phase ii study of accelerated fractionation radiation therapy with carboplatin followed by...
TRANSCRIPT

Pergamon
Int. J. Radiation Oncology Biol. Phys., Vol. 33, No. 2, pp. 357-364, 1995 Copyright 0 1995 Elsevier Science Inc.
Printed in the USA. All rights reserved 0360-3016195 $9.50 + .OO
0360-3016( 95)00160-3
l Clinical Original Contribution
PHASE II STUDY OF ACCELERATED FRACTIONATION RADIATION THERAPY WITH CARBOPLATIN FOLLOWED BY VINCRISTINE CHEMOTHERAPY FOR
THE TREATMENT OF GLIOBLASTOMA MULTIFORME
V. A. LEVIN, M.D.,* M. H. MAOR, M.D.,+ P. F. THALL, PH.D.,$ W. K. A. YUNG, M.D.,* J. BRIJNER, M.D.,” R. SAWAYA, M.D.,l A. P. KYRITSIS, M.D.,* N. LEEDS, M.D.,#
S. Woo, M.D.,** L. RODRIGUEZ, M.D.++ AND M. J. GLEASON, B.S.N.*
Brain Tumor Center and the Departments of *Neuro-Oncology, ‘Radiotherapy, *Biomatbematics, sPathology, ‘Neurosurgery, and #Radiology, The University of Texas M. D. Anderson Cancer Center, Houston, TX, * *Department of Radiotherapy,
Methodist Hospital, Houston, TX, ‘+Department of Neurosurgery, Memorial Hospital, North Hollywood, FL
Purpose: To conduct a Phase II one-arm study to evaiuate the long-term efficacy and safety of accelerated fractionated radiotherapy combined with intravenous carboplatin for patients with previously untreated giioblastoma multXorme tumors. Methods and Materials: Between 1988 and 1992, 83 patients received 1.9-2.0 Gy radiation three times a day with 2-h infusions of 33 mg/m* carboplatin for two 5-day cycles separated by 2 weeks; following radiotherapy, patients received procarbazine, lomustine ( CCNU) , and vincristine (PCV) for 1 year or until tumor progressed. Results: Eighty-three patients were evaiuable for analysis. Seventy-four of the 83 patients (89%) received one or more courses of PCV, their median survival was 55 weeks. Total resection was performed in 20% (15 of 74), subtotal resection in 69% (51 of 74), and biospy in 11% (8 of 74); reoperation (total or subtotal resection) was petformed in 28 patients (37% ). Survival was worst for those z 61 year old (median 35 weeks). Fits of the Cox proportional hazards regression model showed covariates individually predictive of improved survival were younger age (p < O.Ol), smaller log of radiation volume (p = O.OOS), total or subtotal resection vs. biopsy @ = 0.056)) and higher Earnofsky performance status (p = 0.055). A muitivari- ate analysis showed that age @ = 0.013) and extent of initial surgery (p = 0.003) together were predictive of a better survival with no other variables providing additional significance. Only 8.4% (7 of 83) of patients had clinically documented therapy-associated neurotoxicity (“radiation necrosis”). Conclusion: When com- parable selection criteria were applied, the survival in this study is similar to the results currently attainable with other chemoradiation approaches. The relative safety of accelerated fractionated radiotherapy, as used in this study with carbopiatin, enables concomitant full-dose administration of chemotherapy or radiosensitizing agents in glioblastoma multiforme patients.
Carboplathr, Accelerated fractionated radiotherapy, Giioblastoma, PCV.
INTRODUCTION
In the past 20 years, a number of drug-radiation combina- tions have been tried in attempts to improve on the results with radiation alone in patients with glioblastoma multi- fotme (GBM) . Drugs evaluated in an effort to potentiate tumor-cell kill and patient survival are: hydroxyurea (28), metronidazole (39), misonidazole (3, 33), halopyrimid- ines ( 16, 35), and a variety of alkylating agents (30).
The survival benefits of these combined approaches have been marginal when compared to radiotherapy only or with postradiation chemotherapy combinations.
In all these studies, drug toxicity was encountered that limited their administration in an optimal concomittant fashion with the radiation. To allow full-dose drug admin- istration together with the entire course of normal fraction size radiotherapy, we decided to administer the test drug, carboplatin, during accelerated fractionated radiotherapy,
Reprint requests to: Victor A. Levitt, M.D., Department of Neuro-Oncology, University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Box 100, Houston, TX 77030. Acknowledgements-This study was supported in part by Grant CA55261 from the National Cancer Institute, National Institutes of Health, Department of Health and Human Services. We are very appreciative of the many physicians who referred their
patients to us for treatment on this study. In particular, we wish to thank Drs. Richard Moser (Elk Groove Village, IL) and J. Bob Blacklock and Robert Grossman (Baylor College of Medi- tine and Methodist Hospital, Houston, TX). We also wish to thank Barbara Rescbke for editorial suggestions.
Accepted for publication 31 March 1995.
357

358 I. J. Radiation Oncology 0 Biology l Physics Volume 33, Number 2, 1995
thus reducing the overall time required for concomitant chemotherapy administration.
Accelerated fractionation for primary brain tumors has been extensively studied in Europe by Keim et al. (2 1) and by the EORTC Cooperative Group of Radio- therapy ( 19). Between 198 1 and 1984, 340 patients with high-grade gliomas were entered into a random- ized three-arm protocol that evaluated (a) single daily fraction radiation given conventionally in 6 weeks to a 60 Gy total; (b) three daily fractions of 2 Gy/fraction (approximately 4 h between doses) for 1 week, with a 2-week interval break and a second week of the same irradiation; and (c) a third arm that used the same three daily fraction schedule of radiation but added the radio- sensitizer misonidazole. Among the three arms there were no significant differences in total survival rates or duration of survival. Actually, the disease-free survival duration was slightly worse in the misonidazole arm. The quality of survival was no different between pa- tients receiving the conventional 6-week fractionation and those receiving the accelerated fractionation when radiotherapy was administered in a total of 10 days at three fractions of 2 Gy per day (19).
radiation to the ears is combined with cisplatin ( 10). On the other hand, cisplatin is much less myelosuppressive (thrombocytopenia and leukopenia) than carboplatin. In ad- dition to potentiating radiation, cisplatin and carboplatin have shown some efficacy against glioblastoma multiforme in Phase II studies (40, 4 1) .
