richard gorey 21st century rev 016
TRANSCRIPT
MSc in Pharmaceutical Business and Technology
Module:
21st Century Dynamics & Emerging Trends
Lecturer:
Paul Blunnie
Assignment by:
Richard Gorey Student No. 2917956
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey 20/02/2016
Assignment Document:
MSc in Pharmaceutical Business and Technology
21st
Century Dynamics & Emerging Trends
Semester 1 Assignment (100%)
Lecturer: Paul Blunnie
Please prepare a 3000 word assessment of the evolving subject of Personalised Medicine. The assignment should
include a consideration of the following key elements with examples from the literature. Please refer to the recent
publication by the FDA on Personalised Medicine- copy attached.
Element 1: Why is the percentage of patients for whom drugs are ineffective so high ( 38% in Depression - 75% in
Cancer)- a 2001 study showed that the response rates of patients to medications from different therapeutic classes
ranged from ~80% (analgesics) to ~25% (oncology). In addition, an estimated 2.2 million adverse drug reactions occur
each year in the United States, including more than 100,000 deaths.-see Fig 2 Page 12 of attachment.
Element 2: A consideration of why many drugs under development never reach the stage of being submitted to FDA in an
application requesting approval for marketing. High attrition rates stem largely from failure of drugs to meet expected
efficacy levels, to demonstrate improved outcomes over a comparator drug, or to demonstrate sufficient safety to justify
their use. Improving our understanding of the underlying causes of variability in patient response should catalyse an
increase in the numbers of drugs that are shown to be safe and effective and make it to the market.
Element 3: What personalised medicine seeks to accomplish.
Element 4. The success of many personalised medicines fundamentally depends on the identification of biomarkers and
the successful development of diagnostic tests that can be used to accurately stratify the patient population. Illustrate how
this is so.
The publication gives you a very solid working document with excellent research references so there should be no lack of
resources for you.
Please submit a softcopy on Moodle by Friday Feb. 12th. (EDIT RG: DEADLINE CHANGED TO 20/02/2016)
Paul Blunnie
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey 20/02/2016
Assignment Paper:
Assessment of the Evolving
Subject of Personalised Medicine

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey 20/02/2016
Table of Contents
Assumptions & Considerations: 5
1. Assignment Paper - Element 1 of 4 6
2. Assignment Paper - Element 2 of 4 11
3. Assignment Paper - Element 3 of 4 16
4. Assignment Paper - Element 4 of 4 17
References 25
The blockbuster model is “Broken”
"The challenge for us as an industry …is to move more from a blockbuster model to a targeted model”
Sidney Taurel; Chairman, President and CEO, Eli Lilly and Company (2007)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey 20/02/2016
Assumptions & Considerations
The Author (of this assignment paper) assumes and considers the following;
1. As per the assignment document, this assignment paper considers and refers to the publication
by the FDA; Paving the Way for Personalised Medicine - FDA’s Role in a New Era of Medical
Product Development - October 2013
2. This assignment paper also considers and refers to other sources and material.
3. The Author has outlined some of the positive effects which personalised medicine addresses
regarding the issues raised in elements 1 to 4 of the assignment paper.
4. The assignment document instructs the student to prepare a 3000 word assessment of the
evolving subject of Personalised Medicine. The Author (of this assignment paper) assumes that
