role of estrogen, estrogen receptor-α and esr1 polymorphisms in sle
TRANSCRIPT

Columbia International Publishing Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
Review
*Corresponding email: [email protected] 1 Molecular Medicine Center, Medical University-Sofia, 2 Zdrave Street, 1431 Sofia, Bulgaria 2 Department of Clinical Laboratory and Clinical Immunology and Department of Nephrology,
Medical University-Sofia, 1 Georgi Sofijski Street, 1431 Sofia, Bulgaria 3 Department of Dermatology and Venereology, Medical University-Sofia, 1 Georgi Sofijski Street,
1431 Sofia, Bulgaria
28
Role of Estrogen, Estrogen Receptor-α and ESR1 Polymorphisms in SLE
Zornitsa Kamenarska1*, Maria Hristova2, and Lyubomir Dourmishev3
Received 11 February 2014; Published online 28 June 2014 © The author(s) 2014. Published with open access at www.uscip.us
Abstract The etiology of SLE is not clearly understood but strong genetic predisposition has been recognized. Environmental and hormonal factors are known to contribute towards the expression of the disease. Among the above risk factors, female gender is considered to be of greatest significance. Thus estrogens and their receptors have been proposed as obvious candidates to explain this sexual dimorphism. The present review summarizes our experience, as well as previously reported data in literature about the involvement of estrogen, estrogen receptor-α and ESR1 genetic variants in the pathogenesis of SLE, its clinical manifestations and outcome. Keywords: Estrogen; Estrogen Receptor-α; ESR1 polymorphisms; Systemic lupus erythematosus
1. Introduction
The etiology of SLE is not clearly understood but strong genetic predisposition has been recognized. Environmental and hormonal factors are known to contribute towards the expression of the disease. Among the above risk factors, female gender is considered to be of greatest significance (Cervera et al., 1993). The observed female prevalence is highest after puberty. The pre-puberty female to male ratio is 3:1. It increases to 10:1 during the childbearing years and decreases again to 8:1 after menopause. Thus estrogens and their receptors have been proposed as obvious candidates to explain this sexual dimorphism (Lahita, 1999).

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
29
2. Role of Estrogen in Autoimmunity
The typical physiological level of estrogen (E2) is extremely low, in the range of 10–900 pg/ml, and it varies during the age and the physiological status of the individual (Neill, 2005). E2 can produce different effects depending on its concentration but also on the type of target cell, the receptor subtype present on a given cell type, and the timing of administration. During pregnancy E2 inhibits pro-inflammatory pathways such as TNF-α, IL-1β, IL-6, and the activity of natural killer (NK) cells, whereas E2 at the same concentration stimulates anti-inflammatory pathways such as IL-4, IL-10, and TGF-β (Straub, 2007). Thus E2 can influence the Th1, Th2 and Th17 responses which regulation is thought to play a key role in the induction of autoimmune diseases. E2 is also a potential physiological regulatory factor for the peripheral development of CD4+CD25+ Treg cells. E2, at physiological doses, stimulates the conversion of CD4+CD25- T cells into CD4+CD25+ T cells which exhibits enhanced Foxp3 and IL-10 expression in vitro. Such converted CD4+CD25+ T cells have similar regulatory function as naturally occurring Treg cells, as demonstrated by their ability to suppress naïve T cell proliferation in a mixed lymphocyte reaction. The estrogen receptor (ER) was found expressed in the CD4+CD25- T cells and the conversion of CD4+CD25- T cells into CD4+CD25+ T cells, which is stimulated by E2, could be inhibited by ICI182,780, a specific inhibitor of the estrogen receptors. This supports that E2 may directly act on CD4+CD25- T cells via ER(s) (Tai et al., 2008). At lower concentrations, E2 stimulates TNF-α, IFN-γ, IL-1β, and the activity of the NK cells (Straub, 2007).
