prognostic significance of morphological subtypes in canine malignant lymphomas during chemotherapy
TRANSCRIPT
The
The Veterinary Journal 167 (2004) 158–166
Veterinary Journalwww.elsevier.com/locate/tvjl
Prognostic significance of morphological subtypes incanine malignant lymphomas during chemotherapy
Fr�ed�erique Ponce a,b,c,*, Jean-Pierre Magnol c,d, David Ledieu a, Thierry Marchal d,Vanessa Turinelli a, Karine Chalvet-Monfray e, Corinne Fournel-Fleury a
a Hematology-Cytology-Immunology Laboratory, Departement des Animaux de Compagnie, Ecole Nationale V�et�erinaire de Lyon,
1 Avenue Bourgelat, B.P. 83, Marcy L’Etoile 69280, Franceb The Unit of Internal Medicine, Departement des Animaux de Compagnie, Ecole Nationale V�et�erinaire de Lyon,
1 Avenue Bourgelat, B.P. 83, Marcy L’Etoile 69280, Francec The Unit of Oncology, Departement des Animaux de Compagnie, Ecole Nationale V�et�erinaire de Lyon,
1 Avenue Bourgelat, B.P. 83, Marcy L’Etoile 69280, Franced Pathology Laboratory, D�epartment des Animaux de Compagnie, Ecole Nationale V�et�erinaire de Lyon,
1 Avenue Bourgelat, B.P. 83, Marcy L’Etoile 69280, Francee The Unit of Biomathematics and Epidemiology, Ecole Nationale V�et�erinaire de Lyon, Marcy l’Etoile, France
Accepted 6 October 2003
Abstract
The aim of this study was to determine the response of different morphological subtypes of canine lymphoma to a standardized
therapeutic protocol. Diagnosis of lymphoma was based on cytohistological analysis and immunophenotyping with antibodies
against CD3 and CD79a of an enlarged lymph node or an extranodal mass. Fifty-seven cases were classified according to the
updated Kiel classification adapted to the canine species, into 24 B-cell lymphomas (20 centroblastic polymorphic and four Burkitt-
type subtypes), and 33 T-cell lymphomas (10 pleomorphic mixed, 10 lymphoblastic, eight unclassifiable high grade plasmacytoid,
and five small clear-cell subtypes). All dogs were clinically staged at diagnosis. The protocol used LL-asparaginase, vincristine, cy-
clophosphamide, doxorubicin, and prednisone. First remission duration and overall survival time were evaluated. Although the
T-cell phenotype was associated, on the whole, with a poor prognosis, as previously reported in veterinary and human medicine, the
study showed significant prognostic differences between the B- and the T-cell subtypes of canine lymphoma and suggests that cli-
nico-morphological characterization of the disease is justified in dogs, as in humans.
� 2003 Elsevier Ltd. All rights reserved.
Keywords: Dog; Lymphoma; Classification; Oncology; Chemotherapy
1. Introduction
The first studies on non-Hodgkin�s lymphomas
(NHL) in humans showed that the survival of patients
varied from a few months to several years. Furthermore,
the effectiveness of developing therapies clearly varied
with the histological features. Consequently, clinicians
began to demand much more precise and clinically rel-evant histological diagnoses (Harris et al., 1994, 2000;
Solal-Celigny et al., 1997; Armitage, 1999; Isaacson,
* Corresponding author. Tel.: +33-478-872-585; fax: +33-478-872-
617.
E-mail address: [email protected] (F. Ponce).
1090-0233/$ - see front matter � 2003 Elsevier Ltd. All rights reserved.
doi:10.1016/j.tvjl.2003.10.009
2000; Jaffe et al., 2001). In response to this, the last
classifications of human NHL, the new REAL (Revised
European-American classification of Lymphoid neo-
plasms) (Harris et al., 1994) and WHO (Harris et al.,
2000) classifications, take into account epidemiological,
clinical, morphological, immunophenotypic, and genetic
features and define precise disease entities with their own
prognostic and particular therapeutic schemes (Harris,1999; Jaffe et al., 2001). Therefore, a broad spectrum of
therapeutic options is now available for these different
diseases.
The morphological classifications of canine NHL
have been successively based on the different human
classifications (Breuer and Hermanns, 1998). But, most
F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166 159
of the recent studies, regarding responses to differenttherapeutic protocols and evaluation of prognosis of
NHL have been performed without precise morpho-
logical and immunophenotypical characterization of the
disease, considering canine NHL as a unique entity
(Breuer and Hermanns, 1998; Kiupel et al., 1999; Moore
et al., 2001, 1999; Baskin et al., 2000; Boyce and Kitc-
hell, 2000; Chun et al., 2000). Even if immunophenotype
was determined in some of these therapeutic studies,cytohistological subtypes were never correlated with
survival times (Teske et al., 1994a,b; Starrak et al., 1997;
Kiupel et al., 1999; Chun et al., 2000; Phillips et al.,
2000; Dobson et al., 2001). Only three studies distin-
guished various cytohistological subtypes of B and T
NHL (Teske et al., 1994a,b; Fournel-Fleury et al., 1997,
2002). The most recent took into account the different
clinical presentations along with the different morpho-logical subtypes, in the light of the latest human NHL
classifications (Fournel-Fleury et al., 2002). However,
no therapeutic data were reported.
The aim of the present study was to determine the
response of different morphological subtypes of canine
NHL to a standardized therapeutic protocol and to
address the question whether or not the distinction be-
tween the different subtypes of canine lymphomas, ac-
Table 1
Canine NHL subtypes morphological criteria, according to Fournel-Fleury
B-cell NHL Number
of cases
Histological pattern
Centroblastic
polymorphic
20 Diffuse
Burkitt-typea 4 Diffuse starry-sky
T-cell NHL
Small clear-cell 5 T-zone pattern
Pleomorphic mixed 10 Diffuse
Unclassifiable
high-grade plasmacytoid
8 Diffuse
Lymphoblastic 10 Diffuse
Total 57
MMC, macronucleolated medium-sized-cell.a Burkitt-type on the basis of morphological similarities with the human e
cording to the latest classifications, is clinically justifiedin dogs, as in human medicine.
