is essential and ensured under TBcontrol program (NTEP) with an objective to“cure” and prevent “relapse”.
DOTS: Directly Observed TreatmentShort course ensures “no missed doses” andcompliance as the treatment supporter orobserver directly observes the medicationintake by the patient. Patient-centered careinvolves shared management of the illness bythe patient and health care workers
The most important drugs used for thetreatment of drug susceptible TB areIsoniazid(H), Rifampicin(R), Pyrazinamide(Z),and Ethambutol(E) called as first line antitubercular drugs available in fixed-dosecombination (FDC) i.e., all the drugs to beconsumed are contained in a single pill atfixed doses thereby reducing the number ofpills to be taken per day. The number of pillsdepends on weight of the patient according toweight band. Both new as well as previously
treated cases of drug susceptible TB aretreated with same regimen (2HRZE+4HRE)contrary to previous guidelines as the presentguideline simplifies the treatment regimen into “drug susceptible” or “drug resistant”category. To know about the drug resistancepattern of the TB bacilli, rapid molecular testingmethods (CBNAAT or TrueNat) are utilized andcarried out at designated centers in every cornerof the country and states. Besides rapidmolecular tests which give results in hours,thereare other confirmatory tests like culture andDST (both solid culture and liquid culture) withturnaround time in weeks available atIRL(STDC), Cuttack and RMRC, Bhubaneswar.Phases of TreatmentDrug susceptible tuberculosis treatmenthas two phasesi) An initial 2 months of Intensive Phase
(IP) with combination of usually 4 drugs(H,R,Z,E) to eliminate most ofmicroorganisms and reduce the risk oftreatment failure.
ii) The second phase named as ContinuationPhase (CP) of 4 months duration with acombination of usually 3 drugs (H, R, E)to ensure cure.

174 Science Horizon:Volume 7: Issue 4
APRIL, 2022
When to start TB treatmentIt should be as soon as
possible after the diagnosis ofTB is made whether withbacteriological confirmation(microbiologically confirmedTB) or on physician’s decision(clinically diagnosed TB)irrespective of immune status orcomorbidity of the patient.Timing of taking anti-tubercular treatment (ATT)
The pills should preferablybe taken at least half an hour afterbreakfast with a glass of water.No food should be consumed forat least one hour after ATTconsumption.
Common side effectsNausea and vomiting are
commonly reported by patientswhich mostly occurs with takingthe drugs on empty stomach.Urine turns orange in colour thatneed not to be panicked. Someserious side effects include skinrash, jaundice, blindness.
Weight bands and Pill numbers:
wt band (kg) Daily tablets (4FDC) for 2 months-IP Daily tablets(3FDC) for 4 months-CP
25-34 2 2
35-49 3 3
50-64 4 4
65-75 5 5
>75 6 6

175Science Horizon:Volume 7: Issue 4
APRIL, 2022
Treatment of TB in children andadolescents
First line treatment regimen (drugsusceptible) is same as recommended foradults. Adolescents can use adult formulationand may need extra support for adherence.Severe forms of tuberculosis like TBmeningitis, osteo-articular TB (bones andjoints) should have longer duration of treatment(usually 9-12 months). Breastfed babies areencouraged to continue breast feed duringtheir treatment.
Treatment of pregnant and breast-feeding women with TB
The regimen is same as other people.Breast-feeding mothers should continue tobreast feed their baby during anti TB treatmentpreferably just before the mother consumesthe drugs and few hours later.
1Department of Tuberculosis and Respiratory Diseases,
PRM Medical College, Mayurbhanj, Odisha2Department of Tuberculosis and Respiratory Diseases,
SLN Medical College, Koraput, Odisha

176 Science Horizon:Volume 7: Issue 4
APRIL, 2022
7
DRUG-RESISTANTTUBERCULOSIS
Baijayantimala Mishra
Tuberculosis (TB) is a disease caused bybacteria called Mycobacterium tuberculosis.The disease spreads from one infected personto another person through the air. TB mostcommonly affects the lungs, but it can affectother body organs, such as the brain, kidneys,intestine, lymph nodes, or bone.
In most cases, TB is a treatable andcurable disease when treated with the rightdrugs for the right duration at the righttime.However, it can lead to severe illness anddeath without proper treatment.
Drug-resistant Tuberculosis (DRTB)Drug-resistant TB is called when the
infective agent M.tuberculosis (MTB)bacteria become resistant to the drugs usedto treat TB. This means that the drug can nolonger kill the TB bacteria.
Burden and problems of DRTBAccording to the World Health
Organisation (WHO), two billion people areinfected with M.tuberculosis, roughly a quarterof the world’s population. Around 9 millionnew TB cases occur every year, and 1.5million deaths occur due to TB. As per therecent WHO report, around five lakhs peopledevelop drug resistance every year. However,
around 30% of cases were notdiagnosed, and >50% of drug resistancecases were not detected and reported. Thisindicates, many tuberculosis cases stillremain undiagnosed, detection of drugresistance is also missed in a largeproportion of tuberculosis cases, many donot have access to treatment, and lastly,treatment may not be successful in a largeproportion of patients.
India contributes approximately 25%-30% of the world’s tuberculosis cases anddrug resistance, which is the highest globalcontribution by any country. Globally,6.19%of TB cases had MDR-TB, including2.84% among new and 11.62% amongpreviously treated cases. The estimatednumber as of 2019 of multi-drug resistanceTB (MDRTB) in India was124,000, 9.1 per1lakh population. MDR status is the mostimportant parameter as this is the majordeterminant for the type of antituberculartreatment.
So, to handle the TB menace, both earlydiagnosis and early detection of drug resistanceare essential. Appropriate treatment can beinitiated on time, and the maximum possiblecure can be achieved.
177Science Horizon:Volume 7: Issue 4
APRIL, 2022
The Drugs used to Treat TBTB is primarily treated by two groups of
drugs.The first line and second lines ofantitubercular drugs.
First-line antitubercular drugs (FLDs)
Rifampicin, Isoniazid, Ethambutol andPyrazinamide belong to first-line drugs. Whena TB case is detected for the first time,thepatient is treated with the FLDs. Of the fourFLDs, rifampicin and isoniazid are the twomost essential drugs.
Second-line antitubercular drugs
These are the reserved drugs used totreat TB cases resistant to the first-line drugs.,Drugs belonging to fluoroquinolone andaminoglycosidesare among the major second-line antitubercular drugs.
Recently added antitubercular drugs
Bedaquiline, Delamanid and Linezolidare the recently added antitubercular drugsapproved for use in multi-drug resistant cases.
The emergence of strains resistant toeither of these drugs causes major concern, asit leaves the option of less effective drugs,have more toxic side effects, and result inhigher death rates.
Types of DRTBDrug resistance tuberculosis are of two
types based on the status of antituberculardrug intake.
Primary drug resistance
When drug resistance is detected in anewly diagnosed patient who has not beentreated previously with antitubercular drugs
before, it is called “Primary drug resistance”.This is primarily due to infection with a drug-resistant MTB strain.
Secondary drug resistance
When drug resistance is developed in aTB patient who is already under antituberculardrug treatment,it is called “Secondary drugresistance”. In this case, the resistance to thedrug is developed during the treatment.
How Drug Resistance Develop?Development of drug-resistance TB can
occur due to several reasons as mentionedbelow. However, TB drug resistance is mostlya man-made phenomenon due tomismanagement in administering antituberculardrugs, which leads to spontaneous mutations inM. tuberculosis that make a drug ineffectiveagainst the mutant bacteria.
Causes of DRTB developmentImproper use of the antitubercular drug
is the major reason for the development ofdrug resistance. This can be due to severalcauses like:a. Drug is not taken properly as per the
medical instructionb. Inadequate dose or irregularly
administered treatment regimen allowsdrug-resistant mutants to become thedominant strain.
c. Non-completion of the entire course ofthe treatment regimen
d. Health care providers prescribe thewrong or inappropriate treatmentregimen.
e. The wrong dose or wrong duration of the

178 Science Horizon:Volume 7: Issue 4
APRIL, 2022
course of treatment.f. Failure to achieve necessary drug levels
to deal with all populations ofmycobacteria even with appropriatelyadministered drugs.
g. Poor quality drug.
Various types of drug resistance have beendefined based on the pattern of resistance todifferent drugs used for the treatment of TB.
Types of Drug-resistant Tuberculosisa. Mono-resistant TB (MR TB). The
infecting Mycobacterium tuberculosisstrain is resistant to anyone first-lineanti-TB drug.
b. Multidrug-resistant TB (MDR-TB).When the infecting Mycobacteriumtuberculosis strain is resistant to bothIsoniazid and Rifampicin with or withoutresistance to other first-line anti-TBdrugs.
c. Rifampicin resistant TB (RR-TB). Whenthe infecting Mycobacteriumtuberculosis strain is resistant toRifampicin with or without resistance toother anti-TB drugs.It includes anyresistance to Rifampicin:
i. mono-resistance: resistance only to Rifampicin.ii. poly-resistance: MDR or XDR.
d. Pre-extensively drug-resistant TB (Pre-XDR-TB). TB is caused byMycobacterium tuberculosis strains thatfulfil the definition of MDR/RR-TB andare also resistant to any of thefluoroquinolone used for TB(levofloxacin or moxifloxacin).
e. Extensively drug-resistant TB (XDR-TB).TB caused by Mycobacteriumtuberculosis strains that fulfil thedefinition of Pre-XDR-TB and at least oneadditional Group A drug (presently toeither Bedaquiline or linezolid or both)
Of all the above types of DRTB, as a firststep,it is important to find out the status ofresistance to rifampicin and isoniazid or, inother words,to find out the status of MDR inthe patient. These two drugs are the maincomponent of the first-line drugs. Thetreatment regimen will be different if theMTB strain is resistant to these drugs or MDRstrain. So, when a patient is diagnosed for thefirst time, it is simultaneously essential toknow the MDR status.Detection Methods of Drug Resistancein MTB
There are many methods of detection ofresistance. They can be subdivided into:
A) Phenotypic Methods: To performphenotypic drug sensitivity testing (DST),mycobacteria are initially grown in culturemedia. Growth of the bacteria on the solidmedium is identified by the colony characterand on liquid media by fluorescence which isdetected by the automated detection systemof the instrument indicating a reduction inoxygen tension due to bacterial growth.
To determine the susceptibility of anydrug, MTB is grown on the culture media inthe presence of the drug and in the absence ofthe drug.
If there is no growth in the mediumcontaining the drug, it is considered as sensitive

179Science Horizon:Volume 7: Issue 4
APRIL, 2022
to the drug (MTB bacteria will get killed bythe drug).
If MTB growth occurs in the presenceof the drug, it is considered resistant to thedrug.
Examples of Phenotypic Methodsa. BACTEC 460 TB SYSTEM Radiometric
Methodb. Mycobacterial Growth Indicator Tube
(MGIT) Methodc. Versa TREK Method
The main problem with the phenotypicmethod is that it involves handling livebacteria. Hence, a higher level of biosafetymeasures involves handling live bacteria, sohigher biosafety measures are required. Also,as it needs the bacteria to grow and MTB isslow-growing, it takes several weeks to knowthe results.
B. Genotypic Methods:This is done by the
detection of genetic mutations that areresponsible for drug resistance. These aredetected using molecular methods, which arehighly sensitive and specific and take muchless time than that of the phenotypic methods.
Detection of rifampicin resistance isthe most important to be assessed first whendiagnosed with TB. This is because rifampicinresistance acts as a surrogate marker forMDR TB, because>90% of rifampicin-resistant isolates are also resistant toisoniazid. So, the resistance result ofrifampicin indicates the MDR status of theMTB strain. Various diagnostic systems candetect the MTB DNA and the rifampicinresistance.
WHO endorsed Methods Xpert MTB/RIF (Gene XPert,
Cepheid) Cartridge based nucleic acidamplification test (CBNAAT)
Figure 1:CBNAAT for MTB detection and resistance to rifampicin

180 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Truenat (Molbio diagnostics, India) is asimilar chip-based system
Both these systems can detect MTB andrifampicin resistance within 2 hours.
WHO recommends that the CBNAAT(Cartridge based nucleic acid amplificationtest): Xpert MTB/RIF to be used as the initial
diagnostic test for all adults and children withsigns and symptoms of TB, rather thanmicroscopy and culture.
LPAs (Line Probe Assay): This is a WHOendorsed molecular method for detectingrifampicin and isoniazid resistance andresistance against fluoroquinolones in smear–
Truenat system for MTB and Rifampicin resistance detection
Figure 2:TrueNat system for detection of MTB and resistance to rifampicin
Figure 3: Line probe assay (LPA) for detection of resistance to drugs in MTB

181Science Horizon:Volume 7: Issue 4
APRIL, 2022
positive clinical specimens (direct testing) incultured isolates of MTB. The method is basedon PCR and reverses hybridization.
Do We Have Treatment for DRTBTreatment of DRTB is available, and when
taken correctly, it is quite effective. However,the treatment usually is given for a moreprolonged period and involves a combinationof more than four drugs.Recently, oral drugslike Bedaquiline, Delamanid and Linezolidhave been included in the MDR treatmentregimen in place of injectable medications tomake the treatment more compliant.
Patients with DRTB are managed withthe help of a country-wide network of DRTBcentres. The result of DST, history of previousdrugs taken by the patient, and the adversereactions are considered to select theappropriate treatment regimen.
Can DRTB Be Prevented?To a great extent, development of drug
resistance can be prevented.The Governmentof India has initiated several measures throughits national Tuberculosis EliminationProgramme (NTEP) : Selection of proper treatment regimen Development and implementation of a
more effective and compliant treatmentregimen
Easy availabilityof drugs throughout thecountry
Early case detection of TB as well asDRTB by rapid molecular methods
Prevention of airborne transmission byproper biosafety measures, particularlyin crowded hospital premises.
·Key Points The bacteria Mycobacterium
tuberculosis causes TB. Drug resistance to MTB develops due
to the generation of mutation in thebacteria during the treatment
Rapid molecular testing is available todiagnose MTB and detect rifampicinresistance throughout the country byNTEP.
Most common cause of drug resistancedevelopment is non-compliance to drug
DRTB can be prevented by earlydiagnosis and proper treatment withproper monitoring
AII India Institute of Medical Sciences,
Bhubaneswar-751019, India

