parasites and diarrhea. i: protozoans and diarrhea
TRANSCRIPT

Parasites and Diarrhea. I: Protozoans and Diarrhea Rayhan Hashmey, Robert M. Genta, and A. Clinton WhiteJr.
Intestinal parasitism is extremely common, with approximately 70% of all people harboring one or more intestinal parasite. Parasitism and diarrhea are both hyper- endemic in areas where sanitation is suboptimal. Many clinicians assume that the identification of intestinal par- asites in patients with diarrhea implies that the parasites are the cause. This approach is frequently misguided. Some intestinal parasites such as Giardia lamblia and Enta- moeba histolytica certainly do cause diarrhea. Others, for example Entamoeba coli and Ascaris lumbricoides, almost cer- tainly do not. In addition, there are a number of other organisms that have been associated with diarrheal ill- ness in some cases, which may or may not be important pathogens.
In this article, we will review the role ofprotozoans as definite and possible causes of diarrhea. In Part 11, we review the role of helminths in diarrhea.
Protozoans as Definite Causes of Diarrhea
Table 1 lists the major protozoan parasites that have been associated with diarrhea. G. lamblia and E. his- tolytica are well-known causes of diarrheal illness while Cryptosporidium, Isospora belli, microsporidia and Cyclospora species have been increasingly recognized in association with diarrhea, especially in patients with AIDS. Balantidium coli is a well-recognized but less fiequent cause of diar- rhea. Blastocystis horninis and Dientamoebafvagilis have also been identified in diarrheal illness, but their causal role is less clear. Other organisms such as Entamoeba dispar almost certainly do not cause diarrhea.
Giardiasis Organism and Life Cycle
G. lamblia is a binucleate, flagellated intestinal pro- tozoan. Giardia are primitive eukaryotes and lack mito- chondria.The life cycle is simple and consists of cyst and trophozoite stages. The trophozoite, which measures
Rayhan Hashmey, MD, Robert M. Genta, MD, and A. Clinton White Jr., MD: Departments of Medicine, Pathology, and Microbiology and Immunology, Baylor College of Medicine, Houston, Texas.
Reprint requests: A. Clinton White Jr., MD, Department of Infectious Diseases, Baylor College of Medicine, Rm 561E. One Baylor Plaza, Houston, TX 77030.
J Travel Med 1996;4:17-31.
9-21 pm long, is tear-drop shaped and on stained smears has a characteristic face-like appearance, due to the pres- ence of symmetrically placed nuclei with large karyosomes.The dorsal surface is convex, while the ven- tral surface has a cytoskeletal disc made up of microtubules linked by microribbons.'.* Four pairs of posteriorly directed flagella help in 1ocomotion.Trophozoites mul- tiply by longitudinal binary fission. Encystation occurs in the small bowel and is facilitated by neutral pH and bile salts. Ingesting as few as 1G25 mature cysts can estab- lish infection. Excystation requires a low pH as well as the presence of pancreatic enzymes.3 Epidemiology
G. lamblia is one of the major causes of parasitic diar- rhea worldwide. In the developing world giardiasis is pan- demic, with peak prevalence rates of up to 20% in children less than 10 years of age.4 In the United States G. lamblia is among the most frequently isolated intesti- nal parasites and has been identified in up to 7.2% of stool specimens submitted for parasitologic examination.'a6 Giardiasis often occurs in the setting of waterborne out- breaks.' It is an important cause of chronic diarrhea in travelers returning from developing countries.' Most studies estimate infection rates of 1-3% in short-term vis- itors to endemic area^.^.^ In a large series from Switzer-
Table 1 Protozoan Parasites and Diarrhea
Dejnite Causes of Diarrhea
Causing bloody dnrrhea / dysentery Entamoeba kistolytica Balantidium coli Causing watery diarrhea / malabsorption Giardia lamblia Cryptosporidium parvum isospora belli Cyclospora cayetanensis Microsporidia
Possible Causes of Diarrhea
Dientamoeba fragilis Blastocystis hominis
Not Associated with Diarrhea
Entamoeba dispar Entamoeba coli Entamoeba hartmanni iodamoeba biitschlii Endolimax nana Trichomonas horninis

1 8 J o u r n a l of Travel M e d i c i n e , Volume 4, N u m b e r 1
land, G. lamblia was found in 0.4% of returning travelers who had chronic diarrhea."'Travelers usually get infected after consumption of contaminated water." Although infrequent, several outbreaks of giardiasis have been asso- ciated with contaminated f ~ o d . ~ * - ' ~ Person-to-person transmission is also important, especially in groups such as children in day care centers, sexually active male homosexuals, and institutionalized patient^.'^ These groups may have very high cyst carriage rates, up to 50% in some studies, and can transmit disease to friends and family.'' Animal-to-human transmission has been pos- tulated as a common source ofinfection but has only been documented in a Canadian outbreak traced to beavers." Pathology and Pathogenesis
The trophozoite adheres to the mucosal surface using the ventral disc. This results in distortion of the micmvih and disruption of the brush b~rde r . ' ~ . ' ~The par- asite also elaborates several cytopathic substances includ- ing cysteine pmteinases, enterotoxin, and a surface binding l e ~ t i n . ~ J ~ , ' ~ In addition, infiltration of the lamina propria with lymphocytes has been noted and may lead to vil- lus atrophy. These processes contribute to the develop- ment of disaccharidase deficiencies commonly associated with Giardia infection. Isozyme electrophoresis and genetic studies have demonstrated considerable pheno- typic and genotypic heterogeneity among G. lamblia isolates. Analysis of sequential isolates suggests that this heterogeneity is due to the h g h rate of genetic rearrange- ment within the Giardia genome.20 Chronic infection has been associated with hypogammaglobulinemia, protein- calorie malnutrition, previous gastrectomy, and use of immunosuppressive medication.3~'*~19 Both systemic and mucosal antibody production occurs in giardiasis.21 Secre- tory IgA interferes with the adhesion mechanism of the parasite and may help clear the infection. The greater prevalence of disease in younger patients suggests a par- tial imrn~ni ty .~ Clinical Manifestations
The clinical manifestations of giardiasis are remark- ably &verse, including asymptomatic carriage, acute diar- rheal disease, severe chronic diarrhea with malabsorption, and growth failure in Patients with acute symptomatic giardiasis complain of diarrhea, abdominal cramps, bloating, flatulence, malaise, nausea, and anorexia. Stools may be greasy or foul smelling. Fever and tenes- mus are uncommon and point toward other pathogens that are invasive. Extraintestinal manifestations have been described in rare cases and include urticaria, reactive arthritis, and biliary tract di~ease.'~ Chronic infection is associated with profound malaise, lassitude, epigastric discomfort, headaches, and steatorrhea. Patients who develop recurrent diarrhea after treatment for Giardia infection may have associated lactose intolerance rather than relapse of their infection.
Diagnosis The most common method for diagnosis of giar-
diasis is microscopic examination of the stools for tropho- zoites using either wet mount or trichrome ~ ta in .~~Three consecutive stool specimens when properly examined yield a diagnosis in 80-90% of cases.25 Iodine staining is used for better identification of the cysts.The stool sam- ple may be preserved in 10% buffered formalin and examined later using trichrome or iron hematoxylin stains.The duodenal string test (Entero-Test) may increase the yield, but this procedure is not well-tolerated by patients. In selected patients, endoscopic aspiration and biopsy may be considered. Giardia antigen detection assays are commercially available and are highly sensitive and specific.2h Treatment and Prevention
Metronidazole is the most frequently used drug for the treatment of giardiasis in the United States and is asso- ciated with a cure rate of 8c-90%." The adult dosage is 250 mg PO t.i.d. for 5-7 days; children should receive 5 mg/kg PO t.i.d. for 7 days. Quinacrine, which has a comparable efficacy, is associated with far more side effects and is no longer available in the United States. Tinidazole is frequently used worldwide but is not avail- able in the US. It has excellent efficacy when given in a single oral dose of 2 g.28 Furazolidone 25-50 mg PO q.i.d. is available as a liquid suspension. Recommended dura- tion of therapy is for 7 days. It is well-tolerated by chil- dren, but the efficacy is lower. Pregnant women may be treated with paromomycin, a nonabsorbable aminogly- coside, which is effective in 60-70% of cases.Treatment of asymptomatic cyst passers has been advocated in developed countries and returning travelers. Such an approach is futile in hyperendemic areas due to rapid rein- fection.2' Travelers to developing countries should be advised against the ingestion of untreated surface water. Bringing water to boil is adequate to kill Giardia cysts, though boiling for a few minutes may be required at higher altitudes. Halogenation with iodine- or chlorine- based agents is generally effective.6 Person-to-person transmission can be reduced by practicing strict hand- washing. '()
Amebiasis (Entamoeba histolyfica and Entamoeba dispar) Organisms and Life Cycle
Amebiasis is caused by infection with the enteric protozoan E. histolytiru.The existence of pathogenic and nonpathogenic strains of E. kistolytica has been postulated for some time based on studies showing differences in isozyme electrophoretic patterns (zymodemes) .31,32 More recently, genomic differences in DNA polymerase chain reaction amplification products, rRNA probe studies, and cloned genes have confirmed the existence of two dis- tinct species that are morphologically identi~al.~'~"'The non-

H a s h r n e y e t a l . . P a r a s i t e s a n d D i a r r h e a . I : P r o t o z o a n s a n d D i a r r h e a 1 9
pathogenic species, now named Entamoeba dispar, is only associated with the asymptomatic carrier state, while E. histolytica causes tissue invasion and symptomatic disease.
The genus Entamoebu also includes five other species (E. coli, E. gingivulis, E. moshkovskii, E. hartmanni and E. polecki] known to infect humans. None of these species cause disease in humans.34
The life cycle of E. histolyticu includes trophozoite and cystic stages. Cysts are excreted into the environment and can remain viable for several weeks.The mature cyst is quadrinucleate and ranges in size fi-om 8.5-19 prn in diam- eter. Infection is acquired by ingestion of the cyst form. Excystation occurs in the small bowel and results in eight motile trophozoites ranging from 12-60 p.m in size. Epidemiology
Both species have a worldwide distribution with approximately 12% of the world’s population infected with one of the E. dispar has never been associated with disease and does not elicit any specific serologic response. In contrast, E. histolyticu causes serum antiamebic antibody production in -90% of patients with invasive disease.35 Since E. histolytica and E. dispar are morphologically identical, most of the data on preva- lence includes both. In most areas E. dispav is 10 times as common as E. histolyticu. Amebiasis is endemic in countries such as Mexico, India,West and South Africa, and Central and South America, where up to 50% of the population may be infected. Serologic surveys in endemic areas indicate that up to 25% of the population have had prior asymptomatic infection with E. histolyti~a.~~ Epi- demiologic risk factors include lower socioeconomic status, migration from areas of high endemicity, institu- tionalization (especially in mentally retarded individuals) and living in a communal setting. Patients with amebic liver abscess have a high prevalence (>75%) of asymp- tomatic intestinal colonization with E. histolytica that may result in a prolonged carrier state if inappropriately treated.” Invasive amebic disease carries an annual world- wide mortality of 40,000-100,000.