Nitrosourea-based drug combinations appear mini- mally superior to monotherapy for glioblastoma multi- forme in a study comparing postirradiation carmustine (BCNU) to the PCV combination (procarbazine, CCNU, and vincristine) (24, 26). Although the median (50th percentile) time to tumor progression (TlP) and the me- dian survival duration were comparable, the 25th percen- tile durations were 72 (‘lTP) and 94 (survival) weeks for PCV compared to 43 and 71 weeks for BCNU. Hence, for this study, we chose PCV as adjuvant chemotherapy following irradiation.
METHODS AND MATERIALS
Patients
Because the accelerated schedule of three daily fractions of 2 Gy given in two cycles of 5 days with a treatment break of 2 weeks produced equal results to conventional radiation therapy, we chose the acceler- ated schedule, thus reducing the total time of car- boplatin administration to only 10 days.
All patients entered in this study were seen at either The University of Texas M. D. Anderson Cancer Center (MDACC), Houston, TX, or Memorial Hospital, North Hollywood, FL. Eligible patients had to fulfill the follow- ing criteria:
It has been demonstrated that cisplatin or carboplatin, combined with radiation, increases radiation cell kill (9, 13). This effect is greater with infusion schedules than with bolus injections ( 12). Although a number of reasons for the potentiation of the radiation effect have been sug- gested ( 12, 34), inhibition of sublethal radiation-damage repair appears to be the most tenable explanation at this time. Other putative mechanisms are inhibition of poten- tially lethal damage repair, selective radiosensitization of hypoxic cells, and perturbation of cell-cycle kinetics. It is not clear whether inherent sensitivity of tumor cells to cisplatin is an absolute prerequisite to the drug’s radia- tion-potentiating effects. Cells that are sensitive to cis- platin as a cytotoxic agent appear to be unable to repair deoxyribonucleic acid (DNA) -DNA intrastrand cross- links (2). DNA-protein and DNA-inter&rid crosslinking by cis- and truns-platinum diamminedichloride in L1210 leukemia cells was also shown to be directly related to cytotoxicity (42).
1.
2.
3. 4. 5.
histologic diagnosis of glioblastoma multiforme or gli- osarcoma using a modified Ringertz scale (4) normal liver function (serum glutamic-pyruvic trans- aminase, and alkaline phosphatase levels equal or less than two times institutional normal and bilirubin levels I 1.5 mg/dl), creatinine levels I 1.5 mg/dl, and a normal hemogram (absolute neutrophil count z 1500/ mn? and platelet count 2 125,OOO/mm’) age > 16 years Kamofsky performance status 2 60 signed Institutional Review Board-approved informed consent form
6. lack of (a) active infection; (b) pregnancy (adequate contraception required) ; (c) any disease that would obscure toxicity or dangerously alter drug metabolism; and (d) serious intercurrent illness.
Study design This was a single-arm study designed to evaluate carboplatin during accelerated fractionated radia- tion followed by PCV in patients with glioblastoma multi- forme by ‘ITP, survival duration, and toxicity. The treat- ment plan was:
Although most radiosensitization studies have used cis- Radiation therapy The target volume was defined by platin, we decided to use carboplatin, a cis-diammine-cyclo- the tumor volume, as determined by an enhanced mag- butanedicarboxylato platinum II. From all indications, car- netic resonance imaging (MRI) , with a margin of 3 cm. boplatin and cisplatin share a mechanism of cytotoxicity Beam energy was either 6 MV or 18 MV. The fraction resulting from DNA crosslinking, but differ substantially size was 2 Gy given three times a day, with an interfrac- in their pharmacokinetics, dose tolerance, and clinical side tion period of 4 to 5 h. Treatment was administered in 5 effects. Renal toxicity, nausea, and vomiting are predomi- consecutive days, Monday through Friday, in two cycles nant with cisplatin, but minimal with carboplatin (5). Also divided by a 2-week break, for a total dose of 60 Gy. of concern was the ototoxicity and deafness found when Because of MRI patterns of gadolinium contrast enhance-

Glioblastoma multiforme treatments 0 V. A. LEVIN et al. 359
ment (publication in preparation) and reoperation find- ings that suggested radiation late effects in patients on this study and in a parallel anaplastic glioma study, the radiation dose was reduced to 57 Gy, at 1.9 Gy/fraction in the last nine patients. The radiation volume was calcu- lated by multiplying the effective treatment area by the diameter or third dimension at the central axis. Because no correction was made to account for the rounded shape of the head, most radiation volume values are inflated and include tissues outside the central nervous system.
Carboplatin. A dose of 33 mglm’ was administered as a 2-h intravenous (IV) infusion beginning 1.75 h before each radiation therapy (total dose = 990 mg/m’). The schedule used was loosely based on data of Rozencweig et al. (36) who showed that 15-min IV infusions daily for 5 days at a dose of 100 mg /m’/day produced predictable myelosuppression with nadir counts at 22-28 days. Dose modification for myelotoxicity induced by the first week of carboplatin therapy was made during the second 5-day cycle of carboplatin.
