opportunities and challenges in mr-compatible robotics
TRANSCRIPT
©PROJECT NEUROARM,UNIVERSITY OF CALGARY,CALGARY, ALBERTA
Opportunities andChallenges inMR-Compatible Robotics
The last few years have seen fast developments in mag-netic resonance (MR) compatible robotics. On the onehand, we are not far from revolutionary robots guidedby real-time three-dimensional (3-D) magnetic reso-
nance imaging (MRI), allowing reliable and precise minimallyinvasive interventions with reduced recovery time. On theother hand, dedicated robotic interfaces used in conjunctionwith functional MRI (fMRI) will allow neuroscientists toinvestigate the brain mechanisms of manipulation and motorlearning, and to improve rehabilitation therapies for relateddysfunctions. However, the realization of such systems mustaddress major technical challenges due to the strong static andswitching magnetic fields, electromagnetic interference (EMI),the limited space inside MRI scanners, and the physical interac-tion with human subjects/patients. This article gives an over-view of the opportunities offered by this novel technique, thecomponents of MR-compatible robotic systems, the history ofMR-compatible robotics, and the main challenges and direc-tions for future developments.
Compatibility depends on the imaging sequence used for theparticular application (e.g., MRI, fMRI, MR elastography, MRspectroscopy). The term MR compatible, as used in this specialissue, is defined in the introduction to this special issue [1], wherealternative terms corresponding to specific regulations are alsodiscussed.
Promises of MR-Compatible RoboticsRobotic systems are widely used in automation and machiningbecause of the high precision, accuracy, and repeatability thatcan be achieved during positioning or force control tasks[Figure 1(a)]. For the same reasons, many groups have devel-oped robot-assisted interventional systems [e.g., Figure 1(b)],some of which have evolved to commercial systems such asthe Robodoc and Neuromate (Integrated Surgical Systems,Sacramento, California), the da Vinci surgical system (Intui-tive Surgical, Inc., Sunnyvale, California), or the Acrobot(Acrobot Company Ltd., London, United Kingdom). In com-parison with industrial robots, more stringent safety con-straints must be respected, because these systems physicallyinteract with a patient and, in some cases, also with the motion
of the physician; therefore, this interaction must be safe andgentle. At the same time, such systems provide the possibilityof assisting and guiding the motion of the surgeon and improv-ing the performance [2].
Over the past years, efforts have been directed towardusing and combining 3-D data from imaging modalities suchas ultrasound, computed tomography (CT), and, more re-cently, MRI to control robotic systems in interventional posi-tioning tasks, motivated by the promises of more preciseinterventions with smaller incisions and reduced recoverytime. MRI is an excellent modality to image soft tissues withhigh contrast and spatial resolution, does not use ionizingradiation or injection of radioactive liquids, and has alsoestablished itself as a tool in advanced brain research. MRIcan provide high-quality anatomic data for interventionssuch as biopsies or brachytherapy (with increased imageresolution and diagnostic accuracy compared with transrec-tal ultrasound [3]), which both require precise positioning ofa needle, and several projects are underway to migrate angio-plasty procedures from CT to MRI.
The potential of MR-compatible robots lies in their abilityto precisely quantify and control position and forces/torques(with 3-D image guidance), and, e.g., generate guiding forcefields or other haptic cues to assist the surgeon during inter-ventional MRI (iMRI) [4]. However, MRI imposes severeconstraints on the development and use of mechatronic toolsand robotic systems and involves higher costs than other imag-ing modalities.
fMRI, on the other hand, allows clinicians and neuroscient-ists to measure the hemodynamic response linked to changesof neural activation in the brain evoked by external stimuli orcognitive tasks performed by the subject. An fMRI-compatiblerobotic system could provide computer-controlled dynamicenvironments to investigate human motor control and relateddysfunctions. This technology would also allow precise quanti-fication of movements and stimuli (onset, duration, subjectperformance) for (functional) clinical diagnostics.
MR-compatible robotic systems have been proposed for thefollowing applications:� stimulators for somatotopic mapping of the brain and
diagnostic fMRI [5]–[9] (Automated stimulators gener-ate a more reproducible output than what is achievable
BY ROGER GASSERT,ETIENNE BURDET,AND KIYOYUKI CHINZEI
MRI
ROBO
TICS
Reviewing the History, Mechatronic Components,and Future Directions of this Technology
Digital Object Identifier 10.1109/EMB.2007.910265
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE 0739-5175/08/$25.00©2008IEEE MAY/JUNE 2008 15

with manual stimulation, and, thus, reduce variability inbrain activation mapping.)
� mechanical vibrators for MR elastography, using MRI tomeasure wave propagation in tissue to, e.g., diagnosecancer [10]–[12]
� robotic systems and assistive devices for iMRI [13]–[18]and interventional radiology
� haptic interfaces to investigate human motor control dur-ing fMRI [19]–[22], for behavioral neuroscience studiesand for fMRI-based robot-assisted rehabilitation afterstroke [23]–[25].
For further reading on MRI and fMRI, see [26]–[29]. The themeissue on ‘‘fMRI—Our Window onto the Brain’’ [30] gives anoverview on the latter. A gallery of MR-compatible mecha-tronic and robotic systems developed by various groups can befound in [73], and slides on this topic can be found in [74].