3. Animal Models of SLE – Role of Estrogen and Estrogen Receptor-α
Recent studies of anti-DNA antibody transgenic mice clearly demonstrated that an elevation in either estrogen or prolactin breaks tolerance of high affinity DNA-reactive B cells and induces a lupus phenotype (Grimaldi, 2006). It was proved that the induction of the lupus phenotype by estrogen is performed via an estrogen receptor-α-dependent pathway (Feng et al., 2010). The role of ER-α in lupus-like disease has been suggested by different studies carried out on animal models. A study in (NZBxNZW)F1 mice that utilized ER-α-selective and ER-β-selective agonists indicated that the ER-α activation plays an immunostimulatory role in murine lupus, whereas the ER-β activation has mild immunosuppressive effects (Li et al., 2007). The key role of ER-α, but not ER-β, in the pathogenesis of lupus was further confirmed in experiments with ER-α −/− NZM2410 and ER-α −/− MRL/lpr lupus prone mice. ERα-deficient mice manifested significantly less pathologic renal disease and proteinuria and had significantly prolonged survival compared to wild-type mice (Svenson et al., 2008). It was shown that the inflammatory response to toll like receptor (TLR) ligands was significantly impacted by the presence of ER-α despite the absence of estradiol, and may partially explain the protective effect of ER-α deficiency in lupus-prone animals (Cunningham et al., 2012).

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
30
4. Role of Estrogen in SLE Patients There is evidence that E2 plays a role in SLE by altering the thresholds for B cell apoptosis and activation. Earlier it was shown that E2 may polyclonally increase the production of IgG, including IgG anti-dsDNA, in SLE patients' peripheral blood mononuclear cells by enhancing B cell activity and by promoting IL-10 production in monocytes (Kanda et al., 1999). Increased levels of estrogen were reported in men with autoimmune disease including SLE (Doukas et al., 2013). There are data to support the role of sex hormones as a trigger for the disease and a modulator of the disease severity (Cohen-Solal et al., 2008). Hyper estrogenic levels in premenopausal SLE women are associated with increased risk of cardiovascular manifestations (Kaliterna et al., 2014). The role of the hormones in the pathogenesis of the disease has been further clarified by Bernier et al. (2009) who demonstrated that the use of combined oral contraceptives was associated with an increased risk of SLE. The risk was particularly elevated in women who have recently started the contraceptive use. It was also reported that the use of oral contraceptives and the use of hormonal replacement therapy increase the chance of venous thromboembolism in SLE patients, especially in those with antiphospholipid antibodies (Mok et al., 2001). Physicians generally do not prescribe hormone replacement therapy to women with SLE because of the widely held view that such treatment can activate SLE. Safety of Estrogens in Lupus Erythematosus - National Assessment (SELENA) is a body which aims to clarify that issue and set adequate treatment criteria (Furie et al., 2014; Thanou et al., 2014).
5. Role of Estrogen Receptor-α in SLE Patients Estrogen acts through two nuclear receptors—estrogen receptor-α (ER-α) and estrogen receptor-β (ER-β). ER-α is mainly expressed in uterus, prostate (stroma), ovary (theca cells), epididymis, bone, breast, and various regions of the brain, liver and white adipose tissue. ER-β is expressed in colon, prostate (epithelium), ovary (granulosa cells), bone marrow, salivary gland, vascular endothelium and certain regions of the brain. Furthermore, in some tissues, both ERs are expressed albeit in different cell types. The expression of the ERα gene (ESR1) and its protein (ERα) in lupus patients was significantly higher than in healthy controls. The enhanced expression of ERα mRNA and protein in SLE was associated with DNA demethylation within the proximal promoter region located between -232 and +81 base pair relative to transcription start site of human ERα gene (Liu et al., 2014).
6. ESR1 Polymorphisms and SLE
Estrogen receptor-α (ER-α) is coded by ESR1 gene, located on chromosomes 6q25.1. Numerous mRNA splice variants exist for ER-α although their exact function in physiology and human diseases remains to be elucidated. The most extensively studied polymorphisms on terms of SLE are the PvuII P/p and XbaI X/x in intron 1. PvuII P and XbaI X variants were found to enhance the ER-α activity (Alonso et al., 2011; Wang et al., 2010) although these results were challenged by Maruyama et al. (2000). A recent study has proved relationship between the estrogen receptor ESR1 PvuII and XbaI polymorphisms and the Th1 and Th2 cytokine expression in patients with SLE.