“3000 words” is an approximation i.e., not an upper or lower limit. The word count of this paper
is approximately 5,150 words, including a copy of the assignment document and the assignment
paper references section.

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 6 of 26 20/02/2016
1. Assignment Paper - Element 1 of 4:
Element 1: Why is the percentage of patients for whom drugs are ineffective so high ( 38% in Depression
- 75% in Cancer)- a 2001 study showed that the response rates of patients to medications from different
therapeutic classes ranged from ~80% (analgesics) to ~25% (oncology). In addition, an estimated 2.2
million adverse drug reactions occur each year in the United States, including more than 100,000 deaths.-
see Fig 2 Page 12 of attachment.
1.1. Why is the percentage of patients for whom drugs are ineffective so high ( 38% in
Depression - 75% in Cancer)- a 2001 study showed that the response rates of patients to
medications from different therapeutic classes ranged from ~80% (analgesics) to ~25%
(oncology)
Every person has a unique variation of the human genome.(1) Although most of the variation
between individuals has no effect on health, an individual's health stems from genetic
variation with behaviors and influences from the environment.(2)(3)
One way that biological variation among people makes itself clear, is responsiveness to drugs,
e.g.; ADHD medicine only works for one of ten preschoolers, cancer drugs are effective for
25% of patients, and depression drugs work with 6 out of 10 patients.(4)
A 2001 study showed that the response rates of patients to medications from different
therapeutic classes ranged from ~80% (analgesics) to ~25% (oncology). (5)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 7 of 26 20/02/2016
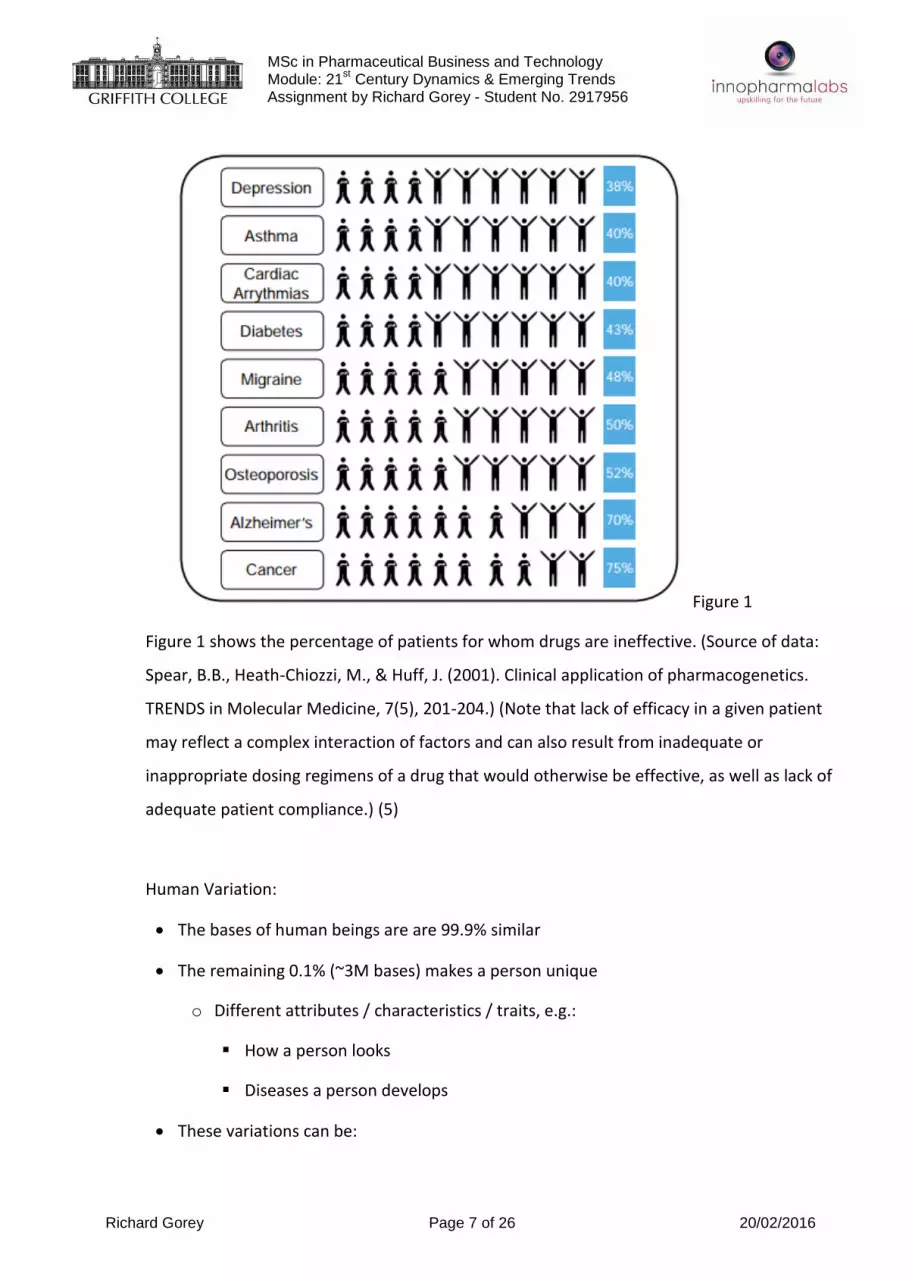
Figure 1
Figure 1 shows the percentage of patients for whom drugs are ineffective. (Source of data:
Spear, B.B., Heath-Chiozzi, M., & Huff, J. (2001). Clinical application of pharmacogenetics.
TRENDS in Molecular Medicine, 7(5), 201-204.) (Note that lack of efficacy in a given patient
may reflect a complex interaction of factors and can also result from inadequate or
inappropriate dosing regimens of a drug that would otherwise be effective, as well as lack of
adequate patient compliance.) (5)
Human Variation:
The bases of human beings are are 99.9% similar
The remaining 0.1% (~3M bases) makes a person unique
o Different attributes / characteristics / traits, e.g.:
How a person looks
Diseases a person develops
These variations can be:
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 8 of 26 20/02/2016
o Harmless (variation in phenotype)
o Harmful (diabetes, cancer, heart disease, Huntington's disease, and hemophilia )
o Latent (variations found in coding and regulatory regions, are not harmful on their
own, and the change in each gene only becomes apparent under certain conditions
e.g. susceptibility to lung cancer) (6)
The safety and effectiveness of a health product may vary from one individual to the next as a
result of genetic and environmental factors, as well as the interaction of these factors. As a
result, there is considerable room for improvement in overall efficacy rates for many products.
(5)
By further elucidating why some patients respond or do not respond to a drug, and why some
experience adverse reactions while others do not, we may be able to use this information to
tailor drug indications to certain populations, thus improving safety and efficacy of drugs by
specifying the population(s) in which they should be used. (5)
1.2. An estimated 2.2 million adverse drug reactions occur each year in the United States,
including more than 100,000 deaths.
