pelvic tilt and truncal inclination
TRANSCRIPT

SPINE Volume 34, Number 17, pp E599–E606©2009, Lippincott Williams & Wilkins
Pelvic Tilt and Truncal InclinationTwo Key Radiographic Parameters in the Setting of Adults WithSpinal Deformity
Virginie Lafage, PhD, Frank Schwab, MD, Ashish Patel, MD, Nicola Hawkinson, NP,and Jean-Pierre Farcy, MD
Study Design. Prospective radiographic and clinicalanalysis.
Objective. Investigate the relationship between spino-pelvic parameters and patient self reported outcomes onadult subjects with spinal deformities.
Summary of Background Data. It is becoming increas-ingly recognized that the study of spinal alignment shouldinclude pelvic position. While pelvic incidence determineslumbar lordosis, pelvic tilt (PT) is a positional parameterreflecting compensation to spinal deformity. Correlationbetween plumbline offset (sagittal vertical axis [SVA]) andHealth Related Quality of Life (HRQOL) measures hasbeen demonstrated, but such a study is lacking for PT.
Methods. This prospective study was carried out on125 adult patients suffering from spinal deformity (meanage: 57 years). Full-length free-standing radiographs in-cluding the spine and pelvis were available for all pa-tients. HRQOL instruments included: Oswestry DisabilityIndex, Short Form-12, Scoliosis Research Society. Corre-lation analysis between radiographic spinopelvic param-eters and HRQOL measures was pursued.
Results. Correlation analysis revealed no significancepertaining to coronal plane parameters. Significant sagit-tal plane correlations were identified. SVA and truncalinclination measured by T1 spinopelvic inclination (T1–SPI) (angle between T1–hip axis and vertical) correlatedwith: Scoliosis Research Society (appearance, activity, to-tal score), Oswestry Disability Index, and Short Form-12(physical component score). Correlation coefficientsranged from 0.42 � r � 0.55 (P � 0.0001). T1–SPI revealedgreater correlation with HRQOL compared to SVA. PTshowed correlation with HRQOL (0.28 � r � 0.42) andwith SVA (r � 0.64, P � 0.0001).
Conclusion. This study confirms that pelvic positionmeasured via PT correlates with HRQOL in the setting ofadult deformity. High values of PT express compensatorypelvic retroversion for sagittal spinal malalignment. Thisstudy also demonstrates significant T1–SPI correlationwith HRQOL measures and outperforms SVA. This pa-rameter carries the advantage of being an angular mea-surement which avoids the error inherent in measuringoffsets in noncalibrated radiographs.
Key words: pelvic tilt, HRQOL, sagittal plane, adult spi-nal deformity, alignment. Spine 2009;34:E599–E606
Spinal deformity (de novo scoliosis, adult adolescent id-iopathic scoliosis and iatrogenic deformities) is a com-plex disorder affecting up to 60% of the aging adultpopulation.1 For most subjects, stable ankylosis of thespine may leave them relatively asymptomatic, butothers are left with significant pain and functional dis-ability. Un-like adolescent idiopathic scoliosis, wheretreatment guidelines are driven by radiologic risk ofprogression, adult spinal deformities must be assessedby the patients self perception of pain/disability.Health-related quality of life (HRQOL) instrumentsare now widely used to evaluate the effect of a spinaldeformity on physical function, pain, mental health,and self-image.
In order to define objective criteria for surgical treat-ment of adult spinal deformities, several authors haveinvestigated the relationship between HRQOL instru-ments and radiographic measurements. In an early studyon 95 patients, Schwab et al2 identified radiologic pa-rameters that correlated with a patient’s perceived pain(measured with a Visual Analog Scale of pain): interver-tebral subluxation (olisthesis), L3 and L4 coronal verte-bral obliquity, and loss of lumbar lordosis. Loss of lor-dosis was also found to be correlated with the lowerShort Form (SF) –36 scores in a later report.3 More re-cently, Glassman et al4,5 investigated the relationship be-tween global alignment (frontal5 and sagittal4,5) withHRQOL measures; the sagittal vertical axis (SVA), mea-sured as the offset between C7 plumbline and the pos-terosuperior corner of S1, was found to be correlatedwith pain and a decrease in function measured by theOswestry Disability Index (ODI), Scoliosis Research So-ciety (SRS) and the SF-12 instruments. Finally an adultdeformity classification was established6 where keys pa-rameters (lumbar lordosis, SVA, and intervertebral sub-luxations) were identified as modifiers, for the dominantfrontal/sagittal deformity type, according to their impacton the HRQOL. These studies identified key radio-graphic parameters correlated with patient pain and dis-ability, but nevertheless, these studies present with a fewdrawbacks: a limited number of radiographic parame-ters investigated, and no parameters related to the pelvis.
It is notable, that since the work published by Mar-nay and Vidal7,8 on the pelvis and the concept of “co-nus of economy” presented by Dubousset,9 numerous
From the NYU Hospital for Joint Diseases, New York, NY.Acknowledgment date: May 21, 2008. Revision date: January 18,2009. Acceptance date: February 23, 2009.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).Corporate/Industry funds were received in support of this work. Nobenefits in any form have been or will be received from a commercialparty related directly or indirectly to the subject of this manuscript.Supported by Medtronic Sofamor Danek.Address correspondence and reprint requests to Virginie Lafage, PhD,NYU Hospital for Joint Diseases, 380 2nd Ave, Suite 1001, New York,NY 10010; E-mail: [email protected]
E599
studies have investigated the role of the pelvis in thecomplexity of the human standing sagittal spinalalignment. Three pelvic parameters have been de-scribed in literature. Pelvic incidence10 (PI) is a mor-phologic parameter which has been demonstrated todefine lumbar alignment. More recently, PI was usedto describe a set of sagittal spinal morphotypes.11,12
Pelvic tilt (PT), is a positional pelvic parameter thatmeasures pelvic version. In some specific cases, thisparameter has been demonstrated to act as a compen-satory mechanism in order to maintain an upright pos-ture with age related changes in sagittal alignment.Finally, Sacral slope (SS), quantifies the sagittal sacralinclination and completes the geometric relationshipwhere “PI � PT � SS.”