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
31
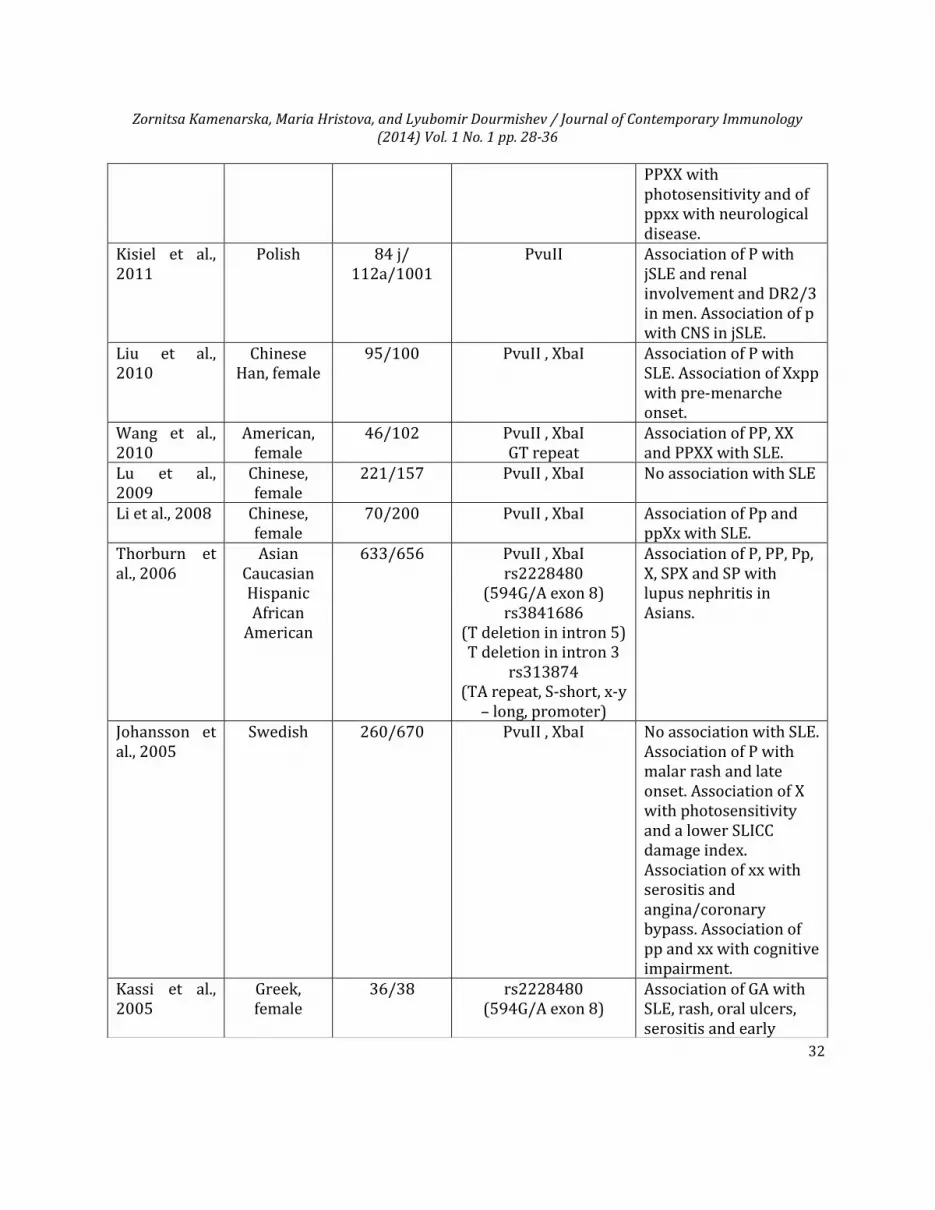
According to the results, the polymorphisms are associated with an alteration in the Th-1/Th-2 balance in favor of Th-2, increasing the susceptibility to SLE. The findings also indicated that ER-α gene polymorphisms could influence the expression of IL-10, IL-4, IL-2 and IFN-γ in SLE, with the Th-2 cell being predominant in patients with PpXx and Ppxx genotypes (Lu et al., 2009). An association between the PvuII P/p and XbaI X/x polymorphisms and SLE has been reported in several studies concerning Asian population (Liu et al., 2010; Li et al., 2008; Thorburn et al., 2006; Lee et al., 2004; Liu et al., 2002, Liu et al., 2000) but most of the studies concerning Europeans have not found any (Kamenarska et al., 2012; Tanev et al., 2011; Thorburn et al., 2006; Johansson et al., 2005). The incompatibility in the results especially those, concerning the allele and genotype distribution among patients and controls might be due to racial, ethnical or gender variation as well as illness classification. It was proved that ethnic variation plays a major role in genetic regulation of estrogen or estrogen receptor activity and related polymorphism to individual diseases (Hsieh et al., 2007). Some authors support the idea that ESR1 polymorphisms are not associated with the disease susceptibility but they rather have a disease modifying role associated with the clinical features and laboratory manifestations. The ESR1 polymorphisms have been related to disease onset (Liu et al., 2010, Johansson et al., 2005, Kassi et al., 2005, Lee et al., 2004). Skin rashes were found more common in patients with the dominant X (Kamenarska et al., 2012) and P alleles (Johansson et al., 2005) and in patients with PpXx genotype (Liu et al., 2002). The P allele and the PPXX genotype appeared associated with photosensitivity (Tanev et al., 2011; Johansson et al., 2005) which is tightly linked to skin rashes. The frequency of hematological abnormalities, hypertension, capillary thrombi and glomerular sclerosis was higher in patients with ppxx genotype (Liu et al., 2002). The neurological disease was higher in patients with ppxx (Tanev et al., 2011), pp and xx genotype (Johansson et al., 2005) and p allele (Kisiel et al., 2011). More detailed information concerning the association of ESR1 polymorphisms with the susceptibility and the clinical manifestations of SLE could be found in Table 1.
