pharmaceuticals - metagenics institute
TRANSCRIPT

MSE2673 - 01/15
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
February - March 2015


3
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Presentation ................................................................................................................................................................................29 Co-Prescribing: The Future of Healthcare .................................................................................................................................... 29 Getting Perspective on Interactions ............................................................................................................................................. 36 Decision Making Framework: EDMC .......................................................................................................................................... 45 Cautions: Changing Drug Levels ................................................................................................................................................ 51 Absorption ................................................................................................................................................................................ 52 Metabolism .............................................................................................................................................................................. 55 Detoxification and Medications ............................................................................................................................................ 57 Cautions: Antagonising Drug Effects ........................................................................................................................................... 63 Immune Suppressants and Anti-inflammatories ...................................................................................................................... 64 Cautions: Adverse Potentiation ............................................................................................................................................................... 76 Antidepressants................................................................................................................................................................... 77 Benzodiazepines ................................................................................................................................................................. 83 Anticoagulant/Antiplatelet Medications ................................................................................................................................. 88 Surgery .............................................................................................................................................................................. 96 Benefits: Positive Potentiation ...................................................................................................................................................... 98 Cardiovascular Medications ................................................................................................................................................ 99 Antihypertensives .............................................................................................................................................................. 101 Lipid-Lowering Medications................................................................................................................................................ 106 Antidiabetic Medications ................................................................................................................................................... 108 Weaning and Poly Pharmacy .............................................................................................................................................. 115 Benefits: Countering Side Effects ........................................................................................................................................................... 118 Antibiotics ........................................................................................................................................................................ 119 NSAIDS............................................................................................................................................................................ 121 Proton Pump Inhibitors ...................................................................................................................................................... 125 Oral Contraceptive Pill ...................................................................................................................................................... 129 Long Term Health Alongside Medications ............................................................................................................................ 132 Summary ................................................................................................................................................................................ 136
CONTENTS
Seminar Summary .........................................................................................................................................................................5 The Future of Healthcare Lies in Co-Prescription ............................................................................................................................ 5 Natural Medicine’s Strengths Can Support Pharmaceuticals’ Weaknesses ........................................................................................ 6 Understanding the Benefits and Cautions ...................................................................................................................................... 6 Putting Interactions in Perspective .................................................................................................................................................. 7 Individuality Causes More Interactions than Natural Medicines ........................................................................................................ 7 Poor Quality Control Tarnishes the Safety of Natural Medicines ....................................................................................................... 8 Deciding Whether to Prescribe – EDMC ........................................................................................................................................ 9 Evidence: What is the Balance? .................................................................................................................................................... 9 Dose Can be Tailored and Monitoring Increased ......................................................................................................................... 10 Communication is a Powerful Interaction-Management Strategy .................................................................................................... 10 Making an Assessment of Multiple Medications ............................................................................................................................ 11 Cautions: Changing Drug Levels ................................................................................................................................................ 12 Drug Absorption is Variable........................................................................................................................................................ 12 Drug Metabolism Enzymes Can be Altered .................................................................................................................................. 12 Treating the Liver and Detoxifying with Drugs ............................................................................................................................... 12 Narrow Therapeutic Window Medications ................................................................................................................................... 13 Antagonising Drug Effects – Conflicting Motives in Autoimmunity .................................................................................................. 13 Augmentation of Anti-inflammatories .......................................................................................................................................... 14 Potentiating Drug Effects in the Nervous System ........................................................................................................................... 15 Sedative Herbs and Drugs .......................................................................................................................................................... 16 Potentiation of Anticoagulants is Not as Common as Once Thought .............................................................................................. 17 Anticoagulant Interactions and Surgery ....................................................................................................................................... 17 Dealing with a Potential Interaction ............................................................................................................................................. 18 Focusing on the Benefits of Co-prescribing .................................................................................................................................. 18 Positive Potentiation in Cardiometabolic Disease .......................................................................................................................... 18 Potentiating Lipid Lowering Medications ...................................................................................................................................... 19 Coprescribing in Diabetics ......................................................................................................................................................... 20 Lipoic Acid is a Primary Adjuvant Therapy for Diabetes ................................................................................................................. 21 Weaning Guidelines .................................................................................................................................................................. 21 Polypharmacy – Where to Start? ................................................................................................................................................. 22 Specific Natural Medicines to Counteract Drug Side Effects........................................................................................................... 23 NSAIDs may Cause Mucosal Damage Through Dysbiosis ............................................................................................................. 24 Counteracting Hidden Nutrient Depletion .................................................................................................................................... 24 Daily Support for OCP Users ...................................................................................................................................................... 25 Maintaining Wellness on Pharmaceuticals ................................................................................................................................... 25 Confident and Safe Prescribing Alongside Pharmaceuticals ........................................................................................................... 26 References ................................................................................................................................................................................ 26

Appendix 1: Co-Prescribing Summary Tables..............................................................................................................................139 Appendix 1A: Natural Medicines with Immune Suppressant/Anti-Inflammatory Medications ........................................................... 139 Appendix 1B: Natural Medicines with Anxiolytic Medications ....................................................................................................... 140 Appendix 1C: Natural Medicines with Antidepressant Medications .............................................................................................. 141 Appendix 1D: Natural Medicines with Anticoagulant/Antiplatelet Medications .............................................................................. 142 Appendix 1E: Natural Medicines with Lipid Lowering Medications ................................................................................................ 143 Appendix 1F: Natural Medicines with Antihypertensive Medications ............................................................................................. 144 Appendix 1G: Natural Medicines with Antidiabetic Medications............................................................................................................... 145 Appendix 1H: Natural Medicines with Antibiotics ....................................................................................................................... 146 Appendix 1I: Natural Medicines with Proton Pump Inhibitors ....................................................................................................... 147 Appendix 1J: Natural Medicines with Hormone Medications ....................................................................................................... 148 Appendix 1K: Natural Medicines with Cancer Treatment ............................................................................................................. 149
Appendix 2: Technical Information .............................................................................................................................................150 High Purity, Low Reflux, Concentrated Fish Oil ............................................................................................................................ 150 Hydroxyapatite and Soy for Osteoporosis .................................................................................................................................. 168 Alpha Lipoic Acid for Antioxidant Support ................................................................................................................................... 184 Mixed Tocopherols & Tocotrienols for Free Radical Defence ......................................................................................................... 193

5
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
SEMINAR SUMMARY
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes
With the majority of Australians and New Zealanders taking at least one pharmaceutical medicine on a regular basis,1 prescribing natural medicines alongside drugs is difficult to avoid. Many practitioners worry about the potential of their prescriptions to cause adverse interactions with these medications, when in fact, the vast majority of research demonstrates the opposite.2
In many cases, a lack of confidence in co-prescribing can constitute a significant missed opportunity for the patient to receive the quality health care that natural medicine can offer. There are many clinical trials demonstrating the effective use of natural medicines alongside pharmaceuticals such as antihypertensives, antidiabetics and antidepressants, just to name a few. On the other hand, there are only a handful of clinical trials and case reports on the potential negative effects of these interactions.3,4 In most cases, depriving our patients of the benefit of natural medicines based on concerns around interactions is not an evidence-based strategy.
THE FUTURE OF HEALTHCARE LIES IN CO-PRESCRIPTION Both natural and pharmaceutical medicine have a lot to offer the health of patients. Pharmaceutical medicines have the powerful ability to control physiological and pathophysiological processes in the body, alleviating symptoms and reducing acute risk for many individuals. Natural medicines, on the other hand, get to the root cause of a disease and help to restore homeostasis. Neither can work effectively alone in a health care system which deals with many types and degrees of health and disease.
The current medical model was forged in the time of deathly infections and injuries, where heroic, lifesaving interventions were celebrated. Now, in a time of chronic disease, high potency narrow target medicines and surgical rescue are less relevant5 (until end stage disease occurs) – it is subtle, broad-acting, safe, and long-term medicine that is needed here. The change in burden of disease from 1900 to 2010 is well illustrated in Figure 1. Chronic disease is not caused by a drug deficiency – natural medicines can bridge the gap between chronic disease and the mainstream health care system. Cardiovascular disease, diabetes and cancer cannot be successfully managed into the future without the use of both groups of medicines side by side. While pharmaceutical medicines can be highly effective, life-saving strategies which reduce risk and control symptomatology, natural medicines and lifestyle change are needed to truly help restore health.
Figure 1. The burden of disease in 1900 compared to 2010.6

6
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NATURAL MEDICINE’S STRENGTHS CAN SUPPORT PHARMACEUTICALS’ WEAKNESSESIn many situations, even the most powerful pharmaceutical drugs are unable to adequately control symptoms of disease, often due to an inability to address underlying factors. Antidepressants have been shown to be not more effective than placebo in many trials.7 Proton-pump inhibitors, designed to relieve gastric symptoms of reflux and ulcers, have been shown to worsen the very symptoms they are designed to treat when a patient attempts to withdraw.8 Further, drugs can result in a wide range of side effects, with over 1.5 million Australians suffering an adverse event from medicines each year, ranging from mild to severe, and including death.9 Even such widely used drugs as the cholesterol-lowering statins, frequently touted as a wonder drug for cardiovascular disease, have hidden dangers – in addition to painful muscle myopathy, they increase the risk of diabetes by 47%.10
Pharmaceutical side effects can often be managed appropriately by natural medicines, allowing the patients to receive the benefit of the drug without the risk. Gut damage from non-steroidal anti-inflammatory drugs (NSAIDs),11, 12 nutrient depletion from metformin13 or cough from antihypertensives14 are all significantly improved with natural medicines. The natural medicine practitioner’s toolbox is perfectly suited to the job of coprescribing. We can replace missing nutrients, protect organ function or correct the drivers of disease which remain unaddressed by the pharmaceuticals. Our treatments are highly effective, broadly acting strategies which address the whole patient, have an excellent safety record and can be tailored to suit the individual patient’s needs. Figure 2 outlines the key benefits which can be achieved with coprescribing.
Figure 2. Benefits of prescribing alongside pharmaceuticals.
Beyond our prescriptions, our knowledge also puts us in an ideal place to help patients comfortably navigate both natural and conventional medical treatment. Most medical practitioners receive minimal training in nutrition and natural health care15, and frequently lack the time to investigate the evidence behind proposed interactions. Many natural health care practitioners consider and research the effects of conventional medicines on a daily basis when they prescribe their treatment. In addition, they offer the time and willingness to listen (to both patients and other health care providers), investigate the options, and tailor the treatment to the individual. By developing our knowledge of interactions and working respectfully alongside medical practitioners, natural health care practitioners can be a trusted resource for our patients and other health care providers.
UNDERSTANDING THE BENEFITS AND CAUTIONSThere are clearly significant benefits to co-prescribing. There are also some potential risks: changing drug levels, antagonising drug effects and negative consequences from potentiating the drug effect (Figure 3). We will examine each of these cautions and benefits in turn – reviewing the evidence, discussing some examples and discerning the real risks from the theory, to determine the responsible, professional course of action.

7
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Figure 3. The potential cautions for prescribing natural medicines alongside pharmaceuticals.
PUTTING INTERACTIONS IN PERSPECTIVEWhen considering information on herb and nutrient interactions with pharmaceuticals, it is important to note that the vast majority are hypothetical, and have never actually been demonstrated to occur in humans. Well-documented herb drug interactions are rare, compared to the thousands of drug-drug interactions reported each year.16
Consider the case of St John’s Wort. Concern peaked in 2001 around the potential of St John’s Wort to modify drug levels of pharmaceutical medications, with stickers issued to be applied to all St John’s Wort-containing natural medicines sold in stores.17 At this point in time, one case of the interaction had been reported.18 Media attention is high on these types of interactions, ensuring that isolated cases receive more attention than the daily numbers of patients admitted to hospital with drug-drug interactions.
Many of the potential interactions listed in the interaction literature are derived from in vitro studies where herbs are placed in test tubes with drug-metabolising enzymes.19 In these types of tests, most herbs will return a positive result, demonstrating inhibition of these important enzymes. However, studies demonstrate that these results rarely translate to significant human clinical effects, and may be due to direct contact effects of herbal constituents, such as tannins, inactivating the proteins within the enzymes, an effect which doesn’t occur when the herb is consumed orally and processed through the digestive system.20 Predictions based on in vitro results can be completely misleading - take St John’s Wort again – in vitro evidence suggested it inhibits a wide range of drug metabolising enzymes, potentially leading to multiple drug toxicity. Human evidence shows a much more limited (although still significant) effect on inducing enzymes, restricted to two, and any effect in humans may be to reduce drug levels, rather than increase them.21
INDIVIDUALITY CAUSES MORE INTERACTIONS THAN NATURAL MEDICINESWhen the effect of natural supplements taken orally by humans is compared to the levels of variation caused by other factors, the effect is small. It is estimated that the average person consumes around 1 tonne of food per year.22 As a result, the amount of foreign compounds we consume through our food and drink supply is far higher in quantity than that from nutritional or herbal supplements. Significant effects on drug levels have been found with common exposures such as broccoli (40-50% reduction), orange juice (76% increase), barbequed meat (75% decrease) and smoking (20-40% decrease).23 Every time a patient eats, drinks or breathes, they can change their drug levels.
Equally significant is the effect of other individual factors such as genetics, age, sex, and organ function, with drug metabolism known to vary over 10-fold between different individuals.24 Figure 4 provides a summary of some key factors which influence drug metabolism and response. Due to severe limitations in being able to predict these idiosyncratic factors, the same drug dosage is typically prescribed to any given individual. If it doesn’t work, the drug dose may be increased. If it causes side effects, the drug dose may be reduced, or less favourably, the side effects may be considered to be a new emerging symptom – for which another drug may be prescribed. The practice of drug dosage is therefore not an exact science, and factors which change drug levels are an unavoidable fact of life.

8
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Figure 4. Factors which impact drug metabolism and response.25
POOR QUALITY CONTROL TARNISHES THE SAFETY OF NATURAL MEDICINES Natural medicines can contain more than what is on the label. Contamination issues are a real problem in Australia and New Zealand, with hundreds of examples of over-the-counter supplements listed on the Safety Advisory Alerts section of the Therapeutic Goods Administration (TGA) website each year. Natural medicines can be contaminated with heavy metals, pesticides, microorganisms, insects, prescription drugs, or cheaper substitute materials.26 In a survey of herbal medicines available for internet and over-the-counter purchase in South Australia, 18% were not registered with the Australian Register of Therapeutic Goods (ARTG), and 60% had differing ingredient concentrations on the website or label compared to their ARTG listing, providing little guarantee of actual active ingredient.27 To guarantee quality products, Health World performs all of its testing on site in its dedicated chemical and microbiology laboratories. The quality assurance and quality control team consists of 35 staff, whose primary responsibility is to ensure the raw materials received and products produced are of high quality, free from contaminants and meet the label claim for potency throughout shelf life and beyond. Every new formulation is tested for stability before launch, as different combinations of ingredients can have unexpected effects in a formulation – a guarantee of potency which the TGA does not require. Table 1 describes the quality measures Health World employs to guarantee high quality, efficacious products.
Table 1. Health World’s unique, industry leading guarantee of quality and efficacy.
QUALITY MEASUREHEALTH WORLD INTERNALLY CONTROLLED PROCESSES
Selection of raw materials based on rigorous evidence review 3On site
Thorough audits of raw material suppliers to ensure quality ingredients 3On site
Identification assays for all raw materials upon receipt to confirm specifications 3On site
Testing of raw materials for heavy metal, pesticide and microbiological contamination 3On site
State of the art manufacturing facility, with stringently controlled processes and environmental conditions for reproducible results
3On site
Live probiotic assays at all product stages – raw material, powder blending, encapsulation, transport trials and shelf life stability
3On site
Temperature controlled and cold-supply chain from raw material to shipping of finished goods to customers 3On site
Strict maintenance of all limits for label claims and rejecting batches out of specification 3On site
Therapeutic Goods Administration-certified compliance for manufacturing and testing facilities maintaining high Good Manufacturing Practice standards
3On site
Ongoing investment in internal method development to accurately quantify ingredients in finished goods 3On site
Full internal stability program providing actual (not theoretical) pre-launch stability on all products, with ongoing real-time stability
3On site
Taste & tolerance testing of finished goods 3On site
Manufacture of ‘food’ products under rigorous Good Manufacturing Practice standards 3On site
Efficacy testing of products and protocols in clinic 3On site

9
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
A lack of quality assurance of levels of actives and presence of contaminants can cause significant issues when attempting to evaluate the validity of a potential interaction. Previous case reports cannot be taken at face value, as many reports of herb-drug interactions are sketchy and lack laboratory analysis to establish a positive identification of the herb involved, and to exclude the effect of contaminants or adulterants.28 Take the example of black cohosh and hepatotoxicity. In 2002, several case reports linked hepatotoxicity to products labelled as containing black cohosh. The case reports were poorly documented and lacking analysis with regard to authentication of black cohosh in the products used by the patients. The final conclusion was that it was most likely substitution of cheaper herbal species in these products and that black cohosh does not present an overt risk of hepatotoxicity. 29
Typically, case reports are also significantly flawed in their reporting of potential interactions, as while the herb or nutrient may have been blamed, upon investigation, it is often found that allergens, new drugs or illnesses were also introduced or experienced, which could have equally or more likely contributed to the interaction.30
DECIDING WHETHER TO PRESCRIBE – EDMCAs we have seen, the vast majority of interactions are based on theoretical, in vitro or unreliable case information which may have little application to everyday clinical practice. When interactions do occur, they may be due to quality issues, or they may be due to individual variability in drug metabolising enzymes or other unique health factors. Many potential interactions are actually likely to be beneficial, such as improving the efficacy of the drug or assisting a patient to manage their disease and associated symptoms. Other potential interactions can be mitigated by simply changing the dosing regimen or increasing the patient monitoring. A framework for weighing up the evidence, deciding whether to prescribe and putting in place a management plan, is the EDMC model: evidence, dosing, monitoring and communication (Figure 5).
Figure 5: A framework for determining whether and how to prescribe natural medicines alongside pharmaceuticals.
EVIDENCE: WHAT IS THE BALANCE?Whenever a potential interaction is flagged in the literature, a practitioner should carefully examine the evidence for the interaction, both positive and negative. On what basis is the interaction proposed? The lowest level of evidence is isolated case reports, being influenced by so many other variables. In vitro or animal studies on the effects of supplements on drug metabolising enzymes carry a little more weight, but are still reasonably theoretical, as in most cases they do not translate to human clinical effects. Human clinical trials using the natural medicine and drug of question, with measured outcomes of drug levels, change in biomarkers or symptomatology provide the highest level of evidence.31, 32 Often, when clinical trials of this nature have been conducted, the outcome demonstrates safety, with no adverse effects, and in many cases a significant observed health benefit.33 Levels of evidence for potential interactions are detailed in Metagenics Technical Data, found at www.metagenics.com.au and www.metagenics.co.nz in the practitioner section, and additional information and advice can be accessed by contacting Metagenics Technical

10
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Support. Other sources of information include online interaction databases such as Natural Standards Database34 and text books such as Herbs & Natural Supplements by Lesley Braun and Marc Cohen.35
The positive and negative evidence can be weighed to determine whether a beneficial or negative outcome is more likely. The other factor which should be taken into account is the potential level of consequence of both potential outcomes –i.e. is the interaction a transient inconvenience, is it easily reversible, or could it cause significant disability, damage or death? For example, if the benefit could be significant (such as fish oil for heart disease) and the interaction unlikely and mild (eg. fish oil and warfarin therapy, which is unlikely to change blood clotting at less than 6.8 g/day combined EPA/DHA)36,37 then this gives a clear rationale to prescribe. On the other hand, if the interaction is potentially life-threatening (such as St John’s Wort reducing drug levels of anti-organ rejection drugs38) and the benefit is comparatively mild (improving mood), it may be best not to prescribe.
DOSE CAN BE TAILORED AND MONITORING INCREASEDOften, a change in dosing strategy can reduce or eliminate the potential for negative interaction. Natural medicines such as minerals and herbs can reduce the absorption of certain medications, and separating the dose by 2 hours eliminates this interaction, making it safe to prescribe.39,40 In other protocols, alternating the drug and natural medicine may be the most useful strategy, such as using natural medicine treatments between cycles of methotrexate, chemotherapy or ovarian stimulation in IVF.
Many potential interactions simply warrant increased monitoring, rather than any change to the prescription. For example, if the natural medicine has the potential to augment effects of medication on reducing blood pressure, the blood pressure can be monitored more regularly to detect whether an interaction is occurring. If the interaction is causing a decrease in blood pressure, there may be potential to refer back to the medical practitioner for reduction of drug dosage. Other interactions may relate to influences on drug levels or pathology markers, and increasing the frequency of test monitoring can detect an interaction early, if it does occur, and the natural medicine or drug dose can be adjusted accordingly. It is important to remember, however, that patients introduce many drug-modifying factors into their diet and lifestyle each day without concomitant monitoring strategies employed. Changes in biomarkers may not necessarily be attributable to the effect of nutrients or herbs, with confirmation sought and due consideration to other factors given before a potentially beneficial natural medicine protocol is withdrawn.
COMMUNICATION IS A POWERFUL INTERACTION-MANAGEMENT STRATEGYCommunication with all parties involved – with the patient, as well as other practitioners involved in their care - is a powerful interaction-management strategy. Before you begin to co-prescribe, ensure you have a clear picture of the individual’s health goals and limitations. Do they want better symptom control, or is their primary goal to wean off their medication? Are they open to a potential change in drug dose or is that not a desirable outcome for them? There are many potential benefits to co-prescribing, and if we understand the patient’s goals, we are more likely to be able to target treatment to achieve them.
Ideally, the patient needs to understand the prescription and take an active role in their care. As practitioners, we can explain the rationale of our treatment, the potential risk versus the potential benefit, and ensure that we have their informed consent to proceed with the treatment. The patient should be able to monitor their symptoms and keep you informed of any progress, positive or negative, and know what signs may indicate that they are experiencing an adverse interaction. They should understand their responsibility to seek and comply with effective monitoring strategies to maximise the benefit and safety of the intervention.
When this is not possible, due to impairments of understanding, awareness, ability or support, this may change the prescription, or other parties will need to take active responsibility for areas of patient limitation. You may need to have the full support of a medical practitioner, who can schedule frequent appointments to monitor symptoms, pathology markers or drug levels. You may also need a family member or carer who can report changes in symptoms to yourself or the medical practitioner.
In any situation where there is a real (albeit often unlikely) risk of an interaction with moderate to severe consequences, it is important to inform the medical prescriber to ensure that both parties are aware of the potential interaction and can bring their own area of expertise to patient monitoring. Approach the communication from a place of confidence, and present your well-thought out rationale, with evidence, to the medical practitioner. Many medical practitioners will not have personally examined the evidence for interactions, perhaps only hearing about well-publicised case reports, and may not realise the risk: benefit analysis lies, in many cases, strongly in the favour of co-prescription. Take the opportunity to provide assistance and network with other practitioners, demonstrating your knowledge and professional conduct in this important area.
An example of the process of the EDMC analysis is represented in Table 2.

11
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Table 2. EDMC analysis on the prescription of Milk Thistle, Green Tea And Amino Acids For Optimal Detoxificationalongside an antihypertensive beta-blocker medication.
In the table above, we can see how the information gathered can be synthesised into a summary of the evidence for risk and benefit, and a summary of the management plan, outlining dosing, monitoring and communication strategies. This type of analysis is ideal to perform and keep on your patient’s file as a record of the decision making process in the prescription of your natural medicine protocol.
MAKING AN ASSESSMENT OF MULTIPLE MEDICATIONSWhen multiple medications are involved, the same decision making process needs to be followed – there are just more natural medicines and drugs to cross check. Each natural medicine to be prescribed should be checked for evidence of potential interactions with each drug (eg. by reading the Cautions and Contraindications section of the Metagenics Technical Data.) Any relevant dosing, monitoring or communication strategies which may affect the prescription can be noted along with the evidence, as in the main body of Table 3. Once the information has been summarised, you can review the net evidence for the safety of each natural medicine at the end of each row. Does the potential benefit outweigh any risk identified? At the bottom of each column you can summarise the management plan to mitigate any potential interaction with each drug.
Table 3. Summarising the EDMC analysis for patients taking multiple natural medicines and pharmaceuticals.
In the model above, we have seen how a number of potential interactions between natural medicines and drugs can be mitigated by implementing some simple clinical strategies. Below, we will examine the three most common types of negative interactions in more detail, explore some examples, discuss important factors for consideration and investigate strategies to reduce the likelihood of interactions.

12
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CAUTIONS: CHANGING DRUG LEVELSThe first type of potentially negative interaction is changing drug levels – classified as a pharmacokinetic interaction, whereby the movement of drugs in the body is changed. Other interactions are pharmacodynamic in nature, altering the effects of the drug rather the level. These will be discussed below. The potential consequences of pharmacokinetic interactions include reduced therapeutic action of the drug (where concentrations are too low to have the desired effect), increased therapeutic action (where concentrations are too high and the effect is too strong), and/or drug toxicity (where high concentrations directly create side effects).
To understand why natural medicines can alter the drug levels, we need to understand a little about the drug metabolising systems in the body. There are two key processes we are interested in – absorption and metabolism.
DRUG ABSORPTION IS VARIABLEA key transporter which regulates the absorption of medications is p-glycoprotein.41 Embedded in the luminal face of the enterocytes, p-glycoprotein’s function is to limit the absorption of foreign compounds by the gut mucosa. When a compound sensed as non-nutritional and potentially toxic is taken up by the enterocyte, the job of p-glycoprotein is to quickly pump it back out into the lumen, for subsequent excretion, before it is absorbed into systemic circulation.42 The numbers of p-glycoprotein are highly influenced by all oral exposures, comprising diet, herbs, drugs and toxins.43 A number of potential interactions are based on the effect of herbs on p-glycoprotein. For example, St Mary’s thistle has been shown to be an inducer of p-glycoprotein in vitro,44 but human data suggests it may actually reduce levels of this enzyme.45 Despite this evidence, no case reports to date have suggested that either action creates a clinically significant effect.
Drug absorption can also be significantly influenced by gut function. The pH of the stomach can range from 1.5 to 3.5,46 between which the absorption of drugs can vary 4 fold, from 20% to 80% of a drug being absorbed.47 When correcting gut function, a potential effect on changing drug levels should be noted for the patient, and drug dosage may be able to be reduced as a consequence. The microbiome of the gut also plays a role in drug levels. Activation of drugs such as digoxin (anti-arrhythmic), sulfasalazine (anti-inflammatory for the gut) and clonazepam (a benzodiazepine for insomnia) can be significantly influenced by the composition of gut flora.48 In the presence of dysbiosis, when drug-activating strains are not present in sufficient amounts, lower drug levels are found entering the blood stream. Further, changes in intestinal transit time can create increases in drug absorption when intestinal transit is slowed, and the contrary effect when transit time is increased.49 Being aware of such potential interactions helps us to identify when changes in symptomatology may be related to changes in drug levels, and how our treatments are impacting this. Other factors which influence drug absorption include meal constituents such as fibre, minerals and tannins, which can bind drugs, and are best taken 2 hours apart.50
DRUG METABOLISING ENZYMES CAN BE ALTEREDThe drug metabolising enzyme system consists primarily of a family of enzymes known as cytochrome P450 enzymes, or CYPs. This system was not originally a drug metabolising enzyme system, as there were no pharmaceuticals or man-made chemicals present during the evolution of humans. The system presumably evolved to deal with the clearance of plant-derived compounds from the food we ingested.51 As a consequence, we can see when plant-derived compounds from the diet are ingested, levels of the different CYPs can be increased or decreased in response to the demand. Many modern pharmaceutical drugs (around 70%) are derived from or have similar structures to plant compounds52, which means the body can process them relatively easily through the same CYPs as dietary and herbal compounds. When an individual on a medication changes their intake of plant compounds, through dietary change or herbal supplements, CYP activity can be affected and drug levels may change.53 However, rarely is this biochemical change reflected in clinical symptomatology. Most drug levels can change significantly throughout the course of the day, and from day to day, with little consequence, due to the highly variable intake of dietary and environmental exposures our patients are exposed to.
TREATING THE LIVER AND DETOXIFYING WITH DRUGSThe potential effect of herbs and nutrients on drug clearance often arises when practitioners consider strategies which act on the liver for their patients. An example scenario is that of a patient on anti-hypertensive medication for whom you wish to prescribe Milk Thistle, Green Tea And Amino Acids For Optimal Detoxification (Table 2). When we look at the various EDMC factors on the interaction, we discover that there are no specific concerns with the prescription of Milk Thistle, Green Tea And Amino Acids For Optimal Detoxification alongside the beta blocker medication, however a general theoretical interaction is noted for monitoring of patients on any medication due to detoxifying effects. Such an interaction is easily mitigated by increasing the frequency of blood pressure monitoring to weekly, to ensure the blood pressure remains under control during the treatment period.
In other patients on medications, you may consider a complete detox program. There are many substances within a detox protocol which can alter drug-metabolising enzymes, however there are many situations where there is significant benefit to be gained by detoxifying patients who are on medications. Toxicity can be a key driver of many chronic diseases, including diabetes, cardiovascular disease, autoimmune conditions, depression and hypothyroidism.54,55

13
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
For most of the key medications these patient groups are taking, detoxification can be a safe strategy to assess the underlying drivers of the condition, restoring the body’s ability to cope with the medication, as well as potentially reducing the need for medication. Several options for detoxification are available, with Integrated Detoxification suitable for most, and the option of a Specialised Liver program being ideal when hepatic function is compromised with the use of many medications.
NARROW THERAPEUTIC WINDOW MEDICATIONSAs a general rule, changing drug levels is only of significant concern when we have a patient taking a drug with a narrow therapeutic index (NTI). This term refers to the drug having a specific window of serum concentrations in which it is effective. Too low, and the drug won’t adequately control the disease processes, and if too high, the drug can quickly turn from effective to toxic. A list of these drugs is provided in Table 4.
Table 4. Drugs with a narrow therapeutic index.56,57
Prescribing natural medicines with potentially metabolism-altering effects alongside NTI drugs is not absolutely contraindicated, however increased medical monitoring is required. The patient should be aware of the potential for adverse consequences, have given their informed consent, and be prepared to actively seek and comply with monitoring strategies to ensure safety. A clinical example of this was the successful detoxification of a patient on warfarin therapy. The patient was being maintained on weekly monitoring of INR levels, with strong indications for detox, including fatigue, weight gain and excessive alcohol and tobacco consumption. The medical practitioner was informed and the regular monitoring frequency of INR was continued. The patient successfully completed the detox without significant changes in INR, achieving beneficial lifestyle change, weight loss, improved energy and digestive function.
ANTAGONISING DRUG EFFECTS – CONFLICTING MOTIVES IN AUTOIMMUNITYNatural medicines also have the potential to have pharmacodynamic-type interactions with drugs – where the natural medicine may not necessarily change the drug levels, but may interfere with its action in the body. This interference may be antagonising or augmenting the drug’s effects.
A potential antagonising effect on drugs which often arises in clinical practice is in the treatment of autoimmunity. In an attempt to gain control of the powerful inflammatory damage occurring in these diseases, conventional medicine uses an array of increasingly immunosuppressive drugs. The gold standard of aggressive therapy for new onset rheumatoid arthritis is triple disease-modifying anti-rheumatic drug (DMARD) therapy – consisting of classical anti-inflammatories such as sulfasalazine, combined with the cell-replication inhibitors methotrexate and hydroxychloroquinone.58,59 When these don’t work, patients become eligible for government subsidies for the highly expensive TNF-alpha inhibitors,60 which effectively ‘shut down’ whole pathways of immune function, providing effective control of autoimmune symptoms in many cases, but also predisposing to infections and cancer (Figure 6).61,62,63

14
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
TNF-α
Cancer prevention
Infection defence
Inflammation
• Macrophage maturation • Neutrophil recruitment• Immune surveillance
TNF-α inhibitor
Figure 6. The effects of TNF-alpha inhibitors on immune functions. 64,65,66
The natural view of treating autoimmune conditions is significantly different. Natural medicine views autoimmunity as a response to an imbalance in the body, and attempts to remove the driver, rather than simply suppress the response. In many cases, autoimmunity is believed to occur in response to a hidden chronic infection – the immune system is constantly activated by the presence of a foreign invader, and resolving the autoimmunity actually requires both balancing and stimulating actions on immune function, to reduce tissue damage while eliminating the pathogen.67
This natural medicine treatment approach presents many theoretical interactions. Any natural medicine we might use with an immune stimulating action – zinc, vitamin C, andrographis, immune-stimulating mushrooms - could provide a potential interaction with powerful immune suppressant pharmaceuticals. A common example is that of the immune-stimulating mushrooms, Cordyceps, Coriolus & Reishi For Immune Stimulation, indicated in the treatment of autoimmune conditions, theoretically contraindicated with TNF-alpha inhibitors. When we take a look at the evidence, there is no data supporting the interaction – no animal or human studies, or case reports of autoimmune disease worsening with the use of these ingredients. Experts in the published literature recommend that these mushrooms are highly indicated in autoimmune conditions, where they ‘pose no threat of autoimmune backlash’.68 The potential benefit outweighs the risk in this situation, and the potential adverse consequences (a worsening of symptoms) can be easily detected, with the treatment adjusted accordingly. Case reports from practitioners using the combination in practice add support to this analysis, with successful symptom control achieved without worsening. Such immune stimulant formulas in autoimmunity are also rarely used in isolation – when supporting such a patient, we often use anti-inflammatory supplements such as turmeric and fish oil, and immune balancing remedies such as probiotics and vitamin D, which add balance to the prescription.
AUGMENTATION OF ANTI-INFLAMMATORIESTurmeric is a well-studied anti-inflammatory for autoimmune diseases, including research in rheumatoid arthritis, where BCM-95® turmeric was shown to be as effective as pharmaceutical anti-inflammatories69, and in ulcerative colitis, where turmeric has been used safely alongside conventional anti-inflammatories including sulfasalazine, alleviating symptoms and preventing relapse.70
Another indispensable adjunct is fish oil. One of the reasons fish oil may be an effective anti-inflammatory in autoimmune disease is that as well as having a generalised anti-inflammatory action, EPA and DHA can also directly inhibit the inflammatory signal (toll-like receptor activation) which is stimulated as a result of infectious pathogens binding to cell-membranes – reducing the inflammatory impact of infectious drivers of autoimmunity. Fish oil has been studied by researchers from the University of Adelaide as an adjunct to triple DMARD therapy for newly diagnosed rheumatoid arthritis. When participants took 5.5 g daily of combined EPA/DHA for 1 year alongside their pharmaceutical medications, they experienced a 40% rate of remission, compared to 19% in the control group. Further, the percent of people considered to fail triple DMARD therapy and require progression to higher risk drugs such as pyrimidine synthesis inhibitors and TNF-alpha inhibitors was only 12% in the fish oil group, compared to 34% in the standard therapy group (Figure 7).71

15
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Figure 7. The impact of adjuvant fish oil prescription in new-onset rheumatoid arthritis – reducing failure of tripleDMARD therapy and improving remission rates. 72
The simple addition of a natural medicine to a pharmaceutical treatment protocol in such a serious disease demonstrated safety but also powerful efficacy, a remarkable benefit for the patient, as well as the taxpayer, avoiding the progression to expensive and potentially risky drugs. Further, in a meta-analysis, the effects of fish oil in other studies in rheumatoid arthritis were found to be directly comparable to the effects of a TNF-alpha inhibitor, for reductions in joint pain intensity, number of painful/tender joints and duration of morning stiffness.73 A further benefit is the lack of side effects – while a number of therapies for autoimmune diseases actually carry an increased risk of chronic disease such as cardiovascular disease or cancer, fish oil consumption does not, and actually provides benefits for risk reduction.74
The impressive results above were achieved with the equivalent of 2 serves a day of the upgraded, higher potency High Purity, Low Reflux Concentrated Fish Oil, now containing 500mg of EPA and 200mg DHA in every 1000mg fish oil. Recently, a review of fish oils in the Australian marketplace, in both the practitioner and retail sectors, demonstrated that there is a substantial variation amongst different brands with different levels of toxins, with higher amounts of DDT, pesticides and other chemicals found in some brands. Other products did not met the label claim for amounts of EPA and DHA. This research indicates that all fish oils are not the same.75 Your patients may tell you they are already taking a fish oil supplement, but they may not be receiving the amount of actives required, and may be getting more than they bargained for with toxins. Switching patients from cheaper supermarket brands to quality practitioner-only supplements can make the difference between an effective treatment protocol and one that fails to deliver results - the most expensive natural medicine is always the one which doesn’t work. More support can be found at www.metagenics.com.au/loyalpatientsforlife, where you will find videos and scripts to assist having these important conversations with their patients.
Appendix 1A provides a summary of some key prescriptions which may be used alongside anti-inflammatory/immunosuppressant medications.
POTENTIATING DRUG EFFECTS IN THE NERVOUS SYSTEMThe other key type of interaction is potentiation, where effects of the drug are enhanced by the natural medicine. While this can often be a positive effect, it has the potential to create adverse symptoms when the effect is augmented too strongly. The potential for this interaction can often arise when a practitioner attempts to treat a symptom or condition for which the patient is also taking medication.
Natural health care practitioners have in recent years shied away from the prescription of any serotonergic compounds alongside antidepressants, due the widespread publicity around St John’s Wort interactions and fear of serotonin syndrome. However, the majority of patients do not receive adequate relief from depressive symptoms on medication, with only 1 to 2 out of 10 achieving a better response than placebo, suggesting that augmentation therapy may be a desired outcome.76 When we examine the evidence, the risk for serotonin syndrome is theoretical only, with a few unsubstantiated case reports in the case of St John’s Wort,77,78 and no case reports with 5-hydroxytryptophan.79 This is less surprising when you consider that in psychiatric practice, multiple antidepressant medications may be used together – and even in the case of these potent medicines, serotonin syndrome is uncommon.
The risk of adverse potentiation is often considered when two medicines have a similar target in the body – and in many cases, this can create an effective treatment protocol when monitoring is in place. Addressing the drivers is

16
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
another strategy, where the natural medicine does not act on the same target as the drug, but instead supports the underlying processes causing the disease. In the case of depression, there are a number of natural medicines which can be used with an excellent safety record and numerous clinical trials alongside anti-depressants. Magnesium is one of these nutrients, with researchers speculating that ‘inadequate dietary magnesium may be the main cause of treatment-resistant depression’80 – a clear mandate for increased use of this nutrient in mood disorders, in medication naïve patients or alongside pharmaceuticals. A variety of magnesium formulas with condition-specific herbs and cofactors are available to address all needs, from fatigue, to anxiety, to mood disorders associated with female hormonal imbalance.
Fish oil is another key adjuvant. In some striking results, research demonstrates how 1 g of EPA daily in medicated patients drops the Hamilton Depression rating scale by 40%, compared to 15% on placebo.81 EPA, not DHA, appears to play the active role in depression, however a combined formula with high levels of EPA will provide the best therapeutic effect, alongside the additional cognitive benefits of DHA. Folic acid is another supplement which has the power to potentiate antidepressants in a positive way, particularly in women. In one study, the addition of just 500 mcg of folic acid to standard treatment with an SSRI increased the response rate to treatment after 10 weeks to 93.9%, compared to only 61.1% with fluoxetine alone.82 Other useful nutrients which have demonstrated efficacy in clinical trials alongside antidepressants are 1500 IU of vitamin D,83 25 mg of zinc,84 and 2 g of N-acetyl cysteine.85 Even though each could be said to have neurotransmitter-altering effects and create a theoretical interaction, these simple nutrition interventions can be prescribed with confidence with clinical trial-demonstrated safety and efficacy alongside antidepressants. Appendix 1B provides a summary of some key options.
SEDATIVE HERBS AND DRUGSA similar concern around negative potentiation can occur when prescribing alongside benzodiazepines (sedative drugs acting on the GABA receptor) used for anxiety and insomnia. Patients on these medications may often present desiring an alternative or an additive medication, for a number of reasons – they may be experiencing drowsiness from taking them during the day for anxiety, or grogginess the next morning from taking them at night, and wish to try something natural. Some may have inadequately controlled anxiety or insomnia and wish to avoid needing to increase their drug dosage. Many of the herbs and nutrients natural health care practitioners prescribe for these conditions have GABA-ergic actions, including herbs such as zizyphus, passionflower and magnolia in Herbal Support for Hyper HPA and Stress, as well as magnesium, creating a potential interaction. Typically, the concern here is increased drowsiness, difficulty driving a car or operating machinery, or more pronounced levels of sedation. However, typically concerns are unwarranted. When we examine the evidence again, this is a theoretical caution only, and while some degree of increased sedation may (often desirably) occur, it is extremely unlikely to cause severe enough sedation to impair function. In one study, passionflower was compared to a benzodiazepine for effects in anxious patients. Passionflower was found to be as effective as the benzodiazepine (Figure 8) without impairing work performance, the main complaint associated with benzodiazepine use.86
Figure 8. The effects of passionflower are comparable to benzodiazepines for reducing anxiety.
The unlikely incidence of adverse potentiation can be further reduced by taking the medicines at different times of day, so that the effect of one will peak at a different time of day to the other. In the case of benzodiazepines, due to their addictive nature and highly sedating side effects, many wish to reduce their drug dosage if adequate control can be

17
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
gained over their symptoms, so some degree of potentiation is a desired effect. Such GABA-ergic supplements may also safely be taken alongside antidepressants, with monitoring.
In one such case, a 53 year old patient presented with recent onset severe anxiety and insomnia due to a recent marriage breakdown. She is already taking an SSRI, with the doctor recommending an increase in dose as well as the addition of a benzodiazepine, to control the recently emerged symptoms. The practitioner prescribed Herbal Support for Hyper HPA and Stress, alongside Rehmannia Complex for Nervous Exhaustion, and valerian, vitamin B5 and vitamin B6. After 4 days, the patient noted she ‘felt a difference in just one day’ for her anxiety, with improvements in insomnia after 2 weeks. Improvements continued and were maintained at 10 weeks, where she reduced her dose of several of the supplements. During the course of treatment, the patient’s general practitioner telephoned the practitioner, impressed, to ask what products the patient was taking and how they worked. Such a case demonstrates how prescribing alongside pharmaceuticals can provide significant benefit for patients who would otherwise need to increase drug numbers or doses, as well as a significant degree of practitioner satisfaction.
POTENTIATION OF ANTICOAGULANTS IS NOT AS COMMON AS ONCE THOUGHTA significant number of natural medicine cautions and contraindications are related to blood coagulation. Many natural ingredients can be shown to have a ‘blood thinning’ action to some degree, as a part of the spectrum of anti-inflammatory properties that herbs and nutrients possess, which has led to a large number of cautions around anticoagulant and antiplatelet drugs. However, it seems that many of these potential concerns are unwarranted. Even three of the most potentially concerning, Gingko, vitamin E and fish oil, all of which are commonly discussed as being contraindicated with warfarin – have been examined in a recent review to be likely safe with warfarin, in conjunction with increased monitoring of international normalised ratio (INR – a measure of blood clotting) at introduction and dose change.87 Vitamin E specifically has been examined in a number of clinical trials, demonstrating no significant change in INR when supplemented at 720 mg/day.88 Research recommends INR is checked 1-2 weeks after starting vitamin E therapy, in a similar protocol to the standard assessment of INR in the week after starting a new drug.89
This confirmed safety of vitamin E in cardiovascular patients prescribed warfarin provides a useful therapeutic strategy to reduce cardiovascular risk. While alpha-tocopherol supplementation has shown poor rates of efficacy in cardiovascular disease, a mixed blend of tocopherols and tocotrienols provides a significantly greater therapeutic effect. For example, mixed tocopherols are more effective than alpha-tocopherol alone in inhibiting platelet aggregation,90 and tocotrienols improve LDL cholesterol, apolipoprotein B and triglyceride levels,91 making the combination a powerful force in the prevention and treatment of cardiovascular disease. Mixed Tocopherols & Tocotrienols For Free Radical Defence consists of a blend of all eight isomers of vitamin E: alpha-, beta-, gamma-, and delta-tocopherols, and alpha-, beta-, gamma-, and delta tocotrienols, for a broad therapeutic activity in cardiovascular disease and other conditions.
Another common example is coenzyme Q10 (CoQ10) and warfarin. Warfarin has its effect on blood coagulation by blocking the formation of vitamin K-dependent clotting factors. CoQ10 (ubiquinone) has a similar structure to vitamin K (phylloquinone), and can theoretically act to counteract the effects of warfarin use. This interaction is commonly cited as a caution, for use only under medical supervision. When we examine the evidence, there are four case reports which identified a possible interaction, however patients were on multiple medications, CoQ10 was self-prescribed at an unknown dose, and their previous history of INR stability was unknown.92 Contrast this to the randomised controlled trial which was conducted, providing CoQ10 100mg daily to 21 patients stable on long term warfarin therapy, where no effects on INR were noted.93 Based on this evidence, CoQ10 is unlikely to create changes in INR in the majority of patients, but monitoring of INR would be prudent at introduction of therapy, weekly for the first few weeks after introduction and monthly for 3 months thereafter. With the introduction of any therapy such as this where there is some risk of a moderate to severe side effect, it is best practice to inform the patient’s prescribing practitioner of the potential interaction, your rationale and evidence for the prescription, and the proposed management plan to monitor. This has the benefit of increasing practitioner awareness, perhaps opening up the benefits to be received by other patients, as well as inspiring team work and networking amongst healthcare practitioners.
Appendix 1C summarises some of the common formulas which may be prescribed in patients taking anticoagulant medications.
ANTICOAGULANT INTERACTIONS AND SURGERYSurgery is a related concern, where herbs and nutrients with potential anticoagulant actions may interact with surgical procedures and increase the risk of bleeding. In these circumstances, it is prudent to discontinue any natural medicines with suspected effects on bleeding one week before and after surgery,94 due to the severity of the potential consequence, and the small benefit that is lost by omitting the natural therapy for a few weeks.
However, when used with the support of the surgical team, natural medicines with potential anticoagulant effects can still have a place in management of surgery. The team at the Alfred Hospital in Melbourne use pre-and post-surgerical administration of fish oil, lipoic acid, magnesium, CoQ10 and selenium, for two months prior to coronary bypass surgery and for one month after, achieving lower levels of cardiac damage and improved rehabilitation post-surgery.95

18
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Coronary bypass surgery involves a high risk of bleeding96, yet these natural medicines are used successfully. The team involved have published their findings, and in situations such as these where there is a published precedent, practitioners may wish to encourage patients to discuss the potential use of such treatment with their cardiac physician.
As we have seen, there are some real cautions with the use of natural medicines alongside pharmaceuticals. However, in many cases, the potential benefit outweighs the risk, and the risk can be effectively reduced by a sound management plan involving correct dosing, responsible monitoring and proactive communication. We have reviewed several scenarios, real life case studies and clinical trials where it is quickly apparent that many of these patients are significantly better off with co-prescribing, than they would have been had the practitioner let lack of confidence get in the way of a beneficial protocol.
DEALING WITH A POTENTIAL INTERACTIONShould a patient report that a potential interaction has occurred, the best course of action is to record as much detail as possible about the event – details about the patient, their reaction, medical history, current medicines being taken, including batch number and expiry date, and other changes in diet, lifestyle or exposures which may have contributed. Manufacturers such as Health World have processes in place to evaluate the potential significance of the interaction, perform any testing of products and, if warranted, report the interaction to the Therapeutic Goods Administration. Many potential interactions can be one-off events, based on the interplay of a number of unknown factors in the patient’s diet/lifestyle or other exposures for that period of time. If suitable, based on the patient situation and the severity of the symptoms, when an interaction has been likely, an ideal protocol is to remove the suspected medicine/s until symptoms resolve, and then reintroduce the medicine/s one at a time under supervision to confirm the reaction. Each individual is biochemically unique, and although the best decisions are made based on the evidence, all idiosyncratic reactions cannot be predicted, and some degree of management of these effects is a part of clinical practice.
FOCUSING ON THE BENEFITS OF CO-PRESCRIBINGCo-prescribing is not just about avoiding interactions and working as far away from the pharmaceuticals as possible - it is about working to provide the patient with the greatest benefit from the combined effects of the natural medicine protocol and the pharmaceutical. Just as we discussed in the section on adverse potentiation, many natural medicines can augment the effects of pharmaceuticals, and although this may be seen as a negative, in most situations it is actually a benefit.97 Positive potentiation can result in improved clinical results for the patient, such as control of a previously uncontrolled symptom, or the ability to reduce their drug dosage or number in the future as the natural medicine is able to take over the role of the drug. Drugs are ideal for strong symptom control and modulation of dangerous pathophysiological processes in the body, however they have their limitations, as we discussed above. Natural medicines can often close the gap between the patient and the drug, addressing the unaddressed drivers of disease, and having broader corrective effects on physiology than a single target drug. By using both together, patients can often get the best that both systems of healthcare have to offer.
POSITIVE POTENTIATION IN CARDIOMETABOLIC DISEASEA common clinical area where drugs do not adequately prevent disease is in the area of cardiometabolic disease. Drugs to treat cardiovascular disease typically target the ‘number’ associated with the disease – reducing blood pressure, lowering lipids, stabilising heartbeat. However the real underlying processes and causes - inflammation and endothelial dysfunction, stemming from fundamental factors such as poor diet, lack of exercise, stress and toxicity, go unaddressed.98 The mechanism of action of antihypertensives is an important case-in-point. The key mechanisms of antihypertensives are to block some of the regulating enzymes (ACE inhibitors, angiotensin receptor antagonists), to drain the body of fluid to reduce blood vessel volume (diuretics), or to block the function of calcium or beta-adrenergic receptors in the vasoconstrictive process (calcium channel and beta blockers). However, an excess of ACE, calcium or fluid is not the cause of hypertension.
Natural medicine protocols, however, are ideal to get to the root cause of these types of disturbances, making a significant impact on disease progression. Magnesium is a perfect example of a pleiotropic nutrient ideally suited to patients with cardiovascular disease. It acts directly on a key driver of hypertension, atherosclerosis and insulin resistance – the endothelial dysfunction – acting to increase the vasodilatory actions of nitric oxide which assist in blood pressure regulation, glucose disposal and reduction in local intimal inflammation, part of the atherosclerotic plaque progression.99 As a result, magnesium can improve diabetic control, acts as an anti-hypertensive, and reduces systemic markers of inflammation such as CRP.100 By dealing with the cause of the problem, we can both reduce biomarkers of disease as well as make a real impact on the health of the patient. When prescribing formulas such as High Potency Taurine, Glycine and Magnesium for Cardiovascular Health, practitioners often worry about the potassium content, as several antihypertensive drugs can increase potassium levels in the body - ACE inhibitors, angiotensin receptor blockers, and potassium sparing diuretics. However, the average patient receives up to 100-fold higher amounts from their diet in an uncontrolled manner. For example, a serve of beef, potato, yoghurt and banana each contain between 300-600 mg potassium, whereas a serve of High Potency Taurine, Glycine and Magnesium for Cardiovascular Health contains 52 mg. The general recommendation for individuals consuming potassium-sparing drugs is to limit their daily potassium intake to 4.7 g.101

