ptja17 - core submission dossier - eunethta
TRANSCRIPT
PTJA17 - Core Submission Dossier
Elivaldogene autotemcel
Cerebral Adrenoleukodystrophy
Submitted by: bluebird bio (Netherlands) B.V.
Stadsplateau 7
WTC Utrecht
3521AZ Utrecht
The Netherlands
Disclaimer: The sole responsibility for the content of this document lies with the submitting
manufacturer and neither the European Commission nor EUnetHTA are responsible for any use that may be made of the information contained therein.
Contact details for administrative purposes
Name of contact person: Ingrid van der Eijk
Add Telephone number: +31 6 1002 6071
Email address: [email protected]
Email address of contact: [email protected]
Telephone number:
Email address:
For agency completion
Date of receipt:
Identifier:
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 2
DOCUMENT HISTORY
Version Date Description
V0.1 09/03/21 Initial Core Submission Dossier
V0.2 26/03/21 Updated Core Submission Dossier based on Missing Items
V0.3 21/05/21 Amended Core Submission Dossier due to CHMP opinion (grace period)
V1.0 16/08/21 Publication of final version (editorial changes only)
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 3
LIST OF ABBREVIATIONS
ADD Addison-only phenotype
Adol-CER Adolescent cerebral ALD
Adult-CER Adult cerebral ALD
AE Adverse events
aGVHD Acute graft-versus-host disease
AI Adrenal insufficiency
ALD Adrenoleukodystrophy
ALDP Adrenoleukodystrophy protein
allo-HSC Allogeneic haematopoietic stem cell
allo-HSCT Allogeneic haematopoietic allogenic stem cell transplant
AMC Academic Medical Center
AMN Adrenomyeloneuropathy
AMN-CER AMN with cerebral adrenoleukodystrophy
ANC Absolute neutrophil count
ATC Anatomical Therapeutic Chemical
ATG Anti-thymocyte globulin
ATG Anti-thymocyte globulin
BMT Bone marrow transplant
BSC Best supportive care
CALD Cerebral adrenoleukodystrophy
CBT Cord blood transplantation
CC-ALD / CCER Childhood cerebral adrenoleukodystrophy
cDNA Complementary deoxyribonucleic acid
cGVHD Chronic graft-versus-host disease
CHIT Chitotriosidase
CHMP Committee for Medicinal Products for Human Use
CI Confidence Interval
CMV Cytomegalovirus
CNS Central nervous system
CONSORT Consolidated Standards Of Reporting Trials
CRF Case report form
CSA Cyclosporin
CSF Cerebrospinal fluid
CSR Clinical study report
CTCAE Common Terminology Criteria for Adverse Events
DMC Data monitoring committee
DMD Duchenne muscular dystrophy
DRS Disability Rating Scale
DSC-MRP Dynamic susceptibility weighted perfusion MRI
DSM Diagnostic and Statistical Manual of Mental Disorders
DTI Diffusion tensor imaging
EBMT European Society for Blood and Marrow Transplant
EBV Epstein-Barr virus
EC European Commission
EEG Electroencephalogram
Eli-cel Elivaldogene autotemcel
EMA European Medicines Agency
EPAR European Public Assessment Report
EudraCT European Union Drug Regulating Authorities Clinical Trials Database
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 4
EUnetHTA European Network for Health Technology Assessment
FDA Food and Drug Administration
FLAIR Fluid-attenuated inversion recovery
FU Follow-up
G-CSF Granulocyte colony-stimulating factor
GdE Gadolinium enhancement
GI Gastrointestinal
GIS Gadolinium intensity scale
GLD Globoid cell leukodystrophy - Krabbe disease
GVHD/ GVH Graft-versus-host disease
HCT Haematopoietic cell transplantation
HHV-6 Human herpesvirus 6
HLA Human leukocyte antigen
HRQoL Health-related quality of life
HSC Haematopoietic stem cells
HSCT Haematopoietic stem cell transplantation
HTA Health Technology Assessment
ICD International Classification of Diseases
ICU Intensive care unit
IQ Intelligence quotient
IQR Interquartile range
IST Immunosuppressive therapy
ITT Intention-to-treat
IV Intravenous
KOL Key opinion leader
LVV Lentiviral vector
M/ mo Months
MAA Marketing Authorisation Application
MAIC Matching-adjusted indirect comparison
MCID Minimal clinically important difference
MFD Major functional disabilities
MLD Metachromatic leukodystrophy
MMF Mycophenolate mofetil
MNC Mononuclear cell collection
MP Methylprednisolone
MPS-IH Mucopolysaccharidosis type I-Hurler
MR Magnetic resonance
MRA Magnetic resonance angiography
MRI Magnetic resonance imaging
MRP magnetic resonance perfusion
MRS Magnetic resonance spectroscopy
MSC Mesenchymal stem cells
MSD Matched sibling donors
MTX Methotrexate
N/A or NA Not available
NAC N-acetyl-L-cysteine
NBS Newborn screening
NCI National cancer institute
NFS Neurologic Function Score
NICE National Institute for Health and Care Excellence
NMA Non-myeloablative conditioning
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 5
NMSD Non-matched sibling donor
NR Not reported
OS Overall survival
PASS Post-authorisation safety study
PBL Peripheral blood leukocytes
PedsQL Paediatric Quality of Life Inventory
PI Principal investigator
PICO Population, intervention, comparator and outcome
PIND Progressive Intellectual Neurodegeneration
PIQ Performance intelligence quotient
PRIME Priority medicines
PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PROMIS Patient-reported outcomes measurement information system
PS Propensity score
QALY Quality-adjusted life year
QoL Quality of life
QTC Qualified Treatment Centres
RCL Replication-competent lentivirus
RCT Randomised Controlled Trial
RDC Retrospective data collection
SAE Serious adverse event
SCT Stem cell transplantation
SD Standard Deviation
SF Short-form
SLR Systematic literature review
SmPC Summary of Product Characteristics
SOC System organ classes
STROBE Strengthening The Reporting of Observational Studies in Epidemiology
TBD To be determined
TP Transplanted population
TPE Eligible transplant population
TPES Strictly eligible transplant population
TRM Transplant-related mortality
UCBT Umbilical cord blood transplantation
VCN Vector copy number
VLCA Very long-chain acid
VLCF Very long-chain fatty
VLCFA Very long-chain fatty acid
VOD Veno-occlusive disease
W/O Without
WBC White blood cell
X-ALD X-linked adrenoleukodystrophy
yo Years old
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 6
TABLE OF CONTENTS
DOCUMENT HISTORY ..................................................................................................................2
LIST OF ABBREVIATIONS ............................................................................................................3
TABLE OF CONTENTS .................................................................................................................6
LIST OF TABLES ..........................................................................................................................8
LIST OF FIGURES....................................................................................................................... 10
EXECUTIVE SUMMARY .............................................................................................................. 11
1 DESCRIPTION AND TECHNICAL CHARACTERISTICS OF THE TECHNOLOGY .................... 14
1.1 SUMMARY OF THE CHARACTERISTICS OF THE TECHNOLOGY ....................................................... 14 1.2 CHARACTERISTICS OF THE TECHNOLOGY ................................................................................ 14 1.3 REGULATORY STATUS OF THE TECHNOLOGY ............................................................................ 18
2 HEALTH PROBLEM AND CURRENT CLINICAL PRACTICE .................................................. 19
2.1 SUMMARY OF ISSUES RELATING TO THE HEALTH PROBLEM AND CURRENT CLINICAL PRACTICE .......... 19 2.2 OVERVIEW OF THE DISEASE OR HEALTH CONDITION .................................................................. 19 2.3 TARGET POPULATION........................................................................................................... 25 2.4 CLINICAL MANAGEMENT OF THE DISEASE OR HEALTH CONDITION ................................................. 27
3 COMPARATORS IN THE ASSESSMENT ............................................................................... 35
4 CURRENT USE OF THE TECHNOLOGY................................................................................ 36
4.1 SUMMARY OF ISSUES RELATING TO CURRENT USE OF THE TECHNOLOGY ...................................... 36 4.2 CURRENT USE OF THE TECHNOLOGY ...................................................................................... 36 4.3 REIMBURSEMENT AND ASSESSMENT STATUS OF THE TECHNOLOGY ............................................. 36
5 INVESTMENTS AND TOOLS REQUIRED............................................................................... 37
5.1 SUMMARY OF ISSUES RELATING TO THE INVESTMENTS AND TOOLS REQUIRED TO INTRODUCE THE
TECHNOLOGY ..................................................................................................................... 37 6 REQUIREMENTS TO USE THE TECHNOLOGY ..................................................................... 38
6.1 IF ANY SPECIAL CONDITIONS ARE ATTACHED TO THE REGULATORY AUTHORISATION, MORE
INFORMATION SHOULD BE PROVIDED HERE INCLUDING REFERENCES TO THE APPROPRIATE
SECTIONS OF ASSOCIATED DOCUMENTS .................................................................................. 38 6.2 DESCRIBE THE EQUIPMENT REQUIRED TO USE THE TECHNOLOGY ................................................ 41 6.3 DESCRIBE THE SUPPLIES REQUIRED TO USE THE TECHNOLOGY ................................................... 42
7 CLINICAL EFFECTIVENESS AND SAFETY ........................................................................... 43
7.1 CHAPTER OUTLINE .............................................................................................................. 43 7.2 SUMMARY OF THE CLINICAL EFFECTIVENESS ............................................................................ 43 7.3 SUMMARY OF SAFETY .......................................................................................................... 43 7.4 IDENTIFICATION AND SELECTION OF RELEVANT STUDIES............................................................. 44 7.5 RELEVANT STUDIES ............................................................................................................. 48 7.6 MAIN CHARACTERISTICS OF STUDIES ...................................................................................... 51 7.7 METHODS OF EVIDENCE SYNTHESIS ....................................................................................... 68 7.8 INDIVIDUAL STUDY RESULTS (CLINICAL OUTCOMES) ................................................................... 71 7.9 INDIVIDUAL STUDY RESULTS (SAFETY OUTCOMES) .................................................................... 98 7.10 CONCLUSIONS ........................................................................................................... 111 7.11 STRENGTHS AND LIMITATIONS ...................................................................................... 112
8 REFERENCES..................................................................................................................... 117
9 APPENDICES...................................................................................................................... 124
9.1 SCOPING PICO ................................................................................................................ 124 9.2 SEARCH STRATEGY ........................................................................................................... 125

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 7
9.3 SLR: INCLUDED STUDIES .................................................................................................... 128 9.4 SLR: MAIN CHARACTERISTICS OF STUDIES ............................................................................ 131 9.5 CLINICAL OUTCOMES DEFINITIONS........................................................................................ 153 9.6 SLR: INDIVIDUAL STUDY RESULTS (CLINICAL OUTCOMES) ......................................................... 162 9.7 SAFETY OUTCOMES DEFINITIONS ......................................................................................... 178 9.8 ELI-CEL CLINICAL DEVELOPMENT PROGRAMME: INDIVIDUAL STUDY RESULTS (SAFETY OUTCOMES) .. 186 9.9 SLR: INDIVIDUAL STUDY RESULTS (SAFETY OUTCOMES) .......................................................... 193 9.10 RISK OF BIAS ASSESSMENT .......................................................................................... 196
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 8
LIST OF TABLES
Table 1.1 Features of the technology ............................................................................................. 14 Table 1.2 Administration and dosing of the technology .................................................................... 15 Table 1.3 Summary of VLCFA in Fasting Serum Over Time (TP) ..................................................... 17 Table 1.4 Regulatory status of eli-cel ............................................................................................. 18 Table 2.1 Incidence at birth of ALD in Norway in 2011 .................................................................... 22 Table 2.2 Total number of allogeneic transplants for CALD patients per year in Europe .................... 27 Table 2.3. Relevant guidelines for diagnosis and management ........................................................ 34 Table 7.1 Inclusion and Exclusion Criteria -SLR PICO .................................................................... 46 Table 7.2 List of all relevant studies – eli-cel clinical development programme ................................. 49 Table 7.3 List of key non-randomized studies identified through the SLR ......................................... 51 Table 7.4 Characteristics of the studies – eli-cel clinical development programme ............................ 52 Table 7.5 Patient flow – eli-cel clinical development programme...................................................... 55 Table 7.6 Analysis populations for ALD-102 and interstudy comparisons ......................................... 57 Table 7.7 Baseline characteristics – eli-cel clinical development programme .................................... 58 Table 7.8 Characteristics of the key studies ................................................................................... 61 Table 7.9 Patient flow of the key studies ........................................................................................ 64 Table 7.10 Baseline characteristics of the key studies..................................................................... 66 Table 7.11 Overview of baseline confounders ................................................................................ 70 Table 7.12 OS with in ALD-102, LTF-304 and ALD-103 .................................................................. 72 Table 7.13 MFD-free survival in ALD-102, LTF-304 and ALD-103 ................................................... 74 Table 7.14 Loes scores in ALD-102 and ALD-103 .......................................................................... 75 Table 7.15 Results summary for eli -cel clinical development programme ......................................... 77 Table 7.16 PedsQL score in ALD-102 and LTF-304........................................................................ 79 Table 7.17 Results summary non-comparative studies – key studies ............................................... 84 Table 7.18 HRQoL outcomes reported in Beckmann et al. .............................................................. 85 Table 7.19 Comparison per outcome for eli-cel, HSCT and BSC studies – OS & mortality................. 86 Table 7.20 Comparison per outcome for eli-cel, HSCT and BSC studies – OS & mortality (cont.) ...... 88 Table 7.21 Comparison per outcome for eli-cel, HSCT and BSC studies – MFD-free survival ............ 89 Table 7.22 Comparison per outcome for eli-cel, HSCT and BSC studies – NFS ............................... 90 Table 7.23 Comparison per outcome for eli-cel, HSCT and BSC studies – Loes score ...................... 92 Table 7.24 Comparison per outcome for eli-cel, HSCT and BSC studies – Loes score (cont.) ........... 94 Table 7.25 Comparison per outcome for eli-cel, HSCT and BSC studies – GdE+.............................. 95 Table 7.26 Comparison per outcome for eli-cel, HSCT and BSC studies – QoL ................................ 97 Table 7.27 Overview of safety outcomes – eli-cel clinical development programme ........................ 100 Table 7.28 Overview of additional safety outcomes reported in key studies .................................... 104 Table 7.29 Overview of GVHD reported in key studies .................................................................. 104 Table 7.30 Overview of adverse events reported in key studies ..................................................... 104 Table 7.31 Comparison of safety for eli -cel, HSCT and BSC studies – adverse events ................... 105 Table 7.32 Comparison of safety for eli -cel, HSCT and BSC studies – adverse events (cont.) ......... 107 Table 7.33 Comparison of safety for eli -cel, HSCT and BSC studies – additional safety outcomes... 108 Table 7.34 Comparison of safety for eli-cel, HSCT and BSC studies – additional safety outcomes
(cont.) .................................................................................................................................. 109 Table 7.35 Comparison of safety for eli -cel, HSCT and BSC studies – GVHD ................................ 110 Table 9.1. Assessment scope: relevant PICO(s) identified for the planned assessment................... 124 Table 9.2. List of all included studies (non-randomised, observational) – SLR ................................ 128 Table 9.3. Characteristics of the studies – SLR ............................................................................ 131 Table 9.4. Patient flow – SLR ...................................................................................................... 141 Table 9.5 Baseline characteristics – SLR ..................................................................................... 147 Table 9.6 Baseline characteristics – SLR (cont.)........................................................................... 149 Table 9.7 Baseline characteristics – SLR (cont.)........................................................................... 151 Table 9.8 Methods of data collection and analysis of clinical outcomes .......................................... 153 Table 9.9 Results summary for overall survival – SLR................................................................... 162 Table 9.10 Results summary for mortality – SLR .......................................................................... 162 Table 9.11 Results summary for NFS and Loes score – SLR ........................................................ 162 Table 9.12 Results summary Gottingen-1985 (non-comparative studies) – SLR ............................. 163 Table 9.13 Results summary for HRQoL – SLR............................................................................ 163 Table 9.14 Results summary Beam et al. 2007 (non-comparative studies)– SLR ............................ 164 Table 9.15 Results summary Bladowska et al. 2015 (non-comparative studies) – SLR ................... 164
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 9
Table 9.16 Results summary Fernandes et al. 2018 (non-comparative studies) – SLR.................... 164 Table 9.17 Results summary Jardim et al. 2010 (non-comparative studies) – SLR.......................... 165 Table 9.18 Results summary Kato et al. 2019 (non-comparative studies) – SLR............................. 165 Table 9.19 Results summary Kühl et al. 2018 (non-comparative studies) – SLR ............................. 166 Table 9.20 Results summary McKinney et al. 2013 (non-comparative studies) – SLR ..................... 166 Table 9.21 Results summary McKinney et al. 2016 (non-comparative studies) – SLR ..................... 166 Table 9.22 Results summary Miller et al. 2016 (non-comparative studies) – SLR............................ 167 Table 9.23 Results summary Miller et al. 2011 (non-comparative studies) – SLR............................ 167 Table 9.24 Results summary Moser et al. 2005 (non-comparative studies) – SLR .......................... 168 Table 9.25 Results summary Orchard et al. 2019 (non-comparative studies) – SLR........................ 168 Table 9.26 Results summary Peters et al. 2004 (non-comparative studies) – SLR .......................... 169 Table 9.27 Results summary Pierpont et al. 2018 (non-comparative studies) – SLR ....................... 169 Table 9.28 Results summary Pierpont et al. 2020 (non-comparative studies) – SLR ....................... 170 Table 9.29 Results summary Polgreen et al. 2011 (non-comparative studies) – SLR ...................... 170 Table 9.30 Results summary Saute et al. 2016 (non-comparative studies) – SLR ........................... 171 Table 9.31 Results summary Shapiro et al. 2000 (non-comparative studies) – SLR ........................ 171 Table 9.32 Results summary Suzuki et al. 2001 (non-comparative studies) – SLR.......................... 171 Table 9.33 Results summary Tran et al. 2017 (non-comparative studies) – SLR............................. 171 Table 9.34 Results summary van den Broek et al. 2018 (non-comparative studies) – SLR .............. 172 Table 9.35 Methods of data collection and analysis of safety outcomes ......................................... 178 Table 9.36 Frequency and severity of adverse events by sys tem organ class – eli-cel clinical
development programme ...................................................................................................... 186 Table 9.37 Overview of adverse events – SLR ............................................................................. 193 Table 9.38 Overview of additional safety outcomes – SLR ............................................................ 194 Table 9.39 Risk of bias assessment ............................................................................................ 196 Table 9.40 Risk of bias assessment (cont.) .................................................................................. 200
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 10
LIST OF FIGURES
Figure 1.1 %ALDP+ cells in peripheral blood over time (boxplot; TP) ............................................... 16 Figure 1.2 NFS over time by subject (TP)....................................................................................... 17 Figure 2.1 Pathophysiology of adrenoleukodystrophy ..................................................................... 20 Figure 2.2 Illustration of rapid neurologic deterioration over the course of 2.5 months ....................... 21 Figure 2.3 Allo-HSCT in CALD by donor type ................................................................................. 29 Figure 2.4 Algorithm for the management of ALD ........................................................................... 32 Figure 6.1 Patient and product journey in the commercial setting..................................................... 38 Figure 7.1 Eli-cel clinical development programme ......................................................................... 44 Figure 7.2 PRISMA flow diagram................................................................................................... 48 Figure 7.3 Patient flow – ALD-102 ................................................................................................. 55 Figure 7.4 Patient flow – ALD-103 ................................................................................................. 56 Figure 7.5 ALD-102 vs ALD-103, time to OS, before and after propensity score adjustment .............. 69 Figure 7.6 ALD-102 vs ALD-103, time to MFD-free survival, before and after propensity score
adjustment ............................................................................................................................. 69 Figure 7.7 OS in ALD-102 and ALD-103 TPES-population without NMSD (i.e., alternative donor) ...... 72 Figure 7.8 MFD-free survival in ALD-102 and ALD-103 TPES population without MSD (i.e.,
alternative donor) ................................................................................................................... 74 Figure 7.9 Loes score over time in ALD-102................................................................................... 75 Figure 7.10 Loes score over time in ALD-103 TPES population ....................................................... 76 Figure 7.11 OS in Kühl et al. (left)* and van den Broek et al. (right)** ............................................... 81 Figure 7.12 MFD-free survival by Kühl et al. ................................................................................... 82 Figure 9.1 Patient flow – Jardim et al. 2010.................................................................................. 142 Figure 9.2 Patient flow – Mahmood et al. 2007 ............................................................................. 143 Figure 9.3 Patient flow – McKinney et al. 2013 ............................................................................. 143 Figure 9.4 Patient flow – McKinney et al. 2016 ............................................................................. 144 Figure 9.5 Patient flow – Pierpont et al. 2020 ............................................................................... 145 Figure 9.6 Patient flow – Polgreen et al. 2011 .............................................................................. 146 Figure 9.7 Patient flow – Tran et al. 2017 ..................................................................................... 146 Figure 9.8 Overall survival – Beam et al. 2007 ............................................................................. 173 Figure 9.9 Overall survival – Kühl et al. 2018................................................................................ 173 Figure 9.10 MFD-free survival – Kühl et al. 2018 .......................................................................... 174 Figure 9.11 Overall survival after development of neurological symptoms – Mahmood et al. 2007 ... 174 Figure 9.12 Overall survival stratified by severity of involvement on baseline MRI – Mahmood et al.
2007 .................................................................................................................................... 175 Figure 9.13 Overall survival after HSCT for the entire cohort – Miller et al. 2011 ............................. 175 Figure 9.14 Overall survival after HSCT based on various patient and HCT characteristics – Miller
et al. 2011 ............................................................................................................................ 176 Figure 9.15 Overall survival after HSCT by number of neurological deficits and MRI severity score
– Peters et al. 2004 .............................................................................................................. 176 Figure 9.16 Six-year overall survival – Van den Broek et al. 2018 .................................................. 176
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 11
EXECUTIVE SUMMARY
Health problem
Cerebral adrenoleukodystrophy (CALD) is a rare, X-linked metabolic, neurodegenerative disorder caused by mutations in the ABCD1 gene.
CALD is characterised by rapidly progressive inflammatory cerebral demyelination, leading to
progressive, irreversible loss of neurologic function and death, if left untreated.
Onset of CALD usually occurs between the ages of 3 and 12 years with peak incidence between 6-8 years of age.1
Untreated patients with CALD typically die within 2–4 years of symptom onset, although patients may survive, sometimes in a profoundly disabled state, for several years.2
Clinical pathway and unmet need
The early stages of CALD are clinically asymptomatic but brain abnormalities can be detected by
magnetic resonance imaging (MRI).2 Nonetheless, confirmatory diagnosis of CALD can be complex and can take time due to unclear symptoms, especially in case of no previous diagnosis of ALD in the family.
Untreated CALD follows a clinical course beginning with mild cognitive and motor deficits followed by a rapidly progressive and devastating inflammatory phase, leading to irreversible brain damage and severe physical and cognitive disability.2,3
Current CALD treatment options are limited due to a lack of approved therapies. Allogeneic- haematopoietic stem cell transplantation (allo-HSCT) is an effective treatment if performed in an early disease phase; however, it has a high-risk profile, including significant immunologic complications, mortality and other adverse events.2-5 Moreover, the success and risk-profile of allo-HSCT is mostly
dependent on the donor source, which can take substantial time to identify, or may not exist, while the disease is irreversibly progressing.
Patients who do not undergo allo-HSCT receive symptomatic and palliative care (best supportive care
[BSC]) as necessary, requiring increasing amounts of care as disability progresses. Various therapies are used in Europe, such as Lorenzo’s oil, but effectiveness evidence is lacking. 6
Given the severity of the disease, rapid irreversible progression and, as a consequence, short window
of opportunity to treat, there is a need for a treatment that is available within a short time period and can stabilise neurologic decline in CALD patients, while also having a favourable risk-benefit profile.
Eli-cel (Skysona)
Eli-cel is a one-time autologous, ex vivo, gene therapy, providing a treatment option for patients less than 18 years of age, with an ABCD1 mutation and early CALD for whom a human leukocyte antigen (HLA)-matched sibling donor (MSD) for allo-HSCT is not available.
Eli-cel adds functional copies of the ABCD1 complimentary deoxyribonucleic acid (cDNA) into patients’
haematopoietic stem cells (HSCs) through transduction of autologous cluster of differentiated 34 (CD34+) cells with Lenti-D lentiviral vector.
Eli-cel is an orphan medicinal product (EU/3/12/1003) and was granted eligibility to the priority
medicines (PRIME) scheme on 26 July 2018 (EMA/PRIME/18/029), enabling this promising therapy to reach patients as early as possible. European full marketing authorisation is currently expected to be granted July 2021.
The efficacy and safety of eli-cel in the treatment of early CALD patients for whom an HLA-MSD for allo-HSCT is not available was demonstrated in ALD-102, a phase 2/3, single-group, open-label study.
Eli-cel is the first therapy specifically developed for treatment of CALD and is expected to offer a lifelong durable treatment effect, owing to stable integration of functional ABCD1 cDNA into long-term
repopulating HSCs.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 12
Identification and synthesis of relevant studies
The evidence provided in this submission for the safety and efficacy of eli-cel was generated through the eli-cel clinical development programme.
The eli-cel clinical development programme consisted of several single-arm trials. To enable
comparison of the key eli-cel clinical trial, ALD-102, with allo-HSCT, an observational trial with a similar study design was set up with allo-HSCT, ALD-103. This was a naïve comparison.7 The validity of this comparison was supported by propensity score adjusted analyses.8
Additionally, a systematic literature review (SLR) identified 27 relevant studies for the comparators considered, allo-HSCT (25 studies) and BSC (two studies). Based on their coverage of the SLR’s PICOs (population, intervention, comparator and outcome), six of these studies were identified as key studies and deemed comparable to the eli-cel clinical development programme.
The studies identified through the SLR and the eli-cel clinical studies were assessed to determine whether the use of statistical methods, i.e. a matching-adjusted indirect comparison (MAIC)9, would comprise a feasible and relevant comparison method. Issues were identified in terms of the sample
size, baseline characteristics, study designs used and reported outcome measures. As such, no statistical methods were undertaken to compare the studies identified through the SLR with the eli -cel clinical development programme.
Results on clinical outcomes
Results to date suggest that early treatment with eli-cel can stabilise the progression of CALD in patients less than 18 years of age with an ABCD1 genetic mutation for whom an HLA-matched sibling
HSC donor is not available.
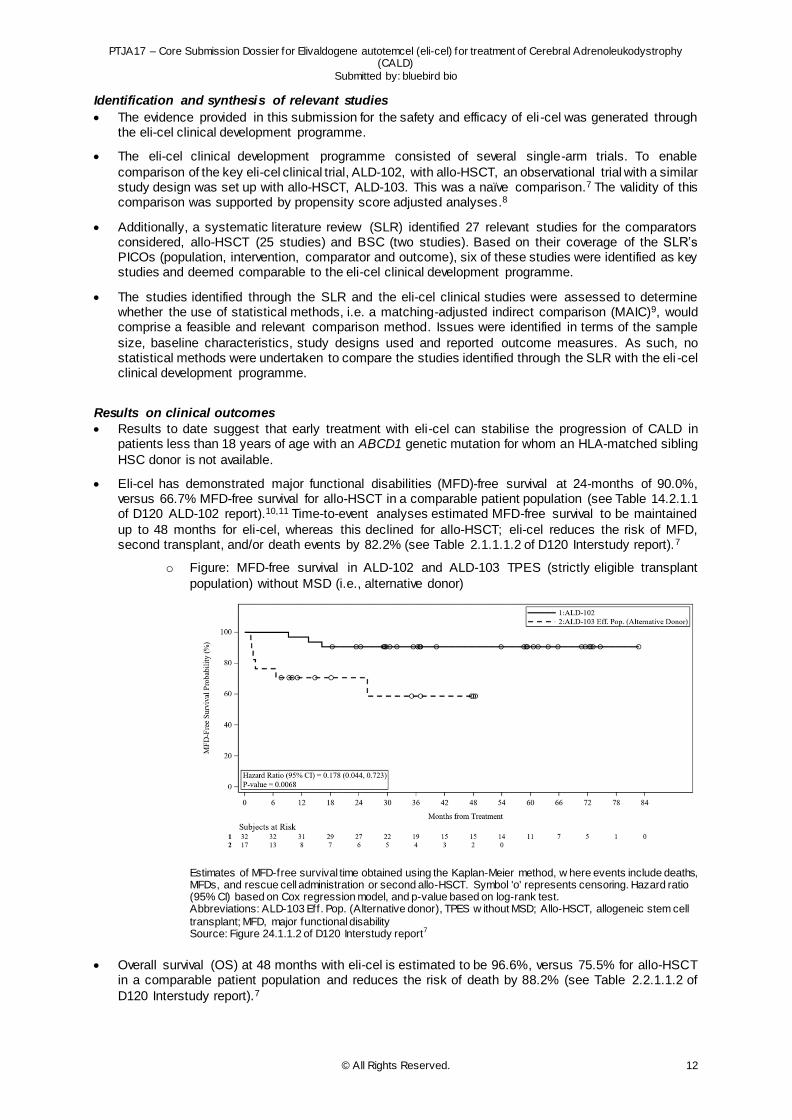
Eli-cel has demonstrated major functional disabilities (MFD)-free survival at 24-months of 90.0%, versus 66.7% MFD-free survival for allo-HSCT in a comparable patient population (see Table 14.2.1.1 of D120 ALD-102 report).10,11 Time-to-event analyses estimated MFD-free survival to be maintained
up to 48 months for eli-cel, whereas this declined for allo-HSCT; eli-cel reduces the risk of MFD, second transplant, and/or death events by 82.2% (see Table 2.1.1.1.2 of D120 Interstudy report).7
o Figure: MFD-free survival in ALD-102 and ALD-103 TPES (strictly eligible transplant
population) without MSD (i.e., alternative donor)
Estimates of MFD-free survival time obtained using the Kaplan-Meier method, w here events include deaths, MFDs, and rescue cell administration or second allo-HSCT. Symbol 'o' represents censoring. Hazard ratio (95% CI) based on Cox regression model, and p-value based on log-rank test. Abbreviations: ALD-103 Eff. Pop. (Alternative donor), TPES w ithout MSD; Allo-HSCT, allogeneic stem cell
transplant; MFD, major functional disability Source: Figure 24.1.1.2 of D120 Interstudy report7
Overall survival (OS) at 48 months with eli-cel is estimated to be 96.6%, versus 75.5% for allo-HSCT in a comparable patient population and reduces the risk of death by 88.2% (see Table 2.2.1.1.2 of
D120 Interstudy report).7
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 13
Eli-cel has demonstrated a similar ability to allo-HSCT to stabilise disease progression, as stable
neurologic function score (NFS) at 24 months has been observed in 96.4% of patients treated with eli-cel and 100% for allo-HSCT (see Table 14.2.4 of D120 ALD-102 report)10,11.
Loes score has been found to remain stable in patients treated with eli-cel, with 21 of 27 (77.8%)
patients reporting no change from baseline to Month 24 (see Table 14.2.5 of D120 ALD-102 report).10
Results on safety outcomes
Eli-cel has a favourable safety profile, with no evidence of acute or chronic graft-versus-host disease (GVHD), graft failure or rejection (see Tables 14.3.2.1 and 14.3.2.2 of D120 ALD-102 report).10
o In contrast, among allo-HSCT patients, ALD-103 found that 52.0% patients experienced acute or chronic GVHD and 26.3% graft failure within 24 months.11
The majority of adverse events with eli-cel administration were consistent with those associated with
mobilisation and myeloablative conditioning performed for allo-HSCT, and resolved with standard measures (see Table 3.4.7 of D120 Interstudy report).7
Only five out of 51 patients (9.8%) experienced adverse events (AEs) that were potentially related to
eli-cel: one with BK-mediated viral cystitis (serious AE grade 3), two with pancytopenia (serious AE grade 3), and two with vomiting (grade 1) (see Tables 3.4.6.1 and 3.4.9 of D120 Interstudy report).7
No treatment-related mortality with eli-cel has been reported, while 17.8% of patients in ALD-103 died
from treatment-related causes within one year of allo-HSCT (see Table 3.2.2.2 of D120 Interstudy report).7
Conclusion
Eli-cel is the first therapy specifically developed for treatment of CALD and is expected to offer a
lifelong durable treatment effect for patients less than 18 years of age with an ABCD1 mutation and early CALD for whom an HLA-MSD for allo-HSCT is not available.
The eli-cel clinical development programme demonstrated that eli-cel stabilises neurologic disease
progression and is generally well-tolerated since no signs of GVHD and graft failure were reported.
Eli-cel is expected to provide a durable long-term MFD-free survival and OS. This is in contrast to allo-HSCT and BSC, which are both associated with worse outcomes than eli-cel.
In summary, eli-cel is a novel, one-time autologous gene therapy which has shown a positive benefit/risk-profile in clinical trials for paediatric patients with early CALD for whom an HLA-matched sibling HSC donor is not available.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 14
1 DESCRIPTION AND TECHNICAL CHARACTERISTICS OF THE
TECHNOLOGY
1.1 Summary of the characteristics of the technology
Elivaldogene autotemcel (eli-cel) is a one-time autologous, ex vivo, gene therapy, providing a
treatment option for patients less than 18 years of age with an ABCD1 mutation and early cerebral adrenoleukodystrophy (CALD) for whom a human leukocyte antigen (HLA)-matched sibling donor (MSD) for allogeneic haematopoietic stem cell transplant (allo-HSCT) is not available. It is the first
therapy specifically developed for treatment of this devastating disease.
Eli-cel adds functional copies of the ABCD1 complimentary deoxyribonucleic acid (cDNA) into patients’ HSCs through transduction of autologous cluster of differentiated 34 (CD34+) cells with Lenti-D
lentiviral vector (LVV; gene addition).
Eli-cel is expected to offer a lifelong durable treatment effect, owing to stable integration of functional ABCD1 cDNA into long-term repopulating haematopoietic stem cells.
Eli-cel has demonstrated the ability to stabilise CALD disease progression as measured by changes in Neurologic Function Score (NFS) at 24 months after administration. Moreover, eli-cel has been shown to be associated with Month 24 MFD-free survival of 90.0% and clinically meaningful overall survival of 96.4%.
Eli-cel has a favourable safety profile, with no evidence of insertional oncogenesis, graft-versus-host disease (GVHD), graft failure or rejection, or treatment-related mortality and only very limited treatment-emergent adverse events.
A full marketing authorisation is to be granted. Eli-cel is an orphan medicinal product (EU/3/12/1003) and was granted eligibility to the priority medicines (PRIME) scheme on 26 July 2018 (EMA/PRIME/18/029), with the intent for this promising therapy to reach patients as early as possible.
1.2 Characteristics of the technology
1.2.1 Provide an overview of the technology
Eli-cel (Skysona) is a one-time autologous gene therapy, providing a treatment option for patients less than 18 years of age, with an ABCD1 mutation and early CALD for whom an HLA-matched sibling
haematopoietic stem cell (HSC) donor for allo-HSCT is not available. A summary of the pharmaceutical technology is given in Table 1.1.
Table 1.1 Features of the technology
Non-proprietary name Elivaldogene autotemcel
Proprietary name Skysona
Marketing authorisation holder bluebird bio
Class Gene therapy
Active substance(s) Elivaldogene autotemcel is a genetically modified autologous CD34+ cell-enriched population that contains HSCs transduced with lentiviral vector (LVV) encoding ABCD1 complementary deoxyribonucleic acid (cDNA) for human adrenoleukodystrophy protein (ALDP) with a strength of 2-30 × 106 cells/mL.
Pharmaceutical formulation(s) Dispersion for infusion. One or more infusion bags, which contain a dispersion of 2 ‑30 × 106 cells/mL suspended in cryopreservative solution. Each infusion bag contains approximately 20 mL of Skysona.
ATC code TBD – will be part of the ATC code: N07 Other nervous system drugs
Mechanism of action Skysona adds functional copies of the ABCD1 cDNA into patients’ HSCs through transduction of autologous CD34+ cells with Lenti -D LVV. After Skysona infusion, transduced CD34+ HSCs engraft in the bone marrow and differentiate into various cell types, including monocytes (CD14+) that migrate to the brain where they further differentiate into macrophages and cerebral microglia that can produce functional ALDP. The functional ALDP can then enable the local degradation of very long-chain fatty acids
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 15
(VLCFAs) in the brain, which in turn can stabilise the disease by preventing further inflammation and demyelination. However, it is not anticipated that Skysona treatment will affect other manifestations of ALD including adrenal insufficiency. Impact of Skysona treatment on adrenomyeloneuropathy has not been s tudied. Following successful engraftment with genetically modified cells, the expression of ALDP is expected to be lifelong.
Abbreviations: ALDP, adrenoleukodystrophy protein; ATC, Anatomical Therapeutic Chemical; cDNA, complementary deoxyribonucleic acid; HSCs, haematopoietic stem cells; LVV, lentiviral vector; VLCFA, very long-chain fatty acid; TBD, to be
determined Source: eli-cel Summary of Product Characteristics (SmPC)12
1.2.2 Summarise the information about administration and dosing of the technology
Table 1.2 Administration and dosing of the technology
Method of administration Eli-cel is an ex vivo gene therapy administered intravenously through infusion. Eli-cel is manufactured from the patient's own, previously harvested, stem cells. After enrichment for CD34+ cells, the cells undergo ex vivo transduction with the Lenti-D LVV. Prior to eli-cel treatment, the patient receives myeloablative conditioning – chemotherapy to clear space in the bone marrow – after which the transduced stem cells, i.e. eli-cel, are infused to repopulate the bone marrow.
Doses The minimum recommended dose of eli-cel is 5.0 × 106 CD34+ cells/kg. In clinical studies doses up to 38.2 × 106 CD34+ cells/kg have been administered.
Dosing frequency Eli-cel is a one-time treatment.
Average length of a course of treatment
Eli-cel is a one-time treatment administered on a single day. However, patients are hospitalised from the beginning of myeloablative conditioning until they achieve neutrophil engraftment or are clinically stable. In clinical study ALD-102, patients spent a median of 29.0 days (range 15–54) in hospital from conditioning through to neutrophil engraftment.
Anticipated average interval between courses of treatments
Not applicable. Eli-cel is a one-time treatment.
Anticipated number of repeat courses of treatments
Not applicable. Eli-cel is a one-time treatment.a
Dose adjustments If the minimum dose of eli-cel 5.0 × 106 CD34+ cells/kg is not met after initial medicinal product manufacturing, the patient may undergo one or more additional cycles of mobilisation and apheresis, separated by at least 14 days, in order to obtain more cells for additional manufacture.
aTo date, no engraftment failure or GVHD has been observed in the trial patient pool (ALD-102 and ALD-104) (see Table 14.3.2.2 of D120 ALD-102 report and Table 14.3.2.2.of D120 ALD-104 report).10,13 Based on the anticipated MoA, additional product administration will not be required because of the stable integration of ABCD1 into long-term repopulating HSCs. In addition, multiple administrations of eli-cel have not been tested in clinical trials.
Abbreviations: LVV, lentiviral vector Source: eli-cel SmPC12
1.2.3 State the context and level of care for the technology
Eli-cel must be administered in a qualified treatment centre (QTC) by a physician(s) with experience in
HSCT transplantation as well as in the treatment of patients with neurological disorders. Patients require close monitoring from the beginning of myeloablative conditioning therapy through to the moment of neutrophil engraftment and/or clinical stability and are hospitalised for this duration. As part of the eli-
cel clinical trial development programme, a median hospitalisation duration of 28 days (range: 15-54 days) was reported (see Table 2.5.1 of D120 Interstudy report).7
The majority of adverse events (AEs) with eli-cel administration were consistent with those associated
with mobilisation and myeloablative conditioning performed for HSCT, and mostly resolved with standard measures during the initial hospitalisation.
1.2.4 State the claimed benefits of the technology
Eli-cel is the first approved therapy developed specifically for patients less than 18 years of age with an ABCD1 genetic mutation and early CALD for whom an HLA-matched sibling HSC donor is not available.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 16
It is an innovative, fully personalised, one-time autologous gene therapy based on a patient’s own HSCs,
to which functional ABCD1 cDNA is integrated via company-patented LVV (Lenti-D LVV). This LVV is designed to address the genetic cause of the disease by targeting the ABCD1 gene. It is projected to achieve this goal by carrying human ABCD1 cDNA-derived sequences that encode the normal human
ALDP. Lenti-D LVV is a replication defective, self-inactivating (SIN), third generation HIV-1 based LVV to ensure genotoxicity is minimised as much as possible. Eli-cel is an autologous gene therapy which eliminates the need for finding a matched and available, ideally sibling, donor. 14 (see Sections 5 and 6.1
for further details regarding the differences in requirements to use eli-cel vs allo-HSCT).
Eli-cel is expected to offer a lifelong durable treatment effect, owing to stable integration of functional ABCD1 cDNA into long-term repopulating haematopoietic stem cells. Eli-cel does not fix the germline
mutation in the ABCD1 gene; it adds functional copies of the ABCD1-cDNA into the genomes of the CD34+ HSCs of the patients, which reconstitute the hematopoietic system of the myeloablated patients.15,16 These HSCs differentiate into various cell types, including monocytes that migrate to the
brain, where they further differentiate into macrophages and cerebral microglia, which produce functional ALDP and enable transport of VLCFAs into cellular peroxisomes for degradation.16,17
Undifferentiated HSCs are critical for life-long blood production and are uniquely defined by their
capacity to durably self-renew and/or generate daughter stem cells that produce healthy red blood cells.18-20 After one-time treatment with eli-cel, modified stem cells can serve as a long-term reservoir for monocytes, ensuring durable and life-long expression.21
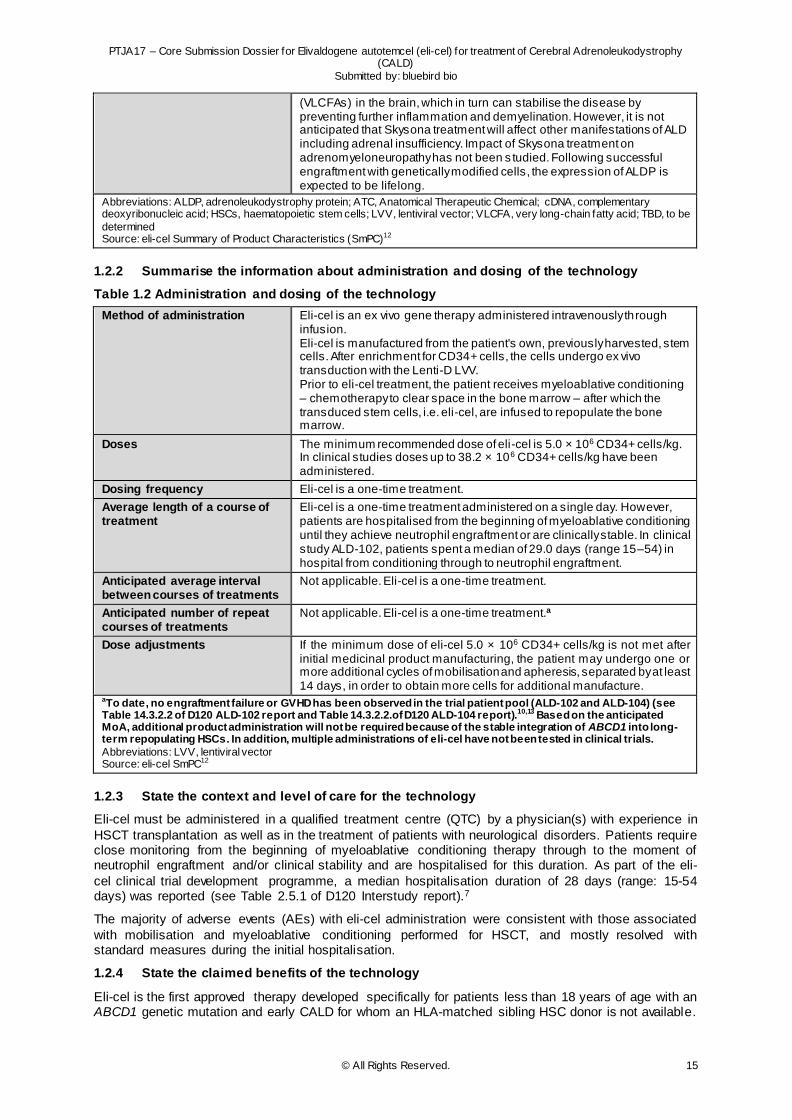
Based on the MoA it is expected that modified cells likely enter the brain quickly after engraftment, based on ALDP measurement in CD14+ cells, which is detectable within 1 month and over the duration of the study period of 24 months (Figure 1.1).22
Figure 1.1 %ALDP+ cells in peripheral blood over time (boxplot; TP)
Note: The LOD for this assay is 1.5% and the LOQ for this assay is 4.0%. Measurements for all samples w ere given as reported, regardless of whether they were above the LOD or LOQ.
Also VLCFA levels over time, as observed in the ALD-102 study, support fast onset of effect as well as sustainability (

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 17
Table 1.3).
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 18
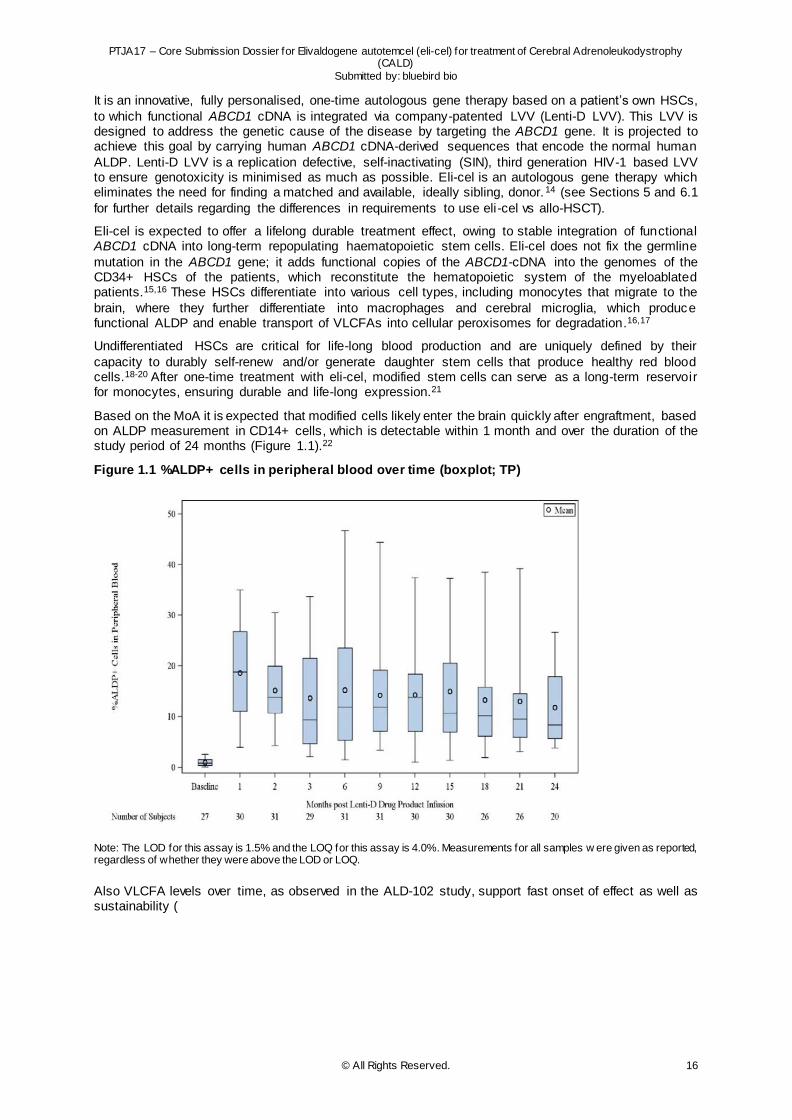
Table 1.3 Summary of VLCFA in Fasting Serum Over Time (TP)
Abbreviations: LysoPC, C26:0 lysophosphatidylcholine; TP, transplant population; VLCFA, very long-chain fatty acids
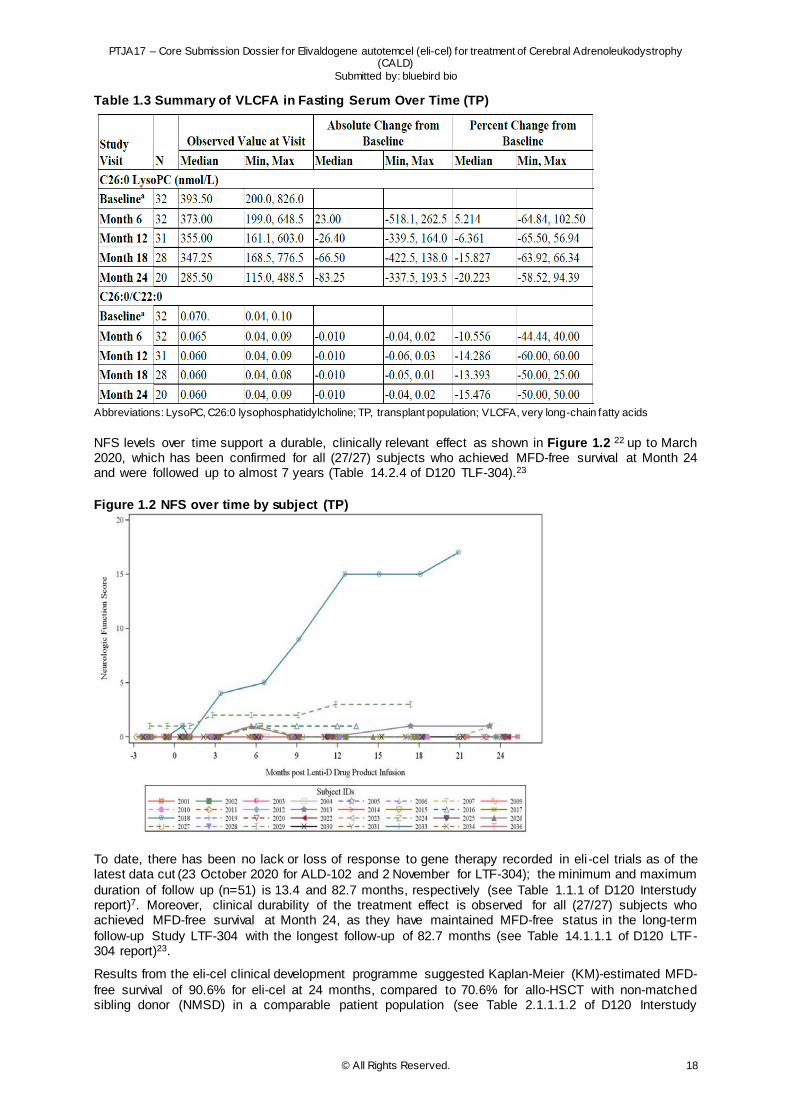
NFS levels over time support a durable, clinically relevant effect as shown in Figure 1.2 22 up to March 2020, which has been confirmed for all (27/27) subjects who achieved MFD-free survival at Month 24 and were followed up to almost 7 years (Table 14.2.4 of D120 TLF-304).23
Figure 1.2 NFS over time by subject (TP)
To date, there has been no lack or loss of response to gene therapy recorded in eli -cel trials as of the latest data cut (23 October 2020 for ALD-102 and 2 November for LTF-304); the minimum and maximum
duration of follow up (n=51) is 13.4 and 82.7 months, respectively (see Table 1.1.1 of D120 Interstudy report)7. Moreover, clinical durability of the treatment effect is observed for all (27/27) subjects who achieved MFD-free survival at Month 24, as they have maintained MFD-free status in the long-term
follow-up Study LTF-304 with the longest follow-up of 82.7 months (see Table 14.1.1.1 of D120 LTF-304 report)23.
Results from the eli-cel clinical development programme suggested Kaplan-Meier (KM)-estimated MFD-
free survival of 90.6% for eli-cel at 24 months, compared to 70.6% for allo-HSCT with non-matched sibling donor (NMSD) in a comparable patient population (see Table 2.1.1.1.2 of D120 Interstudy
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 19
report).7 Similarly, eli-cel was associated with improved overall survival (OS) of 96.6% versus 86.3% for
allo-HSCT with NMSD in a comparable patient population at 24 months (see Table 2.1.1.1.2 of D120 Interstudy report).7 These survival estimations are expected to be maintained between months 24 and 48. In contrast, the estimates for allo-HSCT with NMSD in a comparable patient population are expected
to decrease over this period to an MFD-free survival of 58.8% and OS of 75.5% (see Section 7.8 for further details and clinical benefits of eli-cel vs allo-HSCT).11 This decrease in survival among allo-HSCT with NMSD patients is predominantly driven by the incompatibility of donor and recipient, with failures
due to secondary graft rejection or GVHD causing mortality, each of which are treatment challenges with which eli-cel is not associated.
In line with this and owing to autologous gene therapy with a patient’s own HSCs, eli-cel has a favourable
safety profile. There is currently no evidence of GVHD, graft failure or rejection, or transplant-related mortality, all of which are common safety concerns for CALD patients treated with allo-HSCT. Similarly, eli-cel is associated with fewer treatment-emergent adverse events and infections than have been
reported in comparable patient populations treated with allo-HSCT (see Section 7.9 for further details and clinical benefits of eli-cel vs allo-HSCT).
Patients who do not undergo allo-HSCT receive best supportive care (BSC): symptomatic and palliative
care as necessary, requiring increasing amounts of care as disability progresses. Various therapies are used as supportive care in European countries, but evidence for effectiveness is lacking – so far these have not been demonstrated to have a significant efficacy in limiting disease progression (more details
are presented in section 2.4.1). Therefore, other than allo-HSCT, eli-cel is the only treatment that modifies the underlying disease and, as a result, limits disease progression and improves survival.
1.3 Regulatory status of the technology
Table 1.4 outlines the regulatory status of eli-cel. At present, eli-cel has only been submitted for approval
to the European Medicines Agency (EMA) with an expected European Commission (EC) decision in July 2021.
Table 1.4 Regulatory status of eli-cel
Organisation issuing approval
Verbatim wording of the (expected) indication(s)
(Expected) Date of approval
Launched (yes/no) If no: include proposed date of launch
EMA Eli-cel (Skysona) is indicated for the treatment of early cerebral adrenoleukodystrophy in patients less than 18 years of age, with an ABCD1 genetic mutation, and for whom a human leukocyte antigen (HLA)-matched sibling haematopoietic stem cell (HSC) donor is not available.
EC decision expected July 2021
No; pending EC decision
Abbreviations: EC, European Commission; EMA, European Medicines Agency; HLA, human leukocyte antigen; HSC; haematopoietic stem cell
1.3.1 Other indications for which the technology has marketing authorisation
Eli-cel does not have marketing authorisation for any other indications.
1.3.2 State any contraindications or groups for whom the technology is not recommended
Eli-cel is contraindicated in patients with a hypersensitivity to the active substance or the list of excipients listed in the Summary of Product Characteristics (SmPC). Additionally, contraindications to the
mobilisation agents and the conditioning agents must be considered.12
1.3.3 List other countries in which the technology has marketing authorisation
Eli-cel has no marketing authorisation anywhere in the world but is in MA review in the EU. bluebird bio
is currently exploring paths for marketing authorisation in other countries.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 20
2 HEALTH PROBLEM AND CURRENT CLINICAL PRACTICE
2.1 Summary of issues relating to the health problem and current clinical practice
CALD, an X-linked, rare neurodegenerative disease that predominately affects young boys, is
characterised by rapidly progressive inflammatory cerebral demyelination, leading to progressive, irreversible loss of neurologic function and death, if left untreated.
Onset of CALD usually occurs between the ages of 3 and 12 years with peak incidence between 6-8
years of age.
The clinical burden of CALD is high. The health-related quality of life (HRQoL) of CALD patients has not been well-reported but the devastating nature of the disease with its rapid progression inevitably has a severe impact on not only the patient but also on their family/carers. In case no previous
diagnosis of adrenoleukodystrophy (ALD) has been reported within the family, confirmatory diagnosis of CALD can be complex and can take time due to unclear symptoms. In addition to the relatively late onset in childhood, this sometimes leads to presence of more than one patient in a family.
Current CALD treatment options are limited due to a lack of approved therapies . Allo-HSCT is an effective treatment, however, it has a high-risk profile, including significant immunologic complications, mortality and other AEs. Moreover, finding an HSC compatible donor can take much time or can be
impossible at all, while the disease is irreversibly progressing.
Given a lack of therapeutic options with a favourable risk/benefit ratio in patients with CALD, the use of eli-cel would be appropriate in those diagnosed with early CALD for whom an HLA-matched sibling
HSC donor is not available.
Given the severity of the disease, rapid irreversible progression and, as a consequence, short window of opportunity to treat, it is important that treatment is available on short notice. Eli-cel is available for infusion in about 2 months after a patient’s own cell harvesting via apheresis (see Package leaflet:
Information for the patient or carer in Annex III of the SmPC).12
2.2 Overview of the disease or health condition
2.2.1 Define the disease or health condition in the scope of this assessment
ALD is a rare X-linked metabolic disorder caused by mutations in the ABCD1 gene which codes for the adrenoleukodystrophy protein (ALDP) involved in the peroxisomal degradation of VLCFAs (Figure 2.1). The ABCD1 gene is located on the X chromosome. Females have two X chromosomes, one from each
parent, whereas males have only one X chromosome. Thus, if males inherit the mutation, there is no normal gene to compensate as there is in females. Males therefore typically manifest X-linked disorders most severely. In the absence of functional ALDP, VLCFAs accumulate in plasma and tissues,
particularly those of the adrenal glands and white matter of the brain and spinal cord. 2
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 21
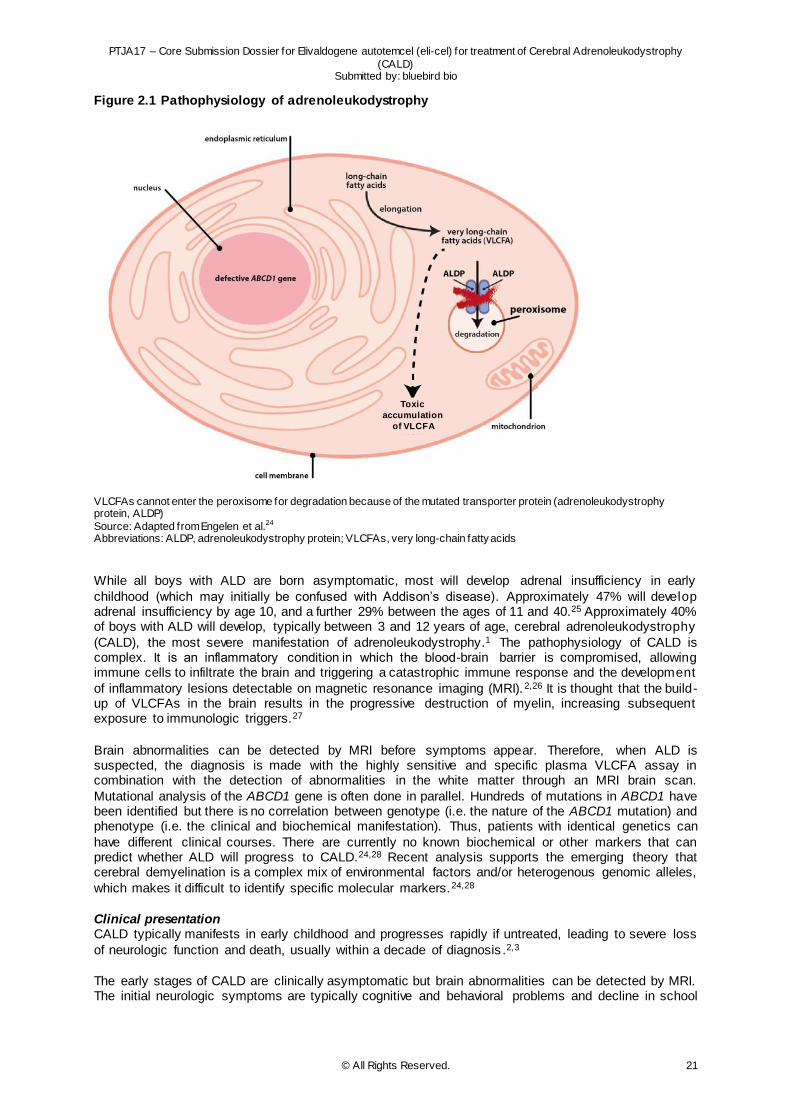
Figure 2.1 Pathophysiology of adrenoleukodystrophy
VLCFAs cannot enter the peroxisome for degradation because of the mutated transporter protein (adrenoleukodystrophy protein, ALDP)
Source: Adapted from Engelen et al.24 Abbreviations: ALDP, adrenoleukodystrophy protein; VLCFAs, very long-chain fatty acids
While all boys with ALD are born asymptomatic, most will develop adrenal insufficiency in early
childhood (which may initially be confused with Addison’s disease). Approximately 47% will develop adrenal insufficiency by age 10, and a further 29% between the ages of 11 and 40.25 Approximately 40% of boys with ALD will develop, typically between 3 and 12 years of age, cerebral adrenoleukodystrophy
(CALD), the most severe manifestation of adrenoleukodystrophy.1 The pathophysiology of CALD is complex. It is an inflammatory condition in which the blood-brain barrier is compromised, allowing immune cells to infiltrate the brain and triggering a catastrophic immune response and the development
of inflammatory lesions detectable on magnetic resonance imaging (MRI).2,26 It is thought that the build-up of VLCFAs in the brain results in the progressive destruction of myelin, increasing subsequent exposure to immunologic triggers.27
Brain abnormalities can be detected by MRI before symptoms appear. Therefore, when ALD is suspected, the diagnosis is made with the highly sensitive and specific plasma VLCFA assay in combination with the detection of abnormalities in the white matter through an MRI brain scan.
Mutational analysis of the ABCD1 gene is often done in parallel. Hundreds of mutations in ABCD1 have been identified but there is no correlation between genotype (i.e. the nature of the ABCD1 mutation) and phenotype (i.e. the clinical and biochemical manifestation). Thus, patients with identical genetics can
have different clinical courses. There are currently no known biochemical or other markers that can predict whether ALD will progress to CALD.24,28 Recent analysis supports the emerging theory that cerebral demyelination is a complex mix of environmental factors and/or heterogenous genomic alleles,
which makes it difficult to identify specific molecular markers.24,28
Clinical presentation CALD typically manifests in early childhood and progresses rapidly if untreated, leading to severe loss
of neurologic function and death, usually within a decade of diagnosis .2,3
The early stages of CALD are clinically asymptomatic but brain abnormalities can be detected by MRI. The initial neurologic symptoms are typically cognitive and behavioral problems and decline in school
Toxic accumulation of
VLCFA
Toxic
accumulation
of VLCFA
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 22
performance in early to mid-childhood (median age 7 years), which may be misdiagnosed as attention
deficit hyperactivity disorder or other more common developmental issues.2,24
As the disease progresses, irreversible brain damage occurs. Affected boys develop more pronounced disabilities, such as hearing and visual difficulties, aphasia (speech and language impairment), apraxia
(difficulty planning motor actions), swallowing dysfunction, walking/running difficulties, episodes of incontinence, and seizures within 6 to 15 months of the first symptom onset.29 Progression at this stage can be rapid and devastating: patients may lose the ability to walk and to understand language within a
period of weeks.2,24
Progression leads to major functional disabilit ies (MFDs). Patients are eventually left profoundly disabled: blind, incontinent, and unable to move, speak, or respond. They require tube feeding and full -
time nursing care.2 This condition has been described as an "apparent vegetative state". 2,3 The six disabilities with the greatest effect on independent functioning (loss of communication, cortical blindness, dependence on tube feeding, wheelchair dependence, no voluntary movement, and total
incontinence) have been designated as MFDs for the purposes of assessing clinical outcomes in CALD.4,30 Death from CALD is almost always inevitable without treatment.
Natural history and prognosis
CALD usually manifests early in childhood, between the ages of 3 and 12 years. However, it can also occur in adolescence and adulthood with similar symptoms and clinical presentation. 2 The mean (± standard deviation [SD]) age of onset in two large published series was 7 ± 1.7 and 7 ± 2 years. 3,31
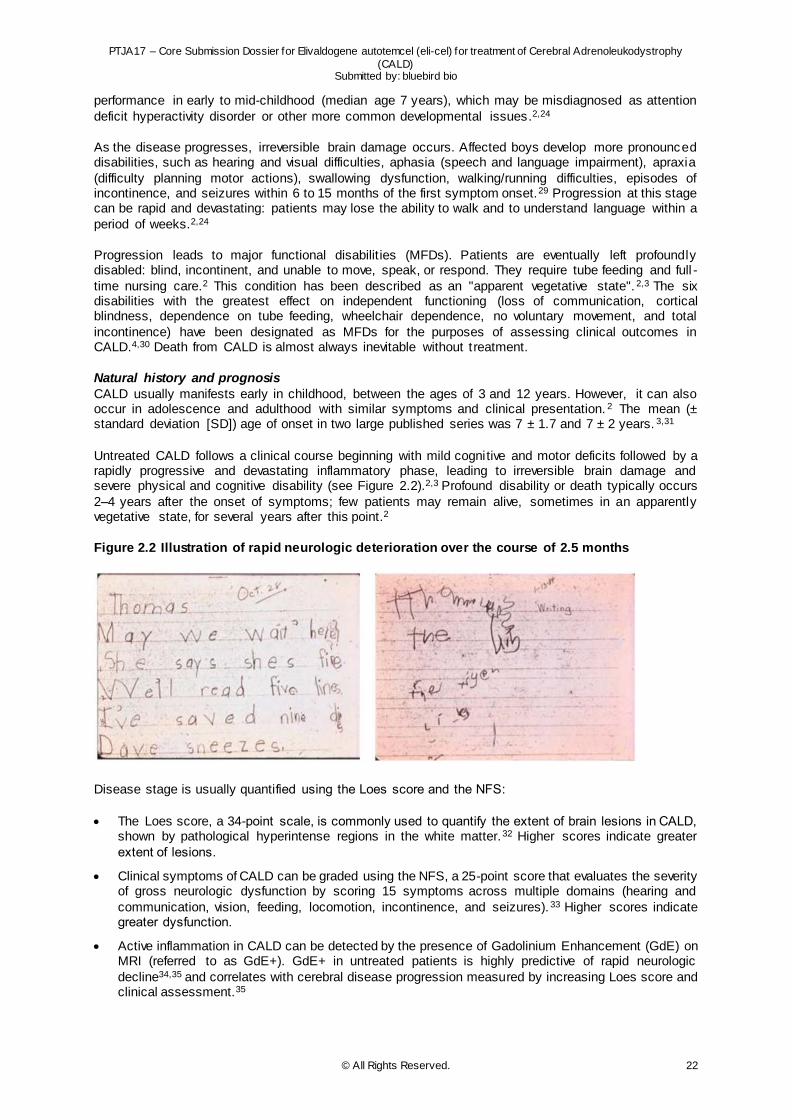
Untreated CALD follows a clinical course beginning with mild cognitive and motor deficits followed by a rapidly progressive and devastating inflammatory phase, leading to irreversible brain damage and severe physical and cognitive disability (see Figure 2.2).2,3 Profound disability or death typically occurs
2–4 years after the onset of symptoms; few patients may remain alive, sometimes in an apparently vegetative state, for several years after this point.2
Figure 2.2 Illustration of rapid neurologic deterioration over the course of 2.5 months
Disease stage is usually quantified using the Loes score and the NFS:
The Loes score, a 34-point scale, is commonly used to quantify the extent of brain lesions in CALD, shown by pathological hyperintense regions in the white matter.32 Higher scores indicate greater
extent of lesions.
Clinical symptoms of CALD can be graded using the NFS, a 25-point score that evaluates the severity of gross neurologic dysfunction by scoring 15 symptoms across multiple domains (hearing and
communication, vision, feeding, locomotion, incontinence, and seizures). 33 Higher scores indicate greater dysfunction.
Active inflammation in CALD can be detected by the presence of Gadolinium Enhancement (GdE) on MRI (referred to as GdE+). GdE+ in untreated patients is highly predictive of rapid neurologic
decline34,35 and correlates with cerebral disease progression measured by increasing Loes score and clinical assessment.35
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 23
The early stage of CALD, where cerebral involvement is limited, is clinically asymptomatic, but brain
abnormalities can be detected by MRI.2 Early stage can generally be defined as NFS score 0 or 1 and a Loes score ≤9 or <10.3-5 More details about NFS, Loes and GdE are presented in section 7.11.1, as these are used as clinical endpoints. The definition of early CALD in the context of the indication of eli-
cel is further explained in section 2.3.1, paragraph “Definition of early CALD”.
In a group of 30 untreated patients in the United States (US) in whom CALD was identified at an early stage (NFS score 0 or 1; Loes score <9), the probability of survival at 5 years was 54%.3 Similarly, in a
retrospective study (ALD-101) sponsored by bluebird bio (described in more detail in section 7.6.1), 55% of 72 untreated patients (i.e. those who did not undergo allo-HSCT) were alive 5 years after CALD diagnosis.4
It has been reported recently that a few patients, mostly diagnosed in late adolescence or adulthood, seem to experience stabilised CALD, in which the disease spontaneously self-stabilises, without evidence of inflammatory progression.36 The underlying processes for this are currently not well
understood and cannot be predicted, as available disease markers are lacking.
No specific ICD-10 code exists for CALD, however the ICD-10 code for ALD is: 2021 ICD-10-CM Diagnosis code E71.529 (“X-linked adrenoleukodystrophy, unspecified type”).
2.2.2 Present an estimate of prevalence and/or incidence for the disease or health condition including recent trends
Limited epidemiology data is available presenting the incidence and prevalence of CALD in Europe. A
few European studies have been identified reporting incidence, prevalence, and proportion of CALD patients in a population of ALD patients.
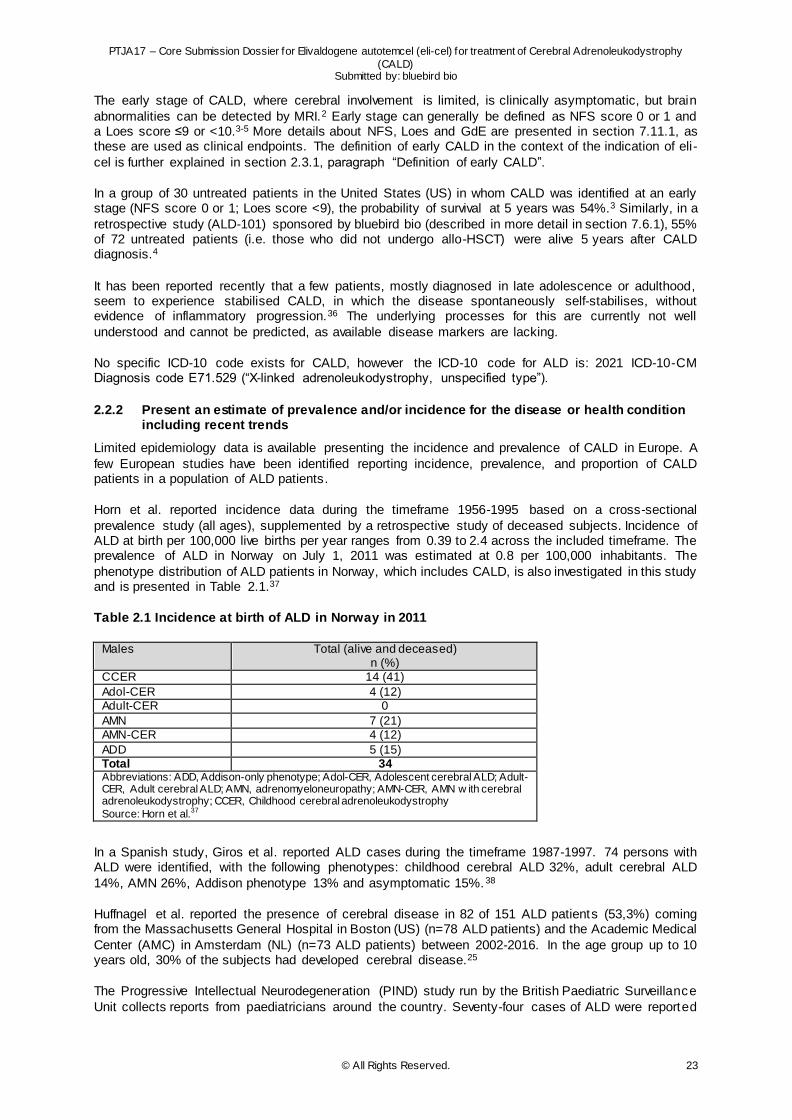
Horn et al. reported incidence data during the timeframe 1956-1995 based on a cross-sectional
prevalence study (all ages), supplemented by a retrospective study of deceased subjects. Incidence of ALD at birth per 100,000 live births per year ranges from 0.39 to 2.4 across the included timeframe. The prevalence of ALD in Norway on July 1, 2011 was estimated at 0.8 per 100,000 inhabitants. The
phenotype distribution of ALD patients in Norway, which includes CALD, is also investigated in this study and is presented in Table 2.1.37
Table 2.1 Incidence at birth of ALD in Norway in 2011
Males Total (alive and deceased) n (%)
CCER 14 (41)
Adol-CER 4 (12) Adult-CER 0
AMN 7 (21) AMN-CER 4 (12)
ADD 5 (15) Total 34 Abbreviations: ADD, Addison-only phenotype; Adol-CER, Adolescent cerebral ALD; Adult-CER, Adult cerebral ALD; AMN, adrenomyeloneuropathy; AMN-CER, AMN w ith cerebral adrenoleukodystrophy; CCER, Childhood cerebral adrenoleukodystrophy
Source: Horn et al.37
In a Spanish study, Giros et al. reported ALD cases during the timeframe 1987-1997. 74 persons with ALD were identified, with the following phenotypes: childhood cerebral ALD 32%, adult cerebral ALD
14%, AMN 26%, Addison phenotype 13% and asymptomatic 15%.38
Huffnagel et al. reported the presence of cerebral disease in 82 of 151 ALD patients (53,3%) coming from the Massachusetts General Hospital in Boston (US) (n=78 ALD patients) and the Academic Medical
Center (AMC) in Amsterdam (NL) (n=73 ALD patients) between 2002-2016. In the age group up to 10 years old, 30% of the subjects had developed cerebral disease.25
The Progressive Intellectual Neurodegeneration (PIND) study run by the British Paediatric Surveillance
Unit collects reports from paediatricians around the country. Seventy-four cases of ALD were reported

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 24
in the period 1997–2014, 19 of which were asymptomatic. This is likely to be an under-reporting of the
true number of children with ALD, however, and is lower than would be expected from the UK birth rate.39
As little country-specific data on CALD incidence are available, the incidence of CALD is estimated,
based on the proportion of males with ALD who are expected to develop CALD. The incidence of ALD among newborn males in the US has been estimated to be approximately 1 in 21,00040 and French investigators have made a similar estimate although figures are reported including both males and
females (1:17.000 including both male and female newborns)41. The estimated incidence of CALD is based on the proportion of males with ALD who are expected to develop CALD; up to 40% of boys with ALD will progress to CALD between the ages of 3 and 18 years (onset before the age of 3 is rare). 1 This
is in line with the proportion of ALD patients presenting the CALD phenotype as described in the country -specific studies above.
Considering 4.2 million live births in the EU (before Brexit), approximately 2.1 million male live
births (based on sex ratio of 1.06 male/female) are expected per year.42,43 Of these, approximately 103 males would have ALD, leading to approximately 40 patients in Europe who develop CALD each year.1,40 There is no evidence that frequency of ALD varies with ethnic background.24 No major
differences in incidence rates of ALD or CALD occur between countries around the world.40,44
This estimation is based on incidence figures only, given the severity of the disease, rapid irreversible progression, and short survival.
2.2.3 Describe the symptoms and burden of the disease or health condition for patients
Survival and mortality Untreated patients with CALD typically die within 2–4 years of symptom onset, although patients may
survive, sometimes in a profoundly disabled state, for several years.2 As also presented in section 2.2.1, 5-year survival rates have been described in two studies: In a group of 30 untreated patients in the US in whom CALD was identified at an early stage (NFS score 0 or 1; Loes score <9), the probability of
survival at 5 years was 54%.3 Similarly, in a retrospective study (ALD-101) sponsored by bluebird bio (described in more detail in section 7.6.1), 55% of 72 untreated patients (95% CI 42.2–65.7%) (i.e. those who did not undergo allo-HSCT) were alive 5 years after CALD diagnosis.4
Survival after treatment with allo-HSCT varies depending on the disease stage at the time of treatment and the level of donor matching. In a cohort of 65 patients in a retrospective study (both early and later-stage disease) who underwent allo-HSCT, 5-year OS was 78% (95% CI 64–86.6%).4 More details about
survival after treatment is reported in section 7.8.
Population mortality rates for CALD are not available because of its rarity.
Symptoms and Patient burden
CALD is a devastating condition for patients and their families. It leads to progressive neurologic and functional deterioration, ending in profound physical and cognitive disability, and leading to death in many cases within a few years. As such, it has a devastating impact on affected boys and their families. 2
The clinical presentation of CALD is described in Section 2.2.1.
CALD is associated with six MFDs that develop as the disease progresses4, and result in the total loss of the underlying ability:
loss of communication
cortical blindness
dependence on tube feeding
wheelchair dependence
loss of voluntary movement
total incontinence.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 25
A study by Furlan et al. analysed data from CALD patients in Brazil and presented the initial signs and
symptoms of CALD, as being: aphasia, hyperactivity, visual disorders, poor school performance, skin hyperpigmentation, impaired motor coordination, sphincter incontinence, memory disorders, aggressiveness, hearing disorders, decreased strength in lower limbs, dysgraphya, uninhibited
behaviour, seizures, difficulty in reading and difficulty in ambulation.45
Other papers have also described symptoms that are related to a decline in neurological and neuropsychological scores, and include being in vegetative state, spastic ity, loss of speech, loss of
vision46,47, deteriorated language skills, motor function deterioration, sensory deficits48, difficulty with basic communication, basic reading or writing tasks, deterioration in IQ/intellect, mobility limitations and seizures49, personality change, gait disturbance, being bedridden50 and dementia51,52.
The devastating nature of CALD means that it has a severe and progressive impact on HRQoL if not treated. Although very few studies of HRQoL in patients with untreated CALD have been identified in the literature, it is evident that the disease has a severe impact on the patient, caregivers and family ,
caused by having to experience a healthy boy deteriorate both physically and cognitively and the sense of guilty of the mothers, who transmitted the defective gene to the sons. Also, children experience significant problems of social isolation, and CALD patients with progressive disease require assistance
24 hours/day which is a huge burden for both the patient and their family.53
Impact on quality of life Utility values can range between 0 and 1, where 0 represents death and 1 represents perfect health.
Utility scores in patients with CALD were not identified in the literature;54 however, patients who develop MFDs will self-evidently have a considerable reduction in utility. To give an indication, a study by Petrou and Kupek using survey data from children with a range of disabilities (not ALD) in the UK assigned a
disutility of –0.452 to ‘vision disorders and blindness’ and –0.541 to ‘muscular dystrophy and spinal muscular atrophy’.55
Bessey et al. estimated the disutility values associated with childhood CALD in the UK, mapping the
ALD-Disability Rating Scale (DRS) onto the EQ-5D-5L. This resulted in an overall quality-adjusted life year (QALY) of 0.682, 0.599, 0.11 and 0.031 for ALD-DRS1, ALD-DRS2, ALD-DRS3 and ALD-DRS4 respectively (a higher ALD-DRS score means more disability).56
In general, treatment with allo-HSCT has a significant short-term impact on HRQoL; Sung and colleagues estimated a disutility of –0.57 for young adults undergoing allo-HSCT (with MSD in Acute Myeloid Leukaemia – not ALD).57 This was confirmed in the observational clinical study ALD-103, where
in the 24 months following allo-HSCT treatment (n = 11), the median Paediatric Quality of Life Inventory (PedsQL) total scale score (0-100 (best)) decreased by 11.67 points (6.0–17.4).11
Caregiver burden
Only two Asian studies of burden or HRQoL in caregivers of children with CALD have been identified.54 Kuratsubo et al. conducted an analysis interviewing 37 parents of patients with CALD in Japan. Many parents felt physical or mental tiredness, and some developed illnesses such as depressive disorder,
irritable colon, facial palsy, autonomic imbalance, duodenal ulcer, lumbar disc hernia and lumbar strain. Also social problems such as difficulties in family relations, change or loss of job and decreased income or increased expenses were reported.58 In another study interviewing 8 mothers of patients with ALD in
Taiwan, psychological impact was also reported, including feeling guilty for being a carrier and powerlessness towards unsatisfactory treatment.59 This was also reported in a study in the UK in another progressive childhood condition with some similarities to CALD; Duchenne muscular dystrophy.60
Given the nature of CALD, it is self-evident that caregivers will face huge psychological and practical burdens in caring for a child with CALD who does not receive successful disease-modifying treatment. After allo-HSCT, it would be expected that caregivers of patients who experience complications (GVHD,
infections) would face a greater continuing burden than those whose children have good functional status and freedom from treatment-related comorbidities.
Economic burden
CALD and its treatment exert a high economic burden on healthcare systems and families. Limited published evidence is available describing the direct and indirect costs of CALD.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 26
In the observational ALD-103 study for CALD patients treated with allo-HSCT (n = 59), the median
cumulative number of hospital inpatient days for the initial treatment period until neutrophil engraftment was 51.0 (range 3–240).11 For 96.6% of patients this time was accrued during a single hospitalisation. The median cumulative number of hospital inpatient days between engraftment and 24 months post -
treatment was 14.0 (3–308). Half of patients (50.0%) had no hospitalisations during this period, 20.7% had one, 19.0% had two, and the remainder had more.11
Direct costs for treatment of CALD were identified in a US claims database study. The median per
patient cost of allo-HSCT and the first year of care post-treatment in a 2012–2018 claims database analysis of 14 patients with CALD in the US was $588,233 (range $118,912–2,327,603).61 Total costs included all those reimbursed by the insurer in the one year period from the point of receiving allo-HSCT,
including initial transplant and hospital stay costs. The wide variation in costs largely reflected differing needs for rehospitalisation (e.g. for subsequent transplant or management of GVHD).61
Costs of allo-HSCT for CALD patients in Europe have not been identified in literature. However,
Blommestein et al. report the costs of HSCT for haematological diseases in general (not CALD specifically) in the Netherlands, which can be assumed to be in line with the costs of allo-HSCT for CALD patients.62 It should be noted that the data is not very recent however (SCTs were performed in
2007-2009). The total costs included selection and harvesting of stem cells, transplantation and 1-year follow-up. The average costs per patient were €101,919 for sibling allo-SCT. The costs of transplantations from unrelated donors were much higher: €171,478 and €254,689 for allo-SCT with a
matched unrelated donor and allo-SCT with umbilical cord blood respectively.62 It is important to note that conditioning regimen and HSCT techniques have advanced specifically for inborn errors since this publication, which also might impact costs.
Bessey et al. published a cost-utility analysis in the UK setting, with the objective to analyse the efficiency of resource allocation in a newborn screening programme for ALD. Per patient costs (for paediatrics ) were reported for the NHS (2014-2015) for symptomatic ALD. Annual healthcare costs were £5,436 for
mild/moderate and £17,621 for moderate/severe. Annual social care costs were £11,056 to £112,662 for mild/moderate and moderate/severe respectively. Transplant-related costs were estimated at £98,147.56
Although not much literature on economic burden is available, it is assumed to be high and increasing with further progression of the disease. In addition to costs for allo-HSCT, costs are incurred for regular visits to the physician/hospital, special needs in terms of school, wheelchair, tube feeding, incontinence,
and, in the severely progressed patients, 24hr nursing at home.
2.3 Target population
2.3.1 Target population
Eli-cel is indicated for the treatment of early cerebral adrenoleukodystrophy in patients less than 18
years of age, with an ABCD1 genetic mutation, and for whom a human leukocyte antigen (HLA)-matched sibling haematopoietic stem cell (HSC) donor is not available.12
Only patients without an available MSD MSD is an instantly recognised category of transplant and the most clear-cut, as far as "best transplants" are concerned for minimising possible HSCT-related complications and, currently, in absence of clear
and solid data on non-HLA factors that could influence transplant outcomes. For CALD, matched related non-sibling donor transplants happen much less often than MSD transplants, as also confirmed in a recent natural history study.4 One of the reasons could be because the mother is excluded by definition,
as she is an ABCD1 carrier. An exclusion criterion for the eli-cel pivotal clinical trial ALD-102 was having a willing 10/10 HLA-MSD, leading to the current wording in the indication.
Age less than 18 years
The indication of treatment in patients less than 18 years of age aligns with the inclusion criteria for
bluebird bio’s clinical studies in CALD. The actual age range of subjects enrolled in the clinical trials
is reflective of the ages at which subjects are most likely to have had a diagnosis of CALD and match
entry criteria for neurologic status in the clinical trial. A recent meta-analysis of CALD studies from 1970
through Sept 10 2019, showed that 90% of patients were diagnosed between 3 and 12 years of
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 27
age.36 Consistent with these results, subjects treated with allo-HSCT in bluebird bio’s clinical studies
(Studies ALD-101 and ALD-103, for more details see section 7.4.1) ranged from 2 to 18 years of age,
and the majority of them were 6 to 11 years old (76.6%).
The benefit/risk of eli-cel therapy is expected to be a function of disease status more rather than numeric
age, biology of CALD and mechanism of eli-cel treatment are not expected to differ by age in patients
who are less than 18 years old, and differences in efficacy or safety across this age range have not
been detected. Thus, treatment should be guided by clinical parameters and be available to eligible
patients less than 18 years of age.
HLA-matched sibling HSC donor
One of the exclusion criteria for the eli-cel pivotal clinical trial ALD-102 (for more details see section
7.4.1) was having a willing, healthy (meaning not carrying ABCD1 mutation) 10/10 human leukocyte
antigen-matched sibling donor, leading to the current wording in the indication. MSD is an instantly
recognised category of transplant and the most clear-cut, as far as "best transplants" are concerned for
minimising possible HCT-related complications and, currently, in absence of clear and solid data on
non-HLA factors that could influence transplant outcomes. The risks of allogeneic HSCT are significantly
higher for subjects who do not have a 10/10 HLA-matched sibling donor, particularly the risks of
engraftment failure, GVHD and overall mortality. To date, the most successful outcomes with allo-HSCT
have been reported when cells from a HLA-matched unaffected HSC sibling donor were used.4,5,49,64
Therefore, patients without an unaffected, willing 10/10 HLA-matched sibling donor have the highest
level of unmet medical need. Moreover, for CALD, matched related non-sibling donor transplants
happen much less often than MSD transplants, as also confirmed in the natural history study ALD-101.4 One of the reasons could be because the mother is excluded by definition, as she is an ABCD1 carrier.
Definition of early CALD
Many measures used for disease assessment of CALD are observations on continuous scales. These include Loes score (0 to 34), NFS (0 to 25), and GdE (typically described as present in bright and/or large amounts, present in dim and/or small amounts, or absent). When making treatment decisions,
healthcare providers consider all of these elements as well as other elements such as neurocognit ive function. There are not one or two factors or measures that clearly and specifically define the disease, but rather it is the full picture of disease that allows for treatment decisions to be made. It is important
to ensure that initial cerebral manifestations of CALD are present, which is typically done through radiographic examination. It is also important to treat as early as possible before more advanced signs of disease have developed as the damage to the brain is irreversible. The clinical study inclusion criteria
for bluebird bio’s Study ALD-102 (described in more detail in section 7.5.1 and 7.6.1) accurately describe the patient population that is consistently offered allo-HSCT in clinical.5,65 Early disease was defined as Loes score between 0.5 and 9.0 and NFS ≤1). Please note that no meaningful differences were found
in subgroup analysis of clinical outcome by mild versus moderate-severe Loes score. Based on the natural history of the disease and known outcomes following allo-HSCT, arresting disease progression early is important to maximising benefit to the patient. Clinical study data demonstrate the benefit to
treatment of subjects across the spectrum of early disease included in eli -cel studies.
2.3.2 Size of target population
The estimated incidence of CALD is based on the proportion of males with ALD who are expected to
develop CALD, as little country-specific data on CALD incidence are available. For Europe, it is estimated that approximately 40 patients per year will develop CALD, without ethnic predisposition (detailed information is provided in section 2.2.2 of this dossier). This estimation is based on incidence
figures only, given the severity of the disease, rapid irreversible progression and, as a consequence, short window of opportunity to treat.
The estimated incidence of CALD does not correspond to the number of patients that are eligible for
treatment with eli-cel, because only cases that are identified at an early stage can be treated. The number of allo-HSCT per year in Europe could be used as a proxy for the number of treatable patients. This information is available from the European Society for Blood and Marrow Transplant (EBMT)
registry.66 The EBMT registry contains patient clinical data, including aspects of the diagnosis and disease, first-line treatments, HSCT procedures, transplant type, donor type, stem cell source, complications and outcome. The data presented here has been based on the following criteria: CALD
diagnosis in European countries, allogeneic transplant in or after 2015 and having age at diagnosis <18
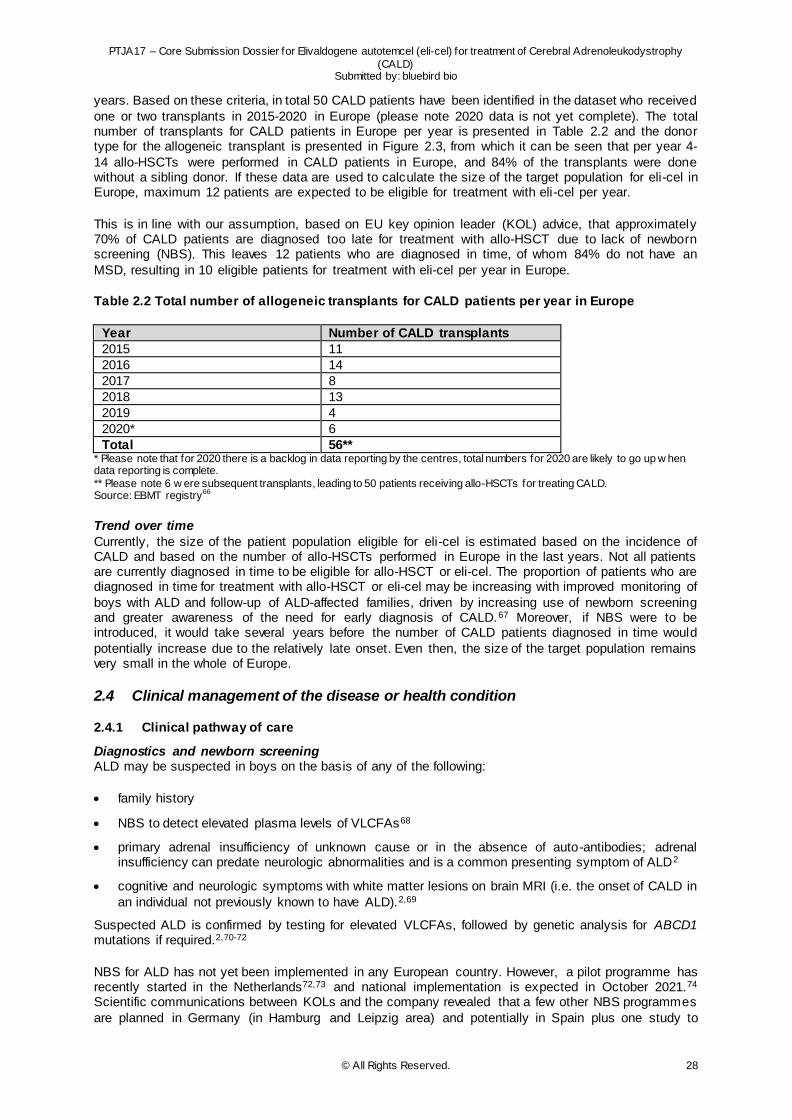
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 28
years. Based on these criteria, in total 50 CALD patients have been identified in the dataset who received
one or two transplants in 2015-2020 in Europe (please note 2020 data is not yet complete). The total number of transplants for CALD patients in Europe per year is presented in Table 2.2 and the donor type for the allogeneic transplant is presented in Figure 2.3, from which it can be seen that per year 4-
14 allo-HSCTs were performed in CALD patients in Europe, and 84% of the transplants were done without a sibling donor. If these data are used to calculate the size of the target population for eli-cel in Europe, maximum 12 patients are expected to be eligible for treatment with eli-cel per year.
This is in line with our assumption, based on EU key opinion leader (KOL) advice, that approximately 70% of CALD patients are diagnosed too late for treatment with allo-HSCT due to lack of newborn screening (NBS). This leaves 12 patients who are diagnosed in time, of whom 84% do not have an
MSD, resulting in 10 eligible patients for treatment with eli-cel per year in Europe.
Table 2.2 Total number of allogeneic transplants for CALD patients per year in Europe
Year Number of CALD transplants
2015 11
2016 14
2017 8
2018 13
2019 4
2020* 6
Total 56** * Please note that for 2020 there is a backlog in data reporting by the centres, total numbers for 2020 are likely to go up w hen data reporting is complete.
** Please note 6 w ere subsequent transplants, leading to 50 patients receiving allo-HSCTs for treating CALD. Source: EBMT registry66
Trend over time
Currently, the size of the patient population eligible for eli-cel is estimated based on the incidence of CALD and based on the number of allo-HSCTs performed in Europe in the last years. Not all patients are currently diagnosed in time to be eligible for allo-HSCT or eli-cel. The proportion of patients who are diagnosed in time for treatment with allo-HSCT or eli-cel may be increasing with improved monitoring of
boys with ALD and follow-up of ALD-affected families, driven by increasing use of newborn screening and greater awareness of the need for early diagnosis of CALD.67 Moreover, if NBS were to be introduced, it would take several years before the number of CALD patients diagnosed in time would
potentially increase due to the relatively late onset. Even then, the size of the target population remains very small in the whole of Europe.
2.4 Clinical management of the disease or health condition
2.4.1 Clinical pathway of care
Diagnostics and newborn screening ALD may be suspected in boys on the basis of any of the following:
family history
NBS to detect elevated plasma levels of VLCFAs68
primary adrenal insufficiency of unknown cause or in the absence of auto-antibodies; adrenal insufficiency can predate neurologic abnormalities and is a common presenting symptom of ALD2
cognitive and neurologic symptoms with white matter lesions on brain MRI (i.e. the onset of CALD in
an individual not previously known to have ALD).2,69
Suspected ALD is confirmed by testing for elevated VLCFAs, followed by genetic analysis for ABCD1 mutations if required.2,70-72
NBS for ALD has not yet been implemented in any European country. However, a pilot programme has recently started in the Netherlands72,73 and national implementation is expected in October 2021.74 Scientific communications between KOLs and the company revealed that a few other NBS programmes
are planned in Germany (in Hamburg and Leipzig area) and potentially in Spain plus one study to
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 29
validate the ALD NBS test through a pilot programme in Italy. An analysis undertaken from the
perspective of the National Health Service in the UK predicted that adding screening of boys for ALD to an existing tandem NBS programme would reduce lifetime costs and improve outcomes for those who develop CALD thus demonstrating the cost-effectiveness of an ALD NBS programme. Cost savings
were driven by estimated reductions in the cost of social care and education.56
CALD may develop in boys already diagnosed with ALD, or it may be the first clinical manifestation of the condition. Once a diagnosis of ALD has been established, diagnosis of CALD is confirmed based
on evidence of characteristic white matter lesions on MRI.75 The extent of cerebral involvement on MRI is measured by the Loes score. GdE on MRI is a marker of active and progressive cerebral inflammatory disease.4,5
Early detection, before the onset of clinical symptoms, is crucial to enable allo-HSCT to be performed at an early stage of the disease, when outcomes are most favourable.2,5
The early stages of CALD can be detected by brain MRI in boys with known ALD before symptoms
develop; treatment guidelines recommend brain MRI every 6 months between the ages of 3 and 12 years, and every 12 months thereafter.2
In boys not known to have ALD, early symptoms of CALD are often misdiagnosed as attention deficit
hyperactivity disorder, and diagnosis may be delayed.2
Loes pattern and scoring measures the extent of demyelination by MRI and is commonly used to determine the extent of cerebral disease.32 GdE is an indicator of active inflammation and is associated
with a poor prognosis in untreated patients.4
Unless there is a known family history of ALD/CALD, or the child is born in a territory where NBS is performed (so far only one NBS pilot has been identified in the Netherlands as described above) 72, the
disease is rarely known before symptoms emerge. The cerebral phenotype (CALD) may be the first clinical manifestation of ALD. Because the initial clinical presentation is often unspecific it can make the diagnosis extremely difficult. Delayed diagnosis is common. A further proportion of boys are diagnosed
too late to be eligible for allo-HSCT. We assume, based on EU KOL advice, that approximately 70% of CALD patients are diagnosed too late for treatment with allo-HSCT.
The rarity of the disease coupled with the lack of NBS programmes, complicates an early diagnosis,
which is key to ensure timely treatment before further damage occurs. Current monitoring guidelines recommend that all boys with ALD who are aged 3 to 12 years be monitored every 6 months with MRI to detect early signs of cerebral involvement (more details are described in section 2.4.2).2 It is important
to note that such a monitoring strategy is necessary since there is currently no test to predict if CALD will develop in boys with ALD.
Clinical pathway
Allo-HSCT Allo-HSCT is currently the only disease-modifying treatment available for CALD patients. Allo-HSCT is an effective treatment for CALD, provided that it is performed at an early stage (i.e. when the patient
has initial and limited cerebral involvement, generally defined as NFS 0 or 1 and Loes score ≤9 or <10).2-
5 However, allo-HSCT is associated with life-threatening risks, including transplant-related mortality, GVHD, graft rejection and opportunistic severe infections related to immunosuppressant usage.
Outcomes are affected by the clinical stage of the patient at transplant, and whether or not there is a well-matched donor.
Allo-HSCT involves administering chemotherapy to clear space in the bone marrow (known as
conditioning), then replenishing with healthy haematopoietic stem cells from a donor. The mechanism of action of allo-HSCT in CALD is not fully understood, but it has been proposed that donor stem cells develop into monocytes that travel to the brain and further differentiate into microglial cells that express
ALDP.30 Processing of VLCFA by these cells is thought to lower local VLCFA levels, preventing further inflammation and demyelination and thereby stabilising the disease.
Transplant protocols and conditioning regimens in CALD vary among cent res but involve the following
components:
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 30
Conditioning – usually this is myeloablative conditioning, a regimen that severely or completely
depletes the bone marrow cells; reduced intensity conditioning is used in some patients particularly in those with more advanced disease30
GVHD prophylaxis – immunosuppressive drugs are given with the aim of preventing GVHD 5
Other supportive care and prophylaxis may be administered in line with institutional protocols.
Burden of treatment with allo-HSCT Allo-HSCT involves myeloablative chemotherapy, requiring several weeks of hospitalisation. It has been indicated by patients and their caregivers that families must pause their lives for up to two years when
a child is undergoing allo-HSCT due to the complex management of transplantation.53 In addition to the burden of the procedure itself, allo-HSCT is associated with life-threatening risks, including opportunistic infections (29% of patients), acute GVHD (31%), GVHD (7%) and graft failure (18%).4 Patients require
long-term immunosuppressive therapy after allo-HSCT, in order to prevent graft rejection and GVHD, although a risk remains. The rate of graft failure or rejection was even 26.3% in the observational ALD-103 study.11
Patients who experience graft failure require a second transplant for survival, adding substantially to the burden of treatment. In some cases, due to rapid disease progression, patients may no longer be eligible for another transplant.
GVHD is a serious complication of allo-HSCT associated with substantial mortality and morbidity, and impaired HRQoL.76,77 It continues to occur despite the use of prophylactic medicines.78 The incidence is highest among patients with mismatched unrelated donors but it can occur with any allogenic donor
type.76
Acute GVHD typically occurs in the first 100 days after transplant. It most commonly manifests as mild to moderate skin rash but may also involve epithelial tissues in the lungs and gastrointestinal (GI) tract.
In severe cases, GVHD can have a devastating effect on the skin, GI tract, and liver. Severe acute GVHD is associated with significant mortality.76
Chronic GVHD is characterised by inflammation and fibrosis.79 It most commonly affects the skin,
eyes, mouth, liver, and GI tract; GI involvement causes anorexia, nausea, vomiting, and diarrhoea.77
Both types of GVHD are associated with decreased HRQoL, impaired functional status, and increased risk of mortality. The need for immunosuppression to prevent or treat GVHD after allo-HSCT exposes
patients to the risk of opportunistic infections, which can be fatal, and is associated with a range of side effects.78,80
Unmet need
Since CALD can rapidly progress and can results in irreversible cerebral damage, there is only a small window of opportunity to modify the disease course with effective treatment; this can only be achieved in patients with early disease (definition of early CALD is explained in more detail in section 2.3.1).
Allo-HSCT offers an effective treatment for CALD if performed early in the disease course, and outcomes are better with well-matched donors. However, because it involves the use of cells from a donor, allo-HSCT carries a significant risk of immune-mediated complications in the form of GVHD and
graft failure or rejection.30 Furthermore, patients require long-term immunosuppression after allo-HSCT, exposing them to the risk of potentially fatal opportunistic infections.78,80
Allo-HSCT can be performed with various types of donors. MSDs carry less safety risks although they
still occur.11,49 An alternative to allo-HSCT is particularly needed for patients for whom an MSD is not available: these patients are at higher risk for graft rejection and GVHD if a mismatched donor has to be used. Allo-HSCT with mismatched unrelated donors is associated with worse outcomes and greater
risks than allo-HSCT with other donor types,4 yet more than 70% of transplants for CALD involve unrelated donors.66 Of 56 transplants reported in the EBMT registry from 2015 to 2020, 84% were performed in patients without an MSD (see 2.3).66
Figure 2.3 Allo-HSCT in CALD by donor type
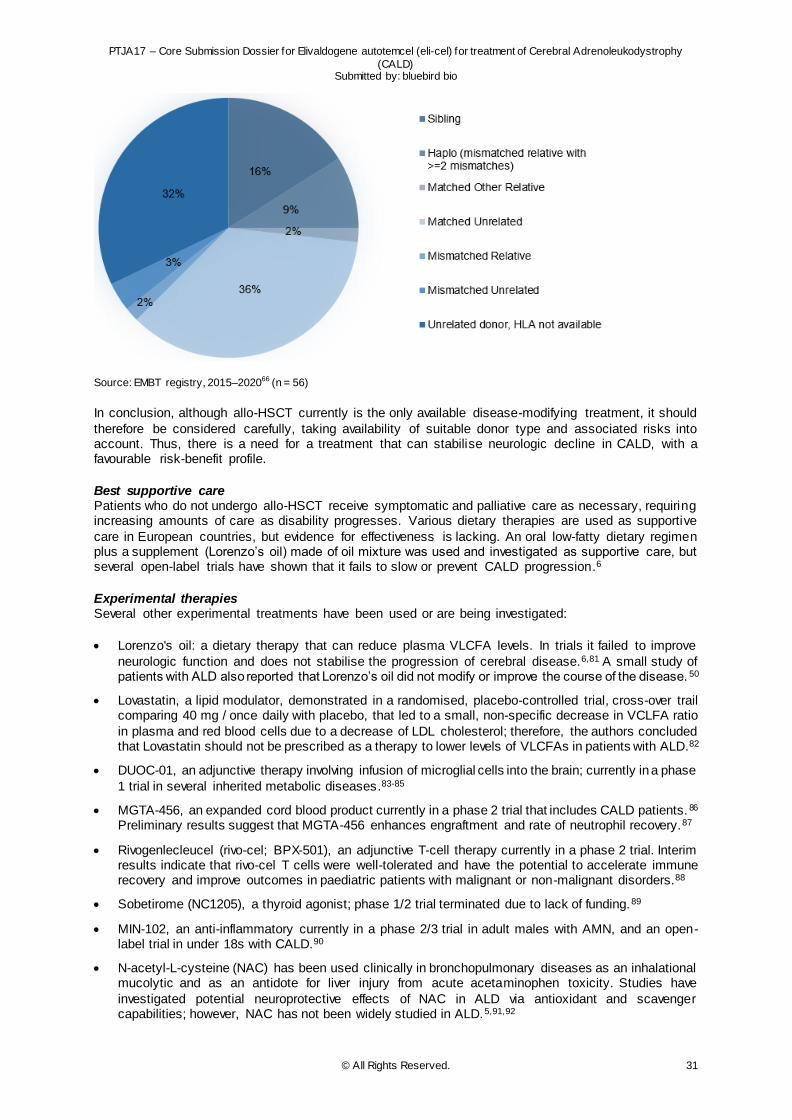
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 31
Source: EMBT registry, 2015–202066 (n = 56)
In conclusion, although allo-HSCT currently is the only available disease-modifying treatment, it should
therefore be considered carefully, taking availability of suitable donor type and associated risks into account. Thus, there is a need for a treatment that can stabilise neurologic decline in CALD, with a favourable risk-benefit profile.