Table 1 Summary of association studies of ESR1 polymorphisms with SLE
Reference Population SLE/Controls Polymorphisms Clinical feature Kamenarska et al., 2012
Bulgarian 45/69 PvuII , XbaI (intron 1)
No association with lupus nephritis. Association of X with malar rash and of X, P, XX+Xx and PP+Pp with hematological disease.
Tanev et al., 2011
Bulgarian, female
112/50 PvuII , XbaI No association with SLE. No association with disease on-set and duration. Association of
Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
32
PPXX with photosensitivity and of ppxx with neurological disease.
Kisiel et al., 2011
Polish 84 j/ 112a/1001
PvuII Association of P with jSLE and renal involvement and DR2/3 in men. Association of p with CNS in jSLE.
Liu et al., 2010
Chinese Han, female
95/100 PvuII , XbaI
Association of P with SLE. Association of Xxpp with pre-menarche onset.
Wang et al., 2010
American, female
46/102 PvuII , XbaI GT repeat
Association of PP, XX and PPXX with SLE.
Lu et al., 2009
Chinese, female
221/157 PvuII , XbaI No association with SLE
Li et al., 2008 Chinese, female
70/200 PvuII , XbaI Association of Pp and ppXx with SLE.
Thorburn et al., 2006
Asian Caucasian Hispanic African
American
633/656 PvuII , XbaI rs2228480
(594G/A exon 8) rs3841686
(T deletion in intron 5) T deletion in intron 3
rs313874 (TA repeat, S-short, x-y
– long, promoter)
Association of P, PP, Pp, X, SPX and SP with lupus nephritis in Asians.
Johansson et al., 2005
Swedish 260/670 PvuII , XbaI
No association with SLE. Association of P with malar rash and late onset. Association of X with photosensitivity and a lower SLICC damage index. Association of xx with serositis and angina/coronary bypass. Association of pp and xx with cognitive impairment.
Kassi et al., 2005
Greek, female
36/38 rs2228480 (594G/A exon 8)
Association of GA with SLE, rash, oral ulcers, serositis and early

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
33
The fundamental studies aiming to clarify the role of ER-α and E2 in SLE were carried out mostly in animal models. There are data which support a role of ER-α in E2-induced autoimmunity in lupus-prone mice, but the results and conclusions may not necessarily be applicable to the development of lupus in humans. Evidently more studies concerning SLE in humans are needed till the data finds application into clinical practice.
