participatory research in public health: creating innovative alliances for health
TRANSCRIPT

ARTICLE IN PRESS
1353-8292/$ - se
doi:10.1016/j.he
�CorrespondE-mail addr
(P. Mantoura).
Health & Place 13 (2007) 440–451
www.elsevier.com/locate/healthplace
Participatory research in public health:Creating innovative alliances for health
Pascale Mantouraa,d,�, Sylvie Gendronb,d, Louise Potvinc,d
aDepartment of Social and Preventive Medicine, Universite de Montreal, C.P. 6128, Succ. Centre-ville, Montreal, Que., Canada H3C 3J7bFaculty of Nursing, Universite de Montreal, Montreal, Que., Canada
cDepartment of Social and Preventive Medicine, Universite de Montreal, Montreal, Que., CanadadCentre de recherche Lea-Roback sur les inegalites sociales de sante de Montreal, Que., Canada
Received 27 September 2005; received in revised form 28 April 2006; accepted 1 May 2006COPY
Abstract
This article discusses alliances within local socio-sanitary space, one in which community sector and health sector actors,
public health researchers and funding bodies meet. The discussion is based on the study of a research space made up of
representatives of actors found at the local level. Both the minutes of the discussions of 12 meetings of the research team,
and the collaborative outputs produced throughout the research initiative provide the empirical data for a qualitative
analysis. The findings reveal a research space concomitantly constituted by aspects of ‘‘non-cooperative games’’ and of
networks based on innovation-fostering knowledge exchanges, which can be viewed, from the perspective of a reflexive
epistemology, as a tool for implementing innovative alliances in local, health-promoting socio-sanitary space.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Local public health; Participatory research; Innovation; Knowledge and learning networks; Game theory PERSONAL
S
R' IntroductionAlliances and coalitions that are inclusive of adiversity of actors are nowadays essential features ofpublic health research and intervention (Bakeret al., 2005; Bilodeau, 2000; Butterfoss and Kegler,2002; Potvin et al., 2003; Green et al., 2001; Israelet al., 1998; Lasker and Weiss, 2003; White et al.,2002). Clearly, no single organization acting on itsown can bring together the knowledge, resources ortrust networks which are required to address the
AUTHO
e front matter r 2006 Elsevier Ltd. All rights reserved
althplace.2006.05.002
ing author. Tel.: +1 514 343 6111 (4556).
ess: [email protected]
wide array of determinants that generate increas-ingly complex problems and issues in public health(Marmot and Wilkinson, 1999; Wilkinson andMarmot, 1998). In response, more public healthorganizations are now engaged in the building oflocal alliances through research as well as pro-gramme development initiatives (Suarez-Balcazar,Harper et al., 2005; Shoultza, Onehab et al., 2006)that are steered by the leitmotiv of innovation
(Fassin, 1998; Health Canada, 2001).Thus, to meet its health objectives, public health
programming increasingly permeates civil society.This movement inevitably (re)designs a socio-sanitary space that, in turn, transforms the practicesand identities of the various actors, as well as their
.
ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451 441
R
projects and interactions. This being said, publichealth theory remains poorly equipped to reflectupon, facilitate and evaluate the changes induced bythis growing tendency to intersect social andsanitary worlds in public health practice (Potvinet al., 2005; McQueen, 2001; Potvin and Chabot,2002).
The aim of this paper is to contribute ideas andempirical observations to the theory and practice ofinnovative alliances for public health. This studyreports on an ongoing participatory researchinitiative that brought together actors from com-munity-based organisations, funding bodies, publichealth and academia. The research endeavourcreated an alliance between local actors from healthand social intervention spheres as well as civilsociety that reproduces present-day emergent formsof socio-sanitary spaces in public health. Weexamined the processes and issues that occurredwithin this space and highlight the salient features ofthese forms of alliance in light of contemporarysocial theory of networks and game theory.
Alliances as networks for innovation
The local production of public health (Fassin,1998), through multi-sector, multi-level and multi-disciplinary networks of actors constitutes animportant locus of innovation. Considered in theseterms, public health does not exist in itself. It isdefined in the processes through which it occurs.Moreover, the dynamics of this local productionreveal what is at stake in the social world and whateventually becomes part of the public health lexicon(Fassin, 1998, p. 13).1 Close observation of localscenes ought to, therefore, uncover evolving alli-ances between various actors, such as professionals,associations and elected officials, who literally invent
public health. In the end, it is those inventions thateffectively translate concerns and issues into publichealth agendas that, in turn, become politicalobjects in the public space (Fassin, 1998) and arelikely to lead to innovations in public health.
Innovations refer to practices and programmesthat replace traditional interventions considered tobe outmoded (Bilodeau et al., 2003). By definition,an innovation is ‘‘an emerging phenomenon builtthrough interactions that are progressively estab-lished between previously unconnected actors,knowledge and goods that become bound together
AUTHOR'S PE
1Our translation.
in a cluster of interdependencies’’ (Callon et al.,1999, p. 14).2 Innovation occurs, therefore, throughaction (Callon et al., 1999). It is fostered byinteraction (Bilodeau et al., 2003; White et al.,2002) and enables the sharing of knowledge andlearning.
The notion of network as developed by Callon etal. (1999) defines innovation dynamics as action,interaction, shared knowledge and learning amongactors of different origins. It can thus serve tocharacterize emergent alliances and inventions inpublic health. These authors conceptualise networksas a complex of translation operations throughwhich actors produce innovative knowledge andpractice. Translation ‘‘makes it possible to establisha certain equivalence that is constantly renegotiated,between distant interests, which are uncertain andunstable. Translation often entails the constructionof new identities and new interests’’ (Callon et al.,1999, p. 41; Callon and Rabeharisoa, 2003).3
Translation therefore facilitates exchange of diverseforms of knowledge and knowing, as well as enablesthe development of shared understanding andinsight between initially foreign universes, which,in turn, gradually reconfigure themselves throughtheir interactions. In a similar vein, Fassin (1998)notes that it is less the existence of new actors thatlocally produces public health, than the develop-ment of different relationships and networks amongactors. Hence, public health innovations can beconstrued as originating in the interactions betweendiverse actors that are, recursively, reconfigured interms of their identities, interests and practices.Such reconsiderations of boundaries, definitions,roles and responsibilities have also been referred toas the creation of new communities of practicearound public health (MacKian et al., 2003; Popayet al., 2004).