The overall prevalence of intestinal amebiasis in the United States was about 4% of clinical stool specimens, but this appears to be decreasing.36 In the southwestern United States there is a higher prevalence of invasive disease, especially among immigrants from Mexico. E. histolytiu is not a common cause of traveler’s diarrhea. How- ever, amebiasis can be a cause of chronic diarrhea in trav- elers returning from developing countries.” The risk of acquiring infection is proportional to the duration of stay in the endemic area. Ninety-five percent of travelers or immigrants who develop liver disease will present within 5 months after returning from an area of endemicity. Pathology and Pathogenesis
E. histolyticu trophozoites attach to the colonic epithelium by means of a galactose inhibitable adherence
lectin (GIAL), a 260 kD surface protein.This adherence lectin protects the parasite against complement-mediated lysis by inhibiting the assembly of C8 and C9 compo- nents with the membrane attack ~ o m p l e x . ’ ~ ~ ~ * ~ ~ ’ The cytolytic activity of E. histolyticu is dependent upon direct contact to the target cell, binding by the GIAL, and the presence of extracellular calcium ions.4” Proteolytic dis- ruption of tissue planes is mediated by a variety of par- asite enzyme^.^^^^^ Proteinases cause extracellular tissue destruction and degradation of secretory 1gA.The spec- trum of colonic lesions range from nonspecific thickening of the mucosa to frank ~lceration.~’The classic descrip- tion of flask-shaped ulcers is seen in less than half of cases. After invadmg the colonic epithelium, the amebic tropho- zoites can reach the liver via the ascending portal venous system. In the liver, extracellular proteinases digest the hepatic tissues, thereby resulting in focal areas of tissue destruction that can coalesce into necrotic areas termed liver abscesses. Immunity to amebic infection is incom- plete, although patients cured of invasive disease rarely have reinfection. Clinical Manifestations
Noninvasive lumenal infection with E. histolytica may result in asymptomatic infection or nonspecific gas- trointestinal complaints such as bloating, cramps, decreased appetite, and flatulence. Amebic colitis on the other hand has a subacute onset characterized by bloody mucoid diarrhea, abdominal pain, weight loss, bloating, tenes- mus, cramps, and fever. Amebic colitis can occur in a chronic nondysenteric syndrome with intermittent diar- rhea, mucus, and abdominal ~ a i n . ~ ’ . ~ ~ Complications of intestinal infection include fulminant colitis, toxic mega- colon, intestinal perforation, stricture formation, and ameboma (annular lesion of the colon, usually near the cecal area, inhstinguishable fi-om carcinoma of the
Chronic amebic colitis is clinically indistinguishable from idiopathic inflammatory bowel disease. Because corticosteroid therapy may result in perforation, stool examination for trophozoites and serologic test for ame- bic disease should be performed prior to making a diag- nosis of inflammatory bowel disease.
Extraintestinal disease most commonly presents as amebic liver abscess. Patients present with fever and right upper quadrant abdominal pain. Laboratory findings include leukocytosis and elevated liver enzymes. Liver abscesses occasionally rupture into the pleural space, resulting in pleural efisions. Extraintestinal disease rarely involves the pericardium, genitourinary system, and the brain. Diagnosis
The diagnosis of intestinal infection is made by finding cysts or trophozoites in the stool. A saline wet mount of the stool should be made kom a fi-esh stool spec- imen, as trophozoites disintegrate in 30 minutes at room

20 Journa l of Trave l Medic ine , V o l u m e 4 , Number 1
temperat~re.~' If immediate evaluation cannot be per- formed, the specimen should be fixed in polyvinyl alco- hol and examined later using trichrome o r iron hematoxylin stains. Stool examination is positive in >85% ofpatients when at least three stool specimens are exam- ined on alternate days.46 Hematophagous trophozoites when seen are pathognomonic of E. h i~ to ly t ica .~ ' Endoscopy with scraping or biopsy is a useful technique in evaluation of difficult to diagnose cases.
In nonendemic areas, serum antiamebic antibody tests may be useful in the diagnosis of invasive disease. Over 85% of patients with biopsy-proven disease have detectable antibody by the seventh day of illness." In endemic areas a positive serology is less helpful. Up to 25% of the population may have serologic evidence of prior infec- t i ~ n . ~ ~ Several new stool and serum antigen detection techniques appear promising in the identification of pathogenic versus nonpathogenic strain^.^'
The presence of an amebic liver abscess is suggested by a history of fever and right upper quadrant pain, hepatic tenderness on physical examination, and an ele- vation in liver enzymes. Diagnosis requires the demon- stration of the abscess by ultrasonography or computerized tomcgraphy scan. Trea tmenf
Amebicidal drugs have been divided into intralu- menal agents (e.g., diloxanide furoate, paromomycin, iodoquinol, and tissue agents metronidazole, tinidazole, and emetine).48Ti~~ue amebicides lull amebae in host tis- sues and organs, whereas the poorly absorbed lumenal amebicides are active only in the intestinal l ~ m e n . ~ '
"E. histolytica" cysts found in the stool of asympto- matic cyst passers are usually those of E. dispar. Since this parasite has never been shown to cause invasive infec- tion, treatment is unnecessary. Serologic tests are nega- tive and cysts are excreted in the stool for a limited per iod , usually 6-8 months. An enzyme-linked immunosorbent assay (ELISA) test to distinguish between E. histolytica and E. dispar is being developed. Symptomatic patients should be treated. In patients without evidence of invasive disease, diloxanide furoate 500 mg P O t.i.d. for I0 days is the therapy of choice. In the United States this drug is available only from the Centers for Disease Control and Prevention (CDC). Iodoquinol 650 mg PO t.i.d. for 20 days is also effective but has bothersome side effects and a longer duration of therapy. Paro- momycin can be used as an alternative for lumenal or mild colonic disease. Invasive disease should be treated with metronidazole 750 mg P O t.i.d. for 10 days (tinida- zole is also available outside the United States) followed by a lumenal amebicidal agent in order to eradicate intestinal disease.'') Tetracycline or erythromycin may be used in patients unable to tolerate metronidazole, but these drugs are not effective in hepatic disease. Dehy-
droemetine is available from the CDC. Due to the occur- rence of serious side effects such as prolongation of the Q-T interval, it should be administered in a monitored hospital setting. Chloroquine may be added to metron- idazole in extraintestinal disease. Fine needle aspiration is indicated in left-sided abscesses and those unrespon- sive to medical therapy.
Cryptosporidium panrum Organism and Life Cycle
The protozoan parasites of the genus Cryptosporid- ium are closely related to other coccidian parasites such as TDxoplasma and Isospora. Although many species were named based on presumed host-species specificity, there is little host specificity for the strains infecting mammals.s1 Most organisms infecting mammals probably belong to a single species, C. parvum.
Humans are infected after ingestion of oocysts (4-6 p,m in diameter).5' After excystation in the s m a l l intestines, the motile sporozoites attach to the host cells via their anterior end.They are enveloped by the microvilli and subsequently develop along the lumenal surface of the enterocyte within a parasitophorous vacuole separated from the host cytoplasm by a dense organelle (intracel- lular but extracytoplasinic).The parasite enlarges to form the trophozoite and divides forming meronts with four to eight nierozoites. When nierozoites are released they invade other host cells, and a portion of the merozoites develop into the sexual forms (macrogamont and micro- gamont) . M e r fertihzation the macrogamont develops into an oocyst, which sporulates in situ. Most of the oocysts are coated with a thick wall and are environmentally hardy. About 20% of the oocysts are thin-walled and may be involved in an autoinfection cycle. Epidemiology
The first human case of cryptosporidiosis was reported as recently as 1976 and only seven human cases were reported prior to 1982.52The number of cases has risen dramatically since the description ofAIDS. Subse- quently, cryptosporidiosis has been identified in over 50 countries on all six inhabited continents in both normal and immunocompromised hosts.s3
When clinical stool specimens are examined for Crptosporidium oocysts, approximately 1-3% are positive in studies from North America and Europe (range 0.1%-14.1%, mean of 1.6 and 2.6%, respectively). In contrast, rates of 4.9-10.4% are typical in developing countries (range 1.3-31 .5%).53.'4 Seroprevalence rates, which presumably reflect active or prior infection, range from 25-35% in developed countries but up to 64% among the urban indigent population in Latin 5 . 5 6
Cryptosporidiosis has been identified as a common cause of diarrhea in developing c ~ u n t r i e s . ~ ~ ~ " ~ ~ Infec-

H a s h m e y e t a l . , P a r a s i t e s a n d D i a r r h e a . I: P r o t o z o a n s a n d D i a r r h e a 2 1
tion is more common in children than in adults, but is rare in breastfed infants.sy,6' Cryptosporidiosis appears to be more prevalent in warm, wet month^.'^^."^ Cryp- tosporidiosis has also been frequently identified as a cause of diarrhea in travelers returning from areas with poor ~anitation.'~+'The oocysts are very hardy and sur- vive for prolonged periods in the environment. Cryp- tosporidiosis is associated with waterborne epidemics of diarrheal Chlorination of water supplies does not appreciably kill the oocysts.