182 Science Horizon:Volume 7: Issue 4
APRIL, 2022
8
HIV AND TB
Prasanta Raghab Mohapatra
Acquired Immune Deficiency Syndrome(AIDS) is a progressive life-threatening diseasecaused by human immunodeficiency virus(HIV) by damaging the body immune (defence)system. Much before HIV infected humans, asimilar virus called simian immunodeficiencyvirus (SIV), originated from naturally infectedold wild-living chimpanzees and gorillas inwest-central Africa. These SIVs were perhapstransmitted to humans when African meat-eaters hunted infected chimpanzees for meatand came in interaction and mucosaltransmission with the infected blood. Overdecades, this disease entity was unknown andslowly spread across Africa and later into otherparts of the world. This was first recognized inthe western world as a new disease during 1981when rising numbers of young homosexualmen developed unfamiliar opportunisticinfections and uncommon cancers. Since then,HIV has become one of the most devastatinginfectious diseases and persistent killers inhuman history. HIV is a virus that weakens theimmune system. If HIV is not treated, it leadsto cause severe damage to the immune systemand manifests with a syndrome which presentsas varied symptoms called AIDS (acquiredimmunodeficiency syndrome).
Tuberculosis (TB) is caused by abacteria called Mycobacteriumtuberculosis, transmitted by aerosol (coughmediated through the air), and unlike AIDS, itis curable with proper treatment. In 1720, forthe first time, the infectious basis of TB wasinferred by Benjamin Marten. Robert Kochisolated the tubercle bacillus in Berlin on 24March 1882.India was the first country tostart a national TB program (NTP) in 1962.The world could not eliminate TB to date, itultimately has been a significant killer overthe centuries till date with the creation ofdrug-resistant TB. TB is (still) the leadingcause of death among AIDS patients worldwide.Among the biggest treatment dilemmas is howto manage TB/HIV at the same time.
With time, HIV has spread worldwide.TB in HIV infected people has been commondue to the ease of transmissibility, compleximmunological response, chronic progressionand the need for long-term treatment and drugresistance. HIV is the most important riskfactor for the progression of latentMycobacterium tuberculosis infection toactive disease. The risk of latent TB infection(LTBI) progression into active TB disease isnearly twenty-fold. The most common cause

183Science Horizon:Volume 7: Issue 4
APRIL, 2022
of death among people living with HIV (PLHIV)is tuberculosis. In HIV TB co-infection, poorimmune defences lead to poor control of the TBinfection, leading to widespread disseminationof various opportunistic infections.
Although the current TB-HIV epidemicis in a declining trend, it is still associatedwith a high social stigma. The difficulty intreating and preventing both has been apermanent challenge for the last few decades.As per the Global TB report 2021, with theemergence of the coronavirus virus disease2019 (COVID-19) pandemic and the resultinglockdown, there has been a significant reductionof TB diagnosis and treatment, which has led toincreased TB deaths, many unnoticed. TheCOVID-19 pandemic has reversed years ofprogress in providing essential TB controlservices. The most obvious impact is a significantglobal drop in the reporting of number of newlydiagnosed cases with TB. India has contributed41% of the worldwide decline during the firstwave of COVID-19 (between 2019 and 2020).Similarly, it has also affected HIV detectionand management adversely.
As per World TB report-2021, therewere 1.3 million TB deaths among HIV-
negative people and an additional 214 000among HIV-positive people. About 34% of thetotal number of TB deaths in HIV-negative andHIV-positive people occurs in India.
As per the recent data from NationalAIDS Control Organisation (NACO), Ministryof Health and Family Welfare, Government ofIndia, the predominant mode of transmissionof HIV infection in India is throughheterosexual contact (94%),and the next modeis by prenatal (parent to child) transmission.Prevalence among some crucial groups ofpopulations, including female sex workers(FSW), men who have sex with men (MSM),transgender (TG), and people who inject drugs(PWID), are 1.56%, 2.6%, 3.14% and6.26%,respectively.Transmission and ClinicalManifestations of AIDS
The virus is usually transmitted throughdefinite contact with infected blood, semen orvaginal fluids. If the virus cannot be eliminated,in a few weeks of getting HIV infection, thevirus replicates in human cells. With theincreased load of virus and decreased bodyimmunity, flu-like symptoms such as low-grade fever, sore throat and fatigue usually
Estimates of TB Burden (WHO 2019) Number Rate per lakh Populationin India
Incidence of TB cases (includes HIV + TB) 2.640 million 193
Incidence (HIV+TB only) 71,000 5.2
Incidence (MDR/RR-TB) 124,000 9.1
Mortality (deaths) (excludes HIV+TB) 436,000 32
Mortality (deaths) (HIV+TB only) 9,500 0.69
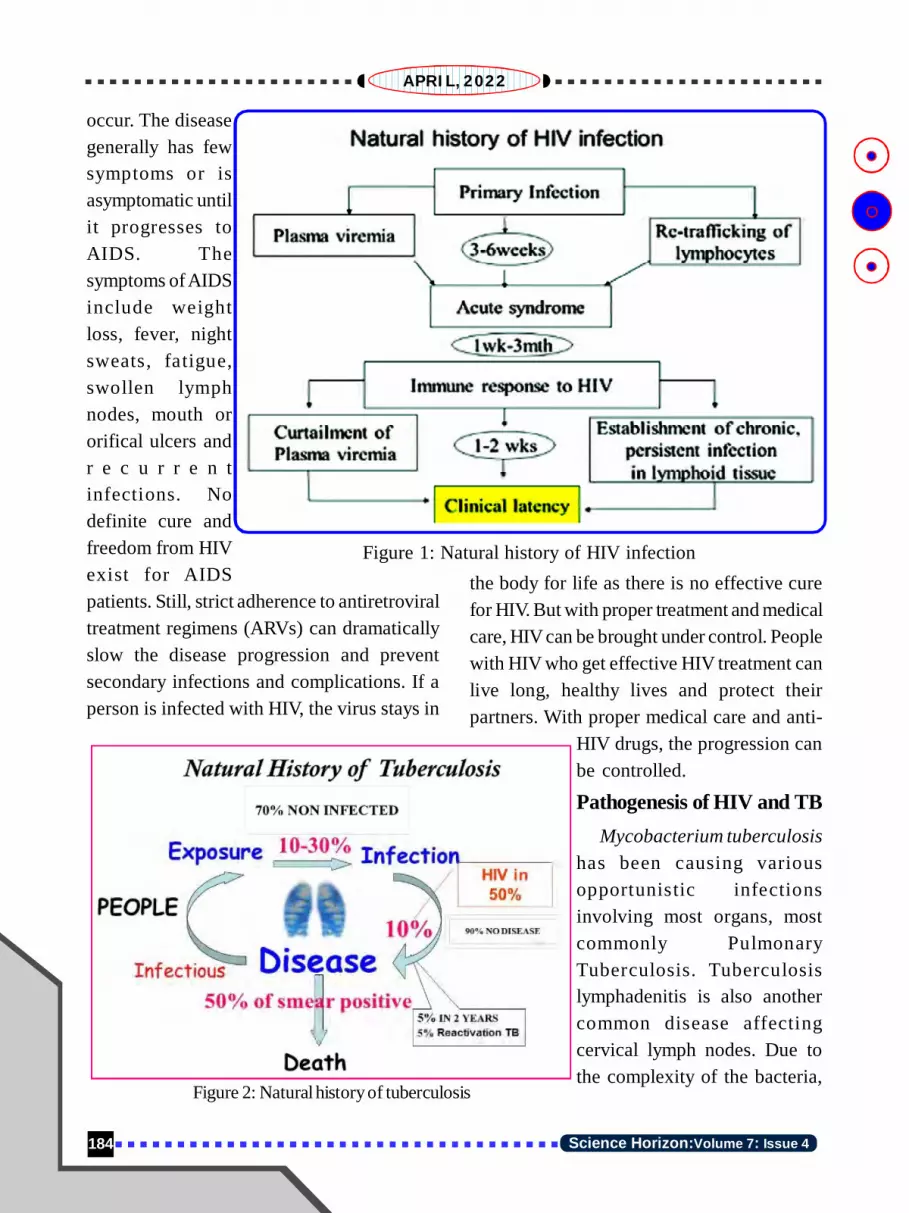
184 Science Horizon:Volume 7: Issue 4
APRIL, 2022
occur. The diseasegenerally has fewsymptoms or isasymptomatic untilit progresses toAIDS. Thesymptoms of AIDSinclude weightloss, fever, nightsweats, fatigue,swollen lymphnodes, mouth ororifical ulcers andr e c u r r e n tinfections. Nodefinite cure andfreedom from HIVexist for AIDSpatients. Still, strict adherence to antiretroviraltreatment regimens (ARVs) can dramaticallyslow the disease progression and preventsecondary infections and complications. If aperson is infected with HIV, the virus stays in
the body for life as there is no effective curefor HIV. But with proper treatment and medicalcare, HIV can be brought under control. Peoplewith HIV who get effective HIV treatment canlive long, healthy lives and protect theirpartners. With proper medical care and anti-
HIV drugs, the progression canbe controlled.
Pathogenesis of HIV and TBMycobacterium tuberculosis
has been causing variousopportunistic infectionsinvolving most organs, mostcommonly PulmonaryTuberculosis. Tuberculosislymphadenitis is also anothercommon disease affectingcervical lymph nodes. Due tothe complexity of the bacteria,
Figure 1: Natural history of HIV infection
Figure 2: Natural history of tuberculosis

185Science Horizon:Volume 7: Issue 4
APRIL, 2022
pathogenesis. Our immune system is regulatedby lymphocytes, a type of white blood cell inour body. Based on the factor called ClusterDeterminant (CD), lymphocytes are of twotypes such as CD4 (helper T cells) and CD8(cytotoxic T cells). CD4 cells are responsiblefor body immunity (cell-mediated) and fightagainst infections. The CD 4+ T helper cellsconfer the Cell-Mediated Immunity (CMI).CD4+ T helper cells also provide the defenceagainst TB infection. The hallmark of HIVinfection is the depletion of CD4+ T helpercells. Once immune suppressed, the bodycannot clear the virus and suffer fromcontinuous viral replication. CD8+lymphocytes have an essential role in theearly control of viremia, but ultimately immunesystem becomes fatigued and dysfunctionalwith persistent viremia. HIV remains a chronicinfection due to genomic integration of thevirus in the human body, its cellular dormancy,and genetic changeability, tendency, andcapability for immune escape. A persistentantigenic stimulation leads to dysfunction ofT cells; therefore, with a decrease of T-helpercells, our body immunity decreases, resultingin reactivation of TB, or ease of re-infectionby exogenous TB bacteria or development ofprogressive primary disease in HIV infection.A poor CMI leads to a weakened defenceagainst TB and is probably the most potentknown risk factor for the development of TB.The interaction between HIV and TB infectionsis bidirectional. Therefore, adequate CMI isrequired to create an immune response againstM. tuberculosis. HIV infection causes CD4+T-cell depletion and failure to impart immune
response to M. tuberculosis. Hence, as theCD4+ cell counts decline, the rate ofreactivation of TB is likely to increase. Thechance of dissemination or spread of TB inthe body also increases as the CD4+ T-cellcounts fall below 200/microliter due to poorimmune response. HIV infected persons arealso at higher risk for progressive diseasefollowing primary TB infection and subsequentTB episodes from exogenous re-infection.
Impact of TB on HIV: There has been asignificant increase in plasma HIV viremiaduring the acute phase of TB disease. There isevidence of accelerated HIV progression partlyattributable to the increased systemic immuneactivation in HIV TB co-infection.
Several other mechanisms in thepresence of tuberculosis infection maycontribute to augmented virus replication. Eventhe local sites of active tuberculosis infectionused to act as epifocal of HIV replicationirrespective of systemic HIV-1 activity. Increased secretion of different pro-
inflammatory cytokines, like tumournecrosis factor (TNFá), has been knownto induce viral replication.
Immune activation due to TB infectionleads to increased expression ofchemoreceptors (CXCR4 and CCR5)leads to increased viral entry into theimmune cells and subsequent highreplication and viremia.
Lipoarabinomannan, a cell wall elementof MTB, trigger virus replication in virus-carrying cells by inducing TNF–á andIL-6 production.

186 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Clinical PresentationThe clinical presentation of HIV
associated tuberculosis is varied and oftenatypical. Clinical presentation of TB in HIVinfected patients largely depends on the levelof immunosuppression. In patients withrelatively preserved immune function (CD4+count > 200 cells/mm3), pulmonary TB (PTB)is seen more frequently than extra pulmonaryTB (EPTB). With progressive depletion ofCD4 count, the clinical presentation oftuberculosis used tobe more atypical. TBfrequently manifest with atypical feature likelower lobe pneumonia, similar to bacterialpneumonia rather than typical fibro-cavitarydiseases of the upper lobes as seen inimmunocompetent persons. As the immunesuppression increases, the chest radiographmay show prominent mediastinal or para-tracheal lymphadenopathy or miliary form oftuberculosis. Extra pulmonary TB accountsfor only 20 percent of cases in HIV negativepersons, but it accounts for half of the cases inHIV positive persons. The disease also tendsto be disseminated, involving two or morenon-contiguous organs concomitantly. Themost common sites of extrapulmonary diseaseare peripheral lymph nodes and pleura. Inlymph nodes, there may be poor granulomaformation with increasing immunosuppression.
Other common extrapulmonary sites arepericardial, peritoneal, abdominal andneurological. The neurological manifestationsof HIV TB co-infection are tuberculousmeningitis (TBM), tuberculomas, andtuberculous brain abscess, meningeal TB beingthe most common of them. Progressive
deterioration in the immune system may alsolead to widespread dissemination oftuberculosis blood circulationleadingtomultiple micro-abscesses, organinvolvement and abdominal lymphadenopathy.
DiagnosisHIV testing:The national programme
uses fourth generation rapid tests which detectp24 antigen as well as antibodies to HIV.Voluntary counselling and testing (VCT) arethe traditional approach towards HIV testingwith emphasis on pre-test counselling, apartfrom provider-initiated testing and counselling.For TB patients, it is desirable that HIV testingbe carried out as an essential (not mandatory)part of TB treatment registration, and it shouldbe done before or at the point of TB diagnosis.In children below 18 months of age, thepersistence of maternal antibodies may leadto false-positive antibody-based tests. In thisage group, the diagnosis of HIV is made bytests that detect HIV nucleic acid (antigen) ona dried blood sample (DBS) from the infant.
As per HIV testing services (HTS)guidelines (2015), the offer of testing is madeto all TB patients (confirmed and suspects),patients with sexually transmitted infections,pregnant women in addition to provider-initiated testing and counselling (PITC).
Diagnosis of TB:The diagnosis ofpulmonary tuberculosis in HIV negativepatients is relatively easy as patients are oftensputum positive for Acid Fast Bacilli (AFB).World Health Organisation recommends TBscreening at the time of diagnosis of HIVbefore ART is started and at regular intervals