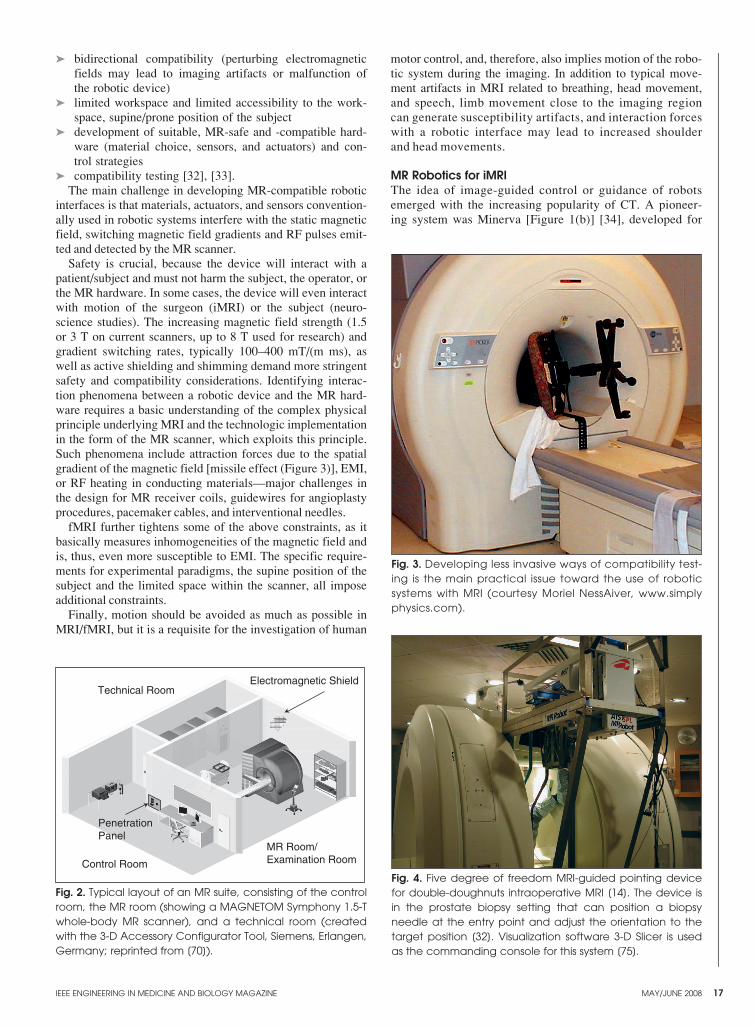
MR Environment and ImagingIn which environment must MR-compatible robots operate? Atypical MR suite consists of a shielded MR room, or examina-tion room, in which the MR scanner is located, a technicalroom, which contains the related control, amplifying, andmeasuring equipment, and a control room from where theequipment is operated (Figure 2). A penetration panel betweenthe MR room and the control room gives access to the earth-grounded shield and typically contains waveguides to pass
cables into the MR room as well as connectors and integratedlow-pass filters for signal and power lines. American Societyfor Testing and Materials (ASTM) F2503-05 (‘‘Standard Prac-tice for Marking Medical Devices and Other Items for Safetyin the Magnetic Resonance Environment,’’ ASTM International)defines the term MR environment as an MR environment-volumewithin the 0.50-mT (5 gauss [G]) line of an MR system,which includes the entire 3-D volume of space surroundingthe MR scanner. If the 0.50-mT line is contained within theFaraday shielded volume, the entire room is considered as anMR environment. This line also delimits the hazard zone toexternal equipment.
The MR room shielding may consist of only a Faraday cage,which prevents outside radio frequency (RF) noise from dis-turbing the imaging, or additionally contain soft iron to divertthe magnetic flux from the main magnet or outside disturban-ces. MRI/fMRI requires high homogeneity and temporalstability of the main magnetic field. There have been reportsof disturbances due to close-by elevators, as well as fromtrucks or trains passing nearby [31].
For the imaging, the subject is placed on a movable bed,and the body part to be imaged is moved into the isocenterof the magnet, where the magnetic field presents the high-est homogeneity. Access to the subject is limited, becausethe bore is a narrow cylinder of about 55 cm in diameter(can be as small as 35 cm for head scanners), typically
1.25–2 m in length.Although Figure 2 shows a
1.5-T short-bore whole-bodyclosed scanner (typically usedfor functional imaging), otherconfigurations such as open/intraoperative low-field scan-ners are used in iMRI. Manu-facturers are also introducinghigh-field scanners with larg-er bore diameters of up to70 cm to promote access tothe patient.
Challenges inMR-Compatible RoboticsThe hardware and imagingmethods of MRI/fMRI createvarious challenges for the de-velopment of MR-compatiblerobotic systems. Theseinclude:� safety (for patient/subject,
operator, medical staff,and equipment)
(a) (b)
Fig. 1. Example of robotic systems in industrial and medical applications. (a) The XR31 parallelDelta robot is a highly dynamic industrial robot. The robot is placing two to three biscuits persecond in blister packs (courtesy Demaurex/Bosch, Romanel sur Lausanne, Switzerland). (b)Minerva, the first comprehensive robotic system for neurosurgery in combination with CT im-aging, was developed for precise needle placement during stereotactic brain biopsy. Minervaperformed 14 successful operations at the University Hospital in Lausanne, Switzerland, between1993 and 1995 (courtesy EPFL, Switzerland).
We are not far from revolutionary robots guided
by real-time three-dimensional magnetic
resonance imaging.
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 200816
� bidirectional compatibility (perturbing electromagneticfields may lead to imaging artifacts or malfunction ofthe robotic device)
� limited workspace and limited accessibility to the work-space, supine/prone position of the subject
� development of suitable, MR-safe and -compatible hard-ware (material choice, sensors, and actuators) and con-trol strategies
� compatibility testing [32], [33].The main challenge in developing MR-compatible robotic
interfaces is that materials, actuators, and sensors convention-ally used in robotic systems interfere with the static magneticfield, switching magnetic field gradients and RF pulses emit-ted and detected by the MR scanner.
Safety is crucial, because the device will interact with apatient/subject and must not harm the subject, the operator, orthe MR hardware. In some cases, the device will even interactwith motion of the surgeon (iMRI) or the subject (neuro-science studies). The increasing magnetic field strength (1.5or 3 T on current scanners, up to 8 T used for research) andgradient switching rates, typically 100–400 mT/(m ms), aswell as active shielding and shimming demand more stringentsafety and compatibility considerations. Identifying interac-tion phenomena between a robotic device and the MR hard-ware requires a basic understanding of the complex physicalprinciple underlying MRI and the technologic implementationin the form of the MR scanner, which exploits this principle.Such phenomena include attraction forces due to the spatialgradient of the magnetic field [missile effect (Figure 3)], EMI,or RF heating in conducting materials—major challenges inthe design for MR receiver coils, guidewires for angioplastyprocedures, pacemaker cables, and interventional needles.
fMRI further tightens some of the above constraints, as itbasically measures inhomogeneities of the magnetic field andis, thus, even more susceptible to EMI. The specific require-ments for experimental paradigms, the supine position of thesubject and the limited space within the scanner, all imposeadditional constraints.
Finally, motion should be avoided as much as possible inMRI/fMRI, but it is a requisite for the investigation of human
motor control, and, therefore, also implies motion of the robo-tic system during the imaging. In addition to typical move-ment artifacts in MRI related to breathing, head movement,and speech, limb movement close to the imaging regioncan generate susceptibility artifacts, and interaction forceswith a robotic interface may lead to increased shoulderand head movements.
MR Robotics for iMRIThe idea of image-guided control or guidance of robotsemerged with the increasing popularity of CT. A pioneer-ing system was Minerva [Figure 1(b)] [34], developed for
Fig. 3. Developing less invasive ways of compatibility test-ing is the main practical issue toward the use of roboticsystems with MRI (courtesy Moriel NessAiver, www.simplyphysics.com).
