rhetorical histories of psychosis
TRANSCRIPT

162
CHAPTER THREE: RHETORICAL HISTORIES OF PSYCHOSIS
“You see, here’s the problem. You don’t know the history of psychiatry. I do.” – Tom Cruise.34
“Science, unlike art, is a system of derivative ideas filtered through centuries. Consequently, originality in science is not only infrequent but unwelcome, and even the most original ideas have a history, often a much longer one than their authors suppose.” – Miriam Siegler & Humphry Osmond35
“Direct selfobservation is not nearly sufficient for us to know ourselves: we require history, for the past continues to flow within us in a hundred waves; we ourselves are, indeed, nothing but that which at every moment we experience of this continual flowing… [To] understand history we have to go in quest of the living remnants of historical epochs – we have to travel, as the father of history, Herodotus, traveled, to other nations – for these are only earlier stages of culture grown firm upon which we can take a stand… But there exists a subtler art and object of travel which does not always require us to move from place to place or to traverse thousands of miles. The last three centuries very probably still continue to live on, in all their cultural colors and cultural refractions, close beside us: they only want to be discovered. In many families, indeed in individual men, the strata still lie neatly and clearly one on top of the other: elsewhere there are dislocations and faults which make understanding more difficult… He who, after long practice in this art of travel, has become a hundredeyed Argos, will in the end be attended everywhere by his Io36 – I mean his ego – and will rediscover the adventurous travels of this ego in process of becoming and transformation.” – Friedrich Nietzsche.37
“Let the credulous and the vulgar continue to believe that all mental woes can be cured by a daily application of old Greek myths to their private parts.” – Vladimir Nabokov.38
***
The public discussion and controversy over DSM5 takes place in the
context of the progressive development of modern medicine generally and the
emergence of modern psychiatry in particular. This chapter draws forward
this context by examining a number of key moves in the histories of medicine
34 Tom Cruise, interviewed by Matt Lauer on NBC’s ‘Today Show’ (“Tom Cruise discusses his views on antidepressants and psychiatry,” 2005, para. 14).35 Miriam Siegler & Humphry Osmond (1974, p. 1).36 According to Greek mythology, Hera sent Argos Panoptes (a primordial giant with 100 eyes) to watch over the cownymph Io in order to guard against any illicit encounters with Zeus (E. Hamilton, 1940).37 Friedrich Nietzsche (1986, sec. II:223, emphasis in the original).38 Vladimir Nabokov (1973, p. 66).
163
and madness. The arc of the chapter is to situate the contemporary context
concerning psychosis risk syndrome (a topic I take up directly in Chapter 4).
The controversy over predictive and diagnostic understandings of risk
syndrome raises a critical issue central to the DSM5 debate: What is the
nature of mental illness and its status as a “real, recognizable, unitary and
stable object of history”? This question raises issues that concern the
ordering of prevention and treatment within a hierarchy of medical values,
the role of likely course and prognosis in psychiatric nosology, and the
importance of (and attributed confidence in) scientific knowledge about the
etiology and pathogenesis of psychotic disorders. Analysis of the issue will
offer insight into the ways in which continuity and discontinuity are
performed rhetorically, the relationship between diagnosis and recommended
treatment, and the perseverance of cultural systems and epistemic
assemblages well beyond their putative abandonment by apparent consensus
(Luque, Berrios, & Villagrán, 2003, p. 111). I explore several interrelated
historical discursive movements that are germane to each of these issues, yet
can be difficult to see in contemporary biomedical discourses without the
right tools.
The chapter is a study in rhetorical history. It moves from what are
regarded as dated theories of pathology to explain contemporary stateofthe
art medical appeals. This critical history shows the contemporary relevance
164
of the residues of thinking which still retain the capacity in some manner to
“organize the chaos” within and around us (Nietzsche, 1874, p. 122).
Through the various twists and turns of material history, alongside adjacent
professional and clinical languages, a perspective on the selfgenerating
processes of discursive formations becomes visible. By the end of the chapter,
the diverse observations made along the path through the dislocations,
faults, and neatly lying strata of the discourses of madness and medicine
should coalesce into themes that set forth the context in which nosological
positions become advocated and contested. My history has three discursive
episodes, each of which I shall preview briefly in order to show the
progressive, cumulative developments of contexts within which DSM5
debates occur.
1. The Humoral Model of Pathology. Humorism (sometimes
'humoralism' or the 'humoral model') constitutes a model that dominated the
articulation of medicine for more than 2,500 years. This discourse offers the
earliest definitions of pathology in the Western medical tradition. Humorism
was for all purposes coequal with medicine as a field of knowledge, into which
all medical discoveries for millennia were integrated. This chapter identifies
basic premises of this model and reads select, foundational texts of medical
science in the Hippocratic corpus and the writings of Galen. Additionally, it
examines nonmedical authorities writing about medicine, especially the

165
Roman Epicurean philosopher Lucretius. His radically material and
biological account of mental illness shares much in common with
contemporary biomedical views. From the very beginning, Hippocrates made
both epistemic and institutional moves as he formulated medical practice.
Modern medicine featured similar rhetorical strategies in defining medicine
and madness. These feature a wide array of relevant discourses, including:
Mesmerism (a protopsychotherapy developed to treat what are now known
as dissociative identity disorders); categories adopted by alienists like
melancholia and mania; twentieth century theories about personality
structures and types; contemporary constructs like Attention Deficit /
Hyperactivity Disorder (ADHD); recurrent institutional squabbles between
psychiatrists and psychologists; the marketing of alternative 'holistic' or
'naturopathic' dietary supplements; and the presentation and rhetorical use
of scans produced with brain imaging technologies. The chapter shows how
traditional concepts were carried forward into modern times.
2. The Rise of Scientific Medicine. For the purposes of this study, I
examine the transition to a 'scientific' approach to medicine as a phenomenon
stretching from the seventeenth century, when the therapeutic effects of the
bark of cinchona trees (which contains quinine, an effective malaria
treatment) were discovered, to the early twentieth century. The
achievements most relevant to the DSM5 debate come from the emergence
166
(and subsequent convergence) of ontological and physiological interpretations
of pathology. Thomas Sydenham, called the 'English Hippocrates,' offers an
example of departure to the modern. His approach to medicine was at once
neoHippocratic and protobiopolitical, retaining certain humoral beliefs.
These beliefs informed his decisions about the variables he included in the
first ever epidemiological study involving data collection and statistical
analysis. Sydenham crafted an ontological distinction, dividing illness into
discrete disease entities that each present as a syndrome with characteristic
clinical signs and symptoms. His empiricist approach (distinguished from
rationalist humorism) was concerned with “semeiosis” rather than diagnosis
(Coulter, 1975, p. 247).39 Sydenham's classification of 'hysteria' as a mental
illness anticipated the contemporary conflict between psychological and
biological explanations in psychiatry. A later generation of physicians
revised this view, arguing that disordered bodily 'vapors' were the source of
hysteria. In turn, twentieth century psychoanalysis reformulated these class,
gender, and sex based outlooks into 'conversion disorder,' an illness that
features psychic tensions giving way to somatic distress. Rudolf Virchow
argued that biological terminology and conceptualization should replace the
ontological understanding of illness. The relationship between
39 Originally, semiotics was a field of medical knowledge concerned with the interpretation of clinical signs, only later acquiring its more generalized identity as the study of signification and meaningmaking (Baer, 1988).
167
psychoanalysis and pharmaceutical intervention thus became contested.
Although its terms were worked out early in the twentieth century, the
modern setting for defining and diagnosing disorder still broadly shapes the
context for DSM5 contestation.
3. The Emergent Assembly of Psychiatry. The final section of this
rhetorical history describes the genesis of psychiatry. JeanÉtienne
Dominique Esquirol, a French alienist, produced the first comprehensive
nosology of mental illness based on the patients he observed while working in
an asylum. Visual representations played a critical role in Esquirol's efforts
to persuade his colleagues of the merits of his classification scheme. Esquirol
appropriated the visual rhetoric of Linnaeus, the father of modern taxonomy.
Esquirol's representations are followed by the semiotic dialectic of 'neurosis'
and 'psychosis,' which unfolded alongside Emil Kraepelin's diagnostic
category 'dementia praecox.' Dementia praecox was a revolutionary
pathological entity because it was defined by its temporal course and
prognosis. This concept of psychotic illness evolved into Bleuler's
'schizophrenia,' which reimagined dementia praecox as a loosening of
associations and a splitting of the mind. The sharp material turn of the last
fifty years gave biological meaning to these two ideas: a loss of associations
between neurons and neurological lesions in gray and white matter.
Developments in psychopharmacology and in brain imaging techniques
168
continue the material turn, which pharmaceutical advertising has carried to
publics. The mixed development of psychiatry combined with public
representations of disease form the context in which DSM5 finds controversy
attributed to the wellbeing of a profession and its publics.
The Humoral Model of Pathology
Humorism is a model of pathology that explains variance in human
health, personality, and drive as a function of the deficiencies and excesses of
four distinct bodily fluids, the humors. Hippocrates compiled humorism into
a system in the fourth century before the Common Era, and some five
centuries later, Claudius Galen integrated it with Aristotelian philosophy
into a comprehensive theory for the science of medicine, defined as “the
knowledge of what is healthy, what is morbid, and what is neither” (Galen,
2004, p. 1).40 Mapped onto the four classic elements that Empedocles (2012)
had described a century before Hippocrates, the humors were structurally
organized in relation to one another according to the qualitative binaries of
hot/cold and wet/dry (Figure 3.1).
40 Galen goes on to clarify that it “makes no difference if one uses the term ‘diseased’ instead of ‘morbid.’ The term ‘knowledge’ is to be understood in its common, not its technical, sense” (2004, p. 1).

169
Source: (Magner, 2002, p. 25)
Figure 3.1: Structural relationships between the humors, temperaments, elements, and qualities
170
While it might seem paradoxical to describe a liquid as ‘dry,’ these
qualities were simultaneously metaphorical and physiological. Hippocrates
observed, for example, that one could become dehydrated as a result of
drinking too much wine.41 Further, he observed that the consumption of wine
often brought a feeling of warmth. Hence, Hippocrates thought of wine as
being both hot and dry. Noting that the sweetness of a wine inversely
correlates with its suppressive effect on salivation, acrid wines were
described as more ‘dry’ than sweet wines, a distinction that persists today
(Norrie, 2003). In a similar manner, we make use of humoral terminology
when we speak of comedy as ‘dry’ (as a deadpan delivery lacks the outward
signs of cheer associated with ‘moist’ sanguine humor) or ‘dark’ (associated
with the melancholy of black bile).
Physicians understood the humors to be “lifegiving moisture,” liquid
incarnations of the vital forces that govern all of the rhythms of life, from the
seasons and the weather all the way down to human health, “a proper
mixture of the humors being as necessary to bodily growth and functioning as
that of the elements to the creation of permanent substances” (Tillyard, 2011,
p. 69). These vital forces deeply penetrate our corporeal nature, circulating
through and ‘coloring’ human bodies, both literally and (as we understand it
41 The various writings attributed to Hippocrates are not all believed to have been authored by him, but rather by subsequent students (King, 1993). Citations of Hippocrates in this chapter should be understood as citations of the Hippocratic corpus, rather than necessarily as direct attributions to the historical Hippocrates.
171
today) metaphorically, as in the reddening of the face associated with both a
sanguine complexion and a sanguine disposition. In other words, they are
visibly present in one’s complexion (the literal result of a ‘complex’ of
humors), level of activity, mood, posture, speech, and temperature (derived
etymologically from the Latin temperare, ‘to mix’). Each humor further
corresponds with a distinctive temperament (also derived from temperare)
and prevailing affective state: black bile (the hidden fluid responsible for
darkening blood and stool, thought to be produced in the spleen or bowel)
with the sad melancholic; choler (yellow bile or gastric juice, thought to be
produced in the liver) with the angry choleric; phlegm (mucus, sweat, tears,
and other colorless secretions, thought to be produced in the brain) with the
sluggish phlegmatic; and blood (a hot red liquid thought to be produced in the
heart) with the cheerful sanguine (Galen, 2004; Gottfried, 1983; Healy, 2008;
Magner, 2002; Noll, 2011).
Though not terribly controversial at the time, the notion that our
personality and behavior are at least partially (if not entirely) determined by
physiological factors was repressed deep within the Western cultural
unconsciousness for millennia, and its return in the nineteenth century
ironically was instrumental in the final rejection of humorism by the medical
establishment in favor of a model of discrete disease states based on
pathological anatomy. The four temperaments, protoWeberian ideal types of
172
characterological dispositions, signify clusters of character tendencies (later
conceptualized as personality traits), the consequences of the humors
tempering one another such that one of the four humors completely
dominates the other three in an individual's body and, thus, character
(Strelau, 2002; Weber, 1949).
In a physically and mentally healthy person, all four humors are in a
state of eucrasia (literally a ‘good mixture’) or balance. Accordingly,
dyscrasia (‘bad mixture’), the acute (sometimes chronic) imbalance of humors,
is the direct cause of most disease. ‘Cause’ here refers to susceptibility, a
disposition or tendency (‘habitus’) toward some specific manifestation of
disease; “habitus phthisicus,” for example, is the Latinized Hippocratic term
used to describe someone who is especially susceptible to what was later
known as pulmonary tuberculosis (R. J. Campbell, 2009, p. 440). Hippocrates
notes:
If the brain is corrupted by phlegm the patients are quiet and silent, if
by bile they are vociferous, malignant and act improperly. If the brain
is heated, terrors, fears, and terrifying dreams occur; if it is too cool the
patients are grieved and troubled. (cited by Diethelm, 1971, p. 16)
Another form of imbalance, either in some singular extrahumoral disposition
or in a crisis associated with an inner conflict between dispositions, produces
an illness state known as ‘distemper,’ paralleling our contemporary notion(s)

173
of the disordered personality (e.g., borderline personality disorder),
distinguished from the acute clinical syndrome (Healy, 2008).42
In some cases, the pathogenic imbalance is not within an individual
human body (agent), but rather the surrounding environment (scene), which
may be a source of some bad odor (‘miasma’) or of contagion, a disease
substance that, unlike miasma, was produced within a human body before
beginning to circulate through corrupted or polluted air (Gottfried, 1983;
Noll, 2011). When predisposition to a particular illness runs in a family, the
imbalance is not a humoral excess or deficiency per se, but rather an intrinsic
imbalance within a single humor—‘bad blood,’ in which the inherited trait, or
perhaps rather heredity as such, is metonymically reduced to the sanguine
humor (Ciobanu, 2012). Infectious disease was communicable even across
the barrier of metaphor, as an imbalance in the ‘body politic’ was known to
render individual human bodies susceptible to leprosy (Douglas, 1992).
Humoral pathology served as a logic that unified the various medical
techniques of diagnosis and intervention. The model provided explanations
of the mechanisms of ancient pharmacotherapy. These explanations spread
to other domains of thought through figures of speech. For example, the
sophist Gorgias of Leontini invoked humoral pathology in his famous
observation about the power of rhetoric:
42 In DSMIV, this is a difference between the second and first axes (respectively) of disorders.

174
The effect of speech upon the soul is comparable to the power of drugs
over the nature of bodies. For just as different drugs dispel different
secretions from the body, and some bring an end to disease and others
to life, so also in the case of speeches: some distress, others delight,
some cause fear, others make the hearers bold, and some drug and
bewitch the soul with a kind of evil persuasion. (Gorgias, 1972, para.
14).
This may be the first articulation of the 'talking cure,' written 2,300 years
before Freud was born, formulated as an argument by analogy to humoral
medicine.
We can see traces of the humoral architectonic in our everyday
language today, as when a chronically irritable person, prone to outbursts of
anger, is said to have a ‘bad temper’ (and is perhaps ‘hotheaded,’ unlike
people who can ‘keep their cool’ when the unexpected occurs) or when a
moody, sensitive, and perhaps erratic individual is said to be
‘temperamental.’ An almost opposite type of character is signified by
‘temperance,’ which invokes notions of moderation and selfcontrol, the result
of a balanced character. Etymologically, the difference between
‘temperament’ and ‘temperance,’ both noun derivatives of the verb temperare,
is that the former contains the Latin suffix –mentum while the latter
contains the Latin suffix –antia. The suffixes –mentum and –antia are
175
extremely similar, both functioning to convert a verb into a noun
representing a state associated with, produced by, or instantiated in the
action signified by the verb. The difference is that –mentum converts the
verb into a concrete state, generally the subject (as in government) or object
(as in firmament) of the verb, while –antia converts the present participle
form of the verb into a noun, emphasizing process rather than source or
outcome (Luschnig & Luschnig, 1982). Temperamental is simply an adjective
derived from temperament. Hence, ‘temperamental’ describes someone prone
to concrete states of character or affect, the outcomes of distinctive humoral
mixtures that are imbalanced in one way or another. In contrast, temperate
(the adjectival form of temperance) describes someone whose character is
moderated by a steady, balanced process of humoral mixing (as well as a
steady, balanced climate). This is how two nearly identical words generated
within a robust semiotic system came to have nearly opposite meanings.43
The difference between concrete states and dynamic processes may
seem merely semantic, but will come to be the pivot point for multiple
revolutions in psychiatric nosology as the conflict between categorical and
dimensional approaches to diagnosis. Indeed, Theodore Millon, a
psychologist who served on both the DSMIII and DSMIV committees, and
43 This also helps to explain how a powerful eighteenth to twentieth century American social movement thoroughly united in opposition to mixed beverages could perhaps paradoxically come to be known as the ‘Temperance Movement.’

176
Erik Simonsen, past president of the International Society on the Study of
Personality Disorders and past chairman of the World Psychiatric
Association section on personality disorders, argue that, while
debates on these issues often degenerate into semantic arguments and
theoretical hairsplitting, it is naïve to assume that metaphysical
verbiage and word quibbling are all that are involved. Nevertheless,
the language that we use, and the assumptions such language reflects,
are very much a part of our scientific disagreements. (Millon &
Simonsen, 2010, p. 50)
How one defines pathology determines how one thinks of individual
disorders: how to measure their presence or absence, what it means to treat
them, and how to distinguish one from another.
Humoral Rhetoric from Antiquity to Modernity
In contrast with certain mystical or religious orientations in which
madness (possession by a demonic or divine force) and physical ailments
(manifestations of the corrupting or defiling nature of sin) are seen in moral
terms as two incommensurate elements of a cosmic theological drama, the
humoral orientation seems strikingly modern. Its concepts of mental and
physical illness both are ‘seen’ (literally and metaphorically) as natural
processes best explained physiologically and, thus, falling within the domain
of medical science. This is very clear in Hippocrates’s treatment of the so

177
called ‘sacred disease,’ today known as epilepsy, in which he presents a
thoroughly secular understanding of mental illness (as epilepsy was regarded
from antiquity until very recently) along with some very prescient claims
about the role and functions of the brain:
I do not believe that the ‘Sacred Disease’ is any more divine or sacred
than any other disease but, on the contrary, has specific characteristics
and a definite cause. Nevertheless, because it is completely different
from other diseases, it has been regarded as a divine visitation by
those who, being only human, view it with ignorance and
astonishment… It is my opinion that those who first called this disease
‘sacred’ were the sort of people we now call witchdoctors, faithhealers,
quacks and charlatans. These are exactly the people who pretend to be
very pious and to be particularly wise. By invoking a divine element
they were able to screen their own failure to give suitable treatment
and so called this a ‘sacred’ malady to conceal their ignorance of its
nature… The brain is the seat of this disease, as it is of other very
violent diseases… It ought to be generally known that the source of
our pleasure, merriment, laughter and amusement, as of our grief,
pain, anxiety and tears, is none other than the brain. It is specially
the organ which enables us to think, see and hear, and to distinguish
the ugly and the beautiful… It is the brain too which is the seat of

178
madness and delirium, of the fears and frights which assail us, often
by night, but sometimes even by day; it is there where lies the cause of
insomnia and sleepwalking, of thoughts that will not come, forgotten
duties and eccentricities. All such things result from an unhealthy
condition of the brain… This socalled ‘sacred disease’ is due to the
same causes as all other diseases… Each has its own nature44 and
character and there is nothing in any disease which is unintelligible or
which is insusceptible to treatment… The physician… could cure this
disease too provided that he could distinguish the right moment for the
application of the remedies. He would not need to resort to
“purifications” and magic spells. (Hippocrates, 1995, pp. 139–144)
This line of argument was centuries ahead of its time, and not only on
account of the “astonishingly prescient” insights about the material nature of
conscious experience located in the brain, for which it justifiably is celebrated
(Zeman, 2006, p. 2).45 This jurisdictional polemic is also evidence that, from
the very beginning, Western medicine has been the site of a discursive
struggle over the politics of medical expertise.
While admitting that the ‘sacred disease’ certainly may seem
supernatural to a nonexpert, Hippocrates positions himself as an expert who 44 The word for nature is physis ( ),φύσις emphasizing that the basis of disease is physiological, not supernatural.45 Aristotle, a virtual contemporary of Hippocrates, suggested that the mind was located in the heart and that the only purpose of the brain was to keep the body from overheating by cooling the blood (Klein & Thorne, 2006).
179
knows better, because he understands that, like other physiological diseases,
the ‘sacred disease’ is caused by organic dysfunction. Further, causal
knowledge should be privileged over other kinds of knowledge because one
cannot effectively treat disease without it. By this justification, Hippocrates
defines the ‘sacred disease’ as a physiological phenomenon.46 The tactic of
arguing from definition “is a very persuasive way to stake out expertise, since
it distinguishes what is within the purview of a particular expert from what
is not” (Hartelius, 2011, p. 113). By embedding a causal argument within an
argument from definition, Hippocrates further strengthens his position by
demonstrating that there is a rational basis for privileging the physiological
expertise of a physician over the theological expertise of a faithhealer.
This novel interpretation of reality became part of medicine's origin
myth, giving rise to a rhetorical form that physicians have employed at
various points in history. In the eighteenth century, the many individuals
who displayed multiple personalities “were understood, within the
explanatory paradigms of their era, to be afflicted with the various Judeo
Christian forms of possession, and were approached therapeutically with the
culturallysanctioned JudeoChristian rituals of exorcism” (Kluft, 1993, p.
87). Franz Mesmer challenged this in 1775 by offering the 'scientific'
46 An unfortunate counterpoint to this line of reasoning, which became evident during the socalled ‘witch craze’ in Europe (spanning the fourteenth to seventeenth centuries), is that if a disease does not respond to medical treatment, that might be evidence that the patient is a victim of witchcraft (Barstow, 1995; R. Porter, 1991).
180
explanation that the phenomenon and its apparent treatment by exorcism
were in fact both the result of 'animal magnetism.' Mesmer advocated a new
technique “to cure patients for very high fees by assembling them around a
container filled with magnetized water” (Ellenberger, 1970, p. 186).
Mesmer's theory, connecting physiology and cosmology, was based on a
universal principle of fluid matter, which occupies all space; and that
as all bodies moving in the world, abound with pores, this fluid matter
introduces itself through the interstices and returns backwards and
forwards, flowing through one body by the currents which issue
therefrom to another, as in a magnet, which produces the phenomenon
we call Animal Magnetism. This fluid consists of fire, air, and spirit,
and like all other fluids tends to an equilibrium... Philosophers have
compared the human body to an electrical machine, they have
supposed the arms the conductors, the fingers the pointers, which any
one may experience by trying. Hold the fingers of both hands for some
time towards the patient's pericardium, and you may easily perceive
all the effects of electricity on the invalid's body. (Wonders of animal
magnetism displayed, 1791, pp. 11–13)
The various magnetic treatments worked best on “thin bilious persons of a
sanguine constitution whose nervous system is irritable” (de Veaumore, 1785,
p. vi).
181
By reinterpreting supernatural possession according to humoral theory
(in a modified form: illness was the result of an imbalance of a magnetic fluid
that circulated through the body), Mesmer echoed Hippocrates'
reinterpretation of the 'sacred disease.' Mesmer slightly modernized the idea
by appealing to a recent technological invention, the Leyden jar, a type of
capacitor that had been invented thirty years earlier (Riskin, 2002). With the
simple addition of magnets, a humoral system could simultaneously possess
the glow of the stateoftheart and the mystique of a received esoteric
tradition: The anonymous author of the 1791 treatise I quoted above reports
that he, speaking of himself in the third person, “is one of the few instances of
exception from the general mysterious oath of secrecy; yet he has the
happiness of being fully instructed in this wonderful system, by a professor of
the first rate abilities” (p. 15).
Even though his theory was quickly rejected as physically and
physiologically absurd, Mesmer's appropriation of the Hippocratic drama in
which modern science triumphs over myth and superstition made it
persuasive, and its persuasiveness persisted after its formal rejection.
Followers of Mesmer explained that the efficacy of his treatment was the
result of suggestion, giving birth to hypnosis, in which one is 'mesmerized' (C.
L. Hull, 1929). In this case, a psychological interpretation replaced an earlier
physical, biological etiology for mental illness. Understood as a mysterious
182
form of persuasion, animal magnetism provided a language in which the
dynamics of political revolution could be expressed: Porter (1985) notes that
“the French Revolution begot 'political Mesmerists,' who hoped the waves of
animal magnetism would radiate a politics of peace, liberty, and health” (p.
23).
The association of magnetism and health continues today in the form
of magnetic therapy. An alternative medicine website (through which
various magnetic products are available for purchase) suggests that magnetic
therapy
is recognized as a nonevasive [sic] natural therapy... [Magnets] are
used in hospitals and clinics... Magnetism is the very foundation of life
on earth. The human body has developed over millions of years within
this magnetic field. Our body is “electric,” it resonates within a
frequency range and is constantly being altered by poor diet, injury,
illness, accidents and the effects of electromagnetic fields. Magnet
therapy products can help to readdress [sic] this imbalance by allowing
the body to repair itself, from within. (MAGNETiC, 2007, para. 2–4)
The website (which is a typical example of this kind of discourse) attempts to
build ethos by referencing the use of magnetism in orthodox medicine,
specifically, magnetic resonance imaging (MRI) and transcranial magnetic
stimulation (TMS). We will see this phenomenon again in the next section,
183
which examines the role of humoral rhetoric in 'naturopathic' marketing
appeals.
A more contemporary reappearance of an Hippocratic rhetorical form,
similarly employing an argument from definition that implicitly is backed by
a claim to superior knowledge about cause and effect, appears in the APA’s
official response to legislation proposing to extend prescribing rights to
clinical psychologists:
The American Psychiatric Association deplores [proposed legislation
that would] permit clinical psychologists to prescribe potent
medication… Psychologists have always had a clear path to prescribing
privileges: medical school. No psychologydesigned and administered
crash course in drug prescribing can substitute for the comprehensive
knowledge and skills physicians achieve through medical education
and rigorous clinical experience… We pledge to continue to oppose all
efforts to jeopardize the public health by allowing persons without a
medical education to practice medicine. (Harding, 2002, para. 1–4, my
emphasis)
Then, as now, disciplinary boundary disputes were contests between
competing theories about the causes and remedies of disease. If madness is
caused by the gods, then its treatment should be the domain of priests; if
instead madness is caused by humoral disturbances, then physicians and