Best supportive care Patients who do not undergo allo-HSCT receive symptomatic and palliative care as necessary, requiring increasing amounts of care as disability progresses. Various dietary therapies are used as supportive
care in European countries, but evidence for effectiveness is lacking. An oral low-fatty dietary regimen plus a supplement (Lorenzo’s oil) made of oil mixture was used and investigated as supportive care, but several open-label trials have shown that it fails to slow or prevent CALD progression.6
Experimental therapies Several other experimental treatments have been used or are being investigated:
Lorenzo's oil: a dietary therapy that can reduce plasma VLCFA levels. In trials it failed to improve
neurologic function and does not stabilise the progression of cerebral disease.6,81 A small study of patients with ALD also reported that Lorenzo’s oil did not modify or improve the course of the disease. 50
Lovastatin, a lipid modulator, demonstrated in a randomised, placebo-controlled trial, cross-over trail comparing 40 mg / once daily with placebo, that led to a small, non-specific decrease in VCLFA ratio
in plasma and red blood cells due to a decrease of LDL cholesterol; therefore, the authors concluded that Lovastatin should not be prescribed as a therapy to lower levels of VLCFAs in patients with ALD.82
DUOC-01, an adjunctive therapy involving infusion of microglial cells into the brain; currently in a phase
1 trial in several inherited metabolic diseases.83-85
MGTA-456, an expanded cord blood product currently in a phase 2 trial that includes CALD patients. 86 Preliminary results suggest that MGTA-456 enhances engraftment and rate of neutrophil recovery.87
Rivogenlecleucel (rivo-cel; BPX-501), an adjunctive T-cell therapy currently in a phase 2 trial. Interim results indicate that rivo-cel T cells were well-tolerated and have the potential to accelerate immune recovery and improve outcomes in paediatric patients with malignant or non-malignant disorders.88
Sobetirome (NC1205), a thyroid agonist; phase 1/2 trial terminated due to lack of funding.89
MIN-102, an anti-inflammatory currently in a phase 2/3 trial in adult males with AMN, and an open-label trial in under 18s with CALD.90
N-acetyl-L-cysteine (NAC) has been used clinically in bronchopulmonary diseases as an inhalational mucolytic and as an antidote for liver injury from acute acetaminophen toxicity. Studies have
investigated potential neuroprotective effects of NAC in ALD via antioxidant and scavenger capabilities; however, NAC has not been widely studied in ALD.5,91,92
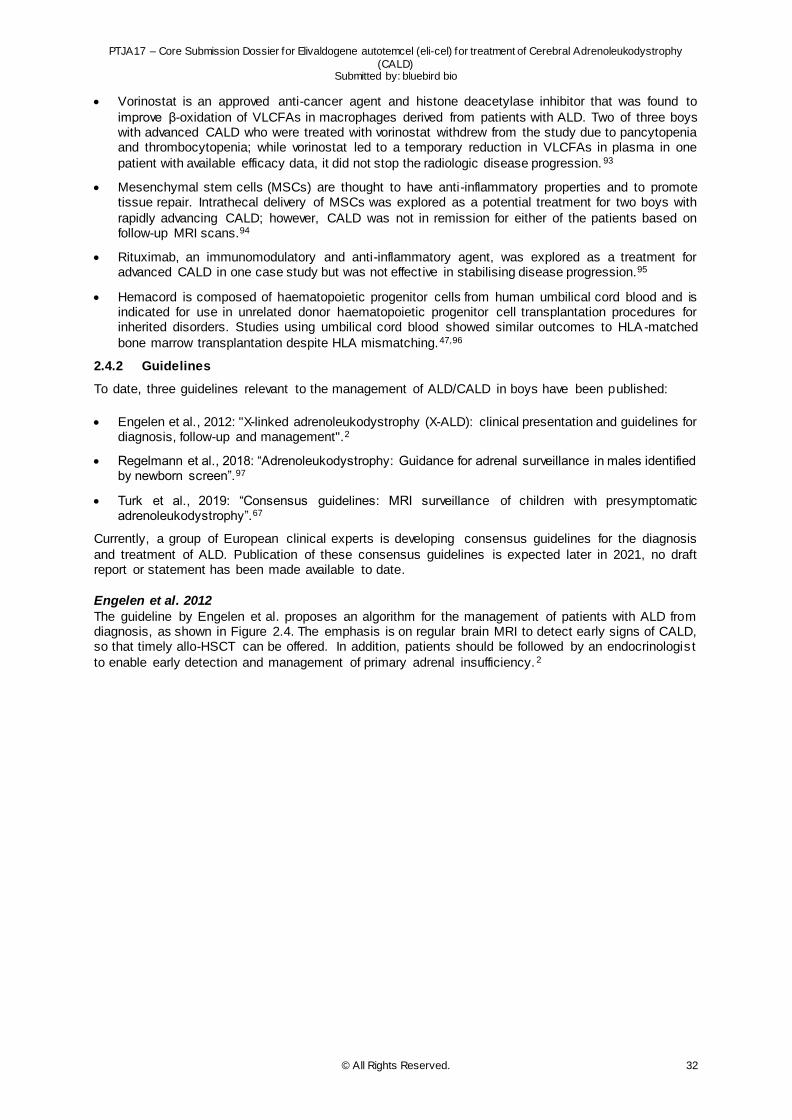
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 32
Vorinostat is an approved anti-cancer agent and histone deacetylase inhibitor that was found to
improve β-oxidation of VLCFAs in macrophages derived from patients with ALD. Two of three boys with advanced CALD who were treated with vorinostat withdrew from the study due to pancytopenia and thrombocytopenia; while vorinostat led to a temporary reduction in VLCFAs in plasma in one
patient with available efficacy data, it did not stop the radiologic disease progression. 93
Mesenchymal stem cells (MSCs) are thought to have anti-inflammatory properties and to promote tissue repair. Intrathecal delivery of MSCs was explored as a potential treatment for two boys with
rapidly advancing CALD; however, CALD was not in remission for either of the patients based on follow-up MRI scans.94
Rituximab, an immunomodulatory and anti-inflammatory agent, was explored as a treatment for advanced CALD in one case study but was not effective in stabilising disease progression.95
Hemacord is composed of haematopoietic progenitor cells from human umbilical cord blood and is indicated for use in unrelated donor haematopoietic progenitor cell transplantation procedures for inherited disorders. Studies using umbilical cord blood showed similar outcomes to HLA-matched
bone marrow transplantation despite HLA mismatching.47,96
2.4.2 Guidelines
To date, three guidelines relevant to the management of ALD/CALD in boys have been published:
Engelen et al., 2012: "X-linked adrenoleukodystrophy (X-ALD): clinical presentation and guidelines for diagnosis, follow-up and management".2
Regelmann et al., 2018: “Adrenoleukodystrophy: Guidance for adrenal surveillance in males identified by newborn screen”.97
Turk et al., 2019: “Consensus guidelines: MRI surveillance of children with presymptomatic adrenoleukodystrophy”.67
Currently, a group of European clinical experts is developing consensus guidelines for the diagnosis
and treatment of ALD. Publication of these consensus guidelines is expected later in 2021, no draft report or statement has been made available to date.
Engelen et al. 2012
The guideline by Engelen et al. proposes an algorithm for the management of patients with ALD from diagnosis, as shown in Figure 2.4. The emphasis is on regular brain MRI to detect early signs of CALD, so that timely allo-HSCT can be offered. In addition, patients should be followed by an endocrinologis t
to enable early detection and management of primary adrenal insufficiency. 2
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 33
Figure 2.4 Algorithm for the management of ALD
* If there is no gadolinium enhancement present, consider arrested cerebral ALD and repeat the MRI in 3 months.
Source: Engelen et al. 2 Abbreviations: ALD, adrenoleukodystrophy; BMT, bone marrow transplant (allogeneic haematopoietic stem cell transplant); MRI, magnetic resonance imaging (of the brain); X-ALD, X-linked adrenoleukodystrophy
The recommendations from this publication2 in relation to CALD can be summarised as follows.
Regular follow-up in boys with ALD is important so that CALD can be detected early enough for allo-HSCT to be offered.
MRI is recommended every 6 months in boys aged 3–12 years and every 12 months thereafter, or as
soon as possible if new symptoms occur.
Despite a significant mortality risk, allo-HSCT remains the only therapeutic intervention that can stabilise the progression of cerebral demyelination in CALD, provided that it is performed very early (i.e. when affected boys or men have no or minor symptoms of CALD).
Because CALD can progress rapidly, it is strongly advised that the possibility of allo-HSCT is discussed as soon as brain MRI abnormalities typical of CALD are detected.
There is no proven treatment for CALD in adults; allo-HSCT can be considered in adults with early
stage CALD.
Regelmann et al. These clinical recommendations address screening by NBS for adrenal insufficiency in boys identified
to have ALD. The authors note that there is limited literature evidence regarding monitoring of evolving adrenal insufficiency in male infants and children with ALD. The recommendations suggest that assessment of adrenal function should be initiated at ALD diagnosis and monitored regularly, so that
boys with adrenal insufficiency can be identified promptly and life-threatening adrenal crisis can be prevented.97
The guidelines do not address CALD. However, they note that allo-HSCT does not prevent progression
of adrenal insufficiency, probably because VLCFA has already accumulated in the adrenal cortex to a damaging degree by the time of transplant. The authors state that it is not known whether gene therapy for CALD would prevent adrenal insufficiency progression, but it is thought to be unlikely.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 34
Turk et al.
These expert consensus guidelines state that boys with ALD identified early in life should be closely monitored with serial brain MRIs during the period of highest risk for conversion to CALD:67
Perform a baseline brain MRI between 12 and 18 months of age.
Perform a second MRI 1 year after the baseline.
Beginning at age 3, obtain an MRI every 6 months until age 12.
Obtain an annual MRI after the age of 12.
To limit gadolinium exposure and duration of sedation, MRIs should be read in real-time to assess for
a cerebral lesion; if a lesion or questionable lesion is seen, then gadolinium should be applied. Gadolinium should be administered if no real-time reading capability is available in those children requiring sedation.
Strong emphasis should be placed on family education in order to maintain the surveillanc e schedule and avoid loss to follow-up.
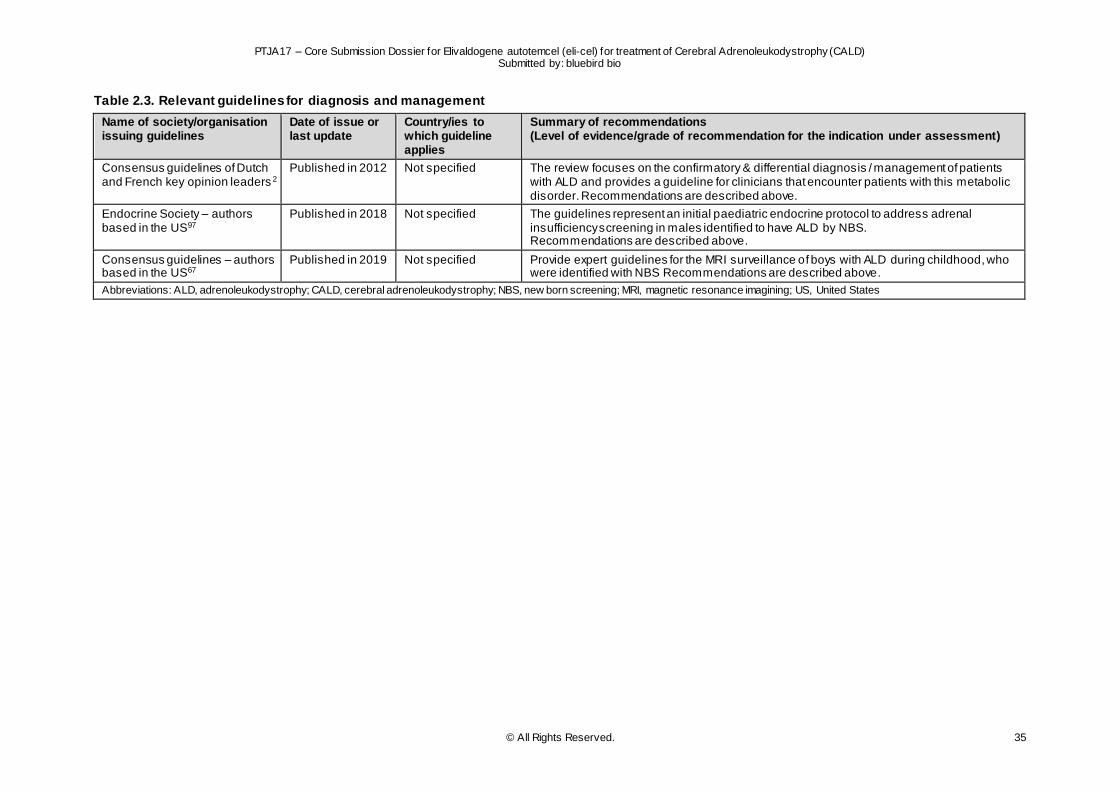
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 35
Table 2.3. Relevant guidelines for diagnosis and management
Name of society/organisation issuing guidelines
Date of issue or last update
Country/ies to which guideline applies
Summary of recommendations (Level of evidence/grade of recommendation for the indication under assessment)
Consensus guidelines of Dutch and French key opinion leaders 2
Published in 2012 Not specified The review focuses on the confirmatory & differential diagnosis / management of patients with ALD and provides a guideline for clinicians that encounter patients with this metabolic disorder. Recommendations are described above.
Endocrine Society – authors based in the US97
Published in 2018 Not specified The guidelines represent an initial paediatric endocrine protocol to address adrenal insufficiency screening in males identified to have ALD by NBS. Recommendations are described above.
Consensus guidelines – authors based in the US67
Published in 2019 Not specified Provide expert guidelines for the MRI surveillance of boys with ALD during childhood, who were identified with NBS Recommendations are described above.
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; NBS, new born screening; MRI, magnetic resonance imagining; US, United States
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 36
3 COMPARATORS IN THE ASSESSMENT
The comparators in the assessment are considered to be:
Allogeneic haematopoietic stem cell transplant (allo-HSCT) excluding those with an HLA-matched sibling donor
Best supportive care for patients that have no access to allo-HSCT - includes any treatment for
symptom relief. May also include treatments that aim to slow/halt disease progression but have not shown effectiveness in clinical trials.
There are no official guidelines for the treatment of CALD in Europe, but the consensus publications of
Engelen et al. (EU), Turk et al. (US) and Regelmann et al. (US) are often quoted.2,67,97 The publication of Engelen et al. outline that in Europe, allo-HSCT remains the only therapeutic intervention that can arrest the progression of cerebral demyelination in ALD patients under the age of 18. Moreover, the
procedure is to be performed very early, i.e., when affected boys have no or minor symptoms due to cerebral demyelinating disease.2
Allo-HSCT
Allo-HSCT is described in more detail in section 2.4.1. In summary, allo-HSCT is currently the only disease-modifying treatment available for CALD patients. Allo-HSCT is an effective treatment for CALD, provided that it is performed at an early stage (i.e. when the patient has limited cerebral involvement,
generally defined as NFS 0 or 1 and Loes score ≤9 or <10).2-5 However, allo-HSCT is associated with life-threatening risks, including transplant-related mortality, GVHD, and graft rejection. Outcomes are affected by the clinical stage of the patient at transplant, and whether or not there is a well -matched
donor.
Within the submitted EU indication for eli-cel, patients are only eligible for eli-cel if an HLA-matched sibling HSC donor is not available.12 MSDs are available in less than 20% of cases (see section Unmet
need in 2.4.1).66
Not all patients receive allo-HSCT, due to several reasons:
the clinical stage of the disease when diagnosed (too far progressed),
the donor search (due to fast progression of the disease, there is a limited time window to successfully perform allo-HSCT),
the availability of a well-matched donor,
the choice of the Health Care Practitioner and/or family due to the risk associated with the allo-HSCT,
especially in the absence of an MSD.
Best supportive care Patients who do not undergo allo-HSCT receive best supportive care: symptomatic and palliative care
as necessary, requiring increasing amounts of care as disability progresses. Various therapies are used as supportive care in European countries, but evidence for effectiveness is lacking – never demonstrated to have a significant efficacy in limiting disease progression.
Open-label trials with Lorenzo’s oil have shown that the disease continues to progress even when plasma VLCFA are normalised by Lorenzo’s oil treatment.6,81,98 The scientific evidence is weak and therefore this treatment is not recommended for use in clinical practice.2
Several attempts were made to investigate therapies that either target the underlying mechanism of
disease, or that improve allo-HSCT outcomes, but so far, no disease-modifying therapy, other than allo-HSCT and eli-cel is available. Other experimental therapies are described in more detail in section Experimental therapies in 2.4.1, however solid data is not available since the respective phase 1-2
trials are ongoing or have stopped.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 37
4 CURRENT USE OF THE TECHNOLOGY
4.1 Summary of issues relating to current use of the technology
Current use of eli-cel is limited to clinical trials (see clinical effectiveness and safety outcomes relating
to eli-cel in section 7).
Eli-cel has been submitted for approval to EMA with an expected EC decision in July 2021.
Eli-cel is currently not commercially available anywhere in the world.
4.2 Current use of the technology
Not applicable.
4.3 Reimbursement and assessment status of the technology
Not applicable.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 38
5 INVESTMENTS AND TOOLS REQUIRED
5.1 Summary of issues relating to the investments and tools required to introduce the technology
Eli-cel is a gene therapy administered as a one-time treatment. It is an individualised gene therapy
which is manufactured using a patient’s own stem cells.
o Subsequently, the harvesting of a patient’s cell versus that of a donor requires different methodologies. Specifically, for eli-cel, the harvesting of a patient’s cells is performed via a
peripheral blood vein after standard mobilisation and apheresis approaches. In contrast, the donor source of allo-HSCT is variable and can be obtained from either the bone marrow or umbilical cord blood.
o Administration of eli-cel follows existing practices associated with HSCT, i.e. myeloablative
conditioning, and is similar to that of its comparator, allo-HSCT, with the main difference being the source of the collected cells (a donor is not needed) and patient’s haematopoietic stem cell manipulation for drug product manufacturing.
Manufacturing of eli-cel occurs via transduction process and ad hoc quality validation and is highly specialised. Manufacturing is centralised at one site for European patients (Minaris Regenerat ive Medicine [previously known as Apceth Biopharma] Munich, Germany). After HSCT collection and
standard donor cell quality checks, it is infused into the recipient, without requirements for further manufacturing processes.
Eli-cel should be stored in the vapour phase of liquid nitrogen at ≤-140°C, i.e. liquid nitrogen tank that
is appropriate for genetically modified organisms, until ready to be thawed for administration. Infusion bag(s) should be kept in in their original metal cassette(s) and should not be refrozen after thawing. The requirement for a separated tank, not mandatory for allo-HSCT, implies that appropriately trained
staff need to be present within the treating centre.
After eli-cel infusion, patients are expected to be enrolled in a non-interventional post-authorisation safety study (PASS), REG-502, for 5 years following the commercial availability of eli-cel, in order to
further characterise and contextualise the long-term safety of eli-cel in patients with CALD. Outcomes will be collected for up to 15-years post-infusion/post-transplant.
Due to the advanced technology and rarity of the disease, t reatment with eli-cel involves highly structured and regulated collaboration between bluebird bio, specialised care centres and the
manufacturing site.
o Eli-cel will be made available to patients through partnership with a small network of referral centres that are qualified for providing this treatment (QTCs).
o QTCs will have a multi-disciplinary team (transplant expert, apheresis experts, cell lab expert, neuro radiologist, etc.), who have to be trained on and aligned with the same stringent quality criteria used for the eli-cel trials (FACT/JACIE≥6), which includes having experience in HSC
transplantation and in the treatment of patients with neurological disorders.
o Patients not living in a country with a QTC will be expected to receive cross -border care.
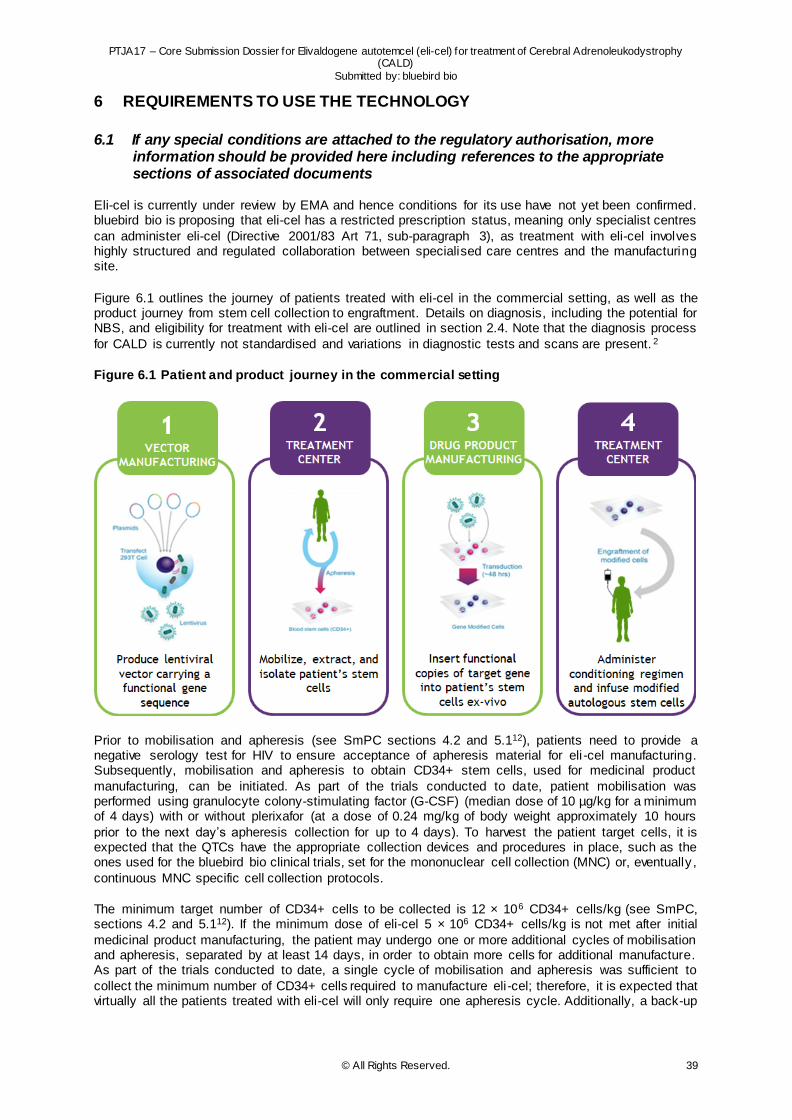
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 39
6 REQUIREMENTS TO USE THE TECHNOLOGY
6.1 If any special conditions are attached to the regulatory authorisation, more information should be provided here including references to the appropriate sections of associated documents
Eli-cel is currently under review by EMA and hence conditions for its use have not yet been confirmed. bluebird bio is proposing that eli-cel has a restricted prescription status, meaning only specialist centres
can administer eli-cel (Directive 2001/83 Art 71, sub-paragraph 3), as treatment with eli-cel involves highly structured and regulated collaboration between specialised care centres and the manufacturing site.
Figure 6.1 outlines the journey of patients treated with eli-cel in the commercial setting, as well as the product journey from stem cell collection to engraftment. Details on diagnosis, including the potential for NBS, and eligibility for treatment with eli-cel are outlined in section 2.4. Note that the diagnosis process
for CALD is currently not standardised and variations in diagnostic tests and scans are present. 2
Figure 6.1 Patient and product journey in the commercial setting
Prior to mobilisation and apheresis (see SmPC sections 4.2 and 5.112), patients need to provide a negative serology test for HIV to ensure acceptance of apheresis material for eli -cel manufacturing. Subsequently, mobilisation and apheresis to obtain CD34+ stem cells, used for medicinal product
manufacturing, can be initiated. As part of the trials conducted to date, patient mobilisation was performed using granulocyte colony-stimulating factor (G-CSF) (median dose of 10 µg/kg for a minimum of 4 days) with or without plerixafor (at a dose of 0.24 mg/kg of body weight approximately 10 hours
prior to the next day’s apheresis collection for up to 4 days). To harvest the patient target cells, it is expected that the QTCs have the appropriate collection devices and procedures in place, such as the ones used for the bluebird bio clinical trials, set for the mononuclear cell collection (MNC) or, eventually ,
continuous MNC specific cell collection protocols.
The minimum target number of CD34+ cells to be collected is 12 × 106 CD34+ cells/kg (see SmPC, sections 4.2 and 5.112). If the minimum dose of eli-cel 5 × 106 CD34+ cells/kg is not met after initial
medicinal product manufacturing, the patient may undergo one or more additional cycles of mobilisation and apheresis, separated by at least 14 days, in order to obtain more cells for additional manufacture. As part of the trials conducted to date, a single cycle of mobilisation and apheresis was sufficient to
collect the minimum number of CD34+ cells required to manufacture eli-cel; therefore, it is expected that virtually all the patients treated with eli-cel will only require one apheresis cycle. Additionally, a back-up
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 40
collection of CD34+ stem cells is required for potential rescue treatment via apheresis or by bone marrow
harvest.
The patient’s cells are transported to the manufacturing practices, where LVV-mediated transduction of CD34+ cells takes place. Manufacturing of eli-cel is centralised at one site in Europe (Germany).
Following formulation, which consists of cryopreservation and quality release, eli-cel is transported back to the QTC to treat the patient.
Prior to eli-cel administration, patients will undergo four days of myeloablative conditioning at the hospital
(see SmPC12 section 5.1). Patients remain at the hospital until neutrophil engraftment is achieved or until they are clinically stable. As part of the eli-cel clinical trial programme, patients received busulfan in conjunction with a lymphodepleting agent (cyclophosphamide or fludarabine), as well as anti -seizure,
anti-fungal and antibiotic prophylaxis in accordance with institutional guidelines. After completion of conditioning, a minimum washout period of 48 hours was required before eli -cel infusion (see SmPC, sections 4.2 and 5.112).
The finished eli-cel product is composed of one or more infusion bags, which contain a dispersion of 2-30 × 106 cells/mL suspended in cryopreservative solution. Each infusion bag contains approximately 20 mL of eli-cel and should be stored in the vapour phase of liquid nitrogen at ≤-140°C, i.e. liquid nitrogen
tanks, adapted for genetically modified organism, until ready to be thawed for administration. Infusion bag(s) should be kept in in their original metal cassette(s) and should not be refrozen after thawing (see SmPC, section 6.412). The requirement for a separated tank, not mandatory for allo-HSCT, implies that
appropriately trained staff need to be present within the QTC. Subsequently, once eli-cel administration has been completed, patients may receive G-CSF per institutional practice.
As highlighted previously, patients will remain in hospital after eli-cel administration for approximately 3-
6 weeks. Neutrophil engraftment is expected by at least day 43 after infusion of eli -cel (see SmPC, section 5.112). In the eli-cel trials, median (min, max) duration of hospitalisation from admission for conditioning through to discharge was 28.0 days (15, 54).7 Patients who experience neutrophil
engraftment failure will receive rescue treatment with the back-up collection of CD34+ cells. Subsequently, patients receive annual monitoring of complete blood counts to monitor for any possible lab sign of insertional oncogenesis, which could lead to leukaemia/lymphoma (see SmPC, annex II,
section D12).
Insertional oncogenesis represents a safety concern associated with gene therapy, especially if retroviral vectors are used. Lenti-D LVV represents, differently, a highly modified self-inactivated (SIV)
LVV designed to minimise the potential for insertional oncogenesis. 99 There was no evidence of genotoxicity in any in vitro or in vivo nonclinical studies conducted within the nonclinical development programme for eli-cel that supported its clinical use for the treatment of paediatric patients with CALD.
Lenti-D LVV bears a significantly reduced risk of insertional oncogenesis which, however, cannot be fully excluded at this point. To date, there is no published evidence of S IN-design LVV-mediated insertional oncogenesis in any eli-cel nonclinical or clinical study.100
Post-authorisation safety study Once patients outside eli-cel clinical trials have completed eli-cel treatment and achieved neutrophil engraftment, they are expected to enrol in a non-interventional post-authorisation safety study (PASS;
REG-502), in order to further characterise and contextualise the long-term safety of eli-cel in patients with CALD. REG-502 will enrol patients in the EBMT registry. Enrolment will be for a duration of 5 years following the commercial availability of eli-cel. Outcomes will be collected for up to 15-years post-
infusion/post-transplant.
Additional risk minimisation materials in form of patient and healthcare professional educational and reminder materials have been proposed in the Marketing Authorisation Application (MAA) dossier.
6.1.1 QTCs and cross-border eli-cel care
Eli-cel care is recommended to be centralised given the rarity of CALD and the high requirements associated with eli-cel treatment, i.e. securing build-up and maintenance of the necessary eli-cel
treatment experience. Therefore, it is bluebird bio’s intention to make eli-cel available to patients through partnership with a small network of referral centres across Europe, known as QTCs, that have been
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 41
confirmed to be trained on and aligned with the same stringent quality criteria used for the eli-cel trials
(FACT/JACIE≥6).101
The requirements necessary to qualify as an eli-cel gene therapy treatment centre are:
1. Experience in cell therapy for usage of HSCT
– Experience in autologous HSCT and allo-HSCT – Experience in the extraction, preparation and storage of cell preparations through to
transport in support of the further processing of eli-cel – Capability to follow bluebird bio Standard Operation Procedure for apheresis, transport
and storage
2. Extensive experience in the treatment of paediatric patients with CALD – Experience in allo-HSCT in paediatric patients with metabolic or neurologic diseases
– Network of excellence to support care for ALD patients – Established (international) referral networks
3. Experience in the management of side effects due to myeloablative conditioning and post-infusion of transplant product
4. Capabilities to participate in an indication based long-term registry for patients with CALD
Specifically, eli-cel must be administered in a QTC by a physician(s) with experience in HSC transplantation and in the treatment of patients with neurological disorders (see draft SmPC, section
4.212).
Patients not living in a country with a QTC will be expected to receive cross -border care through cross-country KOL collaboration, also facilitated by the European Reference Network (ERN). Proactive
scientific collaboration with MetabERN, focused on Hereditary Metabolic Diseases, was initiated by bluebird bio to identify gaps and promote educational initiatives around patient early diagnosis and cross-border referral. Although other routes to access eli-cel may exist thanks to bilateral agreements
and patient flows between regions, the below description focuses on the most common European-wide options available to patients.
On a European-wide scale, there are two main legal frameworks for patients to access planned
treatment abroad102:
(1) Social Security Regulations (EC) 883/2004 and 987/2009, and
(2) Directive 2011/24/EU on patients’ rights in cross-border healthcare.
These routes have various similarities and differences, but the most relevant difference for this consideration is around payment modality. Under the Social Security Regulations (EC) 883/2004 and 987/2009, the health services are paid directly as if the patient is insured by the social security system
of the country of treatment (i.e. according to the tariffs and the payment procedure in force in the country of treatment). However, under Directive 2011/24/EU on patients’ rights in cross -border healthcare, patients have to first pay for treatment and then request reimbursement in the form of a refund in their
home country upon submission of proof of payment. In the case of eli-cel, a one-time gene therapy, such an upfront payment is not a viable solution.
In addition, the European Commission’s Manual for patients (p. 20) states that: “When you apply for
prior authorisation needed to obtain treatment abroad involving an overnight hospital stay or highly specialised and expensive medical equipment, your national health service/ health insurance provider will always first look into the applicability of the Social Security Regulations (EC) 883/2004 and
987/2009”.102
As such, and under the current application of the legal framework, the Social Security Regulations (EC) 883/2004 and 987/2009 are considered the most viable cross-border healthcare route to access eli-cel.
Under the Regulations, a prior authorisation (granted on issuance of the S2 form) needs to be granted by the patient’s national health service / statutory health insurance provider, prior to travel abroad for
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 42
treatment. This S2 form ensures that costs are settled directly between the healthcare provider and the
national health service / health insurance provider.
Finally, the European Commission’s Manual for patients (p. 18) states that: “patients with rare diseases may be offered the possibility under the Social Security Regulations (EC) 883/2004 and 987/2009 to
seek treatment in another EU/EEA Member State or Switzerland even for diagnosis and treatments which are not available in the patient’s home country. As long as the treatment concerned is covered in the country of treatment prior authorisation may be granted." In such a case, where eli-cel would not be
available in the patient’s home country, the granting of this prior authorisation remains at the discretion of the patient’s national health service / health insurance provider.102
In order to support patients looking for treatment abroad, National Contact Points for Cross -border
Healthcare have been established following Directive 2011/24/EU on patients’ rights in cross -border healthcare.103
Although steps to access treatment abroad vary country-by-country, it may be useful to highlight on a
high-level the key steps in a patient’s route to access eli-cel abroad (DISCLAIMER: the exact route a patient would follow to access eli-cel in a cross-border setting may vary by country and on a case-by-case basis)104:
1. The patient’s doctor recommends eli-cel treatment, but eli-cel is not available in the patient’s country. It is available in a specialised and qualified treatment centre in another European country.
2. With the support of their National Contact Point (NCP), the patient/doctor navigates the cross-border system and identifies the appropriate route to planned care abroad.
3. The patient requests their national health service / statutory health insurance provider for
coverage of medical costs to get treated at a defined QTC – this application happens through the ‘S2 form’ (incl. any supporting documents).
4. With the submission of their S2 application, the patient has started the pre-authorisation
decision process.
5. If the patient’s national health service / statutory health insurance provider authorises the S2 request for eli-cel treatment, this means that medical costs will usually directly be covered by
this entity.
6. Potentially with the support of a National Contact Point for Cross-Border Healthcare in the country of treatment and the QTC, the patient needs to affiliate to an appropriate healthcare
payer in the country of treatment to be treated as a local public patient.
7. With the approved S2 form, the patient avoids paying most treatment / medical costs linked to their planned care abroad. However, they must pay any contribution to the cost (i.e. co-
payment) that a local citizen in the country of treatment would normally pay. If applicable, based on the Vanbraekel supplement, the patient may contemplate requesting reimbursement of this co-payment.102
8. At the QTC, the patient is treated with eli-cel in the same way as a local patient.
In order to avoid patients having to travel across borders as much as possible, the company is exploring the possibility that parts of the treatment process, e.g. apheresis or follow-up visits, could be performed
in the countries without QTC. However, this remains subordinated to the local capacity in handling the treatment steps in compliance to eli-cel SmPC requirements and bluebird bio’s high-quality standards as for QTCs.
6.2 Describe the equipment required to use the technology
No additional requirements.

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 43
6.3 Describe the supplies required to use the technology
Supplies required for eli-cel are detailed in section 6.1 and 6.2.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 44
7 CLINICAL EFFECTIVENESS AND SAFETY
7.1 Chapter outline
This chapter outlines the clinical effectiveness and safety of CALD treatments. Evidence is reported
based on the eli-cel clinical development programme and a dedicated systematic literature review (SLR) for relevant comparators. Specifically, this chapter will start with summary statements relating to the clinical effectiveness and safety (sections 7.1 and 7.3). This is followed by a section on the identification
and selection of relevant studies (section 7.4), overview of identified relevant studies (section 7.5), overview of main characteristics per study (section 7.6) and clinical and safety results (section 7.8 and 7.9). Except for the summary sections, each section is split into two, with the first section outl ining the
methodology and/or results in relation to the eli-cel clinical development programme and the second section outlining the same information for the studies identified through the SLR. The tables in the section covering the SLR are limited to the key studies identified through the SLR to further support
comparison between the eli-cel clinical development programme and SLR. Section 7.5.2 outlines which studies were identified as key studies, as well as a justification. A full overview of details pertaining all studies identified through the SLR, their main characteristics and clinical and safety result can be found
in the appendix (sections 9.3 to 9.9).
Note: as part of engagement with EUnetHTA a project plan outlining the assessment scope was
developed. This assessment utilised the population, intervention, comparators and outcomes (PICOs) framework to establish the scope. In the remainder of this document, “scoping PICO” will refer to the assessment scope and designed as part of engagement with EUnetHTA (detailed in the
appendix, section 9.1), whereas “SLR PICO” will refer to the PICO utilised as part of the SLR that was conducted in order to identify relevant evidence of the efficacy and safety of eli -cel versus
comparator therapies (detailed in section 7.4.2).
7.2 Summary of the clinical effectiveness
Results to date suggest that early treatment with eli-cel can stabilise the progression of CALD in patients less than 18 years of age with an ABCD1 genetic mutation for whom an HLA-matched sibling
HSC donor is not available.
Eli-cel has demonstrated an MFD-free survival at 24-months of 90.0%, versus 66.7% MFD-free survival for allo-HSCT in a comparable patient population (see Table 14.2.1.1 of D120 ALD-102
report).10,11 Eli-cel reduces the risk of MFD, second transplant, and/or death events by 82.2% (see Table 2.1.1.1.2 of D120 Interstudy report).7
OS at 48 months with eli-cel is estimated to be 96.6%, versus 75.5% for allo-HSCT in a comparable
patient population and reduces the risk of death by 88.2% (see Table 2.2.1.1.2 of D120 Interstudy report).7
Eli-cel has demonstrated a similar ability to allo-HSCT to stabilise disease progression, as stable NFS at 24 months has been observed in 96.4% of patients treated with eli-cel versus 100% for allo-HSCT)
(see Table 14.2.4 of D120 ALD-102 report).10,11
Loes score has been found to remain stable in patients treated with eli-cel, with 21 of 27 (77.8%) patients reporting no change from baseline to Month 24 (see Table 14.2.5 of D120 ALD-102 report).10
7.3 Summary of safety
Eli-cel has a favourable safety profile, with no evidence of acute or chronic GVHD, graft failure or rejection (see Tables 14.3.2.1 and 14.3.2.2 of D120 ALD-102 report).10
o In contrast, among allo-HSCT patients, ALD-103 found that 52.0% patients experienced acute or
chronic GVHD and 26.3% graft failure within 24 months.11
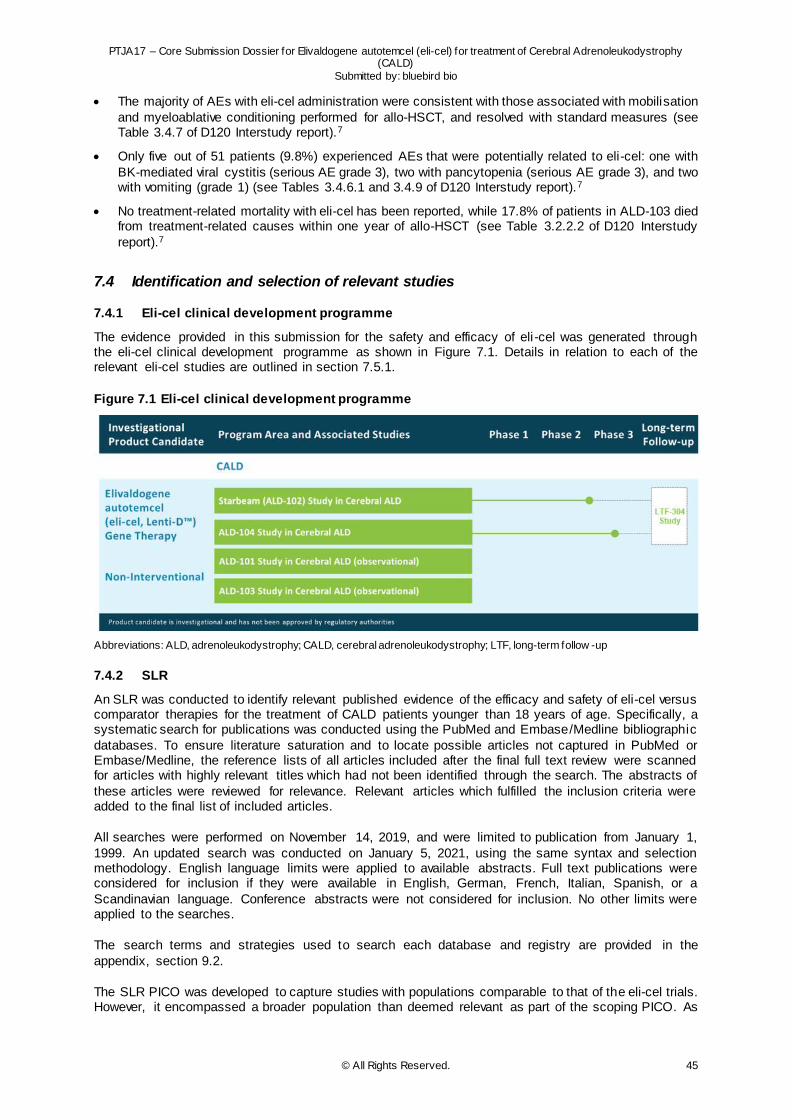
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 45
The majority of AEs with eli-cel administration were consistent with those associated with mobilisation
and myeloablative conditioning performed for allo-HSCT, and resolved with standard measures (see Table 3.4.7 of D120 Interstudy report).7
Only five out of 51 patients (9.8%) experienced AEs that were potentially related to eli-cel: one with
BK-mediated viral cystitis (serious AE grade 3), two with pancytopenia (serious AE grade 3), and two with vomiting (grade 1) (see Tables 3.4.6.1 and 3.4.9 of D120 Interstudy report).7
No treatment-related mortality with eli-cel has been reported, while 17.8% of patients in ALD-103 died from treatment-related causes within one year of allo-HSCT (see Table 3.2.2.2 of D120 Interstudy
report).7
7.4 Identification and selection of relevant studies
7.4.1 Eli-cel clinical development programme
The evidence provided in this submission for the safety and efficacy of eli -cel was generated through the eli-cel clinical development programme as shown in Figure 7.1. Details in relation to each of the relevant eli-cel studies are outlined in section 7.5.1.
Figure 7.1 Eli-cel clinical development programme
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; LTF, long-term follow -up
7.4.2 SLR
An SLR was conducted to identify relevant published evidence of the efficacy and safety of eli-cel versus comparator therapies for the treatment of CALD patients younger than 18 years of age. Specifically, a systematic search for publications was conducted using the PubMed and Embase/Medline bibliographic
databases. To ensure literature saturation and to locate possible articles not captured in PubMed or Embase/Medline, the reference lists of all articles included after the final full text review were scanned for articles with highly relevant titles which had not been identified through the search. The abstracts of
these articles were reviewed for relevance. Relevant articles which fulfilled the inclusion criteria were added to the final list of included articles.
All searches were performed on November 14, 2019, and were limited to publication from January 1,
1999. An updated search was conducted on January 5, 2021, using the same syntax and selection methodology. English language limits were applied to available abstracts. Full text publications were considered for inclusion if they were available in English, German, French, Italian, Spanish, or a
Scandinavian language. Conference abstracts were not considered for inclusion. No other limits were applied to the searches.
The search terms and strategies used to search each database and registry are provided in the
appendix, section 9.2.
The SLR PICO was developed to capture studies with populations comparable to that of the eli-cel trials. However, it encompassed a broader population than deemed relevant as part of the scoping PICO. As
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 46
a result, the following steps outline the methodology used for the SLR, as well as the additional
measures that were taken to ensure the SLR PICO used in this submission is reflective of the scoping PICO. Briefly, the SLR PICO originally also considered adult CALD patients, as well as additional outcomes and study designs. The SLR PICO outlined in Table 7.1 is reflective of the scoping PICO
considered for the present submission.
An additional search on “cerebral adrenoleukodystrophy” was conducted on 25 March 2021 in three clinical trial databases, including all studies of the eli-cel clinical study programme. The search has
resulted in the identification of 2 potentially relevant studies that have no published results yet, but these can be expected in the future:
- ClinicalTrials.gov
17 records were identified, of which 4 were excluded as these were studies from the eli-cel clinical development programme. A further 9 records did not fulfil the PICOS (5 concerned experimental interventions, 4 were non-interventional). Furthermore, 1 study was excluded as
it was withdrawn and 1 was excluded as it concerned an expanded access study for Lorenzo’s oil. Of the 2 remaining relevant studies, 1 concerned a phase 2 trial to haploidentical allo-HSCT
following reduced intensity conditioning. Results are not yet available, but a publication is to be expected in the future. The other study concerned an open label study to the effect of glycerol trierucate (Lorenzo’s oil)
and has results. However, the study has been terminated because of lack of funding, and has moved to expanded access (mentioned above). A publication could be expected in the future.
- ICTRP Search Portal
14 records were identified, of which 5 were excluded as these were studies from the eli-cel clinical development programme. A further 8 records did not fulfil the PICOS (6 concerned experimental interventions, 2 were non-interventional). The remaining relevant study concerned
a phase 2 trial to haploidentical allo-HSCT following reduced intensity conditioning (same as found in other trials databases). Results are not yet available, a publication is to be expected in the future.
- EU CTR 8 records were identified, of which 3 were excluded as these were studies from the eli-cel clinical development programme. All of the remaining records were excluded as they did not fulfil the
PICOS (3 concerned experimental interventions and 2 were in adult patients).
Population To establish comparability between the studies identified through the SLR and the eli-cel clinical
development programme, the criteria for eligible interventions in the SLR PICO were designed to align with the study population in the eli-cel clinical development programme as well as eli-cel’s indication: treatment of early cerebral adrenoleukodystrophy in patients less than 18 years of age, with an ABCD1
genetic mutation, and for whom a HLA-matched sibling HSC donor is not available.
Intervention and Comparator There are no official guidelines for the treatment of CALD in Europe, but consensus publications such
as Engelen et al. are often quoted (see section 2.4.2)2. These outline that, despite the lack of any approved treatment, allo-HSCT can potentially arrest the progression of cerebral demyelination in CALD patients under the age of 18. This treatment is associated with improved efficacy if provided at an early
stage of the disease, i.e. when patients display no or minor symptoms due to cerebral demyelinating disease. For allo-HSCT, the use of an HLA-matched donor is the most appropriate to achieve optimal outcomes. In the case of eli-cel, patients are only eligible for treatment if an HLA-matched sibling HSC
donor is not available. This occurs in over 80% of CALD cases.66 On this basis, allo-HSCT with a different donor than MSD is considered as a comparator to the intervention, eli-cel, assessed in this submission.5
Additionally, BSC in the form of treatments relieving symptoms or treatments which aim to slow or hal t disease progression but have not shown effectiveness in clinical trials, are considered as comparators in this submission. These comprise Lorenzo’s oil, low-fatty dietary regimens and post-HSCT anti-
inflammatory treatments (see section 2.4.1 for further details on relevant comparators).
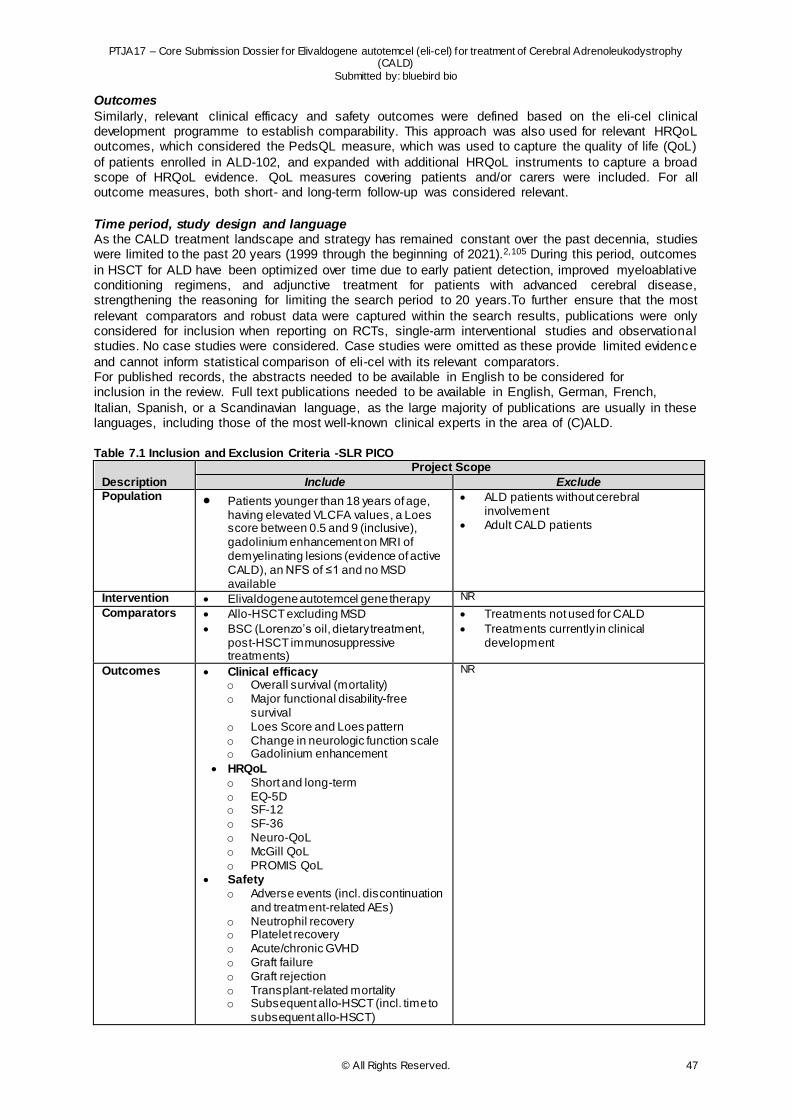
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 47
Outcomes
Similarly, relevant clinical efficacy and safety outcomes were defined based on the eli-cel clinical development programme to establish comparability. This approach was also used for relevant HRQoL outcomes, which considered the PedsQL measure, which was used to capture the quality of life (QoL)
of patients enrolled in ALD-102, and expanded with additional HRQoL instruments to capture a broad scope of HRQoL evidence. QoL measures covering patients and/or carers were included. For all outcome measures, both short- and long-term follow-up was considered relevant.
Time period, study design and language As the CALD treatment landscape and strategy has remained constant over the past decennia, studies were limited to the past 20 years (1999 through the beginning of 2021).2,105 During this period, outcomes
in HSCT for ALD have been optimized over time due to early patient detection, improved myeloablative conditioning regimens, and adjunctive treatment for patients with advanced cerebral disease, strengthening the reasoning for limiting the search period to 20 years.To further ensure that the most
relevant comparators and robust data were captured within the search results, publications were only considered for inclusion when reporting on RCTs, single-arm interventional studies and observational studies. No case studies were considered. Case studies were omitted as these provide limited evidence
and cannot inform statistical comparison of eli-cel with its relevant comparators. For published records, the abstracts needed to be available in English to be considered for inclusion in the review. Full text publications needed to be available in English, German, French,
Italian, Spanish, or a Scandinavian language, as the large majority of publications are usually in these languages, including those of the most well-known clinical experts in the area of (C)ALD. Table 7.1 Inclusion and Exclusion Criteria -SLR PICO
Description
Project Scope
Include Exclude Population Patients younger than 18 years of age,
having elevated VLCFA values, a Loes score between 0.5 and 9 (inclusive), gadolinium enhancement on MRI of demyelinating lesions (evidence of active CALD), an NFS of ≤1 and no MSD available
ALD patients without cerebral involvement
Adult CALD patients
Intervention Elivaldogene autotemcel gene therapy NR
Comparators Allo-HSCT excluding MSD
BSC (Lorenzo’s oil, dietary treatment, post-HSCT immunosuppressive treatments)
Treatments not used for CALD
Treatments currently in clinical development
Outcomes Clinical efficacy o Overall survival (mortality) o Major functional disability-free
survival o Loes Score and Loes pattern o Change in neurologic function scale o Gadolinium enhancement
HRQoL o Short and long-term o EQ-5D o SF-12 o SF-36 o Neuro-QoL o McGill QoL o PROMIS QoL
Safety o Adverse events (incl. discontinuation
and treatment-related AEs) o Neutrophil recovery o Platelet recovery o Acute/chronic GVHD o Graft failure o Graft rejection o Transplant-related mortality o Subsequent allo-HSCT (incl. time to
subsequent allo-HSCT)
NR

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 48
Description Project Scope
Include Exclude
Time Short and long-term follow-up Publications from 1 January 1999 up to
the date of the search
Earlier than 1999
Study design Randomised controlled trials
Single-arm interventional studies
Observational studies
Case studies
Systematic reviews
Other criteria Published in full text
English abstracts, and full text can be in English, German, French, Italian, Spanish, or a Scandinavian language
Non-published material Full text in another language than those
listed
Conference abstracts Abbreviations: AE, adverse event; ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; BSC, best supportive care; GVHD, graft-versus-host disease; HRQoL, health-related quality of life; HSCT, haematopoietic stem cell transplantation; MRI, magnetic resonance imaging; MSD, matched sibling donor; PROMIS, Patient-Reported Outcomes Measurement Information System; QoL, quality of life; SF, short-form; VLCFA, very long-chain fatty acid
As part of both the original and updated search, a total of 517 records were screened by title and abstract, by two independent reviewers following the eligibility criteria specified in Table 7.1. The reviewers resolved any disagreement through discussion, and an arbitrator adjudicated unresolved
disagreements. After exclusions were applied, 91 records remained for the full text review. The full text review excluded an additional 44 records (reason for exclusion are described in Figure 7.2). Four additional records were identified by screening reference lists of the included articles. A total of 51
articles were considered for inclusion as part of the original SLR. Applying additional constraints relating to the population, outcomes, and study design, 28 articles were considered for inclusion and will be further described in this dossier.
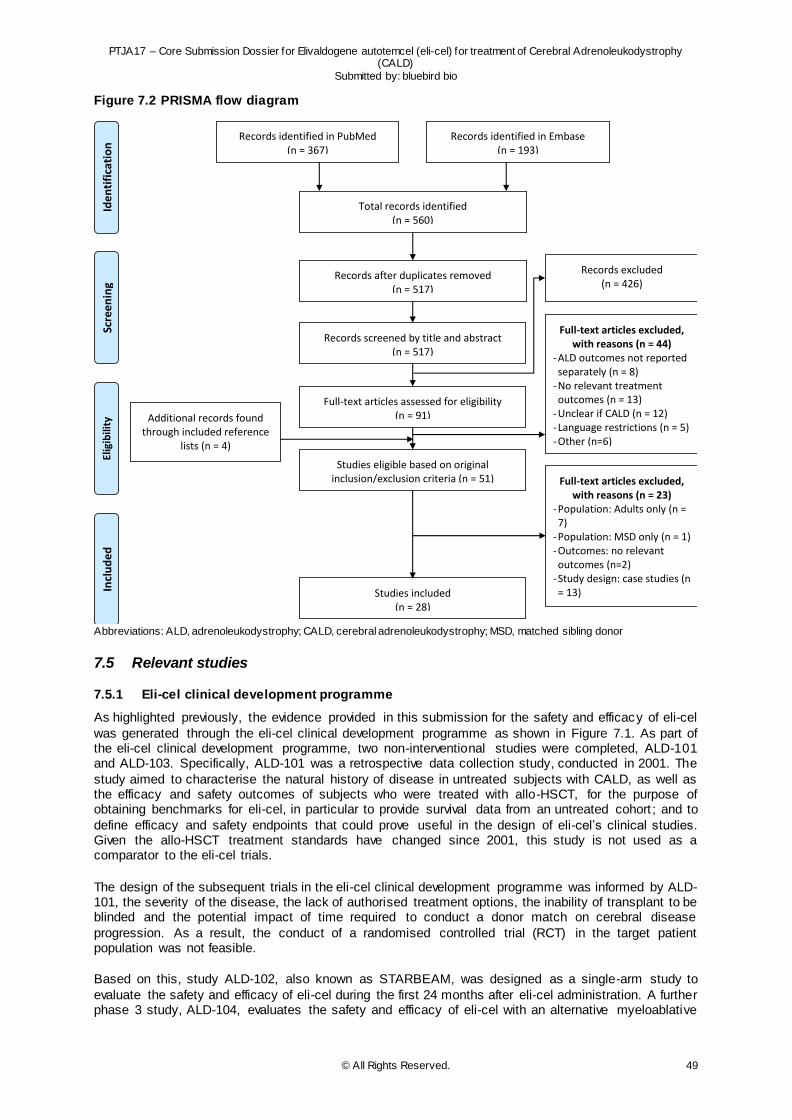
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 49
Figure 7.2 PRISMA flow diagram
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; MSD, matched sibling donor
7.5 Relevant studies
7.5.1 Eli-cel clinical development programme
As highlighted previously, the evidence provided in this submission for the safety and efficacy of eli-cel
was generated through the eli-cel clinical development programme as shown in Figure 7.1. As part of the eli-cel clinical development programme, two non-interventional studies were completed, ALD-101 and ALD-103. Specifically, ALD-101 was a retrospective data collection study, conducted in 2001. The
study aimed to characterise the natural history of disease in untreated subjects with CALD, as well as the efficacy and safety outcomes of subjects who were treated with allo-HSCT, for the purpose of obtaining benchmarks for eli-cel, in particular to provide survival data from an untreated cohort ; and to
define efficacy and safety endpoints that could prove useful in the design of eli-cel’s clinical studies. Given the allo-HSCT treatment standards have changed since 2001, this study is not used as a comparator to the eli-cel trials.
The design of the subsequent trials in the eli-cel clinical development programme was informed by ALD-101, the severity of the disease, the lack of authorised treatment options, the inability of transplant to be blinded and the potential impact of time required to conduct a donor match on cerebral disease
progression. As a result, the conduct of a randomised controlled trial (RCT) in the target patient population was not feasible.
Based on this, study ALD-102, also known as STARBEAM, was designed as a single-arm study to
evaluate the safety and efficacy of eli-cel during the first 24 months after eli-cel administration. A further phase 3 study, ALD-104, evaluates the safety and efficacy of eli-cel with an alternative myeloablative
Scre
enin
g In
clu
ded
El
igib
ility
Id
enti
fica
tio
n Records identified in Embase
(n = 193)
Total records identified (n = 560)
Records after duplicates removed (n = 517)
(n = )
Records excluded (n = 426)
Records screened by title and abstract (n = 517)
Full-text articles excluded, with reasons (n = 44)
- ALD outcomes not reported separately (n = 8)
- No relevant treatment outcomes (n = 13)
- Unclear if CALD (n = 12) - Language restrictions (n = 5) - Other (n=6)
Full-text articles assessed for eligibility (n = 91)
Studies eligible based on original inclusion/exclusion criteria (n = 51)
Records identified in PubMed (n = 367)
Studies included (n = 28)
Additional records found through included reference
lists (n = 4)
Full-text articles excluded, with reasons (n = 23)
- Population: Adults only (n = 7)
- Population: MSD only (n = 1) - Outcomes: no relevant outcomes (n=2)
- Study design: case studies (n = 13)
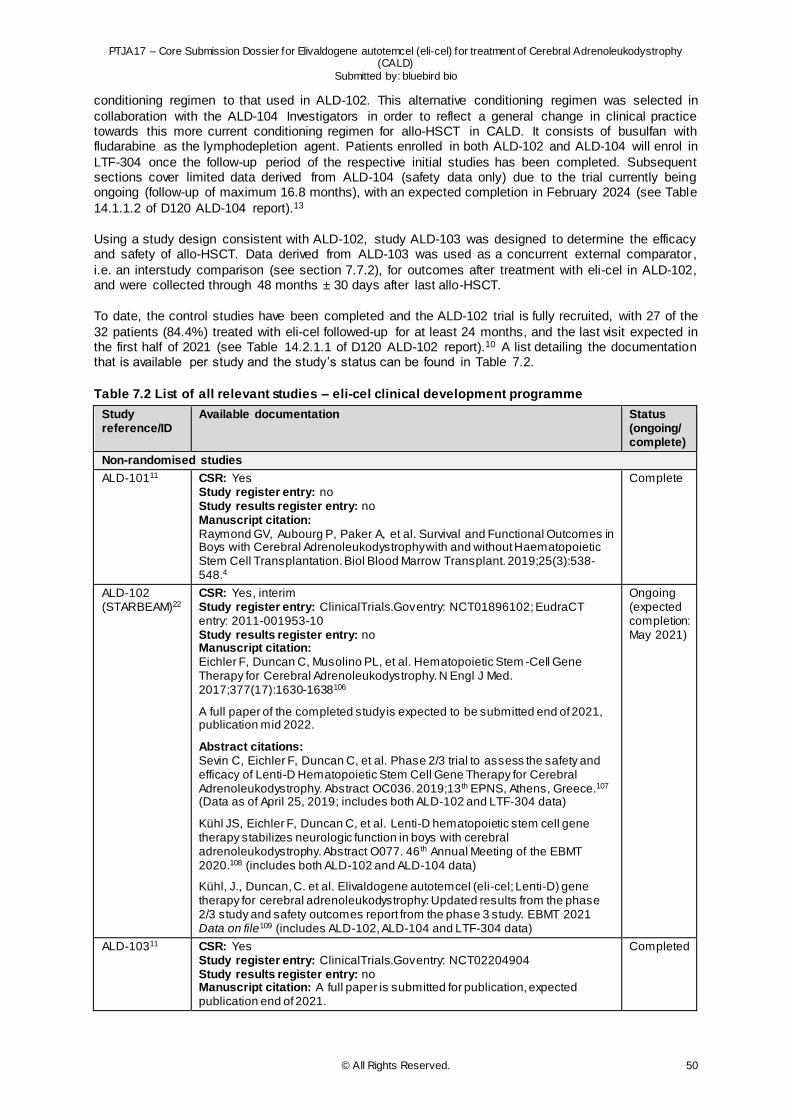
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 50
conditioning regimen to that used in ALD-102. This alternative conditioning regimen was selected in
collaboration with the ALD-104 Investigators in order to reflect a general change in clinical practice towards this more current conditioning regimen for allo-HSCT in CALD. It consists of busulfan with fludarabine as the lymphodepletion agent. Patients enrolled in both ALD-102 and ALD-104 will enrol in
LTF-304 once the follow-up period of the respective initial studies has been completed. Subsequent sections cover limited data derived from ALD-104 (safety data only) due to the trial currently being ongoing (follow-up of maximum 16.8 months), with an expected completion in February 2024 (see Table
14.1.1.2 of D120 ALD-104 report).13
Using a study design consistent with ALD-102, study ALD-103 was designed to determine the efficacy and safety of allo-HSCT. Data derived from ALD-103 was used as a concurrent external comparator ,
i.e. an interstudy comparison (see section 7.7.2), for outcomes after treatment with eli-cel in ALD-102, and were collected through 48 months ± 30 days after last allo-HSCT.
To date, the control studies have been completed and the ALD-102 trial is fully recruited, with 27 of the
32 patients (84.4%) treated with eli-cel followed-up for at least 24 months, and the last visit expected in the first half of 2021 (see Table 14.2.1.1 of D120 ALD-102 report).10 A list detailing the documentation that is available per study and the study’s status can be found in Table 7.2.
Table 7.2 List of all relevant studies – eli-cel clinical development programme
Study reference/ID
Available documentation Status (ongoing/ complete)
Non-randomised studies
ALD-10111 CSR: Yes Study register entry: no Study results register entry: no Manuscript citation: Raymond GV, Aubourg P, Paker A, et al. Survival and Functional Outcomes in Boys with Cerebral Adrenoleukodystrophy with and without Haematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant. 2019;25(3):538-548.4
Complete
ALD-102 (STARBEAM)22
CSR: Yes, interim Study register entry: ClinicalTrials.Gov entry: NCT01896102; EudraCT entry: 2011-001953-10 Study results register entry: no Manuscript citation: Eichler F, Duncan C, Musolino PL, et al. Hematopoietic Stem -Cell Gene Therapy for Cerebral Adrenoleukodystrophy. N Engl J Med. 2017;377(17):1630-1638106
A full paper of the completed study is expected to be submitted end of 2021, publication mid 2022.
Abstract citations: Sevin C, Eichler F, Duncan C, et al. Phase 2/3 trial to assess the safety and efficacy of Lenti-D Hematopoietic Stem Cell Gene Therapy for Cerebral Adrenoleukodystrophy. Abstract OC036. 2019;13 th EPNS, Athens, Greece.107 (Data as of April 25, 2019; includes both ALD-102 and LTF-304 data)
Kühl JS, Eichler F, Duncan C, et al. Lenti-D hematopoietic stem cell gene therapy stabilizes neurologic function in boys with cerebral adrenoleukodystrophy. Abstract O077. 46 th Annual Meeting of the EBMT 2020.108 (includes both ALD-102 and ALD-104 data)
Kühl, J., Duncan, C. et al. Elivaldogene autotemcel (eli-cel; Lenti-D) gene therapy for cerebral adrenoleukodystrophy: Updated results from the phase 2/3 study and safety outcomes report from the phase 3 study. EBMT 2021 Data on file109 (includes ALD-102, ALD-104 and LTF-304 data)
Ongoing (expected completion: May 2021)
ALD-10311 CSR: Yes Study register entry: ClinicalTrials.Gov entry: NCT02204904 Study results register entry: no Manuscript citation: A full paper is submitted for publication, expected publication end of 2021.
Completed
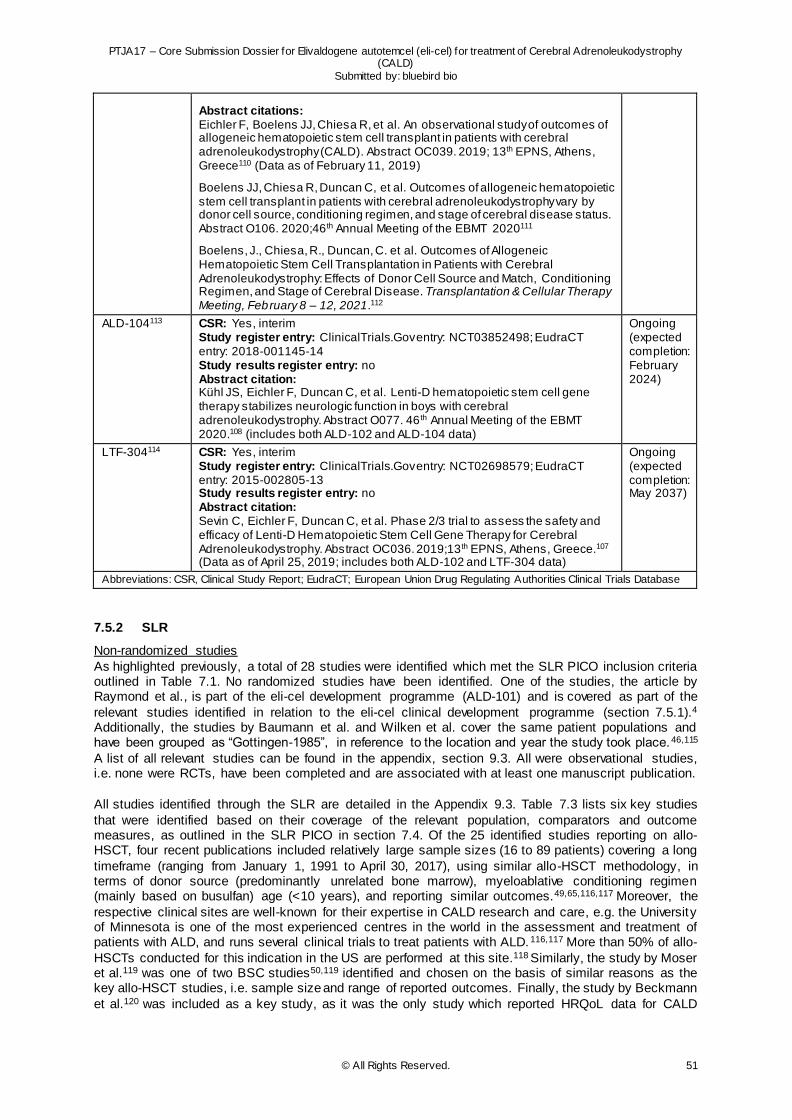
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 51
Abstract citations: Eichler F, Boelens JJ, Chiesa R, et al. An observational study of outcomes of allogeneic hematopoietic stem cell transplant in patients with cerebral adrenoleukodystrophy (CALD). Abstract OC039. 2019; 13th EPNS, Athens, Greece110 (Data as of February 11, 2019)
Boelens JJ, Chiesa R, Duncan C, et al. Outcomes of allogeneic hematopoietic stem cell transplant in patients with cerebral adrenoleukodystrophy vary by donor cell source, conditioning regimen, and stage of cerebral disease status. Abstract O106. 2020;46 th Annual Meeting of the EBMT 2020111
Boelens, J., Chiesa, R., Duncan, C. et al. Outcomes of Allogeneic Hematopoietic Stem Cell Transplantation in Patients with Cerebral Adrenoleukodystrophy: Effects of Donor Cell Source and Match, Conditioning Regimen, and Stage of Cerebral Disease. Transplantation & Cellular Therapy Meeting, February 8 – 12, 2021.112
ALD-104113 CSR: Yes, interim Study register entry: ClinicalTrials.Gov entry: NCT03852498; EudraCT entry: 2018-001145-14 Study results register entry: no Abstract citation: Kühl JS, Eichler F, Duncan C, et al. Lenti-D hematopoietic stem cell gene therapy stabilizes neurologic function in boys with cerebral adrenoleukodystrophy. Abstract O077. 46 th Annual Meeting of the EBMT 2020.108 (includes both ALD-102 and ALD-104 data)
Ongoing (expected completion: February 2024)
LTF-304114 CSR: Yes, interim Study register entry: ClinicalTrials.Gov entry: NCT02698579; EudraCT entry: 2015-002805-13 Study results register entry: no Abstract citation: Sevin C, Eichler F, Duncan C, et al. Phase 2/3 trial to assess the safety and efficacy of Lenti-D Hematopoietic Stem Cell Gene Therapy for Cerebral Adrenoleukodystrophy. Abstract OC036. 2019;13 th EPNS, Athens, Greece.107 (Data as of April 25, 2019; includes both ALD-102 and LTF-304 data)
Ongoing (expected completion: May 2037)
Abbreviations: CSR, Clinical Study Report; EudraCT; European Union Drug Regulating Authorities Clinical Trials Database
7.5.2 SLR
Non-randomized studies
As highlighted previously, a total of 28 studies were identified which met the SLR PICO inclusion criteria outlined in Table 7.1. No randomized studies have been identified. One of the studies, the article by Raymond et al., is part of the eli-cel development programme (ALD-101) and is covered as part of the
relevant studies identified in relation to the eli-cel clinical development programme (section 7.5.1).4 Additionally, the studies by Baumann et al. and Wilken et al. cover the same patient populations and have been grouped as “Gottingen-1985”, in reference to the location and year the study took place.46,115
A list of all relevant studies can be found in the appendix, section 9.3. All were observational studies, i.e. none were RCTs, have been completed and are associated with at least one manuscript publication.
All studies identified through the SLR are detailed in the Appendix 9.3. Table 7.3 lists six key studies
that were identified based on their coverage of the relevant population, comparators and outcome measures, as outlined in the SLR PICO in section 7.4. Of the 25 identified studies reporting on allo-HSCT, four recent publications included relatively large sample sizes (16 to 89 patients) covering a long
timeframe (ranging from January 1, 1991 to April 30, 2017), using similar allo-HSCT methodology, in terms of donor source (predominantly unrelated bone marrow), myeloablative conditioning regimen (mainly based on busulfan) age (<10 years), and reporting similar outcomes.49,65,116,117 Moreover, the
respective clinical sites are well-known for their expertise in CALD research and care, e.g. the University of Minnesota is one of the most experienced centres in the world in the assessment and treatment of patients with ALD, and runs several clinical trials to treat patients with ALD. 116,117 More than 50% of allo-
HSCTs conducted for this indication in the US are performed at this site.118 Similarly, the study by Moser et al.119 was one of two BSC studies50,119 identified and chosen on the basis of similar reasons as the key allo-HSCT studies, i.e. sample size and range of reported outcomes. Finally, the study by Beckmann
et al.120 was included as a key study, as it was the only study which reported HRQoL data for CALD
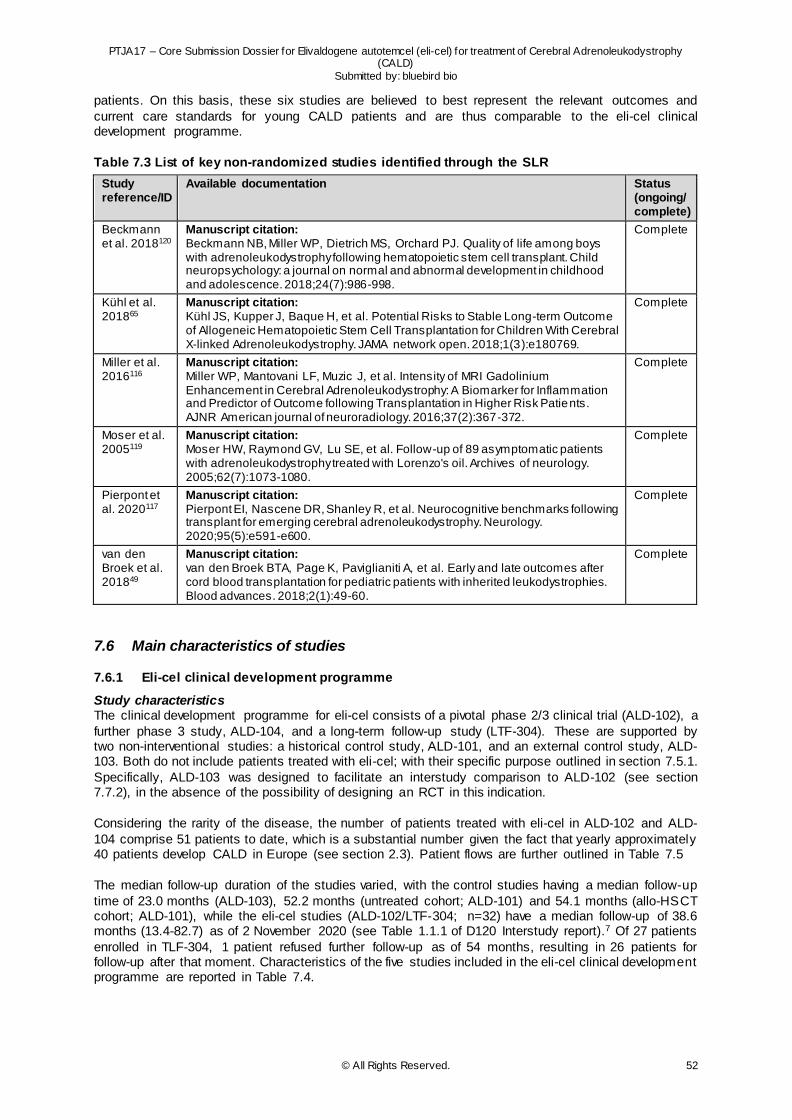
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 52
patients. On this basis, these six studies are believed to best represent the relevant outcomes and
current care standards for young CALD patients and are thus comparable to the eli-cel clinical development programme.
Table 7.3 List of key non-randomized studies identified through the SLR
Study reference/ID
Available documentation Status (ongoing/ complete)
Beckmann et al. 2018120
Manuscript citation: Beckmann NB, Miller WP, Dietrich MS, Orchard PJ. Quality of life among boys with adrenoleukodystrophy following hematopoietic stem cell transplant. Child neuropsychology: a journal on normal and abnormal development in childhood and adolescence. 2018;24(7):986-998.
Complete
Kühl et al. 201865
Manuscript citation: Kühl JS, Kupper J, Baque H, et al. Potential Risks to Stable Long-term Outcome of Allogeneic Hematopoietic Stem Cell Transplantation for Children With Cerebral X-linked Adrenoleukodystrophy. JAMA network open. 2018;1(3):e180769.
Complete
Miller et al. 2016116
Manuscript citation: Miller WP, Mantovani LF, Muzic J, et al. Intensity of MRI Gadolinium Enhancement in Cerebral Adrenoleukodystrophy: A Biomarker for Inflammation and Predictor of Outcome following Transplantation in Higher Risk Patients. AJNR American journal of neuroradiology. 2016;37(2):367-372.
Complete
Moser et al. 2005119
Manuscript citation: Moser HW, Raymond GV, Lu SE, et al. Follow-up of 89 asymptomatic patients with adrenoleukodystrophy treated with Lorenzo's oil. Archives of neurology. 2005;62(7):1073-1080.
Complete
Pierpont et al. 2020117
Manuscript citation: Pierpont EI, Nascene DR, Shanley R, et al. Neurocognitive benchmarks following transplant for emerging cerebral adrenoleukodystrophy. Neurology. 2020;95(5):e591-e600.
Complete
van den Broek et al. 201849
Manuscript citation: van den Broek BTA, Page K, Paviglianiti A, et al. Early and late outcomes after cord blood transplantation for pediatric patients with inherited leukodystrophies. Blood advances. 2018;2(1):49-60.
Complete
7.6 Main characteristics of studies
7.6.1 Eli-cel clinical development programme
Study characteristics The clinical development programme for eli-cel consists of a pivotal phase 2/3 clinical trial (ALD-102), a
further phase 3 study, ALD-104, and a long-term follow-up study (LTF-304). These are supported by two non-interventional studies: a historical control study, ALD-101, and an external control study, ALD-103. Both do not include patients treated with eli-cel; with their specific purpose outlined in section 7.5.1.
Specifically, ALD-103 was designed to facilitate an interstudy comparison to ALD-102 (see section 7.7.2), in the absence of the possibility of designing an RCT in this indication.
Considering the rarity of the disease, the number of patients treated with eli-cel in ALD-102 and ALD-
104 comprise 51 patients to date, which is a substantial number given the fact that yearly approximately 40 patients develop CALD in Europe (see section 2.3). Patient flows are further outlined in Table 7.5
The median follow-up duration of the studies varied, with the control studies having a median follow-up
time of 23.0 months (ALD-103), 52.2 months (untreated cohort; ALD-101) and 54.1 months (allo-HSCT cohort; ALD-101), while the eli-cel studies (ALD-102/LTF-304; n=32) have a median follow-up of 38.6 months (13.4-82.7) as of 2 November 2020 (see Table 1.1.1 of D120 Interstudy report).7 Of 27 patients
enrolled in TLF-304, 1 patient refused further follow-up as of 54 months, resulting in 26 patients for follow-up after that moment. Characteristics of the five studies included in the eli-cel clinical development programme are reported in Table 7.4.
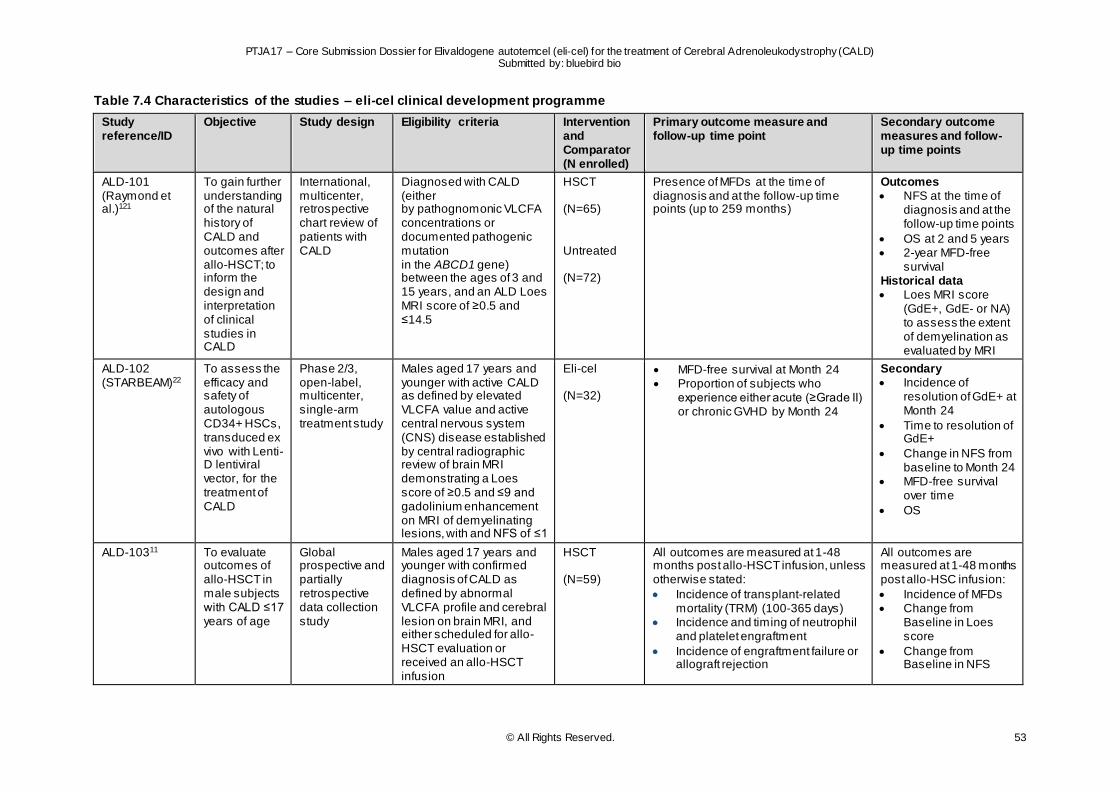
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 53
Table 7.4 Characteristics of the studies – eli-cel clinical development programme
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary outcome measure and follow-up time point
Secondary outcome measures and follow-up time points
ALD-101 (Raymond et al.)121
To gain further understanding of the natural history of CALD and outcomes after allo-HSCT; to inform the design and interpretation of clinical studies in CALD
International, multicenter, retrospective chart review of patients with CALD
Diagnosed with CALD (either by pathognomonic VLCFA concentrations or documented pathogenic mutation in the ABCD1 gene) between the ages of 3 and 15 years, and an ALD Loes MRI score of ≥0.5 and ≤14.5
HSCT (N=65) Untreated (N=72)
Presence of MFDs at the time of diagnosis and at the follow-up time points (up to 259 months)
Outcomes NFS at the time of
diagnosis and at the follow-up time points
OS at 2 and 5 years 2-year MFD-free
survival Historical data Loes MRI score
(GdE+, GdE- or NA) to assess the extent of demyelination as evaluated by MRI
ALD-102 (STARBEAM)22
To assess the efficacy and safety of autologous CD34+ HSCs, transduced ex vivo with Lenti-D lentiviral vector, for the treatment of CALD
Phase 2/3, open-label, multicenter, single-arm treatment study
Males aged 17 years and younger with active CALD as defined by elevated VLCFA value and active central nervous system (CNS) disease established by central radiographic review of brain MRI demonstrating a Loes score of ≥0.5 and ≤9 and gadolinium enhancement on MRI of demyelinating lesions, with and NFS of ≤1
Eli-cel (N=32)
MFD-free survival at Month 24 Proportion of subjects who
experience either acute (≥Grade II) or chronic GVHD by Month 24
Secondary Incidence of
resolution of GdE+ at Month 24
Time to resolution of GdE+
Change in NFS from baseline to Month 24
MFD-free survival over time
OS
ALD-10311 To evaluate outcomes of allo-HSCT in male subjects with CALD ≤17 years of age
Global prospective and partially retrospective data collection study
Males aged 17 years and younger with confirmed diagnosis of CALD as defined by abnormal VLCFA profile and cerebral lesion on brain MRI, and either scheduled for allo-HSCT evaluation or received an allo-HSCT infusion
HSCT (N=59)
All outcomes are measured at 1-48 months post allo-HSCT infusion, unless otherwise stated:
Incidence of transplant-related mortality (TRM) (100-365 days)
Incidence and timing of neutrophil and platelet engraftment
Incidence of engraftment failure or allograft rejection
All outcomes are measured at 1-48 months post allo-HSC infusion:
Incidence of MFDs Change from
Baseline in Loes score
Change from Baseline in NFS
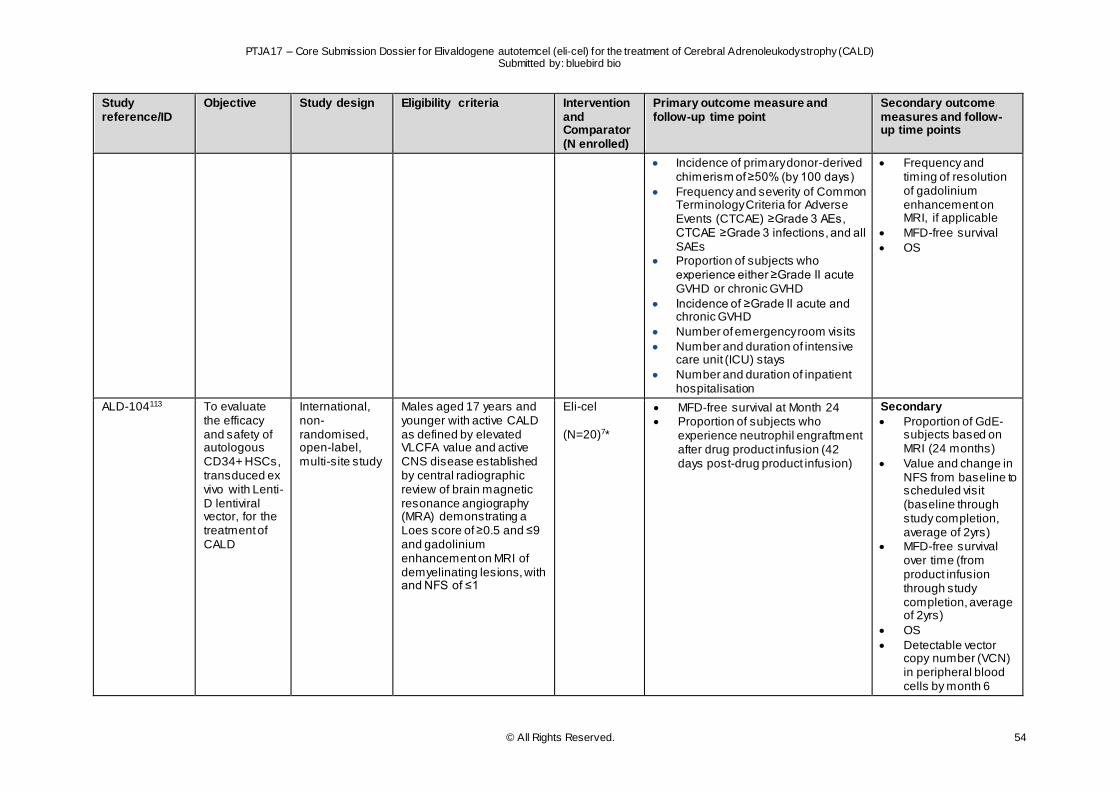
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 54
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary outcome measure and follow-up time point
Secondary outcome measures and follow-up time points
Incidence of primary donor-derived chimerism of ≥50% (by 100 days)
Frequency and severity of Common Terminology Criteria for Adverse Events (CTCAE) ≥Grade 3 AEs, CTCAE ≥Grade 3 infections, and all SAEs
Proportion of subjects who experience either ≥Grade II acute GVHD or chronic GVHD
Incidence of ≥Grade II acute and chronic GVHD
Number of emergency room visits
Number and duration of intensive care unit (ICU) stays
Number and duration of inpatient hospitalisation
Frequency and timing of resolution of gadolinium enhancement on MRI, if applicable
MFD-free survival
OS
ALD-104113 To evaluate the efficacy and safety of autologous CD34+ HSCs, transduced ex vivo with Lenti-D lentiviral vector, for the treatment of CALD
International, non-randomised, open-label, multi-site study
Males aged 17 years and younger with active CALD as defined by elevated VLCFA value and active CNS disease established by central radiographic review of brain magnetic resonance angiography (MRA) demonstrating a Loes score of ≥0.5 and ≤9 and gadolinium enhancement on MRI of demyelinating lesions, with and NFS of ≤1
Eli-cel (N=20)7*
MFD-free survival at Month 24 Proportion of subjects who
experience neutrophil engraftment after drug product infusion (42 days post-drug product infusion)
Secondary
Proportion of GdE- subjects based on MRI (24 months)
Value and change in NFS from baseline to scheduled visit (baseline through study completion, average of 2yrs)
MFD-free survival over time (from product infusion through study completion, average of 2yrs)
OS
Detectable vector copy number (VCN) in peripheral blood cells by month 6
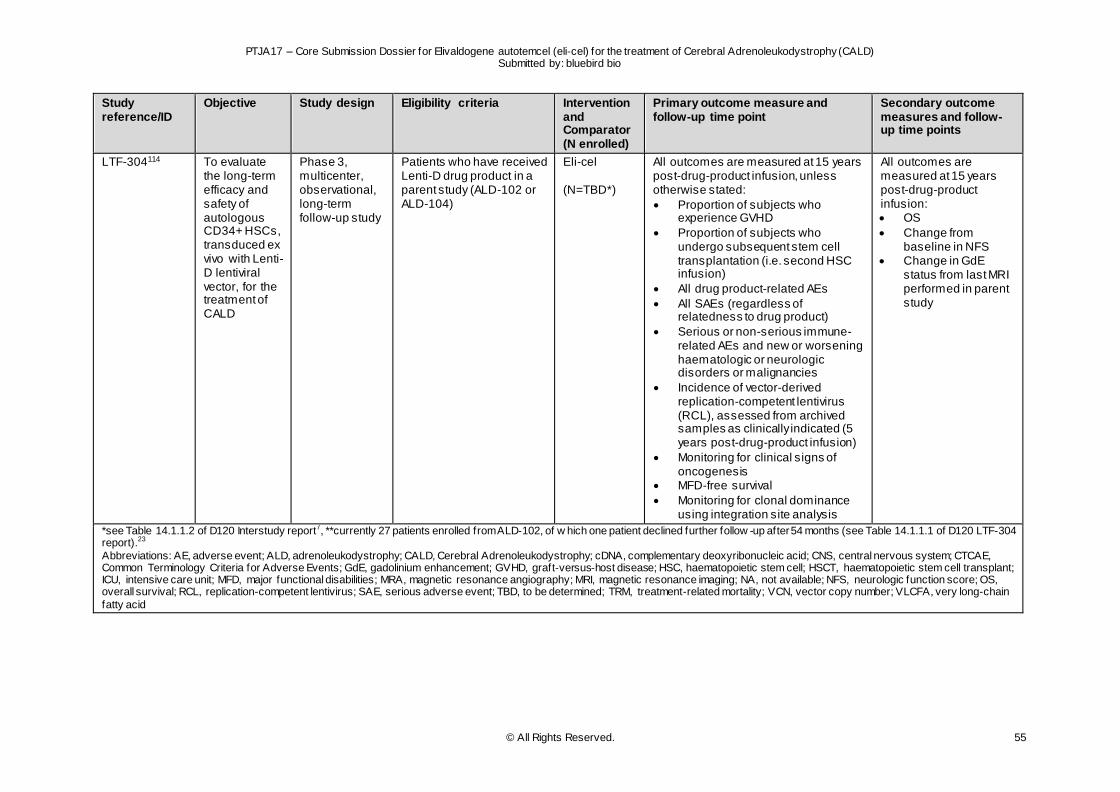
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 55
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary outcome measure and follow-up time point
Secondary outcome measures and follow-up time points
LTF-304114 To evaluate the long-term efficacy and safety of autologous CD34+ HSCs, transduced ex vivo with Lenti-D lentiviral vector, for the treatment of CALD
Phase 3, multicenter, observational, long-term follow-up study
Patients who have received Lenti-D drug product in a parent study (ALD-102 or ALD-104)
Eli-cel (N=TBD*)
All outcomes are measured at 15 years post-drug-product infusion, unless otherwise stated:
Proportion of subjects who experience GVHD
Proportion of subjects who undergo subsequent stem cell transplantation (i.e. second HSC infusion)
All drug product-related AEs
All SAEs (regardless of relatedness to drug product)
Serious or non-serious immune-related AEs and new or worsening haematologic or neurologic disorders or malignancies
Incidence of vector-derived replication-competent lentivirus (RCL), assessed from archived samples as clinically indicated (5 years post-drug-product infusion)
Monitoring for clinical signs of oncogenesis
MFD-free survival
Monitoring for clonal dominance using integration site analysis
All outcomes are measured at 15 years post-drug-product infusion: OS
Change from baseline in NFS
Change in GdE status from last MRI performed in parent study
*see Table 14.1.1.2 of D120 Interstudy report7, **currently 27 patients enrolled from ALD-102, of w hich one patient declined further follow -up after 54 months (see Table 14.1.1.1 of D120 LTF-304 report).23
Abbreviations: AE, adverse event; ALD, adrenoleukodystrophy; CALD, Cerebral Adrenoleukodystrophy; cDNA, complementary deoxyribonucleic acid; CNS, central nervous system; CTCAE, Common Terminology Criteria for Adverse Events; GdE, gadolinium enhancement; GVHD, graft-versus-host disease; HSC, haematopoietic stem cell; HSCT, haematopoietic stem cell transplant; ICU, intensive care unit; MFD, major functional disabilities; MRA, magnetic resonance angiography; MRI, magnetic resonance imaging; NA, not available; NFS, neurologic function score; OS, overall survival; RCL, replication-competent lentivirus; SAE, serious adverse event; TBD, to be determined; TRM, treatment-related mortality; VCN, vector copy number; VLCFA, very long-chain
fatty acid
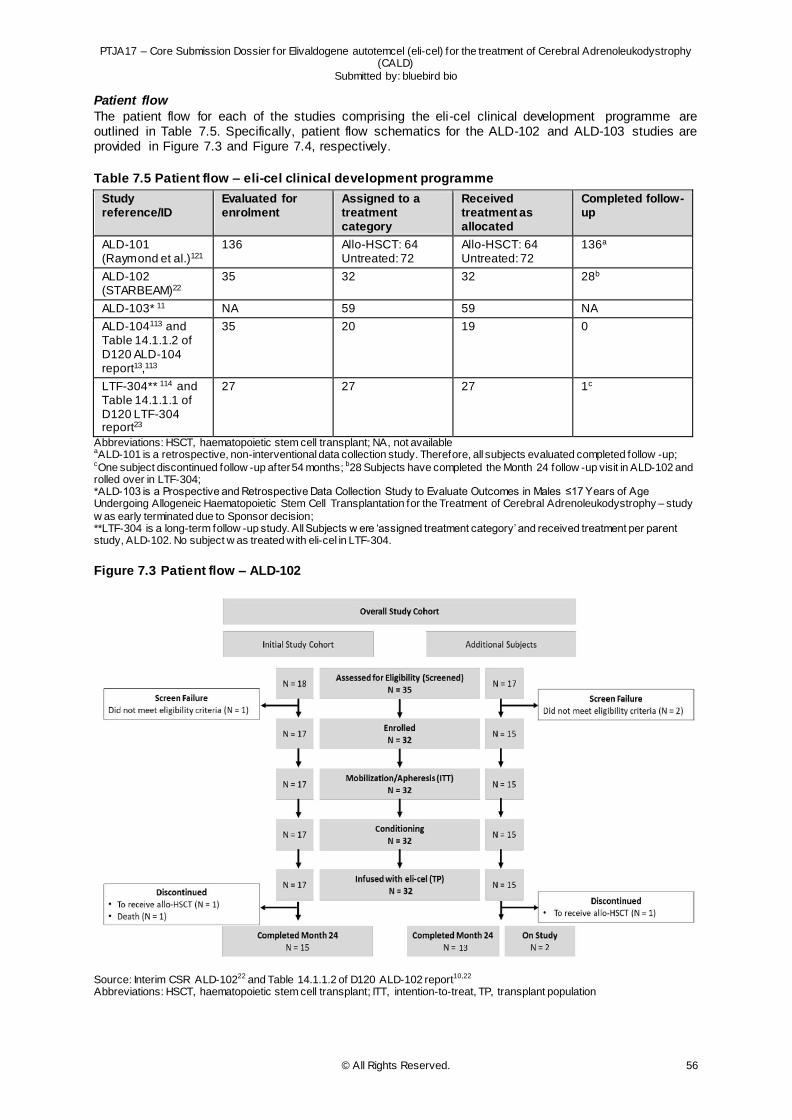
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 56
Patient flow
The patient flow for each of the studies comprising the eli-cel clinical development programme are outlined in Table 7.5. Specifically, patient flow schematics for the ALD-102 and ALD-103 studies are provided in Figure 7.3 and Figure 7.4, respectively.
Table 7.5 Patient flow – eli-cel clinical development programme
Study reference/ID
Evaluated for enrolment
Assigned to a treatment category
Received treatment as allocated
Completed follow-up
ALD-101 (Raymond et al.)121
136 Allo-HSCT: 64 Untreated: 72
Allo-HSCT: 64 Untreated: 72
136a
ALD-102 (STARBEAM)22
35 32 32 28b
ALD-103* 11 NA 59 59 NA
ALD-104113 and Table 14.1.1.2 of D120 ALD-104 report13,113
35 20 19 0
LTF-304** 114 and Table 14.1.1.1 of D120 LTF-304 report23
27 27 27 1c
Abbreviations: HSCT, haematopoietic stem cell transplant; NA, not available aALD-101 is a retrospective, non-interventional data collection study. Therefore, all subjects evaluated completed follow -up; cOne subject discontinued follow -up after 54 months; b28 Subjects have completed the Month 24 follow -up visit in ALD-102 and rolled over in LTF-304; *ALD-103 is a Prospective and Retrospective Data Collection Study to Evaluate Outcomes in Males ≤17 Years of Age Undergoing Allogeneic Haematopoietic Stem Cell Transplantation for the Treatment of Cerebral Adrenoleukodystrophy – study
w as early terminated due to Sponsor decision; **LTF-304 is a long-term follow -up study. All Subjects w ere ‘assigned treatment category’ and received treatment per parent study, ALD-102. No subject w as treated with eli-cel in LTF-304.
Figure 7.3 Patient flow – ALD-102
Source: Interim CSR ALD-10222 and Table 14.1.1.2 of D120 ALD-102 report10,22 Abbreviations: HSCT, haematopoietic stem cell transplant; ITT, intention-to-treat, TP, transplant population
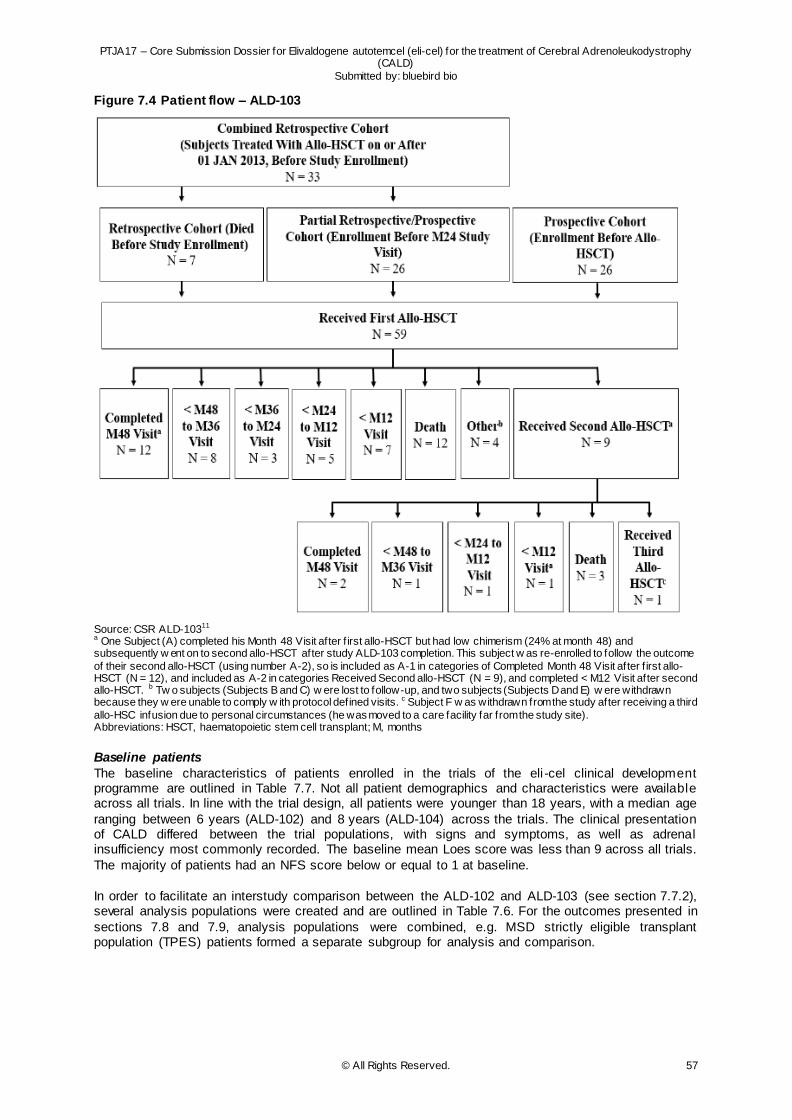
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 57
Figure 7.4 Patient flow – ALD-103
Source: CSR ALD-10311 a One Subject (A) completed his Month 48 Visit after f irst allo-HSCT but had low chimerism (24% at month 48) and subsequently w ent on to second allo-HSCT after study ALD-103 completion. This subject w as re-enrolled to follow the outcome
of their second allo-HSCT (using number A-2), so is included as A-1 in categories of Completed Month 48 Visit after f irst allo-HSCT (N = 12), and included as A-2 in categories Received Second allo-HSCT (N = 9), and completed < M12 Visit after second allo-HSCT. b Tw o subjects (Subjects B and C) w ere lost to follow-up, and two subjects (Subjects D and E) w ere withdrawn because they w ere unable to comply w ith protocol defined visits. c Subject F w as withdrawn from the study after receiving a third
allo-HSC infusion due to personal circumstances (he was moved to a care facility far from the study site). Abbreviations: HSCT, haematopoietic stem cell transplant; M, months
Baseline patients
The baseline characteristics of patients enrolled in the trials of the eli -cel clinical development programme are outlined in Table 7.7. Not all patient demographics and characteristics were available across all trials. In line with the trial design, all patients were younger than 18 years, with a median age
ranging between 6 years (ALD-102) and 8 years (ALD-104) across the trials. The clinical presentation of CALD differed between the trial populations, with signs and symptoms, as well as adrenal insufficiency most commonly recorded. The baseline mean Loes score was less than 9 across all trials.
The majority of patients had an NFS score below or equal to 1 at baseline.
In order to facilitate an interstudy comparison between the ALD-102 and ALD-103 (see section 7.7.2), several analysis populations were created and are outlined in Table 7.6. For the outcomes presented in
sections 7.8 and 7.9, analysis populations were combined, e.g. MSD strictly eligible transplant population (TPES) patients formed a separate subgroup for analysis and comparison.
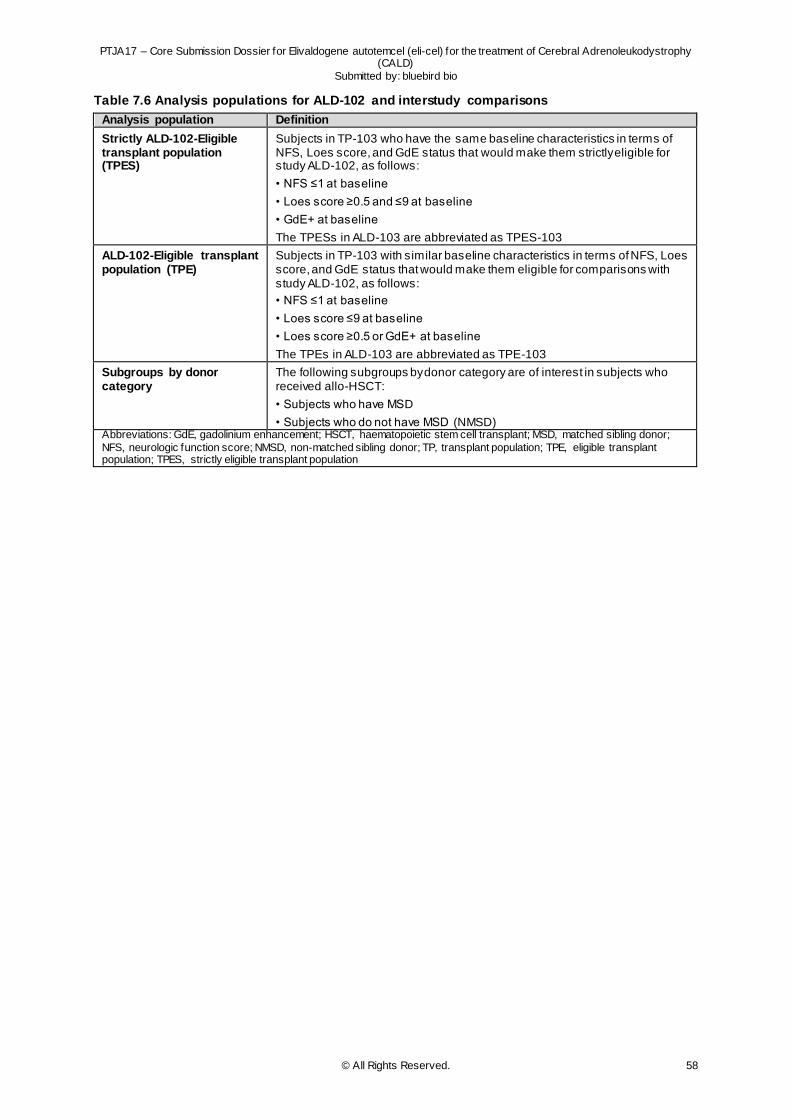
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 58
Table 7.6 Analysis populations for ALD-102 and interstudy comparisons
Analysis population Definition
Strictly ALD-102-Eligible transplant population (TPES)
Subjects in TP-103 who have the same baseline characteristics in terms of NFS, Loes score, and GdE status that would make them strictly eligible for study ALD-102, as follows:
• NFS ≤1 at baseline
• Loes score ≥0.5 and ≤9 at baseline
• GdE+ at baseline
The TPESs in ALD-103 are abbreviated as TPES-103
ALD-102-Eligible transplant population (TPE)
Subjects in TP-103 with similar baseline characteristics in terms of NFS, Loes score, and GdE status that would make them eligible for comparisons with study ALD-102, as follows:
• NFS ≤1 at baseline
• Loes score ≤9 at baseline
• Loes score ≥0.5 or GdE+ at baseline
The TPEs in ALD-103 are abbreviated as TPE-103
Subgroups by donor category
The following subgroups by donor category are of interest in subjects who received allo-HSCT:
• Subjects who have MSD
• Subjects who do not have MSD (NMSD) Abbreviations: GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplant; MSD, matched sibling donor;
NFS, neurologic function score; NMSD, non-matched sibling donor; TP, transplant population; TPE, eligible transplant population; TPES, strictly eligible transplant population
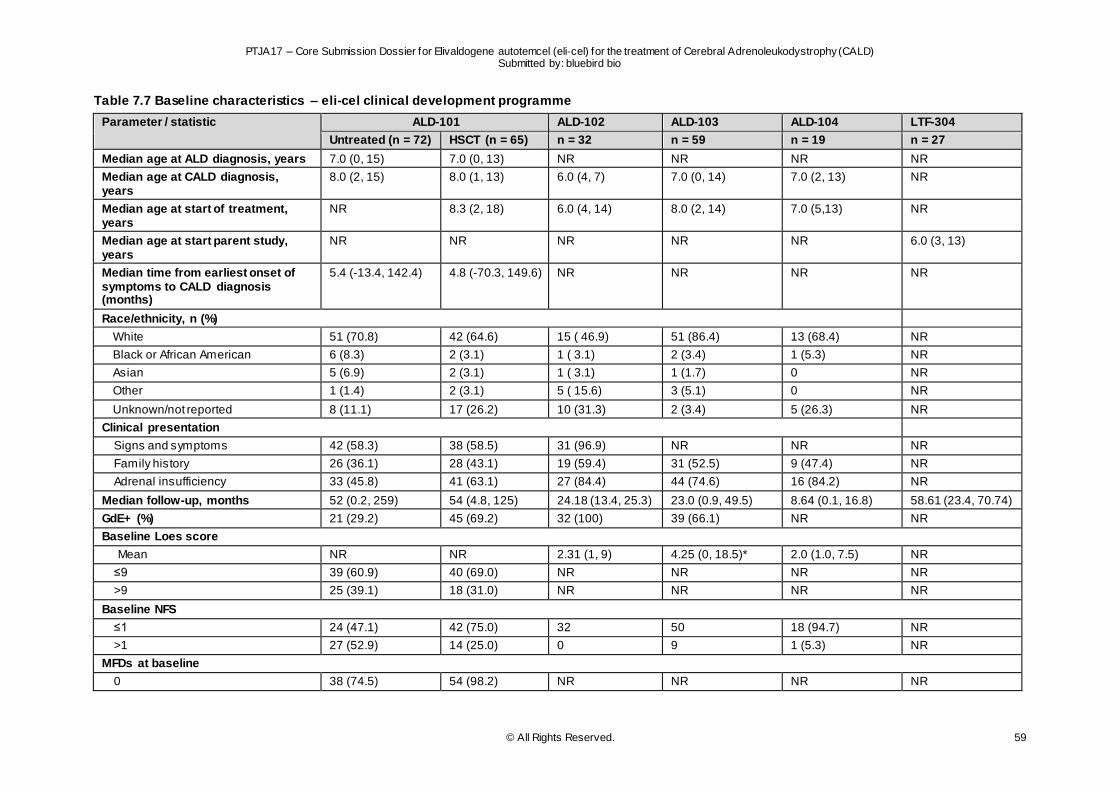
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 59
Table 7.7 Baseline characteristics – eli-cel clinical development programme
Parameter / statistic ALD-101 ALD-102 ALD-103 ALD-104 LTF-304
Untreated (n = 72) HSCT (n = 65) n = 32 n = 59 n = 19 n = 27
Median age at ALD diagnosis, years 7.0 (0, 15) 7.0 (0, 13) NR NR NR NR
Median age at CALD diagnosis, years
8.0 (2, 15) 8.0 (1, 13) 6.0 (4, 7) 7.0 (0, 14) 7.0 (2, 13) NR
Median age at start of treatment, years
NR 8.3 (2, 18) 6.0 (4, 14) 8.0 (2, 14) 7.0 (5,13) NR
Median age at start parent study, years
NR NR NR NR NR 6.0 (3, 13)
Median time from earliest onset of symptoms to CALD diagnosis (months)
5.4 (-13.4, 142.4) 4.8 (-70.3, 149.6) NR NR NR NR
Race/ethnicity, n (%)
White 51 (70.8) 42 (64.6) 15 ( 46.9) 51 (86.4) 13 (68.4) NR
Black or African American 6 (8.3) 2 (3.1) 1 ( 3.1) 2 (3.4) 1 (5.3) NR
Asian 5 (6.9) 2 (3.1) 1 ( 3.1) 1 (1.7) 0 NR
Other 1 (1.4) 2 (3.1) 5 ( 15.6) 3 (5.1) 0 NR
Unknown/not reported 8 (11.1) 17 (26.2) 10 (31.3) 2 (3.4) 5 (26.3) NR
Clinical presentation
Signs and symptoms 42 (58.3) 38 (58.5) 31 (96.9) NR NR NR
Family history 26 (36.1) 28 (43.1) 19 (59.4) 31 (52.5) 9 (47.4) NR
Adrenal insufficiency 33 (45.8) 41 (63.1) 27 (84.4) 44 (74.6) 16 (84.2) NR
Median follow-up, months 52 (0.2, 259) 54 (4.8, 125) 24.18 (13.4, 25.3) 23.0 (0.9, 49.5) 8.64 (0.1, 16.8) 58.61 (23.4, 70.74)
GdE+ (%) 21 (29.2) 45 (69.2) 32 (100) 39 (66.1) NR NR
Baseline Loes score
Mean NR NR 2.31 (1, 9) 4.25 (0, 18.5)* 2.0 (1.0, 7.5) NR
≤9 39 (60.9) 40 (69.0) NR NR NR NR
>9 25 (39.1) 18 (31.0) NR NR NR NR
Baseline NFS
≤1 24 (47.1) 42 (75.0) 32 50 18 (94.7) NR
>1 27 (52.9) 14 (25.0) 0 9 1 (5.3) NR
MFDs at baseline
0 38 (74.5) 54 (98.2) NR NR NR NR

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 60
1 8 (15.7) 1 (1.8) NR NR NR NR
≥2 5 (9.8) 0 NR NR NR NR
*for 56 out of 59 subjects.
