prescription drug use among pregnant women in opioid maintenance treatment
TRANSCRIPT

Prescription drug use among pregnant women inopioid Maintenance Treatment
Ingunn Olea Lund1, Svetlana Skurtveit1,2, Anders Engeland2,3, Kari Furu2,4, Edle Ravndal1 &Marte Handal2
SERAF—Norwegian Centre for Addiction Research, University of Oslo, Oslo, Norway,1 Department of Pharmacoepidemiology, Norwegian institute of PublicHealth, Oslo, Norway,2 Department of Public Health and Primary Health Care, University of Bergen, Oslo, Norway3 and Department of Pharmacy, University ofTromsø, Tromsø, Norway4
ABSTRACT
Aims This study describes the use of prescribed drugs among women in opioid maintenance treatment (OMT)prior to, and during, pregnancy. Design This cohort study was based on data from two nationwide databases:the Medical Birth Registry of Norway and the Norwegian Prescription Database. Setting Norway, 2004–2010.Participants OMT drugs were dispensed to 138 women with 159 pregnancies. Measurements All prescriptiondrugs dispensed to women in OMT three months prior to, and during, pregnancy were studied. Amounts of benzodi-azepines, z-hypnotics and opioid analgesics dispensed during pregnancy were studied and bivariate analysis was usedto study neonatal outcomes of OMT pregnancies with and without such co-medication. Findings The prevalence ofprescription drug use by pregnant OMT women was high both during the three-month period prior to (69%), andduring (81%), pregnancy. The proportion of pregnant women that was dispensed anti-infectives (48%) and/or drugsacting on the nervous system (45%) during any time in pregnancy was especially high. In 21%, 15% and 13% of thepregnancies the women were dispensed benzodiazepine anxiolytics, opioid analgesics or benzodiazepine hypnoticsrespectively. Only 5% of the OMT women were dispensed antidepressants. Malformations were significantly morecommon among children born to mothers in OMT that received co-medication with opioids, benzodiazepines orz-hypnotics. Conclusions A higher proportion of women in opioid maintenance treatment in Norway use prescrip-tion drugs prior to, and during, pregnancy than pregnant women in the general population. Co-medication with drugswith abuse potential may increase the risk of adverse pregnancy outcomes and this need to be further addressed.
Keywords Antidepressants, benzodiazepines, co-medication, maternal outcomes, neonatal outcomes, opioids,opioid maintenance treatment, pregnancy, prescription drugs.
Correspondence to: Ingunn Olea Lund, SERAF—Norwegian Centre for Addiction Research, Postboks 1039 Blindern, 0315 Oslo, Norway.E-mail: [email protected] 25 August 2011; initial review completed 8 October 2011; final version accepted 3 August 2012
INTRODUCTION
Opioid dependence in pregnant women is a major publichealth issue associated with high costs to society and at apersonal level for women and their children [1,2]. OpioidMaintenance treatment (OMT) is considered the besttreatment option for most pregnant women with opioiddependence [3]; several studies have reported that suchtreatment improves pregnancy outcomes [4–8]. OMTduring pregnancy is not without risks, however—adversepregnancy and neonatal outcomes have been described[9–11].
With a high prevalence of psychiatric and somaticproblems [7,12,13], this patient group may be in need
of additional prescription medication. Co-occurringdisorders are common in pregnant OMT women. Theprevalence of depression is especially high—estimatedto 35–73% [7,8,14,15]. Hence, the use of prescriptiondrugs for depression and other conditions is expectedto be high. However, use of drugs during pregnancy isgenerally complicated because of the limited knowledgewith regard to beneficial and possible adverse effectsfor both the mother and the fetus. This is even morecomplicated for the vulnerable patient group thatpregnant OMT women constitute. Knowledge on poten-tial risks from co-medication with other prescriptiondrugs in pregnant OMT women is scarce and existingresearch is based on interviews and questionnaires
RESEARCH REPORT doi:10.1111/j.1360-0443.2012.04049.x
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction

[7,13]. Such self-reported information may be incom-plete and biased.
Owing to limited knowledge about co-medication inpregnant OMT women some women may not receivethe medications they need because physicians fear thatco-medication may further increase the risk of adversepregnancy and neonatal outcomes. However, somewomen may receive co-medication that may be harmful,such as benzodiazepines, which may increase the risksof adverse neonatal outcomes [16–18]. Malformations,such as cleft lip and cleft palate, have been reported[18,19]. Z-hypnotics have similar mechanisms of actionsas benzodiazepines and limited human research has beenconducted on use during pregnancy [18]. Treatment ofpain in OMT patients is challenging because some anal-gesics, like opioids, may predispose to relapse to drug-seeking behavior and over-medication may occur [20].However, the opioid dose which is sufficient to avoid with-drawal symptoms does not contribute to pain relief andeffective pain treatment is therefore required [20]. Bothover- and under-medication endangers the treatment sta-bility and may cause a relapse to illegal substance use.The risk of drug-seeking behavior may increase if womenare prescribed additional medicines with abuse potentialfrom others than the medical doctor prescribing OMT.Additional opioids may also increase the risk of negativeneonatal outcomes [18].
There is a need for a methodological approach thatwill offer detailed information on co-medication amongstpregnant OMT women during pregnancy. Population-based registries of births and dispensed prescribed drugsin Norway offer a unique opportunity to perform prospec-tive studies on prescription drug use in a nationwidecohort of pregnant OMT women.
The main aims of the present study were to describeprescription drug use among women in OMT prior topregnancy and during the first, second and third trim-ester of pregnancy, and to describe in more detail the useof prescribed opioids analgesics, benzodiazepines andz-hypnotics among OMT women. In addition, we wantedto describe maternal and neonatal outcomes followingOMT with and without co-medication with these drugsduring pregnancy.
METHOD
Data sources
The Medical Birth Registry of Norway
The Medical Birth Registry of Norway contains informa-tion on all births in Norway [21]. The registry is based oncompulsory notification on every birth or late abortionfrom 12 weeks of gestation. The medical birth registrycontains information on complications during preg-
nancy and delivery, and length of pregnancy, as well asinformation on the infant, including birth defects andother perinatal problems [21]. A standard antenatal formis completed during prenatal care and the midwife entersadditional data recorded at the time of birth. Follow-updata are added until discharge of hospital births. Latespontaneous abortion was defined as termination ofpregnancy after 12 weeks, but before 22 completed weeksof gestation; stillbirth as birth of a dead fetus after 22completed weeks of gestation; and preterm birth as livebirth after at least 22, but before 37 completed weeks ofgestation. Major malformations were recorded accordingto European Registration of Congenital Anomalies andTwins (EUROCAT) [22]. Neonatal abstinence is describedin the Norwegian Medical Birth Registry as irritabilityand neurological symptoms in neonates born to womenknown to abuse narcotics, alcohol or prescription drugs.Hence, symptoms, not treatment, are registered. Thelength of pregnancy was determined by ultrasound [23]for most cases (97%) and a pregnancy start date wasestimated. Each pregnancy was divided into trimesters;weeks 1–12, weeks 13–26, week 27–birth.