184
their remedies should enjoy privileged status.
In accordance with Hippocrates' physiological model, from antiquity
through the beginning of the nineteenth century, physicians believed that
madness (whether presenting with seizures, delirium, sleepwalking, or any
other ‘very violent’ disease of the brain) was a unitary phenomenon
characterized by a total insanity that interfered with every function of the
mind (generally understood to be unitary in substance), a “delirious and
raving state” that robbed one of all awareness, judgment, and free will
(Healy, 1997, p. 29). Madness could manifest as mania, characterized by
frenzied overactivity, or melancholia, characterized by lugubrious
underactivity, but in either case the insane person was completely dissociated
from reality, whether catatonic or maniacal. This entails many conditions
that would not fall today under the domain of psychiatry, e.g., amnesia,
cerebellar ataxia, delirium, dementia, encephalitis, epilepsy, narcolepsy,
peduncular hallucinosis, stroke, stupor, tertiary syphilis, etc. (Fear, Sharp, &
Healy, 1995).
Hippocrates and Galen both left written ‘case’ descriptions of mental
illnesses, a genre of medical rhetoric which has only recently receded in
prominence in the discourses of institutional psychiatry in favor of the
randomized controlled clinical trial, in which an anonymous sample of
patients stands in for a population (Berkenkotter, 2011). These case
185
descriptions superficially resemble modern constructs of mental illnesses,
which enables the modern practice in which disease constructs as we
understand them today are placed into narratives that project them into the
past, so that their modern development appears natural and inevitable
(Healy, 2008). Against the background of ancient and obscure medical
theories, anything resembling something we can make sense of stands out
and is particularly susceptible to anachronistic misreading.
This tendency may be less pronounced with texts not principally
concerned with the techne of medicine. Titus Lucretius Carus, a Roman
philosopher writing some three centuries after Hippocrates (and about two
centuries before Galen), crafted an argument symptomatic of the orientation
toward mental health and the mind engendered by ancient humoral thinking.
In a polemic against the notion of an afterlife, Lucretius describes an acute
state of frenzy (with features of delirium, psychosis, and the ‘sacred disease’)
grounded in an explicitly material understanding of cognition and the mind
as a natural, nonunitary biological object so deeply interconnected with the
rest of the body as to give rise to something resembling a somatoform
disorder:
When… the mind is upset by some more overwhelming fear, we see all
the spirit in every limb upset in sympathy. Sweat and pallor break out
all over the body. Speech grows inarticulate; the voice fails; the eyes
186
grow dim; the ears buzz; the limbs totter. Often we see men actually
drop down because of the terror that has gripped their minds… The
same reasoning proves that mind and spirit are both composed of
matter. We see them propelling the limbs, rousing the body from
sleep, changing the expression of the face and guiding and steering the
whole man – activities that all clearly involve touch, as touch in turn
involves matter. How then can we deny their material nature? …[As]
the body suffers the horrors of disease and the pangs of pain, so we see
the mind stabbed with anguish, grief, and fear… Often enough in the
body’s illness the mind wanders. It raves and babbles distractedly. At
times it drifts on a tide of drowsiness, with drooping eyelids and
nodding head, into a deep and unbroken sleep… Since the mind is
thus invaded by the contagion of disease, you must acknowledge that it
is destructible… Or it may happen that a man is seized with a sudden
spasm of epilepsy before our eyes. He falls as though struck by
lightning and foams at the mouth. He groans and trembles in every
joint. He raves. He contracts his muscles. He writhes. He gasps
convulsively… The cause of the foaming is that the spirit, torn apart
by the violence of the disease throughout the limbs, riots and whips up
spray… The raving occurs because mind and spirit are dislodged and,
as I have explained, split up and scattered this way and that by the
187
same poison [that is, the excess of the offending humor]. Then, when
the cause of the disease has passed its climax and the morbid secretion
of the distempered body has returned to its secret abode, then the man
rises, swaying unsteadily at first, and returns bit by bit to all his
senses and recovers his vital spirit… Conversely, we see that the
mind, like a sick body, can be healed and directed by medicine… When
you embark on an attempt to alter the mind or to direct any other
natural object, it is fair to suppose that you are adding certain parts or
transposing them or subtracting some trifle at any rate from their
sum. But an immortal object will not let its parts be rearranged or
added to, or the least bit drop off… [Spirit] and mind are held in by
the whole body, intermingled through veins and flesh, sinews and
bones, and are… kept together so as to perform the motions that
generate sentience. (Lucretius, 1994, pp. 70–81)
Early modern anxieties about the distinction between body and mind, the
unitary and/or immortal nature of the latter, and the existence of powerful
affective passions within a morally responsible and rationally sovereign
subject all seem absent in the humoral lifeworld as exemplified in this text.
Despite the Epicurean metaphysical orientation that sees reality as
fundamentally composed of indivisible, discrete atomic units, this discourse
consistently stresses continuity—between illness and health, mind and body,
188
mental and physical disease—along with a radical materialism according to
which all mental and physical pathologies share a proximate biological
pathogenesis. This tension appears in the basic structure of the argument
against the immortality of the soul. Though Lucretius and Hippocrates have
very different objectives, both of their arguments depend on establishing an
identity between mental and physical illness. For Lucretius, this equation
provides evidence that the soul or psyche is entirely material, and, because
the material body evidently is destructible, the soul, therefore, is destructible.
The passage begins with an argument by sign, noting the physiological
changes that accompany intense fear or anxiety. Lucretius points to three
binary clusters of signs: skin disturbances with speech disturbances,
dimming eyes with failing voice, and buzzing ears with tottering limbs. Each
pair contains a spiritual component and a somatic component. The first
cluster is external, visibly evident; the second cluster is relational, a
disturbance in the sick patient’s ability to perceive the outer world and in the
outer world's ability to observe the spirit within; the third is internal,
auditory hallucinations and nonresponsive muscles. The body responds this
way to mental anxiety because the spirit (energy animating body and mind)
is upset in ‘sympathy’ with the mind. Galen further developed this basic idea
when he discovered and named the sympathetic nervous system, which he
believed was the medium for vital energy that has become decoupled from the

189
humors. The connection goes both ways: Just as mental anguish can
manifest in somatic form, so too can physical illness produce mental
symptoms.
The same clustering pattern recurs again in the description of the man
seized with epilepsy. Just before this section, Lucretius associates vocal
utterances with mental activity by positioning the mind as the speaking
subject who ‘raves’ and ‘babbles’ during somatic illness. Lucretius then
presents the symptoms of the ‘sacred disease’ in four clusters of voice (a
movement of the mind) with body motion. The man falls and his mouth
foams; groans while his joints tremble; raves as his muscles contract; and
finally, writhes and gasps. When the seizure ends, physical swaying mirrors
the recovery of senses. Physical motion, Lucretius explains, generates
sentience. The explanation of the common causes of mental and somatic
suffering amplifies their verbal association. The man’s spirit, as physical as
mind and body, has been lacerated by the ‘violence’ in the limbs caused by the
poisonous humoral excess, which also splits his psyche (a complex of mind
and spirit). As we shall see, this metaphor—intended literally—is a
conceptual prodrome of the modern disease entity schizophrenia, a loosening
of associations in the psyche accompanied by neurobiological deficits that
imply a splitting of the mind.
Though Lucretius describes the human body in terms of its discrete

190
parts, made all the more discontinuous as they fissure and separate over the
course of the seizure, the force of the argument comes from the contrast
between this disjunction, on one hand, and the greater underlying unity in
substance and action, on the other. This is expressed in a different way in
the argument from definition at the end of the passage. Immortality may be
predicated only of a composite substance that absolutely resists change, i.e.,
addition, subtraction, or rearrangement of its component parts. Because the
mind can be healed by medicine, it cannot have this property. In this form,
the argument seems redundant, because the fact that the mind can become
sick in the first place also proves it is subject to change. But its minor
premise, the similitude between sick body and sick mind, expresses explicitly
what was implied in the copia of mental and somatic symptom clusters.
Understood as a terministic screen, the humoral model overpowers the
atomistic tendency of Epicureanism to direct attention away from the
continuous. Kenneth Burke explains that “there are two kinds of terms:
terms that put things together and terms that take things apart”;
accordingly, “some systems stress the principle of continuity, some the
principle of discontinuity… All terminologies must implicitly or explicitly
embody choices between the principle of continuity and the principle of
discontinuity” (1966, pp. 49–50). This is what distinguishes a categorical
nosology, which emphasizes differences in kind, from a dimensional nosology,
191
which emphasizes differences in degree. In Lucretius' image of wholebody
madness, we can see not only that the humoral terminology stresses
continuity, but that it does so forcefully, perhaps overwhelmingly, relative to
another terminology. The representations of health and disease manifest
this same ratio of continuity to discontinuity that characterizes the rhetorical
assemblage by which they are produced.
Like body and soul, rhetorical models of health and sickness are
mortal. Their direction or alteration occurs by adding to, subtracting from, or
transposing their component parts. But in the process of change, the parts
are conserved. What is added comes from somewhere, and what is
subtracted goes somewhere, and in this sense they achieve a restricted form
of immortality. For most of history, the process of change occurs through the
informal formation of consensus among members of a rhetorical community.
The DSM, with its formal revision process, institutionalizes the consensus
approved rhetorical model and explicitly defines its component parts and
their arrangement. But however a model is changed, its parts live on as
vestiges of the prior unity, carrying with them the model’s unique tropes and
ability to persuade.
Though humoral pathology has been thoroughly discredited and
explicitly rejected by modern medical science, it maintains a powerful
cultural presence to this day. Humoral tropes, logics, and aesthetics

192
continually show up in modern medical rhetoric. ‘Holistic’ and ‘naturopathic’
medicine today is often marketed in the humoral idiom. As we will see in
subsequent chapters—especially in the next chapter's discussion of ‘disease
branding’ and 'preillnesses'—the effective marketing of a new therapy or
treatment modality often must include constructing a health problem that
the new product can treat. This is simply an application of the more general
strategy in deliberative rhetoric to define or frame a problem in a way that
implies the appropriateness of the advocated solution.47 To market vitamins,
herbs, and other ‘nutritional supplements,’ one also must sell a corresponding
model of pathology. This rhetorical situation is constrained, however, by
FDA rules that strictly regulate the marketing of therapeutic agents
“intended to diagnose, treat, cure, or prevent any disease” (Code of Federal
Regulations, 2012). The naturopathic marketer does not need to make such
claims, however, if instead the product is intended to rectify some sort of
imbalance which may, among other things, contribute to some disease. This
presents an interesting opportunity for interdisciplinary collaboration
between lawyers and marketers as they seek to craft a narrative that
includes everything but the illicit therapeutic claim (upon which the entire
advertisement depends). As the FDA does not regulate the use of
47 Nixon’s ‘Vietnamization’ speech, for example, deploys this strategy to great effect, although his creative reading of the historical record was not appreciated by all critics (K. K. Campbell, 1972; Hill, 1972).
193
enthymemes, presumably this is not illegal.48
An example of this tactic appears in the marketing copy of one
nutritional supplement that relies extensively on the rhetorical resources of
humorism, substituting dietary elements and ‘brain chemistry’ for bodily
fluids. The potential consumer/patient is informed that Attention
Deficit/Hyperactivity Disorder (ADHD) is in fact a group of disorders of
“certain mechanisms in the central nervous system,” and that various food
additives, which can “throw off the balance in the chemistry of the brain,”
often are to blame (2013, para. 1–2). The curious logical jump between these
two sentences underscores the enthymematic status of the therapeutic claim:
Researchers have found that a lack of these nutrients to the brain can
cause from minor to serious mental and emotional imbalances, which
are common symptoms in Adult ADHD. Using a liquid form is
preferable here for best absorption. (The Balance You Need, 2013,
para. 4)
The humoral architectonic provides an organizing rhetorical logic that brings
together a disparate constellation of concerns: the preoccupation with
deficiencies, excesses, and balance (particularly of the neurohumoral 'brain
chemistry'); the references to vital life forces; the observation that the
recommended course of action promotes 'health overall'; and the semiotic
48 Disclaimer: This should not be read as legal advice.

194
pairing, both semantically and iconically, of balance and fluid (Figure 3.2).

195
Figure 3.2: Humoral rhetorical appeals in ‘naturopathic’ marketing
Source: (The Balance You Need, 2013).
196
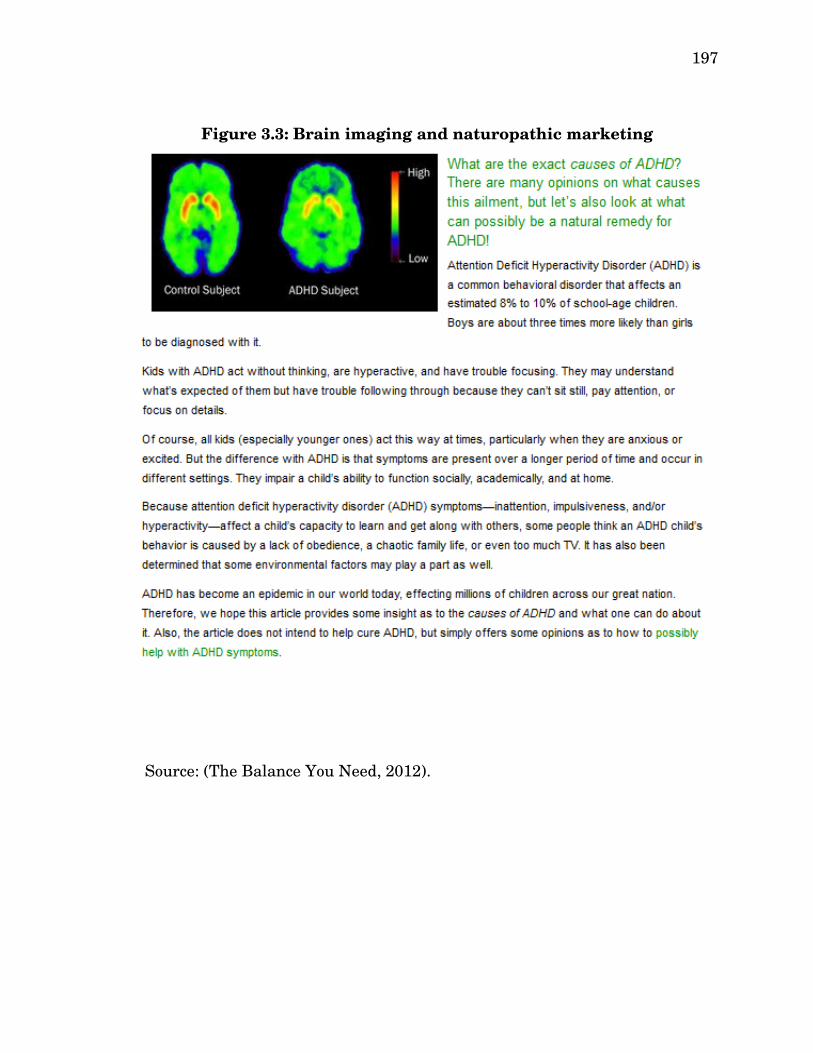
While antimodern tropes about the hazards of technology frequently
appear in naturopathic discourses, it is clear that these discourses have a
catholic nature. Advertisers can incorporate humoralized technoscientific
medical appeals to build credibility. For example, a subpage devoted to
explaining the causes of ADHD contains an image with two sidebyside brain
scans, most likely produced by positron emission tomography (PET) on
subjects who have received injections of radiolabelled raclopride, used to
measure dopamine receptor density (Köhler, Hall, Ögren, & Gawell, 1985;
The Balance You Need, 2012). None of this is explained—indeed, the image
is not even mentioned in passing. The image itself contains no internal
caption or explanation aside from a key by which we can see that certain
areas of the control subject’s brain are variously ‘higher’ and ‘lower’ in some
unspecified respect than the matching areas of the ADHD subject’s brain
(Figure 3.3).
197
Source: (The Balance You Need, 2012).
Figure 3.3: Brain imaging and naturopathic marketing

198
The average member of the public, particularly one who might be
shopping for a ‘natural’ ADHD medicine, probably cannot read PET scans, so
the inclusion of details or some context might not have added anything
meaningful to the message, but with their conspicuous absence the image
clearly must be understood as an enthymeme. This image functions as a
prop that conveys the idea that ADHD is ‘real,’ which is to say a
neurobiological disorder. This was less of a problem when the disorder was
known as 'minimal brain dysfunction' (MBD) or 'minimal brain damage,' a
disease construct based on certain observed similarities between encephalitis
survivors with brain lesions and the wider group of poorly behaved children
(Lakoff, 2000). Physicians diagnosed MBD so frequently that, by the middle
of the 1970s, it had
become an allencompassing, wastebasket diagnosis for any child who
does not quite conform to society's stereotype of normal children...
Children are labeled as such by school psychologists who find
“organicity” on psychological testing or even by teachers who find
certain vague symptoms that they relate to MBD. Labeling troubled
children as having MBD has almost become a national pastime.
(Schmitt, 1975, p. 1313)
Lacking reliable evidence that the disorder was in fact caused by “some
underlying unobservable etiological mechanism in the brain,” and concerned

199
about the stigmatizing effect of labelling children as brain damaged, the
American Psychiatric Association renamed the disorder “attention deficit
disorder (with or without hyperactivity)” in DSMIII and then “attention
deficit hyperactivity disorder” in DSMIIIR (American Psychiatric
Association, 1987, p. 50; Barkley, 2006, p. 8).
If the disorder is nonorganic, parents are less accepting of biological
treatments. This is the attitude that the appeal to brain imaging militates
against. Even though “some people think” that problems with attention and
hyperactivity are caused by bad parenting or television, they are in fact
symptoms of this neurobiological disorder (The Balance You Need, 2012,
para. 5). Additionally, the image reinforces the connection to modern medical
science and its prestige, which makes the website less likely to be read as
quackery. We are also told that the information offered here, which
culminates in a product testimonial for some redacted “liquid organic
product” produced by the also redacted “Company X,” is simply for
educational purposes. Presumably the name of the product ‘Body Balance’
was not included so as to maintain the farcical suggestion that this subpage
of the Body Balance website is for “information purposes only,” though this is
undermined by the fact that the words “liquid organic product” contain a
hyperlink to the main product page. Crucially, nothing on the page is
intended to help anyone treat the medical disorder ADHD, but rather “simply

200
[to] offer some opinions as to how to possibly help with ADHD symptoms.”
Besides recommending the Body Balance product, these opinions also include
the suggestion to perform a “colon cleanse” four times annually; conveniently,
a colon cleansing supplement is also available for sale elsewhere on the
website.49
The discrete disease entity ADHD seems particularly wellsuited to a
humoral reading, given that its defining features are characterized as a
deficiency in ‘attention’ and a surplus of ‘activity.’ Lay explanations of the
supposedly ‘paradoxical’ efficacy of its conventional medical treatment,
psychostimulant therapy—i.e., amphetamine ('Adderall,' 'Dexadrine,'
'Vyvanse'), methamphetamine ('Desoxyn'), or methylphenidate ('Concerta,'
'Focalin,' 'Ritalin')—often resemble the Galenic notion of sympathy.50 This
parallels the biomedical understanding that stimulants are
‘sympathomimetic,’ i.e., capable of arousing the sympathetic nervous system,
increasing blood pressure, body temperature, and heart rate (Grohol, 2012).
Despite universal expert rejection of humoral theory’s scientific validity, its
rhetorical validity depends upon whether potential consumers find such
appeals persuasive. In the world of late capitalism, Body Balance (in liquid
49 Unlike the laundry list of potentially dangerous chemicals—including sugar—that could be the cause of their child’s ADHD, parents are comforted with the incredibly spurious suggestion that “[all] of these products are safe for children since they are all made from plant sources” (The Balance You Need, 2013). 50 The outmoded idea that the therapeutic effect of amphetamine in ADHD is “paradoxical” was first suggested by Bradley (1937).

201
commodity form) can be purchased over the internet. Similarly, the ongoing
suasive force of the therapeutic logic of ‘sympathy’ enables the homeopathy
industry today to market biologically inert placebo remedies to the tune of
more than three billion dollars in annual revenues in the United States alone
(Nahin, Barnes, Stussman, & Bloom, 2009).51 Finally, explanations of the
action of pharmacological agents in terms of ‘sympathy’ (and its inverse,
‘antipathy’) persisted well into the nineteenth century, and physiologists
have retained Galen’s name ‘sympathetic nervous system’ to refer to the
anatomical branch of the autonomic nervous system responsible for
mediating the ‘sympathoadrenal’ (‘fightorflight’) response (Ackerknecht,
1974).
Why did Humorism Succeed?
According to the standards of modern scientific positivism, humorism
is nothing more than pseudoscience, no more legitimate than astrology or
phrenology. It particularly fails the falsifiability criterion, an essential
realitytesting procedure according to which a scientific theory is valid to the
extent that it can make successful predictions (Popper, 1935). It is somewhat
surprising that humorism held sway with the bulk of medical authorities
from the time of Hippocrates through the first part of the nineteenth century.
51 Homeopathy is based on the doctrine proposed by Samuel Hahnemann (1833) that 'like cures like’ – essentially, the theory posits that a substance known to cause a particular symptom can heal that same symptom once it is so severely diluted that not even one molecule of the original substance remains.
202
How is it possible that so few noticed an imbalance between humorism's
theoretical sophistication and its practical failures in developing effective
cures for disease? This was no innocuous form of quackery, merely
promoting harmless absurdities or ineffective but cheap placebos: Many sick
people were given dangerous diaphoretics, laxatives, purgatives, and
diuretics, or needlessly subjected to bloodletting (sometimes with fatal
consequences) in misguided attempts to restore humoral balance. This
mystery can be attributed partly to external causes: persistent confirmation
bias, pervading trust for traditional sources of expert knowledge, and the
fact, as Kuhn (1962) observed, that “once it has achieved the status of
paradigm, a scientific theory is declared invalid only if an alternative
candidate is available to take its place” (p. 77).52 But the primary source of
its suasive persistence, I contend, consists internally in its coherence as an
ideological cultural system (Geertz, 1964). Its preoccupation with
maintaining the proper quantity of each humoral liquid must be understood
in light of the Lacanian dictum concerning the absence of lack in the real—
that is, “every perception of a lack or a surplus (‘not enough of this,’ ‘too much
of that’) always involves a symbolic universe” (Lacan, 1988, p. 313; Žižek,
1994, p. 11, emphasis in original). Humorism has little to no epistemic
52 I say this without necessarily agreeing with Kuhn's idea of how that transition takes place (i.e., revolutionary paradigm shift). See the discussion in the previous chapter on Toulmin's criticism of Kuhn's hypothesis, a criticism which I argue finds considerable support in this study.
203
validity to the extent that its objects of knowledge belong to the order of the
real, but the calculus is much different if its knowledge claims are confined to
symbolic or imaginary objects. Its rhetorical effectiveness as a cultural
system depends upon its ability to obscure this constraint on its referential
capacity while remaining ever faithful to it.
In such cultural systems, the prereflective experience of reality occurs
through, with, and in (recalling the Eucharistic doxology: per ipsum, et cum
ipso, et in ipso) a shared, socially constructed, symbolic order in which
cognitive, normative, and affective registers of meaning are integrated by the
figures of rhetoric into a unitary (perhaps hypostatic) conceptual framework
structured by a grammar of symbols and social facts (Durkheim, 1982; Lévi
Strauss, 1963). The tropes of analogy and metaphor are particularly
important to the overall coherence of a lifeworld conceived in this manner53
because they work structurally to identify the abstract, arbitrary, strange,
and uncertain with the familiar, observable, realitytested, and shared,
providing an underlying basis for common sense, judgments of validity,
legitimation, and persuasiveness. To the extent that distinct bodies of
knowledge—fields like herbalism and nutrition, along with more distant
fields like meteorology and astrology—were integrated into the humoral
symbolic universe, an epistemic ‘multiplier effect’ came into play such that a
53 That is, I am not attempting to be completely faithful to Husserl (1970) in my usage here.
204
modest symbolic outlay may stimulate a great deal of meaning production
mediated through aggregate processes of cultural exchange.54 The mastery of
new knowledge that is epistemically anchored in the humoral symbolic order
serves as a kind of validation of that order (unless the new knowledge turns
out to be a complete flop). Even if the epistemic content of the humoral order
were reduced to mere scholarly custom, this alone might explain its cultural
stability insofar as “the person who does not adapt himself to it is subjected
to both petty and major inconveniences and annoyances as long as the
majority of people he comes in contact with continue to uphold the custom
and conform with it” (Weber, 1978, p. 30). Some annoyances are more
blatant than others; in the sixteenth century, for example, the faculty of
medicine at the University of Leipzig persuaded civil authorities to ban books
written by the medical heretic Paracelsus, whose attempts to overthrow the
traditional humoral orthodoxy often drew comparisons to his contemporary,
Martin Luther (Pagel, 1982). Other inconveniences in the realm of science
communication are more subtle. By failing to use the accepted terminology
and concepts, clarity suffers, there are fewer opportunities for publication or
collaboration, and it becomes more difficult to promote one’s ideas to the
wider public.
54 My aim with this Keynesian subtext is simultaneously to explain and demonstrate (there is an inverse relationship between my success and the degree to which this explanation is necessary) an epistemic process Burke called “verbal ‘atom cracking.’ That is, a word belongs by custom to a certain category—and by rational planning you wrench it loose and metaphorically apply it to a different category” (Burke, 1984a, p. 308).

205
Humorism's robust longevity is thus a testament both to its ubiquitous
embeddedness in other cultural systems (just as, for Lucretius, the psyche
innervates and is embedded in the body), enabling social actors of all levels of
theoretical nuance or expertise to work toward mutual understanding by
means of its symbolic network (reproducing the symbolic order in the
process), and to its casuistic flexibility, i.e., its hermeneutic power to
incorporate and explain a very wide range of phenomena, giving it an
enormous capacity to employ common observations of reality as inventional
resources for encompassing new situations (Burke, 1984a). For example, in
the definitive medical textbook of the medieval period, Avicenna used
humoral concepts to elaborate a theory of “emotional aspects, mental
capacity, moral attitudes, selfawareness, movements and dreams” (Rastogi,
2012, p. 81).55 Similar efforts continued into the twentieth century, notably
including Hans Eysenck’s (1947) fourfactor model of personality in which the
dimensions of extraversion and neuroticism stand in for temperature and
dryness, respectively. Perhaps the epistemic distance between the world of
validated psychometric scales and computerassisted statistical techniques
like orthogonal factor analysis, on one hand, and the 2,500 yearold pre
scientific humoral model, on the other, is smaller than it first seems.
55 Avicenna was also one of the rare few scholars during the medieval period who recognized that both consciousness and behavior are products of organic processes in the brain, and that some somatic symptoms may have psychological explanations (Preul, 1997; Vakili & Gorji, 2006).
206
Why did Humorism Fail?
To explain how humoral pathology eventually came to be rejected, I
would like to extend my earlier analogy between the health of a person and
the health of a model. In cancer, the same physiological processes and
anatomical elements that allowed one to live and thrive become the vehicle of
one’s mortality. In a similar manner, the same features and capacities that
explain the persistence of humorism also facilitated the model’s rhetorical
fragmentation and downfall. The persistence of humorism was due in part to
its capacity for doctrinal development, enabling it to accommodate, explain,
or otherwise account for new, seemingly inconsistent, discoveries. As the
model was challenged by new empirical observations and material social
practices, its adaption process became disordered, leading to an
uncontrollable heterogeneous complexification. Its widespread cultural and
epistemic integration required that the model’s growth be even and
consistent so that changes could diffuse into the general body of social
knowledge. Theoretical developments provoked by different challenges
became inconsistent, slowly splitting the humoral psyche, leading to its
progressive epistemic deterioration.
The serendipitous discovery by Catholic missionaries in 1630 that a
bitter substance in the bark of the cinchona tree, called quinine, can treat
effectively the high fever associated with malaria (from the Italian mala aria,

207
‘bad air,’ once thought to be its source) is one significant example of the kind
of challenges the humoral order faced. At the time, medical authorities
believed that all fevers resulted from an excess of bile, which was thought to
cause fermentation in the blood, for which the (rather ineffective) treatments
of bleeding and purging were indicated.56 Making matters more confusing,
the apparently effective extract is a dry powder derived from a tree native to
the hot climate of Peru. One might expect such a substance to amplify,
rather than ameliorate, the suffering brought about by a surplus of the
quintessentially hot and dry humor. As it turned out, according to leading
seventeenthcentury authorities in humoral medicine, the socalled ‘Jesuit’s
Powder’ stimulated the flow of bilious secretions through the nervous system,
an example of the phenomenon Galen called ‘sympathy,’ which effected a
cure by pushing the malarial fever to its conclusion (Berdoe, 2006).
The plot further thickened when it was discovered that quinine’s
therapeutic efficacy was specific, limited to fevers associated with the discrete
disease entity malaria. Why shouldn’t the same sympathetic process resolve
other forms of fever? Is the category of ‘discrete disease entity’ part of a larger
category that also includes pathology conforming to the old unitary disease
concept, or does this new category conceptually replace the old? Both
56 The new treatment’s effectiveness relative to the then current standard of care was sufficiently impressive that its advocates were able to overcome widespread antiCatholic persecutory delusions that quinine was the first phase of some “Popish plot” against the Protestant nations (Rocco, 2004, p. 103).