To our knowledge, the only report regarding the rela-tionship between patient self reported outcomes and PTwas published by Lazennec et al.13 A population of 81patients who underwent lumbosacral fusion was ana-lyzed for pre and postoperative differences in spinopelvicparameters and postoperative residual pain. The authorsdemonstrated that patients with a larger postoperativePT, increased pelvic retroversion, were more likely todemonstrate residual pain, than patients with a smallerpostoperative PT.
The purpose of this study was to evaluate correlationsbetween coronal and sagittal radiographic parametersand HRQOL measures on a population of adult patientswith spinal deformity.
Materials and Methods
This is a consecutive, prospective study approved by ourhospital’s institutional review board. This radiographic andclinical study involved 125 adult patients presenting for con-sultation at 1 center for pain/disability related to spinal de-formity. Inclusion criteria were any adult (�18 years old)presenting at least 1 of the following radiographic sign ofspinal deformity:
● Coronal Cobb angle curvature �30°,● Sagittal or coronal imbalance,● Thoracic kyphosis greater than 60° (T3 or T5–T12),● Lumbar lordosis less than 30° with scoliosis equal to or
greater than 15°,● Thoracolumbar kyphosis (T10–L2) greater than 20°,● Lumbar kyphosis (equal to or greater than 3 levels)
greater than 10°.
Radiographic data collection consisted of full-length stand-ing coronal and sagittal radiographs obtained in free-standingposture with fingers on the clavicles and shoulders in 45° offorward elevation.14 All images were digitized with a Vidarscanner (Vidar Systems Corp., Herndon, VA), and then ana-lyzed using a validated spine dedicated software15–17 (Spinev-iew, Surgiview, Paris, France). Measurements included over100 spinopelvic parameters including: maximal coronal Cobbangle, global coronal balance (coronal offset between C7 ver-tebral body and the center of S1 endplate), SVA, sagittal T1–and T9 –spino-pelvic inclination (SPI), thoracic kyphosis,thoracolumbar alignment, lumbar lordosis, PI, PT, and SS(Figures 1, 2). Of note, the sagittal spinopelvic parametershave been previously described by Legaye and Duval-Beaupere18 and have appeared in literature under many syn-onyms: T1–T9 sagittal offsets,19 T1–T9 tilting,16 T1–T9tilt,20 T1–T9 sagittal tilt…
Clinical patient analysis based on standard HRQOL mea-sures was collected at the time of radiographic acquisition andincluded the following instruments: ODI, SF-12, SRS-23.While higher scores on the ODI represent increasing disability,the inverse holds true for the SRS instrument and SF-12, wherehigher scores reflect less disability/pain than low scores.
Statistical correlation analysis was pursued to determinecorrelation (Spearman rank order) between radiographic pa-rameters and overall and domain specific scores of HRQOLinstruments.
Results
Group DescriptionThe study group consisted of 29 men and 96 women, theaverage age of the study population was 57 years (range:
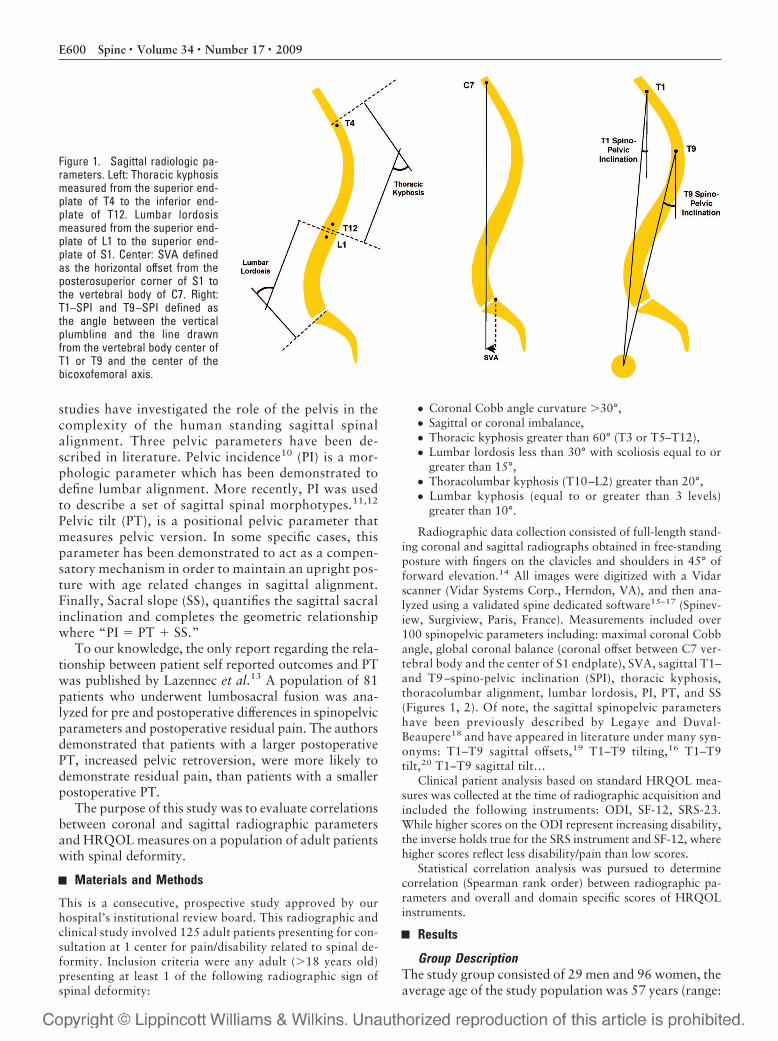
Figure 1. Sagittal radiologic pa-rameters. Left: Thoracic kyphosismeasured from the superior end-plate of T4 to the inferior end-plate of T12. Lumbar lordosismeasured from the superior end-plate of L1 to the superior end-plate of S1. Center: SVA definedas the horizontal offset from theposterosuperior corner of S1 tothe vertebral body of C7. Right:T1–SPI and T9 –SPI defined asthe angle between the verticalplumbline and the line drawnfrom the vertebral body center ofT1 or T9 and the center of thebicoxofemoral axis.
