peripheral markers in testing pathophysiological hypotheses and diagnosing alzheimer's disease
TRANSCRIPT

170892-6638/98/0012-0017/$02.25 Q FASEB
/ 381c 0002 Mp 17 Tuesday Nov 25 11:34 AM LP–FASEB 0002
Peripheral markers in testing pathophysiologicalhypotheses and diagnosing Alzheimer’s disease
L. GASPARINI,* M. RACCHI,* G. BINETTI,* M. TRABUCCHI,† S. B. SOLERTE,‡
D. ALKON,§ R. ETCHEBERRIGARAY,H G. GIBSON,†† J. BLASS,†† R. PAOLETTI,**AND S. GOVONI‡‡,**,1
*I.R.C.C.S San Giovanni di Dio, Alzheimer’s Disease Unit Sacred Heart Hospital-FBF, Brescia;†Department of Experimental Medicine and Biochemical Sciences, University of Roma Tor Vergata;‡Internal Medicine Department, Geriatric Clinic, University of Pavia, Italy; §Laboratory of AdaptiveSystems, National Institute of Neurological Disorders and Stroke, National Institutes of Health,Bethesda, Maryland 20892, USA; HInstitute for Cognitive and Computational Sciences, GeorgetownUniversity Medical Center, Washington D.C. 20007, USA; ††Cornell University Medical College atBurke Medical Research Institute, New York 10605, USA; **Institute of Pharmacological Sciences,University of Milano, and ‡‡University of Pavia, Italy
ABSTRACT Alterations in amyloid precursor pro-tein (APP) metabolism, calcium regulation, oxidativemetabolism, and transduction systems have been im-plicated in Alzheimer’s disease (AD). Limitations tothe use of postmortem brain for examining molecu-lar mechanisms underscore the need to develop ahuman tissue model representative of the pathophys-iological processes that characterize AD. The use ofperipheral tissues, particularly of cultured skin fibro-blasts derived from AD patients, could complementstudies of autopsy samples and provide a useful toolwith which to investigate such dynamic processes assignal transduction systems, ionic homeostasis, oxi-dative metabolism, and APP processing. Peripheralcells as well as body fluids (i.e., plasma and CSF)could also provide peripheral biological markers forthe diagnosis of AD. The criteria required for a def-inite diagnosis of AD presently include clinical crite-ria in association with histopathologic evidenceobtained from biopsy or autopsy. Thus, the use ofperipheral markers as a diagnostic tool, either to pre-dict or at least to confirm a diagnosis, may be of greatimportance.—Gasparini, L., Racchi, M., Binetti, G.,Trabucchi, M., Solerte, S. B., Alkon, D., Etcheberri-garay, R., Gibson, G., Blass, J., Paoletti, R., Govoni,S. Peripheral markers in testing pathophysiologicalhypotheses and diagnosing Alzheimer’s disease.FASEB J. 12, 17–34 (1998)
Key Words: peripheral cells · CSF · plasma · diagnosis
ALZHEIMER’S DISEASE (AD)2 is a progressive neuro-degenerative disorder characterized by irreversiblecognitive and physical deterioration. It is a majorcause of death and a growing public health problemas life expectancy in the general population in-creases. The first case report of Alzheimer’s diseasewas published in 1907 by Alois Alzheimer (1). It de-
scribed the autopsy findings for a woman who diedat age 55 with progressive dementia and in whomnewly available silver stains revealed the presence ofabnormal nerve cells containing tangles of fibers(neurofibrillary tangles) and neuritic plaques in thecerebral cortex.
Much work has been done since then to identifythe etiology and pathophysiological mechanisms thatlead to the premature dysfunction and death of theneurons that characterize Alzheimer’s disease. A mo-lecular characterization of structures that constitutethe neuropathological lesions typical of AD, the neu-ritic plaques and neurofibrillary tangles, are one ap-proach to that question. Extracellular senile plaquesin their classical form represent a compacted amyloiddeposit consisting mainly of b-amyloid (or Ab), a frag-ment of a larger protein defined as amyloid precur-sor protein (APP) (2, 3) that is expressed in allmammalian tissues except in nonnucleated redblood cells (4). Neurofibrillary tangles (NFT) rep-resent intraneuronal bundles of paired helicalfilaments (PHF), which consist mainly of the
1 Correspondence: c/o Institute of Pharmacological Sci-ences, University of Milano, Via Balzaretti 9, 20133 Milano,Italy. E-mail: [email protected]
2 Abbreviations: Ab, b-amyloid; ACTH, adrenocorticotropinhormone; AD, Alzheimer’s disease; ApoE, apolipoprotein E;APP, amyloid precursor protein; BK, bradykinin; CO, cyto-chrome c oxidase; CRH, corticotropin-releasing hormone;CSF, cerebrospinal fluid; DEX, dexamethasone; DS, Down’ssyndrome; FAD, familial Alzheimer’s disease; GHRH, growthhormone-releasing hormone; HPA, hypothalamic-pituitary-adrenal; IL-2, interleukin 2; IFN-b, interferon b; IP3, inositol-(1,4,5)-trisphosphate; NFT, neurofibrillary tangles; NK,natural killer; PHF, paired helical filaments; PKC, protein ki-nase C; PKC-a, protein kinase C a isoform; PRL, prolactin;PS1, presenilin 1; PS2, presenilin 2; sAPP, soluble APP; SLI,somatostatin-like immunoreactivity; TEA, tetraethylammo-nium; TRH/TSH, thyrotropin releasing hormone/thyrotro-pin hormone.

18 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 18 Tuesday Nov 25 11:34 AM LP–FASEB 0002
microtubule-associated tau protein in an abnormallyphosphorylated form and ubiquitin (5, 6). The rea-son why this abnormal accumulation of amyloid andPHF occurs in the AD brain is not yet clear.
Pathophysiological studies and diagnosis of the dis-ease rely in part on the use of brain tissue from dis-eased patients. In particular, confirmation of ADdiagnosis is only possible postmortem by neuro-pathological analysis, despite the lack of completespecificity of central markers such as amyloid plaquesand NFT. Senile plaques and NFT are not unequiv-ocal markers of Alzheimer’s disease. In fact, amyloidplaques can be observed in the brain of normal ageddonors (7). NFT can also be detected in the brain ofother neurodegenerative disorders such as Pick’s dis-ease, progressive supranuclear palsy, and corticobasaldegeneration (8).
Accordingly, there is an active search to identifyaccessible tissues or body fluids that are suitable forexploring pathophysiological hypotheses and thatprovide a biological marker with which to confirmdiagnoses. Although this latter goal still eludes theefforts of the investigators, some relevant data havebeen obtained that contribute to the characterizationof working pathophysiological hypotheses, such as inthe case of amyloid precursor metabolism or oxida-tive metabolism dysfunction.
THE USE OF PERIPHERAL TISSUES:RATIONALE AND METHODOLOGICALCONSTRAINTS
To identify the cellular and molecular abnormalitiesthat cause the characteristic neuropathological le-sions of AD, autopsied brains and extraneural tissueshave been used. The use of peripheral cells is basedon the hypothesis that Alzheimer’s disease might bea systemic disease that affects several tissues in thebody. The specific brain damage could be the ex-pression of a greater sensitivity to injury in postmi-totic cells of the brain. Furthermore, a potentialgenetic defect underlying the disease may be mani-fest in several body tissues that express the gene in-volved.
Peripheral tissues suitable for exploring patho-physiological hypotheses and possibly for providing auseful biological marker for diagnosis of AD includeskin fibroblasts, platelets, lymphocytes, as well as bodyfluids such as plasma or cerebrospinal fluid (CSF).Among these tissues, cultured skin fibroblasts havebeen used successfully to elucidate the molecular andbiochemical bases of many inborn errors of metabo-lism that cause neurological disease, i.e., Refsum’sdisease (9) and Lesch-Nyhan disease (10). Moreover,fibroblasts are an appropriate model for studies ofthose genetic diseases of the nervous system with lateclinical onset, including familial Alzheimer’ s disease,
because they can be easily cultured and stored andcontain the complete genomic information of the or-ganism.
As always when studying the effect of a pathologyon a given tissue, the choice of appropriate controlsand the problem of distinguishing those changes thatare due to the disease from effects related to otheraspects of the patients, such as nutritional status anddrug treatments, are key issues. This problem is mostimportant for cells such as platelets and lymphocytes,which are influenced more by the patients’ condi-tion, but nutritional and drug effects are enormouslydiluted in cultured fibroblasts. When using culturedskin fibroblasts, some technical variables should alsobe considered. Growth properties and in vitro agingof AD and control fibroblast cultures do not differunder standard conditions (11–14), although thistopic is still controversial. Since growth propertiesand biological age in culture can have profound ef-fects on the properties of cells cultured from skin,including the expression of genes (which could berelated to AD) (15), reproducible and interpretableresults with the AD fibroblasts model require atten-tion to the replicability of culture conditions includ-ing, but not limited to, matching AD and control cellsfor age, sex of the donors, and biological age in cul-ture, i.e., cumulative population doubling level andpercentage of life span completed (16). Differentgrowth conditions, aging of cultures in vitro, andstate of confluency of the cells at the time of the ex-periment may account for discrepancies betweendata from different laboratories. Only abnormalitiesreplicated in larger series across different laborato-ries or characterizing subgroups of AD patients arelikely to be of relevance (17) in diagnosing Alzhei-mer’s disease. This diagnosis indeed appears to bethe major challenge posed by AD in its sporadic late-onset form, which still represents the vast majority ofall cases.
On the other hand, data obtained using fibroblastsfrom individuals with known gene defects, althoughrepresenting only a small proportion of all AD cases,could be very informative about the cellular patho-physiology of Alzheimer’s disease. Recent advancesin understanding the genetics of AD allow identifi-cation of families bearing mutations in APP, prese-nilin 1 (PS1), or presenilin 2 (PS2) genes coded onchromosomes 21, 14 and 1, respectively (18). Fibro-blast lines from familial AD patients can now be clas-sified according to the specific gene defect to seewhether a particular genetic abnormality alters cel-lular function in a unique manner (Table 1).
Peripheral cells are therefore useful in identifyingand testing hypotheses on the primary pathophysio-logical mechanisms leading to Alzheimer’s diseaseand for avoiding variables derived from a postmor-tem state. On the other hand, peripheral cells cannotbe used to answer other clinically relevant questions
PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 19
/ 381c 0002 Mp 19 Tuesday Nov 25 11:34 AM LP–FASEB 0002
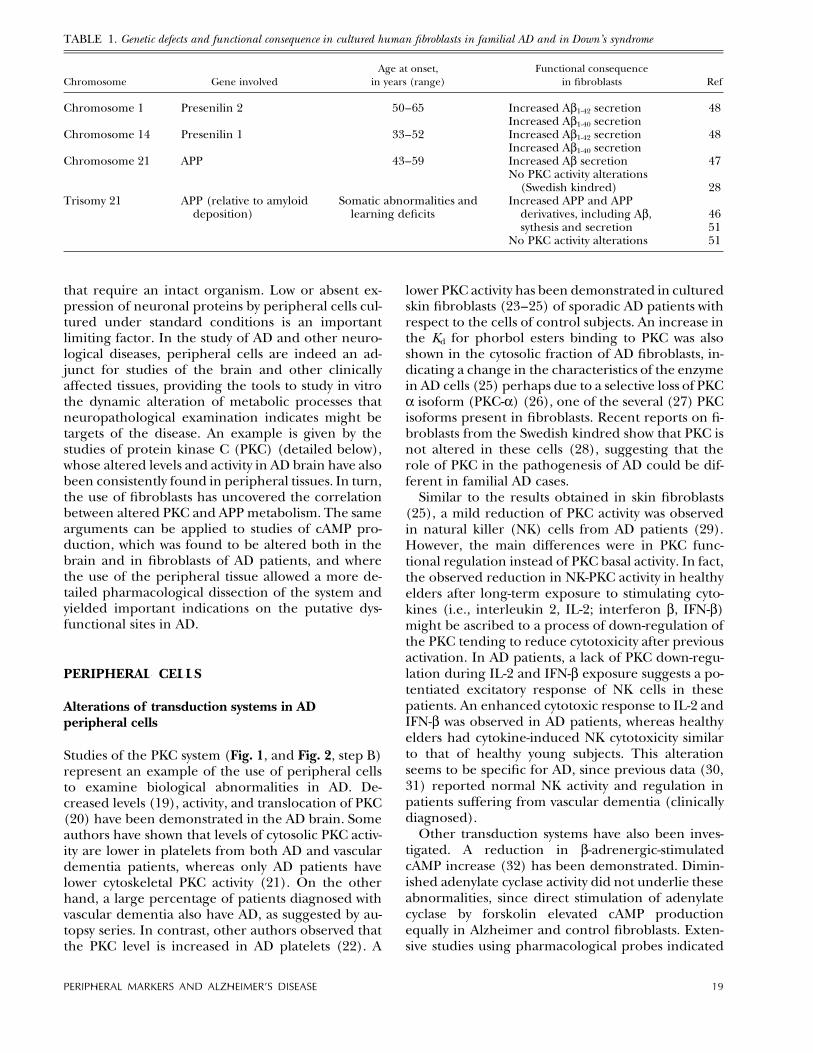
TABLE 1. Genetic defects and functional consequence in cultured human fibroblasts in familial AD and in Down’s syndrome
Chromosome Gene involvedAge at onset,
in years (range)Functional consequence
in fibroblasts Ref
Chromosome 1 Presenilin 2 50–65 Increased Ab1-42 secretion 48Increased Ab1-40 secretion
Chromosome 14 Presenilin 1 33–52 Increased Ab1-42 secretion 48Increased Ab1-40 secretion
Chromosome 21 APP 43–59 Increased Ab secretion 47No PKC activity alterations
(Swedish kindred) 28Trisomy 21 APP (relative to amyloid
deposition)Somatic abnormalities and
learning deficitsIncreased APP and APP
derivatives, including Ab,sythesis and secretion
4651
No PKC activity alterations 51
that require an intact organism. Low or absent ex-pression of neuronal proteins by peripheral cells cul-tured under standard conditions is an importantlimiting factor. In the study of AD and other neuro-logical diseases, peripheral cells are indeed an ad-junct for studies of the brain and other clinicallyaffected tissues, providing the tools to study in vitrothe dynamic alteration of metabolic processes thatneuropathological examination indicates might betargets of the disease. An example is given by thestudies of protein kinase C (PKC) (detailed below),whose altered levels and activity in AD brain have alsobeen consistently found in peripheral tissues. In turn,the use of fibroblasts has uncovered the correlationbetween altered PKC and APP metabolism. The samearguments can be applied to studies of cAMP pro-duction, which was found to be altered both in thebrain and in fibroblasts of AD patients, and wherethe use of the peripheral tissue allowed a more de-tailed pharmacological dissection of the system andyielded important indications on the putative dys-functional sites in AD.
PERIPHERAL CELLS
Alterations of transduction systems in ADperipheral cells
Studies of the PKC system (Fig. 1, and Fig. 2, step B)represent an example of the use of peripheral cellsto examine biological abnormalities in AD. De-creased levels (19), activity, and translocation of PKC(20) have been demonstrated in the AD brain. Someauthors have shown that levels of cytosolic PKC activ-ity are lower in platelets from both AD and vasculardementia patients, whereas only AD patients havelower cytoskeletal PKC activity (21). On the otherhand, a large percentage of patients diagnosed withvascular dementia also have AD, as suggested by au-topsy series. In contrast, other authors observed thatthe PKC level is increased in AD platelets (22). A
lower PKC activity has been demonstrated in culturedskin fibroblasts (23–25) of sporadic AD patients withrespect to the cells of control subjects. An increase inthe Kd for phorbol esters binding to PKC was alsoshown in the cytosolic fraction of AD fibroblasts, in-dicating a change in the characteristics of the enzymein AD cells (25) perhaps due to a selective loss of PKCa isoform (PKC-a) (26), one of the several (27) PKCisoforms present in fibroblasts. Recent reports on fi-broblasts from the Swedish kindred show that PKC isnot altered in these cells (28), suggesting that therole of PKC in the pathogenesis of AD could be dif-ferent in familial AD cases.