References
Alonso, P., Gratacòs, M., Segalàs, C., Escaramís, G., Real, E., Bayés, M., et al. (2011). Variants in estrogen receptor alpha gene are associated with phenotypical expression of obsessive-compulsive disorder. Psychoneuroendocrinology, 36(4), 473-483. http://dx.doi.org/10.1016/j.psyneuen.2010.07.022
Bernier, M. O., Mikaeloff, Y., Hudson, M., & Suissa, S. 2009. Combined oral contraceptive use and the risk of systemic lupus erythematosus. Arthritis & Rheumatism, 61(4), 476-481. http://dx.doi.org/10.1002/art.24398
Cervera, R., Khamashta, M. A., Font, J., Sebastiani, G. D., Gil, A., Lavilla, P., et al. (1993). Systemic lupus erythematosus: clinical and immunologic patterns of disease expression in a cohort of 1,000 patients. The European Working Party on Systemic Lupus Erythematosus. Medicine, 72(2), 113–124. http://dx.doi.org/10.1097/00005792-199303000-00005
Cohen-Solal, J. F., Jeganathan, V., Hill, L., Kawabata, D., Rodriguez-Pinto, D., Grimaldi, C., Diamondm B. (2008). Hormonal regulation of B-cell function and systemic lupus erythematosus. Lupus, 17(6), 528–532.
onset. Lee et al., 2004
Korean, female
137/268 PvuII , XbaI
Association of PP with late onset. Association of Xx and ppXx with early onset.
Liu et al., 2002
Chinese 245/172 PvuII , XbaI
Association of PpXx with lupus nephritis in male, skin rashes and arthritis. Association of ppxx with hematological abnormalities, hypertension, capillary thrombi, glomerular sclerosis. Association of Ppxx with renal vacuitis.
Kassi et al., 2001
Greek, female
19/11 Sequencing of exon 1 and 2
No association with SLE.
Liu et al., 2000
Chinese 245/172 PvuII , XbaI
Association of PpXx with lupus nephritis in male.

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
34
http://dx.doi.org/10.1177/0961203308089402
Cunningham, M. A., Naga, O. S., Eudaly, J. G., Scott, J. L., & Gilkeson, G. S. (2012). Estrogen receptor alpha modulates Toll-like receptor signaling in murine lupus. Clinical Immunology, 144(1), 1-12. http://dx.doi.org/10.1016/j.clim.2012.04.001
Doukas, C., Saltiki, K., Mantzou, A., Cimponeriu, A., Terzidis, K., Sarika, L., Mavrikakis, M., Sfikakis, P., & Alevizaki, M. (2013). Hormonal parameters and sex hormone receptor gene polymorphisms in men with autoimmune diseases. Rheumatology Inernational, 33(3), 575-582. http://dx.doi.org/10.1007/s00296-012-2386-4
Feng, F., Nyland, J., Banyai, M., Tatum, A., Silverstone, A. E., & Gavalchin, J. (2010). The induction of the lupus phenotype by estrogen is via an estrogen receptor-alpha-dependent pathway. Clinical Immunology, 134(2), 226-236. http://dx.doi.org/10.1016/j.clim.2009.10.004
Furie, R. A., Leon, G., Thomas, M., Petri, M. A., Chu, A. D., Hislop, C., et al (2014). A phase 2, randomised, placebo-controlled clinical trial of blisibimod, an inhibitor of B cell activating factor, in patients with moderate-to-severe systemic lupus erythematosus, the PEARL-SC study. Annals of the Rheumatic Diseases, doi: 10.1136/annrheumdis-2013-205144. http://dx.doi.org/10.1136/annrheumdis-2013-205144
Grimaldi, C. M. (2006). Sex and systemic lupus erythematosus: the role of the sex hormones estrogen and prolactin on the regulation of autoreactive B cells. Current Opinion in Rheumatology, 18(5), 456-461. http://dx.doi.org/10.1097/01.bor.0000240354.37927.dd
Hsieh, Y.-Y., Wang, Y.-K., Chang, C.-C., & Lin, C.-S. (2007). Estrogen receptor a-351 XbaI*G and -397 PvuII*C-related genotypes and alleles are associated with higher susceptibilities of endometriosis and leiomyoma. Molecular Human Reproduction, 13(2), 117–122. http://dx.doi.org/10.1093/molehr/gal099
Johansson, M., Ärlestig, L., Möller, B., Smedby T., & Rantapää-Dahlqvist, S. (2005). Oestrogen receptor α gene polymorphisms in systemic lupus erythematosus. Annals of the Rheumatic Diseases, 64(11), 1611-1617. http://dx.doi.org/10.1136/ard.2004.032425
Kaliterna, D. M., Radić, M., & Ljutić, D. (2014). Does estrogen stimulate the pathogenic sort of anticardiolipin antibodies? The Israel Medical Association journal: IMAJ, 16(3), 197-198.
