right ventricular myocardial function in patients with either idiopathic or ischemic dilated...
TRANSCRIPT

Right Ventricular Myocardial Function in Patients withEither Idiopathic or Ischemic Dilated CardiomyopathyWithout Clinical Sign of Right Heart Failure: Effectsof Cardiac Resynchronization TherapyANTONELLO D’ANDREA, M.D.,* GEMMA SALERNO, M.D.,* RAFFAELLA SCARAFILE,M.D.,* LUCIA RIEGLER, M.D.,* RITA GRAVINO, M.D.,* FRANCESCA CASTALDO, M.D.,*ROSANGELA COCCHIA, M.D.,* GIUSEPPE LIMONGELLI, M.D.,* MASSIMO ROMANO,M.D.,† PAOLO CALABRO, M.D.,* GERARDO NIGRO, PROF.,* SERGIO CUOMO, M.D.,*EDUARDO BOSSONE, M.D.,‡ PIO CASO, M.D.,§ and RAFFAELE CALABRO, PROF.*From the *Chair of Cardiology, Second University of Naples, Naples, Italy; †Chair of Internal Medicine, Federico II◦
University, Naples, Naples, Italy; ‡Institute of Respiratory Disease, University of Milan, IRCCS FondazionePoliclinico-Mangiagalli-Regina Elena, Milan, Italy; and §Department of Cardiology, Monaldi Hospital, Naples, Italy
Objective: In dilated cardiomyopathy (DCM), right ventricular (RV) dysfunction has been reportedand attributed both to altered loading conditions and to RV involvement in the myopathic process.The aim of the study was to detect RV myocardial function in DCM using two-dimensional (2D) strainechocardiography and to assess the effects of cardiac resynchronization therapy (CRT) on RV myocardialstrain during a 6-month follow-up.
Methods and Results: A total of 110 patients (mean age: 55.4 ± 11.2 years) with either idiopathic (n =60) or ischemic (n = 50) DCM, without overt clinical signs of RV failure, underwent standard echo and 2Dstrain analysis of RV longitudinal strain in RV septal and lateral walls. The two groups were comparablefor clinical variables (New York Heart Association class III in 81.8%). Left ventricular volumes, ejectionfraction, stroke volume, and mitral valve effective regurgitant orifice were similar between the two groups.No significant differences were evidenced in Doppler mitral and tricuspid inflow measurements. RVdiameters were mildly increased in patients with idiopathic DCM, while RV tricuspid annulus systolicexcursion and Tei-index were comparable between the two groups. RV global longitudinal strain andregional peak myocardial strain were significantly impaired in patients with idiopathic DCM comparedwith those having ischemic DCM (all P < 0.001). Using left ventricular end-systolic volume as marker forresponse to CRT, 70 patients (63.3%) were long-term responders. Ischemic DCM patient responders toCRT showed a significant improvement in RV peak systolic strain. Conversely, in patients with idiopathicDCM and in ischemic patients nonresponders to CRT, no improvement in RV function was evidenced.By multivariable analysis, in the overall population, ischemic etiology of DCM (P < 0.0001), positiveresponse to CRT (P < 0.001), and longitudinal intraventricular dyssynchrony (P <0.01) emerged as theonly independent determinants of RV global longitudinal strain after CRT.
Conclusions: Two-dimensional strain represents a promising noninvasive technique to assess RV my-ocardial function in patients with DCM. RV myocardial deformation at baseline and after CRT are moreimpaired in idiopathic compared with ischemic DCM patients. Future longitudinal studies are warrantedto understand the natural history of RV myocardial function, the extent of reversibility of RV dysfunctionwith CRT, and the possible prognostic impact of such indexes in patients with congestive heart failure.(PACE 2009; 32:1017–1029)
heart failure, resynchronization therapy, idiopathic dilated cardiomyopathy, two-dimensional strainimaging, right ventricle, right ventricular function
Cardiac resynchronization therapy (CRT) isan established therapy for patients with advancedcongestive heart failure associated with electro-
Address for reprints: Antonello D’Andrea, M.D., Via G. Mar-tucci 35, 80121, Naples, Italy. Fax: 390-817-145205; e-mail:[email protected]
Received December 31, 2008; revised March 5, 2009; acceptedMarch 18, 2009.
mechanical dyssyncrony.1,2 Currently, patientsare selected for CRT on the basis of clinical andelectrocardiographic (ECG) criteria and of stan-dard left ventricular (LV) echocardiographic in-dexes.3,4 In dilated cardiomyopathy (DCM), rightventricular (RV) dysfunction has been observedand attributed both to altered loading conditionsowing to LV diastolic impairment and to RV in-volvement in the myopathic process.5–8
C©2009, The Authors. Journal compilation C©2009 Wiley Periodicals, Inc.
PACE, Vol. 32 August 2009 1017

D’ANDREA, ET AL.
To date, few data are available regarding theeffects of CRT on RV function. Previous studies re-ported the beneficial effect of CRT on RV chambersize and on the severity of tricuspid regurgitationand pulmonary artery pressure.9–11
Among various echocardiographic tech-niques, Doppler myocardial imaging and strainrate imaging have gained acceptance by virtueof their ability to define myocardial timing, con-tractility, and deformation in patients with leftbundle branch block and heart failure.3,12–17 Inaddition, Doppler myocardial imaging was alsoshown to be a reliable and reproducible methodof analyzing global and regional RV function18–21
and in providing prognostic information.6–8 How-ever, both this technique and Doppler strain mea-sures are limited by Doppler angle of incidence.A novel approach to quantify regional myocardialfunction from routine grayscale two-dimensional(2D) echocardiographic images, known as speckle-tracking 2D strain echocardiography, calculatesmyocardial strain independent of angle of inci-dence and has been recently validated againstsonomicrometry and tagged magnetic resonanceimaging.22–26
On these grounds, the aims of the presentstudy were: (1) to analyze by speckle-tracking 2Dstrain RV myocardial function in patients with ei-ther idiopathic or ischemic DCM without overtclinical signs of right heart failure, and (2) to assesspossible different effects of CRT on RV myocardialstrain during a 6-month follow-up.
MethodsStudy Population
From January 2006 to December 2007, 625 am-bulatory heart failure patients with known LV sys-tolic dysfunction were referred to our echocardio-graphic laboratory. Patients with QRS < 120 ms(n = 102), overt clinical signs of RV failure (n =130), atrial fibrillation (n = 79), inducible myocar-dial ischemia (n = 25), poor echocardiographicwindow (n = 11), and improved LV ejection frac-tion (>40%; n = 46) were ineligible for our study.Among the remaining 232 patients (112 with id-iopathic DCM and 120 with ischemic DCM), 110patients were prospectively studied and selectedfor CRT for severe heart failure despite optimalpharmacological therapy, and were followed upfor at least 6 months after the implantation.
The final study population therefore included110 patients (mean age: 55.4 ± 11.2 years) witheither idiopathic (60 patients) or ischemic (50 pa-tients) DCM. Inclusion criteria for CRT were NewYork Heart Association (NYHA) class III–IV re-fractory heart failure, LV end-diastolic diameter >55 mm, LV ejection fraction <35%, QRS interval >120 ms, and sinus rhythm.
Exclusion criteria were acute LV congestiveheart failure, overt clinical signs of right heart fail-ure (distended and prominent jugular veins, sig-nificant peripheral edema, hepatomegaly, ascites),coronary artery bypass graft surgery, and myocar-dial infarction within the previous 3 months, pre-vious RV myocardial infarction, valvular stenosis,previous valve replacement or reconstruction, pre-vious pulmonary embolism, and chronic cor pul-monale. This study was approved by the hospitalethics committee, and all patients gave written in-formed consent to participate in the study.
Implantation Technique
CRT was initiated with implantation of abiventricular pacing system (CONTAK CD H115,CD II H119, RENEWAL H135, or III H170, H175,H177, Guidant Corp., Arden Hills, MN, USA;InSync ICD 7272, Marquis 7277, or InSync ICDII, Marquis 7289, Medtronic Inc., Minneapolis,MN, USA). LV leads were positioned as follows:posterior-lateral or lateral in 85 patients and an-terior or anterior-lateral in 25 patients. In orderto optimize benefit from CRT, in the overall pop-ulation of DCM patients we performed an echo-guided positioning of the LV pacing lead, deter-mining by use of Doppler myocardial imagingthe site of latest mechanical activation.3 In ad-dition, among the 50 patients with ischemic car-diomyopathy, preimplantation evaluation of my-ocardial thickness of the region targeted for LVpacing was assessed. As reported by others, weconsidered presence of myocardial scar tissuein case of measurement of end-diastolic wallthickness ≤0.6 cm.27 In our population, myocar-dial scar was observed in the anterior/antero-lateral position in 35 ischemic patients and in theposterior/postero-lateral position in 10 patients,while in five patients normal myocardial thick-ness (>0.6 cm) was measured. As a consequence,in 33 of the 35 patients with anterior/antero-lateralscar, LV lead was implanted in the posterior-lateral position, while in eight of the 10 patientswith posterior/postero-lateral scar, LV lead wasimplanted in anterior-lateral position. Optimalatrioventricular delay was determined first usingRitter’s method followed by optimization of inter-ventricular delay.28 Postoptimization mean atri-oventricular delay was 120 ± 55 ms, with a widevariability of optimized atrioventricular delay in-tervals (60–180 ms) among the patient cohort,while postoptimization mean interventricular de-lay was 35 ± 15 ms.