Although they are generally safe and effective in most instances, current empirical approaches
to pharmaceutical therapy contribute to an estimated 3 million incorrect or ineffective drug
prescriptions annually. One study found that approximately 2.2 million people per year in the
United States experienced an adverse drug reaction (ADR) during a hospital stay or were
admitted to the hospital for an ADR. This study also reported that ADRs account for
approximately 106,000 deaths per year, which would rank ADRs between the fourth and sixth
leading causes of death in the United States, depending on whether liberal or conservative
estimates are used. The economic burden associated with drug-related morbidity and
mortality is substantial, with annual costs estimated earlier this decade at more than $177
billion. ADRs also are the leading cause of market withdrawals of drugs. (7)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 9 of 26 20/02/2016
Few prescribed medications are effective for all who use them, and most ADRs are caused by
an exaggerated effect of a drug on the human body. Drug response can be influenced by
genetically mediated variations that affect the metabolism, transport, distribution, absorption,
and excretion of a drug. Although ADRs can result from a variety of factors, genetic variations
of drug-metabolising enzymes have been highly correlated with ADRs in some instances. (7)
Pharmacogenomics (PGx) is the study of how genes affect a person's response to drugs. This
relatively new field combines pharmacology (the science of drugs) and genomics (the study of
genes and their functions) to develop effective, safe medications and doses that will be
tailored to a person's genetic makeup. (13)
One of the most anticipated potential benefits of PGx is the reduction of ADRs. In vitro
diagnostic tests may be useful in identifying individuals who are more likely to experience
ADRs from particular drugs because of genetic variations in drug targets in the body or in the
enzymes that metabolise drugs. Achieving even modest reductions in the rate of ADRs could
result in substantial improvements in health outcomes and reductions in health care costs. (7)
One group of drug-metabolising enzymes that figures prominently in contemporary and future
PGx applications is cytochrome P450 (CYP450). This enzyme metabolises many of the most
widely prescribed drugs used in the United States, including Adderall®
(amphetamine/dextroamphetamine), Coreg® (carvedilol), Effexor® (venlafaxine), Inderal®
(propranolol), Paxil® (paroxetine), Prozac® (flouxetine), Risperdal® (risperidone), Strattera®
(atomoxetine), Toprol® (metoprolol), Tussionex® (chlorpheniramine and hydrocodone), and
Zofran® (ondansetron). A variant of the CYP2D6 gene, which affects expression of the CYP450
enzyme, is associated with slower metabolism of these drugs and is prevalent at differing rates
among various population groups. The CYP2D6 gene is associated with slower drug
metabolism among approximately 5% to 10% of Caucasians, 1% to 3% of Hispanics, 2% to 5%
of Asians, and 2% to 7% of African Americans. As is the case with similar genetically
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 10 of 26 20/02/2016
determined metabolic traits, conventional racial and ethnic designations are inadequate
markers, and differences in drug metabolism among these groups may be more accurately
identified with PGx testing. (7)

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 11 of 26 20/02/2016
2. Assignment Paper - Element 2 of 4:
Element 2: A consideration of why many drugs under development never reach the stage of being
submitted to FDA in an application requesting approval for marketing. High attrition rates stem largely
from failure of drugs to meet expected efficacy levels, to demonstrate improved outcomes over a
comparator drug, or to demonstrate sufficient safety to justify their use. Improving our understanding of
the underlying causes of variability in patient response should catalyse an increase in the numbers of
drugs that are shown to be safe and effective and make it to the market.
The FDA determines that products are safe and effective before marketing through a careful evaluation
of benefits and risks that considers the available scientific data in the context of the underlying condition
or disease. (5)
Many drugs under development never reach the stage of being submitted to FDA in an application
requesting approval for marketing. High attrition rates stem largely from failure of drugs to meet
expected efficacy levels, to demonstrate improved outcomes over a comparator drug, or to demonstrate
sufficient safety to justify their use. Improving our understanding of the underlying causes of variability
in patient response should catalyse an increase in the numbers of drugs that are shown to be safe and
effective and make it to the market. (5)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 12 of 26 20/02/2016
Figure 2
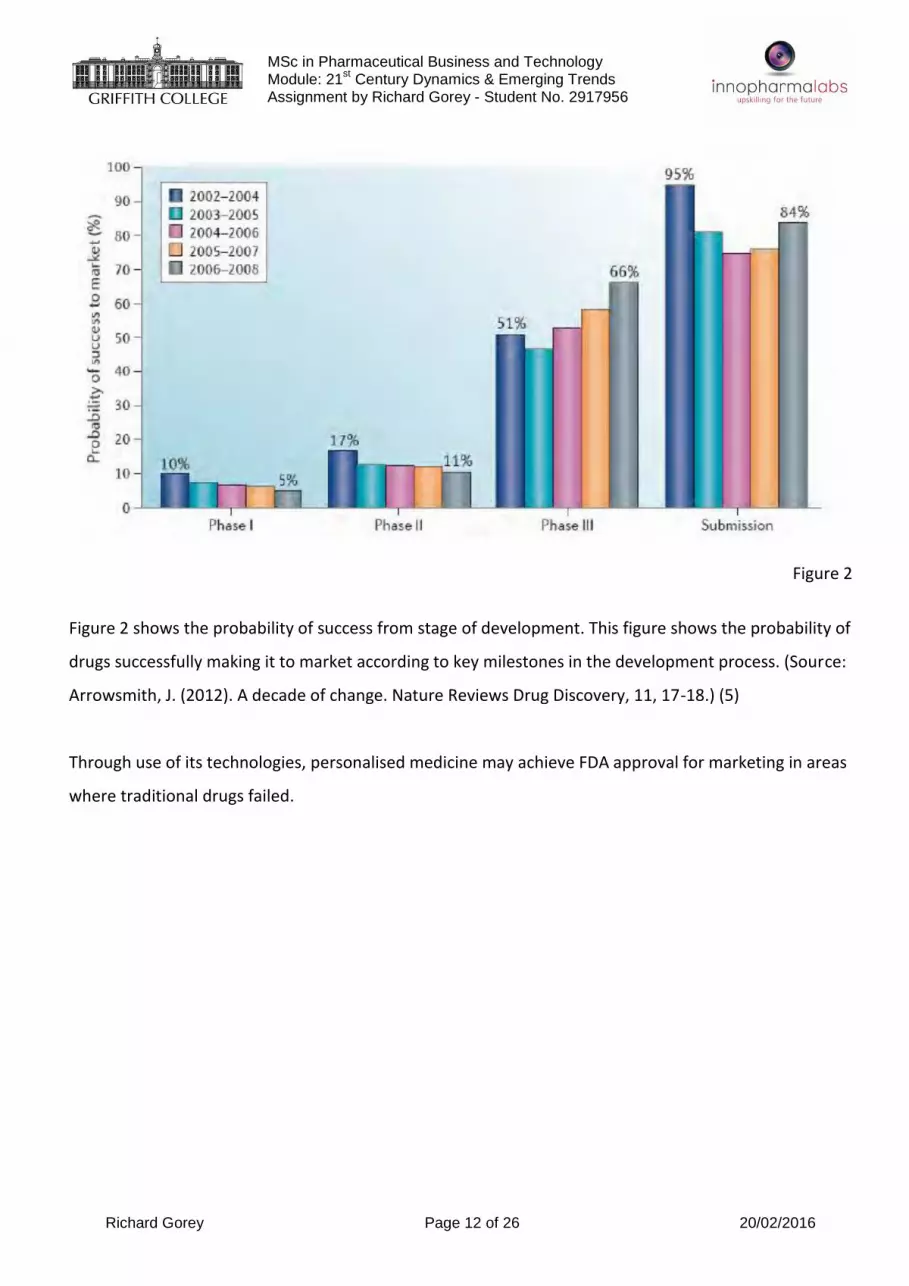
Figure 2 shows the probability of success from stage of development. This figure shows the probability of
drugs successfully making it to market according to key milestones in the development process. (Source:
Arrowsmith, J. (2012). A decade of change. Nature Reviews Drug Discovery, 11, 17-18.) (5)
Through use of its technologies, personalised medicine may achieve FDA approval for marketing in areas
where traditional drugs failed.