187Science Horizon:Volume 7: Issue 4
APRIL, 2022
during follow-up. The sputum microscopy candetect tuberculosis bacteria in HIV infectedpersons in 45 percent of cases. Cartridge-based nucleic acid amplification test(CBNAAT), e.g. Xpert MTB/RIF or TrueNat,has much higher efficacy in detecting TBcases and also can see rifampicin resistance.It provides diagnosis and rifampicin resistanceresults in about 2 hours.
ManagementPrinciples for managing HIV TB co-infected patients: If a patient with TB isdiagnosed to have HIV, the urgency is to startTB treatment as per the treatment guidelines.All HIV TB coinfected patients are to beinitiated on antiretroviral treatment (ART)regardless of the CD4 count. ART reduces theincidence and recurrence of TB and deathrates. Co-trimoxazole, used for prophylaxisto prevent pneumocystis infections, should begiven to all HIV TB patients.
As a routine, all HIV persons need to bescreened regularly for TB using the 4-symptomquestionaries- new-onset cough, fever, weightloss and night sweats among adults duringtheir visit to the ART centre.
The management of active TB disease inboth HIV infected persons and HIV negativepersons is essentially the same with a fewadditional considerations. In HIV infectedperson, ART must be started early duringtreatment to reduce the risk of death.Appropriate management requires combininganti-TB drugs, ART and co-trimoxazole(trimethoprim-sulphamethoxazole) preventivetherapy (CPT) to prevent progression of thedisease and other opportunistic infections
(OI). ART reduces mortality by about 80%(range 64-95%) in patients with drug-susceptible TB, and CPT (co-trimoxazolepreventive therapy) halves mortality risk. Theaddition of TB Preventive Therapy (TPT) amongPLHIV, who do not have active TB, preventsactivation of latent TB to active TB disease.
Deaths occurring in the earlier months(first month) of TB treatment are usually dueto TB, but the late deaths are due to HIVprogression. The national programme of Indiaalso recommends simultaneous initiation ofanti-TB treatment and ART for all coinfectedpatients with a CD4+ count less than 50 cells/mm3 to reduce mortality among severelyimmune-compromised patients. Initiating ARTduring TB treatment was associated withreduced mortality, improved ART complianceand sustained patient retention.
Another significant challenge isdetermining the optimum time to start ARTfor patients on TB treatment, as any delays inART initiation are associated with a substantialrisk of mortality. It has been recommendedthat in coinfected patients, TB treatment shouldbe initiated immediately on diagnosis of TB,and ART should be initiated within the nexteight weeks, irrespective of CD4+ cell count.Patients with CD4+ cell counts of less than50 cells/ìlmustbe given ART within two weeksof initiation of TB treatment for a betteroutcome.
Antiretroviral TherapyThe virus hides in ‘immunological
sanctuaries’ in the body; it is therefore toodifficult to wipe it off. As antiretroviral drugscannot eradicate the HIV infection, the goals

188 Science Horizon:Volume 7: Issue 4
APRIL, 2022
of ART are to achieve suppression of viralreplication with the recovery of the immunesystem and eventual prolongation of life andimproving quality of life. ART also preventstransmission of HIV by suppression of theviral multiplication.
Zidovudine was the first drug effectiveagainst HIV in 1985, but the virus developedresistance quickly with a single drug. TheDiscovery of non-nucleoside reversetranscriptase inhibitors (example: Nevirapineand later Efavirenz) made the therapy simplerand soon became standard of care along withtwo nucleoside reverse transcriptase inhibitors.The availability of different drugs in fixed-dose combination (FDC) by Indianpharmaceutical companies in generic formsmade therapy simpler, reduced the number oftablets to be taken daily, thereby increasingadherence potential. India has contributedlargely for global ART supply at a lowerprice,”a dollar a day” by an Indianpharmaceutical company, which has been thegame-changer in increasing access toantiretroviral (ARV) drugs globally.
For the last two decades, the standardregimen for the treatment of HIV-1 infectionhas been “triple-drug therapy”. In India, theNational AIDS Control Organization (NACO)currently recommends a simple harmonizedART in the form of a single dose /tablet offixed-dose drug combination includingTenofovir, Lamivudine and Dolutegravir to allnewly diagnosed HIV-1 infection regardlessof patients’ CD4+ count or clinical stage.Efavirenz is now provided only for thosewomen who do not want to take dolutegravir
as it is considered safe to be administeredduring pregnancy.
Many times, HIV patients have intractablediarrhoea, and, in such cases, there ismalabsorption of ARV and ATT drugs, whichmay lead to the emergence of drug resistance.
IRISThe condition is commonly known as
“immune reconstitution inflammatorysyndrome” (IRIS). IRIS may present rapidclinical deterioration caused by theinflammatory response due to dysregulatedimmune response. IRIS is a clinical conditionmanifested in some cases of AIDS orimmunosuppression due to recovering bodyimmune response. It paradoxically makes theclinical symptoms of infection worse and, attimes, very severe. Mycobacteriumtuberculosis has been the commonestpathogen associated with IRIS.
HIV & MDR-TBThere were an estimated 484 000
incident cases of multi-drug resistance (MDR)/rifampicin resistance (RR) TB worldwide in2018, with India sharing 27% of the globalburden. HIV and MDRTB co-infection areassociated with much higher morbidity andmortality. During co-treatment of HIV TB,several factors like poor drug absorption, pillburden and overlapping toxicities leading topoor compliance, drug interactions leading tosub-therapeutic drug levels etc, may lead toemergence of drug resistance to anti-TB drugsas resistance to ARVs. Second-line anti-tubercular drugs are more toxic and oftendifficult to tolerate.

189Science Horizon:Volume 7: Issue 4
APRIL, 2022
TB Preventive TherapyTB Preventive Therapy (TPT) involves
the administration of selective anti-TB drugsto TB negative people to prevent activation oflatent TB. The effects of TPT have shown toaugment the impact of ART on reducing theincidence of TB. Under the nationalprogramme, India is presently using Isoniazid(INH) for individuals with suspected latentTB infection so as to prevent progression toactive TB disease.National Framework for Joint HIV/TB Collaborative Programs in India
Implementation of TB and HIVcollaborative activities in India started in 2001to present-day intensified case-finding (ICF),referral to NTEP designated microscopycentres (DMCs) and referral of TB patientswith HIV risk for HIV testing and counselling.
The national policy framework for TB/HIV Collaborative Activities between NationalTuberculosis Elimination Programme (NTEP)and National AIDS Control Programme(NACP)guides establishing mechanisms forcoordination between NACP and NTEP atnational, sub-national and district levels. Thisframework also focused on the cascade ofcare for HIV-TB coinfected patients frominitial suspicion to confirmation of TB andinitiation of anti- tubercular treatment (ATT)and ART with monthly coordination meetingsto review cross-referrals and track lost peopleat some stage of cascade.
HIV-TB Control Early diagnosis Effective TB treatment
Control of infection transmission HIV prevention Inter-sectoral coordination for care for
HIV-TB coinfected
ChallengesSome key challenges in HIV/TB have
been a multi-fold burden of stigma,discrimination and economic loss suffered bypeople and families with the disease. As aresult, there has been gaps between TB andHIV prevention, treatment and care services(e.g., increased access and coverage of HIVscreening for TB patients, access to ART andother interventions) and coordination amongNGOs working in TB and HIV projectsincluding linkage of NGOs working fordifferent high risk population like commercialsex workers (CSW), men who have sex withmen (MSM), and intravenous drug users (IDU)to TB sites.
Some challenges in the management ofHIV-TB infection include so many pill burdens,poor tolerance, poor drug absorption from thestomach, poor adherence, substance abuse,drug-drug interactions, overlapping toxicities,stigmatization and discrimination etc.
In addition to existing programmes, bothNTEP and NACP must find better ways toprioritize service delivery that should focuson the wide-scale deployment of logistics,infrastructure, human resources andsustainability of uninterrupted services.
.......To be Continued at Page No.-194

190 Science Horizon:Volume 7: Issue 4
APRIL, 2022
9
TUBERCULOSIS PREVENTION:VACCINES & BEHAVIOURAL ASPECTS
1Abhinav Sinha2Srikanta Kanungo
“Tuberculosis is a social disease, itsunderstanding demands that the impact ofsocial and economic factors on the individualbe considered as much as the mechanisms bywhich tubercle bacilli cause damage to thehuman body”- Rene.J. Dubos
IntroductionTuberculosis (TB) is an infectious
disease usually caused by Mycobacteriumtuberculosis, transmitted from one person tothe other primarily through droplets whilecoughing, sneezing and spitting etc. It mainlyaffects lungs known as pulmonary tuberculosisbut can also involve other body parts,commonly referred to as extra pulmonarytuberculosis. The most important risk factorsfor TB infection are Human ImmunodeficiencyVirus (HIV), diabetes mellitus, crowding,malnutrition, alcoholism and Hodgkinlymphoma. World Health Organizationdeclared tuberculosis as a public healthemergency in 1993 when it urged governmentsto scale up their efforts to prevent and controlTB. Soon, directly observed treatment, shortcourse (DOTS) was launched. Following theWHO’s mission, India initiated its NationalTuberculosis Programme (NTP) in 1962.Later,in 1997 the strategy was revised with
implementation of DOTS under RevisedNational Tuberculosis Control Programme(RNTCP). A case based web platform ‘Nikshay’was launched in 2012 to electronically reportand keep a track of TB data. Recently IN 2020,National Tuberculosis Elimination Programmewas launched with a vision to achieve ‘TB freeIndia’. Despite being preventable and 60 yearsof efforts, India still has the highesttuberculosis burden and mortality in the world.
Pillars for TB Prevention and ControlTuberculosis can be prevented, treated
and cured with emphasis on three priority areas:1. Identify TB cases, complete their
treatment and render their status as non-infectious.
2. Screen the contacts of active cases todetermine if they are the active diseasethemselves; or whether they have beeninfected; or prophylaxis is requiredespecially for children and other highrisk persons.
3. Screening, testing and treating high riskpopulations such as immunosuppressivedrug users, HIV patients, slum dwellersetc. for latent TB infection.

191Science Horizon:Volume 7: Issue 4
APRIL, 2022
These three strategies not only focus onindividual cases but also fulfill broaderepidemiologic functions by reducing activecase loads and hence, ceasing the transmissionin the community. However India faces dauntingchallenges in TB control due to high latent TBinfection in the community which may re-activate at any time. Additionally, delayeddiagnosis and inadequate treatment alsoaccentuate the issue. Furthermore, the situationbecomes complex among multi-drug resistant(MDR-TB) and extensively drug resistant(XDR-TB) which remains undetected, or afterdetection have poor chances of treatmentsuccess with a high loss to follow up.“Knowing is not enough; we must apply.Willing is not enough; we must do.”- Goethe
Patient Centered TB CareThe End TB strategy recommends a
patient centered approach for care andprevention of TB. This should be locallycontextual, culturally tailored and considerequitable distribution. This can be achievedthrough accessible healthcare facilities;availability of human resources such asdoctors, nurses, laboratory technicians andtreatment supervisors; availability of materialresources such as smear microscopy, x-rayand medicines; quality services; relevance ofservices in harmony with the needs of patientssuch as nutritional, financial and psychosocialsupport; timing and continuity of care, technicalquality and social accountability.
Prevention Strategies“Prevention is better than cure.”
Targeting preventive therapy is the most
effective intervention to control tuberculosis.It is the most comprehensive strategy as onlyappropriate social behavior can address thechallenge of dealing with the large latent casesof TB. Hence, following steps should be takento prevent TB:
Air Borne infection ControlIt aims to minimize the risk of
transmission broadly at two levels: communityand institutional level. At community level,social habits such as spitting, sneezing withoutcovering face, not following cough etiquettes,alcoholism, debilitating or mentally challengedpatients and delay in presenting to the facilitypose a significant challenge. Additionally,special groups such as migrant population;slum dwellers; backward and tribal pockets;institutional setups such as old age homes,destitute homes, children homes and jails;patients having multimorbidity andcomorbidities such as HIV and diabetes are ata higher risk. Environmental pollution alsocontributes to challenges in spreading TB atcommunity level.
At institutional level, patients with chestinfection at outpatient settings and poorventilation while at in patient facility coughscreening, use of mask and counsellingneeds to be focused. Additionally, atinstitutional level certification for AICcompliance should be necessary, fasttracking of cases, provision of N95 masksfor staff, separate facility for positivepatients, infection control measures at ARTclinics, personal protective equipment (PPE)for staff, periodic trainings is necessary.

192 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Contact TracingTransmission from index case to the
contact can happen anytime hence all contactshould be identified with attention tosymptomatic people, children below six yearsof age and other high risk groups.
UndernutritionIt is one of the most common risk factor
for progression of TB in India. Previousevidence suggests TB incidence could declineby 14% with per unit increase in body massindex (BMI). Therefore, we should aim atreducing undernutrition especially among atrisk population. Furthermore, undernutritioncan also lead to severe disease, adverse effectsand higher likelihood of relapse after cure.The NTEP recommends nutritious food and adaily micronutrient supplements. Additionally,TB patients are financially supported for takinggood nutrition under ‘NikshayPoshan Yojana’.
Preventive TherapyChildren below six years of age are more
susceptible to TB infection and hence will beevaluated for active TB. Once active infectionhas been ruled out, a preventive therapy ofisoniazid (INH) irrespective of their BCG
vaccination or nutritional status is started. Theadvised dose for INH is 10mg/kg body weightfor a minimum of six months.
Tuberculosis VaccineSustainable Development Goals (SDG),
WHO End TB Strategy, and the End TB Goalsby Stop TB Partnership targets to end theglobal epidemic of TB by 2035 which remainsa daunting target. Developing an interventionagainst tuberculosis is a crucial global healthpriority. Although, Bacille Calmette Guerin(BCG) vaccine has been successfully used toprotect against childhood TB for almost acentury still adult TB vaccines are in thedevelopment stage. BCG vaccine providesprotection against TB during childhood up to10 years of age but its efficacy wanes duringadolescence with minimal protection againstadult pulmonary TB. Currently, adult TBvaccine candidates are in pipeline for clinicaltrials which can be grouped into two broadcategories: the first being mycobacterial wholecell-derived vaccines and subunit vaccineswhich are directed against some selectedantigens. The various vaccine candidates andtheir current status is provided below:
Vaccine Candidate Clinical Trial PhasePhase 1 Phase 2 Phase 2a Phase 3 Licensed
Mycobacterial Live MTBVAC VPM1002 BCG
whole cell-derived Killed RUTI DAR-901 MIP,
VaccaeTM
Sub-unit Adjuvant Gam ID93+GLA- H56:IC31 M72+AS01E
TBvac SE
Viral Ad5Ag85A, TB/Flu-04LVectored ChAd0x185A