Similar to the results obtained in skin fibroblasts(25), a mild reduction of PKC activity was observedin natural killer (NK) cells from AD patients (29).However, the main differences were in PKC func-tional regulation instead of PKC basal activity. In fact,the observed reduction in NK-PKC activity in healthyelders after long-term exposure to stimulating cyto-kines (i.e., interleukin 2, IL-2; interferon b, IFN-b)might be ascribed to a process of down-regulation ofthe PKC tending to reduce cytotoxicity after previousactivation. In AD patients, a lack of PKC down-regu-lation during IL-2 and IFN-b exposure suggests a po-tentiated excitatory response of NK cells in thesepatients. An enhanced cytotoxic response to IL-2 andIFN-b was observed in AD patients, whereas healthyelders had cytokine-induced NK cytotoxicity similarto that of healthy young subjects. This alterationseems to be specific for AD, since previous data (30,31) reported normal NK activity and regulation inpatients suffering from vascular dementia (clinicallydiagnosed).
Other transduction systems have also been inves-tigated. A reduction in b-adrenergic-stimulatedcAMP increase (32) has been demonstrated. Dimin-ished adenylate cyclase activity did not underlie theseabnormalities, since direct stimulation of adenylatecyclase by forskolin elevated cAMP productionequally in Alzheimer and control fibroblasts. Exten-sive studies using pharmacological probes indicated
20 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 20 Tuesday Nov 25 11:34 AM LP–FASEB 0002
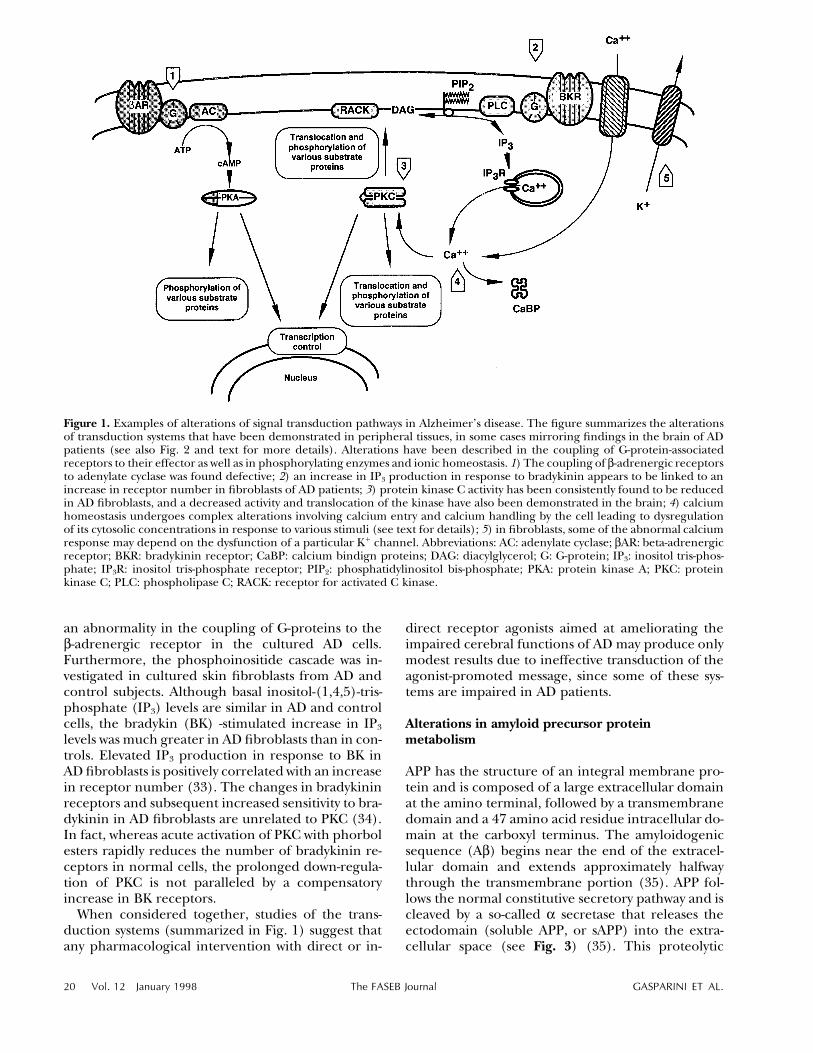
Figure 1. Examples of alterations of signal transduction pathways in Alzheimer’s disease. The figure summarizes the alterationsof transduction systems that have been demonstrated in peripheral tissues, in some cases mirroring findings in the brain of ADpatients (see also Fig. 2 and text for more details). Alterations have been described in the coupling of G-protein-associatedreceptors to their effector as well as in phosphorylating enzymes and ionic homeostasis. 1) The coupling of b-adrenergic receptorsto adenylate cyclase was found defective; 2) an increase in IP3 production in response to bradykinin appears to be linked to anincrease in receptor number in fibroblasts of AD patients; 3) protein kinase C activity has been consistently found to be reducedin AD fibroblasts, and a decreased activity and translocation of the kinase have also been demonstrated in the brain; 4) calciumhomeostasis undergoes complex alterations involving calcium entry and calcium handling by the cell leading to dysregulationof its cytosolic concentrations in response to various stimuli (see text for details); 5) in fibroblasts, some of the abnormal calciumresponse may depend on the dysfunction of a particular K/ channel. Abbreviations: AC: adenylate cyclase; bAR: beta-adrenergicreceptor; BKR: bradykinin receptor; CaBP: calcium bindign proteins; DAG: diacylglycerol; G: G-protein; IP3: inositol tris-phos-phate; IP3R: inositol tris-phosphate receptor; PIP2: phosphatidylinositol bis-phosphate; PKA: protein kinase A; PKC: proteinkinase C; PLC: phospholipase C; RACK: receptor for activated C kinase.
an abnormality in the coupling of G-proteins to theb-adrenergic receptor in the cultured AD cells.Furthermore, the phosphoinositide cascade was in-vestigated in cultured skin fibroblasts from AD andcontrol subjects. Although basal inositol-(1,4,5)-tris-phosphate (IP3) levels are similar in AD and controlcells, the bradykin (BK) -stimulated increase in IP3
levels was much greater in AD fibroblasts than in con-trols. Elevated IP3 production in response to BK inAD fibroblasts is positively correlated with an increasein receptor number (33). The changes in bradykininreceptors and subsequent increased sensitivity to bra-dykinin in AD fibroblasts are unrelated to PKC (34).In fact, whereas acute activation of PKC with phorbolesters rapidly reduces the number of bradykinin re-ceptors in normal cells, the prolonged down-regula-tion of PKC is not paralleled by a compensatoryincrease in BK receptors.
When considered together, studies of the trans-duction systems (summarized in Fig. 1) suggest thatany pharmacological intervention with direct or in-
direct receptor agonists aimed at ameliorating theimpaired cerebral functions of AD may produce onlymodest results due to ineffective transduction of theagonist-promoted message, since some of these sys-tems are impaired in AD patients.
Alterations in amyloid precursor proteinmetabolism
APP has the structure of an integral membrane pro-tein and is composed of a large extracellular domainat the amino terminal, followed by a transmembranedomain and a 47 amino acid residue intracellular do-main at the carboxyl terminus. The amyloidogenicsequence (Ab) begins near the end of the extracel-lular domain and extends approximately halfwaythrough the transmembrane portion (35). APP fol-lows the normal constitutive secretory pathway and iscleaved by a so-called a secretase that releases theectodomain (soluble APP, or sAPP) into the extra-cellular space (see Fig. 3) (35). This proteolytic
PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 21
/ 381c 0002 Mp 21 Tuesday Nov 25 11:34 AM LP–FASEB 0002
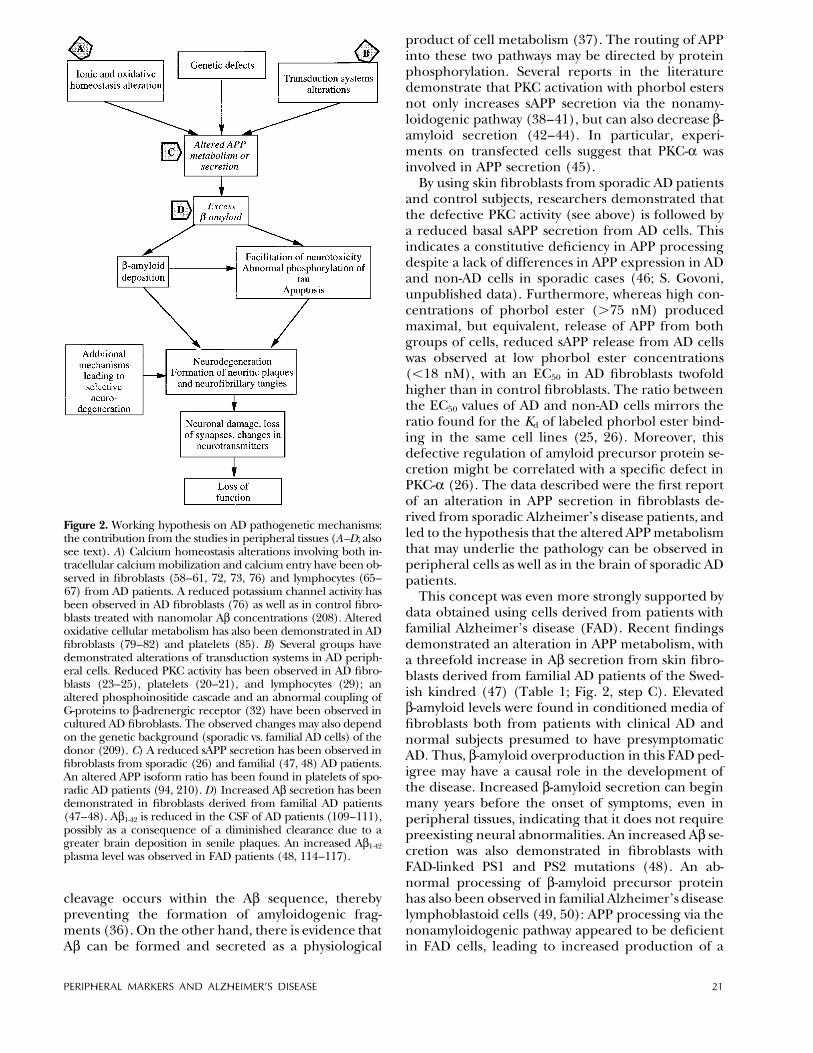
Figure 2. Working hypothesis on AD pathogenetic mechanisms:the contribution from the studies in peripheral tissues (A–D; alsosee text). A) Calcium homeostasis alterations involving both in-tracellular calcium mobilization and calcium entry have been ob-served in fibroblasts (58–61, 72, 73, 76) and lymphocytes (65–67) from AD patients. A reduced potassium channel activity hasbeen observed in AD fibroblasts (76) as well as in control fibro-blasts treated with nanomolar Ab concentrations (208). Alteredoxidative cellular metabolism has also been demonstrated in ADfibroblasts (79–82) and platelets (85). B) Several groups havedemonstrated alterations of transduction systems in AD periph-eral cells. Reduced PKC activity has been observed in AD fibro-blasts (23–25), platelets (20–21), and lymphocytes (29); analtered phosphoinositide cascade and an abnormal coupling ofG-proteins to b-adrenergic receptor (32) have been observed incultured AD fibroblasts. The observed changes may also dependon the genetic background (sporadic vs. familial AD cells) of thedonor (209). C) A reduced sAPP secretion has been observed infibroblasts from sporadic (26) and familial (47, 48) AD patients.An altered APP isoform ratio has been found in platelets of spo-radic AD patients (94, 210). D) Increased Ab secretion has beendemonstrated in fibroblasts derived from familial AD patients(47–48). Ab1-42 is reduced in the CSF of AD patients (109–111),possibly as a consequence of a diminished clearance due to agreater brain deposition in senile plaques. An increased Ab1-42
plasma level was observed in FAD patients (48, 114–117).
cleavage occurs within the Ab sequence, therebypreventing the formation of amyloidogenic frag-ments (36). On the other hand, there is evidence thatAb can be formed and secreted as a physiological
product of cell metabolism (37). The routing of APPinto these two pathways may be directed by proteinphosphorylation. Several reports in the literaturedemonstrate that PKC activation with phorbol estersnot only increases sAPP secretion via the nonamy-loidogenic pathway (38–41), but can also decrease b-amyloid secretion (42–44). In particular, experi-ments on transfected cells suggest that PKC-a wasinvolved in APP secretion (45).
By using skin fibroblasts from sporadic AD patientsand control subjects, researchers demonstrated thatthe defective PKC activity (see above) is followed bya reduced basal sAPP secretion from AD cells. Thisindicates a constitutive deficiency in APP processingdespite a lack of differences in APP expression in ADand non-AD cells in sporadic cases (46; S. Govoni,unpublished data). Furthermore, whereas high con-centrations of phorbol ester (ú75 nM) producedmaximal, but equivalent, release of APP from bothgroups of cells, reduced sAPP release from AD cellswas observed at low phorbol ester concentrations(õ18 nM), with an EC50 in AD fibroblasts twofoldhigher than in control fibroblasts. The ratio betweenthe EC50 values of AD and non-AD cells mirrors theratio found for the Kd of labeled phorbol ester bind-ing in the same cell lines (25, 26). Moreover, thisdefective regulation of amyloid precursor protein se-cretion might be correlated with a specific defect inPKC-a (26). The data described were the first reportof an alteration in APP secretion in fibroblasts de-rived from sporadic Alzheimer’s disease patients, andled to the hypothesis that the altered APP metabolismthat may underlie the pathology can be observed inperipheral cells as well as in the brain of sporadic ADpatients.