In the context of a research initiative or a givenprogramme of action, actors working in isolationhave limited influence in the face of indifferentcolleagues and decision makers (Callon et al., 1999).To stimulate change, they eventually developalliances around provisional projects through whichsome objectives can intersect and converge. Theseprojects are, in fact, the building blocks of emergingnetworks and potential for innovation. As alliancesare established, networks develop, evolve andextend by means of gradual learning, iterations,
SONAL COPY
2Our translation.3Our translation.
ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451442
R
negotiation and adaptation through the knowledgeand know-how that becomes available. In thiscollective process, during which knowledge andcompetencies are generated and ascertained; iden-tities, interests, projects and expectations changeand emerge through the interactions, the evolvingnegotiations and the search of acceptable compro-mise (Callon et al., 1999). In this perspective,programmes of action are inevitably unstable andfrequently revised as knowledge is produced andcombined with the outcomes of past and recon-structed alliances. Innovation therefore emergesfrom a process of knowledge development throughtrial and error, reflexive probing and bricolage
(tinkering)4 throughout alliances that reveal thepath to follow while it is being mapped (Callonet al., 1999).
Knowledge production through learning alliances
Knowledge production thus lies at the heart oflearning alliances that characterise innovation-fostering networks. Knowledge is a higher orderconcept than information. In addition to havinginformation, people with knowledge are able tointegrate and situate new facts, data and informa-tion within the larger context of their experience,expertise and judgment. As such, they are able touse their knowledge in a sophisticated way and totransform it into new knowledge (Meijboom et al.,2004). We have seen that this transformation canoccur through alliances. However, the nature ofthose alliances can influence the knowledge produc-tion process and outcome.
Alliances based on trust, in which ‘‘we’’ is moreimportant than ‘‘I.’’
In their research on the development of healthnetworks in the Netherlands, Meijboom et al. 2004highlight the notion of trust as a key conceptunderlying the organization of knowledge produc-tion and learning. Likewise, Lasker and Weiss(2003) refer to the synergy that must be establishedbetween partners to go beyond their individual andspecific contributions in order to foster knowledgeand learning. As a consequence, knowledge produc-tion and management is a complex activity. It
AUTHOR'S PE
4Although the English substantive tinkering conveys the fact
that a bricolage is an assemblage of disparate elements, it does
not render the meaning that a bricolage is necessarily a work of
creation.
cannot be reduced to rules and mechanisms thatgovern marketplace economy, aim for efficiency orfoster hierarchical interactions (Callon et al., 1999;Adler, 2001; Lewin, 2001). The variety and hetero-geneity intrinsic to emergent networks nurtureinteraction, multiply negotiation processes andrequire arbitration and compromise (Callon et al.,1999, p. 2). Trust and synergy are therefore essentialto counteract and transform power differentials andcontrol dynamics in order to establish innovation-fostering networks that rely on shared norms andvalues (Adler, 2001; Meijboom et al., 2004).However, although alliances based on trust appearpromising, actors and organizations must be moti-vated to take the risk of working together.
Alliances based on opportunism, in which ‘‘I’’ ismore important than ‘‘we.’’
Notwithstanding the value of trust as a means ofregulating knowledge collectives, most alliances inthe health field are guided by more pragmaticintentions. Opportunism and protection of one’sown interests, to the detriment or not of collectiveinterests, is common. Given repeated observation ofthis reality, recent literature suggests that it is moreuseful to conceptualize intersectoral action in termsof the specific interests pursued by individual andorganizational actors and thus to go beyond theideological discourse of health promotion (O’Neillet al., 1997). Such a perspective enables us tounderstand how, at certain moments, strategicalliances use conflict and bargaining instead ofcooperation and problem resolution (Costongs andSpringett, 1997; Bilodeau et al., 2002). As well,organizations that withdraw from alliances are,more often than not, those that do not agree to giveup part of the control they have over their ownresources, not to mention those of others (Greenet al., 2001).
Game theory, applied to community-based healthcoalitions, can help explain such a phenomenon(Ford et al., 2004). This theory was developed tostudy the simultaneous decision-making processesof two or more people. Given that individuals mustmake decisions at the same time in certaincircumstances, and that the overall outcome of acollaborative process depends on the complex ofdecisions made by all actors, the situation may beconstrued as a game. When applied to networksconstituted on a voluntary basis, this theory putsinto perspective the fundamentally unstable natureof strategic alliances, since the future behaviour and
SONAL COPY

ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451 443
R
particular projects of constituent members are, forthe most part, uncertain. Thus, although desirable,mutual cooperation is not automatic, nor predict-able. The actors making up a network can pursuestrategies that appear rational from an individualperspective, but that are suboptimal when consid-ered through a collective lens.
Game theory can thus contribute to our under-standing of network development by the distinctionit draws between the intention to cooperate andstrategic reality. A ‘‘non-cooperation’’ perspectivecould, in fact, be more useful than an assumption ofcooperation to consider the nature of alliances andtheir configuration around health-related issues(Ford et al., 2004).5 Although a ‘‘non-cooperativegame’’ might seem a pejorative expression, in gametheory it describes any situation that does not meetone of the following three conditions: (1) themotivations of all actors involved are knownamongst themselves; (2) legal agreements governthe relationships among the members; and (3) all thebenefits gained from the cooperative venture aredistributed equitably between the members. Suchconditions could be useful to reflect upon socio-sanitary alliances as they frequently include somefeatures of ‘‘non-cooperation’’, such as: incompleteinformation with respect to the intentions of other/partner members, absence of formal contracts,vertical power relations, and variable or unevenbenefit returns to the communities. In the face of‘‘non-cooperative games,’’ it could therefore beappropriate to observe communication and ex-change processes to analyze relationships and fosternetwork stability. In the absence of transparency,actors will tend to pursue their own interests sincethey have little or no clear appreciation regardingothers’ motives. This inevitably threatens theviability of the alliance and collective action (Fordet al., 2004).