Initial descriptions of cryptosporidiosis in normal hosts stressed animal contact;74 however, epidemiologic data have strongly supported only calf-to-human trans- mission."' Subsequent studies suggest that person-to- person transmission is also common, especially in urban area^.^',^^ In developed countries, cryptosporidiosis is a frequent cause of outbreaks of diarrhea in the context of day-care center^.^^^^^^^' Person-to-person transmission has also been documented in secondary cases in house- hold c ~ n t a c t s ~ ~ ~ ~ ~ and among health care ~orkers .~ 'The high prevalence of disease among homosexual males also suggests person-to-person transmission.*" Cryp- tosporidiosis is an increasingly recognized cause of diar- rhea in travelers to developing countries. Cryptosporidium was found to be the cause of diarrhea in 5% of travelers to Leningrad and in short-term Peace Corps workers in West Africa.*',''
T h e prevalence of cryptosporidiosis is high in immunocompromised hosts, particularly in patients with AIDS. In the United States, 3-4% of patients with AIDS have cryptosporidi~sis. '~ In contrast, in Africa more than half of AIDS patients have crypto- sporidi~sis. '~ Prevalence rates in Latin America are intermediate.'s~x6 Pathology and Pathogenesis
Cvyptosporidium has been detected throughout the gastrointestinal tract, in the biliary tract, and even in the respiratory tract.sh Intestinal changes include villus blunt- ing, crypt hyperplasia, and infiltration of the lamina pro- pria with polymorphonuclear leukocytes, lymphocytes, and plasma The parasites are found within the microdus layer within parasitophorous vacuoles.Though most patients exhibit normal duodenal villous architec- ture, high intensity infections, as evidenced by histologic examination of biopsy specimens, were associated with severe morphologic abnormalities."
The pathophysiology of diarrhea in cryptosporidiosis is complex and likely involves both host and parasite fac- tors. Current data suggest that site specific alteration in the function of villus absorptive cells, as evidenced by alteration in glucose-mediated sodium transport and release by the host of proinflammatory cytokines as part ofthe mucosal immune response, are the primary mech-
anism involved." Chloride dependent enterotoxic activ- ity has also been described."
The host immune response in cryptosporidiosis has not been clearly defined. Secretory antibodies have been noted to interfere with sporozoite and merozoite attach- ment, but the development of specific serum and mucosal antibodies in AIDS patients does not effect a In contrast, the cell mediated immune response, specifi- cally CD4 T cells and IFN-y, appear to play an impor- tant role in limiting infection.y4y6 In patients with HIV, the CD4 count is the best marker of the ability of the immune system to clear infection."'
Dose response studies in healthy volunteers, using one strain of C. parvum, have shown a low mean infec- tive dose (ID5,) of 132 oocy~ts; '~ however, it is not known whether immunocompromised individuals are more susceptible to infection than normal hosts.The dose of the inoculum did not influence the incubation period or the severity of illness. Clinical Manifestations
The clinical presentation of cryptosporidiosis varies depending on the host response. In normal hosts, initial symptoms follow an incubation period, usually 7-10 day^.^^.'^,^^^'' Onset is typically abrupt. The most com- monly identified symptom is diarrhea, with watery stools that may be voluminous. Mucus is usually not present. Fecal leukocytes and blood are absent. Abdominal pain and cramping were frequently noted in some series.74," Weight loss, anorexia, and flatulence have been noted. Fever when noted is typically low grade. Nausea and vom- iting are present only in a minority of patients. Respi- ratory symptoms have been frequently noted in some series.5',6Z,99. 100
In travelers and other immunocompetent hosts, symptoms typically resolve in 10-1 4 days.64,74.76," How- ever, C. parvum is among the most common causes of diarrhea persisting for over 2 weeks, and chronic cases lasting over 30 days are well described."" Oocysts are excreted in the stool for 1-2 weeks after resolution of symptoms.98 Cryptosporidiosis has been associated with malabsorption. Whether this reflects Cryptosporidium causing malabsorption or merely the increased severity and recognition of cryptosporidiosis in patients with mal- absorption due to other causes is unclear. Asympto- matic shedding of oocysts has been noted in some
In immunocompromised hosts, disease onset is usually i n s i d i o ~ s . ~ ~ * ~ ~ . ~ ~ , ' " " J " ~ Watery diarrhea may grad- ually increase over weeks to months. Weight loss and profound dehydration are common. Abdominal pain and cramping are also common. Symptoms typically persist unless there is improvement in the immunologic status.
lo'

22 Journal o f Travel Medicine, Volume 4 , Number 1
Diagnosis Since the symptoms of cryptosporidiosis are non-
specific, diagnosis usually depends on the demonstration of oocysts in stool specimens. Considerable experience i5 required to obtain reliable results.The sensitivity of stool examination may be increased by concentration tech- niques or by staining. Sheather's sucrose floatation is the most frequently used concentration te~hnique.'"~"'~
A number ofstaining techniques have been used for Cryptosporidiurn. 525637.103 A cid-fast staining is most com- monly employed (Fig. 1). A number of acid-fast stains are widely used, including modified Kenyoun, diniethyl sulfoxide-modified stains, and fluorescent stains. 'i)1,'iJ4 In patients with diarrhea, oocysts can generally be identi- fied by acid-fast staining without using concentration techniques.
Monoclonal antibody based immunofluorescent tests to detect oocysts in stool specimens are commer- cially available and demonstrate >90% sensitivity and specificity.'"' In comparative studies, the immunofluo- rescence test is both more sensitive and more specific than acid-fast staining technique^."'^^'"^ Widespread applica- tion of this test may be limited by the additional cost. Tissue forms can be detected in biopsy specimens with routine histologic stains including hematoxylin and eosin or Giemsa.In8 Treatment
Fluid and electrolyte replacement are of primary importance in all cases of diarrhea. Attention to nutri- tion may be critical since the immunosuppression asso- ciated with malnutrition may delay recovery."' In compromised hosts, nonspecific antidiarrheal agents such as loperamide or diphenoxylate may be required to limit voluminous fluid losses. In a recent controlled clinical trial,
the somatostatin analogue octreotide was no more effec- tive than placebo.'"'
There are numerous reports of antiparasitic agents used in cryptosporidiosis. Spiramycin, a poorly absorbed macrolide antibiotic, was initially reported to affect cryptosporidiosis in patients with AIDS in anecdotal reports,"' but efficacy has not been demonstrated in con- trolled trials. "*
Paromomycin, a poorly absorbed aminoglycoside antibiotic,"3 achieves effective concentrations along the lumenal surface of the intestines, where the organism is found in vivo."4 A small placebo-controlled trial demon- strated both clinical and parasitologic improvement with paromomycin treatment in patients with AIDS."' Patients experienced significant symptomatic improvement; how- ever, a majority relapsed.
HIV-infected individuals should be advised not to drink water directly from lakes or rivers. Currently there are no recommendations regarding the use of household tap water; however, persons who want to take indepen- dent precautions can reduce the risk of infection by boiling water for 1 minute, by using"abso1ute" 1 micron water filters, or by using high-quality bottled water.- Risk of infection during travel to endemic areas can be reduced by avoiding use of untreated surface and ground water and by boiling water prior to use.
Isospora belli 1. belli is a coccidian parasite closely related to Cryp-
tosporidium. The oocyst is elliptical and measures 22-33 by 10-15 p m in size.Within the oocyst are two sporo- cysts, each ofwhich contains four sporozoites.The sporo- zoites are released in the intestines, invade the intestinal epithelium, and undergo asexual (merogony) and sexual (gametogony) division within cytoplasmic vacuoles of the enterocyte."6 The oocysts are excreted prior to sporu- lation, which occurs outside the host. Epidemiology
1. belli is widely distributed in the animal kingdom. Infections have been described from nearly all the coun- tries in the Americas, as well as in subSaharan Africa, the Middle East,Asia and the Pacific islands, and E ~ r o p e . " ~ , " ~ Studies suggest an increased prevalence in tropical and subtropical climates and in areas with poor sanitation. Little is known about the prevalence of infection in humans. In a limited number of studies employing ade- quate techniques, 0.1-1.8% of stools were positive."' Prevalence among AIDS patients in the United States is approximately 1%."' This may be an underestimate; this organism was not routinely looked for, and cotri- moxazole is frequently prescribed in these patients. In contrast the prevalence rate in less developed countries is as high as 15%.K44,R5J20 The mechanisms of transmis- sion are unknown, although spread from infected ani- mals and humans is suspected.
Figure 1 Oocysts of Cryptosporidiurn are visualized in a stool specimen stained by the modified acid-fast stain (with per- mission from Dr. Lynn Garcia).