Study Protocol
A week before implantation and 6 monthsafter, all the patients underwent a clinical ex-amination, 12-lead ECG, standard Doppler echo,
1018 August 2009 PACE, Vol. 32

RV STRAIN IN IDIOPATHIC VERSUS DILATED CARDIOMYOPATHY AFTER CRT
and 2D strain by Vivid 7 ultrasound system (GEVingmed Ultrasound AS, Horten, Norway). Thepatients were considered as responders to CRT ifLV end-systolic volume decreased by 15% and asnonresponders in all other cases.
Standard Echocardiography
Standard Doppler echocardiography andspeckle-tracking 2D strain were performed withthe subjects in partial left decubitus. A vari-able frequency phased-array transducer (2.5–3.5–4.0 MHz) was used for 2D and Doppler imag-ing. Doppler echocardiographic tracings wererecorded on magneto-optical disk. All the mea-surements were analyzed by two experiencedreaders blind to the etiology and responder statusof DCM patients, on the average of more than threecardiac cycles. Stroke volume was obtained byLV outflow Doppler method as the product be-tween outflow tract area and LV output time-velocity integral.29 LV ejection fraction was mea-sured using a commercially available softwareprogram that applied modified Simpson’s rule onthe two- and four-chamber views.
RV end-diastolic chamber size was accuratelyassessed using four parameters according to theprotocol proposed by Foale et al. and by the Amer-ican Society of Echocardiography guidelines forchamber quantification, integrating apical four-chamber and short-axis views.30,31 Care must betaken to obtain a true nonforeshortened apicalfour-chamber view, oriented to obtain the max-imum RV dimension, before making these mea-surements. Two of the four parameters were themeasurements of the midcavity and basal RV di-ameter in the apical four-chamber view at enddiastole. The third one included the major axisof the RV, and was defined as the distance be-tween the RV apex to the midpoint of the tricus-pid annulus. The last one was the measurementof RV outflow tract at subpulmonary region fromparasternal short-axis view.
Tricuspid annular plane systolic excursion(TAPSE) was calculated as index of RV globalsystolic function by the difference between end-diastolic and end-systolic measurements (in mm).The Tei-index (RV myocardial performance index)was calculated as previously described.32
By pulsed Doppler myocardial imaging, theearly (Ea) and late (Aa) diastolic annular veloc-ities were measured at the lateral corner of themitral and tricuspid annuli, in accordance withthe method proposed by Nagueh et al.33 Mitral Evelocity, corrected for the influence of relaxation(i.e., the E/Ea ratio), was calculated to estimate LVfilling pressures. In order to obtain a measure ofglobal myocardial RV function, peak systolic ve-locity (Sm) obtained at the tricuspid annulus and
base and mid-RV segments were averaged, as re-ported by others.
The proximal flow convergence techniquewas used as a quantitative Doppler method to cal-culate regurgitant volume of flow and orifice area(effective regurgitant orifice [ERO]).34
Two-Dimensional Echocardiographic RV Strain
Two-dimensional strain uses grayscale (B-mode) sector image and is based on frame-by-frame tracking of small rectangular image blockswith stable speckle pattern.22,23,26 A minimumframe rate of 30 Hz was required for reliable op-eration of this program and frame rates of 60–90Hz were used for routine grayscale imaging. Api-cal four-chamber view (the same as the RV diam-eter measurement) was obtained using the sameultrasound system and probe used for standardechocardiography; end systole was chosen as thesingle frame for the endocardial to epicardial re-gion of interest to include maximal wall thicknessfor strain calculation. The “Zoom/RES” feature onthe echocardiographic machine was used to im-prove the accuracy of RV measurements. A circu-lar region of interest was traced on the endocardialcavity interface of the apical four-chamber viewat RV systole (minimum cavity area) by a point-and-click approach. Then, a second, larger con-centric circle was automatically generated, whichwas near the epicardium with a default widthof 15 mm. The region of interest then includedthe entire RV myocardial wall, and a click fea-ture increased or decreased the width of the twocircles for thicker or thinner walls, respectively.The tracking algorithm followed the endocardiumfrom this one frame throughout the cardiac cycle.Accordingly, for RV longitudinal strain, myocar-dial thickening was represented with a negativevalue, color-coded as red; myocardial thinningwas represented with a positive value, color-codedas blue; and then these were superimposed to con-ventional 2D images. The software then automat-ically divided the image into six standard seg-ments and provided an automated tracking score,similar to statistical standard deviation (SD), asfeedback of the stability of the regional speckletracking, ranging from 1.0 to 3.0 in arbitrary units.A tracking score value of <2.5 was determinedas acceptable as previously described, and slightadjustments were made to the placement of theregion of interest in regions with greater SDs toattempt to improve tracking stability. The track-ing process was performed offline in a dedicatedsoftware (EchoPAQ PC 2D strain, GE Healthcare,Milwaukee, WI, USA). Longitudinal strains foreach individual segment were measured and av-eraged for RV septal and lateral walls. In addition,the software calculated RV global longitudinal
PACE, Vol. 32 August 2009 1019

D’ANDREA, ET AL.
strain by averaging local strains along the entireright ventricle.
Analysis of Mechanical Dyssynchrony
In accordance with the Recommendationsfor Performance of Echocardiography for CRT,recently proposed by the American Soci-ety of Echocardiography Dyssynchrony WritingGroup,35 in our study protocol the followingdyssynchrony measures were performed:
1. Interventricular Dyssynchrony (Time dif-ference between RV and LV ejections). This wasdetermined as the time from the onset of pulsedDoppler flow velocities in the LV and RV outflowtracts, respectively.
2. Longitudinal Intraventricular Dyssyn-chrony. From the apical four-chamber, two-chamber, and long-axis views, this index was sim-ply measured by Doppler myocardial imaging asthe time from the Sm wave of one wall to the Smwave of the opposing wall on the same cineloops.
3. Radial Intraventricular Dyssynchrony.By use of speckle tracking applied to routine mid-ventricular short-axis images, baseline speckle-tracking radial dyssynchrony was defined as a timedifference in peak septal wall to posterior wallstrains ≥130 ms.
Statistical Methods
All the analyses were performed using a com-mercially available package (SPSS, Rel 11.0 2002,SPSS Inc., Chicago, IL, USA). Variables are pre-sented as mean ± SD. Two-tailed t-test for pairedand unpaired data was used to assess changes be-tween groups. Linear regression analyses and par-tial correlation test by Pearson’s method were doneto assess univariate relations.
To identify significant independent determi-nants of RV myocardial strain in patients withdilated cardiomyopathy, their individual asso-ciation with clinically relevant and echocardio-graphic variables was assessed by multivariablelinear regression analysis. The following variableswere included into the analysis: clinical data(age, sex, body surface area, mean blood pressure,etiology of heart failure) and echocardiographicmeasurements (LV volumes, RV diameters,Doppler mitral and tricuspid inflow measure-ments, TAPSE, RV Tei-index, mitral valve ERO,pulmonary artery pressure, dyssynchrony in-dexes, response to CRT). These variables were se-lected according to their clinical relevance andpotential impact on RV function, as shown byearlier studies. Variable selection was performedin the multivariable Cox regression as an interac-tive stepwise backward elimination method, each
time excluding the one variable with the highest Pvalue according to Wald statistics. The assumptionof linearity was checked graphically by studyingthe smoothed martingale residuals from the nullmodel plotted against the covariate variables. Thelinearity assumptions were satisfied. The Hosmer-Lemeshow goodness-of-fit test was used to checkthat the model adequately fit the data. The modelalso underwent bootstrap validation (200 runs).36
In order to decrease the inflation of the Type 1 errorrate due to multiple testing, the statistical signifi-cance was defined as two-sided P value <0.01.
Reproducibility of 2D strain measurementswas determined in all the subjects. Inter- andintraobserver variability was examined usingboth Pearson’s bivariate two-tailed correlationsand Bland-Altman analysis. Relation coefficients,95% confidence limits, and percent errors werereported.
ResultsStudy Population
Clinical features of the 110 patients enrolledin the study are shown in Table I. At the time ofCRT system implantation, 82.2% patients were inNYHA functional class III and 17.8% in NYHAclass IV. QRS duration ranged from 120 to 210 ms(mean 149.2 ± 22.1 ms). The two groups were com-parable for most of the clinical variables. However,patients with ischemic DCM were more frequentlysmokers and diabetics.
LV Echocardiography at Baseline
LV volumes, ejection fraction, stroke volume,and mitral valve ERO were comparable betweenthe two groups. No significant differences wereevidenced in Doppler transmitral inflow measure-ments and in the E/Ea ratio (Table II).
RV Dimension and Function at Baseline
RV diameters were mildly increased in pa-tients with idiopathic DCM, while TAPSE, RV Tei-index, and RV Doppler myocardial imaging Smpeaks were comparable between the two groups(Table III).
Overall, RV speckle tracking was possiblein 637 (96.5%) of 660 attempted segments fromthe 110 subjects with technically adequate im-ages, with only 3.5% of segments eliminated withtracking variation scores >2.5. Overall trackingvariation scores were <2.0 in 81%.
RV global and regional peak myocardial strainwere significantly compromised in patients withidiopathic DCM compared with ischemic DCMin both the analyzed RV walls (Table III; Figs. 1and 2).