To summarize, we have seen that the localproduction of public health generates innovation.In turn, innovation promotes knowledge exchangeand learning that are constitutive of originalalliances and networks. Callon et al.’s (1999) notionof translation is useful to situate knowledge devel-opment in a process of network building that brings
AUTHOR'S PE
5It should be noted that this terminology is specific to game
theory, in that we adopt a view of alliances characterized by
relationships of power. Therefore, this expression does not mean
‘‘non-cooperation,’’ but rather refers to a cooperative setting that
embodies unequal forces.
together distant interests and gradually reconfiguresthem. This being said, networks that emergethrough knowledge production and learning requireparticular styles of coordination that are based ontrust and transparency to attenuate restrictivecontrol dynamics and to foster innovative projects.Mutual cooperation is not automatic, however, andalliances are also configured by the particularinterests pursued by each actor. Effectual analysisof network development should therefore differ-entiate between the intention to cooperate and thestrategic reality that permeates its configuration. Inthis vein, game theory distinctively underscores howa non-cooperative perspective (or ‘‘conflictual co-operation’’) can be more informative than anassumption of cooperation when considering so-cio-sanitary alliances. Specifically, the absence oftransparency, communication and trust can inhibitthe sustainability of collaboration.
Our theoretical markers exposed, we now turn toan analysis of our participatory research initiative todraw out the prevailing issues that occurred as wecreated an innovative socio-sanitary alliance forhealth.
Method
This analysis is part of an ongoing participatoryresearch programme on the impacts of social andphysical environments on health. One of our goalsthroughout this programme is to develop theory onintersectoral practices in local public health inter-ventions (Potvin et al., 2001). As such, ourparticipatory research initiative reproduced a localsocio-sanitary alliance that mirrors an innovativealliance for public health as we prepared for andundertook the development of collaborative re-search projects in response to local needs andpriorities. The processes, issues and interests in-volved thus serve as an instrumental case (Stake,1994) to reflect upon and improve our under-standing of local public health innovation andalliance formation.
The alliance under examination is made up ofresearch collaborators from institutional settingssuch as public health (Montreal Public HealthDepartment) and the City of Montreal, commu-nity-based organisations (Neighbourhood collec-tives for sustainable local development, theHunger and Social Development collective) andacademia (university-based researchers in healthand social sciences). Between May 2003 and March
SONAL COPY
ARTICLE IN PRESS
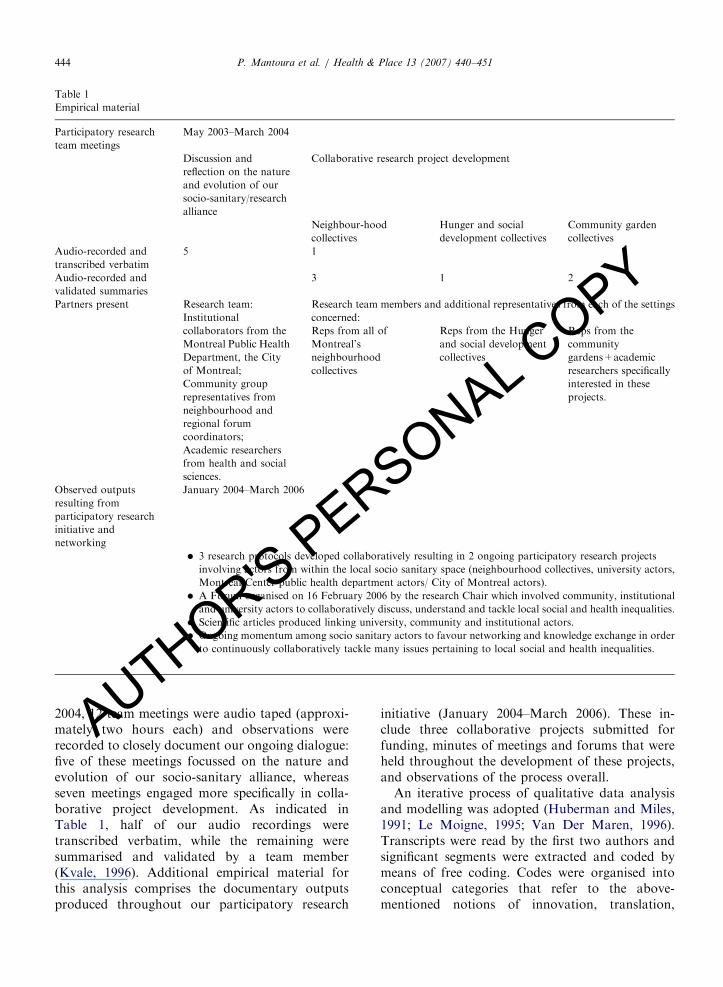
Table 1
Empirical material
Participatory research
team meetings
May 2003–March 2004
Discussion and
reflection on the nature
and evolution of our
socio-sanitary/research
alliance
Collaborative research project development
Neighbour-hood
collectives
Hunger and social
development collectives
Community garden
collectives
Audio-recorded and
transcribed verbatim
5 1
Audio-recorded and
validated summaries
3 1 2
Partners present Research team:
Institutional
collaborators from the
Montreal Public Health
Department, the City
of Montreal;
Community group
representatives from
neighbourhood and
regional forum
coordinators;
Academic researchers
from health and social
sciences.
Research team members and additional representatives from each of the settings
concerned:
Reps from all of
Montreal’s
neighbourhood
collectives
Reps from the Hunger
and social development
collectives
Reps from the
community
gardens+academic
researchers specifically
interested in these
projects.
Observed outputs
resulting from
participatory research
initiative and
networking
January 2004–March 2006
� 3 research protocols developed collaboratively resulting in 2 ongoing participatory research projects
involving actors from within the local socio sanitary space (neighbourhood collectives, university actors,
Montreal-Center public health department actors/ City of Montreal actors).