Postradiation PCV. Four weeks after completing radiation patients started PCV chemotherapy on the fol- lowing schedule: CCNU, 110 mg/m’ orally on day 1; procarbazine, 60 mg/m’ orally on days 8-21; and vin- cristine, 1.4 mg/m’ IV on days 8, 29. PCV courses were repeated at 6-7-week intervals for six courses or until tumor progression.
TIP and survival were measured from the first day of chemoradiation treatment until progression was docu- mented or death occurred. At the time of progression, the patient was offered other treatments if appropriate. These patients continued to be monitored for survival.
The study was designed to detect an increase in median TIP of 1.5-fold (40 to 60 weeks) for patients with gli- oblastoma multiforme. The basis for the null median of 40 weeks was the published TIP and survival curves of protocol patients in the Northern California Oncology Group (NCOG) studies 6G61 (24), 6G91 (25), and 6682-l (35). The survival distributions from all three protocol studies were exponential with median TTP of 37, 41, and 43 weeks, respectively. The sample size re- quired to detect the 1.5-fold increase in median TIP with 90% power at a 5% level of significance, assuming an accrual of 1.5 week and a follow-up of 65 weeks after study closure, is 83 patients (8).
Evaluations Before treatment, patients underwent a (a) physical
and neurologic examination, (b) determination of perfor- mance status, (c) an MRI, or rarely, a computed tomogra- phy (CT) scan, with and without contrast enhancement, (d) complete blood count, differential, and platelet counts, and (e) a chemistry survey. During treatment, complete blood counts, differential, and platelet counts were obtained every week during radiotherapy and every 2 weeks during PCV chemotherapy; neurologic examina- tions, contrast-enhanced MRI scans, and chemistry sur-
veys were evaluated every 6-7 weeks during the first year. During the second year, patients in remission were evaluated with neurologic examinations and contrast-en- hanced MRI scans at 3-month intervals; intervals were extended to every 4 months during the third year and to 6 months in the fourth year.
Determination of response Variables were evaluated based on changes since the
last examination and scans (27). Although neurologic performance was monitored by
grading both symptoms and signs, objective response was based on changes in the contrast-enhanced MRI or CT scans.
Response to therapy was recorded, but was of little value because (a) it was difficult to distinguish resolution of postsurgical artifacts from true response to therapy; (b) some patients had no residual disease to monitor after surgery; and (c) the end points of the study were TIP and survival duration. Stable disease (SD) was defined as no change in the MRI scan with the patient receiving stable or decreasing doses of glucocorticoids; progressive disease (PD) was defined by an increasing tumor volume, provided that the dose of glucocorticoids had not been decreased since the last evaluation period; if the glucocor- ticoid dose was concomitantly decreased, the response was scored SD for that visit.
Data management and quality control All patients were registered and all data were kept
by the MDACC Brain Tumor Center Data Management Office. All relevant information was documented in the patient’s medical record and/or flow sheets and com- puter-based Patient Data Management Systems (PDMS) database.
Designated total and subtotal resections were con- firmed by review of postoperative MRI scans.
Statistical methods Survival analyses were performed on the the 83 pa-
tients who received prescribed radiotherapy and car- boplatin; more detailed analyses were conducted on the 74 patient subset that, in addition, received at least one course of PCV. Unadjusted survival analyses were done using Kaplan-Meier (20) plots, log rank tests, and their generalizations ( 11) . The Cox proportional hazards re- gression model (7) and its generalization to accommo- date time-varying covariates were used to assess the ability of patient covariates to predict survival and TTP. Covariate effects on survival and TTP were first as- sessed individually.
Covariates individually predictive at level of 0.10 were included in a multivariate Cox model, with a final model obtained using backward elimination. Goodness-of-fit was assessed using likelihood statistics, individual covari- ate parameter p-values, Martingale and Schoenfeld resid- ual plots ( 17, 37), the proportionality assumption was

Volume 33. Number 2, 1995 360 I. J. Radiation Oncology 0 Biology 0 Physics
Table 1. Patient characteristics
No PCV patients FCV patients
9 74 Evaluable patients Age, years
Median (range) Karnofsky score
Median 90-100 70-80 < 70
Sww Total resection Subtotal resection Biopsy
Number of surgeries 1 operation 2 operations 3 or more operations
Radiation dose 60 Gy 57 Gy
Radiation tumor volume, cc
Median
Carboplatin dose, mg/m’
Median
66(52-78)
90 7(78%) 1 (11%) 1 (11%)
2 (22%) 7 (78%)
9 (100%)
1185 (722-1724)
958 (660- looo)
55 (19-71)
90 43 (58%) 24 (32%) 7(9%)
15 (20%) 51(69%)
8 (11%)
46(62%) 25 (34%)
3(4%)
65 (88%) 9(12%)
968 (428-4360)
973 (683-1094)
assessed using the test of Grambsch and Themeau ( 17). All residual plots were smoothed using the method of Cleveland (6). All computations were carried out in Splus ( 1) and StatXact (Cytel Software Corporation, Cam- bridge, MA) on a SUN Spare 2 workstation (Sun Micro- systems, Inc., Mountain View, CA). Fits of the Cox model with time) varying covariates were performed us- ing the package of Themeau (38). Pair-wise associations between patient covariates were evaluated using the Fisher exact and generalized exact tests for crosstabulated categorical variables (32)) the Wilcoxon-Mann-Whit- ney test, and the Kruskal-Wallis test.