19
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CoQ10, discussed above as being an adjunct for cardiac surgery, is another nutrient which provides significant potentiating benefit to cardiovascular disease protocols. When compared to placebo, doses of CoQ10 ranging from 34 mg/day to 225 mg/day have been demonstrated in numerous clinical trials to decrease systolic blood pressure by 17mm/Hg, and diastolic by 10mm/Hg (Figure 9).102 Being an antioxidant, it also works on the underlying inflammation and oxidative stress in the blood vessel, as well as assisting in cardiac energy production through its role in the mitochondrial electron transport chain. Raising plasma levels of CoQ10 to an effective value is an important consideration, as 3.0 mg/L has been used as a cut off for desirable antihypertensive effects.103 The Vesisorb form of CoQ10 has been clinically proven to raise plasma levels above 3.0 μg/ml for around 6-8 hours after administration with a peak plasma level of 6.89 μg/mL, compared to 2.24 μg/mL achieved with an oil-based ubiquinone formula.104
Figure 9. A meta-analysis summarises the effects of CoQ10 on hypertension in three studies, demonstrating a 17% reduction in systolic blood pressure.
The combination of these two nutrients, magnesium and CoQ10, with fish oil, was used in the case of a 74 year old male with uncontrolled atrial fibrillation, despite anti-arrhythmic, antihypertensive and antiplatelet medication, as well as magnesium oxide supplementation. The practitioner prescribed the replacement magnesium formula High Potency Taurine, Glycine and Magnesium for Cardiovascular Health, twice daily, containing the more bioavailable form of magnesium, MetaMag® magnesium bisglycinate, as well as Enhanced Bioavailability Co-enzyme Q10 150 mg once daily, and High Potency Ultra Pure EPA/DHA Capsules, two capsules twice daily. After 4 weeks, the frequency and duration of the atrial fibrillation events had reduced, and after 12 weeks, the patient reported no episodes for 4 weeks, with improved energy and sleep. After an appointment with the cardiologist, at which the patient was advised to stop their supplements as they ‘were a waste of money’, the atrial fibrillation returned and the patient was again hospitalised. He restarted his naturopathic treatment, stabilising the atrial fibrillation, and the patient was able to embark on a long awaited caravanning holiday which had been delayed as a result of his unstable health. In this case, without any pharmaceutical dose adjustment, the natural health care practitioner was able to help the patient effectively manage their symptoms alongside the medical treatment.
A summary of natural medicines which are commonly used alongside antihypertensive agents is provided in Appendix 1D.
POTENTIATING LIPID LOWERING MEDICATIONSMost patients with cardiometabolic risk factors take a statin – the number one selling drug in Australia and New Zealand.105 However, the statin’s heyday may just now be passing. Over the last 10 years, statin prescriptions have been skyrocketing, as new research demonstrated them to be a pleiotropic wonder-drug – reducing inflammation, alleviating endothelial dysfunction, and of course, reducing cholesterol. However, as the benefits have been unveiled, so have risks emerged. Statins have been associated with a 47% increase in risk of new onset diabetes, being shown to impair pancreatic beta cell function and impair insulin sensitivity.106,107 Statins are also associated with a relatively common side effect of myopathy, or muscle pain, due to their inhibition of CoQ10 synthesis.108 Another strike for statins has been the increased publicity around the limitations of the lipid hypothesis for cardiovascular disease.
The idea that high LDL cholesterol was the key cause of atherosclerosis - the so-called “lipid hypothesis” of cardiovascular disease - was developed from a sequential association of dietary lipids, cholesterol, and CVD by several researchers
20
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
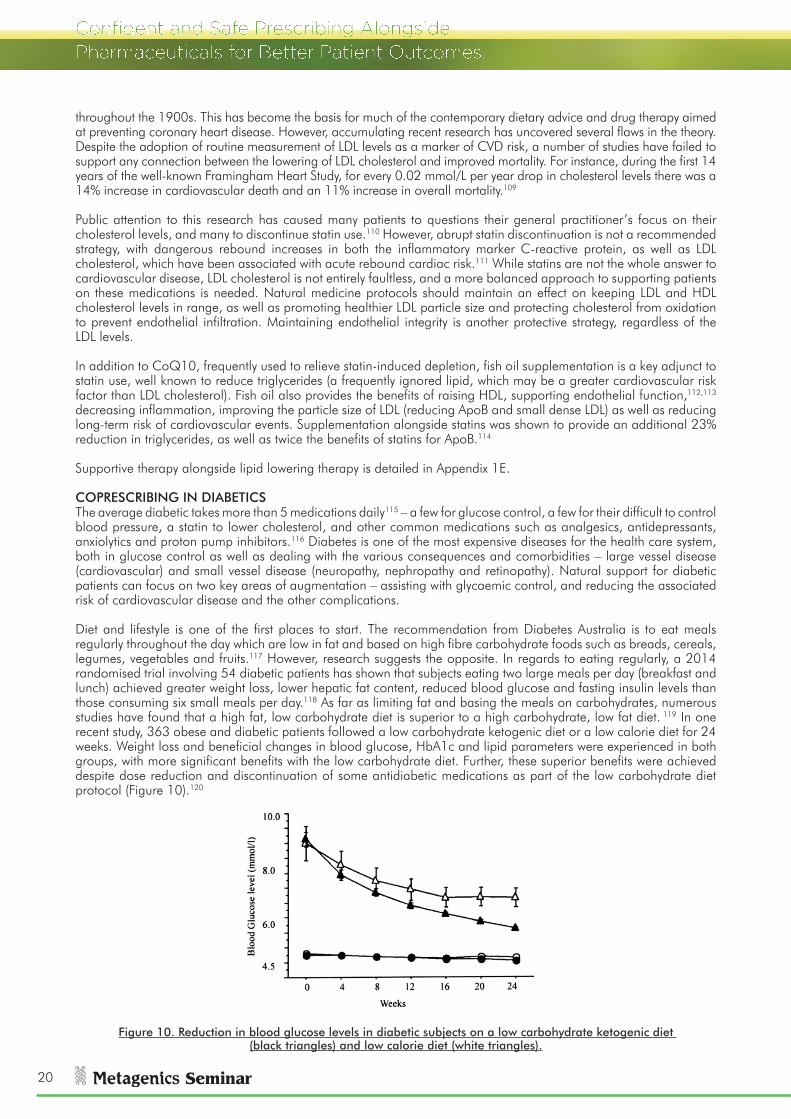
throughout the 1900s. This has become the basis for much of the contemporary dietary advice and drug therapy aimed at preventing coronary heart disease. However, accumulating recent research has uncovered several flaws in the theory. Despite the adoption of routine measurement of LDL levels as a marker of CVD risk, a number of studies have failed to support any connection between the lowering of LDL cholesterol and improved mortality. For instance, during the first 14 years of the well-known Framingham Heart Study, for every 0.02 mmol/L per year drop in cholesterol levels there was a 14% increase in cardiovascular death and an 11% increase in overall mortality.109
Public attention to this research has caused many patients to questions their general practitioner’s focus on their cholesterol levels, and many to discontinue statin use.110 However, abrupt statin discontinuation is not a recommended strategy, with dangerous rebound increases in both the inflammatory marker C-reactive protein, as well as LDL cholesterol, which have been associated with acute rebound cardiac risk.111 While statins are not the whole answer to cardiovascular disease, LDL cholesterol is not entirely faultless, and a more balanced approach to supporting patients on these medications is needed. Natural medicine protocols should maintain an effect on keeping LDL and HDL cholesterol levels in range, as well as promoting healthier LDL particle size and protecting cholesterol from oxidation to prevent endothelial infiltration. Maintaining endothelial integrity is another protective strategy, regardless of the LDL levels.
In addition to CoQ10, frequently used to relieve statin-induced depletion, fish oil supplementation is a key adjunct to statin use, well known to reduce triglycerides (a frequently ignored lipid, which may be a greater cardiovascular risk factor than LDL cholesterol). Fish oil also provides the benefits of raising HDL, supporting endothelial function,112,113 decreasing inflammation, improving the particle size of LDL (reducing ApoB and small dense LDL) as well as reducing long-term risk of cardiovascular events. Supplementation alongside statins was shown to provide an additional 23% reduction in triglycerides, as well as twice the benefits of statins for ApoB.114
Supportive therapy alongside lipid lowering therapy is detailed in Appendix 1E.
COPRESCRIBING IN DIABETICSThe average diabetic takes more than 5 medications daily115 – a few for glucose control, a few for their difficult to control blood pressure, a statin to lower cholesterol, and other common medications such as analgesics, antidepressants, anxiolytics and proton pump inhibitors.116 Diabetes is one of the most expensive diseases for the health care system, both in glucose control as well as dealing with the various consequences and comorbidities – large vessel disease (cardiovascular) and small vessel disease (neuropathy, nephropathy and retinopathy). Natural support for diabetic patients can focus on two key areas of augmentation – assisting with glycaemic control, and reducing the associated risk of cardiovascular disease and the other complications.
Diet and lifestyle is one of the first places to start. The recommendation from Diabetes Australia is to eat meals regularly throughout the day which are low in fat and based on high fibre carbohydrate foods such as breads, cereals, legumes, vegetables and fruits.117 However, research suggests the opposite. In regards to eating regularly, a 2014 randomised trial involving 54 diabetic patients has shown that subjects eating two large meals per day (breakfast and lunch) achieved greater weight loss, lower hepatic fat content, reduced blood glucose and fasting insulin levels than those consuming six small meals per day.118 As far as limiting fat and basing the meals on carbohydrates, numerous studies have found that a high fat, low carbohydrate diet is superior to a high carbohydrate, low fat diet. 119 In one recent study, 363 obese and diabetic patients followed a low carbohydrate ketogenic diet or a low calorie diet for 24 weeks. Weight loss and beneficial changes in blood glucose, HbA1c and lipid parameters were experienced in both groups, with more significant benefits with the low carbohydrate diet. Further, these superior benefits were achieved despite dose reduction and discontinuation of some antidiabetic medications as part of the low carbohydrate diet protocol (Figure 10).120
Figure 10. Reduction in blood glucose levels in diabetic subjects on a low carbohydrate ketogenic diet (black triangles) and low calorie diet (white triangles).

21
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Based on the significant results and the necessity to reduce medication use with such a diet, the conclusion of this study’s authors was that type 2 diabetes patients should be monitored closely when commencing such a diet, as it has the potential to significantly lower blood glucose levels. While this caution should be taken seriously, with increased blood glucose monitoring put in place and the commencement of dietary change communicated to the health care provider, it provides a powerful potential benefit which should not be overlooked because of the need for a management plan. (Such is the case with most of the natural medicines we have reviewed for potentiating benefits.)
Shake It Professional Weight Management System is an easy to implement system for patients to follow a low carbohydrate, ketogenic diet. Complete with patient guides, recipe books, meal replacements and motivational newsletters, the program educates, inspires and supports patients as they follow the dietary plan. In a clinical trial on the program, over 12 weeks, obese patients lost an average of 10 kg, as well as reducing their triglycerides, fasting insulin and CRP levels. Such a program is ideal for use with weight loss patients as well as patients who require better metabolic control – metabolic syndrome, prediabetes and diabetes - with appropriate monitoring.
LIPOIC ACID IS A PRIMARY ADJUVANT THERAPY FOR DIABETESLipoic acid is an invaluable coprescription for diabetic patients, with the potential to improve glycaemic control as well as prevent diabetic complications. Lipoic acid works by stimulating intracellular pathways which promote cellular glucose utilisation, as well as by regenerating glutathione, to protect cells against glucose-induced oxidative stress. 600 mg/day of lipoic acid has been clinically trialled in diabetics in a number of studies, with results demonstrating safety and efficacy alongside metformin to improve insulin sensitivity (Figure 11)121, alongside ACE inhibitors to improve endothelial function,122 and in conjunction with various diabetic medications to relieve symptoms of neuropathy in just 5 weeks.123
Figure 11. 1200 mg lipoic acid increases insulin sensitivity in diabetics on metformin, as measured by glucose disposal.
In a case of a 66 year old male patient with long term type 2 diabetes, recent onset neuropathy and retinopathy caused him to seek natural health care treatment. He was taking multiple medications, including three antihypertensives, two oral hypoglycaemics, as well as four insulin injections daily, a statin and a benzodiazepine. The practitioner prescribed a nutritional support protocol including lipoic acid 600 mg/day, CoQ10 150 mg, fish oil 4000 mg/day, Resveratrol Antioxidant Complex and a multivitamin in the form of Male Nutritional Support with ModucareTM. At six months follow-up, the neuropathy had reduced in frequency, only occurring with alcohol consumption or overexertion, and the ophthalmologist reported stabilisation of retinopthy. After 18 months of treatment, the ophthalmologist shook the patient’s hand and said ‘Congratulations – I don’t know what you’ve done, but you’ve reversed the retinopathy!’ In this case, significant benefits were achieved to alleviate the complications of diabetes, while the glucose control was stable and the patient’s medications remained unchanged. This was well-suited to the patient’s goals, as he had stated that he didn’t want to ‘go through a lot of medication changes.’ As a result, the practitioner did not focus on an insulin sensitising protocol, but instead one which protected cells from diabetic damage.
Common medications which can be prescribed alongside antidiabetic medications are listed in Appendix 1F.
WEANING GUIDELINESA frequent consequence of improving drug efficacy is an ability to reduce drug dosage, or wean off certain drugs altogether.
Before prescribing a potentiating protocol, it is wise to consider the patient’s goals for treatment, as we saw in

22
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
the diabetic case above. While patient goals are important, also important is that the patient understands their responsibility in the process – to monitor their symptoms, comply with regular testing or assessment, and be willing to communicate openly with their primary health care provider about their natural medicine protocol and potential drug dosage adjustment. A guideline for factors to consider before embarking on a weaning plan is presented in Table 5.
Table 5. Guidelines for assessing the appropriateness of a weaning.
If weaning is decided upon as an appropriate goal, then a structured plan should be developed. What are the measures that will be used to determine a patient is ready to begin weaning – e.g. symptom scores or pathology markers that need to be achieved? Over what timeline will the weaning take place, and how will it be monitored?Many medications, providing such strong control over certain physiological pathways, have the potential to produce rebound effects or other side effects when discontinued. Going ‘cold-turkey’ by abruptly ceasing the medication is not advisable for most classes of drugs, and a gradual dose reduction plan is ideal. Overlapping the treatment period is often advisable, as the natural medicine may take a few weeks to begin having a therapeutic effect, at which time it may be able to take over from some of the effects of the drug.
When a suggested weaning plan has been produced, the patient’s prescribing practitioner should be contacted, detailing the natural medicine support plan, the evidence base and patient-specific rationale for weaning, and seeking input on the proposed dose-reduction protocol. In contentious areas, technical data on products and research papers supporting the weaning plan can be provided. The patient and practitioners involved should always keep in mind that if professional opinions differ on the correct course of treatment, in the end it is the patient who has the right to choose their treatment, and the practitioner’s role is to provide the information for them to make an informed decision.
POLYPHARMACY – WHERE TO START?Many patients take multiple medications, and have complex symptom pictures. Imagine the case of a 45 year old male, presenting with fatigue, muscle pain and headaches. He also has dyslipidaemia and hypertension, for which he takes a statin and an ACE inhibitor. He is obese, has a poor diet and drinks excessive amounts of alcohol. He takes an NSAID for generalised muscle pain and is also taking a budget fish oil supplement from the supermarket.In such a patient, you may see multiple goals which need to be achieved - reducing his cholesterol and blood pressure, improving his pain, losing weight, and improving lifestyle. The weight may be contributing to the abnormal cholesterol and blood pressure, whereas the statin drug may be contributing to his muscle pain and prompting NSAID use. While the practitioner may want to get to the root of the cardiovascular risk by tackling the weight, lipids and blood pressure, the patient has actually presented for pain, fatigue and headaches. In situations such as these, embarking on a program involving significant commitment to lifestyle change may not be the ideal first line strategy, as it does not address the patient’s primary complaint, and they may quickly lose motivation and become dissatisfied with treatment. The chance of success for this patient to increase their exercise with their current symptoms of fatigue and pain is also low. Designing the initial treatment protocol with the patient’s primary goals in mind is likely to achieve the best degree of compliance, patient retention, and ability to treat the long term health issues in the future. In this example, the practitioner could prescribe CoQ10 and magnesium, to address the potential statin-induced deficiency and treat the fatigue, pain and headaches, while providing the Wellness diet guidelines to assist the patient to start making healthier choices. Within a month, the patient may find that his pain and energy has improved. At this point, he has experienced some successful results from the changes implemented so far, and gained confidence in the practitioner’s advice. The practitioner may wish to introduce some exercise, and change his fish oil to a high potency, high quality supplement which will begin to address his cardiovascular risk. As the magnesium, CoQ10, fish oil, diet and exercise continue to work, the patient’s blood pressure and lipids may begin to come down over time, and a potential medication reduction may be possible. Should the practitioner change to a dedicated weight loss program such as Shake It Professional Weight Management System, these beneficial changes are even more likely. Such a progression is illustrated in Figure 12.

23
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Baseline 1 month 4 month 6 month
FatigueHeadaches
Muscle painDyslipidaemiaHypertension
Obesity
ACE inhibitorStatins
AnalgesicsGeneric fish oil
DyslipidaemiaHypertension
Obesity
ACE inhibitorStatins
↓ AnalgesicQ10Mag
High strength fish oilExercise
Add: MagnesiumQ10
Wellness diet
Dyslipidaemia↓Hypertension
↓Obesity
↓ACE inhibitorStatins
Q10Mag
High strength fish oilExercise Shake it
↓Dyslipidaemia↓Hypertension
↓Obesity
↓ACE inhibitor↓Statins
Q10Mag
High strength fish oilExercise Shake it
Figure 12. Case scenario of a patient using multiple medications, with proposed treatment and projected results.
As we can see, in a patient taking multiple medications, embarking on an effective natural medicine treatment protocol, involving supplemental support as well as diet and lifestyle change, has the potential to have a flow-on effect to reduce the dose or need for several medications over time. This can occur by tackling one or two issues at a time, and achieving small goals along the way, without overwhelming the patient or recommending aggressive drug withdrawal.
SPECIFIC NATURAL MEDICINES TO COUNTERACT DRUG SIDE EFFECTSIn addition to being able to enhance the efficacy and reduce the dose of pharmaceuticals, the other key benefit of co-prescribing is to be able to counteract some of the side effects of drugs. Natural medicines can restore nutrients which are depleted (such as omega 3 depletion with statins)124, counteract collateral effects on physiology (such as infection risk with corticosteroids)125, and protect tissues from adverse effects (such as gut mucosal damage with NSAIDs).126
A classic example of a co-prescription to counter side effects of a drug is the use of probiotics alongside antibiotics. While antibiotics are extremely useful for killing stubborn or serious infections, they have unavoidable negative consequences on the commensal flora throughout the body, leaving the body vulnerable to such opportunistic infections as candida and antibiotic associated diarrhoea.127 A combination of probiotics including Lactobacillus acidophilus NCFM and Bifidobacterium infantis Bi07 has been shown to minimise the impact of antibiotics on the gut microbiome (Figure 13), in particular promoting the maintenance of Bifidobacteria, the organism most commonly depleted by antibiotics.128
Figure 13. Probiotics containing Lactobacillus acidophilus NCFM and Bifidobacterium infantis Bi07 prevent gut microbiome degradation during antibiotic therapy.129

24
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
While probiotics are effective preventative agents, they are also one of the most effective treatments when side effects do occur. Numerous trials have shown Saccharomyces cerevisiae boullardii to be an effective treatment for antibiotic-associated diarrhoea, and the probiotic yeast has also been well utilised for the treatment of candida overgrowth with drug use.130 Lactobacillus rhamnosus LGG is the most extensively researched probiotic strain in the world, with studies demonstrating it is the probiotic of choice for antibiotic-associated diarrhoea in children, along with many other non-medication related applications.131 Common natural medicines which are recommended alongside antibiotics are detailed in Appendix 1F.
NSAIDS MAY CAUSE MUCOSAL DAMAGE THROUGH DYSBIOSISAs common as antibiotic use is, NSAID use is even more frequent. Despite the fact that these drugs are well-known to cause gut damage with each dose, many individuals are taking these medications not only occasionally but on a daily basis. Many of those with chronic conditions such as osteoarthritis or back pain feel they have no other choice to relieve their pain. Through inhibiting cyclooxygenase, these medications reduce the production of inflammatory prostaglandins and leukotrienes, but also the prostaglandins which mediate epithelial barrier maintenance and cell renewal. To prevent gastric damage in those on long-term NSAID use, a proton pump inhibitor (PPI) is often prescribed, which reduces the incidence of damage in the stomach but actually increases the incidence of small intestinal damage, which is more difficult to detect and can have more severe consequences.132 This is believed to occur because of an iatrogenic intestinal dysbiosis – contributed to by NSAID use but worsened with use of PPIs, associated with a significant intestinal depletion of Bifidobacteria.133 The novel prescription of a probiotic to reduce intestinal bleeding with NSAID use can be combined with the well-known protective effect of glutamine, boswellia and zinc in Glutamine & Boswellia (BosPure Boswellia) for Intestinal Integrity. Such supportive therapy is indicated in any patient taking NSAIDs long term, but may be especially useful where a suspected iatrogenic intestinal permeability and dysbiosis is contributing to other patient symptoms. For those with gastric symptoms associated with anti-inflammatory drug use, the more specific BCM-95 Turmeric and GutGard Liquorice for Heartburn and Reflux protects the stomach from gastritis and ulceration. Appendix 1A provides a summary of natural medicines which may be used alongside NSAIDs.
COUNTERACTING HIDDEN NUTRIENT DEPLETIONThe proton pump inhibitors discussed above are a relatively new drug, whose uptake in the marketplace has been remarkable. In the period from 1995 to 2006, prescription numbers in Australia for PPIs increased 1318% - a period which coincided with the open listing of the drug on the government-subsidised Australian Pharmaceutical Benefits Scheme (PBS).134,135 Currently, there are enough PPIs dispensed to treat 7% of the Australian population every day.136
As we saw above, PPIs are a known cause of intestinal dysbiosis, which can create intestinal damage. In addition, they can cause significant nutrient depletion. Use has been linked in numerous studies to a 30 - 60% increased risk of bone fractures,137 associated with depletion of calcium, as well as lesser known effects on magnesium depletion.138 B12 levels are another potential victim of PPI therapy, with hypochlorhydric individuals failing to be able to liberate the protein-bound B12 found in food.139 The full impact of these nutrient depletions in such a large segment of the population is potentially yet to be realised. A summary of some key considerations alongside PPIs is found in Appendix 1G.
In the situation of nutrient depletion by PPIs, or with any other hidden side effects of medications, the natural health care practitioner may need to proactively discuss these issues with patients. A patient may seek your help for their headaches and fatigue, but you may suspect a potential relationship to the mineral and B vitamin depletion from their PPI medication. Such an underlying problem could prevent you from achieving therapeutic results with the patient, and should be discussed upfront. In other situations, the potential nutrient depletion from their medication may not be linked to their primary complaint, but could be placing them at increased risk of other disease long term – such as the risk of osteoporosis with PPIs. Many patients can be focused on a short term view of their health, motivated by achieving symptom control and taking a ‘pill for an ill’. Helping patients to see the perspective of their long term health, and their crucial role in the management of it, can help patients to make more proactive decisions about their health choices. While providing this balanced viewpoint, it is important to remind patients that they should discuss any prospect of medication dose reduction or discontinuation with their prescriber, to ensure that individual circumstances are taken into account. This particularly applies to the PPI medications, as withdrawal can cause troublesome symptoms, especially in those with certain gastrointestinal conditions.
To support patients with calcium depletion or fracture risk, a new combination of Hydroxyapatite And Soy For Osteoporosis provides the most effective form of calcium for bone rebuilding, with soy isoflavones, and the nutritional cofactors vitamin C, boron, zinc, manganese, vitamin K and D3. Microcrystalline hydroxyapatite is derived from whole bone, and contains crystalline calcium and phosphorus, naturally occurring trace minerals, as well as bone proteins such as type 1 collagen, all of which assist the maintenance of bone health.140,141,142 Use of microcrystalline hydroxyapatite has been shown to protect against osteoporosis with glucocorticoid use,143 as well as augment the bone-building effects of HRT,144 making it a useful adjunct alongside various medications, including PPIs. The addition of an isoflavone-rich soy extract to the formula is a highly evidence based strategy for maximising the uptake and

25
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
utilisation of nutrients by bone.145 Soy isoflavones have been demonstrated in a multitude of studies to increase spine BMD by 2.4% over 6-12 months, a highly significant effect (Figure 14).146,147 Soy decreases inflammation-induced bone breakdown and increases bone synthesis, in part through a synergistic action with vitamin D.148,149 Soy has been subjected to extensive safety reviews, with proven safety for patients of all ages, as well as those at risk of or currently suffering from cancer. As soy binds to the anti-proliferative oestrogen receptor beta, it can have positive oestrogenic effects without affecting oestrogen receptor alpha activity, the receptor usually associated with cancer.150
Figure 14. Meta-analysis summarises the results of many studies demonstrating a 2.4% increase in bone density with soy isoflavones.151
DAILY SUPPORT FOR OCP USERSA little known fact for many women is the effect of their oral contraceptive pill (OCP) on nutrient status. The pill has been associated with widespread nutritional depletion, including vitamins B2, B6, B12, C, E and folate, as well as magnesium, selenium, zinc.152 The reduction in serum magnesium has been proposed to be a significant contributor to the increased risk of thrombosis and vascular events which women who take the pill are exposed to.153 Aside from thrombosis, other side effects of the OCP include nausea, headache and even depression, in a large percentage of women. Supplementation with just 25mg/day of vitamin B6 was shown to significantly reduce the prevalence of such side effects.154 An ideal formula to be prescribed for every woman taking the OCP is Magnesium and Broccoli for Women's Health. This magnesium-rich supplement is specifically designed to provide women with key nutrients which are involved in female health and are commonly deficient. It replenishes the nutrients depleted by the pill, as well as addressing a number of the drivers of female health issues by the addition of anti-inflammatory, detoxifying and stress-relieving herbs. Such a formula provides no known risk of failed contraception when taken alongside the pill, and places women in a more nutritionally replete situation for global health, addressing any underlying female health concerns, or for potential future conception.
MAINTAINING WELLNESS ON PHARMACEUTICALSAs we have seen, drugs cause the depletion of many nutrients – vitamins, minerals, fatty acids and even cofactors such as CoQ10.155 As a general rule, patients are far better off with a nutritional support prescription alongside their medications than no support at all. In fact, leaving patients in a nutritionally depleted state because of a lack of confidence around co-prescribing could be leaving them open to significant harm. Individuals who are nutritionally depleted are more likely to experience adverse drug reactions, with a lack of nutrition linked to poor drug detoxification and binding capacity.156,157,158
An ideal consideration for individuals on long term medication, especially those using polypharmacy for chronic diseases, is the Wellness Program. The Wellness Program is a combination of healthy diet, lifestyle and exercise recommendations, along with the core prescription of health maintenance supplements – multivitamin and mineral formula, high potency fish oil, strain-specific probiotics and phytonutrient-rich antioxidants. This combination has far-reaching benefits for most conditions that patients present with, and has very few interactions with medications. Increased monitoring may be needed in certain situations, due to the potential of such a program to reduce the need for antihypertensive or anti-diabetic medication, as well as for those on narrow therapeutic window drugs.

26
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CONFIDENT AND SAFE PRESCRIBING ALONGSIDE PHARMACEUTICALSWhen treating patients taking pharmaceutical drugs, natural medicine practitioners have a unique opportunity to both improve patient health, and improve their clinical success and satisfaction. Significant gains can be made to improve clinical results when natural medicines are used to augment drug efficacy, address the underlying drivers and counteract the side effects of pharmaceuticals. No other health care practitioner is more ideally positioned to be able to assist patients to receive the benefits of informed natural medicine prescribing alongside their medical practitioner’s treatment.
For practitioners, working in this important area can provide a high level of satisfaction, as more meaningful results can be achieved with patients’ primary health problems. Supporting medicated patients with therapeutic natural medicine protocols has the potential to make a significant impact on the burden of chronic disease in the community, improving outcomes and reducing health care costs. Providing confident and evidence-based advice for patients and achieving successful results can help make natural health care practitioners a trusted resource for patients and medical practitioners alike.
Prescribing alongside pharmaceuticals is a reality for every natural health care practitioner. Embracing and maximising this opportunity is the future of health for all involved.
REFERENCES1. Morgan TK, et al. A national census of medicines use: a 24-hour snapshot of Australians aged 50 years and older. MJA 2012; 196 (1):50-532. Braun L, Cohen M. Herbs & Natural Supplements. 3rd edn. New South Wales: Elsevier; 2010:91 3. Braun L, Cohen M. Herbs & Natural Supplements. 3rd edn. New South Wales: Elsevier; 2010:914. Braun LA, et al. Adverse reactions to complementary medicines: the Australian pharmacy experience. IJPP 2010;18:242–2445. Holman HR. The inadequacy of medical education. Chronic Illn. 2009 Mar;5(1):18-206. Jones DS, et al. The burden of disease and the changing task of medicine. N Engl J Med 2012;366(25):2333-23387. Zarate C, et al. New paradigms for treatment-resistant depression. Ann N Y Acad Sci 2013;1292:21-318. McColl KE, Gillen D. Evidence that proton-pump inhibitor therapy induces the symptoms it is used to treat. Gastroenterology 2009;137(1):20-229. The Royal Australasian College of Physicians. Action needed to reduce medication-related death. Media Release. Friday 22 February, 2013.
http://www.racp.edu.au/download.cfm?DownloadFile=13B6E042-DF13-1154-DC331ADE67E276AC10. Culver AL, et al. Statin use and risk of diabetes mellitus in postmenopausal women in the Women's Health Initiative. Arch Intern Med. 2012 Jan
23;172(2):144-5211. Dehpour AR, et al. The protective effect of liquorice components and their derivatives against gastric ulcer induced by aspirin in rats. J Pharm Pharmacol
1994;46(2):148-912. Sivalingam N, et al. Zinc protects against indomethacin-induced damage in the rat small intestine. Eur J Pharmacol 2011;654(1):106-1613. De Jager J, et al. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B12 deficiency: randomised placebo controlled
trial. BMJ 2010;340:c218114. Bhalla P, et al. Attenuation of angiotensin converting enzyme inhibitor induced cough by iron supplementation: role of nitric oxide. J Renin Angiotensin
Aldosterone Syst. 2011 Dec;12(4):491-715. Zimmermann M, Kretchmer N. Isn't it time to teach nutrition to medical students? Am J Clin Nutr 1993;58:828-82916. Braun L, Cohen, M. Herbs & Natural Supplements. 3rd edn. New South Wales: Elsevier; 2010 17. https://www.tga.gov.au/alert/st-johns-wort-important-interactions-between-st-johns-wort-hypericum-perforatum-preparations-and-prescription-medicines
(Date accessed 2/12/14)18. https://www.tga.gov.au/alert/st-johns-wort-important-interactions-between-st-johns-wort-hypericum-perforatum-preparations-and-prescription-medicines
(Date accessed 2/12/14)19. Posadzki P, Watson L, Ernst E. Herb-drug interactions: an overview of systematic reviews. Br J Clin Pharmacol 2012;75(3):603-61820. Shord SS, et al. Drug-Botanical Interactions: A review of the laboratory, animal, and human data for 8 common botanicals. Integrative Cancer Therapies
2009; 8(3):208–22721. Shord SS, et al. Drug-Botanical Interactions: A review of the laboratory, animal, and human data for 8 common botanicals. Integrative Cancer Therapies
2009; 8(3):208–22722. http://www.livescience.com/18070-food-americans-eat-year-infographic.html (Date accessed 2/12/14)23. Butterweck V, et al. Pharmacokinetic herb-drug interactions: are preventive screenings necessary and appropriate? Planta Med 2004;70:784-79124. Harris RZ, Jang GR, Tsunoda S. Dietary effects on drug metabolism and transport. Clin Pharmacokinet 2003;42(13):1071-8825. What Affects Psychiatric Drug Response? Personalised Medicine Portal. Genomic Medicine Institute. https://elcaminogmi.dnadirect.com/grc/patient-site/
psychiatric-drug-response/what-affects-psychiatric-drug-response.html?1TSygRyYLZj7y3i98o4f0gC26. Byard RW. A review of the potential forensic significance of traditional herbal medicines. J Forensic Sci. 2010 Jan;55(1):89-9227. Blacksell L, Byard RW, Musgrave IF. Forensic problems with the composition and content of herbal medicines. J Forensic Leg Med. 2014 Mar;23:19-21. 28. Fugh-Berman A. Herb-drug interactions. The Lancet 2000;355:134-13829. Teschke R, et al. Herb induced liver injury presumably caused by black cohosh: a survey of initially purported cases and herbal quality specifications. Annals
of Hepatology 2011;10(3):249-5930. Mahady GB. United States Pharmacopeia review of the black cohosh case reports of hepatotoxicity. Menopause 2008; 15(4):628/63831. Neustadt J. Herb-drug interactions: what clinicians need to know. Integrative Medicine 2006;5(1):16-2632. De Smet PAGM. Clinical risk management of herb–drug interactions. Br J Clin Pharmacol 2006;63 (3): 258–26733. Mozaffari-Khosravi H. Eicosapentaenoic acid versus docosahexaenoic acid in mild-to-moderate depression: A randomised, double-blind, placebo-
controlled trial. European Neuropsychopharmacology 2013;23:636–64434. Natural Standards Database. https://naturalmedicines.therapeuticresearch.com/databases.aspx35. Braun L, Cohen M. Herbs & Natural Supplements. 3rd edn. New South Wales: Elsevier; 201036. Bender NK, et al. Effects of marine fish oils on the anticoagulation status of patients receiving chronic warfarin therapy. Journal of thrombosis and
thrombolysis 1998;5:257-26137. Leaf A, et al. Do fish oils prevent restenosis after coronary angioplasty? Circulation 1994;90:2248-225738. Shord SS, et al. Drug-Botanical Interactions: A review of the laboratory, animal, and human data for 8 common botanicals. Integrative Cancer Therapies
2009; 8(3):208–22739. Fleischer D, et al. Drug, meal and formulation interactions influencing drug absorption after oral administration. Clinical Pharmacokinetics 1999;30(3):233-
25440. http://naturaldatabase.therapeuticresearch.com/nd/Search.aspx?cs=&s=ND&pt=100&id=982&ds=interdrug&name=ZINC&searchid=49409437 (Date
accessed 3/12/14)41. Romiti N, et al. Effects of grapefruit juice on the multidrug transporter P-glycoprotein in the human proximal tubular cell line HK-2. Life Sci 2004;76:293–
302

27
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
42. Edwards G. Ivermectin: does P-glycoprotein play a role in neurotoxicity: Filaria Journal 2003;2 Suppl 1:S843. Neustadt J. Herb-drug interactions: what clinicians need to know. Integrative Medicine 2006;5(1):16-2644. Chung SY, et al. Inhibition of P-glycoprotein by natural products in human breast cancer cells. Arch Pharm Res 2005;28.7:823-82845. Zadoyan G, Fuhr U. Phenotyping studies to assess the effects of phytopharmaceuticals on in vivo activity of main human cytochrome P450 enzymes. Planta
Med 2012;78:1428-145746. http://www.nlm.nih.gov/medlineplus/ency/article/003883.htm (Date accessed 4/12/14)47. Mitra A, Kesisoglou F. Impaired drug absorption due to high stomach pH: a review of strategies for mitigation of such effect to enable pharmaceutical
product development. Mol Pharm 2013;10(11):3970-948. Li H, Jia W. Co-metabolism of microbes and host: implications for drug metabolism and drug-induced toxicity. Clin Pharmacol Ther 2013;94(5):574-8149. Davis SS, et al. Alimentary tract and pancreas transit of pharmaceutical dosage forms through the small intestine. Gut 1986; 27:886-89250. Fleischer D, et al. Drug, meal and formulation interactions influencing drug absorption after oral administration. Clinical Pharmacokinetics 1999;30(3):233-25451. Butterweck V, et al. Pharmacokinetic herb-drug interactions: are preventive screenings necessary and appropriate? Planta Med 2004;70:784-79152. Helmstadter A, Staiger C. Traditional use of medicinal agents: a valid source of evidence. Drug Discovery Today 2014;19(1):4-753. Brantley SJ, et al. Herb–Drug Interactions: challenges and opportunities for improved predictions. Drug Metab Dispos 2014;42:301–31754. Lind L, Lind PM. Can persistent organic pollutants and plastic-associated chemicals cause cardiovascular disease? J Intern Med 2012;271(6):537-55355. Lee DK, et al. A strong dose-response relation between serum concentrations of persistent organic pollutants and diabetes: results from the National Health
and Examination Survey 1999-2002. Diabetes Care 2006;29:1638-164456. Pope ND. Generic substitution of narrow therapeutic index drugs. US Pharm 2009;34(6)(Generic Drug Review suppl):12-19 57. https://www.tga.gov.au/alert/st-johns-wort-important-interactions-between-st-johns-wort-hypericum-perforatum-preparations-and-prescription-medicines
(Date accessed 2/12/14)58. Aletaha D, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism
collaborative initiative. Arthritis Rheum. 2010 Sep;62(9):2569-8159. Proudman SM, et al. Fish oil in recent onset rheumatoid arthritis: A randomised, double-blind, controlled trial within algorithm-based drug use. Abstracts of
Pharma Nutrition 2013 / PharmaNutrition 2 (2014) 75–11960. http://www.medicareaustralia.gov.au/provider/pbs/drugs1/crohns.jsp#N10041 (Date accessed 4/12/14)61. McKenna MR, Stobaugh DJ, Deepak P. Melanoma and non-melanoma skin cancer in inflammatory bowel disease patients following tumor necrosis factor-α
inhibitor monotherapy and in combination with thiopurines: analysis of the Food and Drug Administration Adverse Event Reporting System. J Gastrointestin Liver Dis. 2014 Sep;23(3):267-71.
62. Targownik LE, Bernstein CN. Infectious and malignant complications of TNF inhibitor therapy in IBD. Am J Gastroenterol. 2013 Dec;108(12):1835-42, quiz 1843. doi: 10.1038/ajg.2013.294.
63. Moran GW, et al. Review article: dermatological complications of immunosuppressive and anti-TNF therapy in inflammatory bowel disease. Aliment Pharmacol Ther. 2013 Nov;38(9):1002-24.
64. McKenna MR, Stobaugh DJ, Deepak P. Melanoma and non-melanoma skin cancer in inflammatory bowel disease patients following tumor necrosis factor-α inhibitor monotherapy and in combination with thiopurines: analysis of the Food and Drug Administration Adverse Event Reporting System. J Gastrointestin Liver Dis. 2014 Sep;23(3):267-71.
65. Targownik LE, Bernstein CN. Infectious and malignant complications of TNF inhibitor therapy in IBD. Am J Gastroenterol. 2013 Dec;108(12):1835-42, quiz 1843. doi: 10.1038/ajg.2013.294.
66. Moran GW, et al. Review article: dermatological complications of immunosuppressive and anti-TNF therapy in inflammatory bowel disease. Aliment Pharmacol Ther. 2013 Nov;38(9):1002-24.
67. Grammatikos AP, Tsokos GC. Immunodeficiency and autoimmunity: lessons from systemic lupus erythematosus. Trends Mol Med. 2012 Feb;18(2):101-868. Kidd PM. The use of mushroom glucans and proteoglycans in cancer treatment. Alt Med Rev, 2000;5(1):2169. Chandran B, Goel A. A randomised, pilot study to assess the efficacy and safety of curcumin in patients with active rheumatoid arthritis. Phytother Res. 2012
Nov;26(11):1719-25.70. Hanai H, et al. Curcumin maintenance therapy for ulcerative colitis: randomized, multicentre, double-blind, placebo-controlled trial. Clin Gastroenterol
Hepatol 2006;4(12):1502-671. Proudman SM, et al. Fish oil in recent onset rheumatoid arthritis: A randomised, double-blind, controlled trial within algorithm-based drug use. Abstracts of
Pharma Nutrition 2013 / PharmaNutrition 2 (2014) 75–11972. Proudman SM, et al. Fish oil in recent onset rheumatoid arthritis: A randomised, double-blind, controlled trial within algorithm-based drug use. Abstracts of
Pharma Nutrition 2013 / PharmaNutrition 2 (2014) 75–11973. James M, et al. 3rd International Immunonutrition Workshop:Session 3: Fatty acids and the immune system Fish oil and rheumatoid arthritis: past, present
and future. Proc Nutr Soc 2010; 69:316–32374. James M, et al. 3rd International Immunonutrition Workshop:Session 3: Fatty acids and the immune system Fish oil and rheumatoid arthritis: past, present
and future. Proc Nutr Soc 2010; 69:316–32375. Bengston-Nash SM, et al. A nutritional-toxicological assessment of Antarctic krill oil versus fish oil dietary supplements. Nutrition 2014;6:3382-3402 76. Zarate C, et al. New paradigms for treatment-resistant depression. Ann NY Acad Sci 2013;1292:21-3177. Sarris J, et al. Adjuvant use of nutritional and herbal medicines with antidepressants, mood stabilisers and benzodiazepines. J Psychiatr Res 2010;44(1):32-
4178. https://www.tga.gov.au/alert/st-johns-wort-important-interactions-between-st-johns-wort-hypericum-perforatum-preparations-and-prescription-medicines
(Date accessed 2/12/14)79. Qureshi NA, Al-Bedah AM. Mood disorders and complementary and alternative medicine: A literature review. Neuropsychiatr Dis Treat 2013;9:639-5880. Eby GA 3rd, Eby KL. Magnesium for treatment-resistant depression: A review and hypothesis. Med Hypotheses 2010;74(4):649-6081. Mozaffari-Khosravi H. Eicosapentaenoic acid versus docosahexaenoic acid in mild-to-moderate depression: A randomised, double-blind, placebo-
controlled trial. European Neuropsychopharmacology 2013;23:636–64482. Coppen A, Bailey J. Enhancement of the antidepressant action of fluoxetine by folic acid: a randomised, placebo controlled trial. J Affect Disord.
2000;60(2):121-3083. Khoraminya N, et al. Therapeutic effects of vitamin D as adjunctive therapy to fluoxetine in patients with major depressive disorder Aust NZ J Psychiatry
2013;47(3):271-584. Lai J, et al. The efficacy of zinc supplementation in depression: Systematic review of randomised controlled trials. J Affect Disord 2012;136:e31-e3985. Berk M, et al. N-acetylcysteine for depressive symptoms in bipolar disorder – a double-blind randomised placebo-controlled trial. Biol Psychiatry
2008;64:361-368 86. Akhondzadeh S, et al. Passionflower in the treatment of generalised anxiety: A pilot double-blind randomised controlled trial with oxazepam. J Clin Pharm
Ther 2001;26(5):363-7 87. Gardiner P, et al. Concomitant use of prescription medications and dietary supplements in menopausal women: An approach to provider preparedness.
Maturitas 2011;68:251–25588. Kim JM, White RH. Effect of vitamin E on the anticoagulant response to warfarin. Am J Cardiol. 1996 Mar 1;77(7):545-689. Kim JM, White RH. Effect of vitamin E on the anticoagulant response to warfarin. Am J Cardiol. 1996 Mar 1;77(7):545-690. Liu M, et al. Mixed tocopherols inhibit platelet aggregation in humans: potential mechanisms. Am J Clin Nutr, 2003;77:700–70691. Qureshi AA, et al. Dose-dependent suppression of serum cholesterol by tocotrienol-rich fraction (TRF25) of rice bran in hypercholesterolaemic humans.
Atherosclerosis 2002;161:199-20792. Spigset O. Reduced effect of warfarin caused by ubidecarenone. The Lancet 1994;344(12):1372-137393. Engelsen J, Nielsen JD, Winther K. Effect of coenzyme Q10 and Ginkgo biloba on warfarin dosage in stable, long-term warfarin treated outpatients. A
randomised, double blind, placebo-crossover trial. Thromb Haemost 2002;87(6):1075-694. Braun L, Cohen M. Herbs & Natural Supplements. 3rd edn. New South Wales: Elsevier; 2010.95. Braun L, Stanguts C, Spitzer O, et al. A wellness program for cardiac surgery improves clinical outcomes. Advances in Integrative Medicine 2014;1:32-3796. Chu MWA, et al. Does clopidogrel increase blood loss after coronary artery bypass surgery? Ann Thorac Surg 2004;78:1536-154197. Mozaffari-Khosravi H. Eicosapentaenoic acid versus docosahexaenoic acid in mild-to-moderate depression: A randomised, double-blind, placebo-

28
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
controlled trial. European Neuropsychopharmacology 2013;23:636–64498. Houston M. The Life of the Vascular Tunnel: Foundational Vascular Biology for the Clinician. The Institute for Functional Medicine. Annual International
Conference 2012 Scottsdale, AZ99. Maier JA. Endothelial cells and magnesium: implications in atherosclerosis. Clin Sci (Lond). 2012;122(9):397-407100. imental-Mendia LE. Oral magnesium supplementation decreases C-reactive protein levels in subjects with prediabetes and hypomagnesemia: a clinical
randomised double-blind placebo-controlled trial. Arch Med Res 2014;45(4):325-30101. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulphate. The National Academies Press http://www.iom.edu/~/media/Files/
Activity%20Files/Nutrition/DRIs/DRI_Electrolytes_Water.pdf (Date accessed 21/11/14)102. Rosenfeldt FL, et al. Coenzyme Q10 in the treatment of hypertension: a meta-analysis of the clinical trials. J Hum Hypertens 2007;21:297-306103. Langsjoen P, et al. Treatment of essential hypertension with coenzyme Q10. Mol Aspects Med 1994;15 Suppl:S265-72104. Liu ZX, Artmann C. Relative bioavailability comparison of different coenzyme Q10 formulations with a novel delivery system. Altern Ther Health Med. 2009
Mar-Apr;15(2):42-6105. Top 10 drugs. Aust Prescr 2014;37:195 http://www.australianprescriber.com/magazine/37/6/article/1543.pdf (Date accessed 4/12/14)106. Culver AL. et al. Statin use and risk of diabetes mellitus in postmenopausal women in the Women's Health Initiative. Arch Intern Med. 2012 Jan
23;172(2):144-52107. Goldstein MR, Mascitelli L. Do statins cause diabetes? Current Diabetes Reports 2013;10.1007/s11892-013-0368-x108. Rundek T, et al. Atorvastatin decreases the coenzyme Q10 level in the blood of patients at risk for cardiovascular disease and stroke. Arch Neurol
2004;61(6):889-92109. Volk MG. An examination of the evidence supporting the association of dietary cholesterol and saturated fats with serum cholesterol and development of
coronary heart disease. Altern Med Rev. 2007 Sep;12(3):228-45110. http://www.news.com.au/lifestyle/health/abc-tv-show-catalyst-could-cause-3000-heart-attacks/story-fneuzlbd-1226780002493 111. http://stroke.ahajournals.org/content/37/10/2640.full 112. http://www.ncbi.nlm.nih.gov/pubmed/22584102 113. http://www.ncbi.nlm.nih.gov/pubmed/19394939 114. Davidson MH, et al. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: an
8-week, randomised, double-blind, placebo-controlled study. Clinical Therapeutics 2007;29:1354-1367115. Bailey CJ, Kodack M. Patient adherence to medication requirements for therapy for type 2 diabetes. Int J Clin Pract 2011;65(4):314-322116. Bailey CJ, Kodack M. Patient adherence to medication requirements for therapy for type 2 diabetes. Int J Clin Pract 2011;65(4):314-322117. https://www.diabetesaustralia.com.au/Living-with-Diabetes/Eating-Well/Food-What-Should-I-Eat/ 118. Kahleova H, et al. Eating two larger meals a day (breakfast and lunch) is more effective than six smaller meals in a reduced-energy regimen for patients with
type 2 diabetes: a randomised crossover study. Diabetologia. 2014 Aug;57(8):1552-60119. Feinman RD, et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition 2015; 31:1–
13120. Hussain TA, et al. Effect of low-calorie versus low-carbohydrate ketogenic diet in type 2 diabetes. Nutrition, 2012 Oct;28(10):1016-21121. Kamenova P. Improvement of insulin sensitivity in patients with type 2 diabetes mellitus after oral administration of alpha-lipoic acid. Hormones (Athens),
2006;5(4):251-8122. Rahman ST, et al. The impact of lipoic acid on endothelial function and proteinuria in quinapril-treated diabetic patients with stage I hypertension: Results
from the QUALITY study. J Cardiovasc Pharmacol Therapeutics 2012;17(2):139-145123. Zeigler D, et al. Oral treatment with α-Lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes Care 2006;29 (11): 2365-
2370124. De Logeril M, et al. Recent findings on the health effects of omega-3 fatty acids and statins, and their interactions: do statins inhibit omega-3? BMC Med.
2013 Jan 4;11:5125. Brassard P, et al. Oral corticosteroids and the risk of serious infections in patients with elderly-onset inflammatory bowel Diseases. Am J Gastroenterol
2014;109:1795-1802126. Sivalingam N, et al. Zinc protects against indomethacin-induced damage in the rat small intestine. Eur J Pharmacol 2011;654(1):106-16127. Katz JA. Probiotics for the prevention of antibiotic-associated diarrhoea and Clostridium difficile diarrhoea. J Clin Gastroenterol 2006;40(3):249-255128. Engelbrektson AL, et al. Probiotics to minimize the disruption of faecal microbiota in healthy subjects undergoing antibiotic therapy. J Med Microbiol 2009.
58 :663-670129. Engelbrektson AL, et al. Probiotics to minimize the disruption of faecal microbiota in healthy subjects undergoing antibiotic therapy. J Med Microbiol 2009.
58 :663-670130. McFarland LV. Systematic review and meta-analysis of Saccharomyces boulardii in adult patients. World J Gastroenterol 2010; 16(18): 2202-2222 131. Katz JA. Probiotics for the prevention of antibiotic-associated diarrhoea and Clostridium difficile diarrhoea. J Clin Gastroenterol 2006;40(3):249-255132. Syer SD, Wallace JL. Environmental and NSAID-enteropathy: dysbiosis as a common factor. Curr Gastroenterol Rep 2014;16(3):377133. Syer SD, Wallace JL. Environmental and NSAID-enteropathy: dysbiosis as a common factor. Curr Gastroenterol Rep 2014;16(3):377134. http://www.nps.org.au/publications/health-professional/prescribing-practice-review/2006/prescribing-practice-review-25 135. Australian Government. Department of Veterans Affairs. Therapeutic Brief Topic 32: Proton Pump Inhibitors – How much for how long? Accessed online
3/12/14 http://www.veteransmates.net.au/VeteransMATES/documents/module_materials/M32_TherBrief.pdf 136. Australian Government. Department of Veterans Affairs. Therapeutic Brief Topic 32: Proton Pump Inhibitors – How much for how long? Accessed online
3/12/14 http://www.veteransmates.net.au/VeteransMATES/documents/module_materials/M32_TherBrief.pdf 137. http://www.sciencedirect.com/science/article/pii/S0002934311001641138. http://www.fda.gov/Drugs/DrugSafety/ucm245011.htm (Date accessed 11/11/14)139. Wilhelm SM, et al. Perils and pitfalls of long-term effects of proton pump inhibitors. Expert Rev Clin Pharmacol 2013;6(4):443-51140. Anderson GH, Draper HH. Effect of dietary phosphorus on calcium metabolism in intact and parathyroidectomized adult rats. J Nutr. 1972;102:123-132141. Manufacturer’s Information: MCH-Cal Natural Calcium Information Sheet, 2007142. Stepan JJ, et al. Quantitation of growth factors in ossein-mineral-compound. Life Sci 1991;49(13):79-84143. Pines A, et al. Clinical trial of microcrystalline hydroxyapatite compound ('Ossopan') in the prevention of osteoporosis due to corticosteroid therapy. Curr
Med Res Opin 1984;8(10):734-42144. Castelo-Branco C et al. Ossein hydroxyapatite compounds for preventing postmenopausal bone loss. Coadjuvant use with hormone replacement therapy. J
Reprod Med 1999;44(3);241-6145. Atmaca A, et al. Soy isoflavones in the management of postmenopausal osteoporosis. Menopause 2008;15(4 Pt 1):748-57146. Taku K, et al. Effect of soy isoflavone extract supplements on bone mineral density in menopausal women: meta-analysis of randomized controlled trials.
Asia Pac J Clin Nutr. 2010;19(1):33-42147. Harkness LS, et al. Decreased bone resorption with soy isoflavone supplementation in postmenopausal women. J Womens Health (Larchmt).
2004;13:1000-7148. Chang K-L, et al. Combined effect of soy isoflavones and vitamin D3 on bone loss in ovariectomized rats. Nutrition, 2013;29:250–257149. Park CY, Weaver CM. Vitamin D Interactions with soy isoflavones on bone after menopause: a review. Nutrients 2012;4:1610-1621150. Park CY, Weaver CM. Vitamin D Interactions with soy isoflavones on bone after menopause: a review. Nutrients 2012;4:1610-1621151. Taku K, et al. Effect of soy isoflavone extract supplements on bone mineral density in menopausal women: meta-analysis of randomized controlled trials.
Asia Pac J Clin Nutr. 2010;19(1):33-42 152. Palmery M, et al. Oral contraceptives and changes in nutritional requirements. Eur Rev Med Pharmacol Sci 2013;17(13):1804-13153. Palmery M, et al. Oral contraceptives and changes in nutritional requirements. Eur Rev Med Pharmacol Sci 2013;17(13):1804-13154. Var C, et al. Supplementation with vitamin B6 reduces side effects in Cambodian women using oral contraception. Nutrients 2014;6:3353-3362155. Meletis CD, Zabriskie N. Common Nutrient Depletions Caused by Pharmaceuticals. Alternative and Complementary Therapies. February 2007, 13(1): 10-17.156. Pickering G. Frail elderly, nutritional status and drugs. Arch Gerontol Geriatr. 2004 Mar-Apr;38(2):174-80 157. Kutuzova GD. 1,25-Dihydroxyvitamin D3 regulates genes responsible for detoxification in intestine. Toxicol Appl Pharmacol, 2007 Jan 1;218(1):37-44158. Raiten DJ. Nutrition and pharmacology: general principles and implications for patients with HIV. Am J Clin Nutr 2011;94(suppl):1697S-702S