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 13 of 26 20/02/2016
Figure 3
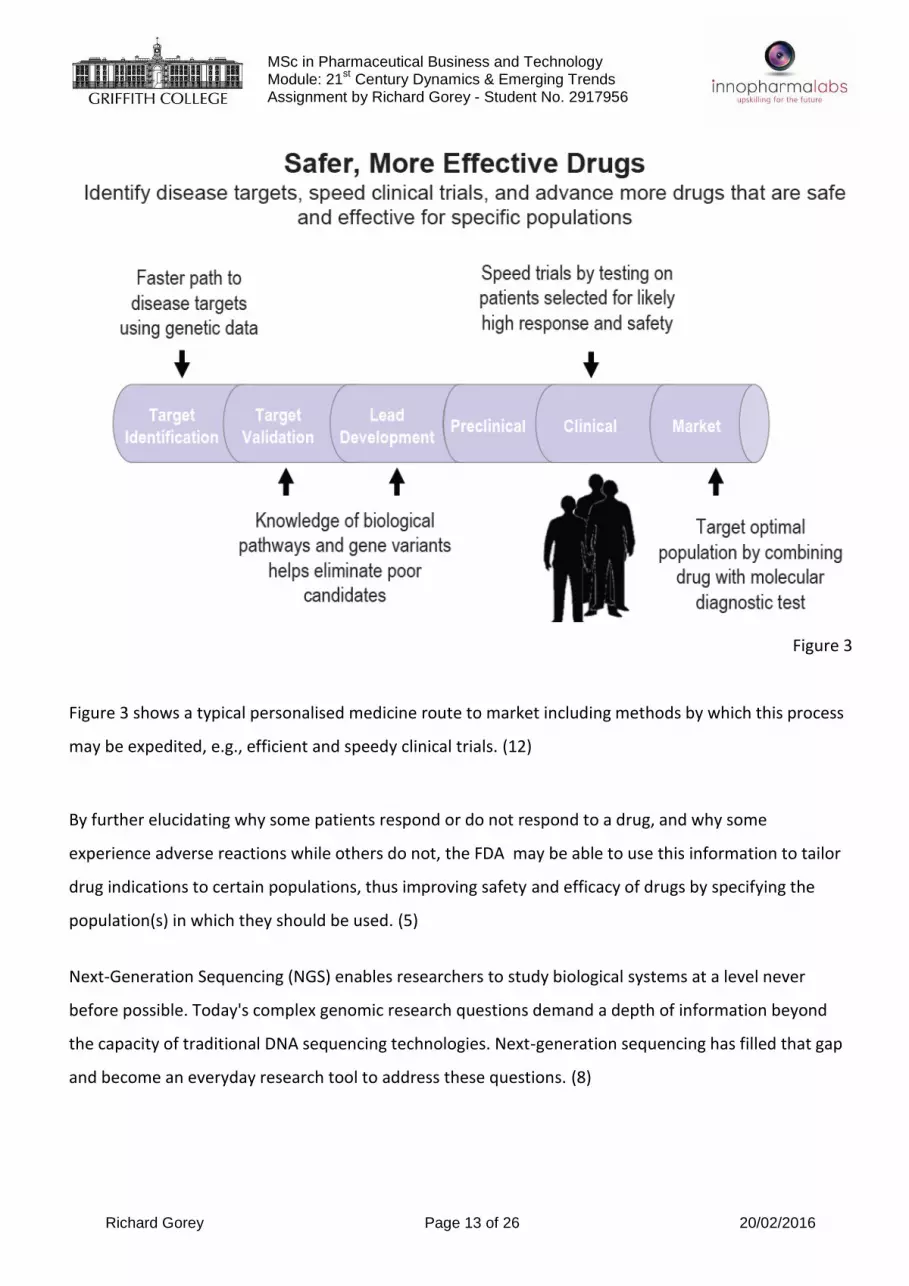
Figure 3 shows a typical personalised medicine route to market including methods by which this process
may be expedited, e.g., efficient and speedy clinical trials. (12)
By further elucidating why some patients respond or do not respond to a drug, and why some
experience adverse reactions while others do not, the FDA may be able to use this information to tailor
drug indications to certain populations, thus improving safety and efficacy of drugs by specifying the
population(s) in which they should be used. (5)
Next-Generation Sequencing (NGS) enables researchers to study biological systems at a level never
before possible. Today's complex genomic research questions demand a depth of information beyond
the capacity of traditional DNA sequencing technologies. Next-generation sequencing has filled that gap
and become an everyday research tool to address these questions. (8)

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 14 of 26 20/02/2016
The FDA’s current premarket review approaches for evaluating a test’s analytical and clinical
performance are designed around the more traditional one-test, one-disease paradigm. However, the
massive amount of data produced in next generation sequencing and the multitude of possible diseases
and conditions which a single genomic sequence might identify, present new challenges for the FDA, and
clearly requires thinking through new approaches that will enable the FDA to fulfil its mission of
protecting and promoting public health. As the FDA evaluates its options and considers what approach it
should take going forward, its work is informed by some real world experience, which it has already had
with the technology. (9)
In late 2013, the FDA granted marketing authorisation to the first NGS sequencing test system, Illumina’s
MiSeqDx instrument platform and two tests that detect DNA changes in the gene that causes cystic
fibrosis (CF). The MiSeqDx compares the patient’s genomic sequence to a reference sequence and
indicates any differences between the patient and the reference sequence. The FDA’s review of these
products employed a practical approach. For analytical performance, the FDA looked at how accurately
the instrument sequenced a representative set of genetic variants across the genome rather than
requiring data on every possible variant. Doing so avoided years of data gathering and unnecessary delay
in the public’s access to the benefits of this technology while still assuring its accuracy and reliability. (9)
The FDA employed similar flexibility in assessing the two CF tests. The FDA did not require that the
company collect new, independent data supporting each mutation’s association with disease in order to
demonstrate clinical performance. (9)
Instead, the company was able to leverage existing information by referring to a well-curated, shared
database of CF mutations to demonstrate its tests’ clinical validity. This database is really a model of