Kanda, N., Tsuchida, T., Tamaki, K. (1999). Estrogen enhancement of anti-double-stranded DNA antibody and immunoglobulin G production in peripheral blood mononuclear cells from patients with systemic lupus erythematosus. Arthritis & Rheumatism, 42(2), 328-337. http://dx.doi.org/10.1002/1529-0131(199902)42:2<328::AID-ANR16>3.0.CO;2-#
Kamenarska, Z., Hristova, M., Dourmishev, L., Andonova, S., Kaneva, R., Mitev, V., Bogov, B., & Savov, A. (2012). Association between estrogen receptor-α gene polymorphisms and lupus nephritis in Bulgarian patients. BANTAO journal, 10(2), 59-62.
Kassi, E., Vlachoyiannopoulos, P. G., Kominakis, A., Kiaris, H., Moutsopoulos, H. M., & Moutsatsou, P., 2005. Estrogen receptor alpha gene polymorphism and systemic lupus erythematosus: a possible risk? Lupus, 14(5), 391-398. http://dx.doi.org/10.1191/0961203305lu2104oa
Kassi, E. N., Vlachoyiannopoulos, P. G., Moutsopoulos, H. M., Sekeris, C. E., & Moutsatsou, P. (2001). Molecular analysis of estrogen receptor alpha and beta in lupus patients. European Journal of Clinical Investigation, 31(1), 86-93. http://dx.doi.org/10.1046/j.1365-2362.2001.00762.x
Lahita, R. G. (1999). The role of sex hormones in systemic lupus erythematosus. Current Opinion in Rheumatology, 11(5), 352–356.

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
35
http://dx.doi.org/10.1097/00002281-199909000-00005
Lee, Y. J., Shin, K. S., Kang, S. W., Lee, C. K., Yoo, B., Cha, H. S., et al. (2004). Association of the oestrogen receptor a gene polymorphisms with disease onset in systemic lupus erythematosus. Annals of the Rheumatic Diseases, 63(10), 1244–1249. http://dx.doi.org/10.1136/ard.2003.012583
Li, F., Che, Zh., Liu, Y., Fu H., Wang, Z., & Lu, Z. (2008). Association between estrogen receptor α gene polymorphisms and systemic lupus erythematosus in Chinese women. Chinese Journal of Clinical Laboratory Science, 2008, 2(2), 112-114.
Li, J., & McMurray, R. W. (2007). Effects of estrogen receptor subtype-selective agonists on autoimmune disease in lupus-prone NZB/NZW F1 mouse model. Clinical Immunology, 123(2), 219-226. http://dx.doi.org/10.1016/j.clim.2007.01.008
Liu, H. W., Lin, H. L., Yen, J. H., Tsai, W. C., Chiou, S. S., Chang, J. G., et al. (2014). Demethylation within the proximal promoter region of human estrogen receptor alpha gene correlates with its enhanced expression: Implications for female bias in lupus. Molecular immunology, 61(1), 28-37. http://dx.doi.org/10.1016/j.molimm.2014.05.002
Liu, O.-G., Huang, Q.-S., Duan, Z.-B., Huang, T.-L., & Liu, Z.-G. (2010). Association between estrogen receptor gene polymorphism and systemic lupus erythematosus in women of Han nationality from Jiangxi province. Chinese Journal of Dermatology, 43(7), 460-462.