2. Materials and methods
2.1. Selection of the dogs
One hundred and forty dogs with NHL were pre-sented to the Oncology Unit at the Lyon Veterinary
School between January 1999 and January 2001. Only
dogs without any treatment before diagnosis and with a
complete clinical follow-up during chemotherapy were
included in the study to ensure a population with a
uniform and rigorous protocol. Finally, 57 dogs were
included in this retrospective study.
2.2. Diagnosis and subtypes of NHL (Table 1)
Each diagnosis of NHL was based on the examina-
tion of fine-needle aspirates (FNA) (stained with
May-Gr€unwald-Giemsa) and biopsy specimens (paraf-
fin-embedded sections, stained with haematoxilin and
eosin) from at least one enlarged lymph node or ex-
tranodal mass. In all cases, the immunophenotype was
et al. (1997, 2002)
Cytological criteria Mitotic
index
Mixture of MMC (<20%), small blastic cells
(up to 80%), centroblasts (20–50%), immunoblasts
(<20%)
High
Medium size High
Round nuclei with highly clumped chromatin,
multiple nucleoli
Scant, deeply basophilic cytoplasm, sometimes
vacuolated
Small size Low
Round or slightly irregular nuclei
Extended, unipolar, pale cytoplasm
Small, medium, and large sizes Medium
to high
Irregular nuclei
Pale cytoplasm
Small, medium, and large sizes High
Round or slightly irregular nuclei
Extended, basophilic, plasmacytoid cytoplasm
Medium size High
Round or convoluted nuclei with dusty chromatin
and inconspicuous nucleoli
Poorly extended and basophilic cytoplasm
ntity.

160 F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166
established on fresh or frozen fine-needle aspirates andparaffin-embedded sections, by the use of a polyclonal
antibody against CD3 as a pan-T marker (Ferrer et al.,
1992) and a monoclonal antibody against CD79a as a
pan-B marker (Jones, 1993; Jones et al., 1993). These
procedures have been previously described (Fournel-
Fleury et al., 1997). The cases were classified according
to the updated Kiel classification (Lennert and Feller,
1991) adapted to canine species, and in the light of thecurrent evolution of the human NHL classifications
(REAL and WHO classifications), as previously de-
scribed (Fournel-Fleury et al., 1997, 2002). Samples
were reviewed independently by a cytologist and a
pathologist.
2.3. Clinical staging
All dogs were first evaluated by physical examination,
complete blood count, serum biochemistry, thoracic
radiography, and abdominal ultrasonography. Bone
marrow aspirate was performed in 53 cases, allowing the
dogs to be completely staged at diagnosis according to
the World Health Organization (WHO) V-stage criteria
for canine lymphomas (Owen, 1980). In addition, dogs
were assigned to substage categories of ‘‘a’’ (withoutsystemic signs of illness) or ‘‘b’’ (with systemic signs of
illness) (Fan and Kitchell, 2002).
2.4. Chemotherapy protocol
The combination chemotherapy utilized LL-asparagi-
nase, vincristine, cyclophosphamide, doxorubicin, and
prednisone and was modified from VELCAP protocol(Ogilvie and Moore, 1995). It was maintained until
death. The doses and schedules are provided in Table 3.
The doses of cyclophosphamide were reduced (by 10–
20%) if the dog became neutropenic (<1500 cells/lL).The induction period was defined as the first 5 weeks of
chemotherapy; subsequent treatments were considered
to be maintenance chemotherapy. At first relapse, the
Table 2
Updated Kiel classification of the canine lymphomas (Fournel-Fleury et al.,
(Jaffe et al., 2001) and the domestic animals WHO classification (Valli et al.
Malignant lymphomas
Updated Kiel Human WHO
B-cell neoplasms
Centroblastic polymorphic Diffuse large B-cell lymphoma
Burkitt-type Burkitt lymphoma
T-cell neoplasms
Low-grade malignancy
Small clear-cell (T-zone) Peripheral T-cell lymphoma, unsp
High-grade malignancy
Pleomorphic mixed Peripheral T-cell lymphoma, unsp
Plasmacytoid Peripheral T-cell lymphoma, unsp
Lymphoblastic Precursor T-cell lymphoblastic lym
previous induction protocol was repeated, and the samemaintenance chemotherapy was then applied until the
second relapse. At second relapse, reinduction was
attempted with LL-asparaginase for the first week and
followed by doxorubicin, as the single-agent chemo-
therapy, 3 weeks later and then as a maintenance ther-
apy every 3 weeks, six times in all.
2.5. Assessment of response, first remission duration, and
overall survival time
The response to chemotherapy was evaluated one
week after initiation of treatment. Lymph nodes were
measured with calipers by the same clinician. Complete
response was defined as a 75–100% resolution of lymph
node enlargement and related clinical signs, and nor-
malization of hypercalcaemia. Partial response was de-fined as 50–75% resolution in the largest dimension of
the site of measurable lymphadenopathy and an im-
provement of clinical signs. Stable disease was defined as
0–50% decrease in measurable lymphadenopathy, with
no change in clinical signs. No response was defined as a
further increase of measurable lymphadenopathy, with
or without a worsening of clinical signs (Lucroy et al.,
1998). Dogs were clinically evaluated every 3 weeksduring maintenance therapy. The duration of the first
remission (FR) was defined as the time (in months) be-
tween the start of treatment and the first relapse (re-
currence of lymphadenopathy or extranodal mass
assessed by cytological examination). Overall survival
time (OST) was defined as the time between the start of
treatment and the death of the dog.