RESULTS 1.0
Patient characteristics Between April 5, 1989 and February 28, 1992, 86 pa-
tients were entered into this study. Three patients were considered not to be evaluable for
response; one was treated with gamma-knife radiotherapy directly after completion of external-beam radiation and without our approval, one was lost completely to follow- up after radiotherapy, and one progressed outside of the radiation field soon after completing radiotherapy and re- quired additional nonprotocol radiotherapy. Table 1 sum- marizes patient characteristics for the 83 evaluable pa- tients: 74 patients received at least one course of PCV, and 9 patients did not receive PCV. Of the nine patients
0.8 - PCV (n=74)
ir 1
- No PCV (n=9)
9
0.6
m 0 0.4
E 0.2
0.0 0 40 80 120 160 200
WEEKS
Fig. 1. Unadjusted time to tumor progression for the 74 patients who received FCV and the 9 patients who did not receive PCV.
who received carboplatin and radiation therapy as pre- scribed, but who did not receive postradiotherapy PCV, all refused to start PCV; of these, four progressed within 9 to 15 weeks. The median age for the 74 evaluable patients who received PCV was 55 years and is compara- ble to that of patients in previous studies (24, 25, 35).
Time to tumor progression (progression-free survival) analyses
As an end point, TTP is less reliable than death. Radiation changes can mimic tumor, reoperation is not always possible, and histologic examination of re- moved tissue can show a mixed pattern of tumor and necrosis. Additionally, one of the hallmarks of glioblas- toma multiforme is necrosis and radiation normally produces additional necrosis in the tumor field (4). For the analysis of TTP, the six patients found to have only necrosis at reoperation were not considered to have progressed at the time of reoperation. Figure 1 is a Kaplan-Meier representation of TTP for the 74 patients that received at least one course of PCV following radi- ation and the nine patients who did not.
The median TTP was 26 weeks; 56 patients progressed and 18 were censored, that is, alive and still in remission at the time of this analysis. Differences in TIP between the three surgery groups were almost significant (p = 0.073). When the biopsy and subtotal resection groups were combined, the difference in TIP between the two groups became significant (p = 0.04) ; median ‘ITP was 52 weeks for the 15 patients who had a total, 25 weeks for the 5 1 patients with a subtotal resection, and 2 1 weeks for the eight patients who had a biopsy.
Survival analyses Among the patients receiving at least one course of
PCV, 68 patients were dead and 6 censored at the time of this analysis. As expected from the explanations as to why patients did not accept postitradiation PCV, the survivals of those 74 patients who did receive PCV were substantially longer (median, 55 weeks; Fig. 2) than the survivals of the nine patients not receiving PCV (median,

Glioblastoma multifonne treatments 0 V. A. LEVIN et al. 361
2 0.8 - PCV (n=74)
0.8 - No PCV (n=9)
0.4
0.2
0.0 0 52 104 158 268 260
WEEKS
Fig. 2. Unadjusted survival time for the 74 patients who received PCV and the 9 patients who did not receive PCV.
20.1 weeks; 7 of 9 dead; p = not significant). The survival of all 83 patients is 53 weeks compared to 55 weeks survival for the 74 patients who received at least one course of PCV. Differences in survival time between the three surgery groups (Fig. 3) were significant (p = 0.003) ; the longest survivals were in the total resection group (median 80 weeks), second longest in the subtotal resection group (median 55 weeks), and shortest in the biopsy group (median 37 weeks).
Table 2 summarizes individually predictive covariates for the 74 patients who received the initial course of PCV. Covariates individually predictive for survival at p I 0.05 were age, extent of surgery, log radiation volume, and number of courses of PCV chemotherapy after week 45; Kamofsky performance score and radiation dose were marginally significant.
The number of reoperations, number of courses of PCV, and performance status each varied over time, be- ginning at first day of chemoradiation treatment. Baseline (nontime-varying) covariates were age, sex, radiation dose, carboplatin dose, and radiation tumor volume. Num- ber of PCV courses and number of reoperations each increased linearly over time, specifically over the first 45 weeks for number of PCV courses and over the first 75 weeks for number of reoperations. Consequently, each of
0.8 - c
Biopsy - Subtotal
2 z 0.6 - Total
3 2 0.4
p 0.2
100 150 200 250 300
WEEKS
Fig. 3. Unadjusted survival time for patients who had total resection ( IZ = 15) and subtotal resection (n = 5 1) , or biopsy only (n = 8) and received PCV chemotherapy.
Table 2. Covariates individually predictive (univariate Cox model) of time to progression or survival time for 74
evaluable patients who received at least one course of PCV
Survival time
Variable Favorable p-Value*
Age Younger 0.013 Kamofsky score Higher 0.055 Surgery Total or subtotal 0.003 Carboplatin dose NS Log RT volume Smaller 0.005 Surgeries after week 75 NS Number of courses of PCV More 0.010
* Based on likelihood ratio statistic for each variable. Abbreviation: NS = not significant; PCV = procarbazine,
CCNU, vincristine.
these two covariates was vacuously predictive of survival and TTP over these time periods, because patients who survived longer were available to have more courses of PCV and more reoperations. A time-shifted Cox regres- sion analysis of number of PCV courses beginning at week 45, based on the 48 patients still alive at this time, indicated that conditional on 45-week survival number of PCV courses was predictive of additional survival (p = 0.001) and TTP (p = 0.011) . Similar analyses of number of reoperations beginning at week 75 were based on 24 patients still alive at that time, and showed no significant prediction of either survival or lTP. Performance status, which varied randomly over time, was not predictive of Tl? (p = 0.86) and was marginally predictive of survival (p = 0.055).
For the three surgical subgroups (total resection, subto- tal resection, and biopsy), only baseline Kamofsky score differed significantly (p < O.OOl), with a total or partial resection more likely in patients with higher Karnofsky score; the number of surgeries, age, carboplatin dose, and log irradiation volume did not differ significantly across the surgical subgroups. Radiation dose was partially con- founded with surgical status in that 9 of the 74 PCV patients who received 57 Gy radiation had total or subtotal resection.