� A Forum organised on 16 February 2006 by the research Chair which involved community, institutional
and university actors to collaboratively discuss, understand and tackle local social and health inequalities.
� Scientific articles produced linking university, community and institutional actors.
� Ongoing momentum among socio sanitary actors to favour networking and knowledge exchange in order
to continuously collaboratively tackle many issues pertaining to local social and health inequalities.
P. Mantoura et al. / Health & Place 13 (2007) 440–451444
THOR'S PERSONAL COPY
2004, 12 team meetings were audio taped (approxi-mately two hours each) and observations wererecorded to closely document our ongoing dialogue:five of these meetings focussed on the nature andevolution of our socio-sanitary alliance, whereasseven meetings engaged more specifically in colla-borative project development. As indicated inTable 1, half of our audio recordings weretranscribed verbatim, while the remaining weresummarised and validated by a team member(Kvale, 1996). Additional empirical material forthis analysis comprises the documentary outputsproduced throughout our participatory research
AU
initiative (January 2004–March 2006). These in-clude three collaborative projects submitted forfunding, minutes of meetings and forums that wereheld throughout the development of these projects,and observations of the process overall.An iterative process of qualitative data analysisand modelling was adopted (Huberman and Miles,1991; Le Moigne, 1995; Van Der Maren, 1996).Transcripts were read by the first two authors andsignificant segments were extracted and coded bymeans of free coding. Codes were organised intoconceptual categories that refer to the above-mentioned notions of innovation, translation,

ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451 445
knowledge-based networks and game theory. Theseconcepts fit the data (Glaser and Strauss, 1967) andmade it possible to understand the dynamics of ouralliance. A report was produced by the first twoauthors to present the elaborated categories withtheir supporting quotations to the local partnersduring a team meeting for validation. The con-ceptual categories were perceived as being a correctrepresentation of the dynamic at hand.
Findings
Content analysis of our research meetings anddiscussions highlights three main characteristics ofour socio-sanitary alliance: (1) it is a non-coopera-tive game space; (2) it stimulates experimentationand innovation; and (3) it enhances knowledgeexchange. Selected quotations illustrate these find-ings.6 Close examination of the collaborative out-puts produced further support the experimentation,innovation and knowledge exchange characteristicsof this socio-sanitary space.
R
A non-cooperative game spaceAs the research collaborators engaged in theprocess, it quickly became apparent that fourfeatures characteristic of a non-cooperative gameemerged through our forming alliance. PE
S
Opportunistic transactionsAll agreed that our process was ‘‘far from beingneutral’’. The research domains, the collaboratorswe invite and the information that is shared are notneutral choices. Thus, it was rapidly establishedamongst ourselves that our transactions, althoughpointing toward some common goals, were largelyopportunities to deliberately achieve our respectivepurposes. For instance:
(y) to think that a researcher is neutral is a bitstupid. A researcher always has a hypothesis inmind, a hypothesis she believes in, and onaccount of which she sets in motion a certainnumber of things, as well as chooses not to triggera whole lot of other things.
AUTHOR'
6For the present purposes, transcripts have been translated
from French to English.
Working with/through distrust
A certain degree of distrust was expressed bysome collaborators with respect to our proposedresearch agenda. Past experience that involvedcommunity, academic and institutional actors hadweakened the trust that is vital to a fruitfulparticipatory research process. In the past, anotherresearch team had set a study in motion despitedisagreement expressed by various representatives,thus without reaching an acceptable compromisefor all those concerned. As a result, our collabora-tors most dedicated to community-oriented organi-sations were worried that our emergent researchprojects would poorly correspond to their issues andpriorities, as it had been the case in the past.
(y) for me, there is an issue here, between us andthe researchers. It takes trust between us. Duringthat other experience, there was no more trust.When you read a report, you need to know youwill trust the authors, you need to trust theirrigor, and the report has to be respectful of allpartners (y.). At the time, although we had saidno, the report described our activities in a way(that did not represent the complexities of ourpractice in context). I don’t want to be nasty, butyou could say they just wore us offy, because inour milieus, at the collective, our coordinatorsoften change. So, basically, it makes you wonderabout their scientific rigor.
Besides distrust conveyed by some regarding theresearch(er) agenda, unawareness of each others’motives was also cause for concern. The wish wasclearly expressed that each actor’s role and institu-tional affiliation be spelled out.
For me, there is a condition to success, and it isto know who is talking here, and about what. Forme, it’s essential to identify everybody’s role.Otherwise, there is no consciencey
Paradoxically, some level of trust had to beestablished among the collaborators before thisdistrust in various agendas was expressed. In turn,this eventually infused a little more trust in theprocess.
Constrained communication and transparency
Communication pathways appear constrainedwhen certain actors meet. For instance, the presenceof actors closely associated with funding agencies
SONAL COPY
ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451446
R
restricted freedom of speech and transparentexpression of viewpoints for some research partners.
(y) I feel a bit awkward discussing this when(representatives of) our funding agencies aresitting here with us at the same table. (y) Iparticipated in a few studies before, and it’s a bitdifficult to talk about what we do, our practice,our issues, and to do it freely, especially withyour sponsors or the people who evaluate yourwork y and that are likely to judge what you aresaying y
Otherwise, technical vocabulary was rather opa-que for several partners:
I have some issues about the vocabularyyforme, this collaborative, inter-sector, multi-sector,multi-network, inter-network vocabularyy.itdoesn’t mean much to mey
Terminology that has no meaning for some, ordifferent meanings for others, thus limited ourdiscussion at some times. Some felt that we oughtto create our own lexicon, and reach some agree-ment around certain terms, to understand eachother and work together.
Perceived inequity: research outcomes for whom?