208
possibilities would raise new, difficult questions. Left unanswered, these
questions threatened the humoral order with legitimation crisis just as other
historical social forces seemed to be aligning against orthodoxy in general
(e.g., widespread and frequently violent religious partisanship; sweeping
changes in society’s mode of production associated with industrialization;
mass dissatisfaction with the institutions of aristocracy and monarchy;
exposure to new cultural forms of knowledge about health and remedies
associated with the Age of Exploration; an intellectual climate associated
with the Enlightenment that favored radical breaks with tradition, etc.).
Remarkably, the humoral symbolic order managed to avert the crisis
and preserve its hegemonic cultural position by successfully performing the
ideological functions of “hiding real contradictions and of reconstituting on an
imaginary level a relatively coherent discourse which serves as the horizon
of… experience” (Poulantzas, 1973, p. 207). In doing so, however, it
sustained serious damage, as the necessary legitimating discourses and
conceptual elaborations were “[reminiscent] of the epicycles used by
astronomers to explain variances within the Ptolemaic universe… [and
which] did not so much overthrow the wobbling paradigm of Galenic humoral
concepts as they supported the ancient edifice with more ‘modern’ knowledge”
(Haller, 1994, p. 18, my emphasis). The epistemic disorder was not cured; it
was simply in remission. Haller’s metaphorical characterization of the order
209
as ‘wobbling’ is particularly insightful because it highlights the degree to
which humoral theory was out of balance, in total variance with its own
ultimate values. The humoral order did not so much neutralize the external
substantive contradiction between theory and observation as transform it
into an internal performative contradiction entailed in the imbalanced and
fragmented form in which the values of balance and unity were defended as
ultimate terms. The first contradiction was constituted by a rupture between
the registers of the Symbolic and the Real; the second contradiction
represented a conflict entirely within the Symbolic, “between a meaning
conveyed explicitly and a meaning conveyed by the act itself of conveying” (D.
Turner, 1983, p. 26).
The hegemonic grip of humorism on the institution of medicine began
to recede as a result not of theoretical development, but rather of changes in
material productive practices and relationships; in other words, base
determined superstructure (Marx, 1904). A vast market existed for new
treatments, including herbs discovered in recently colonized parts of the
world, as well as the purified chemicals and metals promoted by Paracelsus
(1657). These highly profitable treatments could be rendered intelligible only
retrospectively, as medical treatments within the humoral framework.
Medical theory thus “followed the money” (Healy, 2008, p. 15). As more and
more of these treatments were adopted, the medical literature gradually
210
became less focused on pure theory and more interested in empirical
observations (Maehle, 1999). The genre of the ‘case history’ as a medical
topos reappeared. As I shall demonstrate later, the prevalence and emphasis
of the ‘case history’ in medical rhetoric as a ‘place’ to look for substantiating
evidence at any given time can be seen as a barometer of tension between
medical theory and practice. Appeals to the case are relatively more
persuasive to an audience suspicious of the available theoretical paradigm;
their suppression is a rhetorical move made by defenders of an orthodoxy, as
when the editorial board of the American Journal of Psychiatry, following the
promulgation of the new DSMIII nosology, decreed that “single case reports
should be published as Letters to the Editor rather than as Clinical Research
Reports” (Edelson, 1985; “Single Case Reports,” 1984, p. 852).
The ascent of appeals to the case rather than to humoral theory
pointed to the discontinuous nature of disease. From the drama concerning
the introduction of quinine, we can see that a radical discovery alone is
insufficient to bring about a change in intellectual order. Before the
introduction of a powerful new architectonic, the old regime of knowledge
must be delegitimized:
The real revolution in medicine, which set the stage for antibiotics and
whatever else we have in the way of effective therapy today… did not
begin with the introduction of science into medicine. That came years
211
later. Like a good many revolutions, this one began with the
destruction of dogma. It was discovered, sometime in the 1830s, that
the greater part of medicine was nonsense. (Thomas, 1995, p. 159)
How was this aporia achieved? The cacophonous proliferation of cases was
coupled with emerging technologies that facilitated novel ways of ‘seeing’ the
signs of illness, both in human patients and in the old theoretical orthodoxy.
Physicians had long had the ability to look inside the bodies of individuals
postmortem (though were often prohibited from doing so by religious
authorities), but the microscope, the stethoscope, and the practice of histology
opened up a whole new vista of morbidity, “[plunging] the gaze of the
doctor… into the interior of the body,” a shifting of horizon that would be
repeated again in the twentieth century, when new genetic and statistical
techniques allowed scientists to ‘see’ in populations a new array of
pathological objects (Hacking, 1975; Hedgecoe & Martin, 2008; N. S. Rose,
2007, p. 193). A new perceptive technology can show the continuous to be
discontinuous and visaversa, potentially producing terministic rupture,
“since all laboratory instruments of measurements and observation are
devices invented by the symbolusing animal, [and thus] they too necessarily
give interpretations in terms of either continuity or discontinuity” (Burke,
1966, p. 49). Novel technological modes of observation not only enables new
objects of knowledge to be seen, but also reveal the contradictions,
212
limitations, and absurdities of the old theoretical orthodoxy (Hogle, 2008).
The Rise of Scientific Medicine
Like water coming to a boil that is preceded by rising bubbles, this
sudden and dramatic revolution in the nineteenth century was preceded by
nascent microconfigurations of knowledge. These epistemic fragments were
not full models of pathology but, rather, terministic sonograms through
which one can glimpse the modern concept of disease in an embryonic stage.
Two of these emergent frameworks, one emphasizing discontinuity and the
other continuity, were of particular importance: an ‘ontological interpretation’
of disease, and a ‘physiological interpretation’ of disease (KräuplTaylor,
1982). According to the ontological interpretation, the vista of pathology is
subdivided into discrete disease entities that are distinct from the signs and
symptoms revealing their presence. The physiological interpretation instead
focuses on morbid processes as they manifest in the body. Both
interpretations provided important insights necessary for the development of
modern medical science. As medicine moved dialectically from one
interpretation to the other, the conceptual integrity of humoral concepts
became strained, and with each new rearticulation, shifts in meaning were
accompanied by the introduction of emerging modern concepts. Many ideas
and concepts that would become central to modern medical science emerged
centuries before their time, but in combination with archaic vestiges of the
213
old order. These concepts were sometimes discarded or remixed into new
discursive assemblages before being taken up in modern form.
The Ontological Interpretation
Thomas Sydenham (1682), who was heavily influenced by the findings
about quinine and the putative disease entity ‘malaria,’ as well as by the
Methodist school of biological classification that began with Italian physician
and botanist Andrea Caesalpino (1583), made an articulate case for an
“ontological view of disease… [affirming] the existence of natural and
unwavering disease entities, separable from the person, and whose
presentation was uniform across sufferers” (Boyle, 1990, p. 8). In no small
part due to his novel ontological approach to pathology, Sydenham, the so
called “English Hippocrates” (Noll, 2007, p. x), contributed greatly to
medicine. Before Sydenham, many medical authorities had a difficult time
grasping the idea of a discrete disease entity, conflating it with a discrete
disease expression. An illness state involving several distinct symptoms
implied a holistic pathology, especially in the absence of any distinctive
pathological features (e.g., Koplik spots, uniquely characteristic of measles).
Sydenham’s approach to nosology was built around the “presupposition that
clinical findings fall into easily identifiable constellations of signs and
symptoms that can be recognized through their natural histories” (Cutter,
2003, p. 37). Avicenna had hinted at the concept of syndrome (unaltered from

214
the Greek syndromē [ μ ], meaningσυνδρο ή a disorderly crowd running
together), but Sydenham explicitly articulated and significantly developed it
(Millon, 2004).57 The basic idea is that, by closely observing a large number
of patients and keeping precise records of their cooccurring pathological
characteristics, it is possible to identify distinctive forms of disease that share
a common set of causes and, presumably, should respond to the same
treatment (as with malaria and quinine) (Blashfield, 1984).
Sydenham’s views caught on in part because they were popular with
physicians who, transformed into scientists by his revolutionary
methodology, were eager to take up the important job of systematically
recording the wide range of elements that work together to produce the
disease processes in their patients (Boyle, 1990). This shift in medical
research and training resulted in new institutional and professional norms
emphasizing careful, detailed clinical observations (KräuplTaylor, 1979).
These developments prompted a biopolitical reading of the Hippocratic
corpus. Sydenham collected data on major disease outbreaks in London from
16611675 and detected an association between specific syndromes and the
time of year, providing empirical support for an ancient hypothesis, revived
by his contemporary, Robert Boyle, that the seasons (relating to the humors) 57 Having worked out a synthesis of Galenic medicine and the Stoic theory of signs, Avicenna proceeded “to schematize a conditional with multiple antecedents and a common consequent: ‘If this man has a chronic fever, hard cough, labored breathing, shooting pains, and rasping pulse, he has pleurisy.’ Here Avicenna lays a groundwork for the idea of a syndrome as he pioneers in the diagnosis of a specific disease” (Goodman, 2003, p. 155).

215
were epidemiologically significant (D. Porter, 1998).58 The idea of studying
populations to identify risk factors for disease influenced the development in
the following century of an emergent mode of governance involving “the
dramatic expansion in the scope of government, featuring an increase in the
number and size of the governmental calculation mechanisms” (A. Hunt &
Wickham, 1994, p. 76).
As distinctive as Sydenham’s position was, he did not abandon
humorism, routinely resorting to humoral explanations whenever necessary,
particularly for acute conditions that, he posited, often resulted from
atmospheric ‘miasmata’ disturbing the humors (KräuplTaylor, 1979).
Though the discrete disease entity represented a distinct move away from
holistic pathology, Sydenham believed its manifestation as a syndromal
complex pointed to a multifactorial etiology and pathogenesis, with multiple
simultaneous influences acting on a patient and influencing the course of the
morbid process (KräuplTaylor, 1982). Neither an imbalance in the humors,
an invasion of a pathogen (i.e., some inorganic corpuscular substance
originating underground), a distressing life event, nor any other lone
stimulus was sufficient to trigger the onset of an illness, though each could
contribute to one’s susceptibility. Similarly, though the outbreak of
epidemics eluded reliable prediction, he identified several risk factors he
58 The term ‘epidemiology’ first appeared a little more than a century later in Joaquín de Villalba’s (1802) Epidemilogía Española.

216
believed to be significant: excessive humidity or dryness, extremely cold or
hot temperatures, and the presence of “vapors” emanating from “the inward
bowels of the earth” (cited by Dewhurst, 1966, pp. 66–67).
Evolution of Hysteria
These neoHippocratic sources of disease were discarded by subsequent
physicians, only to be rearticulated less than a hundred years later in slightly
revised form. The principles of modern chemistry were applied to the old
humoral framework, fusing moral judgment and somatic pathology within
vaporous imagery:
[In] acid vapors the particles are mobile, and even incapable of rest,
but their activity is weak, without effect; when they are distilled,
nothing remains in the alembic but an insipid phlegm… [One] would
consider the vapors that rise from the blood to the brain and that have
degenerated into an acid and corrosive vapor… [to be] a chemistry of
the humors. …Certain particularly volatile animal spirits are alkaline
salts that move with great speed and transform themselves into vapors
when they become too tenuous; but there are other vapors that are
volatized acids; the ether gives these latter enough movement to carry
them to the brain and the nerves where, ‘encountering the alkalis, they
cause infinite ills.’ Strange, the qualitative instability of these
[vaporous] illnesses; strange, the confusion of their dynamic properties
217
and the secret nature of their chemistry! …The space in which [the
vaporous] assumed its dimensions was…that of the body, in the
coherence of its organic values and its moral values. (Foucault, 2001,
pp. 122, 142–143)
Just as the people of London in Sydenham’s time suffered from an epidemic
brought on by vapors from deep underground, many wealthy and urbane
women living in Paris suffered from an epidemic brought on by vapors that
emanated from their own inward bowels (or furor uterinus, an agitated
womb):
For more than a century, the vapors have been endemic in large cities;
most women who take pleasure in the comforts of life are vaporous,
and one might say that they purchase a series of languid infirmities
with the vast riches that they so enjoy.59 (Raulin, 1758, p. viii, my
translation)
Men were less often afflicted, but when they were it was usually their fault
as well: “Men become vaporous just like women when their nerves lose their
natural firmness;60 it sometimes happens that they were born with their
feeble temperaments, but more often than not they become weak through
acts of debauchery, exhaustion, idleness, mental strain, etc.” (Raulin, 1758, p. 59 “Il y a déja plus d'un siécle que les vapeurs sont endémiques dans les grandes Villes; la plupart des femmes qui jouissent des commodités de la vie sont vaporeuses, on peut dire qu'elles achetent par un suite de langueurs l'agrément des richesses” (Raulin, 1758, p. viii).60 Not just their nerves, as the vapors usually brought on impotency in these effete men (Vila, 1998).
218
42, my translation).61
Some commentators suggested that this epidemic was a form of
disease unique to capitalist modernity: “We have few good books on the
vaporous diseases…[and] the reason is simple; it is that these diseases are
new, their progress having followed that of the vast population of Paris and
its heart of luxury” (Beauchêne, 1783, pp. 8–9, my translation).62 Others
linked the outbreak to older disease states (e.g., melancholia, hysteria), while
still emphasizing its novel epidemic status:
Melancholy is not exactly a new disease, but in no other century was it
so widespread, nor did it have the same level of intensity; thus we can
look at it as a new plague. It is necessary to bring all efforts to destroy
it, as was done successfully for venereal diseases. (Bressy, 1789, pp. ii–
iii, my translation)63
All agreed that this was a bourgeois ‘plague,’ afflicting women whose “mode
of life [was seen by] physicians…as overrefined and soft,” as well as
effeminate men “who had ‘degenerated’ to a similarly delicate temperament”
61 “Les hommes deviennent vaporeux tout comme les femmes lorsque leurs nerfs perdent leur fermeté naturelle; il arrive quelquefois qu'ils sont foibles par une suite du temperament, mais ils le deviennent le plus souvent par la débauche, par l'épuisement, par l'oisiveté, par la contention d'esprit, etc.” (Raulin, 1758, p. 42).62 “On a peu de bons livres sur les maladies vaporeuses… La raison en est simple, c'est que ces maladies sont nouvelles; leurs progres ont suivi coeur du luxe, ceux de l'immense population de Paris” (Beauchêne, 1783, pp. 8–9).63 “La mélancolie n'est pas précisément une maladie nouvelle, mais dans aucun siècle n'avoit été aussi général, & n'avoit eu autant d'intensité; de maniere qu'on peut la regarder comme un fléau nouveau: il faut donc réunir tous les efforts pour l'anéantir, comme on le fait avec succès pour les affections vénériennes” (Bressy, 1789, pp. ii–iii).
219
(Vila, 1998, p. 229). The couches of the Victorian era were designed with the
vaporous woman in mind, as even the slightest stimulus could cause her to
become faint, overwhelmed with emotion; other prominent symptoms
included “edema or hyperemia, …nervousness, insomnia, sensations of
heaviness in the abdomen, muscle spasms, shortness of breath, loss of
appetite for food or sex with the approved male partner, and [a general]
tendency to cause trouble for others” (Maines, 2001, p. 23).
The connection between Sydenham and the pathologically feminine
Parisians of the eighteenth and nineteenth centuries goes far beyond the
suggestion that vapors (of some sort) cause illness. The eighteenth century
vaporous diseases were based on a syndrome Sydenham identified as
hysteria in the seventeenth century, a name it would regain in the nineteenth
century as a focal point of study for JeanMartin Charcot, Pierre Janet, and
Sigmund Freud (Breuer & Freud, 2000; Charcot, 1971; Janet, 1920).
Hysteria is as old as Western medicine itself, but Sydenham was the first to
conceive of hysteria as a disease of the mind (Bronfen, 1998). The
conventional wisdom in 1600 was that it was caused by a malpositioned
womb (Rousseau, 1993). The name ‘hysteria’ comes from the Greek word for
uterus, hystera ( ).ὑστέρα The Hippocratic corpus lists a variety of symptoms
thought to be related to the movements of an excessively dry womb. Sexual
intercourse, in order to add moisture to the womb, was the recommended
220
treatment: Nubat illa et morbus effugiet, ‘let her marry and the disease shall
disappear’ (Kerber, 2005, p. 275, my translation; King, 1993).
Sydenham’s (1682) careful study (particularly his observation that
men and women equally exhibited the constellation of hysterical symptoms)
led him to believe that the problem was not in the womb, but rather in the
brain.64 Nevertheless, the concept could not escape its gendered roots, and
has invited feminist readings, according to which the hysterical women of the
nineteenth century “epitomize universal female oppression” (Showalter, 1998,
p. 10). On the other hand, Herndl (1988) suggested that hysteria “has come
to figure a sort of rudimentary feminism and feminism a kind of articulate
hysteria” (p. 54). The tensions and ambivalences entailed in gendered
diagnoses recur, for example, in the DSM5 diagnoses of compulsive buying
disorder (CBD) and premenstrual dysphoric disorder (PMDD), which some
suggest present women as irrational, with poor impulse control and monthly
episodes of emotional instability (Saedi, 2012).
Sydenham noted that hysteria (understood metaphysically as an
independent disease entity) could simulate the symptoms of several organic
diseases, e.g., convulsions, heart palpitations related to anxiety, paralysis
64 Nevertheless, as we have already seen, the ‘wandering womb’ hypothesis persisted in one form or another through the twentieth century, and directly led to the invention of the vibrator, which began as a device used by physicians to administer socalled ‘medical massage’ (designed to induce ‘hysterical paroxysm,’ a euphemism for orgasm), a standard treatment for hysteria and several eating disorders still common as late as the 1920s (Maines, 2001).
221
similar to that produced by stroke, and unexplained pain similar to kidney
stones. The ontological assumptions that the same symptoms could have
different causes and that the same cause could present with different
symptoms enabled Sydenham to identify and catalogue the various forms of
this disorder as had never been done before (Schneck, 1957). Sydenham
focused less on individual symptoms than the overall syndromal complex,
and his ontological interpretation of disease allowed him to distinguish
between the symptoms and the disorder. Before Sydenham, a physician
observing one case of syncope caused by orthostatic hypotension and another
case of hysterical fainting would not have been able meaningfully to
distinguish between the two manifestations of illness. A recent encomium
testifies to the prescience of Sydenham’s clinical pictures of hysterical
syndromes, and more broadly to the enduring significance and influence of
Sydenham’s approach on contemporary nosological debate in psychiatry:
The careful and systematic manner of his descriptions of hysterical
phenomena was so comprehensive that little can be added today to
what he said three centuries ago. He recognized that hysteria was
among the most common chronic diseases, and… he also suggested
that differential diagnosis between real biological diseases and those
generated by the mind could only be made if the patient’s psychological
state could be thoroughly known. He was among the most successful

222
in illustrating that emotions can generate and simulate physical
disorders. In his efforts to formulate a syndromal pattern for
numerous disorders, he extended the range of his observations to
include not only the patient’s dispositions, emotions, and defenses, but
the family context within which they arose… [in order] to determine
the overall pathogenesis of certain syndromes, largely through the use
of both physical and psychological phenomena. (Millon & Simonsen,
2010, p. 23)
Hence, the concept of vaporous diseases that appeared after Sydenham was a
throwback to a previous era, leading physicians away from the psychogenic
nature of hysteria.
Charcot was less than prescient when he wrote in an 1888 letter to
Freud: “Rest assured, hysteria is coming along, and one day it will occupy
gloriously the important place it deserves in the sun” (cited by Micale, 1993,
p. 496). Nonetheless, the syndrome once associated with the signifier
‘hysteria’ is still a source of diagnostic controversy, and the array of issues
currently under discussion was almost entirely anticipated by Sydenham in
the seventeenth century. There is certainly some truth to Guillain’s (1949)
suggestion that “in reality, the patients have not changed since the time of
Charcot—only the words used to describe them have changed” (p. 147, my

223
translation).65 In the DSMIV and ICD10 nosologies, hysteria is known as
‘conversion disorder’ (classed with the somatoform disorders in the former
and with the dissociative disorders in the later), and is characterized by
“unexplained” symptoms such as (nonepileptic) seizures, unusual
movements, fainting, weakness, and sensory disturbances. While the
symptoms “suggest a neurological or other general medical condition,” in fact
“psychological factors are judged to be associated with the symptoms or
deficits” (American Psychiatric Association, 1994, p. 445). Diagnosis requires
a “thorough medical investigation… to rule out an etiologically neurological
or general medical condition,” as the symptoms of conversion disorder
“typically do not conform to known anatomical pathways and physiological
mechanisms, but instead follow the individual’s conceptualization of a
condition” (1994, sec. 300.11).
The name ‘conversion disorder’ itself refers to the basic hypothesis that
the symbolic resolution of unconscious psychological conflicts can manifest
somatically—in other words, a psychological conflict that cannot be resolved
consciously is ‘converted’ into a complex of physical symptoms (Nicholson &
Kanaan, 2009). The DSM5 Somatic Symptom Disorders Workgroup
65 “Ces malades étaient exactement les mêmes que ceux qui se présentaient aux consultations du temps de Charcot. En réalité, les malades n'ont pas changé depuis Charcot, ce sont les mots pour les désigner qui ont changé” (Guillain, 1949, p. 147). The claim is certainly not absolutely true; patients can and do change, sometimes even because of changes in the words used to describe them. Obviously bored wealthy housewives no longer need fainting couches to make it through the day.
224
recommended that the disorder be renamed ‘functional neurological disorder’
(American Psychiatric Association, 2011b).66 Apparently, the name
‘conversion disorder’ is too closely associated with the old psychoanalytic
heresy:
Although long dominant, the conversion hypothesis… has little
supportive empirical evidence. Even the notion that the etiology of
these symptoms is wholly psychological may be scientifically incorrect.
For example, functional brain imaging studies showing findings such
as contralateral thalamic hypoactivity in hemisensory conversion
encourage us to understand conversion symptoms from a brain as well
as a mind perspective… [The] name “conversion disorder” has not been
widely accepted by either nonpsychiatrists or patients. We therefore
need a name that sidesteps an unhelpful brain/mind dichotomy… For
the majority of patients psychological factors can be identified, but not
for all… In practice, conversion disorder is usually diagnosed after a
neurologist has identified a symptom as “nonorganic” because of
66 The final name of this disorder was “still under active discussion” as of the time that the APA made the draft revisions unavailable in anticipation of the imminent publication of the new edition (American Psychiatric Association, 2011b). In the final draft, as an apparent compromise, the disorder was named “Conversion disorder (functional neurological symptom disorder)” (American Psychiatric Association, 2013, p. 318). According to the explanation of the disorder's diagnostic features: “Many clinicians use the alternative names of 'functional' (referring to abnormal central nervous system function) or 'psychogenic' (referring to an assumed etiology) to describe the symptoms of conversion disorder (functional neurological symptom disorder)” (p. 319). It is unclear why the authors believe that the suggestion that the disorder is caused by “abnormal central nervous system function” is less “etiological” than the suggestion that the disorder is “psychogenic.”
225
clinical findings of incongruity with disease or internal consistency…
[We] suggest that conversion disorder be renamed “functional
neurological disorder” and that the requirement for the exclusion of
feigning and identification of associated psychological factors be
relegated to the accompanying text... Together these changes have the
potential to foster collaboration between psychiatrists and
neurologists. (J. Stone, LaFrance, Levenson, & Sharpe, 2010, pp. 626–
627)
A few brief observations about this official line of reasoning are in order. The
authors take for granted that ‘psychological’ phenomena are nonorganic, as
if the activities of the mind could be wholly independent of the activities of
the brain. Otherwise, the observation that ‘functional brain imaging studies’
show activity of some sort in the brains of patients with conversion disorder
could not serve to refute the claim that the etiology of the symptoms is
“wholly psychological.” This is a vulgar strawperson argument—not even
René Descartes, and most certainly not Freud, would accept the premise that
some “wholly psychological” phenomenon could occur without any
corresponding material/organic activity.67 This reasoning mistake means
that, instead of seeking to elucidate the neurobiological basis of psychological
phenomena, this hypermaterial turn is made seemingly for its own sake.
67 The positions of Descartes and Freud on this matter are discussed in greater detail below.
226
The irony in the subsequent comment concerning the need to sidestep an
“unhelpful brain/mind dichotomy” is almost overwhelming. Over against the
approach of DSM5, Sydenham had strongly resisted the urge to reduce the
syndromal complex to either organic or psychological morbid processes
(Schneck, 1957).
The concern for the patients’ acceptance of the diagnosis is interesting,
although, if the ‘conversion’ hypothesis is correct, attempts to over
accommodate the patients in this regard may be antitherapeutic, as the
incidence of hysteria dramatically declined once the conversion hypothesis
became well known to the public (Micale, 1993). There are many ways to
interpret this finding, but the most parsimonious is that a population is less
vulnerable to hysteria when the latter is understood in psychodynamic terms
than when it is commonly believed to be a neurological disorder. Finally, it is
somewhat strange that a neurologist's failure to discover a neurological
problem would be a defining characteristic of a ‘neurological disorder,’
functional or otherwise.68 In any event, the various twists and turns through
which ‘hysterical affection’ has been ‘converted’ into a neurofunctional
disorder were possible only because of Sydenham’s careful studies, and
though the DSM5 approach rejects a strict ontological interpretation
68 The authors also suggest that the name ‘functional neurological disorder’ would constitute a “return to an older terminology” (p. 626). As evidence for this claim, they cite Wessely, Nimnuan, and Sharpe (1999), who indeed use this terminology, which, they contend, is a better way to discuss the symptoms of conversion disorder and other somatoform disorders. Given the context, the referent for the comparative word ‘older’ is very unclear.
227
pointing toward some vague ineffable physiology, the differences between
Sydenham’s hysteria and the contemporary form are more cosmetic than
substantive.69
The Physiological Interpretation
Why did the seventeenth century mental illness of hysteria change into
a collection of neurological vaporous diseases in the eighteenth century?
There were many factors, but perhaps most important was a growing interest
in and understanding of functional physiological processes that resulted from
the introduction of scientific methodology to medicine. The material practices
that Sydenham inspired gave rise to a terministic screen focused on morbid
physiological processes. A physiological interpretation of pathology appealed
to the postmetaphysical sensibility of the Enlightenment, expressed
famously in 1748 by David Hume:
If we take in our hand any volume; of divinity or school metaphysics,
for instance; let us ask, Does it contain any abstract reasoning
concerning quantity or number? No. Does it contain any experimental
reasoning concerning matter of fact and existence? No. Commit it then
to the flames: for it can contain nothing but sophistry and illusion.
(Hume, 1993, p. 114, emphasis in the original)
69 The biggest difference between Sydenham’s clinical picture and those represented in DSMIV and ICD10 is that Sydenham also included hypochondriasis and melancholia as clinical forms of the hysterical syndrome (Dewhurst, 1966).