The final multivariate Cox model for survival (Table 3), was obtained by backward elimination of the covari-
Table 3. Summary of final Cox proportional hazards model (based on a backward elimination starting at age, Kamofsky
performance score, extent of surgery, and log radiation volume) for predicting survival in 74 evaluable patients
Estimated Variable risk p-Value*
As 1.027 0.013 Total or subtotal original surgery 0.309 0.003
* Likelihood ratio = 13.8 on 2 degrees of freedom. Abbreviation: NS = p = 0.10.
362 I. J. Radiation Oncology 0 Biology 0 Physics Volume 33, Number 2, 1995
ates: age, Karnofsky score, extent of original surgery, and log radiation dose. Age and extent of initial surgery are most important for survival, Kamofsky performance score and log radiation volume are not significant (p 2 0.1) .
Comparison to previous NCOG studies. Visual com- parison of the TTP and survival curves of the 74 patients who received PCV to the comparable groups of patients from NCOG 6G61 (24)) NCOG 6G91 (25)) and NCOG 6082-l (35) led to a decision to not proceed with a formal comparison of the groups. The median (50th per- centile) and 25% ‘M’P and survival are shown in Table 4 for the three NCOG studies and the the current study. Most comparable in survival to our current study are the NCOG 6682-l results.
The latter study evaluated 96-h infusions of bromo- deoxyuridine for 6 weeks of conventional radiation fol- lowed by PCV chemotherapy.
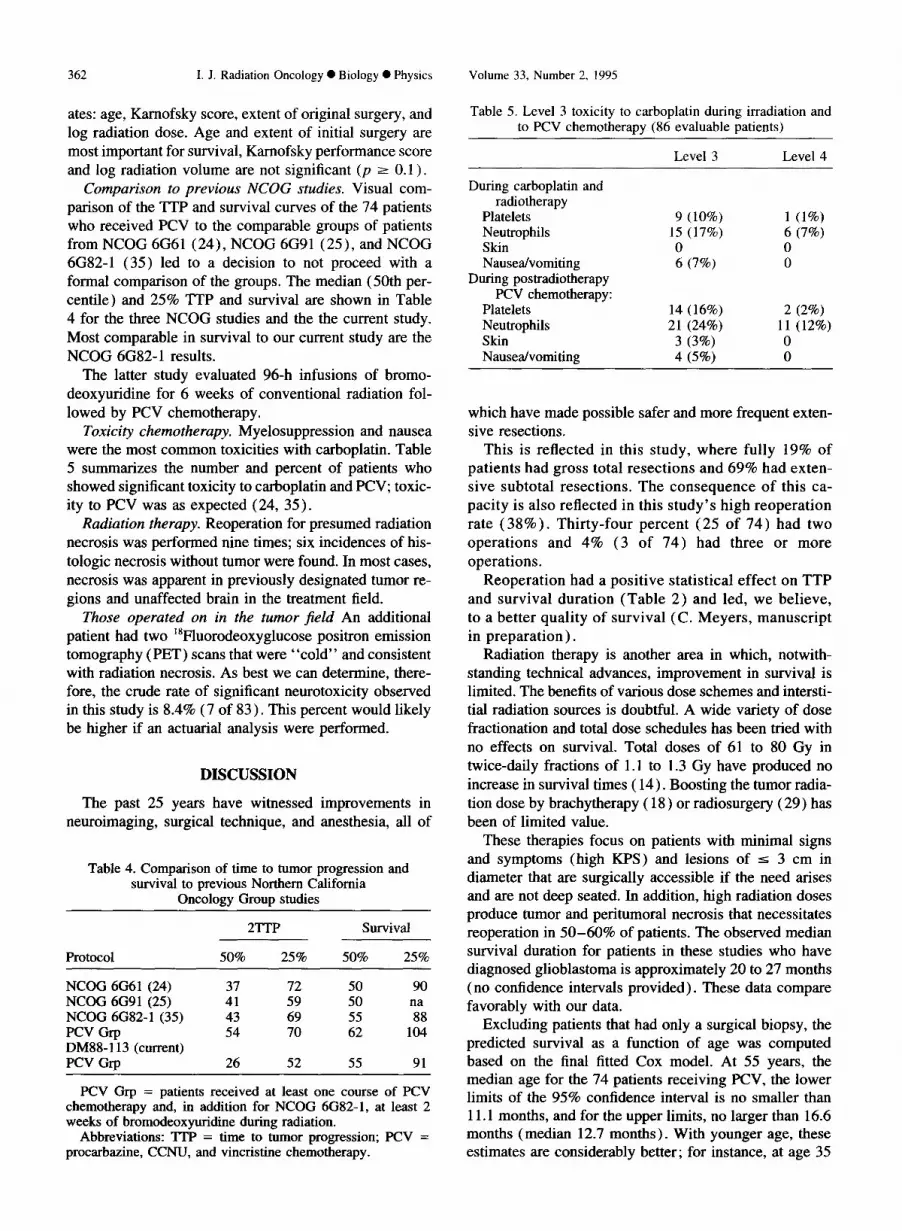
Toxicity chemotherapy. Myelosuppression and nausea were the most common toxicities with carboplatin. Table 5 summarizes the number and percent of patients who showed significant toxicity to carboplatin and PCV; toxic- ity to PCV was as expected (24, 35).
Radiation therapy. Reoperation for presumed radiation necrosis was performed nine times; six incidences of his- tologic necrosis without tumor were found. In most cases, necrosis was apparent in previously designated tumor re- gions and unaffected brain in the treatment field.
Those operated on in the tumor jeld An additional patient had two ‘8Fluorodeoxyglucose positron emission tomography (PET) scans that were “cold” and consistent with radiation necrosis. As best we can determine, there- fore, the crude rate of significant neurotoxicity observed in this study is 8.4% (7 of 83). This percent would likely be higher if an actuarial analysis were performed.