29
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MORE THAN HALF OF AUSTRALIANS TAKE
PHARMACEUTICAL MEDICATIONS
Morgan TK, et al. A national census of medicines use: a 24-hour snapshot of Australians aged 50 years and older. MJA 2012; 196 (1):50-53
Medicines Australia Facts Book. http://medicinesaustralia.com.au/issues-information/publications/facts-book/
CHRONIC DISEASE IS THE NEW EPIDEMIC
Jones DS, et al. The burden of disease and the changing task of medicine.N Engl J Med 2012;366(25):2333-2338
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

30
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
PHARMACEUTICALS DON’T WORK FOR EVERYONE
“The vast majority of drugs only work in 30 or 50% of people”
Allen Roses, vice-president of genetics at GlaxoSmithKline
BMJ. Dec 13, 2003; 327(7428): 1366
Anybody familiar with the notion of “number needed to treat” knows that it's usually necessary
to treat many patients in order for one to benefit.
BMJ. Dec 13, 2003; 327(7428): 0.
TOP 10 AUSTRALIAN MEDICINESDRUG
NUMBER OF PRESCRIPTIONS
USE
Atorvastatin 8 659 127 Lipid modifying agent
Rosuvastatin 7 610 977 Lipid modifying agent
Esomeprazole 6 967 801 For acid related disorders
Paracetamol 6 299 698 Analgesic
Pantoprazole 4 179 926 For acid related disorders
Perindopril 3 951 282 Antihypertensive
Metformin hydrochloride 3 539 513 For obstructive lung disease
Salmeterol and fluticasone 3 168 825 Antihypertensive
Irbesartan 3 032 109 Antihypertensive
Simvastatin 2974 311 Lipid modifying agent
Department of Health, Commonwealth of Australia. Top 10 drugs. Australian Prescriber 2014;37:195.
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

31
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
SIDE EFFECTS FROM PRESCRIPTION MEDICATION CAN BE FATAL
Adverse events, including hospital-borne infections,medication mix-ups, drug side-effects and patientfalls, affect about one in six patients.
Metherel M . Hospital botches kill 4500. The Age; July 27, 2009.http://www.theage.com.au/national/hospital-botches-kill-4500-20090726-dxjm.html
1.5 MILLION AUSTRALIANS SUFFER AN ADVERSE DRUG
REACTION PER YEAR• Over 1.5 million Australians suffer an adverse event from
medicines each year resulting in at least 400,000 visits togeneral practitioners, 190,000 hospital admissions and, insevere cases, death.
• Approximately two to three per cent of all hospital admissionsare medication-related and, of those, approximately 50 percent are preventable.
The Royal Australasian College of Physicians. Action needed to reduce medication-related death. Media Release. Friday 22 February, 2013.
http://www.racp.edu.au/download.cfm?DownloadFile=13B6E042-DF13-1154-DC331ADE67E276AC.
STATINS INCREASE RISK OF DIABETES BY 47% OVER THREE
YEARS
Culver AL. et al. Statin use and risk of diabetes mellitus in postmenopausal women in the Women's Health Initiative. Arch Intern Med. 2012 Jan 23;172(2):144-52
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

32
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CURRENT MEDICAL MODEL NOT EQUIPPED TO MANAGE
CHRONIC DISEASE
‘Medical practice is now confronted by a dominant health problem, chronic disease,
for which it was not designed.’
Holman HR. The inadequacy of medical education. Chronic Illn. 2009 Mar;5(1):18-20
NATURAL MEDICINES BRIDGE THE GAP
Liang X, Li H, Li S. A novel network pharmacology approach to analyse traditional herbal formulae: the Liu-Wei-Di-Huang pill as a case study. Mol Biosyst. 2014 May;10(5):1014-22.
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

33
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
WHAT’S THE REAL RISK OF CO-PRESCRIBING?
THE BENEFITS VERSUS RISK OF CO-PRESCRIBING IS FAVOURABLE
When manufactured and prescribedappropriately, the safety of herbal andnatural medicine is high. Serious adverseeffects and dangerous interactions arerare, particularly in comparison with thethousands of reports attributed topharmaceutical medicines.
Associate Professor Lesley Braun
Braun L, Cohen, M. Herbs & Natural Supplements. 3rd edn. New South Wales: Elsevier; 2010
CHOOSE THE PATH TO SUCCESS
Side effects
Drivers unaddressed
Higher doses, more drugs
Disease progressionImproved
health
Weaning
Better symptom relief
Disease control
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

34
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
BENEFITS FOR THE PRACTITIONER• Large population to treat• Regular, compliant patients keen
for improved results• Networking opportunity with
other health care practitioners• Good source of referrals• Improved confidence• Increased clinical satisfaction
through achieving meaningful results
• Business building
NATURAL HEALTH PRACTITIONERS HAVE THE CLINICAL TOOLBOX TO
CO-PRESCRIBENatural medicine treatments:• Address underlying causes• Act pleiotropically for better
disease management• Are flexible and can be
individualised• Are evidence-based• Have a good safety record• Encourage healthy lifestyles• Are motivating and achievable
THE BENEFITS OF CO-PRESCRIBING
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

35
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CAUTIONS FOR CO-PRESCRIBING
MANY EXAMPLES OF SUCCESSFUL CO-PRESCRIBING
CO-PRESCRIBING: THE FUTURE OF HEALTHCARE

36
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MANY HERB-DRUG INTERACTIONS ARE
HYPOTHETICAL‘In 10 systematic reviews, herb-drug interactionswere hypothetical as the primary research wasbased on in vitro and/or animal studies. Thisoverview suggests that the quality of research onherb-drug interactions is often wanting.’
Posadzki P, et al. Herb-drug interactions: an overview of systematic reviews. Br J ClinPharmacol 2012;75(3):603-618
GETTING PERSPECTIVE ON INTERACTIONS

37
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Shor
dSS
, et a
l. D
rug-
Bota
nica
l Int
erac
tions
: A
Revi
ew o
f the
Lab
orat
ory,
Ani
mal
, and
Hum
an
Dat
a fo
r 8 C
omm
on B
otan
ical
s. I
nteg
rativ
e C
ance
r Th
erap
ies
2009
;8(3
):208
–227
EVID
ENC
E FO
R I
NTE
RA
CTI
ON
S B
ASE
D
ON
MIS
LEA
DIN
G I
N V
ITR
O R
ESU
LTS
GETTING PERSPECTIVE ON INTERACTIONS

38
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Byard RW. A review of the potential forensic significance of traditional herbal medicines. J Forensic Sci. 2010 Jan;55(1):89-92
ADVERSE REACTIONS:
COULD IT BE A QUALITY
CONTROL ISSUE?
What Affects Psychiatric Drug Response? Personlised Medicine Portal. Genomic Medicine Institute. https://elcaminogmi.dnadirect.com/grc/patient-site/psychiatric-drug-response/what-
affects-psychiatric-drug-response.html?1TSygRyYLZj7y3i98o4f0gC
GENES, PHYSIOLOGY, LIFESTYLE AND ENVIRONMENT DICTATE THE
DRUG RESPONSE
GETTING PERSPECTIVE ON INTERACTIONS

39
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
AUSTRALIAN MEDICINES CONTAMINATED WITH HEAVY METALS
AND PRESCRIPTION DRUGS
CASE REPORT: HEAVY METAL TOXICITY FROM HERBAL MEDICINE
• 34 y.o. female • Shortness of breath, palpitations, decreased
exercise tolerance and generalised arthralgia• Taking numerous Ayuvedic herbal formulas from
overseas for infertility• Haemoglobin 66 g/L, basophilic stippling of RBCs• Serum lead 105 μg/dL (<10 μg/dL)• Symptoms and lead levels reduced after chelation
therapy
Hochholzer K, Li W, Gunja N. A heavy burden: remaining vigilant with herbal remedies. Aust Fam Physician 2014;43(8):545-6
GETTING PERSPECTIVE ON INTERACTIONS

40
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
LABELS DON’T MATCH INGREDIENTS IN 60% OF AUSTRALIAN PRODUCTS
Purchasers may be exposed to potentially hazardous concentrations of materials, or be at higher risk of overdose.
Blacksell L, Byard RW, Musgrave IF. Forensic problems with the composition and content of herbal medicines. J Forensic Leg Med. 2014;23:19-21
BEWARE OF PRESCRIBING MEDICINES NOT LISTED WITH
THE TGA• Identity of active ingredients may be incorrect• Potency of active ingredients may be variable• May contain undisclosed contaminants • Not manufactured to appropriate standards• May not be covered by professional indemnity insurance
GETTING PERSPECTIVE ON INTERACTIONS

41
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EUPHRASIA BATCH REJECTED BY METAGENICS QUALITY CONTROL
Euphrasiaofficinalisstandard
Euphrasia officinalisRaw material tested
THE METAGENICS INVESTMENT ENSURES THE HIGHEST
QUALITY PRODUCTS• High Performance Thin Layer Chromatography• Atomic Absorption• Gas Chromatography• High Performance Liquid Chromatography
GETTING PERSPECTIVE ON INTERACTIONS

42
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
IF IT’S NOT UP TO SCRATCHWE REJECT IT
• We reject approximately 45 raw materials per year due to inferior quality
• Each product goes through multiple check points to ensure that it meets our high quality standards.
• Some products have over 300 check points and signatures from different Health World staff before it is deemed ready for sale.
REJECT
CORRECT IDENTIFICATION OF RAW MATERIAL IS ESSENTIAL
FOR QUALITY
• The HPLC-UV profile sample does not conform with reference REF0056
• Comparison with the reference Scutellaria baicalensis indicates the likely source: characteristic flavone glycosides of Scutellariaspp.
Bupleurum cross-contamination with Scutellaria
GETTING PERSPECTIVE ON INTERACTIONS

43
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
REAL TIME STABILITY GUARANTEES THERAPEUTIC
EFFICACY
FAIL
GETTING PERSPECTIVE ON INTERACTIONS

44
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HEA
LTH
WO
RLD
’S U
NIQ
UE,
IN
DU
STR
Y LE
AD
ING
G
UA
RA
NTE
E O
F Q
UA
LITY
AN
D E
FFIC
AC
YQ
UA
LITY
MEA
SURE
HEA
LTH
WO
RLD
Sele
ctio
n of
raw
mat
eria
ls b
ased
on
rigor
ous
evid
ence
rev
iew
O
n si
te
Thor
ough
aud
its o
f raw
mat
eria
l sup
plie
rs to
ens
ure
qual
ity in
gred
ient
s
Off
site
Iden
tific
atio
n as
says
for
all r
aw m
ater
ials
upo
n re
ceip
t to
conf
irm s
peci
ficat
ions
O
n si
te
Test
ing
of r
aw m
ater
ials
for
heav
y m
etal
, pes
ticid
e an
d m
icro
biol
ogic
al c
onta
min
atio
n
On
site
Stat
e of
the
art m
anuf
actu
ring
faci
lity,
with
stri
ngen
tly c
ontro
lled
proc
esse
s an
d en
viro
nmen
tal c
ondi
tions
for
repr
oduc
ible
res
ults
O
n si
te
Live
pro
biot
ic a
ssay
s at
all
prod
uct s
tage
s –
raw
mat
eria
l, po
wde
r bl
endi
ng, e
ncap
sula
tion,
tran
spor
t tria
ls a
nd s
helf
life
stab
ility
O
n si
te
Tem
pera
ture
con
trolle
d an
d co
ld-s
uppl
y ch
ain
from
raw
mat
eria
l to
ship
ping
of f
inis
hed
good
s to
cus
tom
ers
O
n si
te
Stric
t mai
nten
ance
of a
ll lim
its fo
r la
bel c
laim
s an
d re
ject
ing
batc
hes
out o
f spe
cific
atio
n
On
site
Ther
apeu
tic G
oods
Adm
inis
tratio
n-ce
rtifie
d co
mpl
ianc
e fo
r m
anuf
actu
ring
and
test
ing
faci
litie
s m
aint
aini
ng h
igh
Goo
d M
anuf
actu
ring
Prac
tice
stan
dard
s
On
site
Ong
oing
inve
stm
ent i
n in
tern
al m
etho
d de
velo
pmen
t to
accu
rate
ly q
uant
ify in
gred
ient
s in
fini
shed
goo
ds
On
site
Full
inte
rnal
sta
bilit
y pr
ogra
m p
rovi
ding
act
ual (
not t
heor
etic
al) p
re-la
unch
sta
bilit
y on
all
prod
ucts
, with
ong
oing
rea
l-tim
e st
abili
ty
On
site
Tast
e &
tole
ranc
e te
stin
g of
fini
shed
goo
ds
On
site
Man
ufac
ture
of ‘
food
’ pro
duct
s un
der
rigor
ous
Goo
d M
anuf
actu
ring
Prac
tice
stan
dard
s
On
site
Effic
acy
test
ing
of p
rodu
cts
and
prot
ocol
s in
clin
ic
On
site
GETTING PERSPECTIVE ON INTERACTIONS

45
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
DET
ERM
ININ
G W
HET
HER
AN
D
HO
W T
O C
O-P
RES
CR
IBE:
ED
MC
DECISION MAKING FRAMEWORK: EDMC

46
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
RESOURCES FOR REVIEWING EVIDENCE
Evidence for potential interactions
• Metagenics Technical Support Team
• Metagenics Technical Data – Contraindications and Cautions
• Natural Standards Database https://naturalmedicines.therapeuticresearch.com/databases.aspx
• TGA – database of adverse event notifications http://www.tga.gov.au/DAEN/daen-entry.aspx
• Braun L, Cohen, M. Herbs & Natural Supplements. 3rd ed. New South Wales: Elsevier; 2010
Information on medications
• Australian Prescriberhttp://www.australianprescriber.com/
• Drug metabolism pathwayshttp://medicine.iupui.edu/clinpharm/ddis/main-table/
• PubMedhttp://www.ncbi.nlm.nih.gov/pubmed/
• Google Scholarhttp://scholar.google.com.au/
Metagenics product information
• www.metagenics.com.au
• www.metagenics.co.nz
EDMC – EVIDENCEEVIDENCE FOR INTERACTIONS CAN VARY SIGNIFICANTLY
Neustadt J. Herb-drug interactions: what clinicians need to know. Integrative Medicine 2006;5(1):16-26
DECISION MAKING FRAMEWORK: EDMC

47
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
RISK VS BENEFIT ANALYSIS• What is the clinical outcome of an
interaction if it does occur? Minor or major?
Risk vs benefit analysis• Could the benefit be significant and
the interaction mild? (e.g. Fish oil and warfarin)
• Or the benefit be mild and the interaction life threatening? (eg. St John’s Wort and organ rejection)
DOSING CONSIDERATIONS• Timing of administration:
- If potential absorption interaction, separate by 2 hours- If systemic additive effects undesired, separate doses by 6-
12 hours - Dosing may overlap if medication not adequately
controlling symptoms and some additive effects inconsequential/desired
• Duration of use- Is CAM prescription short term, e.g. to relieve symptoms, or
long term, e.g. to prevent nutritional deficiencies- Prescriptions may be separated from cycles of
chemotherapy, methotrexate, IVF, etc.
DETERMINE THE SEVERITY
OF ANY POTENTIAL
INTERACTION
De Smet PAGM. Clinical risk management of herb–drug interactions. Br J Clin Pharmacol2006; 63 (3): 258–267
DECISION MAKING FRAMEWORK: EDMC

48
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
COMMUNICATION: PATIENTS AND PRACTITIONERS
Communication with the patient:• Discuss their goals• Confirm understanding
and compliance - informed consent
• Assess ability and reliability to self monitor
• Assess limiting factors
Communication with the prescribing practitioner:• Optional for low risk
interactions• Inform of any potentially
higher risk interactions and provide the evidence, literature and rationale to support your choice
• Seek involvement in weaning protocols
MONITORING: COMMON TESTS THAT MAY NEED TO BE
MONITOREDQUESTIONS
TO ASK:
WHAT DO YOU NEED TO
MONITOR?
HOW FREQUENTLY DO YOU NEED TO
MONITOR?WHO WILL MONITOR?
EXAMPLES
Symptoms Daily Patient – symptom diary
Blood pressure Weekly Practitioner/Patient
Blood glucose Weekly Practitioner/Patient
HbA1c Three monthly Practitioner
Lipid profile Three monthly initially then every six months to yearly
Practitioner
Drug levels – e.g. digoxin
When CAM introduced, then three to six monthly
Practitioner
Internationalnormalised ratio (INR)
Weekly Practitioner
DECISION MAKING FRAMEWORK: EDMC

49
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSISDRUG:
NAT MED:ANALYSIS
EVIDENCE What is the evidence for a potential interaction –positive/negative, consequences, level of evidence?
DOSING Can the interaction be mitigated by changing the dose regimen?
MONITORING Can the interaction be mitigated by monitoring?
COMMUNICATION What does the patient tell us?What communication is needed?
SUMMARY: EVIDENCE OF RISK/BENEFIT
Based on the evidence and the potential success of a management plan, what is the potential risk vs benefit?
SUMMARY:MANAGEMENT
PLAN
Dosing planMonitoring planCommunication plan
WHAT IS THE MANAGEMENT PLAN?
DECISION MAKING FRAMEWORK: EDMC

50
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
THE BENEFITS OF CO-PRESCRIBING
PRESCRIBING WITH MULTIPLE MEDICATIONS
ACE INHIBITOR ASPIRIN DIGOXIN SUMMARY
High Potency Taurine, Glycine and Magnesium
For Cardiovascular Health
Theoretical additional reduction in BP, likely beneficial. Monitor.
No evidence for interaction
No evidence for interaction Safe to use with
monitoring
Enhanced Bioavailability Co-enzyme Q10 150 mg
Theoretical additional reduction in BP, likely beneficial.Monitor.
No evidence for interaction
Theoretical effects on drug absorption Safe to use with
monitoring and dose separation
High Potency Ultra Pure EPA/DHA Capsules
No evidence for interaction
Theoretical additional antiplatelet effects. Clinical trials demonstrate no effect. Other significant benefits to patient.
No evidence for interaction
Safe to use
Vitamin D3
No evidence for interaction
No evidence for interaction
High doses of vitamin D may increase risk of hypercalcaemia
Safe to use below 2000 IU (50 mcg) per day
MANAGEMENT PLAN Monitor BP None required Monitor digoxin and calcium levels
DECISION MAKING FRAMEWORK: EDMC

51
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
POTENTIAL DRUG-NUTRIENT INTERACTIONS
Boullata JI et al. Drug–nutrient interactions: A broad view withimplications for practice. J Acad of Nutr Diet 2012; 112(4):506-17
CAUTIONS FOR CO-PRESCRIBING
CAUTIONS: CHANGING DRUG LEVELS

52
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EXPRESSION OF P-GLYCOPROTEIN INFLUENCES
ABSORPTION
Edwards G. Ivermectin: does P-glycoprotein play a role in neurotoxicity: Filaria Journal 2003;2 Suppl 1:S8
NATURAL COMPOUNDS MAY AFFECT ABSORPTION AND METABOLISM OF DRUGS
Liu C et al. Herb-drug interactions involving drug metabolising enzymes and transporters. Current Drug Metabolism 2011;12:835-849
CAM
CAM
CAUTIONS: CHANGING DRUG LEVELSABSORPTION

53
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MICROBIOME ACTIVATES MANY DRUGS AND NATURAL
INGREDIENTS
• Sulfasalazine• Digoxin• Clonazepam• Metronidazole• Daidzein• Quercetin
Li H, Jia W. Cometabolism of microbes and host: implications for drug metabolism and drug-induced toxicity. Clin Pharmacol Ther 2013;94(5):574-81. doi: 10.1038/clpt.2013.157
HYPOCHLORHYDRIA MAY REDUCE ABSORPTION OF MEDICATION
Several publications have reported low and variable absorption of weakly basic
drugs under high gastric pH conditions, which can consequently lead to
subtherapeutic exposure
Mitra A, Kesisoglou F. Impaired drug absorption due to high stomach pH: a review of strategies for mitigation of such effect to enable pharmaceutical product development. Mol
Pharm 2013;10(11):3970-9
CAUTIONS: CHANGING DRUG LEVELSABSORPTION

54
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Bisphosphonate :a.m. 30 mins beforeeatingPPI: p.m. 30 minutes before eating
MITIGATE ABSORPTION INTERACTIONS BY SEPARATING
THE DOSE
GENERAL FACTORS AFFECTING DRUG ABSORPTION
FACTOR MECHANISM ACTION
Meal Reduce or increase absorption Check medication manufacturer’s instructions
Fibre May bind drugs and delay transport resulting in decreased bioavailability
Take medication one hour before or two hours after consuming fibre
Minerals May reduce absorption through complex formation
Separate dosing of medication and minerals
Tannins Bind alkaloid drugs Avoid consuming tannins around prescription and mineral dosing
Dysbiosis Gut flora can convert drugs to their active form, and dysbiosis may alter absorption rates
Correct dysbiosis with strain specific probiotic
Transit time If rapid may increase drug clearance and reduce efficacy; if slow may reduce drug clearance and increase side effects
Address too rapid or too slow transit time with dietary change and herbal digestive support
Intestinal permeability May have a negative effect on both nutrient and drug absorption
Correct intestinal permeability
CAUTIONS: CHANGING DRUG LEVELSABSORPTION

55
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MAIN CYPs WHICH DETOXIFY PRESCRIPTION MEDICATIONS
PROPORTION OF DRUGS METABOLISED BY CYPS
CYP3A4/5 36%
CYP2D6 19%
CYP2C8 16%
CYP1A1/2 11%
CYP2C19 8%
NATURAL MEDICINES AND PHARMACEUTICALS SHARE
SIMILAR METABOLIC PATHWAYSMore than two thirds of
the pharmaceutical actives recently
introduced have some relationship to natural
sources and only 30% are of purely synthetic origin.
Helmstadter A, Staiger C. Traditional use of medicinal agents: a valid source of evidence. Drug Discovery Today 2014;19(1):4-7
CAUTIONS: CHANGING DRUG LEVELSMETABOLISM

56
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HER
BS
CA
N A
LTER
DR
UG
LEV
ELS
VIA
D
RU
G M
ETA
BO
LISI
NG
EN
ZYM
ES
Bran
tley
SJ, e
t al.
Her
b–D
rug
Inte
ract
ions
: C
halle
nges
and
Opp
ortu
nitie
s fo
rIm
prov
ed P
redi
ctio
ns. D
rug
Met
abD
ispo
s20
14;4
2:30
1–31
7
CAUTIONS: CHANGING DRUG LEVELSMETABOLISM

57
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
DET
OX
IFIC
ATI
ON
PA
THW
AYS
AN
D
SUP
PO
RTI
VE
NU
TRIE
NTS
PROCESSESU
PTAK
E TR
ANSP
OR
TER
SC
YP 4
50s
Oxi
datio
nR
educ
tion
Hyd
roly
sis
Hyd
ratio
nD
ehal
ogen
atio
n
IMB
ALA
NC
ER
eact
ive
Inte
rmed
iate
s
Nuc
leop
hile
s an
d E
lect
roph
iles
PRO
TEC
TIO
NM
ilk th
istle
Gre
en te
aV
itam
ins
A, C
, ES
elen
ium
Zinc
TRAN
SFER
ASES
Ace
tyla
tion
Met
hyla
tion
Sul
phat
ion
Glu
tath
iona
tion
Glu
curo
nida
tion
Tran
sam
inat
ion
EFFL
UX
TRAN
SPO
RTE
RS
Exc
retio
n of
con
juga
ted
toxi
ns in
to b
ile a
nd u
rine
REQUIREMENTS and PROMOTERS
ATP
(mag
nesi
um, B
-co
mpl
ex)
B2,
B3,
B6,
fola
te, B
12G
luta
thio
ne (g
luta
min
e,
cyst
eine
, gly
cine
)B
ranc
hed-
chai
n am
ino
acid
s fro
m ri
ce p
rote
in
ATP
(mag
nesi
um, B
-co
mpl
ex)
B5
(ace
tyla
tion)
B6
(tran
sam
inat
ion)
Gre
en te
aA
min
o ac
ids
–ric
e pr
otei
nG
luta
min
e, c
yste
ine,
gl
ycin
e (g
luta
thio
ne)
Taur
ine
Sel
eniu
m
ATP
(mag
nesi
um, B
-co
mpl
ex)
Milk
this
tleG
arde
nia
jasm
inoi
des
Taur
ine
Adap
ted
from
Lisk
aD
et a
l. D
etox
ifica
tion
and
biot
rans
form
atio
nali
mba
lanc
es.
Expl
ore
(NY)
200
6;2(
2):1
25
DN
A A
ND
PR
OTE
IN
DA
MA
GE
PHA
SE 0
PHA
SE I
FUN
CTI
ON
ALI
SATI
ON
PHA
SE II
CO
NJU
GA
TIO
N
PHA
SE II
IEL
IMIN
ATI
ON
CAUTIONS: CHANGING DRUG LEVELSDETOXIFICATION AND MEDICATIONS

58
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MEDICATED PATIENTS WHERE TOXICITY MAY BE A DRIVER
CONDITION COMMON MEDICATION POSSIBLE TOXICITY AS A DRIVER
SAFE TO USEDETOXIFICATION
PROGRAMS
Depression SSRIs Dysbiosis and intestinal permeability
Yes, with monitoring ofmood
Hypothyroidism Levothyroxine sodium Xenobiotics, dysbiosis Yes, with monitoring of symptoms
Diabetes Metformin Xenobiotics Yes, with monitoring of blood glucose
Rheumatoidarthritis
Methotrexate, sulfasalazine, TNF-α inhibitors
Dysbiosis Yes, with monitoring of symptoms
Inflammatorybowel disease
Prednisone, TNF-αinhibitors, methotrexate.
Dysbiosis Yes, with monitoring ofsymptoms
Breast cancer Tamoxifen Xenobiotics Yes, short term
Hypertension ACE inhibitor, beta blocker, diuretic
Xenobiotics (heavy metals)
Yes, with monitoring of blood pressure
CAUTIONS: CHANGING DRUG LEVELSDETOXIFICATION AND MEDICATIONS

59
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MET
AG
ENIC
S D
ETO
XIF
ICA
TIO
N P
RO
GR
AM
SCAUTIONS: CHANGING DRUG LEVELS
DETOXIFICATION AND MEDICATIONS

60
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSIS: SUMMARYBETA BLOCKER STATIN BENZODIAZEPINE SUMMARY
Milk Thistle, Green Tea and Amino Acids for
Optimal Detoxification
Unlikely potential to change drug levels and result in changes in blood pressure
Unlikely potential to change drug levels and result in changes in cholesterol
Unlikely potential to change drug levels and result in changes in sedation
Safe to use with monitoring
Detox Greens
No evidence for interaction
Pectin may reduce absorption. Separate dose by two hours
No evidence for interaction
Safe to use with separation of
dosing
Dandelion, Ginger and Meadowsweet for
Healthy Digestion
No evidence for interaction
No evidence for interaction
No evidence for interaction Safe to use
Garlic, Wormwood & Lavender for Dysbiosis
No evidence for interaction
No evidence for interaction
Potential additive sedative effects
Safe to use with monitoring
MANAGEMENT PLANMonitor blood
pressureSeparate dose by
two hoursMonitor symptoms –sedation and sleep
EDMC ANALYSIS: INTEGRATED DETOXIFICATION IN
HYPERTENSION• 43 y.o. male• Headaches, fatigue, muscle pain• Poor diet, excessive alcohol,
overweight• Medications - Beta blocker,
statin and PPI• Scores high in detoxification
questionnaire
EDMC ANALYSIS: EVIDENCE
Milk Thistle, Green Tea & Amino Acids for Optimal Detoxification• No contraindications or cautions for
antihypertensives• Monitor patients on any medication due
to theoretical action milk thistle has on CYPs.
CAUTIONS: CHANGING DRUG LEVELSDETOXIFICATION AND MEDICATIONS

61
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
DRUGS WITH A NARROW THERAPEUTIC INDEX
DRUG PRIMARY USE
Lithium Bipolar disorder (mania)
Warfarin Anticoagulant
Digoxin Antiarrhythmic
Olanzapine Antipsychotic (schizophrenia)
Carbamazepine Anticonvulsant and mood-stabilizing drug used primarily for epilepsy and bipolar disorder
Phenytoin Antiepileptic
Theophylline Bronchodilator for asthma and COPD
Procainamide Antiarrhythmic for atrial fibrillation
Levothyroxine sodium Synthetic T4 for hypothyroidism
Ethosuximide Used only to treat absence (petit mal) seizures
Cyclosporine Immune suppressant for transplants and psoriasis
HIV protease inhibitors, non-nucleoside transcriptase inhibitors Antiretroviral drugs
Pope ND. Generic substitution of narrow therapeutic index drugs. US Pharm 2009;34(6)(Generic Drug Review suppl):12-19
https://www.tga.gov.au/alert/st-johns-wort-important-interactions-between-st-johns-wort-hypericum-perforatum-preparations-and-prescription-medicines (Date accessed 2/12/14)
EDMC ANALYSIS: COMMUNICATION
Inform patient of potential interaction• Interaction is theoretical, no human evidence• If interaction did occur it would pose minimal risk
– blood pressure may elevate or reduce• Ensure patient is willing to monitor blood pressure
regularly, e.g. weekly
CAUTIONS: CHANGING DRUG LEVELSDETOXIFICATION AND MEDICATIONS

62
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: DETOX WITH PATIENT ON WARFARIN
• 25 yo obese male recently hospitalised with deep vein thrombosis in legplus pulmonary embolism
• On warfarin 8 mg/day; weekly INR monitoring
• Wants to lose weight; recently given up alcohol and cigarettes (2 packs/day& 12 stubbies)
• Heartburn, sensitive spicy foods, constipation
• Put on 6 week Detox by Naturopath
• Practitioner checked Metagenics Safety Data before prescribing. Patient INRmonitored closely as outpatient by hospital – advised to inform them of hisprescription and potential for warfarin dose to change
• Outcome: patient successfully completed 6 week detox; no change in INR;experienced weight loss, increased energy, improved digestion, motivated tocontinue with weight loss protocol next
DETOXING WITH DRUGS: CLINICAL GUIDANCE
1. Detoxification can change drug levels2. Changing drug levels may only be of significant
importance in some clinical situations3. Detoxification is a short-term intervention. A risk-
benefit analysis is required. 4. Increasing patient monitoring can assist to
overcome potential interactions.
CAUTIONS: CHANGING DRUG LEVELSDETOXIFICATION AND MEDICATIONS

63
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CONFLICTING GOALS IN AUTOIMMUNE DISEASE?
NATURAL MEDICINE APPROACH• Zinc• Vitamin C• Vitamin D• Cordyceps• Coriolus• Reishi• Andrographis
Immune stimulation
and balance
Immune suppression
CONVENTIONAL MEDICINE APPROACH• NSAIDs• Corticosteroids• Methotrexate• Cyclosporine • TNF-alpha
inhibitors
CAUTIONS FOR CO-PRESCRIBING
CAUTIONS: ANTAGONISING DRUG EFFECTS
IMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

64
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
TNF-α INHIBITORS CAN BLOCK BOTH ADVERSE AND BENEFICIAL FUNCTIONS
McKenna MR, et al. J Gastrointestin Liver Dis. 2014 Sep;23(3):267-71; Targownik LE, Bernstein CN. Am J Gastroenterol. 2013 Dec;108(12):1835-42; Moran GW, et al.
Aliment Pharmacol Ther. 2013 Nov;38(9):1002-24.
POOR IMMUNITY + INFECTION = AUTOIMMUNITY
Grammatikos AP, Tsokos GC. Immunodeficiency and autoimmunity: lessons from systemic lupus erythematosus. Trends Mol Med. 2012 Feb;18(2):101-8
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

65
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
IMMUNE STIMULANT MUSHROOMS CREATE
HOMEOSTASIS IN AUTOIMMUNITYThe bioactive glucans and proteoglycans isolatedfrom mushrooms are currently the most promisingclass of immunoceuticals. Without doubt, they arecapable of simultaneously augmenting all the keypathways of host immunity.These substances are pro-homeostatic, uniquelyeffective immune boosters, which pose no threat ofautoimmune backlash.
Kidd PM. The use of mushroom glucans and proteoglycans in cancer treatment. Alt Med Rev, 2000;5(1):21
EDMC ANALYSIS: CORDYCEPS, CORIOLUS & REISHI FOR IMMUNE
STIMULATION - EVIDENCE
Technical Support:Australia
1800 777 648
New Zealand0508 227 744
EDMC ANALYSIS: CORDYCEPS, CORIOLUS & REISHI FOR IMMUNE
STIMULATION - EVIDENCE
Autoimmune conditions: Evidence indicates these mushrooms are beneficial in autoimmune disease, however the theoretical possibility exists that immune stimulant activity may exacerbate autoimmunity. Monitor.
CORDYCEPS, CORIOLUS & REISHI FOR IMMUNE
STIMULATION
Cordyceps sinensis (Cordyceps), myceliumLentinula edodes (Shiitake), fruiting bodyGanoderma lucidum (Reishi), fruiting bodyTrametes versicolor (Coriolus), mycelium
EDMC ANALYSIS: CORDYCEPS, CORIOLUS & REISHI FOR IMMUNE STIMULATION IN AUTOIMMUNITY
• 48 yo• Rheumatoid arthritis not managed by
medication• Childcare worker – frequent infections• RA symptoms improve if prescribed antibiotics
for respiratory infection• TNF-alpha inhibitor medication
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

66
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSIS: MONITORING
BASELINE WEEK 1 WEEK 2 WEEK 3 WEEK 4 WEEK 5 WEEK 6
Pain 6 7 6 6 5 5 5
Stiffness 8 8 7 7 6 6 5
Mobility 3 3 4 4 5 5 5
Fatigue 7 7 8 7 6 6 6
Other S
Subjective measures: pain and symptom diary
Objective measures:• hsCRP• ESR
• Rheumatoid factor• ANA
EDMC ANALYSIS: WEIGHING UP THE EVIDENCE FOR MUSHROOMS• Theoretical
negative outcome -worsen autoimmunity
• Evidence – none.
• Potential positive outcomes – RA symptoms and infections
• Evidence –mushrooms have homeostatic actions in immune function and do not exacerbate autoimmunity
Kidd PM. The use of mushroom glucans and proteoglycans in cancer treatment. Alt Med Rev, 2000;5(1):21
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

67
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: PATIENT 145 MULTIPLE SCLEROSIS
• Female 40’s• MS diagnosed five years ago after a seizure• Prescribed glatiramer acetate (immune modulator)
and oxcarbazepine (anticonvulsant)• Naturopath prescribed mushrooms to stimulate
immunity• After one year of mushroom treatment: patient
stable, no symptoms, feeling very good.
EDMC ANALYSISDRUG: TNF-ALPHA INHIBITOR
NAT MED: CORDYCEPS, CORIOLUS AND REISHI FOR IMMUNE STIMULATION
ANALYSIS
EVIDENCE Counters immune suppression which may drive chronic infection-induced autoimmunity.
DOSING No dosing considerations
MONITORING Affected parameter (symptoms) can be easily monitored by patient.
COMMUNICATION Patient capable of self-monitoring symptoms.
SUMMARY: EVIDENCE OF RISK/BENEFIT
Natural medicine likely to provide significant benefits to patient’s immune function.An unlikely flare up of autoimmune condition should be detected before adverse consequences occur.
SUMMARY:MANAGEMENT
PLAN
Dosing plan – dose natural medicine twice dailyMonitoring plan – monitor symptoms weeklyCommunication – informing medical prescriber is optional
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

68
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CURCUMIN REDUCES RELAPSE IN ULCERATIVE COLITIS
PATIENTS
Hanai H, et al. Curcumin maintenance therapy for ulcerative colitis: randomized, multicentre, double-blind, placebo-controlled trial. Clin Gastroenterol Hepatol 2006;4(12):1502-6
25 G/DAY BCM-95™ TURMERIC AS EFFECTIVE AS NSAID IN
RHEUMATOID ARTHRITIS
Chandran B, Goel A. A randomised, pilot study to assess the efficacy and safety of curcumin in patients with active rheumatoid arthritis. Phytother Res 2012. doi:
10.1002/ptr.4639
(25 g/day Turmeric)
(25 g/day Turmeric)
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

69
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
5.5 G/DAY EPA AND DHA DOUBLES REMISSION RATE IN RA
Proudman SM, et al. Fish oil in recent onset rheumatoid arthritis: A randomised,double-blind, controlled trial within algorithm-based drug use. Abstracts of Pharma
Nutrition 2013 / PharmaNutrition 2 (2014) 75–119
CURCUMIN SAFE AND EFFECTIVE ADJUVANT IN IBD
Suskind DL, et al. Tolerability of curcumin in paediatric inflammatory bowel disease: A forced-dose titration study. J Pediatr Gastroenterol Nutr 2013;56(3):277-9
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

70
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
2.7 G/DAY FISH OIL REDUCES NSAID USE IN RHEUMATOID
ARTHRITIS
Omega-3 PUFAs at dosages of >2.7 g/day for >3 months may be effective at reducing NSAID use in RA patients
Lee Y, Bae S, Song G. Omega-3 polyunsaturated fatty acids and the treatment of rheumatoid arthritis: a meta-analysis. Archives of Medical Research 2012;43:356-362
FISH OIL COMPARABLE TO TNF ALPHA INHIBITORS FOR RHEUMATOID ARTHRITIS
-0.4
-0.35
-0.3
-0.25
-0.2
-0.15
-0.1
-0.05
0
Cha
nges
in p
ain
from
bas
elin
e(s
tand
ardi
sed
mea
n di
ffere
nce)
TNF alpha inhibitor Fish oil
James M et al. 3rd International Immunonutrition Workshop:Session 3: Fatty acids and the immune system Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc
2010; 69:316–323
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

71
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EPA
AN
D D
HA
HA
VE
NO
VEL
AN
TI-
INFL
AM
MA
TOR
Y M
ECH
AN
ISM
S
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

72
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HIGH PURITY, LOW REFLUX, CONCENTRATED FISH OIL
IN HOUSE FISH OIL TESTING FOR PURITY,
POTENCY AND STABILITY
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

73
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
IM
MU
NE
SUP
PR
ESSA
NT
/AN
TI-I
NFL
AM
MA
TOR
Y M
EDIC
ATI
ON
SCAUTIONS: ANTAGONISING DRUG EFFECTS
IMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

74
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
ENCOURAGING PATIENTS TO SWITCH TO METAGENICS
SUPPLEMENTSSELF-PRESCRIBED SUPPLEMENTRISKS
METAGENICS ADVANTAGE
Fish oil Higher level of toxinsOxidisedAmount of EPA and DHA doesn’t match label
Higher than Australian standards set for contaminants and oxidationHigh strength
CoQ10 Reduced bioavailability Vesisorb for enhanced bioavailability
Calcium Reduced bioavailability Microcrystalline hydroxyapatite for enhanced bone mineralisation
Magnesium Reduced bioavailability Magnesium bisglycinate (Meta MagTM) for enhanced bioavailability
Vitamin D Poor stability Real-time stability to guarantee vitamin D shelf life
Krill oil Potential contamination Purified krill oil
Probiotics Strain not specifiedNo clinical evidenceStability issues due to non-refrigeration
Clinically trialled, strain specific and stability assured
DISCUSS THE BENEFITS OF PRACTITIONER ONLY FORMULAS• How could poor quality products
be contributing to their problems?• Are discounted bulk products cost
effective if they are not therapeutic?
• Are your patients spending their money on unnecessary supplements?
• Are they taking excessive levels of nutrients or the wrong ingredients for their condition?
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

75
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
RESOURCES: LOYAL PATIENTS FOR LIFE
https://www.metagenics.com.au/loyal-patients-for-life
CAUTIONS: ANTAGONISING DRUG EFFECTSIMMUNE SUPPRESSANTS AND ANTI-INFLAMMATORIES

76
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
ST JOHN’S WORT: WILL IT CAUSE SEROTONIN SYNDROME WITH
SSRI USE?• Evidence to support such a concern is weak and is
currently based only on unsubstantiated case reports.• The case studies typically also have concomitant use
of other medications and/or recreational drugs, anda background of cyclothymia
• Caution is warranted in people with a personal orfamily history of bipolar depression
Sarris J, et al. Adjuvant use of nutritional and herbal medicines with antidepressants, mood stabilisers and benzodiazepines. J Psychiatr Res 2010;44(1):32-41
5-HTP SAFE AND EFFECTIVE AS AN ADJUVANT FOR DEPRESSION
No case of serotonin syndrome has beenreported in subjects taking 5-hydroxy-L-tryptophan alone or in combination withSSRIs. Further, no adverse interactionshave been reported between 5-hydroxy-L-tryptophan and the monoamine oxidaseinhibitors.
Qureshi NA, Al-Bedah AM. Mood disorders and complementary and alternative medicine: A literature review. Neuropsychiatr Dis Treat 2013;9:639-58
CAUTIONS FOR CO-PRESCRIBING
CAUTIONS: ADVERSE POTENTIATION
ANTIDEPRESSANTS

77
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MAGNESIUM DEFICIENCY MAY CAUSE TREATMENT RESISTANT
DEPRESSION• Intracellular magnesium levels were found lower in
the brains of treatment resistant depression (TRD)patients than in healthy volunteers.
• There is sufficient evidence to implicate inadequatedietary magnesium as the main cause of TRD, andthat physicians should prescribe magnesium forTRD.
Eby GA 3rd, Eby KL. Magnesium for treatment-resistant depression: A review and hypothesis. Med Hypotheses 2010;74(4):649-60
MANY PATIENTS REQUIRE AUGMENTATION OF
ANTIDEPRESSANT THERAPYUsing antidepressants,
only one to two out of ten patients shows clinical effects beyond those
associated with placebo.
Zarate C, et al. New paradigms for treatment-resistant depression. Ann N Y Acad Sci2013;1292:21-31
CAUTIONS: ADVERSE POTENTIATIONANTIDEPRESSANTS

78
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CH
OO
SE T
HE
RIG
HT
MA
GN
ESIU
M F
OR
YO
UR
PA
TIEN
T
CAUTIONS: ADVERSE POTENTIATIONANTIDEPRESSANTS

79
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
500 μG/DAY FOLIC ACID ENHANCES ANTIDEPRESSANT
ACTION OF FLUOXETINE
Coppen A, Bailey J. Enhancement of the antidepressant action of fluoxetine by folic acid: a randomised, placebo controlled trial. J Affect Disord. 2000;60(2):121-30
EPA ENHANCES RESPONSE TO ANTIDEPRESSANTS
Mozaffari-Khosravi H. Eicosapentaenoic acid versus docosahexaenoic acid in mild-to-moderate depression: A randomised, double-blind, placebo-controlled trial. European
Neuropsychopharmacology 2013;23:636–644
CAUTIONS: ADVERSE POTENTIATIONANTIDEPRESSANTS
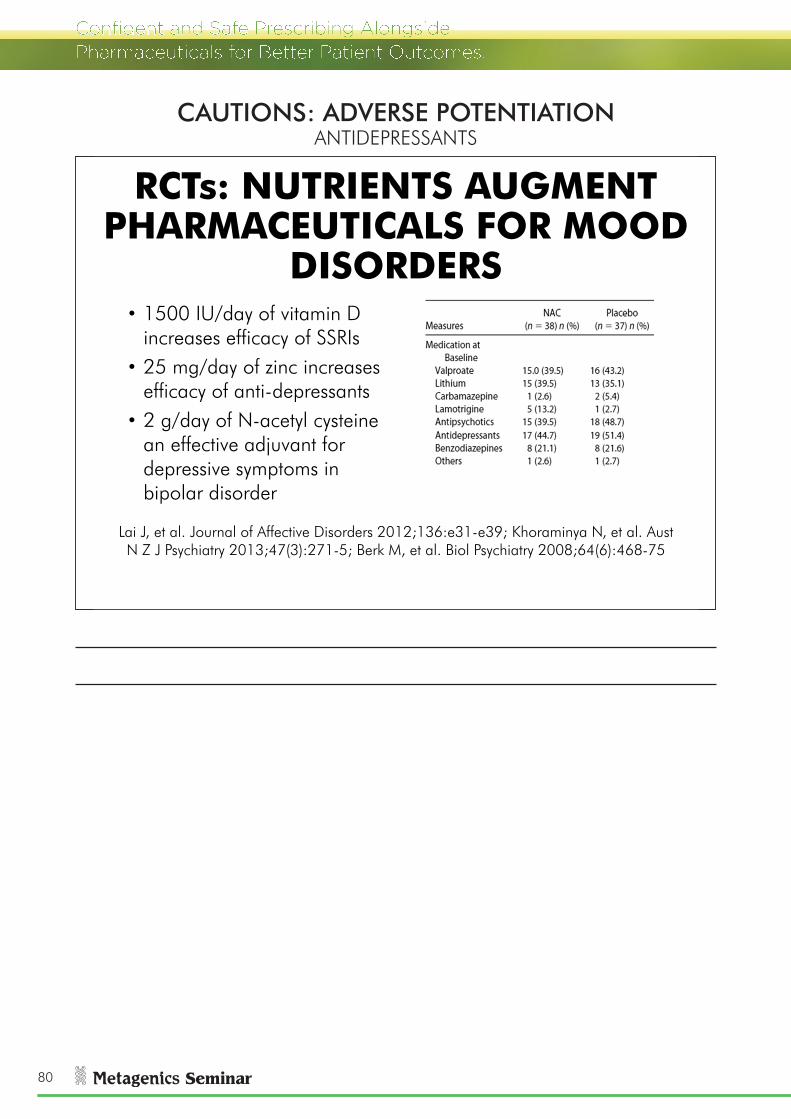
80
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
RCTs: NUTRIENTS AUGMENT PHARMACEUTICALS FOR MOOD
DISORDERS• 1500 IU/day of vitamin D
increases efficacy of SSRIs• 25 mg/day of zinc increases
efficacy of anti-depressants• 2 g/day of N-acetyl cysteine
an effective adjuvant for depressive symptoms in bipolar disorder
Lai J, et al. Journal of Affective Disorders 2012;136:e31-e39; Khoraminya N, et al. AustN Z J Psychiatry 2013;47(3):271-5; Berk M, et al. Biol Psychiatry 2008;64(6):468-75
CAUTIONS: ADVERSE POTENTIATIONANTIDEPRESSANTS