2.6. Statistical analysis
First remission and OST curves were estimated by
Kaplan–Meyer statistics for all the different subtypes of
lymphoma and tested using Mantel�s simplified v2 of thelog-rank test (Laplanche et al., 1997; Petrie and Watson,
2000). Probability values p < 0:05 were considered
1997, 2002): possible correlation with the human WHO classification
, 2002)
Domestic animals WHO
Diffuse large B-cell lymphoma
Burkitt-type lymphoma
ecified Not described
ecified Not described
ecified Not described
phoma/leukemia T-cell lymphoblastic leukemia/lymphoma

Table 3
Chemotherapy protocol
Drug name Dose Route Frequency
Five-week induction phase
LL-Asparaginase 400 IU/kg IM Once weekly, on week 1
Vincristine 0.75 mg/m2 IV Once weekly, on weeks 2–5
Cyclophosphamide 250 mg/m2 PO Once weekly, on weeks 2, 5
Prednisone 1 mg/kg PO Once daily
Maintenance phase during remission
Vincristine 0.75 mg/m2 IV Every 3 weeks
Cyclophosphamide 250 mg/m2 PO Every 3 weeks
Prednisone 1 mg/kg PO Every 2 days
Same protocol after first relapse
Induction phase after second relapse
LL-Asparaginase 400 IU/kg IM Once weekly, on week 1
Maintenance phase after second relapse
Doxorubicin 30 mg/m2 IV On week 4, every 3 weeks
IM, intramuscular; IV, intravenous; and PO, per os.
F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166 161
significant for all statistical tests. All statistical analyses
were done with Microsoft Excel 2000.
3. Results
This series of 57 cases included 24 B-cell and 33 T-cellNHL. Six different morphological subtypes of canine
NHL, two subtypes of the B-cell, and four of the T-cell
lineage, entered in this study (Tables 1 and 2). The main
epidemiological, clinical, and survival data are summa-
rized in Tables 4 and 5 for each morphological subtypes.
Among the B-cell NHL, 20 cases were centroblastic
polymorphic and four were Burkitt-type. The centrob-
Table 4
Epidemiological and clinical data of the 57 cases according to morphologica
Morphological
subtypes
Breed Age (years) Sex Ad
La Med Sm M F Gen
CP (20) 17 2 1 7.8 (4–11) 14 6 20
B (4) 4 0 0 8 (7–10) 3 1 4
SCC (5) 3 2 0 8.9 (6–11) 2 3 3
PM (10) 10 0 0 8.4 (5–15) 5 5 10
P (8) 8 0 0 5.8 (1–11) 4 4 7
LB (10) 10 0 0 5.3 (1–10) 7 3 6
Morphological
subtypes
Clinical stage
I IIa IIb IIIa IIIb IVa IVb
CP (20) 0 0 0 12 0 4 0
B (4) 0 0 0 0 0 0 4
SCC (5) 0 3 0 2 0 0 0
PM (10) 0 0 0 0 9 0 1
P (8) 0 0 0 1 0 0 1
LB (10) 0 0 0 0 0 0 3
CP, centroblastic polymorphic B lymphoma; B, Burkitt-type B lympho
lymphoma; P, plasmacytoid T lymphoma; LB, lymphoblastic T lymphoma;
megaly; gen, generalized; loc, localized; MM, mediastinal mass; BM, bone m
ND, not determined.
lastic polymorphic subtype was associated with a gen-
eralized lymphadenopathy which developed over 1–4
weeks (median, 2 weeks) without any other clinical
signs. Dogs were in clinical stages IIIa–Va. Two dogs
developed gastrointestinal signs (vomiting and diar-
rhoea) during the induction phase after the administra-
tion of cyclophosphamide, but they responded well toantiemetics and intestinal protectants (smectite, Smecta,
Ipsen). One dog became neutropenic during the induc-
tion cycle and had a dose reduction (10%) for
cyclophosphamide.
Concerning the Burkitt-type subtype, in addition to a
generalized lymphadenopathy, all dogs presented with
alimentary infiltration, assessed by cytological
l subtypes of canine lymphoma
MM Hepato-
megaly
Spleno-
megaly
Gut BM Hyper
calcaemiaLoc
0 0 3 7 0 4 0
0 0 4 4 4 ND 1
2 0 0 0 0 0 0
0 0 1 1 0 0 0
1 4 7 7 0 6 4
4 8 3 7 0 7 3
Va Vb
4 0
0 0
0 0
0 0
1 5
0 7
ma; SCC, small clear-cell T lymphoma; PM, pleomorphic mixed T
La, large; Med, medium; Sm, small; M, male; F, female; Ad, adeno-
arrow; and MFR and OST in months except written indication.