DISCUSSION
The past 25 years have witnessed improvements in neuroimaging, surgical technique, and anesthesia, all of
Table 4. Comparison of time to tumor progression and survival to previous Northern California
Oncology Group studies
Protocol
2TrP
50% 25%
Survival
50% 25%
NC00 6G61 (24) NCOG 6G91 (25) NCOG 6G82-1 (35) PCV Grp DM88-113 (current) PCV Grp
37 41 43 54
26
72 59 69 70
52
50 50 55 62
55
90 na 88
104
91
F’CV Grp = patients received at least one course of PCV chemotherapy and, in addition for NCOG 6G82-1, at least 2 weeks of bromodeoxyuridine during radiation.
Abbreviations: TTP = time to tumor progression; PCV = procarbazine, CCNU, and vincristine chemotherapy.
Table 5. Level 3 toxicity to carboplatin during irradiation and to PCV chemotherapy (86 evaluable patients)
Level 3 Level 4
During carboplatin and radiotherapy
Platelets Neutrophils Skin Nausea/vomiting
During postradiotherapy PCV chemotherapy:
Platelets Neutrophils Skin Nausea/vomiting
9 (10%) 1 (1%) 15 (17%) 6 (7%) 0 0 6 (7%) 0
14 (16%) 2 (2%) 21 (24%) 11 (12%)
3 (3%) 0 4 (5%) 0
which have made possible safer and more frequent exten- sive resections.
This is reflected in this study, where fully 19% of patients had gross total resections and 69% had exten- sive subtotal resections. The consequence of this ca- pacity is also reflected in this study’s high reoperation rate (38%). Thirty-four percent (25 of 74) had two operations and 4% (3 of 74) had three or more operations.
Reoperation had a positive statistical effect on TTP and survival duration (Table 2) and led, we believe, to a better quality of survival (C. Meyers, manuscript in preparation).
Radiation therapy is another area in which, notwith- standing technical advances, improvement in survival is limited. The benefits of various dose schemes and intersti- tial radiation sources is doubtful. A wide variety of dose fractionation and total dose schedules has been tried with no effects on survival. Total doses of 61 to 80 Gy in twice-daily fractions of 1.1 to 1.3 Gy have produced no increase in survival times ( 14). Boosting the tumor radia- tion dose by brachytherapy ( 18) or radiosurgery ( 29) has been of limited value.
These therapies focus on patients with minimal signs and symptoms (high KPS ) and lesions of 5 3 cm in diameter that are surgically accessible if the need arises and are not deep seated. In addition, high radiation doses produce tumor and peritumoral necrosis that necessitates reoperation in 50-60% of patients. The observed median survival duration for patients in these studies who have diagnosed glioblastoma is approximately 20 to 27 months (no confidence intervals provided). These data compare favorably with our data.
Excluding patients that had only a surgical biopsy, the predicted survival as a function of age was computed based on the final fitted Cox model. At 55 years, the median age for the 74 patients receiving PCV, the lower limits of the 95% confidence interval is no smaller than 11.1 months, and for the upper limits, no larger than 16.6 months (median 12.7 months). With younger age, these estimates are considerably better; for instance, at age 35

years, the comparable 95% confidence intervals are 13.8 and 28.4 months (median 18.4 months).
Chemotherapeutic potentiation of radiation to effect greater tumor-cell kill and lengthen the survival of pa- tients who have glioma has been the object of investiga- tion for nearly 25 years. Unfortunately, consistent benefit has been either unattainable or modest (30). One reason for this is certainly the fact that chemotherapy given to potentiate 32 days of radiation over 6-7 weeks produces serious systemic dose-limiting toxicity that limits our ability to use effective chemotherapy doses. To overcome this limitation, we embarked on these studies that com- press the time of radiation administration into 10 days to allow for maximal carboplatin dosing and also recovery from drug toxicity during the planned treatment break. For this study, we chose carboplatin because of limited nausea and vomiting, acceptable myelotoxicity, and its capacity to potentiate radiation-induced cell kill (9, 13 ) . Unfortunately, this study failed to demonstrate a potentia- tion by carboplatin at the dose and schedule used.
By pushing the envelop of radiation-chemotherapy po- tentiation, we run the risk of producing more central neu- rotoxicity. For a variety of reasons, autopsies are no longer as obtainable as in past decades. Our capacity, therefore, to have histologic proof of radiation damage is limited to surgical biopsy (with bromodeoxyuridine labeling indices when possible) in selected patients. Addi- tional secondary information from MRI scans, PET, and single photon emission tomography (SPECT) can be helpful, but is not definitive. As best we can determine, the rate of significant neurotoxicity observed in this study is 9.4% (7 of 74). Clinically relevant radiation necrosis has been reported in approximately 3 to 9% of brain
Glioblastoma multifonne treatments l V. A. LEVIN et al. 363
tumor patients (22, 23, 3 1) . Some of these studies may underestimate the true incidence of focal radiation necro- sis, because they were conducted prior to the MRI era; autopsy studies suggest that focal necrosis may be as high as 18%.
Interestingly, the median survival of these seven pa- tients with significant neurotoxicity was 23.3 months (range 8 to +29 months) ; their mean Kamofsky perfor- mance score at the start of treatment, at 6 months, and at 12 months were 90, 87, and 85, respectively. Certainly these “side effects” are tolerable for a disease as devasta- ting and difficult to treat as glioblastoma multiforme. A more systematic study based on serial neuropsychologic testing will be published separately at the completion of the anaplastic glioma stratum of this protocol.
The major conclusions of this study are that aggressive initial surgery and reoperation for patients under the age of 60 years who have glioblastoma can lead to median survivals of 12.7 to 18.4 months, depending on covariates. Although this was not a randomized study comparing brachytherapy or radiosurgery boosts to accelerated frac- tionated external-beam radiation, our data are, neverthe- less, comparable and bring into question the widespread use of more expensive brachytherapy and radiosurgery for treating glioblastoma patients.