On more than one occasion, doubts wereexpressed about our ability to establish genuinelyhorizontal alliances and benefit equitably from ourwork together. Since the encounter of our different‘‘worlds’’ is historically permeated by hierarchicalrelationships, with the institutional system tradi-tionally putting the community sector under closescrutiny, representatives from the latter felt that ourresearch alliance may be less advantageous forthem. Our group was thus challenged to considerlocal public health innovation and alliance forma-tion from a different and wider angle so that ourcollaborative research and theory development onintersectoral practice in the socio-sanitary spacecould be useful for all partners involved.
(y) this research project is not about commu-nity-based organisations, but rather about trans-actions between the community and ‘somethingelse’. I would like to know when there will be astudy about that ‘something else’, about theother side of the interaction. Instead of focussingon the community representatives and organisa-tions, observing its every move, how it reacts
AUTHOR'S PE
during negotiations, and so on and so forth,I wonder if anything similar is done with afocus on other actorsyIt’s as if it were a one wayroad, and this raises questions for meyIf wewant to study that so-called new socio-sanitaryspace...it seems to me that all actors involvedshould be considered, studied and taken intoaccount.
Experimentation and innovation
Despite the dynamics presented above, ouralliance resulted in some experimentation andinnovation. First, our collaborative work wasdeemed to foster distinctively different and uniquediscussions and ideas because the actors engagedfelt freer than usual to express themselves. Thiswas mainly due to the fact that the researchspace involved moderators and instigators whowere neither funding bodies nor evaluators of anykind.
(y) this is a place where people can breath-eythis was the first time a meeting wasorganised by an external body (other thanfunding agencies), and it led to a different kindof interaction.
Second, our research initiative enabled criticalanalysis of complex situations and social change.There was an authentic desire to go beyondtraditional understandings and to devise new waysto implement change and think through ourrealities.
In the institutional system, we often don’t havethe time to engage in a critical analysis of ourwork, in the way that this research project mayhelp us to do (y). We have to imagine otherways of doing things. (yThis project offers thepossibility) to innovate in the way we (implementchange) in our respective settings, particularlywhen it comes to the very demanding aspect ofcreating a successful interface between differentactors.We have to dreamyI invite you to a vision. Ithink the stake here is that despite what ishappening, within the demolition context en-gaged in (our province)y we need to worktogether. I think it’s up to us to describe a worldwe would like to build; we have to write it up, tocreate it. We have to go back to our drawingboards.
SONAL COPY

ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451 447
R
Third, and most importantly, many collaborativeoutputs emerged from this research initiative. Threeresearch protocols were developed and resulted intwo funded participatory research projects that arepresently underway and involving actors fromwithin the local socio sanitary space (neighbour-hood collectives, university actors, Montreal-Centerpublic health department actors/City of Montrealactors). A Forum was also organised by the researchchair and it involved community, institutional anduniversity actors to collaboratively discuss, under-stand and tackle local social and health inequalities.
Comments from this forum are particularlyrevealing:
ywe see the importance of networking andcreating alliancesy and the great value of eventslike this one to put together our ideas and get abigger picture of our reality.This was a great day! It helped us to betterunderstand each other, have a more positiveattitude towards one another, and change ourpreconceived ideas about each other. Lets con-tinue to support this worky and move intoaction!ywe note the usefulness of networking (y)knowing how to work with people and groupswith similar objectives but who are very different.
Enhanced knowledge exchange
Finally, through open discussion and experimen-tation, it was possible to put ‘‘conflicts’’ at anotherlevel, start closing some gaps between our comple-mentary worlds and work alongside one another.This lead to an apparent readjustment of precon-ceived ideas and enhanced knowledge exchange.
This research space is useful for reorientingtensions towards something else. (y) this projectcreates a space that makes it possible, withpeople whose goal is obviously to generateknowledge, to find a neutral territory wheresharing can happeny and through which it’seasier to extrapolate knowledge. It doesn’tsanction. It’s to help reinforce, adjust, improveaction (y) to obtain better results.yYes, we are funding bodies, that, I cannotdeny, but when I see in front of me people whomistrust me as if they were seeing the civil servantwho might be writing a negative remark on thereport they have written and that this will resultin cutting their budgetsyit is all the contrary!
AUTHOR'S PE
What I can say is that the goal is for things towork.
As examples of knowledge exchange outputs,scientific articles have been produced linking uni-versity, community and institutional actors. We arefinally, observing an ongoing momentum amongsocio sanitary actors to favour networking andknowledge exchange in order to continuouslycollaboratively tackle many issues pertaining tolocal social and health inequalities. Specifically therehave already been a few occasions of networkingand working sessions which have been instigated bydifferent local actors in order to tackle a specificproblem, consults on a particular issue, or supportthe writing of a specific working document. Theactors involved during those working sessionsinclude the city of Montreal, researchers andPh.D. students from the university of Montreal,institutional partners from the Montreal PublicHealth Department, and Community group repre-sentatives from neighbourhood collectives.
Discussion
Our findings highlight the issues that occurredduring our ongoing research initiative and that arelikely to characterise emergent socio-sanitary alli-ances: a mixture of non-cooperative games througha network of knowledge exchange, learning andinnovation.
The non-cooperative game aspects stem largelyfrom experiences prior to our research initiative. Inaddition, they refer to features of collaborativeaction that takes place outside the realm of researchper se: opportunism; the potential for individualinterests to hinder the realisation of collective goals;unawareness of each actors’ underlying motives;concern for inequitable distribution of benefitsbetween partners; challenges to clear, transparentand reciprocal communication; and the need toestablish a delicate balance of trust amongst actorsthat may have many reasons, a priori, to bedistrustful of each other. This being said, thesefeatures of ‘‘conflictual collaboration’’ were alle-viated by the input of university partners whofunctioned as mediators as they implemented aparticular format of interaction and ensured on-going discussion around the nature of our alliance.In fact, the research endeavour facilitated dialogue,the expression of concerns and apprehensions aswell as the identification of respective needs as
SONAL COPY

ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451448
R
initially distant universes came closer together withthe support of participant translators. It thusappears that the interactive space created byparticipatory research was beneficial and constitu-tive of our emerging alliance and ensuing networkformation. In particular, our analysis suggests thatunder conditions that are generative of relationshipsbased on trust, transparency and improved com-munication, it is possible to initiate a translationprocess through which knowledge exchange andinnovation take place.