E600 Spine • Volume 34 • Number 17 • 2009
22–88 years old). The breakdown of patients by primarydiagnosis was as follows: 54 Adult Idiopathic Scoliosis,33 Adult de novo scoliosis, 29 iatrogenic sagittal imbal-ance, 4 hyper-kyphosis, 3 congenital kyphosis, 1 thora-columbar kyphosis and 1 coronal imbalance. Fortypatients had undergone previous arthrodesis. Nonopera-tive care (physical therapy, injection, pain medication,bracing) was indicated for 85 patients, whereas surgicaltreatment was proposed to 40 patients.
The 125 patients of this study had the following sum-mary HRQOL scores: mean SRS � 3.1, mean ODI � 45,mean SF-12 physical component score (PCS) � 36.2, andmean SF-12 MCS � 48. Detailed HRQOL scores arereported in Table 1, radiographic values of the entirestudy group are summarized in Table 2.
A summary of correlations found between radio-graphic parameters and HRQOL scores is provided inTable 3. Main findings are discussed hereafter.
Coronal PlaneNo correlation was found between the coronal Cobbangle and any HRQOL measures; the magnitude of thecoronal deformity did not impact pain and disability, asmeasured by HRQOL instrument, in a linear fashion.Interestingly, no correlation was found between clinicaloutcomes and the coronal global balance (offset betweenC7 plumbline and S1).
Regional Sagittal CurvesSignificant correlations between L1–S1 lumbar lordosisand HRQOL measures were identified. L1–S1 lumbar
lordosis was correlated with walking and standing com-ponents of the ODI (respectively, r � �0.344 and r ��0.365; P � 0.001) as well as with the bodily pain andthe PCSs of the SF-12 instrument (respectively, r � 0.314and r � 0.392; P � 0.001). In other words, a loss oflumbar lordosis was correlated with an increase of painand a decrease of function. No correlations were foundbetween thoracic kyphosis, thoracolumbar alignment,and any of the HRQOL scores.
Global Sagittal AlignmentSignificant correlation between sagittal plane parametersand HRQOL measures were identified. The SVA had acorrelation with SRS total score of 0.41 (Spearman cor-relation coefficient, P � 0.001). The correlation coeffi-cient for SRS activity was 0.44 (P � 0.001). The corre-lation between SVA and SF-12 PCS was 0.5 (P � 0.001).In terms of ODI, the strongest correlation with SVA wasnoted for “standing disability” (r � 0.52, P � 0.001).
Interestingly, more significant in its correlation withself-reported HRQOL than SVA was the sagittal T1–SPI.This parameter (mean value � �1°, Standard deviation[SD] � 7°) was found to have the highest correlationwith HRQOL of all radiographic parameters analyzed.
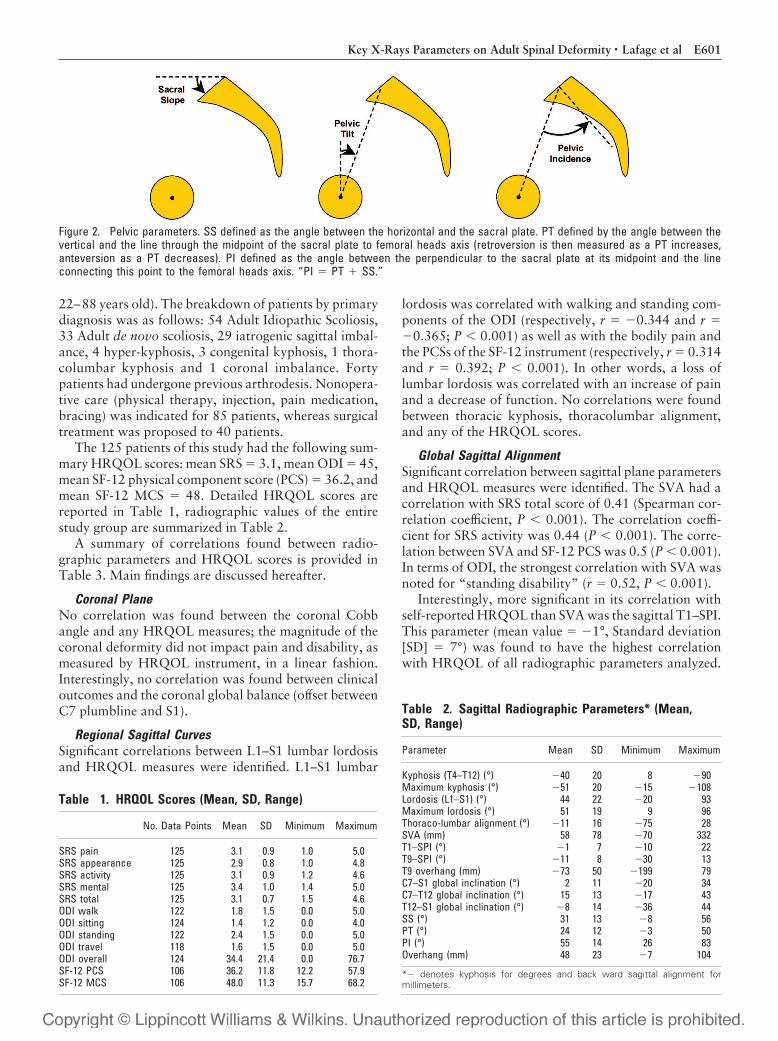
Figure 2. Pelvic parameters. SS defined as the angle between the horizontal and the sacral plate. PT defined by the angle between thevertical and the line through the midpoint of the sacral plate to femoral heads axis (retroversion is then measured as a PT increases,anteversion as a PT decreases). PI defined as the angle between the perpendicular to the sacral plate at its midpoint and the lineconnecting this point to the femoral heads axis. “PI � PT � SS.”