Fig. 4. Five degree of freedom MRI-guided pointing devicefor double-doughnuts intraoperative MRI [14]. The device isin the prostate biopsy setting that can position a biopsyneedle at the entry point and adjust the orientation to thetarget position [32]. Visualization software 3-D Slicer is usedas the commanding console for this system [75].
Technical Room
PenetrationPanel
Control Room
MR Room/Examination Room
Electromagnetic Shield
Fig. 2. Typical layout of an MR suite, consisting of the controlroom, the MR room (showing a MAGNETOM Symphony 1.5-Twhole-body MR scanner), and a technical room (createdwith the 3-D Accessory Configurator Tool, Siemens, Erlangen,Germany; reprinted from [70]).
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 2008 17

precise needle placement during stereotactic brain biopsy.Minerva was designed to work with X-ray CT and was notMR-compatible. The first robotic system to be used withinthe gantry of an MR scanner was developed by Masamuneet al. [13]. The research interest of this group was mainly onthe influence of the machine on the imaging. The system suf-fered from a lack of rigidity, possibly because it was mademainly from polymers, which, in turn, provides a highamount of MR compatibility. Although the targeting accu-racy was evaluated using image guidance, the robot was notdesigned to maneuver during the imaging.
In 1999, Chinzei et al. [32] investigated mechatronic ele-ments for their application in MR environments and devel-oped a 5 degree of freedom (DoF) surgical assist robotactuated over linear drives actuated by ultrasonic motorsand encoders located outside the MR bore, designed tosimultaneously maneuver with imaging (Figure 4). Usingthe inhomogeneity and signal-to-noise ratio within theregion of a spherical phantom, Chinzei et al. [35] numeri-cally demonstrated that the loss of image quality due to therobot was negligible. Hempel et al. presented the first MR-compatible robotic system for cannula insertion to be com-mercialized [36], [37].
The anticipated advantages of MR-compatible roboticsystems for iMRI are: 1) an improved accuracy withrespect to manual interventions; 2) shorter procedure timeby eliminating ineffective interventions, e.g., unsuccessfulbiopsies; 3) better access to the patient inside the gantrywith respect to a direct intervention by a physician; and4) reduction of electromagnetic exposure of staff (occupa-tional health concern [38]), by controlling the robot fromoutside the scanner room.
Clinical practice of robotic assistance in the MR envi-ronment is still limited, and further clinical studies will benecessary to consolidate the advantages of MR-compatiblerobotic systems for iMRI; e.g., with the systems presentedin this special issue. This will also help identify the appli-cations that will profit most from this technology. Todate, the only commercial robotic surgical device ap-proved for use [in the European Union (EU)] is the Inno-motion system [36], [37]. We can also cite the ExAblate2000 system [39], [40], which is an MRI-guided high-intensity focused ultrasound system for tissue ablation. Itcoregisters with the MRI coordinate system and allowsthe physician to select and monitor the region to be treatedon the MR images. Fichtinger et al. developed a roboticsystem for transrectal prostate biopsy under MRI guid-ance [41], demonstrating that it has sufficient accuracy.This system is driven manually, and the tool position ismonitored by encoders mounted on the mechanism jointsas well as by MRI.
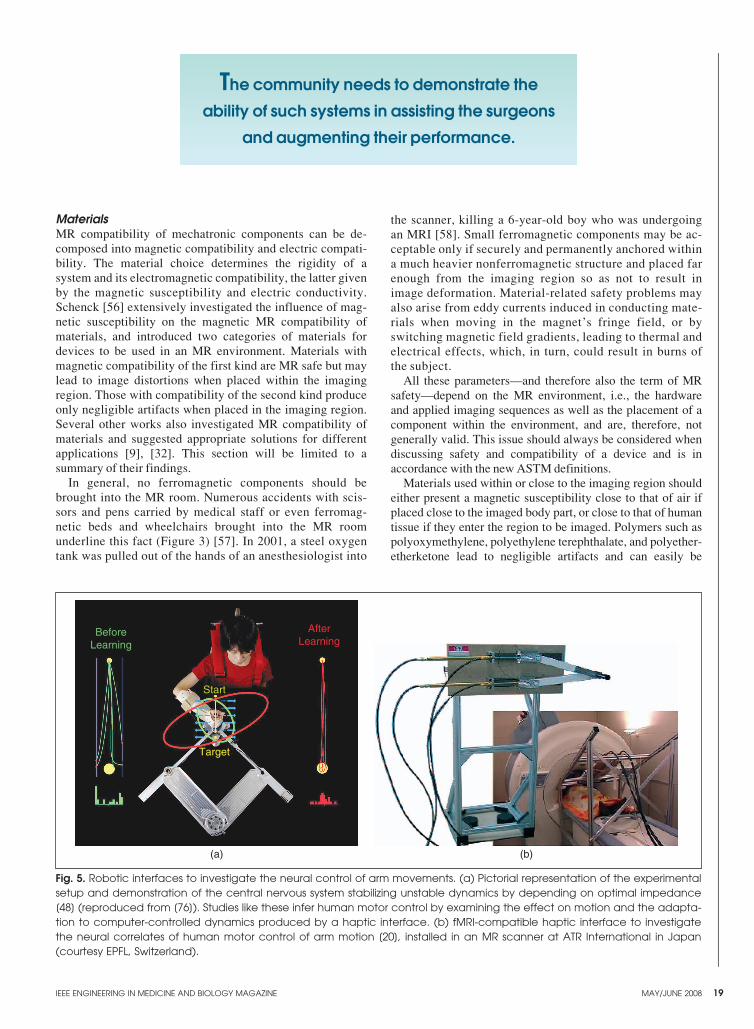
MR-Robotics for Neuroscience and Diagnostic fMRIRobotic interfaces can dynamically interact with humansperforming movements and can be used to study neuromus-cular adaptation [42]–[44]. It, thus, becomes possible to in-vestigate motor control by measuring the interaction force,limb trajectory, and endpoint impedance [45], whereas themotor commands to the muscles can be estimated fromelectromyography [46]. Investigating the adaptation tovirtual dynamic environments produced by such hapticinterfaces has led to major advances in neuroscience [47],[48] [Figure 5(A)]. A haptic interface that could be used inconjunction with fMRI would enable neuroscientists toview and investigate the brain mechanisms involved inhuman motor control [Figure 5(B)] and related dysfunc-tions. This could become a critical tool in neuroscience andrehabilitation.