81
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TID
EPR
ESSA
NT
MED
ICA
TIO
NS
CAUTIONS: ADVERSE POTENTIATIONANTIDEPRESSANTS

82
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
PASSIONFLOWER HAS SIMILAR ACTIVITY TO BENZODIAZEPINES
Akhondzadeh S, et al. Passionflower in the treatment of generalised anxiety: A pilot double-blind randomised controlled trial with oxazepam. J Clin Pharm Ther 2001;26(5):363-7
STRESS LESS PROGRAM
CAUTIONS: ADVERSE POTENTIATIONANTIDEPRESSANTS
BENZODIAZEPINES

83
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSIS: ANXIETY AND BENZODIAZEPINES
• 46 y.o. female• Anxiety throughout the day, panic
attacks, insomnia• On benzodiazepines but interfering
with ability to concentrate at work • Drinking alcohol every night to cope
with stress and anxiety• Other medications: Thyroxine, OCP
HERBAL SUPPORT FORHYPER HPA AND STRESS
Ingredients:Ziziphus jujuba var. spinosa, seed dry (Zizyphus)Pueraria lobata, root dry (Pueraria)Magnolia officinalis, bark dry (Magnolia)Passiflora incarnata, herb dry (Passionflower)
Applications:Anxiety & tensionStress Insomnia Inability to relax Nervous tension
DETERMINING WHETHER AND HOW TO CO-PRESCRIBE
CAUTIONS: ADVERSE POTENTIATIONBENZODIAZEPINES

84
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EMDC ANALYSIS: SUMMARYTHYROXINE OCP BENZODIAZEPINE SUMMARY
Herbal Support for Hyper HPA and Stress
No evidence for interaction
Theoretical possibility kudzu inhibits effect of OCP
Potential additiveeffects
Safe to use with
monitoring and contraception
Magnesium AlkalisingCombination for Stress
No evidence for interaction
No evidence for interaction
Potential additiveeffects Safe to use
Female Nutritional Support with Broccoli
No evidence for interaction. Formula containsiodine
No evidence for interaction
No evidence forinteraction Safe to use
MANAGEMENT PLAN
Normal thyroid monitoring
Monitor mood and advise patient to use barrier methods of
contraception
Monitor mood
EDMC ANALYSIS: EVIDENCE
Cautions
Sedative medications including alcohol:Theoretical concern with sedative herbs as they may potentially have additive sedative effects.
CAUTIONS: ADVERSE POTENTIATIONBENZODIAZEPINES

85
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSIS: DOSING
Thyroxine – 100 mcg in the morningOCP – 1 tablet dailyDiazepam – 5 mg before bed
CAUTIONS: ADVERSE POTENTIATIONBENZODIAZEPINES

86
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
A
NX
IOLY
TIC
MED
ICA
TIO
NS
CAUTIONS: ADVERSE POTENTIATIONBENZODIAZEPINES

87
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: DEPRESSION AND ANXIETY
Week 10• Anxiety well controlled, reduced dose of Herbal Support for
Hyper HPA and Stress to one with breakfast and one before bed. Also use Herbal Support for Hyper HPA and Stress when required if you have a bad day.
• Energy improved now 6/10• Reduced dose of Nutritional Support for Stress to one a
morning • “Thanks for helping me through this, I feel more in control”
CASE STUDY: DEPRESSION AND ANXIETY
Week 3• Anxiety well controlled ”I have stopped Herbal Support for
Hyper HPA and Stress at lunchtime and I am coping well”• Had a few bad nights but generally sleeping wellWeek 6• Anxiety well controlled, “I can think clearer and I am moving
forward”• Sleeping through to 5 a.m.• Started counseling last week• GP rang practitioner to ask what products the patient was
taking and how they worked.
CASE STUDY: DEPRESSION AND ANXIETY
After 4 days:Anxiety is improved “I felt a difference in one day”• Insomnia no real changeWeek 2:• Anxiety much improved “I feel calm and in
control”• Sleeping through to 3-4 a.m.• GP “Stay on supplements if they are helping”
CASE STUDY: DEPRESSION AND ANXIETY
Currently taking:• Venlafaxine (SSRI) 150 mg – in the morning• Fish oil 1000 mg – three times a day• Calcium and magnesium – one tablet twice a day• Antioxidant tablet – one tablet dailyPrescription:• Herbal Support for Hyper HPA and Stress – one tablet three times a
day and two before bed• Rehmannia Complex for Nervous Exhaustion - two tablets twice a day• Nutritional Support for Stress – one tablet twice a day• Mexican Valerian – one tablet before bed
CASE STUDY: DEPRESSION AND ANXIETY
Female, 53• History of depression and antidepressant usePresenting complaints: • Severe anxiety and insomnia caused by recent
marriage breakdown. “I wanted this separation but it is harder than I thought”
• Waking every hour and thinking about things• Low energy the last 3 months - 3/10• GP wants to prescribe a benzodiazepine and increase
dose of antidepressant
CAUTIONS: ADVERSE POTENTIATIONBENZODIAZEPINES

88
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
VITAMIN E SAFE IN WARFARIN USE WITH MONITORING
Kim JM, White RH. Effect of vitamin E on the anticoagulant response to warfarin. Am J Cardiol 1996 ;77(7):545-6
Moderate to large doses of vitamin E can be safelyused in patients receiving warfarin, and treatmentwith vitamin E is not contraindicated in thesepatients. However, because it is always wise toretest the INR or prothrombin time several daysafter starting a new drug, we recommend retestingthe INR approximately one to two weeks afterstarting vitamin E therapy.
NATURAL INGREDIENTS AND WARFARIN – NOT AS RISKY AS
COMMONLY THOUGHT
Gardiner P, et al. Concomitant use of prescription medications and dietary supplements in menopausal women: An approach to provider preparedness.
Maturitas 2011;68:251–255
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

89
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
BROAD SPECTRUM VITAMIN E MAY PROTECT AGAINST CVDThere are 4 different tocopherols (vitamin E), α-, β-, γ-and δ-tocopherols, with minor structural differences.All occur naturally as a mixture in plant-based foods.The tocopherol content in food is inversely associatedwith mortality from cardiovascular disease. The lack ofnatural tocopherols such as γ - and δ -tocopherol inmost vitamin E preparations may be a limiting factorfor promoting health.
Saldeen K, Saldeen T. Importance of tocopherols beyond alpha-tocopherol:evidence from animal and human studies. Nutrition Research 2005;25:877–889
POOR CVD RESULTS WITH ALPHA- TOCOPHEROL ALONE
Jialal I, Devaraj S. Scientific evidence to support a vitamin E and heart disease health claim: research needs. J Nutr 2005;135(2):348-53
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

90
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MIXED TOCOPHEROLS & TOCOTRIENOLS FOR FREE
RADICAL DEFENCE• Tocopherols concentrate – mixed (low alpha type)• Tocotrienols complex – palm
KEY ACTIONS:AntioxidantAnti-inflammatoryImproves membrane fluiditySupports mitochondriaNeuroprotectiveCardioprotectivePrevents DNA damage
KEY APPLICATIONS:Cardiovascular diseaseReproductive healthSkin healthMaintenance of cognitionFibromyalgia
MIXED TOCOTRIENOLS LOWER CRP
Heng EC, et al. Supplementation with tocotrienol-rich fraction alters the plasma levels of Apolipoprotein A-I precursor, Apolipoprotein E precursor, and C-reactive protein precursor from
young and old individuals. Eur J Nutr, 2013;52:1811–1820
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

91
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSIS: COQ10 AND WARFARIN
• 66 year old male• History of stroke and CVD• Medication: warfarin,
antihypertensive and cholesterol lowering medication
• Presents with hypertension, dyslipidaemia, coronary artery disease and poor circulation
DETERMINING WHETHER AND HOW TO CO-PRESCRIBE
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

92
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EDMC ANALYSIS: WARFARIN AND COQ10 EVIDENCE
• 3 individual case reports
• Elderly on multiple medications
• CoQ10 self prescribed and dose unknown
• Stability of oral anticoagulant treatment unknown
• Randomised human clinical trial -100mg CoQ10 daily
• 21 patients on long-term warfarin
• No effects on INR
Engelsen J, Nielsen JD, Winther K. Effect of coenzyme Q10 and Ginkgo biloba on
warfarin dosage in stable, long-term warfarin treated outpatients. A
randomised, double blind, placebo-crossover trial. Thromb Haemost
2002;87(6):1075-6
Spigset O. Reduced effectof warfarin caused by ubidecarenone. The Lancet
1994;344(12):1372-1373
EDMC ANALYSIS: COQ10 AND WARFARIN EVIDENCE
Antihypertensives: CoQ10 can decrease blood pressure and might have additive blood pressure lowering effects when used with antihypertensive drugs. Monitor.
Warfarin: concomitant use of CoQ10 may potentially reduce the anticoagulative effects of warfarin. Three case reports have documented a decrease of the INR (decreased effect of warfarin) in patients who were previously stable. However, a double-blind, randomised controlled trial of 21 patients on long-term warfarin therapy found no effect of 4 weeks of CoQ10 at a dose of 100mg daily. Careful monitoring is recommended.
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

93
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
PATIENTS OFTEN DON’T TELL THEIR DOCTOR THEY ARE USING
NATURAL MEDICINES• Over 40% of Australians over 50 use both
pharmaceutical and natural medicines• Over half of dual modality users do not inform their
medical practitioner they use natural medicines• Reasons given are that the doctor doesn’t ask or
patients feel it’s not important to discloseMorgan TK, et al. A national census of medicines use: a 24-hour snapshot
of Australians aged 50 years and older. MJA 2012; 196: 50–53Yong PW, et al. Consumption of dietary health supplements among
hospitalized patients at an acute tertiary Hospital. Pharmanutrition 2014;2:135–140
HAVE THE CONVERSATION: TELL MEDICAL PRACTITIONERS ABOUT
PRESCRIBING ALONGSIDE PHARMACEUTICALS
• Be proactive and contact the medical practitioner about the co-prescription
• Outline what you have prescribed, why and describe the safety of the combination
• Provide evidence if it may be viewed as contentious co-prescription
EDMC ANALYSIS: COQ10 AND WARFARIN
WARFARIN ACE INHIBITOR STATIN SUMMARY
Enhanced Bioavailability Co-enzyme Q10 100 mg
Case reports suggest interaction but clinical trial at 100 mg/day shows no effect.
CoQ10 may have additive effects. Monitor blood pressure.
No evidence for interaction
Safe to use at 100 mg/day with
monitoring
High Potency Taurine, Glycine and Magnesium for Cardiovascular Health
No evidence of interaction
Magnesium may have additive effects. Monitor blood pressure
No evidence of interaction
Safe to use with monitoring
High Potency Ultra Pure EPA/DHA Liquid
Clinical trials have shown doses of 6.8 g (EPA+DHA)fish oil do not influence anticoagulant effects of warfarin
No evidence of interaction
Fish oil with statins improves lipid parameters and may have additive effects.
Safe to use at maximum dose of 6.8 g per day (EPA+DHA) with
monitoring
MANAGEMENT PLAN
Monitor INR Monitor blood pressure
Monitor lipids
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

94
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Dear Doctor,
I am a Naturopath consulting at Clinic X on the Sunshine Coast. I have recently seen Patient B who sought my advice on improving his health and wellbeing. I noted that he has been prescribed warfarin and has been on this medication for some time.
I have prescribed him Coenzyme Q10 at a dose of 100 mg/day. Based on the unlikely potential of an interaction I would like to suggest that we increase the monitoring of his INR over the next month.
Please find enclosed a copy of a randomised controlled trial which found no adverse effects of CoQ10 at 100 mg/day for four weeks in patients on long term warfarin therapy.
Please do not hesitate to call me if you would like to discuss care of Patient B or require any further information.
Kind regardsNaturopath
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

95
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
A
NTI
CO
AG
ULA
NT/
A
NTI
PLA
TELE
T M
EDIC
ATI
ON
S
CAUTIONS: ADVERSE POTENTIATIONANTICOAGULANT/ANTIPLATELET MEDICATIONS

96
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
GENERAL GUIDELINES FOR PATIENTS UNDERGOING
SURGERY• Recommend natural medicines with known safety
and benefits• Stop use of natural medicines known or suspected
to present a safety risk (e.g. increased bleedingwith vitamin E or fish oils) one week prior tosurgery
• Further information - Braun L, Cohen, M. Herbs &Natural Supplements. 3rd edn. New South Wales:Elsevier; 2010
NUTRITIONAL SUPPORT IMPROVES CLINICAL OUTCOMES OF CARDIAC
SURGERYIntegrative Cardiac Wellness Program at The Alfred Hospital • Coenzyme Q10 100 mg three times daily• Magnesium 400 mg three times daily• Lipoic acid 100 mg three times daily• Omega-3 fatty acids 300 mg three times daily• Selenium 200 mcg per dayPatients follow this protocol for two months prior to surgery and one month after under the guidance of a cardiologist. Outcome –improved redox status, reduced myocardial damage and shortened hospital stay.
Braun L, Stanguts C, Spitzer O, et al. A wellness program for cardiac surgery improves clinical outcomes. Advances in Integrative Medicine 2014;1:32-37
CAUTIONS: ADVERSE POTENTIATIONSURGERY

97
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CO
LLEC
T D
ETA
ILED
R
EPO
RTS
OF
PO
TEN
TIA
L IN
TER
AC
TIO
NS
CAUTIONS: ADVERSE POTENTIATIONSURGERY

98
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CAUTIONS ARE OFTEN EVIDENCE OF AUGMENTATION
http://naturaldatabase.therapeuticresearch.com/nd/Search.aspx?cs=&drg=1&s
=ND&pt=&sh=7&fs=ND#top
THE BENEFITS OF CO-PRESCRIBING
BENEFITS: POSITIVE POTENTIATION

99
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
THE UNDERLYING CAUSE OF CVD IS INFLAMMATION AND
ENDOTHELIAL DYSFUNCTION
Houston M. The Life of the Vascular Tunnel: Foundational Vascular Biology for the Clinician. The Institute for Functional Medicine. Annual International Conference 2012 Scottsdale, AZ
MOST HEART ATTACK SUFFERERS HAVE NORMAL SERUM LIPID
LEVELSOf patients that suffered a heart attack:• 72% had normal lipids• 14% had none of the
conventional risk factors - smoker, diabetes, dyslipidaemia, hypertension or family history
Canto JG, et al. Number of coronary heart disease risk factors and mortality in patients with first myocardial infarction. JAMA. 2011 Nov 16;306(19):2120-7.
BENEFITS: POSITIVE POTENTIATIONCARDIOVASCULAR MEDICATIONS

100
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MAGNESIUM IS AN EFFECTIVE ADJUVANT TO
ANTIHYPERTENSIVESTwo hundred and ninety nine hypertensive subjectstreated at least six months with medications (beta-blockers, Ca channel blockers, ACE inhibitors,diuretics) and receiving magnesium supplements(243-486 mg/day of elemental magnesium). All ofthese eight studies showed a significant decrease inblood pressure.
Rosanoff A. Magnesium supplements may enhance the effect of antihypertensive medications in stage 1 hypertensive patients. Magnesium
Research 2010;23(1):27-40
Evaluation only.Created with Aspose.PowerPoint.Copyright 2004 Aspose Pty Ltd.
MAGNESIUM TARGETS UNADDRESSED ENDOTHELIAL
DYSFUNCTION
Maier JA. Endothelial cells and magnesium: implications in atherosclerosis. Clin Sci (Lond). 2012;122(9):397-407
BENEFITS: POSITIVE POTENTIATIONCARDIOVASCULAR MEDICATIONS
ANTIHYPERTENSIVES

101
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
COQ10 IS A PROVEN ANTIHYPERTENSIVE AGENT
Rosenfeldt FL, et al. Coenzyme Q10 in the treatment of hypertension: a meta-analysisof the clinical trials. Journal of Human Hypertension 2007;21:297-306
Percentage reduction in diastolic blood pressure Percentage reduction in systolic blood pressure
HOW MUCH POTASSIUM CAN BE TAKEN WITH POTASSIUM
SPARING DRUGS?Individuals taking drugs for
cardiovascular disease such as ACE inhibitors, ARBs (Angiotensin Receptor
Blockers), or potassium sparing diuretics may need to consume less
than 4.7 g/day of potassium.
Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulphate. The National
Academies Presshttp://www.iom.edu/~/media/Files/Activity%20Fil
es/Nutrition/DRIs/DRI_Electrolytes_Water.pdf
ITEMPOTASSIUM/SERVE (MG)
Tuna 625
Beef and lamb 625
Potato 470
Spinach 390
Yogurt 390
Banana 350
Almonds 350
Avocado 275
Apple 195
High Potency Taurine, Glycine and Magnesium for Cardiovascular Health
52
BENEFITS: POSITIVE POTENTIATIONANTIHYPERTENSIVES

102
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: ATRIAL FIBRILLATION
Male, 74• Atrial fibrillation (AF); even though on medication it is not well
controlled and different medications have been trialed• 3-4 times a week and is lasting for 2-3 hours, if it lasts longer
hospitalisation. “It leaves me feeling tired and exhausted and isreally affecting my life”
• Cardiologist is recommending cardiac ablation if it cannot becontrolled with medication.
• “I am scared to go out, in case it happens. All I want to do ishook up the van and go travelling.”
CASE STUDY: ATRIAL FIBRILLATION
Currently taking:• Amiodarone 200 mg,• Irbesartan 150 mg• Aspirin 100 mg• Magnesium oxide tablet 300 mg/day• Glucosamine sulphate 750 mg BD
SUPERIOR BIOAVAILABILITY OF COQ10 WITH VESISORB™
Liu ZX, Artmann C. Relative bioavailability comparison of different coenzyme Q10 formulations with a novel delivery system. Altern Ther Health Med 2009;15(2):42-6
- VESIsorb CoQ10
- Emulsified formula
- Solubilised formula
- Emulsified formula
BENEFITS: POSITIVE POTENTIATIONANTIHYPERTENSIVES

103
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: ATRIAL FIBRILLATION
Week 20• Cardiologist appointment 10 days ago, “AF going well, but
stop supplements – you are wasting your money.”• Three days after stopping treatment AF returned and had to be
hospitalised. AF occurred three times in the following week.• Restarted concurrent naturopathic treatment.Week 28• No AF for the last six weeks, had consult with GP “stay on the
supplements they are obviously helping to control your AF”• “Now that I am sorted we leave in two days for a four week
caravanning holiday”
CASE STUDY: ATRIAL FIBRILLATION
Prescription:
• Stop magnesium tablet
• High Potency Taurine, Glycine and Magnesium for Cardiovascular Health – 1scoop twice daily
• Enhanced Bioavailability Co-enzyme Q10 150 mg – 1 capsule daily
• High Potency Ultra Pure EPA/DHA Capsules – 2 capsules twice daily
Week 4
• AF still happening, but not lasting as long and has only occurred twice in thelast 7 days. It lasts for around 30 mins.
Week 12
• No AF for 4 weeks
• A lot more energy
• Sleeping better
BENEFITS: POSITIVE POTENTIATIONANTIHYPERTENSIVES

104
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TIH
YPER
TEN
SIV
E M
EDIC
ATI
ON
SBENEFITS: POSITIVE POTENTIATION
ANTIHYPERTENSIVES

105
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HELP PATIENTS MAKE RESPONSIBLE INFORMED
DECISIONS
The impact of ‘ABC catalyst’ on lipid modifying medication use. The Heart Foundation. November 2013
1.8 G/DAY N-ACETYL CYSTEINE AUGMENTS ACE INHIBITORS
Barrios V, et al. N-acetylcysteine potentiates the antihypertensive effect of ACE inhibitors in hypertensive patients. Blood Press. 2002;11(4):235-9
BENEFITS: POSITIVE POTENTIATIONANTIHYPERTENSIVES
LIPID-LOWERING MEDICATIONS

106
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
4 G/DAY OMEGA 3 WITH SIMVASTATIN REDUCES TRIGLYCERIDES BETTER THAN
SIMVASTATIN ALONE
Davidson MH, et al. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: an 8-week, randomised, double-
blind, placebo-controlled study. Clinical Therapeutics 2007;29:1354-1367
BENEFITS: POSITIVE POTENTIATIONLIPID-LOWERING MEDICATIONS

107
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
LIP
ID
LOW
ERIN
G M
EDIC
ATI
ON
S
BENEFITS: POSITIVE POTENTIATIONLIPID-LOWERING MEDICATIONS

108
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
A LOW CARBOHYDRATE DIET PRODUCES THE MOST BENEFITS
FOR DIABETES
Feinman RD, et al. Dietary carbohydrate restriction as the first
approach in diabetesmanagement: Critical review and evidence base. Nutrition 2015;
31:1–13
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

109
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

110
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
1200 MG LIPOIC ACID INCREASES INSULIN SENSITIVITY IN
DIABETICS ON METFORMIN
0
1
2
3
4
5
6
7
Baseline 4 wk
Glu
cose
disp
osal
(mg/
kg/m
in)
Kamenova P. Improvement of insulin sensitivity in patients with type 2 diabetes mellitus after oral administration of alpha-lipoic acid. Hormones
(Athens). 2006;5(4):251-8
Healthy control levels
SHAKE IT CLINICAL TRIAL PROVES EFFICACY
BASELINE WEEK 12
Weight (kg) 96.8 86.0
Fat mass (kg) 37.7 30.8
Lean mass (kg) 58.8 55.2
Triglycerides (mmol/L) 1.5 1.0
HDL (mmol/L) 1.4 1.5
TG/HDL 1.1 0.7
Insulin (pmol/L) 66.7 22.2
HOMA 2.3 0.7
hs-CRP (mg/L) 4.6 4.1
Lamb J, et al. Validation of a weight management program featuring a protein-sparing food plan and a 10,000-step exercise regimen for obese individuals. Metagenics,
Inc./MetaProteomics LLC
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

111
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
600 MG/DAY LIPOIC ACID REDUCES PERIPHERAL NEUROPATHY IN DIABETICS
Zeigler D, et al. Oral treatment with α-Lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes Care 2006;29 (11): 2365-2370
600 MG/DAY LIPOIC ACID POTENTIATES ACE INHIBITORS IN DIABETICS WITH HYPERTENSION
Rahman ST, et al. The Impact of Lipoic Acid on Endothelial Function and Proteinuria in Quinapril-Treated Diabetic Patients With Stage I Hypertension: Results From the QUALITY Study. Journal of Cardiovascular Pharmacology and Therapeutics 2012;17(2):139-145
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

112
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: DIABETIC NEUROPATHY AND
RETINOPATHYMale, 66
• Type II diabetes for 12 years – well-controlled (HBA1c and fasting glucose <7)
• Hypertension for 20 years – medicated – ranges from 125/60 to 170/80
• Weight – 86.8 kg (elevated waist circumference)
Presenting complaints:
• Peripheral neuropathy – painful burning feet, worse in evening, severe nerve irritation in groin
• Retinopathy – 6 months ago ophthalmologist found ‘few spots of damage’
• Doesn’t want medication interfered with “I don’t want to have to change my insulin around again”
LIPOIC ACID: ACTIONS AND APPLICATIONS
APPLICATIONS:• Type 2 diabetes• Diabetic complications:
– Neuropathy– Nephropathy– Cardiovascular disease– Heavy metal
detoxification
ACTIONS:• Antioxidant• Improves glucose metabolism• Improves cellular energy
production• Protects cardiovascular system• Heavy metal chelation
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

113
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE STUDY: DIABETIC NEUROPATHY AND
RETINOPATHYAfter 18 months:• Ophthalmologist – “Congratulations – I can’t see any
signs of damage - I don’t know what you’ve done, butyou’ve reversed it!”
• Neuropathy improvement maintained• HbA1c, glucose, lipids, BP, kidney function all stable at
previous levels• Weight now maintained at 84kg (lost 2.8kg)• Mood and energy improved – gardening, painting, home
improvement etc.
CASE STUDY: DIABETIC NEUROPATHY AND
RETINOPATHYAfter 6 months:• Only burning feet and groin pain now when drinks alcohol
or overexerted• Ran out of lipoic acid for two weeks – neuropathy returned• Ophthalmologist found stabilisation of retinopathy since
last year• “I think the pain killer and the lipoic acid are really
working well together”
CASE STUDY: DIABETIC NEUROPATHY AND RETINOPATHY
Prescription:• Male Nutritional Support with ModucareTM – 1 daily• Resveratrol Antioxidant Complex – 1 daily• Lipoic Acid: Enhanced Bioavailability, Solvent Free – 1 BD• Enhanced Bioavailability Co-enzyme Q10 150 mg – 1
capsule daily• High Potency, Low Reflux Marine Lipids – 2 BDStarted low dose opioid analgesic at night for pain
CASE STUDY: DIABETIC NEUROPATHY AND RETINOPATHY
Medications:• Insulin – 4 injections daily (3 rapid, 1 overnight)• Oral hypoglycaemics (metformin, thiazolidinedione)• Antihypertensives (Ca channel blocker, Ang II antagonist,
ACE inhibitor)• Statin 40mg• Benzodiazepine 5mg• Magnesium tablet 300 mg – 1 daily• Vitamin C tablet 1000 mg – 1 daily• Glucosamine tablet 1000 mg – 2 BD
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

114
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
A
NTI
DIA
BET
IC M
EDIC
ATI
ON
S
BENEFITS: POSITIVE POTENTIATIONANTIDIABETIC MEDICATIONS

115
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HOW TO WORK WITH GP FOR WEANING
• Write a letter to GP:– Introduce yourself– Briefly discuss your treatment history of patient– Discuss rationale for wanting to wean– Agree on the design and plan of the weaning protocol– Discuss research on potential interactions– Attach relevant papers– Provide tech data on key prescriptions– Offer contact details to encourage ongoing communication
• Educate patient about your treatment approach • Ensure patient knows they have the right to choose their treatment,
i.e. informed consent
PREPARING A WEANING PLAN• Establish the goals• Discuss the necessity for gradual withdrawal and input from
the prescriber• Detail the natural medicine support plan• Detail the supportive evidence/previous case examples
where available• Overlap the treatment period between the natural medicine
and the pharmaceutical where suitable• Determine the measures to be used to assess readiness to
begin weaning• Map the proposed timeline, with markers to achieve for
subsequent dose reduction and drug cessation
TO WEAN OR NOT TO WEAN...
WHEN TO WEAN WHEN NOT TO WEAN• Patient goals include weaning• Compliant patient• Patient is willing to
communicate openly with prescriber
• Patient physically and mentally prepared
• Circumstances support monitored weaning process
• During times of excess stress• Patient unstable• Unwilling to comply with
dosing/monitoring• If introducing other variables
which may affect outcome• Patient unable to give
informed consent
BENEFITS: POSITIVE POTENTIATIONWEANING AND POLYPHARMACY

116
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
DETERMINING THE HEIRARCHY OF TREATMENT IN
POLYPHARMACY PATIENTS• Many patients are on multiple
medications• May be prudent to address one at a
time to ensure safety and gain patients’ confidence
• Determine priority co-prescription based on symptoms and patient’s goals
• Typically providing acute relief is the first objective
POLYPHARMACY: CASE SCENARIO
45 yo male:• Fatigue, muscle pain, headache• Dyslipidaemia, hypertension• Obese, poor diet, smoker, drinker• Current medication:
– Statin– ACE inhibitor– NSAID– Generic fish oil
Dear Doctor,
I am a Naturopath consulting at Clinic X on the Sunshine Coast. I have been seeing Patient C for the last two months, advising him on nutritional and lifestyle support to improve his sleep. He would like to wean off Temazepam as he is finding it contributes to drowsiness during the day which is affecting his work.
I would like to support him with a weaning protocol designed to gradually and safely reduce the dose of Temazepam. This involves reducing the dose incrementally to reduce withdrawal symptoms as outlined below:Week 1 – reduce dose by ¼Week 2 – reduce dose by ¼ Week 3 – reduce dose by ¼ Week 4 – reduce dose by ¼
This is a model I’ve used successfully in the past with another medical practitioner and I would be willing to work with your input and permission.
I am concurrently prescribing a formula containing the herbs passionflower, magnolia, zizyphus and kudzu to assist sleep and support the weaning process. Research demonstrates that these herbs have similar action to benzodiazepines and can be safely used alongside these medications. Please find this research attached as well as technical data provided by the manufacturer of this formula.
Please do not hesitate to contact me if you require any further information or would like to discuss this further.
Yours sincerelyNaturopath
BENEFITS: POSITIVE POTENTIATIONWEANING AND POLYPHARMACY

117
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CASE SCENARIO: PROJECTED TREATMENT PROGRESS
BENEFITS: POSITIVE POTENTIATIONWEANING AND POLYPHARMACY

118
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NCFM AND BIO7 IMPROVE GUT MICROBIOME DURING ANTIBIOTIC
THERAPY
Engelbrektson, AL, et al. Probiotics to minimize the disruption of faecal microbiota in healthy subjects undergoing antibiotic therapy. Journal of Medical Microbiology 2009. 58 :663-670
THE BENEFITS OF CO-PRESCRIBING
BENEFITS: COUNTERING SIDE EFFECTS
ANTIBIOTICS

119
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
A careful review of the literature supports the
efficacy of S. boulardii in the prevention of antibiotic-
associated diarrhoea, whereas LGG is useful in the
treatment of antibiotic-associated diarrhoea in
children.Katz JA. Probiotics for the prevention of antibiotic-associated diarrhea and
Clostridium difficile diarrhea. J Clin Gastroenterol. 2006 Mar;40(3):249-55.
S. BOULARDII AND LGG TREAT ANTIBIOTIC-ASSOCIATED DIARRHOEA
McFarland LV. Systematic review and meta-analysis of Saccharomycesboulardii in adult patients. World J Gastroenterol 2010; 16(18): 2202-2222
SACCHAROMYCES BOULARDII REDUCES INFECTIOUS DIARRHOEA
BENEFITS: COUNTERING SIDE EFFECTSANTIBIOTICS
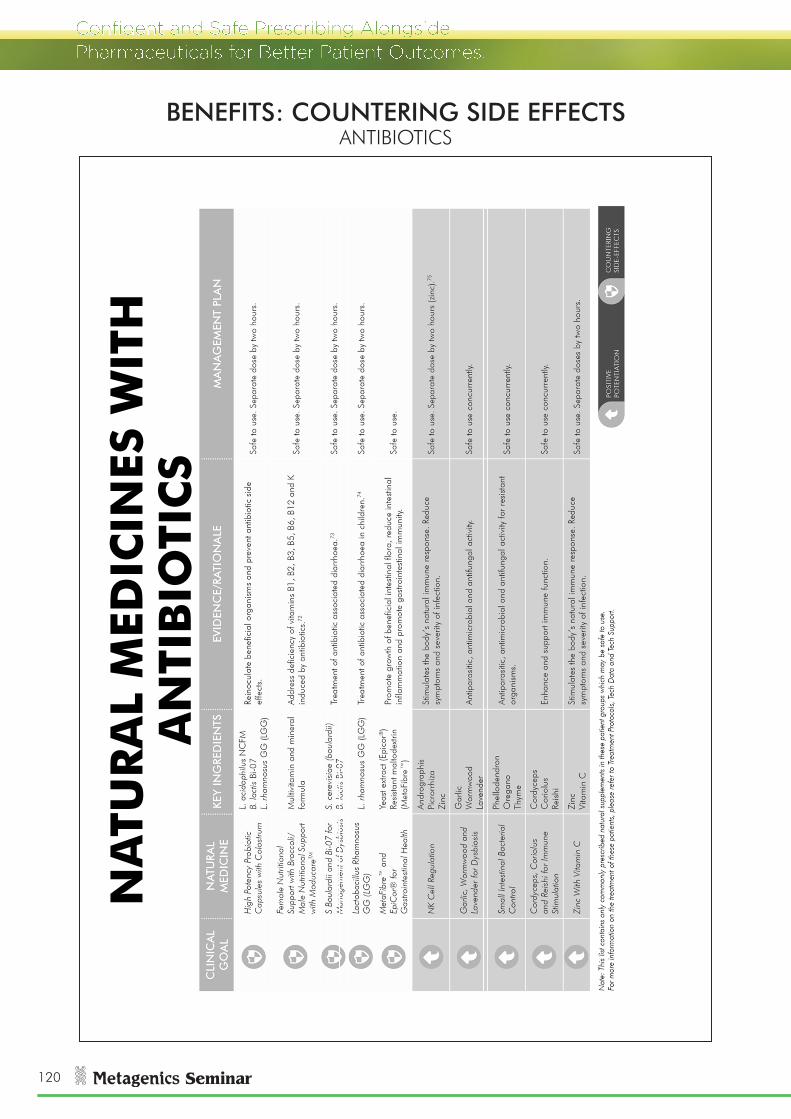
120
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
A
NTI
BIO
TIC
S
BENEFITS: COUNTERING SIDE EFFECTSANTIBIOTICS

121
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
DYSBIOSIS DRIVES NSAID-INDUCED GUT DAMAGE
Syer SD, Wallace JL. Environmental and NSAID-enteropathy: dysbiosis as a common factor. Curr Gastroenterol Rep 2014;16(3):377
• Ibuprofen• Aspirin• Naproxen• Celecoxib
Laine L, et al. Gastric mucosal defense and cytoprotection: bench to bedside. Gastroenterology 2008;135(1):41-60
NON-STEROIDAL ANTI-
INFLAMMATORY DRUGS CAUSE GUT BARRIER
DAMAGE
BENEFITS: COUNTERING SIDE EFFECTSNSAIDS

122
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
ZINC PROTECTS AGAINST NSAID-INDUCED GUT DAMAGE
Pre-treatment with zinc sulphate was found toreduce the extent of indomethacin-induced mucosaldamage. Drug-induced increases in activities of theMMPs and bacterial counts in the intestine werealso attenuated by zinc.
Sivalingam N, et al. Zinc protects against indomethacin-induced damage in the rat small intestine. Eur J Pharmacol 2011;654(1):106-16
Aspirin given with liquorice reduced the number and size of ulcers, reducing the
ulcer index from 1.5 to 0.5 and the incidence from 96% to 46% compared to
aspirin alone.
LIQUORICE REDUCES NSAID-INDUCED GUT DAMAGE
Dehpour AR, et al. The protective effect of liquorice components and their derivatives against gastric ulcer induced by aspirin in rats. J Pharm Pharmacol 1994;46(2):148-9
PROBIOTICS MAY REDUCE PPI AND NSAID-INDUCED GUT DAMAGE
Treatment with a PPI led to a marked loss ofBifidobacteria species. Prevention with dailyadministration of Bifidobacteria resulted ina correction of the dysbiosis and preventionof the increase in intestinal damage andbleeding.
Syer SD, Wallace JL. Environmental and NSAID-enteropathy: dysbiosis as a common factor. Curr Gastroenterol Rep 2014;16(3):377
BENEFITS: COUNTERING SIDE EFFECTSNSAIDS

123
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
IM
MU
NE
SUP
PR
ESSA
NT
/AN
TI-I
NFL
AM
MA
TOR
Y M
EDIC
ATI
ON
SBENEFITS: COUNTERING SIDE EFFECTS
NSAIDS
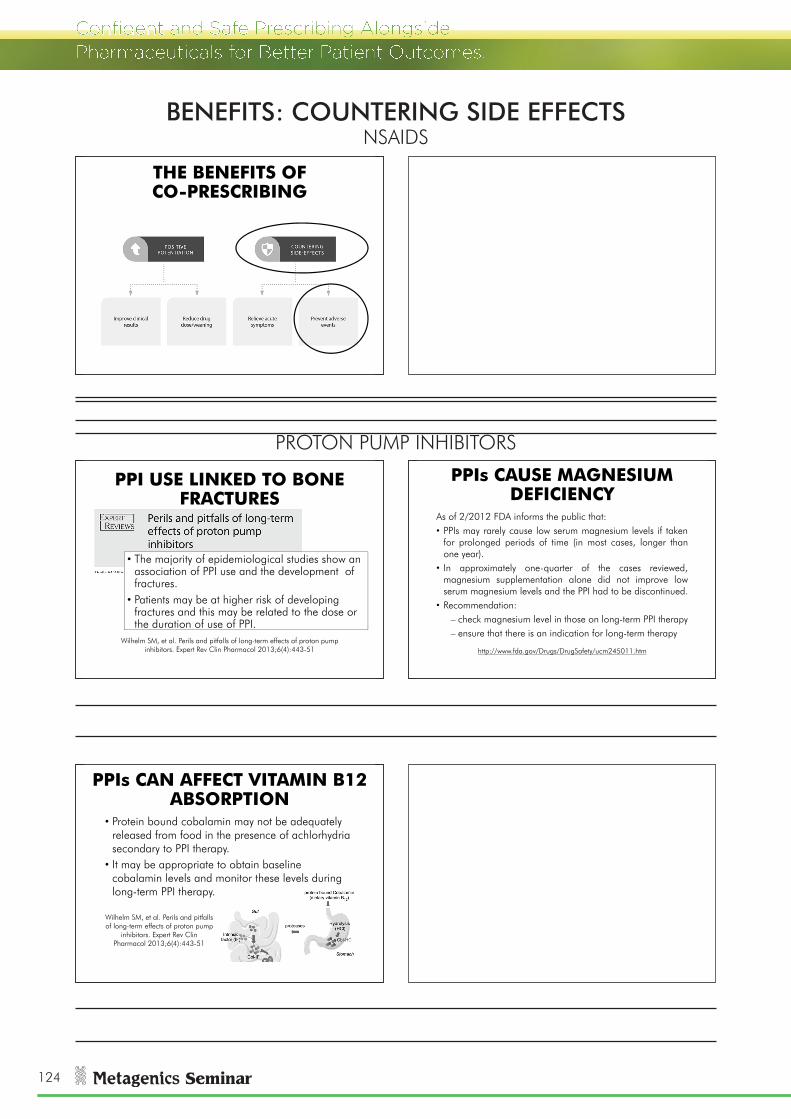
124
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
PPIs CAN AFFECT VITAMIN B12 ABSORPTION
• Protein bound cobalamin may not be adequately released from food in the presence of achlorhydriasecondary to PPI therapy.
• It may be appropriate to obtain baseline cobalamin levels and monitor these levels during long-term PPI therapy.
Wilhelm SM, et al. Perils and pitfalls of long-term effects of proton pump
inhibitors. Expert Rev ClinPharmacol 2013;6(4):443-51
PPIs CAUSE MAGNESIUM DEFICIENCY
As of 2/2012 FDA informs the public that:• PPIs may rarely cause low serum magnesium levels if taken
for prolonged periods of time (in most cases, longer thanone year).
• In approximately one-quarter of the cases reviewed,magnesium supplementation alone did not improve lowserum magnesium levels and the PPI had to be discontinued.
• Recommendation:– check magnesium level in those on long-term PPI therapy– ensure that there is an indication for long-term therapy
http://www.fda.gov/Drugs/DrugSafety/ucm245011.htm
PPI USE LINKED TO BONE FRACTURES
• The majority of epidemiological studies show an association of PPI use and the development of fractures.
• Patients may be at higher risk of developing fractures and this may be related to the dose or the duration of use of PPI.
Wilhelm SM, et al. Perils and pitfalls of long-term effects of proton pump inhibitors. Expert Rev Clin Pharmacol 2013;6(4):443-51
THE BENEFITS OF CO-PRESCRIBING
BENEFITS: COUNTERING SIDE EFFECTSNSAIDS
PROTON PUMP INHIBITORS

125
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
P
RO
TON
PU
MP
IN
HIB
ITO
RS
BENEFITS: COUNTERING SIDE EFFECTSPROTON PUMP INHIBITORS

126
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CREATE A VISUAL FOR THE PATIENT
ALERT PATIENTS TO HIDDEN ADVERSE EFFECTS OF
PRESCRIPTION MEDICATIONS• Patient presents with headaches,
fatigue and cramps• Currently taking PPI for reflux• Could the PPI therapy be
contributing to the symptoms?• What potential side effects do you
need to alert the patient to?
HAVE THE CONVERSATION: THE NEED TO TREAT
• In many cases a practitioner may identify a need to co-prescribe to treat a need outside the patient’s primary complaint.
• How can you best communicate this message to the patient?
BENEFITS: COUNTERING SIDE EFFECTSPROTON PUMP INHIBITORS

127
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
3.2 G/DAY MICROCRYSTALLINE HYDROXYAPATITE IMPROVES
BONE BUILDING EFFECTS OF HRT
-2
-1
0
1
2
3
4
5
BMD
cha
nge
from
ba
selin
e (%
)
Oestrogen Oestrogen + MCHA MHCA Control
Castelo-Branco C et al. Ossein hydroxyapatite compounds for preventing postmenopausal bone loss. Coadjuvant use with hormone replacement therapy. J
Reprod Med 1999;44(3);241-6
MICROCRYSTALLINE HYDROXYAPATITE PREVENTS GLUCOCORTICOID-ASSOCIATED OSTEOPOROSIS
Back painCortical thickness of metacarpals
Pines A, et al. Clinical trial of microcrystalline hydroxyapatite compound ('Ossopan') in the prevention of osteoporosis due to corticosteroid therapy.
Curr Med Res Opin 1984;8(10):734-42
BENEFITS: COUNTERING SIDE EFFECTSPROTON PUMP INHIBITORS

128
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HYDROXYAPATITE AND SOY FOR OSTEOPOROSIS
SOY ISOFLAVONES INCREASE BMD IN MENOPAUSAL WOMEN
Data from 1240 menopausal women revealed that daily
ingestion of an average of 82 mg soy isoflavones for 6-12
months significantly increased spine BMD by an average of 2.38% (p=0.001) compared
with controls
Taku K, et al. Effect of soy isoflavone extract supplements on bone mineral density in menopausal women: meta-analysis of randomized controlled trials. Asia Pac J Clin Nutr.
2010;19(1):33-42.
BENEFITS: COUNTERING SIDE EFFECTSPROTON PUMP INHIBITORS

129
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
HYDROXYAPATITE AND SOY FOR OSTEOPOROSISGlycine max (Soy), seed
providing soy isoflavones
Hydroxyapatite
providing calcium and phosphorus
Ascorbic acid
Borax (sodium borate)
providing boron
Zinc amino acid chelate (Meta Zn® - Zinc bisglycinate)
providing zinc
Manganese amino acid chelate
providing manganese
Phytomenadione (vitamin K1)
Cholecalciferol (vitamin D3)
SOY ISOFLAVONES SELECTIVELY BIND TO OESTROGEN RECEPTOR
BETAThe ERβ is thought to have anti-proliferativeeffects, thus being a possible target pathway toprevent reproductive cancer while enhancing bonehealth in post-menopausal women. Most genisteintreatment effects disappeared from osteoblastswhen ERβ was silenced.
Park CY, Weaver CM. Vitamin D Interactions with soy isoflavones on bone after menopause: a review. Nutrients 2012;4:1610-1621
BENEFITS: COUNTERING SIDE EFFECTSPROTON PUMP INHIBITORS
ORAL CONTRACEPTIVE PILL
OCP REDUCES MAGNESIUM AND MAY CONTRIBUTE TO
THROMBOSISSerum magnesium levels are reduced by the oralcontraceptive pill (OCP). When magnesiumdepletion occurs, it alters the calcium/magnesiumratio which can affect blood coagulability. Thus, ithas been hypothesised that the reduction in serummagnesium levels is one reasons for increased riskof thrombosis while using OCP.
Palmery M, et al. Oral contraceptives and changes in nutritional requirements. Eur Rev Med Pharmacol Sci 2013;17(13):1804-13
OCP LINKED TO NUTRIENT DEPLETION
Key nutrient depletions involve:• Vitamins B2, B6, B12, folate• Vitamin C, E• Magnesium, selenium, zinc
Palmery M, et al. Oral contraceptives and changes in nutritional requirements. EurRev Med Pharmacol Sci 2013;17(13):1804-13

130
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
25 MG/DAY B6 REDUCES SIDE EFFECTS OF OCP
Var C, et al. Supplementation with Vitamin B6 Reduces Side Effects inCambodian Women Using Oral Contraception. Nutrients 2014;6:3353-3362
0
10
20
30
40
50
60
Nausea Headache Depression
Perc
enta
ge o
f wom
en s
uffe
ri g
from
spe
cific
sid
e ef
fect
B6 Control
BENEFITS: COUNTERING SIDE EFFECTSORAL CONTRACEPTIVE PILL

131
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
NA
TUR
AL
MED
ICIN
ES W
ITH
H
OR
MO
NE
MED
ICA
TIO
NS
BENEFITS: COUNTERING SIDE EFFECTSORAL CONTRACEPTIVE PILL

132
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
COMMON MEDICATIONS DEPLETE NUMEROUS NUTRIENTS
DRUG NUTRIENT DEPLETED CATCHPHRASE
Diuretics Magnesium, sodium, potassium and zinc High Absorption Multi Mineral Powder
NSAIDs Vitamin C, folic acid, and iron Female/Male Nutritional Support
Beta-adrenergic CoQ10 Enhanced Bioavailability Co-enzyme Q10 150 mg
Statins CoQ10 Enhanced Bioavailability Co-enzyme Q10 150 mg
PPIs Beta-carotene, vitamin B12, folic acid, vitamin D, calcium, iron and zinc CoQ10,
Female/Male Nutritional Support
Metformin B12, folic acid, and CoQ10 Enhanced Bioavailability Co-enzyme Q10 150 mgOptimal B12/Folate for Cellular Health
HRT Vitamin B2, B6, B12, C, folic acid, magnesium and zinc
Magnesium and Broccoli for Women's Health
Antibiotics Vitamin B1, B2, B3, B5, B6, B12 and K Female/Male Nutritional Support
Corticosteroids Vitamin C, D, calcium, magnesium, potassium, zinc, copper and selenium
Hydroxyapatite and Soy for Osteoporosis
Meletis CD, Zabriskie N. Common Nutrient Depletions Caused by PharmaceuticalsAlternative and Complementary Therapies. February 2007, 13(1): 10-17.
POOR HEALTH AND NUTRITION CAN CAUSE ADVERSE DRUG REACTIONS
HEALTH PARAMETER
BIOLOGICAL CONSEQUENCE
AFFECT ON DRUG
Protein malnutrition
Reduced plasma proteins Increased serum unbound drug fraction
Obesity Increased storage site for lipophilic drugs
Decreased serum levels of lipophilic drugs
Loss of fat free mass
Reduced volume of distribution of medication
Increased serum levels
Low vitamin D Reduced gene expression of detoxification enzymes
Increased serum levels
Pickering G. Arch Gerontol Geriatr. 2004 Mar-Apr;38(2):174-80. Kutuzova GD. Toxicol Appl Pharmacol. 2007 Jan 1;218(1):37-44. Raiten DJ. Am J Clin Nutr
2011;94(suppl):1697S–702S); Cheymol G. Clin Pharmacokinet. 2000;39(3):215-231.
BENEFITS: COUNTERING SIDE EFFECTSLONG TERM HEALTH ALONGSIDE MEDICATIONS

133
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
THE WELLNESS
AND HEALTHY AGEING
PROGRAM
BENEFITS: COUNTERING SIDE EFFECTSLONG TERM HEALTH ALONGSIDE MEDICATIONS

134
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
THE
WEL
LNES
S P
RO
GR
AM
: SU
PP
LEM
ENT
REC
OM
MEN
DA
TIO
NS
BENEFITS: COUNTERING SIDE EFFECTSLONG TERM HEALTH ALONGSIDE MEDICATIONS

135
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
WELLNESS IS SAFE ALONGSIDE MEDICATIONS
Key considerations• Monitor patients on medications for beneficial reductions in
blood pressure, blood glucose or INR• Caution with multivitamins alongside vitamin D sensitive
disorders (histoplasmosis, sarcoidosis, tuberculosis, lymphoma) and folate-sensitive disorders (leukaemia, methotrexate consumption)
• Caution with phytochemical supplements alongside narrow therapeutic index drugs or cancer therapy
BENEFITS: COUNTERING SIDE EFFECTSLONG TERM HEALTH ALONGSIDE MEDICATIONS

136
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
EFFECTIVE COMMUNICATION IS ESSENTIAL
With patients:• Discuss goals• Be aware of concerns and limitations• Create management plans together• Provide education • Present the long-term view of healthWith medical practitioners:• Keep informed• Provide education• Seek involvement• Create health management teams
INCLUDE YOUR PRACTICE IN THE BIGGEST MARKET SHARE
59.1% of Australians takeone or more medications.
ABS National Health Survey: Use of Medications Australia. 4377.0. 1995
NATURAL HEALTH PRACTITIONERS HAVE THE CLINICAL TOOLBOX TO
CO-PRESCRIBE
PRESCRIBING ALONGSIDE PHARMACEUTICALS IS SAFE
AND EFFECTIVE• Most interactions are positive• Adverse interactions are rare• You have the tools and resources to
be the expert in this field• There is a wealth of evidence to
support co-prescribing• Open communication and regular
monitoring makes prescribing alongside pharmaceuticals easy to implement
SUMMARY

137
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
MOST CAUTIONS CAN BE MITIGATED WITH A MANAGEMENT PLAN
CO-PRESCRIBING LEADS TO BETTER CLINICAL OUTCOMES
SUMMARY

138
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CHOOSE THE PATH TO SUCCESS
Side effects
Drivers unaddressed
Higher doses, more drugs
Disease progressionImproved
health
Weaning
Better symptom relief
Disease control
EDMC ANALYSIS: YOUR GUIDE TO MAKING THE BEST DECISIONS
SUMMARY