Table 1. HRQOL Scores (Mean, SD, Range)
No. Data Points Mean SD Minimum Maximum
SRS pain 125 3.1 0.9 1.0 5.0SRS appearance 125 2.9 0.8 1.0 4.8SRS activity 125 3.1 0.9 1.2 4.6SRS mental 125 3.4 1.0 1.4 5.0SRS total 125 3.1 0.7 1.5 4.6ODI walk 122 1.8 1.5 0.0 5.0ODI sitting 124 1.4 1.2 0.0 4.0ODI standing 122 2.4 1.5 0.0 5.0ODI travel 118 1.6 1.5 0.0 5.0ODI overall 124 34.4 21.4 0.0 76.7SF-12 PCS 106 36.2 11.8 12.2 57.9SF-12 MCS 106 48.0 11.3 15.7 68.2
Table 2. Sagittal Radiographic Parameters* (Mean,SD, Range)
Parameter Mean SD Minimum Maximum
Kyphosis (T4–T12) (°) �40 20 8 �90Maximum kyphosis (°) �51 20 �15 �108Lordosis (L1–S1) (°) 44 22 �20 93Maximum lordosis (°) 51 19 9 96Thoraco-lumbar alignment (°) �11 16 �75 28SVA (mm) 58 78 �70 332T1–SPI (°) �1 7 �10 22T9–SPI (°) �11 8 �30 13T9 overhang (mm) �73 50 �199 79C7–S1 global inclination (°) 2 11 �20 34C7–T12 global inclination (°) 15 13 �17 43T12–S1 global inclination (°) �8 14 �36 44SS (°) 31 13 �8 56PT (°) 24 12 �3 50PI (°) 55 14 26 83Overhang (mm) 48 23 �7 104
*� denotes kyphosis for degrees and back ward sagittal alignment formillimeters.
E601Key X-Rays Parameters on Adult Spinal Deformity • Lafage et al
The correlation between T1–SPI and SRS total score wasr � 0.43 (P � 0.001), whereas the correlation with SRSactivity subscore was r � 0.47 (P � 0.001) and correla-tion with SF-12 PCS was r � 0.48 (P � 0.001). In termsof ODI, the strongest correlation was noted with stand-ing disability, as for SVA, but this correlation was stron-ger at r � 0.6 (P � 0.001). Of note a review of ourdatabase21 on 75 asymptomatic adult volunteers (meanage � 48 years old, equally distributed between 20 and79 years old) revealed a mean value of T1–SPI of �6°(SD � 3.8°) without any significant age-related changes.
Pelvic ParametersThe third most significant radiographic parameter corre-lated to HRQOL measures was PT. This parameter ofpelvic position had a mean value of 24° in this studypopulation, which is greater than that reported in a vol-unteer population19 (PT � 13°, SD � 9°). PT had acorrelation with SRS total score of r � 0.28 (P � 0.001).The correlation between PT and SRS activity subscorewas r � 0.35 (P � 0.001) and correlation with SF-12PCS was r � 0.43 (P � 0.001). In terms of ODI, thestrongest correlation was noted with “walking disabil-ity” (r � 0.38, P � 0.001).
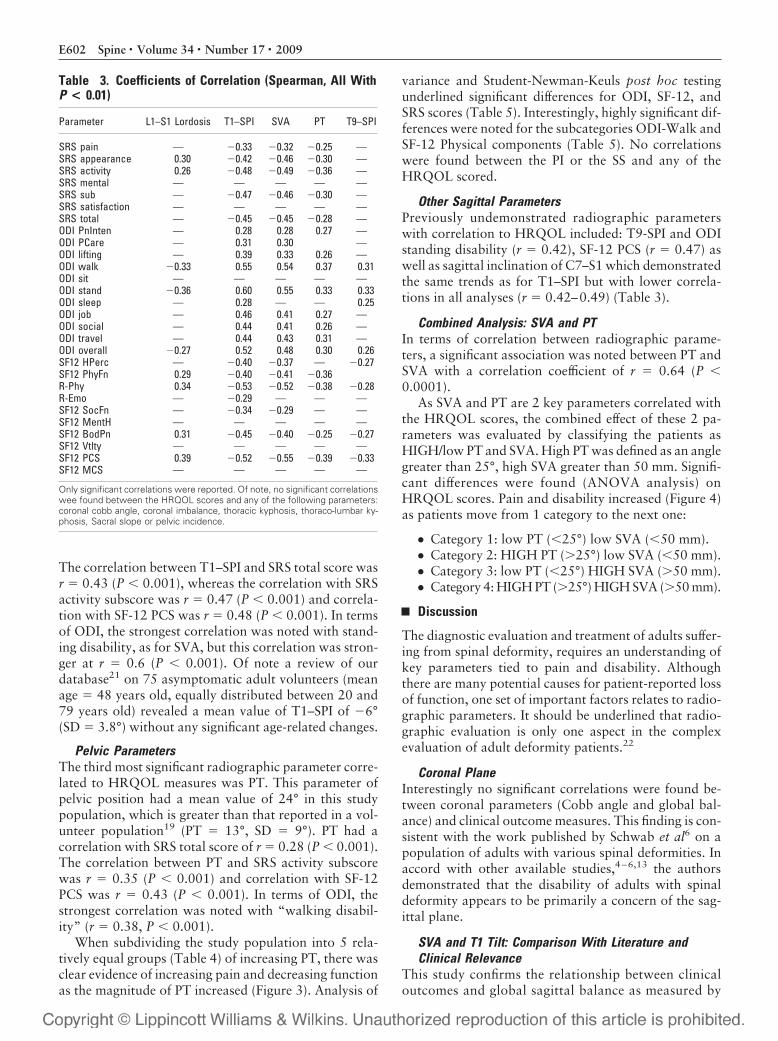
When subdividing the study population into 5 rela-tively equal groups (Table 4) of increasing PT, there wasclear evidence of increasing pain and decreasing functionas the magnitude of PT increased (Figure 3). Analysis of
variance and Student-Newman-Keuls post hoc testingunderlined significant differences for ODI, SF-12, andSRS scores (Table 5). Interestingly, highly significant dif-ferences were noted for the subcategories ODI-Walk andSF-12 Physical components (Table 5). No correlationswere found between the PI or the SS and any of theHRQOL scored.