193Science Horizon:Volume 7: Issue 4
APRIL, 2022
Mycobacterial Whole Cell-derivedVaccines
These vaccines are derived fromMycobacterium tuberculosis, BCG or closelyrelated strains of non-tuberculousmycobacteria. These can further be classifiedinto live vaccines that are attenuated throughgenetic modification and killed orfractionated. These vaccines comprise ofdifferent antigenic components which offera diverse immune response.
Subunit VaccinesThese vaccines target a small number of
selected antigens (six or less). The mainchallenge in developing these vaccines isidentifying the optimal antigen to be included.The current used antigens have been tested inanimal models prior to developing vaccinescandidates.
The significant protection rendered byM72/AS01E candidate during Phase 2b ofclinical trials points towards feasibility andstrongly encourages a brighter future andcontinued efforts in this direction. However,there is an urgent need to develop an effectivevaccine which can be easily administeredand cost-effective so that it is accessiblefor all and especially for marginalizedcommunities such as slum dwellers who areat a h igher risk of contracting TB.Additionally, strategies such as routes ofadministration and vaccine platforms needto be channelized. Lessons learnt on vaccineequity during COVID-19 pandemic should beapplied for egalitarian distribution of TBvaccines especially among LMICs.
ConclusionGiven the magnitude of TB in India and
its associated cost, it cannot be overlooked toachieve Universal Health Coverage. Persistentefforts are required to control and manage TBwith increasing pace.Although, effectivenessof prevention has been long established stillpublic health measures aim at active casefinding and treatment. Hence, preventionshould be at the core of all public healthprogrammes aimed at controlling TB infection.Developing indigenous vaccine candidatesshould be targeted. Political commitmentalong with prioritization of resources can helpin achieving goals. Additionally, at individuallevel people should be vigilant, takeprecautions, report to the health facilities atthe earliest and complete treatment to end TB.Key Messages for AchievingTuberculosis Control in India Provision of cost-effective high quality
rapid diagnostics and treatment for alleverywhere.
Inclusion of high risk populationsincluding close contacts in care throughactive case finding.
Invest in making tuberculosis patientsfinancially stable to achieve fulltreatment.
Increased efforts to acceleratetuberculosis research and developmentof diagnostics, therapeutics and vaccines.
Accountability of stakeholders and keypersonnel in achieving targets.
References MacNeil A, Glaziou P, Sismanidis C, Date A,
Maloney S, Floyd K. Global epidemiology of

194 Science Horizon:Volume 7: Issue 4
APRIL, 2022
tuberculosis and progress toward meetingglobal targets—worldwide, 2018. Morbidityand Mortality Weekly Report. 2020 Mar20;69(11):281.
Bhargava A, Bhargava M, Juneja A. Socialdeterminants of tuberculosis: context,framework, and the way forward to endingTB in India. Expert Review of RespiratoryMedicine. 2021 Jul 3;15(7):867-83.
Reid MJ, Arinaminpathy N, Bloom A, BloomBR, Boehme C, Chaisson R, Chin DP,Churchyard G, Cox H, Ditiu L, Dybul M.Building a tuberculosis-free world: The LancetCommission on tuberculosis. The Lancet. 2019Mar 30;393(10178):1331-84.
Harding E. WHO global progress report ontuberculosis elimination. The LancetRespiratory Medicine. 2020 Jan 1;8(1):19.
Schrager LK, Vekemens J, Drager N,Lewinsohn DM, Olesen OF. The status oftuberculosis vaccine development. TheLancet Infectious Diseases. 2020 Mar1;20(3):e28-37.
Hatherill M, White RG, Hawn TR. Clinicaldevelopment of new TB vaccines: recentadvances and next steps. Frontiers inmicrobiology. 2020 Jan 30;10:3154.
ICMR, Regional Medical Research Centre,
Bhubaneswar, Odisha-751023
.....Continuing from Page No.-189Conclusion
TB is already a leading cause ofmorbidity and mortality and remains asignificant public health problem in thedeveloping world. The present-day COVID-19 pandemic put the control program to adecade back. The HIV epidemic has causeda resurgence of TB. HIV TB co-infectionhas a major impact on human health andthrows unprecedented challenges on thealready strained health care system in mostcountries. The dual epidemic also pushesthe victim to a spiral of poverty, stigma anddiscrimination.
Clinical management of HIV TB co-infection is challenging. There aresignificant issues like pill burden, drug
interactions, toxicities, poor adherence,which may impact the treatment.
Although the HIV TB epidemic scalemay look daunting, sustained efforts throughawareness, preventive strategies, betterdiagnostic tools, newer and less toxic drugs,cutting-edge research, and knowledgesharing have been carrying a positive change.Committed leadership and an integratedapproach are needed to defeat this scourge.We also need to be aware of the setback thatthe recent COVID-19 pandemic had on thesustainability of the collaborative activitiesat all levels of health care and how to reversethese setbacks.
AII India Institute of Medical Sciences,
Bhubaneswar-751019

195Science Horizon:Volume 7: Issue 4
APRIL, 2022
10
TUBERCULOSIS IN DIABETICPOPULATION
Tahziba Hussain
IntroductionType 2 Diabetes Mellitus (T2DM) has
become a pandemic and is in fact the bane ofthe modern times. At present, there are 300million people affected with diabetes globallyand the number is likely to rise two-fold in thefuture five years.
India has the highest burden oftuberculosis (TB) and second highest burdenof diabetes in the world, with annual TBincidence of 2.2 million cases (range 2.0-2.5million) and around 63 million people livingwith diabetes.
About 75% of people with diabeteslive in low- and middle-income countries andabout half of them are unaware of their diabetesstatus. The global increase in type 2 diabetesmellitus (DM) is recognized as a neglected,important and re-emerging risk and challengeto tuberculosis (TB) control. Individuals withDM have three times the risk of developingTB and there are now more individuals withTB-DM co-morbidity than TB-HIV co-infection. India has been dubbed the DiabeticCapital of the world with its huge diabeticpopulation. India has the highest number of TBcases and also the highest number of duallyinfected individuals, in the world. The
association and synergistic rolebetween T2DM and TB in causing humandisease has been recognised since long back.Globally, about 10% of TB cases are associatedwith diabetes. The linkage between T2DM andTB is a challenge for global tuberculosiscontrol. Improved understanding of the bi-directional relationship of the two diseases isnecessary for proper planning and collaborationto reduce the dual burden of diabetes and TB.In people with TB, it may be appropriate toactively screen for DM. Prevention, screening,and treatment of both diseases together ismore effective. A model similar to the TB-HIV program may be the best approach.Recognizing the serious threat posed byDiabetes-TB, the National TuberculosisElimination Program (NTEP) calls forstrengthening collaboration between TB anddiabetes control programs for bettermanagement of diabetic patients with TB andTB patients with diabetes. The diabetesepidemic has a huge impact on the dynamicsof epidemiology of TB and poses severalchallenges to control of TB in a resource-poor country like India. Diabetes/TB burdencan be brought under control by timelydiagnosis of TB among diabetics by intensifiedcase finding, by adequate and effective treatment

196 Science Horizon:Volume 7: Issue 4
APRIL, 2022
of detected cases and preventive therapy.Diabetes epidemic poses a serious threat oncontrol of TB, and the current gaps in knowledgerelated to diagnosis, prevention and treatmentof TB among people with diabetes.
Convergence of countries with highestburden of TB and DM worldwide. Among theten countries with the highest number ofdiabetes patients worldwide, six are also amongthe 22 high-burden countries that contribute80% of the TB cases worldwide.
Bi-directional RelationshipType 2 Diabetes mellitus and
Tuberculosis (TB) often manifest togetherleading to complications at various levels.
Several studies have reported thatdiabetes, smoking and alcohol abuse are therisk factors which can actually raise the riskof developing active TB twice or thrice. It wasobserved from a mathematical modellinganalysis of the effects of smoking on TBinfection and mortality that smoking mightlead to an excess of 18 million TB cases and40 million deaths from TB between 2010 and2050. In India, a major portion of the TB
burden can be attributed to smoking(40%) and DM (15%).
There is a bi-directional relationshipbetween TB and diabetes, and they both impactthe presentation of each other. Diabetes isbeing increasingly recognized as a risk factorfor TB and may affect its presentation, whilstTB may worsen glycemic control or lead toIGT (impaired glucose tolerance) among TBpatients. This relationship demands adjustmentin treatment and the need to employ insulin inthe treatment of hyperglycemia during activeTB infection when required. A review of theanti-glycemic agent(s) is also warranted onceTB treatment is over.
The expected rise in diabetes cases indeveloping countries (driven mainly by type 2diabetes) which also bear the brunt oftuberculosis would increase the influence ofdiabetes on TB in the coming future.
Many studies suggest that DM isassociated with the clinical presentation ofTB. Namely, TB-DM patients (versus TB-noDM) are more likely to present with pulmonary(versus extra-pulmonary), cavitary (versus

197Science Horizon:Volume 7: Issue 4
APRIL, 2022
non-cavitary) and sputum smear-positive TBat diagnosis. During the course of TBtreatment, TB-DM patients take longer toconvert from sputum smear-positive to -negative. Some studies also find that DMpatients are more likely to present with drug-resistant and multi-drug resistant TB, althoughthis relationship is not seen in all studies.
A study using dynamic TB transmissionmodels to analyze the potential effects of DMon TB epidemiology in 13 countries with highburden of TB concluded that stopping the riseof DM would avoid 6 million incident casesand 1.1 million. TB deaths in these countriesin 20 years. Thus, every community worldwideneeds to evaluate the prevalence of DM and itscontribution to TB. This information is variablebetween regions and critical to guide for themost efficient use of limited resources for TBcontrol programs.
Pulmonary Versus Extra-Pulmonary TBPulmonary TB accounts for 70-80% of
the cases, and it is generally accepted thatimmune compromise facilitates hematogenousdissemination of M. tuberculosis, pre-disposing to extra-pulmonary TB. Such is thecase of TB patients with HIV-AIDS or thosetaking TNF blockers. This contrasts with TB-DM patients who are less likely to presentwith extra-pulmonary TB.
This may be due to a hyper-reactive cell-mediated immune response to M. tuberculosisin DM patients that may be suboptimal forcontaining M. tuberculosis growth within thelung, but effective for preventing itsdissemination and reactivation elsewhere.
Cavitary and Smear-positive TBM. tuberculosis induces a strong cell-
mediated immunity leading to the formationof pulmonary granulomas (tubercles) that arethought to be a double-edged sword for thehost. Granulomas initially limit M.tuberculosis growth, but in hosts in whom M.tuberculosis continues to replicate, thesestructures undergo central caseation withrupturing and spilling of thousands of viablebacilli into the airways. This “cavitary TB” isassociated with sputum smear-positivity. TB-DM patients are more likely than TB-no DMto present with cavitary TB that is accompaniedby higher bacillary burden in sputa.
Together, the higher frequency of PTBvs extra-pulmonary TB, cavitary TB, and smear-positive TB at diagnosis and extending duringtreatment, would predict that TB-DM patientsare more infectious than TB-no DM.TB Treatment outcomes in TB-DMPatients
There is growing evidence fromobservational studies that TB-DM is associatedwith an increase in adverse TB treatmentoutcomes, specifically for delays inmycobacterial clearance, treatment failures,death, relapse and re-infection.Delays in Sputum Smear Clearanceand Treatment Failure
TB-DM versus TB-no DM patients aremore likely to remain sputum smear-positiveafter completion of the intensive phase oftreatment, and this outcome is an earlypredictor of treatment failure (sputum smearor culture positivity at five months or later

198 Science Horizon:Volume 7: Issue 4
APRIL, 2022
during treatment), which is also more likely inTB-DM versus TB-no DM.
Relapse and Re-infectionTB-DM patients also appear to have a
higher risk of relapse. The review by Baker etal reported a nearly 4-fold risk of relapse inTB-DM versus TB-no DM. A prospective studyin southern Mexico with 1262 TB patientscharacterized for M. tuberculosis genotypesfurther distinguished between relapses and re-infections, and found higher adjusted odds ofboth outcomes in DM vs no DM.Should TB-DM patients be ManagedDifferently from TB-no DM?
The clinical findings and higher risk ofadverse outcomes in TB-DM patients indicatethe need for prospective cohort studies aimedat confirming these observations andidentifying the underlying factors leading totreatment failures in DM.
ImmunityPeople with a weak immune system as a
result of chronic diseases such as diabetesare at a higher risk of progressing fromlatent to active TB. People with diabeteshave a two to three times higher risk ofgetting infected with TB, compared topeople without diabetes.
Large proportions of people withdiabetes as well as TB remain undiagnosed, orare diagnosed at a late stage. Due to lack ofearly detection and treatment, complicationsfrom TB-diabetes co-morbidity lead to highcost on treatment and out-of-pocketexpenditure. Early detection can help improvecare and control of both diseases.
Diabetes can lengthen the time for sputumculture conversion. Theoretically, this couldlead to the development of drug resistance ifa 4-drug regimen in the intensive phase oftherapy is changed to a 2-drug regimen in thepresence of culture-positive TB.
People with TB and co-existing diabeteshave a four times higher risk of death duringTB treatment and higher risk of TB relapseafter treatment. The World Health Organization(WHO) recommended that TB treatmentsshould be rigorously implemented for peoplewith TB–diabetes co-morbidity.
Diabetes is complicated by the presenceof infectious diseases, including TB. It isimportant that proper care for diabetes beprovided to patients suffering from TB–diabetes co-morbidity.
TB is associated with worseningglycaemic control in people with diabetes. Ithas been argued that good glycemic control inTB patients can improve treatment outcomes.
The precise biological mechanisms thatresult in this interaction between diabetes andTB are still not clear. Epidemiological modelshave shown that diabetes accounts for 20% ofsmear-positive pulmonary TB and recentanalyses have indicated that the increase indiabetes prevalence in India has been animportant obstacle to reducing TB incidencein the country.The Underlying PathophysiologicalMechanisms
The increased risk of TB among diabetespatients is multi-factorial and several putativemechanisms have been proposed. There is

199Science Horizon:Volume 7: Issue 4
APRIL, 2022
decreased cellular immunity due to reduced T-lymphocyte count as well as function and alow neutrophil count. Diabetics show a reducedT-helper 1 (TH 1) cytokine response level,tumor necrosis factor (TNF-alpha and TNF-beta), interleukin-1, and interleukin-6production compared to their non-diabeticcounterparts. The susceptibility of diabetespatients to TB is mainly due to reducednumbers and function of T-lymphocytes.particularly TH1 cytokine inhibitionof Mycobacterium tuberculosis. There ismacrophage dysfunction in diabetes whichresults in impaired production of reactiveoxygen species and phagocytic and chemotacticfunction. Chemotaxis of monocytes is alsoimpaired in patients with diabetes, a defectwhich does not improve with insulin.Hyperglycemia is thought to also impair theforce of respiratory burst in expellingpathogens. Whilst these proposed mechanismsare plausible, it is important that furthermechanistic studies are done to confirm themor otherwise. The stress response to infectionmay also play a role in dysglycemia, a situationmediated by the effect of interleukin-1 (IL-1),interleukin-6 (IL-6), and TNF-alpha. Thistemporal relationship has been demonstratedin some studies where between 19 and 42.6%of active TB patients were discovered to haveIGT or diabetes with a significant reduction orcomplete regression in the rates followingtreatment.
TB may cause TB pancreatitis as wellas pancreatic endocrine hypofunction whichmay lead to IGT or new onset diabetes orworsen its control. TB pancreatitis may
become obvious only after the person developsdiabetes. Lastly, whilst malnutrition has beenproposed as a risk factor for infections anddysglycemia, body mass index has not beenassociated with IGT or diabetes.Understanding the ImmuneDysfunction to Mtb in DM patients
Given that efficient Mtb killing by anti-mycobacterial antibiotics requires cooperationbetween innate and adaptive immuneresponses, the higher frequency of adverseoutcomes in DM patients suggests that thehyper-reactive immune response tomycobacterial antigens in TB-DM patients isnot effective for Mtb killing. There are severalpossible explanations for the contribution ofdysfunctional immunity to these adversetreatment outcomes.1) The higher Th1 and Th17 response is only
present in the peripheral blood of TB-DM patients, while anti-inflammatoryresponses that facilitate Mtb growth onlyoccur in the lungs.
2) There is a higher production of pro-inflammatory cytokines like IFN-ã in thelungs of humans (as observed in mice),but it is not effective for downstreamactivation of macrophages or cytotoxicT-cells that ultimately kill Mtb.
3) The hyper-reaction to Mtb antigens maybe deleterious and contribute to lungtissue damage with more severe TB andthe higher frequency of death in TB-DMpatients.
Understanding this complex relationshipbetween excessive immunity in TB-DM will