Abbreviations: ALD, Adrenoleukodystrophy; CALD, Cerebral Adrenoleukodystrophy; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplant; NFS, neurologic function score; NR, not reported; MFD, major functional disabilities
Sources: CSR ALD-101121, Interim CSR ALD-10222 and D120 ALD-102 report (Tables 14.1.1.2, 14.1.3.1, 14.2.5,)10, CSR ALD-10311, Interim CSR ALD-104113 and D120 ALD-104 report (Tables
14.1.1.2, 14.2.5)3, Interim CSR LTF-304114 and D120 LTF-304 report (Table 14.1.1.1)23
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 61
7.6.2 SLR
Study characteristics Of the key studies selected (see Table 7.8), five covered CALD treatment with allo-HSCT49,65,116,117,120 and one with Lorenzo’s oil (BSC)119.
Allo-HSCT In all five allo-HSCT studies, patients were treated with ISTs alongside their allo-HSCT treatment. Four out of five allo-HSCT studies reported that patients received their donor stem cells from a variety of
different sources,65,116,117,120 while one study reported that all patients received cord blood transplant. 49 Similarly, the donor match was either mixed or unspecified. Follow-up across the studies ranged from one year in the study by Miller et al.116 to nine years in the study by Kühl et al.65 In terms of outcomes,
most of the allo-HSCT studies (n=4) reported a measure of efficacy, two studies outlined safety outcomes and one study reported QoL outcome measures. The outcome measures in these five allo-HSCT studies covered the majority of relevant outcomes identified as part of the SLR’s PICO.
BSC In the study by Moser et al.119 outlining treatment of CALD patients with BSC, specifical ly with Lorenzo’s oil, patients received Lorenzo’s oil in oral form, with a dosage that provided approximately 20% of daily
caloric intake (2-3 mL/kg). Patients were followed-up for approximately seven years, during which 14 patients received treatment with allo-HSCT. In terms of outcomes, the study by Moser et al.119 covered both efficacy and safety outcomes, but no QoL measures.
An overview of the study characteristics of all studies identified through the SLR can be found in the appendix, section 9.4 (Table 9.3). Broadly, the key allo-HSCT studies were reflective of the full scope of allo-HSCT evidence identified. No further studies covering treatment with BSC or outlining QoL
outcomes were identified.
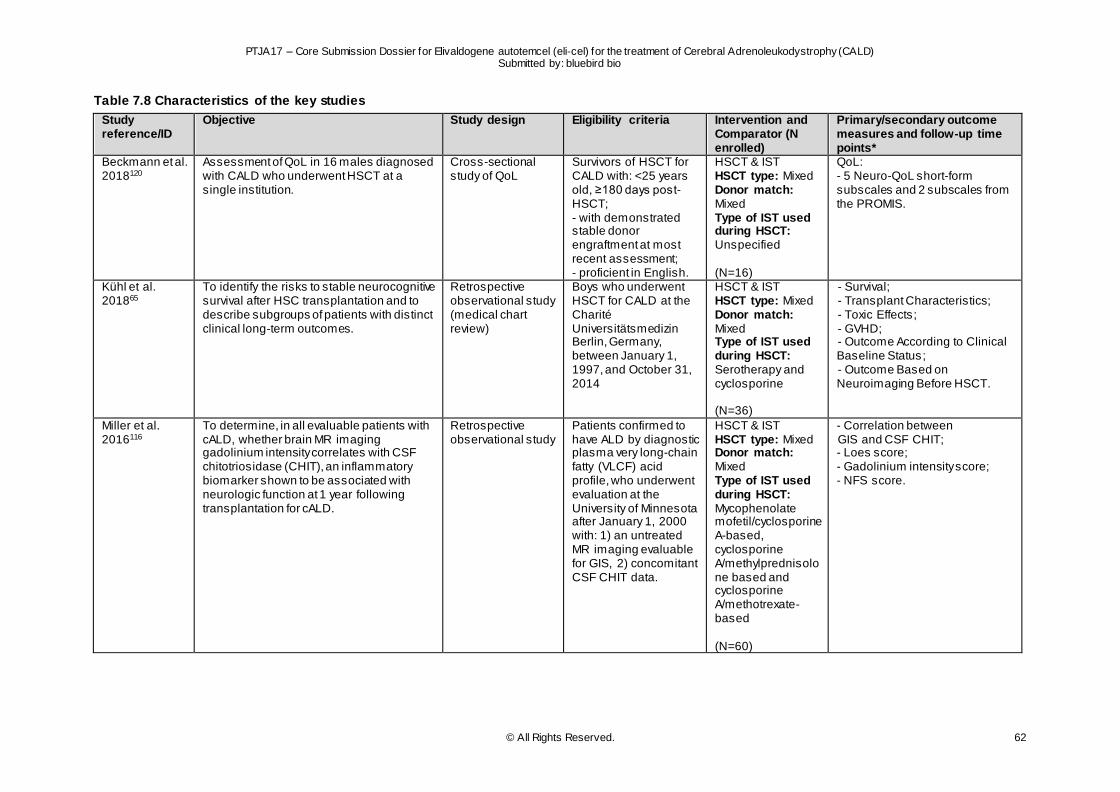
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 62
Table 7.8 Characteristics of the key studies
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
Beckmann et al. 2018120
Assessment of QoL in 16 males diagnosed with CALD who underwent HSCT at a single institution.
Cross-sectional study of QoL
Survivors of HSCT for CALD with: <25 years old, ≥180 days post-HSCT; - with demonstrated stable donor engraftment at most recent assessment; - proficient in English.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Unspecified (N=16)
QoL: - 5 Neuro-QoL short-form subscales and 2 subscales from the PROMIS.
Kühl et al. 201865
To identify the risks to stable neurocognitive survival after HSC transplantation and to describe subgroups of patients with distinct clinical long-term outcomes.
Retrospective observational study (medical chart review)
Boys who underwent HSCT for CALD at the Charité Universitätsmedizin Berlin, Germany, between January 1, 1997, and October 31, 2014
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Serotherapy and cyclosporine (N=36)
- Survival; - Transplant Characteristics; - Toxic Effects; - GVHD; - Outcome According to Clinical Baseline Status; - Outcome Based on Neuroimaging Before HSCT.
Miller et al. 2016116
To determine, in all evaluable patients with cALD, whether brain MR imaging gadolinium intensity correlates with CSF chitotriosidase (CHIT), an inflammatory biomarker shown to be associated with neurologic function at 1 year following transplantation for cALD.
Retrospective observational study
Patients confirmed to have ALD by diagnostic plasma very long-chain fatty (VLCF) acid profile, who underwent evaluation at the University of Minnesota after January 1, 2000 with: 1) an untreated MR imaging evaluable for GIS, 2) concomitant CSF CHIT data.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Mycophenolate mofetil/cyclosporine A-based, cyclosporine A/methylprednisolone based and cyclosporine A/methotrexate-based (N=60)
- Correlation between GIS and CSF CHIT; - Loes score; - Gadolinium intensity score; - NFS score.
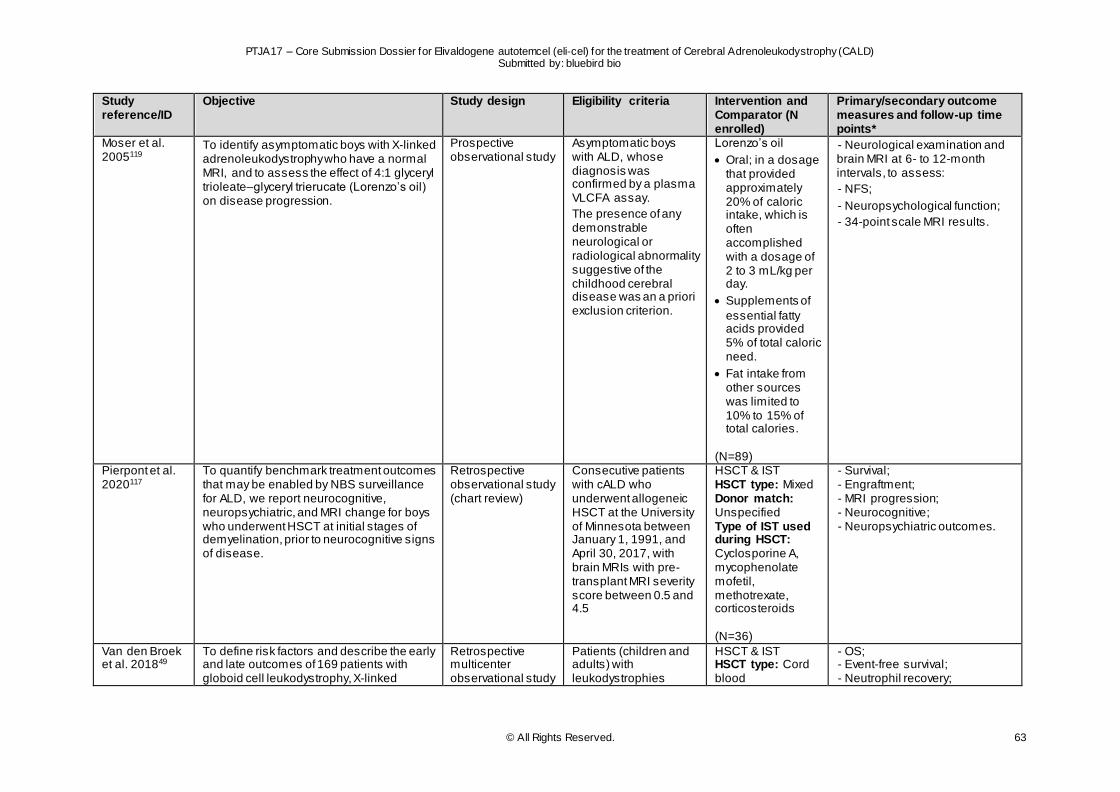
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 63
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
Moser et al. 2005119
To identify asymptomatic boys with X-linked adrenoleukodystrophy who have a normal MRI, and to assess the effect of 4:1 glyceryl trioleate–glyceryl trierucate (Lorenzo’s oil) on disease progression.
Prospective observational study
Asymptomatic boys with ALD, whose diagnosis was confirmed by a plasma VLCFA assay.
The presence of any demonstrable neurological or radiological abnormality suggestive of the childhood cerebral disease was an a priori exclusion criterion.
Lorenzo’s oil
Oral; in a dosage that provided approximately 20% of caloric intake, which is often accomplished with a dosage of 2 to 3 mL/kg per day.
Supplements of
essential fatty acids provided 5% of total caloric need.
Fat intake from other sources was limited to 10% to 15% of total calories.
(N=89)
- Neurological examination and brain MRI at 6- to 12-month intervals, to assess:
- NFS;
- Neuropsychological function;
- 34-point scale MRI results.
Pierpont et al. 2020117
To quantify benchmark treatment outcomes that may be enabled by NBS surveillance for ALD, we report neurocognitive, neuropsychiatric, and MRI change for boys who underwent HSCT at initial stages of demyelination, prior to neurocognitive signs of disease.
Retrospective observational study (chart review)
Consecutive patients with cALD who underwent allogeneic HSCT at the University of Minnesota between January 1, 1991, and April 30, 2017, with brain MRIs with pre-transplant MRI severity score between 0.5 and 4.5
HSCT & IST HSCT type: Mixed Donor match: Unspecified Type of IST used during HSCT: Cyclosporine A, mycophenolate mofetil, methotrexate, corticosteroids (N=36)
- Survival; - Engraftment; - MRI progression; - Neurocognitive; - Neuropsychiatric outcomes.
Van den Broek et al. 201849
To define risk factors and describe the early and late outcomes of 169 patients with globoid cell leukodystrophy, X-linked
Retrospective multicenter observational study
Patients (children and adults) with leukodystrophies
HSCT & IST HSCT type: Cord blood
- OS; - Event-free survival; - Neutrophil recovery;
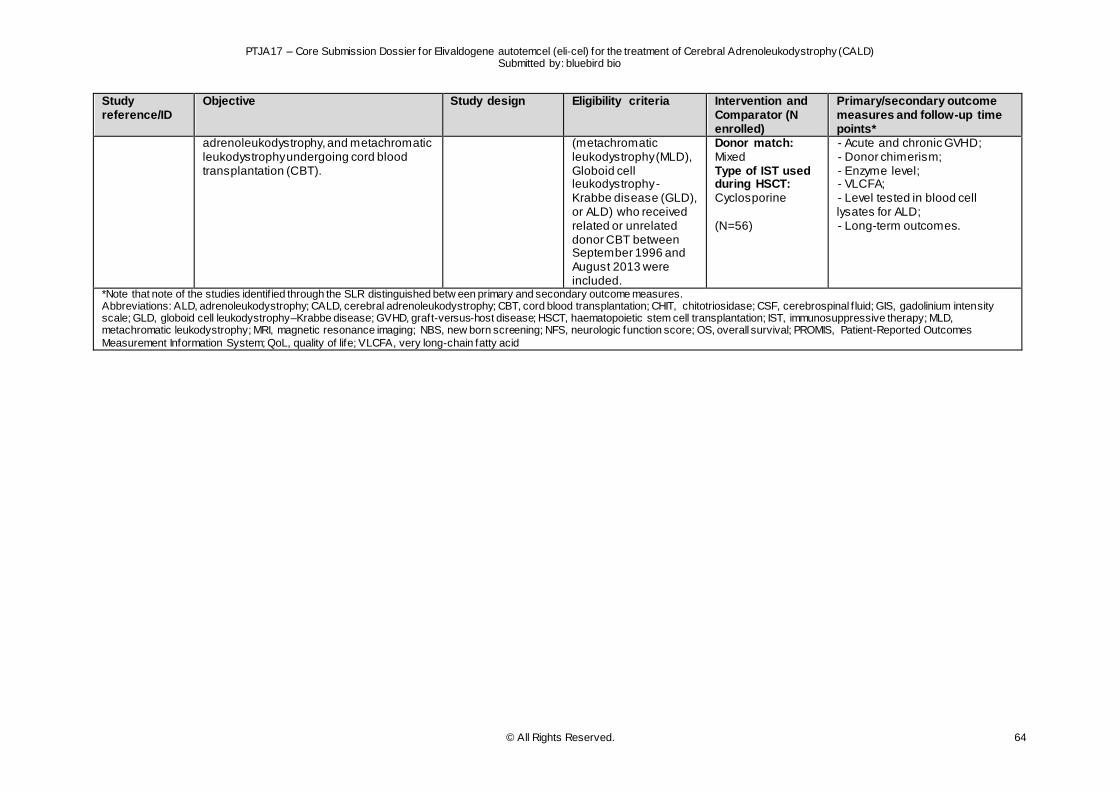
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 64
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
adrenoleukodystrophy, and metachromatic leukodystrophy undergoing cord blood transplantation (CBT).
(metachromatic leukodystrophy (MLD), Globoid cell leukodystrophy - Krabbe disease (GLD), or ALD) who received related or unrelated donor CBT between September 1996 and August 2013 were included.
Donor match: Mixed Type of IST used during HSCT: Cyclosporine (N=56)
- Acute and chronic GVHD; - Donor chimerism; - Enzyme level; - VLCFA; - Level tested in blood cell lysates for ALD; - Long-term outcomes.
*Note that note of the studies identif ied through the SLR distinguished betw een primary and secondary outcome measures. Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; CBT, cord blood transplantation; CHIT, chitotriosidase; CSF, cerebrospinal f luid; GIS, gadolinium intensity scale; GLD, globoid cell leukodystrophy–Krabbe disease; GVHD, graft-versus-host disease; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; MLD, metachromatic leukodystrophy; MRI, magnetic resonance imaging; NBS, new born screening; NFS, neurologic function score; OS, overall survival; PROMIS, Patient-Reported Outcomes
Measurement Information System; QoL, quality of life; VLCFA, very long-chain fatty acid
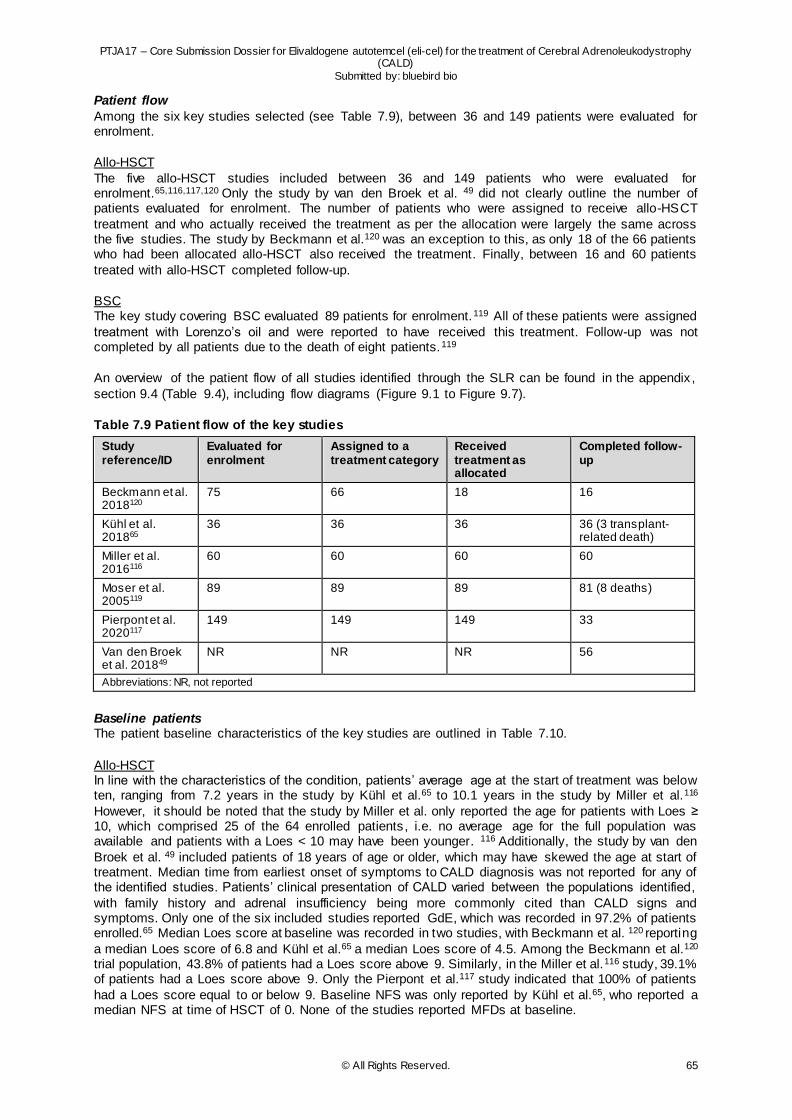
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 65
Patient flow
Among the six key studies selected (see Table 7.9), between 36 and 149 patients were evaluated for enrolment.
Allo-HSCT
The five allo-HSCT studies included between 36 and 149 patients who were evaluated for enrolment.65,116,117,120 Only the study by van den Broek et al. 49 did not clearly outline the number of patients evaluated for enrolment. The number of patients who were assigned to receive allo-HSCT
treatment and who actually received the treatment as per the allocation were largely the same across the five studies. The study by Beckmann et al.120 was an exception to this, as only 18 of the 66 patients who had been allocated allo-HSCT also received the treatment. Finally, between 16 and 60 patients
treated with allo-HSCT completed follow-up.
BSC The key study covering BSC evaluated 89 patients for enrolment.119 All of these patients were assigned
treatment with Lorenzo’s oil and were reported to have received this treatment. Follow-up was not completed by all patients due to the death of eight patients.119
An overview of the patient flow of all studies identified through the SLR can be found in the appendix ,
section 9.4 (Table 9.4), including flow diagrams (Figure 9.1 to Figure 9.7).
Table 7.9 Patient flow of the key studies
Study reference/ID
Evaluated for enrolment
Assigned to a treatment category
Received treatment as allocated
Completed follow-up
Beckmann et al. 2018120
75 66 18 16
Kühl et al. 201865
36 36 36 36 (3 transplant-related death)
Miller et al. 2016116
60 60 60 60
Moser et al. 2005119
89 89 89 81 (8 deaths)
Pierpont et al. 2020117
149 149 149 33
Van den Broek et al. 201849
NR NR NR 56
Abbreviations: NR, not reported
Baseline patients The patient baseline characteristics of the key studies are outlined in Table 7.10.
Allo-HSCT In line with the characteristics of the condition, patients’ average age at the start of treatment was below ten, ranging from 7.2 years in the study by Kühl et al.65 to 10.1 years in the study by Miller et al.116
However, it should be noted that the study by Miller et al. only reported the age for patients with Loes ≥ 10, which comprised 25 of the 64 enrolled patients, i.e. no average age for the full population was available and patients with a Loes < 10 may have been younger. 116 Additionally, the study by van den
Broek et al. 49 included patients of 18 years of age or older, which may have skewed the age at start of treatment. Median time from earliest onset of symptoms to CALD diagnosis was not reported for any of the identified studies. Patients’ clinical presentation of CALD varied between the populations identified,
with family history and adrenal insufficiency being more commonly cited than CALD signs and symptoms. Only one of the six included studies reported GdE, which was recorded in 97.2% of patients enrolled.65 Median Loes score at baseline was recorded in two studies, with Beckmann et al. 120 reporting
a median Loes score of 6.8 and Kühl et al.65 a median Loes score of 4.5. Among the Beckmann et al.120 trial population, 43.8% of patients had a Loes score above 9. Similarly, in the Miller et al.116 study, 39.1% of patients had a Loes score above 9. Only the Pierpont et al.117 study indicated that 100% of patients
had a Loes score equal to or below 9. Baseline NFS was only reported by Kühl et al.65, who reported a median NFS at time of HSCT of 0. None of the studies reported MFDs at baseline.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 66
BSC
Moser et al.119 reported an average age at start of treatment with Lorenzo’s oil of 4.75 years. Clinical presentation of CALD was predominantly based on family history (77%). No GdE, Loes, NFS or MFD score at baseline was reported.119
An overview of the baseline patient characteristics of all studies identified through the SLR can be found in the appendix, section 9.4 (Table 9.5 to Table 9.7).
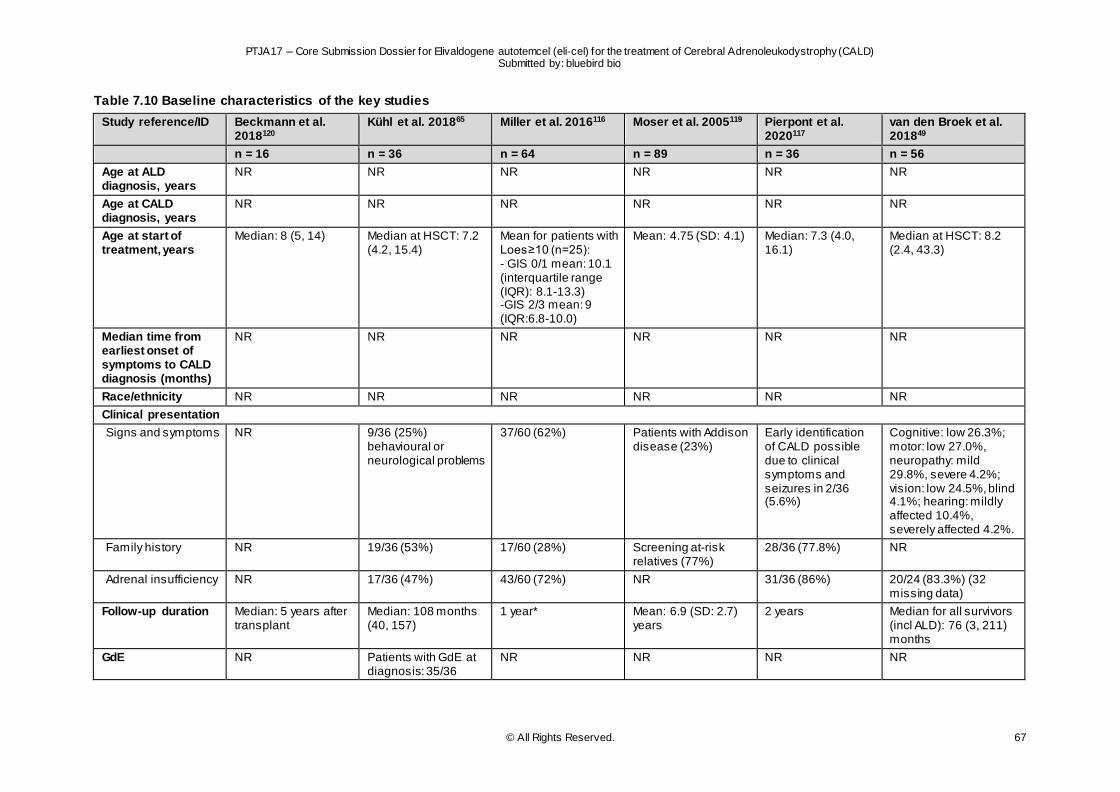
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 67
Table 7.10 Baseline characteristics of the key studies
Study reference/ID Beckmann et al. 2018120
Kühl et al. 201865 Miller et al. 2016116 Moser et al. 2005119 Pierpont et al. 2020117
van den Broek et al. 201849
n = 16 n = 36 n = 64 n = 89 n = 36 n = 56
Age at ALD diagnosis, years
NR NR NR NR NR NR
Age at CALD diagnosis, years
NR NR NR NR NR NR
Age at start of treatment, years
Median: 8 (5, 14) Median at HSCT: 7.2 (4.2, 15.4)
Mean for patients with Loes≥10 (n=25): - GIS 0/1 mean: 10.1 (interquartile range (IQR): 8.1-13.3) -GIS 2/3 mean: 9 (IQR:6.8-10.0)
Mean: 4.75 (SD: 4.1) Median: 7.3 (4.0, 16.1)
Median at HSCT: 8.2 (2.4, 43.3)
Median time from earliest onset of symptoms to CALD diagnosis (months)
NR NR NR NR NR NR
Race/ethnicity NR NR NR NR NR NR
Clinical presentation
Signs and symptoms NR 9/36 (25%) behavioural or neurological problems
37/60 (62%) Patients with Addison disease (23%)
Early identification of CALD possible due to clinical symptoms and seizures in 2/36 (5.6%)
Cognitive: low 26.3%; motor: low 27.0%, neuropathy: mild 29.8%, severe 4.2%; vision: low 24.5%, blind 4.1%; hearing: mildly affected 10.4%, severely affected 4.2%.
Family history NR 19/36 (53%) 17/60 (28%) Screening at-risk relatives (77%)
28/36 (77.8%) NR
Adrenal insufficiency NR 17/36 (47%) 43/60 (72%) NR 31/36 (86%) 20/24 (83.3%) (32 missing data)
Follow-up duration Median: 5 years after transplant
Median: 108 months (40, 157)
1 year* Mean: 6.9 (SD: 2.7) years
2 years Median for all survivors (incl ALD): 76 (3, 211) months
GdE NR Patients with GdE at diagnosis: 35/36
NR NR NR NR
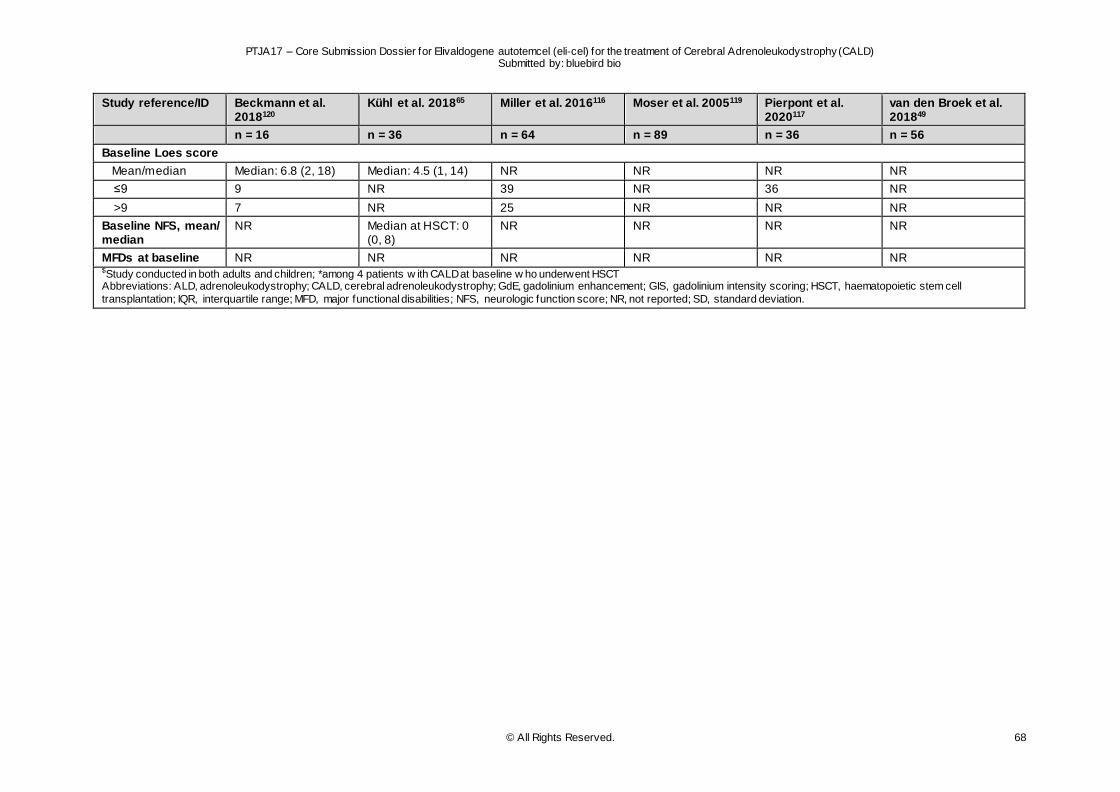
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 68
Study reference/ID Beckmann et al. 2018120
Kühl et al. 201865 Miller et al. 2016116 Moser et al. 2005119 Pierpont et al. 2020117
van den Broek et al. 201849
n = 16 n = 36 n = 64 n = 89 n = 36 n = 56
Baseline Loes score
Mean/median Median: 6.8 (2, 18) Median: 4.5 (1, 14) NR NR NR NR
≤9 9 NR 39 NR 36 NR
>9 7 NR 25 NR NR NR
Baseline NFS, mean/ median
NR Median at HSCT: 0 (0, 8)
NR NR NR NR
MFDs at baseline NR NR NR NR NR NR $Study conducted in both adults and children; *among 4 patients w ith CALD at baseline w ho underwent HSCT Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; GdE, gadolinium enhancement; GIS, gadolinium intensity scoring; HSCT, haematopoietic stem cell
transplantation; IQR, interquartile range; MFD, major functional disabilities; NFS, neurologic function score; NR, not reported; SD, standard deviation.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 69
7.7 Methods of evidence synthesis
7.7.1 Eli-cel clinical development programme evidence synthesis
As highlighted in section 7.5.1, due to the rarity of CALD, it is difficult to conduct an RCT comparing eli-cel with a concurrent control arm in the treatment of CALD patients. As a result, the eli-cel clinical development programme consisted of several single-arm trials. To enable comparison of the key eli-cel
clinical trial, ALD-102, with allo-HSCT, an allo-HSCT observational trial with a similar study design was set up (ALD-103).
Results associated with this comparison of ALD-102 with ALD-103 were summarised in an interstudy
clinical study report and updated following the latest datacut (ALD-102: 23 October 2020, LTF-304: 2 November 2020) and comprise a naïve comparison of the outcomes identified in the two trials.7
To further investigate the accuracy of the comparative effectiveness of this comparison, a heterogeneity
analysis was performed using patient level data from ALD-102 and ALD-103, in the form of propensity score (PS) adjusted analyses.8 These were designed to take into account differences in the baseline characteristic variable distributions between the subset of TPES-103 subjects who did not have an MSD
(i.e. TPES-103-NMSD) and TP-102 subjects. The patient level data used for these analyses date from January 2020; only minor differences are to be expected once the final ALD-102 CSR data are available.
To account for the limited sample sizes of TP-102 (N=32) and TPES-103 NMSD (N=17), 3 specific PS
methods were used:
1. Inverse probability weighting (IPTW; weight being normalized)
2. Overlap weighting (OW; weight being normalized)
3. Use PS as a covariate in the regression model (PS in regression model)
These 3 PS methods make use of all observed data. Simulation studies show that PS methods perform better with larger sample sizes. For studies with limited sample size, such as TP-102 and TPES-103
NMSD, confidence on the adjusted outcome can be strengthened if results from the 3 PS methods are similar and consistent.
A set of seven baseline confounders were identified as being independently correlated with patient
prognosis, based on input from the clinical trials’ investigators and key opinion leaders. Subsequently, these seven confounders were included in the propensity score based adjusted analysis. Specifically, these covered:
Age at baseline
Age at CALD diagnosis
Month from CALD diagnosis to Relative day 1
Loes score at baseline
NFS score at baseline
Loes pattern group at baseline
Presence of Comorbid condition at baseline
Section 7.11.2 outlines the relevance of the Loes and NFS in CALD; while, age and presence of
comorbid conditions are based on the EBMT handbook and the study on the development of the haematopoietic cell transplantation (HCT)-comorbidity index.122,123 Additionally, GdE was considered as it is also a confounder which is correlated with patient prognosis. However, it was excluded because in
ALD-102, its value was always positive (no variation), while in ALD-103, it had both positive and negative values. As such, the variable values did not span the same range which is problematic in propensity score analyses as it would lead to a bias in the analysis.
The propensity score adjusted analyses found consistently that for both efficacy and safety endpoints, comparing ALD-102 and ALD-103 populations, after propensity score adjustment, did not change conclusions originally drawn on the basis of the naïve comparison.8 Two examples demonstrating the
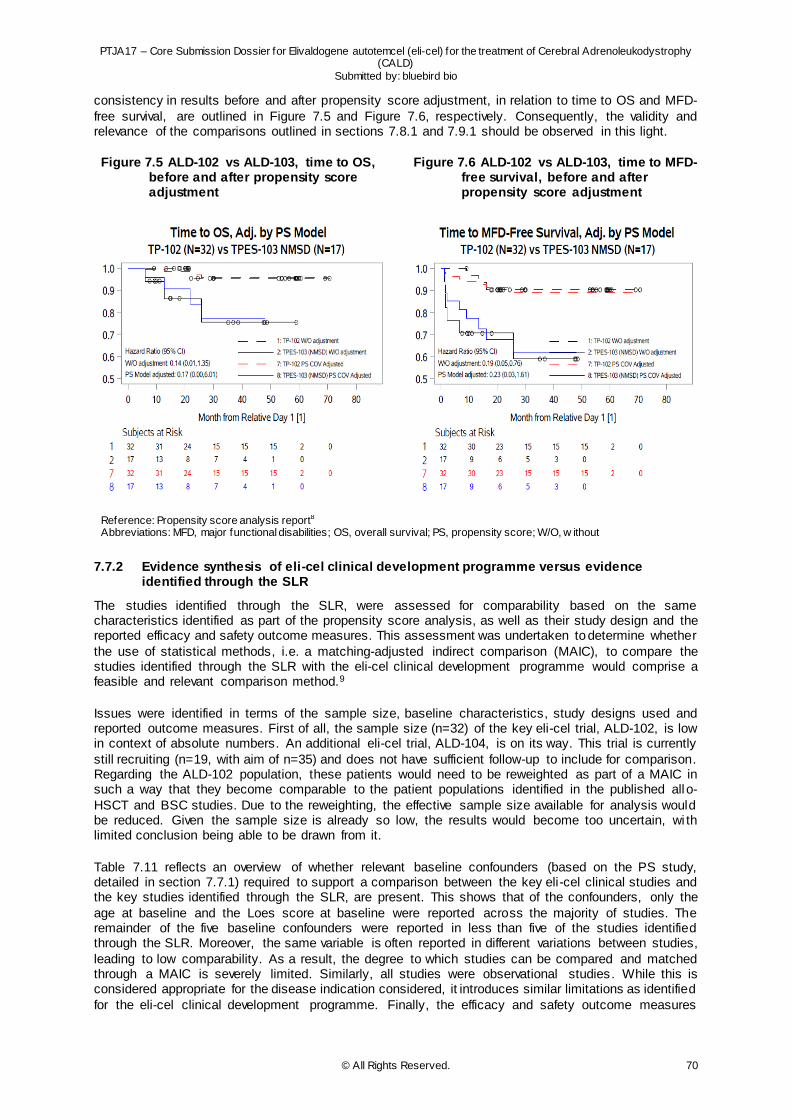
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 70
consistency in results before and after propensity score adjustment, in relation to time to OS and MFD-
free survival, are outlined in Figure 7.5 and Figure 7.6, respectively. Consequently, the validity and relevance of the comparisons outlined in sections 7.8.1 and 7.9.1 should be observed in this light.
Figure 7.5 ALD-102 vs ALD-103, time to OS, before and after propensity score adjustment
Figure 7.6 ALD-102 vs ALD-103, time to MFD-free survival, before and after propensity score adjustment
Reference: Propensity score analysis report8 Abbreviations: MFD, major functional disabilities; OS, overall survival; PS, propensity score; W/O, w ithout
7.7.2 Evidence synthesis of eli-cel clinical development programme versus evidence identified through the SLR
The studies identified through the SLR, were assessed for comparability based on the same characteristics identified as part of the propensity score analysis, as well as their study design and the reported efficacy and safety outcome measures. This assessment was undertaken to determine whether
the use of statistical methods, i.e. a matching-adjusted indirect comparison (MAIC), to compare the studies identified through the SLR with the eli-cel clinical development programme would comprise a feasible and relevant comparison method.9
Issues were identified in terms of the sample size, baseline characteristics, study designs used and reported outcome measures. First of all, the sample size (n=32) of the key eli-cel trial, ALD-102, is low in context of absolute numbers. An additional eli-cel trial, ALD-104, is on its way. This trial is currently
still recruiting (n=19, with aim of n=35) and does not have sufficient follow-up to include for comparison. Regarding the ALD-102 population, these patients would need to be reweighted as part of a MAIC in such a way that they become comparable to the patient populations identified in the published all o-
HSCT and BSC studies. Due to the reweighting, the effective sample size available for analysis would be reduced. Given the sample size is already so low, the results would become too uncertain, wi th limited conclusion being able to be drawn from it.
Table 7.11 reflects an overview of whether relevant baseline confounders (based on the PS study, detailed in section 7.7.1) required to support a comparison between the key eli-cel clinical studies and the key studies identified through the SLR, are present. This shows that of the confounders, only the
age at baseline and the Loes score at baseline were reported across the majority of studies. The remainder of the five baseline confounders were reported in less than five of the studies identified through the SLR. Moreover, the same variable is often reported in different variations between studies,
leading to low comparability. As a result, the degree to which studies can be compared and matched through a MAIC is severely limited. Similarly, all studies were observational studies. While this is considered appropriate for the disease indication considered, it introduces similar limitations as identified
for the eli-cel clinical development programme. Finally, the efficacy and safety outcome measures
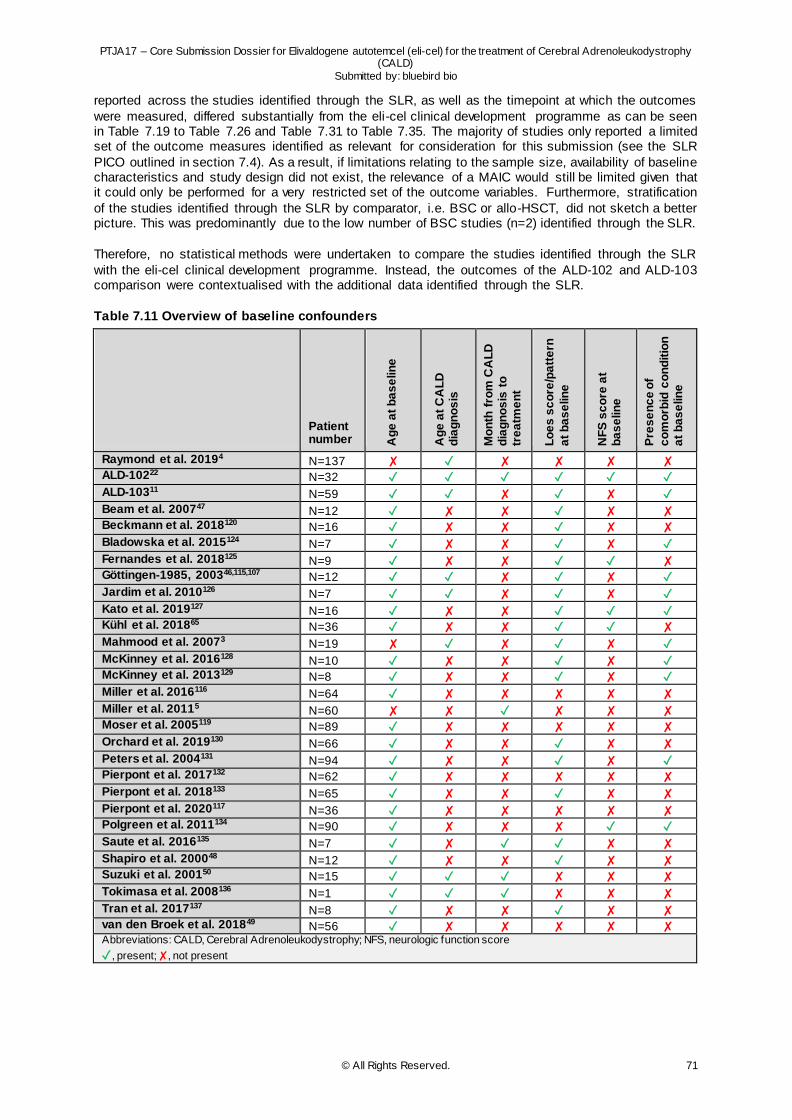
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 71
reported across the studies identified through the SLR, as well as the timepoint at which the outcomes
were measured, differed substantially from the eli-cel clinical development programme as can be seen in Table 7.19 to Table 7.26 and Table 7.31 to Table 7.35. The majority of studies only reported a limited set of the outcome measures identified as relevant for consideration for this submission (see the SLR
PICO outlined in section 7.4). As a result, if limitations relating to the sample size, availability of baseline characteristics and study design did not exist, the relevance of a MAIC would still be limited given that it could only be performed for a very restricted set of the outcome variables. Furthermore, stratification
of the studies identified through the SLR by comparator, i.e. BSC or allo-HSCT, did not sketch a better picture. This was predominantly due to the low number of BSC studies (n=2) identified through the SLR.
Therefore, no statistical methods were undertaken to compare the studies identified through the SLR
with the eli-cel clinical development programme. Instead, the outcomes of the ALD-102 and ALD-103 comparison were contextualised with the additional data identified through the SLR.
Table 7.11 Overview of baseline confounders
Patient number A
ge
at
ba
se
lin
e
Ag
e a
t C
AL
D
dia
gn
os
is
Mo
nth
fro
m C
AL
D
dia
gn
os
is t
o
tre
atm
en
t
Lo
es
sc
ore
/pa
tte
rn
at
ba
se
lin
e
NF
S s
co
re a
t b
as
elin
e
Pre
se
nc
e o
f
co
mo
rbid
co
nd
itio
n
at
ba
se
lin
e
Raymond et al. 20194 N=137 ✘ ✓ ✘ ✘ ✘ ✘ ALD-10222 N=32 ✓ ✓ ✓ ✓ ✓ ✓
ALD-10311 N=59 ✓ ✓ ✘ ✓ ✘ ✓
Beam et al. 200747 N=12 ✓ ✘ ✘ ✓ ✘ ✘ Beckmann et al. 2018120 N=16 ✓ ✘ ✘ ✓ ✘ ✘
Bladowska et al. 2015124 N=7 ✓ ✘ ✘ ✓ ✘ ✓
Fernandes et al. 2018125 N=9 ✓ ✘ ✘ ✓ ✓ ✘ Göttingen-1985, 200346,115,107 N=12 ✓ ✓ ✘ ✓ ✘ ✓
Jardim et al. 2010126 N=7 ✓ ✓ ✘ ✓ ✘ ✓
Kato et al. 2019127 N=16 ✓ ✘ ✘ ✓ ✓ ✓ Kühl et al. 201865 N=36 ✓ ✘ ✘ ✓ ✓ ✘
Mahmood et al. 20073 N=19 ✘ ✓ ✘ ✓ ✘ ✓
McKinney et al. 2016128 N=10 ✓ ✘ ✘ ✓ ✘ ✓ McKinney et al. 2013129 N=8 ✓ ✘ ✘ ✓ ✘ ✓
Miller et al. 2016116 N=64 ✓ ✘ ✘ ✘ ✘ ✘
Miller et al. 20115 N=60 ✘ ✘ ✓ ✘ ✘ ✘ Moser et al. 2005119 N=89 ✓ ✘ ✘ ✘ ✘ ✘
Orchard et al. 2019130 N=66 ✓ ✘ ✘ ✓ ✘ ✘
Peters et al. 2004131 N=94 ✓ ✘ ✘ ✓ ✘ ✓ Pierpont et al. 2017132 N=62 ✓ ✘ ✘ ✘ ✘ ✘
Pierpont et al. 2018133 N=65 ✓ ✘ ✘ ✓ ✘ ✘
Pierpont et al. 2020117 N=36 ✓ ✘ ✘ ✘ ✘ ✘ Polgreen et al. 2011134 N=90 ✓ ✘ ✘ ✘ ✓ ✓
Saute et al. 2016135 N=7 ✓ ✘ ✓ ✓ ✘ ✘
Shapiro et al. 200048 N=12 ✓ ✘ ✘ ✓ ✘ ✘ Suzuki et al. 200150 N=15 ✓ ✓ ✓ ✘ ✘ ✘
Tokimasa et al. 2008136 N=1 ✓ ✓ ✓ ✘ ✘ ✘
Tran et al. 2017137 N=8 ✓ ✘ ✘ ✓ ✘ ✘ van den Broek et al. 201849 N=56 ✓ ✘ ✘ ✘ ✘ ✘ Abbreviations: CALD, Cerebral Adrenoleukodystrophy; NFS, neurologic function score
✓ , present; ✘, not present
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 72
7.8 Individual study results (clinical outcomes)
Clinical outcome definitions and methods of analysis, where available, are presented per study in Table
9.8, in the appendix (section 9.5). In line with the SLR PICO (see section 7.4), the following clinical outcomes were considered:
OS (mortality)
MFD-free survival
Loes score and Loes pattern
Change in NFS
GdE value
HRQoL
An explanation of each of these clinical outcomes is outlined in section 2.2.1 and 2.2.3.
Minimal clinically important difference (MCID) From the literature, there are no generally accepted MCIDs for the clinical outcomes under
consideration, except for HRQoL. For the used instrument, PedsQL, the MCID is 4.5 points.138-140
Based on feedback from regulators including the EMA and FDA, and discussion with clinical experts in the therapeutic area, the objective of Study ALD-101 was to identify the most clinically meaningful
endpoints for the proposed pivotal clinical study, Study ALD-102. Prevention of all six MFDs at Month 24 post-transplant was selected as the primary efficacy endpoint in order to demonstrate that treatment with eli-cel is able to stabilise the disease and preserve the capacity for independent living. The CHMP
has included in their scientific advice (2016) that Study ALD-102 was designed with a number of supportive clinically meaningful secondary endpoints for both efficacy and safety that are precise and objective in their measurement. These same assessments are used today by clinicians to follow patients
with CALD and evaluate factors such as disease progression.
Selection of secondary endpoints for Study ALD-102 was based primarily on data collected in Study ALD-101 and on findings from review of CALD literature, which showed that 1) NFS and Loes scores
are useful and commonly used as confirmatory tools to assess disease status and extent of demyelination, respectively, and 2) GdE in untreated patients was associated with rapid disease progression and resolution of enhancement by Month 6 after allo-HSCT was usually associated with
stabilisation of disease. Thus, NFS, Loes score, and resolution of GdE were determined to be useful and clinically meaningful secondary endpoints. More details on the validity of the endpoints included are outlined in section 7.11.1.
7.8.1 Eli-cel clinical development programme: clinical efficacy outcomes
Table 7.15 outlines a summary of the clinical efficacy outcomes reported as part of the trials included in the eli-cel clinical development programme. Each of the outcomes are outlined in further detail in the
following subsections.
Overall survival As of 23 October 2020, 32 patients had been treated with eli-cel in ALD-102.22 27 of 30 evaluable
patients treated with eli-cel in ALD-102 were alive and MFD-free at Month 24 (90.0%; 95% CI 73.5–97.9) (see Table 14.2.1.1 of D120 ALD-102 report).10 A further two patients had been treated but not reached 24 months of follow-up.
The three patients that did not achieve Month 24 MFD-free survival discontinued from the study. Of these, only one experienced MFDs. This patient experienced rapid disease progression early in the study, which led to MFD and death. The other two withdrew from the study and were censored at the
date of their last visit. One withdrew because of white matter lesion progression and one following MRI evidence of disease progression, who went on to receive allo-HSCT but died from transplant-related complications.141
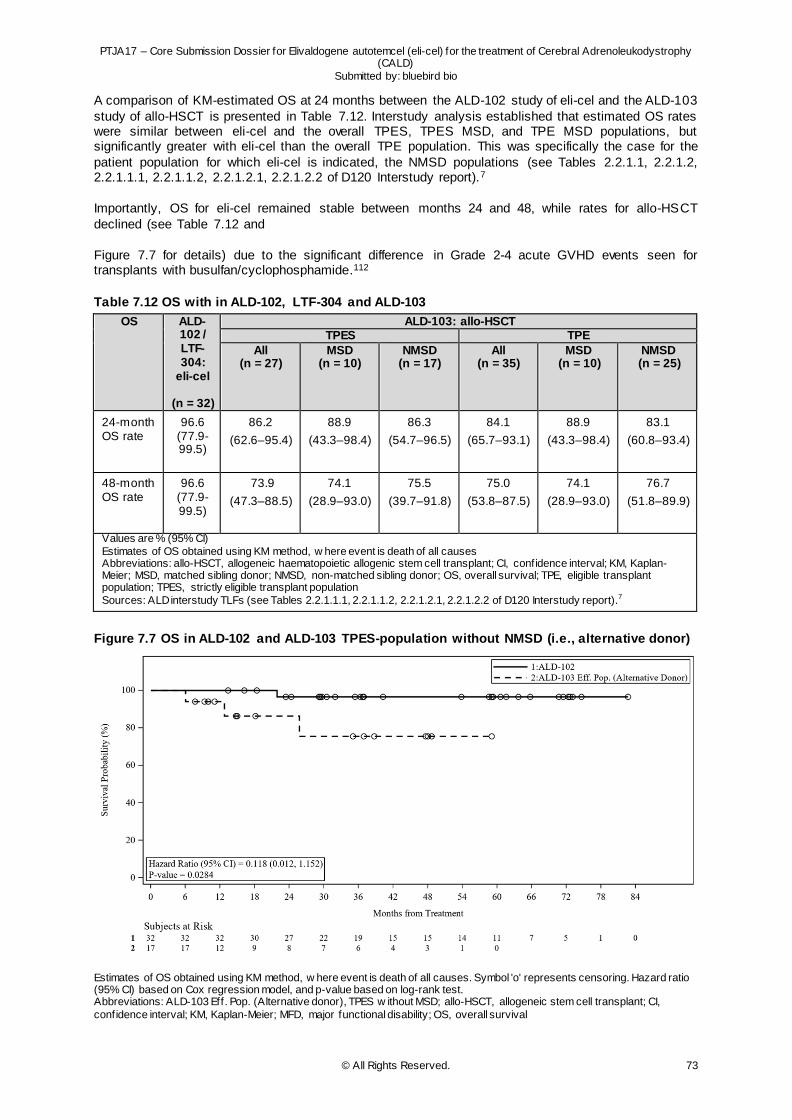
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 73
A comparison of KM-estimated OS at 24 months between the ALD-102 study of eli-cel and the ALD-103
study of allo-HSCT is presented in Table 7.12. Interstudy analysis established that estimated OS rates were similar between eli-cel and the overall TPES, TPES MSD, and TPE MSD populations, but significantly greater with eli-cel than the overall TPE population. This was specifically the case for the
patient population for which eli-cel is indicated, the NMSD populations (see Tables 2.2.1.1, 2.2.1.2, 2.2.1.1.1, 2.2.1.1.2, 2.2.1.2.1, 2.2.1.2.2 of D120 Interstudy report).7
Importantly, OS for eli-cel remained stable between months 24 and 48, while rates for allo-HSCT
declined (see Table 7.12 and
Figure 7.7 for details) due to the significant difference in Grade 2-4 acute GVHD events seen for transplants with busulfan/cyclophosphamide.112
Table 7.12 OS with in ALD-102, LTF-304 and ALD-103
OS ALD-102 / LTF-304:
eli-cel
(n = 32)
ALD-103: allo-HSCT TPES TPE
All (n = 27)
MSD (n = 10)
NMSD (n = 17)
All (n = 35)
MSD (n = 10)
NMSD (n = 25)
24-month OS rate
96.6 (77.9-99.5)
86.2
(62.6–95.4)
88.9
(43.3–98.4)
86.3
(54.7–96.5)
84.1
(65.7–93.1)
88.9
(43.3–98.4)
83.1
(60.8–93.4)
48-month OS rate
96.6 (77.9-99.5)
73.9
(47.3–88.5)
74.1
(28.9–93.0)
75.5
(39.7–91.8)
75.0
(53.8–87.5)
74.1
(28.9–93.0)
76.7
(51.8–89.9)
Values are % (95% CI) Estimates of OS obtained using KM method, w here event is death of all causes Abbreviations: allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, confidence interval; KM, Kaplan-Meier; MSD, matched sibling donor; NMSD, non-matched sibling donor; OS, overall survival; TPE, eligible transplant population; TPES, strictly eligible transplant population
Sources: ALD interstudy TLFs (see Tables 2.2.1.1.1, 2.2.1.1.2, 2.2.1.2.1, 2.2.1.2.2 of D120 Interstudy report).7
Figure 7.7 OS in ALD-102 and ALD-103 TPES-population without NMSD (i.e., alternative donor)
Estimates of OS obtained using KM method, w here event is death of all causes. Symbol 'o' represents censoring. Hazard ratio (95% CI) based on Cox regression model, and p-value based on log-rank test. Abbreviations: ALD-103 Eff. Pop. (Alternative donor), TPES w ithout MSD; allo-HSCT, allogeneic stem cell transplant; CI,
confidence interval; KM, Kaplan-Meier; MFD, major functional disability; OS, overall survival
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 74
Source: ALD Interstudy TLFs (see Figure 24.2.1.2 of D120 Interstudy report)7
In terms of long-term follow-up, eli-cel has demonstrated to be associated with a durable effect on OS in the 27 patients who had enrolled in LTF-304 as of 2 November 2020. All 27 subjects (100%) remained alive at their last follow-up visit, a median of 58.61 months (range 23.4-82.7) from infusion (see Table
14.1.1.1 of D120 LTF-304 report).23
MFD-free survival MFDs are the 6 most severe disabilities - loss of communication, cortical blindness, total incontinence,
no voluntary movement, wheelchair dependence, and tube feeding - typically experienced by boys with CALD, as seen from the natural history of the disease.4 Through consultation with experts in the field and analysis of data from ALD-101 natural history study, MFD-free survival was, therefore, selected as
the composite primary efficacy endpoint in the eli-cel clinical programme to assess time after eli-cel infusion that the patient remains free of clinical manifestation related to those 6 major disabilities of CALD.
27 of 30 evaluable patients were alive and MFD-free at Month 24 (90.0%; 95% CI 73.5–97.9) (see Table 14.2.1.1 of D120 ALD-102 report13). Of the three patients who did not meet the MFD-free survival endpoint, only one experienced MFDs, the other two patients withdrew (see details in the OS section).
MFD-free survival for the 30 evaluable patients was consistent with the predefined efficacy success benchmark.141 As part of this benchmark, the success criterion required the lower bound of the two-sided Month-24 MFD-free survival to be >50%, which was defined as the threshold for the result to be
considered clinically meaningful. 22
MFD-free survival at Month 24 with eli-cel was comparable to that seen in the TPES population (n = 27) treated with allo-HSCT in study ALD-103 (77.8% [95% CI 52.4–93.6]).11 However, within this population
there were clear differences in outcomes based on donor source, with higher rates of MFD-free survival observed in patients who had an MSD (n = 10) (88.9% [51.8–99.7]) than in those who did not (n = 17) (66.7% [29.9–92.5]).11 The latter of which reflects the population considered as part of the eli-cel label.
Consequently, comparing KM-estimated MFD-free survival over time between eli-cel and a broader group of patients in ALD-103, established that MFD-free survival rates were similar between eli-cel and the TPES and TPE MSD populations, but significantly greater with eli -cel than the overall TPES and
TPE populations, as well as each of the NMSD populations (Table 7.13) (see Tables 2.1.1.1.1, 2.1.1.2.1, 2.1.1.1.2, 2.1.1.2, 2.1.1.2.2 and 2.1.1.1.2 of D120 Interstudy report).7
Important to note, is that while MFD-free survival for eli-cel was maintained between Months 24 and
48, estimated rates of MFD-free survival for allo-HSCT declined over this period (
Figure 7.8).7 This decline was mainly due to incompatibility of donor and recipient, with failures due to secondary graft rejection, or GVHD causing mortality.112
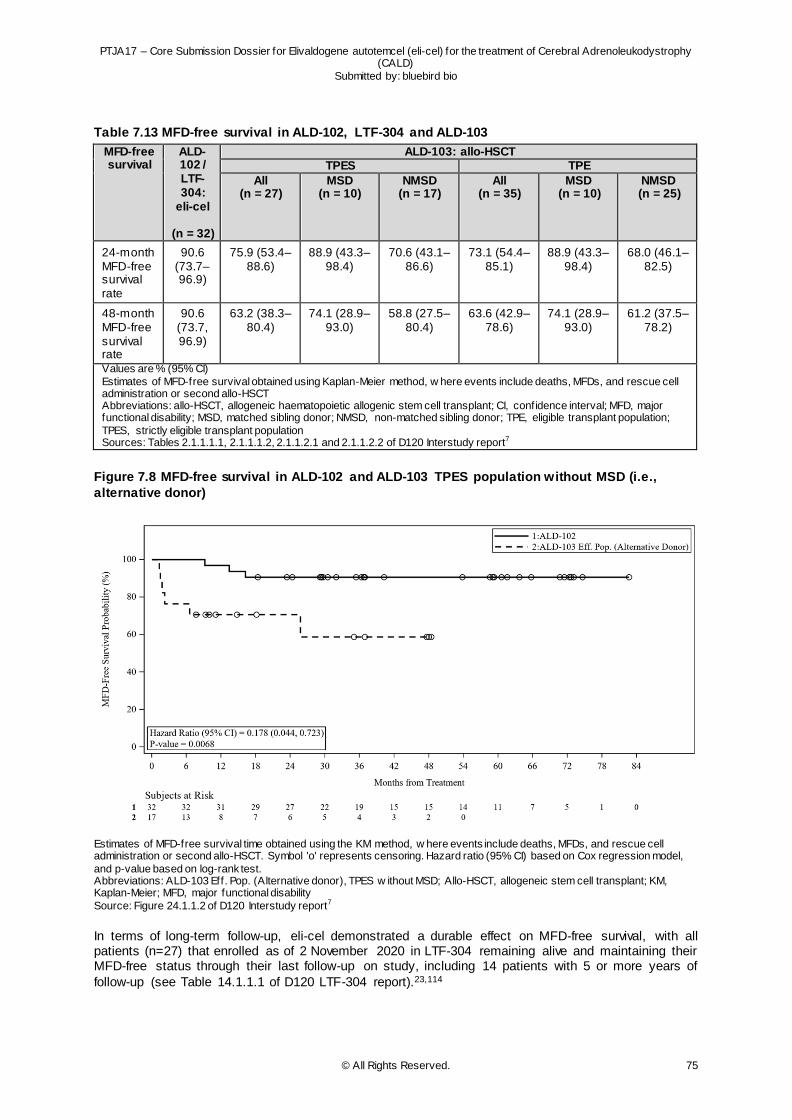
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 75
Table 7.13 MFD-free survival in ALD-102, LTF-304 and ALD-103
MFD-free survival
ALD-102 / LTF-304:
eli-cel
(n = 32)
ALD-103: allo-HSCT TPES TPE
All (n = 27)
MSD (n = 10)
NMSD (n = 17)
All (n = 35)
MSD (n = 10)
NMSD (n = 25)
24-month MFD-free survival rate
90.6 (73.7–96.9)
75.9 (53.4–88.6)
88.9 (43.3–98.4)
70.6 (43.1–86.6)
73.1 (54.4–85.1)
88.9 (43.3–98.4)
68.0 (46.1–82.5)
48-month MFD-free survival rate
90.6 (73.7, 96.9)
63.2 (38.3–80.4)
74.1 (28.9–93.0)
58.8 (27.5–80.4)
63.6 (42.9–78.6)
74.1 (28.9–93.0)
61.2 (37.5–78.2)
Values are % (95% CI) Estimates of MFD-free survival obtained using Kaplan-Meier method, w here events include deaths, MFDs, and rescue cell administration or second allo-HSCT Abbreviations: allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, confidence interval; MFD, major functional disability; MSD, matched sibling donor; NMSD, non-matched sibling donor; TPE, eligible transplant population;
TPES, strictly eligible transplant population Sources: Tables 2.1.1.1.1, 2.1.1.1.2, 2.1.1.2.1 and 2.1.1.2.2 of D120 Interstudy report7
Figure 7.8 MFD-free survival in ALD-102 and ALD-103 TPES population without MSD (i.e.,
alternative donor)
Estimates of MFD-free survival time obtained using the KM method, w here events include deaths, MFDs, and rescue cell administration or second allo-HSCT. Symbol 'o' represents censoring. Hazard ratio (95% CI) based on Cox regression model,
and p-value based on log-rank test. Abbreviations: ALD-103 Eff. Pop. (Alternative donor), TPES w ithout MSD; Allo-HSCT, allogeneic stem cell transplant; KM, Kaplan-Meier; MFD, major functional disability Source: Figure 24.1.1.2 of D120 Interstudy report7
In terms of long-term follow-up, eli-cel demonstrated a durable effect on MFD-free survival, with all patients (n=27) that enrolled as of 2 November 2020 in LTF-304 remaining alive and maintaining their MFD-free status through their last follow-up on study, including 14 patients with 5 or more years of
follow-up (see Table 14.1.1.1 of D120 LTF-304 report).23,114
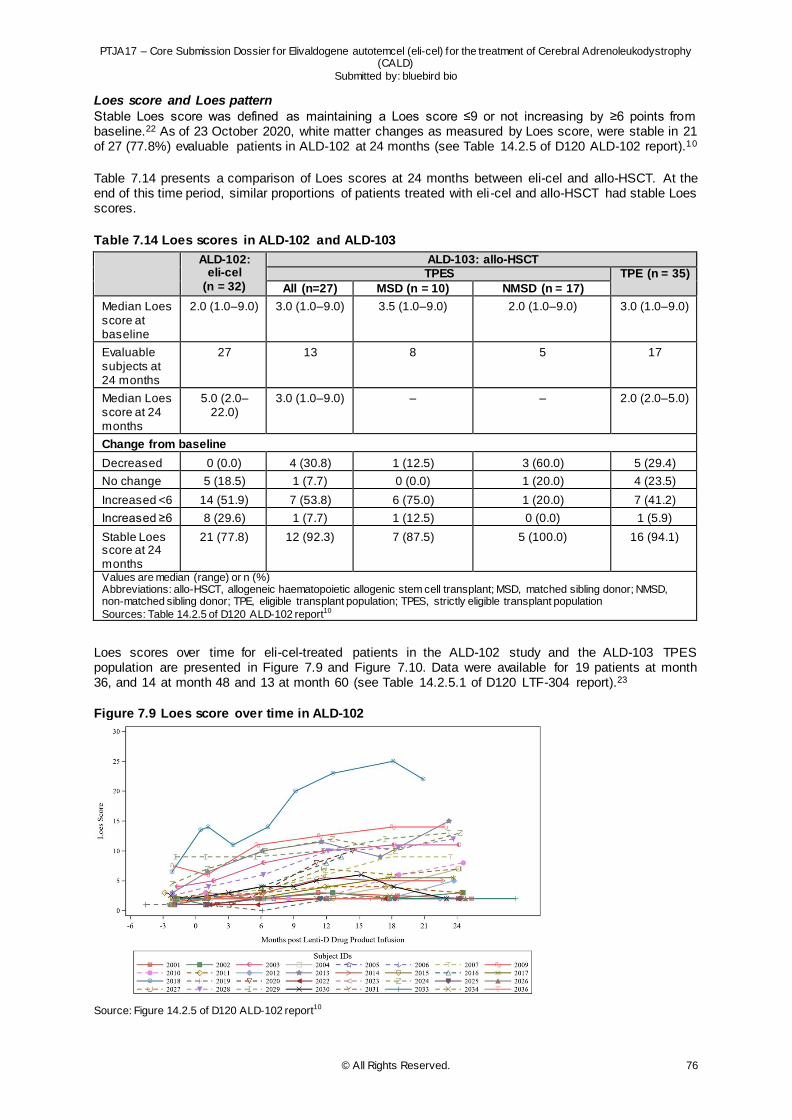
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 76
Loes score and Loes pattern
Stable Loes score was defined as maintaining a Loes score ≤9 or not increasing by ≥6 points from baseline.22 As of 23 October 2020, white matter changes as measured by Loes score, were stable in 21 of 27 (77.8%) evaluable patients in ALD-102 at 24 months (see Table 14.2.5 of D120 ALD-102 report).10
Table 7.14 presents a comparison of Loes scores at 24 months between eli-cel and allo-HSCT. At the end of this time period, similar proportions of patients treated with eli-cel and allo-HSCT had stable Loes scores.
Table 7.14 Loes scores in ALD-102 and ALD-103
ALD-102: eli-cel
(n = 32)
ALD-103: allo-HSCT TPES TPE (n = 35)
All (n=27) MSD (n = 10) NMSD (n = 17)
Median Loes score at baseline
2.0 (1.0–9.0) 3.0 (1.0–9.0) 3.5 (1.0–9.0) 2.0 (1.0–9.0) 3.0 (1.0–9.0)
Evaluable subjects at 24 months
27 13 8 5 17
Median Loes score at 24 months
5.0 (2.0–22.0)
3.0 (1.0–9.0) – – 2.0 (2.0–5.0)
Change from baseline
Decreased 0 (0.0) 4 (30.8) 1 (12.5) 3 (60.0) 5 (29.4)
No change 5 (18.5) 1 (7.7) 0 (0.0) 1 (20.0) 4 (23.5)
Increased <6 14 (51.9) 7 (53.8) 6 (75.0) 1 (20.0) 7 (41.2)
Increased ≥6 8 (29.6) 1 (7.7) 1 (12.5) 0 (0.0) 1 (5.9)
Stable Loes score at 24 months
21 (77.8) 12 (92.3) 7 (87.5) 5 (100.0) 16 (94.1)
Values are median (range) or n (%) Abbreviations: allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; MSD, matched sibling donor; NMSD, non-matched sibling donor; TPE, eligible transplant population; TPES, strictly eligible transplant population
Sources: Table 14.2.5 of D120 ALD-102 report10
Loes scores over time for eli-cel-treated patients in the ALD-102 study and the ALD-103 TPES population are presented in Figure 7.9 and Figure 7.10. Data were available for 19 patients at month 36, and 14 at month 48 and 13 at month 60 (see Table 14.2.5.1 of D120 LTF-304 report).23
Figure 7.9 Loes score over time in ALD-102
Source: Figure 14.2.5 of D120 ALD-102 report10
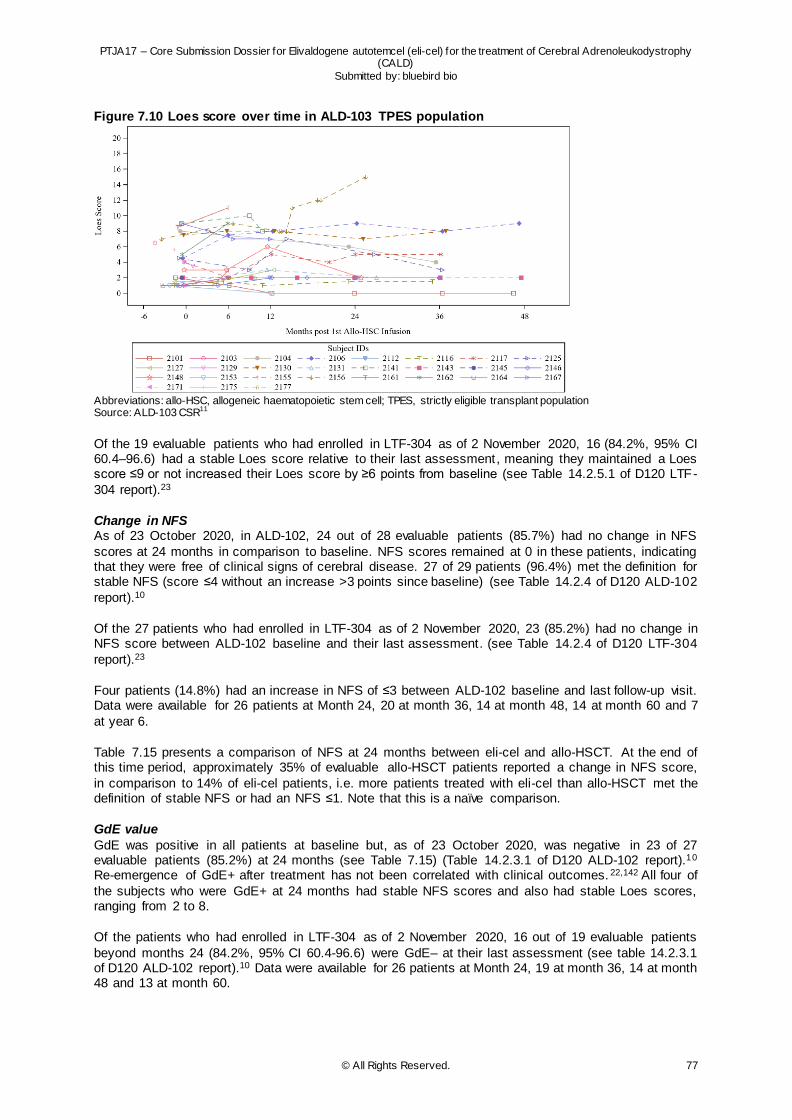
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 77
Figure 7.10 Loes score over time in ALD-103 TPES population
Abbreviations: allo-HSC, allogeneic haematopoietic stem cell; TPES, strictly eligible transplant population Source: ALD-103 CSR11
Of the 19 evaluable patients who had enrolled in LTF-304 as of 2 November 2020, 16 (84.2%, 95% CI 60.4–96.6) had a stable Loes score relative to their last assessment, meaning they maintained a Loes score ≤9 or not increased their Loes score by ≥6 points from baseline (see Table 14.2.5.1 of D120 LTF-
304 report).23
Change in NFS As of 23 October 2020, in ALD-102, 24 out of 28 evaluable patients (85.7%) had no change in NFS
scores at 24 months in comparison to baseline. NFS scores remained at 0 in these patients, indicating that they were free of clinical signs of cerebral disease. 27 of 29 patients (96.4%) met the definition for stable NFS (score ≤4 without an increase >3 points since baseline) (see Table 14.2.4 of D120 ALD-102
report).10
Of the 27 patients who had enrolled in LTF-304 as of 2 November 2020, 23 (85.2%) had no change in NFS score between ALD-102 baseline and their last assessment. (see Table 14.2.4 of D120 LTF-304
report).23
Four patients (14.8%) had an increase in NFS of ≤3 between ALD-102 baseline and last follow-up visit. Data were available for 26 patients at Month 24, 20 at month 36, 14 at month 48, 14 at month 60 and 7
at year 6.
Table 7.15 presents a comparison of NFS at 24 months between eli-cel and allo-HSCT. At the end of this time period, approximately 35% of evaluable allo-HSCT patients reported a change in NFS score,
in comparison to 14% of eli-cel patients, i.e. more patients treated with eli-cel than allo-HSCT met the definition of stable NFS or had an NFS ≤1. Note that this is a naïve comparison.
GdE value
GdE was positive in all patients at baseline but, as of 23 October 2020, was negative in 23 of 27 evaluable patients (85.2%) at 24 months (see Table 7.15) (Table 14.2.3.1 of D120 ALD-102 report).10 Re-emergence of GdE+ after treatment has not been correlated with clinical outcomes. 22,142 All four of
the subjects who were GdE+ at 24 months had stable NFS scores and also had stable Loes scores, ranging from 2 to 8.
Of the patients who had enrolled in LTF-304 as of 2 November 2020, 16 out of 19 evaluable patients
beyond months 24 (84.2%, 95% CI 60.4-96.6) were GdE– at their last assessment (see table 14.2.3.1 of D120 ALD-102 report).10 Data were available for 26 patients at Month 24, 19 at month 36, 14 at month 48 and 13 at month 60.
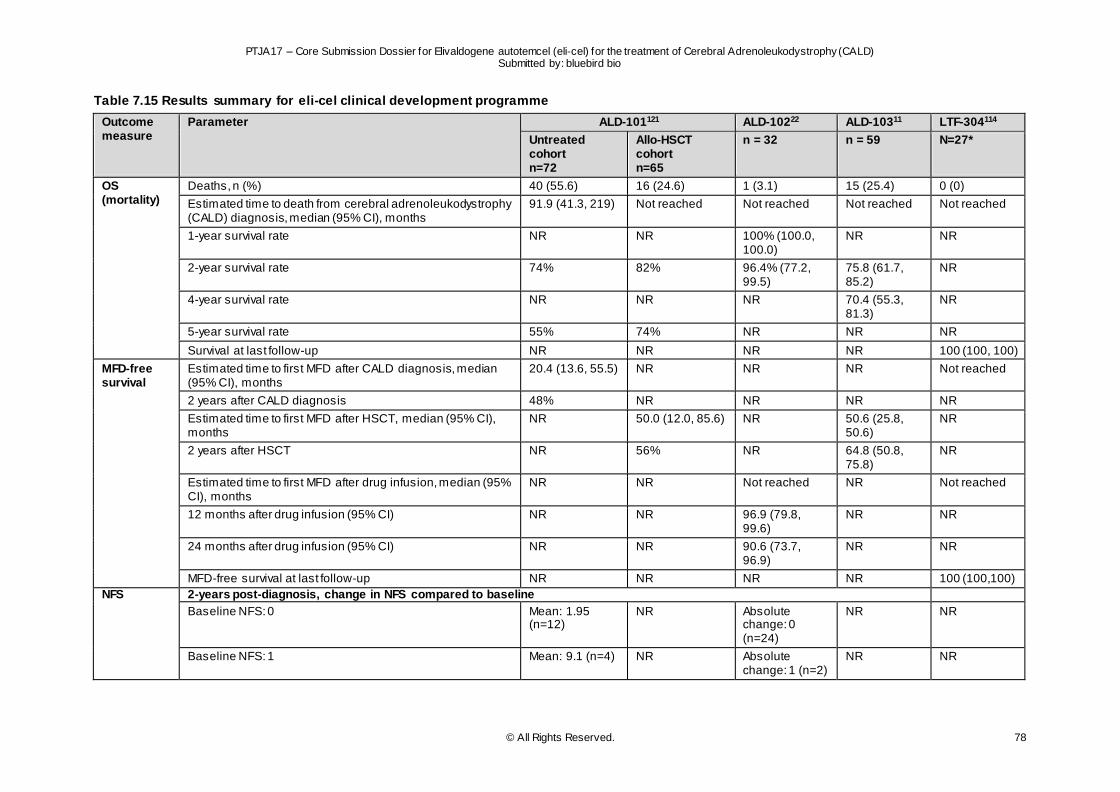
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 78
Table 7.15 Results summary for eli-cel clinical development programme
Outcome measure
Parameter ALD-101121 ALD-10222 ALD-10311 LTF-304114
Untreated cohort n=72
Allo-HSCT cohort n=65
n = 32 n = 59 N=27*
OS (mortality)
Deaths, n (%) 40 (55.6) 16 (24.6) 1 (3.1) 15 (25.4) 0 (0)
Estimated time to death from cerebral adrenoleukodystrophy (CALD) diagnosis, median (95% CI), months
91.9 (41.3, 219) Not reached Not reached Not reached Not reached
1-year survival rate NR NR 100% (100.0, 100.0)
NR NR
2-year survival rate 74% 82% 96.4% (77.2, 99.5)
75.8 (61.7, 85.2)
NR
4-year survival rate NR NR NR 70.4 (55.3, 81.3)
NR
5-year survival rate 55% 74% NR NR NR
Survival at last follow-up NR NR NR NR 100 (100, 100)
MFD-free survival
Estimated time to first MFD after CALD diagnosis, median (95% CI), months
20.4 (13.6, 55.5) NR NR NR Not reached
2 years after CALD diagnosis 48% NR NR NR NR
Estimated time to first MFD after HSCT, median (95% CI), months
NR 50.0 (12.0, 85.6) NR 50.6 (25.8, 50.6)
NR
2 years after HSCT NR 56% NR 64.8 (50.8, 75.8)
NR
Estimated time to first MFD after drug infusion, median (95% CI), months
NR NR Not reached NR Not reached
12 months after drug infusion (95% CI) NR NR 96.9 (79.8, 99.6)
NR NR
24 months after drug infusion (95% CI) NR NR 90.6 (73.7, 96.9)
NR NR
MFD-free survival at last follow-up NR NR NR NR 100 (100,100)
NFS 2-years post-diagnosis, change in NFS compared to baseline
Baseline NFS: 0 Mean: 1.95 (n=12)
NR Absolute change: 0 (n=24)
NR NR
Baseline NFS: 1 Mean: 9.1 (n=4) NR Absolute change: 1 (n=2)
NR NR
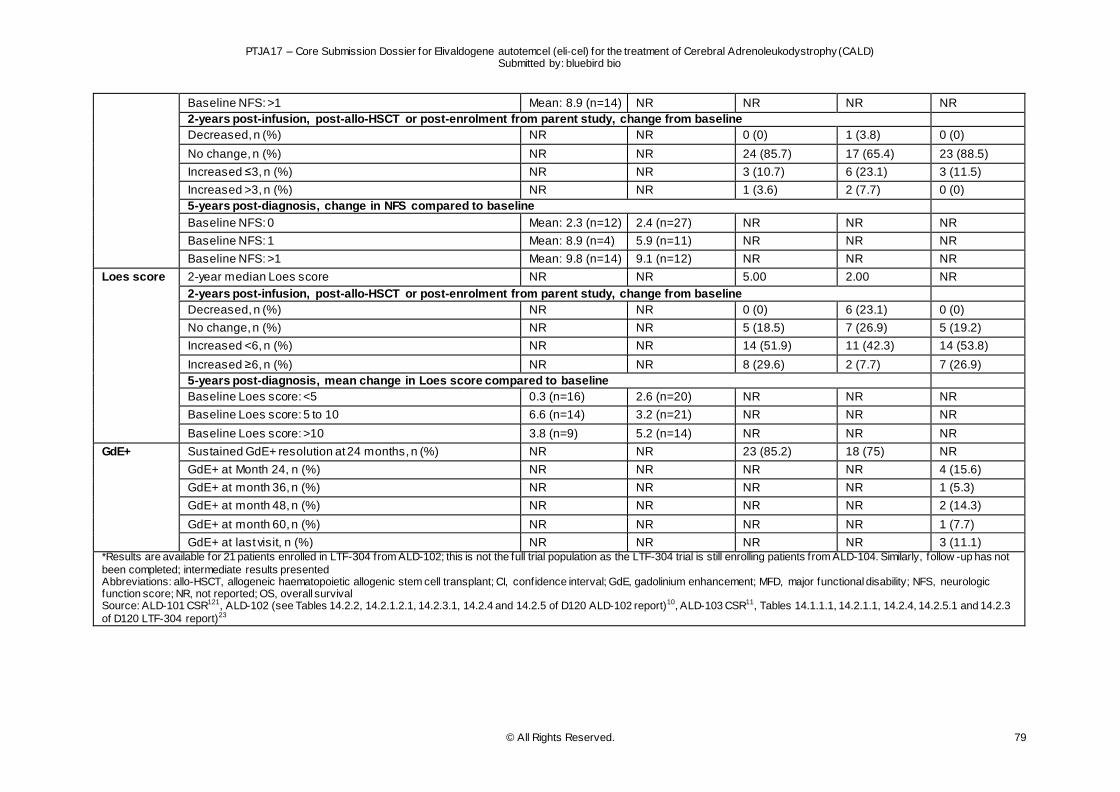
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 79
Baseline NFS: >1 Mean: 8.9 (n=14) NR NR NR NR
2-years post-infusion, post-allo-HSCT or post-enrolment from parent study, change from baseline
Decreased, n (%) NR NR 0 (0) 1 (3.8) 0 (0)
No change, n (%) NR NR 24 (85.7) 17 (65.4) 23 (88.5)
Increased ≤3, n (%) NR NR 3 (10.7) 6 (23.1) 3 (11.5)
Increased >3, n (%) NR NR 1 (3.6) 2 (7.7) 0 (0)
5-years post-diagnosis, change in NFS compared to baseline
Baseline NFS: 0 Mean: 2.3 (n=12) 2.4 (n=27) NR NR NR
Baseline NFS: 1 Mean: 8.9 (n=4) 5.9 (n=11) NR NR NR
Baseline NFS: >1 Mean: 9.8 (n=14) 9.1 (n=12) NR NR NR
Loes score 2-year median Loes score NR NR 5.00 2.00 NR
2-years post-infusion, post-allo-HSCT or post-enrolment from parent study, change from baseline
Decreased, n (%) NR NR 0 (0) 6 (23.1) 0 (0)
No change, n (%) NR NR 5 (18.5) 7 (26.9) 5 (19.2)
Increased <6, n (%) NR NR 14 (51.9) 11 (42.3) 14 (53.8)
Increased ≥6, n (%) NR NR 8 (29.6) 2 (7.7) 7 (26.9)
5-years post-diagnosis, mean change in Loes score compared to baseline
Baseline Loes score: <5 0.3 (n=16) 2.6 (n=20) NR NR NR
Baseline Loes score: 5 to 10 6.6 (n=14) 3.2 (n=21) NR NR NR
Baseline Loes score: >10 3.8 (n=9) 5.2 (n=14) NR NR NR
GdE+ Sustained GdE+ resolution at 24 months, n (%) NR NR 23 (85.2) 18 (75) NR
GdE+ at Month 24, n (%) NR NR NR NR 4 (15.6)
GdE+ at month 36, n (%) NR NR NR NR 1 (5.3)
GdE+ at month 48, n (%) NR NR NR NR 2 (14.3)
GdE+ at month 60, n (%) NR NR NR NR 1 (7.7)
GdE+ at last visit, n (%) NR NR NR NR 3 (11.1) *Results are available for 21 patients enrolled in LTF-304 from ALD-102; this is not the full trial population as the LTF-304 trial is still enrolling patients from ALD-104. Similarly, follow -up has not
been completed; intermediate results presented Abbreviations: allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, confidence interval; GdE, gadolinium enhancement; MFD, major functional disability; NFS, neurologic function score; NR, not reported; OS, overall survival Source: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3
of D120 LTF-304 report)23
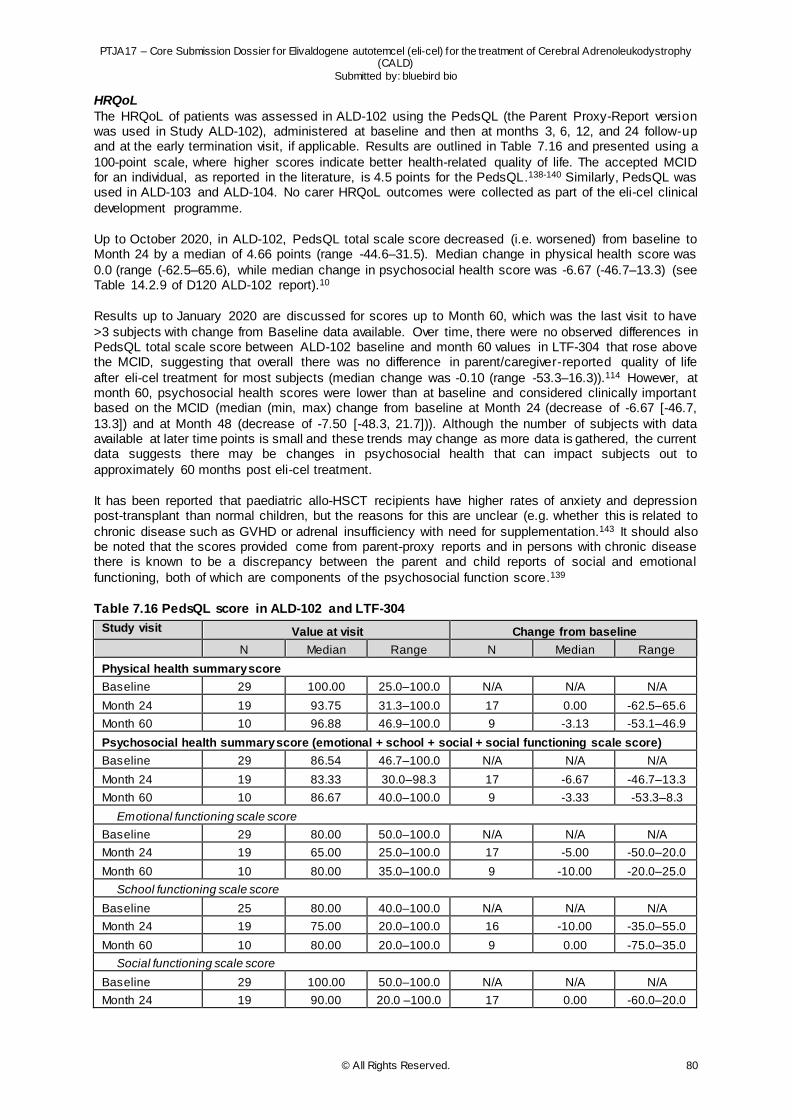
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 80
HRQoL
The HRQoL of patients was assessed in ALD-102 using the PedsQL (the Parent Proxy-Report version was used in Study ALD-102), administered at baseline and then at months 3, 6, 12, and 24 follow-up and at the early termination visit, if applicable. Results are outlined in Table 7.16 and presented using a
100-point scale, where higher scores indicate better health-related quality of life. The accepted MCID for an individual, as reported in the literature, is 4.5 points for the PedsQL.138-140 Similarly, PedsQL was used in ALD-103 and ALD-104. No carer HRQoL outcomes were collected as part of the eli-cel clinical
development programme.
Up to October 2020, in ALD-102, PedsQL total scale score decreased (i.e. worsened) from baseline to Month 24 by a median of 4.66 points (range -44.6–31.5). Median change in physical health score was
0.0 (range (-62.5–65.6), while median change in psychosocial health score was -6.67 (-46.7–13.3) (see Table 14.2.9 of D120 ALD-102 report).10
Results up to January 2020 are discussed for scores up to Month 60, which was the last visit to have
>3 subjects with change from Baseline data available. Over time, there were no observed differences in PedsQL total scale score between ALD-102 baseline and month 60 values in LTF-304 that rose above the MCID, suggesting that overall there was no difference in parent/caregiver-reported quality of life
after eli-cel treatment for most subjects (median change was -0.10 (range -53.3–16.3)).114 However, at month 60, psychosocial health scores were lower than at baseline and considered clinically important based on the MCID (median (min, max) change from baseline at Month 24 (decrease of -6.67 [-46.7,
13.3]) and at Month 48 (decrease of -7.50 [-48.3, 21.7])). Although the number of subjects with data available at later time points is small and these trends may change as more data is gathered, the current data suggests there may be changes in psychosocial health that can impact subjects out to
approximately 60 months post eli-cel treatment.
It has been reported that paediatric allo-HSCT recipients have higher rates of anxiety and depression post-transplant than normal children, but the reasons for this are unclear (e.g. whether this is related to
chronic disease such as GVHD or adrenal insufficiency with need for supplementation.143 It should also be noted that the scores provided come from parent-proxy reports and in persons with chronic disease there is known to be a discrepancy between the parent and child reports of social and emotional
functioning, both of which are components of the psychosocial function score.139
Table 7.16 PedsQL score in ALD-102 and LTF-304
Study visit Value at visit Change from baseline
N Median Range N Median Range
Physical health summary score
Baseline 29 100.00 25.0–100.0 N/A N/A N/A
Month 24 19 93.75 31.3–100.0 17 0.00 -62.5–65.6
Month 60 10 96.88 46.9–100.0 9 -3.13 -53.1–46.9
Psychosocial health summary score (emotional + school + social + social functioning scale score)
Baseline 29 86.54 46.7–100.0 N/A N/A N/A
Month 24 19 83.33 30.0–98.3 17 -6.67 -46.7–13.3
Month 60 10 86.67 40.0–100.0 9 -3.33 -53.3–8.3
Emotional functioning scale score
Baseline 29 80.00 50.0–100.0 N/A N/A N/A
Month 24 19 65.00 25.0–100.0 17 -5.00 -50.0–20.0
Month 60 10 80.00 35.0–100.0 9 -10.00 -20.0–25.0
School functioning scale score
Baseline 25 80.00 40.0–100.0 N/A N/A N/A
Month 24 19 75.00 20.0–100.0 16 -10.00 -35.0–55.0
Month 60 10 80.00 20.0–100.0 9 0.00 -75.0–35.0
Social functioning scale score
Baseline 29 100.00 50.0–100.0 N/A N/A N/A
Month 24 19 90.00 20.0 –100.0 17 0.00 -60.0–20.0
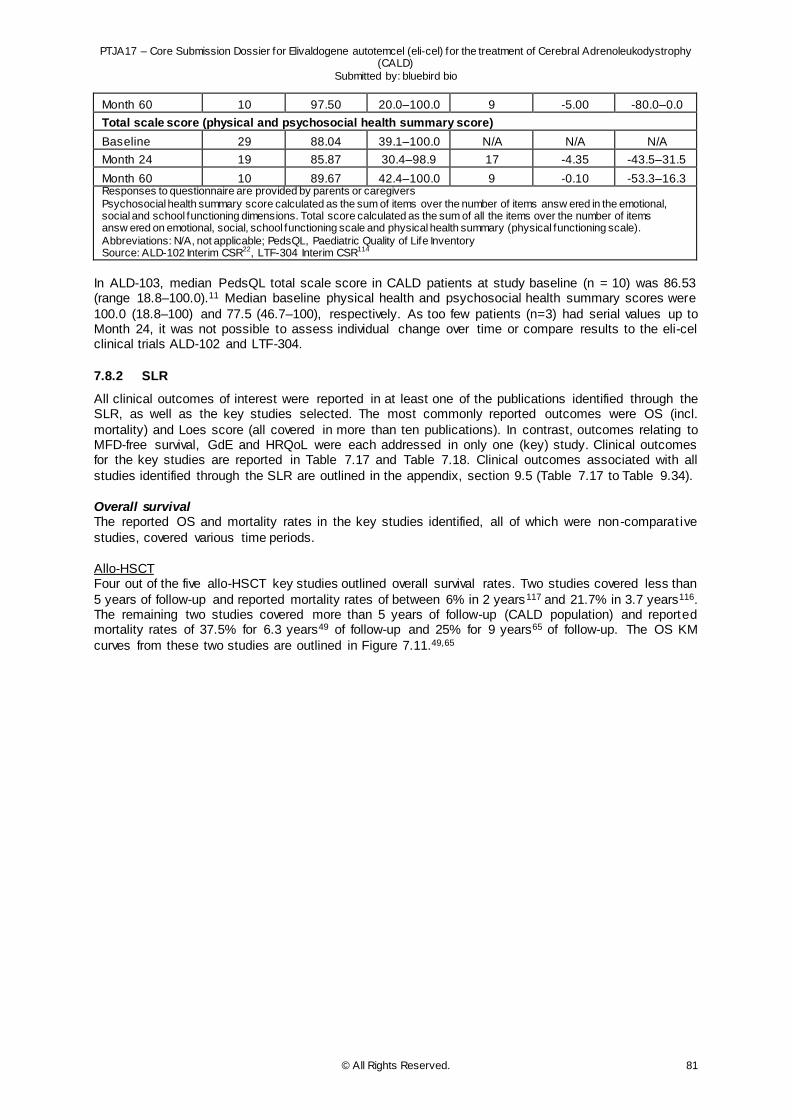
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 81
Month 60 10 97.50 20.0–100.0 9 -5.00 -80.0–0.0
Total scale score (physical and psychosocial health summary score)
Baseline 29 88.04 39.1–100.0 N/A N/A N/A
Month 24 19 85.87 30.4–98.9 17 -4.35 -43.5–31.5
Month 60 10 89.67 42.4–100.0 9 -0.10 -53.3–16.3 Responses to questionnaire are provided by parents or caregivers Psychosocial health summary score calculated as the sum of items over the number of items answ ered in the emotional, social and school functioning dimensions. Total score calculated as the sum of all the items over the number of items answ ered on emotional, social, school functioning scale and physical health summary (physical functioning scale). Abbreviations: N/A, not applicable; PedsQL, Paediatric Quality of Life Inventory Source: ALD-102 Interim CSR22, LTF-304 Interim CSR114
In ALD-103, median PedsQL total scale score in CALD patients at study baseline (n = 10) was 86.53 (range 18.8–100.0).11 Median baseline physical health and psychosocial health summary scores were
100.0 (18.8–100) and 77.5 (46.7–100), respectively. As too few patients (n=3) had serial values up to Month 24, it was not possible to assess individual change over time or compare results to the eli-cel clinical trials ALD-102 and LTF-304.
7.8.2 SLR
All clinical outcomes of interest were reported in at least one of the publications identified through the SLR, as well as the key studies selected. The most commonly reported outcomes were OS (incl.
mortality) and Loes score (all covered in more than ten publications). In contrast, outcomes relating to MFD-free survival, GdE and HRQoL were each addressed in only one (key) study. Clinical outcomes for the key studies are reported in Table 7.17 and Table 7.18. Clinical outcomes associated with all
studies identified through the SLR are outlined in the appendix, section 9.5 (Table 7.17 to Table 9.34).
Overall survival The reported OS and mortality rates in the key studies identified, all of which were non-comparat ive
studies, covered various time periods.
Allo-HSCT Four out of the five allo-HSCT key studies outlined overall survival rates. Two studies covered less than
5 years of follow-up and reported mortality rates of between 6% in 2 years117 and 21.7% in 3.7 years116. The remaining two studies covered more than 5 years of follow-up (CALD population) and reported mortality rates of 37.5% for 6.3 years49 of follow-up and 25% for 9 years65 of follow-up. The OS KM
curves from these two studies are outlined in Figure 7.11.49,65
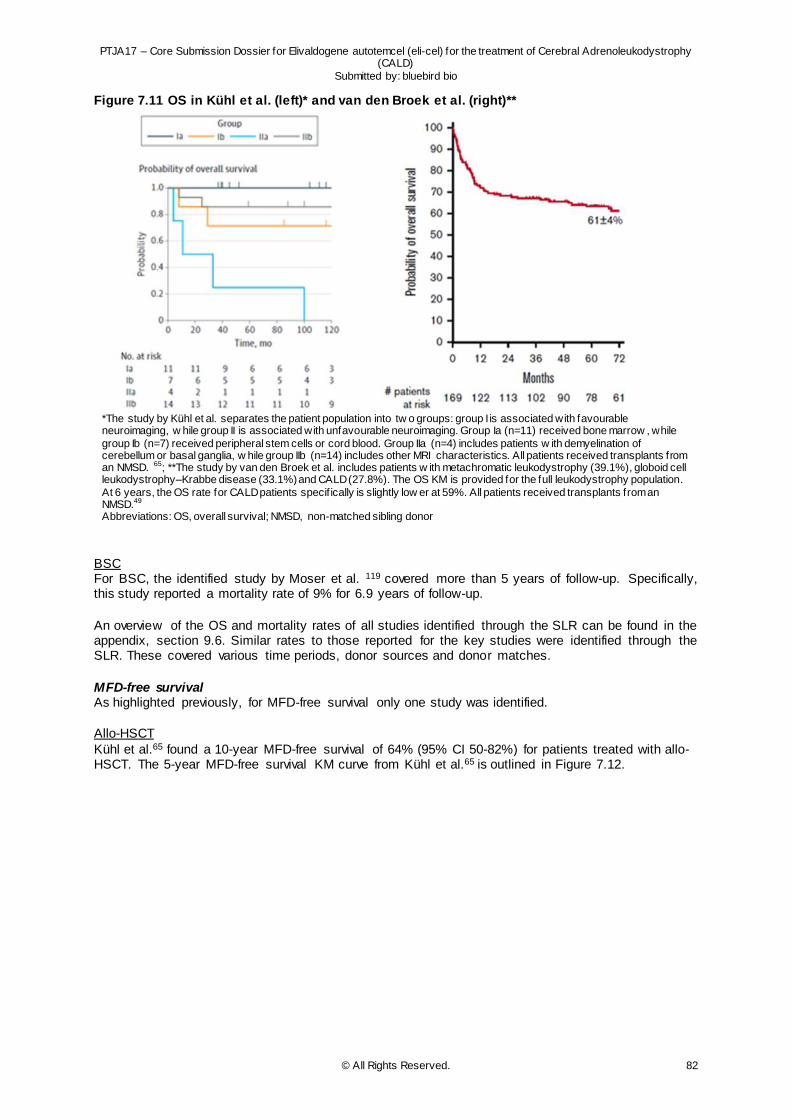
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 82
Figure 7.11 OS in Kühl et al. (left)* and van den Broek et al. (right)**
*The study by Kühl et al. separates the patient population into tw o groups: group I is associated with favourable neuroimaging, w hile group II is associated with unfavourable neuroimaging. Group Ia (n=11) received bone marrow , while
group Ib (n=7) received peripheral stem cells or cord blood. Group IIa (n=4) includes patients w ith demyelination of cerebellum or basal ganglia, w hile group IIb (n=14) includes other MRI characteristics. All patients received transplants from an NMSD. 65; **The study by van den Broek et al. includes patients w ith metachromatic leukodystrophy (39.1%), globoid cell leukodystrophy–Krabbe disease (33.1%) and CALD (27.8%). The OS KM is provided for the full leukodystrophy population.
At 6 years, the OS rate for CALD patients specif ically is slightly low er at 59%. All patients received transplants from an NMSD.49 Abbreviations: OS, overall survival; NMSD, non-matched sibling donor
BSC For BSC, the identified study by Moser et al. 119 covered more than 5 years of follow-up. Specifically, this study reported a mortality rate of 9% for 6.9 years of follow-up.
An overview of the OS and mortality rates of all studies identified through the SLR can be found in the appendix, section 9.6. Similar rates to those reported for the key studies were identified through the SLR. These covered various time periods, donor sources and donor matches.
MFD-free survival As highlighted previously, for MFD-free survival only one study was identified.
Allo-HSCT
Kühl et al.65 found a 10-year MFD-free survival of 64% (95% CI 50-82%) for patients treated with allo-HSCT. The 5-year MFD-free survival KM curve from Kühl et al.65 is outlined in Figure 7.12.
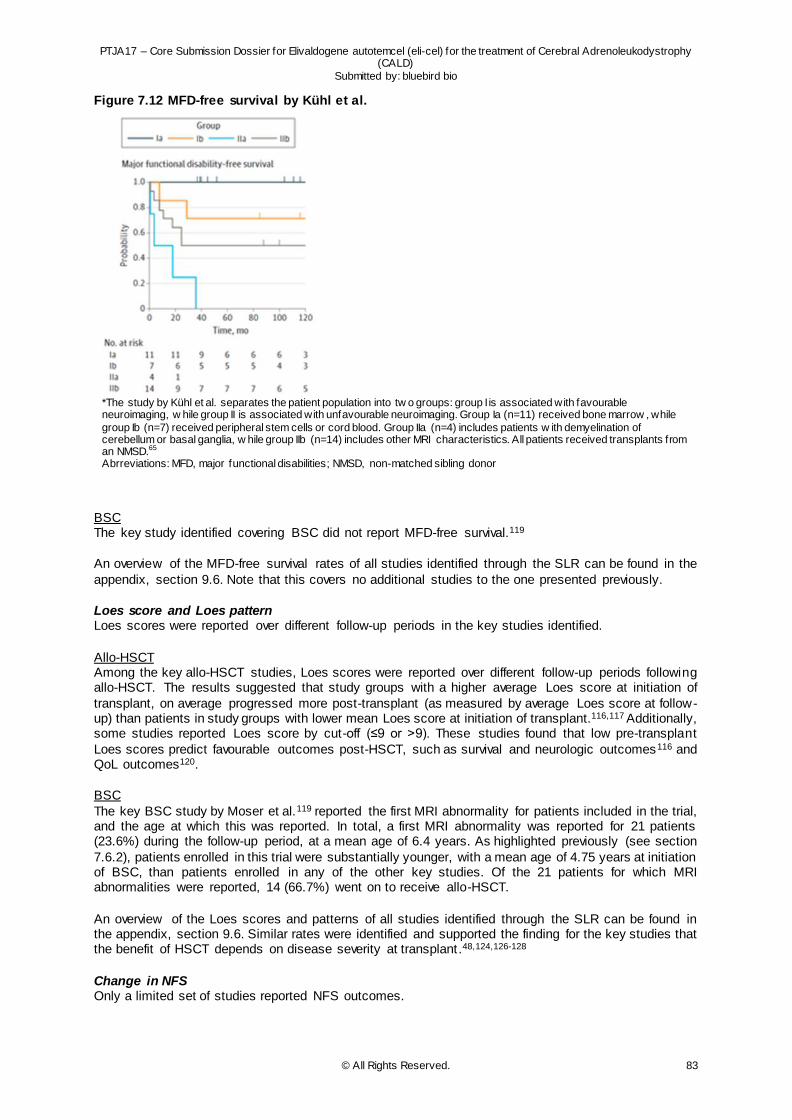
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 83
Figure 7.12 MFD-free survival by Kühl et al.