The first functional studies with robotic interfaces werecarried out with positron emission tomography (PET) [49],[50]. They took advantage of the fact that conventionalrobotic systems from earlier studies could be used, becausePET is not susceptible to EMI from such devices. However,PET requires injection of radioactive tracers, has low tempo-ral resolution (in the order of a minute for oxygen-basedstudies), and has low spatial resolution, making it difficult todifferentiate between activation in functionally differentareas such as the primary motor cortex (M1) and primarysomatosensory cortex (S1) [51], or different regions of thecerebellum [52].
The rapid spread and evolution of MRI and fMRI overthe past years have made this modality attractive for neuro-science investigations and have allowed to overcome theshortcomings of PET. fMRI has a spatial resolution of2–6 mm and a temporal resolution in the order of a second.Time-resolved analysis of neuronal activation may evenreduce the temporal resolution to a few hundred millisec-onds. However, the MR environment precludes the use ofconventional robotic devices with fMRI, both for safety andcompatibility reasons, and fMRI is also very sensitive tohead and limb motion—its main disadvantage comparedwith PET.
Despite the large interest and many developments in thisfield, only few fMRI studies using robotic devices have so farbeen published to our knowledge [19], [53]–[55].
MR-Compatible MechatronicsSeveral robotic systems for specific applications in MRI/fMRI are presented in this special issue, and their mecha-tronic components are also discussed. Here, we briefly dis-cuss basic components to realize MR-compatible roboticsystems, as well as the limitations the design engineerencounters in their choice.
Safety is crucial because the device will
interact with a patient or subject and must not
harm the subject, the operator, or the
MR hardware.
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 200818
MaterialsMR compatibility of mechatronic components can be de-composed into magnetic compatibility and electric compati-bility. The material choice determines the rigidity of asystem and its electromagnetic compatibility, the latter givenby the magnetic susceptibility and electric conductivity.Schenck [56] extensively investigated the influence of mag-netic susceptibility on the magnetic MR compatibility ofmaterials, and introduced two categories of materials fordevices to be used in an MR environment. Materials withmagnetic compatibility of the first kind are MR safe but maylead to image distortions when placed within the imagingregion. Those with compatibility of the second kind produceonly negligible artifacts when placed in the imaging region.Several other works also investigated MR compatibility ofmaterials and suggested appropriate solutions for differentapplications [9], [32]. This section will be limited to asummary of their findings.
In general, no ferromagnetic components should bebrought into the MR room. Numerous accidents with scis-sors and pens carried by medical staff or even ferromag-netic beds and wheelchairs brought into the MR roomunderline this fact (Figure 3) [57]. In 2001, a steel oxygentank was pulled out of the hands of an anesthesiologist into
the scanner, killing a 6-year-old boy who was undergoingan MRI [58]. Small ferromagnetic components may be ac-ceptable only if securely and permanently anchored withina much heavier nonferromagnetic structure and placed farenough from the imaging region so as not to result inimage deformation. Material-related safety problems mayalso arise from eddy currents induced in conducting mate-rials when moving in the magnet’s fringe field, or byswitching magnetic field gradients, leading to thermal andelectrical effects, which, in turn, could result in burns ofthe subject.
All these parameters—and therefore also the term of MRsafety—depend on the MR environment, i.e., the hardwareand applied imaging sequences as well as the placement of acomponent within the environment, and are, therefore, notgenerally valid. This issue should always be considered whendiscussing safety and compatibility of a device and is inaccordance with the new ASTM definitions.
Materials used within or close to the imaging region shouldeither present a magnetic susceptibility close to that of air ifplaced close to the imaged body part, or close to that of humantissue if they enter the region to be imaged. Polymers such aspolyoxymethylene, polyethylene terephthalate, and polyether-etherketone lead to negligible artifacts and can easily be
The community needs to demonstrate the
ability of such systems in assisting the surgeons
and augmenting their performance.
BeforeLearning
(a) (b)
Start
Target
AfterLearning
Fig. 5. Robotic interfaces to investigate the neural control of arm movements. (a) Pictorial representation of the experimentalsetup and demonstration of the central nervous system stabilizing unstable dynamics by depending on optimal impedance[48] (reproduced from [76]). Studies like these infer human motor control by examining the effect on motion and the adapta-tion to computer-controlled dynamics produced by a haptic interface. (b) fMRI-compatible haptic interface to investigatethe neural correlates of human motor control of arm motion [20], installed in an MR scanner at ATR International in Japan(courtesy EPFL, Switzerland).
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 2008 19

machined. It must, however, be considered that even smallamounts of metal introduced during fabrication can lead tosignificant artifacts if the sample is placed within the imagingregion. Fiberglass and carbon fiber profiles present high stiff-ness but are difficult to machine. Within the fringe field, wehave successfully used brass and aluminum components. Notethat brass screws are often used on stereotaxic frames forinterventional neurology procedures.
Several mechanical components, such as linear guides,ball bearings, and pneumatic pistons, are readily availableon the market from MR-safe and -compatible materials(polymers, glass, beryllium-copper, ceramics). Aluminumprofiles and nonferromagnetic fixation elements are alsowidely available.
ActuatorsThe choice of an adequate actuation method is a central issuein the development of any mechatronic device and stronglydetermines the dynamic performances of the system. Thischoice is particularly difficult for robotic systems workingwithin an MR environment because of the imposed safety andcompatibility constraints as discussed earlier. These con-straints are even more severe in the case of fMRI, where actua-tion is also required during imaging, whereas this problem isovercome in some interventional systems by moving betweenimaging phases.
A detailed overview of actuation principles for applicationsin MR environments, covering positioning tasks, vibrotactilestimulation, as well as force feedback is given in [59]. Investi-gated principles include hydrostatic, belt, and cable transmis-sions as well as electrostatic and piezoelectric actuators. Agood solution to a given application often involves a combina-tion of several actuation principles. Systems for iMRI involv-ing positioning task have mainly used commercially availableultrasonic actuators, whereas systems for neuroscience studiesduring fMRI mostly use hydrostatic, pneumatic, or mechani-cal transmissions.
SensorsIn contrast to MR-compatible actuation methods, where per-formance and MR compatibility are in trade-off, MR-compat-ible force sensors with good performances can be developedmore easily [62]. EMI can be avoided by using light transmis-sion over optical fibers, which allows placing sensitive andnoisy electronic components away from the scanner, or evenoutside the MR room. This also prevents the sensor outputfrom being corrupted by the electromagnetic pulses emittedby the MR scanner. The interaction force can, thus, be deter-mined from the deflection of an elastic probe using reflectedor differential light intensity measurement over optical fibers.The sensing element can be made from materials adapted to
the location of use. For these reasons, several groups havechosen this approach [21], [24], [60]–[64]. Because of thelow current supply demand, traditional, commercially avail-able force sensors such as piezoresistive [65] or strain gage[25], [66] sensors have also been used with adequate shield-ing and filtering.