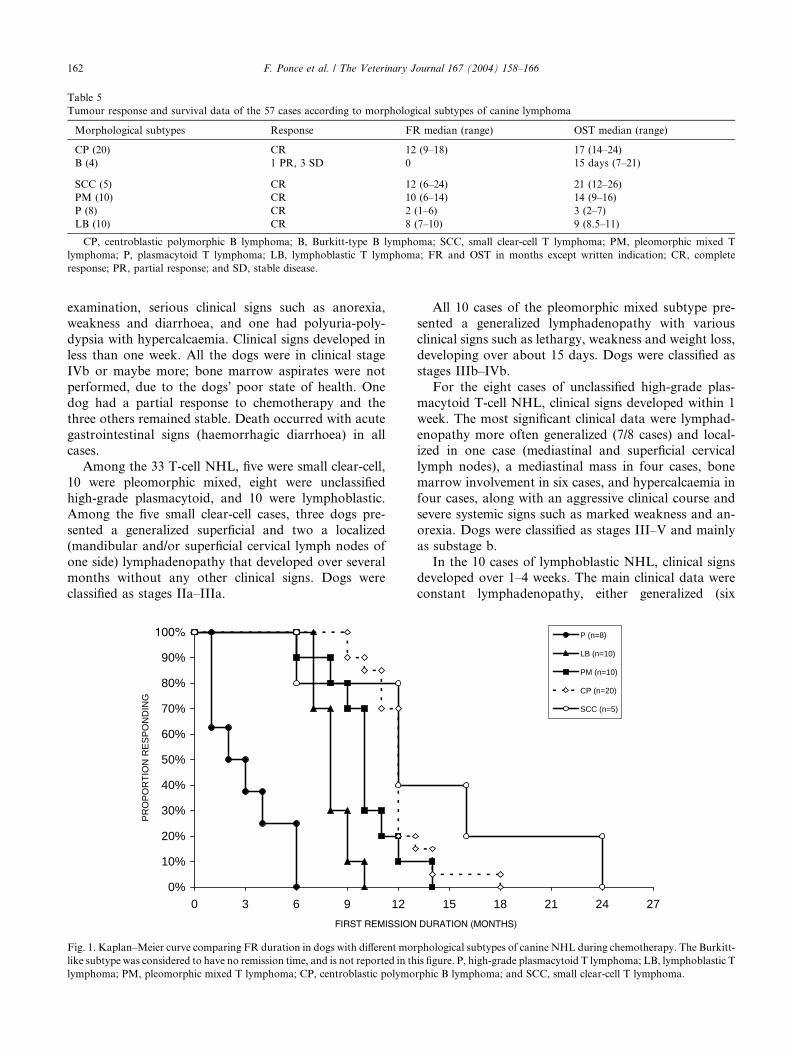
Table 5
Tumour response and survival data of the 57 cases according to morphological subtypes of canine lymphoma
Morphological subtypes Response FR median (range) OST median (range)
CP (20) CR 12 (9–18) 17 (14–24)
B (4) 1 PR, 3 SD 0 15 days (7–21)
SCC (5) CR 12 (6–24) 21 (12–26)
PM (10) CR 10 (6–14) 14 (9–16)
P (8) CR 2 (1–6) 3 (2–7)
LB (10) CR 8 (7–10) 9 (8.5–11)
CP, centroblastic polymorphic B lymphoma; B, Burkitt-type B lymphoma; SCC, small clear-cell T lymphoma; PM, pleomorphic mixed T
lymphoma; P, plasmacytoid T lymphoma; LB, lymphoblastic T lymphoma; FR and OST in months except written indication; CR, complete
response; PR, partial response; and SD, stable disease.
162 F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166
examination, serious clinical signs such as anorexia,weakness and diarrhoea, and one had polyuria-poly-
dypsia with hypercalcaemia. Clinical signs developed in
less than one week. All the dogs were in clinical stage
IVb or maybe more; bone marrow aspirates were not
performed, due to the dogs� poor state of health. One
dog had a partial response to chemotherapy and the
three others remained stable. Death occurred with acute
gastrointestinal signs (haemorrhagic diarrhoea) in allcases.
Among the 33 T-cell NHL, five were small clear-cell,
10 were pleomorphic mixed, eight were unclassified
high-grade plasmacytoid, and 10 were lymphoblastic.
Among the five small clear-cell cases, three dogs pre-
sented a generalized superficial and two a localized
(mandibular and/or superficial cervical lymph nodes of
one side) lymphadenopathy that developed over severalmonths without any other clinical signs. Dogs were
classified as stages IIa–IIIa.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
0 3 6 9 12
PR
OP
OR
TIO
N R
ES
PO
ND
ING
Fig. 1. Kaplan–Meier curve comparing FR duration in dogs with different mor
like subtype was considered to have no remission time, and is not reported in th
lymphoma; PM, pleomorphic mixed T lymphoma; CP, centroblastic polymo
All 10 cases of the pleomorphic mixed subtype pre-sented a generalized lymphadenopathy with various
clinical signs such as lethargy, weakness and weight loss,
developing over about 15 days. Dogs were classified as
stages IIIb–IVb.
For the eight cases of unclassified high-grade plas-
macytoid T-cell NHL, clinical signs developed within 1
week. The most significant clinical data were lymphad-
enopathy more often generalized (7/8 cases) and local-ized in one case (mediastinal and superficial cervical
lymph nodes), a mediastinal mass in four cases, bone
marrow involvement in six cases, and hypercalcaemia in
four cases, along with an aggressive clinical course and
severe systemic signs such as marked weakness and an-
orexia. Dogs were classified as stages III–V and mainly
as substage b.
In the 10 cases of lymphoblastic NHL, clinical signsdeveloped over 1–4 weeks. The main clinical data were
constant lymphadenopathy, either generalized (six
15 18 21 24 27
P (n=8)
LB (n=10)
PM (n=10)
CP (n=20)
SCC (n=5)
phological subtypes of canine NHL during chemotherapy. The Burkitt-
is figure. P, high-grade plasmacytoid T lymphoma; LB, lymphoblastic T
rphic B lymphoma; and SCC, small clear-cell T lymphoma.