139
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1A
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Opt
imal
B12
/Fol
ate
For
Cel
lula
r Hea
lth
B12
Folin
ic a
cid
Pyrid
oxal
-5-p
hosp
hate
Ad
dres
s fo
late
def
icie
ncy
indu
ced
by m
etho
trexa
te.
Safe
to u
se –
sep
arat
e do
se b
y 24
hou
rs a
fter
met
hotre
xate
.1
Hig
h Ab
sorp
tion
Mul
ti M
iner
al P
owde
rM
ultim
iner
al fo
rmul
aAd
dres
s de
ficie
ncy
of c
alci
um, m
agne
sium
, pot
assi
um, z
inc,
and
se
leni
um in
duce
d by
NSA
IDs.
2Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs.
Liqu
id V
itam
in D
Vita
min
D3
Addr
ess
defic
ienc
y of
vita
min
D in
duce
d by
NSA
IDs.
3 Sa
fe to
use
.
Glu
tam
ine
& B
osw
ellia
(B
osPu
re® B
osw
ellia
) for
In
test
inal
Int
egrit
y
Glu
tam
ine
Bosp
ure®
Bos
wel
liaC
ount
er in
test
inal
per
mea
bilit
y an
d m
ucos
al d
amag
e in
duce
d by
N
SAID
s.4
Safe
to u
se c
oncu
rren
tly. S
epar
ate
dose
by
two
hour
s.
BCM
-95®
Tur
mer
ic a
nd
Gut
Gar
d® L
iquo
rice
for
Hea
rtbur
n an
d Re
flux
BCM
-95®
Tur
mer
icG
utG
ard®
Liq
uoric
eC
ount
er g
astri
c m
ucos
al d
amag
e in
duce
d by
NSA
IDs.
5Sa
fe to
use
con
curr
ently
.
Hig
h Po
tenc
y Pr
obio
tic
Cap
sule
s w
ith C
olos
trum
L. a
cido
philu
s N
CFM
B. la
ctis
Bi-0
7L.
rham
nosu
s G
G (L
GG
)
Cou
nter
acts
NSA
ID-in
duce
d dy
sbio
sis
whi
ch m
edia
tes
inte
stin
al
muc
osal
dam
age.
6Sa
fe to
use
con
curr
ently
. Sep
arat
e do
se b
y tw
o ho
urs.
Cor
dyce
ps, C
orio
lus
& R
eish
i For
Imm
une
Stim
ulat
ion
Cor
dyce
psC
orio
lus
Reis
hi
Cou
nter
s im
mun
e su
ppre
ssio
n w
hich
may
driv
e ch
roni
c in
fect
ion-
indu
ced
auto
imm
unity
.7Sa
fe to
use
with
reg
ular
mon
itorin
g of
sym
ptom
s.
Hig
h Pu
rity,
Low
Ref
lux,
C
once
ntra
ted
Fish
Oil
EPA
DH
AC
linic
al tr
ials
dem
onst
rate
fish
oil
can
redu
ce th
e us
e of
TN
F-al
pha
inhi
bito
rs a
nd N
SAID
s.8,
9,10
Sa
fe to
use
con
curr
ently
.
Hig
h Po
tenc
y An
ti-in
flam
mat
ory
Her
bs
BCM
-95®
Tur
mer
icBo
swel
liaW
hite
will
ow b
ark
Supp
ortiv
e an
ti-in
flam
mat
ory
actio
n -
redu
ces
acut
e in
flam
mat
ion,
pai
n an
d sw
ellin
g.
Safe
to u
se c
oncu
rren
tly.
Phel
lode
ndro
n, H
ops
And
Sele
nium
for
Auto
imm
unity
Berb
erin
e (P
hello
dend
ron)
Hop
sSe
leni
um
Dec
reas
es ti
ssue
dam
age,
ant
i-inf
lam
mat
ory,
sup
ports
tiss
ue
inte
grity
and
rep
air.
Safe
to u
se, w
ith m
edic
al m
onito
ring
requ
ired
for
cycl
ospo
rine
leve
ls (b
erbe
rine)
.11 S
epar
ate
dose
s by
2 h
ours
to p
reve
nt
chan
ges
in d
rug
abso
rptio
n (z
inc)
.12
Liqu
id V
itam
in D
Vita
min
D3
Regu
late
imm
une
func
tion
in a
utoi
mm
unity
and
impr
ovin
g im
mun
e de
fenc
e.Sa
fe to
use
exc
ept w
ith c
alci
potri
ol (m
ay c
ause
vita
min
D
toxi
city
).13
Zinc
with
Vita
min
C
Pow
der
Zinc
Vita
min
CFu
ndam
enta
l sup
port
for
imm
une
func
tion
Safe
to u
se -
sep
arat
e do
se b
y 2
hour
s to
pre
vent
cha
nges
in
drug
abs
orpt
ion
(zin
c).14
NA
TUR
AL
MED
ICIN
ES W
ITH
IM
MU
NE
SUP
PR
ESSA
NT
/A
NTI
-IN
FLA
MM
ATO
RY
MED
ICA
TIO
NS
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
IMM
UN
E SU
PPRE
SSA
NT/
AN
TI-I
NFL
AM
MA
TORY
MED
ICA
TIO
NS
• N
SAID
s•
Cor
ticos
tero
ids
• M
etho
trexa
te•
TNF-
alph
a in
hibi
tors
• C
yclo
spor
ine
• Im
mun
oglo
bulin
rep
lace
men
t the
rapy
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS

140
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1B
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Her
bal S
uppo
rt fo
r Hyp
er
HPA
Stre
ss
Zizy
phus
Mag
nolia
Pass
iflor
a
Stud
ies
show
com
para
ble
effe
cts.
Evi
denc
e pa
ssifl
ora
supp
orts
sy
mpt
oms
of o
piat
e w
ithdr
awal
.15Sa
fe to
use
. Sep
arat
e do
se b
y si
x ho
urs
if ad
ditiv
e ef
fect
s un
desi
red.
Mag
nesi
um A
lkal
isin
g C
ombi
natio
n fo
r Stre
ssM
etaM
ag® m
agne
sium
Pota
ssiu
m c
itrat
eSu
ppor
ts G
ABA
sign
allin
g an
d re
duce
s SN
S ac
tivity
. Mag
nesi
um
defic
ienc
y re
duce
s se
roto
nin
leve
ls.
Safe
to u
se c
oncu
rren
tly.
Bupl
euru
m C
ompl
ex F
or
Ner
vous
Ten
sion
And
Irr
itabi
lity
Bupl
euru
mPe
ony
Supp
orts
moo
d an
d be
nefic
ial f
or ir
ritab
ility,
anx
iety
and
stre
ss.
Safe
to u
se c
oncu
rren
tly.
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
XIO
LYTI
C M
EDIC
ATI
ON
S
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
AN
XIO
LYTI
C M
EDIC
ATI
ON
S
• Be
nzod
iaze
pine
s•
Beta
blo
cker
s•
Alph
a bl
ocke
rs
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS

141
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1C
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Hig
h Pu
rity,
Low
Ref
lux,
C
once
ntra
ted
Fish
Oil
EPA
DH
ARC
T ev
iden
ce fi
sh o
il au
gmen
ts e
ffica
cy o
f ant
idep
ress
ants
with
po
tent
ial t
o lo
wer
dos
e.16
,17
Safe
to u
se c
oncu
rren
tly.
Hig
h Po
tenc
y M
agne
sium
, Chr
omiu
m
and
Sele
nium
Met
aMag
® M
agne
sium
Taur
ine
Glu
tam
ine
Evid
ence
for
augm
enta
tion
of a
ntid
epre
ssan
t the
rapy
and
se
roto
nin
leve
ls.18
,19
Safe
to u
se c
oncu
rren
tly.
N-a
cety
lcys
tein
eN
-ace
tylc
yste
ine
Stud
ies
show
N-a
cety
lcys
tein
e re
duce
s se
verit
y of
dep
ress
ion
whe
n us
ed a
s ad
junc
tive
ther
apy.
20Sa
fe to
use
con
curr
ently
.
Zinc
with
Vita
min
CZi
ncVi
tam
in C
RCTs
sho
w z
inc
augm
ents
effi
cacy
of a
ntid
epre
ssan
ts.21
,22
Safe
to u
se c
oncu
rren
tly.
Opt
imal
B12
/Fol
ate
For
Cel
lula
r Hea
lth
B12
Folin
ic a
cid
Pyrid
oxal
-5-p
hosp
hate
RCTs
sho
w fo
late
enh
ance
s ac
tivity
of a
ntid
epre
ssan
ts, e
sp. w
ith
high
hom
ocys
tein
e (a
bove
11
μmol
/litr
e).23
,24
Safe
to u
se c
oncu
rren
tly.
Liqu
id V
itam
in D
Vita
min
D3
Evid
ence
sug
gest
s vi
tam
in D
def
icie
ncy
may
pla
y a
role
in
depr
essi
on.25
Safe
to u
se c
oncu
rren
tly.
Hig
h Po
tenc
y An
ti-in
flam
mat
ory
Her
bs
BCM
-95®
Tur
mer
icBo
swel
liaW
hite
will
ow b
ark
RCT
evid
ence
cur
cum
in a
ugm
ents
effi
cacy
of a
ntid
epre
ssan
ts.26
Safe
to u
se c
oncu
rren
tly.
Moo
d, A
dren
al a
nd
Thyr
oid
Supp
ort
St J
ohn’
s w
ort
With
ania
SAM
ePo
tent
ially
sig
nific
ant b
enef
it as
adj
uvan
t with
ant
idep
ress
ants
.27
A th
erap
eutic
tria
l may
be
war
rant
ed w
ith a
ctiv
e m
onito
ring
of
moo
d (S
t Joh
n’s
Wor
t, SA
Me)
and
blo
od p
ress
ure
(tyro
sine
).28,2
9
Hyd
roxy
trypt
opha
n C
ompl
ex
5-H
TPSA
Me
Phen
ylal
anin
ePo
tent
ially
sig
nific
ant b
enef
it as
adj
uvan
t with
ant
idep
ress
ants
.30
A th
erap
eutic
tria
l may
be
war
rant
ed w
ith a
ctiv
e m
onito
ring
of
moo
d (5
-HTP
) and
blo
od p
ress
ure
(phe
nyla
lani
ne).31
,32
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TID
EPR
ESSA
NT
MED
ICA
TIO
NS
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
AN
TID
EPRE
SSA
NT
MED
ICA
TIO
NS
• Se
lect
ive
sero
toni
n re
upta
ke in
hibi
tors
(SSR
Is)
• Se
lect
ive
sero
toni
n an
d no
radr
enal
ine
reup
take
in
hibi
tors
(SN
RIs)
• N
orad
rena
line
reup
take
inhi
bito
rs•
Tric
yclic
ant
idep
ress
ants
• Re
vers
ible
inhi
bito
rs o
f mon
oam
ine
oxid
ase
A (R
IMAs
)•
Tetra
cycl
ic a
ntid
epre
ssan
ts•
Tetra
cylic
ana
logu
es o
f mia
nser
in (n
orad
ren-
ergi
c an
d sp
ecifi
c se
roto
nerg
ic a
ntid
epre
ssan
t [N
aSSA
])•
Mel
aton
ergi
c an
tidep
ress
ants
• M
onoa
min
e ox
idas
e in
hibi
tors
(MAO
Is)
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS

142
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Hig
h Pu
rity,
Low
Ref
lux,
C
once
ntra
ted
Fish
Oil
EPA
DH
A
Redu
ces
card
iova
scul
ar r
isk
- an
tiarr
hyth
mic
, im
prov
es
endo
thel
ial f
unct
ion,
lipi
d-lo
wer
ing,
inhi
bits
pla
tele
t ag
greg
atio
n.33
Safe
to u
se c
oncu
rren
tly a
t tot
al fa
tty a
cid
inta
ke (E
PA +
D
HA)
of 6
.8 g
dai
ly.34
,35
Mon
itor
INR
wee
kly
for
first
mon
th o
f su
pple
men
tatio
n.
Hig
h Po
tenc
y Ta
urin
e,
Gly
cine
and
Mag
nesi
um
for C
ardi
ovas
cula
r Hea
lth
Met
aMag
® m
agne
sium
Taur
ine
Redu
ces
hype
rtens
ion,
sup
ports
end
othe
lial f
unct
ion
and
card
iova
scul
ar h
ealth
.Sa
fe to
use
con
curr
ently
.
Enha
nced
Bio
avai
labi
lity
Co-
enzy
me
Q10
100
mg
CoQ
10 w
ith V
ESIs
orb
Redu
ces
hype
rtens
ion,
impr
oves
car
diac
ene
rgy
prod
uctio
n.Sa
fe to
use
con
curr
ently
at 1
00 m
g pe
r da
y w
ith m
onito
ring
of
INR
wee
kly
for
first
mon
th o
f sup
plem
enta
tion.
36
Mix
ed T
ocop
hero
ls &
To
cotri
enol
s fo
r Fre
e Ra
dica
l Def
ence
Mix
ed to
coph
erol
sM
ixed
toco
trien
ols
Supp
orts
car
diov
ascu
lar
heal
th, a
nti-t
hrom
botic
, lip
id-lo
wer
ing,
an
tioxi
dant
and
ant
i-inf
lam
mat
ory.
Safe
to u
se c
oncu
rren
tly b
elow
720
mg/
day,
with
mon
itorin
g of
IN
R w
eekl
y fo
r fir
st m
onth
of s
uppl
emen
tatio
n.37
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TIC
OA
GU
LAN
T/
AN
TIP
LATE
LET
MED
ICA
TIO
NS
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
IMM
UN
E SU
PPRE
SSA
NT/
AN
TI-I
NFL
AM
MA
TORY
MED
ICA
TIO
NS
• W
arfa
rin (v
itam
in K
ant
agon
ist)
• As
pirin
(CO
X-1
inhi
bito
r)•
Clo
pido
grel
(ant
ipla
tele
t)•
Apix
aban
(Fac
tor
Xa in
hibi
tor)
• D
abig
atra
n et
exila
te (T
hrom
bin
inhi
bito
r)
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS
APPENDIX 1D

143
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1E
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Enha
nced
Bio
avai
labi
lity
Co-
enzy
me
Q10
150
mg
CoQ
10 w
ith V
ESIs
orb
Addr
ess
defic
ienc
y of
CoQ
10 a
nd d
efic
ienc
y-re
late
d m
yopa
thy
indu
ced
by s
tatin
s.38
Safe
to u
se c
oncu
rren
tly.
Hea
lthy
Glu
cose
M
etab
olis
m
Hop
sAc
acia
Chr
omiu
mM
ay a
ssis
t to
coun
tera
ct s
tatin
-indu
ced
insu
lin r
esis
tanc
e.39
Sa
fe to
use
con
curr
ently
.
Liqu
id V
itam
in D
3Vi
tam
in D
3C
ount
erac
ts s
tatin
-ass
ocia
ted
myo
path
y in
92%
of c
ases
whe
n vi
tam
in D
def
icie
nt.40
Safe
to u
se c
oncu
rren
tly.
Hig
h Pu
rity,
Low
Ref
lux,
C
once
ntra
ted
Fish
Oil
EPA
DH
AAd
dres
s om
ega
3 de
ficie
ncy
indu
ced
by s
tatin
s.41
RC
Ts
dem
onst
rate
aug
men
tatio
n of
lipi
d-lo
wer
ing
drug
s.42
,43
Safe
to u
se c
oncu
rren
tly. M
onito
r se
rum
lipi
ds 3
-6 m
onth
ly.
Antio
xida
nt
Cho
lest
erol
Su
ppor
t Com
plex
Citr
us b
iofla
vono
ids
Toco
trien
ols
Low
ers
LDL
and
trigl
ycer
ides
.44Sa
fe to
use
con
curr
ently
. Mon
itor
seru
m li
pids
3-6
mon
thly.
Om
ega-
3 an
d As
taxa
nthi
n C
ompl
exKr
ill o
ilRe
duce
s to
tal c
hole
ster
ol, L
DL,
and
trig
lyce
rides
, and
incr
ease
s H
DL
leve
ls.45
Safe
to u
se c
oncu
rren
tly. M
onito
r se
rum
lipi
ds 3
-6 m
onth
ly.
Mix
ed T
ocop
hero
ls &
To
cotri
enol
s fo
r Fre
e Ra
dica
l Def
ence
Mix
ed to
coph
erol
sM
ixed
toco
trien
ols
Impr
oves
leve
ls o
f LD
L ch
oles
tero
l, ap
olip
opro
tein
B a
nd
trigl
ycer
ides
.46
Safe
to u
se c
oncu
rren
tly.
NA
TUR
AL
MED
ICIN
ES W
ITH
LIP
ID L
OW
ERIN
G M
EDIC
ATI
ON
S
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
IMM
UN
E SU
PPRE
SSA
NT/
AN
TI-I
NFL
AM
MA
TORY
MED
ICA
TIO
NS
• St
atin
s•
Fibr
ates
• Bi
le a
cid
sequ
estra
nts
• Ez
etim
ibe
(cho
lest
erol
abs
orpt
ion
inhi
bito
r)
• Lo
mita
pide
(VLD
L sy
nthe
sis
inhi
bito
r)•
Orli
stat
(gas
tric
and
panc
reat
ic li
pase
inhi
bito
r)
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS

144
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Hig
h Po
tenc
y Iro
n an
d C
ofac
tors
Iron
bisg
lyci
nate
Chi
ckw
eed
B6, B
12, V
it C
Iron
supp
ress
es A
CE
inhi
bito
r-in
duce
d co
ugh.
47Sa
fe to
use
con
curr
ently
. Sep
arat
e do
se b
y tw
o ho
urs.
Zinc
with
Vita
min
CZi
ncVi
tam
in C
Addr
ess
zinc
def
icie
ncy
indu
ced
by A
CE
inhi
bito
rs a
nd th
iazi
de
diur
etic
s.48
,49
Safe
to u
se c
oncu
rren
tly. S
epar
ate
dose
by
two
hour
s.
Hig
h Ab
sorp
tion
Mul
ti M
iner
al P
owde
rM
ultim
iner
al fo
rmul
aAd
dres
s po
tass
ium
, mag
nesi
um, c
alci
um a
nd z
inc
defic
ienc
y in
duce
d by
loop
diu
retic
s.50
Safe
to u
se c
oncu
rren
tly. S
epar
ate
dose
by
two
hour
s.
Fem
ale
Nut
ritio
nal
Supp
ort w
ith B
rocc
oli/
M
ale
Nut
ritio
nal S
uppo
rt w
ith M
oduc
areTM
Mul
tivita
min
and
min
eral
fo
rmul
a
Addr
ess
pyrid
oxin
e, th
iam
ine
and
asco
rbic
aci
d de
ficie
ncy
indu
ced
by lo
op d
iure
tics.
51 C
ount
erac
t thi
amin
e de
ficie
ncy
and
incr
ease
d ho
moc
yste
ine
with
thia
zide
diu
retic
s.52
,53
Safe
to u
se c
oncu
rren
tly. S
epar
ate
dose
by
two
hour
s.
Hea
lthy
Glu
cose
M
etab
olis
m
Hop
sAc
acia
Chr
omiu
m
May
ass
ist t
o co
unte
ract
bet
a bl
ocke
r-in
duce
d gl
ucos
e in
tole
ranc
e an
d in
crea
sed
risk
diab
etes
.54Sa
fe to
use
con
curr
ently
.
Her
bal L
axat
ive
Gin
ger
Cha
mom
ileC
asca
ra
Impr
ove
mot
ility
in th
e ca
se o
f cal
cium
cha
nnel
blo
cker
s ca
usin
g na
usea
and
con
stip
atio
n.55
Safe
to u
se c
oncu
rren
tly.
Enha
nced
Bio
avai
labi
lity
Co-
enzy
me
Q10
150
mg
CoQ
10 w
ith V
ESIs
orb
Cou
nter
dep
letio
n of
CoQ
10 in
the
myo
card
ium
by
beta
bl
ocke
rs.56
Red
uces
hyp
erte
nsio
n as
a m
onot
hera
py o
r in
co
njun
ctio
n w
ith a
ntih
yper
tens
ives
.57
Safe
to u
se c
oncu
rren
tly w
ith b
lood
pre
ssur
e m
onito
ring.
58
Hig
h Po
tenc
y Ta
urin
e,
Gly
cine
and
Mag
nesi
um
for C
ardi
ovas
cula
r Hea
lth
Met
aMag
® m
agne
sium
Taur
ine
Addr
ess
mag
nesi
um d
efic
ienc
y in
duce
d by
thia
zide
diu
retic
s.59
RC
Ts s
how
aug
men
tatio
n of
ant
ihyp
erte
nsiv
es.60
,61
Safe
to u
se c
oncu
rren
tly w
ith b
lood
pre
ssur
e m
onito
ring.
Nut
ritio
nal a
nd H
erba
l Su
ppor
t for
a H
ealth
y H
eart
Purp
le s
age
Haw
thor
nC
oQ10
Folic
aci
dB1
2
Redu
ces
hype
rtens
ion
as a
mon
othe
rapy
or
in c
onju
nctio
n w
ith
antih
yper
tens
ives
.62Sa
fe to
use
con
curr
ently
with
blo
od p
ress
ure
mon
itorin
g.63
,64
Hig
h Pu
rity,
Low
Ref
lux,
C
once
ntra
ted
Fish
Oil
EPA
DH
ARe
duce
s ca
rdio
vasc
ular
risk
- a
ntia
rrhy
thm
ic, i
mpr
oves
end
othe
lial
func
tion,
lipi
d-lo
wer
ing,
inhi
bits
pla
tele
t agg
rega
tion.
65Sa
fe to
use
con
curr
ently
.
N-a
cety
lcys
tein
eN
-ace
tylc
yste
ine
Stud
ies
show
N-a
cety
lcys
tein
e po
tent
iate
s ac
tion
of
antih
yper
tens
ives
.66Sa
fe to
use
con
curr
ently
with
blo
od p
ress
ure
mon
itorin
g.
Alph
a Li
poic
Aci
d fo
r An
tioxi
dant
Sup
port
Lipo
ic a
cid
Stud
ies
show
lipo
ic a
cid
pote
ntia
tes
actio
ns o
f ant
ihyp
erte
nsiv
es
in d
iabe
tics,
as
wel
l as
impr
ovin
g in
sulin
sen
sitiv
ity.67
Safe
to u
se c
oncu
rren
tly w
ith b
lood
pre
ssur
e m
onito
ring.
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TIH
YPER
TEN
SIV
E M
EDIC
ATI
ON
S
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
IMM
UN
E SU
PPRE
SSA
NT/
AN
TI-I
NFL
AM
MA
TORY
MED
ICA
TIO
NS
• AC
E In
hibi
tors
• C
alci
um c
hann
el b
lock
ers
• Al
pha
bloc
kers
• Be
ta b
lock
ers
• Th
iazi
de d
iure
tics
• Lo
op d
iure
tics
• An
giot
ensi
n-II
anta
goni
sts
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS
APPENDIX 1F

145
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1G
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Enha
nced
Bio
avai
labi
lity
Co-
enzy
me
Q10
150
mg
CoQ
10 w
ith V
ESIs
orb
Addr
ess
CoQ
10 d
efic
ienc
y in
duce
d by
met
form
in.68
Safe
to u
se c
oncu
rren
tly.
Opt
imal
B12
/Fol
ate
For
Cel
lula
r Hea
lth
B12
Folin
ic a
cid
Pyrid
oxal
-5-p
hosp
hate
Addr
ess
fola
te a
nd B
12 d
efic
ienc
y in
duce
d by
met
form
in.69
Safe
to u
se c
oncu
rren
tly.
Alph
a Li
poic
Aci
d fo
r An
tioxi
dant
Sup
port
Lipo
ic a
cid
Evid
ence
dem
onst
rate
s sa
fe a
nd e
ffect
ive
adju
nctiv
e an
tidia
betic
ag
ent,
trea
tmen
t and
pre
vent
ion
of d
iabe
tic n
euro
path
y an
d di
abet
ic h
yper
tens
ion.
70
Safe
to u
se c
oncu
rren
tly. M
onito
r bl
ood
gluc
ose
wee
kly
and
HbA
1c e
very
thre
e m
onth
s.
Hig
h Po
tenc
y Ta
urin
e,
Gly
cine
and
Mag
nesi
um
for C
ardi
ovas
cula
r Hea
lth
Met
aMag
® m
agne
sium
Taur
ine
Enha
nces
insu
lin s
ensi
tivity
, sup
ports
car
diov
ascu
lar
heal
th.
Safe
to u
se c
oncu
rren
tly. M
onito
r bl
ood
gluc
ose
wee
kly
and
HbA
1c e
very
thre
e m
onth
s.
Hea
lthy
Glu
cose
M
etab
olis
m
Hop
sAc
acia
Chr
omiu
m
Supp
orts
insu
lin s
ensi
tivity
, glu
cose
met
abol
ism
and
hea
lthy
lipid
s.Sa
fe to
use
con
curr
ently
. Mon
itor
bloo
d gl
ucos
e w
eekl
y an
d H
bA1c
eve
ry th
ree
mon
ths.
Resv
erat
rol A
ntio
xida
nt
Com
plex
age
ing
Resv
erat
rol
BCM
-95®
Tur
mer
icEv
iden
ce o
f syn
ergi
stic
act
ions
with
met
form
in.
Safe
to u
se c
oncu
rren
tly. M
onito
r bl
ood
gluc
ose
wee
kly
and
HbA
1c e
very
thre
e m
onth
s.
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TID
IAB
ETIC
MED
ICA
TIO
NS
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.
AN
TID
IABE
TIC
MED
ICA
TIO
NS
• M
etfo
rmin
(big
uani
de)
• Th
iazo
lidin
edio
nes
• Su
lfony
lure
as•
Alph
a-gl
ucos
idas
e in
hibi
tors
• In
sulin
POSI
TIVE
PO
TEN
TIAT
ION
CO
UN
TERI
NG
SI
DE-
EFFE
CTS

146
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Hig
h Po
tenc
y Pr
obio
tic
Cap
sule
s w
ith C
olos
trum
L. a
cido
philu
s N
CFM
B. la
ctis
Bi-0
7L.
rham
nosu
s G
G (L
GG
)
Rein
ocul
ate
bene
ficia
l org
anis
ms
and
prev
ent a
ntib
iotic
sid
e ef
fect
s.Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs.
Fem
ale
Nut
ritio
nal
Supp
ort w
ith B
rocc
oli/
M
ale
Nut
ritio
nal S
uppo
rt w
ith M
oduc
areTM
Mul
tivita
min
and
min
eral
fo
rmul
aAd
dres
s de
ficie
ncy
of v
itam
ins
B1, B
2, B
3, B
5, B
6, B
12 a
nd K
in
duce
d by
ant
ibio
tics.
72Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs.
S Bo
ular
dii a
nd B
i-07
for
Man
agem
ent o
f Dys
bios
isS.
cer
evis
iae
(bou
lard
ii)B.
lact
is B
i-07
Trea
tmen
t of a
ntib
iotic
ass
ocia
ted
diar
rhoe
a.73
Safe
to u
se. S
epar
ate
dose
by
two
hour
s.
Lact
obac
illus
Rha
mno
sus
GG
(LG
G)
L. rh
amno
sus
GG
(LG
G)
Trea
tmen
t of a
ntib
iotic
ass
ocia
ted
diar
rhoe
a in
chi
ldre
n.74
Safe
to u
se. S
epar
ate
dose
by
two
hour
s.
Met
aFib
re™
and
Ep
iCor
® fo
r G
astro
inte
stin
al H
ealth
Yeas
t ext
ract
(Epi
cor®
)Re
sist
ant m
alto
dext
rin
(Met
aFib
re™
)
Prom
ote
grow
th o
f ben
efic
ial i
ntes
tinal
flor
a, r
educ
e in
test
inal
in
flam
mat
ion
and
prom
ote
gast
roin
test
inal
imm
unity
.Sa
fe to
use
.
NK
Cel
l Reg
ulat
ion
Andr
ogra
phis
Picr
orrh
iza
Zinc
Stim
ulat
es th
e bo
dy’s
nat
ural
imm
une
resp
onse
. Red
uce
sym
ptom
s an
d se
verit
y of
infe
ctio
n.Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs
(zin
c).75
Gar
lic, W
orm
woo
d an
d La
vend
er fo
r Dys
bios
is
Gar
licW
orm
woo
dLa
vend
erAn
tipar
asiti
c, a
ntim
icro
bial
and
ant
ifung
al a
ctiv
ity.
Safe
to u
se c
oncu
rren
tly.
Smal
l Int
estin
al B
acte
rial
Con
trol
Phel
lode
ndro
nO
rega
noTh
yme
Antip
aras
itic,
ant
imic
robi
al a
nd a
ntifu
ngal
act
ivity
for
resi
stan
t or
gani
sms.
Safe
to u
se c
oncu
rren
tly.
Cor
dyce
ps, C
orio
lus
and
Reis
hi fo
r Im
mun
e St
imul
atio
n
Cor
dyce
psC
orio
lus
Reis
hiEn
hanc
e an
d su
ppor
t im
mun
e fu
nctio
n.Sa
fe to
use
con
curr
ently
.
Zinc
With
Vita
min
CZi
ncVi
tam
in C
Stim
ulat
es th
e bo
dy’s
nat
ural
imm
une
resp
onse
. Red
uce
sym
ptom
s an
d se
verit
y of
infe
ctio
n.Sa
fe to
use
. Sep
arat
e do
ses
by tw
o ho
urs.
NA
TUR
AL
MED
ICIN
ES W
ITH
AN
TIB
IOTI
CS
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.PO
SITI
VE
POTE
NTI
ATIO
NC
OU
NTE
RIN
G
SID
E-EF
FEC
TS
APPENDIX 1H

147
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1I
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Hig
h Ab
sorp
tion
Mul
ti M
iner
al P
owde
rM
ultim
iner
al fo
rmul
aAd
dres
s m
agne
sium
, cal
cium
, iro
n an
d zi
nc d
efic
ienc
y in
duce
d by
PPI
s.76
,77
Safe
to u
se. S
epar
ate
dose
by
two
hour
s.
Fem
ale
Nut
ritio
nal
Supp
ort w
ith B
rocc
oli/
M
ale
Nut
ritio
nal S
uppo
rt w
ith M
oduc
areTM
Mul
tivita
min
and
min
eral
fo
rmul
aAd
dres
s vi
tam
in B
12, C
, and
D d
efic
ienc
y in
duce
d by
PPI
s.78
,79,
80Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs.
Hyd
roxy
apat
ite a
nd S
oy
for O
steo
poro
sis
Hyd
roxy
apat
iteSo
y is
ofla
vone
sAd
dres
s ca
lciu
m a
nd v
itam
in D
def
icie
ncy
indu
ced
by P
PIs,
w
here
bon
e de
nsity
may
be
at r
isk.
81Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs.
Enha
nced
Bio
avai
labi
lity
Co-
enzy
me
Q10
150
mg
CoQ
10 w
ith V
ESIs
orb
Addr
ess
CoQ
10 d
efic
ienc
y in
duce
d by
PPI
s.Sa
fe to
use
. Sep
arat
e do
se b
y tw
o ho
urs.
BCM
-95®
Tur
mer
ic a
nd
Gut
Gar
d® L
iquo
rice
for
Hea
rtbur
n an
d Re
flux
BCM
-95®
Tur
mer
icG
utG
ard®
Liq
uoric
eRe
duce
s gu
t inf
lam
mat
ion
and
faci
litat
es P
PI w
ithdr
awal
.82Sa
fe to
use
con
curr
ently
.
NA
TUR
AL
MED
ICIN
ES W
ITH
PR
OTO
N P
UM
P I
NH
IBIT
OR
S
PRO
TON
PU
MP
INH
IBIT
ORS
• O
mep
razo
le•
Esom
epra
zole
• La
nsop
razo
le•
Rabe
praz
ole
• Pa
ntop
razo
le•
Dex
lans
opra
zole
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.PO
SITI
VE
POTE
NTI
ATIO
NC
OU
NTE
RIN
G
SID
E-EF
FEC
TS

148
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Mag
nesi
um a
nd B
rocc
oli
for W
omen
's H
ealth
Met
aMag
® m
agne
sium
BosP
ure®
Bos
wel
liaC
ham
omile
Addr
ess
mag
nesi
um, v
itam
in B
6, B
12, f
olat
e, v
itam
in C
and
zin
c de
ficie
ncy
indu
ced
by O
CP
and
HRT
.83,8
4,85
Sa
fe to
use
.
Fem
ale
Nut
ritio
nal
Supp
ort w
ith B
rocc
oli
Mul
tivita
min
and
min
eral
fo
rmul
aAd
dres
s vi
tam
in B
6, B
12, f
olat
e, v
itam
in C
, vita
min
E a
nd z
inc
defic
ienc
y in
duce
d by
the
OC
P an
d H
RT.86
,87,
88
Safe
to u
se.
Hig
h Po
tenc
y Pr
obio
tic
Cap
sule
s w
ith C
olos
trum
L. a
cido
philu
s N
CFM
B. la
ctis
Bi-0
7L.
rham
nosu
s G
G (L
GG
)
Rein
ocul
ate
bene
ficia
l org
anis
ms
and
rest
ore
heal
thy
mic
robi
ome.
Safe
to u
se. S
epar
ate
dose
by
two
hour
s.
Vite
x, G
inge
r and
W
ithan
ia to
Incr
ease
Pr
oges
tero
ne
Vite
xG
inge
rW
ithan
ia
Alle
viat
es s
ympt
oms
of P
MS
and
othe
r co
nditi
ons
for
whi
ch th
e O
CP
may
be
pres
crib
ed.
May
red
uce
OC
P ef
ficac
y -
reco
mm
end
barr
ier
met
hods
of
cont
race
ptio
n du
ring
conc
urre
nt u
se.
Oes
troge
n Li
fting
Her
bsRe
hman
nia
Six
Zizy
phyu
sAn
emar
rhen
a
Incr
ease
s oe
stro
gen
leve
ls, s
uppo
rts n
ervo
us s
yste
m a
nd
adap
tatio
n to
alte
red
horm
one
leve
ls d
urin
g an
d po
st
men
opau
se.
Safe
to u
se c
oncu
rren
tly.
NA
TUR
AL
MED
ICIN
ES W
ITH
HO
RM
ON
E M
EDIC
ATI
ON
S
HO
RMO
NE
MED
ICA
TIO
NS
• O
ral c
ontra
cept
ive
pill
(OC
P)•
Hor
mon
e re
plac
emen
t the
rapy
(HRT
)
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.PO
SITI
VE
POTE
NTI
ATIO
NC
OU
NTE
RIN
G
SID
E-EF
FEC
TS
APPENDIX 1J

149
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
APPENDIX 1K
CLI
NIC
AL
GO
AL
NA
TURA
L M
EDIC
INE
KEY
ING
RED
IEN
TSEV
IDEN
CE/
RATI
ON
ALE
MA
NA
GEM
ENT
PLA
N
Cor
dyce
ps, C
orio
lus
& R
eish
i For
Imm
une
Stim
ulat
ion
Cor
dyce
psC
orio
lus
Reis
hi
Redu
ce c
hem
othe
rapy
and
rad
ioth
erap
y si
de e
ffect
s, im
prov
e th
e ef
fect
iven
ess
and
supp
ort i
mm
une
surv
eilla
nce1,
2,3,
4
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy5
and
chem
othe
rape
utic
dru
gs in
clud
ing
mito
myc
in-C
, cy
clop
hosp
ham
ide
and
fluor
oura
cil.6,
7,8
No
evid
ence
of h
arm
with
oth
er d
rug
clas
ses.
Cel
l Sig
nalli
ng,
Det
oxifi
catio
n an
d An
tioxi
dant
Sup
port
for
DN
A Re
plic
atio
n
Resv
erat
rol
Gre
en te
aBC
M-9
5® T
urm
eric
Redu
ces
drug
res
ista
nce,
incr
ease
s ef
ficac
y an
d re
duce
s si
de
effe
cts
with
som
e dr
ug c
lass
es.9,
10,1
1,12
,13
Mai
ntai
ns a
ntio
xida
nt
stat
us, r
egul
ates
cel
l cyc
les,
red
uces
ang
ioge
nesi
s an
d de
crea
ses
met
asta
tic p
oten
tial.14
,15
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy16
,17,
18 a
nd
chem
othe
rape
utic
dru
gs in
clud
ing
etop
osid
e,19
cis
plat
in,20
bl
eom
ycin
21 a
nd p
aclit
axel
22 b
ut n
ot w
ith c
yclo
phos
pham
ide,
23
doxo
rubi
cin,
24 c
ampt
othe
cin
and
mec
hlor
etha
min
e (c
urcu
min
)25
and
boro
nic
acid
-bas
ed p
rote
asom
e in
hibi
tors
(gre
en te
a).26
N-a
cety
lcys
tein
eN
-ace
tylc
yste
ine
Redu
ce s
ide
effe
cts
of r
adio
ther
apy27
and
che
mot
hera
py a
nd
prev
ents
form
atio
n of
DN
A ad
duct
s.28
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy29
and
ch
emot
hera
peut
ic d
rugs
incl
udin
g do
xoru
bici
n30 a
nd c
ispl
atin
.31
Sepa
rate
dos
e by
four
hou
rs a
fter
cisp
latin
.32
No
evid
ence
of h
arm
with
oth
er d
rug
clas
ses.
Enha
nced
Bio
avai
labi
lity
Co-
enzy
me
Q10
150
mg
CoQ
10 w
ith V
ESIs
orb
Redu
ces
fatig
ue a
nd c
ardi
otox
icity
with
che
mot
hera
py e
sp. w
ith
doxo
rubu
cin.
33 S
uppo
rts h
ealth
y ce
ll si
gnal
ling,
apo
ptos
is a
nd
antio
xida
nt d
efen
ce.34
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy35
and
ch
emot
hera
peut
ic d
rugs
incl
udin
g an
thra
cycl
ines
,36
cam
ptot
heci
n37 a
nd d
oxor
ubic
in.38
No
evid
ence
of h
arm
with
oth
er d
rug
clas
ses.
Lipi
ds a
nd T
ocot
rieno
ls fo
r H
ealth
y C
ell M
embr
anes
an
d C
ogni
tion
Fish
oil
Phos
phat
idyl
serin
eTo
cotri
enol
s
Redu
ces
fatig
ue a
nd n
ause
a; im
prov
es r
espo
nse
rate
to
chem
othe
rapy
and
sur
viva
l rat
e in
pat
ient
s af
ter
treat
men
t.39
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy40
and
ch
emot
hera
peut
ic d
rugs
incl
udin
g do
xoru
bici
n,41
car
bopl
atin
, an
thra
cycl
ines
, vin
orel
bine
and
gem
cita
bine
.42
No
evid
ence
of h
arm
with
oth
er d
rug
clas
ses.
Gin
seng
and
Dan
g G
ui
Ten
Gin
seng
Redu
ces
drug
-indu
ced
kidn
ey d
amag
e an
d pr
even
ts d
amag
e to
th
e bo
ne m
arro
w, th
ymus
and
spl
een
durin
g ra
diot
hera
py.43
,44
Supp
orts
imm
une
func
tion
thro
ugh
the
prod
uctio
n of
nat
ural
ki
ller
cells
and
inte
rleuk
ins.
45
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy
and
chem
othe
rape
utic
dr
ugs
such
as
mito
myc
in, c
ispl
atin
, cyc
loph
osph
amid
e an
d flu
orou
raci
l.46,4
7
No
evid
ence
of h
arm
with
oth
er d
rug
clas
ses.
Nut
rient
s an
d H
erbs
for
Mito
chon
dria
l Fun
ctio
n
Gre
en te
aYe
rba
mat
eKo
rean
gin
seng
Enha
nces
the
sens
itivi
ty o
f tum
ours
and
dru
g-re
sist
ant c
ance
r ce
lls to
che
mot
hera
py.48
,49
Addr
ess
mito
chon
dria
l dys
func
tion
in
canc
er a
nd r
educ
e da
mag
e fro
m o
xida
tive
stre
ss.50
Safe
to u
se c
oncu
rren
tly w
ith r
adio
ther
apy51
and
ch
emot
hera
peut
ic d
rugs
suc
h as
dox
orub
icin
52 a
nd p
aclit
axel
,53
but n
ot w
ith b
oron
ic a
cid-
base
d pr
otea
som
e in
hibi
tors
(gre
en
tea)
.54
No
evid
ence
of h
arm
with
oth
er d
rug
clas
ses.
NA
TUR
AL
MED
ICIN
ES W
ITH
CA
NC
ER T
REA
TMEN
T
Not
e: T
his
list c
onta
ins
only
com
mon
ly p
resc
ribed
nat
ural
sup
plem
ents
in th
ese
patie
nt g
roup
s w
hich
may
be
safe
to u
se.
For m
ore
info
rmat
ion
on th
e tre
atm
ent o
f the
se p
atie
nts,
ple
ase
refe
r to
Trea
tmen
t Pro
toco
ls, T
ech
Dat
a an
d Te
ch S
uppo
rt.PO
SITI
VE
POTE
NTI
ATIO
NC
OU
NTE
RIN
G
SID
E-EF
FEC
TS

150
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 1
High Purity, Low Reflux, Concentrated Fish Oil High Purity, Low Reflux, Concentrated Fish Oil contains high potency omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) produced through state of the art manufacturing techniques to ensure optimal purity. It is an ideal supplement for supporting cardiovascular health and brain function, and reducing inflammation. EPA has benefits for cardiovascular health and lipids, has been shown to play a role in the stabilisation of mood and has an anti-inflammatory effect that may assist in the management of inflammatory conditions such as arthritis. DHA plays a role in lowering triglycerides and has a cardioprotective function. It is also one of the major structural building blocks in brain membrane phospholipids and is required for normal neuronal function. NUTRIENTS THAT MAY ASSIST Concentrated omega-3 triglycerides - fish oil
Providing eicosapentaenoic acid (EPA) Providing docosahexaenoic acid (DHA)
CLINICAL APPLICATIONS BACKGROUND/TECHNICAL INFORMATION EPA and DHA: EPA (20:5 omega3) and DHA (22:6 omega3) are long chain unsaturated fatty acids that are important for cell membrane structure and function (Figure 1). They undergo interconversion in the body, and are important anti-inflammatory agents via modulation of the production of eicosanoids and cytokines.
KEY ACTIONS Anti-inflammatory Cardioprotective – reduces triglycerides, raises HDL, anti-hypertensive,
improves endothelial function, reduces atherosclerosis, antithrombotic and antiplatelet, anti-arrythmic
Nervous system support – supports neurotransmission, reduces amyloid accumulation, supports neural development
KEY APPLICATIONS Inflammatory conditions:
o Autoimmune disease (adjuvant therapy – anti-inflammatories and immunosuppressants)
o Rheumatoid arthritis o Osteoarthritis
Cardiovascular disease: o Dyslipidaemia (adjuvant therapy – statins) o Atherosclerosis o Hypertension o Coronary artery disease
Neural development o During pregnancy and infancy to enhance infant neural development/
cognitive function Mood disorders
o Depression (adjuvant therapy – depression) o Bipolar disorder
Cognitive decline and dementia o Ageing and cognitive decline o Alzheimer’s disease and dementia
APPENDIX 2: TECHNICAL INFORMATION

151
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 2
Figure 1. EPA is a 20 carbon chain with five cis double bonds; the first double bond is located at the third
carbon from the omega end. DHA is a 22 carbon chain with six cis double bonds: the first at the third carbon from the omega end.
Although commonly referred to as essential fatty acids (EFAs), EPA and DHA and are not technically essential as they can be formed in the body via the conversion of alpha-linolenic acid. This conversion process, however, can be very slow, and may be inadequate in certain circumstances: elevated dietary saturated fats, cholesterol, trans-fatty acids, protein deficiency, a glucose-rich diet, alcohol, adrenaline, glucocorticoids, age, diabetes and deficiencies of pyridoxine, zinc and magnesium, which inhibit the desaturase enzymes required for the endogenous formation of EPA and DHA.1 This makes EPA and DHA conditionally essential; meaning that under certain conditions the requirements for these fatty acids may exceed the individual's capacity to synthesise them. The most significant dietary source of EPA and DHA is marine fish: in western societies the rate of fish consumption is often low. Supplementation with EPA and DHA is therefore ideal to optimise the body’s levels of these fatty acids. Australian diet lacks sufficient omega-3 Studies show that most Australian people are not consuming enough omega-3 fatty acids for optimal health, including most Australian children.2,3 The National Heart Foundation of Australia (NHFA) recommends that children should receive the adult recommendation of 500 mg per day of combined EPA and DHA.4 Most Australians, however, fall short of the recommended daily intake, three in five Australians don’t eat the recommended two to three serves of 150 g of oily fish per week required for good heart health5 and less than 10% of children meet these recommendations.6 This dietary deficiency of EFAs is significant as scientific evidence demonstrates that one of the major health benefits of EFAs is the prevention of cardiovascular disease (CVD). In Japan, for example, the incidence of CVD is significantly lower than in countries like Australia where the intake of EFAs is five times lower than Japanese intakes.7 Given the evident health benefits of regular consumption of EPA and DHA and the tendency of the Australian population to consume more meat in preference to fish, supplementation with fish oil is an ideal way to ensure the recommended daily intake of 500 mg of EPA/DHA can be easily met. High Purity, Low Reflux, Concentrated Fish Oil ideally meet this need with an ideal ratio of EPA: DHA providing 500 mg and 200 mg respectively of each per capsule. Requirements during pregnancy The need for EFAs during pregnancy for foetal neurological growth and development is also well recognised, with an additional 200 mg per day of DHA during pregnancy and lactation recommended above the normal adult requirement. Evidence suggests that Australian pregnant and breastfeeding women do not receive adequate DHA, which may affect their own and their babies’ health. For example, Australian women of child bearing age have been found to consume only 80-90 mg a day of DHA.8,9 The developing foetus accumulates approximately 67 mg per day of DHA,10 and researchers suggest DHA will be preferentially diverted from maternal stores to the foetus, which may increase the mother’s risk for post-natal depression. Therefore, a low intake of DHA during pregnancy may place both mother and baby at risk. Requirements during breastfeeding In addition, evidence shows that Australian breastfeeding mothers may not have adequate DHA levels in their breast milk. Studies show that the breast milk of Australian mothers is consistently

152
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 3
lower than the World Health Organisation’s (WHO) recommended level of 0.35% of total fatty acids11 (Figure 2). This is essential not only to reduce the mother’s risk of postpartum depression but also to ensure sufficient fatty acid levels for infant cognitive and physical development.
Figure 2. Australian breast milk DHA content is consistently lower than recommended levels.12 It is also vital to ensure that babies who are not breastfed receive sufficient EPA and DHA for normal growth and development. Fortification of infant formulas with EPA and DHA is not a mandatory requirement in Australia and many contain only low levels, so many babies may need additional supplementary EPA/DHA. Of those infant formulas which do contain added EFA, there is also the potential for these polyunsaturated fatty acids (PUFAs) to be oxidised. Infant formula has been found to contain high amounts of 4-hydroxyhexenal (HHE), a byproduct of lipid peroxidation, with cytotoxic effects potentially damaging to infant metabolism.13,14 INGREDIENTS High quality, purified fish oils: Metagenics uses only high quality, molecularly distilled fish oil as a source of EPA and DHA to ensure purity and batch consistency with low levels of contaminants. In accordance with our leading stance on quality and purity, we have ensured that the fish oil concentrates used in our fish oil products contain well below the Australian allowable levels of pesticides, solvents and heavy metals. The batch testing results for High Purity, Low Reflux, Concentrated Fish Oil are shown compared to the Australian Standard (Table 1).
Table 1: Contaminants levels in High Purity, Low Reflux, Concentrated Fish Oil compared to Australian Standard.
Contaminant High Purity, Low Reflux, Concentrated Fish Oil Australian Standard
Dioxins, Furans, Dioxin-like PCBs 2.83 pg/g 10 pg/g
Heavy Metals Arsenic Lead Cadmium Mercury
None detected None detected None detected 0.01ppm
1.0 ppm 0.5 ppm 0.5 ppm 0.5 ppm
Pesticides (DDT, DDD, DDE) < 0.006 mg/kg 1.0 mg/kg Peroxide Value (PV) <3.0 meq/kg 10 meq/kg Anisidine Value (AV) 4.3 meq/kg 30 meq/kg
0.21 0.21 0.20
0.26 0.260.23
0.35
DHA % IN BREAST MILK
1995 1998 1992 2002 2004 2006 WHO recommended level

153
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 4
Sustainable fishing Metagenics supports sustainable fishing and marine conservation by only sourcing small fish species using sustainable fishing practices. Metagenics fish oils are certified by Friend of the Sea, an independent organisation that audits and certifies products that practice sustainable fishing and reduce their environmental impact. ACTIONS ANTI-INFLAMMATORY Metabolism of long chain PUFAs The dietary intake of fish oil modulates the production of eicosanoids, cytokines and other factors such as peroxisome proliferator-activated receptors (PPARs)* which regulate the inflammatory response. Arachidonic acid (AA) is an omega-6 fatty acid which is a direct precursor to a variety of proinflammatory mediators. Conversion of AA via the cyclooxygenase (COX) enzymes produces the pro-inflammatory series 2 prostanoids (such as prostaglandin E2 [PGE2] prostacyclin 2 [PGI2]) and thromboxanes [TXs], while the lipoxygenases (LOX) system produces the pro-inflammatory series 4 leukotrienes from AA. In contrast, omega-3 fatty acids are incorporated into cell membranes partly at the expense of AA. This leaves less substrate for conversion to inflammatory mediators. The mediators produced from EPA have a different structure from those derived from AA, giving rise to the anti-inflammatory series 3 PGs and TXs and to series 5 LXs (Figure 5). Prostanoids The series 2 prostaglandins derived from AA play a role in swelling and inflammation at sites of injury and excessive levels are associated with many inflammatory conditions. Series 2 prostaglandins also seem to play a role in inducing birth, and in regulating temperature, blood pressure and platelet aggregation and clotting. The series 3 prostaglandins derived from EPA/DHA have anti-inflammatory and antiatherogenic effects and work to attenuate excessive series 2 production. Adequate production of the series 3 prostaglandins confers protection against heart attack and stroke as well as certain inflammatory diseases like arthritis, lupus and asthma. Fish oil enhances suppressive action of paracetamol on series 2 prostanoids A study with rheumatoid arthritis (RA) patients demonstrated that suppression of PGE2 by paracetamol is enhanced by fish oil. Nineteen RA patients were divided into high EPA and low EPA groups as defined by measurement of their serum EPA levels, after consuming a dose of supplemental EPA (providing EPA 2.7 g and DHA 1.8 g daily). Blood samples were then taken immediately before and one hour after ingestion of 1 g paracetamol. The outcome measured was COX-2 generated PGE2 and COX-1 generated TXA2. Paracetamol suppressed the synthesis of these eicosanoids and the suppression was greater in the high EPA group (Figure 3). The authors suggest that the combination of fish oil and paracetamol suppresses PGE2 synthesis by an amount comparable to that from maximum therapeutic doses of non-steroidal anti-inflammatory drugs (NSAIDs).15
*PPARs are members of the nuclear hormone receptor superfamily of ligand-dependent transcription factors which play an important role in the control of numerous cellular processes, including lipid metabolism, glucose homeostasis, cell cycle progression, cell differentiation, inflammation, and extracellular matrix remodeling. PPAR- is implicated in fatty acid metabolism, while PPAR- is important in lipoprotein metabolism, adipogenesis, and insulin sensitivity.