Although not demonstrating a benefit for carboplatin potentiation of radiation therapy, our study shows the feasability and relative safety of combining accelerated fractionated radiotherapy with chemotherapy. Future plans are to complete the anaplastic glioma stratum of this protocol and complete an ongoing Phase II study of high-dose bromodeoxyuridine with accelerated fraction- ated radiotherapy for patients with glioblastoma multi- forme.
REFERENCES
1. Becker, R. A.; Chambers, J. M.; Wilks, A. R. The new S language. Pacific Grove, CA: Wadsworth; 1988.
2. Bedford, P.; Fichtinger-Schepman, A. M. J.; Shellard, S. A.; Walker, M. C.; Hill, B. T. Differential repair of platinum-DNA adducts in human bladder and testicular tu- mor continuous cell lines. Cancer. Res. 48:3019-3024; 1988.
3. Bleehen, N. W.; Wiltshire, G. R.; Plowman, P. N.; Watson, J. V.; Gleave, J. R.; Holmes, A. E.; Lcwin, W. S.; Treip, C. S. A randomized study of misonidazole and radiotherapy for grade 3 and 4 cerebral astrocytomas. Br. J. Cancer. 43:436-442; 1981.
4. Burger, P. C.; Scheithauer, B. W.; Vogel, F. S.: Surgical pAthology of the nervous system and its coverings. 3rd ed. New York Churchill Livingstone; 1991:214-234.
5. Canetta, R.; Franks, C.; Smaldone, L.; Bragman, K.; Rozen- cweig, M.: Clinical status of carboplatin. Oncology 1:61- 69; 1987.
6. Cleveland, W. S. Robust locally weighted regression and smoothing scatterplots. J. Am. Stat. Assoc. 74596-610; 1979.
7. Cox, D. R. Regression models and life tables. J. R. Stat. Sot. 34~187-220; 1972.
8. Dixon, D. 0.; Simon, R. Sample size considerations for
studies comparing survival curves using histroical controls. J. Clin. Epidemiol. 41:1209-1213; 1988.
9. Douple, E. B.; Richmond, R. C.; OHara, J. A.; Coughlin, C. T. Carhoplatin as a potentiator of radiation therapy. Can- cer. Treat, Rev. 12: 1 1 l- 124; 1985.
10. Feun, L. G.; Stewart, D. J.; Maor, M. H.; Leavens, M.; Savaraj, N.; Burgess, M. A.; Yung, W. K.; Benjamin, R. S. A pilot study of cis-diamminedichloroplatinum and radiation therapy in high grade astrocytomas. J. Neuroon- col. 1:109-113; 1983.
11. Fleming, T. R.; Harrington, D. P. Counting processes and survival analysis. New York John Wiley & Sons; 1991.
12. Fu, K. K.; Lam, K. N.; Rayner, P. A. The influence of time sequence of cisplatin administration and continuous low dose rate irradiation (CLDRI) on their combined effects on a murine squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 11:2119-2124; 1985.
13. Fu, K. K.; Rayner, P. A.; Lam, K. N. Modification of the effects of continuous low dose rate irradiation by concurrent chemotherapy infusion. Int. J. Radiat. Oncol. Biol. Phys. 10:1473-1478; 1984.
14. Fulton, D. S.; Urtasun, R. C.; Scott-Brown, I.; Johnson, E. S.; Mielke, B.; Curry, B.; Huyser-Wierenga, D.; Hanson, J.; Feldstein, M. Increasing radiation dose intensity using

364 I. J. Radiation Oncology l Biology l Physics Volume 33, Number 2, 1995
hyperfractionation in patients with malignant glioma. Final report of a prospective phase I-II dose response study. J. Neurooncol. 14:63-72; 1992.
15. George, S. L.; Desu, M. M. Planning the size and duration of a clinical trial studying the time to some critical event. J. Chron. Dis. 27:15-24; 1974.
16. Goffman, T. E.; Dachowski, L. J.; Bobo, H.; Oldfield, E. H.; Steinberg, S. M.; Cook, J.; Mitchell, J. B.; Katz, C.; Smith, R.; Glatstein, E. Long-term follow-up on National Cancer Institute phase I/II study of glioblastoma multi- forme treated with iododeoxyuridine and hyperfractionated irradiation. J. Clin. Oncol. 10:264-268; 1992.
17. Grambsch, P. M.; Themeau, T. M. Proportional hazards tests and diagnostics based on weighted residuals. Biome- trika 81:515-52; 1994.
18. Gutin, P. H.; Prados, M. D.; Phillips, T. L.; Wara, W. M.; Larson, D. A.; Leibel, S. A.; Sneed, P. K.; Levin, V. A.; Weaver, K. A.; Silver, P. External irradiation followed by an interstitial high activity iodine-125 implant “boost” in the initial treatment of malignant gliomas: NCOG study 66-82-2. Int. J. Radiat. Oncol. Biol. Phys. 21:601-606; 1991.
19. Horiot, J. C.; van den Bogaert, W.; Ang, K. K.; Van der Schueren, E.; Bartelink, H.; Gonzalez, D.; de Pauw, M.; van Glabbeke, M. European organization for research on treatment of cancer trials using radiotherapy with multiple fractions per day. Front. Radiat. Ther. Oncol. 22:149- 161; 1988.
20. Kaplan, E. L.; Meier, P.: Nonparametric estimates from incomplete observations. J. Am. Stat. Assoc. 53:457-481; 1958.
21. Keim, H.; Potthoff, K.; Schmidt, K.; Schiebusch, M.; Neiss, A.; Trott, K. R. Survival and quality of life after continuous accelerated radiotherapy of glioblastoma. Radiother. Oncol. 9:21-26; 1987.