H a s h r n e y e t a l . , P a r a s i t e s a n d D i a r r h e a . I : P r o t o z o a n s a n d D i a r r h e a 2 3
Pathology and Pathogenesis Biopsy and autopsy specimens show villus atrophy,
crypt hyperplasia, and infiltration of the lamina propria with inflammatory cells, in particular eosinophils."'J2' All of the life cycle stages are visible within biopsy speci- mens.The mechanisms responsible for diarrhea are not clear, but may relate to malabsorption, which has been well described in both normal and compromised
Clinical Features The clinical features of isosporiasis in immuno-
competent hosts have been well defined by several large series and from experimental and laboratory-acquired infections.'1x~'22-'zs Aft er an incubation period (6-12 days in experimental and laboratory infections), patients typically present with an acute onset of fever, headache, and malaise. Gastrointestinal complaints include diarrhea (both frequent and watery stools), abdominal pain, nau- sea, and vomiting. Initially the stools are watery, but subsequently they may be fatty. Stool specimens do not contain fecal leukocytes but frequently contain Charcot- Leyden crystals and fat. Peripheral eosinophilia is fi-equent. While symptoms are usually self limited, patients are often ill for 6 weeks to 6 months. Even in apparently normal hosts, a portion of patients go on to develop chronic diar- rhea and malabsorption, which may persist for years.' l6.l2'
Patients with AIDS and isosporiasis present with an insidious onset of diarrhea, weight loss, and abdominal
Fever and vomiting are less frequently noted. Symptoms are usually present for months prior to dia- gnosis. Biliary disease, acalculous cholecystitis, and ulcer- ative colitis have been r e p ~ r t e d . ' ~ ~ . ' ' ~ Diagnosis
Diagnosis depends on the identification of organ- isms in stool or biopsy specimens.While the oocysts can be identified in wet mounts of stool specimens, stool examinations are frequently negative unless they are concentrated. Zinc sulfate floatation has been highly successful in some laboratories.'23 Acid-fast stains appear to increase the sensitivity of stool examination.'2y Treatment
Isosporiasis responds promptly to therapy with antifolate d r ~ g s . ' ~ " , ' ~ ' , ' ~ ~ , ' ~ ' Trimethoprim (160 mg) com- bined with sulfamethoxazole (800 mg) four times a day for 10 days leads to prompt resolution of symptoms in normal hosts and in patients with AIDS. For AIDS patients, approximately half will relapse if not placed on secondary prophylaxis. Both trimethoprim (TMP)/sulfa- methoxazole (SMX) (160 mg/800 mg three times a week) and sulfadoxine/pyrimethamine (500 mg/25 mg) once weekly can prevent relapse.'30 Cyclospora
Cyclospora cayetanensis, a coccidian parasite, has recently been identified as causing human infe~ti0n.l~'
Before its identification as a coccidian parasite, Cyclospora had been referred to as cyanobacteria-like bodies (CLB) and blue-green algae.132-'35 The appearance of oocysts is similar to those of Cryptosporidium, but the size is slightly larger (9-10 pm). Each oocyst contains two sporocysts, each of which contain two sporozoites.I3' Epidemiology
There is a wide geographic hstribution of Cyclospora. Most of the reported cases have originated in tropical countries such as India, Nepal, and South America. Cases have been identified in travelers returning from the trop- i c ~ . ' ~ ~ . ' " ~ ' ~ ' Gascon et al. found Cyclospora in 2.8% of patients with traveler's diarrhea in their ~1inic.l~' Trans- mission occurs via the oral route, and local outbreaks have been traced to contaminated water or food supply. An outbreak of relapsing diarrhea among 17 physicians and three hospital employees in a Chicago hospital was traced to a contaminated water s o ~ r c e . ' ~ ~ ~ ~ ' ~ ' Most outbreaks occur during the summer season. Pathology and Pathogenesis
The site ofinfection is the sma l l intestine. Endoscopic biopsy specimens show a diffuse inflammatory response, with an increase in intraepithelial leukocytes, mild to severe villus atrophy, and crypt hyperplasia. '42The patho- genesis of these lesions and the mechanism of diarrhea are unclear; however, both invasion as well as toxin pro- duction have been p~s tu l a t ed . '~~ Clinical Presentation
The clinical presentation is similar to that of Cryp- tosporidium and Isospora infections. Clinically, patients present with watery diarrhea, anorexia, and malaise. Approximately half experience abdominal cramps and up to a third have nausea, vomiting, and fever. Symptoms often wax and wane.The duration of illness in immuno- competent patients is variable but typically lasts several weeks (mean duration 43 days in one series).I3' In AIDS patients, Cyclospora results in chronic intestinal infection with prolonged diarrhea.137 Duration of symptoms cor- relates with the presence of Cyclospora in the stool. Con- trol groups either with other causes of diarrhea or without symptoms only rarely have the organism in their stools. C. cayetanensis may be associated with bil- iary tract disease.'43 Diagnosis and Treatment
Diagnosis requires a high index of suspicion. Diag- nosis is dependent on microscopic demonstration of morphologic characteristics, staining properties, and auto- fluorescence under ultraviolet light. In contrast to Crypto- sporidium, staining is variable with the modified acid-fast stain (Fig. 2). Oocysts autofluoresce when examined under ultraviolet light and do not cross-react with immunologic tests specific for C r ~ p t o ~ p o r i d i u m . ' ~ ~ . ' ~ ~ Measurement of oocysts is recommended to distinguish Cyclospora from Cryptosporidium.'44,'45 Cotrimoxazole

2 4 Journa l o f Travel M e d i c i n e , Volume 4, Number 1
Figure 2 A stool specimen demonstrating a variable uptake of modified acid-fast stain by oocysts of Cyclospara (kindly pro- vided by Dr. Charles Stager).
(TMP 160 mg/SMX 800 mg) PO b.i.d. for 5-7 days is the treatment of choice, with recent studies reporting a significant response to therapy and improvement in both clinical and parasitologic parameter^.^'.'"^'^",'^'
Microsporid ia ( Enterocytozoon bieneusi and Encephalitozoon intestinalis) Organism and Life Cycle
Microsporidia are a group of obligate intracellular protozoan parasites belonging to the phylum Microspora, which consists of more than one hundred genera and over a thousand 14' Human infection was first reported in 1959 and thus far four genera have been impli- cated in human disease: Enterocytozoon sp. (E . bieneusz], Encephalitozoon sp. (E . hellurn, E . canaliculi, E. intestinalis), Nosema sp. (N. connori, N. ocularurn, N. corneurn), and Pleistophora sp.149a15fl The major species associated with enteric infection are Enterocytozoon bieneusi and Encephal- itozoon intestinalis (previously called Septata intestinalis).
Microsporidia are primitive eukaryotic unicellular parasites.They lack mitochondria and golgi membranes and possess small prokaryotic-sized rRNA.'" They pro- duce environmentally resistant spores that are charac- terized by coiled polar tubules. After entering the hosts, the polar tubules inject the sporoplasm (nucleus and cytoplasm) into the host cell.'48,149,152 Although there is significant intergeneric variation, the life cycle has three distinct phases: first, the spore or infective stage; second, the proliferative stage during which the organism divides by merogony (schizogony); and lastly, sporogony, the spore-forming stage. Epidemiology
Little is known about the epidemiology of human microsporidiosis. Serologic surveys suggest that infection with these organisms is widespread. Spread of the organ-
isms through environmental, person-to-person (fecal-oral, aerosolized respiratory secretions), and animal-to-person transmission have been postulated.'5"J53 Although there are few reported cases of microsporidial infection in nonHIV patients, these organisms are increasingly being recognized as etiologic agents of chronic disseminated dis- ease in HIV-positive individuals. E. bieneusi and E. intesti- nalis have both been associated with chronic diarrhea in AIDS patients. However, studies have not been unani- mous in demonstrating this association. In one case- controlled prospective study, the investigators did not find a significant difference in the presence of microsporidia on intestinal biopsy specimens when comparing HIV infected patients with and without diarrhea.'54 In con- trast, others have noted a clear association between infec- tion and altered d-xylose absorption.'"* In the normal host, microsporidia have been associated with traveler's diarrhea.'55 It has been suggested that microsporidia transiently infect immunocompetent individuals causing disease only in immunosuppressed p a t i e n t ~ . ' ~ ~ , ' ~ ~ J ~ ~ Pathology and Pathogenesis
E. bieneusi infections generally appear to be limited to the intestinal and biliary epithelium. The organisms are primarily found in the tips of the villi. Meronts are 4-6 p m in diameter. E. bieneusi was initially identified by electron m i c r o s ~ o p y . ~ ~ ~ ~ ' ~ ~ E. bieneusi infections are lim- ited to the intestinal and biliary epithelium. Histopatho- logic changes range from normal villus architecture to severe d u s atrophy. Infiltration of the lamina propria with mononuclear cells has been noted. Little is known about t he pathogenic basis o f diarrhea in intestinal microsporidiosis. Malabsorption of both carbohydrates and fats has been d e m o n ~ t r a t e d . ~ " ~ ~ ' ~ ~ * ' ~ ~
E . intestinalis infects enterocytes, macrophages, fibro- blasts, and endothelial cells of the lamina propria. In contrast to E. bieneusi, widespread dissemination often
Clinical Presentation Microsporidia have been associated with a self-lini-
ited diarrheal illness in a few apparently immunocom- petent patients. 155 Ophthalmologic involvement and central nervous system disease have also been reported. E. bieneusi appears to be associated with chronic diarrhea in AIDS patients.Is4 In this group, the clinical presenta- tion consists of diarrhea that is watery, without blood or mucus, and of variable volume. Weight loss is common. Since diagnosis was initially limited to patients who underwent intestinal biopsy, self-limited cases and milder cases may have been overlooked. Asymptomatic intesti- nal colonization by microsporidia has also been reported. lS4 Microsporidial infection of the biliary mucosa is associated with AIDS ~holangiopathy.'~'~'~ Clinical pre- sentation of E. intestinalis resembles that of E. bieneusi, except that extraintestinal disease is common.'6'
H a s h m e y e t a l . , P a r a s i t e s a n d D i a r r h e a . I: P r o t o z o a n s a n d D i a r r h e a 25
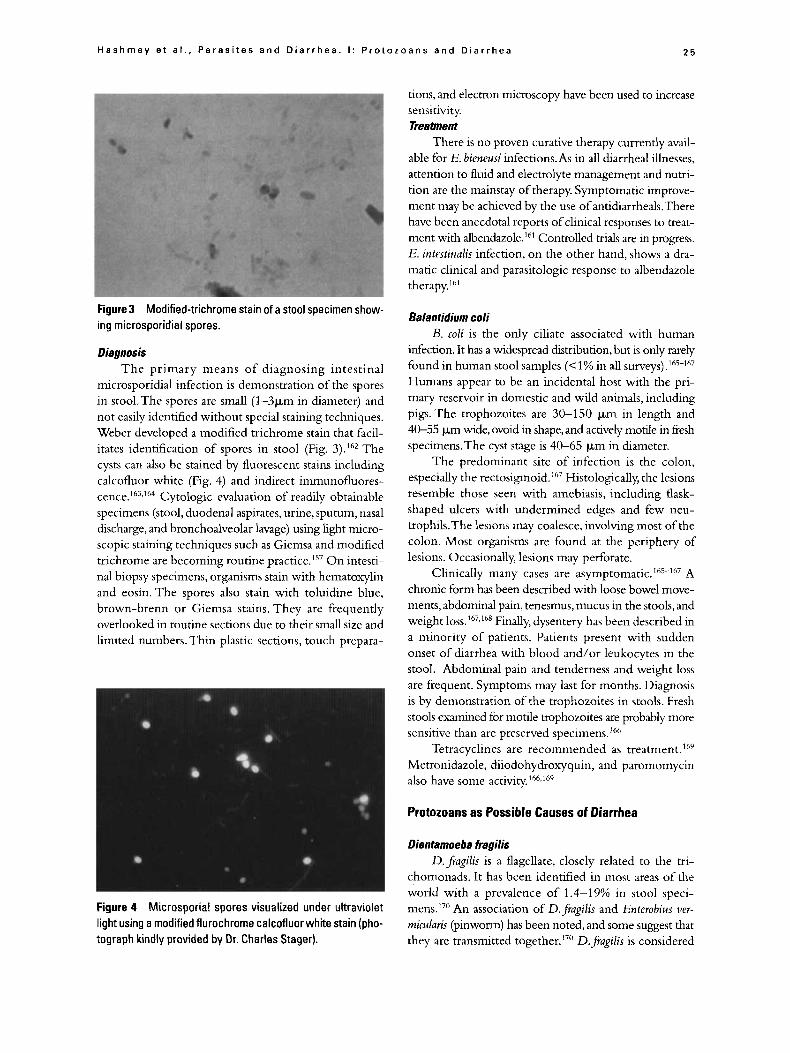
Figure 3 Modified-trichrorne stain of a stool specimen show- ing microsporidial spores.