*The study by Kühl et al. separates the patient population into tw o groups: group I is associated with favourable neuroimaging, w hile group II is associated with unfavourable neuroimaging. Group Ia (n=11) received bone marrow , while
group Ib (n=7) received peripheral stem cells or cord blood. Group IIa (n=4) includes patients w ith demyelination of cerebellum or basal ganglia, w hile group IIb (n=14) includes other MRI characteristics. All patients received transplants from an NMSD.65 Abrreviations: MFD, major functional disabilities; NMSD, non-matched sibling donor
BSC The key study identified covering BSC did not report MFD-free survival.119
An overview of the MFD-free survival rates of all studies identified through the SLR can be found in the
appendix, section 9.6. Note that this covers no additional studies to the one presented previously.
Loes score and Loes pattern Loes scores were reported over different follow-up periods in the key studies identified.
Allo-HSCT Among the key allo-HSCT studies, Loes scores were reported over different follow-up periods following allo-HSCT. The results suggested that study groups with a higher average Loes score at initiation of
transplant, on average progressed more post-transplant (as measured by average Loes score at follow-up) than patients in study groups with lower mean Loes score at initiation of transplant.116,117 Additionally, some studies reported Loes score by cut-off (≤9 or >9). These studies found that low pre-transplant
Loes scores predict favourable outcomes post-HSCT, such as survival and neurologic outcomes116 and QoL outcomes120.
BSC
The key BSC study by Moser et al.119 reported the first MRI abnormality for patients included in the trial, and the age at which this was reported. In total, a first MRI abnormality was reported for 21 patients (23.6%) during the follow-up period, at a mean age of 6.4 years. As highlighted previously (see section
7.6.2), patients enrolled in this trial were substantially younger, with a mean age of 4.75 years at initiation of BSC, than patients enrolled in any of the other key studies. Of the 21 patients for which MRI abnormalities were reported, 14 (66.7%) went on to receive allo-HSCT.
An overview of the Loes scores and patterns of all studies identified through the SLR can be found in the appendix, section 9.6. Similar rates were identified and supported the finding for the key studies that the benefit of HSCT depends on disease severity at transplant.48,124,126-128
Change in NFS Only a limited set of studies reported NFS outcomes.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 84
Allo-HSCT
Of the key allo-HSCT studies, Miller et al.116 and Kühl et al.65 reported an increase in NFS during follow-up. Both studies indicated a progression of symptoms over time following allo-HSCT and suggested this change was more substantial for patients with a higher NFS at baseline. In the study by Kühl, 15/36
patients had stable neuroimaging and event-free survival after the transplant, while, in contrast, the other 18 patients presented more extended demyelination.65
BSC
Moser et al.119 reported that ten patients (11%) developed neurological abnormalities. For four patients, this developed after allo-HSCT, i.e. these patients were initially started on BSC but received allo-HSCT during the follow-up period.
Section 9.6 in the appendix outlines NFS results for the remaining studies identified through the SLR. Note that for the majority of studies, NFS was reported at baseline only.
GdE value
As highlighted previously, only one of the key studies reported GdE.
Allo-HSCT Kühl et al. reported that 35 out of 36 patients showed GdE at baseline.65 At >6 months after HSCT, 2
out of 36 patients showed GdE, indicating that the treatment resolved white matter lesions in most patients.65
BSC
The key study identified covering BSC did not report GdE.119
An overview of GdE results across all studies identified through the SLR can be found in the appendix , section 9.6. Note that the majority of studies reporting GdE values only reported these at baseline, not
at follow-up.
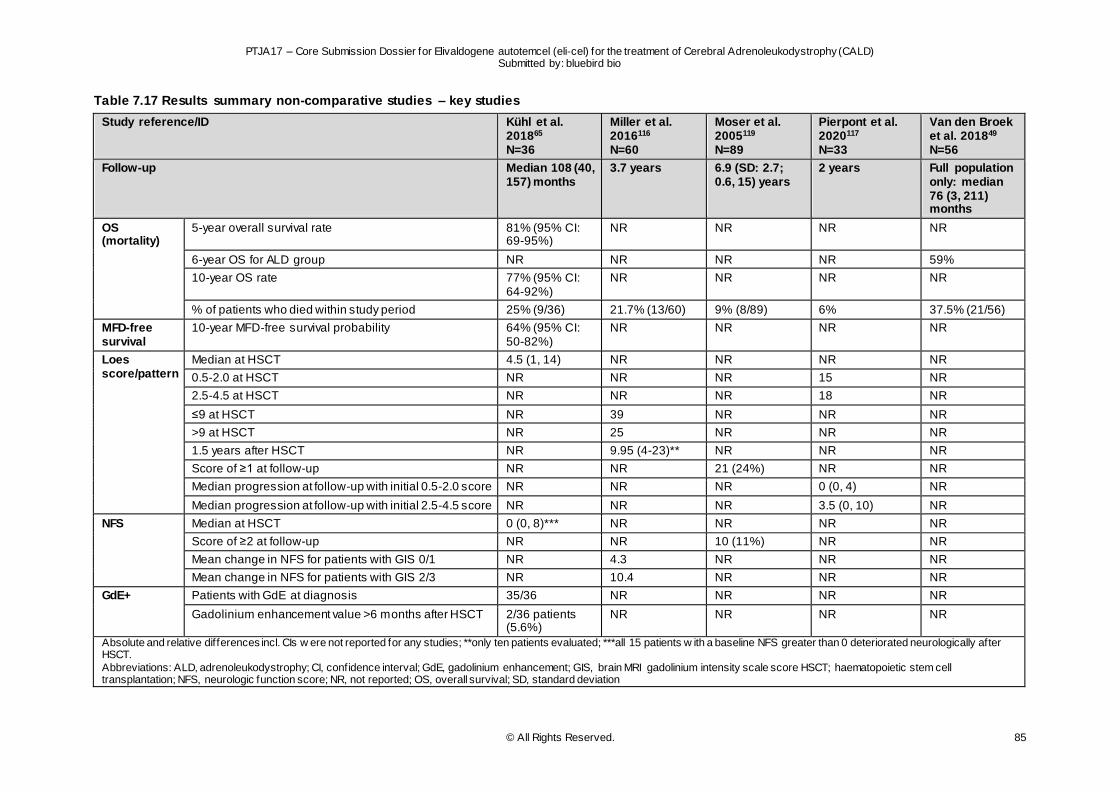
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 85
Table 7.17 Results summary non-comparative studies – key studies
Study reference/ID Kühl et al. 201865 N=36
Miller et al. 2016116 N=60
Moser et al. 2005119 N=89
Pierpont et al. 2020117 N=33
Van den Broek et al. 201849 N=56
Follow-up Median 108 (40, 157) months
3.7 years 6.9 (SD: 2.7; 0.6, 15) years
2 years Full population only: median 76 (3, 211) months
OS (mortality)
5-year overall survival rate 81% (95% CI: 69-95%)
NR NR NR NR
6-year OS for ALD group NR NR NR NR 59%
10-year OS rate 77% (95% CI: 64-92%)
NR NR NR NR
% of patients who died within study period 25% (9/36) 21.7% (13/60) 9% (8/89) 6% 37.5% (21/56)
MFD-free survival
10-year MFD-free survival probability 64% (95% CI: 50-82%)
NR NR NR NR
Loes score/pattern
Median at HSCT 4.5 (1, 14) NR NR NR NR
0.5-2.0 at HSCT NR NR NR 15 NR
2.5-4.5 at HSCT NR NR NR 18 NR
≤9 at HSCT NR 39 NR NR NR
>9 at HSCT NR 25 NR NR NR
1.5 years after HSCT NR 9.95 (4-23)** NR NR NR
Score of ≥1 at follow-up NR NR 21 (24%) NR NR
Median progression at follow-up with initial 0.5-2.0 score NR NR NR 0 (0, 4) NR
Median progression at follow-up with initial 2.5-4.5 score NR NR NR 3.5 (0, 10) NR
NFS Median at HSCT 0 (0, 8)*** NR NR NR NR
Score of ≥2 at follow-up NR NR 10 (11%) NR NR
Mean change in NFS for patients with GIS 0/1 NR 4.3 NR NR NR
Mean change in NFS for patients with GIS 2/3 NR 10.4 NR NR NR
GdE+ Patients with GdE at diagnosis 35/36 NR NR NR NR
Gadolinium enhancement value >6 months after HSCT
2/36 patients (5.6%)
NR NR NR NR
Absolute and relative differences incl. CIs w ere not reported for any studies; **only ten patients evaluated; ***all 15 patients w ith a baseline NFS greater than 0 deteriorated neurologically after HSCT.
Abbreviations: ALD, adrenoleukodystrophy; CI, confidence interval; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score HSCT; haematopoietic stem cell transplantation; NFS, neurologic function score; NR, not reported; OS, overall survival; SD, standard deviation
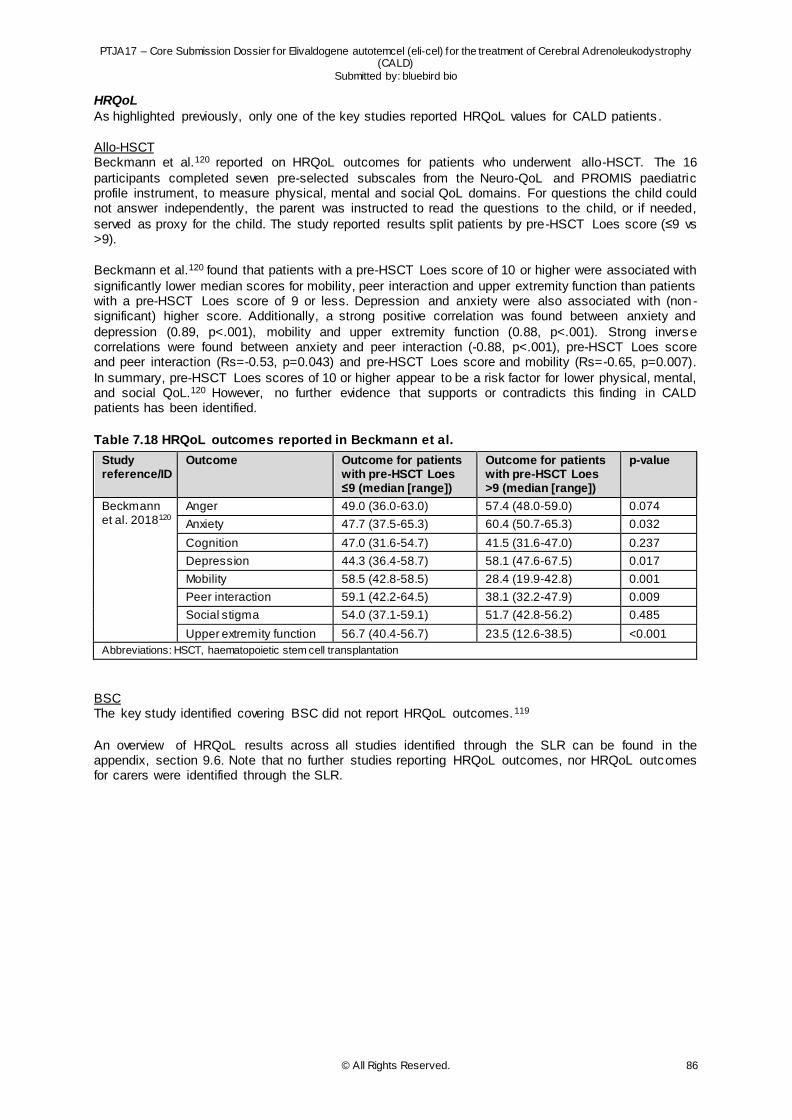
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 86
HRQoL
As highlighted previously, only one of the key studies reported HRQoL values for CALD patients .
Allo-HSCT Beckmann et al.120 reported on HRQoL outcomes for patients who underwent allo-HSCT. The 16
participants completed seven pre-selected subscales from the Neuro-QoL and PROMIS paediatric profile instrument, to measure physical, mental and social QoL domains. For questions the child could not answer independently, the parent was instructed to read the questions to the child, or if needed,
served as proxy for the child. The study reported results split patients by pre-HSCT Loes score (≤9 vs >9).
Beckmann et al.120 found that patients with a pre-HSCT Loes score of 10 or higher were associated with
significantly lower median scores for mobility, peer interaction and upper extremity function than patients with a pre-HSCT Loes score of 9 or less. Depression and anxiety were also associated with (non -significant) higher score. Additionally, a strong positive correlation was found between anxiety and
depression (0.89, p<.001), mobility and upper extremity function (0.88, p<.001). Strong inverse correlations were found between anxiety and peer interaction (-0.88, p<.001), pre-HSCT Loes score and peer interaction (Rs=-0.53, p=0.043) and pre-HSCT Loes score and mobility (Rs=-0.65, p=0.007).
In summary, pre-HSCT Loes scores of 10 or higher appear to be a risk factor for lower physical, mental, and social QoL.120 However, no further evidence that supports or contradicts this finding in CALD patients has been identified.
Table 7.18 HRQoL outcomes reported in Beckmann et al.
Study reference/ID
Outcome Outcome for patients with pre-HSCT Loes ≤9 (median [range])
Outcome for patients with pre-HSCT Loes >9 (median [range])
p-value
Beckmann et al. 2018120
Anger 49.0 (36.0-63.0) 57.4 (48.0-59.0) 0.074
Anxiety 47.7 (37.5-65.3) 60.4 (50.7-65.3) 0.032
Cognition 47.0 (31.6-54.7) 41.5 (31.6-47.0) 0.237
Depression 44.3 (36.4-58.7) 58.1 (47.6-67.5) 0.017
Mobility 58.5 (42.8-58.5) 28.4 (19.9-42.8) 0.001
Peer interaction 59.1 (42.2-64.5) 38.1 (32.2-47.9) 0.009
Social stigma 54.0 (37.1-59.1) 51.7 (42.8-56.2) 0.485
Upper extremity function 56.7 (40.4-56.7) 23.5 (12.6-38.5) <0.001
Abbreviations: HSCT, haematopoietic stem cell transplantation
BSC The key study identified covering BSC did not report HRQoL outcomes.119
An overview of HRQoL results across all studies identified through the SLR can be found in the appendix, section 9.6. Note that no further studies reporting HRQoL outcomes, nor HRQoL outcomes for carers were identified through the SLR.
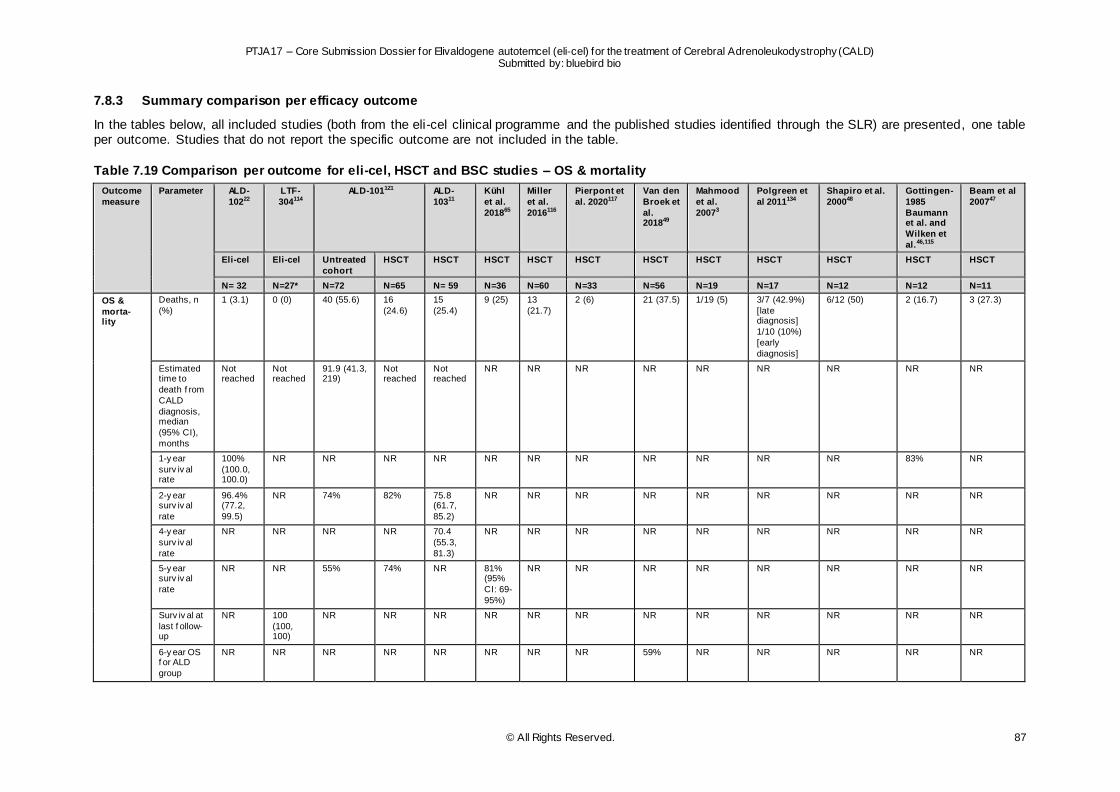
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 87
7.8.3 Summary comparison per efficacy outcome
In the tables below, all included studies (both from the eli-cel clinical programme and the published studies identified through the SLR) are presented, one table per outcome. Studies that do not report the specific outcome are not included in the table.
Table 7.19 Comparison per outcome for eli-cel, HSCT and BSC studies – OS & mortality
Outcome
measure
Parameter ALD-
10222
LTF-
304114
ALD-101121 ALD-
10311
Kühl
et al.
201865
Miller
et al.
2016116
Pierpont et
al. 2020117
Van den
Broek et
al. 201849
Mahmood
et al.
20073
Polgreen et
al 2011134
Shapiro et al.
200048
Gottingen-
1985
Baumann et al. and
Wilken et
al.46,115
Beam et al
200747
Eli-cel Eli-cel Untreated
cohort
HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=36 N=60 N=33 N=56 N=19 N=17 N=12 N=12 N=11
OS &
morta- lity
Deaths, n
(%)
1 (3.1) 0 (0) 40 (55.6) 16
(24.6)
15
(25.4)
9 (25) 13
(21.7)
2 (6) 21 (37.5) 1/19 (5) 3/7 (42.9%)
[late diagnosis]
1/10 (10%)
[early
diagnosis]
6/12 (50) 2 (16.7) 3 (27.3)
Estimated time to
death f rom
CALD
diagnosis, median
(95% CI),
months
Not reached
Not reached
91.9 (41.3, 219)
Not reached
Not reached
NR NR NR NR NR NR NR NR NR
1-y ear
surv iv al rate
100%
(100.0, 100.0)
NR NR NR NR NR NR NR NR NR NR NR 83% NR
2-y ear surv iv al
rate
96.4% (77.2,
99.5)
NR 74% 82% 75.8 (61.7,
85.2)
NR NR NR NR NR NR NR NR NR
4-y ear
surv iv al
rate
NR NR NR NR 70.4
(55.3,
81.3)
NR NR NR NR NR NR NR NR NR
5-y ear surv iv al
rate
NR NR 55% 74% NR 81% (95%
CI: 69-
95%)
NR NR NR NR NR NR NR NR
Surv iv al at
last f ollow-up
NR 100
(100, 100)
NR NR NR NR NR NR NR NR NR NR NR NR
6-y ear OS f or ALD
group
NR NR NR NR NR NR NR NR 59% NR NR NR NR NR
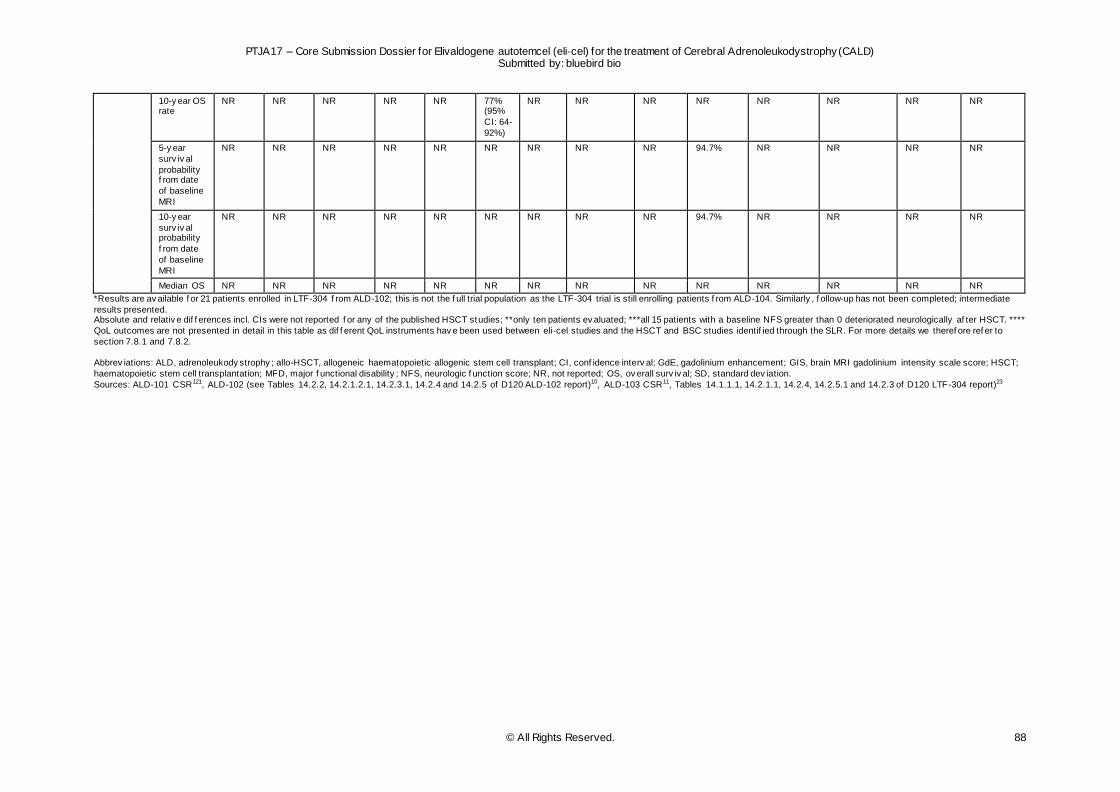
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 88
10-y ear OS rate
NR NR NR NR NR 77% (95%
CI: 64-
92%)
NR NR NR NR NR NR NR NR
5-y ear
surv iv al
probability f rom date
of baseline
MRI
NR NR NR NR NR NR NR NR NR 94.7% NR NR NR NR
10-y ear
surv iv al probability
f rom date
of baseline
MRI
NR NR NR NR NR NR NR NR NR 94.7% NR NR NR NR
Median OS NR NR NR NR NR NR NR NR NR NR NR NR NR NR
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed; intermediate
results presented. Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies; **only ten patients ev aluated; ***all 15 patients with a baseline NFS greater than 0 deteriorated neurologically af ter HSCT. ****
QoL outcomes are not presented in detail in this table as dif f erent QoL instruments hav e been used between eli-cel studies and the HSCT and BSC studies identif ied through the SLR. For more details we theref ore ref er to
section 7.8.1 and 7.8.2.
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score; HSCT;
haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation.
Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
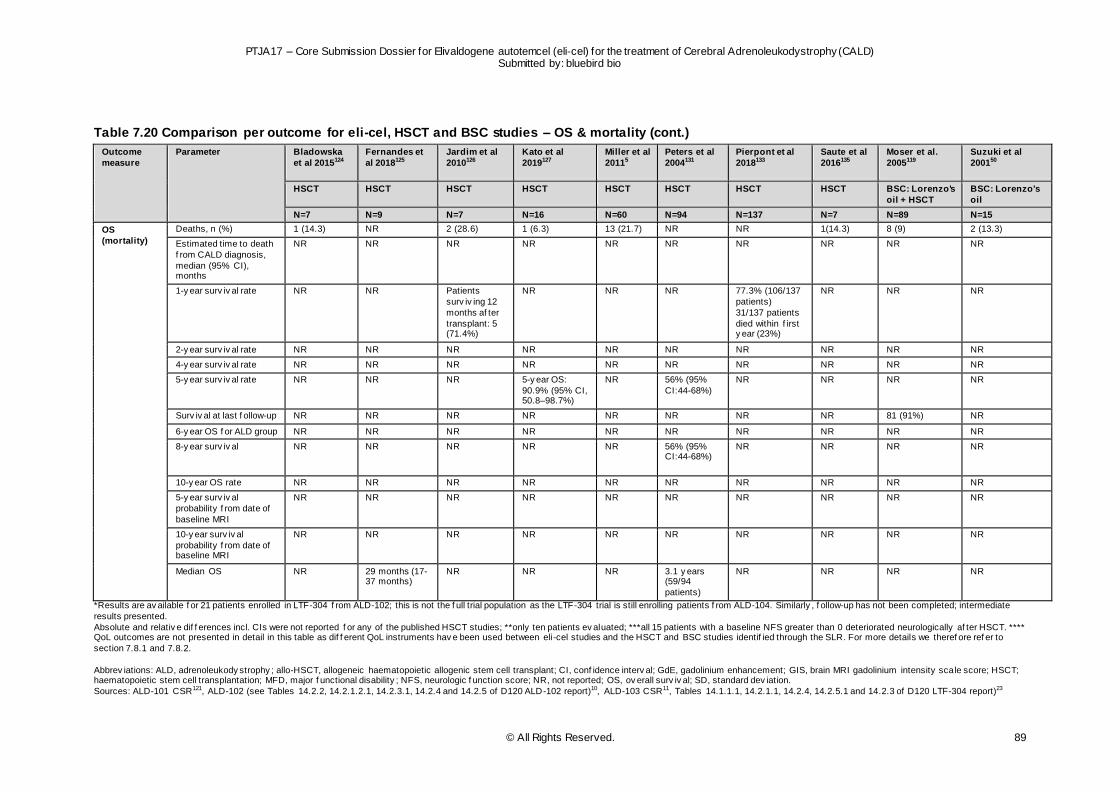
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 89
Table 7.20 Comparison per outcome for eli-cel, HSCT and BSC studies – OS & mortality (cont.)
Outcome
measure
Parameter Bladowska
et al 2015124
Fernandes et
al 2018125
Jardim et al
2010126
Kato et al
2019127
Miller et al
20115
Peters et al
2004131
Pierpont et al
2018133
Saute et al
2016135
Moser et al.
2005119
Suzuki et al
200150
HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT BSC: Lorenzo's
oil + HSCT
BSC: Lorenzo's
oil
N=7 N=9 N=7 N=16 N=60 N=94 N=137 N=7 N=89 N=15
OS
(mortality)
Deaths, n (%) 1 (14.3) NR 2 (28.6) 1 (6.3) 13 (21.7) NR NR 1(14.3) 8 (9) 2 (13.3)
Estimated time to death
f rom CALD diagnosis,
median (95% CI), months
NR NR NR NR NR NR NR NR NR NR
1-y ear surv iv al rate NR NR Patients
surv iv ing 12
months af ter
transplant: 5 (71.4%)
NR NR NR 77.3% (106/137
patients)
31/137 patients
died within f irst y ear (23%)
NR NR NR
2-y ear surv iv al rate NR NR NR NR NR NR NR NR NR NR
4-y ear surv iv al rate NR NR NR NR NR NR NR NR NR NR
5-y ear surv iv al rate NR NR NR 5-y ear OS:
90.9% (95% CI, 50.8–98.7%)
NR 56% (95%
CI:44-68%)
NR NR NR NR
Surv iv al at last f ollow-up NR NR NR NR NR NR NR NR 81 (91%) NR
6-y ear OS f or ALD group NR NR NR NR NR NR NR NR NR NR
8-y ear surv iv al NR NR NR NR NR 56% (95% CI:44-68%)
NR NR NR NR
10-y ear OS rate NR NR NR NR NR NR NR NR NR NR
5-y ear surv iv al
probability f rom date of
baseline MRI
NR NR NR NR NR NR NR NR NR NR
10-y ear surv iv al
probability f rom date of baseline MRI
NR NR NR NR NR NR NR NR NR NR
Median OS NR 29 months (17-37 months)
NR NR NR 3.1 y ears (59/94
patients)
NR NR NR NR
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed; intermediate
results presented.
Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies; **only ten patients ev aluated; ***all 15 patients with a baseline NFS greater than 0 deteriorated neurologically af ter HSCT. **** QoL outcomes are not presented in detail in this table as dif f erent QoL instruments hav e been used between eli-cel studies and the HSCT and BSC studies identif ied through the SLR. For more details we theref ore ref er to
section 7.8.1 and 7.8.2.
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score; HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation.
Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
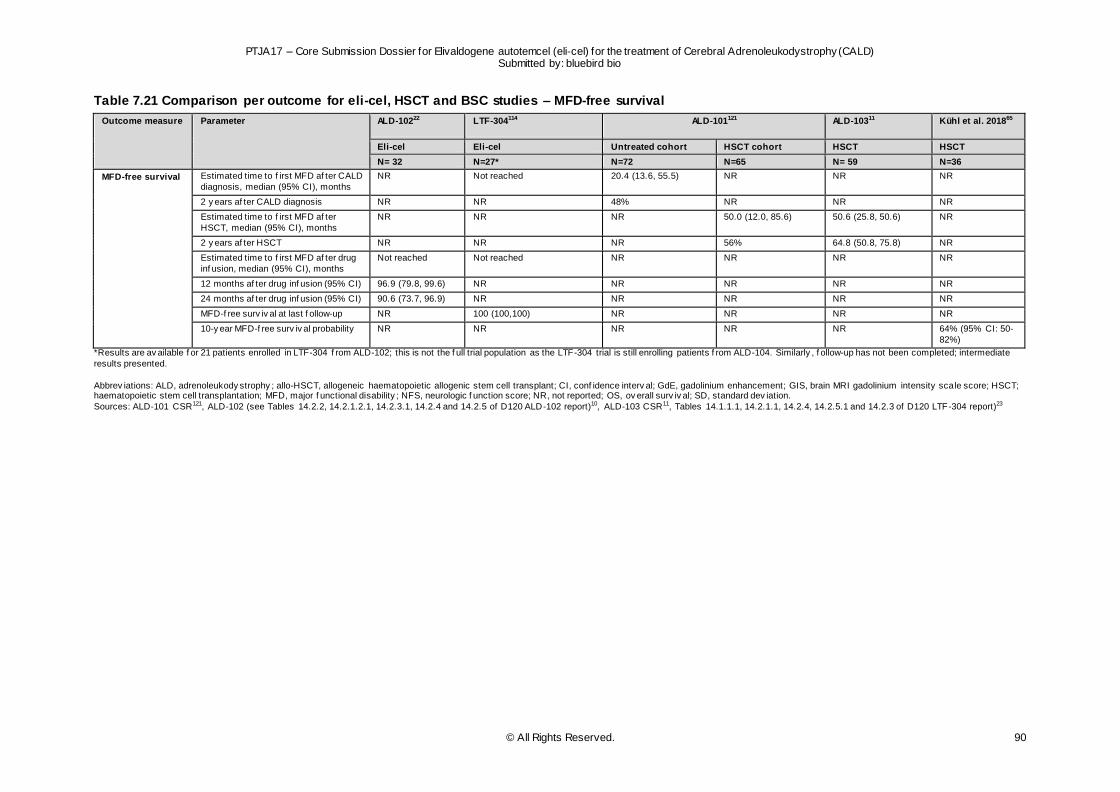
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 90
Table 7.21 Comparison per outcome for eli-cel, HSCT and BSC studies – MFD-free survival
Outcome measure Parameter ALD-10222 LTF-304114 ALD-101121 ALD-10311 Kühl et al. 201865
Eli-cel Eli-cel Untreated cohort HSCT cohort HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=36
MFD-free survival Estimated time to f irst MFD af ter CALD
diagnosis, median (95% CI), months
NR Not reached 20.4 (13.6, 55.5) NR NR NR
2 y ears af ter CALD diagnosis NR NR 48% NR NR NR
Estimated time to f irst MFD af ter
HSCT, median (95% CI), months
NR NR NR 50.0 (12.0, 85.6) 50.6 (25.8, 50.6) NR
2 y ears af ter HSCT NR NR NR 56% 64.8 (50.8, 75.8) NR
Estimated time to f irst MFD af ter drug
inf usion, median (95% CI), months
Not reached Not reached NR NR NR NR
12 months af ter drug inf usion (95% CI) 96.9 (79.8, 99.6) NR NR NR NR NR
24 months af ter drug inf usion (95% CI) 90.6 (73.7, 96.9) NR NR NR NR NR
MFD-f ree surv iv al at last f ollow-up NR 100 (100,100) NR NR NR NR
10-y ear MFD-f ree surv iv al probability NR NR NR NR NR 64% (95% CI: 50-
82%)
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed; intermediate
results presented.
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score; HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation.
Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
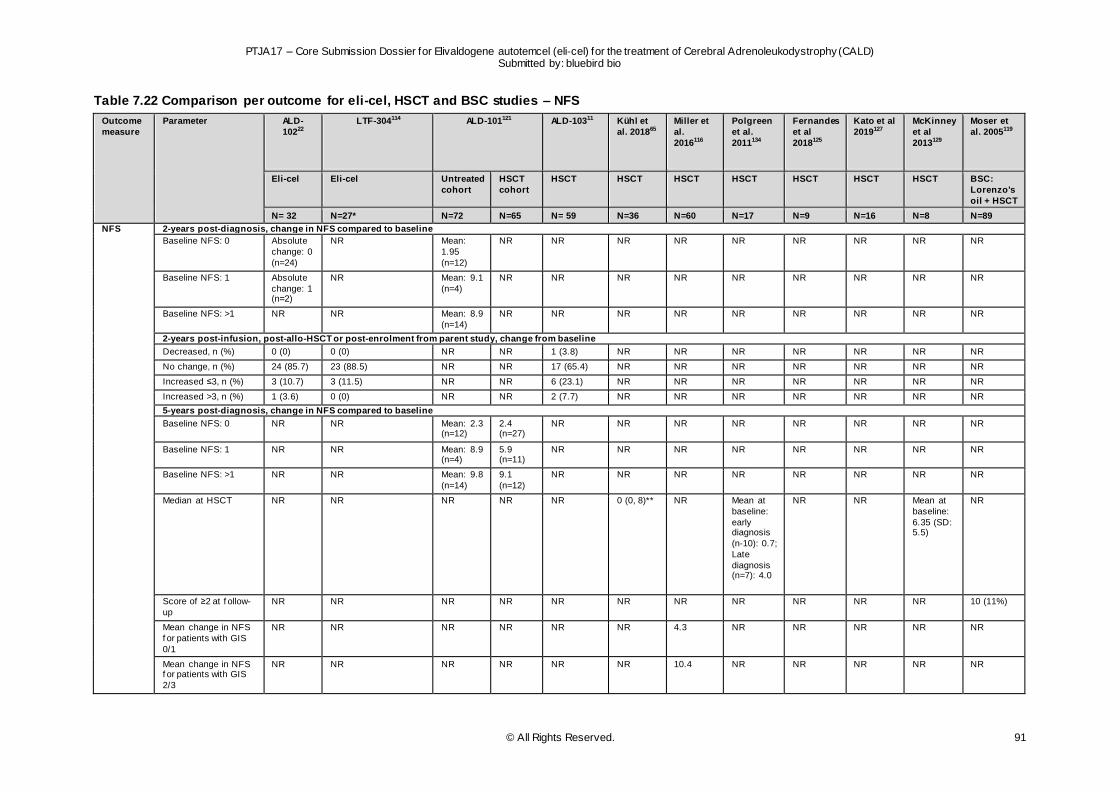
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 91
Table 7.22 Comparison per outcome for eli-cel, HSCT and BSC studies – NFS
Outcome
measure
Parameter ALD-
10222
LTF-304114 ALD-101121 ALD-10311 Kühl et
al. 201865
Miller et
al.
2016116
Polgreen
et al.
2011134
Fernandes
et al
2018125
Kato et al
2019127
McKinney
et al
2013129
Moser et
al. 2005119
Eli-cel Eli-cel Untreated
cohort
HSCT
cohort
HSCT HSCT HSCT HSCT HSCT HSCT HSCT BSC:
Lorenzo's
oil + HSCT
N= 32 N=27* N=72 N=65 N= 59 N=36 N=60 N=17 N=9 N=16 N=8 N=89
NFS 2-years post-diagnosis, change in NFS compared to baseline
Baseline NFS: 0 Absolute
change: 0
(n=24)
NR Mean:
1.95
(n=12)
NR NR NR NR NR NR NR NR NR
Baseline NFS: 1 Absolute
change: 1 (n=2)
NR Mean: 9.1
(n=4)
NR NR NR NR NR NR NR NR NR
Baseline NFS: >1 NR NR Mean: 8.9
(n=14)
NR NR NR NR NR NR NR NR NR
2-years post-infusion, post-allo-HSCT or post-enrolment from parent study, change from baseline
Decreased, n (%) 0 (0) 0 (0) NR NR 1 (3.8) NR NR NR NR NR NR NR
No change, n (%) 24 (85.7) 23 (88.5) NR NR 17 (65.4) NR NR NR NR NR NR NR
Increased ≤3, n (%) 3 (10.7) 3 (11.5) NR NR 6 (23.1) NR NR NR NR NR NR NR
Increased >3, n (%) 1 (3.6) 0 (0) NR NR 2 (7.7) NR NR NR NR NR NR NR
5-years post-diagnosis, change in NFS compared to baseline
Baseline NFS: 0 NR NR Mean: 2.3 (n=12)
2.4 (n=27)
NR NR NR NR NR NR NR NR
Baseline NFS: 1 NR NR Mean: 8.9 (n=4)
5.9 (n=11)
NR NR NR NR NR NR NR NR
Baseline NFS: >1 NR NR Mean: 9.8
(n=14)
9.1
(n=12)
NR NR NR NR NR NR NR NR
Median at HSCT NR NR NR NR NR 0 (0, 8)** NR Mean at
baseline:
early diagnosis
(n-10): 0.7;
Late
diagnosis (n=7): 4.0
NR NR Mean at
baseline:
6.35 (SD: 5.5)
NR
Score of ≥2 at f ollow-
up
NR NR NR NR NR NR NR NR NR NR NR 10 (11%)
Mean change in NFS
f or patients with GIS
0/1
NR NR NR NR NR NR 4.3 NR NR NR NR NR
Mean change in NFS f or patients with GIS
2/3
NR NR NR NR NR NR 10.4 NR NR NR NR NR
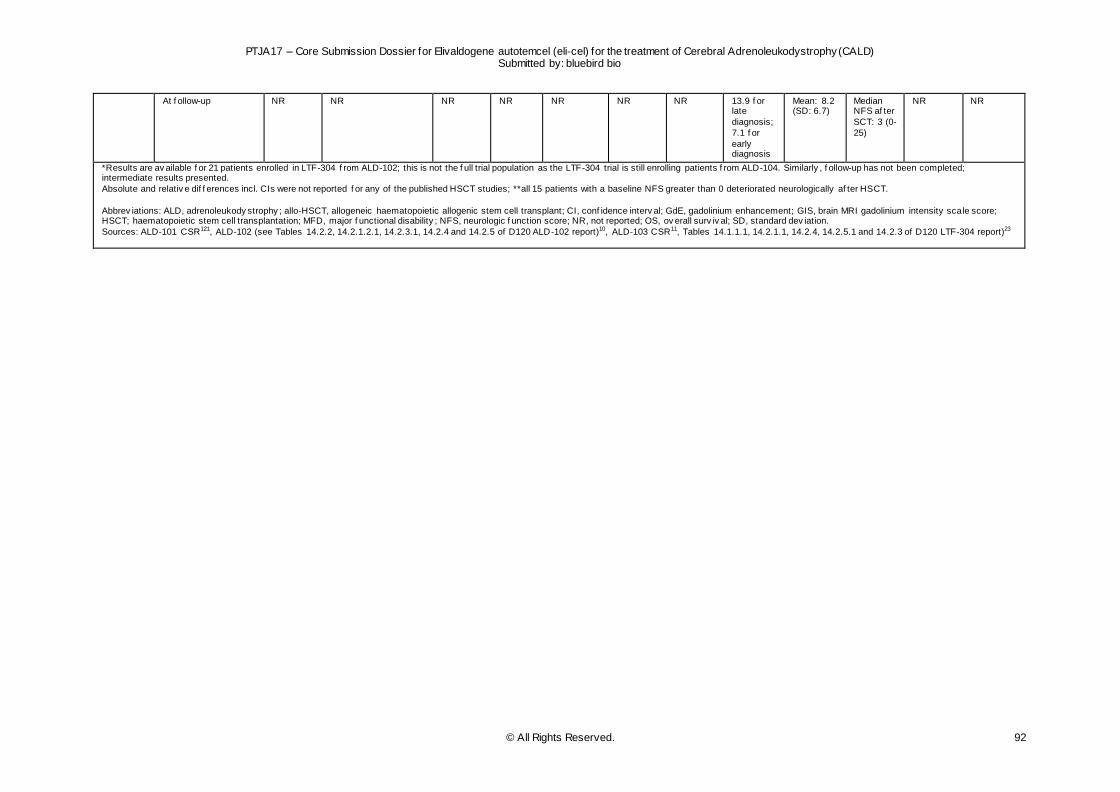
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 92
At f ollow-up NR NR NR NR NR NR NR 13.9 f or late
diagnosis;
7.1 f or
early diagnosis
Mean: 8.2 (SD: 6.7)
Median NFS af ter
SCT: 3 (0-
25)
NR NR
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed; intermediate results presented.
Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies; **all 15 patients with a baseline NFS greater than 0 deteriorated neurologically af ter HSCT.
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score; HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation.
Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
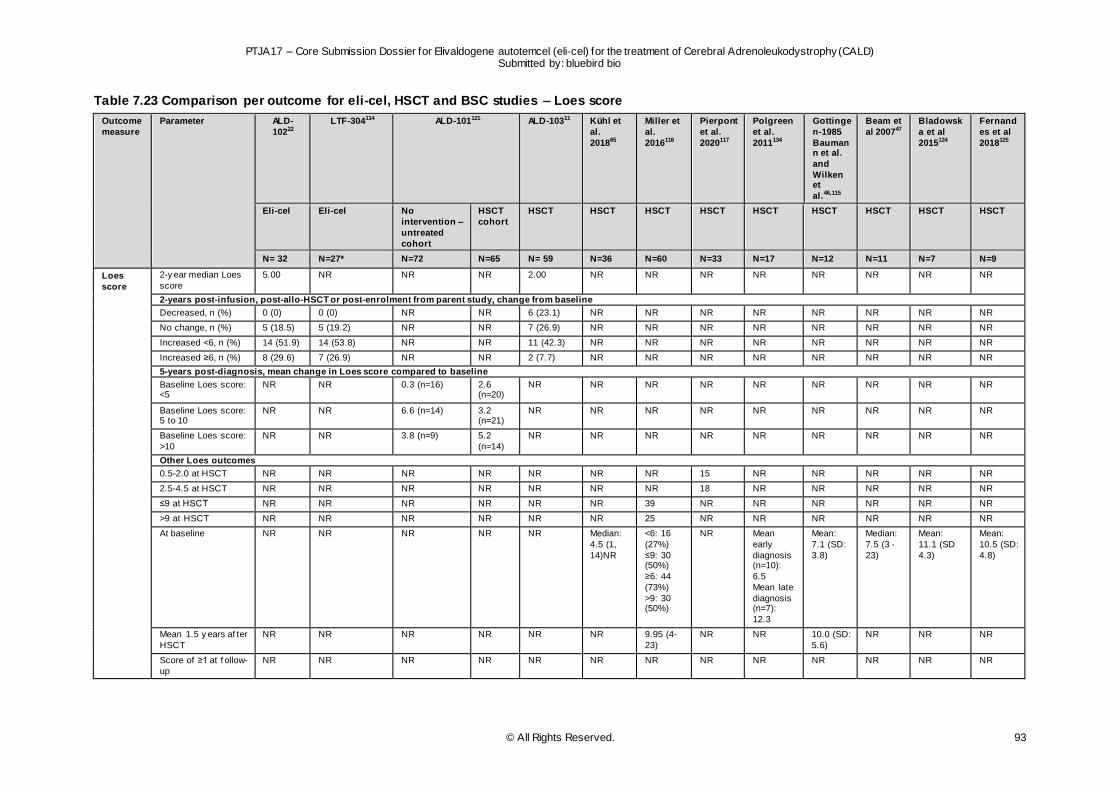
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 93
Table 7.23 Comparison per outcome for eli-cel, HSCT and BSC studies – Loes score
Outcome
measure
Parameter ALD-
10222
LTF-304114 ALD-101121 ALD-10311 Kühl et
al.
201865
Miller et
al.
2016116
Pierpont
et al.
2020117
Polgreen
et al.
2011134
Gottinge
n-1985
Baumann et al.
and
Wilken et
al.46,115
Beam et
al 200747
Bladowsk
a et al
2015124
Fernand
es et al
2018125
Eli-cel Eli-cel No
intervention –
untreated
cohort
HSCT
cohort
HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=36 N=60 N=33 N=17 N=12 N=11 N=7 N=9
Loes
score
2-y ear median Loes
score
5.00 NR NR NR 2.00 NR NR NR NR NR NR NR NR
2-years post-infusion, post-allo-HSCT or post-enrolment from parent study, change from baseline
Decreased, n (%) 0 (0) 0 (0) NR NR 6 (23.1) NR NR NR NR NR NR NR NR
No change, n (%) 5 (18.5) 5 (19.2) NR NR 7 (26.9) NR NR NR NR NR NR NR NR
Increased <6, n (%) 14 (51.9) 14 (53.8) NR NR 11 (42.3) NR NR NR NR NR NR NR NR
Increased ≥6, n (%) 8 (29.6) 7 (26.9) NR NR 2 (7.7) NR NR NR NR NR NR NR NR
5-years post-diagnosis, mean change in Loes score compared to baseline
Baseline Loes score: <5
NR NR 0.3 (n=16) 2.6 (n=20)
NR NR NR NR NR NR NR NR NR
Baseline Loes score: 5 to 10
NR NR 6.6 (n=14) 3.2 (n=21)
NR NR NR NR NR NR NR NR NR
Baseline Loes score:
>10
NR NR 3.8 (n=9) 5.2
(n=14)
NR NR NR NR NR NR NR NR NR
Other Loes outcomes
0.5-2.0 at HSCT NR NR NR NR NR NR NR 15 NR NR NR NR NR
2.5-4.5 at HSCT NR NR NR NR NR NR NR 18 NR NR NR NR NR
≤9 at HSCT NR NR NR NR NR NR 39 NR NR NR NR NR NR
>9 at HSCT NR NR NR NR NR NR 25 NR NR NR NR NR NR
At baseline NR NR NR NR NR Median:
4.5 (1,
14)NR
<6: 16
(27%)
≤9: 30 (50%)
≥6: 44
(73%)
>9: 30 (50%)
NR Mean
early
diagnosis (n=10):
6.5
Mean late
diagnosis (n=7):
12.3
Mean:
7.1 (SD:
3.8)
Median:
7.5 (3 -
23)
Mean:
11.1 (SD
4.3)
Mean:
10.5 (SD:
4.8)
Mean 1.5 y ears af ter
HSCT
NR NR NR NR NR NR 9.95 (4-
23)
NR NR 10.0 (SD:
5.6)
NR NR NR
Score of ≥1 at f ollow-
up
NR NR NR NR NR NR NR NR NR NR NR NR NR
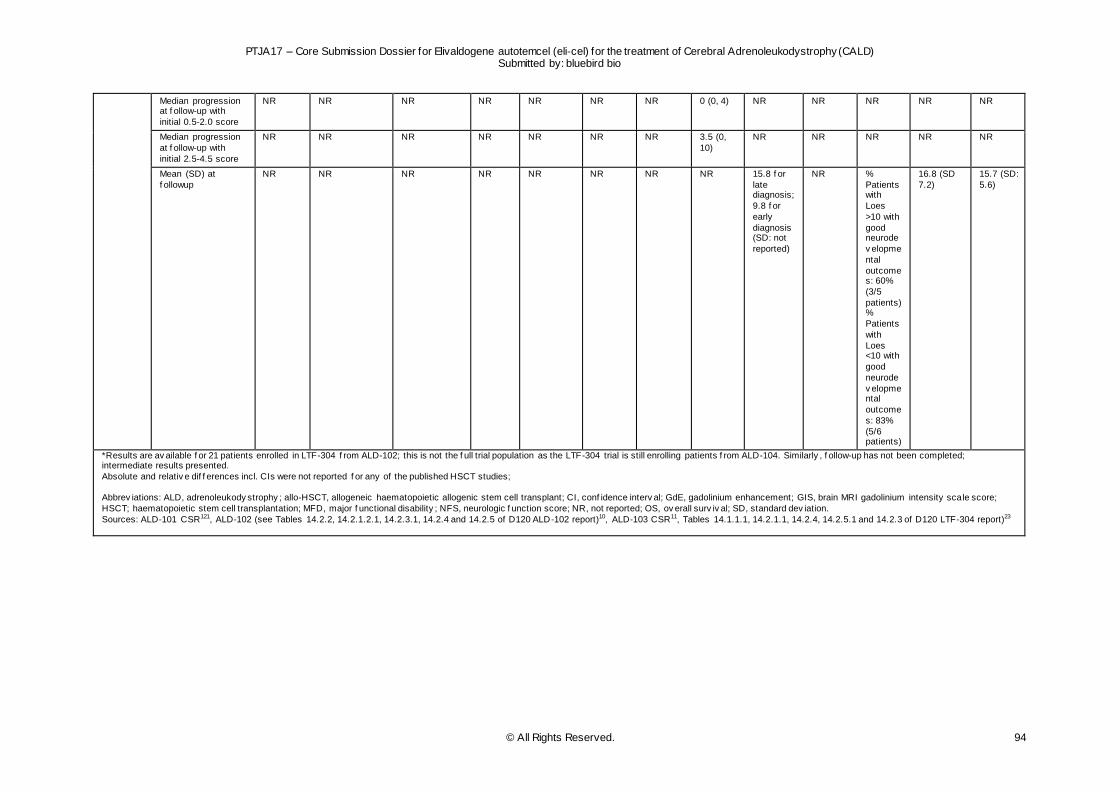
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 94
Median progression at f ollow-up with
initial 0.5-2.0 score
NR NR NR NR NR NR NR 0 (0, 4) NR NR NR NR NR
Median progression
at f ollow-up with
initial 2.5-4.5 score
NR NR NR NR NR NR NR 3.5 (0,
10)
NR NR NR NR NR
Mean (SD) at
f ollowup
NR NR NR NR NR NR NR NR 15.8 f or
late diagnosis;
9.8 f or
early
diagnosis (SD: not
reported)
NR %
Patients with
Loes
>10 with
good neurode
v elopme
ntal
outcomes: 60%
(3/5
patients) %
Patients
with
Loes <10 with
good
neurode
v elopmental
outcome
s: 83%
(5/6 patients)
16.8 (SD
7.2)
15.7 (SD:
5.6)
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed; intermediate results presented.
Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies;
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score;
HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation.
Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
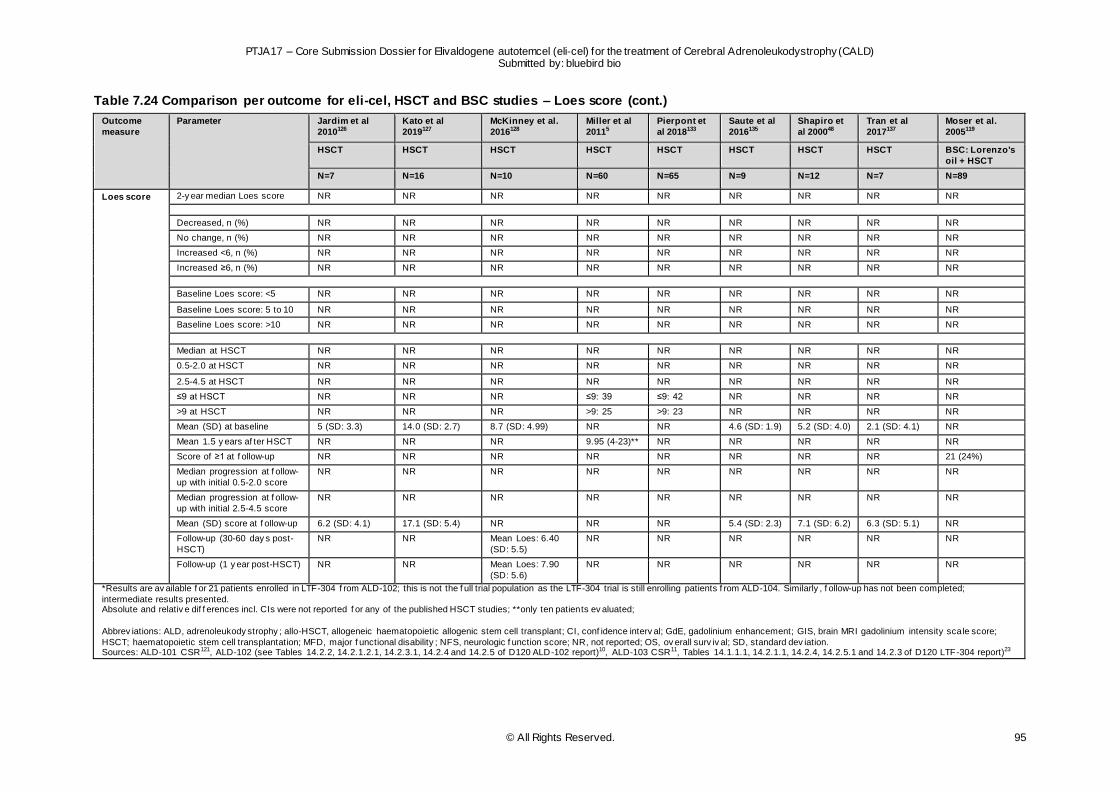
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 95
Table 7.24 Comparison per outcome for eli-cel, HSCT and BSC studies – Loes score (cont.)
Outcome
measure
Parameter Jardim et al
2010126
Kato et al
2019127
McKinney et al.
2016128
Miller et al
20115
Pierpont et
al 2018133
Saute et al
2016135
Shapiro et
al 200048
Tran et al
2017137
Moser et al.
2005119
HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT BSC: Lorenzo's
oil + HSCT
N=7 N=16 N=10 N=60 N=65 N=9 N=12 N=7 N=89
Loes score 2-y ear median Loes score NR NR NR NR NR NR NR NR NR
Decreased, n (%) NR NR NR NR NR NR NR NR NR
No change, n (%) NR NR NR NR NR NR NR NR NR
Increased <6, n (%) NR NR NR NR NR NR NR NR NR
Increased ≥6, n (%) NR NR NR NR NR NR NR NR NR
Baseline Loes score: <5 NR NR NR NR NR NR NR NR NR
Baseline Loes score: 5 to 10 NR NR NR NR NR NR NR NR NR
Baseline Loes score: >10 NR NR NR NR NR NR NR NR NR
Median at HSCT NR NR NR NR NR NR NR NR NR
0.5-2.0 at HSCT NR NR NR NR NR NR NR NR NR
2.5-4.5 at HSCT NR NR NR NR NR NR NR NR NR
≤9 at HSCT NR NR NR ≤9: 39 ≤9: 42 NR NR NR NR
>9 at HSCT NR NR NR >9: 25 >9: 23 NR NR NR NR
Mean (SD) at baseline 5 (SD: 3.3) 14.0 (SD: 2.7) 8.7 (SD: 4.99) NR NR 4.6 (SD: 1.9) 5.2 (SD: 4.0) 2.1 (SD: 4.1) NR
Mean 1.5 y ears af ter HSCT NR NR NR 9.95 (4-23)** NR NR NR NR NR
Score of ≥1 at f ollow-up NR NR NR NR NR NR NR NR 21 (24%)
Median progression at f ollow-
up with initial 0.5-2.0 score
NR NR NR NR NR NR NR NR NR
Median progression at f ollow-
up with initial 2.5-4.5 score
NR NR NR NR NR NR NR NR NR
Mean (SD) score at f ollow-up 6.2 (SD: 4.1) 17.1 (SD: 5.4) NR NR NR 5.4 (SD: 2.3) 7.1 (SD: 6.2) 6.3 (SD: 5.1) NR
Follow-up (30-60 day s post-
HSCT)
NR NR Mean Loes: 6.40
(SD: 5.5)
NR NR NR NR NR NR
Follow-up (1 y ear post-HSCT) NR NR Mean Loes: 7.90
(SD: 5.6)
NR NR NR NR NR NR
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed;
intermediate results presented. Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies; **only ten patients ev aluated;
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score;
HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation. Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
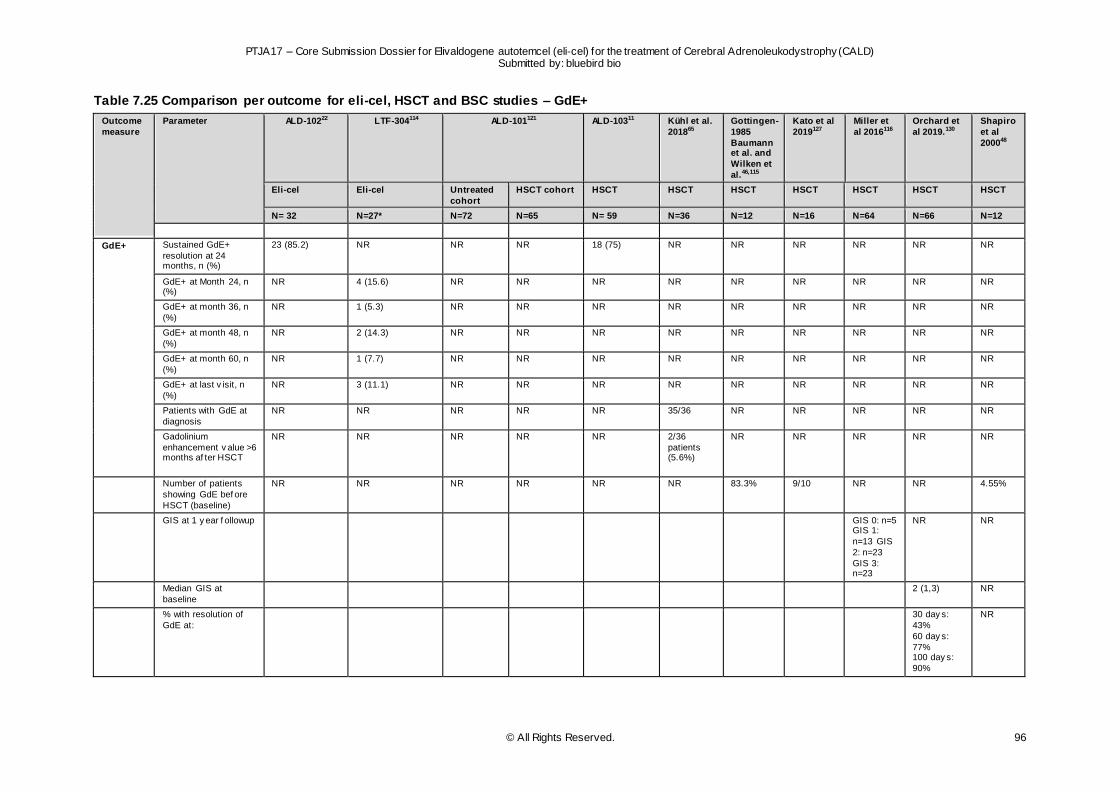
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 96
Table 7.25 Comparison per outcome for eli-cel, HSCT and BSC studies – GdE+
Outcome
measure
Parameter ALD-10222 LTF-304114 ALD-101121 ALD-10311 Kühl et al.
201865
Gottingen-
1985
Baumann et al. and
Wilken et
al.46,115
Kato et al
2019127
Miller et
al 2016116
Orchard et
al 2019.130
Shapiro
et al
200048
Eli-cel Eli-cel Untreated
cohort
HSCT cohort HSCT HSCT HSCT HSCT HSCT HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=36 N=12 N=16 N=64 N=66 N=12
GdE+ Sustained GdE+
resolution at 24 months, n (%)
23 (85.2) NR NR NR 18 (75) NR NR NR NR NR NR
GdE+ at Month 24, n (%)
NR 4 (15.6) NR NR NR NR NR NR NR NR NR
GdE+ at month 36, n
(%)
NR 1 (5.3) NR NR NR NR NR NR NR NR NR
GdE+ at month 48, n
(%)
NR 2 (14.3) NR NR NR NR NR NR NR NR NR
GdE+ at month 60, n
(%)
NR 1 (7.7) NR NR NR NR NR NR NR NR NR
GdE+ at last v isit, n
(%)
NR 3 (11.1) NR NR NR NR NR NR NR NR NR
Patients with GdE at
diagnosis
NR NR NR NR NR 35/36 NR NR NR NR NR
Gadolinium
enhancement v alue >6 months af ter HSCT
NR NR NR NR NR 2/36
patients (5.6%)
NR NR NR NR NR
Number of patients
showing GdE bef ore
HSCT (baseline)
NR NR NR NR NR NR 83.3% 9/10 NR NR 4.55%
GIS at 1 y ear f ollowup GIS 0: n=5 GIS 1:
n=13 GIS
2: n=23
GIS 3: n=23
NR NR
Median GIS at
baseline
2 (1,3) NR
% with resolution of
GdE at:
30 day s:
43%
60 day s:
77% 100 day s:
90%
NR
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 97
180 day s: 94%
365 day s:
98%
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed;
intermediate results presented.
Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score;
HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation.
Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
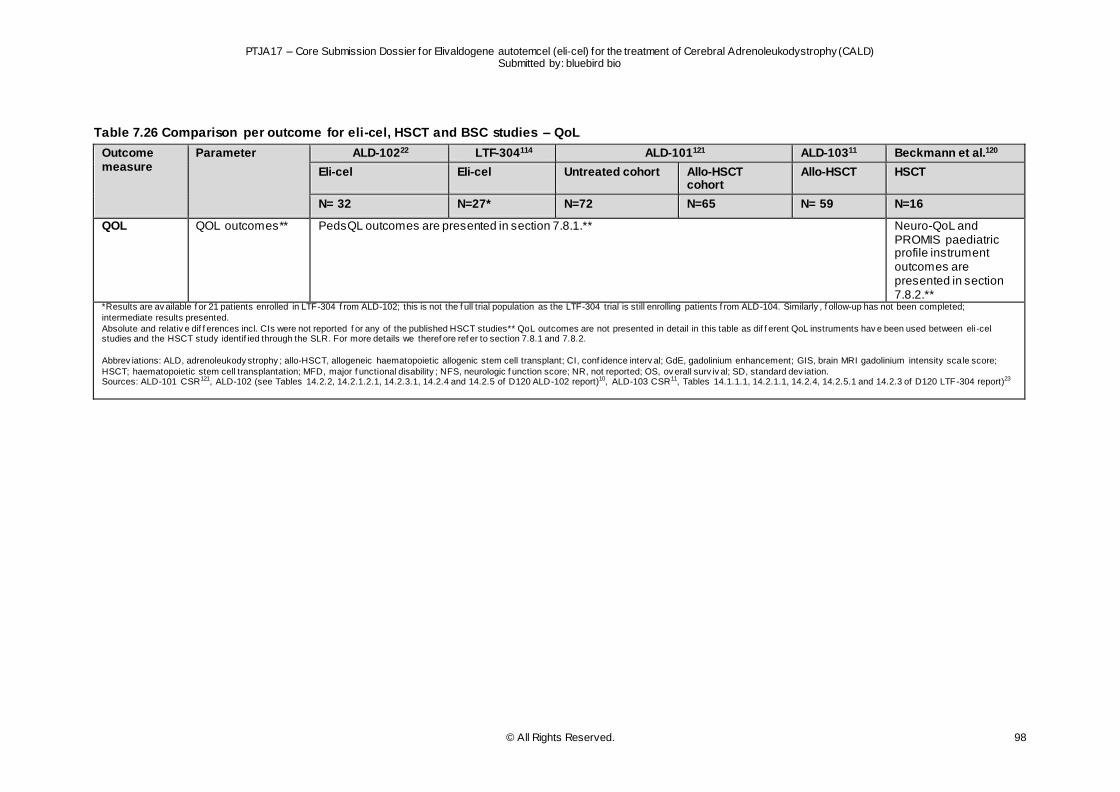
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 98
Table 7.26 Comparison per outcome for eli-cel, HSCT and BSC studies – QoL
Outcome measure
Parameter ALD-10222 LTF-304114 ALD-101121 ALD-10311 Beckmann et al.120
Eli-cel Eli-cel Untreated cohort Allo-HSCT cohort
Allo-HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=16
QOL QOL outcomes** PedsQL outcomes are presented in section 7.8.1.**
Neuro-QoL and PROMIS paediatric profile instrument outcomes are presented in section 7.8.2.**
*Results are av ailable f or 21 patients enrolled in LTF-304 f rom ALD-102; this is not the f ull trial population as the LTF-304 trial is still enrolling patients f rom ALD-104. Similarly , f ollow-up has not been completed;
intermediate results presented.
Absolute and relativ e dif f erences incl. CIs were not reported f or any of the published HSCT studies** QoL outcomes are not presented in detail in this table as dif f erent QoL instruments hav e been used between eli-cel studies and the HSCT study identif ied through the SLR. For more details we theref ore ref er to section 7.8.1 and 7.8.2.
Abbrev iations: ALD, adrenoleukody strophy ; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; CI, conf idence interv al; GdE, gadolinium enhancement; GIS, brain MRI gadolinium intensity scale score;
HSCT; haematopoietic stem cell transplantation; MFD, major f unctional disability ; NFS, neurologic f unction score; NR, not reported; OS, ov erall surv iv al; SD, standard dev iation. Sources: ALD-101 CSR121, ALD-102 (see Tables 14.2.2, 14.2.1.2.1, 14.2.3.1, 14.2.4 and 14.2.5 of D120 ALD-102 report)10, ALD-103 CSR11, Tables 14.1.1.1, 14.2.1.1, 14.2.4, 14.2.5.1 and 14.2.3 of D120 LTF-304 report)23
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 99
7.9 Individual study results (safety outcomes)
Safety outcome definitions and methods of analysis, where available, are presented per study in Table 9.35, in the appendix (section 9.7). Overall, the following safety outcomes were considered:
Neutrophil recovery
Platelet recovery
Graft failure
Graft rejection
GVHD (acute/chronic)
TRM
Subsequent allo-HSCT (incl. time to subsequent allo-HSCT)
AEs (incl. discontinuation and treatment-related AEs)
An explanation of CALD-specific safety outcomes is outlined in section 2.4.1.
7.9.1 Eli-cel clinical development programme: safety outcomes
Table 7.27 outlines the safety outcomes reported as part of the trials included in the eli-cel clinical
development programme.
Neutrophil and platelet recovery As of 23 October 2020, all 32 patients treated with eli-cel in ALD-102 had successful engraftment . Median time to neutrophil and platelet engraftment was 13.0 (range 11.0–41.0) and 32.0 (16.0–60.0)
days, respectively.22 Similar rates were reported for the 19 patients treated with eli-cel in ALD-104, with median time to neutrophil and platelet recovery at 13.0 (range 12.0-31.0) and 29.0 (14.0-108.0), respectively (see Table 14.3.2.2 of D120 ALD-104 report).13 Of the patients treated, 2 patients had a
serious event of pancytopenia approximately 2 months post-elivaldogene autotemcel infusion, which were considered possibly related to elivaldogene autotemcel. The events were diagnosed post-neutrophil engraftment and platelet engraftment was achieved on Day 104 and 108, respectively. Both
patients were treated for pancytopenia and neither experienced bleeding events. Treatment included G-CSF (n=2), platelet infusion (n=2), eltrombopag (n=2, ongoing as of February 2020), packed red blood cell transfusions (n=2), and intravenous immune globulin (n=1). As of last visit, approximately 13 months
post-infusion, low platelet persisted in both patients and white blood count/ANC fluctuated within lower limit of normal in 1 patient.109
In patients treated with allo-HSCT in ALD-103 (n=59), median time to neutrophil recovery was slightly
higher at 17.0 days (range 12.0-36.0), while this was similar to the rates reported in ALD-102 and ALD-104 for platelet recovery, at 26.0 days (13.0-67.0).11
Graft failure and graft rejection
There were no cases of graft failure or graft rejection in patients treated with eli -cel.22,113 This can be explained by the fact that treatment with eli-cel involves autologous gene therapy rather than allo-HSCT. As part of the ALD-103 trial ten out of 38 evaluable patients treated with allo-HSCT (26.3%) experienced
graft failure or allograft rejection.11 All ten patients received allo-HSCT from an NMSD.
GVHD There were no cases of GVHD in patients treated with eli-cel (see Table 3.1.1.2.2.of D120 Interstudy
report).7,22,113 Similar to graft failure and graft rejection, this can be explained by the fact that treatment with eli-cel involves autologous gene therapy rather than allo-HSCT. In the ALD-103 trial, half of the evaluable allo-HSCT treated patients (26 out of 50 [52.0%]) had either grade II or higher acute or chronic
GVHD.11 Five of these patients died, four due to grade II or higher GVHD and one due to chronic GVHD. All GVHD events occurred by Month 24. Specifically, GVHD affected greater proportions of patients who

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 100
received allo-HSCT from an NMSD (23 out of 40 [57.5%]), than those who received allo-HSCT from an
MSD (three out of ten [30.0%]).11
Transplant-related mortality No TRM with eli-cel has been reported to date (see Table 3.2.1 of D120 Interstudy report).7,22,113 In
contrast, 17.8% of patients in ALD-103 died from transplant-related causes within one year of allo-HSCT.11 All deaths occurred in patients who lacked an MSD (ALD-103, NMSD: n=48, 1-year treatment -related mortality: 22.2%).11
Subsequent allo-HSCT (incl. time to subsequent allo-HSCT) Among eli-cel treated patients (n=51), subsequent allo-HSCT occurred in two patients until last follow-up (3.9%). Both patients withdrew from the study (ALD-102) to receive allo-HSCT per Investigator’s
recommendation (see Table 34.7.1 of the D120 Interstudy report).7 As part of ALD-103, subsequent allo-HSCT occurred in 35.3% of NMSD patients in a comparable population, leading to a relative risk of 0.177 (95% CI 0.040-0.784). Time to subsequent allo-HSCT was not reported as part of the endpoints
in the eli-cel clinical development program, however, for the purposes of comparison with ALD-103, time point of study withdrawal was taken as proxy. Comparison analysis resulted in an HR of 0.095 (95 %CI 0.018-0.516), indicating that eli-cel reduces the risk of subsequent allo-HSCT with 90.5%. Importantly ,
a higher incidence of AEs was observed after second allo-HSCT than after first allo-HSCT (see Table 34.7.2 of the D120 Interstudy report).7
Adverse events (incl. discontinuation and TRAEs)
The majority of AEs with eli-cel administration were consistent with those associated with mobilisation and myeloablative conditioning performed for HSCT and resolved with standard measures. To date, patients (9.8%) in ALD-102 had experienced AEs that were potentially related to eli-cel: these were one
case of BK-mediated viral cystitis (serious AE grade 3), two cases of pancytopenia (serious AE grade 3) and two cases of vomiting (grade 1). In ALD-104 two patients experienced AEs potentially related to eli-cel, both were cases of pancytopenia (serious AE grade 3) (see Tables 3.4.9, 3.4.6.1.of D120
Interstudy report; Table 14.3.1.6 of D120 ALD-102 report; table 14.3.1.3.1 of D120 ALD-104 report).7,10,13 None of the reported AEs led to discontinuation of the studies (see Table 1.1.1 of D120 Interstudy report).7 In comparison, treatment-related AEs were more common among allo-HSCT patients, as
reported in ALD-103. Of 59 subjects in the transplanted population (TP), > 40% experienced treatment -emergent adverse events (TEAEs) in the following system organ classes (SOCs): blood and lymphatic system disorders (38/59 [64.4%] subjects), infection and infestations (35/59 [59.3%] subjects),
gastrointestinal disorders (34/59 [57.6%] subjects), vascular disorders (29/59 [49.2%] subjects), and metabolism and nutrition disorders (28/59 [47.5%] subjects).11 Table 9.36 outlines (serious) AEs per SOC, as observed in the eli-cel clinical development programme.
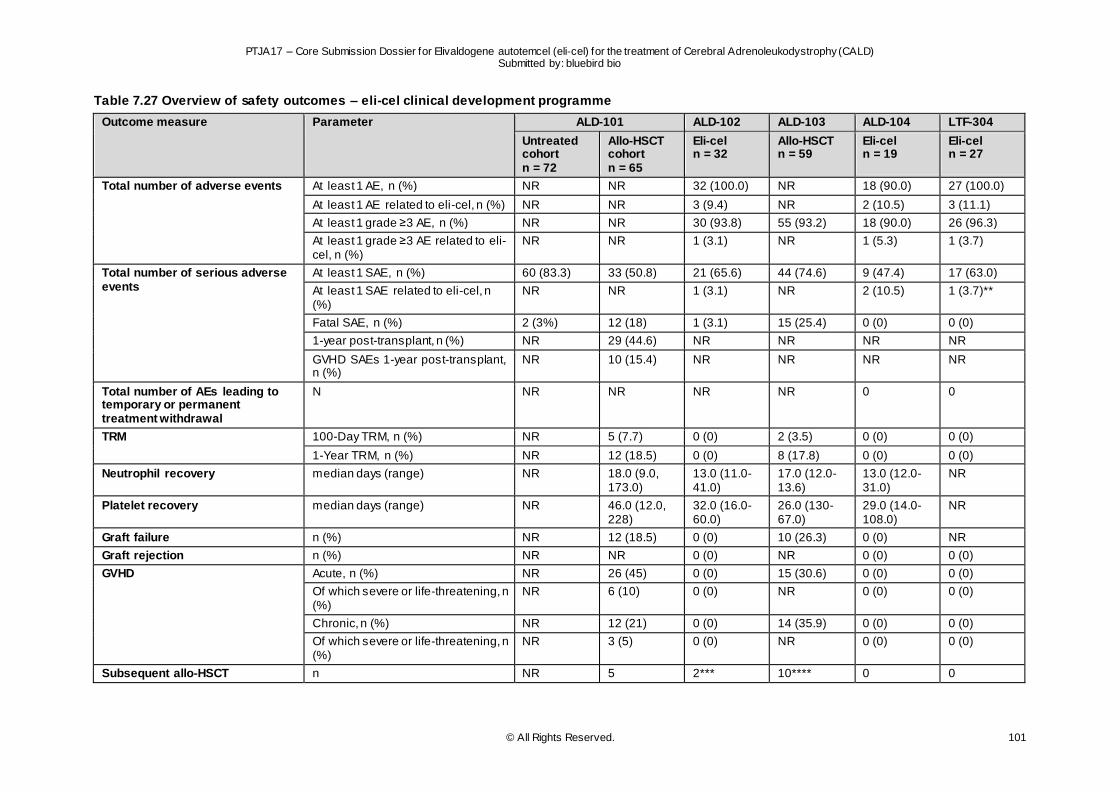
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 101
Table 7.27 Overview of safety outcomes – eli-cel clinical development programme
Outcome measure Parameter ALD-101 ALD-102 ALD-103 ALD-104 LTF-304
Untreated cohort n = 72
Allo-HSCT cohort n = 65
Eli-cel n = 32
Allo-HSCT n = 59
Eli-cel n = 19
Eli-cel n = 27
Total number of adverse events At least 1 AE, n (%) NR NR 32 (100.0) NR 18 (90.0) 27 (100.0)
At least 1 AE related to eli-cel, n (%) NR NR 3 (9.4) NR 2 (10.5) 3 (11.1)
At least 1 grade ≥3 AE, n (%) NR NR 30 (93.8) 55 (93.2) 18 (90.0) 26 (96.3)
At least 1 grade ≥3 AE related to eli-cel, n (%)
NR NR 1 (3.1) NR 1 (5.3) 1 (3.7)
Total number of serious adverse events
At least 1 SAE, n (%) 60 (83.3) 33 (50.8) 21 (65.6) 44 (74.6) 9 (47.4) 17 (63.0)
At least 1 SAE related to eli-cel, n (%)
NR NR 1 (3.1) NR 2 (10.5) 1 (3.7)**
Fatal SAE, n (%) 2 (3%) 12 (18) 1 (3.1) 15 (25.4) 0 (0) 0 (0)
1-year post-transplant, n (%) NR 29 (44.6) NR NR NR NR
GVHD SAEs 1-year post-transplant, n (%)
NR 10 (15.4) NR NR NR NR
Total number of AEs leading to temporary or permanent treatment withdrawal
N NR NR NR NR 0 0
TRM 100-Day TRM, n (%) NR 5 (7.7) 0 (0) 2 (3.5) 0 (0) 0 (0)
1-Year TRM, n (%) NR 12 (18.5) 0 (0) 8 (17.8) 0 (0) 0 (0)
Neutrophil recovery median days (range) NR 18.0 (9.0, 173.0)
13.0 (11.0-41.0)
17.0 (12.0-13.6)
13.0 (12.0-31.0)
NR
Platelet recovery median days (range) NR 46.0 (12.0, 228)
32.0 (16.0-60.0)
26.0 (130-67.0)
29.0 (14.0-108.0)
NR
Graft failure n (%) NR 12 (18.5) 0 (0) 10 (26.3) 0 (0) NR
Graft rejection n (%) NR NR 0 (0) NR 0 (0) 0 (0)
GVHD Acute, n (%) NR 26 (45) 0 (0) 15 (30.6) 0 (0) 0 (0)
Of which severe or life-threatening, n (%)
NR 6 (10) 0 (0) NR 0 (0) 0 (0)
Chronic, n (%) NR 12 (21) 0 (0) 14 (35.9) 0 (0) 0 (0)
Of which severe or life-threatening, n (%)
NR 3 (5) 0 (0) NR 0 (0) 0 (0)
Subsequent allo-HSCT n NR 5 2*** 10**** 0 0
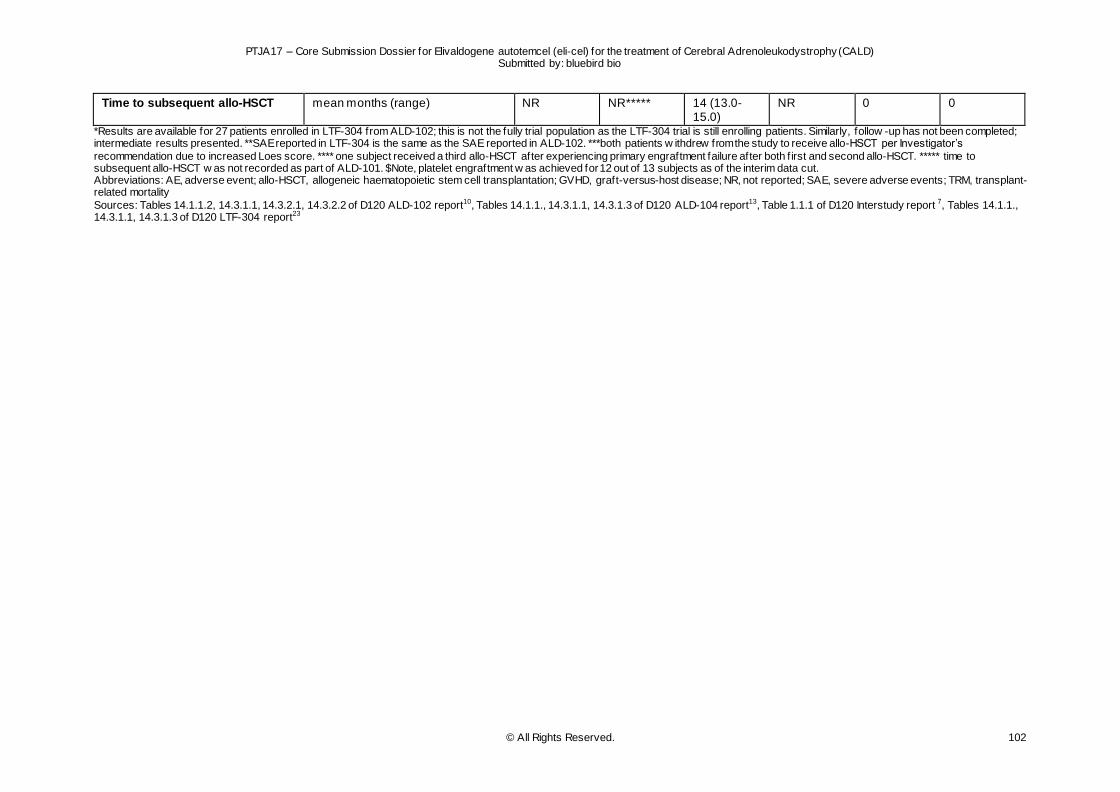
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 102
Time to subsequent allo-HSCT mean months (range) NR NR***** 14 (13.0-15.0)
NR 0 0
*Results are available for 27 patients enrolled in LTF-304 from ALD-102; this is not the fully trial population as the LTF-304 trial is still enrolling patients. Similarly, follow -up has not been completed; intermediate results presented. **SAE reported in LTF-304 is the same as the SAE reported in ALD-102. ***both patients w ithdrew from the study to receive allo-HSCT per Investigator’s
recommendation due to increased Loes score. **** one subject received a third allo-HSCT after experiencing primary engraftment failure after both f irst and second allo-HSCT. ***** time to subsequent allo-HSCT w as not recorded as part of ALD-101. $Note, platelet engraftment w as achieved for 12 out of 13 subjects as of the interim data cut. Abbreviations: AE, adverse event; allo-HSCT, allogeneic haematopoietic stem cell transplantation; GVHD, graft-versus-host disease; NR, not reported; SAE, severe adverse events; TRM, transplant-related mortality
Sources: Tables 14.1.1.2, 14.3.1.1, 14.3.2.1, 14.3.2.2 of D120 ALD-102 report10, Tables 14.1.1., 14.3.1.1, 14.3.1.3 of D120 ALD-104 report13, Table 1.1.1 of D120 Interstudy report 7, Tables 14.1.1., 14.3.1.1, 14.3.1.3 of D120 LTF-304 report23
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 103
7.9.2 SLR
All safety outcomes of interest were reported in at least one of the publications identified through the SLR, and covered by the majority of key studies. The most commonly reported outcomes were GVHD, graft failure and transplantation-related mortality. In contrast, graft rejection was only addressed in two
studies, neither one of which was a key study.124,125 Safety outcomes for the key studies are reported in Table 7.30. Safety outcomes associated with all studies identified through the SLR are outlined in the appendix, section 9.7 (Table 9.37 to Table 9.38).
Neutrophil and platelet recovery Only a limited set of studies reported neutrophil and platelet outcomes.49,65
Allo-HSCT
Specifically, two of the key studies49,65 reported time to neutrophil recovery after allo-HSCT (see Table 7.28), with one of these49 also reporting platelet recovery time. The median days for neutrophil recovery varied between 19.565 and 21 days49, while platelet recovery took longer at a median of 52 days.65
BSC Given the nature of treatment with Lorenzo’s oil, neutrophil and platelet recovery times were not considered a relevant outcome measure as part of the Moser et al. study.119
An overview of neutrophil and platelet recover times across all studies identified through the SLR can be found in the appendix, section 9.9. These values were similar to those reported in the key studies.
Graft failure and graft rejection
Half of the key studies reported on graft failure, while none reported graft rejection results. 49,65,117
Allo-HSCT Graft failure was reported in three of the key studies49,65,117 (see Table 7.28), and varied between 0%65
and 8%49. All patients received transplants from an NMSD. Graft rejection was not reported in the key studies.
BSC
Given the nature of treatment with Lorenzo’s oil, graft failure and graft rejection were not reported for Lorenzo’s oil as part of the Moser et al.119 study.
Section 9.9 in the appendix outlines graft failure and graft rejection results for the remaining studies
identified through the SLR. On average, the graft failure rates reported in the key studies were lower than the graft failure rates reported across all studies identified through the SLR (see appendix, section 9.7, Table 9.38). In terms of graft rejection, only in two studies124,125 identified through the SLR reported
on these, both of which had small sample sizes.
GVHD A common and potentially serious adverse event for patients treated with allo-HSCT is GVHD. GVHD
outcomes were reported for the majority of the key studies identified.49,65,117,119 In Table 7.29, the number of patients who contracted various forms of GVHD are reported for the key studies.
Allo-HSCT
Three49,65,117 of the allo-HSCT key studies outlined GVHD results. These were not comparable as they reflected different definitions of GVHD, i.e. Kühl et al. 201865 reported that 25.0% of patients experienced acute GVHD of grade II or higher, while 22.2% were reported to experience chronic GVHD. On the other
hand, Pierpont et al. 2020117 only report severe GVHD, which occurred in one patient (3.0%). Finally, Van den Broek et al. 201849 reported the GVHD cumulative incidence for grade II-IV and grade III-IV GVHD, which were 35.3% and 20.2%, respectively. In general, this indicated a substantial part of allo-
HSCT patients in the key studies experienced GVHD.
BSC While the nature of treatment with Lorenzo’s oil does not result in GVHD, a subset of 14 patients enrolled
in the study by Moser et al.119 were reported to have received allo-HSCT during follow-up. Of these
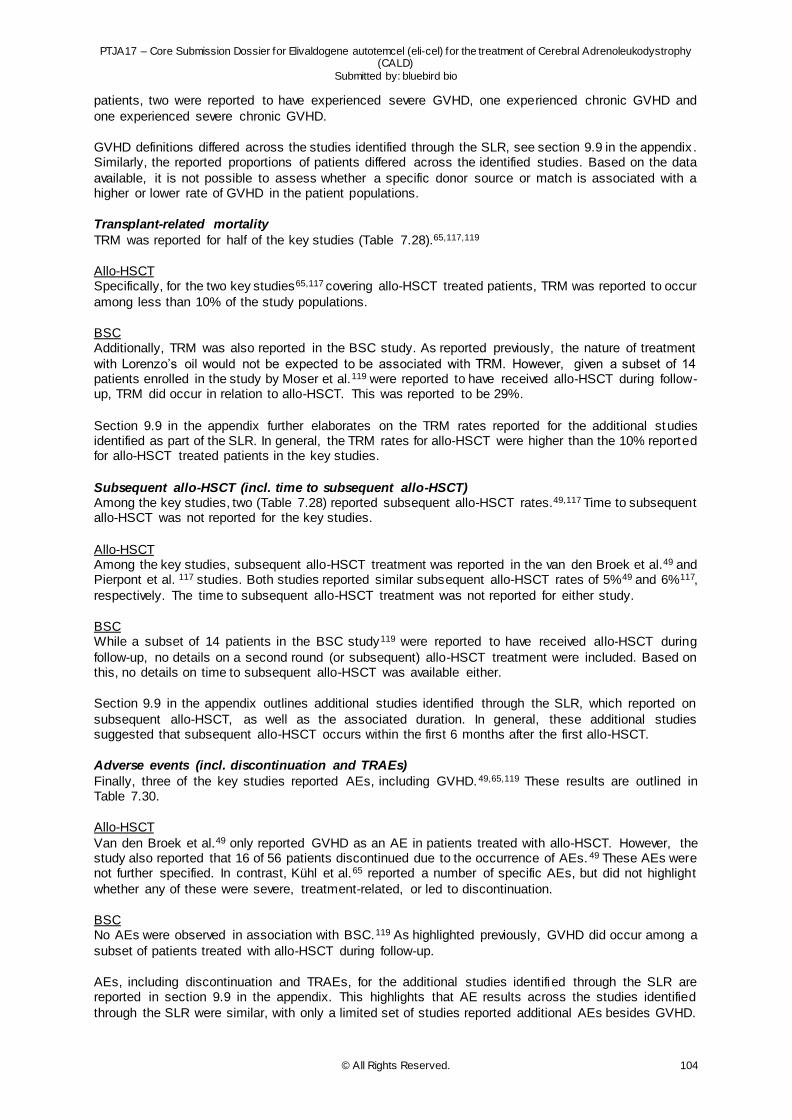
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 104
patients, two were reported to have experienced severe GVHD, one experienced chronic GVHD and
one experienced severe chronic GVHD.
GVHD definitions differed across the studies identified through the SLR, see section 9.9 in the appendix . Similarly, the reported proportions of patients differed across the identified studies. Based on the data
available, it is not possible to assess whether a specific donor source or match is associated with a higher or lower rate of GVHD in the patient populations.
Transplant-related mortality
TRM was reported for half of the key studies (Table 7.28).65,117,119
Allo-HSCT Specifically, for the two key studies65,117 covering allo-HSCT treated patients, TRM was reported to occur
among less than 10% of the study populations.
BSC Additionally, TRM was also reported in the BSC study. As reported previously, the nature of treatment
with Lorenzo’s oil would not be expected to be associated with TRM. However, given a subset of 14 patients enrolled in the study by Moser et al.119 were reported to have received allo-HSCT during follow-up, TRM did occur in relation to allo-HSCT. This was reported to be 29%.
Section 9.9 in the appendix further elaborates on the TRM rates reported for the additional studies identified as part of the SLR. In general, the TRM rates for allo-HSCT were higher than the 10% reported for allo-HSCT treated patients in the key studies.
Subsequent allo-HSCT (incl. time to subsequent allo-HSCT) Among the key studies, two (Table 7.28) reported subsequent allo-HSCT rates.49,117 Time to subsequent allo-HSCT was not reported for the key studies.
Allo-HSCT Among the key studies, subsequent allo-HSCT treatment was reported in the van den Broek et al.49 and Pierpont et al. 117 studies. Both studies reported similar subsequent allo-HSCT rates of 5%49 and 6%117,
respectively. The time to subsequent allo-HSCT treatment was not reported for either study.
BSC While a subset of 14 patients in the BSC study119 were reported to have received allo-HSCT during
follow-up, no details on a second round (or subsequent) allo-HSCT treatment were included. Based on this, no details on time to subsequent allo-HSCT was available either.
Section 9.9 in the appendix outlines additional studies identified through the SLR, which reported on
subsequent allo-HSCT, as well as the associated duration. In general, these additional studies suggested that subsequent allo-HSCT occurs within the first 6 months after the first allo-HSCT.
Adverse events (incl. discontinuation and TRAEs)
Finally, three of the key studies reported AEs, including GVHD.49,65,119 These results are outlined in Table 7.30.
Allo-HSCT
Van den Broek et al.49 only reported GVHD as an AE in patients treated with allo-HSCT. However, the study also reported that 16 of 56 patients discontinued due to the occurrence of AEs. 49 These AEs were not further specified. In contrast, Kühl et al.65 reported a number of specific AEs, but did not highlight
whether any of these were severe, treatment-related, or led to discontinuation.
BSC No AEs were observed in association with BSC.119 As highlighted previously, GVHD did occur among a
subset of patients treated with allo-HSCT during follow-up.
AEs, including discontinuation and TRAEs, for the additional studies identified through the SLR are reported in section 9.9 in the appendix. This highlights that AE results across the studies identified
through the SLR were similar, with only a limited set of studies reported additional AEs besides GVHD.
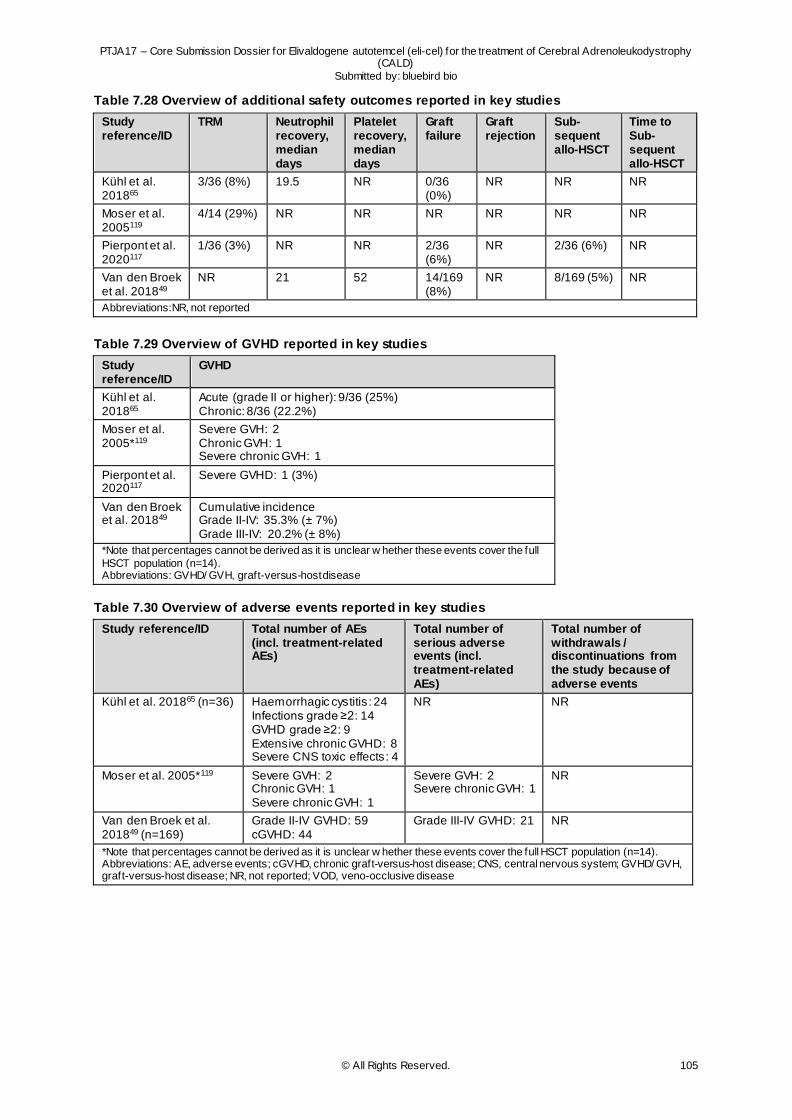
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 105
Table 7.28 Overview of additional safety outcomes reported in key studies
Study reference/ID
TRM Neutrophil recovery, median days
Platelet recovery, median days
Graft failure
Graft rejection
Sub-sequent allo-HSCT
Time to Sub-sequent allo-HSCT
Kühl et al. 201865
3/36 (8%) 19.5 NR 0/36 (0%)
NR NR NR
Moser et al. 2005119
4/14 (29%) NR NR NR NR NR NR
Pierpont et al. 2020117
1/36 (3%) NR NR 2/36 (6%)
NR 2/36 (6%) NR
Van den Broek et al. 201849
NR 21 52 14/169 (8%)
NR 8/169 (5%) NR
Abbreviations:NR, not reported
Table 7.29 Overview of GVHD reported in key studies
Study reference/ID
GVHD
Kühl et al. 201865
Acute (grade II or higher): 9/36 (25%) Chronic: 8/36 (22.2%)
Moser et al. 2005*119
Severe GVH: 2 Chronic GVH: 1 Severe chronic GVH: 1
Pierpont et al. 2020117
Severe GVHD: 1 (3%)
Van den Broek et al. 201849
Cumulative incidence Grade II-IV: 35.3% (± 7%) Grade III-IV: 20.2% (± 8%)
*Note that percentages cannot be derived as it is unclear w hether these events cover the full
HSCT population (n=14). Abbreviations: GVHD/ GVH, graft-versus-host disease
Table 7.30 Overview of adverse events reported in key studies
Study reference/ID Total number of AEs (incl. treatment-related AEs)
Total number of serious adverse events (incl. treatment-related AEs)
Total number of withdrawals / discontinuations from the study because of adverse events
Kühl et al. 201865 (n=36) Haemorrhagic cystitis : 24 Infections grade ≥2: 14 GVHD grade ≥2: 9 Extensive chronic GVHD: 8 Severe CNS toxic effects: 4
NR NR
Moser et al. 2005*119 Severe GVH: 2 Chronic GVH: 1 Severe chronic GVH: 1
Severe GVH: 2 Severe chronic GVH: 1
NR
Van den Broek et al. 201849 (n=169)
Grade II-IV GVHD: 59 cGVHD: 44
Grade III-IV GVHD: 21 NR
*Note that percentages cannot be derived as it is unclear w hether these events cover the full HSCT population (n=14). Abbreviations: AE, adverse events; cGVHD, chronic graft-versus-host disease; CNS, central nervous system; GVHD/ GVH, graft-versus-host disease; NR, not reported; VOD, veno-occlusive disease
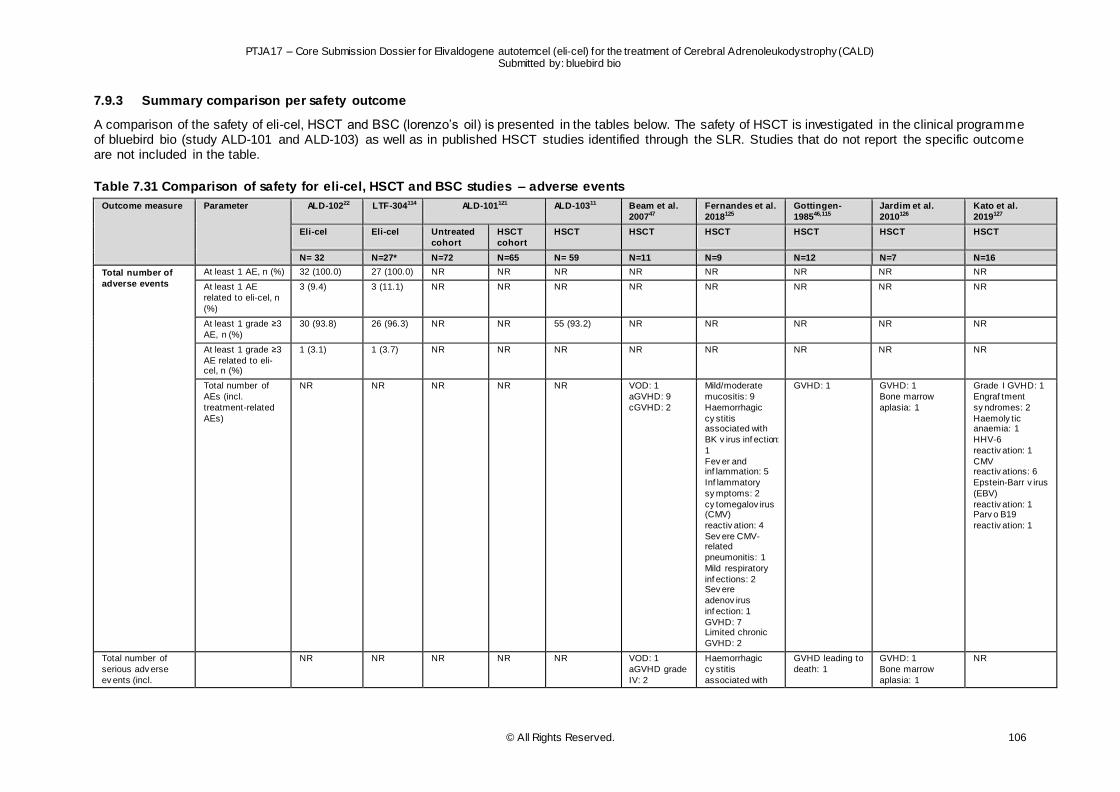
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 106
7.9.3 Summary comparison per safety outcome
A comparison of the safety of eli-cel, HSCT and BSC (lorenzo’s oil) is presented in the tables below. The safety of HSCT is investigated in the clinical programme of bluebird bio (study ALD-101 and ALD-103) as well as in published HSCT studies identified through the SLR. Studies that do not report the specific outcome are not included in the table.
Table 7.31 Comparison of safety for eli-cel, HSCT and BSC studies – adverse events
Outcome measure Parameter ALD-10222 LTF-304114 ALD-101121 ALD-10311 Beam et al.
200747
Fernandes et al.
2018125
Gottingen-
198546,115
Jardim et al.
2010126
Kato et al.
2019127
Eli-cel Eli-cel Untreated
cohort
HSCT
cohort
HSCT HSCT HSCT HSCT HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=11 N=9 N=12 N=7 N=16
Total number of
adverse events
At least 1 AE, n (%) 32 (100.0) 27 (100.0) NR NR NR NR NR NR NR NR
At least 1 AE
related to eli-cel, n
(%)
3 (9.4) 3 (11.1) NR NR NR NR NR NR NR NR
At least 1 grade ≥3
AE, n (%)
30 (93.8) 26 (96.3) NR NR 55 (93.2) NR NR NR NR NR
At least 1 grade ≥3
AE related to eli-cel, n (%)
1 (3.1) 1 (3.7) NR NR NR NR NR NR NR NR
Total number of
AEs (incl.
treatment-related
AEs)
NR NR NR NR NR VOD: 1
aGVHD: 9
cGVHD: 2
Mild/moderate
mucositis: 9
Haemorrhagic
cy stitis associated with
BK v irus inf ection:
1
Fev er and inf lammation: 5
Inf lammatory
sy mptoms: 2
cy tomegalov irus (CMV)
reactiv ation: 4
Sev ere CMV-related
pneumonitis: 1
Mild respiratory
inf ections: 2 Sev ere
adenov irus
inf ection: 1
GVHD: 7 Limited chronic
GVHD: 2
GVHD: 1 GVHD: 1
Bone marrow
aplasia: 1
Grade I GVHD: 1
Engraf tment
sy ndromes: 2
Haemoly tic anaemia: 1
HHV-6
reactiv ation: 1
CMV reactiv ations: 6
Epstein-Barr v irus
(EBV)
reactiv ation: 1 Parv o B19
reactiv ation: 1
Total number of
serious adv erse
ev ents (incl.
NR NR NR NR NR VOD: 1
aGVHD grade
IV: 2
Haemorrhagic
cy stitis
associated with
GVHD leading to
death: 1
GVHD: 1
Bone marrow
aplasia: 1
NR
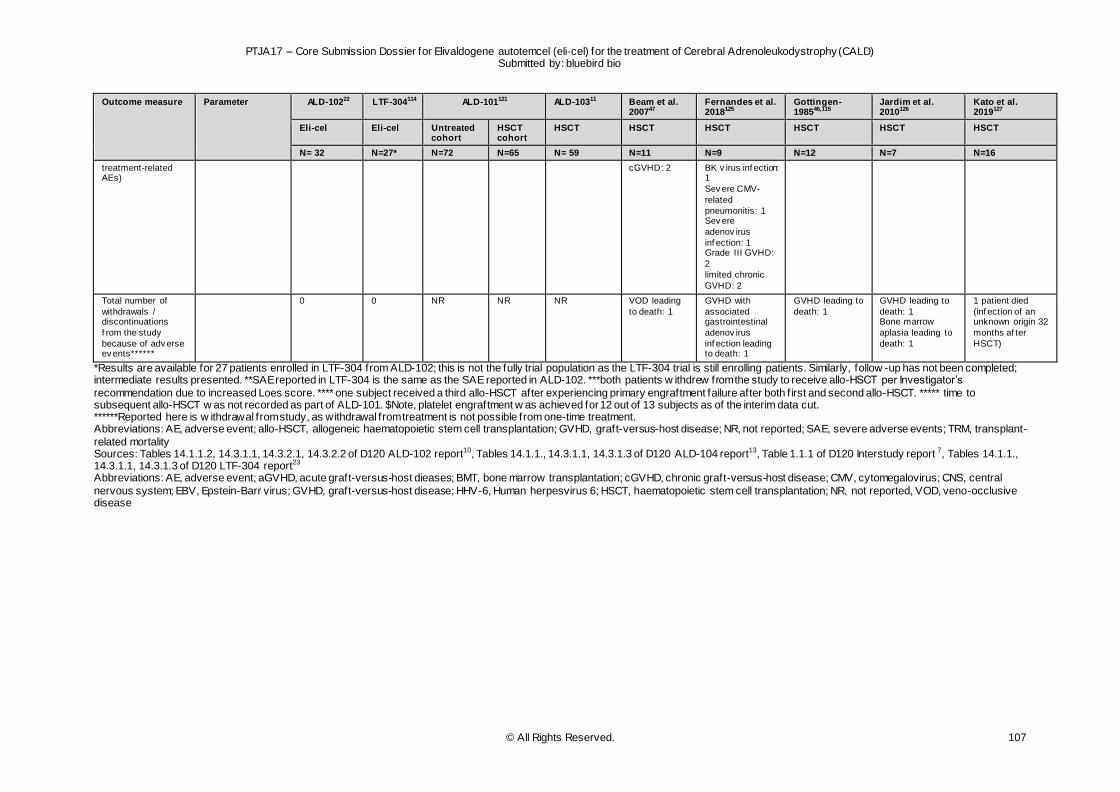
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 107
Outcome measure Parameter ALD-10222 LTF-304114 ALD-101121 ALD-10311 Beam et al. 200747
Fernandes et al. 2018125
Gottingen-198546,115
Jardim et al. 2010126
Kato et al. 2019127
Eli-cel Eli-cel Untreated cohort
HSCT cohort
HSCT HSCT HSCT HSCT HSCT HSCT
N= 32 N=27* N=72 N=65 N= 59 N=11 N=9 N=12 N=7 N=16
treatment-related AEs)
cGVHD: 2 BK v irus inf ection: 1
Sev ere CMV-
related
pneumonitis: 1 Sev ere
adenov irus
inf ection: 1 Grade III GVHD:
2
limited chronic
GVHD: 2
Total number of
withdrawals / discontinuations
f rom the study
because of adv erse ev ents******
0 0 NR NR NR VOD leading
to death: 1
GVHD with
associated gastrointestinal
adenov irus
inf ection leading to death: 1
GVHD leading to
death: 1
GVHD leading to
death: 1 Bone marrow
aplasia leading to
death: 1
1 patient died
(inf ection of an unknown origin 32
months af ter
HSCT)
*Results are available for 27 patients enrolled in LTF-304 from ALD-102; this is not the fully trial population as the LTF-304 trial is still enrolling patients. Similarly, follow -up has not been completed; intermediate results presented. **SAE reported in LTF-304 is the same as the SAE reported in ALD-102. ***both patients w ithdrew from the study to receive allo-HSCT per Investigator’s
recommendation due to increased Loes score. **** one subject received a third allo-HSCT after experiencing primary engraftment failure after both f irst and second allo-HSCT. ***** time to subsequent allo-HSCT w as not recorded as part of ALD-101. $Note, platelet engraftment w as achieved for 12 out of 13 subjects as of the interim data cut. ******Reported here is w ithdrawal from study, as withdrawal from treatment is not possible from one-time treatment. Abbreviations: AE, adverse event; allo-HSCT, allogeneic haematopoietic stem cell transplantation; GVHD, graft-versus-host disease; NR, not reported; SAE, severe adverse events; TRM, transplant-
related mortality Sources: Tables 14.1.1.2, 14.3.1.1, 14.3.2.1, 14.3.2.2 of D120 ALD-102 report10, Tables 14.1.1., 14.3.1.1, 14.3.1.3 of D120 ALD-104 report13, Table 1.1.1 of D120 Interstudy report 7, Tables 14.1.1., 14.3.1.1, 14.3.1.3 of D120 LTF-304 report23 Abbreviations: AE, adverse event; aGVHD, acute graft-versus-host dieases; BMT, bone marrow transplantation; cGVHD, chronic graft-versus-host disease; CMV, cytomegalovirus; CNS, central
nervous system; EBV, Epstein-Barr virus; GVHD, graft-versus-host disease; HHV-6, Human herpesvirus 6; HSCT, haematopoietic stem cell transplantation; NR, not reported, VOD, veno-occlusive disease
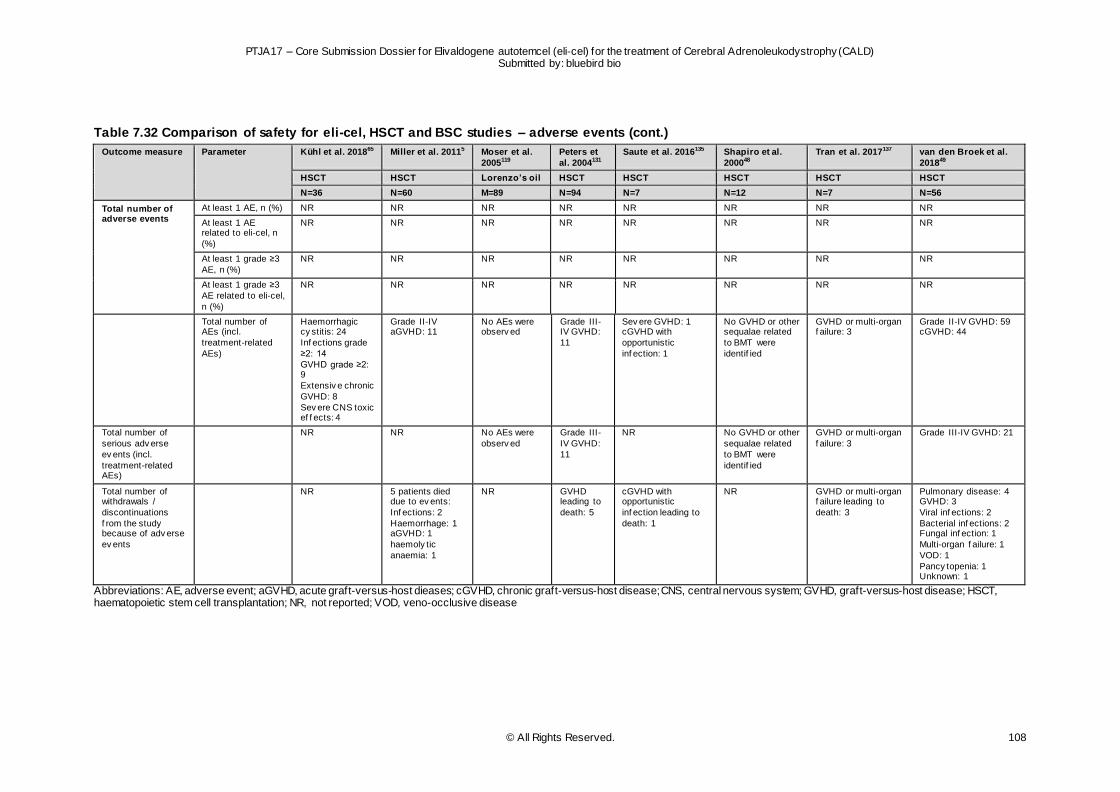
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 108
Table 7.32 Comparison of safety for eli-cel, HSCT and BSC studies – adverse events (cont.)