22. Leibel, S. A.; Sheline, G. E. Radiation therapy for neo- plasms of the brain. J. Neurosurg. 66:1-22; 1987.
23. Levin, V. A.; Gutin, P. H.; Leibel, S. Neoplasms of the central nervous system. In: DeVita, V. T., Jr.; Hellman, S.; Rosenberg, S. A., eds. Cancer. Principles and practice of oncology, 4th ed. Philadelphia, PA: J. B. Lippincott; 1993: 1679- 1737.
24. Levin, V. A.; Silver, P.; Hannigan, J.; Wara, W. M.; Gutin, P. H.; Davis, R. L.; Wilson, C. B. Superiority of postradio- therapy adjuvant chemotherapy with CCNU, procarbazine, and vincristine (PCV) over BCNU for anaplastic gliomas: NCOG 6G61 final report. Int. J. Radiat. Oncol. Biol. Phys. 18:321-324; 1990.
25. Levin, V. A.; Wara, W. M.; Davis, R. L.; Silver P.; Resser, K. J.; Yatsko, K.; Nutik, S.; Gutin, P. H.; Wilson, C. B. NCOG protocol 6G91: Seven drug chemotherapy and irra- diation for patients with glioblastoma multiforme. Cancer Treat. Rep. 70:739-744; 1986,
26. Levin, V. A.; Wara, W. M.; Davis, R. L.; Vestnys, P.; Resser, K. J.; Yatsko, K.; Nut&, S.; Gutin, P. H.; Wilson, C. B. Phase III comparison of BCNU and the combination of procarbazine, CCNU, and vincristine administered after radiotherapy with hydroxyurea for malignant gliomas. J. Neurosurg. 63:218-223; 1985:
27. Levin, V. A.; Crafts, D. C.; Norman, D. M.; Hoffer, P. B.; Spire, J. P.; Wilson, C. B. Criteria for evaluating malignant
brain tumor patients undergong chemotherapy. J. Neuro- surg. 47:329-335; 1977.
28. Levin, V. A.; Wilson, C. B.; Davis, R.; Wara, W. M.; Pischer, T. L.; Irwin, L. A phase III comparison of BCNU, hydroxyurea, and radiation therapy to BCNU and hydroxy- urea for primary malignant gliomas. J. Neurosurg. 5 1:526- 532; 1979.
29. Loeffler, J. S.; Alexander, E.; Shea, W. M.; Wen, P. Y.; Fine, H. A.; Kooy, H. M.; Black, P. M. Radiosurgery as part of the initial management of patients with malignant gliomas. J. Clin. Oncol. 10:1379-1385; 1992.
30. Maor, M. H.; Levin, V. A. Combination of radiotherapy and drugs for the treatment of malignant gliomas. In: John, M. J.; Philips, T.; Legha, S., eds. Chemoradiation: An inte- grated approach to cancer treatment. Philadelphia, PA: Lea & Febiger; 1993:191-203.
3 1. Marks, J. E.; Baglan, R. J.; Prassad, S. C.; Blank, W. F. Cerebral radio-necrosis: Incidence and risk in relation to dose, time, fractionation and volume. Int. J. Radiat. Oncol. Biol. Phys. 7:243-252; 1981.
32. Mehta, C. R. The exact analysis of contingency tables in medical research. Stat. Methods Med. Res. 3:135-156; 1994.
33. Nelson, D. F.; Diener-West, M.; Weinstein, A. S.; Schoen- feld, D.; Nelson, J. S.; Sause, W. T.; Chang, C. H.; Good- man, R.; Carabell, S. A randomized comparison of misoni- dazole sensitized radiotherapy plus BCNU and radiotherapy plus BCNU for treatment of malignant glioma after surgery: Final report of an RTOG study. Int. J. Radiat. Oncol. Biol. Phys. 12:1793-1800; 1986.
34. Nias, A. H. Radiation and platinum drug interaction. Int. J. Radiat. Biol. 48:297-314; 1985.
35. Phillips, T. L.; Levin, V. A.; Ahn, D. K.; Gutin, P. H.; Davis, R. L.; Wilson, C. B.; Prados, M. D.; Wara, W. M.; Flam, M. S. Evaluation of bromodeoxyuridine in glioblas- toma multiforme: A Northern California cancer center phase II study. Int. J. Radiat. Oncol. Biol. Phys. 21:709- 714; 1991.
36. Rozencweig, M.; Nicaise, C.; Beer, M.; Crespeigne, N.; Van Rijmenant, M.; Lenaz, L.; Kenis, Y. Phase I study of carboplatin given on a five-day intravenous schedule. J. Clin. Oncol. 1:621-626; 1983.
37. Themeau, T. M.; Grambsch, P. M.; Fleming, T. R. Martin- gale-based residuals for Survival Models. Biometrika 77:147-160; 1990.
38. Themeau, T. M. A package for survival analysis in S. Mayo foundation; 1994.
39. Urtasun, R. C.; Feldstein, M. L.; Partington, T. Radiation and nitroimidazoles in supratentorial high grade gliomas: A second clinical trial. Br. J. Cancer 46:101-108; 1982.
40. Walker, R. W.; Allen, J. C. Cisplatin in the treatment of rcurrent childhood primary brain tumors. J. Clin. Oncol. 6:62-66; 1988.
41. Yung, W. K. A.; Mechtler, L.; Gleason, M. J. Intravenous carboplatin for recurrent malignant gliomas: A phase II study. J. Clin. Oncol. 9:860-864; 1991.
42. Zwelling, L. A.; Anderson, T.; Kohn, K. W. DNA-protein and DNA interstrand cross-linking by cis- and trans-plati- num (II) diamminedichloride in L1210 mouse leukemia cells and relation to cytotoxicity. Cancer. Res. 39:365-369; 1979.