1020 August 2009 PACE, Vol. 32
RV STRAIN IN IDIOPATHIC VERSUS DILATED CARDIOMYOPATHY AFTER CRT
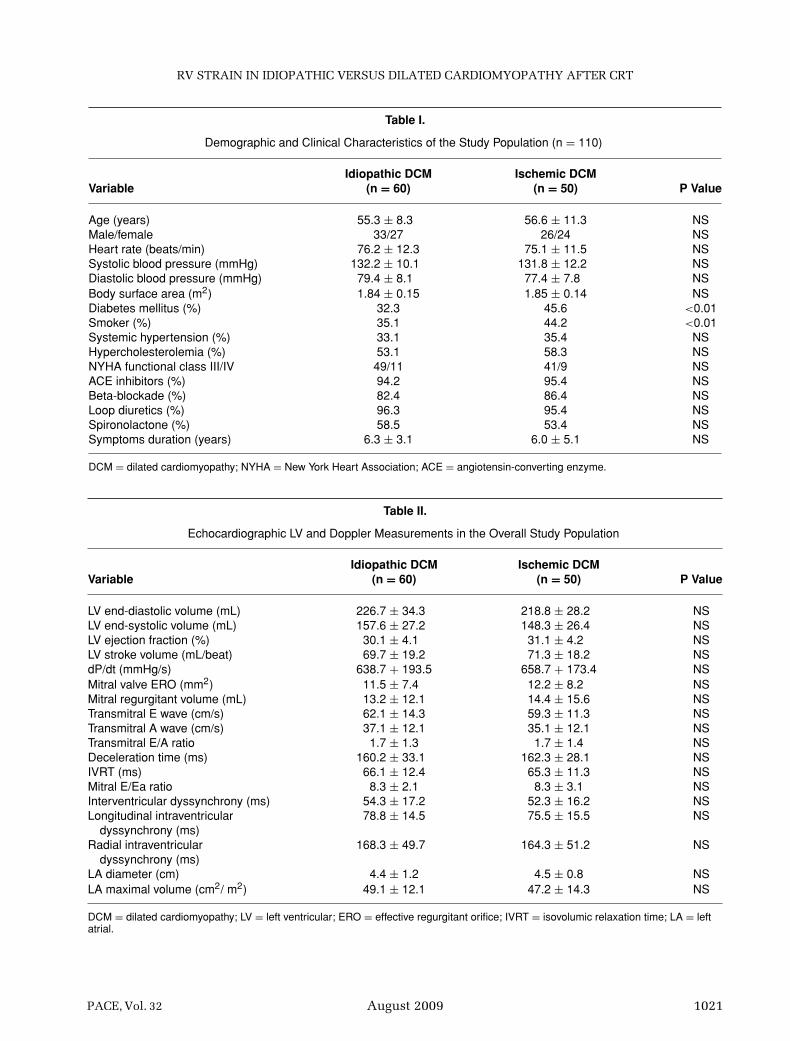
Table I.
Demographic and Clinical Characteristics of the Study Population (n = 110)
Idiopathic DCM Ischemic DCMVariable (n = 60) (n = 50) P Value
Age (years) 55.3 ± 8.3 56.6 ± 11.3 NSMale/female 33/27 26/24 NSHeart rate (beats/min) 76.2 ± 12.3 75.1 ± 11.5 NSSystolic blood pressure (mmHg) 132.2 ± 10.1 131.8 ± 12.2 NSDiastolic blood pressure (mmHg) 79.4 ± 8.1 77.4 ± 7.8 NSBody surface area (m2) 1.84 ± 0.15 1.85 ± 0.14 NSDiabetes mellitus (%) 32.3 45.6 <0.01Smoker (%) 35.1 44.2 <0.01Systemic hypertension (%) 33.1 35.4 NSHypercholesterolemia (%) 53.1 58.3 NSNYHA functional class III/IV 49/11 41/9 NSACE inhibitors (%) 94.2 95.4 NSBeta-blockade (%) 82.4 86.4 NSLoop diuretics (%) 96.3 95.4 NSSpironolactone (%) 58.5 53.4 NSSymptoms duration (years) 6.3 ± 3.1 6.0 ± 5.1 NS
DCM = dilated cardiomyopathy; NYHA = New York Heart Association; ACE = angiotensin-converting enzyme.
Table II.
Echocardiographic LV and Doppler Measurements in the Overall Study Population
Idiopathic DCM Ischemic DCMVariable (n = 60) (n = 50) P Value
LV end-diastolic volume (mL) 226.7 ± 34.3 218.8 ± 28.2 NSLV end-systolic volume (mL) 157.6 ± 27.2 148.3 ± 26.4 NSLV ejection fraction (%) 30.1 ± 4.1 31.1 ± 4.2 NSLV stroke volume (mL/beat) 69.7 ± 19.2 71.3 ± 18.2 NSdP/dt (mmHg/s) 638.7 + 193.5 658.7 + 173.4 NSMitral valve ERO (mm2) 11.5 ± 7.4 12.2 ± 8.2 NSMitral regurgitant volume (mL) 13.2 ± 12.1 14.4 ± 15.6 NSTransmitral E wave (cm/s) 62.1 ± 14.3 59.3 ± 11.3 NSTransmitral A wave (cm/s) 37.1 ± 12.1 35.1 ± 12.1 NSTransmitral E/A ratio 1.7 ± 1.3 1.7 ± 1.4 NSDeceleration time (ms) 160.2 ± 33.1 162.3 ± 28.1 NSIVRT (ms) 66.1 ± 12.4 65.3 ± 11.3 NSMitral E/Ea ratio 8.3 ± 2.1 8.3 ± 3.1 NSInterventricular dyssynchrony (ms) 54.3 ± 17.2 52.3 ± 16.2 NSLongitudinal intraventricular 78.8 ± 14.5 75.5 ± 15.5 NS
dyssynchrony (ms)Radial intraventricular 168.3 ± 49.7 164.3 ± 51.2 NS
dyssynchrony (ms)LA diameter (cm) 4.4 ± 1.2 4.5 ± 0.8 NSLA maximal volume (cm2/ m2) 49.1 ± 12.1 47.2 ± 14.3 NS
DCM = dilated cardiomyopathy; LV = left ventricular; ERO = effective regurgitant orifice; IVRT = isovolumic relaxation time; LA = leftatrial.
PACE, Vol. 32 August 2009 1021
D’ANDREA, ET AL.
Table III.
RV Standard Echo and 2D Strain Measurements at Baseline in the Overall Study Population
Idiopathic DCM Ischemic DCMVariable (n = 60) (n = 50) P Value
RV diameter (four-chamber annulus) (cm) 3.4 ± 0.6 2.9 ± 0.5 <0.01RV diameter (four-chamber middle ventricle) (cm) 3.4 ± 0.6 3.1 ± 0.3 <0.05RV long-axis diameters (four-chamber) (cm) 9.2 ± 0.8 8.6 ± 0.7 <0.05RVOT diameter (short-axis) (cm) 2.8 ± 0.5 2.7 ± 0.8 NSTricuspid regurgitation velocity (m/s) 2.2 ± 0.4 2.4 ± 0.5 NSRV fractional area change (%) 33.2 ± 2.4 34.2 ± 1.4 NSTAPSE (cm) 1.67 ± 0.33 1.71 ± 0.35 NSRV Tei-index 0.41 ± 0.04 0.39 ± 0.06 NSDoppler myocardial imaging RV Sm peak velocity (m/s) 5.4 ± 2.1 5.7 ± 3.1 NSTricuspid E/Ea ratio 5.1 ± 2.3 5.2 ± 2.4 NSRV lateral wall mean 2D strain (%) −9.3 ± 2.1 −15.4 ± 2.8 <0.001RV septal wall mean 2D strain (%) −8.2 ± 2.5 −14.4 ± 2.4 <0.001RV global longitudinal 2D strain (%) −8.8 ± 2.7 −14.6 ± 2.6 <0.001
RV = right ventricle; RVOT = right ventricular outflow tract; TAPSE = tricuspid annular plane systolic excursion.
Clinical and Echocardiographic Responseto CRT
Six months after CRT, 78 patients (71%)were in NYHA functional class I–II, while 20(18.1%) and 12 (10.9%) were in NYHA classIII and IV, respectively. QRS duration was sig-nificantly reduced from 149.2 ± 22.1 to 126 ±22 ms (P <0.001), while a significant increase in6-minute walking distance was seen (from 220.7 ±18 to 348 ± 75 m; P < 0.001).
All the patients had echocardiographic stud-ies 6 months after CRT to determine long-term re-sponse. When LV end-systolic volume was usedas the principal outcome marker for response toCRT, 70 patients (63.3%; 41 with idiopathic DCM,29 with ischemic DCM) were long-term respon-ders, and 40 (36.7%; 19 with idiopathic DCM, 21with ischemic DCM) were nonresponders.
Overall, significant changes in the entire CRTgroup were observed. A significant increase wasdetected in LV ejection fraction and LV stroke vol-ume, while mitral regurgitation decreased. In ad-dition, RV diameters decreased and indexes of RVsystolic function increased. Individual responses,however, were variable.