patient participation, created with support from the Cystic Fibrosis Foundation. With Illumina as the
trailblazer, subsequent sequencing platforms of the same type are exempt from premarket review. The
FDA’s primary focus will be the tests that are developed and performed on these platforms. (9)
The FDA is committed to regulating medical products based on the most advanced scientific information
available. It intends use the breakthroughs resulting from NGS technology to accelerate development of

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 15 of 26 20/02/2016
a practical and nimble approach that will allow medical advances in the field of genomics to be
implemented as soon as possible, using its regulatory flexibility and the power of the information placed
into high-quality databases. The FDA published a preliminary discussion paper on how to optimise its
regulation of NGS technology to assure that tests are not only safe and effective, but are available for
patients as soon as possible. (9)
NGS technology is integral to the future of personalised medicine. Whatever approach FDA ultimately
adopts must be selected with care to ensure continued innovation in this still evolving technology and
the advancement of the public health. (9)
President Obama’s 2016 budget proposal included a request for an additional $10 million for FDA work
on Next Generation Sequencing. This funding, which is part of the Precision Medicine Initiative, will help
the FDA acquire the additional tools and expertise that it needs to develop new approaches and to
advance the development of high quality, curated databases akin to the one that was used for the
review of the two Illumina tests for cystic fibrosis. (9)
Ultimately, The FDA’s actions and policies must be based on the best available science, while ensuring
that these breakthrough technologies are part of a foundation of basic medical care by doctors and
other providers that are safe, effective, and focus on meeting the needs of individual patients. (9)
“As the field advances, we expect to see more efficient clinical trials based on a more thorough
understanding of the genetic basis of disease. We also anticipate that some previously failed medications
will be recognised as safe and effective and will be approved for subgroups of patients with specific
genetic markers.” - Margaret Hamburg, M.D.Commissioner, U.S. Food and Drug Administration, Francis
Collins, M.D., Ph.D.Director, National Institutes of Health - The Case for Personalised Medicine 3rd
Edition - Personalised Medicine Coalition (9)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 16 of 26 20/02/2016
3. Assignment Paper - Element 3 of 4:
Element 3: What personalised medicine seeks to accomplish.
By using molecular analysis to achieve optimum medical outcomes in the management of a patient’s
disease or disease predisposition, personalised medicine promises to introduce a new standard of
healthcare. (10)
The concept of personalised medicine, that medical care can be tailored to the genomic and molecular
profile of the individual has repercussions that extend far beyond the technology that makes it possible.