The Norwegian Prescription Database
The Norwegian Prescription Database includes all pre-scribed drugs dispensed in Norway since 1 January 2004.It covers the entire Norwegian population of 4.9 million[21]. The prescription database contains information onall prescribed drugs in Norway dispensed at pharmaciesto individual patients outside hospitals and in-patienttreatment facilities. Data on use among institutionalizedpatients in hospitals and other institutions are also col-lected, though as the data is aggregated at institutionallevel, it is not included in our study. For each prescription,dispensing date and detailed information on the drug isregistered. The indication for prescribing is not registered,but, when present, the code of reimbursement isrecorded, which may function as a proxy of diagnosis.
Linkage of registry data
Data in the Medical Birth Registry of Norway was linkedto the Norwegian Prescription Database based on the per-sonal identity number that is assigned to each person inNorway at birth or immigration.
Setting
The national OMT program in Norway is operatedthrough regional centers that coordinates all OMT admis-sions. The program is a high threshold one with strictadmission criteria and high social control [24]. Prescrip-tion of methadone and buprenorphine in Norway may beprescribed by a medical doctor in specialist health-care
2 Ingunn Olea Lund et al.
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction

services or by a general practitioner. If prescribed by ageneral practitioner, he or she should collaborate closelywith the specialist health-care services to make sure thatthe patient receives the care they need for optimal physi-cal, psychological, social and occupational functioning[25].
There is, in principle, zero tolerance to the use ofillegal drugs and alcohol during pregnancy in OMTwomen. If voluntary measures to help pregnant OMTwomen to stop using illegal drugs during pregnancydo not help, treatment providers are obliged by law totake action and women may be detained in in-patienttreatment during the entire, or parts of, the pregnancy[26].
Study population
Pregnancies
All singleton pregnancies registered in the Medical BirthRegistry beginning from 30 March 2004 and ending nolater than 31 December 2010 (349 020 pregnancies)were included. There may be more pregnancy and neo-natal complications in twin pregnancies so they were,therefore, excluded. Pregnancies where the mother’sidentity was unknown or she was living outside ofNorway at the time of birth were excluded. After allexclusions the number of pregnancies was 345 703.
To be defined as an OMT patient the pregnant womanhad to be dispensed methadone mixture [AnatomicalTherapeutic Chemical (ATC) classification system codeN07BC02], buprenorphine sublingual tablets (Subutex®/ATC code N07BC01) or buprenorphine–naloxone com-bined sublingual tablets (Subuxone®/N07BC51) from apharmacy at least once during pregnancy. Women thatreceived methadone drugs with the reimbursement codefor palliative treatment of malignant disease wereexcluded from the study. Methadone tablets or capsulescan be used in Norway in pain therapy, but this did notapply for any of the women in our study [27]. With theserequirements, our study consisted of 159 pregnancies in138 women in OMT treatment. According to numbersreported to the Norwegian Directorate of Health ofwomen in OMT giving birth during the study period, thestudy covers three quarters of all births from women inOMT in Norway.
Drugs
All drugs in Norway are classified according to the ATCclassification system [28]. The amount of drug dispensedis measured as defined daily doses (DDDs), a quantitybased on the assigned average dose per day on the medi-cations main indication for adults [28]. All ATC groupswere studied as an expression of comorbidity. In addi-
tion, some drugs acting on the nervous system (ATCgroup N) were studied more closely than other druggroups. Table 1 shows the DDDs for the different genericsubstances classified as benzodiazepine anti-epileptics,benzodiazepine anxiolytics, benzodiazepine hypnotics,z-hypnotics, and weak and strong opioids that werestudied in more detail. Drugs for opioid maintenancetreatment (methadone, buprenorphine and buprenor-phine combination) are excluded, both when describinguse of prescription drugs in general and when describingdrugs acting on the nervous system in more detail. Useof benzodiazepines refers to at least one prescription ofbenzodiazepine: anxiolytics, hypnotics or anti-epileptics(Table 1). Opioid analgesics were identified by the ATCcode N02A [28]. Opioid analgesics are usually catego-rized into two groups: week or strong opioids. Codeine,tramadol and dextropropoxyphene combinations arecategorized as weak opioid analgesics, whereas theremainider (ketobemidone, morphine, fentanyl,buprenorphine, hydromorhone, oxycodone, pethidine,dihydrocodeine, pentazocine) are classified as strongopioid analgesics.
Dispensing periods
Data on dispensed drugs from January 2004 to the end ofDecember 2010 were used to ensure the inclusion of alldrugs dispensed up to three months before pregnancy forall women in our sample whose pregnancies started from30 March 2004. The three months prior to pregnancywere included to enable us to evaluate a change in drugsdispensed as a result of pregnancy. Drugs dispensedduring this period may have been used by the women inthe early stages of pregnancy. The three-month time-frame was chosen to correspond to the duration of thethree trimesters of pregnancy.
Statistics
Period prevalence, means, medians, interquartile range(IQR) and confidence intervals (CI) are presented whereappropriate. CIs for proportions were calculated usingthe corrected version of the score [29]. The effect ofco-medication on pregnant OMT women on adverse preg-nancy and neonatal outcomes was studied by bivariateanalysis: t test and c2 test as appropriate. A cohort of159 pregnancies where approximately one third of thewomen received co-medication have low power to studythe effects of such medication in pregnant OMT women.As an example, an increase in the proportion of new-borns with abstinence from 50% to 61%, as observed inthis sample, has a power of 26% to be significant at analpha level of 0.05. Statistical analyses were conductedusing SPSS for Windows, version 18.0.
Pregnant women in OMT: prescription drug use 3
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction

Ethics
The Norwegian Data Inspectorate was notified before theMedical Birth Registry and the Norwegian PrescriptionDatabase were linked, as required by the Norwegian lawfor national health registries. The linkage generatedanonymous files for research purposes.
RESULTS
Background characteristics of the OMT women
The mean age of the pregnant OMT women was 32 yearsand 64% had one or more children prior to the studyperiod. In total, 51% of the women were dispensed metha-done, 49% buprenorphine and 10% buprenorphine–naloxone combinations during pregnancy. All thewomen that used buprenorphine–naloxone combinationsswitched to buprenorphine.
Prescription drugs dispensed to pregnant OMT women
Apart from OMT drugs, 69% of the women were dispensedother drugs in the 3 months prior to, and 81% were dis-pensed prescription drugs during, pregnancy (Table 2).Use of anti-infectives for systemic use (48%) and prescrip-tion drugs acting on the nervous system (45%) were themost frequently used drugs during pregnancy.