Outcome measure Parameter Kühl et al. 201865 Miller et al. 20115 Moser et al.
2005119
Peters et
al. 2004131
Saute et al. 2016135 Shapiro et al.
200048
Tran et al. 2017137 van den Broek et al.
201849
HSCT HSCT Lorenzo’s oil HSCT HSCT HSCT HSCT HSCT
N=36 N=60 M=89 N=94 N=7 N=12 N=7 N=56
Total number of adverse events
At least 1 AE, n (%) NR NR NR NR NR NR NR NR
At least 1 AE related to eli-cel, n
(%)
NR NR NR NR NR NR NR NR
At least 1 grade ≥3
AE, n (%)
NR NR NR NR NR NR NR NR
At least 1 grade ≥3
AE related to eli-cel,
n (%)
NR NR NR NR NR NR NR NR
Total number of AEs (incl.
treatment-related
AEs)
Haemorrhagic cy stitis: 24
Inf ections grade
≥2: 14
GVHD grade ≥2: 9
Extensiv e chronic
GVHD: 8
Sev ere CNS toxic ef f ects: 4
Grade II-IV aGVHD: 11
No AEs were observ ed
Grade III-IV GVHD:
11
Sev ere GVHD: 1 cGVHD with
opportunistic
inf ection: 1
No GVHD or other sequalae related
to BMT were
identif ied
GVHD or multi-organ f ailure: 3
Grade II-IV GVHD: 59 cGVHD: 44
Total number of
serious adv erse
ev ents (incl.
treatment-related AEs)
NR NR No AEs were
observ ed
Grade III-
IV GVHD:
11
NR No GVHD or other
sequalae related
to BMT were
identif ied
GVHD or multi-organ
f ailure: 3
Grade III-IV GVHD: 21
Total number of withdrawals /
discontinuations
f rom the study because of adv erse
ev ents
NR 5 patients died due to ev ents:
Inf ections: 2
Haemorrhage: 1 aGVHD: 1
haemoly tic
anaemia: 1
NR GVHD leading to
death: 5
cGVHD with opportunistic
inf ection leading to
death: 1
NR GVHD or multi-organ f ailure leading to
death: 3
Pulmonary disease: 4 GVHD: 3
Viral inf ections: 2
Bacterial inf ections: 2 Fungal inf ection: 1
Multi-organ f ailure: 1
VOD: 1
Pancy topenia: 1 Unknown: 1
Abbreviations: AE, adverse event; aGVHD, acute graft-versus-host dieases; cGVHD, chronic graft-versus-host disease; CNS, central nervous system; GVHD, graft-versus-host disease; HSCT, haematopoietic stem cell transplantation; NR, not reported; VOD, veno-occlusive disease
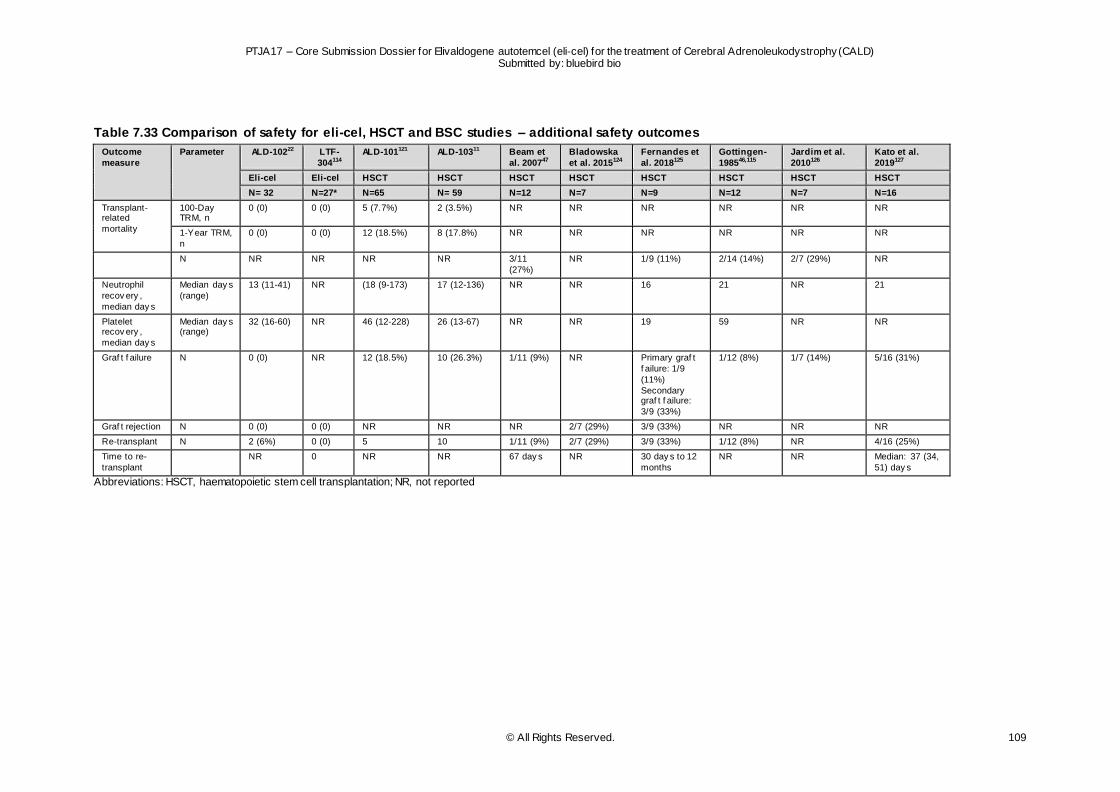
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 109
Table 7.33 Comparison of safety for eli-cel, HSCT and BSC studies – additional safety outcomes
Outcome
measure
Parameter ALD-10222 LTF-
304114
ALD-101121 ALD-10311 Beam et
al. 200747
Bladowska
et al. 2015124
Fernandes et
al. 2018125
Gottingen-
198546,115
Jardim et al.
2010126
Kato et al.
2019127
Eli-cel Eli-cel HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT
N= 32 N=27* N=65 N= 59 N=12 N=7 N=9 N=12 N=7 N=16
Transplant-related
mortality
100-Day TRM, n
0 (0) 0 (0) 5 (7.7%) 2 (3.5%) NR NR NR NR NR NR
1-Year TRM,
n
0 (0) 0 (0) 12 (18.5%) 8 (17.8%) NR NR NR NR NR NR
N NR NR NR NR 3/11
(27%)
NR 1/9 (11%) 2/14 (14%) 2/7 (29%) NR
Neutrophil
recov ery ,
median day s
Median day s
(range)
13 (11-41) NR (18 (9-173) 17 (12-136) NR NR 16 21 NR 21
Platelet recov ery ,
median day s
Median day s (range)
32 (16-60) NR 46 (12-228) 26 (13-67) NR NR 19 59 NR NR
Graf t f ailure N 0 (0) NR 12 (18.5%) 10 (26.3%) 1/11 (9%) NR Primary graf t
f ailure: 1/9
(11%)
Secondary graf t f ailure:
3/9 (33%)
1/12 (8%) 1/7 (14%) 5/16 (31%)
Graf t rejection N 0 (0) 0 (0) NR NR NR 2/7 (29%) 3/9 (33%) NR NR NR
Re-transplant N 2 (6%) 0 (0) 5 10 1/11 (9%) 2/7 (29%) 3/9 (33%) 1/12 (8%) NR 4/16 (25%)
Time to re-
transplant
NR 0 NR NR 67 day s NR 30 day s to 12
months
NR NR Median: 37 (34,
51) day s
Abbreviations: HSCT, haematopoietic stem cell transplantation; NR, not reported
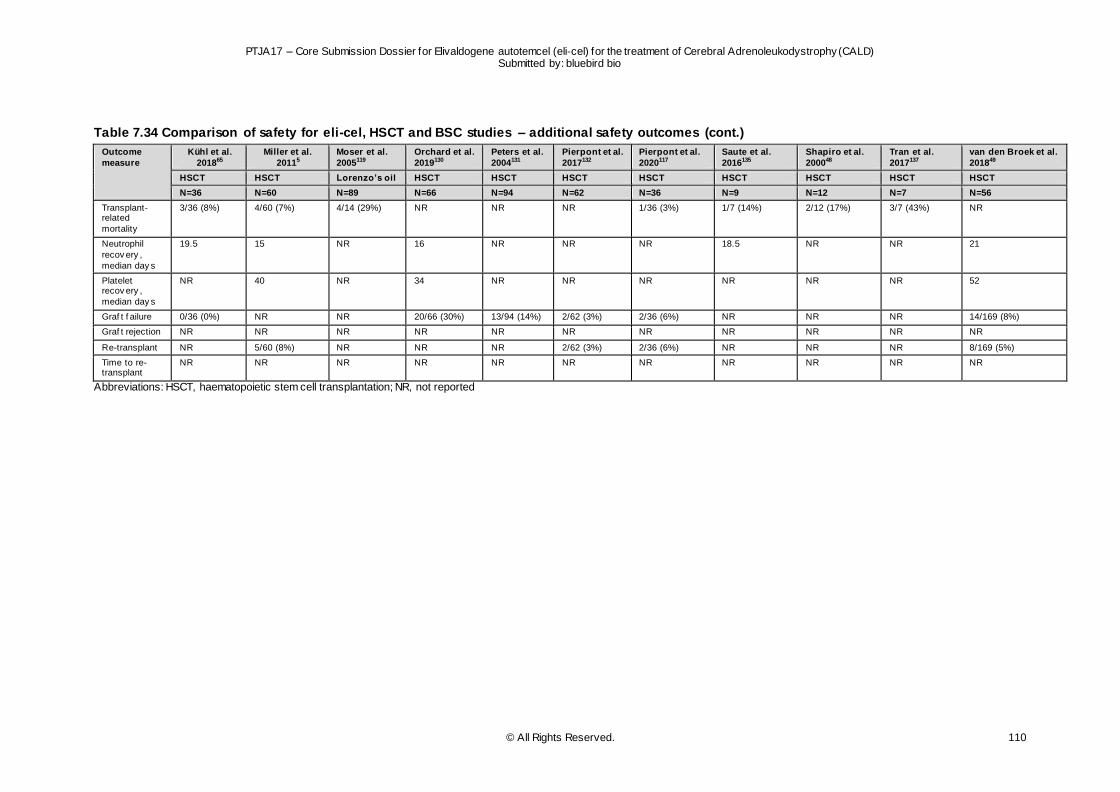
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 110
Table 7.34 Comparison of safety for eli-cel, HSCT and BSC studies – additional safety outcomes (cont.)
Outcome
measure
Kühl et al.
201865
Miller et al.
20115
Moser et al.
2005119
Orchard et al.
2019130
Peters et al.
2004131
Pierpont et al.
2017132
Pierpont et al.
2020117
Saute et al.
2016135
Shapiro et al.
200048
Tran et al.
2017137
van den Broek et al.
201849
HSCT HSCT Lorenzo’s oil HSCT HSCT HSCT HSCT HSCT HSCT HSCT HSCT
N=36 N=60 N=89 N=66 N=94 N=62 N=36 N=9 N=12 N=7 N=56
Transplant-related
mortality
3/36 (8%) 4/60 (7%) 4/14 (29%) NR NR NR 1/36 (3%) 1/7 (14%) 2/12 (17%) 3/7 (43%) NR
Neutrophil
recov ery ,
median day s
19.5 15 NR 16 NR NR NR 18.5 NR NR 21
Platelet recov ery ,
median day s
NR 40 NR 34 NR NR NR NR NR NR 52
Graf t f ailure 0/36 (0%) NR NR 20/66 (30%) 13/94 (14%) 2/62 (3%) 2/36 (6%) NR NR NR 14/169 (8%)
Graf t rejection NR NR NR NR NR NR NR NR NR NR NR
Re-transplant NR 5/60 (8%) NR NR NR 2/62 (3%) 2/36 (6%) NR NR NR 8/169 (5%)
Time to re-transplant
NR NR NR NR NR NR NR NR NR NR NR
Abbreviations: HSCT, haematopoietic stem cell transplantation; NR, not reported
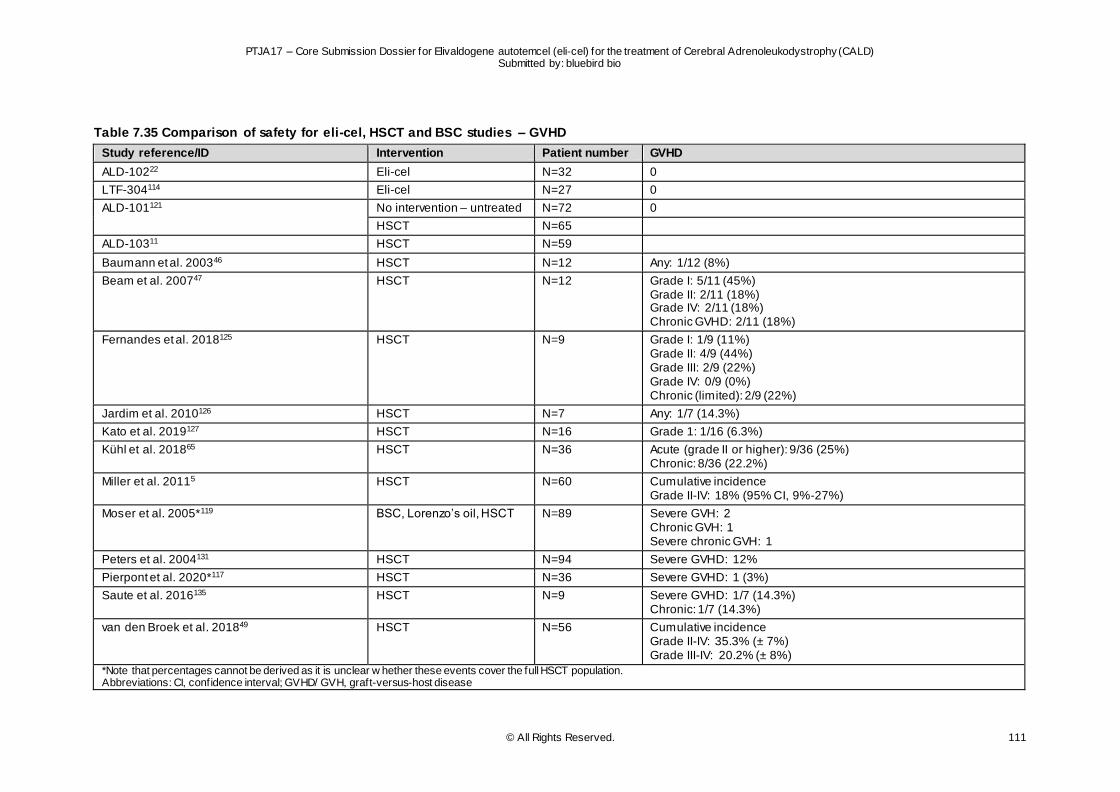
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 111
Table 7.35 Comparison of safety for eli-cel, HSCT and BSC studies – GVHD
Study reference/ID Intervention Patient number GVHD
ALD-10222 Eli-cel N=32 0
LTF-304114 Eli-cel N=27 0
ALD-101121 No intervention – untreated N=72 0
HSCT N=65
ALD-10311 HSCT N=59
Baumann et al. 200346 HSCT N=12 Any: 1/12 (8%)
Beam et al. 200747 HSCT N=12 Grade I: 5/11 (45%) Grade II: 2/11 (18%) Grade IV: 2/11 (18%) Chronic GVHD: 2/11 (18%)
Fernandes et al. 2018125 HSCT N=9 Grade I: 1/9 (11%) Grade II: 4/9 (44%) Grade III: 2/9 (22%) Grade IV: 0/9 (0%) Chronic (limited): 2/9 (22%)
Jardim et al. 2010126 HSCT N=7 Any: 1/7 (14.3%)
Kato et al. 2019127 HSCT N=16 Grade 1: 1/16 (6.3%)
Kühl et al. 201865 HSCT N=36 Acute (grade II or higher): 9/36 (25%) Chronic: 8/36 (22.2%)
Miller et al. 20115 HSCT N=60 Cumulative incidence Grade II-IV: 18% (95% CI, 9%-27%)
Moser et al. 2005*119 BSC, Lorenzo’s oil, HSCT N=89 Severe GVH: 2 Chronic GVH: 1 Severe chronic GVH: 1
Peters et al. 2004131 HSCT N=94 Severe GVHD: 12%
Pierpont et al. 2020*117 HSCT N=36 Severe GVHD: 1 (3%)
Saute et al. 2016135 HSCT N=9 Severe GVHD: 1/7 (14.3%) Chronic: 1/7 (14.3%)
van den Broek et al. 201849 HSCT N=56 Cumulative incidence Grade II-IV: 35.3% (± 7%) Grade III-IV: 20.2% (± 8%)
*Note that percentages cannot be derived as it is unclear w hether these events cover the full HSCT population. Abbreviations: CI, confidence interval; GVHD/ GVH, graft-versus-host disease
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 112
7.10 Conclusions
Eli-cel is a novel, one-time autologous gene therapy which has shown a positive benefit/risk-profile in clinical trials for paediatric patients with early CALD for whom an HLA-matched sibling HSC donor is not available. The eli-cel clinical studies demonstrate that eli-cel stabilises neurologic disease progression
and is generally well-tolerated since no signs of GVHD and graft failure were reported. Eli-cel is expected to provide a durable long-term MFD-free survival and OS. This is in contrast to allo-HSCT and BSC, which are both associated with worse outcomes than eli-cel.
7.10.1 Benefits associated with eli-cel relative to its comparators
Eli-cel is a modified autologous CD34+ cell-enriched population containing stem cells transduced with an LVV that encodes ABCD1 cDNA for human ALDP. In recognition of its beneficial potential, eli-cel
was granted Breakthrough Therapy designation by the US Food and Drug Administration (FDA) in May 2018 for the treatment of CALD and was granted access to the PRIME scheme by EMA in July 2018. Eli-cel also has an orphan drug designation from both the FDA and EMA. An MAA has been submitted
to the EMA for eli-cel and the procedure is currently ongoing under accelerated review.
The primary and most relevant source of data currently available for the safety and efficacy of eli -cel for the indication under consideration is the ALD-102 trial22 and its associated long-term follow-up trial, LTF-
304 (median follow-up not reached).114 Data for control patients receiving allo-HSCT were obtained through a single-arm trial, ALD-103,11 specifically designed with the purpose of being an external control for comparison to ALD-102.22 Additionally, data for comparators (allo-HSCT and BSC) were obtained
through a dedicated SLR (see section 7.8 and 7.9).
Results to date suggest that early treatment with eli-cel can stabilise disease progression in patients with CALD, thereby offering the first authorised, promising, effective and safe treatment option for
patients less than 18 years of age and have an ABCD1 genetic mutation and early CALD, for whom an HLA-matched sibling HSC donor is not available.22 In the ALD-102 and LTF-304 trials,22,114 eli-cel demonstrated sustained MFD-free survival and OS. Specifically, eli-cel demonstrated Month 24 MFD-
free survival of 90.0%10 versus 66.7% for allo-HSCT in a comparable patient population and was estimated to be 90.6% versus 58.8% at 48 months (see table 14.2.1.1 and 14.2.1.2.1 of D120 ALD-102 report).10,11,22,114 Evidence from the SLR (see section 7.8) found similar MFD-free survival outcomes for
allo-HSCT treated patients, while no MFD-free survival outcomes for BSC were identified. In terms of OS, this was estimated to be 96.6%7 for patients treated with eli-cel, versus 75.5% for allo-HSCT patients in a comparable patient population at 48 months (see Table 2.2.1.1.2 of D120 Interstudy
report).7,11,22,114 The studies identified through the SLR (see section 7.8) reported similar survival rates to those reported in ALD-103 for allo-HSCT.11 For patients treated with BSC, the SLR reported a lower mortality rate than reported for patients treated with allo-HSCT (see section 7.8). However, it is important
to note that the patient population treated with BSC was younger and generally in better health than the CALD populations included in the allo-HSCT studies. Other clinical and safety outcomes, including Loes score, change in NFS, GVHD and subsequent allo-HSCT requirements, were associated with similar
benefits for patients treated with eli-cel versus those treated with either allo-HSCT or BSC based on evidence from both the eli-cel clinical development programme, as well as the SLR (see section 7.8 and 7.9) (see Table 14.2.4 and 14.2.5 of D120 ALD-102 report; Tables 14.2.4 and 14.2.5.1 of D120 LTF-
304 report; Tables 3.1.1.2.2, Tables 34.7.1 and 34.7.2 of D120 Interstudy report).7,10,23 Notably, in terms of risk reduction, eli-cel reduces the risk of death by 88.2% (see Table 2.2.1.1.2 of D120 Interstudy report)7 and the risk of MFD, subsequent transplant, and/or death events by 82.2% versus allo-HSCT
(see Table 2.1.1.1.2 of D120 Interstudy report)7. No such comparison could be made versus BSC due to lack of data and comparable populations.
These benefits further underscore the potential clinically meaningful benefit of eli-cel versus treatment
options currently in place for CALD patients; substantially reducing the risk of death, MFD and subsequent transplant in comparison to both allo-HSCT and BSC.
7.10.2 Harms associated with eli-cel relative to its comparators
Results from the ALD-102, ALD-104 and LTF-304 trials suggest that CALD patients treated with eli-cel exhibit a substantially lower risk of experiencing serious safety events, such as acute and chronic GVHD,
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 113
engraftment failure and 1-year TRM, than CALD patients treated with allo-HSCT (see Tables 3.1.1.2.2,
3.2.2.2 and 3.3.2.2 of D120 Interstudy report).7 In fact, no such events have been reported to date for patients treated with eli-cel (ALD-102, ALD-104 and LTF-304).7 In contrast, acute GVHD, chronic GVHD, graft failure and 1-year TRM have been reported to be 30.6%, 35.9%, 26.3% and 17.8%, respectively ,
among allo-HSCT treated patients in a comparable patient population.11 As part of the SLR, similar safety rates to those reported in ALD-103 were reported for allo-HSCT treatment (see section 7.9).
Given the nature of BSC, specifically Lorenzo’s oil, these events were not reported as the treatment
does not involve procedures which can lead to engraftment failure or GVHD. While 1-year TRM was reported for patients receiving BSC, this was for a specific subpopulation who received allo-HSCT during follow-up. Results for this subpopulation were in line with those of patients treated with allo-HSCT (see
section 7.9).119
Treatment with eli-cel is well-tolerated, with a favourable and well-manageable safety profile. In the ALD-102 and ALD-104 clinical studies 60.8% of patients experienced at least one SAE versus 74.6% of allo-
HSCT treated patients in a comparable patient population (see Table 3.4.9 of D120 Interstudy report)7,11 however, the incidence of SAEs related to eli-cel was 5.9% (n=3) and entailed a case of BK-mediated viral cystitis and two cases of pancytopenia (see Table 3.4.6.1 of D120 Interstudy report).7 The events
were diagnosed post-neutrophil engraftment and platelet engraftment was achieved on Day 104 and 108, respectively. As of last visit, approximately 13 months post-infusion, low platelet persisted in both patients and white blood count/ANC fluctuated within lower limit of normal in 1 patient.109 The patient
with BK-mediated viral cystitis died as a result of their SAE; this was the only patient who received eli-cel and died as a result of an SAE. In contrast, 25.4% of patients treated with allo-HSCT died as a result of a treatment-related SAE in a comparable patient population.11 Only limited evidence on SAEs and
deaths associated with SAEs was identified through the SLR for both allo-HSCT and BSC (see section 7.9).
7.11 Strengths and limitations
7.11.1 Validity of the evidence base
Study quality Eli-cel clinical development programme The evidence provided in this submission for the safety and efficacy of eli -cel was generated through
the eli-cel clinical development programme.
As part of the eli-cel clinical development programme, two non-interventional studies were completed, ALD-101 and ALD-103.11,121 The retrospective data collection study, ALD-101 was conducted to
characterise the natural history of disease in untreated subjects with CALD, as well as the efficacy and safety outcomes of subjects who were treated with allo-HSCT, for the purpose of defining efficacy and safety endpoints that could prove useful in the design of clinical studies.121
ALD-101 was crucial in the development of future ALD studies; the data helped define the efficacy endpoints for ALD-102, ALD-103, and ALD-104, allowing identification of the six MFDs that are unambiguous indicators of disease progression.
Study ALD-103 was consequently designed to collect prospective and retrospective data on CALD patients who underwent contemporary allo-HSCT, using a study design consistent with that described in study ALD-102 with respect to efficacy assessments and their timing. Suitability for allo-HSCT and
choice of treatment protocol was determined by the subjects' treating physician as per institutional policies/protocols and other local treatment guidelines.11
Data derived from ALD-103 were intended to be used as a concurrent external comparator for outcomes
after treatment with eli-cel, and were collected through 48 months ± 30 days after last allo-HSCT.11
The severity of CALD, the rarity of the disease, the lack of authorised treatment options, the inability of transplant to be blinded, and the potential impact of time required to conduct a donor match on cerebral
disease progression, precluded the conduct of an RCT in the target patient population. Additionally, the natural history of CALD in patients with GdE (an inclusion criterion for ALD-102) is well-defined, with untreated patients experiencing predictable progressive morbidity and high mortality. GdE is a
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 114
prognostic biomarker of rapid disease progression; the vast majority of untreated CALD patients with
GdE will experience rapid neurological decline and develop MFDs resulting in either a vegetative state or death within a short period of symptom onset (in approximately 1.9 + /- 2 years).4 Therefore, a single-arm, 24-month study design for pivotal ALD-102 was deemed appropriate for generating sufficient
evidence to establish effectiveness of eli-cel for the treatment of CALD when compared to the well-defined natural history of the disease. Specifically, to establish eli-cel benefit, a clinically meaningful benchmark for the primary endpoint of 24-month MFD-free survival was defined, supported by results
from untreated subjects in natural history ALD-101 and data from disease-specific literature that reports on OS. In order to provide additional supportive evidence and confirm the treatment benefit of eli -cel, analyses were defined to make comparisons with concurrently collected data from allo-HSCT-treated
subjects in ALD-103 as well as with historically-collected data from allo-HSCT-treated subjects in ALD-101 (see section 7.7).11,121
Intervention at the early stage of cerebral involvement (i.e., NFS ≤ 1, Loes score ≤ 9) has been shown
to lead to more favourable outcomes,1,131 and development of contrast agent enhancement (GdE+) on brain MRI is indicative of future poor prognosis in untreated patients .4,35 Therefore, eligibility for ALD-102 and ALD-104 included GdE+ at baseline, NFS ≤1 at baseline, and Loes score ≥0.5 to ≤9 at baseline,
defining a population with early stage cerebral disease and poor prognosis without treatment, who could maximally benefit from gene therapy treatment. Eligibility of subjects for inclusion into data collection and non-interventional studies for allo-HSCT was broader than this, to provide an overall understanding of the
natural history of the disease in untreated subjects (ALD-101) as well as an understanding of the disease course in allo-HSCT treated subjects (ALD-101, ALD-103). Thus, subpopulations and subgroups of subjects in ALD-101 and ALD-103 are used for interstudy efficacy comparisons.
The risk of bias assessment was done for the eli-cel clinical trial program (including for the HSCT studies in that program). Specifically, the checklist for observational research, developed by Berger et al. was used.144 This checklist assesses the relevance and credibility of the studies identified. The questionnaire
consists of 33 questions related to the relevance and credibility of an observational study. Each question was scored with Yes / No / Can’t Answer (including comment, such as ‘not applicable’). Relevance questions relate to usefulness of the observational study to inform health care decision making. Based
on the scoring of the individual questions, the overall relevance of the observational study was to be judged as Sufficient or Insufficient. If the observational study was considered sufficiently relevant, the credibility was assessed. The credibility was captured with questions in the following 6 domains: Design,
Data, Analysis, Reporting, Interpretation, and Conflict of interest. Details and key considerations associated with this checklist are described in the original checklist by Berger et al. 144
More details of the risk of bias assessment are presented in appendix 9.10.
SLR Safety and efficacy evidence for the relevant comparators, allo-HSCT and BSC, were derived from both the eli-cel clinical development programme (control studies, discussed as part of the eli-cel clinical
development programme) and an SLR.
Validity of the eli-cel clinical development programme was outlined previously. In relation to the studies identified and included through the SLR, a risk of bias assessment was conducted with the same
checklist by Berger et al.144
Out of the 27 evaluated studies, 20 studies (74%) received ≥70% positive responses in the assessment, indicating a lower risk of bias based on the Berger et al.144 checklist. All studies, independent of the risk
of bias, were included in the synthesis of efficacy and safety outcomes. Of the seven studies scoring below 70%, the lowest score was 60%, suggesting that while the risk of bias was more substantial for this study than for others, it was still relatively limited.126
More details of the risk of bias assessment are presented in appendix 9.10.
As noted previously (see section 7.7), the included studies have study populations of different sizes and backgrounds. They have also formulated their research questions differently, which is likely to affect the
study population chosen and the outcome measures obtained. This reduces the comparability of the outcome measures obtained across the different studies, as well as the feasibility of conducting a comparison based on statistical methods, i.e. a MAIC.9 As a result, no statistical methods were
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 115
undertaken to compare the studies identified through the SLR with the eli -cel clinical development
programme. Instead, the outcomes of the ALD-102 and ALD-103 comparison were contextualised with the additional data identified through the SLR.
Validity of the endpoints
Clinical endpoints The relevance and clinical meaningfulness of the endpoints included in the SLR and the eli-cel clinical development programme are outlined below. As part of refining the eli-cel clinical development
programme, these were discussed with the EMA/CHMP (Committee for Medicinal Products for Human Use) and FDA in the context of scientific advice in 2015 (FDA Type C meeting on 17 Nov 2015), 2016 (CHMP scientific advice letter dated 25 Feb 2016 [EMEA/H/SA/2080/2/2015/PA/SME/ADT/III]) and
2018 (FDA Type C meeting on 22 Feb 2018 and Breakthrough Therapy Designation meeting on 15 Nov 2018; CHMP scientific advice letter dated 22 February 2018 [EMEA/H/SA/2080/2/FU/1/2018/PA/ADT/ PED/II]).
Overall survival OS is a standard measure to assess efficacy of transplantation procedures.
MFD-free survival
Based on a comprehensive chart review of ALD-101 data, a group of CALD experts identified six MFDs that were chosen based on their clinical significance and impact on independent functioning. Prevent ion of the development of MFDs, which represent neurologic deterioration, has been recognised as an
important clinical benefit and is expected to significantly reduce the burden on the patient, the patients’ families and healthcare resources.4 MFDs include loss of communication, cortical blindness, tube feeding, total incontinence, wheelchair dependence, and complete loss of voluntary movement .
Loes score and Loes pattern The Loes score is a 34-point scale used to evaluate and describe disease burden throughout the brain in patients with CALD by scoring MRI findings based on severity.32 The score presents information on
overall severity of white matter atrophy as well as the location of the myelin damage. The Loes pattern is also associated with prognosis. Patterns 1 (parieto-occipital white matter), 2 (frontal white matter), and 5 (concomitant parieto-occipital and frontal white matter) are associated with faster progression;
age and GdE were important co-variates for Patterns 1 and 2. Patterns 3 (corticospinal tract) and 4 (cerebellar white matter) are associated with slower progression.
Change in NFS
The NFS scale is a 25-point composite scale that assesses functional disabilities.33 It was designed specifically for the consistent and reproducible clinical evaluation of patients with CALD. It assesses 15 functional domains affected by the disease and is the most common clinical evaluation tool used by
clinical specialists caring for these patients.5,33 Higher NFS at baseline are also associated with worse prognosis post allo-HSCT.4,5
GdE
Presence of contrast agent enhancement on MRI (frequently involving the use of gadolinium-based agents, and thus referred to as GdE+) represents a clinically important, radiographic biomarker of active neuroinflammatory disease and poor prognosis in untreated patients. These patients experience the
most rapid progression of disease, have more MFDs, and have a higher mortality rate due to disease progression.4,35 GdE+ is frequently used to indicate the necessity for transplantation.
Quality of life
The HRQoL of patients was assessed in ALD-102, ALD-103 and ALD-103 using the PedsQL (the Parent Proxy-Report version was used on Study ALD-102), administered at baseline and then at months 3, 6, 12, and 24 follow-up and at the early termination visit, if applicable. Parents were asked to evaluate their
child in the following four dimensions for the past one month: Physical, Emotional, Social and School Functioning. Results are presented using a 100-point scale, where higher scores indicate better HRQoL. The accepted MCID for an individual, as reported in the literature, is 4.5 points for the PedsQL.138-140 No
carer HRQoL outcomes were collected as part of the eli-cel clinical development programme.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 116
Safety endpoints
The safety outcomes measures investigated as part of the eli-cel clinical development programme and SLR are recognised as the standard assessments for the management of subjects with CALD either prior to or after HSCT.
Neutrophil/platelet recovery Successful HSCT, both autologous and allogeneic, requires a rapid and durable engraftment, with neutrophil and platelet reconstitution. Therefore, recovery of neutrophils and platelets are appropriate
safety outcomes to include.145
Graft failure or rejection/subsequent allo-HSCT/GVHD There is a 10% to 30% risk of failure or rejection of engraftment, and acute and chronic GVHD in patients
treated with allo-HSCT (across donor types),146 with the risk of GVHD being approximately 30% in CALD patients147; therefore, it is appropriate to assess these safety events. Similarly, a consequence of graft rejection and/or failure may be subsequent allo-HSCT and is thus included as a relevant safety outcome.
TRM Although allo-HSCT early in the course of CALD is considered the standard of care, based on experience with allo-HSCT for metabolic disorders, even in the most experienced centres, the TRM rate
is roughly 15%.1,131 Therefore, survival after allo-HSCT is an appropriate safety outcome to include.
(S)AEs Standard safety assessments included clinical and laboratory assessments. Clinical assessments
performed to monitor the safety of subjects enrolled in the eli-cel clinical development programme included medical history, physical examination, vital signs, collection of AEs (including serious AEs, specific eli-cel-related AEs and GVHD), and concomitant therapy and procedures. Standard laboratory
assessments were also performed, including haematology, blood chemistry, liver function tests, and adrenal function tests. Haematology measurements enabled day of neutrophil and platelet engraftment to be calculated. To enable comparison, similar outcomes were extracted from the studies identified
through the SLR, which indicated similar reasons for inclusion of standard safety assessments.
Overall, the evidence provided in this dossier supports the clinical benefit of eli-cel as a treatment option for patients with early CALD diagnosis for whom an HLA-matched sibling HSC donor is not available.
7.11.2 Relevance of the evidence
The results of ALD-102 demonstrate the clinical benefit and safety of eli-cel. The bias potential of the evidence base of eli-cel and allo-HSCT was outlined previously.
The study population of ALD-102 included paediatric CALD patients (less than 18 years of age) with early disease, as measured by Loes score ≥0.5 to ≤9.0 and NFS ≤1, who did not have an MSD for allo-HSCT. This corresponds to the target population of eli-cel according to the label indication and is
transferable to the European health care context with regard to both general patient characteristics and disease-specific criteria (see section 7.6 and section 2.3).
The clinical effectiveness and safety of eli-cel was compared to allo-HSCT, which represents the current
standard of care,2 through an interstudy comparison (see section 7.7.2), as well as evidence obtained through an SLR (see sections 7.8 and 7.9). Very limited evidence in relation to BSC (see section 7.5) was identified and, similar to SLR evidence on allo-HSCT, did not support comparison to eli-cel by
means of statistical methods, e.g. meta-analysis.9 Specifically, this was driven by differing baseline characteristics across studies, as well as variations in research questions and outcomes measures obtained (see section 7.7). Nonetheless, all efficacy and safety endpoints outlined in this assessment
are patient-relevant (see sections 7.8 and 7.9), were collected using valid instruments and analysed using adequate methods.
7.11.3 Limitations of comparisons
Due to the rarity of the disease, the number of patients at risk are low to start with. Obviously, in comparisons over time, like overall survival and MFD-free survival, these numbers will further decrease. One of the reasons that this specifically happens quickly for allo-HSCT, are the risks associated with
this treatment.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 117
Additionally, a difference in number of subjects with missing data could also contribute to this rapid
decrease, as analyses of proportion of MFD-free survival, NFS, Loes score, and GdE status performed across the submitted studies are based on non-missing observations. However, MFD-free survival analysed by Kaplan-Meier method was included in all studies as one of the key secondary endpoints to
account for missing data (by censoring) and provide unbiased estimation and inference.
For proportion-based endpoints, a common method is to pre-define missing as failure based on an ITT approach. Based on Study ALD-102 data as of 23 October 2020, 2/32 subjects are missing data
because they are still ongoing in the study. The missing rate for TP-102 is 6.2%, which is far lower than 9/27 (33.3%) for TPES-103 final data. These subjects were not Month 24 evaluable because they did not complete the Month 24 Visit in the defined time period. Since Study ALD-102 has a lower proportion
of subjects with missing data, MFD free survival rate at Month 24 based on observed case analysis is conservative and the bias is likely against the TP-102 cohort.
To investigate the effect of ALD-102 having a lower proportion of subjects with missing data versus ALD-
103, two additional analyses have been performed:148
1) counting TP-102 missing data as a negative outcome for selected primary and secondary efficacy endpoints, while missing data for TPES-101 and TPES-103 were imputed as a success for these
endpoints. This is the most conservative approach of missing data imputation.
2) to account for varying time of follow-up in subjects, the efficacy endpoints were analysed at the last available assessment.
These additional analyses did not change the conclusions on the comparable benefit between eli-cel and allo-HSCT. Additionally, analysis of the data at last assessment suggests that if current trends continue, the eli-cel dataset will only become stronger as the data matures.
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 118
8 REFERENCES
1 Moser, H. W. et al. X-linked adrenoleukodystrophy. Nature clinical practice. Neurology 3, 140-151, doi:10.1038/ncpneuro0421 (2007).
2 Engelen, M. et al. X-linked adrenoleukodystrophy (X-ALD): clinical presentation and guidelines for diagnosis, follow-up and management. Orphanet journal of rare diseases 7, 51, doi:10.1186/1750-1172-7-51 (2012).
3 Mahmood, A. et al. Survival analysis of haematopoietic cell transplantation for childhood cerebral X-linked adrenoleukodystrophy: a comparison study. The Lancet. Neurology 6, 687-692, doi:10.1016/s1474-4422(07)70177-1 (2007).
4 Raymond, G. V. et al. Survival and Functional Outcomes in Boys with Cerebral Adrenoleukodystrophy with and without Hematopoietic Stem Cell Transplantation. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow
Transplantation 25, 538-548, doi:10.1016/j.bbmt.2018.09.036 (2019). 5 Miller, W. P. et al. Outcomes after allogeneic hematopoietic cell transplantation for childhood
cerebral adrenoleukodystrophy: the largest single-institution cohort report. Blood 118, 1971-
1978, doi:10.1182/blood-2011-01-329235 (2011). 6 van Geel BM, A. J., Haverkort EB. Progression of abnormalities in adrenomyeloneuropathy
and neurologically asymptomatic X-linked adrenoleukodystrophy despite treatment with
“Lorenzo’s oil. J Neurol Neurosurg Psychiatry 67, 290-299 (1999). 7 bluebird bio Inc. TLFs Interstudy D120 MAA. Data on file (2021). 8 bluebird bio Inc. Propensity Scored Analysis Report Data on file.
9 Phillippo, D. M. et al. NICE DSU Technical support Document 18: Methods for Population-Adjusted Indirect Comparison in Submissions to NICE (2016).
10 bluebird bio Inc. TLFs ALD-102 D120 MAA. Data on file (2021).
11 bluebird bio Inc. Clinical Study Report ALD-103 (bluebird Bio Inc., 2020). 12 bluebird bio inc. Elivaldogene autotemcel Summary of Product Characteristics (2021). 13 bluebird bio Inc. TLFs ALD-104 D120 MAA Data on file (2021).
14 Ciurea, S. O. et al. Is a matched unrelated donor search needed for all allogeneic transplant candidates? Blood advances 2, 2254-2261, doi:10.1182/bloodadvances.2018021899 (2018).
15 Doerflinger, N. et al. Retroviral transfer and long-term expression of the adrenoleukodystrophy
gene in human CD34+ cells. Hum Gene Ther. 9, 1025-1036 (1998). 16 Cartier, N. et al. Retroviral-mediated gene transfer corrects very-long-chain fatty acid
metabolism in adrenoleukodystrophy fibroblasts. Proc Natl AcadSci U S A 92, 1674-1678
(1995). 17 Benhamida, S. et al. Transduced CD34+ cells from adrenoleukodystrophy patients with HIV-
derived vector mediate long-term engraftment of NOD/SCID mice. Mol Ther. 7, 317-324 (2003).
18 Mansilla-Soto, J. et al. Cell and Gene Therapy for the Beta-Thalassemias: Advances and Prospects Hum Gene Ther. 27, 295-304 (2016).
19 Srivastava, A. et al. Cure for thalassemia major - from allogeneic hematopoietic stem cell
transplantation to gene therapy Haematologica 102, 214-223 (2017). 20 Dong, A. et al. Gene Addition Strategies for β-Thalassemia and Sickle Cell Anemia Adv Exp
Med Biol 1013, 155-176 (2017).
21 Doulatov, S. et al. Hematopoiesis: a human perspective Cell Stem Cell 10, 120-136 (2012). 22 bluebird bio Inc. Interim clinical study report ALD-102. Data on file (2020). 23 bluebird bio Inc. TLFs LTF-304 D120 MAA. Data on file (2021).
24 Engelen, M., et al.,. Facts on ALD. ALD Info. https://adrenoleukodystrophy.info/clinical-diagnosis/facts-on-ald. Published 2018. Accessed 30 June 2018. (2018).
25 Huffnagel, I. C. et al. The Natural History of Adrenal Insufficiency in X-Linked
Adrenoleukodystrophy: An International Collaboration. The Journal of clinical endocrinology and metabolism 104, 118-126, doi:10.1210/jc.2018-01307 (2019).
26 Kemp, S., et al., . ALD Info: Clinical presentations (2019).
27 Musolino, P. L. et al. Brain endothelial dysfunction in cerebral adrenoleukodystrophy. Brain : a journal of neurology 138, 3206-3220, doi:10.1093/brain/awv250 (2015).
28 Richmond, P. A. et al. Multi-Omic Approach to Identify Phenotypic Modifiers Underlying
Cerebral Demyelination in X-Linked Adrenoleukodystrophy. Frontiers in cell and developmental biology 8, 520, doi:10.3389/fcell.2020.00520 (2020).
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 119
29 Suzuki, Y. et al. Natural history of X-linked adrenoleukodystrophy in Japan. Brain &
development 27, 353-357, doi:10.1016/j.braindev.2004.09.008 (2005). 30 Miller, W. Stem cell-transplantation therapy for adrenoleukodystrophy: current perspectives.
Journal of Neurorestoratology 5, 5-19, doi:https://doi.org/10.2147/JN.S99304 (2017).
31 Moser, H. W. et al. The adrenoleukodystrophies. Critical reviews in neurobiology 3, 29-88 (1987).
32 Loes, D. J. et al. Adrenoleukodystrophy: a scoring method for brain MR observations.
American Journal of Neuroradiology 15, 1761 (1994). 33 Moser, H. W. et al. X-Linked adrenoleukodystrophy: overview and prognosis as a function of
age and brain magnetic resonance imaging abnormality. A study involving 372 patients.
Neuropediatrics 31, 227-239, doi:10.1055/s-2000-9236 (2000). 34 Loes, D. J. et al. Analysis of MRI patterns aids prediction of progression in X-linked
adrenoleukodystrophy. Neurology 61, 369-374, doi:10.1212/01.wnl.0000079050.91337.83
(2003). 35 Melhem, E. R. et al. X-linked adrenoleukodystrophy: the role of contrast-enhanced MR
imaging in predicting disease progression. AJNR. American journal of neuroradiology 21, 839-
844 (2000). 36 Mallack, E. J. et al. Clinical and radiographic course of arrested cerebral
adrenoleukodystrophy. Neurology 94, e2499-e2507, doi:10.1212/wnl.0000000000009626
(2020). 37 Horn, M. A. et al. Adrenoleukodystrophy in Norway: high rate of de novo mutations and age-
dependent penetrance. Pediatric neurology 48, 212-219,
doi:10.1016/j.pediatrneurol.2012.12.007 (2013). 38 Girós-Blasco, M. R., M; Ribes, A; Pàmpols-Ros, T. Diagnosis of peroxisomal diseases in
Spain in the period 1987-1997. Rev Neurol 28 (S1), 40-40 (1999).
39 Stellitano, L. A. et al. Leukodystrophies and genetic leukoencephalopathies in childhood: a national epidemiological study. Developmental medicine and child neurology 58, 680-689, doi:10.1111/dmcn.13027 (2016).
40 Bezman, L. et al. Incidence of X-linked adrenoleukodystrophy and the relative frequency of its phenotypes. American journal of medical genetics 76, 415-419 (1998).
41 Aubourg, P. [X-linked adrenoleukodystrophy]. Annales d'endocrinologie 68, 403-411,
doi:10.1016/j.ando.2007.04.002 (2007). 42 Eurostat data from 2018 <https://ec.europa.eu/eurostat/statistics-
explained/index.php/Fertility_statistics;> (
43 European Union Demographics Profile 2018, <https://www.indexmundi.com/european_union/demographics_profile.html (visited September 2020)> (
44 Wiesinger, C. et al. The genetic landscape of X-linked adrenoleukodystrophy: inheritance, mutations, modifier genes, and diagnosis. The application of clinical genetics 8, 109-121, doi:10.2147/tacg.S49590 (2015).
45 Furlan, F. L. S. et al. X-LINKED ADRENOLEUKODYSTROPHY IN BRAZIL: A CASE SERIES. Rev Paul Pediatr 37, 465-471, doi:10.1590/1984-0462/;2019;37;4;00015 (2019).
46 Baumann, M. et al. Haematopoietic stem cell transplantation in 12 patients with cerebral X-
linked adrenoleukodystrophy. European journal of pediatrics 162, 6-14, doi:10.1007/s00431-002-1097-3 (2003).
47 Beam, D. et al. Outcomes of unrelated umbilical cord blood transplantation for X-linked
adrenoleukodystrophy. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation 13, 665-674, doi:10.1016/j.bbmt.2007.01.082 (2007).
48 Shapiro, E. et al. Long-term effect of bone-marrow transplantation for childhood-onset cerebral X-linked adrenoleukodystrophy. Lancet (London, England) 356, 713-718, doi:10.1016/s0140-6736(00)02629-5 (2000).
49 van den Broek, B. T. A. et al. Early and late outcomes after cord blood transplantation for pediatric patients with inherited leukodystrophies. Blood advances 2, 49-60, doi:10.1182/bloodadvances.2017010645 (2018).
50 Suzuki, Y. et al. The clinical course of childhood and adolescent adrenoleukodystrophy before and after Lorenzo's oil. Brain & development 23, 30-33, doi:10.1016/s0387-7604(00)00196-0 (2001).

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 120
51 Ping, L. L. et al. The genotype and phenotype studies of 40 Chinese patients with X-linked
adrenoleukodystrophy (X-ALD). Beijing da xue xue bao. Yi xue ban = Journal of Pek ing University. Health sciences 38, 66-70 (2006).
52 Winstone, A. et al. The presentation and diagnosis of UK children with X-linked
adrenoleukodystrophy ascertained over 17 years. Developmental medicine and child neurology 57 SUPPL. 1 (2015).
53 AIALD, O. a. A. Health Technology Assessment on drug for CALD answered by the
associations of patients. 15 December 2020 (2020). 54 Health Economics and Technology Assessment Research. Burden of disease of Cerebral
Adrenoleukodystrophy (CALD): Protocol for a Systematic Literature Review - Final report.
Data on file 55 Petrou, S. et al. Estimating Preference-Based Health Utilities Index Mark 3 Utility Scores for
Childhood Conditions in England and Scotland. Medical Decision Making 29, 291-303,
doi:10.1177/0272989x08327398 (2009). 56 Bessey, A. et al. Economic impact of screening for X-linked Adrenoleukodystrophy within a
newborn blood spot screening programme. Orphanet journal of rare diseases 13, 179,
doi:10.1186/s13023-018-0921-4 (2018). 57 Sung, L. et al. Treatment options for patients with acute myeloid leukemia with a matched
sibling donor: a decision analysis. Cancer 97, 592-600, doi:10.1002/cncr.11098 (2003).
58 Kuratsubo, I. et al. Parents of childhood X-linked adrenoleukodystrophy: high risk for depression and neurosis. Brain & development 30, 477-482, doi:10.1016/j.braindev.2007.12.012 (2008).
59 Lee, T. Y. et al. The lived experience of Taiwanese mothers of a child diagnosed with adrenoleukodystrophy. Journal of health psychology 19, 195-206, doi:10.1177/1359105312467388 (2014).
60 National Institute for Health and Care Excellence (NICE). Highly Specialised Technologies Evaluation. Ataluren for treating Duchenne muscular dystrophy caused by a nonsense mutation in the dystrophin gene [ID 428]. . Committee Papers (2015).
61 Paramore C, D. A., Boulanger L. . Costs of Episodes of Care for Allogeneic Transplant for the Treatment of Cerebral Adrenoleukodystrophy in the U.S. Virtual ISPOR 2020 (2020).
62 Blommestein, H. M. et al. Real-world costs of autologous and allogeneic stem cell
transplantations for haematological diseases: a multicentre study. Annals of hematology 91, 1945-1952, doi:10.1007/s00277-012-1530-2 (2012).
63 Poduslo, S. E. et al. Myelin development in infant brain. Neurochemical research 9, 1615-
1626, doi:10.1007/bf00964595 (1984). 64 Mallhi, K. K. et al. Allele-Level HLA Matching Impacts Key Outcomes Following Umbilical Cord
Blood Transplantation for Inherited Metabolic Disorders. Biology of blood and marrow
transplantation : journal of the American Society for Blood and Marrow Transplantation 23, 119-125, doi:10.1016/j.bbmt.2016.10.019 (2017).
65 Kühl, J.-S. et al. Potential Risks to Stable Long-term Outcome of Allogeneic Hematopoietic
Stem Cell Transplantation for Children With Cerebral X-linked Adrenoleukodystrophy. JAMA Network Open 1, e180769-e180769, doi:10.1001/jamanetworkopen.2018.0769 (2018).
66 bluebird bio Inc. EBMT Registry CALD allo-HSCT 2015-2020. Data on file (2021).
67 Turk B, M. E., Adang L. Consensus Guidelines: MRI Surveillance of Children with Presymptomatic Adrenoleukodystrophy Neurology 92, 46-47 (2019).
68 Hubbard, W. C. et al. Newborn screening for X-linked adrenoleukodystrophy (X-ALD):
validation of a combined liquid chromatography-tandem mass spectrometric (LC-MS/MS) method. Molecular genetics and metabolism 97, 212-220, doi:10.1016/j.ymgme.2009.03.010 (2009).
69 Kemp, S. et al. Adrenoleukodystrophy - neuroendocrine pathogenesis and redefinition of natural history. Nature reviews. Endocrinology 12, 606-615, doi:10.1038/nrendo.2016.90 (2016).
70 Wiens, K. et al. A report on state-wide implementation of newborn screening for X-linked Adrenoleukodystrophy. American journal of medical genetics. Part A 179, 1205-1213, doi:10.1002/ajmg.a.61171 (2019).
71 Lee, S. et al. Evaluation of X-Linked Adrenoleukodystrophy Newborn Screening in North Carolina. JAMA Netw Open 3, e1920356, doi:10.1001/jamanetworkopen.2019.20356 (2020).
72 Barendsen, R. W. et al. Adrenoleukodystrophy Newborn Screening in the Netherlands (SCAN
Study): The X-Factor. Frontiers in cell and developmental biology 8, doi:10.3389/fcell.2020.00499 (2020).

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 121
73 SCAN-studie. Screening op adrenoleukodystrofie (ALD) in Nederland via de hielprik ,
<https://scanstudie.nl/> (n.d). 74 National Institute for Health and Environment Ministry of Health, W. a. S. Extension of the heel
prick , <https://www.pns.nl/hielprik/professionals/uitbreiding> (2017).
75 Engelen, M., et al., . X-linked adrenoleukodystrophy: pathogenesis and treatment. Current neurology and neuroscience reports 14, 486, doi:10.1007/s11910-014-0486-0 (2014).
76 Sung, A. D. et al. Concise review: acute graft-versus-host disease: immunobiology,
prevention, and treatment. Stem cells translational medicine 2, 25-32, doi:10.5966/sctm.2012-0115 (2013).
77 Pidala, J. Graft-vs-host disease following allogeneic hematopoietic cell transplantation. Cancer
control : journal of the Moffitt Cancer Center 18, 268-276, doi:10.1177/107327481101800407 (2011).
78 Hill, L. et al. New and emerging therapies for acute and chronic graft versus host disease.
Therapeutic advances in hematology 9, 21-46, doi:10.1177/2040620717741860 (2018). 79 Zeiser, R. et al. Pathophysiology of Chronic Graft-versus-Host Disease and Therapeutic
Targets. The New England journal of medicine 377, 2565-2579, doi:10.1056/NEJMra1703472
(2017). 80 García-Cadenas, I. et al. Patterns of infection and infection-related mortality in patients with
steroid-refractory acute graft versus host disease. Bone marrow transplantation 52, 107-113,
doi:10.1038/bmt.2016.225 (2017). 81 Aubourg, P. et al. A Two-Year Trial of Oleic and Erucic Acids (“Lorenzo's Oil”) as Treatment
for Adrenomyeloneuropathy. New England Journal of Medicine 329, 745-752,
doi:10.1056/nejm199309093291101 (1993). 82 Engelen M, O. R., Dijkgraaf MGW, Hijzen M, van der Wardt LA, van Geel BM, de Visser M,
Wanders RJA, Tien Poll-The B, Kemp S. Lovastatin in X-Linked Adrenoleukodystrophy. The
New England journal of medicine 362, 276-277, doi:DOI: 10.1056/NEJMc0907735 (2010). 83 Kurtzberg, J. et al. Preclinical characterization of DUOC-01, a cell therapy product derived
from banked umbilical cord blood for use as an adjuvant to umbilical cord blood
transplantation for treatment of inherited metabolic diseases. Cytotherapy 17, 803-815, doi:10.1016/j.jcyt.2015.02.006 (2015).
84 Saha, A. et al. A cord blood monocyte-derived cell therapy product accelerates brain
remyelination. JCI insight 1, e86667, doi:10.1172/jci.insight.86667 (2016). 85 ClinicalTrials.gov. UCB derived oligodendrocyte-like cells (DUOC-01).
https://clinicaltrials.gov/ct2/show/NCT02254863. Published 2019. Updated December 2019.
Accessed 2020. (2019). 86 ClinicalTrials.gov. MGTA-456 in patients with inherited metabolic disorders undergoing
hematopoietic stem cell transplantation (HSCT).
https://clinicaltrials.gov/ct2/show/NCT03406962. Published 2020. Updated June 2020. Accessed 2020. Published 2020. Updated June 2020. Accessed 2020. (2020).
87 Orchard, P. J. et al. Robust Engraftment with Mgta-456, a CD34<sup>+</sup> Expanded Cell
Therapy Product in Patients with Inherited Metabolic Disorders (IMD): Preliminary Phase 2 Trial Results. Biology of Blood and Marrow Transplantation 25, S91-S92, doi:10.1016/j.bbmt.2018.12.171 (2019).
88 Galaverna, F. et al. Administration of BPX-501 Cells Following T and B-Cell-Depleted HLA-Haploidentical HSCT (haplo-HSCT) in Children with Malignant or Non-Malignant Disorders. Biology of Blood and Marrow Transplantation 25, S13-S14, doi:10.1016/j.bbmt.2018.12.080
(2019). 89 ClinicalTrials.gov. Safety, pharmacokinetics and pharmacodynamics of NV1205 in pediatric
male subjects with adrenoleukodystrophy. https://clinicaltrials.gov/ct2/show/NCT03196765.
Published 2019. Updated March 2019. Accessed 2020. (2019). 90 ClinicalTrials.gov. A clinical study to evaluate the efficacy and safety of MIN-102 (IMP) in male
AMN patients. https://clinicaltrials.gov/ct2/show/NCT03231878. Published 2019. Updated
March 2019. Accessed 2020. (2019). 91 ClinicalTrials.gov. A study to evaluate the safety, tolerability, and pharmacokinetics of OP-101
after intravenous administration in healthy volunteers.
https://clinicaltrials.gov/ct2/show/NCT03500627. Published 2018. Updated September 2018. Accessed 2020. (2018).
92 Tolar, J. et al. N-acetyl-L-cysteine improves outcome of advanced cerebral
adrenoleukodystrophy. Bone marrow transplantation 39, 211-215, doi:10.1038/sj.bmt.1705571 (2007).
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 122
93 Zierfuss, B. et al. Vorinostat in the acute neuroinflammatory form of X-linked
adrenoleukodystrophy. Ann Clin Transl Neurol 7, 639-652, doi:10.1002/acn3.51015 (2020). 94 Gupta, A. et al. Failure of intrathecal allogeneic mesenchymal stem cells to halt progressive
demyelination in two boys with cerebral adrenoleukodystrophy. Stem cells translational
medicine 9, 554-558, doi:10.1002/sctm.19-0304 (2020). 95 Rosewich, H. et al. B cell depletion can be effective in multiple sclerosis but failed in a patient
with advanced childhood cerebral X-linked adrenoleukodystrophy. Therapeutic advances in
neurological disorders 12, 1756286419868133, doi:10.1177/1756286419868133 (2019). 96 Prasad, V. K. et al. Unrelated donor umbilical cord blood transplantation for inherited
metabolic disorders in 159 pediatric patients from a single center: influence of cellular
composition of the graft on transplantation outcomes. Blood 112, 2979-2989, doi:10.1182/blood-2008-03-140830 (2008).
97 Regelmann, M. O. et al. Adrenoleukodystrophy: Guidance for Adrenal Surveillance in Males
Identified by Newborn Screen. The Journal of clinical endocrinology and metabolism 103, 4324-4331, doi:10.1210/jc.2018-00920 (2018).
98 Moser, H. W. et al. Evaluation of the preventive effect of glyceryl trioleate- trierucate
("Lorenzo's oil") therapy in X-linked adrenoleukodystrophy: Results of two concurrent trials. (2003) PEROXISOMAL DISORDERS AND REGULATION OF GENES (2003).
99 Biffi, A. et al. Gene therapy for leukodystrophies. Human molecular genetics 20, R42-53,
doi:10.1093/hmg/ddr142 (2011). 100 bluebird bio Inc. EU-Risk Management Plan for Skysona (elivaldogene autotemcel) Part II
Module SVII. (2021).
101 Foundation for the accreditation of cellular therapy (FACT) Joint accrediatation commitee ISCT and EBMT (JACIE). FACT-JACEI International Standards for Hematopoitic Cellular Therapy Product Collection, Processing, and Administration. (2018).
102 European Commission. Manual for patients: patient's right to accessing healthcare in any EU/EAA country. https://ec.europa.eu/health/sites/health/files/cross_border_care/docs/2019_ncptoolbox_manua
lpatients_en.pdf. Accessed 2020. 103 European Union. Information points: planned medical treatment abroad,
<https://europa.eu/youreurope/citizens/health/planned-healthcare/get-more-
info/index_en.htm> ( 104 EU-Patienten-DE. Assumption of costs in case of planned treatment as if you had statutory
health insurance in Germany (form E 112 or S2). https://www.eu-
patienten.de/en/behandlung_deutschland/geplante_behandlung/wer_traegt_die_kosten/behandlung_wie_gesetzlich_krankenversicherte_2/behandlung_wie_gesetzlich_krankenversicherte_4.jsp Published 2017. Accessed 26.01.2021. (2017).
105 Mallack, E. J. et al. The Landscape of Hematopoietic Stem Cell Transplant and Gene Therapy for X-Linked Adrenoleukodystrophy. Current treatment options in neurology 21, 61, doi:10.1007/s11940-019-0605-y (2019).
106 Eichler, F. et al. Hematopoietic Stem-Cell Gene Therapy for Cerebral Adrenoleukodystrophy. The New England journal of medicine 377, 1630-1638, doi:10.1056/NEJMoa1700554 (2017).
107 Sevin, C., et al.,. Phase 2/3 trial to assess the safety and efficacy of Lenti -D Hematopoietic
Stem Cell Gene Therapy for Cerebral Adrenoleukodystrophy. Abstract OC036 13th EPNS, Athens, Greece. (2019).
108 Kühl, J., et al., . Lenti-D hematopoietic stem cell gene therapy stabilizes neurologic function in
boys with cerebral adrenoleukodystrophy. Abstract O077 46th Annual Meeting of the EBMT (2020).
109 Kühl, J. et al. Elivaldogene autotemcel (eli-cel; Lenti-D) gene therapy for cerebral
adrenoleukodystrophy: Updated results from the phase 2/3 study and safety outcomes report from the phase 3 study. EBMT 2021 Data on file (2021).
110 Eichler, F., et al., . An observational study of outcomes of allogeneic hematopoietic stem cell
transplant in patients with cerebral adrenoleukodystrophy (CALD). Abstract OC039. 13th EPNS, Athens, Greece (2019).
111 Boelens, J., et al.,. Outcomes of allogeneic hematopoietic stem cell transplant in patients with
cerebral adrenoleukodystrophy vary by donor cell source, conditioning regimen, and stage of cerebral disease status. Abstract O106 46th Annual Meeting of the EBMT (2020).
112 Boelens, J. et al. Outcomes of Allogeneic Hematopoietic Stem Cell Transplantation in Patients
with Cerebral Adrenoleukodystrophy: Effects of Donor Cell Source and Match, Conditioning
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 123
Regimen, and Stage of Cerebral Disease. Transplantation & Cellular Therapy Meeting,
February 8 – 12, 2021 (2021). 113 bluebird bio Inc. Interim clinical study report ALD-104. Data on file (2020). 114 bluebird bio Inc. Interim clinical study report LTF-304. Data on file (2020).
115 Wilken, B. et al. Quantitative proton magnetic resonance spectroscopy of children with adrenoleukodystrophy before and after hematopoietic stem cell transplantation. Neuropediatrics 34, 237-246, doi:10.1055/s-2003-43254 (2003).
116 Miller, W. P. et al. Intensity of MRI Gadolinium Enhancement in Cerebral Adrenoleukodystrophy: A Biomarker for Inflammation and Predictor of Outcome following Transplantation in Higher Risk Patients. AJNR. American journal of neuroradiology 37, 367-
372, doi:10.3174/ajnr.A4500 (2016). 117 Pierpont, E. I. et al. Neurocognitive benchmarks following transplant for emerging cerebral
adrenoleukodystrophy. Neurology 95, e591-e600, doi:10.1212/wnl.0000000000009929
(2020). 118 National Bone Marrow Program: Be the Match. Transplants by Disease Category at Each U.S.
NMDP Transplant Center,
<https://bethematch.org/uploadedfiles/bethematchcontent/patients_and_families/before_transplant/choosing_a_transplant_center/transplants_by_disease_charts/metabolic.pdf> (2018).
119 Moser, H. W. et al. Follow-up of 89 asymptomatic patients with adrenoleukodystrophy treated
with Lorenzo's oil. Archives of neurology 62, 1073-1080, doi:10.1001/archneur.62.7.1073 (2005).
120 Beckmann, N. B. et al. Quality of life among boys with adrenoleukodystrophy following
hematopoietic stem cell transplant. Child neuropsychology : a journal on normal and abnormal development in childhood and adolescence 24, 986-998, doi:10.1080/09297049.2017.1380176 (2018).
121 bluebird bio Inc. Clinical Study Report ALD-101. Data on file (2015). 122 Carreras, E. et al. The EBMT Handbook . (2019). 123 Sorror, M. L. et al. Development and Validation of a Novel Acute Myeloid Leukemia-
Composite Model to Estimate Risks of Mortality. JAMA oncology 3, 1675-1682, doi:10.1001/jamaoncol.2017.2714 (2017).
124 Bladowska, J. et al. The Role of MR Imaging in the Assessment of Clinical Outcomes in
Children with X-Linked Adrenoleukodystrophy after Allogeneic Haematopoietic Stem Cell Transplantation. Pol J Radiol 80, 181-190, doi:10.12659/PJR.893285 (2015).
125 Fernandes, J. F. et al. Haploidentical bone marrow transplantation with post transplant
cyclophosphamide for patients with X-linked adrenoleukodystrophy: a suitable choice in an urgent situation. Bone marrow transplantation 53, 392-399, doi:10.1038/s41409-017-0015-2 (2018).
126 Jardim, L. B. et al. X-linked adrenoleukodystrophy: clinical course and minimal incidence in South Brazil. Brain & development 32, 180-190, doi:10.1016/j.braindev.2009.02.002 (2010).
127 Kato, K. et al. Allogeneic stem cell transplantation with reduced intensity conditioning for
patients with adrenoleukodystrophy. Molecular genetics and metabolism reports 18, 1-6, doi:10.1016/j.ymgmr.2018.11.001 (2019).
128 McKinney, A. M. et al. Childhood Cerebral Adrenoleukodystrophy: MR Perfusion
Measurements and Their Use in Predicting Clinical Outcome after Hematopoietic Stem Cell Transplantation. American Journal of Neuroradiology 37, 1713, doi:10.3174/ajnr.A4773 (2016).
129 McKinney, A. M. et al. Childhood Cerebral X-Linked Adrenoleukodystrophy: Diffusion Tensor Imaging Measurements for Prediction of Clinical Outcome after Hematopoietic Stem Cell Transplantation. American Journal of Neuroradiology 34, 641, doi:10.3174/ajnr.A3232 (2013).
130 Orchard, P. J. et al. Successful donor engraftment and repair of the blood-brain barrier in cerebral adrenoleukodystrophy. Blood 133, 1378-1381, doi:10.1182/blood-2018-11-887240 (2019).
131 Peters, C. et al. Cerebral X-linked adrenoleukodystrophy: the international hematopoietic cell transplantation experience from 1982 to 1999. Blood 104, 881-888, doi:10.1182/blood-2003-10-3402 (2004).
132 Pierpont, E. I. et al. Neurocognitive Trajectory of Boys Who Received a Hematopoietic Stem Cell Transplant at an Early Stage of Childhood Cerebral Adrenoleukodystrophy. JAMA neurology 74, 710-717, doi:10.1001/jamaneurol.2017.0013 (2017).
133 Pierpont, E. I. et al. Post-transplant adaptive function in childhood cerebral adrenoleukodystrophy. Ann Clin Transl Neurol 5, 252-261, doi:10.1002/acn3.526 (2018).
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 124
134 Polgreen, L. E. et al. Early diagnosis of cerebral X-linked adrenoleukodystrophy in boys with
Addison's disease improves survival and neurological outcomes. European journal of pediatrics 170, 1049-1054, doi:10.1007/s00431-011-1401-1 (2011).
135 Saute, J. A. et al. Neurological outcomes after hematopoietic stem cell transplantation for
cerebral X-linked adrenoleukodystrophy, late onset metachromatic leukodystrophy and Hurler syndrome. Arquivos de neuro-psiquiatria 74, 953-966, doi:10.1590/0004-282x20160155 (2016).
136 Tokimasa, S. et al. Umbilical cord-blood transplantations from unrelated donors in patients with inherited metabolic diseases: Single-institute experience. Pediatric transplantation 12, 672-676, doi:10.1111/j.1399-3046.2007.00876.x (2008).
137 Tran, C. et al. Long-term outcome of patients with X-linked adrenoleukodystrophy: A retrospective cohort study. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society 21, 600-609, doi:10.1016/j.ejpn.2017.02.006
(2017). 138 Seid, M. et al. The impact of realized access to care on health-related quality of life: a two-
year prospective cohort study of children in the California State Children's Health Insurance
Program. The Journal of pediatrics 149, 354-361, doi:10.1016/j.jpeds.2006.04.024 (2006). 139 Varni, J. W. et al. The PedsQL 4.0 as a pediatric population health measure: feasibility,
reliability, and validity. Ambulatory pediatrics : the official journal of the Ambulatory Pediatric
Association 3, 329-341, doi:10.1367/1539-4409(2003)003<0329:tpaapp>2.0.co;2 (2003). 140 Vetter, T. R. et al. An observational study of patient versus parental perceptions of health-
related quality of life in children and adolescents with a chronic pain condition: who should the
clinician believe? Health and quality of life outcomes 10, 85, doi:10.1186/1477-7525-10-85 (2012).
141 De Oliveira S, E. F., Duncan C, et al. . Autologous hematopoietic stem cell gene therapy for
cerebral adrenoleukodystrophy –Results of an international Phase 2/3 trial. SMID 2018 (2018).
142 bluebird bio Inc. Clinical study protocol ALD-102. Data on file (2017).
143 Di Giuseppe, G. et al. Anxiety, depression, and mental health-related quality of life in survivors of pediatric allogeneic hematopoietic stem cell transplantation: a systematic review. Bone marrow transplantation 55, 1240-1254, doi:10.1038/s41409-020-0782-z (2020).
144 Berger, M. L. et al. A questionnaire to assess the relevance and credibility of observational studies to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value in health : the journal of the International Society for Pharmacoeconomics
and Outcomes Research 17, 143-156, doi:10.1016/j.jval.2013.12.011 (2014). 145 Gonçalves, T. L. et al. Specific factors influence the success of autologous and allogeneic
hematopoietic stem cell transplantation. Oxid Med Cell Longev 2, 82-87,
doi:10.4161/oxim.2.2.8355 (2009). 146 Hahn, T. et al. Risk factors for acute graft-versus-host disease after human leukocyte antigen-
identical sibling transplants for adults with leukemia. Journal of clinical oncology : official
journal of the American Society of Clinical Oncology 26, 5728-5734, doi:10.1200/jco.2008.17.6545 (2008).
147 Carlens, S. et al. Risk factors for chronic graft-versus-host disease after bone marrow
transplantation: a retrospective single centre analysis. Bone marrow transplantation 22, 755-761, doi:10.1038/sj.bmt.1701423 (1998).
148 bluebird bio Inc. Low evaluability numbers. D120 submission. (2021).
149 Loes, D. J. et al. Adrenoleukodystrophy: a scoring method for brain MR observations. AJNR
Am J Neuroradiol 15, 1761-1766 (1994).
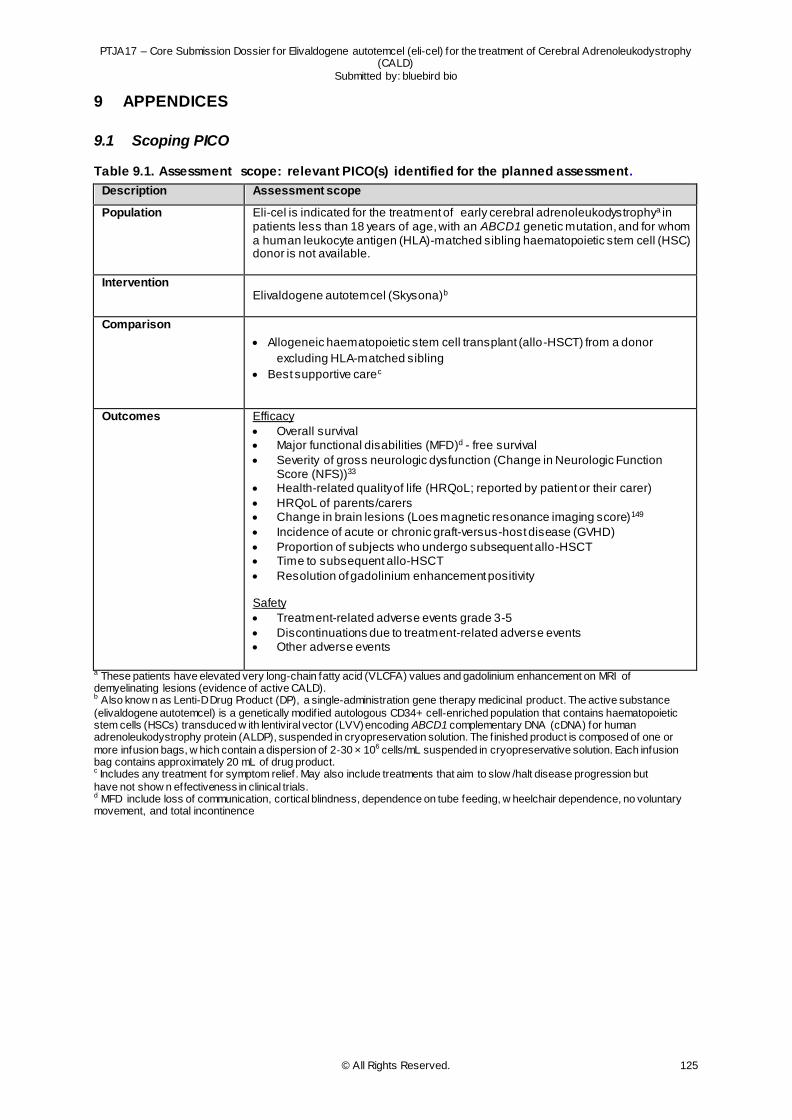
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 125
9 APPENDICES
9.1 Scoping PICO
Table 9.1. Assessment scope: relevant PICO(s) identified for the planned assessment.
Description Assessment scope
Population
Eli-cel is indicated for the treatment of early cerebral adrenoleukodystrophya in patients less than 18 years of age, with an ABCD1 genetic mutation, and for whom a human leukocyte antigen (HLA)-matched sibling haematopoietic stem cell (HSC) donor is not available.
Intervention
Elivaldogene autotemcel (Skysona)b
Comparison
Allogeneic haematopoietic stem cell transplant (allo-HSCT) from a donor
excluding HLA-matched sibling
Best supportive carec
Outcomes
Efficacy
Overall survival Major functional disabilities (MFD)d - free survival
Severity of gross neurologic dysfunction (Change in Neurologic Function Score (NFS))33
Health-related quality of life (HRQoL; reported by patient or their carer)
HRQoL of parents/carers Change in brain lesions (Loes magnetic resonance imaging score)149
Incidence of acute or chronic graft-versus-host disease (GVHD)
Proportion of subjects who undergo subsequent allo-HSCT Time to subsequent allo-HSCT
Resolution of gadolinium enhancement positivity Safety
Treatment-related adverse events grade 3-5
Discontinuations due to treatment-related adverse events Other adverse events
a These patients have elevated very long-chain fatty acid (VLCFA) values and gadolinium enhancement on MRI of demyelinating lesions (evidence of active CALD). b Also know n as Lenti-D Drug Product (DP), a single-administration gene therapy medicinal product. The active substance
(elivaldogene autotemcel) is a genetically modif ied autologous CD34+ cell‑enriched population that contains haematopoietic stem cells (HSCs) transduced w ith lentiviral vector (LVV) encoding ABCD1 complementary DNA (cDNA) for human adrenoleukodystrophy protein (ALDP), suspended in cryopreservation solution. The f inished product is composed of one or
more infusion bags, w hich contain a dispersion of 2‑30 × 106 cells/mL suspended in cryopreservative solution. Each infusion bag contains approximately 20 mL of drug product. c Includes any treatment for symptom relief. May also include treatments that aim to slow /halt disease progression but
have not show n effectiveness in clinical trials. d MFD include loss of communication, cortical blindness, dependence on tube feeding, w heelchair dependence, no voluntary movement, and total incontinence
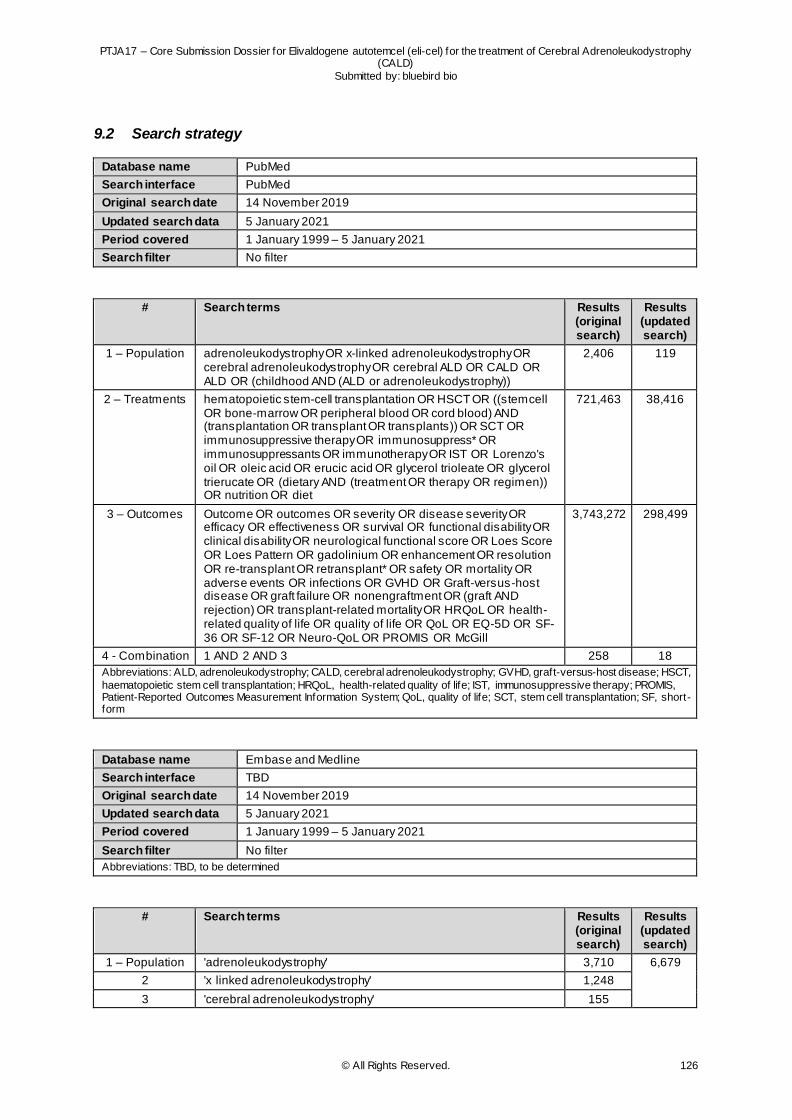
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 126
9.2 Search strategy
Database name PubMed
Search interface PubMed
Original search date 14 November 2019
Updated search data 5 January 2021
Period covered 1 January 1999 – 5 January 2021
Search filter No filter
# Search terms Results (original search)
Results (updated search)
1 – Population adrenoleukodystrophy OR x-linked adrenoleukodystrophy OR cerebral adrenoleukodystrophy OR cerebral ALD OR CALD OR ALD OR (childhood AND (ALD or adrenoleukodystrophy))
2,406 119
2 – Treatments hematopoietic stem-cell transplantation OR HSCT OR ((stemcell OR bone-marrow OR peripheral blood OR cord blood) AND (transplantation OR transplant OR transplants)) OR SCT OR immunosuppressive therapy OR immunosuppress* OR immunosuppressants OR immunotherapy OR IST OR Lorenzo's oil OR oleic acid OR erucic acid OR glycerol trioleate OR glycerol trierucate OR (dietary AND (treatment OR therapy OR regimen)) OR nutrition OR diet
721,463 38,416
3 – Outcomes Outcome OR outcomes OR severity OR disease severity OR efficacy OR effectiveness OR survival OR functional disability OR clinical disability OR neurological functional score OR Loes Score OR Loes Pattern OR gadolinium OR enhancement OR resolution OR re-transplant OR retransplant* OR safety OR mortality OR adverse events OR infections OR GVHD OR Graft-versus-host disease OR graft failure OR nonengraftment OR (graft AND rejection) OR transplant-related mortality OR HRQoL OR health-related quality of life OR quality of life OR QoL OR EQ-5D OR SF-36 OR SF-12 OR Neuro-QoL OR PROMIS OR McGill
3,743,272 298,499
4 - Combination 1 AND 2 AND 3 258 18
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; GVHD, graft-versus-host disease; HSCT,
haematopoietic stem cell transplantation; HRQoL, health-related quality of life; IST, immunosuppressive therapy; PROMIS, Patient-Reported Outcomes Measurement Information System; QoL, quality of life; SCT, stem cell transplantation; SF, short-form
Database name Embase and Medline
Search interface TBD
Original search date 14 November 2019
Updated search data 5 January 2021
Period covered 1 January 1999 – 5 January 2021
Search filter No filter
Abbreviations: TBD, to be determined
# Search terms Results (original search)
Results (updated search)
1 – Population 'adrenoleukodystrophy' 3,710 6,679
2 'x linked adrenoleukodystrophy' 1,248
3 'cerebral adrenoleukodystrophy' 155
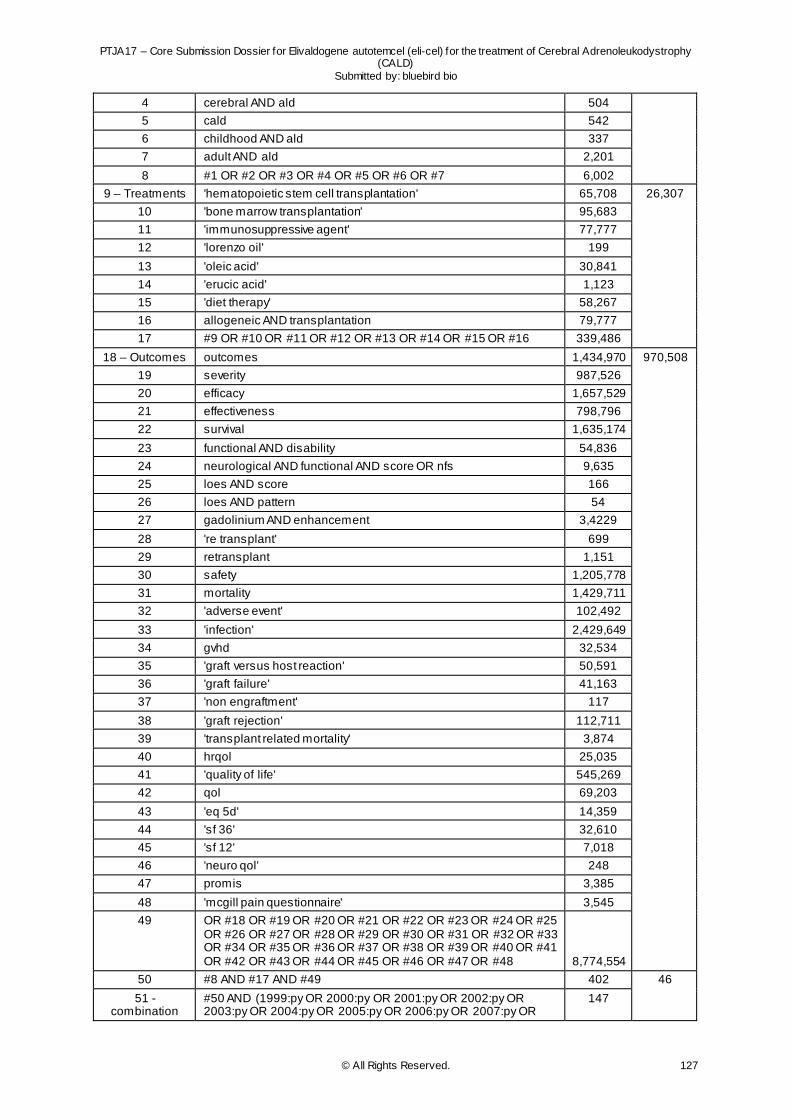
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 127
4 cerebral AND ald 504
5 cald 542
6 childhood AND ald 337
7 adult AND ald 2,201
8 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 6,002
9 – Treatments 'hematopoietic stem cell transplantation' 65,708 26,307
10 'bone marrow transplantation' 95,683
11 'immunosuppressive agent' 77,777
12 'lorenzo oil' 199
13 'oleic acid' 30,841
14 'erucic acid' 1,123
15 'diet therapy' 58,267
16 allogeneic AND transplantation 79,777
17 #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 339,486
18 – Outcomes outcomes 1,434,970 970,508
19 severity 987,526
20 efficacy 1,657,529
21 effectiveness 798,796
22 survival 1,635,174
23 functional AND disability 54,836
24 neurological AND functional AND score OR nfs 9,635
25 loes AND score 166
26 loes AND pattern 54
27 gadolinium AND enhancement 3,4229
28 're transplant' 699
29 retransplant 1,151
30 safety 1,205,778
31 mortality 1,429,711
32 'adverse event' 102,492
33 'infection' 2,429,649
34 gvhd 32,534
35 'graft versus host reaction' 50,591
36 'graft failure' 41,163
37 'non engraftment' 117
38 'graft rejection' 112,711
39 'transplant related mortality' 3,874
40 hrqol 25,035
41 'quality of life' 545,269
42 qol 69,203
43 'eq 5d' 14,359
44 'sf 36' 32,610
45 'sf 12' 7,018
46 'neuro qol' 248
47 promis 3,385
48 'mcgill pain questionnaire' 3,545
49 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 OR #48 8,774,554
50 #8 AND #17 AND #49 402 46
51 - combination
#50 AND (1999:py OR 2000:py OR 2001:py OR 2002:py OR 2003:py OR 2004:py OR 2005:py OR 2006:py OR 2007:py OR
147
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 128
2008:py OR 2009:py OR 2010:py OR 2011:py OR 2012:py OR 2013:py OR 2014:py OR 2015:py OR 2016:py OR 2017:py OR 2018:py OR 2019:py) AND [embase]/lim NOT ([embase]/lim AND [medline]/lim)
[covering 2019-2021]
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; GVHD, graft-versus-host disease; HRQoL, health-related quality of life; NFS, neurologic function score; PROMIS, Patient-Reported Outcomes Measurement Information System; QoL, quality of life; SF, short-form
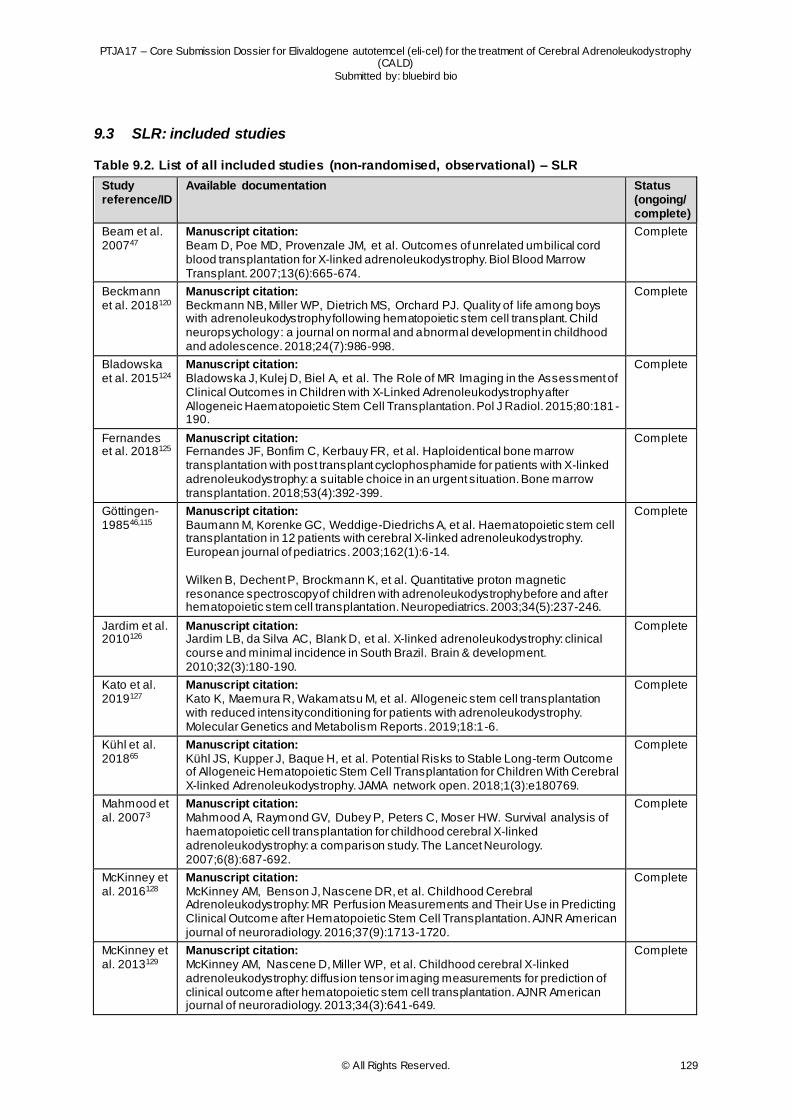
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 129
9.3 SLR: included studies
Table 9.2. List of all included studies (non-randomised, observational) – SLR
Study reference/ID
Available documentation Status (ongoing/ complete)
Beam et al. 200747
Manuscript citation: Beam D, Poe MD, Provenzale JM, et al. Outcomes of unrelated umbilical cord blood transplantation for X-linked adrenoleukodystrophy. Biol Blood Marrow Transplant. 2007;13(6):665-674.
Complete
Beckmann et al. 2018120
Manuscript citation: Beckmann NB, Miller WP, Dietrich MS, Orchard PJ. Quality of life among boys with adrenoleukodystrophy following hematopoietic stem cell transplant. Child neuropsychology : a journal on normal and abnormal development in childhood and adolescence. 2018;24(7):986-998.
Complete
Bladowska et al. 2015124
Manuscript citation: Bladowska J, Kulej D, Biel A, et al. The Role of MR Imaging in the Assessment of Clinical Outcomes in Children with X-Linked Adrenoleukodystrophy after Allogeneic Haematopoietic Stem Cell Transplantation. Pol J Radiol. 2015;80:181 -190.
Complete
Fernandes et al. 2018125
Manuscript citation: Fernandes JF, Bonfim C, Kerbauy FR, et al. Haploidentical bone marrow transplantation with post transplant cyclophosphamide for patients with X-linked adrenoleukodystrophy: a suitable choice in an urgent situation. Bone marrow transplantation. 2018;53(4):392-399.
Complete
Göttingen-198546,115
Manuscript citation: Baumann M, Korenke GC, Weddige-Diedrichs A, et al. Haematopoietic stem cell transplantation in 12 patients with cerebral X-linked adrenoleukodystrophy. European journal of pediatrics. 2003;162(1):6-14. Wilken B, Dechent P, Brockmann K, et al. Quantitative proton magnetic resonance spectroscopy of children with adrenoleukodystrophy before and after hematopoietic stem cell transplantation. Neuropediatrics. 2003;34(5):237-246.
Complete
Jardim et al. 2010126
Manuscript citation: Jardim LB, da Silva AC, Blank D, et al. X-linked adrenoleukodystrophy: clinical course and minimal incidence in South Brazil. Brain & development. 2010;32(3):180-190.
Complete
Kato et al. 2019127
Manuscript citation: Kato K, Maemura R, Wakamatsu M, et al. Allogeneic stem cell transplantation with reduced intensity conditioning for patients with adrenoleukodystrophy. Molecular Genetics and Metabolism Reports. 2019;18:1-6.
Complete
Kühl et al. 201865
Manuscript citation: Kühl JS, Kupper J, Baque H, et al. Potential Risks to Stable Long-term Outcome of Allogeneic Hematopoietic Stem Cell Transplantation for Children With Cerebral X-linked Adrenoleukodystrophy. JAMA network open. 2018;1(3):e180769.
Complete
Mahmood et al. 20073
Manuscript citation: Mahmood A, Raymond GV, Dubey P, Peters C, Moser HW. Survival analysis of haematopoietic cell transplantation for childhood cerebral X-linked adrenoleukodystrophy: a comparison study. The Lancet Neurology. 2007;6(8):687-692.
Complete
McKinney et al. 2016128
Manuscript citation: McKinney AM, Benson J, Nascene DR, et al. Childhood Cerebral Adrenoleukodystrophy: MR Perfusion Measurements and Their Use in Predicting Clinical Outcome after Hematopoietic Stem Cell Transplantation. AJNR American journal of neuroradiology. 2016;37(9):1713-1720.
Complete
McKinney et al. 2013129
Manuscript citation: McKinney AM, Nascene D, Miller WP, et al. Childhood cerebral X-linked adrenoleukodystrophy: diffusion tensor imaging measurements for prediction of clinical outcome after hematopoietic stem cell transplantation. AJNR American journal of neuroradiology. 2013;34(3):641-649.
Complete
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 130
Miller et al. 2016*116
Manuscript citation: Miller WP, Mantovani LF, Muzic J, et al. Intensity of MRI Gadolinium Enhancement in Cerebral Adrenoleukodystrophy: A Biomarker for Inflammation and Predictor of Outcome following Transplantation in Higher Risk Patients. AJNR American journal of neuroradiology. 2016;37(2):367-372. * A portion of these patients are also reported in Orchard et al. 2019
Complete
Miller et al. 20115
Manuscript citation: Miller WP, Rothman SM, Nascene D, et al. Outcomes after allogeneic hematopoietic cell transplantation for childhood cerebral adrenoleukodystrophy: the largest singleinstitution cohort report. Blood. 2011;118(7):1971-1978.
Complete
Moser et al. 2005119
Manuscript citation: Moser HW, Raymond GV, Lu SE, et al. Follow-up of 89 asymptomatic patients with adrenoleukodystrophy treated with Lorenzo's oil. Archives of neurology. 2005;62(7):1073-1080.
Complete
Orchard et al. 2019*130
Manuscript citation: Orchard PJ, Nascene DR, Miller WP, Gupta A, Kenney-Jung D, Lund TC. Successful donor engraftment and repair of the blood-brain barrier in cerebral adrenoleukodystrophy. Blood. 2019;133(12):1378-1381. * A portion of these patients were previously reported in Miller et al. 2016
Complete
Peters et al. 2004131
Manuscript citation: Peters C, Charnas LR, Tan Y, et al. Cerebral X-linked adrenoleukodystrophy: the international hematopoietic cell transplantation experience from 1982 to 1999. Blood. 2004;104(3):881-888.
Complete
Pierpont et al. 2017*132
Manuscript citation: Pierpont EI, Eisengart JB, Shanley R, et al. Neurocognitive Trajectory of Boys Who Received a Hematopoietic Stem Cell Transplant at an Early Stage of Childhood Cerebral Adrenoleukodystrophy. JAMA neurology. 2017;74(6):710-717. * Similar subjects may have been included in Pierpont et al. 2018 and Pierpont et al. 2020, however, this was not part of the same study aim .
Complete
Pierpont et al. 2018*133
Manuscript citation: Pierpont EI, McCoy E, King KE, et al. Post-transplant adaptive function in childhood cerebral adrenoleukodystrophy. Annals of Clinical and Translational Neurology. 2018;5(3):252-261. * Similar subjects may have been included in Pierpont et al. 2017 and Pierpont et al. 2020, however, this was not part of the same study aim .
Complete
Pierpont et al. 2020*117
Manuscript citation: Pierpont EI, Nascene DR, Shanley R, et al. Neurocognitive benchmarks following transplant for emerging cerebral adrenoleukodystrophy. Neurology. 2020;95(5):e591-e600. * Similar subjects may have been included in Pierpont et al. 2017 and Pierpont et al. 2018, however, this was not part of the same study aim .
Complete
Polgreen et al. 2011134
Manuscript citation: Polgreen LE, Chahla S, Miller W, et al. Early diagnosis of cerebral X-linked adrenoleukodystrophy in boys with Addison's disease improves survival and neurological outcomes. European journal of pediatrics. 2011;170(8):1049-1054.
Complete
Saute et al. 2016135
Manuscript citation: Saute JA, Souza CF, Poswar FO, et al. Neurological outcomes after hematopoietic stem cell transplantation for cerebral X-linked adrenoleukodystrophy, late onset metachromatic leukodystrophy and Hurler syndrome. Arquivos de neuro-psiquiatria. 2016;74(12):953-966.
Complete
Shapiro et al. 200048
Manuscript citation: Shapiro E, Krivit W, Lockman L, et al. Long-term effect of bone-marrow transplantation for childhood-onset cerebral X-linked adrenoleukodystrophy. Lancet (London, England). 2000;356(9231):713-718.
Complete
Suzuki et al. 200150
Manuscript citation: Suzuki Y, Imamura A, Shimozawa N, Kondo N. The clinical course of childhood and adolescent adrenoleukodystrophy before and after Lorenzo's oil. Brain & development. 2001;23(1):30-33.
Complete
Tokimasa et al. 2008136
Manuscript citation: Tokimasa S, Ohta H, Takizawa S, et al. Umbilical cord-blood transplantations from unrelated donors in patients with inherited metabolic diseases: Single -institute experience. Pediatric transplantation. 2008;12(6):672-676.
Complete

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 131
Tran et al. 2017137
Manuscript citation: Tran C, Patel J, Stacy H, et al. Long-term outcome of patients with X-linked adrenoleukodystrophy: A retrospective cohort study. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society. 2017;21(4):600-609.
Complete
van den Broek et al. 201849
Manuscript citation: van den Broek BTA, Page K, Paviglianiti A, et al. Early and late outcomes after cord blood transplantation for pediatric patients with inherited leukodystrophies. Blood advances. 2018;2(1):49-60.
Complete
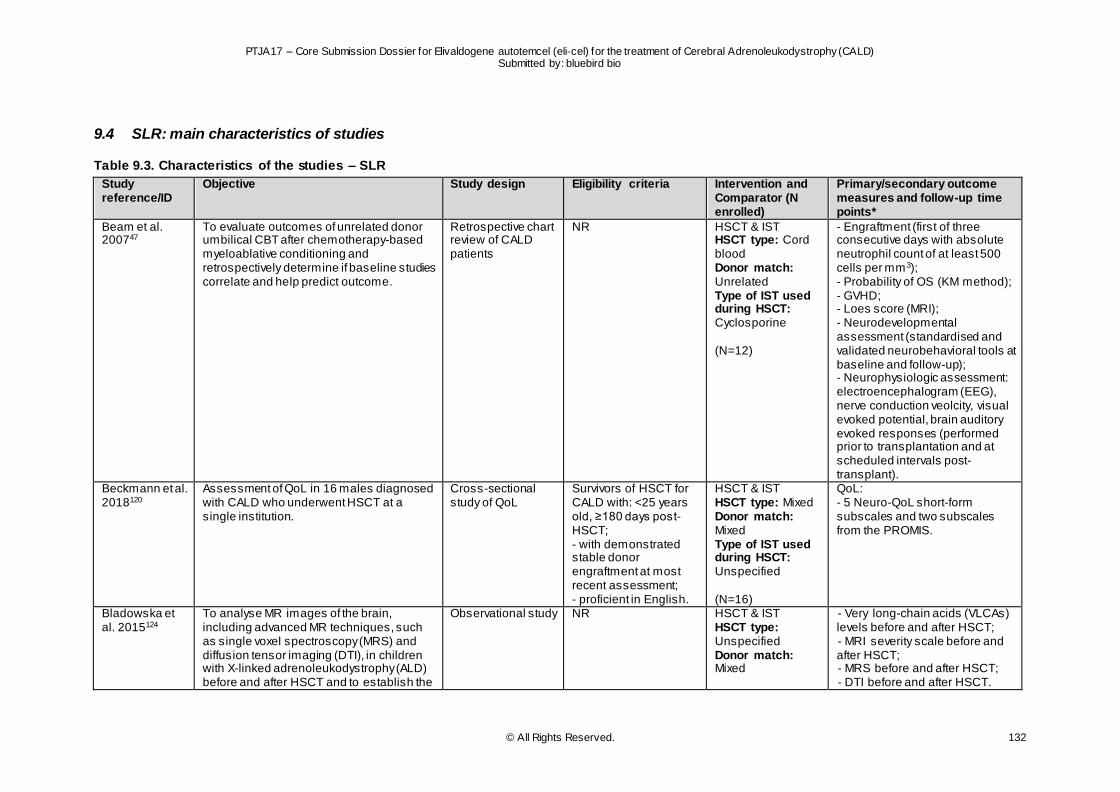
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 132
9.4 SLR: main characteristics of studies
Table 9.3. Characteristics of the studies – SLR
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
Beam et al. 200747
To evaluate outcomes of unrelated donor umbilical CBT after chemotherapy-based myeloablative conditioning and retrospectively determine if baseline studies correlate and help predict outcome.
Retrospective chart review of CALD patients
NR HSCT & IST HSCT type: Cord blood Donor match: Unrelated Type of IST used during HSCT: Cyclosporine (N=12)
- Engraftment (first of three consecutive days with absolute neutrophil count of at least 500 cells per mm3); - Probability of OS (KM method); - GVHD; - Loes score (MRI); - Neurodevelopmental assessment (standardised and validated neurobehavioral tools at baseline and follow-up); - Neurophysiologic assessment: electroencephalogram (EEG), nerve conduction veolcity, visual evoked potential, brain auditory evoked responses (performed prior to transplantation and at scheduled intervals post-transplant).
Beckmann et al. 2018120
Assessment of QoL in 16 males diagnosed with CALD who underwent HSCT at a single institution.
Cross-sectional study of QoL
Survivors of HSCT for CALD with: <25 years old, ≥180 days post-HSCT; - with demonstrated stable donor engraftment at most recent assessment; - proficient in English.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Unspecified (N=16)
QoL: - 5 Neuro-QoL short-form subscales and two subscales from the PROMIS.
Bladowska et al. 2015124
To analyse MR images of the brain, including advanced MR techniques, such as single voxel spectroscopy (MRS) and diffusion tensor imaging (DTI), in children with X-linked adrenoleukodystrophy (ALD) before and after HSCT and to establish the
Observational study NR HSCT & IST HSCT type: Unspecified Donor match: Mixed
- Very long-chain acids (VLCAs) levels before and after HSCT; - MRI severity scale before and after HSCT; - MRS before and after HSCT; - DTI before and after HSCT.