Diagnosis The primary means of diagnosing intestinal
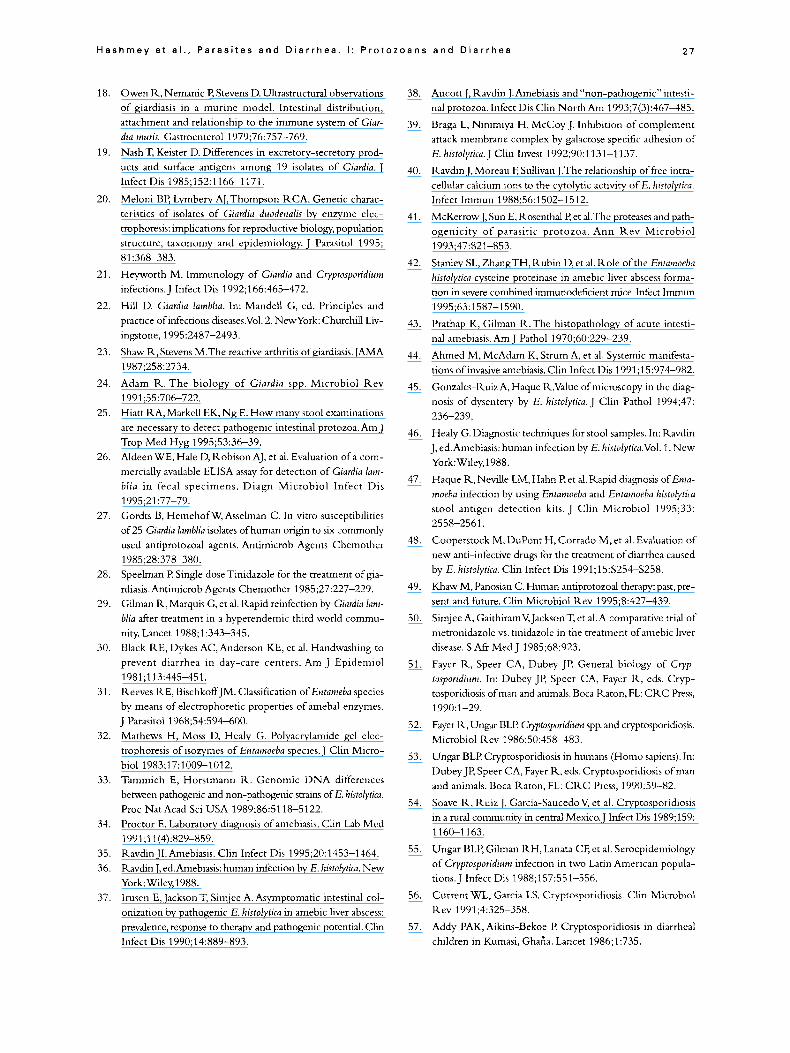
microsporidial infection is demonstration of the spores in stool.The spores are small (1-3pm in diameter) and not easily identified without special staining techniques. Weber developed a modified trichrome stain that facil- itates identification of spores in stool (Fig. 3).'62 The cysts can also be stained by fluorescent stains including calcofluor white (Fig. 4) and indirect immunofluores- ~ e n c e . ' ~ ' , ~ ~ ~ Cytologic evaluation of readily obtainable specimens (stool, duodenal aspirates, urine, sputum, nasal discharge, and bronchoalveolar lavage) using light micro- scopic staining techniques such as Giemsa and modified trichrome are becoming routine practice.I5' O n intesti- nal biopsy specimens, organisms stain with hematoxylin and eosin. The spores also stain with toluidine blue, brown-brenn or Giemsa stains. They are frequently overlooked in routine sections due to their small size and limited numbers. Thin plastic sections, touch prepara-
Figure 4 Microsporial spores visualized under ultraviolet light using a modified flurochrome calcofluor white stain (pho- tograph kindly provided by Dr. Charles Stager).
tions, and electron microscopy have been used to increase sensitivity. Treatment
There is no proven curative therapy currently avail- able for E. bieneusi infections.As in all diarrheal illnesses, attention to fluid and electrolyte management and nutri- tion are the mainstay of therapy. Symptomatic improve- ment may be achieved by the use of antidiarrheals.There have been anecdotal reports of clinical responses to treat- ment with albendazole.16' Controlled trials are in progress. E. intestinulis infection, on the other hand, shows a dra- matic clinical and parasitologic response to albendazole therapy.16'
Balanfidium coli B. coli is the only ciliate associated with human
infection. It has a widespread distribution, but is only rarely found in human stool samples (<1% in all surveys).'65-167 Humans appear to be an incidental host with the pri- mary reservoir in domestic and wild animals, including pigs. The trophozoites are 30-150 p,m in length and 40-55 p,m wide, ovoid in shape, and actively motile in fi-esh specimens.The cyst stage is 40-65 p,m in diameter.
The predominant site of infection is the colon, especially the rectosigmoid. 167 Histologically, the lesions resemble those seen with amebiasis, including flask- shaped ulcers with undermined edges and few neu- trophils.The lesions may coalesce, involving most of the colon. Most organisms are found at the periphery of lesions. Occasionally, lesions may perforate.
Clinically many cases are a~ymptornatic. '"~'~~ A chronic form has been described with loose bowel move- ments, abdominal pain, tenesmus, mucus in the stools, and weight ~ o s s . ~ ~ ~ J ~ ~ Finally, dysentery has been described in a minority of patients. Patients present with sudden onset of diarrhea with blood and/or leukocytes in the stool. Abdominal pain and tenderness and weight loss are frequent. Symptoms may last for months. Diagnosis is by demonstration of the trophozoites in stools. Fresh stools examined for motile trophozoites are probably more sensitive than are preserved specimens.'66
Tetracyclines are recommended as treatment.'69 Metronidazole, diiodohydroxyquin, and paromomycin also have some activity.'66a160
Protozoans as Possible Causes of Diarrhea
Dienfamoeba fragilis D.fragilis is a flagellate, closely related to the tri-
chomonads. It has been identified in most areas of the world with a prevalence of 1.4-19% in stool speci- m e n ~ . ~ ~ " An association of D.fragi!is and Enterobius uer- micularis (pinworm) has been noted, and some suggest that they are transmitted t~gether. '~" D.jagUis is considered

26 Journa l of T r a v e l Medicine, Volume 4, Number 1
by some to be a cause of diarrheal illness. Most infor- mation on D.frugi/is-associated illness comes from ret- rospective studies. Several studies identified the organism in stool samples of patients that lacked other recognized pathogen~.'~+''~ In a recent survey, D.jiagilis was the only parasite found in two-thirds of the cases.173 It occurred more frequently in children 5-9 years old. Eighty per- cent of the patients reported diarrheal symptoms. Anal pr~ritis'~",'~' and eosinophilia have been reported in a sub- stantial portion of c a ~ e s . ' ~ ~ ~ ' ~ ~ T h e s e symptoms may in part be due to concomitant pinworm infection.
None of these studies looked carefully for other organisms that might have accounted for the symptoms (e.g., Esherichia coli, Stronnloides stercoralis, G. lamblia, Ctypto- sporidium, and Isospora) . Furthermore, D.jiagilis has never been shown to be invasive.While pathologic abnormal- ities have been described in infected patients (e.g., fibrosis of the appendix),I7* other explanations seem more likely than parasitism.Therapy with metronidazole, iodoquinol, or paromomycin is effective, but eradicating the organ- ism has only inconsistent effects on ~ y m p t o m s . ' ~ " , ' ~ ~
Blastocystis hominis B. hominis is a common component of the human
intestinal flora. In the past, it was mistakenly believed to be a yeast. Elegant studies, primarily by Zierdt and coworkers, have conclusively demonstrated that B. hoininis is a protozoan.'74
The role of t h s organism in the pathogenesis of diar- rhea is contr~versial. '~~ B. hominis is present in 10-20% of stools from both normal and ill populations. Several series have been reported of patients with B. hominis in their stools, the absence of other identified pathogens, and gastrointestinal symptoms.'7"'7y A recent prospective case-controlled study among tourists in Nepal failed to show a difference in prevalence or heavy colonization (> I0 organisms per high power field) of B. hominis between study subjects and controls.'X".'X' Symptoms attributed to B. hominis include diarrhea, abdominal pain and bloating, and anorexia. Duration of illness has been variable. Eosinophilia has been noted in some cases. Response to therapy with antiprotozoal agents has been variable. Eradication of the organism does not correlate well with clinical response.
Not all commonly recognized pathogens were sought in these studies, nor were noninfectious causes of diarrhea excluded. O n careful evaluation, three groups found that most patients with diarrhea and Blastocystis in their stool have another explanation for their symp- t o m ~ . ' ~ ' - ' ~ ~ Biopsy specimens have usually shown nor- mal t i ~ s u e . " ~ Studies in gnotobiotic animals have demonstrated colonization only when infected with other stool organisms as well as B. hominis. Finally,
purportedly infected humans lacked a significant sero- logic response to the organism."'
Other Protozoa A number of nonpathogenic protozoa may be identi-
fied by routine parasitologic examination of stool speci- mens. The most frequently encountered are Endolimax nana and Entamoeba coli, each identified in approximately 4% of specimens. Others include Entamoeba hartmanrzi, Iodamoeba butchlii and Trichomonas hominis.'
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
0.
1.
2.
13.
14.
15.
16.
17.
Soltys B, Gupta R . Immunoelectron microscopy of Giardia lamblia cytoskeleton using antibody to acetylated alpha-tubu- lin. J Eukar Microbiol 1994;41(6):625-632. Chavez B, Martinezpalonio A. Ciardia lanrblia: freeze fracture structure of the ventral disc plasma membrane. J Eukar Microbiol 1995;42:136-141. Farthing M. Diarrheal disease: current concepts and future challenges. Pathogenesis of giardiasis.Trans R SOC Trop Med
Gilman R , Brown K. Epidemiology and serology of Giardia lamblia in a developing country: Bangladesh 1985.Trans 1\ SOC Trop Med Hyg 1985;79:469-473. Kappus KD, Lundgen KJ,Juranek D, et al. Intestinal parasitism in the United States: update on a continuing problem. Am J Trop Med Hyg 1994;50:705-713. Hill 13 Giardiasis: itsues in diagnosis and management. Infect Dis Clin North Am 1994;7(3):503-525. Craun G. Waterborne giardkasis in the United States. Lancet
Kelsall BL, Guerrant RL. Evaluation of diarrhea in the return- ing traveler. Infect Dis Clin North Am 1992;6:413-425. Brodsky K, Spencer HJ, Schultz M. Giardiasis in American travelers to the Soviet Union. J Infect Dis 1974;130:319. Steffan R , Richenback M,Wilheni U. Health problems after travel to developing countries. J Infect Dis 1987;156:84-93. Gray SE Kouse AR. Giaraiasisa cause of travellers' diarrhoea. CDK Review 1992;2:R45-47. Mintz ED, Hudson-Wragg M, Mshar D, et al. Foodborne giardiasis in a corporate ofice setting. J Infect Dis 1993; 167:250-253. Quick R , Paugh K,Addiss D, et al. Restaurant-associated out- break of giardiasis. J Infect Dis 1992;166:673-676. PorterJD, Gathey C, Heymann D, et al. Food-borne outbreak of Giardia lamblia.Am J Public Health 1990;80:1259-1260. Pickering L,Woodward W, DuPont H. Occurrence of Giardia larnblia in children in day care centers. J Pediatr 1984;
Dykes A, Ihranek D. Municipal waterborne giardiasis: an epi- demiological investigation. Beavers implicated as a possible reservoir. Ann Intern Med 1978;92:165-170. Balasz M, Szaltocky E. Electron microscopic examination of the mucosa of the small intestine in infection due to Giardia lamblia. Path Kes Pract 1978;163:250-260.