Prescriptions of drugs acting on the nervous system
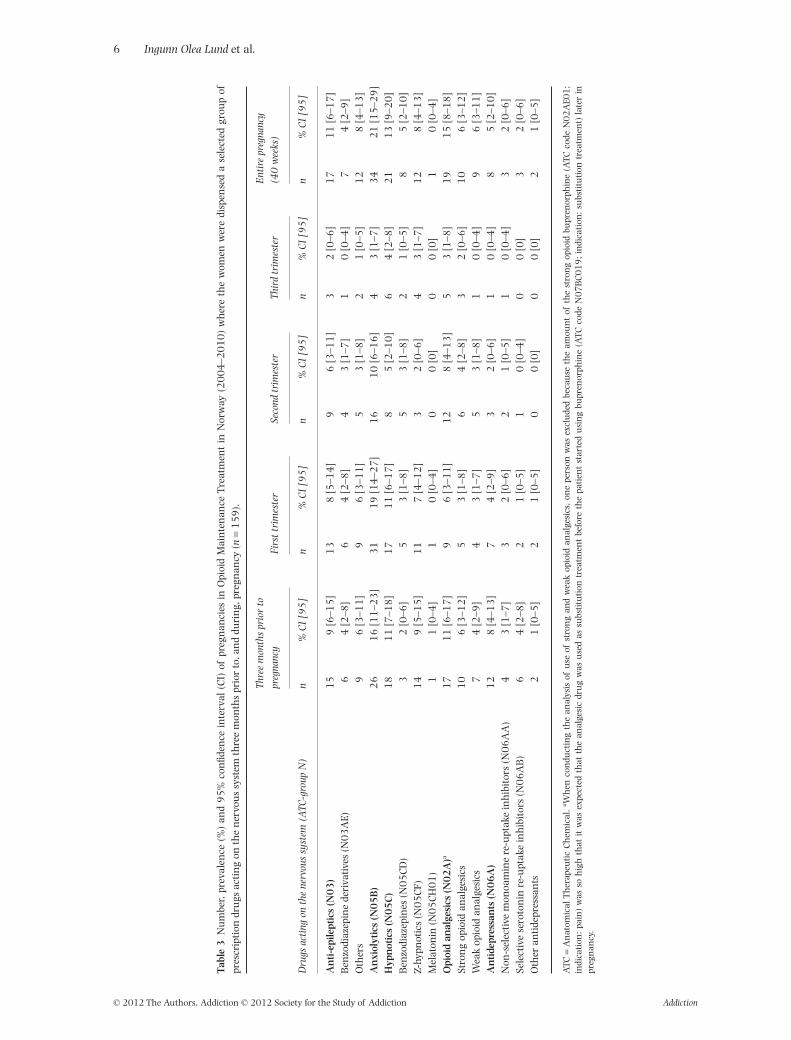
In total, 42 pregnant women [26.4% (95% CI 20–34)]used benzodiazepines (anti-epileptics, anxiolytics orhypnotics) during the entire pregnancy and 6 [4%,(2–8)] during the last trimester. In 21% and 13% of thepregnancies the women were dispensed benzodiazepineanxiolytics and benzodiazepine hypnotics respectively.All groups of benzodiazepines and z-hypnotics werereduced from the period prior to pregnancy to the thirdtrimester of pregnancy; benzodiazepine anti-epilepticsfrom 4% to 0%, benzodiazepine anxiolytics from 16%to 3%, benzodiazepine hypnotics from 2% to 1% andz-hypnotics from 9% to 3% (Table 3). Opioid analgesicswere used by 15% of the women during pregnancy(Table 3). Use was reduced from 11% in last 3 monthsprior to pregnancy to 3% during the last trimester. Anti-depressants were used by 5% of pregnant women duringpregnancy.
Benzodiazepines, z-hypnotics and opioids were notalways prescribed by the same physician that prescribedOMT during pregnancy; 17 of 30 women were pre-scribed opioid analgesics (N02A) from another physi-cian, 6 of 8 benzodiazepine anti-epileptics (N03AE01),20 of 42 benzodiazepine anxiolytics (N05B), 7 of 8benzodiazepine hypnotics (N05CD) and 11 of 16z-hypnotics (N05CF).
Table 1 Defined daily dose (DDD) of benzodiazepines, z-hypnotics and opioid analgesics used by pregnant women in opioid mainte-nance treatment in Norway (2004–2010).
ATC code DDD (oral administration)
BenzodiazepinesAnti-epileptics
Clonazepam N03AE01 8 mgAnxiolytics
Diazepam N05BA01 10 mgOxazepam N05BA04 50 mgAlprazolam N05BA12 1 mg
HypnoticsNitrazepam N05CD02 5 mgFlunitrazepam N05CD03 1 mg
Z-hypnoticsZopiclone N05CF01 7.5 mgZolpidem N05CF02 10 mgOpioid analgesicsOpioid analgesics (strong)
Morphine N02AA01 100 mgOxycodone N02AA05 30 mgBuprenorphine N02AE01 1.2 mga
Opioid analgesics (weak)Codeine N02AA59 b
ATC = Anatomical Therapeutic Chemical. aParenteral, sublingual and transdermal administration only. bAll codeine products are fixed combinationswith acetaminophen. For the product containing 400 mg paracetamol, one DDD will represent 120 mg codeine and 1600 mg paracetamol. For productscontaining 500 mg paracetamol, one DDD will represent 90 mg codeine and 1500 mg paracetamol.
4 Ingunn Olea Lund et al.
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction

Tabl
e2
Nu
mbe
r,pr
eval
ence
(%)a
nd
95
%co
nfid
ence
inte
rval
(CI)
ofpr
egn
anci
esin
opio
idm
ain
ten
ance
trea
tmen
tin
Nor
way
(20
04
–20
10
)wh
ere
the
wom
enw
ere
disp
ense
dpr
escr
ipti
ondr
ugs
thre
em
onth
spr
ior
to,a
nd
duri
ng,
preg
nan
cy(n
=1
59
).