This concept was even more strongly supported bydata obtained using cells derived from patients withfamilial Alzheimer’s disease (FAD). Recent findingsdemonstrated an alteration in APP metabolism, witha threefold increase in Ab secretion from skin fibro-blasts derived from familial AD patients of the Swed-ish kindred (47) (Table 1; Fig. 2, step C). Elevatedb-amyloid levels were found in conditioned media offibroblasts both from patients with clinical AD andnormal subjects presumed to have presymptomaticAD. Thus, b-amyloid overproduction in this FAD ped-igree may have a causal role in the development ofthe disease. Increased b-amyloid secretion can beginmany years before the onset of symptoms, even inperipheral tissues, indicating that it does not requirepreexisting neural abnormalities. An increased Ab se-cretion was also demonstrated in fibroblasts withFAD-linked PS1 and PS2 mutations (48). An ab-normal processing of b-amyloid precursor proteinhas also been observed in familial Alzheimer’s diseaselymphoblastoid cells (49, 50): APP processing via thenonamyloidogenic pathway appeared to be deficientin FAD cells, leading to increased production of a
22 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 22 Tuesday Nov 25 11:34 AM LP–FASEB 0002
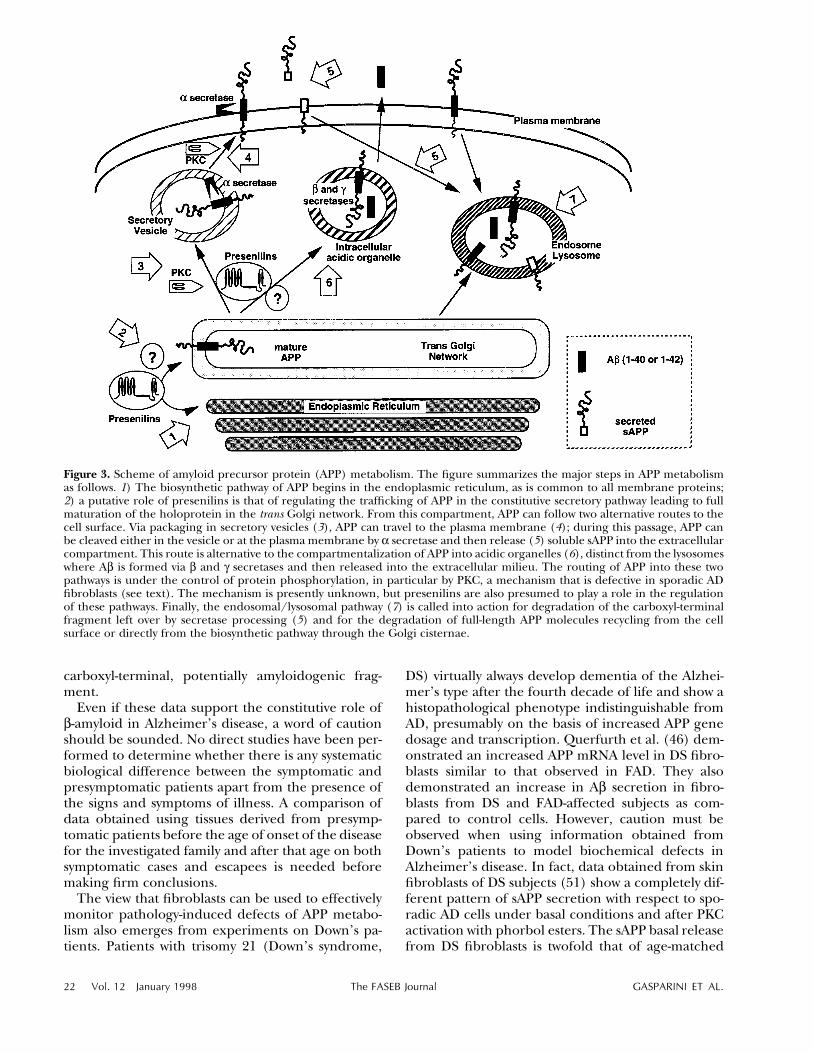
Figure 3. Scheme of amyloid precursor protein (APP) metabolism. The figure summarizes the major steps in APP metabolismas follows. 1) The biosynthetic pathway of APP begins in the endoplasmic reticulum, as is common to all membrane proteins;2) a putative role of presenilins is that of regulating the trafficking of APP in the constitutive secretory pathway leading to fullmaturation of the holoprotein in the trans Golgi network. From this compartment, APP can follow two alternative routes to thecell surface. Via packaging in secretory vesicles (3), APP can travel to the plasma membrane (4); during this passage, APP canbe cleaved either in the vesicle or at the plasma membrane by a secretase and then release (5) soluble sAPP into the extracellularcompartment. This route is alternative to the compartmentalization of APP into acidic organelles (6), distinct from the lysosomeswhere Ab is formed via b and g secretases and then released into the extracellular milieu. The routing of APP into these twopathways is under the control of protein phosphorylation, in particular by PKC, a mechanism that is defective in sporadic ADfibroblasts (see text). The mechanism is presently unknown, but presenilins are also presumed to play a role in the regulationof these pathways. Finally, the endosomal/lysosomal pathway (7) is called into action for degradation of the carboxyl-terminalfragment left over by secretase processing (5) and for the degradation of full-length APP molecules recycling from the cellsurface or directly from the biosynthetic pathway through the Golgi cisternae.
carboxyl-terminal, potentially amyloidogenic frag-ment.
Even if these data support the constitutive role ofb-amyloid in Alzheimer’s disease, a word of cautionshould be sounded. No direct studies have been per-formed to determine whether there is any systematicbiological difference between the symptomatic andpresymptomatic patients apart from the presence ofthe signs and symptoms of illness. A comparison ofdata obtained using tissues derived from presymp-tomatic patients before the age of onset of the diseasefor the investigated family and after that age on bothsymptomatic cases and escapees is needed beforemaking firm conclusions.
The view that fibroblasts can be used to effectivelymonitor pathology-induced defects of APP metabo-lism also emerges from experiments on Down’s pa-tients. Patients with trisomy 21 (Down’s syndrome,
DS) virtually always develop dementia of the Alzhei-mer’s type after the fourth decade of life and show ahistopathological phenotype indistinguishable fromAD, presumably on the basis of increased APP genedosage and transcription. Querfurth et al. (46) dem-onstrated an increased APP mRNA level in DS fibro-blasts similar to that observed in FAD. They alsodemonstrated an increase in Ab secretion in fibro-blasts from DS and FAD-affected subjects as com-pared to control cells. However, caution must beobserved when using information obtained fromDown’s patients to model biochemical defects inAlzheimer’s disease. In fact, data obtained from skinfibroblasts of DS subjects (51) show a completely dif-ferent pattern of sAPP secretion with respect to spo-radic AD cells under basal conditions and after PKCactivation with phorbol esters. The sAPP basal releasefrom DS fibroblasts is twofold that of age-matched

PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 23
/ 381c 0002 Mp 23 Tuesday Nov 25 11:34 AM LP–FASEB 0002
control cells. Moreover, stimulated APP release is al-ready maximal at low phorbol ester concentrations(9 nM), and the peak response is lower on a per-centage basis than in control fibroblasts because ofhigher basal release. Thus, in DS fibroblasts, PKC-sensitive secretion can be stimulated only modestly,indicating a saturation of this pathway due to thehigher APP content of DS cells when compared tocontrol and AD fibroblasts. These results also indi-cate that the PKC-sensitive mechanisms that controlAPP release might be saturated and might dependon the level of APP expression. These observationstress the importance of evaluating APP expressionafter pharmacological treatments with a potential ef-fect on APP secretion, since changes in this parame-ter may reset the system and affect the pool of theprecursor available for secretion under basal or stim-ulated conditions.
Altered calcium homeostasis in AD peripheral cells
Several findings (for review, see ref 52) support thehypothesis that altered processing of the b-amyloidprecursor protein contributes to loss of neuronal cal-cium homeostasis and thus to neurofibrillary degen-eration. These data suggest that a shift in APPprocessing, in favor of increased liberation of b-am-yloid and reduced release of sAPP, should destabilizeintracellular calcium concentration ([Ca2/]
i) and en-danger neurons in two ways: 1) increased levels of b-amyloid would make neurons more vulnerable to ex-citotoxicity (53); on the other hand, 2) reduced levelsof sAPP would deprive neurons of a neuroprotectivesubstance that can stabilize [Ca2/]i (54–57).
Alterations in calcium homeostasis have also beenfound in peripheral cells (Fig. 2, step A). The firststudy utilizing fibroblasts from AD patients revealedthat calcium uptake declines (58). Total membrane-bound calcium increases in fibroblasts in normal ag-ing and is elevated even further in those withAlzheimer’s disease (59). Other reports suggest thatcytosolic free calcium decreases; however, this hasnot been replicated (60, 61). Cytosolic free calciumconcentration is increased in platelets (62) and lym-phocytes derived from AD patients (63), but not inlymphoblasts (64). In addition, freshly prepared hu-man lymphocytes showed elevated mitogen-inducedcalcium responses after exposure to b-amyloid (65–67). A diminished response of cytosolic free calciumto drugs such as bradykinin has been found in ADfibroblasts by some (61, 68, 69) but not all groups(70–73). The discrepancy may be due to the concen-tration of bradykinin used; Huang et al. (70) and Itoet al. (73) have observed an exaggerated response tolow (nanomolar concentrations) BK concentrationsby using AD fibroblasts.
Altered internal calcium stores have been demon-strated by different treatments in AD fibroblasts.
Bombesin elevates cytosolic free calcium more incells from AD patients than in controls (73). The cal-cium pool released by A23187 after treatment withhigh bradykinin concentrations is higher in AD thanin control fibroblasts (74). Another study that dem-onstrated altered internal calcium pools in Alzhei-mer fibroblasts revealed that mitochondria from ADfibroblasts had decreased calcium uptake (75).
A greatly diminished response of cytosolic freecalcium to high concentrations of the potassiumchannel blocker tetraethylammomium (TEA) alsosuggests that regulation of calcium entry is abnormalin AD fibroblasts. Patch clamp studies indicate thatthis abnormal calcium response reflects the func-tional absence of a particular K/ channel (76).
The apparent lack of replicability with fibroblastshas been particularly striking for the study of calciumhomeostasis. Many laboratories are equipped to mea-sure calcium, but methodological variations aregreat. In addition, controlling all the variables of tis-sue culture (presence or absence of antibiotics, syn-chrony of the cell cycle, cumulative populationdoubling level at the time of the experiments, inter-val between seeding and when the measurement ismade, seeding density) is extremely difficult. In fact,the reduced resting calcium and the diminished re-sponse to bradykinin previously observed in AD fi-broblasts (60, 68) have been difficult to replicate (70,73). The inability to repeat these findings may havebeen partially related to the cell phase in which thevarious studies were performed. Recent results rep-licated the decreased response to bradykinin, vaso-pressin, or serum in familial AD cells if the cells werestudied in S phase (69). No AD/control differenceoccurs after bradykinin stimulation when the cells arein G2 or M phase. Similarly, if cells are studied 7 daysafter plating, 40–60% decreases are apparent in theAD fibroblasts (69). Another measure of calcium ho-meostasis where the method of measurement ac-counts for the apparent discrepancies is where thepotassium channel blocker TEA elevates cytosolicfree calcium in controls, but not AD fibroblasts. Inthe original report, addition of TEA distinguishedAD cell lines from controls (76). However, a recentreport did not find this measure to discriminate be-tween AD and controls (77). Methodological differ-ences may account for the discrepancies. Theoriginal study used microscopic imaging to examineindividual cells and calculate the percent of respond-ing cells (76). However, experiments from Matsu-yama et al. (77) averaged microscopic fields thatcontained many cells, which severely limits resolutionand sensitivity.
Experiments on the bradykinin-induced IP3 re-sponse provide an example in which treatment of thecells accounts for the lack of replicability betweenstudies. The initial study found no differences in IP3
formation in control and AD cells when IP3 release

24 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 24 Tuesday Nov 25 11:34 AM LP–FASEB 0002
was measured after 3H-inositide in serum free me-dium for 4 days (70). Subsequent studies in the samelaboratory revealed enhanced IP3 formation in ADcells compared to controls in cells that had notbeen serum deprived (33). Subsequent experimentsshowed that IP3 formation was enhanced in AD cellsregardless of the method of measurement, as long asthe treatment did not include prolonged serum de-privation (33). These discrepancies (also reviewed inref 78) should not be viewed as a reason to dismissthis approach. Research on fibroblasts has pro-gressed to a stage that elucidating the underlyingmechanistic basis of any of these discrepancies is pos-sible if adequate attention is paid to the details ofexperimental techniques used.
Alterations in oxidative metabolism in AD peripheral cells
Cellular calcium and oxidative metabolism are closelylinked in fibroblasts, as in other tissues, and variousparameters of altered energy metabolism have beenreported in peripheral cells (particularly in fibro-blasts) from Alzheimer patients.
Increased lactate production and altered glucoseutilization occur (59, 79, 80) in AD fibroblasts. Theactivities of key mitchondrial enzymes such as a-ke-toglutarate dehydrogenase are diminished eitherslightly (81) or by as much as 40% (82) in Alzheimerfibroblasts. This last result has been confirmed in anindependent series of experiments showing inherentdefect of the a-ketoglutarate dehydrogenase com-plex (83). Glutamine oxidation also declines (59, 79,80) in AD cells, although not always (84). Further-more, reduced cytochrome c oxidase (CO) activitywas demonstrated in platelets derived from AD pa-tients (85) and also in AD fibroblasts from our bank(Govoni et al., unpublished results). Recently pub-lished data (86) describe genetic defects in the mi-tochondrial DNA coding for CO subunits CO1 andCO2. However, these results await independent con-firmation in a different series of patients. These re-sults are all consistent with the hypothesis thatabnormal oxidation in AD brain is not just secondaryto neurodegeneration, but the hypothesis needs tobe investigated further. Finally, abnormalities in ce-rebral metabolism of oxygen and glucose can be ex-pected to interact synergistically with cerebrovascularfactors in causing brain damage in AD.
Use of peripheral cells as an aid in diagnosingdisease
Peripheral cells—and in particular cultured skin fi-broblasts from AD patients—might provide a usefulaid in AD diagnosis. Today, the criteria needed for aconclusive diagnosis of AD include clinical criteria inassociation with histopathologic evidence obtainedfrom a biopsy or autopsy. Thus, the use of peripheral
cells as a diagnostic tool, either to predict or at leastto confirm the diagnosis, may be of great importance.None of the alterations described in peripheral cellscan now be used as a diagnostic tool if consideredalone. One possible approach to achieve this goal isto combine more than one set of data and therebyprovide a profile for AD cells distinguishable fromthat of controls.
The first attempt in this direction was made by Hir-ashima et al. (87). Previous findings by the same au-thors demonstrated the absence of a specificpotassium channel and of TEA-induced calcium in-crease in AD fibroblasts (76). The stimulation of cal-cium release from intracellular stores in response tobombesin or low BK concentrations was greatly en-hanced in AD fibroblasts compared with cells fromcontrol donors (73). On the basis of these results,Hirashima (87) introduced a scoring system that in-tegrated altered and normal responses to low BK con-centrations, bombesin, and TEA stimulation ofintracellular calcium elevation in AD vs. control fi-broblasts. This scoring system also takes into accountthe degree of responsiveness and/or unresponsive-ness of each particular cell line. It generated an indexdistinguishing AD patients from controls with bothhigh specificity and sensitivity (87). The authors havealso examined many non-Alzheimer’s dementia con-trols and still found complete specificity. These re-sults indicate that by taking the overall profile ofresponses into account, it is possible to enhance thediagnostic value of these cellular alterations. Further-more, the diagnostic measurements obtained in fi-broblasts appear to be closely correlated for twopopulations of patients living in distant geographicareas, since cells used for the study described wereobtained from Coriell Cell Repository (Camden,N.J.) and a fibroblast bank established in Brescia, It-aly (Project Ministry of Health #500.7 AG/4.8455/Regione Lombardia). Moreover, specificity and sen-sitivity of the assay should be established by includingpatients bearing different kinds of neurological dis-eases in order to determine the ability of the markerto distinguish AD from normal aging and from otherdementias. Severity and length of the illness are otherimportant factors to consider to determine whetherthe parameters measured also allow identification ofstages of the disease.
Studies of platelets also suggest that it may be pos-sible to detect alterations of APP synthesis/metabo-lism of potential diagnostic significance in sporadicAD patients. In fact, the presence of APP in plateletgranules has generated great interest in the study ofplatelet function and biochemistry in AD patients.Several laboratories have shown that human plateletscontain full-length APP (88–93) and are suitable forthe study of APP processing. It has also been pro-posed that platelets may serve as a possible source ofthe Ab sequence (93), providing one mechanism by

PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 25
/ 381c 0002 Mp 25 Tuesday Nov 25 11:34 AM LP–FASEB 0002
which cerebral amyloid might be derived from thecirculation and contribute to cerebral or cerebrovas-cular amyloidosis. According to Van Nostrand et al.(88–90), the protease inhibitor protease nexin-2, thesecreted form of APP that contains the Kunitz pro-tease inhibitor domain, may play a role in regulatingblood coagulation by inhibiting blood coagulationfactor IXa, and platelets may serve as a vehicle to de-liver this protein to sites of vascular injury. A recentstudy (94) has demonstrated the existence of a con-sistent alteration in platelet APP isoforms in AD andDown’s syndrome (i.e., a lower 130–106/110 kDa ra-tio) that is of potential value as a biochemical markerof the disease.