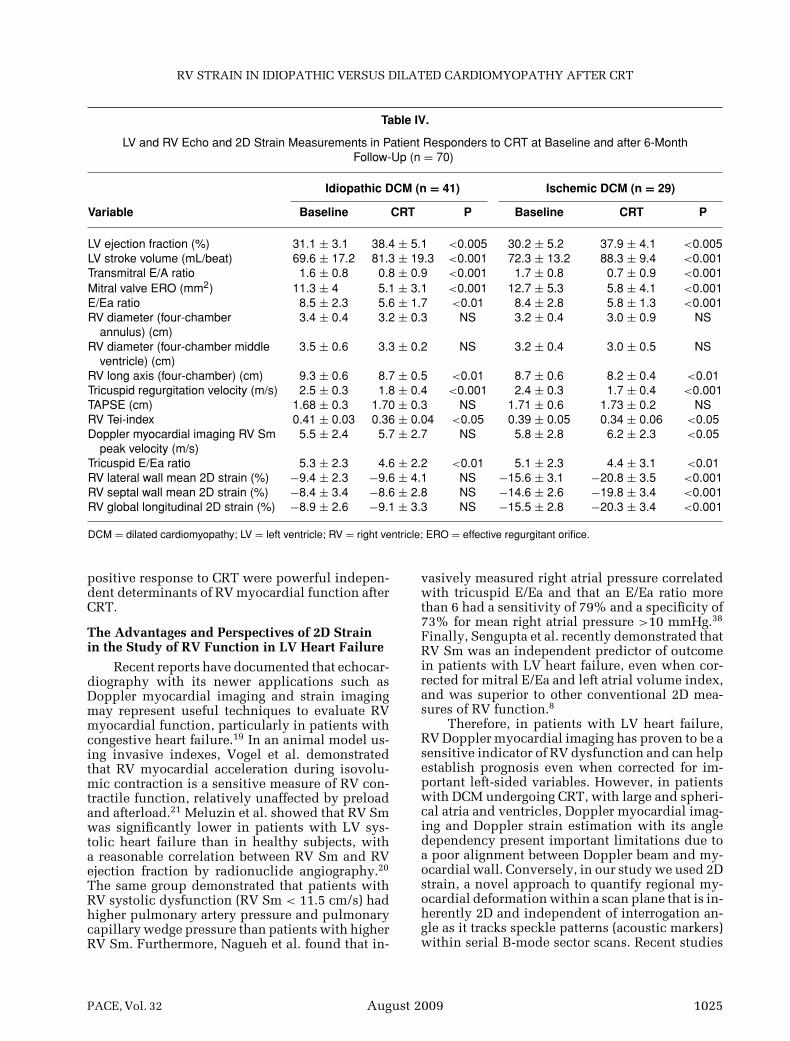
Responders to CRT
Among patient responders to CRT, patientswith ischemic DCM showed a mild but signifi-cant improvement in RV long-axis diameter and inboth RV Doppler myocardial imaging Sm peak andRV Tei-index. In addition, an improvement in RVpeak systolic strain and global longitudinal strain
was observed in 25 of the 29 (86.2%) ischemic pa-tients and only in 12 of the 41 (29.2%) idiopathicpatients (Table IV). Significant inverse correlationbetween changes in myocardial RV global longitu-dinal strain and both changes in mitral valve ERO(r = –0.56, P < 0.001) and changes in transmitralE/A ratio (r = –0.53, P < 0.005) were observed.Conversely, in patients with idiopathic DCM nosignificant differences were found before and afterCRT for both standard and 2D strain indexes of RVsystolic function, while a mild but significant de-crease in RV diameters was observed (Table IV).
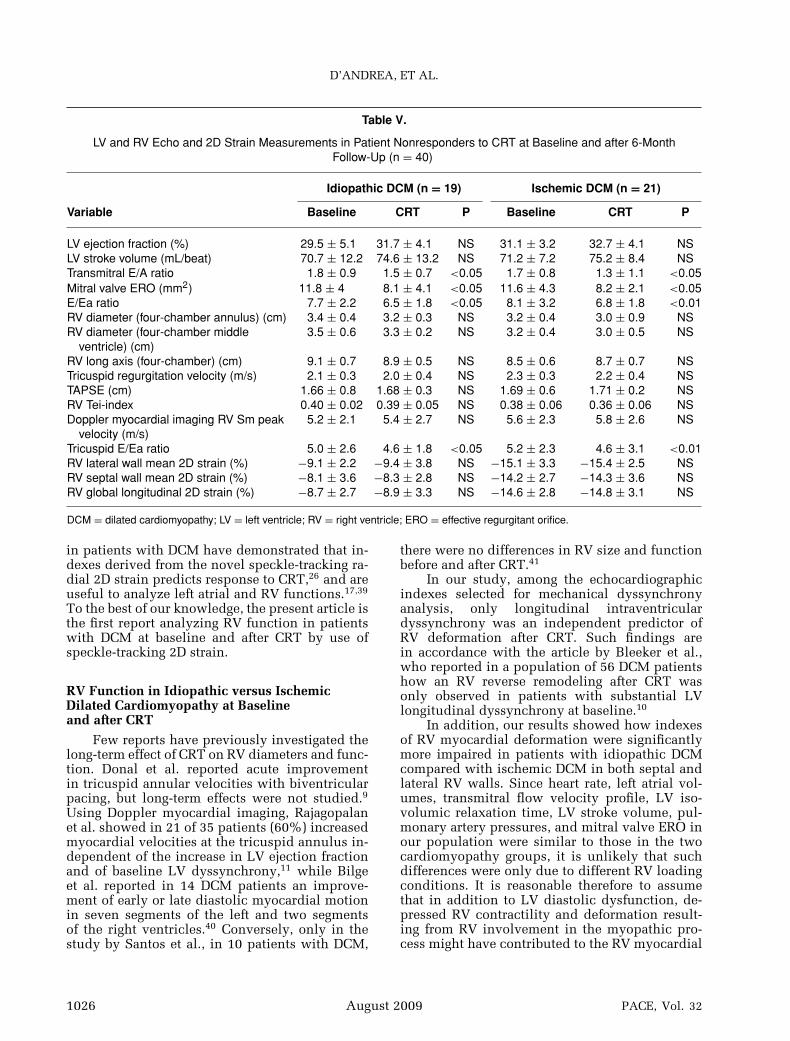
Nonresponders to CRT
In patients nonresponders to CRT, no im-provement in RV diameters and function was ev-idenced in patients with both idiopathic and is-chemic etiology of DCM (Table V). In addition, nosignificant correlation was found between changesin RV global longitudinal strain and changes ineither mitral valve ERO (r = −0.2, P = 0.21) ortransmitral E/A ratio (r = −0.23, P = 0.24).
By multivariable analysis, after adjustingfor potential determinants, in the overall pop-ulation of patients, ischemic etiology of DCM(β-coefficient in the final model = 0.58; P < 0.0001;β-coefficient estimate averaged across bootstrapsamples = 0.57; P < 0.0001), longitudinal intra-ventricular dyssynchrony (β-coefficient in the fi-nal model = 0.36; P < 0.01; β-coefficient estimateaveraged across bootstrap samples = 0.35; P <0.01), and positive response to CRT (β-coefficientin the final model = 0.46; P < 0.001; β-coefficient
1022 August 2009 PACE, Vol. 32
RV STRAIN IN IDIOPATHIC VERSUS DILATED CARDIOMYOPATHY AFTER CRT
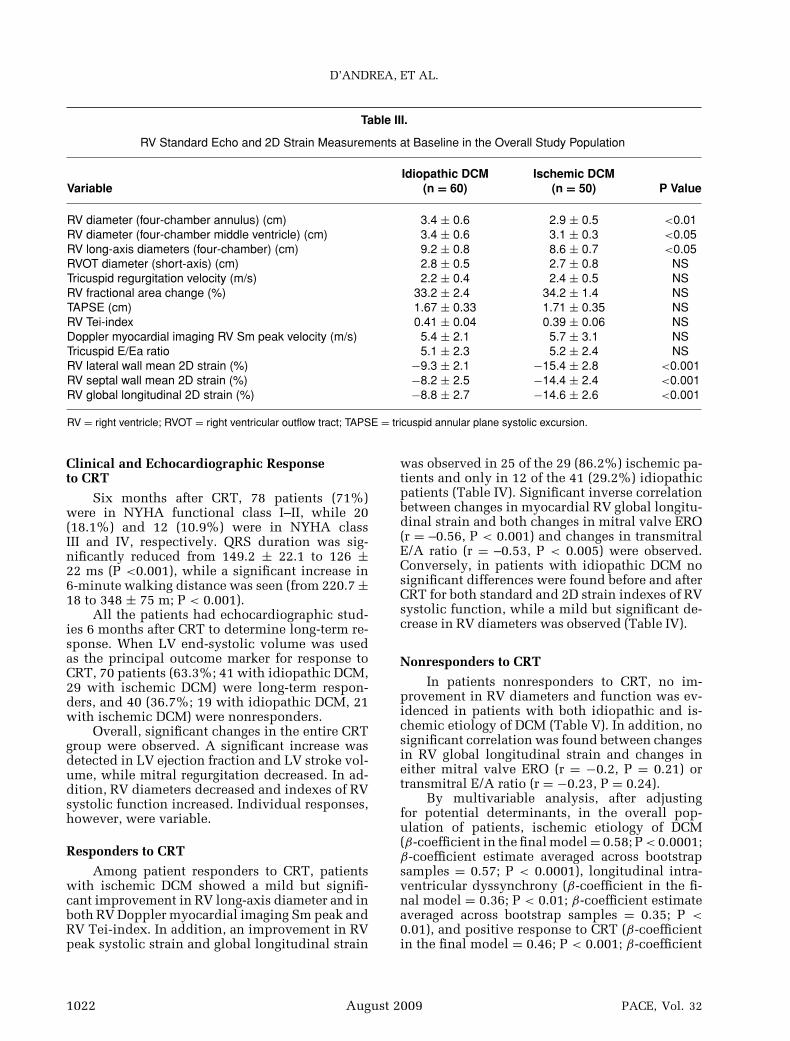
Figure 1. An example of RV longitudinal 2D strain in a patient with idiopathic DCM from an apical four-chamberview. The curve is color-coded by the defined myocardial segment as depicted in the figure. Note the severe impairmentof RV deformation, with an RV global longitudinal strain of –9.2%.
estimate averaged across bootstrap samples = 0.47;P < 0.001) emerged as the only independent de-terminants of RV global longitudinal strain afterCRT.