Dru
ggr
oups
(ATC
grou
p)
Thre
em
onth
sbe
fore
topr
egna
ncy
Firs
ttr
imes
ter
Seco
ndtr
imes
ter
Thir
dtr
imes
ter
Ent
ire
preg
nanc
y(4
0w
eeks
)
n%
CI
[95
]n
%C
I[9
5]
n%
CI
[95
]n
%C
I[9
5]
n%
CI
[95
]
Alim
enta
rytr
act
and
met
abol
ism
(A)
64
[2–8
]2
11
3[9
–20
]1
28
[4–1
3]
74
[2–9
]3
01
9[1
3–2
6]
Blo
odan
dbl
ood
form
ing
orga
ns
(B)
74
[2–9
]1
06
[3–1
2]
13
8[5
–14
]9
6[3
–11
]2
11
3[9
–20
]C
ardi
ovas
cula
rsy
stem
(C)
74
[2–9
]7
4[2
–9]
21
[0–5
]6
4[2
–8]
13
8[5
–14
]D
erm
atol
ogic
als
(D)
12
8[4
–13
]9
6[3
–11
]8
5[2
–10
]7
4[2
–9]
18
11
[7–1
8]
Gen
itou
rin
ary
syst
eman
dse
xh
orm
ones
(G)
15
9[6
–15
]6
4[2
–8]
64
[2–8
]0
0[0
]1
28
[4–1
3]
Syst
emic
hor
mon
alpr
epar
atio
ns
excl
.sex
hor
mon
esan
din
sulin
’s(H
)1
06
[3–1
2]
43
[1–7
]9
6[3
–11
]7
4[2
–9]
11
7[4
–12
]A
nti
-in
fect
ives
for
syst
emic
use
(J)
36
23
[17
–30
]3
01
9[1
3–2
6]
40
25
[19
–33
]3
11
9[1
4–2
7]
77
48
[40
–56
]A
nti
neo
plas
tic
and
imm
un
omod
ula
tin
gag
ents
(L)
21
[0–5
]1
0[0
–4]
00
[0]
00
[0]
10
[0–4
]M
usc
oske
leta
lsys
tem
(M)
18
11
[7–1
8]
96
[3–1
1]
32
[0–6
]0
0[0
]1
28
[4–1
3]
Ner
vou
ssy
stem
(N)
excl
.dru
gsu
sed
inop
ioid
depe
nde
nce
71
45
[37
–53
]5
93
7[3
0–4
5]
41
26
[19
–33
]2
11
3[9
–20
]7
14
5[3
7–5
3]
An
tipa
rasi
tic
prod
uct
s,in
sect
icid
esan
dre
pelle
nts
(P)
43
[1–7
]2
1[0
–5]
00
[0]
00
[0]
21
[0–5
]R
espi
rato
rysy
stem
(R)
29
18
[13
–25
]2
11
3[9
–20
]2
01
3[8
–19
]1
96
[3–1
1]
40
25
[19
–33
]Se
nso
ryor
gan
san
dva
riou
s(S
+V
)7
4[2
–9]
43
[1–7
]2
1[0
–5]
64
[2–8
]1
17
[4–1
2]
Tota
l1
10
69
[61
–76
]9
66
0[5
2–6
8]
10
06
3[5
5–7
0]
74
47
[39
–55
]1
29
81
[74
–87
]
ATC
=A
nat
omic
alT
her
apeu
tic
Ch
emic
al.
Pregnant women in OMT: prescription drug use 5
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction
Tabl
e3
Nu
mbe
r,pr
eval
ence
(%)
and
95
%co
nfid
ence
inte
rval
(CI)
ofpr
egn
anci
esin
Opi
oid
Mai
nte
nan
ceT
reat
men
tin
Nor
way
(20
04
–20
10
)w
her
eth
ew
omen
wer
edi
spen
sed
ase
lect
edgr
oup
ofpr
escr
ipti
ondr
ugs
acti
ng
onth
en
ervo
us
syst
emth
ree
mon
ths
prio
rto
,an
ddu
rin
g,pr
egn
ancy
(n=
15
9).
Dru
gsac
ting
onth
ene
rvou
ssy
stem
(ATC
-gro
upN
)
Thre
em
onth
spr
ior
topr
egna
ncy
Firs
ttr
imes
ter
Seco
ndtr
imes
ter
Thir
dtr
imes
ter
Ent
ire
preg
nanc
y(4
0w
eeks
)
n%
CI
[95
]n
%C
I[9
5]
n%
CI
[95
]n
%C
I[9
5]
n%
CI
[95
]
An
ti-e
pile
ptic
s(N
03
)1
59
[6–1
5]
13
8[5
–14
]9
6[3
–11
]3
2[0
–6]
17
11
[6–1
7]
Ben
zodi
azep
ine
deri
vativ
es(N
03
AE)
64
[2–8
]6
4[2
–8]
43
[1–7
]1
0[0
–4]
74
[2–9
]O
ther
s9
6[3
–11
]9
6[3
–11
]5
3[1
–8]
21
[0–5
]1
28
[4–1
3]
An
xiol
ytic
s(N
05
B)
26
16
[11
–23
]3
11
9[1
4–2
7]
16
10
[6–1
6]
43
[1–7
]3
42
1[1
5–2
9]
Hyp
not
ics
(N0
5C
)1
81
1[7
–18
]1
71
1[6
–17
]8
5[2
–10
]6
4[2
–8]
21
13
[9–2
0]
Ben
zodi
azep
ines
(N0
5C
D)
32
[0–6
]5
3[1
–8]
53
[1–8
]2
1[0
–5]
85
[2–1
0]
Z-hy
pnot
ics
(N0
5C
F)1
49
[5–1
5]
11
7[4
–12
]3
2[0
–6]
43
[1–7
]1
28
[4–1
3]
Mel
aton
in(N
05
CH
01
)1
1[0
–4]
10
[0–4
]0
0[0
]0
0[0
]1
0[0
–4]
Opi
oid
anal
gesi
cs(N
02
A)a
17
11
[6–1
7]
96
[3–1
1]
12
8[4
–13
]5
3[1
–8]
19
15
[8–1
8]
Stro
ng
opio
idan
alge
sics
10
6[3
–12
]5
3[1
–8]
64
[2–8
]3
2[0
–6]
10
6[3
–12
]W
eak
opio
idan
alge
sics
74
[2–9
]4
3[1
–7]
53
[1–8
]1
0[0
–4]
96
[3–1
1]
An
tide
pres
san
ts(N
06
A)
12
8[4
–13
]7
4[2
–9]
32
[0–6
]1
0[0
–4]
85
[2–1
0]
Non
-sel
ectiv
em
onoa
min
ere
-upt
ake
inh
ibit
ors
(N0
6A
A)
43
[1–7
]3
2[0
–6]
21
[0–5
]1
0[0
–4]
32
[0–6
]Se
lect
ive
sero
ton
inre
-upt
ake
inh
ibit
ors
(N0
6A
B)
64
[2–8
]2
1[0
–5]
10
[0–4
]0
0[0
]3
2[0
–6]
Oth
eran
tide
pres
san
ts2
1[0
–5]
21
[0–5
]0
0[0
]0
0[0
]2
1[0
–5]
ATC
=A
nat
omic
alT
her
apeu
tic
Ch
emic
al.
a Wh
enco
ndu
ctin
gth
ean
alys
isof
use
ofst
ron
gan
dw
eak
opio
idan
alge
sics
,on
epe
rson
was
excl
ude
dbe
cau
seth
eam
oun
tof
the
stro
ng
opio
idbu
pren
orph
ine
(ATC
code
N0
2A
E01
;in
dica
tion
:pa
in)
was
soh
igh
that
itw
asex
pect
edth
atth
ean
alge
sic
dru
gw
asu
sed
assu
bsti
tuti
ontr
eatm
ent
befo
reth
epa
tien
tst
arte
du
sin
gbu
pren
orph
ine
(ATC
code
N0
7B
C0
19
;in
dica
tion
:su
bsti
tuti
ontr
eatm
ent)
late
rin
preg
nan
cy.