228
Ontological interpretations in general were no longer in vogue with the
intelligentsia by the eighteenth century. Thirteen years after Hume
published his Enquiry concerning human understanding, Giovanni Morgagni,
now regarded as the father of anatomical pathology, identified lesions in the
organs, rather than humoral imbalance, as the cause of disease (Morgagni,
1903). In 1761, he published his pathbreaking text De sedibus et causis
morborum, in which he aggregated the physiological data extant in the
literature along with the anatomical observations he and his teacher, Antonio
Valsalva had made in the preceding decades.70 Its publication revolutionized
medicine: By placing anatomy at the foundation of general pathology,
“medicine was elevated to the rank of a natural science” (Virchow, 1958a, p.
178).
In 1858, less than a century later, after cataloging the various kinds of
tissue and their cellular natures, Rudolph Virchow delivered a series of
famous lectures in which he established a new model of disease based on
cellular pathology that quickly became dominant within the new modern
institution of clinical medicine (Turk, 1993). In his early days, Virchow
explicitly rejected the ontological view of disease in favor of a physiological
conception. According to this essentially nominalist view, diseases do not 70 Antonio Valsalva, a physician and anatomist from Bologna whose research predominately focused on the ear, is known today for inventing the ‘Valsalva maneuver’ whereby with a closed mouth and a pinched nose one attempts to exhale in order to equalize the pressure between the ears and sinuses, a technique commonly performed today by divers and airplane passengers.

229
exist independently, but, rather, subsist in dysfunctional bodily processes.
The old humoral model was essentially physiological, though not scientific.
Instead of seeing discrete disease entities with their own unique course and
treatment, a physiologist sees somatic processes that deviate from the norm,
lying in a continuous spectrum from healthy to diseased. For the 26yearold
Virchow, seeking in 1847 to define ‘scientific medicine,’ disease entities are
“neither selfsubsistent, circumscribed, autonomous organisms, nor entities
which have forced their way into the body, nor parasites rooted on it, but…
[rather] they represent only the course of physiological phenomena under
altered conditions” (Virchow, 1958b, p. 26). When he reached the age of 73,
however, Virchow felt less of a need to militate against ontological readings of
his cellular model:
Aside from cells, there are no histogenetic or organopoietic substances.
This conception is expressly ontological. That is its merit, not its
deficiency. There is in actuality an ens morbi [disease entity], just as
there is an ens vitae [living entity]; in both instances a cell or cell
complex has the claim to be thus designated. (Virchow, 1958a, p. 207)
Essentially, then, Virchow read realism into the nominalist ontological
interpretation. Discrete disease entities exist and are coequal with
physiological disordered processes.
To understand how Virchow was able to advance these seemingly

230
contradictory positions about pathology, one must take note of his ultimate
driving concern, precisely the same concern held by the developers of DSM5:
the development of a conceptual framework of pathology best suited to “pave
the way for muchneeded scientific progress” (Hyman, 2011, p. 5). If disease
is understood ontologically, where is it located and what is its nature? The
elder Virchow in 1895 drew a connection between serum therapy (in which a
serum from an immunized animal is used to treat a disease) and the old
humoral model:
Enthusiasts see here a final triumph of humoral pathology, although a
humoral pathology quite different from any preceding it. The old
humoral pathology cannot come into question at all, but only one of the
later forms—hematopathology [i.e., a branch of cellular pathology that
focuses on hematopoietic cells, which originate in bone marrow and
give rise to red and white blood cells and platelets], to be precise… The
doctrine of putrid infections (septicemia) had gradually passed over
into general knowledge; everyone assumed that putrescent substances
exerted a harmful effect and sometimes caused new putrefactive
processes in the body. But no one had the right to conclude from this
doctrine that the tissues of the body—let us say the cells for brevity—
could be disregarded, and that a putrid infection was nothing more
than an abnormal condition of the blood. The blood only contains the

231
causes of the tissue disturbance; the disease is not the blood, but is
rather the effect of the cause on the cells or tissues. (1958a, p. 213)
The humoral (functional) pathology had located disease in the fluids of the
body, while the anatomical (ontological) pathology had located disease in the
body’s solid parts. The physical properties of solidity and fluidity seem to
stand in respectively for the concrete discontinuity of the ontological
perspective and the dynamic continuity of the physiological perspective.
Virchow reconciled these conflicting views by first locating life within
the cell, composed of solid organelles immersed in cytoplasmic fluid and
surrounded by a membrane. The cell is thus the scene of a biological drama
in which cellular components are agents engaging in the various acts that
constitute and sustain life. Its entelic ‘purpose,’ understood as an
Aristotelian final cause, is to continue living, and thus the acts must proceed
in an orderly fashion consistent with the ‘normal’ vital mode of operation for
a cell of its type. When, for whatever reason, the dynamic cellular processes
or structures of the cell deviate from this norm, that deviation constitutes
disease. Disease is directly identified with the disordered cell, rather than
depicted as a pattern of various signs and symptoms. Instead of ‘tobacco
smoking syndrome,’ we have a cancerous lung. Though it becomes a bit more
complicated when applied to behavior rather than apparent cellular
structure, this interpretation of pathology provides a relatively objective

232
criterion with which one can detect the presence of disease: dysfunctional
deviancy.71
According to this perspective, life is simultaneously a process and a
concrete material entity (that is, the living cell, which comes from a pre
existing cell). Thus, the disordered (unordentliche, sometimes translated as
‘deranged’) cell serves as the concrete representation of disease (Virchow,
1958b, p. 37). The pathological cellular condition comprised for Virchow the
disease entity, and the point of diagnosis was to identify and name the
cellular abnormality. This contrasts with the bacteriological view that had
emerged by the end of the nineteenth century, according to which a disease
entity was defined by the cause of pathological changes—invading bacteria—
regardless of the particular presentation of the illness. This model of
pathology, which is ontological in nature, introduced the idea that a single
disease entity could produce an array of pathological changes, such that in
two individual patients, the same disease might present with completely
different symptoms or even be asymptomatic. As we will see in the next
section, these various terministic screens influenced those attempting to
make sense of madness, even though there was no corresponding way to
differentiate forms of madness on the basis of cellular abnormalities (and
even today mental illness by and large cannot be diagnosed on the basis of
71 It was not yet known that cells could be quite deviant without actually presenting any medical problem, as can often be the case with some benign tumors.

233
physiological testing).
Reconciliation of Ontology and Physiology
As advances in medical science changed the way we measured and
observed disease, an ontological interpretation was applied whenever disease
could be linked to an external referent—either etiological, e.g., an invading
microbe, or pathogenetic, e.g., a characteristic course over time (as its
temporal extension is external to its manifestation physiologically at any
single point in time). Its usefulness depends on how well a given disease
entity seems to fit its external anchor given the constraints of state of the art
medical technology. The less physicians could predict about the cause or
course of an illness, the more carefully they attended to the observed
physiological phenomena. It has often been the case that a successful
ontological interpretation points to a new physiological area of interest to
study, and a successful physiological interpretation leads to an ontological
interpretation of the same disorder based on the newly grasped knowledge.
As a terministic screen with an expansive circumference, the
ontological interpretation today pervades everyday speech:
Usually, we do not give it a second thought, when we talk of ‘catching’
a disease, of being ‘attacked’ by it, ‘struck’ by it (‘stroke,’ ‘apoplexy’),
‘seized’ by it (‘seizure,’ ‘epilepsy’). We speak of disease ‘carriers’ who
are not ill themselves, of diseases which are ‘transmitted’ from person
234
to person or parent to child, which move as ‘epidemics’ from place to
place or lurk as ‘endemic’ dangers waiting for the unimmunized
traveler. (KräuplTaylor, 1979, p. 6)
These idioms are so appealing in part because they helps us ‘order the chaos’
caused by medical ailments, providing some psychological comfort by offering
“a reassuringly simply solution to the apparent chaos of physical suffering: a
number of seemingly disparate phenomena can be accounted for and perhaps
abolished by reference to one underlying cause” (Boyle, 1990, p. 9). No
matter how advanced our knowledge of physiology becomes, it will be difficult
to stray too far from an ontological understanding of disease because of how
embedded it is in our linguistic lifeworld. On the other hand, advances in our
understanding of human biological processes at the molecular and genomic
levels make the physiological interpretation equally entrenched. Changing
paradigms in modern medicine is therefore less about adopting an ontological
or physiological interpretation than choosing which of the two to prioritize.
Scientific discussions of novel disease constructs can shift back and forth
between an ontological or physiological emphasis, often without any apparent
insight about this indeterminacy on the part of the discussants. We will see
this phenomenon in the next chapter, as those debating early interventions
in psychosis cannot seem to decide if they are discussing a psychosis risk
syndrome or the prodromal phase of a psychotic disorder. Both terministic

235
screens are required to navigate the contemporary discourses of medicine.
The most successful paradigms in medicine integrate both ontological
and physiological terminologies. This is true even more generally: The
discovery of calculus by Newton and Leibniz, for example, brought the
continuous and discrete together in a single terminology, solving Zeno’s
paradoxes and providing the mathematical framework for modern Newtonian
physics (Kondratieva, 2007). Similarly, continuous and discrete physical
terminologies are integrated in the theories of quantum physics. At the risk
of drawing Alan Sokal's (1996) ire, I would suggest that, notwithstanding the
objective physical reality of particlewave duality, there is a discursive
phenomenon at work that is operating at an even more general level of
abstraction than the physical or mathematical. Reality, whether physical or
social, is neither discrete nor continuous until it is rendered so in language.
Our terminologies come into being not as a result of discovering
significant objects (that is, objects to be signified) that actually are
continuous or discrete in themselves, but rather as a result of humanity's
invention of the negative (Burke, 1963). As eighteenth century naturalist
Charles Bonnet put it, “If there are no cleavages in nature, it is evident that
our classifications are not hers” (as cited in Lovejoy, 1936, p. 230). Similarly,
Cassirer (1944) suggests, “Nature as such only contains individual and
diversified phenomena. If we subsume these phenomena under class
236
concepts and general laws we do not describe facts of nature. Every system is
a work of art—a result of conscious creative activity” (p. 209). Either kind of
terminology might be more or less ‘accurate’—that is, capable of
encompassing a situation in a way that satisfies the rhetorical motives giving
rise to the symbolic action in the first place (Burke, 1974). While noumenal
objects are neither discontinuous nor continuous, phenomenal objects obey
the structure we give to them. An account of some phenomenon that is
produced wholly within a single terminology is bound to be an incomplete,
partial reading. Therefore, epistemic revolutions tend to come at times when
rhetors have discovered a new terminology that accounts for and reconciles
two distinct terminologies by which discontinuous and discrete approaches
had been divided.
Any successful integration must organize the symbolic field clearly and
efficiently so that the terminologies are appropriate to the situations that call
for their use without redundancy. It must find a way around the confusion
and miscommunication associated with incompatible epistemologies. The
integrated terminologies must be made to enrich and complement, rather
than cancel, one another. The new terminology certainly will still emphasize
either continuity or discontinuity, but in a way that transcends the
differences of the older terminologies, a “dialectical resolution by reduction to
an ultimate order” (Burke, 1969b, p. 207). What is needed is a new way of
237
understanding the world that can be condensed, if only metaphorically, into
some ultimate symbol under which the previous terminologies can organize.
The new terminology must be clear to all parties, something that everyone
can access for the first time at once, and which promises to be epistemically
productive. As this chapter continues, we will see how these criteria apply to
later epistemic developments on the road to psychiatric modernity.
For biological medicine in the nineteenth century, cellular pathology
provided a terminology that reconciles the ontological and physiological
interpretations. It is not merely a variant of the old humoral order with an
updated empirical grounding; rather, it is a new model in which disease is a
disturbance not of the whole body but of one discrete part. Any present
humoral rhetoric circulates around an ontological terminology of discrete
disease entities, and though a disease is not defined by its cause or course, it
is recognized that diseases have specific causes and courses. The signs and
symptoms of a syndromal complex were joined with a physiological
understanding of morbid processes within the unifying image of the deranged
cell.
Psychiatric Antecedents
Despite the achievements of cellular pathology, it seemed more or less
inapplicable to mental illness. The Cartesian mind was unitary and
immaterial; that madness could result from disordered brain cells was

238
inconceivable.72 Two major historical developments produced the epistemic
shift that facilitated the birth of psychiatry. First, an alternative view of the
mind emerged from the Scottish Enlightenment in the form of faculty
psychology. Developed by Thomas Reid as an epistemological theory, faculty
psychology was based on the assumption that each individual operation of
the mind (e.g., perception, emotion, memory, will, appetite, etc.) was driven
by an independent mental faculty (Reid, 1785). These ideas were taken up by
French alienists and were influential in discussions about the nature of
madness in the early 19th century, in addition to forming the basis of the
phrenology movement (Boutroux, 1897; Brooks, 1976; Marková, 2005). Both
alienism and the phrenology movement also were influenced by the growing
physiognomic tradition, according to which one could infer an individual's
personality and character systematically from his or her external appearance
(Lavater, 1789).
The phrenologists suggested that different mental functions were
located in different regions of the brain (primarily around its outer surface),
and that variations of these functions corresponded to the external
72 It must be noted however that Descartes contributed significantly to the modern understanding of neuroanatomy, including particularly his suggestion that the soul was materially connected to the body via the pineal gland, and his assumption that the organization and material structure of the nervous system, which mediated the connection between the intentions of the will and the behavior of the body, reflected established habits of behavior (LeDoux, 2003; G. Murphy, 1956). His neuroanatomical instincts were incorrect, for the most part, but the very fact that he conceived of the problem in these terms was highly significant.
239
topography of the skull (Kosslyn & Andersen, 1995). Though the latter
assumption was discredited, phrenology was “the first ‘scientific’ effort made
to analyze the underlying brain structure from which character and
personality might be derived” (Millon & Simonsen, 2010, p. 21). In a series of
lectures throughout Europe at the beginning of the nineteenth century, an
early exponent of phrenology, Franz Joseph Gall, introduced to a wide
audience the idea that cognitive functions are localized in neuroanatomy
(Breidbach, 2001). A few decades later, anatomical discoveries about the
structure and function of the dorsal and ventral roots of the spinal nerve led
to an anatomical exegesis of the reflex arc, demonstrating that the nervous
system was the source of at least some human behaviors (Hall, 1843). Two
decades later, with the discovery that the destruction of a specific region of
the brain causes aphasia, this finding was extrapolated to brain function
(Sechenov, 1863). The functionally differentiated mind of faculty psychology
and the efforts by alienists and phrenologists to study its physiological
implications lined up with the discovery of the functionally localized central
nervous system to forge a new category of epistemological figures and objects
of knowledge.
The second major development was institutional, namely, the
“establishment at the beginning of the [nineteenth] century of a new mode of
exclusion and confinement of the madman in a psychiatric hospital”
240
(Foucault, 1972, p. 40). This development had its roots in the seventeenth
century, when those deemed to be mad (that is, unemployed) were
imprisoned and forced to labor so that they would not remain ‘idle’ (Foucault,
2001). Madness was regarded as a source of danger and a sign of
inhumanity, understood neither medically nor morally, for “the disturbance
of his reason restored the madman to the immediate kindness of nature by a
return to animality” (p. 75). At the end of the eighteenth century, the first
hospitals came into existence, spurred by the moral movement in medicine
that sought to transform “hostels where the sick went to die [into]
institutions dedicated to providing a therapeutic milieu” (Healy, 1997, p. 32).
Corresponding to this development, Philippe Pinel is usually credited with
unchaining the inmates of l'Hôpital Bicêtre (an asylum near Paris), though
this was actually the work of JeanBaptiste Pussin, who was superintendent
in 1797. Pinel, after having apprenticed himself to Pussin at Bicêtre, became
superintendent of the Hospice de la Salpêtrière in 1795 and in 1800, shocked
by the inhumane treatment of the mentally ill (so the typical narrative goes),
followed in Pussin’s footsteps by banning the use of chains as restraints
(Cousin, Garrabe, & Morozov, 2008; Gerard, 1997; Pinel, 2008; Walsh,
1913).73
73 Inversely, Pussin also followed in Pinel’s footsteps by joining him at Salpêtrière a few years later as his special assistant. Pussin’s interest in treating asylum inmates began not in medical school—he was not a physician, but a tanner by trade—but rather during his own experience as patient at Bicêtre suffering from scrofula (lymphadenopathy of the neck related to tuberculosis). After his recovery, he took a staff position at Bicêtre in 1771, and 13

241
The new institution of the psychiatric hospital facilitated the
transformation of the asylum inmate into a new object of medical knowledge,
the mentally ill patient. Rose and AbiRached (2013) suggest that these
institutions “seemed to confer some homogeneity upon those disparate
individuals—displaced, desolate, despairing, deranged—who were collected
within its walls” (p. 115). Two important features of the new clinical gaze
allowed madness to be seen differently than ever before. First, asylums
enabled alienists to observe pathological processes temporally, drawing
attention to another aspect of disease: its course over time. Second, observing
the mad alongside one another revealed clearly that insanity manifested in
many distinct ways (Healy, 1997; N. S. Rose, 2007). For the first time, it
became possible to observe the symptoms, course, and outcome of a large
sample of mentally ill patients, leading Pinel (1807) to advocate the use of
data driven experimental methods and statistical analysis in medical
research:
years later he became superintendent of the mental ward, despite his lack of medical education. His social status perhaps explains why he was insufficiently credited for his role in the founding of psychiatry. Despite Pinel’s explicit crediting of Pussin in the 1809 second edition of his Treatise on Insanity, his contemporaries insisted on crediting Pinel for Pussin’s initiative. Various etchings and a painting in 1876 by Tony RobertFleury, in which Pinel was depicted as “singlehandedly unchaining the mentally ill,” almost certainly helped to promote this myth (Noll, 2007, p. 56). Subsequent historians have for the most part passed on the error without correction. Michel Foucault in Madness & Civilization notes (with some irony) that “Pinel, according to tradition, had ‘liberated’ the insane of Bicêtre” (2001, p. 240), and David Healy reports that “Philippe Pinel, one of the first physicians to work in a lunatic asylum, unlocked the chains binding the lunatics in the Bicêtre” (2004b, p. 10). In fact, in 1797, two years after Pinel left Bicêtre, Pussin instituted a reform that permanently banned the use of chains as restraints, and three years later, once Pussin had joined Pinel at Salpêtrière, a similar reform was instituted (Gerard, 1997; Pinel, 2008).
242
In medicine it is difficult to come to any agreement if we do not attach
a precise meaning to the word ‘experiment,’ since everyone praises his
own results and more or less only cites the facts in their favor. For an
experiment to be genuine and conclusive and serve as a solid basis for
any method of treatment, it must be carried out on a large number of
patients following the same general rules and a predetermined order.
It must also be based on a consistent series of observations made with
extreme care and repeated for a number of years with some kind of
regularity. Finally, it should report all of the findings, assigning as
much weight to results that are favorable as to results that are not.74
Suffice it to say a medical experiment must be founded on the theory of
probabilities, which has already been applied so successfully to civil
life, and on which the methods of treating the sick must henceforth
rely if they are to be established on a solid foundation.75 (pp. 169–170,
my translation)
74 Selective publication of positive results is still a major problem for private sector pharmaceutical research (Goldacre, 2013; Healy, 2000b, 2004a; Washington, 2011).75 “Il est difficile de s'entendre en médecine si on n'attache un sens précis au mot expérience, puisque chacun vante les résultats de la sienne propre, et qu'il cite plus ou moins de faits en sa faveur. Une expérience, pour être authentique et concluante, et servir de fondement solide à une méthode quelconque de traitement, doit être faite sur un grand nombrr de malades, asservia à des règles générales et dirigés suivant un ordre déterminé. Elle doit être aussi établie sur une succession régulière d'observations constatées avec un soin extrêmè et répétées pendant un certain nombre d'années avec une sorte de conformité. Enfin elle doit rapporter également les événemens favorables comme ceux qui sont contraires, assigner leurs nombres respectifs, et instruire autant par les uns que par les autres. C'est assez dire qu'elle doit être fondée sur la théorie des probabilités déjà si heureusement appliquée à plusieurs objets de la vie civile, et sur laquelle doivent désormais porter les méthodes de traitment des maladies, si on veut les établir sur un fondement solide” (Pinel, 1807, pp. 169–170).

243
These four changes—the new idea that disease was varied in kind and could
be classified on the basis of deranged anatomy (down to the cellular level);
the new understanding that the mind was differentiated in function and,
anatomically, so was the brain; the realization that at least some (if not all)
behaviors were mediated by activity in the central nervous system; and the
ability repeatedly to observe large numbers of mentally ill patients whose
symptoms over time appeared quite varied, regularly record the findings, and
compare data over time—converged to inspire the first modern systematic
attempts to articulate a nosology of madness within the framework of
institutional practices that “came to be known as clinical medicine” (T. D.
Murphy, 1981, p. 308, emphasis in the original).
The Emergent Assembly of Psychiatry
The first major classification system to emerge from this convergent
set of factors was Pinel’s 1806 Treatise on Insanity, which divided madness
into five categories: dementia, idiocy, mania with delirium, mania without
delirium, and melancholia (P. J. Cowen, Harrison, & Burns, 2012). In all
cases, however, Pinel thought the patient completely insane. This changed
with the nosological system produced by Pinel’s student JeanÉtienne
Dominique Esquirol. After distinguishing madness from the humoral
temperaments that were not pathological (although they might increase one’s
susceptibility to psychopathology), Esquirol (1838b) divided mental illness
244
into two categories, insanity and partial insanity. The latter group included
monomania (‘partial delirium’) and lypemania (‘melancholy with delirium’),
chronic cerebral affections, unattended by fever, and characterized by
a partial lesion of the intelligence, affections or will. At one time, the
intellectual disorder is confined to a single object, or a limited number
of objects. The patients seize upon a false principle, which they pursue
without deviating from logical reasonings, and from which they deduce
legitimate consequences, which modify their affections, and the acts of
their will. Aside from this partial delirium, they think, reason and act,
like other men… [Among those suffering from affective monomania,
by] plausible motives, [and] by very reasonable explanations, they
justify the actual condition of their sentiments, and excuse the
strangeness and inconsistency of their conduct… In a third class of
cases, a lesion of the will exists. The patient is drawn away from his
accustomed course, to the commission of acts, to which neither reason
nor sentiment determine, which conscience rebukes, and which the will
has no longer the power to restrain. The actions are involuntary,
instinctive, irresistible… The monomaniac is gay, petulant, rash,
audacious. The lypemaniac is sorrowful, calm, diffident, fearful... The
course of monomania is more acute, its duration shorter, and its
termination more favorable, unless there are complications. The

245
contrary holds true in lypemania. In this, the delirium seems to
depend more particularly upon some abdominal lesion; while in the
other, it appears to be caused more immediately, by the anormal
condition of the brain… [We] need not confound these two pathological
conditions, nor impose upon them the same name, if we desire
precision in medical language… Partial delirium is a phenomenon so
remarkable, that the more we observe it, the more we are astonished,
that a man who feels, reasons, and acts, like the rest of the world,
should feel, reason and act no more like other men, upon a single
point? (Esquirol, 1838b, pp. 320–321)
Several things about this division are noteworthy. Esquirol assumes that the
subvarieties of monomania correspond to psychic ‘lesions’ (the extent to
which this was meant metaphorically is unclear), and his division of intellect,
will, and affect match the original treble division of Reid’s psychological
faculties, and can be seen still in the contemporary categories of cognitive,
affective, and conduct disorders. Esquirol provides an early example of the
strained attempt to combine psychological and neurological objects in one
nosological system. The explicit rationale for this nosology, with its category
errors, is the need for ‘precision in medical language.’ Through this precision,
a form of illness that no one has been able to see before becomes remarkably,
even astonishingly, clear. Like the stethoscope, this classification is designed

246
to be a technology for seeing a hybrid object of medical knowledge.
Second, Esquirol justifies the principle division between monomania
and lypemania on the basis of their course and prognosis. This represents a
significant development of the syndrome concept, which originally denoted a
synchronic semiotic pattern. This innovation will become very important in
the development of dementia praecox, to which I shall turn shortly.
Esquirol's treatment of the category of temporal course contains an echo of
humoral thinking:
After Hippocrates, Areteus and Celsus assure us, that summer and
autumn produce rage... Dementia appears in winter. Charles VI
became insane after having been exposed to the sun... Excess cold
causes the same disorders; a truth illustrated in the experience of our
troops during their disastrous retreat from Russia, when many French
soldiers were seized with phrenetic delirium, and even mania... Heat,
like cold, acts upon the insane, with this difference, that the
continuance of warmth augments the excitement, while cold prolongs
the depression. Great atmospheric commotions excite and exasperate
the insane. A house for the insane is most disturbed... at the period of
the equinoxes... The influence of the seasons extends even to the
course of the insanity. There are individuals who pass the summer in
a state of prostration or agitation; whilst in the winter they are in an
247
opposite condition... Insanity, which appears in spring and summer,
has an acute course. If not speedily cured, it terminates in the winter.
The monomania and mania of autumn, terminate only in the spring.
Summer is more favorable to the cure of dementia... (Esquirol, 1838b,
pp. 31–32)
Esquirol based these conclusions on observational data recorded at the
Salpêtrière hospital over a nine year period by alienists following Sydenham's
suggestions to look for relationships between clinical signs and the time of
year.
Third, Esquirol implies that any behavior resulting from one of these
mental ‘lesions’ is beyond the patient's control. This remains the core legal
principle by which defendants can avoid culpability for crimes associated
with psychiatric illness (‘not guilty by reason of mental disease or defect’). So
many of the varieties of monomania Esquirol identifies are associated with
criminality, including murder, theft, and rape, or as the DSM5 Paraphilias
Subworkgroup proposed to call it, ‘coercive paraphilia,’ which I discuss
extensively in Chapter 4 (D. Thornton, 2010).
Fourth, the very idea of lypemania, literally a 'sadnessmania,' inverts
the traditional traditional binary opposition between melancholia and mania
that traces back to Hippocrates. In this way, it is stunningly modern. Healy
suggests that in proposing “a selective disorder of mood, Esquirol all but
248
created modernity. This was the cornerstone on which the modern edifice of
depression has since been erected” (1997, p. 33). Although the concept of
monomania is no longer extant scientifically, it remains in the popular
culture in words like ‘pyromania,’ ‘kleptomania,’ and ‘nymphomania’: “[The]
survival to this day of this use of the mania suffix indicates where one of the
corpses on the road to modernity is buried” (Healy, 1997, p. 33). But as
radical as Esquirol's monomania concept was, traces of the humoral model
appear in his invocation of melancholy, along with the suggestion that
lypemania (‘sadnessmania’) involves some problem in the stomach.
Finally, Esquirol is aware of great epistemic tensions. He notices the
discordance between categorical and dimensional diagnostic concepts, a
distinction which was central to the DSMIII nosological revolution in 1980
and which animates many of the DSM5 controversies today. Furthermore,
Esquirol reveals the inner conflict he feels between honoring the received
wisdom of the past and embracing the empirical science of the present:
Does the moon exercise any influence upon the insane? ...The English,
and almost all the moderns, give to the insane the name of lunatics...
Certain isolated facts and phenomena observed in many nervous
diseases would seem to justify this opinion. I have been unable to
verify this influence, though I have been at some pains to assure
myself of it... At Hospital Salpêtrière, where practical truths have