154
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 5
Figure 3. Fish oil enhances analgesic effects of paracetamol.16
Augments actions of NSAIDs In patients with rheumatoid arthritis, long term use of fish oil has been shown to reduce discretionary use of NSAIDs by 40%.17 NSAIDs, paracetamol and omega-3 fatty acids in fish oil, can, in different ways, all inhibit COX, through which the nociceptive eicosanoid PGE2 is produced (Figure 4).18
Figure 4. Mechanisms of inhibition of COX by NSAIDs, long chain omega-3 fatty acids (EPA) and paracetamol.19 Leukotrienes Leukotrienes are a family of proinflammatory lipid mediators of the innate immune response and are important signalling molecules in inflammatory and allergic conditions. The series 4 LTs, such as LTB4, derived from AA, are powerful chemotactic agents (i.e. promote pro-inflammatory leukocyte migration to site of inflammation), whereas LTC4 induces smooth muscle contractions, for example in the airways causing bronchoconstriction in asthmatic patients. The series 5 LTs derived from EPA reduce series 4 LT production (both compete for COX) and are leukotriene receptors antagonists (Figure 5).20 Resolvins and protectins More recently, other EPA and DHA anti-inflammatory metabolites have been identified. Notably from EPA metabolism is resolvin e1 (RvE1), derived from the series 5 LOX. It is generated during the resolution phase of inflammation by dampening of LTB4 signaling on leukocytes.21 DHA-derived inflammation resolving mediator classes include resolvin D2 (RvD2) and protectin D1 (PD1). The production of these DHA-derived lipid mediators are increased in the later stages of an inflammatory response, at which time they enhance the removal of neutrophils and blunt proinflammatory cytokine expression. 22,23

155
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 6
Arachidonic acid
Linoleic acid
EPA
Alpha linolenic acid
DHA
Deep sea fish, grass fed animal products
Diet
and
met
abol
ismM
etab
olite
sCe
ll m
embr
ane
Arachidonic acid EPA
AgeingAlcoholStress
High fat dietNutrient
deficiencies
DHA
PLA2
EPA/DHA free fatty acid
PGE3, PGI3, TXA3,
PGE3, PGF3α
LTB5, FTC5, LTD5,
LTE5
RvE1 RvD2, PD1
Prostanoids
Leukotrienes
Resolvins and protectins
COXLOX
PGE2, PGI2, TXA2,
PGE2, PGF2α
LTB4, FTC4, LTD4,
LTE4
AA derived EPA derived DHA derived
Vegetable oils
Grain fed animal
products
Inflammatory Anti-inflammatory
Anti-inflammatory
PPARTLR
Nf-κB
Anti-inflammatoryAc
tions
Vegetable oils
Figure 5. Metabolism of EFAs and effects on inflammation.
Unmetabolised EPA/DHA display anti-inflammatory properties In addition to modulating ‘downstream’ mediators of inflammation, such as prostaglandins, recent research shows that unmetabolised EPA and DHA regulate ‘upstream’ mediators of inflammation, highlighting a broad spectrum and potent anti-inflammatory action. Nuclear factor kappa B (NF-κB) is a transcription factor known to be a master regulator of inflammation. Activation of NF-κB triggers the expression of numerous pro-inflammatory mediators such as COX 2, interleukin 1 beta (IL-1β) and tumour necrosis factor alpha (TNF-α). Studies show that EPA/DHA attenuate NF-κB via two mechanisms. One key trigger of NF-κB activity is stimulation of transmembrane proteins, toll-like receptors (TLRs). Pathogens, such as lipopolysaccharide (LPS) from gram-negative bacteria, bind to TLRs and induce inflammation via NF-κB. It has been found that the free EPA/DHA fatty acids (i.e. those not metabolised by COX or LOX) act as “safety signals” for TLR in which they bind to the receptor but do not elicit an inflammatory response, i.e. TLR antagonists.24 The other key mechanism of EPA/DHA attenuating NF-κB is via activation of proliferator-activated receptors (PPARs). Stimulation of PPAR blunts NF-κB activity and studies show that free EPA
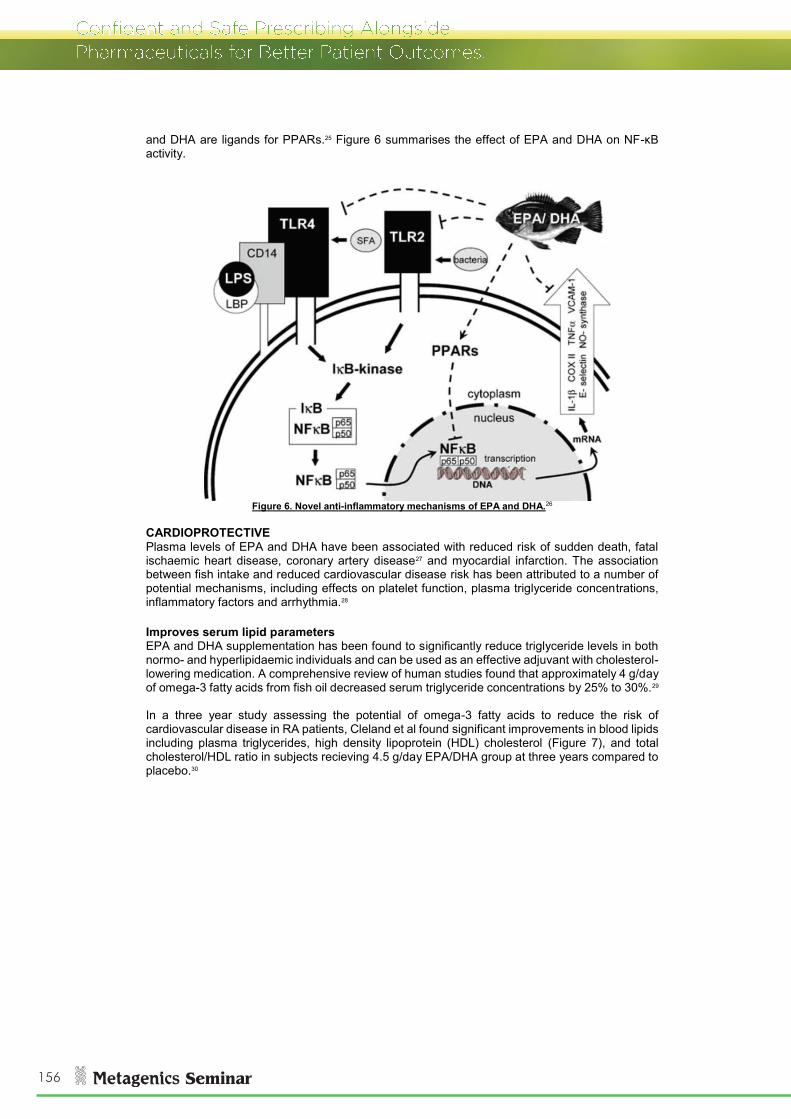
156
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 7
and DHA are ligands for PPARs.25 Figure 6 summarises the effect of EPA and DHA on NF-κB activity.
Figure 6. Novel anti-inflammatory mechanisms of EPA and DHA.26
CARDIOPROTECTIVE Plasma levels of EPA and DHA have been associated with reduced risk of sudden death, fatal ischaemic heart disease, coronary artery disease27 and myocardial infarction. The association between fish intake and reduced cardiovascular disease risk has been attributed to a number of potential mechanisms, including effects on platelet function, plasma triglyceride concentrations, inflammatory factors and arrhythmia.28 Improves serum lipid parameters EPA and DHA supplementation has been found to significantly reduce triglyceride levels in both normo- and hyperlipidaemic individuals and can be used as an effective adjuvant with cholesterol-lowering medication. A comprehensive review of human studies found that approximately 4 g/day of omega-3 fatty acids from fish oil decreased serum triglyceride concentrations by 25% to 30%.29 In a three year study assessing the potential of omega-3 fatty acids to reduce the risk of cardiovascular disease in RA patients, Cleland et al found significant improvements in blood lipids including plasma triglycerides, high density lipoprotein (HDL) cholesterol (Figure 7), and total cholesterol/HDL ratio in subjects recieving 4.5 g/day EPA/DHA group at three years compared to placebo.30

157
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 8
Figure 7. Changes in HDL and triglycerides in subjects receiving 4.5 g/day EPA/DHA (fish oil) compared to a control group.31
In a randomised controlled trial, 44 obese type 2 diabetic patients with metabolic syndrome were treated for three months with either diet alone (the control group) or diet plus EPA 1.8 g daily. Significant reductions of total cholesterol, LDL cholesterol, triglycerides, and remnant lipoprotein particle (RLP)* cholesterol were observed in the EPA group.32 Fish oil enhances action of statins Barter and Ginsberg demonstrated in a meta-analysis the effectiveness of a combination of omega-3 fatty acids with statins in the treatment of hyperlipidaemia, with fish oil enhancing not only the statin-induced reduction of low density lipoprotein (LDL) but also producing additional beneficial changes in other lipid parameters such as high density lipoprotein (HDL), triglycerides and lipoprotein particle size.33 For example, in a randomised, controlled trial, 254 hypertriglyceridemic patients who had received more than eight weeks of stable statin therapy were enrolled to assess the efficacy of adding 4 g/day omega-3 fatty acids to 40 mg/day simvastatin for eight weeks. The main outcome measure was the percent change in non-high-density lipoprotein cholesterol (non-HDL-C) levels from baseline to the end of treatment. It was found that the combination of simvastatin and omega-3, in conjunction with dietary counselling, improved non-HDL-C and other lipid and lipoprotein parameters to a greater extent than simvastatin alone (Figure 8).34
Figure 8. Median percent change in non-high-density lipoprotein cholesterol (non-HDL-C), triglycerides (TG), calculated very-low-density lipoprotein cholesterol (VLDL-C), and low-density lipoprotein cholesterol (LDL-C)
from baseline to the end of treatment.35 * Remnant lipoprotein particles (RLP), also known as remnant lipoproteins or remnant-like particles, are derived from very low density lipoproteins (VLDL) and chylomicrons which are the major carriers of plasma triglycerides. Compared with the nascent triglyceride-rich lipoproteins, RLPs are smaller particles with a higher density and more cholesteryl ester, which gives them more potential atherogenic properties.
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
Control Fish oil Control Fish oil
mm
ol/L
Baseline 3 years
Omega-3 + statin
Placebo + statin
*
*
HDL Triglycerides

158
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 9
Anti-hypertensive Studies in healthy individuals have demonstrated that DHA has an antihypertensive effect. For example, a meta-analysis including 36 studies, 22 of which were double-blind designed and with a duration of over two weeks, showed a significant 4.0 mmHg reduction in systolic blood pressure (SBP) and 2.7 mmHg diastolic blood pressure (DBP) in hypertensive patients (BP >140/90 mmHg), with a median consumption of 3.7 g/day of fish oil. The effect was notably higher in subjects >45 years (Figure 9).36
Figure 9. Average reductions in systolic blood pressure (SBP) and diastolic blood pressure (DBP) in 36
randomised trials of fish oil and blood pressure, grouped by age and hypertension status.37 Bars represent mean, weighted differences in blood pressure change during fish oil supplementation between
the intervention and control groups. The blood pressure-lowering effects of DHA may, in part, be attributed to vasorelaxant properties via modulation of intracellular calcium release and calcium channels in vascular smooth muscle cells and possibly also through the modulation of vasodilatory prostanoids that activate potassium channels.38 Further mechanisms proposed for lowering blood pressure include EPA stimulation of prostacyclin synthesis and increased nitric oxide (NO) production, both of which result in vasodilation.39 Improves endothelial function Fish oils can improve endothelial relaxation by enhancing NO- and non-NO-induced vasodilatation.40 They also protect the endothelium from injury, inhibiting new plaque development as described in the following section. Reduces atherosclerosis development Hyperlipidaemia, hypertension and diabetes mellitus increase the risk of damage to the arterial endothelium. In response, the endothelial cells secrete more prothrombotic factors as well as cytokines and growth factors which attract mononuclear cells and macrophages into the intima. Macrophages then become lipid-rich foam cells, and in conjunction with other changes, a “fatty streak” develops. Proliferation of smooth muscles follows and a “fibrofatty lesion” develops. This is a chronic inflammatory process leading to increased risk of cardiovascular events such as heart attack and stroke. The key players in the development of atherosclerosis are platelet-derived growth factors-A and –B (PDGF-A and PDGF-B) and monocyte chemoattractant protein-1 (MCP-1). Omega-3 fatty acids have been found to reduce PDGF-A and apolipoprotein B mRNA (B mRNA), demonstrating the antiatherosclerotic potential of omega-3 in terms of reduced arterial lumen encroachment.41 Omega-3 fish oil reduces the number of macrophages in atherosclerotic plaque, increasing stability and reducing the likelihood of rupture.42

159
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 10
Antithrombotic and antiplatelet Omega-3 fatty acids decrease platelet aggregation by inducing increased production of PGI3 and suppressing the synthesis of LTB4 and TXA2, both of which promote chemotactic platelet adhesion.43 There is also evidence that fish oil supplementation may enhance fibrinolysis,44 reducing the development of atherosclerotic disease. Anti-arrhythmic DHA is the major omega-3 fatty acid incorporated into myocardial membranes, suggesting an important role for DHA in cardiac function.45 Animal studies with administration of DHA,46 and DHA/EPA47 have been found to have significant anti-arrhythmic effects be due to effects on modulating cardiac electrolyte transport, thromboxane production, and reducing ischaemic acidosis.45,48 NERVOUS SYSTEM SUPPORT DHA comprises 30-40% of the phospholipids of the cerebral cortex and retina, and is an important contributor to membrane fluidity.49 DHA affects neurotransmission, membrane-bound enzyme and ion channel activities, gene expression, and synaptic plasticity; and its deficiency is associated Alzheimer’s disease, hyperactivity and schizophrenia.50 EPA has important roles with neural signalling and synapse formation, and has been shown to help with depressive symptoms.51 Support neurotransmission Research has discovered that the fluidity of neural membranes can modulate several important intracellular events resulting in alteration of the activity of neurotransmitters. Membrane fluidity is largely a function of the amount of DHA incorporated into it, and has been found to affect the binding of enzymes involved in intracellular transduction. Further, membrane fluidity is believed to also influence the response receptors have to their ligands, including receptors for cytokines, neurotransmitters and growth factors. For example, DHA has been shown to affect noradrenergic and serotonergic neurotransmission and is suggested to have a positive effect on behaviour.52 Reduces amyloid accumulation Animal models of Alzheimer’s disease have shown that DHA reduces the intraneuronal accumulation of both amyloid-β and tau – two proteins associated with the development and progression of the disease.53,54,55,55 In support of these findings, additional research shows that DHA-derived neuroprotective signalling helps to counteract proinflammatory, cell-damaging events triggered by cytokine and amyloid peptide factors associated witht this condition. In particular, neuroprotectin D1 regulates the secretion of amyloid-β peptides, resulting in the modulation of inflammatory signalling, neuronal survival, and the preservation of brain cell function.56 PROMOTES NEURAL DEVELOPMENT DHA is a major structural lipid of the brain, and studies have demonstrated that DHA promotes neurogenesis, enhancing brain development in utero.57 Omega-3 fatty acid deprivation may affect brain development at multiple levels, from membrane biogenesis, through gene expression, protection against oxidative stress, and altered neurotransmission. Due to the fact that DHA accretion relative to brain weight is greatest during foetal development and early infancy (Figure 10), it is generally considered that this reflects a critical time during which deficiency of DHA may have long-term consequences for later brain function. From this it is very clear that the critical time for DHA supplementation is the first two years of life.58

160
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 11
Figure 10. DHA (22:6 omega-3) deposits rapidly in the brain in utero and in early childhood.59
APPLICATIONS INFLAMMATORY CONDITIONS AUTOIMMUNE DISEASE Several clinical trials have investigated the benefits of fish oil supplementation in inflammatory conditions which are characterised by a high level of inflammatory cytokines such as interleukin 1 (IL-1) and LTB4. Examples of these conditions include Crohn’s disease, ulcerative colitis, lupus erythematosus, endometriosis and migraine headaches.60,61,62 Belluzi et al, conducted a one year study with 78 patients with inflammatory bowel disease (IBD) who had been in clinical remission for <24 months to assess the effect of fish oil supplementation on their risk of relapse. Patients of this type have about 75% greater risk of relapse in comparison with patients who have been in remission longer. The patients were randomly assigned to receive either 1.8 g EPA and 0.9 g DHA or a placebo. After one year of treatment, 59% of the patients in the fish oil group were still in remission compared with only 26% in the placebo group. RHEUMATOID ARTHRITIS Eicosanoids derived from the omega-6 arachidonic acid play a role in RA, and the efficacy of NSAIDs in the treatment of RA indicates the importance of the pro-inflammatory COX pathway in the pathophysiology of the disease. Several studies have reported anti-inflammatory effects of fish oil in patients with RA, such as decreased LTB4, PGE2 and inflammatory cytokine production, and reduced serum CRP levels.63 There have been a number of clinical trials in RA reporting clinical improvements with fish oil. A meta-analysis of 17 randomised controlled trials assessed the pain relieving effects of omega-3 fatty acids in patients with RA or joint pain secondary to IBD and dysmenorrhoea. The results showed that supplementation for three to four months with a minimum of 2.7 g of combined EPA and DHA significantly reduced patient reported joint pain intensity, duration of morning stiffness, number of painful and/or tender joints, and NSAID consumption. Therefore, for arthritis patients, at least 2.7 g of EPA/DHA is recommended.64,65 A more recent meta-analysis (2012) supported the above results. The authors examined 10 randomised controlled trials involving 183 RA patients and 187 placebo-treated RA controls to assess the effects of omega-3 fatty acids on clinical outcomes in patients with RA. The results demonstrated a reduction in clinical symptoms of RA (as outlined in the previous study) at a minimum dose of 2.7 g/day for a minimum of three months and particularly noted the reduction in NSAID use in RA patients over this time frame.66 Fish oil has also been studied as an adjunct to triple disease-modifying antirheumatic drugs (DMARD) therapy for newly diagnosed rheumatoid arthritis. When participants took 5.5 g daily of combined EPA/DHA for one year alongside their pharmaceutical medication, they experienced a

161
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 12
40% rate of remission, compared to 19% in the control group. Further, the percent of people considered to fail triple DMARD therapy and require progression to higher risk drugs such as pyrimidine synthesis inhibitors and TNF-α inhibitors was only 12% in the fish oil group, compared to 34% in the standard therapy group (Figure 11).67
Figure 11. The impact of adjuvant fish oil prescription in new-onset rheumatoid arthritis – reducing failure of
triple DMARD therapy and improving remission rates. 68 OSTEOARTHRITIS Inflammation is also a characteristic of osteoarthritis (OA). Inflammatory cytokines found in osteoarthritic joints can intensify the pathophysiological processes that result in joint damage. EPA and DHA compete with AA for access to eicosanoid forming enzymes, demonstrating the potential to reduce inflammation.69 A study investigated the relationship between plasma levels of long chain omega-6 and omega-3 fatty acids and MRI evidence of synovitis in the knees of patients with OA. Increased levels of AA were found in those with moderate-to-severe synovitis, whilst an inverse relationship was seen between patellofemoral cartilage loss and total omega-3 levels.70 In a study where animal chondrocytes were challenged with the inflammatory cytokines characteristic in the pathogenesis of OA, such as IL-1 and tumour necrosis factor–alpha (TNF-α), EFAs were found to reduce mRNA expression of these inflammatory cytokines as well as cartilage-degrading proteinases (aggrecanases, matrixmetalloproteinases [MMPs]).71 Further, EFAs also reduce the expression of the inflammatory COX-2 but not the important COX-1, and thus produce a more favourable outcome than NSAIDs, where both are reduced.72 The potential for fish oil to reduce the use of NSAIDs is important, as these drugs – whilst providing a rapid analgesic effect – have not been shown to improve long term outcomes in arthritic patients. In addition, they act as an irritant to the gastrointestinal mucosa with long term use. Further, the suppression of COX activity, specifically the inhibition of PGE2 synthesis by paracetamol – the preferred analgesic for OA - is enhanced by fish oil, with the combined synergistic effect comparable to NSAIDs.73 CARDIOVASCULAR DISEASE ATHEROSCLEROSIS A controlled study with 223 patients, with evidence of lesions detected at coronary angiography, demonstrated a clinically significant benefit from fish oil on the reduction of atherosclerosis, comparable to other measures such as cholesterol-lowering with medication, lifestyle changes and vigorous exercise. This study found that a dose of 1.5 g omega-3 fatty acids per day for two years reduced progression and increased regression of atherosclerotic plaques in those with established coronary disease.74

162
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 13
CORONARY ARTERY DISEASE In a prospective cohort study of postmenopausal women with established coronary artery disease, (n=228) over three years, those with a higher reported fish intake and higher levels of plasma triglyceride and plasma phospholipid DHA had less progression of coronary atherosclerosis.75 In a randomised controlled trial, patients with a total cholesterol of 6.5 mmol/L or greater received either 1.8 g of EPA daily with statin medication (EPA group; n=9326) or statin only (controls; n=9319) with a five-year follow-up. There was a 19% relative reduction in major coronary events in the EPA group, compared with 10% reduction in the control group. Unstable angina and non-fatal coronary events were also significantly reduced in the EPA group. Triglycerides decreased significantly by 9% from baseline in the EPA group and by 4% in controls.76 PREVENT FURTHER CVD EVENTS POST INFARCTION A large scale clinical trial of patients surviving recent myocardial infarction, the GISSI-Prevenzione trial, investigated the efficacy of 1 g/day of omega-3 fatty acids in reducing overall and cardiovascular, cardiac, and coronary mortality. In this study, 11,323 patients were randomly assigned to receive omega-3 fatty acids or no treatment (control) in conjunction with pharmacological treatment and lifestyle advice for 3.5 years.The results found an early (by 90 days) and significant reduction in total mortality reduction compared to controls (Figure 12). Likewise, there was a significant reduction in cardiovascular, cardiac, and coronary deaths after six to eight months in the fish oil group compared to the controls. 77
Figure 12. The early and sustained effect of omega-3 fatty acids on total mortality in patients surviving recent myocardial infarction 78
In a randomised controlled trial, 18 men with a history of myocardial infarction were randomised to placebo or 225 mg of EPA and 585 mg of DHA and daily for four months. The omega-3 fatty acids decreased resting heart rate by 7%, improved heart rate recovery after exercise by 19%, and increased heart rate variability. These changes were described to be consistent with the observed decrease in risk for sudden cardiac death seen with omega-3 fatty acid supplementation.79 Fish oil has shown benefit in randomised controlled trials for the prevention of potentially fatal cardiac arrhythmia. In one study individuals with a recent history of myocardial infarction, given a daily dose of approximately 290 mg EPA and 580 mg DHA, had a significantly lower risk of death (particularly cardiovascular death), non-fatal myocardial infarction, or stroke.80 While, in a trial of 402 patients with a history of ventricular arrhythmias and implanted with cardioverter/defibrillators,* treatment with 2.6 g total of EPA/DHA per day prolonged the time to * An implantable cardioverter defibrillator is used in patients at risk for recurrent, sustained ventricular tachycardia or fibrillation.

163
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 14
the first event (ventricular tachycardia or ventricular fibrillation) and reduced the risk of death from any cause. In the subset of 236 patients who completed 11 months on treatment, there was a 48% reduction in sudden cardiac death compared to controls.81 Postoperative atrial fibrillation (AF) is a common complication of coronary artery bypass graft. Fish oils have been found to significantly reduce the incidence of postoperative AF, and shorten the hospital stay.82 NEURAL DEVELOPMENT AND COGNITIVE FUNCTION Neurodevelopment during pregnancy A review of eight randomised controlled trials comparing cognitive development in controls and in children whose mother received fish oil supplementation was used to extrapolate the results to prenatal intake. It was estimated that increasing maternal DHA intake by 1 g/day increases a child’s IQ by 1.3 points.83 In a randomised controlled trial, pregnant women consumed 300 mg DHA five times a week or placebo from 24 weeks of gestation until delivery. Tests of problem solving and recognition memory were administered to infants at nine months of age. Treatment had significant effects on the performance of problem-solving tasks.84 Another double-blind, randomised, placebo-controlled trial found fish oil during pregnancy has beneficial effects for cognitive development, particularly hand-eye coordination. Ninety eight pregnant women received supplementation with fish oil (2.2 g DHA plus 1.1 g EPA/day) or olive oil from 20 weeks gestation until delivery. Their infants were assessed at 2.5 years of age. Children in the fish oil supplemented group attained a significantly higher score for hand-eye coordination than the placebo group. Eye-hand coordination scores correlated with omega-3 fatty acid levels in cord blood erythrocytes and inversely correlated with omega-6 PUFA.85 Also consistent with evidence suggesting a link between DHA and cognitive development in infancy is a study where toddlers of mothers with higher levels of DHA at birth showed more mature developmental profiles on single-object attention measures and more optimal performance on distractibility assessments than toddlers from mothers with lower DHA (Figure 13).86
Figure 13. Distractability indexes for high- and low- DHA infants.87 Left – percentage of children who turned to the distracting stimulus. Right – duration of looking at the
distracting stimulus. Neurodevelopment during infancy Numerous studies have found positive correlations between blood DHA levels and improvements in cognitive or visual function in infants.88,89,90 A meta-analysis of DHA supplementation of infant formula has also found a significant relation between total DHA and visual acuity at four months of age.91 Trials with formulae providing close to the world wide human milk mean of 0.32% DHA are more likely to yield functional benefits attributable to DHA.92 The device is connected to leads positioned inside the heart: these leads sense the cardiac rhythm, delivering electrical shocks to the heart to restore the normal rhythm.

164
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 15
Neurodevelopment during childhood A study on EPA and DHA found significant benefit in a group of seven to nine year old South African schoolchildren. In this randomised controlled trial, 183 children were instructed to consume 25 g/day of a sandwich spread containing either a DHA-rich fish paste (providing 82 mg EPA and 192 mg DHA/day) or a control paste for six months. The children were subjected to a battery of cognitive tests during the intervention, which measured verbal learning, reading and spelling capabilities. At the end of the trial those receiving the fish paste showed significant improvement in verbal learning scores for recognition and discrimination, significant benefit in spelling tests and a trend for improvement in reading test.93 A randomised controlled trial in four year old children from North America found a similar relationship between cognitive function and DHA levels. In this study, 87 children received either 400 mg/day DHA or placebo for four months. The researchers conducted several cognitive tests on the children at baseline and upon completion of the trial. The primary end point results found that there was no difference between those receiving DHA and the placebo group. The researchers suggest their testing methods may have been too easy as they observed a large “ceiling effect” in several of the measures (i.e. both groups achieved high scores). However, in those receiving DHA, regression analysis revealed a statistically significant positive association between blood level of DHA and higher scores on the Peabody Picture Vocabulary Test (PPVT, Figure 14), a test reflecting listing comprehension and vocabulary acquisition.94
Figure 14. Regression analysis of Peabody Picture Vocabulary Test (PPVT) score versus DHA
blood level in children treated with 400 mg/day DHA at the end of the four month intervention.36
MOOD DISORDERS Animal studies have indicated the mood-regulating effects of EPA in inflammation-associated changes in stress and anxiety behaviour.95 Studies have also shown that people with depression are likely to have a lower serum level of omega-3 fatty acids.96 Depression is also associated with a noted elevation of pro-inflammatory eicosanoids from AA. As EPA competes with AA and inhibits the action of phospholipase A2 it therefore decreases the production of AA pro-inflammatory mediators. These effects may play important roles in the psychophysiology of depression and several studies have demonstrated the benefits of omega-3 fatty acids in conjunction with standard medications improving the overall outcome for patients.97,98,99 DEPRESSION EFAs have been investigated for their efficacy, alone or in combination with selective serotonin reuptake inhibitors (SSRIs) for the treatment of major depression. A meta-analysis revealed that EPA (or higher ratio of EPA to DHA) supplementation may have a stronger antidepressant effect than DHA, with supplements containing more than 50% EPA significantly better than placebo, whereas there was no significant difference with DHA when used as a single therapy.100

165
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 16
EPA enhances response to antidepressant treatment A randomised, controlled trial was conducted to compare the efficacy of EPA versus DHA as adjuvants to maintenance medication treatments for mild-to-moderate depression. Eighty-one mild-to-moderately depressed patients were randomly assigned to receive either 1g/day of EPA or DHA or placebo (coconut oil) for 12 weeks. The primary outcome measure was the Hamilton Depression Rating Scale (HDRS) final score. Patients in the EPA group showed a significantly lower mean HDRS score at study endpoint compared with those in the DHA or placebo groups (Figure 15). Furthermore, response to treatment (defined as a >50% decrease from the baseline HDRS score) was observed in six patients receiving EPA, while none of the patients in the DHA or placebo groups responded to treatment. Overall, these data suggest greater efficacy of EPA compared to DHA or placebo as an adjunctive treatment in mild-to-moderate depression.101
Figure 15. Effectiveness of EPA as an adjuvant to antidepressant medication.102
In another trial, patients with major depressive disorder participated in a four week trial involving the addition of either EPA 2 g/day or placebo to ongoing antidepressant therapy. The effect of EPA was significant from week two of treatment, similar to the time course for effectiveness of antidepressants. The mean reduction of HDRS score in patients receiving EPA was 12.4 points, compared with 1.6 in patients receiving placebo - a clinically meaningful difference.103 Further, an eight week trial was conducted with 28 patients with major depressive disorder, comparing omega-3 fatty acids (9.6 g/day) with placebo, in conjunction with their usual treatment. Those in the treatment group had a significantly decreased score on the HDRS than those in the placebo group.104 Monotherapy in children Depressed children may also benefit from fish oil. Twenty-eight children with diagnosed depression, aged between six and twelve years, were randomised to receive either 380-400 mg EPA and 180-200 mg DHA daily or placebo. The results showed highly significant effects of EPA and DHA on symptoms using the Children’s Depression Rating Scale (CDRS) (Figure 16).105 Among the children on EPA and DHA treatment, seven out of ten had a greater than 50% reduction in CDRS scores compared with zero out of ten of those on placebo. Four out of ten children in the EPA plus DHA group met remission criteria at study exit; no subject in the placebo group met this criteria.

166
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 17
Figure 16. CDRS during 16 weeks of omega-3 or placebo treatment.
Omega-3 versus placebo was significantly different at weeks 8, and weeks 12 and 16.106
BIPOLAR DISORDER In a small open-label study, EPA was also shown to have potential as an adjunctive treatment in the depressive phase of bipolar I disorder (where depression alternates with mania). Twelve bipolar type I patients with diagnosed depressive symptoms were treated with 1.5 to 2 g of EPA for up to six months. Ten patients completed at least one month of therapy. At least a 50% reduction in depression, as measured by the HDRS, was achieved by eight of these within one month, and by another patient within two months.107 High dose fish oil (9.6 g/day) has also shown to improve the short-term course of illness in bipolar disorder with the treatment group having a significantly longer period of remission than the placebo group.108 COGNITIVE DECLINE A prospective study of dietary intake of DHA and EPA was conducted in 210 elderly men (aged 70–89 years). Participants who ate fish had significantly less five year cognitive decline than did non consumers. A significant dose-response relationship was noted between the combined intake of EPA and DHA and cognitive decline, with an intake of EPA/DHA 380 mg/day associated with a 1.1-point difference in cognitive decline as measured via the Mini-Mental State Examination (MMSE).109 A randomised controlled trial has also shown DHA can be useful for the management of age related cognitive decline (ARCD).* Four hundred and eighty five subjects aged ≥55 were randomly assigned 900 mg/day of DHA or a placebo for 24 weeks. The primary measure was changes from baseline in Cambridge Neuropsychological battery (CANTAB) paired associate learning (PAL), a validated visuospatial learning and episodic memory test. The results found that those receiving DHA demonstrated significantly fewer PAL errors compared to the placebo. DHA supplementation was also associated with improved immediate and delayed verbal recognition memory scores. In addition, the cognitive changes were significantly correlated with plasma DHA levels at the end of the trial (Figure 17). The researchers report that the results in CANTAB data from the study indicate an improvement equivalent to being seven years younger in PAL test performance in those administered DHA, compared to a 3.6 year improvement from the placebo (which may be due re-test effect). That is,
* The Diagnostics and Statistical Manual (DSM IV) defines ARCD as an ‘‘objectively identified decline in cognitive functioning consequent to the ageing process that is within normal limits given a person’s age”.

167
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 18
after treatment, the PAL test performance in the DHA group was almost 200% better than that seen in the placebo group. 110
Figure 17. Correlation between plasma DHA levels and changes in paired associate learning (PAL) test in
subjects with age-related cognitive decline (p=0.024).111 ALZHEIMER’S DISEASE AND DEMENTIA The content of DHA has been shown to be decreased in the brain and plasma of patients with dementia. The world-renowned Framingham Heart Study found that low plasma phosphatidylcholine DHA levels are strongly associated with the development of dementia, including Alzheimer’s disease. The top quartile of plasma phosphatidylcholine DHA level was associated with a significant 47% reduction in the risk of developing dementia.112 In a randomised controlled trial, 204 patients with Alzheimer’s disease on acetylcholine esterase inhibitor treatment with an MMSE score of 15 points or more* were randomised to 0.6 g EPA and 1.7 g DHA daily, or placebo, for six months, after which both groups received omega -3 fatty acid supplementation for an additional six months. Although, overall, there was no change in patients with more severe Alzheimer’s disease between the two treatment groups, positive results were seen in a small subgroup (n=32) with very mild Alzheimer’s disease (MMSE >27 points). A reduction in cognitive decline was observed between six and twelve months in this group when receiving omega-3 fatty acid supplementation.113
CAUTIONS/CONTRAINDICATIONS CONTRAINDICATIONS Allergies and Sensitivities: Avoid in people with allergies to fish.114
o Although the fish oil in this formula is highly purified, those with extreme fish allergy (anaphylaxis) would be advised to avoid.
CAUTIONS Anticoagulant/antiplatelet drugs: Clinical trials have shown high-dose fish oil omega-3 fatty
acid consumption to be safe, even when concurrently administered with other agents that may increase bleeding (i.e. antiplatelet or antithrombotic medications such as aspirin and warfarin). The clinical trial evidence suggests that if such an increased bleeding risk exists, the risk is very small and not of clinical significance. For example, 6.8 g of EPA/DHA daily for 6 months showed no adverse effects. However, it is reasonable to monitor patients treated with fish oils and anticoagulants for international normalised ratio (INR) as well as potential adverse bleeding experiences.115,116
* The MMSE is a brief 30-point questionnaire test that is used to assess cognition. The maximum score is 30. A score of 23 or lower is indicative of cognitive impairment.
For full technical data including Cautions and Contraindications and References, go to www.metagenics.com.au (Australia), or www.metagenics.co.nz (New Zealand).

168
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 1
Hydroxyapatite and Soy for Osteoporosis Hydroxyapatite and Soy for Osteoporosis is a high quality calcium supplement for the prevention and treatment of osteoporosis. It contains a range of vitamin and mineral cofactors to support bone health and the integrity of bone extracellular matrix components such as collagen. It consists of a highly bioavailable microcrystalline hydroxyapatite bone extract; an isoflavone-rich extract of soy beans; plus the vitamins and minerals known to contribute to the maintenance of bone density. It is an ideal supplement for both genders, from adolescence, through adulthood, menopause and into the elderly years, and may also assist in the prevention of osteoporosis associated with corticosteroid therapy. HERBS AND NUTRIENTS THAT MAY ASSIST
Glycine max (Soy), seed providing soy isoflavones Hydroxyapatite
providing calcium and phosphorus Ascorbic acid Borax (sodium borate)
providing boron Zinc amino acid chelate (Meta Zn® - Zinc bisglycinate)
providing zinc Manganese amino acid chelate
providing manganese Phytomenadione (vitamin K1) Cholecalciferol (vitamin D3)
ACTIONS AND APPLICATIONS BACKGROUND TECHNICAL INFORMATION
KEY ACTIONS: Reduces bone resorption Promotes bone-building Reduces inflammation Balances oestrogen signalling Promotes calcium absorption and retention Promotes collagen synthesis Promotes bone growth factors
KEY APPLICATIONS:
Osteoporosis Optimising bone growth and improving bone mass Protects against bone loss in corticosteroid therapy Reduces risk of falls and fractures

169
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 2
BONE STRUCTURE AND CONSTITUENTS Bone is a complex connective tissue. Anatomically, there are two types of bone:
Compact bone (also known as cortical bone), which contains dense deposits of minerals, chiefly calcium phosphate, along with type 1 collagen and other long structural molecules called glycosamino-glycans (GAGs). These are arranged in concentric circles around a central osteonic canal which contains the blood and lymph vessels and nerves (Figure 1).
Spongy bone (also known as trabecular or cancellous bone) has the mineral deposits arranged as a system of struts, with bone marrow filling the spaces between (Figure 1). Bone marrow contains the stem cells that gives rise to all the types of blood cells.
Bones are covered with a tissue – the periosteum – which supplies blood and lymph vessels, as well as nerves.
Calcium Calcium is the most abundant divalent cation in the body: the average 70 kg adult contains about 1,000 to 1,400 g of calcium, with 99% of this contained in the bones and teeth.2 This calcium must be obtained from the diet. Sources in the Western diet are primarily dairy foods (yogurt, cheese, milk, etc.); fish eaten with their bones, such as sardines and salmon; and green leafy vegetables such as kale, turnip greens and cabbage.3 Most Australians don’t get enough calcium The average dietary calcium intake in Australia is below the recommended daily intake (see below), particularly in young women and in the elderly of both genders. Additionally, the period of rapid skeletal growth in children is often a time of inadequate calcium intake.4 Nearly half of the adult skeletal mass is accrued during adolescence. In youth, a positive calcium balance is necessary in order to achieve the maximum peak of bone mass and, even when longitudinal growth of bone is completed, the process of mineralisation can last a further four years. This life stage is a window of opportunity for influencing peak bone mass and reducing the risk of osteoporosis in later life.5,6 Absorption of dietary calcium is relatively low in adults: while growing children may absorb up to 75% of the calcium in their diet, adults average only about 30% absorption. Dietary factors that may inhibit calcium absorption include:
Excessive fibre (through binding or increased transit time) Phytates and oxalates (binding) Excessive divalent cations such as zinc or magnesium (which may compete for intestinal absorption) Unabsorbed dietary fatty acids (complex formation) Excretion of calcium by the kidneys may be increased by excessive sodium or caffeine.7
The recommended daily intake (RDI) for calcium for 12-18 year olds, women over 50 years, and men over 70 years is 1300 mg daily. The RDI for men aged 19-70 years and women 19-50 years is 1000 mg daily.8 The recommendation for increased calcium intake in women over 50 and men over 70 is an attempt to offset the impact of osteoporosis, a condition that predominantly affects these age groups. Collagen Collagen is the main component of connective tissue, constituting from 25% to 35% of the protein content of the whole body, and around 28% of bone. While the minerals in bone provide the stiffness, the collagen fibres provide the ability to absorb impacts, i.e., the toughness or resilience.9 Consequently, while bone mineral density (BMD, see below) is certainly a major parameter influencing bone strength, and measurement of BMD is commonly used in that regard, it is not the only factor. Total bone strength derives from the individual contributions from the three-dimensional organisation of the trabeculae (the micro-architecture, see Figure 3),
Figure 1. Bone structure1

170
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 3
mechanical stresses from the way the bones fit together, any micro-damage that may have occurred, and the intrinsic properties of the mineral and collagen matrix.10 Bone is a living, dynamic tissue It is easy to regard bone as a fixed and unchanging ‘scaffolding’ inside the body, but in fact, like every other tissue, it is a site of continual metabolic turnover through the actions of the cells within it. These are responsible for bone production, modelling, and remodelling (maintenance) (Figure 2):
Osteoblasts are derived from mesenchymal stem cells and are responsible for bone matrix synthesis and its subsequent mineralisation. They produce osteoid, comprised of type I collagen (~94%) and osteocalcin, a non-collagenous polypeptide used in the building of the bone matrix. The hardness and rigidity of bone is due to the deposition of hydroxyapatite in the osteoid matrix, forming a crystalline complex of calcium and phosphate. Calcified bone contains about 25% organic matrix (2-5% of which are cells), 5% water and 70% inorganic mineral (hydroxyapatite).
Osteocytes are osteoblasts that become incorporated within the newly formed osteoid, which eventually becomes calcified bone. Osteocytes situated deep in bone matrix maintain contact with newly incorporated osteocytes in osteoid, and with osteoblasts and bone lining cells on the bone surfaces, through an extensive network of cell processes (canaliculi). They are thought to be ideally situated to respond to changes in physical forces upon bone and to transduce messages to cells on the bone surface, directing them to initiate resorption or formation responses.
Osteoclasts are large multinucleated cells, like macrophages, derived from the same haematopoietic lineage as immune white blood cells. Osteoclasts function in the breakdown and resorption of bone and are found attached to the bone surface at sites of active bone resorption. Their characteristic feature is a ruffled edge where active resorption takes place with the secretion of bone-resorbing enzymes, which digest bone matrix.11
In the adult skeleton, the majority of bone surfaces that are not undergoing formation or resorption (i.e. not being remodelled) are lined by bone lining cells.
Figure 2. Bone cells.12
Bone mineral density (BMD) This is the term referring to the amount of mineral matter per square centimetre of bone.13 BMD measurements are most commonly conducted on the lumbar spine and over the upper part of the hip, typically using dual-energy X-ray absorptiometry (DEXA).14 The yearly decline in bone mineral density (BMD) of the lumbar spine and hip in postmenopausal women is reported to be at least 1% and up to 2.4%.15 Therefore, an intervention that reports a small percentage positive change in BMD from baseline (such as a 1% increase), which at f irst may appear negligible, is in fact a clinically significant outcome. OSTEOPOROSIS Although the greatest focus has generally been on post-menopausal women, osteoporosis is a condition which actually affects both men and women. It is characterised by a decline in the amount of bone (Figure 3) and an increase in the susceptibility to fractures.17 Prevalence of osteoporosis Estimates from the Australian Bureau of Statistics’ 2004-05 National Health Survey suggest that about 600,000 Australians
Figure 3. The trabeculae or microarchitecture of healthy vs.
osteoporotic bone16

171
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 4
(3% of the population) have diagnosed osteoporosis. Of these, 85% are women. Osteoporosis is uncommon before the age of 45 years, after which its prevalence significantly increases over time (Figure 4).
Figure 4. Prevalence of osteoporosis, by age group, 2004–05
Based on self-reports of having a doctor’s diagnosis of osteoporosis.18
Osteoporosis often symptomless The actual number of people with osteoporosis is likely to be significantly higher than reported because many people do not know they have it. Osteoporotic bone loss is subtle and often without overt symptoms until a fracture occurs. PATHOPHYSIOLOGY OF OSTEOPOROSIS Fundamentally, osteoporosis occurs when the bone-resorption activity of osteoclasts exceeds the bone-building activity of osteoblasts. As with so many chronic diseases, the fundamental driver of this condition is inflammation: osteoclast function has been shown to be up-regulated through the interaction of the pro-inflammatory cytokine known as the receptor activator of nuclear factor-kappa-B ligand (RANKL) with its functional receptor (RANK). How activation of the RANK/RANKL pathway contributes to osteoporosis (Figure 5):
RANK is a membrane-bound tumour necrosis factor receptor expressed on the cell membrane of osteoclasts.
RANKL (the ligand) binds to RANK (the receptor) on the pre-fusion osteoclast cell’s surface, triggering osteoclast activation. RANKL is considered the key osteoclastogenic cytokine, essential for osteoclast differentiation, activation and survival.19
Osteoprotegerin (OPG) is a secreted decoy receptor of RANKL that serves as a physiological inhibitor of RANKL-driven osteoclast activities.20
Figure 5: The RANK–RANKL-OPG signalling pathway. To generate activated osteoclasts, RANKL is secreted by osteoblasts
and osteocytes in bone, and these bind to its natural receptor, RANK, on the surface of pre-fusion osteoclasts. To fine-balance this activation system, osteoblasts and osteocytes also secrete OPG, which is a natural decoy receptor for RANKL and
prevents binding of RANKL to RANK.21

172
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 5
In bone, osteoblasts are the predominant gatekeepers of bone resorption signals. In response to various endocrine, paracrine and cytokine signals (probably including mechanical stress), osteoblasts, osteocytes and/or marrow stromal cells modulate the production of OPG and RANKL, with the ratio of these factors ultimately governing the level of osteoclast activity. The resorptive effect reflects the binding of non-OPG-bound, membrane-associated or soluble RANKL to RANK on osteoclasts and/or their precursors.22 The inflammatory trigger for this process can be traced back to oestrogen deficiency In the typical menopausal onset of osteoporosis, the inflammatory trigger that activates RANKL is provided by oestrogen deficiency. Oestrogen normally stimulates OPG production in osteoblasts and thus exerts anti-resorptive effects on bone.24 A lack of oestrogen removes this inhibitory effect of OPG on bone breakdown, and also results in T cell activation and subsequent secretion of numerous cytokines, including RANKL and TNF-α, two cytokines with pronounced osteoclastogenic activity (Figure 6).25 Oestrogen receptor beta activation is desirable for bone health Oestrogen can bind to two receptor types: alpha (α) or beta (β), through which it modulates the expression of genes, stimulating DNA transcription and subsequent protein and enzyme production. Oestrogen receptor alpha (ERα) is expressed throughout the body, being found in particularly high amounts within the endometrium, breast, hypothalamus and ovary.26 It is pro-inflammatory and associated with aberrant cell proliferation and malignancy, i.e., oestrogen-dependent cancers.27 ERβ is primarily found within the kidneys, brain, bone, heart, lungs, endothelial cells and intestinal mucosa.28 It opposes ERα activation and enhances oestrogen detoxification, thereby having a beneficial anti-inflammatory (and therefore anti-osteoporotic) effect.29 Less active polymorphisms of ERβ have been associated with an increased risk of osteoporosis.30 Oestrogen deficiency causes calcium losses and induces secondary hyperparathyroidism The extra-skeletal effects of oestrogen deficiency on bone loss are mainly due to increased renal calcium excretion and decreased intestinal calcium absorption. Oestrogen deficiency is accompanied by a continuous increase in serum parathyroid hormone (PTH) levels: oestrogen seems to have a direct depressive action on the parathyroid gland, which is lost in oestrogen-deficient conditions. Additionally, oestrogen deficiency increases the sensitivity of bone to PTH. The action of PTH is to mobilise calcium from bone stores through up-regulating RANKL to increase osteoclast activity.31 INGREDIENTS MICROCRYSTALLINE HYDROXYAPATITE Hydroxyapatite and Soy for Osteoporosis contains microcrystalline hydroxyapatite (MCHA) concentrate, a superior source of high quality and highly bioavailable natural calcium with several advantages over other bone health supplements. Itself derived from whole bone, MCHA is obviously the ideal starting material for the construction – or reconstruction - of bone. It contains all the natural elements of healthy bone in a protein-mineral complex. MCHA is a crystalline calcium and
Immune cells
Osteoclasts
Osteoblasts
RANKL
RANK
ER
OESTROGEN
ER
OPGInflammatory
cytokines
Bone resorption
Figure 6. A model of the effects of oestrogen on bone loss.23
ER = oestrogen receptor; OPG = osteoprotegerin; RANKL = receptor activator of nuclear factor-kappa-B ligand; RANK =
receptor activator of nuclear factor-kappa-B
Table 1: A typical breakdown of hydroxyapatite32
Calcium 26 % Type 1 collagen 23% Phosphorus 12% Glycosaminoglycans 3.7% Magnesium 0.4 % Zinc 0.0064% Iron 0.00039% Boron 0.00014%

173
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 6
phosphorus matrix that contains, on average, 26% calcium as calcium phosphate: providing calcium and phosphorus in the ideal 2:1 physiological ratio of these elements (Table 1).33 MCHA is processed by freeze drying so that the low temperatures maintain the naturally occurring nutrients and minerals in their original form.34 Trace minerals come ‘pre-packaged’ in MCHA In addition to the key biologically active constituents in MCHA, it also contains a range of naturally occurring trace minerals, including zinc, iron, boron, chromium, copper, manganese, silicon, sulfur and others, in the same physiological proportions as found in healthy bone.35 Some of these are of particular importance to bone health and have been supplementally boosted in this formula. Proteins and growth factors enhance the effectiveness of MCHA MCHA is more than just a calcium mineral supplement, and its clinical success is associated with the presence of specific bone proteins found naturally within the bone matrix. These comprise type 1 collagen, bone amino acids, growth factors and glycosaminoglycan molecules. Properly processed, a whole bone extract contains a quantifiable spectrum of these protein constituents.36 This is important because research has emphasised the link between intact proteins in finished bone extracts and positive effects on bone density.37 MCHA is 23% type 1 collagen, the predominant type of collagen found naturally in healthy bone. The glycosaminoglycan molecules include chondroitin sulphate, and the predominant amino acids are glycine, hydroxyproline, proline and glutamic acid. Growth factors identified in whole bone extracts such as microcrystalline hydroxyapatite include transforming growth factor- -like growth factors I and II.38,39 Vacuum drying retains the integrity of heat sensitive proteins, including growth factors, maximising the effectiveness of MCHA.40 MCHA quality and purity The raw material for our MCHA concentrate is sourced from New Zealand pasture-fed cattle that are raised without the use of antibiotics or hormones, and government veterinary-signed health certificates accompany each batch of product to verify the safety and disease-free status of the product.* MCHA has been independently tested, by the most sensitive laboratory methods available, for heavy metals (Table 2), for microbial contaminants, and to ensure there are no residues of commonly used veterinarian-administered therapeutic antibiotics and hormone growth promoters.
Table 2: Analysis of naturally occurring heavy metals in MCHA compared to standard
Specification standard MCHA41 Lead Cadmium Mercury
<0.8 ppm <0.1 ppm <0.05 ppm
0.24 ppm <0.01 ppm
<0.05 ppm
SOY ISOFLAVONES Glycine max (Soy Isoflav-OneTM) extract is a non-genetically modified soybean extract containing a minimum of 40% isoflavones. Isoflavones are more accurately classified as selective oestrogen receptor modulators (SERMs) than as phytoestrogens. Rather than exerting a direct oestrogen-like action, they have an amphoteric effect, decreasing the impact of oestrogen dominance (as in the reduction of hormonally-driven cancers42,43), yet increasing oestrogenic stimulation in deficient conditions, such as osteoporosis. This selectivity of action of isoflavones may stem in part from their preferential binding to and activation of oestrogen receptor-beta (ERβ) compared with oestrogen receptor-alpha (ERα).44 Binding of isoflavones such as genistein and daidzein to ERβ is thought to be the mechanism behind both their anti-proliferative effects and the enhancement of bone health in post-menopausal women.45 In an in vitro study, it was found that most of the treatment effects of genistein disappeared from rat osteoblasts when ERβ was silenced, which identifies ERβ as the receptor mediating the beneficial effects.46
* For example, this product is certified free of bovine spongiform encephalopathy (BSE).
174
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 7
OTHER COFACTORS This formula contains additional cofactors – zinc, boron, manganese, vitamins C, D3 and K1 – which, in addition to their many other valuable functions, are important for healthy bones. Zinc is a mineral that is involved in around 300 enzyme reactions in the body, including many antioxidant enzymes required for protection of body tissues against free radical-induced damage. Zinc is also part of the ‘zinc finger motifs’* within DNA transcription factors, and is thus important for building new tissue.47 Signs of zinc deficiency include growth retardation, skeletal abnormalities and defective collagen synthesis.48 Dietary zinc intake and plasma zinc concentrations have been found to be correlated with BMD; and were found to be lower in men with osteoporosis.49 Boron has important roles in bone health and may be significant in the prevention of osteoporosis. It interacts with calcium, vitamin D and magnesium – all nutrients that are vital for bone health. It also has roles in cell membrane function and stability, metabolic regulation, and mediation of the inflammatory response.50 Manganese is another important cofactor for bone health. It is required for the biosynthesis of glycosaminoglycans in bone matrix formation, and is a cofactor for several enzymes in bone.51 Manganese deficiency is associated with increases in serum calcium, phosphorus and alkaline phosphatase.†,52 Vitamin C is essential for normal collagen formation. It is required for the synthesis of collagen components hydroxyproline and hydroxylysine. Hydroxyproline serves to stabilise the collagen triple helix and its absence results in structurally unstable collagen, whilst hydroxylysine is necessary for formation of intermolecular crosslinks between collagen fibres. Failure of hydroxylation due to vitamin C deficiency results in tissue breakdown, epitomised by the ascorbate deficiency disease scurvy, characterised by bleeding gums, tooth loss and joint damage.53 Vitamin D3 (cholecalciferol) intake has long been associated with bone mineral density and bone turnover, skeletal growth and bone strength. Vitamin D insufficiency occurs with high frequency throughout Australia.54 Deficiency is associated with:
Rickets - softening of the bones in children leading to weakness, deformity and fractures Osteomalacia - softening of the bones due to defective bone mineralisation in adults Osteoporosis - reduced BMD and disrupted bone micro-architecture, which predisposes to fracture;
and Muscle weakness that may contribute to falls in the elderly, which – when associated with
osteoporosis – increases the likelihood of fractures.55,56 The precursor for vitamin D, cholecalciferol, is obtained from the diet or formed in the skin, and is subsequently hydroxylated first in the liver to 25-OH D3 (calcidiol); then again in the kidney to form the active vitamin D metabolite 1,25-(OH)2 D3 (calcitriol). Calcitriol facilitates the active absorption of calcium in the intestine by stimulating the synthesis of calcium binding protein (calbindin), and, along with parathyroid hormone, it helps regulate blood calcium and phosphorus concentrations, acting on bone, intestine and kidney.57 Vitamin K1: Phytomenadione Phytomenadione (vitamin K1, also called phytonadione or phylloquinone) is the naturally-occurring plant form of vitamin K, a fat-soluble vitamin that belongs to a family of structurally similar compounds. Vitamin K is an essential requirement for bone development and maintenance. It is an important cofactor in the action of the enzyme γ-carboxylase, whose carboxylating action activates a number of proteins, such as elements of the blood clotting cascade. It is also an essential requirement for the conversion of osteocalcin, the principal non-collagenous matrix protein in bone, to its functional form, which appears to act as a deposition site for hydroxyapatite crystals.58 Vitamin K deficiency leads to an increase in under-carboxylated osteocalcin, a less functional form detected in osteoporotic patients that is used as a predictor for risk of fracture.59 Poor vitamin K status has been associated with the low BMD and high prevalence of osteoporosis found in Crohn’s disease patients.60 The presence of subclinical vitamin K deficiency is emerging as a widespread issue, and is exaggerated by an ageing population.61.
* Zinc fingers are small protein structures that use one or more zinc ions to help stabilise their folds. They are classified into several different structural families (zinc finger proteins) and typically function as interaction modules that bind DNA, RNA, proteins, or small molecules. † Alkaline phosphatase is a zinc-dependent enzyme involved in phosphate metabolism. Increased levels are associated with skeletal bone changes.