6 Ingunn Olea Lund et al.
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction
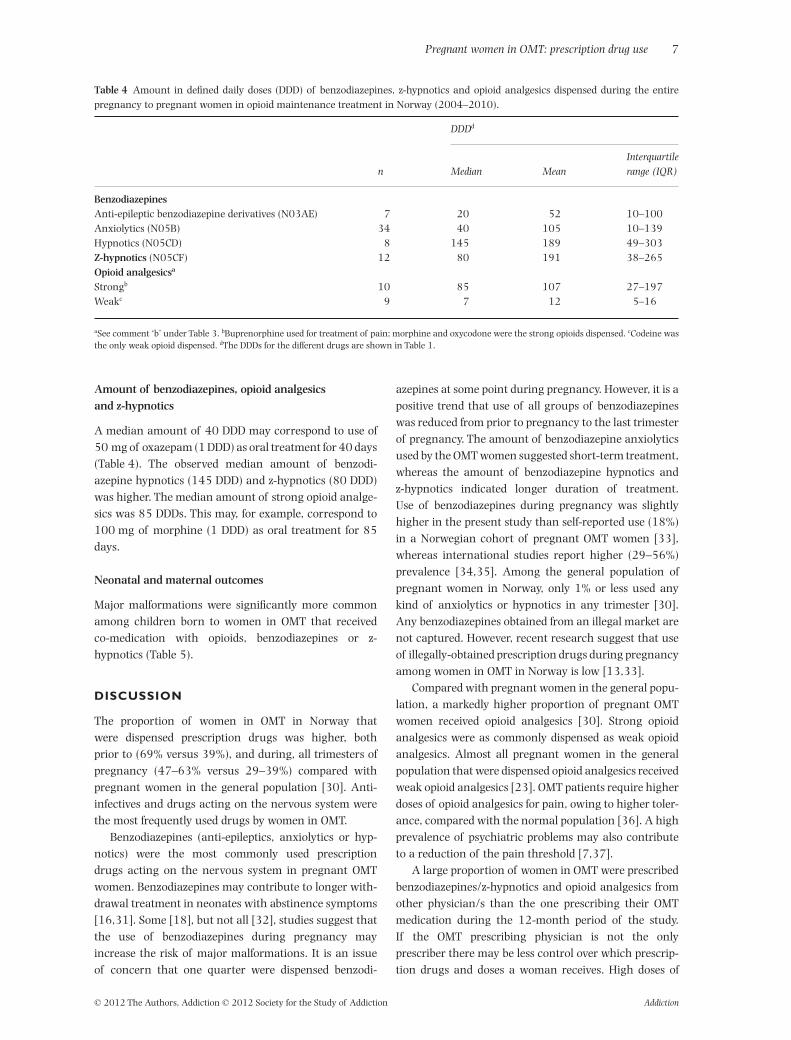
Amount of benzodiazepines, opioid analgesicsand z-hypnotics
A median amount of 40 DDD may correspond to use of50 mg of oxazepam (1 DDD) as oral treatment for 40 days(Table 4). The observed median amount of benzodi-azepine hypnotics (145 DDD) and z-hypnotics (80 DDD)was higher. The median amount of strong opioid analge-sics was 85 DDDs. This may, for example, correspond to100 mg of morphine (1 DDD) as oral treatment for 85days.
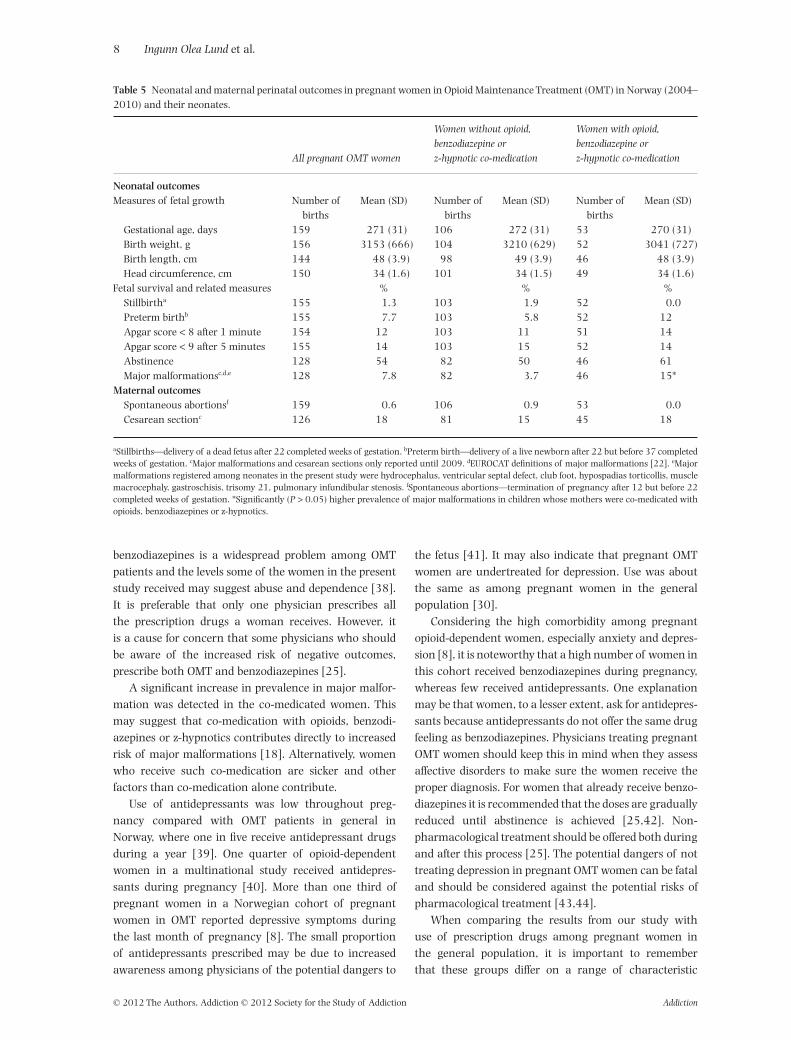
Neonatal and maternal outcomes
Major malformations were significantly more commonamong children born to women in OMT that receivedco-medication with opioids, benzodiazepines or z-hypnotics (Table 5).