249
become, in some sort known, among the inmates of the house, they
have no longer any suspicions of lunar influence. The same is true of
the Bicêtre... Nevertheless, an opinion which has existed for ages,
which is spread abroad through all lands, and which is consecrated by
finding a place in the vocabulary of every tongue, demands the most
careful attention of observers. (pp. 3233, my emphasis)
This hardly seems like the writing of a revolutionary, though that he was.
Inventional Visual Rhetoric
Alongside a description of the characteristic symptoms and their
observed course, Esquirol provided an illustrative case history for each
diagnostic category in his textbook. Each of these histories includes a
description of how the patients typically appear physically, including such
features as posture and skin color, and a handdrawn image of a patient
exemplifying the physical ‘look’ associated with the diagnosis (Figure 3.4).
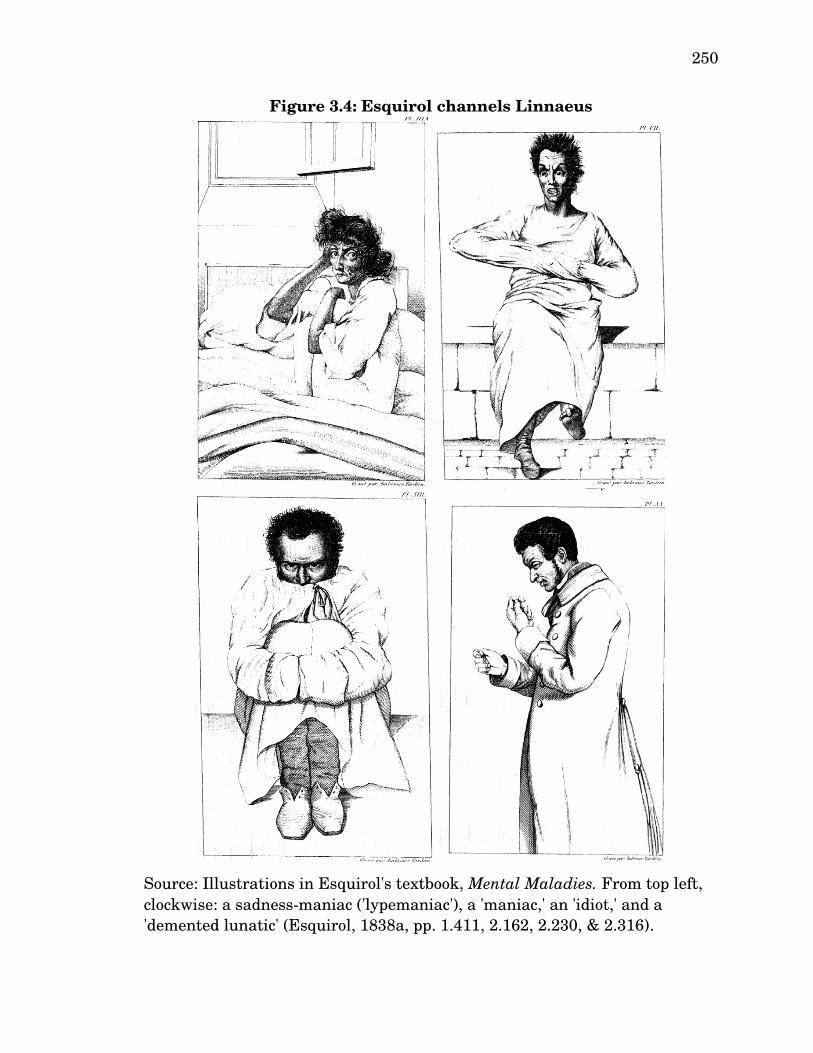
250
Source: Illustrations in Esquirol's textbook, Mental Maladies. From top left, clockwise: a sadnessmaniac ('lypemaniac'), a 'maniac,' an 'idiot,' and a 'demented lunatic' (Esquirol, 1838a, pp. 1.411, 2.162, 2.230, & 2.316).
Figure 3.4: Esquirol channels Linnaeus

251
These images were drawn in a style reminiscent of Linnaeus' (1735)
renderings of plant species a century earlier (Gilman, 1982).76 Linnaeus's
classificatory illustrations have stood in for the specificity of modern medicine
in terms of both diagnosis and treatment, in contrast to the holistic nature of
the humoral model. An illuminating example of this is found in an
advertisement (Figure 3.5) in the American Journal of Psychiatry, which
compares the specificity of bee communication, as represented by Linnaeus,
to the specificity of the minor tranquilizer 'Librium' (Roche, 1981, pp. A36–
A37).
76 The link between Linneaus and psychiatric nosology is also apparent in the work of François Boissier de Sauvages de Lacroix, a botanist and physician who created the first nosological framework for disease by synthesizing the work of Sydenham and Linneaus in his threevolume magnum opus, Nosologia Methodica, published in 1763, which incorporated much of the substantive content from his 1731 Treatise de Nouvelles Classes de Maladies, a work that focused on madness. His approach to madness strongly influenced Pinel’s thinking, and more broadly, his Nosologia “was used as an orderly classification for decades, if not centuries, to come” (Millon & Simonsen, 2010, p. 25).

252
Source: An advertisement in the American Journal of Psychiatry (Roche,
1981, pp. A36–A37).
Figure 3.5: Linnaeus invoked to emphasize specificity of 'Librium'
253
Influenced by Pinel, Esquirol considered physical features to be very
important in classifying ‘specimens’ of madness, a physiognomic epistemic
orientation shared with the phrenologists. This grounded psychopathology in
physical biology, helping to anchor primitive psychiatry in the larger
institutional domain of medicine. Subsequent alienists of the nineteenth
century continued to regard patients' physical appearance as diagnostically
relevant, to the extent that “the visual image was central to the clinical
practice of individuating the pathology” (N. S. Rose, 2007, p. 193).
Kenneth Burke provides a hint about the underlying rhetorical
motives when he suggests that a preoccupation with images can be associated
with a “mystical transcendence of the person in generalizing the concept of
role to the point where the realistic or dramatistic notion of people in
situations retreats behind the pure lyric of imagistic suggestion” (1969a, p.
300). Certainly, the visual always lies within a web of signification (Geertz,
1973). Images also seem especially wellsuited to be significant symbols upon
which a new, transcendent, ultimate order can be constructed. A new
organizing object is introduced within a visual epistemic field which has not
yet been reduced to either continuous or discontinuous terms. Its visibility,
accessible to all, announces the possible formation of a new epistemic
paradigm.
Along these lines, I contend that the prominent inclusion of images
254
within the nosological text implies a dissatisfaction with a purely symbolic
level of signification, which Esquirol felt the need to supplement with
illustrations that are at once iconic, in that they are meant to resemble or
imitate the signified, and indexical, in that there is supposedly an actual
relationship between psychopathology and posture, facial expression,
complexion, and other similar physical attributes (Peirce, 1868). Each of
these levels of signification should be understood in light of the rhetorical
canon of elocutio, by which Esquirol ornamented his new epistemic objects.
During the nineteenth century, the teaching of rhetoric became scientized,
leading to the “elocutionary sciences of chironomia (descriptive gesturing),
chirologia (emotional gesturing), proxemics (body positioning), facial display,
and bodily action” (Gronbeck, 2008, p. xxiv). In Esquirol we have a
fascinating example of symmetry whereby the teaching of science becomes
rhetoricized along precisely the same lines: His illustrations emphasize
“appearance, complexion… posture, gestures, and movements of the entire
figure” (Gilman, 1982, p. 12). The strategy of elaborating a scientific concept
by means of visual copia is a common way to enhance a concept's sense of
reality (Burri & Dumit, 2008). Publication of Esquirol's images historicized
the new clinical gaze and the distinctive form in which psychopathology, in
all its varieties, appears to this gaze.
Humoral pathology also featured a strong visual component. Its

255
therapies were, more often than not, worse than useless, but they were
persuasive nevertheless. Bleeding a feverish patient produced an immediate
change in complexion and body temperature that all could see and feel. This
may not have corresponded with a cure, but it did not need to. No one can
see a cure itself; it is always mysterious and hidden (just as causation was
accessible only intuitively, as Hume argued). The patient either gets better
or dies, and if either includes a visual change, our compulsively reasonable
(but often irrational) minds cannot help assigning meaning to the imagined
association between the two. The visual evidence that we have at least some
mastery over the natural world appeals to our gnostic desire for some secret,
ineffable knowledge by which we can be saved from the imperfection, flaws,
dangers, and evil embedded in the material world of disease and death. Our
cognitive biases belie a fantasy of mastery over an uncontrollable situation.
This is how the ‘functional neurological’ hypothesis of hysteria, which
explains nothing at all (quite explicitly) but involves visible fMRI evidence,
could become preferred over the conversion hypothesis, which provides a
complete explanation and suggests an invisible, but often successful method
of treatment. An explanation that makes sense but is invisible generally will
be suspect. Explanations can be wrong, especially those built on the premise
that our unconscious minds play tricks on us, intentionally deceiving us in
order to avoid staring into the abyss of our neuroses, preferring even bodily
256
suffering over confronting an inner conflict.
Much like the cultural return of the humoral ultimate order in the
marketing of alternative medicine, visual displays of madness have made a
great return in the neurobiological discourses of psychopathology. For
example, psychiatrist Daniel Amen runs a clinic that specializes in single
photon emission computerized tomography (SPECT) imaging techniques,
with which he claims he can classify subtypes of mental disorders that are
not currently recognized by mainstream psychiatry. Amen also claims that
such images can aid differential diagnosis between accepted disorder
categories, as well as inform medication decisions and monitor treatment
outcomes. The website presents sample SPECT images for a variety of
disorders, accompanied by explanatory captions and adjoining case histories
(Figures 3.6 and 3.7). Much like Esquirol’s illustrations, captions tell the
reader what is supposedly evident in the image, though perhaps ‘Ce n'est pas
une maladie mentale’ would be better (Magritte, 1929; Figure 3.8).

257
Figure 3.6: SPECT images of schizophrenia constitute a modernday reenactment of Esquirol’s illustrated nosology
Source: (The Amen Clinics, 2012c, sec. SCHIZOPHRENIA).
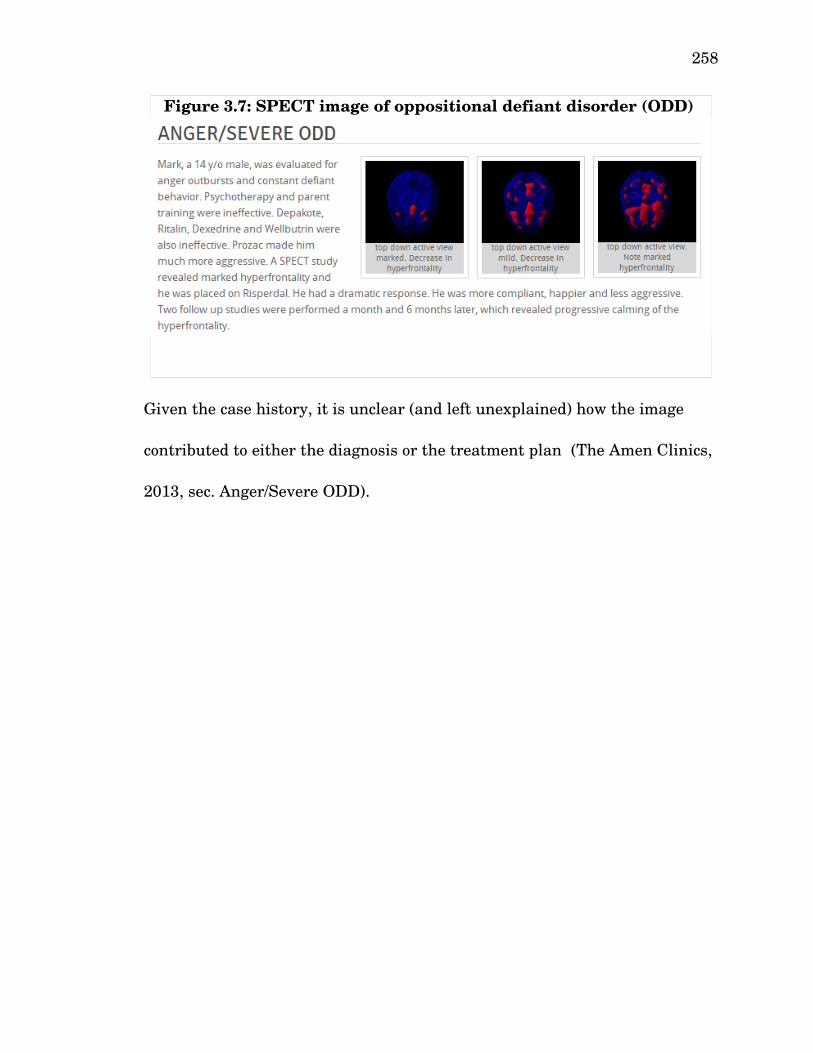
258
Figure 3.7: SPECT image of oppositional defiant disorder (ODD)
Given the case history, it is unclear (and left unexplained) how the image
contributed to either the diagnosis or the treatment plan (The Amen Clinics,
2013, sec. Anger/Severe ODD).

259
Figure 3.8: The Treachery of Neuroimaging

260
In his gallery of SPECT images, Amen sees what Esquirol saw in his
asylum: specific patterns, diversity in what once was thought to be a unity,
and a corresponding new means of classification. Accompanying each of his
images are descriptions of the essential features of the putative diagnostic
category and the typical features one will ‘see’ in the SPECT images. Yet,
ambiguity pervades the pseudoprecision of this neophrenological exercise.
For example, in ‘Temporal lobe ADD,’ “SPECT imaging typically shows
decreased or increased activity in the temporal lobes with decreased
prefrontal cortex activity” (The Amen Clinics, 2012b, sec. Temporal Lobe
ADD, my emphasis). The ‘insights’ provided by the images are not always
very insightful; for example, SPECT imaging helped to diagnose a child
presenting with “angry outbursts and constant defiant behavior” with
oppositional defiant disorder (ODD), and helped select a medication that was
of a different class than the five drugs that had already been tried
unsuccessfully (The Amen Clinics, 2013, sec. Anger/Severe ODD).
The website of the Amen Clinics revealingly suggests that “SPECT can
specifically help people with ADHD by: Helping evaluate whether or not the
person is ADHD; Helping determine the type of ADHD to inform treatment
decisions; …Reducing emotional pain and stigma by demonstrating that
symptoms and behaviors are not imaginary; Increasing treatment compliance
by showing pictures of results; Helping families gain a better understanding
261
of the illness through visuals” (The Amen Clinics, 2012a, sec. SPECT
IMAGING, my emphasis). Not only is the imaging technology said to
increase diagnostic precision, it can do so while reducing stigma, increasing
compliance, and facilitating public understanding.
Neurosis and Psychosis
Just as physicians during the nineteenth century began charting the
developments and changes of symptoms in the presentation of an illness over
time, critics can study the longitudinal course of terminologies of mental
illness. The terminologies at any given point during this period for the most
part stress discontinuity; similarly, these terminologies enact discontinuity in
their changes, interactions, and moments of selfreference. The terms
‘neurosis’ and ‘psychosis’ emerged in the eighteenth and nineteenth centuries
(respectively), but the relatively constant flux in meaning through the early
twentieth century makes it very difficult to read psychiatric discourses from
this period on their own terms.
At first, ‘neurosis’ designated any disease of the nervous system, while
‘psychosis’ initially referred to the psychic dimension of a brain disease and
entailed a total disorder of the personality coupled with an organic brain
pathology (Janzarik, 2003; Knoff, 1970; SchmidtDegenhard, 1988). Neither
Pinel nor Esquirol used the term neurosis, as neuroses were within the
general domain of the physician and distinct from insanity (and, for Esquirol,

262
partial insanity). When the concept of neurosis first appeared in the late
eighteenth century, it signified a lesion of the nerves, in accordance with the
anatomical model of pathology. In contrast to ‘neuritis,’ in which one could
see visibly damaged nerves upon autopsy, the neurological damage associated
with neurosis was invisible but presumed, and the prevailing belief was that
“in due course scientific advances would locate the invisible pathology”
(Healy, 1997, p. 39). Epilepsy (explicitly defined as a neurosis in the late
nineteenth century) and neuropathy are diseases that capture the original
meaning of the term. Perhaps ironically, the best modern example of a
psychiatric disorder believed to be an invisible neurological disorder is
‘functional neurological disorder.’ The DSM5 conversion of hysteria into
functional neurological disorder brings psychiatry full circle, reintroducing
the original concept of neurosis for the historically important hysterical
condition (although the somatoform disorder work group would undoubtedly
be horrified by the suggestion that they reintroduced the concept of neurosis).
Karl Friedrich Canstatt introduced the concept of psychosis in 1841 as
a synonym for ‘psychic neurosis’ (Bürgy, 2008; Canstatt, 1841; Scharfetter,
1987).77 Feuchtersleben (1845) stressed the importance of both the somatic
and the psychic in understanding psychosis, and deployed the term as a
subset of the larger category of neurosis:
77 Many sources incorrectly claim that Baron Ernst Maria Johann Karl Freiherr von Feuchtersleben (1845) first introduced the term ‘psychosis.’
263
Every psychosis is, at the same time, a neurosis; because, without the
intervention of nervous action, no change of the psychical action
becomes manifest, but every neurosis is not a psychosis, of which
convulsions and pain afford sufficient examples. Agreeably to this
notion is the popular view that a madman is not called mad because
his brain is overexcited, but because he judges and acts absurdly.
(Feuchtersleben, 1847, p. 246)
During the second half of the nineteenth century, ‘psychosis’ frequently
appeared in the psychiatric literature, generally used as a “synonym for
terms such as mental disorder, mental illness, and insanity” (Bürgy, 2008, p.
1201). While efforts, following the discovery of the reflex arc, to locate
increasingly higher nervous system functions in the brain enjoyed much
success, belief lingered that nonmaterial sources of the highest functions
associated with conscious judgment would be discovered. The emerging
distinction between ‘psychosis’ and ‘neurosis’ reflects this belief in that the
former was a disorder of the mind while the latter was a disorder of the
nervous system (Beer, 1995, 1996). Of course, every disorder of the central
nervous system implicates the mind in some manner, and vice versa.
Classification of a disorder as one or the other unavoidably introduces
assumptions about etiology, implying the causal priority of either mind or
brain. These distinctions became more pronounced once the concept of

264
neurosis narrowed, resulting in a discursive decoupling of the two into
distinct, mutually exclusive categories.
Freud (1893b, 1924a) reintroduced this same distinction within the
concept of neurosis itself, distinguishing ‘psychoneuroses’ (later, just
‘neuroses’ unqualified) that were psychological in nature from ‘actual
neuroses’ that entailed physical damage to the nerves. Freud suggested that
the most common cause of this damage was masturbation, which Esquirol
(1838b) referred to as “that scourge of human kind” (p. 41). With respect to
therapeutic outcomes, risk management, and preventive psychiatry, Freud
(1893b) viewed 'actual neurosis' very much as psychosis is understood today,
and regarded it as psychoanalytically untreatable. Freud’s understanding of
‘neurosis’ (qua ‘psychoneurosis,’ not ‘actual neurosis’) radically transforms
what was once a “rigid boundary” between the sane and the insane by
“creating a new class of neurotic behaviors and linking it with normal rather
than psychotic behavior” (Horowitz, 2002, p. 53). Freudian neuroses imply a
fluid and dynamic nosology in which the difference between normality and
neurosis is a matter of degree, not kind. Rather than the discontinuous
categories of healthy and diseased, we have a continuous spectrum arrayed
dimensionally. This nosological view came to dominate the psychodynamic
tradition in much of the twentieth century, although, as discussed in Chapter
1, it fell out of favor in mainstream psychiatry with the 1980 publication of
265
DSMIII. In Chapter 4, we will see how this repressed perspective has
returned in contemporary psychiatric discourse about the nature, treatment,
and prevention of psychotic disorders.
The cyclic alternation of the meaning of ‘neurosis’ (actual or otherwise)
and ‘psychosis’ created some confusion: everyone meant something definite by
each term, but these meanings often were idiosyncratic, not shared. Since
Freud believed that only the (psycho)neuroses could be treated effectively
with psychoanalysis, the term came to be associated with the psychoanalytic
tradition and its dimensional nosologies. Psychosis was something more
extreme, left to the asylum psychiatrists who treated large confined groups of
mentally ill patients rather than spending six hours per week with individual
patients, as Freud did (Freud, 1913a). In part because of this division,
neuroses became associated with disordered psychological functioning, and
psychoses with gross nervous system dysfunction. Pierre Janet (1920)
identified a loss of la fonction du réel (‘the reality function’) as the defining
characteristic of neurosis; similarly, Freud suggested that neurotic patients
“turn away from reality because they find it unbearable—either the whole or
parts of it” (Freud, 1911, p. 301). Though both neurosis and psychosis were
associated with impaired reality testing, in psychosis this impairment was
absolute (Kantrowitz, Katz, Paolitto, Sashin, & Solomon, 1987). Freud, for
whom acute florid hallucination “is perhaps the most extreme and striking
266
form of psychosis,” conceptualized psychosis as a state in which “either the
external world is not perceived at all, or the perception of it has no effect”
(Freud, 1924a, p. 151). In contrast, the loss of insight was milder in a
neurotic break with reality, although it could progress to psychosis,
suggesting more of a continuum than a strict etiological and pathogenic
division:
[At] a final stage in the evolution of a neuroses [sic], the feeling of
unreality may pass over into that falsification of reality which we label
delusion. Hypochondriacal fear, such as the common one of heart
disease, may evolve by quantitative increase into the feeling that the
heart is literally gone, or actually broken. In this case, fear and
anxiety have developed into delusion. Another example may be cited;
in groping for the cause of his illness, a sufferer may conclude that he
is sick because he has violated the rules, as he understands them, of
health. Later on, as he becomes hopeless concerning his recovery, he
may deny that he is ill and state that his sins have found him out or
even that he is being punished by God. (Myerson, 1936, p. 263)
Clearly, the psychotic patient suffers from a total disconnection from reality,
with a complete lack of insight. At the end of the nineteenth century, this
break with reality became associated with a new diagnostic category, the
emergence of which coincided with a nosological development that serves as
267
the foundation for the modern (DSMIII) approach to the classification of
mental illness.
Dementia Praecox: Prognosis as Diagnosis
Unlike the forms of mental illness known in some manner since
antiquity (e.g., melancholia), dementia praecox did not become an object of
knowledge until the midnineteenth century, when alienists began noticing
among the masses of generally insane patients a group of predominately
young people who suffered from a chronic, progressive decline in mental
faculties with no apparent cause. Emil Kraepelin provided the first
systematic treatment of dementia praecox, literally precocious or premature
dementia, the precursor to what is now called ‘schizophrenia’ (Kraepelin,
1896). Kraepelin appropriated the basic idea for dementia praecox from
BénédictAugustin Morel, who in 1852 described (in passing) a disorder he
called ‘démence précoce’ occurring in young patients who were ‘stuporous,’
appearing at first to have a good prognosis but nevertheless descending
inevitably into incurable dementia (Morel, 1852). Thomas Clouston named a
similar disorder the “hereditary insanity of adolescence,” which he later
shortened to “adolescent insanity,” not to be confused with (for Clouston) the
closely related “masturbational insanity,” a diagnosis he continued to
champion well after it fell out of vogue (Clark, 2004; Clouston, 1891, p. 111).
Based on work by his student, Ewald Hecker, Karl Kahlbaum described a

268
form of ‘jugendliche irresein’ (juvenile madness) that often developed into
catatonia, a syndrome he studied extensively, as well as hebephrenia, a
syndrome characterized by severely disorganized speech and behavior
(Hecker, 1871; Kahlbaum, 1863).
Kraepelin integrated these varied clinical pictures and their seemingly
unrelated categories of symptoms (e.g., catatonia, confusion, delusions,
disorganized behavior, grandiosity, hallucinations, impaired communication
ranging from strange to completely incoherent, unusual thought patterns,
etc.) into the unified nosological entity dementia praecox. The common
organizing feature of dementia praecox was a marked deterioration in
personal/social behavioral and cognitive functioning from which the patient
was unlikely to recover. Kraepelin accounted for the diverse phenotypes of
disease expression by positing nine distinct ‘clinical forms’ of his new disease
entity: “We meet everywhere the same fundamental disorders in the different
forms of dementia praecox… in very varied conjunctions, even though the
clinical picture may appear at first sight ever so divergent” (cited by
Jablensky, 2011, pp. 3–4).78
In the foreword to the fifth edition of his revolutionary textbook,
Lehrbuch der Psychiatrie, Kraepelin emphasized the importance of the course
78 Kraepelin’s ‘clinical forms’ include ‘dementia praecox simplex,’ ‘hebephrenia, ‘depressive dementia praecox (simple and delusional form),’ ‘circular dementia praecox,’ ‘agitated dementia praecox,’ ‘periodic dementia praecox,’ ‘catatonia, paranoid dementia (mild and severe form),’ and ‘schizophasia (confusional speech dementia praecox)’ (Kraepelin, 1896).