Hyg 1993;87:17-21.
1 986;2: 5 13-5 14.
104:522-526.
Hashrney e t a l . , P a r a s i t e s a n d D i a r r h e a . I : P r o t o z o a n s a n d D i a r r h e a 2 7
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28
29
30.
31
32
33
34
35 36
37
Owen R, Nemanic F’, Stevens D. Ultrastructural observations o f giardiasis in a murine model. Intestinal distribution, attachment and relationship to the immune system of Giar- dia muris. Gastroenterol 1979;76:757-769. Nash T, Keister D. Differences in excretory-secretory prod- ucts and surface antigens among 19 isolates of Giardia. J Infect Dis 1985;152:1166-1171.
Meloni BP, Lymbery AJ,Thompson RCA. Genetic charac- teristics of isolates of Giardia duodenalis by enzyme elec- trophoresis: implications for reproductive biology, population structure, taxonomy and epidemiology. J Parasitol 1995; 81 :368-383. Heyworth M. Immunology o f Ciardia and Cryptosporidium infections. J Infect Dis 1992;166:465-472.
Hill D. Giardia tamblia. In: Mandell G, ed. Principles and practice of infectious &seases.Vol. 2. NewYork: Churchill Liv- ingstone, 1995:2487-2493. Shaw R, Stevens M.The reactive arthritis of giardiasis. JAMA 1987;258:2734. Adam R. The biology of Giardia spp. Microbiol Rev
Hiatt RA, Markell EK, Ng E. How many stool examinations are necessary to detect pathogenic intestinal protozoa. Am J Trop Med Hyg 1995;53:36-39. Aldeen WE, Hale D, Robison AJ, et al. Evaluation of a com- mercially available ELISA assay for detection of Giardia lam- biia in fecal specimens. Diagn Microbiol Infect Dis
Gordts B, HemehofW, Asselman C. In vitro susceptibilities of 25 Giardia lamblia isolates of human origin to six commonly used antiprotozoal agents. Antimicrob Agents Chemother
Speelman €? Single doseTinidazole for the treatment of gia- rdiasis. Antimicrob Agents Chemother 1 985;27:227-229. Gilman R, Marquis G, et al. Rapid reinfection by Giardia [am- blia after treatment in a hyperendemic third world commu- nity. Lancet 1988;1:343-345. Black RE, Dykes AC, Anderson KE, et al. Handwashing to prevent diarrhea in day-care centers. Am J Epideniiol
Reeves RE, BischkoffJM. Classification o f Entameba species by means of electrophoretic properties of ameba1 enzymes. J Parasitol 1968;54:594-600. Mathews H , Moss D, Healy G. Polyacrylamide gel elec- trophoresis o f isozymes of Entamoeba species. J Clin Micro- biol 1983;17:1009-1012. Tammich E, Horstmann R. Genomic DNA differences between pathogenic and non-pathogenic strains of E. hktolytica. Proc Nat Acad Sci USA 1989;86:5118-5122. Proctor E. Laboratory diagnosis of amebiasis. Clin Lab Med
Ravdin JI. Amebiasis. Clin Infect Dis 1995;20:1453-1464. Ravdin J, ed.Amebiasis: human infection by E. histolytica. New York: Wiley,1988. Irusen E, Jackson T, Simjee A. Asymptomatic intestinal col- onization by pathogenic E. histolytica in amebic liver abscess: prevalence, response to therapy and pathogenic potential. Clin Infect Dis 1990;14:889-893.
1991;55:706-722.
1995;21:77-79.
1985;28:378-380.
1981 ;113:445-451.
1991;11(4):829-859.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
Aucott J. Ravdin J. Amebiasis and “non-pathogenic” intesti- nal protozoa. Infect Dis Clin North Am 1993;7(3):467-485.
Braga L, Ninimiya H, McCoy J. Inhibition of complement attack membrane complex by galactose specific adhesion o f
E. histolytica. J Clin Invest 1992;90:1131-1137.
Ravdin J. Moreau F, Sullivan J.The relationship of free intra- cellular calcium ions to the cytolytic activity of E. histoiytiru. Infect Immun 1988;56:1502-1512.
McKerrowJ, Sun E, Rosenthal P, et al.The proteases and path- ogenicity of parasitic protozoa. Ann Rev Microbiol 1993;47:821-853.
Stanley SL, ZhangTH, Rubin D, et al. Role o f the Entamoeba histolytica cysteine proteinase in amebic liver abscess forma- tion in severe combined immunodeficient mice. Infect Immun 1995;63: 1587-1 590. Prathap K, Gilman R . The histopathology o f acute intesti- nal amebiasis.Am J Pathol 1970;60:229-239.
Ahmed M, McAdam K, Strum A, et al. Systemic manifesta- tions ofinvasive amebiasis. Clin Infect Dis 1991 ;15:974-982.
Gonzales-Ruiz A, Haque R.Value of microscopy in the diag- nosis of dysentery by E. histolytica. J Clin Pathol 1994;47: 236-239.
Healy G. Diagnostic techniques for stool samples. In: Ravdin J, ed.Amebiasis: human infection by E. histolytica.Vo1. 1. New York:Wiley,l988.
Haque R, NeviUe LM, Hahn P, et al. Rapid hagnosis of Enfa- moeba infection by using Entamoeba and Entamoeba histolytica stool antigen detection kits. J Clin Microbiol 1995;33: 2558-2561,
Cooperstock M, DuPont H, Corrado M, et al. Evaluation of new anti-infective drugs for the treatment o f diarrhea caused by E. histolytica. Clin Infect Dis 1991;15:S254-S258.
Khaw M, Panosian C. Human antiprotozoal therapy: past, pre- sent and future. Clin Microbiol Rev 1995;8:427-439.
Simjee A, GaithiramV,JacksonT, et a1.A comparative trial o f
metronidazole vs. tinidazole in the treatment of amebic liver disease. S Afr Med J 1985;68:923.
Fayer R , Speer CA, Dubey JP. General biology of Cryp- tosporidium. In: Dubey JP, Speer CA, Fayer K, eds. Cryp- tosporidiosis of man and animals. Boca Raton, FL: CKC Press, 199O:l-29.
Fayer R, Ungar BLP Cryptosporidium spp. and cryptosporidiosis. Microbiol Rev 1986;50:458-483.
Ungar BLP. Cryptosporidiosis in humans (Homo sapiens). In: Ihbey JP, Speer CA, Fayer R,eds. Cryptosporidiosis ofman and animals. Boca Raton, FL: C R C Press, 1990:59-82.
Soave R, Ruiz J, Garcia-Saucedo V, et al. Cryptosporidiosis in a rural community in central Mexic0.J Infect Dis 1989;159: 1160-1163.
Ungar BLP, Gilman RH, Lanata CF, et al. Seroepidenmiology of Cryptosporidium infection in two Latin American popula- tions. J Infect Dis 1988;157:551-556.
Current WL, Garcia LS. Cryptosporidiosis. Clin Microbiol Rev 1991 ;4:325-358. Addy PAK, Aikins-Bekoe I! Cryptosporidiosis in diarrheal children in Kumasi, Gharia. Lancet 1986;1:735.
2 8 Journa l o f Travel Medic ine , V o l u m e 4, Number 1
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
Bogaerts J, Lepage P, Rouvony D, et al. Cryptosporidium species, a frequent cause of diarrhoea in Central Africa. J Clin Microbiol 1984;20:874-876. Mata L, Bolanos H, Pizarro D, et al. Cryptosporidiosis in chd- dren from some highland Costa Rican rural and urban areas. Am J Trop Med Hyg 1984;33:24-29. Mathan MM,Venkatesan S, George R, et al. Cryptosporidiosis and diarrhoea in southern Indian children. Lancet 1985;2:1172-1175. Pape JW, Levine E, Beaulieu ME, et al. Cryptosporidiosis in Haitian children. Am J Trop Med Hyg 1987;36:333-337. Shahid NS, Rahman ASMH, Anderson BC, et al. Cryp- tosporidiosis in Bangladesh. BMJ 1985;290:114-115. Weikel CS, Johnston L, DeSousa A, et al. Cryptosporidiosis in northeastern Brazil. J Infect Dis 1985;151:963-965. Wolfion JS, Richter JM,Waldron MA, et al. Cryptosporidiosis in immunocompetent hosts. N Engl J Med 1985;312:
Soave R, Ma E? Cryptosporidiosis.Trave1er’s diarrhea in two families. Arch Intern Med 1985;145:70-72. Ma P, Kaufman DL, Helmick CG, et al. Cryptosporidiosis in tourists returning from the Caribbean. N Engl J Med
Jokipii L, Pohjola S,Jokipii AMM. Cryptosporidium: a frequent finding in patients with gastrointestinal symptoms. Lancet
Juranek DD. Cryptosporidiosissources of infection and guidelines for prevention. Clin Infect Dis 1995;21:S57-S61. Smith HV, PattersonWJ,Hardie R, et al.An outbreak ofwater- borne cryptosporidiosis caused by post-treatment contami- nation. Epidemiol Infect 1989;103:703-715. Hayes EB, Matte TD, O’Brien TR, et al. Large community outbreak of cryptosporidiosis due to contamination of a fil- tered public water supply. N Engl J Med 1989;3201372-1376. D’Antonio RG,Win RE,Taylor JP, et al. A waterborne out- break of cryptosporidiosis in normal hosts. Ann Intern Med
MacKenzie WR, ScheU WL, Blair KA, et a]. Massive outbreak of waterborne Cryptosporidium infection in Milwaukee, WI: recurrence of illness and risk of secondary transmission. Clin Infect Dis 1995;21:57-62. MackenzieWR,Addiss DG, Davis JP. Cryptosporidium and the public water supply - reply. N Engl J Med 1994;331:1530. Current WL, Reese NC, Ernst JV, et al. Human cryp- tosporidiosis in immunocompetent and immunodeficient persons: studies of an outbreak and experimental transmis- sion. N Engl J Med 1983;308:1252-1257. MacKenziem, Hoxie NJ, Proctor ME, et a1.A massive out- break of Cryptosporidium infection transmitted through the public water supply. N Engl J Med 1994;331:161-167. Anonymous. Cryptosporidiosis in England andWales: preva- lence and clinical and epidemiological features. Public Health Laboratory Service Study Group. BMJ 1990;300:774-777. Alpert G, Bell LM, Kirkpatrick CE, et al. Outbreak of cryp- tospori&osis in a day-care center. Pediatrics 1986;77:152-157. Anonymous. Cryptosporidiosis among children attending day-care centers-Georgia, Pennsylvania, Michigan, Cali- fornia, New Mexico. MMWR 1984;33:599-601.