In contrast to force sensing, which requires a sensor as closeas possible to the output of the system, the problem of EMIcan be significantly reduced for position sensing. Opticalencoders or an optical tracking system can be placed at a cer-tain distance away from the scanner, or reflected/differentiallight intensity measurement over optical fibers can be used tomeasure displacement close to the imaging region. Kimmiget al. [67] presented an MR eye-tracking system based on asimilar principle.
Several groups have also successfully used optical encodersin the vicinity of or within an MR scanner [19], [20], [25]. Inaddition, our work has shown that a shielded optical trackingsystem with active markers can also be used in the fringe fieldof an MR scanner to track hand and finger motion [68]. How-ever, bringing any electronic components into the MR roomcan result in compatibility problems and can be a delicateissue to resolve. Compatibility of such devices can be im-proved by carrying light pulses over optical fibers instead ofpowering light emitting diodes over electric cables.
ConclusionThe development of MR-compatible robotic systems is acomplex task and demands knowledge in various fields ofscience. Thus, information exchange and collaboration be-tween mechatronics engineers, MR physicists, clinicians,and psychologists is one of the major challenges in develop-ing and evaluating such systems. The complexity of roboticsystems, especially if they are to operate within an MR envi-ronment, makes certification and acceptance by medical staffdifficult. Guidelines not only need to be developed to facili-tate information exchange, but researchers also require sim-ple and clear testing protocols to evaluate the safety andcompatibility of their systems. Only with such guidelineswill we see more systems come to clinical evaluation inthe future. Finally, as with all robotic systems for medicalapplications, the community needs to demonstrate the abil-ity of such systems in assisting surgeons and augmentingtheir performance.
Further ReadingWe have touched several fields that could not be treated indetail in this article. Readers interested in surgical roboticsmay see [69], and further aspects of MR-compatible roboticsare treated in [70]. An overview of robotic systems for appli-cations in MRI and fMRI can be found in [59], [71], [72].
The potential of MR-compatible robots lies
in their ability to precisely quantify
and control position and forces/torques
(with 3-D image guidance).
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 200820

AcknowledgmentsThe MR/T Robot project is a collaboration between the Surgi-cal Planning Laboratory (SPL) of Brigham and Women’sHospital, Johns Hopkins University, under NSF EngineeringResearch Center ‘‘Computer Integrated Surgical Systems andTechnology,’’ and National Institute of Advanced IndustrialScience and Technology (AIST). This research was funded byUS NIH P41 RR13218, P01 CA67165, R01 EB000304, USNSF ERC 9731748, Japan NEDO 02A47019b. The MR-compatible robotics project to investigate human motor con-trol is a collaboration project between the Ecole Polytechni-que Federale de Lausanne, Switzerland, and Imperial CollegeLondon, United Kingdom. This research was funded by ATRInternational in Japan, the Ecole Polytechnique Federale deLausanne (EPFL), the National University of Singapore, theEU-CEC Touch-HapSys project, and the Swiss National Sci-ence Foundation grant FNS-205321-104292/1. Roger Gassertis supported by the Swiss National Science Foundation, SNSFproject Nr. PBEL2-114427.
Roger Gassert received a M.Sc. in micro-engineering and a Ph.D. in robotics andneuroscience from the EPFL in 2002 and2006, respectively. He is currently a post-doctoral fellow in the Department of Bio-engineering at Imperial College, London,United Kingdom. He has developed thetechnology for MR-compatible robotic
devices to interact with human motion. His main researchinterests are in assistive devices, medical robotics, and neuro-science. He is a Member of the IEEE.
Etienne Burdet obtained an M.S. inmathematics in 1990, an M.S. in physicsin 1991, and a Ph.D. in robotics in 1996,all from Eidgenossische TechnischeHochschule (ETH) Zurich, Switzerland.He is currently a senior lecturer at Impe-rial College, London. He is doing researchat the interface of robotics and bioengineer-
ing, and his main research interest is human–machine interac-tion. He has contributions in various fields from human motorcontrol to virtual reality-based training systems, assistive devi-ces, and micro robotics for life sciences. He is a Member ofthe IEEE.
Kiyoyuki Chinzei obtained his M.Eng inprecision machinery engineering in 1989and a Ph.D in medical machinery engineer-ing in 1993 from the University of Tokyo.He is currently the leader of the SurgicalAssist Technology Group of the NationalInstitute of Advanced Industrial Scienceand Technology (AIST), Japan. His main
interest is in surgical robotics and its integration with medicalimaging and surgical planning. He is also active in soft tissuebiomechanics.
Address for Correspondence: Roger Gassert, Department ofBioengineering, Imperial College London, SW7 2AZ London,UK. E-mail: [email protected].