200 Science Horizon:Volume 7: Issue 4
APRIL, 2022
help improve the clinical management of TBpatients, regardless of their DM status.
Bi-directional ScreeningIn India, the screening of TB patients for
diabetes is relatively easy and a high rate ofdetection of DM, ranging from 10%-44% inTB patients has been observed in many studiesin different states. However, screening for TBamong diabetes patients is less easy, withseveral studies reporting challenges such asless registration of patients and reluctance toprovide sputum specimens. The doctors and/or technical staff, on the other hand, arereluctant for this additional work and do notrecord the screening systematically. Routinescreening for dysglycemia should be done forall TB patients, especially at the time ofdiagnosis. Among patients with diabetes, thereis a stronger case to be made for screening forTB routinely or at the least suspicion.Diagnosed patients should promptly bereferred to a TB centre for treatment. Strategiesfor the prevention of TB must continually beemphasized. These include improvements inhousing and nutrition, poverty reduction,treatment of HIV/AIDS, and above all theavailability of diagnostic tools such as sputumsmear microscopy, X-rays, and automatedmolecular tests
OdishaGood geographical coverage of the TB
control programme in Odisha with emphasison universal access to active TB case finding inthe community is probably the reason. Severalstudies have reported that Diabetes makes asubstantial contribution to incidence of TB. TB
control efforts might be benefited from activecase finding and treatment of latent TB inpeople with diabetes and increased efforts todiagnose and treat diabetes in populationswhere diabetes affects the risk of TB to alarger extent. In India, the growing problem ofdiabetes in this high-risk group population couldmake prevention of tuberculosis, a priority areain the future. Further research is needed todetermine this and ascertain the average timingof TB screening among diabetes patients. Moreresearch is warranted to investigate how theincidence of TB impacts diabetes controlefforts in this state.
ConclusionScreening for TB among T2DM patients
in diabetes clinics would lead to earlierdetection of TB, which in turn, would help inearly treatment while decreasing the risk ofnosocomial transmission. It will further leadto better TB-specific treatment outcomes andprevention of diabetes complications. We,therefore, feel that screening T2DM patients,irrespective of their complaints and symptoms,at regular intervals, for signs and symptoms ofTB would go a long way in early detection ofthe Tuberculosis.
Publications Related to Diabetes :1. Elina Das, Shritam Das, SK Kar, VS Yadav,
Tahziba Hussain. (2017). Prevalence & riskfactors of pre-diabetes & diabetes amongpatients with active TB disease attending threeRNTCP centres in Odisha. InternationalJournal of Diabetes in DevelopingCountries. 37 (2) : 141 - 147.
.......To be Continued at Page No.-206

201Science Horizon:Volume 7: Issue 4
APRIL, 2022
11
COVID-19 AND TUBERCULOSIS:TACKLING THE DUAL PROBLEM
IN FUTURE
Sampat Dash
A Merger of an Age-old Pandemic witha New One
December 2019 will always beremembered in history as the date that changedthe world and Wuhan, the place from which itall started. However, before the CoronavirusDisease 2019 (COVID-19) pandemic, we inIndia were struggling with many othercommunicable disease pandemics of whichtuberculosis (TB) is the most aged one.Description about this is also present in ourVedas as “Rajyakshama” which means to decay.Prior to the discovery of TB bacilli by RobertKoch,the disease was considered to be due tobad air and poor hygiene of the surroundingenvironment.However, on 24 March 1882,after the bacilli was discovered, ourunderstanding of this disease became clearer.So, this day is celebrated every year as “Worldtuberculosis day” to create awareness andcontinue our effort to fight this pandemic.India and China are the two most populouscountries in the world and both are developingcountries with population density being muchmore than the western world. Hence, thenumber of TB cases are way more than anypart of the world and one out of four TB casesare found in India. This is not limited to drug
sensitive TB cases but also drugresistant ones. So,a huge amount of healthcare resources in both these countries aremobilised to fight this pandemic even beforethe COVID-19 pandemic. But with COVID-19coming to this part of world, it further strainedthe health care system leading to opening ofmany dimensions about management oftuberculosis pandemic.What COVID-19 Has Done to The World
Severe acute respiratory syndromecoronavirus 2 (SARS-CoV-2) virus, whichcauses COVID-19, is considered to be azoonotic virus that has transferred from thebats to the humans and was first detected inWuhan province of China. Initially, the WorldHealth Organization (WHO) never thoughtabout the severity of this disease,howeverwith its rapid spread all throughout the world,it was declared as a pandemic on “11 March2020”. Initially it was considered to spreadonly by fomites, but with time ourunderstanding of this disease, it was found tobe spreading by fomites and aerosols also.The spread started fromChinato Europe,andthen to America, and finally the south eastAsiasubcontinent. And obviously with apopulation of millions, this disease caused

202 Science Horizon:Volume 7: Issue 4
APRIL, 2022
havoc in all possible dimension including lockdown to diverting all resources and manpowerfor this disease hence creating a deficit in allother disease management that has beenpreviously being taken care of. This caused agross mismatch between the COVID-19disease and all other disease of publicsignificance.Similarities of this DUO (COVID-19and Tuberculosis)
Both of these diseases primarily affectthe respiratory tract to start with fever, coughand both can present with breathlessness toblood in sputum (Figure 1). TB and COVID-19severity mainly depend on the ability of thebody’s immunity to fight any infectiousdiseases. So, patients with multiplecomorbidities like diabetes mellitus (DM),cardiac issues and people having any chronicdisease of kidney, liver, brain are the ones whosuffer more and land up in a serious state tothe hospital. Hence, even though these diseasesaffect people of all age groups, those withpoor immunological status are the ones thatbecome sick enough to cause hospitalizationand death. One more factor that also play animportant role in India is the huge number ofchronic respiratory disease patients likechronic obstructive pulmonary disease(COPD), uncontrolled asthma, people workingin many industrial areas with poor air quality,as all these factors makes the local immunityof the lungs to work in a poor state makingthem prone to all types of respiratory diseaseincluding both COVID-19 and tuberculosis(Figure 2). COVID-19 also causes a moreserious state in people who are already
suffering from tuberculosis as their lungs arealready in a bad shape. So, for countries likeIndia, this Duo of COVID-19 and TB appearsto be more stressful than other parts of worldwhere they don’t have TB.The Adverse Effects of This Duo (TBand COVID-19)
The fright of COVID-19 made the worldto put many restrictions, to start from stoppinginternational flights to locking down the wholecountries. This created a stigma for patientswith respiratory complaints to come forconsultation and treatment of their diseasesincluding tuberculosis. The fear of COVID-19 also caused many institutions to shutdown regular OPD services and divert alltheir resources for COVID-19 management.All these events hampered not only the newcases of tuberculosis from getting diagnosedbut also the previously diagnosed cases fromgetting treated properly. Hence the pandemicof COVID-19 actually increased the severityof tuberculosis pandemic because of poorcase findings and patients not getting propertreatment.
There is Always a Ray of HopeThe advice of “physical distancing, use
of masks, and hand hygiene” has become anorm in this COVID-19 era. This has definitelycaused a sense of awareness among the publicabout respiratory hygiene and avoiding anytype of activities that cause crowding wherethere is a high chance of spreading anyrespiratory disease, hence tuberculosisprevention got a direct benefit. Not only thesemeasures but also shutting down all type oflocomotives, factories and other industries

203Science Horizon:Volume 7: Issue 4
APRIL, 2022
for a significant time cause the air quality toimprove significantly and hence disease whichdeteriorate due to of air pollution like COPDand Asthma exacerbation has definitely comedown leading to significant amount ofimprovement of the health condition of thesepatients.This led to less hospital visit andexposure to COVID-19 environment. COVID-19 pandemic has made the authorities of allcountries to understand the importance ofhealth care system and the need of hour is toprepare the health system not only on thebasis of manpower but also with infrastructureto be always ready for any such pandemic incoming days. Medical personnel have alsounderstood the importance of personalprotective measures while taking care ofseriously ill respiratory cases like ARDS toprevent all aerosols generating procedures.The coordination between different healthsystems with lab networking includingtransporting seriously ill patients from oneplace to another improved a lot. ECMOunderstanding has also improved among themedical fraternity and this will definitely beof help in coming days to be used in deservingpatients not limited to COVID-19. Peoplealso understood the importance of good healthand the need of hour is to maintain good
health and taking care of their comorbidities.All these will definitely improve in comingdays the health care system and the health ofthe public leading to better control of notonly COVID-19 but also other pandemicincluding tuberculosis both in outpatientmanagement as well as taking care of thosegetting admitted with respiratorycomplications.
Where We are NowWe also need to look into the gain we
achieved in this pandemic. Even though theloss is huge both in form of life and livelihood,but this pandemic also opened our eyes for anew tomorrow. We came to know about thegaps in health care system in terms ofinfrastructure, manpower, coordinationbetween different departments involved inhealth care management, the need of publicprivate relationship in managingCOVID-19pandemic. Hence, it is the need of the hour touse the knowledge we gained duringthisCOVID-19 pandemic to counter the age-oldtuberculosisfight to make a bettertomorrow.
Consultant Pulmonology & Critical Care
Ashwini Lung Institute, ChandrasekharpurBhubaneswar, Odisha
In the article: NOBEL LAUREATE SIR C.V. RAMAN AND HISDISCOVERY published in February 2022 issue of the magazine, therewas a typographical error in the year of birth of Sir C.V. Raman. It shouldbe 1888. The error is regretted.
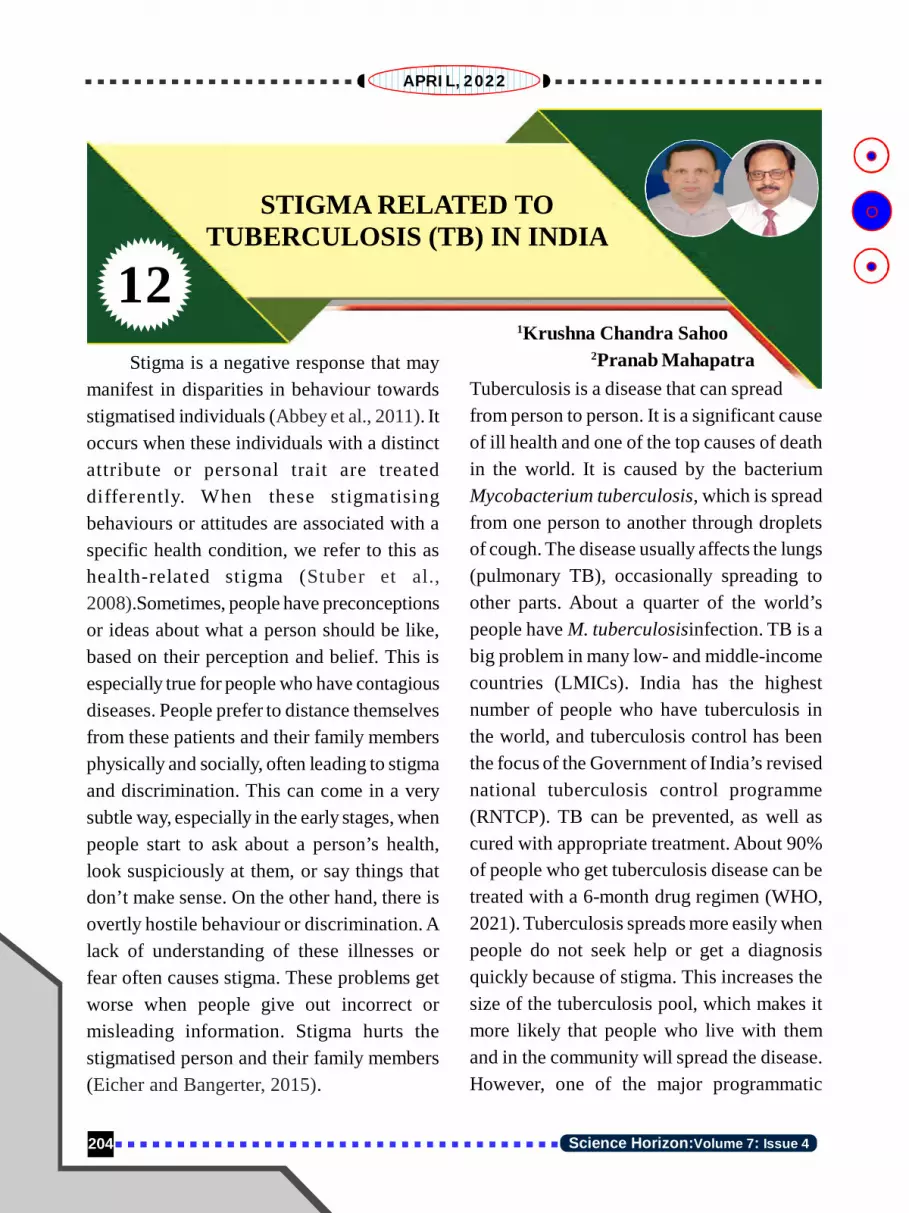
204 Science Horizon:Volume 7: Issue 4
APRIL, 2022
12
STIGMA RELATED TOTUBERCULOSIS (TB) IN INDIA
1Krushna Chandra Sahoo2Pranab MahapatraStigma is a negative response that may
manifest in disparities in behaviour towardsstigmatised individuals (Abbey et al., 2011). Itoccurs when these individuals with a distinctattribute or personal trait are treateddifferently. When these stigmatisingbehaviours or attitudes are associated with aspecific health condition, we refer to this ashealth-related stigma (Stuber et al.,2008).Sometimes, people have preconceptionsor ideas about what a person should be like,based on their perception and belief. This isespecially true for people who have contagiousdiseases. People prefer to distance themselvesfrom these patients and their family membersphysically and socially, often leading to stigmaand discrimination. This can come in a verysubtle way, especially in the early stages, whenpeople start to ask about a person’s health,look suspiciously at them, or say things thatdon’t make sense. On the other hand, there isovertly hostile behaviour or discrimination. Alack of understanding of these illnesses orfear often causes stigma. These problems getworse when people give out incorrect ormisleading information. Stigma hurts thestigmatised person and their family members(Eicher and Bangerter, 2015).
Tuberculosis is a disease that can spreadfrom person to person. It is a significant causeof ill health and one of the top causes of deathin the world. It is caused by the bacteriumMycobacterium tuberculosis, which is spreadfrom one person to another through dropletsof cough. The disease usually affects the lungs(pulmonary TB), occasionally spreading toother parts. About a quarter of the world’speople have M. tuberculosisinfection. TB is abig problem in many low- and middle-incomecountries (LMICs). India has the highestnumber of people who have tuberculosis inthe world, and tuberculosis control has beenthe focus of the Government of India’s revisednational tuberculosis control programme(RNTCP). TB can be prevented, as well ascured with appropriate treatment. About 90%of people who get tuberculosis disease can betreated with a 6-month drug regimen (WHO,2021). Tuberculosis spreads more easily whenpeople do not seek help or get a diagnosisquickly because of stigma. This increases thesize of the tuberculosis pool, which makes itmore likely that people who live with themand in the community will spread the disease.However, one of the major programmatic