DISCUSSION
The proportion of women in OMT in Norway thatwere dispensed prescription drugs was higher, bothprior to (69% versus 39%), and during, all trimesters ofpregnancy (47–63% versus 29–39%) compared withpregnant women in the general population [30]. Anti-infectives and drugs acting on the nervous system werethe most frequently used drugs by women in OMT.
Benzodiazepines (anti-epileptics, anxiolytics or hyp-notics) were the most commonly used prescriptiondrugs acting on the nervous system in pregnant OMTwomen. Benzodiazepines may contribute to longer with-drawal treatment in neonates with abstinence symptoms[16,31]. Some [18], but not all [32], studies suggest thatthe use of benzodiazepines during pregnancy mayincrease the risk of major malformations. It is an issueof concern that one quarter were dispensed benzodi-
azepines at some point during pregnancy. However, it is apositive trend that use of all groups of benzodiazepineswas reduced from prior to pregnancy to the last trimesterof pregnancy. The amount of benzodiazepine anxiolyticsused by the OMT women suggested short-term treatment,whereas the amount of benzodiazepine hypnotics andz-hypnotics indicated longer duration of treatment.Use of benzodiazepines during pregnancy was slightlyhigher in the present study than self-reported use (18%)in a Norwegian cohort of pregnant OMT women [33],whereas international studies report higher (29–56%)prevalence [34,35]. Among the general population ofpregnant women in Norway, only 1% or less used anykind of anxiolytics or hypnotics in any trimester [30].Any benzodiazepines obtained from an illegal market arenot captured. However, recent research suggest that useof illegally-obtained prescription drugs during pregnancyamong women in OMT in Norway is low [13,33].
Compared with pregnant women in the general popu-lation, a markedly higher proportion of pregnant OMTwomen received opioid analgesics [30]. Strong opioidanalgesics were as commonly dispensed as weak opioidanalgesics. Almost all pregnant women in the generalpopulation that were dispensed opioid analgesics receivedweak opioid analgesics [23]. OMT patients require higherdoses of opioid analgesics for pain, owing to higher toler-ance, compared with the normal population [36]. A highprevalence of psychiatric problems may also contributeto a reduction of the pain threshold [7,37].
A large proportion of women in OMT were prescribedbenzodiazepines/z-hypnotics and opioid analgesics fromother physician/s than the one prescribing their OMTmedication during the 12-month period of the study.If the OMT prescribing physician is not the onlyprescriber there may be less control over which prescrip-tion drugs and doses a woman receives. High doses of
Table 4 Amount in defined daily doses (DDD) of benzodiazepines, z-hypnotics and opioid analgesics dispensed during the entirepregnancy to pregnant women in opioid maintenance treatment in Norway (2004–2010).
n
DDDd
Median MeanInterquartilerange (IQR)
BenzodiazepinesAnti-epileptic benzodiazepine derivatives (N03AE) 7 20 52 10–100Anxiolytics (N05B) 34 40 105 10–139Hypnotics (N05CD) 8 145 189 49–303Z-hypnotics (N05CF) 12 80 191 38–265Opioid analgesicsa
Strongb 10 85 107 27–197Weakc 9 7 12 5–16
aSee comment ‘b’ under Table 3. bBuprenorphine used for treatment of pain; morphine and oxycodone were the strong opioids dispensed. cCodeine wasthe only weak opioid dispensed. dThe DDDs for the different drugs are shown in Table 1.
Pregnant women in OMT: prescription drug use 7
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction
benzodiazepines is a widespread problem among OMTpatients and the levels some of the women in the presentstudy received may suggest abuse and dependence [38].It is preferable that only one physician prescribes allthe prescription drugs a woman receives. However, itis a cause for concern that some physicians who shouldbe aware of the increased risk of negative outcomes,prescribe both OMT and benzodiazepines [25].
A significant increase in prevalence in major malfor-mation was detected in the co-medicated women. Thismay suggest that co-medication with opioids, benzodi-azepines or z-hypnotics contributes directly to increasedrisk of major malformations [18]. Alternatively, womenwho receive such co-medication are sicker and otherfactors than co-medication alone contribute.
Use of antidepressants was low throughout preg-nancy compared with OMT patients in general inNorway, where one in five receive antidepressant drugsduring a year [39]. One quarter of opioid-dependentwomen in a multinational study received antidepres-sants during pregnancy [40]. More than one third ofpregnant women in a Norwegian cohort of pregnantwomen in OMT reported depressive symptoms duringthe last month of pregnancy [8]. The small proportionof antidepressants prescribed may be due to increasedawareness among physicians of the potential dangers to
the fetus [41]. It may also indicate that pregnant OMTwomen are undertreated for depression. Use was aboutthe same as among pregnant women in the generalpopulation [30].
Considering the high comorbidity among pregnantopioid-dependent women, especially anxiety and depres-sion [8], it is noteworthy that a high number of women inthis cohort received benzodiazepines during pregnancy,whereas few received antidepressants. One explanationmay be that women, to a lesser extent, ask for antidepres-sants because antidepressants do not offer the same drugfeeling as benzodiazepines. Physicians treating pregnantOMT women should keep this in mind when they assessaffective disorders to make sure the women receive theproper diagnosis. For women that already receive benzo-diazepines it is recommended that the doses are graduallyreduced until abstinence is achieved [25,42]. Non-pharmacological treatment should be offered both duringand after this process [25]. The potential dangers of nottreating depression in pregnant OMT women can be fataland should be considered against the potential risks ofpharmacological treatment [43,44].
When comparing the results from our study withuse of prescription drugs among pregnant women inthe general population, it is important to rememberthat these groups differ on a range of characteristic
Table 5 Neonatal and maternal perinatal outcomes in pregnant women in Opioid Maintenance Treatment (OMT) in Norway (2004–2010) and their neonates.
All pregnant OMT women
Women without opioid,benzodiazepine orz-hypnotic co-medication
Women with opioid,benzodiazepine orz-hypnotic co-medication
Neonatal outcomesMeasures of fetal growth Number of
birthsMean (SD) Number of
birthsMean (SD) Number of
birthsMean (SD)
Gestational age, days 159 271 (31) 106 272 (31) 53 270 (31)Birth weight, g 156 3153 (666) 104 3210 (629) 52 3041 (727)Birth length, cm 144 48 (3.9) 98 49 (3.9) 46 48 (3.9)Head circumference, cm 150 34 (1.6) 101 34 (1.5) 49 34 (1.6)
Fetal survival and related measures % % %Stillbirtha 155 1.3 103 1.9 52 0.0Preterm birthb 155 7.7 103 5.8 52 12Apgar score < 8 after 1 minute 154 12 103 11 51 14Apgar score < 9 after 5 minutes 155 14 103 15 52 14Abstinence 128 54 82 50 46 61Major malformationsc,d,e 128 7.8 82 3.7 46 15*
Maternal outcomesSpontaneous abortionsf 159 0.6 106 0.9 53 0.0Cesarean sectionc 126 18 81 15 45 18
aStillbirths—delivery of a dead fetus after 22 completed weeks of gestation. bPreterm birth—delivery of a live newborn after 22 but before 37 completedweeks of gestation. cMajor malformations and cesarean sections only reported until 2009. dEUROCAT definitions of major malformations [22]. eMajormalformations registered among neonates in the present study were hydrocephalus, ventricular septal defect, club foot, hypospadias torticollis, musclemacrocephaly, gastroschisis, trisomy 21, pulmonary infundibular stenosis. fSpontaneous abortions—termination of pregnancy after 12 but before 22completed weeks of gestation. *Significantly (P > 0.05) higher prevalence of major malformations in children whose mothers were co-medicated withopioids, benzodiazepines or z-hypnotics.