For the model about RV global longitudinalstrain, each of the variables in the final modelsappeared in the bootstrap models over 90% ofthe time. According to model validation statis-tics, discrimination of the model was adequate:c-statistic = 0.771; calibration, shrinkage coeffi-cient = 0.77; Hosmer-Lemeshow P value = 0.82.
To define the optimal cut-off value of RVglobal strain to predict RV remodeling afterCRT (i.e., significant decrease in RV diame-ters), a receiver operating characteristic curveanalysis was performed. An RV global lon-gitudinal strain <12% at baseline showed asensitivity and a specificity, respectively, of83.7% and 87.8% (area under the curve: 0.83;95% confidence interval [CI] 0.78–0.93; P <
0.0001) to predict RV lack of response toCRT.
Reproducibility of RV 2D StrainIntraobserver Variability
Pearson’s correlations: RV lateral wall, r =0.86, P < 0.00001; RV septal wall, r = 0.88, P <0.00001; RV global longitudinal strain, r = 0.84,P < 0.00001.
Bland-Altman analysis: RV lateral wall (95%CI ± 1.8; percent error 3.3), RV septal wall (95%CI ± 1.2; percent error 3.2%), RV global longitudi-nal strain (95% CI ± 1.5; percent error 3.2%).
Interobserver Variability
Pearson’s correlations: RV lateral wall, r =0.86, P < 0.00001; RV septal wall, r = 0.86, P <0.00001; RV global longitudinal strain, r = 0.84,P < 0.00001.
PACE, Vol. 32 August 2009 1023
D’ANDREA, ET AL.
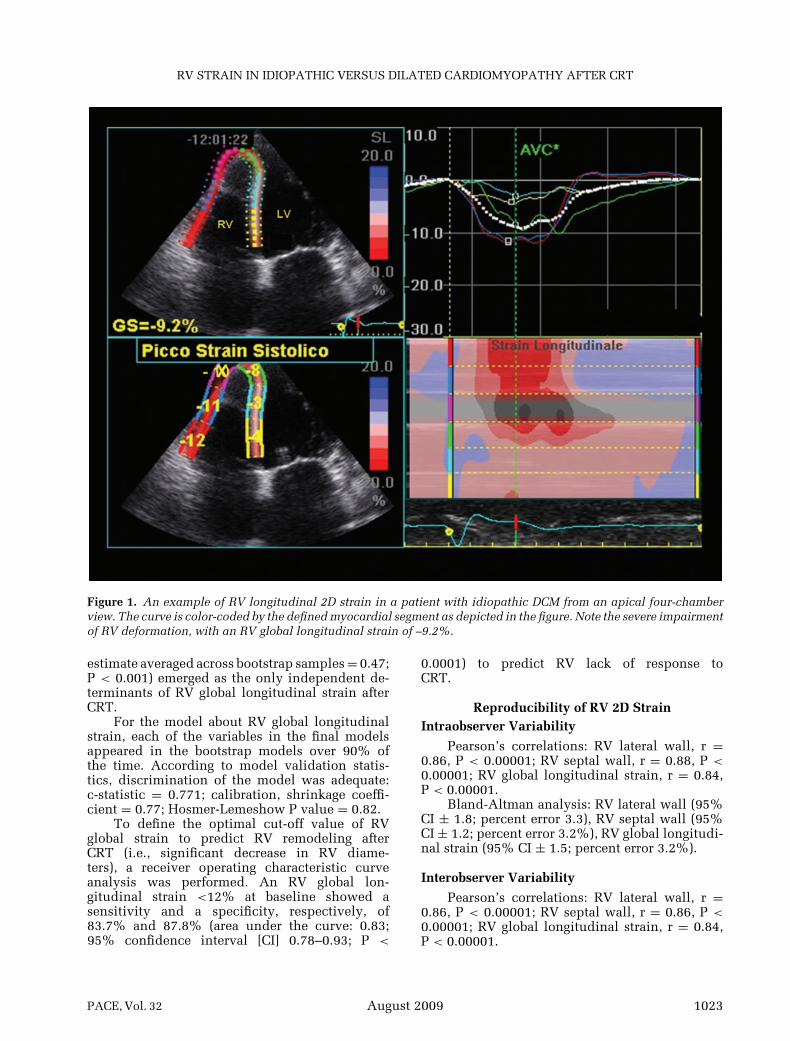
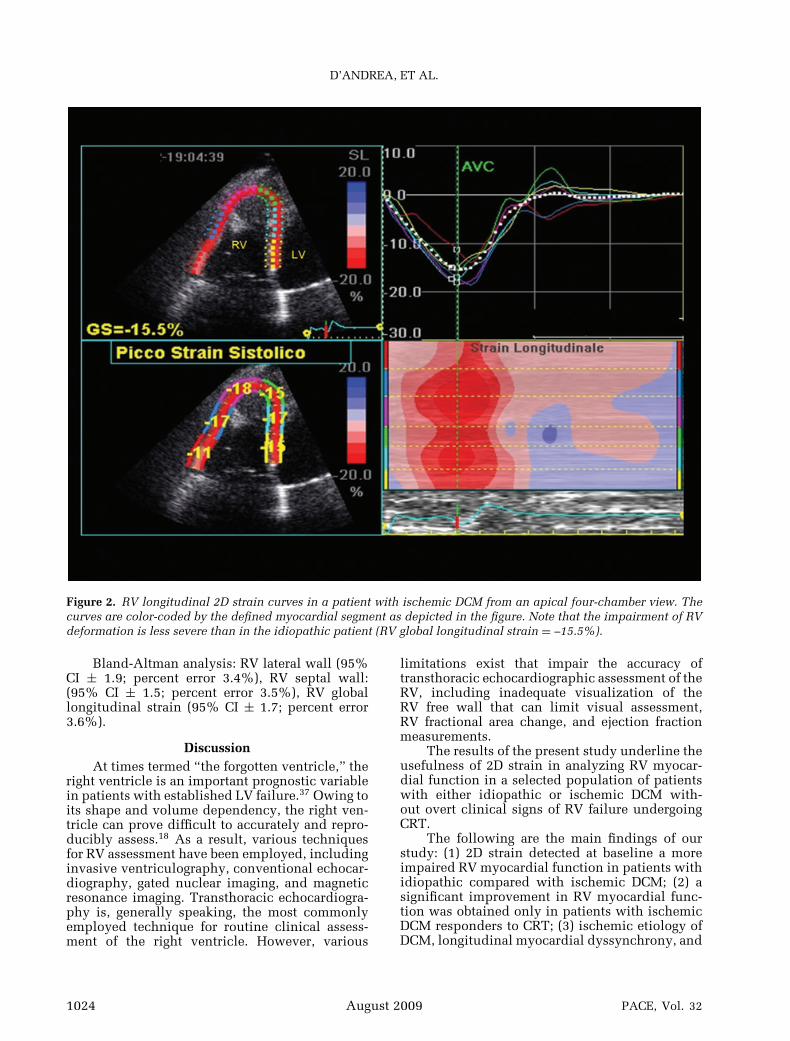
Figure 2. RV longitudinal 2D strain curves in a patient with ischemic DCM from an apical four-chamber view. Thecurves are color-coded by the defined myocardial segment as depicted in the figure. Note that the impairment of RVdeformation is less severe than in the idiopathic patient (RV global longitudinal strain = –15.5%).
Bland-Altman analysis: RV lateral wall (95%CI ± 1.9; percent error 3.4%), RV septal wall:(95% CI ± 1.5; percent error 3.5%), RV globallongitudinal strain (95% CI ± 1.7; percent error3.6%).
DiscussionAt times termed “the forgotten ventricle,” the
right ventricle is an important prognostic variablein patients with established LV failure.37 Owing toits shape and volume dependency, the right ven-tricle can prove difficult to accurately and repro-ducibly assess.18 As a result, various techniquesfor RV assessment have been employed, includinginvasive ventriculography, conventional echocar-diography, gated nuclear imaging, and magneticresonance imaging. Transthoracic echocardiogra-phy is, generally speaking, the most commonlyemployed technique for routine clinical assess-ment of the right ventricle. However, various
limitations exist that impair the accuracy oftransthoracic echocardiographic assessment of theRV, including inadequate visualization of theRV free wall that can limit visual assessment,RV fractional area change, and ejection fractionmeasurements.
The results of the present study underline theusefulness of 2D strain in analyzing RV myocar-dial function in a selected population of patientswith either idiopathic or ischemic DCM with-out overt clinical signs of RV failure undergoingCRT.