205Science Horizon:Volume 7: Issue 4
APRIL, 2022
challenges is stigma related to tuberculosis(Chakrabartty et al. 2018; Thomas andStephen, 2021).
Stigma is often a roadblock in the pathof appropriate health care for tuberculosis,delaying diagnosis and making it morechallenging to manage and treat illnesses.People’s perceptions and beliefs abouttuberculosis influence how patients seekhealth care. The stigma around tuberculosiswas caused by people being afraid of thedisease itself, but it was also based on people’sbeliefs. More than half of people withtuberculosis experience stigma after beingdiagnosed, which causes them to stop takingtheir medication (Thomas and Stephen, 2021).Moreover, patients with TB are afraid of thespread of disease, so they don’t prefer to go toa public place to avoid verbal abuse.
In India, both men and women facedifferent problems because of the stigma.Tuberculosis-related stigma was highest inunmarried, economically inactive women withlow socioeconomic status who were morelikely to be stigmatised. Women had moretuberculosis stigma than men. Unmarriedwomen with TB feel that they will face achallenge in getting a partner for theirmarriage. Those who are married at the timeof TB diagnosis, were afraid of separation,divorce, isolation, and rejection from theirfamilies, especially their in-laws. Men werestigmatised and feared losing their jobs(Somma et al., 2008; Thomas and Stephen,2021). The married women put off gettingchecked out and getting treatment becausethey don’t want their husbands to find out
about the disease and leave them. For men,stigma caused them to lose their jobs.
It’s essential to look at the gender aspectof the illness it has a significant influence oncareseeking all along the course of the disease.The social meanings associated with the gendercan affect the response to illness and continuedtreatment. A careful look at the things thatkeep or break down stigma could help guideefforts to reduce its adverse effects and turnstigma into support.
Stigma and discrimination can worsensymptoms and make it more difficult to gettreatment. Patients lost hope and had lowerself-esteem because of stigma, which led tomore psychiatric symptoms, problems withsocial relationships, and less likelihood tostay with treatment. Other adverse effects ofstigma are unwillingness for treatment, stayingaway from family, friends, or co-workers,thus getting deprived of the support fortreatment. It also makes it more difficult tofind work, school, or social activities, and finda place to live where they can be protectedfrom harassment. There are a lot of issues thataren’t taken into account in the tuberculosiscontrol program in India. There needs to be aparticipatory community approach wherecommunities are involved at every stage forsensitisation and prevention of stigma.Thereare still problems in all tuberculosis controlefforts because of the stigma around TB. Thisneeds to be dealt with across multi-layers inthe tuberculosis care cascade and requirespsychosocial interventions that are patient-centred and health provider-centred. We needhuman-friendly, stigma-free, need-based

206 Science Horizon:Volume 7: Issue 4
APRIL, 2022
psychosocial interventions in addition toclinical interventions because tuberculosis isnot just a medical disease but also a socialdisease, and we need to treat both the aspectsat the same time.
People should learn how to deal withtuberculosis patients. Tuberculosis relatedstigma can hurt the patient and their family,and it may cause them to stay away fromsociety because of shame and fear. There is aneed for education to provide practical adviceto people and families and teach communitiesto support people with tuberculosis.
References1) Abbey S, Charbonneau M, Tranulis C, Moss
P, Baici W, Dabby L, Gautam M, Paré M.Stigma and discrimination. Can J Psychiatry.2011 Oct;56(10):1-9.
2) Chakrabartty A, Basu P, Ali KM, SarkarAK, Ghosh D. Tuberculosis related stigmaand its effect on the delay for sputumexamination under the Revised NationalTuberculosis Control Program in India. IndianJournal of Tuberculosis. 2018 Apr1;65(2):145-51.
3) Eicher V, Bangerter A. Social representationsof infectious diseases. Handbook of socialrepresentations. 2015:385-96.
4) Somma, D., Thomas, B.E., Karim, F., Kemp,J., Arias, N., Auer, C., Gosoniu, G.D.,Abouihia, A. and Weiss, M.G., 2008. Genderand socio-cultural determinants of TB-relatedstigma in Bangladesh, India, Malawi andColombia [Special section on gender andTB]. The International Journal ofTuberculosis and Lung Disease, 12(7),pp.856-866.
5) Stuber J, Meyer I, Link B. Stigma, prejudice,discrimination and health. Social science &medicine (1982). 2008 Aug;67(3):351.
6) Thomas BE, Stephen A. Tuberculosis relatedstigma in India: roadblocks and the wayforward. Expert Review of RespiratoryMedicine. 2021 Jul 3;15(7):859-61.
7) World Health Organization. Global tuberculosisreport 2021. Geneva: WHO; 2021.
1Regional Medical Research Centre, Indian Council of
Medical Research, Bhubaneswar – 7510232Department of Psychiatry, Kalinga Institute of Medical
Sciences, Bhubaneswar – 751024
2. Shritam Das, Elina Das, Kashyap Bhuyan,Biswajita Prusty, Minaketan Barik,V.S.Yadav# & Tahziba Hussain (2017).Bi-directional Screening of Tuberculosispatients for Type 2 Diabetes Mellitus andDiabetes patients for Tuberculosis inBhubaneswar, Odisha. InternationalJournal of Community Medicine &Public Health. 4 (7) : 2435 - 2442.
3. Tahziba Hussain, Kashyap Bhuyan,Biswajita Prusty, Minaketan Barik, ShritamDas, V.S.Yadav and Sanghamitra Pati.
(2018). Incidence and risk factors ofTuberculosis among patients with Type 2Diabetes mellitus attending a tertiary carehospital in Bhubaneswar, Odisha. NationalJournal of Medical Research. 8 (2) : 69- 75.
ICMR-Regional Medical Research Centre,
Bhubaneswar - 751023. Odisha
.....Continuing from Page No.-200
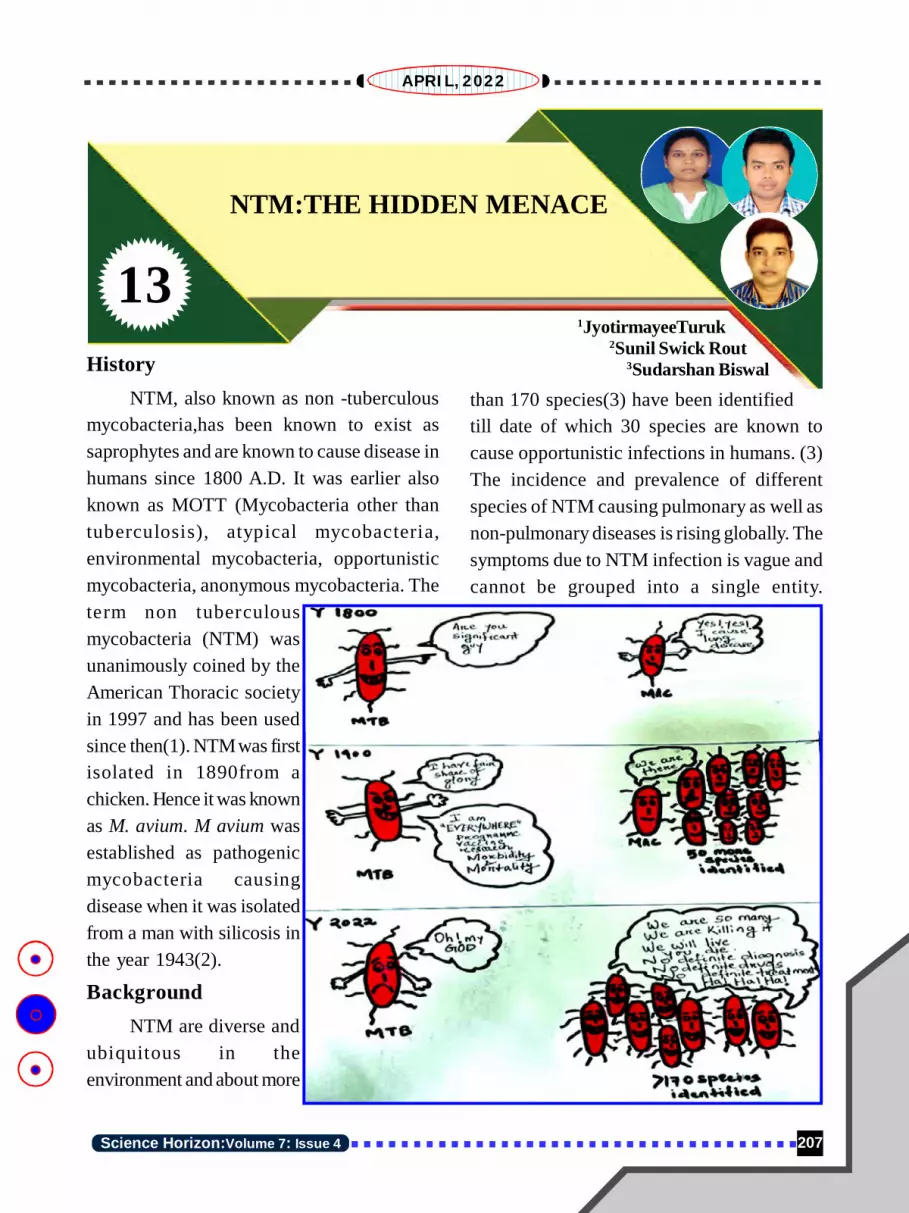
207Science Horizon:Volume 7: Issue 4
APRIL, 2022
13
NTM:THE HIDDEN MENACE
1JyotirmayeeTuruk2Sunil Swick Rout
3Sudarshan BiswalHistoryNTM, also known as non -tuberculous
mycobacteria,has been known to exist assaprophytes and are known to cause disease inhumans since 1800 A.D. It was earlier alsoknown as MOTT (Mycobacteria other thantuberculosis), atypical mycobacteria,environmental mycobacteria, opportunisticmycobacteria, anonymous mycobacteria. Theterm non tuberculousmycobacteria (NTM) wasunanimously coined by theAmerican Thoracic societyin 1997 and has been usedsince then(1). NTM was firstisolated in 1890from achicken. Hence it was knownas M. avium. M avium wasestablished as pathogenicmycobacteria causingdisease when it was isolatedfrom a man with silicosis inthe year 1943(2).
BackgroundNTM are diverse and
ubiquitous in theenvironment and about more
than 170 species(3) have been identifiedtill date of which 30 species are known tocause opportunistic infections in humans. (3)The incidence and prevalence of differentspecies of NTM causing pulmonary as well asnon-pulmonary diseases is rising globally. Thesymptoms due to NTM infection is vague andcannot be grouped into a single entity.

208 Science Horizon:Volume 7: Issue 4
APRIL, 2022
Therefore, any bacteria causing tuberculosislike illness other than MTB was grouped asbacteria causing Mycobacteriosis.Mycobacteriosis was used to excludetuberculosis disease from any other illnesses.
NTM causes opportunistic infection inimmune compromised individuals and was mostcommonly isolated from HIV patients. Nearlyabout 30 species of NTM have been confirmedto cause human disease but human-humantransmission is not commonly seen in NTMinfection. They are also emerging asmycobacterium causing fatal illness as mostof the species are difficult to treat due to theirintrinsic resistance to common antibioticsavailable as well as non-availability of acommon drug regimen for their treatment.
NTM is widely distributed in theenvironment, including soil, tap water, mud,food stuff. NTM has been isolated from manynatural sources. Therefore, the man-made
changes will greatly affect the biology of theorganism and may increase the risk forcausation of disease.
MicroscopyNTM are acid fast bacilli(pink in
colour).The microscopic picture of NTMshows that they do not have the typicalmorphology(i.e. bacilli which are long slenderwith nodules) as of that of Mycobacteriumtuberculosis (MTB), and can vary from beingshort AFB to filamentous in nature.
CultureMost of the NTM are easy to culture and
can be grown in media like Lowenstein Jensen(LJ), Middlebrook and Dubos broth/agar. SomeNTM may require special ingredients likeblood or supplements like ferric ammoniumsulphate. Most of the NTM grow intemperature between 25°C and 37°C but somelike Mycobacterium xenopi may require

209Science Horizon:Volume 7: Issue 4
APRIL, 2022
higher temperature like 45°C for its growth.The NTM can be identified by theircharacteristic growth pattern, pigmentation andrate of growth.
They have been classified into 4 typesdepending on the culture characteristics asper the Runyonclassification.
Identification to the Species LevelIdentification of NTM up to its species
level can be done by using different techniques:
1. Biochemical tests2. HPLC (High performance liquid
chromatography)3. Isoenzyme and protein
electrophoregrams4. Gene probes5. Gene amplification methods6. DNA fingerprinting7. Commercial kits using line probe assay
(LPA)


211Science Horizon:Volume 7: Issue 4
APRIL, 2022
Flowchart for diagnosis of NTM which can be known by performing the drugsensitivity testing.
4.Toxicity monitoring of drugs: Many drugsprescribed for treatment of NTM infectionhave considerable toxicity. Therefore, it isadvisable to look after side effects like visualimpairedness, kidney function test, liverfunction test, ototoxicity, any skin reactions.
References1. Griffith DE, Aksamit T, Brown-Elliott BA,
Catanzaro A, Daley C, Gordin F, et al. AnOfficial ATS/IDSA Statement: Diagnosis,Treatment, and Prevention of NontuberculousMycobacterial Diseases. Am J Respir Crit CareMed. 2007 Feb 15;175(4):367–416.
2. Nontuberculous Mycobacteria (NTM):History [Internet]. [cited 2022 Jan 5]. Availablefrom: https://www.nationaljewish.org/conditions/ntm-nontuberculous-mycobacteria/ntm-nontuberculous-mycobacteria-overview/history
3. Zulu M, Monde N, Nkhoma P, Malama S,Munyeme M. Nontuberculous Mycobacteriain Humans, Animals, and Water in Zambia: ASystematic Review. Front Trop Dis. 2021 Jul1;2:679501.
ICMR- Regional MedicalResearch Centre,
Bhubaneswar