The adoption of personalised medicine will require changes in healthcare infrastructure, diagnostics and
therapeutics business models, reimbursement policy from government and private payers, and a
different approach to regulatory oversight. Personalised medicine will shift medical practices upstream
from the reactive treatment of disease, to proactive healthcare management including screening, early
treatment, and prevention, and will alter the roles of both physician and patient. It will create a greater
reliance on electronic medical records and decision support systems in an industry that has a long history
of resistance to information technology. Personalised medicine requires a systems approach to
implementation. However, in a healthcare economy that is highly decentralised and market driven, it is
incumbent upon the stakeholders themselves to advocate for a consistent set of policies and legislation
that pave the way for the adoption of personalised medicine. (14)
Personalised medicine seeks to:
Detect disease at an earlier stage, when it is easier to treat effectively
Enable the selection of optimal therapy and reduce trial-and error prescribing
Reduce adverse drug reactions
Increase patient compliance with therapy
Improve the selection of targets for drug discovery
Reduce the time, cost, and failure rate of clinical trials
Revive drugs that failed clinical trials or were withdrawn from the market
Avoid withdrawal of marketed drugs
Shift the emphasis in medicine from reaction to prevention
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 17 of 26 20/02/2016
Reduce the overall cost of healthcare
(12)
Figure 4
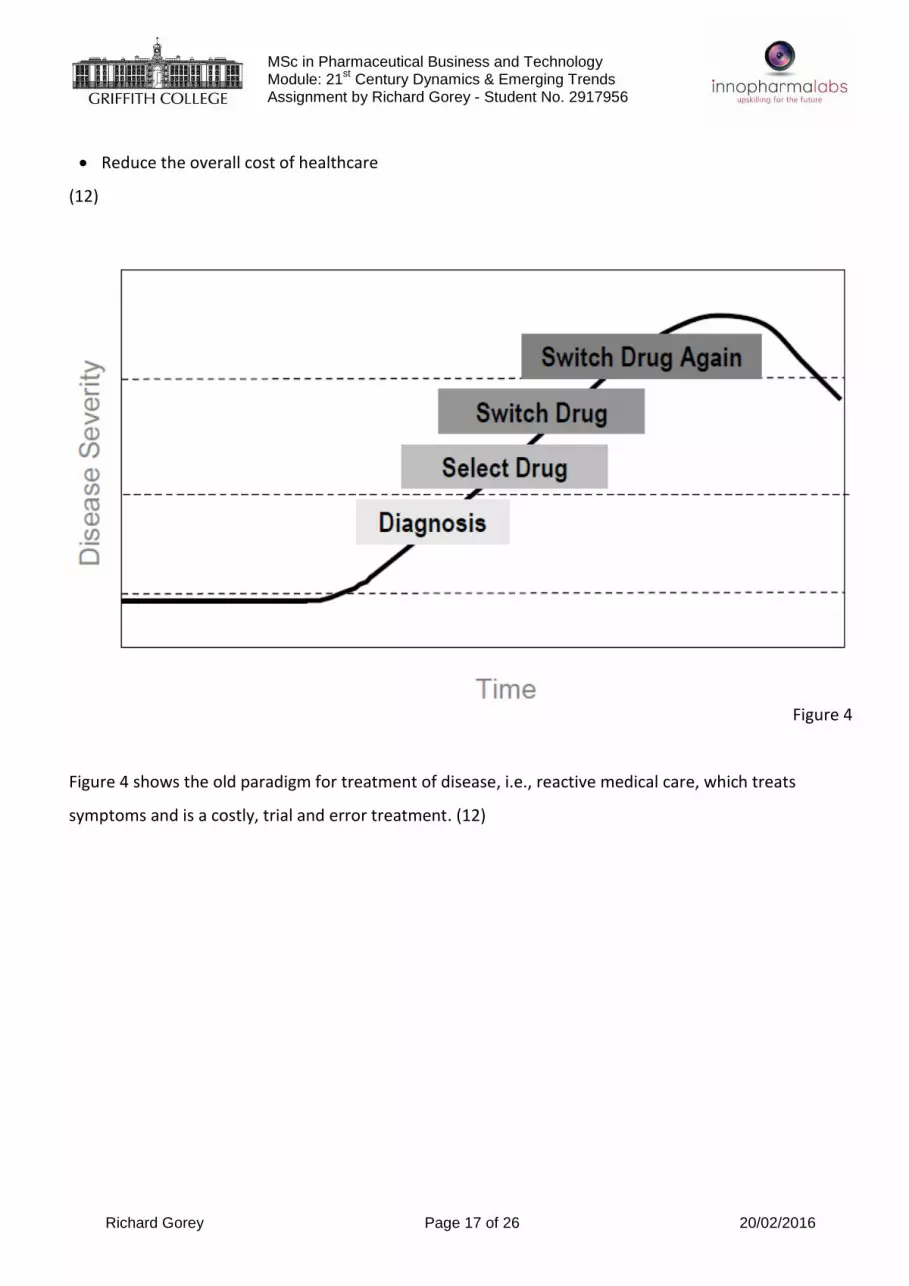
Figure 4 shows the old paradigm for treatment of disease, i.e., reactive medical care, which treats
symptoms and is a costly, trial and error treatment. (12)

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 18 of 26 20/02/2016
Figure 5
Figure 5 shows the personalised medicine paradigm for health management, i.e., efficient medical care,
which includes molecular screening, early detection, rapid effective treatment and improved quality of
care. (12)

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 19 of 26 20/02/2016
Figure 6
Figure 6 shows the personalised medicine paradigm for preventive medical care, which incorporates
predisposition guides for prevention, identification of molecular markers and healthcare cost reduction.
(12)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 20 of 26 20/02/2016
4. Assignment Paper - Element 4 of 4:
Element 4; The success of many personalised medicines fundamentally depends on the identification of
biomarkers and the successful development of diagnostic tests that can be used to accurately stratify the
patient population. Illustrate how this is so.
Biomarkers are defined as any molecule derived from a biological sample that can indicate current
disease status, evaluate progression of the disease, or assess potential responsiveness to a particular
medication. (11)
There is significant interest in the prediction and early detection of disease through the analysis of
biological markers, or biomarkers, which have the potential to significantly improve clinical outcomes.
(11)
Biomarkers come in many forms including DNA mutations, proteins, and messenger RNA (mRNA)
transcripts. For example, ratios of aspartate/alanine aminotransferase are used as a reliable biomarker
for liver fibrosis, protein levels of S100-beta are used as a biomarker of treatment response for
malignant melanoma, while mutations of the genes BRCA1 and BRCA2 are well known biomarkers
predicting the development of breast cancer. DNA methylation is also a well-studied biomarker.