1278-1 282.
1985;312:647-648.
1983;2:358-361.
1986;103:886-888.
79. Koch KL, Phillips DJ, Aber RC, et al. Cryptosporidiosis in hospital personnel: evidence for person-to-person transmis- sion. Ann Intern Med 1984;102:593-596. Soave R, Danner RL, Honig CL, et al. Cryptosporidiosis in homosexual males. Ann Intern Med 1984;100:504-511.
81, Jokipii L, Pohjola S,Jokipii AM. Cryptospori&osis associated with traveling and giardiasis. Gastroenterol 1985;89:838-842. Ungar BL, Mulligan M, Nutman TB. Serologic evidence of Cryptosporidium infection in US volunteers before and dur- ing Peace Corps service in Africa. Arch Intern Med
Navin T R , Hardy AM. Cryptosporidiosis in patients with AIDS. J Infect Dis 1987;155:150. Sewankambo N, Mugenva RD, Goodgame R, et al. Entero- pathic AIDS in Uganda: an endoscopic, histologic, and micro- biologic study. AIDS 1987; 1:9-13. Sanchez-Mejorada G, Ponce-de-Leon S,Vilarcompte D, et al. AIDS in Mexico 1983-1990: changing clinical trends. 31st Interscience Conference on Antimicrobial Agents and Chemotherapy, Chicago, 1991. Diaz RMDS, Mangini ACS, Torres DMAGV, et al. Cryp- tosporidiosis among patients with acquired immunodefi- ciency syndrome (AIDS) in the county of Sio Paulo, Brazil. Rev Inst MedTrop Sao Paul0 1988;30:310-312.
87. CurrentWL. Cryptosporidium spp. 1n:Walzer PD, Genta RM, eds. Parasitic infections in the compromised host. NewYork: Marcel Dekker, Inc., 1989:281-341.
88. Genta RM, Chappell CL,White AC Jr, et al. Duodenal mor- phology and intensity of infection in AIDS-related cryp- tosporidiosis. Gastroenterol 1993; 105: 1769-1 775.
89. Goodgame RW, Kimball K, O u CN, et al. Intestinal function and injury in AIDS-related cryptosporidiosis. Gastroenterol
90. Martins CAP, Guerrant RL. Cryptosporidium and cryp- tosporidiosis. Parasitol Today 1995;11:434-436.
91. Guarino A, Canani RB, Casola A, et al. Human intestinal cryp- tosporidiosis: secretory diarrhea and enterotoxic activity in Caco-2 cells. J Infect Dis 1995;171:976-983.
92. Flanigan TE? Human immunodeficiency virus infection and cryptosporidiosis: protective immune responses. Am J Trop Med Hyg 1994;50:29-35.
93. BenhamouY, Kapel N, Hoang C, et al. Inefficacy of intesti- nal secretory immune response to Cryptosporidium in the Acquired Immunodeficiency Syndrome. Gastroenterol
94. FlaniganTeWhalen C,Turner J, et al. Cryptosporidium infec- tion and CD4 count.Ann Intern Med 1992;116:840-842.
95. Ungar BLP, Kao T-C, Burris JA, et al. Cryptosporidium infec- tion in an adult mouse model. Independant roles for IFN-g and CD4+T lymphocytes in protective immunity.J Immunol 199 1 ; 147: 1014-1022.
96. Chen W, Harp JA, Harmsen AG. Requirement for CD4+ cells and gamma interferon in resolution of established Cryp- tosporidium pawurn infection in mice. Infect Immun 1993;61:
97. Dupont HL, Chappell CL, Sterling CR, et al.The infectiv- ity of Cyptosporidium pawurn in healthy volunteers. N Engl J Med 1995;332:855-859.
80.
82.
1989; 149:894-897. 83.
84.
85.
86.
1995;108:1075-1082.
1995;108:627-635.
3928-3932.
H a s h m e y e t a l . , P a r a s i t e s a n d D i a r r h e a . 1 : P r o t o z o a n s a n d D i a r r h e a 2 9
98. Jokipii L, Jolului AMM.Timing of symptoms and oocyst excre- tion in human cryptosporidiosis. N Engl J Med 1986;315:
99. Egger M, Mausezahl D, Odermatt P, et al. Symptoms and trans- mission of intestinal cryptosporidiosis. Arch Dis Child
100. Soave R . Cryptosporidiosis and isosporiasis in patients with AIDS. Infect Dis Clin North Am 1988;2:485-493.
101. Fang GD, Lima AAM, Martins CV, et al. Etiology and epi- demiology of persistent diarrhea in Northeastern Brazil: a hos- pital-based, prospective, case-controlled study. J Pediatr Gastroenterol Nutr 1995;21:137-144.
102. Roberts WG, Green PHR, Ma J, et a]. Prevalence of cryp- tosporidiosis in patients undergoing endoscopy: evidence for an asymptomatic carrier state.Am J Med 1989;87:537-539.
103. Garcia LS, Current WL. Cryptosporidiosis: clinical features and diagnosis. Crit Rev Clin Lab Sci 1989;6:439-460.
104. CurrentWL.Techniques in laboratory maintenance of Cryp- tosporidium. In: Dubey JP, Speer CA, Fayer R , eds. Crypto- sporidiosis of man and animals. Boca Raton, FL: C R C Press,
105. Zimmerman S, Needham C. Comparison of conventional stool concentration and preserved smear methods with Mer- iflour Cryptosporidium/ Giardia direct immunofluorescence assay and Prospect Giardia EZ microplate assay for detection of Giardia lambia. J Clin Microbiol 1995;33:1942-1943.
106. Garcia LS, Brewer TC, Bruckner DA. Fluorescence detection of Cryptosporidium oocysts in human fecal specimens by using monoclonal antibodies. J Clin Microbiol 1987;25:119-121.
107. Arrowood MJ, Sterling CR. Comparison of conventional staining methods and monoclonal antibody-based methods for Crpfospon’dium oocyst detection. J C h Microbiol 1989;27: 149G1495.
108. Kotler DP, Francisco A, Clayton E et al. Small intestinal injury and parasitic diseases in AIDS.Ann Intern Med 1990;113: 444-449.
109. Sallon S, Deckelbaum RJ, Schmid 11, et al. Cryptosporidium, malnutrition, and chronic diarrhea. Am J Dis Child 1988;
110. Simon DM, Cello JP, Valenzuela J. Multicenter trial of octreotide in patients with refractory Acquired Immunode- ficiency Syndrome-associated diarrhea. Gastroenterol 1995;
111. Portnoy D, Whiteside ME, Buckley E, et al. Treatment of intestinal cryptosporidiosis with spiramycin. Ann Intern Med
112. Soave R , Armstrong D. Cryptosporidium and cryp- tosporidiosis. Rev Infect Dis 1986;8:1012-1023.
113. Gathe J, Piot D, Hawkins K, et al.Treatment of gastrointesti- nal cryptosporidiosis with paromomycin.VIth Annual Con- ference on AIDS, San Francisco, 1990.Vol. 2. London:Welcome Foundation, 1990.
1643-1 647.
1990;65:445-447.
1990:31-49.
142:312-315.
108~1753-1760.
1984;101:202-204.
114. Marshall RJ, Flanigan TP. Paromomycin inhibits Cryp- tosporidium infection of a human enterocyte cell line. J Infect Dis 1992;165:772-774.
11 5. White AC Jr, Chappell CL, Hayat CS, et al. Paromomycin for cryptosporidiosis in AIDS: a prospective, double-blind trial. J Infect Dis 1994;170:419-424.
1 16. Brandborg LL, Goldberg SB, Briedenbach WC. Human coc- cidia-a possible cause of malabsorption. The life cycle in small-bowel mucosal biopsies as a diagnostic feature. N Engl J Med 1970;283:1306-1313.
117. Faust EC, Giraldo LE, Caidedo G, et al. Human isosporiasis in the western hemisphere.Am JTrop Med Hyg 1961;lO: 343-349.
118. Smitskamp H, Dey-Muller E. Geographic distribution and clinical significance of human coccidiosis. Trop Geogr Med 1966;18:133-136.
119. Sorvillo FJ, Lieb LE, Seidel J, et al. Epidemiology of isospo- riasis among persons with Acquired Immunodeficiency Syn- drome in Los Angeles County.Am JTrop Med Hyg 1995;53:
20. DeHovitz JA, Pape JW, Boncy M, et al. Clinical manifesta- tions and therapy of Isusporu belli infection in patients with the Acquired Immunodeficiency Syndrome. N Engl J Med
21. TrierJS, Moxey PC, Schimmel EM, et al. Chronic intestinal coccidiosis in man: intestinal morphology and response to treatment. Gastroenterol 1974;66:923-935.
122. Barksdale WL, Routh CF. Isospora homiMis infections among American personnel in the southwest Pacific. Am J Trop Med 1948;28:639-644.
123. Henderson HE, Gillespie GW, Kaplan P, et al. The human
124. Jarpa Gana A. Coccidiosis humana. Biologica (Santiago)
125. Matsubayashi H, NozawaT. Experimental infection of Isuspora hominis in man.Am J Trop Med 1948;28:633-637.
126. Sorvillo F, Lieb L, Iwakoshi. Isospora belli and the Acquired Immune Deficiency Syndrome. N Engl J Med l990;322131.
127. Benator D, French A, Beaudet L, et al. Cyclospara infection associated with cholecystitis in a patient withAIDS.Ann Intern Med 1994;121:663-664.