212 Science Horizon:Volume 7: Issue 4
APRIL, 2022
14Jaya Krushna Panigrahi
IntroductionA disease is considered as any harmful
deviation from the normal structural orfunctional state of an organism, generallyassociated with certain signs and symptoms,and differing in nature from externalphysical injury. A disease is indicative of theabnormal state of an organism commonlyexhibiting specific symptoms. In a diseasedcondition, the normal functioning of the cells,tissues, and organs of a person deteriorates.Non-infectious or non-communicable diseases(NCDs), sometimes also referred to aschronic diseases, remain confined to thepersons who have contracted them and don’tgettransmitted to others. These are caused by avariety of circumstantial factors includinginfection by pathogens, nutritionaldeficiencies, genetic defects, environmentalcauses,lifestyle, gender and age-relatedproblems of the individuals. Four major typesof non-communicable diseases have beenidentified by the World Health Organization(WHO): cancer, cardiovasculardisease(e.g., heart attack, stroke), chronic respiratorydisease (e.g., asthma), and diabetes mellitus.As per the WHO estimation, combinedtogether, these four groups of
TUBERCULOSIS ANDENVIRONMENT
conditions,resulting in non-communicable diseases, account forabout 82 percent of all deaths.These can alsoarise from environmental exposures or fromgenetically determined abnormalities, whichmay be evident at birth or which may becomeapparent later in life. Diseases like diabetes,high-blood pressure, hemophilia, anemia,goiter, Down syndrome and cardio-vasculardisorders come under this category.
On the contrary, the infectious orcommunicable or transmissible diseases (IDs)are transmitted from person-to-person, i.e.from infected persons or hosts to healthypersons through the transfer of variouspathogenic agents such as viruses, bacteria,fungi or animal parasites, directly or indirectly.Transmission or dissemination of suchinfection happens either by direct contactorthrough any medium. Such spread isan ecological phenomenon, the host servingas the environment in which the parasite lives;complexity arises when the parasite occurs inmore than one host species (Burrows, 2022).Tuberculosis, malaria, chickenpox, cholera,colds, influenza, herpes, measles and COVID-19are examples of common infectiousdiseases.The burden of infectious diseases

213Science Horizon:Volume 7: Issue 4
APRIL, 2022
(IDs), especially of tuberculosis (TB), remainshigh in low and middle income countries(LMIC). Although the true dimensions of thisco-morbidity have not yet been fullyunderstood, there is a growing amount of data,over the last 10 years that suggest a clearassociation between NCDs and TB (Puchneret al., 2019).Tuberculosis as a CommunicableDisease
Tuberculosis, caused by a bacteriumcalled Mycobacterium tuberculosis,is one ofthe deadliest, chronic communicable diseasesof humans, which is also prevalent in livestockand wildlife. It is still considered a seriouspublic health concern, in addition to itseconomic and social significance. Though theTB bacterium primarily attacks the humanlungs, but it can also infect any other part ofthe body such as the kidney, brain and spine.The historical importance of this lethalinfection is that it has been discovered to beexistent in our immediate ancestor, Homoerectus, as has been recorded from thefossil skeleton of half a million years old.
As the WHO estimates, a total of 1.5million people died from TB in 2020 (including2,14,000 people with HIV infection). Thus, thismakes TB the 13th leading cause of death andthe second leading infectious killer diseaseafter the COVID-19 (above HIV/AIDS)worldwide.It spreads through microscopicdroplets,containing the pathogen, released intothe air when someone with untreated, activeform of tuberculosis of the lungs or throatcoughs, speaks or sings and people nearbybreathe in these bacteria and become infected.
It is also a fact that although tuberculosis iscontagious, it’s not easy to diagnose.
Risk Factors InvolvedFor intervening and reducing the
infection transmission of this chronic humandisease, we need to understand the risk factorsassociated with it.Narasimhan et al. (2013)state that the risk of progression from exposureto the tuberculosis bacilli to the developmentof active disease is a two-stage processgoverned by both exogenous and endogenousrisk factors. Exogenous factors play a keyrole in accentuating the progression fromexposure to infection, among which thebacillary load in the sputum and the proximityof an individual to an infectious TB case arekey factors. Similarly, endogenous factors leadto the progression from infection to active TBdisease. They further opine that along withwell-established risk factors (such as humanimmunodeficiency virus (HIV), malnutrition,and young age), emerging variables such asdiabetes, indoor air pollution, alcohol, use ofimmunosuppressive drugs, and tobacco smokeplay a significant role at both the individualand the population levels. Further,socioeconomic and behavioral factors as wellas specific groups such as health care workersand certain indigenous population are alsoshown to have increased susceptibility to TBinfection and disease. The followingillustration explains the various aspects andlinks of the risk factors involved.
Environmental FactorsTuberculosis as a contagious disease
spreads from person to person. It has been

214 Science Horizon:Volume 7: Issue 4
APRIL, 2022
noted over the years that increased risk of TBis linked with certain environmental riskfactors.However, poverty has a goodconnection with the increased incidence ofTB as more and more poverty-ridden people,mostly from the developing world, have beenhistorically the worst sufferers of the disease.Schmidt (2008) has opined that for centuries,TB has been linked anecdotally withenvironmental risk factors that go hand-in-hand with poverty, such as indoor air pollution,tobacco smoke, malnutrition, overcrowdedliving conditions and excessive alcoholuse.The WHO report that the low- and middle-income countries (LMICs) of the worldaccount for about 98% of the reported TBcases entirely corroborates suchpropositions.Hence, experts in the field oftuberculosis are aptly focusing their attentionatpresent to confront these underlying risk
factors through theTB eradicationprogrammes so as tolimit the spreadingof the disease.
For theprevailing bettere n v i r o n m e n t a lconditions in thedeveloped or richnations of the globe,the prevalence ofTB is of much lessproportion thatremains confinedthere to the poor,mostly in urban
neighbourhoods. Demographic, socio-economic and environmental factors, to whichpeople are exposed, together play a significantrole in the incidence of the disease. Accordingto the analyses made by Dye and colleaguesworking at the WHO Stop TB Department,malnutrition, indoor air pollution from usedsolid fuels, and active smoking constitute thethree top population-attributable TB risksglobally, followed by HIV infection, diabetes,and excessive drinking. The WHO agrees tothe proposition that poverty and urbanizationcreate the perfect conditions for thetransmission of tuberculosis.Some top mostenvironmental risk factors are discussed herewith additional focus.
a. Household Environment: One significantreason behind India carrying the biggest burdenof this disease is the significant influence ofthe physical household environment where the
Fig 1: Risk factors for tuberculosis infection and disease (Narasimhan et al., 2013)

215Science Horizon:Volume 7: Issue 4
APRIL, 2022
people reside. The socio-economicconditions of the people of lower andlower-middle income groups beingbelow the desired level, they mostly livein unhygienic environments withinadequate sanitary system whereindoor air pollution is of commonoccurrence. In a study conducted bySingh et al. (2018), prevalence of TBwas found to be the highest amongelderly people (0.9%), people with noeducation (0.4%) and people belonging to thepoorest wealth quintile (0.53%). Crowding orhigher population density has been consideredas a crucial infection threat in bothindustrialized and non-industrialized countries.It includes overcrowded houses or congestedrooms where enough space is not available tothe people residing in such places. Suchovercrowding scenarios are of commonoccurrence in slum areas of cities indeveloping nations, where the living conditionsof the inhabitants are very much cramped. Incase of prevalence of TB in such communities,the risk of disease transmission from infectedpatients to others is of higher degree.
Further, hospital admissions in coldermonths are significantly higher than in warmermonths. As access to healthcare facilities aswell as label of awareness is of low magnitude,the chance of early cure of this infectiousdisease remains low. It has been reported thatin India, TB prevalence rates are consistentlyhigher among urban children in comparison tothe same group of the rural areas.Migrantpeople with increased mobility and seekingtemporary works in different places fall victim
to the disease very often as they spend theirtime in crowded, unhygienic living conditions.In many cases, the DOTS (Directly ObservedTreatment, Short-course) protocol for TBdetection and treatment are not adhered to thatmakes the bacterium more resistant and helpsin progression of the disease.
b. Smoking: Many observations have led tothe conclusion that smoking has the capacityto trigger more cases of the onset oftuberculosis. Though such cases of occurrenceare certainly less than the cases caused by theHIV/AIDS, but considering the high number ofpersons addicted to smoking in a population,its impact on the magnitude of TB infection iscertainly higher than that of the HIV. This iscorroborated by Donald Enarson, senioradvisor to the International Union AgainstTuberculosis and Lung Disease, Paris, whohence suggests for cessation of smoking.Schmidt (2008) quotes him stating thatalthough smoking’s capacity to trigger TBinfection among individuals is surely less thanthat of HIV/AIDS, it might actually engendermore TB cases on a population basis becausepeople who smoke far outnumber those
Fig 2: Crowded slum housing in cities

216 Science Horizon:Volume 7: Issue 4
APRIL, 2022
infected with HIV.Smoking of cigarettes, bidis,hookah and other tobacco materials has a goodlink with the occurrence of TB, which remainswell documented. Singh et al. (2018) notedfrom their observation that the family memberswho were regularly (daily) exposed to smoke(second-hand smoke) inside the house weremore prone to getting tuberculosis ascompared to the households where people donot smoke inside the house.
Another important aspect is that almosthalf the world’s population and 90% of ruralhouseholds, as WHO estimates, depend ontraditional stoves or open fires for cookingand heating, being fueled by low-cost, easilyavailable kerosene; biomass such as animaldung, crop residues, wood and charcoal;andcoal. These fuels release smoke for inefficientburning that is laden with health-damagingpollutants such as respirable particulate mattersand carbon dioxide,causing indoor air pollutionin poorly ventilated spaces. The women in thedeveloping world being mostly involved in thecooking process, such pollution greatly affectstheir health. Thus, while tobacco smoking hasadverse impacts mostly on the men, the indoorair pollution caused by smoke pollution from
solid fuels exerts detrimental impacts on thewomen’s health. Both these types of smokes,including second hand tobacco smoke, act asthe TB risk factors affecting both the sexes.This happens as smoke impairs the ability ofthe lung ciliato clear the bacteria from therespiratory tract, thus resulting in infection.The medical practitioners hence advisesimultaneous DOTS treatment and smokingcessation, as these might complement eachother.
c. Alcohol Consumption: Another significantfactor that induces TB incidence and enhancesits progression is excessive consumption ofalcohol. The immune response of the bodydeclines in the diseased condition, whilealcoholism in the scenario of risky socialinteractions with infected persons paves theway for increased transmission of the disease.When smoking tobacco and drinking alcoholtend to go hand-in-hand, the combined impactsof both make the person highly vulnerable tothe disease as both act as strong risk factors.Concerning the alcohol dosage, Imtiaz et al.(2017) observed that tuberculosis risk rose asethanol intake increased, with evidence of athreshold effect. Alcohol consumption caused22.02 incident cases and 2.35 deaths per1,00,000 people from tuberculosis in 2014.They also recorded that alcohol-attributabletuberculosis incidence increased between2000 and 2014 in most high tuberculosisburden countries, whereas mortality decreased.A study has indicated that consumption of heavyamount of alcohol on regular basis (more than40 g of ethanol per day or diagnosis of analcohol use disorder) resulted in a nearly three-
Fig 3: Smoking substantially increases the risk of TB

217Science Horizon:Volume 7: Issue 4
APRIL, 2022
fold increase in the risk of tuberculosis.Thus,researchers consider alcohol use, alcoholdosage,and alcohol-related problems as riskfactors for tuberculosis.
d. Malnutrition: The bidirectionalassociation between malnutrition andtuberculosis incidence is a well-establishedfact. This has been evidently established inpopulations affected by poverty, famine, war,natural disasters, mass migration, andconfinement in prisons or ghettos. Schmidt(2008) opines that given that it’s usuallyimpossible to retrospectively discernnutritional status in patients before their TBdisease, it is hard to determine whethermalnutrition led to TB or vice versa. Thiscan only be done reliably through cohortstudies that follow healthy subjects overtime after determining nutrition status atbaseline. Thus, it is a vicious cycle betweenmalnutrition and occurrence of tuberculosis.Undernutrition can lead to progression of thelatent infection to tuberculosis and TB worsensundernutrition, which in turn increases theseverity of the TB disease. Thus, the need is toimprove the nutritional status of the patient
greatly so as to reduce the impacts oftuberculosis.Focus has to be given on thesupply of adequate amounts of micro-and macronutrients, such as proteins andvitamins, so that natural immunityagainst the disease can be boosted. Therole of proteins is illustrated by the factthat they not only fortify the immunefunction, but also strengthen the lungtissues by collagen proteins. To cite acase of vitamins, vitamin D helps with
macrophage function, and macrophages helpto clear TB bacteria. Many authors suggestthat enhanced nutritional support of theundernourished populations at high risk of TBmay reduce the incidence of the disease insuch groups.
The Way Forward
In the context of the global burden ofdisease (GBD), The Lancet journal states thatthe latest global disease estimates reveal aperfect storm of rising chronic diseases andpublic health failures.This has been fuellingthe COVID-19 pandemic to acquire greaterproportion.The most comprehensive globalstudy - analyzing 286 causes of death, 369
Fig 4: Alcoholism behind the rise of TB
Fig 5: Malnutrition often induces TB incidence