Methylated cytosine residues have been associated with several diseases, including cancer and
neurological disorders. (11)
Over the years, non-coding RNAs (ncRNAs) have become the focus of biomarker research, an approach
that has been favorably used in the investigation of response to treatment for several medical
conditions. There are several types of ncRNAs, of which microRNAs (miRNAs) are the best known and the
most frequently assessed for their potential role as biomarkers. MiRNAs have been proposed as
molecular biomarkers in cancer, liver and cardiovascular disease, and central nervous system disorders,
among many others. MiRNAs are small ncRNAs molecules that follow a well characterized biogenesis
pathway that includes processing through the DGCR8/ DROSHA, Exportin-5, Dicer and RISC molecular
complexes . Through post-transcriptional activity, these small, single-stranded, 19–25-base RNA

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 21 of 26 20/02/2016
transcripts regulate the expression of numerous genes. Binding of the miRNA to the complementary
sequence of a target mRNA relies on recognition of the seed region, the 2–8 nucleotides located at the
3′end of the miRNA, which leads to either mRNA degradation or translational repression. (11)
Other ncRNA species such as PIWI-interacting RNAs (piRNAs), small nucleolar RNAs (snoRNAs), small
nuclear RNAs (snRNAs) and long non-coding RNAs are also gaining support as key components of cellular
regulation, and thus might be potentially assessed as biomarkers of disease. PiRNAs are small ncRNAs of
24–31 nt length. In contrast to miRNAs, these are Dicer-independent and interact with the PIWI
subfamily of Argonaute proteins involved in the regulation of genome stability. PIWI proteins are
involved in gene regulation through RNA degradation and have been linked to DNA methylation. In
addition, piRNAs have been reported as potential biomarkers for bladder, breast, and gastric cancers.
SnoRNAs are key components of the small ribonucleoproteins (snoRNPs) which are responsible for
sequence-specific 2′-O-Methylation of ribosomal RNA (rRNA). SnoRNAs have been shown to participate
in post-transcriptional regulation of rRNA by targeting snoRNPs in the nucleus. In addition, snoRNAs have
been proposed as potential biomarkers for several forms of human cancers. Long non-coding RNAs are
another class of ncRNAs that have gained a lot of attention recently as potential biomarkers. They
comprise a heterogeneous group of ncRNAs larger than 200 nt, which includes long non-coding RNAs
(lncRNAs), large intergenic non-coding RNAs (lincRNAs) and transcribed ultraconserved regions (T-UCRs),
among others. LncRNAs are known to regulate DNA methylation by recruiting chromatin remodeling
complexes. LincRNAs have been associated with active transcription in regions of transcriptional
elongation. Finally, while the function of T-UCRs is still unknown, they have been demonstrated to
interact with microRNAs and might have a role in the development of disease. T-UCRs have been
recently postulated as potential diagnostic and prognostic biomarkers in colorectal cancer patients. (11)
While any ncRNA is a putative biomarker, miRNAs have received the most attention because they
possess several features that render them especially powerful :
i.) they are highly conserved, and evolutionary complexity correlates with miRNA complexity, which
suggests an important biological function;
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 22 of 26 20/02/2016
ii.) there are a relatively small number of individual miRNAs with a large dynamic range of
expression;
iii.) they are secreted into circulation and can be measured in all biological fluids;
iv.) they are not easily degraded and are thus highly stable in clinical samples;
v.) they are involved in pathway regulation, as one miRNA can target many genes, and a single gene
can be regulated by many different miRNAs;
vi.) miRNAs show tissue and cell specific expression profiles; and
vii.) there is a large body of literature supporting their role in the pathophysiology of disease. (11)
Most ncRNA quantification studies performed to date rely on qRT-PCR, in situ hybridization, or
microarray techniques. These methods have several strengths, but also contain some important
limitations. These include: the number of miRNA molecules that can be analyzed simultaneously, the
amount of RNA required for the analysis of multiple targets, the quality and source of the RNA, the
sensitivity of detection, and the need for previous knowledge of targets. Next generation sequencing
(NGS) provides researchers with a powerful tool for the detection of RNA molecules in biological
samples. NGS offers methodological advantages such as increased throughput, decreased RNA input,
consistency and quality of data, higher detection depth, analysis of all RNA populations, and discovery of
novel molecules. Furthermore, length of protocols, sequencing time, and prices are continuously
dropping, making NGS an ideal tool for biomarker research. (11)
While scientific discoveries across multiple fields have led to an explosion of biological information, the
development of diagnostics and their translation into clinical practice pose a number of scientific and
regulatory challenges. Inadequate performance of a diagnostic test that is used to guide treatment
decisions can have severe therapeutic consequences. For example, with an incorrect diagnostic result, an
unsuitable drug may be given to a patient who will, as a result, be harmed or will not benefit, because
the drug will cause an other wise avoidable adverse event, will be ineffective for that patient, or both. (5)

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 23 of 26 20/02/2016
Diagnostic tests are intended to measure (as in the case of in vitro diagnostics), or evaluate (as in the
case of electrocardiogram tracings or imaging technologies), an indicator of a normal biological process,
pathogenic process, or response to a therapeutic intervention. In the case of in vitro diagnostic test
development, biomarker discovery and evaluation of the biomarker are critical initial steps. If the
biomarker is not significantly correlated with the clinical state – for example, a particular genetic
mutation with a disease – a diagnostic test that measures that biomarker will not produce meaningful
results for that disease. (5)
Diagnostic tests generally fall under the FDA’s medical device authority and are classified and regulated
in a risk-based manner. Risk determination includes the risk of an erroneous result, and the harm to a
patient that might be incurred based on an incorrect test result when the test is used as intended.
Diagnostic test results can be incorrect in two major ways: they can report a positive result when the
result is actually negative (false positive), or they can report a negative result when the actual result was
positive (false negative). Tests that measure the amount of a substance can report values that are falsely
high or low. False test results and their consequences are evaluated for their risk of harm to patients. For
example, a false positive test result that could lead to a patient undergoing an invasive medical
procedure or a therapy with toxic side effects would generally be considered high risk. Similarly, a false
negative test result that might alter medical management and delay appropriate intervention for a life-
threatening condition might also be considered high risk. (5)
In evaluating a diagnostic device, FDA looks at its analytical validity as well as its clinical validity.