References[1] R. Gassert, E. Burdet, and K. Chinzei, ‘‘MR-compatible robotics—A criticaltool for image guided interventions, clinical diagnostics and neuroscience,’’ Eng.Med. Biol. Mag., vol. 8, no. 3, pp. 12–14, 2008.[2] B. Davies, S. Harris, W. Lin, R. Hibberd, R. Middleton, and J. Cobb,‘‘Active compliance in robotic surgery—The use of force control as a dy-namic constraint,’’ Proc. Inst. Mech. Eng., H, vol. 211, no. 4, pp. 285–292,1997.[3] A. Krieger, R. C. Susil, C. Menard, J. A. Coleman, G. Fichtinger, E. Atalar,and L. L. Whitcomb, ‘‘Design of a novel MRI compatible manipulator for imageguided prostate interventions,’’ IEEE Trans. Biomed. Eng., vol. 52, no. 2,pp. 306–313, 2005.[4] J. Troccaz, M. Peshkin, and B. Davies, ‘‘Guiding systems for computerassisted surgery: Introducing synergistic devices,’’ Med. Image Anal., vol. 2,no. 2, pp. 101–119, 1998.[5] S. Graham, W. Staines, A. Nelson, D. Plewes, and W. McIlroy, ‘‘New devicesto deliver somatosensory stimuli during functional MRI,’’ Magn. Reson. Med.,vol. 46, no. 3, pp. 436–442, 2001.[6] S. Golaszewski, C. Siedentopf, E. Baldauf, F. Koppelstaetter, W. Eisner,J. Unterrainer, G. Guendisch, F. Mottaghy, and S. Felber, ‘‘Functional magneticresonance imaging of the human sensorimotor cortex using a novel vibrotactilestimulator,’’ NeuroImage, vol. 17, no. 1, pp. 421–430, 2002.[7] R. Briggs, I. Dy-Liacco, P. Malcolm, H. Lee, K. Peck, K. Gopinath,N. Himes, D. Soltysik, P. Browne, and R. Tran-Son-Tay, ‘‘A pneumatic vibrotac-tile stimulation device for fMRI,’’ J. Magn. Reson. Med., vol. 51, no. 3, pp. 640–643, 2004.[8] A. Zappe, T. Maucher, K. Meier, and C. Scheiber, ‘‘Evaluation of a pneumati-cally driven tactile stimulator device for vision substitution during fMRI studies,’’J. Magn. Reson. Med., vol. 51, no. 4, pp. 828–834, 2004.[9] R. Gassert, N. Vanello, D. Chapuis, V. Hartwig, E. Scilingo, A. Bicchi,L. Landini, E. Burdet, and H. Bleuler, ‘‘Active mechatronic interface for hapticperception studies with functional magnetic resonance imaging: Compatibilityand design criteria,’’ in Proc. IEEE Int. Conf. Robotics and Automation (ICRA),2006, pp. 3832–3837.[10] J. Bishop, G. Poole, M. Leitch, and D. Plewes, ‘‘Magnetic resonance imagingof shear wave propagation in excised tissue,’’ J. Magn. Reson. Imaging, vol. 8,no. 6, pp. 1257–1265, 1998.[11] J. Bishop, A. Samani, J. Sciarretta, and D. Plewes, ‘‘Two-dimensional MRelastography with linear inversion reconstruction: Methodology and noise analy-sis,’’ J. Phys. Med. Biol., vol. 45, no. 8, pp. 2081–2091, 2000.[12] K. Uffmann, C. Abicht, W. Grote, H. Quick, and M. Ladd, ‘‘Design of anMR-compatible piezoelectric actuator for MR elastography,’’ Concepts Magn.Reson., vol. 15, no. 4, pp. 239–254, 2002.[13] K. Masamune, E. Kobayashi, Y. Masutani, M. Suzuki, T. Dohi, H. Iseki, andK. Takakura, ‘‘Development of an MRI-compatible needle insertion manipulatorfor stereotactic neurosurgery,’’ J. Image Guided Surg., vol. 1, no. 4, pp. 242–248,1995.[14] K. Chinzei, N. Hata, F. Jolesz, and R. Kikinis, ‘‘MR compatible surgical assistrobot: System integration and preliminary feasibility study,’’ presented at the Int.Conf. Medical Image Computing and Computer-Assisted Intervention (MICCAI),Pittsburgh, PA, USA, 2000.[15] B. T. Larson, A. G. Erdman, N. V. Tsekos, E. Yacoub, P. V. Tsekos, andI. G. Koutlas, ‘‘Design of an MRI-compatible robotic stereotactic device for mini-mally invasive interventions in the breast,’’ J. Biomech. Eng., vol. 126, no. 4,pp. 458–465, 2004.[16] K. Harada, K. Tsubouchi, M. Fujie, and T. Chiba, ‘‘Micro manipulators forintrauterine fetal surgery in an open MRI,’’ presented at the IEEE Int. Conf.Robotics and Automation (ICRA), Barcelona, Spain, 2005.[17] N. Hata, R. Hashimoto, and J. Tokuda, ‘‘Needle guiding robot for MR-guidedmicrowave thermotherapy of liver tumor using motorized remote-center-of-motionconstraint,’’ presented at the IEEE Int. Conf. Robotics and Automation (ICRA),Barcelona, Spain, 2005.[18] M. Muntener, A. Patriciu, D. Petrisor, D. Mazilu, H. Bagga, L. Kavoussi,K. Cleary, and D. Stoianovici, ‘‘Magnetic resonance imaging compatible roboticsystem for fully automated brachytherapy seed placement,’’ Urology, vol. 68,no. 6, pp. 1313–1317, 2006.[19] J. Diedrichsen, Y. Hashambhoy, T. Rane, and R. Shadmehr, ‘‘Neural corre-lates of reach errors,’’ J. Neurosci., vol. 25, no. 43, pp. 9919–9931, 2005.[20] R. Gassert, L. Dovat, O. Lambercy, Y. Ruffieux, D. Chapuis, G. Ganesh,E. Burdet, and H. Bleuler, ‘‘A 2-DOF fMRI compatible haptic interface to interactwith arm movements,’’ presented at the IEEE Int. Conf. Robotics and Automation(ICRA), Orlando, Florida, USA, 2006.[21] R. Gassert, R. Moser, E. Burdet, and H. Bleuler, ‘‘MRI/fMRI-compatiblerobotic system with force feedback for interaction with human motion,’’ IEEE-ASME Trans. Mechatron., vol. 11, no. 2, pp. 216–224, 2006.[22] A. J. Suminski, J. L. Zimbelman, and R. A. Scheidt, ‘‘Design and validationof a MR-compatible pneumatic manipulandum,’’ J. Neurosci. Methods, vol. 163,no. 2, pp. 255–266, 2007.[23] N. Hogan. MRI compatible wrist robot [Online]. Available: http://web.mit.edu/hogan/www/Projects/MRI_Wrist_Robot.htm[24] R. Riener, T. Villgrattner, R. Kleiser, T. Nef, and S. Kollias, ‘‘fMRI-compatible electromagnetic haptic interface,’’ presented at the 27th Annual Int.Conf. IEEE Engineering in Medicine and Biology Society (EMBC), Shanghai,China, 2005.