CSF AND PLASMA. APP, Ab, TAU PROTEIN,AND OTHER MARKER PROTEINS
Amyloid precursor protein or Ab and other APP frag-ments are detectable in cerebospinal fluid. LowerCSF APP levels in AD patients with respect to controlswere demonstrated by several groups (95–98). LowsAPP concentrations were also detected by Farlow etal. (97) in CSF from AD patients who carry a pointmutation at codon 717 in exon 17 of the APP gene.However, it has not been systematically studiedwhether the defect is specific to Alzheimer’s disease.The concentrations of the soluble extracellular por-tion of APP (sAPP) are also decreased in AD patientswhen compared to healthy control subjects (99) anddemented non-Alzheimer-type patients (100). Almkv-ist et al. (101) observed an association between lowlevels of a-sAPP and poor performance on neuro-psychological tests in individuals from a Swedish fam-ily with AD and a double mutation at codons 670/671 of APP gene.
Seubert et al. (102) first isolated and quantified Abfrom human biological fluids (i.e., CSF and plasma).Alterations of CSF Ab levels were reported in AD pa-tients. Nakamura et al. (103) found a significant el-evation in the level of Ab in the CSF of early-onsetAD patients. On the other hand, Nitsch et al. (104)found that Ab levels in the CSF of AD patients wereinversely correlated both to cognitive and functionalmeasures of dementia severity. Lannfelt et al. (105)demonstrated a correlation between decreased solu-ble Ab levels and duration of illness, but found nodifferences in CSF levels of Ab between APP670/671mutation carriers and noncarriers from the Swedishfamily they studied. Comparable amounts of Ab inAD and control CSF were found by other laboratories(106–108), indicating that the total CSF Ab level isnot a useful marker for current diagnosis of AD.
Ab1-42 CSF levels seem to be a more specificmarker of AD pathology than total Ab. In fact, CSFAb1-42 levels were significantly lower in AD patientsrelative to a non-AD group (109–111). However,
some overlapping of the control Ab1-42 levels withAD values (109) was present. Ab1-42 has recentlybeen shown to deposit in the brain tissue of pa-tients with AD (112, 113), suggesting that dimin-ished clearance may account for its reduction in ADCSF. The peptide may be elevated early in the dis-ease and decrease during progression (Lannfelt,working group on biological markers of AD, Alz-heimer’s Association).
Ab concentration also seems to be altered inplasma from AD patients. Song et al. (114) observedthat plasma Ab1-42 is increased in carriers of familialAD linked to chromosome 14. Plasma Ab is also in-creased in carriers of the 670-671 mutation from theSwedish kindred (115). No differences in Ab levelswere seen between symptomatic and presymptomaticcarriers, which shows that the increase of Ab levelsmight be a very early event in the disease, at least inthe Swedish kindred. On the other hand, it cannotbe excluded that the increase in Ab levels is unrelatedto the pathogenesis of the disease, being indistinctlyelevated both in patients and in asymptomatic indi-viduals. Follow-up studies investigating whether theelevated Ab levels in subjects with no symptoms arepredictive of a future development of the illness willhelp to clarify this point. This observation has beeninterpreted as indicating a potential importance ofplasma Ab as an early marker for identifying individ-uals who will develop AD because of elevated Ab con-centrations, at least in cases of FAD. MoreoverYounkin et al. (116) observed that an elevated plasmaconcentration of Ab1-42 may also play a role in somepatients with sporadic AD cases and that, in at leastsome of these patients, Ab1-42 may be elevated beforethe onset of symptoms. This observation has not beenreplicated by other authors (see below); additionalresults are clearly needed before drawing any conclu-sions about the risk for AD that is conferred by ele-vation of plasma Ab1-42. Scheuner et al. (48)demontrated an increased Ab1-42 level in plasma fromsubjects with FAD-linked PS1, PS2, APPK670N,M671L, and APPV717I mutations. Plasma Ab1-42 levelis also elevated in presymptomatic carriers of PS1 andPS2 mutations. Kosaka et al. (117) found an in-creased percentage of plasma amyloid ending atAb42(43) in patients with the bAPP717 mutation. Anincreased Ab1-40 plasma level was also observed incarriers of the APPK670N, M671L mutation. In con-trast, Ab1-42 was not statisically increased in subjectswith late-onset sporadic AD compared with age-matched control subjects. This observation and thefinding that Ab1-42 was significantly increased in allpresymptomatic gene carriers indicate that the in-creased Ab1-42 observed in subjects with FAD-linkedAPP and PS1 or PS2 mutations occurs as a direct con-sequence of the mutations and not as an indirectmanifestation of the AD state. The diagnostic signif-icance of levels of Ab1-42 in these cases obviously is

26 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 26 Tuesday Nov 25 11:34 AM LP–FASEB 0002
secondary to the finding of the pathogenetic muta-tion.
Tau protein, the main component of neurofibril-lary tangles, can also be detected in CSF. Tau levelsin the CSF of AD cases are significantly elevated com-pared to healthy control individuals, vascular demen-tia patients, and neurological control subjects (118–127). It is debated whether tau levels are also elevatedin other kinds of neurological diseases where neu-ronal death or damage occurs. In particular, in-creased CSF levels of tau are found in a definiteproportion (10–20%) of neurological controls (119,122, 123). Furthermore, there is an overlap betweenAD and other forms of dementia, reducing the pre-dictive value of elevated CSF tau. The simultaneousanalysis of tau and Ab1-42 in the same CSF sample ap-pears to be of particular interest. In fact, the presenceof elevated tau levels and reduced Ab1-42 seems to behighly predictive of AD (specificity 96%). Conversely,high Ab1-42 and low tau were observed only in controlpatients (specificity 100%). However, the combinedCSF tau and Ab1-42 measurements were not informa-tive in those patients who fell into the low Ab1-42/lowtau group. The diagnostic potential of these resultsneeds to be evaluated further (109, 110).
Among other proteins that are unrelated to themajor Alzheimer’s markers, such as Ab or tau, theiron binding protein p97 has recently been proposedas a possible diagnostic marker for the disease (128).Its level has been found to be significantly increasedin freshly prepared plasma samples from AD patients.The data are promising because of the virtual ab-sence of overlaps with the levels measured in theplasma of control subjects, including individuals suf-fering from other neuropathologies. As for manyother proposed diagnostic markers for AD, theplasma level of p97 awaits a complete validation on alarge number of patients in carefully designed mul-ticenter studies.
NEUROENDOCRINE SYSTEM
The neuropathological hallmarks of Alzheimer’s dis-ease are very prominent in the hippocampus (129,130), a brain site that is pivotal for regulation of thehypothalamic-pituitary-adrenal (HPA) system. In ratsand primates, lesions of the hippocampus result inhypersecretion of glucocorticoid under resting andstress conditions (131), whereas hippocampal stim-ulation inhibits this system (132). There is agreementin the literature about an age-associated reduction inthe number of hippocampal corticosteroid recep-tors, mainly mineralcorticoid receptors, resulting inan age-related increase in HPA system activity(133–135).
Studies (136) in healthy elderly humans suggestthat with aging, the human HPA system becomes
more disinhibited, showing an age-related increase inHPA system activity. Thus, one would expect that, inpatients with AD, the age-associated HPA systemchanges are aggravated by the disease process itself.However, studies of HPA system function in AD pa-tients have so far yielded controversial findings. Hat-zinger et al. (137) demonstrated profoundly alteredregulation of the HPA system in patients with AD. Infact, they demonstrated that patients with AD had sig-nificantly higher basal cortisol concentrations, and ahigher percentage of AD patients escaped the dexa-methasone (DEX) suppression of cortisol releasewhen compared to elderly controls. On the otherhand, the DEX suppression test is typically abnormalin depression, so the observed changes cannot beconsidered specific for dementia. The alteration ofthe HPA axis in AD patients is further supported bya significantly lower adrenocorticotropin hormone(ACTH) and cortisol release after administration ofadditional corticotropin-releasing hormone (CRH),as compared with the control group. In addition, itwas demonstrated that CRH and ACTH levels are sig-nificantly reduced in the CSF of AD patients (138–140) in the absence of differences in plasma levels ofCRH, ACTH, and cortisol (141). However, none ofthe patients showed evidence of pituitary-adrenal dys-function, suggesting an involvement of extrahypo-thalamic CRH (138). Several studies indicate a re-duction in CRH-like immunoreactivity in the cerebralcortex of AD patients (142–144), particularly in tem-poral, frontal, and occipital areas. In the same corti-cal areas, an increased CRH receptor number wasreported (142). Nevertheless, these findings are notspecific to Alzheimer’s dementia. In fact, reduced lev-els of CRH in CSF were also demonstrated in patientswith vascular dementia (139–141), and reducedCRH-like immunoreactivity at the level of the cere-bral cortex level was also found in Parkinson’s diseaseand progressive supranuclear palsy (143, 145). Otheralterations in the neuroendocrine system of AD pa-tients have also been reported. An attenuated growthhormone-releasing hormone (GHRH) -inducedgrowth hormone response specific to AD was dem-onstrated by Lesh et al. (146) and Ghiso et al. (147),but not by others (148, 149). Furthermore, a reduc-tion in CSF levels of antidiuretic hormone was ob-served not only in AD patients, but also in patientswith frontal lobe dementia (150). No alteration ofthe thyrotropin-releasing hormone/thyrotropin hor-mone (TRH/TSH) and prolactin (PRL) systems wasreported in AD patients (151, 152).
A reduced somatostatin-like immunoreactivity(SLI) in some regions of the AD brain was reportedby several groups (153–156). However, a reductionis also detectable in the brain of patients with Parkin-son’s disease (154, 155) or major depression (155).Also, one report (157) shows an increased SLI inboth AD and vascular dementia. Several papers (150,

PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 27
/ 381c 0002 Mp 27 Tuesday Nov 25 11:34 AM LP–FASEB 0002
158–165) even demonstrated reduced SLI in the CSFof AD patients at early stages of the disease, whereasjust one group found no differences between AD andcontrol subjects (165). However, low SLI values inCSF are not specific to AD; in fact, reduced SLI wasdemonstrated in the CSF of patients affected not onlyby neurological disorders such as frontal lobe de-mentia (150), Parkinson disease (166), vascular de-mentia, normal pressure hydrocephalus (161, 167),senile dementia of the Lewy body type (168), demen-tia with frontotemporal degeneration (154), and de-mentia associated with alcoholism (164), but also inpsychiatric diseases like major depression (158) andschizophrenia (156). Therefore, the measurement ofSLI in CSF in demented patients may not be helpfulin the diagnostic procedure. These observations donot support the existence of a specific neuroendo-crine pattern for AD patients. However, the newfindings on the relationship between AD and inflam-mation and estrogens and AD risk in postmenopausalwomen strongly suggest the need to explore furtherthe potential neuroendocrine alterations in this dis-ease (169–173).
APOLIPOPROTEIN E AND DEMENTIA
An important chapter in Alzheimer’s disease re-search regards the role of apolipoprotein E (ApoE)isoforms in the disease. ApoE is a plasma protein in-volved in cholesterol transport (174). In the centralnervous system, ApoE is produced by astrocytes (175)and is implicated in the growth and repair of the ner-vous system during development or after injury (176–178). ApoE is also increased in several chronicneurodegenerative diseases. In AD, ApoE is bound toextracellular senile plaques, to intracellular neurofi-brillary tangles, and at sites of cerebral vessel congo-philic angiopathy (179). Immunoreactivity for ApoEis also detectable in cerebral amyloid deposits andneurofibrillary tangles in kuru and in amyloidplaques of Creutzfeld-Jacob disease (179).
The ApoE gene is localized on chromosome 19 andpresents three alleles—e2, e3, and e4—that deter-mine ApoE polymorphism. Analysis of ApoE allelesin AD and control subjects demonstrated a highly sig-nificant association of ApoE type 4 allele (ApoE e4)and late-onset familial Alzheimer’s disease (180).The allele frequency of ApoE e4 in 30 random af-fected patients, each from a different AD family, was0.50 { 0.06 vs. a frequency of 0.16 { 0.03 in 91 age-matched nonrelated controls. The analysis was thenextended to sporadic late-onset AD patients by Saun-ders et al. (181): the same kind of association withallele e4 was demonstrated in living and autopsy-doc-umented AD patients vs. controls. The increased fre-quency of the e4 allele in late-onset sporadic and
familial AD was demonstrated in U.S. (180–182) aswell as Japanese, Finnish, and Italian populations(183–187). Furthermore, the frequency of the e4 al-lele also seems to be increased in early onset sporadicAD patients in a Japanese and a Dutch population(188, 189).
The inheritance of one or two ApoE e4 alleles seemsto influence Alzheimer pathology in a gene dose-de-pendent manner: the amount of histologically iden-tified Ab in vessels and plaques in the cerebral cortexof patients with sporadic late-onset AD is a directfunction of their ApoE genotype. Increased amyloiddeposits in vessels and increased density of stronglyAb immunoreactive plaques in patients homozygousfor ApoE e4 compared with patients homozygous forApoE e3 have been demonstrated, although the topicis controversial (185). ApoE e3/e4 patients have anintermediate phenotype (190). A gene dose effectcan also be detected in the age of onset of AD. In-heritance of the ApoE e4 allele is associated with anearlier onset of the disease: the median age at onsetamong AD patients decreased from 83 to 78 to 74years as the number of ApoE e4 alleles increased from0 to 1 to 2, respectively (191). These findings led tothe hypothesis of ApoE e4 as a risk factor for Alzhei-mer’s disease and suggested a potential use of ApoEgenotype as a diagnostic test, although the issue is stillcontroversial (192–194).
Recently it has been demonstrated that the fre-quency of ApoE e4 allele is increased not only in AD,but also in other types of dementia. Frisoni et al.(186) confirmed increased ApoE e4 allele frequencyin 93 sporadic AD patients, but also demonstrated asimilar increase in e4 frequency in 23 vascular de-mentia patients. Moreover, it has been demonstratedthat e4 frequency is also increased in patients affectedby Creutzfeld-Jacob disease (195) and by Lewy bodydementia (196), but not in Down’s demented sub-jects (197, 198).
Therefore, the association of the ApoE e4 allele isnot unique to Alzheimer’s disease. The use of ApoEgenotype as a diagnostic test in symptom-free individ-uals has insufficient epidemiological support at pres-ent to be useful. In fact, it cannot predict when, orif, an individual with ApoE e4/4 will get Alzheimer’sdisease. On the other hand, the genotype may beused to confirm that patients with early dementiahave Alzheimer’s disease. ApoE genotyping may alsobe used to subdivide symptomatic patients by bio-logical risk in order to foresee the response to drugtreatment (199) and the clinical progression of thepathology (200), since the proportion of patientswith slow progression seems to increase with increas-ing e4 gene dose, suggesting that disease durationmight be longer in e4 carriers (201).
In addition to genotyping, several groups havemeasured ApoE levels in CSF alone or in conjunctionwith tau and Ab1-42. Various authors found reduced

28 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 28 Tuesday Nov 25 11:34 AM LP–FASEB 0002
CSF ApoE concentrations in AD patients, irrespectiveof the ApoE genotype (202–204). However, contrast-ing results have been published; one recent reportfound no difference (205) in CSF ApoE concentra-tions, and another found an increase (206). The de-crease of CSF ApoE, on the other hand, does notappear to be limited to AD and, rather, may representan unspecific marker for neurodegenerative disor-ders (204). It is tempting to speculate that since li-poproteins participate in lipid transport during cellrepair, the relative lack of ApoE may impair repairmechanisms, making the brain more susceptible todamage. In studies that measured CSF levels of Ab1-
42 (reduced in AD) or tau (which increases in AD),the two parameters were found to be independent(102, 107) of ApoE genotype. However, in a recentstudy (207) of a limited number of AD patients fol-lowed for 14 months, the ApoE e4 carriers presentedincreasing tau CSF levels. While this observationawaits confirmation, it may suggest that there areApoE isoform-specific differences in the regulationof the homeostasis of tau.