218 Science Horizon:Volume 7: Issue 4
APRIL, 2022
diseases and injuries, and 87 risk factors in204 countries and territories - reveals howwell the world’s population were prepared interms of underlying health for the impact ofthe COVID-19 pandemic. In such a situation,the health systems across the globe, mostimportantly in the developing world, need tobe improved and disparities are eliminated.Though a good progress has been made in thearena of prevention and treatment of infectiousdiseases worldwide to reduce mortality, thereis still a huge unfinished agenda to containdiseases like tuberculosis. The need of thehour is much greater synergies amongpopulation health, prevention, treatment andcare, and development efforts, besides politicalcommitment and funding for the cause. AsTracey Burton states, vulnerable people aroundthe world affected by TB cannot wait anylonger for quality testing, treatment and care.Though many organizations, including WHO;Global Fund to Fight AIDS, TB and Malaria;Stop TB Partnership and UNDP, are workingto address the urgent threat of TB menace, weneed to undertake further stringent actions inthis direction. Policy planners and decisionmakers need to focus additional attentiontowards the prevention and treatmentinterventions. Environmental factors boostingthe TB incidences must be tackled with addedattention. Our concerted efforts will translate
into reality the targets of achieving the GlobalPlan to End TB 2018-2022, and the SustainableDevelopment Goal target to end TB by 2030.
References1) Burrows W (2022) Disease. Available online
on https://www.britannica.com/science/disease; visited on 03.02.2022.
2) Imtiaz S, Shield K D, RoereckeM,Samokhvalov A V, Lönnroth K and RehmJ (2017) Alcohol consumption as a risk factorfor tuberculosis: meta-analyses and burden ofdisease. European Respiratory Journal, 50(1), 28705947.
3) Narasimhan P, Wood J, MacIntyre C Rand Mathai D (2013) Risk Factors forTuberculosis. Pulmonary Medicine, SpecialIssue (Available online on https://doi.org/10.1155/2013/828939).
4) Puchner K P, Rodriguez-Fernandez R, OliverM and Solomos Z (2019) Non-communicablediseases and tuberculosis: Anticipating theimpending global storm.Glob Public Health,14(9), 1372-1381.
5) Schmidt C W (2008) Linking TB and theEnvironment: An Overlooked MitigationStrategy. Environ Health Perspectives,116(11): A478–A485.
6) Singh S K, Kashyap G C and Puri P (2018)Potential effect of household environment onprevalence of tuberculosis in India: evidencefrom the recent round of a cross-sectionalsurvey. BMC Pulmonary Medicine, 18, 66.
Odisha Environmental Society,
Bhubaneswar

219Science Horizon:Volume 7: Issue 4
APRIL, 2022
8
ROLE OF ICMR- REGIONALMEDICAL RESEARCH CENTRE
(RMRC), BHUBANESWAR INTUBERCULOSIS CONTROL AND
PREVENTION1Sidhartha Giri, 2JyotirmayeeTuruk,
3Dasarathi Das, 4Sanghamitra PatiThe Indian Council of Medical
Research (ICMR) is the supreme body for theformulation, coordination and promotionof medical research in India. At the same time,it is considered to be one of the oldest andlargest medical research bodies in the world.The ICMR is funded by the Government ofIndia through the Department of HealthResearch (DHR), Ministry of Health andFamily Welfare (MoHFW).
ICMR has a network of 26 institutes, theheadquarter being located in New Delhi. ICMRhas made outstanding contribution as aknowledge generating agency and contributedin understanding various diseases of nationalimportance such as malaria, Japaneseencephalitis, tuberculosis, AIDS, Kala-azar,Filariasis, Leprosy and Poliomyelitis.Additionally, ICMR has made extensivecontributions in the areas of nutrition,reproduction and maternal and child health,occupational and environmental health andresearch complimenting health systems. ICMRregional medical research institutes/ centreshave been contributing in tackling regionalhealth problems. Training and capacity buildingof young investigators, medical and alliedhealth professionals and providing funding
support for research projects toinvestigators all over the country are othervery unique and significant contributions ofICMR. ICMR continues to provide extramuralfunding to strengthen research capabilitieswithin the institutes of the council as well asother research institutes, medical collegesand non-Governmental organizations forvarious research projects.ICMR- Regional Medical ResearchCentre (RMRC), Bhubaneswar
Out of the total 26 institutes, ICMR-RMRC Bhubaneswar is one of the renownedand well developed research institute in easternIndia which is focussed on communicableand non-communicable diseases, humanresource development, other basic , appliedand translational research and has collaboratedwith other ICMR and non-ICMRinstitutionsincluding the State Government ofOdisha, NVBDCP, Delhi, Gates Foundation,DBT, AIIMS New Delhi, IVI, DST, for enhancedresearch, skill improvement and mutualexchange of scientific viewpoints.From thebeginning, the institute has various facilitiessuch as insectariums, animal house, libraryand information, biomedical informatics

220 Science Horizon:Volume 7: Issue 4
APRIL, 2022
centre, national reference laboratoryfor TB and virology network laboratory.National Reference Laboratoryfor Tuberculosis at ICMR-RMRC, Bhubaneswar
In 1997, India launched theRevised National TB ControlProgramme (RNTCP), based on theinternationally recommended DirectlyObserved Treatment Short-course(DOTS) strategy. RNTCP expandedacross the country in a phased mannerwith support from World Bank andother development partners. In March2006, full nation-wide coverage wasachieved, covering over a billionpopulation. The main strategy indetection of TB cases is quality assureddiagnosis. The RNTCP network oflaboratories for TB is composed ofNational Reference Laboratories(NRLs), state level Intermediatereference laboratories (IRLs) andCulture & Drug Susceptibility Testing (C &DST) laboratories and peripheral levellaboratories as designated microscopy centres(DMCs). Effective implementation of DOTSand DOTS Plus strategy is the key componentof RNTCP under Central TB Division of theMinistry of Health and Family Welfare,Government of India. For ease of supervisionand monitoring work, ICMR-RMRC,Bhubaneswar was designated as a NationalReference Laboratory (NRL) for tuberculosisin 2013.
In India, there are six designated NRLsnamely National Institute for Research in
Tuberculosis (NIRT), Chennai; NationalTuberculosis Institute (NTI) Bangalore;National Institute of TB & RespiratoryDiseases (NIRTD) New Delhi; Central JALMAInstitute of Leprosy other Mycobacterialdiseases, Agra; Regional Medical ResearchCentre (RMRC), Bhubaneswar; and BhopalMemorial Hospital and Research Centre,(BMHRC) Bhopal.
The NRL for TB at RMRC, Bhubaneswarwas assigned 10 states namely Odisha, WestBengal, Assam, Meghalaya, Mizoram, Manipur,Nagaland, Sikkim, Tripura and ArunachalPradesh.
Figure 1: National Reference Laboratory (NRL)for tuberculosis at ICMR-RMRC, Bhubaneswar

221Science Horizon:Volume 7: Issue 4
APRIL, 2022
The main focus of the activitiesof the NRL includes: Quality assessment of
smear microscopy(EQA)
Quality assurance ofculture and drugsusceptibility testing oflaboratories under it
Providing support tolaboratories for capacitybuilding
Impart training to statelaboratories ontechnologies used for TB diagnosis
Providing support to DOTS plus centerswith laboratory support
Projects on Tuberculosis Conductedby ICMR-RMRC, Bhubaneswar
During 2009 to 2011, ICMR RMRCBhubaneswar carried out a project on diagnosisof pulmonary TB using culture in solid media(LJ) and carry out drug sensitivity pattern ofthe isolates. The diagnosis of pulmonarytuberculosis under Directly ObservedTreatment Short-course (DOTS) programmewas based on clinical symptoms, radiologicalfindings and sputum microscopy. However, thesputum microscopy fails to detect the low orpaucibacillary infections and an estimated5000 to 10000 bacilli per ml is required fordiagnosis of TB using AFB staining. The AFBstaining also can not differentiate betweenMycobacterium tuberculosis and othermycobacterium. Though the culture ofMycobacterium tuberculosis in solid LJ mediatakes 6-8 weeks to grow, it provides definitive
diagnosis and study of its drug sensitivityfurther helps in the control of the disease moreeffectively. The study was carried out incollaboration with Capital Hospital,Bhubaneswar.
RMRC Bhubaneswar conducted a studyon drug resistance among sputum positivetuberculosis patients in Rayagada district from2011 to 2013. The study estimated theprevalence of drug resistance amongtuberculosis patients in a tribal district ofOdisha inhabited by 57% tribal population. Thisstudy provided the much-needed drugresistance information during the start ofprogrammatic management of drug-resistantTB (PMDT) services at Odisha after a gap of10 years from the first study in Mayurbhanjdistrict in 2000-2001. The prevalence ofmulti-drug resistant TB (MDR TB) was 0%and 7.0% among new and previously treatedpatients in this study. The low prevalence ofdrug resistance observed in this area was a
Figure 2: Studies on tuberculosis in tribal populations

222 Science Horizon:Volume 7: Issue 4
APRIL, 2022
good indicator of RNTCP programme beingimplemented in the Rayagada district.
In September 2013, RMRC initiated aproject on performance of Light EmittingDiode microscope in different settings for aTB diagnosis. As microscopic examination ofsputum smears is the main tool for thediagnosis of pulmonary tuberculosis in TBcontrol programmes, newer microscopicmethods were compared with the conventionalZN microscopy. The project was conducted incollaboration with Capital Hospital,Bhubaneswar, in which sputum specimens,along with consent form and patientinformation form, were collected fromsuspected pulmonary TB patients andprocessed for ZN, FM, LED microscopy (3different methods) and solid culture with LJmedium.The results of the study showed thatcompared to ZN microscopy, LED FM wasmore sensitive in detecting TB bacilli.
During 2013 to 2016, RMRCBhubaneswar conducted a prospective studyto determine the incidence of tuberculosisamong patients with Type 2 Diabetes Mellitus.In this study, 1200 patients with Type 2Diabetes mellitus were screened for signs &symptoms of TB. Blood samples from thesepatients were analyzed for various biochemicalparameters and HbA1C. Socio-demographicand clinical data were collected from alldiabetes patients using standardized forms.Clinical evaluation of each patient included adetailed history of duration and chronology ofchest symptoms like cough, dyspnoea, fever,chest pain, and haemoptysis. Out of 1200patients, only 13 (1.08%) patients had TB
active disease. The results showed that theincidence of TB among patients with diabeteswas less than that reported from other regions.
During 2015 to 2017, RMRCBhubaneswar was involved in a multi-centricstudy to estimate the burden of TB among thetribal population and develop an innovativehealth system model to strengthen TB controlin the tribal areas. Odisha has 62 distinct tribalgroups, making it the largest collection oftribal people in a single state in the country.Each of these tribal groups has its ownindigenous customs and continues to practicethem even today. More than half of theirpopulation is concentrated in four districts ofBalangir, Dhenkanal, Kandhamal andMayurbhanj. RMRC Bhubaneswar conductedanother study on targeted Intervention toexpand and strengthen TB Control in tribalpopulations under the Revised NationalTuberculosis Control Programme (RNTCP),India, during 2016 to 2018.
Undernutrition is both an important riskfactor for, and a common consequence of, TB.It is therefore a common comorbid conditionfor people with active TB and is associatedwith increased risk of mortality and poortreatment outcome. Most individuals withactive TB are in a catabolic state and experienceweight loss and some show signs of vitaminand mineral deficiencies at diagnosis. Weightloss among those with TB can be caused byseveral factors, including reduced food intakedue to loss of appetite, nausea and abdominalpain; nutrient losses from vomiting andmetabolic alterations caused by the disease.During 2016 to 2018, RMRC Bhubaneswar

223Science Horizon:Volume 7: Issue 4
APRIL, 2022
conducted a study on the effectiveness offood supplementation on treatment outcomesand nutritional status of adults with pulmonarytuberculosis in Odisha.
From 2019 to 2021, RMRCBhubaneswar was involved in a national surveyfor state-wise prevalence of microbiologicallyconfirmed pulmonary tuberculosis in India,where RMRC was responsible for Chhattisgarhstate. This ambitious study was planned toestimate the point prevalence ofmicrobiologically confirmed pulmonary TBamong persons aged e”15 years in India for 20states / state groups.To estimate the burden ofhuman pulmonary paragonimiasis in crab eatingcommunities and smear negative suspectedTB cases from some states of India, RMRCBhubaneswar conducted a pilot study in twodistricts of Odisha, Nayagarh and Mayurbhanj.These districts were selected based on numberof TB cases, geography and crab eating
behaviour.
In a recently initiated study, RMRCBhubaneswar will map hotspots of MDR-TBin Assam, Tripura and Sikkim using genomicsapproaches. The main objective of the projectis to employ whole genome sequencing andtraditional genotyping for mapping hotspotsof primary MDR-TB in Assam, Tripura andSikkim and to identify transmission patternsand source/s of MDR-TB using molecularepidemiology and clinical epidemiology.
In another study, RMRC Bhubaneswar,evaluated the burden of Atypical Mycobacteriaor non-tuberculous mycobacteria (NTM) incausing respiratory infections. When evaluatedclinically, it was found that the most of thepatients had symptoms and signs as that oftuberculosis. The chest X-Ray imagesmimicked pulmonary tuberculosis but thepatients did not respond to the common drugregimen for M. tuberculosis. As the diagnosis
of NTM are importantfor therapeutic purpose,the project for diagnosisof non - tuberculousmycobacteria wasundertaken in March2018 considering onlythe pulmonary samples.Gradually extrapulmonary sampleswere also tested forpresence of NTM. In thisproject, NTM has beenisolated from 42 clinicalsamples (bothpulmonary and extraFigure 3: Studies on human pulmonary paragonimiasis by RMRC, BBSR

224 Science Horizon:Volume 7: Issue 4
APRIL, 2022
pulmonary). M. chelonae, M.fortuitum, M. gordonae, M.abscessus, M. mageritenseareamong the different isolatesfrom the clinical samples.
In the recent years, RMRCBhubaneswar has been part ofseveral multi-centric trials onTB diagnosis, therapy, andprevention. In a multicentre trialto assess the performance ofcentralized assay solutions fordetection of MTB andresistance to Rifampin andIsoniazid, the institute willestimate the diagnostic accuracy of centralizedassay solutions for MTB detection for smear-positive and smear-negative TB, includingXpert MTB/RIF (or Ultra) as a comparatorand culture as the reference standard. Theinstitute is part of an open-label, non-randomized, two-stage, dose-finding study ofverapamil tablet formulation in adulttuberculosis patients in continuation phase ofanti-tuberculosis treatment. The project aimsto determine the compensatory increase inverapamil dose that can offset the increasedmetabolism of verapamil when it is co-administered with rifampicin to TB patients attheir sixth month of treatment. The study alsoaims to confirm the safety and tolerability ofverapamil in patients with TB withoutunderlying cardiac disease. The study is beingconducted as a collaborative project betweenRMRC, Bhubaneswar and SCB medicalcollege, Cuttack. RMRC Bhubaneswar is alsopart of a phase III, randomized, double-blind,
placebo controlled trial to evaluate the efficacyand safety of VPM1002 and ImmunovacVaccines in preventing TB in healthy householdcontacts of newly diagnosed sputum positivepulmonary TB patients.
To conclude, ICMR-RMRCBhubaneswar has conducted studies on severalaspects of tuberculosis during the last twodecades. This includes evaluating the burdenof tuberculosis, including MDR TB, in Odishaand other states. Special focus has been givento understand the burden of TB in specificpopulations such as tribal groups,malnourished, and people with diabetesmellitus. Several trials have also beenconducted by RMRC Bhubaneswar to studythe effects of anti-tubercular drugs andvaccines.
ICMR- Regional Medical Research Centre,
Bhubaneswar
Figure 4:Studies on tuberculosis vaccines by RMRC, BBSR