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 2008 21

[25] A. Khanicheh, A. Muto, C. Triantafyllou, B. Weinberg, L. Astrakas,A. Tzika, and C. Mavroidis, ‘‘fMRI-compatible rehabilitation hand device,’’ J.Neuroeng. Rehabil., vol. 3, no. 24, pp. 24–24, 2006.[26] D. Stark and W. Bradley, Magnetic Resonance Imaging, 3rd ed. St. Louis,MO: C.V. Mosby, 1999.[27] J. Hornak (2006). The Basics of MRI. [Online]. Available: http://www.cis.rit.edu/htbooks/mri/[28] E. Amaro and G. Barker, ‘‘Study design in fMRI: Basic principles,’’ BrainCogn., vol. 60, no. 3, pp. 220–232, 2006.[29] Functional MRI (fMRI): Links and information (2008, Mar. 28). [Online].Available: http://www.functionalmri.org/[30] T. Adali and V. D. Calhoun, (editors), ‘‘Functional MRI: Our window ontothe brain, theme issue,’’ IEEE Eng. Med. Biol. Mag., vol. 25, no. 2, Mar./Apr. 2006.[31] E. Durand, P. F. van de Moortele, M. Pachot-Clouard, and D. Le Bihan,‘‘Artifact due to B(0) fluctuations in fMRI: Correction using the k-space centralline,’’ Magn. Reson. Med., vol. 46, no. 1, pp. 198–201, 2001.[32] K. Chinzei, R. Kikinis, and A. Jolesz, ‘‘MR compatibility of mechatronicdevices: Design criteria,’’ Proc. 2nd Int. Conf. Medical Image Computing andComputer-assisted Interventions (MICCAI), Cambridge, UK, pp. 1020–1030,1999.[33] G. Schaefers, ‘‘Overview: Methods and current standards for magnetic reso-nance (MR) safety and compatibility testing for medical robotic and manipulatordevices used in MR environments,’’ Eng. Med. Biol. Mag., IEEE, vol. 27, no. 3,pp. 23–27.[34] H. Fankhauser, D. Glauser, P. Flury, Y. Piguet, M. Epitaux, J. Favre, andR. A. Meuli, ‘‘Robot for CT-guided stereotactic neurosurgery,’’ Stereotact. Funct.Neurosurg., vol. 63, pp. 93–98, 1994.[35] K. Chinzei, K. Yoshinaka, and T. Washio, ‘‘Numerical simulations and labtests for design of MR-compatible robots,’’ presented at the IEEE Int. Conf.Robotics and Automation (ICRA), Orlando, Florida, USA, 2006.[36] E. Hempel, H. Fischer, L. Gumb, T. Hohn, H. Krause, U. Voges,H. Breitwieser, B. Gutmann, J. Durke, M. Bock, and A. Melzer, ‘‘An MRI-compatible surgical robot for precise radiological interventions,’’ Comput. AidedSurg., vol. 8, no. 4, pp. 180–191, 2003.[37] INNOMEDIC—Touch the future (2008, Mar. 28). [Online]. Available:http://www.innomedic.de/[38] S. F. Keevil, W. Gedroyc, P. Gowland, D. L. G. Hill, M. O. Leach,C. N. Ludman, K. McLeish, D. W. McRobbie, R. S. Razavi, and I. R. Young,‘‘Electromagnetic field exposure limitation and the future of MRI,’’ Br. J. Radiol.,vol. 78, no. 935, pp. 973–975, 2005.[39] Z. R. Cohen, J. Zaubermann, S. Harnof, Y. Mardor, D. Nass, E. Zadicario,A. Hananel, D. Castel, M. Faibel, and Z. Ram, ‘‘Magnetic resonance imaging-guided focused ultrasound for thermal ablation in the brain: A feasibility study ina swine model,’’ Neurosurgery, vol. 60, no. 4, pp. 593–600, 2007.[40] K. Hynynen, N. McDannold, G. Clement, F. A. Jolesz, E. Zadicario,R. Killiany, T. Moore, and D. Rosen, ‘‘Pre-clinical testing of a phased array ultra-sound system for MRI-guided noninvasive surgery of the brain—A primatestudy,’’ Eur. J. Radiol., vol. 59, no. 2, pp. 149–156, 2006.[41] G. Fichtinger, A. Krieger, R. Susil, A. Tanacs, L. Whitcomb, and E. Atalar,‘‘Transrectal prostate biopsy inside closed MRI scanner with remote actuation,under real-time image guidance,’’ presented at the 5th Int. Conf. on MedicalImage Computing and Computer-Assisted Intervention (MICCAI), Tokyo, Japan,2002.[42] E. de Vlugt, A. C. Schouten, F. C. van der Helm, P. C. Teerhuis, andG. G. Brouwn, ‘‘A force-controlled planar haptic device for movement controlanalysis of the human arm,’’ J. Neurosci. Methods, vol. 129, no. 2, pp. 151–168,2003.[43] H. I. Krebs, B. T. Volpe, M. L. Aisen, and N. Hogan, ‘‘Increasing productiv-ity and quality of care: Robot-aided neuro-rehabilitation,’’ J. Rehabil. Res. Dev.,vol. 37, no. 6, pp. 639–652, 2000.[44] H. Gomi and M. Kawato, ‘‘Equilibrium-point control hypothesis examinedby measured arm stiffness during multijoint movement,’’ Science, vol. 272,no. 5258, pp. 117–120, 1996.[45] E. Burdet, R. Osu, D. W. Franklin, T. Yoshioka, T. E. Milner, andM. Kawato, ‘‘A method for measuring endpoint stiffness during multi-joint armmovements,’’ J. Biomech., vol. 33, no. 12, pp. 1705–1709, 2000.[46] D. W. Franklin, R. Osu, E. Burdet, M. Kawato, and T. E. Milner, ‘‘Adapta-tion to stable and unstable dynamics achieved by combined impedance control andinverse dynamics model,’’ J. Neurophysiol., vol. 90, no. 5, pp. 3270–3282, 2003.[47] R. Shadmehr and F. A. Mussa-Ivaldi, ‘‘Adaptive representation of dynamicsduring learning of a motor task,’’ J. Neurosci., vol. 14, no. 5, pp. 3208–3224,1994.[48] E. Burdet, R. Osu, D. W. Franklin, T. E. Milner, and M. Kawato, ‘‘The cen-tral nervous system stabilizes unstable dynamics by learning optimal impedance,’’Nature, vol. 414, no. 6862, pp. 446–449, 2001.[49] R. Shadmehr and H. H. Holcomb, ‘‘Neural correlates of motor memory con-solidation,’’ Science, vol. 277, no. 5327, pp. 821–825, 1997.[50] H. I. Krebs, T. Brashers-Krug, S. L. Rauch, C. R. Savage, N. Hogan,R. H. Rubin, A. J. Fischman, and N. M. Alpert, ‘‘Robot-aided functional imaging:Application to a motor learning study,’’ Hum. Brain Mapp., vol. 6, no. 1, pp. 59–72, 1998.[51] M. Lotze, P. Montoya, M. Erb, E. Hulsmann, H. Flor, U. Klose,N. Birbaumer, and W. Grodd, ‘‘Activation of cortical and cerebellar motor areas