175
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 8
ACTIONS INHIBITS BONE RESORPTION Soy isoflavones decrease bone resorption The effects of isoflavones on bone are thought to be through direct effects on the bone cells, rather than from influences on calcium absorption. Isoflavones have been shown to inhibit osteoclast proliferation and decrease bone resorption by osteoclasts.62 Also, by binding to ERβ in osteoblastic cells, isoflavones induce production of OPG, which competes with RANKL and prevents bone resorption. PROMOTES BONE BUILDING MCHA builds better bone The benefit of a whole bone extract with preserved organic factors has been shown in an animal study that compared MCHA to both a bone mineral complex (obtained by reducing MCHA to ash to remove its organic constituents), and to simple calcium carbonate, in the healing of standardised bony defects produced in the distal femoral epiphyses of rabbits.
Control group: 84th day After clearly delayed bone formation, some coarse trabeculae with irregular shape and poor mineralisation developed. Only a small reaction occurred in the surrounding spongiosa.
Calcium carbonate group: 84th day The concentric growth of a dense trabecular meshwork began early but made little progress. Fibrous cartilage occupies the centre of the defect
Bone mineral group: 84th day An irregular, partly delayed, formation of coarse bone fills about 75% of the defect
MCHA group: 84th day The newly formed bone in the defect is already largely remodelled and the wide-meshed cancellous bone is now connected with the surrounding spongiosa.
Figure 7: Photomicrographs of femoral sections, prepared using a fluorescent microscope, showing that only treatment with MCHA resulted in significant improvements in bone healing.63
All three active treatment groups showed significantly improved mineralisation compared to an untreated control group (Figure 7). However, only MCHA resulted in significant improvements in the pattern and quality of bone healing. This indicates that MCHA has a beneficial effect on the process of bone healing; an effect lost if the organic components of the compound are destroyed, or if pure calcium carbonate is substituted. This strongly supports the osteogenic effects of the organic (protein) components of MCHA, enhancing the utilisation of mineral intake.64

176
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 9
MCHA increases markers of bone building Osteoblasts produce osteocalcin as part of bone-building, a process dependent on vitamins D and K.65 In a three year clinical trial, women aged over 65 years with osteoporosis of the lumbar spine or femoral neck were given either 712 mg elemental calcium/day from MCHA or 1000 mg elemental calcium/day from calcium carbonate. Both groups also received a vitamin D supplement.66 The results found that levels of serum osteocalcin increased to a greater extent in the MCHA group compared with the calcium carbonate group (Figure 8).
Figure 8: Changes over time and between-group differences in mean serum osteocalcin levels.67
CC=calcium carbonate; MCHA = microcrystalline hydroxyapatite. * p < 0.05 vs CC; ** p < 0.05 vs baseline.
Isoflavones promote osteoblast proliferation and activity Bone cell cultures have shown that isoflavones induce pre-osteoblasts to differentiate into osteoblasts and increase osteoblast mineralisation.68 The combination of soy with vitamin D improves bone mineralisation Combining isoflavones with vitamin D3 increases the proliferation of cultured pre-osteoblasts.69 One proposed mechanism is that phytoestrogens increase vitamin D receptor (VDR) and vitamin D metabolites in bone cells. Genistein, for instance, has been shown to up-regulate VDR transcription and expression.70 It is proposed that soy phytoestrogens, in combination with vitamin D, may synergistically induce osteoblast activation and prevent pre-osteoclast and osteoclast differentiation, through the increase of vitamin D metabolites, VDR, and ER actions (Figure 9).
Figure 9. Possible mechanisms of the effect of soy isoflavones and vitamin D on bone metabolism.
Soy isoflavones and vitamin D (VD) can synergistically stimulate bone formation through inducing 1,25(OH)2-D synthesis and receptor (VDR) expression. Binding of VD to VDRs can induce osteoblast activity and bone formation. Also, bone resorption may be reduced through inducing oestrogen receptor (ER) expression, which is affected by VD and soy isoflavones. An increase in ER can lead to an increase in OPG formation and thus prevent osteoclast (OC) maturation, resulting in less bone resorption.71
MCHA

177
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 10
REDUCES INFLAMMATION In animal studies, a soy-derived isoflavone-rich powder and the isolated isoflavone genistein were effective in decreasing the leukocyte number in mouse blood and lowering the secretions of inflammatory markers, including IL-1, IL-6, NO, and PGE2. Possible mechanisms are:
Activation of PPAR-γ, a transcription factor that reduces pro-inflammatory gene expression Inhibition of cyclooxygenase-2 (COX-2), a major pro-inflammatory enzyme Reduced iNOS protein expression.72
Anti-inflammatory actions of vitamin D Vitamin D deficiency has been linked to various inflammatory diseases. A recent study showed that physiologic levels of vitamin D (75-125 nmol/L of 25(OH)D3) can modulate LPS-induced inflammatory cytokine (IL-6 and TNF-α) production in human monocytes. The study identified the up-regulation of MAPK phosphatase-1 as a novel mechanism by which vitamin D inhibits inflammation. The authors concluded that patients with chronic inflammatory diseases that are vitamin D deficient (<50 nmol/L) may benefit from oral supplementation of vitamin D to get their serum vitamin D level above 75 nmol/L.*73 BALANCES OESTROGEN SIGNALLING Isoflavones are ERβ agonists Genistein is a phytoestrogen which binds to ERs with an affinity for ERβ of 87% and just 4% for ERα, compared to oestradiol. As ERβ activation down-regulates ERα activity, genistein is therefore able to decrease ERα activation and block the binding of more potent oestrogens at the same time.74,75As discussed earlier (page 5), up-regulation of ERβ is beneficial for bone health and enhances bone mineral density.76 PROMOTES CALCIUM ABSORPTION AND RETENTION Better bioavailability and absorption with MCHA MCHA has been shown to be superior to calcium gluconate in enhancing calcium uptake in a study of 15 elderly osteoporotic patients. The participants were first given calcium gluconate, delivering 93 mg elemental calcium, and two weeks later MCHA, delivering 78 mg elemental calcium. Calcium absorption was measured by using a calcium tracer (47Ca). Absorption of the tracer was significantly greater in the MCHA group than in the calcium gluconate group at both of the time intervals (both p<0.001; Figure 10). Possible explanations of the enhanced absorption of calcium from MCHA include the fact that it contains phosphorus (which the gluconate does not), or that components of the organic matrix in MCHA may increase absorption.78 Vitamin D controls calcium homeostasis and bone metabolism. It increases the absorption from the gut of both calcium and phosphorous, and together with parathyroid hormone, regulates calcium and phosphorous metabolism. These actions raise plasma levels to support bone mineralisation and prevent hypocalcaemia. 79 Boron plays a role in calcium balance through a number of different mechanisms, in particular, helping to reduce urinary calcium excretion and enhancing calcium absorption.80 Its influence on vitamin D and magnesium metabolism may be influenced by its effects on cell membrane activity.81 In addition, boron’s influence on steroid hormone production may enhance its role in bone support through the reduction of calcium and magnesium excretion.82
* Our general recommendation is to aim for serum levels of vitamin D between 100 and 150 nmol/L
Figure 10: Mean 47Ca absorption results expressed as percentage of administered dose per litre of plasma.77
After 30minutes
After 2hours
Calcium gluconate 0.52 1.3MCHA 1.21 2.11
0
0.5
1
1.5
2
2.5
% d
ose
abso
rbed

178
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 11
Vitamin K supplementation reduces urinary calcium excretion and bone resorption, and increases bone mass.83 PROMOTES COLLAGEN SYNTHESIS Vitamin C is essential for the synthesis of the key bone protein, collagen. The major amino acid constituents of collagen are glycine, proline, hydroxyproline and hydroxylysine. The formation of these last two requires iron to carry out the oxidation, and use ascorbic acid (vitamin C) to return the iron to its oxidised state. Deprivation of ascorbate leads to deficiencies in proline hydroxylation, which leads to less stable collagen that can manifest as the disease scurvy. The assembly of the triple-helix collagen fibril is an elegant and complex process. Other nutritional requirements include zinc and manganese. Zinc appears to reduce the activity of collagenase enzymes, which degrade type 1 collagen, thereby promoting increased collagen levels.84 Manganese is required for the activation of prolidase, an enzyme that functions to provide proline for collagen formation.85 PROMOTES BONE GROWTH FACTORS Zinc can increase bone growth factors and bone matrix protein, which are involved in the stimulation of bone formation and proliferation of osteoblastic cells. Zinc may modulate the anabolic effect of insulin-like growth factor I (IGF-1) in osteoblasts, and may enhance the proliferative effect of oestrogen on these cells.86 The process of osteoporosis and the interaction of these herbs and nutrients in Hydroxyapatite and Soy for Osteoporosis with these processes are illustrated in Figure 11.
Osteoblasts
Calcium absorption and
deposition
MCHA proteinsZinc
ManganeseVitamin C
Immune cells
Bone matrix formation
Osteoclasts
RANKL PTH
Bone Mineral Density
Soy isoflavonesMCHA calcium
Vitamin DVitamin K
Boron
Bone growth factors
RANK
ERVDR
ZincOPG
Inflammation
Bone resorption Bone growth and repair
- +
ER
Soy isoflavonesVitamin D
Key: StimulatesInhibitsFacilitates
Soy isoflavones
Figure 11: A summary of the processes involved in the regulation of bone growth and loss, and the actions of Hydroxyapatite and Soy for Osteoporosis
VDR = vitamin D receptor; ER = oestrogen receptor; PTH = parathyroid hormone; RANKL = receptor activator of NFκB ligand; RANK = receptor activator of nuclear factor-kappa-B; OPG = osteoprotegerin

179
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 12
APPLICATIONS OSTEOPOROSIS Calcium supplementation is a proven therapy to prevent bone loss A meta-analysis of 15 trials of at least 12 months in duration, involving a total of 1806 postmenopausal patients, has confirmed that calcium supplementation is correlated with a positive effect on bone density post-menopause, with a mean 2.05% increase in total body bone density over two years, a 1.66% increase in the lumbar spine, and 1.91% in the distal radius.*87 MCHA is the most effective form of calcium Prevention of osteoporosis through slowing of post-menopausal bone loss has been found to be achieved more significantly with MCHA than with calcium carbonate.88,89,90 A three year study was conducted to compare the effects of MCHA to calcium carbonate on BMD in women with osteoporosis. Subjects were women aged over 65 years with osteoporosis of the lumbar spine or femoral neck. The treatment group received MCHA at a dose of two 830 mg tablets every 12 hours (712 mg elemental calcium per day).† The control group received calcium carbonate at a dose of 500 mg of elemental calcium every 12 hours (1000 mg elemental calcium per day). Both groups also received a vitamin D supplement.92 The results found that BMD reduction was significantly less over three years for the hydroxyapatite group than for those on calcium carbonate (Figure 12). The conclusions of the study were that MCHA has a greater anabolic effect on bone than calcium carbonate, and that treatment was shown to be more effective in increasing serum osteocalcin levels than calcium carbonate. Subsequent improvement in bone quality could potentially lead to a reduction in fracture risk.93 Long-term treatment with MCHA safe and effective Long term benefits and safety of MCHA are confirmed by a retrospective four-year follow-up study of a cohort of 112 post-menopausal women in an osteoporosis program that included health and dietary advice, plus supplementation with 3.32 g MCHA daily.† A progressive and statistically significant increase in distal forearm BMD was observed with mean trabecular T-scores‡ increasing from baseline values of -1.27, to -0.86 at the end of the four-year follow-up period. These results indicate significant improvements in BMD in these patients.94 MCHA augments the effects of hormone replacement therapy on BMD MCHA at 3.32 g daily (712 mg elemental calcium)† has been shown to give further effects in increasing vertebral bone mass in postmenopausal women, when given in conjunction with oestradiol hormone replacement therapy. Over the 12 month treatment period, the oestrogen and MCHA group achieved a 4.7% increase in BMD at the lumbar spine – more than twice that of the oestrogen alone group (2.2%). There was a 1.1% decrease in BMD in the control group.95
* See earlier note on BMD (page 4) to understand the significance of these results † Hydroxyapatite and Soy for Osteoporosis provides 4 g MCHA and 1000 mg elemental calcium daily ‡ A T-score is the measurement of an individual’s bone density relative to that of a healthy 30-year-old.
Figure 12: Changes in mean BMD at the lumbar spine.91
CC=calcium carbonate; MCHA = microcrystalline hydroxyapatite
MCHA CC

180
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 13
Meta-analysis confirms soy isoflavones increase BMD A meta-analysis including data from1240 menopausal women revealed that daily ingestion of an average of 82 mg soy isoflavones* for 6-12 months significantly increased spine BMD by an average of 2.38% (p=0.001) compared with controls (Figure 13).97 Representative of these studies is a randomised, placebo-controlled clinical trial by Harkness et al, in which a crossover design was used to test the effect of soy isoflavones (110 mg/day of a combination of genistein/daidzein/glycitein) on bone formation, bone resorption, bone mineral content, and BMD for 6 months.98 Those subjects supplemented with isoflavones showed an average decrease in urinary concentrations of type 1 collagen α1-chain helical peptide (HP), a marker of bone resorption, of 37%. This decrease in bone resorption represents a return to urinary HP levels found in premenopausal women.99 Overall, the isoflavone treatment had a positive effect on bone mineral content and BMD. It produced a 3.5% increase in total spine bone mineral content compared with pretreatment levels. In addition, there were significant treatment effects at select lumbar sites, including L2 and L3 spine BMD, and a 1% increase in total spine BMD with treatment. These results are similar to those achieved with low-dose conjugated oestrogens (hormone replacement therapy).100 Vitamin D improves effects of calcium on bone density Vitamin D supplementation may decrease bone turnover and increase bone mineral density. Several randomised placebo-controlled trials with vitamin D and calcium show a significant decrease in fracture incidence.101 In association with calcium, vitamin D may be beneficial for the improvement of BMD in elderly patients with recognised vitamin D deficiency. A randomised double-blind placebo-controlled study found that combined supplementation with 1000 mg of elemental calcium (as carbonate) and 800 IU of vitamin D daily† for 12 months, in women over the age of 65 years with vitamin D deficiency (median serum level of just 17.5 nmol/L)‡, resulted in substantial increases in BMD. Forty-six per cent of the participants had osteoporosis. The median increase in BMD was significantly greater in the supplemented group than in the placebo group (Figure 14). Similarly, markers of bone turnover were significantly reduced in the treated group compared to the placebo group.102
* Hydroxyapatite and Soy for Osteoporosis provides 90 mg isoflavones daily, including daidzin, glycitin, genestin, daidzein, glycetein, and genestein. † Hydroxyapatite and Soy for Osteoporosis provides 1000 IU vitamin D daily. ‡ A vitamin D blood serum level of 17.5 nmol/L is severely deficient – ideal levels are 100-150 nmol/L
Figure 13: Effects of soy isoflavones on spine BMD (%).96
Total (95% CI)

181
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 14
Figure 14: Percent change in BMD over 12 months of supplementation with vitamin D and
calcium103 Calcium supplementation can also improve premenopausal bone mass Sufficient calcium intake has benefits for bone mass, not just in post-menopausal women, but also pre-menopausally. Evidence confirms that calcium intake is positively associated with bone mass in premenopausal adult females.104 Calcium supplementation can benefit men as well as women In both men and women, a calcium supplement of 750 mg daily has been found to prevent loss of BMD, reduce femoral medullary expansion, secondary hyperparathyroidism, and high bone turnover.105 OPTIMISING BONE GROWTH AND IMPROVING BONE MASS Adolescence The following randomised controlled trials illustrate the benefits of calcium and vitamin D supplementation in adolescence. Calcium supplementation of adolescent boys increases skeletal growth, resulting in greater stature and bone mineral acquisition, while in girls it enhances BMD.
In 143 boys aged 16-18 years, compared to placebo, 1000 mg calcium per day (as carbonate) for 13 months resulted in changes in anthropomorphic measurements, such as greater height (+0.4%, equivalent to an average of 7 mm), lean mass (+1.3%), and lumbar spine bone area (+1.5%). These changes were associated with greater bone mineral content throughout the body as measured via dual-energy x-ray absorptiometry, with effects proportionate to the increase in growth.106
A 15-month study of 144 adolescent girls, with an average age of 17.3 years, found calcium supplementation (1000 mg calcium per day as carbonate) significantly increased size-adjusted bone mineral content by an average of 2.6%. Individual increments were: lumbar spine, 1.9%; ultradistal radius, 1.3%; total hip, 2.7%; femoral neck, 2.2%; trochanter, 4.8%.107
Another example of the enhancement of BMD in female adolescents with calcium supplementation has been found in a study of forty-two pairs of twins. One of each twin (mean age 14 years) was given calcium 1000 mg (as carbonate). At the end of the first 6 months, there was a significant within-pair difference of 1.53% at the spine and 1.27% at the hip. The greatest effect was seen in the first 6 months; thereafter the difference was maintained for the 18 months of the study.108
Vitamin D3 can also augment BMD in adolescents. In a randomised controlled trial of 228 adolescent girls (mean age 11.4 years), vitamin D3 supplementation with 400 IU daily for one year was found to significantly augment bone mineral content in the measured locations of femur (+17.2%) and lumbar spine (+12.5%). It appeared to do this mostly by decreasing bone resorption, as indicated by the concentration of biochemical markers.109
PROTECTS AGAINST BONE LOSS IN CORTICOSTEROID THERAPY Long-term treatment with exogenous corticosteroids is associated with osteoporosis. Calcium supplementation may reduce the loss of bone mass that occurs with this treatment. A controlled clinical trial of 40 patients at
2.98
1.19
0.86 0.
99
-0.2
1
-0.8
3 -0.5
6
0.11
Vitamin D plus Calcium Placebo
L2-L4 FEMORAL NECK TROCHANTER WHOLE BODY

182
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 15
risk of osteoporosis because of long-term treatment with prednisolone (5 to 20 mg/day) compared treatment with 6 to 8 g MCHA for 12 months (n=32) to untreated controls (n=8). Just over two-thirds of the patients had back pain prior to the trial. In the MCHA-treated group, there was a dramatic and significant reduction in pain, with only 10% of the patients with initial back pain having continued pain after 12-months' MCHA treatment (Figure 15). In comparison, in the control group, back pain severity increased during the trial in three patients and was unchanged in a fourth. Measures of cortical thickness showed small, insignificant decreases during MCHA treatment, compared to more marked decreases in the control group (Figure 16).110
Figure 15: Mean back pain severity scores before
and during the trial period in 23 patients111 Figure 16: Change in mean cortical thickness
during the trial112 MCHA has also been found to have a significant prophylactic effect in preventing the development of osteoporosis in corticosteroid-treated rheumatoid patients. In a controlled study of 72 individuals, those given MCHA 6 g daily for 12 months had significantly less reduction in stem height (crown-to-seat distance whilst sitting) and radial BMD than the control group.113 REDUCES RISK OF FALLS AND FRACTURES Patients with nonspecific muscle weakness, muscle aches and pains, and bone pain are often found to have low vitamin D. Similarly, vitamin D deficiency has been associated with reversible myopathy in patients with osteomalacia. Several studies support the hypothesis that vitamin D inadequacy contributes to age-related muscle weakness and falls. A compelling meta-analysis of RCTs showed a greater than 20% reduced risk of falls among older individuals treated with vitamin D supplements. Additional supporting evidence comes from a study that investigated factors leading to fracture in postmenopausal women with osteoporosis; vitamin D inadequacy was associated with increased body sway, increased risk of falls, and fall-related fractures.115 A prospective study that examined factors associated with falls in 637 institutionalised ambulatory subjects reported that a low baseline serum 25(OH)D level was significantly associated with increased risk of falling. In a randomised, double-blind trial, treatment with vitamin D plus calcium daily for 3 months reduced the risk of falling by 49% compared with calcium alone among elderly women in long-stay geriatric care (Figure 17).116 Similarly, a study of elderly adults in Switzerland showed that treatment with vitamin D significantly reduced the number of falls for individuals with calcium intake of more than 512 mg/d.
Risk
of f
all
Ca only Ca + D
-49%
Figure 17: Relative to therapy with 1200 mg/d of calcium for 12 weeks, daily therapy with 800 IU of vitamin D and 1200 mg of calcium accounted for a 49% reduction in the relative risk of falls among older women (mean age, 85.3 years) in long-term geriatric care. Ca = calcium; Ca + D = Ca plus vitamin D.114

183
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 16
These studies suggest that adequate serum vitamin D may prevent fractures not only by improving calcium homeostasis but also by improving musculoskeletal function. Other recent evidence suggests that vitamin D inadequacy may be a factor in loss of muscle mass and muscle strength (sarcopenia). One population-based study reported that vitamin D levels between 40 and 94 nmol/L were associated with better musculoskeletal function in the lower extremities of both active and sedentary ambulatory adults 60 years or older compared with levels less than 40 nmol/L.117 In an examination of 13 meta-analyses, 11 found a significantly decreased fracture incidence in the supplemented groups. It was concluded that a vitamin D supplement of 800 IU per day, in combination with calcium, may decrease the incidence of non-vertebral fractures by about 10 to 20%, especially in persons in the older age groups having low-baseline vitamin D status and low calcium intake and showing good compliance.118 CAUTIONS AND CONTRAINDICATIONS CONTRAINDICATIONS Allergies and Sensitivities: Avoid in individuals with known allergy or hypersensitivity to soy, and/or
members of the Fabaceae (pea) family.119 CAUTIONS Alendronate: Calcium causes decreased absorption of this drug.120 Separate doses by at least 2 hours. Amiloride: Conflicting information exists regarding the potential interactions between amiloride and zinc.
Amiloride has been reported to both reduce zinc excretion (leading to zinc accumulation),121 and lead to zinc deficiency.122 Monitor zinc status.
Antibiotics: Both zinc and manganese may form insoluble complexes with certain antibiotic medications. Separate doses by at least 2 hours.123,124,125,126
Anticoagulant/Antiplatelet drugs: Vitamin K increases coagulation. Concomitant use of vitamin K and antiplatelet or antithrombotic medications such as aspirin and warfarin might increase thrombus risk. Use with caution and monitor INR in patients taking warfarin.127
Atenolol: Calcium may form insoluble complexes with this medication reducing absorption. Separate dose by at least 2 hours.128
Bisphosphonates: Calcium may decrease bisphosphonate absorption. Separate doses by at least 2 hours.129,130
Calcium channel blockers: Use with caution in patients on calcium channel blockers. o Hypercalcaemia due to high doses of vitamin D can reduce the effectiveness of such medications
in atrial fibrillation. Avoid vitamin D doses above 2000 IU (50 µg) daily and monitor.131 o Hypercalcaemia may result if used concurrently with high doses of calcium (i.e. doses > 2000
mg/day). Increased serum calcium may have an antagonistic effect that could precipitate the re-emergence of arrhythmias and/or an increase in blood pressure.132,133
Cardiac glycosides/Digoxin: Hypercalcaemia induced by high doses of vitamin D (i.e. doses > 2000 IU/day or 50 µg/day) or calcium (i.e. doses > 2000 mg/day) can increase the risk of fatal cardiac arrhythmias with cardiac glycosides. Avoid high doses of calcium and/or vitamin D and use under medical supervision only. 134
Chemotherapy/Radiotherapy: Vitamin C and zinc may affect efficacy of chemotherapy. Use with caution and only under the supervision of a patient’s oncologist. It has generally been thought that antioxidants may interfere with chemotherapy and/or radiotherapy by decreasing the efficacy of the treatment, recent studies have found that antioxidants are safe to use in conjunction with these treatments. However, it is still advisable to check with a patient’s oncologist before recommending a formula containing antioxidants.135
Haemochromatosis and other diseases of iron accumulation: Vitamin C increases iron absorption; use with caution in cases of uncontrolled haemochromatosis, thalassaemia, sideroblastic anaemia or erythrocyte G6PD deficiency.136
Hypercalcaemia: High dose calcium supplementation (i.e. doses > 2000 mg/day) and/or vitamin D doses above 2000 IU (50 µg) daily should be avoided due to the risk of increased calcium accumulation.137 Use with caution and only under medical supervision.
For full technical data including Cautions and Contraindications and References, go to www.metagenics.com.au (Australia), or www.metagenics.co.nz (New Zealand).

184
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 1
Alpha Lipoic Acid for Antioxidant Support
Alpha lipoic acid (ALA) is an important fat- and water-soluble, intracellular antioxidant which can be used in the management and prevention of diabetes and diabetic complications such as neuropathy, nephropathy and cardiovascular disease. ALA also possesses key biological activities outside of its antioxidant effect, such as improving insulin sensitivity, supporting mitochondrial energy production and chelating heavy metals. HERBS AND NUTRIENTS THAT MAY ASSIST R,S-alpha lipoic acid CLINICAL APPLICATIONS
BACKGROUND TECHNICAL INFORMATION Type 2 diabetes Type 2 diabetes is a chronic metabolic disorder characterised by absolute or relative deficiencies in insulin secretion and/or action and associated with dysfunction in metabolic pathways. As a consequence, various complications develop including both macro- and micro-vascular dysfunction.1 Both diabetes type 1 and 2 are associated with a number of complications including peripheral neuropathy, nephropathy, and retinopathy. Peripheral neuropathy is a particularly common complication of diabetes, affecting one in four diabetic patients and presenting a significant cause of morbidity and mortality.2 Pain and sleep interference are the two main symptoms in conjunction with paraesthesia and sensory loss. Disturbed glucose metabolism in type 2 diabetes Type 2 diabetes is condition with widespread metabolic dysfunction including hyperglycaemia, glycation reactions and insulin resistance. Several key cellular components and processes have been identified to be involved in the development of insulin resistance, such as the function of the insulin receptor, the kinase signalling coupled to the insulin receptor and the expression and translocation of glucose transporters. One critical component of the intracellular signalling involved in metabolic function is activated protein kinase (AMPK). This kinase acts as a metabolic master switch regulating several intracellular systems including the cellular uptake of glucose, the β-oxidation of fatty acids, the biogenesis of mitochondria and the activity of glucose transporter type 4 (GLUT4).3 The net result of activating AMPK is enhanced glucose oxidation and cellular bioenergetics.4 Evidence shows that AMPK signalling is dysregulated in subjects with metabolic syndrome and type II diabetes and that AMPK stimulation can improve insulin sensitivity and metabolic function.5
KEY ACTIONS: Antioxidant Improves glucose metabolism Improves cellular energy production Protects cardiovascular system Heavy metal chelation
KEY APPLICATIONS:
Type 2 diabetes Diabetic complications:
o Neuropathy o Nephropathy o Cardiovascular disease
Heavy metal detoxification

185
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 2
Oxidative stress in type II diabetics Oxidative stress plays a significant role in the pathogenesis of diabetic complications, including peripheral neuropathy and cataract formation. Diabetics have increased levels of lipid hydroperoxides, DNA adducts* and protein carbonyls†. Increased oxidative stress in diabetes appears to be due mainly to hyperglycaemia, which results in decreased synthesis of glutathione, disturbing the redox balance and driving the development of co-morbidities in diabetes.6 Cardiovascular disease in type II diabetics The development of cardiovascular disease (CVD) is a known risk associated with type 2 diabetes, and endothelial dysfunction is an early and crucial event in the pathogenesis of atherosclerosis and CVD. Reduced endothelium-derived nitric oxide (NO) is thought to contribute to endothelial dysfunction and atherosclerosis through the loss of the vasodilatory, anti-inflammatory and antiproliferative properties of NO. Elevated blood glucose increases the production of reactive oxygen species (ROS), which damages endothelial cells, causing a decreased production of NO.7,8
INGREDIENTS Alpha-lipoic acid (ALA) is an endogenous thiol compound which may also be obtained from both animal and plant sources. ALA is more abundant in animal-derived foods such as red meat and organ meats, whilst the highest plant sources include spinach, broccoli, brussel sprouts, potatoes, peas and rice bran.9 Humans can synthesise ALA de novo from fatty acids and cysteine, however only in very small amounts, therefore ALA needs to be provided by exogenous sources.10 ALA converts easily to its reduced form, dihydrolipoic acid (DHLA) by nicotinamide adenine dinucleotide (NADH) or nicotinamide adenine dinucleotide phosphate (NADPH) in many tissues of the body (Figure 1).11 DHLA has shown greater antioxidant activities than LA, with the ability to neutralise free radicals and regenerate vitamins C and E from their reduced forms.12
Figure 1. Oxidised (LA) and reduced forms (DHLA) of lipoic acid,13
ALA comes in two isomers: R-lipoic acid (R-ALA) and S-lipoic acid (S-ALA). Naturally occurring ALA is in the R form, whilst supplemental form is often a racemic mixture (R,S-ALA). R,S-ALA has shown excellent bioavailability compared to the R form, as well as clinical efficacy, being the most well-studied form.14,15‡ No hexane or solvents are used in the production of R,S-alpha lipoic acid to ensure the purity of this compound. ACTIONS ANTIOXIDANT ALA is an important fat- and water-soluble, intracellular antioxidant that is critical for protection against free radical damage. ALA is the primary antioxidant in the body’s antioxidant defence cascade; as in the form of DHLA, it is responsible for reducing vitamin C, glutathione and coenzyme Q10 from their oxidised forms. These antioxidants in turn can each regenerate vitamin E from its oxidised form. Ultimately, ALA is the fundamental antioxidant that assist with vitamin E neutralising free radicals (Figure 2).16
* DNA adducts are altered forms of DNA which reflect exposure to known carcinogens and methylating agents † Protein carbonyls serve as markers of oxidative stress ‡ Alpha Lipoic Acid for Antioxidant Support contains R,S-alpha lipoic acid

186
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 3
Figure 2. ALA reduces the oxidised forms of vitamin C (semi-dehydroascorbate), glutathione (GSSG) and coenzyme Q10 (ubisemiquinone) which results in reducing oxidised vitamin E and ultimately assists in neutralising free radicals (e.g.
superoxide [ROO●]).17 Lipoic acid reduces oxidative stress in both healthy adults and those with diabetes. Daily supplementation with 600 mg of lipoic acid for three months was found to significantly reduce lipid-hydroperoxide formation, significantly improving the imbalance between increased oxidative stress and antioxidant defence even in patients with poor glycaemic control.18 IMPROVES GLUCOSE METABOLISM Animal and human studies have shown ALA to have the following actions on glucose metabolism: Increases glucose uptake and glycogen synthesis Improves glucose oxidation Reduces plasma insulin and free fatty acids Prevents glycation reactions in some proteins19,20.21, 22 Protects against β-cell destruction
One key intracellular mechanism of ALA in improving metabolic function is that it stimulates the translocation from the cytosol of GLUT-4 to the plasma membrane.23 Specifically, ALA augments the activity of components of the intracellular insulin signalling cascade: insulin receptor, insulin receptor substrate-1, phosphatidylinositol (PI) 3-kinase, Akt1, and p38 mitogen-activate protein kinase
(p38 MAPK) (Figure 3). These compounds act to translocate GLUT-4 to the plasma membrane to promote uptake of glucose from the serum into the cell. 24,25
Figure 3. Facilitation of glucose uptake by lipoic acid.26
As previously stated, AMPK acts as a master switch for glucose and thus energy metabolism. Diabetes-prone obese rats and control rats were given ALA for three days whilst skeletal AMPK was tested. It was found that ALA significantly increased AMPK in skeletal muscle in diabetic and control rats, which also correlated with an increase in insulin-stimulated glucose uptake. These results suggest that the insulin sensitising effects of ALA may also be due to its ability to activate AMPK.27 IMPROVES CELLULAR ENERGY PRODUCTION ALA is an important cofactor for three enzyme complexes* required for mitochondrial energy metabolism. Supplementation with ALA helps to support the activities of these enzymes, thereby promoting oxidative phospohorylation and increasing energy metabolism.28,29 In addition to supporting mitochondrial enzymes, ALA also can improve cellular energy production by promoting key regulators of mitochondrial function. Peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α) is a transcriptional regulator of mitochondrial function and biogenesis and thus
* Pyruvate dehydrogenase (PDH), α-ketoglutarate dehydrogenase (KGDH), and branched chain α-ketoacid dehydrogenase (BCKDH)

187
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 4
a critical regulator of energy homeostasis, blood pressure, cholesterol homoeostasis, and itself is stimulated by AMPK. ALA has been found to increase energy metabolism and mitochondrial biogenesis in animals by increasing the phosphorylation of AMPK and subsequent expression of PGC-1α, further supporting its important role in energy metabolism.30 PROTECTS CARDIOVASCULAR SYSTEM ALA protects against oxidative damage to the cardiovascular system in animal models and human subjects with diabetes. This may mitigate the development of cardiovascular disease that frequently develops in diabetic patients. For example, a study on subjects with metabolic syndrome receiving 300 mg/day of ALA showed a statistically significant reduction in plasma levels of interleukin-6 and plasminogen activator-1 (PAI-1), both important markers of inflammation implicated in the pathogenesis of atherosclerosis (Figure 4).31
Figure 4. Reduction of IL-6 and PAI-1 levels by ALA.32
In another trial investigating endothelial function, 35 patients with diabetes were given 600 mg/day ALA for 18 months and were compared to 49 diabetics who served as control. The researchers measured the subject’s plasma thrombomodulin levels during the trial, which is a marker of endothelial damage. At the end to the trial there was a significant increase in thrombomodulin from baseline (i.e. worsening) in the control group whilst the ALA group showed a significant decrease (Table 1).33
Table 1. Changes in thrombomodulin in diabetic patients treated with ALA compared untreated diabetics who served as a controls. 34
ALA Control Baseline Control Baseline Control Thrombomodulin (ng/ml) 37.5 30.9* 35.9 39.7*
*p<0.01 from baseline
In diabetic animals, ALA significantly reversed endothelial dysfunction and reduced the development of atherosclerotic lesions. Diabetic rats when consuming a control diet showed the presence of intracellular lipid droplet accumulation only in the intima layer of arteries. In contrast, these lesions extended to the other layers in the diabetic rats who were fed an atherogenic diet. Supplementation with ALA to diabetic rats consuming a atherogenic diet prevented the decrease in endothelial NO and the enhancement of atherosclerosis (Figure 5), such as preventing lipid accumulating in layers beyond the intima as indicated by a lower atherogenic index.35,36

188
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 5
AD AD + LA AD AD + LA Figure 5. ALA improved NO levels and atherogenic index.37,38
Left: Effect of ALA on NO levels. Right: Effects of ALA on atherogenic index. AD – atherogenic diet; AD + ALA – atherogenic diet plus alpha lipoic acid
HEAVY METAL CHELATION Due to the presence of two thiol groups, ALA and DHLA both have metal chelating properties (Figure 6).39 They are absorbed into the intracellular environment and complex metals previously bound to other sulphydryl proteins, preventing cellular damage. ALA is most effective in chelating copper, zinc and lead, while DHLA also forms complexes with these three metals as well as iron and mercury.40 This ensures that excess levels of these metals and minerals are monitored. The recycling of antioxidants such as vitamin E, C and glutathione by DHLA further reduces the potential for cellular damage, and glutathione itself is a heavy metal chelator.
Figure 6. Metal chelation by lipoic acid.41
M = Heavy metal eg. lead, cadmium, mercury
APPLICATIONS TYPE 2 DIABETES ALA has been shown to have a number of beneficial effects, both in the treatment of type 2 diabetes and its related complications. ALA’s effect on insulin sensitivity was evaluated in a four week randomised controlled trial in 74 patients with type 2 diabetes. Patients were randomised into one of four groups, placebo or active treatment of 600 mg of ALA once daily, twice daily or three times daily. The results found significantly more subjects had an increase in insulin-stimulated glucose disposal in all ALA treatment groups compared to controls.42 Interestingly, there was no dose effect seen in the three different treatment groups, indicating 600 mg a day is the preferred dose. Therefore, all subjects receiving ALA were combined in a collective “active” group and then compared to placebo. These results revealed significantly different changes in glucose disposal after treatment. It was found that insulin stimulated glucose disposal decreased by 10% in the placebo group and improved by 27% in the active group (Figure 7).43

189
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 6
Figure 7. Treatment with ALA acid significantly increased insulin stimulated glucose uptake in diabetic individuals compared to placebo.44
A randomised, placebo-controlled trial was conducted to assess the effectiveness of ALA supplementation on glycaemic status in thirty eight patients with type 2 diabetes. ALA at 300, 600, 900 or 1200 mg daily or a placebo was given for six months. The results showed a decrease in haemoglobin A1c (HbA1c) and fasting blood glucose (Figure 8) in the combined groups receiving ALA, demonstrating that supplementation could improve glycaemic status. The authors also found demonstrable evidence for the adjuvant use of ALA in type 2 diabetics taking oral hypoglycaemic medication.45
Figure 8. Changes in fasting blood glucose (FBG) in type 2 diabetes patients after six months of ALA treatment compared to placebo.46
Results from another trial showed long-term prevention of blood glucose worsening in diabetics when administered ALA. Thirty five patients with diabetes were given 600 mg/day ALA for 18 months and were compared to 49 diabetics who served as control. At the end to the trial there was significant increase in HbA1c from baseline (i.e. worsening) in the control group (8.4 to 8.8%) whilst the ALA group showed no significant change from baseline (8.4 to 8.5%).47 PREVENTION DIABETIC COMPLICATIONS Neuropathy Several studies have confirmed that ALA is an effective treatment for diabetic peripheral neuropathy.48,49,50,51 For example, a randomised controlled trial was conducted with 181 diabetic patients with distal symmetric polyneuropathy (DSP).* Patients received 600 mg, 1,200 mg, or 1,800 mg of ALA or placebo for five weeks. The primary outcome measure was the change from baseline of the Total Symptom Score (TSS), including stabbing pain, burning pain, paraesthesia, and numbness of the feet. The results demonstrated that TSS was significantly reduced in all the ALA groups versus placebo at by week two, suggesting a rapid effect of * Distal symmetric polyneuropathy is associated with excruciating neuropathic pain in the extremeties and is responsible for both substantial morbidity and increased mortality.
-15%
-10%
-5%
0%
5%
10%
15%
20%
25%
30%
Chan
ge fr
om b
asel
ine
in in
sulin
st
imul
ated
glu
cose
upt
ake
Placebo ALA

190
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 7
ALA.(Figure 9) The improvements remained significant for the remaining weeks and the authors suggested 600 mg is the ideal dose.52
Figure 9. Mean Total Symptom Score (TSS) levels in diabetic patients with distal symmetric polyneuropathy (DSP) on a weekly
basis during the placebo run-in and the randomised double-blind period of the trial.53 More recently, the NATHAN 1 trial was conducted to assess the safety and efficacy of ALA over a four year period. This was a randomised double-blind trial with 460 patients with mild to moderate diabetic distal symmetric sensorimotor polyneuropathy where the subjects were randomly assigned to treatment with 600 mg ALA daily or placebo. After four years the neuropathy impairment score (NIS) and muscular weakness subscore improved significantly on ALA and worsened on placebo.54 Nephropathy Evidence shows that ALA treatment reduces biomarkers of kidney pathology in diabetic patients. In one study, 35 patients with diabetes were given 600 mg/day ALA for 18 months and were compared to 49 diabetics who served as control. The results showed that the control group recorded worsening of kidney function over the 18 months, with their urinary albumin concentration (UAC)* significantly increasing (21 to 37 ng/l), whilst the ALA group showed non-significant reduction in UAC (29 to 15 ng/L). These results indicate that ALA prevents worsening of glomerular dysfunction in diabetics.55 Another trial investigated the effect of a combination of angiotensin-converting enzyme inhibitors (ACEIs) with or without ALA on urinary albumin concentrations in diabetics with hypertension. Forty diabetic patients were given quinapril (QUI) 40 mg/day or QUI plus ALA 600 mg/day for eight weeks and the results found an additive effect of ALA on lowering AUC (Figure 10).56
* The presence of excessive levels of albumin in the urine is an indication of glomerular damage, as large molecules such as the albumin protein are able to pass into the urine. In diabetics, the oxidative stress is thought to be the cause of the glomerular damage.

191
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 8
Figure 10. Levels of urinary albumin in diabetic patients receiving quinapril or quinapril plus ALA. 57
Cardiovascular disease Results from a comparative trial showed stabilisation of blood pressure in diabetics given ALA whilst the control group recorded an increase in blood pressure. Thirty five patients with diabetes were given 600 mg/day ALA for 18 months and were compared to 49 diabetics who served as control. At the end of the trial there was a significant increase in both systolic and diastolic blood pressure from baseline (i.e. worsening) in the control group whilst the ALA group showed no change from baseline (Table 2).58 Table 2. Changes in blood pressure in diabetic patients treated with ALA compared with untreated diabetics who served as a
controls. 59 ALA Control Baseline Control Baseline Control Systolic 126 133 132 142* Diastolic 77 76 76 80*
*p<0.01 from baseline A study investigated the effects of a combination of irbesartan, an angiotensin receptor blocker, and ALA on endothelial function in patients with metabolic syndrome. Fifty eight subjects were randomly allocated either irbesartan 150 mg/day, ALA 300 mg/day, both irbesartan and ALA, or matching placebo for four weeks was measured. The results showed that endothelial-dependent flow-mediated dilation (FMD) was increased significantly by 44% in the ALA alone group and by 75% in the irbesartan and ALA group (Figure 11).60 The authors conclude that irbesartan and/or ALA to patients with the metabolic syndrome improves endothelial dysfunction; a factor that is implicated in the pathogenesis of atherosclerosis.
Figure 11. Improvements in endothelial function with irbesartan and ALA.61
01020304050607080
FMD
% c
hang
e fr
om b
asel
ine
Placebo ALA ALA + irbesartan

192
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 9
Another randomised controlled trial was conducted with 40 diabetic patients with stage 1 hypertension* to investigate the effects of a combination of ACEIs and ALA on blood pressure and endothelial function. Patients were given quinapril (QUI) 40 mg/day for eight weeks or QUI plus ALA 600 mg/day for eight weeks and FMD was assessed. The combination of ALA and QUI demonstrated a substantial increase in FMD by 116% (see Figure 12), indicating improved endothelial function.62
Figure 12. Effect of quinapril and ALA on flow-mediated dilation.63
METAL DETOXIFICATION The presence of heavy metals can cause significant lipid peroxidation in the brain.64 Evidence shows there is an age-dependent reaction with excess brain metal (namely copper, iron and zinc), which induces β-amyloid to precipitate into metal-enriched plaques.65 Animal studies have shown that DHLA attenuated age-related accumulation of iron in the brain (see Figure 13), whilst also improving antioxidant status.66 DHLA-mediated chelation of iron and copper in the brain had a positive effect by reducing the free radical damage contributing to Alzheimer’s disease.67
Figure 13. LA supplementation reverses the age-related increase in iron levels.68
An animal model of mercury toxicity found that administration of ALA led to a significantly increased biliary excretion of inorganic mercury (12- to 37-fold) than a placebo, highlighting a detoxifying effect of ALA.69
Protecting against heavy metal toxicity Numerous animal models show that administration of ALA attenuates the oxidative damage from heavy metal toxicity, such as lead, mercury, cadmium and arsenic.70,71,72,73,74 For example, an animal study demonstrated that lipoic acid affords protection against the oxidative stress generated by experimental cadmium intoxication. The liver and the kidney of those animals administered the metal showed elevated levels of hydroxyl radicals and malondialdehyde and a corresponding decrease in
* Stage 1 hypertension was defined as having systolic blood pressure >125 mm Hg.
Metagenics Technical Team December 2014 9
Another randomised controlled trial was conducted with 40 diabetic patients with stage 1 hypertension* to investigate the effects of a combination of ACEIs and ALA on blood pressure and endothelial function. Patients were given quinapril (QUI) 40 mg/day for eight weeks or QUI plus ALA 600 mg/day for eight weeks and FMD was assessed. The combination of ALA and QUI demonstrated a substantial increase in FMD by 116% (see Figure 12), indicating improved endothelial function.62
Figure 12. Effect of quinapril and ALA on flow-mediated dilation.63
METAL DETOXIFICATION The presence of heavy metals can cause significant lipid peroxidation in the brain.64 Evidence shows there is an age-dependent reaction with excess brain metal (namely copper, iron and zinc), which induces β-amyloid to precipitate into metal-enriched plaques.65 Animal studies have shown that DHLA attenuated age-related accumulation of iron in the brain (see Figure 13), whilst also improving antioxidant status.66 DHLA-mediated chelation of iron and copper in the brain had a positive effect by reducing the free radical damage contributing to Alzheimer’s disease.67
Figure 13. LA supplementation reverses the age-related increase in iron levels.68
An animal model of mercury toxicity found that administration of ALA led to a significantly increased biliary excretion of inorganic mercury (12- to 37-fold) than a placebo, highlighting a detoxifying effect of ALA.69
Protecting against heavy metal toxicity Numerous animal models show that administration of ALA attenuates the oxidative damage from heavy metal toxicity, such as lead, mercury, cadmium and arsenic.70,71,72,73,74 For example, an animal study demonstrated that lipoic acid affords protection against the oxidative stress generated by experimental cadmium intoxication. The liver and the kidney of those animals administered the metal showed elevated levels of hydroxyl radicals and malondialdehyde and a corresponding decrease in
* Stage 1 hypertension was defined as having systolic blood pressure >125 mm Hg.
Metagenics Technical Team December 2014 10
antioxidants, reduced glutathione, total thiols and other antioxidant nutrients and enzymes. Supplementation with ALA changed the tissue redox state directly by quenching the free radicals and indirectly by bolstering the antioxidants and antioxidant enzyme defences.75 CAUTIONS AND CONTRAINDICATIONS CONTRAINDICATIONS
N/A CAUTIONS
Anti-hypertensive medication: Concurrent use of lipoic acid can produce an additive or synergistic response and may support patients with metabolic syndrome, hypertension and dyslipidaemia. Monitor blood pressure.76
Chemotherapy and radiotherapy: Theoretically concomitant use might decrease effectiveness of chemotherapy. The use of lipoic acid and other antioxidants is controversial during radiation and chemotherapy though positive interactions are also reported. Use under medical supervision.77
Oral hypoglycaemic agents and insulin: Concurrent use of lipoic acid could produce an additive or synergistic response, resulting in hypoglycaemia. However, lipoic acid supplementation should be encouraged in many cases as it effectively reduces the risk of diabetic complications. Monitor blood glucose levels.78,79
Thiamine deficiency: Lipoic acid should not be administered in high doses to patients suspected of having a thiamine deficiency (commonly seen in alcoholics) unless the thiamine deficiency is corrected.80,81
PREGNANCY AND BREASTFEEDING
Pregnancy: There is no evidence of harm when used during pregnancy. Likely safe when used at the recommended dosage.82,83
Breastfeeding: Likely safe when used at the recommended dosage.84,85 REFERENCES 1 Golbidi S, Badran M, Laher I. Diabetes and alpha lipoic acid. Frontiers in Pharmacology 2011;2:1-15. 2 Vasudevan D, Naik MM, Mukaddam QI. Efficacy and safety of methylcobalamin, alpha lipoic acid and pregabalin combination versus pregabalin monotherapy in improving pain and nerve conduction velocity in type 2 diabetes associated impaired peripheral neuropathic condition. [MAINTAIN]: Results of a pilot study. Annals of Indian Academy of Neurology 2014;17(1):19-24. 3 Winder WW, Hardie DG. AMP-activated protein kinase, a metabolic master switch: possible roles in type 2 diabetes. Am J Physiol.1999 Jul;277(1 Pt 1):E1-10. 4 Pang J, Choi Y, Park T. Ilex paraguariensis extract ameliorates obesity induced by high-fat diet: potential role of AMPK in the visceral adipose tissue. Arch Biochem Biophys. 2008 Aug 15;476(2):178-85. 5 Coughlan KA, Valentine RJ, Ruderman NB, Saha AK. AMPK activation: a therapeutic target for type 2 diabetes? Diabetes Metab Syndr Obes. 2014(24);7:241-53. 6 Packer L, Kraemer K, Rimbach G. Molecular aspects of lipoic acid in the prevention of diabetes complications. Nutrition 2001;17:888-895. 7 Heinisch BB, et al. Alpha-lipoic acid improves vascular endothelial function in patients with type 2 diabetes: a placebo controlled randomised trial. European Journal of Clinical Investigation 2009;40:148-154. 8 Sena CM, et al. Effects of alpha-lipoic acid on endothelial function in aged diabetic and high-fat fed rats. Br J Pharmacol 2008;153:894-906. 9 Goraca A, et al. Lipoic acid – biological activity and therapeutic potential. Pharmacological Reports 2011;63:849-858. 10 Goraca A et al. Lipoic acid – biological activity and therapeutic potential. Pharmacological Reports 2011;63:849-858. 11 Alpha-lipoic acid. Monograph. Alt Med Review 2006;11(3):232-237. 12 Flora SJS. Structural, chemical and biological aspects of antioxidants for strategies against metal and metalloid exposure. Oxidative Medicine and Cellular Longevity 2009;2(4):191-206. 13 Gomes MB, Negrato CA. Alpha-lipoic acid as a pleiotropic compound with potential therapeutic use in diabetes and other chronic diseases. Diabetol Metab Syndr. 2014 Jul 28;6(1):80. 14 Keith DJ, et al. Age and gender dependent bioavailability of R- and R,S-α-lipoic acid: a pilot study. Pharmacol Res 2012;66(3):199-206 15 Mignini F, et al. Single dose bioavailability and pharmacokinetic study of an innovative formulation of α-lipoic acid (ALA600) in healthy volunteers. Minerva Med 2011;102(6):475-82. 16 Ghibu S, et al. Antioxidant properties of an endogenous thiol: alpha-lipoic acid, useful in the prevention of cardiovascular diseases. J Cardiovasc Pharmacol 2009;54(5):391-398. 17 Packer L, Kraemer K, Rimbach G. Molecular aspects of lipoic acid in the prevention of diabetes complications. Nutrition 2001;17:888-895. 18 Borcea V, et al. Alpha-lipoic acid decreases oxidative stress even in diabetic patients with poor glyacaemic control and albuminuria. Free Radic Biol Med 1999;26:1495. 19 Jacob S, et al. The antioxidant alpha-lipoic acid enhances insulin-stimulated glucose metabolism in insulin resistant rat skeletal muscle. Diabetes 1996;45:1024.
For full technical data including Cautions and Contraindications and References, go to www.metagenics.com.au (Australia), or www.metagenics.co.nz (New Zealand).