8 Ingunn Olea Lund et al.
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction

besides OMT that might have affected medication use—socioeconomic status, smoking and comorbidity.
Limitations
Drugs dispensed at hospitals and other institutions arenot registered at an individual level. Patients who aredispensed drugs at pharmacies may be more stable andless prone to use drugs with abuse potential than patientsthat are dispensed OMT drugs at OMT centers. Hence, itmay be that our study underestimates the prevalence ofprescription drug use. Data on indication is not registeredin studies based on prescription databases and the dis-pensed drugs are not necessarily consumed by the recipi-ents. Some drugs may be taken sporadically upon theappearance of symptoms which could re-occur long afterthe dispensing date. The medication may be re-sold onthe illegal market and some women may have boughtprescriptions drugs from the illegal market [45].
To compare the effects of co-medication on adversepregnancy and neonatal outcomes we used bivariateanalysis, which means that we did not adjust for potentialconfounders.
Strengths
The study covers a national cohort of outpatient preg-nant OMT women in Norway. The data is not based onself-reports or interviews, hence recall biases are elimi-nated. The unique personal identity number andpopulation-based registries on birth, deaths, emigrationsand prescriptions provide high quality linkages betweenthe high quality registries in Norway.
CONCLUSION
Pregnant OMT women use more prescription drugs thanpregnant women in the general population [30]. Anti-infectives and drugs acting on the nervous system werethe most commonly used prescription drugs among preg-nant OMT women. The use of prescription drugs withabuse potential were reduced as pregnancy proceeded.The low use of antidepressants may indicate that womenin OMT in Norway are undertreated for depression.Co-medication may increase the risk of adverse preg-nancy outcomes and this needs to be further addressed.The findings provide invaluable knowledge for physiciansworking with this patient group and may form the basisfor developing clinical guidelines for co-medication inpregnant OMT women.
Declarations of interest
None.
Acknowledgements
Thanks to Gabrielle Welle-Strand, Norwegian Centrefor Addiction Research and Norwegian Directorate ofHealth, and Hendree Jones, RTI International and JohnsHopkins Medicine for invaluable help in reading andcommenting on the manuscript.
References
1. Unger A., Metz V., Fischer G. Opioid dependent and preg-nant: what are the best options for mothers and neonates?Obstet Gynecol Int; DOI: 10.1155/2012/195954.
2. Finnegan L. P., Hagan T., Kaltenbach K. A. Scientific foun-dation of clinical practice: opiate use in pregnant women.Bull N Y Acad Med 1991; 67: 223–39.
3. Jones H. E., O’Grady K. E., Malfi D., Tuten M. Methadonemaintenance versus methadone taper during pregnancy:maternal and neonatal outcomes. Am J Addict 2008; 17:372–86.
4. Jansson L. M., Svikis D. S., Velez M., Fitzgerald E., Jones H. E.The impact of managed care on drug-dependent pregnantand postpartum women and their children. Subst UseMisuse 2007; 42: 961–74.
5. Winklbaur B., Kopf N., Ebner N., Jung E., Thau K., Fischer G.Treating pregnant women dependent on opioids is not thesame as treating pregnancy and opioid dependence: aknowledge synthesis for better treatment for women andneonates. Addiction 2008; 103: 1429–40.
6. Benningfield M. M., Arria A. M., Kaltenbach K., Heil S. H.,Stine S. M., Coyle M. G. et al. Co-occurring psychiatric symp-toms are associated with increased psychological, social,and medical impairment in opioid dependent pregnantwomen. Am J Addict 2010; 19: 416–21.
7. Tuten M., Fitzsimons H., Chisolm M., Jones H., Heil S.,O’Grady K. The impact of mood disorders on the deliveryand neonatal outcomes of methadone-maintained preg-nant patients. Am J Drug Alcohol Abuse 2009; 35: 358–63.
8. Lund I. O., Skurtveit S., Sarfi M., Bakstad B., Welle-StrandG., Ravndal E. A two-year prospective study of psychologicaldistress among a national cohort of pregnant women inopioid maintenance treatment and their partners. J SubstUse; DOI: 10.3109/14659891.2011.642928.
9. Jones H. E., Kaltenbach K., Heil S. H., Stine S. M., CoyleM. G., Arria A. M. et al. Neonatal abstinence syndrome aftermethadone or buprenorphine exposure. N Engl J Med 2010;363: 2320–31.
10. Burns L., Mattick R. P., Lim K., Wallace C. Methadone inpregnancy: treatment retention and neonatal outcomes.Addiction 2007; 102: 264–70.
11. Lejeune C., Simmat-Durand L., Gourarier L., Aubisson S.Prospective multicenter observational study of 260 infantsborn to 259 opiate-dependent mothers on methadone orhigh-dose buprenophine substitution. Drug Alcohol Depend2006; 82: 250–7.
12. Skeie I., Brekke M., Lindbæk M., Waal H. Somatic healthamong heroin addicts before and during opioid mainte-nance treatment: a retrospective cohort study. BMC PublicHealth 2008; 8: 43.
13. Lund I. O., Skurtveit S., Sarfi M., Bakstad B., Welle-StrandG., Ravndal E. Substance use during and after pregnancyamong a national cohort of pregnant women in opioidmaintenance treatment and their partners. J Subst Use2012; 17: 277–86.
Pregnant women in OMT: prescription drug use 9
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction

14. Fitzsimons H. E., Tuten M., Vaidya V., Jones H. E. Mood dis-orders affect drug treatment success of drug-dependentpregnant women. J Subst Abuse Treat 2007; 32: 19–25.
15. Haller D. L., Knisely J. S., Dawson K. S., Schnoll S. H. Peri-natal substance abusers: psychological and social charac-teristics. J Nerv Ment Dis 1993; 181: 509–13.
16. Seligman N. S., Salva N., Hayes E. J., Dysart K. C., PequignotE. C., Baxter J. K. Predicting length of treatment for neonatalabstinence syndrome in methadone-exposed neonates. Am JObstet Gynecol 2008; 199: 396.