The following are the main findings of ourstudy: (1) 2D strain detected at baseline a moreimpaired RV myocardial function in patients withidiopathic compared with ischemic DCM; (2) asignificant improvement in RV myocardial func-tion was obtained only in patients with ischemicDCM responders to CRT; (3) ischemic etiology ofDCM, longitudinal myocardial dyssynchrony, and
1024 August 2009 PACE, Vol. 32
RV STRAIN IN IDIOPATHIC VERSUS DILATED CARDIOMYOPATHY AFTER CRT
Table IV.
LV and RV Echo and 2D Strain Measurements in Patient Responders to CRT at Baseline and after 6-MonthFollow-Up (n = 70)
Idiopathic DCM (n = 41) Ischemic DCM (n = 29)
Variable Baseline CRT P Baseline CRT P
LV ejection fraction (%) 31.1 ± 3.1 38.4 ± 5.1 <0.005 30.2 ± 5.2 37.9 ± 4.1 <0.005LV stroke volume (mL/beat) 69.6 ± 17.2 81.3 ± 19.3 <0.001 72.3 ± 13.2 88.3 ± 9.4 <0.001Transmitral E/A ratio 1.6 ± 0.8 0.8 ± 0.9 <0.001 1.7 ± 0.8 0.7 ± 0.9 <0.001Mitral valve ERO (mm2) 11.3 ± 4 5.1 ± 3.1 <0.001 12.7 ± 5.3 5.8 ± 4.1 <0.001E/Ea ratio 8.5 ± 2.3 5.6 ± 1.7 <0.01 8.4 ± 2.8 5.8 ± 1.3 <0.001RV diameter (four-chamber
annulus) (cm)3.4 ± 0.4 3.2 ± 0.3 NS 3.2 ± 0.4 3.0 ± 0.9 NS
RV diameter (four-chamber middleventricle) (cm)
3.5 ± 0.6 3.3 ± 0.2 NS 3.2 ± 0.4 3.0 ± 0.5 NS
RV long axis (four-chamber) (cm) 9.3 ± 0.6 8.7 ± 0.5 <0.01 8.7 ± 0.6 8.2 ± 0.4 <0.01Tricuspid regurgitation velocity (m/s) 2.5 ± 0.3 1.8 ± 0.4 <0.001 2.4 ± 0.3 1.7 ± 0.4 <0.001TAPSE (cm) 1.68 ± 0.3 1.70 ± 0.3 NS 1.71 ± 0.6 1.73 ± 0.2 NSRV Tei-index 0.41 ± 0.03 0.36 ± 0.04 <0.05 0.39 ± 0.05 0.34 ± 0.06 <0.05Doppler myocardial imaging RV Sm
peak velocity (m/s)5.5 ± 2.4 5.7 ± 2.7 NS 5.8 ± 2.8 6.2 ± 2.3 <0.05
Tricuspid E/Ea ratio 5.3 ± 2.3 4.6 ± 2.2 <0.01 5.1 ± 2.3 4.4 ± 3.1 <0.01RV lateral wall mean 2D strain (%) −9.4 ± 2.3 −9.6 ± 4.1 NS −15.6 ± 3.1 −20.8 ± 3.5 <0.001RV septal wall mean 2D strain (%) −8.4 ± 3.4 −8.6 ± 2.8 NS −14.6 ± 2.6 −19.8 ± 3.4 <0.001RV global longitudinal 2D strain (%) −8.9 ± 2.6 −9.1 ± 3.3 NS −15.5 ± 2.8 −20.3 ± 3.4 <0.001
DCM = dilated cardiomyopathy; LV = left ventricle; RV = right ventricle; ERO = effective regurgitant orifice.
positive response to CRT were powerful indepen-dent determinants of RV myocardial function afterCRT.
The Advantages and Perspectives of 2D Strainin the Study of RV Function in LV Heart Failure
Recent reports have documented that echocar-diography with its newer applications such asDoppler myocardial imaging and strain imagingmay represent useful techniques to evaluate RVmyocardial function, particularly in patients withcongestive heart failure.19 In an animal model us-ing invasive indexes, Vogel et al. demonstratedthat RV myocardial acceleration during isovolu-mic contraction is a sensitive measure of RV con-tractile function, relatively unaffected by preloadand afterload.21 Meluzin et al. showed that RV Smwas significantly lower in patients with LV sys-tolic heart failure than in healthy subjects, witha reasonable correlation between RV Sm and RVejection fraction by radionuclide angiography.20
The same group demonstrated that patients withRV systolic dysfunction (RV Sm < 11.5 cm/s) hadhigher pulmonary artery pressure and pulmonarycapillary wedge pressure than patients with higherRV Sm. Furthermore, Nagueh et al. found that in-
vasively measured right atrial pressure correlatedwith tricuspid E/Ea and that an E/Ea ratio morethan 6 had a sensitivity of 79% and a specificity of73% for mean right atrial pressure >10 mmHg.38
Finally, Sengupta et al. recently demonstrated thatRV Sm was an independent predictor of outcomein patients with LV heart failure, even when cor-rected for mitral E/Ea and left atrial volume index,and was superior to other conventional 2D mea-sures of RV function.8
Therefore, in patients with LV heart failure,RV Doppler myocardial imaging has proven to be asensitive indicator of RV dysfunction and can helpestablish prognosis even when corrected for im-portant left-sided variables. However, in patientswith DCM undergoing CRT, with large and spheri-cal atria and ventricles, Doppler myocardial imag-ing and Doppler strain estimation with its angledependency present important limitations due toa poor alignment between Doppler beam and my-ocardial wall. Conversely, in our study we used 2Dstrain, a novel approach to quantify regional my-ocardial deformation within a scan plane that is in-herently 2D and independent of interrogation an-gle as it tracks speckle patterns (acoustic markers)within serial B-mode sector scans. Recent studies
PACE, Vol. 32 August 2009 1025
D’ANDREA, ET AL.
Table V.
LV and RV Echo and 2D Strain Measurements in Patient Nonresponders to CRT at Baseline and after 6-MonthFollow-Up (n = 40)
Idiopathic DCM (n = 19) Ischemic DCM (n = 21)
Variable Baseline CRT P Baseline CRT P
LV ejection fraction (%) 29.5 ± 5.1 31.7 ± 4.1 NS 31.1 ± 3.2 32.7 ± 4.1 NSLV stroke volume (mL/beat) 70.7 ± 12.2 74.6 ± 13.2 NS 71.2 ± 7.2 75.2 ± 8.4 NSTransmitral E/A ratio 1.8 ± 0.9 1.5 ± 0.7 <0.05 1.7 ± 0.8 1.3 ± 1.1 <0.05Mitral valve ERO (mm2) 11.8 ± 4 8.1 ± 4.1 <0.05 11.6 ± 4.3 8.2 ± 2.1 <0.05E/Ea ratio 7.7 ± 2.2 6.5 ± 1.8 <0.05 8.1 ± 3.2 6.8 ± 1.8 <0.01RV diameter (four-chamber annulus) (cm) 3.4 ± 0.4 3.2 ± 0.3 NS 3.2 ± 0.4 3.0 ± 0.9 NSRV diameter (four-chamber middle
ventricle) (cm)3.5 ± 0.6 3.3 ± 0.2 NS 3.2 ± 0.4 3.0 ± 0.5 NS
RV long axis (four-chamber) (cm) 9.1 ± 0.7 8.9 ± 0.5 NS 8.5 ± 0.6 8.7 ± 0.7 NSTricuspid regurgitation velocity (m/s) 2.1 ± 0.3 2.0 ± 0.4 NS 2.3 ± 0.3 2.2 ± 0.4 NSTAPSE (cm) 1.66 ± 0.8 1.68 ± 0.3 NS 1.69 ± 0.6 1.71 ± 0.2 NSRV Tei-index 0.40 ± 0.02 0.39 ± 0.05 NS 0.38 ± 0.06 0.36 ± 0.06 NSDoppler myocardial imaging RV Sm peak
velocity (m/s)5.2 ± 2.1 5.4 ± 2.7 NS 5.6 ± 2.3 5.8 ± 2.6 NS
Tricuspid E/Ea ratio 5.0 ± 2.6 4.6 ± 1.8 <0.05 5.2 ± 2.3 4.6 ± 3.1 <0.01RV lateral wall mean 2D strain (%) −9.1 ± 2.2 −9.4 ± 3.8 NS −15.1 ± 3.3 −15.4 ± 2.5 NSRV septal wall mean 2D strain (%) −8.1 ± 3.6 −8.3 ± 2.8 NS −14.2 ± 2.7 −14.3 ± 3.6 NSRV global longitudinal 2D strain (%) −8.7 ± 2.7 −8.9 ± 3.3 NS −14.6 ± 2.8 −14.8 ± 3.1 NS
DCM = dilated cardiomyopathy; LV = left ventricle; RV = right ventricle; ERO = effective regurgitant orifice.
in patients with DCM have demonstrated that in-dexes derived from the novel speckle-tracking ra-dial 2D strain predicts response to CRT,26 and areuseful to analyze left atrial and RV functions.17,39
To the best of our knowledge, the present article isthe first report analyzing RV function in patientswith DCM at baseline and after CRT by use ofspeckle-tracking 2D strain.