To further understand and illustrate how partici-patory research can create such conditions, let usconsider the prisoner’s dilemma—a metaphor takenfrom game theory. The prisoner’s dilemma describesa situation in which an actor’s individual interestsmay correspond to collective interests if certainconditions are met. We are first introduced to twoprisoners who are under arrest for a given situationand questioned separately. If they confirm eachother’s counterfeit story, both will be assigned arather minor punishment. If, however, one prisoner‘‘tells the tale’’ but is betrayed by the other, he willbe severely punished while the other will be set free.Otherwise, if they betray one another, they will bothbe severely punished. Under these conditions, onecan see how these prisoners could take advantage ofmutual trust; how they could potentially maximizetheir own interests through betrayal; or how theycould harm each other through reciprocal betrayal.This being said, in the absence of trust, or withoutknowledge of what the other will do, each prisoneris most likely to pursue his own interests and betraythe other, even though they would both be better offif they cooperated with one another (Ford et al.,2004). If, however, the prisoners could negotiatebefore their arrest, talk to one another after beingarrested, establish some kind of contractual agree-ment, or read each others’ statements, their capacityto know what behaviour to expect from the otherwould be much more refined and their desire tocollaborate would greatly increase. Negotiation,interaction, and establishment of contracts andverification mechanisms, through dynamics of open-ness and transparency, hence become means forestablishing trust in non-cooperative game situa-tions.
With regard to our participatory research initia-tive, we can see that the conditions and needsexpressed by our partners to create a productivealliance are similar to the features inherent in thepotential resolution of the prisoner’s dilemma.
AUTHOR'S PE
Indeed, trust, transparency and communicationare means of tackling the ‘‘alliance dilemma.’’ Ifour team was able to engage in open dialogue,experimentation, knowledge exchange and innova-tion, it is no doubt because some of these elementswere part and parcel of our ‘‘research partnershipframework’’ that guided its development: we have awritten document (contract), that anyone couldconsult at any time, and which spells out the valuesand principles we adhere to as well as the roles andobligations of each partner (Bernier et al., in press).Moreover, all our discussions and exchanges wererecorded, and detailed summaries were producedfollowing each meeting, which made consultationpossible if the need arose (verification and transpar-ency). Finally, according to our observations,communication and negotiation abilities were pro-gressively developing. Trust and transparency,however, take time to develop and are built throughrepeated interaction and collaborative action (Israelet al., 1998; Suarez-Balcazar, Harper et al., 2005).The collaborative research work and funded parti-cipatory research projects generated from ouralliance are credible illustrations of such (inter)ac-tions which, in turn, are effective building blocksthat iteratively reinforce transparency and trust.
Local socio-sanitary alliances for health and thedistinctive features of a participatory researchinitiative.
The development of a socio-sanitary alliancewithin a participatory research initiative can thuspresent a significant advantage. In essence, theresearch structure and methodology can helpsmooth over disagreements and dissipate conflicts,as well as provide a discussion platform that canattenuate cultural differences and correct precon-ceptions. In other words, under specific conditions,the research context may foster dialogue within alocal socio-sanitary alliance and open the door tomutual learning, knowledge exchange and the openexpression of concerns.
However, the presence of an academic oruniversity-based partner within such a local socio-sanitary alliance is not automatically positive, as itmay situate the process and outcomes within theframework of a specific discipline or realm of adistinct sector. This specific location is not idealsince the development of synergetic action forms(Lasker and Weiss, 2003) depends on an ‘‘inter-sectoral’’ effort that can define the prevailing issuein an innovative way, via the creation of anautonomous action space which is not dependent
SONAL COPY

ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451 449
R
on any one or all of the sectors involved (White etal., 2002). In our case, even though the host-academic partner (the chair) was situated withinthe general framework of a social and preventivemedicine department, the academic actors involvedwithin the chair were rooted in a multitude ofsectors and disciplines, namely, sociology, urbanismand public health. Therefore, in our experience, avariety of academic partners brought together by achair whose goal is, amongst other things, to openpublic health to the social sciences, carried a certainnumber of possibilities for innovation which couldhave been different had the academic actor beencomposed of one preponderant sector and disci-pline.
The type of action a research initiative involves(even if participatory), must also be considered.Research-generated action is mostly of a dialogicalnature, and thus is largely of a different kind thanthe action underlying local interventions. Bearing inmind Callon et al. (1999) pragmatist notion that onemust engage in action to understand, as well asWhite et al. (2002) claim that the best strategy todeal with the challenge of intersectoral relationshipsis to move as quickly as possible from discussion toaction proper, it therefore appears that researchpartners should not remain for too long in adiscursive mode. They must ensure the rapidaddition of a more intense action dimension todevelop more sophisticated knowledge as well as tomobilise and sustain the engagement in intersectoralaction. The literature on university–communityalliances provides further confirmation of this(Baker et al., 1999; Lantz et al., 2001; O’Neillet al., 1997; Butterfoss and Kegler, 2002). In theinitial phases of alliance formation, action oftentends to focus on structural arrangements andprocedural development rather than on the issuesof concern. An important lesson learned, however,is that a balance must be rapidly achieved, duringthe first development phases of alliance formation,between action aimed at infrastructure and proce-dures and action geared to the resolution ofproblems or concerns. On the one hand, this fosterstrust among the members; and on the other, itenables some of the partners, especially thoseengaged in direct (inter)action in the field, toimmediately appreciate the benefits of collaboration(Baker et al., 1999; Buckeridge et al., 2002; Lantz etal., 2001). Our participatory research initiativestarted generating interesting outputs, such aspractical, locally based collaborative projects, when
AUTHOR'S PE
diverse partners became more engaged in the actualdevelopment of the projects, rather than theirdiscussion.