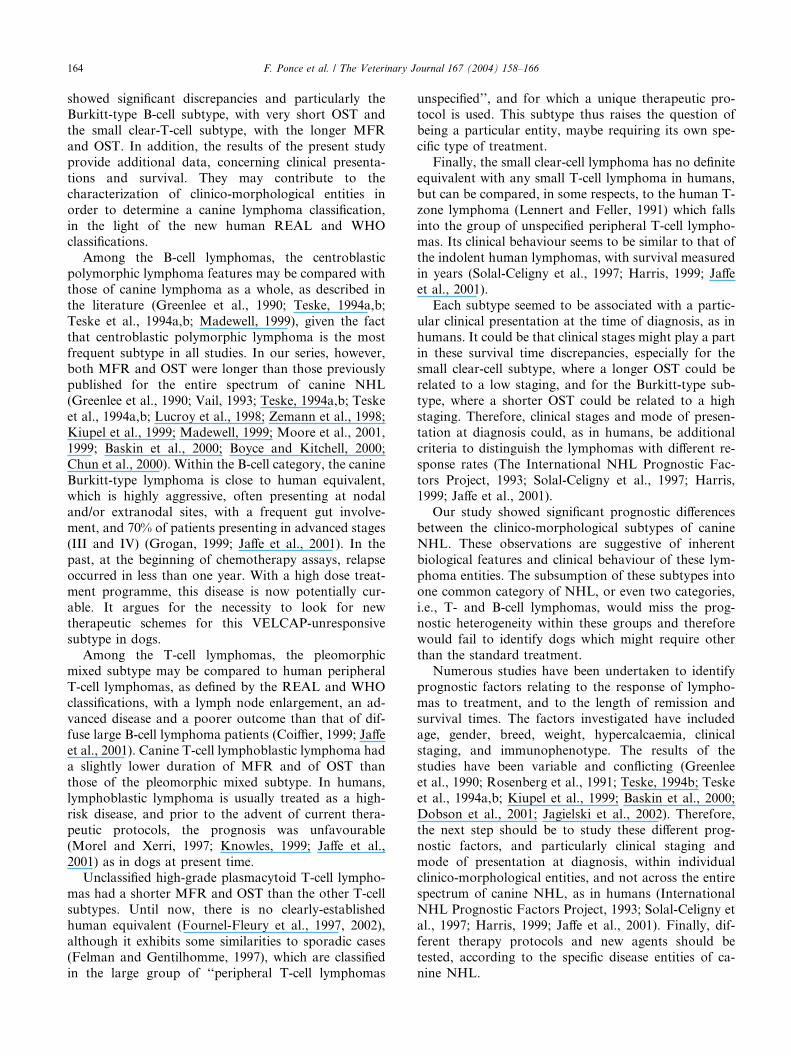
Fig. 2. Kaplan–Meier curve comparing OST in dogs with different morphological subtypes of canine NHL during chemotherapy. B, Burkitt-type B
lymphoma; P, high-grade plasmacytoid T lymphoma; LB, lymphoblastic T lymphoma; PM, pleomorphic mixed T lymphoma; CP, centroblastic
polymorphic B lymphoma; and SCC, small clear-cell T lymphoma.
F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166 163
cases) or localized (four cases with mandibular, super-
ficial cervical or mesenteric lymphadenopathy), a me-
diastinal mass in eight cases, bone marrow involvement
in seven cases, and hypercalcaemia in three cases. Seri-ous clinical signs such as weakness, anorexia, weight
loss, dyspnoea, and vomiting were noticed. Dogs were
classified as stages IVb–Vb.
The observed discrepancies between MFR or OST of
the different subtypes, based on the survival curves
(Figs. 1 and 2), were significant (p < 0:05).
4. Discussion
In human medicine, the oncologist�s common goal
has been to find a lymphoma classification that predictsoutcomes and responses to chemotherapy. Hence, in the
group of human NHL, there are a lot of distinct diseases
with their own prognostic relevance, associated with
distinctive responses to therapy, and for which unique
treatments are appropriate (Jaffe et al., 2001). For ex-
ample, gastric lymphomas often respond to the eradi-
cation of Helicobacter pylori, Burkitt�s lymphoma is
treated with a high dose treatment programme, whereasindolent lymphomas without pejorative prognostic fac-
tors are not treated until transformation to a high-grade
type (Solal-Celigny et al., 1997; Armitage, 1999; Isaac-
son, 2000; Jaffe et al., 2001).
In contrast, many canine lymphoma therapies have
been tested over the last 30 years without any distinction
between morphological subtypes (Greenlee et al., 1990;
Vail, 1993; Teske, 1994a,b; Teske et al., 1994a,b; Lucroy
et al., 1998; Zemann et al., 1998; Kiupel et al., 1999;
Madewell, 1999; Moore et al., 2001, 1999; Baskin et al.,2000; Boyce and Kitchell, 2000; Chun et al., 2000), ex-
cept for only one recent study on 49 cases of canine
lymphoma (Dobson et al., 2001). Nevertheless, in this
last study, the absence of low grade tumours, the low
percentage of T-cell lymphomas (13%), the questionable
grouping of the Burkitt, and the lymphoblastic subtypes
may be responsible for the lack of significant prognostic
differences between the identified morphological sub-types. In the present study, median OST was 14 months,
which is close to the majority of previously reported
veterinary data.
T-cell lymphomas, both in humans (Melnyk et al.,
1997; Solal-Celigny et al., 1997; Gisselbrecht et al., 1998;
Jaffe et al., 2001) and in dogs (Teske et al., 1994a,b;
Ruslander et al., 1997; Starrak et al., 1997; Kiupel et al.,
1999; Phillips et al., 2000; Dobson et al., 2001), are as-sociated with a poor prognosis. In our study, a com-
parison between the most frequently encountered canine
B and T-cell subtypes (i.e., the centroblastic polymor-
phic B-cell lymphoma and the pleomorphic mixed T-cell
lymphoma) showed that the MFR and OST were
significantly shorter for the latter. Consequently, com-
parisons between these most frequent subtypes con-
firmed that T-cell phenotype may be a prognostic factorassociated with a poor outcome. However, within each
group of B- and T-cell lymphomas, the various subtypes
164 F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166
showed significant discrepancies and particularly theBurkitt-type B-cell subtype, with very short OST and
the small clear-T-cell subtype, with the longer MFR
and OST. In addition, the results of the present study
provide additional data, concerning clinical presenta-
tions and survival. They may contribute to the
characterization of clinico-morphological entities in
order to determine a canine lymphoma classification,
in the light of the new human REAL and WHOclassifications.