128. Alfandari S,Ajana F, Senneville E, et al. Haemorrhagic ulcer- ative colitis due to Isospora belli in AIDS. Int J STD AIDS 1995;6:216.
129. Ng E, Markell EK, Fleming RL, et al. Demonstration of Isospora belli by acid-fast stain in a patient with Acquired Immunodeficiency Syndrome. J Clin Microbiol 1984;20: 384-386.
656-659.
1986;315:87-90.
1sospora.Am J Hyg 1963;78:302-309.
1966;39:3-26.
130. Pape JW,Verdier R-I, Johnson W D Jr. Treatment and pro- phylaxis of Isospora belli infection in patients with the Acquired Immunodeficiency Syndrome. N Engl J Med 1989;320:
131. Westerman EL, Christensen KP. Chronic Isospora belli infec- tion treated with co-trimoxazole.Ann Intern Med 1979;91:
1044-1 047.
4 13-41 4. 132. Himy R,Villard 0, Kremer M. Cyclosporida: a review.JTravel
133. Pollock K, Bendall R , Moody A.Traveler’s diarrhea associ- ated with cyanobacterium like bodies. Lancet 1992;341:
134. Bendall K, Lucas S, Moody A. Diarrhea associated with cyanobacterium like bodies: a new coccidian enteritis of man. Lancet 1993;341:59@592.
Med 1993;2:33-36.
556-557.
30 J o u r n a l of T r a v e l Medic ine , Volume 4 , Number 1
135. OrtegaY, Sterling C, Gilmaii R. Cyclospora species: a new protozoal pathogen of humans. N Engl J Med 1993;328:
136. OrtegaYR, Gilman RH, Sterling CR.A new coccidian par- asite (Apicomplexa: Eimeriidae) from humans. J Parasitol
137. PaprW,Verdier R , Boncy M. Cyclospora infections in adults infected with HIV. Clinical manifestations, treatment and prophylaxis. Ann Intern Med 1994;121:654-657.
138. Hope C, Shlim D, Rajah R. Epidemiology of diarrheal ill- ness associated with a coccidian like organism among trav- ellers and foreign residents in Nepal. Lancet 1993;341:
139. Gascon J, Corachan M, Bombi JA, et al. Cyclospora in patients with travellers harrhea. Scand J Infect Dis 1995;27:511-514.
140. Anonymous. Outbreaks of diarrheal illness associated with Cyanobacteria (blue-green algae)-like bodies-Chicago and Nepal, 1989 and 1990. MMWR 1991;40:325-327.
141. Huang P,Weber JT, Sosin DM, et al.The first reported out- break of diarrheal illness associated with Cyclospora in the United States. Ann Intern Med 1995;123:409-414.
142. Conner B, Shlim D, ScholesV. Pathologic changes in small bowel in nine patients with diarrhea associated with a coc- cidia like body. Ann intern Med 1993;119:377-382.
143. Sifuentesosornio J, Porrascortes G, Bendall RE et al. Cyclospora cayetanensis infection in patients with and without AIDS- biliary disease as another clinical manifestation. Clin Infect Dis 1995;21:1092-1097.
144. Long EG,White EH, Carmichael WW, et al. Morphologic and staining characteristics of a cyanobacterium-like organ- ism associated with harrhea.J infect Dis 1991;164:199-202.
145. Topazian M, Bia E New parasites around the block emerg- ing intestinal protozoa. Gastroenterol 1994;2:147-159.
146. Madico G, Gilman R , Miranda E.Treatment of Cyclospora infections with cotrimoxazole. Lancet 1993;342:122-123.
147. Hoge CW, Shlim DR, Ghimire M, et al. Placebo-controlled trial of co-trimoxazole for Cyclospora infections among travellers and foreign residents in Nepal. Lancet 1995;345:
148. Bryan RT. Microsporidia. in: Mandell G, Benett J, D o h R, eds. Principles and practice of infectious diseases.Vo1. 2. New York: Churchill Livingstone, 1995.
149. Weber R , Bryan RT, Schwartz DA, et al. Human microsporidial infections. Clin Microbiol Rev 1994;7:
150. Canning E, HolListerW. Human lnfectiom with Microsporiha.
151. Vossbrinck C, Barker M, Didier C, et al. Ribosomal RNA sequence suggests microsporidia are extremely primitive eukaryotes. Nature 1987;326:411-414.
152. Muscat I . Human microspori&osis.J Infect 1990;21:125-129. 153. Canning EU, Hollister WS. Enterocytozoon bieneusi
(microsporida): prevalence and pathogenicity in AIDS patients. Trans R SocTrop Med Hyg 1990;84:181-186.
154. Rabeneck L, Gyorkey F, Genta R M , et al.The role of microsporima in the pathogenesis of HIV-related chronic diar- rhea.Ann Intern Med 1993;119:895-899.
1308-1312.
1994;80:625-629.
1175-1179.
691-693.
426-461.
Rev Med Microbiol 1992;3:35-42.
155. Sandfort J, Hannemann A, Gelderblom H, et al. Enterocyto- zoon bieneusi infection in an immunocompetent patient who had acute diarrhea and who was not infected with the Human Immunodeficiency Virus. Clin Infect Dis 1994;lY: 5 14-51 6.
156. Cali A. General microsporidian features and recent findings on AIDS isolates. J Protozool 1991;38:625-630.
157. Schwartz DA,Bryan RT,Weber K, et al. Microsporidiosis in HIV positive patients: current methods for diagnosis using biopsy, cytologic, ultrastructural, immunologcal, and tissue cd- ture techniques. Folia Parasitol 1994;41: 101-1 09.
158. Orenstien J, Dieterich D, Kotler D. Systemic dissemination of a newly recognized intestinal Microsporidia species in
159. Cello J. AIDS cholangiopathy: spectrum of disease. Ann Intern Med 1986; 105:207-210.
160. Pol S, Romana C, Richard S. Microsporidia infection in patients with AIDS and unexplained cholangitis. N Engl J Med
161. Dore GJ, Marriott DJ, Hing MC, et al. Disseminated microsporidiosis due to Septata intestinalis in nine patients infected with the Human ImmunodeficiencyVirus - response to therapy with albendazole. Clin Infect Dis 1995;21:7&76.
162. Weber R, Bryan R, Owen R, et al. Improved light-micro- scopical detection of microsporidial spores in stool and duo- denal aspirates. N Engl J Med 1992;326:161-166
163. Didier ES, Orenstein JM, Aldras A, et al. Comparison of three staining methods for detecting microsporidia in fluids. J Clin Microbiol 1995;33:3138-3145.
164. LunaVA, Stewart BK, Bergeron DL, et al. Use of the fluo- rochrome calcofluor white in the screening of stool speci- mens for spores of microsporidia.Am J Clin Pathol1995;103:
165. Walzer PD, Judson FN, Murphy KB, et al. Balantidiasis out- break inTruk.Am JTrop Med Hyg 1973;22:33-41.
166. Lee RV, Prowten AW, Sidney A, et al.Typhlitis due to Balan- tidium coli in captive lowland gordas. Rev Infect Dis 1990;12:
167. ArhanVM, Koppisch E. Balantidiasis: a review and report of
168. Swartzwelder JC. Balantidiasis. Am J Digest Dis 1950;17:
169. Anonymous. Drugs for parasitic infections.The Medical Let- ter 1995;37:99-108.
170. Yang J, Scholten T. Dientamoeba fragilis: a review noted on its epidemiology, pathogenicity, mode of transmission, and hag- nosis.Am JTrop Med Hyg 1977;26:16-22.
171. Spencer MJ, Garcia LS, Chapin MR. Dientamoeba fragilis: an intestinal pathogen in chddren?Am J Dis Child 1979;133: 390-393.
172. Kean BH, Malloch CL.The neglected ameba: Dientamoeba fragilis: a report of 100 “pure” infections. Am J Digest Dis
173. Grendon JH, Digiacomo RE Frost FJ. Descriptive features of Dientamoeba fragilis infections. J Trop Med Hyg 1995;98:
174. Zierdt CH. Blastocystis hominis-past and future. Clin
AIDSAIIX 1992;6:1143-1150.
1993;328:95-99.
656-659.
1052-1059.
cases.Am J Pathoi 1956;32:1089-1115.
173-179.
1966;11:735-746.
309-31 5.
Microbiol Rev 1991;4:61-79.
H a s h m e y e t a l . , P a r a s i t e s a n d D i a r r h e a . I : P r o t o z o a n s a n d D i a r r h e a 3 1
175. Anonymous. Blastocystis hominis: commensal or pathogen? Lancet 1991 ;337:521-522.
176. Doyle PW, Helgason MM, Mathias RG, et al. Epidemiology and pathogenicity of Blastocystis hominis. J Clin Microbiol
177. Kain KC, Noble MA, Freeman HJ, et al. Epidemiologic and clinical features associated with Blastocystis hominis infec- tion. Diagn Microbiol Infect 1 3 s 1987;8:235-244.
178. Phillips BP, Zierdt CH. Blastocystis hominis: pathogenic potential in human patients and gnotobiotes. Exp Parasitol
179. Sheehan DJ, Raucher BG, McKitrick JC.Association ofBlas- tocystis hominis with signs and symptoms of human disease. J Clin Microbiol 1986;24:548-550.
1990; 28:116-121.
1976;39: 358-364.
180. Shlim DK, Hoge CW, Rajah R , et al. Is Blastocystis hominis a cause of diarrhea in travelers-a prospective controlled study in Nepal. Clin Infect Dis 1995;21:97-101.181, Keystone JS. Editorial-Blastocystis hominis and travelers dar- rhea. Clin Infect Dis 1995;21:102-103.
182. Sun T, Katz S,Tanenbaum B, et al. Questionable significance of Blastocystis hominis infection. Am J Gastro 1989;84:
183. Markell EK, Udkow MI? Blastocystis hominis: pathogen or fellow traveler.Am JTrop Med Hyg 1986;35:1023-1026.
184. Miller RA, Minshew BH. Blastocystis hominis: an organism in search of a disease. Rev Infect Dis 1988;10:930-938.
185. Chen J,Vaudry WL, Kowlewska K , et al. Lack of seruni immune response to Blastocystis honiinis. Lancet 1987;2:1021.
1543-1 547.
Hard work on a coffee plant in Avare, near SFio Paulo, Brazil. Submitted by Danielle Guyrech, M.D., and Julian Schilling, M.D.