Analytical validity refers to how well the test measures what it is supposed to measure, whereas clinical
validity looks at how well the test predicts who has or does not have a disease or condition for which it is
being tested. In personalised medicine, where the diagnostic test is often a biomarker-based assay, such
as a genetic test, the clinical validity of the test refers to how well the test works in helping to identify
people who will or will not respond to a therapy (or who will or will not suffer adverse consequences).
(5)
In addition to analytical and clinical validity, stakeholders in personalised medicine are also interested to
know the clinical utility of new diagnostics. “Clinical utility” is a term that describes the relevance and

MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 24 of 26 20/02/2016
usefulness of an intervention in patient care; in other words, how much value does it add? When a
diagnostic test informs the use of a medical treatment, the test has clinical utility if its use improves the
treatment outcome. While the accuracy of a diagnostic test used to individualise treatment or an
intervention is evaluated by measuring its analytical and clinical validity, the usefulness of the test is
typically evaluated by its clinical utility. There is considerable debate about the methods of
demonstrating clinical utility and the level of evidence – in terms of quantity, quality, and type – that
should be obtained for any new diagnostic test to be introduced into routine clinical practice. (5)
Many of the diagnostic tests used in personalised medicine are in vitro diagnostic devices (IVDs), also
called clinical laboratory tests, which test body substances from patients for alterations in levels of
biomarkers (e.g., proteins) and the presence/absence of genetic susceptibility biomarkers. The
development and validation of IVDs for use in guiding therapeutic treatment pose a number of particular
challenges. First, the sheer pace of the development of IVDs over the past decade has been staggering.
Volumes of information arising out of the human genome project combined with a dramatic decrease in
costs of DNA sequencing, for example, are giving way to an explosion of publications linking particular
genetic markers to diseases or conditions and a rapid application of this information in the development
of new molecular diagnostic tests. How best to integrate rapidly evolving genomic information into
clinical care while ensuring safety and efficacy is a topic of considerable public debate and discussion. For
the FDA, the evaluation of these tests, and the development of standards for levels of evidence required
to demonstrate the validity of the test, are especially complicated when the meaning of a given genetic
association may be poorly understood or change over time. Moreover, the complexity of these tests is
ever evolving, as single marker tests have given way to tests that measure multiple markers
simultaneously, such as complex gene panels. Extensive DNA and RNA sequencing across multiple genes
or the whole genome are already being used in clinical practice. (5)
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 25 of 26 20/02/2016
References
1. Dudley, J; Karczewski, K. (2014). Exploring Personal Genomics. Oxford: Oxford University Press.
2. "Personalized Medicine 101: The Science". Personalized Medicine Coalition. Retrieved 26 April 2014.
3. Lu, YF; Goldstein, DB; Angrist, M; Cavalleri, G (24 July 2014). "Personalized medicine and human
genetic diversity". Cold Spring Harbor perspectives in medicine 4 (9): a008581.
doi:10.1101/cshperspect.a008581. PMID 25059740.
4. "When Healthcare and Computer Science Collide". University of Illinois at Chicago. University of
Illinois at Chicago Health Information Management Department.
5. Paving the Way for Personalized Medicine - FDA’s Role in a New Era of Medical Product
Development - October 2013
6. Dumontier::BIOL4301:Personalized Medicine Personalized Medicine Michel Dumontier, Ph.D.
Associate Professor of Bioinformatics Department of Biology, Institute of Biochemistry, School of
Computer Science Carleton University Ottawa Institute for Systems Biology Ottawa-Carleton Institute
for Biomedical Engineering Nov 18, 2010
7. Realizing the Potential of Pharmacogenomics: Opportunities and Challenges - Report of the
Secretary’s Advisory Committee on Genetics, Health, and Society – 2008
8. http://www.illumina.com/technology/next-generation-sequencing.html
9. “Optimizing FDA's Regulatory Oversight of Next Generation Sequencing Diagnostic Tests” - Remarks
by Margaret A. Hamburg, M.D. Commissioner of Food and Drugs - National Institutes of Health -
February 20, 2015
10. https://www.aacc.org/~/media/files/divisions/lvd/personalized_medicine_lvd_division.pdf?la=en
The Case for Personalized Medicine - Personalized Medicine Coalition
11. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4487992/
Biomarker discovery: quantification of microRNAs and other small non-coding RNAs using next
generation sequencing - Juan Pablo Lopez, Alpha Diallo, Cristiana Cruceanu, Laura M. Fiori, Sylvie
Laboissiere, Isabelle Guillet, Joelle Fontaine, Jiannis Ragoussis, Vladimir Benes, Gustavo
Turecki, and Carl Ernst
12. https://www.aacc.org/~/media/files/divisions/lvd/personalized_medicine_lvd_division.pdf?la=en
MSc in Pharmaceutical Business and Technology Module: 21
st Century Dynamics & Emerging Trends
Assignment by Richard Gorey - Student No. 2917956
Richard Gorey Page 26 of 26 20/02/2016
Personalized Medicine: The Changing Landscape of Healthcare - American Association of Clinical
Chemistry Annual MeetingSan Diego, California July 14th, 2007 Edward Abrahams, Ph.D.Executive
Director Personalized Medicine Coalition
13. http://ghr.nlm.nih.gov/handbook/genomicresearch/pharmacogenomics
What is pharmacogenomics?
14. http://www.ncbi.nlm.nih.gov/pubmed/16336000
The Personalized Medicine Coalition: goals and strategies.
Abrahams E1, Ginsburg GS, Silver M.
Personalized Medicine Coalition, Washington, DC 20005, USA.