Among the B-cell lymphomas, the centroblastic
polymorphic lymphoma features may be compared with
those of canine lymphoma as a whole, as described in
the literature (Greenlee et al., 1990; Teske, 1994a,b;
Teske et al., 1994a,b; Madewell, 1999), given the fact
that centroblastic polymorphic lymphoma is the most
frequent subtype in all studies. In our series, however,both MFR and OST were longer than those previously
published for the entire spectrum of canine NHL
(Greenlee et al., 1990; Vail, 1993; Teske, 1994a,b; Teske
et al., 1994a,b; Lucroy et al., 1998; Zemann et al., 1998;
Kiupel et al., 1999; Madewell, 1999; Moore et al., 2001,
1999; Baskin et al., 2000; Boyce and Kitchell, 2000;
Chun et al., 2000). Within the B-cell category, the canine
Burkitt-type lymphoma is close to human equivalent,which is highly aggressive, often presenting at nodal
and/or extranodal sites, with a frequent gut involve-
ment, and 70% of patients presenting in advanced stages
(III and IV) (Grogan, 1999; Jaffe et al., 2001). In the
past, at the beginning of chemotherapy assays, relapse
occurred in less than one year. With a high dose treat-
ment programme, this disease is now potentially cur-
able. It argues for the necessity to look for newtherapeutic schemes for this VELCAP-unresponsive
subtype in dogs.
Among the T-cell lymphomas, the pleomorphic
mixed subtype may be compared to human peripheral
T-cell lymphomas, as defined by the REAL and WHO
classifications, with a lymph node enlargement, an ad-
vanced disease and a poorer outcome than that of dif-
fuse large B-cell lymphoma patients (Coiffier, 1999; Jaffeet al., 2001). Canine T-cell lymphoblastic lymphoma had
a slightly lower duration of MFR and of OST than
those of the pleomorphic mixed subtype. In humans,
lymphoblastic lymphoma is usually treated as a high-
risk disease, and prior to the advent of current thera-
peutic protocols, the prognosis was unfavourable
(Morel and Xerri, 1997; Knowles, 1999; Jaffe et al.,
2001) as in dogs at present time.Unclassified high-grade plasmacytoid T-cell lympho-
mas had a shorter MFR and OST than the other T-cell
subtypes. Until now, there is no clearly-established
human equivalent (Fournel-Fleury et al., 1997, 2002),
although it exhibits some similarities to sporadic cases
(Felman and Gentilhomme, 1997), which are classified
in the large group of ‘‘peripheral T-cell lymphomas
unspecified’’, and for which a unique therapeutic pro-tocol is used. This subtype thus raises the question of
being a particular entity, maybe requiring its own spe-
cific type of treatment.
Finally, the small clear-cell lymphoma has no definite
equivalent with any small T-cell lymphoma in humans,
but can be compared, in some respects, to the human T-
zone lymphoma (Lennert and Feller, 1991) which falls
into the group of unspecified peripheral T-cell lympho-mas. Its clinical behaviour seems to be similar to that of
the indolent human lymphomas, with survival measured
in years (Solal-Celigny et al., 1997; Harris, 1999; Jaffe
et al., 2001).
Each subtype seemed to be associated with a partic-
ular clinical presentation at the time of diagnosis, as in
humans. It could be that clinical stages might play a part
in these survival time discrepancies, especially for thesmall clear-cell subtype, where a longer OST could be
related to a low staging, and for the Burkitt-type sub-
type, where a shorter OST could be related to a high
staging. Therefore, clinical stages and mode of presen-
tation at diagnosis could, as in humans, be additional
criteria to distinguish the lymphomas with different re-
sponse rates (The International NHL Prognostic Fac-
tors Project, 1993; Solal-Celigny et al., 1997; Harris,1999; Jaffe et al., 2001).
Our study showed significant prognostic differences
between the clinico-morphological subtypes of canine
NHL. These observations are suggestive of inherent
biological features and clinical behaviour of these lym-
phoma entities. The subsumption of these subtypes into
one common category of NHL, or even two categories,
i.e., T- and B-cell lymphomas, would miss the prog-nostic heterogeneity within these groups and therefore
would fail to identify dogs which might require other
than the standard treatment.
Numerous studies have been undertaken to identify
prognostic factors relating to the response of lympho-
mas to treatment, and to the length of remission and
survival times. The factors investigated have included
age, gender, breed, weight, hypercalcaemia, clinicalstaging, and immunophenotype. The results of the
studies have been variable and conflicting (Greenlee
et al., 1990; Rosenberg et al., 1991; Teske, 1994b; Teske
et al., 1994a,b; Kiupel et al., 1999; Baskin et al., 2000;
Dobson et al., 2001; Jagielski et al., 2002). Therefore,
the next step should be to study these different prog-
nostic factors, and particularly clinical staging and
mode of presentation at diagnosis, within individualclinico-morphological entities, and not across the entire
spectrum of canine NHL, as in humans (International
NHL Prognostic Factors Project, 1993; Solal-Celigny et
al., 1997; Harris, 1999; Jaffe et al., 2001). Finally, dif-
ferent therapy protocols and new agents should be
tested, according to the specific disease entities of ca-
nine NHL.
F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166 165
References
Armitage, J.O., 1999. Goals of a lymphoma classification for the
oncologist. In: Mason, D.Y., Harris, N.L. (Eds.), Human Lym-
phoma: Clinical Implications of the REAL Classification. Springer-
Verlag, London, p. 3(1-4).
Baskin, C.R., Couto, C.G., Wittum, T.E., 2000. Factors influencing
first remission and survival in 145 dogs with lymphoma: a
retrospective study. Journal of American Animal Hospital Asso-
ciation 36, 404–409.
Boyce, K.L., Kitchell, B.E., 2000. Treatment of canine lymphoma with
COPLA/LVP. Journal of American Animal Hospital Association
36, 395–403.
Breuer, W., Hermanns, W., 1998. Classification of lymphohaemopoi-
etic neoplasias (LHN) in dogs and cats. European Journal of
Veterinary Pathology 4, 5–20.
Chun, R., Garrett, L.D., Vail, D.M., 2000. Evaluation of a high-dose
chemotherapy protocol with no maintenance therapy for dogs with
lymphoma. Journal of Veterinary Internal Medicine 14, 120–124.