Liu, Z. H., Cheng, Z. H., Gong, R. J., Liu, H., Liu, D., & Li, L. S. (2002). Sex differences in estrogen receptor gene polymorphism and its association with lupus nephritis in Chinese. Nephron 90(2), 174–178. http://dx.doi.org/10.1159/000049039
Liu, H., Liu, Z., Chen, Z., Liu, D., & Li, L., (2000). Estrogen receptor gene polymorphism and its association with clinicopathological manifestation of lupus nephritis. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 17(4), 266-269.
Lu, Z.-M., Wang, Z.-E, Liu, Y.-Q., Wu, Ch.-X., Wang, Ch.-Y., Zhang, B.-Ch., et al. (2009). Association of estrogen receptor α gene polymorphisms with cytokine genes expression in systemic lupus erythematosus. Croatian Medical Journal, 50(2), 117–123. http://dx.doi.org/10.3325/cmj.2009.50.117
Maruyama, H., Toji, H., Harrington, C. R., Sasaki, K., Izumi, Y., Ohnuma, T., et al. (2000). Lack of an association of estrogen receptor alpha gene polymorphisms and transcriptional activity with Alzheimer disease. Archives of Neurology, 57(2), 236–240. http://dx.doi.org/10.1001/archneur.57.2.236
Mok, C. C., Lau, C. S., & Wong, R. W. (2001). Use of exogenous estrogens in systemic lupus erythematosus. Seminars in Arthritis and Rheumatism, 30(6), 426-435. http://dx.doi.org/10.1053/sarh.2001.22498
Neill, J. D. (2005). Knobil and Neill's physiology of reproduction (3rd ed). Academic Press, New York.
Straub, R. H. (2007). The complex role of estrogens in inflammation. Endocrine Reviews, 28(5), 521-574. http://dx.doi.org/10.1210/er.2007-0001
Svenson, J. L., EuDaly, J., Ruiz, P., Korach, K. S., & Gilkeson, G. S. (2008). Impact of estrogen receptor deficiency on disease expression in the NZM2410 lupus prone mouse. Clinical Immunology, 128(2), 259-268. http://dx.doi.org/10.1016/j.clim.2008.03.508
Tai, P., Wang, J., Jin, H., Song, X., Yan, J., Kang, Y., et al. (2008). Induction of regulatory T cells by physiological level estrogen. Journal of Cellular Physiology, 214(2), 456-464. http://dx.doi.org/10.1002/jcp.21221
Tanev D., Robeva R., Andonova S., Nikolova M., Stoycheva М., Tomova A., et al. (2011). Systemic lupus erythematosus and estrogen receptor polymorphism in Bulgarian women. Rheumatology (Sofia), 19(3), 59-64.

Zornitsa Kamenarska, Maria Hristova, and Lyubomir Dourmishev / Journal of Contemporary Immunology (2014) Vol. 1 No. 1 pp. 28-36
36
Thanou, A., Chakravarty, E., James, J. A., & Merrill, J. T. (2014). How should lupus flares be measured? Deconstruction of the Safety of Estrogen in Lupus Erythematosus National Assessment-Systemic Lupus Erythematosus Disease Activity Index flare index. Rheumatology (Oxford), doi: 10.1093/rheumatology/keu153. http://dx.doi.org/10.1093/rheumatology/keu153
Thorburn, Ch. M., Pawlikowska, L., Woo, J. M., Taylor, K., Carlson, El., Kwok, P.-Y., et al. (2006). Confirmation of Esr1 Polymorphism Association with Lupus Nephritis in a Multi-Ethnic Case-Control Cohort. 10-15.11.2006 Washington, 2006 ACR/ARHP Scientific Meeting Program Book, 641.
Wang, J., Nuite, M., & McAlindon, T. E. (2010). Association of estrogen and aromatase gene polymorphisms with systemic lupus erythematosus. Association of estrogen and aromatase gene polymorphisms with systemic lupus erythematosus. Lupus, 19(6), 734-740. http://dx.doi.org/10.1177/0961203309359517