In the end, although a socio-sanitary alliancesituated within a participatory research context doesimpose some limits on the nature of action and itscourse, it creates an interesting opportunity forreflexive practice and innovation. A reflexiveepistemology suggests that action is permanentlysituating itself in space (geographic, social, political,and cultural) and time (historical). In other words,reflexive practice locates action in a space that iscontinually being transformed, most notablythrough social interactions (Potvin et al., 2005).Through a reflexive dynamic, participatory researchtherefore has the potential to transform interactionsamong the actors involved and thus foster thedevelopment of locally innovative partnershippractices. In public health, these ‘‘new relationshipmodes between agents’’ (Fassin, 1998), or ‘‘newactors’’ (Callon et al., 1999), are at the heart ofinnovative practice in the local socio-sanitarysphere. As we have learned from our experience,the actors involved in our participatory researchinitiative developed innovative socio-sanitary alli-ances which, in turn, modified some of theirpractices, changed some perceptions and views of‘‘the other’’, and fostered the establishment ofrelationships based on trust and transparency. Asthese and additional actors continue to tackleshared problems through a network of collabora-tively developed (research) projects, we can expectfurther transformation of local practice and iden-tities. A reflexive stance is thus an essentialingredient to cultivate in participatory approachesin public health. In our opinion, participatoryresearch that reflexively brings together the socialand sanitary worlds to address the increasinglycomplex issues that confront our rapidly changingsocieties is key to innovative alliances and practicesfor health. Such local alliances and partnerships notonly refer to the call for partnerships suggested bythe Ottawa (1986) and Bangkok Charters (2005),but they also represent the local production andconfigurations of Public Health (Fassin, 1998)which are the locus for innovation for PublicHealth.
Conclusion
Public health’s interest in infiltrating local socialspace fosters interventions which are more likely to
SONAL COPY
ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451450
R
promote health. The establishment of alliancesabout socio-sanitary issues thus becomes a practicalmechanism for grasping issues in a comprehensive,innovative way. At the local level, these alliances arenot produced without their share of problems, andthere is still need for more studies of the issuessurrounding the local production of public health.
The present study has drawn out that theinteractive space created by a participatory researchinvolving socio sanitary actors not only enabled abetter understanding of socio sanitary networkformation, but also was beneficial and constitutiveof such network formation. Our analysis suggeststhat under specific conditions that are generative ofrelationships based on trust, transparency andimproved communication, it is possible to initiatea translation process through which the ‘‘alliancesdilemma’’ is attenuated and knowledge exchangeand innovation take place.
In the end, the creation of a reflexive spacethrough a participatory research makes it possibleto view the participatory socio sanitary researchalliance as a tool with the potential for fostering theimplementation of the trust, transparency andcommunication favourable to the local developmentof innovative networks based on knowledge ex-change. In this light, under precise conditions,participatory research can be viewed as a tool whichcontributes to nurturing public health practices inlocal spaces through the creation of innovativealliances for the production and promotion ofhealth.
Acknowledgements
The authors wish to thank the local partners fortheir engagement in the participatory work that leadto this paper and for validating the manuscriptthroughout the writing process. The final versionhas been submitted to all partners for revision.
The authors wish to thank as well StephaneVibert, Angele Bilodeau and Jocelyne Bernier fortheir useful comments on previous drafts.
Louise Potvin is Chair of ‘‘Community Ap-proaches to Inequalities in Health’’, a research andteaching chair funded by the Canadian HealthServices Research Foundation (CHSRF/CIHR no.CP1-0526-05).
Part of the analysis and writing of this article wasmade possible through funding from the CanadianInstitutes for Health Research (CIHR): DoctoralFellowship (MFE-58109) obtained by Pascale Man-
AUTHOR'S PE
toura; Postdoctoral Fellowship (765-2000-0092)obtained by Sylvie Gendron.
References
Adler, P., 2001. Market, Hierarchy, and Trust. The knowledge
economy and the future of capitalism. Organization Science
12 (2), 215–234.
Baker, E., Homan, S., Schonhoff, R., Kreuter, M., 1999.
Principles of Practice for Academic/Practice/Community
Research Partnerships. American Journal of Preventive
Medicine 16 (3S), 86–93.
Baker, E., Metzler, M., Galea, S., 2005. Addressing social
determinants of health inequities: learning from doing.
American Journal of Public Health 95 (4), 553–555.
Bernier, J., Rock, M., Roy, M., Bujold, R., Potvin, L., in press.
Structuring an inter-sector research partnership: a negotiated
zone. Social and Preventive Medicine.
Bilodeau, A., Chamberland, C., et al., 2002. L’innovation sociale,
une condition pour accroıtre la qualite de l’action en
partenariat dans le champ de la sante publique. Canadian
Journal of Program Evaluation 17 (2), 59–88.
Bilodeau, A., 2000. Les conditions de qualite de la planification
participative et de l’action en partenariat en sante publique.
Le cas des priorites regionales 1995–1998 de Montreal-
Centre., Programme de sciences humaines appliquees. Faculte
des etudes superieures. Universite de Montreal, Montreal,
p. 358.
Bilodeau, A., Lapierre, S., Marchand, Y., 2003. Le partenariat:
comment c-a marche? Mieux s’outiller pour reussir. Montreal:
Regie regionale de la sante et des services sociaux de
Montreal-Centre—Direction de la sante publique. Down
loaded http://www.santepub-mtl.qc.ca/Publication/pdfautre/
guidepartenariat.pdf on April 17 2006.
Buckeridge, D.L., Mason, R., Robertson, A., Frank, J., Glazier,
R., Purdon, L., Amrhein, C.G., Chaudhuri, N., Fuller-
Thomson, E., Gozdyra, P., Hulchanski, D., Moldofsky, B.,
Thompson, M., Wright, R., 2002. Making health data maps:
a case study of a community/university research collabora-
tion. Social Science & Medicine 55, 1189–1206.
Butterfoss, F.D., Kegler, M.C., 2002. Toward a comprehensive
understanding of community coalitions. In: DiClemente, R.J.,
Crosby, R.A., Kegler, M.C. (Eds.), Emerging Theories in
Health Promotion Practice and Research. Strategies
for Improving Public Health. Jossey-Bass, San Francisco,
pp. 157–193.