Coiffier, B., 1999. Optimal treatment strategies for peripheral T cell
lymphoma (unspecified category). In: Mason, D.Y., Harris, N.L.
(Eds.), Human Lymphoma: Clinical Implications of the REAL
Classification. Springer-Verlag, London, p. 29(1-5).
Dobson, J.M., Blackwood, L.B., Mc Innes, E.F., Bostock, D.E.,
Nicholls, P., Hoather, T.M., Tom, B.D., 2001. Prognostic variables
in canine multicentric lymphosarcoma. Journal of Small Animal
Practice 42, 377–384.
Fan, T.M., Kitchell, B.E., 2002. An update on diagnosis and treating
canine lymphosarcoma. Veterinary Medicine, 58–67.
Felman, P., Gentilhomme, O., 1997. In: Arnette (Ed.), Atlas de
cytopathologie ganglionnaire. Paris, France.
Ferrer, L., Fondevila, D., Rabanal, R., Ramis, A., 1992. Detection of
T lymphocytes in canine tissue embedded in paraffin wax by means
of antibody to CD3 antigen. Journal of Comparative Pathology
106, 311–314.
Fournel-Fleury, C., Magnol, J.P., Bricaire, P., Marchal, T., Chabanne,
L., Delverdier, A., Bryon, P.A., Felman, P., 1997. Cytohistological
and immunological classification of canine malignant lymphomas.
Comparison with human non-Hodgkin�s lymphomas. Journal of
Comparative Pathology 117, 35–39.
Fournel-Fleury, C., Ponce, F., Felman, P., Blavier, A., Bonnefont, C.,
Chabanne, L., Marchal, T., Cadore, J.L., Goy-Thollot, I., Ledieu,
D., Ghernati, I., Magnol, J.P., 2002. Canine T-cell lymphomas: a
morphological, immunological, and clinical study of 46 new cases.
Veterinary Pathology 39, 92–109.
Gisselbrecht, C., Gaulard, P., Lepage, E., Coiffier, B., Briere, J.,
Haioun, C., Cazals-Hatem, D., Bosly, A., Xerri, L., Tilly, H.,
Berger, F., Bouhabdallah, R., Diebold, J., 1998. Prognostic
significance of T-cell phenotype in aggressive non-Hodgkin�slymphomas. Blood 92, 76–82.
Greenlee, P.G., Filippa, D.A., Quimby, F.W., Patnaik, A.K., Calvano,
S.E., Matus, R.E., Kimmel, M., Hurvitz, A.I., Lieberman, P.H.,
1990. Lymphomas in dogs. A morphologic, immunologic and
clinical study. Cancer 66, 480–490.
Grogan, T.M., 1999. Morphologic, immunologic and genetic features
of Burkitt�s and Burkitt-like lymphomas. In: Mason, D.Y., Harris,
N.L. (Eds.), Human Lymphoma: Clinical Implications of the
REAL Classification. Springer-Verlag, London, p. 41(1-7).
Harris, N.L., 1999. Introduction and rationale for the REAL
classification. In: Mason, D.Y., Harris, N.L. (Eds.), Human
Lymphoma: Clinical Implications of the REAL Classification.
Springer-Verlag, London, p. 1(1-7).
Harris, N.L., Jaffe, E.S., Diebold, J., Flandrin, G., Muller-Hermeling,
H.K., Vardiman, J., Lister, T.A., Bloomfield, C.D., 2000. The
World Health Organization classification of neoplasms of the
hematopoietic and lymphoid tissues: report of the clinical advisory
committee meeting, Airlie house, Virginia, November, 1997. The
Hematology Journal 1, 53–66.
Harris, N.L., Jaffe, E.S., Stein, H., Banks, P.M., Chan, J.K.C., Cleary,
M.L., Delsol, G., De Woolf-Peeters, C., Falini, B., Gatter, K.C.,
Grogan, T.M., Isaacson, P.G., Knowles, D.M., Mason, D.Y.,
Muller-Hermeling, H.K., Pileri, S.A., Piris, M.A., Ralphkiaer, E.,
Warnke, R.A., 1994. A revised European-American classification
of lymphoid neoplasms: a proposal from the international study
group. Blood 84, 1361–1392.
Isaacson, P.G., 2000. The current status of lymphoma classification. A
review. British Journal of Haematology 109, 258–266.
Jaffe, E.S., Harris, N.L., Stein, H., Vardiman, J.W. (Eds.), 2001. World
Health Organization Classification of Tumours. Pathology and
Genetics of Tumours of Haematopoietic and Lymphoid Tissues.
IARC Press, Lyon, France, p. 351.
Jagielski, D., Lechowski, R., Hoffmann-Jagielska, M., Winiarczyk, S.,
2002. A retrospective study of the incidence and prognostic factors
of multicentric lymphoma in dogs (1998–2000). Journal of Veter-
inary Mededicine A 49, 419–424.
Jones, M., 1993. Peptide Immunisation as a Source of Cross-species
Reactive Antisera Recognizing Leukocyte Differentiation Anti-
gens. Immunological Reagents for the Study of Disease in
Companion Animals. The Wellcome Trust, London.
Jones, M., Cordell, J.L., Beyers, A.D., Tse, A.G.D., Mason, D.Y.,
1993. Detection of T and B cells in many animal species using
cross-reactive anti-peptide antibodies. Journal of Immunol 150,
5429–5435.
Kiupel, M., Teske, E., Bostock, D., 1999. Pronostic factors for
treated canine malignant lymphoma. Veterinary Pathology 36,
292–300.
Knowles, D.M., 1999. Morphologic, immunologic and genetic features
of precursor T and B cell neoplasms. In: Mason, D.Y., Harris, N.L.
(Eds.), Human Lymphoma: Clinical Implications of the REAL
Classification, vol. 43. Springer, London, pp. 1–2.
Laplanche, A., ComNougu�e, C., Flamant, R., 1997. M�ethodes
Statistiques Appliqu�ees �a la Recherche Clinique. M�edecine-Sci-
ences Flammarion, 164.