Other Sagittal ParametersPreviously undemonstrated radiographic parameterswith correlation to HRQOL included: T9-SPI and ODIstanding disability (r � 0.42), SF-12 PCS (r � 0.47) aswell as sagittal inclination of C7–S1 which demonstratedthe same trends as for T1–SPI but with lower correla-tions in all analyses (r � 0.42–0.49) (Table 3).
Combined Analysis: SVA and PTIn terms of correlation between radiographic parame-ters, a significant association was noted between PT andSVA with a correlation coefficient of r � 0.64 (P �0.0001).
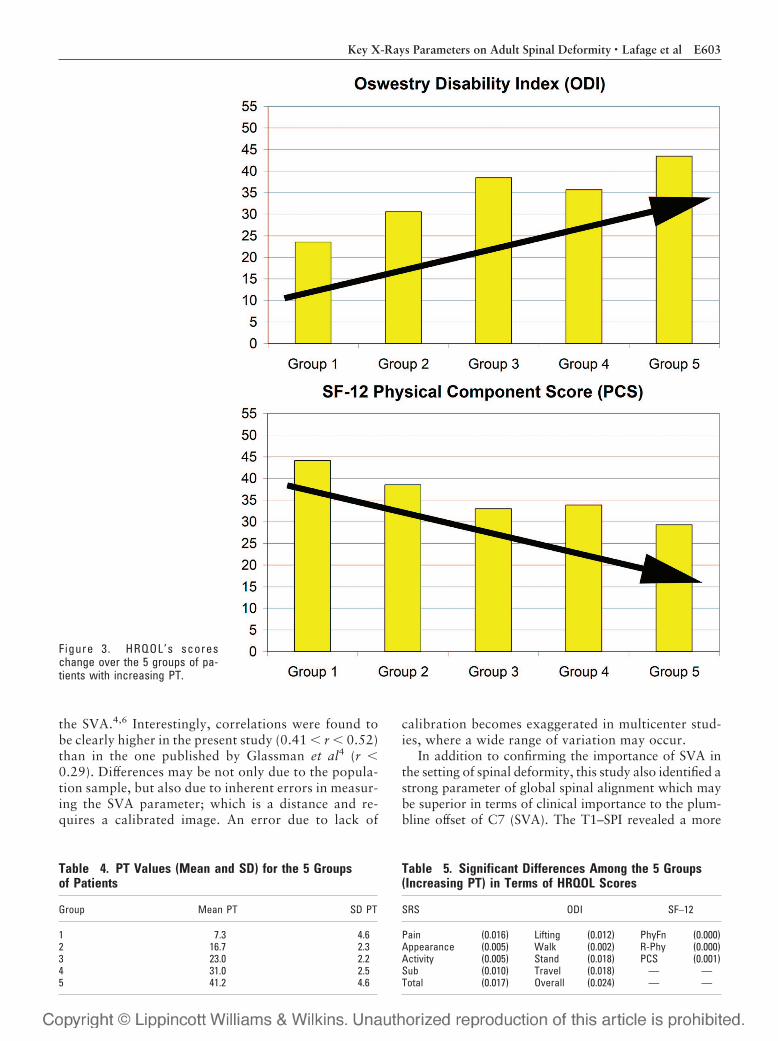
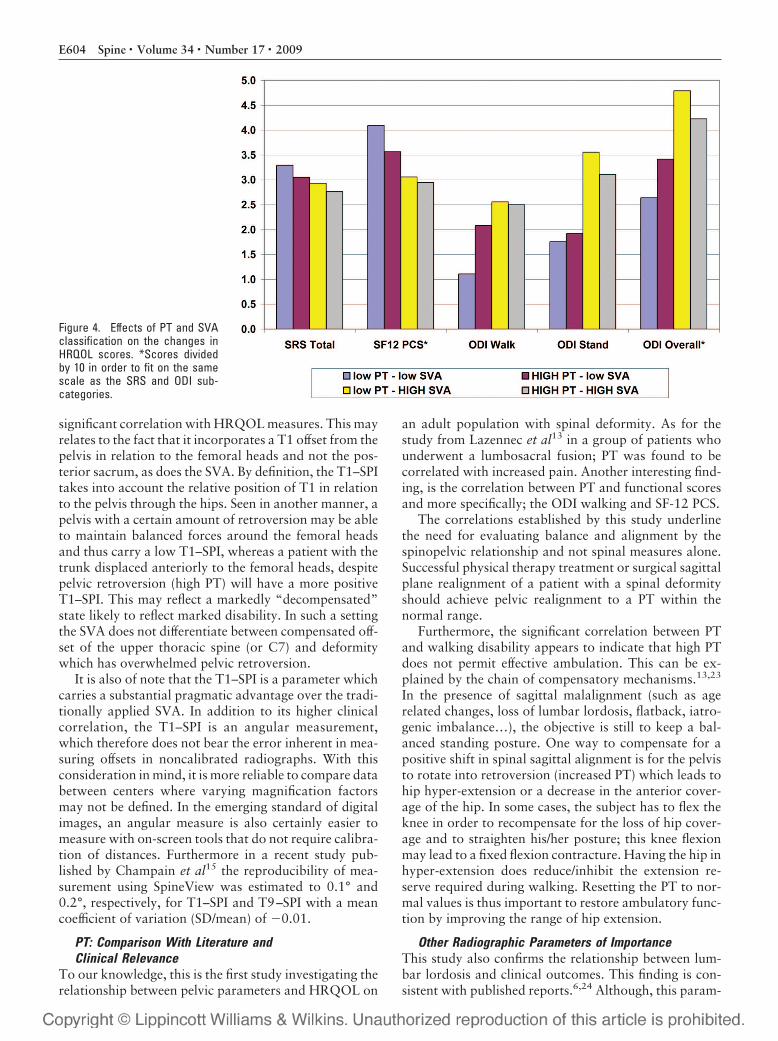
As SVA and PT are 2 key parameters correlated withthe HRQOL scores, the combined effect of these 2 pa-rameters was evaluated by classifying the patients asHIGH/low PT and SVA. High PT was defined as an anglegreater than 25°, high SVA greater than 50 mm. Signifi-cant differences were found (ANOVA analysis) onHRQOL scores. Pain and disability increased (Figure 4)as patients move from 1 category to the next one:
● Category 1: low PT (�25°) low SVA (�50 mm).● Category 2: HIGH PT (�25°) low SVA (�50 mm).● Category 3: low PT (�25°) HIGH SVA (�50 mm).● Category 4: HIGH PT (�25°) HIGH SVA (�50 mm).
Discussion
The diagnostic evaluation and treatment of adults suffer-ing from spinal deformity, requires an understanding ofkey parameters tied to pain and disability. Althoughthere are many potential causes for patient-reported lossof function, one set of important factors relates to radio-graphic parameters. It should be underlined that radio-graphic evaluation is only one aspect in the complexevaluation of adult deformity patients.22
Coronal PlaneInterestingly no significant correlations were found be-tween coronal parameters (Cobb angle and global bal-ance) and clinical outcome measures. This finding is con-sistent with the work published by Schwab et al6 on apopulation of adults with various spinal deformities. Inaccord with other available studies,4–6,13 the authorsdemonstrated that the disability of adults with spinaldeformity appears to be primarily a concern of the sag-ittal plane.
SVA and T1 Tilt: Comparison With Literature andClinical Relevance