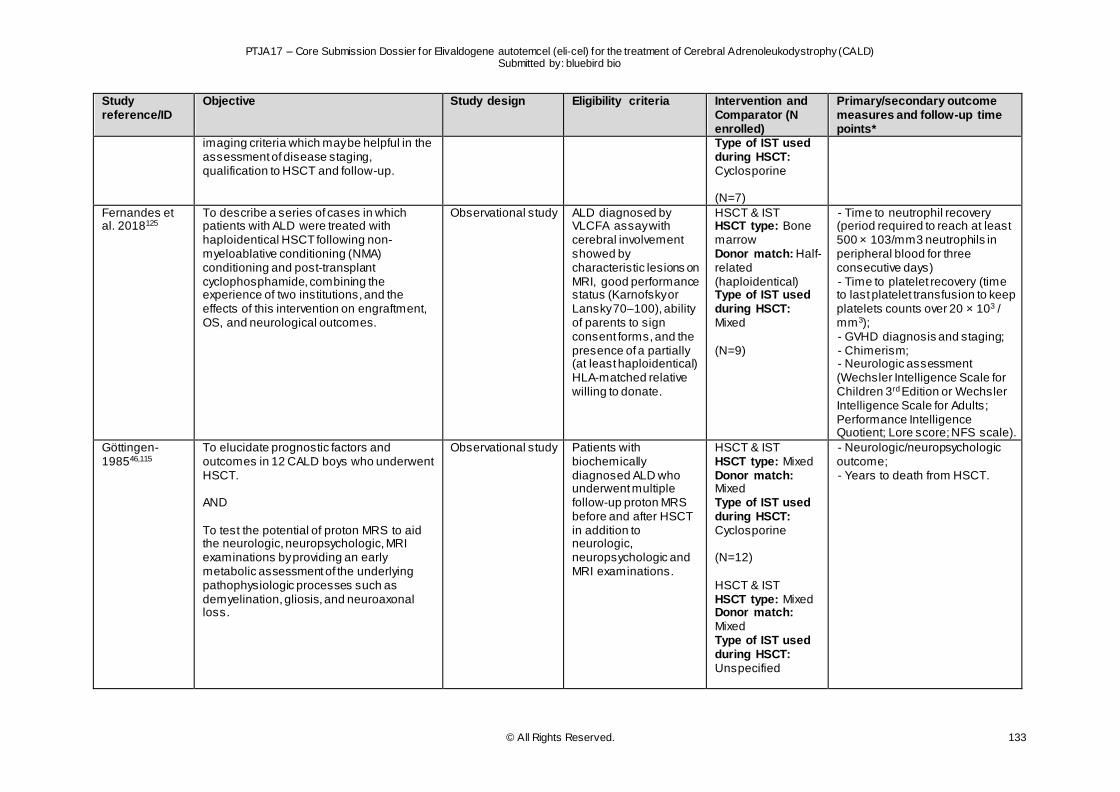
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 133
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
imaging criteria which may be helpful in the assessment of disease staging, qualification to HSCT and follow-up.
Type of IST used during HSCT: Cyclosporine (N=7)
Fernandes et al. 2018125
To describe a series of cases in which patients with ALD were treated with haploidentical HSCT following non-myeloablative conditioning (NMA) conditioning and post-transplant cyclophosphamide, combining the experience of two institutions, and the effects of this intervention on engraftment, OS, and neurological outcomes.
Observational study ALD diagnosed by VLCFA assay with cerebral involvement showed by characteristic lesions on MRI, good performance status (Karnofsky or Lansky 70–100), ability of parents to sign consent forms, and the presence of a partially (at least haploidentical) HLA-matched relative willing to donate.
HSCT & IST HSCT type: Bone marrow Donor match: Half-related (haploidentical) Type of IST used during HSCT: Mixed (N=9)
- Time to neutrophil recovery (period required to reach at least 500 × 103/mm3 neutrophils in peripheral blood for three consecutive days) - Time to platelet recovery (time to last platelet transfusion to keep platelets counts over 20 × 103 / mm3); - GVHD diagnosis and staging; - Chimerism; - Neurologic assessment (Wechsler Intelligence Scale for Children 3rd Edition or Wechsler Intelligence Scale for Adults; Performance Intelligence Quotient; Lore score; NFS scale).
Göttingen-198546,115
To elucidate prognostic factors and outcomes in 12 CALD boys who underwent HSCT. AND To test the potential of proton MRS to aid the neurologic, neuropsychologic, MRI examinations by providing an early metabolic assessment of the underlying pathophysiologic processes such as demyelination, gliosis, and neuroaxonal loss.
Observational study Patients with biochemically diagnosed ALD who underwent multiple follow-up proton MRS before and after HSCT in addition to neurologic, neuropsychologic and MRI examinations.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Cyclosporine (N=12) HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Unspecified
- Neurologic/neuropsychologic outcome; - Years to death from HSCT.
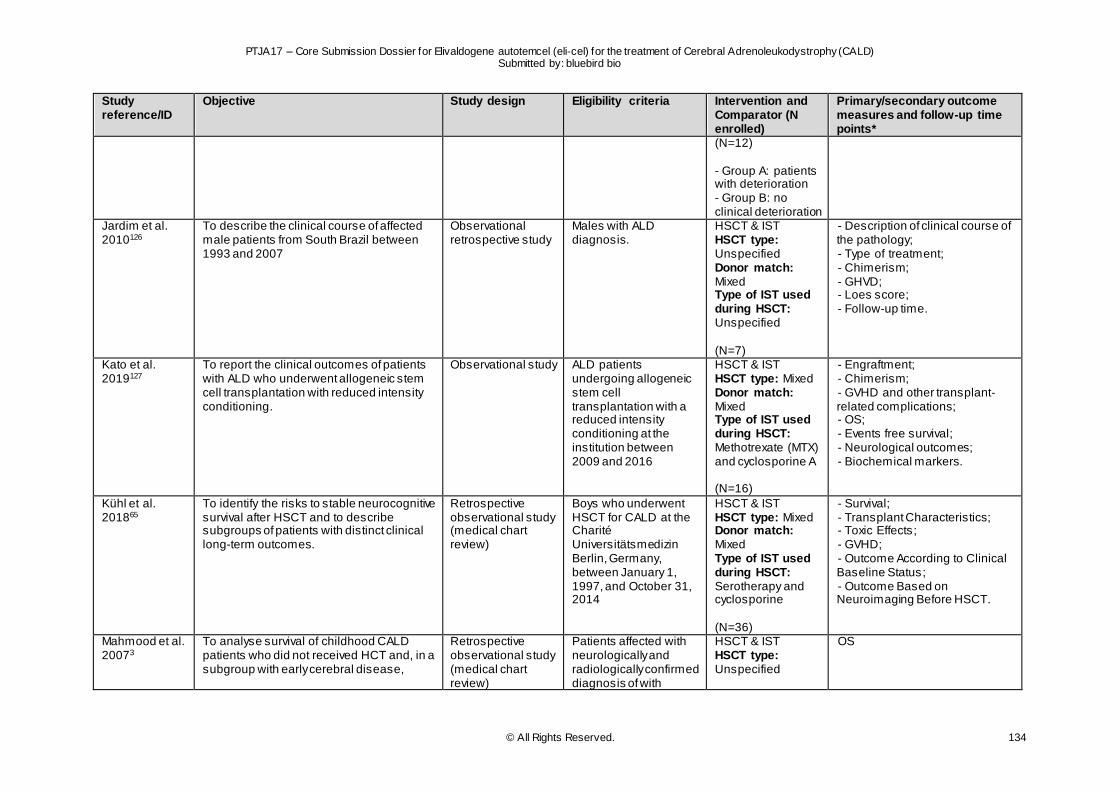
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 134
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
(N=12) - Group A: patients with deterioration - Group B: no clinical deterioration
Jardim et al. 2010126
To describe the clinical course of affected male patients from South Brazil between 1993 and 2007
Observational retrospective study
Males with ALD diagnosis.
HSCT & IST HSCT type: Unspecified Donor match: Mixed Type of IST used during HSCT: Unspecified (N=7)
- Description of clinical course of the pathology; - Type of treatment; - Chimerism; - GHVD; - Loes score; - Follow-up time.
Kato et al. 2019127
To report the clinical outcomes of patients with ALD who underwent allogeneic stem cell transplantation with reduced intensity conditioning.
Observational study ALD patients undergoing allogeneic stem cell transplantation with a reduced intensity conditioning at the institution between 2009 and 2016
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Methotrexate (MTX) and cyclosporine A (N=16)
- Engraftment; - Chimerism; - GVHD and other transplant-related complications; - OS; - Events free survival; - Neurological outcomes; - Biochemical markers.
Kühl et al. 201865
To identify the risks to stable neurocognitive survival after HSCT and to describe subgroups of patients with distinct clinical long-term outcomes.
Retrospective observational study (medical chart review)
Boys who underwent HSCT for CALD at the Charité Universitätsmedizin Berlin, Germany, between January 1, 1997, and October 31, 2014
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Serotherapy and cyclosporine (N=36)
- Survival; - Transplant Characteristics; - Toxic Effects; - GVHD; - Outcome According to Clinical Baseline Status; - Outcome Based on Neuroimaging Before HSCT.
Mahmood et al. 20073
To analyse survival of childhood CALD patients who did not received HCT and, in a subgroup with early cerebral disease,
Retrospective observational study (medical chart review)
Patients affected with neurologically and radiologically confirmed diagnosis of with
HSCT & IST HSCT type: Unspecified
OS
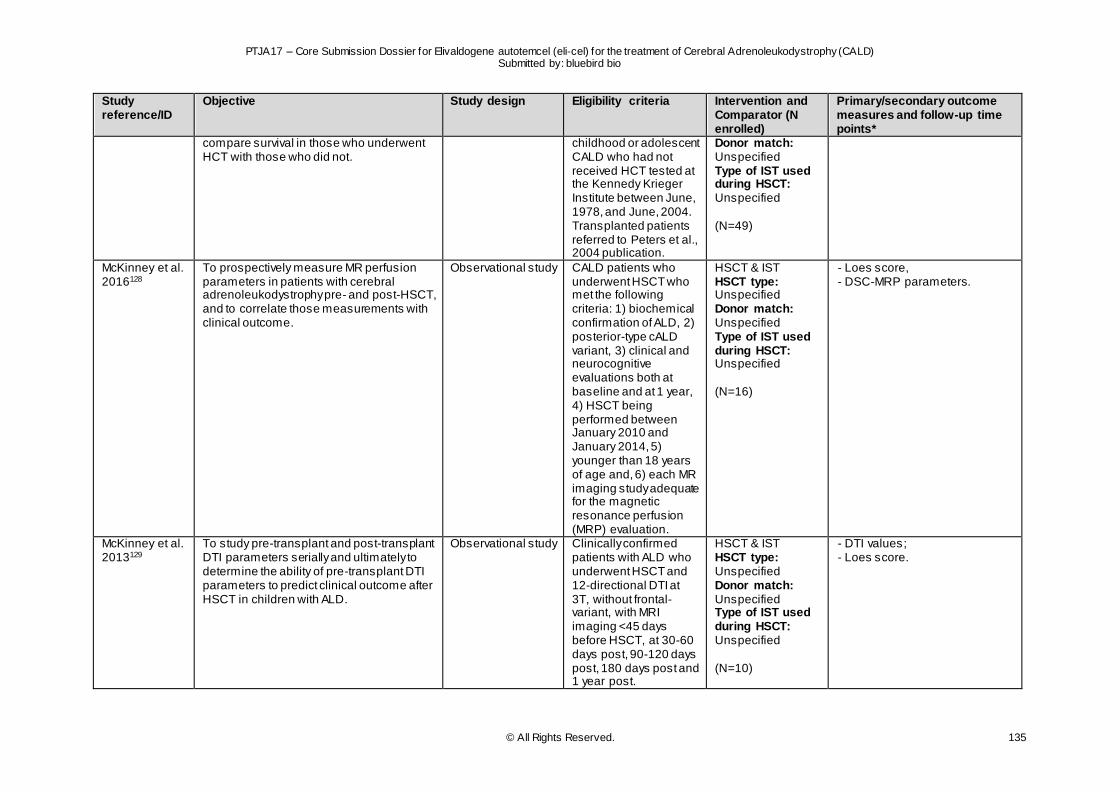
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 135
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
compare survival in those who underwent HCT with those who did not.
childhood or adolescent CALD who had not received HCT tested at the Kennedy Krieger Institute between June, 1978, and June, 2004. Transplanted patients referred to Peters et al., 2004 publication.
Donor match: Unspecified Type of IST used during HSCT: Unspecified (N=49)
McKinney et al. 2016128
To prospectively measure MR perfusion parameters in patients with cerebral adrenoleukodystrophy pre- and post-HSCT, and to correlate those measurements with clinical outcome.
Observational study CALD patients who underwent HSCT who met the following criteria: 1) biochemical confirmation of ALD, 2) posterior-type cALD variant, 3) clinical and neurocognitive evaluations both at baseline and at 1 year, 4) HSCT being performed between January 2010 and January 2014, 5) younger than 18 years of age and, 6) each MR imaging study adequate for the magnetic resonance perfusion (MRP) evaluation.
HSCT & IST HSCT type: Unspecified Donor match: Unspecified Type of IST used during HSCT: Unspecified (N=16)
- Loes score, - DSC-MRP parameters.
McKinney et al. 2013129
To study pre-transplant and post-transplant DTI parameters serially and ultimately to determine the ability of pre-transplant DTI parameters to predict clinical outcome after HSCT in children with ALD.
Observational study Clinically confirmed patients with ALD who underwent HSCT and 12-directional DTI at 3T, without frontal-variant, with MRI imaging <45 days before HSCT, at 30-60 days post, 90-120 days post, 180 days post and 1 year post.
HSCT & IST HSCT type: Unspecified Donor match: Unspecified Type of IST used during HSCT: Unspecified (N=10)
- DTI values; - Loes score.
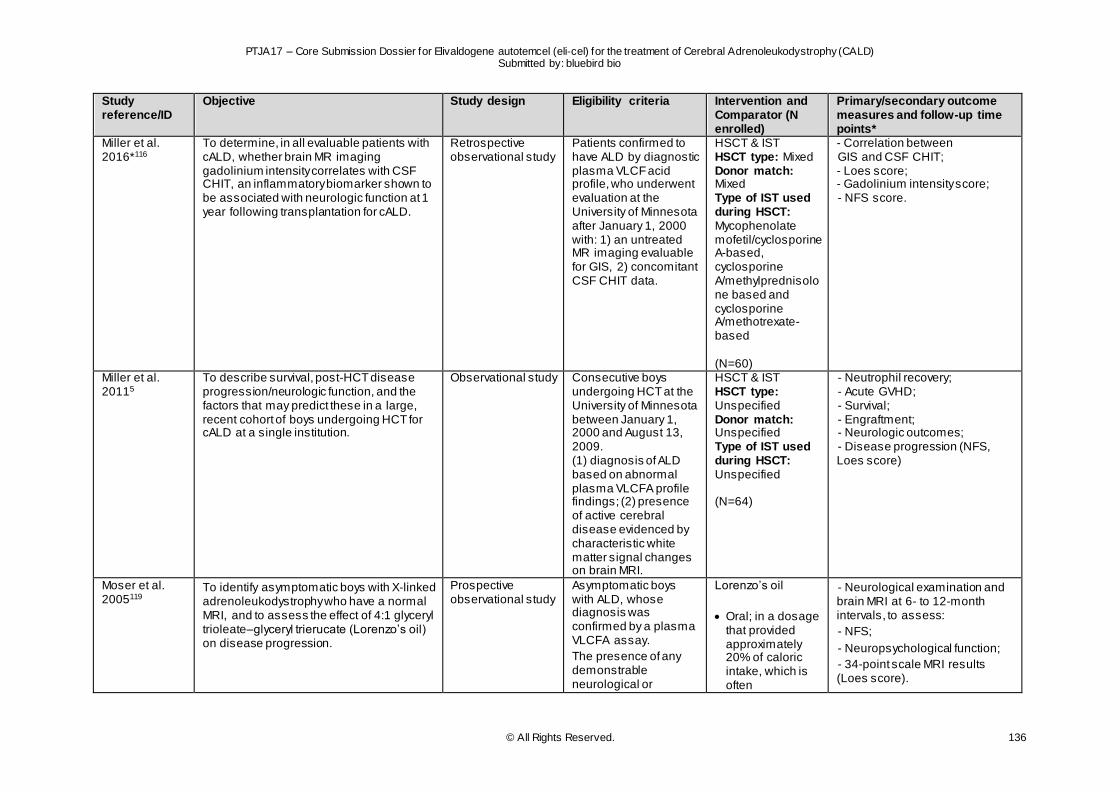
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 136
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
Miller et al. 2016*116
To determine, in all evaluable patients with cALD, whether brain MR imaging gadolinium intensity correlates with CSF CHIT, an inflammatory biomarker shown to be associated with neurologic function at 1 year following transplantation for cALD.
Retrospective observational study
Patients confirmed to have ALD by diagnostic plasma VLCF acid profile, who underwent evaluation at the University of Minnesota after January 1, 2000 with: 1) an untreated MR imaging evaluable for GIS, 2) concomitant CSF CHIT data.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Mycophenolate mofetil/cyclosporine A-based, cyclosporine A/methylprednisolone based and cyclosporine A/methotrexate-based (N=60)
- Correlation between GIS and CSF CHIT; - Loes score; - Gadolinium intensity score; - NFS score.
Miller et al. 20115
To describe survival, post-HCT disease progression/neurologic function, and the factors that may predict these in a large, recent cohort of boys undergoing HCT for cALD at a single institution.
Observational study Consecutive boys undergoing HCT at the University of Minnesota between January 1, 2000 and August 13, 2009. (1) diagnosis of ALD based on abnormal plasma VLCFA profile findings; (2) presence of active cerebral disease evidenced by characteristic white matter signal changes on brain MRI.
HSCT & IST HSCT type: Unspecified Donor match: Unspecified Type of IST used during HSCT: Unspecified (N=64)
- Neutrophil recovery; - Acute GVHD; - Survival; - Engraftment; - Neurologic outcomes; - Disease progression (NFS, Loes score)
Moser et al. 2005119
To identify asymptomatic boys with X-linked adrenoleukodystrophy who have a normal MRI, and to assess the effect of 4:1 glyceryl trioleate–glyceryl trierucate (Lorenzo’s oil) on disease progression.
Prospective observational study
Asymptomatic boys with ALD, whose diagnosis was confirmed by a plasma VLCFA assay.
The presence of any demonstrable neurological or
Lorenzo’s oil
Oral; in a dosage that provided approximately 20% of caloric intake, which is often
- Neurological examination and brain MRI at 6- to 12-month intervals, to assess:
- NFS;
- Neuropsychological function;
- 34-point scale MRI results (Loes score).
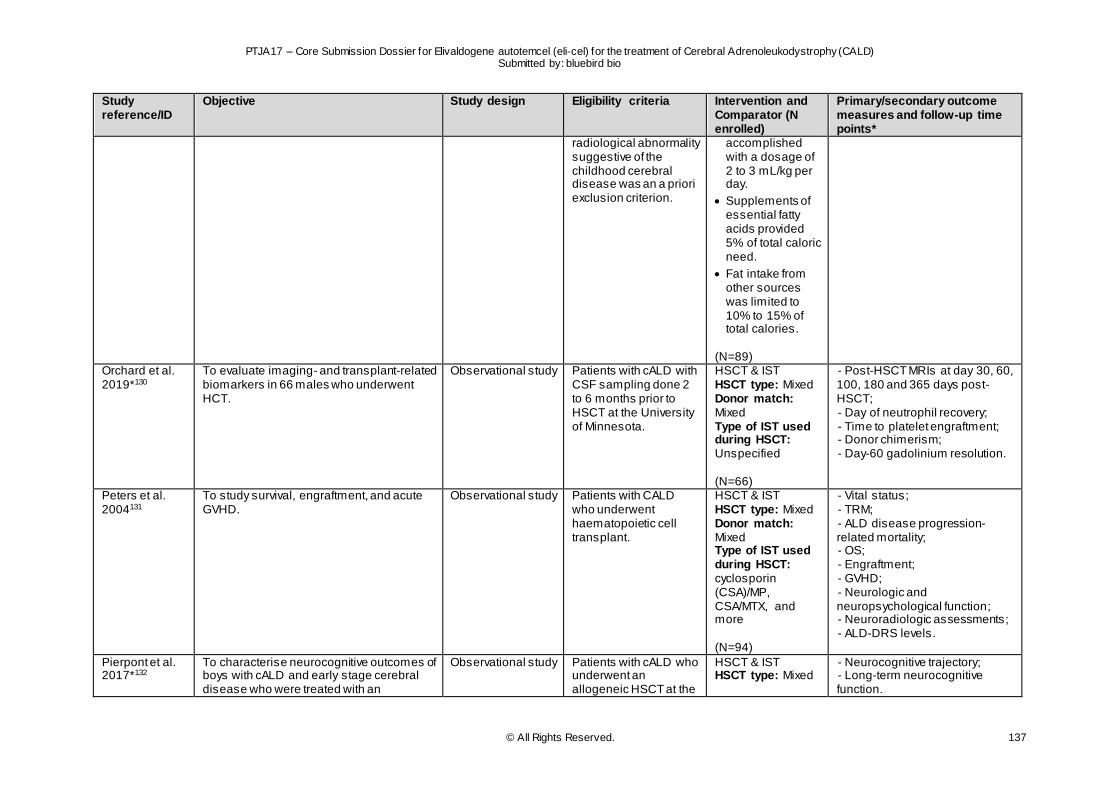
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 137
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
radiological abnormality suggestive of the childhood cerebral disease was an a priori exclusion criterion.
accomplished with a dosage of 2 to 3 mL/kg per day.
Supplements of essential fatty acids provided 5% of total caloric need.
Fat intake from other sources was limited to 10% to 15% of total calories.
(N=89)
Orchard et al. 2019*130
To evaluate imaging- and transplant-related biomarkers in 66 males who underwent HCT.
Observational study Patients with cALD with CSF sampling done 2 to 6 months prior to HSCT at the University of Minnesota.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: Unspecified (N=66)
- Post-HSCT MRIs at day 30, 60, 100, 180 and 365 days post-HSCT; - Day of neutrophil recovery; - Time to platelet engraftment; - Donor chimerism; - Day-60 gadolinium resolution.
Peters et al. 2004131
To study survival, engraftment, and acute GVHD.
Observational study Patients with CALD who underwent haematopoietic cell transplant.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: cyclosporin (CSA)/MP, CSA/MTX, and more (N=94)
- Vital status; - TRM; - ALD disease progression-related mortality; - OS; - Engraftment; - GVHD; - Neurologic and neuropsychological function; - Neuroradiologic assessments; - ALD-DRS levels.
Pierpont et al. 2017*132
To characterise neurocognitive outcomes of boys with cALD and early stage cerebral disease who were treated with an
Observational study Patients with cALD who underwent an allogeneic HSCT at the
HSCT & IST HSCT type: Mixed
- Neurocognitive trajectory; - Long-term neurocognitive function.
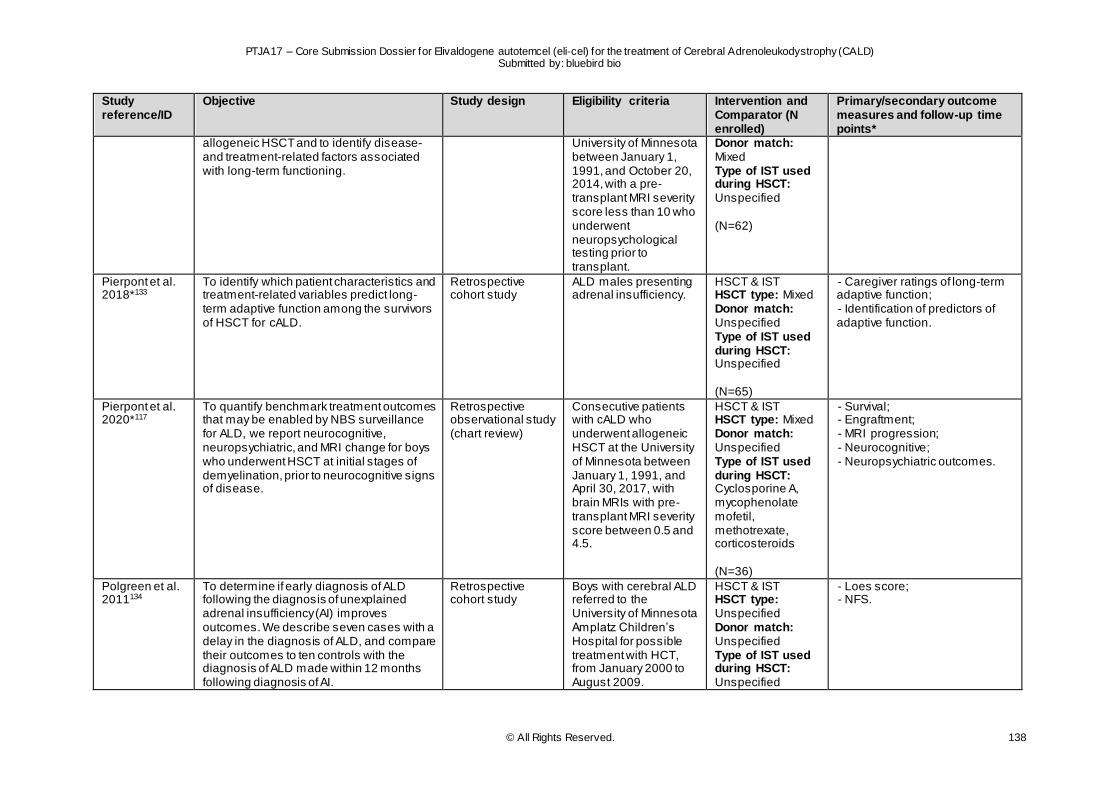
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 138
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
allogeneic HSCT and to identify disease- and treatment-related factors associated with long-term functioning.
University of Minnesota between January 1, 1991, and October 20, 2014, with a pre-transplant MRI severity score less than 10 who underwent neuropsychological testing prior to transplant.
Donor match: Mixed Type of IST used during HSCT: Unspecified (N=62)
Pierpont et al. 2018*133
To identify which patient characteristics and treatment-related variables predict long-term adaptive function among the survivors of HSCT for cALD.
Retrospective cohort study
ALD males presenting adrenal insufficiency.
HSCT & IST HSCT type: Mixed Donor match: Unspecified Type of IST used during HSCT: Unspecified (N=65)
- Caregiver ratings of long-term adaptive function; - Identification of predictors of adaptive function.
Pierpont et al. 2020*117
To quantify benchmark treatment outcomes that may be enabled by NBS surveillance for ALD, we report neurocognitive, neuropsychiatric, and MRI change for boys who underwent HSCT at initial stages of demyelination, prior to neurocognitive signs of disease.
Retrospective observational study (chart review)
Consecutive patients with cALD who underwent allogeneic HSCT at the University of Minnesota between January 1, 1991, and April 30, 2017, with brain MRIs with pre-transplant MRI severity score between 0.5 and 4.5.
HSCT & IST HSCT type: Mixed Donor match: Unspecified Type of IST used during HSCT: Cyclosporine A, mycophenolate mofetil, methotrexate, corticosteroids (N=36)
- Survival; - Engraftment; - MRI progression; - Neurocognitive; - Neuropsychiatric outcomes.
Polgreen et al. 2011134
To determine if early diagnosis of ALD following the diagnosis of unexplained adrenal insufficiency (AI) improves outcomes. We describe seven cases with a delay in the diagnosis of ALD, and compare their outcomes to ten controls with the diagnosis of ALD made within 12 months following diagnosis of AI.
Retrospective cohort study
Boys with cerebral ALD referred to the University of Minnesota Amplatz Children’s Hospital for possible treatment with HCT, from January 2000 to August 2009.
HSCT & IST HSCT type: Unspecified Donor match: Unspecified Type of IST used during HSCT: Unspecified
- Loes score; - NFS.
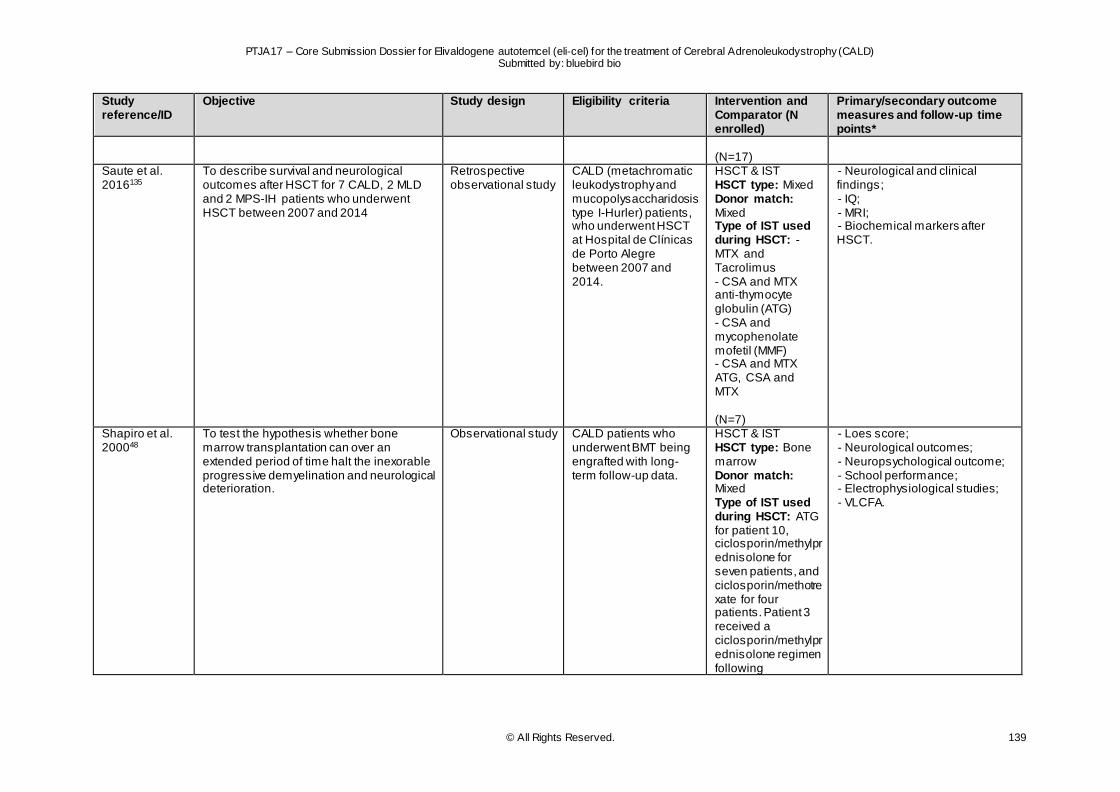
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 139
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
(N=17)
Saute et al. 2016135
To describe survival and neurological outcomes after HSCT for 7 CALD, 2 MLD and 2 MPS-IH patients who underwent HSCT between 2007 and 2014
Retrospective observational study
CALD (metachromatic leukodystrophy and mucopolysaccharidosis type I-Hurler) patients, who underwent HSCT at Hospital de Clínicas de Porto Alegre between 2007 and 2014.
HSCT & IST HSCT type: Mixed Donor match: Mixed Type of IST used during HSCT: - MTX and Tacrolimus - CSA and MTX anti-thymocyte globulin (ATG) - CSA and mycophenolate mofetil (MMF) - CSA and MTX ATG, CSA and MTX (N=7)
- Neurological and clinical findings; - IQ; - MRI; - Biochemical markers after HSCT.
Shapiro et al. 200048
To test the hypothesis whether bone marrow transplantation can over an extended period of time halt the inexorable progressive demyelination and neurological deterioration.
Observational study CALD patients who underwent BMT being engrafted with long-term follow-up data.
HSCT & IST HSCT type: Bone marrow Donor match: Mixed Type of IST used during HSCT: ATG for patient 10, ciclosporin/methylprednisolone for seven patients, and ciclosporin/methotrexate for four patients. Patient 3 received a ciclosporin/methylprednisolone regimen following
- Loes score; - Neurological outcomes; - Neuropsychological outcome; - School performance; - Electrophysiological studies; - VLCFA.
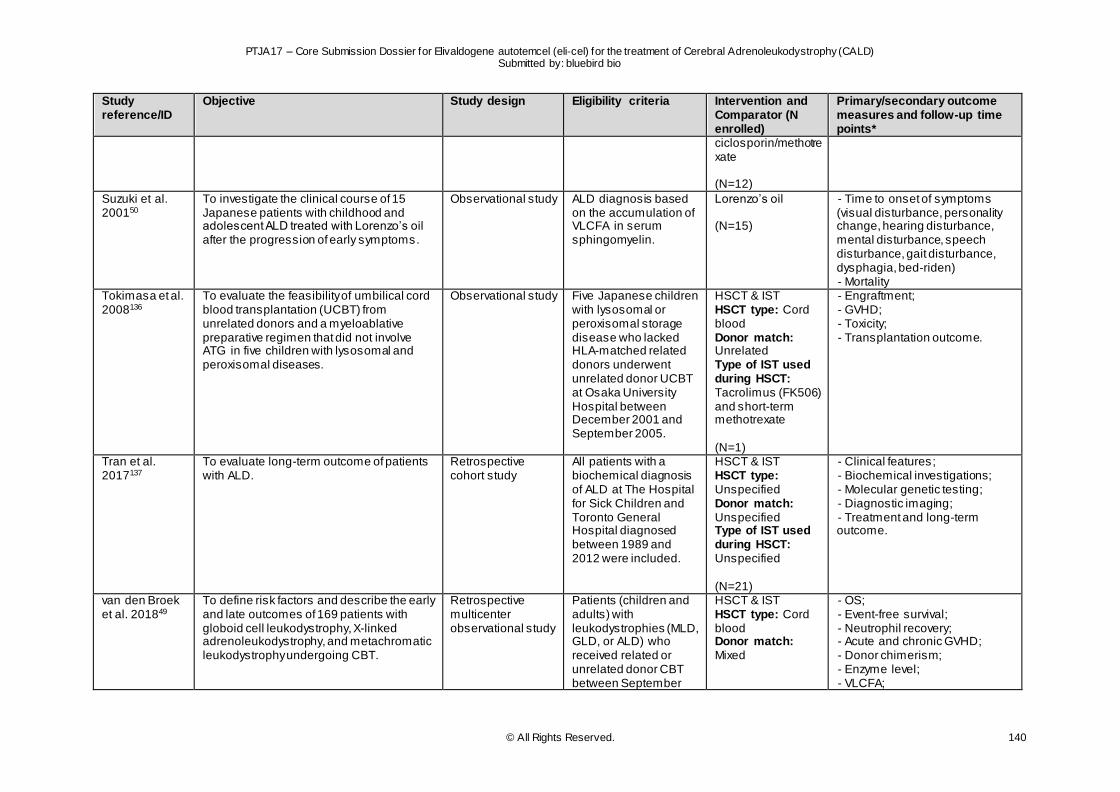
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 140
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
ciclosporin/methotrexate (N=12)
Suzuki et al. 200150
To investigate the clinical course of 15 Japanese patients with childhood and adolescent ALD treated with Lorenzo’s oil after the progression of early symptoms.
Observational study ALD diagnosis based on the accumulation of VLCFA in serum sphingomyelin.
Lorenzo’s oil (N=15)
- Time to onset of symptoms (visual disturbance, personality change, hearing disturbance, mental disturbance, speech disturbance, gait disturbance, dysphagia, bed-riden) - Mortality
Tokimasa et al. 2008136
To evaluate the feasibility of umbilical cord blood transplantation (UCBT) from unrelated donors and a myeloablative preparative regimen that did not involve ATG in five children with lysosomal and peroxisomal diseases.
Observational study Five Japanese children with lysosomal or peroxisomal storage disease who lacked HLA-matched related donors underwent unrelated donor UCBT at Osaka University Hospital between December 2001 and September 2005.
HSCT & IST HSCT type: Cord blood Donor match: Unrelated Type of IST used during HSCT: Tacrolimus (FK506) and short-term methotrexate (N=1)
- Engraftment; - GVHD; - Toxicity; - Transplantation outcome.
Tran et al. 2017137
To evaluate long-term outcome of patients with ALD.
Retrospective cohort study
All patients with a biochemical diagnosis of ALD at The Hospital for Sick Children and Toronto General Hospital diagnosed between 1989 and 2012 were included.
HSCT & IST HSCT type: Unspecified Donor match: Unspecified Type of IST used during HSCT: Unspecified (N=21)
- Clinical features; - Biochemical investigations; - Molecular genetic testing; - Diagnostic imaging; - Treatment and long-term outcome.
van den Broek et al. 201849
To define risk factors and describe the early and late outcomes of 169 patients with globoid cell leukodystrophy, X-linked adrenoleukodystrophy, and metachromatic leukodystrophy undergoing CBT.
Retrospective multicenter observational study
Patients (children and adults) with leukodystrophies (MLD, GLD, or ALD) who received related or unrelated donor CBT between September
HSCT & IST HSCT type: Cord blood Donor match: Mixed
- OS; - Event-free survival; - Neutrophil recovery; - Acute and chronic GVHD; - Donor chimerism; - Enzyme level; - VLCFA;
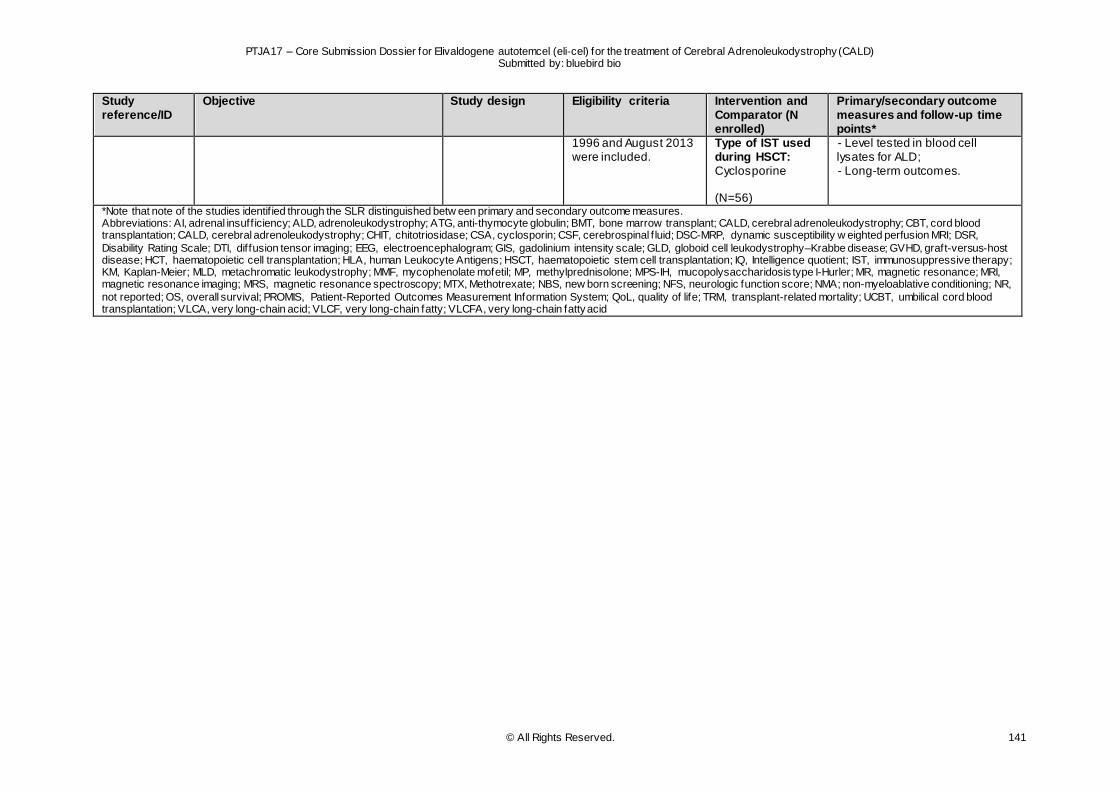
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 141
Study reference/ID
Objective Study design Eligibility criteria Intervention and Comparator (N enrolled)
Primary/secondary outcome measures and follow-up time points*
1996 and August 2013 were included.
Type of IST used during HSCT: Cyclosporine (N=56)
- Level tested in blood cell lysates for ALD; - Long-term outcomes.
*Note that note of the studies identif ied through the SLR distinguished betw een primary and secondary outcome measures. Abbreviations: AI, adrenal insuff iciency; ALD, adrenoleukodystrophy; ATG, anti-thymocyte globulin; BMT, bone marrow transplant; CALD, cerebral adrenoleukodystrophy; CBT, cord blood transplantation; CALD, cerebral adrenoleukodystrophy; CHIT, chitotriosidase; CSA, cyclosporin; CSF, cerebrospinal f luid; DSC-MRP, dynamic susceptibility w eighted perfusion MRI; DSR,
Disability Rating Scale; DTI, diffusion tensor imaging; EEG, electroencephalogram; GIS, gadolinium intensity scale; GLD, globoid cell leukodystrophy–Krabbe disease; GVHD, graft-versus-host disease; HCT, haematopoietic cell transplantation; HLA, human Leukocyte Antigens; HSCT, haematopoietic stem cell transplantation; IQ, Intelligence quotient; IST, immunosuppressive therapy; KM, Kaplan-Meier; MLD, metachromatic leukodystrophy; MMF, mycophenolate mofetil; MP, methylprednisolone; MPS-IH, mucopolysaccharidosis type I-Hurler; MR, magnetic resonance; MRI, magnetic resonance imaging; MRS, magnetic resonance spectroscopy; MTX, Methotrexate; NBS, new born screening; NFS, neurologic function score; NMA; non-myeloablative conditioning; NR,
not reported; OS, overall survival; PROMIS, Patient-Reported Outcomes Measurement Information System; QoL, quality of life; TRM, transplant-related mortality; UCBT, umbilical cord blood transplantation; VLCA, very long-chain acid; VLCF, very long-chain fatty; VLCFA, very long-chain fatty acid
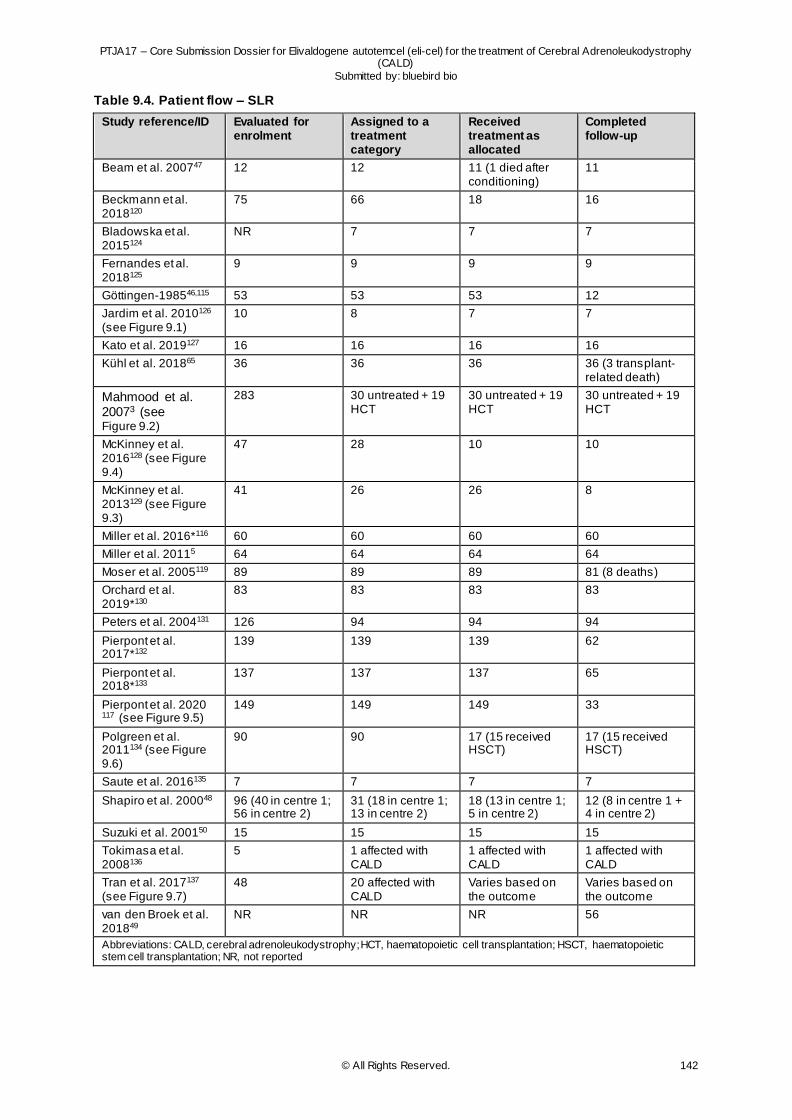
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 142
Table 9.4. Patient flow – SLR
Study reference/ID Evaluated for enrolment
Assigned to a treatment category
Received treatment as allocated
Completed follow-up
Beam et al. 200747 12 12 11 (1 died after conditioning)
11
Beckmann et al. 2018120
75 66 18 16
Bladowska et al. 2015124
NR 7 7 7
Fernandes et al. 2018125
9 9 9 9
Göttingen-198546,115 53 53 53 12
Jardim et al. 2010126 (see Figure 9.1)
10 8 7 7
Kato et al. 2019127 16 16 16 16
Kühl et al. 201865 36 36 36 36 (3 transplant-related death)
Mahmood et al. 20073 (see Figure 9.2)
283 30 untreated + 19 HCT
30 untreated + 19 HCT
30 untreated + 19 HCT
McKinney et al. 2016128 (see Figure 9.4)
47 28 10 10
McKinney et al. 2013129 (see Figure 9.3)
41 26 26 8
Miller et al. 2016*116 60 60 60 60
Miller et al. 20115 64 64 64 64
Moser et al. 2005119 89 89 89 81 (8 deaths)
Orchard et al. 2019*130
83 83 83 83
Peters et al. 2004131 126 94 94 94
Pierpont et al. 2017*132
139 139 139 62
Pierpont et al. 2018*133
137 137 137 65
Pierpont et al. 2020 117 (see Figure 9.5)
149 149 149 33
Polgreen et al. 2011134 (see Figure 9.6)
90 90 17 (15 received HSCT)
17 (15 received HSCT)
Saute et al. 2016135 7 7 7 7
Shapiro et al. 200048 96 (40 in centre 1; 56 in centre 2)
31 (18 in centre 1; 13 in centre 2)
18 (13 in centre 1; 5 in centre 2)
12 (8 in centre 1 + 4 in centre 2)
Suzuki et al. 200150 15 15 15 15
Tokimasa et al. 2008136
5 1 affected with CALD
1 affected with CALD
1 affected with CALD
Tran et al. 2017137 (see Figure 9.7)
48 20 affected with CALD
Varies based on the outcome
Varies based on the outcome
van den Broek et al. 201849
NR NR NR 56
Abbreviations: CALD, cerebral adrenoleukodystrophy; HCT, haematopoietic cell transplantation; HSCT, haematopoietic stem cell transplantation; NR, not reported
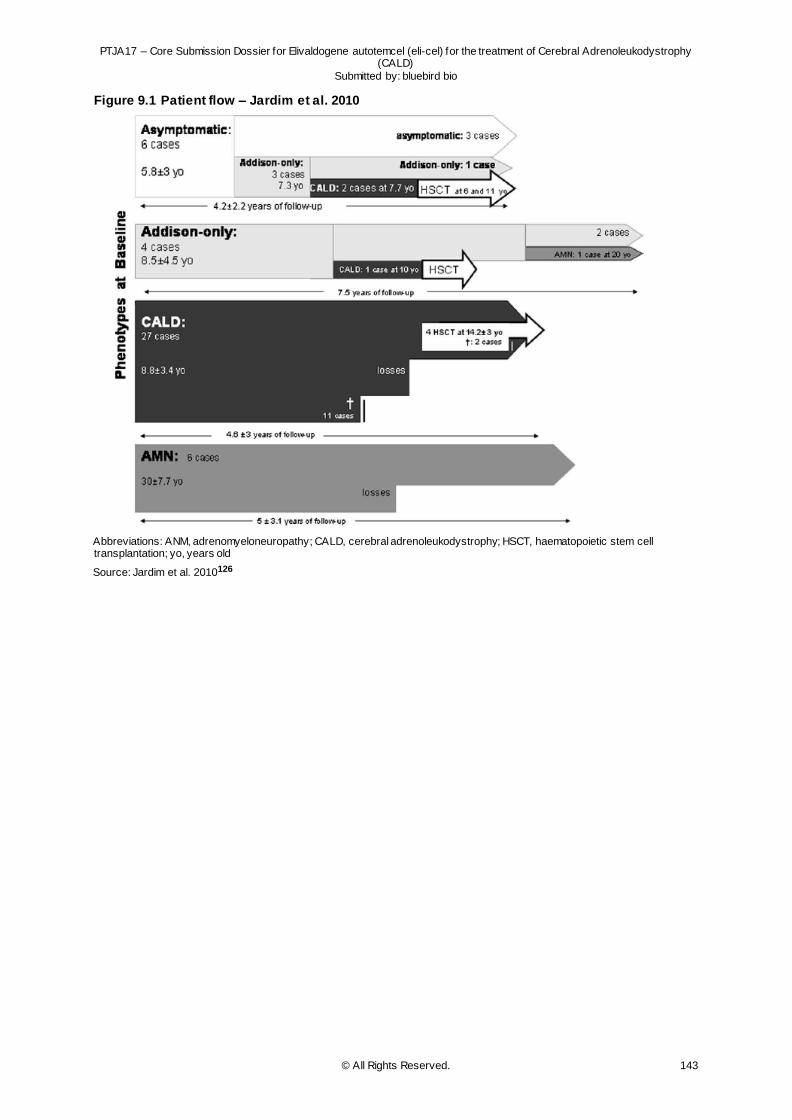
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 143
Figure 9.1 Patient flow – Jardim et al. 2010
Abbreviations: ANM, adrenomyeloneuropathy; CALD, cerebral adrenoleukodystrophy; HSCT, haematopoietic stem cell transplantation; yo, years old
Source: Jardim et al. 2010126
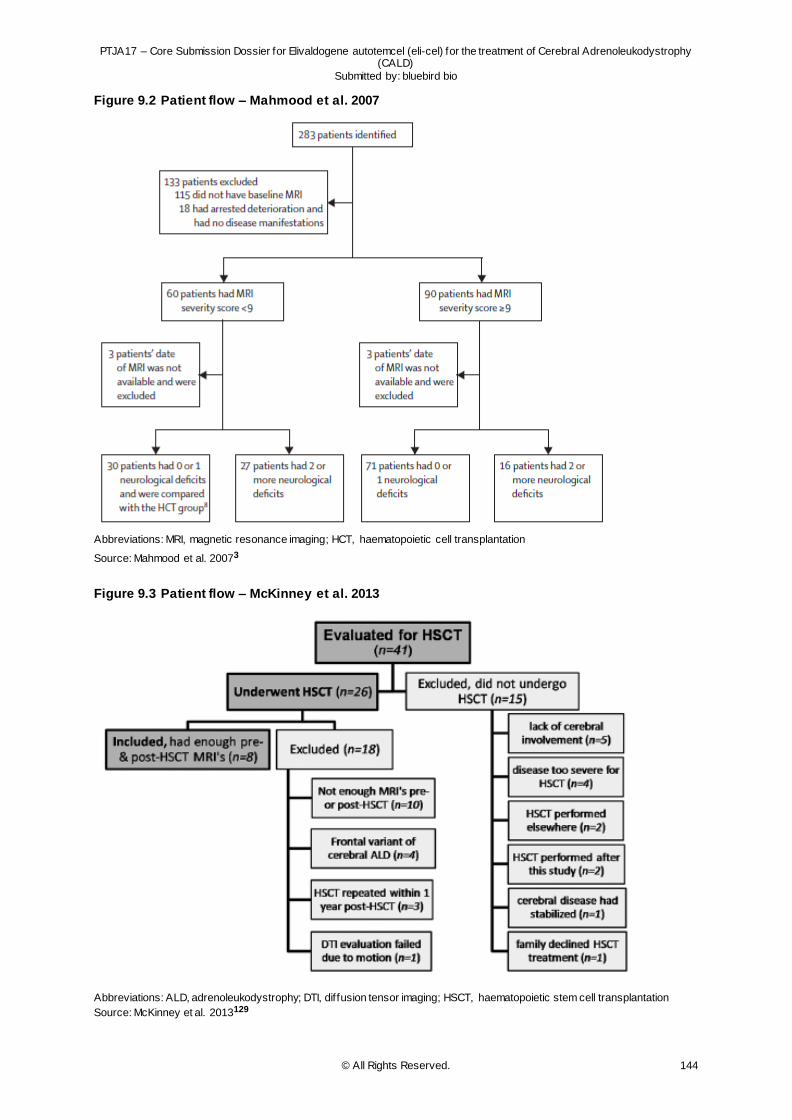
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 144
Figure 9.2 Patient flow – Mahmood et al. 2007
Abbreviations: MRI, magnetic resonance imaging; HCT, haematopoietic cell transplantation
Source: Mahmood et al. 20073
Figure 9.3 Patient flow – McKinney et al. 2013
Abbreviations: ALD, adrenoleukodystrophy; DTI, diffusion tensor imaging; HSCT, haematopoietic stem cell transplantation
Source: McKinney et al. 2013129
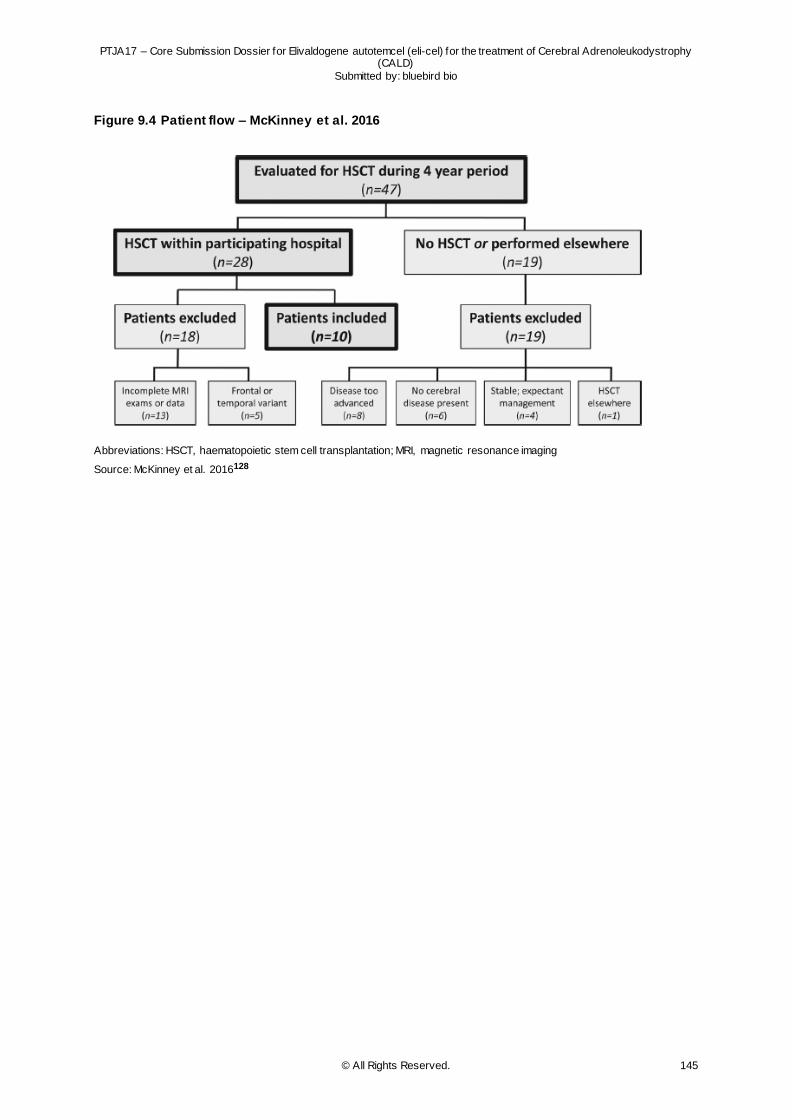
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 145
Figure 9.4 Patient flow – McKinney et al. 2016
Abbreviations: HSCT, haematopoietic stem cell transplantation; MRI, magnetic resonance imaging
Source: McKinney et al. 2016128
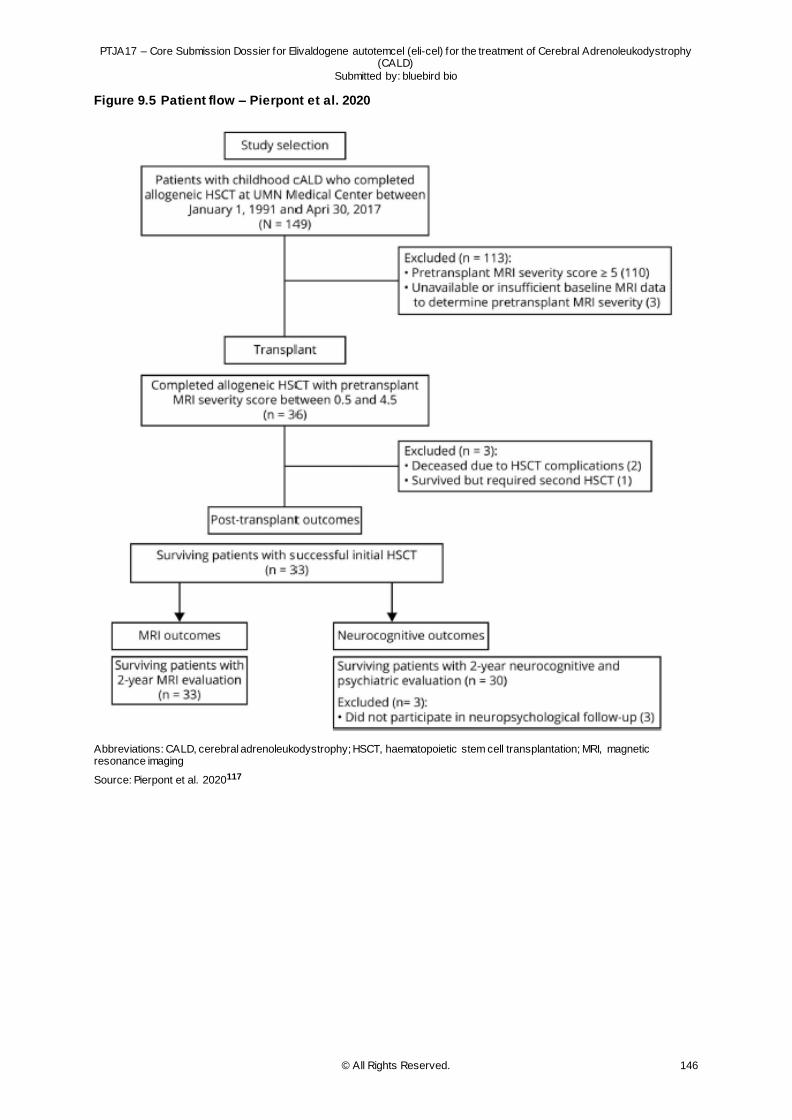
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 146
Figure 9.5 Patient flow – Pierpont et al. 2020
Abbreviations: CALD, cerebral adrenoleukodystrophy; HSCT, haematopoietic stem cell transplantation; MRI, magnetic resonance imaging
Source: Pierpont et al. 2020117
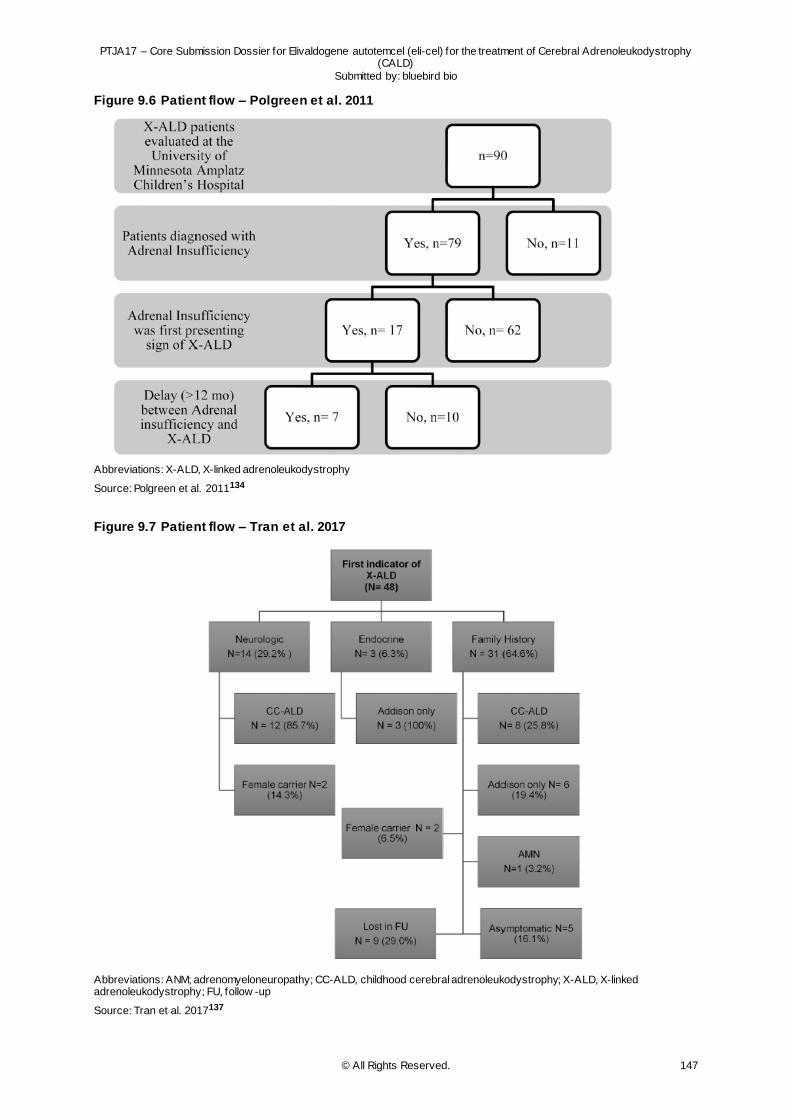
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 147
Figure 9.6 Patient flow – Polgreen et al. 2011
Abbreviations: X-ALD, X-linked adrenoleukodystrophy
Source: Polgreen et al. 2011134
Figure 9.7 Patient flow – Tran et al. 2017
Abbreviations: ANM; adrenomyeloneuropathy; CC-ALD, childhood cerebral adrenoleukodystrophy; X-ALD, X-linked adrenoleukodystrophy; FU, follow -up
Source: Tran et al. 2017137
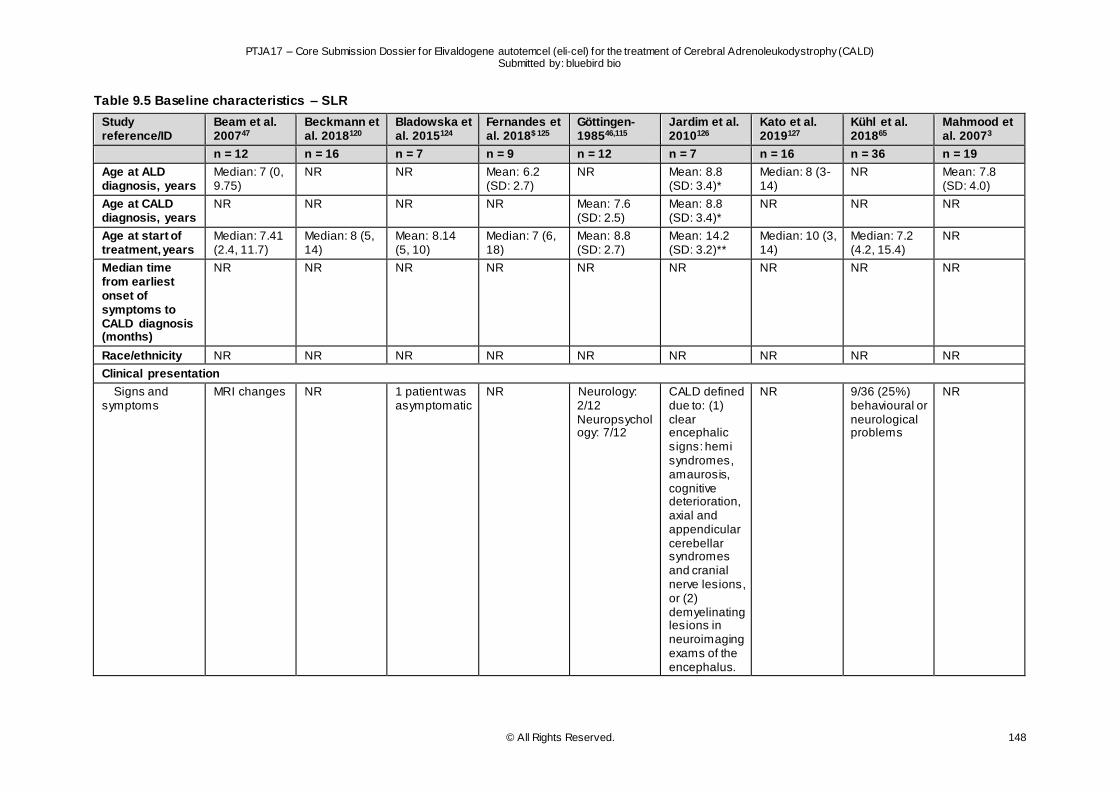
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 148
Table 9.5 Baseline characteristics – SLR
Study reference/ID
Beam et al. 200747
Beckmann et al. 2018120
Bladowska et al. 2015124
Fernandes et al. 2018$ 125
Göttingen-198546,115
Jardim et al. 2010126
Kato et al. 2019127
Kühl et al. 201865
Mahmood et al. 20073
n = 12 n = 16 n = 7 n = 9 n = 12 n = 7 n = 16 n = 36 n = 19
Age at ALD diagnosis, years
Median: 7 (0, 9.75)
NR NR Mean: 6.2 (SD: 2.7)
NR Mean: 8.8 (SD: 3.4)*
Median: 8 (3-14)
NR Mean: 7.8 (SD: 4.0)
Age at CALD diagnosis, years
NR NR NR NR Mean: 7.6 (SD: 2.5)
Mean: 8.8 (SD: 3.4)*
NR NR NR
Age at start of treatment, years
Median: 7.41 (2.4, 11.7)
Median: 8 (5, 14)
Mean: 8.14 (5, 10)
Median: 7 (6, 18)
Mean: 8.8 (SD: 2.7)
Mean: 14.2 (SD: 3.2)**
Median: 10 (3, 14)
Median: 7.2 (4.2, 15.4)
NR
Median time from earliest onset of symptoms to CALD diagnosis (months)
NR NR NR NR NR NR NR NR NR
Race/ethnicity NR NR NR NR NR NR NR NR NR
Clinical presentation
Signs and symptoms
MRI changes NR 1 patient was asymptomatic
NR Neurology: 2/12 Neuropsychology: 7/12
CALD defined due to: (1) clear encephalic signs: hemi syndromes, amaurosis, cognitive deterioration, axial and appendicular cerebellar syndromes and cranial nerve lesions, or (2) demyelinating lesions in neuroimaging exams of the encephalus.
NR 9/36 (25%) behavioural or neurological problems
NR
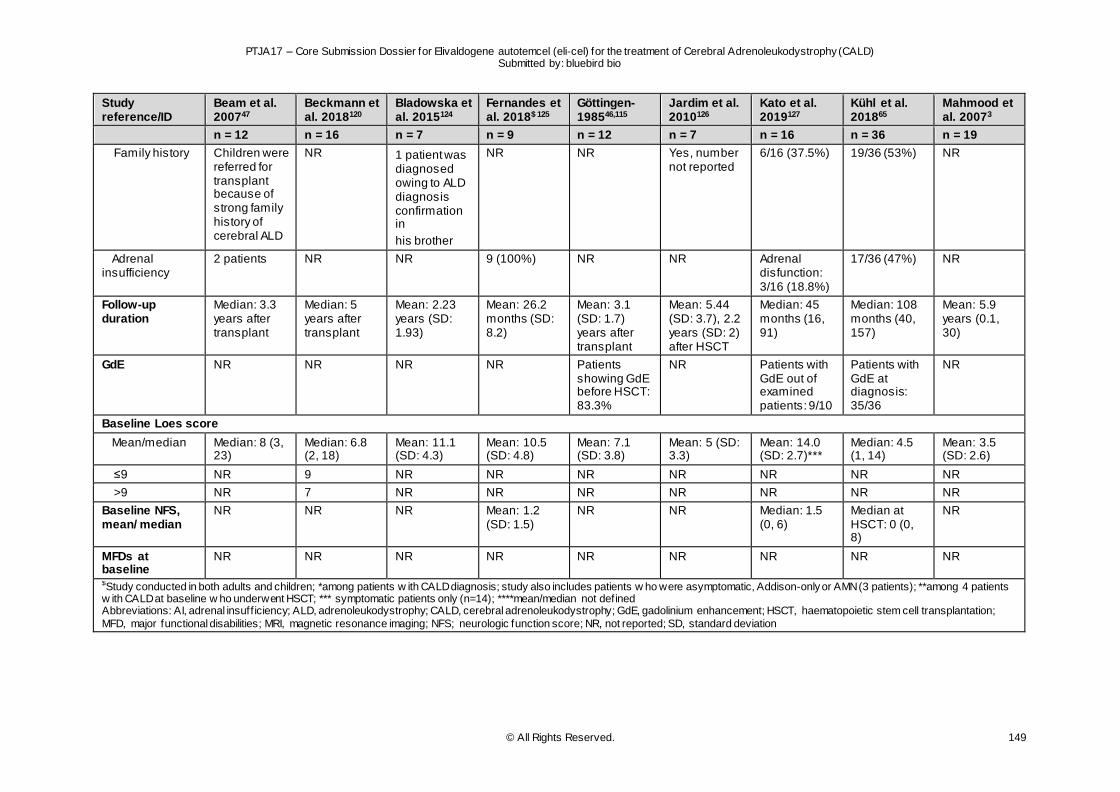
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 149
Study reference/ID
Beam et al. 200747
Beckmann et al. 2018120
Bladowska et al. 2015124
Fernandes et al. 2018$ 125
Göttingen-198546,115
Jardim et al. 2010126
Kato et al. 2019127
Kühl et al. 201865
Mahmood et al. 20073
n = 12 n = 16 n = 7 n = 9 n = 12 n = 7 n = 16 n = 36 n = 19
Family history Children were referred for transplant because of strong family history of cerebral ALD
NR 1 patient was diagnosed owing to ALD diagnosis confirmation in
his brother
NR NR Yes, number not reported
6/16 (37.5%) 19/36 (53%) NR
Adrenal insufficiency
2 patients NR NR 9 (100%) NR NR Adrenal disfunction: 3/16 (18.8%)
17/36 (47%) NR
Follow-up duration
Median: 3.3 years after transplant
Median: 5 years after transplant
Mean: 2.23 years (SD: 1.93)
Mean: 26.2 months (SD: 8.2)
Mean: 3.1 (SD: 1.7) years after transplant
Mean: 5.44 (SD: 3.7), 2.2 years (SD: 2) after HSCT
Median: 45 months (16, 91)
Median: 108 months (40, 157)
Mean: 5.9 years (0.1, 30)
GdE NR NR NR NR Patients showing GdE before HSCT: 83.3%
NR Patients with GdE out of examined patients: 9/10
Patients with GdE at diagnosis: 35/36
NR
Baseline Loes score
Mean/median Median: 8 (3, 23)
Median: 6.8 (2, 18)
Mean: 11.1 (SD: 4.3)
Mean: 10.5 (SD: 4.8)
Mean: 7.1 (SD: 3.8)
Mean: 5 (SD: 3.3)
Mean: 14.0 (SD: 2.7)***
Median: 4.5 (1, 14)
Mean: 3.5 (SD: 2.6)
≤9 NR 9 NR NR NR NR NR NR NR
>9 NR 7 NR NR NR NR NR NR NR
Baseline NFS, mean/ median
NR NR NR Mean: 1.2 (SD: 1.5)
NR NR Median: 1.5 (0, 6)
Median at HSCT: 0 (0, 8)
NR
MFDs at baseline
NR NR NR NR NR NR NR NR NR
$Study conducted in both adults and children; *among patients w ith CALD diagnosis; study also includes patients w ho were asymptomatic, Addison-only or AMN (3 patients); **among 4 patients w ith CALD at baseline w ho underwent HSCT; *** symptomatic patients only (n=14); ****mean/median not defined Abbreviations: AI, adrenal insuff iciency; ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplantation;
MFD, major functional disabilities; MRI, magnetic resonance imaging; NFS; neurologic function score; NR, not reported; SD, standard deviation
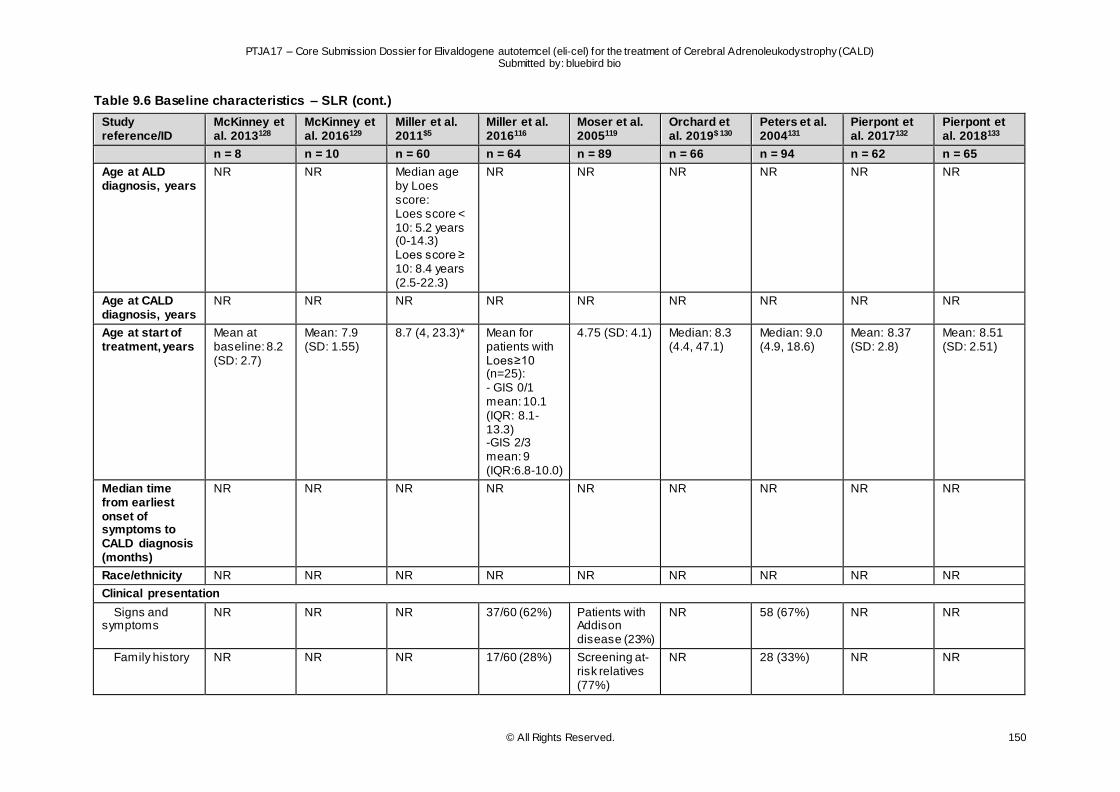
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 150
Table 9.6 Baseline characteristics – SLR (cont.)
Study reference/ID
McKinney et al. 2013128
McKinney et al. 2016129
Miller et al. 2011$5
Miller et al. 2016116
Moser et al. 2005119
Orchard et al. 2019$ 130
Peters et al. 2004131
Pierpont et al. 2017132
Pierpont et al. 2018133
n = 8 n = 10 n = 60 n = 64 n = 89 n = 66 n = 94 n = 62 n = 65
Age at ALD diagnosis, years
NR NR Median age by Loes score: Loes score < 10: 5.2 years (0-14.3) Loes score ≥ 10: 8.4 years (2.5-22.3)
NR NR NR NR NR NR
Age at CALD diagnosis, years
NR NR NR NR NR NR NR NR NR
Age at start of treatment, years
Mean at baseline: 8.2 (SD: 2.7)
Mean: 7.9 (SD: 1.55)
8.7 (4, 23.3)* Mean for patients with Loes≥10 (n=25): - GIS 0/1 mean: 10.1 (IQR: 8.1-13.3) -GIS 2/3 mean: 9 (IQR:6.8-10.0)
4.75 (SD: 4.1) Median: 8.3 (4.4, 47.1)
Median: 9.0 (4.9, 18.6)
Mean: 8.37 (SD: 2.8)
Mean: 8.51 (SD: 2.51)
Median time from earliest onset of symptoms to CALD diagnosis (months)
NR NR NR NR NR NR NR NR NR
Race/ethnicity NR NR NR NR NR NR NR NR NR
Clinical presentation
Signs and symptoms
NR NR NR 37/60 (62%) Patients with Addison disease (23%)
NR 58 (67%) NR NR
Family history NR NR NR 17/60 (28%) Screening at-risk relatives (77%)
NR 28 (33%) NR NR

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 151
Study reference/ID
McKinney et al. 2013128
McKinney et al. 2016129
Miller et al. 2011$5
Miller et al. 2016116
Moser et al. 2005119
Orchard et al. 2019$ 130
Peters et al. 2004131
Pierpont et al. 2017132
Pierpont et al. 2018133
n = 8 n = 10 n = 60 n = 64 n = 89 n = 66 n = 94 n = 62 n = 65
Adrenal insufficiency
NR NR NR 43/60 (72%) NR NR NR NR NR
Follow-up duration
1 year** 1 year** Median: 3.7 (0.7, 9.6) years after HSCT
1 year** 6.9 (SD: 2.7) years
180 days** 8 years** Median: 4.2 (1.8, 25.4) years
Mean: 4.6 (1.0, 24.1) years
GdE NR NR NR NR NR Median gadolinium intensity score: 2 (1, 3)
NR NR NR
Baseline Loes score
Mean/median Mean: 6.35 (SD: 5.5)
Mean: 8.7 (SD: 4.99)
NR NR NR Median: 9 (1, 19.5)
Median Loes for patients w ith Performance Intelligence
Quotient (PIQ) < 80: 12.8 (range: 8-19) Median Loes for
patients w ith PIQ ≥ 80: 8 (range: 0-23.5)
NR Mean: 7.52 (SD: 5.02)
<6 NR NR 16 (27%) NR NR NR NR NR NR
≤9 NR NR 30 (50%) 39 NR NR NR NR 42
≥6 NR NR 44 (73%) NR NR NR NR NR NR
>9 NR NR 30 (50%) 25 NR NR NR NR 23
Baseline NFS
mean/ median NR NR NR NR NR NR NR NR NR
≤1 NR NR 30 (60%) NR NR NR NR NR NR
>1 NR NR 20 (40%) NR NR NR NR NR NR
MFDs at baseline
NR NR NR NR NR NR NR NR NR
$Study conducted in both adults and children; *undefined unit; **mean/median not defined
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; GdE, gadolinium enhancement; GIS, gadolinium intensity scale; HSCT, haematopoietic stem cell transplantation; IQR, interquartile range; MFD, major functional disabilities; NFS, neurologic function scale; NR, not reported; SD, standard deviation; PIQ, Performance Intelligence Quotient
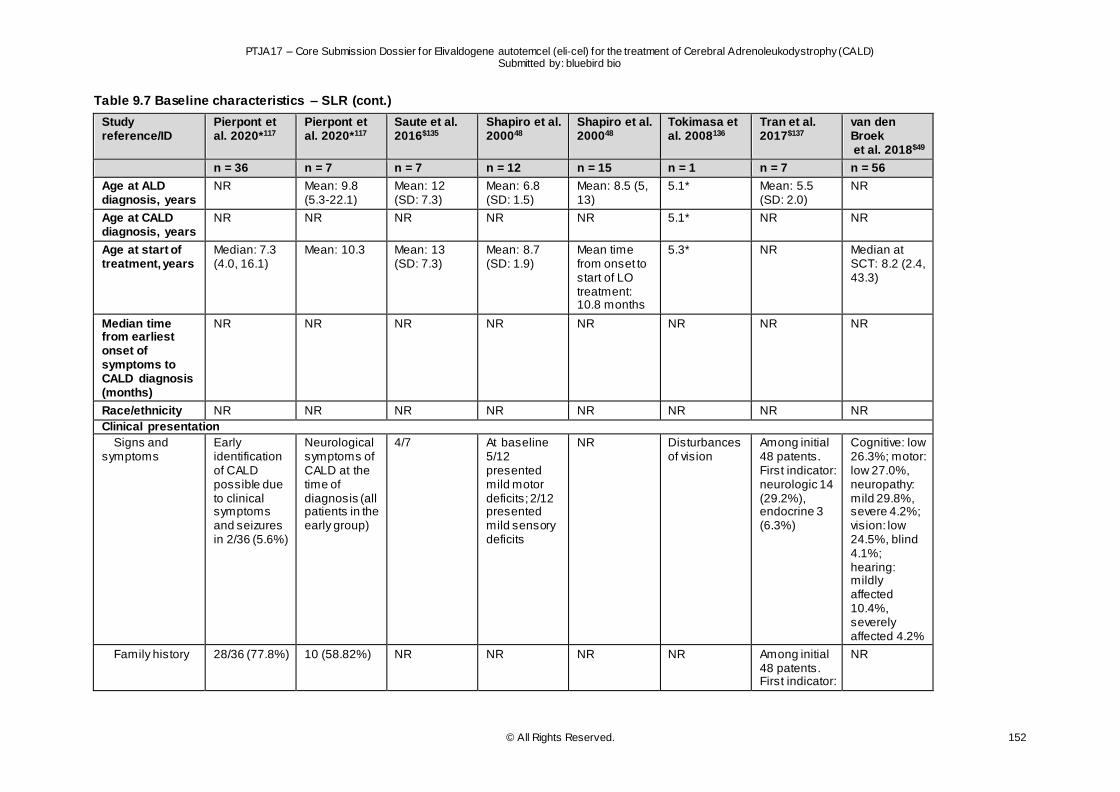
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 152
Table 9.7 Baseline characteristics – SLR (cont.)
Study reference/ID
Pierpont et al. 2020*117
Pierpont et al. 2020*117
Saute et al. 2016$135
Shapiro et al. 200048
Shapiro et al. 200048
Tokimasa et al. 2008136
Tran et al. 2017$137
van den Broek et al. 2018$49
n = 36 n = 7 n = 7 n = 12 n = 15 n = 1 n = 7 n = 56
Age at ALD diagnosis, years
NR Mean: 9.8 (5.3-22.1)
Mean: 12 (SD: 7.3)
Mean: 6.8 (SD: 1.5)
Mean: 8.5 (5, 13)
5.1* Mean: 5.5 (SD: 2.0)
NR
Age at CALD diagnosis, years
NR NR NR NR NR 5.1* NR NR
Age at start of treatment, years
Median: 7.3 (4.0, 16.1)
Mean: 10.3 Mean: 13 (SD: 7.3)
Mean: 8.7 (SD: 1.9)
Mean time from onset to start of LO treatment: 10.8 months
5.3* NR Median at SCT: 8.2 (2.4, 43.3)
Median time from earliest onset of symptoms to CALD diagnosis (months)
NR NR NR NR NR NR NR NR
Race/ethnicity NR NR NR NR NR NR NR NR
Clinical presentation
Signs and symptoms
Early identification of CALD possible due to clinical symptoms and seizures in 2/36 (5.6%)
Neurological symptoms of CALD at the time of diagnosis (all patients in the early group)
4/7 At baseline 5/12 presented mild motor deficits; 2/12 presented mild sensory deficits
NR Disturbances of vision
Among initial 48 patents. First indicator: neurologic 14 (29.2%), endocrine 3 (6.3%)
Cognitive: low 26.3%; motor: low 27.0%, neuropathy: mild 29.8%, severe 4.2%; vision: low 24.5%, blind 4.1%; hearing: mildly affected 10.4%, severely affected 4.2%
Family history 28/36 (77.8%) 10 (58.82%) NR NR NR NR Among initial 48 patents. First indicator:
NR
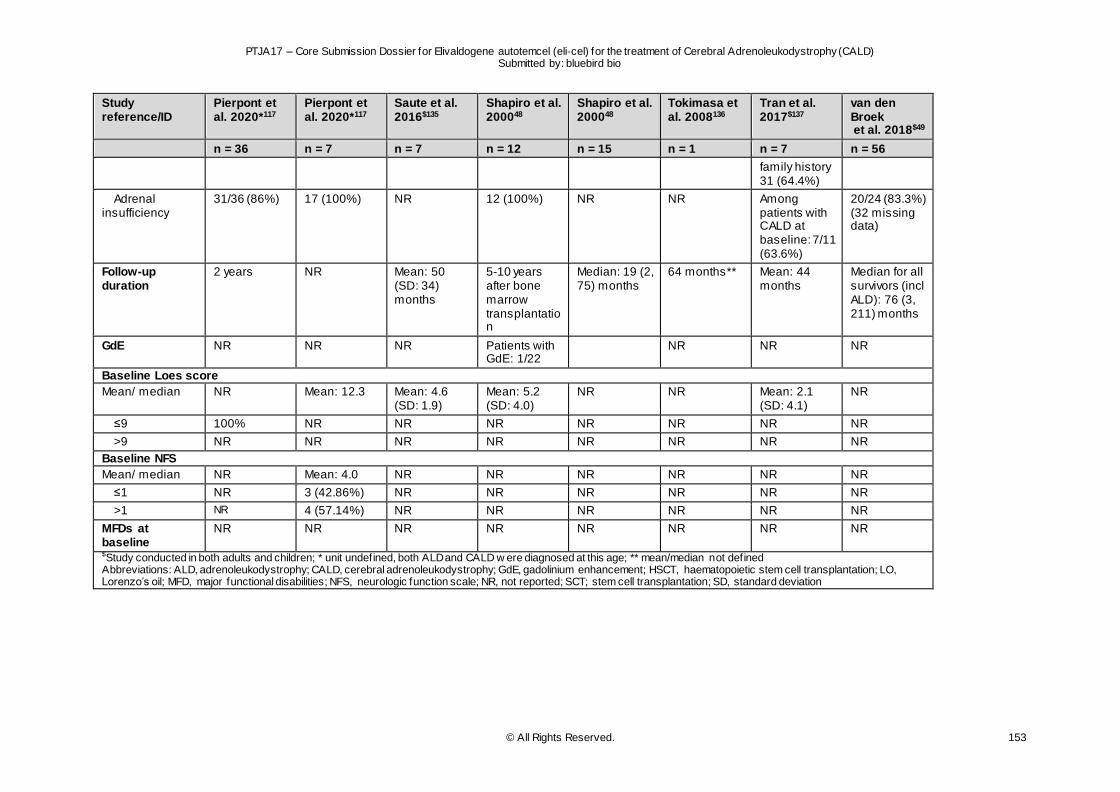
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD) Submitted by: bluebird bio
© All Rights Reserved. 153
Study reference/ID
Pierpont et al. 2020*117
Pierpont et al. 2020*117
Saute et al. 2016$135
Shapiro et al. 200048
Shapiro et al. 200048
Tokimasa et al. 2008136
Tran et al. 2017$137
van den Broek et al. 2018$49
n = 36 n = 7 n = 7 n = 12 n = 15 n = 1 n = 7 n = 56
family history 31 (64.4%)
Adrenal insufficiency
31/36 (86%) 17 (100%) NR 12 (100%) NR NR Among patients with CALD at baseline: 7/11 (63.6%)
20/24 (83.3%) (32 missing data)
Follow-up duration
2 years NR Mean: 50 (SD: 34) months
5-10 years after bone marrow transplantation
Median: 19 (2, 75) months
64 months** Mean: 44 months
Median for all survivors (incl ALD): 76 (3, 211) months
GdE NR NR NR Patients with GdE: 1/22
NR NR NR
Baseline Loes score
Mean/ median NR Mean: 12.3 Mean: 4.6 (SD: 1.9)
Mean: 5.2 (SD: 4.0)
NR NR Mean: 2.1 (SD: 4.1)
NR
≤9 100% NR NR NR NR NR NR NR
>9 NR NR NR NR NR NR NR NR
Baseline NFS
Mean/ median NR Mean: 4.0 NR NR NR NR NR NR
≤1 NR 3 (42.86%) NR NR NR NR NR NR
>1 NR 4 (57.14%) NR NR NR NR NR NR
MFDs at baseline
NR NR NR NR NR NR NR NR
$Study conducted in both adults and children; * unit undefined, both ALD and CALD w ere diagnosed at this age; ** mean/median not defined Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplantation; LO, Lorenzo’s oil; MFD, major functional disabilities; NFS, neurologic function scale; NR, not reported; SCT; stem cell transplantation; SD, standard deviation
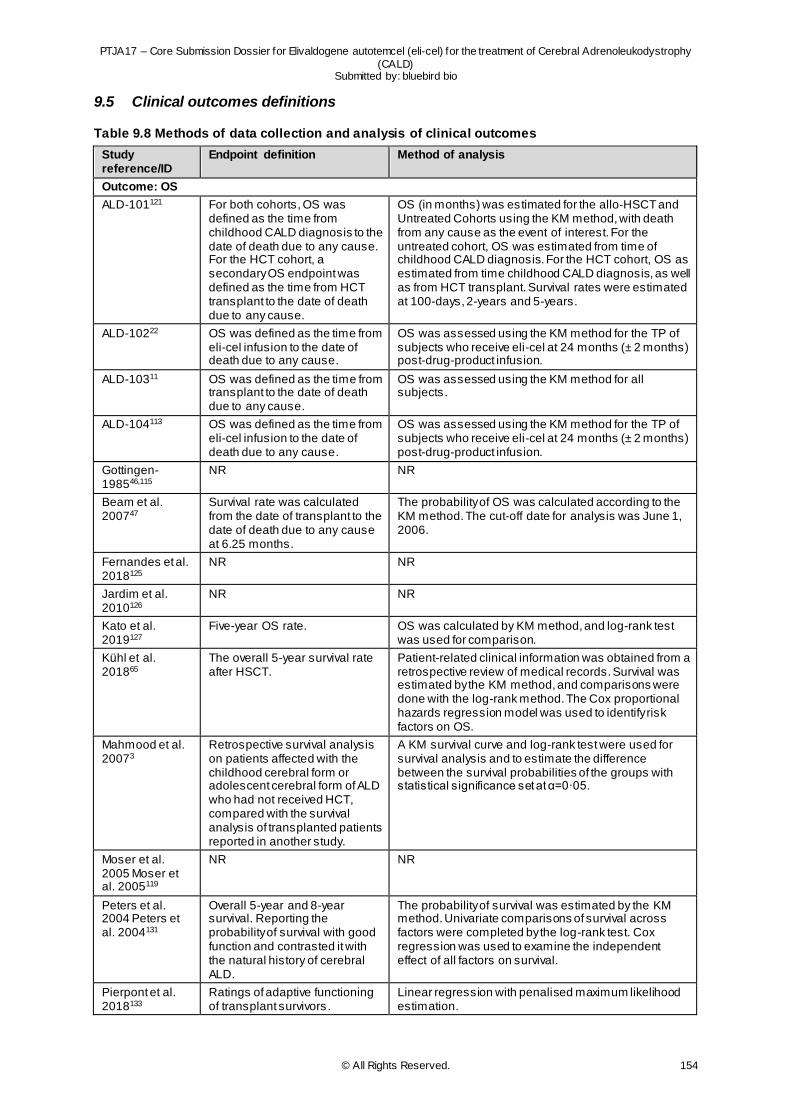
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 154
9.5 Clinical outcomes definitions
Table 9.8 Methods of data collection and analysis of clinical outcomes
Study reference/ID
Endpoint definition Method of analysis
Outcome: OS
ALD-101121 For both cohorts, OS was defined as the time from childhood CALD diagnosis to the date of death due to any cause. For the HCT cohort, a secondary OS endpoint was defined as the time from HCT transplant to the date of death due to any cause.
OS (in months) was estimated for the allo-HSCT and Untreated Cohorts using the KM method, with death from any cause as the event of interest. For the untreated cohort, OS was estimated from time of childhood CALD diagnosis. For the HCT cohort, OS as estimated from time childhood CALD diagnosis, as well as from HCT transplant. Survival rates were estimated at 100-days, 2-years and 5-years.
ALD-10222 OS was defined as the time from eli-cel infusion to the date of death due to any cause.
OS was assessed using the KM method for the TP of subjects who receive eli-cel at 24 months (± 2 months) post-drug-product infusion.
ALD-10311 OS was defined as the time from transplant to the date of death due to any cause.
OS was assessed using the KM method for all subjects.
ALD-104113 OS was defined as the time from eli-cel infusion to the date of death due to any cause.
OS was assessed using the KM method for the TP of subjects who receive eli-cel at 24 months (± 2 months) post-drug-product infusion.
Gottingen-198546,115
NR NR
Beam et al. 200747
Survival rate was calculated from the date of transplant to the date of death due to any cause at 6.25 months.
The probability of OS was calculated according to the KM method. The cut-off date for analysis was June 1, 2006.
Fernandes et al. 2018125
NR NR
Jardim et al. 2010126
NR NR
Kato et al. 2019127
Five-year OS rate. OS was calculated by KM method, and log-rank test was used for comparison.
Kühl et al. 201865
The overall 5-year survival rate after HSCT.
Patient-related clinical information was obtained from a retrospective review of medical records. Survival was estimated by the KM method, and comparisons were done with the log-rank method. The Cox proportional hazards regression model was used to identify risk factors on OS.
Mahmood et al. 20073
Retrospective survival analysis on patients affected with the childhood cerebral form or adolescent cerebral form of ALD who had not received HCT, compared with the survival analysis of transplanted patients reported in another study.
A KM survival curve and log-rank test were used for survival analysis and to estimate the difference between the survival probabilities of the groups with statistical significance set at α=0·05.
Moser et al. 2005 Moser et al. 2005119
NR NR
Peters et al. 2004 Peters et al. 2004131
Overall 5-year and 8-year survival. Reporting the probability of survival with good function and contrasted it with the natural history of cerebral ALD.
The probability of survival was estimated by the KM method. Univariate comparisons of survival across factors were completed by the log-rank test. Cox regression was used to examine the independent effect of all factors on survival.
Pierpont et al. 2018133
Ratings of adaptive functioning of transplant survivors .
Linear regression with penalised maximum likelihood estimation.
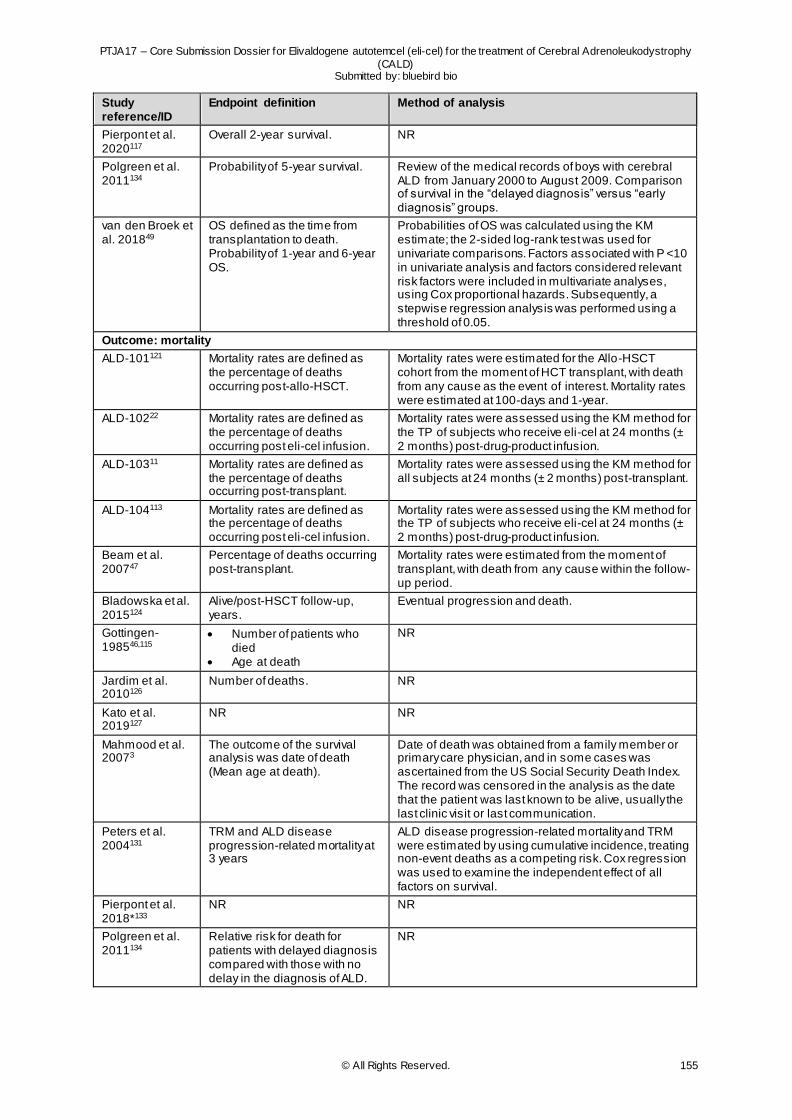
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 155
Study reference/ID
Endpoint definition Method of analysis
Pierpont et al. 2020117
Overall 2-year survival. NR
Polgreen et al. 2011134
Probability of 5-year survival. Review of the medical records of boys with cerebral ALD from January 2000 to August 2009. Comparison of survival in the “delayed diagnosis” versus “early diagnosis” groups.
van den Broek et al. 201849
OS defined as the time from transplantation to death. Probability of 1-year and 6-year OS.
Probabilities of OS was calculated using the KM estimate; the 2-sided log-rank test was used for univariate comparisons. Factors associated with P <10 in univariate analysis and factors considered relevant risk factors were included in multivariate analyses, using Cox proportional hazards. Subsequently, a stepwise regression analysis was performed using a threshold of 0.05.
Outcome: mortality
ALD-101121 Mortality rates are defined as the percentage of deaths occurring post-allo-HSCT.
Mortality rates were estimated for the Allo-HSCT cohort from the moment of HCT transplant, with death from any cause as the event of interest. Mortality rates were estimated at 100-days and 1-year.
ALD-10222 Mortality rates are defined as the percentage of deaths occurring post eli-cel infusion.
Mortality rates were assessed using the KM method for the TP of subjects who receive eli-cel at 24 months (± 2 months) post-drug-product infusion.
ALD-10311 Mortality rates are defined as the percentage of deaths occurring post-transplant.
Mortality rates were assessed using the KM method for all subjects at 24 months (± 2 months) post-transplant.
ALD-104113 Mortality rates are defined as the percentage of deaths occurring post eli-cel infusion.
Mortality rates were assessed using the KM method for the TP of subjects who receive eli-cel at 24 months (± 2 months) post-drug-product infusion.
Beam et al. 200747
Percentage of deaths occurring post-transplant.
Mortality rates were estimated from the moment of transplant, with death from any cause within the follow-up period.
Bladowska et al. 2015124
Alive/post-HSCT follow-up, years.
Eventual progression and death.
Gottingen-198546,115
Number of patients who died
Age at death
NR
Jardim et al. 2010126
Number of deaths. NR
Kato et al. 2019127
NR NR
Mahmood et al. 20073
The outcome of the survival analysis was date of death (Mean age at death).
Date of death was obtained from a family member or primary care physician, and in some cases was ascertained from the US Social Security Death Index. The record was censored in the analysis as the date that the patient was last known to be alive, usually the last clinic visit or last communication.
Peters et al. 2004131
TRM and ALD disease progression-related mortality at 3 years
ALD disease progression-related mortality and TRM were estimated by using cumulative incidence, treating non-event deaths as a competing risk. Cox regression was used to examine the independent effect of all factors on survival.
Pierpont et al. 2018*133
NR NR
Polgreen et al. 2011134
Relative risk for death for patients with delayed diagnosis compared with those with no delay in the diagnosis of ALD.
NR
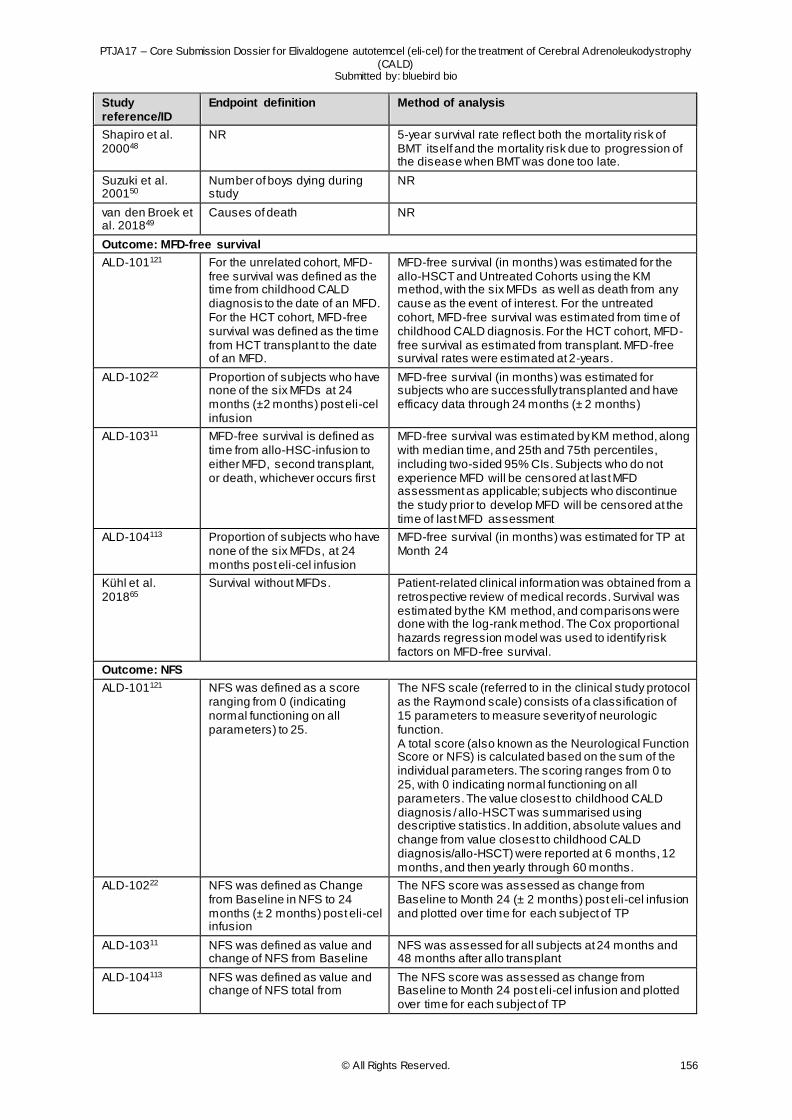
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 156
Study reference/ID
Endpoint definition Method of analysis
Shapiro et al. 200048
NR 5-year survival rate reflect both the mortality risk of BMT itself and the mortality risk due to progression of the disease when BMT was done too late.
Suzuki et al. 200150
Number of boys dying during study
NR
van den Broek et al. 201849
Causes of death NR
Outcome: MFD-free survival
ALD-101121 For the unrelated cohort, MFD-free survival was defined as the time from childhood CALD diagnosis to the date of an MFD. For the HCT cohort, MFD-free survival was defined as the time from HCT transplant to the date of an MFD.
MFD-free survival (in months) was estimated for the allo-HSCT and Untreated Cohorts using the KM method, with the six MFDs as well as death from any cause as the event of interest. For the untreated cohort, MFD-free survival was estimated from time of childhood CALD diagnosis. For the HCT cohort, MFD-free survival as estimated from transplant. MFD-free survival rates were estimated at 2-years.
ALD-10222 Proportion of subjects who have none of the six MFDs at 24 months (±2 months) post eli-cel infusion
MFD-free survival (in months) was estimated for subjects who are successfully transplanted and have efficacy data through 24 months (± 2 months)
ALD-10311 MFD-free survival is defined as time from allo-HSC-infusion to either MFD, second transplant, or death, whichever occurs first
MFD-free survival was estimated by KM method, along with median time, and 25th and 75th percentiles, including two-sided 95% CIs. Subjects who do not experience MFD will be censored at last MFD assessment as applicable; subjects who discontinue the study prior to develop MFD will be censored at the time of last MFD assessment
ALD-104113 Proportion of subjects who have none of the six MFDs, at 24 months post eli-cel infusion
MFD-free survival (in months) was estimated for TP at Month 24
Kühl et al. 201865
Survival without MFDs. Patient-related clinical information was obtained from a retrospective review of medical records. Survival was estimated by the KM method, and comparisons were done with the log-rank method. The Cox proportional hazards regression model was used to identify risk factors on MFD-free survival.
Outcome: NFS
ALD-101121 NFS was defined as a score ranging from 0 (indicating normal functioning on all parameters) to 25.
The NFS scale (referred to in the clinical study protocol as the Raymond scale) consists of a classification of 15 parameters to measure severity of neurologic function. A total score (also known as the Neurological Function Score or NFS) is calculated based on the sum of the individual parameters. The scoring ranges from 0 to 25, with 0 indicating normal functioning on all parameters. The value closest to childhood CALD diagnosis / allo-HSCT was summarised using descriptive statistics. In addition, absolute values and change from value closest to childhood CALD diagnosis/allo-HSCT) were reported at 6 months, 12 months, and then yearly through 60 months.
ALD-10222 NFS was defined as Change from Baseline in NFS to 24 months (± 2 months) post eli-cel infusion
The NFS score was assessed as change from Baseline to Month 24 (± 2 months) post eli-cel infusion and plotted over time for each subject of TP
ALD-10311 NFS was defined as value and change of NFS from Baseline
NFS was assessed for all subjects at 24 months and 48 months after allo transplant
ALD-104113 NFS was defined as value and change of NFS total from
The NFS score was assessed as change from Baseline to Month 24 post eli-cel infusion and plotted over time for each subject of TP
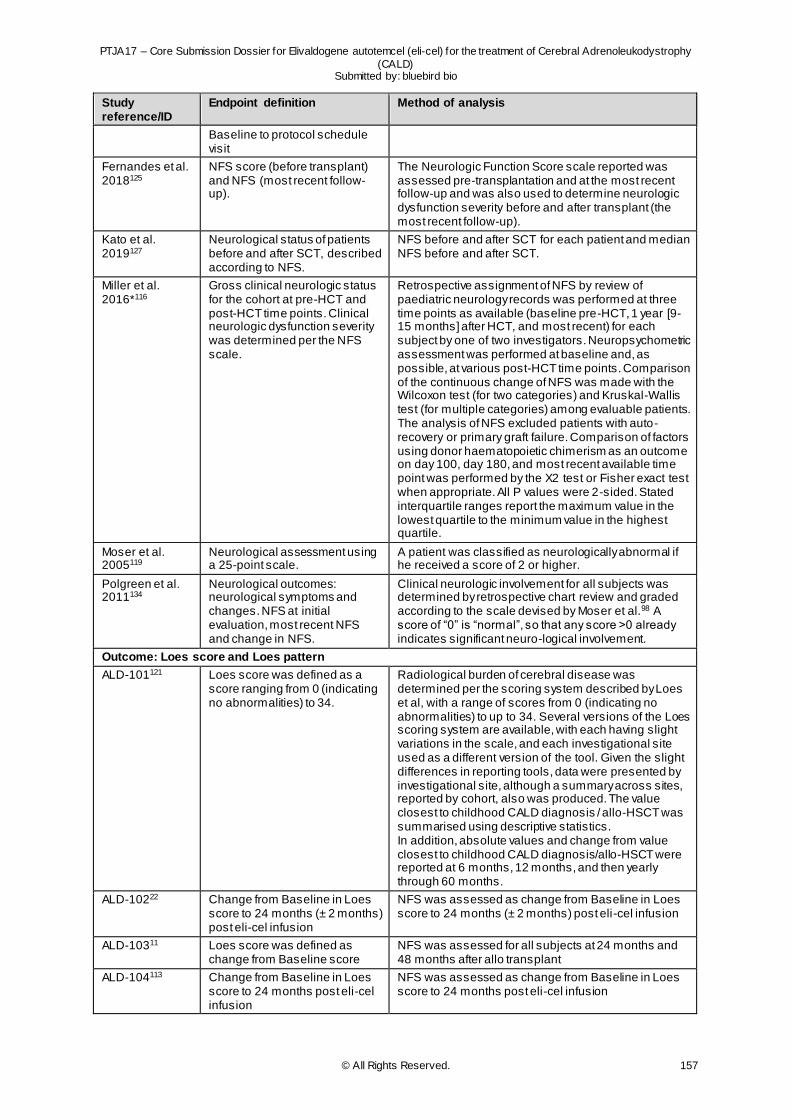
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 157
Study reference/ID
Endpoint definition Method of analysis
Baseline to protocol schedule visit
Fernandes et al. 2018125
NFS score (before transplant) and NFS (most recent follow-up).