Lennert, K., Feller, C.A., 1991. Histologie des Lymphomes Malins
NonHodgkiniens selon la Classification de Kiel Actualis�ee. Doin,
Paris, p. 307.
Lucroy, M.D., Phillips, B.S., Kraegel, S.A., Simonson, E.R., Made-
well, B., 1998. Evaluation of single-agent Mitoxantrone as chemo-
therapy for relapsing canine lymphoma. Journal of Veterinary
Internal Medicine 12, 325–329.
Madewell, B.R., 1999. Diagnosis, assessment of prognosis, and
treatment of dogs with lymphoma: the sentinel changes (1973–
1999). Journal of Veterinary Internal Medicine 13, 393–394.
Melnyk, A., Rodriguez, W.C., Pugh, W.C., Cabannillas, F., 1997.
Evaluation of the revised European-American lymphoma classifi-
cation confirms the clinical relevance of immunophenotype in 560
cases of aggressive non-Hodgkin�s lymphoma. Blood 89, 4514–
4520.
Moore, A.S., Cotter, S.M., Rand, W.M., Wood, C.A., Williams, L.E.,
London, C.A., Frimberger, A.E., L�Heureux, D.A., 2001. Evalu-
ation of a discontinuous treatment protocol (VELCAP-S) for
canine lymphoma. Journal of Veterinary Internal Medicine 15,
348–354.
Moore, A.S., London, C.A., Wood, C.A., Williams, L.E., Cotter,
S.M., L�Heureux, D.A., Frimberger, A.E., 1999. Lomustine
(CCNU) for the treatment of resistant lymphoma in dogs. Journal
of Veterinary Internal Medicine 13, 395–398.
Morel, P., Xerri, L., 1997. Lymphomes lymphoblastiques. In: Solal-
Celigny, Ph., Brousse, N., Ferm�e, Ch., Gisselbrecht, Ch., Reyes, F.,
Coiffier, B. (Eds.), Lymphomes. Frison Roche, Paris, pp. 266–272.
Ogilvie, G.K., Moore, A.S., 1995. Management of specific diseases:
lymphoma. In: Managing the Veterinary Cancer Patient. Veteri-
nary Learning Systems, Trenton, NJ, pp. 228–259.

166 F. Ponce et al. / The Veterinary Journal 167 (2004) 158–166
Owen, L.N., 1980. WHO. In: Owen, L.N. (Ed.), TNM Classification of
Tumors in Domestic Animals. Geneva, p. 47.
Petrie, A., Watson, P., 2000. Statistics for Veterinary and Animal
Science, second ed. Blackwell Science, London. p. 243.
Phillips, B.S., Kass, P.H., Naydan, D.K., Winthrop, M.D., Griffey,
S.M., Madewell, B.R., 2000. Apoptotic and proliferation indexes in
canine lymphoma. Journal of Veterinary Diagnostic Investigation
12, 111–117.
Rosenberg, M.P., Matus, R.E., Patnaik, A.K., 1991. Prognostic
factors in dogs with lymphoma and associated hypercalcemia.
Journal of Veterinary Internal Medicine 5, 268–271.
Ruslander, D.A., Gebhard, D.H., Tompkins, M.B., Grindem, C.B.,
Page, R.L., 1997. Immunophenotypic characterization of canine
lymphoproliferative disorders. In Vivo 11, 169–172.
Solal-Celigny, P., Brousse, N., Ferm�e, C., Gisselbrecht, C., Reyes, F.,
Coiffier, B., 1997. Lymphomes. Lymphomes NonHodgkiniens –
Maladie de Hodgkin, 3�eme ed. Frison-Roche, Paris, p. 527.
Starrak, G.S., Berry, C.R., Page, R.L., Johnson, J.L., Thrall, D.E.,
1997. Correlation between thoracic radiographic changes and
remission/survival duration in 270 dogs with lymphosarcoma.
Veterinary Radiology Ultrasound 38, 411–418.
Teske, E., 1994a. Canine malignant lymphoma: a review and compar-
ison with human non-Hodgkin�s lymphomas. Veterinary Quarterly
16, 209–219.
Teske, E., 1994b. Prognostic factors for malignant lymphoma in the
dog: an update. Veterinary Quarterly 16 (suppl. 1), 29s–31s.
Teske, E., Van Heerde, P., Rutteman, G.R., Kurzman, I.D., Moore,
P.F., Mac Ewen, G., 1994a. Prognostic factors for treatment of
malignant lymphoma in dogs. Journal of American Veterinary
Medical Association 205, 1722–1728.
Teske, E., Wisman, P., Moore, P.F., Van Heerde, P., 1994b. Histologic
classification and immuno-phenotyping of canine non-Hodgkin�slymphomas: unexpected high frequency of T-cell lymphomas with
B-cell morphology. Experimental Haematology 22, 1179–1187.
The International Non-Hodgkin�s Lymphoma Prognostic Factors
Project, 1993. A predictive model for aggressive non-Hodgkin�slymphoma. New England Journal of Medicine 329, 987.
Vail, D.M., 1993. Recent advances in chemotherapy for lymphoma of
dogs and cats. Compendium of Continuing Education 15, 1031.
Valli, V.E., Jacobs, R.M., Parodi, A.L., Vernau, W., Moore, PF.,
2002. WHO International Histological Classification of Hemato-
poietic Tumors of Domestic Animals. Second series, vol. VIII.
Armed Forces Institute of Pathology, Washington, DC, p. 190.
Zemann, B.I., Moore, A.S., Rand, W.M., Mason, G., Ruslander,
D.M., Frimberger, A.E., Wood, C.A., L�Heureux, D.A., Gliatto,
J., Cotter, S.M., 1998. A combination chemotherapy protocol
(VELCAP-L) for dogs with lymphoma. Journal of Veterinary
Internal Medicine 12, 465–470.