Callon, M., Rabeharisoa, V., 2003. Research in the ‘‘wild’’ and
the shaping of new social identities. Technology in Society 25,
193–204.
Callon, M., Cohendet, P., Curien, N., Dalle, J.-M., Eymard-
Duvernay, F., Foray, D., Schenk, E., 1999. Reseau
et coordination. Paris.
Costongs, C., Springett, J., 1997. Joint working and the
production of a City Plan: The Liverpool experience. Health
Promotion International 12 (1), 9–19.
Fassin, D., 1998. La politique des corps et le gouvernement des
villes. La production locale de sante publique. In: Fassin, D.
(Ed.), Les figures urbaines de la sante publique. Enquetes sur
des experiences locales. La Decouverte, Paris, pp. 7–46.
SONAL COPY

ARTICLE IN PRESSP. Mantoura et al. / Health & Place 13 (2007) 440–451 451
R
Ford, E.W., Wells, R., Bailey, B., 2004. Sustainable network
advantages: a game theoretic approach to community-based
health care coalitions. Health Care Management Review 29
(2), 159–169.
Green, L.W., Daniel, M., Novick, L., 2001. Partnerships and
coalitions for community-based research. Public Health
Reports 116 (Supp.1), 20–31.
Glaser, G.G., Strauss, A.L., 1967. The Discovery of Grounded
Theory. Aldine, Chicago.
Huberman, A.M., Miles, M.B., 1991. Analyse des donnees
qualitatives. Recueil de nouvelles methodes. De Boeck-
Wesmael, Bruxelles.
Israel, B.A., Schulz, A.J., Parker, E.A., Becker, A.B., 1998.
Review of community-based research: assessing partnership
approaches to improve public health. Annual Review of
Public Health 19, 173–202.
Kvale, S., 1996. Interviews: An Introduction to Qualitative
Research Interviewing. Sage Publications, Thousand Oaks,
CA.
Lantz, P.M., Viruell-Fuentes, E., Israel, B.A., Softley, D.,
Guzman, R., 2001. Can communities and academia work
together on public health research? Evaluation results from a
community-based participatory research partnership in De-
troit. Journal of Urban Health: Bulletin of the New York
Academy of Medicine 78 (3), 495–507.
Lasker, R.D., Weiss, E.S., 2003. Broadening participation in
community problem solving: a multidisciplinary model to
support collaborative practice research. Journal of Urban
Health: Bulletin of the New York Academy of Medicine 80
(1), 14–60.
Lewin, A.Y., 2001. Crossroads. Organization Science 12 (2), 214.
Le Moigne, J.-L., 1995. Les epistemologies constructivistes.
Presses universitaires de France, Paris.
MacKian, S., Elliott, H., Busby, H., Popay, J., 2003. Everywhere
and nowhere: locating and understanding the ‘‘new’’ public
health. Health & Place 9, 219–229.
Marmot, M., Wilkinson, R.G., 1999. Social Determinants of
Health. Oxford University Press, Oxford.
McQueen, D.V., 2001. Strengthening the evidence base for health
promotion. Health Promotion International 16, 261–268.
Meijboom, B., de Haan, J., Verheyen, P., 2004. Networks for
integrated care provision: an economic approach based on
opportunism and trust. Health Policy 69, 33–43.
O’Neill, M., Lemieux, V., Groleau, G., Fortin, J.P., Lamarche,
P., 1997. Coalition theory as a framework for understandingHOR'S PE
and implementing intersectoral health-related interventions.
Health Promotion International 12 (1), 79–87.
Popay, J., Mallinson, S., Kowarzik, U., 2004. Developing public
health work in local health systems. Primary Health Care
Research and Development 5, 338–350.
Potvin, L., Chabot, P., 2002. Splendor and misery of epidemiol-
ogy for the evaluation of health promotion. Revista Brasileria
de Epidemiologica 5 (1), 1–13.
Potvin, L., Lessard, R., Fournier, P., 2001. Inegalites sociales de
sante. Un partenariat de recherche et de formation. Revue
canadienne de sante publique 93 (2), 134–137.
Potvin, L., Cargo, M., McComber, A., Delormier, T., Macaulay,
A., 2003. Implementing participatory intervention and
research in communities: lessons from the Kahnawake
Schools Diabetes Prevention Project. Social Science &
Medicine 56, 1295–1305.
Potvin, L., Gendron, S., Bilodeau, A., Chabot, P., 2005.
Integrating social theory into public health practice. Amer-
ican Journal of Public Health 95 (4), 591–595.
Sante Canada, 2001. The population health template: key elements
and actions that define the population health approach.
Stake, R.E., 1994. Case studies. In: Denzin, N.K., Lincoln, Y.S.
(Eds.), Handbook of Qualitative Research. Sages, Thousand
Oaks, pp. 236–247.
Shoultza, J., Onehab, M.F., et al., 2006. Finding solutions to
challenges faced in community-based participatory research
between academic and community organizations. Journal of
Interprofessional Care 20 (2), 33–144.
Suarez-Balcazar, Y., Harper, G.W., et al., 2005. An interactive
and contextual model of community–university collabora-
tions for research and action. Health Education Behaviour 32
(1), 84–101.
Van Der Maren, J.M., 1996. Methodes de recherche pour
l’education, 2e edition Bruxelles. Presses Universitaires de
l’Universite de Montreal, De Boeck Universite.
White, D., Jobin, L., McCann, D., Morin, P., 2002. Pour sortir
des sentiers battus. L’action intersectorielle en sante mentale.
Les publications du Quebec, Sainte-Foy.
WHO, 1986. Ottawa Charter for Health Promotion. http://
www.euro.who.int/AboutWHO/Policy/20010827_2
WHO, 2005. The Bangkok Charter for Health Promotion in a
Globalized World. http://www.who.int/healthpromotion/con-
ferences/6gchp/bangkok_charter/en/
Wilkinson, R., Marmot, M., 1998. The solid facts: social
determinants of health. In: E. WHO Regional Office (Ed.).
SONAL COPY
T
AU