This study confirms the relationship between clinicaloutcomes and global sagittal balance as measured by
Table 3. Coefficients of Correlation (Spearman, All WithP < 0.01)
Parameter L1–S1 Lordosis T1–SPI SVA PT T9–SPI
SRS pain — �0.33 �0.32 �0.25 —SRS appearance 0.30 �0.42 �0.46 �0.30 —SRS activity 0.26 �0.48 �0.49 �0.36 —SRS mental — — — — —SRS sub — �0.47 �0.46 �0.30 —SRS satisfaction — — — — —SRS total — �0.45 �0.45 �0.28 —ODI PnInten — 0.28 0.28 0.27 —ODI PCare — 0.31 0.30 —ODI lifting — 0.39 0.33 0.26 —ODI walk �0.33 0.55 0.54 0.37 0.31ODI sit — — — — —ODI stand �0.36 0.60 0.55 0.33 0.33ODI sleep — 0.28 — — 0.25ODI job — 0.46 0.41 0.27 —ODI social — 0.44 0.41 0.26 —ODI travel — 0.44 0.43 0.31 —ODI overall �0.27 0.52 0.48 0.30 0.26SF12 HPerc — �0.40 �0.37 — �0.27SF12 PhyFn 0.29 �0.40 �0.41 �0.36R-Phy 0.34 �0.53 �0.52 �0.38 �0.28R-Emo — �0.29 — — —SF12 SocFn — �0.34 �0.29 — —SF12 MentH — — — — —SF12 BodPn 0.31 �0.45 �0.40 �0.25 �0.27SF12 Vtlty — — — — —SF12 PCS 0.39 �0.52 �0.55 �0.39 �0.33SF12 MCS — — — — —
Only significant correlations were reported. Of note, no significant correlationswee found between the HRQOL scores and any of the following parameters:coronal cobb angle, coronal imbalance, thoracic kyphosis, thoraco-lumbar ky-phosis, Sacral slope or pelvic incidence.
E602 Spine • Volume 34 • Number 17 • 2009
the SVA.4,6 Interestingly, correlations were found tobe clearly higher in the present study (0.41 � r � 0.52)than in the one published by Glassman et al4 (r �0.29). Differences may be not only due to the popula-tion sample, but also due to inherent errors in measur-ing the SVA parameter; which is a distance and re-quires a calibrated image. An error due to lack of
calibration becomes exaggerated in multicenter stud-ies, where a wide range of variation may occur.
In addition to confirming the importance of SVA inthe setting of spinal deformity, this study also identified astrong parameter of global spinal alignment which maybe superior in terms of clinical importance to the plum-bline offset of C7 (SVA). The T1–SPI revealed a more
Figure 3. HRQOL’s scoreschange over the 5 groups of pa-tients with increasing PT.