RV Function in Idiopathic versus IschemicDilated Cardiomyopathy at Baselineand after CRT
Few reports have previously investigated thelong-term effect of CRT on RV diameters and func-tion. Donal et al. reported acute improvementin tricuspid annular velocities with biventricularpacing, but long-term effects were not studied.9Using Doppler myocardial imaging, Rajagopalanet al. showed in 21 of 35 patients (60%) increasedmyocardial velocities at the tricuspid annulus in-dependent of the increase in LV ejection fractionand of baseline LV dyssynchrony,11 while Bilgeet al. reported in 14 DCM patients an improve-ment of early or late diastolic myocardial motionin seven segments of the left and two segmentsof the right ventricles.40 Conversely, only in thestudy by Santos et al., in 10 patients with DCM,
there were no differences in RV size and functionbefore and after CRT.41
In our study, among the echocardiographicindexes selected for mechanical dyssynchronyanalysis, only longitudinal intraventriculardyssynchrony was an independent predictor ofRV deformation after CRT. Such findings arein accordance with the article by Bleeker et al.,who reported in a population of 56 DCM patientshow an RV reverse remodeling after CRT wasonly observed in patients with substantial LVlongitudinal dyssynchrony at baseline.10
In addition, our results showed how indexesof RV myocardial deformation were significantlymore impaired in patients with idiopathic DCMcompared with ischemic DCM in both septal andlateral RV walls. Since heart rate, left atrial vol-umes, transmitral flow velocity profile, LV iso-volumic relaxation time, LV stroke volume, pul-monary artery pressures, and mitral valve ERO inour population were similar to those in the twocardiomyopathy groups, it is unlikely that suchdifferences were only due to different RV loadingconditions. It is reasonable therefore to assumethat in addition to LV diastolic dysfunction, de-pressed RV contractility and deformation result-ing from RV involvement in the myopathic pro-cess might have contributed to the RV myocardial
1026 August 2009 PACE, Vol. 32

RV STRAIN IN IDIOPATHIC VERSUS DILATED CARDIOMYOPATHY AFTER CRT
dysfunction in our patients with idiopathic DCM,even before the appearance of symptoms and signsof RV failure. However, because of substantial dif-ferences in methods, it was difficult to compareprevious studies on RV function with ours.
In our population, a significant improvementin RV myocardial function after CRT was obtainedonly in patients with ischemic DCM responders toCRT. Such reversible RV dysfunction in ischemicpatients may further confirm that the initial RVdysfunction was mainly due to RV afterload mis-match rather than intrinsic RV disease. In fact,in our patients, changes in lateral RV strain werestrongly associated with changes in mitral valveERO and in Doppler transmitral E/A ratio afterCRT. Therefore, in these patients, the improve-ment in mitral regurgitation due to CRT can leadto lower pulmonary artery pressures and therebydecrease RV afterload and improve systolic func-tion.42 Another possible mechanism is the benefi-cial effects of CRT on LV remodeling and dilation.In fact, a decrease in LV dilation can improve RVdiastolic filling and thereby improve RV systolicfunction.43
Conversely, in idiopathic DCM, our findingsdetected an irreversible impairment of RV defor-mation even after improvement of loading condi-tions during CRT. The lack of association betweenchanges in RV strain and improvement in diastolicmeasurements may confirm the presence in idio-pathic DCM patients of a larger involvement of RVstructure and function in the myopathic process.Since RV dimension and function are importantprognostic variables in patients with establishedLV failure, our results may have important clin-ical implications on the evaluation of long-termeffects of pharmacological therapy and of CRT inpatients with DCM.
Study LimitationsOur study has several limitations. RV strain is
influenced by loading conditions; thus, the com-parisons of RV deformation properties betweenidiopathic and ischemic patients may have beeninfluenced by preload and by RV wall stress. How-ever, even if our study protocol did not includeany invasive hemodynamic measurement, our pa-tients with DCM presented similar mean heartrates, left atrial and LV volumes, and Doppler in-dexes of global diastolic function. As a result, thisconfounding factor should not detract from thevalue of RV strain analysis.
Another limitation is the lack of a gold stan-dard for assessing baseline RV function. Althoughprevious studies used TAPSE, RV Tei-index, andDoppler myocardial imaging to assess RV func-tion,19–21 more data are needed, particularly in
correlating echocardiographic data with invasivemeasures of RV function.
As previously specified, this is the first reportanalyzing RV function in patients with DCM byuse of speckle-tracking 2D strain. In particular, weused for 2D strain analysis EchoPAC PC programfrom GE Healthcare. Since a definite software forRV 2D strain has not yet been provided, we ap-plied a program of 2D strain for LV to analyzealso RV strain. The feasibility and reproducibil-ity of RV strain patterns and measurements weregood. However, in future studies changes of thesoftware may be needed in order to improve thetracking ability of the speckle-tracking system forRV functional study.
A technical limitation is that speckle-trackingechocardiography is dependent on frame rate andimage resolution. Low frame rate results in thespeckle pattern changing too much from frame toframe, which prevents the precise characterizationof regional myocardial motion and impacts theoverall temporal resolution of the regional strainmap. In contrast, increasing the frame rate reducesscan line density that reduces image resolution.Frame rate in our setting ranged from 60 to 90frames/s; this value is lower than frame rate avail-able with Doppler strain; however, indexes of RVfunction used in this study did not rely on differ-ence in the timing of contraction.
Our analysis was limited by data collectionfrom the apical four-chamber view, as this wasthe only image plane that provided reliable in-formation on longitudinal RV deformation in asufficient number of patients. It would be desir-able to obtain information on RV deformation fromthe complete RV cavity. However, in the presentstudy, RV radial strain was not calculated from theparasternal short- and long-axis views because theRV wall is too thin to be properly analyzed in theseviews.
Finally, sample size limited our ability todraw definitive conclusions regarding the benefitof CRT in selected patient subsets.
ConclusionsThis study demonstrates for the first time
that a novel speckle-tracking algorithm applied toroutine grayscale 2D images represents a promis-ing and feasible noninvasive technique to assessRV myocardial dysfunction in patients with DCMwithout overt RV failure.
RV deformation both at baseline and after CRTis more impaired in idiopathic compared with is-chemic DCM. Since both the appearance of signsof right heart failure and RV functional parame-ters have been proposed as powerful predictorsof common cardiovascular outcomes in heart fail-ure patients,6–8,19 future longitudinal studies are
PACE, Vol. 32 August 2009 1027
D’ANDREA, ET AL.
warranted to further our understanding of the nat-ural history of RV myocardial deformation, the ex-tent of reversibility of RV dysfunction with med-
ical therapy and/or CRT, and the possible long-term impact of such changes on outcomes in pa-tients with congestive heart failure.
References1. Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E,
Kocovic DZ, et al., MIRACLE Study Group. Multicenter InSync ran-domized clinical evaluation. Cardiac resynchronization in chronicheart failure. N Engl J Med 2002; 346:1845–1852.
2. Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kap-penberger L, Tavazzi L; Cardiac Resynchronization-Heart Failure(CARE-HF) Study Investigators. The effect of cardiac resynchro-nization on morbidity and mortality in heart failure N. Engl J Med2005; 352:1539–1549.
3. Bax JJ, Abraham T, Barold SS, Breithardt OA, Fung JW, GarrigueS, Gorcsan J 3rd, et al. Cardiac resynchronization therapy: Part 1–issues before device implantation. J Am Coll Cardiol 2005; 20:2153–2167.
4. Hawkins NM, Petrie MC, MacDonald MR, Hogg KJ, McMurrayJJ. Selecting patients for cardiac resynchronization therapy: Elec-trical or mechanical dyssynchrony? Eur Heart J 2006; 27:1270–1281.
5. Spinarova L, Meluzın J, Toman J, Hude P, Krejcı J, Vıtovec J. Rightventricular dysfunction in chronic heart failure patients. Eur J HeartFail 2005; 7:485–489.
6. Meluzın J, Spinarova L, Dusek L, Toman J, Hude P, Krejcı J. Prognos-tic importance of the right ventricular function assessed by Dopplertissue imaging. Eur J Echocardiogr 2003; 4:262–271.
7. Meluzin J, Spinarova L, Hude P, Krejcı J, Kincl V, Panovsky R, DusekL. Prognostic importance of various echocardiographic right ven-tricular functional parameters in patients with symptomatic heartfailure. J Am Soc Echocardiogr 2005; 18:435–444.
8. Sengupta R, Patel R, Dokainish H. Right ventricular tissue Doppleris an independent predictor of outcome in patients with left ven-tricular heart failure. J Am Soc Echocardiogr 2006; 19:624a.
9. Donal E, Vignat N, De Place C, Leray E, Crocq C, Mabo P, DaubertJC, et al. Acute effects of biventricular pacing on right ventricularfunction assessed by tissue Doppler imaging. Europace 2007; 9:108–112.
10. Bleeker GB, Schalij MJ, Nihoyannopoulos P, Steendijk P, MolhoekSG, van Erven L, Bootsma M, et al. Left ventricular dyssynchronypredicts right ventricular remodelling after cardiac resynchroniza-tion therapy. J Am Coll Cardiol 2005; 46:2264–2269.
11. Rajagopalan N, Suffoletto MS, Tanabe M, Miske G, Thomas NC,Simon MA, Bazaz R, et al. Right ventricular function followingcardiac resynchronization therapy. Am J Cardiol 2007; 100:1434–1436.
12. D’Andrea A, Ducceschi V, Caso P, Galderisi M, Mercurio B, Lic-cardo B, Sarubbi B, et al. Usefulness of Doppler tissue imaging forthe assessment of right and left ventricular myocardial function inpatients with dual-chamber pacing. Int J Cardiol 2001; 81:75–83.