The Neurologic Function Score scale reported was assessed pre-transplantation and at the most recent follow-up and was also used to determine neurologic dysfunction severity before and after transplant (the most recent follow-up).
Kato et al. 2019127
Neurological status of patients before and after SCT, described according to NFS.
NFS before and after SCT for each patient and median NFS before and after SCT.
Miller et al. 2016*116
Gross clinical neurologic status for the cohort at pre-HCT and post-HCT time points. Clinical neurologic dysfunction severity was determined per the NFS scale.
Retrospective assignment of NFS by review of paediatric neurology records was performed at three time points as available (baseline pre-HCT, 1 year [9-15 months] after HCT, and most recent) for each subject by one of two investigators. Neuropsychometric assessment was performed at baseline and, as possible, at various post-HCT time points. Comparison of the continuous change of NFS was made with the Wilcoxon test (for two categories) and Kruskal-Wallis test (for multiple categories) among evaluable patients. The analysis of NFS excluded patients with auto-recovery or primary graft failure. Comparison of factors using donor haematopoietic chimerism as an outcome on day 100, day 180, and most recent available time point was performed by the X2 test or Fisher exact test when appropriate. All P values were 2-sided. Stated interquartile ranges report the maximum value in the lowest quartile to the minimum value in the highest quartile.
Moser et al. 2005119
Neurological assessment using a 25-point scale.
A patient was classified as neurologically abnormal if he received a score of 2 or higher.
Polgreen et al. 2011134
Neurological outcomes: neurological symptoms and changes. NFS at initial evaluation, most recent NFS and change in NFS.
Clinical neurologic involvement for all subjects was determined by retrospective chart review and graded according to the scale devised by Moser et al.98 A score of “0” is “normal”, so that any score >0 already indicates significant neuro-logical involvement.
Outcome: Loes score and Loes pattern
ALD-101121 Loes score was defined as a score ranging from 0 (indicating no abnormalities) to 34.
Radiological burden of cerebral disease was determined per the scoring system described by Loes et al, with a range of scores from 0 (indicating no abnormalities) to up to 34. Several versions of the Loes scoring system are available, with each having slight variations in the scale, and each investigational site used as a different version of the tool. Given the slight differences in reporting tools, data were presented by investigational site, although a summary across sites, reported by cohort, also was produced. The value closest to childhood CALD diagnosis / allo-HSCT was summarised using descriptive statistics. In addition, absolute values and change from value closest to childhood CALD diagnosis/allo-HSCT were reported at 6 months, 12 months, and then yearly through 60 months.
ALD-10222 Change from Baseline in Loes score to 24 months (± 2 months) post eli-cel infusion
NFS was assessed as change from Baseline in Loes score to 24 months (± 2 months) post eli-cel infusion
ALD-10311 Loes score was defined as change from Baseline score
NFS was assessed for all subjects at 24 months and 48 months after allo transplant
ALD-104113 Change from Baseline in Loes score to 24 months post eli-cel infusion
NFS was assessed as change from Baseline in Loes score to 24 months post eli-cel infusion
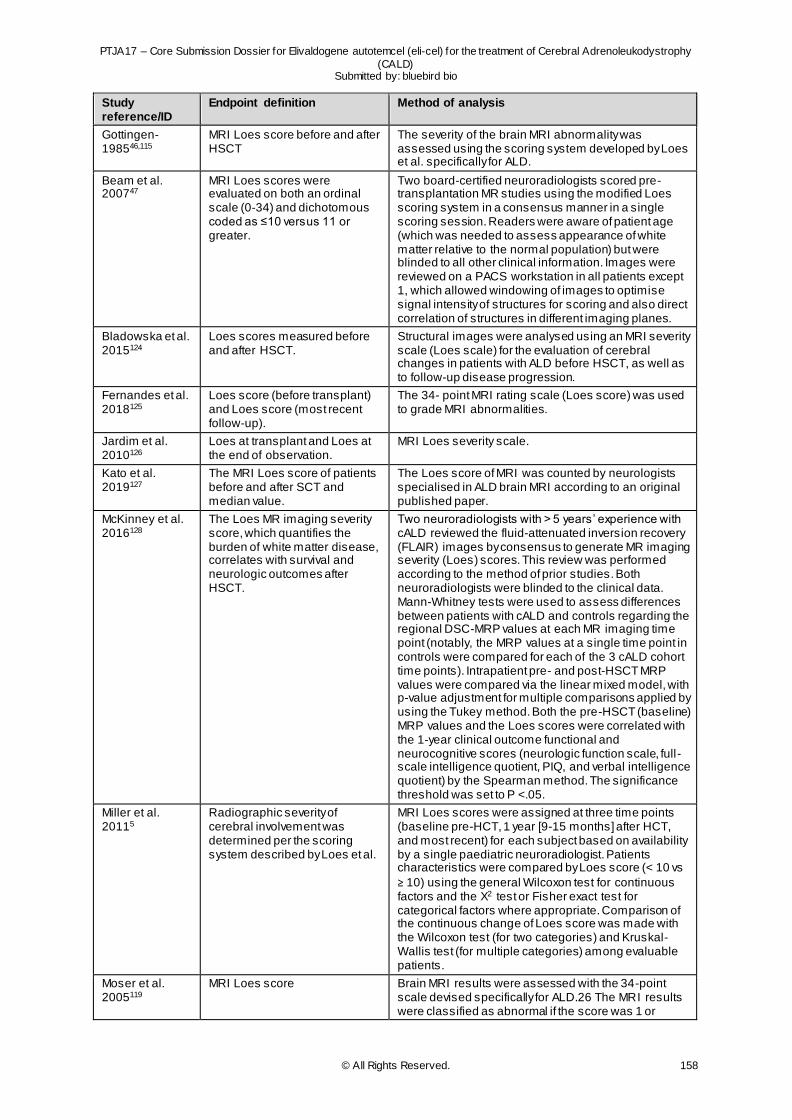
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 158
Study reference/ID
Endpoint definition Method of analysis
Gottingen-198546,115
MRI Loes score before and after HSCT
The severity of the brain MRI abnormality was assessed using the scoring system developed by Loes et al. specifically for ALD.
Beam et al. 200747
MRI Loes scores were evaluated on both an ordinal scale (0-34) and dichotomous coded as ≤10 versus 11 or greater.
Two board-certified neuroradiologists scored pre-transplantation MR studies using the modified Loes scoring system in a consensus manner in a single scoring session. Readers were aware of patient age (which was needed to assess appearance of white matter relative to the normal population) but were blinded to all other clinical information. Images were reviewed on a PACS workstation in all patients except 1, which allowed windowing of images to optimise signal intensity of structures for scoring and also direct correlation of structures in different imaging planes.
Bladowska et al. 2015124
Loes scores measured before and after HSCT.
Structural images were analysed using an MRI severity scale (Loes scale) for the evaluation of cerebral changes in patients with ALD before HSCT, as well as to follow-up disease progression.
Fernandes et al. 2018125
Loes score (before transplant) and Loes score (most recent follow-up).
The 34- point MRI rating scale (Loes score) was used to grade MRI abnormalities.
Jardim et al. 2010126
Loes at transplant and Loes at the end of observation.
MRI Loes severity scale.
Kato et al. 2019127
The MRI Loes score of patients before and after SCT and median value.
The Loes score of MRI was counted by neurologists specialised in ALD brain MRI according to an original published paper.
McKinney et al. 2016128
The Loes MR imaging severity score, which quantifies the burden of white matter disease, correlates with survival and neurologic outcomes after HSCT.
Two neuroradiologists with > 5 years’ experience with cALD reviewed the fluid-attenuated inversion recovery (FLAIR) images by consensus to generate MR imaging severity (Loes) scores. This review was performed according to the method of prior studies. Both neuroradiologists were blinded to the clinical data. Mann-Whitney tests were used to assess differences between patients with cALD and controls regarding the regional DSC-MRP values at each MR imaging time point (notably, the MRP values at a single time point in controls were compared for each of the 3 cALD cohort time points). Intrapatient pre- and post-HSCT MRP values were compared via the linear mixed model, with p-value adjustment for multiple comparisons applied by using the Tukey method. Both the pre-HSCT (baseline) MRP values and the Loes scores were correlated with the 1-year clinical outcome functional and neurocognitive scores (neurologic function scale, full-scale intelligence quotient, PIQ, and verbal intelligence quotient) by the Spearman method. The significance threshold was set to P <.05.
Miller et al. 20115
Radiographic severity of cerebral involvement was determined per the scoring system described by Loes et al.
MRI Loes scores were assigned at three time points (baseline pre-HCT, 1 year [9-15 months] after HCT, and most recent) for each subject based on availability by a single paediatric neuroradiologist. Patients characteristics were compared by Loes score (< 10 vs
≥ 10) using the general Wilcoxon test for continuous factors and the X2 test or Fisher exact test for categorical factors where appropriate. Comparison of the continuous change of Loes score was made with the Wilcoxon test (for two categories) and Kruskal-Wallis test (for multiple categories) among evaluable patients.
Moser et al. 2005119
MRI Loes score Brain MRI results were assessed with the 34-point scale devised specifically for ALD.26 The MRI results were classified as abnormal if the score was 1 or
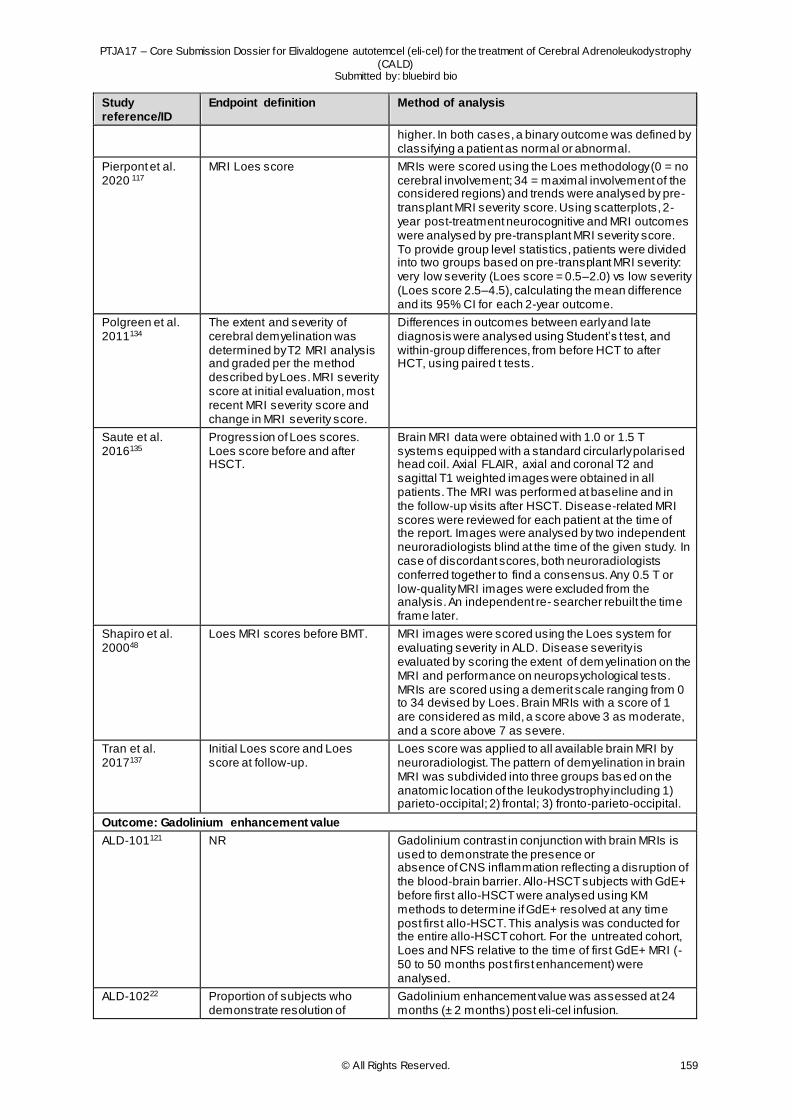
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 159
Study reference/ID
Endpoint definition Method of analysis
higher. In both cases, a binary outcome was defined by classifying a patient as normal or abnormal.
Pierpont et al. 2020 117
MRI Loes score MRIs were scored using the Loes methodology (0 = no cerebral involvement; 34 = maximal involvement of the considered regions) and trends were analysed by pre-transplant MRI severity score. Using scatterplots, 2-year post-treatment neurocognitive and MRI outcomes were analysed by pre-transplant MRI severity score. To provide group level statistics, patients were divided into two groups based on pre-transplant MRI severity: very low severity (Loes score = 0.5–2.0) vs low severity (Loes score 2.5–4.5), calculating the mean difference and its 95% CI for each 2-year outcome.
Polgreen et al. 2011134
The extent and severity of cerebral demyelination was determined by T2 MRI analysis and graded per the method described by Loes. MRI severity score at initial evaluation, most recent MRI severity score and change in MRI severity score.
Differences in outcomes between early and late diagnosis were analysed using Student’s t test, and within-group differences, from before HCT to after HCT, using paired t tests.
Saute et al. 2016135
Progression of Loes scores. Loes score before and after HSCT.
Brain MRI data were obtained with 1.0 or 1.5 T systems equipped with a standard circularly polarised head coil. Axial FLAIR, axial and coronal T2 and sagittal T1 weighted images were obtained in all patients. The MRI was performed at baseline and in the follow-up visits after HSCT. Disease-related MRI scores were reviewed for each patient at the time of the report. Images were analysed by two independent neuroradiologists blind at the time of the given study. In case of discordant scores, both neuroradiologists conferred together to find a consensus. Any 0.5 T or low-quality MRI images were excluded from the analysis. An independent re- searcher rebuilt the time frame later.
Shapiro et al. 200048
Loes MRI scores before BMT. MRI images were scored using the Loes system for evaluating severity in ALD. Disease severity is evaluated by scoring the extent of demyelination on the MRI and performance on neuropsychological tests. MRIs are scored using a demerit scale ranging from 0 to 34 devised by Loes. Brain MRIs with a score of 1 are considered as mild, a score above 3 as moderate, and a score above 7 as severe.
Tran et al. 2017137
Initial Loes score and Loes score at follow-up.
Loes score was applied to all available brain MRI by neuroradiologist. The pattern of demyelination in brain MRI was subdivided into three groups based on the anatomic location of the leukodystrophy including 1) parieto-occipital; 2) frontal; 3) fronto-parieto-occipital.
Outcome: Gadolinium enhancement value
ALD-101121 NR Gadolinium contrast in conjunction with brain MRIs is used to demonstrate the presence or absence of CNS inflammation reflecting a disruption of the blood-brain barrier. Allo-HSCT subjects with GdE+ before first allo-HSCT were analysed using KM methods to determine if GdE+ resolved at any time post first allo-HSCT. This analysis was conducted for the entire allo-HSCT cohort. For the untreated cohort, Loes and NFS relative to the time of first GdE+ MRI (-50 to 50 months post first enhancement) were analysed.
ALD-10222 Proportion of subjects who demonstrate resolution of
Gadolinium enhancement value was assessed at 24 months (± 2 months) post eli-cel infusion.
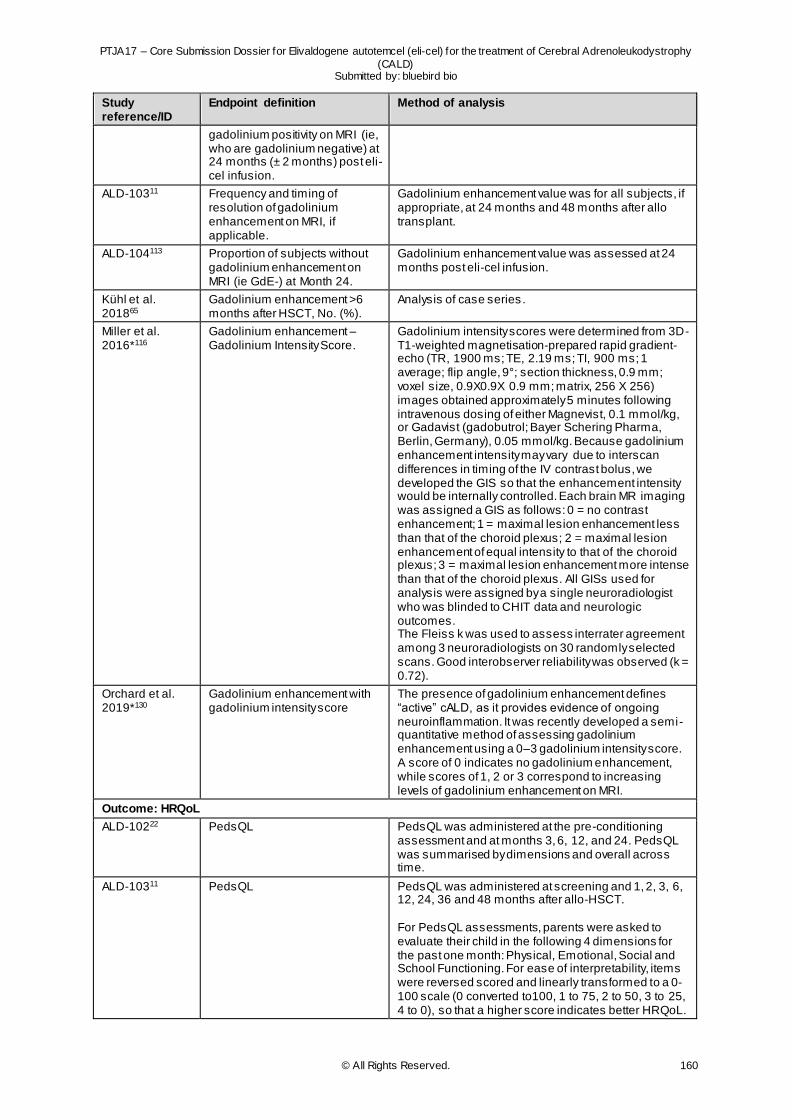
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 160
Study reference/ID
Endpoint definition Method of analysis
gadolinium positivity on MRI (ie, who are gadolinium negative) at 24 months (± 2 months) post eli-cel infusion.
ALD-10311 Frequency and timing of resolution of gadolinium enhancement on MRI, if applicable.
Gadolinium enhancement value was for all subjects, if appropriate, at 24 months and 48 months after allo transplant.
ALD-104113 Proportion of subjects without gadolinium enhancement on MRI (ie GdE-) at Month 24.
Gadolinium enhancement value was assessed at 24 months post eli-cel infusion.
Kühl et al. 201865
Gadolinium enhancement >6 months after HSCT, No. (%).
Analysis of case series .
Miller et al. 2016*116
Gadolinium enhancement – Gadolinium Intensity Score.
Gadolinium intensity scores were determined from 3D-T1-weighted magnetisation-prepared rapid gradient-echo (TR, 1900 ms; TE, 2.19 ms; TI, 900 ms; 1 average; flip angle, 9°; section thickness, 0.9 mm; voxel size, 0.9X0.9X 0.9 mm; matrix, 256 X 256) images obtained approximately 5 minutes following intravenous dosing of either Magnevist, 0.1 mmol/kg, or Gadavist (gadobutrol; Bayer Schering Pharma, Berlin, Germany), 0.05 mmol/kg. Because gadolinium enhancement intensity may vary due to interscan differences in timing of the IV contrast bolus, we developed the GIS so that the enhancement intensity would be internally controlled. Each brain MR imaging was assigned a GIS as follows: 0 = no contrast enhancement; 1 = maximal lesion enhancement less than that of the choroid plexus; 2 = maximal lesion enhancement of equal intensity to that of the choroid plexus; 3 = maximal lesion enhancement more intense than that of the choroid plexus. All GISs used for analysis were assigned by a single neuroradiologist who was blinded to CHIT data and neurologic outcomes. The Fleiss k was used to assess interrater agreement among 3 neuroradiologists on 30 randomly selected scans. Good interobserver reliability was observed (k = 0.72).
Orchard et al. 2019*130
Gadolinium enhancement with gadolinium intensity score
The presence of gadolinium enhancement defines “active” cALD, as it provides evidence of ongoing neuroinflammation. It was recently developed a semi-quantitative method of assessing gadolinium enhancement using a 0–3 gadolinium intensity score. A score of 0 indicates no gadolinium enhancement, while scores of 1, 2 or 3 correspond to increasing levels of gadolinium enhancement on MRI.
Outcome: HRQoL
ALD-10222 PedsQL PedsQL was administered at the pre-conditioning assessment and at months 3, 6, 12, and 24. PedsQL was summarised by dimensions and overall across time.
ALD-10311 PedsQL PedsQL was administered at screening and 1, 2, 3, 6, 12, 24, 36 and 48 months after allo-HSCT. For PedsQL assessments, parents were asked to evaluate their child in the following 4 dimensions for the past one month: Physical, Emotional, Social and School Functioning. For ease of interpretability, items were reversed scored and linearly transformed to a 0-100 scale (0 converted to100, 1 to 75, 2 to 50, 3 to 25, 4 to 0), so that a higher score indicates better HRQoL.
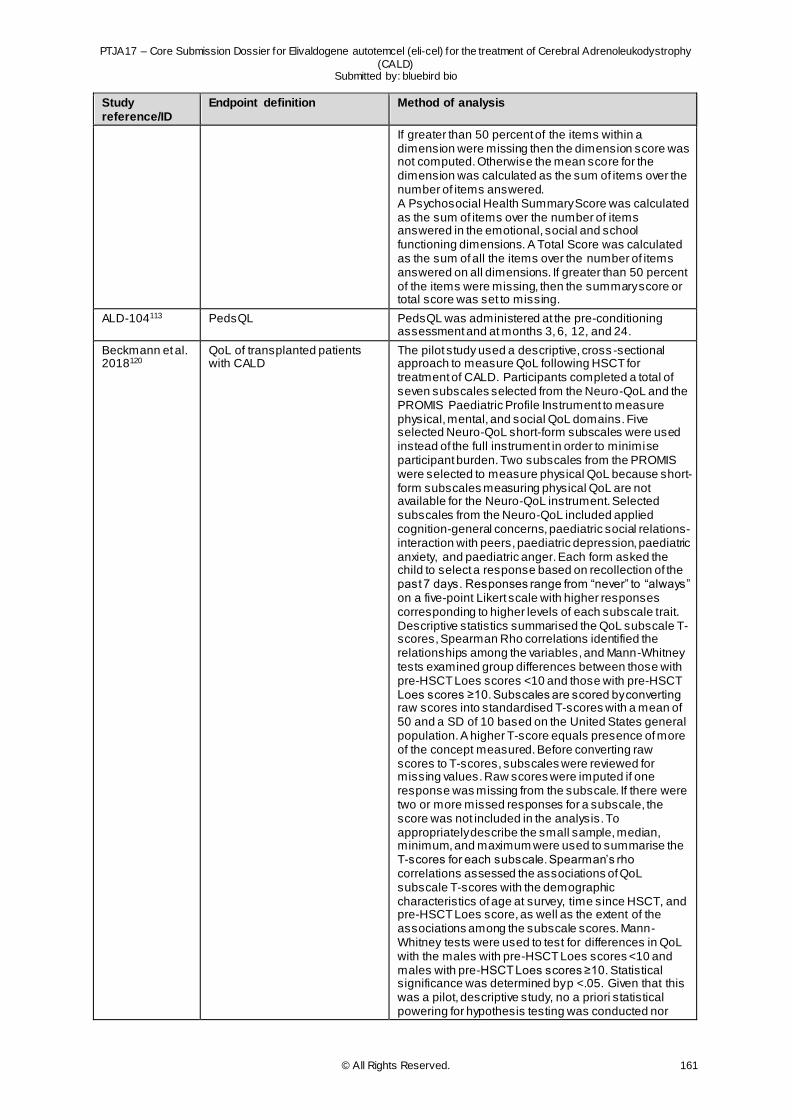
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 161
Study reference/ID
Endpoint definition Method of analysis
If greater than 50 percent of the items within a dimension were missing then the dimension score was not computed. Otherwise the mean score for the dimension was calculated as the sum of items over the number of items answered. A Psychosocial Health Summary Score was calculated as the sum of items over the number of items answered in the emotional, social and school functioning dimensions. A Total Score was calculated as the sum of all the items over the number of items answered on all dimensions. If greater than 50 percent of the items were missing, then the summary score or total score was set to missing.
ALD-104113 PedsQL PedsQL was administered at the pre-conditioning assessment and at months 3, 6, 12, and 24.
Beckmann et al. 2018120
QoL of transplanted patients with CALD
The pilot study used a descriptive, cross -sectional approach to measure QoL following HSCT for treatment of CALD. Participants completed a total of seven subscales selected from the Neuro-QoL and the PROMIS Paediatric Profile Instrument to measure physical, mental, and social QoL domains. Five selected Neuro-QoL short-form subscales were used instead of the full instrument in order to minimise participant burden. Two subscales from the PROMIS were selected to measure physical QoL because short-form subscales measuring physical QoL are not available for the Neuro-QoL instrument. Selected subscales from the Neuro-QoL included applied cognition-general concerns, paediatric social relations-interaction with peers, paediatric depression, paediatric anxiety, and paediatric anger. Each form asked the child to select a response based on recollection of the past 7 days. Responses range from “never” to “always” on a five-point Likert scale with higher responses corresponding to higher levels of each subscale trait. Descriptive statistics summarised the QoL subscale T-scores, Spearman Rho correlations identified the relationships among the variables, and Mann-Whitney tests examined group differences between those with pre-HSCT Loes scores <10 and those with pre-HSCT Loes scores ≥10. Subscales are scored by converting raw scores into standardised T-scores with a mean of 50 and a SD of 10 based on the United States general population. A higher T-score equals presence of more of the concept measured. Before converting raw scores to T-scores, subscales were reviewed for missing values. Raw scores were imputed if one response was missing from the subscale. If there were two or more missed responses for a subscale, the score was not included in the analysis. To appropriately describe the small sample, median, minimum, and maximum were used to summarise the T-scores for each subscale. Spearman’s rho correlations assessed the associations of QoL subscale T-scores with the demographic characteristics of age at survey, time since HSCT, and pre-HSCT Loes score, as well as the extent of the associations among the subscale scores. Mann-Whitney tests were used to test for differences in QoL with the males with pre-HSCT Loes scores <10 and males with pre-HSCT Loes scores ≥10. Statistical significance was determined by p <.05. Given that this was a pilot, descriptive study, no a priori statistical powering for hypothesis testing was conducted nor

PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 162
Study reference/ID
Endpoint definition Method of analysis
were there any corrections to the alpha for multiple tests. The magnitude of the effect sizes (group differences and correlations) was the primary focus.
Abbreviations: ALD, adrenoleukodystrophy; allo-HSCT, allogeneic haematopoietic allogenic stem cell transplant; BMT, bone marrow transplant; CALD, cerebral adrenoleukodystrophy; CHIT, chitotriosidase; CI, confidence interval; CNS, central nervous system; DSC-MRP, dynamic susceptibility w eighted perfusion MRI; FLAIR, f luid-attenuated inversion recovery;
GdE, gadolinium enhancement; GIS, gadolinium intensity scale; HCT, haematopoietic cell transplantation; HRQoL, health-related quality of life; IV, intravenous; KM, Kaplan-Meier; MFD, major functional disabilities; MRI, magnetic resonance imaging; MR, magnetic resonance; NFS, neurologic function score; NR, not reported; OS, overall survival; PedsQL, Paediatric Quality of Life Inventory; PIQ, performance intelligence quotient; PROMIS, Patient-Reported Outcomes
Measurement Information System; QoL, quality of life; SCT, stem cell transplantation; SD, standard, deviation; TP, transplanted population; TRM, transplant-related mortality; UNMQL, University of Minneapolis Quality of Life Inventory
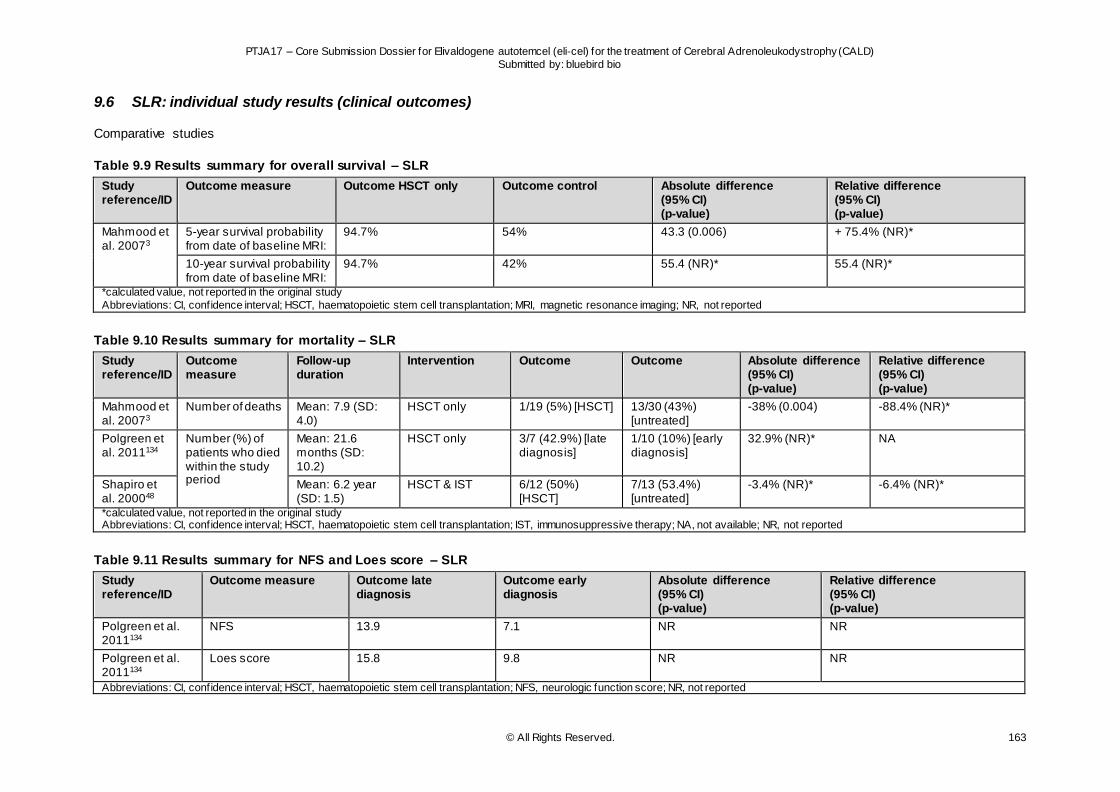
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 163
9.6 SLR: individual study results (clinical outcomes)
Comparative studies
Table 9.9 Results summary for overall survival – SLR
Study reference/ID
Outcome measure Outcome HSCT only Outcome control
Absolute difference (95% CI) (p-value)
Relative difference (95% CI) (p-value)
Mahmood et al. 20073
5-year survival probability from date of baseline MRI:
94.7% 54% 43.3 (0.006) + 75.4% (NR)*
10-year survival probability from date of baseline MRI:
94.7% 42% 55.4 (NR)* 55.4 (NR)*
*calculated value, not reported in the original study
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; MRI, magnetic resonance imaging; NR, not reported
Table 9.10 Results summary for mortality – SLR
Study reference/ID
Outcome measure
Follow-up duration
Intervention Outcome Outcome
Absolute difference (95% CI) (p-value)
Relative difference (95% CI) (p-value)
Mahmood et al. 20073
Number of deaths Mean: 7.9 (SD: 4.0)
HSCT only 1/19 (5%) [HSCT] 13/30 (43%) [untreated]
-38% (0.004) -88.4% (NR)*
Polgreen et al. 2011134
Number (%) of patients who died within the study period
Mean: 21.6 months (SD: 10.2)
HSCT only 3/7 (42.9%) [late diagnosis]
1/10 (10%) [early diagnosis]
32.9% (NR)* NA
Shapiro et al. 200048
Mean: 6.2 year (SD: 1.5)
HSCT & IST 6/12 (50%) [HSCT]
7/13 (53.4%) [untreated]
-3.4% (NR)* -6.4% (NR)*
*calculated value, not reported in the original study Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NA, not available; NR, not reported
Table 9.11 Results summary for NFS and Loes score – SLR
Study reference/ID
Outcome measure Outcome late diagnosis
Outcome early diagnosis
Absolute difference (95% CI) (p-value)
Relative difference (95% CI) (p-value)
Polgreen et al. 2011134
NFS 13.9 7.1 NR NR
Polgreen et al. 2011134
Loes score 15.8 9.8 NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; NFS, neurologic function score; NR, not reported
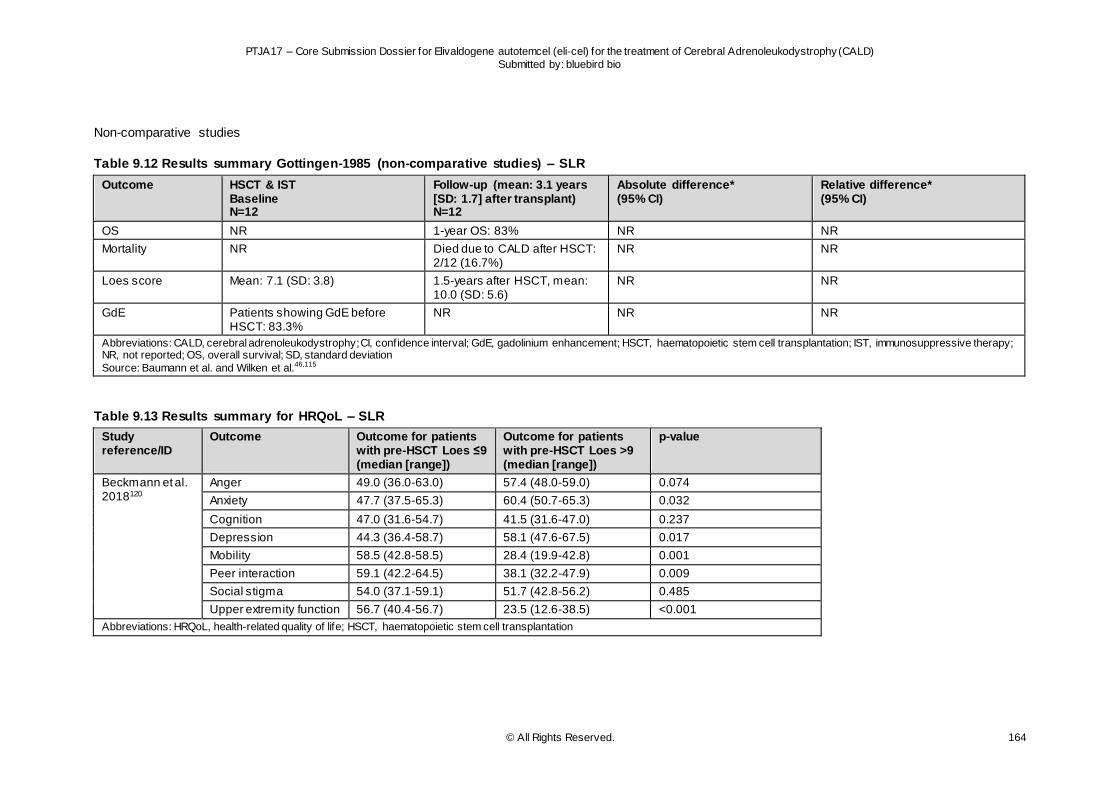
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 164
Non-comparative studies
Table 9.12 Results summary Gottingen-1985 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=12
Follow-up (mean: 3.1 years [SD: 1.7] after transplant) N=12
Absolute difference* (95% CI)
Relative difference* (95% CI)
OS NR 1-year OS: 83% NR NR
Mortality NR Died due to CALD after HSCT: 2/12 (16.7%)
NR NR
Loes score Mean: 7.1 (SD: 3.8) 1.5-years after HSCT, mean: 10.0 (SD: 5.6)
NR NR
GdE Patients showing GdE before HSCT: 83.3%
NR NR NR
Abbreviations: CALD, cerebral adrenoleukodystrophy; CI, confidence interval; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; OS, overall survival; SD, standard deviation
Source: Baumann et al. and Wilken et al.46,115
Table 9.13 Results summary for HRQoL – SLR
Study reference/ID
Outcome Outcome for patients with pre-HSCT Loes ≤9 (median [range])
Outcome for patients with pre-HSCT Loes >9 (median [range])
p-value
Beckmann et al. 2018120
Anger 49.0 (36.0-63.0) 57.4 (48.0-59.0) 0.074
Anxiety 47.7 (37.5-65.3) 60.4 (50.7-65.3) 0.032
Cognition 47.0 (31.6-54.7) 41.5 (31.6-47.0) 0.237
Depression 44.3 (36.4-58.7) 58.1 (47.6-67.5) 0.017
Mobility 58.5 (42.8-58.5) 28.4 (19.9-42.8) 0.001
Peer interaction 59.1 (42.2-64.5) 38.1 (32.2-47.9) 0.009
Social stigma 54.0 (37.1-59.1) 51.7 (42.8-56.2) 0.485
Upper extremity function 56.7 (40.4-56.7) 23.5 (12.6-38.5) <0.001
Abbreviations: HRQoL, health-related quality of life; HSCT, haematopoietic stem cell transplantation
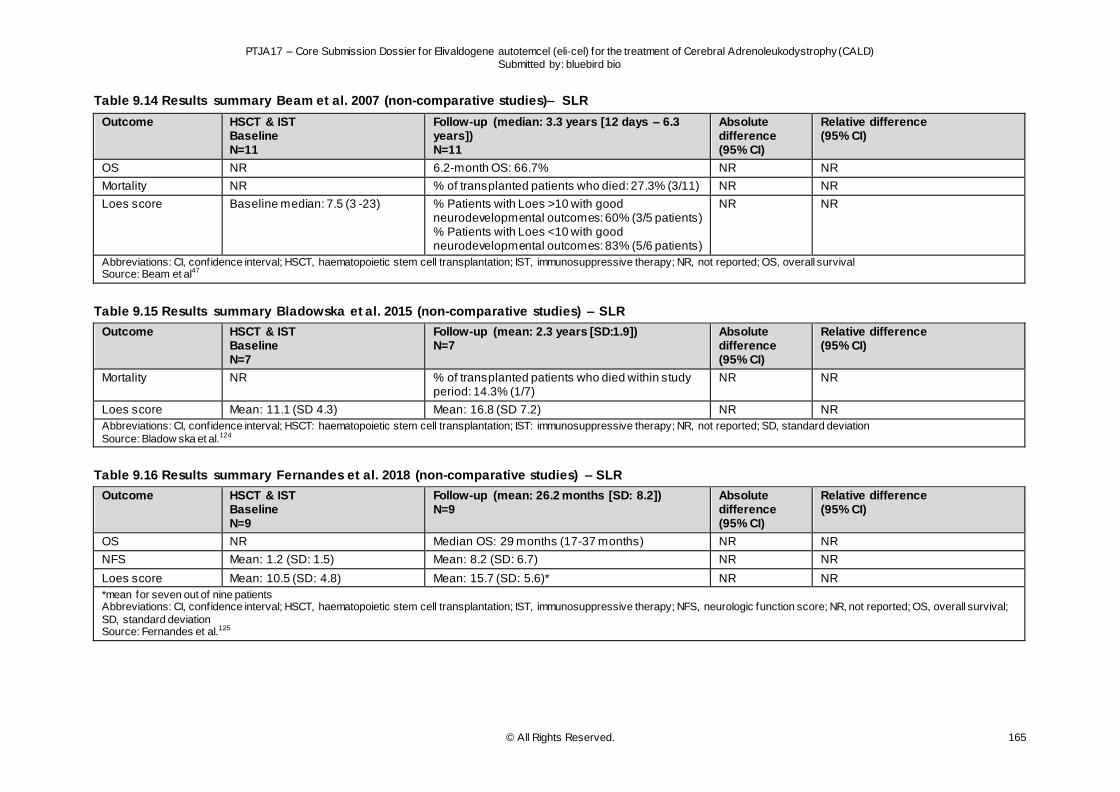
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 165
Table 9.14 Results summary Beam et al. 2007 (non-comparative studies)– SLR
Outcome
HSCT & IST Baseline N=11
Follow-up (median: 3.3 years [12 days – 6.3 years]) N=11
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR 6.2-month OS: 66.7% NR NR
Mortality NR % of transplanted patients who died: 27.3% (3/11) NR NR
Loes score Baseline median: 7.5 (3 -23) % Patients with Loes >10 with good neurodevelopmental outcomes: 60% (3/5 patients) % Patients with Loes <10 with good neurodevelopmental outcomes: 83% (5/6 patients)
NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; OS, overall survival Source: Beam et al47
Table 9.15 Results summary Bladowska et al. 2015 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=7
Follow-up (mean: 2.3 years [SD:1.9]) N=7
Absolute difference (95% CI)
Relative difference (95% CI)
Mortality NR % of transplanted patients who died within study period: 14.3% (1/7)
NR NR
Loes score Mean: 11.1 (SD 4.3) Mean: 16.8 (SD 7.2) NR NR
Abbreviations: CI, confidence interval; HSCT: haematopoietic stem cell transplantation; IST: immunosuppressive therapy; NR, not reported; SD, standard deviation
Source: Bladow ska et al.124
Table 9.16 Results summary Fernandes et al. 2018 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=9
Follow-up (mean: 26.2 months [SD: 8.2]) N=9
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR Median OS: 29 months (17-37 months) NR NR
NFS Mean: 1.2 (SD: 1.5) Mean: 8.2 (SD: 6.7) NR NR
Loes score Mean: 10.5 (SD: 4.8) Mean: 15.7 (SD: 5.6)* NR NR
*mean for seven out of nine patients Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NFS, neurologic function score; NR, not reported; OS, overall survival;
SD, standard deviation Source: Fernandes et al.125
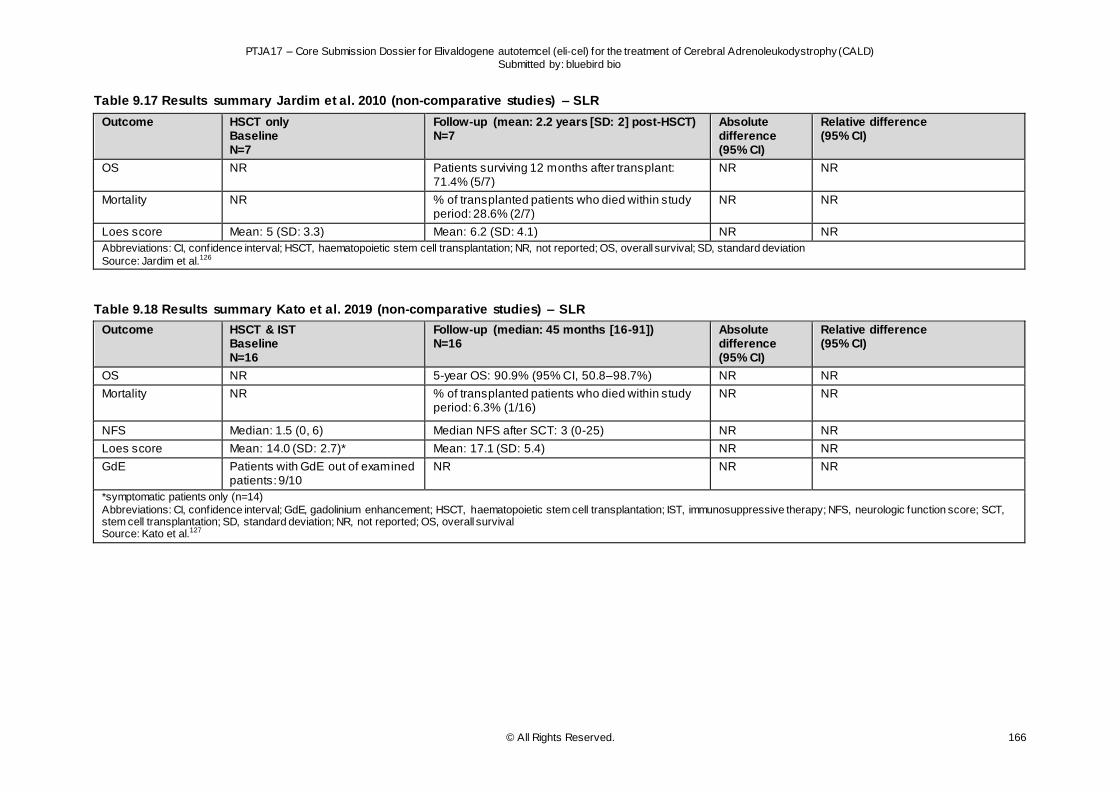
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 166
Table 9.17 Results summary Jardim et al. 2010 (non-comparative studies) – SLR
Outcome
HSCT only Baseline N=7
Follow-up (mean: 2.2 years [SD: 2] post-HSCT) N=7
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR Patients surviving 12 months after transplant: 71.4% (5/7)
NR NR
Mortality NR % of transplanted patients who died within study period: 28.6% (2/7)
NR NR
Loes score Mean: 5 (SD: 3.3) Mean: 6.2 (SD: 4.1) NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; NR, not reported; OS, overall survival; SD, standard deviation
Source: Jardim et al.126
Table 9.18 Results summary Kato et al. 2019 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=16
Follow-up (median: 45 months [16-91]) N=16
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR 5-year OS: 90.9% (95% CI, 50.8–98.7%) NR NR
Mortality NR % of transplanted patients who died within study period: 6.3% (1/16)
NR NR
NFS Median: 1.5 (0, 6) Median NFS after SCT: 3 (0-25) NR NR
Loes score Mean: 14.0 (SD: 2.7)* Mean: 17.1 (SD: 5.4) NR NR
GdE Patients with GdE out of examined patients: 9/10
NR NR NR
*symptomatic patients only (n=14)
Abbreviations: CI, confidence interval; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NFS, neurologic function score; SCT, stem cell transplantation; SD, standard deviation; NR, not reported; OS, overall survival Source: Kato et al.127
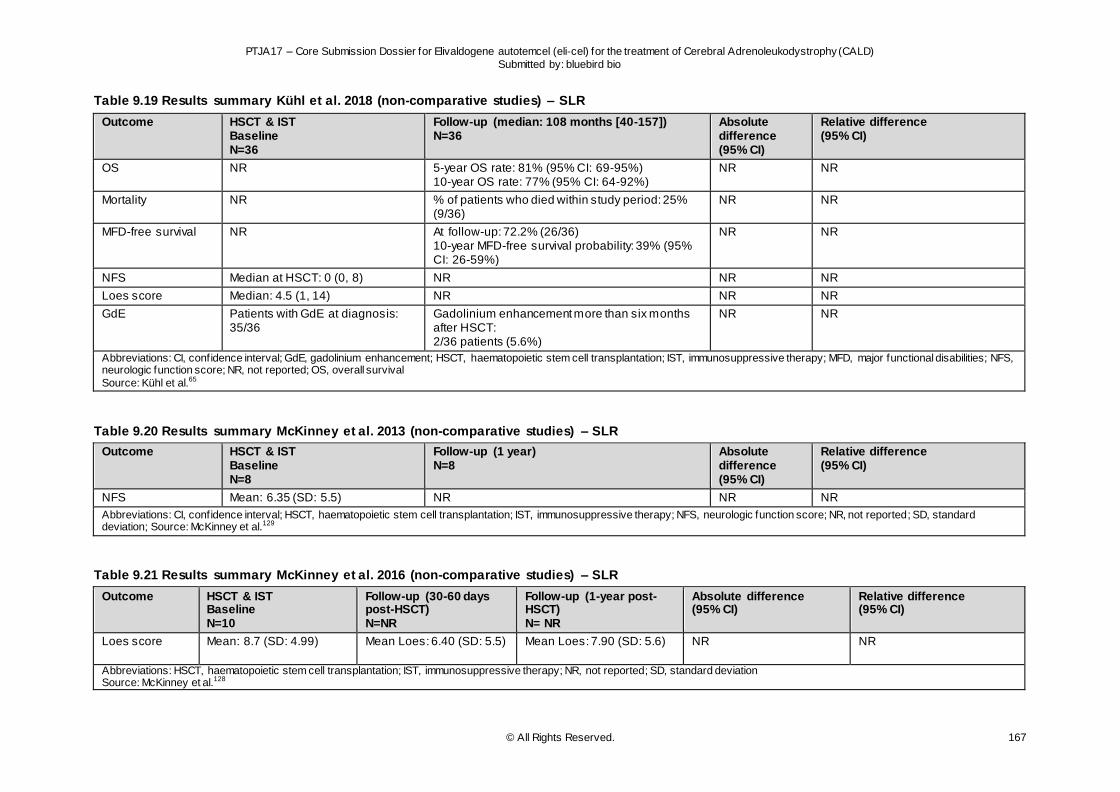
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 167
Table 9.19 Results summary Kühl et al. 2018 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=36
Follow-up (median: 108 months [40-157]) N=36
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR 5-year OS rate: 81% (95% CI: 69-95%) 10-year OS rate: 77% (95% CI: 64-92%)
NR NR
Mortality NR % of patients who died within study period: 25% (9/36)
NR NR
MFD-free survival NR At follow-up: 72.2% (26/36) 10-year MFD-free survival probability: 39% (95% CI: 26-59%)
NR NR
NFS Median at HSCT: 0 (0, 8) NR NR NR
Loes score Median: 4.5 (1, 14) NR NR NR
GdE Patients with GdE at diagnosis: 35/36
Gadolinium enhancement more than six months after HSCT: 2/36 patients (5.6%)
NR NR
Abbreviations: CI, confidence interval; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; MFD, major functional disabilities; NFS, neurologic function score; NR, not reported; OS, overall survival
Source: Kühl et al.65
Table 9.20 Results summary McKinney et al. 2013 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=8
Follow-up (1 year) N=8
Absolute difference (95% CI)
Relative difference (95% CI)
NFS Mean: 6.35 (SD: 5.5) NR NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NFS, neurologic function score; NR, not reported; SD, standard deviation; Source: McKinney et al.129
Table 9.21 Results summary McKinney et al. 2016 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=10
Follow-up (30-60 days post-HSCT) N=NR
Follow-up (1-year post-HSCT) N= NR
Absolute difference (95% CI)
Relative difference (95% CI)
Loes score Mean: 8.7 (SD: 4.99) Mean Loes: 6.40 (SD: 5.5)
Mean Loes: 7.90 (SD: 5.6) NR NR
Abbreviations: HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; SD, standard deviation Source: McKinney et al.128
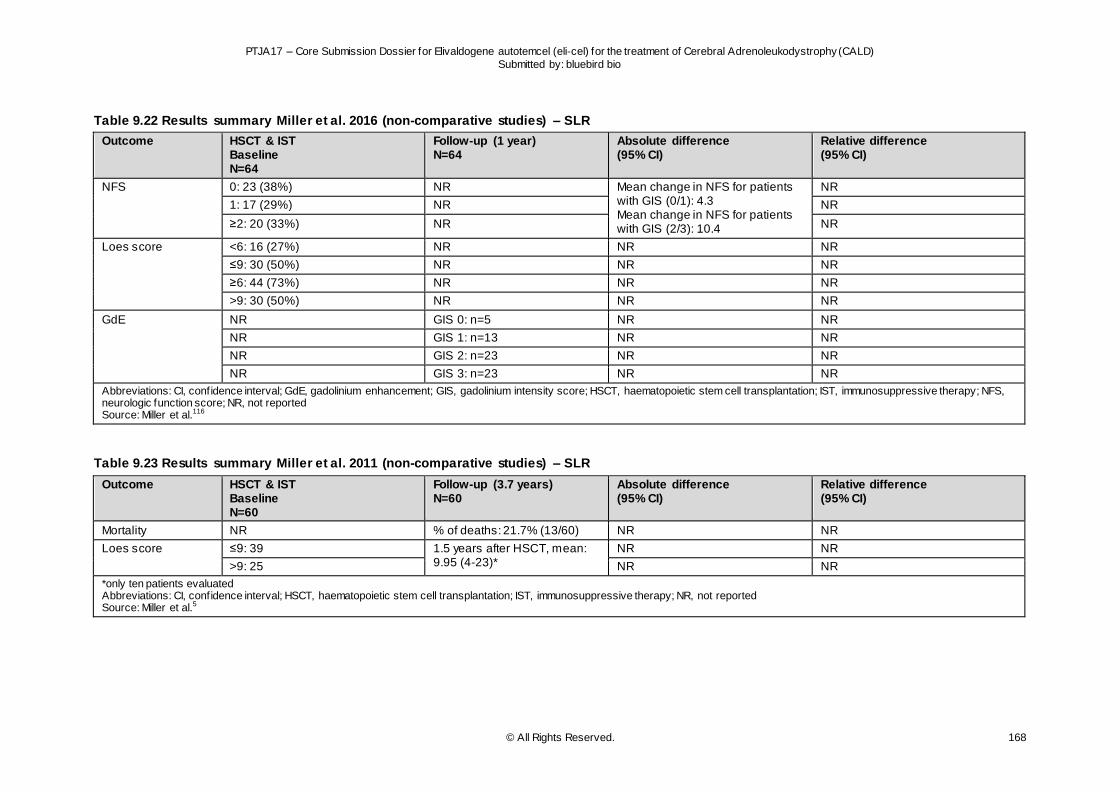
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 168
Table 9.22 Results summary Miller et al. 2016 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=64
Follow-up (1 year) N=64
Absolute difference (95% CI)
Relative difference (95% CI)
NFS 0: 23 (38%) NR Mean change in NFS for patients with GIS (0/1): 4.3 Mean change in NFS for patients with GIS (2/3): 10.4
NR
1: 17 (29%) NR NR
≥2: 20 (33%) NR NR
Loes score <6: 16 (27%) NR NR NR
≤9: 30 (50%) NR NR NR
≥6: 44 (73%) NR NR NR
>9: 30 (50%) NR NR NR
GdE NR GIS 0: n=5 NR NR
NR GIS 1: n=13 NR NR
NR GIS 2: n=23 NR NR
NR GIS 3: n=23 NR NR
Abbreviations: CI, confidence interval; GdE, gadolinium enhancement; GIS, gadolinium intensity score; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NFS, neurologic function score; NR, not reported Source: Miller et al.116
Table 9.23 Results summary Miller et al. 2011 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=60
Follow-up (3.7 years) N=60
Absolute difference (95% CI)
Relative difference (95% CI)
Mortality NR % of deaths: 21.7% (13/60) NR NR
Loes score ≤9: 39 1.5 years after HSCT, mean: 9.95 (4-23)*
NR NR
>9: 25 NR NR
*only ten patients evaluated Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported Source: Miller et al.5
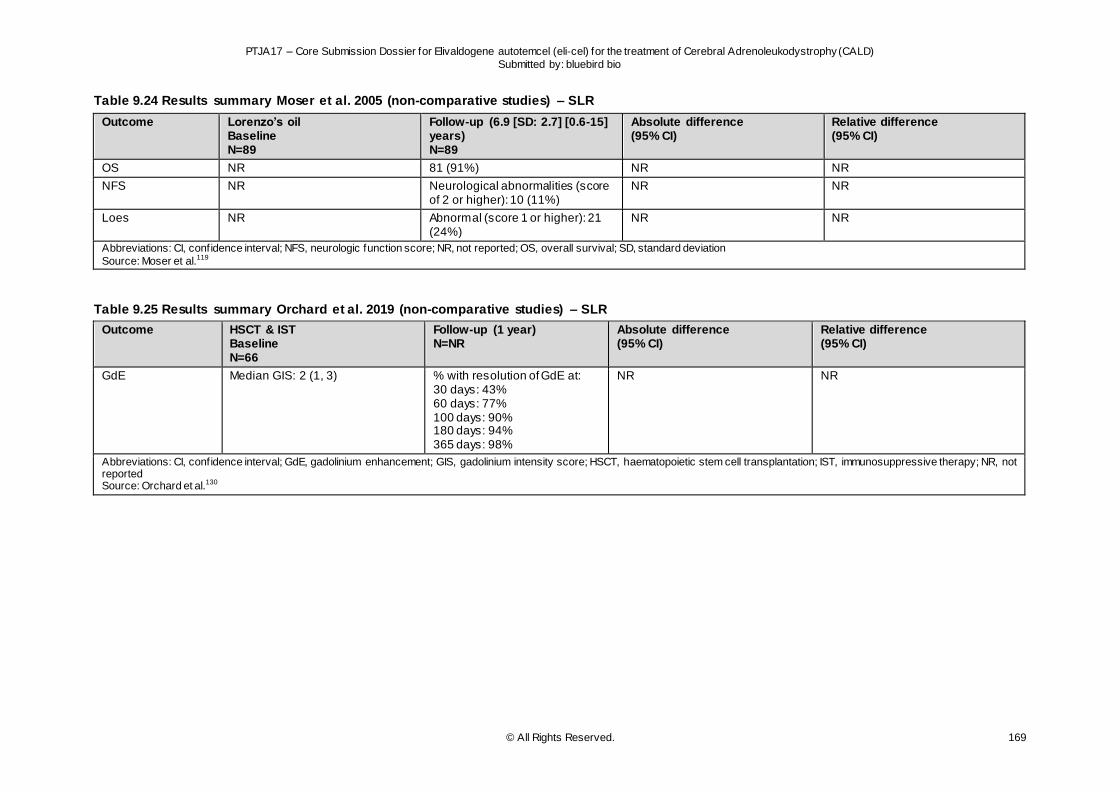
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 169
Table 9.24 Results summary Moser et al. 2005 (non-comparative studies) – SLR
Outcome
Lorenzo’s oil Baseline N=89
Follow-up (6.9 [SD: 2.7] [0.6-15] years) N=89
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR 81 (91%) NR NR
NFS NR Neurological abnormalities (score of 2 or higher): 10 (11%)
NR NR
Loes NR Abnormal (score 1 or higher): 21 (24%)
NR NR
Abbreviations: CI, confidence interval; NFS, neurologic function score; NR, not reported; OS, overall survival; SD, standard deviation
Source: Moser et al.119
Table 9.25 Results summary Orchard et al. 2019 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=66
Follow-up (1 year) N=NR
Absolute difference (95% CI)
Relative difference (95% CI)
GdE Median GIS: 2 (1, 3) % with resolution of GdE at: 30 days: 43% 60 days: 77% 100 days: 90% 180 days: 94% 365 days: 98%
NR NR
Abbreviations: CI, confidence interval; GdE, gadolinium enhancement; GIS, gadolinium intensity score; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported Source: Orchard et al.130
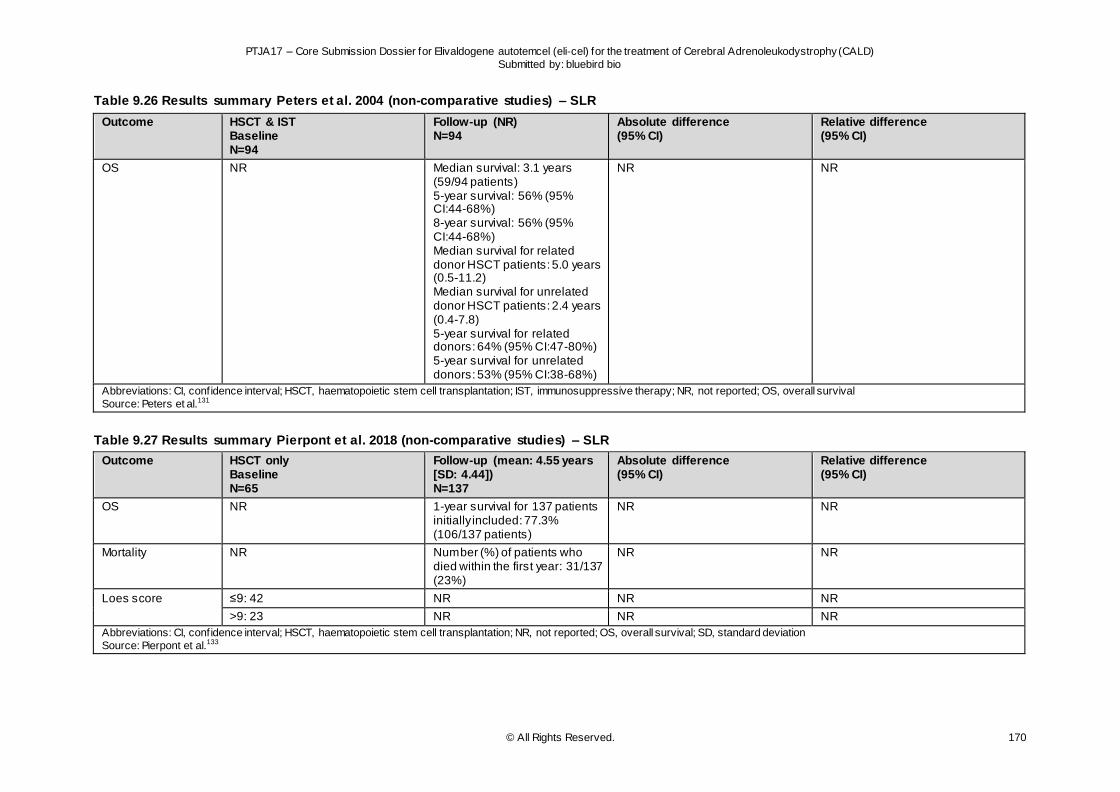
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 170
Table 9.26 Results summary Peters et al. 2004 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=94
Follow-up (NR) N=94
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR Median survival: 3.1 years (59/94 patients) 5-year survival: 56% (95% CI:44-68%) 8-year survival: 56% (95% CI:44-68%) Median survival for related donor HSCT patients: 5.0 years (0.5-11.2) Median survival for unrelated donor HSCT patients: 2.4 years (0.4-7.8) 5-year survival for related donors: 64% (95% CI:47-80%) 5-year survival for unrelated donors: 53% (95% CI:38-68%)
NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; OS, overall survival
Source: Peters et al.131
Table 9.27 Results summary Pierpont et al. 2018 (non-comparative studies) – SLR
Outcome
HSCT only Baseline N=65
Follow-up (mean: 4.55 years [SD: 4.44]) N=137
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR 1-year survival for 137 patients initially included: 77.3% (106/137 patients)
NR NR
Mortality NR Number (%) of patients who died within the first year: 31/137 (23%)
NR NR
Loes score ≤9: 42 NR NR NR
>9: 23 NR NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; NR, not reported; OS, overall survival; SD, standard deviation
Source: Pierpont et al.133
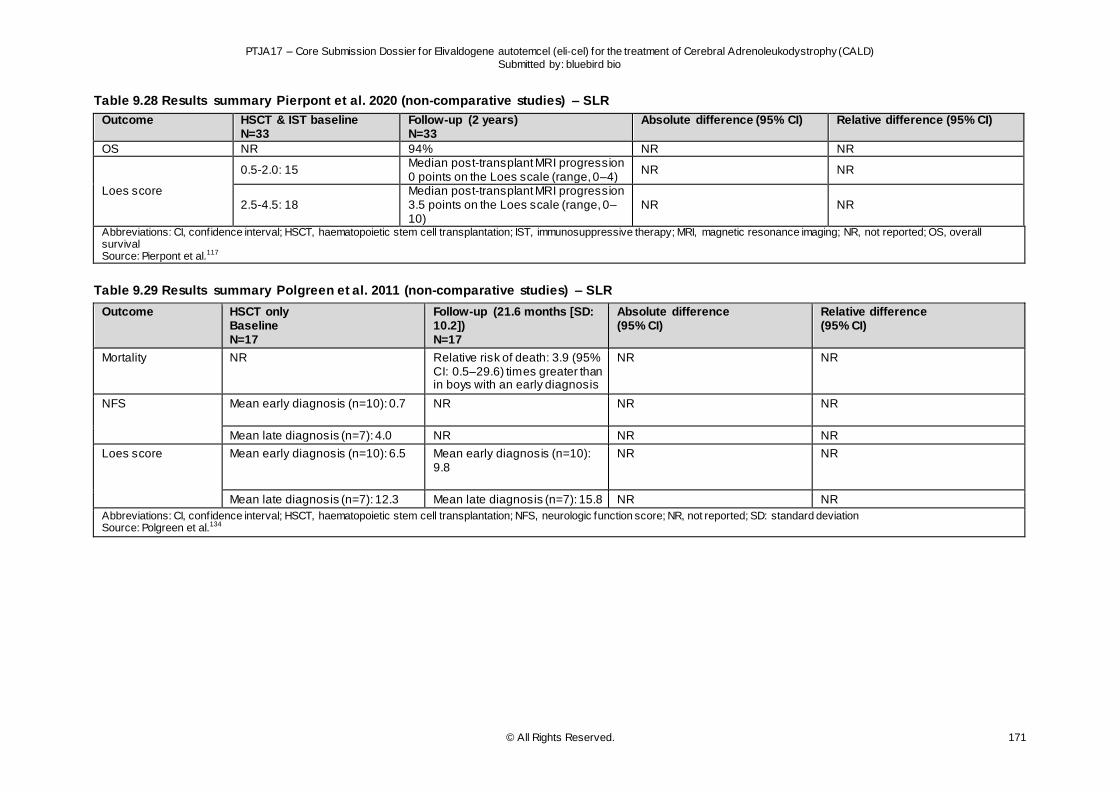
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 171
Table 9.28 Results summary Pierpont et al. 2020 (non-comparative studies) – SLR
Outcome HSCT & IST baseline N=33
Follow-up (2 years) N=33
Absolute difference (95% CI) Relative difference (95% CI)
OS NR 94% NR NR
Loes score
0.5-2.0: 15 Median post-transplant MRI progression 0 points on the Loes scale (range, 0–4)
NR NR
2.5-4.5: 18 Median post-transplant MRI progression 3.5 points on the Loes scale (range, 0–10)
NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; MRI, magnetic resonance imaging; NR, not reported; OS, overall survival Source: Pierpont et al.117
Table 9.29 Results summary Polgreen et al. 2011 (non-comparative studies) – SLR
Outcome
HSCT only Baseline N=17
Follow-up (21.6 months [SD: 10.2]) N=17
Absolute difference (95% CI)
Relative difference (95% CI)
Mortality NR Relative risk of death: 3.9 (95% CI: 0.5–29.6) times greater than in boys with an early diagnosis
NR NR
NFS Mean early diagnosis (n=10): 0.7
NR NR NR
Mean late diagnosis (n=7): 4.0 NR NR NR
Loes score Mean early diagnosis (n=10): 6.5
Mean early diagnosis (n=10): 9.8
NR NR
Mean late diagnosis (n=7): 12.3 Mean late diagnosis (n=7): 15.8 NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; NFS, neurologic function score; NR, not reported; SD: standard deviation Source: Polgreen et al.134
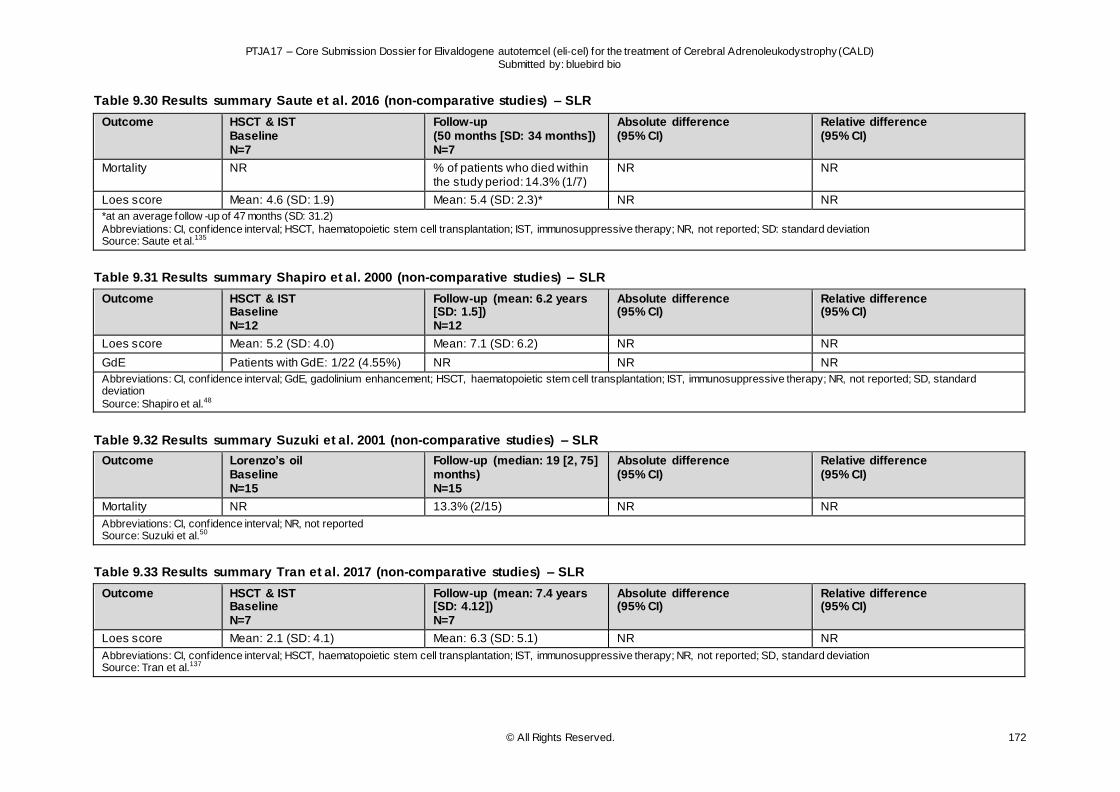
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 172
Table 9.30 Results summary Saute et al. 2016 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=7
Follow-up (50 months [SD: 34 months]) N=7
Absolute difference (95% CI)
Relative difference (95% CI)
Mortality NR % of patients who died within the study period: 14.3% (1/7)
NR NR
Loes score Mean: 4.6 (SD: 1.9) Mean: 5.4 (SD: 2.3)* NR NR
*at an average follow -up of 47 months (SD: 31.2)
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; SD: standard deviation Source: Saute et al.135
Table 9.31 Results summary Shapiro et al. 2000 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=12
Follow-up (mean: 6.2 years [SD: 1.5]) N=12
Absolute difference (95% CI)
Relative difference (95% CI)
Loes score Mean: 5.2 (SD: 4.0) Mean: 7.1 (SD: 6.2) NR NR
GdE Patients with GdE: 1/22 (4.55%) NR NR NR
Abbreviations: CI, confidence interval; GdE, gadolinium enhancement; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; SD, standard deviation
Source: Shapiro et al.48
Table 9.32 Results summary Suzuki et al. 2001 (non-comparative studies) – SLR
Outcome
Lorenzo’s oil Baseline N=15
Follow-up (median: 19 [2, 75] months) N=15
Absolute difference (95% CI)
Relative difference (95% CI)
Mortality NR 13.3% (2/15) NR NR
Abbreviations: CI, confidence interval; NR, not reported Source: Suzuki et al.50
Table 9.33 Results summary Tran et al. 2017 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=7
Follow-up (mean: 7.4 years [SD: 4.12]) N=7
Absolute difference (95% CI)
Relative difference (95% CI)
Loes score Mean: 2.1 (SD: 4.1) Mean: 6.3 (SD: 5.1) NR NR
Abbreviations: CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; SD, standard deviation Source: Tran et al.137
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 173
Table 9.34 Results summary van den Broek et al. 2018 (non-comparative studies) – SLR
Outcome
HSCT & IST Baseline N=56
Follow-up (NR for CALD only, for full population: median: 76 months [3-211]) N=56
Absolute difference (95% CI)
Relative difference (95% CI)
OS NR 6-year OS for ALD group: 59% NR NR
Mortality NR % of ALD patients who died during study period: 37.5% (21/56)
NR NR
Abbreviations: ALD, adrenoleukodystrophy; CALD, cerebral adrenoleukodystrophy; CI, confidence interval; HSCT, haematopoietic stem cell transplantation; IST, immunosuppressive therapy; NR, not reported; OS, overall survival Source: van den Broek et al.49
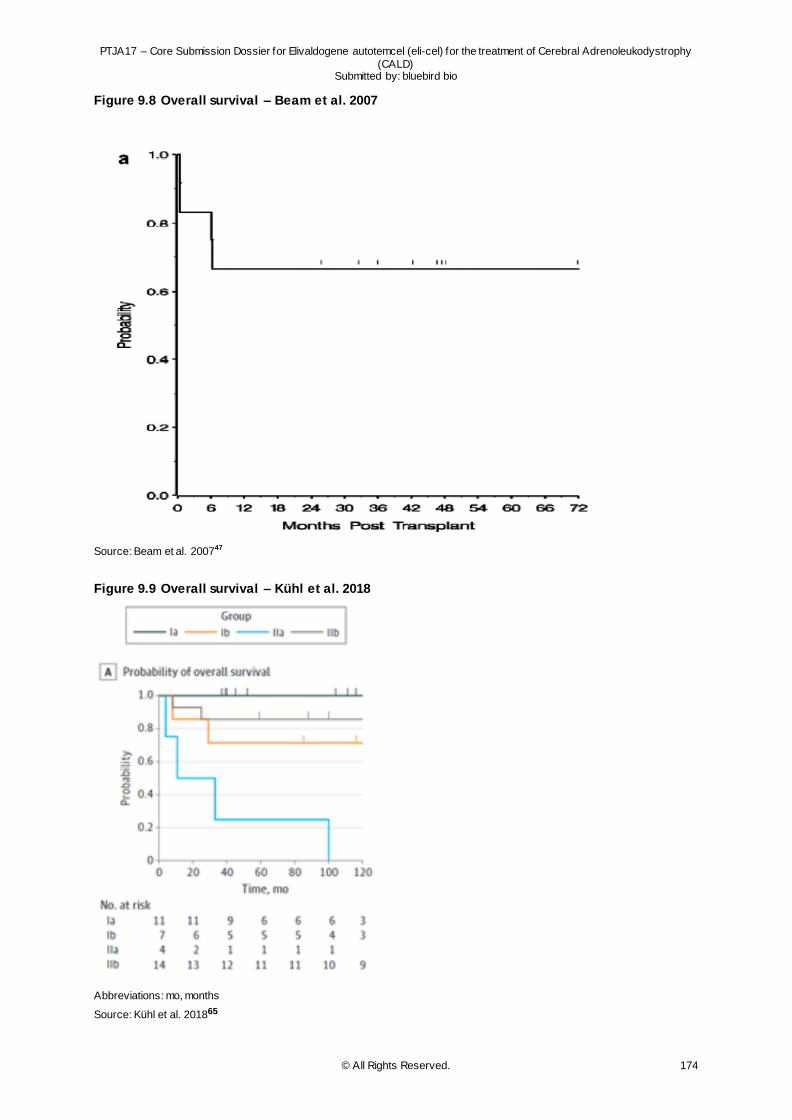
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 174
Figure 9.8 Overall survival – Beam et al. 2007
Source: Beam et al. 200747
Figure 9.9 Overall survival – Kühl et al. 2018
Abbreviations: mo, months
Source: Kühl et al. 201865
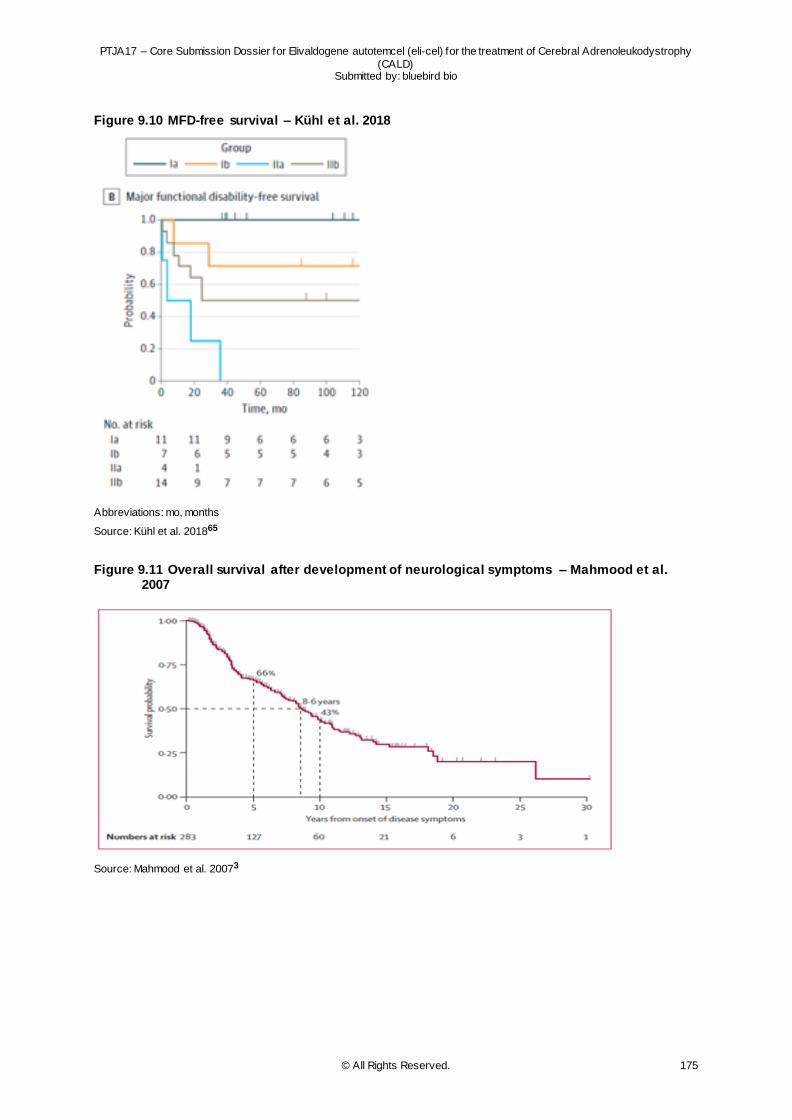
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 175
Figure 9.10 MFD-free survival – Kühl et al. 2018
Abbreviations: mo, months
Source: Kühl et al. 201865
Figure 9.11 Overall survival after development of neurological symptoms – Mahmood et al. 2007
Source: Mahmood et al. 20073
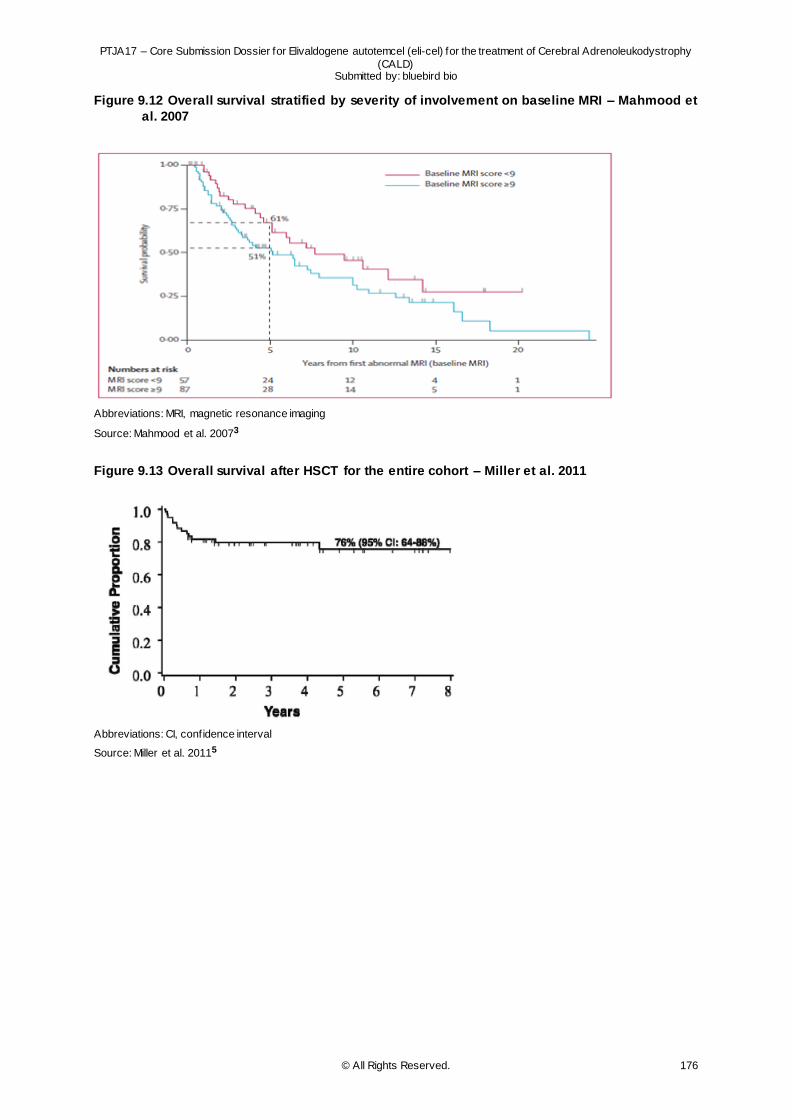
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 176
Figure 9.12 Overall survival stratified by severity of involvement on baseline MRI – Mahmood et
al. 2007
Abbreviations: MRI, magnetic resonance imaging
Source: Mahmood et al. 20073
Figure 9.13 Overall survival after HSCT for the entire cohort – Miller et al. 2011
Abbreviations: CI, confidence interval
Source: Miller et al. 20115
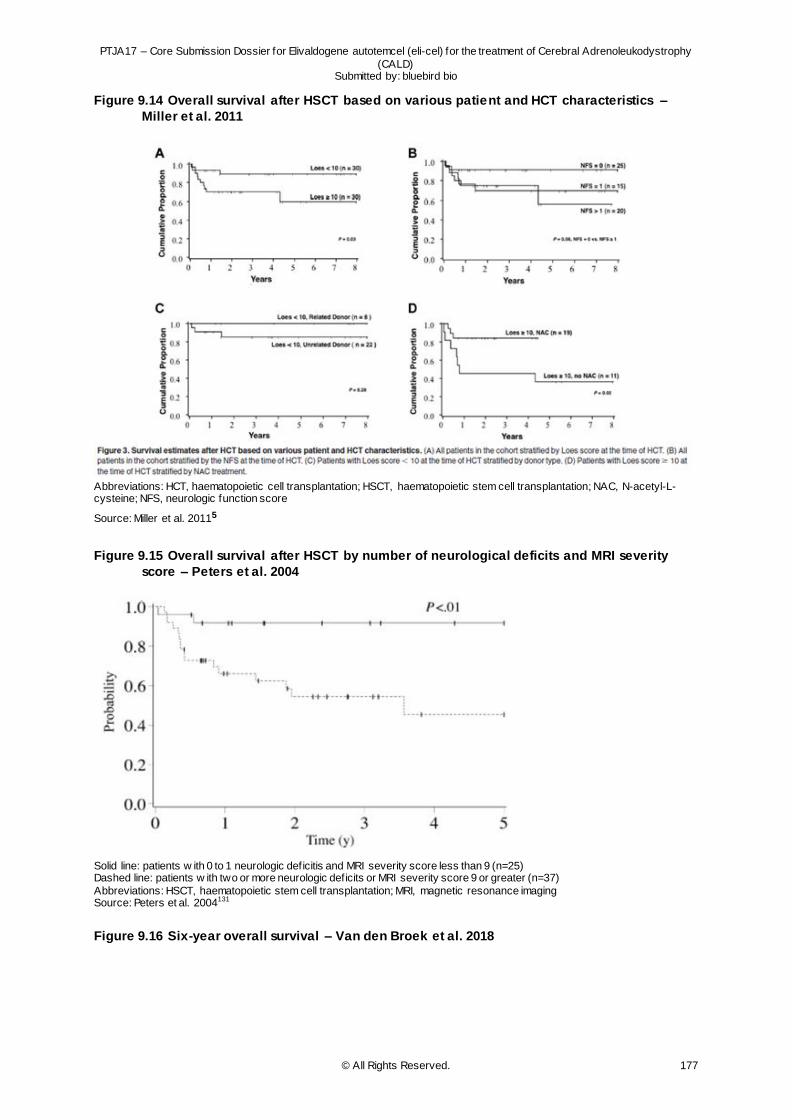
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 177
Figure 9.14 Overall survival after HSCT based on various patient and HCT characteristics –
Miller et al. 2011
Abbreviations: HCT, haematopoietic cell transplantation; HSCT, haematopoietic stem cell transplantation; NAC, N-acetyl-L-cysteine; NFS, neurologic function score
Source: Miller et al. 20115
Figure 9.15 Overall survival after HSCT by number of neurological deficits and MRI severity
score – Peters et al. 2004
Solid line: patients w ith 0 to 1 neurologic deficitis and MRI severity score less than 9 (n=25) Dashed line: patients w ith two or more neurologic deficits or MRI severity score 9 or greater (n=37)
Abbreviations: HSCT, haematopoietic stem cell transplantation; MRI, magnetic resonance imaging Source: Peters et al. 2004131
Figure 9.16 Six-year overall survival – Van den Broek et al. 2018
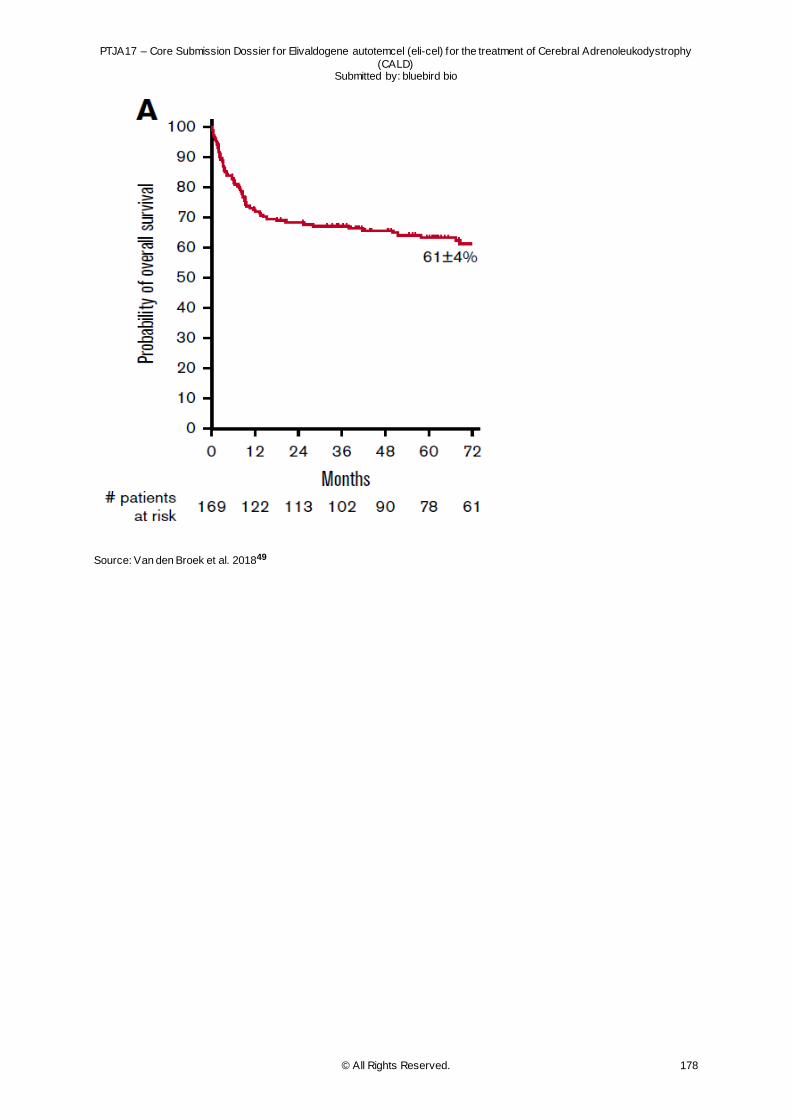
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 178
Source: Van den Broek et al. 201849
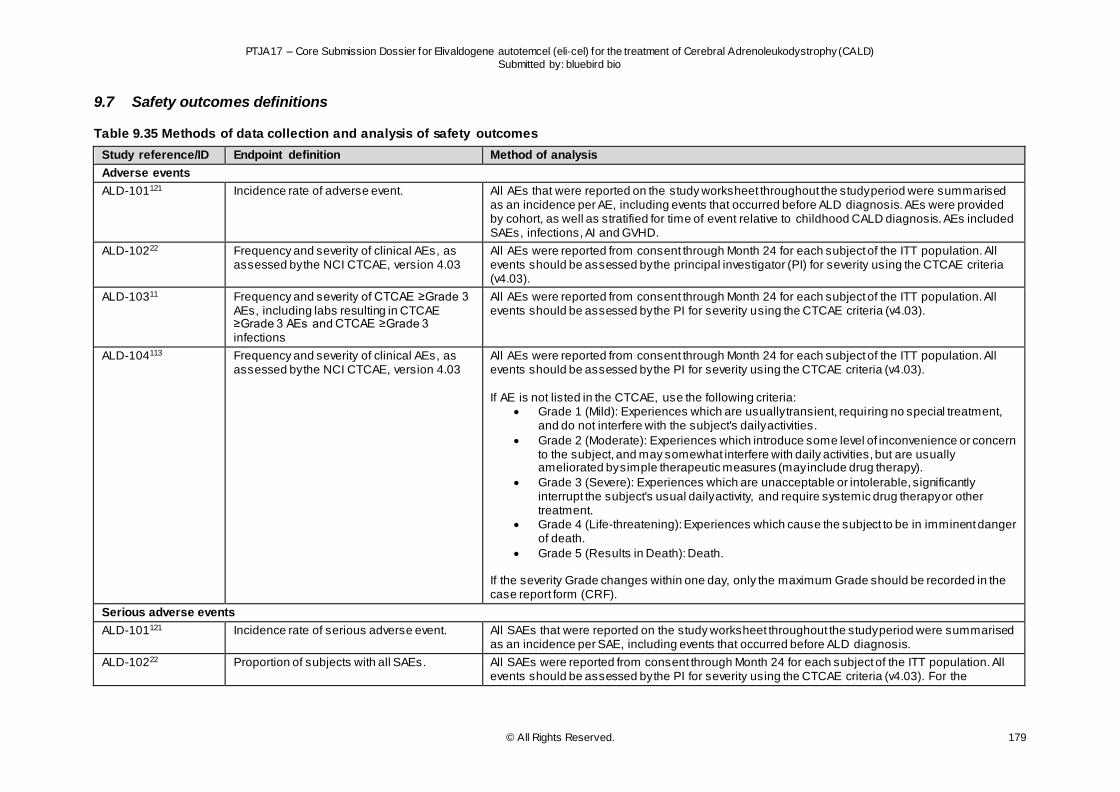
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 179
9.7 Safety outcomes definitions
Table 9.35 Methods of data collection and analysis of safety outcomes
Study reference/ID Endpoint definition Method of analysis
Adverse events
ALD-101121 Incidence rate of adverse event. All AEs that were reported on the study worksheet throughout the study period were summarised as an incidence per AE, including events that occurred before ALD diagnosis. AEs were provided by cohort, as well as stratified for time of event relative to childhood CALD diagnosis. AEs included SAEs, infections, AI and GVHD.
ALD-10222 Frequency and severity of clinical AEs, as assessed by the NCI CTCAE, version 4.03
All AEs were reported from consent through Month 24 for each subject of the ITT population. All events should be assessed by the principal investigator (PI) for severity using the CTCAE criteria (v4.03).
ALD-10311 Frequency and severity of CTCAE ≥Grade 3 AEs, including labs resulting in CTCAE ≥Grade 3 AEs and CTCAE ≥Grade 3 infections
All AEs were reported from consent through Month 24 for each subject of the ITT population. All events should be assessed by the PI for severity using the CTCAE criteria (v4.03).
ALD-104113 Frequency and severity of clinical AEs, as assessed by the NCI CTCAE, version 4.03
All AEs were reported from consent through Month 24 for each subject of the ITT population. All events should be assessed by the PI for severity using the CTCAE criteria (v4.03). If AE is not listed in the CTCAE, use the following criteria:
Grade 1 (Mild): Experiences which are usually transient, requiring no special treatment, and do not interfere with the subject's daily activities.
Grade 2 (Moderate): Experiences which introduce some level of inconvenience or concern to the subject, and may somewhat interfere with daily activities, but are usually ameliorated by simple therapeutic measures (may include drug therapy).
Grade 3 (Severe): Experiences which are unacceptable or intolerable, significantly interrupt the subject's usual daily activity, and require systemic drug therapy or other treatment.
Grade 4 (Life-threatening): Experiences which cause the subject to be in imminent danger of death.
Grade 5 (Results in Death): Death. If the severity Grade changes within one day, only the maximum Grade should be recorded in the case report form (CRF).
Serious adverse events
ALD-101121 Incidence rate of serious adverse event. All SAEs that were reported on the study worksheet throughout the study period were summarised as an incidence per SAE, including events that occurred before ALD diagnosis.
ALD-10222 Proportion of subjects with all SAEs. All SAEs were reported from consent through Month 24 for each subject of the ITT population. All events should be assessed by the PI for severity using the CTCAE criteria (v4.03). For the
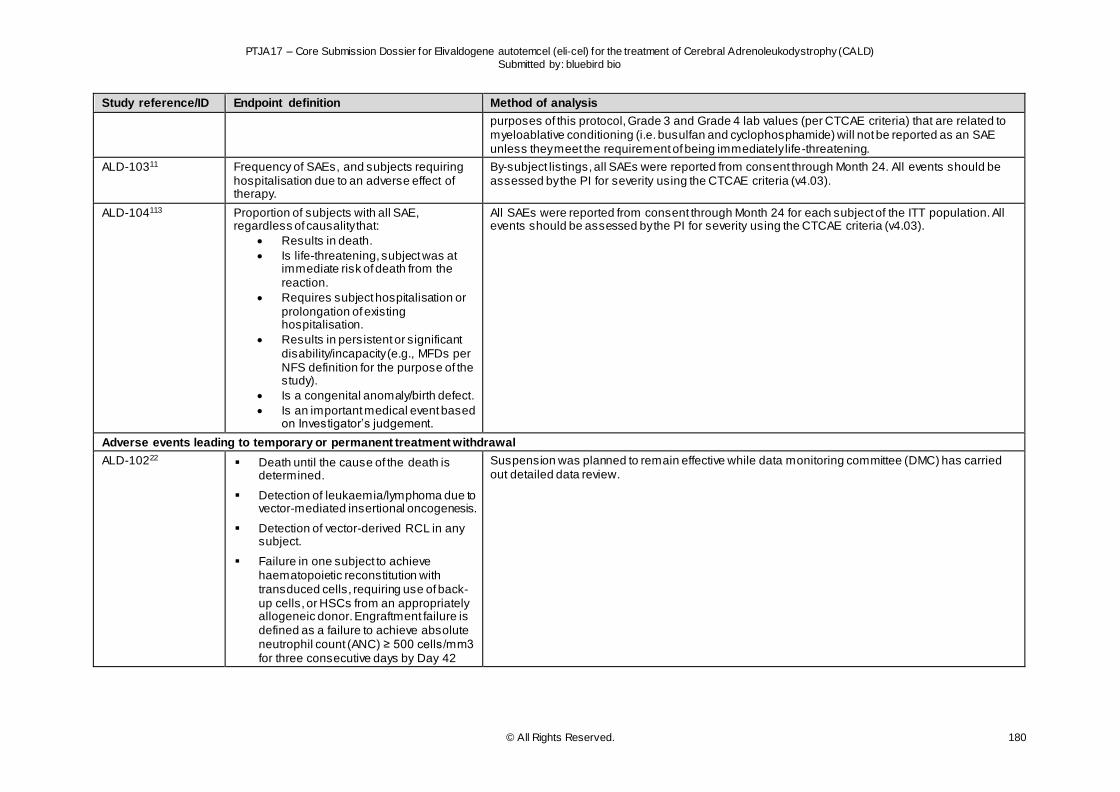
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 180
Study reference/ID Endpoint definition Method of analysis
purposes of this protocol, Grade 3 and Grade 4 lab values (per CTCAE criteria) that are related to myeloablative conditioning (i.e. busulfan and cyclophosphamide) will not be reported as an SAE unless they meet the requirement of being immediately life-threatening.
ALD-10311 Frequency of SAEs, and subjects requiring hospitalisation due to an adverse effect of therapy.
By-subject listings, all SAEs were reported from consent through Month 24. All events should be assessed by the PI for severity using the CTCAE criteria (v4.03).
ALD-104113 Proportion of subjects with all SAE, regardless of causality that:
Results in death.
Is life-threatening, subject was at immediate risk of death from the reaction.
Requires subject hospitalisation or prolongation of existing hospitalisation.
Results in persistent or significant disability/incapacity (e.g., MFDs per NFS definition for the purpose of the study).
Is a congenital anomaly/birth defect.
Is an important medical event based on Investigator’s judgement.
All SAEs were reported from consent through Month 24 for each subject of the ITT population. All events should be assessed by the PI for severity using the CTCAE criteria (v4.03).
Adverse events leading to temporary or permanent treatment withdrawal
ALD-10222 Death until the cause of the death is determined.
Detection of leukaemia/lymphoma due to vector-mediated insertional oncogenesis.
Detection of vector-derived RCL in any subject.
Failure in one subject to achieve haematopoietic reconstitution with transduced cells, requiring use of back-up cells, or HSCs from an appropriately allogeneic donor. Engraftment failure is defined as a failure to achieve absolute neutrophil count (ANC) ≥ 500 cells/mm3 for three consecutive days by Day 42
Suspension was planned to remain effective while data monitoring committee (DMC) has carried out detailed data review.
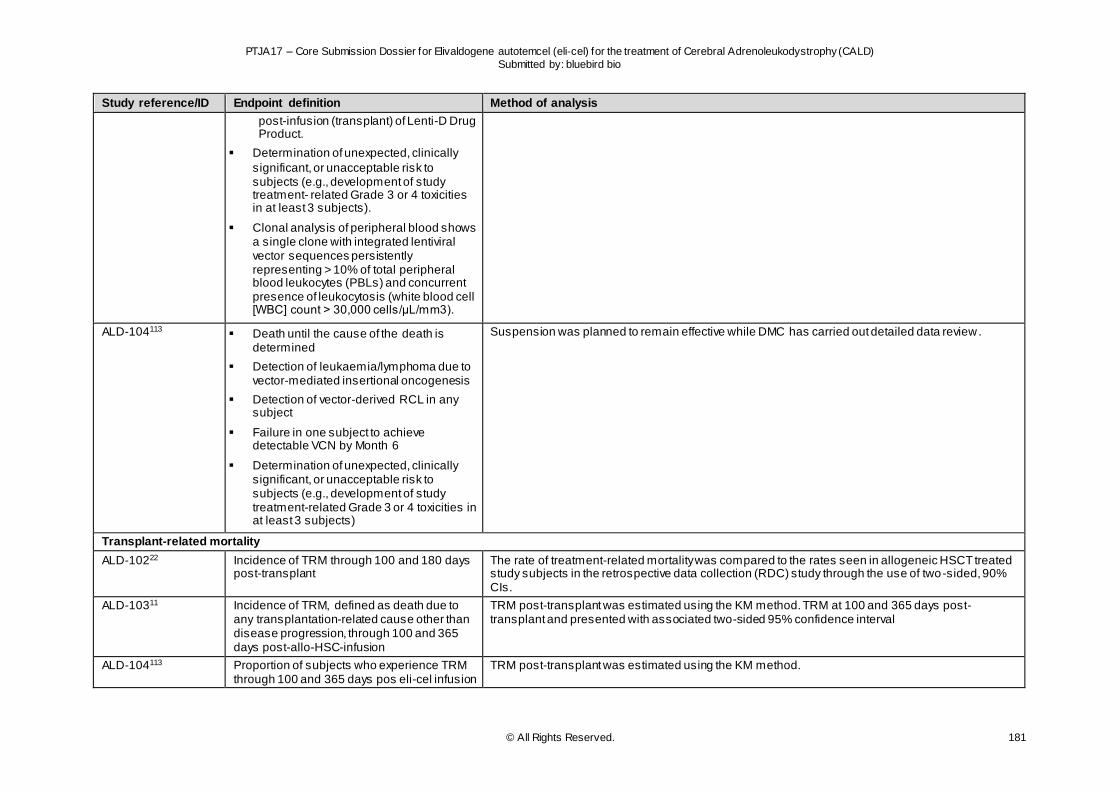
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 181
Study reference/ID Endpoint definition Method of analysis
post-infusion (transplant) of Lenti-D Drug Product.
Determination of unexpected, clinically
significant, or unacceptable risk to subjects (e.g., development of study treatment- related Grade 3 or 4 toxicities in at least 3 subjects).
Clonal analysis of peripheral blood shows a single clone with integrated lentiviral vector sequences persistently representing > 10% of total peripheral blood leukocytes (PBLs) and concurrent presence of leukocytosis (white blood cell [WBC] count > 30,000 cells/μL/mm3).
ALD-104113 Death until the cause of the death is determined
Detection of leukaemia/lymphoma due to vector-mediated insertional oncogenesis
Detection of vector-derived RCL in any subject
Failure in one subject to achieve detectable VCN by Month 6
Determination of unexpected, clinically significant, or unacceptable risk to subjects (e.g., development of study treatment-related Grade 3 or 4 toxicities in at least 3 subjects)
Suspension was planned to remain effective while DMC has carried out detailed data review.
Transplant-related mortality
ALD-10222 Incidence of TRM through 100 and 180 days post-transplant
The rate of treatment-related mortality was compared to the rates seen in allogeneic HSCT treated study subjects in the retrospective data collection (RDC) study through the use of two-sided, 90% CIs.
ALD-10311 Incidence of TRM, defined as death due to any transplantation-related cause other than disease progression, through 100 and 365 days post-allo-HSC-infusion
TRM post-transplant was estimated using the KM method. TRM at 100 and 365 days post-transplant and presented with associated two-sided 95% confidence interval
ALD-104113 Proportion of subjects who experience TRM through 100 and 365 days pos eli-cel infusion
TRM post-transplant was estimated using the KM method.
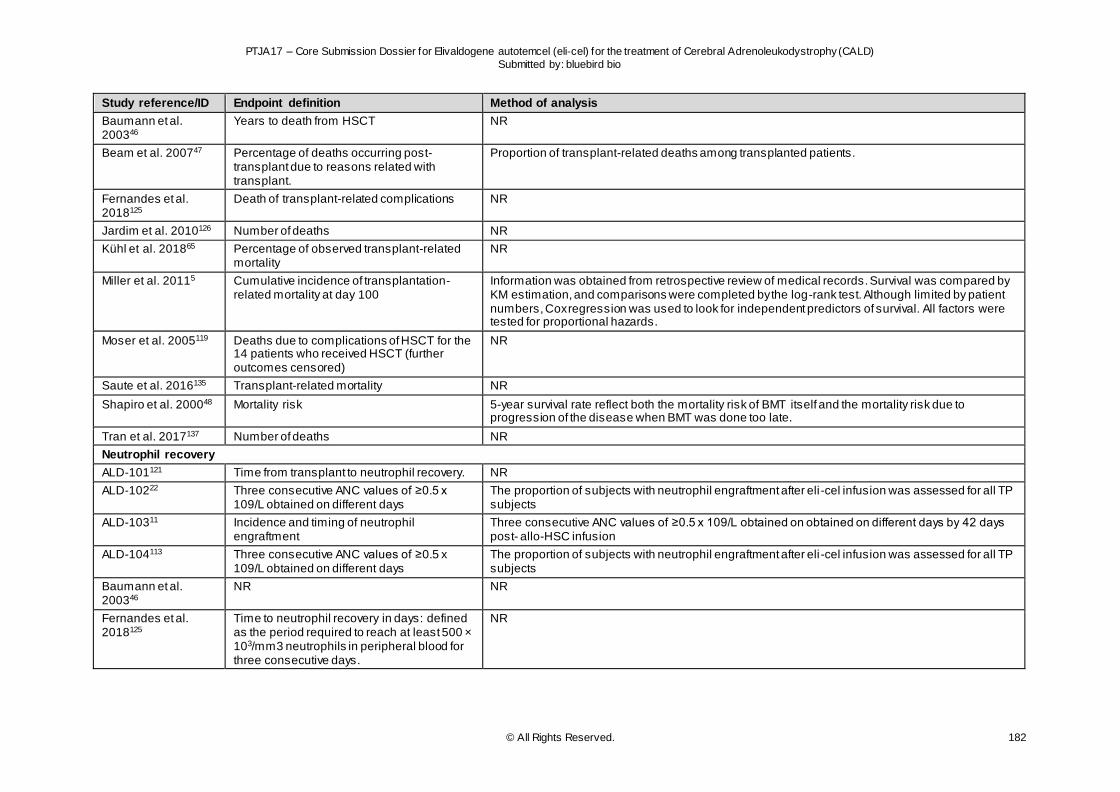
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 182
Study reference/ID Endpoint definition Method of analysis
Baumann et al. 200346
Years to death from HSCT NR
Beam et al. 200747 Percentage of deaths occurring post-transplant due to reasons related with transplant.
Proportion of transplant-related deaths among transplanted patients.
Fernandes et al. 2018125
Death of transplant-related complications NR
Jardim et al. 2010126 Number of deaths NR
Kühl et al. 201865 Percentage of observed transplant-related mortality
NR
Miller et al. 20115 Cumulative incidence of transplantation- related mortality at day 100
Information was obtained from retrospective review of medical records. Survival was compared by KM estimation, and comparisons were completed by the log-rank test. Although limited by patient numbers, Cox regression was used to look for independent predictors of survival. All factors were tested for proportional hazards.