Table 4. PT Values (Mean and SD) for the 5 Groupsof Patients
Group Mean PT SD PT
1 7.3 4.62 16.7 2.33 23.0 2.24 31.0 2.55 41.2 4.6
Table 5. Significant Differences Among the 5 Groups(Increasing PT) in Terms of HRQOL Scores
SRS ODI SF–12
Pain (0.016) Lifting (0.012) PhyFn (0.000)Appearance (0.005) Walk (0.002) R-Phy (0.000)Activity (0.005) Stand (0.018) PCS (0.001)Sub (0.010) Travel (0.018) — —Total (0.017) Overall (0.024) — —
E603Key X-Rays Parameters on Adult Spinal Deformity • Lafage et al
significant correlation with HRQOL measures. This mayrelates to the fact that it incorporates a T1 offset from thepelvis in relation to the femoral heads and not the pos-terior sacrum, as does the SVA. By definition, the T1–SPItakes into account the relative position of T1 in relationto the pelvis through the hips. Seen in another manner, apelvis with a certain amount of retroversion may be ableto maintain balanced forces around the femoral headsand thus carry a low T1–SPI, whereas a patient with thetrunk displaced anteriorly to the femoral heads, despitepelvic retroversion (high PT) will have a more positiveT1–SPI. This may reflect a markedly “decompensated”state likely to reflect marked disability. In such a settingthe SVA does not differentiate between compensated off-set of the upper thoracic spine (or C7) and deformitywhich has overwhelmed pelvic retroversion.
It is also of note that the T1–SPI is a parameter whichcarries a substantial pragmatic advantage over the tradi-tionally applied SVA. In addition to its higher clinicalcorrelation, the T1–SPI is an angular measurement,which therefore does not bear the error inherent in mea-suring offsets in noncalibrated radiographs. With thisconsideration in mind, it is more reliable to compare databetween centers where varying magnification factorsmay not be defined. In the emerging standard of digitalimages, an angular measure is also certainly easier tomeasure with on-screen tools that do not require calibra-tion of distances. Furthermore in a recent study pub-lished by Champain et al15 the reproducibility of mea-surement using SpineView was estimated to 0.1° and0.2°, respectively, for T1–SPI and T9–SPI with a meancoefficient of variation (SD/mean) of �0.01.
PT: Comparison With Literature andClinical Relevance
To our knowledge, this is the first study investigating therelationship between pelvic parameters and HRQOL on
an adult population with spinal deformity. As for thestudy from Lazennec et al13 in a group of patients whounderwent a lumbosacral fusion; PT was found to becorrelated with increased pain. Another interesting find-ing, is the correlation between PT and functional scoresand more specifically; the ODI walking and SF-12 PCS.
The correlations established by this study underlinethe need for evaluating balance and alignment by thespinopelvic relationship and not spinal measures alone.Successful physical therapy treatment or surgical sagittalplane realignment of a patient with a spinal deformityshould achieve pelvic realignment to a PT within thenormal range.
Furthermore, the significant correlation between PTand walking disability appears to indicate that high PTdoes not permit effective ambulation. This can be ex-plained by the chain of compensatory mechanisms.13,23
In the presence of sagittal malalignment (such as agerelated changes, loss of lumbar lordosis, flatback, iatro-genic imbalance…), the objective is still to keep a bal-anced standing posture. One way to compensate for apositive shift in spinal sagittal alignment is for the pelvisto rotate into retroversion (increased PT) which leads tohip hyper-extension or a decrease in the anterior cover-age of the hip. In some cases, the subject has to flex theknee in order to recompensate for the loss of hip cover-age and to straighten his/her posture; this knee flexionmay lead to a fixed flexion contracture. Having the hip inhyper-extension does reduce/inhibit the extension re-serve required during walking. Resetting the PT to nor-mal values is thus important to restore ambulatory func-tion by improving the range of hip extension.
Other Radiographic Parameters of ImportanceThis study also confirms the relationship between lum-bar lordosis and clinical outcomes. This finding is con-sistent with published reports.6,24 Although, this param-
Figure 4. Effects of PT and SVAclassification on the changes inHRQOL scores. *Scores dividedby 10 in order to fit on the samescale as the SRS and ODI sub-categories.
E604 Spine • Volume 34 • Number 17 • 2009

eter appeared to present with the lowest coefficient ofcorrelation with HRQOL measures within this investi-gation, it is nevertheless a key parameter to take intoaccount when analyzing radiographic alignment.
Global AnalysisAnalysis by classifying patients according to their globalsagittal balance (SVA) and pelvic version (PT) demon-strated that pain and disability increased when patientsmoved from a lower category to a higher one. Category 1corresponds to patients with SVA and PT within normallimits; these patients were included in the study for localspinal deformities (low lumbar lordosis, high thoracickyphosis…). Category 2 corresponds to patients whomay have developed pelvic retroversion (high PT) tocompensate for an underling spinal malalignment in or-der to maintain their head over the pelvis (low SVA);therefore evaluating their sagittal alignment by SVAalone would not have identified their sagittal malalign-ment. Interestingly, patients in Category 3 present a sig-nificant anterior malalignment (high SVA) but do notdevelop pelvic retroversion (low PT) to compensate forthis spinal malalignment; this lack of pelvic compensa-tion is a challenging issue in the context of orthopediccare since one must understand the underlying mecha-nisms (soft tissue issues, hip anteversion…) before con-sidering any treatment. Finally, patients in Category 4present with the highest level of self reported pain anddisability; despite pelvic retroversion (high PT) these pa-tients are not able to maintain their head over the pelvis(high SVA).
This article established the relationship between pel-vic retroversion and/or loss of spinal alignment and clin-ical outcomes. The ability of a patient to compensate fora spinal malalignment via an increase of pelvic retrover-sion is of primary importance in the clinical evaluation.Nevertheless one should keep in mind that pelvic retro-version may also be the primary cause of sagittal mal-alignment if a patient presents with some specific softtissue or lower extremity disorder (shortening of thehamstring, hip flexion contracture, hip deformity).
Conclusion
A primary goal in nonoperative or surgical treatment ofadult spinal deformity is achieving proper alignment forergonomic standing. To achieve this, the surgeon mustensure global spinal balance as well as normalized pelvicposition. The data from this investigation underlines theclinical significance of PT and also offers a pragmaticparameter for assessment of global spinal alignment, theT1–SPI.