17. Pritham U. A., Paul J. A., Hayes M. J. Opioid dependency inpregnancy and length of stay for neonatal abstinence syn-drome. J Obstet Gynecol Neonatal Nurs 2012; 41: 180–90.
18. Briggs G. G., Freeman R. K., Yaffe S. J. Drugs in Pregnancy andLactation Shaw R., editor. 8 edn. Philadelphia: LippincottWilliams & Wilkins; 2008, p. 419, 1251.
19. Daae L., Holene E., Jacobsen D., Wiik Johansen P.,Figenschou Soleng A., Spigset O. et al. Felleskatalogen[Catalog of Medicinial Products Markeded in Norway]. Oslo:Fagbokforlaget; 2011.
20. Fredheim O. M. S., Borchgrevink P. C., Nordstrand B.,Clausen T., Skurtveit S. Prescription of analgesics topatients in opioid maintenance therapy: a pharmaco-epidemiological study. Drug Alcohol Depend 2011; 116:158–62.
21. Furu K., Wettermark B., Andersen M., Martikainen J. E.,Almarsdottir A. B., Sørensen H. T. The Nordic countries as acohort for pharmacoepidemiological research. Basic ClinPharmacol Toxicol 2010; 106: 86–94.
22. EUROCAT. 15 Years of Surveillance of Congenital Anomalitiesin Europe 1980–1992. Eurocat Central Registry Brussels:Institute of Hygiene and Epidemiology; 1997.
23. Handal M., Engeland A., Rønning M., Skurtveit S., Furu K.Use of prescribed opioid analgesics and co-medication withbenzodiazepines in women before, during, and after preg-nancy: a population-based cohort study. Eur J Clin Pharma-col 2011; 67: 953–60.
24. Waal H. Merits and problems in high-threshold methadonemaintenance treatment. Eur Addict Res 2007; 13: 66–73.
25. Bakstad B., Welle-Strand G. National Guidelines for PregnantWomen in Opioid Maintenenace Treatment (OMT) andFollow-Up of Their Families until the Children Reach Schoolage[In Norwegian only]. Oslo: Norwegian Directorate ofHealth; 2011.
26. Lovdata, lov 1999, nr 61, Sosialtjenesteloven § 6-2a.Tilbakeholdelse av gravide rusmisbrukere [Social ServicesAct § 6-2a Retention of substance dependent pregnantwomen in institutions], 1999.
27. Fredheim O. M. S., Kaasa S., Dale O., Klepstad P., LandrøN. I., Borchgrevink P. C. Opioid switching from oral slowrelease morphine to oral methadone may improve paincontrol in chronic non-malignant pain: a nine-monthfollow-up study. Palliat Med 2006; 20: 35.
28. WHO. WHO Collaborating Centre for Drug StatisticsMethodology. ATC Classification Index with DDDs 2010. Oslo:Norwegian institute of Public Health; 2010.
29. Vollset S. E. Confidence intervals for a binomial proportion.Stat Med 1993; 12: 809–24.
30. Engeland A., Bramness J. G., Daltveit A. K., Rønning M.,Skurtveit S., Furu K. Prescription drug use among fathers
and mothers before and during pregnancy. A population-based cohort study of 106 000 pregnancies in Norway2004–2006. Br J Clin Pharmacol 2008; 65: 653–60.
31. Berghella V., Lim P. J., Hill M. K., Cherpes J., Chennat J.,Kaltenbach K. Maternal methadone dose and neonatalwithdrawal. Am J Obstet Gynecol 2003; 189: 312–7.
32. Wikner B. N., Stiller C. O., Bergman U., Asker C., Källén B.Use of benzodiazepines and benzodiazepine receptor ago-nists during pregnancy: neonatal outcome and congenitalmalformations. Pharmacoepidemiol Drug Saf 2007; 16:1203–10.
33. Bakstad B. S., Sarfi M., Welle-Strand G. K., Ravndal E. Opioidmaintenance treatment during pregnancy: occurrence andseverity of neonatal abstinence syndrome. Eur Addict Res2009; 15: 128–34.
34. Metz V., Jagsch R., Ebner N., Würzl J., Pribasnig A.,Aschauer C. et al. Impact of treatment approach on mater-nal and neonatal outcome in pregnant opioid-maintainedwomen. Hum Psychopharmacol 2011; 26: 412–21.
35. Lacroix I., Berrebi A., Garipuy D., Schmitt L., Hammou Y.,Chaumerliac C. et al. Buprenorphine versus methadonein pregnant opioid-dependent women: a prospective multi-center study. Eur J Clin Pharmacol 2011; 67: 10531059.
36. Meyer M., Wagner K., Benvenuto A., Plante D., Howard D.Intrapartum and postpartum analgesia for women main-tained on methadone during pregnancy. Obstet Gynecol2007; 110: 261.
37. Chiu Y., Silman A., Macfarlane G., Ray D., Gupta A., DickensC. et al. Poor sleep and depression are independently associ-ated with a reduced pain threshold. Results of a populationbased study. Pain 2005; 115: 316–21.
38. Backmund M., Meyer K., Soyka M., Reimer J., Schütz C. G.Co-consumption of benzodiazepines in heroin users,methadone-substituted and codeine-substituted patients.J Addict Dis 2006; 24: 17–29.
39. Hartz I., Bramness J., Skurtveit S. Prescription of antide-pressants to patients on opioid maintenance therapy—apharmacoepidemiological study. Nor J Epidemiol 2011; 21:77–83.
40. Martin P. R., Arria A. M., Fischer G., Kaltenbach K., HeilS. H., Stine S. M. et al. Psychopharmacologic managementof opioid-dependent women during pregnancy. Am J Addict2009; 18: 148–56.
41. Tuccori M., Testi A., Antonioli L., Fornai M., Montagnani S.,Ghisu N. et al. Safety concerns associated with the use ofserotonin reuptake inhibitors and other serotonergic/noradrenergic antidepressants during pregnancy: a review.Clin Ther 2009; 31: 1426–53.
42. Metz V., Köchl B., Fischer G. Should pregnant women withsubstance use disorders be managed differently? Neuro-psychiatry 2012; 2: 29–41.
43. Lewis G. The women who died 2006–2008. BJOG 2011;118 (suppl): 30–56.
44. Oates M., Cantwell R. Deaths from psychiatric causes. BJOG2011; 118 (suppl): 132–42.
45. Waal H., Clausen T., Haaseth A., Lillevold P. Seraf rapport1/2010 Siste år med gamle retningslinjer. Statusrapport 2009.[Seraf report 1/2010. Final year with old guidelines. Statusreport 2009]. Oslo: Norwegian Centre for AddictionResearch; 2010.
10 Ingunn Olea Lund et al.
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction Addiction