269
of disease progression over time to his new conception of psychiatric disease:
“What convinced me of the superiority of the clinical method of diagnosis…
over the traditional one, was the certainty with which we could predict, on
the basis of our new concept of disease, the future course of events” (cited by
Noll, 2011, p. 66). In the case of dementia praecox, the “importance of our
diagnosis would therefore consist in this: that we are now able, at the very
beginning of the illness, to predict its resulting in a characteristic state of
feebleness” (Kraepelin, 1917, pp. 28–29). The sixth edition culminated in a
major insight that would define his nosological system: There are ultimately
two categories of insanity, one that terminates in dementia (dementia
praecox was the classic exemplar of this category) and one that does not
(exemplified by manicdepressive insanity, based on the concept in French
alienism of folie circulaire, or ‘circular insanity’). The ability to observe the
course of the illness, made systematically possible scarcely fifty years earlier,
became central to the organization of Kraepelin’s nosology, later serving as
the ideological basis for DSMIII. Just as the ‘neoKraepelinian’ categorical
DSMIII is now giving way to the more dimensional DSM5, Kraepelin,
toward the end of his life, discussed the possibility of replacing his
dichotomous categorical nosology with a dimensional model in which the
syndromes associated with his two categories of insanity “do not represent
the expression of particular pathological processes, but rather indicate the

270
areas of our personality in which these processes unfold” (Kraepelin, 1974, p.
12).
Kraepelin’s approach was revolutionary for several reasons. First, he
replaced the Sydenhamian ‘syndrome’ (i.e., “a cluster of signs and symptoms
that would remain consistent regardless of outcome”) with ‘prognosis’ as the
key term under which disease entities were organized (Noll, 2011, p. 66).79
This move made it possible, years later, for the term ‘syndrome’ to be
transformed such that the idea of a ‘risk syndrome’ was intelligible. Second,
his methodology involved statistical analysis of longitudinal data generated
from thousands of cases, setting the stage for the biopolitical turn in the 20th
century. Third, he explicitly appropriated the clinical language of medicine
to fashion psychiatry as its own medical specialty that treated naturally
occurring (provisional) discrete disease entities, each of which was
understood to have an underlying (but as of yet unknown) biological aetiology
and pathophysiology. Appeals to imagery no longer were needed to serve this
institutional linking function. For dementia praecox, the “nature of the
disease process… is not known, but it seems probable, judging from the
clinical course, and especially in those cases where there has been a rapid
deterioration, that there is a definite disease process in the brain, involving
the cortical neurones”: indeed in a few cases, “anatomical lesions have been
79 Syndrome will indeed return, as we shall see shortly, but in a revised form that incorporates the ideas of course and prognosis.

271
found which can be explained only upon such a basis” (Kraepelin, 1907, p.
221). This finding confirmed suspicions that Kraepelin had voiced a decade
earlier:
The real nature of dementia praecox is totally obscure… It is hard to
see why an organism which has hitherto developed in a healthy or
even energetic way should suddenly, and for no particular reason, not
only come to a standstill but even deteriorate into chronic sickness… I
consider it more likely that what we have here is a tangible morbid
process occurring in the brain… It is true that morbid anatomy has so
far been quite unable to help us here, but we should not forget that
reliable methods have not yet been employed in a serious search for
morbid changes. (Kraepelin, 1987, p. 23)
Kraepelin already had found evidence that such lesions constituted the
organic basis of what we now know as Alzheimer’s disease. As dementia
praecox was for Kraepelin essentially an earlyonset variant of the same
disorder (as they both develop the same putatively terminal course), he
assumed it was only a matter of time before the parallel organic brain
pathology would be mapped out for dementia praecox (Metzl, 2009).
One important caveat must be noted here. That mental diseases have
a biological basis does not imply that that their causes can be reduced
entirely to physical defects of the brain; Kraepelin dismissed attempts to do
272
so as brain mythology (‘hirnmythologie’).80 Nor does it imply the irrelevance
of psychological factors: the appendix to Kraepelin’s lectures on clinical
psychiatry asserts that this field “must include a study of the personality
itself, the temperament and general reactions, and also an analysis of the
aspirations, wishes, and conflicts, which have preceded the outbreak of
definite mental disorder, and in a great measure determine its occurrence”
(T. Johnstone, 1917, p. 357).81 Kraepelin believed it was important to chart
all observed clinical variants carefully, but he fiercely resisted ascribing
etiological significance to their division, and left open the question whether
these clinical variants manifested an underlying unitary pathogenesis or,
instead, represented multiple disease states (Jablensky, 2010). Still,
Kraepelin believed that the evidence justified provisionally “regarding the
majority at least of the clinical pictures which are brought together here as
the expression of a single morbid process, though outwardly they often
diverge very far from on another” (Kraepelin, 1919, p. 3). Unfortunately,
Kraepelin’s hopes of finding distinctive organic antecedents and
80 This approach was particularly associated with Theodor Meynert (1890) and Carl Wernicke (1906), who attempted to build an overall system of organic and mechanistic psychiatry. But they often supplemented their objective findings with hypotheses on the anatomical and physiologic substratum of psychic activity… [formulating] psychopathological disturbances in terms borrowed from brain anatomy” (Ellenberger, 1970, p. 284).81 Contrast this with what came to be known in the 1970s as the neoKraepelinian model, which “disregards etiology and dismisses conflicting theoretical standpoints… The neoKraepelinians do not disregard etiology as much as history, whether personal or social. They would most likely be satisfied with some form of genetic and biochemical etiology, which is in fact what they aim for. The neoKraepelinians simply do not want to deal with any form of social etiology” (P. Brown, 1990).
273
neurobiological pathological mechanisms associated with behavioral clusters
never were realized (Boyle, 1990; Gottesman & Shields, 1982; Jaspers, 1963;
Kendell, 1975; Wing, 1978).
Like Esquirol, Kraepelin had identified a new way of looking at mental
illness, although unlike Esquirol, visual observation did not figure heavily in
this new technology of seeing. Kraepelin and Freud both
mark a move away from the eye. Each opens the interior of the patient
to medical knowledge by demoting observation in favor of
interpretation. Kraepelin… illustrated his textbook liberally with
illustrations, but they were just that—illustrations. Their diagnostic
role had been taken over by the case history: the chronology of
symptomatology, etiology, and prognosis that was the diagnostic key.
(N. S. Rose, 2007, pp. 193–194)
Just as Kraepelin rejects Esquirol’s prioritization of visual observation, Freud
disparages his teacher, JeanMartin Charcot, as “not a reflective man, not a
thinker: he had the nature of an artist—he was, as he himself said, a
‘visuel,’—a man who sees” (Freud, 1893a, p. 49). What Kraepelin (and Freud)
made visible was subtle, easy to miss – indeed, the “whole disturbance
[associated with dementia praecox] can be so very gradual and the symptoms
so illdefined that relatives see them only as the result of an unfortunate
development or perhaps a weakness in character” (Kraepelin, 1987, p. 13).
274
Further, the clinical pictures82 of the different forms of dementia praecox
were so variegated that Kraepelin went on for some seventy pages outlining
the various psychic symptoms he had observed. Yet these symptoms could be
divided into two broad groups to form the “general psychic clinical picture” of
dementia praecox (Kraepelin, 1919, p. 74). The first roughly corresponds
with what we now consider ‘negative symptoms,’ primarily flat affect, alogia,
avolition, and anhedonia:
One the one hand, we observe a weakening of those emotional activities
which permanently form the mainsprings of volition. In connection
with this, mental activity and instinct for occupation become mute.
The result of this part of the morbid process is emotional dullness,
failure of mental activities, loss of mastery over volition, of endeavor,
and of ability for independent action. The essence of personality is
thereby destroyed, the best and most precious part of its being, as
[German asylum reformer, neurologist, and psychiatrist Wilhelm]
Griesinger once expressed it, torn from her… The rapidity with which
deepseated and permanent dementia sometimes develops in the
domain of intellectual work makes the suggestion easy, that it also
may itself be drawn by the disease into a sympathetic morbid state,
even though it is invariably encroached on to a much less degree than
82 The ubiquity of the 'clinical picture' metaphor in medical literature also testifies to the emphasis on the visual in diagnosis.
275
emotion and volition. (Kraepelin, 1919, p. 74, emphasis in original)
One cannot fail to notice here the tripartite division of the psyche—intellect,
affect, and will—inherited from the faculty psychology tradition of the
Scottish Enlightenment.
Kraepelin’s second group includes much of what we now call ‘positive
symptoms,’ which include delusions, hallucinations, ideas of reference,
grandiose thinking, disorganized speech, bizarre thoughts, and bizarre
psychomotor behavior (e.g., catatonia). Rather than focus on the signs and
symptoms here, Kraepelin describes what he sees as their underlying psychic
basis:
The second group of disorders... gives dementia praecox its peculiar
stamp… It consists of the loss of the inner unity of the activities of
intellect, emotion, and volition in themselves and among one another...
This annihilation presents itself to us in the disorders of association…
in incoherence of the train of thought, in the sharp changes of moods
as well as in desultoriness and derailments in practical work. But
further the near connection between thinking and feeling, between
deliberation and emotional activity on the one hand, and practical
work on the other is more or less lost. Emotions do not correspond to
ideas. The patients laugh and weep without cause, without any
relation to their circumstances and their experiences, smile while they
276
narrate the tale of their attempts at suicide: they are very much
pleased that they “chatter so foolishly,” and must remain permanently
in the institution, on the most insignificant occasions they fail into
violent terror or outbursts of rage, and then immediately break out
into a neighing laugh. It is just this disagreement between idea and
emotion that gives their behavior the stamp of “silliness.” (Kraepelin,
1919, pp. 74–75, emphasis in original)
Kraepelin was following an idea developed by Erwin Stransky, a Viennese
neurologist who devised an explanatory model of dementia praecox involving
“inaffectivity” due to the loss of “intrapsychical coordination,” i.e., loosening
of the connection between the “noopsyche” and the “thymopsyche”
(Kretzschmar & Petit, 1994, p. 377).83 Kraepelin believed further in a
connection between negative and positive symptoms:
As it seems to me, there exists an inner connection between the two
groups of disorders, which are here distinguished. What fashions our
experiences into a firmly mortised building, in which each part must
fit the other and subordinate itself to the general plan, are general
conceptions and ideas. The even calm of our temper, the swift victory
83 Despite the conceptual richness of this model, Stransky later adopted an atheoretical perspective that would later still come to be associated with neoKraepelinianism: “…the mere fact that I have to work through the pompous, arrogant, and puffy language of most mediocre philosophers [publishing in psychiatric journals]… causes considerable, almost physical discomfort in me… Every totally mindless brain cobbler or spine cutter does more research work than recent philosophers all taken together” (cited by M. Spitzer, 1991, p. 763; Stransky, 1923, pp. 251–252, 259).
277
over sudden shocks, are guaranteed by the higher general emotions; on
the one hand they give to the background of our mood a definite
coloring even when no emotional stimuli are caused by special internal
or external experiences. Lastly, the inner unity of our will is
conditioned by the general trend of volition which is always alive in us,
and which is the product of our racial and personal development. We
may therefore expect that a weakening or annihilation of the influence
which general conceptions, higher emotions, and the permanent
general trend of volition exercise on our thinking, feeling, and acting,
must draw after it that inner disintegration, those “schizophrenic”
disorders, which we meet with in dementia praecox. It seems to me
that the disorders observed in the patients and the complaints to
which they give utterance, point exactly to injury to the general
scheme of our psychic development, as it fixes the substance of our
personality. The general trend of volition and also the higher emotions
might form the first point of attack. But further the instrument of
general conceptions with its regulating influence on the train of
thought would then also become worthless, if the will were no longer
capable of using it. (Kraepelin, 1919, pp. 75–76, emphasis in original)
Here, we see the influence of Kantian psychology (according to which
concepts and sense perception are inseparably connected through intuition)
278
on Kraepelin’s understanding of the psychopathology of dementia praecox
(Sedler, 1994).
Schizophrenia: A Continuum of Discontinuity
Dementia praecox underwent one more important transformation
under Paul Eugen Bleuler, who conceptualized the disorder as a ‘loosening of
associations,’ leading him to propose the name ‘schizophrenia’ (to which
Kraepelin refers in the passage quoted above). A decade after the publication
of Kraepelin’s classic text, Bleuler criticized the concept of dementia praecox
as antiquated and untimely:
The older term is a product of a time when not only the very concept of
dementia, but, also that of precocity, was applicable to all cases at
hand. But it hardly fits our contemporary ideas of the scope of this
diseaseentity. (Bleuler, 1911a, p. 7)
Scarcely a century earlier, 2,500yearold terms were still current; by the
beginning of the twentieth century, terms scarcely a single decade old were
seen as ancient and out of touch, historical artifacts from a bygone era. Just
as psychiatry became attuned to the continuous course of disease over time,
its diseaseconcepts seemed to follow a rather discontinuous temporal course,
a diachronic loosening of nosological associations. The discontinuous nature
of the knowledgeproduction process became reflected in the knowledge
produced, and dementia praecox became schizophrenia. This term combined

279
the Greek words for ‘to split’ (schizein, σχίζειν) and ‘mind’ (phrēn, φρήν),
because, while it is not “possible to find a perfect name for a concept which is
still developing and changing… the ‘splitting’ of different psychic functions is
one of its most important characteristics” (p. 8). In light of schizophrenia’s
role in establishing a psychiatric nosology in which insanity has been divided
into discrete disease entities, featuring a splitting mind, which, like insanity,
once had been regarded as unitary, seems fitting.
Historians of medicine usually attribute the notion that schizophrenia
is irreversible to Kraepelin, often as a way to distinguish him from Bleuler,
but this is backwards.84 In typically careful, measured scientific prose,
Kraepelin notes: “[The] possibility cannot in the present state of our
knowledge be disputed, that a certain number of cases of dementia praecox
attain to complete and permanent recovery, and also the relations to the
period of youth do not appear without exception” (Kraepelin, 1919, p. 4). For
Bleuler, however, a patient's seemingly permanent recovery is almost
certainly illusory:
[Whenever] I have been able to examine any of those who have been
pronounced cured I have found a residue of the illness. The diagnosis
of a cure has often been rash… I know patients whose achievements in
84 As a representative example, Jablensky suggests that “Eugen Bleuler… modified Kraepelin’s original concept by adding to the scope of dementia praecox clinical illnesses that did not evolve into a ‘terminal state’ of deterioration” (Jablensky, 2011, p. 4).

280
life have been outstanding… [including] business men who
independently build up large and successful businesses, civil servants,
parsons, a poet and a scholar of international renown. The last of
these had suffered two attacks of catatonia before writing a new
scientific work. It was a pleasure to discuss scientific matters with
him even when he was still suffering from genuine delusional ideas.
But when I finally considered him completely ready to resume work, he
was still making crude logical mistakes when one spoke to him about
the complexes which had played a part in his illness. I would not like
to accept as a genuine cure a state in which some parts of the mental
apparatus are permanently inaccessible to logic… When the disease
process flares up, it is more correct, in my view, to talk in terms of
deteriorating attacks, rather than its recurrence. Of course the term
recurrence is more comforting to the patient and his relatives than the
notion of progressively deteriorating attacks. (Bleuler, 1987, pp. 61–62)
In this passage we glimpse the totalizing character of Bleuler’s
schizophrenia, and the strict criteria with which he evaluates a patient's
sanity. Were a cure effected, the patient no longer make ‘crude logical
mistakes’ relating to some past traumatic event or subject of disordered
reasoning. Bleuler is able to take pleasure in discussing stateoftheart
science with a scholar whom he judges to be acutely psychotic. The final
281
insight, that patients are troubled by the likelihood (in his opinion) that
deterioration is inevitable, raises the additional question whether to
prioritize epistemic or therapeutic values, particularly if providing hope and
comfort to a mentally ill patient improves treatment outcomes (Anthony,
1993; Kleinman, Eisenberg, & Good, 1978; Slade, 2010). Kraepelin is
agnostic regarding recovery. Bleuler, however, explicitly excludes the
possibility: “By the term ‘dementia praecox’ or ‘schizophrenia’ we designate a
group of psychoses whose course is at times chronic, at times marked by
intermittent attacks, and which can stop or retrograde at any stage but does
not permit a full restitutio ad integrum” (Bleuler, 1911a, p. 9).
Further, despite a clear nominal discontinuity between ‘schizophrenia’
and ‘dementia praecox,’ Bleuler stresses that they are different labels for the
same fundamental disease entity:
In using the term dementia praecox I would like it to mean what the
creator of the concept meant it to mean. To treat the subject from any
other point of view would serve no purpose, but I would like to
emphasize that Kraepelin’s dementia praecox is not necessarily either
a form of dementia or a disorder of early onset. For this reason, and
because there is no adjective or noun that can be derived from the term
dementia praecox, I am taking the liberty of using the word
schizophrenia to denote Kraepelin’s concept. I believe that the tearing
282
apart or splitting of psychic functions is a prominent symptom of the
whole group and I will give my reasons elsewhere. (Bleuler, 1987, p.
59, emphasis in the original)
In other words: I am using the concept in the same way as Kraepelin did,
meaning what he meant, except that he got it entirely wrong and, even
worse, his neologism is not very catchy, so I have given it a new name and
supplied a new meaning. Of course, to some extent this is simply the
inevitable consequence of making sense of a text (for certainly a nosological
category and its accompanying diagnostic criteria constitute a text imbued
with a surplus of meaning ripe for interpretation) by putting it in other
words; as biblical scholar Bart Ehrman has observed, “to read a text is,
necessarily, to change a text” (2005, p. 217). Given Kraepelin’s emphasis on
prognosis, it is interesting that the title of Bleuler’s article is ‘Die prognose
der dementia praecox: Schizophreniegruppe’ (‘The prognosis of dementia
praecox: Group of schizophrenias’): this suggests that the concept of
schizophrenia developed over time just as the course of schizophrenia
develops in an individual case over time. Further, Bleuler uses the plural
‘schizophrenias’ because he does not view schizophrenia “as a disease in the
narrower sense but as a disease group, about analogous with the group of the
organic dementias, which are divided into paresis, senile forms, etc. One
should, therefore, really speak of schizophrenias in the plural” (Bleuler, 1924,

283
p. 373). This move, justified on the grounds that it facilitated newly possible
‘studies of heredity,’ presaged the later notion of schizophrenia spectrum
disorders (e.g., delusional disorder, psychotic depression, schizotypal
personality disorder, schizophreniform disorder, schizoaffective disorder, and
importantly for the next chapter, psychosis risk syndrome).
Today, schizophrenia often misleadingly suggests something akin to
‘multiple personality disorder’ to a lay audience (interpreting ‘splitmind’ to
mean a psyche divided between more than one personality, rather than
psychic functions undergoing a process of splitting).85 In Bleuler’s time,
however, the name ‘schizophrenia’ hit the right cord as a psychiatric
ideograph (McGee, 1980), containing a powerful combination of precision and
ambiguity:
The term schizophrenia and the idea of a loosening of associations
caught on in part because people thought they knew what was meant
by a loosening of associations but also in part because an adjective
could be made of the term in a way that it couldn’t be made of
dementia praecox. Once coined, words like schizophrenia, neurosis,
85 This misunderstanding is particularly understandable in light of Bleuler’s explanation that “[it] is not alone in hysteria that one finds an arrangement of different personalities one succeeding the other; through similar mechanisms schizophrenia produces different personalities existing side by side” (Bleuler, 1924, p. 134, emphasis in the original German). this passage has sometimes been construed to claim that Bleuler included multiple personality disorder within his broader concept of schizophrenia (Rosenbaum, 1980), Bleuler’s italicization suggests this is a misreading, an argument made most persuasively by Ian Hacking (1998) in a rather scathing criticism of Rosenbaum’s interpretation of Bleuler’s work.
284
and psychosis can be like harpoons; if they go in they can be very
difficult to get out. On such details can important aspects of the
history of medicine turn. (Healy, 1997, p. 35)
Something about the concept of loosening associations was easy for people to
see in others. Helpfully, Bleuler also incorporated the “imagery and
vocabulary of syphilology… [by writing about] ‘severe cases’ requiring
confinement, and ‘latent cases’ lurking about without the patient realizing
that he is ill” (Szasz, 1976, p. 11). Like other mental disorders of its day, as a
‘disease’ schizophrenia was a working hypothesis that may not meet the
criteria of a unified etiology or pathogenesis. The transformation of dementia
praecox into schizophrenia, however, entailed a subtle but very important
change: No longer fixed as a Kraepelinian provisional natural disease entity,
one could conceive of schizophrenia, like the various ‘clinical forms’ from
which it was constructed, as a clustering of signs and symptoms—that is, as a
syndrome (J. N. Morris, 1978).
Conceptually, Bleuler’s schizophrenia extended Kraepelin’s dementia
praecox fairly faithfully, while simultaneously integrating several important
psychoanalytic ideas about the nature of the illness. Three years after it was
published, Swiss psychiatrist and founder of analytic psychology, Carl Jung,
praised Bleuler's formulation as similar to his own:
It is particularly gratifying to me that a psychiatrist of Bleuler’s
285
standing has fully accepted, in his great monograph on the disease, all
the essential points in my work. The chief difference between us is as
to whether the psychological disturbance should be regarded as
primary or secondary in relation to the physiological basis. (Jung,
1960b, p. 155)
Furthermore, Bleuler invokes concepts popularized by Pierre Janet (who, like
Freud, trained under Charcot at Salpêtrière) in order to explain the process
of psychic splitting (‘spaltung’):
In every case, we are confronted with a more or less clearcut splitting
of the psychic functions. If the disease is marked, the personality loses
its unity; at different times different psychic complexes seem to
represent the personality… one set of complexes dominates the
personality for a time, while other groups of ideas or drives are ‘split
off’ and seem either partly or completely impotent… It is the splitting
which gives the peculiar stamp to the entire symptomatology.
However, behind this systematic splitting into definite ideacomplexes,
we have found a previous primary loosening of the associational
structure which can lead to an irregular fragmentation of such solidly
established elements as concrete ideas. The term, schizophrenia,
refers to both kinds of splitting, which often fuse in their effects.
(Bleuler, 1911a, pp. 9, 362)
286
Here, again, the discontinuous gives way to a conceptual continuity, as
Bleuler (loosely?) associates the concept of 'complexes' with fragmented ideas,
and integrates psychodynamic concepts into the Kraepelinian disease
construct. Bleuler appears to have been influenced by Janet’s concept of
désagrégation (dissociation), a fragmentation of the psyche under sharp
affective stress that results in a fixed idea complex (Ellenberger, 1970; Janet
& Raymond, 1903). The term ‘complex,’ of course, is a throwback to a
humoral rhetoric in which disorders of the personality proceed from an
imbalanced complex of vital fluids; in modern times, it first appears in the
work of Karl Kahlbaum’s student, Georg Theodor Ziehen, as ‘gefühlsbetonter
vorstellungskomplex’ (‘emotionallycharged representational complex,’
roughly), and makes its way to Bleuler by way of Carl Jung in 1904 (Freud &
Jung, 1974; Moskowitz & Heim, 2011).86 Though not introduced with a literal
illustration, Jung metaphorically invokes the inventional power of the image
in scientific discourse in his clearest exposition of the appropriated concept:
What then, scientifically speaking, is a “feelingtoned complex?” It is
the image of a certain psychic situation which is strongly accentuated
emotionally and is, moreover, incompatible with the habitual attitude
of consciousness. This image has a powerful inner coherence, it has its
own wholeness and, in addition, a relatively high degree of autonomy,
86 After his final mental break in 1889, Friedrich Nietzsche became Ziehen’s most famous patient at the Jena psychiatric hospital (Wilkes, 2000).

287
that it is subject to the control of the conscious mind to only a limited
extent, and therefore behaves like an animated foreign body in the
sphere of consciousness… My findings in regard to complexes
corroborate [a] somewhat disquieting picture of the possibilities of
psychic disintegration, for fundamentally there is no difference in
principle between a fragmentary personality and a complex. They
have all the essential features in common, until we come to the
delicate question of fragmented consciousness. Personality fragments
undoubtedly have their own consciousness, but whether some psychic
fragments as complexes are also capable of a consciousness of their
own is a still unanswered question… We observe… in certain
psychoses… [that] the complexes get “loud” and appear as “voices”
having a thoroughly personal character. Today we can take it as
moderately certain that complexes are in fact “splinter psyches.” The
aetiology of their origin is frequently a socalled trauma, an emotional
shock or some such thing, that splits off a bit of the psyche. Certainly
one of the commonest causes is a moral conflict, which ultimately
derives from the apparent impossibility of affirming the whole of one’s
nature. (Jung, 1960b, pp. 96–98, emphasis in the original)
This explanation parallels Janet’s etiological account of the ‘subconscious
fixed idea’ (Ellenberger, 1970; Van der Hart & Friedman, 1989; Van der Kolk,

288
Brown, & Van der Hart, 1989; Van der Kolk & Van der Hart, 1989). Bleuler’s
suggestion that a “loosening of associational structure” is behind the
“splitting into definite ideacomplexes” further parallels Janet’s suggestion
that a “weakening of the synthetic activity of the mind” is behind the mental
weakness of psychasthenia (Bleuler, 1911a, p. 362; Janet, 1930; Janet &
Raymond, 1903; Perry & Laurence, 1984, p. 33).87
AntiPsychotics and History
The categories of continuity and discontinuity, as we have seen, can be
extended temporally. So far in this chapter, I have presented an historical
account of the development of psychosis. But that account would be
incomplete without considering how history appears within the rhetorical
economy of psychiatry. I therefore now turn to a brief discussion about the
various temporal orientations that the pharmaceutical industry articulated
through its marketing of phenothiazine antipsychotic drugs. The industry
has imagined and reimagined the history of contemporary psychiatry, along
with the temporal course of psychosis as an object of knowledge, in its efforts
to deal with the contradictions of continuity and discontinuity in the late
capitalist marketplace.
87 Psychasthenia, the disease entity Janet is most known for establishing, is to neurasthenia as Freud’s psychoneurosis is to actual neurosis (Janet & Raymond, 1903). Ellenberger (1970) argues that Bleuler’s schizophrenia is more or less a “transposition” of Janet’s psychasthenia (p. 406). Moskowitz & Heim (2011) argue for an even closer affinity, noting parallel key terms (e.g., ‘lowering,’ ‘leveling,’ ‘weakening,’ and ‘synthesis’) and the features of inherited premorbid susceptibility and mental weakness resulting in the destruction of an individual’s ability to restrain and order the more primitive and chaotic elements of the psyche.