13. D’Andrea A, Caso P, Cuomo S, Scarafile R, Salerno G, LimongelliG, Di Salvo G, et al. Effect of dynamic myocardial dyssynchrony onmitral regurgitation during supine bicycle exercise stress echocar-diography in patients with idiopathic dilated cardiomyopathy and‘narrow’ QRS. Eur Heart J 2007; 28:1004–1011.
14. Yu C-M, Fung JW-H, Zhang Q, Chan C-K, Chan Y-S, Lin H, KumLCC, et al. Tissue Doppler imaging is superior to strain rate imagingand postsystolic shortening on the prediction of reverse remodel-ing in both ischaemic and nonischaemic heart failure after cardiacresynchronization therapy. Circulation 2004; 110:66–73
15. Yu CM, Zhang Q, Wing-Hong Fung J, Chi-Kin Chan H, Chan YS,Wai-Kwok Yip G, Kong SL, et al. A novel tool to assess systolicasynchrony and identify responders of cardiac resynchronizationtherapy by tissue synchronization imaging. J Am Coll Cardiol 2005;45:677–684.
16. Mele D, Pasanisi G, Capasso F, De Simone A, Morales MA, Pog-gio D, Capucci A, et al. Left intraventricular myocardial deforma-tion dyssynchrony identifies responders to cardiac resynchroniza-tion therapy in patients with heart failure. Eur Heart J 2006 May;27:1070–1078.
17. D’Andrea A, Caso P, Romano S, Scarafile R, Riegler L, Salerno G,Limongelli G, et al. Different effects of cardiac resynchronizationtherapy on left atrial function in patients with either idiopathicor ischaemic dilated cardiomyopathy: A two-dimensional specklestrain study. Eur Heart J 2007; 28:2738–2748.
18. Tulevski II, Romkes H, Dodge-Khatami A, van der Wall EE,Groenink M, van Veldhuisen DJ, Mulder BJ. Quantitative assess-ment of the pressure and volume overloaded right ventricle: Imag-ing is a real challenge. Int J Cardiovasc Imaging 2002; 18:41–51.
19. Gondi S, Dokainish H. Right ventricular tissue Doppler and strainimaging: Ready for clinical use? Echocardiography 2007; 24:522–532.
20. Meluzın J, Spinarova L, Bakala J, Toman J, Krejcı J, Hude P, KaraT, et al. Pulsed Doppler tissue imaging of the velocity of tricuspidannular systolic motion; a new, rapid and non-invasive methodof evaluating right ventricular systolic function. Eur Heart J 2001;22:280–282
21. Vogel M, Schmidt MR, Kristiansen SB, Cheung M, White PA,Sorensen K, Redington AN. Validation of myocardial accelerationduring isovolumic contraction as a novel noninvasive index of rightventricular contractility: Comparison with ventricular pressure-volume relations in an animal model. Circulation 2002; 105:1693–1699.
22. Korinek J, Kjaergaard J, Sengupta PP, Yoshifuku S, McMahon EM,Cha SS, Khandheria BK, et al. High spatial resolution speckle track-ing improves accuracy of 2-dimensional strain measurements: Anupdate on a new method in functional echocardiography. J Am SocEchocardiogr 2007; 20:165–170.
23. Reisner SA, Lysyansky P, Agmon Y, Mutlak D, Lessick J, Fried-man Z. Global longitudinal strain: A novel index of left ventricularsystolic function. J Am Soc Echocardiogr 2004; 17:630–633.
24. Belghiti H, Brette S, Lafitte S, Reant P, Picard F, Serri K, Lafitte M,et al. Automated function imaging: A new operator-independentstrain method for assessing left ventricular function. Arch Cardio-vasc Dis 2008; 101:163–169.
25. Amundsen BH, Helle-Valle T, Edvardsen T, Torp H, Crosby J, Ly-seggen E, Stoylen A, et al. Noninvasive myocardial strain measure-ment by speckle tracking echocardiography: Validation against so-nomicrometry and tagged magnetic resonance imaging. J Am CollCardiol 2006; 47:789–793.
26. Suffoletto MS, Dohi K, Cannesson M, Saba S, Gorcsan J 3rd.Novel speckle-tracking radial strain from routine black-and-whiteechocardiographic images to quantify dyssynchrony and predictresponse to cardiac resynchronization therapy. Circulation 2006;113:960–968.
27. Cwajg JM, Cwajg E, Nagueh SF, He ZX, Qureshi U, Olmos LI,Quinones MA, et al. End-diastolic wall thickness as a predictorof recovery of function in myocardial hibernation: Relation to rest-redistribution T1–201 tomography and dobutamine stress echocar-diography. J Am Coll Cardiol 2000; 35:1152–1161.
28. Ritter P, Padeletti L, Gillio-Meina L, Gaggini G. Determination of theoptimal atrioventricular delay in DDD pacing. Comparison betweenecho and peak endocardial acceleration measurements. Europace1999; 1:126–130.
29. Dubin J, Wallerson DC, Cody RJ, Devereux RB. Comparative ac-curacy of Doppler echocardiographic methods for clinical strokevolume determination. Am Heart J 1990; 120:116–123.
30. Foale RA, Nihoyannopoulos P, Mc Kenna W. Echocardiographicmeasurement of normal adult right ventricle. Br Heart J 1986; 56:33–44.
31. Lang M, Bierig M, Devereux RB, Flachskampf FA, Foster E, PellikkaPA, Picard MH, et al. Recommendations for Chamber Quantifica-tion: A Report from the American Society of Echocardiography’sGuidelines and Standards Committee and the Chamber Quantifica-tion Writing Group, developed in conjunction with the EuropeanAssociation of Echocardiography, a branch of the European Societyof Cardiology. J Am Society Echo 2005; 18:1440–1463.
32. Miller D, Farah MG, Liner A, Fox K, Schluchter M, Hoit BD. Therelation between quantitative right ventricular ejection fraction andindices of tricuspid annular motion and myocardial performance. JAm Soc Echocardiogr 2004; 17:443–447.
33. Nagueh SF, Sun H, Kopelen HA, Middleton KJ, Khoury DS. Hemo-dynamic determinants of the mitral annulus diastolic velocities bytissue Doppler. J Am Coll Cardiol 2001; 37:278–285.
34. Enriquez-Sarano M, Miller F, Hayes S, Bailey K, Tajik A, SewardJ. Effective mitral regurgitant orifice area: Clinical use and pitfalls
1028 August 2009 PACE, Vol. 32
RV STRAIN IN IDIOPATHIC VERSUS DILATED CARDIOMYOPATHY AFTER CRT
of the proximal isovelocity surface area method. J Am Coll Cardiol1995; 25:703–709
35. Gorcsan J 3rd, Abraham T, Agler DA, Bax JJ, Derumeaux G,Grimm RA, Martin R, et al., American Society of Echocardiogra-phy Dyssynchrony Writing Group. Echocardiography for cardiacresynchronization therapy: Recommendations for performance andreporting–a report from the American Society of EchocardiographyDyssynchrony Writing Group endorsed by the Heart Rhythm Soci-ety. J Am Soc Echocardiogr 2008; 21:191–213.
36. Weitzen S, Lapane KL, Toledano AY, Hume AL, Mor V. Princi-ples for modeling propensity scores in medical research: A system-atic literature review. Pharmacoepidemiol Drug Saf 2004; 13:855–857.
37. Rigolin VH, Robiolio PA, Wilson JS, Harrison JK, Bashore TM. Theforgotten chamber: The importance of the right ventricle. CathetCardiovasc Diagn 1995; 35:18–28.
38. Nageh MF, Kopelen HA, Zoghbi WA, Quinones MA, Nagueh SF. Es-timation of mean right atrial pressure using tissue Doppler imaging.Am J Cardiol 1999; 84:1448–1451.
39. Borges AC, Knebel F, Eddicks S, Panda A, Schattke S, Witt C, Bau-mann G. Right ventricular function assessed by two-dimensionalstrain and tissue Doppler echocardiography in patients with pul-
monary arterial hypertension and effect of vasodilator therapy. AmJ Cardiol 2006; 98:530–534.
40. Bilge AK, Ozben B, Ozyigit T, Acar D, Hunerel D, Adalet K, NisanciY. Assessment of early changes in the segmental functions of the leftand the right ventricles after biventricular pacing in heart failure:A study with tissue Doppler imaging. Angiology 2008; 59:179–184.
41. Santos JF, Caetano F, Parreira L, Madeira J, Cardoso P, Fonseca N,Segurado F, et al. Effects of cardiac resynchronization therapy onright ventricular function. Evaluation with tissue Doppler echocar-diography. Rev Port Cardiol 2003; 22:1347–1355.
42. Kanzaki H, Bazaz R, Schwartzman D, Dohi K, Sade LE, GorcsanJ. A mechanism for immediate reduction in mitral regurgitationafter cardiac resynchronization therapy: Insights from mechani-cal activation strain mapping. J Am Coll Cardiol 2004; 44:1619–1625.
43. Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Mel-drum DR, Dupuis J, et al., National Heart, Lung, and Blood InstituteWorking Group on Cellular and Molecular Mechanisms of RightHeart Failure. Right ventricular function and failure: Report of aNational Heart, Lung, and Blood Institute Working Group on Cellu-lar and Molecular Mechanisms of Right Heart Failure. Circulation2006; 114:1883–1891.
PACE, Vol. 32 August 2009 1029