193
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 1
Mixed Tocopherols & Tocotrienols for Free Radical Defence Mixed Tocopherols & Tocotrienols for Free Radical Defence is a vitamin E supplement of the highest potency and broadest range of activity. It consists of all eight isomers of vitamin E: alpha-, beta-, gamma-, and delta-tocopherols, and alpha-, beta-, gamma-, and delta-tocotrienols. The synergy of these mixed tocopherols and tocotrienols produces a broader therapeutic activity than a single tocopherol. Mixed Tocopherols & Tocotrienols for Free Radical Defence is a lipid-soluble antioxidant specifically formulated to provide antioxidant support in the cardiovascular system, male and female reproductive systems, and the skin. NUTRIENTS THAT MAY ASSIST
Tocopherols concentrate – mixed (low alpha type) Tocotrienols complex - palm
ACTIONS AND APPLICATIONS INGREDIENTS Vitamin E is one of nature’s most potent fat soluble antioxidants, and is essential to the proper function of all major tissues and organ systems in the body. Many studies indicate that antioxidant inadequacy from depleted dietary vitamin E is associated with an increase in reactive oxygen species (ROS), cell injuries, and subsequent disorders in the affected tissues, including accelerated ageing. Humans are unable to synthesise their own vitamin E and must rely on oral (dietary and supplemental) or topical (in the case of skin and mucous membranes)1, delivery. There are eight forms of vitamin E Vitamin E occurs naturally as a mixture of four tocopherols and four tocotrienols, both quartets known as alpha, beta, gamma and delta (Figure 1).
KEY ACTIONS: Antioxidant Anti-inflammatory Improves membrane fluidity Supports mitochondria Neuroprotective Cardioprotective Prevents DNA damage (carcinoprotective)
KEY APPLICATIONS:
Cardiovascular disease o Hypertension o Dyslipidaemia
Reproductive health Maintenance of cognition Skin health Conditions associated with oxidative stress
o Fibromyalgia

194
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 2
Figure 1: Vitamin E: Structure of tocopherols compared to tocotrienols. Tocotrienols possess
three double bonds in the side chain which is thought to be the reason tocotrienols demonstrated different biological actions to tocopherols.2,3
MIXED TOCOPHEROLS – low alpha type Mixed Tocopherols & Tocotrienols for Free Radical Defence employs a low-alpha type mixed tocopherol concentrate derived from certified non-genetically modified soy oil,* with the following breakdown of tocopherols:
D-alpha-tocopherol 14% D-beta-tocopherol 2% D-gamma-tocopherol 60% D-delta-tocopherol 24%
Mixed tocopherols better than alpha-tocopherol alone The synergy of the four mixed tocopherols produces a far broader and superior therapeutic activity than a single tocopherol concentrate.4 Evidence indicates that the mixed tocopherols have additive and synergistic activities that support their broader beneficial biologic functions, and that gamma-tocopherol in particular is superior to alpha-tocopherol for key functions of vitamin E such as reducing platelet aggregation, reducing lipid peroxidation and low density lipoprotein (LDL) oxidation, and increasing superoxide dismutase (SOD) antioxidant activity. It is important, therefore, to ensure that supplemental vitamin E contains high levels of gamma-tocopherol when prescribing it for patients with, or at risk of developing, cardiovascular disease.5 Overall, researchers have found that a preparation of mixed tocopherols containing higher levels of gamma- and delta-tocopherol in comparison to a lower level of alpha-tocopherol (hence “low-alpha type”), has better antioxidant and anti-inflammatory actions than alpha-tocopherol alone.6 MIXED TOCOTRIENOLS - palm The tocotrienols are the four unsaturated members of the vitamin E family: alpha-, beta-, gamma- and delta-tocotrienol. As shown above in Figure 1, tocotrienols are structurally different from the tocopherols in having three trans double-bonds in the hydrocarbon tail.7 The tocotrienols in Mixed Tocopherols & Tocotrienols for Free Radical Defence are derived from certified non-genetically modified, sustainably sourced palm oil,8 which provides mixed tocotrienols with the following breakdown:
D-alpha-tocotrienol 37% D-beta-tocotrienol 4% D-gamma-tocotrienol 45% D-delta-tocotrienol 14%
Tocotrienols broaden the potential activity Tocotrienols have been shown to rectify vitamin E deficiency states, exhibiting potent free radical scavenging properties, and regulating numerous transcription factors and receptors.9 As with the tocopherols, an extract of mixed tocotrienols provides the optimal range of actions, including powerful hypocholesterolaemic, anticancer and neuroprotective properties that enhance and complement the actions of the tocopherols.10
* The extract contains no soy protein.

195
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 3
ACTIONS ANTIOXIDANT As one of nature’s most potent fat-soluble antioxidants, vitamin E - as both tocopherols and tocotrienols - prevents unsaturated linkages in complex lipids from undergoing auto-oxidation, peroxide formation and destructive free radical pathology. Because of this fundamental protective role, it gives continued protection and integrity to all cellular and subcellular membranes, and is ultimately involved in the proper function of all major organ systems in the body.11,12,13,14,15,16 In cell membranes, vitamin E prevents oxidative damage to the polyunsaturated fatty acids within the phospholipid layer. This is achieved by reacting with free radical molecules to form tocopheroxyl radicals, which leave the cell membrane and enter the aqueous environment outside the membrane, where they react with vitamin C (or other hydrogen donors such as glutathione) to become reduced and therefore regenerated.17 Alpha-tocopherol increases expression of Nrf2 In addition to its own antioxidant activity, alpha-tocopherol has been shown to activate the Keap1/Nrf2 pathway† by increasing Nrf2 expression (Figure 2) and inducing its translocation to the nucleus. This increases the expression and/or activity of numerous antioxidant and phase II (detoxifying) enzymes, including:
Glutamate cysteine ligase (GCL) NAD(P)H:quinone oxidoreductase 1 (NQO1) Heme oxygenase-1 (HO-1) Glutathione S-transferase (GST) Superoxide dismutase (SOD)
In addition, total antioxidant capacity and glutathione are also increased.19 Gamma-tocopherol is a powerful nucleophile that traps electrophilic mutagens in lipophilic compartments. It thus complements glutathione, which similarly scavenges electrophilic mutagens in the aqueous phase of the cell. In particular, gamma-tocopherol is a potent quencher of peroxynitrite, a highly damaging electrophilic mutagen and free radical, and may protect lipids, DNA, and proteins from peroxynitrite-dependent damage.20,21 Mixed tocopherols more effective than just alpha-tocopherol A study compared the effectiveness of alpha-tocopherol against a mixed tocopherol preparation on hydrogen peroxide-induced lipid peroxidation (measured by malondialdehyde (MDA) concentrations) in human erythrocytes. While both alpha-tocopherol and the tocopherol mixture protected the cells from lipid peroxidation, it was obvious that the uptake of gamma- and delta-tocopherols was much higher than that of alpha-tocopherol, and that the mixture was much more potent than alpha-tocopherol alone (Figure 3).22
† Kelch-like ECH-associated protein 1 (Keap-1) is a protein that interacts with nuclear factor (erythroid-derived 2)-like 2 (Nrf2), a transcription factor that induces many cytoprotective enzymes.
Figure 2: Effects of alpha-tocopherol (α-T) on total and nuclear Nrf2 expression.18

196
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 4
Tocotrienols improve oxidative status in healthy older subjects In a study to determine the effects of tocotrienol supplementation on the oxidative status in healthy older individuals, 62 subjects were recruited from two age groups, 35-49 years (n = 31) and over 50 years (n = 31), and randomly assigned to receive either 160 mg/day of a mixed tocotrienol complex or identical placebo for six months. Blood samples were obtained at onset, three and six months. It was found that:
The plasma ratio of HDL-C to total cholesterol improved in both younger and older groups with supplementation.
Protein carbonyl contents (a marker for oxidative damage) were markedly decreased, and advanced glycation end-products (AGEs) levels were lower, in the supplemented >50 year-old group, indicating reduced oxidative damage in tissues.
In the supplemented older group, SOD activity was decreased after three and six months of supplementation, indicating a reduction in oxidative stress.
The observed reductions in protein damage, AGE and antioxidant enzyme levels may indicate a restoration of redox balance after tocotrienol supplementation, particularly in individuals over 50 years of age.24 Tocotrienols inhibit lipid peroxidation When individual components of a tocotrienol-rich fraction were examined for their ability to prevent damage, researchers observed maximum inhibition of lipid peroxidation by gamma-tocotrienol, followed by alpha-tocotrienol, delta-tocotrienol and alpha-tocopherol. Compared to alpha-tocopherol, tocotrienols exhibit superior protective abilities against oxidative damage, in terms of lipid peroxidation and protein oxidation in brain mitochondria.25
Figure 3: Erythrocyte MDA levels after stimulation with hydrogen peroxide (H2O2). Pretreatment with mixed tocopherols showed a stronger inhibitory effect than pretreatment with alpha-tocopherol. Data based on six experiments.23 T: Tocopherol. *p < 0.05, **p < 0.001 vs. alpha-tocopherol. ¤p < 0.05, ¤¤p < 0.01, ¤¤¤p < 0.001 vs. 30 uM.

197
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 5
Figure 4 demonstrates the inhibitory effect of tocotrienol-rich fraction (TRF) on lipid peroxidation and protein oxidation in mitochondria exposed to an oxidising agent. TRF at 5 micromolar (5 mM) concentration significantly inhibited the formation of thiobarbituric acid reactive substances (TBARS) – a marker for oxidative damage. The inhibition of peroxidation obtained was 17% with alpha-tocopherol and 44% with TRF. Enhanced formation of protein carbonyls induced by ascorbate Fe2+ was also effectively inhibited by TRF: inhibition obtained by alpha-tocopherol and TRF were 57% and 69% respectively. When individual components of TRF were examined for their ability to prevent damage, maximum inhibition of lipid peroxidation was observed by gamma-tocotrienol, followed by alpha-tocotrienol, delta-tocotrienol and alpha-tocopherol.27 PROTECTS AGAINST DNA DAMAGE AND CANCER Antioxidant support may also reduce the risk of cancer by preventing DNA damage. It is known that the more DNA damage that occurs, the greater the chance that errors in repair will happen. This can lead to recombination errors during DNA replication, which are associated with carcinogenesis. Tocotrienols reduce DNA damage A randomised, double-blind placebo-controlled study was performed to determine the efficacy of tocotrienol supplementation on levels of DNA damage in adults. Sixty four subjects aged 37 to 78 years were administered a tocotrienol supplement (containing approximately 120 mg/day of mixed tocotrienols) for six months. The subjects had blood and urine samples taken at baseline, three and six months to measure a number of markers of DNA damage.‡ The results show that those receiving tocotrienols had significantly less total DNA damage after three months, and this remained low after six months. (Figure 5).29 This suggests that tocotrienols offer broad protection against DNA damage, and ultimately protection against carcinogenesis.30 Mixed tocopherols reduce number and size of induced tumours To investigate the inhibitory effect of a tocopherol mixture against mammary tumorigenesis, female rats were treated with a carcinogen (N-methyl-N-nitroso-urea, NMU), and then fed diets containing 0.1%, 0.3%, or 0.5% mixed tocopherols rich in gamma- and delta-tocopherols for 9 weeks. Tumour burden and multiplicity were determined, and the levels of markers of inflammation, proliferation, and apoptosis were evaluated. The regulation of nuclear receptor signalling by tocopherols was also studied.
‡ Markers used were the frequency of sister chromatid exchange (SCE), the comet assay, chromosome 4 aberrations and urinary 8-hydroxy-2’-deoxyguanosine (8-OHdG) levels. The comet assay is considered a marker of both single strand breaks (SSBs) and double strand breaks (DSBs) of DNA, while SCE is suggested to be evidence of repair of damaged DSBs.
Figure 4: Effect of tocotrienol-rich-fraction (TRF) and alpha-tocopherol (5 mM) on lipid peroxidation and protein oxidation in rat brain mitochondria induced by ascorbate-Fe2+. TBARS = Thiobarbituric acid reactive substances.26
Figure 5: Amount of DNA damage in leukocytes during a six month trial of tocotrienols compared to
placebo.28
** p<0.01
Placebo Tocotrienols

198
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 6
It was found that dietary administration of 0.1%, 0.3%, or 0.5% mixed tocopherols suppressed mammary tumour growth by 38%, 50% or 80%, respectively. Tumour multiplicity was also significantly reduced in all three mixed tocopherol groups. Mixed tocopherols activated peroxisome proliferator activated receptor-gamma and antagonised oestrogen action, suggesting that gamma- and delta-tocopherols may be effective agents for the prevention of breast cancer (Figure 6). ANTI-INFLAMMATORY Both tocopherols and tocotrienols exhibit anti-inflammatory actions Mechanistic studies have demonstrated that in epithelial cells, macrophages and neutrophils, specific forms of vitamin E such as gamma- and delta-tocopherol, and the tocotrienols (especially gamma-tocotrienol), modestly inhibit inflammatory cytokines such as prostaglandin E2 (PGE2) and leukotriene B4 (LTB4), without inhibiting cyclooxygenase (COX) and lipoxygenase (5-LOX) activity. In lung epithelial cells, macrophages, and some cancer cells, gamma-tocotrienol has been shown to inhibit the activation of inflammatory transcription factor nuclear factor kappa-B (NFκB), as well as its regulated genes, including cytokines and chemokines.31 Tocotrienols are potent anti-inflammatories The anti-inflammatory effects of tocotrienols were investigated by assessing the capacity of dietary supplementation to block lipopolysaccharide (LPS)-induced TNF-α secretion in mice. Alpha-, gamma- and delta-tocotrienols all produced significant dose-dependent inhibition (20% to 48%) of LPS-induced serum TNF-α levels as compared to control diets (Figure 7). These results demonstrate that tocotrienols block production of key pro-inflammatory cytokines induced by LPS, most probably via inhibition of NFkB. They also show delta-tocotrienol to be the most effective anti-inflammatory isomer. Maximal inhibition of LPS-induced TNF-α was obtained with relatively low concentrations of delta-tocotrienol, which were also found to block LPS-induced gene expression of inflammatory mediators IL-1β, IL-6 and iNOS.33 Vitamin E reduces expression of acute-phase proteins C-reactive protein (CRP) is an acute-phase protein whose expression has been shown to be regulated in response to tissue injury, infection, or other inflammatory stimuli.
Figure 6: Mixed tocopherols (MT) inhibit mammary tumour growth in a dose-dependent manner. C: Average tumour burden in the groups fed mixed tocopherols (0.1%, 0.3% and 0.5% in the diet) was reduced
by 37.9%, 50.0%, and 80.3%, respectively. D: Tumour multiplicity of the group fed 0.1%, 0.3% and 0.5% mixed tocopherols in the diet was reduced by
39.6%, 47.9%, and 62.5% respectively. Significant difference between groups fed control and mixed tocopherol diets was determined by Student’s t-test (#P =0. 05, *P < 0.05, **P < 0.01, *** P < 0.001).
Figure 7: Effect of alpha-tocopherol and various concentrations of tocotrienols (2.5, 5 and 10 mcg/Kg) on serum TNF-α levels in LPS-stimulated mice.32

199
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 7
Alpha-tocopherol reduces hsCRP The effect of alpha-tocopherol supplementation (1200 IU/d) was tested on plasma CRP and interleukin-6 (IL-6) release from activated monocytes in type 2 diabetic patients with and without macrovascular complications compared to matched controls. Plasma high sensitive CRP (hs-CRP) and monocyte IL-6 were assayed at baseline, following 3 months of supplementation, and following a 2 month washout phase. Diabetic subjects had elevated hsCRP and monocyte IL-6 compared to controls. The alpha-tocopherol supplementation supplementation significantly lowered levels of C-reactive protein and monocyte interleukin-6 in all three groups (Figure 8).34
Figure 8: Effect of alpha-tocopherol (AT) supplementation on hs-CRP: hs-CRP was measured at baseline, following alpha-tocopherol supplementation and after the washout phase. *p<0.02 compared to baseline and washout phases; (a) p<0.02 compared to C; (b) p<0.02 compared to type 2 diabetics, with (DM2-MV) or without (DM) macrovascular complications.35
Tocotrienols reduce CRP Subjects in another study were assigned a tocotrienol-rich oil supplement (78% tocotrienols and 22% tocopherols, 150 mg/day) or placebo capsules for 6 months. Fasting plasma samples were obtained at 0, 3, and 6 months, and plasma tocopherol and tocotrienol levels, apolipoprotein A-I precursor, apolipoprotein E precursor, and CRP were determined. Tocotrienol supplementation was shown to increase APOA1 and APOE levels (see later) and lower CRP levels (Figure 9).36
Figure 9: Impact of tocotrienol supplementation on expression of CRP37
IMPROVES MEMBRANE FLUIDITY Because it is fat-soluble and can insert into lipid bilayers, vitamin E (in general) is vital to membrane fluidity and is also the premier membrane antioxidant. Membrane function is absolutely vital to cellular functions in every tissue of the body. Research shows tocotrienols distribute better than tocopherols in the fatty layers of
Baseline
10000
15000
20000
25000
30000
35000
40000
3 month 6 month
Relativ
e intensity
*
*
CRP expression
Placebo Tocotrienols
5000
Baseline
Placebo
3 month
Tocotrienols
Baseline
Placebo

200
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 8
the cell membrane, and that their unsaturated side chain allows for more efficient penetration into tissues that contain saturated fatty layers, such as the brain and liver.38 When tocotrienols insert into lipid bilayer membranes, the shape of their unsaturated side chain also produces greater flexibility than tocopherols (Figure 10).39 This increased flexibility and fluidity of the membrane provided by tocotrienols may enhance membrane function such as cell signalling and neural transmission. This may, in turn, partly explain the observed neuroprotective effects of tocotrienols.40,41
Figure 10: Movement and flexibility in lipid membranes of tocopherols (left) compared to tocotrienols (right).
Tocotrienols have three double bonds in their side chain which provides greater flexibility and may promote membrane function such as cell signalling and neural transmission.42
SUPPORTS MITOCHONDRIAL FUNCTION Tocotrienols protect mitochondria through several mechanisms The surge of free radicals during oxidant exposure can trigger an opening of the mitochondrial permeability transition (MPT) pore, resulting in mitochondrial depolarisation, decreased ATP synthesis and reduced energy availability to power cell functions. Tocotrienols inhibit oxidant-induced MPT opening and mitochondrial depolarisation, and improve the mitochondrial flow of electrons.43 As such, tocotrienols improve mitochondrial function during oxidative stress. Gamma-tocotrienol has been shown to protect against oxidative stress-induced mitochondrial dysfunction and cell injury. In a study where tert-butyl hydroperoxide (TBHP) injury was induced to selective cell cultures, gamma-tocotrienol (GT3) was found to decrease the production of ROS, improve mitochondrial respiration, maintain ATP levels (as measured by ATP-ase activity) and prevent cell death (Figure 11).45 NEURONAL PROTECTION All previous actions - antioxidant, anti-inflammatory, improving membrane fluidity and mitochondrial function – will contribute to neuronal protection. Alpha-tocopherol reduces neural damage in epilepsy Vitamin E (as alpha-tocopherol) has been shown to have beneficial effects in epilepsy, mainly ascribed to its antioxidant properties. Besides radical-induced neurotoxicity, neuro-inflammation is also involved in the pathophysiology of epilepsy, since neuroglial activation and cytokine production exacerbate seizure-induced neurotoxicity and contribute to epileptogenesis. Oral supplementation with alpha-tocopherol has been shown to markedly reduce astrocytic and microglial activation, neuronal cell death and oxidative stress in the hippocampus, as observed 4 days after seizure.46 Tocotrienols prevent neuronal damage Alpha-tocotrienol has been shown to prevent neurodegeneration in mice and rat neurons, by regulating specific mediators of cell death. In fact, alpha-tocotrienol attenuates the arachidonic acid cascade leading to oxidative brain injury and inhibits the glutamate-induced neurotoxicity by modulating phospholipase A2 activity. 47 The highly destructive free radical peroxynitrite has been implicated in the development of excitoneurotoxicity48 through the oxidative destruction of post-synaptic glutamate transporters.49 Gamma-tocotrienol, in particular,
Figure 11: Gamma-tocotrienol (GT3) preserves mitochondrial function 4 hours after TBHP
exposure.44 TBHP= tert-butyl hydroperoxide

201
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 9
is a potent quencher of peroxynitrite.50,51 In another in vitro study, a tocotrienol-rich fraction of palm oil significantly inhibited hydrogen peroxide-induced neuronal death.52 Again, the increased flexibility and fluidity of membranes conferred by tocotrienols may enhance cell signalling and neural transmission, which may partly explain the observed neuroprotective effects of tocotrienols.53,54 CARDIOPROTECTIVE Again all the actions listed above - antioxidant, anti-inflammatory, improving membrane fluidity, and especially supporting mitochondrial function - contribute to the cardioprotective capacity of vitamin E. Most research on the actions of vitamin E in cardiovascular disease has concentrated on the form with the highest apparent biological activity, namely alpha-tocopherol. However, it is well known that gamma-tocopherol is more effective in the detoxification of reactive nitrogen species and exhibits better anti-oxidative properties in food lipids than alpha-tocopherol.55 Tocopherols and tocotrienols reduce cholesterol synthesis and low-density lipoprotein (LDL) peroxidation Tocopherols and tocotrienols have both been shown to inhibit 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, the hepatic enzyme responsible for cholesterol synthesis.56 However, the problem in CVD is not cholesterol as such, but oxidised cholesterol. Peroxidation of LDL-lipids has emerged as the initiating step in the pathogenesis of atherosclerosis,57,58 with LDL oxidation leading to monocyte adhesion and their accumulation as lipid-laden foam cells in the arterial intima, which form the fatty streaks that over time become atheromatous plaque. Clinical trials with vitamin E§ suggest that it may decrease the susceptibility of LDL to oxidation by free radicals, thereby having an early positive effect on cardiovascular health.59 Tocopherols and tocotrienols inhibit monocytic adhesion The adherence of monocytes to the vascular endothelium is an important early event in atherogenesis. Endothelial vascular cell adhesion molecule-1 (VCAM-1), intercellular adhesion molecule-1 (ICAM-1), and endothelial leukocyte adhesion molecule-1 (E-selectin) are all expressed in human atherosclerotic plaques and appear to play a role in atherosclerosis and the risk of future myocardial infarction.60
Alpha-tocopherol has been shown to inhibit monocyte adhesion by inhibiting the surface expression of these endothelial adhesion molecules.61
Tocotrienols also reduce endothelial expression of adhesion molecules and adhesion of monocytes, with delta-tocotrienol exhibiting the highest inhibitory action on monocytic cell adherence.62
Tocotrienols reduce atherogenic apolipoprotein-B Clinical evidence has strongly supported the concept that apolipoprotein-B (apoB) is a better index of atherogenic risk than total or LDL cholesterol. Several epidemiological studies have shown that tocotrienols reduce atherogenic apoB plasma levels by a significant 10-15%.63 Tocopherols and tocotrienols increase beneficial apolipoprotein-A1 This apolipoprotein has a major role in the functions of high-density lipoprotein (HDL) during the transport of excess cholesterol from peripheral tissues toward the liver for excretion. In addition, APOA1 interacts with paraoxonase, an enzyme located on HDL that reduces oxidative modification of LDL, thereby decreasing the occurrence of atherosclerosis. APOA1 was found to be significantly increased following both alpha-tocopherol64 and tocotrienol65 supplementation. Tocotrienols increase apolipoprotein-E to help clear cholesterol from circulation Tocotrienol supplementation also increased serum levels of APOE, an apolipoprotein with roles in reverse cholesterol transport (removal of cholesterol from circulation) and plasma lipoprotein metabolism. It can serve as a ligand for the LDL receptor and for specific APOE receptors in the liver. APOE functions in the clearance of VLDL and chylomicron remnants, thus affecting circulating concentrations of lipoproteins and plasma levels of cholesterol. Low concentrations of APOE represent a risk of developing CVD.66 Tocotrienols reduce atherosclerosis through modulating PPAR activity Alpha-tocopherol alone has been shown to be unable to prevent atherosclerosis formation in apolipoprotein E-heterozygous (ApoE+/−) mice on a cholesterol diet; whereas a mixture of alpha-tocopherol and tocotrienols reduced liver cholesterol levels and atheroma formation.
§ Type of vitamin E unspecified, so probably alpha-tocopherol

202
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 10
Mice fed a high-cholesterol atherogenic diet supplemented with soy bean oil as vehicle, plus 0.1% (w/w) rosiglitazone (an insulin-sensitising antidiabetic medication), 0.05% (w/w) or 0.2% (w/w) tocotrienols for 16 weeks. Cross-sections of the proximal aorta were examined for atherosclerotic lesions. The average lesion area for the mice on vehicle (soybean oil) alone was 46.7%; rosiglitazone treatment reduced the area to 39.0%; while the 0.05% and 0.2% tocotrienol treatments reduced the lesion area to 35.5% and 28.4% respectively (Figure 12), strongly indicating that tocotrienols can attenuate the development of atherosclerosis. The peroxisome proliferator-activated receptors (PPARs) are ligand-regulated transcription factors that play essential preventive roles in the development of atherosclerosis through regulating energy metabolism and inflammation. Further analysis demonstrated that the tocotrienols enhanced PPAR activities (α-tocopherol did not), strongly suggesting that the tocotrienols are acting like PPAR ligands.68 Anti-inflammatory actions support cardiovascular health Inflammation is involved with every stage of CVD, from the initial lesion to acute coronary syndromes such as plaque rupture. The acute phase protein C-reactive protein (CRP) has been proposed as a predictive and prognostic marker for cardiovascular events including atherosclerosis, stroke, and thrombosis. CRP directly exhibits pro-inflammatory effects on peripheral vascular cells such as activation of the classical complement pathway, increase in cellular adhesion, and reduction of endothelial nitric oxide. A strong correlation between increased plasma CRP levels and impaired endothelial function has been reported in patients with coronary artery disease.70 The anti-inflammatory properties of vitamin E are discussed above.71 Tocopherols and tocotrienols are anti-thrombotic Tocopherols inhibit platelet adhesion and aggregation.72 These anti-thrombotic effects have been shown to be due to the inhibition of the synthesis of the eicosanoid thromboxane B2. In addition, supplemental tocotrienols have also been shown to suppress plasma levels of platelet factor 4 through inhibition of phospholipase A2, an enzyme that potentiates the release of arachidonic acid from membrane-bound phospholipids to various eicosanoids.73 Mixed tocopherols are more effective than alpha-tocopherol alone in inhibiting platelet aggregation Forty-six subjects were randomly divided into three groups receiving either alpha-tocopherol (100 mg); natural mixed tocopherols (gamma- 100 mg, delta- 40 mg and alpha- 20 mg)**; or placebo. A series of factors were measured before and after eight weeks administration of these tocopherols, and it was noted that: NO release and SOD protein content in platelets increased
in both tocopherol-treated groups PKC activation in platelets was markedly decreased in
both tocopherol-treated groups ADP-induced platelet aggregation decreased significantly in the mixed tocopherol group, but not in the
alpha-tocopherol and control groups (Figure 13).
** Mixed Tocopherols & Tocotrienols for Free Radical Defence provides alpha-tocopherol 75 mg, gamma-tocopherol 270 mg and delta-tocopherol 106 mg daily.
Figure 12: Tocotrienols attenuate atherosclerosis in ApoE−/− mice. Quantitative analyses of the atherosclerotic lesion areas in the four groups (n = 5). (Rosi = rosiglitazone, insulin-sensitising antidiabetic drug)67
Figure 13: Mean ADP-induced platelet aggregation before and after supplementation for 8 weeks with alpha-tocopherol (α-Toc) or mixed tocopherols (Mixed), showing superior
action of the mixed tocopherols over the alpha-tocopherol alone.69

203
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 11
From this it may be concluded that mixed tocopherols are more potent in preventing platelet aggregation than alpha-tocopherol alone.74
SUMMARY OF THE MAJOR ACTIONS OF VITAMIN E Tocopherols Tocotrienols Antioxidant ++ ++ Anti-inflammatory + + Mitochondrial function + Neuroprotective + ++ Cardioprotective ++ ++ Carcinoprotective + +
APPLICATIONS CARDIOVASCULAR DISEASE Vitamin E reduces cardiovascular disease Two large long-term studies, the Prospective Nurses’ Health Study and the Health Professionals’ Follow-Up Study, reported that, compared to non-users, vitamin E†† supplementation at a minimum dose of 67 mg per day for at least two years significantly reduced the risk of coronary disease by an estimated 40%.75,76 The Cambridge Heart Antioxidant Study (CHAOS) involved 2002 patients with proven coronary atherosclerosis and compared the effects of two different strengths of vitamin E (alpha-tocopherol) supplementation (268 and 536 mg)‡‡ and a placebo over 510 days. Treatment with either dose of vitamin E was demonstrated to reduce the risk of cardiovascular death and non-fatal myocardial infarction by over 75%, with effects lasting after 12 months.77 Other randomised controlled trials on vitamin E have found:
A reduction of up to 41% in CVD mortality risk in women who took 402 mg of natural vitamin E every other day during a 10-year follow-up period.
A significant 54% reduction of major CVD events and 65% reduction in non-fatal myocardial infarction among high risk subjects who had been randomly assigned to take 536 mg of alpha-tocopherol.78
Survey of literature shows vitamin E beneficial to CVD A survey of 59 published reports, including observational studies, retrospective and prospective randomised clinical trials, meta-analyses, and pooling analyses revealed:
Seven studies that reported a reduction in risk of coronary heart disease (CHD) varying from 5 to 65%; Four analyses that found reductions in the risk of stroke varying from 15 to 60%; Three meta-analyses of cohort studies that reported a significant inverse association between
increased vitamin E intake and CVD, with a 4 to 44% reduction; Most case-control studies conducted in European countries found an inverse relationship between
vitamin E in blood plasma or serum and CVD events; Similarly, risk of angina pectoris was inversely associated with plasma alpha-tocopherol
concentrations in another four case-control studies.79 Tocotrienols also effective for CVD Dietary tocotrienol supplements have been shown to prevent atherosclerosis development in patients and preclinical animal models. They are particularly noteworthy for the ability to reverse arterial blockage.80
†† The “vitamin E” in these studies is unspecified, but most probably alpha-tocopherol, as this was considered the representative active form in the 1980s ‡‡ Mixed Tocopherols & Tocotrienols for Free Radical Defence provides around 460 mg mixed natural tocopherols daily as alpha-tocopherol 75 mg, beta-tocopherol 9.6 mg, gamma-tocopherol 270 mg and delta-tocopherol 106 mg daily.
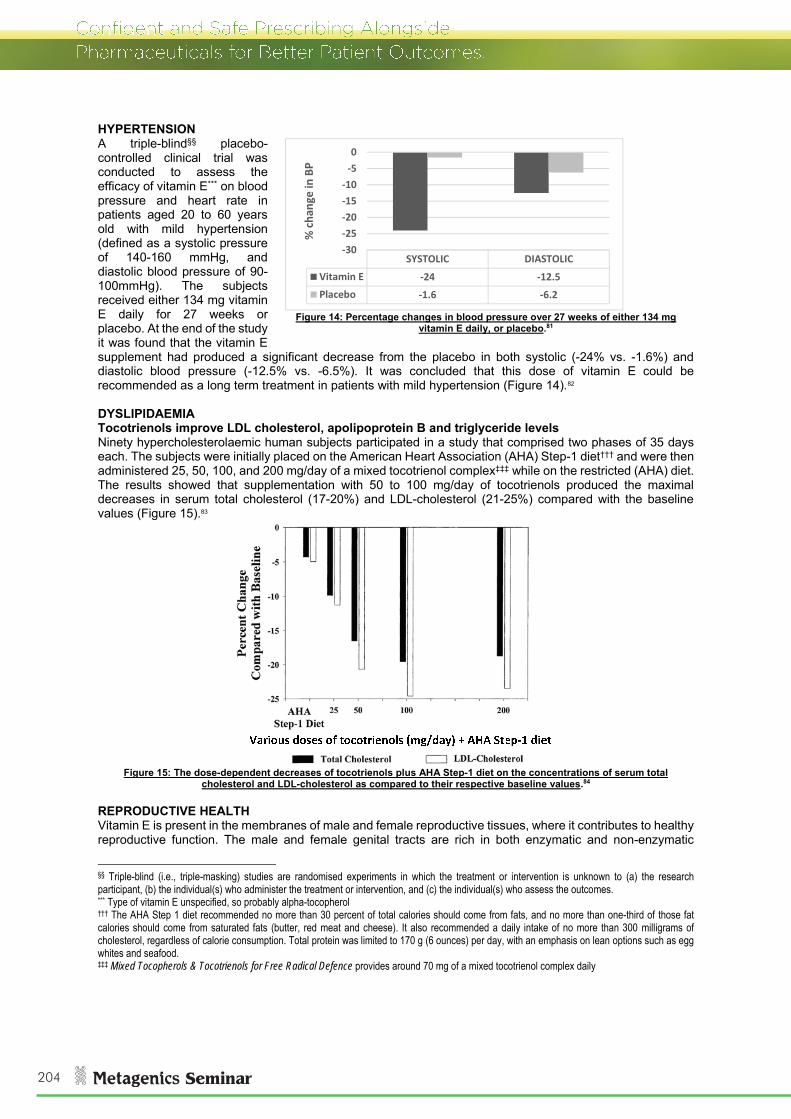
204
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 12
HYPERTENSION A triple-blind§§ placebo-controlled clinical trial was conducted to assess the efficacy of vitamin E*** on blood pressure and heart rate in patients aged 20 to 60 years old with mild hypertension (defined as a systolic pressure of 140-160 mmHg, and diastolic blood pressure of 90-100mmHg). The subjects received either 134 mg vitamin E daily for 27 weeks or placebo. At the end of the study it was found that the vitamin E supplement had produced a significant decrease from the placebo in both systolic (-24% vs. -1.6%) and diastolic blood pressure (-12.5% vs. -6.5%). It was concluded that this dose of vitamin E could be recommended as a long term treatment in patients with mild hypertension (Figure 14).82 DYSLIPIDAEMIA Tocotrienols improve LDL cholesterol, apolipoprotein B and triglyceride levels Ninety hypercholesterolaemic human subjects participated in a study that comprised two phases of 35 days each. The subjects were initially placed on the American Heart Association (AHA) Step-1 diet††† and were then administered 25, 50, 100, and 200 mg/day of a mixed tocotrienol complex‡‡‡ while on the restricted (AHA) diet. The results showed that supplementation with 50 to 100 mg/day of tocotrienols produced the maximal decreases in serum total cholesterol (17-20%) and LDL-cholesterol (21-25%) compared with the baseline values (Figure 15).83
Figure 15: The dose-dependent decreases of tocotrienols plus AHA Step-1 diet on the concentrations of serum total
cholesterol and LDL-cholesterol as compared to their respective baseline values.84 REPRODUCTIVE HEALTH Vitamin E is present in the membranes of male and female reproductive tissues, where it contributes to healthy reproductive function. The male and female genital tracts are rich in both enzymatic and non-enzymatic
§§ Triple-blind (i.e., triple-masking) studies are randomised experiments in which the treatment or intervention is unknown to (a) the research participant, (b) the individual(s) who administer the treatment or intervention, and (c) the individual(s) who assess the outcomes. *** Type of vitamin E unspecified, so probably alpha-tocopherol ††† The AHA Step 1 diet recommended no more than 30 percent of total calories should come from fats, and no more than one-third of those fat calories should come from saturated fats (butter, red meat and cheese). It also recommended a daily intake of no more than 300 milligrams of cholesterol, regardless of calorie consumption. Total protein was limited to 170 g (6 ounces) per day, with an emphasis on lean options such as egg whites and seafood. ‡‡‡ Mixed Tocopherols & Tocotrienols for Free Radical Defence provides around 70 mg of a mixed tocotrienol complex daily
Figure 14: Percentage changes in blood pressure over 27 weeks of either 134 mg
vitamin E daily, or placebo.81
SYSTOLIC DIASTOLICVitamin E ‐24 ‐12.5Placebo ‐1.6 ‐6.2
‐30‐25‐20‐15‐10‐50
% cha
nge in BP

205
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 13
antioxidants. Vitamin E acts as a chain-breaking antioxidant, in that it not only scavenges oxygen radicals from within the membrane, but also intercepts peroxyl and alkoxyl radicals which are generated during the conversion of lipid hydroperoxides that fuel the peroxidative chain reaction, thereby preventing this damaging process from propagating through plasma membrane.85,86 Vitamin E supports progesterone levels in PMS and infertiltiy Regression of the corpus luteum is mediated in part by oxidative reactions, and excess oxidative stress can lead to premature degradation and low progesterone production due to luteal defect. Vitamin E is present in high levels in ovarian cells, human follicular fluid, and the corpus luteum, and serves a vital role in attenuating the potentially toxic effects of oxidative stress by scavenging lipid peroxides. This may be useful in progesterone-deficient women’s health conditions such as premenstrual syndrome and infertility.87,88,89 Vitamin E improves luteal phase defect In a study to investigate whether luteal function in women with luteal phase defect§§§ can be improved by increasing blood flow to the corpus luteum, patients were given 600 mg/day vitamin E during the luteal phase of the subsequent menstrual cycle. After the next cycle, the control group, who received no medication, showed improvement in only 3 of the 11 patients (27%). In contrast, of the 18 patients who received vitamin E, 15 (83%) showed improvement in luteal circulation and 12 (67%) in luteal function (as indicated by increased progesterone production). These results confirm that luteal blood flow is a critical factor for the healthy function of the corpus luteum, and that vitamin E treatment improves luteal function by improving blood flow.90 Vitamin E supports sperm viability in male infertility Vitamin E supplementation appears to be especially warranted for male fertility because this vitamin is the main antioxidant in various cell membranes, including those surrounding sperm. Free radicals lead to peroxidation of phospholipids in the mitochondria of the sperm, making the sperm immotile. Vitamin E has been shown to play an essential role in inhibiting free radical damage to the unsaturated fatty acids of the sperm membrane. Additionally, it has been shown to protect the DNA within sperm from damage.92 An in vitro investigation into the efficacy of vitamin E to protect sperm against ROS-mediated damage showed a dose-dependent improvement in both motility and viability.93 This study showed a gradual decrease in spermatozoal motility and viability in stored sperm from 0.5 to 6 hours, which was attributed to oxidative stress to which spermatozoa are subjected to during storage. Lipid peroxidation also impairs the fertilizing potential of sperm. Vitamin E treatment in vitro produced a significant improvement in sperm motility and viability (Figure 16).94 MAINTENANCE OF COGNITION Tocopherols and tocotrienols reduce risk of developing Alzheimer’s disease Low levels of tocopherols and tocotrienols have been associated with cognitive decline and Alzheimer’s disease. A study was conducted to assess the relationship between all plasma forms of vitamin E and markers of oxidative damage to mild cognitive impairment (MCI) and Alzheimer’s disease (AD). Compared with cognitively normal subjects, patients with AD and MCI had lower levels of tocopherols, tocotrienols (Figure 17) and total vitamin E. Both MCI and AD cases were 85% less likely to be in the highest tertile of total tocopherols and total vitamin E, and 92 to 94% less likely to be in the highest tertile of total tocotrienols.95 This study shows that high plasma vitamin E levels are associated with reduced likelihood of developing MCI and AD. Reduced levels of alpha- and gamma-tocopherols were associated with increased indexes of their utilisation due to reaction with free radicals, suggesting that vitamin E depletion could be due to increased utilisation due to oxidative stress.
§§§ Luteal phase defect is a condition in which the corpus luteum is dysfunctional, and produces reduced amounts of progesterone, leading to shorter periods (the second, luteal, phase is curtailed). It may be associated with infertility.
Figure 16: Dose-dependent preservation of sperm motility (A) and viability (B) after 6 hours in solution, with various concentrations of vitamin E (RT = Ringer-Tyrode solution plus 0.1, 1 or 2 mmol/L vitamin E.91

206
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 14
Tocotrieno
ls (nM/m
mol ch
olesterol)
Tocopherols (μmol/m
mol cholesterol)
0
1.25
2.5
3.75
5
6.25
7.5
8.75* p<0.0001 vs. control
**
**
Figure 17: Low tocopherols and tocotrienols in cognitive impairment.96
DERMAL PROTECTION Vitamin E protects the skin from oxidative damage As the outermost organ of the body, in addition to combatting normal endogenous generation of ROS, the skin is frequently and directly exposed to a pro-oxidative environment, including ultraviolet radiation, chemicals, and air pollutants. The induction of oxidative damage by environmental stimuli such as UVA, UVB, and ozone has been demonstrated to occur in skin lipids, proteins and DNA. To counteract such oxidative injury, human skin is equipped with a network of enzymatic and non-enzymatic antioxidant systems. Vitamin E is the major naturally-occurring lipid-soluble non-enzymatic antioxidant protecting the skin from the adverse effects of oxidative stress.97 Many studies indicate that antioxidant inadequacy from depleted dietary vitamin E is associated with accelerated ageing of the skin.98,99 It has been demonstrated, for instance, that the stratum corneum, which maintains the barrier function of skin, is highly susceptible to vitamin E depletion and lipid peroxidation induced by UVA and UVB. Vitamin E is a significant constituent of human sebum, which is continuously secreted at cheek and forehead sites. Researchers have concluded that sebaceous gland secretion is a relevant physiologic pathway for the delivery of vitamin E to upper layers of the facial skin. This mechanism may serve to protect skin surface lipids and the upper stratum corneum from harmful oxidation.100 Vitamin E alleviates atopic dermatitis In a randomised, double-blind, placebo-controlled trial investigating the effect of vitamin E on dermatitis, atopic dermatitis patients received 400 mg (600 IU) alpha-tocopherol daily for 60 days and their clinical improvement was evaluated by SCORing Atopic Dermatitis (SCORAD). Over the course of trial, the average SCORAD reduced by 35.7%, and a significant negative association between plasma alpha-tocopherol and SCORAD, intensity, objective and extent was identified.101

207
Confident and Safe Prescribing Alongside Pharmaceuticals for Better Patient Outcomes.
Metagenics Technical Team December 2014 15
FIBROMYALGIA Fibromyalgia patients deficient in vitamin E There is an increased risk of fat soluble vitamin deficiency in individuals with disorders associated with suboptimal mitochondrial function, such as fibromyalgia (FM) and chronic fatigue syndrome (CFS). ROS are thought to play a role in the aetiology and pathogenesis of fibromyalgia, indicating the need for greater antioxidant protection. A study of 30 female fibromyalgia patients investigated the levels of plasma antioxidant vitamins, lipid peroxidation and nitric oxide (NO) in comparison to controls. It was found that concentrations of vitamin E were significantly lower in patients with FM than controls, and lipid peroxidation concentrations were significantly higher in the plasma of the FM patients than in controls (Figure 18).102
Figure 18: Low vitamin E in patients
with fibromyalgia103 CAUTIONS/CONTRAINDICATIONS CONTRAINDICATIONS Allergies and sensitivities: Avoid with known allergy or hypersensitivity to palm oil or derivative
thereof.104 CAUTIONS Anticoagulant/Antiplatelet drugs: Concomitant use alongside anticoagulant or antiplatelet agents such
as aspirin and warfarin might increase the risk of bleeding. Use with caution and monitor INR in patients taking warfarin.
o Tocopherols and tocotrienols have antiplatelet effects. These effects are only likely to be clinically significant when supplementing with 536 mg/day (800 IU) or more of mixed tocopherol and tocotrienols.105,106
Bleeding disorders: Due to the anticoagulant properties of tocopherols and tocotrienols there have been safety concerns in regards to the risk of increased bleeding tendency. These effects are only likely to be clinically significant when supplementing with a total of 536 mg/day (800 IU) or more. To minimise the risk of exacerbation of these bleeding events it is recommended to: 107,108,109,110,111,112
o Use supplemental vitamin E cautiously in those patients with bleeding disorders. o Discontinue use of supplemental vitamin E during acute bleeding episodes, such as during and
immediately after a haemorrhagic stroke, or in patients who are at high risk for haemorrhagic stroke.
Chemotherapy/radiotherapy: Vitamin E may affect the efficacy of chemotherapy. Use with caution and only under the supervision of a patient’s oncologist. It has generally been thought that antioxidants may interfere with chemotherapy and/or radiotherapy by decreasing the efficacy of the treatment, recent studies have found that antioxidants are safe to use in conjunction with these treatments. However, it is still advisable to check with a patient’s oncologist before recommending a formula containing antioxidants.113
Surgery: Stop treatment at least 1 week prior to major surgery as tocopherols and tocotrienols may have antiplatelet effects. These effects are only likely to be clinically significant when supplementing with 536 mg/day (800 IU) or more of mixed tocopherol and tocotrienols.114,115
PREGNANCY AND BREASTFEEDING Pregnancy: Likely safe when used at recommended doses. Breastfeeding: Likely safe when used at recommended doses. REFERENCES 1 Thiele JJ, Ekanayake-Mudiyanselage S. Vitamin E in human skin: Organ-specific physiology and considerations for its use in dermatology. Mol Aspects Med, 2007; 28 (5): 646-67. 2 Sen CK, Khanna S, Roy S. Tocotrienols: Vitamin E beyond tocopherols. Life Sci. 2006 Mar 27; 78(18): 2088-98. 3 Aggarwal BB, Sundaram C, Prasad S, Kannappan R. Tocotrienols, the vitamin E of the 21st century: its potential against cancer and other chronic diseases. Biochem Pharmacol. 2010 Dec 1; 80(11): 1613-31.
CO
NTR
OL
FIBR
OM
YALGIA
For full technical data including Cautions and Contraindications and References, go to www.metagenics.com.au (Australia), or www.metagenics.co.nz (New Zealand).