289
As a selfreferential epistemic field, scientific legitimation depends in
part on temporal narratives. While progress in science “is widely recognized
as nonlinear,” and, moreover, only “in hindsight does the development [of
knowledge] appear to have the coherence that creates a sense of a linear,
inexorable path,” it is nevertheless the case that scientific discourses tend to
presuppose a linear flow of time (National Research Council, 2006, p. 73).
The arrow of epistemic progress almost always points toward the future (R.
Morris, 1985).
Time is an epistemic category with a social origin that arises from the
rhythms of our social interactions and institutional practices (Durkheim,
2001; Nowotny, 1992; Sorokin & Merton, 1937). The typical argument form
of scientific rhetoric is temporal—one establishes a link to the past by
summarizing the state of relevant knowledge prior to research, then explains
how the findings update that state, and finally suggests the next steps future
research might take (Fahnestock, 2004; C. R. Miller, 1992; Toulmin &
Goodfield, 1965). Furthermore, an epistemic logic that aims at elucidating
causal relationships entails specific temporal commitments. For these
reasons, scientific authority and institutional legitimation are bound up in
narratives that establish temporal ethos (Kisiel, 1997; Lenzo, 1995;
Suchman, 1995).
Specifically, I examine advertisements for these drugs published in

290
medical journals, and I address two complementary but distinct temporal
maneuvers guided by 'pharmaceutical reason' (Lakoff, 2005). First, I present
a series of advertisements by which the figure of the antipsychotic gets
deployed as a framing device that positions psychiatric modernity as a radical
rupture with the primitive past. 'Western psychiatry' made this sudden
break with the discovery of the antipsychotic properties of the phenothiazine
drug chlorpromazine ('Thorazine'). Everything coming before this discovery
was utterly 'primitive' and barbaric. Messages reflecting this move
metonymically use phenothiazine compounds, especially Thorazine, to
represent scientific progress and the birth of pharmaceutical reason. Kendall
(2011) notes that what was identified here was the “beginnings of the new
science of psychiatry... that married the chemists' laboratory with the
psychiatric ward,” adding a cautionary note: “It is easy to miss an important
fact here: this also marks the birth of a new industry” (p. 267).
Second, I examine how those same drugs get positioned temporally
three decades after their discovery, when other newer antipsychotics
complicated attempts to appeal to the stateoftheart. The central claim is
that the medications discovered in the 1950s by the 'pioneers' are timeless
classics that difficult to improve upon. The latter move is, for obvious
reasons, less commonly found in pharmaceutical marketing copy today, but
shows up in the discourses of psychiatrists. Though these two moves are

291
complementary, they are also in tension, as on one hand the emphasis is on
the discontinuous nature of scientific progress and the temporal ruptures it
produced, while on the other, progress seems to have stopped at the
beginning of the new golden era of scientific psychiatry. As pharmaceutical
reason is the “strategic logic... that links chemical intervention to diagnostic
representation according to the norm of disease specificity,” these rhetorical
embodiments of particular attitudes toward history recur in the context of
nosological controversy (Lakoff, 2005, p. 176).
Phenothiazines as the Discontinuous New
In a twopage advertisement for Thorazine (Figure 3.9), one of a
series, the leftpage caption, “Basic tools of Primitive psychiatry,” appears
above photographs of two museum artifacts: a totem from Zaire, “used to
'drive out' an illness,” and a mask from Nigeria that “honors dead ancestors
and enforces the law” (Smith, Kline, & French Laboratories, 1975a, pp. 406–
407). The opposing caption reads: “Basic tool of Western psychiatry,” under
which appears the name “Thorazine,” along with an abbreviated version of
the prescribing information insert for physicians in small print.
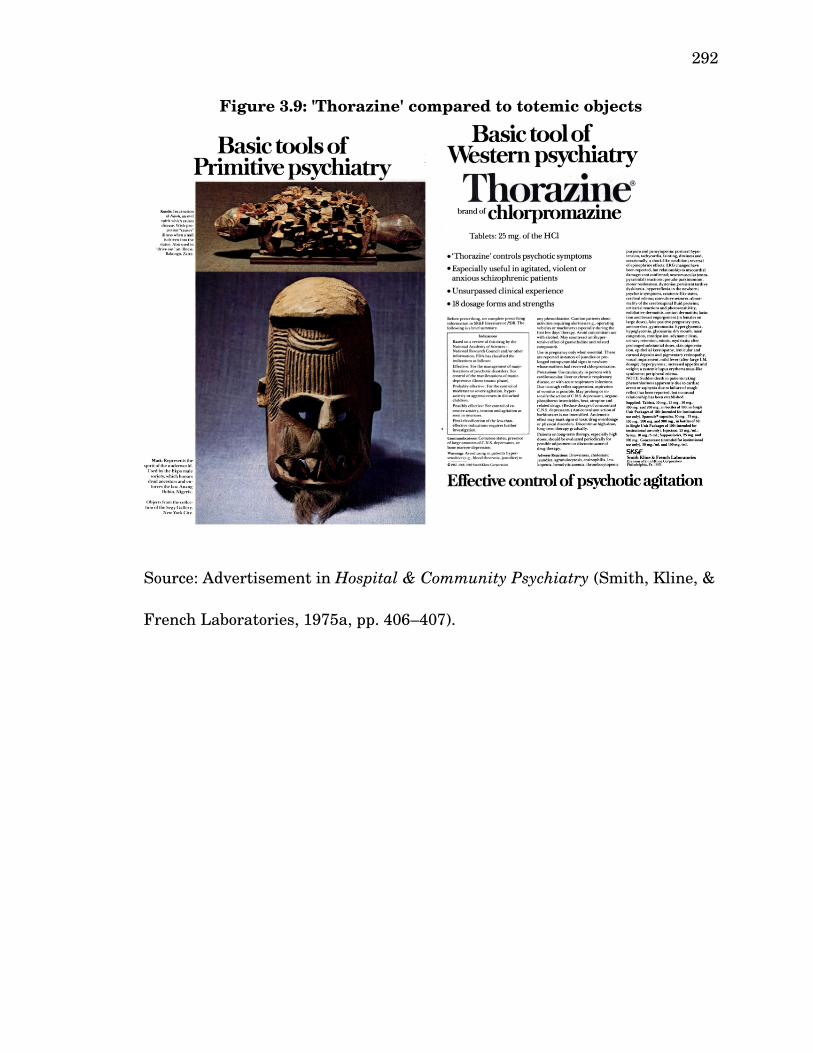
292
Source: Advertisement in Hospital & Community Psychiatry (Smith, Kline, &
French Laboratories, 1975a, pp. 406–407).
Figure 3.9: 'Thorazine' compared to totemic objects

293
A similar advertisement (Figure 3.10), part of a different series, for
another phenothiazine antipsychotic, trifluorperazine ('Stelazine'), features a
photograph of a painted mask found in Mexico on the left page (Smith, Kline,
& French Laboratories, 1975b, pp. 329–330). On the opposing page, the
slogan “Lift the Mask of Psychotic Withdrawal” appears above an abbreviated
version of the prescribing information sheet for Stelazine in small print. The
effect is to emphasize the 'transcultural' nature of the illness treated by
Stelazine, while playing on the dissonance between an image of a tribal mask
and the pageantry of modern psychopharmacological science. The
advertisement also illustrates how pharmaceutical reason reconfigured the
category of psychotherapeutic intervention: The audience is told that
“psychotic withdrawal,” treatable with Stelazine, “can make [schizophrenic
patients] inaccessible to therapy.” In this way, administration of an
antipsychotic is both a therapeutic technique and a “disciplinary technology”
which works “on the body, in order to help produce the subject as a speaking
being” (Lakoff, 2005, p. 84).
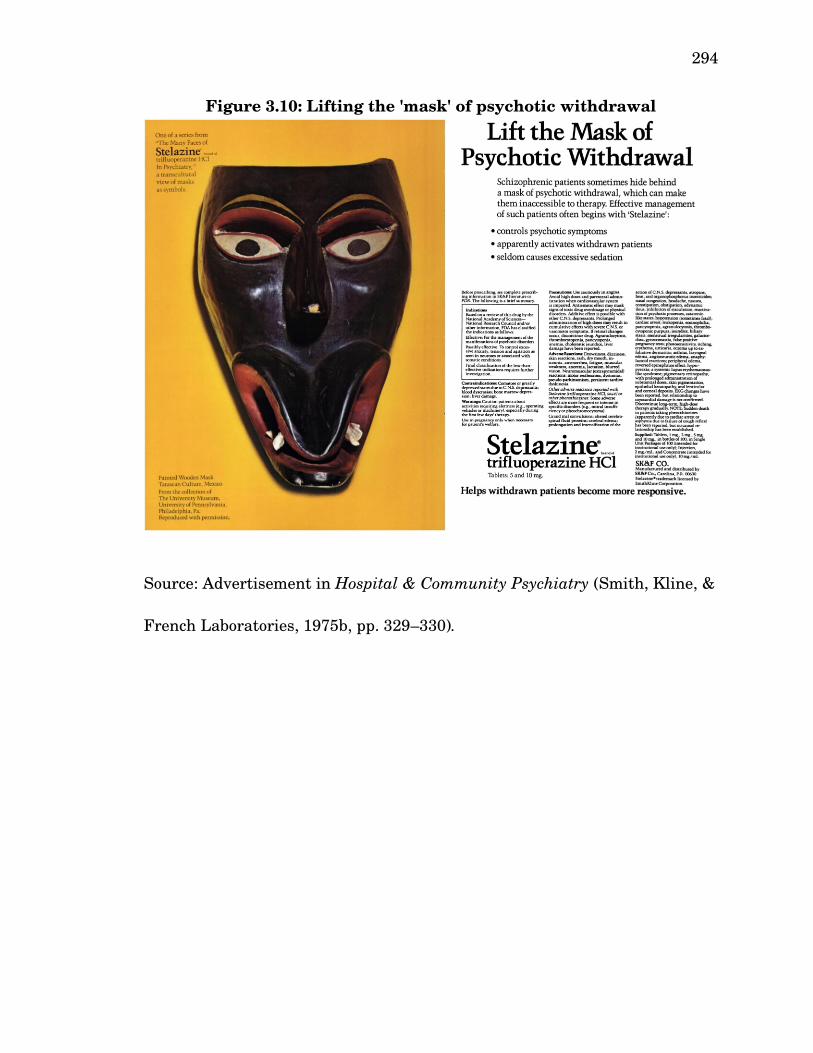
294
Source: Advertisement in Hospital & Community Psychiatry (Smith, Kline, &
French Laboratories, 1975b, pp. 329–330).
Figure 3.10: Lifting the 'mask' of psychotic withdrawal

295
Another advertisement for Thorazine (Figure 3.11), printed sixteen
years earlier, contains an image from a wood engraving depicting a “surprise
bath,” supposedly “used in colonial times 'to restore the distracted to their
senses'” (Smith, Kline, & French Laboratories, 1959, pp. 52–53). A second
illustration demonstrates how this 'treatment' worked: a lever is pulled,
which results in a presumably mentally ill man falling through a trap door in
the floor into a pool of water. The advertisement explains: “Less than 200
years ago, the mentally ill were bled, purged, beaten, and sometimes nearly
drowned in efforts to restore them to their senses. The treatment of mental
illness has progressed far beyond methods such as these.”
Thorazine is described as a “fundamental drug” and a kind of
“chemotherapy” for mental illness. It owes its significance to both its
unparalleled therapeutic efficacy and its role in “the development of related
drugs which offer the psychiatrist opportunities to help an even greater
number of patients.” This drug that now restores one's senses had been used
only a few years earlier as a general anesthetic, branded as 'Largactil,'
reflecting “initial perceptions of its likely large range of action” (Healy, 1997,
p. 181, emphasis in original). While in this advertisement, Thorazine is still a
general treatment for “mental illness,” it is just a few years from being
understood as a highly specific treatment for schizophrenia (or even more
specifically as a treatment for “psychotic agitation,” as in Figure 3.9).
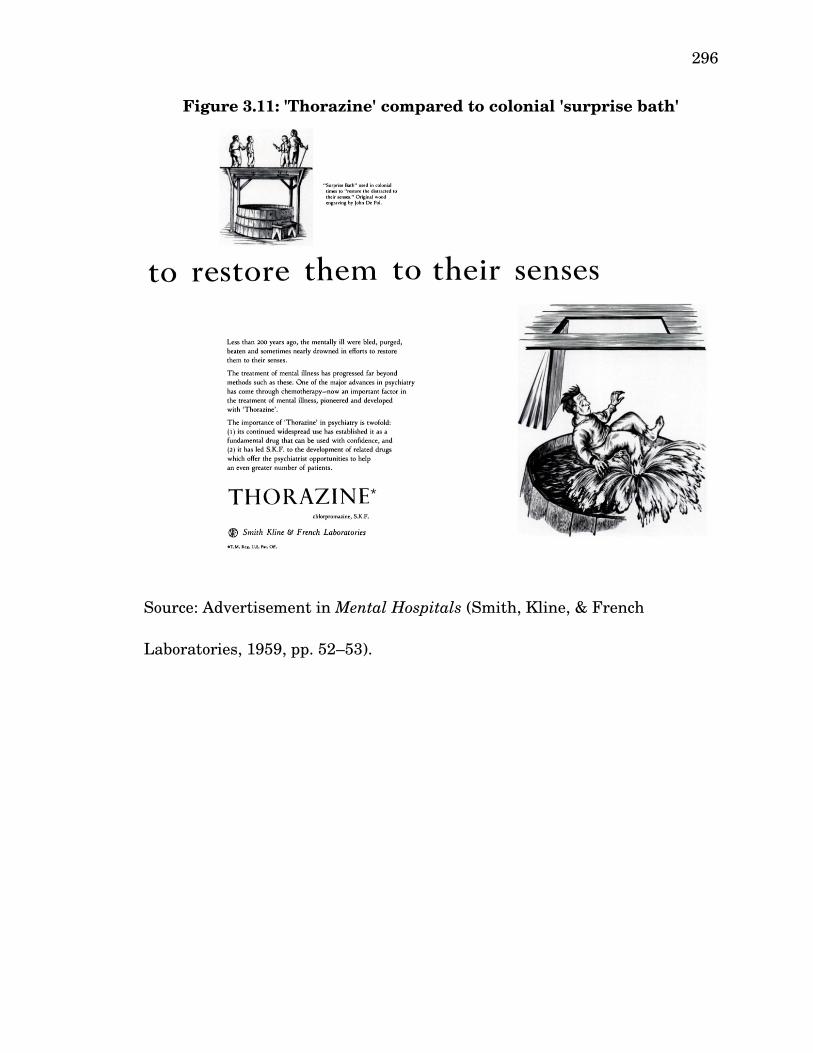
296
Source: Advertisement in Mental Hospitals (Smith, Kline, & French
Laboratories, 1959, pp. 52–53).
Figure 3.11: 'Thorazine' compared to colonial 'surprise bath'

297
All three of these advertisements show how the pharmaceutical
industry cultivated an attitude toward antipsychotic drugs, the discovery of
which inaugurated an era profoundly discontinuous with psychiatry's archaic
past. Taking advantage of the emphasis in modern science on the linearity of
time, these advertisements exemplify a strategy by which one emphasizes the
novelty of some idea, technique, or product by dissociating it from its
historical antecedents.88 This strategy is not without its hazards:
Because linear time is sequential and progressive, any ‘cracks’ in the
dissociative strategy, i.e., any lingering continuities between past and
present, may render current issues as outmoded as the history they
echo. That is, associations between past and present may cast the
88 This dissociative strategy is by no means unique to science, or even to the modern world. St. Paul employed it in his conflict with James, Peter, and the Jerusalem church, concerning Jewish dietary law and circumcision:
I want you to know, brothers and sisters, that the gospel I preached is not of human origin. I did not receive it from any man, nor was I taught it; rather, I received it by revelation from Jesus Christ. For you have heard of my previous way of life... I was advancing in Judaism beyond many of my own age among my people and was extremely zealous for the traditions of my fathers. But when God... was pleased to reveal his Son in me so that I might preach him among the Gentiles, my immediate response was not to consult any human being. I did not go up to Jerusalem to see those who were apostles before I was, but I went into Arabia... I assure you before God that what I am writing you is no lie. (Galatians 1:1120, New International Version)
Paul establishes ethos by referring to his knowledge of the traditions which he now rejects, and by emphasizing the novelty of his teaching, insisting, rather vehemently, that he did not consult anyone who actually met Jesus for years. This break with the past was so radical that it inspired one of Paul's secondcentury followers, Marcion of Sinope, to proclaim that the god of the Torah is an evil demiurge, and Jesus (and his one and only apostle, Paul) revealed the existence of a god who had previously been completely unknown. This in turn, according to Tyson (2006), led secondcentury protoorthodox Christians to author the Acts of the Apostles, which explicitly contradicts Paul's claims in his Epistle to the Galatians, quoted here (see, for example, Acts 9:131). This example illustrates the wide range of the rhetorical topics of historical continuity, and the discontinuity of ingenium.
298
present as retrogressive as the past, rather than coloring the past as
progressive as the present. (Lake, 1991, p. 128)
Fear of the consequences of insufficient temporal dissociation almost led the
group of psychiatrists associated with 'neoKraepelinism' to reject that label:
We didn't like it for a long time. I think we were afraid it would seem
too oldfashioned an idea, even though we insisted that all our
residents read Kraepelin's monographs and emphasized his work with
the medical students. But we were worried that the label didn't point
in the right direction. (Guze, 2000, p. 405, my emphasis)
Similarly, I read the drive to root out lingering psychodynamic diagnoses
(e.g., conversion disorder) from the DSM in light of this concern. Their
presence seems archaic, and since a neuropsychiatric analogue has yet to be
discovered, the only option is to come up with new names.
Pharmaceutical companies faced a similar problem as new medications
accumulated. In the 1950s and early 1960s, psychopharmacologists
discovered an array of extraordinarily effective psychiatric medications. By
and large, the medications discovered since then have not exceeded their
predecessors in efficacy (Healy, 1997, 2004b; Hyman, 2013; N. S. Rose, 2007;
Taylor, 2013). This is not a fact generally highlighted by the pharmaceutical
industry, but it arose in the 1980s in the context of marketing some of the
older drugs.

299
Phenothiazines as the Continuous Old
Three decades after the discovery of the antipsychotic effects of
chlorpromazine, with newer antipsychotics on the market, advertisements for
the older drugs ceased emphasizing the importance of novelty. Marketers
rebranded the same drugs that once had been heralded as a radically
discontinuous break with a hopelessly primitive past as timeless classics.
Two similar advertisements in the American Journal of Psychiatry recast
'Stelazine' as classic, traditional, and perhaps even an historical masterpiece.
In one (Figure 3.12), a photograph showing a bust of Beethoven contains the
text: “Some things are hard to improve upon.” On the opposing page, the
message “'Stelazine' A Classic Antipsychotic” stands above a comparison
between trifluorperazine and Beethoven's Fifth Symphony (Smith, Kline, &
French Laboratories, 1981a, pp. A46–A47). One is tempted to take this as a
highly ironic affirmation of a point made almost four decades earlier by
Horkheimer and Adorno (2002), dismissing the phenomenon of 'metoo'
antipsychotics as a sort of “caricature of style” that contrasts with the
“genuine style of the... great [psychopharmacological] artists... who adopted
style as a rigor to set against the chaotic expression of suffering” (p. 103). An
advertisement (Figure 3.13) appearing a few months later similarly compared
trifluorperazine to Homer's Iliad (Smith, Kline, & French Laboratories,
1981b, pp. A30–A31).
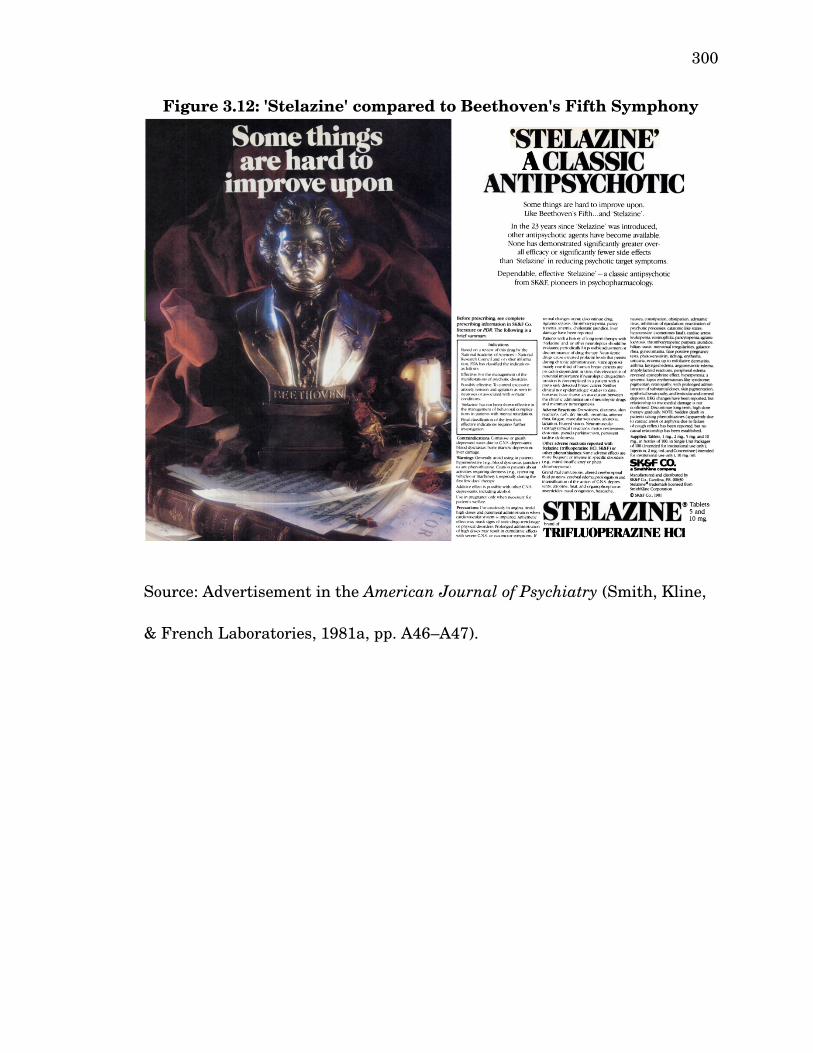
300
Source: Advertisement in the American Journal of Psychiatry (Smith, Kline,
& French Laboratories, 1981a, pp. A46–A47).
Figure 3.12: 'Stelazine' compared to Beethoven's Fifth Symphony

301
Source: Advertisement in the American Journal of Psychiatry (Smith, Kline,
& French Laboratories, 1981b, pp. A30–A31).
Figure 3.13: 'Stelazine' compared to Homer's Iliad

302
Today, with the patents long expired on these drugs, pharmaceutical
companies are much less eager to come to the defense of these canonical
classics of modern medicine. Instead, they now champion the 'atypical' class
of antipsychotics, modeled after the dibenzodiazapine drug clozapine
('Clozaril'), a remarkably effective drug that was relatively less likely to
produce extrapyramidal symptoms (EPS) like tardive dyskinesia, the bane of
patients treated with traditional antipsychotics.89 Psychiatrists today,
however, sometimes discuss the difficulty in improving on the classic
antipsychotics, as in Michael Taylor's jeremiad against the “malignant
influence of the pharmaceutical industry on the prescribing of psychotropic
agents”:
Another fiction is that medical psychiatric treatments are better today
than they were 40 years ago... The newer antidepressant medications,
mood stabilizers, and antipsychotic agents have no greater efficacy
than the older agents. The secondgeneration TCAs and lithium still
have the best efficacy data and side effect profile... Psychiatrists accept
the promotional fictions of industry and insist that unlike the rest of
89 Unfortunately, a different sideeffect led to clozapine's quick withdrawal from the market in 1975, when eight patients being treated with clozapine in Finland died from agranulocytosis, a condition in which one's immune system becomes severely compromised (Kendall, 2011). Clozapine was eventually reintroduced in 1989 in light of its reported effectiveness in 'atypical' cases of schizophrenia in which the symptoms were “treatmentresistant” (Kane, Honigfeld, Singer, & Meltzer, 1988, p. 789). The emergence of 'treatment resistance' as a diagnostic category is a clear example of the tendency, under the regime of pharmaceutical reason, whereby “[illness] comes gradually to be defined in terms of that to which it 'responds'” (Lakoff, 2005, p. 7).
303
human kind we are not influenced by advertising. We are. (Taylor,
2013, p. 146)90
Similarly, referring to the genetic categories of 'firstgeneration
antipsychotics' (FGAs) and 'secondgeneration antipsychotics' (SGAs),
Kendall (2011) argues, on the basis of a metaanalysis of 150 studies
comparing antipsychotic drugs, that “there are no consistent differences
between atypicals and typicals, SGAs and FGAs... The story of the atypicals
and the SGAs is not the story of clinical discovery and progress; it is the story
of fabricated classes, money and marketing” (p. 267). His conclusion,
affirming that “they are all just plain antipsychotics,” reinforces the idea that
like, perhaps, epic lyric poetry, some things are just hard to improve upon (p.
268)
The pharmaceutical industry obviously has no need to maintain
consistency in its messaging and, as I noted, the messages do complement
one another in emphasizing the fundamental distinctiveness of the
psychiatric drugs discovered in the 1950s. “Rhetoremes” recirculate through
the historical discourses of pharmaceutical reason, rewriting psychiatry's
relationship with its past (Salazar, 2011, p. 103). Chapter 4 will explore the
negative effects of the temporal dislocation that accompanies the
reconfiguration of diagnostic categories for the controversy over 'psychosis
90 This problem is hardly unique to psychiatry. No pharmaceutical treatment for acute heart failure developed over the last two decades has decreased mortality (Jauhar, 2014).

304
risk.' These advertisements reveal the ways in which modern psychiatry
views its own historical timeline, and illustrates how the forms of past
appeals can reemerge, presenting rhetorical liabilities and opportunities.
Schizophrenia & Psychosis Today
As the concept of schizophrenia developed over the course of the 20th
century, it became closely paired with the concept of psychosis. In DSM5, it
appears in the section ‘Schizophrenia Spectrum and Other Psychotic
Disorders’ (American Psychiatric Association, 2012b). Like the DSMIV and
ICD10 classifications, the DSM5 classification of schizophrenia is firmly
within the (neo)Kraepelinian tradition, built upon the concept of the disease
entity, and with the basic assumption that clinical symptoms, longitudinal
course and prognosis, and brain pathology are closely linked. Furthermore,
the modern conceptual understanding of psychosis descends from Erwin
Stransky's notion of intrapsychical discoordination, which Eugen Bleuler
popularized as a loosening of associations within the psyche. Once the will,
emotions, and cognitions of a patient are disconnected in the context of a
‘formal thought disorder,’ the patient is fundamentally disconnected from
reality.
This break with reality is key to the modern understanding of
schizophrenia and psychosis. Bleuler’s formulation of schizophrenia resides
not in the contemporary psychotic disorders so much as in the dissociative
305
disorders, which are characterized by “a disruption in the usually integrated
functions of consciousness, memory, identity, or perception of the
environment” (American Psychiatric Association, 1994, p. 477). Whether by
perceiving objects that do not exist (hallucinations), believing things that are
manifestly false (delusions), speaking so incoherently that meaningful
intersubjective interaction cannot occur (disorganized communication), or
withdrawal from the world in emotion (flat affect) and intention (avolition),
psychosis manifests as a loss of contact with reality. The critical test is
whether an individual maintains ‘reality testing’ procedures. For example, if
a patient hears voices but attempts to verify whether the source is external
(recognizing the possibility that the ‘voices’ are in fact auditory
hallucinations), the patient is not psychotic; if, on the other hand, the patient
cannot be convinced (having ‘delusional conviction’) that his or her
hallucinatory perceptions are unreal, the patient suffers from 'frank
psychosis.'
This modern idea of psychosis is a rearticulation of the ancient idea of
madness. The psychotic patient is out of reach, disconnected from the
objective material world by delusions and perceptual disturbances, from the
intersubjective world by grossly disorganized communication, from the
subjective world by affective flattening and other negative symptoms, and
from the industrialized modern world by severe functional impairments.
306
Before Hippocrates, such a disconnection was brought about by divine or
alien intrusion into the human body; for Hippocrates, by an imbalance of
liquids within the body creating a disturbance within the brain; and for
nineteenth and twentiethcentury alienists and psychiatrists influenced by
faculty psychology, by a loosening of intrapsychic associations. Today, the
pathophysiology of psychosis is understood largely as it was in the past,
albeit expressed in the technoscientific language of neurobiology and
materiality. Just as Hippocrates and Galen converted the spiritualized
accounts of disease into physiological ones, modern neurobiologists have done
the same to the older psychodynamic explanations that seemingly have
passed away. Instead of imbalanced humors, we see disturbed
neurotransmission postulated by the dopamine hypothesis (too much
dopamine) and the glutamate hypothesis (not enough glutamate) of
schizophrenia (Laruelle, Kegeles, & AbiDargham, 2003; Moghaddam &
Javitt, 2011; J. M. Stone, Morrison, & Pilowsky, 2007; Swerdlow & Koob,
1987).91
91 These hypotheses, which I have dramatically oversimplified, are interestingly enough in part the products of extreme substance abuse. The recognition that overactivity in the mesolimbic dopaminergic pathway plays a role in psychosis came after observing the psychosis associated with very large doses of stimulant drugs (e.g., cocaine, methamphetamine) and certain treatments for Parkinson’s disease (e.g., LDOPA), both of which facilitate the transmission of dopamine in the central nervous system. This discovery led to the elucidation of the pharmacological mechanism of chlorpromazine and the other neuroleptic drugs (namely, antagonism of the D2 family of dopamine receptors). Neuroleptics, especially the newer ‘atypical’ class that began with clozapine, also antagonize 5HT2A (a subtype of serotonin) receptors, through which the effects of Lysergic acid diethylamide (LSD) and psilocybin (the active hallucinogenic ingredient in socalled ‘magic mushrooms’ are mediated. Likewise, observations of the psychotic states associated with phencyclidine (PCP),
307
As we have come to expect, these hypotheses lend themselves to iconic
representation:
[Molecular] brain processes had become accepted enough to be
represented in conventionalized visual simulations, ...replete with
images simulating the neuronal processes underlying different
pathologies... In Stahl’s iconography, each neurotransmitter is allotted
a distinct icon—norepinephrine, for example is a triangle—and each
receptor is illustrated with a reciprocal icon—in this case a rectangle
with a triangle shape cut out—into which the neurotransmitter fits
like a key into a lock… These powerful and compelling simulations
combine a matteroffact materiality, iconic character, and languid
truthfulness. They also diagram a molecular specificity of different
types of disorder. Once imagined in this way, pathologies can be
illustrated visually as variations from this “normal” state…
Schizophrenia can be…illustrated with a moving image of a synapse
with dopamine molecules jumping across it—clearly an excess of them
in the “schizophrenic brain.” (N. S. Rose, 2007, pp. 200–201)
These illustrations of madness lack any representations of the mentally ill
patient, but reintroduce a human element by anthropomorphizing some of
the molecular elements.
a drug that blocks the NmethylDaspartate (NDMA) glutamate receptors, led to the glutamate hypothesis of schizophrenia.