CONCLUSION
The use of peripheral tissues and body fluids fromAD patients has contributed a considerable amountof evidence toward the evaluation of working patho-physiological hypotheses for this disease, the one de-picted in Fig. 2 being an example. According to datareviewed here, a defect in transduction systems mightplay a key role in the pathogenesis of Alzheimer’sdisease. For example, the reduced PKC activityobserved in AD fibroblasts might influence APPmetabolism and reduce APP processing via the non-amyloidogenic pathway with an increased formationof Ab. Many events could follow enhanced Ab pro-duction (Ab deposition, facilitation of neurotoxicity,disruption of calcium homeostasis, abnormal tauphosphorylation), resulting in the neurodegenera-tive pattern and loss of function typical of ADpatients. However, this hypothesis needs to be inves-tigated further, and peripheral tissues could be animportant tool in the clarification of several otherpoints.
The search for a biological marker that could helpin predicting or confirming AD diagnosis is still a richarea for research. The attempt to build a biological pro-file that is characteristic of AD cells, with the associationof different variables, seems a more promising ap-proach (87, 110), at least for sporadic cases. Further-more, the initial data indicate a need to design studiesthat are carefully targetted at detecting the diagnosticpotential of observed biological differences. A moreclinically oriented experimental design, with double-
blind and multicenter tests with preestablished inclu-sion criteria, should be adopted.
REFERENCES
1. Alzheimer, A. (1907) Uber eine eigenartige Erkrangkung derHimrinde. All. Z. Psychiatr. 64, 146–148
2. Hass, C., and Selkoe, D. J. (1993) Cellular processing of b-am-yloid precursor protein and the genesis of amyloid b-peptide.Cell 75, 1039–1042
3. Kang, J., Lemaire, H. G., Unterbeck, A., Salbaum, J. M., Masters,C. L., Grzaeschik, K. H., Multhaup, G., Beyreuther, K., andMueller-Hill, B. (1987) The precursor of Alzheimer’s diseaseamyloid A4 protein resembles a cell surface receptor. Nature(London) 325, 733–736
4. Glenner, G. G. (1988) Alzheimer’s disease: its problems andgenes. Cell 52, 307–308
5. Grundke-Iqbal, I., Iqbal, K., Tung, Y. C., Quinlan, M., Wis-niewski, H. M., and Binder, L. I. (1986) Abnormal phosphor-ylation of the microtubule-associated protein tau in Alzheimercytoskeletal pathology. Proc. Natl. Acad. Sci. USA 83, 4913–4917
6. Mori, H., Kondo, J., and Ihara, Y. (1987) Ubiquitin is a com-ponent of paired helical filaments in Alzheimer’s disease. Sci-ence 235, 1641–1644
7. Dickson, D. W., Crystal, H. A., Mattiace L. A., Masur, D. M.,Blau, A., Davies, P., Yen, S.-H., and Aronson M. K. (1992) Iden-tification of normal and pathological aging in prospectivelystudied nondemented elderly humans. Neurobiol. Aging 13, 1–11
8. Feany, M. B., and Dickson D. W. (1996) Neurodegenerativedisorders with extensive tau pathology: a comparative study andreview. Ann. Neurol. 40, 139–148
9. Steinberg, D. (1983) Phytanic acid storage disease (Refsum’sdisease). In The Metabolic Basis of Inherited Disease (Stanbury,J. B., Wyngaarden, J. B., Fredrickson, D. S., Goldstein, J. L., andBrown, M. S., eds) 5th Ed, pp. 731–747, McGraw Hill, New York
10. Stanbury, B., Wyngaarden, J. B., Fredrickson, D. S., Goldstein,J. L., and Brown, M. S. (eds) (1983) The Metabolic Basis of Inher-ited Disease, 5th Ed, McGraw Hill, New York
11. Balin, A. K., Baker, A. C., Leong, I. C., and Blass, J. P. (1988)Normal replicative lifespan of Alzheimer skin fibroblasts. Neu-robiol. Aging 9, 195–198
12. Carmeliet, G., Hauman, R., Dom, R., David, G., Fryns, J.-P., VanDer Berghe, H., and Cassiman, J.-J. (1990) Growth propertiesand in vitro lifespan of Alzheimer disease and Down syndromefibroblasts. A blind study. Mech. Ageing Dev. 53, 17–33
13. Carmeliet, G., David, G., and Cassiman, J.-J. (1991) Cellular age-ing of Alzheimer’s disease and Down syndrome cells in culture.Mutat. Res. 256, 221–231
14. Tesco, G., Vergelli, M., Amaducci, L., and Sorbi, S. (1993)Growth properties of familial Alzheimer skin fibroblasts duringin vitro aging. Exp. Gerontol. 28, 51–58
15. Adler, M. J., Coronel, C., Shelton, E., Seegmiller, J. E., and De-wji, N. N. (1991) Increased gene expression of Alzheimer dis-ease b-amyloid precursor protein in senescent culturedfibroblasts. Proc. Natl. Acad. Sci. USA 88, 16–20
16. Tofel-Grehl, B., Blass, J. P., and Gibson, G. E. (1992) Hetero-geneity in CDPL to phase out among fibroblasts from differentAlzheimer families. Mol. Biol. Cell 35, 1898
17. Blass, J. P., Baker, A. C., Sheu, K.-F. R., Black, R. S., and Smith,A. (1989) Use of cultured skin fibroblasts in studies of Alzhei-mer’ s disease. In Biological Markers of Alzheimer’s Disease (Boller,F., Katzman, R., Rascol, A., Signoret, J. L., and Christen, Y., eds)pp. 153–162, Springer-Verlag, New York
18. Sandbrink, R., Hartmann, T., Masters, C. L., and Beyreuther,K. (1996) Genes contributing to Alzheimer’s disease. Mol. Psy-chiat. 1, 27–40
19. Cole, G., Dobkins, K. R., Hansen, L. A., Terry, R. D., and Saitoh,T. (1988) Decreased levels of protein kinase C in Alzheimerbrain. Brain Res. 452, 165–174
20. Wang, H.-Y., Pisano, M. R., and Friedman, E. (1994) Attenuatedprotein kinase C activity and translocation in Alzheimer’s dis-ease brain. Neurobiol. Aging 15, 293–298
PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 29
/ 381c 0002 Mp 29 Tuesday Nov 25 11:34 AM LP–FASEB 0002
21. Bosman, G. J., Schurmans-Stekhoven, J. H., Melenhorst, J. J.,Van Zuylen, A. J., Bartholomeus, I. G., Van Kalmthout, P. J.,and De Grip, W. J. (1992) Are thrombocyte membranes alteredin Alzheimer’s disease? A morphometric and biochemicalstudy. Neurobiol. Aging 13, 711–716
22. Matsushima, H., Shimohama, S., Tanaka, S., Taniguchi, T.,Hagiwara, M., Hidaka, H., and Kimura, J. (1994) Platelet pro-tein kinase C levels in Alzheimer’s disease. Neurobiol. Aging 15,671–674
23. Van Huyn, T., Cole, G., Katzman, R., Huang, K.-P., and Saitoh,T. (1989) Reduced protein kinase C immunoreactivity and al-tered protein phosphorylation in Alzheimer’s disease fibro-blasts. Arch. Neurol. 46, 1195–1199
24. Bruel, A., Cherqui, G., Columelli, S., Margelin, D., Roudier, M.,Sinet, P.-M., Prieur, M., Perignon, J.-L., and Delabar, J. (1991)Reduced protein kinase C activity in sporadic Alzheimer’s dis-ease fibroblasts. Neurosci. Lett. 133, 89–92
25. Govoni,, S., Bergamaschi, S., Racchi, M., Battaini, F., Binetti, G.,Bianchetti, A., and Trabucchi, M. (1993) Cytosol protein kinaseC downregulation in fibroblasts from Alzheimer’s disease pa-tients. Neurology 43, 2581–2586
26. Bergamaschi, S., Binetti, G., Govoni, S., Wetsel, W. C., Battaini,F., Trabucchi, M., Bianchetti, A., and Racchi, M. (1995) Defec-tive phorbol ester-stimulated secretion of b-amyloid precursorprotein from Alzheimer’s disease fibroblasts. Neurosci. Lett. 201,1–4
27. Racchi, M., Bergamaschi, S., Govoni, S., Wetsel, W. C., Bian-chetti, A., Binetti, G., Battaini, F., and Trabucchi, M. (1994)Characterization and distribution of protein kinase C isoformsin human skin fibroblasts. Arch. Biochem. Biophys. 314, 107–111
28. Vestling, M., Adem, M., Lannfelt, L., and Cowburn, R. F. (1995)Protein kinase C levels and activity in cultured skin fibroblastsfrom affected and non-affected members of the Swedish familywith the amyloid precursor protein 670/671 mutation. Soc. Neu-rosci. Abstr. 21, 774.14
29. Solerte, S. B., Pascale, A., Fortino, I., Battaini, F., Ferrari, E.,Fioravanti, M., and Govoni, S. (1996) Cortisol and cytokinesmodulatory effects on cytosolytic and protein kinase C activitiesof natural killer in Alzheimer’s disease. Neurobiol. Aging 17, 4S,S169
30. Solerte, S. B, Fioravanti, M., Severgnini, M., Cerutti, N., Loca-telli, M., Terenzi, F., Cottinelli, M., Pezza, N., and Ferrari, E.(1996) Cortisol, DHEA-sulphate (DEAS) and natural killer(NK) cell functions in the clinical characterization of Alzhei-mer’s disease. J. Endocrinol. Invest. 19, 52
31. Solerte, S. B., Fioravanti, M., Severgnini, S., Locatelli, M., Ren-zullo, M., Pezza, N., Cerutti, N., and Ferrari, E. (1996) En-hanced cytotoxic response of natural killer cells to interleukin-2in Alzheimer’s disease. Dementia 7, 343–348
32. Huang, H.-M., and Gibson, G. E. (1993) Altered b-adrenergicreceptor stimulated cAMP formation in cultured skin fibro-blasts from Alzheimer donors. J. Biol. Chem. 268, 14616–14621
33. Huang, H.-M., Lin, T.-A., Sun, G. Y., and Gibson, G. E. (1995)Increased inositol 1,4,5-triphosphate accumulation correlateswith an up-regulation of bradykinin receptors in Alzheimer’sdisease. J. Neurochem. 64, 761–766
34. Huang, H. M., and Gibson, G. (1996) Regulation of bradykinin-induced Ins(1,4,5)P3 formation by protein kinase C in humanfibroblasts. Life Sci. 59, 1533–1543
35. Selkoe, D. J. (1994) Cell biology of the amyloid b-protein pre-cursor and the mechanism of Alzheimer’s disease. Annu. Rev.Cell. Biol. 10, 373–403
36. Sisodia, S. S. (1992) Beta-amyloid precursor protein cleavageby a membrane bound protease. Proc. Natl. Acad. Sci. USA 89,6075–6079
37. Shoji, M., Golde, T. E., Ghiso, J., Cheung, T. T., Estus S., Shaf-fer, L. M., Cai, X.-D., McKay, D. M., Tintner, R., Frangione, B.,and Younkin S.,G. (1992) Production of the Alzheimer amyloidb protein by normal proteolytic processing. Science 258, 126–129
38. Buxbaum, J. D., Gandy, S. E., Cicchetti, P., Ehrlich, M. E., Czer-nik, A. J., Fracasso, R. P., Ramabhadran, T. V., Unterbeck,A. J., and Greengard, P. (1990) Processing of Alzheimer b/A4amyloid precursor protein: modulation by agents that regulateprotein phosphorylation. Proc. Natl. Acad. Sci. USA 87, 6003–6006
39. Gillespie, S. L., Golde, T. E., and Younkin, S. G. (1992) Secre-tory processing of the Alzheimer amyloid b/A4 precursor isincreased by protein phosphorylation. Biochem. Biophys. Res.Commun. 187, 1285–1290
40. Caporaso, G. L., Gandy, S. E., Buxbaum, J. D., Ramabhadran,T. V., and Greengard, P. (1992) Protein phosphorylation reg-ulates secretion of Alzheimer b/A4 amyloid precursor protein.Proc. Natl. Acad. Sci. USA 89, 3055–3059
41. Loffler, J., and Huber, G. (1993) Modulation of b-amyloid pre-cursor protein secretion in differentiated and nondifferen-tiated cells. Biochem. Biophys. Res. Commun. 195, 97–103
42. Hung, A. Y., Haass, C., Nitsch, R. M., Qui, W. Q., Citron, M.,Wurtman, R. J., Growdon, J. H., and Selkoe, D. J. (1993) Acti-vation of protein kinase C inhibits cellular production of theamyloid b-protein. J. Biol. Chem. 268, 22959–22962
43. Gabuzda, D., Busciglio, J., and Yankner, B. A. (1993) Inhibitionof b-amyloid production by activation of protein kinase C. J.Neurochem. 61, 2326–2329
44. Buxbaum, J. D., Koo, E. H., and Greengard, P. (1993) Proteinphosphorylation inhibits production of Alzheimer amyloid b/A4 peptide. Proc. Natl. Acad. Sci. USA 90, 9195–9198
45. Slack, B. E., Nitsch, R. M., Livneh, E., Kunz, G. M., Jr., Breu, J.,Eldar, H., and Wurtman, R. J. (1993) Regulation by phorbolesters of amyloid precursor protein release from Swiss 3T3 fi-broblasts overexpressing protein kinase Ca. J. Biol. Chem. 268,21097–21101
46. Querfurth, H. W., Wijsman, E. M., St. George-Hyslop, P. H.,and Selkoe, D. J. (1995) bAPP mRNA transcription is increasedin cultured fibroblasts from the familial Alzheimer’s disease-1family. Mol Brain Res. 28, 319–337
47. Citron, M., Vigo-Pelfrey, C., Teplow, D. B., Miller, C., Schenk,D., Johnston, J., Winblad, B., Venizelos, N., Lannfelt, L., andSelkoe, D. J. (1994) Excessive production of amyloid b-proteinby peripheral cells of symptomatic and presymptomatic pa-tients carrying the swedish familial Alzheimer disease mutation.Proc. Natl. Acad. Sci. USA 91, 11993–11997
48. Scheuner, D., Eckman, C., Jensen, M., Song, X., Citron, M.,Suzuki, N., Bird, T. D., Hardy, J., Hutton, M., Kukull, W., Lar-son, E., Levy-Lahad, E., Vitanen, M., Peskind E., Poorkaj P.,Schellenberg, G., Tanzi, R., Wasco, W., Lannfelt, L., Selkoe, D.,and Younkin S. (1996) Secreted amyloid b-protein similar tothat in the senile plaques of Alzheimer’s disease is increased invivo by the presenilin 1 and 2 and APP mutations linked tofamilial Alzheimer’s disease. Nat. Med. 2, 864–870
49. Matsumoto, A., and Fujiwara, Y. (1991) Abnormal and deficientprocessing of beta-amyloid precursor protein in familial Alz-heimer’s disease lymphoblastoid cells. Biochem. Biophys. Res.Commun. 175, 361–365
50. Matsumoto, A., and Fujiwara, Y. (1993) Aberrant proteolysis ofthe beta-amyloid precursor protein in familial Alzheimer’s dis-ease lymphoblastoid cells. Eur. J. Biochem. 217, 21–27