Moser et al. 2005119 Deaths due to complications of HSCT for the 14 patients who received HSCT (further outcomes censored)
NR
Saute et al. 2016135 Transplant-related mortality NR
Shapiro et al. 200048 Mortality risk 5-year survival rate reflect both the mortality risk of BMT itself and the mortality risk due to progression of the disease when BMT was done too late.
Tran et al. 2017137 Number of deaths NR
Neutrophil recovery
ALD-101121 Time from transplant to neutrophil recovery. NR
ALD-10222 Three consecutive ANC values of ≥0.5 x 109/L obtained on different days
The proportion of subjects with neutrophil engraftment after eli -cel infusion was assessed for all TP subjects
ALD-10311 Incidence and timing of neutrophil engraftment
Three consecutive ANC values of ≥0.5 x 109/L obtained on obtained on different days by 42 days post- allo-HSC infusion
ALD-104113 Three consecutive ANC values of ≥0.5 x 109/L obtained on different days
The proportion of subjects with neutrophil engraftment after eli -cel infusion was assessed for all TP subjects
Baumann et al. 200346
NR NR
Fernandes et al. 2018125
Time to neutrophil recovery in days: defined as the period required to reach at least 500 × 103/mm3 neutrophils in peripheral blood for three consecutive days.
NR
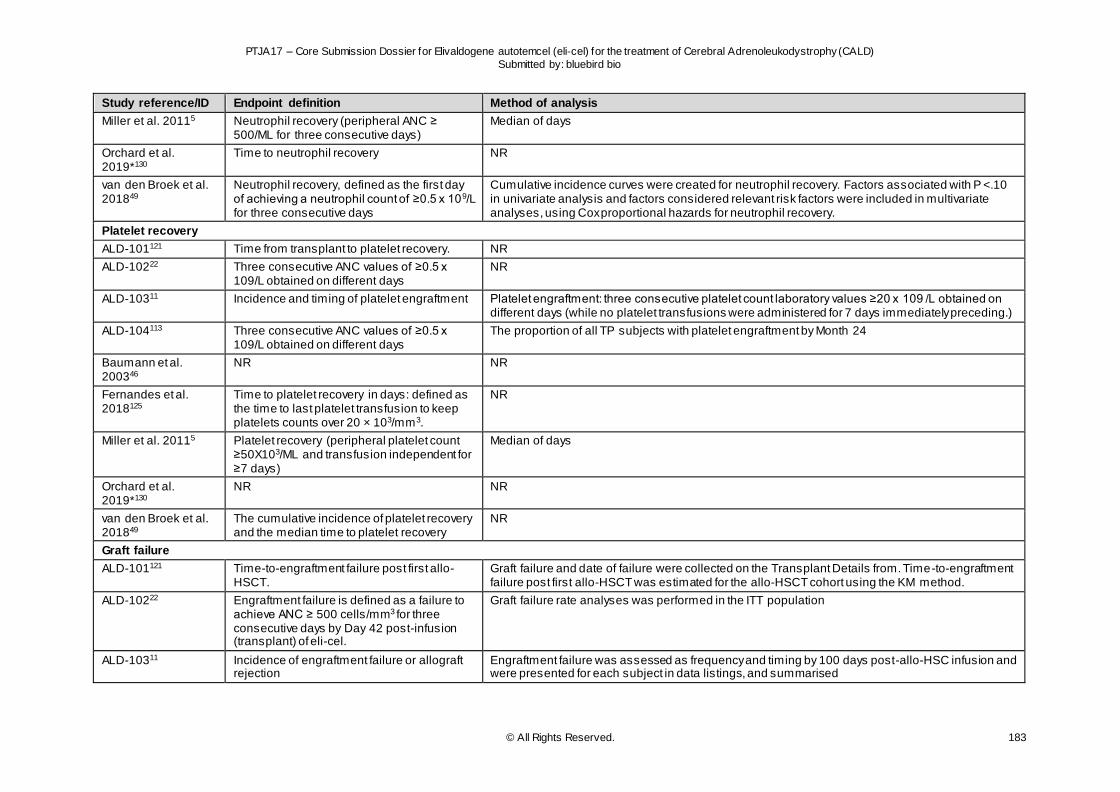
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 183
Study reference/ID Endpoint definition Method of analysis
Miller et al. 20115 Neutrophil recovery (peripheral ANC ≥ 500/ML for three consecutive days)
Median of days
Orchard et al. 2019*130
Time to neutrophil recovery NR
van den Broek et al. 201849
Neutrophil recovery, defined as the first day of achieving a neutrophil count of ≥0.5 x 109/L for three consecutive days
Cumulative incidence curves were created for neutrophil recovery. Factors associated with P <.10 in univariate analysis and factors considered relevant risk factors were included in multivariate analyses, using Cox proportional hazards for neutrophil recovery.
Platelet recovery
ALD-101121 Time from transplant to platelet recovery. NR
ALD-10222 Three consecutive ANC values of ≥0.5 x 109/L obtained on different days
NR
ALD-10311 Incidence and timing of platelet engraftment Platelet engraftment: three consecutive platelet count laboratory values ≥20 x 109 /L obtained on different days (while no platelet transfusions were administered for 7 days immediately preceding.)
ALD-104113 Three consecutive ANC values of ≥0.5 x 109/L obtained on different days
The proportion of all TP subjects with platelet engraftment by Month 24
Baumann et al. 200346
NR NR
Fernandes et al. 2018125
Time to platelet recovery in days: defined as the time to last platelet transfusion to keep platelets counts over 20 × 103/mm3.
NR
Miller et al. 20115 Platelet recovery (peripheral platelet count ≥50X103/ML and transfusion independent for ≥7 days)
Median of days
Orchard et al. 2019*130
NR NR
van den Broek et al. 201849
The cumulative incidence of platelet recovery and the median time to platelet recovery
NR
Graft failure
ALD-101121 Time-to-engraftment failure post first allo-HSCT.
Graft failure and date of failure were collected on the Transplant Details from. Time-to-engraftment failure post first allo-HSCT was estimated for the allo-HSCT cohort using the KM method.
ALD-10222 Engraftment failure is defined as a failure to achieve ANC ≥ 500 cells/mm3 for three consecutive days by Day 42 post-infusion (transplant) of eli-cel.
Graft failure rate analyses was performed in the ITT population
ALD-10311 Incidence of engraftment failure or allograft rejection
Engraftment failure was assessed as frequency and timing by 100 days post-allo-HSC infusion and were presented for each subject in data listings, and summarised
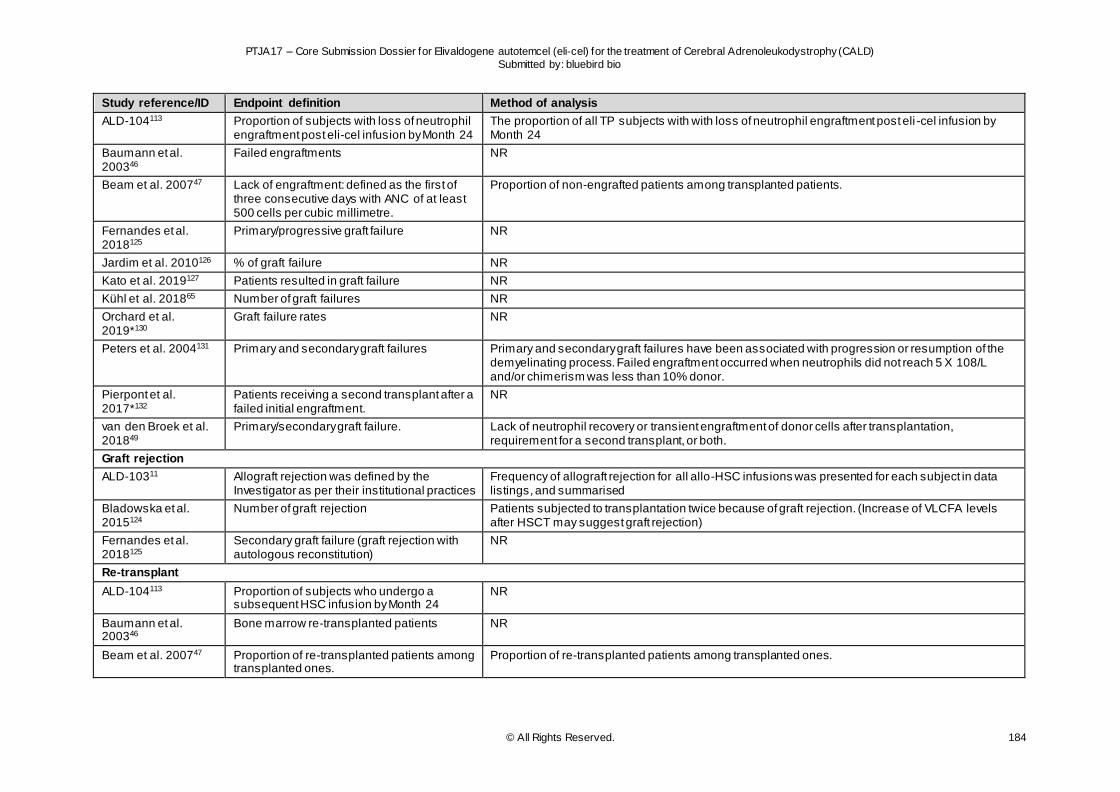
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 184
Study reference/ID Endpoint definition Method of analysis
ALD-104113 Proportion of subjects with loss of neutrophil engraftment post eli-cel infusion by Month 24
The proportion of all TP subjects with with loss of neutrophil engraftment post eli -cel infusion by Month 24
Baumann et al. 200346
Failed engraftments NR
Beam et al. 200747 Lack of engraftment: defined as the first of three consecutive days with ANC of at least 500 cells per cubic millimetre.
Proportion of non-engrafted patients among transplanted patients.
Fernandes et al. 2018125
Primary/progressive graft failure NR
Jardim et al. 2010126 % of graft failure NR
Kato et al. 2019127 Patients resulted in graft failure NR
Kühl et al. 201865 Number of graft failures NR
Orchard et al. 2019*130
Graft failure rates NR
Peters et al. 2004131 Primary and secondary graft failures Primary and secondary graft failures have been associated with progression or resumption of the demyelinating process. Failed engraftment occurred when neutrophils did not reach 5 X 108/L and/or chimerism was less than 10% donor.
Pierpont et al. 2017*132
Patients receiving a second transplant after a failed initial engraftment.
NR
van den Broek et al. 201849
Primary/secondary graft failure. Lack of neutrophil recovery or transient engraftment of donor cells after transplantation, requirement for a second transplant, or both.
Graft rejection
ALD-10311 Allograft rejection was defined by the Investigator as per their institutional practices
Frequency of allograft rejection for all allo-HSC infusions was presented for each subject in data listings, and summarised
Bladowska et al. 2015124
Number of graft rejection Patients subjected to transplantation twice because of graft rejection. (Increase of VLCFA levels after HSCT may suggest graft rejection)
Fernandes et al. 2018125
Secondary graft failure (graft rejection with autologous reconstitution)
NR
Re-transplant
ALD-104113 Proportion of subjects who undergo a subsequent HSC infusion by Month 24
NR
Baumann et al. 200346
Bone marrow re-transplanted patients NR
Beam et al. 200747 Proportion of re-transplanted patients among transplanted ones.
Proportion of re-transplanted patients among transplanted ones.
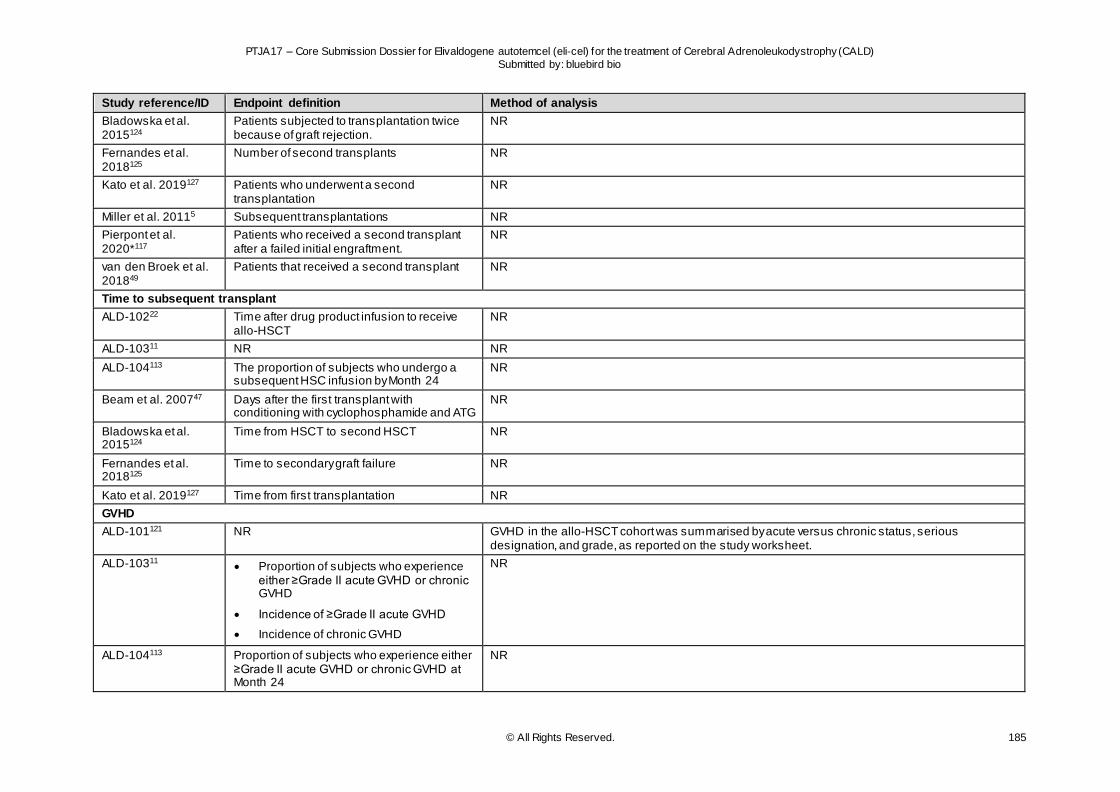
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 185
Study reference/ID Endpoint definition Method of analysis
Bladowska et al. 2015124
Patients subjected to transplantation twice because of graft rejection.
NR
Fernandes et al. 2018125
Number of second transplants NR
Kato et al. 2019127 Patients who underwent a second transplantation
NR
Miller et al. 20115 Subsequent transplantations NR
Pierpont et al. 2020*117
Patients who received a second transplant after a failed initial engraftment.
NR
van den Broek et al. 201849
Patients that received a second transplant NR
Time to subsequent transplant
ALD-10222 Time after drug product infusion to receive allo-HSCT
NR
ALD-10311 NR NR
ALD-104113 The proportion of subjects who undergo a subsequent HSC infusion by Month 24
NR
Beam et al. 200747 Days after the first transplant with conditioning with cyclophosphamide and ATG
NR
Bladowska et al. 2015124
Time from HSCT to second HSCT NR
Fernandes et al. 2018125
Time to secondary graft failure NR
Kato et al. 2019127 Time from first transplantation NR
GVHD
ALD-101121 NR GVHD in the allo-HSCT cohort was summarised by acute versus chronic status, serious designation, and grade, as reported on the study worksheet.
ALD-10311 Proportion of subjects who experience either ≥Grade II acute GVHD or chronic GVHD
Incidence of ≥Grade II acute GVHD
Incidence of chronic GVHD
NR
ALD-104113 Proportion of subjects who experience either ≥Grade II acute GVHD or chronic GVHD at Month 24
NR
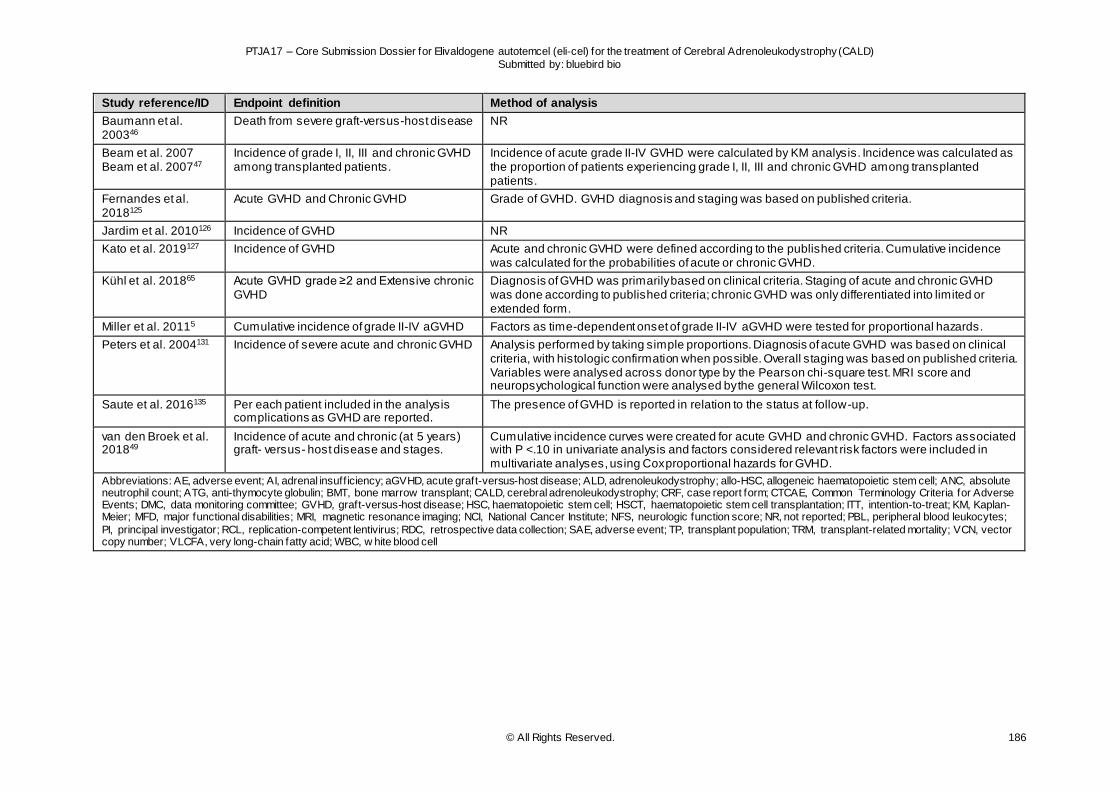
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 186
Study reference/ID Endpoint definition Method of analysis
Baumann et al. 200346
Death from severe graft-versus-host disease NR
Beam et al. 2007 Beam et al. 200747
Incidence of grade I, II, III and chronic GVHD among transplanted patients.
Incidence of acute grade II-IV GVHD were calculated by KM analysis. Incidence was calculated as the proportion of patients experiencing grade I, II, III and chronic GVHD among transplanted patients.
Fernandes et al. 2018125
Acute GVHD and Chronic GVHD Grade of GVHD. GVHD diagnosis and staging was based on published criteria.
Jardim et al. 2010126 Incidence of GVHD NR
Kato et al. 2019127 Incidence of GVHD Acute and chronic GVHD were defined according to the published criteria. Cumulative incidence was calculated for the probabilities of acute or chronic GVHD.
Kühl et al. 201865 Acute GVHD grade ≥2 and Extensive chronic GVHD
Diagnosis of GVHD was primarily based on clinical criteria. Staging of acute and chronic GVHD was done according to published criteria; chronic GVHD was only differentiated into limited or extended form.
Miller et al. 20115 Cumulative incidence of grade II-IV aGVHD Factors as time-dependent onset of grade II-IV aGVHD were tested for proportional hazards.
Peters et al. 2004131 Incidence of severe acute and chronic GVHD Analysis performed by taking simple proportions. Diagnosis of acute GVHD was based on clinical criteria, with histologic confirmation when possible. Overall staging was based on published criteria. Variables were analysed across donor type by the Pearson chi-square test. MRI score and neuropsychological function were analysed by the general Wilcoxon test.
Saute et al. 2016135 Per each patient included in the analysis complications as GVHD are reported.
The presence of GVHD is reported in relation to the status at follow-up.
van den Broek et al. 201849
Incidence of acute and chronic (at 5 years) graft- versus- host disease and stages.
Cumulative incidence curves were created for acute GVHD and chronic GVHD. Factors associated with P <.10 in univariate analysis and factors considered relevant risk factors were included in multivariate analyses, using Cox proportional hazards for GVHD.
Abbreviations: AE, adverse event; AI, adrenal insuff iciency; aGVHD, acute graft-versus-host disease; ALD, adrenoleukodystrophy; allo-HSC, allogeneic haematopoietic stem cell; ANC, absolute neutrophil count; ATG, anti-thymocyte globulin; BMT, bone marrow transplant; CALD, cerebral adrenoleukodystrophy; CRF, case report form; CTCAE, Common Terminology Criteria for Adverse Events; DMC, data monitoring committee; GVHD, graft-versus-host disease; HSC, haematopoietic stem cell; HSCT, haematopoietic stem cell transplantation; ITT, intention-to-treat; KM, Kaplan-Meier; MFD, major functional disabilities; MRI, magnetic resonance imaging; NCI, National Cancer Institute; NFS, neurologic function score; NR, not reported; PBL, peripheral blood leukocytes;
PI, principal investigator; RCL, replication-competent lentivirus; RDC, retrospective data collection; SAE, adverse event; TP, transplant population; TRM, transplant-related mortality; VCN, vector copy number; VLCFA, very long-chain fatty acid; WBC, w hite blood cell
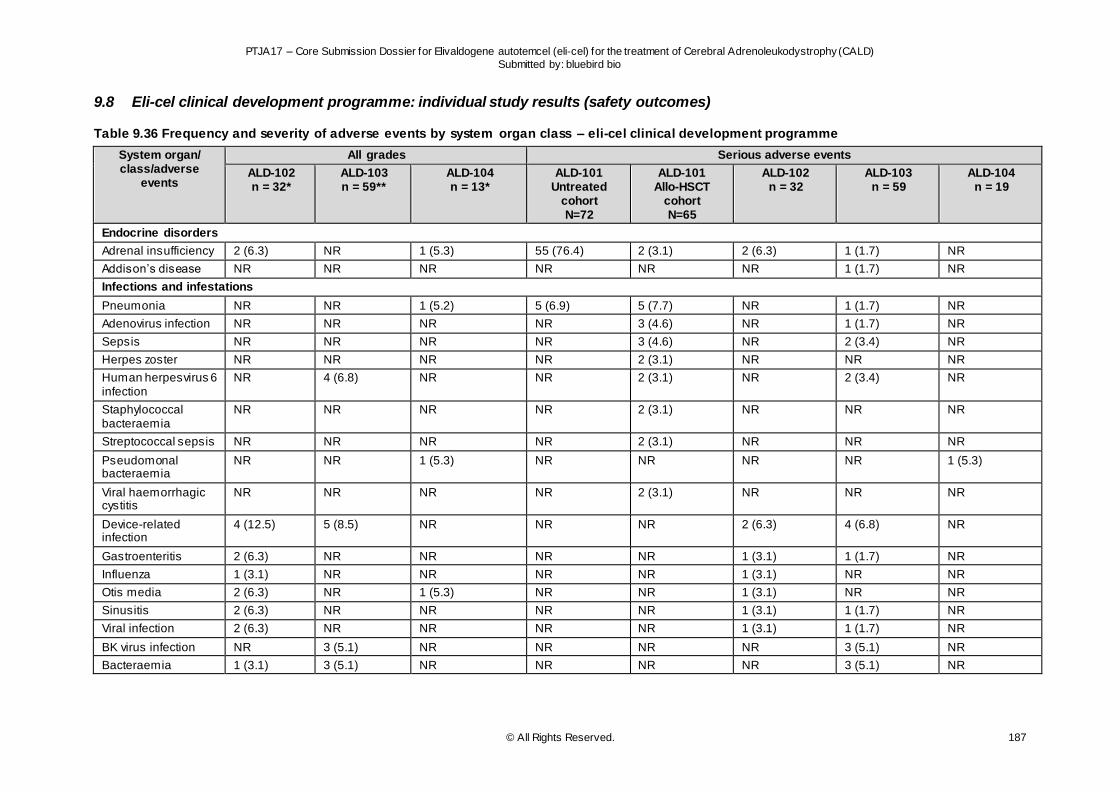
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 187
9.8 Eli-cel clinical development programme: individual study results (safety outcomes)
Table 9.36 Frequency and severity of adverse events by system organ class – eli-cel clinical development programme
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Endocrine disorders
Adrenal insufficiency 2 (6.3) NR 1 (5.3) 55 (76.4) 2 (3.1) 2 (6.3) 1 (1.7) NR
Addison’s disease NR NR NR NR NR NR 1 (1.7) NR
Infections and infestations
Pneumonia NR NR 1 (5.2) 5 (6.9) 5 (7.7) NR 1 (1.7) NR
Adenovirus infection NR NR NR NR 3 (4.6) NR 1 (1.7) NR
Sepsis NR NR NR NR 3 (4.6) NR 2 (3.4) NR
Herpes zoster NR NR NR NR 2 (3.1) NR NR NR
Human herpesvirus 6 infection
NR 4 (6.8) NR NR 2 (3.1) NR 2 (3.4) NR
Staphylococcal bacteraemia
NR NR NR NR 2 (3.1) NR NR NR
Streptococcal sepsis NR NR NR NR 2 (3.1) NR NR NR
Pseudomonal bacteraemia
NR NR 1 (5.3) NR NR NR NR 1 (5.3)
Viral haemorrhagic cystitis
NR NR NR NR 2 (3.1) NR NR NR
Device-related infection
4 (12.5) 5 (8.5) NR NR NR 2 (6.3) 4 (6.8) NR
Gastroenteritis 2 (6.3) NR NR NR NR 1 (3.1) 1 (1.7) NR
Influenza 1 (3.1) NR NR NR NR 1 (3.1) NR NR
Otis media 2 (6.3) NR 1 (5.3) NR NR 1 (3.1) NR NR
Sinusitis 2 (6.3) NR NR NR NR 1 (3.1) 1 (1.7) NR
Viral infection 2 (6.3) NR NR NR NR 1 (3.1) 1 (1.7) NR
BK virus infection NR 3 (5.1) NR NR NR NR 3 (5.1) NR
Bacteraemia 1 (3.1) 3 (5.1) NR NR NR NR 3 (5.1) NR
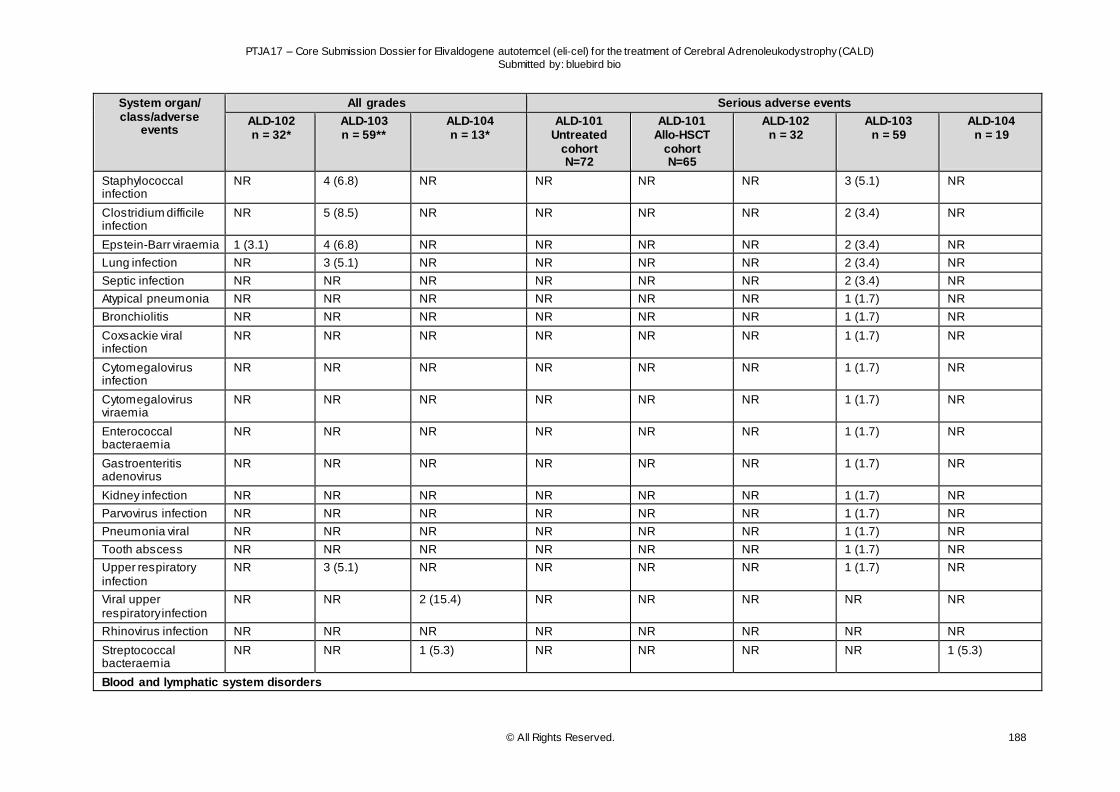
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 188
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Staphylococcal infection
NR 4 (6.8) NR NR NR NR 3 (5.1) NR
Clostridium difficile infection
NR 5 (8.5) NR NR NR NR 2 (3.4) NR
Epstein-Barr viraemia 1 (3.1) 4 (6.8) NR NR NR NR 2 (3.4) NR
Lung infection NR 3 (5.1) NR NR NR NR 2 (3.4) NR
Septic infection NR NR NR NR NR NR 2 (3.4) NR
Atypical pneumonia NR NR NR NR NR NR 1 (1.7) NR
Bronchiolitis NR NR NR NR NR NR 1 (1.7) NR
Coxsackie viral infection
NR NR NR NR NR NR 1 (1.7) NR
Cytomegalovirus infection
NR NR NR NR NR NR 1 (1.7) NR
Cytomegalovirus viraemia
NR NR NR NR NR NR 1 (1.7) NR
Enterococcal bacteraemia
NR NR NR NR NR NR 1 (1.7) NR
Gastroenteritis adenovirus
NR NR NR NR NR NR 1 (1.7) NR
Kidney infection NR NR NR NR NR NR 1 (1.7) NR
Parvovirus infection NR NR NR NR NR NR 1 (1.7) NR
Pneumonia viral NR NR NR NR NR NR 1 (1.7) NR
Tooth abscess NR NR NR NR NR NR 1 (1.7) NR
Upper respiratory infection
NR 3 (5.1) NR NR NR NR 1 (1.7) NR
Viral upper respiratory infection
NR NR 2 (15.4) NR NR NR NR NR
Rhinovirus infection NR NR NR NR NR NR NR NR
Streptococcal bacteraemia
NR NR 1 (5.3) NR NR NR NR 1 (5.3)
Blood and lymphatic system disorders
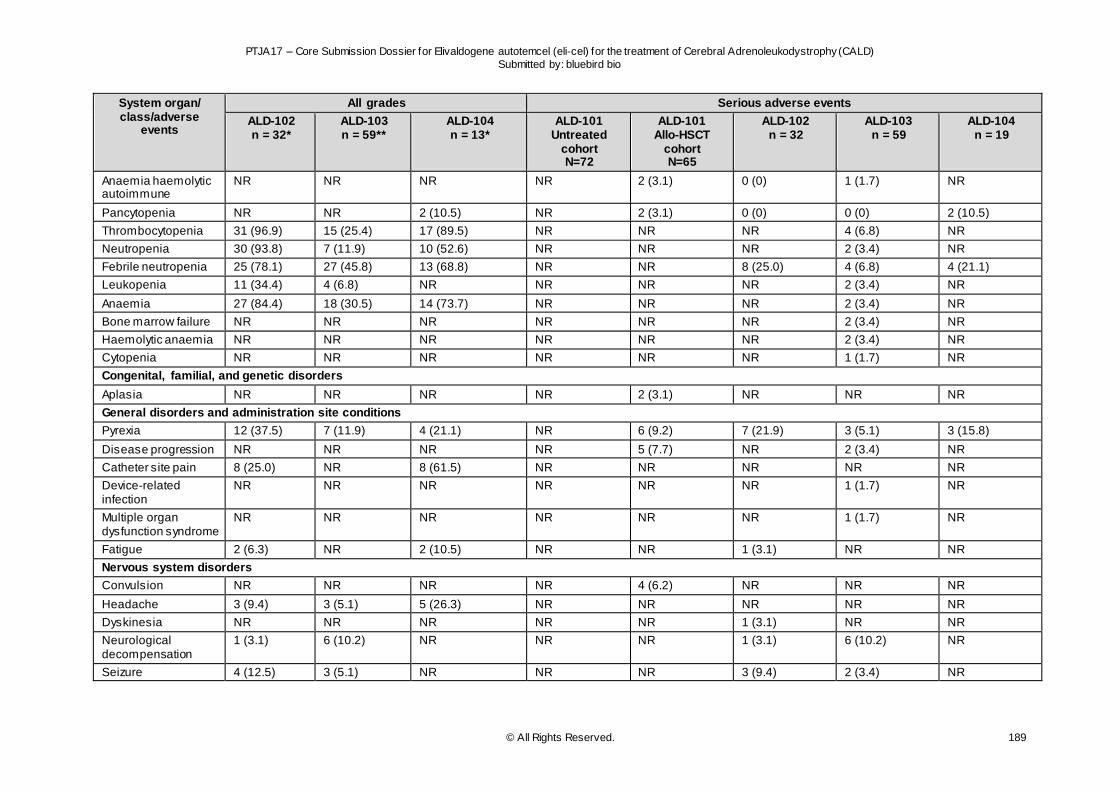
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 189
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Anaemia haemolytic autoimmune
NR NR NR NR 2 (3.1) 0 (0) 1 (1.7) NR
Pancytopenia NR NR 2 (10.5) NR 2 (3.1) 0 (0) 0 (0) 2 (10.5)
Thrombocytopenia 31 (96.9) 15 (25.4) 17 (89.5) NR NR NR 4 (6.8) NR
Neutropenia 30 (93.8) 7 (11.9) 10 (52.6) NR NR NR 2 (3.4) NR
Febrile neutropenia 25 (78.1) 27 (45.8) 13 (68.8) NR NR 8 (25.0) 4 (6.8) 4 (21.1)
Leukopenia 11 (34.4) 4 (6.8) NR NR NR NR 2 (3.4) NR
Anaemia 27 (84.4) 18 (30.5) 14 (73.7) NR NR NR 2 (3.4) NR
Bone marrow failure NR NR NR NR NR NR 2 (3.4) NR
Haemolytic anaemia NR NR NR NR NR NR 2 (3.4) NR
Cytopenia NR NR NR NR NR NR 1 (1.7) NR
Congenital, familial, and genetic disorders
Aplasia NR NR NR NR 2 (3.1) NR NR NR
General disorders and administration site conditions
Pyrexia 12 (37.5) 7 (11.9) 4 (21.1) NR 6 (9.2) 7 (21.9) 3 (5.1) 3 (15.8)
Disease progression NR NR NR NR 5 (7.7) NR 2 (3.4) NR
Catheter site pain 8 (25.0) NR 8 (61.5) NR NR NR NR NR
Device-related infection
NR NR NR NR NR NR 1 (1.7) NR
Multiple organ dysfunction syndrome
NR NR NR NR NR NR 1 (1.7) NR
Fatigue 2 (6.3) NR 2 (10.5) NR NR 1 (3.1) NR NR
Nervous system disorders
Convulsion NR NR NR NR 4 (6.2) NR NR NR
Headache 3 (9.4) 3 (5.1) 5 (26.3) NR NR NR NR NR
Dyskinesia NR NR NR NR NR 1 (3.1) NR NR
Neurological decompensation
1 (3.1) 6 (10.2) NR NR NR 1 (3.1) 6 (10.2) NR
Seizure 4 (12.5) 3 (5.1) NR NR NR 3 (9.4) 2 (3.4) NR
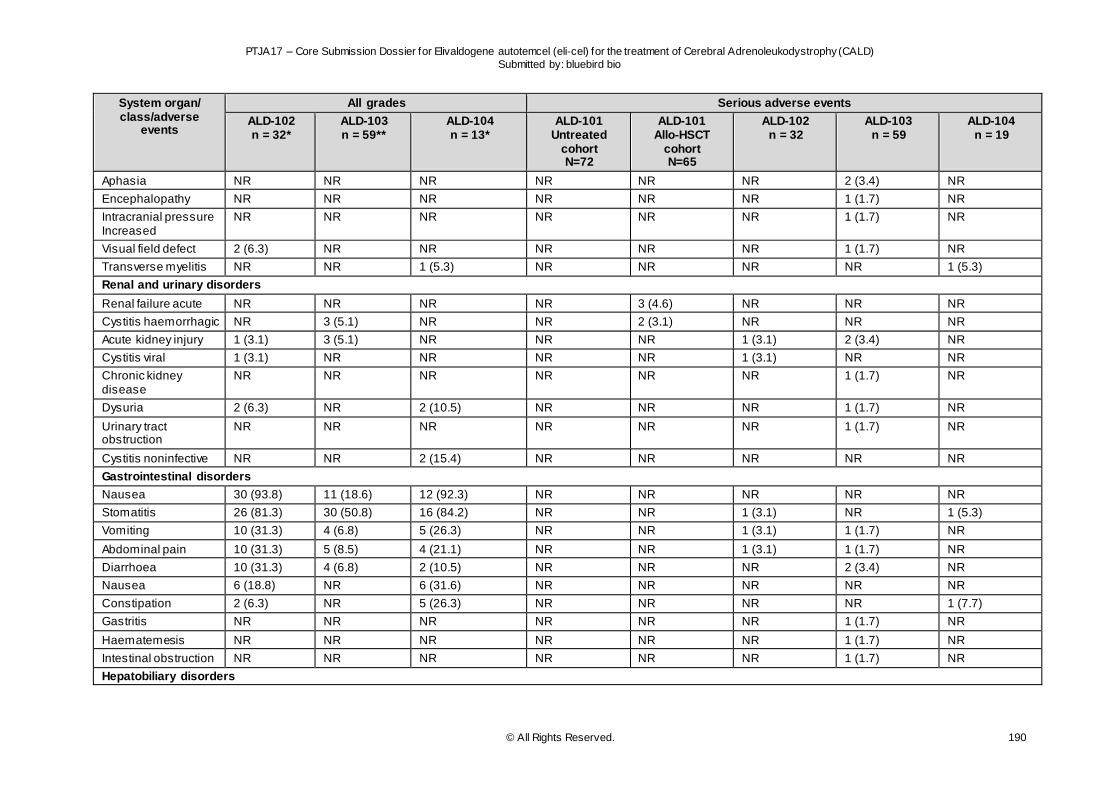
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 190
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Aphasia NR NR NR NR NR NR 2 (3.4) NR
Encephalopathy NR NR NR NR NR NR 1 (1.7) NR
Intracranial pressure Increased
NR NR NR NR NR NR 1 (1.7) NR
Visual field defect 2 (6.3) NR NR NR NR NR 1 (1.7) NR
Transverse myelitis NR NR 1 (5.3) NR NR NR NR 1 (5.3)
Renal and urinary disorders
Renal failure acute NR NR NR NR 3 (4.6) NR NR NR
Cystitis haemorrhagic NR 3 (5.1) NR NR 2 (3.1) NR NR NR
Acute kidney injury 1 (3.1) 3 (5.1) NR NR NR 1 (3.1) 2 (3.4) NR
Cystitis viral 1 (3.1) NR NR NR NR 1 (3.1) NR NR
Chronic kidney disease
NR NR NR NR NR NR 1 (1.7) NR
Dysuria 2 (6.3) NR 2 (10.5) NR NR NR 1 (1.7) NR
Urinary tract obstruction
NR NR NR NR NR NR 1 (1.7) NR
Cystitis noninfective NR NR 2 (15.4) NR NR NR NR NR
Gastrointestinal disorders
Nausea 30 (93.8) 11 (18.6) 12 (92.3) NR NR NR NR NR
Stomatitis 26 (81.3) 30 (50.8) 16 (84.2) NR NR 1 (3.1) NR 1 (5.3)
Vomiting 10 (31.3) 4 (6.8) 5 (26.3) NR NR 1 (3.1) 1 (1.7) NR
Abdominal pain 10 (31.3) 5 (8.5) 4 (21.1) NR NR 1 (3.1) 1 (1.7) NR
Diarrhoea 10 (31.3) 4 (6.8) 2 (10.5) NR NR NR 2 (3.4) NR
Nausea 6 (18.8) NR 6 (31.6) NR NR NR NR NR
Constipation 2 (6.3) NR 5 (26.3) NR NR NR NR 1 (7.7)
Gastritis NR NR NR NR NR NR 1 (1.7) NR
Haematemesis NR NR NR NR NR NR 1 (1.7) NR
Intestinal obstruction NR NR NR NR NR NR 1 (1.7) NR
Hepatobiliary disorders
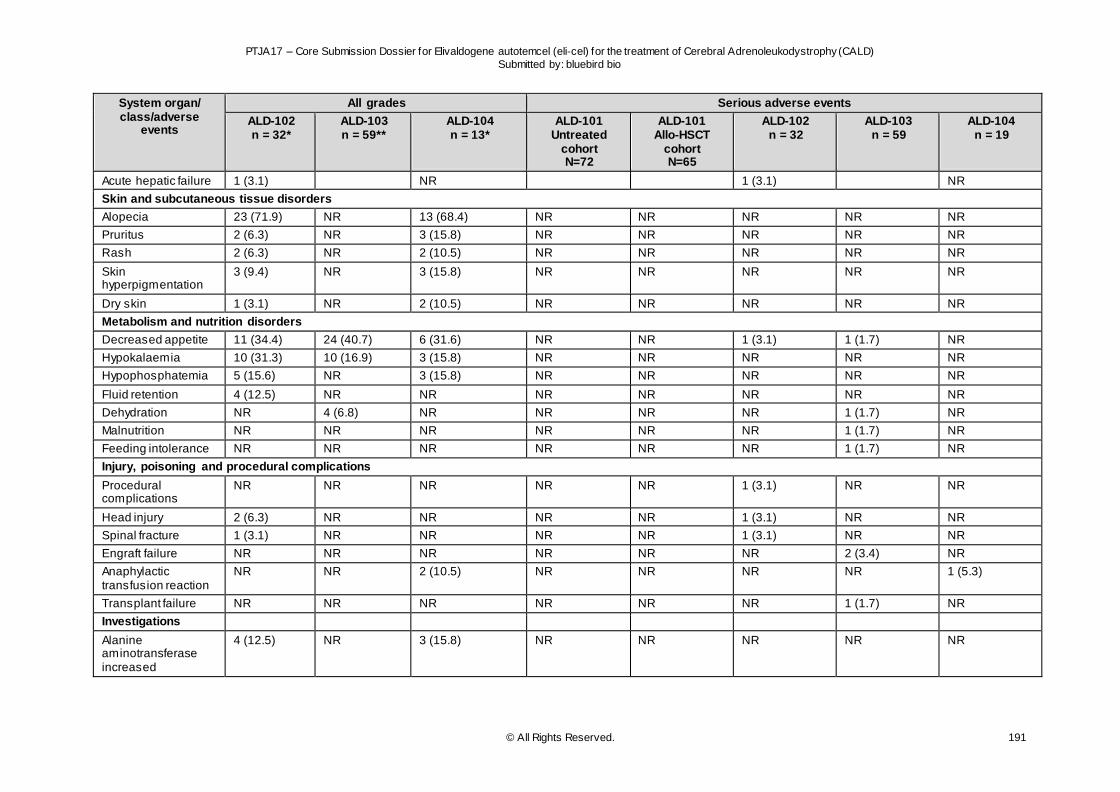
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 191
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Acute hepatic failure 1 (3.1) NR 1 (3.1) NR
Skin and subcutaneous tissue disorders
Alopecia 23 (71.9) NR 13 (68.4) NR NR NR NR NR
Pruritus 2 (6.3) NR 3 (15.8) NR NR NR NR NR
Rash 2 (6.3) NR 2 (10.5) NR NR NR NR NR
Skin hyperpigmentation
3 (9.4) NR 3 (15.8) NR NR NR NR NR
Dry skin 1 (3.1) NR 2 (10.5) NR NR NR NR NR
Metabolism and nutrition disorders
Decreased appetite 11 (34.4) 24 (40.7) 6 (31.6) NR NR 1 (3.1) 1 (1.7) NR
Hypokalaemia 10 (31.3) 10 (16.9) 3 (15.8) NR NR NR NR NR
Hypophosphatemia 5 (15.6) NR 3 (15.8) NR NR NR NR NR
Fluid retention 4 (12.5) NR NR NR NR NR NR NR
Dehydration NR 4 (6.8) NR NR NR NR 1 (1.7) NR
Malnutrition NR NR NR NR NR NR 1 (1.7) NR
Feeding intolerance NR NR NR NR NR NR 1 (1.7) NR
Injury, poisoning and procedural complications
Procedural complications
NR NR NR NR NR 1 (3.1) NR NR
Head injury 2 (6.3) NR NR NR NR 1 (3.1) NR NR
Spinal fracture 1 (3.1) NR NR NR NR 1 (3.1) NR NR
Engraft failure NR NR NR NR NR NR 2 (3.4) NR
Anaphylactic transfusion reaction
NR NR 2 (10.5) NR NR NR NR 1 (5.3)
Transplant failure NR NR NR NR NR NR 1 (1.7) NR
Investigations
Alanine aminotransferase increased
4 (12.5) NR 3 (15.8) NR NR NR NR NR
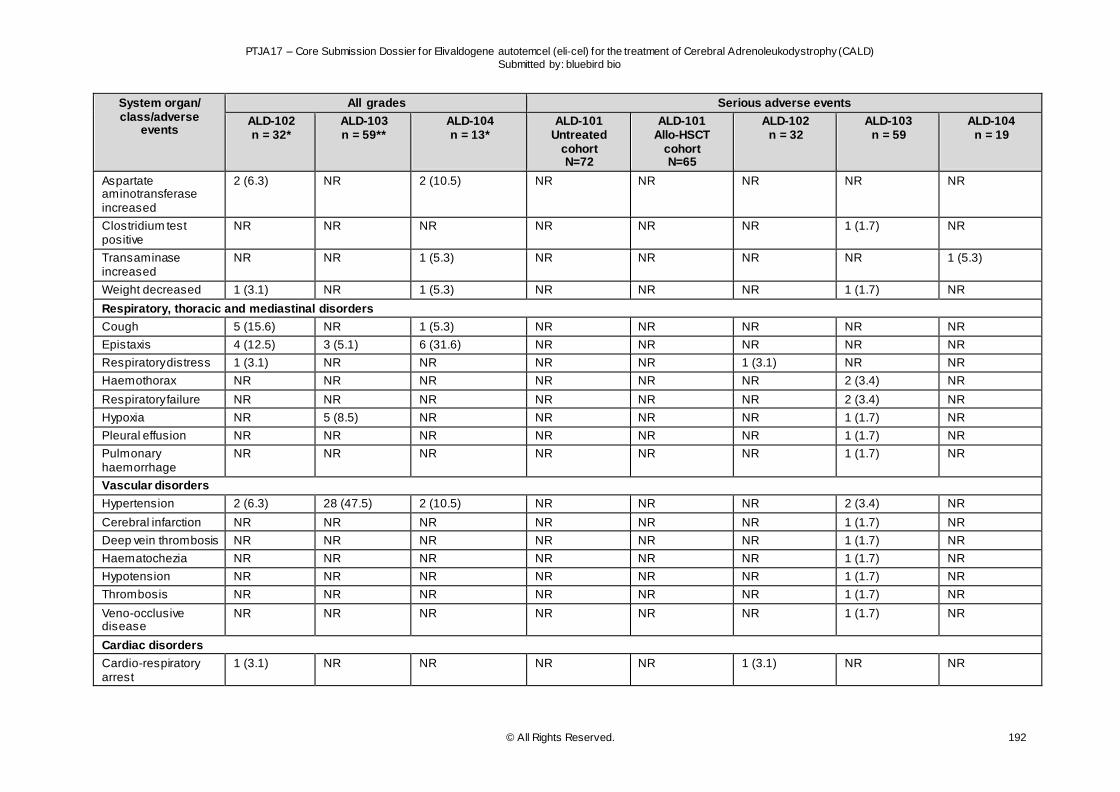
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 192
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Aspartate aminotransferase increased
2 (6.3) NR 2 (10.5) NR NR NR NR NR
Clostridium test positive
NR NR NR NR NR NR 1 (1.7) NR
Transaminase increased
NR NR 1 (5.3) NR NR NR NR 1 (5.3)
Weight decreased 1 (3.1) NR 1 (5.3) NR NR NR 1 (1.7) NR
Respiratory, thoracic and mediastinal disorders
Cough 5 (15.6) NR 1 (5.3) NR NR NR NR NR
Epistaxis 4 (12.5) 3 (5.1) 6 (31.6) NR NR NR NR NR
Respiratory distress 1 (3.1) NR NR NR NR 1 (3.1) NR NR
Haemothorax NR NR NR NR NR NR 2 (3.4) NR
Respiratory failure NR NR NR NR NR NR 2 (3.4) NR
Hypoxia NR 5 (8.5) NR NR NR NR 1 (1.7) NR
Pleural effusion NR NR NR NR NR NR 1 (1.7) NR
Pulmonary haemorrhage
NR NR NR NR NR NR 1 (1.7) NR
Vascular disorders
Hypertension 2 (6.3) 28 (47.5) 2 (10.5) NR NR NR 2 (3.4) NR
Cerebral infarction NR NR NR NR NR NR 1 (1.7) NR
Deep vein thrombosis NR NR NR NR NR NR 1 (1.7) NR
Haematochezia NR NR NR NR NR NR 1 (1.7) NR
Hypotension NR NR NR NR NR NR 1 (1.7) NR
Thrombosis NR NR NR NR NR NR 1 (1.7) NR
Veno-occlusive disease
NR NR NR NR NR NR 1 (1.7) NR
Cardiac disorders
Cardio-respiratory arrest
1 (3.1) NR NR NR NR 1 (3.1) NR NR
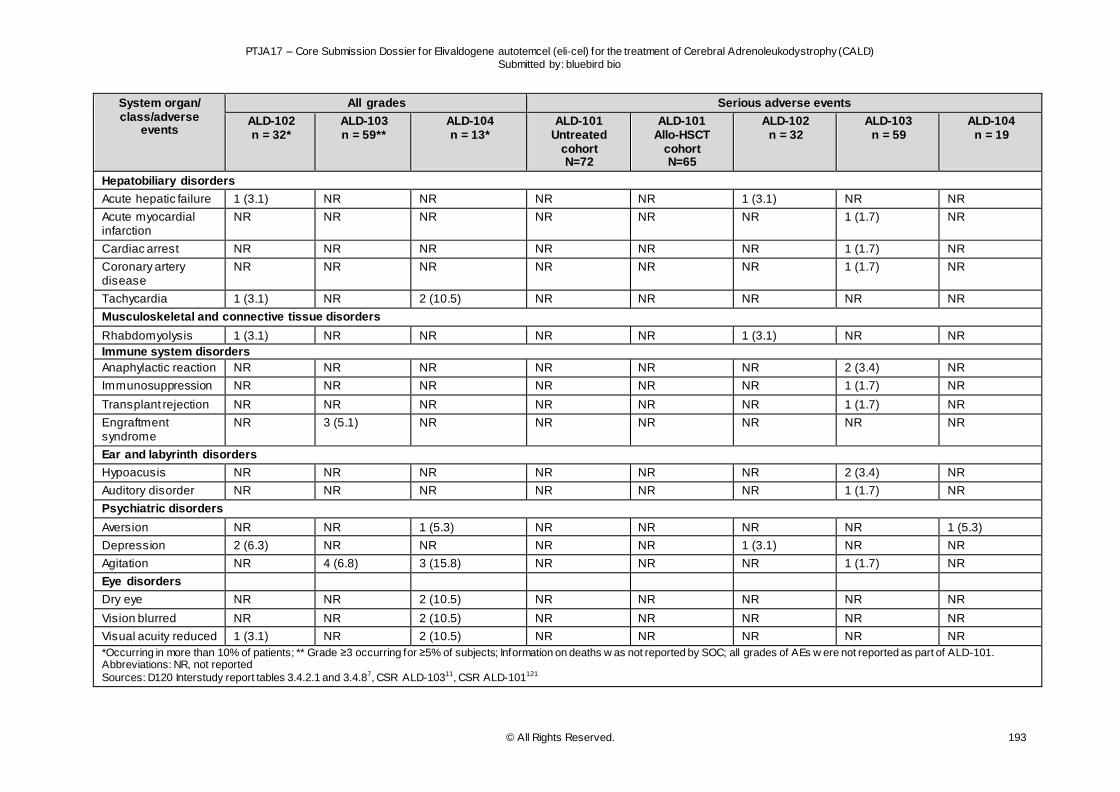
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 193
System organ/ class/adverse
events
All grades Serious adverse events
ALD-102 n = 32*
ALD-103 n = 59**
ALD-104 n = 13*
ALD-101 Untreated
cohort N=72
ALD-101 Allo-HSCT
cohort N=65
ALD-102 n = 32
ALD-103 n = 59
ALD-104 n = 19
Hepatobiliary disorders
Acute hepatic failure 1 (3.1) NR NR NR NR 1 (3.1) NR NR
Acute myocardial infarction
NR NR NR NR NR NR 1 (1.7) NR
Cardiac arrest NR NR NR NR NR NR 1 (1.7) NR
Coronary artery disease
NR NR NR NR NR NR 1 (1.7) NR
Tachycardia 1 (3.1) NR 2 (10.5) NR NR NR NR NR
Musculoskeletal and connective tissue disorders
Rhabdomyolysis 1 (3.1) NR NR NR NR 1 (3.1) NR NR
Immune system disorders
Anaphylactic reaction NR NR NR NR NR NR 2 (3.4) NR
Immunosuppression NR NR NR NR NR NR 1 (1.7) NR
Transplant rejection NR NR NR NR NR NR 1 (1.7) NR
Engraftment syndrome
NR 3 (5.1) NR NR NR NR NR NR
Ear and labyrinth disorders
Hypoacusis NR NR NR NR NR NR 2 (3.4) NR
Auditory disorder NR NR NR NR NR NR 1 (1.7) NR
Psychiatric disorders
Aversion NR NR 1 (5.3) NR NR NR NR 1 (5.3)
Depression 2 (6.3) NR NR NR NR 1 (3.1) NR NR
Agitation NR 4 (6.8) 3 (15.8) NR NR NR 1 (1.7) NR
Eye disorders
Dry eye NR NR 2 (10.5) NR NR NR NR NR
Vision blurred NR NR 2 (10.5) NR NR NR NR NR
Visual acuity reduced 1 (3.1) NR 2 (10.5) NR NR NR NR NR
*Occurring in more than 10% of patients; ** Grade ≥3 occurring for ≥5% of subjects; Information on deaths w as not reported by SOC; all grades of AEs w ere not reported as part of ALD-101. Abbreviations: NR, not reported
Sources: D120 Interstudy report tables 3.4.2.1 and 3.4.87, CSR ALD-10311, CSR ALD-101121
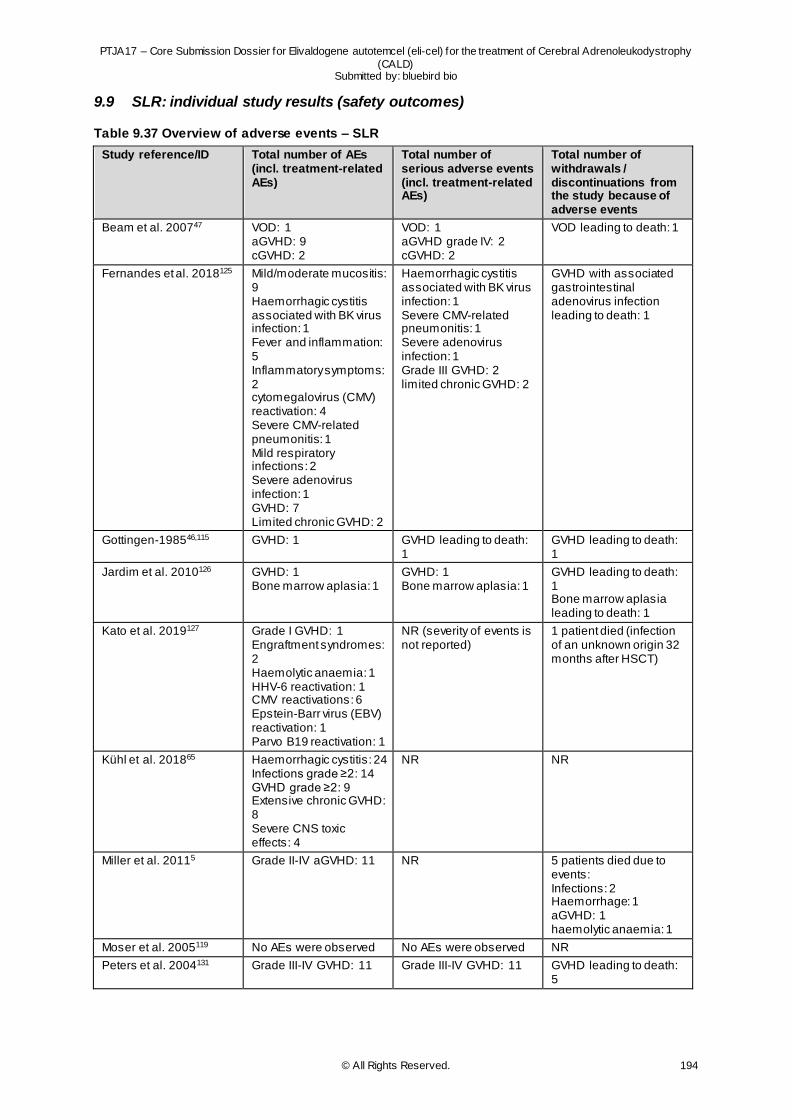
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 194
9.9 SLR: individual study results (safety outcomes)
Table 9.37 Overview of adverse events – SLR
Study reference/ID Total number of AEs (incl. treatment-related AEs)
Total number of serious adverse events (incl. treatment-related AEs)
Total number of withdrawals / discontinuations from the study because of adverse events
Beam et al. 200747 VOD: 1 aGVHD: 9 cGVHD: 2
VOD: 1 aGVHD grade IV: 2 cGVHD: 2
VOD leading to death: 1
Fernandes et al. 2018125 Mild/moderate mucositis: 9 Haemorrhagic cystitis associated with BK virus infection: 1 Fever and inflammation: 5 Inflammatory symptoms: 2 cytomegalovirus (CMV) reactivation: 4 Severe CMV-related pneumonitis: 1 Mild respiratory infections: 2 Severe adenovirus infection: 1 GVHD: 7 Limited chronic GVHD: 2
Haemorrhagic cystitis associated with BK virus infection: 1 Severe CMV-related pneumonitis: 1 Severe adenovirus infection: 1 Grade III GVHD: 2 limited chronic GVHD: 2
GVHD with associated gastrointestinal adenovirus infection leading to death: 1
Gottingen-198546,115 GVHD: 1 GVHD leading to death: 1
GVHD leading to death: 1
Jardim et al. 2010126 GVHD: 1 Bone marrow aplasia: 1
GVHD: 1 Bone marrow aplasia: 1
GVHD leading to death: 1 Bone marrow aplasia leading to death: 1
Kato et al. 2019127 Grade I GVHD: 1 Engraftment syndromes: 2 Haemolytic anaemia: 1 HHV-6 reactivation: 1 CMV reactivations: 6 Epstein-Barr virus (EBV) reactivation: 1 Parvo B19 reactivation: 1
NR (severity of events is not reported)
1 patient died (infection of an unknown origin 32 months after HSCT)
Kühl et al. 201865 Haemorrhagic cystitis: 24 Infections grade ≥2: 14 GVHD grade ≥2: 9 Extensive chronic GVHD: 8 Severe CNS toxic effects: 4
NR NR
Miller et al. 20115 Grade II-IV aGVHD: 11 NR 5 patients died due to events: Infections: 2 Haemorrhage: 1 aGVHD: 1 haemolytic anaemia: 1
Moser et al. 2005119 No AEs were observed No AEs were observed NR
Peters et al. 2004131 Grade III-IV GVHD: 11 Grade III-IV GVHD: 11 GVHD leading to death: 5
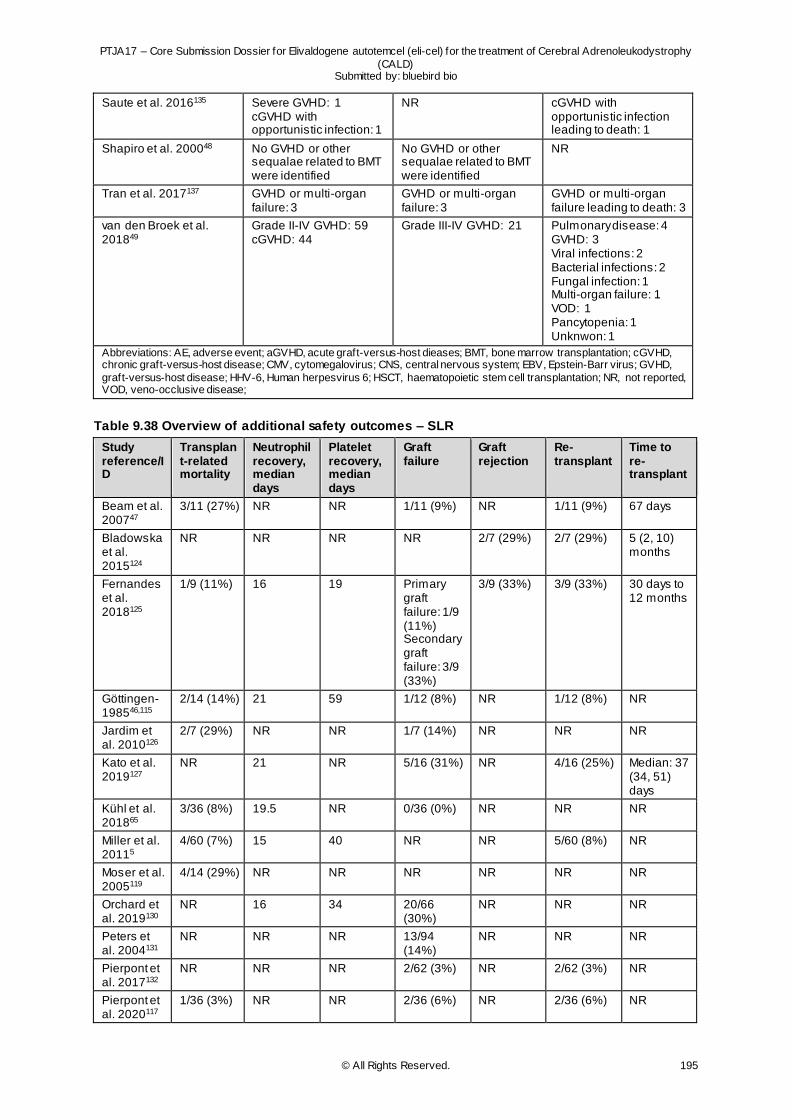
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 195
Saute et al. 2016135 Severe GVHD: 1 cGVHD with opportunistic infection: 1
NR cGVHD with opportunistic infection leading to death: 1
Shapiro et al. 200048 No GVHD or other sequalae related to BMT were identified
No GVHD or other sequalae related to BMT were identified
NR
Tran et al. 2017137 GVHD or multi-organ failure: 3
GVHD or multi-organ failure: 3
GVHD or multi-organ failure leading to death: 3
van den Broek et al. 201849
Grade II-IV GVHD: 59 cGVHD: 44
Grade III-IV GVHD: 21 Pulmonary disease: 4 GVHD: 3 Viral infections: 2 Bacterial infections: 2 Fungal infection: 1 Multi-organ failure: 1 VOD: 1 Pancytopenia: 1 Unknwon: 1
Abbreviations: AE, adverse event; aGVHD, acute graft-versus-host dieases; BMT, bone marrow transplantation; cGVHD, chronic graft-versus-host disease; CMV, cytomegalovirus; CNS, central nervous system; EBV, Epstein-Barr virus; GVHD,
graft-versus-host disease; HHV-6, Human herpesvirus 6; HSCT, haematopoietic stem cell transplantation; NR, not reported, VOD, veno-occlusive disease;
Table 9.38 Overview of additional safety outcomes – SLR
Study reference/ID
Transplant-related mortality
Neutrophil recovery, median days
Platelet recovery, median days
Graft failure
Graft rejection
Re-transplant
Time to re-transplant
Beam et al. 200747
3/11 (27%) NR NR 1/11 (9%) NR 1/11 (9%) 67 days
Bladowska et al. 2015124
NR NR NR NR 2/7 (29%) 2/7 (29%) 5 (2, 10) months
Fernandes et al. 2018125
1/9 (11%) 16 19 Primary graft failure: 1/9 (11%) Secondary graft failure: 3/9 (33%)
3/9 (33%) 3/9 (33%) 30 days to 12 months
Göttingen-198546,115
2/14 (14%) 21 59 1/12 (8%) NR 1/12 (8%) NR
Jardim et al. 2010126
2/7 (29%) NR NR 1/7 (14%) NR NR NR
Kato et al. 2019127
NR 21 NR 5/16 (31%) NR 4/16 (25%) Median: 37 (34, 51) days
Kühl et al. 201865
3/36 (8%) 19.5 NR 0/36 (0%) NR NR NR
Miller et al. 20115
4/60 (7%) 15 40 NR NR 5/60 (8%) NR
Moser et al. 2005119
4/14 (29%) NR NR NR NR NR NR
Orchard et al. 2019130
NR 16 34 20/66 (30%)
NR NR NR
Peters et al. 2004131
NR NR NR 13/94 (14%)
NR NR NR
Pierpont et al. 2017132
NR NR NR 2/62 (3%) NR 2/62 (3%) NR
Pierpont et al. 2020117
1/36 (3%) NR NR 2/36 (6%) NR 2/36 (6%) NR
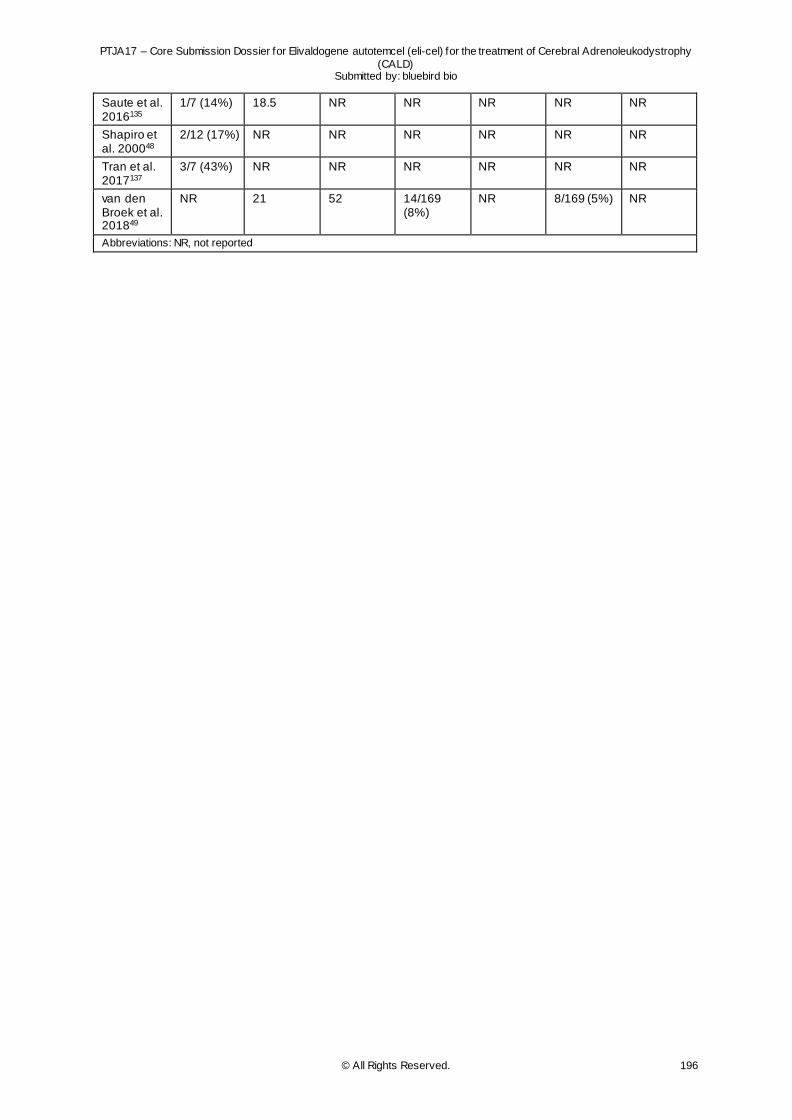
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy
(CALD) Submitted by: bluebird bio
© All Rights Reserved. 196
Saute et al. 2016135
1/7 (14%) 18.5 NR NR NR NR NR
Shapiro et al. 200048
2/12 (17%) NR NR NR NR NR NR
Tran et al. 2017137
3/7 (43%) NR NR NR NR NR NR
van den Broek et al. 201849
NR 21 52 14/169 (8%)
NR 8/169 (5%) NR
Abbreviations: NR, not reported
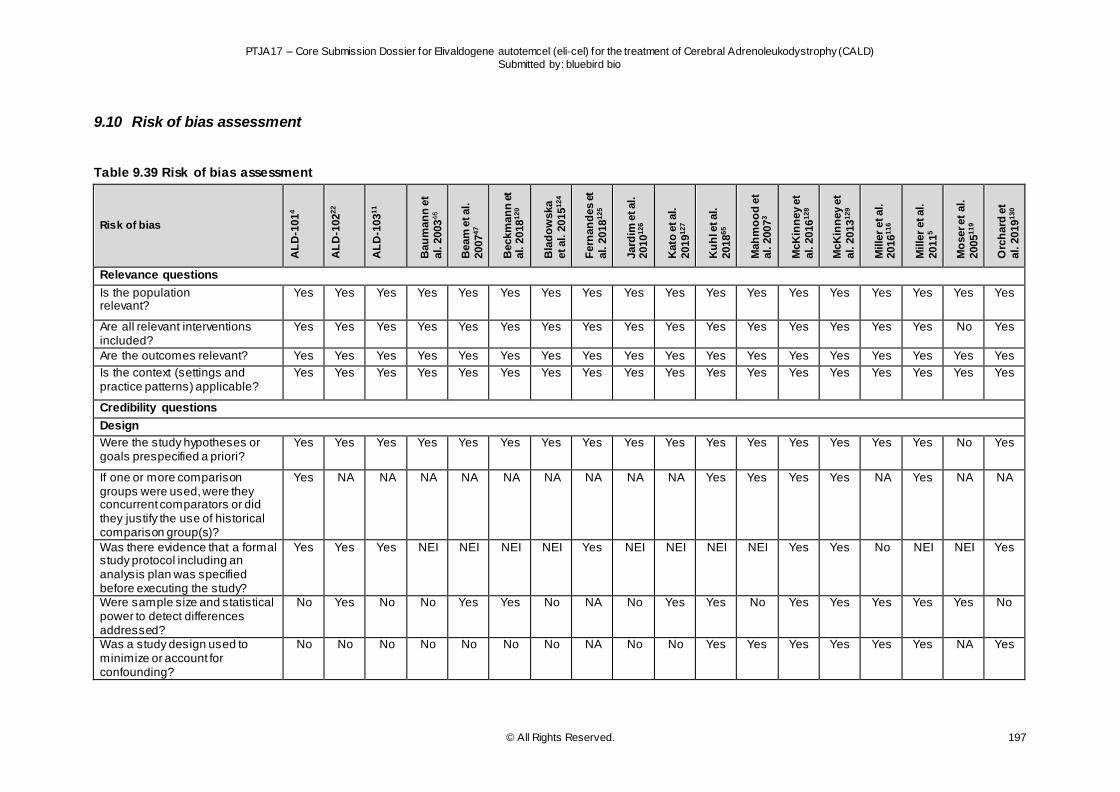
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 197
9.10 Risk of bias assessment
Table 9.39 Risk of bias assessment
Risk of bias
AL
D-1
01
4
AL
D-1
02
22
AL
D-1
03
11
Bau
man
n e
t
al. 2
003
46
Beam
et al.
2007
47
Beckm
an
n e
t al. 2
018
12
0
Bla
do
wska
et al. 2
015
12
4
Fern
an
des e
t
al. 2
018
12
5
Jard
im e
t al.
2010
12
6
Kato
et al.
2019
12
7
Ku
hl e
t al.
2018
65
Mah
mo
od
et
al. 2
007
3
McK
inn
ey e
t
al. 2
016
12
8
McK
inn
ey e
t
al. 2
013
12
9
Mille
r et al.
2016
11
6
Mille
r et al.
2011
5
Mo
ser et
al.
2005
11
9
Orc
hard
et
al. 2
019
13
0
Relevance questions
Is the population relevant?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are all relevant interventions included?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes
Are the outcomes relevant? Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Is the context (settings and practice patterns) applicable?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Credibility questions
Design
Were the study hypotheses or goals prespecified a priori?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes
If one or more comparison groups were used, were they concurrent comparators or did they justify the use of historical comparison group(s)?
Yes NA NA NA NA NA NA NA NA NA Yes Yes Yes Yes NA Yes NA NA
Was there evidence that a formal study protocol including an analysis plan was specified before executing the study?
Yes Yes Yes NEI NEI NEI NEI Yes NEI NEI NEI NEI Yes Yes No NEI NEI Yes
Were sample size and statistical power to detect differences addressed?
No Yes No No Yes Yes No NA No Yes Yes No Yes Yes Yes Yes Yes No
Was a study design used to minimize or account for confounding?
No No No No No No No NA No No Yes Yes Yes Yes Yes Yes NA Yes
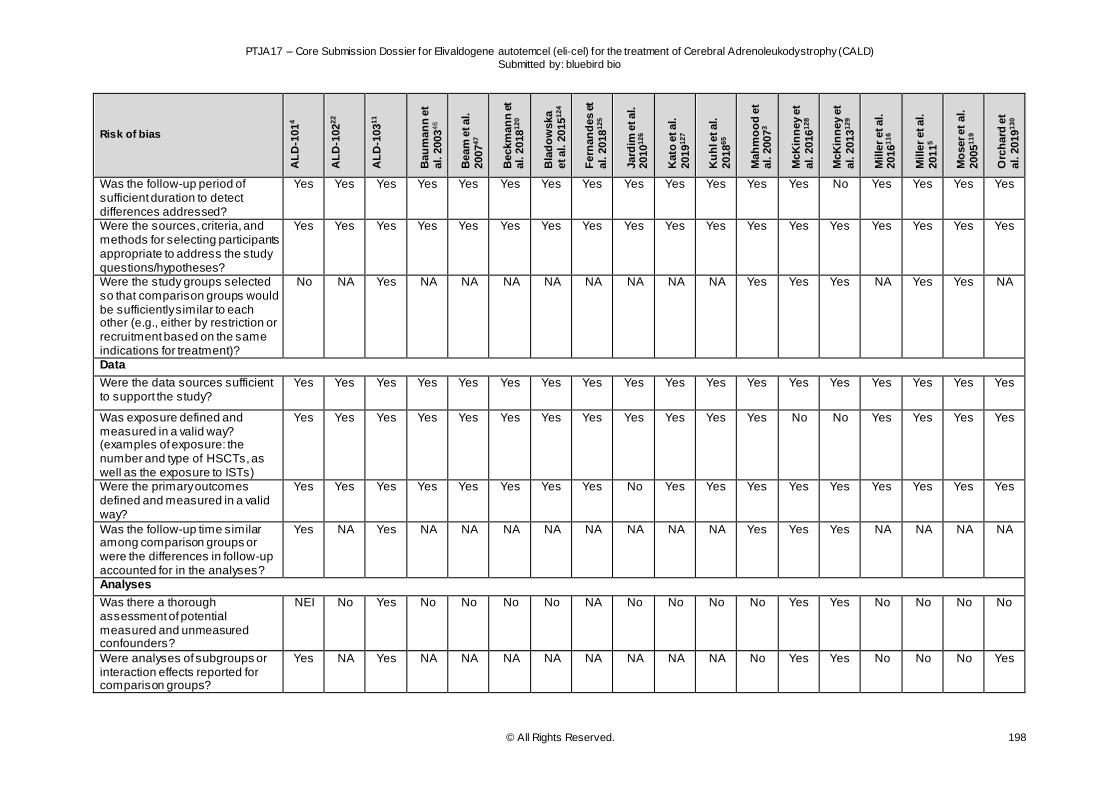
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 198
Risk of bias
AL
D-1
01
4
AL
D-1
02
22
AL
D-1
03
11
Bau
man
n e
t
al. 2
003
46
Beam
et al.
2007
47
Beckm
an
n e
t al. 2
018
12
0
Bla
do
wska
et al. 2
015
12
4
Fern
an
des e
t
al. 2
018
12
5
Jard
im e
t al.
2010
12
6
Kato
et al.
2019
12
7
Ku
hl e
t al.
2018
65
Mah
mo
od
et
al. 2
007
3
McK
inn
ey e
t
al. 2
016
12
8
McK
inn
ey e
t
al. 2
013
12
9
Mille
r et al.
2016
11
6
Mille
r et al.
2011
5
Mo
ser et
al.
2005
11
9
Orc
hard
et
al. 2
019
13
0
Was the follow-up period of sufficient duration to detect differences addressed?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes Yes Yes Yes
Were the sources, criteria, and methods for selecting participants appropriate to address the study questions/hypotheses?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Were the study groups selected so that comparison groups would be sufficiently similar to each other (e.g., either by restriction or recruitment based on the same indications for treatment)?
No NA Yes NA NA NA NA NA NA NA NA Yes Yes Yes NA Yes Yes NA
Data
Were the data sources sufficient to support the study?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Was exposure defined and measured in a valid way? (examples of exposure: the number and type of HSCTs, as well as the exposure to ISTs)
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No Yes Yes Yes Yes
Were the primary outcomes defined and measured in a valid way?
Yes Yes Yes Yes Yes Yes Yes Yes No Yes Yes Yes Yes Yes Yes Yes Yes Yes
Was the follow-up time similar among comparison groups or were the differences in follow-up accounted for in the analyses?
Yes NA Yes NA NA NA NA NA NA NA NA Yes Yes Yes NA NA NA NA
Analyses
Was there a thorough assessment of potential measured and unmeasured confounders?
NEI No Yes No No No No NA No No No No Yes Yes No No No No
Were analyses of subgroups or interaction effects reported for comparison groups?
Yes NA Yes NA NA NA NA NA NA NA NA No Yes Yes No No No Yes
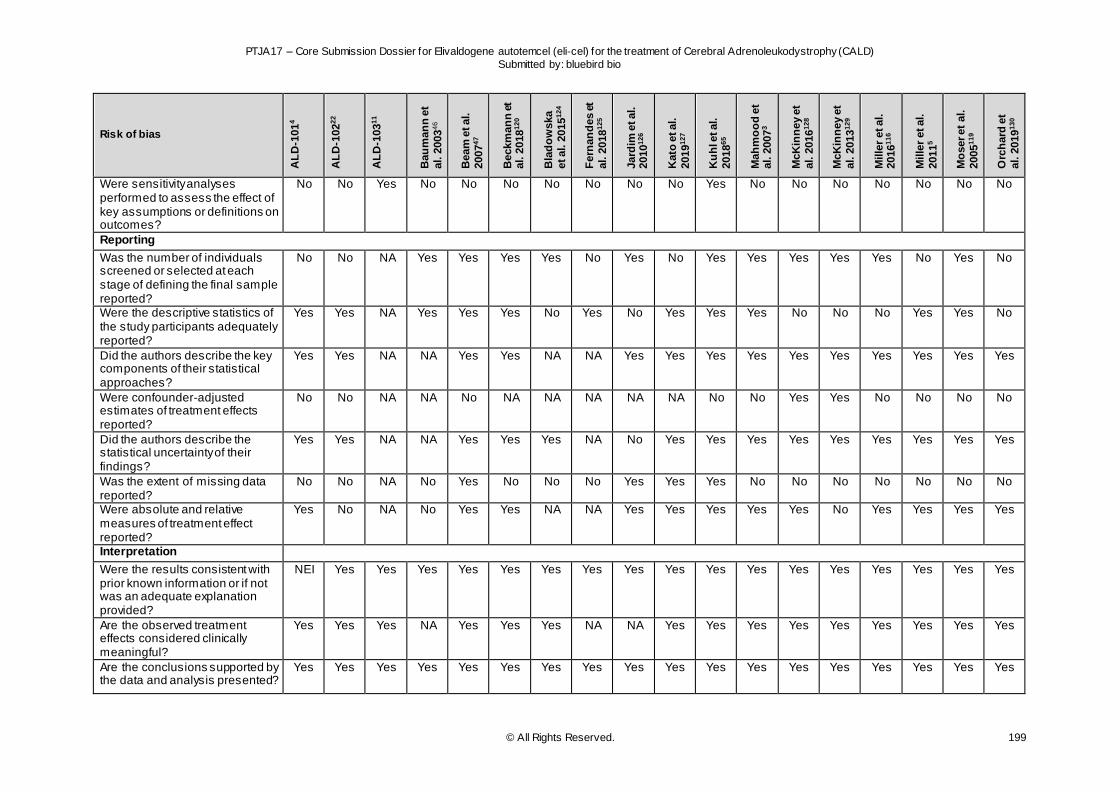
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 199
Risk of bias
AL
D-1
01
4
AL
D-1
02
22
AL
D-1
03
11
Bau
man
n e
t
al. 2
003
46
Beam
et al.
2007
47
Beckm
an
n e
t al. 2
018
12
0
Bla
do
wska
et al. 2
015
12
4
Fern
an
des e
t
al. 2
018
12
5
Jard
im e
t al.
2010
12
6
Kato
et al.
2019
12
7
Ku
hl e
t al.
2018
65
Mah
mo
od
et
al. 2
007
3
McK
inn
ey e
t
al. 2
016
12
8
McK
inn
ey e
t
al. 2
013
12
9
Mille
r et al.
2016
11
6
Mille
r et al.
2011
5
Mo
ser et
al.
2005
11
9
Orc
hard
et
al. 2
019
13
0
Were sensitivity analyses performed to assess the effect of key assumptions or definitions on outcomes?
No No Yes No No No No No No No Yes No No No No No No No
Reporting
Was the number of individuals screened or selected at each stage of defining the final sample reported?
No No NA Yes Yes Yes Yes No Yes No Yes Yes Yes Yes Yes No Yes No
Were the descriptive statistics of the study participants adequately reported?
Yes Yes NA Yes Yes Yes No Yes No Yes Yes Yes No No No Yes Yes No
Did the authors describe the key components of their statistical approaches?
Yes Yes NA NA Yes Yes NA NA Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Were confounder-adjusted estimates of treatment effects reported?
No No NA NA No NA NA NA NA NA No No Yes Yes No No No No
Did the authors describe the statistical uncertainty of their findings?
Yes Yes NA NA Yes Yes Yes NA No Yes Yes Yes Yes Yes Yes Yes Yes Yes
Was the extent of missing data reported?
No No NA No Yes No No No Yes Yes Yes No No No No No No No
Were absolute and relative measures of treatment effect reported?
Yes No NA No Yes Yes NA NA Yes Yes Yes Yes Yes No Yes Yes Yes Yes
Interpretation
Were the results consistent with prior known information or if not was an adequate explanation provided?
NEI Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are the observed treatment effects considered clinically meaningful?
Yes Yes Yes NA Yes Yes Yes NA NA Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are the conclusions supported by the data and analysis presented?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
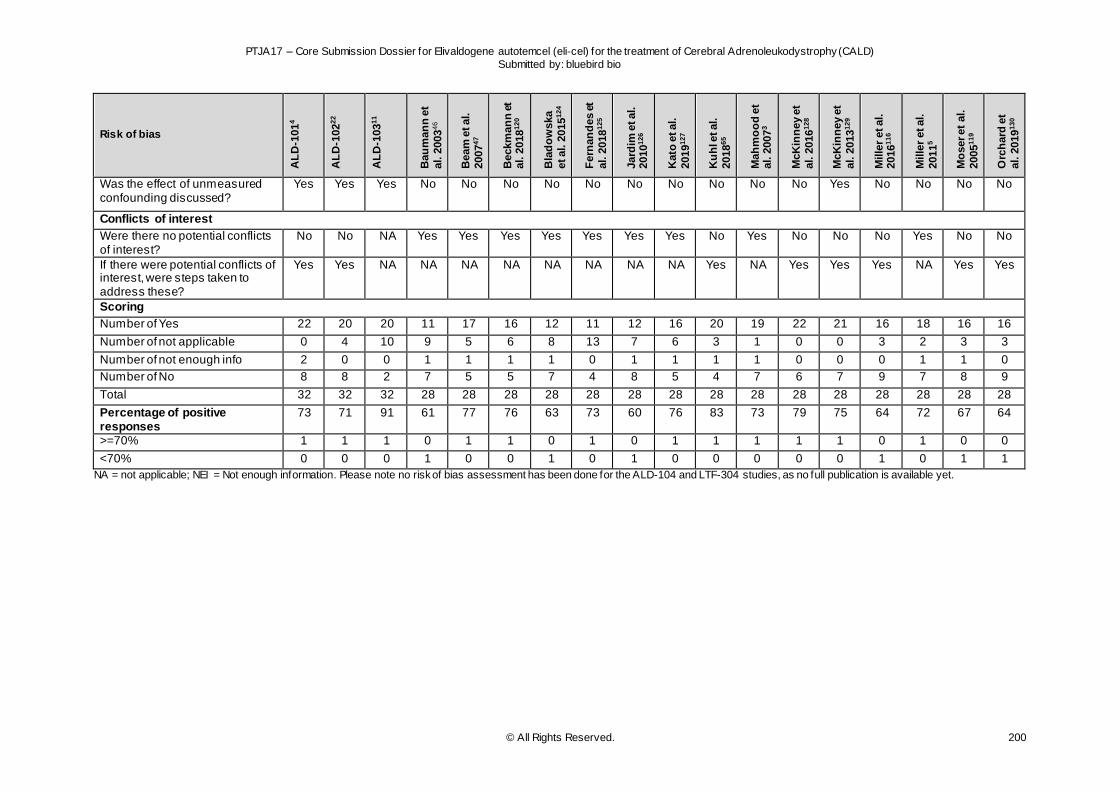
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 200
Risk of bias
AL
D-1
01
4
AL
D-1
02
22
AL
D-1
03
11
Bau
man
n e
t
al. 2
003
46
Beam
et al.
2007
47
Beckm
an
n e
t al. 2
018
12
0
Bla
do
wska
et al. 2
015
12
4
Fern
an
des e
t
al. 2
018
12
5
Jard
im e
t al.
2010
12
6
Kato
et al.
2019
12
7
Ku
hl e
t al.
2018
65
Mah
mo
od
et
al. 2
007
3
McK
inn
ey e
t
al. 2
016
12
8
McK
inn
ey e
t
al. 2
013
12
9
Mille
r et al.
2016
11
6
Mille
r et al.
2011
5
Mo
ser et
al.
2005
11
9
Orc
hard
et
al. 2
019
13
0
Was the effect of unmeasured confounding discussed?
Yes Yes Yes No No No No No No No No No No Yes No No No No
Conflicts of interest
Were there no potential conflicts of interest?
No No NA Yes Yes Yes Yes Yes Yes Yes No Yes No No No Yes No No
If there were potential conflicts of interest, were steps taken to address these?
Yes Yes NA NA NA NA NA NA NA NA Yes NA Yes Yes Yes NA Yes Yes
Scoring
Number of Yes 22 20 20 11 17 16 12 11 12 16 20 19 22 21 16 18 16 16
Number of not applicable 0 4 10 9 5 6 8 13 7 6 3 1 0 0 3 2 3 3
Number of not enough info 2 0 0 1 1 1 1 0 1 1 1 1 0 0 0 1 1 0
Number of No 8 8 2 7 5 5 7 4 8 5 4 7 6 7 9 7 8 9
Total 32 32 32 28 28 28 28 28 28 28 28 28 28 28 28 28 28 28
Percentage of positive responses
73 71 91 61 77 76 63 73 60 76 83 73 79 75 64 72 67 64
>=70% 1 1 1 0 1 1 0 1 0 1 1 1 1 1 0 1 0 0
<70% 0 0 0 1 0 0 1 0 1 0 0 0 0 0 1 0 1 1
NA = not applicable; NEI = Not enough information. Please note no risk of bias assessment has been done for the ALD-104 and LTF-304 studies, as no full publication is available yet.
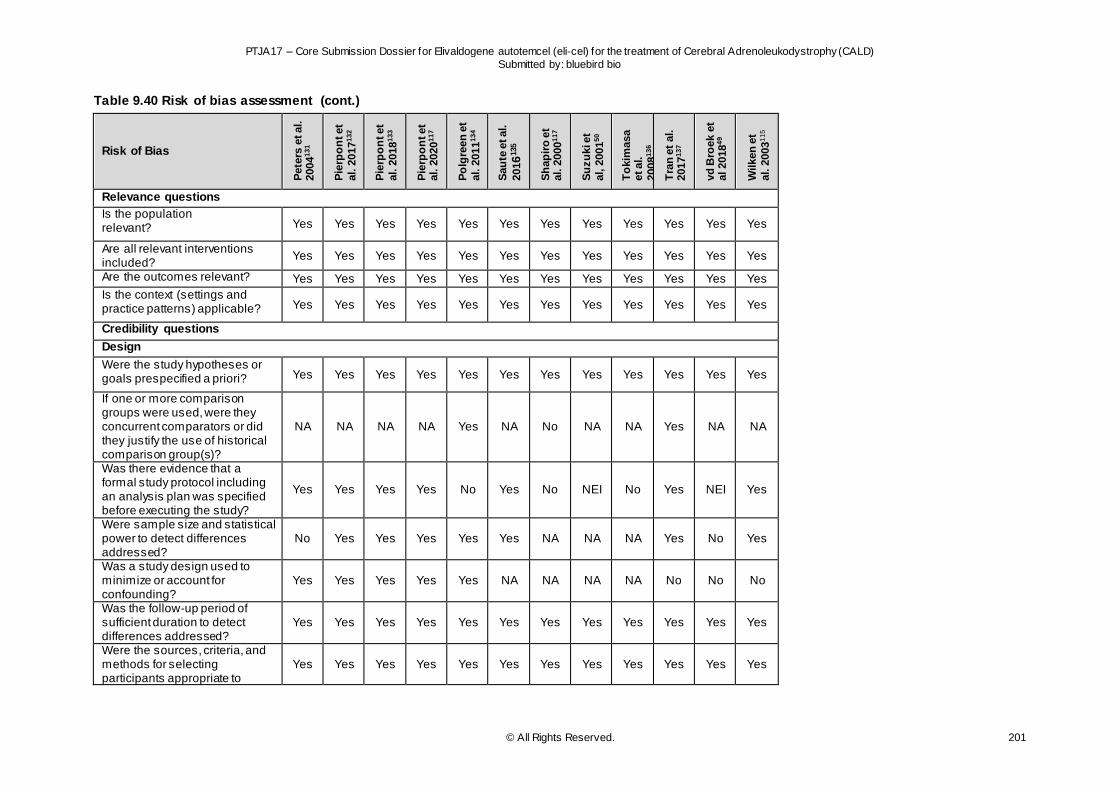
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 201
Table 9.40 Risk of bias assessment (cont.)
Risk of Bias
Pete
rs e
t al.
2004
13
1
Pie
rpo
nt et
al. 2
017
13
2
Pie
rpo
nt et
al. 2
018
13
3
Pie
rpo
nt et
al. 2
020
11
7
Po
lgre
en
et
al. 2
011
13
4
Sau
te e
t al.
2016
135
Sh
ap
iro
et
al. 2
000
11
7
Su
zu
ki e
t
al, 2
001
50
To
kim
asa
et al.
2008
13
6
Tra
n e
t al.
2017
13
7
vd
Bro
ek e
t al 2018
49
Wilken
et
al. 2
003
11
5
Relevance questions
Is the population relevant? Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are all relevant interventions included?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are the outcomes relevant? Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Is the context (settings and practice patterns) applicable? Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Credibility questions
Design
Were the study hypotheses or goals prespecified a priori? Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
If one or more comparison groups were used, were they concurrent comparators or did they justify the use of historical comparison group(s)?
NA NA NA NA Yes NA No NA NA Yes NA NA
Was there evidence that a formal study protocol including an analysis plan was specified before executing the study?
Yes Yes Yes Yes No Yes No NEI No Yes NEI Yes
Were sample size and statistical power to detect differences addressed?
No Yes Yes Yes Yes Yes NA NA NA Yes No Yes
Was a study design used to minimize or account for confounding?
Yes Yes Yes Yes Yes NA NA NA NA No No No
Was the follow-up period of sufficient duration to detect differences addressed?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Were the sources, criteria, and methods for selecting participants appropriate to
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
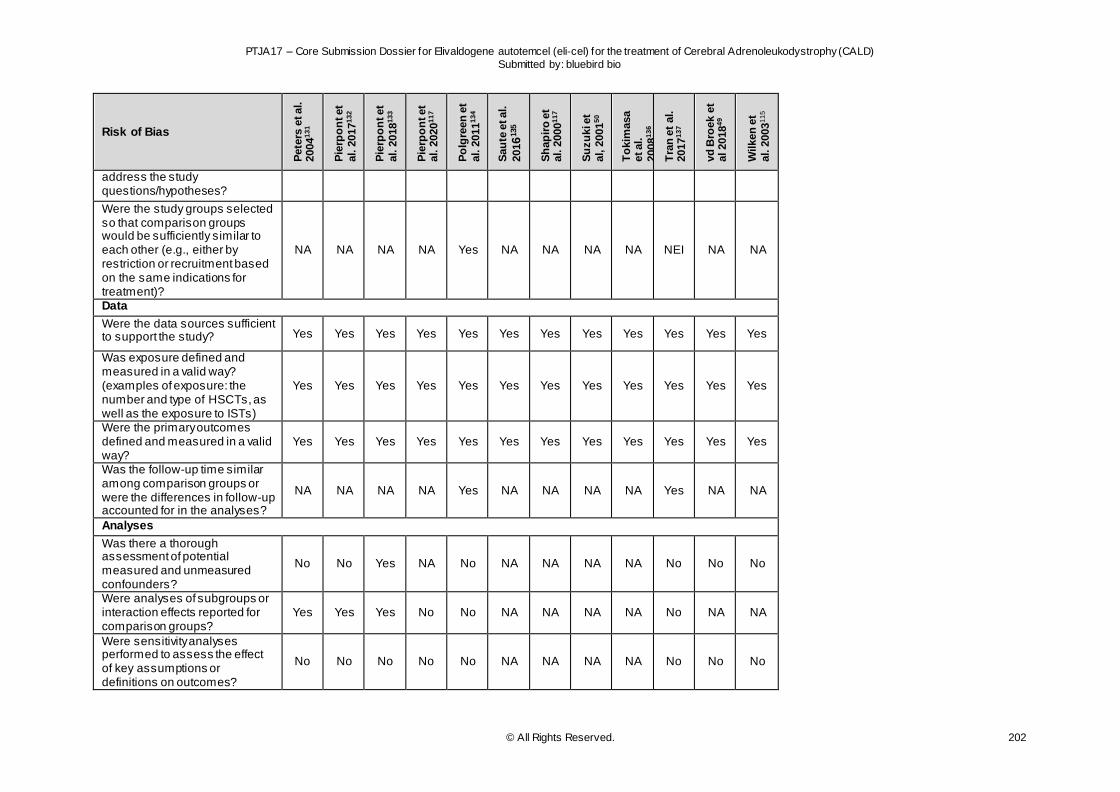
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 202
Risk of Bias
Pete
rs e
t al.
2004
13
1
Pie
rpo
nt et
al. 2
017
13
2
Pie
rpo
nt et
al. 2
018
13
3
Pie
rpo
nt et
al. 2
020
11
7
Po
lgre
en
et
al. 2
011
13
4
Sau
te e
t al.
2016
135
Sh
ap
iro
et
al. 2
000
11
7
Su
zu
ki e
t
al, 2
001
50
To
kim
asa
et al.
2008
13
6
Tra
n e
t al.
2017
13
7
vd
Bro
ek e
t al 2018
49
Wilken
et
al. 2
003
11
5
address the study questions/hypotheses?
Were the study groups selected so that comparison groups would be sufficiently similar to each other (e.g., either by restriction or recruitment based on the same indications for treatment)?
NA NA NA NA Yes NA NA NA NA NEI NA NA
Data
Were the data sources sufficient to support the study? Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Was exposure defined and measured in a valid way? (examples of exposure: the number and type of HSCTs, as well as the exposure to ISTs)
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Were the primary outcomes defined and measured in a valid way?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Was the follow-up time similar among comparison groups or were the differences in follow-up accounted for in the analyses?
NA NA NA NA Yes NA NA NA NA Yes NA NA
Analyses
Was there a thorough assessment of potential measured and unmeasured confounders?
No No Yes NA No NA NA NA NA No No No
Were analyses of subgroups or interaction effects reported for comparison groups?
Yes Yes Yes No No NA NA NA NA No NA NA
Were sensitivity analyses performed to assess the effect of key assumptions or definitions on outcomes?
No No No No No NA NA NA NA No No No
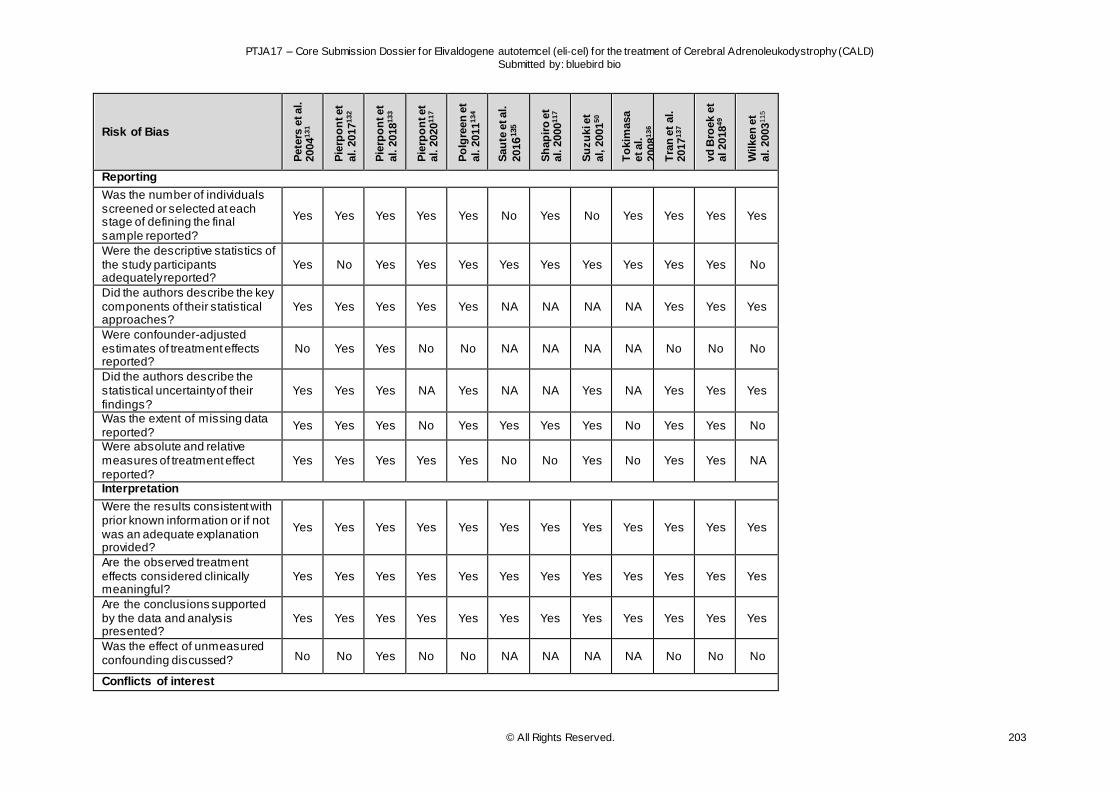
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 203
Risk of Bias
Pete
rs e
t al.
2004
13
1
Pie
rpo
nt et
al. 2
017
13
2
Pie
rpo
nt et
al. 2
018
13
3
Pie
rpo
nt et
al. 2
020
11
7
Po
lgre
en
et
al. 2
011
13
4
Sau
te e
t al.
2016
135
Sh
ap
iro
et
al. 2
000
11
7
Su
zu
ki e
t
al, 2
001
50
To
kim
asa
et al.
2008
13
6
Tra
n e
t al.
2017
13
7
vd
Bro
ek e
t al 2018
49
Wilken
et
al. 2
003
11
5
Reporting
Was the number of individuals screened or selected at each stage of defining the final sample reported?
Yes Yes Yes Yes Yes No Yes No Yes Yes Yes Yes
Were the descriptive statistics of the study participants adequately reported?
Yes No Yes Yes Yes Yes Yes Yes Yes Yes Yes No
Did the authors describe the key components of their statistical approaches?
Yes Yes Yes Yes Yes NA NA NA NA Yes Yes Yes
Were confounder-adjusted estimates of treatment effects reported?
No Yes Yes No No NA NA NA NA No No No
Did the authors describe the statistical uncertainty of their findings?
Yes Yes Yes NA Yes NA NA Yes NA Yes Yes Yes
Was the extent of missing data reported?
Yes Yes Yes No Yes Yes Yes Yes No Yes Yes No
Were absolute and relative measures of treatment effect reported?
Yes Yes Yes Yes Yes No No Yes No Yes Yes NA
Interpretation
Were the results consistent with prior known information or if not was an adequate explanation provided?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are the observed treatment effects considered clinically meaningful?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Are the conclusions supported by the data and analysis presented?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Was the effect of unmeasured confounding discussed? No No Yes No No NA NA NA NA No No No
Conflicts of interest
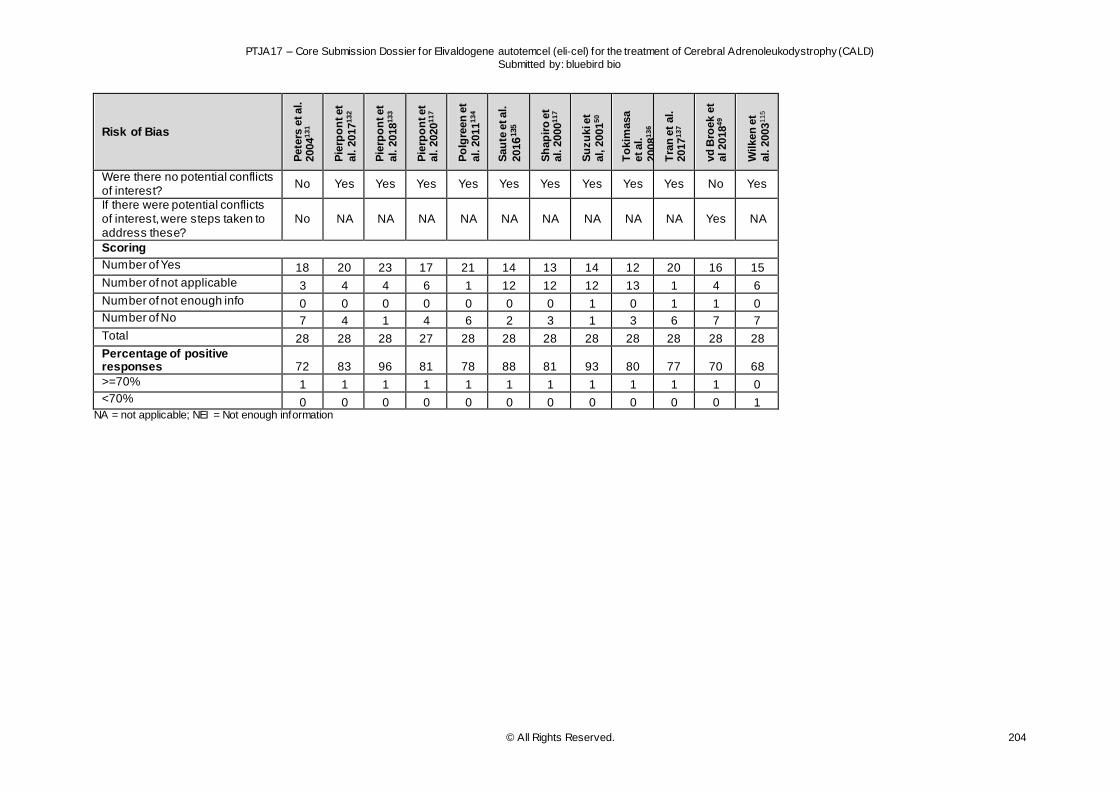
PTJA17 – Core Submission Dossier for Elivaldogene autotemcel (eli-cel) for the treatment of Cerebral Adrenoleukodystrophy (CALD)
Submitted by: bluebird bio
© All Rights Reserved. 204
Risk of Bias
Pete
rs e
t al.
2004
13
1
Pie
rpo
nt et
al. 2
017
13
2
Pie
rpo
nt et
al. 2
018
13
3
Pie
rpo
nt et
al. 2
020
11
7
Po
lgre
en
et
al. 2
011
13
4
Sau
te e
t al.
2016
135
Sh
ap
iro
et
al. 2
000
11
7
Su
zu
ki e
t
al, 2
001
50
To
kim
asa
et al.
2008
13
6
Tra
n e
t al.
2017
13
7
vd
Bro
ek e
t al 2018
49
Wilken
et
al. 2
003
11
5
Were there no potential conflicts of interest?
No Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes
If there were potential conflicts of interest, were steps taken to address these?
No NA NA NA NA NA NA NA NA NA Yes NA
Scoring
Number of Yes 18 20 23 17 21 14 13 14 12 20 16 15
Number of not applicable 3 4 4 6 1 12 12 12 13 1 4 6
Number of not enough info 0 0 0 0 0 0 0 1 0 1 1 0 Number of No 7 4 1 4 6 2 3 1 3 6 7 7
Total 28 28 28 27 28 28 28 28 28 28 28 28
Percentage of positive responses 72 83 96 81 78 88 81 93 80 77 70 68
>=70% 1 1 1 1 1 1 1 1 1 1 1 0 <70% 0 0 0 0 0 0 0 0 0 0 0 1
NA = not applicable; NEI = Not enough information