308
Stahl’s (2008) illustration of a variant of the glutamate hypothesis
(Figure 3.14) provides a fascinating example of this kind of move. For
reasons that are not entirely clear, walking individuals each holding a sign—
politically ‘radical’ protesters, perhaps—stand in for “toxic free radicals” that
have been “generated in the neurodegenerative process of excitotoxicity”
(Stahl, 2008, p. 442). The “neuroprotective” drug—a “free radical
scavenger”—that comes to the rescue appears to be PacMan’s evil twin, a
yellow spherical monster with sharp teeth and eerie red eyes. The limp
corpse of one activist, still hanging from the jaws of one of these
neuroprotective agents, no longer capable of grasping the sign that has now
fallen to the ground, evidences the effectiveness of this “novel glutamatergic
treatment” supposedly depicted in the scene of carnage. All of this action
takes place presumably on the surface of a neuron, next to a massive
structure apparently representing the NmethylDaspartate (NMDA)
receptor protein and ligandgated ion channel. The small yellow circles
represent the ultimate source of the free radicals: calcium ions (Ca2+) flowing
into the neuron. Another illustration (Figure 3.15) signifies this process
whereby “dangerous enzymes... produce troublesome free radicals” (p. 306).
A third depicts a scenario in which free radicals are left unchecked (Figure
3.16). This illustration connects a molecular event to a lesioned neuron,
which is associated with nearby icons representing psychotic symptoms.
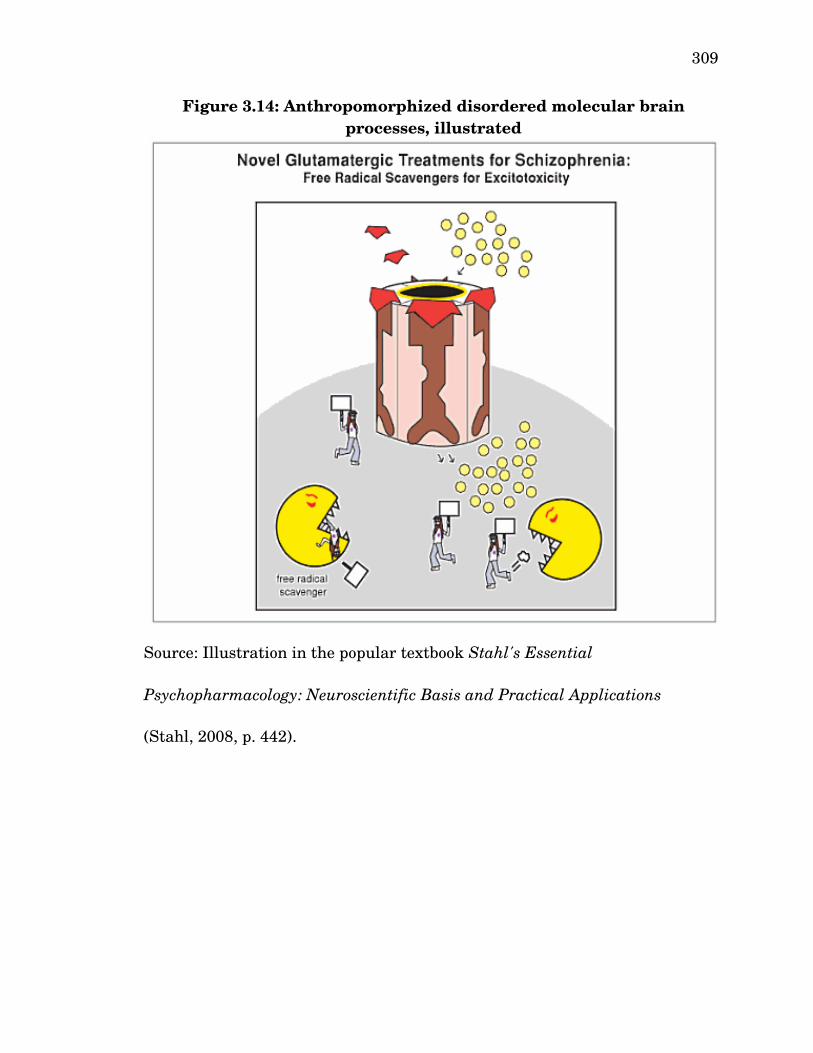
309
Figure 3.14: Anthropomorphized disordered molecular brain processes, illustrated
Source: Illustration in the popular textbook Stahl's Essential
Psychopharmacology: Neuroscientific Basis and Practical Applications
(Stahl, 2008, p. 442).
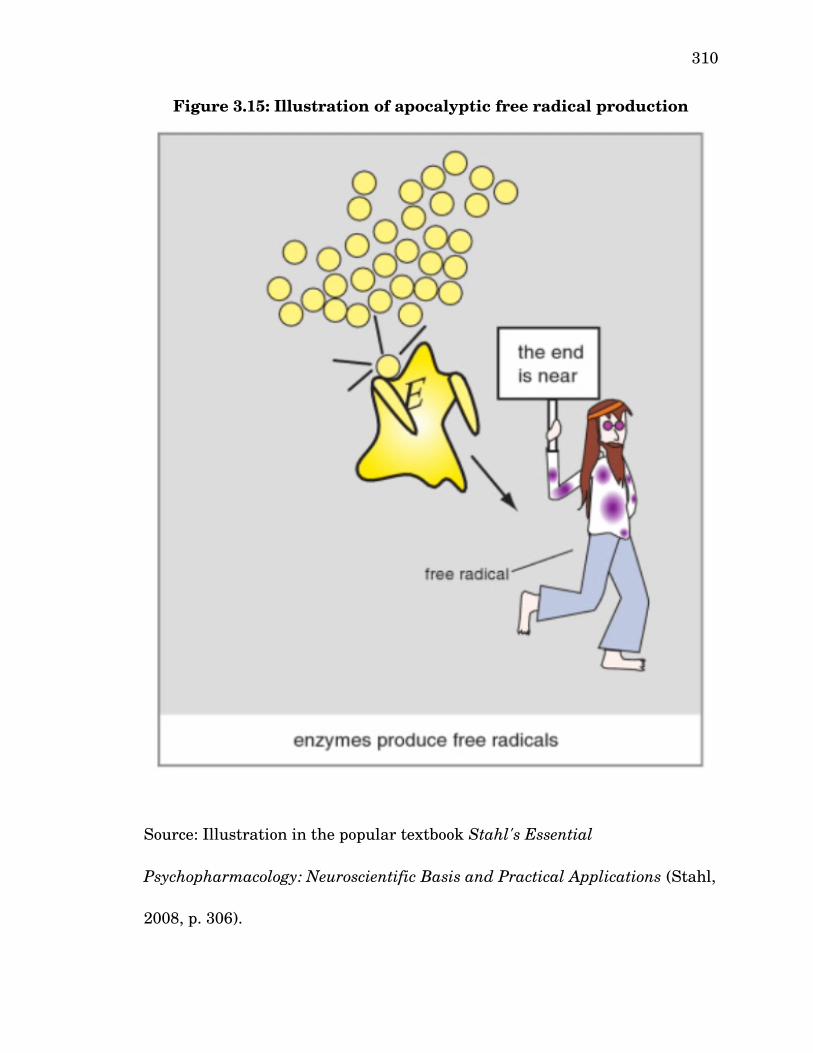
310
Source: Illustration in the popular textbook Stahl's Essential
Psychopharmacology: Neuroscientific Basis and Practical Applications (Stahl,
2008, p. 306).
Figure 3.15: Illustration of apocalyptic free radical production

311
Source: Illustration in the popular textbook Stahl's Essential
Psychopharmacology: Neuroscientific Basis and Practical Applications (Stahl,
2008, p. 307).
Figure 3.16: Excitotoxicity, cell death, and psychotic symptoms
312
Ideas about the health of the individual and ideas about the health of a
society tend to be closely related, which is why healthrelated metaphors
show up so frequently in sociopolitical discussions. Paradigmatically, in his
Republic, Plato contrasts a ‘healthy’ city with a ‘feverish’ one (Plato, 1997d,
sec. 372e–373a). In Stahl's illustrations, we see the same move in reverse,
with a sociopolitical metaphor showing up in expert biomedical discourse
(specifically, in a technical textbook for medical students, physicians,
psychopharmacologists, and neuroscientists—not a lay audience). Are Stahl's
degenerate ‘radicals,’ walking a picket line or attending a political rally, a
toxic source of madness afflicting our society? The images certainly contain
authoritarian overtones that recall a time when, some believed, psychiatry
stood simply for the involuntarily confinement of social deviants. Other
illustrations in the text suggest that Stahl understands the molecular action
of pharmaceutical agents in disciplinary terms. For example, his icon for
donepezil ('Aricept'), a reversible acetylcholinesterase inhibitor used to
manage the symptoms of Alzheimer's disease, is a straitjacket marked with
the American and Japanese flags (Figure 3.17). The flags, which distinguish
donepezil from the other compounds also iconically reduced to straitjackets,
were presumably chosen because the Japanese pharmaceutical company
Eisai developed the drug, and the Americanbased multinational
pharmaceutical corporation Pfizer marketed it.
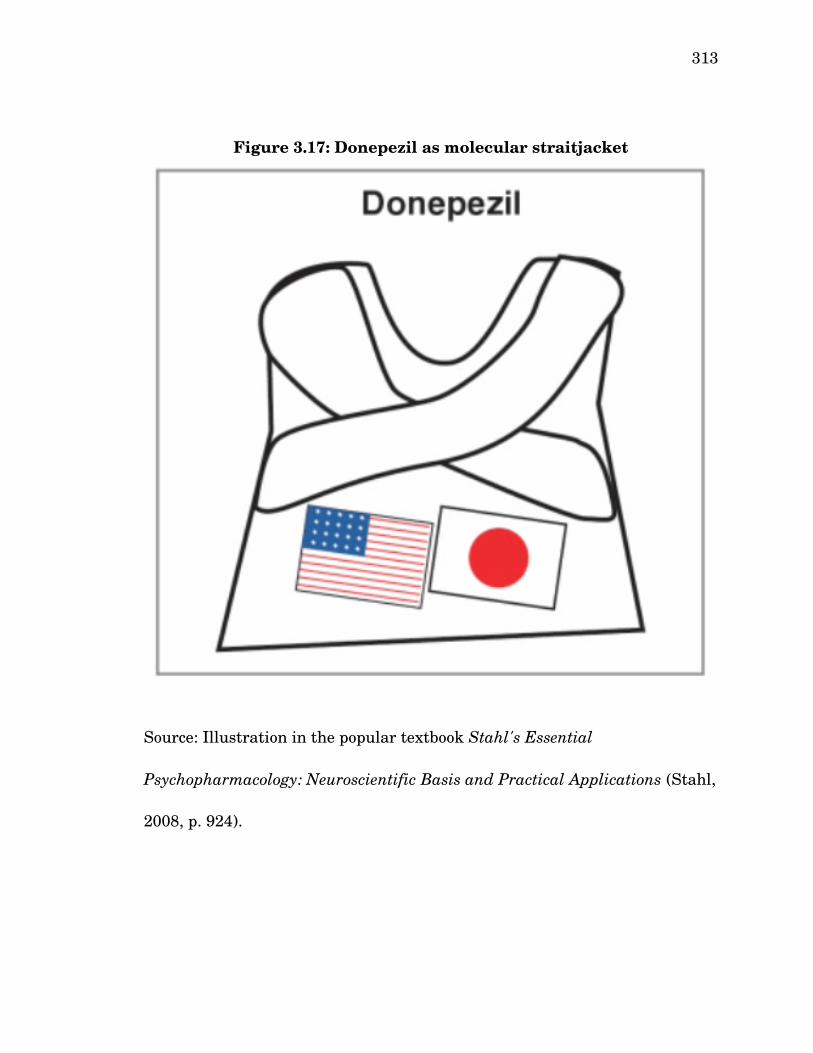
313
Source: Illustration in the popular textbook Stahl's Essential
Psychopharmacology: Neuroscientific Basis and Practical Applications (Stahl,
2008, p. 924).
Figure 3.17: Donepezil as molecular straitjacket

314
Just as humoral rhetoric finds contemporary application in the
representations of molecular neurotransmission dysfunction, the residues of
the rhetorical histories of medicine form an epistemic assemblage with
structural magnetic resonance imaging (MRI) technologies, which encourage
researchers to see the brain in terms of deficiencies and excesses of white and
gray matter and in terms of normal or abnormal anatomical structures. The
discursively constructed MRI imagery works to persuade the world that the
psychic ‘lesions’ of schizophrenia take the material form of deficiencies in the
volume of gray matter in the medial temporal lobe, heteromodal association
cortex, and superior temporal gyrus (Falkai, Schmitt, & Cannon, 2011).
Channeling Virchow, these deficits were conceived initially as cellular lesions
(E. C. Johnstone, Frith, Crow, Husband, & Kreel, 1976), but newer
developments in neuroimaging technology, including diffusion tensor imaging
(DTI) and in vivo functional MRI (fMRI), revealed problems with the myelin
or axonal membrane in cortical regions, as well as unusually low white
matter anistrophy, all of which suggested to neuroscientists that the neural
networks of psychotic patients were losing connections between neurons
(Davis et al., 2003; Jafri, Pearlson, Stevens, & Calhoun, 2008; Josin & Liddle,
2001; Kubicki et al., 2007; Vercammen, Knegtering, den Boer, Liemburg, &
Aleman, 2010). With this, a mechanistic physiological account—the
“disconnection hypothesis of schizophrenia”—of schizophrenia's conceptual

315
‘loosening of associations’ was born (Friston, 1998, p. 115).92
Conclusion
Before moving to the next chapter, I shall summarize this chapter's
key findings. First, we examined the enduring presence of old epistemic
models as the field of medicine developed, the first and primary example of
which was humorism. I argue that the humoral model's longevity was not
due to its 'accuracy,' in the positivist sense of enabling one to make falsifiable
predictions. Rather, I explain its success rhetorically. Humorism provided
an architectonic communicative structure to the field of medicine that
infiltrated linguistic structures and other fields of knowledge, effectively used
visual appeals to justify its claims, and was remarkably robust in adapting to
new findings, innovations, and situations through a process of “casuistic
stretching,” that is, “introducing new principles while theoretically remaining
faithful to old principles” (Burke, 1984a, p. 229). This capacity was not
unlimited, and, eventually, the model became so unbalanced that it no longer
was tenable. The modern 'scientific' approaches to medicine displaced the
humoral architectonic. As I argue, humorism survives today in fragmented
hybrid discourses that contribute to the overall polytechtonic rhetoric of
contemporary psychiatric nosology.
One major finding is that a persuasive epistemic model that manages
92 These issues will be discussed further in the next chapter in the context of psychosis risk syndrome.
316
to stay persuasive from one generation to the next—i.e., that successfully
reproduces itself—does so by spreading through cultural channels, using
figures of speech to travel between contexts and fields. That the humoral
model of pathology was so successful speaks to the persuasiveness of the
rhetorical forms to which it gave rise. By embedding itself in the language of
everyday life, its forms continue to circulate today: when we frame pathology
in terms of imbalance, deficiency, and excess; when we speak of personality
as temperament; when we appeal to synechdochic imagery to communicate
ideas about new disease constructs; when we buy and sell the endless array
of dietary supplements available to the health consumer; when we sip a dry
wine while watching a dark comedy. In these examples we see some of the
substantive ideas of humoral pathology (illness is caused by chemical
imbalance), its ordering structure (health is holistic and continuous), and its
implications (a disordered personality is as much a health issue as a
disordered organ, and moreover, its cause is a disordered organ). It has
infiltrated our language to such a degree that we no longer have any idea
that words like temperature, temperament, and temperate have anything to
do with one another, let alone that they originate in humoral pathology.
As successful as humorism was (and is), it is even more remarkable
that the more mythical understanding of illness that it supplanted also
remains with us today. We refer, for example, to a convulsive episode as a
317
'seizure' even though we do not believe it to be the result of a supernatural
entity taking temporary possession of the body. The transition from this
mythical view to the more 'scientific' humoral model also remains as an ideal.
Yet what remains of the mythical are not merely the fossilized linguistic
remnants of a forgotten age, but an enduring point of contact. Consider, for
example, the history of the dissociative disorders (DD). We have already
examined the rise and fall of animal magnetism, which Mesmer positioned as
a 'scientific' alternative to possession and exorcism. As for the underlying
disorder, it made its way into DSMIII:
With a change in the dominant paradigms for understanding (and
expressing) mental illness, the possession states did not abruptly cease
to exist. Instead, what we now call MPD [multiple personality
disorder] and DDNOS [dissociative disorder not otherwise specified]
began to be described in the literature without a supernatural
explanation... [These] conditions are no more than the secular
expression of the same psychological structures that were found in the
JudeoChristian possession syndromes. MPD is the contemporary
demystified form of an anthropological commonplace. (Kluft, 1993, p.
88)
Noll (2014) suggests that this nosological move constituted an expansion of
“the jurisdictional boundary of 'scientific' psychiatry and [colonization of] the
318
supernatural,” but “the blurring of this boundary” that allowed psychiatrists
to claim “superior therapeutic expertise for techniques that had formerly
been the province of magicoreligious practioners (exorcists)... would backfire,
pulling many of them into the rip tide of Satanic panic” (p. 2).93 This 'Satanic
panic' came in the form of thousands of MPD patients who, through hypnosis,
'recovered' memories of Satanic ritual abuse from their childhood, which they
had 'repressed.' Institutionalizing the diagnosis of MPD did not supplant the
mythical notion that people could be possessed by evil spirits; to the contrary,
it simply created a hybrid scientificsupernatural construct which validated
the mythical idea along with the ensuing moral panic about Satanic cults. As
Allen Frances remarked in a comment on Noll's article on April 3, 2014,
“modern man has acquired remarkable knowledge but is still capable of
remarkably primitive thinking and cruel action.”94
The early modern transitional period during which humorism lost its
hegemonic grip on medical science began with Thomas Sydenham, who
93 In a very heated reply, Richard Kluft argues: “While Dr. Noll accuses me of promoting the colonization of the supernatural, an alternative explanation might be that I have studied the literatures of anthropology and the history of psychiatry to appreciate the wisdom of understanding DID [Dissociative Identity Disorder] as a secularized expression of possession syndromes... What Dr. Noll excoriates may be understood, alternatively, as a crosscultural sensitivity increasingly embraced by our profession” (Kluft, 2014, p. 4). In the same reply, Kluft makes use of apophasis to respond to what he perceived as personal attacks: “In my response I will not counterattack Dr. Noll for his egregious and regrettable ad hominem remarks. Here I will simply state my aversion to attacks against individuals, and my conviction that they distract from rather than enhance one's argument (p. 3).94 Frances also explains here that his vocal opposition to DSM5 was partly motivated by guilt about his failure to use his position as Chair of the DSMIV Task Force to oppose the satanic ritual abuse false epidemic.
319
popularized quinine as a treatment for malaria, founded the field of
epidemiology, and introduced the ontological concepts of syndrome and
discrete disease entity. Sydenham challenged the prevailing association
between hysteria and the uterus. Equipped with the ontological
interpretation, Sydenham distinguished between symptoms and disease
entities, which led to his insight that hysteria was most likely a mental
illness. Later physicians, who rejected this view, reimagined the illness in
terms of bodily 'vapors.' The vapors became an immensely popular illness in
the eighteenth and nineteenth centuries, and the phenomenon attracted
epidemiological social critique that associated it with gender, sexual
behavior, and social class. Twentiethcentury psychoanalysts reformulated
the disorder again as 'conversion disorder,' an illness in which inner psychic
tension 'converts' into somatic distress. Finally, the DSM5 Somatic Distress
Disorders Work Group (later renamed the Somatic Symptoms Disorders
Work Group) attempted to rebrand the disorder as 'functional neurological
disorder.' Each transition point represents a major shift in substantive
theory and rhetorical form. The DSM5 controversy concerned how
psychiatry should come to terms with these accumulated theories and forms,
rather than any genuinely scientific matter.
Rudolph Virchow's physiological interpretation of pathology helps
explain how hysteria became vaporous. In the wake of major developments

320
in the science of human anatomy down to the cellular level, physiological
pathology represented a backlash against the metaphysical elements of the
ontological interpretation. Similar to humorism, the physiological
interpretation cast pathology as the result of disordered processes in the
body, which often manifested as visible organic lesions. Physicians looked for
physiological damage proximate to the clinical signs and symptoms. Hysteria
causes a wide range of symptoms in every area of body, so the unseen
physiological cause must be something that could move throughout the body
from one organ system to another. Hence, the vapors.
Rudolph Virchow had originally conceived of the physiological
interpretation as an alternative to the ontological interpretation, but by the
end of his career, he argued that the two interpretations were actually
compatible. Therefore, I analyzed the integration of the two terministic
screens, one emphasizing continuity, the other discontinuity. As this strange
discursive permutation came into existence, the influence of faculty
psychology enabled physicians to apply the physiological model
metaphorically to the mind. A greater understand of neuroanatomy partially
undid this metaphor by suggesting disorders of the mind were in fact
disorders of the brain. These developments coincided with the conceptual
transformation of the asylum from a prison to a hospital at the turn of the
nineteenth century. All together, I argue, these antecedents brought the field

321
of psychiatry into existence.
My analysis of psychosis reveals that it does not have a single
rhetorical history, but several. As an object of knowledge, psychosis only
came into existence in late modernity, and only after early psychiatrists
(alienists) realized that they could break down madness into nosological sub
categories. Physicians working in other specialties of medicine (which,
indeed, had only recently acquired multiple specialties) had fairly recently
carried out similar projects in their subfields. The first major systematizing
effort we examined was by Esquirol, who made extensive use of visual
rhetoric to persuade his colleagues that he had identified a useful new way of
'seeing' madness. After Esquirol, the varieties of madness continued to
proliferate. The next major systematizing effort we examined was by
Kraepelin, who joined together several disparate recently identified varieties
of madness into the common diagnosis of dementia praecox, a syndrome
unified by a new pathological category: prognostic course over time.
Psychosis thus was first fragmented into variants that then were re
associated with one another by reference to temporal deterioration. Finally,
Bleuler, focusing on the splitting of intrapsychic associations, rebranded the
quintessential psychotic disorder as schizophrenia.
A striking feature of this development is the blurring of form and
content. A new way of seeing becomes accepted as an innovation if
322
knowledge workers in a field are persuaded of its worth. Thus, the
innovative theōria ( )θεωρία becomes a epistemic stock upon which rhetorical
forms may trade. The microscope enables one to see a cell, but in that image
of the microscopic, the microscope itself is visible. So also with nosologies.
Longitudinal observation of the ill allows one to distinguish one form of
illness from another, but soon the idea of temporal course itself becomes a
category of illness.
The cases in this chapter highlight the importance of visual appeals in
epistemic rhetoric. Esquirol's illustrations of his patients were effective not
because they showed anyone anything about mental illness, but because they
worked enthymematically to suggest that, with the aid of this new epistemic
system, readers could now 'see' a new object of knowledge that had previously
been invisible. Subsequent advocates of nosological models in psychiatry
(including pharmaceutical marketing departments) over the past two
centuries made use of the same rhetorical form. I have provided several
examples of this phenomenon, the occurrence of which is all the more
remarkable because these visual appeals contain no useful scientific
information.
The analyses in this chapter suggest that as new scientific models and
theories develop, they supplement old theories rather than overturn them.
Like humorism, this is true of the modern posthumoral terministic screens

323
of pathology, the ontological and physiological interpretations. Within
psychiatric nosologies, this is true of psychodynamic and biomedical
approaches. Each new model that reveals something that had been invisible
provides an enduring set of rhetorical forms through which advocates render
scientific (and pseudoscientific) theories persuasive. In this sense, the
accumulation of these rhetorical residues facilitates communication. But in a
different way, it inhibits communication by introducing incommensurate
objects of knowledge, often sharing a common name. As Lakoff's (2005) study
of psychiatric clinical practices in Argentina demonstrates, this can create
confusion when clinicians with very different nosological orientations come
together to discuss particular cases. By the same token, these points of
confusion also become the seeds of controversy. It is tough to find consensus
when the field teeters between two ends, but the contest gets worse when
aggressive or restrictive judgments are debated as to whether to name new
diseases or rename old ones.
As the next chapter will show, the strategic ambiguity needed to forge
consensus can later result in irresolvable dissensus if the meaning of a key
term remains unclarified. In the case of psychosis risk syndrome, sometimes
researchers will, in the same publication, express two mutually exclusive
understandings of the meaning of risk, a consequence of the etiological
nihilism introduced in DSMIII.