during executed and imagined hand movements: An fMRI study,’’ J. Cogn. Neu-rosci., vol. 11, no. 5, pp. 491–501, 1999.[52] W. Grodd, E. Hulsmann, M. Lotze, D. Wildgruber, and M. Erb, ‘‘Sensorimo-tor Mapping of the Human Cerebellum: fMRI evidence of somatotopic organiza-tion,’’ Hum. Brain Mapp., vol. 13, no. 2, pp. 55–73, 2001.[53] A. Van de Winckel, S. Sunaert, N. Wenderoth, R. Peeters, P.Van Hecke, H. Feys, E. Horemans, G. Marchal, S. P. Swinnen, C. Perfetti,and W. De Weerdt, ‘‘Passive somatosensory discrimination tasks in healthyvolunteers: Differential networks involved in familiar versus unfamiliarshape and length discrimination,’’ Neuroimage, vol. 26, no. 2, pp. 441–453,2005.[54] L.L.C.D. Bursztyn, G. Ganesh, H. Imamizu, M. Kawato, and J. R. Flanagan,‘‘Neural correlates of internal-model loading,’’ Curr. Biol., vol. 16, no. 24,pp. 2440–2445, 2006.[55] A. J. Suminski, S. M. Rao, K. M. Mosier, and R. A. Scheidt, ‘‘Neural andelectromyographic correlates of wrist posture control,’’ J. Neurophysiol., vol. 97,no. 2, pp. 1527–1545, 2007.[56] J. F. Schenck, ‘‘The role of magnetic susceptibility in magnetic resonanceimaging: MRI magnetic compatibility of the first and second kinds,’’ Med. Phys.,vol. 23, no. 6, pp. 815–850, 1996.[57] G. Starck, B. Vikhoff-Baaz, K. Lagerstrand, E. Forssell-Aronsson, andS. Ekholm, ‘‘Phantom study of the lethal hazards involving ferromagnetic objectsin the magnetic field of a clinical MR scanner,’’ presented at the European Soci-ety for Magnetic Resonance in Medicine and Biology (ESMRMB), Copenhagen,Denmark, 2004.[58] ABC News. (2005, Aug.). ‘‘MRI scanner accidents on the rise,’’ [Online].Available: http://abcnews.go.com/GMA/story?id=1057960[59] R. Gassert, A. Yamamoto, D. Chapuis, L. Dovat, H. Bleuler, and E. Burdet,‘‘Actuation methods for applications in MR environments,’’ Concepts Magn.Reson. B: Magn. Reson. Eng., vol. 29B, no. 4, pp. 191–209, 2006.[60] M. Tada, S. Sasaki, and T. Ogasawara, ‘‘Development of an optical 2-axisforce sensor usable in MRI environments,’’ in Proc. IEEE sensors, Orlando, Flor-ida, 2002, vol. 1, pp. 253–258.[61] N. Takahashi, M. Tada, J. Ueda, Y. Matsumoto, and T. Ogasawara, ‘‘Anoptical 6-axis force sensor for brain function analysis using fMRI,’’ in Proc. IEEESensors, Toronto, Canada, 2003, vol. 1, pp. 253–258.[62] R. Gassert, D. Chapuis, H. Bleuler, and E. Burdet, ‘‘Sensors for applica-tions in magnetic resonance environments,’’ IEEE-ASME Trans. Mechatron.,vol. 13, no. 3, June 2008, in press.[63] M. Tada and T. Kanade, ‘‘Development of an MR-compatible optical forcesensor,’’ in Proc. 26th Annu. Int. Conf. IEEE EMBS (EMBC), San Francisco, CA,2004, vol. 3, pp. 2022–2025.[64] M. Tada and T. Kanade, ‘‘Design of an MR-compatible three-axis force sen-sor,’’ in Proc. IEEE/RSJ Int. Conf. Intelligent Robots and Systems (IROS), Alberta,Canada, 2005, pp. 3505–3510.[65] N. S. Ward, J. M. Newton, O. B. C. Swayne, L. Lee, A. J. Thompson, R.J. Greenwood, J. C. Rothwell, and R. S. J. Frackowiak, ‘‘Motor system activationafter subcortical stroke depends on corticospinal system integrity,’’ Brain, vol. 129,no. 3, pp. 809–819, 2006.[66] J. Hidler, T. Hodics, B. Xu, B. Dobkin, and L. G. Cohen, ‘‘MR compatibleforce sensing system for real-time monitoring of wrist moments during fMRI test-ing,’’ J. Neurosci. Methods, vol. 155, no. 2, pp. 300–307, 2006.[67] H. Kimmig, M. Greenlee, F. Huethe, and T. Mergner, ‘‘MR-eyetracker: Anew method for eye movement recording in functional magnetic resonance imag-ing,’’ Exp. Brain Res., vol. 126, no. 3, pp. 443–449, 1999.[68] M. Klarhofer, M. Haelg, R. Gassert, S. Haller, and K. Scheffler, ‘‘MR-compatible optical tracking device with active markers,’’ presented at the Int.Society of Magnetic Resonance in Medicine, Miami, Florida, USA, 2005.[69] K. Cleary and C. Nguyen, ‘‘State of the art in surgical robotics: Clinicalapplications and technology challenges,’’ Comput. Aided Surg., vol. 6, no. 6,pp. 312–328, 2001.[70] R. Gassert, ‘‘MR-compatible robotics to investigate human motor control,’’Ph.D. dissertation, Ecole Polytechnique Federale de Lausanne (EPFL), Lausanne,Switzerland, 2006.[71] H. Elhawary, A. Zivanovic, B. Davies, Lamp, and M. Lamperth, ‘‘A reviewof magnetic resonance imaging compatible manipulators in surgery,’’ in Proc.Inst. Mech Eng. H, J. Eng. Med., vol. 220, no. 3, pp. 413–424, 2006.[72] N. V. Tsekos, A. Khanicheh, E. Christoforou, and C. Mavroidis, ‘‘Magneticresonance-compatible robotic and mechatronics systems for image-guided inter-ventions and rehabilitation: A review study,’’ Annu. Rev. Biomed. Eng., vol. 9,pp. 351–387, 2007.[73] MR-Robotics Gallery (2007, October 9) [Online]. Available: http://mrrobo-tics.epfl.ch/gallery[74] ‘‘MRI/fMRI compatible robot technology––A critical tool for neuroscienceand image guided intervention’’ [Online]. Available: http://mrrobotics.epfl.ch/ICRA[75] S. DiMaio, S. Pieper, K. Chinzei, N. Hata, S. Haker, D. Kacher,G. Fichtinger, C. Tempany, and R. Kikinis, ‘‘Robot-assisted needle placement inopen-MRI: System architecture, integration and validation,’’ Comput. Aid. Surg.vol. 12, no. 1, pp. 15–24, 2007.[76] R. Gassert, L. Dovat, G. Ganesh, E. Burdet, H. Imamizu, T. Milner, andH. Bleuler, ‘‘Multijoint arm movements to investigate motor control with fMRI,’’in Proc. IEEE EMBC, Shanghai, China, 2005, pp. 4488–4491.
IEEE ENGINEERING IN MEDICINE AND BIOLOGY MAGAZINE MAY/JUNE 200822