51. Govoni, S., Bergamaschi, S., Gasparini, L., Quaglia, C., Racchi,M., Cattaneo, E., Binetti, G., Bianchetti, A., Giovetti, F., Battaini,F., and Trabucchi, M. (1996) Fibroblasts of patients affected byDown’s syndrome oversevrete amyloid precursor protein andare hyporesponsive to protein kinase C stimulation. Neurology47, 1–7
52. Mattson, M. P., Barger, S. W., Cheng, B., Lieberburg, I., Smith-Swintosky, V. L., and Rydel, R. E. (1993) b-Amyloid precursorprotein metabolites and loss of neuronal Ca2/ homeostasis inAlzheimer’s disease. Trends Neurosci. 16, 409–414
53. Mattson, M. P., Cheng, B., Culwell, A. R., Esch, F. S., Lieber-burg, I., and Rydell, R. E. (1993) Evidence for excitoprotectiveand intraneuronal calcium-regulating roles for secreted formsof beta-amyloid precursor protein. Neuron 10, 243–254
54. Mattson, M. P., Cheng, B., Davis, D., Bryant, K., Lieberburg, I.,and Rydell, R. E. (1992) Beta amyloid peptides destabilize cal-cium homeostasis and render human cortical neurons vulner-able to excitotoxicity. J. Neurosci. 12, 376–389
55. Mattson, M. P., Tomaselli, K., and Rydell, R. E. (1993) Calciumdestabilizing and neurodegenerative effects of aggregated beta-amyloid peptide are attenuated by basic FGF. Brain Res. 621,34–49
56. Yankner, B. A., Duffy, L. K., and Kirschner, D. A. (1990) Neu-rotrophic and neurotoxic effects of amyloid beta protein: re-versal by tachykinin neuropeptides. Science 250, 279–282
30 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 30 Tuesday Nov 25 11:34 AM LP–FASEB 0002
57. Pike, C., Walencewicz, A., Glabe, C., and Cotman, C. (1991) Invitro aging of beta-amyloid protein causes peptide aggregationand neurotoxicity. Brain Res. 563, 311–314
58. Peterson, C., Gibson, G. E., and Blass, J. P. (1985) Altered cal-cium uptake in cultured skin fibroblasts from patients with Alz-heimer’s disease. N. Engl. J. Med. 312, 1063–1064
59. Peterson, C., and Goldman, J. E. (1986) Alterations in calciumcontent and biochemical processes in cultured skin fibroblastsfrom aged and Alzheimer donors. Proc. Natl. Acad. Sci. USA 83,2758–2762
60. Peterson, C., Ratan, R. R., Shelanski, M., and Goldman G. E.(1986) Cytosolic free calcium and cell spreading decrease infibroblasts from aged and Alzheimer donors. Proc. Natl. Acad.Sci. USA 83, 7999–8001
61. Peterson, C., Ratan, R. R., Shelanski, M., and Goldman, G. E.(1988) Altered response of fibroblasts from aged and Alzhei-mer donors to drugs that elevate cytosolic free calcium. Neuro-biol. Aging 9, 261–266
62. Le Quan Sang, K. H., Mignot, E., Gilbert, J. C., Huguet, R.,Aquino, J. P., Regnier, O., and Devynck, M. A. (1993) Plateletcytosolic free calcium concentration is increased in aging andAlzheimer’s disease. Biol. Psychiatry 33, 391–393
63. Adunsky, A., Baram, D., Hershkowitz, M., and Mekori, Y. A.(1991) Increased cytosolic free calcium in lymphocytes of Alz-heimer patients. J. Neuroimmunol. 33, 167–172
64. Gibson G.E., and Toral-Barza L. (1992) Cytosolic free calciumin lymphoblasts from young, eged and Alzheimer’s disease sub-jects. Mech. Ageing Dev. 63, 1–9
65. Eckert, A., Hartmann, H., and Muller, W. E. (1993) Beta-amy-loid protein enhances the mitogen-induced calcium responsein circulating human lymphocytes. FEBS Lett. 330, 49–52
66. Eckert, A., Hartmann, H., Forstl, H., and Muller, W. E. (1994)Alterations of intracellular calcium regulation during aging andAlzheimer’s disease in nonneuronal cells. Life Sci. 55, 2019–2029
67. Hartmann, H., Eckert, A., and Muller, W. E. (1994) Apolipo-protein E and cholesterol affect neuronal calcium signalling:the possible relationship to beta-amyloid neurotoxicity.Biochem. Biophys. Res. Commun. 200, 1185–1192
68. McCoy, K. R., Mullins, R. D., Newcomb, T. G., Ng, G. M., Pav-linkova, G., Polinsky, R. J., Nee, L. E., and Sisken, J. E. (1993)Serum- and bradykinin-induced calcium transient in familialAlzheimer’s fibroblasts. Neurobiol. Aging 14, 447–455
69. Tatebayashi, Y., Takeda, M., Kashiwaggi, Y., Okochi, M., Kuru-madani, T., Sekiyama, A., Kanayama, G, Hariguchi, S., andNishimura, T. (1995) Cell cycle-dependent abnormal calciumresponse in fibroblasts from patients with familial Alzheimer’sdisease. Dementia 6, 9–16
70. Huang, H. M., Toral-Barza, L., Thaler, H., Tofel-Grehl, B., andGibson, G. E. (1991) Inositol phosphates and intracellular cal-cium after bradykinin stimulation in fibroblasts from young,normal aged and Alzheimer donors. Neurobiol. Aging 12, 469–473
71. Borden, L. A., Maxfield, F. R., Goldman, J. E., and Shelanski,M. L. (1992) Resting (Ca2/)i and (Ca2/)i transients are similarin fibroblasts from normal and Alzheimer’s donors. Neurobiol.Aging 13, 33–38
72. Bondy, B., Klages, U., Muller-Spahn, F., and Hock, C. (1994)Cytosolic free (Ca2/) in mononuclear blood cells from de-mented patients and healthy controls. Eur. Arch. Psychiatry ClinNeurosci. 243, 224–228
73. Ito, E., Oka, K., Etcheberrigaray, R., Nelson, T. J., McPhie,D. L., Tofel-Grehl, B., Gibson, G. E., and Alkon, D. L. (1994)Internal Ca2/ mobilization is altered in fibroblasts from patientswith Alzheimer disease. Proc. Natl. Acad. Sci. USA 91, 534–538
74. Gibson, G. E., Zhang, H., Toral-Barza, L., Szolosi, S., and Tofel-Grehl, B. (1996) Calcium stores in cultured fibroblasts andtheir changes with Alzheimer’s disease. Biochim Biophys Acta1316, 71–77
75. Kumar, U., Dunlop, D. M., and Richardson, J.S. (1994) Mito-chondria from Alzheimer’s fibroblasts show a decreased uptakeof calcium and increased sensitivity to free radicals. Life Sci. 54,1855–1860
76. Etcheberrigaray, R., Ito, E., Oka, K., Tofel-Grehl, B., Gibson,G. E., and Alkon, D. L. (1993) Potassium channel dysfunctionin fibroblasts identifies patients with Alzheimer disease. Proc.Natl. Acad. Sci. USA 90, 8209–8213
77. Matsuyama, S. S., Yamaguchi, D. T., Vegara, J., and Jarvik, L. F.(1995) Tetraethylammonium-induced calcium concentrationchanges in skin fibroblasts from patients with Alzheimer’s dis-ease. Dementia 6, 241–244
78. Gibson, G. E., Martins, R., Blass, J., and Gandy, S. (1996) Al-tered oxydation and signal transduction systems in fibroblastsfrom Alzheimer’s patients. Life Sci. 59, 477–490
79. Sims, N. R., Finegan, J. M., and Blass, J. P. (1987) Altered met-abolic properties of cultured skin fibroblasts in Alzheimer’s dis-ease. Ann. Neurol. 21, 451–456
80. Sorbi, S., Piacentini, S., Latorraca, S., Piersanti P., and Amad-ucci, L. (1995) Alterations in metabolic properties in fibroblastsin Alzheimer’s disease. Alzheimers Dis. Assoc. Disord. 9, 73–77
81. Gibson, G. E., Sheu, K.-F. R., Blass, J. P., Baker, A., Carlson,K. C., Harding, B., and Perrino, P. (1988) Reduced activity ofthiamine-dependent enzymes in the brains and peripheral tis-sues of patients with Alzheimer’s disease. Arch. Neurol. 45, 836–840
82. Sheu, K. R., Cooper, A. J. L., Koike, K., Koike, M., Lindsay, G.,and Blass, J. P. (1994) Abnormality of the a-ketoglutarate de-hydrogenase complex in fibroblasts from Alzheimer’s disease.Ann. Neurol. 35, 312–318
83. Blass J. P., Kwan-Fu, R. S., Piacentini, S., and Sorbi, S. (1997)Inherent abnormalities in oxidative metabolism in AD: inter-action with vascular abnormalities. In press
84. Cooper A. L., Sheu K. F., and Blass J. P. (1996) Normal gluta-mate metabolism inAlzheimer’s disease fibroblasts deficient inalpha-ketoglutarate dehydrogenase complex activity. Dev. Neu-rosci. 18, 499–504, 1996
85. Parker, W. D., Filley, C. M., and Parks J. K. (1990) Cytochromec oxidase deficiency in Alzheimer’s disease. Neurology 40, 1302–1303
86. Davis, R. E., Miller, S., Herrnstadt, C., Ghosh S. S., Fahy, E.,Shinobu, L. A., Galasko, D., Thal, L. J., Beal, M. F., Howell, N.,Parker, D. W. (1997) Mutations in mitochondrial cytochromec oxidase genes segregate with late onset Alzheimer’s disease(1997) Proc. Natl. Acad. Sci. USA 94, 4526–4531
87. Hirashima, N., Etcheberrigaray, R., Bergamaschi, S., Racchi,M., Battaini, F., Binetti, G., Govoni, S., and Alkon, D. L. (1996)Calcium responses in human fibroblasts: a diagnostic molecularprofile for Alzheimer’s disease. Neurobiol Aging 17, 549–555
88. Van Nostrand, W. E., Schmaier, A. H., and Wagner, S. L. (1992)Potential role of protease nexin-2/amyloid beta-protein pre-cursor as cerebral anticoagulant. Ann. N.Y. Acad. Sci. 674, 243–252
89. Van Nostrand, W. E., Schmaier, A. H., Farrow, J. S., and Cun-ningham, D. D. (1990) Protease nexin-II (amyloid beta-proteinprecursor): a platelet alpha-granule protein. Science 248, 745–748
90. Van Nostrand, W. E., Wagner, S. L., Suzuki, M., Choi, B. H.,Farrow, J. S., Geddes, J. W., Cotman, C. W., and Cunningham,D. D. (1989) Protease nexin-II, a potent antichymotrypsin,shows identity to amyloid beta-protein precursor. Nature (Lon-don) 341, 546–549
91. Li, Q. X., Evin, G., Small, D. H., Multhaup, G., Beyreuther, K.,and Masters, C. L. (1995) Proteolytic processing of Alzheimer’sdisease beta A4 amyloid precursor protein in human platelets.J. Biol. Chem. 270, 14140–14147
92. Li, Q. X. Berndt, M. C., Bush, A. I., Rumble, B., Mackenzie, I.,Friedhuber, A., Beyreuther, K., and Masters, C. L. (1994)Membrane-associated forms of the beta A4 amyloid protein pre-cursor of Alzheimer’s disease in human platelet and brain:surface expression on the activated human platelet. Blood 84,133–142
93. Gardella, J. E., Gorgone, G. A., Munoz, P. C., Ghiso, J., Fran-gione, B., and Gorevic, P. D. (1992) Beta protein precursorexpression in human platelets and a megakaryocyte cell line.Possible implications for the origin of cerebral amyloidosis inAlzheimer’s disease. Lab. Invest. 67, 303–313
94. Di Luca, M., Pastorino, L., Cattabeni, F., Zanardi, R., Racagni,G., Smeraldi, E., and Perez, J. (1996) Abnormal pattern ofplatelet APP isoforms in Alzheimer’s disease and Down syn-drome. Arch. Neurol. 53, 1162–1166
95. Henriksson, T., Barbour, R. M., Braa, S., Ward, P., Fritz, L. C.,Johnson-Wood, K., Chung, H. D., Burke, W., Reinikainen,K. J., Riekkinen, P., and Schenk, D. B. (1991) Analysis andquantitation of the b-amyloid precursor protein in the cerebro-
PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 31
/ 381c 0002 Mp 31 Tuesday Nov 25 11:34 AM LP–FASEB 0002
spinal fluid of Alzheimer’s disease patients with a monoclonalantibody-based immunoassay. J. Neurochem. 56, 1037–1042
96. Prior, R., Monning, U., Schreiter-Gasser, U., Weidemann, Blen-now, K, Gottfries, C. G., Masters, C. L., and Beyreuther, K.(1991) Quantitative changes in the amyloid bA4 precursor pro-tein in Alzheimer cerebrospinal fluid. Neurosci. Lett. 124, 69–73
97. Farlow, M., Ghetti, B., Benson, M. D., Farrow, J. S., Van Nos-trand, W. E., and Wagner, S. L. (1992) Low cerebrospinal-fluidconcentrations of soluble amyloid b-protein precursor inhereditary Alzheimer’s disease. Lancet 340, 453–454
98. Lannfelt, L., Basun, B., Wahlund, L.-O., Rowe, B. A., Wagner,S. (1995) decreased cerebrospinal fluid alpha-secretase cleavedamyloid precursor protein as diagnostic marker for Alzheimer’sdisease. Nature Med. 1, 829–832
99. Palmert, M. R., Usiak, M., Mayeux, R., Raskind, M., Tuortel-lotte, W. W., and Younkin, S. G. (1990) Soluble derivatives ofthe b amyloid protein precursor in cerebrospinal fluid: altera-tions in normal aging and in Alzheimer’s disease. Neurology 40,1028–1034
100. Van Nostrand, W. E., Wagner, S. L., Shankle, W. R., Farrow,J. S., Dick, M., Rozemuller, J. M. Kuiper, M. A., Wolters, E. C.,Zimmerman, J., Cotman, C. W., and Cunningham, D. D. (1992)Decreased levels of soluble amyloid b-protein precursor in ce-rebrospinal fluid of live Alzheimer disease patients. Proc. Natl.Acad. Sci USA 89,2551–2555
101. Almkvist, O., Basun, H., Wagner, S. L., Rowe, B. A., Wahlund,L.-O., and Lannfelt, L. (1997) Cerebrospinal fluid levels of al-pha secretase cleaved soluble amyloid precursor protein mirrorcognition in Swedish family with Alzheimer’s disease and agene mutation. Arch. Neurol. 54, 641–647
102. Seubert, P., Vigo-Pelfrey, C., Esch, F., Lee, M., Dovey, H., Davis,D., Sinha, S., Schlossmacher, Whaley, J., Swindlehurst, C., Mc-Cormack, R., Wolfert, R., Selkoe, D. J., Lieberburg, I., andSchenk, D. (1992) Isolation and quantification of soluble Alz-heimer’s b-peptide from biological fluid. Nature (London) 359,325–327
103. Nakamura, T., Shoji, M., Harigaya, Y., Watanabe, M., Hosoda,K., Cheung, T. T., Shaffer, L. M., Golde, T. E., Younkin, L. H.,Younkin, S. G., and Shunsaku, H. (1994) Amyloid b-proteinlevels in cerebrospinal fluid are elevated in early onset Alzhei-mer’s disease. Ann. Neurol. 36, 903–911