The significant findings regarding the T1–SPI param-eter indicates the usefulness of this relatively unknownparameter in the analysis of patients suffering from spi-nal deformity. Coupled with PT, 2 key parameters; onespinopelvic and the other pelvic, are captured and offeressential information on the sagittal alignment of stand-ing patients with spinal deformity.
Further work will assist in clarifying the relationshipand interaction between pelvic and spinal parameters inthe setting of surgical realignment. This work will helpdevelop patient-specific formulas to assist planning ofspinal realignment and offer pragmatic tools for thetreatment of complex adult deformity.
Key Points
● Self reported disability increases with anteriorsagittal balance.● T1–SPI (angular measurement) revealed a moresignificant correlation with clinical outcomes mea-sures than the sagittal plumbline.● Severity of disability increases with pelvic retro-version.● Analysis of sagittal plane must integrate not onlyspinal parameters but also those related to thepelvis.
References
1. Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, andnutritional parameters in an elderly volunteer population. Spine 2005;30:1082–5.
2. Schwab FJ, Smith VA, Biserni M, et al. Adult scoliosis: a quantitative radio-graphic and clinical analysis. Spine 2002;27:387–92.
3. Schwab F, Dubey A, Pagala M, et al. Adult scoliosis: a health assessmentanalysis by SF-36. Spine 2003;28:602–6.
4. Glassman SD, Bridwell K, Dimar JR, et al. The impact of positive sagittalbalance in adult spinal deformity. Spine 2005;30:2024–9.
5. Glassman SD, Berven S, Bridwell K, et al. Correlation of radiographic pa-rameters and clinical symptoms in adult scoliosis. Spine 2005;30:682–8.
6. Schwab F, Farcy JP, Bridwell K, et al. A clinical impact classification ofscoliosis in the adult. Spine 2006;31:2109–14.
7. Vidal J, Marnay T. Sagittal deviations of the spine, and trial of classificationas a function of the pelvic balance [in French]. Rev Chir Orthop ReparatriceAppar Mot 1984;70(suppl 2):124–6.
8. Vidal J, Marnay T. Morphology and anteroposterior body equilibrium inspondylolisthesis L5–S1 [in French]. Rev Chir Orthop Reparatrice ApparMot 1983;69:17–28.
9. Dubousset J. Three-dimensional analysis of the scoliotic deformity. In: Wein-stein SL, ed. Pediatric Spine: Principles and Practice. New York, NY: RavenPress; 1994.
10. Legaye J, Duval-Beaupere G, Hecquet J, et al. Pelvic incidence: a fundamen-tal pelvic parameter for three-dimensional regulation of spinal sagittalcurves. Eur Spine J 1998;7:99–103.
11. Roussouly P, Berthonnaud E, Dimnet J. Geometrical and mechanical analy-sis of lumbar lordosis in an asymptomatic population: proposed classifica-tion [in French]. Rev Chir Orthop Reparatrice Appar Mot 2003;89:632–9.
12. Roussouly P, Gollogly S, Berthonnaud E, et al. Classification of the normalvariation in the sagittal alignment of the human lumbar spine and pelvis inthe standing position. Spine 2005;30:346–53.
13. Lazennec JY, Ramare S, Arafati N, et al. Sagittal alignment in lumbosacralfusion: relations between radiological parameters and pain. Eur Spine J2000;9:47–55.
14. Horton WC, Brown CW, Bridwell KH, et al. Is there an optimal patientstance for obtaining a lateral 36� radiograph? A critical comparison of threetechniques. Spine 2005;30:427–33.
15. Champain S, Benchikh K, Nogier A, et al. Validation of new clinical quan-titative analysis software applicable in spine orthopaedic studies. Eur Spine J2006;15:982–91.
16. Rajnics P, Pomero V, Templier A, et al. Computer-assisted assessment ofspinal sagittal plane radiographs. J Spinal Disord 2001;14:135–42.
17. Vialle R, Ilharreborde B, Dauzac C, et al. Intra and inter-observer reliabilityof determining degree of pelvic incidence in high-grade spondylolisthesisusing a computer assisted method. Eur Spine J 2006;15:1449–53.
18. Legaye J, Hecquet J, Marty C, et al. Equilibre sagittal du rachis. Relationsentre bassin et courbures rachidiennes sagittales en position debout. Rachis1993;5:215–26.
E605Key X-Rays Parameters on Adult Spinal Deformity • Lafage et al

19. Vialle R, Levassor N, Rillardon L, et al. Radiographic analysis of the sagittalalignment and balance of the spine in asymptomatic subjects. J Bone JointSurg Am 2005;87:260–7.
20. Legaye J, Duval-Beaupere G. Sagittal plane alignment of the spine and grav-ity: a radiological and clinical evaluation. Acta Orthop Belg 2005;71:213–20.
21. Schwab F, Lafage V, Boyce R, et al. Gravity line analysis in adult volunteers:age-related correlation with spinal parameters, pelvic parameters, and footposition. Spine 2006;31:E959–67.
22. Schwab F, Lafage V, Farcy J, et al. Predicting Outcome and Complications inSurgical Treatment of Adult Scoliosis: An Analysis of 109 Patients at 2-YearFollow Up. Edinburgh, Scotland: SRS; 2007.
23. Yoshimoto H, Sato S, Masuda T, et al. Spinopelvic alignment in patientswith osteoarthrosis of the hip: a radiographic comparison to patients withlow back pain. Spine 2005;30:1650–7.
24. Jang JS, Lee SH, Kim JM, et al. Can patients with sagittally well-compensated lumbar degenerative kyphosis benefit from surgical treatmentfor intractable back pain? Neurosurgery 2009;64:115–21; discussion 121.
E606 Spine • Volume 34 • Number 17 • 2009