104. Nitsch, R. M., Rebeck, G. W., Deng, M., Richardson, U. I., Ten-nis, M., Schenk, D. B., Vigo-Pelfrey, C., Lieberburg, I., Wurt-man, R. J., Hyman, B. T., and Growdon, J. H. (1995)Cerebrospinal fluid levels of amyloid b-protein in Alzheimer’sdisease: inverse correlation with severity of dementia and effectof apolipoprotein E genotype. Ann. Neurol. 37, 512–518
105. Lannfelt, L., Basun, H., Vigo-Pelfrey, C., Wahlund, L.O., Win-blad, B., Lieberburg, I., and Schenk, D. (1995) Amyloid b-pep-tide in cerebrospinal fluid in individuals with the SwedishAlzheimer amyloid precursor protein mutation. Neurosci. Lett.199, 203–206
106. Tabaton, M., Nunzi, M. G., Xue, R., Usiak, M., Autilio-Gambetti,L., and Gambetti, P. (1994) Soluble amyloid b-protein is amarker of Alzheimer amyloid in brain but not in cerebrospinalfluid. Biochem. Biophys. Res. Commun. 200, 1598–603
107. Southwick, P. C., Yamagata, S. K., Echols, C. L., Jr., Higson,G. J., Neynaber, S. A., Parson, R. E., and Munroe, W. A. (1996)Assessment of amyloid b protein in cerebrospinal fluid as anaid in the diagnosis of Alzheimer’s disease. J. Neurochem. 66,259–265
108. Van Gool, W. A., Kuiper, M. A., Walstra, G. J. M., Wolters,E. C., and Bolhuis, P. A. (1995) Concentrations of amyloid bprotein in cerebrospinal fluid of patients with Alzheimer’s dis-ease. Ann. Neurol. 37, 277–279
109. Motter, R., Vigo-Pelfrey, C., Kholodenko, D., Barbour, R., John-son-Wood, K., Galasko, D., Chang, L., Miller, B., Clark, C.,Green, R., Olson, D., Southwick, P., Wolfert, R., Munroe, B.,Lieberburg, I., Seubert, P., and Schenk, D. (1995) Reductionof b-amyloid peptide 42 in the cerebrospinal fluid of patientswith Alzheimer’s disease. Ann. Neurol. 38, 643–648
110. Schenk, D., Motter, R., Kholodenko, D., Lieberburg, I., andSeubert, P. (1996) Ab 42 and tau as markers of Alzheimer’sdisease. Neurobiol. Aging 17, S1
111. Ida, N., Hartmann, T., Pantel, J., Schroder, J., Zerfass, R., Forstl,H., Sandbrink, R., Masters, C. L., and Beyreuther, K. (1996)Analysis of heterogeneous bA4 peptides in human cerebrospi-
nal fluid and blood by a newly developed sensitive western blotassay. J. Biol. Chem. 271, 22908–22914
112. Iwatsubo, T., Odaka, A., Suzuki, N., Mizusawa, H., Nukina, N.,and Ihara, Y. (1994) Visualization of Ab42(43) and Ab40 insenile plaques with end-specific monoclonals: evidence that aninitially deposited species is Ab42(43). Neuron 13, 45–52
113. Roher, A., Lowenson, J., Clarke, S., Wolkow, C., Wang, R., Cot-ter, R. J, Reardon, I. M, Zurcher-Neely, H. A, Heinrikson, R. L.,Ball, M. J., et al. (1993) Structural alterations in the peptidebackbone of b-amyloid core protein may account for its depo-sition and stability in Alzheimer’s disease. J. Biol. Chem. 268,3072–3083
114. Song, X. H., Suzuki, N., Bird, T., Peskind, E., Schellenberg, G.,and Younkin, S. G. (1995) Plasma amyloid b protein (Ab) end-ing at Ab42(43) is increased in carriers of familial AD (FAD)linked to chromosome 14. Soc. Neurosci. Abstr. 21, 1501
115. Jensen, M., Song, X. H. Suzuki, N., Lannfelt, L., and Younkin,S. G. (1995) The bAPP670/671 Alzheimer mutation (Swedish)increases plasma amyloid b protein concentration. Soc. Neurosci.Abstr. 21, 1501
116. Younkin, L. H., Eckman, C. B., Yager, D., Graff-Rafford, N., andYounkin, S. G. (1996) Analysis of plasma Ab concentration insporadic AD patients and non-demented subjects of all ages.Neurobiol. Aging 17, S167
117. Kosaka, T., Imagawa, M., Seki, K., Arai, H., Sasaki, H., Tsuji, S.,Asami-Odaka, A., Fukushima, T., Ima, K., and Iwatsubo, T.(1997) The bAPP717 Alzheimer mutation increases the per-centage of plasma amyloid-b protein ending at Ab42(43). Neu-rology 48, 741–745
118. Tato, R. E., Frank, A., and Hernanz, A. (1995) Tau proteinconcentrations in cerebrospinal fluid of patients with dementiaof the Alzheimer type. J. Neurol. Neurosurg. Psychiat. 59, 280–283
119. Vigo-Pelfrey, C., Seubert, P., Barbour, R., Blomquist, C., Lee,M., Lee, D., Coria, F., Chang, L., Miller, B., Lieberburg, I., etal. Elevation of microtubule-associated protein tau in the ce-rebrospinal fluid of patients with Alzheimer’s disease. (1995)Neurology 45, 788–793
120. Munroe, W. A., Southwick, P. C., Chang, L., Scharre, D. W.,Echols, C. L., Jr., and Fu, P. C. (1995) Tau protein in cerebro-spinal fluid as an aid in the diagnosis of Alzheimer’s disease.Ann. Clin. Lab. Sci. 25, 207–217
121. Vandermeeren, M., Mrecken, M., Vanmechelen, E., Six, J., Vande Voorde, A., Martin, J. J., and Cras, P. (1993) Detection of tproteins in normal and Alzheimer’s disease cerebrospinal fluidwith a sensitive sandwich enzyme-linked immunoassorbent as-say. J. Neurochem. 61, 1828–1834
122. Jensen, M., Basun, H., and Lannfelt, L. (1995) Increased ce-rebrospinal fluid tau in patients with Alzheimer’s disease. Neu-rosci. Lett. 186, 189–191
123. Arai, H., Terajima, M., Miura, M., Higuchi, S., Muramatsu, T.,Machida, N., Seiki, H., Takase, S., Clark, C. M., Lee, V. M.-Y.,Trojanowski, J. Q., and Sasaki, H. (1995) Tau in cerebrospinalfluid: a potential diagnostic marker in Alzheimer’s disease.Ann. Neurol. 38, 649–652
124. Galasko, D., Clark, C., Chang, L., Miller, B., Green, R. C., Mot-ter, R., and Seubert P. (1997) Assessment of cerebrospinal fluidlevels of tau in mildly demented patients with Alzheimer’s dis-ease. Neurology 48, 632–635
125. Blomberg, M., Jensen, M., Basun, H., Lannfelt, L., and Wah-lund, L.-O. (1996) Increased of CSF tau levels in most Alzhei-mer patients during 15 months follow-up. Neurobiol. Aging 17,S167
126. Johnson, G. V. W., Seubert, P., Cox, T. M., Motter, R., Brown,J. P., and Galasko, D. (1997) The tau protein in human cere-brospinal fluid in alzheimers disease consists of proteolyticallyderived fragments. J. Neurochem. 68, 430–433
127. Blennow, K., Wallin, A., Agren, H., Spenger, C., Siegfried, J.,and Vanmechelen, E. (1995) Tau protein in cerebrospinalfluid. A biochemical marker for axonal degeneration in Alz-heimer’s disease? Mol. Chem. Neuropathol. 26, 231–245
128. Kennard, M. L., Feldman, H., Yamada, T., and Jefferies, W. A.(1996) Serum levels of the iron binding protein p97 are ele-vated in Alzheimer’s disease. Nat. Med. 2, 1230–1235
129. Ball, M. J. (1978) Topographic distribution of neurofibrillarytangles and granulovacuolar degeneration in hippocampal cor-tex of aging and demented patients. A quantitative study. ActaNeuropathol. 42, 73–80
32 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 32 Tuesday Nov 25 11:34 AM LP–FASEB 0002
130. Coleman, P. D., and Flood, D. G. (1987) Neuron numbers anddendritic extent in normal aging and Alzheimer’s disease. Neu-robiol. Aging 8, 521–545
131. Sapolski, R. M., Zolan-Morgan, S., and Squire, L. R. (1991) In-hibition of glucocorticoid secretion by the hippocampal for-mation in the primate. J. Neurosci. 11, 3695–3704
132. Dunn, I. D., and Orr, S. E. (1984) Differential plasma cortico-sterone responses to hippocampal stimulation. Brain Res. 54, 1–8
133. Lorens, S. A., Hata, N., Handa, R. J., Van de Kar, L. D., Gusch-wanb, M., Goral, J., Lee, J. M., Hamiltor, M. E., Bethea, C. L.,and Clancy, J. (1990) Neurochemical, endocrine and immu-nological response to stress in young and old Fisher 344 malerats. Neurobiol. Aging 11, 139–150
134. Reul, J. M., Tonnaer, J. A. D. M., and de Kloet, E. R. (1988)Neurotropic ACTH analog promotes plasticity of type I corti-costeroid receptors in brain of senescent rats. Neurobiol. Aging9, 253–260
135. Reul, J. M. H. M., Rothuizen, J., and de Kloet, E. R. (1991) Age-related changes in the dog hypothalamic-pituitary-adrenocor-tical system: neuroendocrine activity and corticosteroidreceptors. J. Steroid Biochem. Mol. Biol. 40, 63–69
136. Heuser, I. J., Gotthardt, U., Schweiger, U., Schmider, J., Lam-mers, C. H., Dettling, M., and Holsboer, F. (1994) Age-associ-ated changes of pituitary-adrenocortical hormone regulation inhumans: importance of gender. Neurobiol. Aging 15, 227–231
137. Hatzinger, M., Z’Brun, A., Hemmeter, U., Seifritz, E, Baumann,F., Holsboer-trachsler, E., and Heuser, I. J. (1995) Hypotha-lamic-pituitary-adrenal system function in patients with Alzhei-mer’s disease. Neurobiol. Aging 16, 205–209
138. May, C., Rapoport, S. I., Tomai, T. P., Chrousos, G. P., and Gold,P. W. (1987) Cerebrospinal fluid concentrations of corticotro-pin-releasing hormone (CRH) and corticotropin (ACTH) arereduced in patients with Alzheimer’s disease. Neurology 37, 535–538
139. Facchinetti, F., Nappi, G., Petraglia, F., Martignoni, E., Sinfor-iani, E., and Genazzani, A. R. (1984) Central ACTH deficit indegenerative and vascular dementia. Life Sci. 35, 1691–1697
140. Suemaru, S., Suemaru, K., Hashimoto, K., Ogasa, T., Hirasawa,R., Makino, S., and Kageyama, J. (1993) Cerebrospinal fluidcorticotropin-releasing hormone and ACTH, and peripherallycirculating choline-containing phospholipid in senile demen-tia. Life Sci. 53, 697–706
141. Suemaru, S., Hashimoto, K., Ogasa, T., Hirasawa, R. V., Makino,S., Ota, Z., Kageyama, J., and Suemaru, K. (1991) Cerebrospinalfluid and plasma corticotropin-releasing hormone in senile de-mentia. Life Sci. 48, 1871–1879
142. De Souza, E. B., Whitehouse, P. J., Kuhar, M. J., Price, D. L. V.,and Vale, W. W. (1986) Reciprocal changes in corticotropin-releasing factor (CRF)-like immunoreactivity and CRF recep-tors in cerebral cortex of Alzheimer’s disease. Nature (London)319, 593–595
143. Whitehouse, P. J, Vale, W. W., Zweig, R. M. V., Singer, H. S,Mayeux, R., Kuhar, M. J., Price, D. L., and De Souza, E. B.(1987) Reductions in corticotropin releasing factor-like im-munoreactivity in cerebral cortex in Alzheimer’s disease, Par-kinson’s disease, and progressive supranuclear palsy. Neurology37, 905–909
144. Bissette, G., Reynolds, G. P., Kilts, C. D., Widerlov, E., and Nem-eroff, C. B. (1985) Corticotropin-releasing factor-like immu-noreactivity in senile dementia of the Alzheimer type. J. Am.Med. Assoc. 254, 3067–3069
145. De Souza, E. B., Whitehouse, P. J., Price, D. L., and Vale, W. W.(1987) Abnormalities in corticotropin-releasing hormone(CRH) in Alzheimer’s disease and other human disorders. Ann.N.Y. Acad. Sci. 512, 236–247
146. Lesch, K. P., Ihl, R., Frolich, L., Rupprecht, R., Muller, U.,Schulte, H.M., and Maurer, K. (1990) Endocrine responses togrowth hormone releasing hormone and corticotropin releas-ing hormone in early-onset Alzheimer’s disease. Psychiatry Res.33, 107–112
147. Ghiso, E., Nicolosi, M., Arvat, E., Marcone, A., Danelon, F.,Mucci, M., Franceschi, M., Smirne, S., and Camanni, F. (1993)Growth hormone secretion in Alzheimer’s disease: studies withgrowth hormone releasing hormone alone and combined withpyridostigmine or arginine. Dementia 4, 315–320
148. Murialdo, G., Zerbi, F., Filippi, U., Tosca, P., Fonzi, F., Di Paolo,E., Costelli, P., Porro, S., Polleri, A., and Savoldi, F. (1990) Cho-linergic modulation of growth hormone-releasing hormoneeffects on growth hormone secretion in dementia. Neuropsycho-biology 24, 129–314
149. Gomez, J. M., Aguilar, M., Navarro, M. A., Ortola, J., and Soler,J. (1994) Secretion of growth hormone and thyroid-stimulatinghormone in patients with dementia. Clin. Invest. 72, 489–493
150. Edvinsson, L., Minthon, L., Ekman, R., and Gustafson, L.(1993) Neuropeptides in cerebrospinal fluid of patients withAlzheimer’s disease and dementia with frontotemporal lobe de-generation. Dementia 4, 167–171
151. Albert, M., Jenike, M., Nixon, R., and Nobel, K. (1993) Thyro-tropin response to thyrotropin-releasing hormone in patientswith dementia of the Alzheimer type. Biol. Psychiatry 33, 267–271
152. Dysken, M. W., Falk, A., Pew, B., Kuskowski, M., and Krahn,D. D. (1990) Gender differences in TRH-stimulated TSH andprolactin in primary degenerative dementia and elderly con-trols. Biol. Psychiatry 28, 144–150
153. Bierer, L. M., Haroutunian, V., Gabriel, S., Knott, P. J., Carlin,L. S., Purohit, D. P., Perl, D. P., Schmeidler, J., Kanof, P., andDavis, K. L. (1995) Neurochemical correlates of dementia se-verity in Alzheimer’s disease: relative importance of the cholin-ergic deficits. J. Neurochem. 64, 749–760
154. Beal, M. F. (1990) Somatostatin in neurodegenerative illnesses.Metabolism 39, 116–119
155. Leake, A., and Ferrier, I. N. (1993) Alterations in neuropep-tides in aging and disease. Pathophysiology and potential forclinical intervention. Drugs Aging 3, 408–27
156. Reinikainen, K. J., Koponen, H., Jolkkonen, J., and Riekkinen,P. J. (1990) Decreased somatostatin-like immunoreactivity inthe cerebrospinal fluid of chronic schizophrenic patients withcognitive impairment. Psychiatry Res. 33, 307–312
157. Wallin, A., Carlsson, A. V., Ekman, R., Gottfries, C. G., Karlsson,I., Svennerholm, L., and Widerlov, E. (1991) Hypothalamicmonoamines and neuropeptides in dementia. Eur. Neuropsycho-pharmacol. 1, 165–168
158. Molchan, S. E., Hill, J. L., Martinez, R. A., Lawlor, B. A., Mellow,A. M., Rubinow, D. R., Bissette, G. V., Nemeroff, C. B., andSunderland, T. (1993) CSF somatostatin in Alzheimer’s diseaseand major depression relationship to hypothalamic-pituitary-adrenal axis and clinical measures. Psychoneuroendocrinology 18,509–519
159. Yasuda, M., Minamitani, N., and Maeda, K. (1993) Peptide his-tidine methionine in cerebrospinal fluid of patients with seniledementia of the Alzheimer type. Jpn. J. Psychiatry Neurol. 47, 85–90
160. Hartikainen, P., Reinikainen, K. J., Soininen, H., Sirvio, J., Soik-keli, R., and Riekkinen, P. J. (1992) Neurochemical markers inthe cerebrospinal fluid of patients with Alzheimer’s disease,Parkinson’s disease and amyotrophic lateral sclerosis and nor-mal controls. J. Neural Trans. Parkinson Dis. Dement. Sect. 4, 53–68
161. Wikkelso, C., Ekman, R., Westergren, I., and Johansson, B.(1991) Neuropeptides in cerebrospinal fluid in normal pres-sure hydrocephalus and dementia. Eur. Neurol. 31, 88–93
162. Minthon, L., Edvinsson, L., Ekman, R., and Gustafson, L.(1990) Neuropeptide levels in Alzheimer’s disease and demen-tia with frontotemporal degeneration. J. Neural Trans. Suppl. 30,57–67
163. Reinikainen, K. J., Soininen, H., and Riekkinen, P. J. (1990)(A)Neurotrasmitter changes in Alzheimer’s disease: implicationsto diagnostics and therapy. J. Neurosci. Res. 27, 576–586
164. Koponen, H., Reinikainen, K. J., Jolkkonen, J. Y., and Riekki-nen, P. J. (1990) Somatostatin-like immunoreactivity in the CSFof patients with dementia associated with alcoholism. Acta Neu-rol. Scand. 82, 289–291
165. Banki, C. M., Karmacsi, L., Bissette, G., and Nemeroff, C. B.(1992) Cerebrospinal fluid neuropeptides in mood disorderand dementia. J. Affective Disord. 25, 39–45
166. Strittmatter, M. M., and Cramer, H. (1992) Parkinson’s diseaseand dementia: clinical and neurochemical correlations. Neu-roreport 3, 413–416
167. Molins, A., Catalan, R., Sahuquillo, J., Castellanos, J. M., Codina,A., and Galard, R. (1991) Somatostatin cerebrospinal fluid lev-els in dementia. J. Neurol. 238, 168–170
PERIPHERAL MARKERS AND ALZHEIMER’S DISEASE 33
/ 381c 0002 Mp 33 Tuesday Nov 25 11:34 AM LP–FASEB 0002
168. Leake, A., Perry, E. K., Perry, R. H., Jabeen, S., Fairbairn, A. F.,McKeith, I. G., and Ferrier, I. N. (1991) Neocortical concentra-tions of neuropeptides in senile dementia of the Alzheimer andLewy body type: comparison with Parkinson’s disease and se-verity correlations. Biol. Psychiatry 29, 357–364
169. Tang, M. X., Jacobs, D., Stern Y., Marder, K., Schofield, P., Gur-land, P., Andrews, H., and Mayeux, R. (1996) Effect of estrogenduring menopause on risk and age at onset of Alzheimer’s dis-ease. Lancet 348, 429–432
170. Henderson, V. W., Paganini-Hill, A., Emanuel, C. D., Dunn,M. E., and Buckwater, J. G. (1994) Estrogen replacement ther-apy in older women: comparison between Alzheimer’s diseasecases and non-demented controls. Arch. Neurol. 51, 896–899
171. Eikelenboom, P., and Veerhuis, R. (1996) The role of comple-ment and activated microglia in the pathogenesis of Alzhei-mer’s disease. Neurobiol. Aging 17, 673–680
172. Roger, J., Webster, S., Fue, L.-F., Brachova, L., Civin, W. H.,Emmerling, M., Shivers, B., Walker, D., and McGeer, P. (1996)Inflammation and Alzheimer’s disease. Neurobiol. Aging 17,681–686
173. Kalaria, R. N., Harshbarger-Kelly, M., Coher, D. L., and Pre-mkumar, D. R. D. (1996) Molecular aspects of inflammatoryand immume responses in Alzheimer’s disease. Neurobiol. Aging17, 687–694
174. Weisgraber, K. H., Roses, A. D., and Strittmatter, W. J. (1994)The role of apolipoprotein E in the nervous system. Curr. Opin.Lipidol. 5, 110–116
175. Pitas, R. E., Boyles, J. K., Lee, S. H., Foss, D., and Mahley, R. W.(1987)Astrocytes synthesize apolipoprotein E and metabolizeapolipoprotein E-containing lipoproteins. Biochem. Biophys. Acta917, 148–161
176. Poirier, J. (1994) Apolipoprotein E in animal models of CNSinjury and in Alzheimer’s disease. Trends Neurosci. 17, 525–530
177. Ignatius, M. J., Gebicke-Harter, P. J., Skene, J. H. P., Schilling,J. W., Weisgraber, K. H., Mahley, R. W., and Shooter, E. M.(1986) Expression of apolipoprotein E during nerve degener-ation and regeneration. Proc. Natl. Acad. Sci. USA 83, 1125–1129
178. Snipes, G. J. V., McGuire, C. B., Norden, J. J., and Freeman,J. A. (1986) Nerve injury stimulates the secretion of apolipo-protein E by nonneuronal cells. Proc. Natl. Acad. Sci. USA 83,1130–1134
179. Namba, Y., Tomonaga, M., Kawasaki, H., Otomo, E., and Ikeda,K. (1991) Apolipoprotein E immunoreactivity in cerebral am-yloid deposits and neurofibrillary tangles in Alzheimer’s diseaseand kuru plaque amyloid in Creutzfeldt-Jacob disease. BrainRes. 41, 163–166
180. Strittmatter, W. J, Saunders, A. M., Schmechel, D., Pericak-Vance, M., Enghild, J., Salvesen, G. S., and Roses, A. D. (1993)Apolipoprotein E-high avidity binding to b-amyloid and in-creased frequency of type 4 allele in late-onset familial Alzhei-mer disease. Proc. Natl. Acad. Sci. USA 90, 1977–1981
181. Saunders, A. M., Strittmatter, W. J., Schmechel, D., St. George-Hyslop, P. H., Pericak-Vance, M. A., Joo, S. H., Rosi, B. L., Gu-sella, J. F., Crapper-MacLachlan, D. R., Alberts, M. J., Hulette,C., Crain, B., Goldgaber, D., and Roses, A. D. (1993) Associa-tion of apolipoprotein E allele e4 with late-onset familial andsporadic Alzheimer’s disease. Neurology 43, 1467–1472
182. Peacock, M. L., and Fink, J. K. (1994) ApoE e4 allelic associationwith Alzheimer’s disease: independent confirmation using de-neturing gradient gel electrophoresis. Neurology 44, 339–341
183. Ueki, A., Kawano, M., Namba, Y., Kawakami, M., and Ikeda, K.(1993) A high frequency of apolipoprotein E4 isoprotein inJapanese patients with late-onset nonfamilial Alzheimer’s dis-ease. Neurosci. Lett. 163, 166–168
184. Kuusisto, J., Koivisto, K., Kervinen, K., Mykkanen, L., Helkala,E. L., Vanhanen, M., Hanninan, T., Pyorala, K., Kesaniemi,Y. A., Riekkinen, P., and Laakso, M. (1994) Association of apo-lipoprotein E phenotypes with late onset Alzheimer’s disease:population based study. Br. Med. J. 309, 636–638
185. Heinonen, O., Lehtovirta, M., Soininen, H., Helisalmi, S, Man-nermaa, A., Sorvari, H., Kosunen, O., Paljarvi, L., Ryynanen,M., and Riekkinen, P. J. (1995) Alzheimer pathology of patientscarrying apolipoprotein E epsilon 4 allele. Neurobiol. Aging 16,505–513
186. Frisoni, G. B., Calabresi, L., Geroldi, C., Bianchetti, A.,D’Acquarica, A. L., Govoni, S., Sirtori, C. R., Trabucchi, M., and
Franceschini, G. (1994) Apolipoprotein E e4 allele in Alzhei-mer’s disease and vascular dementia. Dementia 5, 240–242
187. Sorbi, S., Nacmias, B., Forleo, P., Latorraca, S., Gobbini, I.,Bracco, L., Piacentini, S., and Amaducci, L. (1994) ApoE allelefrequencies in Italian sporadic and familial Alzheimer’s disease.Neurosci.Lett. 177, 100–102
188. Dai, X. Y., Nanko, S., Hattori, M., Fukuda, R., Nagata, K., Isse,K., Ueki, A., and Kazamatsuri, H. (1994) Association of apoli-poprotein E4 with sporadic Alzheimer’s disease is more pro-nounced in early onset type. Neurosci. Lett. 175, 74–76
189. Van Duijn, C. M., de Knijff, P., Cruts, M., Wehnert, A., Havekes,L. M., Hofman, A., and Van Broeckhoven, C. (1994) Apolipo-protein E4 allele in a population-based study of early-onset Alz-heimer’s disease. Nat. Genet. 7, 74–78
190. Schmechel, D. E., Saunders, A. M., Strittmatter, W. J., Crain,B. J., Hulette, C. M., Joo, S. H., Pericak-Vance, M. A., Goldgaber,D., and Roses, A. D. (1993) Increased amyloid b-peptide de-position in cerebral cortex as a consequence of apolipoproteinE genotype in late-onset Alzheimer disease. Proc. Natl. Acad. Sci.USA 90, 9649–9653
191. Tsal, M. S., Tangalos, E. G., Petersen, R. C., Smith, G. E., Schald,D. J., Kokmen, E., Ivnik, R. J., and Thibodeau, S. N. (1994)Apolipoprotein E: risk factor for Alzheimer disease. Am. J. Hum.Genet. 54, 643–649
192. Saunders, A. M., Hulette, C., Welsh-Bohmer, K. A., Schmechel,D. E., Crain, B., Burke, J. R., Alberts, M. J., Strittmatter, W. J.,Breitner, J. C. S., Rosenberg, C., Scott, S. V., Gaskell, P. C., Jr.,Pericak-Vance, M. A., and Roses, A. D. (1996) Specificity, sen-sitivity, and predictive value of apolipoprotein-E genotyping forsporadic Alzheimer’s disease. Lancet 348, 90–93
193. Frisoni, G. B., Geroldi, C., Bianchetti, A., Binetti, G., and Tra-bucchi, M. (1996) The gain of apolipoprotein E genotyping toseparate Alzheimer’s disease from normal individuals: rele-vance to community studies. Dementia 7, 336–342
194. Frisoni, G. B., Bianchetti, A., Govoni, S., and Trabucchi, M.(1996) Diagnostic usefulness of apolipoprotein E e4 in the di-agnosis of the dementia (letter). J. Neurol. Neurosurg. Psychiat.60, 699–700
195. Amouyel, P., Vidal, O., Launay, J. M., and Laplanche, J. L.(1994) The apolipoprotein E alleles as major susceptibility fac-tors for Creutzfeldt-Jacob disease. Lancet 344, 1315–1318
196. St. Clair, D., Norrman, J., Perry, R., Yates, C., Wilcock, G., andBrookes, A. (1994) Apolipoprotein E e4 allele frequency in pa-tients with Lewy body dementia, Alzheimer’s disease and age-matched controls. Neurosci. Lett. 176, 45–46
197. Van Gool, W. A., Evenhuis, H. M., and van Duijn, C. M., onbehalf of the Dutch Study Group on Down’s syndrome andAgeing. (1995) A case-control study of apolipoprotein E ge-notypes in Alzheimer’s disease associated with Down’s syn-drome. Ann. Neurol. 38, 225–230
198. Mann, D. M. A., Pickering-Brown, S. M., Siddons, M. A., Iwat-subo, T., Ihara, Y., Asami-Okada, A., and Suzuki, N. (1995) Theextent of amyloid deposition in brain in patients with Down’ssyndrome does not depend upon the apolipoprotein E geno-type. Neurosci Lett. 196, 105–108
199. Poirier, J., Delisle, M.-C., Quirion, R., Aubert, I., Farlow, M.,Lahiri, D., Hui, S., Bertrand, P., Nalbantoglu, J., Gilfix, B. M.,and Gauthier, S. (1995) Apolipoprotein E4 allele as a predictorof cholinergic deficits and treatment outcome in Alzheimer dis-ease. Proc. Natl. Acad. Sci. USA 92, 12260–12264
200. Roses, A. D, Strittmatter, W. J., and Pericak-Vance, M. A. (1994)Clinical application of apolipoprotein E genotyping to Alzhei-mer’s disease. Lancet 343, 1564–1565
201. Frisoni, G. B., Geroldi, C., Bianchetti, A., Calabresi, L., Fran-ceschini, G., and Trabucchi, M. (1995) Gene dose of the e4allele of apolipoprotein E and disease progression in sporadiclate-onset Alzhiemer’s disease. Ann. Neurol. 37, 596–604
202. Blennow, K., Hesse, C., and Fredman, P. (1994) Cerebrospinalfluid apolipoprotein E is reduced in Alzheimer’s disease. Neu-roreport 5, 2534–2536
203. Lehtimaki, T., Pirttila, T., Mehta, P. D., Wisniewski, H. M., Frey,H., and Nikkari, T. (1995) Apolipoprotein E (apoE) polymor-phism and its influence on ApoE concentrations in the cere-brospinal fluid in Finnish patients with Alzheimer’s disease.Human Genet. 95, 39–42
204. Landen, M., Hesse, C., Fredman, P., Regland, B., Wallin, A.,and Blennow, K. (1996) Apolipoprotein E in cerebrospinal

34 Vol. 12 January 1998 The FASEB Journal GASPARINI ET AL.
/ 381c 0002 Mp 34 Tuesday Nov 25 11:35 AM LP–FASEB 0002
fluid from patients with Alzheimer’s disease and other formsof dementia is reduced but without any correlation to theapoE4 isoform. Dementia 7, 273–278
205. Hahne, S., Nordstedt, C., Ahlin, A., and Nyback, H. (1997) Lev-els of cerebrospinal fluid apolipoprotein E in patients with Alz-heimer’s disease and healthy controls. Neurosci. Lett. 224, 99–102
206. Merched, A., Blain, H., Visvikis, S., Herbeth, B., Jeandel, C., andSiest, G. (1997) Cerebrospinal fluid apolipoprotein E level isincreased in late-onset Alzheimer’s disease. J. Neurol. Sci. 145,33–39
207. Blomberg, M., Jensen, M., Basun, H., Lannfelt, L., and Wah-lund, L. O. (1996) Increasing cerebrospinal fluid tau levels ina subgroup of Alzheimer patients with apolipoprotein E allele
epsilon 4 during 14 months follow-up. Neurosci. Lett. 214, 163–166
208. Etcheberrigaray, R., Ito, E., Kim, C. S., and Alkon, D. L. (1994)Soluble b-amyloid induction of Alzheimer’s phenotype for hu-man fibroblast K/ channels. Science 264, 276–279
209. Vestling, M., Adem, A., Racchi, M., Gibson, G. E., Lannfelt, L.,and Cowburn, R. F. (1997) Differential regulation of adenylylcyclase in fibroblasts from sporadic and familial Alzheimer’sdisease cases with PS1 and APP mutations. Neuroreport 8, 127–130
210. Rosenberg, R. N., Baskin, F., Fosmire, J. A., Risser, R., Adams,P., Svetlik, D., Honig, L. S., Cullum, M. C., and Weiner, M. F.(1997) Altered amyloid processing in platelets of patients withAlzheimer’s disease. Arch. Neurol. 54, 139–144